
Eating Patterns in a Population-Based Sample of Children Aged 5 to 7 Years: Association With...
7
Eating disorders symptoms in pregnancy: A longitudinal study of women with recent and past eating disorders and obesity Nadia Micali 4 , Janet Treasure, Emily Simonoff King’s College London, Institute of Psychiatry, Department of Child and Adolescent Psychiatry, London, United Kingdom Received 31 October 2006; received in revised form 22 March 2007; accepted 1 May 2007 Abstract Objective: To determine the impact of pregnancy on eating disorders (ED) symptoms using data from a large prospective, community-based cohort study. Methods: Women (12,254) were classified according to whether they had a recent or past history of ED, were obese before pregnancy, or constituted part of the general population control group. We evaluated self-induced vomiting (SIV), laxative use, exercise behavior, and appraisals about weight gain during pregnancy, as well as dieting, and shape and weight concern before and during pregnancy. Results: Women with a recent episode of ED dieted, used laxatives, reported SIV, and exercised more than other groups during pregnancy. They were also more likely to report ED cognitions in pregnancy and their weight and shape concern scores remained high during pregnancy. Women with past ED were also more likely than controls to have some ED behaviors and/ or concerns about weight gain during pregnancy. Conclusions: Women with a recent ED continued to have some ED symptoms in pregnancy, albeit fewer compared to before pregnancy. Although at a lower level, women with a past history of ED also had ED symptoms in pregnancy. Screening for ED symptoms during pregnancy may provide a useful opportunity for engagement in treatment and to reduce behaviors that might be detrimental to the foetus. D 2007 Elsevier Inc. All rights reserved. Keywords: Eating disorders; Pregnancy; Obesity; ALSPAC Introduction Eating disorders (ED) affect about 5–7% of women of child-bearing age. Previous studies have tried to clarify the impact of pregnancy on ED symptoms; however, this largely remains unclear. Two different hypotheses have been postulated and have resulted from previous literature. The first is that eating behaviors (and associated symptoms if relevant) will improve during the early part of the pregnancy because of concern for the well-being of the foetus. The second is that the weight gain during pregnancy may exacerbate or rekindle latent weight and shape concerns which may lead to a relapse of the ED in the post-partum period. In general, previous studies have shown a decrease in ED symptoms between the first and third trimester of pregnancy in women with an active ED at conception (in particular bulimia nervosa—BN) [1–3]. One study on 15 women with ED, however, reported a worsening or continuation of symptoms in pregnancy in women with either anorexia nervosa (AN) or BN who were symptomatic at conception [4]. Three recent longitudinal studies followed up women treated for ED. One investigated women who had received treatment for AN (26 pregnancies) and BN (56 pregnan- cies), some of whom had an active ED at conception [5] and found that in the majority of cases bulimic symptoms improved during pregnancy and for a period of time after the birth. However, some ED behaviors did not change significantly, i.e., self-induced vomiting (SIV), overconcern 0022-3999/07/$ – see front matter D 2007 Elsevier Inc. All rights reserved. doi:10.1016/j.jpsychores.2007.05.003 4 Corresponding author. Child and Adolescent Psychiatry, Box PO85, Institute of Psychiatry, De Crespigny Park, SE5 8AF London, United Kingdom. Tel.: +44 0207 848 0468; fax: +44 0207 708 5800. E-mail address: [email protected] (N. Micali). Journal of Psychosomatic Research 63 (2007) 297 – 303
-
Upload
southerndenmark -
Category
Documents
-
view
1 -
download
0
Transcript of Eating Patterns in a Population-Based Sample of Children Aged 5 to 7 Years: Association With...
Journal of Psychosomatic Res
Eating disorders symptoms in pregnancy: A longitudinal study of women
with recent and past eating disorders and obesity
Nadia Micali4, Janet Treasure, Emily Simonoff
King’s College London, Institute of Psychiatry, Department of Child and Adolescent Psychiatry, London, United Kingdom
Received 31 October 2006; received in revised form 22 March 2007; accepted 1 May 2007
Abstract
Objective: To determine the impact of pregnancy on eating
disorders (ED) symptoms using data from a large prospective,
community-based cohort study. Methods: Women (12,254) were
classified according to whether they had a recent or past history
of ED, were obese before pregnancy, or constituted part of the
general population control group. We evaluated self-induced
vomiting (SIV), laxative use, exercise behavior, and appraisals
about weight gain during pregnancy, as well as dieting, and
shape and weight concern before and during pregnancy. Results:
Women with a recent episode of ED dieted, used laxatives,
reported SIV, and exercised more than other groups during
pregnancy. They were also more likely to report ED cognitions
0022-3999/07/$ – see front matter D 2007 Elsevier Inc. All rights reserved.
doi:10.1016/j.jpsychores.2007.05.003
4 Corresponding author. Child and Adolescent Psychiatry, Box PO85,
Institute of Psychiatry, De Crespigny Park, SE5 8AF London, United
Kingdom. Tel.: +44 0207 848 0468; fax: +44 0207 708 5800.
E-mail address: [email protected] (N. Micali).
in pregnancy and their weight and shape concern scores
remained high during pregnancy. Women with past ED were
also more likely than controls to have some ED behaviors and/
or concerns about weight gain during pregnancy. Conclusions:
Women with a recent ED continued to have some ED symptoms
in pregnancy, albeit fewer compared to before pregnancy.
Although at a lower level, women with a past history of ED
also had ED symptoms in pregnancy. Screening for ED
symptoms during pregnancy may provide a useful opportunity
for engagement in treatment and to reduce behaviors that might
be detrimental to the foetus.
D 2007 Elsevier Inc. All rights reserved.
Keywords: Eating disorders; Pregnancy; Obesity; ALSPAC
Introduction
Eating disorders (ED) affect about 5–7% of women of
child-bearing age. Previous studies have tried to clarify the
impact of pregnancy on ED symptoms; however, this
largely remains unclear. Two different hypotheses have
been postulated and have resulted from previous literature.
The first is that eating behaviors (and associated symptoms
if relevant) will improve during the early part of the
pregnancy because of concern for the well-being of the
foetus. The second is that the weight gain during pregnancy
may exacerbate or rekindle latent weight and shape
concerns which may lead to a relapse of the ED in the
post-partum period.
In general, previous studies have shown a decrease in
ED symptoms between the first and third trimester of
pregnancy in women with an active ED at conception (in
particular bulimia nervosa—BN) [1–3]. One study on 15
women with ED, however, reported a worsening or
continuation of symptoms in pregnancy in women with
either anorexia nervosa (AN) or BN who were symptomatic
at conception [4].
Three recent longitudinal studies followed up women
treated for ED. One investigated women who had received
treatment for AN (26 pregnancies) and BN (56 pregnan-
cies), some of whom had an active ED at conception [5] and
found that in the majority of cases bulimic symptoms
improved during pregnancy and for a period of time after
the birth. However, some ED behaviors did not change
significantly, i.e., self-induced vomiting (SIV), overconcern
earch 63 (2007) 297–303

N. Micali et al. / Journal of Psychosomatic Research 63 (2007) 297–303298
with body image, compulsive exercise, and restrictive
eating. ED symptoms did not decrease during pregnancy
in women with AN. The other two studies followed up
women who had received treatment for BN and investigated
the changes in bulimic symptoms during pregnancy. In one,
although bingeing and purging improved during pregnancy,
the number of women completely abstinent from these
behaviors did not change with pregnancy and body
dissatisfaction worsened during pregnancy [6]. The second
reported a nonsignificant decrease in ED symptomatology
in the year of childbirth, with a trend towards lower levels of
symptomatology [7].
Most studies in the literature are difficult to interpret as
they rely on small samples, with heterogeneous, poorly
described cases, and often use retrospective outcome
measures or reports of ED symptomatology. There are
many unanswered questions: there is little information on
pregnancy outcomes in women with AN and it is uncertain
what the outcomes are for women with a past vs. a recent
history of ED. Moreover, only one study has compared
women with ED to control subjects.
This study sought to examine the presence in pregnancy
of ED behaviors, as well as levels of shape and weight
concern in women with a recent episode of ED, women with
a past history of ED, and obese and nonobese controls. Our
secondary aim was to compare the risk of occurrence of ED
behaviors and cognitions in pregnancy amongst subgroups
of women with different ED. In order to do so we used data
from a well-characterized longitudinal cohort (the Avon
Longitudinal Study of Parents and Children—ALSPAC).
The inclusion of an obese control group aimed to determine
whether the effect of pregnancy on eating behaviors and
weight and shape concerns is specific to eating disordered
women or shared by women at high risk for weight and
shape concern (obese women). We hypothesized that
women with a recent episode of ED would be more likely
to report ED behaviors in pregnancy compared to other
groups; and that obese women would have lower rates of
ED behaviors. We also hypothesized that women with
recent and past ED and obese women would report similar
levels of weight and shape concern and abnormal cognitions
about weight gain in pregnancy. We also hypothesized that
amongst women with ED, women with recent AN or BN
would be more likely to report ED symptoms and cognitions
compared to women with past AN or BN.
Methods
Participants and procedures
The ALSPAC is a longitudinal, prospective study of
women and pregnancy [8]. All pregnant women living in
the geographical area of Avon, United Kingdom, who were
expected to deliver their baby between 1st April 1991 and
31st December 1992 were recruited. The sample has been
shown to be representative of the British population. Data
were obtained on 14,472 women via postal questionnaires.
At 12 weeks of pregnancy women were asked if they had
any recent occurrence or past history of psychiatric
problems, including depression, schizophrenia, alcohol
abuse, AN, BN or any other disorder. They also reported
their pre-pregnancy weight and height. Women were
excluded from the current study if they had not answered
this questionnaire (n=2019).
We included 12,252 women in the current study.
Amongst women who reported a history of ED 57 reported
a recent episode of ED (6 AN, 51 BN). Three hundred and
ninety-five (395) women had a past history of ED (167 of
AN, 158 of BN, 70 both AN and BN). These groups were
compared to obese women (n=618) [i.e., women who had a
body mass index (BMI) N30 kg/m2 before pregnancy] and
general population nonobese controls (n=11,184).
Measures
Socio-demographic data were obtained during preg-
nancy; BMI was calculated as pre-pregnant weight/height2.
18 weeks of pregnancy: Women were asked about SIV
and laxative use for weight loss at any time before
pregnancy and during pregnancy. At 18 weeks, women
were also asked how much exercise they engaged in per
week during pregnancy. They were given a list of exercise
activities, i.e., jogging, aerobics, squash, tennis, swimming,
weight training, cycling, etc., and were asked how many
hours per week they engaged in that type of exercise
during the first 18 weeks of pregnancy. These data were
categorized to have an index of bhigh exerciseQ. Women
who engaged in more than 1 h per day of moderate–hard
exercise (jogging, aerobics, squash, tennis, swimming,
weight training, cycling) during pregnancy were classified
as bhigh exercisersQ.Selected items from two subscales of the Eating
Disorder Examination questionnaire (EDE-Q) [9] were
administered to all women relating to the 3 months before
pregnancy and the previous 4 weeks. Five items from the
bweight concernQ and five items from the bshape concernQsubscales were used. Good reliability of these shortened
subscales has been shown [10]. Mean scores for each
subscale were calculated. The weight and shape concern
scales were analysed separately. Differences between mean
pregnancy and mean pre-pregnancy EDE-Q scores were
calculated to determine score changes. These bchangescoresQ were compared across groups.
32 weeks of pregnancy (third trimester): Women were
asked the following questions: bHave you had a strong
desire to lose weight this pregnancy?Q, bHave you felt a loss
of control over eating this pregnancy?Q, bDo you feel you
put on too much weight this pregnancy?Q, bHave you been
on a diet to slim this pregnancy?Q, bHave you ever been on a
diet to slim before this pregnancy?Q. All items were
dichotomous (Yes/No).
N. Micali et al. / Journal of Psychosomatic Research 63 (2007) 297–303 299
Statistical analysis
Women with a recent episode of ED were compared to
women with past ED, obese and nonobese controls. Group
comparisons used parametric (one-way analysis of var-
iance–ANOVA) and nonparametric tests as appropriate,
after testing for normality. Bivariate linear regression
models tested for predictors of continuous outcomes. Binary
logistic regression models were used for binary outcomes.
Post hoc comparisons of odds ratios (OR) amongst groups
were performed. For each analysis, we checked for selective
attrition; none was found.
All analyses were performed using Stata (version 8 for
Windows; STATACorp, College Station, TX, USA) and
SPSS (version 12 for Windows; SPSS Inc., Chicago, IL,
USA). All statistical tests presented are two tailed. Statistical
significance was defined as a P value of less than .05.
Ethical approval
The study was approved by the Institute of Psy-
chiatry Ethics committee (Ref. 110/02) and the ALSPAC
Law and Ethics committee and the Local Research
ethics Committees.
Results
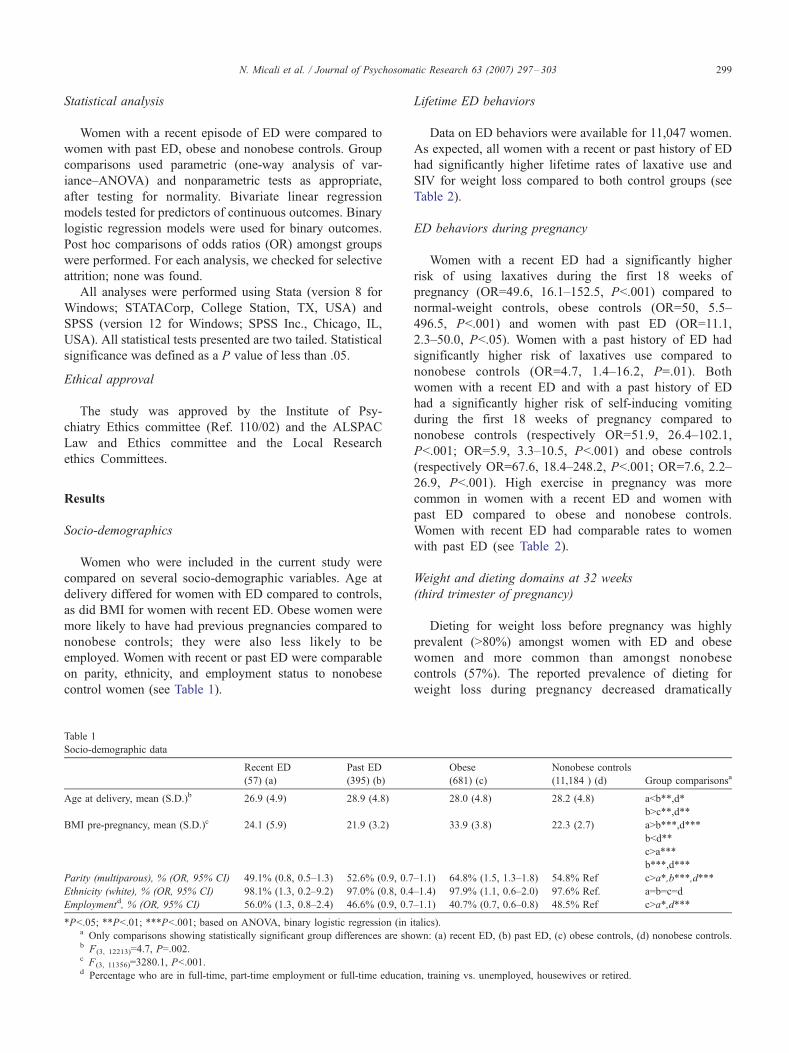
Socio-demographics
Women who were included in the current study were
compared on several socio-demographic variables. Age at
delivery differed for women with ED compared to controls,
as did BMI for women with recent ED. Obese women were
more likely to have had previous pregnancies compared to
nonobese controls; they were also less likely to be
employed. Women with recent or past ED were comparable
on parity, ethnicity, and employment status to nonobese
control women (see Table 1).
Table 1
Socio-demographic data
Recent ED
(57) (a)
Past ED
(395) (b)
Age at delivery, mean (S.D.)b 26.9 (4.9) 28.9 (4.8)
BMI pre-pregnancy, mean (S.D.)c 24.1 (5.9) 21.9 (3.2)
Parity (multiparous), % (OR, 95% CI) 49.1% (0.8, 0.5–1.3) 52.6% (0.9, 0.7
Ethnicity (white), % (OR, 95% CI) 98.1% (1.3, 0.2–9.2) 97.0% (0.8, 0.4
Employmentd, % (OR, 95% CI) 56.0% (1.3, 0.8–2.4) 46.6% (0.9, 0.7
*Pb.05; **Pb.01; ***Pb.001; based on ANOVA, binary logistic regression (ina Only comparisons showing statistically significant group differences are shb F(3, 12213)=4.7, P=.002.c F(3, 11356)=3280.1, Pb.001.d Percentage who are in full-time, part-time employment or full-time educati
Lifetime ED behaviors
Data on ED behaviors were available for 11,047 women.
As expected, all women with a recent or past history of ED
had significantly higher lifetime rates of laxative use and
SIV for weight loss compared to both control groups (see
Table 2).
ED behaviors during pregnancy
Women with a recent ED had a significantly higher
risk of using laxatives during the first 18 weeks of
pregnancy (OR=49.6, 16.1–152.5, Pb.001) compared to
normal-weight controls, obese controls (OR=50, 5.5–
496.5, Pb.001) and women with past ED (OR=11.1,
2.3–50.0, Pb.05). Women with a past history of ED had
significantly higher risk of laxatives use compared to
nonobese controls (OR=4.7, 1.4–16.2, P=.01). Both
women with a recent ED and with a past history of ED
had a significantly higher risk of self-inducing vomiting
during the first 18 weeks of pregnancy compared to
nonobese controls (respectively OR=51.9, 26.4–102.1,
Pb.001; OR=5.9, 3.3–10.5, Pb.001) and obese controls
(respectively OR=67.6, 18.4–248.2, Pb.001; OR=7.6, 2.2–
26.9, Pb.001). High exercise in pregnancy was more
common in women with a recent ED and women with
past ED compared to obese and nonobese controls.
Women with recent ED had comparable rates to women
with past ED (see Table 2).
Weight and dieting domains at 32 weeks
(third trimester of pregnancy)
Dieting for weight loss before pregnancy was highly
prevalent (N80%) amongst women with ED and obese
women and more common than amongst nonobese
controls (57%). The reported prevalence of dieting for
weight loss during pregnancy decreased dramatically
Obese
(681) (c)
Nonobese controls
(11,184 ) (d) Group comparisonsa
28.0 (4.8) 28.2 (4.8) abb**,d*
bNc**,d**
33.9 (3.8) 22.3 (2.7) aNb***,d***
bbd**
cNa***
b***,d***
–1.1) 64.8% (1.5, 1.3–1.8) 54.8% Ref cNa*,b***,d***
–1.4) 97.9% (1.1, 0.6–2.0) 97.6% Ref. a=b=c=d
–1.1) 40.7% (0.7, 0.6–0.8) 48.5% Ref cNa*,d***
italics).
own: (a) recent ED, (b) past ED, (c) obese controls, (d) nonobese controls.
on, training vs. unemployed, housewives or retired.

N. Micali et al. / Journal of Psychosomatic Research 63 (2007) 297–303300
(about four times lower) in all groups. Women with ED
(recent ED: OR=5.1, 2.1–11.9, Pb.001; past ED: OR=1.8,
1.1–3.1, Pb.05) and obese (OR=3.4, 2.5–4.8, Pb.001)
were more likely to diet in pregnancy than nonobese
controls. Women with recent ED had the highest preva-
lence of dieting, followed by obese women and women
with past ED (see Table 2).
At 32 weeks in pregnancy women with recent or past
ED were more likely to report a strong desire to lose
weight (respectively OR=6.1, 3.4–10.7, Pb.001; OR=1.6,
1.3–2.0, Pb.001), that they bfelt they had put on too
much weightQ (respectively OR=2.5, 1.3–4.8, Pb.01;
OR=1.4, 1.1–1.7, Pb.01), a loss of control over eating
(respectively OR=4.6, 2.5–8.6, Pb.001; OR=1.3, 1.1–1.6,
Pb.01), and a high concern about weight gain (respec-
tively OR=2.4, 1.2–4.7, Pb.01; OR=1.3, 1.0–1.6, Pb.05)
compared to nonobese controls. Obese women shared a
strong likelihood of bfeeling they had put on too much
weightQ with women with recent or past ED compared to
nonobese controls (62%, OR=1.2, 1.1–1.5, Pb.01) and a
strong desire to lose weight (OR=2.1, 1.7–2.5, Pb.001)
(Table 2). More women with recent ED had negative
cognitions about weight gain compared to women with
past ED and obese women.
Table 2
ED behaviors before (lifetime) and during pregnancy (18 weeks), dieting and weig
regression and pairwise comparisons
Recent ED
(57) (a)
Past ED
(395) (b)
Lifetime laxative use 42.9% (OR=20.6, 11.6–36.6) 35.1% (OR=14.8, 11.6–1
Lifetime SIV 59.2% (OR=35.8, 20.1–64.0) 49.0% (OR=23.7, 18.9–3
18 weeks
Pregnancy laxative
use (twice or more)
8.2% (OR=49.6, 16.1–152.5) 0.8% (OR=4.7, 1.4–16.2
Pregnancy SIV
(twice or more)
26.5% (OR=51.9, 26.4–102.1) 3.9% (OR=5.9, 3.3–10.5
High exercise
in pregnancy
32.7% (OR=1.8, 1.0–3.3) 31.2% (OR=1.7, 1.3–2.1
32 weeks
Dieting in pregnancy 11.3% (OR=5.1, 2.1–11.9) 4.4% (OR=1.8, 1.1–3.1)
Strong desire to
lose weight
63.5% (OR=6.1, 3.4–10.7) 31.4% (OR=1.6, 1.3–2.0
Put on too much
weight
76.9% (OR=2.5, 1.3–4.8) 64.9% (OR=1.4, 1.1–1.7
Loss of control
over eating
72.5% (OR=4.6, 2.5–8.6) 42.8% (OR=1.3, 1.1–1.6
Concern about
weight gain
78.8% (OR=2.4, 1.2–4.7) 66.1% (OR=1.3, 1.0–1.6
*Pb.05, **Pb.01, ***Pb.001.
Odds ratios are presented for comparisons between index groups and general popa Only comparisons showing statistically significant group differences are sh
EDE-Q scores in pregnancy
Complete weight concern data were available on 10,962
women. Mean weight concern scores pre-pregnancy and
during pregnancy were significantly higher for all ED groups
and obese women compared to nonobese controls (overall
F(3, 10986)=234.68, Pb.001 for pre-pregnancy scores; overall
F(3, 11091)=126.90, Pb.001 for pregnancy scores). Weight
concern scores decreased in pregnancy in all groups.
However, the change score over time was significantly
different in the recent ED group (b coefficient: �0.1,Pb.05) and the obese group (b coefficient: �0.2, Pb.001)only. These two groups changed in a comparable fashion
(Fig. 1) and differently from the other two groups.
Complete shape concern data were available on 10,955
women. Mean shape concern scores pre-pregnancy and
during pregnancy were higher for all groups (ED groups
and obese controls) compared to nonobese controls (overall
F(3, 10983)=231.52, Pb.001 for pre-pregnancy scores, overall
F(3, 11085)=65.43, Pb.001 for during pregnancy scores).
Shape concern scores decreased in pregnancy for obese
women and women with recent ED; the change score was
different for women with recent ED (b coefficient: �0.2,P=.003) and obese women (b coefficient: �0.3, Pb.001)
ht perception at 32 weeks: prevalence and odds ratios (OR), binary logistic
Obese controls
(618) (c)
Nonobese controls
(11,184) (d) Group comparisonsa
8.9) 4.8% (OR=1.4, 0.9–2.0) 3.5% aNc***,d***
bNc***,d***
0.0) 4.6% (OR=1.2, 0.8–1.8) 3.9% aNc***,d***
bNc***,d***
) 0.2% (OR=0.9, 0.1–7.4) 0.2% aNb*, c**,d***
bNd*
) 0.5% (OR=0.8, 0.2–2.4) 0.7% aNb***, c***,d***
bNc***,d***
) 19.7% (OR=0.9, 0.7–1.1) 21.2% aNc*,d*
bNc***,d***
8.0% (OR=3.4, 2.5–4.8) 2.5% aNb*,d***
cNb*,d***
bNd*
) 37.3% (OR=2.1, 1.7–2.5) 22.2% aNb***, c***,d***
bNd*** ,cNd***
) 62.0% (OR=1.2, 1.1–1.5) 56.9% aNc*,d**
bNd**, cNd**
) 33.8% (OR=0.9, 0.7–1.1) 36.1% aNb***, c***,d***
bNc**,d**
) 62.6% (OR=1.1, 0.9–1.3) 60.5% aNc**,d**
bNd*
ulation controls.
own: (a) recent ED, (b) past ED, (c) obese controls, (d) nonobese controls.
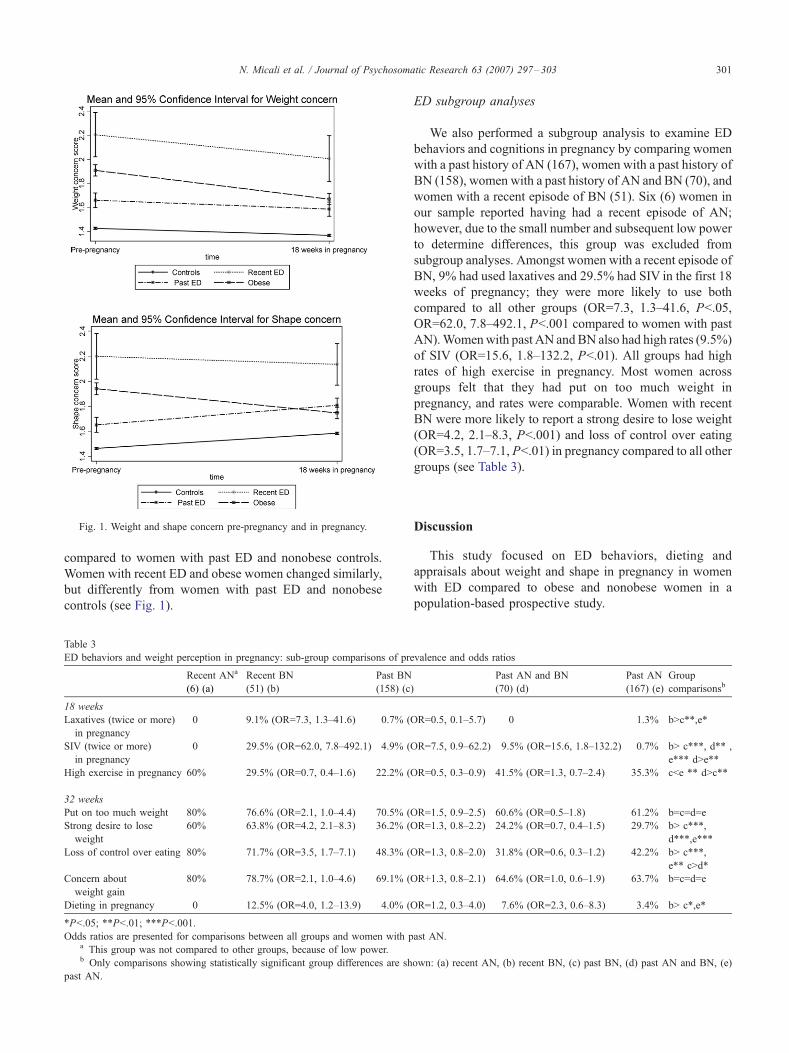
Fig. 1. Weight and shape concern pre-pregnancy and in pregnancy.
N. Micali et al. / Journal of Psychosomatic Research 63 (2007) 297–303 301
compared to women with past ED and nonobese controls.
Women with recent ED and obese women changed similarly,
but differently from women with past ED and nonobese
controls (see Fig. 1).
Table 3
ED behaviors and weight perception in pregnancy: sub-group comparisons of pr
Recent ANa
(6) (a)
Recent BN
(51) (b)
Past BN
(158) (c
18 weeks
Laxatives (twice or more)
in pregnancy
0 9.1% (OR=7.3, 1.3–41.6) 0.7% (
SIV (twice or more)
in pregnancy
0 29.5% (OR=62.0, 7.8–492.1) 4.9% (
High exercise in pregnancy 60% 29.5% (OR=0.7, 0.4–1.6) 22.2% (
32 weeks
Put on too much weight 80% 76.6% (OR=2.1, 1.0–4.4) 70.5% (
Strong desire to lose
weight
60% 63.8% (OR=4.2, 2.1–8.3) 36.2% (
Loss of control over eating 80% 71.7% (OR=3.5, 1.7–7.1) 48.3% (
Concern about
weight gain
80% 78.7% (OR=2.1, 1.0–4.6) 69.1% (
Dieting in pregnancy 0 12.5% (OR=4.0, 1.2–13.9) 4.0% (
*Pb.05; **Pb.01; ***Pb.001.
Odds ratios are presented for comparisons between all groups and women with pa This group was not compared to other groups, because of low power.b Only comparisons showing statistically significant group differences are sh
past AN.
ED subgroup analyses
We also performed a subgroup analysis to examine ED
behaviors and cognitions in pregnancy by comparing women
with a past history of AN (167), women with a past history of
BN (158), women with a past history of AN and BN (70), and
women with a recent episode of BN (51). Six (6) women in
our sample reported having had a recent episode of AN;
however, due to the small number and subsequent low power
to determine differences, this group was excluded from
subgroup analyses. Amongst women with a recent episode of
BN, 9% had used laxatives and 29.5% had SIV in the first 18
weeks of pregnancy; they were more likely to use both
compared to all other groups (OR=7.3, 1.3–41.6, Pb.05,
OR=62.0, 7.8–492.1, Pb.001 compared to women with past
AN).Womenwith past AN andBN also had high rates (9.5%)
of SIV (OR=15.6, 1.8–132.2, Pb.01). All groups had high
rates of high exercise in pregnancy. Most women across
groups felt that they had put on too much weight in
pregnancy, and rates were comparable. Women with recent
BN were more likely to report a strong desire to lose weight
(OR=4.2, 2.1–8.3, Pb.001) and loss of control over eating
(OR=3.5, 1.7–7.1, Pb.01) in pregnancy compared to all other
groups (see Table 3).
Discussion
This study focused on ED behaviors, dieting and
appraisals about weight and shape in pregnancy in women
with ED compared to obese and nonobese women in a
population-based prospective study.
evalence and odds ratios
)
Past AN and BN
(70) (d)
Past AN
(167) (e)
Group
comparisonsb
OR=0.5, 0.1–5.7) 0 1.3% bNc**,e*
OR=7.5, 0.9–62.2) 9.5% (OR=15.6, 1.8–132.2) 0.7% bN c***, d** ,
e*** dNe**
OR=0.5, 0.3–0.9) 41.5% (OR=1.3, 0.7–2.4) 35.3% cbe ** dNc**
OR=1.5, 0.9–2.5) 60.6% (OR=0.5–1.8) 61.2% b=c=d=e
OR=1.3, 0.8–2.2) 24.2% (OR=0.7, 0.4–1.5) 29.7% bN c***,
d***,e***
OR=1.3, 0.8–2.0) 31.8% (OR=0.6, 0.3–1.2) 42.2% bN c***,
e** cNd*
OR+1.3, 0.8–2.1) 64.6% (OR=1.0, 0.6–1.9) 63.7% b=c=d=e
OR=1.2, 0.3–4.0) 7.6% (OR=2.3, 0.6–8.3) 3.4% bN c*,e*
ast AN.
own: (a) recent AN, (b) recent BN, (c) past BN, (d) past AN and BN, (e)
N. Micali et al. / Journal of Psychosomatic Research 63 (2007) 297–303302
Recent ED
We found that, as hypothesized, over a quarter of women
with a recent ED purged during pregnancy (in particular,
women with recent BN reported high rates of purging
behaviors in the first trimester). About 10% of women with
recent ED also reported dieting for weight loss at 32 weeks,
and high rates of concern about weight gain during the third
trimester of pregnancy. In fact, their EDE-Q shape and
weight concerns, although decreased compared to pre-
pregnancy, remained above those of controls during
pregnancy. This finding is consistent with previous studies,
which have shown that most ED behaviors are present
although not common in pregnancy in women with active
ED [1,3,11]. In our study, laxative use was less common,
compared to SIV in pregnancy. This is in line with the
studies of Blais et al. [5] and Crow et al. [6], which showed
a decreased risk of laxative use in pregnancy, but some risk
of continuing to self-induce vomiting.
As expected women with recent ED had the highest rates
of dieting, of concerns about weight gain, and the highest
EDE-Q subscale scores in pregnancy. These findings
suggest that women with recent ED might benefit from
increased support and help during pregnancy aimed at
stopping or reducing their ED behaviors and cognitions.
Past ED
Compensatory behaviors (i.e., SIV, laxative use, and
excessive exercise) were present in women who had had an
ED in the past; nearly 10% of women with a past history of
ED had purged in the first 18 weeks of pregnancy. Although
lower than previous studies, this finding parallels those by
Mitchell et al. [12] that a high percentage of women with a
history of ED continued to vomit and 15% did so at least
once daily in pregnancy. Regarding weight perception in
pregnancy, these women had similar concerns to obese
women, although higher compared to nonobese controls.
As highlighted by previous studies [4,5], high levels
of some ED symptoms (i.e., high exercise and SIV) can
be present in pregnancy in women with a history of AN
(including those who also had BN in the past). Concerns
about weight gain (in particular a sense of loss of control
over eating) and high EDE-Q shape concern scores in
pregnancy were also very common in these women and
increased in pregnancy compared to pre-pregnancy. This
suggests that negative cognitions about weight gain might
be rekindled during pregnancy in this group. This is an
important group clinically, as these women might not be
linked to services and therefore less likely to have access
to specialist help. Perinatal services should be alerted to
the possibility of ED symptoms resurfacing in pregnant
women with a past ED history, especially given that
women are reluctant to admit to ED to their obstetricians
[2]. Research is needed to determine whether this is just
a temporary resurgence of symptoms with a spontaneous
remission in the post-partum or whether it may lead
to relapse.
No previous studies have compared women with ED to
obese women. Our study suggests that weight gain during
pregnancy might trigger different cognitions in women who
have a history of ED and obese women. As hypothesized,
obese women had low rates of compensatory behaviors in
pregnancy. However, subjective dissatisfaction with weight
gain, desire to lose weight, and dieting in pregnancy were
more common in obese women than in nonobese controls.
Although EDE-Q shape and weight concern scores were
significantly higher in this group in pregnancy than in
nonobese controls, they decreased significantly in preg-
nancy compared to pre-pregnancy. This might suggest that
perhaps the well-being of the baby takes precedence over
these concerns in pregnancy in this group of women.
A number of methodological strengths and weaknesses
warrant mention. This is the first study to investigate ED
symptoms and behaviors in pregnancy in a large prospective
population sample with a sufficient number of cases with a
lifetime ED history and the opportunity to have obese and
nonobese weight comparison groups. The main weakness of
this study is that women were classified according to self-
report of a past or recent ED. It is possible that this
represents an underestimate of cases, given the tendency of
screening measures for ED in community samples to miss
cases. The self-reported lifetime ED behaviors and BMI pre-
pregnancy to an extent confirm the self-reported diagnosis.
Moreover, in a recent study, self-report of ED has been
shown to be comparable to longer and widely used ED
screening instruments for screening purposes in general
population studies [13].
Data on lifetime rates of laxative use and SIV for weight
loss and weight and shape concern were obtained contem-
poraneously to pregnancy data, possibly introducing a recall
bias. No data are available on the exact timing of the
occurrence of the ED, apart from self-reported timing of the
ED described as recent or past. It would have been
interesting to collect data on weight gain in pregnancy or
ED symptoms in the post-natal period, given that some
studies have shown that, although there is a symptom
reduction during pregnancy, ED symptoms will recur after
delivery [3,5,14].
In summary, our findings indicate that, although preg-
nancy might have the effect of improving ED symptoms in
women with a recent onset ED, ED symptoms and
cognitions remain elevated in this group of women. More-
over, women with a past history of ED do experience some
ED symptoms and cognitions during pregnancy. It remains
to be established how significant these are in terms of a
relapse of the ED or the effects on the foetus. In a study on
this same sample, we found that babies of women with a
history of AN were significantly smaller than babies of
controls [15].
Our study suggests that although the appraisal of weight
gain and desire to lose weight in obese women is higher

N. Micali et al. / Journal of Psychosomatic Research 63 (2007) 297–303 303
compared to nonobese women, these women have fewer
concerns compared to eating disordered women. Moreover,
weight and shape concern decline in pregnancy in this group
of women, although they still remain more similar in values
to ED women than nonobese controls, suggesting pregnancy
might have a similar effect on weight and shape concern in
obese women and ED women. It remains to be clarified
what the effects of the high weight and shape concerns
might be in this group, in particular as one study suggested
pregnancy is a risk factor for the development of binge-
eating disorder [16].
Our findings have important clinical implications.
Some researchers have reported that pregnancy might
be a good time to engage women with ED in treatment
[6] as they might be motivated to start changing their
eating behaviors. This could also prevent the recrudes-
cence of symptoms that has been reported to occur in the
post-partum period [1–3]. The recent National Institute of
Clinical Excellence (NICE) guidelines for EDs [17] have
suggested that pregnant women with an ED may need
more intensive prenatal care to ensure adequate prenatal
nutrition and foetal development. In view of our results,
women with a past history of ED should also receive
more intensive prenatal care as this may avoid detrimen-
tal outcomes to the foetus, as well as decrease post-
partum resurgence of ED symptoms. Further studies are
needed to clarify the longitudinal aspect of ED sympto-
matology in women with past and recent AN and BN in
the general population.
Acknowledgments
We are extremely grateful to all the families who took
part in this study, the midwives for their help in recruiting
them, and the whole ALSPAC team, which includes
interviewers, computer and laboratory technicians, clerical
workers, research scientists, volunteers, managers, recep-
tionists, and nurses. The UK Medical Research Council, the
Wellcome Trust, and the University of Bristol provide core
support for ALSPAC. This publication is the responsibility
of the authors. Nadia Micali will serve as guarantor for the
contents of this paper. This research was specifically funded
by the National Alliance for Schizophrenia and Depression
(NARSAD) and the Psychiatry Research Trust. We would
specifically like to thank Dr. Sam Leary for her help with the
data and Prof. Alan Stein for selecting the screening
questions for ED symptomatology that were included in
the questionnaires.
References
[1] Lacey JH, Smith G. Bulimia nervosa. The impact of pregnancy on
mother and baby. Br J Psychiatry 1987;150:777–81.
[2] Lemberg R, Phillip J, Phillips R. The impact of pregnancy on anorexia
nervosa and bulimia. Int J Eat Disord 1989;8:285–95.
[3] Morgan JF, Lacey JH, Sedgwick PM. Impact of pregnancy on bulimia
nervosa. Br J Psychiatry 1999;174:135–40.
[4] Stewart DE, Raskin J, Garfinkel PE, MacDonald OL, Robinson GE.
Anorexia nervosa, bulimia, and pregnancy. Am J Obstet Gynecol
1987;157:1194–8.
[5] Blais MA, Becker AE, Burwell RA, Flores AT, Nussbaum KM,
Greenwood DN, et al. Pregnancy: outcome and impact on sympto-
matology in a cohort of eating-disordered women. Int J Eat Disord
2000;27:140–9.
[6] Crow SJ, Keel PK, Thuras P, Mitchell JE. Bulimia symptoms and
other risk behaviors during pregnancy in women with bulimia
nervosa. Int J Eat Disord 2004;36:220–3.
[7] Carter FA, McIntosh VVW, Joyce PR, Frampton CM, Bulik CM.
Bulimia nervosa, childbirth, and psychopathology. J Psychosom Res
2003;55:357–61.
[8] Golding J, Pembrey M, Jones R. ALSPAC—the Avon Longitudinal
Study of Parents and Children: I Study methodology. Paediatr Perinat
Epidemiol 2001;15:74–87.
[9] Fairburn C, Beglin S. Assessment of eating disorders: interview or
self-report questionnaire? Int J Eat Disord 1994;16:363–70.
[10] Stein A, Stein J, Walters E. Eating habits and attitudes amongst
mothers of children with feeding disorders. Br Med J 1995;310:228.
[11] Rocco PL, Orbitello B, Perini L, Pera V, Ciano RP, Balestrieri M.
Effects of pregnancy on eating attitudes and disorders: a prospective
study. J Psychosom Res 2005;59:175–9.
[12] Mitchell JE, Seim HC, Glotter D, Soll EA, Pyle RL. A
retrospective study of pregnancy in bulimia nervosa. Int J Eat
Disord 1991;10:209–14.
[13] Keski-Rahkonen A, Sihvola E, Raevuori A, Kaukoranta J, Bulik CM,
Hoek HW, Rissanen A, Kaprio J. Reliability of self-reported eating
disorders: optimizing population screening. Int J Eat Disord 2006;
39:754–62.
[14] Stein A, Fairburn CG. Eating habits and attitudes in the postpartum
period. Psychosom Med 1996;58:321–5.
[15] Micali N, Simonoff E, Treasure J, ALSPAC. Risk of adverse perinatal
outcomes inwomenwith eating disorders. Br J Psychiatry 2007;255–9.
[16] Fairburn CG, Doll HA, Welch SL, Hay PJ, Davies BA, O’Connor
ME. Risk factors for binge eating disorder: a community-based, case-
control study. Arch Gen Psychiatry 1998;55:425–32.
[17] National Collaborating Centre for Mental Health. Core interventions in
the treatment and management of anorexia nervosa, bulimia nervosa
and related eating disorders. Eat Disord 2004 [Clinical Guideline 9].




















