
Pharmacologic alternatives to antidepressants in posttraumatic stress disorder: A systematic review
Upload
universitaeuropeadiromaCategory
view
3download
0
human psychopharmacology
Hum. Psychopharmacol Clin Exp 2009; 24: 177–190.
Published online 11 February 2009 in Wiley InterScience
(www.interscience.wiley.com) DOI: 10.1002/hup.1005
REVIEW ARTICLE
Duloxetine in acute major depression: review of comparisons toplacebo and standard antidepressants using dissimilar methods
Paolo Girardi1, Maurizio Pompili1,2*, Marco Innamorati3, Michele Mancini4, Gianluca Serafini1,Lorenzo Mazzarini1, Antonio Del Casale1, Roberto Tatarelli1 and Ross J. Baldessarini2
1Department of Psychiatry, Sant’Andrea Hospital, Sapienza University of Rome, Rome, Italy2Department of Psychiatry, Harvard Medical School, Psychopharmacology Program & International Consortium for Mood and PsychoticDisorders Research, McLean Division of Massachusetts General Hospital, Belmont, Massachusetts 02478-1906, USA3Universita di Europea di Roma, Rome, Italy4Eli Lilly Medical Center, Florence, Italy
Background Randomized controlled trials (RCTs) of duloxetine (DLX), an inhibitor of both norepinephrine and serotonin transporters (SNRI),have tested its efficacy in acute major depressive disorder (MDD) versus placebo (PBO) or standard serotonin-reuptake inhibitors (SRIs) andrequire review, comparing analytical methods.Method Computerized searching to identify reports of RCTs of DLX in adult, acute MDD patients permitted meta-analytic pooling toestimate overall response and remission rates, to compare mixed-model, repeated measures (MMRM) versus last-observations-carried-forward (LOCF) analytical methods, and to assess relations of DLX dose to efficacy and adverse outcomes.Results We identified 17 RCTs involving 22 comparisons (DLX versus PBO [n¼ 17) and DLX versus an SRI [n¼ 16]), based on MMRMand LOCF methods that allowed estimates of response (�50% improvement of depression scores) or remission (final depression score �7).There was a large overall DLX/PBO contrast (LOCF, RR¼ 1.42 [CI: 1.31–1.53], p< 0.0001, with a success rate of 65% [11/17]), andsomewhat larger effects with MMRM in both response (MMRM: RR¼ 1.48 [95%CI: 1.31–1.66] versus LOCF: RR¼ 1.41 [CI: 1.28–1.56];NNT 4.8 versus 6.5) and remission (MMRM: RR¼ 1.61 [CI: 1.41–1.85] versus LOCF: RR¼ 1.44 [CI: 1.27–1.63]; NNT¼ 5.9 versus 8.9).Based on LOCF methods, dropout rates were similar with DLX and PBO (RR¼ 1.04 [CI: 0.94–1.15]); DLX response was dose-dependent(r¼þ0.72, p¼ 0.001), and RCT-dropout rates were inversely related to DLX dose, but possibly artifactually.Limitations RCTs involving DLX are limited, with few direct comparisons to standard antidepressants.Conclusions DLX has good evidence of efficacy in acute, adult MDD, especially at doses of 80–120mg/day, but remains inadequatelytested against standard alternatives. MMRM analyses yielded slightly superior FLX/PBO contrasts than older LOCF methods. Copyright#2009 John Wiley & Sons, Ltd.
key words—antidepressants; depression; duloxetine; meta-analysis; short-term treatment; SNRIs
INTRODUCTION
Duloxetine hydrochloride (DLX; LY-246916, Cym-balta1, Yentreve1, and others), or S-(þ)-N-methyl-g-(1-naphthyloxy)-2-thiophenepropylamine hydrochlo-ride (Figure 1), was synthesized in 1988 at the EliLilly Research Center by David Wong and JosephKrushinski, who with Frank Bymaster also led theinvention and preclinical development of R,S-fluox-etine hydrochloride (Prozac1), the first clinically and
*Correspondence to: M. Pompili, Department of Psychiatry, Sant’AndreaHospital, Via di Grottarossa, 1035, 00189 Rome, Italy.E-mails: [email protected]; [email protected]
Copyright # 2009 John Wiley & Sons, Ltd.
commercially successful selective serotonin–reuptakeinhibitor (SRI; Baldessarini, 2005; Wong et al., 1988).Considered a mixed serotonin–norepinephrine reuptakeinhibitor (SNRI), DLX is a potent inhibitor of theinactivation by neuronal reuptake of both serotonin (5-hyroxytryptamine; 5-HT) and norepinephrine (NE),with similarly high (nM) affinity for their transporterproteins (SERT and NET) in brain and other tissues(Bymaster et al., 2001, 2005). The drug hasconsiderably less affinity for the dopamine transporter(DAT), and low affinity for other transporters or forhistaminic, adrenergic, cholinergic, serotoninergic,opioid, and other receptors (Bymaster et al., 2001,2005). The growing group of SNRI antidepressants
Received 7 September 2008
Accepted 19 December 2008
Figure 1. Chemical structure of DLX
178 p. girardi ET AL.
includes bicifadine, clomipramine, milnacipran, highdoses of venlafaxine, norvenlafaxine, and the anti-obesity agent sibutramine (Baldessarini, 2005).DLX was approved for the treatment of major
depressive disorder (MDD) in the US in August 2004,treatment of diabetic neuropathic pain in September 2004,with evidence of analgesic effects from several studies,and gained FDA approval for long-term use in MDD inlate 2007 (Anonymous, 2008). In Europe, the drug wasapproved for use in MDD soon after initial US approval,and also for urinary stress incontinence, for which it alsohas several supportive studies (Anonymous, 2008).FDA approval of DLX for the treatment ofMDDwas
supported by at least 17 controlled trials, including twoproof-of-concept studies, two short-term dose-findingtrials, four phase-III short- and long-term trials, andone relapse-prevention trial (Goldstein et al., 2002,2004; Detke et al., 2002a,b, 2004; Eli Lilly andCompany, 2004c,f, 2006e; Brannan et al., 2005; Burtet al., 2005; Perahia et al., 2006a,b, 2008; Brecht et al.,2007; Khan et al., 2007; Lee et al., 2007; Nierenberget al., 2007; Raskin et al., 2007, 2008a,b; Wade et al.,2007). At least three of these trials remain unpublishedin peer-reviewed journals; two did not find statisticalsuperiority of relatively low doses of DLX over PBO(Eli Lilly and Company, 2004c,f). Most of these studiesalso have brief summary reports provided on theInternet (at www.lillytrials.com) by the manufacturer(Eli Lilly & Company 2004–2008). In addition,before European registration, a 52-week, open-labelstudy was conducted primarily to gather safety data(Raskin et al., 2003). Several post-marketing trials andreviews support both efficacy and safety of DLX in theshort-term treatment for MDD (Cowen et al., 2005;Hudson et al., 2005; Frampton and Plosker, 2007;Nierenberg et al., 2007).
Copyright # 2009 John Wiley & Sons, Ltd.
Despite this extensive research support for short-termuse of DLX in adult MDD, there remains considerableuncertainty about its relative efficacy and safetycompared to other modern antidepressants, its optimaldosing, and the specific clinical value or risks of bothshort- and long-term combined potentiation of both 5-HTand NE with DLX, compared to SRIs or other typesof antidepressants (Thase et al., 2001; Nemeroff et al.,2002; Mallinckrodt et al., 2005; Mann, 2005; Stahlet al., 2005; Ballesteros et al., 2007; Dworkin et al.,2007; Papakostas et al., 2007; Pritchett et al., 2007).Nevertheless, agents with prominent NE-transportinhibiting effects (NRIs) or mixed SNRI properties,in contrast to selective SRIs, may be more likely toprovide analgesic effects, notably for chronic, neuro-pathic pain (Baldessarini, 2005; Saarto and Wiffen,2005; Finnerup et al., 2007; Thase et al., 2007).Given the need to update and critically evaluate the
current status of evidence pertaining to the efficacy andsafety of DLX as an antidepressant with unusualpharmacological properties, we carried out a systematicreview and meta-analyses to evaluate both published andother manufacturer-file reports of research findings fromshort-term trials of DLX in acute MDD episodes inadults.We now report on assessments of rates of response,remission, and adverse events, as well as dose–effectrelationships, based on 17 available double-blind,randomized controlled trial (RCT) comparisons ofDLX with placebo (PBO), as well as 16 activecomparator (SRI)-controlled, trials. We also comparedfindings from analyses based on traditional butquestionable last-observation-carried-forward (LOCF)methods versus potentially superior mixed-modelrepeated-measures (MMRM) approaches (Hennen,2003; Simpson et al., 2008).
MATERIALS AND METHODS
Search strategy
We searched the Medline1 computerized database (toAugust 2008) to identify RCTs of DLX as a treatmentfor adult patients diagnosed with MDD by moderncriteria (DSM-IVor ICD-9/10). Search terms includedcombinations of DLX and MDD or depression, usingRCT as the publication type, as recommended byGlanville et al. (2006). In addition, we hand-reviewedbibliographies of identified reports, and sought accessto both published and unpublished reports of trialsconducted or supported by the manufacturer, Eli Lillyand Company. Two of the co-authors (MP and MI)independently reviewed all citations retrieved toachieve a consensus on trial inclusion, consulting athird co-author (PG) in rare instances of initial
Hum. Psychopharmacol Clin Exp 2009; 24: 177–190.DOI: 10.1002/hup
duloxetine for acute depression 179
disagreement. Studies included were required to havebeen reported in a peer-reviewed journal and to have ascore of 4 or 5 on a 5-point-maximum quality ratingscale (Jadad et al., 1996), as determined by the sameco-authors; in addition, we included several reports ofunpublished studies on file with the manufacturer thatotherwise appeared to meet inclusion criteria.
Variables
Outcome measures were contrasts between DLX andother treatments as proportions (and their ratios ordifferences) of patient–subjects showing: (a) response(reduction of depression severity by �50% betweenintake and end point) based on a standard depressionsymptom rating scale (in the included studies, eitherthe Hamilton Depression Rating Scale [HDRS];[Hamilton, 1960] or the Montgomery-Asberg Depres-sion Rating Scale [MADRS]; [Montgomery andAsberg, 1979]), or (b) remission (final score of �7on the same scales), and (c) rates of early discontinu-ation or dropout prior to the nominal end of each trial aswell as several specific, potentially clinically importantadverse response (ADR) rates, with rates of alldropouts and those related to ADRs, includingsustained hypertension (defined either as systolic bloodpressure (BP) �140mm Hg and �10mm abovebaseline BP over three consecutive visits, or asdiastolic BP of �90mm Hg and �10mm abovebaseline over three consecutive visits). Differencesbetween DLX and PBO or SRIs were expressed as RateRatios (RR); values>1.0 indicate a superior efficacy orinferior tolerability with DLX than with PBO or SRIs.
Statistical analysis
Meta-analyses used random-effects modeling, with orwithout between-trial heterogeneity based on prelimi-nary Q-tests (DerSimonian and Laird, 1986). Meta-analyses included estimates of pooled rate ratios (RR)or rate differences (RD) and their 95% confidenceintervals (CI). Reciprocals of pooled RD values wereused to estimate number-needed-to-treat (NNT; intherapeutic trials) or number-needed-to-harm (NNH;for ADR rates), and their 95%CIs. We also tested forrelationships of mean maximum daily dose of DLXversus response and dropout rates, using linearcorrelations (r). Statistical significance is indicatedby non-overlapping 95% CIs of compared pooled RRor RD values for DLX versus controls, or resultsotherwise yielding two-sided p< 0.05. Data analyseswere based on standard commercial statistical pro-grams (Stata.81, StataCorp, College Station, TX;Statview.51, SAS, Cary, NC).
Copyright # 2009 John Wiley & Sons, Ltd.
RESULTS
Characteristics of trials and subjects
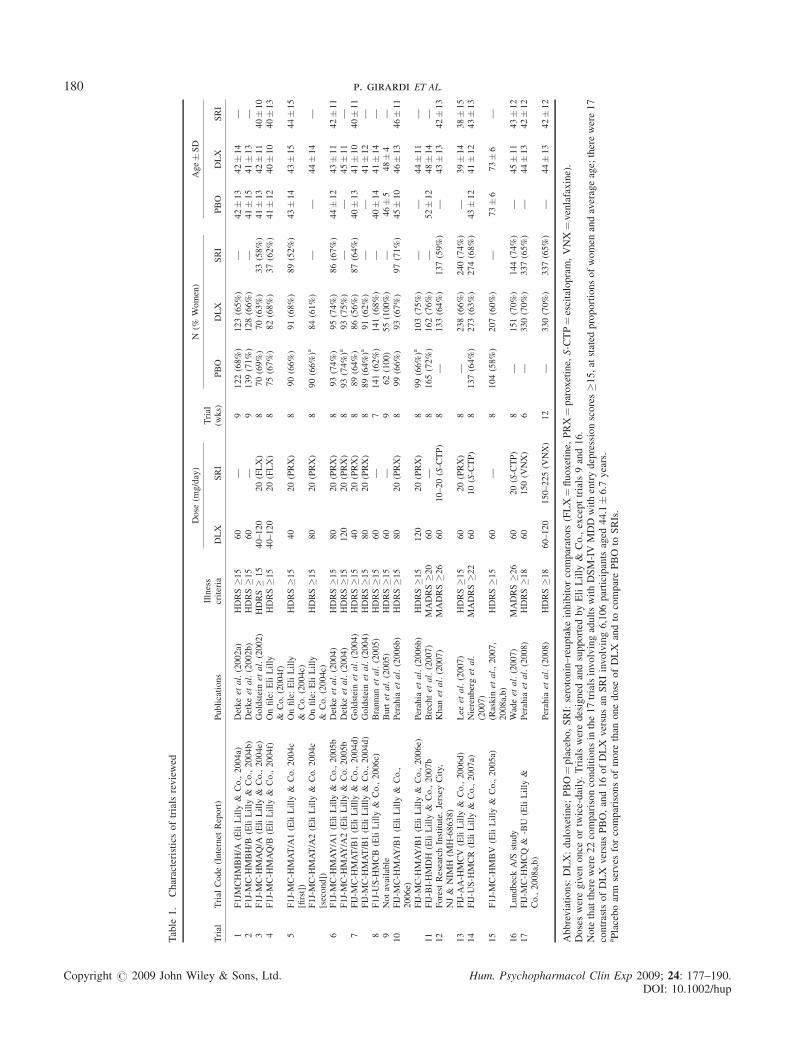
The search strategy identified 42 potential studies, ofwhich only 17, involving a total of 22 comparisons ofDLX doses versus controls (all reported between 2002and 2008) were consistent with selection criteria andincluded in meta-analyses (Detke et al., 2002a,b, 2004[with two doses of DLX]; Goldstein et al., 2002, 2004(two doses); Brannan et al., 2005; Burt et al., 2005;Perahia et al., 2006b [two doses], 2008 [two doses];Brecht et al., 2007; Khan et al., 2007; Lee et al., 2007;Nierenberg et al., 2007; Raskin et al., 2007, 2008a,b;Wade et al., 2007) as well as two trials, involving threedose comparisons, on file at Eli Lilly and Company,2004 (Table 1). We excluded non-MDD patients (withdiabetes, fibromyalgia, or other pain-associated dis-orders, or urinary-incontinence). The RCTs identifiedinvolved multicenter, parallel, double-blind, RCTdesigns among adult outpatients meeting DSM-IVcriteria for an acute episode of MDD, with variablelead-in phases involving use of PBO to washoutpreviously administered psychotropic medicines and toestablish baseline depression ratings.The 17 reports and 22 total comparison trials
analyzed (Table 1) involved adult patients in acuteepisodes of MDD, randomized to PBO versus dailydoses of DLX ranging from 40 to 120mg (average:73.5mg) for 6–12 weeks (mean: 8.2� 1.1 weeks). Ofthese studies, 13 used the 17-item HDRS to evaluateseverity of depressive symptoms, and four employedthe MADRS scale. Most trials included directcomparisons of outcomes estimated by the use of bothMMRM and LOCF methods (Tables 2 and 3). Ageaveraged 44.1� 6.7 years; one trial selected patientsaveraging 73 years of age (reported in Raskin et al.,2007, 2008a,b). Baseline depression rating scores averaged20.4� 4.1 (HDRS, all initially �15) or 40.0� 4.3(MADRS, all initially�20). Subject numbers varied inDLX (n¼ 70–330), SRI (n¼ 33–337) and PBO arms(n¼ 62–165), with 3159 subjects randomized to DLX(in 22 comparisons), 1561 given an SRI in 16 com-parisons, and 1386 treated with PBO in 17 comparisons(total N¼ 6106 non-overlapping patient–subjects;Table 1).
Clinical outcome: response rates
Crude response rates (by MMRM and LOCF analyses)for DLX were 48.8%–59.6% versus PBO at 35.0%–42.2%, yielding an average of 40% superiority of DLX/PBO responses (54.2%/38.6%¼ 1.40), and indicatingclear superiority of DLX over PBO (Table 2). We also
Hum. Psychopharmacol Clin Exp 2009; 24: 177–190.DOI: 10.1002/hup
Table
1.
Characteristicsoftrialsreviewed
Trial
Trial
Code(Internet
Report)
Publications
Illness
criteria
Dose
(mg/day)
Trial
(wks)
N(%
Women)
Age�SD
DLX
SRI
PBO
DLX
SRI
PBO
DLX
SRI
1F1JM
CHMBH/A
(EliLilly
&Co.,2004a)
Detkeet
al.(2002a)
HDRS�15
60
—9
122(68%)
123(65%)
—42�13
42�14
—2
F1J-MC-H
MBH/B
(EliLilly
&Co.,2004b)
Detkeet
al.(2002b)
HDRS�15
60
—9
139(71%)
128(66%)
—41�15
41�13
—3
F1J-MC-H
MAQ/A
(EliLilly
&Co.,2004e)
Goldsteinet
al.(2002)
HDRS�
15
40–120
20(FLX)
870(69%)
70(63%)
33(58%)
41�13
42�11
40�10
4F1J-MC-H
MAQ/B
(EliLilly
&Co.,2004f)
Onfile:EliLilly
&Co.(2004f)
HDRS�15
40–120
20(FLX)
875(67%)
82(68%)
37(62%)
41�12
40�10
40�13
5F1J-MC-H
MAT/A1(EliLilly
&Co.2004c
[first])
Onfile:EliLilly
&Co.(2004c)
HDRS�15
40
20(PRX)
890(66%)
91(68%)
89(52%)
43�14
43�15
44�15
F1J-MC-H
MAT/A2(EliLilly
&Co.2004c
[second])
Onfile:EliLilly
&Co.(2004c)
HDRS�15
80
20(PRX)
890(66%)a
84(61%)
——
44�14
—
6F1J-MC-H
MAY/A1(EliLilly
&Co.,2005b
Detkeet
al.(2004)
HDRS�15
80
20(PRX)
893(74%)
95(74%)
86(67%)
44�12
43�11
42�11
F1J-MC-H
MAY/A2(EliLilly
&Co.2005b
Detkeet
al.(2004)
HDRS�15
120
20(PRX)
893(74%)a
93(75%)
——
45�11
—7
FIJ-M
C-H
MAT/B1(EliLillly&
Co.,2004d)
Goldsteinet
al.(2004)
HDRS�15
40
20(PRX)
889(64%)
86(56%)
87(64%)
40�13
41�10
40�11
FIJ-M
C-H
MAT/B1(EliLillly&
Co.,2004d)
Goldsteinet
al.(2004)
HDRS�15
80
20(PRX)
889(64%)a
91(62%)
——
41�12
—8
F1J-US-H
MCB
(EliLilly
&Co.,2006c)
Brannan
etal.(2005)
HDRS�15
60
—7
141(62%)
141(68%)
—40�14
41�14
—9
Notavailable
Burtet
al.(2005)
HDRS�15
60
—9
62(100)
55(100%)
—46�5
48�4
—10
FIJ-M
C-H
MAY/B1(EliLilly
&Co.,
2006e)
Perahia
etal.(2006b)
HDRS�15
80
20(PRX)
899(66%)
93(67%)
97(71%)
45�10
46�13
46�11
FIJ-M
C-H
MAY/B1(EliLilly
&Co.,2006e)
Perahia
etal.(2006b)
HDRS�15
120
20(PRX)
899(66%)a
103(75%)
——
44�11
—11
FIJ-BI-HMDH
(EliLilly
&Co.,2007b
Brechtet
al.(2007)
MADRS�20
60
—8
165(72%)
162(76%)
—52�12
48�14
—12
Forest
ResearchInstitute.Jersey
City,
NJ&
NIM
H(M
H-68638)
Khan
etal.(2007)
MADRS�26
60
10–20(S-CTP)
8—
133(64%)
137(59%)
—43�13
42�13
13
FIJ-A
A-H
MCV
(EliLilly
&Co.,2006d)
Lee
etal.(2007)
HDRS�15
60
20(PRX)
8—
238(66%)
240(74%)
—39�14
38�15
14
FIJ-U
S-H
MCR
(EliLilly
&Co.,2007a)
Nierenberget
al.
(2007)
MADRS�22
60
10(S-CTP)
8137(64%)
273(63%)
274(68%)
43�12
41�12
43�13
15
F1J-MC-H
MBV
(EliLilly
&Co.,2005a)
(Raskin
etal.,2007,
2008a,b)
HDRS�15
60
—8
104(58%)
207(60%)
—73�6
73�6
—
16
LundbeckA/S
study
Wadeet
al.(2007)
MADRS�26
60
20(S-CTP)
8—
151(70%)
144(74%)
—45�11
43�12
17
FIJ-M
C-H
MCQ
&-BU
(EliLilly
&Co.,2008a,b)
Perahia
etal.(2008)
HDRS�18
60
150(V
NX)
6—
330(70%)
337(65%)
—44�13
42�12
Perahia
etal.(2008)
HDRS�18
60–120
150–225(V
NX)
12
—330(70%)
337(65%)
—44�13
42�12
Abbreviations:DLX:duloxetine;
PBO¼placebo,SRI:serotonin–reuptakeinhibitorcomparators
(FLX¼fluoxetine,
PRX¼paroxetine,
S-CTP¼escitalopram,VNX¼venlafaxine).
Dosesweregiven
once
ortwice-daily.Trialsweredesigned
andsupported
byEliLilly
&Co.,excepttrials9and16.
Notethattherewere22comparisonconditionsin
the17trialsinvolvingadultswithDSM-IVMDDwithentrydepressionscores�15,atstated
proportionsofwomen
andaverageage;therewere17
contrasts
ofDLX
versusPBO,and16ofDLX
versusan
SRIinvolving6,106participants
aged
44.1�6.7
years.
aPlaceboarm
serves
forcomparisonsofmore
than
onedose
ofDLX
andto
comparePBO
toSRIs.
Copyright # 2009 John Wiley & Sons, Ltd. Hum. Psychopharmacol Clin Exp 2009; 24: 177–190.DOI: 10.1002/hup
180 p. girardi ET AL.

Table
2.
RCTsofDLX
versusaPBO
withratesofresponse
andremissionanalyzedbyLOCFversusMMRM
methods
Trials
DLX
Dose
(mg/day)
Trial
(wks)
Response
Rate(n/N
[%])
Rem
issionRate(n/N
[%])
LOCF
MMRM
LOCF
MMRM
DLX
PBO
DLX
PBO
DLX
PBO
DLX
PBO
Detkeet
al.(2002a)
60
954/121(44.6)
26/115(22.6)
75/121(62.0)
33/115(28.7)
38/121(23.1)
17/115(14.8)
53/121(43.8)
18/115(15.7)
Detkeet
al.(2002b)
60
964/128(50.0)
49/139(35.3)
83/128(64.8)
58/139(41.7)
41/128(32.0)
33/139(23.7)
55/128(43.0)
39/139(28.1)
Goldsteinet
al.(2002)
40–120
832/66(48.5)
24/68(35.3)
42/66(63.6)
33/68(48.5)
28/66(42.4)
18/68(26.5)
37/66(56.1)
22/68(32.4)
Detkeet
al.(2004)(a)
80
860/93(64.5)
41/93(44.1)
65/93(69.9)
44/93(47.3)
43/93(46.2)
28/93(30.1)
47/93(50.5)
28/93(30.1)
Detkeet
al.(2004)(b)
120
866/93(71.0)
41/93(44.1)a
72/93(77.4)
44/93(47.3)a
48/93(51.6)
28/93(30.1)a
54/93(58.1)
28/93(30.1)a
F1J-MC-H
MAQ/B
(EliLilly
&Co.,2004f)
40–120
840/81(49.4)
28/72(38.9)
——
32/81(39.5)
21/72(29.2)
——
F1J-MC-H
MAT/A1
(EliLilly
&Co.,2004c)
40
824/90(26.7)
24/89(27.0)
——
22/90(24.4)
18/89(20.2)
——
F1J-MC-H
MAT/A2
(EliLilly
&Co.,2004c)
80
828/81(34.6)
24/89(27.0)a
——
23/81(24.8)
18/89(20.2)a
——
Goldsteinet
al.(2004)
40
837/84(44.0)
27/88(30.7)
——
29/84(34.5)
26/88(29.5)
——
Goldsteinet
al.(2004)
80
844/86(51.2)
27/88(30.7)a
——
43/86(50.0)
26/88(29.5)a
——
Brannan
etal.(2005)
60
755/132(41.7)
54/136(39.7)
74/132(56.1)
69/136(50.7)
30/132(22.7)
33/136(24.3)
46/132(34.8)
43/136(31.6)
Burtet
al.(2005)
60
932/55(58..2)
19/59(32.2)
41/55(74.5)
28/59(47.5)
19/55(34.5)
11/59(18.6)
23/55(41.8)
14/59(23.7)
Perahia
etal.(2006b)
80
860/93(64.5)
51/99(51.5)
64/93(68.8)
53/99(53.5)
41/93(44.1)
33/99(33.3)
46/93(49.5)
33/99(33.3)
Perahia
etal.(2006b)
120
869/102(67.6)
51/99(51.5)a
75/102(73.5)
53/99(53.5)a
41/102(40.2)
33/99(33.3)a
46/102(45.1)
33/99(33.3)a
Brechtet
al.(2007)
60
889/162(54.9)
58/165(35.2)
——
85/162(52.5)
48/165(29.1)
——
Nierenberget
al.(2007)
60
8113/262(43.1)
43/135(31.9)
128/262(48.9)
50/135(37.0)
97/262(37.0)
36/135(26.7)
105/262(40.1)
37/135(27.4)
(Raskin
etal.,2007,
2008a,b)
60
875/201(37.3)
19/102(18.6)
87/207(42.0)
16/104(15.4)
55/201(53.9)
15/102(14.7)
67/207(32.4)
16/104(15.4)
Totals,Means
72.9�23.1
8.1�0.5
942/1930(48.8%)
606/1729(35.0%)
806/1352(59.6%)
481/1140(42.2%)
715/1930(37.0%)
442/1729(25.6%)
579/1352(42.8%)
311/1140(27.3%)
Abbreviations:
DLX,duloxetine;
PBO,placebo;SRI,serotonin–reuptakeinhibitorcomparators
(FLX¼fluoxetine,
PRX¼paroxetine,
S-CTP¼escitalopram,VNX¼venlafaxine).
Thereare17comparisonsofDLXversusPBO(see
Table1),byone(LOCF)ortwomethodsofanalysis(LOCFversusMMRM).Rates
arevalues
ofrespondersorthose
inremission(n)over
subjects
providingdata(N
)andthecorrespondingproportions(%
).aSomePBOresponsesareusedmore
than
once
intrialswithmore
than
onedose
ofDLX.Crudeestimates
ofRRsforDLX/PBO,based
ontotalsshownwere:
Response
MMRM/LOCF¼1.41/1.39;
Rem
issionMMRM/LOCF¼1.57/1.45.
Copyright # 2009 John Wiley & Sons, Ltd. Hum. Psychopharmacol Clin Exp 2009; 24: 177–190DOI: 10.1002/hup
duloxetine for acute depression 181
.
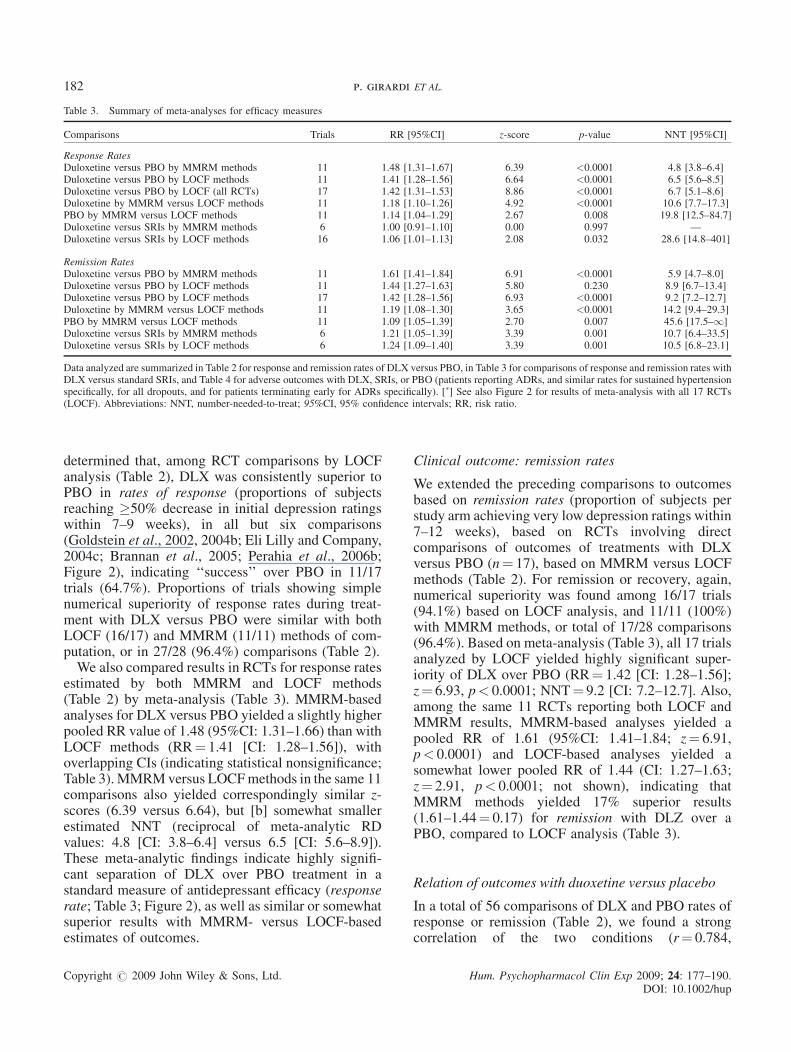
Table 3. Summary of meta-analyses for efficacy measures
Comparisons Trials RR [95%CI] z-score p-value NNT [95%CI]
Response RatesDuloxetine versus PBO by MMRM methods 11 1.48 [1.31–1.67] 6.39 <0.0001 4.8 [3.8–6.4]Duloxetine versus PBO by LOCF methods 11 1.41 [1.28–1.56] 6.64 <0.0001 6.5 [5.6–8.5]Duloxetine versus PBO by LOCF (all RCTs) 17 1.42 [1.31–1.53] 8.86 <0.0001 6.7 [5.1–8.6]Duloxetine by MMRM versus LOCF methods 11 1.18 [1.10–1.26] 4.92 <0.0001 10.6 [7.7–17.3]PBO by MMRM versus LOCF methods 11 1.14 [1.04–1.29] 2.67 0.008 19.8 [12.5–84.7]Duloxetine versus SRIs by MMRM methods 6 1.00 [0.91–1.10] 0.00 0.997 —Duloxetine versus SRIs by LOCF methods 16 1.06 [1.01–1.13] 2.08 0.032 28.6 [14.8–401]
Remission RatesDuloxetine versus PBO by MMRM methods 11 1.61 [1.41–1.84] 6.91 <0.0001 5.9 [4.7–8.0]Duloxetine versus PBO by LOCF methods 11 1.44 [1.27–1.63] 5.80 0.230 8.9 [6.7–13.4]Duloxetine versus PBO by LOCF methods 17 1.42 [1.28–1.56] 6.93 <0.0001 9.2 [7.2–12.7]Duloxetine by MMRM versus LOCF methods 11 1.19 [1.08–1.30] 3.65 <0.0001 14.2 [9.4–29.3]PBO by MMRM versus LOCF methods 11 1.09 [1.05–1.39] 2.70 0.007 45.6 [17.5–1]Duloxetine versus SRIs by MMRM methods 6 1.21 [1.05–1.39] 3.39 0.001 10.7 [6.4–33.5]Duloxetine versus SRIs by LOCF methods 6 1.24 [1.09–1.40] 3.39 0.001 10.5 [6.8–23.1]
Data analyzed are summarized in Table 2 for response and remission rates of DLX versus PBO, in Table 3 for comparisons of response and remission rates withDLX versus standard SRIs, and Table 4 for adverse outcomes with DLX, SRIs, or PBO (patients reporting ADRs, and similar rates for sustained hypertensionspecifically, for all dropouts, and for patients terminating early for ADRs specifically). [�] See also Figure 2 for results of meta-analysis with all 17 RCTs(LOCF). Abbreviations: NNT, number-needed-to-treat; 95%CI, 95% confidence intervals; RR, risk ratio.
182 p. girardi ET AL.
determined that, among RCT comparisons by LOCFanalysis (Table 2), DLX was consistently superior toPBO in rates of response (proportions of subjectsreaching �50% decrease in initial depression ratingswithin 7–9 weeks), in all but six comparisons(Goldstein et al., 2002, 2004b; Eli Lilly and Company,2004c; Brannan et al., 2005; Perahia et al., 2006b;Figure 2), indicating ‘‘success’’ over PBO in 11/17trials (64.7%). Proportions of trials showing simplenumerical superiority of response rates during treat-ment with DLX versus PBO were similar with bothLOCF (16/17) and MMRM (11/11) methods of com-putation, or in 27/28 (96.4%) comparisons (Table 2).We also compared results in RCTs for response rates
estimated by both MMRM and LOCF methods(Table 2) by meta-analysis (Table 3). MMRM-basedanalyses for DLX versus PBO yielded a slightly higherpooled RR value of 1.48 (95%CI: 1.31–1.66) than withLOCF methods (RR¼ 1.41 [CI: 1.28–1.56]), withoverlapping CIs (indicating statistical nonsignificance;Table 3). MMRMversus LOCFmethods in the same 11comparisons also yielded correspondingly similar z-scores (6.39 versus 6.64), but [b] somewhat smallerestimated NNT (reciprocal of meta-analytic RDvalues: 4.8 [CI: 3.8–6.4] versus 6.5 [CI: 5.6–8.9]).These meta-analytic findings indicate highly signifi-cant separation of DLX over PBO treatment in astandard measure of antidepressant efficacy (responserate; Table 3; Figure 2), as well as similar or somewhatsuperior results with MMRM- versus LOCF-basedestimates of outcomes.
Copyright # 2009 John Wiley & Sons, Ltd.
Clinical outcome: remission rates
We extended the preceding comparisons to outcomesbased on remission rates (proportion of subjects perstudy arm achieving very low depression ratings within7–12 weeks), based on RCTs involving directcomparisons of outcomes of treatments with DLXversus PBO (n¼ 17), based on MMRM versus LOCFmethods (Table 2). For remission or recovery, again,numerical superiority was found among 16/17 trials(94.1%) based on LOCF analysis, and 11/11 (100%)with MMRM methods, or total of 17/28 comparisons(96.4%). Based on meta-analysis (Table 3), all 17 trialsanalyzed by LOCF yielded highly significant super-iority of DLX over PBO (RR¼ 1.42 [CI: 1.28–1.56];z¼ 6.93, p< 0.0001; NNT¼ 9.2 [CI: 7.2–12.7]. Also,among the same 11 RCTs reporting both LOCF andMMRM results, MMRM-based analyses yielded apooled RR of 1.61 (95%CI: 1.41–1.84; z¼ 6.91,p< 0.0001) and LOCF-based analyses yielded asomewhat lower pooled RR of 1.44 (CI: 1.27–1.63;z¼ 2.91, p< 0.0001; not shown), indicating thatMMRM methods yielded 17% superior results(1.61–1.44¼ 0.17) for remission with DLZ over aPBO, compared to LOCF analysis (Table 3).
Relation of outcomes with duoxetine versus placebo
In a total of 56 comparisons of DLX and PBO rates ofresponse or remission (Table 2), we found a strongcorrelation of the two conditions (r¼ 0.784,
Hum. Psychopharmacol Clin Exp 2009; 24: 177–190.DOI: 10.1002/hup
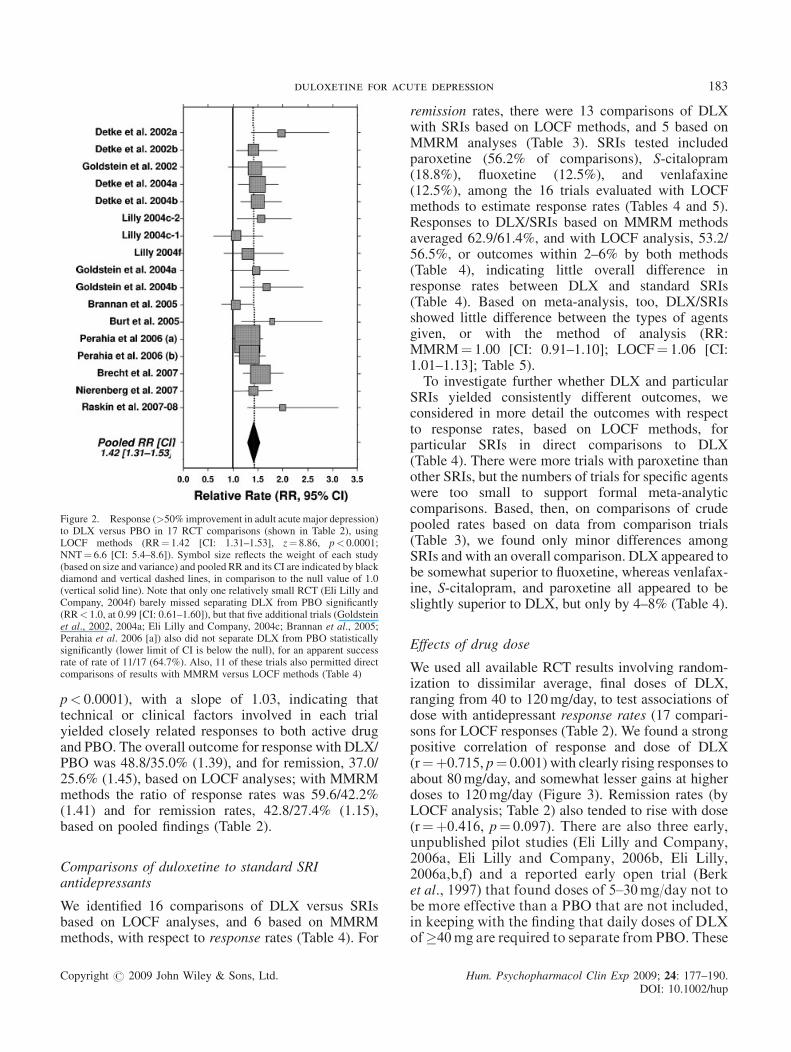
Figure 2. Response (>50% improvement in adult acute major depression)to DLX versus PBO in 17 RCT comparisons (shown in Table 2), usingLOCF methods (RR¼ 1.42 [CI: 1.31–1.53], z¼ 8.86, p< 0.0001;NNT¼ 6.6 [CI: 5.4–8.6]). Symbol size reflects the weight of each study(based on size and variance) and pooled RR and its CI are indicated by blackdiamond and vertical dashed lines, in comparison to the null value of 1.0(vertical solid line). Note that only one relatively small RCT (Eli Lilly andCompany, 2004f) barely missed separating DLX from PBO significantly(RR< 1.0, at 0.99 [CI: 0.61–1.60]), but that five additional trials (Goldsteinet al., 2002, 2004a; Eli Lilly and Company, 2004c; Brannan et al., 2005;Perahia et al. 2006 [a]) also did not separate DLX from PBO statisticallysignificantly (lower limit of CI is below the null), for an apparent successrate of rate of 11/17 (64.7%). Also, 11 of these trials also permitted directcomparisons of results with MMRM versus LOCF methods (Table 4)
duloxetine for acute depression 183
p< 0.0001), with a slope of 1.03, indicating thattechnical or clinical factors involved in each trialyielded closely related responses to both active drugand PBO. The overall outcome for response with DLX/PBO was 48.8/35.0% (1.39), and for remission, 37.0/25.6% (1.45), based on LOCF analyses; with MMRMmethods the ratio of response rates was 59.6/42.2%(1.41) and for remission rates, 42.8/27.4% (1.15),based on pooled findings (Table 2).
Comparisons of duloxetine to standard SRIantidepressants
We identified 16 comparisons of DLX versus SRIsbased on LOCF analyses, and 6 based on MMRMmethods, with respect to response rates (Table 4). For
Copyright # 2009 John Wiley & Sons, Ltd.
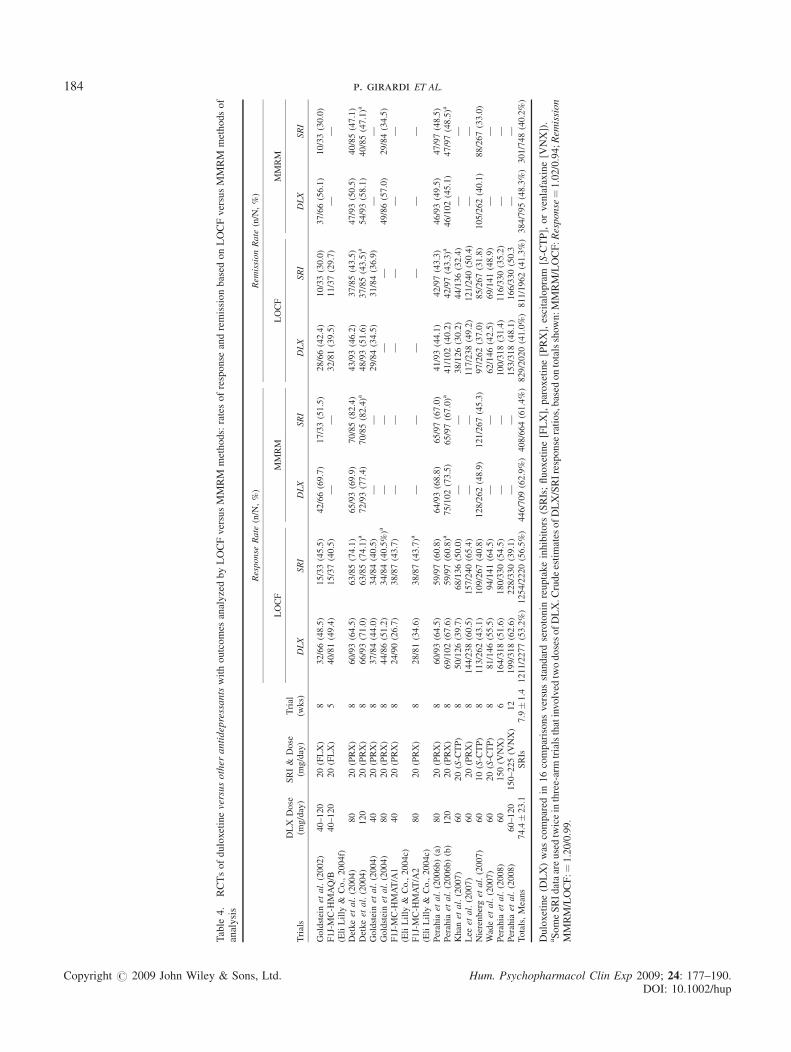
remission rates, there were 13 comparisons of DLXwith SRIs based on LOCF methods, and 5 based onMMRM analyses (Table 3). SRIs tested includedparoxetine (56.2% of comparisons), S-citalopram(18.8%), fluoxetine (12.5%), and venlafaxine(12.5%), among the 16 trials evaluated with LOCFmethods to estimate response rates (Tables 4 and 5).Responses to DLX/SRIs based on MMRM methodsaveraged 62.9/61.4%, and with LOCF analysis, 53.2/56.5%, or outcomes within 2–6% by both methods(Table 4), indicating little overall difference inresponse rates between DLX and standard SRIs(Table 4). Based on meta-analysis, too, DLX/SRIsshowed little difference between the types of agentsgiven, or with the method of analysis (RR:MMRM¼ 1.00 [CI: 0.91–1.10]; LOCF¼ 1.06 [CI:1.01–1.13]; Table 5).To investigate further whether DLX and particular
SRIs yielded consistently different outcomes, weconsidered in more detail the outcomes with respectto response rates, based on LOCF methods, forparticular SRIs in direct comparisons to DLX(Table 4). There were more trials with paroxetine thanother SRIs, but the numbers of trials for specific agentswere too small to support formal meta-analyticcomparisons. Based, then, on comparisons of crudepooled rates based on data from comparison trials(Table 3), we found only minor differences amongSRIs and with an overall comparison. DLX appeared tobe somewhat superior to fluoxetine, whereas venlafax-ine, S-citalopram, and paroxetine all appeared to beslightly superior to DLX, but only by 4–8% (Table 4).
Effects of drug dose
We used all available RCT results involving random-ization to dissimilar average, final doses of DLX,ranging from 40 to 120mg/day, to test associations ofdose with antidepressant response rates (17 compari-sons for LOCF responses (Table 2). We found a strongpositive correlation of response and dose of DLX(r¼þ0.715, p¼ 0.001) with clearly rising responses toabout 80mg/day, and somewhat lesser gains at higherdoses to 120mg/day (Figure 3). Remission rates (byLOCF analysis; Table 2) also tended to rise with dose(r¼þ0.416, p¼ 0.097). There are also three early,unpublished pilot studies (Eli Lilly and Company,2006a, Eli Lilly and Company, 2006b, Eli Lilly,2006a,b,f) and a reported early open trial (Berket al., 1997) that found doses of 5–30mg/day not tobe more effective than a PBO that are not included,in keeping with the finding that daily doses of DLXof�40mg are required to separate fromPBO. These
Hum. Psychopharmacol Clin Exp 2009; 24: 177–190.DOI: 10.1002/hup
Table
4.
RCTsofduloxetineversusother
antidepressantswithoutcomes
analyzedbyLOCFversusMMRM
methods:ratesofresponse
andremissionbased
onLOCFversusMMRM
methodsof
analysis
Trials
DLX
Dose
(mg/day)
SRI&
Dose
(mg/day)
Trial
(wks)
Response
Rate
(n/N,%)
Rem
issionRate
(n/N,%)
LOCF
MMRM
LOCF
MMRM
DLX
SRI
DLX
SRI
DLX
SRI
DLX
SRI
Goldsteinet
al.(2002)
40–120
20(FLX)
832/66(48.5)
15/33(45.5)
42/66(69.7)
17/33(51.5)
28/66(42.4)
10/33(30.0)
37/66(56.1)
10/33(30.0)
F1J-MC-H
MAQ/B
(EliLilly
&Co.,2004f)
40–120
20(FLX)
540/81(49.4)
15/37(40.5)
——
32/81(39.5)
11/37(29.7)
——
Detkeet
al.(2004)
80
20(PRX)
860/93(64.5)
63/85(74.1)
65/93(69.9)
70/85(82.4)
43/93(46.2)
37/85(43.5)
47/93(50.5)
40/85(47.1)
Detkeet
al.(2004)
120
20(PRX)
866/93(71.0)
63/85(74.1)a
72/93(77.4)
70/85(82.4)a
48/93(51.6)
37/85(43.5)a
54/93(58.1)
40/85(47.1)a
Goldsteinet
al.(2004)
40
20(PRX)
837/84(44.0)
34/84(40.5)
——
29/84(34.5)
31/84(36.9)
——
Goldsteinet
al.(2004)
80
20(PRX)
844/86(51.2)
34/84(40.5%)a
——
——
49/86(57.0)
29/84(34.5)
F1J-MC-H
MAT/A1
(EliLilly
&Co.,2004c)
40
20(PRX)
824/90(26.7)
38/87(43.7)
——
——
——
F1J-MC-H
MAT/A2
(EliLilly
&Co.,2004c)
80
20(PRX)
828/81(34.6)
38/87(43.7)a
——
——
——
Perahia
etal.(2006b)(a)
80
20(PRX)
860/93(64.5)
59/97(60.8)
64/93(68.8)
65/97(67.0)
41/93(44.1)
42/97(43.3)
46/93(49.5)
47/97(48.5)
Perahia
etal.(2006b)(b)
120
20(PRX)
869/102(67.6)
59/97(60.8)a
75/102(73.5)
65/97(67.0)a
41/102(40.2)
42/97(43.3)a
46/102(45.1)
47/97(48.5)a
Khan
etal.(2007)
60
20(S-CTP)
850/126(39.7)
68/136(50.0)
——
38/126(30.2)
44/136(32.4)
——
Lee
etal.(2007)
60
20(PRX)
8144/238(60.5)
157/240(65.4)
——
117/238(49.2)
121/240(50.4)
——
Nierenberget
al.(2007)
60
10(S-CTP)
8113/262(43.1)
109/267(40.8)
128/262(48.9)
121/267(45.3)
97/262(37.0)
85/267(31.8)
105/262(40.1)
88/267(33.0)
Wadeet
al.(2007)
60
20(S-CTP)
881/146(55.5)
94/141(64.5)
——
62/146(42.5)
69/141(48.9)
——
Perahia
etal.(2008)
60
150(V
NX)
6164/318(51.6)
180/330(54.5)
——
100/318(31.4)
116/330(35.2)
——
Perahia
etal.(2008)
60–120
150–225(V
NX)
12
199/318(62.6)
228/330(39.1)
——
153/318(48.1)
166/330(50.3
——
Totals,Means
74.4�23.1
SRIs
7.9�1.4
1211/2277(53.2%)1254/2220(56.5%)
446/709(62.9%)408/664(61.4%)829/2020(41.0%)811/1962(41.3%)384/795(48.3%)301/748(40.2%)
Duloxetine(D
LX)was
compared
in16comparisonsversusstandardserotonin
reuptakeinhibitors
(SRIs;fluoxetine[FLX],paroxetine[PRX],escitalopram
[S-CTP],orvenlafaxine[V
NX]).
aSomeSRIdataareusedtwiceinthree-armtrialsthatinvolved
twodosesofDLX.C
rudeestimates
ofDLX/SRIresponse
ratios,based
ontotalsshown:MMRM/LOCF:Response¼1.02/0.94;Rem
ission
MMRM/LOCF:¼
1.20/0.99.
Copyright # 2009 John Wiley & Sons, Ltd. Hum. Psychopharmacol Clin Exp 2009; 24: 177–190.DOI: 10.1002/hup
184 p. girardi ET AL.

Table 5. Comparisons of duloxetine versus SRIs in adult acute major depression
Comparators (SRIs) Trials (n) Duration (weeks)
Doses (mg/day) Response Rates (responsers/subjects) Crude
DLX SRIs DLX SRIs RR
Paroxetine 9 8.0 78 20 632/958 (55.5%) 545/946 (57.6%) 0.96S-Citalopram 3 8.0 60 17 244/534 (45.7%) 271/554 (48.9%) 0.93Fluoxetine 2 6.5 80 20 52/70 (74.3%) 30/70 (42.9%) 1.73Venlafaxine 2 9.0 75 330 363/636 (57.1%) 408/660 (61.8%) 0.92All SRIs 16 7.9 63.5 — 1291/2198 (58.7%) 1254/2230 (56.2%) 1.04
Based on simple pooling (sums) of data for response rates (n/N) from Table 3, based on LOCF analyses. Durations and total daily DLX doses are based onaverages weighted by trial numbers (n) for each condition; doses of SRIs vary widely and are not averaged. Comparisons suggest only minor overall differencesbetween DLX versus SRIs, but based on few trials of most comparators, possible superiority of DLX over fluoxetine, but possible slight (4%–8%) inferiority ofDLX versus other SRIs (based on crude RR <1.0).
duloxetine for acute depression 185
early findings are not included in the presentanalyses (Figure 3).There was also an unexpected, substantial associ-
ation of PBO response rates with the dose of DLX incorresponding active-treatment arms in the same trials(r¼þ0.638, p< 0.006). Accordingly, we computedresponse as the difference in response rates associatedwith DLX versus PBO, which did not increase withDLX dose (r¼þ0.370, p¼ 0.144; not shown). Thesefindings suggest that there may be unaccountedfactors (perhaps related to patient-mix or othercircumstances of the RCTs), and that the relation-ship of dose to effect might be artifactual.
Figure 3. Effects of DLX dose (total mg/day) versus response rates asdefined for Figure 2 (n¼ 20 comparisons from Table 2; simple linearregression r¼ 0.715, p¼ 0.001, but data are shown as curve-fit to alogarithmic function since doses >80mg/day appear to exert lesser effectsper 20mg increase). Not included are data from three early, unpublishedpilot studies and a reported early open trial that found doses of 5–30mg/daynot to be more effective than a PBO, and are discussed in the text. There wasalso an apparent inverse correlation with dose versus dropout rate, than maybe artifactual, as discussed in the text
Copyright # 2009 John Wiley & Sons, Ltd.
An additional unexpected finding was that dropoutrate also correlated inversely with DLX dose(r¼ –0.616, p¼ 0.004 for 20 trials summarized inTable 6). Usually, higher doses of antidepressants bringmore adverse effects, less tolerability, and higherdropout rates (Mavissakalian and Perel, 1989; Bal-dessarini, 2005). However, the observed relationship ofhigher dose of DLX with less dropout risk may wellrepresent an artifact of the method of dosing, in thatmost trials involved initially low doses that weregradually increased as tolerated, to attain a finalmaximum dose, with longer times required for higherdoses. That is, having to try and tolerate lower doses toremain in a trial aiming at relatively high final dosesprobably selects for subjects who remain in trialslonger, even following random assignment to treatmentor dose. This finding was not associated significantlywith rates of overall ADRs, sustained hypertension, orpremature dropouts associated with any ADR (notshown).
Risks of adverse effects
Notable (�10% incidence) adverse effects reported inassociation with DLX-treatment the cited studies(Table 1) ranked: diarrhea � asthenia � fatigue �insomnia � dizziness � nausea � constipation �somnolence � anorexia � nervousness � vomiting �dry mouth � sweating (not shown). Incidence rangedfrom high values of 19% to a low of 14% (mean:17.2� 8.2%). For the same symptoms, paired trialarms with randomization to PBO were associated withan average incidence of 4.36� 3.3%, to yield anoverall risk ratio of over fivefold greater risk ofcomplaints of side effects with DLX than with PBO.Dropout rates could be estimated for 17 of the
comparisons (Table 6). The overall meta-analyticestimate of RR for leaving DLX arms of 15 trialsbefore their targeted completion times, for any reason,and more than with PBO, was 1.04 (95%CI: 0.94–1.15;
Hum. Psychopharmacol Clin Exp 2009; 24: 177–190.DOI: 10.1002/hup

Table
6.
Tolerabilityandadverse
effectsofduloxetineversusSRIs
andPBO
Study
Dose
(mg/day)
Trial
(wks)
Adverse
Responses
Sustained
Hypertension
DropoutsforADRs
AllDropouts
DLX
SRI
PBO
DLX
SRI
PBO
DLX
SRI
PBO
DLX
SRI
PBO
DLX
SRI
Detkeet
al.(2002a)
60
—9
92/122(75.4)
118/123(95.9)
—0/12(0.00)
1/123(0.81)
—3/122(2.45)
17/123(13.8)
—36/122(29.5)
43/123(35.0)
—Detkeet
al.(2002b)
60
—9
108/139(77.7)
111/128(86.7)
—0/139(0.00)
1/128(0.78)
—4/139(2.88)
16/128(12.5)
—49/139(35.3)
50/128(39.1)
—Goldsteinet
al.(2002)
40–120
20(FLX)
858/70(82.9)
62/70(88.6)
30/33(90.9)
4/70(5.71)
3/70(4.29)
1/33(3.03)
3/70(4.29)
7/70(10.0)
1/33(3.03)
24/70(34.3)
24/70(34.4)
12/33(36.4)
Detkeet
al.(2004)
80
20(PRX)
835/93(37.6)
49/95(51.6)
39/86(45.3)
1/93(1.08)
3/93(3.23)
1/86(1.16)
3/93(3.23)
4/95(4.21)
3/86(3.49)
18/93(19.4)
12/95(12.6)
10/86(11.6)
Detkeet
al.(2004)
120
20(PRX)
835/93(37.6)a
47/93(50.5)
39/86(45.3)a
1/93(1.08)a
1/95(1.06)
1/86(1.16)
3/93(3.23)a
3/93(3.23)a
3/86(3.49)a
18/93(19.4)a
9/93(9.68)
10/86(11/6)a
F1J-MCHMAT/A1
(EliLilly
&Co.,2004c)
40
20(PRX)
863/90(70.0)
78/91(85.7)
71/89(79.8)
——
—3/90(3.33)
11/91(12.1)
10/89(11.2)
29/90(32.2)
30/91(33.0)
31/89(34.8)
F1J-MCHMAT/A2
(EliLilly
&Co.,2004c)
80
20(PRX)
863/90(70.0)a
75/84(89.3)
71/89(79.8)a
——
—3/90(3.33)a
13/84(15.5)
10/89(11.2)a
29/90(32.2)a
28/84(33.3)
31/89(34.8)a
F1J-MC-H
MAQ/B
(EliLilly
&Co.,2004f)
40–120
20(FLX)
855/75(73.3)
73/82(89.0)
32/37(86.5)
3/75(4.00)
1/82(1.22)
1/37(2.70)
——
—31/75(41.3)
25/82(30.5)
14/37(37.8)
Goldsteinet
al.(2004)
40
20(FLX)
861/89(68.5)
73/86(84.9)
76/87(87.4)
2/89(2.25)
0/86(0.00)
0/87(0.00)
8/89(8.99)
10/86(11.6)
8/87(9.20)
37/89(41.6)
31/86(36.0)
38/87(43.7
Goldsteinet
al.(2004)
80
20(FLX)
861/89(68.5)a
76/91(83.5)
76/87(87.4)a
2/89(2.25)a
2/91(2.20)
0/87(0.00)a
8/89(8.99)a
14/91(15.4)
8/87(9.20)a
37/89(41.6)a
38/91(41.8)
38/87(43.7)a
Brannan
etal.(2005)
60
—7
——
—1/141(0.71)
1/141(0.71)
—3/141(2.13)
20/141(14.2)
—40/139(28.8)
54/141(38.3)
—Perahia
etal.(2006b)
80
20(PRX)
829/99(29.3)
39/93(41.9)
35/97(36.1)
3/99(3.03)
1/93(1.08)
0/97(0.00)
1/99(1.01)
4/93(2.05)
1/97(1.03)
9/99(9.09)
10/93(10.8)
11/97(11.3)
Perahia
etal.(2006b)
120
20(PRX)
829/99(29.3)a
34/103(33.0)
35/97(36.1)a
3/99(3.03)a
4/103(3.88)
0/97(0.00)a
1/99(1.01)a
2/103(1.94)
1/97(1.03)a
9/99(9.09)a
13/103(0.71)
11/97(11.3)a
Brechtet
al.(2007)
60
—8
75/165(45.5)
90/162(55.6)
——
——
9/165(5.45)
17/162(10.5)
___
37/165(22.4)
41/162(25.3)
—Khan
etal.(2007)
60
10–20(S-CTP)
8—
106/133(79.7)
110/137(80.3)
——
——
17/133(12.8)
3/137(2.19)
—41/133(30.8)
18/137(13.1)
Lee
etal.(2007)
60
20(PRX)
8—
185/237(78.1)
168/239(70.3)
——
——
20/238(8.40)
17/240(7.08)
—72/238(30.3)
57/240(23.8)
Nierenberget
al.(2007)
60
10(S-CTP)
8107/137(78.1)
234/273(85.7)
222/274(81.0)
1/137(0.73)
1/273(0.37)
1/274(0.36)
8/137(5.84)
20/273(7.33)
14/274(5.11)
40/137(29.2)
85/273(31.1)
66/274(24.1)
(Raskin
etal.,2007,
2008a,b)
60
—8
67/104(64.4)
145/207(70.0)
—1/104(0.96)
1/207(0.48)
—9/104(8.65)
20/207(9.66)
—24/104(23.1)
45/207(21.7)
—
Perahia
etal.(2008)
60
150(V
NX)
6—
276/330(83.6)
272/337(80.7)
—1/139(0.72)
4/329(1.22)
—40/330(12.1)
21/337(6.23)
—79/330(23.9)
59/337(17.5)
Perahia
etal.(2008)
60–120
150–225(V
NX)
12
—283/330(85.8)
293/337(86.9)
—6/319(1.88)
8/329(2.43)
—48/330(14.5)
31/337(9.20%)
—116/330(35.2)
86/337(25.5)
Means,Totals
72.5�21.2
SRIs
8.2�1.1
938/1555
(60.3%)
2154/2811
(76.6%)
1569/2112
(74.3%)
22/1240
(1.77%)
27/2043
(1.32%)
17/1542
(1.10%)
69/1620
(4.26%)
303/2871
(10.6%)
131/2076
(6.31%)
467/1693
(27.6%)
846/2953
(28.6%)
492/2113
(23.3%)
Studies(n
¼20)comparingvariousaspectsoftolerabilityofDLX
withserotonin–reuptakeinhibitors
(SRIs)andPBO.ADRs¼adverse
responsesassociated
withdrugtreatm
ent.Dataareratesof
patients
withadverse
effects(n)over
those
providinginform
ation(N
)andtheproportion(%
).aSomecontrolsandcomparatorvalues
arerepeatedin
three-arm
trialsinvolvingtwodosesofDLX.Abbreviations:DLX,duloxetine;
PBO,placebo;SRI,serotonin–reuptakeinhibitor.
Copyright # 2009 John Wiley & Sons, Ltd. Hum. Psychopharmacol Clin Exp 2009; 24: 177–190.DOI: 10.1002/hup
186 p. girardi ET AL.
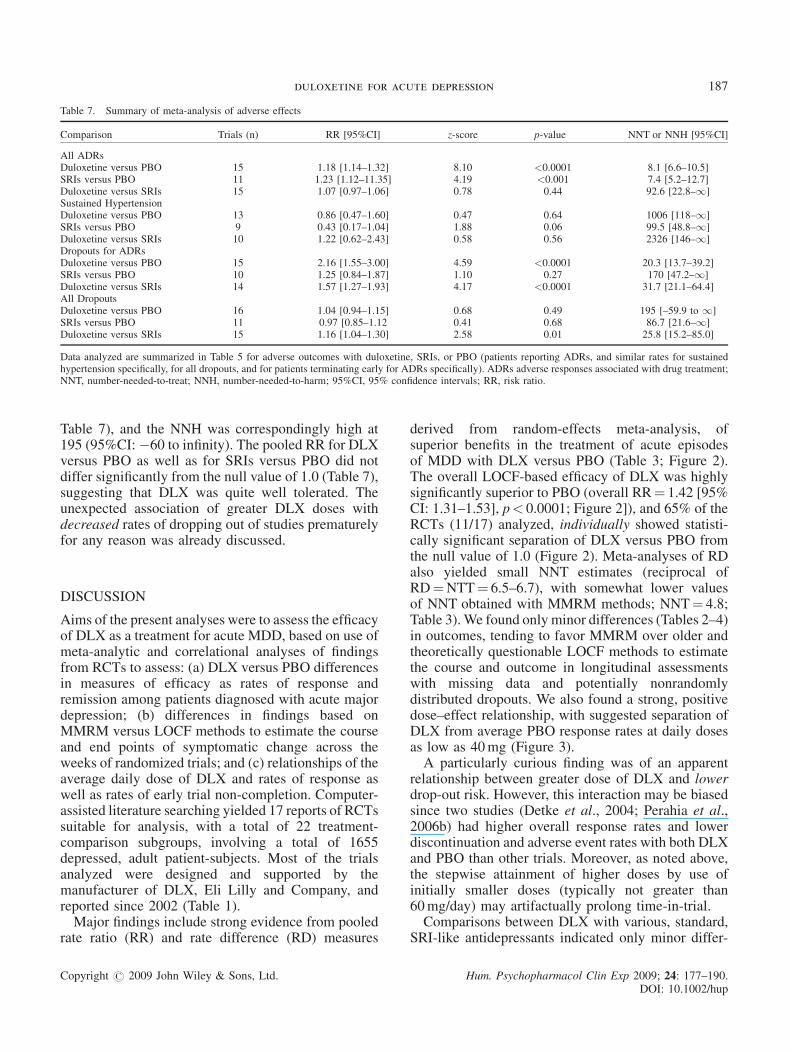
Table 7. Summary of meta-analysis of adverse effects
Comparison Trials (n) RR [95%CI] z-score p-value NNT or NNH [95%CI]
All ADRsDuloxetine versus PBO 15 1.18 [1.14–1.32] 8.10 <0.0001 8.1 [6.6–10.5]SRIs versus PBO 11 1.23 [1.12–11.35] 4.19 <0.001 7.4 [5.2–12.7]Duloxetine versus SRIs 15 1.07 [0.97–1.06] 0.78 0.44 92.6 [22.8–1]Sustained HypertensionDuloxetine versus PBO 13 0.86 [0.47–1.60] 0.47 0.64 1006 [118–1]SRIs versus PBO 9 0.43 [0.17–1.04] 1.88 0.06 99.5 [48.8–1]Duloxetine versus SRIs 10 1.22 [0.62–2.43] 0.58 0.56 2326 [146–1]Dropouts for ADRsDuloxetine versus PBO 15 2.16 [1.55–3.00] 4.59 <0.0001 20.3 [13.7–39.2]SRIs versus PBO 10 1.25 [0.84–1.87] 1.10 0.27 170 [47.2–1]Duloxetine versus SRIs 14 1.57 [1.27–1.93] 4.17 <0.0001 31.7 [21.1–64.4]All DropoutsDuloxetine versus PBO 16 1.04 [0.94–1.15] 0.68 0.49 195 [–59.9 to 1]SRIs versus PBO 11 0.97 [0.85–1.12 0.41 0.68 86.7 [21.6–1]Duloxetine versus SRIs 15 1.16 [1.04–1.30] 2.58 0.01 25.8 [15.2–85.0]
Data analyzed are summarized in Table 5 for adverse outcomes with duloxetine, SRIs, or PBO (patients reporting ADRs, and similar rates for sustainedhypertension specifically, for all dropouts, and for patients terminating early for ADRs specifically). ADRs adverse responses associated with drug treatment;NNT, number-needed-to-treat; NNH, number-needed-to-harm; 95%CI, 95% confidence intervals; RR, risk ratio.
duloxetine for acute depression 187
Table 7), and the NNH was correspondingly high at195 (95%CI:�60 to infinity). The pooled RR for DLXversus PBO as well as for SRIs versus PBO did notdiffer significantly from the null value of 1.0 (Table 7),suggesting that DLX was quite well tolerated. Theunexpected association of greater DLX doses withdecreased rates of dropping out of studies prematurelyfor any reason was already discussed.
DISCUSSION
Aims of the present analyses were to assess the efficacyof DLX as a treatment for acute MDD, based on use ofmeta-analytic and correlational analyses of findingsfrom RCTs to assess: (a) DLX versus PBO differencesin measures of efficacy as rates of response andremission among patients diagnosed with acute majordepression; (b) differences in findings based onMMRM versus LOCF methods to estimate the courseand end points of symptomatic change across theweeks of randomized trials; and (c) relationships of theaverage daily dose of DLX and rates of response aswell as rates of early trial non-completion. Computer-assisted literature searching yielded 17 reports of RCTssuitable for analysis, with a total of 22 treatment-comparison subgroups, involving a total of 1655depressed, adult patient-subjects. Most of the trialsanalyzed were designed and supported by themanufacturer of DLX, Eli Lilly and Company, andreported since 2002 (Table 1).Major findings include strong evidence from pooled
rate ratio (RR) and rate difference (RD) measures
Copyright # 2009 John Wiley & Sons, Ltd.
derived from random-effects meta-analysis, ofsuperior benefits in the treatment of acute episodesof MDD with DLX versus PBO (Table 3; Figure 2).The overall LOCF-based efficacy of DLX was highlysignificantly superior to PBO (overall RR¼ 1.42 [95%CI: 1.31–1.53], p< 0.0001; Figure 2]), and 65% of theRCTs (11/17) analyzed, individually showed statisti-cally significant separation of DLX versus PBO fromthe null value of 1.0 (Figure 2). Meta-analyses of RDalso yielded small NNT estimates (reciprocal ofRD¼NTT¼ 6.5–6.7), with somewhat lower valuesof NNT obtained with MMRM methods; NNT¼ 4.8;Table 3).We found only minor differences (Tables 2–4)in outcomes, tending to favor MMRM over older andtheoretically questionable LOCF methods to estimatethe course and outcome in longitudinal assessmentswith missing data and potentially nonrandomlydistributed dropouts. We also found a strong, positivedose–effect relationship, with suggested separation ofDLX from average PBO response rates at daily dosesas low as 40mg (Figure 3).A particularly curious finding was of an apparent
relationship between greater dose of DLX and lowerdrop-out risk. However, this interaction may be biasedsince two studies (Detke et al., 2004; Perahia et al.,2006b) had higher overall response rates and lowerdiscontinuation and adverse event rates with both DLXand PBO than other trials. Moreover, as noted above,the stepwise attainment of higher doses by use ofinitially smaller doses (typically not greater than60mg/day) may artifactually prolong time-in-trial.Comparisons between DLX with various, standard,
SRI-like antidepressants indicated only minor differ-
Hum. Psychopharmacol Clin Exp 2009; 24: 177–190.DOI: 10.1002/hup

188 p. girardi ET AL.
ences in efficacy or tolerability compared to DLX,particularly as reflected in rates of early dropouts due toADRs (Tables 6 and 7). Both SRIs and DLX yieldedmore reports of ADRs than with PBO, whereas nodifference was apparent among active drugs. With60mg/day of DLX in elderly MDD patients, the mostfrequently reported ADRs were dry mouth andmoderate nausea, and at rates similar to those reportedwith several SRIs in older patients, and withoutappreciable increases or decreases in blood pressure orpulse than with a PBO or SRIs (Raskin et al., 2008a).However, other studies have reported higher rates oftreatment-related nausea with DLX than PBO or SRIs(Detke et al., 2002a,b; Goldstein et al., 2004; Brannanet al., 2005; Perahia et al., 2006b, 2008; Brecht et al.,2007; Lee et al., 2007; Nierenberg et al., 2007; Dunneret al., 2008). In one open label trial with moreprolonged treatment with DLX, newly arising ADRswere rare, but some symptoms have been reported(Dunner et al., 2008) to begin or increase (e.g.,decreased libido, abnormal orgasms, weight-gain or -loss, hypersomnia, night–sweats, nightmares or earlyawakening, increased blood pressure, tachycardia,tremor, dizziness or unsteadiness, aggression, hypo-mania, or suicidal ideation).Notable limitations of the present analyses include
the modest number of RCTs to analyze, an evensmaller number of contrasts between DLX and PBObased on applications of both MMRM and LOCFmethods of data–analysis in the same trials, impreciseestimates of retention times in each trial arm so as toassure precise matching, a limited range of comparisonagents and doses, and the risk of artifactual increase intime-in-trials owing to stepwise achievement ofrelative high doses of DLX, as tolerated.
CONCLUSIONS
The present findings add to the impression that DLX isan effective antidepressant in comparison with PBO,and similarly effective as various SRIs. Additionaltrials and analyses are required to clarify the efficacy,tolerability, and optimal dosing of DLX versus otherantidepressants in common clinical use. Future trialsalso should clarify the potential value of DLX forpreventing relapses in preventing recurrences of MDD,and for indications other than depression, such asanalgesic and anti-incontinence effects that have beenascribed to DLX (Finnerup et al. 2007; Basu andDuckett 2008; Bump et al. 2008; Saarto and Wiffen2008; Schagen van Leeuwen et al. 2008), as well asquantifying relapse risks that follow abrupt versusgradual discontinuation of DLX.
Copyright # 2009 John Wiley & Sons, Ltd.
DISCLOSURES
The authors received no financial support fromproducers of DLX, nor are there any commercialinterests involved in this report. Drs. Innamorati, DelCasale and Mazzarini have no relevant disclosures.Dr Girardi has served as a consultant to, or has engagedin research collaborations with Organon, Eli Lilly,Janssen, Merck, Bristol-Myers Squibb, Astra-Zeneca.Dr Pompili has served as a consultant to, or hasengaged in research collaborations with Eli Lilly, andOrganon Corporations of Italy. Dr Tatarelli has servedas a consultant to, or engaged in research collabor-ations with Eli Lilly, Janssen, Merck, Bristol-MyersSquibb, and Servier Corporations. Dr Serafini hasserved as a consultant to, or engaged in researchcollaborations with Bristol-Myers Squibb. Dr Manciniis an employee and shareholder of Eli Lilly Italy.Dr Baldessarini has served as a consultant to, orengaged in collaborative, investigator-initiatedresearch with Auritec, Biotrofix, Eli Lilly, IFI, JanssenPharmaceutical, JDS-Noven, Luitpold, Merck, Neuro-Healing, Novartis, Pfizer and Solvay Corporations. Noauthor is a member of pharmaceutical speakers’ panels,nor do they or any family member hold equity positionsin pharmaceutical or biotechnology companies.
ACKNOWLEDGEMENTS
Supported, in part, by a grant from the Bruce J. AndersonFoundation and the McLean Hospital Private Donors’Research Fund for Psychopharmacology Research (to RJB).
REFERENCES
Anonymous. 2008. Duloxetine. At: http://en.wikipedia.org/wiki/Duloxetine(Accessed 07/21/2008).
Baldessarini RJ. 2005. Drug therapy of depression and anxiety disorders. InGoodman and Gilman’s the Pharmacological Basis of Therapeutics,Chapter 17 Brunton LL, Lazo JS, Parker KL (eds). McGraw Hill: NewYork; 429–459.
Ballesteros J, Callado LF, Gutierrez M. 2007. An independent meta-analysisusing summary data for clinical response, remission, and discontinuation forany reason from the 6 pivotal phase III randomized clinical trials of duloxetinein major depressive disorder. J Clin Psychopharmacol 27: 219–221.
Berk M, du Plessis AD, Berkett M, Richardt D. 1997. Open-label study ofduloxetine hydrochloride, a mixed serotonin and norepinephrine reuptakeinhibitor, in patients with DSM-III-R major depressive disorder. Int ClinPsychopharmacol 12: 137–140.
Brannan SK, Mallinckrodt CH, Brown EB, et al. 2005. Duloxetine 60mgonce-daily in the treatment of painful physical symptoms in patients withmajor depressive disorder. J Psychiatr Res 39: 43–53.
Brecht S, Courtecuisse C, Debieuvre C, et al. 2007. Efficacy and safety ofduloxetine 60mg once daily in the treatment of pain in patients withmajor depressive disorder and at least moderate pain of unknownetiology: a randomized controlled trial. J Clin Psychiatry 68: 1707–1716.
Burt VK, Wohlreich MM, Mallinckrodt CH, et al. 2005. Duloxetine for thetreatment of major depressive disorder in women ages 40 to 55 years.Psychosomatics 46: 345–354.
Bymaster FP, Dreshfield-Ahmad LJ, Threlkeld PG, et al. 2001. Comparativeaffinity of duloxetine and venlafaxine for serotonin and norepinephrine
Hum. Psychopharmacol Clin Exp 2009; 24: 177–190.DOI: 10.1002/hup
duloxetine for acute depression 189
transporters in vitro and in vivo, human serotonin receptor subtypes, andother neuronal receptors. Neuropsychopharmacology 25: 871–880.
Bymaster FP, Lee TC, Knadler MP, et al. 2005. The dual transporterinhibitor duloxetine: a review of its preclinical pharmacology, pharma-cokinetic profile, and clinical results in depression. Curr Pharm Des 11:1475–1493.
Cowen PJ, Ogilvie AD, Gama J. 2005. Efficacy, safety and tolerability ofduloxetine 60mg once daily in major depression. Curr Med Res Opin 21:345–356.
DerSimonian R, Laird N. 1986. Meta-analysis in clinical trials.Control ClinTrials 7: 177–188.
Detke MJ, Lu Y, Goldstein DJ, et al. 2002a. Duloxetine, 60mg once daily,for major depressive disorder: a randomized double-blind placebo-con-trolled trial. J Clin Psychiatry 63: 308–315.
Detke MJ, Lu Y, Goldstein DJ, et al. 2002b. Duloxetine 60mg once dailydosing versus placebo in the acute treatment of major depression.J Psychiatr Res 36: 383–390.
Detke MJ, Wiltse CG, Mallinckrodt CH, et al. 2004. Duloxetine in the acuteand long-term treatment of major depressive disorder: a placebo- andparoxetine-controlled trial. Eur Neuropsychopharmacol 14: 457–470.
Dunner DL, Wilson M, Fava M, et al. 2008. Long-term tolerability andeffectiveness of duloxetine in the treatment of major depressive disorder.Depress Anxietys 25: E1–8.
Dworkin RH, O’Connor AB, Backonja M, et al. 2007. Pharmacologicmanagement of neuropathic pain: evidence-based recommendations.Pain 132: 237–251.
Eli Lilly and Company. 2004b. Duloxetine once-daily dosing versus placeboin the acute treatment of major depression. Clinical study summary:Study f1j-mc-hmbh study group b. At: http://www.clinicalstudyresult-s.org/documents/company-study_142_0.pdf (Accessed 05/21/2008).
Eli Lilly and Company. 2004c. Duloxetine versus placebo and paroxetine inthe acute treatment of major depression. Clinical study summary: Studyf1j-mc-hmat study group a. At: http://www.clinicalstudyresults.org/docu-ments/company-study_170_0.pdf (Accessed 05/21/2008).
Eli Lilly and Company. 2004d. Duloxetine versus placebo and paroxetine inthe acute treatment of major depression. Clinical study summary: Studyf1j-mc-hmat study group b. At: http://www.clinicalstudyresults.org/docu-ments/company-study_139_0.pdf (Accessed 05/21/2008).
Eli Lilly and Company. 2004e. Duloxetine versus placebo in the treatmentof major depression. Clinical study summary: Study f1j-mc-hmaq studygroup a. At: http://www.clinicalstudyresults.org/documents/company-study_137_0.pdf (Accessed 05/21/2008).
Eli Lilly and Company. 2004f. Duloxetine versus placebo in the treatment ofmajor depression. Clinical study summary: Study f1j-mc-hmaq studygroup b. At: http://www.clinicalstudyresults.org/documents/company-study_138_0.pdf (Accessed 05/21/2008).
Eli Lilly and Company. 2005a. Duloxetine versus placebo in the treatmentof elderly patients with major depressive disorder. Clinical study sum-mary: Study f1j-mc-hmbv. At: http://www.clinicalstudyresults.org/docu-ments/company-study_2651_0.pdf (Accessed 05/21/2008).
Eli Lilly and Company. 2005b. Duloxetine versus placebo and paroxetinein the treatment of major depression. Clinical study summary: StudyFLJ, MC-HMAY Study Group a. At: http://pdf.clinicalstudyresults.org/documents/company-study_887_0.pdf (Accessed 05/21/2008).
Eli Lilly and Company. 2006a. A double-blind, placebo- and clomipramine-controlled study in duloxetine patients with major depression: Clinicalstudy summary: Study f1j-mc-hmai. At: http://pdf.clinicalstudyresults.org/documents/company-study_4148_0.pdf (Accessed 11/14/2008).
Eli Lilly and Company. 2006b. Duloxetine 20/30mg versus Placebo inmajor depression: Clinical study summary: Study f1j-mc-hmah. At:http://pdf.clinicalstudyresults.org/documents/company-study_4147_0.pdf(Accessed 11/4/2008).
Eli Lilly and Company. 2006c. Duloxetine once-daily dosing versus placeboin patients with major depression and pain. Clinical study summary: F1j-us-hmcb. At: http://www.clinicalstudyresults.org/documents/company-study_1038_0.pdf (Accessed 05/21/2008).
Eli Lilly and Company. 2006d. Duloxetine versus paroxetine in the acutetreatment of major depression. Clinical study summary: Study f1j-aa-hmcv. At: http://www.clinicalstudyresults.org/documents/company-study_2402_0.pdf (Accessed 05/21/2008).
Copyright # 2009 John Wiley & Sons, Ltd.
Eli Lilly and Company. 2006e. Duloxetine versus placebo and paroxetinein the treatment of major depression. Clinical study summary: Studyf1j-mc-hmay study group b. At: http://www.clinicalstudyresults.org/documents/company-study_1618_0.pdf (Accessed 05/21/2008).
Eli Lilly and Company. 2006f. Duloxetine/placebo in major depressivedisorder: Clinical study summary: Study f1j-mc-hmag. At: http://pdf.cli-nicalstudyresults.org/documents/company-study_4146_0.pdf (Accessed11/14/2008).
Eli Lilly and Company. 2007a. Duloxetine versus escitalopram and placeboin the treatment of patients with major depression. Clinical studysummary: Study f1j-us-hmcr. At: http://www.clinicalstudyresults.org/documents/company-study_2182_0.pdf (Accessed 05/21/2008).
Eli Lilly and Company. 2007b. A ten-week, randomized, double-blind studyevaluating the efficacy of duloxetine 60mg once daily versus placebo inoutpatients with major depressive disorder and pain. Clinical studysummary: Study f1j-bi-hmdh. At: http://www.clinicalstudyresults.org/documents/company-study_3498_0.pdf (Accessed 05/21/2008).
Eli Lilly and Company. 2008a. Duloxetine versus venlafaxine extendedrelease in the treatment of major depressive disorder. Clinical studysummary: Study f1j-mc-hmbu. At: http://www.clinicalstudyresults.org/documents/company-study_3107_0.pdf (Accessed 05/21/2008).
Eli Lilly and Company. 2008b. Duloxetine versus venlafaxine extendedrelease in the treatment of major depressive disorder. Clinical studysummary: Study f1j-mc-hmcq. At: http://www.clinicalstudyresults.org/documents/company-study_3108_0.pdf (Accessed 06/06/2008).
Finnerup NB, Otto M, Jensen TS, et al. 2007. An evidence-based algorithmfor the treatment of neuropathic pain. MedGenMed 9: 36–47.
Frampton JE, Plosker GL. 2007. Duloxetine: review of its use in thetreatment of major depressive disorder. CNS Drugs 21: 581–609.
Glanville JM, Lefebvre C, Miles JN, et al. 2006. How to identify randomizedcontrolled trials in medline: ten years on. J Med Libr Assoc 94: 130–136.
Goldstein DJ, Lu Y, Detke MJ, et al. 2004. Duloxetine in the treatment ofdepression: double-blind placebo-controlled comparison with paroxetine.J Clin Psychopharmacol 24: 389–399.
Goldstein DJ, Mallinckrodt C, Lu Y, et al. 2002. Duloxetine in the treatmentof major depressive disorder: double-blind clinical trial. J Clin Psychiatry63: 225–231.
Hamilton M. 1960. A rating scale for depression. J Neurol NeurosurgPsychiatry 23: 56–62.
Hennen J. 2003. Statistical methods for longitudinal research on bipolardisorders. Bipolar Disord 5: 156–168.
Hudson JI, Wohlreich MM, Kajdasz DK, et al. 2005. Safety and tolerabilityof duloxetine in the treatment of major depressive disorder: analysis ofpooled data from eight placebo-controlled clinical trials. Hum Psycho-pharmacol 20: 327–341.
Jadad AR,Moore RA, Carroll D, et al. 1996. Assessing the quality of reportsof randomized clinical trials: is blinding necessary? Control Clin Trials17: 1–12.
Khan A, Bose A, Alexopoulos GS, et al. 2007. Double-blind comparison ofescitalopram and duloxetine in the acute treatment of major depressivedisorder. Clin Drug Investig 27: 481–492.
Lee P, Shu L, Xu X, et al. 2007. Once-daily duloxetine 60mg in thetreatment of major depressive disorder: Multicenter, double-blind,randomized, paroxetine-controlled, non-inferiority trial in China, Korea,Taiwan and Brazil. Psychiatry Clin Neurosci 61: 295–307.
Mallinckrodt CH,Watkin JG, Liu C, et al. 2005. Duloxetine in the treatmentof major depressive disorder: a comparison of efficacy in patients withand without melancholic features. BMC Psychiatry 5: 1.
Mann JJ. 2005. Medical management of depression. N Engl J Med 353:1819–1834.
Mavissakalian MR, Perel JM. 1989. Imipramine dose-response relationshipin panic disorder with agoraphobia. Arch Gen Psychiatry 46: 127–131.
Montgomery SA, Asberg M. 1979. New depression scale designed to besensitive to change. Br J Psychiatry 134: 382–389.
Nemeroff CB, Schatzberg AF, Goldstein DJ, et al. 2002. Duloxetine for thetreatment of major depressive disorder. Psychopharmacol Bull 36: 106–132.
Nierenberg AA, Greist JH, Mallinckrodt CH, et al. 2007. Duloxetine versusescitalopram and placebo in the treatment of patients with major depress-ive disorder: onset of antidepressant action, a non-inferiority study. CurrMed Res Opin 23: 401–416.
Hum. Psychopharmacol Clin Exp 2009; 24: 177–190.DOI: 10.1002/hup

190 p. girardi ET AL.
Papakostas GI, Thase ME, Fava M, et al. 2007. Are antidepressant drugsthat combine serotonergic and noradrenergic mechanisms of action moreeffective than the selective serotonin reuptake inhibitors in treating majordepressive disorder? A meta-analysis of studies of newer agents. BiolPsychiatry 62: 1217–1227.
Perahia DG, Gilaberte I, Wang F, et al. 2006a. Duloxetine in the preventionof relapse of major depressive disorder: double-blind placebo-controlledstudy. Br J Psychiatry 188: 346–353.
Perahia DG, Pritchett YL, Kajdasz DK, et al. 2008. Randomized,double-blind comparison of duloxetine and venlafaxine in the treatmentof patients with major depressive disorder. J Psychiatr Res 42:22–34.
Perahia DG, Wang F, Mallinckrodt CH, et al. 2006b. Duloxetine in thetreatment of major depressive disorder: placebo- and paroxetine-con-trolled trial. Eur Psychiatry 21: 367–378.
Pritchett YL, Marciniak MD, Corey-Lisle PK, et al. 2007. Use of effect sizeto determine optimal dose of duloxetine in major depressive disorder.J Psychiatr Res 41: 311–318.
Raskin J, Goldstein DJ, Mallinckrodt CH, et al. 2003. Duloxetine in thelong-term treatment of major depressive disorder. J Clin Psychiatry 64:1237–1244.
Raskin J, Wiltse CG, Dinkel JJ, et al. 2008a. Safety and tolerability ofduloxetine at 60mg once daily in elderly patients with major depressivedisorder. J Clin Psychopharmacol 28: 32–38.
Raskin J, Wiltse CG, Siegal A, et al. 2007. Efficacy of duloxetine oncognition, depression, and pain in elderly patients with major depressive
Copyright # 2009 John Wiley & Sons, Ltd.
disorder: 8-week, double-blind, placebo-controlled trial. Am J Psychiatry164: 900–909.
Raskin J, Xu JY, Kajdasz DK. 2008b. Time to response for duloxetine 60mgonce daily versus placebo in elderly patients with major depressivedisorder. Int Psychogeriatr 20: 309–327.
Saarto T, Wiffen PJ. 2007. Antidepressants for neuropathic pain. CochraneDatabase Syst Rev (issue 4): C D005454.
Simpson HB, Petkova E, Cheng J, et al. 2008. Statistical choices can affectinferences about treatment efficacy: a case study from obsessive-com-pulsive disorder research. J Psychiatr Res 42: 631–638.
Stahl SM, Grady MM, Moret C, et al. 2005. Snris: their pharmacology,clinical efficacy, and tolerability in comparison with other classes ofantidepressants. CNS Spectr 10: 732–747.
Thase ME, Entsuah AR, Rudolph RL. 2001. Remission rates duringtreatment with venlafaxine or selective serotonin reuptake inhibitors.Br J Psychiatry 178: 234–241.
ThaseME, Pritchett YL, OssannaMJ, et al. 2007. Efficacy of duloxetine andselective serotonin reuptake inhibitors: comparisons as assessed byremission rates in patients with major depressive disorder. J Clin Psy-chopharmacol 27: 672–676.
Wade A, Gembert K, Florea I. 2007. A comparative study of the efficacy ofacute and continuation treatment with escitalopram versus duloxetine inpatientswithmajor depressive disorder.CurrMedResOpin 23: 1605–1614.
Wong DT, Robertson DW, Bymaster FP, et al. 1988. Ly227942, an inhibitorof serotonin and norepinephrine uptake: biochemical pharmacology of apotential antidepressant drug. Life Sci 43: 2049–2057.
Hum. Psychopharmacol Clin Exp 2009; 24: 177–190.DOI: 10.1002/hup
Copyright © 2022 FDOKUMEN




















