
Earthquakes and People's Health
206
Earthquakes and People's Health
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of Earthquakes and People's Health

Earthquakes and People's Health

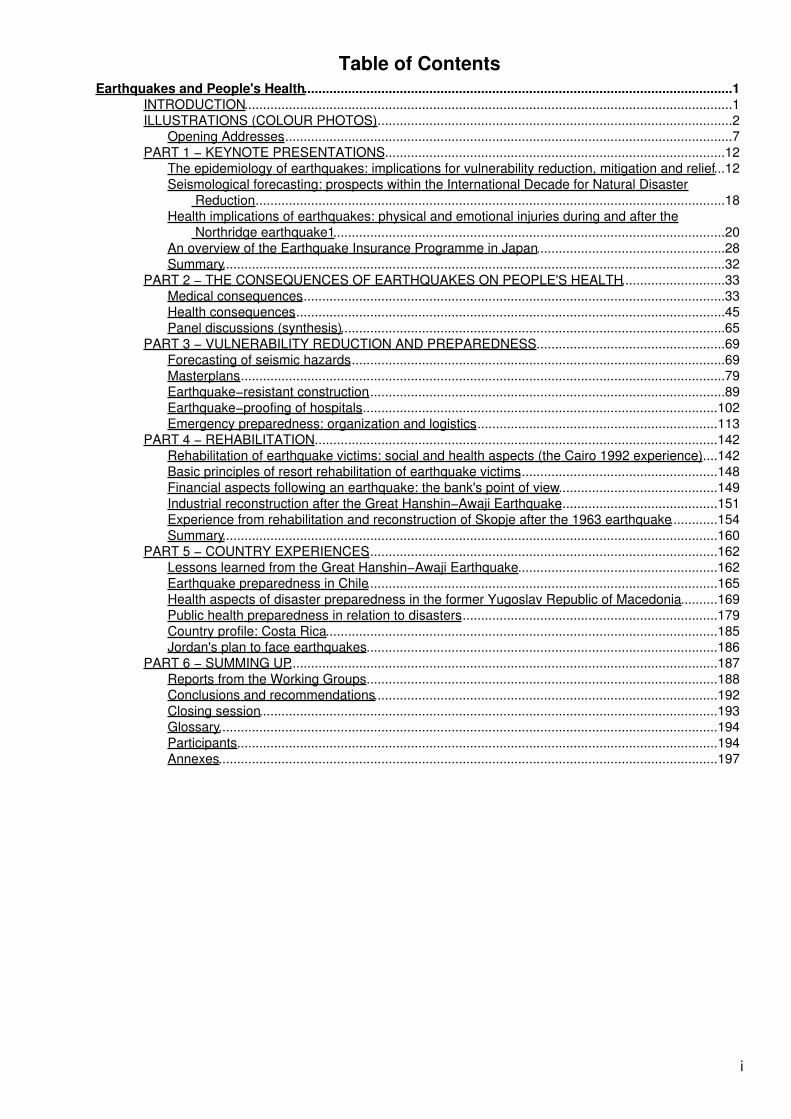
Table of ContentsEarthquakes and People's Health....................................................................................................................1
INTRODUCTION....................................................................................................................................1ILLUSTRATIONS (COLOUR PHOTOS).................................................................................................2
Opening Addresses..........................................................................................................................7PART 1 − KEYNOTE PRESENTATIONS............................................................................................12
The epidemiology of earthquakes: implications for vulnerability reduction, mitigation and relief...12Seismological forecasting: prospects within the International Decade for Natural Disaster
Reduction................................................................................................................................18Health implications of earthquakes: physical and emotional injuries during and after the
Northridge earthquake1..........................................................................................................20An overview of the Earthquake Insurance Programme in Japan...................................................28Summary........................................................................................................................................32
PART 2 − THE CONSEQUENCES OF EARTHQUAKES ON PEOPLE'S HEALTH............................33Medical consequences...................................................................................................................33Health consequences.....................................................................................................................45Panel discussions (synthesis)........................................................................................................65
PART 3 − VULNERABILITY REDUCTION AND PREPAREDNESS...................................................69Forecasting of seismic hazards......................................................................................................69Masterplans....................................................................................................................................79Earthquake−resistant construction.................................................................................................89Earthquake−proofing of hospitals.................................................................................................102Emergency preparedness: organization and logistics..................................................................113
PART 4 − REHABILITATION.............................................................................................................142Rehabilitation of earthquake victims: social and health aspects (the Cairo 1992 experience).....142Basic principles of resort rehabilitation of earthquake victims......................................................148Financial aspects following an earthquake: the bank's point of view...........................................149Industrial reconstruction after the Great Hanshin−Awaji Earthquake...........................................151Experience from rehabilitation and reconstruction of Skopje after the 1963 earthquake.............154Summary......................................................................................................................................160
PART 5 − COUNTRY EXPERIENCES...............................................................................................162Lessons learned from the Great Hanshin−Awaji Earthquake......................................................162Earthquake preparedness in Chile...............................................................................................165Health aspects of disaster preparedness in the former Yugoslav Republic of Macedonia..........169Public health preparedness in relation to disasters......................................................................179Country profile: Costa Rica..........................................................................................................185Jordan's plan to face earthquakes...............................................................................................186
PART 6 − SUMMING UP....................................................................................................................187Reports from the Working Groups...............................................................................................188Conclusions and recommendations.............................................................................................192Closing session............................................................................................................................193Glossary.......................................................................................................................................194Participants..................................................................................................................................194Annexes.......................................................................................................................................197
i

ii

Earthquakes and People's Health
WHO/WCK/SYM/97.1ENGLISH ONLYDISTR: GENERAL
WORLD HEALTH ORGANIZATIONCENTRE FOR HEALTH DEVELOPMENT
KOBE, JAPAN
Earthquakes and People's HealthVulnerability Reduction, Preparedness and Rehabilitation
PROCEEDINGS OF A WHO SYMPOSIUMKOBE, 27−30 JANUARY 1997
World Health Organization1997
This document is not a formal publication of the World Health Organization (WHO), and all rights are reservedby the Organization. The document may, however, be freely reviewed, abstracted, reproduced or translated,in part or in whole, but not for sale or for use in conjunction with commercial purposes.
The texts in this document by named authors are based on their presentations at the WHO Symposium
"Earthquakes and People's Health − Vulnerability Reduction, Preparedness and Rehabilitation" held at Kobe,Japan, 27−30 January 1997.
The views expressed in documents by named authors are solely the responsibility of those authors.
INTRODUCTION
The International Symposium on Earthquakes and People's Health, held in Kobe from 27 to 30 January 1997,was an important event for three main reasons.
Firstly, the symposium commemorated the second anniversary of the Great Hanshin−Awaji Earthquake whichstruck the urban areas of Kobe, leaving 6300 people dead, 30 000 injured and 300 000 homeless. Distressingas they may be, statistics of human and material loss can never adequately express the extent of sufferingand disruption caused by such disasters which call for the utmost sympathy and support.
The amount of casualties and damage caused by earthquakes worldwide has increased markedly over thelast decades. Urbanization and modern technology have brought with them many benefits for our daily livesbut they also increase specific risks for people's health and the environment. Such risks must be carefullyassessed and taken into account by town planners as urbanization is expected to grow steadily. It isestimated that by the year 2000 half of the world's population will live in urban areas.
Secondly, this was already the second symposium held by the WHO Kobe Centre for Health Developmentduring its first year of existence. I wish to acknowledge the generous support of the Hyogo−Kobe communityto the Centre which made it possible to organize this symposium and express my gratitude to the HyogoPrefecture, the City of Kobe and Kobe Steel Ltd. As a result of the symposium, the WHO Centre itself is nowbetter equipped to enhance its research and cooperation activities in support of health development bothlocally and worldwide.
Thirdly, the symposium attracted 190 participants from 21 countries, five international organizations and alarge variety of disciplines. Representation was truly intersectoral and useful proposals were made for tacklingnot only the health consequences of earthquakes but also issues related to vulnerability reduction. Theseinclude recommendations for improved structural standards, organization and logistics. The importance ofcommunity participation was stressed to enable rapid and effective emergency response, particularly in thefirst hours after an earthquake. This requires careful planning, management and training, far ahead of time.
1
Coordination must be ensured, between central and local governments as well as with the local people andvolunteers. Similarly, the long−term harm done by disasters can be overcome more quickly if rehabilitationactivities are well coordinated and involve consultation and participation of the local communities.
Guidelines on the rapid assessment of health needs in cases of emergency, and on community preparedness,are being prepared by WHO in close cooperation with UNHCR, UNICEF, the Red Cross and Red CrescentSocieties and Médecins Sans Frontières.
The International Symposium on Earthquakes and People's Health, held by the WHO Kobe Centre for HealthDevelopment, has made an important contribution to WHO’s overall activities in the areas of standard−setting,technical cooperation and public information, which are all essential parts of its Constitutional mandate.
Hiroshi Nakajima, M.D., Ph.D.Director−General
ILLUSTRATIONS (COLOUR PHOTOS)
Photo credits
Fig. 1: Collapsed elevated freeway in center of Kobe, courtesy of The Japan Society of Civil Engineers
Fig. 2: Central part of Kobe destroyed by fire, courtesy of Swiss Reinsurance Company, Zurich, Switzerlandand Christian Brauner, Freiburg i. Breisgau, Germany
2
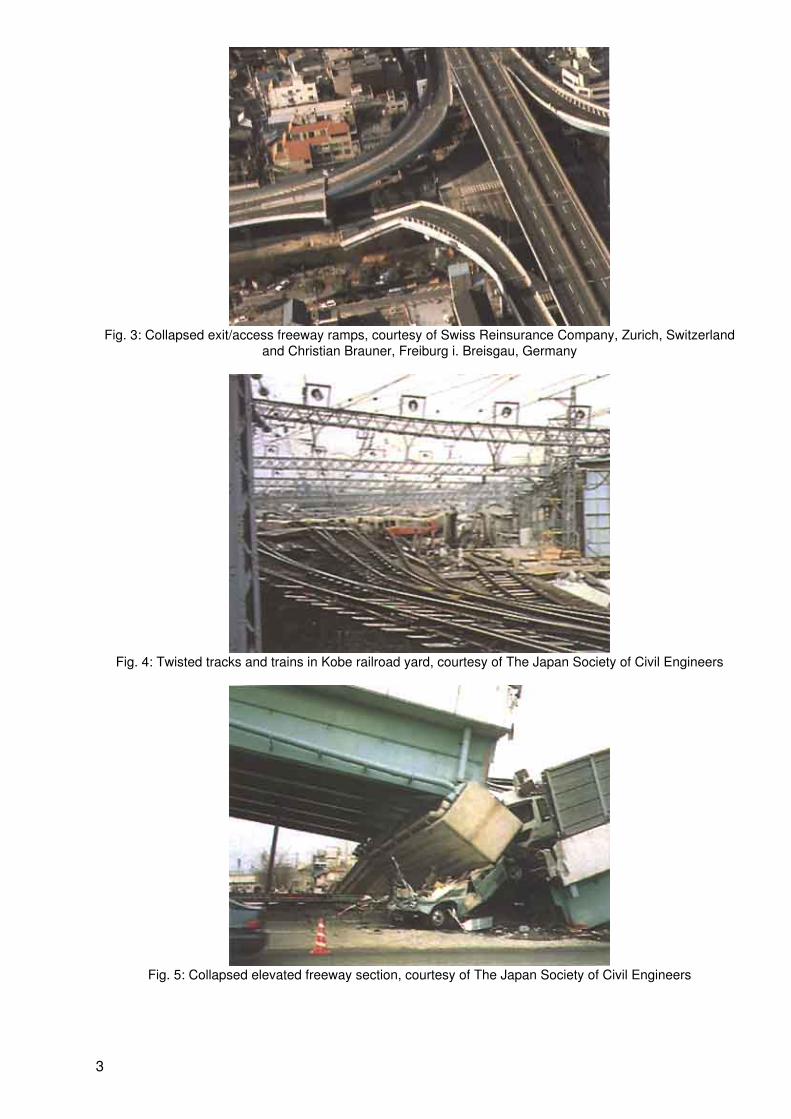
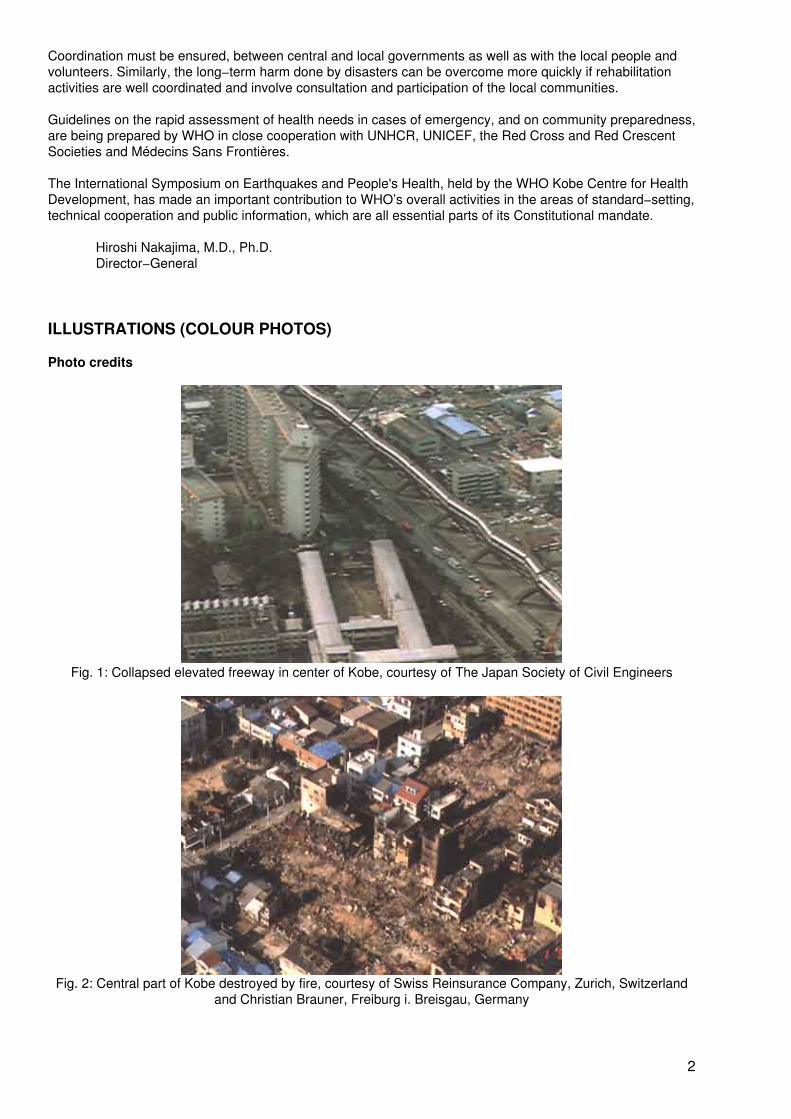
Fig. 3: Collapsed exit/access freeway ramps, courtesy of Swiss Reinsurance Company, Zurich, Switzerlandand Christian Brauner, Freiburg i. Breisgau, Germany
Fig. 4: Twisted tracks and trains in Kobe railroad yard, courtesy of The Japan Society of Civil Engineers
Fig. 5: Collapsed elevated freeway section, courtesy of The Japan Society of Civil Engineers
3
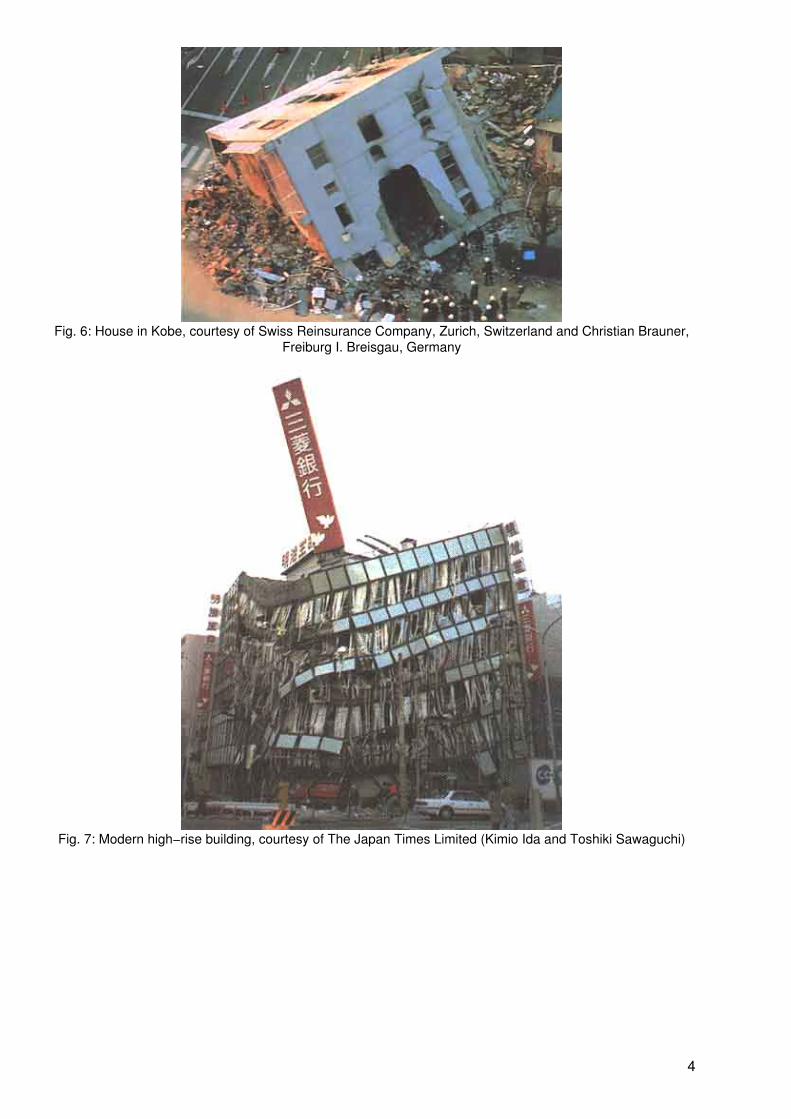
Fig. 6: House in Kobe, courtesy of Swiss Reinsurance Company, Zurich, Switzerland and Christian Brauner,Freiburg I. Breisgau, Germany
Fig. 7: Modern high−rise building, courtesy of The Japan Times Limited (Kimio Ida and Toshiki Sawaguchi)
4
Fig. 8: Port facilities, courtesy of The Japan Society of Civil Engineers
Fig. 9: Concrete building, courtesy of Prof. Nagasawa, Tokyo University
5
Fig. 10: Document storage, courtesy of Prof. Nagasawa, Tokyo University
Fig. 11: X−ray equipment, courtesy of Prof. Nagasawa, Tokyo University
6
Fig. 12: Computer equipment, courtesy of Prof. Nagasawa, Tokyo University
Front cover: View of Kobe, courtesy of Hyogo Prefectural Government
Back cover: Kobe Street, courtesy of Swiss Reinsurance Company, Zurich, Switzerland and ChristianBrauner, Freiburg i. Breisgau, Germany
Opening Addresses
A. Wojtczak, Director, WHO Centre for Health Development
The topic of the International Symposium on Earthquakes and People's Health is of global significance andmarks the second anniversary of the Great Hanshin−Awaji Earthquake which struck Kobe in 1995.
In different parts of the world tragic disasters due to earthquakes or cyclones quite often occur, and effectiveemergency preparedness today goes beyond what the health sector can do alone. Therefore, if we want theimpact of disasters to be reduced, institutional and sectoral barriers have to be broken down, and planningand implementation of emergency preparedness should from its inception involve all sectors andorganizations that have a role to play when disaster strikes.
Disasters also have long−term effects on the physical and mental health of the population, and these effectshave not attracted enough attention from the point of view of preventive measures. Therefore, the aim of oursymposium is to cover both short−term and long−term aspects of health, based on national and internationalexperiences. The symposium provides a forum for the exchange of cross−sectoral and multidisciplinaryknowledge on issues related to earthquakes and health. In addition, there will be an opportunity to learn fromKobe's earthquake experience.
The subtitle of the symposium, "Vulnerability Reduction, Preparedness and Rehabilitation" states quite clearlywhere we would like to see the lessons learned being applied in the future. The keynote presentationsintroduce the most important underlying issues, followed by more details on short−term and long−term effectsas well as rehabilitation and prevention.
The three−and−a−half day programme features six plenary sessions, four panel discussions, three parallelworkshops and a field visit to the Kobe earthquake sites. The outcomes of the symposium should provideadvice to policy−makers and experts in the field and should identify areas where further research may berequired.
The organization of this international symposium is an expression of our deep appreciation to the people andthe authorities of the Hyogo−Kobe community which, despite the disastrous effects of the earthquake whichstruck this city, went ahead and established this Centre. It is also a symbol of the determination of the people
7
of Kobe and a contribution to the health of people throughout the world. Therefore, I should like to express ourthanks to the people of Kobe and our admiration to Hyogo Prefecture and Kobe City administrations for theirmodem and far−sighted vision that resulted in a speedy recovery from this disaster.
H. Nakajima, Director−General, World Health Organization
I am pleased to welcome you all to this international symposium, the second to be organized by the WHOCentre for Health Development in Kobe since it was inaugurated in March 1996.
During this symposium you will deal with the subject of earthquakes and people's health, a topic of majorimportance to the global community and to the people of Japan in particular. Two years ago, the GreatHanshin−Awaji Earthquake struck the urban area of Kobe. It is difficult to adequately express the extent ofsuffering and disruption caused by such disasters which endure for a long time.
In the last decade, several highly destructive earthquakes have hit urban areas: Mexico City in 1985, Spitak(Armenia) in 1988, Loma Prieta (USA) in 1990, Erzincan (Turkey) in 1992, Northridge in 1994 and finally Kobein 1995. These earthquakes have shown the devastating impact disasters can have on areas with highpopulation densities. An additional and major factor of risk for people's health in these areas is theconcentration of industrial hazards such as chemical or nuclear plants. This underscores the importance ofplanning and coordinating carefully at all stages of urban development, so as to reduce the city's overallvulnerability to both natural and man−made disasters.
The United Nations General Assembly designated the 1990s as the International Decade of Natural DisasterReduction, focusing on the cycle of prevention, mitigitation, preparedness, response and recovery. Within itsown area of competence, WHO has been an active partner in this international cooperation effort. Inparticular, it has promoted multisectoral approaches to emergency management, vulnerability analysis andplanning. These include designing frameworks for country programmes, working out technical standards andindicators, and providing support for training.
WHO has a global network of collaborating centres which is an extremely valuable source of expertise onspecific aspects of emergency preparedness and response. Since 1992, a WHO expert panel has advisedMember States on emergency−related issues and humanitarian action. We have been developing closeworking relations with various partners in the public and private sectors, including intergovernmental,nongovernmental and community−based organizations.
One important part of WHO’s work in the area of vulnerability reduction and emergency preparedness is thedefinition of standards and guidelines and their dissemination through the publication of manuals on technicalmatters related to this area of responsibility. A number of these manuals are prepared in partnership with suchbodies as the Office of the United Nations High Commissioner for Refugees (UNHCR), UNICEF, theInternational Committee of the Red Cross, the International Federation of Red Cross and Red CrescentSocieties and Médecins Sans Frontières. At present we are preparing guidelines on:
− rapid health assessment, to ensure an effective response to the immediate health needs ofthe population in an emergency;
− community preparedness, to assist local government, planning officers and communityleaders in building up their capacity to prepare for and respond to emergencies.
The work cosponsored by WHO also covers issues such as environmental health, nutritional needs, andgeneric specifications for emergency relief items. These specifications include guidelines for drug donation.WHO has repeatedly drawn attention to the need to ensure that donated emergency medical aid should beappropriate, safe and effective. This standardization work must be done in advance, as part of emergencypreparedness, so that precious time and manpower are not wasted on sorting out donations when disastersoccur and thousands of people have to be cared for urgently with safe and effective drugs and equipment.
There are many illustrations of the need for such standardization. After the Armenian earthquake in 1988,5000 tonnes of medical supplies and drugs were donated. Of the 2500 tonnes of drugs sent, only one−thirdwas immediately usable; nearly a quarter had to be rejected or destroyed upon arrival, and one−fifth wasinappropriate for an emergency. In the recent Rwandan crisis, a large donation of unwanted and unrequestedantibiotics was sent. Aid workers and local health officials then had to find a way to destroy six million tablets,
8
which presented an added risk of producing multidrug resistance in the local population. Clearly, internationalagreement is needed on which medical supplies and drugs are most necessary in the early phases of anemergency. This will contribute to providing care, avoiding waste, and improving the effectiveness andcoordination of national and international action.
Another important part of our work is related to prevention. In earthquake−prone areas, particularly largecities, this involves advocating and supporting the improvement of construction standards and reinforcementof infrastructure such as bridges, elevated roads and railway lines. I know that the Japan Civil EngineeringAssociation, for example, is devoting much of its attention to this very difficult problem, learning from the tragicKobe experience. "Cities at risk" was the 1996 theme of the United Nations International Decade for NaturalDisaster Reduction. The theme was part of the Habitat II agenda, which dealt with the more general issue ofhuman settlements and town planning for the next century. Cities are growing rapidly, especially in thedeveloping countries: by the year 2000, half the world's population will be living in urban areas, and by theyear 2025, 80% of these urban areas will be in the developing world.
There are many ways in which the health sector can contribute to making cities less vulnerable. These includeclose cooperation with town planners and local government to prevent the development in urban areas ofindustries that would present major health risks in an emergency. Preparedness in the health sector shouldinclude training health professionals to deal with emergencies, ensuring proper construction and maintenanceof, and access to hospitals and health care centres, enlisting community participation in identifying risks, andproviding information and resources to deal with them. In 1994, the World Conference on Natural DisasterReduction adopted the Yokohama Strategy and Plan of Action for a Safer World in the 21st Century. Toachieve vulnerability reduction, the strategy highlights the importance of community−based approaches,training, and involvement at all stages of intervention, including planning. The strategy stresses thatpreventive measures are most effective when they involve participation at all levels, from the local community,through national government, to the international community. Well−prepared communities can stopemergencies from turning into disasters.
The mission of the WHO Kobe Centre for Health Development is to carry out research on the relationsbetween health and its determinants, including social, demographic, economic, technological andenvironmental factors. As emphasized by its Executive Board, WHO has an essential role to play in facilitatingthe exchange of information, knowledge and know−how among various partners from both the public and theprivate sectors, including civil society, and drawing on the wealth of scientific data, expertise and experiencethat is available around the world. The Executive Board particularly stressed the importance of taking fulladvantage of WHO’s network of collaborating centres. A key function of the WHO Centre in Kobe should be toserve as a hub for such networking.
The first symposium held by the WHO Kobe Centre in March 1996 focused on urbanization and the complexchallenge it presents worldwide. It dealt with the public management of urban health, including theorganization of health systems and services, and the problems linked to housing, water, sanitation and wastemanagement. It also touched on the issue of health emergencies in large−scale urban disasters. TheInternational Symposium on Earthquakes and People's Health takes up many of these issues again but with aslightly different perspective.
At the end of 1996, WHO devoted an issue of its World Health magazine to health needs in natural andman−made emergencies. As the magazine rightly puts it, we live in a world fraught with danger. And while wemust keep up our effort to improve preventive measures and early warning systems, we must also be awarethat some risk will always remain. In the face of danger, preparedness and response can be effective only ifwe join forces and act together. Solidarity and coordination at local, national and international levels areindispensable for reducing vulnerability, caring for the afflicted, and restoring the life and hope of the wholecommunity.
The strong support of the Kobe community and officials, the Hyogo Prefecture, and the Japanese governmentfor this WHO Centre demonstrates their determination to be part of this movement for international solidarityand coordination in support of health research and development. I should like to express our sincere gratitudeto them all and our firm commitment to the Kobe Centre and its objectives.
9
S.T. Han, Regional Director, WHO Regional Office for the Western Pacific
It is a great pleasure for me to join the Director−General, Dr Nakajima, in congratulating the WHO Centre forHealth Development for organizing this important symposium. I also wish to add my personal thanks and myendorsement for this important initiative.
History has shown that humanity is indeed extremely vulnerable to earthquakes, cyclones, epidemics, famine,floods and other such natural disasters. A large number of countries of the Western Pacific Region are part ofthe ring of fire of the Pacific and are particularly vulnerable to earthquakes, tsunamis and volcanic eruptions−We are currently acutely aware of this as we continue to see the suffering from the 1991 volcanic eruption ofMount Pinatubo in the Philippines and of course from the Great Hanshin−Awaji Earthquake in Japan. Thesewere two of the largest natural disasters to affect our planet in recent years.
On the more positive side, recent history has also shown us that the impact of disasters can often besignificantly mitigated by careful planning and preparedness and through efficient coordination of relief efforts.
We are fortunate in this Region that the international community is most generous in providing emergencyrelief in the form of supplies, helpers, financial aid and valuable experience. Post−disaster action is normallyexpensive and inefficient when compared to a sustained effort of prevention and mitigation. The MountPinatubo eruption and the Kobe earthquake have clearly illustrated the devastating long−term impact ofdisasters. We also recognize that these two events were of an extremely major scale and cannot be taken asthe norm.
The objective of the WHO programme on emergency and humanitarian action in the Western Pacific Regionis to promote and strengthen disaster preparedness in the Member States and to provide a prompt responseto emergencies and disasters in coordination with other organizations.
At this point, I should like to take the opportunity to publicly thank the Government of Japan for the generouscontribution which has enabled us to further this objective. With their support we have been able to developactivities at country level and employ a full−time emergency coordinator.
The experience from the Great Hanshin−Awaji Earthquake demonstrated what concerted and planned actionby the government, communities and individuals is able to achieve. From this experience we can learnlessons for other parts of the Region and other parts of the world.
In order to address the problem, there are a few simple things that we need to focus on. We need to increasethe level of awareness within all sectors of government, within the health authorities, and among the public ofthe need for emergency preparedness and planning with a special emphasis at the community level. We needto see emergency preparedness integrated with overall national development plans, which are so important inthe early post−disaster phase and which should have adequate resources and be well coordinated with allsectors. Finally, I wish to propose that regionally and globally we should look for more effective ways tosupport the training and research that is needed in this important area.
This latter goal touches directly upon the purpose of this meeting and this is why I am very enthusiastic aboutthe potential of this initiative. The topics being addressed regarding the latest information on the epidemiologyof disasters, on planning, logistics, rescue and medical care are all valuable contributions. I am veryencouraged by the opportunity for all of us to further share our experiences and ideas as lessons for thefuture.
Finally, I wish to emphasize my desire to work closely with the WHO Centre in Kobe to support our regionalemergency and humanitarian action programme. I trust that in the near future our staff will have theopportunity to work with you on developing specific forms of joint collaboration. I believe that this collaborationwill have a significant benefit for the people of the Region not only in emergency preparedness but also inother areas of development where we share common goals and vision.
Again I wish to thank the WHO Centre for Health Development for this excellent initiative.
10
T. Kaihara, Governor, Hyogo Prefecture
As a representative of the area affected by the Great Hanshin−Awaji Earthquake, and on behalf of the citizensof Hyogo Prefecture, I should like to thank the WHO Kobe Centre for Health Development for holding theInternational Symposium on Earthquakes and People's Health in commemoration of the second anniversaryof the earthquake.
I should also like to extend a very warm welcome to all of you who have come from all over Japan, as well asfrom around the world, to participate in this symposium.
Two years have already passed since the earthquake. Following the disaster, we received support from thenational government as well as tremendous cooperation from local municipalities and residents, foreigngovernments, and volunteers. I should like to take this opportunity to express our deep gratitude for thekindness. Strengthened by your encouragement, we have been working hard to restore and reconstruct theregion.
While restoring infrastructure such as ports and roads, we have been carrying out various measures toconstruct permanent housing and to assist those who were affected by the earthquake with rebuilding theirlives.
As we enter our third year of reconstruction, we must build on our previous efforts to work towards economicrevitalization and the full restoration of normal life. However, we must not merely return things to the way theywere before the earthquake. We must work to resolve the various issues facing Japan, such as populationageing and the need to create new industries that are suitable for an increasingly global economy. All ourefforts must be based on a brand new concept that paves the way to a more mature society in the 21stcentury.
It is especially significant that the WHO Centre for Health Development should hold an internationalsymposium to exchange knowledge and experience on earthquakes and health. There will be a field visit toareas affected by the Great Hanshin−Awaji Earthquake, as well as a panel discussion on experiences relatingto the earthquake. I hope that observations made during the field visit will contribute to that discussion− I wishthis symposium success and hope that all of you will find your participation both professionally and personallyrewarding.
K. Sasayama, Mayor, Kobe City
I am very pleased that so many participants from Japan and overseas have come to attend the WHOSymposium here in Kobe, and I should like to welcome you sincerely on behalf of our city.
Two years have already passed since the Great Hanshin−Awaji Earthquake. In this time, we in Kobe havecome to more fully understand the importance of gestures of compassion, caring and kindness during times ofgreat difficulty. We can never fully express how much we appreciated and were encouraged by the supportand heartening words we received from all over Japan and around the world while we were facing this mostdifficult time. I thank you all very much for your help and encouragement.
This symposium is intended to provide a forum for experts on health policy and disaster preventive measuresin earthquake−stricken countries to exchange opinions and information. I hope that, as Kobe's experience isconsidered here, the lessons that can be gleaned from our successes and failures will prove valuable forpolicy−making in other areas of the world.
Throughout its history, the city of Kobe has developed and grown with the introduction of foreign culturesthrough its port. This year we celebrate the 130th anniversary of the opening of the Port of Kobe tointernational trade. Now that we are rebuilding the city and preparing to face the challenges of a new century,it is especially significant that we take advantage of our international connections and create opportunities toexchange ideas with people from all over the world.
As we in Kobe learn from your expertise and experience in other regions, I hope that you also will learn muchabout Kobe. I hope that you will take some time to see the recovery work that has been completed, as well asthe projects that are still under way. As we continue this rebuilding process, I ask once again for yourcontinued understanding and support.
11
J. Koizumi, Minister of Health and Welfare, Japan
I wish to offer you my sincere congratulations on the opening of the International Symposium on Earthquakesand People's Health and also to extend my best wishes for the continued success and development of theWHO Kobe Centre.
PART 1 − KEYNOTE PRESENTATIONS
The epidemiology of earthquakes: implications for vulnerability reduction, mitigation and relief
E.K. Noji1
1E.K. Noji M.D., M.P.H, is Chief of the International Emergency and Refugee HealthPrograms, Centers for Disease Control and Prevention (CDC), Atlanta, GA, USA.
Better epidemiological knowledge of the causes of death and types of injuries and illnesses caused byearthquakes is clearly essential for determining what relief supplies are appropriate and what equipment andpersonnel are needed to respond effectively to such situations, as well as to improve preparedness andreduce vulnerability to the effects of future earthquakes. The overall objective of the epidemiology of disastersis to scientifically measure and describe their health effects and the factors that contribute to these effects,with the goals of assessing the needs of disaster−affected populations, efficiently matching resources toneeds, preventing further adverse health effects, evaluating programme effectiveness, and carrying outcontingency planning.
This presentation focuses on the medical and public health impact of earthquakes and outlines a number ofimportant areas where the science of epidemiology can reduce overall vulnerability to earthquakes and cancontribute to improved disaster preparedness and mitigation.
Major components of vulnerability
Until earthquake prevention and control measures are adopted and mitigation actions implementedthroughout the world, a single severe earthquake can cause tens of thousands of deaths and serious injuriesand enormous economic losses.
During the past 20 years, earthquakes alone have caused more than a million deaths worldwide (1). Ninecountries account for more than 80% of all fatalities this century and almost half of all earthquake deaths inthe world during this period have occurred in just one country − China (Fig. 1.1). On 28 July 1976, at 3.42a.m., an earthquake of magnitude 7.8 occurred in Tangshan in the northeastern part of China. In a matter ofseconds, an industrial city of a million people was reduced to rubble and more than 240 000 people werekilled (2). Recent accelerated urbanization in other seismically active parts of the world where populationdensities reach 20 000−60 000 inhabitants per square kilometre underscores the vulnerability of such areas tosimilar catastrophic numbers of earthquake−related deaths and injuries. In the past 10 years the world haswitnessed four catastrophic earthquakes resulting in great loss of life: in Mexico City in 1985 (10 000 deaths);in Armenia in 1988 (25 000 deaths); in Iran in 1990 (40 000 deaths); and in India in 1993 (10 000 deaths)(Table 1.1). The United States has been relatively fortunate in terms of earthquake−related casualties so far(3). Only an estimated 1600 deaths in the USA have been attributed to earthquakes since colonial times, withover 60% of these having been recorded in California. The most serious earthquake in terms of loss of lifewas the 1906 San Francisco earthquake and fire that killed an estimated 700 people.
12
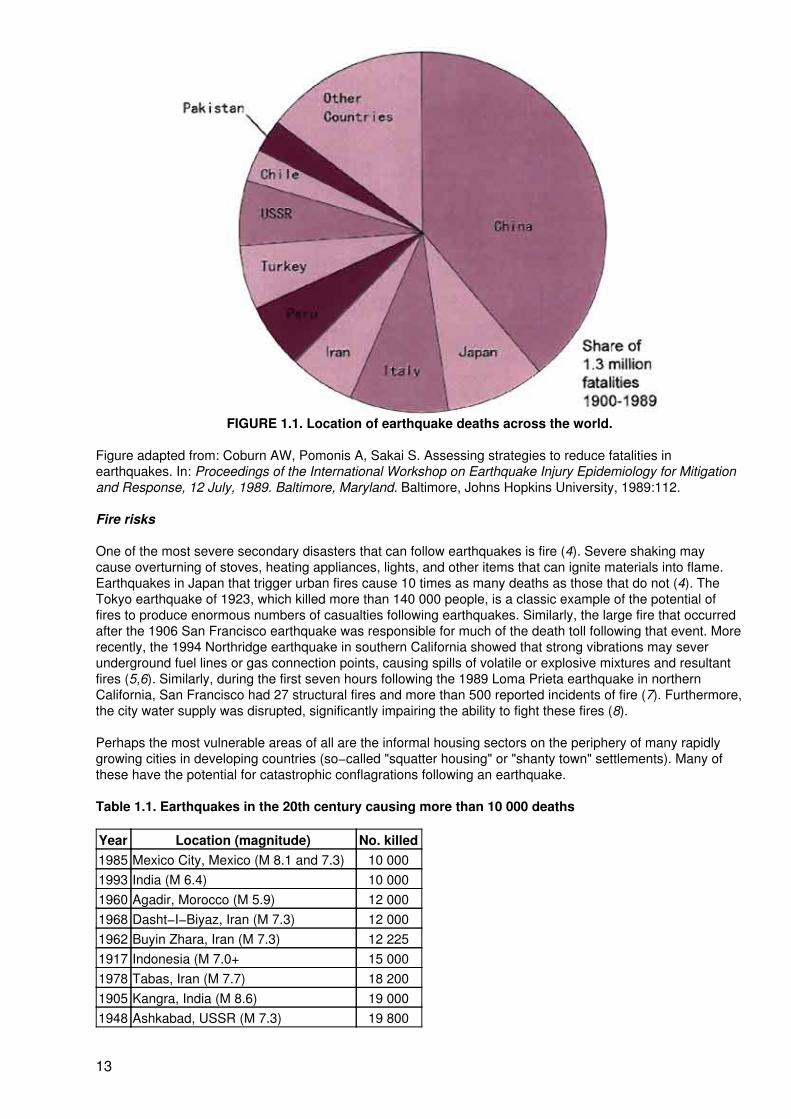
FIGURE 1.1. Location of earthquake deaths across the world.
Figure adapted from: Coburn AW, Pomonis A, Sakai S. Assessing strategies to reduce fatalities inearthquakes. In: Proceedings of the International Workshop on Earthquake Injury Epidemiology for Mitigationand Response, 12 July, 1989. Baltimore, Maryland. Baltimore, Johns Hopkins University, 1989:112.
Fire risks
One of the most severe secondary disasters that can follow earthquakes is fire (4). Severe shaking maycause overturning of stoves, heating appliances, lights, and other items that can ignite materials into flame.Earthquakes in Japan that trigger urban fires cause 10 times as many deaths as those that do not (4). TheTokyo earthquake of 1923, which killed more than 140 000 people, is a classic example of the potential offires to produce enormous numbers of casualties following earthquakes. Similarly, the large fire that occurredafter the 1906 San Francisco earthquake was responsible for much of the death toll following that event. Morerecently, the 1994 Northridge earthquake in southern California showed that strong vibrations may severunderground fuel lines or gas connection points, causing spills of volatile or explosive mixtures and resultantfires (5,6). Similarly, during the first seven hours following the 1989 Loma Prieta earthquake in northernCalifornia, San Francisco had 27 structural fires and more than 500 reported incidents of fire (7). Furthermore,the city water supply was disrupted, significantly impairing the ability to fight these fires (8).
Perhaps the most vulnerable areas of all are the informal housing sectors on the periphery of many rapidlygrowing cities in developing countries (so−called "squatter housing" or "shanty town" settlements). Many ofthese have the potential for catastrophic conflagrations following an earthquake.
Table 1.1. Earthquakes in the 20th century causing more than 10 000 deaths
Year Location (magnitude) No. killed1985 Mexico City, Mexico (M 8.1 and 7.3) 10 0001993 India (M 6.4) 10 0001960 Agadir, Morocco (M 5.9) 12 0001968 Dasht−I−Biyaz, Iran (M 7.3) 12 0001962 Buyin Zhara, Iran (M 7.3) 12 2251917 Indonesia (M 7.0+ 15 0001978 Tabas, Iran (M 7.7) 18 2001905 Kangra, India (M 8.6) 19 0001948 Ashkabad, USSR (M 7.3) 19 800
13
1974 China (M 6.8) 20 0001976 Guatemala City (M 7.5) 23 0001988 Armenia, USSR (M 6.9) 25 0001935 Quetta, Pakistan (M 7.5) 25 0001923 Concepcion, Chile (M 8.3) 25 0001939 Chilián, Chile (M 8.3) 28 0001915 Avezzano, Italy (M 7.5) 32 6101939 Erzincan, Turkey (M 8.0) 32 7001990 Iran (M 7.7) 40 0001927 Tsinghai, China (M 8.0) 40 9121908 Messina, Italy (M 7.5) 58 0001970 Ankash, Peru (M 8.3) 66 7941923 Kanto, Japan (M 8.3) 142 8071920 Kansu, China (M 8.5) 200 0001976 Tangshan, China (M 7.8) 242 000Total Approximately 1 500 000Dams
Dams may also fail, threatening communities downstream. A standard procedure after any sizeableearthquake should be an immediate damage inspection of all dams in the vicinity and a rapid reduction ofwater levels in reservoirs behind any dam suspected of having incurred structural damage.
Structural factors
Trauma caused by partial or complete collapse of man−made structures is overwhelmingly the most commoncause of death and injury in most earthquakes (1). About 75% of fatalities attributed to earthquakes thiscentury were caused by the collapse of buildings that were not adequately designed for earthquakeresistance, were built with inadequate materials, or were poorly constructed (9). Results of field surveysfollowing earthquakes have demonstrated that different building types and structural systems deteriorate indifferent ways when subjected to strong earthquake ground−motion vibration. There is also evidence thatdifferent types of buildings inflict injuries in different ways and to different degrees of severity when theycollapse (10,11,12).
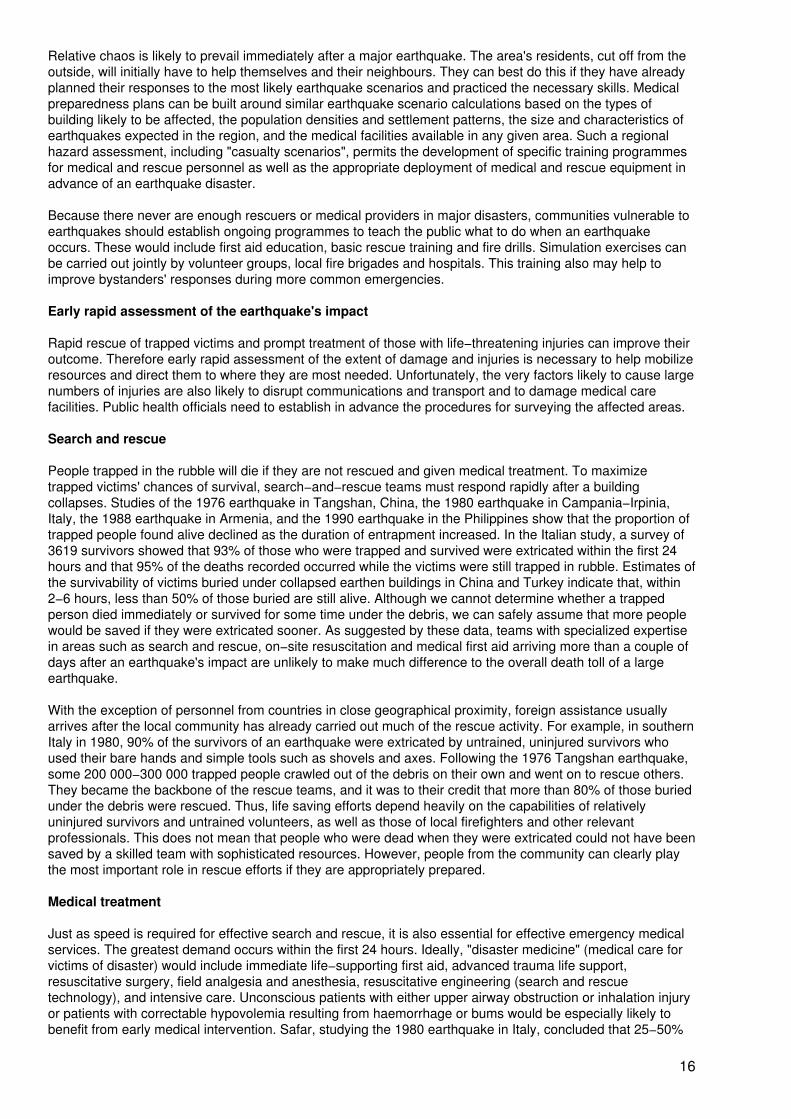
Glass was one of the first in 1976 to apply epidemiology to the study of building collapse (13). He identifiedthe type of housing construction as a major risk factor for injuries. Those living in the newer−style adobehouses were at highest risk for injury or death, while those living in the traditional mud−and−stick houses wereat least risk. Figure 1.2 shows the breakdown of earthquake fatalities by cause for each half of this century. Byfar the greatest proportion of victims died in the collapse of reinforced masonry buildings (e.g. adobe, rubblestone or rammed earth) or unreinforced fired−brick and concrete−block masonry buildings that can collapseeven at low intensities of ground−shaking and will collapse very rapidly at high intensities. Adobe structures inmany highly seismic parts of the world (e.g. Iran, Pakistan, eastern Turkey, Latin America) not only havecollapse−prone walls but also very heavy roofs (13,14). When they collapse, these heavy walls and roofs tendto kill many of the people inside (15,16). Unreinforced masonry buildings abound throughoutearthquake−prone regions of the central United States (e.g., the New Madrid seismic zone). Most of theseunreinforced masonry buildings are not equivalent to ancient construction (like Roman masonry) and remainessentially without retrofits and adequate seismic safety.
14
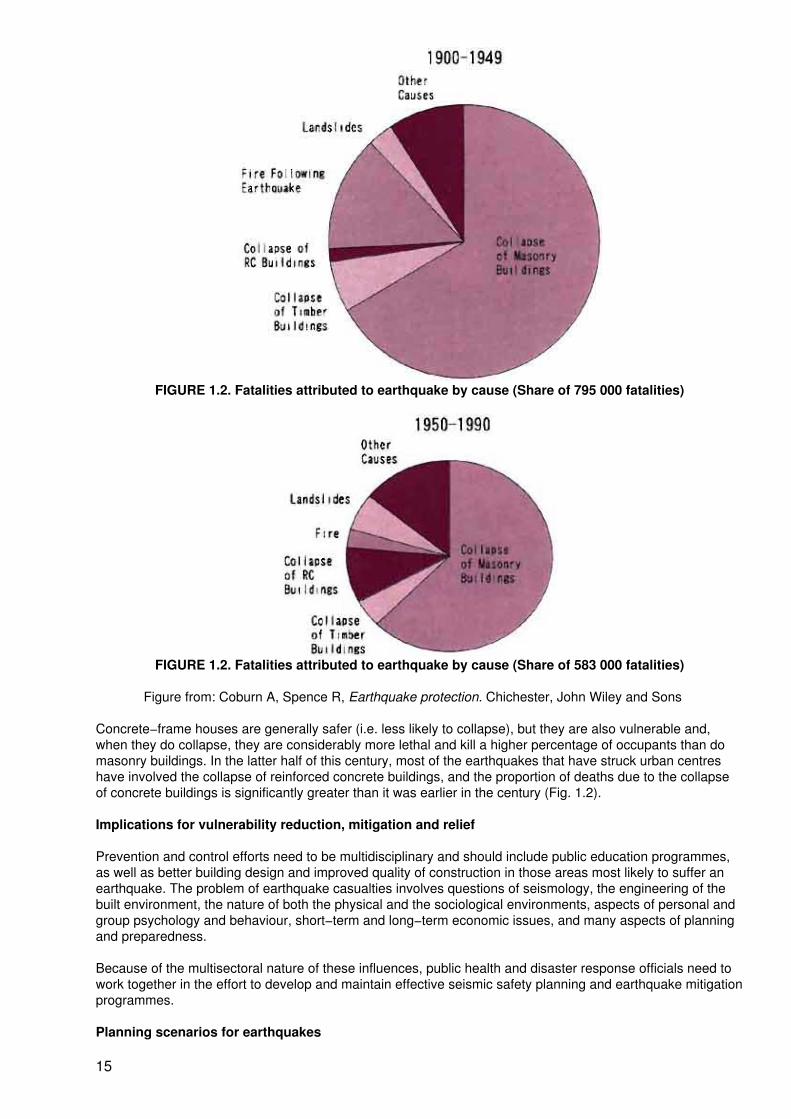
FIGURE 1.2. Fatalities attributed to earthquake by cause (Share of 795 000 fatalities)
FIGURE 1.2. Fatalities attributed to earthquake by cause (Share of 583 000 fatalities)
Figure from: Coburn A, Spence R, Earthquake protection. Chichester, John Wiley and Sons
Concrete−frame houses are generally safer (i.e. less likely to collapse), but they are also vulnerable and,when they do collapse, they are considerably more lethal and kill a higher percentage of occupants than domasonry buildings. In the latter half of this century, most of the earthquakes that have struck urban centreshave involved the collapse of reinforced concrete buildings, and the proportion of deaths due to the collapseof concrete buildings is significantly greater than it was earlier in the century (Fig. 1.2).
Implications for vulnerability reduction, mitigation and relief
Prevention and control efforts need to be multidisciplinary and should include public education programmes,as well as better building design and improved quality of construction in those areas most likely to suffer anearthquake. The problem of earthquake casualties involves questions of seismology, the engineering of thebuilt environment, the nature of both the physical and the sociological environments, aspects of personal andgroup psychology and behaviour, short−term and long−term economic issues, and many aspects of planningand preparedness.
Because of the multisectoral nature of these influences, public health and disaster response officials need towork together in the effort to develop and maintain effective seismic safety planning and earthquake mitigationprogrammes.
Planning scenarios for earthquakes
15
Relative chaos is likely to prevail immediately after a major earthquake. The area's residents, cut off from theoutside, will initially have to help themselves and their neighbours. They can best do this if they have alreadyplanned their responses to the most likely earthquake scenarios and practiced the necessary skills. Medicalpreparedness plans can be built around similar earthquake scenario calculations based on the types ofbuilding likely to be affected, the population densities and settlement patterns, the size and characteristics ofearthquakes expected in the region, and the medical facilities available in any given area. Such a regionalhazard assessment, including "casualty scenarios", permits the development of specific training programmesfor medical and rescue personnel as well as the appropriate deployment of medical and rescue equipment inadvance of an earthquake disaster.
Because there never are enough rescuers or medical providers in major disasters, communities vulnerable toearthquakes should establish ongoing programmes to teach the public what to do when an earthquakeoccurs. These would include first aid education, basic rescue training and fire drills. Simulation exercises canbe carried out jointly by volunteer groups, local fire brigades and hospitals. This training also may help toimprove bystanders' responses during more common emergencies.
Early rapid assessment of the earthquake's impact
Rapid rescue of trapped victims and prompt treatment of those with life−threatening injuries can improve theiroutcome. Therefore early rapid assessment of the extent of damage and injuries is necessary to help mobilizeresources and direct them to where they are most needed. Unfortunately, the very factors likely to cause largenumbers of injuries are also likely to disrupt communications and transport and to damage medical carefacilities. Public health officials need to establish in advance the procedures for surveying the affected areas.
Search and rescue
People trapped in the rubble will die if they are not rescued and given medical treatment. To maximizetrapped victims' chances of survival, search−and−rescue teams must respond rapidly after a buildingcollapses. Studies of the 1976 earthquake in Tangshan, China, the 1980 earthquake in Campania−Irpinia,Italy, the 1988 earthquake in Armenia, and the 1990 earthquake in the Philippines show that the proportion oftrapped people found alive declined as the duration of entrapment increased. In the Italian study, a survey of3619 survivors showed that 93% of those who were trapped and survived were extricated within the first 24hours and that 95% of the deaths recorded occurred while the victims were still trapped in rubble. Estimates ofthe survivability of victims buried under collapsed earthen buildings in China and Turkey indicate that, within2−6 hours, less than 50% of those buried are still alive. Although we cannot determine whether a trappedperson died immediately or survived for some time under the debris, we can safely assume that more peoplewould be saved if they were extricated sooner. As suggested by these data, teams with specialized expertisein areas such as search and rescue, on−site resuscitation and medical first aid arriving more than a couple ofdays after an earthquake's impact are unlikely to make much difference to the overall death toll of a largeearthquake.
With the exception of personnel from countries in close geographical proximity, foreign assistance usuallyarrives after the local community has already carried out much of the rescue activity. For example, in southernItaly in 1980, 90% of the survivors of an earthquake were extricated by untrained, uninjured survivors whoused their bare hands and simple tools such as shovels and axes. Following the 1976 Tangshan earthquake,some 200 000−300 000 trapped people crawled out of the debris on their own and went on to rescue others.They became the backbone of the rescue teams, and it was to their credit that more than 80% of those buriedunder the debris were rescued. Thus, life saving efforts depend heavily on the capabilities of relativelyuninjured survivors and untrained volunteers, as well as those of local firefighters and other relevantprofessionals. This does not mean that people who were dead when they were extricated could not have beensaved by a skilled team with sophisticated resources. However, people from the community can clearly playthe most important role in rescue efforts if they are appropriately prepared.
Medical treatment
Just as speed is required for effective search and rescue, it is also essential for effective emergency medicalservices. The greatest demand occurs within the first 24 hours. Ideally, "disaster medicine" (medical care forvictims of disaster) would include immediate life−supporting first aid, advanced trauma life support,resuscitative surgery, field analgesia and anesthesia, resuscitative engineering (search and rescuetechnology), and intensive care. Unconscious patients with either upper airway obstruction or inhalation injuryor patients with correctable hypovolemia resulting from haemorrhage or bums would be especially likely tobenefit from early medical intervention. Safar, studying the 1980 earthquake in Italy, concluded that 25−50%
16

of victims who were injured and died slowly could have been saved if life−saving first aid had been renderedimmediately.
Data from the 1976 earthquake in Guatemala, the 1985 Mexico City earthquake, the 1988 Armenianearthquake and the 1992 earthquake in Egypt showed that injured people usually seek emergency medicalattention only during the first 3−5 days following the earthquake, after which hospital case patterns returnalmost to normal. From the sixth day onward, the need for emergency medical attention declined rapidly andthe majority of the injured required only ambulatory medical attention, indicating that specialized field hospitalsthat arrive one week or more after an earthquake are generally too late to help during the emergency phase.Following the 1992 earthquake in Egypt, nearly 70% of all patients with earthquake−related injuries wereadmitted within the first 36 hours.
The medical and public health impact of a severe earthquake may well be compounded by significant damageto medical facilities, hospitals, clinics and supply stores within the affected area. In the worst−case scenario, ahospital building may itself be damaged by the earthquake, and the hospital staff may have to continueemergency treatment without using the buildings. For example, on 17 January 1994, at 4:31 a.m. PacificStandard Time, an earthquake registering 6.8 on the Richter scale occurred in a previously unrecognized faultin Los Angeles County's San Fernando Valley, killing at least 60 people. The earthquake caused considerabledamage to health facilities and significant health service disruption. Immediately after the shaking stopped,structural and nonstructural damage forced several hospitals to evacuate patients and move operationsoutside. Structural damage forced several older hospitals and medical buildings to cease or reduceoperations. During the 1985 Mexico City earthquake, which killed an estimated 7000 people, a total of 4397hospital beds were lost (about one in four of those available in the metropolitan Mexico City area). Hospitalemergency plans in earthquake areas should provide for the contingency of evacuating patients from thewards; safely removing critical equipment from operating theaters, radiology departments, and other parts ofthe hospital; and re−establishing routine services for patient care.
Summary
A major earthquake in a major urban area ranks as the largest potential natural disaster in highly seismicparts of the world. Most of what can be done to mitigate injuries must be done before the earthquake occurs.Researchers have identified a number of potentially important risk factors for injuries associated (eitherdirectly or indirectly) with earthquakes. Because structural collapse is the single greatest risk factor, priorityshould be given to seismic safety both in planning land use and in the design and construction of saferbuildings.
The integration of epidemiological studies with those of other disciplines such as engineering, architecture,social science and medical sciences is essential for improved understanding of the injuries that followearthquakes. Better epidemiological knowledge of the risk factors for death and the type of injuries andillnesses caused by earthquakes is clearly an essential requirement for determining what relief supplies,equipment, and personnel are needed to respond effectively.
Strengthening communities' self−reliance in disaster preparedness is the most fruitful way to improve theeffectiveness of relief operations. In disaster−prone areas, training and education in basic first aid and rescuemethods should be an integral part of any community preparedness programme. Unfortunately, because ofthe relatively long periods between major earthquakes, the public health community faces a special challengein effectively communicating the hazards posed by potential earthquakes and the need to plan and take actionbefore an earthquake occurs.
References
1. Coburn A, Spence R, Earthquake protection. Chichester, John Wiley and Sons Ltd., 1992:2−12, 74−80,277−284.
2. Chen Y, Tsoi KL, Chen F, et al. The Great Tangshan Earthquake of 1976: an anatomy of disaster. Oxford,Pergamon Press, 1988.
3. U.S. Department of Commerce, National Oceanic and Atmospheric Administration, and U.S. Department ofInterior, Geological Survey. Boulder, CO, 1982, (Pub. no. 41−1). Earthquake history of the United Statesrevised edition with supplement for 197140.
17
4. Coburn A, Murakami HO, Ohta Y. Factors affecting fatalities and injury in earthquakes. Internal Report,Engineering Seismology and Earthquake Disaster Prevention Planning. Hokkaido, Hokkaido University, 1987.
5. Goltz JD. The Northridge, California, earthquake of January 17, 1994: general resconnaissance report.Buffalo, NY, National Centre for Earthquake Engineering Research, 1994 (Technical Report NCEER94−0005).
6. Hall JF. The January 17, 1994 Northridge, California earthquake: an EQE summary report. San Francisco,EQE International, 1994.
7. Benuska L, (ed.). Loma Prieta earthquake reconnaissance report. Earthquake Spectra, 1990,6 (Suppl.):1−448.
8. EQE Engineering. The October 17, 1989 Loma Prieta earthquake: a quick look report. San Francisco, EQEEngineering, 1989.
9. Coburn A, Spence RJS, Pomonis A. Factors determining human casualty levels in earthquakes: mortalityprediction in building collapse. In: Proceedings of the First International Forum on Earthquake−RelatedCasualties, Madrid, Spain, July 1992. Reston, VA, U.S. Geological Survey, 1992.
10. Noji EK, Kelen GD, Armenian HK, et al. The 1988 earthquake in Soviet Armenia: a case study. Annals ofEmergency Medicine, 1990,19:891−897.
11. Armenian HK, Noji EK, Organessian AP. Case control study of injuries due to the earthquake in SovietArmenia. Bull. World Health Organ. 1992,70:251−257.
12. Roces MC, White ME, Dayrit MM, Durkin ME. Risk factors for injuries due to the 1990 earthquake inLuzon, Philippines, Bull. World Health Organ. 1992,70:509−514.
13. Glass RI, Urrutia JJ, Sibony S, et al. Earthquake injuries related to housing in a Guatemalan village.Science 1977,197:638−643.
14. Mitchell WA, Wolniewicz R, Kolars JF. Predicting casualties and damages caused by earthquakes inTurkey. A preliminary report. Colorado Springs, CO, U.S. Air Force Academy, 1983.
15. Mehrain M. A reconnaissance report on the Iran earthquake. National Centre for Earthquake EngineeringResearch Bulletin 1991,5:1−4.
16. Coburn A, Petrovski J, Ristic D, et al. Mission report and technical review of the impact of the earthquakeof 21 June 1990 in the provinces of Gilan and Zanjan. Earthquake reconstruction program formulation missionto the Islamic Republic of Iran. Geneva, United Nations Disaster Relief Office, 1990.
17. Ceciliano N, Pretto E, Watoh Y, et al. The earthquake in Turkey in 1992: a mortality study. Prehospital andDisaster Medicine, 1993,8:S 139.
Seismological forecasting: prospects within the International Decade for Natural Disaster Reduction
R.L. Kintanar1
1R.L. Kintanar is Chairman, International Decade for Natural Disaster Reduction, Manila,Philippines.
The United Nations International Decade for Disaster Reduction (IDNDR) officially started on 1 January 1990.The Scientific and Technical Committee which I now chair determines the policy and programme of theIDNDR but the bulk of its activities and projects are regional or national in nature.
The Philippines lies in the same Pacific ring of fire as Japan and is also affected by many of the same hazardsthat affect Japan. Among these are earthquakes, volcanic eruptions, typhoons, floods, droughts, wildfires andlandslides. I had the personal experience of conducting a technical survey of the damage from the earthquakein Lamao on the island of Mindanao on 1 April 1955. Those who witnessed the effects of the Kobe earthquake
18
will agree with me that such an episode leaves a permanent impression and is an experience never to beforgotten.
Project RADIUS
At the beginning of the IDNDR it seemed difficult to comprehend the international dimension of disasterpreparedness and to change attitudes and counter the lack of interest. Time and the increasing impact ofnatural disasters in a fast−developing world have made their impact on more and more of the nationalleaderships and on the people themselves. The IDNDR secretariat launched the RADIUS project in 1996 torealize the concept of the IDNDR and the Yokohama Strategy and Plan of Action that was developed in 1994.
The RADIUS project aims to promote worldwide activities for the reduction of seismic disasters in urbanareas, particularly in developing countries, so that the countries of the world will be able to face the newmillennium with greater security against natural disasters. The project will develop common methodologiesand collect state−of−the−art technologies for seismic risk assessment in urban areas in order to raise publicawareness and provide direction for disaster mitigation. It is expected that many of these technologies willcome from among those developed and used in Japan.
Personal earthquake drills
Earthquake drills have been very useful in informing large numbers of the population on the proper action tobe taken in the few seconds after the onset of a strong tremor. The correct reaction to a strong tremor maymake the difference between major or minor injuries to the person concerned.
The main problem with earthquake drills is the large amount of work required to organize, prepare andimplement them. Anyone who has had a hand in organizing such a drill, or who has been involved as aparticipant, knows why these drills cannot be widely utilized.
In an urban centre like Manila, large−scale earthquake drills are next to impossible and no drills of wideapplication have been attempted. In the early 1970s, after a few very strong earthquakes affected Manila, wetried to institutionalize earthquake drills. The best we could do was to propose an alternative − the personalearthquake drill. The government undertook an information campaign to make available to as many of thepopulation as possible the various simple pieces of advice for personal reaction in case of an earthquake.
In the personal earthquake drill we stress the importance of personal reactions. We ask people to identifywhere they spend the greater amount of their time. We then ask them to imagine a strong tremor and to clarifythe appropriate reaction they should have considering their location when the earthquake occurs. We askthem to repeat this procedure for their own security every few weeks or so. We explain that this mentalexercise need take only a few minutes. We also suggest that the exercise could be usefully repeated eachtime they find themselves in a new situation, such as in a movie−house or restaurant or department store.
It is difficult to assess the effectiveness of this mental earthquake drill, but even if it serves only to remindpeople of the risk around them it may well be worth the few minutes of mental exercise.
Forecasting and warning
Even short−term forecasts of the time of an earthquake's occurrence, its magnitude and the area of its impactneed a lot more study and intensified research. Only very few examples of reasonably successful predictionshave been known, as for example in China, France, and the Caribbean and Mediterranean areas. Studieshave identified the Pacific as the area most susceptible to earthquakes. Furthermore, areas of inner−plateseismic faults have been identified, which can be the focus of scientific studies and research. Severalprecursors of earthquakes have been identified, but these cannot as yet be easily used as predictors. Detailedanalysis of seismographic measurements (e.g. by advanced pattern−recognition technology) andobservations of animal behaviour are among these. Another promising tool for earthquake forecasting is themeasurement of the wave velocity in the ground which is known to change drastically before an earthquakeoccurs. Monitoring of the velocity of these waves is currently being undertaken in four areas of the world.
Looking to the future
It is now time to consolidate all activities for natural disaster reduction. The multisectoral components of thissymposium will certainly help in this endeavour. The United Nations efforts embodied in the IDNDR willformally terminate on 31 December 1999. When that time comes we hope that the national, regional and
19
international leadership in disaster reduction that has developed during the decade will continue to prosper.
Health implications of earthquakes: physical and emotional injuries during and after the Northridgeearthquake1
L.B. Bourque,2 C. Peek−Asa,3 M. Mahue,4 L.H. Nguyen,5 K.I. Shoaf,6 J.F. Kraus,7 B. Weiss,8 D.Davenport9 and M. Saruwatari10
1Data were collected and processed with funds from the National Science Foundation (Nos.CMS−9416470 and CMS−9411982), the Los Angeles County Department of Health(Purchase Order R41867 and Award No. 953124), and the California State Department ofHealth Services (Award No. 95−23008).
2L.B. Bourque Ph.D. is Professor, Department of Community Health Sciences, School ofPublic Health and Southern California Injury Prevention Research Center (SCIPRC),University of California, Los Angeles, USA.
3C. Peek−Asa Ph.D. is Adjunct Assistant Professor, Department of Epidemiology, School ofPublic Health and SCIPRC, University of California, Los Angeles, USA.
4M. Mahue M.S. is Epidemiologist, Injury and Violence Prevention Program, Los AngelesCounty Department of Health Services, Los Angeles, USA.
5L.H. Nguyen M.P.H., MSW is Project Coordinator, Department of Community HealthSciences, School of Public Health, University of California, Los Angeles, USA.
6K.I. Shoaf M.P.H, is Project Director, Department of Community Health Sciences, School ofPublic Health and Center for Health Policy Research, University of California, Los Angeles,USA.
7J.F. Kraus Ph.D. is Professor, Department of Epidemiology, School of Public Health andDirector, SCIPRC, University of California, Los Angeles, USA.
8B. Weiss M.P.H, is Director, Injury and Violence Prevention Program, Los Angeles CountyDepartment of Health Services, Los Angeles, USA.
9D. Davenport M.S., R.N., P.H.N. is District Nurse Manager, Los Angeles County CommunityHealth Services, Public Health Programs and Services, Los Angeles, USA−
10M. Saruwatari M.P.H, is Senior Disaster Services Analyst, Los Angeles County HealthServices Administration, Los Angeles, USA.
The number of deaths and the number and severity of physical injuries following an earthquake have beenhypothesized to vary with the magnitude of an earthquake, proximity to the epicenter, soil conditions,characteristics of buildings and other man−made structures, density and distribution of population in the area,environmental conditions, people's location and behaviour, the level of preparedness and hazard mitigation,the time of day, day of the week, season, opportunity for warning, and socioeconomic resources availablewithin family units and communities. Mahoney (1987) suggested that earthquakes exceeding 6 on the Richterscale usually result in death and injuries if they occur in populated areas (7). It has been repeatedly assertedthat the ratio of injuries to deaths is between 3 and 4 to 1, with this average ratio varying "...within the contextof a single catastrophic earthquake along a continuum from many deaths and relatively few injuries close tothe epicenter to the opposite at the periphery of the affected area" (2).
Table 1.2 summarizes reported injuries and deaths in 14 earthquakes during the last 50 years. Here theestimated ratio of injuries to deaths ranges from a high of three deaths for every two injuries in Tangshan,China, to a low of one death for every 450 injuries in Whittier Narrows, California. Clearly, the numbers ofdeaths and injuries vary directly with the number of severely damaged buildings, the number of peopletrapped in buildings, and the efficiency, appropriateness and availability of post−earthquake medical services,and inversely with the efficiency of search−and−rescue opportunities. The amount and severity of damage tobuildings, in turn, is dependent on the extent to which a community has chosen to invest in hazard mitigation
20
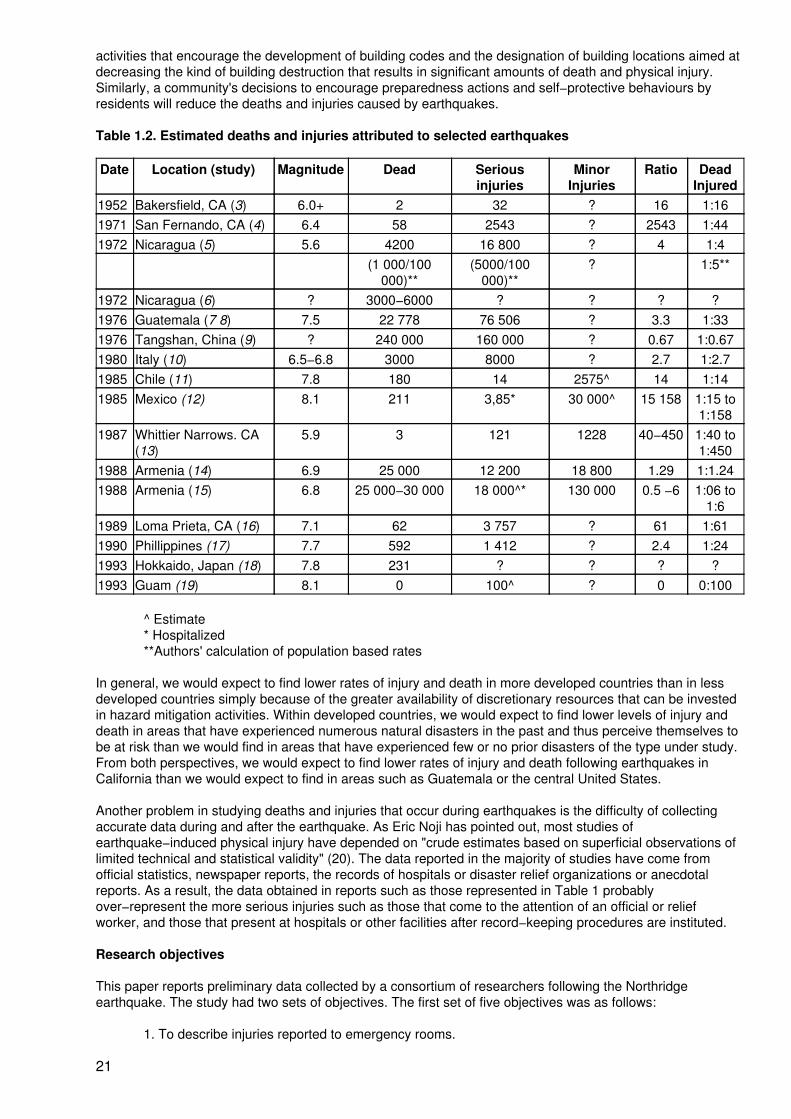
activities that encourage the development of building codes and the designation of building locations aimed atdecreasing the kind of building destruction that results in significant amounts of death and physical injury.Similarly, a community's decisions to encourage preparedness actions and self−protective behaviours byresidents will reduce the deaths and injuries caused by earthquakes.
Table 1.2. Estimated deaths and injuries attributed to selected earthquakes
Date Location (study) Magnitude Dead Seriousinjuries
MinorInjuries
Ratio DeadInjured
1952 Bakersfield, CA (3) 6.0+ 2 32 ? 16 1:161971 San Fernando, CA (4) 6.4 58 2543 ? 2543 1:441972 Nicaragua (5) 5.6 4200 16 800 ? 4 1:4
(1 000/100000)**
(5000/100000)**
? 1:5**
1972 Nicaragua (6) ? 3000−6000 ? ? ? ?1976 Guatemala (7 8) 7.5 22 778 76 506 ? 3.3 1:331976 Tangshan, China (9) ? 240 000 160 000 ? 0.67 1:0.671980 Italy (10) 6.5−6.8 3000 8000 ? 2.7 1:2.71985 Chile (11) 7.8 180 14 2575^ 14 1:141985 Mexico (12) 8.1 211 3,85* 30 000^ 15 158 1:15 to
1:1581987 Whittier Narrows. CA
(13)5.9 3 121 1228 40−450 1:40 to
1:4501988 Armenia (14) 6.9 25 000 12 200 18 800 1.29 1:1.241988 Armenia (15) 6.8 25 000−30 000 18 000^* 130 000 0.5 −6 1:06 to
1:61989 Loma Prieta, CA (16) 7.1 62 3 757 ? 61 1:611990 Phillippines (17) 7.7 592 1 412 ? 2.4 1:241993 Hokkaido, Japan (18) 7.8 231 ? ? ? ?1993 Guam (19) 8.1 0 100^ ? 0 0:100
^ Estimate* Hospitalized**Authors' calculation of population based rates
In general, we would expect to find lower rates of injury and death in more developed countries than in lessdeveloped countries simply because of the greater availability of discretionary resources that can be investedin hazard mitigation activities. Within developed countries, we would expect to find lower levels of injury anddeath in areas that have experienced numerous natural disasters in the past and thus perceive themselves tobe at risk than we would find in areas that have experienced few or no prior disasters of the type under study.From both perspectives, we would expect to find lower rates of injury and death following earthquakes inCalifornia than we would expect to find in areas such as Guatemala or the central United States.
Another problem in studying deaths and injuries that occur during earthquakes is the difficulty of collectingaccurate data during and after the earthquake. As Eric Noji has pointed out, most studies ofearthquake−induced physical injury have depended on "crude estimates based on superficial observations oflimited technical and statistical validity" (20). The data reported in the majority of studies have come fromofficial statistics, newspaper reports, the records of hospitals or disaster relief organizations or anecdotalreports. As a result, the data obtained in reports such as those represented in Table 1 probablyover−represent the more serious injuries such as those that come to the attention of an official or reliefworker, and those that present at hospitals or other facilities after record−keeping procedures are instituted.
Research objectives
This paper reports preliminary data collected by a consortium of researchers following the Northridgeearthquake. The study had two sets of objectives. The first set of five objectives was as follows:
1. To describe injuries reported to emergency rooms.
21
2. To describe the incidence and characteristics of fatal physical injuries.
3. To describe the incidence and characteristics of severe physical injuries which resulted inhospitalization.
4. To describe the incidence and characteristics of self−reported physical injuries.
5. To describe the incidence and characteristics of self−reported emotional injuries.Concentrating only on the self−reported injuries, for which more data are available,
the second set of three additional objectives was:
6. To examine the extent to which injured persons differ from non−injured.
7. To examine who seeks care for physical and emotional injuries.
8. To examine the extent to which patterns of injury vary with people's reports ofpreparedness and hazard mitigation activities.
In reviewing all data presented, it must be emphasized that these data are preliminary and some of theobservations presented may change after further, more sophisticated analysis.
Data sources
The Northridge earthquake occurred at 4:31 a.m. on 17 January 1994, which was Martin Luther King Day, alegal state and federal holiday. The earthquake had a magnitude of 6.7 on the Richter scale and was locatedon a previously unidentified thrust fault in the San Fernando Valley. The most severe shaking wasexperienced in the west San Fernando Valley but the earthquake was felt throughout Los Angeles County andinto Ventura County.
The data presented were of four types: emergency room data, fatalities and hospitalized injuries,self−reported physical injuries, and self−reported emotional injuries.
Emergency room data
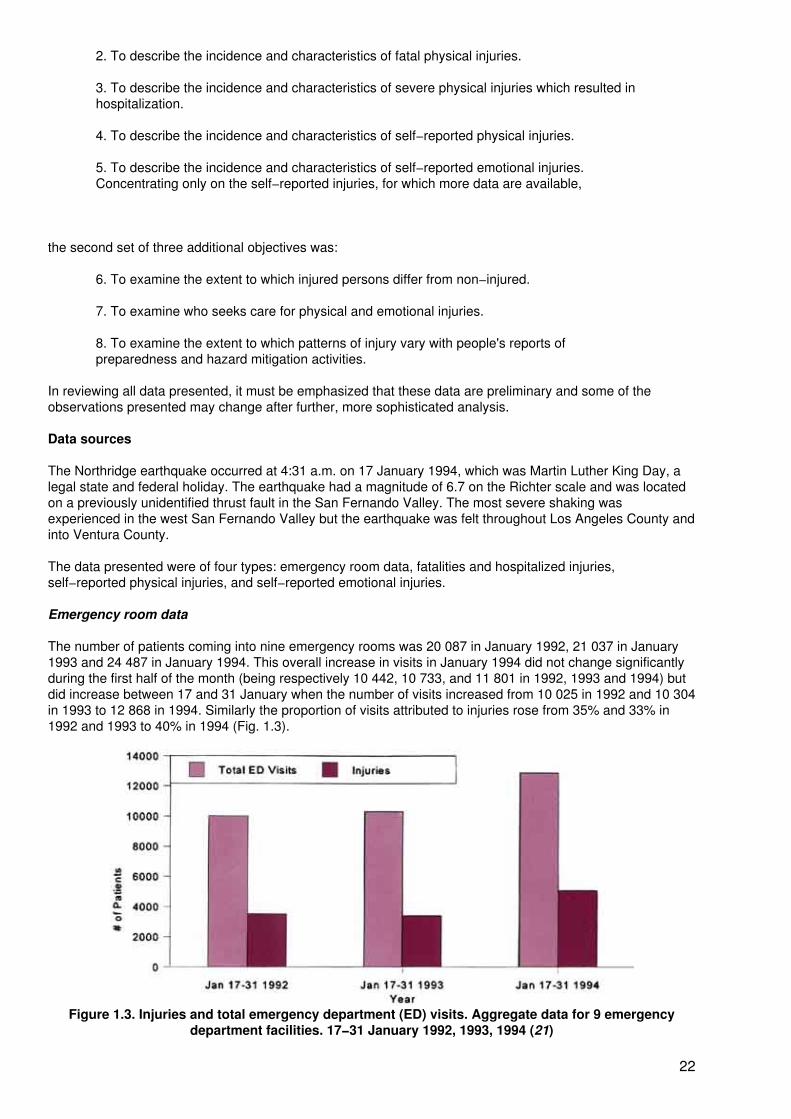
The number of patients coming into nine emergency rooms was 20 087 in January 1992, 21 037 in January1993 and 24 487 in January 1994. This overall increase in visits in January 1994 did not change significantlyduring the first half of the month (being respectively 10 442, 10 733, and 11 801 in 1992, 1993 and 1994) butdid increase between 17 and 31 January when the number of visits increased from 10 025 in 1992 and 10 304in 1993 to 12 868 in 1994. Similarly the proportion of visits attributed to injuries rose from 35% and 33% in1992 and 1993 to 40% in 1994 (Fig. 1.3).
Figure 1.3. Injuries and total emergency department (ED) visits. Aggregate data for 9 emergencydepartment facilities. 17−31 January 1992, 1993, 1994 (21)
22
Looking only at injured patients, both the age distribution and the gender distribution of patients with injuriesshifted between 1992−1993 and 1994. Whereas most injured patients were under 30 in 1992−1993, themajority of injured patients in 1994 were over 30 years of age. Similarly, women were as likely as males topresent as injured in 1994 whereas males were more likely to present with injuries in earlier years.
The number of injuries to the lower and upper extremities increased substantially between 1992−1993 and1994. Injuries to the lower extremities doubled, rising from 764 in 1992 and 756 in 1993 to 1550 in 1994.Injuries to the upper extremities similarly increased, up from 975 in 1992 and 906 in 1993 to 1312 in 1994.The method by which the injury occurred also shifted in 1994 with more than twice as many patients reportingthat they were cut by something (48 to 139), struck by something (23 to 63), or injured through exposure to aplant, insect or animal (59 to 113).
Fatalities and hospitalized injuries
Fatal injuries were pre−identified by the Los Angeles County Coroner's Office to be "earthquake−related", andwere defined as any death from physical injury. Deaths from heart attacks and other non−injury events wereexcluded from this study. Severe injuries were defined as those injuries that required hospital admission fortreatment. Of the 78 hospitals approached, 16 reported admitting one or more earthquake−related injuriesbetween 17 and 31 January 1994. All medical records were individually reviewed in those 16 hospitals.
Through these methods 171 earthquake−related injuries were identified in Los Angeles County. Thirty−threeof these injuries led to fatality and 138 led to hospitalization. The overall injury rates were 1.93 per 100 000residents, with a fatality rate of 0.37 per 100 000 and a rate of 1.56 hospital−admitted injuries per 100 000.For every fatality there were 4.2 hospital−admitted injuries. Unlike other injury rates which are consistentlyhigher for males, the injury rate for females after the Northridge earthquake (2.09 per 100 000) wasnon−significantly higher than the injury rate for males (1.74 per 100 000 residents). There was a dramaticincrease in severe earthquake−related injuries with age, with the fatalities showing a linear increase with ageand the hospitalized injuries showing an almost quadratic increase with age. All of the fatal injuries occurredon the day of the earthquake and 83% occurred within minutes of the earthquake's onset.
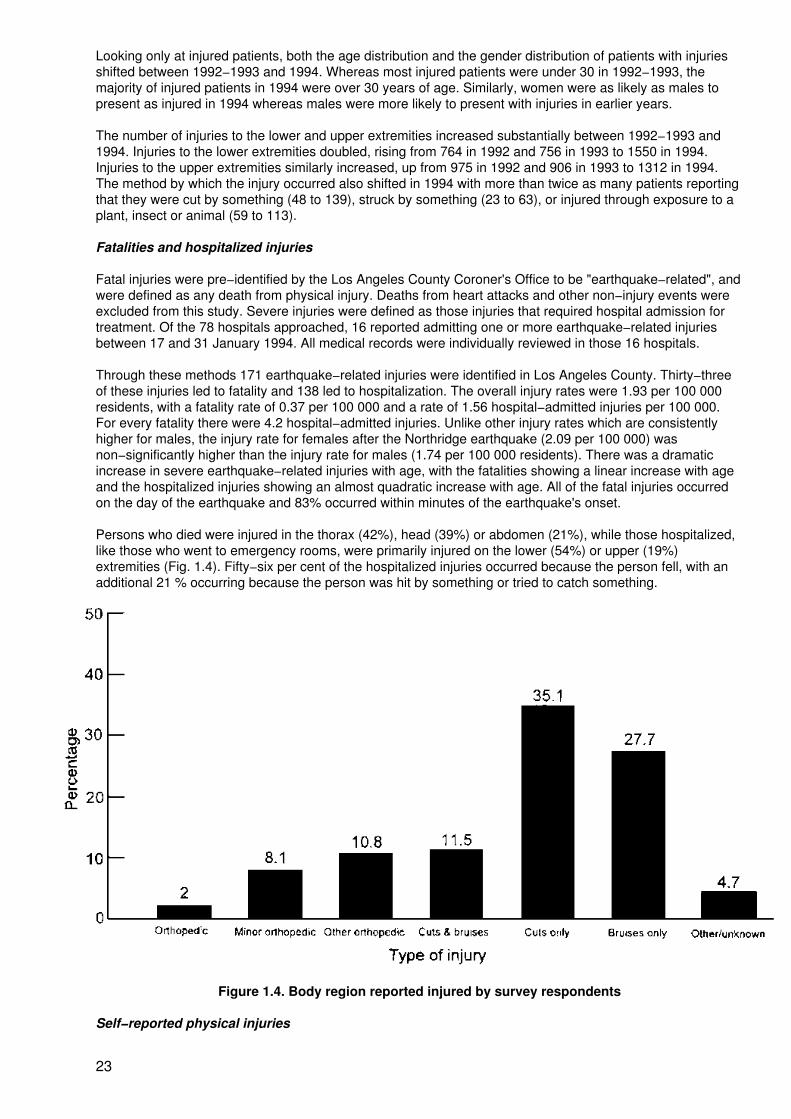
Persons who died were injured in the thorax (42%), head (39%) or abdomen (21%), while those hospitalized,like those who went to emergency rooms, were primarily injured on the lower (54%) or upper (19%)extremities (Fig. 1.4). Fifty−six per cent of the hospitalized injuries occurred because the person fell, with anadditional 21 % occurring because the person was hit by something or tried to catch something.
Figure 1.4. Body region reported injured by survey respondents
Self−reported physical injuries
23
Following the Northridge earthquake, three successive probability samples of Los Angeles County residentswere asked the following questions:
1. Did you have any physical injuries − even minor cuts and bruises − as a result of thisearthquake?
2. When exactly were you injured? Were you injured during the earthquake itself, immediatelyafter the earthquake, within the first 48 hours after the earthquake, during an aftershock, orsome other time?
3. Can you tell me the date and time of the injury?
4. Can you describe exactly what happened to cause your (injury/injuries)?
5. What exactly (was/were) your (injury/injuries)?
6. What parts of your body were injured?
7. Did you seek medical care for your injury?
Eight per cent (N = 149) of the 1830 respondents reported physical injuries. If we extrapolate that to the 3million households in Los Angeles County, it means that 243 000 households had at least one injured adultafter the Northridge earthquake.
Persons in areas at the time of the earthquake where the Mercalli intensity was 8 (20% = 50/252) or 9 (23% =38/168) were more likely to be injured than were those in modified Mercalli intensity (MMI) areas of 6 (2% =6/380) or 7 (5% = 55/1030). Reported physical injuries varied with the amount of damage a respondentreported, whether or not the respondent's house had been inspected and the amount of damage inspectorsfound. Thirty−three per cent (N = 5/15) of persons who reported that red tags (see Annex 2) were put on theirhomes reported that they were injured, while 45% (N = 17/40) of persons with yellow tags, 28% (N = 34/123)of those with green tags, 16% (N = 41/276) of those whose house was inspected but who was not tagged,10% (N = 21/227) of those who reported damage but did not have inspections, and 2% (N = 23/854) of thosewho reported no damage to their homes reported they were injured.
Over half of the injuries occurred because of objects that fell or were broken (54%; N = 81); 15% (N = 22) ofinjuries were caused by the person's own behaviour − for example, they ran, they jumped out of a window, orthey tried to catch something like a television set. Most of the injuries were cuts and/or bruises (74%; N = 110)and, as we saw with the injuries that were hospitalized and showed up in emergency rooms, most of theinjuries occurred to the lower extremities − feet, ankles and legs (Fig. 1.4).
Demographic characteristics that might differentiate injured from non−injured were examined. Like thehospitalized cases, females were more likely to be injured than males (10% vs. 7%; p < .05) but, unlikehospitalized cases, injured persons were more likely to be younger rather than older (37 vs. 41 years; p <−01). The injured also had more education than the non−injured (14 vs. 13 years; p < .01). The injured did notdiffer from the non−injured in income, the number of years they had lived in California, or in the size of theirhousehold.
Ten per cent (N = 15) of the injured sought care for their injuries with five seeking care at hospitals, threegoing to clinics, three going to their private doctor, and two seeking care from relatives, friends or the RedCross. Injured persons who sought care were less likely to be married (23% vs. 39%; p < .05), more likely tobe born in the United States and, thus, less likely to be immigrants (86% vs. 67%; p < .05), and more likely tohave children under 18 (1.5 vs. 0.8 children; p < .05). Persons who sought care for their injuries did not differin age, education, gender, income, ethnicity or years lived in California from those who did not seek care.
Self−reported emotional injuries
In telephone interviews, respondents were asked four questions about emotional injuries:
1. What about emotional injuries? Would you say that you had any emotional injuries as aresult of this earthquake?
2. Can you tell me about that?
24
3. When did you first decide that you were emotionally injured as a result of the earthquake?
4. Did you seek medical or other help for your emotional injuries?
Thirty−four per cent (N= 613) of the 1830 respondents of Los Angeles County reported that they had anemotional injury. As with the physical injuries, if we extrapolate that to the 3 million households in Los AngelesCounty, at least one adult in 1 020 000 households felt they had an emotional injury after the Northridgeearthquake.
Persons in areas with higher Mercalli intensities were more likely to report an emotional injury, but thedifferences across areas defined by MMIs were much less dramatic than they were for physical injuries.Fifty−six per cent (N = 94) of persons in areas with an MMI of 9 reported an emotional injury, while 41% (N =102) of those in MMIs of 8, 31% (N = 314) of those in MMIs of 7, and 27% (N = 103) of those in MMIs of 6reported emotional injury. Similarly, emotional injury varied with the amount of damage reported, but againdifferences were less dramatic across the categories.
Persons who said they were emotionally injured were more likely to be female (66% vs. 48%; p < .05), to havemore children under 18 years of age in the household (1.1 child vs. 0.9 child; p < .05), to be born outside theUnited States (42% vs. 34%; p < .05), and to have lower average education (12.6 years vs. 13.3 years; p <.05). They also had lower household incomes ($35,503 vs. $44,548; p < .05), were less likely to own theirhome (40% vs. 50%; p < .05), and had lived in California for fewer years (25 years vs. 27 years; p < .05). Theemotionally injured did not differ from those not emotionally injured in age, marital status or number of adultsin the household.
Three per cent (N = 59) of the emotionally injured sought some kind of care, but we have no information aboutwhere they went for this. Care−seekers were older (44 vs. 40 years; p < .05), had more education (14 vs. 12years; p < .05), had fewer dependents under 18 years of age (0.8 vs. 1.2; p < .05), and were less likely to beborn outside the United States (22% vs. 44%; p < .05). Those who sought care for emotional injuries did notdiffer from those who did not seek care by sex, marital status, length of time they had lived in California,number of adults in the household, home ownership or average income.
Post−traumatic stress disorder
People have been interested in knowing whether post−traumatic stress disorder or PTSD occurs as a result ofnatural disasters such as earthquakes. The Mississippi Scale of Post−Traumatic Stress Disorder was includedin the first of the three surveys conducted after the Northridge earthquake in order to find out whether PTSDlevels increased with earthquake−related experiences (22,25). The scale includes 35 questions with apossible range from 35, which indicates no PTSD, to 175, the highest level of PTSD. For the 423 persons forwhom complete PTSD data were available following the Northridge earthquake, the range was 40 to 119, witha mean of 64.3 and median of 63.
When examined in relationship to MMIs, PTSD levels varied only slightly with MMIs and damage/inspectiongroups of their homes. Similarly, levels of PTSD did not differ with whether or not respondents reported aphysical injury and whether or not they sought care for the injury.
In contrast, PTSD scores did vary slightly with respondents' reports of having an emotional injury. Personswith no emotional injury had an average score of 62.7; those who had an emotional injury and did not seekcare for it had an average score of 66.7; and those who sought care for an emotional injury had an averagePTSD score of 70.4 (p < .001). Thus, there is little evidence that people experienced high levels of PTSD as aresult of their experiences during the Northridge earthquake.
Preparedness and injuries
Groups in California have invested time and money to give people information about what to do before andduring earthquakes to protect themselves and their property. Over the last 20 years California residents haveincreased the level of their preparedness activities −particularly those that are easiest to do (24). Using dataavailable from these surveys we examined whether people who have invested in preparedness activities wereless likely to report being injured or report damage to their homes. Fig. 1.5 shows the percentage of personswho reported that they had done 12 different preparedness activities prior to the Northridge earthquake. Ofthese 12 things, respondents were most likely to state that they had learned first aid and had a first aid kit intheir homes, and least likely to say that they had invested in structural support for their homes or rearrangedcupboards. On average, respondents had done only two of the 12 preparedness activities before the
25
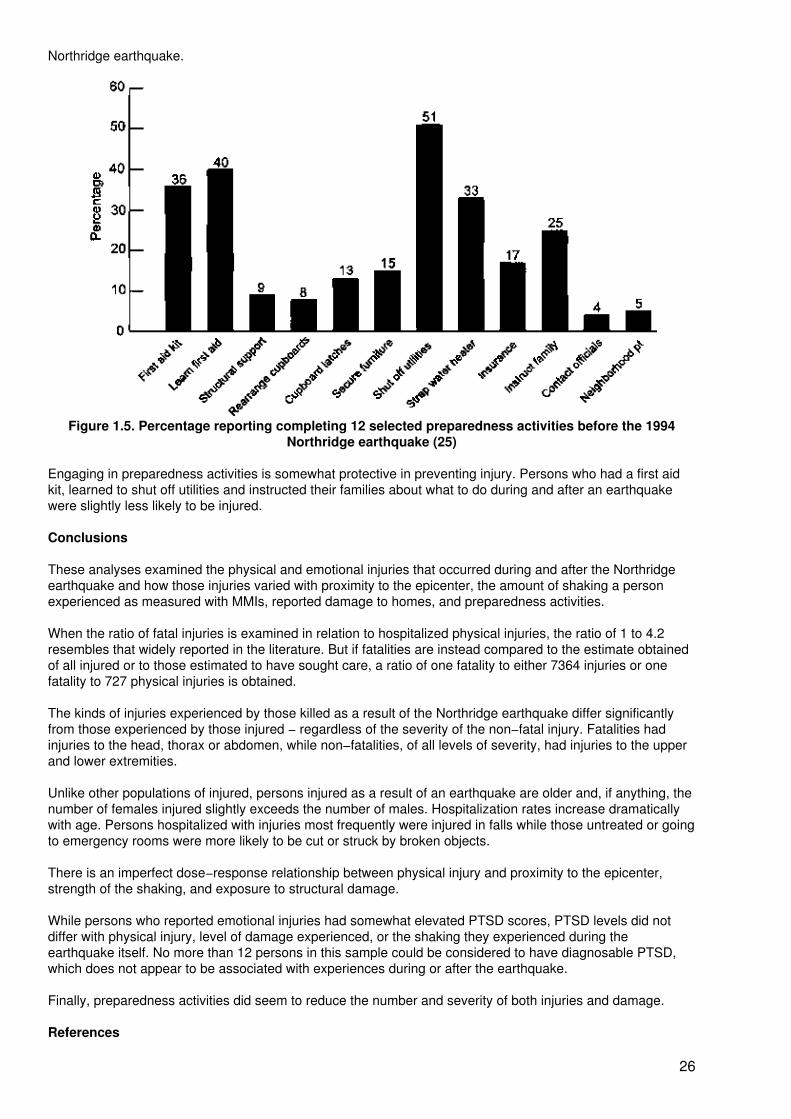
Northridge earthquake.
Figure 1.5. Percentage reporting completing 12 selected preparedness activities before the 1994Northridge earthquake (25)
Engaging in preparedness activities is somewhat protective in preventing injury. Persons who had a first aidkit, learned to shut off utilities and instructed their families about what to do during and after an earthquakewere slightly less likely to be injured.
Conclusions
These analyses examined the physical and emotional injuries that occurred during and after the Northridgeearthquake and how those injuries varied with proximity to the epicenter, the amount of shaking a personexperienced as measured with MMIs, reported damage to homes, and preparedness activities.
When the ratio of fatal injuries is examined in relation to hospitalized physical injuries, the ratio of 1 to 4.2resembles that widely reported in the literature. But if fatalities are instead compared to the estimate obtainedof all injured or to those estimated to have sought care, a ratio of one fatality to either 7364 injuries or onefatality to 727 physical injuries is obtained.
The kinds of injuries experienced by those killed as a result of the Northridge earthquake differ significantlyfrom those experienced by those injured − regardless of the severity of the non−fatal injury. Fatalities hadinjuries to the head, thorax or abdomen, while non−fatalities, of all levels of severity, had injuries to the upperand lower extremities.
Unlike other populations of injured, persons injured as a result of an earthquake are older and, if anything, thenumber of females injured slightly exceeds the number of males. Hospitalization rates increase dramaticallywith age. Persons hospitalized with injuries most frequently were injured in falls while those untreated or goingto emergency rooms were more likely to be cut or struck by broken objects.
There is an imperfect dose−response relationship between physical injury and proximity to the epicenter,strength of the shaking, and exposure to structural damage.
While persons who reported emotional injuries had somewhat elevated PTSD scores, PTSD levels did notdiffer with physical injury, level of damage experienced, or the shaking they experienced during theearthquake itself. No more than 12 persons in this sample could be considered to have diagnosable PTSD,which does not appear to be associated with experiences during or after the earthquake.
Finally, preparedness activities did seem to reduce the number and severity of both injuries and damage.
References
26
1. Mahoney LE. Catastrophic disasters and the design of disaster medical care systems. Annals ofEmergency Medicine, 1987, 16:1085−1091.
2. Alexander D. Death and injury in earthquakes. Disasters, 1985, 9:57−60.
3. Marks ES, Fritz CE. Human reactions in disaster situations. Science, 1954, 182:981−990.
4. Bourque L.B, Reeder LG, Cherlin A, Raven BH, Walton DM. The unpredictable disaster in a metropolis:public response to the Los Angeles earthquake of February, 1971. Los Angeles, UCLA Survey ResearchCenter, 1973.
5. Kates RW, Haas JE, Amaral DJ, Olson RA, Ramos R, Olson R. Human impact of the Managua earthquake.Science, 1973,182:981−990.
6. Whittaker R, Fareed D, Green P, Barry P, Borge A, Fletes−Barrios R. Earthquake disaster in Nicaragua:reflections on the initial management of massive casualties. Journal of Trauma, 1974, 14:37−43.
7. Glass RI, Urrutia JJ, Sibony S, Smith H, Garcia B, Rizzo L. Earthquake injuries related to housing in aGuatemalan village. Science, 1977,197:638−643.
8. de Ville de Goyet C, del Cid E, Romero A, Jeannee E, Lechat M. Earthquake in Guatemala: epidemiologicevaluation of the relief effort. PAHO Bulletin, 1976, 10:95−109.
9. Li J. Social responses to the Tangshan earthquake. Paper presented at the UCLA International Conferenceon the Impact of Natural Disasters, Los Angeles, CA, 9−12 July 1991.
10. Alexander D. Disease epidemiology and earthquake disaster: the example of southern Italy after the 23November 1980 earthquake. Social Science and Medicine, 1982, 16:1959−1969.
11. Ortiz MR, Roman MR, Latorre AV, Soto JZ. Brief description of the effects on health of the earthquake of3rd March 1985, Chile. Disasters, 1986, 10:125−126.
12. Zeballos JL. Health aspects of the Mexico earthquake, 19th September 1985. Disasters, 1986,70:141−149.
13. Tierney K. Social aspects. Earthquake Spectra, 1988,4:11−24.
14. Noji EK, Kelen GD, Armenian HK, Oganessian A, Jones NP, Sivertson KT. The 1988 earthquake in SovietArmenia: a case study. Annals of Emergency Medicine, 1990, 19:891−897.
15. Wyllie LA, Filson JR. Armenian earthquake reconnaissance report. Earthquake Spectra, 1989(Supplement).
16. Benuska K.L. Loma Prieta earthquake reconnaissance report. Earthquake Spectra, 1990, 9 (Supplement).
17. MMWR. Earthquake disaster: Luzon, Philippines. Morbidity and Mortality Weekly Report, 1990,39:573−577.
18. Chung RM. Hokkaido−Nansei−Oki earthquake and tsunami of July 12, 1993 reconnaissance report.Earthquake Spectra, 1995, 11 (Supplement A).
19. Comartin CD. Guam earthquake of August 8, 1993 reconnaissance report. Earthquake Spectra, 1995, 11(Supplement B).
20. Noji E. The 1988 earthquake in Soviet Armenia: implications for earthquake preparedness. Disasters,1989, 13:255−262.
21. Mahue ML, Johnson J, Hartman C, Giangrecco CA, Weiss BP. Injuries resulting from the 1994 Northridgeearthquake, impact on Los Angeles County emergency departments. Abstracts. American Public HealthAssociation 124th Annual Meeting and Exposition, New York, 1996:392,
27
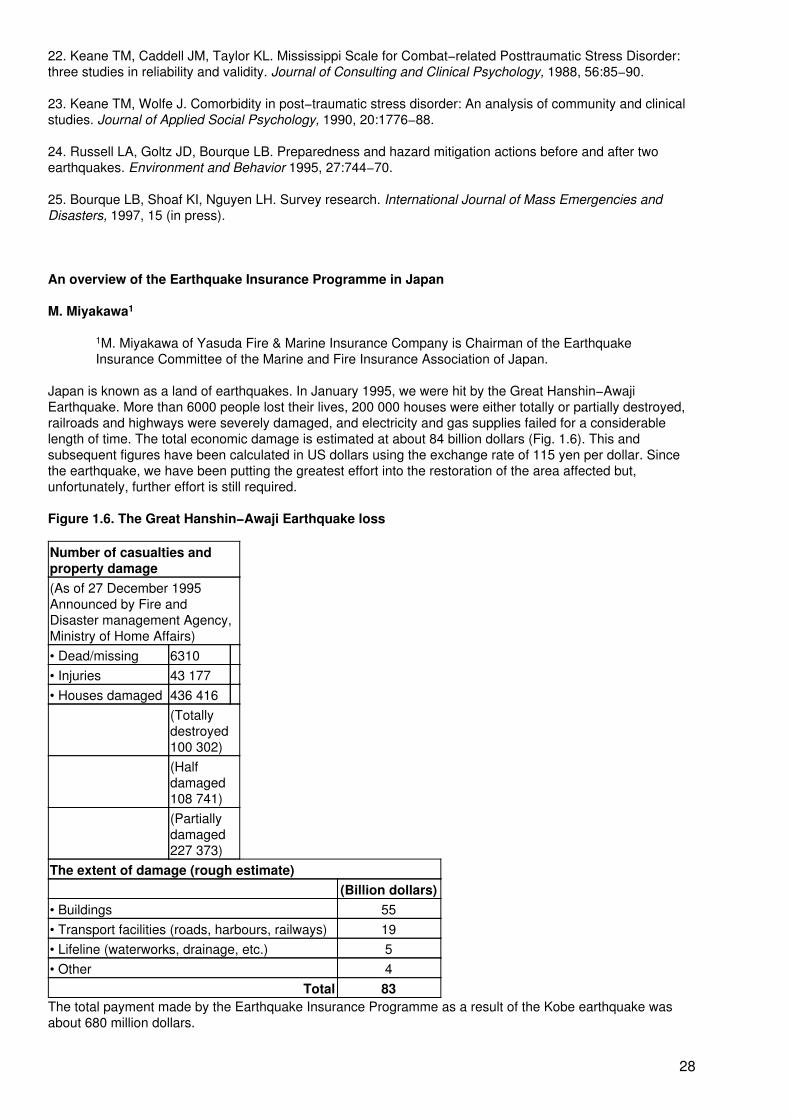
22. Keane TM, Caddell JM, Taylor KL. Mississippi Scale for Combat−related Posttraumatic Stress Disorder:three studies in reliability and validity. Journal of Consulting and Clinical Psychology, 1988, 56:85−90.
23. Keane TM, Wolfe J. Comorbidity in post−traumatic stress disorder: An analysis of community and clinicalstudies. Journal of Applied Social Psychology, 1990, 20:1776−88.
24. Russell LA, Goltz JD, Bourque LB. Preparedness and hazard mitigation actions before and after twoearthquakes. Environment and Behavior 1995, 27:744−70.
25. Bourque LB, Shoaf KI, Nguyen LH. Survey research. International Journal of Mass Emergencies andDisasters, 1997, 15 (in press).
An overview of the Earthquake Insurance Programme in Japan
M. Miyakawa1
1M. Miyakawa of Yasuda Fire & Marine Insurance Company is Chairman of the EarthquakeInsurance Committee of the Marine and Fire Insurance Association of Japan.
Japan is known as a land of earthquakes. In January 1995, we were hit by the Great Hanshin−AwajiEarthquake. More than 6000 people lost their lives, 200 000 houses were either totally or partially destroyed,railroads and highways were severely damaged, and electricity and gas supplies failed for a considerablelength of time. The total economic damage is estimated at about 84 billion dollars (Fig. 1.6). This andsubsequent figures have been calculated in US dollars using the exchange rate of 115 yen per dollar. Sincethe earthquake, we have been putting the greatest effort into the restoration of the area affected but,unfortunately, further effort is still required.
Figure 1.6. The Great Hanshin−Awaji Earthquake loss
Number of casualties andproperty damage(As of 27 December 1995Announced by Fire andDisaster management Agency,Ministry of Home Affairs)• Dead/missing 6310• Injuries 43 177• Houses damaged 436 416
(Totallydestroyed100 302)(Halfdamaged108 741)(Partiallydamaged227 373)
The extent of damage (rough estimate)(Billion dollars)
• Buildings 55• Transport facilities (roads, harbours, railways) 19• Lifeline (waterworks, drainage, etc.) 5• Other 4
Total 83The total payment made by the Earthquake Insurance Programme as a result of the Kobe earthquake wasabout 680 million dollars.
28

Since strong earthquakes hit Japan periodically which caused enormous damages, presented in Fig. 1.7 (intoday's dollars), there are compelling needs for earthquake insurance cover. However, private insurancecompanies were very reluctant to underwrite earthquake risks and until 1964 wrote limited earthquake coverfor commercial property only. There are three main reasons for this. The first is that once a strong earthquakeoccurs the loss is catastrophic, far beyond the capacity of the private insurance industry. Secondly, thefrequency and severity of earthquakes hits large numbers of people so it is difficult to spread the risk, which isthe basis of the private insurance business. The third reason is that there is the risk of adverse selection,which sometimes makes it difficult to limit the insurance only to risks susceptible to earthquake damage.
Figure 1.7. Earthquake damage for the past 500 years − Amount of claims paid (based on data as of 31March 1996)
The 1964 Niigata earthquake changed the situation. Due to the serious damage caused by that earthquake,the need for earthquake insurance became a serious social matter and the "Law concerning EarthquakeInsurance" was implemented in 1966. Under the law, the Earthquake Insurance Programme was introducedwhereby government plays a major role as the re−insurer of the programme. The Earthquake InsuranceProgramme provided only limited cover at the beginning. However, keeping pace with accumulating reserves,we have been constantly improving the programme to the best of our abilities. Most recently, following theKobe earthquake we improved the programme by raising the maximum limit of liability and improving thecoverage for household property. The programme has seven main features.
First, the property covered by the Earthquake Insurance Programme is dwelling−houses and their contentsonly, and commercial property is not covered under the programme. This is because the purpose of the "Lawconcerning Earthquake Insurance" is to help bring greater stability to people's lives.
The second feature is risk covered under the programme. The Earthquake Insurance Programme covers lossor damage by fire, shock, sinking or landslide caused by earthquake, volcanic eruption and tsunami (a tidalwave caused by an earthquake).
One point is worth noting here: fire insurance policies available in Japan exclude fire losses caused byearthquake. In other words, you need to buy both fire insurance and earthquake insurance to cover all firelosses. The reason fire insurance excludes fire losses caused by earthquakes is because dwelling−houses inJapan, especially in urban areas like Tokyo, are very densely concentrated and most of them are made ofwood. A major earthquake is likely to cause many outbreaks of fire, and such fires quickly spread over a widearea and can lead to losses beyond the capacity of the private insurance industry.
The third feature of the programme is how we sell the earthquake insurance. To fulfil the purpose behind the"Law concerning Earthquake Insurance", we sell earthquake insurance in combination with fire insurancewithout exception. In other words, we do not sell earthquake insurance by itself; it is always sold together withfire insurance. However, a customer who does not wish to buy earthquake insurance but only fire insurancemay do so.
29
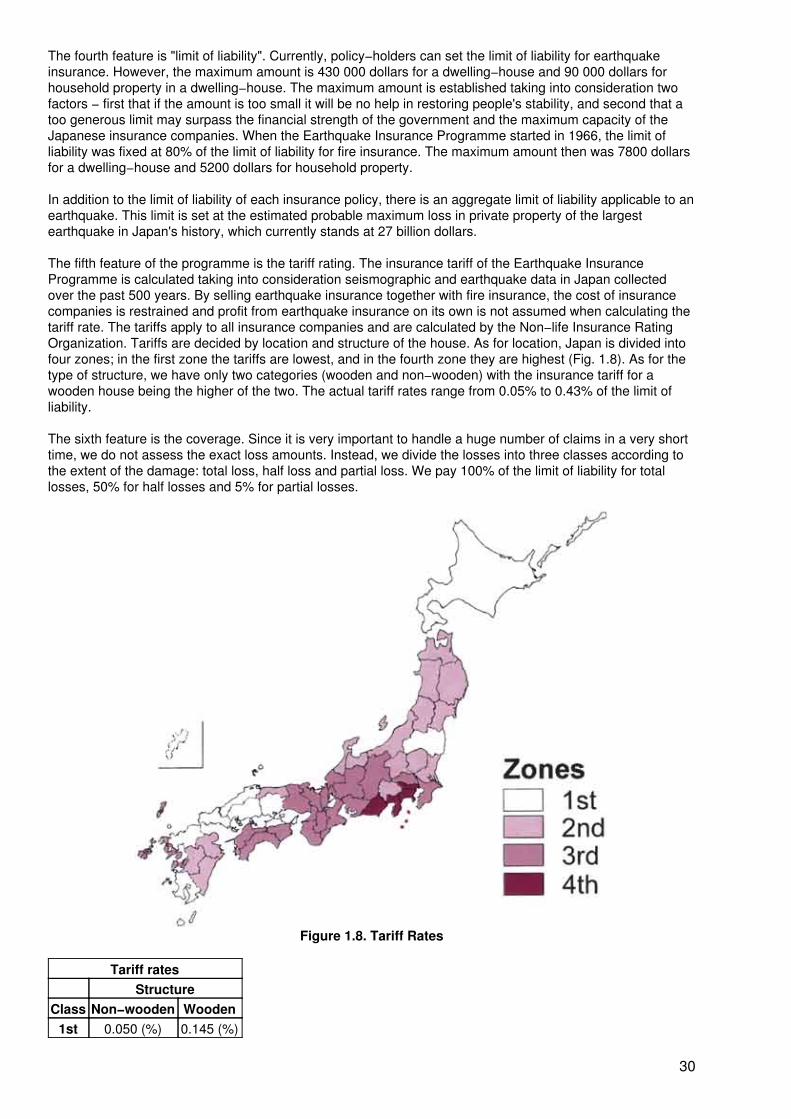
The fourth feature is "limit of liability". Currently, policy−holders can set the limit of liability for earthquakeinsurance. However, the maximum amount is 430 000 dollars for a dwelling−house and 90 000 dollars forhousehold property in a dwelling−house. The maximum amount is established taking into consideration twofactors − first that if the amount is too small it will be no help in restoring people's stability, and second that atoo generous limit may surpass the financial strength of the government and the maximum capacity of theJapanese insurance companies. When the Earthquake Insurance Programme started in 1966, the limit ofliability was fixed at 80% of the limit of liability for fire insurance. The maximum amount then was 7800 dollarsfor a dwelling−house and 5200 dollars for household property.
In addition to the limit of liability of each insurance policy, there is an aggregate limit of liability applicable to anearthquake. This limit is set at the estimated probable maximum loss in private property of the largestearthquake in Japan's history, which currently stands at 27 billion dollars.
The fifth feature of the programme is the tariff rating. The insurance tariff of the Earthquake InsuranceProgramme is calculated taking into consideration seismographic and earthquake data in Japan collectedover the past 500 years. By selling earthquake insurance together with fire insurance, the cost of insurancecompanies is restrained and profit from earthquake insurance on its own is not assumed when calculating thetariff rate. The tariffs apply to all insurance companies and are calculated by the Non−life Insurance RatingOrganization. Tariffs are decided by location and structure of the house. As for location, Japan is divided intofour zones; in the first zone the tariffs are lowest, and in the fourth zone they are highest (Fig. 1.8). As for thetype of structure, we have only two categories (wooden and non−wooden) with the insurance tariff for awooden house being the higher of the two. The actual tariff rates range from 0.05% to 0.43% of the limit ofliability.
The sixth feature is the coverage. Since it is very important to handle a huge number of claims in a very shorttime, we do not assess the exact loss amounts. Instead, we divide the losses into three classes according tothe extent of the damage: total loss, half loss and partial loss. We pay 100% of the limit of liability for totallosses, 50% for half losses and 5% for partial losses.
Figure 1.8. Tariff Rates
Tariff ratesStructure
Class Non−wooden Wooden1st 0.050 (%) 0.145 (%)
30
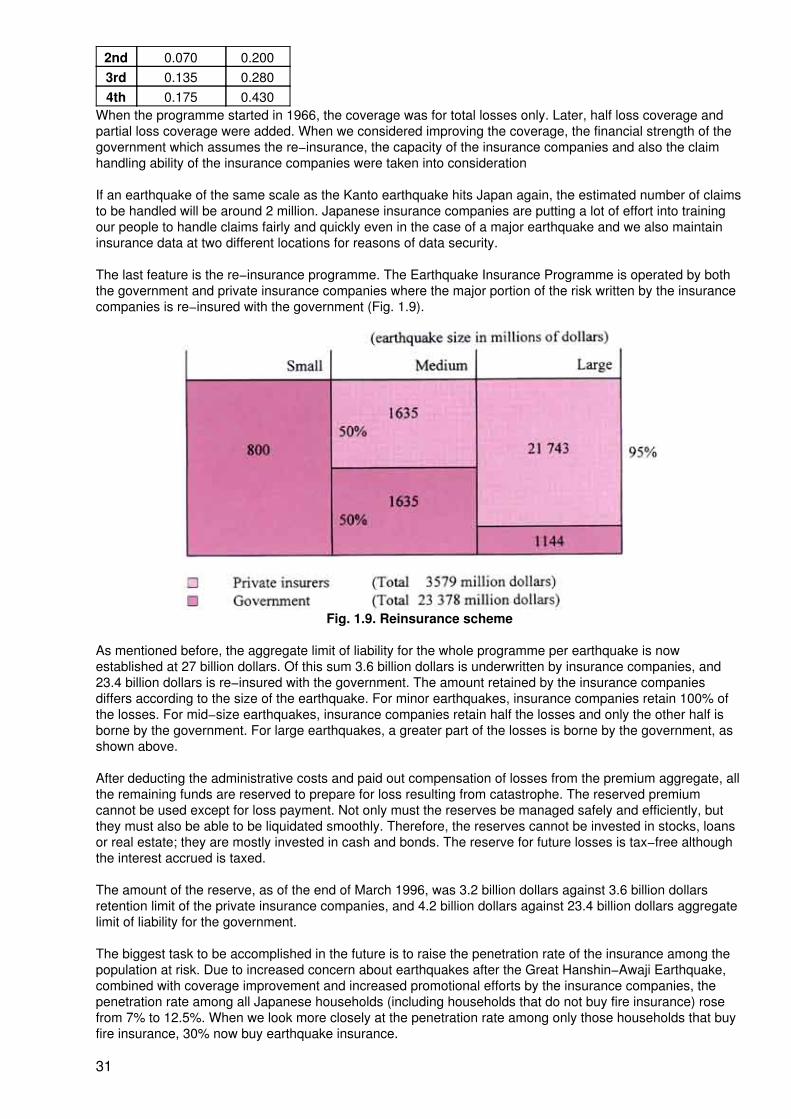
2nd 0.070 0.2003rd 0.135 0.2804th 0.175 0.430
When the programme started in 1966, the coverage was for total losses only. Later, half loss coverage andpartial loss coverage were added. When we considered improving the coverage, the financial strength of thegovernment which assumes the re−insurance, the capacity of the insurance companies and also the claimhandling ability of the insurance companies were taken into consideration
If an earthquake of the same scale as the Kanto earthquake hits Japan again, the estimated number of claimsto be handled will be around 2 million. Japanese insurance companies are putting a lot of effort into trainingour people to handle claims fairly and quickly even in the case of a major earthquake and we also maintaininsurance data at two different locations for reasons of data security.
The last feature is the re−insurance programme. The Earthquake Insurance Programme is operated by boththe government and private insurance companies where the major portion of the risk written by the insurancecompanies is re−insured with the government (Fig. 1.9).
Fig. 1.9. Reinsurance scheme
As mentioned before, the aggregate limit of liability for the whole programme per earthquake is nowestablished at 27 billion dollars. Of this sum 3.6 billion dollars is underwritten by insurance companies, and23.4 billion dollars is re−insured with the government. The amount retained by the insurance companiesdiffers according to the size of the earthquake. For minor earthquakes, insurance companies retain 100% ofthe losses. For mid−size earthquakes, insurance companies retain half the losses and only the other half isborne by the government. For large earthquakes, a greater part of the losses is borne by the government, asshown above.
After deducting the administrative costs and paid out compensation of losses from the premium aggregate, allthe remaining funds are reserved to prepare for loss resulting from catastrophe. The reserved premiumcannot be used except for loss payment. Not only must the reserves be managed safely and efficiently, butthey must also be able to be liquidated smoothly. Therefore, the reserves cannot be invested in stocks, loansor real estate; they are mostly invested in cash and bonds. The reserve for future losses is tax−free althoughthe interest accrued is taxed.
The amount of the reserve, as of the end of March 1996, was 3.2 billion dollars against 3.6 billion dollarsretention limit of the private insurance companies, and 4.2 billion dollars against 23.4 billion dollars aggregatelimit of liability for the government.
The biggest task to be accomplished in the future is to raise the penetration rate of the insurance among thepopulation at risk. Due to increased concern about earthquakes after the Great Hanshin−Awaji Earthquake,combined with coverage improvement and increased promotional efforts by the insurance companies, thepenetration rate among all Japanese households (including households that do not buy fire insurance) rosefrom 7% to 12.5%. When we look more closely at the penetration rate among only those households that buyfire insurance, 30% now buy earthquake insurance.
31

When we compare the penetration rate between zones, we discover that the higher the risk and thereforeinsurance rates the higher the rate of penetration. In the fourth zone penetration rate is highest with 20%among all households and 40% among holders of fire insurance policies.
We feel that it is our duty to further promote earthquake insurance. On the coverage side, we shall alsocontinue our efforts for improvement, such as raising the limit of liability. These tasks and improvements mustbe accomplished by understanding the needs of the Japanese people, while at the same time taking intoconsideration the financial strength of both the government and the private insurance companies. I hope thatthe experience of Japan's Earthquake Insurance Programme will be of help in the consideration of aworldwide indemnity programme for natural disasters.
Summary
Y. Nagasawa1
1Y. Nagasawa, Dr. Engr., Dipl. HFP, JIA, is from the Department of Architecture, GraduateSchool of Engineering, University of Tokyo, Tokyo, Japan.
Dr Eric K. Noji, Chief, International Emergency and Refugee Health Programs, Centers for Disease Controland Prevention, Atlanta, USA presented the epidemiology of earthquakes and its implications for vulnerabilityreduction, mitigation and relief. He indicated that 1.3 million died from major earthquakes during the presentcentury and that eight countries in the world account for about 75% of these fatalities; among these Chinaaccounted for 50%. The science of epidemiology involves a number of important areas which, if properlystudied and integrated with other disciplines of engineering, architecture and social and medical science, canreduce overall vulnerability to earthquakes and contribute to improved disaster preparedness and mitigation.Mortality and morbidity vary according to an earthquake's magnitude, duration and time of occurrence, humanresponse to the incident, and the type and construction of houses and buildings. The major risk factors are tolarge extent outside the medical realm. The collapse of buildings can lead to many types of injury, amongwhich multisystem injuries are quite common. Also the inhalation of the dust resulting from the collapse cancause severe morbidity and pose a challenge to rescue personnel and medical teams.
Demand for emergency medical assistance after an earthquake declines rapidly and is rarely needed after thesecond day of the disaster. Therefore, the utility of international teams which arrive later has to be examined.Good training must be prepared, including such important advice as staying in or outside buildings, whichdepends on the situation. Dr Noji concluded with a plea to researchers and practitioners to come together andshare their knowledge.
Dr Roman Kintanar, Coordinator, Typhoon Committee Secretariat and Chairman, Seismic TechnicalCommittee, International Decade for Natural Disaster Reduction (IDNDR), Quezon City, Philippines, made thesecond keynote presentation on seismological forecasting. He also explained the origin and role of IDNDR.
Dr Kintanar stated that even short−term forecasts of the time of an earthquake's occurrence, its magnitudeand the area of its impact need a lot more study and intensified research. Only very few examples ofreasonably successful predictions have become known, for example, in China, France, the Caribbean andMediterranean areas. A promising tool for earthquake forecasting is being developed by the measurement ofthe wave velocity in the ground which is known to change drastically before an earthquake occurs. Monitoringof the velocity of these waves is presently undertaken in four areas of the world.
Dr Linda B. Bourque, Professor, Department of Community Health Sciences, School of Public Health,University of California, USA, made the third keynote presentation on "Health implications of earthquakes:physical and emotional injuries after the Northbridge earthquake". Dr Bourque introduced her presentation bydefining the many factors that determine the number and severity of physical injuries following an earthquake.The findings of her research were based on a set of interconnected studies conducted by a consortium ofresearchers following the Northbridge earthquake of 17 January 1994 in Los Angeles, California. This studyaimed to more accurately count and assess the severity of physical and emotional injuries attributable to theearthquake, and was supported by data from coroners' reports, hospital admission records, hospitalemergency room records and three telephone surveys of Los Angeles County residents (amounting to a totalof 1849 telephone interviews) conducted during the period from August 1994 to June 1996. In many casesthere had to be examination of whether injuries were really earthquake−related or not. Also inhabitants ofadjacent areas not directly affected by the earthquake were found to have experienced widespread emotional
32
stress. While the number of 63 deaths directly attributable to structural failure and the number of injuries whichrequired hospitalization were remarkably low in the densely populated area of Los Angeles, it was estimatedthat some 240 000 persons out of the entire population of Los Angeles County experienced at least a minorinjury. Thirty thousand of these sought formal or informal medical care. Psychological effects were particularlysevere in persons who lost property, and in immigrants and women with children.
Mr Masao Miyakawa, Chairman, Fire and Earthquake Insurance Committee and Managing Director, YasudaFire and Marine Insurance Company Ltd., Tokyo, Japan, presented an overview of the Earthquake InsuranceProgramme in Japan. He stressed the need for an earthquake insurance coverage programme in a countrylike Japan, which is known to be periodically hit by strong earthquakes. However, private insurancecompanies were reluctant to take the risk of being involved in earthquake insurance until 1964. Only after thecatastrophic Niigata earthquake, when the government agreed to be a partner as the re−insurer againstearthquake risks and passed the "Law concerning Earthquake Insurance", has insurance become possible,but the penetration rate is still low. Since 1966 progressive improvements have been made to raise themaximum limit of liability and improve the coverage for household property. The main features of thisprogramme to cover the loss of private property are: that earthquake insurance is sold only in combinationwith fire insurance, that coverage is limited to around US$ 430 000 for a private house and around US$ 90000 for its contents, and that tariffs applicable are universal for all insurance companies and range between0.05% and 0.43% of insurance value.
He stressed that private citizens must be better prepared for self−help, i.e. by making sure that heavy furniturein their apartments is securely fixed and by being trained what to do first and how to help. He also hoped thatthe Japanese Earthquake Insurance Programme could be a model for the initiation of a worldwide indemnityprogramme for natural disasters.
During the joint discussion of the keynote presentations by the audience, the following issues werehighlighted:
− There is a need to further study animal behaviour as a predictor of earthquakes.
− It is necessary to organize community members in terms of immediate response to disasterand to orient them as to their important role in vulnerability reduction.
− There is a need to strengthen the organization of emergency medical services as theirfailure results in an increased number of casualties.
PART 2 − THE CONSEQUENCES OF EARTHQUAKES ON PEOPLE'S HEALTH
Medical consequences
Medical consequences of earthquake disasters in Russia
S.F. Goncharov1
1S.F. Goncharov, M.D., is Professor, All−Russian Centre for Disaster Medicine "Zaschita",Moscow, Russian Federation.
Practical daily experience in Russia strongly suggested the need for organizational and functional integrationof all health resources and manpower concerned with the medical response to disaster. Hence theAll−Russian Disaster Medical Service was set up. The structure of the service and the principles of itsoperation are still being developed. The service is concerned with the forecast of health consequences ofearthquakes and with the formation of a system of medical support to populations during relief operations(1,2,3,4).
Most studies of earthquake problems are devoted to trying to forecast the place and time of occurrence and todeveloping appropriate protective measures (normally relating to architecture and construction aspects) (5,6).
33
At the same time, apparently insufficient attention has been given to scientific study of earthquake reliefoperations and, in particular, to the organization of medical support. Though some specific aspects of thatproblem are described in a number of works (2,5,7,8,9,10), several aspects of the problem have not been fullyinvestigated, such as:
− the development of medical services in the aftermath of an earthquake;− the pattern of casualties and of evacuation of the injured;− the working conditions of medical units and facilities at the site of the earthquake;− the system of medical support to earthquake relief operations.
To clarify these issues we studied 2560 variants of earthquake occurrence and the corresponding medicalresponse, using mathematical computer simulation. In the course of these studies we took into considerationseismic intensity (from V to XII on the MSK−64 scale), three types of population centre (metropolis, city,town), 20 types of building design, different variants of population location at the moment of the earthquakeand different rates of extrication of the victims from the ruins (3,6, and 10 days).
Our own experience with earthquakes (Ashkhabad, 1948; Tashkent, 1967; Armenia, 1988; Neftegorsk, 1995)was of great help to us, as was the data on earthquakes in Japan, the USA and other countries(4,5,7,8,9,11,12). I wish to express my appreciation to the American and Japanese scientists for the valuableinformation obtained from them concerning, for example, the study of earthquakes in Loma Prieta (1989) andKobe (1995) (5,8,9).
The results of the research showed that the medical response in the aftermath of an earthquake is primarilyfaced with the practically instantaneous appearance of a large number of victims with traumatic injuries. Theamount and pattern of casualties among the population depend on the seismic intensity and where peoplewere at the moment the earthquake occurred (in an open place, in various types of buildings). The type oftraumatic injury also depends on the situation a person is in at the moment of injury (1,2,13,14).
We obtained a comprehensive picture of human casualties at the moment of an earthquake according totypes of building collapse and different seismic intensities. A quantitative relationship was established,demonstrating that greater seismic intensity causes larger numbers of casualties. It was shown that in themost devastating earthquakes of intensity XI to XII on the MSK−64 scale, the number of persons who manageto survive decreases. The data also indicate that the given mean indices can be applied to make averagepredictions for any populated area (if there is no definite information on the type of buildings), as shown by thefact that variations by different localities are very small (0.01% at seismic intensity 5 to 1.13% at seismicintensity 9). In the research we looked at how casualty values among people depend on their location (withthe proportion of people indoors ranging from 10% to 100%). These indices follow a distinct dependence: ifthe number of persons indoors increases, the number of casualties increases correspondingly.
Table 2.1. Possible delay of death of victims in the ruins, as a % of the given group of the victims(expert estimate)
Time after theearthquake
Proportion of delayed deaths within given group, normalized to total fatalitiesof that group
Seriously injured With injuries of moderateseverity
With life−threateninginjuries
With injuries notlife−threatening
Hours:>6 60
6−12 2013−24 2025−48 1048−72 3 10
Days:4−6 60 207−10 20 7511−12 10 5
34
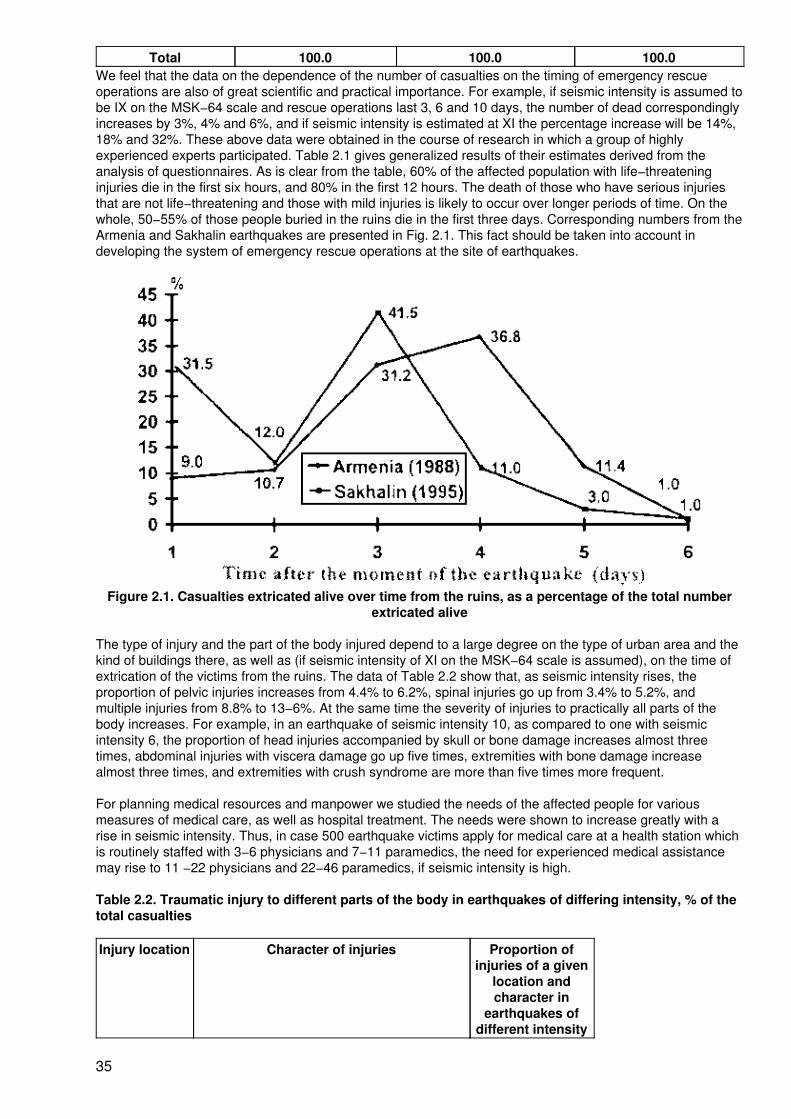
Total 100.0 100.0 100.0We feel that the data on the dependence of the number of casualties on the timing of emergency rescueoperations are also of great scientific and practical importance. For example, if seismic intensity is assumed tobe IX on the MSK−64 scale and rescue operations last 3, 6 and 10 days, the number of dead correspondinglyincreases by 3%, 4% and 6%, and if seismic intensity is estimated at XI the percentage increase will be 14%,18% and 32%. These above data were obtained in the course of research in which a group of highlyexperienced experts participated. Table 2.1 gives generalized results of their estimates derived from theanalysis of questionnaires. As is clear from the table, 60% of the affected population with life−threateninginjuries die in the first six hours, and 80% in the first 12 hours. The death of those who have serious injuriesthat are not life−threatening and those with mild injuries is likely to occur over longer periods of time. On thewhole, 50−55% of those people buried in the ruins die in the first three days. Corresponding numbers from theArmenia and Sakhalin earthquakes are presented in Fig. 2.1. This fact should be taken into account indeveloping the system of emergency rescue operations at the site of earthquakes.
Figure 2.1. Casualties extricated alive over time from the ruins, as a percentage of the total numberextricated alive
The type of injury and the part of the body injured depend to a large degree on the type of urban area and thekind of buildings there, as well as (if seismic intensity of XI on the MSK−64 scale is assumed), on the time ofextrication of the victims from the ruins. The data of Table 2.2 show that, as seismic intensity rises, theproportion of pelvic injuries increases from 4.4% to 6.2%, spinal injuries go up from 3.4% to 5.2%, andmultiple injuries from 8.8% to 13−6%. At the same time the severity of injuries to practically all parts of thebody increases. For example, in an earthquake of seismic intensity 10, as compared to one with seismicintensity 6, the proportion of head injuries accompanied by skull or bone damage increases almost threetimes, abdominal injuries with viscera damage go up five times, extremities with bone damage increasealmost three times, and extremities with crush syndrome are more than five times more frequent.
For planning medical resources and manpower we studied the needs of the affected people for variousmeasures of medical care, as well as hospital treatment. The needs were shown to increase greatly with arise in seismic intensity. Thus, in case 500 earthquake victims apply for medical care at a health station whichis routinely staffed with 3−6 physicians and 7−11 paramedics, the need for experienced medical assistancemay rise to 11 −22 physicians and 22−46 paramedics, if seismic intensity is high.
Table 2.2. Traumatic injury to different parts of the body in earthquakes of differing intensity, % of thetotal casualties
Injury location Character of injuries Proportion ofinjuries of a given
location andcharacter in
earthquakes ofdifferent intensity
35

6 8 10 12Head Total 19.0 19.0 18.3 18.2
Including bone injuries 0.6 1.3 3.3 3.6Thorax Total 8.8 8.5 7.7 7.6
Including bone injuries 0.8 1.1 2.2 2.3Abdomen Total 1.0 1.0 1.0 1.0
Including viscera injuries 0.04 0.07 0.20 0.20Pelvis Total 4.4 4.8 6.0 6.2
Including bone injuries and urogenital organs 0.4 1.0 2.6 2.8Spine Total 3.4 3.8 5.0 5.2
Including bone injuries 0.5 1.0 2.7 2.9Extremities Total 54.6 53.2 48.8 48.2
Including bone injuries 5.2 7.5 14.9 16.0Including crush syndrome 2.3 2.8 12.6 14.0
Multiple 8.8 9.7 13.2 13.6Including crush syndrome 0.6 1.3 3.3 3.6
If seismic intensity is estimated at XI to XII on the MSK−64 scale, more than 50% of the injured requirehospital treatment. In relation to the total population, the maximum relative need for hospital beds arises atseismic intensities of 9−10. One should pay attention to the fact that − according to our research − the relativenumber of hospital beds remains fairly stable at different seismic intensities and various locations.
Our experience and research led to the formulation of a system of medical support in response toearthquakes. The system has to a considerable degree been tested in practice (1,4,11). Its main features arethe following:
1. In the organization and provision of medical support, the All−Russian Disaster MedicalService:
− takes part in deliver)' of first aid and in the evacuation of casualties from thesite of an earthquake (general−purpose emergency rescue teams must carryout the search for the injured, their extrication from the ruins, delivery of firstaid at the site of the disaster and removal of casualties);
− organizes and delivers emergency medical care to the injured atprehospital and hospital stages;
− organizes transportation of casualties between stages of medicalevacuation.
2. All medical facilities of a given administrative region, irrespective of their type, are involvedin medical emergency response to help the victims of an earthquake (see Fig. 2.2).
3. Medical support in earthquake relief operations is organized as a chain of medicaltreatment, with competent medical care provided to patients throughout their evacuation tohospitals. Depending on the type of earthquake and the state the relief operations are in,different medical measures are necessary.
4. Hospital medical facilities within the system of the Disaster Medical Service in the zone ofan earthquake, as well as teams of medical experts attached to other medical facilities,operate under the system for up to 15 days− After this period of time the treatment of thedisaster victims and their rehabilitation are taken care of by the public health system.
5. An effective system will be set up for the dispatch and medical escort of the injured whenevacuating and transporting casualties.
36
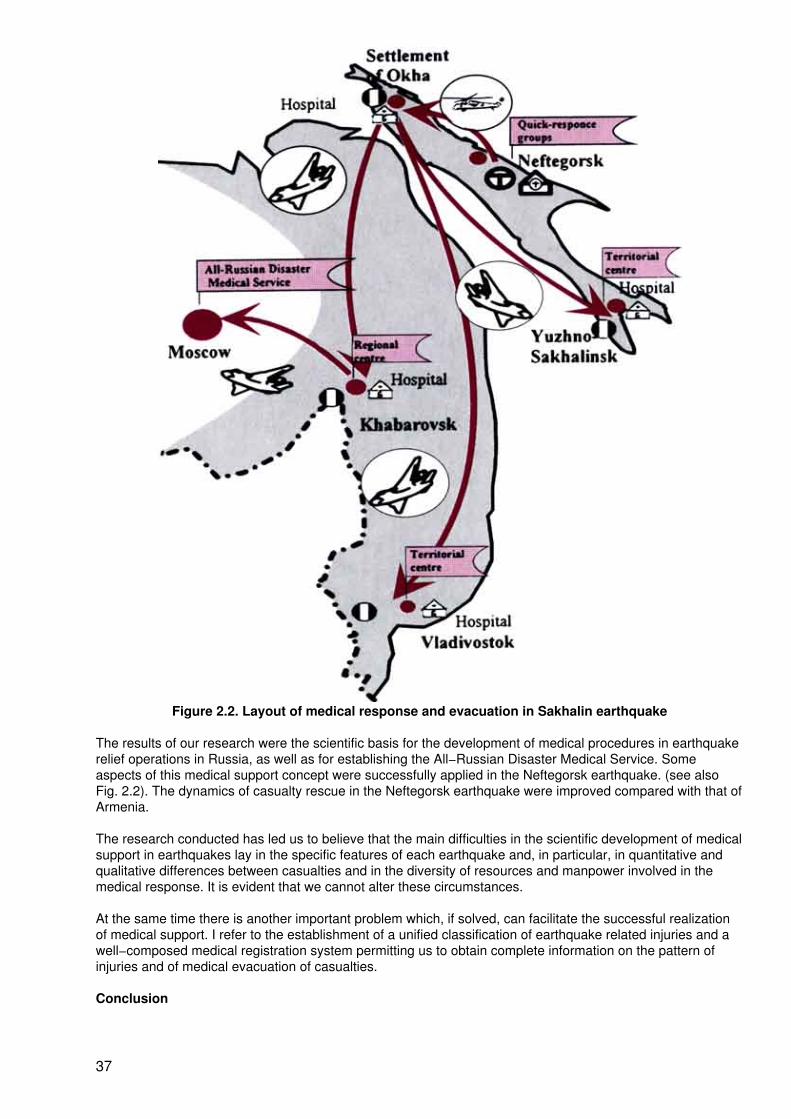
Figure 2.2. Layout of medical response and evacuation in Sakhalin earthquake
The results of our research were the scientific basis for the development of medical procedures in earthquakerelief operations in Russia, as well as for establishing the All−Russian Disaster Medical Service. Someaspects of this medical support concept were successfully applied in the Neftegorsk earthquake. (see alsoFig. 2.2). The dynamics of casualty rescue in the Neftegorsk earthquake were improved compared with that ofArmenia.
The research conducted has led us to believe that the main difficulties in the scientific development of medicalsupport in earthquakes lay in the specific features of each earthquake and, in particular, in quantitative andqualitative differences between casualties and in the diversity of resources and manpower involved in themedical response. It is evident that we cannot alter these circumstances.
At the same time there is another important problem which, if solved, can facilitate the successful realizationof medical support. I refer to the establishment of a unified classification of earthquake related injuries and awell−composed medical registration system permitting us to obtain complete information on the pattern ofinjuries and of medical evacuation of casualties.
Conclusion
37
Despite many investigations into the problem of earthquakes, the medical aftermath, the casualty patterns andthe system of medical support at the site of an earthquake have been insufficiently studied. Our researchlooked at 2560 variants of earthquakes (varying seismic intensity, different types of building design, populationactivities, location of the population at the moment of the earthquake, and speed of emergency rescueoperations). The medical follow−up to an earthquake is characterized primarily by a practically instantaneousappearance of a great number of victims with traumatic injuries. Some 50−55% of victims buried in the ruinsdie in the first three days, and this fact should be taken into account when developing emergency rescueoperations. According to our models we predicted casualties among populations that coincide with actual datafrom the earthquakes in Spitak and Neftegorsk.
Our research and experience led to the formulation of the concept of the All−Russian Medical Support Systemfor earthquake−stricken areas. We should like to recommend our findings and recommendations forapplication in other countries.
References
1. Goncharov SF. Medical support of population in earthquake relief operations. 15−16.11.1995. Tashkent, 1995.
2. Goncharov SF, Lobanov GP. Regularities in development of medico−sanitary aftermath of earthquakes.Forecast technique of probable casualties among population in earthquakes.
20.11.1995. 1995.
3. Nechaev EA, Farshatov MN. Military medicine and peacetime disasters. Moscow, 1994.
4. On life and health protection of RF population in emergencies of man−made and natural origin: Ordinanceof the Government of the Russian Federation # 420, dated 3 May 1994.
5. The Great Hanshin−Awaji (Kobe) Earthquake in Japan: on site relief and international response. UnitedNations Department of Humanitarian Affairs, February 28 −March 10, 1995, Geneva. 1995, 23(7).
6. Ulomov V.I. Seismic hazard and earthquake "syndrome". 1996, 13(1):72−80.
7. Avdokhin VP. The San Francisco earthquake medical response. , 1990,4:27−33.
8. Durkin ME et al. Injuries and emergency medical response in the Loma Prieta earthquake. Bulletin of theSeismological Society of America, 1991.
9. Thiel CC (Ed.). Competing against time: report to the Governor from The Board of Inquiry on the 1989Loma Prieta Earthquake, Sacramento, State of California, Office of Planning and Research, 1990.
10. United States Geological Survey. Proc. Conf. XLIX: A Meeting of the US Ad Hoc Working Group on"Earthquake−Related Casualties", USGS Open−File Report 90−244, 1990.
11. Goncharov SF. Medical support of population in earthquake relief operations on Sakhalin Island.23−24.10.1995, Moscow, 1995.
12. The Earthquake in Japan. (109), Moscow, 1995.
13. Nechaev EA (ed.). Crush syndrome. Moscow, 1989.
14. Nikogosyan RV. The Armenia earthquake: experience, conclusions, problems. 1990, 9:7−9.
38
Acute diseases during and after the Great Hanshin−Awaji Earthquake
K. Tatemichi1
1K. Tatemichi is Director, Emergency Department, Kobe City General Hospital, Kobe, Japan.
Background
In this century there have been 18 major earthquakes in Japan. Eight of them killed more than 1000 people.The Great Hanshin−Awaji Earthquake had the second largest number of victims, exceeded only by the Kantoearthquake of 1923 in which 140 000 people died, most of them from fire. The epicentre of the earthquakewas just near the centre of the modem city of Kobe in a highly populated area. The maximum ground motionof 3m was the severest in the history of Japan.
In the Great Hanshin−Awaji Earthquake, more than 70% of the victims died immediately and more than 90%died within the first day. Seventy−nine per cent of the deaths were from suffocation, crushing and burns (1).Patients presenting themselves with acute diseases after the earthquake came chiefly from home (51.6%),from refugee centres (27.7%) and from hospitals (14.9%) which had admitted 2−3 times more patients thanthey had capacity for (2). We saw 2978 patients during the four weeks after the disaster, and 475 acutely illpatients were hospitalized (3).
The Kobe City General Hospital emergency department is the only tertiary level trauma and medical centre inKobe (population 1.4 million). Before the earthquake more than 3000 people with trauma or acute diseaseshad been admitted annually. About one−third of all serious cases in the whole city were brought to this centre.
The hospital has 1000 beds. Its functioning was severely disrupted by the earthquake which destroyedvarious apparatus, cut off basic services and damaged the bridge which was the only way onto the artificialisland where the hospital was built, thus restricting access. Making the most of what was possible, 137patients were treated (including six who underwent surgery) during the first week after the earthquake and475 patients were treated within a month. These 475 patients comprised 333 with acute diseases and 142with trauma.
Objective and methods
This paper aims to analyse the acute diseases during and after the earthquake compared with the data in atypical month before the disaster.
All the patients hospitalized in the Kobe City General Hospital from 17 January to 13 February (four weeks)were listed, and cases of respiratory, cardiac, gastric and central nervous system illness were studied.
Results
Classification and incidence
In the phase during and just after the disaster, respiratory disease was the most frequent, with 24 patients inthe first week, 28 in the second and a total of 106 within the four−week period under study. Cardiac casesamounted to 18 in the first week, 20 in the next and a total of 68 within four weeks. There were no cases ofgastric illness in the first week, but there were 13 in the next, 17 in the third and 26 in the fourth week, giving atotal of 56 within four weeks.
The early appearance of respiratory disease, followed by cardiac problems and the later increase in gastricillness seems a significant tendency (Fig. 2.3). Patients with central nervous system diseases were few innumber and appeared late in the fourth week after the disaster.
39
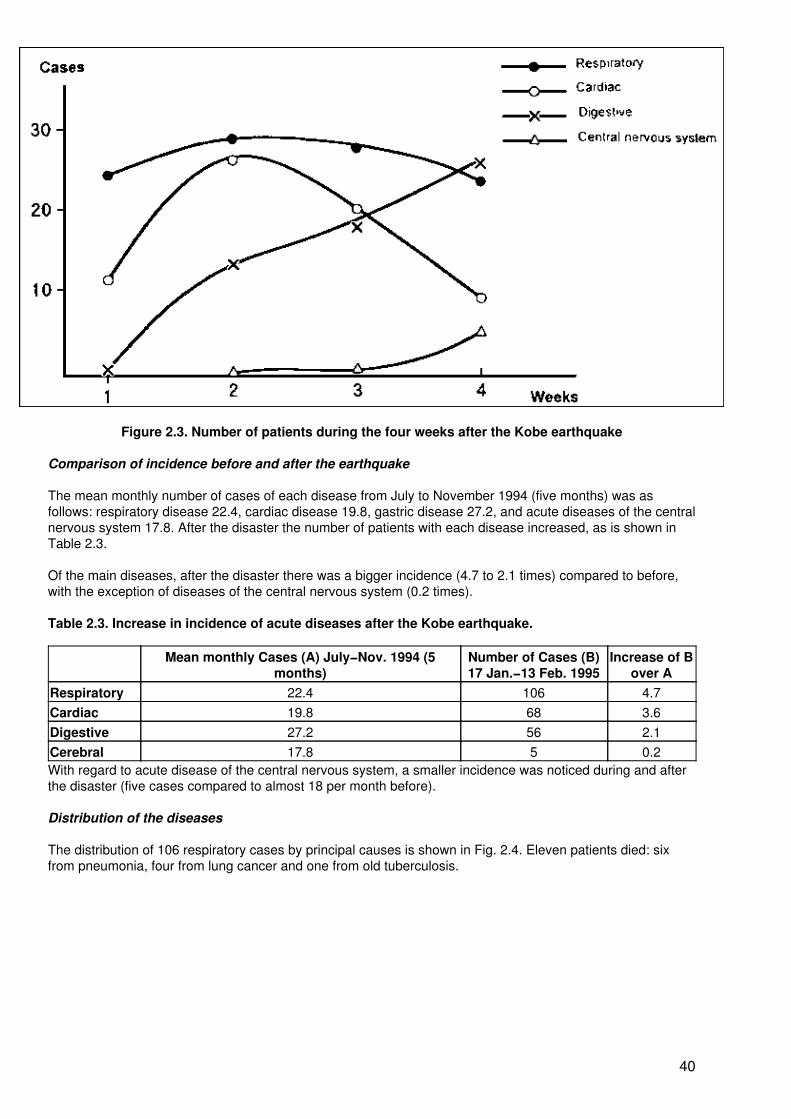
Figure 2.3. Number of patients during the four weeks after the Kobe earthquake
Comparison of incidence before and after the earthquake
The mean monthly number of cases of each disease from July to November 1994 (five months) was asfollows: respiratory disease 22.4, cardiac disease 19.8, gastric disease 27.2, and acute diseases of the centralnervous system 17.8. After the disaster the number of patients with each disease increased, as is shown inTable 2.3.
Of the main diseases, after the disaster there was a bigger incidence (4.7 to 2.1 times) compared to before,with the exception of diseases of the central nervous system (0.2 times).
Table 2.3. Increase in incidence of acute diseases after the Kobe earthquake.
Mean monthly Cases (A) July−Nov. 1994 (5months)
Number of Cases (B)17 Jan.−13 Feb. 1995
Increase of Bover A
Respiratory 22.4 106 4.7Cardiac 19.8 68 3.6Digestive 27.2 56 2.1Cerebral 17.8 5 0.2With regard to acute disease of the central nervous system, a smaller incidence was noticed during and afterthe disaster (five cases compared to almost 18 per month before).
Distribution of the diseases
The distribution of 106 respiratory cases by principal causes is shown in Fig. 2.4. Eleven patients died: sixfrom pneumonia, four from lung cancer and one from old tuberculosis.
40
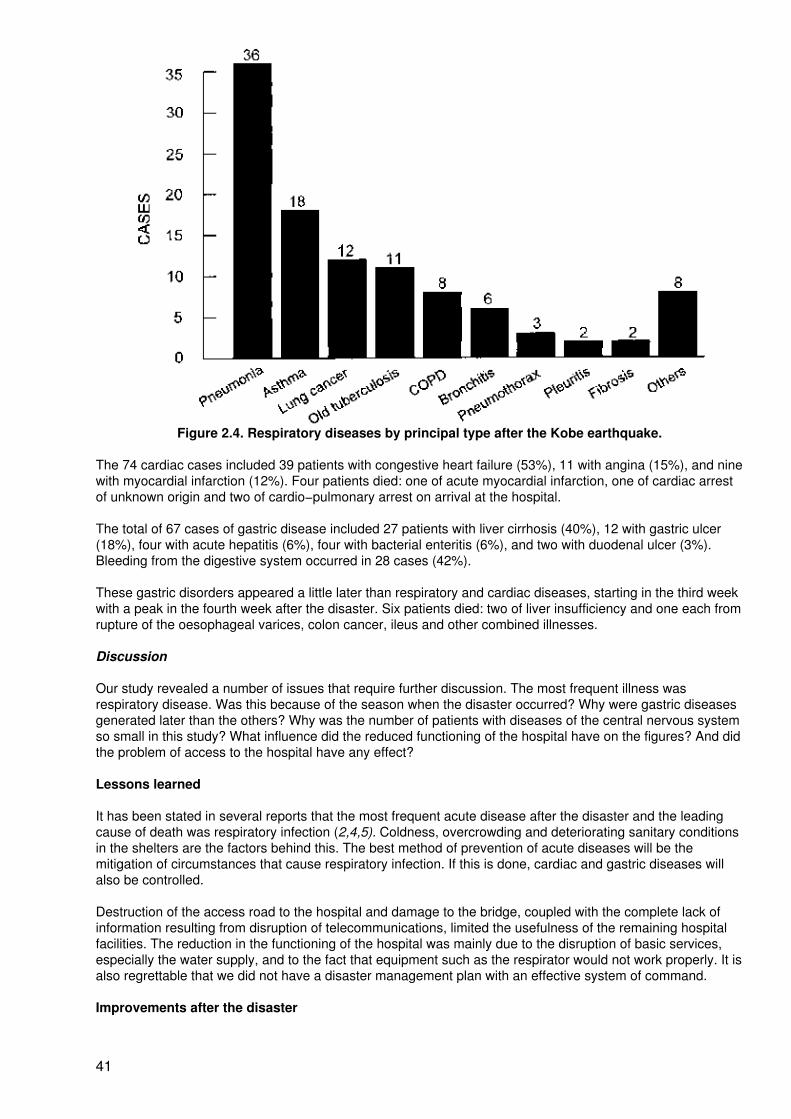
Figure 2.4. Respiratory diseases by principal type after the Kobe earthquake.
The 74 cardiac cases included 39 patients with congestive heart failure (53%), 11 with angina (15%), and ninewith myocardial infarction (12%). Four patients died: one of acute myocardial infarction, one of cardiac arrestof unknown origin and two of cardio−pulmonary arrest on arrival at the hospital.
The total of 67 cases of gastric disease included 27 patients with liver cirrhosis (40%), 12 with gastric ulcer(18%), four with acute hepatitis (6%), four with bacterial enteritis (6%), and two with duodenal ulcer (3%).Bleeding from the digestive system occurred in 28 cases (42%).
These gastric disorders appeared a little later than respiratory and cardiac diseases, starting in the third weekwith a peak in the fourth week after the disaster. Six patients died: two of liver insufficiency and one each fromrupture of the oesophageal varices, colon cancer, ileus and other combined illnesses.
Discussion
Our study revealed a number of issues that require further discussion. The most frequent illness wasrespiratory disease. Was this because of the season when the disaster occurred? Why were gastric diseasesgenerated later than the others? Why was the number of patients with diseases of the central nervous systemso small in this study? What influence did the reduced functioning of the hospital have on the figures? And didthe problem of access to the hospital have any effect?
Lessons learned
It has been stated in several reports that the most frequent acute disease after the disaster and the leadingcause of death was respiratory infection (2,4,5). Coldness, overcrowding and deteriorating sanitary conditionsin the shelters are the factors behind this. The best method of prevention of acute diseases will be themitigation of circumstances that cause respiratory infection. If this is done, cardiac and gastric diseases willalso be controlled.
Destruction of the access road to the hospital and damage to the bridge, coupled with the complete lack ofinformation resulting from disruption of telecommunications, limited the usefulness of the remaining hospitalfacilities. The reduction in the functioning of the hospital was mainly due to the disruption of basic services,especially the water supply, and to the fact that equipment such as the respirator would not work properly. It isalso regrettable that we did not have a disaster management plan with an effective system of command.
Improvements after the disaster
41
Respiratory diseases will be well controlled by comfortable shelters with sufficient sanitation, protection fromcold, and relief materials. Additional measures that either have already been implemented or are plannedinclude a helicopter transportation system, a strong hospital with aseismic equipment and flexible links to thewater, electricity and telecommunications systems, a tunnel under the sea as another access to the islandhospital, and an effective disaster management plan.
References
1. Internal report of the Community Health Division, Public Health and Environment Department, HyogoPrefecture, 1995.
2. Report by the research project on early medical response to the Great Hanshin−Awaji Earthquake.Government of Japan, 1996.
3. Tatemichi K. Early medical response to the Great Hansihn−Awaji Earthquake (Japanese). Kobe MunicipalHospital Bulletin (special ed.), 17 January 1996:45−57.
4. Kario K, Ohhashi T. A follow−up study on cardiovascular disease at the time of the Hanshin AwajiEarthquake. Medicine & Global Survival, 1995, 2(4):191−201.
5. Kunii O, Akagi M, Kita E. The medical and public health response to the Great Hanshin Awaji Earthquake inJapan: a case study in disaster planning. Medicine & Global Survival, 1995, 2(4):210−226.
Long−term studies of mortality and morbidity following the Armenian earthquake
A.K. Melkonian1, H.K. Armenian2 and A.P. Hovanesian3
1A.K. Melkonian, M.D., is from the Republican Information and Computer Centre, Ministry ofHealth, Armenia.
2H.K. Armenian, M.D., Ph.D., is from the Department of Epidemiology, School of Hygiene andPublic Health, Johns Hopkins University, Baltimore, USA.
3A.P. Hovanesian, Ph.D., is from the Republican Information and Computer Centre, Ministryof Health, Armenia.
Most investigations that have studied mortality from earthquakes have used cross−sectional field surveytechniques or case−control methods and have limited the investigation to the period immediately following thedisaster (1−5). Follow−up data from previous earthquakes suggest that there may be an increase in mortalityduring the post−earthquake period, particularly from coronary heart disease. Looking at mortality data fromdeath registration, Katsouyanni et al (6) compared death rates on three consecutive days following theearthquake in Thessaloniki, Greece, to mortality at other times. They estimated that exposure to theearthquake increased the risk of deaths from cardiac origin three−fold and death from all causes 1.6 times.
An earthquake registering 6.9 on the Richter scale hit the northern part of the Armenian Republic of the SovietUnion at 11:41 a.m. on 7 December 1988 (7). Between half a million and 700 000 people were madehomeless, with deaths estimated at 25 000. More than 21 000 homes were destroyed (8)− As part of a specialinformation system project that collected data about the population in the aftermath of the earthquake, weinitiated a number of epidemiological studies that would provide the necessary data about structural riskfactors and appropriate protective behaviour in the immediate period following the earthquake (9). Acase−control study was conducted in the summer of 1989 in the city of Gumri (known as Leninakan at thetime of the earthquake) involving 189 cases of hospitalized injuries and 156 controls who emerged from theexperience unscathed (10). This case−control study identified a higher risk of injuries for persons who were intaller buildings and who were located on the higher floors of these buildings, as well as for those who wereindoors during the earthquake. On the basis of these initial findings from the case−control study, a large−scalecohort study was started to study these risk factors from a population perspective, to monitor the long−termhealth effects of one of the worst natural disasters of the 20th century on the health conditions of the affectedpopulation and to ascertain continuing needs for health services.
Research methods
42
Following a search for an appropriate study population that could provide a list of persons on the daypreceding the earthquake, it was decided to use the employees of the Ministry of Health living in theearthquake region on 6 December 1988, plus their immediate families, as our study population. Lists of theseemployees were obtained from the payroll and personnel sections as well as from the Republican Informationand Computer Centre of the Ministry of Health in Yerevan. From an initial list of 9017 employees, 7016continuing as well as 705 new employees and their families were identified, usually at their workplace,although some were also interviewed at home. Of the employees that we were not able to contact, 927 hadmoved outside the earthquake region without leaving a follow−up address, 73 had died and their families hadrelocated, 106 refused to be interviewed, and for 895 names on the initial list no information was available orno contact could be established after a number of attempts. For each of the employees that could not belocated a special effort was made by colleagues to get information. A comparison of the information availablefrom the original lists revealed that the group of persons who could not be traced included a larger proportionof physicians in the city of Gumri (Leninakan) compared to the group that could be located.
The study population eventually included 35 043 persons − the 7016 interviewed employees and theirimmediate families, plus the 705 new employees and their families. Each of these employees and their familymembers were contacted twice in two series of interviews. These interviews were conducted during the period1990−1992. In addition, a psychiatric interview was conducted on a random subsample of 2100 persons fromthis same population of age 17−65. Following a definition of the variables of interest, a questionnaire wasdeveloped in Armenian and pretested on a small sample of employees. Each of the questionnaires was codedand entered into a computer format for processing and analysis. In view of the fact that the respondents to theinterview for this analysis were either health professionals or employees of the Ministry of Health with betterthan average access to the health care system and to diagnostic facilities, the information on causes ofmorbidity and mortality was very detailed and involved over 1000 different diagnoses or categories.
Simple frequency distributions and cross−tabulations provided an initial approach to the analysis. In order toadjust for the various factors, a multivariate logistic regression analysis was used. In addition to theadjustments, various other multivariate models were used to test potential interactions between the differentvariables. Incidence density matching with a SAS computer programme (11) was used to select controls forincident cases of coronary heart disease in order to overcome biases caused by coronary heart diseasedeaths.
Conclusion
This is the first analytic study of post−earthquake mortality that uses a population−based follow−up of a cohortby defining a study population for the day before the earthquake and tracing the outcomes in that same groupfollowing the disaster. Although an initial increase of mortality was observed during the first six months of thedisaster, the increase could not be explained by higher exposure to earthquake stressors, except that therewas a higher risk of death for persons who were located inside a building at the moment of the earthquake.
There are a number of potential problems that one has to refer to in reviewing the results of the current study.Ascertainment of deaths is one such potential problem. Although reported cause of death may have a lowdegree of validity in other studies, such reports by health professionals, as in this study, with a higher thanaverage access to the health care system and its diagnostic facilities is probably more valid than causes ofdeath obtained from lay interviewees. The possibility that some deaths during the first few days and weeksfollowing the disaster were missed by the interview process was minimized in this study by identifying ourstudy population on the day before the earthquake and identifying all deaths that occurred after that.
Our inability to establish important links between earthquake stressors and post−disaster mortality may bedue to inappropriate measurement of these stressors or loss as a result of the earthquake.
This study in the post−event phase of the earthquake allows us to identify risk factors of mortality andmorbidity and thus help reduce the long−term consequences of the disaster. Stressors have been identifiedas causes of mortality and morbidity, particularly for coronary artery disease, in other types of disaster. Ourown study of arteriographically determined coronary artery disease in Beirut during the civil war demonstratedthat persons with a higher exposure to war stressors had significantly more coronary artery obstruction (12).
This epidemiological study represents a step in the process of refining disaster research methodology for theinvestigation of the complex relationship between factors related to survival following earthquakes (13).
In this first longitudinal follow−up study of a population−based cohort, we investigated the long−term risk ofmorbidity, in particular for incident coronary heart disease, in persons exposed to stressors. People with a
43
profile of exposure to such stressors as a result of the disaster should be monitored intensively. Preventivemeasures should be considered in the post−disaster period for such persons.
References
1. Spence RJ, Coburn AW, Sakai S, Pomonis A. Reducing human casualties in building collapse: methods ofoptimising disaster plans to reduce injury levels. Cambridge, Martin Centre for Architectural and UrbanStudies, Cambridge University, 1991:1−55.
2. De Bruycker M, Greco D, Lechat MF. The 1980 earthquake in southern Italy: morbidity and mortality.International Journal of Epidemiology, 1985, 14(1):113−17.
3. Glass RI, Urrutia JJ, Sibony S et al. Earthquake injuries related to housing in a Guatemalan village.Science, 1977,197:638−43.
4. Roces MC, White ME, Dayrit MM, Durkin ME. Risk factors for injuries due to the 1990 earthquake in Luzon,Philippines. Bull. World Health Organ., 1992, 70:509−514.
5. Pretto EA, Ricci E, Klain M et al. Disaster reanimatology potentials: structured interview study in ArmeniaIII. Results, conclusions, and recommendations. Prehospital and disaster medicine, 1992, 7:327−338.
6. Katsouyanni K, Kogevinas M, Trichopoulos D. Earthquake related stress and cardiac mortality. Internationaljournal of epidemiology, 1986, 15:326−30.
7. Karapetian NK, Agbabian M, Chilingarian GV. Earthquakes of the Armenian highlands (seismic setting).Los Angeles, University of Southern California, 1991:1.
8. UNDRO. Multisectoral study on disaster and management planing in Armenia. Geneva, UNDRO, 1990.
9. Noji EK, Kelen GD, Armenian HK et al. The 1988 earthquake in Soviet Armenia: case study. Annals ofEmergency Medicine, 1990, 19:891−897.
10. Armenian HK, Noji EK, Oganessian AP. Case control study of injuries due to the earthquake in SovietArmenia. Bull. World Health Organ., 1992, 70:251−257.
11. Pearce N. Incidence density matching with a simple SAS computer program. International journal ofepidemiology, 1989, 18(4):981−84.
12. Sibai AM, Armenian HK, Alam S. Wartime determinants of arteriographically confirmed coronary arterydisease in Beirut. American journal of epidemiology, 1989:130:623−631.
13. Armenian HK. Methodologic issues in the epidemiologic studies of disasters. Proceedings of theInternational Workshop on Earthquake Injury Epidemiology for Mitigation and Response. Baltimore, MD,Johns Hopkins University, 1989: 95−106.
Summary
E. Pretto1and J. Levett2
1 E.A. Pretto M.D., M.P.H. is Principal Investigator, Disaster Reanimatology Study Group andAssociate Director Safar Center for Resuscitation Research, University of Pittsburgh Schoolof Medicine, Pittsburgh, USA.
2 J. Levett is Director of International Affairs, National School of Public Health, Ministry ofHealth and Welfare, Athens, Greece.
Professor Sergey Goncharov, Director, All−Russian Centre for Disaster Medicine, Ministry' of Public Healthand Medical Industry, Moscow, Russian Federation, presented data on the relationship between seismicintensity of earthquakes and casualties in his presentation entitled "Health Consequences of DisastrousEarthquakes in Russia". The experience in the Russian Federation and the former Soviet Union has been that
44
most fatalities occurred within six hours of the disaster and most injuries within three day's. The presentationand a supporting videotape showed a well−equipped system of field−hospitals which were developed fromarmy technology and were installed at the Neftegorsk earthquake within one day.
He also advocated the adoption of a universal classification of earthquake−related injuries and theestablishment of corresponding registries.
Dr Kiyoshi Tatemichi, Director, Emergency Department, Kobe City General Hospital, Kobe, Japan,mentioned that there was no developed plan for disaster management of hospitals before the earthquake. InKobe, 40 out of 80 hospitals were damaged. He described several types of non−traumatic diseases seenamong 475 patients treated at Kobe City General Hospital after the 1995 earthquake. The incidence of acuterespiratory diseases appeared early and continued high for a couple of months (up to 4.7 times normallevels). Besides respiratory diseases, cardiac, neurological and gastric diseases also increased.
Dr Arthur K. Melkonian presented a paper on "Long−term Studies of Mortality and Morbidity following theArmenian Earthquake". After the Spitak earthquake in Armenia which caused some 25 000 deaths and thedestruction of more than 25 000 houses, cohort studies were organized in association with the Notre DameUniversity in the United States. According to these studies, the risk of death from cardiac origin increasedthree times and death due to other causes rose 1.6 times. A special information system project was initiatedsoon after the Armenian earthquake and a case−control study in 1989. Based on these findings thelarge−scale cohort study was established. After four years the data showed that elderly, smokers, people whodo not exercise, drinkers of alcohol and people who tend to stay inside houses had a higher death rate fromcoronary and other causes.
Health consequences
Long−term effects of the Great Hanshin−Awaji Earthquake on urban public health
S. Sato1
1S. Sato is Professor, Department of Hygiene, Kobe University School of Medicine, Kobe,Japan
The long−term effects on public health of the Great Hanshin−Awaji Earthquake, which affected Kobe City andsurrounding areas on 17 January 1995, are discussed in this article from three standpoints. One is the resultof statutory health check−ups for infants and adults at various health centers in Hyogo Prefecture in the 15months after the earthquake. Long−term health problems are further discussed in relation to the numbers ofdeaths of people in Hyogo Prefecture in 1995, in comparison with those in 1994. The physical andpsychological problems of people living in temporary accommodation are also briefly discussed under thisheading.
The second topic of discussion is air pollution in Hyogo Prefecture, including Kobe City, after the earthquakewith reference to concentrations of NO2, SO2 and asbestos. An assessment of these air pollutants at variouspoints in the region is made and their effects on health are discussed.
Health problems not directly related to the earthquake but relevant to Kobe City and Hyogo Prefecture, andthat require improvement especially during the period of recovery from the earthquake, are also discussed.Under this topic the situation of some infectious diseases and ambient conditions is described.
Results of health check−ups and other surveys
In Japan there exists a system of statutory health check−ups for infants at the ages of 18 months and threeyears. The check−ups are required by the Maternal and Child Health Law. Items to be checked are mainlythose related to psychological and somatic developments and the check−up is implemented by municipalgovernments− When conditions requiring attention are found, infants are followed up by or referred tohospitals.
45
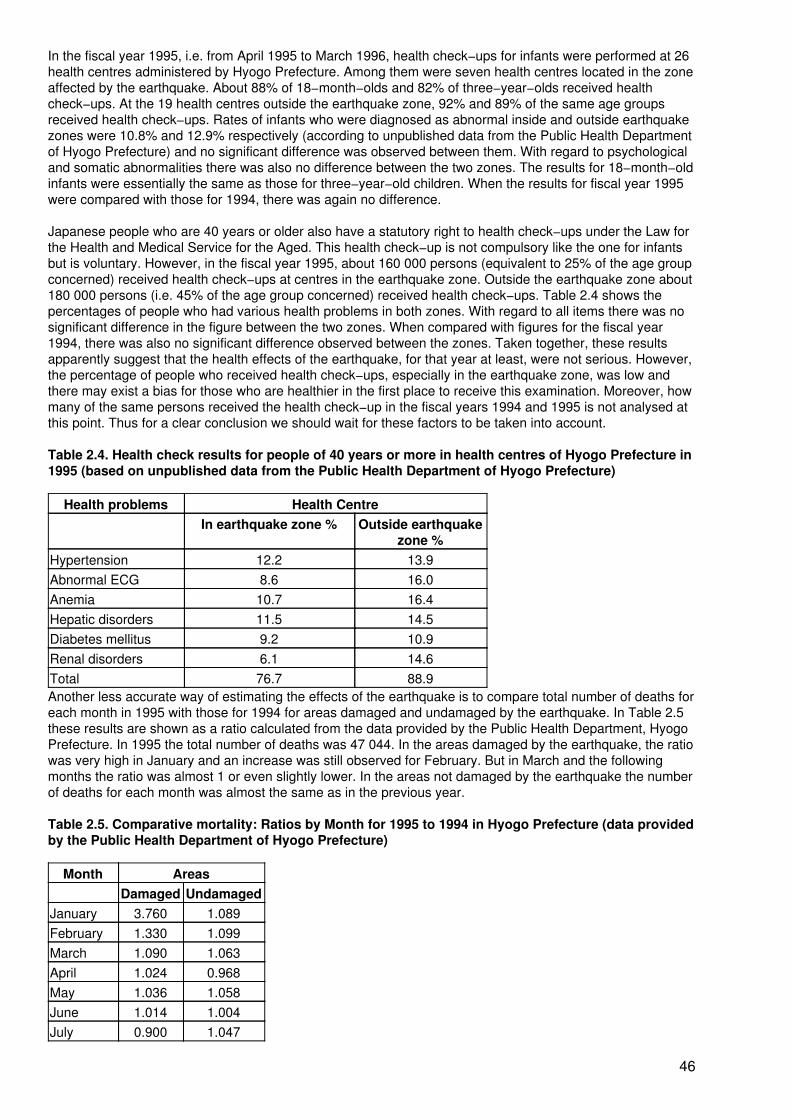
In the fiscal year 1995, i.e. from April 1995 to March 1996, health check−ups for infants were performed at 26health centres administered by Hyogo Prefecture. Among them were seven health centres located in the zoneaffected by the earthquake. About 88% of 18−month−olds and 82% of three−year−olds received healthcheck−ups. At the 19 health centres outside the earthquake zone, 92% and 89% of the same age groupsreceived health check−ups. Rates of infants who were diagnosed as abnormal inside and outside earthquakezones were 10.8% and 12.9% respectively (according to unpublished data from the Public Health Departmentof Hyogo Prefecture) and no significant difference was observed between them. With regard to psychologicaland somatic abnormalities there was also no difference between the two zones. The results for 18−month−oldinfants were essentially the same as those for three−year−old children. When the results for fiscal year 1995were compared with those for 1994, there was again no difference.
Japanese people who are 40 years or older also have a statutory right to health check−ups under the Law forthe Health and Medical Service for the Aged. This health check−up is not compulsory like the one for infantsbut is voluntary. However, in the fiscal year 1995, about 160 000 persons (equivalent to 25% of the age groupconcerned) received health check−ups at centres in the earthquake zone. Outside the earthquake zone about180 000 persons (i.e. 45% of the age group concerned) received health check−ups. Table 2.4 shows thepercentages of people who had various health problems in both zones. With regard to all items there was nosignificant difference in the figure between the two zones. When compared with figures for the fiscal year1994, there was also no significant difference observed between the zones. Taken together, these resultsapparently suggest that the health effects of the earthquake, for that year at least, were not serious. However,the percentage of people who received health check−ups, especially in the earthquake zone, was low andthere may exist a bias for those who are healthier in the first place to receive this examination. Moreover, howmany of the same persons received the health check−up in the fiscal years 1994 and 1995 is not analysed atthis point. Thus for a clear conclusion we should wait for these factors to be taken into account.
Table 2.4. Health check results for people of 40 years or more in health centres of Hyogo Prefecture in1995 (based on unpublished data from the Public Health Department of Hyogo Prefecture)
Health problems Health CentreIn earthquake zone % Outside earthquake
zone %Hypertension 12.2 13.9Abnormal ECG 8.6 16.0Anemia 10.7 16.4Hepatic disorders 11.5 14.5Diabetes mellitus 9.2 10.9Renal disorders 6.1 14.6Total 76.7 88.9Another less accurate way of estimating the effects of the earthquake is to compare total number of deaths foreach month in 1995 with those for 1994 for areas damaged and undamaged by the earthquake. In Table 2.5these results are shown as a ratio calculated from the data provided by the Public Health Department, HyogoPrefecture. In 1995 the total number of deaths was 47 044. In the areas damaged by the earthquake, the ratiowas very high in January and an increase was still observed for February. But in March and the followingmonths the ratio was almost 1 or even slightly lower. In the areas not damaged by the earthquake the numberof deaths for each month was almost the same as in the previous year.
Table 2.5. Comparative mortality: Ratios by Month for 1995 to 1994 in Hyogo Prefecture (data providedby the Public Health Department of Hyogo Prefecture)
Month AreasDamaged Undamaged
January 3.760 1.089February 1.330 1.099March 1.090 1.063April 1.024 0.968May 1.036 1.058June 1.014 1.004July 0.900 1.047
46
August 0.964 1.084September 0.951 1.018October 0.979 1.014November 0.933 1.065December 0.976 1.038For those living in temporary accommodation, rates of physical and psychological disorders are apparentlyhigh. As of April 1996, 37 378 people were living in temporary accommodation in Hyogo Prefecture and KobeCity. About 10% of them, i.e. 3565 people, had adult diseases such as cardiovascular and cerebrovasculardiseases and hypertension. Of these, 155 were suffering from tuberculosis, 512 from psychological problemsand 630 from psychosomatic disorders. The number of people with other disorders was 1294, according tothe Public Health Department of Hyogo Prefecture. Exact comparison of these figures with those of a controlgroup matched in sex and age but living in "ordinary" conditions was not done, but the rates of these disordersseem to be much higher for those living in temporary accommodation. If this is true, and when the results ofhealth check−ups are considered, the detrimental effects of the earthquake on health seem to have beenrather indirect, i.e. they were mainly due to poor living conditions. In fact a survey of nutritional intake ofpeople living in some temporary accommodation showed lower consumptions of meat, fish, eggs, milk, dairyproducts, fresh vegetables and oil.
Air pollution
Air pollution is continuously monitored at about 50 checkpoints in Hyogo Prefecture, including Kobe City, bythe Environment Bureau of the Lifestyle and Culture Department of the prefecture. The main items monitoredare NO2, SO2 and suspended particulate matter. At some points CO concentration is also monitored inrelation to pollution caused by engine exhaust fumes. In 1995 after the earthquake a further 19 hazardouschemicals in the air, such as ammonia, HF, HCN, formaldehyde, phenol, benzene and so on, were alsodetermined in February and July. Asbestos concentrations were measured seven times at 61 points wherebuildings were being destroyed and nine times at another 17 checkpoints in the same year.
Chronological changes of average concentrations of NO2 and SO2 at areas damaged and undamaged by theearthquake are shown in Fig. 2.5. Although less than the environmental standard of 0.04 ppm, NO;concentrations were always higher in damaged areas. This is mainly due to traffic congestion. Not muchdifference was seen with SO; between the two areas and its concentration was always below theenvironmental standard of 0.04 ppm. The concentrations of suspended particulate matter in damaged areaswere a little higher than those in undamaged areas until March 1995 but later they became almost the same inthe two areas (Fig. 2.6). Concentrations of other hazardous chemicals in the air were almost within the rangefound at other cities in Japan. Asbestos concentrations at points where building destruction was done wererather high until June 1995, i.e. 3.0−4.5 fibres/litre as average with a maximum value of 19.9 fibres/litre, butlater they decreased to 0.7 fibre/litre. At other points average values were 1.2 to 0.4 fibre/litre. These averagevalues were less than the Japanese environmental standard of 10 fibres/litre. The standardized mortality ratioof people exposed to asbestos for 25 years was reported to increase linearly depending upon theconcentration of asbestos. Suppose this dose response is linear at very low concentrations of asbestos,exposure to 10 fibres/litre of asbestos for 25 years would yield a standardized mortality ratio of one in 100000. Exposure to 1 fibre/litre, a concentration observed at the points where no building destruction was done,would only increase the standardized mortality ratio by 6 ×10−6. These air pollution results after theearthquake suggest no significant adverse health effects.
47
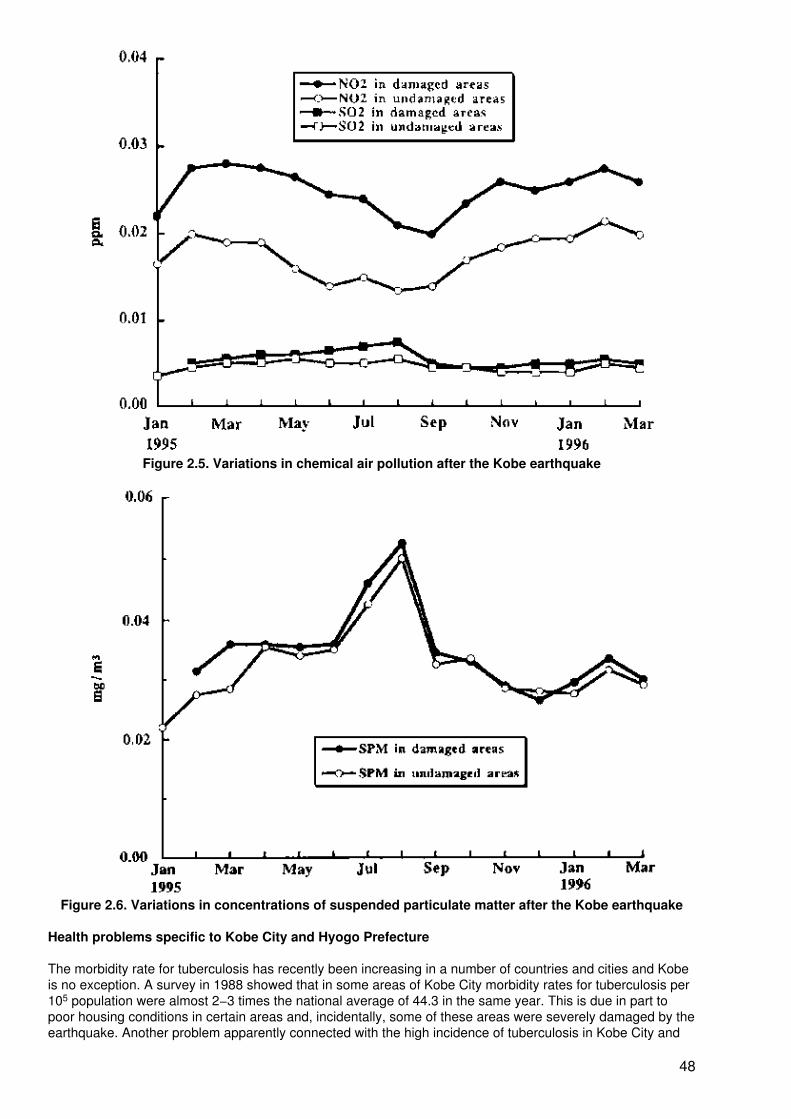
Figure 2.5. Variations in chemical air pollution after the Kobe earthquake
Figure 2.6. Variations in concentrations of suspended particulate matter after the Kobe earthquake
Health problems specific to Kobe City and Hyogo Prefecture
The morbidity rate for tuberculosis has recently been increasing in a number of countries and cities and Kobeis no exception. A survey in 1988 showed that in some areas of Kobe City morbidity rates for tuberculosis per105 population were almost 2−3 times the national average of 44.3 in the same year. This is due in part topoor housing conditions in certain areas and, incidentally, some of these areas were severely damaged by theearthquake. Another problem apparently connected with the high incidence of tuberculosis in Kobe City and
48

Hyogo Prefecture is the high incidences of liver diseases and hepatocellular carcinoma, possibly due tohepatitis C virus (HCV) infection. Preliminary data from a case−control study on the causative factors ofhepatocellular carcinoma in Hyogo Prefecture being carried out by our group show that bachelorhood inmales, past history of blood transfusion in both males and females and family history of HCV hepatitis inmales are significantly correlated with this type of cancer. The presence of the HCV antibody was found in83% of male and 92% of female cases. HCV is thought to be transmitted by blood transfusion or in a relatedmanner, but mother−to−infant, spouse−to−spouse, or intrafamilial transmission is also thought to beimportant. Links with drug abuse and tattooing are also discussed. Moreover, HCV is detectable also in thesaliva or urine of some HCV carriers, and HCV infection has recently been recognized as one of the sexuallytransmitted diseases. Accordingly, prevention of HCV infection may be improved via environmental controlsand changes in sexual behaviour. In this context, improving the sewage disposal system should be a priorityfollowing the earthquake. As of March 1995, average availability of mainline sewage disposal in HyogoPrefecture was 67.4%. Although in Kobe City it was nearly 100%, the average in the urban areas was still78.7% and the average in the rural areas only 6.7%. Improvement of this infrastructure should therefore playan important role in improving human health conditions, and the period of recovery from the earthquake is agood time to do this.
Discussion
In this article the long−term health effects of the earthquake were discussed first with reference to the resultsof health check−ups for infants and adults. On the basis of the relatively high rate of such examinations, i.e.more than 80%, it can be stated that serious psychological or somatic abnormalities were not seen in infantsliving in the earthquake zone at least within that fiscal year. However, there was redistribution of populationafter the earthquake and this was particularly the case with pregnant women, infants and elderly people. Therate of health checks was slightly lower in the earthquake zone than outside it. These facts should beconsidered before a clear conclusion is made. Significantly higher cases of abnormal delivery and retardedgrowth of delivered babies were reported with pregnant women who suffered in some way from theearthquake. The rate of health check−ups of elderly people was also low in the earthquake zone. Furtheranalysis of people who received the health check−up is necessary. For example, comparison of the incidenceof each health problem in people who received the examination both in 1995 and in previous years should bemade. In fact, the number of cases of myocardial infarction increased on Awaji Island in January and February1995.
Comparison of apparent results from health check−ups and apparently higher incidences of various disordersamong people living in temporary accommodation may suggest that the direct effects of the earthquake onhealth were not so serious− Rather, they were indirect and due to poor living conditions after the earthquakethat affected people both physically and psychologically. If so, the provision and maintenance of good livingconditions as soon as possible after a disaster would help with long−term health. Air pollution within a yearafter the earthquake was not serious although higher than usual concentrations of some pollutants were foundin some areas. Poor environmental or other conditions unfavourable for health should also be improved duringthe recovery from the earthquake. The Great Hanshin−Awaji Earthquake was a real tragedy in a number ofways, including human health, but it is hoped that we can learn from it and improve urban health in the future.
Acknowledgement. The author is deeply indebted to Hyogo Prefectural and Kobe City governments for theirkind provision of published as well as unpublised data relevant to the health effects of the GreatHanshin−Awaji Earthquake.
Mental health condition and mental health care of children after the Great Hanshin−Awaji Earthquake: the experience ofNishinomiya City
S. Shirataki1, Y. Matsukawa1 and H. Kashiwagi1
1Department of Psychiatry and Neurology, Kobe University School of Medicine, Kobe, Japan.
Over 6300 people were killed by the Great Hanshin−Awaji Earthquake. Some died immediately whenbuildings collapsed and wooden houses caught fire, and some died only several months later. The magnitudeof the earthquake and the extent of the area affected exceeded past experience in Japan. In this report wefocus attention particularly on the young generation and their mental reactions to the disaster. We alsopropose a school mental health promotion system that was not only useful in such an urgent situation as thisgreat earthquake but can also be applied to routine mental health in schools in Japan.
49
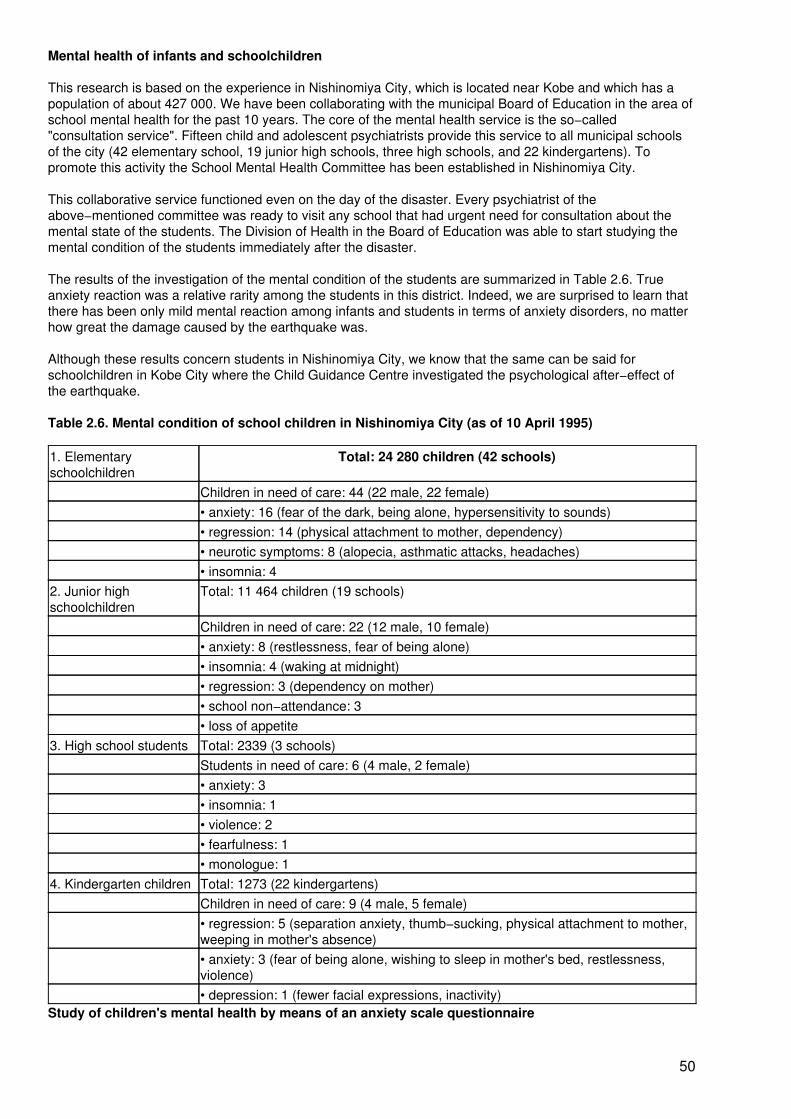
Mental health of infants and schoolchildren
This research is based on the experience in Nishinomiya City, which is located near Kobe and which has apopulation of about 427 000. We have been collaborating with the municipal Board of Education in the area ofschool mental health for the past 10 years. The core of the mental health service is the so−called"consultation service". Fifteen child and adolescent psychiatrists provide this service to all municipal schoolsof the city (42 elementary school, 19 junior high schools, three high schools, and 22 kindergartens). Topromote this activity the School Mental Health Committee has been established in Nishinomiya City.
This collaborative service functioned even on the day of the disaster. Every psychiatrist of theabove−mentioned committee was ready to visit any school that had urgent need for consultation about themental state of the students. The Division of Health in the Board of Education was able to start studying themental condition of the students immediately after the disaster.
The results of the investigation of the mental condition of the students are summarized in Table 2.6. Trueanxiety reaction was a relative rarity among the students in this district. Indeed, we are surprised to learn thatthere has been only mild mental reaction among infants and students in terms of anxiety disorders, no matterhow great the damage caused by the earthquake was.
Although these results concern students in Nishinomiya City, we know that the same can be said forschoolchildren in Kobe City where the Child Guidance Centre investigated the psychological after−effect ofthe earthquake.
Table 2.6. Mental condition of school children in Nishinomiya City (as of 10 April 1995)
1. Elementaryschoolchildren
Total: 24 280 children (42 schools)
Children in need of care: 44 (22 male, 22 female)• anxiety: 16 (fear of the dark, being alone, hypersensitivity to sounds)• regression: 14 (physical attachment to mother, dependency)• neurotic symptoms: 8 (alopecia, asthmatic attacks, headaches)• insomnia: 4
2. Junior highschoolchildren
Total: 11 464 children (19 schools)
Children in need of care: 22 (12 male, 10 female)• anxiety: 8 (restlessness, fear of being alone)• insomnia: 4 (waking at midnight)• regression: 3 (dependency on mother)• school non−attendance: 3• loss of appetite
3. High school students Total: 2339 (3 schools)Students in need of care: 6 (4 male, 2 female)• anxiety: 3• insomnia: 1• violence: 2• fearfulness: 1• monologue: 1
4. Kindergarten children Total: 1273 (22 kindergartens)Children in need of care: 9 (4 male, 5 female)• regression: 5 (separation anxiety, thumb−sucking, physical attachment to mother,weeping in mother's absence)• anxiety: 3 (fear of being alone, wishing to sleep in mother's bed, restlessness,violence)• depression: 1 (fewer facial expressions, inactivity)
Study of children's mental health by means of an anxiety scale questionnaire
50
While there has been only slight mental reaction in terms of anxiety disorder in infants and schoolchildren inthe area affected by the earthquake, it has been obvious that there are many mental problems amongschoolchildren in Japan, such as non−attendance at school, eating disorders and bullying. A great effort hasbeen made by Japanese child and adolescent psychiatrists to participate in treatment teams for theseproblems throughout the country. In Nishinomiya City these problems have also been the main focus of ourconcern. We have been speculating that anxiety could lie behind these mental problems in children.
Because of these considerations we decided to measure the degree of anxiety in every infant, school−childand student in Nishinomiya City. We drew up an anxiety scale questionnaire to be answered by children atkindergarten, elementary school, junior high school, and high school. We modified the original scale by A.Castaneda (1956) to fit the Japanese situation.
Fig. 2.7 shows the distribution of the anxiety score for second grade junior high school students, as anexample. First and third grades were also studied. From this distribution graph, we can statistically establishthe line above which the score indicates increased anxiety of students. This line was calculated from theaverage plus one standard deviation (SD) and defines a warning threshold for teachers.
Furthermore, if physical damage such as full or partial destruction of the home of a student can be correlatedwith the anxiety score, we shall know the extent of the mental aftereffect caused by the great earthquake. Thisquestionnaire study is now being undertaken in Nishinomiya City.
Results have so far been only partially analysed, but we can see from Table 2.7 that the items which studentschecked most frequently are concerns about school performance or their future after graduation. It seemshere again that anxiety which can be regarded as resulting from the experience of the great disaster does notfigure so prominently. This would confirm the results of the analysis using other kinds of information.
Conclusion
We believe that the reason for the relative rarity of severe mental after−effects of the earthquake amongchildren thus studied is, firstly, that suffering children were in physical contact with their mothers all day longand could share the same bed at night, and secondly, that adults and young people gathered in nearbyshelters, mostly school rooms or sports halls. Everyone slept on the floor in these places with thin mats placedclosely side by side. This may have greatly relieved the anxiety of the adults who could also relieve anxiety ofthe young by allowing them to have very close contact. The traditional mother−infant dependency had beenregarded as a thing of the past due to the effect of nurturing guidelines imported from outside Japan, but thishas been proved to still survive in present−day Japan.
As a mental after−effect of the great disaster, the occurrence of post−traumatic stress disorder is very oftenmentioned. However, we observed almost no cases of this disorder in children. Furthermore, we found thedefinition of the concept of post−traumatic stress disorder too vague to apply to young children.
We know that the mechanism that leads to a mental reaction defined as post−traumatic stress disorder afterdisaster is not so simple as to be determined by only two factors − disaster as a cause and post−traumaticstress disorder as an effect. Many other factors are of course involved, including the developmental stage andstatus of the children and various factors that may intervene immediately after the disaster.
51
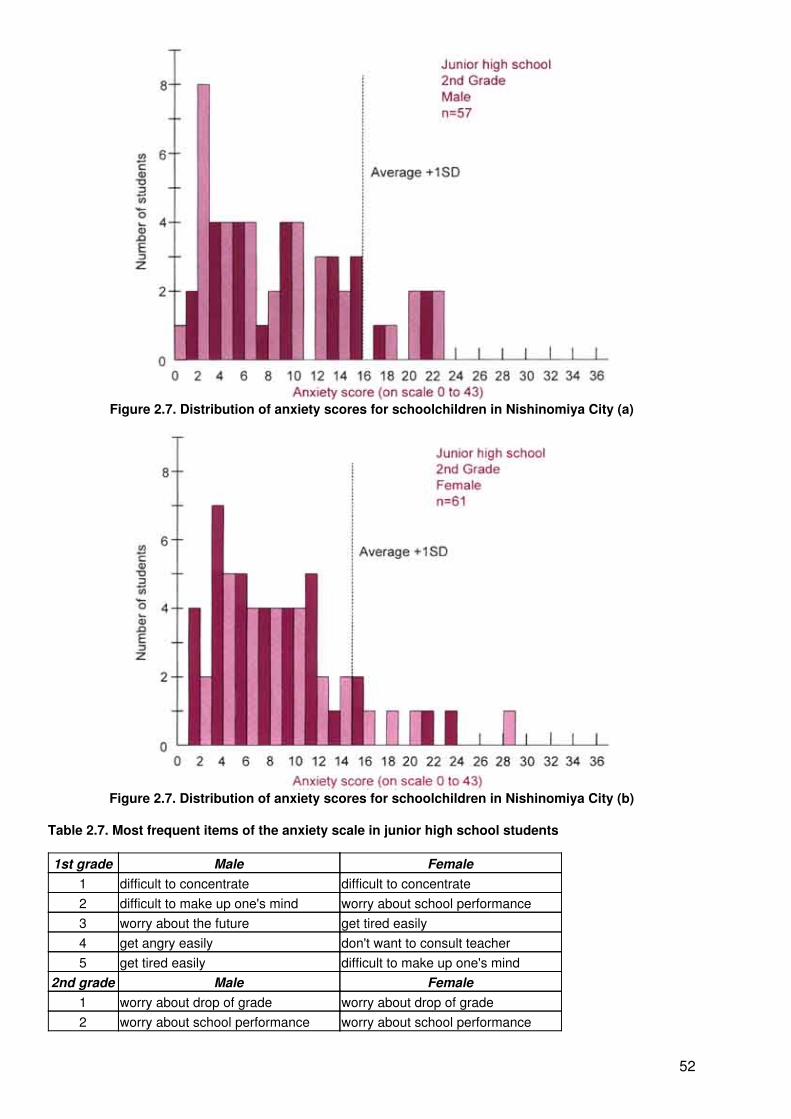
Figure 2.7. Distribution of anxiety scores for schoolchildren in Nishinomiya City (a)
Figure 2.7. Distribution of anxiety scores for schoolchildren in Nishinomiya City (b)
Table 2.7. Most frequent items of the anxiety scale in junior high school students
1st grade Male Female1 difficult to concentrate difficult to concentrate2 difficult to make up one's mind worry about school performance3 worry about the future get tired easily4 get angry easily don't want to consult teacher5 get tired easily difficult to make up one's mind
2nd grade Male Female1 worry about drop of grade worry about drop of grade2 worry about school performance worry about school performance
52
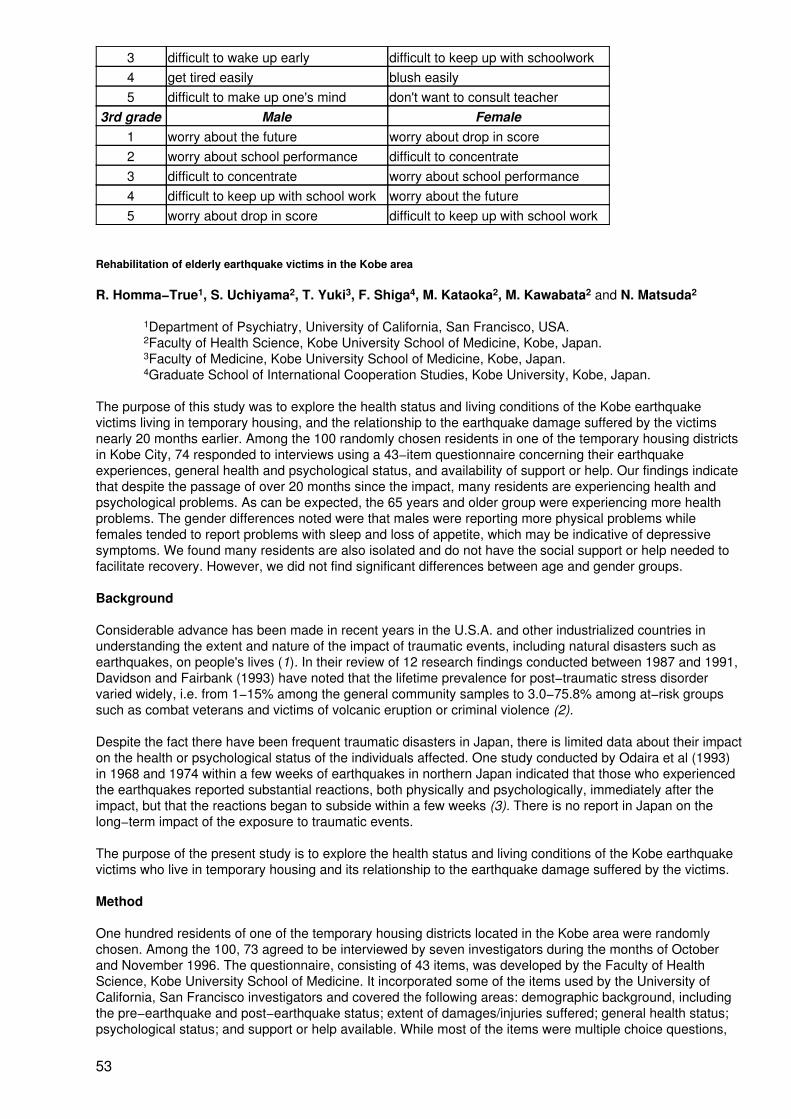
3 difficult to wake up early difficult to keep up with schoolwork4 get tired easily blush easily5 difficult to make up one's mind don't want to consult teacher
3rd grade Male Female1 worry about the future worry about drop in score2 worry about school performance difficult to concentrate3 difficult to concentrate worry about school performance4 difficult to keep up with school work worry about the future5 worry about drop in score difficult to keep up with school work
Rehabilitation of elderly earthquake victims in the Kobe area
R. Homma−True1, S. Uchiyama2, T. Yuki3, F. Shiga4, M. Kataoka2, M. Kawabata2 and N. Matsuda2
1Department of Psychiatry, University of California, San Francisco, USA.2Faculty of Health Science, Kobe University School of Medicine, Kobe, Japan.3Faculty of Medicine, Kobe University School of Medicine, Kobe, Japan.4Graduate School of International Cooperation Studies, Kobe University, Kobe, Japan.
The purpose of this study was to explore the health status and living conditions of the Kobe earthquakevictims living in temporary housing, and the relationship to the earthquake damage suffered by the victimsnearly 20 months earlier. Among the 100 randomly chosen residents in one of the temporary housing districtsin Kobe City, 74 responded to interviews using a 43−item questionnaire concerning their earthquakeexperiences, general health and psychological status, and availability of support or help. Our findings indicatethat despite the passage of over 20 months since the impact, many residents are experiencing health andpsychological problems. As can be expected, the 65 years and older group were experiencing more healthproblems. The gender differences noted were that males were reporting more physical problems whilefemales tended to report problems with sleep and loss of appetite, which may be indicative of depressivesymptoms. We found many residents are also isolated and do not have the social support or help needed tofacilitate recovery. However, we did not find significant differences between age and gender groups.
Background
Considerable advance has been made in recent years in the U.S.A. and other industrialized countries inunderstanding the extent and nature of the impact of traumatic events, including natural disasters such asearthquakes, on people's lives (1). In their review of 12 research findings conducted between 1987 and 1991,Davidson and Fairbank (1993) have noted that the lifetime prevalence for post−traumatic stress disordervaried widely, i.e. from 1−15% among the general community samples to 3.0−75.8% among at−risk groupssuch as combat veterans and victims of volcanic eruption or criminal violence (2).
Despite the fact there have been frequent traumatic disasters in Japan, there is limited data about their impacton the health or psychological status of the individuals affected. One study conducted by Odaira et al (1993)in 1968 and 1974 within a few weeks of earthquakes in northern Japan indicated that those who experiencedthe earthquakes reported substantial reactions, both physically and psychologically, immediately after theimpact, but that the reactions began to subside within a few weeks (3). There is no report in Japan on thelong−term impact of the exposure to traumatic events.
The purpose of the present study is to explore the health status and living conditions of the Kobe earthquakevictims who live in temporary housing and its relationship to the earthquake damage suffered by the victims.
Method
One hundred residents of one of the temporary housing districts located in the Kobe area were randomlychosen. Among the 100, 73 agreed to be interviewed by seven investigators during the months of Octoberand November 1996. The questionnaire, consisting of 43 items, was developed by the Faculty of HealthScience, Kobe University School of Medicine. It incorporated some of the items used by the University ofCalifornia, San Francisco investigators and covered the following areas: demographic background, includingthe pre−earthquake and post−earthquake status; extent of damages/injuries suffered; general health status;psychological status; and support or help available. While most of the items were multiple choice questions,
53
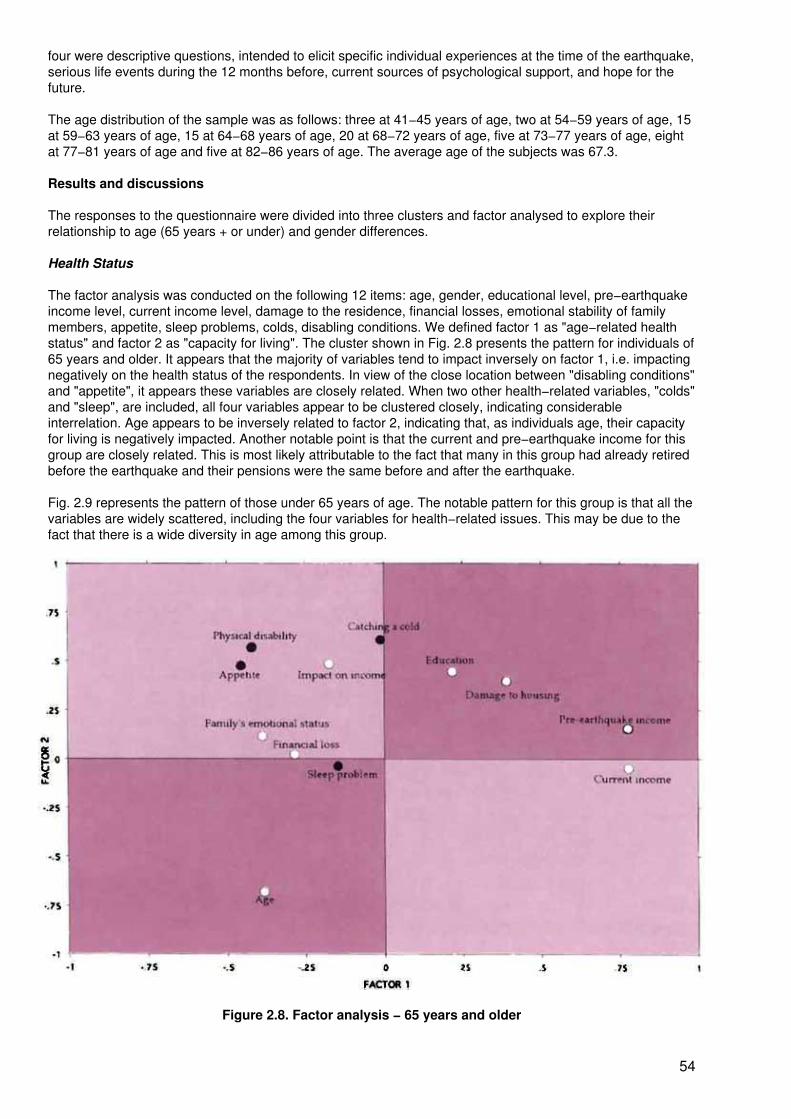
four were descriptive questions, intended to elicit specific individual experiences at the time of the earthquake,serious life events during the 12 months before, current sources of psychological support, and hope for thefuture.
The age distribution of the sample was as follows: three at 41−45 years of age, two at 54−59 years of age, 15at 59−63 years of age, 15 at 64−68 years of age, 20 at 68−72 years of age, five at 73−77 years of age, eightat 77−81 years of age and five at 82−86 years of age. The average age of the subjects was 67.3.
Results and discussions
The responses to the questionnaire were divided into three clusters and factor analysed to explore theirrelationship to age (65 years + or under) and gender differences.
Health Status
The factor analysis was conducted on the following 12 items: age, gender, educational level, pre−earthquakeincome level, current income level, damage to the residence, financial losses, emotional stability of familymembers, appetite, sleep problems, colds, disabling conditions. We defined factor 1 as "age−related healthstatus" and factor 2 as "capacity for living". The cluster shown in Fig. 2.8 presents the pattern for individuals of65 years and older. It appears that the majority of variables tend to impact inversely on factor 1, i.e. impactingnegatively on the health status of the respondents. In view of the close location between "disabling conditions"and "appetite", it appears these variables are closely related. When two other health−related variables, "colds"and "sleep", are included, all four variables appear to be clustered closely, indicating considerableinterrelation. Age appears to be inversely related to factor 2, indicating that, as individuals age, their capacityfor living is negatively impacted. Another notable point is that the current and pre−earthquake income for thisgroup are closely related. This is most likely attributable to the fact that many in this group had already retiredbefore the earthquake and their pensions were the same before and after the earthquake.
Fig. 2.9 represents the pattern of those under 65 years of age. The notable pattern for this group is that all thevariables are widely scattered, including the four variables for health−related issues. This may be due to thefact that there is a wide diversity in age among this group.
Figure 2.8. Factor analysis − 65 years and older
54
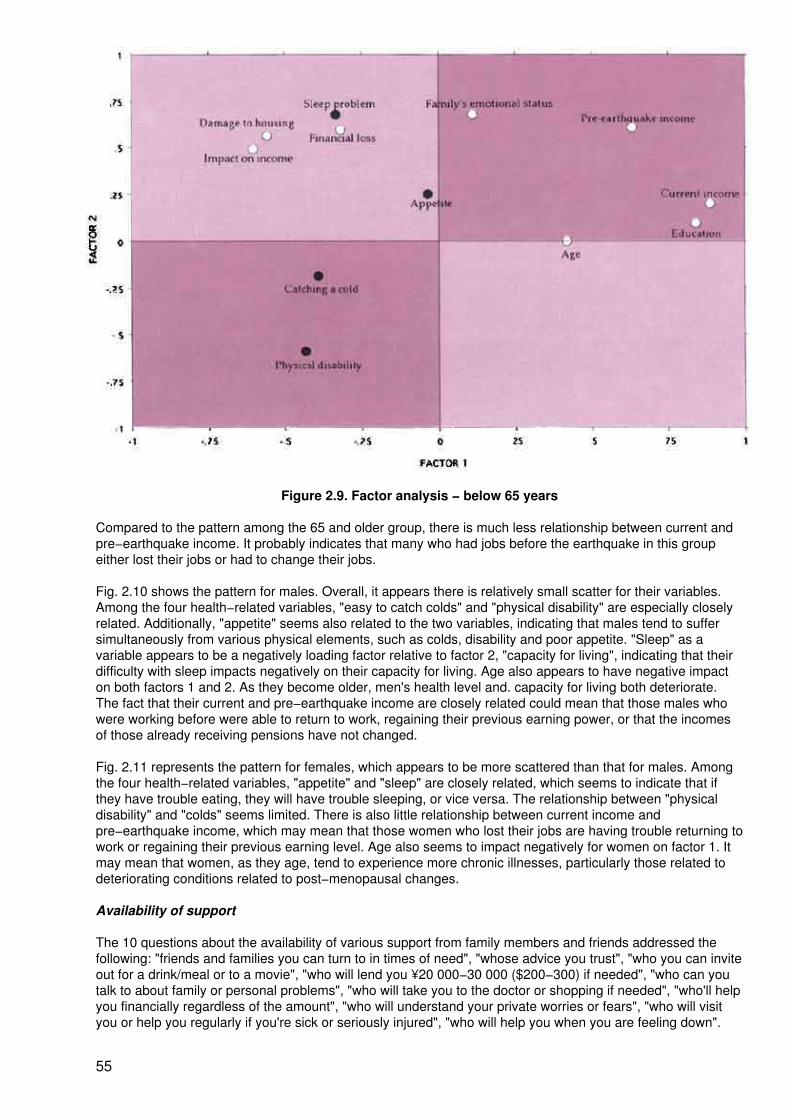
Figure 2.9. Factor analysis − below 65 years
Compared to the pattern among the 65 and older group, there is much less relationship between current andpre−earthquake income. It probably indicates that many who had jobs before the earthquake in this groupeither lost their jobs or had to change their jobs.
Fig. 2.10 shows the pattern for males. Overall, it appears there is relatively small scatter for their variables.Among the four health−related variables, "easy to catch colds" and "physical disability" are especially closelyrelated. Additionally, "appetite" seems also related to the two variables, indicating that males tend to suffersimultaneously from various physical elements, such as colds, disability and poor appetite. "Sleep" as avariable appears to be a negatively loading factor relative to factor 2, "capacity for living", indicating that theirdifficulty with sleep impacts negatively on their capacity for living. Age also appears to have negative impacton both factors 1 and 2. As they become older, men's health level and. capacity for living both deteriorate.The fact that their current and pre−earthquake income are closely related could mean that those males whowere working before were able to return to work, regaining their previous earning power, or that the incomesof those already receiving pensions have not changed.
Fig. 2.11 represents the pattern for females, which appears to be more scattered than that for males. Amongthe four health−related variables, "appetite" and "sleep" are closely related, which seems to indicate that ifthey have trouble eating, they will have trouble sleeping, or vice versa. The relationship between "physicaldisability" and "colds" seems limited. There is also little relationship between current income andpre−earthquake income, which may mean that those women who lost their jobs are having trouble returning towork or regaining their previous earning level. Age also seems to impact negatively for women on factor 1. Itmay mean that women, as they age, tend to experience more chronic illnesses, particularly those related todeteriorating conditions related to post−menopausal changes.
Availability of support
The 10 questions about the availability of various support from family members and friends addressed thefollowing: "friends and families you can turn to in times of need", "whose advice you trust", "who you can inviteout for a drink/meal or to a movie", "who will lend you ¥20 000−30 000 ($200−300) if needed", "who can youtalk to about family or personal problems", "who will take you to the doctor or shopping if needed", "who'll helpyou financially regardless of the amount", "who will understand your private worries or fears", "who will visityou or help you regularly if you're sick or seriously injured", "who will help you when you are feeling down".
55
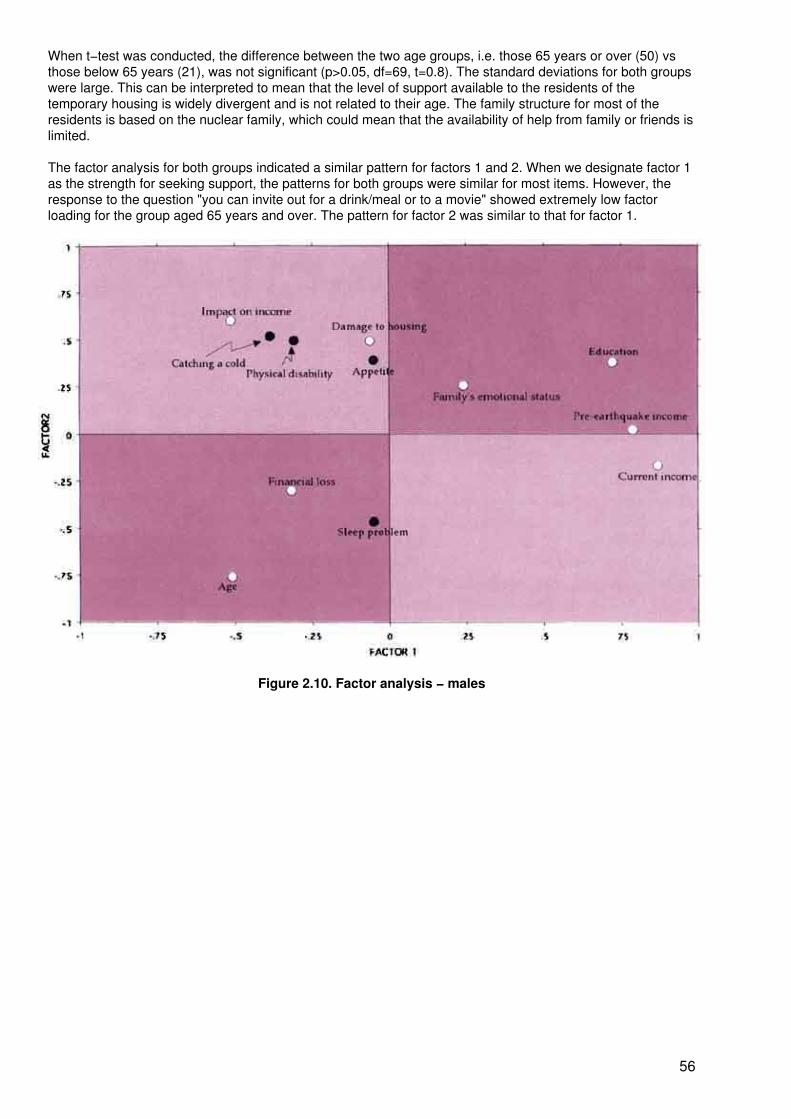
When t−test was conducted, the difference between the two age groups, i.e. those 65 years or over (50) vsthose below 65 years (21), was not significant (p>0.05, df=69, t=0.8). The standard deviations for both groupswere large. This can be interpreted to mean that the level of support available to the residents of thetemporary housing is widely divergent and is not related to their age. The family structure for most of theresidents is based on the nuclear family, which could mean that the availability of help from family or friends islimited.
The factor analysis for both groups indicated a similar pattern for factors 1 and 2. When we designate factor 1as the strength for seeking support, the patterns for both groups were similar for most items. However, theresponse to the question "you can invite out for a drink/meal or to a movie" showed extremely low factorloading for the group aged 65 years and over. The pattern for factor 2 was similar to that for factor 1.
Figure 2.10. Factor analysis − males
56
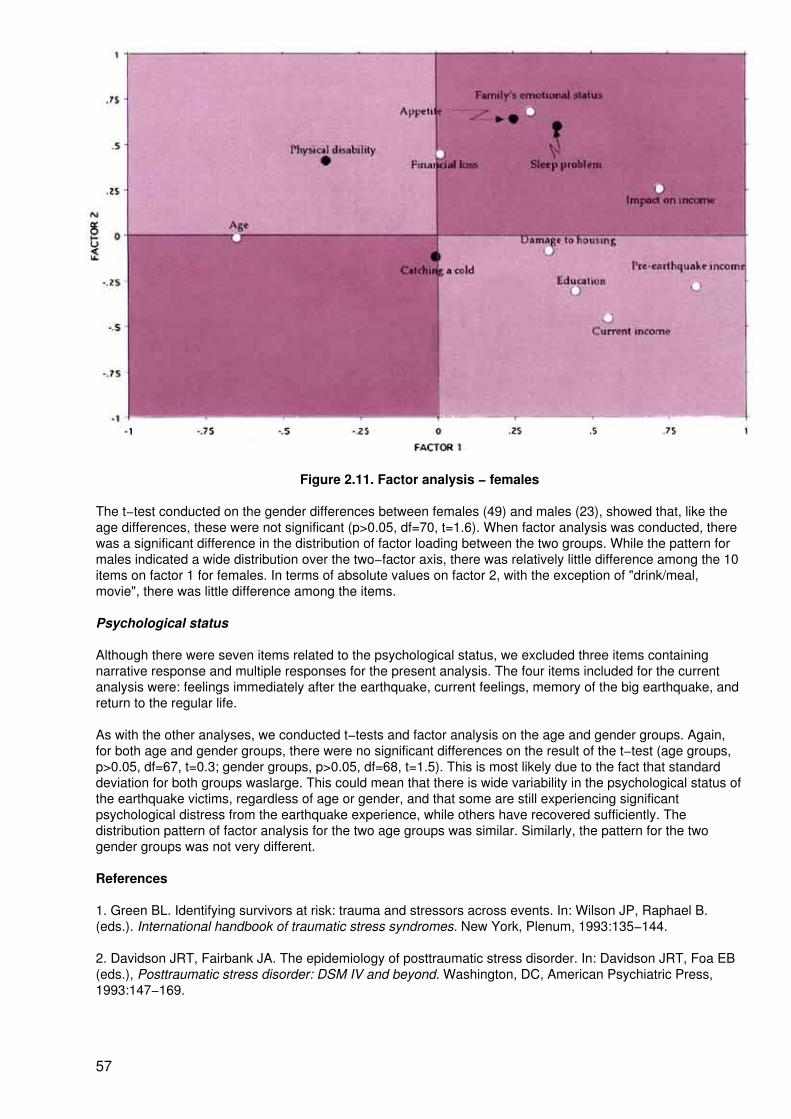
Figure 2.11. Factor analysis − females
The t−test conducted on the gender differences between females (49) and males (23), showed that, like theage differences, these were not significant (p>0.05, df=70, t=1.6). When factor analysis was conducted, therewas a significant difference in the distribution of factor loading between the two groups. While the pattern formales indicated a wide distribution over the two−factor axis, there was relatively little difference among the 10items on factor 1 for females. In terms of absolute values on factor 2, with the exception of "drink/meal,movie", there was little difference among the items.
Psychological status
Although there were seven items related to the psychological status, we excluded three items containingnarrative response and multiple responses for the present analysis. The four items included for the currentanalysis were: feelings immediately after the earthquake, current feelings, memory of the big earthquake, andreturn to the regular life.
As with the other analyses, we conducted t−tests and factor analysis on the age and gender groups. Again,for both age and gender groups, there were no significant differences on the result of the t−test (age groups,p>0.05, df=67, t=0.3; gender groups, p>0.05, df=68, t=1.5). This is most likely due to the fact that standarddeviation for both groups waslarge. This could mean that there is wide variability in the psychological status ofthe earthquake victims, regardless of age or gender, and that some are still experiencing significantpsychological distress from the earthquake experience, while others have recovered sufficiently. Thedistribution pattern of factor analysis for the two age groups was similar. Similarly, the pattern for the twogender groups was not very different.
References
1. Green BL. Identifying survivors at risk: trauma and stressors across events. In: Wilson JP, Raphael B.(eds.). International handbook of traumatic stress syndromes. New York, Plenum, 1993:135−144.
2. Davidson JRT, Fairbank JA. The epidemiology of posttraumatic stress disorder. In: Davidson JRT, Foa EB(eds.), Posttraumatic stress disorder: DSM IV and beyond. Washington, DC, American Psychiatric Press,1993:147−169.
57
3. Odaira T, Iwadate T, Raphael B. Earthquake and traumatic stress: early human reactions in Japanesesociety. In: Wilson JP, Raphael B. (eds.). International handbook of traumatic stress syndromes. New York,Plenum, 1993.
Sustaining rescue personnel: reducing vulnerability to stress
S.M. Platt1
1S.M. Platt MSW is Director for External Relations, Community and Family ServicesInternational, Makati City, Metro Manila, Philippines and New York, United States of America.
Disaster stress and the rescue effort
Planned earthquake response includes an element of systematic attention to the health and welfare of therescue and relief workforce over the entire course of the earthquake event. This is important because thisassembled workforce must be able to respond to the needs of victims for as long as the services they provideare required.
Elements of the rescue and helper workforce responding to an earthquake may include:
Search and rescue Heavy equipment operators FirefightersMedical Body identification/morgue PoliceSocial service Mental health Community
volunteersInternational relief workers Clergy Survivor−volunteersThis varied group of people come with skills, work styles, protocols and training that may or may not haveprepared them for the stress involved in meeting the demands of disaster response in unpredictableearthquake situations. Often they are unaware of disaster stress as a phenomenon which can affect workability and performance.
The intense effort of initial rescue activities, continued contact with victims, and involvement in the slow andoften frustrating recovery effort, predictably expose the responding workforce to extreme stress. This stress isoccupational in nature. While reactions are to be expected, and are seen as normal responses to an abnormalsituation, stress can pose problems both for individuals and for the rescue effort.
Reducing worker vulnerability to the effects of stress involves a process of applying knowledge of disasterstress, understanding its general and particular sources in the earthquake situation, and anticipating howstress responses may affect workers and their work at various stages of the disaster response. Plans canthen be put in place to anticipate, manage and mitigate the negative effects of disaster stress. The positiveaspects of mobilizing to cope with an extremely challenging experience can also be noted and acknowledged.
Three sources of stress affecting the rescue workforce
The earthquake event
Stress results from:
− sudden exposure to dead, dying, injured, mutilated or traumatized victims;
− the sights, sounds and odours of mass destruction;
− personal threat posed by the dangerous post−earthquake environment of collapsed orunstable structures amidst aftershocks;
− certain features of the individual earthquake, such as intense cold, large numbers of childvictims, extremely mangled bodies that are hard to extract, remote or difficult access to site,low rate of live survivor rescues, occurrence in the holiday season.
The nature of the work
58
The stressful aspects of earthquake response work can include:
− intense time pressure to effect rescue while victims are still alive, and to extract bodies foranguished survivors;
− triage work; overload of responsibility involving life and death;
− extremely long hours and heavy workload of difficult, often unfamiliar tasks;
− unfamiliar roles, sometimes multiple and/or conflicting;
− uncomfortable, unsanitary working and living conditions;
− concern about own family;
− mission failure, human error resulting in loss of life or increased misery;
− close media coverage of work;
− equipment failure;
− communication and/or coordination problems.
Organizational problems in earthquake response
Stress affecting workers results from:
− conflicting policies and/or instructions;− inter/intra−organization conflict and competition;− lack of emergency planning;− leadership problems;− political concerns that stall the rescue effort;− inadequate support of staff;− stress management not a priority;− low recognition of worker accomplishment.
In varying combinations, these sources of stress can exert a powerful effect on members of the respondingworkforce. Their characteristically high expectations for their own performance also add pressure. It is notsurprising that disaster workers are sometimes called "hidden victims". It is also unsurprising that they aresubject to stress reactions.
Immediate stress reactions
Exposure to trauma tends to shatter both individual and community sense of well−being and security. Theintense reactions of shock, horror, pain and despair experienced by primary victims of earthquakes create anemotionally demanding context for those attempting to respond to their needs. Workers, including those whomay themselves be victims, often find that they must suppress their own reactions simply to get the work doneduring the different phases. Familiarity with the range of stress responses that workers may experience duringand after their earthquake assignment is important both for the workers themselves and for those insupervisory and leadership roles.
Stress is experienced in a highly individualized manner. Age, life and work experience, training and previouspersonal trauma are some variables which may affect the intensity of reactions of people exposed to anysudden and violent event beyond the usual range of human experience, such as an earthquake. Table 2.8does not represent an all−inclusive list, but it provides examples of what workers may experience in the initialphases of disaster response.
Table 2.8. Immediate reactions to a sudden and violent event
Physical reactions Emotional reactionsnausea, gastrointestinal distress numbness, anxiety, fear
59
sweating, shiveringfaintness, dizzinessmuscle tremors, weaknesselevated heartbeat, respiration, blood pressureuncoordinated movementsoverwhelmedextreme fatigue, exhaustionheadachenarrowed visual field.
rapidly shifting emotionsguilt, survivor guiltexhilaration, survivor joyanger, sadnesshelplessness, feelingdetachmentfeeling unrealdisorientationfeeling out of controldenial, constriction offeelingsstrong identification withvictims.
Cognitive reactions Behavioural reactionsdifficulty concentratingracing, circular thoughtsslowed thinkingmemory problemsconfusion, difficulty naming objectsimpaired problem−solving, calculationsdifficulty making decisionsintrusive images of disasterloss of perspectiveloss of ability to conceptualize, prioritize.
startled reaction,restlessnesssleep and appetitedisturbancesdifficulty expressingoneselfconstant talkingarguments, angryoutburstswithdrawal, apathyexaggerated "gallows"humourslowed reactions,accident−proneinability to rest or let goincreased use of alcohol,tobacco.
Spiritual reactionsintense use of prayer
loss of faith in selfprofound loss of trust.
Total involvement in the work at hand leads workers to ignore their own stress signals. Experiencing a few ofthe effects listed is to be expected. However, if an individual has several responses in each category, jobperformance may be diminishing, causing risk to the worker, colleagues and the rescue effort. Supervisorsmonitor worker stress levels by observing task efficiency and judgement. Decline in these functions indicatesthat stress is excessive and assistance is needed.
Delayed stress reactions
Many workers are surprised by their reactions in the aftermath of a disaster. They wish the disaster to be over,and are unaware that persistent or delayed reactions are common after an intensely meaningful experiencewhich may have been positive as well as painful. People whose responsibilities or coping style require a highdegree of emotional control during the disaster may find themselves reacting at any time afterwards in someof the ways noted below. For most people, reactions gradually decrease until they feel more or less likethemselves in a few weeks. The reappearance of reactions around the anniversary of the earthquake or inresponse to another traumatic event is not uncommon.
Table 2.9. Delayed reactions
Physical reactionssleep disturbances, nightmaresaches and painsappetite and digestive changeslowered resistance to colds and infectionpersistent fatigue.
Emotional reactionsirritability, hostilitymood swings, feeling unstableanxiety, fear of recurrencedepression, grief, angerself−blame, shamefragility, feeling vulnerable
60
numbness, detachment.Cognitive reactionsintrusive memoriesreactivation of previous traumatic eventspreoccupation with earthquake event.
Behavioural reactionsavoidance of event reminderssocial relationship disturbancesdifficulty relating to family and"outsiders"lowered activity levelincreased use of alcohol, drugsconstant need to talk aboutearthquake experience.
Spiritual reactions"Why me" struggleincreased cynicism, disillusionmentloss or gain of self−confidenceloss or renewal of purposerenewed faith in higher beingprofound existential questioning.Complicated, confusing and contradictory responses to a powerful experience are not unusual. Their timingafter the work is completed reflects workers' tendency to cope with traumatic exposure by denying orsuppressing feelings which interfere with getting the job done. Assistance may be needed if delayed reactionsare intense, disturbing and are affecting functioning at regular work or in the family over a period of severalweeks or months after the event. Consultation with a mental health professional well versed in traumapsychology should be considered.
Reducing worker stress vulnerability during the initial rescue effort
Alleviation
Supportive organizations provide workers affected by stressful aspects of their disaster work with a variety ofpost−incident interventions as needed. Workers are prepared to be offered these forms of assistance (moredetails are provided in Annex 3). Interventions may be carried out by staff with appropriate training, or byconsultants, and may include:
− mental health consultation and stress assessment assistance provided to managers;− stress awareness training;− on−scene support services for workers;− stress debriefing;− individual consultations;− referral for additional help with stress reactions.
Policies and procedures for the administration and provision of stress management support need to pay closeattention to worker concerns about confidentiality. When this important aspect is appropriately handled, theservices will be utilized.
Supportive leadership style
In many earthquake rescue and relief efforts, line supervisors and team leaders are the key providers ofstress management support for the workers. Their leadership practices and style can either add to or modifythe stress of those for whom they are responsible. Stress−reducing leadership characteristics include thefollowing (adapted from 7):
Open communication. Stress is significantly reduced when workers feel they have access tofacts about the situation, an effective way of checking out rumours and avenues foraddressing immediate concerns.
Awareness of reactions. Stress is alleviated when supervisors can anticipate a variety ofstress reactions among their workers and respond helpfully. This requires sensitivity tocultural traditions and gender roles.
Availability. Visible leadership in times of crisis is reassuring. Workers respond positively tovisits to their workstations, as well as other forms of encouragement. Reminders of how each
61
worker's task is contributing to the whole rescue and relief effort are appreciated.
Acknowledgment of loss. Timely, formal acknowledgment of deaths and loss enables theworkers to begin mourning. Culturally sensitive grief leadership is highly supportive ofworkers.
Appreciation of efforts. Workers need to feel that their work has been noticed andappreciated. It is important that recognition be timely as well as accurate.
Managing transition in the aftermath of the earthquake
The completion of the emergency phase of earthquake rescue and the transition to slower and morefrustrating recovery work cause their own kind of stress. Workers leaving the scene and those staying butaddressing different tasks experience stress as they "shift gears". Supervisors can arrange supportiveactivities and make changes themselves which will model ways of coping with the stress of the let−downperiod after an intense rescue experience.
• Arrange for an opportunity for the members of the team to discuss their personalexperiences during the impact rescue period. Formal stress debriefing is an option if anappropriate trained facilitator is available.
• Hold "lessons learned" sessions to provide constructive opportunities for workers at alllevels to discuss, evaluate and analyse procedures and the work.
• Assist in re−establishing regular work and personal routines as soon as possible.
• Set an example for fellow workers through self−care, recognizing limits and gettingnecessary sleep.
• Make time for regular recreational or "time out" activities and encourage others to do so tohelp overcome post−event reactions.
• Give recognition and appreciation for work performed.
• Attend to the possible need for ceremonies or rituals to honour losses.
• Encourage team members to reconnect with family and friends.
• Provide information and a handout to help explain disaster stress.
Individual stress management for difficult assignments
When starting a challenging work assignment such as earthquake rescue, it is important for each individual tobe aware that stress will be present at all stages of the work. Disasters expose everyone involved to traumaticand distressing sights, sounds and situations. The spectacle of massive death and destruction, the sufferingof survivors and the intense pressure surrounding the rescue effort takes its toll.
Experienced disaster workers offer the following suggestions to ease passage through the assignmentexperience.
Brief yourself
• Ask for information on the situation and what is most difficult and disturbing about the workand living conditions.
• Determine the amount of self−sufficiency necessary so you can obtain equipment andsupplies to maintain yourself.
• Find an experienced mentor for the settling−in period.
Use reliable strategies to cope with difficult circumstances
62
• Compartmentalize, focus on the task at hand.• Adopt a small tasks, small goals, "one day (or hour) at a time" approach.• Monitor self−talk, avoid negative comments to yourself, use self−encouragement.• Work in pairs with a "buddy agreement" to keep an eye on each other.• Adhere to regular shifts and breaks for water, food and rest.• Know your personal signs of stress and exhaustion.• Agree to periodic leave away from the worksite.
Remember stress survival skills
• Use portable forms of exercise, i.e. calisthenics, jump rope.
• Practice simple relaxation techniques such as deep breathing and stretching.
• Pay attention to nutrition; take care with alcohol, caffeine, sugar.
• Get sufficient sleep to avoid an overdraft in your "sleep bank account".
• Develop and use a repertoire of comforting time−out activities that change your focus(books, music, knitting).
Recognize critical events
Sudden, violent occurrences which present a threat to personal safety and assault one's sense of security andpredictability in life are sometimes called critical events.
Examples include:
− witnessing the death or serious injury of another human being;− involvement in actual or potentially life−threatening situations;− injury or death of a co−worker in the line of duty;− dealing with serious injuries and/or deaths of children;− exposure to mass casualties;− involvement with any event described as an atrocity.
Such events cause stress reactions which are less disturbing with the knowledge that they are normalresponses to an abnormal event. If your work involves possible exposure to critical events, you may find ithelpful to be aware of what you or others might experience in the period following the event. You mayexperience:
− a periodic feeling of unreality, events seeming dream−like;− heightened response to loud noises, reminders of the event scene, or any other surprise;− discomfort at being alone;− discomfort being in a group;− difficulty concentrating on what to do next;− difficulty making decisions and thinking creatively;− difficulty relating to those who were not part of the event;− difficulty resting and sleeping, fear of nightmares;− increase or decrease in appetite;− discomfort being in places that seem unsafe to you;− feeling vulnerable, afraid of losing control;− feeling frightened, sad, angry, irritable, confused;− feeling and being exhausted.
If you have been busy performing necessary tasks after the event, you may not react until you have less todo. A delayed reaction is common, but puts you on a different timetable from others. The suggestions belowmay be of help.
Managing critical event stress
• Take care of yourself. Try to eat regular, easy−to−digest meals. Avoid sugar and caffeinewhen mood swings are a problem. Monitor alcohol use.
63
• Re−establish exercise routine. Even a 20−minute walk will bum off some of the chemicalbyproducts of intense stress which remain in your body and contribute to fatigue and tension.
• Rest by choosing from your repertoire of soothing, distracting activities.
• Communicate about your experience in ways that feel comfortable. Writing an account ofwhat happened and your reactions to it can be helpful.
• Do what you need to do to feel safe. Review security with a qualified colleague.
• Respect your feelings and ways of handling things and those of others. People copedifferently.
• Check out how you are doing with a trusted person. Feedback as you begin to feel more likeyourself can be helpful.
• Take part in debriefings and other recovery activities.
• Reconnect with sources of social and spiritual support.
Reflect on your experience and move on
Intense assignments are rarely over when you leave the site. In the aftermath some people experience anelevated mood that lasts for days or weeks. Others find the let−down sudden and may go through a grievingprocess and feel depressed. For some, flashbacks and intrusive images of disturbing events bring anxiety andcontinued stress which makes it hard to let go and move on to new activities. People may dwell on theirperformance, wishing they had been more effective. They may want to share what happened with those closeto them or may find this painful. If, after a few weeks, discomfort persists and you are still not able to return toyour normal routine, obtain a referral for assistance from a trauma−trained professional.
Many find that, once the assignment is over, life gradually becomes normal and with normality comes a senseof new beginning born of having survived a challenging and dangerous experience. These people may beaware of new skills and competence acquired in coping with the disaster situation and feel satisfaction aboutthis.
Most people eventually accept the notion that disaster experiences have positive as well as negative aspectsand that memories of these become part of one's life. They become accustomed to reactions surfacing fromtime to time in response to subsequent disturbing occurrences or on the anniversary of the disaster event.They accept what happened and their role in it, but focus on the future. They move on.
Reference
1. Lewis J. Critical incident stress and trauma in the workplace. Accelerated Development Inc., Muncie, IN,USA, 1994.
Summary
J. Levett1 Y. Oka2 and K. Shoaf3
1J. Levett is Director of International Affairs, National School of Public Health, Ministry ofHealth and Welfare, Athens, Greece.
2Y. Oka is a Research Associate from the Department of Architecture, University of Tokyo,Tokyo, Japan.
3K. Shoaf is from the Department of Community Health Sciences, School of Public Health,University of California, Los Angeles, USA.
Professor Shigeaki Sato spoke about the "Long−term effects of the Great Hanshin−Awaji Earthquake onurban public health". He described the health check−up system of infants and children under three years of
64
age after the earthquake, and mentioned that problems revealed in earthquake areas were not significantlydifferent from those in nearby non−earthquake areas. He also presented data on people above 40 years ofage in the two types of area and concluded that their conditions also were not significantly different. However,comparatively more people living in shelters had hypertension, heart disease, respiratory ailments,psychological problems, psychosomatic disorders and tuberculosis. Professor Sato concluded that theseconditions are indirect effects of the poor living conditions of the shelters.
Professor Sato also presented data on air quality: after the earthquake, showing that particulate matter wasalmost twice the normal level. However, the asbestos levels stayed generally low and below permissiblelimits.
Professor Sadaaki Shirataki et al. presented a poster on the mental health effects of the Great HanshinEarthquake on children. A study looked at the mental health effects of the earthquake on children. The surveyof elementary, junior high and senior high school students found little anxiety in children as a result of theearthquake and no instances of post−traumatic stress disorder. Possible explanations for this were thatevacuation centres were generally schools that children were familiar with and where they felt comfortable,that in the centres children slept close to their mothers, and that having their children close by decreasedanxiety in adults and thereby reduced it in children too.
The study contradicts much of the literature on the mental health effects of disasters on children. A largenumber of articles suggest that children suffer from post−traumatic stress disorder after disasters of thismagnitude. This study, however, has some methodological advantages over some of the others. First of all, itis a survey of a large number of children using an adaptation of a standard instrument for children. Secondly,the researchers looked at a wide range of psychological distress, including anxiety, and not just atpost−traumatic stress disorder. Other studies tended to be case studies of affected children and not surveysof the general population of children. One concern of the chairperson remains, namely that the explanationsfor the lack of anxiety/post−traumatic stress disorder in children do not appear to have been checked againstappropriate control groups.
Dr Reiko Homma−True et al. explored the health status and living conditions of earthquake victims living intemporary housing in a poster on rehabilitation of elderly earthquake victims in the Kobe area, and therelationship to the earthquake damage suffered by the victims nearly 20 months earlier. Among the 100randomly chosen residents in one of the temporary housing districts in Kobe City, 74 responded to interviewsusing a 43−item questionnaire concerning their earthquake experiences, general health and psychologicalstatus, and availability of support or help. The findings indicate that, despite the passage of more than 20months since the event, many residents are experiencing health and psychological problems. As can beexpected, the 65 years and older group were experiencing more health problems. The gender differencesnoted were that males were reporting more physical problems while females tended to report problems withsleep and loss of appetite, which may be indicative of depressive symptoms. It was found that many residentsare also isolated and do not have the social support or help needed to facilitate recovery.
Ms Sheila Platt described the stress which affects disaster workers as well as a programme for protectingrescue and health care personnel from the adverse affects of their work. The poster emphasized that such astress response is a natural and protective reaction to a negative and potentially hazardous workenvironment. Pathologizing such a response and providing clinical interventions are not necessary to reducethe potential negative impact of the response. However, there are some important steps that can decrease thenegative impact of the stress. These steps include: education of all workers (from the top down) about thenature of disaster work and potential signs of stress; awareness by supervisors of potential stress and stressreactions and having a plan to deal with them; giving workers an opportunity to have regular meals andbreaks from work; providing workers with an opportunity for debriefing.
Panel discussions (synthesis)
Holistic view of major short−term consequences
Panelists: E. Pretto,1 ModeratorM. Erdik2
65
S. Goncharov3
S. Platt4
D.E. Rodriguez5
S. Suganami6
1Associate Director, Safar Center for Resuscitation Research, University of Pittsburgh,Pittsburgh, USA.
2Professor and Chairman, Department of Earthquake Engineering. Bogazici University,Kandilli Observatory and Earthquake Research Institute, Istanbul, Turkey.
3Director of All−Russian Centre for Disaster Medicine "Zaschita", Ministry of Public Healthand Medical Industry, Moscow, Russian Federation.
4Director for External Relations, Community & Family Services International, Makati City,Metro Manila, Philippines and New York, USA.
5Chief, Department of Medicine, Calderon Guardia Hospital, San Jose, Costa Rica.
6President, Association of Medical Doctors of ASIA (AMDA), Okayama, Japan.
Dr Pretto introduced the issue of age distribution in earthquake victims, which usually shows a high risk forchildren and old people but depends on many factors. In Kobe, for example, there were many young people,but some were living in old houses and thus became victims because these houses were particularlyvulnerable. Then three panelists introduced additional issues, which were commented on by another panelistand then opened for audience discussion as follows:
D.E.Rodriguez:
Successful short−term measures based on actual experience in Costa Rica.
M. Erdik: The feasibility of rapid assessment of structural integrity of hospitals following earthquakes.S. Platt: Psychological support of professional rescuers and other health care professionals during
and after disaster response.Dr Rodriguez presented a brief summary of concrete actions that have been taken in Costa Rica to preparefor, mitigate and respond to disasters. He stated that Costa Rica is a poor and disaster−prone country and,therefore, there is a lot of awareness in society of the need for good systems for disaster response. Emphasisis on training courses for health personnel, schools and communal organizations. Also the community must beintegrated in preparedness planning, Commission, an agency of the Costa Rica Government whichcoordinates disaster preparedness, mitigation and response activities throughout the country. He stated thatthis agency was still in development at the time of the 22 April 1991 earthquake and, therefore, had not beenfully prepared for the consequences of that earthquake. However, he stated that the organization has sincestrengthened capacity to respond, including focusing on legislation aimed at the following:
− empowering disaster officials to make decisions regarding rapid allocation of financial andmaterial resources without a lot of bureaucratic red tape at the time of the event and withclearly established assignments;
− strengthening the nation's emergency health care system by developing a pre−hospitalemergency care system, public education in first aid, and vigorous guidelines for thestructural and non−structural preparedness of hospitals;
− developing coordinated networks of volunteer groups in the community;
− making equipment and drugs available which should be pre−purchased, stored or otherwiseavailable in a standardized and unbureaucratic way, making use of past experiences and newWHO guidelines.
Dr Erdik stated that rapid structural and non−structural assessment of hospitals affected by earthquakes iscomplex but might be feasible shortly after the event by specially−trained hospital personnel. He stated thatthis capability could be developed but the need to perform sophisticated tests for an ultimate judgement onstructural integrity would remain and would have to await a more comprehensive analysis by engineers. Initial
66
construction should always emphasize building to adequate standards and protecting lifelines, which can alsobe done as a later upgrade. A 1994 article from Osaka summarized this fairly well but was not implemented.Equipment and furniture can be checked for safety and adequate installation, as a part of preparedness.
Ms Platt stressed the need for more psychological support of health care workers operating in extremeconditions, since they also become victims and need counseling to cope with the consequences of the event.The occupational risk of stress stems above all from:
− witnessing the extent of the disaster;− extracting dead or badly injured from the rubble;− long hours of work;− personal neglect (lack of recognition, organization, proper eating habits, isolation, etc.).
In particular, supervisors are asked to recognize and mitigate these problems. According to Ms Platt,supportive leadership plays an important part in vulnerability reduction and preparedness by appropriate priorbriefings of the workforce and monitoring to ensure adequate healthy living habits during a disaster, such asresting, eating, exercising, etc.
Dr Pretto concluded that the multisectoral interventions to mitigate the short−term effects of earthquakes, asdiscussed in this session, covered three areas or phases:
− pre−hospital responses;− hospital response;− psychological support for rescue personnel.
Mitigating long−term effects
Panelists: J. Levett1, ModeratorM. Gabr2
A.K. Melkonian3
B. Mulyadi4
S. Sato5
K.I. Shoaf6
1Professor and Director, International Affairs, National School of Public Health, Ministry ofHealth & Welfare, Athens, Greece.
2Professor of Pediatrics, Cairo University; Secretary General, Egyptian Red Crescent;Immediate Past Present Global ACHR, WHO, Cairo, Egypt.
3Republican Information and Computer Centre, Ministry of Health, Yerevan, Armenia.
4Director, Private and Specialty Hospitals, Directorate Genera] of Medical Care, Ministry ofHealth, Jakarta, Indonesia.
5 Professor and Chairman, Department of Hygiene, Kobe University School of Medicine,Kobe, Japan.
6 Department of Community Health Sciences, School of Public Health, University ofCalifornia, Los Angeles, USA.
The moderator, Professor Levett, put forward the following main issues for discussion:
− physical and mental health;− socioeconomic effects and long−term recovery;− public health function;− future research.
67
Dr Melkonian was asked to introduce the first issue and mentioned that many initial casualties could beprevented if intervention was made very early and efficiently. Such an effort would have a particular impact onpreventing deaths due to coronary heart disease. He suggested that antidepressant drugs and even placeboscould be used with much benefit.
Dr Mulyadi related to the first and other issues by his remarks, entitled '"Physical and mental health effects:how they can be mitigated". He concurred with the importance of dealing with the emotional needs ofindividual victims. During the rehabilitation phase, support and care to victims, such as provision of adequateshelter, is important to combat aggressiveness and/or depression. He said that the role of the psychiatrist inpsychosocial problems was important and such people should be included in the emergency managementteam. He added, "above all the people of the community should be made to understand the inevitable natureof damages, losses and fatalities as a consequence of disaster, to be psychologically prepared."
In conclusion, Dr Mulyadi supported the notion that the clarification and optimization of the roles ofpsychologists and psychiatrists in disaster relief need more research and data.
Professor Gabr spoke on the "Socioeconomic effect and long−term recovery". He mentioned that insufficientresources in the family, in the community and even at government level remained a major constraint duringdisasters. He added that lack of infrastructure and sometimes the low level of education of people atcommunity level posed additional problems. The restoration of lifelines (such as water supply and electricity)would sometimes take a long time in developing countries.
According to Professor Gabr, in most countries the insurance system and rental rates for replacement housingare prohibitive. Government could help people by providing soft loans, subsidies, housing and new localemployment facilities. He also mentioned that elderly and socially disadvantaged groups may need particularattention, in particular if there are casualties in the supporting family.
Ms Shoaf pointed out that an impression seemed to prevail that assistance in industrialized countries wasgenerally quickly forthcoming. In fact, it was not always the case. Not everybody who deserved help wasgetting it. In addition, if help is given to those who do not need it, it causes frustration and unnecessarypsychological distress. Therefore, she suggested that it was necessary to assess if appropriate reliefmeasures were available to the right people at the right time; such assistance should carefully be checked asto its utility and must be culturally acceptable. In summary, internal and external sources should be used toenhance people's fast recovery from disasters.
Ms Shoaf also suggested a need of psychosocial research on the misuse of relief at the acute stage.Collection of information for such research could be started immediately. She also added that people in manydeveloping countries were already living in stress and may experience no significant additional psychosocialproblems from disasters.
Focusing on the public health function, Ms Shoaf felt that public health would not be a problem soon afterdisaster and vaccination would not be much help. However, people who are regularly taking remedial drugsand may have lost them during the disaster needed to be helped. She suggested that this neededcorresponding preparedness in the family and community, and even at government level.
Dr Mulyadi speaking on the public health function mentioned that water supply, sanitation and housingneeded to be given top priority during disasters. Also, community members need to be trained accordingly.
Responses and comments from the audience concerned training. Dr E. Noji mentioned that although nouniversity was conducting a separate course on emergency preparedness activities, Johns Hopkins offers arelated course on refugees and a few other courses also include disaster issues. Some aspects have alsobeen included in social science courses, but he felt that the social aspects of disasters should be the subjectof research programmes. In the Pan American Health Organization, the New Frontier programme includes thepublic health aspect in disaster training. It was also mentioned that the facilities of the Internet could be usedin the future to publicize quickly realistic damage assessments and the real needs for support.
Dr Hayashi, Director of the Kobe Public Health Research Institute, emphasized strengthening the laboratoryservices during disaster so they could provide early reports. Similarly, disease surveillance and screeningneeded to be started early and immunization should be considered, where effective. Safe water and adequatenutrition would be equally important and particular attention should be paid to adequate sanitary conditions intemporary shelters, particularly the provision of toilets.
68
Professor Sato spoke on "future research". He mentioned that research on long−term and short−term healtheffects, physical and emotional, as well as identification of direct and indirect effects on health needed moreattention, as did studies on people living in temporary housing. The mechanisms of these effects may verywell be explored by cohort studies. They would be costly and much expertise would be needed. A catalyticinfluence of such studies is seen and different sectors should be involved. Careful evaluation of progress maymake such studies possible; research in education and training should be included. He warned, however, thatfollow−up studies were difficult even in industrialized countries because people eventually do not want to bequestioned further.
PART 3 − VULNERABILITY REDUCTION AND PREPAREDNESS
Forecasting of seismic hazards
Monitoring of seismic hazards and earthquake prediction in Kazakstan
A.V. Kravchuk1and S.A. Mazhkenov2
1A.V. Kravchuk is Chief, Main Administration of Emergency Prevention, State EmergencyCommittee of the Republic of Kazakstan, Almaty, Kazakstan.
2S.A. Mazhkenov is Head, Department of Natural Disaster Reduction Division, StateEmergency Committee of the Republic of Kazakstan, Almaty, Kazakstan.
In the Republic of Kazakstan there are natural seismic hazards of an intensity of IX on the MSK−64 scale andhigher in the city of Almaty and in six other areas (East Kazakstan, Semipalatinsk, Taldykorgan, Almaty,Zhambyl and South Kazakstan). The overall area subject to seismic risk covers some 450 000 km2 (Fig. 3−1).
69
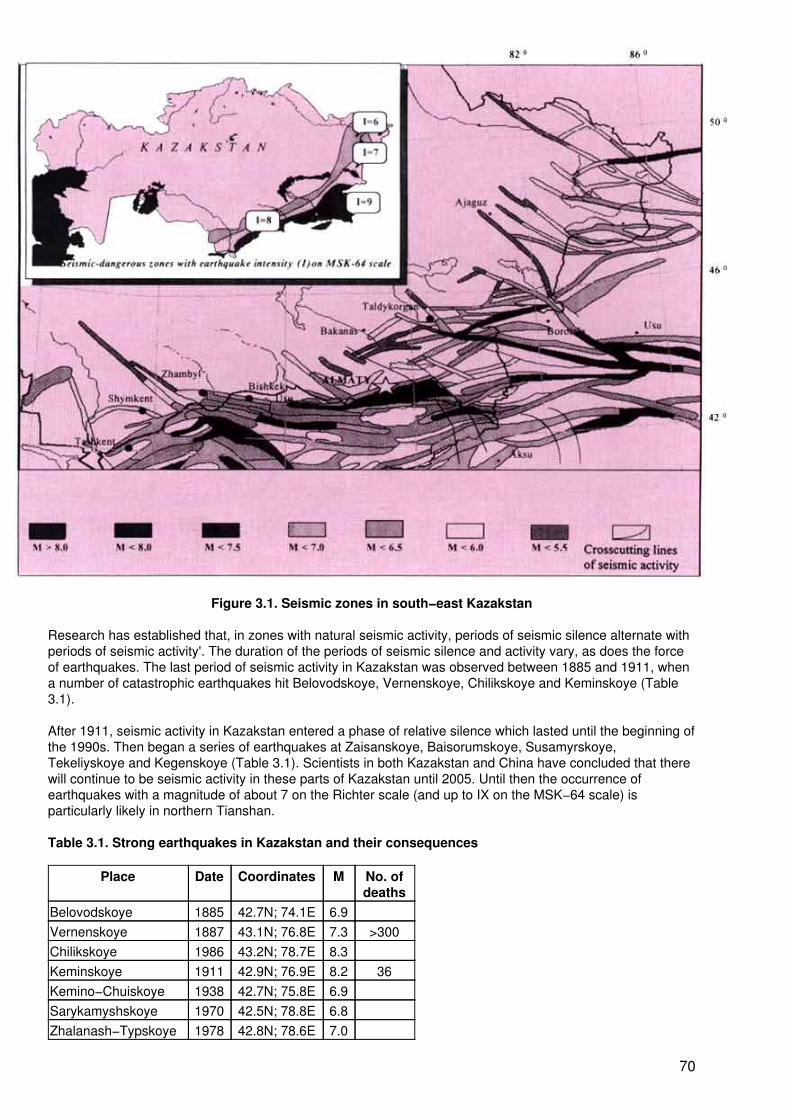
Figure 3.1. Seismic zones in south−east Kazakstan
Research has established that, in zones with natural seismic activity, periods of seismic silence alternate withperiods of seismic activity'. The duration of the periods of seismic silence and activity vary, as does the forceof earthquakes. The last period of seismic activity in Kazakstan was observed between 1885 and 1911, whena number of catastrophic earthquakes hit Belovodskoye, Vernenskoye, Chilikskoye and Keminskoye (Table3.1).
After 1911, seismic activity in Kazakstan entered a phase of relative silence which lasted until the beginning ofthe 1990s. Then began a series of earthquakes at Zaisanskoye, Baisorumskoye, Susamyrskoye,Tekeliyskoye and Kegenskoye (Table 3.1). Scientists in both Kazakstan and China have concluded that therewill continue to be seismic activity in these parts of Kazakstan until 2005. Until then the occurrence ofearthquakes with a magnitude of about 7 on the Richter scale (and up to IX on the MSK−64 scale) isparticularly likely in northern Tianshan.
Table 3.1. Strong earthquakes in Kazakstan and their consequences
Place Date Coordinates M No. ofdeaths
Belovodskoye 1885 42.7N; 74.1E 6.9Vernenskoye 1887 43.1N; 76.8E 7.3 >300Chilikskoye 1986 43.2N; 78.7E 8.3Keminskoye 1911 42.9N; 76.9E 8.2 36Kemino−Chuiskoye 1938 42.7N; 75.8E 6.9Sarykamyshskoye 1970 42.5N; 78.8E 6.8Zhalanash−Typskoye 1978 42.8N; 78.6E 7.0
70
Zaisanskoye 1990 45.5N; 85.2E 7.0 1Baisorumskoye 1991 43.5N; 78.8E 6.3Susamyrskoye 1992 42.0N; 73.3E 7.2Tekeliyskoye 1993 44.7N; 79.0E 6.5Kegenskoye 1994 42.8N; 80.4E 6.0If a destructive earthquake with an intensity of IX on the MSK−64 scale occurred, the Almaty region and thecity of Almaty together could have 300 000 people affected, including killed and injured. The anticipatedconsequences of such an earthquake would amount to a national disaster.
In order to ensure the safety of the population and to preserve its health, the government in 1989 set up anational system of seismological observation and earthquake prediction. Within this system there are today 11scientific organizations, namely the Institute of Seismology, the Institute of Ionosphere, the Institute ofGeophysical Research, the Seismological Expedition, Enterprise "Forecast", the Hydrogeological Expeditionof the Ministry of Geology, the Faculty of Biophysics of Kazak University, the Complex Expedition, the specialgroup of the Geodetic Committee, the Hydrometeorological Bureau, and the Institute of Seismo−ResistantConstruction and Architecture.
The basic tasks of this national system are:
− determining the place, time and parameters of earthquake occurrence;
− monitoring the seismic hazards and predicting earthquake risks;
− seismic zoning of territory and estimating the potential seismic risk in each area;
− developing normative documents on protection of the population material, property and landfrom the effects of earthquakes.
The observations are made by 78 stations in 11 areas of the republic. Currently about 900 persons work forthe system, among them nine doctors and 44 scientists.
Within Kazakstan's national system, seismic monitoring is provided by 27 seismic stations (22 run by theSeismological Expedition and five run by the Institute of Geophysical Research). This seismic network iscapable of monitoring earthquakes with a magnitude of more than 2 (on the Richter scale) for northernTianshan and more than 3 for eastern Tianshan.
The strategy of earthquake prediction has two stages. In the first stage, periods of seismic activity and areasof activity are predicted. A map of the long−term prediction of earthquakes has been made for the region ofnorthern Tianshan, where six zones (South Jungarian, Turgenskaja, Kastekskaja, Narynkolskaja,Kochkorskaja, Kadzhisaiskaja) are identified as having seismic activity until the year 2000 (Fig. 3.1). Data ofthe Kazakstan National Academy Institute of Seismology shows that the occurrence of earthquakes ofmagnitude 6 and more (on the Richter scale) is possible in the specified zones in the next 35 years. Theepicentres of the earthquakes that occurred in the last five years in the south−east of Kazakstan lay within theidentified zones. In the second stage, the place and time of occurrence of earthquakes are forecast. Thescientists of Kazakstan have developed new methods of predicting earthquakes on the basis of an analysis ofseismological, geophysical, ground deformation, hydro−geochemical and other data.
The data from all stations is submitted daily for processing and analysis. Each week these data are discussedin a session of an Interdepartmental Commission on Earthquake Prediction, in which experts from allorganizations doing research on earthquakes are included. After discussion of all data, the conclusions of thecommission are transferred to the State Emergency Committee. In case of the threat of occurrence of adestructive earthquake, the committee announces its decision to the population.
Seismic hazard and risk in Ljubljana, Slovenia
R. Vidrih1, and M. Godec2
1R. Vidrih M.Sc. is Counsellor, Ministry of Environment and Physical Planning, GeophysicalSurvey, Government of the Republic of Slovenia, Ljubljana, Slovenia.
71
2M. Godec B.Sc. is Counsellor, Ministry of Environment and Physical Planning, GeophysicalSurvey, Government of the Republic of Slovenia, Ljubljana, Slovenia.
The city of Ljubljana, Slovenia, is situated in the Ljubljana seismic block which is a part of theGorenjska−Ljubljana seismic region. This region is ranked higher than the Idrija and Krško−Breice regions interms of potential for seismic energy release. A total of 59 earthquakes registering more than IV on the MSKscale have taken place in this region in the past. Of these, 31 earthquakes reached an intensity of VI MSK,nine others were between VI and VII MSK, 10 earthquakes had an intensity of VII MSK, four measuredbetween VII and VIII MSK, another four measured VIII MSK, and one earthquake had an intensity of betweenVIII and IX MSK. The most powerful earthquake occurred on 14 April 1895 and measured 5.8 on the Richterscale. It caused material damage and also claimed 10 lives. On the basis of the seismological records of pastearthquakes, seismological data and geological structure, a map of earthquake microzonation has beendrawn up for planning the action of civil defence units.
We evaluated the seismic hazard on the basis of this microzonation map and information about seismicvulnerability of the buildings in Ljubljana. The map shows losses to be expected within a fixed period in acertain area. We have used these results for the area of Ljubljana centre where the data about the buildingsand their occupants was collected.
In estimating seismic risk, it is assumed that an earthquake occurs in the evening, while residents are usuallyat home and business premises are empty.
The position of Ljubljana
Ljubljana and its suburbs are situated in an area where numerous faults cross. The faults extend in four maindirections. Apart from older faults which extend in an east−west direction, the region is also crossed by thenumerous Dinaric and transverse Dinaric faults which are mostly seismically very active. Similarly active arethe north−south faults. These complex fault crossings and boundaries define some other blocks which in turnproduce a good deal of sporadic seismic activity as a result of their vertical and horizontal movements. Themost important seismic blocks are those at Tošc, the Polhograjski Dolomites, Horjul, the Ljubljana marshland,Kamniško polje, central Ljubljana, and Posavje (1,2).
The land south of Ljubljana emerged during the Quaternary period, the west and the east regions having atendency to rise and the north being made of Miocene depressions which emerged during the Pliocene andQuaternary periods.
Seismotectonic characteristics
Prognostic characteristics were calculated for separate seismic blocks as well as for the wholeGorenjska−Ljubljana seismic region.
Also important for seismic hazard in Ljubljana are the tectonic zones that directly cross this region. We needto emphasize the importance of the Dobrepolje fault that runs from northwest to south−east, and which hasbeen active since the mid−Pliocene. The Idrija fault is also significant although slightly more distant. It hashuge seismotectonic potential and many powerful earthquakes up to an intensity of X on the MSK scale haveoccurred around it.
Seismogeological characteristics
The majority of tectonic blocks are made of seismogeologically unfavourable rock, and only in certain partsare they moderately favourable. Predominantly, there are swamp sediments with low seismoacousticimpedance, shallow underground water, low capability and bad stability, all of which intensify theconsequences of an earthquake. Gravel detritus and conglomerates of which the northern parts of the regionare constructed represent a slightly better foundation. The thickness of the Quaternary detritus is from 10metres to more than 100 metres. The rock foundation is mainly carboniferous, mostly limestone and dolomitesdescending gradually towards the south−west. In certain places the foundation is slate and marl (3).
Strong earthquakes in the past
A total of 59 earthquakes registering higher than IV MSK have taken place in the Ljubljana region since theyear 792. The magnitude of the earthquakes in this region is represented in Fig. 3.2, while their intensities areseen in Fig. 3.3.
72
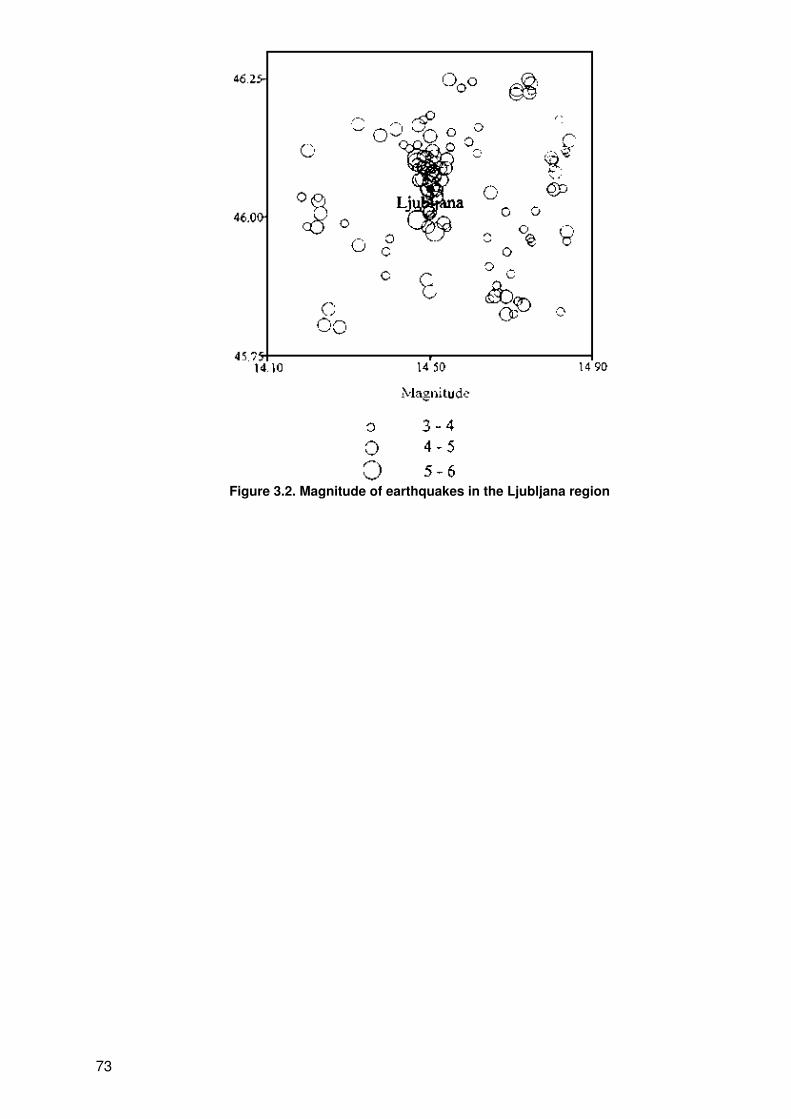
Figure 3.2. Magnitude of earthquakes in the Ljubljana region
73
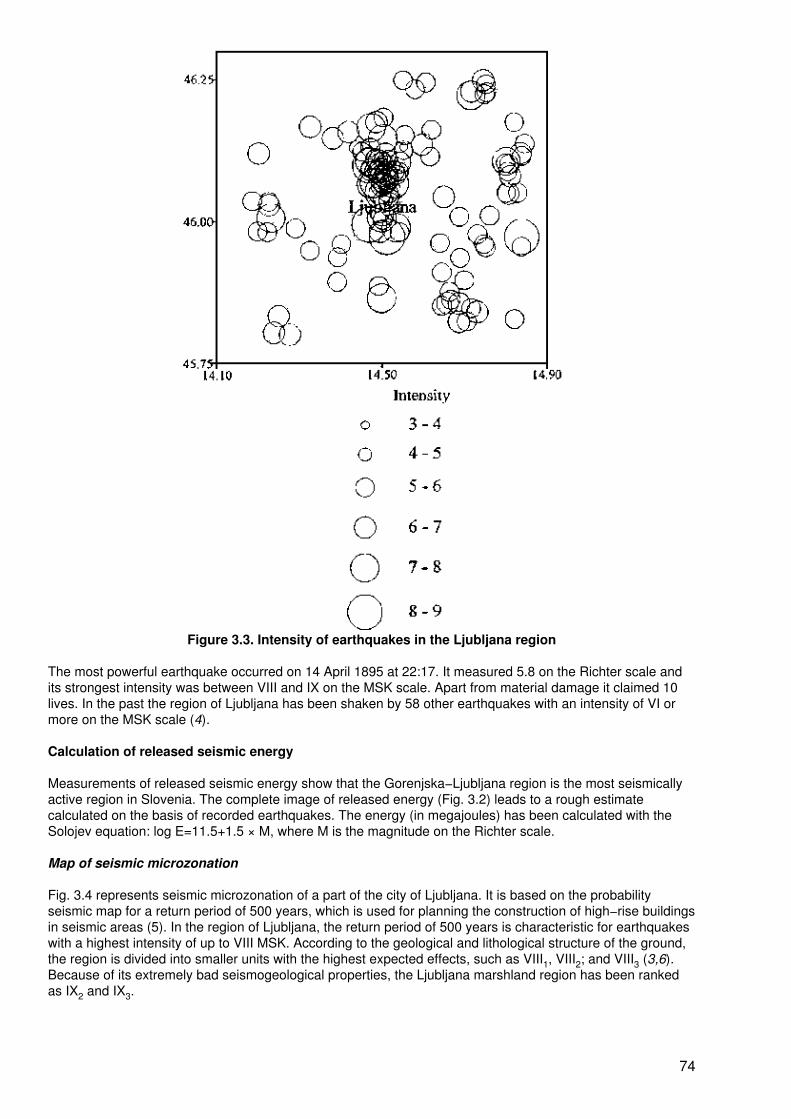
Figure 3.3. Intensity of earthquakes in the Ljubljana region
The most powerful earthquake occurred on 14 April 1895 at 22:17. It measured 5.8 on the Richter scale andits strongest intensity was between VIII and IX on the MSK scale. Apart from material damage it claimed 10lives. In the past the region of Ljubljana has been shaken by 58 other earthquakes with an intensity of VI ormore on the MSK scale (4).
Calculation of released seismic energy
Measurements of released seismic energy show that the Gorenjska−Ljubljana region is the most seismicallyactive region in Slovenia. The complete image of released energy (Fig. 3.2) leads to a rough estimatecalculated on the basis of recorded earthquakes. The energy (in megajoules) has been calculated with theSolojev equation: log E=11.5+1.5 × M, where M is the magnitude on the Richter scale.
Map of seismic microzonation
Fig. 3.4 represents seismic microzonation of a part of the city of Ljubljana. It is based on the probabilityseismic map for a return period of 500 years, which is used for planning the construction of high−rise buildingsin seismic areas (5). In the region of Ljubljana, the return period of 500 years is characteristic for earthquakeswith a highest intensity of up to VIII MSK. According to the geological and lithological structure of the ground,the region is divided into smaller units with the highest expected effects, such as VIII1, VIII2; and VIII3 (3,6).Because of its extremely bad seismogeological properties, the Ljubljana marshland region has been rankedas IX2 and IX3.
74
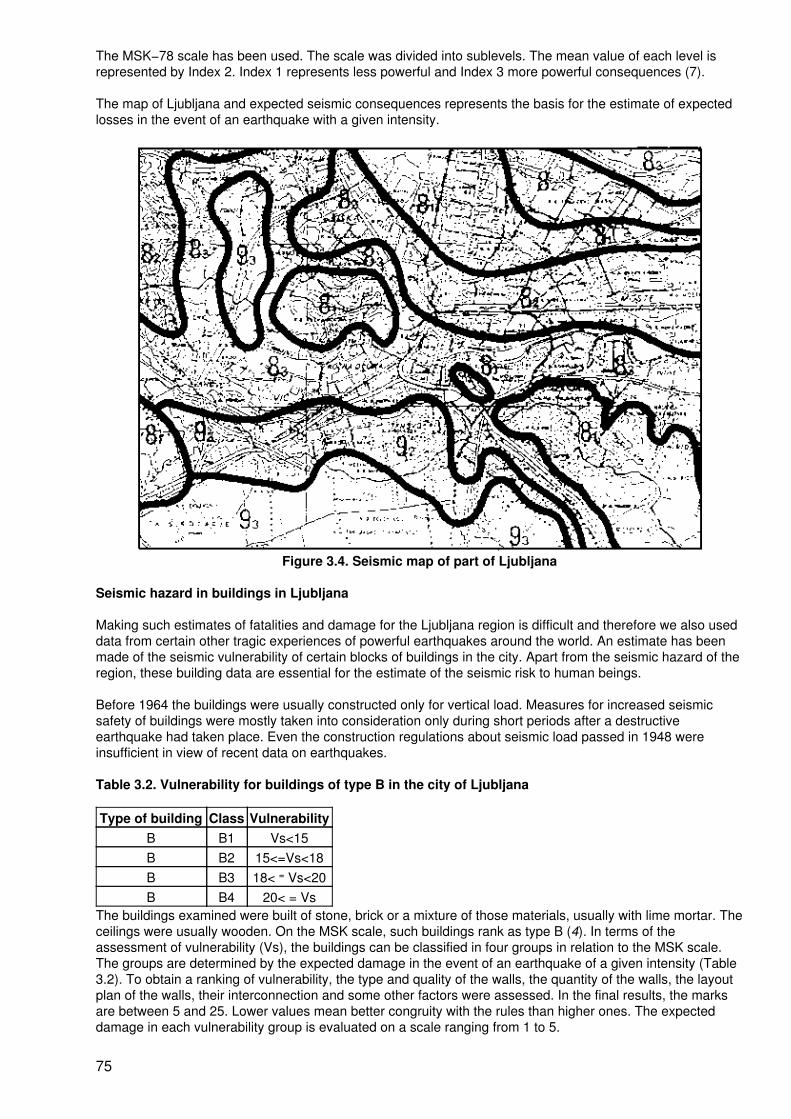
The MSK−78 scale has been used. The scale was divided into sublevels. The mean value of each level isrepresented by Index 2. Index 1 represents less powerful and Index 3 more powerful consequences (7).
The map of Ljubljana and expected seismic consequences represents the basis for the estimate of expectedlosses in the event of an earthquake with a given intensity.
Figure 3.4. Seismic map of part of Ljubljana
Seismic hazard in buildings in Ljubljana
Making such estimates of fatalities and damage for the Ljubljana region is difficult and therefore we also useddata from certain other tragic experiences of powerful earthquakes around the world. An estimate has beenmade of the seismic vulnerability of certain blocks of buildings in the city. Apart from the seismic hazard of theregion, these building data are essential for the estimate of the seismic risk to human beings.
Before 1964 the buildings were usually constructed only for vertical load. Measures for increased seismicsafety of buildings were mostly taken into consideration only during short periods after a destructiveearthquake had taken place. Even the construction regulations about seismic load passed in 1948 wereinsufficient in view of recent data on earthquakes.
Table 3.2. Vulnerability for buildings of type B in the city of Ljubljana
Type of building Class VulnerabilityB B1 Vs<15B B2 15<=Vs<18B B3 18< = Vs<20B B4 20< = Vs
The buildings examined were built of stone, brick or a mixture of those materials, usually with lime mortar. Theceilings were usually wooden. On the MSK scale, such buildings rank as type B (4). In terms of theassessment of vulnerability (Vs), the buildings can be classified in four groups in relation to the MSK scale.The groups are determined by the expected damage in the event of an earthquake of a given intensity (Table3.2). To obtain a ranking of vulnerability, the type and quality of the walls, the quantity of the walls, the layoutplan of the walls, their interconnection and some other factors were assessed. In the final results, the marksare between 5 and 25. Lower values mean better congruity with the rules than higher ones. The expecteddamage in each vulnerability group is evaluated on a scale ranging from 1 to 5.
75
A total of 113 buildings were assessed. Although they are all classified as type B on the MSK scale, theexamination indicated substantial differences. In relation to the expected damage in the event of anearthquake, we can distinguish at least two groups of buildings depending on the period when they wereconstructed. Had we examined more buildings, there would have been even more groups. The buildings oftype B were divided into those built before 1895 (48 buildings), those built between 1896 and 1965 (65buildings) and the third group of buildings built after 1965 (Table 3.3). The year 1895 represents aturning−point in safer building, after the Ljubljana earthquake. Therefore, more damage is anticipated to thebuildings constructed before 1895. Additional modem regulations on construction in seismic regions wereintroduced in 1965.
Table 3.3. Numbers of apartments and residents in buildings of type B in Ljublijana centre, ranked byearthquake risk
ApartmentsIntensity Residents up to 1895 1896−1965 after 1965 Total
VIII1 207 39 4 5 48VIII2 12 235 793 2101 738 3632VIII3 24 583 3489 3617 1394 8500
The seismic risk for the central district of Ljubljana is assessed using the results of the assessment of 113buildings. The assumptions are based on an earthquake measuring VIII on the MSK scale on average soilconditions at night (Fig. 3.5). Quite a large quantity of data for the analysis of such predicted developments inLjubljana Centre had to be gathered (8). The anticipated time of an earthquake means that at such an hourpeople would be back at home, and that offices, factories, schools and shops would be empty.
Classification of the expected damage in the event of various earthquakes was made in relation to theMSK−78 scale and the results of the vulnerability examination. It was established that in the centre ofLjubljana there are no buildings that could be classified as type A on the MSK scale. After further assessment,the same fact was established for the whole central part of Ljubljana.
Therefore all the buildings in this district constructed before 1965 ranked as type B on the MSK scale.Information about the age of the buildings in Ljubljana centre was then gathered for the period before 1900,the period from 1901 to 1963 and the buildings built after 1964. Unfortunately this classification is at odds withthat of the periods defined by the turning−points in the construction safety. However, since the differences aresmall, we assumed that the characteristics of the buildings built before 1895 meet those of all the buildingsconstructed before 1900 and that the characteristics of the buildings from the period between 1896 and 1965equal the characteristics of all the buildings built between 1901 and 1963. The information on the residents ofthese buildings is from 1985. The current situation may be different.
76
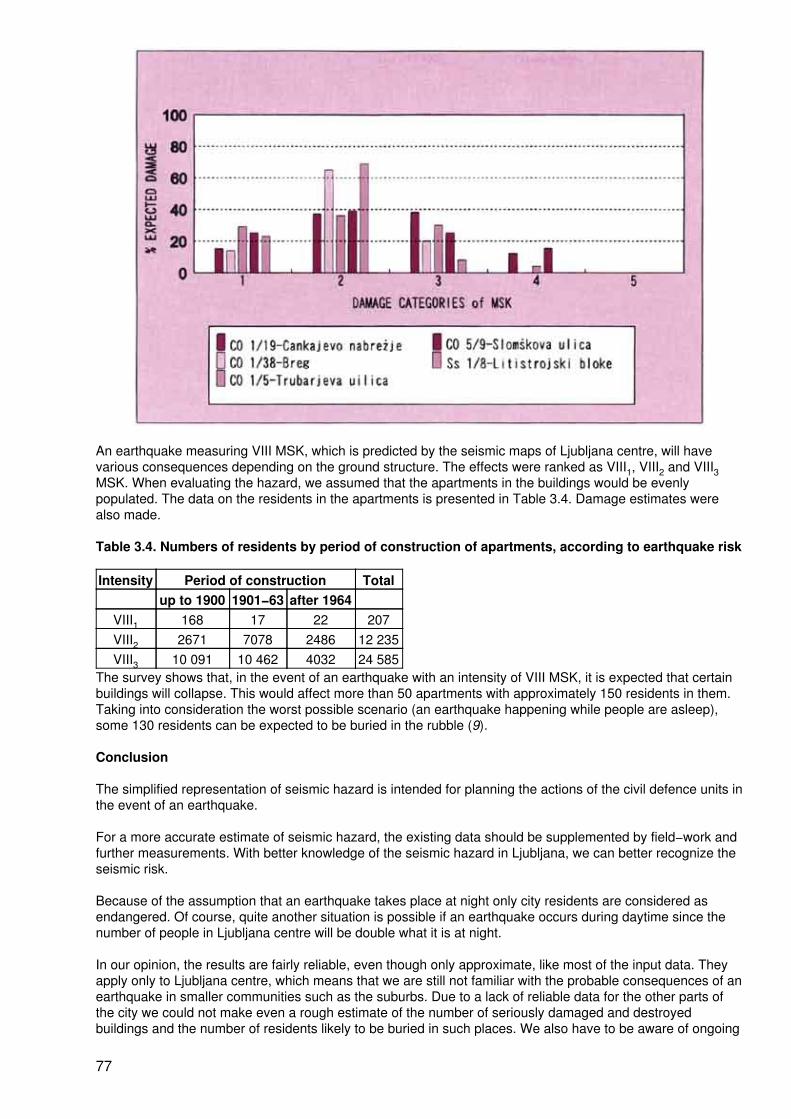
An earthquake measuring VIII MSK, which is predicted by the seismic maps of Ljubljana centre, will havevarious consequences depending on the ground structure. The effects were ranked as VIII1, VIII2 and VIII3MSK. When evaluating the hazard, we assumed that the apartments in the buildings would be evenlypopulated. The data on the residents in the apartments is presented in Table 3.4. Damage estimates werealso made.
Table 3.4. Numbers of residents by period of construction of apartments, according to earthquake risk
Intensity Period of construction Totalup to 1900 1901−63 after 1964
VIII1 168 17 22 207VIII2 2671 7078 2486 12 235VIII3 10 091 10 462 4032 24 585
The survey shows that, in the event of an earthquake with an intensity of VIII MSK, it is expected that certainbuildings will collapse. This would affect more than 50 apartments with approximately 150 residents in them.Taking into consideration the worst possible scenario (an earthquake happening while people are asleep),some 130 residents can be expected to be buried in the rubble (9).
Conclusion
The simplified representation of seismic hazard is intended for planning the actions of the civil defence units inthe event of an earthquake.
For a more accurate estimate of seismic hazard, the existing data should be supplemented by field−work andfurther measurements. With better knowledge of the seismic hazard in Ljubljana, we can better recognize theseismic risk.
Because of the assumption that an earthquake takes place at night only city residents are considered asendangered. Of course, quite another situation is possible if an earthquake occurs during daytime since thenumber of people in Ljubljana centre will be double what it is at night.
In our opinion, the results are fairly reliable, even though only approximate, like most of the input data. Theyapply only to Ljubljana centre, which means that we are still not familiar with the probable consequences of anearthquake in smaller communities such as the suburbs. Due to a lack of reliable data for the other parts ofthe city we could not make even a rough estimate of the number of seriously damaged and destroyedbuildings and the number of residents likely to be buried in such places. We also have to be aware of ongoing
77
changes in buildings as well as in numbers of residents and other users of these buildings.
References
1. Sikošek B. Tektonika, neotektonika in seizmotektonika SR Slovenije. Ljublijana, Publikacije Seizmološkegazavoda SR Slovenije, 1982.
2. Vidrih R, Godec M. Potresna nevarnost Ljubljane. Ujma, 1992, 6:78−81.
3. Vidrih R, Godec M. Lapajne J. Potresna ogroenost Slovenije − obcine Breice, Idrija, Krško, Tolmin inljubljanske obcine. Ljubljana. Seizmološki zavod Slovenije, 1991.
4. Ribaric V. Seizmicnost Slovenije, Katalog potresov (792−1981). Ljubljana, Publikacije Seizmološkegazavoda SR Slovenije, 1982.
5. Ribaric V et al. Seizmološke karte za povratne periode 50, 100, 200, 500, 1000 in 10000 let. Belgrade,Zajednica za seizmologiju SFRJ, 1987.
6. Tomaevic M, Lapajne J, Sheppard P, Bergant M, Lutman M, Godec M, Vidrih R. Potresna ogroenost mestaLjubljana I in II, Ljubljana, Seizmološki zavod Slovenije, 1991.
7. Lapajne J. Potresna lestvica MSK. Ujma Ót, 1989, 3:62−66.
8. Souvan T et al. 1985. ISUP Ljubljana Centre. Urbanisticni inštitut SRS in Zavod za izgradnjo Ljubljane.Ljubljana, ISUP, 1985.
9. Sakai S, Coburn A, Spence R. Human casualties in building collapse, literature review. Cambridge, MartineCentre for Architectural and Urban Studies, 1990.
Summary
Secretariat
Dr V. Kravchuk and Dr SA. Mazhkenov reported on the monitoring of seismic hazards and earthquakeprediction in Kazakstan. The Republic of Kazakstan expects a decade of increased seismic activity, based onhistorical records and geophysical data. Because of the high vulnerability of the country, and in particularbecause of construction during the past decades, various sectors and institutes are collaborating in aforecasting, warning and rescue system. Each week new findings and data are discussed by anInterdepartmental Commission of Earthquake Prediction. Conclusions are directly relayed to the StateEmergency Committee for appropriate action.
Mr M. Godec and Mr R. Vidrih made a presentation on seismic hazard and risk in Ljubljana, Slovenia. Thecity of Ljubljana is situated in the Ljubljana seismic block which is a part of the Gorenjska−Ljubljana seismicregion. This region ranks above the Idrija and Krško−Breice regions in terms of released seismic energy. Atotal of 59 earthquakes registering higher than IV MSK took place in this region in the past. Of these, 31earthquakes reached an intensity of VII MSK, four of them measured between VII and VIII, another fourmeasured VIII, and one earthquake had an intensity of between VIII and IX MSK. The most powerfulearthquake occurred on 14 April 1895, measuring 5.8 degrees on the Richter scale. It caused materialdamage and also claimed 10 lives.
The seismic hazards in Ljubljana were evaluated on the basis of a microzonation map and information aboutthe seismic vulnerability of buildings. The map of earthquake microzonation was prepared on the basis ofseismological records of past earthquakes, seismological data and geological structure in order to help inplanning the action of civil defence units. The map showed expected losses within a fixed period in a certainarea. These results were used for central Ljubljana where all the data about the buildings and their users wascollected. This estimate of seismic hazard was based on an earthquake occurring in the evening whileresidents are usually at home and business premises are empty.
78

Masterplans
Urban earthquake masterplans: social and health aspects
M. Erdik1and J. Swift−Avci2
1M. Erdik is Professor and Chair, Department of Earthquake Engineering, KandilliObservatory and Earthquake Engineering, Bogazici University, Istanbul, Turkey.
2J. Swift−Avci is Senior Research Engineer, Department of Earthquake Engineering, KandilliObservatory and Earthquake Engineering, Bogazici University, Istanbul, Turkey.
Background
In recent decades earthquake disaster risks have increased in urban centres of both developed anddeveloping countries. The increase in the developed countries is due to ageing urban systems and population,greater dependence on technology, and more valuable elements exposed to risk. In developing countries themain increase in seismic risk can be attributed to overcrowding, faulty land−use planning and construction,inadequate infrastructure and services, and environmental degradation. Recent destructive events in MexicoCity (1985, M8.1); Spitak, Armenia (1988, M7.0); Loma Prieta, USA (1989, M7.1); Manjil, Iran (1990, M7.7);the Philippines (1990, M7.8); Erzincan, Turkey (1992, M6.9); Northridge (1994, M6.8); and Kobe (1995, M6.9)have exemplified the consequences of earthquake risk in urban areas and have 'attracted increasing attentionfrom the world at large.
In earthquake−prone urban centres it is imperative that certain preparedness and emergency procedures bedeveloped in case of and prior to an inevitable earthquake disaster. The seismic risk is best portrayed andquantified through the preparation of "earthquake damage and loss scenarios". In urban centres thesescenarios are essential for risk mitigation, emergency response planning and the associated resourceallocation/retrofit prioritization. The first element of such scenarios is the assessment of the hazard, usuallyportrayed in terms of microzonation maps. The vulnerabilities and the damage statistics in terms of lives,structures, systems and the socioeconomic structure constitute the second element. Earthquake damagescenarios are based on the intelligent consideration and combination of original hazards, secondary hazardsand the vulnerability. "Earthquake Masterplans" represent the combination of these scenarios with theappropriate strategies for emergency response planning and risk mitigation.
Earthquake hazard assessment (microzonation)
The assessment of the urban earthquake hazard comprises the specification of the earthquake scenario,compilation of information on propagation path characteristics, topographical, geological and geotechnicaldata, and the identification of the proper attenuation and site response analysis models. Urban earthquakes,notably the 1985 Mexico City and the 1989 Loma Prieta earthquakes, have demonstrated that, in addition tosource distance, the wave propagation characteristics and site conditions play a deterministic role on thedistribution of losses. This shows the importance of macro−scale and micro−scale hazard assessment in theanalysis of urban seismic risk.
In addition to vibratory ground motion, urban seismic hazard assessments should encompass tsunamiinundation, soil failures, terrain movements and surface fault ruptures as appropriate. Although a rationalhazard assessment methodology should obviously provide for uncertainties associated with the inputparameters, most past applications are based on scenario events with minimum quantification or evenqualitative treatment of uncertainty. Pertinent issues are discussed below.
Earthquake scenario
Geological and seismological information forms the basis for choosing the appropriate earthquake scenario,which is usually given in broad terms involving rupture length, location and magnitude. The earthquake(s) maybe associated with local, near and distant sources. For worst−case scenarios the maximum event size isadopted. The earthquake scenario has also been defined as the largest earthquake(s) expected within areasonable period of time (generally 500 years). A rational procedure for the selection of an earthquakescenario in future investigations can be based on the de−aggregation of the hazard to show which eventscontribute most to the loss (1).
79
Attenuation relationships
Attenuation models provide for changes in ground motion severity with source mechanism, distance and localgeology. Currently reliable empirical models exist in terms of peak ground acceleration, velocity anddisplacement (PGA, PGV and PGD) and pseudo−spectral velocity (PSV), at specific frequencies and dampingratios for a given earthquake magnitude, distance, fault mechanism and local geology (2,3). In addition, basedon macroseismic data obtained from past earthquakes, the availability of intensity−based vulnerabilityinformation has dictated the use of site−specific intensity' attenuation relationships.
Modification of ground motion by site conditions
For the quantitative representation of the modification of ground motion by site conditions in microzonationmaps, there exist analytical and empirical approaches. It has been found (4) that the reliability of anynumerical model depends significantly on the measurements of the nonlinear characteristics of soils, whichinherently exhibit large uncertainties. This fact will tend to prohibit the application of purelyanalytical−numerical procedures in future developments of earthquake loss scenarios.
Earthquake−induced ground failures
For proper assessment of the seismic risk in urban centres the potential of the earthquake−induced groundfailure hazard, such as liquefaction, landsliding and surface fault rupture needs to be determined. Groundfailure potential is defined as the probability of occurrence given the susceptibility of the ground and theopportunity exhibited by the severity of ground motion. Because of their high cost and the need for extensivedata, in most of the earthquake loss scenario applications the liquefaction susceptibility has been identified onthe basis of geotechnical/geomorphic criteria (5,6).
Techniques for the site−specific assessment of landslide susceptibility based on engineering parameters havealso been developed (7). In earthquake loss scenario developments, however, the most commonly usedindicators of susceptibility have been based on geomorphic criteria (8). The probability that a landslide will betriggered on a particular slope during a particular earthquake is a function of both the pre−earthquake stabilityof the slope and the severity of the earthquake ground motion.
Elements at risk
In urban areas the population, structures, utilities, systems and socioeconomic activities constitute the"elements at risk". Preparation of urban earthquake damage/loss scenarios relies on the compilation ofinformation in Geographic Information System (GIS) databases on the following: demographic structure fordifferent times of the day; building stock and its typification; lifeline and infrastructure (major roads, railroads,bridges, overpasses, public transportation, power distribution, water, sewage, telephone and natural gasdistribution systems) including their nodal points (stations, pumps, switchyards, storage systems, transmissiontowers, treatment plants, airports, marine ports, etc.); major and critical facilities (dams, power plants, largechemical and fuel storage tanks). Unfortunately the general incompleteness, if not lack of availability, of suchinformation creates a serious bottleneck for urban earthquake loss assessments. The building classificationsystems used in inventories (and eventually in vulnerability matrices) are country−specific, and evenregion−specific, and cannot be applied uniformly in all major urban centres. The information on lifelines andmajor facilities is easier to obtain and the related design and construction practices may have moreinternational conformity.
Earthquake vulnerability
Vulnerability is defined as the degree of loss to a given element at risk, or to a set of such elements, resultingfrom the occurrence of a hazard. The vulnerabilities of lives, structures, systems and the socioeconomicstructure are the main factors influencing earthquake risk and losses in urban areas. More details areprovided in Annex 4 (9−12).
Turkish case study on the social and health aspects of urban earthquakes (1992 Erzincan earthquake)
Although Turkey has enacted and enforced laws and regulations to lower earthquake disaster vulnerability inurban areas, pressures of population growth have partly resulted in unregulated settlements with unsafebuildings on unsafe land. Furthermore, to encourage industrial development and employment opportunities,these controls were not adequately applied in the past and penalties for noncompliance were small. Thus, theincreased social and physical vulnerability contributes substantially to the increase in earthquake disaster risk.
80
The Erzincan earthquake of 1992 underscored the importance of preparedness for such a disaster.Emergency plans and scenarios were ready at government level but they had not been rehearsed andpractised. This resulted in an ineffective response during the first days after the earthquake. The ProvincialRescue and Relief Committee set up as part of the disaster response plan of the city became effective onlyafter the second day of the earthquake. The rescue and relief efforts in the first days of the earthquake werehandled in an ad hoc manner by military personnel. With the arrival of the national and international rescueteams, the rescue efforts became more professional.
The first problem faced after the earthquake was the inadequacy of tents for temporary settlements.Unreliable information disseminated in the first days of the earthquake, especially regarding the quantity anddistribution of tents, hampered the relief activities. This implies that, in urban areas after a disaster, thefriction, potential competition and the likelihood of disturbances among the urban poor will probably increaseand the delivery of emergency assistance may be hindered. The biggest drawback for the social andcommunity services has been the request from the medical and educational personnel for re−appointment tocities outside the disaster area.
In the Erzincan earthquake 677 people were killed and about 4000 persons were injured. Deaths wereconcentrated in collapsed public buildings at the centre of the city. The number of casualties wascomparatively low since the earthquake occurred on a Friday evening when most people were at home. TheThird Army, stationed in Erzincan, started rescue operations with the participation of the people of the citywithin two hours of the earthquake. This took place in darkness, without sufficient equipment, tools orexperience− The lives of close to 300 persons were saved during the night. After 23:00 hours, teams fromneighbouring communities such as Erzurum joined the operation which went on for 48 hours without a break.The foreign rescue teams arrived only days after the event. During the rescue operations which lasted 12days, 378 persons were saved from under the debris. About 1000 vehicles and heavy equipment and some3000 persons took part in the rescue operation and debris removal.
There were three major public hospitals in Erzincan City, two private hospitals and seven clinics. In thesuburbs, there were 41 small hospitals. Most of these hospitals were severely damaged and none could beutilized fully after the earthquake. All of the injured persons were transported to hospitals in other provinces,such as Erzurum and Sivas. Approximately 800 injured persons were treated in Erzurum within the first twodays (500 in the first night). A total of 10 Public Health Ministry teams visited all of the districts andcommunities to render first aid and to dispense medicines. Mobile hospitals were set up by the Ministry ofHealth, the Red Crescent Society, international organizations, and by the countries which providedassistance. These mobile hospitals performed only polyclinic and first aid services. The more seriously injuredwere transported to Erzurum for treatment. Within two days after the earthquake 331 physicians, 187 nursesand 120 ambulances were sent to the disaster area from the neighbouring provinces.
A Red Crescent camp was set up in the soccer stadium in the centre of the city 15 hours after the earthquaketo provide first aid treatment and other basic needs. Emergency materials from other branches of the RedCrescent Society (Erzurum, Elazig and Adana) arrived 5−6 hours after the earthquake. Within 10 hours, thehead office in Ankara sent emergency goods to the city. The medical staff of the camp consisted of a chiefphysician, an assistant chief physician, four temporary physicians, a chief nurse, an assistant chief nurse, fivenurses and 11 temporary nurses. During the first few days, however, there were 20 physicians in the camp.The facilities included an operating room, a delivery room and 200 beds. During the first 15 days after theearthquake, a total of 6633 people received treatment. The number of people treated for injuries was 1865;victims of bums numbered 781; trauma victims, 481; and persons with various infections, 600. There are tworeasons for the large number of persons with burns: most homes were using heaters due to the very coldweather and people were preparing a meal when the earthquake struck. Most of the bums victims werescalded by boiling water. Many children were also burned. A large number of people also suffered fromrespiratory infections caused mainly by inhaling dust from the collapsed buildings and by exposure to the coldweather.
Earthquake damage and loss scenarios
The concept of risk, in the parlance of the Office of the United Nations Disaster Relief Coordinator (UNDRO),means expected levels of loss due to a specific hazard for a given geographic area over a specific timeinterval, given the average return period of the hazard. An earthquake risk analysis based on probability takesinto account the uncertainties inherent in the earth sciences (hazard) and the engineering information(vulnerability) and estimates the probability of the adverse physical, economic and social effects of anearthquake or series of earthquakes in a given urban centre. For example, to compute the expected numberof casualties due to earthquakes in a given city within a given period of time, the following factors need to be
81
combined: the earthquake intensity return period for the given region; the distribution of building types in thegiven region; the vulnerability function of each building type; and the number of casualties expected for eachdamage degree for each building type (i.e. lethality factor).
In the context of damage scenarios, risk can be defined as the loss to the elements at risk that can result fromthe occurrence of earthquake scenarios. Damage scenarios are the vehicles to portray these risks.
Oyo Corporation, for example, has produced earthquake damage scenarios for several localities (e.g.Kawasaki City, Saitama Prefecture, Kanagawa Prefecture) in Japan (13−16). These scenario analysesconsist of several steps in which natural sciences, social sciences and government have roles. As a secondexample, under the general title of "Planning Scenario", the California Department of Conservation Division ofMines and Geology has prepared earthquake damage scenarios for several areas in California (17−19).
Mitigation of urban earthquake risk
Disasters, regardless of the causative element, can be viewed as a break from the normal socioeconomicsystem. Thus the people, institutions and the other elements of life which, by nature, function effectivelyduring normal times, cannot necessarily function effectively during the abnormal conditions created by thedisaster. The need for return to normalcy necessitates appropriate disaster response (disaster management)before disaster happens. Thereby a community will be able to reduce the recurrence of problems duringperiods of disaster−induced abnormality and will be able eventually to serve the disaster victim in a moreefficient manner in order to bring his or her life back to what is referred to as normal. In this context,earthquake disaster mitigation becomes the process of anticipating and planning for damage that a majorearthquake would eventually create.
In general, earthquake risk mitigation options can be analysed under two main headings: non−structural andstructural. Non−structural options encompass the following: the introduction or improvement of disasterlegislation and institutions; the introduction of incentives such as lower insurance premiums for buildings withbetter hazard resistance; and awareness−building, education and training. Structural measures include thereduction of the physical vulnerability of structures and the improvement of urban settlements. The reductionof structural vulnerability can entail retrofitting of existing buildings, other structures and infrastructure forimproved earthquake performance. The effectiveness of public expenditures to be utilized for such activitiesshould be compared with the cost of repair after the disaster. Urban settlements can be improved by changingthe functional characteristics of the settlements through land−use planning and increasing the redundancy ofthe infrastructure, such as building an additional bridge at a strategic crossing.
Specific mitigation issues
In technical terms, earthquake risk is the probability of expected earthquake losses (such as lives, injuries,physical damage and socioeconomic loss). Earthquake damage scenarios are tools for the assessment ofthese losses. Adoption of seismic zonation and land−use planning and enforcement of earthquake design andconstruction codes depend closely on increased public awareness realized through the dissemination ofinformation on vulnerability and risk.
For mitigation of urban earthquake risks the necessary plans, programmes and activities can be listedaccording to the pre−earthquake, co−earthquake and post−earthquake phases.
The pre−earthquake measures that should be implemented in urban centres prone to earthquake risk include:
− pre−disaster planning and management activities and techniques;− disaster awareness, public information, education and training;− legislative and regulatory measures for land−use management;− development of earthquake−resistant design codes and construction standards;− retrofitting of hazardous buildings and facilities;− repair and strengthening of non−engineered low−strength constructions;− hazardous material management;− response readiness;− logistical planning for rescue, first aid and health care;− resource management and stockpiling;− mobile command and communication operations.
82
The emergency activities that should be implemented in urban centres right after an earthquake disasterinclude:
− emergency rescue, evacuation, transportation and communication;− quick assessment of physical damage and socioeconomic losses;− debris removal;− recovery and disposal of dead bodies;− emergency provision of health care, shelter, water, food and utilities;− human response and information management;− law enforcement;− planning and coordination of disaster assistance.
The post−earthquake steps that should be taken in urban centres in the period following earthquake disastersinclude:
− detailed surveys regarding repair, restoration and condemnation decisions;− assessment of socioeconomic conditions, resources and needs;− measures and policies for relief, resettlement, rehabilitation and redevelopment;− planning and coordination of rehabilitation and reconstruction assistance;− siting of new settlements and communities;− retrofit of design codes and construction standards.
Important mitigation activities and emergency health aspects
Disaster emergencies require the services of well−trained, disciplined and well−organized rescue teamsequipped with special instruments. Past earthquake disasters have repeatedly shown the impossibility ofcarrying out effective emergency rescue and assistance operations with untrained personnel. The voluntaryassistance groups and the civil defence personnel are not effective unless they are trained and accompaniedby specialists.
To varying degrees, past urban earthquakes provide evidence regarding the effectiveness of public educationprogrammes on disaster preparedness. While efforts have often been made to develop disaster responseplanning at the government level, at the time of an earthquake there is often no effective response plan inplace. Inadequate reconnaissance and damage assessment has often led to serious delays in full mobilizationand application of national and international response capabilities. The lack of earthquake disaster responseplans has constrained both the efficiency and effectiveness of initial disaster responses. For any earthquakedisaster management programme, the building of public awareness, information dissemination and thetraining of personnel constitute the fundamental ingredients of success (20). For public educationprogrammes in earthquake disaster mitigation the target audience consists of specific sections of thecommunity exposed to earthquakes. The training encompasses public awareness programmes to developand/or to maintain a desired level of awareness and earthquake disaster preparedness.
The urban facilities that are essential for the operation of the socioeconomic system (health services, sanitaryservices, utilities etc.) should be designed with the lowest vulnerability levels. In this respect, the functionalityof the hospitals needs to be ensured during earthquakes. Past experience indicates that 25−50% of deathscan be avoided if emergency health care is available immediately after the earthquake. The immediacy of theneed underscores the importance of external medical assistance, which usually arrives too late to prevent thefirst mortalities. For planning of emergency health care after an earthquake a three−phase plan can beimplemented (21). During the first phase, which encompasses the first hour after the earthquake, immediateaction by all available physicians, on an individual basis and within their vicinity, through their emergencypacks and kits is foreseen. In the second phase, during the first 12 hours, health care can be provided byso−called "emergency health centres". These centres can be planned to be set up at convenient locations(fire stations, schools, clinics etc.) distributed at about equal spacing within the urban area. The spacingshould be approximately 4 km (about 1 hour's walking distance). Each centre should have three physicians(two on a 12−hour rotation basis, and one backup) to conduct the first triage of the victims and to provide theneeded care. Critical patients must be separated for transfer to casualty collection centres or to large hospitalsthat are still functioning. The casualty collection centres constitute the third phase of the emergency healthcare. These centres can be planned to be built in large open spaces, such as sports fields and shoppingcentres, with adequate temporary medical facilities.
Toppozada et al. (18), for instance, addressed the need for functional acute care facilities including staff,blood banks, medical resources and ambulance services in an earthquake planning scenario for the San
83
Bernardino area in California. The vulnerability concentrated on the local acute care hospitals in the zone ofpotentially damaging ground−shaking− assuming that the hospitals in the less vulnerable areas would have tohandle the increased patient load. For planning purposes, operational capabilities of the hospital facilitieswere reviewed from the following perspectives: building damage; injuries and loss of life to patients and staff;loss of medical equipment and supplies; loss of hospital functionality because of access/transportationproblems and/or disrupted infrastructure; and evacuation of hospitals by staff or the public due to loss ofconfidence or other reasons. The potential loss was summarized by estimating loss of hospital beds (ratherthan building damage only) due to an earthquake of a given intensity.
Conclusion
The largest recent earthquakes to hit modem urban environments include the M6.7 Northridge and M6.9 Kobeearthquakes. Both events have shown that urban earthquakes can be highly damaging with the potential todisrupt our lifeline systems and socioeconomic structure and cause economic losses reaching 100 billion USdollars. Yet the loss figure estimated should a future Tokyo earthquake occur is in the vicinity of 1 trillion USdollars (22). Such a disaster can obviously have not only national but severe global repercussions.
Future earthquakes will have more urban centres and exposed valuable elements to target. Industrializationcreates more potential sources of disaster in the form of dangerous spills, explosions and fires. Increaseddependence on computers also brings complexities into the earthquake risks. However, we can also be betterarmed in assessing the physical and socioeconomic impact of urban earthquakes and in proper allocation ofresources towards mitigation of these impacts. The extensive research being carried out on the developmentof earthquake risk assessment methodologies guides our expectations for the future. We can increase ourefforts for the assessment of earthquake risk in urban centres and widely disseminate the results. Severalinternational institutions, programmes and initiatives such as: the World Bank, the World Health Organization(WHO), the International Decade for National Disaster Reduction (IDNDR), the Global Seismic HazardAssessment Program (GSHAP) and the World Seismic Safety Initiative will serve as a catalysts in this regard.
What will be needed in the future is the dissemination of urban earthquake loss information in understandableformats to increase the awareness of the general public, to sensitize top−level decision−makers and to arriveat rational risk mitigation plans.
References
1. McGuire RK. Characterizing active faults as input to seismic hazard studies. Ettore majorana centre forscientific culture istituto nazionale di geofisica 11th course: Active faulting studies for seismic hazardassessment, extended abstracts, 1995.
2. Boore DM et al. Estimation of response spectra and peak accelerations from western North Americanearthquakes: an interim report. USGS Open file report 93−509. Menlo Park, CA, United States GeologicalSurvey, 1993.
3. Campbell KW, Bozorognia Y. Near−source attenuation of peak horizontal acceleration from worldwideaccelerogram recorded from 1957 to 1993. Proceedings of the 5th United States national conference onearthquake engineering, Chicago, IL. 1994.
4. European Macroseismic Scale 1992. Luxembourg, European Seismological Commission, 1993.
5. Youd LT et al. Liquefaction potential map of San Fernando, California. Progress on seismic zonation in theSan Francisco Bay region. USGS Circular No. 807. Menlo Park, CA, United States Geological Survey, 1979.
6. Youd LT, Perkins DM. Mapping of liquefaction induced ground failure potential. Journal of geotechnicalengineering, 1978, 104 (4):433−446.
7. Reducing earthquake hazards: lessons learned from earthquakes, EERI Publication No: 86−02. SanFrancisco, CA, EERI, 1986.
8. Wilson C, Keefer DK. Predicting aerial limits of earthquake induced landsliding. Evaluating earthquakehazards in the Los Angeles region. USGS Professional Paper No. 1360, Washington, DC, United StatesGovernment Printing Office, 1985:317−346.
9. Coburn A. Spence R. Earthquake protection. Chichester, John Wiley and Sons Ltd, 1992.
84
10. Rgelfe (Research Group for Estimating Losses from Future Earthquakes). Estimating losses fromearthquakes in China in the forthcoming 50 Years. Beijing, State seismological bureau, Seismological Press,1992.
11. ATC−13. Earthquake damage evaluation data for California, ATC−13 Report. Redwood City, CA, AppliedTechnology Council, 1985.
12. Ambraseys NN, Jackson JA. Earthquake hazard and vulnerability in the northeastern Mediterranean: theCorinth earthquake sequence of February−March 1981. Disasters, 1981,5(4):355−368.
13. Special publication for seismic microzoning techniques: a case study for Kawasaki City, Japan. OyoCorporation, 1988.
14. Kaneko F, Yamada T. Earthquake scenarios prepared from seismic microzoning studies − a recentexample in Japan. Oyo Corporation, 1992.
15. Kaneko, F. Earthquake disaster countermeasures in Saitama Prefecture, Japan. Issues in urbanearthquake risk. Netherlands, Kluwer Academic Publishers, 1994.
16. Komaru Y et al. Development of an earthquake damage estimation system. Proceedings of the 5thinternational conference on seismic zonation, Nice, Franc. AFPS and EERI, 1995, 1:273−280.
17. Toppozada RT et al. Planning scenario for a major earthquake on the Newport−Inglewood Fault Zone,Special publication No. 102. Sacramento, CA, California Dept. of Conservation, Division of Mines andGeology, 1988.
18. Toppozada RT et al. Planning scenario for a major earthquake on the San Jacinto Fault in the SanBernardino area, Special Publication No. 102. Sacramento, CA, California Dept. of Conservation, Division ofMines and Geology, 1993.
19. Toppozada RT et al. Planning scenario for a major earthquake on the Rodgers Creek Fault in theNorthern San Francisco Bay area, Special Publication No. 112. Sacramento, CA, California Dept. ofConservation, Division of Mines and Geology, 1994.
20. Erdik M. Training and education for disaster preparedness. Regional Development Dialogue, UnitedNations Centre for Regional Development, Nagoya, Japan, 1987, 9(1):36−48.
21. Schultz CH et al. A medical disaster response to reduce immediate mortality after an earthquake. NewEngland journal of medicine, 1996,334:438−444.
22. Berz G, Smolka A. Urban earthquake loss potential: economic and insurance aspects. Proceedings of the10th European conference on earthquake engineering, 1995, 2:127−1134.
Seismic activity and the mitigation of its consequences in Kazakstan
State Emergency Committee of the Republic of Kazakstan
The Republic of Kazakstan in central Asia is the country with the ninth largest area in the world (2717 millionkm2). It has common borders with China, Kyrgyzstan, Russia, Turkmenistan and Uzbekistan. The naturalenvironment and Kazakstan's history have led to an uneven development of the country. Up to 40% ofindustrial facilities are concentrated in the south, south−eastern and eastern regions of the country. There are27 large towns and cities, including the capital, Almaty, 450 villages and a population of 6 million. These urbanareas are in the most active earthquake zones which constitute a high seismic hazard.
Both historical information and modem data testify to a huge potential for the release of energy in the earth'scrust in south−east Kazakstan. A sharp rise in seismic activity took place at the end of the last century and thebeginning of the present one when a series of seismic catastrophes occurred.
In 1885, the Belovodsk earthquake of magnitude 6.9 occurred on the northern slope of the Kyrgyz range. Inthe mountains there were large landslides and ruptures over a total distance of more than 20 km. The extent
85

of vertical movement reached 1 m.
On 9 June 1887, the Vernyi earthquake with a magnitude of 7.3 caused extensive landslides over a largearea. The epicentre was located 35 km from Vernyi (now Almaty). The effects of the earthquake were spreadover an area of 175 km2. There were numerous cracks, escarpments, landshifts and landslides. Theconsequences of the earthquake for the city of Vernyi were terrible. In just one minute, all but one of 1799brick buildings were completely destroyed. Some stone houses had only their wooden frames left standing.About 500 people died.
In the Chilik earthquake of 1889 (magnitude 8.4) the length of breaks in the epicentral zone reached 20 km,and the extent of horizontal movement was up to 5 m. This earthquake was also accompanied by buildingcollapses and landslides in the region of the Chilik and Charyn rivers.
The epicentral zone of the Kemin earthquake of 1911 (magnitude 8.2) occupied a narrow strip that extendedalong the valleys of the rivers Bolshoi, Kemin and Chilik between the Zaili and Kungei Alatau ranges. A seriesof ruptures was formed for up to 200 km from west to east. Vertical movement reached 5 m. In Vernyi, wherethe intensity of the shock reached IX on the MSK−64 scale, all brick buildings were destroyed and 36 peopledied.
All these earthquakes occurred in zones that are prone to seismic activity and were all accompanied by aseries of strong aftershocks. Thus, after the Kemin earthquake of 1911, there were 300 appreciableaftershocks during the next six months.
After the Kemin−Chuiskoje earthquake of 1938 (magnitude 6.9) no further earthquakes with a magnitude ofmore than 4.5 were observed until 1970 when a new stage of seismic activity began. Among the largeearthquakes that followed were those at Turaigyrskoje in 1975 (magnitude 5.0), Sarykamyshskoje in 1970(magnitude 6.6), Zhalanash−Tjupskoje in 1978 (magnitude 7.0) and Almatinskoje in 1982 (magnitude 5.6).
In June 1990 the Zaisan earthquake (magnitude 7.0) took place in the East Kazakstan region. The destructiveconsequences of the earthquake were seen over an extensive area in the Zaisan depression and also inneighbouring parts of China. In 120 settlements, 8874 inhabited buildings were destroyed (about 70% of allstructures) and 36 000 people were left without shelter.
Analysis of historical information and materials by seismologists in Kazakstan has allowed them to understandthe basic seismic structure and to determine the seismic potential of the north Tianshan, Jungar,Chingiz−Tarbagatai and Altai mountain systems (Fig. 3.1).
A map of the long−term forecast of earthquakes for the region of northern Tianshan shows six zones (1 −South Jungarian, 2 − Turgenskaja, 3 − Kastekskaja, 4 − Narynkolskaja, 5 −Kochkorskaja, 6 − Kadzhisaiskaja)where seismic activity is predicted until the year 2000 (Fig. 3.6). Data of the Kazakstan National AcademyInstitute of Seismology show that in the specified zones the occurrence of earthquakes with a magnitude of6.0 and more is possible in the next 3−5 years. The earthquake epicentres during the past five years in thesouth−east of the republic have all been within the identified zones.
86
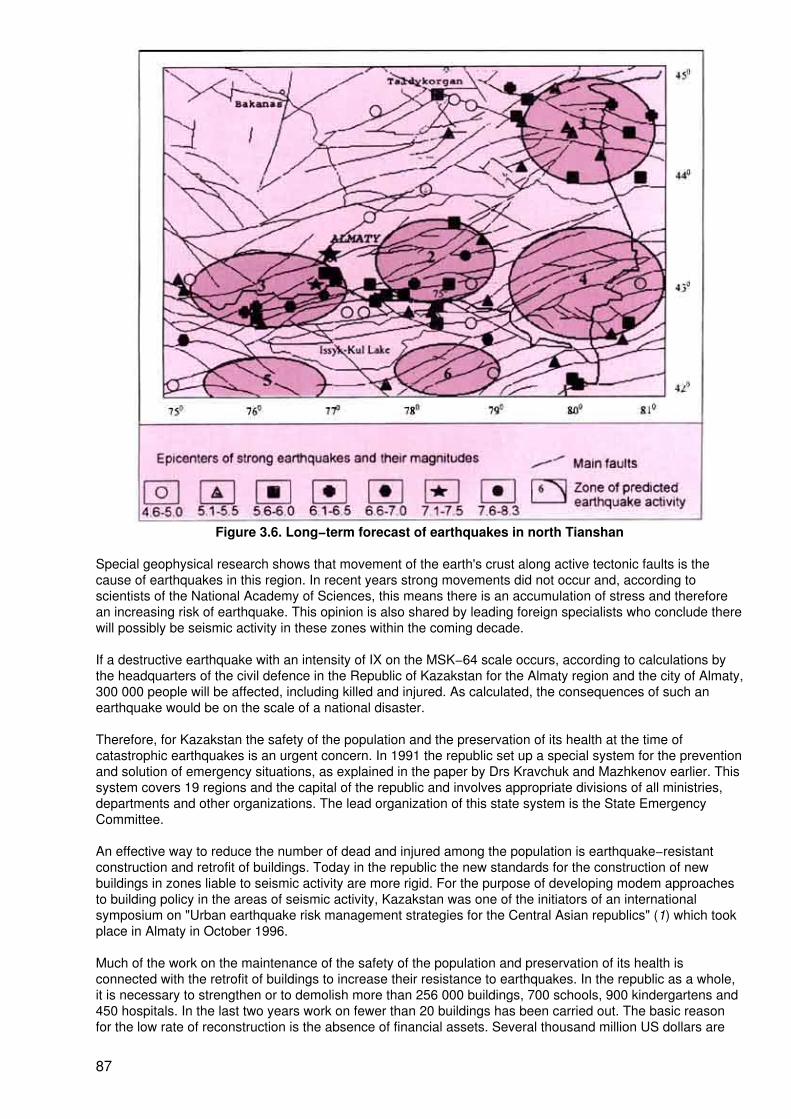
Figure 3.6. Long−term forecast of earthquakes in north Tianshan
Special geophysical research shows that movement of the earth's crust along active tectonic faults is thecause of earthquakes in this region. In recent years strong movements did not occur and, according toscientists of the National Academy of Sciences, this means there is an accumulation of stress and thereforean increasing risk of earthquake. This opinion is also shared by leading foreign specialists who conclude therewill possibly be seismic activity in these zones within the coming decade.
If a destructive earthquake with an intensity of IX on the MSK−64 scale occurs, according to calculations bythe headquarters of the civil defence in the Republic of Kazakstan for the Almaty region and the city of Almaty,300 000 people will be affected, including killed and injured. As calculated, the consequences of such anearthquake would be on the scale of a national disaster.
Therefore, for Kazakstan the safety of the population and the preservation of its health at the time ofcatastrophic earthquakes is an urgent concern. In 1991 the republic set up a special system for the preventionand solution of emergency situations, as explained in the paper by Drs Kravchuk and Mazhkenov earlier. Thissystem covers 19 regions and the capital of the republic and involves appropriate divisions of all ministries,departments and other organizations. The lead organization of this state system is the State EmergencyCommittee.
An effective way to reduce the number of dead and injured among the population is earthquake−resistantconstruction and retrofit of buildings. Today in the republic the new standards for the construction of newbuildings in zones liable to seismic activity are more rigid. For the purpose of developing modem approachesto building policy in the areas of seismic activity, Kazakstan was one of the initiators of an internationalsymposium on "Urban earthquake risk management strategies for the Central Asian republics" (1) which tookplace in Almaty in October 1996.
Much of the work on the maintenance of the safety of the population and preservation of its health isconnected with the retrofit of buildings to increase their resistance to earthquakes. In the republic as a whole,it is necessary to strengthen or to demolish more than 256 000 buildings, 700 schools, 900 kindergartens and450 hospitals. In the last two years work on fewer than 20 buildings has been carried out. The basic reasonfor the low rate of reconstruction is the absence of financial assets. Several thousand million US dollars are
87

needed.
The preservation of people's health is closely connected to the maintenance of "lifelines" of public utilities incase of earthquake. In Kazakstan we have set up a system which allows us to disconnect the electric powerwhen the earthquake strikes and to transfer storage facilities of natural gas from the earthquake zone to saferlocations.
With the purpose of duly informing the population of the threat of earthquake and how to prepare for it, anational system of communication (television, radio, mobile loud−speaker units) has been set up.
Taking into account the very real threat of earthquake for the inhabitants of Kazakstan, the State EmergencyCommittee has announced that training and preparation of the population will be carried out in 1996 and1997. A system of national education in the field of preparation and response in emergency situations hasbeen created. Last year in the republic 50 000 persons completed this course. Information about protectionfrom earthquakes appears regularly in newspapers, on the radio, and on television. An educational film aboutearthquake preparation has been made and special brochures have been issued. Various organizations,schools and kindergartens have regular training on what to do in case of earthquake. The complex training inprevention and response in emergency situations at national level will be carried out annually.
The national plan for the mitigation of the consequences of earthquake is based on a scenario of anearthquake of intensity IX on the MSK−64 scale and the resulting number of dead and injured, damagedhomes and industrial buildings and structures, and disrupted "lifeline" utilities and transport communications.Special attention in the plan is given to losses among medical personnel and condition of medical facilities.
The plan includes a calculation of the needs in terms of medical, search−and−rescue and reconstructionservices, firefighting teams, the military, and types and quantity of equipment necessary to mitigate theconsequences of the earthquake. The necessary assistance should arrive from the nearest parts of therepublic within the first day. Similar plans of protection are available for local governments.
The creation of five professional rescue groups is planned; two are already operating. Local governmentshave created 269 special volunteer groups for emergencies. In businesses and organizations, more than 48000 groups are available for emergencies.
The national emergency medical service has divisions in all areas of the republic. A state medical epidemicand quarantine service has also been set up. Reserves of medical equipment and materials have beencreated at both state and local levels.
In the field of international cooperation, Kazakstan has established on its territory a regional warehouse ofsupplies with the United Nations. The government of Japan provided grants for area seismology and retrofit ofbuildings and other constructions, after finding poor conditions of health and inadequate quality of drinkingwater supply for the population. A joint declaration of the Republic of Kazakstan and Germany aboutrendering mutual help in case of natural disasters and accidents is on the point of signature. After thedestructive earthquake in Un−Nan in 1996, Kazakstan rendered China humanitarian help in the form ofmedicines.
We realize that a state must take responsibility for dealing with this complex problem. Therefore internationalcooperation and mutual aid are nowhere more necessary than in the area of protection from earthquakes. Inthis plan we especially count on the help of developed countries such as the Federal Republic of Germany,Japan and the United States of America, among others.
Reference
1. A NATO Advanced Research Workshop. Urban earthquake risk management strategies for the centralAsian republics: avoiding repetition of the 1988 Armenian and the 1995 Sakhalin disasters. Almaty,Kazakstan. 22−25 October 1996.
Summary
E. Pretto1and Secretariat
88
1E.A. Pretto M.D., M.P.H. is Principal Investigator, Disaster Reanimatology Study Group andAssociate Director Safar Center for Resuscitation Research, University of Pittsburgh Schoolof Medicine, Pittsburgh, USA.
Professor Mustafa Erdik, Chairman, Department of Earthquake Engineering, Bogazici University, KandilliObservatory and Earthquake Research Institute, Istanbul, Turkey, dealt with urban earthquake masterplans,and their social and health aspects. He mentioned that, while developing country cities are generally quitevulnerable because of poor construction quality and/or non−enforced codes and standards, cities indeveloped countries are also vulnerable. Ageing urban technical infrastructures, together with ageingpopulations, increase vulnerability. This is accompanied by a greater dependence on technology andgenerally more capital values are exposed to risk; their loss can lead to financial ruin.
A special inventory of exposed values, utilities, special systems and socioeconomic institutions which arevulnerable would be useful to have but is difficult to obtain, according to Dr Erdik.
He emphasized the importance of structural and non−structural measures to reduce mortality and morbidity.He said these measures must be applied to hospitals, lifelines, and medical supplies as well as to houses.Effective non−structural measures also require legislation and training for those who are responsible fordisaster management. His figures for providing urban planners and emergency organizations with a crediblescenario for a severe earthquake in the densely populated and densely industrialized area of the Bosporouswere alarming. Without additional measures taken to reinforce structures and emergency planning, anearthquake in that area would not only cause many deaths and injuries but would also be a devastating blowto the entire Turkish economy.
The State Emergency Committee of the Republic of Kazakstan reported on "Seismic activity and themitigation of its consequences in Kazakstan". Taking into account the very real threat of earthquake for theinhabitants of Kazakstan, the State Emergency Committee has announced preparedness training of thepopulation in 1996 and 1997. A system of national education in the field of preparation and response inemergency situations has been set up. Last year in the republic more than 50 000 people completed thepreparation course. In the newspapers, on the radio and on television, educational materials on protectionagainst earthquakes are constantly made available. A film "Earthquake: up to, in time, after" has been made,and special brochures are issued. Various organizations, schools and kindergartens have regular training onaction to be taken in case of threat or occurrence of an earthquakes. The complex training at national level forprevention and response in the emergency situation of a catastrophic earthquake will be carried out annually.
The plan of action is based on an estimation of possible conditions after the occurrence of an earthquake withintensity IX on the MSK−64 scale, and the resulting number of dead and injured, condition of inhabited andindustrial buildings and structures, state of "lifeline" utilities and transport communications. The plan givesspecial attention to losses among the medical personnel and to the condition of medical facilities.
The plan includes a calculation of the quantity of medical, search−and−rescue and reconstruction services,firefighting teams, military, and kinds and quantity of equipment necessary for mitigation of the consequencesof the earthquake. The specified assistance should arrive from the nearest areas of republic within the firstday. Similar plans of protection are available for local governments.
Five professional rescue groups are planned and two are already in operation. Local governments have setup 269 special groups of volunteers for emergencies, and businesses and organizations have more than 48000 similar groups available.
International cooperation and mutual aid are nowhere more necessary than in the field of earthquakeprotection. In this plan, Kazakstan especially counts on the help of the more developed countries such as theFederal Republic of Germany, Japan, and the United States of America, among others.
Earthquake−resistant construction
89
Regulations for earthquake−resistant construction
H.P. Wölfel1, M.V. Schalk2, and F.O. Henkel3
1Dr H.P. Wölfel is Professor of Mechanical Engineering, Technical University of Darmstadt,Darmstadt, Federal Republic of Germany, and is a member of the European Committee forStandardization.
2Dr M.V. Schalk is Authorized Manager, Wölfel Consulting Engineers, Höchberg, FederalRepublic of Germany.
3Dr F.O. Henkel is General Manager, Wölfel Consulting Engineers, Höchberg, FederalRepublic of Germany.
Regulations for earthquake−resistant construction have resulted from experience and, as is the caseeverywhere in building history, were earlier handed down from builder to builder. The punishment for errorswas the collapse of the building during an earthquake.
When earthquake engineering became a science on its own, experience and state−of−the−art practice werecast in rules and regulations and thus made available to all specialist colleagues. Today more than 40 stateshave written earthquake regulations which are published regularly by the International Association ofEarthquake Engineering (IAEE) as the "World List of Earthquake Engineering" (7) which currently lists thefollowing countries:
Albania Egypt MexicoAlgeria El Salvador New ZealandArgentina Ethiopia NicaraguaAustralia France PeruAustria Germany PhilippinesBulgaria Greece PortugalCanada India RomaniaChile Indonesia Russian FederationChina Iran SloveniaColumbia Israel SpainCosta Rica Italy TurkeyCroatia Japan United States of AmericaCuba The former Yugoslav Venezuela.Dominican Republic Republic of MacedoniaDespite these regulations and the progress made in science and building technology, losses in lives andproperty have not declined over the last decades. On the contrary, there has even been an increase.Impressive examples of this are the devastating earthquakes in Tangshan, China in 1976, with approximately250 000 deaths, in Mexico in 1985 with damage to a value of US$ 6 billion, and the Kobe earthquake in 1995.On the other hand earthquake activity has not increased worldwide: the average released seismic energyevery year has remained almost constant (2).
Have engineers failed, are the regulations useless, and are all efforts being made in vain? Certainly not, butthe vulnerability of our infrastructure has increased as a result of the growing population density and greatertechnical complexity. Secondary damage through dams bursting, lifelines being destroyed, fires, emission oftoxic substances or radioactivity can be greater that the direct damage caused by the collapse of buildings.
We are clearly racing against urban expansion and technology in our efforts to achieve earthquake−resistantconstruction. The United Nations, with its International Decade of Natural Disaster Reduction (IDNDR), hascalled upon us to make a dash towards the finish−line in this race worldwide (3). The IAEE has taken up thechallenge with the World Seismic Safety Initiative (WSSI) (4). The European Standards Organization (CEN) iscurrently issuing a comprehensive set of guidelines (15), which cover a wide range of member states' needsand can be considered exemplary.
A few aspects of the role that regulations have to play in this race are discussed below. Regulations areunderstood to include all guidelines, directives, recommendations and rules which the state, as the body
90
responsible for public safety, has declared as the basis for approval procedures in construction.
Whether these regulations are right and applicable will be reflected in how the buildings and other structuresbuilt to these regulations withstand the next earthquake. However, since earthquakes and thus such practicaltests are seldom, worldwide cooperation and exchange of experience at the international level are called for.This is ensured through the special conferences of the IAEE (5,6) and the national and continental subgroups,as well as by the International Association for Structure Mechanics in Reactor Technology (IASMRT) foratomic power stations (7). Further initiatives in this direction have also been developed by the IDNDR.
Even countries experiencing very little seismic activity should closely follow progress with regard toearthquakes. Such countries may also be involved indirectly due to international economic links, whether bythe delivery' of industrial plants to seismic areas, by building activity or production in these countries, or byparticipation in disaster relief.
Risk and earthquake protection
Before going into greater detail on standards, the question arises as to what extent earthquake safety ordesign costs are reasonable. The aim of design is to limit the seismic risk:
Risk = H × R × C
where
H = Probability of occurrence of an earthquake of a specific intensity at a site (seismic hazardanalysis)
R = Probability of such intensity initiating a critical course of events (seismic response andfragility evaluation)
C = Extent of damage and losses in such a course of events (consequence analysis).
The risks given at all stages of intensity for all courses of events and damage are to be added together todetermine the total risk in a seismic zone from buildings, plants and infrastructure units as well as from therespective course of events and type of damage.
The probability of occurrence H (of an earthquake of a specific intensity) is stipulated by nature. This must bedetermined, or rather estimated, by seismologists. Figure 3.7 shows the characteristics of probability curves:one falling line with increasing slope on a logarithmic scale, reaching in a first approximation a limit whichcannot be exceeded due to seismotectonic conditions.
91
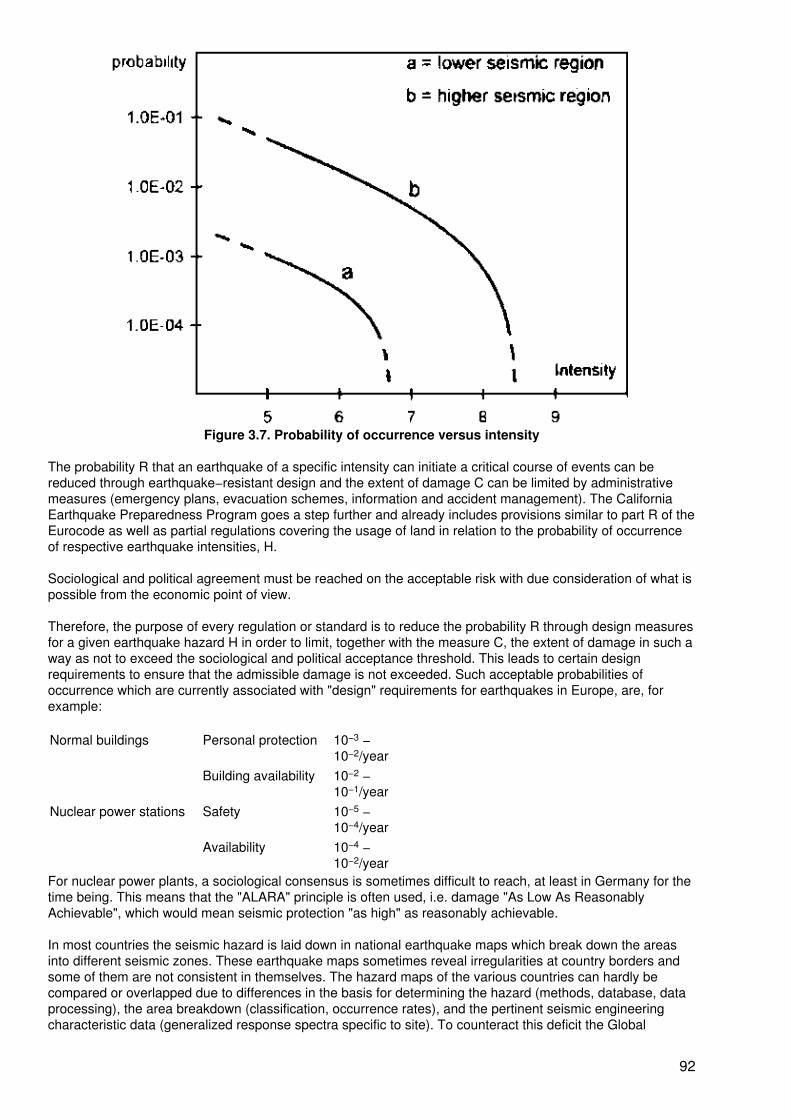
Figure 3.7. Probability of occurrence versus intensity
The probability R that an earthquake of a specific intensity can initiate a critical course of events can bereduced through earthquake−resistant design and the extent of damage C can be limited by administrativemeasures (emergency plans, evacuation schemes, information and accident management). The CaliforniaEarthquake Preparedness Program goes a step further and already includes provisions similar to part R of theEurocode as well as partial regulations covering the usage of land in relation to the probability of occurrenceof respective earthquake intensities, H.
Sociological and political agreement must be reached on the acceptable risk with due consideration of what ispossible from the economic point of view.
Therefore, the purpose of every regulation or standard is to reduce the probability R through design measuresfor a given earthquake hazard H in order to limit, together with the measure C, the extent of damage in such away as not to exceed the sociological and political acceptance threshold. This leads to certain designrequirements to ensure that the admissible damage is not exceeded. Such acceptable probabilities ofoccurrence which are currently associated with "design" requirements for earthquakes in Europe, are, forexample:
Normal buildings Personal protection 10−3 −10−2/year
Building availability 10−2 −10−1/year
Nuclear power stations Safety 10−5 −10−4/year
Availability 10−4 −10−2/year
For nuclear power plants, a sociological consensus is sometimes difficult to reach, at least in Germany for thetime being. This means that the "ALARA" principle is often used, i.e. damage "As Low As ReasonablyAchievable", which would mean seismic protection "as high" as reasonably achievable.
In most countries the seismic hazard is laid down in national earthquake maps which break down the areasinto different seismic zones. These earthquake maps sometimes reveal irregularities at country borders andsome of them are not consistent in themselves. The hazard maps of the various countries can hardly becompared or overlapped due to differences in the basis for determining the hazard (methods, database, dataprocessing), the area breakdown (classification, occurrence rates), and the pertinent seismic engineeringcharacteristic data (generalized response spectra specific to site). To counteract this deficit the Global
92
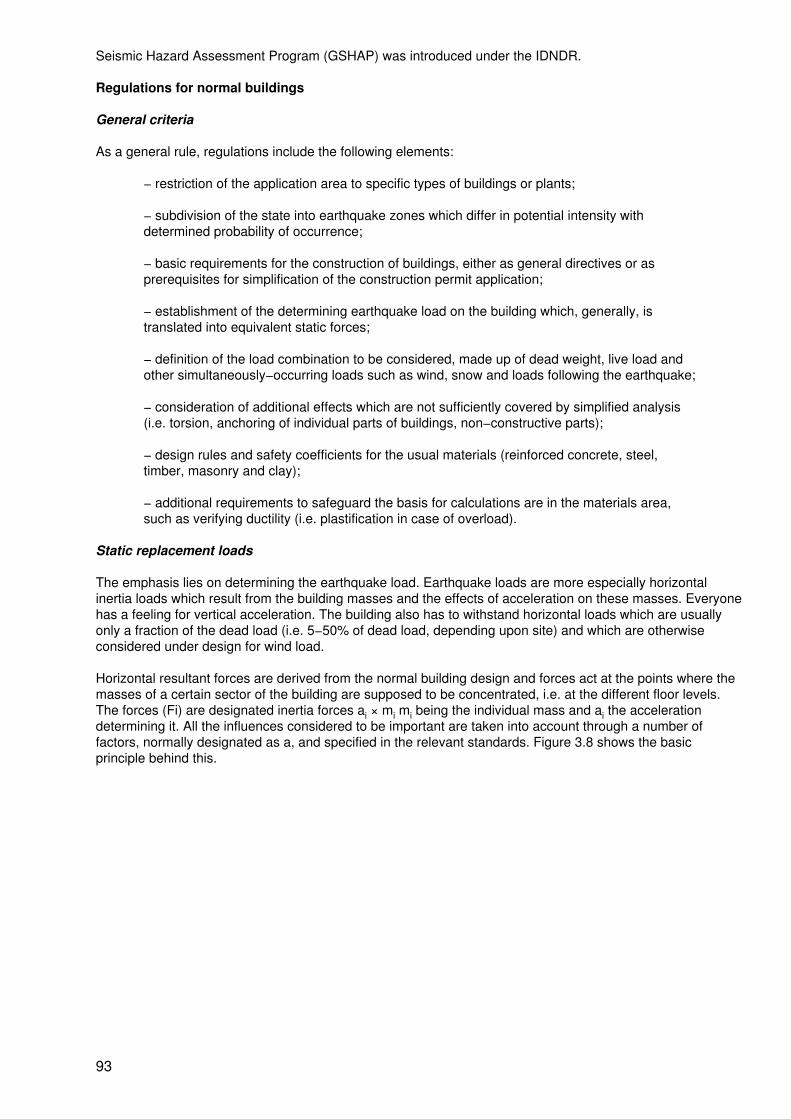
Seismic Hazard Assessment Program (GSHAP) was introduced under the IDNDR.
Regulations for normal buildings
General criteria
As a general rule, regulations include the following elements:
− restriction of the application area to specific types of buildings or plants;
− subdivision of the state into earthquake zones which differ in potential intensity withdetermined probability of occurrence;
− basic requirements for the construction of buildings, either as general directives or asprerequisites for simplification of the construction permit application;
− establishment of the determining earthquake load on the building which, generally, istranslated into equivalent static forces;
− definition of the load combination to be considered, made up of dead weight, live load andother simultaneously−occurring loads such as wind, snow and loads following the earthquake;
− consideration of additional effects which are not sufficiently covered by simplified analysis(i.e. torsion, anchoring of individual parts of buildings, non−constructive parts);
− design rules and safety coefficients for the usual materials (reinforced concrete, steel,timber, masonry and clay);
− additional requirements to safeguard the basis for calculations are in the materials area,such as verifying ductility (i.e. plastification in case of overload).
Static replacement loads
The emphasis lies on determining the earthquake load. Earthquake loads are more especially horizontalinertia loads which result from the building masses and the effects of acceleration on these masses. Everyonehas a feeling for vertical acceleration. The building also has to withstand horizontal loads which are usuallyonly a fraction of the dead load (i.e. 5−50% of dead load, depending upon site) and which are otherwiseconsidered under design for wind load.
Horizontal resultant forces are derived from the normal building design and forces act at the points where themasses of a certain sector of the building are supposed to be concentrated, i.e. at the different floor levels.The forces (Fi) are designated inertia forces ai × mi mi being the individual mass and ai the accelerationdetermining it. All the influences considered to be important are taken into account through a number offactors, normally designated as a, and specified in the relevant standards. Figure 3.8 shows the basicprinciple behind this.
93
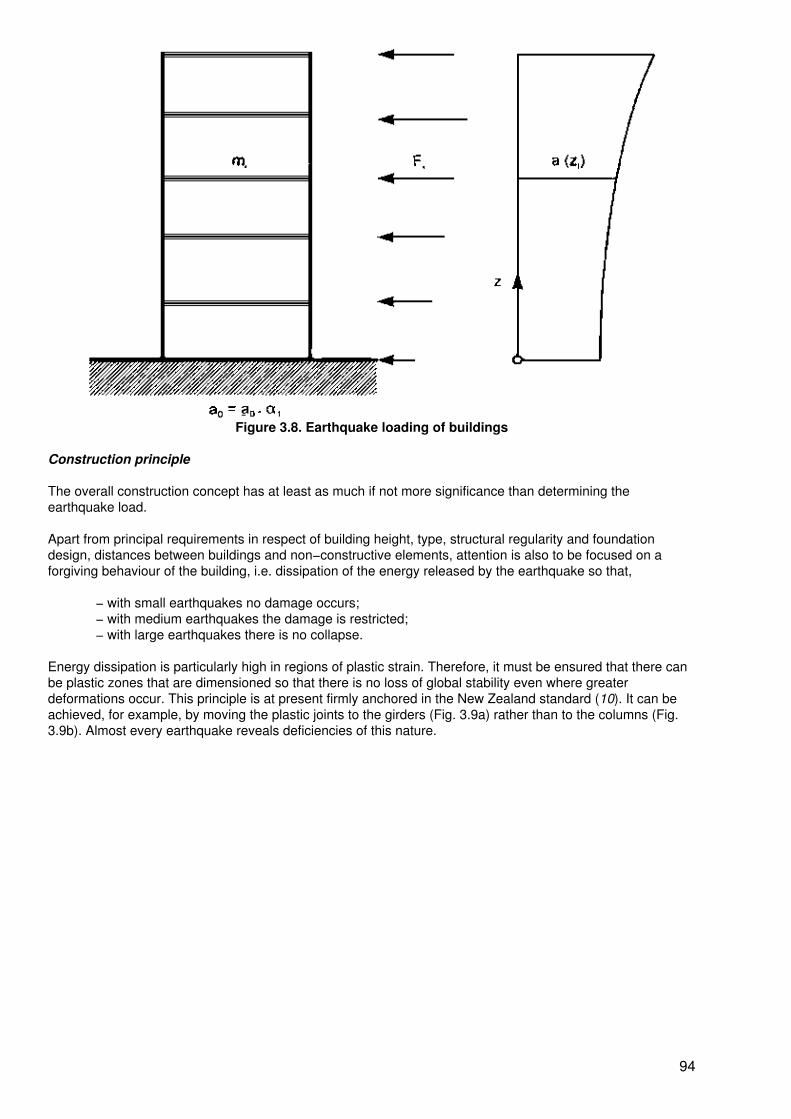
Figure 3.8. Earthquake loading of buildings
Construction principle
The overall construction concept has at least as much if not more significance than determining theearthquake load.
Apart from principal requirements in respect of building height, type, structural regularity and foundationdesign, distances between buildings and non−constructive elements, attention is also to be focused on aforgiving behaviour of the building, i.e. dissipation of the energy released by the earthquake so that,
− with small earthquakes no damage occurs;− with medium earthquakes the damage is restricted;− with large earthquakes there is no collapse.
Energy dissipation is particularly high in regions of plastic strain. Therefore, it must be ensured that there canbe plastic zones that are dimensioned so that there is no loss of global stability even where greaterdeformations occur. This principle is at present firmly anchored in the New Zealand standard (10). It can beachieved, for example, by moving the plastic joints to the girders (Fig. 3.9a) rather than to the columns (Fig.3.9b). Almost every earthquake reveals deficiencies of this nature.
94
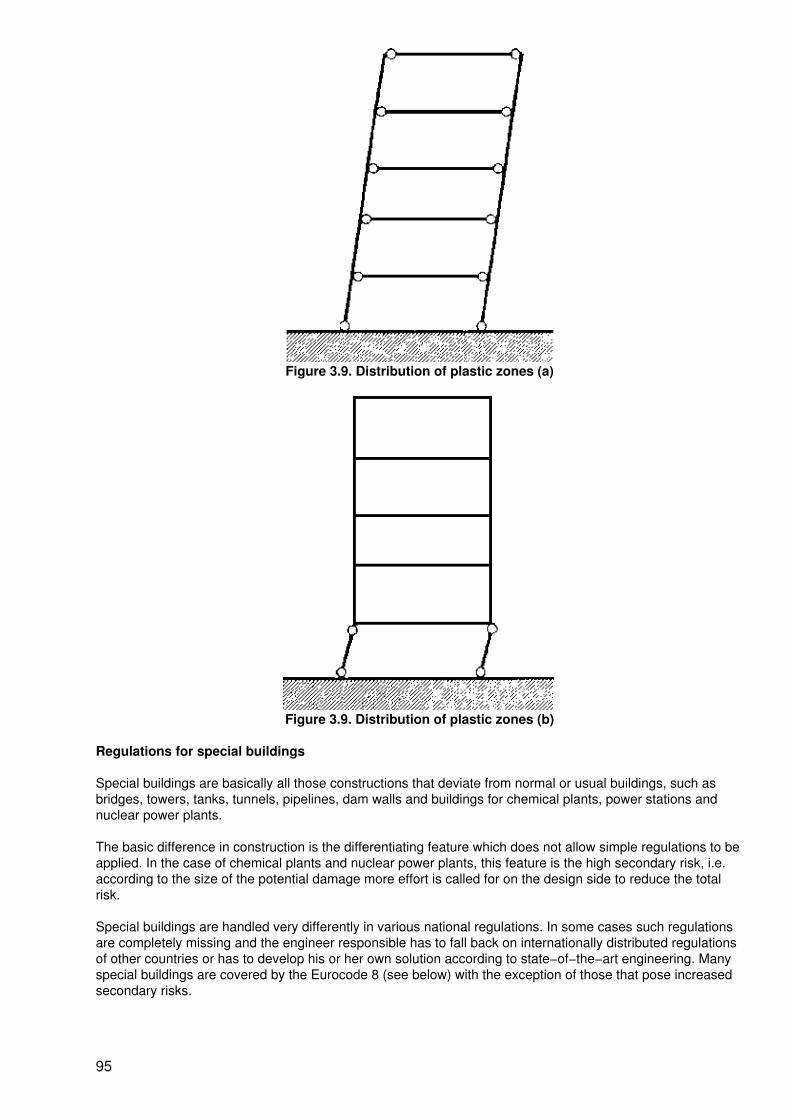
Figure 3.9. Distribution of plastic zones (a)
Figure 3.9. Distribution of plastic zones (b)
Regulations for special buildings
Special buildings are basically all those constructions that deviate from normal or usual buildings, such asbridges, towers, tanks, tunnels, pipelines, dam walls and buildings for chemical plants, power stations andnuclear power plants.
The basic difference in construction is the differentiating feature which does not allow simple regulations to beapplied. In the case of chemical plants and nuclear power plants, this feature is the high secondary risk, i.e.according to the size of the potential damage more effort is called for on the design side to reduce the totalrisk.
Special buildings are handled very differently in various national regulations. In some cases such regulationsare completely missing and the engineer responsible has to fall back on internationally distributed regulationsof other countries or has to develop his or her own solution according to state−of−the−art engineering. Manyspecial buildings are covered by the Eurocode 8 (see below) with the exception of those that pose increasedsecondary risks.
95
As far as we are aware, apart from nuclear technology, there is a lack of suitable regulations or supplementsto existing regulations which deal explicitly with construction work in this sector and take into consideration theamount of possible damage. In practice a solution is generally sought which falls between the standard codeand the regulations for nuclear engineering
Usually very detailed regulations for earthquake−resistant design of nuclear power plants are given incountries with peaceful utilization of atomic energy. In this respect, the following regulations apply:
− US Nuclear Regulatory Commission regulatory guides, USA (11)
− International Atomic Energy Authority (IAEA) safety guides (12) and subsequent technicaldocuments
− Kerntechnischer Ausschuss regulations, Germany (13)
− NSC guides, Japan (14)
Eurocode 8
Overview
Eurocode 8 will comprise design provisions for earthquake resistance of structures (75). It will be one of themost comprehensive earthquake standards to be produced and is part of the complete new standards for theEuropean building industry (EC 1 −9) which are currently in preparation. Eurocode 8 will be published in 1998.Its contents are as follows:
Part 1 − GENERAL RULES
Part 1.1 − Seismic actions and general requirements for structuresPart 1.2 − General rules for buildingsPart 1.3 − Specific rules for various materials and elementsPart 1.4(*) − Strengthening and repair of buildingsPart 2 (*) − BRIDGESPart 3 (*) − TOWERS, MASTS AND CHIMNEYSPart 4 (*) − SILOS, TANKS AND PIPELINESPart 5 − FOUNDATIONS, RETAINING STRUCTURES AND GEOTECHNICAL ASPECTS
The parts marked with an asterisk (*) are still in preparation; the others are virtually complete.
The compilation of Eurocode 8 is being supported by major research projects in different member states. Inthese projects:
− fundamentals and levels of knowledge are being determined and processed;− basic studies on constructions and evidence concepts are being carried out;− draft regulations are being drawn up.
These drafts are discussed and agreed in national committee meetings. Eurocode 8 is to be valid in allEuropean Community and European Free Trade Association countries in the future. However, there is still nodate in sight for the introduction of Eurocode 8. In some countries provisional parts of Eurocode 8 will be putinto practice in the years to come by means of national application documents (NAD).
However, it is essential to point out that Eurocode 8, unlike many other earthquake codes, also expresslycovers some special buildings and excludes only those which have a higher secondary risk. Buildingcomponents and equipment are the only elements not found in Eurocode 8.
Regulations for equipment
All the usual codes aim primarily at load, design and construction of buildings in earthquake areas. They donot regulate (or do so only to a certain extent) the design of components and equipment of buildings andplants against earthquakes. Eurocode 8 at least covers silos, tanks and pipelines but not the inside ofbuildings− Pipelines also represent life−lines but there is no further detail on these,
96

At first sight this appears to be plausible when one assumes that component failure leads to no greaterdamage to persons and avoidance of local economic damage is not primarily the purpose of the buildingcode. However, this is a wrong conclusion. Economic damage through destruction of components in industrialand process engineering plants, and subsequent interruption in operation, can quickly take on dimensions thatare hard to bear. And the risk in the case of high energy components (e.g. pressure and temperature) andthose with toxic substance content are certainly underestimated at present. This is why the German RiskAnalysis Ordinance (based on the European "Seveso" guideline) addresses earthquake loading but gives noconsideration to expert directives (16). Specific instructions for particular branches are also available (17−19).
Regulations for old buildings
All regulations discussed up to now are aimed at the design of new buildings and plants. It is certainly rightthat all present available engineering knowledge should be invested in new buildings. However, old buildingsstill make up the largest part of our heritage. The 1950s saw the beginning of earthquake engineering and thefirst simple earthquake regulations with but few exceptions (Japan and California). It was only in the 1970sand 1980s that adequate, more sophisticated state−of−the−art engineering was developed with dueconsideration to the dynamic behaviour of structures. As a result, protection of most old buildings, is notplanned and they are safeguarded against earthquakes at the most by the experience of the builder. Thismeans that the greatest damage is likely to occur in old buildings as the earthquake here in Kobe revealed ina tragic way.
There is no lack of attempts to establish regulations for strengthening and reinforcing existing structures or forthe repair of buildings after an earthquake. However, the required level of applicability has still to be achieved.
Outlook
Thanks to existing national earthquake regulations, the race between increasing damage potential and theefforts to reduce the probability of damage through design is not lost yet. However, if spectacular earthquakedamage occurs over and over again, this can have only two causes:
− systematic deficiencies in the earthquake regulations both for the assessment of seismicrisk and in the design to reduce this risk;
− deficiencies in putting such regulations into practice and enforcing them, especially on thebuilding site.
Examples of the first cause are the 1976 earthquake in China which occurred in an area previously not knownto be endangered by earthquakes and the 1995 Kobe earthquake which was not expected to have suchintensity. Examples of buildings which failed despite being designed to the given regulations were found in the1985 Mexico earthquake and others where columns plasticized and collapsed. One example of the secondcause is the 1988 Armenian earthquake where it was obvious that the reinforcement planned for theconnection between floor and wall slabs and many ring anchors were simply missing. Here both the buildersand building supervisory authorities failed. More work is needed, particularly with regard to the following:
− establishing of uniform, consistent earthquake maps;
− supplementation of standard regulations for normal buildings with regulations for specialbuildings such as hospitals, bridges, lifelines, chemical plants and tanks in so far as this hasnot already been done;
− regulations for equipment in buildings;
− stricter supervision of building work;
− harmonization of standard regulations so that they can be compared with each other;
− drawing up of guidelines for low−cost housing according to region and type;
− drawing up of regulations for retrofit strengthening of buildings;
− regulations covering the repair of buildings damaged by earthquakes;
97
− development and distribution of recommendations for people's response, depending on thebuilding type.
References
1. International Association for Earthquake Engineering. Earthquake resistant regulations, a world list. 1996,Tokyo.
2. DGEB: Various damage reports from members of the Deutsche Gesellschaft fur Erdbebeningenieurwesenund Baudynamik (DGEB) or their Austrian and Swiss Sister Organisations, published in the news sheets orpresented at conferences.
3. Deutsche Forschungsgemeinschaft: Natural catastrophies and catastrophe prevention, recommendationsto the IDNDR, 1991.
4. Shah HC, Katayama T. WSSI − A dream, a challenge and a time for action. Proceedings of the 10thEuropean Conference in Earthquake Engineering. A.A. Balkema, Rotterdam, Brookfield, 1995:3−10.
5. WCEE Conferences (1958−1996), Proceedings.
6. ECEE Conferences (1971−1995), Proceedings.
7. SMiRT Conferences (1971−1995), Transactions.
8. Paulay T, Bachmann M, Moser K. Earthquake resistant design of concrete structures. Birkhäuser−Verlag,1990, Basel, Boston, Berlin.
9. DIN 4149: Buildings in German earthquake areas; design loads, analysis and structural design, usualbuildings, Version: April 1981.
10. NZS 4203: New Zealand Standard: General Structure Design and Design Loadings for Buildings, 1992.Standard Association of New Zealand, Wellington.
11. USNRC Regulatory Guides, US Nuclear Regulatory Commission, Washington, D.C.
12. IAEA Safety Guides, International Atomic Energy Agency, Vienna.
13. KTA 2201: Design of nuclear power stations against seismic influences, Kerntechnischer Ausschuss,Bundesamt für Strahlenschutz, Braunschweig, Germany.
Part 1: Basics, June 1990.Part 2: Foundations, June 1990.Part 3: Design of civil structures, draft June 1990.Part 4: Requirements for earthquake safety for mechanical and electrotechnical plant equipment, June 1990.
14. NSC Guides: Standards for Seismic Civil Engineering Construction in Japan, 1980. Earthquake ResistantDesign Method for Buildings, 1981, Nuclear Safety Commission and Ministry of Construction, Tokyo, Japan.
15. Eurocode 8: Design Provisions for Earthquake Resistance of Structures, respective current status.European Committee for Standardization, Central Secretariat, rue de Stassart, 36, B−1050 Brussels. October1994.
16. Twelfth Amendment to the Federal German Immission Protection Law (Industrial Hazards Ordinance) −12. BImSchV (May 1991), Bundesgesetzblatt, Bonn.
17. API Standard 650 "Welded Steel Tanks for Oil Storage", Nov. 1980. American Petrol Institute,Washington, D.C.
18. Fischer FD, Rammerstorfer FG, Scharf K. Earthquake resistant design of anchored and unanchored liquidstorage tanks under three−dimensional earthquake excitation. In: Schueller GT (ed.). Structural dynamics,recent advances. Springer, Heidelberg, Germany, 1990.
98

19. Wölfel H, Schalk M. The earthquake on the Swabian Alp − theory and reality of earthquake design. THDSchriftenreihe "Wissenschaft und Technik 16" (Karl−Maguerre Gedächtnis Kolloquium), Technical University,Darmstadt, Germany, 1980.
Experimental verification of anti−seismic designs: The Institute of Earthquake Engineering and Engineering Seismology(IZIIS), as an example
D. Jurukovski1and L. Krstevska2
1Professor D. Jurukovski is Director of the Institute of Earthquake Engineering andEngineering Seismology (IZIS), University "St Cyril and Methodius", Skopje, The formerYugoslav Republic of Macedonia
2Mrs L. Krstevska, M.Sc. is Research Assistant at the Institute of Earthquake Engineering andEngineering Seismology (IZIS), University "St Cyril and Methodius", Skopje, The formerYugoslav Republic of Macedonia
The Institute of Earthquake Engineering and Engineering Seismology (IZIIS) was established in 1965 as aninstitution within the University "St. Cyril and Methodius", Skopje, in the former Yugoslav Republic ofMacedonia. The aim of the institute was to organize research and training in the area of earthquakeengineering and engineering seismology. In following these tasks, the institute received support from theUnited Nations and its specialized agencies, UNDP and UNESCO, for many years following the disastrousSkopje earthquake of 26 July 1963. While meeting the immediate needs for reconstruction of the city, theinstitute created conditions favourable to permanent progress in research and in training of scientific staff andengineers. During its development the institute has thus not only achieved its main objective but has grown, ina relatively short period, into a recognized national and international institution of earthquake engineering andengineering seismology.
Personnel
Throughout the development of the institute, particular attention has been paid to increasing and training thepersonnel since this is one of the major factors determining the quality of the research and the educationalactivities of the institute. Out of the 56 scientific staff members, 15 have Ph.D. degrees and 23 Master'sdegrees in technical sciences, while the remaining 18 staff members are graduate civil engineers, geologists,electrical engineers, physicists, economists and philologists.
Fifteen professors, associate professors and assistant professors from the institute are lecturing andsupervising the postgraduate studies. Most of the scientific staff have, at one time or the other, worked at theuniversities in Japan, USA and other countries as visiting professors or research fellows, or as United Nationsexperts in earthquake engineering or engineering seismology in developing countries.
Scope of the work
The scope of the work of the institute consists mainly of postgraduate studies, scientific research, and appliedresearch and consultancy. Economic development and the threat of catastrophic earthquakes result in anincreasing demand for specialists in earthquake engineering and engineering seismology at Master's anddoctoral degree level. To meet the needs for specialists in these fields, the Institute of EarthquakeEngineering and Engineering Seismology, as an international training centre, organizes postgraduate studiesin various branches and at various levels. During its 30−year experience of training earthquake engineers andspecialists in engineering seismology, courses have been organized for 250 candidates for the Master'sdegree in technical sciences. In addition to this, the institute organizes special courses for engineers fromdeveloping countries.
The scientific research activities of the institute are aimed chiefly at defining the technical basis for thereduction of the consequences of earthquakes. A large number of projects have been carried out on thefollowing subjects:
− study of strong earthquake occurrence, definition and improvement of the methods ofearthquake risk assessment, study of the seismicity and evaluation of the risk of futureearthquake damage;
99
− determination of the dynamic properties of materials and structures in order to establishconsistent scientific criteria for the stability of civil engineering structures under variousdynamic effects;
− establishment of optimum economic and technical criteria for evaluation of theconsequences of strong earthquakes, and optimization of the economic value of structureswith respect to earthquake intensity, frequency of occurrence, expected lifetime and purpose;
− conditions for economic and rational construction using industrialized construction methodsand systems, adequate materials, pre−cast elements and structural systems;
− establishment of the scientific and technical basis for updating and improving constructioncodes compatible with the level of economic development of the country.
The institute carries out a large number of applied and development research projects and provides consultingservices for design and analysis of more sophisticated civil engineering structures. On the average, 100−150applied research projects are completed each year by the institute.
Considering the fact that organized international cooperation provides conditions for more efficient andcomplex scientific research, the institute ensures solid and permanent scientific cooperation with universitiesand research institutions from various countries as one of its priorities for development. This has led to afruitful exchange of scientific information and has maintained the international reputation of the institute whichcooperates with more than 20 universities and centres all over the world.
Facilities
Since equipment is an essential prerequisite for advanced engineering and research, the institute hasinvested heavily in equipment for its laboratories, the value of which is estimated at more than 4 million USdollars. The equipment is located in the five IZIIS laboratories as follows:
• The dynamic testing laboratory is equipped with a number of seismic shaking tables (seeexample Fig. 3.10)
• The soil dynamics laboratory is equipped for carrying out tests to determine the dynamicproperties of soil materials. These tests are necessary to obtain the dynamic strength andstability of soils, the soil liquefaction potential and soil−structure interaction, for in situ testingof foundation models, and other specific testing in the field of soil and foundation dynamics.The latter are carried out in cooperation with the other laboratories of the institute.
• The laboratory for microzoning and geophysical studies is adequately equipped for certainfield measurements in engineering seismology and geophysics, such as seismic refraction,reflection and polar surveys, and measurements of microseismic noise and geoelectricalresistivity.
• The strong motion laboratory is mainly concerned with technical preparation for theinstallation and maintenance of the strong−motion instrument network covering the territory ofthe former Yugoslav Republic of Macedonia and consisting of over 100 accelerographs. Ofthese, more than 60 have been installed on civil engineering structures, and the rest onbedrock or characteristic soil. In order to accomplish these important tasks successfully, thelaboratory has the necessary equipment for calibration, servicing, maintenance and repair ofthe strong−motion instruments.
• The laboratory for special seismological studies is equipped for research into the effects,location and character of small and strong earthquakes and their influence on the soil mediumand structures.
100
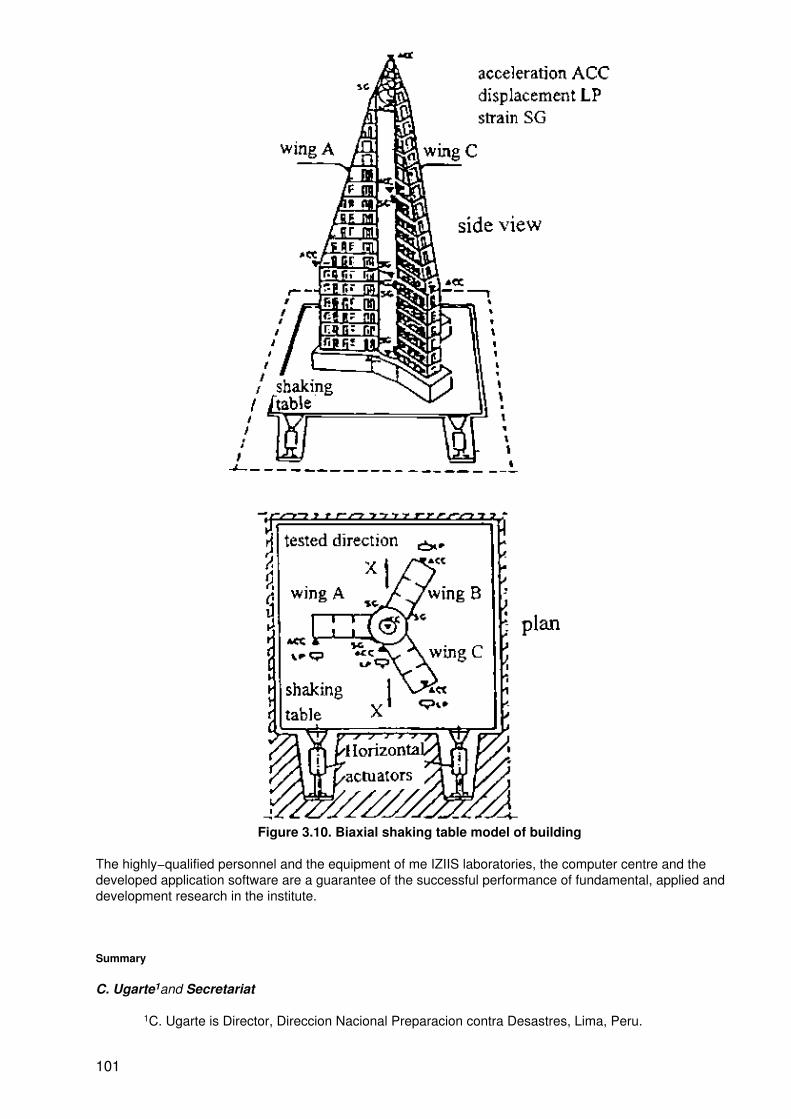
Figure 3.10. Biaxial shaking table model of building
The highly−qualified personnel and the equipment of me IZIIS laboratories, the computer centre and thedeveloped application software are a guarantee of the successful performance of fundamental, applied anddevelopment research in the institute.
Summary
C. Ugarte1and Secretariat
1C. Ugarte is Director, Direccion Nacional Preparacion contra Desastres, Lima, Peru.
101

Professor H.P. Wölfel, Professor of Mechanical Engineering, Technical University of Darmstadt, Germanyand a member of the European Committee for Standardization (CEN), made the first presentation onearthquake−resistant construction. He described mechanisms that structural engineers adopt to definebuilding safety. According to Professor Wölfel, earthquakes have neither become more frequent nor morevicious in recent times; in fact the data show a nearly constant average release of energy from earthquakesover the decades. The key problem is seen in the increase of the density and vulnerability of the structuresmankind has built in risk areas. On the other hand, he emphasized the now well−developed state−of−the−artin structural engineering and that technical standards and norms have resulted in an adequate body ofregulations which nowadays can provide a high degree of preventive protection. However, only 40 countrieshave established national earthquake resistance regulations. Professor Wölfel defined as a principal cause ofstructural failures in recent earthquakes either a lack of regulations or deficiencies in the application andenforcement of these regulations. In the European Union, the Committee for Standardization ('CEN) isdeveloping a comprehensive guide for standard regulations, covering the quite different situations in all itsMember States.
Professor D. Jurukovski and Mrs L. Krstevska presented a paper on the Institute of EarthquakeEngineering and Engineering Seismology (IZIIS). The institute was established in 1965 within the University"St. Cyril and Methodius", Skopje, the former Yugoslav Republic of Macedonia, to organize research andtraining in the area of earthquake engineering and engineering seismology. In following these tasks theinstitute received support from the United Nations and its specialized agencies, UNDP and UNESCO, formany years following the disastrous Skopje earthquake of 26 July 1963. While meeting immediate needs forreconstruction of the city, the institute created conditions favourable to permanent progress in research and intraining of scientific staff and engineers. During its development the institute has thus not only achieved itsmain objective but has grown, in a relatively short period, into a recognized national and internationalinstitution of earthquake engineering and engineering seismology.
In order to respond successfully to the need for a high level of research in these fields, as well as educationand training of engineers, the institute has specialized research sections. This flexible mode of organizationwas necessary because of the scope of work which the institute was called upon to undertake. It covers thefollowing research areas: regional studies (seismology, seismotectonics and geophysics); local soil studiesand soil dynamics; vulnerability analysis; seismic stability of engineering structures; seismic stability ofbuilding structures and engineering materials; nuclear engineering and reliability of structures; and controlengineering.
Earthquake−proofing of hospitals
Safe hospitals: the Mexican strategy to face natural hazards
J. Rodríguez1and J. Oviedo2
1J. Rodriguez is General Director, Preventive Medicine, Ministry of Health, Mexico, D.F.,Mexico.
2 J. Oviedo is Director, Injury Prevention and Control and Health Care in DisasterProgrammes, Ministry of Health, Mexico, D.F., Mexico.
Mexico's natural hazards
Mexico is located in a high risk area of natural hazards such as earthquakes, hurricanes and volcaniceruptions that cause damage to people, buildings and the economy every year.
There are six plates that cause earthquakes in 28 of the 32 Mexican states (more than 90% of the country'sarea). Mexico has about 90 earthquakes higher than 4 on the Richter scale every year. These earthquakeshave caused 15 867 deaths, 46 000 injured and have affected 95 600 people in the last 20 years.
Most of the earthquakes higher than 7 on the Richter scale occur on the Pacific coast (Jalisco, Colima,Michoacan, Guerrero and Oaxaca).
102

Tropical cyclones bring disasters to Mexico's coastlines and islands. In 1996, there were 30 deaths, 763injured and 203 437 people affected due to four hurricanes. The hurricanes affect both the Pacific and Atlanticcoasts.
There are also 16 active volcanoes that may affect more than 6 million people (7.5% of Mexico's population).The Popocatepetl volcano, located 90 km east of Mexico City, has increased its activity since 1994.
The earthquakes in September 1985
The earthquakes that struck Mexico City in 1985 were part of a series of catastrophic earthquakes in LatinAmerica. Mexico City lost 5100 hospital beds (30% of the available beds in the city) and 10 000 deaths werereported that year due to an earthquake of 8.1 on the Richter scale (1).
Chile registered an earthquake of 7.5 on the Richter scale in 1985 also. That caused 2373 hospital beds to belost and 180 deaths.
In San Salvador 1800 hospital beds were lost and 1200 deaths were caused by an earthquake of 5.4 on theRichter scale. Although Costa Rica registered two earthquakes in 1990 and 1991, the damage was restrictedto one hospital.
It was estimated that damage in Mexico amounted to 550 000 million US dollars, while in El Salvador it was97 000 million US dollars. In Mexico 22 urban hospitals were damaged, while in Chile and El Salvador a totalof 20 were damaged in both urban and rural areas (2) (Table 3.5).
Table 3.5. Earthquakes in Latin America
Mexico Chile El Salvador Costa RicaYear 1985 1985 1986 1996−1991
Intensity 8.1 and 7.5 7.5 5.4 6.8, 5, 6.4 and 7.4Beds lost No./% 5100/30%*** 3271/16.6% − 60%**
Deaths 10 000 180 1200 −Injured people 30 000 2500 10 000 −
Costs 550* − 97* 220*
Source: Bitran B. Impacto Económico de los Desastres Naturales en la Infraestructura deSalud. WHO − LC/MEX/1.291 January, 1996.
*Thousands of million US dollars.**One hospital.***Zeballos J. Earthquake in Mexico September 19 and 20, 1985 In PAHO DisasterChronicles, N°3.
Health care in disaster programmes in Mexico
In Mexico two of the most important hospitals − Juárez hospital and General hospital − collapsed. Some 20%of the total deaths were doctors, nurses and patients in those hospitals. The most important hospitals inMexico City could not offer any health care because of damage they sustained (Table 3.6).
After the experience of the earthquake, the Mexican government opened an office to plan and implementstrategies to minimize the effects of natural hazards in the health sector and population. The office is part ofthe Ministry of Health. Its objective is to regulate and supervise the development of regional programmes inboth hospitals and communities.
The new Juárez hospital has developed a plan to reduce the vulnerability of earthquakes since 1987. The newhospital was built according to the new construction regulations for the city. There is also a plan to coordinateactivities before, during and after a disaster. Hospital employees carry out disaster exercises twice a year (3).
Table 3.6. Number of deaths in Juárez Hospitals and General Hospital
Deaths General Hospital Juárez Hospital Total
103
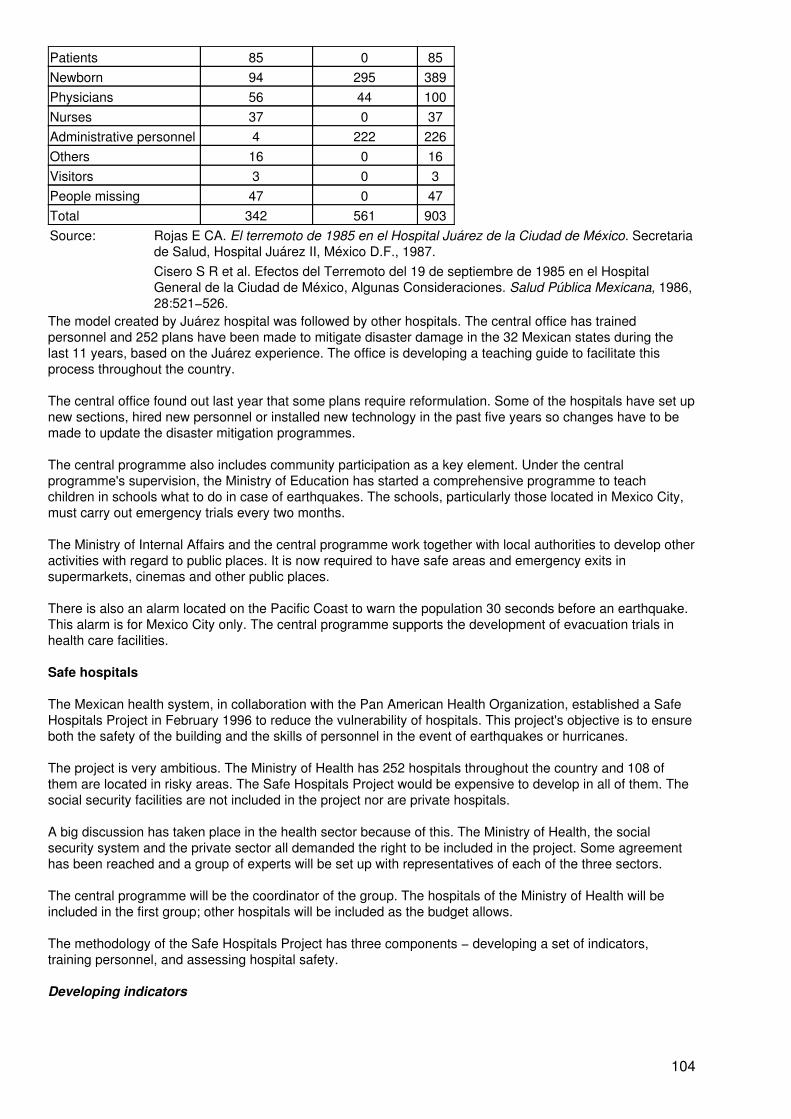
Patients 85 0 85Newborn 94 295 389Physicians 56 44 100Nurses 37 0 37Administrative personnel 4 222 226Others 16 0 16Visitors 3 0 3People missing 47 0 47Total 342 561 903Source: Rojas E CA. El terremoto de 1985 en el Hospital Juárez de la Ciudad de México. Secretaria
de Salud, Hospital Juárez II, México D.F., 1987.Cisero S R et al. Efectos del Terremoto del 19 de septiembre de 1985 en el HospitalGeneral de la Ciudad de México, Algunas Consideraciones. Salud Pública Mexicana, 1986,28:521−526.
The model created by Juárez hospital was followed by other hospitals. The central office has trainedpersonnel and 252 plans have been made to mitigate disaster damage in the 32 Mexican states during thelast 11 years, based on the Juárez experience. The office is developing a teaching guide to facilitate thisprocess throughout the country.
The central office found out last year that some plans require reformulation. Some of the hospitals have set upnew sections, hired new personnel or installed new technology in the past five years so changes have to bemade to update the disaster mitigation programmes.
The central programme also includes community participation as a key element. Under the centralprogramme's supervision, the Ministry of Education has started a comprehensive programme to teachchildren in schools what to do in case of earthquakes. The schools, particularly those located in Mexico City,must carry out emergency trials every two months.
The Ministry of Internal Affairs and the central programme work together with local authorities to develop otheractivities with regard to public places. It is now required to have safe areas and emergency exits insupermarkets, cinemas and other public places.
There is also an alarm located on the Pacific Coast to warn the population 30 seconds before an earthquake.This alarm is for Mexico City only. The central programme supports the development of evacuation trials inhealth care facilities.
Safe hospitals
The Mexican health system, in collaboration with the Pan American Health Organization, established a SafeHospitals Project in February 1996 to reduce the vulnerability of hospitals. This project's objective is to ensureboth the safety of the building and the skills of personnel in the event of earthquakes or hurricanes.
The project is very ambitious. The Ministry of Health has 252 hospitals throughout the country and 108 ofthem are located in risky areas. The Safe Hospitals Project would be expensive to develop in all of them. Thesocial security facilities are not included in the project nor are private hospitals.
A big discussion has taken place in the health sector because of this. The Ministry of Health, the socialsecurity system and the private sector all demanded the right to be included in the project. Some agreementhas been reached and a group of experts will be set up with representatives of each of the three sectors.
The central programme will be the coordinator of the group. The hospitals of the Ministry of Health will beincluded in the first group; other hospitals will be included as the budget allows.
The methodology of the Safe Hospitals Project has three components − developing a set of indicators,training personnel, and assessing hospital safety.
Developing indicators
104
A group of professionals is going to develop a set of indicators to evaluate hospitals. They will take intoaccount the building, the equipment and supplies and the hospital organization.
A group of engineers will decide the indicators to guarantee the security of the building. The foundations andthe rest of the construction must be strong enough to support the hazards of the area. The building itself mustbe a secure place for medical care. Mexico City's construction law is the main input in the discussion.Although the law is not specific to hospitals, the indicators are going to be taken into account. This is perhapsthe most complicated phase to develop. There are two different groups to work with − public health engineersand health managers.
Hospitals require sophisticated technology and supplies to work with that must be located in a safe place. Alsothe equipment and supplies should not be themselves a hazard for people in hospitals. A set of indicators willbe developed regarding the safety and safe positioning of equipment and supplies.
Hospital workers ought to know the specific hazards of the region. They must react according to those risksefficiently. They have specific functions to perform when a disaster occurs. A set of indicators will analyse ifthe hospital organization is prepared in case of disaster. A teaching guide will be provided to hospitaldirectors, as will technical support in planning, information systems, evaluation and rehabilitation.
The guide is in progress. A set of articles has been selected from both national and international literature.They have been classified in three sections − before, during and after. Each section has a set of objectives, areading guide and reading materials. At the end the users are expected to develop a comprehensive plan todeal with hazards.
The three groups of indicators will be printed in a manual. The hospital workers and public health engineerswill be able to follow the indicators to evaluate the hospital's safety.
Training
The second component of the Safe Hospitals Project includes the selection of hospitals and a trainingprogramme for hospital workers. After the hospitals in the most risky areas have been selected, the personneland public health engineers will be trained to evaluate hospitals. The manual referred to above will be used inthe assessment.
The selection process has already started. The central office chose 108 hospitals of the 252. A letter was sentto state health authorities to ask them to decide, according to certain indicators, which state hospitals shouldbe incorporated in the study. A guide for selecting the hospitals has been developed. The indicators weretaken from Boroschek's methodology and modified according to the Mexican context. We have selected 22hospitals to start working with (4).
Certifying safety
A group of professionals will check each hospital's assessment. A certificate will be issued to all hospitals thatmeet the manual's requirements. Both the Mexican Government and the Pan American Health Organizationwill certify the process.
Conclusion
New projects give you new problems to solve. The decentralization of the health sector in Mexico wasreinforced a year ago and the Safe Hospitals Project started at the same time. Some states are ready to goahead and some others are in the process of learning what to do. This has given the central offices a new wayto approach local needs. Many hours have been spent in meetings and negotiation, and more will have to bespent before we can certificate the first group of safe hospitals− The main point, however, is that we havealready started.
References
1. Zeballos J. Earthquake in Mexico. September 19 and 20, 1985. PAHO Disaster Chronicles, 3 1987.
2. Bitrrán BD. Impacto Económico de los Desastres Naturales en la Infraestructura de Salud. ConferenciaInternacional Sobre Mitigación de Desastres en Instalaciones de Salud, 1996.
105
3. Hospital Juárez Centro. Plan Hospitalario para Casos de Desastre. Secretaría de Salud, 1994.
4. Boroschek KR et al. Establecimiento de un Plan Nacional para la Reducción de los Efectos Sísmicos enSistemas de Salud. Conferencia Internacional Sobre Mitigación de Desastres en Instalaciones de Salud,1996.
Earthquake damage to hospitals and clinics in Kobe, Japan
Y. Nagasawa1and G. Sweitzer2
1Y. Nagasawa, Dr. Eng. Dip. HFP, JIA is Professor of the Department of Architecture,Graduate School of Engineering University of Tokyo, Tokyo, Japan.
2G. Sweitzer Ph.D. is from the Department of Architecture, Graduate School of Engineering,University of Tokyo, Tokyo, Japan.
A great earthquake
At 5:46 in the morning on 17 January 1995, a devastating earthquake of 7.2 on the Richter scale hit Japan'smajor port of Kobe and surrounding areas and destroyed or damaged many buildings (Fig. 9). The epicentrewas located about 15 km south−west of Kobe City at the northern tip of Awaji Island at a shallow focal depthof about 14 km (1). Within the 15 second duration of the earthquake, most structures along adensely−populated 40 km length of the bilateral rupture were severely damaged, if not totally destroyed.
Within the two months following the earthquake, more than 5500 were counted dead, 36 000 injured, andmore than 300 000 homeless. More than 185 000 homes were severely damaged or totally destroyed (2).After six months, a newspaper reported the death toll at over 6000, including those who had been admitted tohospitals or clinics and later died as well as those still counted missing− This disaster has come to be calledthe Great Hanshin−Awaji Earthquake, after the area of Hanshin and the island of Awaji.
Damage surveys
A team was formed to assess damage to the health facilities in Kobe affected by the earthquake. The teammembers represented six organizations − the National Institute of Health Services Management, the JapanInstitute of Health Care Architecture, the Japanese Association of Hospital Engineering, the Japanese Societyof Hospital Administration, the Architectural Institute of Japan (AIJ), and the Japan Institute of Architects (JIA).
The team first made a preliminary survey of four hospitals on 2 and 3 February 1995. This effort was incollaboration with the Environment/Health Division of Hyogo Prefecture and the temporary field office of theMinistry of Health and Welfare. Following this, a more in−depth interview survey format was developed; thisfocused on the physical and management situations in hospitals during and after the earthquake. The surveywas later administered in 22 hospitals between April and June. The findings are summarized later in thispaper (3).
Representatives of architectural, building construction and equipment manufacturing concerns reported theirrespective interests independently (4−7). In addition, on 2 March, the Hyogo Prefecture office distributed aquestionnaire to 3223 medical organizations: 224 hospitals and 2999 clinics located in 10 cities and 10 townsin the prefecture. In Japan a hospital has 20 or more beds while a clinic has 19 beds or less, or even no beds.The latter typically have one doctor and one nurse. By 15 March 1995, 182 of the hospitals (81%) and 1845 ofthe clinics (61%) had responded. During June 1995, the Hyogo Prefecture office reported the findings of thisquestionnaire (8); these are summarized below.
Questionnaire survey findings − hospitals and clinics
Responses to the questionnaire administered by the Hyogo Prefecture office are presented as percentages,for hospitals and clinics respectively.
Most of the hospitals (96%) and clinics (57%) were considered to be seismic−resistant structures; most ofthese (68% and 64% respectively), however, were completed before the seismic requirements in the buildingcode were upgraded in 1981. Less than half of the hospitals (45%) but most of the clinics (95%) reported their
106
structures as having 1−4 storeys. Correspondingly, a little over half of the hospitals (52%) but only a few ofthe clinics (5%) reported their structures as being five to nine storeys high. A few of the hospitals (3%) andmost of the clinics (91%), meanwhile, reported a floor area of less than 1000 m2, while 38% of the hospitalsand 9% of the clinics reported a floor area of 1000−3000 m2.
In general, the hospitals were better equipped than were the clinics for this emergency. For instance,emergency (primarily diesel) electric generators were present in 75% of hospitals compared to 3% of clinics.The respective percentages for water reserve containers were 47% compared to 10%, for well−waterprovisions they were 18% and 6%, for LP gas provisions 10% and 5%, for emergency reserves of food 29%and 4%, for drugs 34% and 16%, and for hot−line communication to the fire department the percentages were25% and 2%. Nevertheless, 52% of the hospitals reported their situation to the fire department by othermeans, (e.g. on foot or by bicycle) while 65% of the clinics did not report because their personnel wereoverburdened.
Although most facilities (83% of hospitals and 84% of clinics) did not suffer fire damage, one hospital wascompletely burned down and two others suffered extensive damage. While most facilities reported no deathsor injuries inside the buildings during the first three days (hospitals 81%, clinics 95%) such cases involvinginpatients (hospitals 3, clinics 7) and staff (hospitals 1, clinics 27) were reported later.
Most of the hospitals and many of the clinics (61% and 42% respectively), however, were otherwise severelydamaged or needed extensive repairs. Many of these (39% of hospitals, 54% of clinics) were unable toprovide ordinary surgeries or services in their respective facilities (operating theatres, consultation rooms,examination rooms). In addition, most hospitals and clinics reported damage to their equipment: magneticresonance imaging (MRI) (70%), X−ray equipment (65%), computed tomography (CT) scanners (30%) andcommunication equipment (25%). It is also noteworthy that emergency sprinkler systems in hospitalsmalfunctioned when triggered in 32% of the cases.
Nikkei health care magazine, representing the health care community in Japan, reported the case of KobeNishi (West) municipal hospital, a 370−bed facility (9). Here one inpatient died due to the collapse of the fifthfloor. Originally, this hospital was built as a five−storey structure in 1960; floors 6 and 7 were added in 1967.On the day of the earthquake, the 255 inpatients in the hospital were being cared for by 23 nurses. In thedamaged fifth floor ward, there were 44 inpatients and three nurses. It required one full day before all of thepatients and staff could be rescued from the crushed floor, by which time one patient had died.
Of the total staff associated with the reporting hospitals and clinics, most of the doctors (59% in hospitals,66% in clinics) and many of the nurses (44% in hospitals, 39% in clinics) were working on the day of theearthquake. During the seven days following the earthquake, a few of these facilities (19% of hospitals, 2% ofclinics) requested additional medical and nursing staff. In response, additional doctors were accepted: 178into 19 hospitals and nine into clinics. Likewise, additional nurses were accepted: 282 into 15 hospitals and 14into eight clinics.
In addition, on the day of the earthquake most of the reporting hospitals (98%) and clinics (66%) providedin−house emergency medical services to slightly−injured or ill patients. Hemodialysis services, for example,were provided in 47% of hospitals and 36% of clinics. Although many of the hospitals (44%) postedinformation concerning the availability of clinical OPD services, many clinics (46%) did not. Surgicaloperations meanwhile were performed in 43% of the hospitals; most of the operating theatres receivedelectricity from emergency generators.
Five hospitals and 28 clinics provided clinical services in temporary tents on the day of the earthquake. Withinthe seven days after the earthquake, many physicians from these facilities (903 from hospitals, 2450 fromclinics) were sent to temporary clinics in locations of refuge.
During the first week, thousands of patients were treated, 50 655 in hospitals and 103 440 in clinics. Thesefigures include inpatients (8167 in hospitals and 1718 in clinics) and patients who later deceased (749 inhospitals and 439 in clinics). Among the total number of facilities, 66% of the hospitals and 32% of the clinicsrequested transportation for inpatients to other institutions and the overwhelming majority of these patients(hospitals 95%, clinics 99%) were transported. Nevertheless, six hospitals and two clinics could not securetimely transportation for their patients. This was apparently due to failures of communication with either localgovernment or ambulance service agencies (65% of both types could not be served).
Through all of this, the primary means of transportation for these hospital and clinic patients was via threemeans: private cars (hospital 799, clinics 690), hospital ambulances (hospitals 739, clinics 36) and by fire
107
department ambulances (hospitals 507, clinics 125). Meanwhile, there was great disparity between thehospitals and clinics concerning their knowledge of the availability of helicopters as a means of patienttransportation (hospitals 49%, clinics 20%) as well as the obligation of a physician to accompany each flight(hospitals 52%, clinics 14%). Not surprisingly, therefore, only 46 patients from 22 hospitals and one patientfrom one clinic were transported via helicopter. The one clinic requested helicopter transportation servicesdirectly via the fire department ambulance service agency. For the hospital patients, helicopters typicallylanded at nearby parks or other outdoor spaces (58%); meanwhile most clinics (67%) reported there were nosuitable landing areas nearby.
Also during the first week following the earthquake, most of the facilities had to recover from a lack of water(57% of hospitals, 64% of clinics) and city gas (59% of hospitals, 64% of clinics). In addition, from thebeginning, the majority of facilities (72% of hospitals, 21% of clinics) asked municipal/township governmentsfor provision of water and heating fuels, including LP gas− Many other facilities (34% of hospitals and 35% ofclinics) meanwhile asked private vendors for the same supplies. Nevertheless, 10% of hospitals and 34% ofclinics did not succeed in obtaining adequate provisions for heating and were forced to close for that reasonalone. Most of the facilities (86% of hospitals, 85% of clinics) requested additional provisions of drugs fromprivate vendors.
Two of the three hospitals that had not recovered as of 15 March 1995 held no immediate prospect to resumetheir services. The other hospital meanwhile did not expect to resume services until September 1995, mainlydue to a lack of funds. Otherwise, 80% of the hospitals and 57% of the clinics were expected to complete fullrecovery by the end of March, 1995. Of these, 53% of hospitals and 42% of clinics were consideringupgrading the seismic resistance of their buildings while only a few (14% of hospitals and 9% of clinics) haddecided to install emergency water preservation containers. Emergency drug preservation measures,meanwhile, were under way or are being considered by 67% of hospitals and 43% of clinics. Most of thehospitals and clinics, however, considered alternative communication systems (hospitals 93%, clinics 80%)such as to fire and police departments; information systems (hospitals 93%, clinics 75%), within and outsideof hospital and clinic facilities; and emergency medical service systems (hospitals 95%, clinics 93%),especially regional policy revisions.
Interview survey findings − hospitals
Detailed interviews were administered by the survey team from 6 April to 16 June 1995 in 13 public hospitals(102−1000 beds) and nine private hospitals (151−1250 beds). Each interview team included hospitalarchitects, engineers and administrators.
Several hospitals reported partial structural damage, including cracks in reinforced concrete columns, beamsand walls. One hospital, for instance, reported the repair of the hooping of four columns marked by shearingcracks by using 12 nun−thick reinforced steel plates. In addition, cracks were found in exterior walls, roofs,verandas, chimneys, interior walls, floor slabs and expansion joints. About half of the hospitals reportedbroken windows and many reported broken electric lamps. Most unrestrained shelves or containers holdingbooks, files, X−ray films or patient records were overturned (Figs. 10 and 11). Likewise, most (typicallyunrestrained) television sets on tables fell to the floor. Beds and wagons meanwhile moved horizontally andhit walls; beds with castors were found to be safer for the patients in them.
Most of the hospitals surveyed suffered from the interruption of electric power. While the available emergencyelectric generators (those not damaged by the earthquake) functioned efficiently, some of the water−cooledunits were limited by a lack of water. Accordingly, the air−cooled units proved more effective.
In addition, water supplies were suspended for 2−3 weeks in several of the hospitals surveyed. Damage torooftop water tanks and piping was especially widespread. In one case, water leaked from a rooftop tank intoan elevator shaft, preventing use of the elevator. As a result, the nursing staff of this hospital had to carrywater to the upper floors.
Where piped water was cut off, drinking water was supplied mainly from water wagons operated by localgovernments, voluntary groups and other hospitals. In one hospital where the temporary water was suppliedfrom a fire hydrant, the water was first sterilized before use. Two−thirds of the hospitals surveyed experiencedsuspension of hot water supply due to the water shortage. In addition, the shortage of tap water along with thedestruction of sewage piping limited use of lavatories, especially on upper floors. Three of the hospitals thusaffected requested provision of prefabricated lavatory units from their local governments; these were received.Meanwhile, more than half of the hospitals surveyed suffered from suspension of the city gas supply forperiods from a few weeks up to three months. Restoration of the city gas supply proved much more difficult
108
than restoration of electricity and water.
During the first few days following the earthquake, telephone communication was difficult, especially to localareas. Meanwhile, central heating systems failed to work for up to 40 days in some hospitals due to watershortage and damage to boilers and piping. Portable electric and oil heaters were substituted.
Damaged or broken elevators were found in most of the hospitals surveyed. Almost all of the elevatorsstopped just after the earthquake, as designed. Most of the undamaged units were restarted followinginspection by maintenance crews, as required.
Most (unrestrained) desktop computer terminals meanwhile fell to the floor, although resulting system failuresoccurred less often than expected (Fig. 12). In addition, there was little damage to medical gas piping. Severalrespirators, meanwhile, were operated manually.
Heavy radiological equipment, however, such as CT, MRI and X−ray units, often moved 30−40 cm and evenas far as 1 m. Such units typically required at least one week to be repositioned and recalibrated. In onehospital an angiography unit suspended from the ceiling fell to the floor.
Most of the hospitals surveyed stopped ordinary surgical operations for about one month. Likewise, manylaboratories curtailed operations, reportedly due to damaged files, specimens, instruments and supplies, aswell as the shortage of water. The lack of water also limited hemodialysis (which needs a great amount ofwater), autoclave operation, and the development of X−ray film.
Conclusion
Local government reports stated that medical services were limited primarily by the lack of water andtelecommunications. In addition, the survey team interviews revealed that the facilities that escaped structuraldamage nonetheless could provide only limited medical services for inpatients and outpatients. This was duemainly to non−structural damage, such as to medical and building service equipment. In addition, urbanlifelines were interrupted, including potable water, electric power, energy sources, and water and sewagesystems.
These breakdowns confirmed the need for improved non−structural restraints in conjunction with structuralprovisions. In addition, it suggested the need for an emergency plan that can be implemented immediatelyfollowing earthquake disasters. Admittedly, this approach represented a departure from the current approach,which emphasized improved structural resistance of buildings.
Likewise, it appeared worthwhile to reconsider the current recommendations, which are based on surveys ofpast disasters (10−12).
A basis for developing new recommendations has been initiated by the AIJ. Its members include architects,structural and mechanical engineers, general contractors and academic researchers. In response to theearthquake, AIJ representatives of these groups began to review each field of architectural and urbanplanning. In conjunction, a special research committee proposed to upgrade measures to prevent disasters inbuildings and urban areas. This proposal assumes that the main problem is a lack of preparedness, fromurban and regional perspectives as well as for individual users of buildings. The proposal focuses on fiveareas: urban planning to consider disaster scenarios; seismic−resistant measures for existing buildings notaddressed by current regulations; planning for improved structural design policies; establishment of disasterinformation systems; and basic research to prevent and reduce the impact of earthquake−related disasters.The outstanding challenge, however, is to apply these to existing buildings that do not comply with the oldregulations as well as to new constructions.
The Ministry of Health and Welfare budgeted an additional 25.46 billion yen for the fiscal year 1995 towardsreconstruction of the earthquake−affected areas in Kobe. This was intended to provide for both safer andmore comfortable living environments.
References
1. Shinozuka M. Summary of the earthquake. NCEER Bulletin, 1995, 9(1): Special supplement.
2. Japanese National IDNDR Committee. The Great Hanshin−Awaji Earthquake. Damages and response.Stop disasters, 1995,23.
109
3. Japan Institute of Health Care Architecture, Survey of physical facilities and management of health carefacilities during and after the Great Hanshin−Awaji Earthquake. 1995:7 (preliminary report).
4. Japan Institute of Architects. JIA Special Committee on Urban Disasters, February 1995 preliminary reporton Hyogo Nanbu (South) earthquake. 1995:34.
5. Takenaka−Komuten Ltd. Survey report on the Hanshin Daishinsai (Great Hanshin−Awaji Earthquake).No.1, January 1995:118.
6. Takenaka−Komuten Ltd. Survey Report on the Hanshin Daishinsai (Great Hanshin−Awaji Earthquake).No.2, February 1995:226.
7. Mitsui Home Co Ltd. Performance of 3568 (2 × 4) homes during the Great Hanshin−Awaji Earthquake.1995:126.
8. Hyogo Prefecture Office/Environmental Health Division. Survey results of medical services during the GreatHanshin−Awaji Earthquake. 1995:87.
9. Nikkei Healthcare. Hospitals in the great earthquake. 1995:10−47.
10. Hashimoto S, Nagasawa Y et al. Report on seismic−resistant counter−measures in hospitals. NationalInstitute of Hospital Administration, 1976:118.
11. Kakehi K et al. Seismic−resistance guidelines for medical equipment and medical piping. Tokyo, JapanBuilding Centre, 1980:65.
12. Matsumoto A, Nagasawa Y. A method to estimate sustainability of hospital and medical services in largeurban areas impacted by earthquakes. Tokyo, National Institute of Hospital Administration, 1988:55.
Guidelines for disaster prevention manuals in hospitals
Working Group in the Ministry of Health and Welfare of Japan1
1Health Policy Bureau, Ministry of Health and Welfare, Tokyo, 2 October 1996 (also includedin The Medical System for Emergencies in the 21st Century, Health Publications, Tokyo,1996)
Implementation of disaster prevention in hospitals
In order to ensure effective disaster prevention activities in hospitals, it is desirable that a hospital disasterprevention manual should be prepared by the Committee for Disaster Management in each hospital, and thatdisaster prevention training be implemented based on the manual.
Committee for Disaster Management
It is required that a Committee for Disaster Management be established in each hospital with the hospitaldirector as leader. The committee prepares a disaster prevention manual for the hospital to be ready torespond to real situations of disaster at any time. The committee should also function as a disastermanagement headquarters in the event that a disaster should occur.
Disaster prevention manuals should be reviewed and revised periodically by the committee.
Disaster prevention training
It is desirable to hold disaster prevention training once or more every year, as well as biannual training for fireincluding the cooperation with the local administration and local residents.
Locations and operation methods of communication equipment and disaster prevention facilities, as well asmethods for transporting patients, should be well understood by the personnel.
110
Preparing disaster prevention manuals
Disaster prevention manuals based on simulations
Classification of disasters
• Simulations based on high frequency classification.• Natural disaster: earthquake, volcanic eruption, etc.• Man−made disaster: accident, explosion, etc.
Condition of hospitals (damage, etc.)
• When the hospital is damaged.• When the hospital has no damage.• When the hospital is crowded with patients.
Items to be included in disaster prevention manuals
Disaster management system
• Securement of lifelines.• Stockpile of medical supplies, food, etc.• Handling of hazardous items such as isotopes, etc.• Ensuring cooperation of other supporting hospitals.• Ensuring availability of places for patients to be transferred and transportation methods.
Emergency measures during disaster
• Establishment of internal communication and instruction system.• Ensuring availability of staff and establishment of communication network.• Collection of information (internal and external) and dissemination of information.• Prevention of secondary disaster in hospital caused by leakage of gas, hazardous items,etc.
Handling of inpatients
• Priority must be given to inpatients in every respect.
• Practical needs for serious cases, infusion, artificial respiration must be specificallyrecognized.
• Transfer of patients and transfer methods must be rehearsed.
Measures for accepting patients into hospital
• Establishment of triage/hospitalization system.• Assurance of sufficient manpower.
Items to be considered when the hospital sends a relief/party
• Confirm the functions in the disaster prevention plan in the community.
• Organization of relief party (place to assemble, ensure medical supplies, method oftransportation).
• Necessity of self−supported assistance (medical equipment, medical supplies, medicaltools, as well as preparation of sleeping bags, preserved food, drinking water, portablecooking stoves).
• Preparation of medical record format at medical relief station.
Other items to be noted in preparing the disaster prevention manual
111
• Prevent falling down of shelves on which drugs and medical equipment are stored.
• Reserve the nearest heliport for emergencies and ensure contacts for arrangements forhelicopter.
• It is desirable to preserve manually−operated medical equipment in case of power failure.
• Operation of emergency power generator and distribution circuit must be checked.
Summary
C. Ugarte1, Y. Oka2, K. Shoaf3and Secretariat
1C. Ugarte is Director, Direccion Nacional Preparacion contra Desastres, Lima, Peru.
2Y. Oka is a Research Associate from the Department of Architecture, University of Tokyo,Tokyo, Japan.
3K. Shoaf is from the Department of Community Health Sciences, School of Public Health,University of California, Los Angeles, USA.
Dr J. Oviedo made a presentation on the Mexican strategy to face natural hazards. Dr Oviedo highlighted thevulnerability of Mexico to earthquakes and other types of disasters and the various steps his country took inplanning for disaster management. He emphasized the fact that the Ministry of Health is now focusing on avulnerability reduction programme in hospitals. The programme has three major components: issuing amanual of indicators of vulnerability, starting a training process and performing an assessment. It focuses oninfrastructure, equipment and organization. In principle, hospitals must be safe places to survive disasters,and should have safe and reliable equipment and secure lifelines.
Preparedness, or stressing what to do in an emergency, is also important, and corresponding training at thecommunity level, in hospitals and medical schools is planned. However, Dr Oviedo concluded that moreefforts are needed to convince all partners of the value of the project and to build partnerships with them.
Another issue is where and when outside help should arrive. Using helicopter transport of the injured is alsoimportant and has to be organized. In general, such preparedness must be planned and practised inexercises ahead of time; when the disaster strikes it is too late.
Professor Y. Nagasawa made a poster presentation on earthquake damages to hospitals and clinics inKobe, Japan. After the Great Hanshin−Awaji Earthquake on 17 January 1995, a comprehensive survey teamwas formed to assess damage to the health facilities affected by the earthquake in Kobe City. The teammembers represented six organizations: the National Institute of Health Services Management; the JapanInstitute of Health Care Architecture; the Japanese Association of Hospital Engineering; the Japanese Societyof Hospital Administration; the Architectural Institute of Japan; and the Japan Institute of Architects.
The team first made a preliminary survey of four hospitals, on 2 and 3 February 1995. This effort was incollaboration with the Environment/Health Division of Hyogo Prefecture and the temporary field office of theMinistry of Health and Welfare. Afterwards, a more in−depth interview survey format was developed, focusingon the physical and management situations in hospitals during and after the earthquake. This survey was lateradministered in 22 hospitals from April to June 1995.
Highlights of the findings, which were presented in detail, are as follows:
Local government reports stated that medical services were limited primarily by the lack of water andtelecommunications. In addition, the survey team interviews revealed that the facilities that escaped structuraldamage nonetheless could provide only limited medical services for inpatients and outpatients. This was duemainly to non−structural damage, such as to medical and building service equipment. In addition, urbanlifelines were interrupted, including potable water, electric power, energy sources, and water and sewagesystems.
112
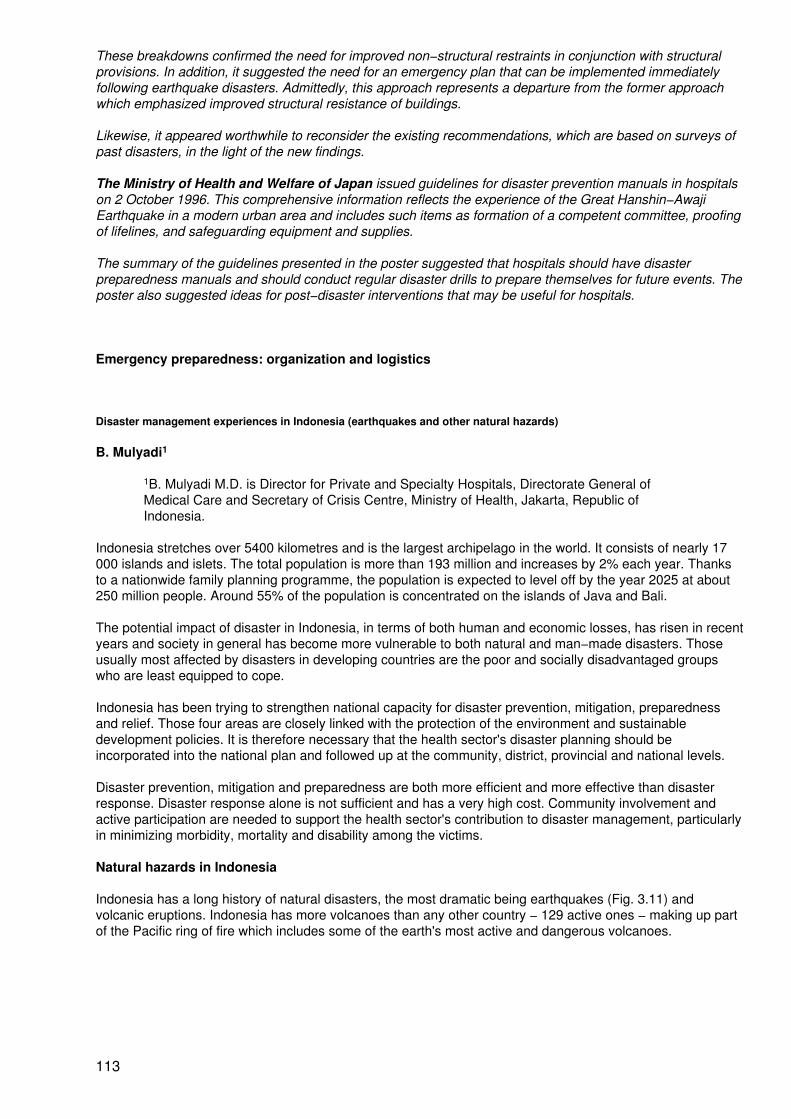
These breakdowns confirmed the need for improved non−structural restraints in conjunction with structuralprovisions. In addition, it suggested the need for an emergency plan that can be implemented immediatelyfollowing earthquake disasters. Admittedly, this approach represents a departure from the former approachwhich emphasized improved structural resistance of buildings.
Likewise, it appeared worthwhile to reconsider the existing recommendations, which are based on surveys ofpast disasters, in the light of the new findings.
The Ministry of Health and Welfare of Japan issued guidelines for disaster prevention manuals in hospitalson 2 October 1996. This comprehensive information reflects the experience of the Great Hanshin−AwajiEarthquake in a modern urban area and includes such items as formation of a competent committee, proofingof lifelines, and safeguarding equipment and supplies.
The summary of the guidelines presented in the poster suggested that hospitals should have disasterpreparedness manuals and should conduct regular disaster drills to prepare themselves for future events. Theposter also suggested ideas for post−disaster interventions that may be useful for hospitals.
Emergency preparedness: organization and logistics
Disaster management experiences in Indonesia (earthquakes and other natural hazards)
B. Mulyadi1
1B. Mulyadi M.D. is Director for Private and Specialty Hospitals, Directorate General ofMedical Care and Secretary of Crisis Centre, Ministry of Health, Jakarta, Republic ofIndonesia.
Indonesia stretches over 5400 kilometres and is the largest archipelago in the world. It consists of nearly 17000 islands and islets. The total population is more than 193 million and increases by 2% each year. Thanksto a nationwide family planning programme, the population is expected to level off by the year 2025 at about250 million people. Around 55% of the population is concentrated on the islands of Java and Bali.
The potential impact of disaster in Indonesia, in terms of both human and economic losses, has risen in recentyears and society in general has become more vulnerable to both natural and man−made disasters. Thoseusually most affected by disasters in developing countries are the poor and socially disadvantaged groupswho are least equipped to cope.
Indonesia has been trying to strengthen national capacity for disaster prevention, mitigation, preparednessand relief. Those four areas are closely linked with the protection of the environment and sustainabledevelopment policies. It is therefore necessary that the health sector's disaster planning should beincorporated into the national plan and followed up at the community, district, provincial and national levels.
Disaster prevention, mitigation and preparedness are both more efficient and more effective than disasterresponse. Disaster response alone is not sufficient and has a very high cost. Community involvement andactive participation are needed to support the health sector's contribution to disaster management, particularlyin minimizing morbidity, mortality and disability among the victims.
Natural hazards in Indonesia
Indonesia has a long history of natural disasters, the most dramatic being earthquakes (Fig. 3.11) andvolcanic eruptions. Indonesia has more volcanoes than any other country − 129 active ones − making up partof the Pacific ring of fire which includes some of the earth's most active and dangerous volcanoes.
113

Figure 3.11. Seismotectonic map of Indonesia
Mount Krakatau, for example, is most famous for its 1883 eruption which killed 35 000 people and caused aglobal weather change. Mount Tambora's eruption in 1816 killed more than 76 000 people. Mount Agung inBali last erupted in 1963 killing 4500 people. Mount Merapi killed nearly 80 people in 1994. Other recent majordisasters are shown in Table 3.7.
The percentage of earthquakes worldwide causing over 1000 fatalities has increased by 10% since the year1910. The total death toll of 1.4 million lives is due, in part, to increased population density in seismic regionsof the world. Indonesia is earthquake−prone because of its position at the junction of the earth's plates.Volcanic activity also provokes earthquakes in the area around the active volcano. Landslides occur whenearthquakes strike mountainous areas or major ground displacement has taken place along a fault.Earthquakes and tsunamis, or tidal waves, are highly dangerous to those living in coastal areas.
The national health system
As in many other Asia−Pacific countries, the main objective of Indonesia's national health system is in linewith the WHO strategy of "Health for All by the Year 2000". Since the 1970s the public health service inIndonesia has supported the development of a community−based health programme as the key approach toimproving the effectiveness, efficiency and equity of health care. The primary health care approach inIndonesia addresses the problems of availability, accessibility and appropriateness of health services to awidely divergent population which is still only 30 % urban and 70% rural.
At the critical subdistrict level (Fig. 3.12), there are nearly 7000 health centres and more than 120 000community health posts (out of a planned 200 000). These health posts will be the focus of an Indonesianprimary health care delivery system.
The medical delivery system, of which the emergency medical services are just a part, is topped by fournational referral hospitals located in Jakarta, Surabaya, Medan and Ujing Pandang. These are designatedclass A hospitals and provide for both specialist and subspecialist referral. The Class B hospitals located inthe 27 provinces provide comprehensive specialist services. The Class C hospitals in the 258 districts providethe basic specialist services. In addition there are numerous Class D hospitals at the district level whichprovide less than the specialist level of services. The health centres and health subcentres are managed andpromoted by general practitioners. This system, at which different levels have distinct yet supportive roles indisaster management, has proved to be the answer to the need for health care in a vast island nation such asIndonesia.
114
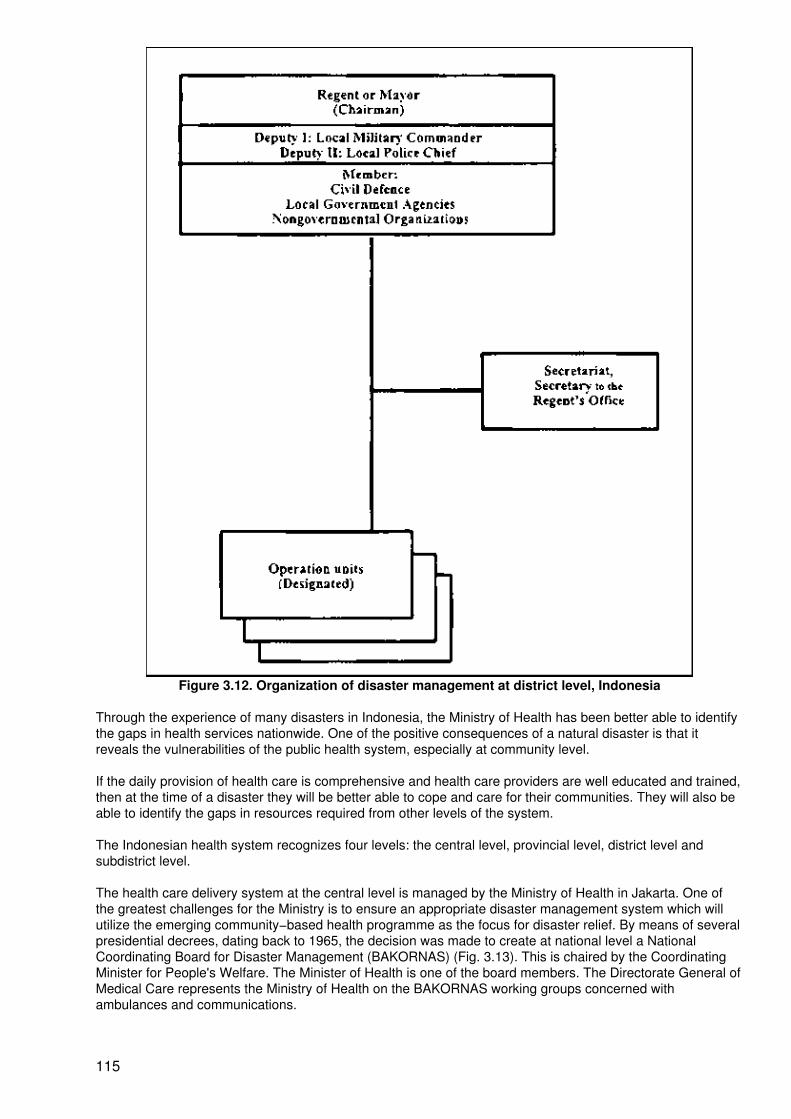
Figure 3.12. Organization of disaster management at district level, Indonesia
Through the experience of many disasters in Indonesia, the Ministry of Health has been better able to identifythe gaps in health services nationwide. One of the positive consequences of a natural disaster is that itreveals the vulnerabilities of the public health system, especially at community level.
If the daily provision of health care is comprehensive and health care providers are well educated and trained,then at the time of a disaster they will be better able to cope and care for their communities. They will also beable to identify the gaps in resources required from other levels of the system.
The Indonesian health system recognizes four levels: the central level, provincial level, district level andsubdistrict level.
The health care delivery system at the central level is managed by the Ministry of Health in Jakarta. One ofthe greatest challenges for the Ministry is to ensure an appropriate disaster management system which willutilize the emerging community−based health programme as the focus for disaster relief. By means of severalpresidential decrees, dating back to 1965, the decision was made to create at national level a NationalCoordinating Board for Disaster Management (BAKORNAS) (Fig. 3.13). This is chaired by the CoordinatingMinister for People's Welfare. The Minister of Health is one of the board members. The Directorate General ofMedical Care represents the Ministry of Health on the BAKORNAS working groups concerned withambulances and communications.
115
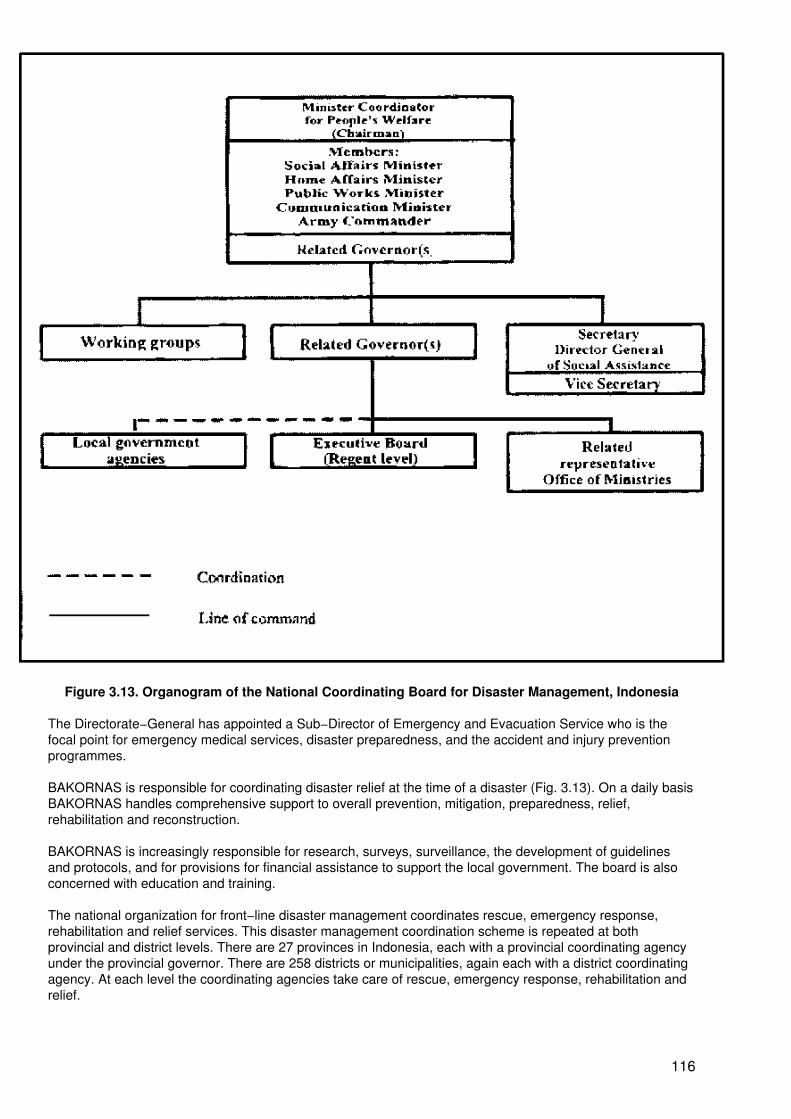
Figure 3.13. Organogram of the National Coordinating Board for Disaster Management, Indonesia
The Directorate−General has appointed a Sub−Director of Emergency and Evacuation Service who is thefocal point for emergency medical services, disaster preparedness, and the accident and injury preventionprogrammes.
BAKORNAS is responsible for coordinating disaster relief at the time of a disaster (Fig. 3.13). On a daily basisBAKORNAS handles comprehensive support to overall prevention, mitigation, preparedness, relief,rehabilitation and reconstruction.
BAKORNAS is increasingly responsible for research, surveys, surveillance, the development of guidelinesand protocols, and for provisions for financial assistance to support the local government. The board is alsoconcerned with education and training.
The national organization for front−line disaster management coordinates rescue, emergency response,rehabilitation and relief services. This disaster management coordination scheme is repeated at bothprovincial and district levels. There are 27 provinces in Indonesia, each with a provincial coordinating agencyunder the provincial governor. There are 258 districts or municipalities, again each with a district coordinatingagency. At each level the coordinating agencies take care of rescue, emergency response, rehabilitation andrelief.
116
An emergency phone number (118) can be used to seek emergency help. Every hospital in the country islinked to this system which needs central management to improve the response time.
Even though Indonesia has a domestic satellite communications system, public telecommunications groundfacilities are prone to disruption in times of disaster. This makes over 140 000 amateur radio stationsthroughout Indonesia a strategic resource. Amateur radio and armed forces communications systems are vitallinks in the communications network, with contingency plans for back−up, during times of major disaster. Oneof the major additions to the national or central level capabilities is the recently developed Crisis Centre beingestablished by the Ministry of Health. This centre, which coordinates all health−related issues at the strategiclevel, will utilize emerging technologies to communicate with the vital provincial and district medical assistanceteams at the time of a disaster.
The basic requirements for successful disaster management
There are many definitions for disaster used by different centres. In this paper, disaster is defined as an eventthat causes many victims that need medical help immediately that cannot be provided by the existing healthfacilities in their routine mode of operation.
With regard to that definition, several important characteristics of disasters should be mentioned:
− there are many casualties and many of them are in serious and critical condition;
− all casualties occur in a relatively short period of time;
− they need emergency medical help immediately;
− the existing health facilities and routine plans of work are not adequate and additional helpis needed.
In response to these characteristics, a basic requirement for a successful disaster management operation canbe proposed. There must be an effective disaster management organization that is able to carry out thefollowing functions:
− it must be capable of obtaining the earliest information about the occurrence of the disaster;
− it must be capable of mobilizing appropriate and adequate resources to cope effectively andefficiently with the disaster;
− it must be capable of coordinating the resources that are mobilized;
− it must be capable of mobilizing and coordinating the resources in the shortest possibletime; it must have all the supporting facilities to carry out the above functions (i.e.communication, transportation, budget).
The organizational framework for disaster management
There are three basic organizational frameworks for managing disasters in Indonesia, namely:
− the referral system− the emergency medical service system− the disaster management organization.
The referral system
As described in the section on the national health system above, the referral system in Indonesia has severallevels. These are: the community health centre and health subcentre, and the Class A, B and C hospitals. Inaddition there are many Class D hospitals.
The emergency medical service system
The Indonesian Ministry of Health requires each hospital in the country to have an emergency department. Ineach region of the referral system in Indonesia, these emergency departments work in cooperation with each
117
other. The cooperation involves all hospitals (government, private and armed forces hospitals) and is thebasis for the emergency medical service system. When disaster strikes this basic referral framework becomesthe emergency medical service and the Crisis Centre is activated to mobilize and to coordinate all resourcesneeded for disaster management.
The disaster management organization
Indonesia's National Coordinating Board for Disaster Management involves, at provincial and district levels, allsectors that participate in disaster management. The participating components include hospitals, theIndonesian Red Cross, regional health officers, the armed forces, the police, the boy scouts, the civil defenceorganization, the Indonesian Amateur Radio Association and the Indonesia Search and Rescue Organization.
The Role of the National Coordinating Board for Disaster Management is:
− to develop basic policy for disaster management;
− to strengthen activities that are considered necessary for successful disaster management,such as standardization, registration and development of personnel, equipment of healthfacilities, and other logistics;
− training and education for medical, paramedical personnel and volunteers to strengthenefforts for disaster prevention, preparedness and mitigation.
The disaster management team and how it works
When disaster strikes the disaster management team comes into action. The team has several components:the field post, the front post, the command post and the severe emergency reception posts. The field post isthe health centre in the affected area that coordinates the teams that give help at the site of disaster. The frontpost is the nearest hospital. If there is no hospital nearby, we construct a field hospital near the site of thedisaster in cooperation with the military health service. The front post's role is to provide further help to themore seriously injured.
The command post is the central referral hospital. Its role is to coordinate the disaster management operationand at the same time it functions as the highest referral hospital to provide further help to the most severevictims.
The severe emergency reception posts are the hospitals that receive victims in a situation when the disaster issuch that very many people are injured and need hospitalization.
The disaster management operation is activated in five phases:
− the alert phase− the initial phase− the planning phase− the operation phase− the post−operation/evaluation phase.
The communication system
The role of the communication system is as follows:
• During the alert and initial phases, the communication system is used to report, to give ascomplete a description as possible of the disaster, including the location, the estimatednumber of victims, and the likelihood of further disastrous events.
• At the planning phase the communication system is used to inform health units that will beinvolved at the operation stage.
• At the operation stage the communication system is used to coordinate the activities of thedifferent components of the disaster management system.
118
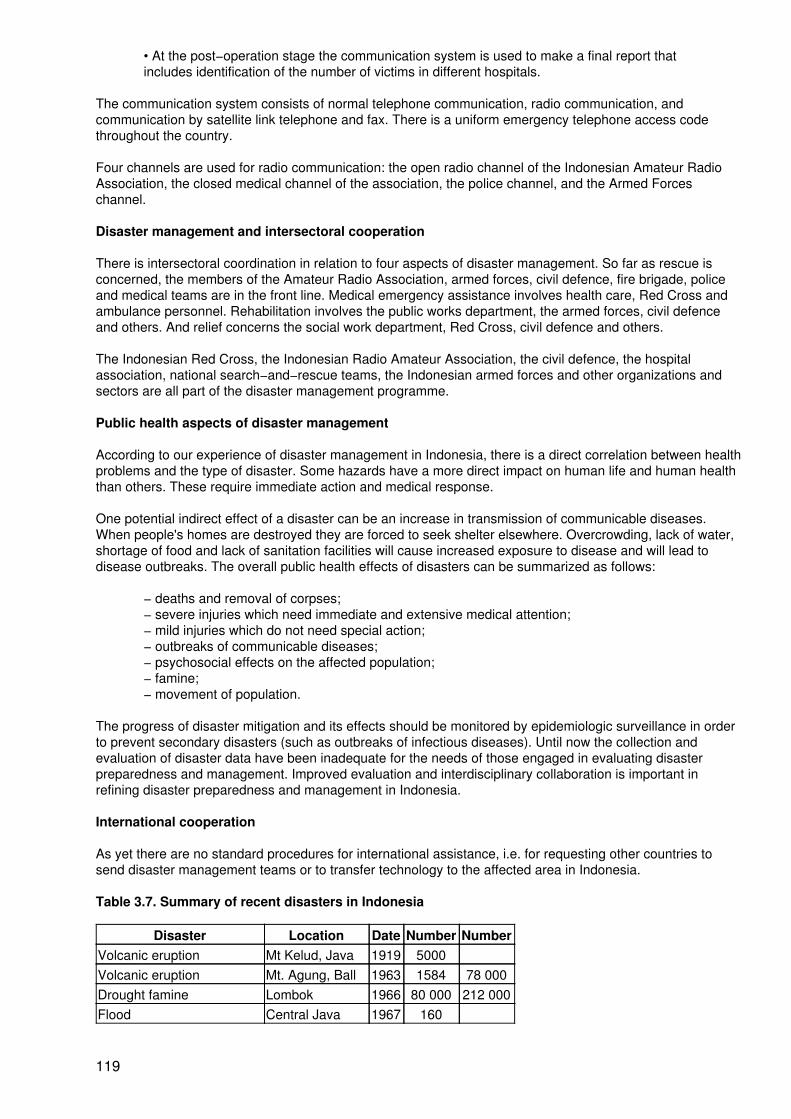
• At the post−operation stage the communication system is used to make a final report thatincludes identification of the number of victims in different hospitals.
The communication system consists of normal telephone communication, radio communication, andcommunication by satellite link telephone and fax. There is a uniform emergency telephone access codethroughout the country.
Four channels are used for radio communication: the open radio channel of the Indonesian Amateur RadioAssociation, the closed medical channel of the association, the police channel, and the Armed Forceschannel.
Disaster management and intersectoral cooperation
There is intersectoral coordination in relation to four aspects of disaster management. So far as rescue isconcerned, the members of the Amateur Radio Association, armed forces, civil defence, fire brigade, policeand medical teams are in the front line. Medical emergency assistance involves health care, Red Cross andambulance personnel. Rehabilitation involves the public works department, the armed forces, civil defenceand others. And relief concerns the social work department, Red Cross, civil defence and others.
The Indonesian Red Cross, the Indonesian Radio Amateur Association, the civil defence, the hospitalassociation, national search−and−rescue teams, the Indonesian armed forces and other organizations andsectors are all part of the disaster management programme.
Public health aspects of disaster management
According to our experience of disaster management in Indonesia, there is a direct correlation between healthproblems and the type of disaster. Some hazards have a more direct impact on human life and human healththan others. These require immediate action and medical response.
One potential indirect effect of a disaster can be an increase in transmission of communicable diseases.When people's homes are destroyed they are forced to seek shelter elsewhere. Overcrowding, lack of water,shortage of food and lack of sanitation facilities will cause increased exposure to disease and will lead todisease outbreaks. The overall public health effects of disasters can be summarized as follows:
− deaths and removal of corpses;− severe injuries which need immediate and extensive medical attention;− mild injuries which do not need special action;− outbreaks of communicable diseases;− psychosocial effects on the affected population;− famine;− movement of population.
The progress of disaster mitigation and its effects should be monitored by epidemiologic surveillance in orderto prevent secondary disasters (such as outbreaks of infectious diseases). Until now the collection andevaluation of disaster data have been inadequate for the needs of those engaged in evaluating disasterpreparedness and management. Improved evaluation and interdisciplinary collaboration is important inrefining disaster preparedness and management in Indonesia.
International cooperation
As yet there are no standard procedures for international assistance, i.e. for requesting other countries tosend disaster management teams or to transfer technology to the affected area in Indonesia.
Table 3.7. Summary of recent disasters in Indonesia
Disaster Location Date Number NumberVolcanic eruption Mt Kelud, Java 1919 5000Volcanic eruption Mt. Agung, Ball 1963 1584 78 000Drought famine Lombok 1966 80 000 212 000Flood Central Java 1967 160
119
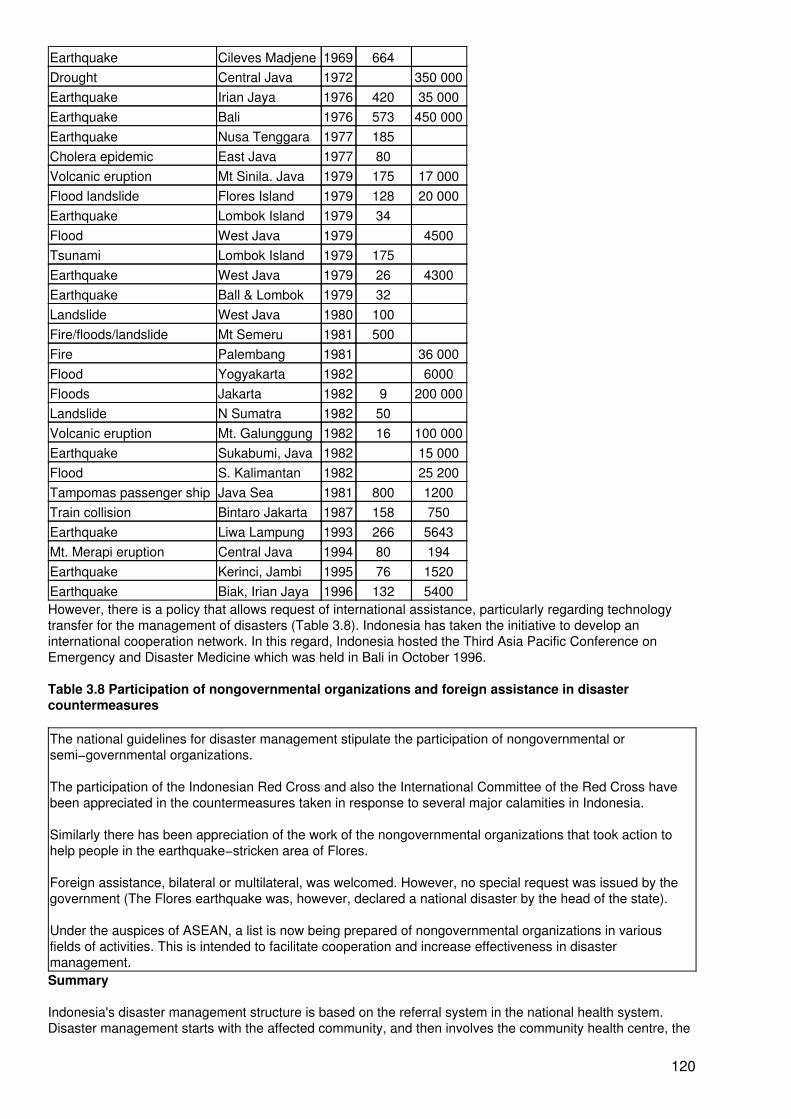
Earthquake Cileves Madjene 1969 664Drought Central Java 1972 350 000Earthquake Irian Jaya 1976 420 35 000Earthquake Bali 1976 573 450 000Earthquake Nusa Tenggara 1977 185Cholera epidemic East Java 1977 80Volcanic eruption Mt Sinila. Java 1979 175 17 000Flood landslide Flores Island 1979 128 20 000Earthquake Lombok Island 1979 34Flood West Java 1979 4500Tsunami Lombok Island 1979 175Earthquake West Java 1979 26 4300Earthquake Ball & Lombok 1979 32Landslide West Java 1980 100Fire/floods/landslide Mt Semeru 1981 500Fire Palembang 1981 36 000Flood Yogyakarta 1982 6000Floods Jakarta 1982 9 200 000Landslide N Sumatra 1982 50Volcanic eruption Mt. Galunggung 1982 16 100 000Earthquake Sukabumi, Java 1982 15 000Flood S. Kalimantan 1982 25 200Tampomas passenger ship Java Sea 1981 800 1200Train collision Bintaro Jakarta 1987 158 750Earthquake Liwa Lampung 1993 266 5643Mt. Merapi eruption Central Java 1994 80 194Earthquake Kerinci, Jambi 1995 76 1520Earthquake Biak, Irian Jaya 1996 132 5400However, there is a policy that allows request of international assistance, particularly regarding technologytransfer for the management of disasters (Table 3.8). Indonesia has taken the initiative to develop aninternational cooperation network. In this regard, Indonesia hosted the Third Asia Pacific Conference onEmergency and Disaster Medicine which was held in Bali in October 1996.
Table 3.8 Participation of nongovernmental organizations and foreign assistance in disastercountermeasures
The national guidelines for disaster management stipulate the participation of nongovernmental orsemi−governmental organizations.
The participation of the Indonesian Red Cross and also the International Committee of the Red Cross havebeen appreciated in the countermeasures taken in response to several major calamities in Indonesia.
Similarly there has been appreciation of the work of the nongovernmental organizations that took action tohelp people in the earthquake−stricken area of Flores.
Foreign assistance, bilateral or multilateral, was welcomed. However, no special request was issued by thegovernment (The Flores earthquake was, however, declared a national disaster by the head of the state).
Under the auspices of ASEAN, a list is now being prepared of nongovernmental organizations in variousfields of activities. This is intended to facilitate cooperation and increase effectiveness in disastermanagement.Summary
Indonesia's disaster management structure is based on the referral system in the national health system.Disaster management starts with the affected community, and then involves the community health centre, the
120
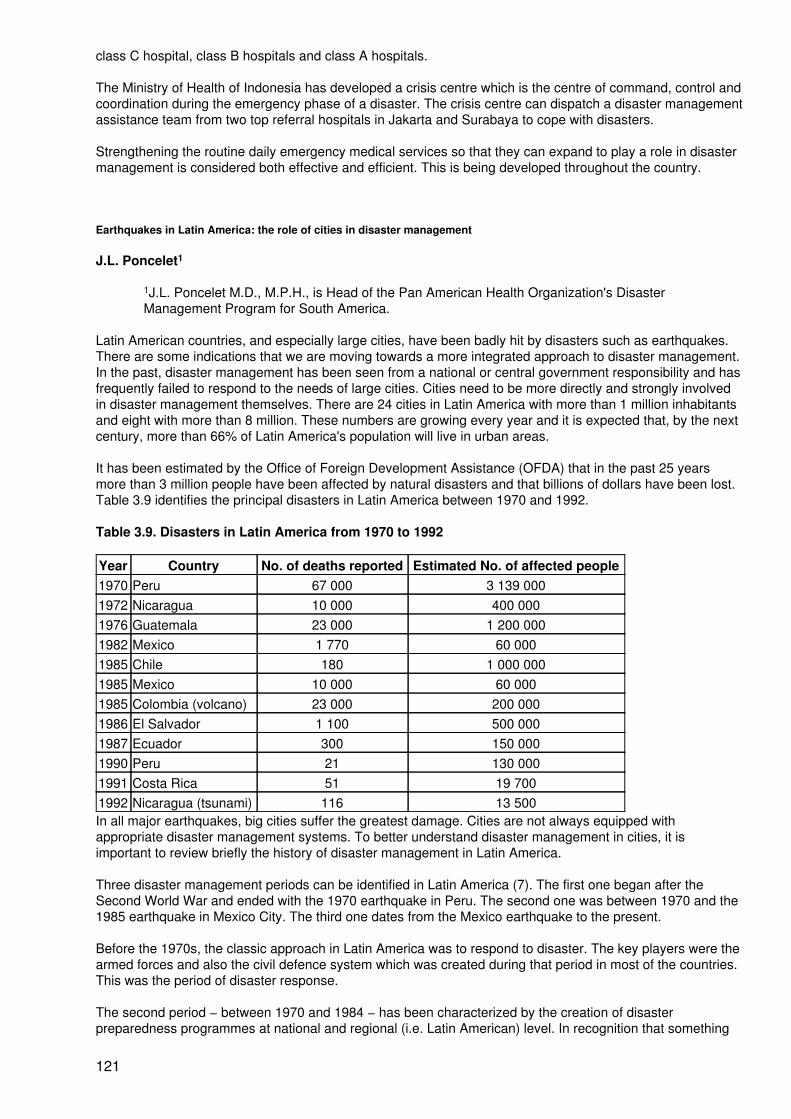
class C hospital, class B hospitals and class A hospitals.
The Ministry of Health of Indonesia has developed a crisis centre which is the centre of command, control andcoordination during the emergency phase of a disaster. The crisis centre can dispatch a disaster managementassistance team from two top referral hospitals in Jakarta and Surabaya to cope with disasters.
Strengthening the routine daily emergency medical services so that they can expand to play a role in disastermanagement is considered both effective and efficient. This is being developed throughout the country.
Earthquakes in Latin America: the role of cities in disaster management
J.L. Poncelet1
1J.L. Poncelet M.D., M.P.H., is Head of the Pan American Health Organization's DisasterManagement Program for South America.
Latin American countries, and especially large cities, have been badly hit by disasters such as earthquakes.There are some indications that we are moving towards a more integrated approach to disaster management.In the past, disaster management has been seen from a national or central government responsibility and hasfrequently failed to respond to the needs of large cities. Cities need to be more directly and strongly involvedin disaster management themselves. There are 24 cities in Latin America with more than 1 million inhabitantsand eight with more than 8 million. These numbers are growing every year and it is expected that, by the nextcentury, more than 66% of Latin America's population will live in urban areas.
It has been estimated by the Office of Foreign Development Assistance (OFDA) that in the past 25 yearsmore than 3 million people have been affected by natural disasters and that billions of dollars have been lost.Table 3.9 identifies the principal disasters in Latin America between 1970 and 1992.
Table 3.9. Disasters in Latin America from 1970 to 1992
Year Country No. of deaths reported Estimated No. of affected people1970 Peru 67 000 3 139 0001972 Nicaragua 10 000 400 0001976 Guatemala 23 000 1 200 0001982 Mexico 1 770 60 0001985 Chile 180 1 000 0001985 Mexico 10 000 60 0001985 Colombia (volcano) 23 000 200 0001986 El Salvador 1 100 500 0001987 Ecuador 300 150 0001990 Peru 21 130 0001991 Costa Rica 51 19 7001992 Nicaragua (tsunami) 116 13 500In all major earthquakes, big cities suffer the greatest damage. Cities are not always equipped withappropriate disaster management systems. To better understand disaster management in cities, it isimportant to review briefly the history of disaster management in Latin America.
Three disaster management periods can be identified in Latin America (7). The first one began after theSecond World War and ended with the 1970 earthquake in Peru. The second one was between 1970 and the1985 earthquake in Mexico City. The third one dates from the Mexico earthquake to the present.
Before the 1970s, the classic approach in Latin America was to respond to disaster. The key players were thearmed forces and also the civil defence system which was created during that period in most of the countries.This was the period of disaster response.
The second period − between 1970 and 1984 − has been characterized by the creation of disasterpreparedness programmes at national and regional (i.e. Latin American) level. In recognition that something
121
had to be done to improve disaster response at the national level, the civil defence organizations werestrengthened and disaster preparedness coordinators were designated in all the ministries of health. Thenational Red Cross Societies also began disaster preparedness programmes in most of the countries.Emergency drills and other disaster management activities started to become familiar to a larger sector ofsociety.
At regional level, the International Federation of Red Cross and Red Crescent Societies created a disastermanagement department. At the request of its general assembly, the Pan American Health Organization(PAHO), created a disaster management programme in 1976 with main financial support from Canada, laterfrom Japan and the United Kingdom; Belgium, France, Germany and the Netherlands now also participatesignificantly. This was the period of disaster preparedness.
The third period − from 1985 to the present − was influenced by the Mexico earthquake and the Nevado delRuiz volcanic eruption. The disaster preparedness officers realized after those major events that preparing acountry was not enough. Some measures had to be taken to reduce the vulnerability of society.
The health sector, which had been one of the best prepared for disaster, was terribly affected by the collapseof the Juarez Hospital in Mexico City, killing not only 295 patients but also the 266 health and administrativestaff (2). In addition, the hospital could not be used to treat the injured. It was clear that regardless of thepreparedness level of a hospital, its collapse would impede the provision of medical aid. The idea of disastermitigation began to take shape.
The International Decade for Natural Disaster Reduction and particularly the 1994 IDNDR conference inYokohama supported the idea of disaster mitigation. It was realized that reducing the impact of a disasterthrough mitigation and prevention would resolve most disaster−related problems. This was the disastermitigation and prevention period.
Each of the above three periods emphasized certain aspects of disaster management. The 1995 GreatHanshin−Awaji Earthquake gave Latin America the initial impression that disaster mitigation was useless.How could a developing country pretend to reduce its vulnerability if Japan failed to do so? A couple ofmonths later it appeared that the Great Hanshin−Awaji Earthquake did not represent the failure of disastermitigation in general but rather the failure of some aspects of it. Other components of disaster responseworked well but were not emphasized by the international press. For example, the existence of a buildingcode did not imply − even for one of the richest societies − that all existing buildings would be reinforcedimmediately. Therefore it had to be expected that buildings which remained vulnerable would collapse.
Another example was the absence of a full−time person in charge of coordinating sectoral preparedness inthe municipality of Kobe before the earthquake1. The Great Hanshin−Awaji Earthquake vigorouslydemonstrated that disaster mitigation could become meaningless if it was not part of a comprehensivedisaster management programme. It also highlighted the importance of appropriate involvement of the cityauthorities.
1Personal conversation with city officials after the 1995 Kobe earthquake.
The disaster management community in Latin America felt that it was an opportune time to evaluate moreprecisely the status of their efforts, as was done recently for the Andean region (Table 3.10). They also startedthinking of ways to improve not only each classic aspect of disaster management (such as disaster response,preparedness and mitigation) but also disaster management per se by ensuring stronger coordination amongall disaster management areas.
One solution is to identify disaster managers: people who have the confidence of the top political level, whohave been trained and who have some disaster experience. In addition, a disaster manager should be able tounderstand and coordinate the work of various disaster specialists and other experts. Coordination of theseexperts is essential in order for disaster management to have a greater impact. There should be disastermanagers at both national and local levels.
Colombia, Costa Rica and Mexico have created or modified their institutions during the last 10 years in orderto establish a body with an overall perspective of disaster management in society. These institutions cover amuch wider spectrum of concerns than the classic civil defence mandate which concentrated primarily on anefficient response. These extremely positive initiatives encourage the integration of different sectors ofsociety. However, these national disaster coordination units are not able to respond to all problems. One ofthe major prerequisites for their efficiency is the existence of a good disaster management network in large
122

cities and elsewhere in the country, and another is the political will in the ministries and in local government.
Following an earthquake in a remote area of Colombia in 1994, it took some time to organize the response. Asimilar problem was observed in the Great Hanshin−Awaji Earthquake where the authorization of centralgovernment was required to mobilize important resources.
That issue is not specific to disaster. Most Latin American governments feel that some kind of decentralizationmust take place in order to offer a more flexible and more rapid response to local problems. Several movesare taking place along these lines. The top priority of the Andean Ministers of Health is the reform of thehealth sector which is driven by the decentralization process. A meeting of health secretaries of LatinAmerican municipalities is foreseen for June 1997. In March, representatives of municipalities of CentralAmerica met in Panama to analyse the role of mayors in disaster management.
A number of national disaster management entities are looking at strengthening their units in large cities aswell as at the provincial level, not only in the area of response but also in disaster mitigation. Peru's civildefence organization is providing access to Internet to their provincial offices. In Argentina and Brazil, theprovinces are the first responders to disaster and the central level intervenes only on request.
Table 3.10. Status of disaster management in the Andean region, December 1996
Bolivia Chile Columbia Ecuador Peru VenezuelaInstitutional CapacityProgramme Name [2] [4] [5] [6] [8] [10]Full−time staff 1 7 4 5 8 5Budget in US$ 00 NR 1 300 000 65 583 26 000 NRPosition Director
GeneralMinisterCabinet
MinistryDirection
DirectorGeneral
Minister Cabinet MinisterCabinet
PreparationsLast sectoral plan update 1996 1989 1996 1996 1996 NRLast provincial planupdate
NR 1996 1996 1996 1996 NR
% of hospitals withdisaster plan updated
NR 26% in1996
46% 26% 50% Yes 18%
% of hospitals with drill 3% 80% 20% 14% 100% Yes 9%% of hospitals withprehospital drill
0% NR 20% 0% 10% Yes NR
MitigationVulnerability analysis, Noof hospitals
No 14/26 41 in progress
16 12 15
No of refurbishedhospitals
No 1/26 3 0 1 2/11
Disaster building code NR Si Yes, 1984Update 1996
In progress Yes Yes
Inclusion of mitigation inMinistry of Health workplan
Yes NR Yes Yes Yes NR
TrainingFaculty withpostgraduate training
9 University No 3 postgraduate Medicine Medicine NursingEngineering
NR
University training >40hours
NR Yes NR Yes NR Yes 10 Yes 5 University Yes NR
No of civil servantstrained
80 Yes NR 800 Yes 25 Yes 600 Yes NR
Source: Information provided by Ministry of Health representatives at the VIII Health DisasterCoordinators Meeting, México, 1996.
123
[2] Política Nacional de Salud para Atención en Casos de Desastre, Bolivia[4] Departamento de Asuntos de Emergencia y Catástrofes, Chile[5] SubDirección de Urgencias, Emergencias y Desastres, Colombia[6] Dirección de Planeamiento de la Seguridad para el Desarrollo, Ecuador[8] Dirección Nacional de Preparación contra Desastres, Perú[10] Oficina de Defensa Civil, Ministerio de Sanidad y Asistencia Social, Venezuela.NR: Not Reported
Large cities have specific problems. Buenos Aires in Argentina and Sao Paolo in Brazil, which have more than12 million inhabitants each, are affected by major flooding which is the result of lack of planning as the citieshave grown. The sewerage systems cannot cope with the quantity of water draining from roofs and roads.Disaster response time has increased in a number of cities such as Rio de Janeiro or Santiago de Chile dueto traffic problems. New emergency response systems are being developed in those cities to reach the injuredmore quickly by better distributing disaster response resources throughout the cities and by improving thestandard of disaster response personnel.
Water distribution systems are an increasing problem in cities in Latin America. For several months, a largesector of Santiago de Chile has suffered water shortages. More and more water sources are further from largecities and therefore more vulnerable to disasters. After the 1985 Mexico City earthquake more than 2 millionpersons were without water.
Hospitals are becoming more vulnerable due to the lack of maintenance. Most hospitals were built before therecent efforts to review building codes in the light of existing hazards. The 1996 International Conference onHospital Vulnerability Reduction was an opportunity to demonstrate the cost−effectiveness of disastermitigation and to obtain the commitment of national authorities.
Latin America is strengthening its economy through industrialization. Most of this takes place in large citiesdue to the availability of manpower there. Cities are becoming surrounded and overcrowded by industrialparks. Access is difficult and the risk of accidents (whether linked to earthquakes or not) is increasing daily aslegislation is often inadequate to deal with the situation. This may be a new challenge for large Latin Americancities in the next century.
Lifelines are another critical issue. For several years the towns of Quito and Guayaquil, Ecuador havesuffered power shortages. Around 60% of the power generated in Ecuador comes from one hydroelectricplant. In 1993 a large−scale landslide blocked the river upstream from the dam and seriously reduced itscapacity by filling it with large quantities of debris and soil.
Big cities need specific solutions which must be identified with their own resources. Central government canensure coordination in the area of norms, laws and general procedures but the cities themselves are closer tothe reality and must improve their disaster management capability. In La Paz, Bolivia; Cali, Colombia andQuito, Ecuador; and in a number of other towns, the mayors decided to nominate a full−time person in chargeof disaster management. In Caracas, Venezuela, the mayor provided funds to reduce the vulnerability of poorareas of the city which are extremely vulnerable to landslides. In Valencia, the mayor set up an emergencyresponse unit that included firemen, physicians and police. That unit attends to daily emergencies but alsoincludes civil defence and other entities which are more specifically concerned with disaster response.
In the area of urban planning some isolated decisions have been taken to reduce vulnerability in cities.Managua, Nicaragua was completely reorganized after the 1972 earthquake in order to reduce the number ofhigh−rise buildings and facilitate road access. Lima, Peru drew−up microzonification maps. Guayaquil,Ecuador, created a committee to look at a building code which will be adapted to the city.
In some case the mayor does not always have the authority or the funds to respond to a disaster. He or shemay have to go to the central government to obtain an emergency budget. Caracas and Quito are now in theprocess of voting on a municipal law which will create a disaster management body and an emergency fundwhich could be used with flexibility in case of disaster.
Conclusion
Latin America has probably made the most progress in disaster management among the developingcountries. However, no system is perfect. Much has been accomplished in building a comprehensiveapproach to disaster management, but this approach has tended to focus on national concerns rather than onthose of the local authorities in spite of the fact that they are the ones closest to the impact of disaster.
124
Large cities in Latin America are vulnerable to many hazards and are exposed to a high degree of risk. Thisrisk has increased over the years due to the explosive growth of the cities.
Disasters in large cities, such as the earthquake in Mexico City in 1995, have influenced disastermanagement in the region. The Great Hanshin−Awaji Earthquake also reminded Latin America of the need forcomprehensive disaster management and for some level of responsibility to be given to the main cities.
The largest number of victims and the greatest losses after earthquakes are concentrated in the large cities.The mayor of a large city should be seen as having overall responsibility for disaster management for his city;he may assume this function himself or delegate it to a preassigned, capable person, like the local fire chief.National and international institutions should therefore strongly support a more direct participation of localauthorities in disaster management.
References
1. A world safe from natural disasters. Washington, DC, Pan American Health Organization,1994.
2. Cronicas de Desastres. Washington, DC, Pan American Health Organization, 1985.
Essential elements for community and hospital earthquake preparedness: summary of earthquake studies
E.A. Pretto1
1E.A. Pretto M.D., M.P.H, is Principal Investigator, Disaster Reanimatology Study Group andAssociate Director, Safar Center for Resuscitation Research, University of Pittsburgh Schoolof Medicine, Pittsburgh, USA.
Conceptual Framework
Health disasters can be defined as mass casualty events that overwhelm or destroy local emergency healthcare delivery systems. Until recently, "medical" response in disaster was limited to public health support ofuninjured survivors. Disaster medicine research was the domain solely of epidemiology and sociology.Earthquake research involved mostly preventive and structural engineering. Early observations of death inearthquakes suggested there might be a population of victims who survive the initial impact but who die hoursor days later from life−threatening injuries and delay in emergency medical care. We theorized that asignificant proportion of these deaths could be prevented with more rapid and better organized resuscitationefforts starting with uninjured co−victims giving the first assistance.
Armenia
The Pittsburgh Group initiated the first interdisciplinary evaluation study of a catastrophe earthquake (1−3). Amajor lesson from this experience was that evaluation of the medical response in a disaster is indeed feasiblealthough complex.
Costa Rica
In this study, a research team conducted a survey of lay survivors and health care professionals whoresponded on 22 April 1991 (4,5). Fifty−four deaths occurred prior to hospitalization (crude death rate =0.4/1000 pop.). Seventeen per cent of these deaths (9/54) were in casualties who survived the initial impactbut died at the scene or while being transported. Twenty−two per cent (2/9) of deaths were judgedpreventable if earlier emergency medical care had been available. Autopsies performed on victims revealedcrush injury as the cause of death. The rapid institution of life−supporting first aid and pre−hospital emergencymedical care would have had significant life−saving potential but was not initiated in a timely manner.
Turkey
In this study, we described mortality and its relationship to building collapse patterns and initial medicalresponse following the earthquake of 12 March 1992 (6). Among 54 witnessed deaths, 55% (n = 28) of thevictims had died slowly, most of whom (n = 26) were pinned or trapped. Medical aid and search−and−rescue
125
arrived after most deaths had occurred. Life−saving first aid and rescue training increased the success ofrescue efforts and could have improved survival. A large proportion of the victims died at the scene of injury.
Japan
The health consequences of tsunamis have not been fully investigated. We conducted a survey amongsurvivors of the 12 July 1993 earthquake−tsunami that affected Okushiri Island (7). The survey yielded dataon a total of 136 people. Among these, 17 were near−drowning survivors and 11 died from drowning. Age,female sex and prior earthquake−related injury (but not geographic location) were important risk factors fordeath. Rescue efforts were hampered by tsunamis which struck coastal villages minutes after the earthquake,causing landslides that blocked roads. A surprisingly large number of victims survived near−drowning. Factorsthat hampered people's ability to rapidly evacuate low−lying coastal areas hit by the tsunami greatly reducedchances of survival.
Summary
Our data suggest that for emergency medical response to be effective (life−saving), it must rely heavily onprofessionals and non−professionals in the local community. Therefore, a significant percentage of apopulation at risk must be educated and trained to respond. Likewise, health care providers at risk should alsobe trained in health disaster management. This assumption is based on the fact that there will not be enoughprofessional rescuers available to respond appropriately to prevent unnecessary deaths.
Conclusion
We strongly encourage the teaching of life−saving first aid to all people, starting in kindergarten andcontinuing into adulthood as part of the training and licensing process for drivers. Because these skills haverelevance for everyday emergencies, and since earthquakes occur infrequently, training must focus on theeveryday emergency response of bystanders. Currently, populations at risk are vulnerable due to lack ofpreparedness. Gaining support for preparedness or mitigation programmes is difficult due to the infrequentnature of disasters, the lack of resources or awareness of risk, and apathy. To overcome these obstacles,health ministries, international health organizations and development agencies must coordinate efforts toestablish a consensus and implement a global strategy of earthquake preparedness, mitigation and response.
References
1. Klain M, Ricci E, Safar P, Semenov V, Pretto E, et al. Prehospital and disaster medicine, 1989,4:135−152.
2. Ricci E, Pretto E, Safar P. Prehospital and disaster medicine 1991, 6(2): 159−166.
3. Pretto E, Ricci E, Safar P, et al. Prehospital and disaster medicine, 1992, 7(4):327−338.
4. Pretto E, Angus D, Abrams J, et al. Prehospital and disaster medicine, 1994, 9:96−106.
5. Bissell RRA, Pretto EA, Angus DC, et al. Prehospital and disaster medicine, 1994, 9:107−117.
6. Angus DC, Pretto E, Abrams J, et al. Epidemiologic assessment of earthquake mortality, building collapsepattern, and medical response after the 13 March 1992 earthquake in Erzincan, Turkey. Prehospital andDisaster Med, in press, July−September, 1997.
7. Pretto E, Kai T. Watoh Y, et al. (unpublished data).
The system of emergency medical care in disasters and catastrophes in Armenia
A.M. Minasyan1
1A.M. Minasyan Ph.D. is Chairman of the Emergency Medical Scientific Centre and Chief ofthe Emergency School, National Institute of Health, Yerevan, Republic of Armenia.
Scientifically based and efficient organization of emergency medical care is considered to be a decisive factorin saving the lives of victims in disasters and catastrophes. During the first hour after a disaster occurs, the
126
three phases of disaster medicine management must be organized. Because it is difficult to estimate thenumber of victims and casualties, a situational evaluation should be included in the first phase. On the basisof this, the second and third phases of disaster management can be made more effective. I define the threephases as follows:
1. Organizational−methodological phase: At this stage all disaster medicine activities in thewake of the disaster are planned and organized.
2. Regional phase: This phase is most important to mitigate disasters which can strikeanywhere. It concerns the local process of eliminating the consequences of disaster and issupported by provisions from the first phase.
3. Primary phase: This is the phase during which individuals and organizations performspecific, urgent functions in extreme situations at the site of the disaster.
The first two phases of disaster medicine management are implemented by the Disaster Committee of theMinistry of Health of Armenia.
Since the elimination of the consequences of disaster is a complex business, calling for special skills andequipment and highly specialized rescue teams, disaster medicine is understandably a national concern. In allthe republics of the former Soviet Union, the provision of emergency medical care following disasters was theresponsibility of the medical branch of the civil defence organization. In practice, this was not very successful,as became clear after the accident at the Chernobyl nuclear power station in 1986 and after the Spitakearthquake in Armenia in 1988. Shortly after these events, special committees for dealing with extremesituations were set up.
With a view to developing an efficient structure for disaster medicine modeled on local disaster needs, a studyof data on the Spitak earthquake was carried out. This study has resulted in disaster medicine in Armeniahaving the following four main directions:
− provision of qualified medical care, with provision of specialized care as close as possible tothe disaster zone;
− coordination of the work of emergency medical teams with damage repair and rescueservices;
− use of specialized ground and air transport to evacuate casualties to hospitals with differentservices;
− identification of medical institutions that are in a position of deliver specialized medical care,and of those institutions that can be turned into specialized hospitals in the shortest time.
Currently, the structure of the disaster medicine service in Armenia has three levels: federal government, theDisaster Committee of the Ministry of Health, and the emergency services. The activities of disaster medicineinclude specific response to the above four items which were studied. One such example is the plan formoving ambulance staff from Yerevan and from nearby regions to the site of a disaster, together withquick−response medical teams.
Our investigations of the health care resources and skills available in Yerevan and other parts of the republic,our review of numerous studies on the medical consequences of disaster (including the Spitak earthquake in1988), and an assessment of the risk factors characteristic of Armenia, all led us to the conclusion that almostall catastrophes and natural disasters in Armenia will be accompanied by numerous casualties. In thisconnection, our suggestions for central disaster medical services are near to the maximum of what canmeaningfully be dispatched to a local geographically limited situation.
As the result of our studies, we recommended the following measures to the Ministry's Disaster Committee:
− to consider the suggested structure and conceptual approaches of disaster medicine andobtain concurrence, where necessary, from the Government of the Republic of Armenia;
− to integrate emergency medical services with rescue service and civil defence servicesusing the Emergency Medical Scientific Centre and ambulance stations in Yerevan and
127
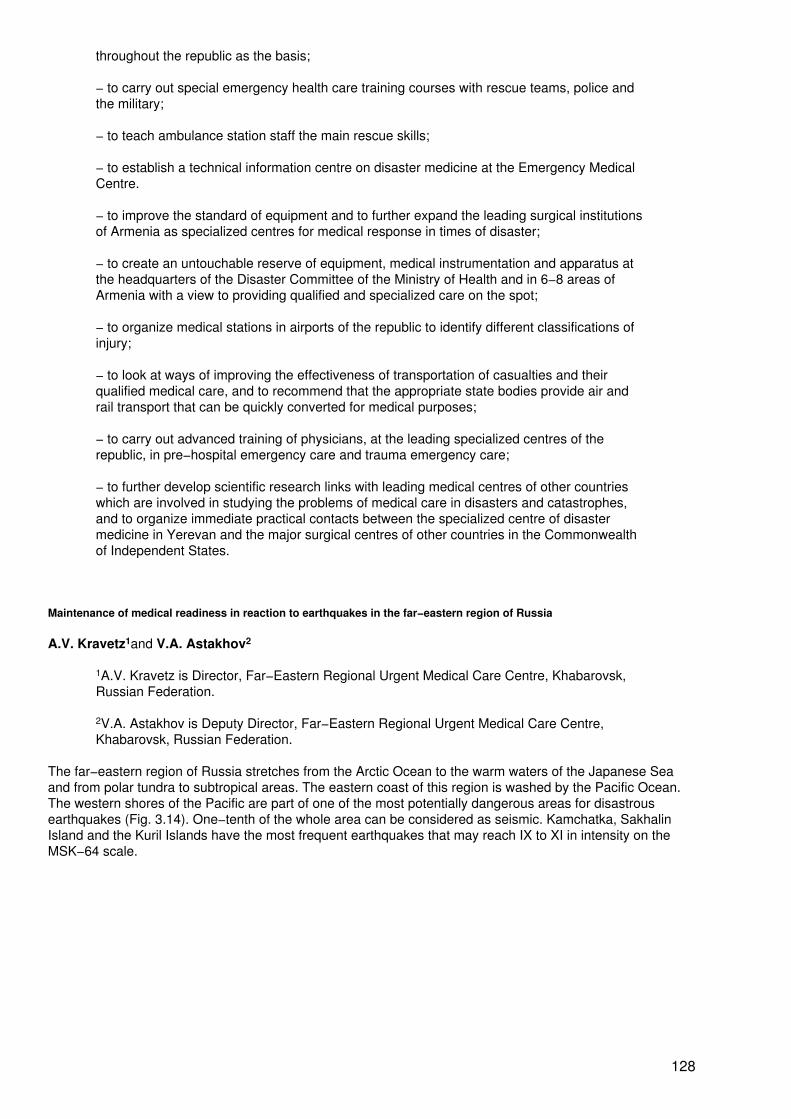
throughout the republic as the basis;
− to carry out special emergency health care training courses with rescue teams, police andthe military;
− to teach ambulance station staff the main rescue skills;
− to establish a technical information centre on disaster medicine at the Emergency MedicalCentre.
− to improve the standard of equipment and to further expand the leading surgical institutionsof Armenia as specialized centres for medical response in times of disaster;
− to create an untouchable reserve of equipment, medical instrumentation and apparatus atthe headquarters of the Disaster Committee of the Ministry of Health and in 6−8 areas ofArmenia with a view to providing qualified and specialized care on the spot;
− to organize medical stations in airports of the republic to identify different classifications ofinjury;
− to look at ways of improving the effectiveness of transportation of casualties and theirqualified medical care, and to recommend that the appropriate state bodies provide air andrail transport that can be quickly converted for medical purposes;
− to carry out advanced training of physicians, at the leading specialized centres of therepublic, in pre−hospital emergency care and trauma emergency care;
− to further develop scientific research links with leading medical centres of other countrieswhich are involved in studying the problems of medical care in disasters and catastrophes,and to organize immediate practical contacts between the specialized centre of disastermedicine in Yerevan and the major surgical centres of other countries in the Commonwealthof Independent States.
Maintenance of medical readiness in reaction to earthquakes in the far−eastern region of Russia
A.V. Kravetz1and V.A. Astakhov2
1A.V. Kravetz is Director, Far−Eastern Regional Urgent Medical Care Centre, Khabarovsk,Russian Federation.
2V.A. Astakhov is Deputy Director, Far−Eastern Regional Urgent Medical Care Centre,Khabarovsk, Russian Federation.
The far−eastern region of Russia stretches from the Arctic Ocean to the warm waters of the Japanese Seaand from polar tundra to subtropical areas. The eastern coast of this region is washed by the Pacific Ocean.The western shores of the Pacific are part of one of the most potentially dangerous areas for disastrousearthquakes (Fig. 3.14). One−tenth of the whole area can be considered as seismic. Kamchatka, SakhalinIsland and the Kuril Islands have the most frequent earthquakes that may reach IX to XI in intensity on theMSK−64 scale.
128
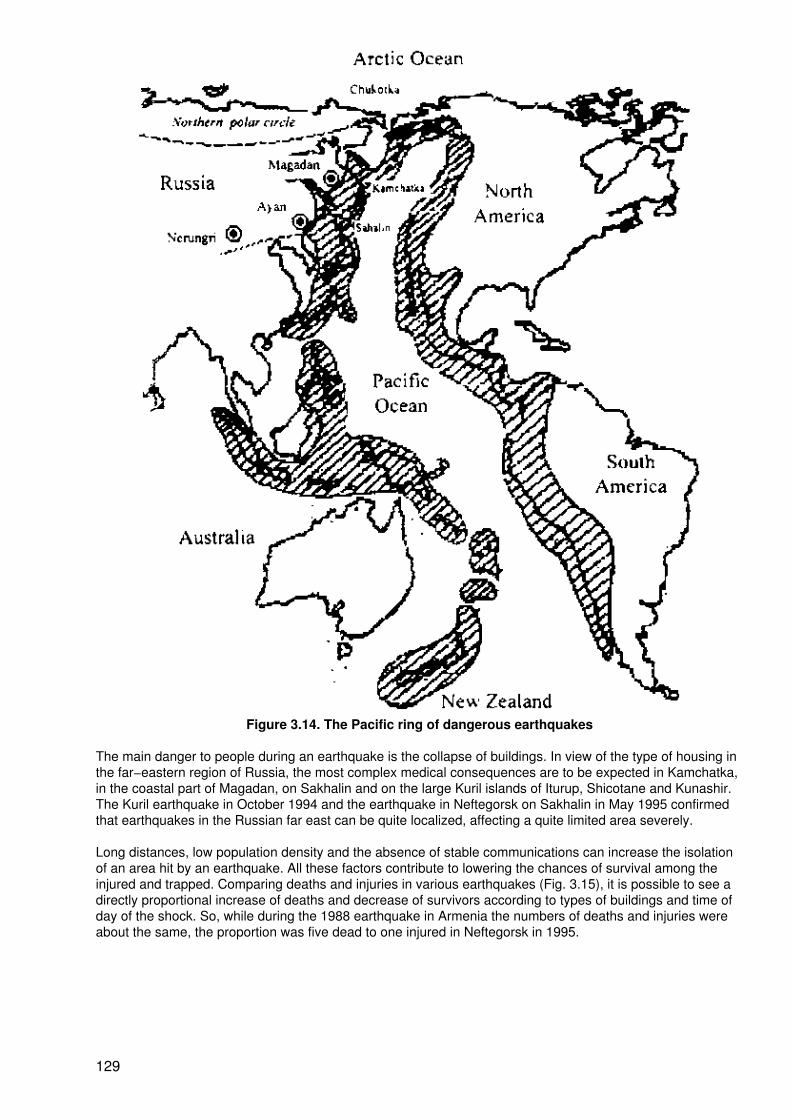
Figure 3.14. The Pacific ring of dangerous earthquakes
The main danger to people during an earthquake is the collapse of buildings. In view of the type of housing inthe far−eastern region of Russia, the most complex medical consequences are to be expected in Kamchatka,in the coastal part of Magadan, on Sakhalin and on the large Kuril islands of Iturup, Shicotane and Kunashir.The Kuril earthquake in October 1994 and the earthquake in Neftegorsk on Sakhalin in May 1995 confirmedthat earthquakes in the Russian far east can be quite localized, affecting a quite limited area severely.
Long distances, low population density and the absence of stable communications can increase the isolationof an area hit by an earthquake. All these factors contribute to lowering the chances of survival among theinjured and trapped. Comparing deaths and injuries in various earthquakes (Fig. 3.15), it is possible to see adirectly proportional increase of deaths and decrease of survivors according to types of buildings and time ofday of the shock. So, while during the 1988 earthquake in Armenia the numbers of deaths and injuries wereabout the same, the proportion was five dead to one injured in Neftegorsk in 1995.
129
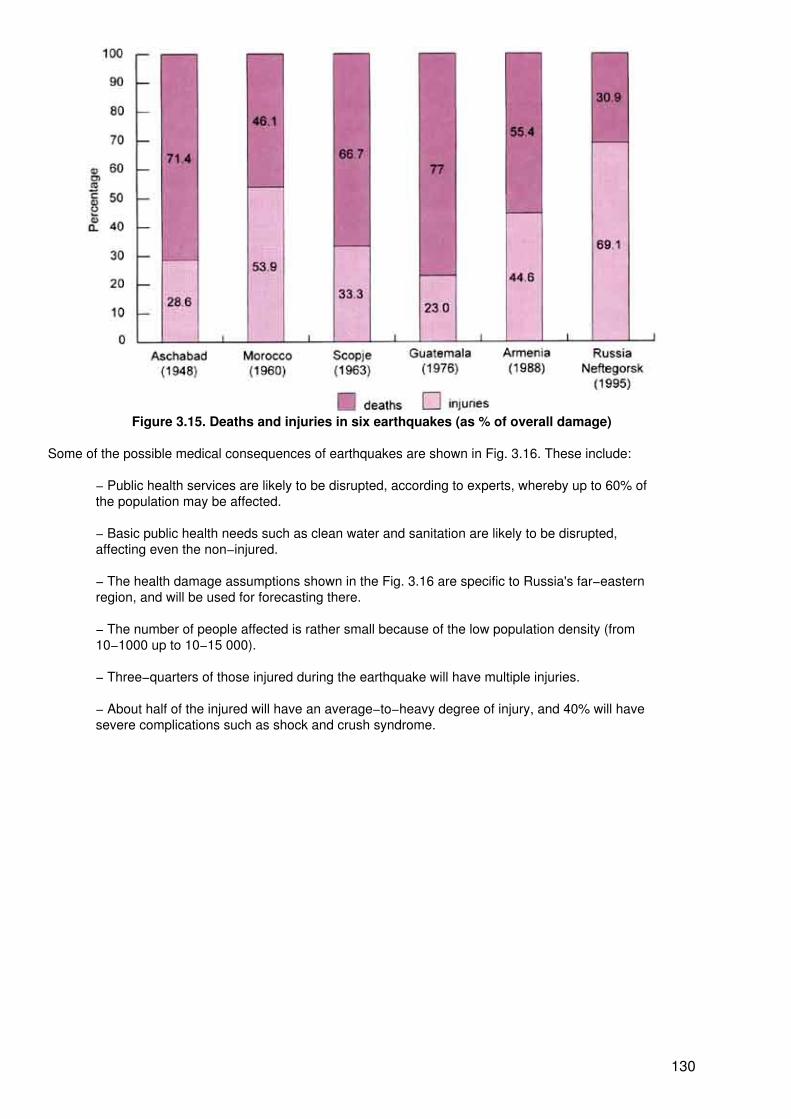
Figure 3.15. Deaths and injuries in six earthquakes (as % of overall damage)
Some of the possible medical consequences of earthquakes are shown in Fig. 3.16. These include:
− Public health services are likely to be disrupted, according to experts, whereby up to 60% ofthe population may be affected.
− Basic public health needs such as clean water and sanitation are likely to be disrupted,affecting even the non−injured.
− The health damage assumptions shown in the Fig. 3.16 are specific to Russia's far−easternregion, and will be used for forecasting there.
− The number of people affected is rather small because of the low population density (from10−1000 up to 10−15 000).
− Three−quarters of those injured during the earthquake will have multiple injuries.
− About half of the injured will have an average−to−heavy degree of injury, and 40% will havesevere complications such as shock and crush syndrome.
130
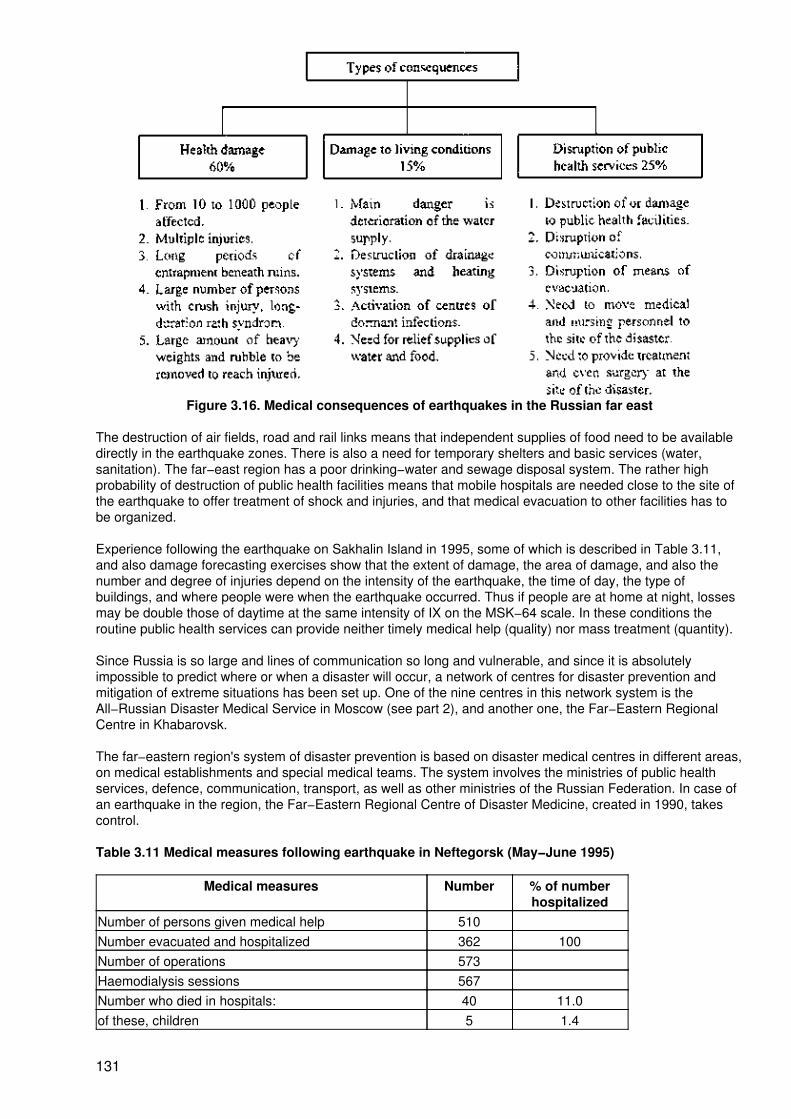
Figure 3.16. Medical consequences of earthquakes in the Russian far east
The destruction of air fields, road and rail links means that independent supplies of food need to be availabledirectly in the earthquake zones. There is also a need for temporary shelters and basic services (water,sanitation). The far−east region has a poor drinking−water and sewage disposal system. The rather highprobability of destruction of public health facilities means that mobile hospitals are needed close to the site ofthe earthquake to offer treatment of shock and injuries, and that medical evacuation to other facilities has tobe organized.
Experience following the earthquake on Sakhalin Island in 1995, some of which is described in Table 3.11,and also damage forecasting exercises show that the extent of damage, the area of damage, and also thenumber and degree of injuries depend on the intensity of the earthquake, the time of day, the type ofbuildings, and where people were when the earthquake occurred. Thus if people are at home at night, lossesmay be double those of daytime at the same intensity of IX on the MSK−64 scale. In these conditions theroutine public health services can provide neither timely medical help (quality) nor mass treatment (quantity).
Since Russia is so large and lines of communication so long and vulnerable, and since it is absolutelyimpossible to predict where or when a disaster will occur, a network of centres for disaster prevention andmitigation of extreme situations has been set up. One of the nine centres in this network system is theAll−Russian Disaster Medical Service in Moscow (see part 2), and another one, the Far−Eastern RegionalCentre in Khabarovsk.
The far−eastern region's system of disaster prevention is based on disaster medical centres in different areas,on medical establishments and special medical teams. The system involves the ministries of public healthservices, defence, communication, transport, as well as other ministries of the Russian Federation. In case ofan earthquake in the region, the Far−Eastern Regional Centre of Disaster Medicine, created in 1990, takescontrol.
Table 3.11 Medical measures following earthquake in Neftegorsk (May−June 1995)
Medical measures Number % of numberhospitalized
Number of persons given medical help 510Number evacuated and hospitalized 362 100Number of operations 573Haemodialysis sessions 567Number who died in hospitals: 40 11.0of these, children 5 1.4
131
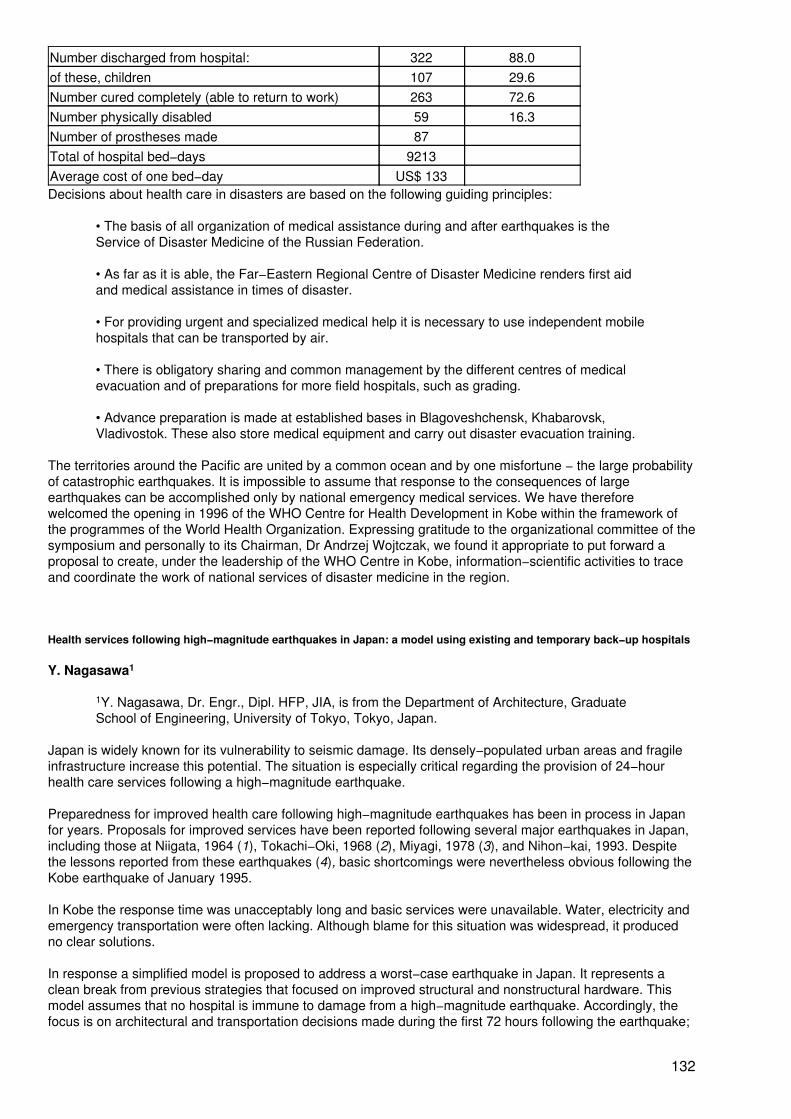
Number discharged from hospital: 322 88.0of these, children 107 29.6Number cured completely (able to return to work) 263 72.6Number physically disabled 59 16.3Number of prostheses made 87Total of hospital bed−days 9213Average cost of one bed−day US$ 133Decisions about health care in disasters are based on the following guiding principles:
• The basis of all organization of medical assistance during and after earthquakes is theService of Disaster Medicine of the Russian Federation.
• As far as it is able, the Far−Eastern Regional Centre of Disaster Medicine renders first aidand medical assistance in times of disaster.
• For providing urgent and specialized medical help it is necessary to use independent mobilehospitals that can be transported by air.
• There is obligatory sharing and common management by the different centres of medicalevacuation and of preparations for more field hospitals, such as grading.
• Advance preparation is made at established bases in Blagoveshchensk, Khabarovsk,Vladivostok. These also store medical equipment and carry out disaster evacuation training.
The territories around the Pacific are united by a common ocean and by one misfortune − the large probabilityof catastrophic earthquakes. It is impossible to assume that response to the consequences of largeearthquakes can be accomplished only by national emergency medical services. We have thereforewelcomed the opening in 1996 of the WHO Centre for Health Development in Kobe within the framework ofthe programmes of the World Health Organization. Expressing gratitude to the organizational committee of thesymposium and personally to its Chairman, Dr Andrzej Wojtczak, we found it appropriate to put forward aproposal to create, under the leadership of the WHO Centre in Kobe, information−scientific activities to traceand coordinate the work of national services of disaster medicine in the region.
Health services following high−magnitude earthquakes in Japan: a model using existing and temporary back−up hospitals
Y. Nagasawa1
1Y. Nagasawa, Dr. Engr., Dipl. HFP, JIA, is from the Department of Architecture, GraduateSchool of Engineering, University of Tokyo, Tokyo, Japan.
Japan is widely known for its vulnerability to seismic damage. Its densely−populated urban areas and fragileinfrastructure increase this potential. The situation is especially critical regarding the provision of 24−hourhealth care services following a high−magnitude earthquake.
Preparedness for improved health care following high−magnitude earthquakes has been in process in Japanfor years. Proposals for improved services have been reported following several major earthquakes in Japan,including those at Niigata, 1964 (1), Tokachi−Oki, 1968 (2), Miyagi, 1978 (3), and Nihon−kai, 1993. Despitethe lessons reported from these earthquakes (4), basic shortcomings were nevertheless obvious following theKobe earthquake of January 1995.
In Kobe the response time was unacceptably long and basic services were unavailable. Water, electricity andemergency transportation were often lacking. Although blame for this situation was widespread, it producedno clear solutions.
In response a simplified model is proposed to address a worst−case earthquake in Japan. It represents aclean break from previous strategies that focused on improved structural and nonstructural hardware. Thismodel assumes that no hospital is immune to damage from a high−magnitude earthquake. Accordingly, thefocus is on architectural and transportation decisions made during the first 72 hours following the earthquake;
132

special emphasis is given to decisions made during the first 12 hours.
Proposed Model
The proposed model is based on the available resources of three similarly−equipped state−of−the−arthospitals, each twinned with a pre−identified temporary back−up hospital, all directed by one administration(see Fig. 3.17). The intent is to serve most injured earthquake victims locally as well as continue service toexisting inpatients and outpatients. This approach is intended to limit both confusion and resourceexpenditures during this traumatic period.
The model assumes that, shortly after the earthquake, hospital A, nearest to the epicenter, is confirmed to beseverely damaged and must be completely evacuated. Adjacent hospital B meanwhile is confirmed to bepartially damaged and must be partially evacuated. The third hospital, hospital C, is considered to beundamaged. Accordingly, critical care inpatients from A are evacuated and transferred immediately byhelicopter (e.g. from National Self−Defence Forces) to C. Critical inpatients that cannot be well−served at Bare also transferred by helicopter to C.
Figure 3.17. Earthquake hospital model
Meanwhile, earthquake victims near to hospitals A and B are gathered at nearby designated open collectionpoints, accessible by helicopter, where triage is performed; critically−injured earthquake victims are alsotransferred by helicopter to C. All critical inpatients from A and B transferred to C are also to be admittedthere.
The obvious capacity problems which may result are to be alleviated by temporary backup hospitals to beprovided near each hospital (A, B, C) during the first 12−hour period, unless threatened by fire or otherpost−earthquake hazards. Each back−up hospital includes accommodation (e.g. a portable tent structure orexisting available space in a school or hospital); portable water supply; portable electricity generators;emergency medical supplies; trained doctors and nurses; and local volunteer navigators to assist in guidingthe injured. Medical services are provided at these same locations as well as they can be until they are fullyfunctional as back−up hospitals.
Accordingly, staff at hospital A are assumed to be occupied with total evacuation of their hospital, includingtransfer of critical patients to C and transfer of non−critical patients to their back−up hospital. In addition, thesestaff must sort and care for local earthquake victims, constituting a worst−case workload. At the same timestaff at hospital B are assumed to be occupied with existing services, partial evacuation, transfer of criticalinpatients to hospital C, and sorting and caring for local earthquake victims while erecting their back−uphospital. Medical staff at C meanwhile are assumed to be occupied with existing services, caring for incomingcritical patients from A and B, and erecting their back−up hospital.
By the end of the 12−hour period, hospital A is assumed to be completely evacuated and to have a fully
133
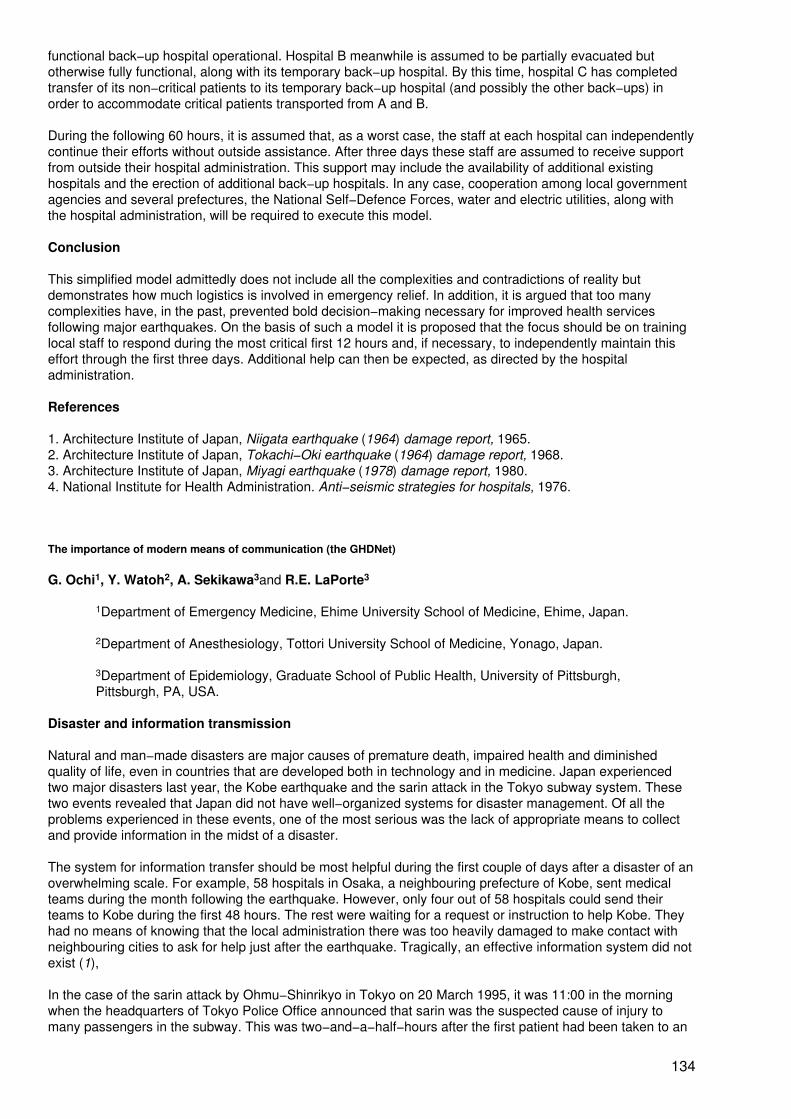
functional back−up hospital operational. Hospital B meanwhile is assumed to be partially evacuated butotherwise fully functional, along with its temporary back−up hospital. By this time, hospital C has completedtransfer of its non−critical patients to its temporary back−up hospital (and possibly the other back−ups) inorder to accommodate critical patients transported from A and B.
During the following 60 hours, it is assumed that, as a worst case, the staff at each hospital can independentlycontinue their efforts without outside assistance. After three days these staff are assumed to receive supportfrom outside their hospital administration. This support may include the availability of additional existinghospitals and the erection of additional back−up hospitals. In any case, cooperation among local governmentagencies and several prefectures, the National Self−Defence Forces, water and electric utilities, along withthe hospital administration, will be required to execute this model.
Conclusion
This simplified model admittedly does not include all the complexities and contradictions of reality butdemonstrates how much logistics is involved in emergency relief. In addition, it is argued that too manycomplexities have, in the past, prevented bold decision−making necessary for improved health servicesfollowing major earthquakes. On the basis of such a model it is proposed that the focus should be on traininglocal staff to respond during the most critical first 12 hours and, if necessary, to independently maintain thiseffort through the first three days. Additional help can then be expected, as directed by the hospitaladministration.
References
1. Architecture Institute of Japan, Niigata earthquake (1964) damage report, 1965.2. Architecture Institute of Japan, Tokachi−Oki earthquake (1964) damage report, 1968.3. Architecture Institute of Japan, Miyagi earthquake (1978) damage report, 1980.4. National Institute for Health Administration. Anti−seismic strategies for hospitals, 1976.
The importance of modern means of communication (the GHDNet)
G. Ochi1, Y. Watoh2, A. Sekikawa3and R.E. LaPorte3
1Department of Emergency Medicine, Ehime University School of Medicine, Ehime, Japan.
2Department of Anesthesiology, Tottori University School of Medicine, Yonago, Japan.
3Department of Epidemiology, Graduate School of Public Health, University of Pittsburgh,Pittsburgh, PA, USA.
Disaster and information transmission
Natural and man−made disasters are major causes of premature death, impaired health and diminishedquality of life, even in countries that are developed both in technology and in medicine. Japan experiencedtwo major disasters last year, the Kobe earthquake and the sarin attack in the Tokyo subway system. Thesetwo events revealed that Japan did not have well−organized systems for disaster management. Of all theproblems experienced in these events, one of the most serious was the lack of appropriate means to collectand provide information in the midst of a disaster.
The system for information transfer should be most helpful during the first couple of days after a disaster of anoverwhelming scale. For example, 58 hospitals in Osaka, a neighbouring prefecture of Kobe, sent medicalteams during the month following the earthquake. However, only four out of 58 hospitals could send theirteams to Kobe during the first 48 hours. The rest were waiting for a request or instruction to help Kobe. Theyhad no means of knowing that the local administration there was too heavily damaged to make contact withneighbouring cities to ask for help just after the earthquake. Tragically, an effective information system did notexist (1),
In the case of the sarin attack by Ohmu−Shinrikyo in Tokyo on 20 March 1995, it was 11:00 in the morningwhen the headquarters of Tokyo Police Office announced that sarin was the suspected cause of injury tomany passengers in the subway. This was two−and−a−half−hours after the first patient had been taken to an
134
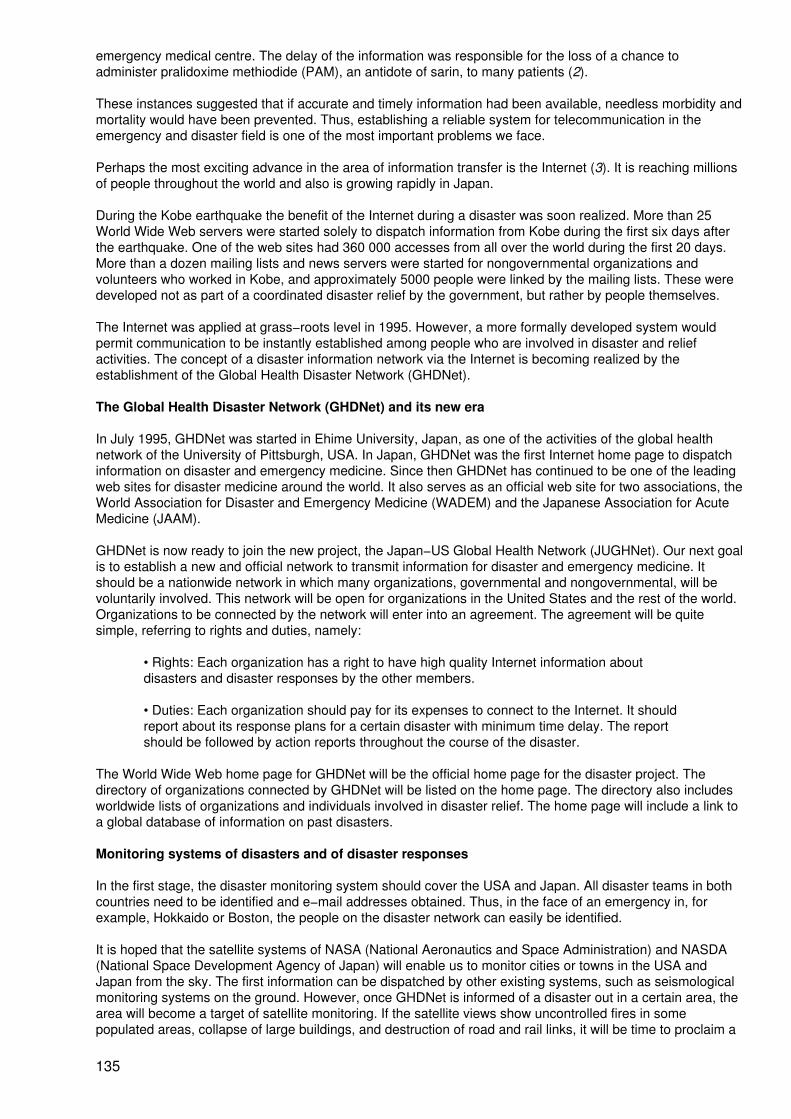
emergency medical centre. The delay of the information was responsible for the loss of a chance toadminister pralidoxime methiodide (PAM), an antidote of sarin, to many patients (2).
These instances suggested that if accurate and timely information had been available, needless morbidity andmortality would have been prevented. Thus, establishing a reliable system for telecommunication in theemergency and disaster field is one of the most important problems we face.
Perhaps the most exciting advance in the area of information transfer is the Internet (3). It is reaching millionsof people throughout the world and also is growing rapidly in Japan.
During the Kobe earthquake the benefit of the Internet during a disaster was soon realized. More than 25World Wide Web servers were started solely to dispatch information from Kobe during the first six days afterthe earthquake. One of the web sites had 360 000 accesses from all over the world during the first 20 days.More than a dozen mailing lists and news servers were started for nongovernmental organizations andvolunteers who worked in Kobe, and approximately 5000 people were linked by the mailing lists. These weredeveloped not as part of a coordinated disaster relief by the government, but rather by people themselves.
The Internet was applied at grass−roots level in 1995. However, a more formally developed system wouldpermit communication to be instantly established among people who are involved in disaster and reliefactivities. The concept of a disaster information network via the Internet is becoming realized by theestablishment of the Global Health Disaster Network (GHDNet).
The Global Health Disaster Network (GHDNet) and its new era
In July 1995, GHDNet was started in Ehime University, Japan, as one of the activities of the global healthnetwork of the University of Pittsburgh, USA. In Japan, GHDNet was the first Internet home page to dispatchinformation on disaster and emergency medicine. Since then GHDNet has continued to be one of the leadingweb sites for disaster medicine around the world. It also serves as an official web site for two associations, theWorld Association for Disaster and Emergency Medicine (WADEM) and the Japanese Association for AcuteMedicine (JAAM).
GHDNet is now ready to join the new project, the Japan−US Global Health Network (JUGHNet). Our next goalis to establish a new and official network to transmit information for disaster and emergency medicine. Itshould be a nationwide network in which many organizations, governmental and nongovernmental, will bevoluntarily involved. This network will be open for organizations in the United States and the rest of the world.Organizations to be connected by the network will enter into an agreement. The agreement will be quitesimple, referring to rights and duties, namely:
• Rights: Each organization has a right to have high quality Internet information aboutdisasters and disaster responses by the other members.
• Duties: Each organization should pay for its expenses to connect to the Internet. It shouldreport about its response plans for a certain disaster with minimum time delay. The reportshould be followed by action reports throughout the course of the disaster.
The World Wide Web home page for GHDNet will be the official home page for the disaster project. Thedirectory of organizations connected by GHDNet will be listed on the home page. The directory also includesworldwide lists of organizations and individuals involved in disaster relief. The home page will include a link toa global database of information on past disasters.
Monitoring systems of disasters and of disaster responses
In the first stage, the disaster monitoring system should cover the USA and Japan. All disaster teams in bothcountries need to be identified and e−mail addresses obtained. Thus, in the face of an emergency in, forexample, Hokkaido or Boston, the people on the disaster network can easily be identified.
It is hoped that the satellite systems of NASA (National Aeronautics and Space Administration) and NASDA(National Space Development Agency of Japan) will enable us to monitor cities or towns in the USA andJapan from the sky. The first information can be dispatched by other existing systems, such as seismologicalmonitoring systems on the ground. However, once GHDNet is informed of a disaster out in a certain area, thearea will become a target of satellite monitoring. If the satellite views show uncontrolled fires in somepopulated areas, collapse of large buildings, and destruction of road and rail links, it will be time to proclaim a
135
state of emergency. Each organization connected to GHDNet will start its response according to plansdecided beforehand.
In the second stage, disaster monitoring by NASA would be able to cover the whole world. The satelliteimages of disaster areas will be sent to some organizations connected to GHDNet. The information will helpthe organizations, national or international, governmental or nongovernmental, to react rapidly in sending theirteams to help people in the disaster area. Some Japanese organizations concerned with internationalassistance, such as Japan Disaster Relief (JDR), the Japan Red Cross (JRC), and the Association of MedicalDoctors of Asia (AMDA), will be good candidates for connecting to the international GHDNet.
Among the several components of GHDNet, transmission of information about disasters is one of the mostimportant. This is the mission assigned to GHDNet in Japan. GHDNet is expected to help individuals andorganizations, irrespective of country or official status, to communicate with each other in case of disaster.
References
1. Kai T. Disaster plans for hospitals. Emergency nursing (special edition). Spring 1996:176−9.
2. Shirakawa Y, Oguri K, Shintani S. An investigation of the information exchange in the Sarin attack in Tokyosubway system. Abstract of the Symposium in the 18th Annual Meeting of Japanese Association forToxicology, 1996.
3. Libman IM, LaPorte RE, Akazawa S, et al. The need for a global health disaster network. Prehospital anddisaster medicine, 1996, 16 (in press).
The problems of hygiene and sanitation after the Great Hanshin−Awaji Earthquake
K. Hayashi1, M. Inoue2and M. Shinya3
1K. Hayashi is Director of the Kobe Institute of Health, Bureau of Health and Welfare, Kobe,Japan.
2M. Inoue is Director of the Kobe Environmental Research Institute, Kobe, Japan.
3M. Shinya is Manager of the Ward Administration, General Affairs Bureau, Kobe, Japan.
We are alive and therefore we eat and excrete. However, people tend to forget the last part of ourmetabolism, probably because it is dirty, loathsome, dark, stinky, abhorrent and so on. Even after the greatHanshin−Awaji Earthquake, the initial reaction of people was to look for food and find a place to stay. Manyneglected the filthy part of human metabolism. But shortly after the shockwave, many people had acompelling urge to excrete. The question was: where?
After the earthquake, all flush toilets in downtown Kobe were out of service because sewage channels weretotally broken. Tapped water was stopped and there were no portable or mobile toilets in the initial phase ofthe aftermath. Over 300 000 people were accommodated in shelters in very unhygienic congested conditions.With few portable toilets available, they created a small mound of faeces in a few hours.
People struggled to arrange toilet facilities, but the next problems were how to dispose of the waste and keepthe toilet clean. Under these conditions, we feared the outbreak of the epidemics caused by toxigenic,bacterial and/or viral gastroenteritis. In fact, influenza started to prevail in the disaster areas. This reportproposes some ideas to improve sanitation and hygiene on the basis of lessons learned during and after theGreat Hanshin−Awaji Earthquake. It also describes preventive measures against epidemics of infectiousdisease at the site of a disaster.
Where can we excrete?
Immediately after the big shock, the tapped water supply in most of the downtown Kobe area stopped.Sewage channels were broken down (Fig. 3.18). Walls of the sedimenting pond in the Higashinada sewageplant were toppled and it temporarily used the nearby sea canal as a processing pond. People rushed toshelters such as schools, health centres, the City Hall or other big buildings because of fear of the aftershock
136
and to escape fire. In some places, more than 3000 people were in very congested dirty areas. Toilet basinsin the shelters were transformed into mounds of faeces one day after the disaster. People could not use thetoilet and some refugees became sick because the situation was so desperate. They ate very little and drankalmost nothing and were exhausted. In the night−time, the situation got worse. People tried to manage withoutgoing to excrete because they were afraid to disturb other people's sleep by getting up and finding their wayacross the very congested floor to the toilet. In the shelter, two persons to an area of 1.65 square metres wasnot uncommon during the night−time.
Figure 3.18. Map of damaged sewage channels (shaded areas)
People made great efforts to provide toilet facilities. Some dug a trough in the ground. Others tried to cleanflush toilets with buckets of water but this did not work long because of the broken sewage channels. Onesuccessful example is shown in Fig. 3.19 which is a toilet built on a manhole over the sewage channel. Unliketoilets with a bucket, this solved the problem of disposal and worked very well as long as the water in thechannel was running. On the basis of this experience, the Kobe city government has now prepared a type ofportable toilet that can be placed on the top of a manhole.
137

Figure 3.19. A toilet on a manhole over a sewage channel
Eventually many portable toilets were supplied. Initially the Kobe authorities estimated that 300 of them wouldbe enough, but in fact needed 3000 toilets, one for every 60−100 people (Fig. 3.20).
In the shelter, where good systematic management or initiative was established, people tried themselves toclean toilets and collected waste regularly without contaminating the area. They sprayed disinfectant andkilled odour. Many items useful for cleaning and disinfection were supplied and a number of volunteerscleaned toilets. This worked in those shelters where the management system functioned smoothly. However,in shelters, where the management was poorer or even non−existent, volunteers were not accepted or had ahard time to find a way to work with the homeless resulting in filthy toilets and contamination of thesurroundings.
138
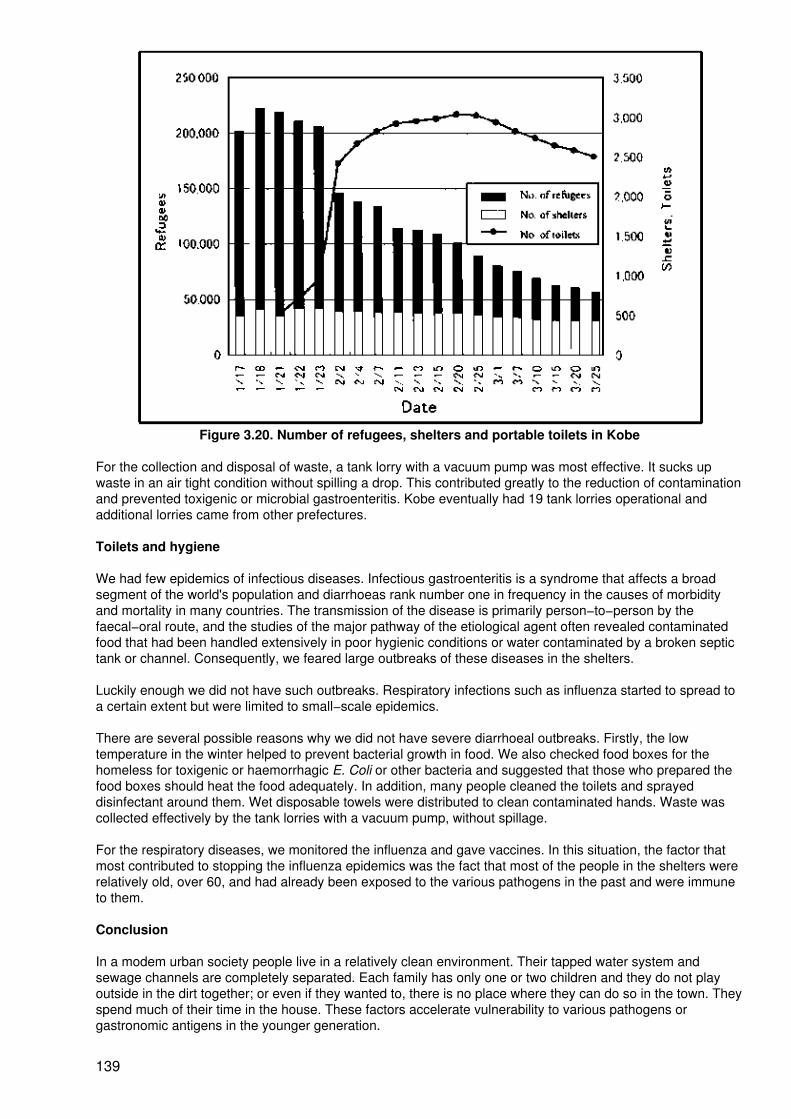
Figure 3.20. Number of refugees, shelters and portable toilets in Kobe
For the collection and disposal of waste, a tank lorry with a vacuum pump was most effective. It sucks upwaste in an air tight condition without spilling a drop. This contributed greatly to the reduction of contaminationand prevented toxigenic or microbial gastroenteritis. Kobe eventually had 19 tank lorries operational andadditional lorries came from other prefectures.
Toilets and hygiene
We had few epidemics of infectious diseases. Infectious gastroenteritis is a syndrome that affects a broadsegment of the world's population and diarrhoeas rank number one in frequency in the causes of morbidityand mortality in many countries. The transmission of the disease is primarily person−to−person by thefaecal−oral route, and the studies of the major pathway of the etiological agent often revealed contaminatedfood that had been handled extensively in poor hygienic conditions or water contaminated by a broken septictank or channel. Consequently, we feared large outbreaks of these diseases in the shelters.
Luckily enough we did not have such outbreaks. Respiratory infections such as influenza started to spread toa certain extent but were limited to small−scale epidemics.
There are several possible reasons why we did not have severe diarrhoeal outbreaks. Firstly, the lowtemperature in the winter helped to prevent bacterial growth in food. We also checked food boxes for thehomeless for toxigenic or haemorrhagic E. Coli or other bacteria and suggested that those who prepared thefood boxes should heat the food adequately. In addition, many people cleaned the toilets and sprayeddisinfectant around them. Wet disposable towels were distributed to clean contaminated hands. Waste wascollected effectively by the tank lorries with a vacuum pump, without spillage.
For the respiratory diseases, we monitored the influenza and gave vaccines. In this situation, the factor thatmost contributed to stopping the influenza epidemics was the fact that most of the people in the shelters wererelatively old, over 60, and had already been exposed to the various pathogens in the past and were immuneto them.
Conclusion
In a modem urban society people live in a relatively clean environment. Their tapped water system andsewage channels are completely separated. Each family has only one or two children and they do not playoutside in the dirt together; or even if they wanted to, there is no place where they can do so in the town. Theyspend much of their time in the house. These factors accelerate vulnerability to various pathogens orgastronomic antigens in the younger generation.
139

Therefore, to prevent epidemics of infectious diseases in future disasters, we have to survey people's immunestatus continually, and a proper vaccination programme has to be carried out by the public health sector of thelocal and/or central government. Clean, easy−to−handle portable toilets with a good disposal system have tobe developed. Each municipal government or public health sector has to prepare and stock these items foremergency use. In the shelters, a good management system has to be established.
The local health research institute has to monitor infectious agents in a disaster. For this purpose, it musthave anti−seismic biohazard facilities. We have developed a model of an anti−seismic biohazard room1 whichis designed to be retrofitted into an existing biohazard facility.
1Acknowledgment: We thank Mr Shigeru Toyoda, Takasago Research & DevelopmentCentre, and Kobe Shipyard & Engine Works, Mitsubishi Heavy Industries Co. Ltd. for thedevelopment of an anti−seismic biohazard room.
Summary
Immediately after the Great Hanshin−Awaji Earthquake, people faced the problems of where to excrete, howto keep toilets clean and how to dispose of waste. They struggled to make toilets. A tank lorry with a vacuumpump collected waste effectively without contaminating the area. Shelters where good management wasestablished were well organized and toilets were clean. Together with the low temperature in the winter, thesefactors contributed to prevent diarrhoeal diseases. Most of the people in the shelters were over 60, and thiswas also effective to a certain extent in preventing a large outbreak of influenza because many hadimmunities. Daily surveillance of the people's immune status and a vaccination programme are essential inthe preparation for future disasters.
Summary
E. Pretto1, C. Ugarte2, J. Levett3, Y. Oka4, K. Shoaf5and Secretariat
1E.A. Pretto M.D., M.P.H, is Principal Investigator, Disaster Reanimatology Study Group andAssociate Director, Safar Center for Resuscitation Research, University of Pittsburgh Schoolof Medicine, Pittsburgh, USA.
2C. Ugarte is Director, Direccion Nacional Preparacion contra Desastres, Lima, Peru.
3J. Levett is Director of International Affairs, National School of Public Health, Ministry ofHealth and Welfare, Athens, Greece.
4Y. Oka is a Research Associate from the Department of Architecture, University of Tokyo,Tokyo, Japan.
5K. Shoaf is from the Department of Community Health Sciences, School of Public Health,University of California, Los Angeles, USA.
Dr B. Mulyadi, Director for Private and Specialty Hospitals, Directorate General of Medical Care andSecretary of the Crisis Centre, Ministry of Health, Jakarta, Indonesia, presented a case study from his country.He explained the vulnerability factors that make his country one of the areas of the world most prone todisasters and described a comprehensive emergency management system for the health sector which is builton a model of "escalation" from daily routine emergencies to full−fledged disaster management. He alsotouched on the multisectoral distribution of roles and responsibilities and focused on those of the health sectorand the means it has to implement these tasks in collaboration with the military and volunteer organizations.He concluded that the main reason behind the success of the disaster management system in Indonesia is itsdecentralization to community level and its fully integrated approach from vulnerability reduction through thewhole range of emergency management.
Dr J.L. Poncelet, Head, Disaster Preparedness Program for South America, PAHO/WHO, Quito, Ecuador,spoke about the impact of earthquakes on Latin American countries and cities and the development ofmanagement policies being adopted in those countries. The emphasis has shifted over the years fromdisaster response to preparedness and now to mitigation. In this development it was found that plans forpreparedness often existed but failed because of lack of skills or clearly defined responsibilities. Also, the
140

increasing specialization among disaster experts creates new problems of coordination for preparedness.Within this coordination, tasks should be delegated to each sector which will have its own responsibilities.
He stated that the emphasis for disaster management is also changing from the national to the regional andcommunity level. Waiting for government orders before reacting and employing resources is a frequent anddeadly phenomenon after disasters. Local authorities, such as the mayor, should be empowered to make thenecessary decisions, based on local input and timing. He also stated that natural disasters are not really allthat natural because a large part of the vulnerability is created by humanity. In the future, nationalmechanisms must be adapted to this delegation of authority, and managerial functions at different levelsshould be defined. Training programmes should include behavioural aspects during disasters. However,obtaining support from the top political level remains important and should be obtained with information,training and involvement.
In the brief discussion on this paper it was re−emphasized by Dr Poncelet that medical and public healthspecialists, as well as those from other sectors, have to speak to politicians and administrators to obtain theirconcurrence and support ahead of the disaster. Dr Goncharov added that politicians want to save and notspend money; some would rather wait until the disaster happens.
Dr E. Pretto presented a poster entitled "Essential elements for community and hospital earthquakepreparedness". Health disasters can be defined as mass casualty events that overwhelm or destroy localemergency health care delivery systems. Until recently, "medical" response in disaster was limited to publichealth support of uninjured survivors. Disaster medicine research was the domain solely of epidemiology andsociology. Earthquake research involved mostly preventive and structural engineering. Early observations ofdeath in earthquakes suggested there might be a population of victims who survive the initial impact but whodie hours to days later from life−threatening injuries and a delay in receiving emergency medical care. It wassuggested that a significant proportion of these deaths could be prevented with more rapid and betterorganized resuscitation efforts starting with uninjured co−victims as the ones giving the initial help.
The chairperson (poster session rapporteur) comments that mass training in first aid of the communities atrisk is an important idea, but that it has largely been untested. Little research into the effectiveness of traininglay persons in first aid has been done. The little research that does exist indicates that training may not besufficient to prepare an individual to react in an emergency situation. It would be good to see a project like thisfunded to an extent that the idea is not only piloted but truly tested as to its possible effectiveness in a disastersituation.
Professor A. Minasyan from Armenia spoke on "The system of emergency medical care in disasters andcatastrophes in Armenia". He began his presentation by reminding the audience of the Chernobyl accidentand the resulting immediate and long−term effects on the health of the people. He stressed that scientificallybased and efficient organization of medical care during emergencies is a decisive factor in saving lives.Professor Minasyan added that during the first hour of a disaster, quick situation analysis should be followedby prompt relief measures provided to the victims. All these measures are possible at present in Armenia withthe formation of disaster committees at three levels and an efficient preparedness plan for all disasters whichwas developed after the Chernobyl nuclear power station accident and the Spitak earthquake in Armenia. Themajor objective of this plan is to provide early, efficient and specialized medical care, with an early rescueservice using surface and air transport.
Professor Minasyan suggested a further number of activities such as training of health and rescue staff,stockpiling appropriate emergency drugs, strengthening the information system and carrying out researchactivities. In response to a question from the audience, Professor Minasyan said that training in disastermedicine is being provided to medical and non−medical personnel in emergency schooling supported by theUnited States Agency for International Development.
Dr V.A. Astakhov, Deputy Director, Far−Eastern Regional Urgent Medical Care Centre, Khabarovsk, RussianFederation, highlighted features of the medical consequences of earthquakes in the far−east region of Russia,an area quite heavily at risk. He advocated the establishment of an Asia−Pacific Centre for DisasterManagement and suggested that the WHO Centre for Health Development, Kobe, should play an importantrole in such a centre.
Professor Y. Nagasawa presented an interesting poster mainly concerned with logistics which, however,some participants found difficult to understand. It was also said that the actual condition and situation of healthcare facilities (after the earthquake) was not as clear or simple as was shown by the model.
141
The model showed several problems concerning the provision of health care after a large disaster: facilities,communication system (telephone, radio, etc.), transportation of patients, and triage. These problems areinterrelated and cannot be discussed without mentioning others.
Dr G. Ochi of the Department of Emergency Medicine, Ehime University School of Medicine, Ehime, Japan,et al presented a poster "The Importance of Modern Means of Communication (the GHDNet)" with a proposalfor various media being utilized for information management during a disaster situation. The proposalpresented ideas for utilizing satellite broadcasts, wireless devices and the Internet, as well as traditionalmedia, for both coordination during a disaster and transmitting information to the public. This projectapparently has been designed in and for Kobe but is adaptable for other places.
Such a system for information transfer should be most helpful during the first two days after a disaster ofoverwhelming scale. For example, 58 hospitals in Osaka, a neighbouring prefecture of Kobe, sent medicalteams during the month following the earthquake. However, only four of the 58 sent their teams to Kobeduring the first 48 hours. The remainder waited for a request or command to help Kobe. They had no way ofknowing that the local government there was too heavily damaged to make contact with surrounding cities toask for help just after the earthquake. Tragically, the information systems did not exist.
In the case of the sarin attack by Ohmu−Shinrikyo in Tokyo in March in 1995, the headquarters of TokyoPolice Office announced at 11:00 a.m. that sarin was suspected of causing the injuries to the subwaypassengers. This was two−and−a−half−hours after the first patient had been taken to an emergency medicalcentre. The delay in the information meant that the chance to administer pralidoxime methiodide, an antidoteof sarin to many patients, was lost.
If accurate and timely information were available in disasters, needless morbidity and mortality would beprevented. Thus, establishing a reliable system for telecommunication in the emergency and disaster field isone of the most important problems we face.
Professor K. Hayashi, Director, Public Health Research Institute, Kobe, Japan, et al, presented a poster onthe problems of hygiene and sanitation after the Great Hanshin−Awaji Earthquake. This poster presented avery important topic. As the sewage system was destroyed by the Kobe earthquake, sanitation became aserious problem quickly. Pictures and data were presented about the lack of sanitary facilities after theearthquake in Hyogo Prefecture. Planning for the disruption of sewage is an important component of adisaster plan. An available source of portable latrines and special collection vehicles are ways of planning forsuch an eventuality. Ordinary waste−collecting vehicles cannot carry toilet waste.
Additional plans might include education of the public about alternative means of disposing of both solid andliquid waste in the aftermath of an earthquake, such as having a supply of plastic garbage bags on hand forwaste disposal. It is also important that public health agencies have a plan for screening water and sanitationfacilities and the authority to shut down those that pose a hazard. After the Northridge earthquake, a majoractivity of the environmental health department of the Los Angeles County Department of Health Services wasto shut off drinking fountains and water−dispensing machines that may have been contaminated.
In the discussion an argument proposed by Professor Wölfel, "The model's case should not occur:engineering can solve the problem" was countered by another opinion, "Even with modern technology, it isimpossible to fully protect all the hospital functions from an earthquake, if it occurs just below it. The point is todecentralize functions of disaster medical care rather than putting up a large Disaster Medical Centre".
PART 4 − REHABILITATION
Rehabilitation of earthquake victims: social and health aspects (the Cairo 1992 experience)
M. Gabr1
1 M. Gabr is Professor of Pediatrics, Cairo University; past president of the AdvisoryCommittee on Health Research, WHO; immediate past president of the International PediatricAssociation; and Secretary General of the Egyptian Red Crescent Society, Cairo, Egypt.
142
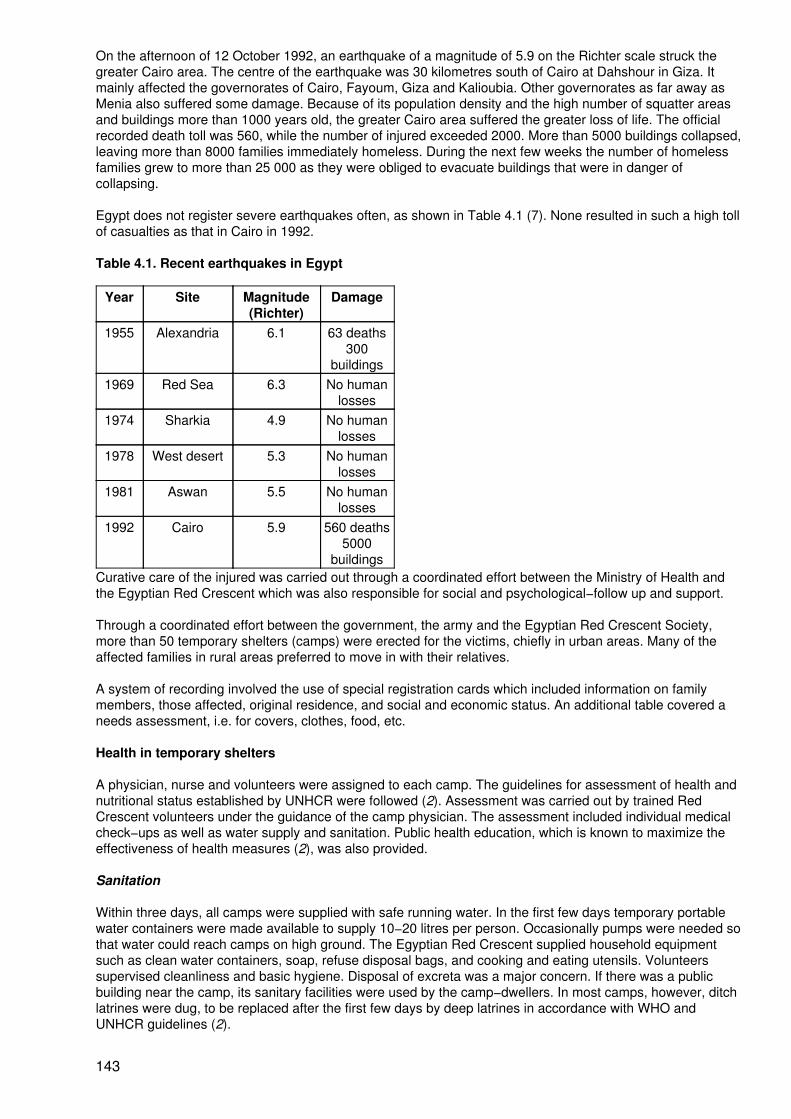
On the afternoon of 12 October 1992, an earthquake of a magnitude of 5.9 on the Richter scale struck thegreater Cairo area. The centre of the earthquake was 30 kilometres south of Cairo at Dahshour in Giza. Itmainly affected the governorates of Cairo, Fayoum, Giza and Kalioubia. Other governorates as far away asMenia also suffered some damage. Because of its population density and the high number of squatter areasand buildings more than 1000 years old, the greater Cairo area suffered the greater loss of life. The officialrecorded death toll was 560, while the number of injured exceeded 2000. More than 5000 buildings collapsed,leaving more than 8000 families immediately homeless. During the next few weeks the number of homelessfamilies grew to more than 25 000 as they were obliged to evacuate buildings that were in danger ofcollapsing.
Egypt does not register severe earthquakes often, as shown in Table 4.1 (7). None resulted in such a high tollof casualties as that in Cairo in 1992.
Table 4.1. Recent earthquakes in Egypt
Year Site Magnitude(Richter)
Damage
1955 Alexandria 6.1 63 deaths300
buildings1969 Red Sea 6.3 No human
losses1974 Sharkia 4.9 No human
losses1978 West desert 5.3 No human
losses1981 Aswan 5.5 No human
losses1992 Cairo 5.9 560 deaths
5000buildings
Curative care of the injured was carried out through a coordinated effort between the Ministry of Health andthe Egyptian Red Crescent which was also responsible for social and psychological−follow up and support.
Through a coordinated effort between the government, the army and the Egyptian Red Crescent Society,more than 50 temporary shelters (camps) were erected for the victims, chiefly in urban areas. Many of theaffected families in rural areas preferred to move in with their relatives.
A system of recording involved the use of special registration cards which included information on familymembers, those affected, original residence, and social and economic status. An additional table covered aneeds assessment, i.e. for covers, clothes, food, etc.
Health in temporary shelters
A physician, nurse and volunteers were assigned to each camp. The guidelines for assessment of health andnutritional status established by UNHCR were followed (2). Assessment was carried out by trained RedCrescent volunteers under the guidance of the camp physician. The assessment included individual medicalcheck−ups as well as water supply and sanitation. Public health education, which is known to maximize theeffectiveness of health measures (2), was also provided.
Sanitation
Within three days, all camps were supplied with safe running water. In the first few days temporary portablewater containers were made available to supply 10−20 litres per person. Occasionally pumps were needed sothat water could reach camps on high ground. The Egyptian Red Crescent supplied household equipmentsuch as clean water containers, soap, refuse disposal bags, and cooking and eating utensils. Volunteerssupervised cleanliness and basic hygiene. Disposal of excreta was a major concern. If there was a publicbuilding near the camp, its sanitary facilities were used by the camp−dwellers. In most camps, however, ditchlatrines were dug, to be replaced after the first few days by deep latrines in accordance with WHO andUNHCR guidelines (2).
143
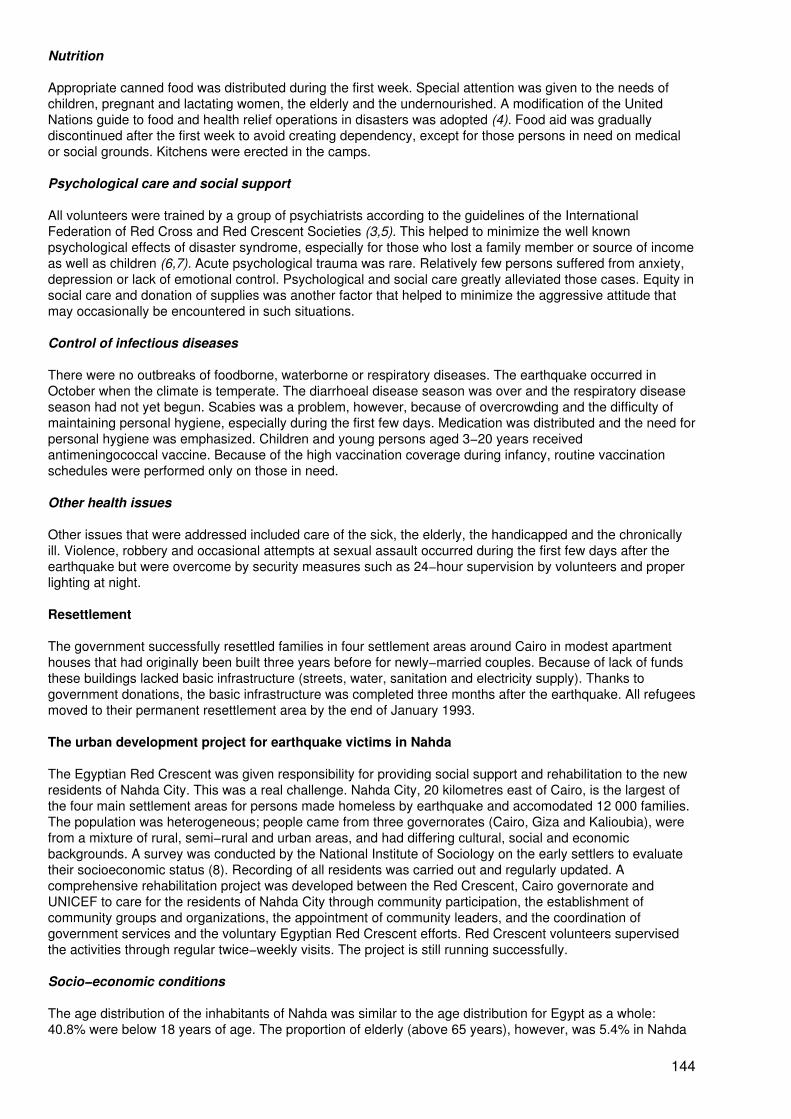
Nutrition
Appropriate canned food was distributed during the first week. Special attention was given to the needs ofchildren, pregnant and lactating women, the elderly and the undernourished. A modification of the UnitedNations guide to food and health relief operations in disasters was adopted (4). Food aid was graduallydiscontinued after the first week to avoid creating dependency, except for those persons in need on medicalor social grounds. Kitchens were erected in the camps.
Psychological care and social support
All volunteers were trained by a group of psychiatrists according to the guidelines of the InternationalFederation of Red Cross and Red Crescent Societies (3,5). This helped to minimize the well knownpsychological effects of disaster syndrome, especially for those who lost a family member or source of incomeas well as children (6,7). Acute psychological trauma was rare. Relatively few persons suffered from anxiety,depression or lack of emotional control. Psychological and social care greatly alleviated those cases. Equity insocial care and donation of supplies was another factor that helped to minimize the aggressive attitude thatmay occasionally be encountered in such situations.
Control of infectious diseases
There were no outbreaks of foodborne, waterborne or respiratory diseases. The earthquake occurred inOctober when the climate is temperate. The diarrhoeal disease season was over and the respiratory diseaseseason had not yet begun. Scabies was a problem, however, because of overcrowding and the difficulty ofmaintaining personal hygiene, especially during the first few days. Medication was distributed and the need forpersonal hygiene was emphasized. Children and young persons aged 3−20 years receivedantimeningococcal vaccine. Because of the high vaccination coverage during infancy, routine vaccinationschedules were performed only on those in need.
Other health issues
Other issues that were addressed included care of the sick, the elderly, the handicapped and the chronicallyill. Violence, robbery and occasional attempts at sexual assault occurred during the first few days after theearthquake but were overcome by security measures such as 24−hour supervision by volunteers and properlighting at night.
Resettlement
The government successfully resettled families in four settlement areas around Cairo in modest apartmenthouses that had originally been built three years before for newly−married couples. Because of lack of fundsthese buildings lacked basic infrastructure (streets, water, sanitation and electricity supply). Thanks togovernment donations, the basic infrastructure was completed three months after the earthquake. All refugeesmoved to their permanent resettlement area by the end of January 1993.
The urban development project for earthquake victims in Nahda
The Egyptian Red Crescent was given responsibility for providing social support and rehabilitation to the newresidents of Nahda City. This was a real challenge. Nahda City, 20 kilometres east of Cairo, is the largest ofthe four main settlement areas for persons made homeless by earthquake and accomodated 12 000 families.The population was heterogeneous; people came from three governorates (Cairo, Giza and Kalioubia), werefrom a mixture of rural, semi−rural and urban areas, and had differing cultural, social and economicbackgrounds. A survey was conducted by the National Institute of Sociology on the early settlers to evaluatetheir socioeconomic status (8). Recording of all residents was carried out and regularly updated. Acomprehensive rehabilitation project was developed between the Red Crescent, Cairo governorate andUNICEF to care for the residents of Nahda City through community participation, the establishment ofcommunity groups and organizations, the appointment of community leaders, and the coordination ofgovernment services and the voluntary Egyptian Red Crescent efforts. Red Crescent volunteers supervisedthe activities through regular twice−weekly visits. The project is still running successfully.
Socio−economic conditions
The age distribution of the inhabitants of Nahda was similar to the age distribution for Egypt as a whole:40.8% were below 18 years of age. The proportion of elderly (above 65 years), however, was 5.4% in Nahda
144
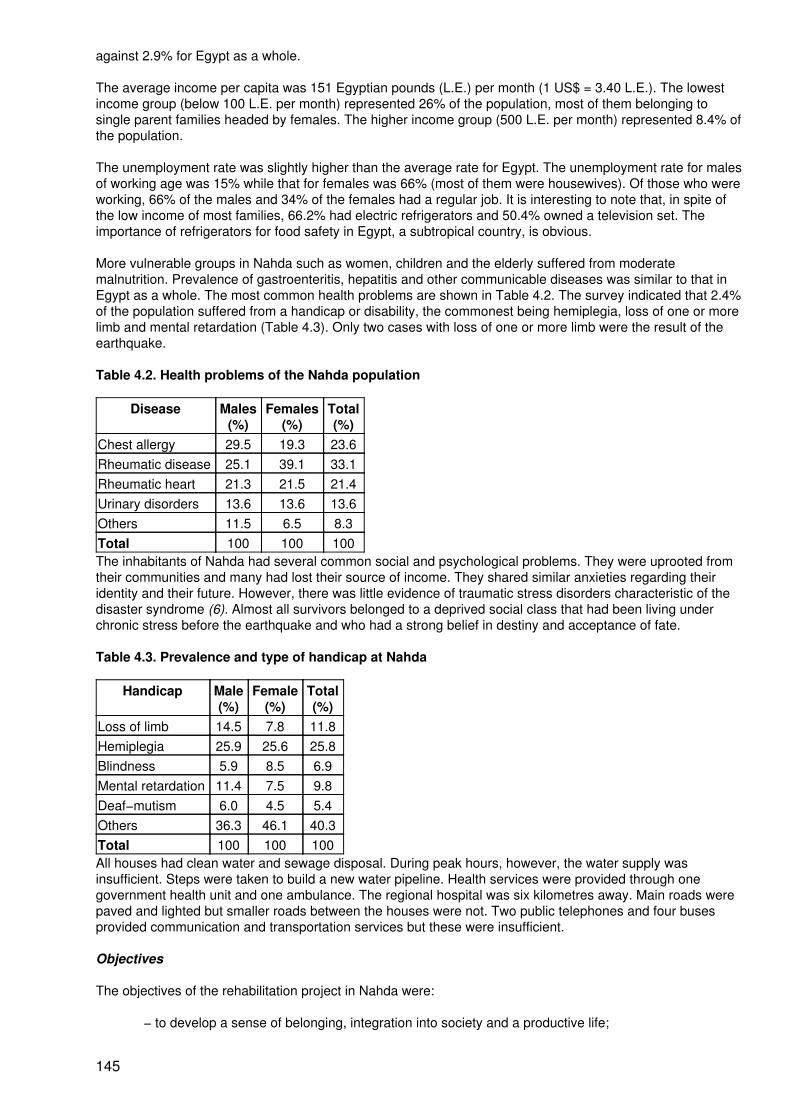
against 2.9% for Egypt as a whole.
The average income per capita was 151 Egyptian pounds (L.E.) per month (1 US$ = 3.40 L.E.). The lowestincome group (below 100 L.E. per month) represented 26% of the population, most of them belonging tosingle parent families headed by females. The higher income group (500 L.E. per month) represented 8.4% ofthe population.
The unemployment rate was slightly higher than the average rate for Egypt. The unemployment rate for malesof working age was 15% while that for females was 66% (most of them were housewives). Of those who wereworking, 66% of the males and 34% of the females had a regular job. It is interesting to note that, in spite ofthe low income of most families, 66.2% had electric refrigerators and 50.4% owned a television set. Theimportance of refrigerators for food safety in Egypt, a subtropical country, is obvious.
More vulnerable groups in Nahda such as women, children and the elderly suffered from moderatemalnutrition. Prevalence of gastroenteritis, hepatitis and other communicable diseases was similar to that inEgypt as a whole. The most common health problems are shown in Table 4.2. The survey indicated that 2.4%of the population suffered from a handicap or disability, the commonest being hemiplegia, loss of one or morelimb and mental retardation (Table 4.3). Only two cases with loss of one or more limb were the result of theearthquake.
Table 4.2. Health problems of the Nahda population
Disease Males(%)
Females(%)
Total(%)
Chest allergy 29.5 19.3 23.6Rheumatic disease 25.1 39.1 33.1Rheumatic heart 21.3 21.5 21.4Urinary disorders 13.6 13.6 13.6Others 11.5 6.5 8.3Total 100 100 100The inhabitants of Nahda had several common social and psychological problems. They were uprooted fromtheir communities and many had lost their source of income. They shared similar anxieties regarding theiridentity and their future. However, there was little evidence of traumatic stress disorders characteristic of thedisaster syndrome (6). Almost all survivors belonged to a deprived social class that had been living underchronic stress before the earthquake and who had a strong belief in destiny and acceptance of fate.
Table 4.3. Prevalence and type of handicap at Nahda
Handicap Male(%)
Female(%)
Total(%)
Loss of limb 14.5 7.8 11.8Hemiplegia 25.9 25.6 25.8Blindness 5.9 8.5 6.9Mental retardation 11.4 7.5 9.8Deaf−mutism 6.0 4.5 5.4Others 36.3 46.1 40.3Total 100 100 100All houses had clean water and sewage disposal. During peak hours, however, the water supply wasinsufficient. Steps were taken to build a new water pipeline. Health services were provided through onegovernment health unit and one ambulance. The regional hospital was six kilometres away. Main roads werepaved and lighted but smaller roads between the houses were not. Two public telephones and four busesprovided communication and transportation services but these were insufficient.
Objectives
The objectives of the rehabilitation project in Nahda were:
− to develop a sense of belonging, integration into society and a productive life;
145
− to carry out cultural, recreational and communal activities to bridge the gaps of alienationand anonymity;
− to help the people to define their problems and find relevant solutions through self−help incooperation with government services;
− to improve the standard of living through the creation of job opportunities, combatingilliteracy, promoting better health, improving nutrition, and improving the social andenvironmental situation.
Implementation
A project director was appointed and community coordinators were selected from among the young people ofNahda. A geographical area was assigned to each coordinator. Residents elected community leaders for eachcluster of apartment houses and organized local committees. Each committee elected a representative to be amember of the regional committee which met every month and included the project director, the chiefEgyptian Red Cross volunteer and the chairman of the local government council− A Supreme Committee forPlanning, Supervision and Evaluation chaired by the governor of Cairo and representatives from the regionalcommittees and local authorities met every three months. Rehabilitation plans were developed on an annualbasis.
The Egyptian Red Crescent erected a social health centre which served as headquarters for the project.Training and educational activities for the trainers were carried out there. Rehabilitation activities were carriedout in 12 smaller centres throughout the Nahda area.
Consultants developed a comprehensive rehabilitation programme. Community participation was mandatoryduring the planning and implementation of the programme. Whenever possible, trainers were selected fromamong the community and given proper training by consultants and professionals. Evaluation was built intothe project.
Three sociocultural clubs were established for children, women and the elderly. Three public libraries and 30mobile libraries began functioning within six months. Recreational trips for children, young people, housewivesand the elderly were carried out with great success. Social programmes to promote better living habits wereconducted regularly, and theatre shows and other artistic activities were performed.
Many of the young people of Nahda were organized into sports teams − football, table tennis, volleyball,handball, basketball and so on. More than 100 tournaments were carried out. Prizes and incentives from thelocal community were offered to the winners. This was very effective in distracting the young people fromharmful activities such as drugs and violence. Although the Nahda area was notorious for its drug−dealersbefore the resettlement they have now completely disappeared.
An indoor gymnasium was opened for women in the women's club and was surprisingly successful. It is veryrare in Egypt for women of this social class to get involved in gymnastic activities. Its results reflectedpositively on their health.
Because of the high illiteracy rate, 22 literacy classes were established in different areas of Nahda.Astonishingly, most of those who enrolled were housewives. More than 650 received literacy education. Againthe positive reflection on health of this activity is evident. Tuition classes for school children needing support,as well as for drop−outs from compulsory primary education, were carried out and have served more than3000 pupils during the past three years. A number of efforts were made to promote upgrading of theenvironment. These included seminars, involvement of young people in environmental projects, theestablishment of a refuse disposal system by the community, school programmes, and care for trees andgreen areas.
Attempts to overcome the poverty and high unemployment were carried out through various innovativevocational training and educational programmes aimed at encouraging income−generating activities. Trainingcovered topics such as home repairs, food preservation, computers, electronics, and electrician's andplumber's skills. Programmes to train young girls as babysitters and to take care of the elderly andhandicapped were highly successful.
Many of these activities reflected positively on health. A system to promote better health nutrition and familyplanning through community participation was established. Female community health leaders were selected
146
from among the community, taking into consideration age, educational background, willingness to serve andgeographical distribution. The training of 100 female health leaders was carried out by consultants through atwo−week special programme involving household hygiene, primary health care, first aid, psychologicalsupport, appropriate nutrition, promotion of family planning, drug abuse, AIDS and so on. Apart from publicseminars on health education by professionals, female community health leaders greatly facilitated healthpromotion through direct communication.
At the beginning, only the free government health unit existed but within six months five private clinics and twopharmacies had started functioning. The Egyptian Red Crescent's social health centre was inaugurated oneyear later and provided health care at nominal fees as well as a 24−hour first aid ambulance service to thenearby hospital. This centre provided services to more than 1500 persons a month. As an example of thesuccess of the health component of the project, 2567 women of child−bearing age sought the use ofcontraceptives in the social health centre during 1996. Vaccination coverage exceeded 90%.
Disabled persons received social care. The Red Crescent supplied wheelchairs and basic physiotherapyequipment. Young women from the community, trained in the care of persons with handicaps, facilitated theirhome care. Cases needing advanced physiotherapy or surgical intervention were referred to appropriatehospitals.
Depression, insomnia, agitation and other psychological manifestations of post−disaster syndrome (5) wererarely encountered. Only occasionally did people need psychological support, which was provided by thetrained community health leaders. This was more successful and reassuring than consulting a professionalpsychiatrist whose role was limited to diagnosis, advice and follow−up.
Evaluation, constraints and solutions
The Nahda resettlement project faced a number of constraints but efforts were made to overcome them. Forinstance, the supply of clean piped water was insufficient at the beginning but was remedied within 18months. Two new bus lines were established at an affordable fare. This greatly facilitated transportation ofpupils to their original schools until new schools were established. The telephone and telegraphcommunication system was also strengthened.
Health and environmental education changed the behaviour of the inhabitants in respect to hygiene andcleanliness. The Egyptian Red Crescent's social health centre supported a comprehensive health, familyplanning and nutrition education programme through a network of voluntary female community health leaders,as well as providing health care at nominal fees.
Housing thousands of families from different social, cultural, economic and geographical backgrounds in onenew settlement area was a unique experience. Community development is still proceeding with great success.This success is related to community participation at all stages of the project, and regular meetings betweenthe government authorities and the social, health, educational, cultural and recreational programmes. Theresidents of the area today are proud to say that they belong to Nahda.
References
1. Sedki A. Report of the Egyptian Prime Minister to the Senate. Cairo, Press of the Egyptian Parliament, 12Nov. 1992.
2. Handbook for emergencies, Geneva, UNHCR, 1982.
3. Disaster rehabilitation and reconstruction. Geneva, IFRC, 1994.
4. Protein Advisory Caloric Group of the United Nations. A guide to food and health relief operations fordisasters. New York, 1977.
5. Guidelines to develop psychological support programs for disaster victims. Geneva, IFRC, 1993.
6. Lazarus RS, Folkman S. Stress Appraisal and Coping. New York, Springer, 1984:578−615.
7. Coping with Natural disasters: the role of health personnel and the community. Geneva, WHO, 1989.
147
8. Fahmy N. Comprehensive survey of the population of Nahda City. Cairo, National Institute of Childhoodand Motherhood Publications, 1993.
Basic principles of resort rehabilitation of earthquake victims
V.N. Zavgorudko1 and T.I. Zavgorudko2
1V.N. Zavgorudko is Doctor of Medical Sciences, Professor, Head of Department of MedicalRehabilitation and Physical Therapy, Far−Eastern Medical University, Honoured Physician ofthe Russian Federation, Khabarovsk, Russian Federation.
2T.I. Zavgorudko is Candidate of Medical Sciences, Associate Professor, Honoured Physicianof the Russian Federation, Khabarovsk, Russian Federation.
Having studied the experience of those who work in the area of disaster medicine, including experience inNeftegorsk, we have noticed that one universally accepted type of rehabilitation programme was absent.Analysis of the health status of Neftegorsk earthquake victims, both those who had been buried under theruins and those who had not, has demonstrated the need to provide, in certain cases, urgent rehabilitationprocedures for those who experience a catastrophe ranging from psychotherapy to complex physical and spatherapy. This applies both to the victims and to those persons who are involved in disaster relief.
Resort rehabilitation is based on active non−medication therapy, that is, unfortunately, rarely used and notwell studied by clinicians, especially those who work in emergency and catastrophe medicine. A resortnormally has both the capacity and excellent facilities to provide rehabilitation. It has enough hospital beds,which sometimes can easily be increased; also specialized wards can be organized to provide special typesof services according to the needs of the patients. There are also plenty of low−cost but highly effectivenatural curative remedies such as mineral waters and therapeutic mud. A resort has well−developed transportroutes and is administratively independent in the Russian Federation.
Rehabilitation is, under present legislation, a compulsory component of measures provided to render aid toand to restore health to victims of catastrophes. Health care at the resort level, the non−medication therapyincludes balneological and mud treatment, physical therapy, curative exercising, massage, psychotherapy,acupuncture, bioenergy usage and climate treatment.
Such rehabilitation of earthquake victims can be combined with clinical medicine at every stage, using all thelatest medical knowledge and technologies. The organization and provision of medical procedures should notbe restricted or influenced by bureaucracy. The benefits of rehabilitation at a resort include the following:
− treatment of certain types of injuries under the special conditions of the locality;
− treatment of the longer−term consequences of injury after specialized aid has already beenapplied;
− enhancement of previously applied medical procedures;
− achievement of steady recovery;
− prevention of recurrence of illness;
− restoration of lost functions;
− prevention of disability or limitation of the disability to an acceptable level;
− reduced impact of persistent, recurrent post−traumatic phantom pains;
− improvement of capacity for work;
− psychological rehabilitation and stress reduction;
− increase of immunological resistance.
148

In areas of high seismic activity nature often provides thermal waters with nitrogeneous−silicous propertiesthat are beneficial to our health. Our studies have shown multiple benefits of those waters on patients.Approaches to treatment may be based on the illness, the symptoms or the nature of the injury, or on acombination of these factors. Patients very rarely have just one condition, and disaster victims are noexception. They usually have many conditions, directly or indirectly caused by the injuries they have suffered.Three hundred diseases and traumas have indications for treatment at resorts with thermal waters. This typeof rehabilitation leads to positive results in 90−95% of victims.
Financial aspects following an earthquake: the bank's point of view
Y. Yasuda1
1 Y. Yasuda is General Manager, Kansai Project Development Division, The Sakura BankLimited, Kobe, Japan.
I am General Manager of Sakura Bank's Kansai Project Development Division which is supporting localgovernments and other bodies in redeveloping certain areas in western parts of Japan, including the Kansaidistrict.
Sakura Bank during the Great Hanshin−Awaji Earthquake
Sakura Bank was established in 1990 by the merger of Taiyo Kobe Bank and Mitsui Bank. It is one of theleading Japanese banks with total assets of US$ 498 billion. It has 530 domestic branches and 46 overseasoffices.
Hyogo Prefecture, including Kobe City, is one of our bank's most important markets. That is the reason whythe former Taiyo Kobe Bank's head office was here and Sakura Bank still has 121 branches here.
Due to the earthquake, most of the branches in Kobe City and the Hanshin area (the area from Kobe toOsaka) were damaged. Five branches completely collapsed and a further 20 branches were seriouslydamaged.
On that day, 119 out of 186 branches in the Kansai region were unable to operate as the result of failure ofelectric power and telecommunications services.
The restoration of the bank's facilities
Sakura Bank was fully equipped with computer systems. The main host computer was located in KanagawaPrefecture near Tokyo and the second host computer in Kobe. The design of these computer systems tookinto account that even if one of them broke down, the other should provide the bank with all its normalelectronic services. Despite the earthquake, however, both computer systems remained functional. Theycontinued to work very well, although they were affected by the disruption of the electric power supply and ofdamages in the communication network between the headquarters and branches.
However, the bank faced another serious difficulty. Equipment and documents were scattered all over theoffices. Only a few bank personnel came to the office that day. In addition, the bank suffered from thedestruction of the lifelines.
Under these circumstances, the staff tried very hard to restore the bank's facilities, considering that manypeople affected by the earthquake needed money and relied on the bank. Due to the rapid and hard work ofour employees, the computer network systems were working again two days after the earthquake and on 23January all branches were able to operate fully. Thus most of our customers felt relieved and there was norush to the bank offices. In fact, it was said that most people felt relieved to see the bank's headquarters safeamong so many destroyed buildings.
Crisis management
In Japan, it is generally said that banks are built so strong that they can resist earthquakes. But this myth wasdestroyed by this earthquake. I had lived here for a year and a half, and I saw things after the earthquake fromthe point of view of a victim as well as that of a bank employee. Crisis unexpectedly attacks our lives and our
149
property and we should prepare ourselves against such crises and emergencies in both public and privateaffairs.
Like other companies, Sakura bank had a manual for emergency management. It was thorough but could notcover everything. Therefore the bank staff needed to act with flexibility in response to the real situation.
The bank's actions
On the day of the earthquake, the transportation systems were completely paralyzed and only 10 out of 600employees were able to arrive at the bank's headquarters by 8 o'clock in the morning. However, as soon asemployees arrived, the bank formed an emergency command centre both in Kobe and in Tokyo and tried bothto check whether other employees were safe and to confirm what damage had been done to the branches inthe area. It was difficult to do these things because of the lack of electricity, disrupted telecommunicationsystems and the shortage of staff. Most of the bank staff were, however, enthusiastic enough to come to theiroffices, some travelling three or four hours on foot, to restore the bank's facilities. As a result, out of 119branches that were closed on 17 January, 75 were open by the next day.
The Bank of Japan gave top priority to supplying enough cash for all the banks in the area of destruction; staffwere kept busy paying out cash. As a result we avoided social disorder. Sakura Bank kept three times asmuch cash reserve as normal for several days after the earthquake in order to pay customers whatever theyneeded to withdraw. The bank also had about 10 staff members dealing exclusively with customers' phoneinquiries, both in Kobe and also in Tokyo, since it was not always easy to use phones in the Kobe area.
Besides these activities, Sakura Bank called on its employees and customers outside the disaster area tomake donations on behalf of the victims. Donations by the bank's employees amounted to 25 million yen.
Treatment of depositors
This huge earthquake threatened Japan's banking system, with its dependence on on−line computers, for thefirst time. It made us realize the importance of the stability of the banking system in a modem urbanenvironment. I believe that the special emergency procedures laid down and practised by the Ministry ofFinance and the Bank of Japan reassured the earthquake victims. These procedures required that:
− even if the customer's passbook and other documents were lost or burned, the bank shouldtake proper steps to check the person's identity and be ready to pay out;
− the bank should pay out fixed−term deposits even prior to the maturity date, as long as thiswas acceptable to the bank;
− the bank should open on Saturdays and Sundays to attend to the needs of customers;
− the bank should make special arrangements for new loans related to recovery from thedisaster.
Sakura Bank and other banks tried very hard to comply with these procedures. The Kobe branch of the Bankof Japan and the Kobe main office of Sakura Bank also offered space to other banks, whose offices were toobadly damaged to open, and helped them carry out their business.
Treatment of customers with loans
On 18 January, Sakura Bank announced special arrangements for rescheduling repayment of loans, forextension of loan periods and for lowering the interest rate in cases of necessity. In addition, low interest loanswere introduced for individuals and enterprises who had suffered in the earthquake.
The bank also released its collateral interest in destroyed or fire−damaged houses that were security forloans, and allowed the owners to use the fire and earthquake insurance money for the specific purpose ofbuilding new residences.
Helping earthquake victims to rebuild their lives
Sakura Bank established three kinds of loans for the earthquake victims. Firstly, the bank set up home loansso that those who had lost their homes could build new ones. These were 40−year loans with a three−year
150
grace period at an interest rate 0.7% lower than for normal home loans. Secondly, the bank set up homerepair loans for repairing damaged residences. Interest on these loans is 2.25% lower than for normal loans ofthis kind. Thirdly, there were loans for support of living, without security, to help earthquake victims getthrough the difficult situation. This kind of loan was up to 3 million yen for a period of seven years, with aone−year grace period at an interest rate 4% lower than normal. The bank also allowed persons with existinghome loans with mortgage to apply for the new home loans.
The Housing Loan Corporation, a government agency, also set up the same kind of special home loans. Sothose in need were able to choose from many kinds of loans. However, these special arrangements were notapplied to elderly people or to those with low incomes. This is still a big problem today.
For customers planning to reconstruct apartment buildings, Sakura Bank took the lead in discussing financingloans and agreed to suspend mortgage obligations temporarily in some cases. According to a survey by thebank, 117 of 232 damaged apartment buildings needed to be reconstructed. Among them, however,agreement about reconstruction among the usual multiple owners was reached for only 78 buildings. (I amafraid that it will take a long time to reach agreement on reconstruction of the rest.)
Sakura Bank set up special counters at all its branches in the Kansai area to give advice to people in need ofloans.
Support for reconstruction
After the earthquake, the government and local authorities worked hard at rescue, near−term survival andplans for reconstruction. On 1 February, Sakura Bank formed a task force for reconstruction open tocooperation with the authorities. The task force set up its own working fund to assist small and medium−sizedenterprises in addition to the local government's financial help.
On 1 March, the bank established a Reconstruction Promotion Department in Tokyo and a ReconstructionProject Department at the headquarters in Kobe. These took the place of the task force in cooperating withgovernment and local authorities. Since then the bank and its affiliated Sakura Research Institute has madevarious proposals for reconstruction.
Now the local governments of Hyogo Prefecture and Kobe City, and other bodies, have four big nationalprojects for reconstruction. These are the promotion of trade and relationships between Kobe, Shanghai andthe Yangtze valley, the construction of a health care park (in the same development area where the newheadquarters of the WHO Centre will be located), the creation of new industries, and memorial events of theGreat Hanshin−Awaji Earthquake. These projects will be carried out by the governments, the local authoritiesand private companies.
As a leading bank in Kobe, Sakura Bank has committed itself to cooperating with and supporting the saidbodies in carrying out these reconstruction projects in the near future.
Industrial reconstruction after the Great Hanshin−Awaji Earthquake
H. Kuramochi1
1 H. Kuramochi is Director General, Commerce and Industry Department, Hyogo PrefecturalGovernment, Kobe, Japan
Impact of the earthquake on industry
Industrial activity has a wide range of impacts on personal and social life through employment and vocation inaddition to the part it plays in the economy. The Great Hanshin−Awaji Earthquake had a particularly importantimpact on industrial activities in two ways.
First, the disaster−stricken area was a highly industrialized one, and consequently the damage inflicted uponindustry was enormous and serious. Key industries such as transport, machinery and steel, and various otherindustries such as sake distillation, fashion and tourism were located in the Hanshin−Awaji area− This areawas producing around 10 trillion yen of Gross Domestic Product, and two−thirds of all economic activities ofHyogo Prefecture took place here.
151
The cost of the damage to the area's industry is estimated to be around 5 trillion yen, of which direct damageto business property and equipment accounted for some 2.5 trillion yen and indirect damage, such asbusiness closures, a further 2.5 trillion.
The second prominent feature of this earthquake's impact was that it occurred at a time when the area'sindustrial structure was in the process of change. A shift was under way from heavy industry to industriesmore oriented to development, services and information. The premature closure of large factories and thedestruction of small and medium−sized ones which were the spearhead of local industrial development as aconsequence of the earthquake has disturbed and slowed down the speed of industrial restructuring.
These two features lead us to the challenges that we have to face and deal with after the earthquake. In theshort term, we need to stop a downward spiral of the local economy by confidence and quick restoration, andin the medium and long−term, we need to promote the necessary future changes in the area's industrialstructure and integrate it into the reconstruction process.
Restoration
Emergency measures to restore industry
Our primary challenge is the earliest possible recovery of industrial activity in the severely damagedHanshin−Awaji area. In order to ensure this, various emergency measures have been put into operation.These include, for example:
− the establishment of a comprehensive consultation centre for small and medium−sizedcompanies, (offering advice on problems faced by businesses hit by the disaster, such asfund−raising, the procurement of business premises, and legal problems, including thesettlement of promissory notes);
− the establishment of loans from an emergency restoration fund at an extremely low interestrate of 2.5% and with no interest payment in the first three years;
− the provision of business premises by constructing temporary factories and cooperativeretail stores;
− tax deferment, reduction and exemption;
− campaigns and events to wipe out the negative image of the area and to renew tourism.
To implement these emergency measures, a trans−organizational reconstruction headquarters wasestablished by the national and local governments immediately after the earthquake, and special budgetaryarrangements were made by both. So far the national government has enacted 16 special laws andestablished a 3.5 trillion yen budget (starting with the original budget for fiscal year 1996). The HyogoPrefectural government has also established a budget of approximately 2 trillion yen for reconstruction so far.
Restoring economic activity
Industry in the affected area was rapidly restored within about six months of the disaster, thanks to the untiringefforts made by both private and public sectors. Although the rate of progress towards full−scale restorationhas subsequently slowed down, it is nevertheless continuing steadily. By the end of 1996, it is estimated thateconomic activity as a whole had been restored to 90% of its pre−earthquake level.
There are, however, increasingly striking differences in the rates of recovery according to types of business.Of course, there has been some delay in restoring some of the local industries which were most severelyaffected by the disaster, such as the synthetic footwear industry. As far as the manufacturing industry isconcerned, production figures generally have been restored to pre−disaster levels thanks to the successfulrevival of major companies, including those in the steel industry.
On the other hand, the retail, service and tourism industries, which had accounted for about 65% of the netturnover of the disaster−stricken area before the earthquake, are still being affected, mainly because of themovement of people away from the area and because of the decline in tourist traffic. For example, theestimated number of tourists visiting Kobe City in October 1996 was 80% of the level of the same month in1994. As a result, hotel room occupancies have not yet fully recovered. After implementing the emergency
152
restoration measures, we have begun our initiative to achieve complete reconstruction as follows:
Reconstruction strategy
Our basic strategy for industrial reconstruction is two−fold. First, the full−scale reconstruction projects shouldaim to construct a new industrial structure that is suited to a society in the 21st century, and not simply restorethe region's industry to its pre−earthquake status. Otherwise the economy of this region will not be able tocompete either in domestic or in international markets. Second, the favourable characteristics of the regionshould be used to enhance reconstruction.
Situated almost in the centre of the Japanese archipelago, the Hanshin−Awaji area is an important junction fortraffic. The area has also developed as a centre of international trade, with the Port of Kobe. It currently has97 000 residents of 97 nationalities, 19 foreign schools serve its foreign residents, and it has a good basis forthe development of international contacts. The aim of our industrial reconstruction, therefore, is theconstruction of a new industrial centre that utilizes the economic links with other countries.
Reconstruction plan
A long−term plan for bringing about the reconstruction outlined was formulated in July 1995. That is the GreatHanshin−Awaji Earthquake Reconstruction Plan (we call it the Hyogo Phoenix Plan). It comprises manyprojects, of which I shall describe several main ones.
First is the creation of an Enterprise Zone. In order to enhance the long−term reforms in industrial structurewithin the process of reconstruction, industrial activity in the earthquake−stricken area needs to become evenmore vigorous than it was before the earthquake. The Enterprise Zone project may be regarded as thenucleus of the industrial reconstruction schemes. Under the Enterprise Zone scheme, appropriate sites in thedisaster−stricken area are designated as special zones entitled to deregulation and tax incentives as a meansof freeing corporate activities for domestic and foreign investment, thus leading to the creation of newindustries.
For this purpose, local taxes (real estate acquisition tax and municipal fixed assets tax) will be reduced andderegulatory measures will be introduced. The Enterprise Zone is also expected to function as a marketwhere, as a result of deregulation, imported high−quality goods can be purchased at lower prices, thusencouraging imports and attracting more customers and businesses to the zone. Hyogo Prefecture and KobeCity have already established ordinances which permit the application of special incentive measures tocompanies located in the zone.
Next, one of the national reconstruction projects proposed last year by the Japanese government'sHanshin−Awaji Reconstruction Commission is the fostering of economic exchanges between theShanghai−Yangtze Valley economic bloc, which is expected to become an Asian growth centre, and theHanshin−Kobe economic bloc zone, thus contributing to the economic development of both Japan and China.The project aims to promote direct trade between Japan and China by achieving a substantial reduction intransport costs. To be more concrete, this project includes developing river boats to transport freight directlybetween the two regions in China and also includes establishing an exclusive berth in the Port of Kobe tofacilitate trade. We also plan to construct a new China town nearby the port, with a view to encouragingcultural exchanges as well as economic exchanges.
Beside the Phoenix Plan, there are a lot of projects proposed by the private sector. One of them is knownprovisionally as the New Industry Creation Research Organization. The object of this project, which operatesin collaboration with the Massachusetts Institute of Technology in the USA, is to promote research and tosupport the development of new industries. Business sectors have come to feel that the process of industrialreconstruction must improve the ability for creative research and development by making use of technologiesaccumulated in this area and by strengthening collaboration and cooperation with universities and researchorganizations both in Japan and abroad. After the medium−sized companies within Hyogo Prefecture havecompleted their assessment of the project, including, for instance, the types of business to be covered by theorganization and the scale of research and development, a public corporation will be formed to act as theparent body charged with the promotion of the project. In order to ensure the smooth progress of thesevarious reconstruction projects, the Organization for the Promotion of Hanshin−Awaji IndustrialReconstruction was established in December 1995 jointly administered by the public and private sectors andforming a bridge between them. It supports the commercialization of basic technologies accumulated in thestricken area, it organizes various public relations campaigns and other events to attract customers andtourists, and it promotes investment in the area by Japanese and foreign companies.
153
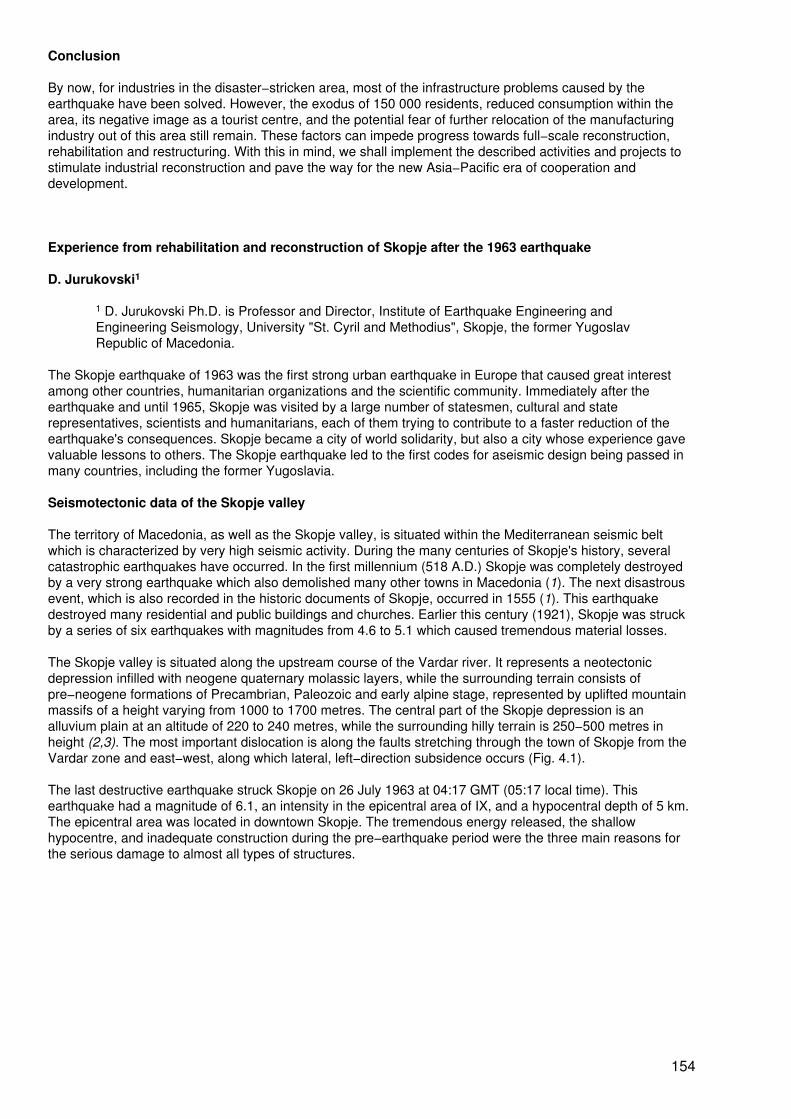
Conclusion
By now, for industries in the disaster−stricken area, most of the infrastructure problems caused by theearthquake have been solved. However, the exodus of 150 000 residents, reduced consumption within thearea, its negative image as a tourist centre, and the potential fear of further relocation of the manufacturingindustry out of this area still remain. These factors can impede progress towards full−scale reconstruction,rehabilitation and restructuring. With this in mind, we shall implement the described activities and projects tostimulate industrial reconstruction and pave the way for the new Asia−Pacific era of cooperation anddevelopment.
Experience from rehabilitation and reconstruction of Skopje after the 1963 earthquake
D. Jurukovski1
1 D. Jurukovski Ph.D. is Professor and Director, Institute of Earthquake Engineering andEngineering Seismology, University "St. Cyril and Methodius", Skopje, the former YugoslavRepublic of Macedonia.
The Skopje earthquake of 1963 was the first strong urban earthquake in Europe that caused great interestamong other countries, humanitarian organizations and the scientific community. Immediately after theearthquake and until 1965, Skopje was visited by a large number of statesmen, cultural and staterepresentatives, scientists and humanitarians, each of them trying to contribute to a faster reduction of theearthquake's consequences. Skopje became a city of world solidarity, but also a city whose experience gavevaluable lessons to others. The Skopje earthquake led to the first codes for aseismic design being passed inmany countries, including the former Yugoslavia.
Seismotectonic data of the Skopje valley
The territory of Macedonia, as well as the Skopje valley, is situated within the Mediterranean seismic beltwhich is characterized by very high seismic activity. During the many centuries of Skopje's history, severalcatastrophic earthquakes have occurred. In the first millennium (518 A.D.) Skopje was completely destroyedby a very strong earthquake which also demolished many other towns in Macedonia (1). The next disastrousevent, which is also recorded in the historic documents of Skopje, occurred in 1555 (1). This earthquakedestroyed many residential and public buildings and churches. Earlier this century (1921), Skopje was struckby a series of six earthquakes with magnitudes from 4.6 to 5.1 which caused tremendous material losses.
The Skopje valley is situated along the upstream course of the Vardar river. It represents a neotectonicdepression infilled with neogene quaternary molassic layers, while the surrounding terrain consists ofpre−neogene formations of Precambrian, Paleozoic and early alpine stage, represented by uplifted mountainmassifs of a height varying from 1000 to 1700 metres. The central part of the Skopje depression is analluvium plain at an altitude of 220 to 240 metres, while the surrounding hilly terrain is 250−500 metres inheight (2,3). The most important dislocation is along the faults stretching through the town of Skopje from theVardar zone and east−west, along which lateral, left−direction subsidence occurs (Fig. 4.1).
The last destructive earthquake struck Skopje on 26 July 1963 at 04:17 GMT (05:17 local time). Thisearthquake had a magnitude of 6.1, an intensity in the epicentral area of IX, and a hypocentral depth of 5 km.The epicentral area was located in downtown Skopje. The tremendous energy released, the shallowhypocentre, and inadequate construction during the pre−earthquake period were the three main reasons forthe serious damage to almost all types of structures.
154
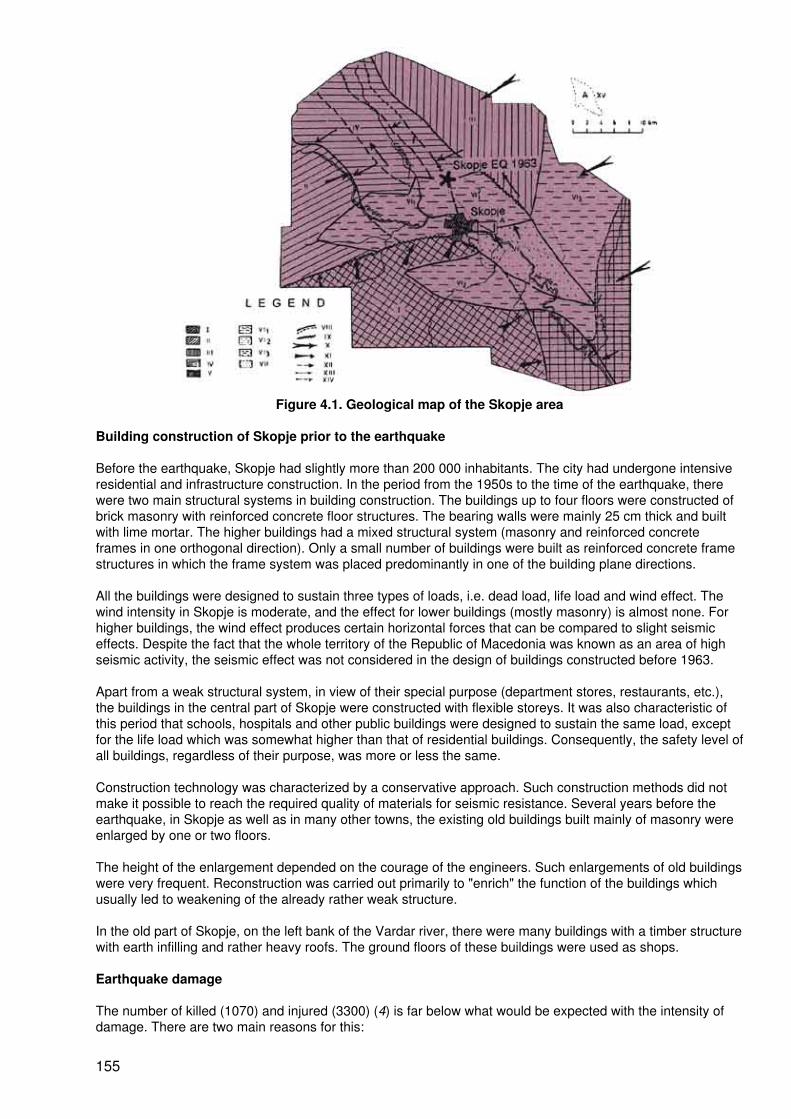
Figure 4.1. Geological map of the Skopje area
Building construction of Skopje prior to the earthquake
Before the earthquake, Skopje had slightly more than 200 000 inhabitants. The city had undergone intensiveresidential and infrastructure construction. In the period from the 1950s to the time of the earthquake, therewere two main structural systems in building construction. The buildings up to four floors were constructed ofbrick masonry with reinforced concrete floor structures. The bearing walls were mainly 25 cm thick and builtwith lime mortar. The higher buildings had a mixed structural system (masonry and reinforced concreteframes in one orthogonal direction). Only a small number of buildings were built as reinforced concrete framestructures in which the frame system was placed predominantly in one of the building plane directions.
All the buildings were designed to sustain three types of loads, i.e. dead load, life load and wind effect. Thewind intensity in Skopje is moderate, and the effect for lower buildings (mostly masonry) is almost none. Forhigher buildings, the wind effect produces certain horizontal forces that can be compared to slight seismiceffects. Despite the fact that the whole territory of the Republic of Macedonia was known as an area of highseismic activity, the seismic effect was not considered in the design of buildings constructed before 1963.
Apart from a weak structural system, in view of their special purpose (department stores, restaurants, etc.),the buildings in the central part of Skopje were constructed with flexible storeys. It was also characteristic ofthis period that schools, hospitals and other public buildings were designed to sustain the same load, exceptfor the life load which was somewhat higher than that of residential buildings. Consequently, the safety level ofall buildings, regardless of their purpose, was more or less the same.
Construction technology was characterized by a conservative approach. Such construction methods did notmake it possible to reach the required quality of materials for seismic resistance. Several years before theearthquake, in Skopje as well as in many other towns, the existing old buildings built mainly of masonry wereenlarged by one or two floors.
The height of the enlargement depended on the courage of the engineers. Such enlargements of old buildingswere very frequent. Reconstruction was carried out primarily to "enrich" the function of the buildings whichusually led to weakening of the already rather weak structure.
In the old part of Skopje, on the left bank of the Vardar river, there were many buildings with a timber structurewith earth infilling and rather heavy roofs. The ground floors of these buildings were used as shops.
Earthquake damage
The number of killed (1070) and injured (3300) (4) is far below what would be expected with the intensity ofdamage. There are two main reasons for this:
155
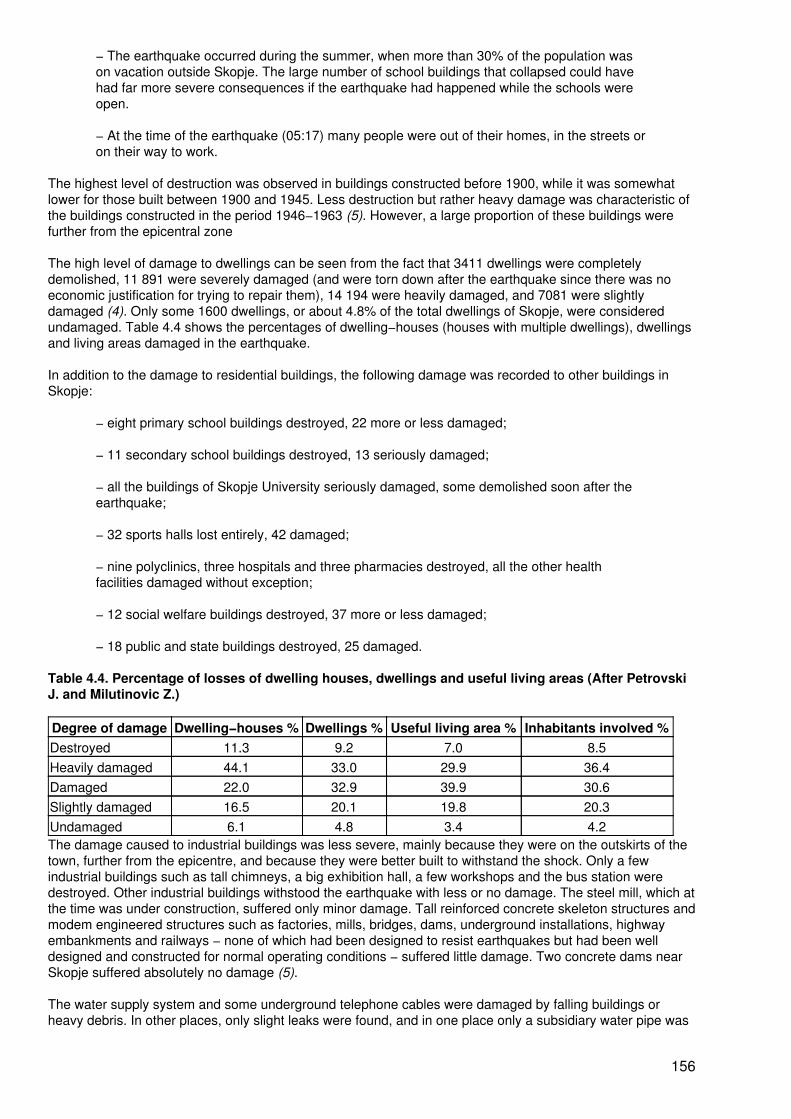
− The earthquake occurred during the summer, when more than 30% of the population wason vacation outside Skopje. The large number of school buildings that collapsed could havehad far more severe consequences if the earthquake had happened while the schools wereopen.
− At the time of the earthquake (05:17) many people were out of their homes, in the streets oron their way to work.
The highest level of destruction was observed in buildings constructed before 1900, while it was somewhatlower for those built between 1900 and 1945. Less destruction but rather heavy damage was characteristic ofthe buildings constructed in the period 1946−1963 (5). However, a large proportion of these buildings werefurther from the epicentral zone
The high level of damage to dwellings can be seen from the fact that 3411 dwellings were completelydemolished, 11 891 were severely damaged (and were torn down after the earthquake since there was noeconomic justification for trying to repair them), 14 194 were heavily damaged, and 7081 were slightlydamaged (4). Only some 1600 dwellings, or about 4.8% of the total dwellings of Skopje, were consideredundamaged. Table 4.4 shows the percentages of dwelling−houses (houses with multiple dwellings), dwellingsand living areas damaged in the earthquake.
In addition to the damage to residential buildings, the following damage was recorded to other buildings inSkopje:
− eight primary school buildings destroyed, 22 more or less damaged;
− 11 secondary school buildings destroyed, 13 seriously damaged;
− all the buildings of Skopje University seriously damaged, some demolished soon after theearthquake;
− 32 sports halls lost entirely, 42 damaged;
− nine polyclinics, three hospitals and three pharmacies destroyed, all the other healthfacilities damaged without exception;
− 12 social welfare buildings destroyed, 37 more or less damaged;
− 18 public and state buildings destroyed, 25 damaged.
Table 4.4. Percentage of losses of dwelling houses, dwellings and useful living areas (After PetrovskiJ. and Milutinovic Z.)
Degree of damage Dwelling−houses % Dwellings % Useful living area % Inhabitants involved %Destroyed 11.3 9.2 7.0 8.5Heavily damaged 44.1 33.0 29.9 36.4Damaged 22.0 32.9 39.9 30.6Slightly damaged 16.5 20.1 19.8 20.3Undamaged 6.1 4.8 3.4 4.2The damage caused to industrial buildings was less severe, mainly because they were on the outskirts of thetown, further from the epicentre, and because they were better built to withstand the shock. Only a fewindustrial buildings such as tall chimneys, a big exhibition hall, a few workshops and the bus station weredestroyed. Other industrial buildings withstood the earthquake with less or no damage. The steel mill, which atthe time was under construction, suffered only minor damage. Tall reinforced concrete skeleton structures andmodem engineered structures such as factories, mills, bridges, dams, underground installations, highwayembankments and railways − none of which had been designed to resist earthquakes but had been welldesigned and constructed for normal operating conditions − suffered little damage. Two concrete dams nearSkopje suffered absolutely no damage (5).
The water supply system and some underground telephone cables were damaged by falling buildings orheavy debris. In other places, only slight leaks were found, and in one place only a subsidiary water pipe was
156
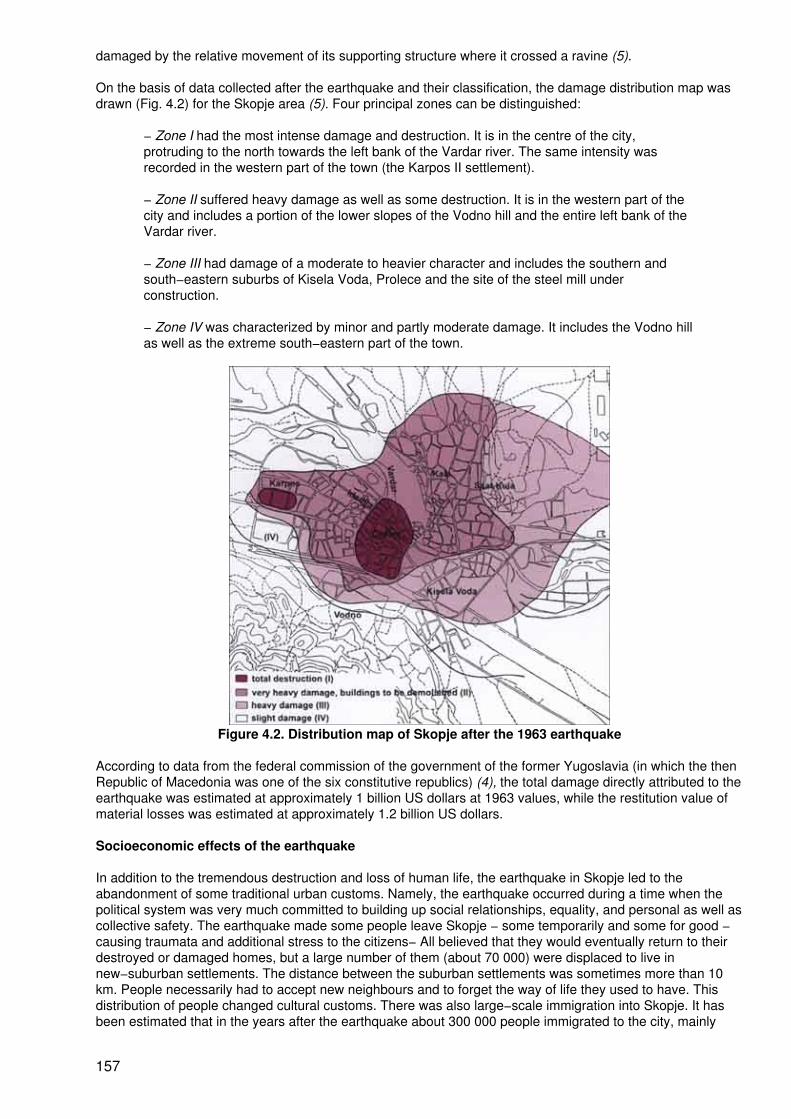
damaged by the relative movement of its supporting structure where it crossed a ravine (5).
On the basis of data collected after the earthquake and their classification, the damage distribution map wasdrawn (Fig. 4.2) for the Skopje area (5). Four principal zones can be distinguished:
− Zone I had the most intense damage and destruction. It is in the centre of the city,protruding to the north towards the left bank of the Vardar river. The same intensity wasrecorded in the western part of the town (the Karpos II settlement).
− Zone II suffered heavy damage as well as some destruction. It is in the western part of thecity and includes a portion of the lower slopes of the Vodno hill and the entire left bank of theVardar river.
− Zone III had damage of a moderate to heavier character and includes the southern andsouth−eastern suburbs of Kisela Voda, Prolece and the site of the steel mill underconstruction.
− Zone IV was characterized by minor and partly moderate damage. It includes the Vodno hillas well as the extreme south−eastern part of the town.
Figure 4.2. Distribution map of Skopje after the 1963 earthquake
According to data from the federal commission of the government of the former Yugoslavia (in which the thenRepublic of Macedonia was one of the six constitutive republics) (4), the total damage directly attributed to theearthquake was estimated at approximately 1 billion US dollars at 1963 values, while the restitution value ofmaterial losses was estimated at approximately 1.2 billion US dollars.
Socioeconomic effects of the earthquake
In addition to the tremendous destruction and loss of human life, the earthquake in Skopje led to theabandonment of some traditional urban customs. Namely, the earthquake occurred during a time when thepolitical system was very much committed to building up social relationships, equality, and personal as well ascollective safety. The earthquake made some people leave Skopje − some temporarily and some for good −causing traumata and additional stress to the citizens− All believed that they would eventually return to theirdestroyed or damaged homes, but a large number of them (about 70 000) were displaced to live innew−suburban settlements. The distance between the suburban settlements was sometimes more than 10km. People necessarily had to accept new neighbours and to forget the way of life they used to have. Thisdistribution of people changed cultural customs. There was also large−scale immigration into Skopje. It hasbeen estimated that in the years after the earthquake about 300 000 people immigrated to the city, mainly
157

from poor areas. For many years after the earthquake, Skopje had little distinct character. City life and citycustoms only returned during the last 20 years.
However, the earthquake created possibilities for many of the citizens to improve their economic and socialconditions. Those in the new suburban settlements were given houses and land at very low prices, whilenowadays the value of that property has risen considerably. The earthquake also led to change incommunication between people. Skopje became a city which people travelled from or which they visited,providing many possibilities to meet other people and exchange experience and knowledge.
Rescue operations
The system of civil protection in the former Yugoslav Republic of Macedonia was organized in a semi−militarystyle, directly under the government of the governing party at that time, the Communist Union. Although thecitizens of Macedonia and the rescue services had no practical experience of rescue operations under suchconditions, according to the documents of the time (4), they moved into action quickly and mobilizedefficiently. However, the fact remains, and was emphasized by the media, that in a large number of cases thecitizens organized themselves. The army also took a considerable part in the rescue operation.
The earthquake caused tremendous damage to health facilities, particularly hospitals. During the first fewhours after the earthquake, the injured were cared for outdoors, and even complex surgery was performed intemperatures as high as 40°C until tents could be erected. In the first post−earthquake hours, the heavilyinjured were transported to the hospitals of the neighbouring towns of Kumanovo, Veles and Tetovo. Twodays after the earthquake, a 200−bed hospital with 209 medical staff was installed in the vicinity of Skopje bythe US Army.
In addition to the emergency medical measures, the following operations were undertaken:
− Rescue of people buried under debris, according to some sources, amounted to as manyas 10 000 (4). Apart from rescue teams from Skopje, those from several neighbouring townsand from all over Yugoslavia began to arrive after a delay of several hours. A team fromFrance joined the efforts to help find survivors under the debris. Besides the national army,the armies of several other countries, such as Germany, the Soviet Union, the USA andothers, were also involved.
− The dead had to be identified and then buried promptly since temperatures were high. Onthe first day about 300 people were buried.
− In parks and other open areas a large number of tent shelters were set up in the first fewdays. By the end of August, about 40 000 shelters had been set up in Skopje. People stayedin the tents from several days to as long as several months. By 1 January 1964, only 104families were still in temporary shelters (4).
− There are not sufficient data on whether drinking water was polluted. However, thepopulation was instructed to use only water that had been boiled. Food distribution wasorganized for a large number of people.
− In Skopje, disinfection was carried out continuously for many days. Also, vaccination of thepopulation was organized. Despite the favourable conditions for epidemics, none wasobserved in Skopje.
− The decision of the Government of Macedonia and the city of Skopje to evacuate children,the elderly and all other people who could not actively take part in the rescue operationsseemed justified under the conditions at the time. A large number of people were evacuatedfor periods varying from several weeks to several months. A number of evacuees of 150 000quoted in some documents seems to be too high.
− The classification of buildings according to level of damage, and the clearing of debris,began immediately after the rescue operations. A large number of experts arrived in Skopjefrom France, Italy, Japan, the Soviet Union, the USA and other countries, offeringprofessional assistance to local engineers. Red markers were used to identify buildings thatshould be torn down; yellow markers were used for buildings that would have to be repairedand strengthened; and green markers were used for slightly damaged buildings and those
158
that could still be used.
Reconstruction of Skopje
As soon as the emergency was under control, it was time to face the problem of Skopje's future. In the mindof the citizens there was never any doubt that Skopje must be rebuilt on the same location − and rebuilt as anexpanding, earthquake−proof metropolis that was greater and more glorious than ever. Because of that, oneweek after the earthquake a decision was made by the federal government of former Yugoslavia thattemporary accommodation for 120 000 Skopje citizens should be provided by the end of the year − 50 000 inrepaired buildings and 70 000 in prefabricated dwellings (6).
By October 1963, moreover, the British scientist Professor N.N. Ambrasey (6) had completed his preliminaryinvestigations for UNESCO and reported that there were no valid seismological grounds for a change of thesite − provided that the Vardar river was regulated so as to prevent its flooding waters from weakening thefoundations of Skopje's buildings and provided that all new buildings in Skopje were designed to resist lateralloads. In this connection, he recommended the establishment in Skopje of Europe's first Institute ofEarthquake Engineering. Meanwhile, the Japanese Government sent a three−person team to advise Skopjecity council on earthquake−resistant construction. Many other experts from Czechoslovakia, France, theformer Soviet Union, the United Kingdom, the USA and other countries came to the same conclusion thatSkopje should be rebuilt on the same site.
The first map of seismic microzonation of the wider urban region of Skopje city was prepared in 1964. In thesame year the former Yugoslavia published its first code for aseismic design and construction. One of the verycomplex and rather costly activities was to repair and strengthen the damaged buildings marked with yellow(salvageable) and green (lightly damaged) within a very short time. Because of our own lack of experience,professional assistance was requested from countries that had faced the problem of urban reconstruction inthe past. Expert knowledge gathered from the reconstruction of cities damaged by bombardment during theSecond World War was useful to us.
It was only after the enactment of the first code for aseismic design and construction in 1964 that activitieswere undertaken to strengthen a number of vital structures. The seismic horizontal forces of such structureshad to be increased by 50% compared to regular residential structures.
A federal law passed towards the end of 1963 allocated the equivalent of 900 million US dollars forreconstruction of Skopje over the next 10 years. In this period, 98.6% of this was spent. The construction ofSkopje after 1973 was financed by the city itself and by the Government of Macedonia.
The enormous destruction caused by the earthquake and the recognized need for new economicdevelopment called for a new city plan. Under the auspices of the United Nations, the city plan was developedby local experts with the participation of two urban planning companies (from Greece and Poland). To preparefor this, research was carried out into the geographical and geological characteristics of the Skopje area,natural barriers to urban expansion, future development trends in the region, land values, location ofhouseholds, and the need for services. Planning was based on the assumption that Skopje by 1981 wouldhave 350 000 inhabitants. This was an underestimate; since 1981 the city counted about 550 000.
Construction in Skopje after 1965
Two events significantly affected the improvement of the quality of construction in Skopje after the 1963earthquake. The first was the adoption of the first temporary regulations in the form of a law for aseismicdesign and construction in seismic regions in the former Yugoslavia− The second was the establishment ofthe Institute of Earthquake Engineering and Engineering Seismology in Skopje, which started work on 1October 1965.
Just how were the provisions of the new code implemented, bearing in mind that up to 1963 structuralengineers had no training in earthquake−resistant construction? The gap in knowledge had to be covered bythe newly established institute. Immediately after its establishment, the institute began a two−year course inearthquake engineering, leading to a Master's degree. The lectures were given by eminent experts in the fieldof earthquake engineering, mainly from Japan and the USA, and by specialists from Canada, India, Italy, NewZealand, Romania, the Soviet Union, the United Kingdom and elsewhere.
Conclusion
159
The experience from Skopje, gathered during the earthquake and during the reconstruction of the city, isextremely important to the wider international community. Several conclusions are particularly relevant:
− Neither the population nor the authorities were prepared for an adequate response in caseof such a disaster. However, people organized themselves on their own initiative, and therelevant services were mobilized very quickly. There is no precise information on the actualefficiency of the official authorities in dealing with the consequences of the earthquake.
− Skopje agreed to construct temporary settlements to accommodate 70 000 citizens, butthese settlements became permanent later on. This allowed the city to increase to anunnatural size from 200 000 in 1963 to 650 000 today. This increase has caused seriouseconomic, cultural, social and residential problems. Also, very useful agricultural land was lostforever.
− The reconstruction work and the construction of the new Skopje was carried out inaccordance with the requirements of the science of earthquake engineering and the advice ofexperts in this field. Therefore, the quality of the buildings guarantees a high safety level forthe citizens. Unfortunately, human memories are short. Nowadays, construction is becomingpoorer. Old buildings are being reconstructed without upgrading their seismic safety,inspection during design and construction is becoming less thorough. In Skopje as elsewhere,it is seen that profit often counts more than the safety of human life.
References
1. Skopje (monograph in five languages). Skopje, Assembly of Skopje, 1983.
2. Arsovski M, Hadzievski D. Generation of the Skopje earthquake according to tectonic and seismologicalobservations (original in Serbo−Croatian). Proceedings of II Yugoslav Symposium of Rock Mechanics andUnderground Construction, Skopje, Republic of Macedonia, 1967.
3. Arsovski M. et al. Seismological investigations of the Skopje valley and the territory of Skopje city, (originalin Serbo−Croatian). Belgrade, Geological Institute of Belgrade, 1964.
4. Jordanovski K. Skopje − catastrophe − reconstruction − experience (original in Macedonian). Skopje,Matica Makedonska, 1993.
5. Petrovski J, Milutinovic Z. Development of vulnerability functions and models for assessment of urban risk.Report for the Commission of the European Committees. Skopje, IZIIS, 1987.
6. Skopje resurgent. New York, United Nations, 1970.
Summary
J. Levett1, C. Ugarte2 and Secretariat
1 J. Levett is Director of International Affairs, National School of Public Health, Ministry ofHealth and Welfare, Athens, Greece.
2 C. Ugarte is Director, Direccion Nacional Preparacion contra Desastres, Lima, Peru.
Professor M. Gabr of Egypt presented his paper on "Rehabilitation of earthquake victims: social and healthaspects (the Cairo 1992 experience)". He first described the consequences of an earthquake of 5.9 on theRichter scale which occurred on 12 October 1992. He mentioned that Cairo sustained the highest damagewith the loss of 560 lives, more than 2000 injured and more than 5000 buildings collapsed. Since Egypt is notdescribed as a high−risk earthquake country, Professor Gabr described the event as a rare disaster. Thisearthquake affected chiefly the districts and administrations of Cairo, Fayoum, Giza, and Kalioubia.
The response and related measures were immediately started by the Ministry of Health with the help of theEgyptian Red Crescent which was responsible for social and psychological follow−up and support of victims.Professor Gabr mentioned that about 50 temporary shelters were immediately constructed for the victims and
160
for health services for them. Strict public health measures were taken and safe running water, soap, refusedisposal bags, and cooking and eating utensils were supplied. Steps were taken to ensure adequate nutrition,psychological care and social support, control of infectious diseases and other health measures.
Subsequently some modest apartments built in Cairo but still vacant, as well as another settlement, wereused to house the earthquake victims. The new community was helped to organize sports, adult literacyclasses, care for the handicapped, social gatherings and other activities. These activities greatly distractedyoung people from harmful activities such as drug abuse and violence. Some of the health measures includedpsychological counselling, nutrition, family planning, vaccinations and AIDS education. As a result, conditionssuch as depression, insomnia, agitation and other psychological manifestations often seen among disastervictims were not seen. Constraints like bad roads, lack of transport facilities, lack of schools, and securityproblems were all dealt with within about six months and earthquake victims were provided with an almostmore comfortable life than before. Professor Gabr added that the Red Crescent, using some initial seedmoney, developed a recovery project that financially was virtually self−sustaining.
V.N. Zavgorudko and T.I. Zavgorudko presented a poster entitled "Basic principles of resort rehabilitation ofearthquake victims". Having studied the experience of those who work in disaster medicine, includingexperience after the Neftegorsk earthquake in Russia, they noticed that one universally accepted type ofrehabilitation programme was missing. The health status of the Neftegorsk victims demonstrated the need toprovide a range of rehabilitation measures, from psychotherapy to complex physical and spa therapy. Suchrehabilitation, they argued, is necessary both for the victims and for the rescue workers and others whoprovide aid in disasters.
Rehabilitation based on active non−medication therapy is rarely used and not well studied by clinicians. Aresort has ideal capacity and excellent facilities to provide rehabilitation to disaster victims. It has enoughhospital beds, the number of beds can be easily increased, and specialized wards can be organized toprovide special types of services according to the needs of the patients. There are also plenty of virtually freebut highly effective natural curative remedies such as mineral waters and the therapeutic use of mud. A resortin Russia has well developed transport links and is administratively independent.
Mr Y. Yasuda, General Manager, Kansai Project Development Division, The Sakura Bank Limited, Kobe,Japan, described the aftermath of an earthquake from a bank's point of view. This description was based onthe experience of his bank during the Kobe earthquake. Mr Yasuda related how the bank's activities wereparalysed during and immediately after the earthquake. This was due mainly to the failure of lifeline servicessuch as electrical power and communication. This means that even if the buildings are strong, one is stillvulnerable to major risks and therefore one needs to be prepared. A small number of banks were operationalimmediately after the earthquake and some provided services on behalf of other banks whose buildings hadbeen destroyed. Special cash supplies were provided from Tokyo and, because there was no shortage ofcash, panic or tension never developed.
Mr Yasuda then described the bank's emergency actions, ranging from staff care to making cash available tothe public in the shortest time possible. He concluded with a number of lessons learned andrecommendations for the future, ranging from the psychological importance of early recovery of cash suppliesin a modern society, to help with low−interest loans for emergency spending and reconstruction.
Mr H. Kuramochi of the Hyogo Prefectural Government spoke on "Industrial reconstruction after the GreatHanshin−Awaji Earthquake". Considering that there were existing emergency preparedness plans, the sizeand extent of the damage took all by surprise. Many lifelines, such as railways, roads, electricity and gas lines,were damaged for months and even years afterwards, and the financial consequences of around 10 trillionyen affected not only Kobe or Japan but to some extent the whole world.
Mr Kuramochi added that early action was taken after the earthquake to invite opinions on rehabilitation fromall concerned, including the business community. Support was provided in the form of funds, subsidies, theerection of temporary factories and other measures. He stressed that the industries should not just aim toreconstruct to their pre−earthquake status, but should consider growth and/or diversification for the future. MrKuramochi mentioned that such plans included major reconstruction promotion projects such as theEnterprise Zone, KIMEC (Kobe International Multimedia and Entertainment City), a large new conventioncentre, an import mart and a move from heavy industry to high−technology oriented enterprises and services.Most members of the Great Hanshin−Awaji Economic Revitalization Plan which was formed in December1995 come from the business community. Within these plans, although still dependent on support from thegovernment, private companies play an important part in Kobe's recovery.
161
The Prefecture's PHOENIX reconstruction plan has among its aims:
− to attract foreign industry by tax rebates;− to provide additional incentives to come to Kobe;− to strengthen the traditional Kobe−Shanghai link;− to construct a new China town.
Mr Kuramochi mentioned constraints, such as the 1.6 trillion yen shortfall in tax revenues in the next 10 years,the fall in consumer demand associated with reconstruction expenses, and the movement of population fromthe affected areas. So far, residency has reached only 80% of the pre−earthquake level. Suitable remedialmeasures also have to be taken to deal with this problem and the solidarity of the whole country is stillneeded.
Dr D. Jurukovski, Director, Institute of Earthquake Engineering and Engineering Seismology, University "StCyril and Methodius", Skopje, the former Yugoslav Republic of Macedonia, then described the rehabilitationand reconstruction of Skopje after the 1963 earthquake and the lessons learned from this destructive event.The main conclusions from his presentation were:
• There is a need for an overall coordination of multisectoral efforts that could be performedby a civil protection organization.
• Self−organized communities form a crucial element in the success of relief operations afterearthquakes.
• Public health issues related to hygiene, food distribution and epidemic control should havethe greatest priority after the initial relief phase.
• Lessons learned need to be captured, documented and applied to future developmentplanning.
PART 5 − COUNTRY EXPERIENCES
Lessons learned from the Great Hanshin−Awaji Earthquake
Panelists: S. Baba1, ModeratorY. Nagasawa2, Co−moderatorS. Seo3
H. Minami4
Y. Yasuda5
S. Araki6
S. Ben Yahmed7, Rapporteur
1 S. Baba is Chairman, International Institute for Diabetes Education and Study, HonoraryPresident of International Diabetes Federation and Professor Emeritus, Kobe University,Kobe, Japan.
2Y. Nagasawa, is Professor, Department of Architecture, Graduate School of Engineering,The University of Tokyo, Tokyo, Japan.
3 S. Seo is President, Hyogo Medical Doctors Association, Kobe, Japan.
4 H. Minami is President, College of Nursing, Art and Science, Kobe, Japan.
5 Y. Yasuda is General Manager, Kansai Project Development Division, The Sakura BankLimited, Kobe, Japan.
162
6 S. Araki is Director, The Kobe Chamber of Commerce and Industry, Kobe, Japan.
7 S. Ben Yahmed is responsible for Emergency Preparedness, World Health Organization,Geneva, Switzerland.
The issues
Question 1: What are the factors that were a surprise in the earthquake?
Dr S. Seo, President, Hyogo Medical Doctors Association, Japan, addressed this question saying:
− deaths from fires and injuries were higher than normal;
− most of the deaths occurred in the first day, if not in the first half−day, before any externalsupport was possible;
− no cases needed haemodialysis among the victims who suffered crush syndrome in the firstday. However, after two days, cases of crush syndrome rapidly increased so that urgenttreatment and also haemodialysis was needed.
Dr Seo also said that medical doctors, among others, were not well−prepared for disaster. It was assumedthat the medical facilities would not be damaged during a disaster, which turned out to be untrue. There wasalso a lack of understanding of the difference between medical treatment in emergencies and disasters, suchas first aid and triage for treatment. Communication was impaired, lifelines for water, electricity and gas werebroken, and access to medical facilities was also often not possible. There was also a shortage of medicineand equipment.
New systems of communication should be built for emergencies. WHO should play a role in vulnerabilityreduction and not only in hospital care. Problems should be anticipated because hospitals cannot be built tobe 100% safe. Emotional upset is different from post−traumatic stress disorder and must be approacheddifferently. Finally, the mobilization of and cooperation with volunteers should be strengthened andreorganized.
Mr Yasuda said that people were not prepared for the disaster and that the command lines for help had notbeen clear (between local and central authorities). Also− in streets crowded with private and businessvehicles, there was no priority for the fire brigade. He also felt that economic activity should be temporarilysuspended in such a situation.
A comment from the floor suggested that 70% of the people alive were rescued by neighbours before thearrival of the local rescue services.
Dr Pretto asked if autopsies were the basis for Dr Seo's data, and this was confirmed.
Question 2: Which effects have most impact on the health and well−being of sufferers?
Professor H. Minami mentioned that among care−providers, post−traumatic stress disorder was observedlargely among the nurses. She said that care−providers tend to resist help, they become overtired, neglectprivate needs and eventually display aggressive behaviour. She said that, when not cared for, they becameaccident−prone.
Dr Seo added that disaster nursing had already been introduced as a new teaching discipline. He also saidthat 76% of the deaths were instant. Within the first 24 hours, 4460 people died in the morning and 440 duringthe afternoon, most of them by suffocation.
Dr Hayashi mentioned from the floor that there were actually few cases of infectious disease becausetemperatures were low. However, human waste became a problem. The simple matters of finding a toilet anddisposing of waste became major issues. Temporary solutions were authorization to use manholes of thesewerage system and the installation of simple, portable toilets.
Question 3: What are the economic and infrastructural measures to enhance vulnerability reductionand emergency preparedness?
163
The two participants from the business and banking sector, Mr Yasuda and Mr Araki, emphasized the factthat initially companies were busy checking the health situation of their employees. They also helped establisha relief and aid fund to which employees and companies contributed. The Kobe Chamber of Commerce andIndustry carried out surveys of infrastructure damage, including port facilities, and organized new sites formarkets.
The next priority was the re−establishment of production systems to permit a speedy socioeconomic recoveryof the whole area. Some 100 000 people moved out of the area and attractive conditions have to be offered topersuade international companies to move into the area. There are still too many regulations obstructingrecovery, in their opinion.
Question 4: What are the measures in the health sector to reduce vulnerability and enhancepreparedness?
Dr Seo emphasized that, although of vital importance to the victims, the role of doctors is not yet seen asimportant when it comes to national disaster management and planning. This fact prevents the healthcommunity from promoting effective vulnerability reduction and preparedness concerning the health effects ofdisasters.
Question 5: What are the most important lessons for future earthquakes in the Hanshin region andelsewhere?
Dr Seo felt that receiving the right information quickly would be most important lesson for the future. Alsowater supplies for essential functions should be safeguarded.
Dr Minami thought that public and professional education for disaster management were most important.Also, research in this field should be better networked and public health centres used in preparednessprogrammes.
Mr Yasuda said that government and banks must coordinate their actions and practise emergency measures.More initial subsidies and improved insurance schemes should be provided.
Mr Araki felt that infrastructures should be strengthened and bureaucracy reduced to help more effectively inthe future. The risk of dependence on computers must be reduced by better safeguarding these machines orby developing a system that makes them redundant. Power failures and provision of necessary back−upswere also a problem and must be improved.
Professor Baba felt that elderly and lonely people should receive more attention to save them from becomingdemoralized or even committing suicide. Measures should be taken to make such persons useful in therecovery process.
Moderator's summary
The Great Hanshin−Awaji Earthquake exposed some serious flaws in emergency preparedness, according toProfessor Baba. However, a great deal of medical, health, social and engineering knowledge was acquiredas a result of the earthquake.
Since then there have been other major earthquakes (e.g. in Sakhalin, Russia and in China) and more willoccur. A worldwide strategy needs to be drawn up for disaster relief efforts to be carried out more effectively.
Types and phases of damages
Large−scale disasters change somewhat as time goes on, but the course of damage usually follows a patterncomprising:
− primary damage (danger due to collapse of houses and other buildings);
− secondary damage (increasing damage due to fire from electricity and sparks);
− tertiary damage (panic due to damage to lifelines, roads, shops and medical facilities,followed by a breakdown of family life, worsening conditions of hygiene, and the spread ofinfectious diseases);
164

− quaternary damage (economic, social and cultural damage affecting the whole country).
Detailed policies for city disaster relief efforts should be planned and implemented on the basis of the abovefour phases.
Crucial issues regarding the Great Hanshin−Awaji Earthquake
There appeared to be various crucial issues regarding the Great Hanshin−Awaji Earthquake. They were:
− disruption of the information system;
− collapse of the transportation system;
− destruction of lifelines;
− lack of medical instruments and drugs;
− problems of the elderly, disabled people, and bereaved families;
− the rebuilding of communities (a task both challenging and rewarding);
− issues concerning temporary housing units (deaths among persons living alone,psychological and emotional aspects);
− survivors still searching for ways to re−establish their lives (security for tomorrow,seed−money to get started);
− relating the rare earthquake experience to the next generation.
Vulnerability reduction for the future
The moderator noted that vulnerability reduction measures should not be confined to hospitals or to centraladministrations but should above all be further decentralized to the community level.
He also stressed that funding of vulnerability reduction measures by private sector funds in addition to publicones should be encouraged. Members of the audience made several suggestions of which the most importantpoints can be summarized as follows:
− A disaster management centre was proposed which is to focus on an integrated informationsystem and test the decision−making system under conditions of urgency.
− The rebuilding of communities requires re−adjustment plans for land and jointly ownedproperties, coexistence of all ages, of bereaved family, the elderly, the disabled, etc. andfail−safe planning of community systems comprising basic design, an adapted civil defencesystem, and a city design that promotes health and sustainable development at thecommunity level.
Earthquake preparedness in Chile
G.N. Solar1
1 G.N. Solar M.D. is Medico Coordinador, Comité de Emergencias, Servicio de SaludMetropolitano Occidente, Santiago, Chile.
Chile is located in the south−west part of South America. It has a continental surface of 756 000 km2, notincluding an Antarctic Territory, and is 4200 km long. Chile is one of the countries situated on the Pacific ringof fire and is therefore frequently affected by high intensity earthquakes of up to VII on the Mercali scale. From1570 until today, more than 100 earthquakes of this severity have shaken the country, and in the last centuryalone more than 75 important earthquakes have happened.
165
Chile may be divided into three areas of seismic activity. Within the large geographical extension between thecity of Arica in the north and the Taitao peninsula (Lat 18°S to 48 °S) in the southern part of the country, theseismic hazard is greater in the north. Seismic intensity is also higher at the coast than in the high mountains.These differences are explained by the displacement of the Nazca plate under the continent. The area withthe lowest seismic activity is known as Area I and comprises the Andes Region. It is also characterized by lowpopulation density.
Area III, with the highest seismic activity, is the coastal zone indicated that includes cities with a highpopulation density. The density is 150 inhabitants per hectare in Santiago and 40−60 inhabitants per hectarein other cities of this area which have frequently been seriously affected by earthquakes and tsunamis.Fortunately, human loss and injury has been low. The largest recent earthquakes in this area were those inArica (1987, magnitude 7.0), Antofagasta (1995, magnitude 7.0), Valparaiso (1985, magnitude 7.8), Santiago(1985, magnitude 7.8), Concepción (1975, magnitude 7.8). The most severe earthquake was registered inChillan City in 1939 (magnitude 9.0 on the Richter scale) and caused 30 000 victims. In that city, situated inArea III, 62% of the houses were made of adobe and 70% of these were destroyed completely. Half of thebrick buildings were also destroyed, but only 11 % of masonry buildings were damaged and 20% of reinforcedconcrete buildings were partially damaged. Chillan City was almost completely rebuilt and today there is littleof the old city remaining.
As a result of this event, strict building codes were introduced and have proved their worth in laterearthquakes in the same area, such as the 1960 earthquake with a magnitude of 7.0. In later earthquakes,however, some reinforced concrete buildings were partially affected because of poor construction quality.
Preparedness of health services
Hospitals must be ready to provide the best services they can. Therefore there must be prior training byworking in a mock emergency situation which includes the structural, organizational and social vulnerabilities.Emergency exercises should then be evaluated to reveal weaknesses. To do this, we have consideredvarious emergency scenarios involving people, hospital installations, public and private institutions, housesand industrial buildings.
Information from such theoretical exercises should be incorporated into regional maps of risk, indicatingstrengths and weaknesses. These should incorporate the environmental health risk, technological risks,natural risks, epidemiological indicators of chronic and acute pathologies, biodemographic structure of thepopulation, and regional industry since all of these may affect the capacity to maintain a continuous responseto population needs. Stocks of critical supplies should also be planned according to known needs. A regionalmap can thus show both risks and resources. The objective of this procedure is to guarantee the capacity ofthe regions to help themselves in case of disaster, using a database of permanent stock and its locationsthroughout the country.
Hospitals in earthquakes
In 1985, an earthquake hit the ports of San Antonio and Valparaiso, as well as the cities of Santiago, Talcaand Concepción. There was enormous damage to hospitals and other buildings. Of 536 hospitals in theaffected zone, 108 received serious (defined as 33.3%) damage. As a consequence 2796 hospitals beds outof 19 581 (14.3%) were not available. Both large and small hospitals were affected. Repair of the structuraldamage to hospitals required an extensive investment programme amounting to 18 800 million US dollars forrebuilding 31 500 m2 of hospital space and to repair 134 000 m2. The 1995 earthquake which affectedAntofagasta city led to economic losses of only US$ 600 000.
The magnitude of earthquakes, the financial limits of the health sector and the vulnerability of hospitalstructures have led to the development of preventive strategies defined to protect hospitals and theirequipment in case of disasters. We are concerned not just with protecting the buildings and the people inthem but with ensuring that the hospital can continue to function when a disaster occurs.
With the premise that proper construction and organization of hospitals can produce a high degree ofprotection, the Health Ministry of Chile and the Civil Engineering Department of the University of Chile, withthe support of PAHO and ECHO−3, have started a project to develop a health care system with controlledrisks.
The primary health care approach
166
Primary health care has been developed in the public sector over a number of decades. Emergency educationand treatment centres at primary level can help reduce much of the demand on higher levels of emergencycare and are a significant help in disaster situations. Experience shows the value of the primary health careapproach in communities, as well as in the interaction between public and private institutions. These primarylevel centres do reduce morbidity in disaster situations. They also help in reintegrating injured persons intocommunity life.
Civil Defence Organization
The Chilean civil defence system is the country's means for disaster response. It involves civil administration,state resources, legislation, nongovernmental organizations, the scientific community and organized groups ofthe population. One of the elements of the civil defence system is the national emergency plan in which allministries and state organisms have a role.
The Interior Affairs Ministry is the main support and the home for the civil defence system and responsibilityfor it falls on the Minister of Interior Affairs. The system relies on a technical organism, the NationalEmergency Bureau (ONEMI), which by law is appointed "to plan, coordinate and execute the activitiesdestined to prevent or to solve problems derived from earthquakes or disasters". ONEMI today has formalrepresentation throughout the country. It functions at national, regional, provincial and community levels.Given the administrative decentralization of the country, this integrated and coordinated structure is of majorimportance. For instance, the role of the community with its city hall and its local authority is vital because thisis at the level where the initial impact of a disaster is felt and it is here that an immediate response has to bemade.
Local coordination and planning are the responsibility of community emergency committees on which arerepresented all groups likely to be involved. This is the best guarantee of adequate management in case of anemergency. The participation of the armed forces, police, public works departments, civil defence, Red Cross,fire department, community organizations and businesses is fundamental to these committees so that risks,vulnerabilities, resources, inventories and coordinated responses can all be evaluated. The civil defencesystem is based on the two fundamental principles of self−help and use of resources in phases. For instance,we do not expect an affected borough to ask for immediate help from the national level if it has not used theresources of non−affected boroughs at the regional level.
The role of the health sector in disaster situations
The health sector plays an important role in the civil defence system for many reasons. It must makeadequate preparation to assist the victims of a disaster, it has to give medical assistance to the injured, itprovides regular care to the non−affected population, and it has to make sure that the environment does nothave a negative effect on people's health after the disaster has occurred. The role of the Public HealthMinistry in relation to the national emergency plan is elaborated in Fig. 5.1.
Tasks of the Public Health Ministry in case of emergency or disaster
These tasks include:
− planning at Ministry level and with regional secretaries of health services and hospitals andcoordinating with the primary care level;
− coordination of the use of private and public capacities;
− giving priority to emergency needs and ensuring the necessary human and mentalresources;
− establishing rules to qualify facilities to serve as back−up hospital wards;
− epidemiological surveillance of infectious and parasitic diseases and their control; designand control of emergency stocks and ensuring rapid distribution;
− control and maintenance of the level of health and the standard of the environment;
− ensuring adequate coordination of ground, air and sea evacuation;
167
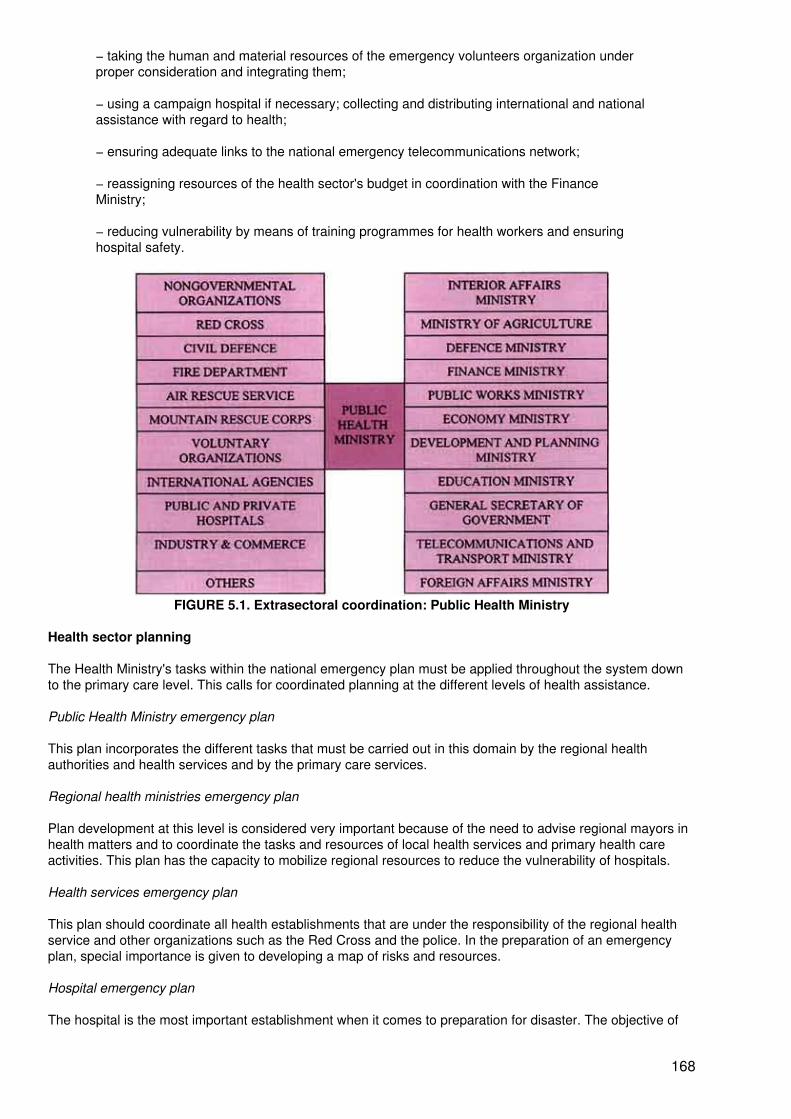
− taking the human and material resources of the emergency volunteers organization underproper consideration and integrating them;
− using a campaign hospital if necessary; collecting and distributing international and nationalassistance with regard to health;
− ensuring adequate links to the national emergency telecommunications network;
− reassigning resources of the health sector's budget in coordination with the FinanceMinistry;
− reducing vulnerability by means of training programmes for health workers and ensuringhospital safety.
FIGURE 5.1. Extrasectoral coordination: Public Health Ministry
Health sector planning
The Health Ministry's tasks within the national emergency plan must be applied throughout the system downto the primary care level. This calls for coordinated planning at the different levels of health assistance.
Public Health Ministry emergency plan
This plan incorporates the different tasks that must be carried out in this domain by the regional healthauthorities and health services and by the primary care services.
Regional health ministries emergency plan
Plan development at this level is considered very important because of the need to advise regional mayors inhealth matters and to coordinate the tasks and resources of local health services and primary health careactivities. This plan has the capacity to mobilize regional resources to reduce the vulnerability of hospitals.
Health services emergency plan
This plan should coordinate all health establishments that are under the responsibility of the regional healthservice and other organizations such as the Red Cross and the police. In the preparation of an emergencyplan, special importance is given to developing a map of risks and resources.
Hospital emergency plan
The hospital is the most important establishment when it comes to preparation for disaster. The objective of
168
the hospital is to assist the victims of the disaster while continuing to care for patients hospitalized before thedisaster occurred. The hospital emergency plan is the responsibility of the local emergency committee whichworks with the local emergency service.
Pre−hospital care plan
In regions with more than one hospital, it is necessary to define a process of triage of victims to the differenthealth facilities. For this purpose, two models of pre−hospital emergency care have been developed, one forthe metropolitan and fifth−region area, essentially relying on ambulances to transport victims to hospitals andanother one for the rest of the country using primary care emergency centres.
Primary care emergency plan
In a disaster situation primary care has strategic importance. This is the level at which first medical help isgiven. With professional resources it provides help to trauma victims, and reduces excessive demand atreferral hospitals. At community level, social problems that result from disasters are often best taken care ofwithin the context of primary health care.
Conclusion
− Planning for disasters must necessarily involves intersectoral coordination in order to defineclearly the roles of different bodies involved in the emergency plan and to specify the meansby which these roles will be fulfilled.
− The emergency plan must be reviewed periodically in the light of changes to the communityand its environment.
− The civil defence system must be strengthened at all levels, which requires majorcoordination with the health sector.
− Training should be provided to improve the skills of different levels of emergencymanagement.
− Risk maps should be drawn up and reviewed regularly. This task requires intersectoralorientation, adequate technical resources, reliable sources of information and modeminformatics approaches. This is an area that is still under development.
− Integrated information and uniform indicators associated with vulnerability criteria should beused in preparing disaster scenarios.
− It is crucial to have efficient management and information on supplies at the national andregional levels, as well as information on emergency stocks in neighbouring countries.
Health aspects of disaster preparedness in the former Yugoslav Republic of Macedonia
Z.V. Milutinovic1
1 Z.V. Milutinovic is Professor, Section for Risk and Disaster Management, Institute ofEarthquake Engineering and Engineering Seismology, University "St. Cyril and Methodius",Skopje, The former Yugoslav Republic of Macedonia.
The former Yugoslav Republic of Macedonia is situated in the central part of the Balkan peninsula. It coversan area of 25 713 km2 and borders on Bulgaria to the east, Greece to the south, Albania to the west andYugoslavia to the north.
According to the 1994 census, the former Yugoslav Republic of Macedonia has 2 001 368 inhabitants, 479808 households, 553 213 dwellings and 167 568 agricultural holdings. There are 1753 settlements, of which29 are large urban areas. The capital of the former Yugoslav Republic of Macedonia is Skopje (450 000inhabitants).
169
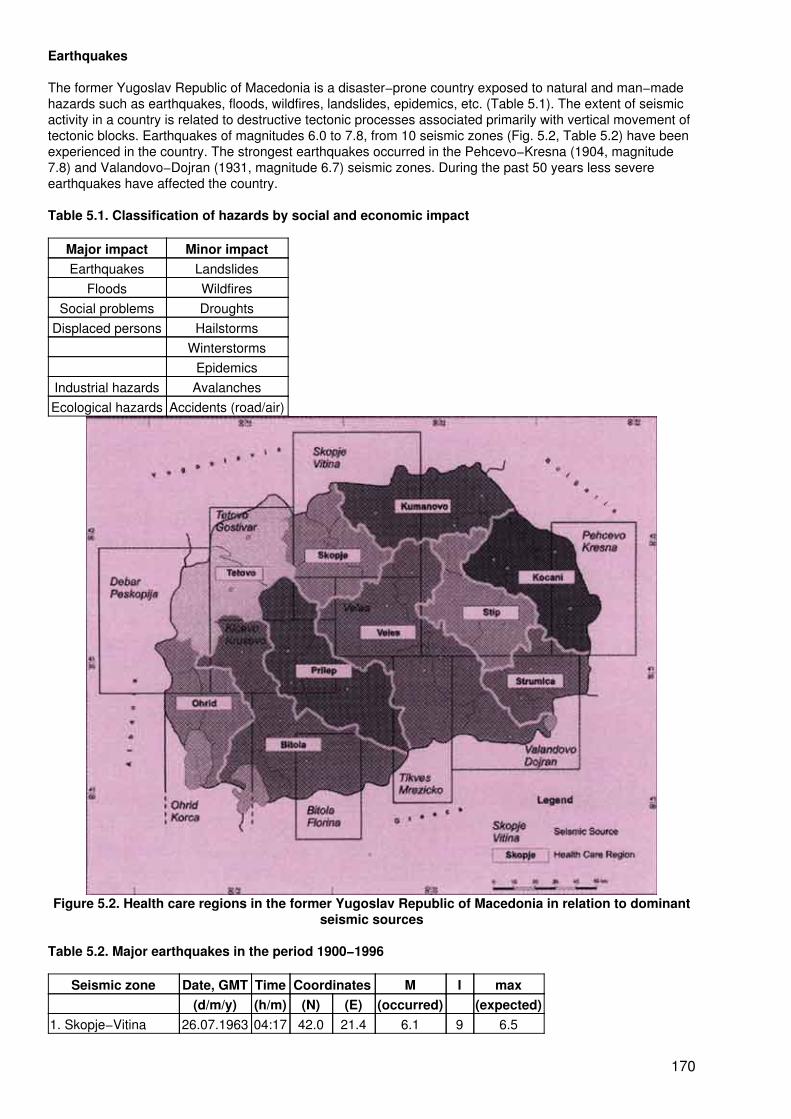
Earthquakes
The former Yugoslav Republic of Macedonia is a disaster−prone country exposed to natural and man−madehazards such as earthquakes, floods, wildfires, landslides, epidemics, etc. (Table 5.1). The extent of seismicactivity in a country is related to destructive tectonic processes associated primarily with vertical movement oftectonic blocks. Earthquakes of magnitudes 6.0 to 7.8, from 10 seismic zones (Fig. 5.2, Table 5.2) have beenexperienced in the country. The strongest earthquakes occurred in the Pehcevo−Kresna (1904, magnitude7.8) and Valandovo−Dojran (1931, magnitude 6.7) seismic zones. During the past 50 years less severeearthquakes have affected the country.
Table 5.1. Classification of hazards by social and economic impact
Major impact Minor impactEarthquakes Landslides
Floods WildfiresSocial problems Droughts
Displaced persons HailstormsWinterstorms
EpidemicsIndustrial hazards AvalanchesEcological hazards Accidents (road/air)
Figure 5.2. Health care regions in the former Yugoslav Republic of Macedonia in relation to dominantseismic sources
Table 5.2. Major earthquakes in the period 1900−1996
Seismic zone Date, GMT Time Coordinates M I max(d/m/y) (h/m) (N) (E) (occurred) (expected)
1. Skopje−Vitina 26.07.1963 04:17 42.0 21.4 6.1 9 6.5
170
2. Tetovo−Gostivar 12.03.1960 11:54 41.9 20.9 5.7 8 6.13. Debar−Peskopija 30.11.1967 07:23 41.4 20.5 6.6 9 6.94. Ohrid−Korca 18.02.1911 21:35 40.9 20.8 6.7 9 6.95. Valandovo−Dojran 08.03.1931 01:50 41.3 22.5 6.7 10 6.96. Pehcevo−Kresna 04.04.1904 10:25 41.8 23.1 7.8 10 7.97. Titov Veles 14.09.1922 16:37 41.7 21.4 5.5 7−8 5.88. Kicevo−Krusevo 21.10.1988 02:18 41.3 21.0 4.4 6−7 5.89. Bitola−Florina 14.09.1920 02:09 41.0 21.4 5.3 7 5.710. Tikves−Mrezicko 09.07.1955 23:53 40.9 22.1 5.1 7−8 6.0
M − Magnitude (Richter Scale), I − Epicentral Intensity (Mercalli Scale)
Vulnerability and seismic risk
Although some degree of general risk awareness exists among the people − and among professionals,planners and authorities − a composite risk assessment for the former Yugoslav Republic of Macedonia hasnot been yet undertaken on a systematic basis or applied to rigorous disaster management and preparednessplanning. With the exception of very general hazard maps, maps showing the severity, frequency and durationof hazardous natural phenomena (except for earthquakes) are not available; this is also the case forintegrated vulnerability and risk assessment in physical and economic terms.
Probabilistic seismic hazard and risk studies are carried out to estimate disaster demands in terms ofphysical/functional losses of residential and public buildings, potential human casualties (morbidity andmortality), accessibility of major and minor transportation routes. Studies are also used to establishrisk−consistent and economically justified emergency preparedness elements at national, regional andmunicipal levels. These are performed for three characteristic levels of expected seismic action that complywith the seismic hazard levels incorporated in the existing legislation for design and construction in theterritory of the former Yugoslav Republic of Macedonia. These levels are:
− FSE: frequent scale earthquake, or earthquake of five years return period;− MSE: moderate scale earthquake, or earthquake of 10 years return period;− LSE: large scale earthquake, or earthquake of 50 years return period.
Residential buildings
There are five main types of residential and public buildings, including individual family dwellings (Table 5.3) inthe territory. Due to the high vulnerability of buildings of weak masonry and of traditional stone or brickconstruction, significant physical damage (in both extent and severity), causing substantial economic losses,is to be expected in moderately strong earthquakes (5.2 < M < 5.9) or shallow earthquakes (h = 10 − 15 km).1In strong to catastrophic earthquakes (M > 6.0 on the Richter scale, I > VIII on the Mercalli scale), the physicallosses for the above building types will be exceptionally high, causing significant human casualties andphysical and economic losses.
1 A typical example is the Bitola earthquake of 1 September 1994 (M = 5.4, I = VII+) whichcaused heavy damages to 4309 buildings and direct economic loss of 2 205 040 thousanddenars (45 million US Dollars), i.e. 3.4% of GNP of The former Yugoslav Republic ofMacedonia for 1993
A significant level of earthquake protection for newly constructed buildings was achieved with theimplementation of the 1964 and 1981 Codes for Design and Construction of Buildings in Seismically ActiveRegions (1). However, both codes represent compromises that reflect not only the planned level of protection,but also the development needs and the economic power and potential of the country. Consequently, acertain degree of vulnerability and potential for generating physical losses is also to be expected in theaseismically designed and constructed buildings, particularly when exposed to catastrophic earthquakes.
The Skopje−Vitina seismic zone has the highest physical and economic loss potential, as well as evacuationand shelter needs (Fig. 5.3). This is not because of the expected severity of the earthquakes but due to thevery high concentration of population and property. Because of the prevalence of highly vulnerablenon−resistant buildings in the region of Eastern Macedonia, the Pehcevo−Kresna seismic zone has thepotential for human casualties (Fig. 5.4) in moderately strong earthquakes.
171
Table 5.3. Population and residential floor area by structural typology and urbanization patterns
STRUCTURAL TYPE Total Urban areas Rural areasPopulation Floor
areaPopulation Floor
areaPopulation Floor
areaEarthquake non−resistant 869 722 17 256
163468 948 9 100 670 400 775 8 155 492
Weak masonry constructed prior to1960
241 215 4 826 257 87 296 1 694 115 153 919 3 132 141
Masonry constructed prior to 1971 628 507 12 429906
381 652 7 406 555 246 856 5 023 351
Earthquake resistant 1 164 243 23 019567
712 787 13 832767
451 456 9 186 800
Strengthened masonry 873 703 17 333164
473 181 9 182 833 400 522 8 150 331
RC* Frame systems 184 002 3 589 647 164 069 3 184 024 19 933 405 623RC Shear wall systems 106 538 2 096 756 106 538 2 096 756Total 2 033 964 40 275
7311 181 735 22 933
437852 231 17 338
292
*RC = reinforced concrete
Health care facilities and the health care system
The network of health care institutions covers the territory of the former Yugoslav Republic of Macedonia in anapproximately uniform manner, with a slightly increased concentration in the region of Skopje where theClinical Centre and the Military Health Care Centre (large army hospital facility) are located. The network ofhealth care institutions is shown in Table 5.4.
Table 5.4. Health care institutions in the former Yugoslav Republic of Macedonia
Type of institution NumberMedical centres 16Health care centres 16Public health stations (Units) 7General hospitals 17Clinics under the Clinical Centre of Skopje 18Clinics under the Faculty of Stomatology 7Specialized hospitals for tuberculosis and other lung diseases 3Specialized hospitals for mental care 3Institutes for orthopaedics and traumatology 1Centres for rehabilitation and prolonged care 7Specialized hospitals 2Specialized hospitals 10Regional health protection institutes 10National (Republic) Health Protection Institute 1The medical units operating in rural regions of the country are associated either with the regional medicalcentres or the health care centres. Out of the total number of 297 rural medical units, 188 provide permanentMD service, whereas 109 provide limited MD service by visiting doctors. The medical centres, health centresand the outpatient stations provide primary health care through 43 5 general practitioner services, 113occupational health services, 157 paediatric health care services for children up to six years of age, 80 healthcare services for children over six years of age, 62 health services for women, 27 health services forprotection against tuberculosis, and seven health services for skin and venereal diseases.
The total bed capacity in the country is about 10 645 beds or 5.5 for every 1000 inhabitants. Of these beds,4849 are in the general hospitals, 4695 in specialized hospitals, 685 in centres for cure and rehabilitation, 280
172
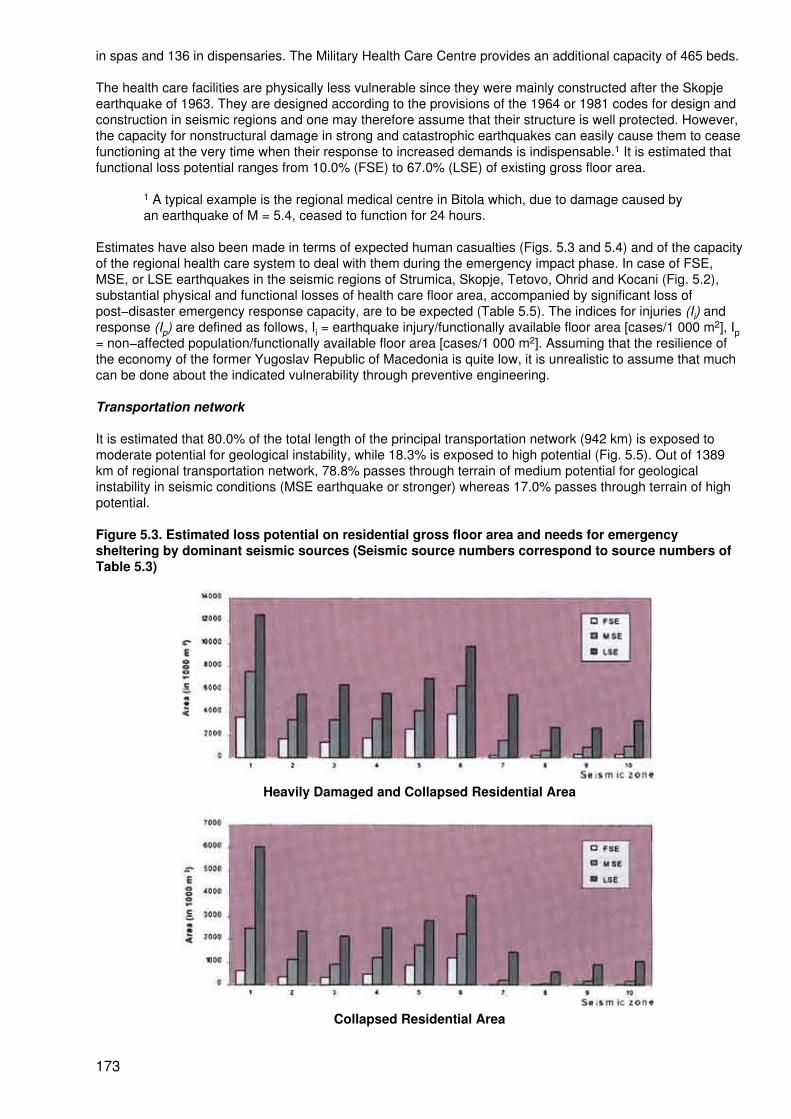
in spas and 136 in dispensaries. The Military Health Care Centre provides an additional capacity of 465 beds.
The health care facilities are physically less vulnerable since they were mainly constructed after the Skopjeearthquake of 1963. They are designed according to the provisions of the 1964 or 1981 codes for design andconstruction in seismic regions and one may therefore assume that their structure is well protected. However,the capacity for nonstructural damage in strong and catastrophic earthquakes can easily cause them to ceasefunctioning at the very time when their response to increased demands is indispensable.1 It is estimated thatfunctional loss potential ranges from 10.0% (FSE) to 67.0% (LSE) of existing gross floor area.
1 A typical example is the regional medical centre in Bitola which, due to damage caused byan earthquake of M = 5.4, ceased to function for 24 hours.
Estimates have also been made in terms of expected human casualties (Figs. 5.3 and 5.4) and of the capacityof the regional health care system to deal with them during the emergency impact phase. In case of FSE,MSE, or LSE earthquakes in the seismic regions of Strumica, Skopje, Tetovo, Ohrid and Kocani (Fig. 5.2),substantial physical and functional losses of health care floor area, accompanied by significant loss ofpost−disaster emergency response capacity, are to be expected (Table 5.5). The indices for injuries (Ii) andresponse (Ip) are defined as follows, Ii = earthquake injury/functionally available floor area [cases/1 000 m2], Ip= non−affected population/functionally available floor area [cases/1 000 m2]. Assuming that the resilience ofthe economy of the former Yugoslav Republic of Macedonia is quite low, it is unrealistic to assume that muchcan be done about the indicated vulnerability through preventive engineering.
Transportation network
It is estimated that 80.0% of the total length of the principal transportation network (942 km) is exposed tomoderate potential for geological instability, while 18.3% is exposed to high potential (Fig. 5.5). Out of 1389km of regional transportation network, 78.8% passes through terrain of medium potential for geologicalinstability in seismic conditions (MSE earthquake or stronger) whereas 17.0% passes through terrain of highpotential.
Figure 5.3. Estimated loss potential on residential gross floor area and needs for emergencysheltering by dominant seismic sources (Seismic source numbers correspond to source numbers ofTable 5.3)
Heavily Damaged and Collapsed Residential Area
Collapsed Residential Area
173
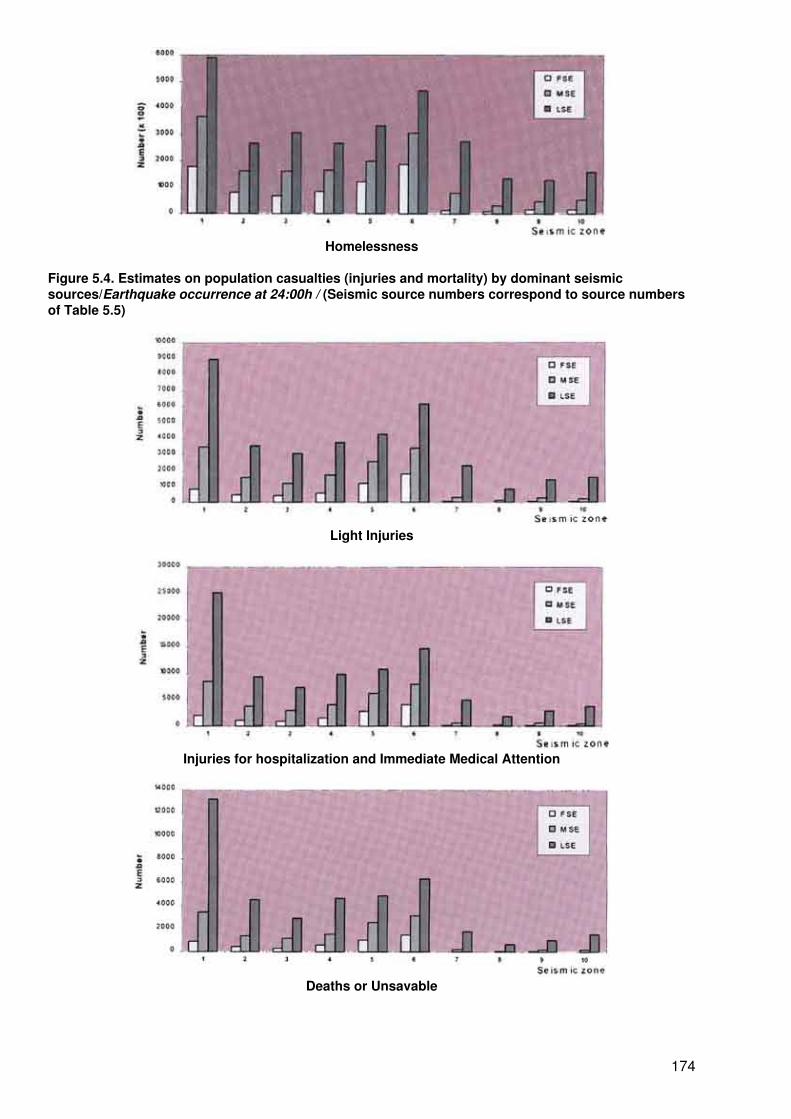
Homelessness
Figure 5.4. Estimates on population casualties (injuries and mortality) by dominant seismicsources/Earthquake occurrence at 24:00h / (Seismic source numbers correspond to source numbersof Table 5.5)
Light Injuries
Injuries for hospitalization and Immediate Medical Attention
Deaths or Unsavable
174
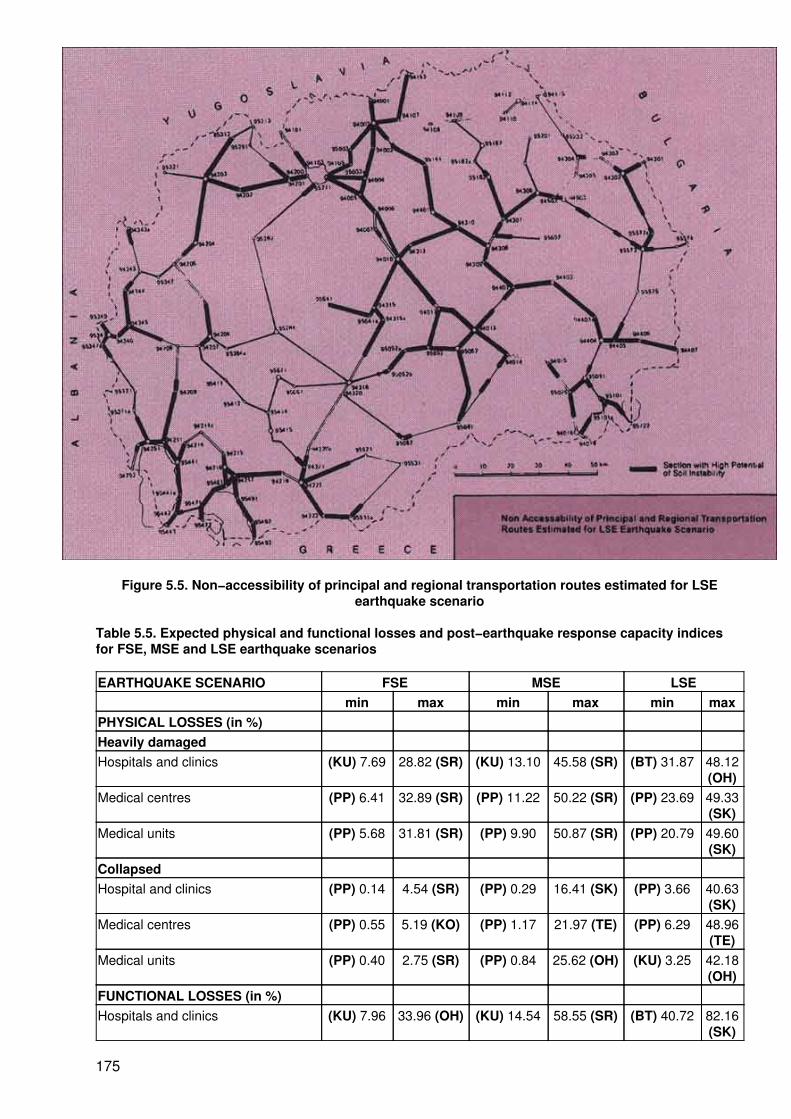
Figure 5.5. Non−accessibility of principal and regional transportation routes estimated for LSEearthquake scenario
Table 5.5. Expected physical and functional losses and post−earthquake response capacity indicesfor FSE, MSE and LSE earthquake scenarios
EARTHQUAKE SCENARIO FSE MSE LSEmin max min max min max
PHYSICAL LOSSES (in %)Heavily damagedHospitals and clinics (KU) 7.69 28.82 (SR) (KU) 13.10 45.58 (SR) (BT) 31.87 48.12
(OH)Medical centres (PP) 6.41 32.89 (SR) (PP) 11.22 50.22 (SR) (PP) 23.69 49.33
(SK)Medical units (PP) 5.68 31.81 (SR) (PP) 9.90 50.87 (SR) (PP) 20.79 49.60
(SK)CollapsedHospital and clinics (PP) 0.14 4.54 (SR) (PP) 0.29 16.41 (SK) (PP) 3.66 40.63
(SK)Medical centres (PP) 0.55 5.19 (KO) (PP) 1.17 21.97 (TE) (PP) 6.29 48.96
(TE)Medical units (PP) 0.40 2.75 (SR) (PP) 0.84 25.62 (OH) (KU) 3.25 42.18
(OH)FUNCTIONAL LOSSES (in %)Hospitals and clinics (KU) 7.96 33.96 (OH) (KU) 14.54 58.55 (SR) (BT) 40.72 82.16
(SK)
175
Medical centres (PP) 6.97 36.95 (KO) (PP) 12.39 64.25 (ST) (PP) 29.29 82.01(TE)
Medical units (PP) 6.08 34.56 (SR) (PP) 10.74 63.63 (OH) (PP) 25.62 79.09(OH)
RESPONSE CAPACITYInjury index, IiHospital, clinics and medical centres (PP) 3 219 (SR) (PP) 7 667 (SR) (PP) 4 1142
(SR)Medical units (PP) 9 848 (SR) (PP) 29 2528 (SR) (PP) 135 4106
(SR)Response index, IpHospital, clinics and medical centres (ST) 3 12 (SR) (ST) 3 19 (SR) (PP) 5 25
(SR)Medical units (SK) 3 70 (SR) (SK) 4 115 (SR) (SK) 8 160
(SR)
Note: Physical and functional losses are presented in % of total existing health care region(HCR) floor area of corresponding medical building classes
High risk HCRs: SR−Strumica, SK−Skopje, OH−Ohrid, Ko−Kocani,TE−TetovoLower risk HCRs: KU−Kumanovo, BT−Bitola, PP−Prilep, ST−Stip
Disaster management in the former Yugoslav Republic of Macedonia
Traditionally, each large−scale disaster in the territory of Macedonia within the former Yugoslavia washandled separately by specially−formed committees and directorates responsible for physical reconstructionand rehabilitation of disaster−stricken regions and revitalization of economic and social functions.Interdisciplinary disaster management, including prevention and preparedness, is a relatively new conceptused for efficient and effective mitigation of the expected destructive effects of natural and man−madedisasters.
Preventive engineering
Standard legislation defining the procedures and the requirements for seismic protection chiefly refer to theissue of mitigating damage to buildings, engineering structures and other facilities. The first Regulations forConstruction of Buildings in Seismically Active Regions1 (as reported above) were introduced in 1964 after thecatastrophic Skopje earthquake of July 1963. The technical measures for repair, strengthening andreconstruction of high−rise buildings (reinforced concrete and masonry structures) are defined in varioustechnical regulations.2(2−4).
1 Official gazette of SFRY, 39/64.2 Official gazette of SFRY, 52/85.
Protection of the population, material property and the entire living environment of the former YugoslavRepublic of Macedonia against other natural or man−made disasters is regulated by abundant legislation.This includes laws on water3, on protection against fires4, on protection against explosions,5 on health care,6on protection of animals against contagious diseases,7 and on protection of flora against diseases anddamage.8 These lawa are accompanied by extensive complementary regulations and ordinances.
3 Official register of SRM, 28/87.4 Official register of SRM 43/86, 37/87, 51/88 and official register of RM, 12/93.5 Official register of SRM 4/7 8, 10/78, 51/88, 36/90 and official register of RM, 12/93.6 Official register of RM, 38/91.7 Official register of RM, 83/92.8 Official register of RM, 83/92.
Emergency management
176
Protection of lives and public health as well as of property against natural disasters (earthquakes, floods,landslides, avalanches, heavy storms, droughts, and other disasters) is regulated by the provisions of the Lawon Protection Against Natural Disasters9 and the Law on Defence.1 The civil defence forces are organized bythe government and are to be used for emergencies as defined by an ordinance of the government.2 Theduties of the civil defence headquarters are defined by the Law on Protection Against Natural Disasters.3
9 Official gazette of SFRY, 39/77, 47/89.1 Official register of SRM, 8/92.2 Official register of SRM, 8/92, chapter VI.3 Official register of SRM, 3 9/77, chapter V.
Activities to mitigate or eliminate a threat or effects created by a natural disaster are defined in disastermanagement plans. The content of the disaster management plans is precisely defined by the Law onProtection Against Natural Disasters.4
4 Official register of SRM, 39/77, article 48.
At municipal level (Fig. 5.6) disaster management plans are enforced and administered by the municipalityalthough the government is involved in developing and coordinating them. Criteria for planned and organizedevacuation of the population in case of, or under the threat of, a military conflict as well as natural orman−made disasters are defined within the Regulations for Criteria for Evacuation of the Population of S.R.Macedonia.5
5 Official register of SRM, 34/87
Relief system
In case of large−scale natural or man−made disasters or epidemics, a state of emergency may be declaredfor the entire territory or part of it, in accordance with the Constitutional Law of the former Yugoslav Republicof Macedonia.6 The state of emergency shall be declared by the parliament by a two−thirds majority, uponrequest of the President, the Government or a minimum of 30 (out of 120−140) members of the parliament.The validity of the decree is 30 days. During the state of emergency, the Government can order directly, orthrough the headquarters of the civil defence, the mobilization of the civil defence forces. First the publicservice for monitoring, warning and information is initiated. Then designated persons in the population itself,as well as any other measures which are necessary according to the Law on Protection Against NaturalDisasters, are mobilized for effective and efficient protection of people and property.
6 Official register of RM, 52/91
Protection and rescue measures are being planned, prepared and executed to minimize and mitigate theconsequences of disaster. These measures include warning the population; evacuation; sheltering; rescuefrom ruins, floods and explosions; medical first aid and fire protection. For military events additional measuressuch as camouflage would be organized.
Civil protection forces are responsible for undertaking all humanitarian activities and tasks related to effectiveand efficient protection and rescue of the population and property in the country, as well as for providingconditions for direct and immediate intervention to prevent disaster. The civil protection forces consist of localforces (headquarters, commissioners and units) and manoeuver forces (headquarters and specialized units).
Local civil protection forces (Fig. 4.7), formed within the companies, public institutions and services and unitsof the local self−management authorities, are also involved in protection and rescue operations inneighbouring endangered areas close to the municipality/region where they have been formed.
Civil protection manoeuver forces are formed as special units and headquartered at state level as well aswithin businesses and facilities of vital interest. They are specially equipped, trained and prepared forperforming complex and comprehensive tasks, primarily in the region where they have been formed and, ifrequired elsewhere, in the territory.
177
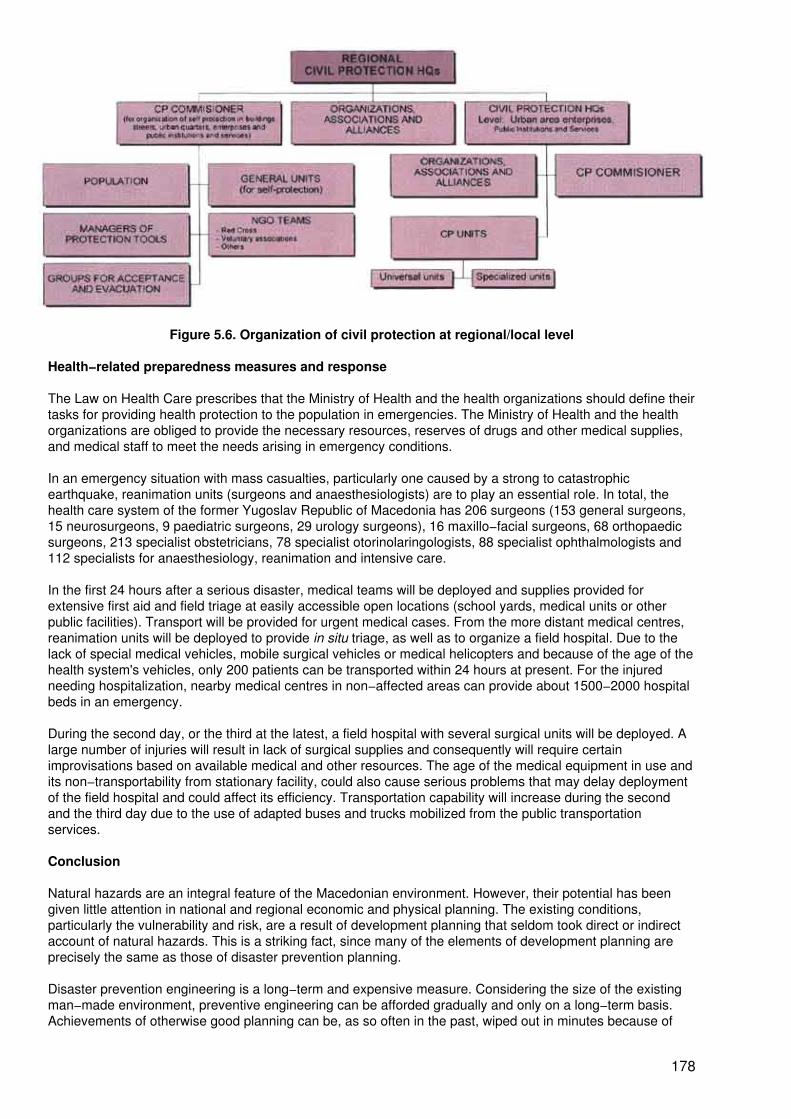
Figure 5.6. Organization of civil protection at regional/local level
Health−related preparedness measures and response
The Law on Health Care prescribes that the Ministry of Health and the health organizations should define theirtasks for providing health protection to the population in emergencies. The Ministry of Health and the healthorganizations are obliged to provide the necessary resources, reserves of drugs and other medical supplies,and medical staff to meet the needs arising in emergency conditions.
In an emergency situation with mass casualties, particularly one caused by a strong to catastrophicearthquake, reanimation units (surgeons and anaesthesiologists) are to play an essential role. In total, thehealth care system of the former Yugoslav Republic of Macedonia has 206 surgeons (153 general surgeons,15 neurosurgeons, 9 paediatric surgeons, 29 urology surgeons), 16 maxillo−facial surgeons, 68 orthopaedicsurgeons, 213 specialist obstetricians, 78 specialist otorinolaringologists, 88 specialist ophthalmologists and112 specialists for anaesthesiology, reanimation and intensive care.
In the first 24 hours after a serious disaster, medical teams will be deployed and supplies provided forextensive first aid and field triage at easily accessible open locations (school yards, medical units or otherpublic facilities). Transport will be provided for urgent medical cases. From the more distant medical centres,reanimation units will be deployed to provide in situ triage, as well as to organize a field hospital. Due to thelack of special medical vehicles, mobile surgical vehicles or medical helicopters and because of the age of thehealth system's vehicles, only 200 patients can be transported within 24 hours at present. For the injuredneeding hospitalization, nearby medical centres in non−affected areas can provide about 1500−2000 hospitalbeds in an emergency.
During the second day, or the third at the latest, a field hospital with several surgical units will be deployed. Alarge number of injuries will result in lack of surgical supplies and consequently will require certainimprovisations based on available medical and other resources. The age of the medical equipment in use andits non−transportability from stationary facility, could also cause serious problems that may delay deploymentof the field hospital and could affect its efficiency. Transportation capability will increase during the secondand the third day due to the use of adapted buses and trucks mobilized from the public transportationservices.
Conclusion
Natural hazards are an integral feature of the Macedonian environment. However, their potential has beengiven little attention in national and regional economic and physical planning. The existing conditions,particularly the vulnerability and risk, are a result of development planning that seldom took direct or indirectaccount of natural hazards. This is a striking fact, since many of the elements of development planning areprecisely the same as those of disaster prevention planning.
Disaster prevention engineering is a long−term and expensive measure. Considering the size of the existingman−made environment, preventive engineering can be afforded gradually and only on a long−term basis.Achievements of otherwise good planning can be, as so often in the past, wiped out in minutes because of
178
failure to account for the disaster potential of natural hazards.
Presently, the economy of the former Yugoslav Republic of Macedonia lacks the capacity and resilience forundertaking consistent long−term preventive engineering measures and absorbing the potential lossesresulting from large−scale disaster. Consequently, emergency preparedness is aimed at substantiallyreducing the impact of disasters on a cost−efficient basis that is affordable in the present economicconditions.
The health care system presently does not have the capacity and equipment to manage efficiently majoremergencies of MSE and LSE scale or even for an FSE emergency. Thus appeals for speedy assistance fromthe international community will probably be required in case of a major disaster in this area.
Acknowledgements
The results, statements and conclusions presented are based on studies carried out for the InternationalFederation of Red Cross and Red Crescent Societies, Geneva, the Macedonian Red Cross, and the WorldHealth Organization Regional Office for Europe, Copenhagen. The results presented have been achievedthrough joint efforts between the author and many of his colleagues, in particular those from the Section forRisk and Disaster Management of the Institute of Earthquake Engineering and Engineering Seismology,University "St. Cyril and Methodius", Skopje, as well as through fruitful and constructive discussions withrepresentatives of the Ministry of Health and Ministry of Defence of the Government of the former YugoslavRepublic of Macedonia.
References
1. Petrovski J, Milutinovic Z. Earthquake damage prediction modeling for the needs of physical and urbanplanning. Report IZIIS 84−084. Skopje, Institute of Earthquake Engineering and Engineering Seismology,1984.
2. Gorevski V. Attitude of the former Yugoslav Republic of Macedonia toward disaster management.Proceedings of the multinational exercise Rescuer '96, Ohrid, 21−25 October 1996.
3. Sutinovski Z. Organization, disaster response capacity and problems of the health care system of theformer Yugoslav Republic of Macedonia. Proceedings of the multinational exercise Rescuer '96, Ohrid, 21−25October 1996.
4. Tasevski B. Disaster relief system of the former Yugoslav Republic of Macedonia. Proceedings of themultinational exercise Rescuer '96, Ohrid, 21−25 October 1996.
Public health preparedness in relation to disasters
J. Levett1
1 J. Levett is Director, International Affairs, National School of Public Health, Athens, Greece
Misfortunes, calamities and catastrophes of varying magnitudes are all too often a part of life. The most recentdisaster to hit Greece occurred earlier this year when several areas suffered catastrophic flooding. Itdestroyed property and took lives. This followed close on the heels of the tragic capsizing of a Greek ship inrough seas in late 1996, trapping all but one of the 21 passengers.
A perusal of the international press or an evening viewing television reveals the enormity of such problemsthat face organized society worldwide − a train crashes, a bridge collapses, a bomb explodes, the earthtrembles. Not infrequently, terrorist acts occur and waves of vulnerable immigrants create seriouscross−border health problems for the nations that receive them. Radioactive fall−out from such nuclearaccidents as those at Three Mile Island or Chernobyl can affect large geographical areas.
Emerging situations demand an immediate assessment, and they need to be optimally contained. Rapidoverall response must be ensured and follow−up reconstruction and rehabilitation must be a part of disastermitigation. When catastrophe strikes, infrastructure is damaged or destroyed, agriculture is impaired, violencemay erupt and health problems occur. The uncontrolled violence which can erupt after a disaster compounds
179
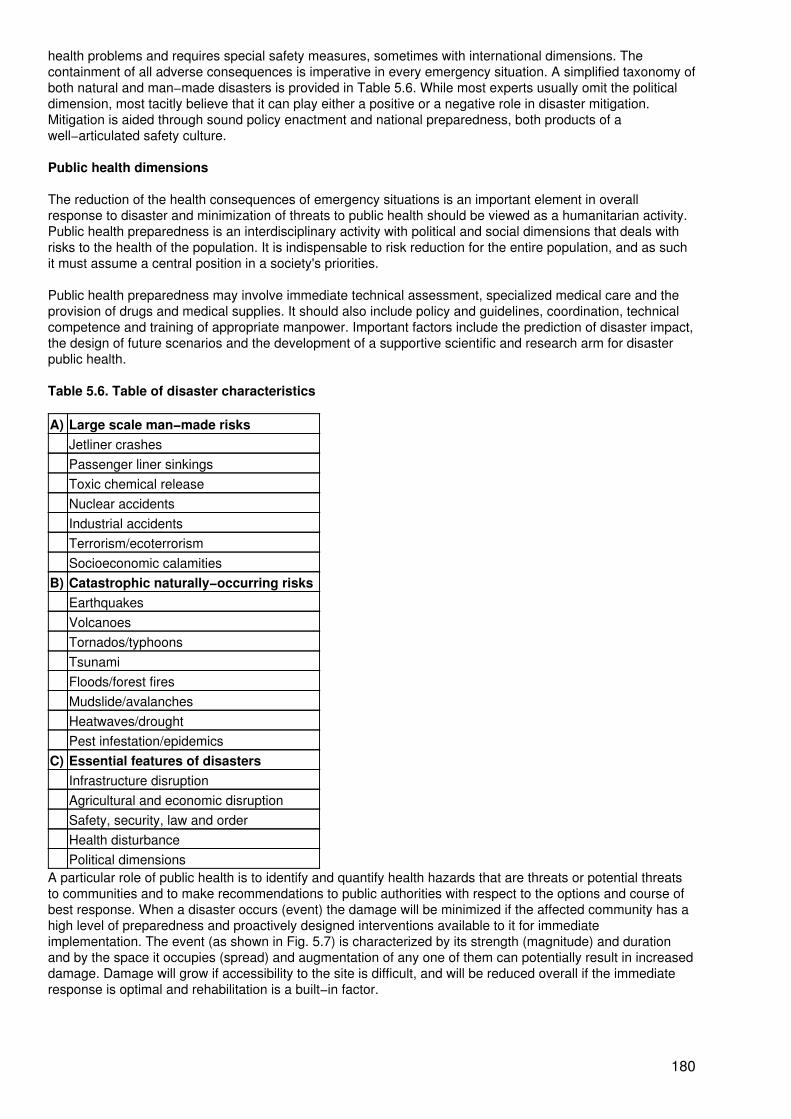
health problems and requires special safety measures, sometimes with international dimensions. Thecontainment of all adverse consequences is imperative in every emergency situation. A simplified taxonomy ofboth natural and man−made disasters is provided in Table 5.6. While most experts usually omit the politicaldimension, most tacitly believe that it can play either a positive or a negative role in disaster mitigation.Mitigation is aided through sound policy enactment and national preparedness, both products of awell−articulated safety culture.
Public health dimensions
The reduction of the health consequences of emergency situations is an important element in overallresponse to disaster and minimization of threats to public health should be viewed as a humanitarian activity.Public health preparedness is an interdisciplinary activity with political and social dimensions that deals withrisks to the health of the population. It is indispensable to risk reduction for the entire population, and as suchit must assume a central position in a society's priorities.
Public health preparedness may involve immediate technical assessment, specialized medical care and theprovision of drugs and medical supplies. It should also include policy and guidelines, coordination, technicalcompetence and training of appropriate manpower. Important factors include the prediction of disaster impact,the design of future scenarios and the development of a supportive scientific and research arm for disasterpublic health.
Table 5.6. Table of disaster characteristics
A) Large scale man−made risksJetliner crashesPassenger liner sinkingsToxic chemical releaseNuclear accidentsIndustrial accidentsTerrorism/ecoterrorismSocioeconomic calamities
B) Catastrophic naturally−occurring risksEarthquakesVolcanoesTornados/typhoonsTsunamiFloods/forest firesMudslide/avalanchesHeatwaves/droughtPest infestation/epidemics
C) Essential features of disastersInfrastructure disruptionAgricultural and economic disruptionSafety, security, law and orderHealth disturbancePolitical dimensions
A particular role of public health is to identify and quantify health hazards that are threats or potential threatsto communities and to make recommendations to public authorities with respect to the options and course ofbest response. When a disaster occurs (event) the damage will be minimized if the affected community has ahigh level of preparedness and proactively designed interventions available to it for immediateimplementation. The event (as shown in Fig. 5.7) is characterized by its strength (magnitude) and durationand by the space it occupies (spread) and augmentation of any one of them can potentially result in increaseddamage. Damage will grow if accessibility to the site is difficult, and will be reduced overall if the immediateresponse is optimal and rehabilitation is a built−in factor.
180
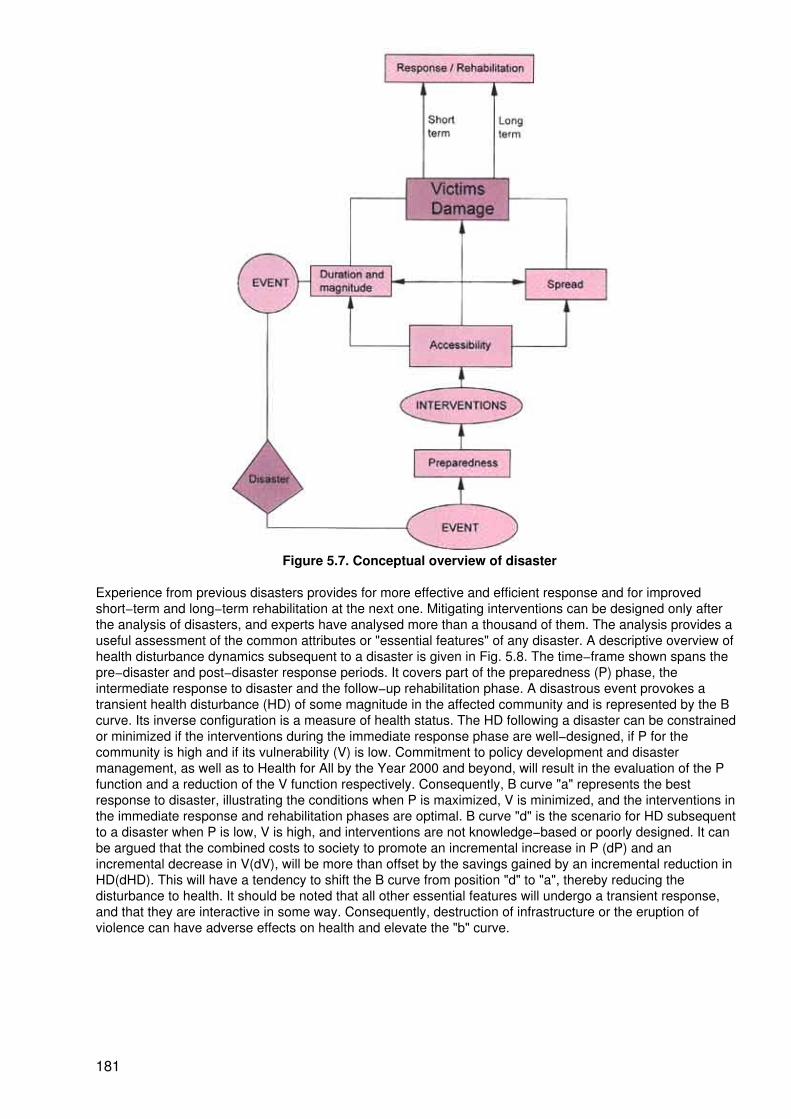
Figure 5.7. Conceptual overview of disaster
Experience from previous disasters provides for more effective and efficient response and for improvedshort−term and long−term rehabilitation at the next one. Mitigating interventions can be designed only afterthe analysis of disasters, and experts have analysed more than a thousand of them. The analysis provides auseful assessment of the common attributes or "essential features" of any disaster. A descriptive overview ofhealth disturbance dynamics subsequent to a disaster is given in Fig. 5.8. The time−frame shown spans thepre−disaster and post−disaster response periods. It covers part of the preparedness (P) phase, theintermediate response to disaster and the follow−up rehabilitation phase. A disastrous event provokes atransient health disturbance (HD) of some magnitude in the affected community and is represented by the Bcurve. Its inverse configuration is a measure of health status. The HD following a disaster can be constrainedor minimized if the interventions during the immediate response phase are well−designed, if P for thecommunity is high and if its vulnerability (V) is low. Commitment to policy development and disastermanagement, as well as to Health for All by the Year 2000 and beyond, will result in the evaluation of the Pfunction and a reduction of the V function respectively. Consequently, B curve "a" represents the bestresponse to disaster, illustrating the conditions when P is maximized, V is minimized, and the interventions inthe immediate response and rehabilitation phases are optimal. B curve "d" is the scenario for HD subsequentto a disaster when P is low, V is high, and interventions are not knowledge−based or poorly designed. It canbe argued that the combined costs to society to promote an incremental increase in P (dP) and anincremental decrease in V(dV), will be more than offset by the savings gained by an incremental reduction inHD(dHD). This will have a tendency to shift the B curve from position "d" to "a", thereby reducing thedisturbance to health. It should be noted that all other essential features will undergo a transient response,and that they are interactive in some way. Consequently, destruction of infrastructure or the eruption ofviolence can have adverse effects on health and elevate the "b" curve.
181
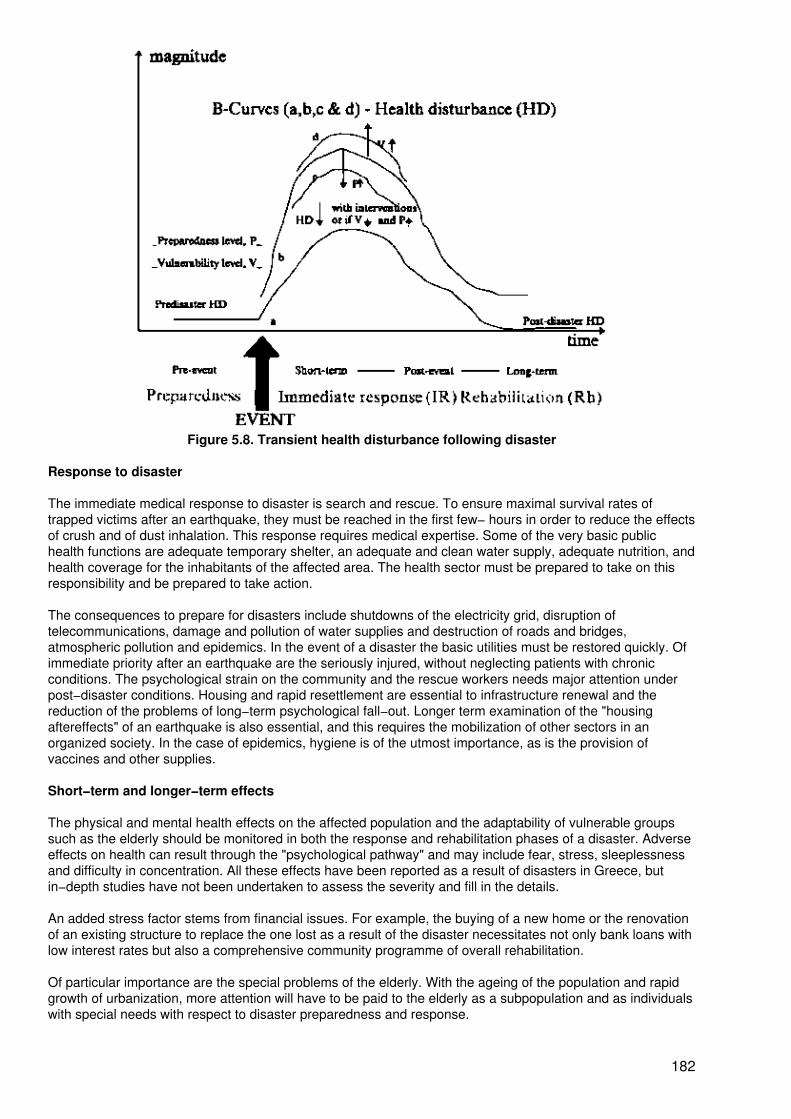
Figure 5.8. Transient health disturbance following disaster
Response to disaster
The immediate medical response to disaster is search and rescue. To ensure maximal survival rates oftrapped victims after an earthquake, they must be reached in the first few− hours in order to reduce the effectsof crush and of dust inhalation. This response requires medical expertise. Some of the very basic publichealth functions are adequate temporary shelter, an adequate and clean water supply, adequate nutrition, andhealth coverage for the inhabitants of the affected area. The health sector must be prepared to take on thisresponsibility and be prepared to take action.
The consequences to prepare for disasters include shutdowns of the electricity grid, disruption oftelecommunications, damage and pollution of water supplies and destruction of roads and bridges,atmospheric pollution and epidemics. In the event of a disaster the basic utilities must be restored quickly. Ofimmediate priority after an earthquake are the seriously injured, without neglecting patients with chronicconditions. The psychological strain on the community and the rescue workers needs major attention underpost−disaster conditions. Housing and rapid resettlement are essential to infrastructure renewal and thereduction of the problems of long−term psychological fall−out. Longer term examination of the "housingaftereffects" of an earthquake is also essential, and this requires the mobilization of other sectors in anorganized society. In the case of epidemics, hygiene is of the utmost importance, as is the provision ofvaccines and other supplies.
Short−term and longer−term effects
The physical and mental health effects on the affected population and the adaptability of vulnerable groupssuch as the elderly should be monitored in both the response and rehabilitation phases of a disaster. Adverseeffects on health can result through the "psychological pathway" and may include fear, stress, sleeplessnessand difficulty in concentration. All these effects have been reported as a result of disasters in Greece, butin−depth studies have not been undertaken to assess the severity and fill in the details.
An added stress factor stems from financial issues. For example, the buying of a new home or the renovationof an existing structure to replace the one lost as a result of the disaster necessitates not only bank loans withlow interest rates but also a comprehensive community programme of overall rehabilitation.
Of particular importance are the special problems of the elderly. With the ageing of the population and rapidgrowth of urbanization, more attention will have to be paid to the elderly as a subpopulation and as individualswith special needs with respect to disaster preparedness and response.
182
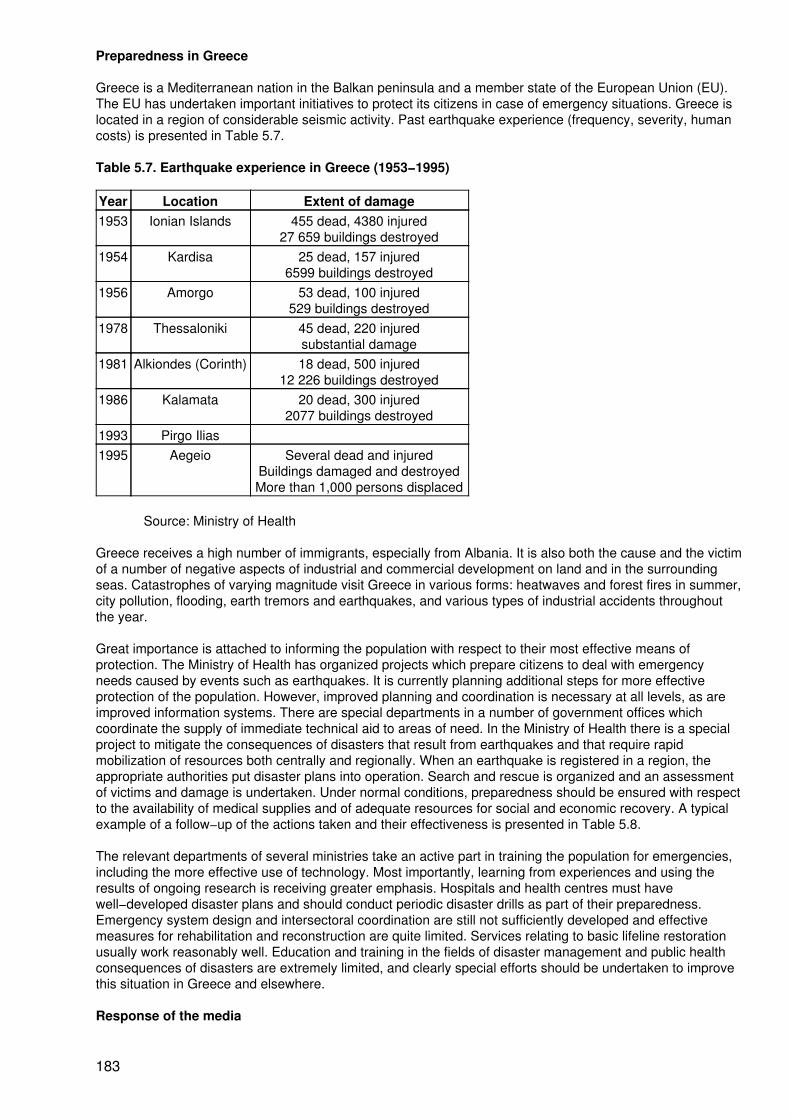
Preparedness in Greece
Greece is a Mediterranean nation in the Balkan peninsula and a member state of the European Union (EU).The EU has undertaken important initiatives to protect its citizens in case of emergency situations. Greece islocated in a region of considerable seismic activity. Past earthquake experience (frequency, severity, humancosts) is presented in Table 5.7.
Table 5.7. Earthquake experience in Greece (1953−1995)
Year Location Extent of damage1953 Ionian Islands 455 dead, 4380 injured
27 659 buildings destroyed1954 Kardisa 25 dead, 157 injured
6599 buildings destroyed1956 Amorgo 53 dead, 100 injured
529 buildings destroyed1978 Thessaloniki 45 dead, 220 injured
substantial damage1981 Alkiondes (Corinth) 18 dead, 500 injured
12 226 buildings destroyed1986 Kalamata 20 dead, 300 injured
2077 buildings destroyed1993 Pirgo Ilias1995 Aegeio Several dead and injured
Buildings damaged and destroyedMore than 1,000 persons displaced
Source: Ministry of Health
Greece receives a high number of immigrants, especially from Albania. It is also both the cause and the victimof a number of negative aspects of industrial and commercial development on land and in the surroundingseas. Catastrophes of varying magnitude visit Greece in various forms: heatwaves and forest fires in summer,city pollution, flooding, earth tremors and earthquakes, and various types of industrial accidents throughoutthe year.
Great importance is attached to informing the population with respect to their most effective means ofprotection. The Ministry of Health has organized projects which prepare citizens to deal with emergencyneeds caused by events such as earthquakes. It is currently planning additional steps for more effectiveprotection of the population. However, improved planning and coordination is necessary at all levels, as areimproved information systems. There are special departments in a number of government offices whichcoordinate the supply of immediate technical aid to areas of need. In the Ministry of Health there is a specialproject to mitigate the consequences of disasters that result from earthquakes and that require rapidmobilization of resources both centrally and regionally. When an earthquake is registered in a region, theappropriate authorities put disaster plans into operation. Search and rescue is organized and an assessmentof victims and damage is undertaken. Under normal conditions, preparedness should be ensured with respectto the availability of medical supplies and of adequate resources for social and economic recovery. A typicalexample of a follow−up of the actions taken and their effectiveness is presented in Table 5.8.
The relevant departments of several ministries take an active part in training the population for emergencies,including the more effective use of technology. Most importantly, learning from experiences and using theresults of ongoing research is receiving greater emphasis. Hospitals and health centres must havewell−developed disaster plans and should conduct periodic disaster drills as part of their preparedness.Emergency system design and intersectoral coordination are still not sufficiently developed and effectivemeasures for rehabilitation and reconstruction are quite limited. Services relating to basic lifeline restorationusually work reasonably well. Education and training in the fields of disaster management and public healthconsequences of disasters are extremely limited, and clearly special efforts should be undertaken to improvethis situation in Greece and elsewhere.
Response of the media
183
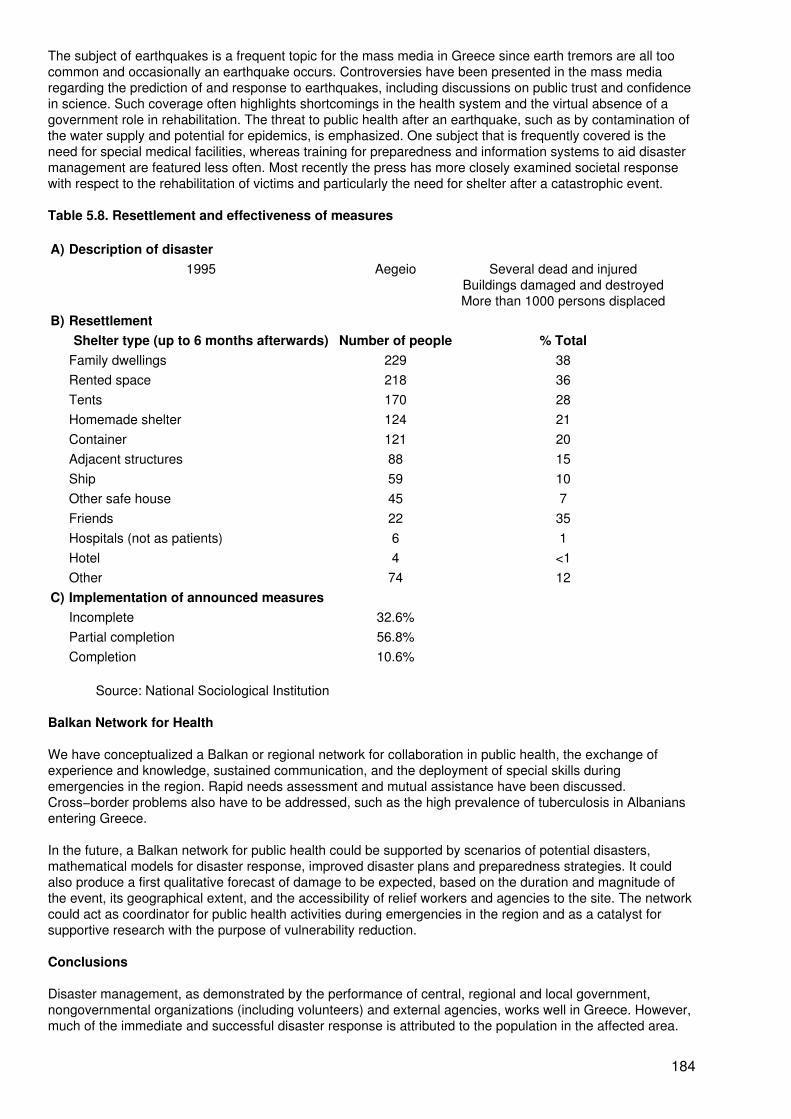
The subject of earthquakes is a frequent topic for the mass media in Greece since earth tremors are all toocommon and occasionally an earthquake occurs. Controversies have been presented in the mass mediaregarding the prediction of and response to earthquakes, including discussions on public trust and confidencein science. Such coverage often highlights shortcomings in the health system and the virtual absence of agovernment role in rehabilitation. The threat to public health after an earthquake, such as by contamination ofthe water supply and potential for epidemics, is emphasized. One subject that is frequently covered is theneed for special medical facilities, whereas training for preparedness and information systems to aid disastermanagement are featured less often. Most recently the press has more closely examined societal responsewith respect to the rehabilitation of victims and particularly the need for shelter after a catastrophic event.
Table 5.8. Resettlement and effectiveness of measures
A) Description of disaster1995 Aegeio Several dead and injured
Buildings damaged and destroyedMore than 1000 persons displaced
B) ResettlementShelter type (up to 6 months afterwards) Number of people % Total
Family dwellings 229 38Rented space 218 36Tents 170 28Homemade shelter 124 21Container 121 20Adjacent structures 88 15Ship 59 10Other safe house 45 7Friends 22 35Hospitals (not as patients) 6 1Hotel 4 <1Other 74 12
C) Implementation of announced measuresIncomplete 32.6%Partial completion 56.8%Completion 10.6%
Source: National Sociological Institution
Balkan Network for Health
We have conceptualized a Balkan or regional network for collaboration in public health, the exchange ofexperience and knowledge, sustained communication, and the deployment of special skills duringemergencies in the region. Rapid needs assessment and mutual assistance have been discussed.Cross−border problems also have to be addressed, such as the high prevalence of tuberculosis in Albaniansentering Greece.
In the future, a Balkan network for public health could be supported by scenarios of potential disasters,mathematical models for disaster response, improved disaster plans and preparedness strategies. It couldalso produce a first qualitative forecast of damage to be expected, based on the duration and magnitude ofthe event, its geographical extent, and the accessibility of relief workers and agencies to the site. The networkcould act as coordinator for public health activities during emergencies in the region and as a catalyst forsupportive research with the purpose of vulnerability reduction.
Conclusions
Disaster management, as demonstrated by the performance of central, regional and local government,nongovernmental organizations (including volunteers) and external agencies, works well in Greece. However,much of the immediate and successful disaster response is attributed to the population in the affected area.
184
Therefore, communities at high risk should have access to preparedness training. According to the Ministry ofHealth response profile following the 1986 earthquake in Kalamata, sanitary conditions and sanitation wererestored, food supplies were ensured and infectious disease was under control within a few days of thedisaster.
However, training in disaster management needs to be developed further and longer−term rehabilitationproblems still persist. The National School of Public Health has also been strengthened as a resource of theministry. As a teaching, service and research institution it could provide considerable support for training ofpersonnel with respect to disasters and could serve as a focus for the development of regional partnerships.More precisely, it could be the focus for the inauguration of graduate level training in disaster managementand public health and would become an integral part of overall preparedness.
Country profile: Costa Rica
D.E. Rodriguez1
1 D.E. Rodriguez is Chief, Department of Medicine, Calderon Guardia Hospital, San Jose,Costa Rica.
The Republic of Costa Rica is located in the Central American isthmus between the Atlantic and Pacificoceans. Its territory covers 51 100 km2 and its geographic position, narrow isthmus, tropical climate andmountain systems account for the risk from natural phenomena such as hurricanes, floods, landslides,earthquakes and volcanic eruptions. In Costa Rica, seismic events are caused by three mechanisms:interplate events, intraplate (local) faults and volcanic activity.
The seismic activity along the Pacific coast is due mainly to the direct influence of interaction of theCoco−Caribe plates. Historically, although these earthquakes have reached magnitudes of 7.7 on the Richterscale, they have not been very destructive because the activity occurs at depths greater than 20 km and theepicentres have not been close to the main population centres. Examples of this type of seismic activity havebeen the Tempisque River earthquake in 1950 with a magnitude of 7.7 on the Richter scale, which occurred inthe northern region of the Pacific coast, and the Golfito earthquake in 1983 with a magnitude of 7.3 on theRichter scale which occurred in the southern region of the Pacific coast.
In the valleys and mountains in the interior of the country, the seismic activity is due to local fault lines. Theseearthquakes have been the most destructive and lethal in spite of their moderate magnitudes (less than 6.5 onthe Richter scale), because the activity is superficial (less than 20 km deep) and the epicentres have beenclose to population centres.
Examples of this activity are the Cartago earthquakes which have destroyed the old capital several times, thelast one being in 1910 with a magnitude of 5.5; the Tilarán earthquake in 1973 which had a magnitude of 6.5and reached an intensity of IX; and the Perez Zeledón earthquake in 1983 which had a magnitude of 6.1,reached an intensity of IX and caused severe damage to the local hospital which had to be rebuilt. The Limónearthquake in 1991 had a magnitude of 7.5 on the Richter scale and caused widespread destruction alongmore than 100 km of the Atlantic coastline, damaging more than 10 000 houses and over 309 km of roadsand destroying five major bridges. The regional hospital and several local clinics had to be evacuated due tosevere damage and were later rebuilt. There was also destruction to lifelines and agriculture due toliquefaction of the soil and landslides and an elevation of the coastline of up to 2 m. All of these disastersaltered the ecology of the regions they affected. The volcanic activity occurs mainly near the volcanic conesand has caused landslides.
The frequency of earthquakes, and the destruction and death that they have caused, have led to the passingof laws concerning construction techniques and siting of buildings, earthquake and fire hazard prevention andmitigation, and disaster preparedness education.
Recently the seismic building code of 1977 was updated to incorporate what was learned from earthquakes inCalifornia. Specifically, three of the major hospitals of Costa Rica underwent structural reinforcement becausethey had been built according to an older and less strict code.
The country's response to disasters is coordinated through the National Emergency Commission which wasestablished in 1969. It is guided by a board of directors representing several government institutions, including
185
the Ministry of Health and the Costa Rican Social Security, as well as the Costa Rican Red Cross. TheCommission and its various divisions and advisory committees include representatives not only from theseinstitutions but also from international organizations such as the Pan American Health Organization.
The fundamental role of the National Emergency Commission is to coordinate the efforts of public and privateinstitutions to cope adequately with disasters through a national emergency plan. The plan has appendicesrelating to the role of several sectors (including the health sector). Regional and local committees, withrepresentatives of the institutions that form the board of directors and from local organizations, function in allregions and most towns of the country.
This organization has stood the test of time and several natural disasters. For a country with very limitedresources, no armed forces and significant vulnerability, the approach to disasters has improved over theyears and the advances have been recognized by national and international institutions. Costa Rica wasawarded the Sasakawa Prize in 1994 for work in this area.
The health sector comprises the Ministry of Health which is responsible for the prevention of ill−health and thepromotion of health, the Costa Rican Social Security which is responsible for medical care in hospitals andclinics, the Costa Rican Red Cross which is responsible for pre−hospital and work−related illnesses, theUniversity of Costa Rica which promotes disaster−related education, and the Water and Ducts Institute whichis responsible for the supply of water and maintenance of the infrastructure. The Pan American HealthOrganization is represented by an Emergency and Disasters subregional office in San Jose and givestechnical advice to the national health institutions.
The health services have done their job well during disasters, mainly because they have functioned as a"system" in which hospitals support each other. There are weaknesses because the financial and materialresources are very limited. In the pre−hospital setting we have identified weaknesses in training, in equipmentand in materials. There is also a significant lack of transportation capabilities, especially by air, which hasbecome clear when entire regions were cut off due to damage to roads and railroads. Another weakness thatwas identified was the inadequate direct communication links between hospitals and health centres by meansother than telephone. This has been partially solved with the assignment of a radio frequency exclusively fordisaster and medical emergency care.
In conclusion, Costa Rica is a small country that is not industrialized and is at risk from multiple natural as wellas technological disasters. The country has organized itself to cope with disasters using the resources ofdifferent public and private institutions in a coordinated way by means of the National Emergency Commissionand the national emergency plan.
The health sector has responded adequately during disasters and has taken the lead in prevention,preparedness and education for disasters. Nevertheless, weaknesses have been identified, especially withregard to the lack of equipment, materials and training for the pre−hospital stage and the lack of airtransportation.
Jordan's plan to face earthquakes
F. Al Tawil1
1F. Al Tawil is Director General, Treatment Services, Ministry of Health, Amman, Jordan.
Our concern about earthquakes began after the earthquake that shook the area of the Middle East in the earlymorning of 22 November 1995. It affected areas of Egypt, Israel, Jordan and Saudi Arabia causing amoderate number of deaths, injuries and building collapses. Its magnitude ranged between 5.7 and 7.2 on theRichter scale. The damage was moderate because its epicentre was about 110 kilometres south of Aqaba,Jordan, in the Red Sea.
This earthquake made us open our eyes and we established a national plan to face such disasters in thefuture. The Ministry of Health in Jordan, with its 680 health centres and 22 hospitals, was the major participantin this plan. However, it also incorporates, as far as possible, the contributions of other participants such asthe Ministry of Internal Affairs and the Royal Armed Forces. The plan has 12 segments corresponding to the12 governorates of Jordan. It covers three phases: the pre−disaster phase, the disaster phase itself, and thepost−disaster phase.
186
Pre−disaster phase
The pre−disaster phase of the national plan concentrates on preparation to face the situation when theearthquake happens. It begins with the initiation of a small central committee of five members. Its place is inthe Ministry of Health and through its instructions another 12 similar committees are established in the 12governorates. The task of these committees in general is to ensure:
− that ambulances in particular and transport vehicles in general are safe and ready to beused when needed at any time, and that communications facilities (especially those that donot require ground wire links) are ready for use in times of disaster;.
− that there is an efficient technical procedure for putting these facilities into action;
− that electric motors are functioning and that simple means of providing back−up power,such as emergency generators and batteries, are available for providing light and power;
− that there is enough potable water, canned food and stock of petroleum to suffice for oneweek at least, and that the stock of medicines will suffice for at least one month.
The results of the observations of the governorate committees on readiness are to transmitted to the centralcommittee four times a year.
Disaster phase
Once the natural disaster occurs, the above−mentioned committees are replaced automatically by disastercommittees with the same names. These are larger (the central disaster committee has 10 members) as wellas higher in rank and therefore capable of decision−making.
These disaster committees, led by the central one, begin by studying and analysing the new situation usingthe preparatory information collected by the previous committees and taking into consideration the actualextent of damage and losses communicated by the committee or committees of the region where the disasterhas taken place.
The next step is to direct all efforts to the disaster zone. Unused resources in the disaster area and above allof the unaffected areas are now directed towards the disaster. The health centres and hospitals in the affectedarea are contacted in case they are damaged. New field hospitals may be set up (with the help of the army)and schools and large government buildings transformed into temporary hospitals if necessary. Thesemeasures depend on the efficient use of sufficient manpower, especially medical staff. They must be carriedout rapidly and must ensure easy accessibility to the medical facilities.
In case of very severe losses, a referring hospital or centre should be designated, or even newly set up, nearthe affected area. The requirements of manpower or technical facilities should be met from any resource inthe country, whether in the public or private sector.
To deal with the new situations efficiently, secondary committees are nominated. These would include apatient admission committee, a referring committee, health safety committees, an education committee andan information committee.
Post disaster phase
This phase could be the most dangerous and an even greater threat to health than the natural disaster itself, ifneglected. Damage to the infrastructure of the area and pollution of the environment may allow for the spreadof endemic and/or epidemic diseases. To mitigate these consequences is the task of the committees.
PART 6 − SUMMING UP
187
Reports from the Working Groups
During the symposium three working groups met to discuss the three phases of disaster management:vulnerability reduction, preparedness and rehabilitation. The chairpersons and rapporteurs of the threeworking groups presented their summary reports to a plenary session. The health and well−being of peopleduring and after earthquakes can be unproved if appropriate measures are taken in all three phases ofdisaster management. It is clear that some overlap exists.
Report from the Working Group on Vulnerability Reduction
Introducing the issue
Vulnerability reduction is a term mainly used in disaster and emergency management.
The working group focused on two main areas: the planning and execution of preventive engineeringmeasures, such as constructing to strict codes; and the selection, planning and preparation of organizationalmeasures, with corresponding training programmes.
Major findings
Levels of hazard
As hazards and the risk of earthquakes prevail in many countries, these countries are encouraged to updateseismic hazard maps and apply them to the local situation. A country's history of earthquakes and methods ofmodern geology and seismology can be used to establish such maps.
Structural and engineering measures
A hazard analysis for specific natural and man−made risks should be provided as an input to the planningprocess which should include, among other things, formulation of building codes, their adoption andenforcement, and design of lifelines and vital systems such as hospitals, water supply, sanitation, electricitysupply, gas supply, communication, transportation and fire prevention, to a higher level of safety. Simplestructures (wood, clay, plaster) should be made more resistant. Retrofit of old structures, insufficientlydesigned, with appropriate reinforcements is also possible and should be based on risk assessment.Strengthening hospitals or special hospital rooms, and/or protecting essential hospital contents, such asdiagnostic or surgical equipment, against earthquakes should be considered.
Logistics, training and public health measures
The group also identified a number of non−engineering measures relating to preparation for future disastersby learning from the past, establishing effective organizational structures and providing training and drills.
Report from the Working Group on Preparedness
Introducing the issue
Preparedness is a much more generally accepted and understandable term than vulnerability reduction.However, in the context of earthquakes and people's health, it requires some explanation to differentiate itfrom rehabilitation and vulnerability reduction, with emphasis on the latter. Whereas longer−term preparationto deal with the effects of earthquakes, (such as training), is defined as a vulnerability reduction issue, most ofthe execution of such measures in an emergency is seen as a preparedness issue in the context of theworking groups. Therefore, in terms of the health and well−being of the affected persons, preparednessinvolves both the prior organization of an effective reaction to an earthquake and the actions that areimmediately necessary during and after an earthquake. This is reflected in the findings of the group.
Major findings
Public information
188

Public awareness programmes utilizing all possible media should constitute an integral and fundamental partof the disaster preparedness programme. Particular attention should be paid to vulnerable groups.
Appropriate procedures should be established for the management of public information, includingmechanisms for rumour control and regular situation updates.
Communication
There should be communication systems, parallel to or backed up by secondary systems, in order to collectand disseminate information, mobilize resources and pass on orders.
Safeguarding lifelines
When necessary, temporary cut−off of dangerous or endangered supply lines, such as railways, gas, waterand electricity, must be initiated.
Rescue operations
Local and voluntary resources must be organized and mobilized to carry out the vital early rescue of peopleburied in debris and to provide first aid. Search and rescue operations are to be coordinated and logistics andequipment support is to be provided. Logistics support should include stopping regular traffic and routineactivities to give priority to rescue
Rapid assessment
Tools and instruments for the rapid assessment of casualties, as well as of damage to health facilities andsystems, should be instituted with provision of training at the local level.
Methods should be included to authorize damaged hospitals to continue functioning where possible in order toavoid unnecessary evacuation.
Mitigating consequences
Early detection and mitigation (fighting) of secondary effects, particularly fires, traffic jams, floods andlandslides, are necessary. The outbreak of communicable diseases must be avoided and the necessarystandards of sanitation maintained. Temporary shelter, food, sanitation, transportation and money supplyshould be provided.
Psychological support
Mitigation of the observed consequences of psychological factors on the affected population and rescueworkers must be an integral part of preparedness.
Report from the Working Group on Rehabilitation
Introducing the issue
Rehabilitation, as with preparedness, is self−explanatory and generally understood. In the context ofearthquakes, the term rehabilitation applies to the group of medium−term and long−term measures that aretaken after an earthquake to support a healthy life for the people affected and to make such effortssustainable. Short−term measures, on the other hand, are largely treated under preparedness. Particularissues which require long lead−times to be effective in the rehabilitation phase, such as insurance, are alsotreated under vulnerability reduction.
Major findings
Overall objectives for rehabilitation
There are two main overall objectives. The first is to achieve a sustainable state of health and well−being thatis at least as good as before the disaster using self−reliance as far as is possible.
189
The second objective is to learn from past events and make the community both less vulnerable and betterprepared for similar events in the future.
Health services
Breakdowns in the system of health services must be avoided. If interruptions occur, the services must berestored. Priority must be given to re−establishing routine basic health and social services to the strickencommunity and to launching community consolidation mechanisms as a way of preventing social andbehavioural complications and dealing with post−traumatic stress disorder and earthquake psychosis.
Reconstruction
Reconstruction and rehabilitation forces should be mobilized by encouraging and coordinating initiatives ofindividuals, industry, volunteer organizations and government, paying particular attention to those who aresocially isolated or economically weak.
Infrastructures such as transportation must be reorganized and safe waste disposal provided. Tertiarydamage, such as loss of living accommodation, property, jobs, confidence and future perspective, must bemitigated.
Rehabilitation activities should be based on a project management approach and should preferably betime−limited.
Financial aspects
In the pre−disaster phase, governments and local authorities should establish contingency funds for relief andrehabilitation, directing external aid towards priority activities concerned with community participation.Successful models of financial solidarity with victims, such as the loss−balancing scheme of post−warGermany (see Annex 5), were discussed and acknowledged. But certain relief operations should be limited induration to avoid people becoming dependent on them.
How to integrate earthquake vulnerability reduction, preparedness and rehabilitation into a holistic and intersectoralapproach
Panelists: L.B. Bourque1, ModeratorM. Gabr2, Co−moderatorJ. Oviedo3
M. Erdik4
K. Hayashi5
B. Mulyadi6
M. Meyers7, Rapporteur
1 L.B. Bourque Ph.D. is Professor, Department of Community Health Sciences, School ofPublic Health and Southern California Injury Prevention Research Center (SCIPRC),University of California, Los Angeles, USA.
2 M. Gabr is Professor of Pediatrics, Cairo University; past president of the AdvisoryCommittee on Health Research, WHO; immediate past president of the International PediatricAssociation; and Secretary General of the Egyptian Red Crescent Society, Cairo, Egypt.
3 J. Oviedo is General Director, Preventive Medicine, Ministry of Health, Mexico, D.F.,Mexico.
4 M. Erdik is Professor and Chair, Department of Earthquake Engineering, KandilliObservatory and Earthquake Engineering, Bogazici University, Istanbul, Turkey.
5 K. Hayashi is Director of the Kobe Institute of Health, Bureau of Health and Welfare, Kobe,Japan.
190
6 B. Mulyadi, M.D., is Director for Private and Specialty Hospitals, Directorate General ofMedical Care and Secretary of Crisis Centre, Ministry of Health, Jakarta, Republic ofIndonesia.
7 M. Meyers is Assistant Director, WHO Centre for Health Development, Kobe, Japan
Panelists were asked to give their "sense" of what had evolved (as consensus or diversity of views) during thefour−day conference, rather than giving their own opinion or presenting their own experiences. The topic wasthen opened to the audience for comment and discussion.
The panel theme was discussed under five questions, as follows:
Question 1: How can interactions between the health sector and other sectors be improved?
All panelists indicated that intersectoral interactions should occur and needed to be improved and that suchinteractions had to be undertaken in a systematic manner before a disaster occurs.
Dr Pretto called for the establishment of a clear intersectoral management structure which had as a majorobjective the facilitation of communications between the different sectors that, of necessity, must be involvedin the response to any disaster. Professor Erdik indicated that such a structure could be facilitated by firstidentifying the problem(s) to be dealt with and the areas of mutual interest across the sectors. On the basis ofthis, multisectoral means of handling these problems could be identified and specified at symposiums similarto this one. Dr Mulyadi stated that small, high−level groups were most appropriate for deciding which sectorsand individuals should be involved, what should be done and what kinds of support each sector or groupcould and would supply. Dr Oviedo mentioned the need to develop common concepts, definitions andlanguage in discussing disasters so that intersectoral communication could more efficiently and productivelytake place. He noted that doctors and engineers in Mexico City have been engaged in increasing intersectoralcommunication about how and when to strengthen hospitals, with an emphasis on learning from each other.Finally, Dr Hayashi noted that part of the problem of lack of intersectoral interaction in Japan came from theinflexibility of bureaucrats with differing responsibilities. The audience also noted that various governmentalagencies first need to coordinate amongst themselves and then to bring in other groups (e.g. the privatesector, nongovernmental organizations, etc.). The key to successful intersectoral interaction isdecentralization and coordination.
Dr Verma mentioned that it was very difficult to compensate for losses. The government's role is importanthere to help provide long−term loans to support housing and recovery. It was mentioned that WHO coulddevelop guidance concerning the methodology for such support.
Question 2: How do vulnerability reduction, preparedness and rehabilitation interface, and what roledo they play in the enhancement of health and public health?
All panel members agreed that vulnerability reduction, preparedness and rehabilitation are part of acontinuum. This continuum represents different phases of the same process which begins before the eventand is active before, during and after the event. In planning, all three must be considered simultaneously; andthe parties responsible within the various sectors at the national, provincial and district levels must beidentified and a chain of command established. In order to plan properly within each area, we must break theplanning process down into extremely small parts to examine needs closely and see how they can best bemet. To the greatest extent possible, rehabilitation should be undertaken autonomously by the people affectedby the disaster.
Dr Noji (from the audience) agreed that all three phases must be carried out with the overriding goal ofdecreasing the vulnerability of human beings to death and injury, and rehabilitation must be done in such away that the community's resilience in dealing with future emergencies is enhanced. Dr Ben Yahmed (fromthe audience) pointed out that vulnerability reduction and preparedness should be carried out as part of theeconomic and social development process.
Question 3: Who should be trained, in what, and by whom?
The panel considered training in its broadest sense and concluded that all categories of persons and groupsneed more and better training. These include medical personnel, professionals from other (non−health)sectors who are involved in dealing with disasters, the community and politicians who should be sensitized tothe need for funding to facilitate adequate training. Members of the public need to be made aware of the
191

overall risk to better enable them to understand the need for increased investment in vulnerability reduction,preparedness and rehabilitation planning. They also need to be given training in what they should and coulddo at the time of a disaster, with particular attention to training in basic first aid. Dr Pretto pointed out thattraining is expensive and, therefore, not everyone can be trained. Thus, training priorities need to beestablished, selected and focused, with emphasis being placed on training that can be used every day byprofessionals in their routine work − not just in the event of a disaster or emergency.
The audience pointed out that obviously those involved in disaster rescue − such as police, fire fighters anddoctors − had to be trained. The need for volunteers to be trained in advance of an earthquake or otherevents was emphasized. Widening the range of training, it was pointed out that people need to be identifiedand trained to formulate disaster−relevant policy and practice. The emphasis throughout the discussion wason training at the community level.
Question 4: What are the major gaps in knowledge and what areas and types of research should beinitiated or increased?
All panel members agreed that existing knowledge about earthquakes is extensive. Much of the information is,however, found within a single sector; and it is often documented in conference proceedings and other poorlydisseminated materials. Thus, there is a critical need to better synthesize, disseminate and implement theinformation. Dr Oviedo suggested the possibility of a website on the Internet. Some specific gaps inknowledge that were noted included: how to identify and have available what would be needed; how toevaluate and assess the methods to provide adequate sanitation systems and means for removing generalwaste, rubble and biohazards; and cost−effectiveness studies of vulnerability reduction and preparedness inless developed countries.
The public health role in disaster situations is not very well understood and must be strengthened in order toprevent short−term and long−term effects by
− maintaining adequate immunization levels at all times;− care of diabetes and hypertension;− good sanitation facilities with reduced vulnerability.
Preparedness should also rely more on public health than on medical emergency, through training,awareness and coordination of supplies.
It was suggested that further study of how to move people after a disaster (e.g. mass transport) when normalroads and railroads are disrupted would be useful. It was also recommended that medical operating teamsundergo training and drills with emphasis on how to perform in a hostile environment (e.g. without electricity,water, etc.).
Question 5: Are disasters always a disaster? What, if anything, can we learn from them?
There was a general consensus that a disaster is an emergency that has been handled badly (see alsodefinition by WHO/EHA/95.1). Every disaster provides opportunities for learning how to gather data better andhow to utilize them better. If adequate vulnerability reduction and preparedness is carried out before thedisaster and a good rehabilitation programme has been planned, a community can actually turn a disaster toits advantage. Post−disaster social and economic development can move along at a faster pace in theaffected area than it otherwise would have moved.
Conclusions and recommendations
• Although earthquakes and other disasters are part of life and therefore are to be expected,proper planning of preventive measures ahead of time can reduce deaths and damagesignificantly. These measures should be agreed upon, broadly publicized, and carried out byall sectors involved. National, international and nongovernmental organizations, if includedfrom the initial planning stages, can make meaningful and timely contributions. Public healthmust also play an important role.
• Well−coordinated planning and decision−making from beginning to end needs to bedecentralized through appropriate delegation to the local level in order to help earthquake
192
victims quickly and effectively. Local officials must be given sufficient resources beforehandand be empowered to make decisions without further consultation, both during planning andafter the disaster strikes.
• The great majority of earthquake victims are saved by other family members or neighbours.The local community/district/neighbourhood must, therefore, be fully engaged inpreparations to reduce vulnerability in case of disaster and be involved in the preparednessplanning. Local volunteers should be organized and integrated into emergency teams,periodic drills conducted, and adequate search−and−rescue and first−aid training given.Ordinary citizens can play a meaningful role by securing household appliances and furniture,storing sufficient supplies of water and joining in rescue drills.
• Hospital preparedness should be improved by adopting and observing appropriate designcodes, by upgrading the safety of essential rooms and equipment, by stocking adequatesupplies of relevant medication and by creating safe and/or redundant lifelines for water,electricity, gas, communication, sanitation and fire protection. Alternative means oftransporting victims and routes of access to hospitals must be planned.
• Psychological stress will affect not only victims but also health care providers (such asdoctors and nurses) and volunteers. In order to combat this, it is therefore necessary toprepare these providers to deal with disasters through education during their studies,postgraduate courses and counselling sessions. These courses should be included inpreparedness planning. When dealing with the general population, special attention should begiven to particularly vulnerable groups such as children, the elderly, the socially isolated andthe mentally and physically handicapped.
• The establishment of comprehensive and affordable insurance against the consequencesof disaster should be encouraged through the solidarity of adequately large groups at risk,government−sponsored re−insurance, discounts for the application of adequate designcodes, etc. Where necessary, such insurance programmes could be supplemented byeffective financial support, such as "seed money" for accountable private and businessrecovery plans.
Closing session
Dr A. Wojtczak and Mr R. Schmidt, of the WHO Centre for Health Development, chaired a session in whichparticipants were given the opportunity to make closing remarks. Dr Wojtczak asked a selection of participantsfrom different regions and disciplines to offer concluding comments and suggestions. In addition toemphasizing support for the general recommendations, participants stressed that the symposium had been anopportunity for intersectoral and interdisciplinary interaction with insight into health community issues. Theterm "vulnerability reduction" had for the first time clearly been applied to public health. Because of this, thesymposium was seen to represent a unique forum in bringing together so many disciplines and in definingtheir roles in the context of reducing human vulnerability (namely deaths and injuries).
It was felt that the complexity of the multisectoral tasks associated with earthquakes and people's healthwould require a systems approach which, if successfully applied to future research, could lead to anextraordinary opportunity to transform society.
A wide distribution of the results of the symposium to governments and nongovernmental organizations andthe active role of the WHO Centre for Health Development as an information centre in disaster managementwas strongly recommended.
In closing the symposium, Dr Wojtczak thanked all the participants for their valuable contributions and veryactive participation. He explained the role of the WHO Centre for Health Development in collecting anddisseminating information and emphasized the Centre's mission as a catalyst for research. He announcedthat complete proceedings were planned for publication by mid−1997.
193
Glossary
Terms
Preparedness: Activities designed to minimize loss of lives and damage, and facilitate timely and effectiverescue relief and rehabilitation.
Rehabilitation: The operations and decisions taken after a disaster with a view to restoring a strickencommunity to its former living conditions, whilst encouraging and facilitating the necessary adjustments to thechanges caused by the disaster.
Relief: (In most cases response is considered as a synonym to relief by most organizations): Assistanceand/or intervention during or after disaster to meet the life preservation and basic subsistence needs.
Vulnerability: Potential degree of loss resulting from a damaging phenomenon likely to occur in that specificarea.
Abbreviations
ATLS Advanced trauma life supportGIS Geographic Information SystemI Intensity used in several of the Mercalli type scalesGSHAP Global Seismic Hazard Assessment ProgramLSFA Life−supporting first−aidM Magnitude on the Richter scaleMCS Mercalli − Cancani − Sieberg scaleMMI Modified Mercalli Intensity areas (MMIs) are determined by reports from U.S. Post Office
employees who estimate the amount of shaking in the area around a post office and theextent and type of damage sustained by major structures (roads, freeways, houses,apartments, commercial buildings). Damage and intensity are classified using a scale fromI − XII, where I represents "Not felt except by a very few under especially favorablecircumstances," and XII represents "Total damage".
MSK−64 A special scale, related and close to the MMI scaleNASA National Aeronautics and Space AdministrationNASDA National Space Development Agency of JapanRGELFE Research Group for Estimating Losses from Future EarthquakesWSSI World Seismic Safety Initiative
Participants
Speakers/Chairpersons/Moderators
Dr Falah Al Tawil, Director General, Treatment Services, Ministry of Health, Amman, Jordan
Dr Vladimir A. Astakhov, Deputy Director, Far−Eastern Regional Urgent Medical Care Centre, Khabarovsk,Russian Federation
Professor Shigeaki Baba, Professor Emeritus, Kobe University, Chairman, International Institute forDiabetes Education and Study and Honorary President, International Diabetes Federation, Kobe, Japan
Professor Linda B. Bourque, Department of Community Health Sciences, School of Public Health,University of California, Los Angeles, United States of America
Professor Mustafa Erdik, Chairman, Department of Earthquake Engineering, Bogazici University, KandilliObservatory and Earthquake Research Institute, Istanbul, Turkey
Professor Mamdouh Gabr, Professor of Pediatrics, Cairo University and Secretary General, Egyptian RedCrescent, Cairo, Egypt
194
Professor Sergey Goncharov, Director, All−Russian Centre for Disaster Medicine "Zaschita", Ministry ofPublic Health and Medical Industry, Moscow, Russian Federation
Professor Dimitar Jurukovski, Director, Institute of Earthquake Engineering and Engineering Seismology,University "St Cyril and Methodius", Skopje, The former Yugoslav Republic of Macedonia
Dr Roman Kintanar, Coordinator, Typhoon Committee Secretariat and Chairman, Seismic TechnicalCommittee, International Decade for Natural Disaster Reduction, Quezon City, Philippines
Mr Haruhiko Kuramochi, Director General, Commerce and Industry Department, Hyogo PrefecturalGovernment, Kobe, Japan
Professor Jeffrey Levett, Director, International Affairs, National School of Public Health, Ministry of Healthand Welfare, Athens, Greece
Dr Arthur K. Melkonian, Republican Information and Computer Centre, Ministry of Health, Yerevan, Armenia
Professor Ara M. Minasyan, Chairman, Emergency Medical Scientific Centre, Ministry of Health, Yerevan,Armenia
Mr Masao Miyakawa, Chairman, Earthquake Insurance Committee, The Marine and Fire InsuranceAssociation of Japan, Inc. and Managing Director, Yasuda Fire and Marine Insurance Company Ltd., Tokyo,Japan
Dr Bagus Mulyadi, Director, Private and Specialty Hospitals, Directorate General of Medical Care andSecretary of Crisis Centre, Ministry of Health, Jakarta, Indonesia
Professor Yasushi Nagasawa, Department of Architecture, Graduate School of Engineering, The Universityof Tokyo, Tokyo, Japan
Dr Eric K. Noji, Chief, International Emergency and Refugee Health Programs, Centers for Disease Controland Prevention, Atlanta, United States of America
Dr Jorge Oviedo Arce, Director, Injury Prevention and Control and Health Care in Disaster Programmes,Ministry of Health, Mexico DF, Mexico
Dr Jean Luc Poncelet, Head, Disaster Management Program for South America, WHO/Pan American HealthOrganization, Quito, Ecuador
Dr Ernesto Pretto, Associate Director, Safar Center for Resuscitation Research, University of Pittsburgh,Pittsburgh, United States of America
Professor Shigeaki Sato, Chairman, Department of Hygiene, Kobe University School of Medicine, Kobe,Japan
Dr G.N. Solar Oyanedel, Medico Coordinador, Comité de Emergencias, Servicio de Salud MetropolitanoOccidente, Santiago, Chile
Dr Kiyoshi Tatemichi, Director, Emergency Department, Kobe City General Hospital, Kobe, Japan
Dr Ciro Ugarte Casafranca, Director, Disaster Preparedness and Response Division, Ministry of Health,Lima, Peru
Professor H. P. Wölfel, Professor of Mechanical Engineering, Technical University of Darmstadt, Germanyand member of European Committee for Standardization (CEN)
Mr Yasuyuki Yasuda, General Manager, Kansai Project Development Division, The Sakura Bank Limited,Kobe, Japan
Panelists
195
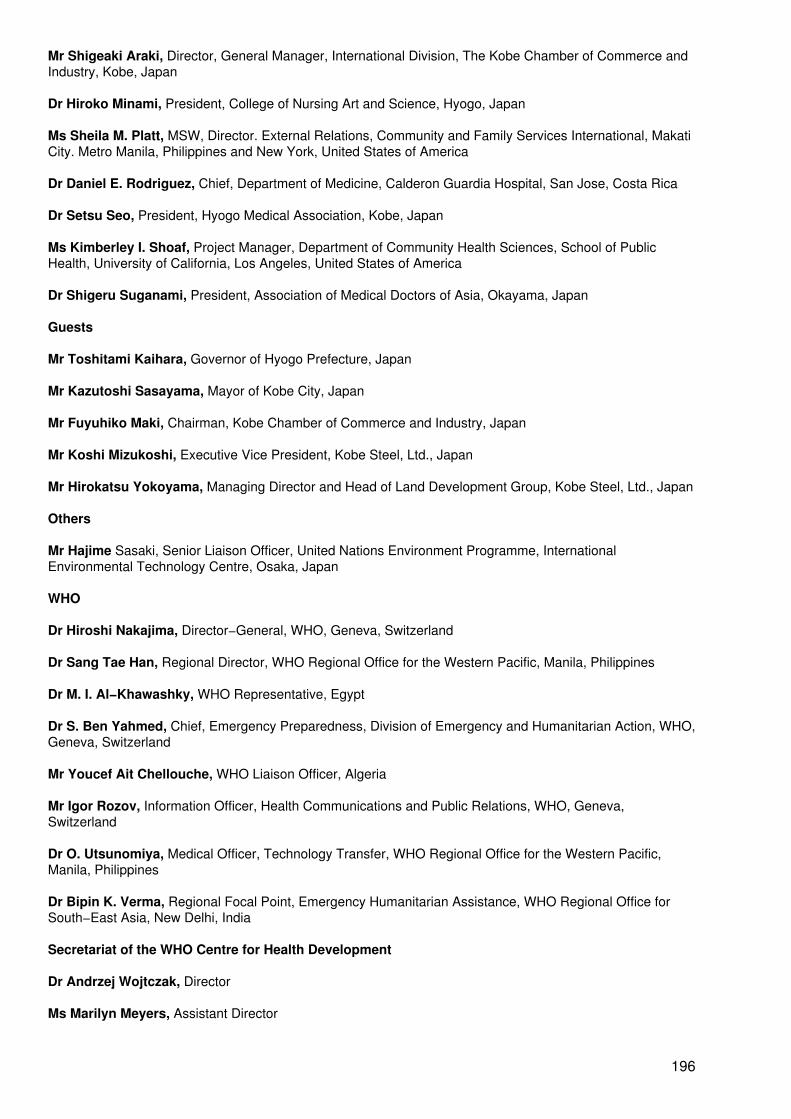
Mr Shigeaki Araki, Director, General Manager, International Division, The Kobe Chamber of Commerce andIndustry, Kobe, Japan
Dr Hiroko Minami, President, College of Nursing Art and Science, Hyogo, Japan
Ms Sheila M. Platt, MSW, Director. External Relations, Community and Family Services International, MakatiCity. Metro Manila, Philippines and New York, United States of America
Dr Daniel E. Rodriguez, Chief, Department of Medicine, Calderon Guardia Hospital, San Jose, Costa Rica
Dr Setsu Seo, President, Hyogo Medical Association, Kobe, Japan
Ms Kimberley I. Shoaf, Project Manager, Department of Community Health Sciences, School of PublicHealth, University of California, Los Angeles, United States of America
Dr Shigeru Suganami, President, Association of Medical Doctors of Asia, Okayama, Japan
Guests
Mr Toshitami Kaihara, Governor of Hyogo Prefecture, Japan
Mr Kazutoshi Sasayama, Mayor of Kobe City, Japan
Mr Fuyuhiko Maki, Chairman, Kobe Chamber of Commerce and Industry, Japan
Mr Koshi Mizukoshi, Executive Vice President, Kobe Steel, Ltd., Japan
Mr Hirokatsu Yokoyama, Managing Director and Head of Land Development Group, Kobe Steel, Ltd., Japan
Others
Mr Hajime Sasaki, Senior Liaison Officer, United Nations Environment Programme, InternationalEnvironmental Technology Centre, Osaka, Japan
WHO
Dr Hiroshi Nakajima, Director−General, WHO, Geneva, Switzerland
Dr Sang Tae Han, Regional Director, WHO Regional Office for the Western Pacific, Manila, Philippines
Dr M. I. Al−Khawashky, WHO Representative, Egypt
Dr S. Ben Yahmed, Chief, Emergency Preparedness, Division of Emergency and Humanitarian Action, WHO,Geneva, Switzerland
Mr Youcef Ait Chellouche, WHO Liaison Officer, Algeria
Mr Igor Rozov, Information Officer, Health Communications and Public Relations, WHO, Geneva,Switzerland
Dr O. Utsunomiya, Medical Officer, Technology Transfer, WHO Regional Office for the Western Pacific,Manila, Philippines
Dr Bipin K. Verma, Regional Focal Point, Emergency Humanitarian Assistance, WHO Regional Office forSouth−East Asia, New Delhi, India
Secretariat of the WHO Centre for Health Development
Dr Andrzej Wojtczak, Director
Ms Marilyn Meyers, Assistant Director
196
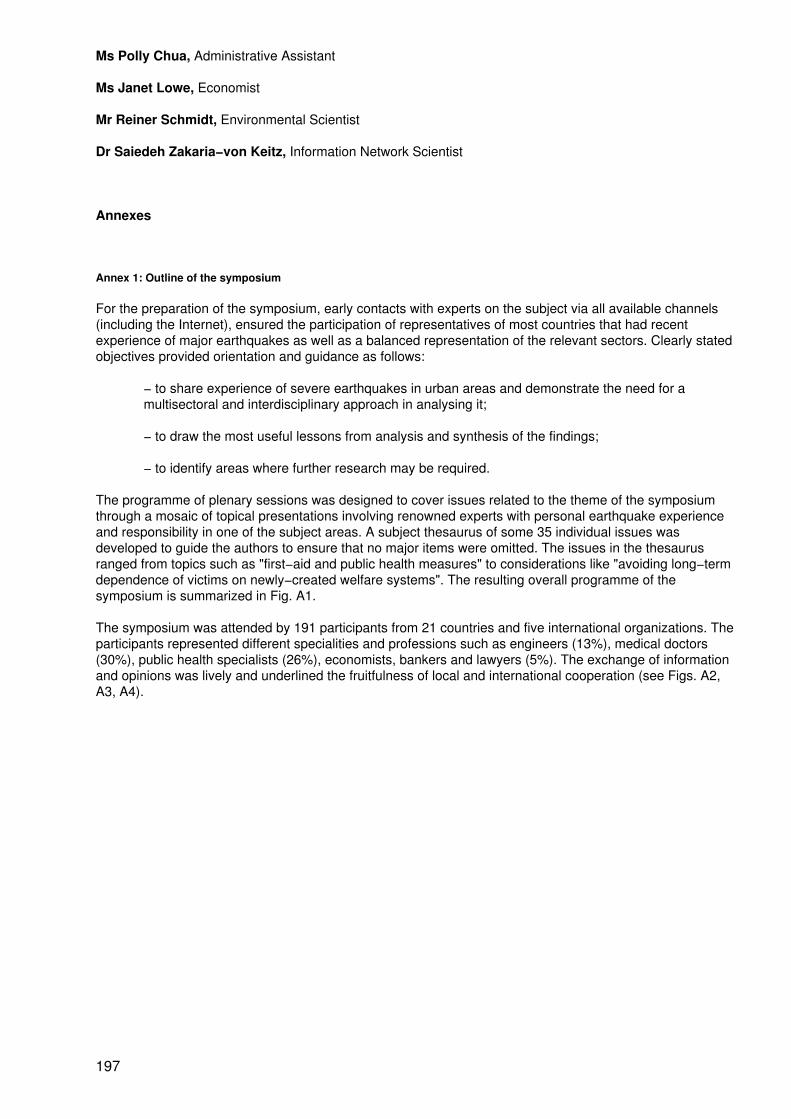
Ms Polly Chua, Administrative Assistant
Ms Janet Lowe, Economist
Mr Reiner Schmidt, Environmental Scientist
Dr Saiedeh Zakaria−von Keitz, Information Network Scientist
Annexes
Annex 1: Outline of the symposium
For the preparation of the symposium, early contacts with experts on the subject via all available channels(including the Internet), ensured the participation of representatives of most countries that had recentexperience of major earthquakes as well as a balanced representation of the relevant sectors. Clearly statedobjectives provided orientation and guidance as follows:
− to share experience of severe earthquakes in urban areas and demonstrate the need for amultisectoral and interdisciplinary approach in analysing it;
− to draw the most useful lessons from analysis and synthesis of the findings;
− to identify areas where further research may be required.
The programme of plenary sessions was designed to cover issues related to the theme of the symposiumthrough a mosaic of topical presentations involving renowned experts with personal earthquake experienceand responsibility in one of the subject areas. A subject thesaurus of some 35 individual issues wasdeveloped to guide the authors to ensure that no major items were omitted. The issues in the thesaurusranged from topics such as "first−aid and public health measures" to considerations like "avoiding long−termdependence of victims on newly−created welfare systems". The resulting overall programme of thesymposium is summarized in Fig. A1.
The symposium was attended by 191 participants from 21 countries and five international organizations. Theparticipants represented different specialities and professions such as engineers (13%), medical doctors(30%), public health specialists (26%), economists, bankers and lawyers (5%). The exchange of informationand opinions was lively and underlined the fruitfulness of local and international cooperation (see Figs. A2,A3, A4).
197
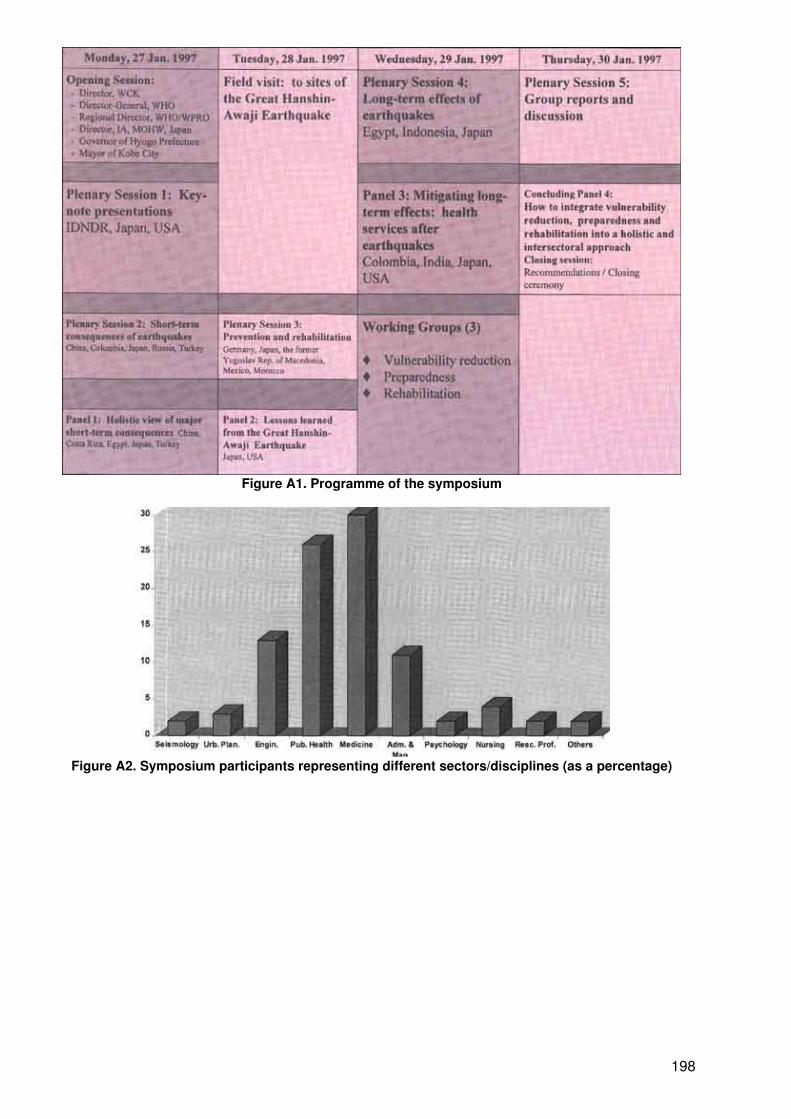
Figure A1. Programme of the symposium
Figure A2. Symposium participants representing different sectors/disciplines (as a percentage)
198
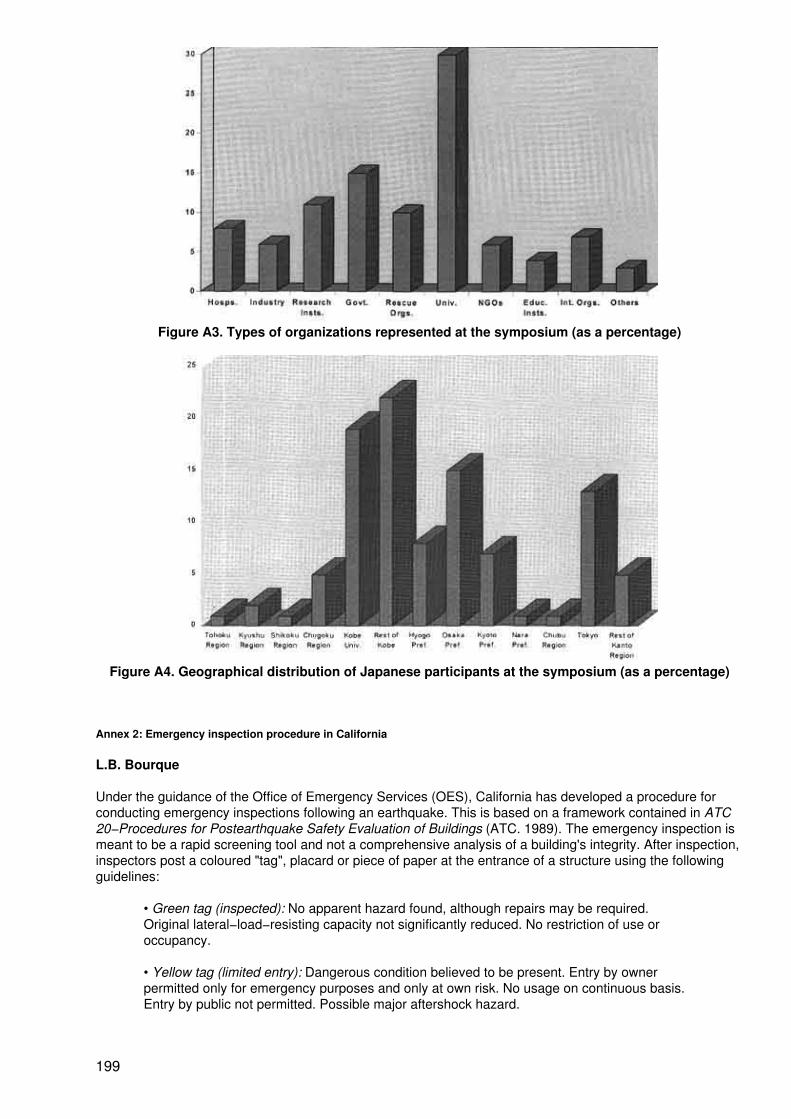
Figure A3. Types of organizations represented at the symposium (as a percentage)
Figure A4. Geographical distribution of Japanese participants at the symposium (as a percentage)
Annex 2: Emergency inspection procedure in California
L.B. Bourque
Under the guidance of the Office of Emergency Services (OES), California has developed a procedure forconducting emergency inspections following an earthquake. This is based on a framework contained in ATC20−Procedures for Postearthquake Safety Evaluation of Buildings (ATC. 1989). The emergency inspection ismeant to be a rapid screening tool and not a comprehensive analysis of a building's integrity. After inspection,inspectors post a coloured "tag", placard or piece of paper at the entrance of a structure using the followingguidelines:
• Green tag (inspected): No apparent hazard found, although repairs may be required.Original lateral−load−resisting capacity not significantly reduced. No restriction of use oroccupancy.
• Yellow tag (limited entry): Dangerous condition believed to be present. Entry by ownerpermitted only for emergency purposes and only at own risk. No usage on continuous basis.Entry by public not permitted. Possible major aftershock hazard.
199
• Red tag (unsafe): Extreme hazard, may collapse. Imminent danger of collapse from anaftershock. Unsafe for occupancy or entry, except by authorities.
For futher details, see Holmes and Somers, January 1996; EQE International, Inc. and The GeographicInformation Systems Group of the Governor's Office of Emergency Services, May 1995; and Ranous, 1995.
Annex 3: Advance planning to reduce emergency workers' vulnerability to stress
S. Platt
Awareness of the need to minimize, manage and alleviate the effects of disaster stress on the respondingworkforce suggests that preparation for worker stress management be considered an integral element ofdisaster preparedness and response plans.
Preparation
In countries where mental health services are well developed, disaster mental health training involving crisisintervention, post−traumatic stress and grief reactions, and disaster psychology is provided to mental healthworkers who participate in disaster response. Opportunities to join practice drills and exercises withcolleagues from emergency organizations are arranged, and mental health workers plan to take majorresponsibility for the support of the disaster workforce. They must adopt a low−key, practical, educationalapproach, avoiding the use of mental health terminology, if their services are to be accepted by rescueworkers.
In addition, emergency organizations teach their workers to expect disaster stress as an occupational hazard,to identify its sources in specific disaster scenarios, and to recognize both their own stress responses andthose of colleagues. Emergency workers and their supervisors learn and practise coping and stressmanagement techniques that can be used for mutual support during rescue work assignments.
All members of the emergency organization are familiar with the elements of stress management support thatare routinely offered during and after rescue operations. These may include:
− end−of−shift meetings that provide information on the rescue effort along with a snack,drink and brief reminders about stress responses and their management;
− informal defusing sessions, presenting periodic opportunities to discuss how the work isgoing, share reactions and receive support;
− formal stress debriefings conducted by a mental health professional for members of a workunit in order to provide a structured opportunity to process personal experience in the rescueeffort and to receive support for managing the stress that is associated with it;
− mental health consultation as needed when intense stress responses are causing distressor interfering with functioning.
In environments where mental health professionals and services are limited, plans can be made for medicaland health workers to receive basic training about physical and psychological responses to disaster. They canthen share this knowledge with disaster response planners so that support for the rescue workforce withregard to stress can be integrated into disaster health planning.
Organizational stress management planning
Organizations committed to instituting an occupational stress management programme engage in a processwhich may have three phases.
Prevention
This involves commitment by the leadership and line management to an approach to occupational safety andsecurity which includes stress management as an integral part of occupational health. Training in elements ofdisaster dynamics and stress response appropriate to different levels of responsibility is a first step towards
200
minimizing workforce vulnerability to the adverse effects of disaster stress.
Preparation
Comprehensive stress management programmes may include elements such as the following:
− recruitment and selection procedures which consider hardiness and resilience;
− orientation and briefing which integrate concepts of stress management and safety;
− provision of accurate job descriptions, including preparation for the ambiguity, lack ofstructure, isolation and personal demands of disaster work (Paton, D. 1994);
− supervisor training in elements of coaching, team−building, stress education and stressmanagement practices;
− development of stress management plans, including support for both normal "wear andtear" and traumatic critical events.
Annex 4: Vulnerability analysis
M. Erdik
A vulnerability analysis involves the elements at risk (physical, social and economic) and the type of risk (suchas damage to structures and systems and human casualties). Vulnerability assessments are usually based onpast earthquake damage (observed vulnerability) and, to a lesser degree, on analytical investigations(predicted vulnerability). Primary physical vulnerabilities are associated with buildings, infrastructure andlifelines. These vulnerabilities are agent− and site−specific. Furthermore, they depend on design, constructionand maintenance particularities. Secondary physical vulnerabilities are associated with consequential damageand losses. Only limited vulnerability models exist for damage resulting from secondary hazards, such aspost−earthquake fire, release of hazardous materials, explosions and water inundation. Socioeconomicvulnerabilities refer to risks to socioeconomic assets and systems, such as damage to social infrastructure,impact on production and employment, change of wealth distribution, and inflation. Socioeconomicvulnerabilities also include casualties and traumas.
In addition to the direct physical damage and casualties from ground−shaking and collateral hazards, indirecteconomic losses constitute a major portion of the total earthquake loss. Indirect economic losses arise as aresult of the discontinued service of damaged facilities. These losses include:
− production and/or sales lost by firms in damaged buildings;− production and/or sales lost by firms unable to receive supplies from other damagedfacilities;− production and/or sales lost by firms due to damaged lifelines;− losses arising from tax revenues and increased unemployment compensations.
Socioeconomic vulnerabilities
In addition to physical vulnerability, the socioeconomic vulnerability of the urban system also needs to beassessed in terms of casualties, social disruption and economic loss for a comprehensive earthquake damageand loss scenario. Casualties in earthquakes arise mostly from structural collapses and from collateralhazards. Lethality per collapsed building for a given class of buildings can be estimated by the combination offactors representing the population per building, occupancy at the time of the earthquake, occupants trappedby collapse, mortality at collapse and post−collapse mortality. Future research and data acquisition will beneeded to decrease the large uncertainties regarding casualty estimates. Social disruption needs to bemeasured in both quantitative (e.g. number of displaced families) and qualitative terms. The ethnoculturalcontext of social disruption should also be considered. Past earthquake disaster experiences indicate thatsingle−parent families, women, handicapped people, children and the elderly constitute the most vulnerablesocial groups.
201
RGELFE provides the urban earthquake lethality rates of 0.0014%, 0.031%, 0.48% and 6.8% respectively forintensities VI, VII, VIII and IX. The lethality rate for intensity VIII coincides with data for the 1992 Erzincan(Turkey) earthquake. The serious injury rate (requiring hospitalization) is given as four times the death rate,and the minor injury rate is 30 times the death rate. Ambraseys & Jackson, using data from Turkey andGreece, provide the following statistics regarding the number of people killed per 100 houses destroyed byearthquakes of magnitude 5 on the Richter scale: rubble masonry houses = 17; adobe houses =11; masonryand reinforced adobe houses = 2; timber and brick houses = 1; reinforced concrete frame houses = 1. Datafrom the 1992 Erzincan earthquake indicate that, on the average, there was one death and three hospitalizedinjuries for each heavily−damaged or collapsed reinforced concrete building.
Annex 5: Sharing losses among citizens: The example of post−war Germany
The German example was introduced in connection with a visit of the Consul General1 to Okinawa at a time ofheated discussions on the subject of indemnity to landowners whose land had been leased to the US militaryunder Japanese−US Security arrangements and who, therefore, had no chance to pursue more lucrativeopportunities. This has been an issue of widespread Japanese public interest. According to theConsul−General's presentation, a somewhat analogous situation, but concerning larger−scale damages,arose in post−World War II Germany. At the Teheran and Yalta conferences, the Allied powers decided tochange many boundaries which set in motion millions of people, among them Germans, who lived east of theOder−Neisse line. The first wave of refugees from these areas arrived in West Germany in June 1945 andsuch immigration continued to the end of 1947. Some 13.6 million Germans lost their land and assets in thisway.
1 Information adapted from a speech in Okinawa in 1995, courtesy of Dr Nils Grueber,German Consul General, Osaka. Full text of the bill appeared in the German FederalRegister, Bundesgesetzblatt of 18 August 1952, No. 34, Part I.
The enactment in 1952 of the "Burden Adjustment Bill" was, therefore, one of the most important legislativeacts for the new Federal Republic (of the West German states). The objective of this bill was to help thevictims of destruction, expulsion and even of currency reform, to find new land, homes and jobs. As financialresources were scarce in the war−torn country, and poverty and misery were widespread, a drastic(large−scale) solution was sought and needed. It was decided that the financial equivalent of 50% of theentire capital assets of the country would be re−distributed. At the time, 50% of total assets left after the waramounted to 35 billion DM. Adjusted to today's value, 50% would be about 500 billion DM or 300 billion USdollars, an immense programme.
In accordance with the new law, both corporations and individuals who were lucky enough to still havepossessions and had their domicile in the federal states or West Berlin had to share 50% of their assets via aspecial tax. The payment schedule, however, could be spread out so that the total of 50% could be paid in 10yearly installments of 5% each. Such measures were employed so as to avoid the threat to the economicviability of taxpaying citizens and organizations. Tax payments were collected into a Burden Adjustment Fund,from which, upon application and careful examination, compensatory payments were made to the victims ofthe war, for homes, land, businesses, household goods, lost savings and disabilities. The Burden AdjustmentAgency was established under the Minister of Finance. The substantial sums which were paid out to manyapplicants not only provided them with financial and psychological relief from their plight, but also greatlyfacilitated the resettlement of people and generally furthered the solidarity among citizens. Often thecompensation received was used as substantial seed money to establish new businesses and resulted in anenterpreneurial boom in post−war Germany.
This unique experience of post−war Germany could contribute to the solution of other burden−sharingsituations which could arise when man−made or natural disasters strike innocent people.
202




















