Naga Hills and Manipur - Search the history of over 682 billion ...
Upload
independentCategory
view
2download
0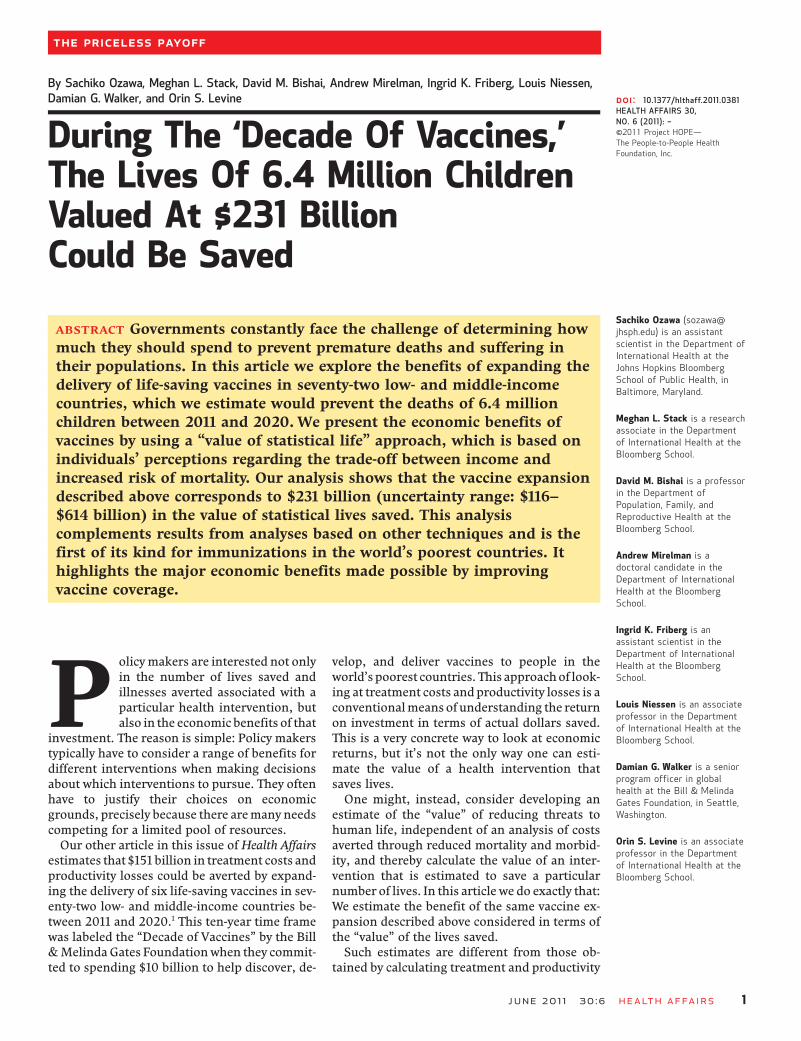
By Sachiko Ozawa, Meghan L. Stack, David M. Bishai, Andrew Mirelman, Ingrid K. Friberg, Louis Niessen,Damian G. Walker, and Orin S. Levine
During The ‘Decade Of Vaccines,’The Lives Of 6.4 Million ChildrenValued At $231 BillionCould Be Saved
ABSTRACT Governments constantly face the challenge of determining howmuch they should spend to prevent premature deaths and suffering intheir populations. In this article we explore the benefits of expanding thedelivery of life-saving vaccines in seventy-two low- and middle-incomecountries, which we estimate would prevent the deaths of 6.4 millionchildren between 2011 and 2020. We present the economic benefits ofvaccines by using a “value of statistical life” approach, which is based onindividuals’ perceptions regarding the trade-off between income andincreased risk of mortality. Our analysis shows that the vaccine expansiondescribed above corresponds to $231 billion (uncertainty range: $116–$614 billion) in the value of statistical lives saved. This analysiscomplements results from analyses based on other techniques and is thefirst of its kind for immunizations in the world’s poorest countries. Ithighlights the major economic benefits made possible by improvingvaccine coverage.
Policymakers are interested not onlyin the number of lives saved andillnesses averted associated with aparticular health intervention, butalso in the economic benefits of that
investment. The reason is simple: Policy makerstypically have to consider a range of benefits fordifferent interventions when making decisionsabout which interventions to pursue. They oftenhave to justify their choices on economicgrounds, precisely because there aremany needscompeting for a limited pool of resources.Our other article in this issue of Health Affairs
estimates that $151 billion in treatment costs andproductivity losses could be averted by expand-ing the delivery of six life-saving vaccines in sev-enty-two low- and middle-income countries be-tween 2011 and 2020.1 This ten-year time framewas labeled the “Decade of Vaccines” by the Bill&MelindaGates Foundationwhen they commit-ted to spending $10 billion to help discover, de-
velop, and deliver vaccines to people in theworld’spoorest countries. This approachof look-ing at treatment costs andproductivity losses is aconventionalmeansof understanding the returnon investment in terms of actual dollars saved.This is a very concrete way to look at economicreturns, but it’s not the only way one can esti-mate the value of a health intervention thatsaves lives.One might, instead, consider developing an
estimate of the “value” of reducing threats tohuman life, independent of an analysis of costsaverted through reduced mortality and morbid-ity, and thereby calculate the value of an inter-vention that is estimated to save a particularnumber of lives. In this article we do exactly that:We estimate the benefit of the same vaccine ex-pansion described above considered in terms ofthe “value” of the lives saved.Such estimates are different from those ob-
tained by calculating treatment and productivity
doi: 10.1377/hlthaff.2011.0381HEALTH AFFAIRS 30,NO. 6 (2011): –©2011 Project HOPE—The People-to-People HealthFoundation, Inc.
Sachiko Ozawa ([email protected]) is an assistantscientist in the Department ofInternational Health at theJohns Hopkins BloombergSchool of Public Health, inBaltimore, Maryland.
Meghan L. Stack is a researchassociate in the Departmentof International Health at theBloomberg School.
David M. Bishai is a professorin the Department ofPopulation, Family, andReproductive Health at theBloomberg School.
Andrew Mirelman is adoctoral candidate in theDepartment of InternationalHealth at the BloombergSchool.
Ingrid K. Friberg is anassistant scientist in theDepartment of InternationalHealth at the BloombergSchool.
Louis Niessen is an associateprofessor in the Departmentof International Health at theBloomberg School.
Damian G. Walker is a seniorprogram officer in globalhealth at the Bill & MelindaGates Foundation, in Seattle,Washington.
Orin S. Levine is an associateprofessor in the Departmentof International Health at theBloomberg School.
June 2011 30:6 Health Affairs 1
The Priceless Payoff

costs, because they also capture the value thatpeople place on their own lives. They are no lessreal, and should not be discounted, because theyare derived from individual judgments of trade-offs between financial rewards and increasedmortality risk. We present such estimates here,butwe first describemore fully the concept of the“value of statistical life.”
Value Of Statistical LifeIndividuals make trade-offs every day betweenhealth and risks of death, such as driving a ve-hicle, smoking a cigarette, and eating unhealthyfood.2 The value of statistical life is based on theidea that peoplemake trade-offs between risks ofdeath and income.3 It is generated from the esti-mated amount of income a typical individual iswilling to trade off to reduce the risk of death.4
Values are derived from both wage risk stud-ies, which use labor-market data, and statedpopulation preference studies, which ask indi-viduals howmuch they arewilling to pay to avoidcertain risks of death.5–7 The reductions in risksare multiplied across a large population. Forexample, if each member of a population of10,000 is willing to pay $670 on average for aone in 10,000decrease inhis or her risk of dying,the value of statistical life is calculated as$6,700,000 (670 × 10;000).Estimating the value of statistical life helps
policy makers determine how much they shouldspend on programs that prevent deaths in theirpopulations. The results are used widely in eco-nomics and regulatory assessments to representthe worth of population-level interventions thatreduce the number of expected deaths by one.
An intervention is undertaken if it costs less toprevent one death than the country’s specific percapita value of statistical life. For example, if ahealth program in the United States costs lessthan the US value of $6.7million to save a child’slife, then it may be considered a worthy in-vestment.Such estimates are frequently applied in high-
income countries to assess investments in pre-venting road traffic accidents or drowning, or inensuring clean air and safe drinking water.9,10
Specifically, the United States has presidentialexecutive orders encouraging the use of value ofstatistical life in policy evaluation and cost-benefit analyses by the Department of Transpor-tation and the Environmental ProtectionAgency.11–14 The value-of-statistical-life conceptis similarly used in the context of policy analysisof Canadian programs15 and is implicitly appliedin European countries.16–18
In the United States, there has been a reluc-tance to quantify life savings in money in the
health sector. However, value-of-statistical-lifemethods are starting to be applied in othercountries to measure the benefits of health in-terventions. Some examples of interventionswhose value has been estimated this way includea cancer risk prevention program in China,19
tuberculosis control strategies in sub-SaharanAfrica,8 and voluntary counseling and testingfor HIV/AIDS in Tanzania.20
Governments and people are already makingtrade-offs between health and money, eitherexplicitly or implicitly.21 Informedpolicymakingrequires a methodology that allows these trade-offs to be captured and quantified in health pol-icy analyses.Vaccines are considered among the most cost-
effective public health interventions.22–24 Theeconomic argument for purchasing vaccines iscompelling when one considers the costs ofvaccination against the immediate benefits ofillness averted and treatment costs saved.Although these short-term health benefits arewell known, there are many other benefits—especially long-term economic ones—that havebeen given inadequate consideration. Very fewarticles todatehavemeasured value-of-statisticallife savings from vaccines.25,26
This article presents the economic benefitsof saving lives from improving coverage ofpneumococcal, rotavirus, pertussis, measles,Haemophilus influenzae type b (Hib), andmalariavaccines in seventy-two of the world’s poorestcountries between 2011 and 2020. Our analysisgoes beyond the economic benefits broughtabout by treatment cost savings and productivitylosses averted by capturing how people valuetheir lives andwouldpay todelaypainand suffer-ing from death.
Study Data And MethodsDeaths Averted In this study we used the LivesSaved Tool to estimate the number of deathsaverted from vaccines.27 The Lives Saved Toolis a freely available child survival modeling tool(http://www.futuresinstitute.org).28,29
The model estimates the impact of specificpublic health interventions on cause-specificneonatal, under-five, and maternal mortality.It uses the most current country-specific esti-mates of demography, mortality rates,30 causesof death,31 health status, rates at which interven-tions are provided, and peer-reviewed effects ofinterventions.32 The model accounts for compet-ing risks among interventions.Our analysis examined the impact of improved
childhood vaccination coverage (pneumococcal,rotavirus, pertussis, measles, Hib, and malaria)in the seventy-two countries eligible to receive
The Priceless Payoff
2 Health Affairs June 2011 30:6

support from theGAVIAlliance (formerly knownas the Global Alliance for Vaccines and Immuni-zation), a global health partnership committedto ensuring access to low-cost immunizations indeveloping countries.33 Vaccination coverage es-timates for 2009 were obtained from the WorldHealth Organization (WHO).34
Based on vaccination targets set by the WHOGlobal Immunization Vision and Strategy, weincreased the rate of immunization linearly to90 percent by 2015 and held the rate constantbetween 2015 and 2020.35 In addition, we as-sumed that a malaria vaccine with an effective-ness of 45 percent36 would be introduced in 2015in malaria-affected countries, with rates of vac-cination increasing linearly to 90 percent by2020 (see details in the online Appendix).37
Benchmark Value Of Statistical Life Fol-lowing the standard rules used by the USCongressional Budget Office38 and the most re-cent literature in the field, we adopted a bench-mark value of statistical life for the United Statesof $6.7 million per life saved, in 2009 dollars.This estimate is based on studies of compensat-ing wage differentials among jobs with varyingrisks of death and interview-based approachesfrom sixty articles in ten high-income coun-tries,6,39 adjusted for inflation and real incomegrowth.4 This figure lies between the value usedby the US Department of Transportation($6.2 million in 2009 dollars)14 and the estimateadopted by the US Environmental ProtectionAgency ($8.1 million in 2009 dollars).40
Benefits Transfer Todate, there are very fewstudies from low-income countries on people’swillingness to pay for mortality risk reductions.To the extent that they exist, results from low-income country studies provide evidence on anincome elasticity of the value of statistical lifethat accounts for differences in per capitaincome, development levels, and aversion torisk between the US and each low-incomecountry.4,8,19,20,25
The method, known as benefits transfer, usesthe income elasticity of the value of life—that is,
the sensitivity of mortality-risk aversion tochanges in income—to estimate the value of stat-istical life in low-income countries as some pro-portion of the United States value of statisti-cal life.Specifically, to determine the value of statisti-
cal life for each low-income country, we firstcalculated an “adjustment factor” by taking theratioof that country’s income toUS income, thenraised that ratio to a power of 1.5, which repre-sents the income elasticity of the value of sta-tistical life between the United States and low-income countries. The US value of statistical lifewas then multiplied by this adjustment factor toprovide the low-income country’s value of sta-tistical life (the equation is provided in standardmathematical shorthand in the online Ap-pendix).37
An income elasticity of 1 assumes that peopleare willing to pay the same proportion of theirincome to reduce mortality risk regardless ofincome level. However, elasticities are oftenfound to be greater than 1 in countries facingearlier stages of economic development. Specifi-cally, studies in low-income countries suggestthat people with lower incomes are willing totake on greater occupational mortality risk thanthose with greater incomes.4,41
Therefore, this study used a baseline incomeelasticity of 1.5 with an uncertainty range be-tween 1 and 2. The higher the income elasticity,the more the value of statistical life in a low-income country is reduced relative to the valueof statistical life in the United States.Value-of-statistical-life adjustments were
made using per capita projected gross domesticproduct figures for the United States and eachlow-income country. Per capita gross domesticproduct projections for 2010–15 were adoptedfrom the International Monetary Fund42 andtrended forward for the years 2016–20 basedon the past five years. To calculate the overallvalue-of-statistical-life values, the number oflives saved as a result of scaling up vaccineswas multiplied by the value of statistical lifefor each country.The sums of these values across seventy-two
countries represent the total value-of-statistical-life figures. This can be interpreted as the aggre-gate amount that families with children at risk ofdeath are willing to pay to lower their risk byimproving childhood immunization coverage.Uncertainty Range We conducted sensitivity
analyses to show the uncertainty ranges aroundeach value-of-statistical-life estimate in themodel.We carried out computer simulations us-ing the Monte Carlo method, varying three keyvariables: (1) the benchmark value-of-statistical-life value (which varied from $6.2 million to
Vaccines areconsidered among themost cost-effectivepublic healthinterventions.
June 2011 30:6 Health Affairs 3

$8.1 million), (2) the income elasticity (whichvaried from 1 to 2), and (3) the mortality esti-mates from the Lives Saved Tool (which variedfrom 30 percent to 297 percent of the baseline;see details in the online Appendix).37 A proba-bility distribution was applied to each variablewhere 10,000 iterations of the model were runusing @RISK software (version 5.7).Limitations There are important limitations
to note with the approach. First, the value-of-statistical-life methodology was developed tomeasure trade-offs in working-age adults. Forthis analysis, value-of-statistical-life values hadto be applied to vaccines that target childrenunder age five. Although the trade-offs parentsmake betweenmoney and risk of death on behalfof their childrenmaybedistinct fromthosemadein the adult wage market, there is no conclusiveevidence that the value would be higher or lowerfor children.43
Second, empirical data on the value of statis-tical life are limited in low-income countries. Inaddition, differences in the extent of the avail-ability and cost of health services may influencewage-risk trade-offs in these countries. The ben-efits-transfer method tries to adjust for cross-country differences in per capita income andstages of economic development. However, fur-ther empirical studies are needed to elicit anddocument the actual value of statistical lifeamong targeted populations.Another limitation is that the approach of es-
timating statistical lives does not include greatersocietal benefits such as economic returns fromdemographic transitions and preventing diseaseoutbreaks. Because the value-of-statistical-lifemethod asks individuals to consider their owntrade-offs between money and risks of death,these societal-level benefits that have external-ities, or other effects, might not be fully consid-ered. These benefitsmaybedwarfed by the value-of-statistical-life numbers, but they are stillimportant to consider if one wishes to paint amore accurate picture of vaccine benefits.The Lives Saved Tool analysis does not capture
the so-called herd immunity benefits that accrueamongpopulationsolder thanage five. These arethe benefits that result when large groups ofpeople have immunity to a particular disease,and therefore are far less likely to pass thedisease to unvaccinated members of the popula-tion—thus keeping the “herd” safe.For example, in countries such as the United
States, large disease reductions have been ob-served among older children and adults fromadministeringpneumococcal vaccine to childrenunder age five.44 Not capturing these benefitswould tend to make our estimates in this articleconservative.
Finally, although this analysis estimated thepotential benefits of vaccination, it did not esti-mate the costs of scalingup thevaccineprograms(including vaccine purchases). However, by es-timating the benefits that may accrue from scal-ing up vaccines, our analysis provides a bench-mark for policy makers to consider.In short, if the expected costs of scaling up are
less than or equal to the projected benefits, thenthe program can be considered to convey netbenefits. Additional work on the costs of scalingup, and especially the distribution of these costsamong payers, would be a useful adjunct to thisanalysis.
ResultsOverall, improving coverage of a package of life-saving childhood vaccines in seventy-two GAVI-eligible countries to 90 percent coverage be-tween 2011 and 2020 would prevent the deathsof approximately 6.4 million children under agefive and would represent $231 billion (uncer-tainty range: $116–$614 billion) in the value ofstatistical lives. In other words, we estimate thebenefits of averting 6.4 million vaccine-prevent-able child deaths in the Decade of Vaccines to beworth $231 billion to those who are at riskof death.The value-of-statistical-life benefits are per-
haps easier to appreciate on an annual basis.The average benefit over the decade was $23 bil-lion per year, corresponding to an average of640,000 lives saved per year. The benefits in-creased over the years, ranging from a low of$3.5 billion in 2011 to a high of $40 billion in2020. This corresponds to saving 130,000 chil-dren’s lives in 2011 and 970,000 children’s livesin 2020 with improved immunization ratesacross the seventy-two GAVI-eligible countries.The largest value-of-statistical-life benefits
were from pneumococcal and Hib vaccines,contributing $105 billion (uncertainty range:
By estimating thebenefits that mayaccrue from scaling upvaccines, our analysisprovides a benchmarkfor policy makers.
The Priceless Payoff
4 Health Affairs June 2011 30:6

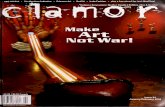
$52–$270 billion) from pneumonia and $14 bil-lion ($7–$36 billion) from meningitis cases. Ro-tavirus vaccine ($54 billion; $27–$138 billion)and malaria vaccine ($28 billion; $14–$76 bil-lion) were the next-largest contributors tovalue-of-statistical-life estimates.Malaria vaccine savings increased rapidly as-
suming its introduction in 2015 (see Exhibit 1).Scaling up the two remaining vaccines yieldedvalue-of-statistical-life benefits of $16 billion($8–$44 billion) from pertussis and $14 billion($7–$38billion) frommeasles.When the share ofeligible people vaccinated is estimated to reach90 percent for all of these vaccines in 2020, oneyear of vaccination is estimated to contributeaggregated value-of-statistical-life benefits of$16 billion from averting pneumonia, $9 billionfrom malaria, and $8 billion from diarrhea.On a regional basis, Africa and South and East
Asia accounted for 88 percent of value-of-statis-tical-life benefits.Within sub-Saharan Africa, to-tal value of statistical life ranged from $28 mil-lion in Lesotho to $42 billion in Angola over thisten-year period. The ranges were even greater inSouth and East Asia, with $16 million value-of-statistical-life benefits in Timor-Leste comparedto $68 billion in India.At the country level, the highest benefits of
vaccinationwere found in India ($68 billion; un-certainty range: $33–$184 billion), Angola($42 billion, $24–$85 billion), Nigeria ($36 bil-lion, $17–$98 billion), and Indonesia ($21 bil-lion, $11–$47 billion). Angola also had the high-est benefit per vaccine-targeted cohort of $5,000with one of the highest per capita gross domesticproducts among the seventy-two countries.Many smaller countries also gained more than$500 in value-of-statistical-life benefits per sur-viving infant; these included Azerbaijan, Bhu-tan, Congo, Indonesia, Nigeria, and Sudan.To help decision makers appreciate what one
year’s worth of benefits would be, we preparedestimates centered on benefits that would accruejust in 2015, whenmost vaccines are scaled up tothepoint that 90percent of the target populationhas been vaccinated (except for the malaria vac-cine). In 2015 there would be $7.5 billion (un-certainty range: $3.5–$20.6 billion) value-of-statistical-life benefits from India, $4.1 billion($2.3–$8.5 billion) from Angola, $3.6 billion($1.7–$10 billion) from Nigeria, and $2.4 billion($1.3–$5.5 billion) from Indonesia.Comparing the values in 2015, we see that
countries such as Angola have high total valueof statistical life because of high value of statis-tical life per capita ($326,300) but fewer livessaved (12,700).By contrast, other countries suchas India have many lives saved (181,300) withlow value of statistical life per capita ($41,100)
(Exhibit 2).The per capita value-of-statistical-life values in
the seventy-two GAVI-eligible countries in 2015ranged from $550,000 in Cuba to $1,700 inBurundi. These values were derived from coun-tries’ respective per capita gross domestic prod-uct—$10,500 in Cuba and $225 in Burundi—forecast for 2015. Among the GAVI Alliancecountries in 2015, child deaths prevented fromscaling up vaccines ranged from 181,300 in Indiato 11 in Cuba.In 2015 the average total value-of-statistical-
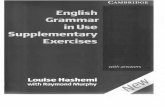
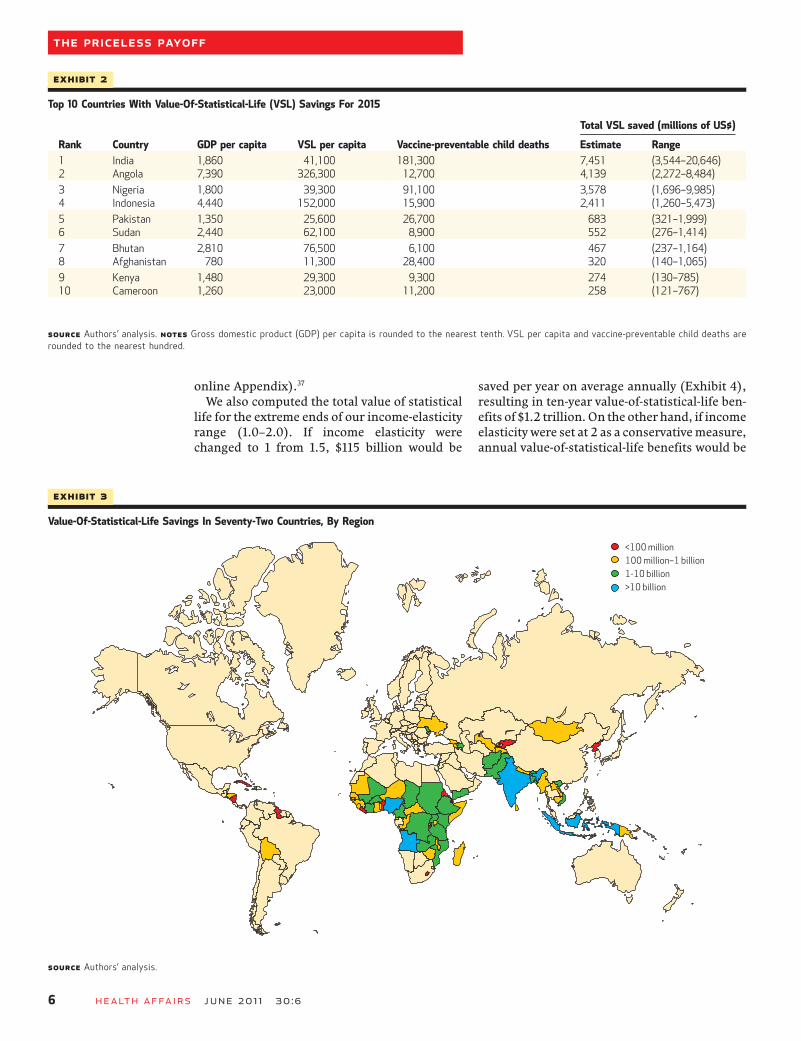
life benefit for a country in sub-Saharan Africawas $298 million across thirty-six countries,compared to an average of $1.2 billion acrossnine countries in South and East Asia. On thewhole, most countries observed between$100million and $1 billion (31 countries, 43 per-cent) or between $1 billion and $10 billion (24countries, 33 percent) in total value-of-statisti-cal-life benefits over the decade (Exhibit 3).Sensitivity analysis found that income elastic-
ity contributed the most to the uncertaintyaround the value-of-statistical-life estimate,ranging the estimate from$72billion to $929bil-lion. The next contributor was the mortality es-timates from the Lives Saved Tool, ranging thevalue of statistical life between $79 billion and$517 billion. The uncertainty around the mortal-ity estimates was driven by a number of inputssuch as the under-five mortality rate, vaccineefficacy, and percentage of deaths due to pneu-monia anddiarrhea. Lastly, the benchmark valueof statistical life ($6.7 million) varied the value-of-statistical-life estimate between $219 billionand $250 billion. In a computer simulation, wecombined these uncertainty ranges to estimate atotal value-of-statistical-life uncertainty rangebetween $116 billion and $614 billion (see the
Exhibit 1
Annual Value-Of-Statistical-Life Savings, By Vaccine-Preventable Disease, 2011–20
Billi
ons o
f dol
lars
PneumoniaMalariaDiarrheaPertussisMeaslesMeningitis
SOURCE Authors’ analysis.
June 2011 30:6 Health Affairs 5
online Appendix).37
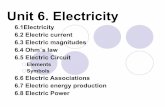
We also computed the total value of statisticallife for the extreme ends of our income-elasticityrange (1.0–2.0). If income elasticity werechanged to 1 from 1.5, $115 billion would be
saved per year on average annually (Exhibit 4),resulting in ten-year value-of-statistical-life ben-efits of $1.2 trillion.On the other hand, if incomeelasticity were set at 2 as a conservativemeasure,annual value-of-statistical-life benefits would be
Exhibit 3
Value-Of-Statistical-Life Savings In Seventy-Two Countries, By Region
SOURCE Authors’ analysis.
Exhibit 2
Top 10 Countries With Value-Of-Statistical-Life (VSL) Savings For 2015
Total VSL saved (millions of US$)
Rank Country GDP per capita VSL per capita Vaccine-preventable child deaths Estimate Range1 India 1,860 41,100 181,300 7,451 (3,544–20,646)2 Angola 7,390 326,300 12,700 4,139 (2,272–8,484)
3 Nigeria 1,800 39,300 91,100 3,578 (1,696–9,985)4 Indonesia 4,440 152,000 15,900 2,411 (1,260–5,473)
5 Pakistan 1,350 25,600 26,700 683 (321–1,999)6 Sudan 2,440 62,100 8,900 552 (276–1,414)
7 Bhutan 2,810 76,500 6,100 467 (237–1,164)8 Afghanistan 780 11,300 28,400 320 (140–1,065)
9 Kenya 1,480 29,300 9,300 274 (130–785)10 Cameroon 1,260 23,000 11,200 258 (121–767)
SOURCE Authors’ analysis. NOTES Gross domestic product (GDP) per capita is rounded to the nearest tenth. VSL per capita and vaccine-preventable child deaths arerounded to the nearest hundred.
The Priceless Payoff
6 Health Affairs June 2011 30:6
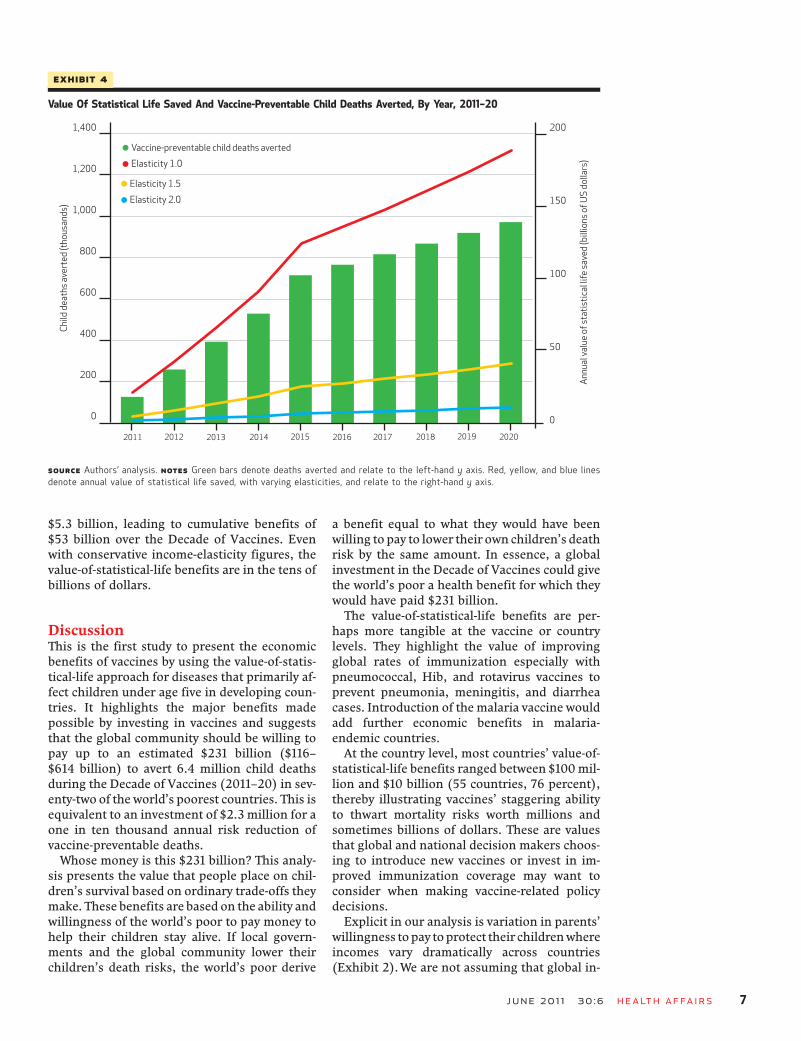
$5.3 billion, leading to cumulative benefits of$53 billion over the Decade of Vaccines. Evenwith conservative income-elasticity figures, thevalue-of-statistical-life benefits are in the tens ofbillions of dollars.
DiscussionThis is the first study to present the economicbenefits of vaccines by using the value-of-statis-tical-life approach for diseases that primarily af-fect children under age five in developing coun-tries. It highlights the major benefits madepossible by investing in vaccines and suggeststhat the global community should be willing topay up to an estimated $231 billion ($116–$614 billion) to avert 6.4 million child deathsduring the Decade of Vaccines (2011–20) in sev-enty-two of the world’s poorest countries. This isequivalent to an investment of $2.3 million for aone in ten thousand annual risk reduction ofvaccine-preventable deaths.Whose money is this $231 billion? This analy-
sis presents the value that people place on chil-dren’s survival based on ordinary trade-offs theymake. These benefits are based on the ability andwillingness of the world’s poor to pay money tohelp their children stay alive. If local govern-ments and the global community lower theirchildren’s death risks, the world’s poor derive
a benefit equal to what they would have beenwilling to pay to lower their own children’s deathrisk by the same amount. In essence, a globalinvestment in the Decade of Vaccines could givethe world’s poor a health benefit for which theywould have paid $231 billion.The value-of-statistical-life benefits are per-
haps more tangible at the vaccine or countrylevels. They highlight the value of improvingglobal rates of immunization especially withpneumococcal, Hib, and rotavirus vaccines toprevent pneumonia, meningitis, and diarrheacases. Introduction of the malaria vaccine wouldadd further economic benefits in malaria-endemic countries.At the country level, most countries’ value-of-
statistical-life benefits ranged between $100mil-lion and $10 billion (55 countries, 76 percent),thereby illustrating vaccines’ staggering abilityto thwart mortality risks worth millions andsometimes billions of dollars. These are valuesthat global and national decision makers choos-ing to introduce new vaccines or invest in im-proved immunization coverage may want toconsider when making vaccine-related policydecisions.Explicit in our analysis is variation in parents’
willingness topay toprotect their childrenwhereincomes vary dramatically across countries(Exhibit 2).We are not assuming that global in-
Exhibit 4
Value Of Statistical Life Saved And Vaccine-Preventable Child Deaths Averted, By Year, 2011–20
Child
dea
ths a
vert
ed (t
hous
ands
)
Annu
al va
lue
of st
atis
tical
life
save
d (b
illio
ns o
f US
dolla
rs)
SOURCE Authors’ analysis. NOTES Green bars denote deaths averted and relate to the left-hand y axis. Red, yellow, and blue linesdenote annual value of statistical life saved, with varying elasticities, and relate to the right-hand y axis.
June 2011 30:6 Health Affairs 7

come disparities and their consequences are de-sirable. However, what each person’s life isworth in practice is what each individual andothers are willing to pay to protect it, implicitlyor explicitly. Global investments in vaccines ac-tually move the world closer to a point at whichall lives have equal value.The value-of-statistical-life estimates found in
our analysis appear comparable to value-of-stat-istical-life values presented in other papers.Raminan Laxminarayan and colleagues foundthat the economic benefit of tuberculosis treat-ment in sub-Saharan Africa was estimated to be$129 billion (uncertainty range: $113–$146 bil-lion),8 which is in the same ballpark as the ben-efits we found in our vaccine analysis.However, this comparison must be made cau-
tiously, because the two studies’ results are notdirectly comparable. There are many differingassumptions, including the number of years oflife saved, countries and years of the analysis,and other key assumptions. Note especially thatthe income-elasticity assumption of 1 used intheir analysis has a large impact on the projectedvalueof statistical life per capita, and it generatesestimates that are higher than when using anelasticity value of 1.5, as we have done in thisanalysis.In examining the benefits of human papillo-
mavirus vaccine in Taiwan, Chih-Hsien Liao andcolleagues found that the per capita value of stat-istical life was estimated at $0.65–$4.09 millionfor vaccinating daughters and $0.56–$3.16 mil-lion for vaccinating mothers.25 Applying ourmethodology with Taiwan’s per capita gross do-mestic product, we estimated a per capita valueof statistical life of $1.7 million for Taiwan in2011, which falls within the range presented inthis study. Although the two studies assess value-of-statistical-life benefits for very different out-comes and countries, the similar scale of theresults reinforces the validity of our findings.
ConclusionOverall, this analysis provides a robust projec-tion of the potential economic benefits that maybe accrued from expanding access to life-savingchildhood vaccines during the Decade of Vac-cines. In its use of the value-of-statistical-life ap-proach, the study represents the first analysis ofits sort for vaccination programs in developingcountries. The sensitivity analyses indicate thatthe benefits accrue to tens of billions of dollarseven under the most conservative set of assump-tions. They also provide a useful indication ofwhere further empiric validation of estimateswould be most valuable. ▪
This study was performed with financialsupport from the Bill & Melinda GatesFoundation. The views expressed hereinare those of the authors and do not
necessarily reflect the official policy orposition of the Bill & Melinda GatesFoundation. The authors thank the LivesSaved Tool team at the Johns Hopkins
Bloomberg School of Public Health,particularly Yvonne Tam and NeffWalker for their support in the provisionof mortality estimates.
NOTES
1 Stack ML, Ozawa S, Bishai DM,Mirelman A, Tam Y, Niessen L, et al.Estimated economic benefits duringthe “Decade of Vaccines”: $6.2 bil-lion in treatment savings, $145 bil-lion in higher output. Health Aff(Millwood). 2011;30(6):xx–xx.
2 Bloom D, Canning D, Jamison D.Health, wealth, and welfare. FinanDevel. 2004;41(1):10–5.
3 Viscusi WK. How to value a life. JEcon Finance. 2008;32:311–23.
4 ICF International. Final report: sub-Saharan Africa refinery projecthealth study. Vol. 1-B Appendices[Internet]. Lexington (MA): ICFInternational; 2009 Jun [cited 2011Mar 1]. Available from: http://hqweb.unep.org/transport/pcfv/PDF/Health_Study_Volume_I-B_6-4-09.pdf
5 Klose T. The contingent valuationmethod in health care. Health Policy.1999;47(2):97–123.
6 Viscusi WK. The value of life: esti-mates with risks by occupation andindustry. Econ Inq. 2004;42(1):
29–48.7 Alberini A. What is a life worth?
Robustness of VSL values from con-tingent valuation surveys. Risk Anal.2005;25(4):783–800.
8 Laxminarayan R, Klein EY, Darley S,Adeyi O. Global investments in TBcontrol: economic benefits. HealthAff (Millwood). 2009;28(4):w730–42. DOI: 10.1377/hlthaff.28.4.w730.
9 De Blaeij A, Florax RJ, Rietveld P,Verhoef E. The value of statistical lifein road safety: a meta-analysis. AccidAnal Prev. 2003;35(6):973–86.
10 Carlsson F, Daruvala D, Jaldell H.Value of statistical life and cause ofaccident: a choice experiment. RiskAnal. 2010;30(6):975–86.
11 Dockins C, Maguire K, Simon N,Sullivan M. Value of statistical lifeanalysis and environmental policy: awhite paper [Internet]. Washington(DC): Environmental ProtectionAgency, National Center for Envi-ronmental Economics; 2004 [cited2011 Mar 1]. Available from: http://yosemite.epa.gov/ee/epa/eerm.nsf/
vwAN/EE-0483-01.pdf/$file/EE-0483-01.pdf
12 Environmental Protection Agency.Guidelines for preparing economicanalyses [Internet]. Washington(DC): EPA; 2010 Dec [cited 2011May 11]. Available from: http://yosemite.epa.gov/ee/epa/eed.nsf/pages/Guidelines.html/$file/Guidelines.pdf
13 Robinson LA. Valuing mortality riskreductions in homeland securityregulatory analyses [Internet].Washington (DC): US Customs andBorder Protection, Department ofHomeland Security; 2008 Jun [cited2011 Mar 1]. Available from: http://www.regulatory-analysis.com/robinson-dhs-mortality-risk-2008.pdf
14 Office of the Secretary, Departmentof Transportation. Memorandum:treatment of the economic value of astatistical life in departmentalanalyses [Internet]. Washington(DC): Office of the Assistant Secre-tary for Transportation Policy; 2010
The Priceless Payoff
8 Health Affairs June 2011 30:6

[cited 2011 May 11]. Available from:http://ostpxweb.dot.gov/policy/reports/080205.htm
15 Chestnut L, De Civita P. Economicvaluation of mortality risk reduc-tion—review and recommendationsfor policy and regulatory analysis:research paper [Internet]. Ottawa(ON): Government of Canada, PolicyResearch Initiative; 2009 Mar [cited2011 Mar 1]. Available from: http://www.policyresearch.gc.ca/doclib/2009-0012-eng.pdf
16 Goebbels AF, Ament AJ, Novak A,Veraart CP, Severens JL. Estimatingthe implicit value of statistical lifebased on public interventionsimplemented in the Netherlands. IntJ Technol Assess Health Care.2008;24(4):495–501.
17 SvenssonM. The value of a statisticallife in Sweden: estimates from twostudies using the “Certainty Ap-proach” calibration. Accid Anal Prev.2009;41(3):430–7.
18 Bellavance F, Dionne G, Lebeau M.The value of a statistical life: a meta-analysis with a mixed effects re-gression model. J Health Econ.2009;28(2):444–64.
19 Wang H, He J. The value of statisticallife: a contingent investigation inChina. Washington (DC): WorldBank; 2010. Policy Research Work-ing Paper Series, No. 5421.
20 Brent RJ. A social cost-benefit cri-terion for evaluating voluntarycounseling and testing with an ap-plication to Tanzania. Health Econ.2010;19(2):154–72.
21 Cutler D, Miller G. The role of publichealth improvements in health ad-vances: the twentieth-century UnitedStates. Demography. 2005;42(1):1–22.
22 Sinha A, Levine O, Knoll MD, MuhibF, Lieu TA. Cost-effectiveness ofpneumococcal conjugate vaccinationin the prevention of child mortality:an international economic analysis.Lancet. 2007;369(9559):389–96.
23 Griffiths UK, Miners A. Economicevaluations of Haemophilus influen-zae type b vaccine: systematic reviewof the literature. Expert Rev Phar-macoecon Outcomes Res. 2009;9(4):333–46.
24 Rheingans RD, Antil L, Dreibelbis R,Podewils LJ, Bresee JS, Parashar UD.Economic costs of rotavirus gastro-enteritis and cost-effectiveness ofvaccination in developing countries.J Infect Dis. 2009;200(Suppl 1):S16–27.
25 Liao CH, Liu JT, Pwu RF, You SL,Chow I, Tang CH. Valuation of the
economic benefits of human papil-lomavirus vaccine in Taiwan. ValueHealth. 2009;12(suppl 3):S74–7.
26 Palanca-Tan R. Value of statisticallife estimates for children in metroManila, inferred from parents’ will-ingness to pay for dengue vaccines[Internet]. Singapore: InternationalDevelopment Research Center; 2008[cited 2011 May 24]. Available from:http://hdl.handle.net/10625/46114
27 Johns Hopkins University Bloom-berg School of Public Health, De-partment of International Health.Lives Saved Tool (LiST): an evidence-based tool for estimating interven-tion impact [Internet]. Baltimore(MD): Johns Hopkins University;2010 [cited 2011 Mar 1]. Availablefrom: http://www.jhsph.edu/dept/ih/IIP/list/index.html
28 Boschi-Pinto C, Black RE. Develop-ment and use of the Lives Saved Tool(LiST): a model to estimate the im-pact of scaling up proven interven-tions on maternal, neonatal, andchild mortality. Int J Epidemiol.2011;40(2):520–1.
29 Stover J, McKinnon R, Winfrey B.Spectrum: a model platform forlinking maternal and child survivalinterventions with AIDS, familyplanning, and demographic projec-tions. Int J Epidemiol. 2010;39(suppl 1):i7–10.
30 United Nations Inter-agency Groupon Child Mortality Estimation. CMEInfo database [Internet]. New York(NY): UNICEF, World HealthOrganization, World Bank, UnitedNations Population Division; 2010Sep 15 [cited 2011 May 11]. Availablefor download from: http://www.childmortality.org/cmeMain.html
31 Black RE, Cousens S, Johnson HL,Lawn JE, Rudan I, Bassani DG, et al.Global, regional, and national causesof child mortality in 2008: a sys-tematic analysis. Lancet. 2010;375(9730):1969–87.
32 Walker N, Fischer-Walker C, Bryce J,Bahl R, Cousens S. Standards forCHERG reviews of intervention ef-fects on child survival. Int J Epide-miol. 2010;39(suppl 1):i21–31.
33 GAVI Alliance. Eligible countries[Internet]. Geneva; GAVI Alliance;2010 [cited 2011 May 11]. Availablefrom: http://www.gavialliance.org/support/who/eligible/index.php
34 World Health Organization. Immu-nization surveillance, assessment,and monitoring: WHO/UNICEF es-timates of national immunizationcoverage [Internet]. Geneva: WHO;2010 [cited 2010 Oct 15]. Available
from: http://www.who.int/immunization_monitoring/routine/immunization_coverage/en/index4.html
35 World Health Organization. Globalimmunization vision and strategy:report by the secretariat [Internet].Geneva: WHO; 2010 Nov [cited 2011Mar 1]. Available from: http://apps.who.int/gb/ebwha/pdf_files/EB128/B128_9-en.pdf
36 Olotu A, Lusingu J, Leach A, LievensM, Vekemans J, Msham S, et al. Ef-ficacy of RTS,S/AS01E malaria vac-cine and exploratory analysis onanti-circumsporozoite antibodytitres and protection in childrenaged 5–17 months in Kenya andTanzania: a randomised controlledtrial. Lancet Infect Dis. 2011;11(2):102–9.
37 To access the Appendix, click on theAppendix link in the box to the rightof the article online.
38 Congressional Budget Office. Re-storing the Value of Every Americanin Environmental Decisions Act; costestimate, reported by the SenateCommittee on Environment andPublic Works. Washington (DC):CBO; 2008.
39 Viscusi WK, Aldy JE. The value of astatistical life: a critical review ofmarket estimates throughout theworld. J Risk Uncertainty. 2003;27(1):5–76.
40 Environmental Protection Agency.Frequently asked questions onmortality risk valuation [Internet].Washington (DC): EPA; 2010 [cited2011 May 11]. Available from: http://yosemite.epa.gov/ee/epa/eed.nsf/pages/MortalityRiskValuation.html
41 Guo X, Hammitt J. Compensatingwage differentials with unemploy-ment: evidence from China. EnvironResour Econ. 2009;42:187–209.
42 International Monetary Fund.WorldEconomic Outlook database. Wash-ington (DC): IMF; 2010 Oct [cited2011 May 11]. Available from: http://www.imf.org/external/pubs/ft/weo/2010/02/weodata/index.aspx
43 Leung J, Guria J. Value of statisticallife: adults versus children. AccidAnal Prev. 2006;38(6):1208–17.
44 Simonsen L, Taylor RJ, Young-Xu Y,Haber M, May L, Klugman KP. Im-pact of pneumococcal conjugatevaccination of infants on pneumoniaand influenza hospitalization andmortality in all age groups in theUnited States. MBio. 2011;2(1):e00309–10.
June 2011 30:6 Health Affairs 9

ABOUT THE AUTHORS: SACHIKO OZAWA, MEGHAN L. STACK,DAVID M. BISHAI, ANDREW MIRELMAN, INGRID K. FRIBERG,LOUIS NIESSEN, DAMIAN G. WALKER, ORIN S. LEVINE & YVONNE TAM
Sachiko Ozawa isan assistantscientist at theJohns HopkinsBloomberg Schoolof Public Health.
In this issue of Health Affairs,Sachiko Ozawa, Meghan Stack, andtheir coauthors present two papersassessing the benefits of vaccines,focusing on the impact of a$10 billion, ten-year investment bythe Bill & Melinda GatesFoundation to expand access tovaccines among children in someof the world’s poorest countries.
The paper on which Ozawa is thelead author employs a “value ofstatistical life” analysis, concludingthat expanding access to vaccineswould prevent the deaths of 6.4million children over the next tenyears. The paper also estimates a$231 billion benefit in terms of thevalue placed on the lives ofchildren who would otherwise die.
The paper on which Stack is thelead author uses a more traditionalmeasure of savings in treatmentcosts and economic output, findingthat $6.2 billion in treatment costsand $145 billion in productivitylosses would be averted by theexpansion of access to vaccines.
Ozawa is an assistant scientist atthe Department of InternationalHealth, Johns Hopkins BloombergSchool of Public Health. Herresearch focuses on examiningeconomic benefits of public healthinterventions, scaling up healthfinancing schemes, and examiningthe role of trust and social capitalin health care systems. In 2010 shewas awarded a faculty grant inglobal health research from theJohns Hopkins Center for Global
Health, and a research grant fromthe Toyota Foundation. Shereceived both her doctorate andmaster’s degrees in health systemsfrom the Bloomberg School, withspecialization in internationalhealth economics.
Meghan L. Stack isa researchassociate at theBloomberg School.
Stack is a research associate inthe Department of InternationalHealth at the Bloomberg School.She serves as a monitoring andevaluation specialist at the school’sInternational Vaccine AccessCenter. Stack received master’sdegrees in international affairs andin international health from JohnsHopkins. Stack also received the2010 Bill & Melinda GatesFoundation Award from the Schoolof Advanced International Studies.
David M. Bishai isa professor at theBloomberg School.
David Bishai is a professor in theDepartment of Population, Family,and Reproductive Health at theBloomberg School. He useseconomics to study how publichealth interventions affectpopulation health, and he directsthe school’s interdepartmentalhealth economics program. He is
also a fellow of both the AmericanAcademy of Pediatrics and theAmerican College of Physicians.Bishai received his doctorate inhealth care systems from theWharton School of Business at theUniversity of Pennsylvania and hismedical degree from the Universityof California, San Diego.
Andrew Mirelman isa doctoralcandidate at theBloomberg School.
Andrew Mirelman is a doctoralstudent in the Health Systemsprogram of the Bloomberg School’sDepartment of InternationalHealth. He also received a masterof public health degree from theBloomberg School.
Ingrid K. Friberg isan assistantscientist at theBloomberg School.
Ingrid K. Friberg is an assistantscientist at the Bloomberg School.She received her doctorate fromthe Bloomberg School, focusing onglobal disease epidemiology andcontrol in international health.
The Priceless Payoff
10 Health Affairs June 2011 30:6
Yvonne Tam is aresearch associateat the BloombergSchool.
Yvonne Tam is a researchassociate at the Bloomberg Schoolof Public Health, having receivedher master’s in international healthfrom the school in 2010.
Louis Niessen is anassociate professorat the BloombergSchool.
Louis Niessen is an associateprofessor in international health,health economics, and chronic andinfectious diseases at theBloomberg School. He also servesas the acting codirector of theHealth Systems and InfectiousDisease Division and head of the
National Institutes of Health’sCenters of Excellence “Centre forControl of Chronic Diseases,” bothat International Centre for theControl of Diarrheal Disease,Bangladesh, and as codirector ofthe Bloomberg School’sInterdepartmental Master of HealthSciences in Health Economics.Niessen received a doctorate inhealth economic and demographicmodeling from the University ofGroningen Population ResearchCentre in the Netherlands. Hereceived his medical degree fromErasmus University, in Rotterdam.
Damian G. Walkeris a senior programofficer at the Bill &Melinda GatesFoundation.
Damian Walker is a seniorprogram officer for global healthdelivery at the Bill & MelindaGates Foundation. He is a healtheconomist with more than thirteenyears’ experience in internationalhealth economics, with a specific
focus on the economic evaluationof public health programs in low-and middle-income countries.Walker has a doctorate in healtheconomics from the London Schoolof Hygiene and Tropical Medicineand a master’s in health economicsfrom the University of York.
Orin S. Levine is anassociate professorat the BloombergSchool.
Orin Levine is the executivedirector of the Bloomberg School’sInternational Vaccine Access Centerand an associate professor at theschool’s Department ofInternational Health. He alsoserves as a steering committeemember for the Johns HopkinsVaccine Initiative. Levine receivedhis doctorate in epidemiology fromJohns Hopkins. He served as theexpert adviser on this thematicissue of Health Affairs.
June 2011 30:6 Health Affairs 11
Copyright © 2022 FDOKUMEN