
education - The BMJ
10
324 27 February 2021 | the bmj Vitamin D for covid-19 I am not an expert in vitamin D nor in covid-19, but the connection isn’t intuitive. But when in doubt, do a randomised controlled trial. Murai and colleagues randomised 240 hospital inpatients in Brazil with moderate to severe covid-19 to a one-off dose of 200 000 units of vitamin D in a double-blind fashion. There was no difference in length of hospital stay (the primary endpoint) between groups. This is not to say that vitamin D isn’t vital in immune function or indeed other bodily functions. It just means supplementation in this way was not helpful. One can hypothesise that vitamin D needs to be replaced earlier in the disease course, or even before the infection, but I doubt it. JAMA doi:10.1001/jama.2020.26848 Moderna’s covid vaccine and variants Whether covid-19 variants will be resistant to vaccines is the big question of the moment, as the answer determines the world’s short term future. In some senses, only time will tell, but this can be evaluated. Wu and colleagues tested serum from participants who received the Moderna vaccine in the phase I trial. They assessed the neutralising activity of the serum against a number of mutations using a pseudovirus (safer than using real virus). Here, the pseudovirus is recombinant vesicular stomatitis virus— this isn’t an important detail, more good to know. Serum neutralising activity was not altered with the B.1.1.7 variant (the Kent variant) but may have been reduced with the B.1.351 variant (the South African variant). The conclusion was that further work is needed investigating the South African variant. N Engl J Med doi:10.1056/NEJMc2102179 What about the Pfizer vaccine? Lui and colleagues tested serum from 15 participants in the efficacy trial for Pfizer’s vaccine. The neutralising power of the serum was reduced by two thirds against B.1.351 (the South African variant) compared with other forms of the virus. This type of assessment may make immunological sense but is not the same as testing whether recipients of the vaccine are protected from the variant compared with those who got a placebo. This is because the vaccine does more than just generate neutralising antibodies—other immune mechanisms would come into play that weren’t measured in this study. Additionally, it would be valuable to know if the vaccine prevents severe disease from variants as opposed to infections. Perhaps challenge trials education FROM THE JOURNALS Edited highlights of weekly research reviews on https://bit.ly/2PLtil8 Alex Nowbar is a clinical research fellow at Imperial College London will be able to test vaccine efficacy against variants. While challenge trials carry risk, I am proud that the UK is the first country to ethically approve such a trial. N Engl J Med doi:10.1056/NEJMc2102017 Immune checkpoint inhibitors in autoimmune disease Immune checkpoint inhibitors are used to treat advanced melanoma. People with autoimmune disease have historically been excluded from trials of these medications for fear of immune related adverse events, so this Dutch cohort study provides some much needed evidence on the safety of these drugs in people with autoimmune disease. Van der Kooij and colleagues studied 228 people with advanced melanoma and autoimmune disease treated with an immune checkpoint inhibitor compared with 2546 people with advanced melanoma but no autoimmune disease. There was no difference in the incidence of immune related adverse events. There was also no difference in survival with and without an autoimmune disease. This evidence supports the use of immune checkpoint inhibitors in people with autoimmune disease, although we don’t know how bad the autoimmune disease was in the individuals studied. Perhaps people with more severe autoimmune disease were not given the medication, so we still don’t really know how safe this is. Ann Intern Med doi:10.7326/M20-3419 Efficacy for bleeding fibroids? The LIBERTY trials randomised women with fibroid-associated heavy menstrual bleeding to relugolix combination therapy for six months in a double-blind fashion. Response was defined as volume of menstrual blood loss <80 mL and a ≥50% reduction in volume from baseline. The response rate (which was the primary endpoint) was over 70% with the treatment and less than 20% with placebo, with preservation of bone mineral density and without concerning adverse events. The secondary endpoints also favoured the treatment, including a greater improvement in the Bleeding and Pelvic Discomfort scale score. Relugolix is an oral gonadotropin-releasing hormone receptor antagonist, and it was combined with estradiol and norethindrone acetate (that is, oestrogen and progesterone). Overtly, this is a success for the therapy, but the study design does seem weighted in its favour—the control was placebo rather than other medications that might be considered standard care. N Engl J Med doi:10.1056/NEJMoa2008283
-
Upload
khangminh22 -
Category
Documents
-
view
5 -
download
0
Transcript of education - The BMJ

324 27 February 2021 | the bmj
education
Vitamin D for covid-19I am not an expert in vitamin D nor in covid-19, but the connection isn’t intuitive. But when in doubt, do a randomised controlled trial. Murai and colleagues randomised 240 hospital inpatients in Brazil with moderate to severe covid-19 to a one-off dose of 200 000 units of vitamin D in a double-blind fashion. There was no diff erence in length of hospital stay (the primary endpoint) between groups. This is not to say that vitamin D isn’t vital in immune function or indeed other bodily functions. It just means supplementation in this way was not helpful. One can hypothesise that vitamin D needs to be replaced earlier in the disease course, or even before the infection, but I doubt it.
� JAMA doi:10.1001/jama.2020.26848
Moderna’s covid vaccine and variantsWhether covid-19 variants will be resistant to vaccines is the big question of the moment, as the answer determines the world’s short term future. In some senses, only time will tell, but this can be evaluated. Wu and colleagues tested serum from participants who received the Moderna vaccine in the phase I trial. They assessed the neutralising activity of the serum against a number of mutations using a pseudovirus (safer than using real virus). Here, the pseudovirus is recombinant vesicular stomatitis virus—this isn’t an important detail, more good to know. Serum neutralising activity was not altered with the B.1.1.7 variant (the Kent variant) but may have been reduced with the B.1.351 variant (the South African variant). The conclusion was that further work is needed investigating the South African variant.
� N Engl J Med doi:10.1056/NEJMc2102179
What about the Pfizer vaccine?Lui and colleagues tested serum from 15 participants in the effi cacy trial for Pfi zer’s vaccine. The neutralising power of the serum was reduced by two thirds against B.1.351 (the South African variant) compared with other forms of the virus. This type of assessment may make immunological sense but is not the same as testing whether recipients of the vaccine are protected from the variant compared with those who got a placebo. This is because the vaccine does more than just generate neutralising antibodies—other immune mechanisms would come into play that weren’t measured in this study. Additionally, it would be valuable to know if the vaccine prevents severe disease from variants as opposed to infections. Perhaps challenge trials
educationFROM THE JOURNALS Edited highlights of weekly research reviews on https://bit.ly/2PLtil8
Alex Nowbar is a clinical research fellow at Imperial College London
will be able to test vaccine effi cacy against variants. While challenge trials carry risk, I am proud that the UK is the fi rst country to ethically approve such a trial.
� N Engl J Med doi:10.1056/NEJMc2102017
Immune checkpoint inhibitors in autoimmune diseaseImmune checkpoint inhibitors are used to treat advanced melanoma. People with autoimmune disease have historically been excluded from trials of these medications for fear of immune related adverse events, so this Dutch cohort study provides some much needed evidence on the safety of these drugs in people with autoimmune disease. Van der Kooij and colleagues studied 228 people with advanced melanoma and autoimmune disease treated with an immune checkpoint inhibitor compared with 2546 people with advanced melanoma but no autoimmune disease. There was no diff erence in the incidence of immune related adverse events. There was also no diff erence in survival with and without an autoimmune disease. This evidence supports the use of immune checkpoint inhibitors in people with autoimmune disease, although we don’t know how bad the autoimmune disease was in the individuals studied. Perhaps people with more severe autoimmune disease were not given the medication, so we still don’t really know how safe this is.
� Ann Intern Med doi:10.7326/M20-3419
Efficacy for bleeding fibroids?The LIBERTY trials randomised women with fi broid-associated heavy menstrual bleeding to relugolix combination therapy for six months in a double-blind fashion. Response was defi ned as volume of menstrual blood loss <80 mL and a ≥50% reduction in volume from baseline. The response rate (which was the primary endpoint) was over 70% with the treatment and less than 20% with placebo, with preservation of bone mineral density and without concerning adverse events. The secondary endpoints also favoured the treatment, including a greater improvement in the Bleeding and Pelvic Discomfort scale score. Relugolix is an oral gonadotropin-releasing hormone receptor antagonist, and it was combined with estradiol and norethindrone acetate (that is, oestrogen and progesterone). Overtly, this is a success for the therapy, but the study design does seem weighted in its favour—the control was placebo rather than other medications that might be considered standard care.
� N Engl J Med doi:10.1056/NEJMoa2008283

the bmj | 27 February 2021 325
WHAT YOU NEED TO KNOW
• Discussing incontinence is embarrassing and scary, so avoid using phrases that suggest these feelings are irrational
• Telling a patient you don’t have all of the answers, sharing frustration, and learning together can help patients feel supported
• Even experienced patients sometimes need help prioritising and support with diffi cult conversations
ROSE
LLO
YD
I became incontinent at the age of 30, after the birth of my fi rst baby, with urge and stress incontinence. Initially, both conditions
responded well to bladder training and physiotherapy, but after the birth of my second child, the stress incontinence became increasingly problematic. Since then I have had many treatments, with varying success.
Incontinence seeps into every area of my life. I am tired from the logistics, the shame, the spare clothes, the laundry, from drowning in drudge, multiple appointments, and health admin.
Facing an appointment I have faced lots of embarrassing problems, and have had many vaginal examinations. Even now I’m struck by a kind of pity for my GP, that they have to look at my body, get close to it, or touch it.
I try to be confi dent, but even as an old-timer, sometimes I am scared or really embarrassed. I am afraid of farting or leaking in examinations, and of clinicians fi nding something new. Doctors ask me to summarise and prioritise my symptoms, which is hard. I don’t know what is “normal,” what I am allowed to complain about, or whether I am making a fuss.
During consultations, I often feel stupid, even though I’ve been a continence patient for a long time. I sometimes rush and I can’t tell when I am the expert or when my GP knows more than I do. I don’t want to waste their time.
The importance of language Health professionals sometimes say “don’t be embarrassed” or “I’ve seen it all before” to reassure me and destigmatise. Perhaps that works for some patients,
but for me, it feels indiff erent. We are socially conditioned to be embarrassed of our genitals. It is a big deal to show someone else or bring up intimate details. I’m always relieved when professionals acknowledge that it isn’t very easy to talk about. It is also reassuring when they say they want to help, and the examination will help us understand what is going on to move forward.
Sometimes I feel like health professionals are afraid of saying they don’t know the answers. During one appointment a GP told me he didn’t know and needed to fi nd out more. It was scary, but it was also reassuring—nobody knows everything. He listened, and we worked together to fi gure
out what to do next. He said he had learned from me, which was useful. It showed me he was on my side and prepared to learn.
Something else I have found helpful is being told that I have been really unlucky to get so many issues so young. Hearing that another health professional I saw was frustrated for me and wished she could do more made me feel less like a failure for getting overwhelmed.
Incontinence is lonely. Sometimes my GP is the only person who knows the worst bits. Especially the day-to-day and ongoing issues and the way multiple embarrassing problems are hard to untangle. I’m lucky they understand that talking is hard and that sometimes I need help prioritising. Correspondence to: L Brett [email protected] Twitter @lucebrett Cite this as: BMJ 2021;372:n207
Sometimes my GP is the Sometimes my GP is the only person who knowsonly person who knows the worst bits the worst bits
READING
0.5 HOURS
EDUCATION INTO PRACTICE • How could you ensure a patient feels welcome and supported to talk
about difficult topics, including incontinence? • What language and techniques can you use to lessen stigma and provide
reassurance when a patient feels embarrassed? • How can you help a patient prioritise different elements of their health
when trying to create a plan together for their care?
ADDITIONAL INFORMATION www.whenyouarethatwoman.co.uk Luce Brett’s memoir, which explores incontinence, birth trauma, postnatal depression, resilience, and survival, is out now. PMSL: Or How I Literally Pissed Myself Laughing and Survived the Last Taboo to Tell the Tale . https://www.bloomsbury.com/uk/pmsl-or-how-i-literally-pissed-myself-laughing-and-survived-the-last-taboo-to-tell-the-tale-9781472977489/
Luce Brett shares what it is like to speak with a healthcare professional about incontinence
WHAT YOUR PATIENT IS THINKING
Incontinence is lonely and hard to talk about

326 27 February 2021 | the bmj
1 Faculty of Health Sciences and Sport, University of Stirling, Stirling, UK
2 Warrell Unit, St Mary’s Hospital, Manchester University NHS Trust, Manchester Academic Health
Science Centre, Manchester, UK
3 Division of Developmental Biology and Medicine, School of Medical Sciences, University of
Manchester, Manchester, UK
4 Nursing, Midwifery and Allied Health Professions Research Unit, Glasgow Caledonian
University, Glasgow, UK
Correspondence to: C Bugge [email protected] This is one of a series of occasional articles that highlight areas of practice where
management lacks convincing supporting evidence. The series advisers are Sera Tort, clinical
editor, and Nai Ming Lai, clinical editor. You can read more about how to prepare and submit
an Education article on our Instructions for Authors pages: https://www.bmj.com/about-bmj/
resources-authors/article-types
Pelvic organ prolapse is common in women over the age of
50 and negatively aff ects their quality of life. 1 Management
includes lifestyle modifi cation, pelvic fl oor muscle training,
vaginal pessary, or surgery. 2 Pessaries may be preferred by
women as an alternative to surgery or while they await surgery.
In an observational study in the UK (680 women), two thirds
of women initially preferred conservative management with
pessaries. Women were more likely to consider surgery if they
were bothered by severe symptoms aff ecting bowel emptying,
sexual function, and quality of life. 3
READING
0.5 HOURS
WHAT YOU NEED TO KNOW
• Self-management of vaginal pessary for pelvic organ prolapse may enable patient autonomy over when to remove and insert the pessary (for example, to remove before intercourse) and may reduce the number of clinic appointments
• Limited evidence from small observational studies suggests that self-management may improve the length of time a woman uses a pessary for, her satisfaction, and her quality of life, without increasing complication rates, but it is diffi cult to generalise from this evidence
• During the covid-19 pandemic, reassure women who may need a pessary change that a delay of a few months is acceptable as long as they are not experiencing any problems such as vaginal bleeding, discharge, or pain
A pessary is inserted into the vagina to hold up the vaginal walls and pelvic organs and to relieve symptoms of prolapse (the fi gure shows types of pessary). Two types of pessary are commonly used: support pessaries—such as rings—and space occupying pessaries—such as Gellhorn or shelf pessaries. Pessaries can be inserted by general practitioners, specialist nurses, specialist physiotherapists, or gynaecologists. Guidance from the National Institute for Health and Care Excellence (NICE) recommends removing and replacing the pessary at least every six months to prevent and detect complications such as vaginal ulceration. 2 NICE guidance does not mention pessary self-management, whereas US guidelines suggest that, where possible, women should be taught to self-manage. 4 Neglected pessaries can result in incarceration or the development of vesicovaginal or rectovaginal fi stulae. In light of the covid-19 pandemic, the British Society of Urogynaecology recommends telephone consultations and a delayed review for women needing a pessary change and having no symptoms. 5
Follow-up care can be through self-management or at a clinic. In clinic based care, women have an appointment every 4-6 months to have their pessary removed, their vaginal tissues inspected, and a new pessary inserted. 6
Pessary complications such as erosions can be identifi ed and treated early. With pessary self-management, however, a woman can remove, clean, and re-insert the pessary herself by following instructions provided by a healthcare professional. This reduces the need for clinic visits and enables fl exibility on the timing of removal—for example, before having sexual intercourse. Reduced outpatient visits can have substantial cost implications for the health service. Not all practices off er pessary self-management to their patients.
It is uncertain if self-management of pessary is safe and improves quality of life for women with prolapse compared with clinic based care.
UNCERTAINTIES
Does self-management of vaginal pessaries improve care for women with pelvic organ prolapse? Carol Bugge ,
1 Melanie Dembinsky ,
1 Rohna Kearney ,
2 3
Suzanne Hagen 4
HOW PATIENTS WERE INVOLVED IN THIS ARTICLE A patient reviewed this manuscript. She highlighted the importance of having telephone support available when self-managing a pessary. This would help ease her concerns in the time between vaginal examinations every two years. Telephone support as a component of self-management has been suggested in the manuscript. We are grateful for the patient’s input.
P

the bmj | 27 February 2021 327
What is the evidence of uncertainty?
Evidence on pessary self-management is very limited and from small non-randomised studies 7 - 11 (table 1, bmj.com). The studies mainly report on the length of time for which women continue to use a pessary. Overall, self-management may improve pessary continuation rates and enhance patient satisfaction and quality of life, but it is diffi cult to generalise these fi ndings. The studies were conducted in diff erent populations, were small, and lacked randomised comparison groups. 7 - 11 Uncertainty exists over optimal follow-up intervals, if they are required, for women who are self-managing.
Is ongoing research likely to provide relevant evidence?
We searched the US National Library of Medicine database and ISRCTN and ANZCTR registries most recently on 8 February 2021 for ongoing trials on pelvic organ prolapse. We identifi ed two trials on pessary self-management. These trials are expected to provide some evidence on the safety and acceptability of self-management, but do not address uncertainties such as optimal follow-up times, potential diff erences in managing pessaries made of diff erent materials, and patient acceptability and satisfaction.
The TOPSY study (ISRCTN62510577) 12 is an ongoing randomised controlled trial in the UK that compares clinic based care with a self-management intervention for women with any type and stage of prolapse using various pessary types (340 participants recruited; expected to report in February 2022). The primary outcome measure is prolapse specifi c quality of life at 18 months. The second study (ACTRN12618000416291) compares self-management for PVC ring pessary with a silicon irregular hexagon pessary. The primary outcome is retention of the pessary at six and 12 months post-randomisation.
What should we do in light of the uncertainty?
The stage of prolapse, impact on quality of life, and patient preferences and characteristics guide decisions on management. In women considering pessary use, discuss options of self-management and clinic based care. Explain the importance of pessary removal and re-insertion to reduce the risk of complications. Self-management is unsuitable for women with cognitive impairment or a physical diffi culty, 2 such as those who do not have the manual dexterity required for pessary handling. If a woman wishes to self-manage her pessary, provide clear instructions (box).
Evidence for length of time between follow-up visits for clinic based care is uncertain, 13 14 with six monthly visits being common in the UK. 6 No evidence based timeframe exists for a clinician’s review if a woman is self-managing and not experiencing problems. A follow-up appointment every two years is reasonable in the absence of further guidelines. Provide a telephone number to call if the woman experiences any problems. Competing interests: CB, SH, and MD declare that there are none. RK was the topic lead for
prolapse on the NICE guidelines (National, Guideline Alliance UK. Urinary incontinence and pelvic
organ prolapse in women: management. 2019).
Cite this as: BMJ 2021;372:n310 Find the full version with references at http://dx.doi.org/10.1136/bmj. n310
WHAT TO DISCUSS WITH WOMEN BEFORE PESSARY USE 2
• Discuss all options for managing symptoms, including lifestyle modifications, pelvic floor muscle training, vaginal pessary, and surgery
• Explain that pessary use requires regular pessary changes, at least once every six months
• Self-management has the potential benefits of being able to remove and insert the pessary when desired—for example, before intercourse—and may also mean reduced clinic appointments
• If the woman prefers self-management of pessary, provide instructions on
– removal and re-insertion technique, ensuring she understands the pelvic anatomy
– cleaning of the pessary, with a short explanation of the material of the pessary
– how to receive a replacement pessary – how she should access support if she experiences problems, such as a phone number to call
• Ensure the type of pessary is appropriate for sexual activity if the woman wishes to be sexually active. Vaginal intercourse is possible with a ring pessary in place but not possible with other types of pessary in place. Self-management of space occupying pessaries tends to be more difficult than for ring and sieve pessaries
• Explain that it may take more than one fitting to achieve a successful pessary fit. The woman may need to try a pessary to find one that is most suitable. Ensure women can void after first fitting before leaving the clinical area.
• Common complications include vaginal discharge, ulceration, bleeding, and expulsion. These can occur if a pessary is not changed regularly. Less commonly, incarceration can occur, which requires pessary removal under anaesthetic. Other complications include rectovaginal or vesicovaginal fistula, and very rarely vaginal, squamous cell cancer.
EDUCATION INTO PRACTICE • How would you discuss the options of self-management and clinic based
management with a woman considering pessary use for prolapse? • What guidance would you provide to a woman opting for self-management of
vaginal pessary?
328 27 February 2021 | the bmj
Raffles Children’s Centre, Raffles Hospital, Singapore
Correspondence to: JH Chong chong_jinho@raff lesmedical.com
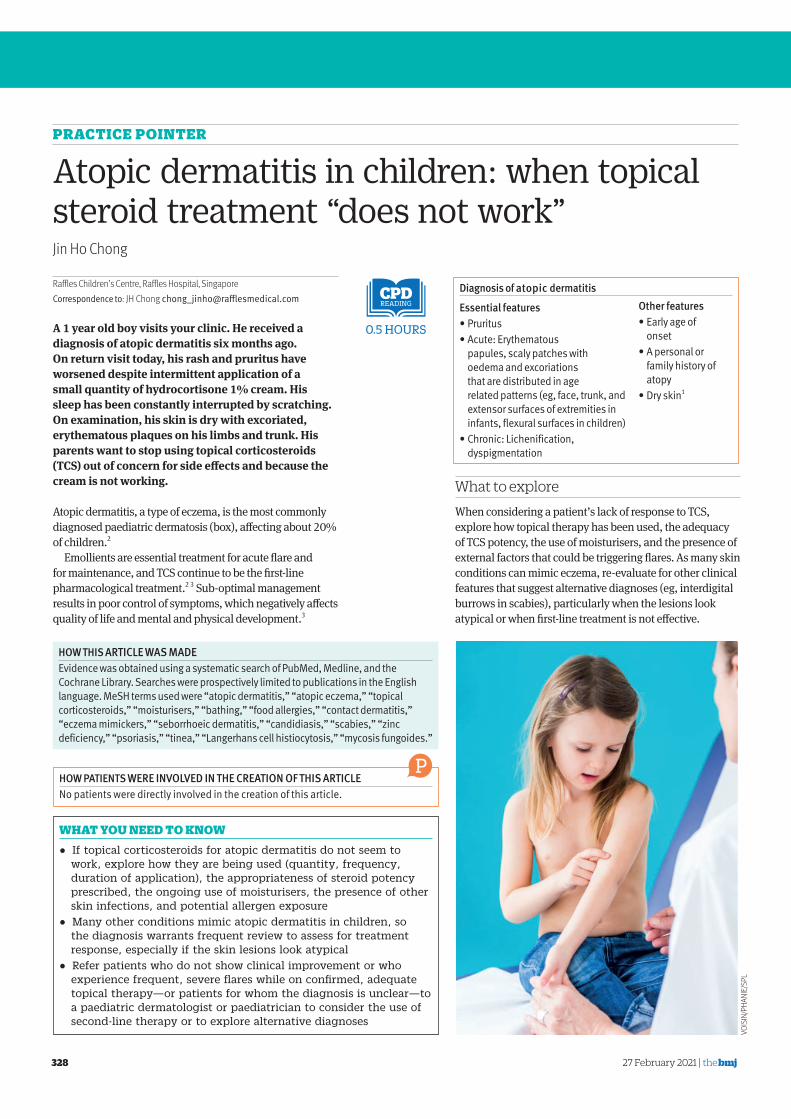
A 1 year old boy visits your clinic. He received a
diagnosis of atopic dermatitis six months ago.
On return visit today, his rash and pruritus have
worsened despite intermittent application of a
small quantity of hydrocortisone 1% cream. His
sleep has been constantly interrupted by scratching.
On examination, his skin is dry with excoriated,
erythematous plaques on his limbs and trunk. His
parents want to stop using topical corticosteroids
(TCS) out of concern for side eff ects and because the
cream is not working.
Atopic dermatitis, a type of eczema, is the most commonly diagnosed paediatric dermatosis (box), aff ecting about 20% of children. 2
Emollients are essential treatment for acute fl are and for maintenance, and TCS continue to be the fi rst-line pharmacological treatment. 2 3 Sub-optimal management results in poor control of symptoms, which negatively aff ects quality of life and mental and physical development. 3
READING
0.5 HOURS
WHAT YOU NEED TO KNOW
• If topical corticosteroids for atopic dermatitis do not seem to work, explore how they are being used (quantity, frequency, duration of application), the appropriateness of steroid potency prescribed, the ongoing use of moisturisers, the presence of other skin infections, and potential allergen exposure
• Many other conditions mimic atopic dermatitis in children, so the diagnosis warrants frequent review to assess for treatment response, especially if the skin lesions look atypical
• Refer patients who do not show clinical improvement or who experience frequent, severe fl ares while on confi rmed, adequate topical therapy—or patients for whom the diagnosis is unclear—to a paediatric dermatologist or paediatrician to consider the use of second-line therapy or to explore alternative diagnoses
What to explore
When considering a patient’s lack of response to TCS, explore how topical therapy has been used, the adequacy of TCS potency, the use of moisturisers, and the presence of external factors that could be triggering fl ares. As many skin conditions can mimic eczema, re-evaluate for other clinical features that suggest alternative diagnoses (eg, interdigital burrows in scabies), particularly when the lesions look atypical or when fi rst-line treatment is not eff ective.
PRACTICE POINTER
Atopic dermatitis in children: when topical steroid treatment “does not work” Jin Ho Chong
Diagnosis of atopic dermatitis Essential features • Pruritus • Acute: Erythematous
papules, scaly patches with oedema and excoriations that are distributed in age related patterns (eg, face, trunk, and extensor surfaces of extremities in infants, flexural surfaces in children)
• Chronic: Lichenification, dyspigmentation
HOW PATIENTS WERE INVOLVED IN THE CREATION OF THIS ARTICLE No patients were directly involved in the creation of this article.
P
HOW THIS ARTICLE WAS MADE Evidence was obtained using a systematic search of PubMed, Medline, and the Cochrane Library. Searches were prospectively limited to publications in the English language. MeSH terms used were “atopic dermatitis,” “atopic eczema,” “topical corticosteroids,” “moisturisers,” “bathing,” “food allergies,” “contact dermatitis,” “eczema mimickers,” “seborrhoeic dermatitis,” “candidiasis,” “scabies,” “zinc deficiency,” “psoriasis,” “tinea,” “Langerhans cell histiocytosis,” “mycosis fungoides.”
Other features • Early age of
onset • A personal or
family history of atopy
• Dry skin 1
VOISIN/PHANIE/SPL

the bmj | 27 February 2021 329
lesions are smooth to touch, not erythematous, and not itchy. 10 11 Conversely, if there is no clinical improvement after one or two weeks of use, re-evaluation is needed to verify use of TCS and emollients, adjust TCS potency, or reconsider the diagnosis. 10 11
Was the appropriate potency prescribed? TCS formulations come in diff erent potencies (table 1) and may not work if an inappropriate potency was prescribed. 3 Mild potency TCS are used for young infants, on mild lesions for older children or large surface areas of eczema and on thin skin sites (face, neck, skin folds), 13 where there is a greater risk of steroid penetration and higher likelihood for systemic absorption. 3 - 14 Conversely, more potent corticosteroids can be used on acute, severe lesions and on thick skin sites such as the palms and soles to arrest severe fl ares more quickly, which in turn reduces the duration of TCS use. 7 - 15 Physicians may refer to the fi gure for a site-based TCS potency guide. Ointments sting less during application on broken skin 14 and are more potent compared with creams. 7
How are moisturisers being applied? Liberal and frequent application of moisturisers, including lotions, creams, gels, and ointments, is not an adjunctive but a cornerstone treatment for atopic dermatitis. Moisturisers exert a steroid sparing eff ect by repairing the compromised skin barrier, alleviating symptoms, preventing fl ares, and possibly even preventing the onset of atopic dermatitis altogether in infants with a family history of atopy. 2 16 No consensus exists for the optimal time interval between the application of TCS and moisturisers, or which is to be applied fi rst. 17 The “best moisturiser” is the one that the patient prefers, works best for the patient, and is aff ordable. 18
Treatment with TCS may be ineff ective if they were applied too sparingly, too infrequently, or for too short a duration. 4 Patient and caregiver concerns about the side eff ects of TCS are associated with reduced use of these medications and warrant open discussion. 5 Systemic side eff ects of topical TCS such as glaucoma and adrenal insuffi ciency and local reactions such as skin atrophy and striae are unlikely to occur with judicious use of TCS. 6
Quantity and frequency Patients and caregivers may be reluctant to apply TCS out of concern for the side eff ects of TCS, so much so that the “thin layer” they apply may be sub-therapeutic. 5 The fi ngertip unit (FTU) guidance for quantity (the amount of cream or ointment squeezed from the fi ngertip to the fi rst crease of the fi nger should cover a skin area equivalent to two palms) is challenging for parents to follow because of the varying sizes of lesions. 7 The dose may be further reduced if the cream is rubbed off on upholstery, clothing, bed linen, or other articles throughout the day. Therefore, better guidance to parents might be to apply enough cream or ointment on active eczema so that there is a visible or glistening layer seen, even on broken skin. Clinicians can help by prescribing a suffi cient number of tubes of TCS, especially if large body surface areas need to be covered. TCS may be applied once or twice daily. 8 9
Duration The period for what is considered “suffi cient” use of TCS varies even for diff erent fl are-ups in the same patient, depending on the severity of lesions, the potency of TCS prescribed, and adherence to regimens of moisturising and TCS treatment. Expect noticeable clinical response within three to fi ve days of application if the TCS prescription is appropriate, and advise patients not to stop TCS use until
Table 1 | Potency of various formulations of topical corticosteroids (adapted with permission from Tay et al. 12 ) This may vary across different classification systems Potency Generic name Strength % FormulationSuper
potent
Betamethasone
dipropionate
0.05 Ointment
Clobetasol propionate 0.05 Ointment, cream,
lotion, shampoo
Mometasone furoate 0.1 Ointment
Potent Betamethasone
dipropionate
0.05 Cream
Betamethasone valerate 0.1 Ointment, cream,
lotion
Mometasone furoate 0.1 Cream, lotion
Hydrocortisone aceponate 0.127 Lipocream
Fluticasone propionate 0.05 Cream
Fluocinolone acetonide 0.05 Cream
Diflucortolone valerate 0.1 Ointment, cream
Triamcinolone acetonide 0.1 Oral paste
Moderate Betamethasone valerate 0.025 Ointment, cream
Fluocinolone acetonide 0.025 Cream
Clobetasol butyrate 0.05 Cream
Desonide 0.05 Cream, lotion
Mild Hydrocortisone 1 Ointment, cream
TCS: Topical corticosteroidsTCI: Topical calcineurin inhibitors
*Prescribe only low potency TCS for infants under 1 year as far as possible
Face
Low potency TCS
TCI
Crisaborole
Scalp
Low-to-high potency TCS
TCI
Crisaborole
Palms/soles
Mid-to-high potency TCS
TCI
Crisaborole
Eyelids
TCI
Crisaborole
Anogenital area
Low potency TCS
TCI
Crisaborole
Trunk/extremities
Low-to-high potency TCS
TCI
Crisaborole
Guide to site based topical treatments for atopic dermatitis. (Reproduced with permission from Yang EJ et al. 3 TCS=topical corticosteroids, TCI=topical calcineurin inhibitors (pimecrolimus, tacrolimus), Crisaborole: phosphodiesterase-4 inhibitor (TCI are generally licensed for children over 2)
How have topical corticosteroids been used?

330 27 February 2021 | the bmj
Is there an underlying food allergy?
Regardless of topical steroid response, underlying food allergies are a common parental concern. Food allergies may coexist with atopic dermatitis or, less frequently, trigger fl ares in those with moderate-severe disease. 11 - 24 In patients with immediate food induced reactions, SPT or specifi c immunoglobulin E tests can confi rm allergens. 12 Patients with suspected delayed reactions causing dermatitis 6-48 hours after ingestion of particular foods—and especially those with gastrointestinal symptoms or faltering growth 12 —would likely benefi t from referral to an allergist to consider oral food challenges. 24
Concern among caregivers about possible food allergies can be signifi cant. It is important that these concerns are heard and that patients still maintain proper skin care if potential food allergies are investigated. Improved control of atopic dermatitis not only improves quality of life, but emerging evidence suggests it may also reduce the incidence or severity of food allergies by preventing penetrance of potential allergens. 16
Are coexisting cutaneous infections hindering successful treatment?
Cutaneous Staphylococcus aureus colonisation may trigger frequent fl ares and super-infections of eczematous lesions, as enterotoxins and scratching break down the skin barrier. 3 25 The presence of fever, pain, pus, discharge, or crusts is consistent with bacterial infection. Obtain swab cultures from lesions that appear infected, nares, or skin folds to identify the bacteria and treat according to culture results. 25 Children with recurrent skin infections may benefi t from a bleach bath. 26
Consider eczema herpeticum (herpes virus infection) in patients with painful vesicles and punched out erosions with dermatitis. 12 25 Eczema herpeticum requires urgent referral and acyclovir treatment as it can lead to meningoencephalitis and fatality. 10 - 25 Seborrhoeic dermatitis (malassezia yeast infection) presents with a head-neck distribution of pink patches with greasy white or yellow scales and is treated with antifungal agents. 27
When should I reconsider the diagnosis of atopic dermatitis?
Table 2 shows a non-exhaustive list of mimickers of paediatric eczema. Dermatitis, especially in children with faltering growth, recurrent severe infections, or dysmorphic features, can also be part of a broader syndrome, such as Netherton, hyper-IgE, Omenn, Wiskott-Aldrich, and trichohepatoenteric 42 syndromes. Some eczema mimics, such as Langerhan’s cell histiocytosis or mycosis fungoides, can have signifi cant consequences if left undiagnosed and untreated.
What are parental expectations and concerns?
Recurrence of fl ares after initially successful treatment with TCS may be interpreted as treatment failure, leading some patients or caregivers to stop using TCS. Eff ective patient education on atopic dermatitis includes an explanation of the chronic relapsing-remitting nature of atopic dermatitis so that patients can anticipate, recognise, and promptly resume use of TCS in the event of a fl are-up. 19 Eliciting and responding to concerns about TCS side eff ects, reviewing proper use of topical medication(s), and providing emotional support are key to agreeing and carrying out an eff ective treatment regimen. 4 19 This, in turn, extends periods of remission and reduces the severity of fl ares. 2 14 Patient education interventions (nurse or multi-professional led) may reduce disease severity and improve quality of life for patients and caregivers. 20
Schedule early or frequent reviews for newly diagnosed patients, especially if their condition is severe, to check for treatment response and to reaffi rm the diagnosis. This also off ers an opportunity to guide topical treatment, to alleviate parental anxiety, and to reassure parents by monitoring for potential side eff ects.
Non-steroidal topical alternatives
For some children older than 2, topical calcineurin inhibitors (TCI) may be a steroid-sparing topical treatment alternative, especially at sites with thin skin. 6 TCI are more costly, may sting on application, and they carry a black box warning for theoretical carcinogenicity. 2 10 The National Institute for Health and Care Excellence (NICE) recommends TCI as a second-line treatment option for children over 2 with moderate to severe eczema who did not have a satisfactory response to TCS, when there is serious risk of important adverse eff ects caused by TCS, such as irreversible skin atrophy. 10 Crisaborole, a topical phosphodiesterase-4 inhibitor, is another non-steroidal alternative that is currently under appraisal by NICE for use in children over 2 years of age. 21
Are environmental and other triggers limiting treatment effectiveness?
Flares may persist or recur with persistent exposure to aggravating factors including heat, sweat, and stress despite optimal use of TCS and moisturiser. 12 22 Allergen avoidance prevents frequent relapses of atopic dermatitis. 2 Patients with moderate to severe disease are more sensitised to common aeroallergens, including house dust mites (HDM), pollen, fungi, and animal dander, 22 some of which can be identifi ed by skin prick tests (SPT). 2 HDM-allergic patients should follow HDM avoidance strategies, including the use of anti-HDM covers. 23 Patients should avoid possible contact allergens, such as metals, fragrances, preservatives, dyes, or even TCS—which may be confi rmed by patch testing—as they trigger recurrent dermatitis. 2 22
The presence of fever, pain, pus, discharge, or The presence of fever, pain, pus, discharge, or crusts is consistent with bacterial infection. Obtain crusts is consistent with bacterial infection. Obtain swab cultures from lesions that appear infected swab cultures from lesions that appear infected

the bmj | 27 February 2021 331
Refer patients who do not show clinical improvement or who experience frequent, severe fl ares while on confi rmed, adequate therapy—or patients for whom the diagnosis is unclear, especially if the lesions look atypical—to a paediatric dermatologist or paediatrician to consider the use of second-line therapy such as phototherapy or immunosuppresants 43 or to explore alternative diagnoses.
Outcome The infant’s condition improves after a more potent TCS is applied in suffi cient quantities, alongside frequent application of moisturiser. TCS application is later re-initiated early upon fl are recurrence. He scratches less and sleeps well. Appropriate use of the correct topical treatment has led to better control of his atopic dermatitis and has improved his quality of life.
EDUCATION INTO PRACTICE • How can you explore the concerns and expectations
of parents and caregivers when prescribing topical corticosteroids for children?
• What concerns do you have about prescribing TCS? How do you decide the correct potency for the patient, and how do you ensure the treatment is used correctly?
• Think of your last paediatric patient with atopic dermatitis. Did you review TCS and emollient use? If the patient did not show clinical improvement, should the diagnosis be reconsidered?
Competing interests: None declared.
Cite this as: BMJ 2021;372:n297 Find the full version with references at http://dx.doi.org/10.1136/bmj. .n297
Table 2 | Paediatric eczema mimickers Diagnosis Common sites Morphology Investigations Complications/notesTinea
(superficial
fungal/
dermatophyte
infections)
corporis
Body, limbs Asymmetric pruritic patches/plaques with
scaly annular borders 28
Microscopy and fungal
culture of hair and skin
scrapings 29
• Frequently misdiagnosed as tinea in infants although tinea
rarely occurs in infants, especially neonates 30
• Misdiagnosis of atopic dermatitis in patients with tinea
can result in “tinea incognito” with persistence of symptoms
despite a less scaly and less annular appearance 31
after the
inappropriate use of topical corticosteroids, which further
delays diagnosis
• A generalised eczematous eruption called
autoeczematisation or interface dermatitis reaction can occur
after antifungal treatment 32
Tinea capitis Scalp Pruritic fine scaly plaques, patchy circular
alopecia, 33
lymphadenopathy
Scabies Web spaces of the fingers,
volar wrists, extensor surfaces
of elbows, axillae, waist,
navel, abdomen, buttocks,
genitals
Erythematous papular eruption, with
serpiginous burrows and intense, intractable
pruritus
Skin scrapings if clinical
diagnosis is in doubt
• Transmitted via close prolonged skin-to-skin contact
• Prevalent in unhygienic, overcrowded conditions
• Can spread to the community if not treated early
• Usually other family members with the same itchy rash 34
Plaque
psoriasis
Diaper area, scalp Sharply demarcated pink plaques Skin biopsy if clinical
diagnosis is in doubt
• Nail involvement: pitting, oil spots, onycholysis, subungual
hyperkeratosis, onychodystrophy
• Responds to topical corticosteroids, other treatment
includes topical vitamin D analogues and retinoids 35
• May be associated with metabolic syndrome (obesity,
hyperlipidaemia, hypertension, diabetes) 36
Guttate
psoriasis
Trunk Monomorphic truncal scaly papules 2 weeks
after a β-haemolytic streptococcal or viral
infection
·
Pustular
psoriasis
Generalised Superficial sterile pustules, fever, malaise, and
arthralgia
Zinc deficiency Acral, periorificial and
anogenital regions 37
Well defined eczematous or psoriasiform
plaques with peripheral scaling and crusts
• Low zinc serum level
• Low alkaline
phosphatase level
• May present with irritability, faltering growth, diarrhoea,
alopecia 38
• Two types:
(1) acrodermatitis enteropathica: an intestinal enzyme defect
results in abnormal zinc absorption,
(2) transient neonatal zinc deficiency: an impaired function
of the maternal zinc transporter leads to low zinc levels in
breastmilk and subsequent zinc deficiency in breastfed
infant 37
Neonatal lupus Facial (especially periorbital
“raccoon eye” distribution)
and scalp
Papulosquamous red and scaly annular
plaques
• Autoantibodies
• Electrocardiogram
• 2D echocardiogram
• Full blood count
• Liver function test
• Congenital heart block may lead to mortality
• Possible multisystemic involvement, including hepatic and
haematologic al
• May be a maternal history of connective tissue disease 39
Langerhans cell
histiocytosis
(LCH)
Scalp, abdomen, chest, back Seborrhoeic or eczematous papules, plaques,
or patches with petechiae or purpura,
hypopigmented macules, umbilicated or
hypopigmented papules, vesicles or bullae,
pustules, nodules or blueberry muffin spots.
Ulceration at intertriginous areas
• Skin biopsy
• May need staging (chest,
abdomen, or intracranial
imaging, skeletal survey)
• A group of diseases caused by Langerhans cells derived
from myeloid progenitor cells
• First sign of LCH in about 80% of cases
• May have multisystem involvement, including diabetes
insipidus 40
Mycosis
fungoides (MF)
Any body part but frequently
localises to sun-protected
areas
Hypopigmented patches, follicular or
acneiform papules, scaly erythematous
patches
• Skin biopsy
• Full blood count with
Sézary cell analysis
• Imaging studies
• Most common primary cutaneous lymphoma in children
• Age of onset spans almost the entire paediatric age range
• Runs an indolent course, may not be diagnosed for months
to years
• Delayed diagnosis can be associated with poor long term
prognosis owing to disease progression 41
When should I refer?

332 27 February 2021 | the bmj
You can record CPD points for reading any article. We suggest half an hour to read and refl ect on each.
Articles with a “learning module” logo have a linked BMJ Learning module at http://learning.bmj.com.
LEARNINGMODULEREADING
0.5 HOURS
A woman in her late teens presented with cutaneous lesions on both feet after a seven day trip to a beach destination in Brazil, where she walked barefoot most of the time. On examination, she had multiple serpiginous erythematous tracks that were intensely itchy and had been slowly migrating for the past few days (figure).
What is the diagnosis?
Submitted by Carole Eldin and Philippe Gautret Patient consent obtained. Cite this as: BMJ 2021;372:n231
SPOT DIAGNOSIS Multiple itchy lesions after recent travel
ENDGAMES
Multiple serpiginous lesions on left foot (a) and serpiginous lesion on sole of right foot (b)
answ
ers
What is the diagnosis? Cutaneous larva migrans (CLM).
CLM is a parasitic disease that occurs in tropical and subtropical regions. It is caused by skin penetration of hookworm larvae that usually infest cats, dogs, and other animals. After a short incubation period (1-5 days), tracks typically appear on the feet or other unprotected parts of the body that might come into contact with contaminated animal faeces. CLM is a clinical diagnosis, presenting as
pruritic serpiginous tracks that migrate 1-2 cm daily. Vesiculobullous lesions occur in 9-15% of cases and sometimes reach a large size (several centimetres in diameter). Bacterial superinfection is possible (9-24% of cases in Brazil), commonly as a result of lesions being scratched.
Antihelminth treatments include ivermectin (200 μg/kg once daily for 1-2 days) and oral albendazole (400 mg once daily for three days).
SPOT DIAGNOSIS Multiple itchy lesions after recent travel
LEARNING POINT Consider CLM in patients with an itchy, serpiginous, migrating cutaneous tracking rash, especially if they have walked barefoot in areas with large numbers of cats and dogs, as commonly occurs at informal beachside bars and restaurants in tropical and subtropical countries.
PATIENT OUTCOMEOur patient received antihistamine and antihelminth treatment and complete healing occurred within a few days. Coincidentally, an unrelated traveller returning from the same region also presented with CLM, suggesting that CLM was prevalent in this area at the time of these presentations.
ONLINE NOW – VACCINES FOR OLDER ADULTS:A STATE OF THE ART REVIEWA State of the Art Review published this week on bmj.com (https://www.bmj.com/content/372/bmj.n188) considers recent improvements to vaccines for older adults, either through the addition of novel adjuvants or by increasing antigen concentration. The review examines the evidence for current best use of vaccines against infl uenza, pneumococcal disease, and herpes zoster and identifi es evidence gaps and potential directions for future research. See other clinical reviews at https://www.bmj.com/education/clinical-review

the bmj | 27 February 2021 333
MINERVA
Death following a heart attack Combining data from 10 European longitudinal studies identifi ed nearly 30 000 people who experienced a heart attack. Around 5000 (18%) died within 28 days and, of these, 3000 (62%) died instantly. Risk of sudden death was infl uenced by past levels of physical activity. People who, at the time of recruitment, reported moderate or high levels of leisure time exercise reduced their risk by 33% and 45%, respectively ( Eur J Prevent Cardiol doi: 10.1093/eurjpc/zwaa146 ).
Fish oil supplements A few years ago, a Cochrane review reckoned that omega-3 fi sh oils had no worthwhile cardiovascular protective eff ect ( Cochrane Database Syst Rev doi: 10.1002/14651858.CD003177.pub3/full ). A 2 year trial in people aged 70 to 80 who had survived an acute myocardial infarction showed that older people are no exception. Cardiovascular events were as frequent in those randomised to fi sh oil supplements as in those taking a corn oil placebo ( Circulation doi: 10.1161/CIRCULATIONAHA.120.052209 ).
Job security improves mental health A longitudinal survey of 20 000 people over 14 years in Australia reports that improvements in job security were strongly linked to a reduction in symptoms of depression and anxiety ( Am J Epidemiol doi: 10.1093/aje/kwaa038 ). Minerva wouldn’t have been surprised by this except
If you would like to write a Minerva picture case, please see our author guidelines at http://bit.ly/29HCBAL and submit online at http://bit.ly/29yyGSx
Lichen amyloidosis of the legs This is lichen amyloidosis on the leg of a man in his 60s. He presented with a 20 year history of multiple hyperpigmented itchy lesions on his arms, legs, and buttocks that were papulonodular and coalesced, forming plaques. Thioflavin T and Congo red staining of biopsy sample were consistent with lichen amyloidosis, which is characterised by cutaneous deposition of amyloid proteins with no systemic involvement. 1 Lichen amyloidosis can be associated with multiple endocrine neoplasia type 2A, 2 3 but, as is often the case, the cause in this patient was idiopathic.
Medical history consisted solely of well managed HIV, which was not thought to have predisposed to the lichen amyloidosis.
The focus of management is on symptom control; evidence for treatment is limited. This man received topical corticosteroids and phototherapy. The pruritus improved without any change to the clinical appearance. Ewa Kloczko ( [email protected] ) ; Wedad Abdelrahman , Guy’s and St Thomas’ NHS Trust, London, UK Patient consent obtained. Cite this as: BMJ 2021;372:n315
that she had recently noted another survey, also from Australia, which found that health outcomes for casual workers were no worse than for those in permanent employment ( Occup Environ Med doi: 10.1136/oemed-2020-106568 ).
Frailty increases mortality after surgery Frailty is the condition of older people at high risk of adverse outcomes such as falls, disability, admission to hospital, or the need for long term care. It’s not surprising then, that in a cross sectional analysis of 900 000 admissions for emergency general surgery in the US, frailty was associated with mortality ( JAMA Surg doi: 10.1001/jamasurg.2020.5397 ). Overall, mortality in the 28 days after surgery was 4.5%. Among those classifi ed as frail, which was just over 10%, mortality was double.
Mesenchymal stem cells in multiple sclerosis Mesenchymal stem cells are pluripotent precursor cells isolated from bone marrow. Their repair promoting properties in animal models make them a potential treatment for several neurological diseases. A phase II study in 48 patients with active multiple sclerosis reports that treatment with autologous mesenchymal stem cells was well tolerated and that it induced short term improvements ( Brain doi: 10.1093/brain/awaa333 ).
Herd immunity Covid-19 vaccines are performing better than anyone could have expected. Even so, they may not be able to prevent transmission of the virus, which is crucial for herd immunity. Herd immunity is like having wet logs in a campfi re. If there’s enough water in the logs— enough immunity in a population—a fi re won’t start. A spark might land—a case might arrive—but without dry fuel, the fi re can’t get going ( https://www.theatlantic.com/health/archive/2021/02/herd-immunity-might-be-impossible-even-vaccines/617973 ).
Vaccines On the same subject, a short video from Science explains the diff erent types of vaccines and how they are made. A deeper understanding of how vaccines induce immunity could shortcut the need for large randomised trials to demonstrate effi cacy. But, at the moment, the most urgent problems concern vaccine supply and equity of access ( https://www.sciencemag.org/news/2021/01/how-leading-covid-19-vaccines-work ). Cite this as: BMJ 2021;372:n470




















