
Effect of adding different thickening agents on the viscosity properties and in vitro mineral...
7
Effect of adding different thickening agents on the viscosity properties and in vitro mineral availability of infant formula Carlos A. González-Bermúdez ⇑ , Carmen Frontela-Saseta, Rubén López-Nicolás, Gaspar Ros-Berruezo, Carmen Martínez-Graciá Department of Food Science and Nutrition, Faculty of Veterinary Sciences, Regional Campus of International Excellence ‘‘Campus Mare Nostrum’’, University of Murcia, Spain article info Article history: Received 29 November 2013 Received in revised form 17 February 2014 Accepted 27 February 2014 Available online 12 March 2014 Keywords: Infant formula Thickeners In vitro digestion Calcium Mineral availability Viscosity Phytate content abstract The effect of adding different thickening agents (locust bean gum (LBG), modified corn and rice starches (MCS, MRS)) to an infant formula on both in vitro mineral availability (Ca, Fe and Zn), quantified by atomic absorption spectrophotometry (AAS), and formula viscosity, after in vitro gastrointestinal digestion, was investigated. LBG was the most effective agent to increase formula thickness. However, it showed a neg- ative effect on Ca, Fe and Zn in vitro solubility and dialysability. MCS and MRS only affected calcium sol- ubility and dialysability when they were used at P50% of the maximum legal limit. No negative effect was observed for Fe and Zn when modified starches were added at the different concentrations assessed. The phytate content in the thickening ingredients was also analysed. Despite finding a considerable amount of phytic acid in the raw ingredients, its final concentration in the infant formula was insufficient to decrease in vitro mineral availability. Ó 2014 Elsevier Ltd. All rights reserved. 1. Introduction Reflux episodes are frequent in infants, although most of them are mild and brief. However, when this passage of gastric content into the oesophagus is accompanied by abdominal pain, oesopha- gitis or inspiratory disorders, as well as others pathological conse- quences, therapeutic intervention becomes necessary (Horvath, Dziechciarz, & Szajewska, 2008). In this regard, a variety of approaches have been proposed, including pharmacological and non-pharmacological therapies. In the treatment of non-compli- cated gastroesophageal reflux, thickening of infant formulas has commonly been recommended (Vandenplas, Hauser, Devreker, Mahler, Degreef & Veereman-Wauters, 2013). Thickening agents, such as locust bean gum (LBG) or modified starches, have fre- quently been added to infant formulas with the aim of increasing their viscosity. The efficacy of thickening agents depends on their ability to increase gastric retention time, avoiding a return to the oesophagus during the first digestion phase, and reducing almost consistently the frequency and volume of regurgitation (Corvaglia, Martini, Aceti, Arcuri, Rossini, & Faldella, 2013). Nevertheless, the number of studies on the effect of thickening agents on rheological properties of infant formulas is very limited, and those that do exist have not made reference to the ideal viscosity value that will lead to a positive effect on children (Bosscher, Van Caillie-Bertrand, & Deelstra, 2003a; Miyazawa, Tomomasa, Kaneko, Arakawa, & Morikawa, 2007; Miyazawa, Tomomasa, Kaneko, & Morikawa, 2004; Vanderhooh, Moran, Harris, Merkel, & Orenstein, 2003). These types of products are commercialised under the name of antireflux or antiregurgitation (AR) infant formulas, and are promoted with the claim that they benefit infants who have gastroesophageal reflux or who spit up regularly (Pina, Llach, Ariño-Armengol, & Iglesias, 2008; Vandenplas, 2008; Vanderhooh et al., 2003). The use of AR formulas has been recommended by the North American and the European Society for Pediatric Gastro- enterology, Hepatology, and Nutrition (NASPGHAN and ESPGHAN, respectively) (Vandenplas et al., 2009) as far as it has been demon- strated that these products significantly reduce regurgitation in infants with recurrent vomiting. (Agget et al., 2002; Chao & Vandenplas, 2007; Vandeplas, 2008; Vanderhooh et al., 2003) Locust bean gum and modified starches, as ingredients for AR formulas, are legally allowed in Europe, where different maximum concentrations have been established for each group (European Parliament and Council, 1995; European Parliament and Council, 2006). According to this legislation, modified starches may be added to infant formulas up to either 30% of total carbohydrates or 2 g/100 mL. In the case of LBG, it may be added up to a maximum level of 10 g/L from birth onwards. These maximum levels are sim- ilar to those recommended by ESPGHAN in its Global Standard for the Composition of Infant Formula (Koletzko et al., 2005) and by http://dx.doi.org/10.1016/j.foodchem.2014.02.168 0308-8146/Ó 2014 Elsevier Ltd. All rights reserved. ⇑ Corresponding author. Tel.: +34 868 88 47 98; fax: +34 868 88 84 97. E-mail address: [email protected] (C.A. González-Bermúdez). Food Chemistry 159 (2014) 5–11 Contents lists available at ScienceDirect Food Chemistry journal homepage: www.elsevier.com/locate/foodchem
Transcript of Effect of adding different thickening agents on the viscosity properties and in vitro mineral...

Food Chemistry 159 (2014) 5–11
Contents lists available at ScienceDirect
Food Chemistry
journal homepage: www.elsevier .com/locate / foodchem
Effect of adding different thickening agents on the viscosity propertiesand in vitro mineral availability of infant formula
http://dx.doi.org/10.1016/j.foodchem.2014.02.1680308-8146/� 2014 Elsevier Ltd. All rights reserved.
⇑ Corresponding author. Tel.: +34 868 88 47 98; fax: +34 868 88 84 97.E-mail address: [email protected] (C.A. González-Bermúdez).
Carlos A. González-Bermúdez ⇑, Carmen Frontela-Saseta, Rubén López-Nicolás, Gaspar Ros-Berruezo,Carmen Martínez-GraciáDepartment of Food Science and Nutrition, Faculty of Veterinary Sciences, Regional Campus of International Excellence ‘‘Campus Mare Nostrum’’, University of Murcia, Spain
a r t i c l e i n f o a b s t r a c t
Article history:Received 29 November 2013Received in revised form 17 February 2014Accepted 27 February 2014Available online 12 March 2014
Keywords:Infant formulaThickenersIn vitro digestionCalciumMineral availabilityViscosityPhytate content
The effect of adding different thickening agents (locust bean gum (LBG), modified corn and rice starches(MCS, MRS)) to an infant formula on both in vitro mineral availability (Ca, Fe and Zn), quantified by atomicabsorption spectrophotometry (AAS), and formula viscosity, after in vitro gastrointestinal digestion, wasinvestigated. LBG was the most effective agent to increase formula thickness. However, it showed a neg-ative effect on Ca, Fe and Zn in vitro solubility and dialysability. MCS and MRS only affected calcium sol-ubility and dialysability when they were used at P50% of the maximum legal limit. No negative effectwas observed for Fe and Zn when modified starches were added at the different concentrations assessed.The phytate content in the thickening ingredients was also analysed. Despite finding a considerableamount of phytic acid in the raw ingredients, its final concentration in the infant formula was insufficientto decrease in vitro mineral availability.
� 2014 Elsevier Ltd. All rights reserved.
1. Introduction lead to a positive effect on children (Bosscher, Van Caillie-Bertrand,
Reflux episodes are frequent in infants, although most of themare mild and brief. However, when this passage of gastric contentinto the oesophagus is accompanied by abdominal pain, oesopha-gitis or inspiratory disorders, as well as others pathological conse-quences, therapeutic intervention becomes necessary (Horvath,Dziechciarz, & Szajewska, 2008). In this regard, a variety ofapproaches have been proposed, including pharmacological andnon-pharmacological therapies. In the treatment of non-compli-cated gastroesophageal reflux, thickening of infant formulas hascommonly been recommended (Vandenplas, Hauser, Devreker,Mahler, Degreef & Veereman-Wauters, 2013). Thickening agents,such as locust bean gum (LBG) or modified starches, have fre-quently been added to infant formulas with the aim of increasingtheir viscosity. The efficacy of thickening agents depends on theirability to increase gastric retention time, avoiding a return to theoesophagus during the first digestion phase, and reducing almostconsistently the frequency and volume of regurgitation (Corvaglia,Martini, Aceti, Arcuri, Rossini, & Faldella, 2013). Nevertheless, thenumber of studies on the effect of thickening agents on rheologicalproperties of infant formulas is very limited, and those that doexist have not made reference to the ideal viscosity value that will
& Deelstra, 2003a; Miyazawa, Tomomasa, Kaneko, Arakawa, &Morikawa, 2007; Miyazawa, Tomomasa, Kaneko, & Morikawa,2004; Vanderhooh, Moran, Harris, Merkel, & Orenstein, 2003).These types of products are commercialised under the name ofantireflux or antiregurgitation (AR) infant formulas, and arepromoted with the claim that they benefit infants who havegastroesophageal reflux or who spit up regularly (Pina, Llach,Ariño-Armengol, & Iglesias, 2008; Vandenplas, 2008; Vanderhoohet al., 2003). The use of AR formulas has been recommended bythe North American and the European Society for Pediatric Gastro-enterology, Hepatology, and Nutrition (NASPGHAN and ESPGHAN,respectively) (Vandenplas et al., 2009) as far as it has been demon-strated that these products significantly reduce regurgitation ininfants with recurrent vomiting. (Agget et al., 2002; Chao &Vandenplas, 2007; Vandeplas, 2008; Vanderhooh et al., 2003)
Locust bean gum and modified starches, as ingredients for ARformulas, are legally allowed in Europe, where different maximumconcentrations have been established for each group (EuropeanParliament and Council, 1995; European Parliament and Council,2006). According to this legislation, modified starches may beadded to infant formulas up to either 30% of total carbohydratesor 2 g/100 mL. In the case of LBG, it may be added up to a maximumlevel of 10 g/L from birth onwards. These maximum levels are sim-ilar to those recommended by ESPGHAN in its Global Standard forthe Composition of Infant Formula (Koletzko et al., 2005) and by
6 C.A. González-Bermúdez et al. / Food Chemistry 159 (2014) 5–11
the European Commission Scientific Committee for Food (1997).Moreover, several authors have indicated the need to explorefurther the effect of these ingredients on the nutrition and healthof infants, as some studies using an in vitro model have suggestedthat the bioavailability of calcium, iron and zinc may be affectedby thickening agents and probably also by the presence of certainantinutrients, such as phytic acid (Bosscher et al., 2000, 2003a;Vandenplas et al., 2013). In particular, this antinutrient has beenreported as a strong chelator of multivalent metal ions, specificallyiron, zinc and calcium (Frontela, Haro, Ros, & Martinez, 2008).
With this background, the aim of this study was to evaluate theeffect of different concentrations of LBG and pregelatinised cornand rice starches added to a commercial infant formula on bothviscosity and mineral (calcium, iron and zinc) availability in vitro.
2. Materials and methods
2.1. Samples
Standard infant formula (Hero Baby� 1) was provided by HeroEspaña SA (Alcantarilla, Murcia, Spain). As thickening agents,locust bean gum (Grinsted LBG 860, Danisco, Portugal), modifiedcorn starch (MCS; Multi-Thick�, Abbott Nutrition, Spain) andmodified rice starch (MRS; Beneo-Remy Industries, Belgium) wereselected. For the infant formula reconstitution, 200 mL of deionisedwater were mixed with 30 g of powder according to the manufac-turer’s instructions.
2.2. Materials and reagents
Deionised water (MilliQ; Millipore, Bedford, MA) was usedthroughout the study. Pepsin (P-7000, from porcine stomach muco-sa), bile salts (B-8756) and pancreatin (P-1750, from porcine pan-creas) were purchased from Sigma (St. Louis, MO). To simulatethe gastrointestinal conditions of children less than 6 months ofage, pepsin solution was prepared by dissolving 1.6 g of pepsin in10 mL of 0.1 N HCl. The pancreatin-bile extract solution was pre-pared by dissolving 0.2 g of pancreatin and 1.25 g of bile in 50 mLof 0.1 M NaHCO3. The working solutions of these enzymes wereprepared immediately before use. For mineral dialysis assays, dial-ysis membranes with molecular mass cut-offs (MMCO) of12,000 Da were purchased from Medicell Intl Ltd., London, UK).Ca, Fe and Zn contents were determined by flame atomic absorptionspectroscopy (AAS) according to the AOAC method (Jorhem 2000).The glass material was washed with detergent, soaked in concen-trated nitric acid (SG 1.41) and rinsed three times with distilleddeionised water before use. In the case of calcium determination,
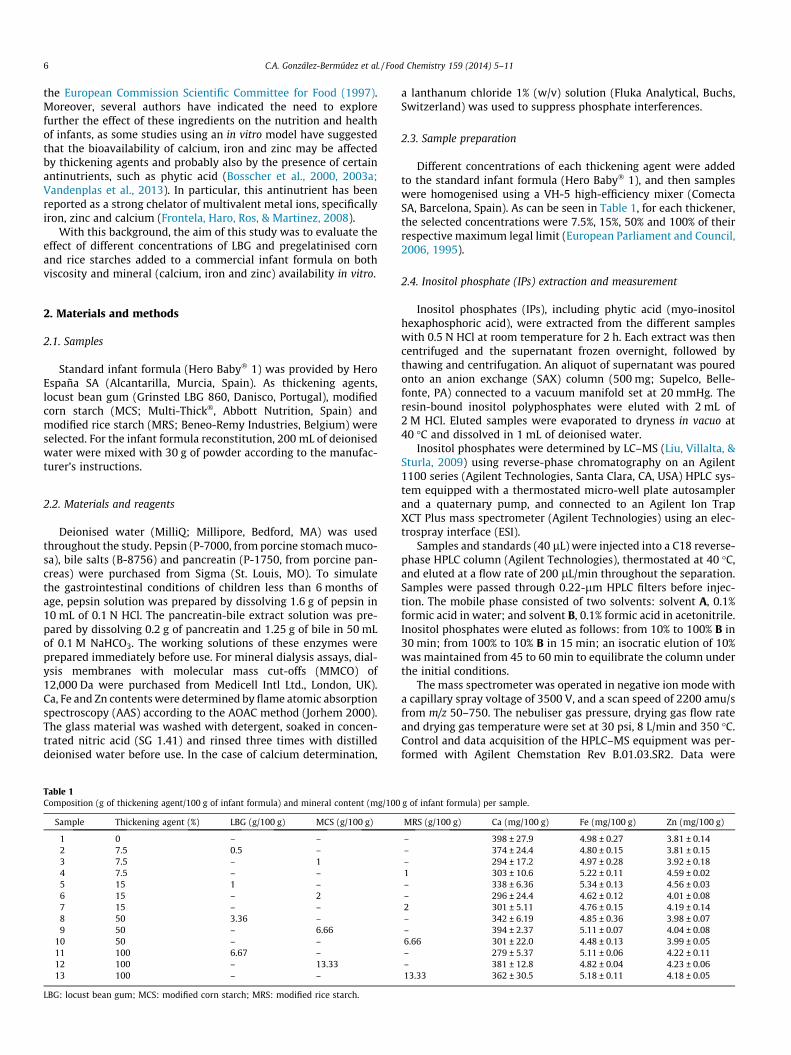
Table 1Composition (g of thickening agent/100 g of infant formula) and mineral content (mg/100
Sample Thickening agent (%) LBG (g/100 g) MCS (g/100 g)
1 0 – –2 7.5 0.5 –3 7.5 – 14 7.5 – –5 15 1 –6 15 – 27 15 – –8 50 3.36 –9 50 – 6.66
10 50 – –11 100 6.67 –12 100 – 13.3313 100 – –
LBG: locust bean gum; MCS: modified corn starch; MRS: modified rice starch.
a lanthanum chloride 1% (w/v) solution (Fluka Analytical, Buchs,Switzerland) was used to suppress phosphate interferences.
2.3. Sample preparation
Different concentrations of each thickening agent were addedto the standard infant formula (Hero Baby� 1), and then sampleswere homogenised using a VH-5 high-efficiency mixer (ComectaSA, Barcelona, Spain). As can be seen in Table 1, for each thickener,the selected concentrations were 7.5%, 15%, 50% and 100% of theirrespective maximum legal limit (European Parliament and Council,2006, 1995).
2.4. Inositol phosphate (IPs) extraction and measurement
Inositol phosphates (IPs), including phytic acid (myo-inositolhexaphosphoric acid), were extracted from the different sampleswith 0.5 N HCl at room temperature for 2 h. Each extract was thencentrifuged and the supernatant frozen overnight, followed bythawing and centrifugation. An aliquot of supernatant was pouredonto an anion exchange (SAX) column (500 mg; Supelco, Belle-fonte, PA) connected to a vacuum manifold set at 20 mmHg. Theresin-bound inositol polyphosphates were eluted with 2 mL of2 M HCl. Eluted samples were evaporated to dryness in vacuo at40 �C and dissolved in 1 mL of deionised water.
Inositol phosphates were determined by LC–MS (Liu, Villalta, &Sturla, 2009) using reverse-phase chromatography on an Agilent1100 series (Agilent Technologies, Santa Clara, CA, USA) HPLC sys-tem equipped with a thermostated micro-well plate autosamplerand a quaternary pump, and connected to an Agilent Ion TrapXCT Plus mass spectrometer (Agilent Technologies) using an elec-trospray interface (ESI).
Samples and standards (40 lL) were injected into a C18 reverse-phase HPLC column (Agilent Technologies), thermostated at 40 �C,and eluted at a flow rate of 200 lL/min throughout the separation.Samples were passed through 0.22-lm HPLC filters before injec-tion. The mobile phase consisted of two solvents: solvent A, 0.1%formic acid in water; and solvent B, 0.1% formic acid in acetonitrile.Inositol phosphates were eluted as follows: from 10% to 100% B in30 min; from 100% to 10% B in 15 min; an isocratic elution of 10%was maintained from 45 to 60 min to equilibrate the column underthe initial conditions.
The mass spectrometer was operated in negative ion mode witha capillary spray voltage of 3500 V, and a scan speed of 2200 amu/sfrom m/z 50–750. The nebuliser gas pressure, drying gas flow rateand drying gas temperature were set at 30 psi, 8 L/min and 350 �C.Control and data acquisition of the HPLC–MS equipment was per-formed with Agilent Chemstation Rev B.01.03.SR2. Data were
g of infant formula) per sample.
MRS (g/100 g) Ca (mg/100 g) Fe (mg/100 g) Zn (mg/100 g)
– 398 ± 27.9 4.98 ± 0.27 3.81 ± 0.14– 374 ± 24.4 4.80 ± 0.15 3.81 ± 0.15– 294 ± 17.2 4.97 ± 0.28 3.92 ± 0.181 303 ± 10.6 5.22 ± 0.11 4.59 ± 0.02– 338 ± 6.36 5.34 ± 0.13 4.56 ± 0.03– 296 ± 24.4 4.62 ± 0.12 4.01 ± 0.082 301 ± 5.11 4.76 ± 0.15 4.19 ± 0.14– 342 ± 6.19 4.85 ± 0.36 3.98 ± 0.07– 394 ± 2.37 5.11 ± 0.07 4.04 ± 0.086.66 301 ± 22.0 4.48 ± 0.13 3.99 ± 0.05– 279 ± 5.37 5.11 ± 0.06 4.22 ± 0.11– 381 ± 12.8 4.82 ± 0.04 4.23 ± 0.0613.33 362 ± 30.5 5.18 ± 0.11 4.18 ± 0.05

C.A. González-Bermúdez et al. / Food Chemistry 159 (2014) 5–11 7
processed using the data analysis software for LC/MSD Trap ver-sion 3.3 (BrukerDaltomik, GmbH, Bremen, Germany) provided bythe manufacturer.
2.5. In vitro digestion
To measure the solubility and dialysability of iron, calcium, andzinc, each sample was reconstituted in rapidly stirring and pre-heated (37 �C) deionised water according to the manufacturer’srecommendations. After reconstitution, samples were digestedusing the widespread in vitro method described by Boato, Wortley,Liu, and Glahn (2002), with modifications aimed at reducing theamounts of enzymes used, since the gastrointestinal tract in theearly stages of life is not yet fully developed (Frontela, Ros, &Martinez, 2009; Frontela et al., 2008). The in vitro digestion pro-cess, which consists of gastric and intestinal stages, was performedat 37 �C. At the end of the intestinal stage, aliquots of 20 g of sam-ple were transferred to 50-mL polypropylene centrifuge tubes(Costar Corning Europe, Badhoevedorp, Netherlands) and then cen-trifuged (Eppendorf 5804-R Centrifuge, Hamburg, Germany) at3500g for 1 h at 4 �C. The supernatant (soluble fraction) was usedto determine the mineral content. Dialysis comprised the gastricstage, followed by an intestinal step in which a dialysis bag con-taining 50 mL of deionised distilled water and an amount ofNaHCO3 equivalent to the titratable acidity (previously measured)was placed in flasks containing 20-g aliquots of the pepsin digest.The iron, calcium and zinc dialysed through the semipermeablemembrane represent the bio-available fraction (expressed as a per-centage) of the total minerals present in the sample (Etcheverry,Grusak, & Fleige, 2012; Frontela, Ros, & Martínez, 2011).
2.6. Determination of mineral content
The Fe, Ca and Zn concentrations in samples and the mineralsoluble and dialysable fractions were determined by AAS (ThermoScientific AA Spectrometer S Series; Thermo, Waltham, MA). Priorto analyses, the organic matter was destroyed in an ashing oven(Nabertherm, Lilienthal, Germany) at 525 �C for 32 h. Three millili-tres of HNO3 were then added to the ashes and the samples wereheated to dryness. After cooling, the residue was dissolved with1 mL of HCl (SG 1.9), and the solution was transferred to a 10-mLvolumetric flask and made to volume with water. The mineral con-tent in the diluted, acidified samples was determined against Fe, Caand Zn standard solutions (Merck, Germany). The calibrationcurves obtained were between 1 and 15 ppm for Ca, 0.25 and5 ppm for Fe and 0.25 and 2 for Zn, and showed an acceptable lin-earity with correlation coefficients greater than 0.995. Mineral sol-ubility and dialysability (%) were calculated as follows (Frontelaet al., 2011):
Soluble ð%Þ ¼ Soluble mineral content ðmg=100 gÞTotal mineral content of the sample ðmg=100 gÞ� 100
Dialysable ð%Þ¼ Dialysable mineral content ðmg=100 gÞTotal mineral content of the sample ðmg=100 gÞ�100
2.7. Validation criteria for the AAS technique
The reference material obtained from the International AtomicEnergy Agency (IAEA) 153-Milk Powder (Vienna, Austria) was usedas a control to test the method for accuracy. Fe, Ca and Zn wereanalysed in the reference material. The measured mean values
(n = 3) for Fe, Ca and Zn were 2.04, 13125 and 37.98 lg/grespectively, which were in accordance with the certified rangeof 2.56 ± 1.28 lg/g for Fe, 12855 ± 445 lg/g for Ca, and 39.45 ±2.52 lg/g for Zn. The precision of the method was calculated fromthe results obtained in the analysis of the soluble mineral fractionfrom six aliquots of a sample. The values expressed as coefficient ofvariation (%), were 1.19 for iron, 0.99 for calcium and 1.00 for zinc.
2.8. Viscosity measurement during in vitro gastric digestion
Viscosity, understood as a quantitative rheological measure-ment of frictional resistance to shear in a fluid, was measured ineach sample, as well as in the standard formula (Hero Baby� 1).This was done using a rotational viscometer (Haake ViscotesterVT6L plus, Thermo Electron Corporation, Germany) with a number1 spindle at 60 rpm and 37 �C. With the aim of characterising therheology of each agent added to the standard formula, four mea-surements were made for each sample during the first stage ofin vitro digestion: immediately after reconstitution (0), just afterpH adjustment and enzyme addition (beginning of digestion) (1),after 30 min (2), after 60 min (3), and after 120 min (4) ofin vitro gastric digestion.
2.9. Statistical analysis
All experiments were carried out six times, and the results werereported as means ± SD. After confirming the data normality usingthe Kolmogorov–Smirnov test and homoscedasticity by the Levenetest, solubility and dialysability of the samples were compared byone-way analysis of variance (ANOVA) and a Tukey post-test formultiple comparisons to determine the significance of the effectsof different thickening agents used at the same legal concentrationlevel (p < 0.05). For each level, the results were compared with thestandard formula. Pearson’s correlation test was performed toinvestigate the relationship between the concentration of eachthickening agent’s viscosity values, phytate content and Ca, Feand Zn solubility and dialysability. Values of p < 0.05 (two-tailed)were considered significant. All statistical analyses were per-formed with the Statistical Package for the Social Sciences (SPSSversion 14.0; SPSS Inc., Chicago, IL).
3. Results and discussion
3.1. Effect of different concentrations of thickening agents on in vitromineral availability in infant formulas
The three measured minerals (Ca, Fe and Zn) assessed in infantformula were aligned to the levels recommended by infant formularegulation (Commission Directive, 2006). Differences observed inmineral content between samples can be considered negligibleand are attributed to the different proportions of thickening agentsused (Table 1). The effect of the concentration of each thickeningagent on Ca, Fe and Zn solubility and dialysability percentages ofinfant formulas are shown in Figs. 1 and 2, respectively.
Regarding mineral solubility, calcium was the only mineral neg-atively affected by the three thickening agents when they wereadded in high concentrations (>50% of maximum legal limit) com-pared with the standard formula (Hero Baby� 1 without thickeningagents). This negative effect was significantly higher (p < 0.05) forLBG than for modified starches at the same concentration (100%).This could be explained by the higher amount of IP6 (myoinositolhexaphosphoric acid) in LBG (47.3 mg/100 g) compared withamounts observed in modified starches (19.2 mg/100 g in MCSand 17.5 mg/100 g in MRS). In this regard, it must also be noted
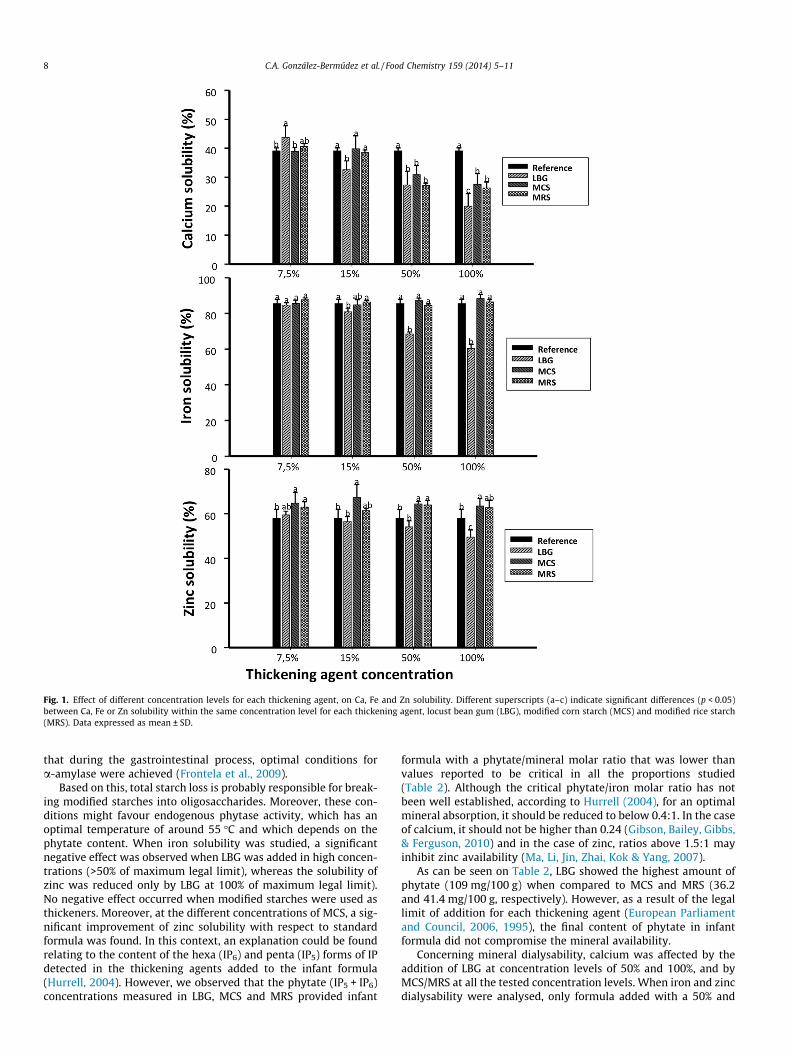
Fig. 1. Effect of different concentration levels for each thickening agent, on Ca, Fe and Zn solubility. Different superscripts (a–c) indicate significant differences (p < 0.05)between Ca, Fe or Zn solubility within the same concentration level for each thickening agent, locust bean gum (LBG), modified corn starch (MCS) and modified rice starch(MRS). Data expressed as mean ± SD.
8 C.A. González-Bermúdez et al. / Food Chemistry 159 (2014) 5–11
that during the gastrointestinal process, optimal conditions fora-amylase were achieved (Frontela et al., 2009).
Based on this, total starch loss is probably responsible for break-ing modified starches into oligosaccharides. Moreover, these con-ditions might favour endogenous phytase activity, which has anoptimal temperature of around 55 �C and which depends on thephytate content. When iron solubility was studied, a significantnegative effect was observed when LBG was added in high concen-trations (>50% of maximum legal limit), whereas the solubility ofzinc was reduced only by LBG at 100% of maximum legal limit).No negative effect occurred when modified starches were used asthickeners. Moreover, at the different concentrations of MCS, a sig-nificant improvement of zinc solubility with respect to standardformula was found. In this context, an explanation could be foundrelating to the content of the hexa (IP6) and penta (IP5) forms of IPdetected in the thickening agents added to the infant formula(Hurrell, 2004). However, we observed that the phytate (IP5 + IP6)concentrations measured in LBG, MCS and MRS provided infant
formula with a phytate/mineral molar ratio that was lower thanvalues reported to be critical in all the proportions studied(Table 2). Although the critical phytate/iron molar ratio has notbeen well established, according to Hurrell (2004), for an optimalmineral absorption, it should be reduced to below 0.4:1. In the caseof calcium, it should not be higher than 0.24 (Gibson, Bailey, Gibbs,& Ferguson, 2010) and in the case of zinc, ratios above 1.5:1 mayinhibit zinc availability (Ma, Li, Jin, Zhai, Kok & Yang, 2007).
As can be seen on Table 2, LBG showed the highest amount ofphytate (109 mg/100 g) when compared to MCS and MRS (36.2and 41.4 mg/100 g, respectively). However, as a result of the legallimit of addition for each thickening agent (European Parliamentand Council, 2006, 1995), the final content of phytate in infantformula did not compromise the mineral availability.
Concerning mineral dialysability, calcium was affected by theaddition of LBG at concentration levels of 50% and 100%, and byMCS/MRS at all the tested concentration levels. When iron and zincdialysability were analysed, only formula added with a 50% and
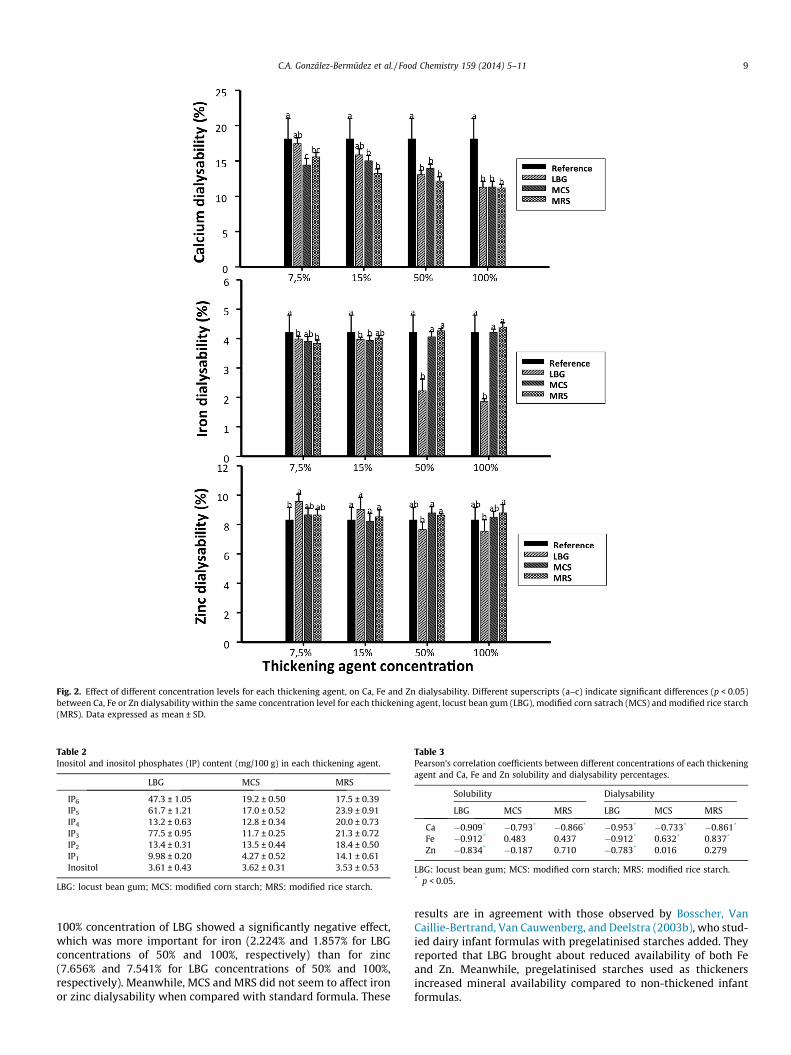
Fig. 2. Effect of different concentration levels for each thickening agent, on Ca, Fe and Zn dialysability. Different superscripts (a–c) indicate significant differences (p < 0.05)between Ca, Fe or Zn dialysability within the same concentration level for each thickening agent, locust bean gum (LBG), modified corn satrach (MCS) and modified rice starch(MRS). Data expressed as mean ± SD.
Table 2Inositol and inositol phosphates (IP) content (mg/100 g) in each thickening agent.
LBG MCS MRS
IP6 47.3 ± 1.05 19.2 ± 0.50 17.5 ± 0.39IP5 61.7 ± 1.21 17.0 ± 0.52 23.9 ± 0.91IP4 13.2 ± 0.63 12.8 ± 0.34 20.0 ± 0.73IP3 77.5 ± 0.95 11.7 ± 0.25 21.3 ± 0.72IP2 13.4 ± 0.31 13.5 ± 0.44 18.4 ± 0.50IP1 9.98 ± 0.20 4.27 ± 0.52 14.1 ± 0.61Inositol 3.61 ± 0.43 3.62 ± 0.31 3.53 ± 0.53
LBG: locust bean gum; MCS: modified corn starch; MRS: modified rice starch.
Table 3Pearson’s correlation coefficients between different concentrations of each thickeningagent and Ca, Fe and Zn solubility and dialysability percentages.
Solubility Dialysability
LBG MCS MRS LBG MCS MRS
Ca �0.909* �0.793* �0.866* �0.953* �0.733* �0.861*
Fe �0.912* 0.483 0.437 �0.912* 0.632* 0.837*
Zn �0.834* �0.187 0.710 �0.783* 0.016 0.279
LBG: locust bean gum; MCS: modified corn starch; MRS: modified rice starch.* p < 0.05.
C.A. González-Bermúdez et al. / Food Chemistry 159 (2014) 5–11 9
100% concentration of LBG showed a significantly negative effect,which was more important for iron (2.224% and 1.857% for LBGconcentrations of 50% and 100%, respectively) than for zinc(7.656% and 7.541% for LBG concentrations of 50% and 100%,respectively). Meanwhile, MCS and MRS did not seem to affect ironor zinc dialysability when compared with standard formula. These
results are in agreement with those observed by Bosscher, VanCaillie-Bertrand, Van Cauwenberg, and Deelstra (2003b), who stud-ied dairy infant formulas with pregelatinised starches added. Theyreported that LBG brought about reduced availability of both Feand Zn. Meanwhile, pregelatinised starches used as thickenersincreased mineral availability compared to non-thickened infantformulas.

Table 4Viscosity of formulas (cps) with different under maximum legal limits (7.5%, 15%, 50% and 100%) of thickening agents during in vitro gastric digestion.
Concentration (%) Thickening agent After reconstitution Beginning of digestion 30 min 60 min 120 min
Time of measurement0 LBG 1.27 ± 0.140 2.13 ± 0.052 2.46 ± 0.057 1.90 ± 0.086 1.64 ± 0.127
7.5 LBG 2.65 ± 0.174b 3.42 ± 0.342b 3.44 ± 0.204b 3.01 ± 0.158b 2.97 ± 0.132b
MCS 3.39 ± 0.169a 4.08 ± 0.180a 3.99 ± 0.113a 3.94 ± 0.082a 3.7 ± 0.228a
MRS 3.67 ± 0.126a 4.24 ± 0.063a 4.03 ± 0.092a 3.77 ± 0.152a 3.64 ± 0.199a
15 LBG 5.09 ± 0.201a 6.13 ± 0.123a 5.90 ± 0.094a 5.75 ± 0.193a 5.56 ± 0.144a
MCS 4.67 ± 0.233b 6.57 ± 0.281a 4.96 ± 0.135b 4.97 ± 0.190b 4.56 ± 0.239b
MRS 4.01 ± 0.161c 5.47 ± 0.247b 5.00 ± 0.126b 4.72 ± 0.139b 4.43 ± 0.160b
50 LBG 68.61 ± 1.214a 86.6 ± 1.279a 74.14 ± 1.862a 67.57 ± 2.878a 60.2 ± 1.574a
MCS 18.36 ± 0.463b 26.9 ± 0.301b 25.59 ± 0.506b 23.23 ± 0.507b 21.5 ± 0.963b
MRS 18.59 ± 0.369b 22.6 ± 0.955c 22.00 ± 0.104c 21.98 ± 0.273b 21.9 ± 0.170b
100 LBG 109.2 ± 6.337a 136 ± 4.475a 130.66 ± 5.376a 119.96 ± 5.201a 102 ± 3.252a
MCS 22.43 ± 0.494b 29.3 ± 0.274b 33.18 ± 0.345b 30.27 ± 0.656b 27.1 ± 0.158b
MRS 25.7 ± 0.212b 30.4 ± 0.455b 28.06 ± 0.185b 27.98 ± 0.111b 27.1 ± 0.222b
Within the same concentration level, different superscripts (a–c) for the same time of measurement, indicate significant differences (p < 0.05) between thickeners.LBG: locust bean gum; MCS: modified corn starch; MRS: modified rice starch.
10 C.A. González-Bermúdez et al. / Food Chemistry 159 (2014) 5–11
To determine a possible linear relationship between the differentconcentrations of each thickening agent added to infant formula andCa, Fe and Zn solubility and dialysability, a Pearson correlation wasrun. The results are shown in Tables 3 and 4. A significant negativecorrelation was found for Ca, Fe and Zn solubility (�0.909, �0.912and �0.834, respectively) and dialysability (�0.953, �0.912 and�0.783, respectively) when LBG was used as a thickening agent.These results are in accordance with the negative effect of LBG onmineral availability observed in the present study. However, thissignificant negative effect was only found for Ca when MCS andMRS were added to the standard infant formula, but not for Fe orZn. The explanation for these findings could be that, due to the pres-ence of ionisable groups, LBG could bind Ca, Fe and Zn, formingunabsorbable complexes and decreasing mineral solubility and dial-ysability. In addition, LBG might decrease the availabilities of Ca, Feand Zn as a consequence of its gel-forming capacities. This will cre-ate a viscous environment in the small intestine, and thus impair thedigestion of food components. Related to this, Bosscher et al. (2003b)suggested that LBG could form strong complexes with metal ions,rendering them unavailable for absorption.
Regarding modified or pregelatinised starches, MCS and MRSmight be considered digestible carbohydrates. According to thispossibility, during digestion process, bound minerals could bereleased to the intestinal lumen, increasing mineral availability incomparison with LBG. Nevertheless, the in vitro availability of cal-cium seems to be decreased, which could be due to the formationof unabsorbable complexes (Agget et al., 2002; CommissionDirective, 2006). The results of similar published in vitro studiesalso suggest that the bioavailability of Ca, Fe and Zn in infantformula may be decreased by thickened formulas with non-digestible carbohydrates such as LBG, but not by those withmodified starches added (Bosscher et al., 2000, 2003a; CommissionDirective, 2006).
3.2. Effect of thickening agent concentrations on in vitro viscosity
The viscosity values of infant formulas mixed with different con-centrations of each thickening agent are presented in Table 4. Theresults are grouped according to the time of measurement and con-centration of the thickening agent. Overall, after pH adjustment to 4with 6 N HCL, the viscosity of formulas increased in relation to theirrespective viscosities just after reconstitution, being more evidentat a higher concentration of thickening agents (15% or greater). Thisfinding has been also described by other authors (Vanderhooh et al.,2003). Although the viscosity-increasing mechanism does not seemto be well-known, it might have to do with the physical interaction
between the thickening agents and protein components in theassayed product.
Comparing viscosity values, standard infant formula with a LBGconcentration of 15% or greater, showed a significantly higher(p < 0.05) viscosity value than that for the standard infant formulawith MCS and MRS added. Focusing on the viscosity provided byLBG, it reached values higher than 60 cps and 100 cps for a 50%and 100% concentration, respectively, under the maximum legallimit (3.36 g or 6.67 g of LBG per 100 g of infant formula). In con-trast with these values, MCS and MRS provided viscosity valueshigher than 20 cps and 27 cps for a 50% and 100% concentration,respectively, under the maximum legal limit (6.66 g or 13.33 g ofstarches per 100 g of formula).
Due to the lack of clinical trials or in vivo assays, no minimumviscosity limits for infant regurgitation management in childrencan be fixed. Nevertheless, a viscosity higher than 100 cps could ex-ert a negative effect, since oesophageal clearance of refluxed mate-rial would be reduced (Infante-Pina, Lara-Villoslada, López-Ginés, &Morales-Hernández, 2010). This would affect the oesophageal acidexposure time, increasing the risk of oesophagitis secondary togastric content reflux (Corvaglia et al., 2013). Moreover, if the vis-cosity of infant formula is too high, infants could reject it, since theymay have trouble sucking such a formula through a standardnipple.
4. Conclusions
LBG, MCS and MRS are frequently used as thickening ingredi-ents in AR-infant formulas. In the present study, the effect of theiraddition to a standard infant formula on both, mineral in vitroavailability (solubility and dialysability percentages measured byAAS) and viscosity has been determined. Analysing the viscosityresults, it can be concluded that LBG is more effective as a thicken-ing agent than MCS or MRS when added to infant formula underthe legal limits. However, LBG negatively affects the availabilityof calcium, iron and zinc in vitro, decreasing mineral solubilityand dialysability, whereas MCS and MRS only affect calcium solu-bility and dialysability in a negative way. These findings should betaken into account when developing an antiregurgitation infantformula, since the acceptance of foods by infants and mineralrequirements could be potentially compromised. A possible solu-tion could be the adequate combination of these thickening agentsto minimise the negative effect on mineral availability while max-imising the effect on formula viscosity.
With the aim of characterising the in vivo effects of these ingre-dients, it would be necessary to conduct clinical trials or in vivo
C.A. González-Bermúdez et al. / Food Chemistry 159 (2014) 5–11 11
assays in infants. This would lead not only to a better understand-ing of the nutritional management of infant regurgitation, but alsoto the establishment of an effective thickening agent concentrationwhich leading to a reduction in regurgitation episodes. In thesetypes of studies, an interesting and innovative focus will be to ana-lyse the effect of thickening agents on colonic microbiota.
Acknowledgements
We would like to thank Hero España S.A. (Alcantarilla, Murcia,Spain) for providing the samples for this study. We would like tothank also to Dr. Alejandro Torrecillas from CAID (University ofMurcia, Spain) for the performance of the HPLC/MS analysis. Thisstudy was supported by the Seneca Foundation and Science andTechnology Agency (Murcia Region, Spain) through the Project(11978/PI/09). Carlos A. González Bermúdez was supported by apredoctoral grant from the University of Murcia.
References
Agget, P. J., Agostoni, C., Goulet, O., Hernell, O., Berthold, K., Lafaber, H. L., et al.(2002). Antireflux or antiregurgitation milk products for infants and youngchildren: A commentary by the ESPGHAN Committee on Nutrition. Journal ofPediatric Gastroenterology and Nutrition, 34, 496–498.
Boato, F., Wortley, G. M., Liu, R. H., & Glahn, R. P. (2002). Red grape juice inhibits ironavailability: Application of an in vitro digestion/Caco-2 cell model. Journal ofAgricultural and Food Chemistry, 50, 6935–6938.
Bosscher, D., Van Caillie-Bertrand, M., & Deelstra, H. (2003a). Do thickeningproperties of locust bean gum affect the amount of calcium, iron and zincavailable for absorption from infant formula? In vitro studies. InternationalJournal of Food Science and Nutrition, 54, 261–268.
Bosscher, D., Van Caillie-Bertrand, M., Van Cauwenberg, R., & Deelstra, H. (2003b).Availability of calcium, iron and zinc from dairy infant formulas is affected bysoluble dietary fibers and modified starch fractions. Nutrition, 19, 641–645.
Bosscher, D., Van Caillie-Bertrand, M., Van Dyck, K., Robberecht, H., VanCauwenbergh, R., & Deelstra, H. (2000). Thickening infant formula withdigestible and indigestible carbohydrate: Availability of calcium, iron, andzinc in vitro. Journal of Pediatric Gastroenterology and Nutrition, 30, 373–378.
Chao, H. C., & Vandenplas, Y. (2007). Comparison of the effect of a cornstarchthickened formula and strengthened regular formula on regurgitation, gastricemptying and weight gain in infantile regurgitation. Diseases of the Esophagus,20, 155–160.
Commission Directive 2006/141/EC of 22 December 2006 on infant formulae andfollow-on formulae and amending Directive 1999/21/EC. <http://eur-lex.europa.eu/en/index.htm>.
Corvaglia, L., Martini, S., Aceti, A., Arcuri, S., Rossini, R., & Faldella, G. (2013).Nonpharmacological management of gastroesophageal reflux in preterminfants. BioMed Research International, 2013, 1–7.
Etcheverry, P., Grusak, M. A., & Fleige, L. E. (2012). Applications of in vitrobioaccessibility and bioavailability methods for calcium, carotenoids, folate,iron, magnesium, polyphenols, zinc and vitamins B6, B12, D and E. Frontiers inPhysiology, 3, 1–22.
European Commission Scientific Committee for Food (1997). Opinion on certainadditives to foods for infants and young children in good health and in foods forspecial medical purposes for infants and young children: Locust bean gum.Document XXIV/1270/97. Annex II.
European Parliament and Council Directive 2006/141/EC on infant formulae andfollow-on formulae. <http://ec.europa.eu/food>.
European Parliament and Council Directive 95/2/EC of 20 February 1995 on foodadditives other than colours and sweeteners. <http://ec.europa.eu/food>.
Frontela, C., Haro, J. F., Ros, G., & Martinez, C. (2008). Effect of dephytinization andfollow-on formula addition on in vitro iron, calcium, and zinc availability frominfant cereals. Journal of Agricultural and Food Chemistry, 56, 3805–3811.
Frontela, C., Ros, G., & Martinez, C. (2009). Iron and calcium availability fromdigestion of infant cereals by Caco-2 cells. European Food Research andTechnology, 228, 789–797.
Frontela, C., Ros, G., & Martínez, C. (2011). Phytic acid content and ‘‘in vitro’’ iron,calcium and zinc bioavailability in bakery products: The effect of processing.Journal of Cereal Science, 54, 173–179.
Gibson, R. S., Bailey, K. B., Gibbs, M., & Ferguson, E. L. (2010). A review of phytate,iron, zinc, and calcium concentrations in plant-based complementary foodsused in low-income countries and implications for bioavailability. Food andNutrition Bulletin, 31, 134–146.
Horvath, A., Dziechciarz, P., & Szajewska, H. (2008). The effect of thickened-feedinterventions on gastroesophageal reflux in infants: Systematic review andmeta-analysis of randomized, controlled trials. Pediatrics, 122, 1268–1277.
Hurrell, R. F. (2004). Phytic acid degradation as a means of improving ironabsorption. International Journal for Vitamin and Nutrition Research, 74, 445–452.
Infante-Pina, D., Lara-Villoslada, F., López-Ginés, G., & Morales-Hernández, M. E.(2010). Thickened infant formula, rheological study of the ‘‘in vitro’’ properties.Anales de Pediatria (Barcelona), 72, 302–308.
Koletzko, B., Baker, S., Cleghorn, G., Neto, U. F., Gopalan, S., Hernell, O., et al. (2005).Global standard for the composition of infant formula: Recommendations of anESPGHAN coordinated international expert group. Journal of PediatricGastroenterology and Nutrition, 41, 584–599.
Liu, X., Villalta, P. W., & Sturla, S. J. (2009). Simultaneous determination of inositoland inositol phosphates in complex biological matrices: Quantitative ion-exchange chromatography/tandem mass spectrometry. Rapid Communicationsin Mass Spectrometry, 23, 705–712.
Ma, G., Li, Y., Jin, Y., Zhai, F., Kok, F. J., & Yang, X. (2007). Phytate intake and molarratios of phytate to zinc, iron and calcium in the diets of people in China.European Journal of Clinical Nutrition, 61, 368–374.
Miyazawa, R., Tomomasa, T., Kaneko, H., Arakawa, H., & Morikawa, A. (2007). Effectof formula thickened with reduced concentration of locust bean gum ongastroesophageal reflux. Acta Pædiatrica, 96, 910–914.
Miyazawa, R., Tomomasa, T., Kaneko, H., & Morikawa, A. (2004). Effect of locustbean gum in Anti-regurgitant milk on the regurgitation in uncomplicatedgastroesophageal reflux. Journal of Pediatric Gastroenterology and Nutrition, 38,479–483.
Pina, D. I., Llach, X. B., Ariño-Armengol, B., & Iglesias, V. V. (2008). Prevalence anddietetic management of mild gastrointestinal disorders in milk-fed infants.World Journal of Gastroenterology, 14, 248–254.
Vandenplas, Y. (2008). Thickened infant formula does what it has to do: Decreaseregurgitation. Pediatrics, 123, 549–550.
Vandenplas, Y., Hauser, B., Devreker, T., Mahler, T., Degreef, E., & Veereman-Wauters, G. (2013). Gastro-esophageal reflux in children: Symptoms, diagnosisand treatment. Journal of Pediatric Sciences, 3, 1–20.
Vandenplas, Y., Rudolph, C., DiLorenzo, C., Hassall, E., Liptak, G., Mazur, L., et al.(2009). Pediatric gastroesophageal reflux clinical practice guidelines: Jointrecommendations of the North American Society for PediatricGastroenterology, Hepatology, and Nutrition (NASPGHAN) and the EuropeanSociety for Pediatric Gastroenterology, Hepatology, and Nutrition (ESPGHAN).Journal of Pediatric Gastroenterology and Nutrition, 49, 498–547.
Vanderhooh, J. A., Moran, J. R., Harris, C. L., Merkel, K. L., & Orenstein, S. R. (2003).Efficacy of a pre-thickened infant formula: A multicenter, double-blind,randomized, placebo-controlled parallel group trial in 104 infants withsymptomatic gastroesophageal reflux. Clinical Pediatrics, 42, 483–495.




















