
A randomized placebo-controlled trial of gabapentin for cocaine dependence
8
Drug and Alcohol Dependence 81 (2006) 267–274 A randomized placebo-controlled trial of gabapentin for cocaine dependence Adam Bisaga ∗ , Efrat Aharonovich, Fatima Garawi, Frances R. Levin, Eric Rubin, Wilfrid N. Raby, Edward V. Nunes Department of Psychiatry, Columbia University College of Physicians and Surgeons, New York, NY, USA Received 23 May 2005; received in revised form 25 July 2005; accepted 25 July 2005 Abstract Background: In laboratory animals, augmentation of GABA neurotransmission results in inhibition of cocaine self-administration and inhibition of reinstatement to cocaine-seeking behaviors. If parallel effects were observed in humans, GABA-ergic medication should be effective both in the abstinence–induction as well as in the relapse-prevention phase of cocaine dependence treatment. Gabapentin is an anticonvulsant medication that increases human brain GABA levels. We evaluated the safety and efficacy of gabapentin combined with relapse-prevention therapy in the treatment of cocaine-dependent individuals. Design: The study involved 129 individuals with cocaine dependence. Of the 99 participants, who were randomized into a double-blind trial 88% were males, 66% were minorities and with an average age of 39 years (range 22–58 years). After 2 weeks of placebo lead-in, participants were randomized to receive either gabapentin 3200 mg (1600 mg bid) or placebo for 12 weeks, followed by 2 weeks of placebo lead-out. Prior to randomization, participants were stratified into four groups based on the principal route of cocaine use (smokers versus intranasal users) and the level of cocaine use during the 2 weeks of lead-in (high level versus low level). Throughout the 16 weeks study, participants received weekly individual relapse-prevention therapy. The outcome measures included: days of cocaine use and a binary indicator of abstinence based on urine toxicology test, self-reported cocaine craving and retention in treatment. Results: Forty-nine percent of randomized patients completed 12 weeks of the trial. Retention did not differ by treatment group but cocaine-smokers dropped out of treatment at a significantly faster rate than intranasal users. For the entire sample, odds of cocaine use over the course of the study did not differ between gabapentin- and placebo-treated individuals. There was a significant difference in the odds of cocaine use between high and low-use groups, with the odds in high-use groups decreasing over time and odds in the low-use groups gradually increasing over the course of the study, such that by the end of the study low and high users were similarly likely to use cocaine. In the low-use group, there was a non-significant trend suggesting that gabapentin-treated subjects had more favorable outcome compared to placebo-treated individuals. There was no treatment effect on abstinence rates, craving or other substance use. Gabapentin at 3200 mg/day was very well tolerated in this group of cocaine-dependent participants. Conclusions: When combined with weekly individual relapse-prevention therapy, gabapentin 1600mg bid was no more effective than placebo in the treatment of cocaine dependence. When reviewed in conjunction with other published studies, gabapentin and other GABA enhancing anticonvulsant medications may deserve further study as relapse-preventive agents in cocaine-dependent individuals who achieve abstinence early in treatment. © 2005 Elsevier Ireland Ltd. All rights reserved. Keywords: Cocaine dependence; Pharmacotherapy trials; Gabapentin; Relapse-prevention therapy; Placebo lead-in 1. Introduction Cocaine exerts its acute effects through augmentation of dopaminergic (DA) neurotransmission and these dopaminer- ∗ Corresponding author. Present address: New York State Psychiatric Institute, 1051 Riverside Dr., Unit #120, New York, NY 10032, USA. Tel.: +1 212 543 6542; fax: +1 212 543 5991. E-mail address: [email protected] (A. Bisaga). gic effects are thought to contribute both to cocaine’s acute effects on brain metabolism (London et al., 1990) and to the maintenance of cocaine addiction (Kuhar et al., 1991). Further- more, regular cocaine use is associated with long-term alter- ations in brain function including chronic changes in neural metabolism (Volkow et al., 1992), abnormal dopamine trans- mission (Goldstein and Volkow, 2002; Martinez et al., 2004) and structural alterations (London et al., 1999) involving key elements in the circuitry regulating drug-reinforced behaviors. 0376-8716/$ – see front matter © 2005 Elsevier Ireland Ltd. All rights reserved. doi:10.1016/j.drugalcdep.2005.07.009
-
Upload
venicejewishstudies -
Category
Documents
-
view
6 -
download
0
Transcript of A randomized placebo-controlled trial of gabapentin for cocaine dependence

Drug and Alcohol Dependence 81 (2006) 267–274
A randomized placebo-controlled trial of gabapentin for cocaine dependence
Adam Bisaga∗, Efrat Aharonovich, Fatima Garawi, Frances R. Levin, Eric Rubin,Wilfrid N. Raby, Edward V. Nunes
Department of Psychiatry, Columbia University College of Physicians and Surgeons, New York, NY, USA
Received 23 May 2005; received in revised form 25 July 2005; accepted 25 July 2005
Abstract
Background: In laboratory animals, augmentation of GABA neurotransmission results in inhibition of cocaine self-administration and inhibitionof reinstatement to cocaine-seeking behaviors. If parallel effects were observed in humans, GABA-ergic medication should be effective both inthe abstinence–induction as well as in the relapse-prevention phase of cocaine dependence treatment. Gabapentin is an anticonvulsant medicationthat increases human brain GABA levels. We evaluated the safety and efficacy of gabapentin combined with relapse-prevention therapy in thetreatment of cocaine-dependent individuals.Design: The study involved 129 individuals with cocaine dependence. Of the 99 participants, who were randomized into a double-blind trial8 participantsw -out. Priort l users) andt ed weeklyi sed on urinetR e-smokersd e of the studyd en high andl ourse of thes -significantt no treatmente e-dependentpC n placeboi enhancinga stinence earli©
K
1
d
1T
cute
alter-urals-04
iors.
0d
8% were males, 66% were minorities and with an average age of 39 years (range 22–58 years). After 2 weeks of placebo lead-in,ere randomized to receive either gabapentin 3200 mg (1600 mg bid) or placebo for 12 weeks, followed by 2 weeks of placebo lead
o randomization, participants were stratified into four groups based on the principal route of cocaine use (smokers versus intranasahe level of cocaine use during the 2 weeks of lead-in (high level versus low level). Throughout the 16 weeks study, participants receivndividual relapse-prevention therapy. The outcome measures included: days of cocaine use and a binary indicator of abstinence baoxicology test, self-reported cocaine craving and retention in treatment.esults: Forty-nine percent of randomized patients completed 12 weeks of the trial. Retention did not differ by treatment group but cocainropped out of treatment at a significantly faster rate than intranasal users. For the entire sample, odds of cocaine use over the coursid not differ between gabapentin- and placebo-treated individuals. There was a significant difference in the odds of cocaine use betwe
ow-use groups, with the odds in high-use groups decreasing over time and odds in the low-use groups gradually increasing over the ctudy, such that by the end of the study low and high users were similarly likely to use cocaine. In the low-use group, there was a nonrend suggesting that gabapentin-treated subjects had more favorable outcome compared to placebo-treated individuals. There wasffect on abstinence rates, craving or other substance use. Gabapentin at 3200 mg/day was very well tolerated in this group of cocainarticipants.onclusions: When combined with weekly individual relapse-prevention therapy, gabapentin 1600 mg bid was no more effective tha
n the treatment of cocaine dependence. When reviewed in conjunction with other published studies, gabapentin and other GABAnticonvulsant medications may deserve further study as relapse-preventive agents in cocaine-dependent individuals who achieve aby
n treatment.2005 Elsevier Ireland Ltd. All rights reserved.
eywords: Cocaine dependence; Pharmacotherapy trials; Gabapentin; Relapse-prevention therapy; Placebo lead-in
. Introduction
Cocaine exerts its acute effects through augmentation ofopaminergic (DA) neurotransmission and these dopaminer-
∗ Corresponding author. Present address: New York State Psychiatric Institute,051 Riverside Dr., Unit #120, New York, NY 10032, USA.el.: +1 212 543 6542; fax: +1 212 543 5991.
E-mail address: [email protected] (A. Bisaga).
gic effects are thought to contribute both to cocaine’s aeffects on brain metabolism (London et al., 1990) and to themaintenance of cocaine addiction (Kuhar et al., 1991). Further-more, regular cocaine use is associated with long-termations in brain function including chronic changes in nemetabolism (Volkow et al., 1992), abnormal dopamine tranmission (Goldstein and Volkow, 2002; Martinez et al., 20)and structural alterations (London et al., 1999) involving keyelements in the circuitry regulating drug-reinforced behav
376-8716/$ – see front matter © 2005 Elsevier Ireland Ltd. All rights reserved.oi:10.1016/j.drugalcdep.2005.07.009

268 A. Bisaga et al. / Drug and Alcohol Dependence 81 (2006) 267–274
In addition to effects on DA within this circuitry, chronic cocaineuse also disrupts gamma-aminobutyric acid (GABA) function-ing in the central nervous system (Xi et al., 2003). Specifi-cally, it appears that GABA-ergic neurotransmission within themesolimbic system tonically inhibits DA function (Lacey, 1993).Disruption of GABA in these regulatory pathways by chroniccocaine use could possibly result in a disinhibition of DA neu-rons, thereby enhancing cocaine’s dopaminergic effects.
To date, most of the pharmacological strategies to treatcocaine dependence have directly targeted DA and other mono-aminergic neurotransmission, by either mimicking effects ofcocaine on DA reuptake or blocking dopaminergic effects ofcocaine with DA receptor antagonists. Unfortunately, theseinterventions have been ineffective in controlled trials (Soareset al., 2001). As suggested above, an alternative approach tomodulating cocaine’s dopaminergic effects could derive fromaugmentation of GABA-ergic neurotransmission. In supportof this idea, treatment with GABA agonists as well as aug-mentation of GABA neurotransmission resulted in decreasedcocaine self-administration in laboratory animals (Campbell etal., 1999; Kushner et al., 1999; Roberts et al., 1996; Stromberget al., 2001). GABA-ergic mechanisms have also been identifiedin cocaine-primed, stress and conditioned-cue induced drug-seeking behavior in an animal reinstatement model of relapse(Campbell et al., 1999; Fuchs et al., 2004; McFarland et al.,2004; McFarland and Kalivas, 2001). Therefore, under labora-t l asr dicat rgicm ctiona
atea lledc 3;K 03E tientwa eline(
rgicm s. Thma anb r,a minoa ts oc in,2 dlyd iating -l ntind e us(H subj ainew ekinc
We included a placebo lead-in period prior to randomizationin part to remove non-compliant patients and reduce attritionduring the controlled trial (seeBisaga et al., 2005, for discus-sion of the use of a lead-in period in addiction pharmacotherapytrials). The purpose was also to divide the sample into those whobecome abstinent initially from those who continue to use. Theresultant subgroups (low versus high cocaine use during the lead-in) may have different responsiveness to medication, depend-ing on whether the medication works by preventing relapse inpatients who are able to become abstinent initially or by inducingabstinence in active users.
We now report results from a 12-week double-blind trial com-paring effects of a high dose of gabapentin (3200 mg/day) andplacebo in cocaine-dependent individuals. The primary goal ofthe study was to examine whether treatment with gabapentinwould result in a reduction of cocaine use and craving. The sec-ondary goal was to examine whether gabapentin may be moreeffective in patients who are able to achieve abstinence duringa lead-in period, compared to those who cannot quit during thelead-in, suggesting a primarily relapse-preventive mechanismsof medication action.
2. Methods
2.1. Participants
er-s ) Out-p itedf psy-c M-I buses tests,E Mena rentc ays int ajora there iates,s en-d ropica ysicald reg-n
2
long,s om-i ientsw ther-a mplesd ed too sifyp ber ofn wasf nts
ory conditions, inhibition of both self-administration as weleinstatement can be accomplished using GABA-ergic meion. If parallel effects were observed in humans, GABA-eedication should be effective both in the abstinence–indus well as in the relapse-prevention phase of treatment.
GABA-active medications, including baclofen, topiramnd tiagabine, have shown efficacy in preliminary controlinical trials for cocaine dependence (Gonzalez et al., 200ampman et al., 2004; Ling et al., 1998; Shoptaw et al., 20).fficacy of these medications has been shown both in paith a high level of cocaine use at baseline (Shoptaw et al., 2003)s well as in patients with a low level of cocaine use at basKampman et al., 2004).
In this report, we examine gabapentin, another GABA-eodulator that has been the subject of several recent studieedication facilitates GABA-ergic neurotransmission (Kocsisnd Honmou, 1994; Loscher et al., 1991) and increases humrain GABA levels (Petroff et al., 1996). Gabapentin, howevelso affects other receptor systems including excitatory acids and noradrenaline, as well as exerting direct effecalcium and potassium ion channels (Surges and Feuerste002; Taylor et al., 1998). Two case reports describe markeecreased cocaine cravings and cocaine use after initabapentin (Markowitz et al., 1997; Raby, 2000). In two open
abel trials, treatment with 800–2400 mg of daily gabapeecreased cocaine cravings and urine-confirmed cocainMyrick et al., 2001; Raby and Coomaraswamy, 2004). Finally,art et al. (2004)reported that gabapentin decreased the
ective effects but not self-administration of smoked cochen given at a dose of 1200 mg a day to non-treatment seocaine users.
-
s
is
n
g
e
-
g
Individuals who applied for treatment at Columbia Univity’s Substance Treatment and Research Service (STARSatient Research Clinic in New York City, USA, were recru
or this study. Clinical screening was conducted by clinicalhologists and included structured clinical interview for DSV (SCID I/P) and a clinical interview assessing substance aeverity. Medical assessment included history, laboratoryCG, a physical examination and a psychiatric evaluation.nd women, 18–60-year old, who met DSM criteria for curocaine dependence and had used cocaine at least 4 dhe previous month and were included. Individuals with mffective or psychotic disorder or ADHD were excluded. Oxclusion criteria included: (1) physical dependence on opedative-hypnotics or alcohol or if the principal drug of depence was not cocaine; (2) ongoing treatment with psychotgents or other substance use treatment; (3) unstable phisorders, which might make participation hazardous; (4) pancy or lactation.
.2. Study procedures
Following study consent, patients entered a 2-week-ingle-blind placebo lead-in period. To be eligible for randzation and continued participation in the treatment, patere required to attend at least one (out of two scheduled)py sessions and submit four (out of six scheduled) urine sauring the 2 weeks of lead-in. This requirement was designbtain sufficient number of urine samples to correctly clasatients’ lead-in level of cocaine use and to reduce the numon-compliant patients prior to randomization. The lead-in
ollowed by the 12-week double-blind trial in which patie

A. Bisaga et al. / Drug and Alcohol Dependence 81 (2006) 267–274 269
were randomized to receive placebo or gabapentin. After com-pleting the 12 weeks of a double-blind trial, patients entered a2-week long, single-blind medication taper and placebo lead-out phase. Patients who did not come for a visit to submit aurine sample for 14 consecutive days were classified as studydrop-outs and their participation in the study was discontinued.
Gabapentin 400 mg and matching placebo capsules were pro-vided by Parke-Davis Pharmaceuticals Ltd. A matching capsulecontaining 50 mg of riboflavin (added as urine marker to assesscompliance; see below) and lactose filler was manufactured bythe research pharmacy of the New York State Psychiatric Insti-tute. Throughout the 16 weeks of the study, participants receivedtwo medication bottles per day, the morning dose included fourmedication/placebo capsules and a capsule with riboflavin andthe evening dose included four medication/placebo capsules.Gabapentin dose was gradually increased to a target dose of1600 mg bid over the period of 15 days and at the treatmentcompletion was gradually stopped over a period of 7 days.
Participants were required to attend the clinic three times perweek. During each visit, patients gave an observed urine speci-men and completed self-reported measures of drug use, cravingand mood. At each visit, a research nurse obtained vital signs,inquired about side-effects, collected unused medication anddispensed a new supply of medication. During the lead-in period,urine samples were tested on site using on trak test sticks (Roche)for cocaine and these results were used for stratification (seeb set entE ndeU indic ntiono pantw strum 5 fof
ienta inicap eekl rap( t-m iorars apist t. Ats withr treatm nce
2
vest om-i g tot cainu use)T orm grou
included patients who provided one or no cocaine-negative urinespecimens. We hypothesize that there might be a differentialeffect of gabapentin in patients who are actively using cocaineat the time of medication initiation (i.e. abstinence–inductioneffect) versus patients who were abstinent at the time of medi-cation initiation (relapse-prevention effect). In addition, cocaineuse at the initiation of the study has been found to be predictive oftreatment outcome (Alterman et al., 1997; Ehrman et al., 2001).The second parameter was the principal route of cocaine admin-istration (smoking versus intranasal), which has also been foundto be predictive of treatment outcome (Nunes et al., 1995). Thedistribution of the subjects across the four groups was as follows:29 and 23 for smokers (high and low); 27 and 20 for intranasalusers (high and low).
2.4. Outcome measures
The primary outcome measure was a binary response(cocaine use/no cocaine use) indicating whether a new episodeof cocaine use occurred for each day of the trial. This was deter-mined using the method ofPreston et al. (1997), which appliespharmacokinetic criteria to semi-quantitative data on benzoylec-gonine concentration to identify occasions of new drug use.Urine samples that are cocaine positive but do not meet criteriafor a new use day are considered a carry-over from a previoususe episode, thereby preventing overestimation of drug use.
daysp num-b ving.I (1:a of non reat-m yondt
2
tiona ancel oupsu istic.A Time-c treat-m cainec oddso lizede OC-G tw eablea sistenta st, wee rs int ntry)c Next,w levela oundn d
elow). During the treatment phase, urine specimens wereo the laboratory for quantitative benzoylecgonine assessmach urine sample submitted during the trial was observed uV light for fluorescence and any absence of fluorescence,ating medication non-compliance, was brought to the attef treatment team and was discussed with patient. Particiere reimbursed for the time taken to complete research inents, US$ 10 per week during the treatment and US$ 2
ollow-up visits.Once per week throughout 16 weeks of treatment, pat
ttended an individual therapy session conducted by a clsychologist. The first two therapy sessions during the 2-w
ead-in included elements of motivational enhancement theMiller and Rollnick, 1991) and for the remainder of treaent participants received manual-guided cognitive-behav
elapse-prevention intervention (Carroll et al., 1994). Randomessions were audio taped and reviewed by the team of thero provide ongoing supervision and prevent therapeutic driftudy consent and every 2 weeks thereafter, patients metesearch psychiatrist who monitored patients’ progress inent including the review of medication safety and adhere
.3. Stratification
A research pharmacist who was independent of the inigative team conducted randomization. Prior to the randzation, patients were stratified into four groups accordinwo parameters. The first parameter was the level of cose during the 2 weeks of lead-in (low use versus highhe low-use group included patients who provided twoore cocaine-negative urine specimens and the high-use
nts.r-
s-r
sl
y
l
ts
a-.
-
e.
p
The secondary outcome measure was the proportion ofer week craving cocaine. This was based on self-reporteder of days in which participants experienced cocaine cra
n addition, we examined a binary indicator of abstinencebstinent; 0: otherwise), defined as 3 consecutive weeksew cocaine use at any time during the trial and retention in tent, defined as the number of study weeks completed be
he 2-week lead-in (range 1–12 weeks).
.5. Data analyses
All analyses were performed on the intent-to-treat populand all statistical tests were two-tailed at the .05 signific
evel. Retention in treatment was compared between grsing Kaplan–Meier survival curves and the Log-Rank statbstinence rates were compared using chi-square test.ourse analyses were performed to examine the effects ofent and stratification assignment on cocaine use and co
raving, over the 84 days of the study. We modeled thef cocaine use over the course of the study using generastimating equations (GEE, as implemented by SAS’s PRENMOD) with logit link function. Models with differenorking correlations were specified (independent, exchangnd autoregressive) and the estimates obtained were concross all structures. Robust estimates are reported. Firxamined a model with treatment condition and day as factohe model adjusted for baseline (30 days prior to treatment eocaine use (dollar amount per week spent on cocaine).e examined the effect of the stratification assignment (nd route) on the outcome. Route of administration was fot to be predictive (p > .20, for all terms involving route) an
270 A. Bisaga et al. / Drug and Alcohol Dependence 81 (2006) 267–274
was excluded from the model. Age and baseline dollar amountspent on cocaine were examined as a potential confounders inthe model with treatment and level of use as predictors, but werefound not to correlate with the outcome or interact with the otherfactors in the model and were subsequently removed. The finalmodel included treatment condition, lead-in level of use and timeas factors in the model. Model fit was assessed using devianceand Pearson chi-square criteria as well as examination of resid-ual plots. The craving outcome was similarly analyzed usingGEE, with constant variance and identity link function.
3. Results
3.1. Sample description
We screened 1063 individuals for eligibility. Of thosescreened in person, 349 did not meet study inclusion criteria and585 failed to complete the evaluation or were unable to committo thrice weekly study visits. Presence of comorbid psychiatricdisorders (mainly major depression and ADHD), a low level ofcocaine use and coexisting medical conditions were the mostcommon reasons for exclusion from study participation. A totalof 129 individuals consented to the study and entered the singleblind, placebo lead-in phase. Thirty participants who consentedwere not eligible for randomization due to non-compliance withstudy requirements during a 2-week long, single-blind placebol
ales4 20%w rang2 were or tos ollaa US
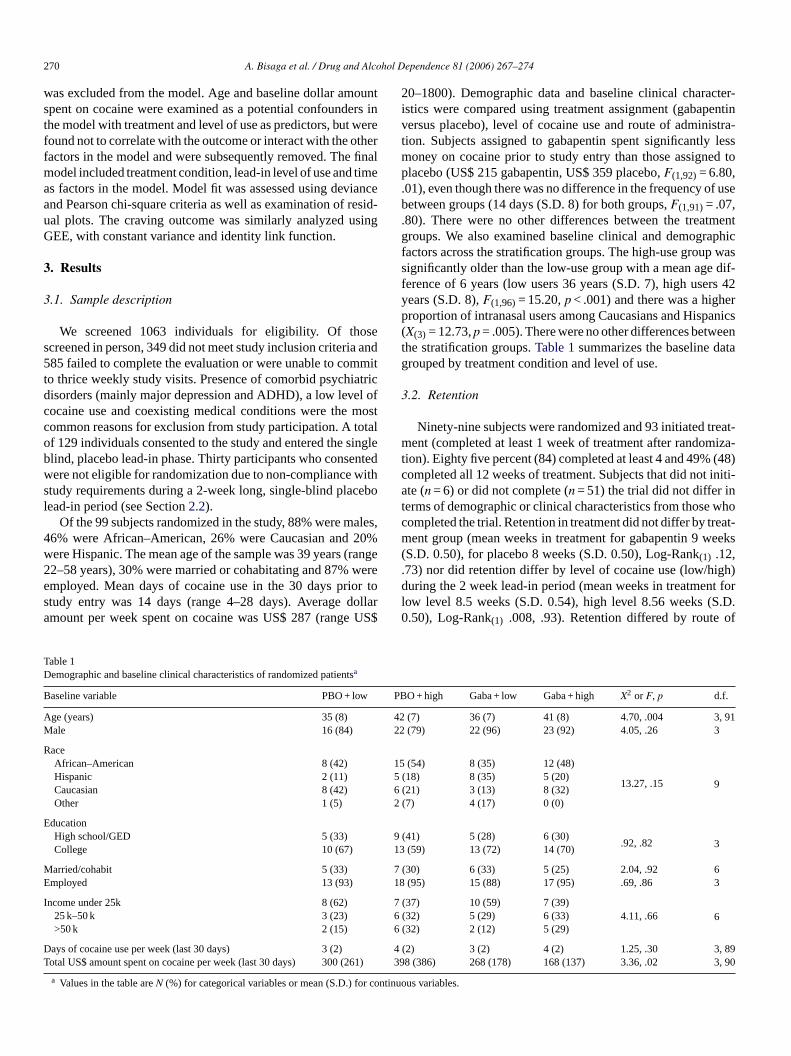
20–1800). Demographic data and baseline clinical character-istics were compared using treatment assignment (gabapentinversus placebo), level of cocaine use and route of administra-tion. Subjects assigned to gabapentin spent significantly lessmoney on cocaine prior to study entry than those assigned toplacebo (US$ 215 gabapentin, US$ 359 placebo,F(1,92)= 6.80,.01), even though there was no difference in the frequency of usebetween groups (14 days (S.D. 8) for both groups,F(1,91)= .07,.80). There were no other differences between the treatmentgroups. We also examined baseline clinical and demographicfactors across the stratification groups. The high-use group wassignificantly older than the low-use group with a mean age dif-ference of 6 years (low users 36 years (S.D. 7), high users 42years (S.D. 8),F(1,96)= 15.20,p < .001) and there was a higherproportion of intranasal users among Caucasians and Hispanics(X(3) = 12.73,p = .005). There were no other differences betweenthe stratification groups.Table 1summarizes the baseline datagrouped by treatment condition and level of use.
3.2. Retention
Ninety-nine subjects were randomized and 93 initiated treat-ment (completed at least 1 week of treatment after randomiza-tion). Eighty five percent (84) completed at least 4 and 49% (48)completed all 12 weeks of treatment. Subjects that did not initi-ate (n = 6) or did not complete (n = 51) the trial did not differ int whoc eat-m eeks(. gh)d t forl .D.0 of
TD s
B
A 4 , 91M 2
R15
2
E91
M 7E 1
I66
D 3, 89T 1) 3, 90
r con
ead-in period (see Section2.2).Of the 99 subjects randomized in the study, 88% were m
6% were African–American, 26% were Caucasian andere Hispanic. The mean age of the sample was 39 years (2–58 years), 30% were married or cohabitating and 87%mployed. Mean days of cocaine use in the 30 days pritudy entry was 14 days (range 4–28 days). Average dmount per week spent on cocaine was US$ 287 (range
able 1emographic and baseline clinical characteristics of randomized patienta
aseline variable PBO + low
ge (years) 35 (8)ale 16 (84)
aceAfrican–American 8 (42)Hispanic 2 (11)Caucasian 8 (42)Other 1 (5)
ducationHigh school/GED 5 (33)College 10 (67)
arried/cohabit 5 (33)mployed 13 (93)
ncome under 25k 8 (62)25 k–50 k 3 (23)>50 k 2 (15)
ays of cocaine use per week (last 30 days) 3 (2)otal US$ amount spent on cocaine per week (last 30 days) 300 (26
a Values in the table areN (%) for categorical variables or mean (S.D.) fo
,
ee
r$
erms of demographic or clinical characteristics from thoseompleted the trial. Retention in treatment did not differ by trent group (mean weeks in treatment for gabapentin 9 w
S.D. 0.50), for placebo 8 weeks (S.D. 0.50), Log-Rank(1) .12,73) nor did retention differ by level of cocaine use (low/hiuring the 2 week lead-in period (mean weeks in treatmen
ow level 8.5 weeks (S.D. 0.54), high level 8.56 weeks (S.50), Log-Rank(1) .008, .93). Retention differed by route
PBO + high Gaba + low Gaba + high X2 or F, p d.f.
2 (7) 36 (7) 41 (8) 4.70, .004 32 (79) 22 (96) 23 (92) 4.05, .26 3
5 (54) 8 (35) 12 (48)
13.27, .15 9(18) 8 (35) 5 (20)
6 (21) 3 (13) 8 (32)(7) 4 (17) 0 (0)
(41) 5 (28) 6 (30).92, .82 33 (59) 13 (72) 14 (70)
(30) 6 (33) 5 (25) 2.04, .92 68 (95) 15 (88) 17 (95) .69, .86 3
7 (37) 10 (59) 7 (39)4.11, .66 6(32) 5 (29) 6 (33)
(32) 2 (12) 5 (29)
4 (2) 3 (2) 4 (2) 1.25, .30398 (386) 268 (178) 168 (137) 3.36, .02
tinuous variables.
A. Bisaga et al. / Drug and Alcohol Dependence 81 (2006) 267–274 271
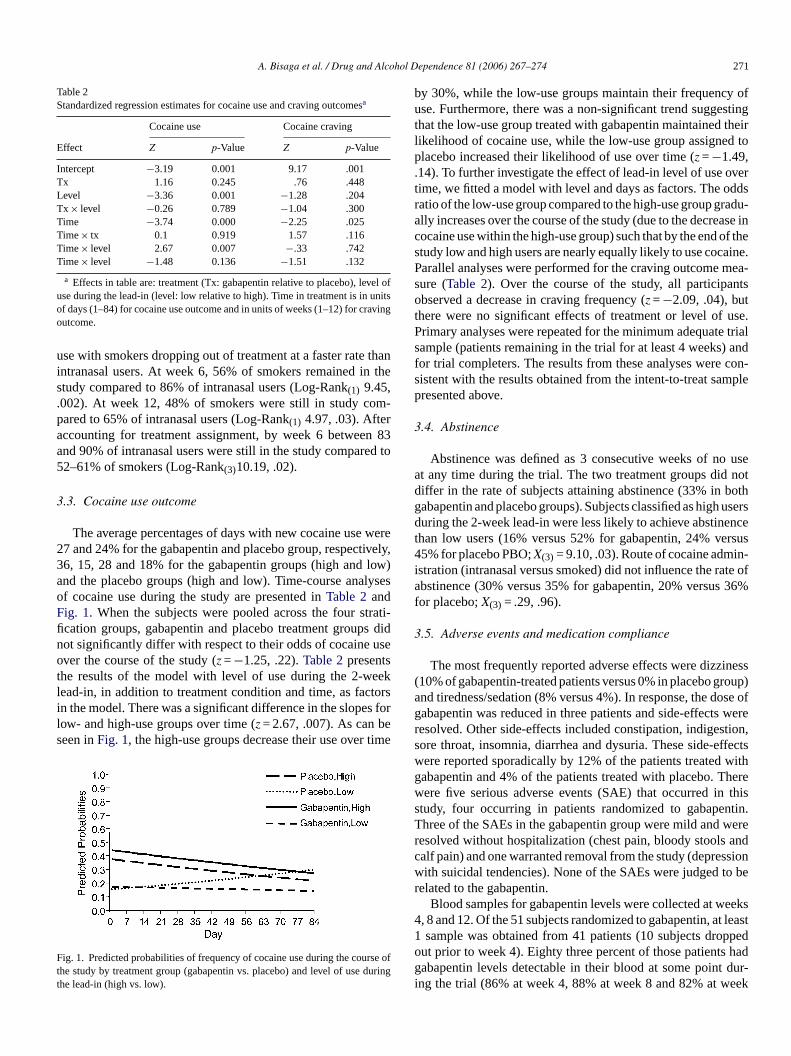
Table 2Standardized regression estimates for cocaine use and craving outcomesa
Cocaine use Cocaine craving
Effect Z p-Value Z p-Value
Intercept −3.19 0.001 9.17 .001Tx 1.16 0.245 .76 .448Level −3.36 0.001 −1.28 .204Tx × level −0.26 0.789 −1.04 .300Time −3.74 0.000 −2.25 .025Time× tx 0.1 0.919 1.57 .116Time× level 2.67 0.007 −.33 .742Time× level −1.48 0.136 −1.51 .132
a Effects in table are: treatment (Tx: gabapentin relative to placebo), level ofuse during the lead-in (level: low relative to high). Time in treatment is in unitsof days (1–84) for cocaine use outcome and in units of weeks (1–12) for cravingoutcome.
use with smokers dropping out of treatment at a faster rate thanintranasal users. At week 6, 56% of smokers remained in thestudy compared to 86% of intranasal users (Log-Rank(1) 9.45,.002). At week 12, 48% of smokers were still in study com-pared to 65% of intranasal users (Log-Rank(1) 4.97, .03). Afteraccounting for treatment assignment, by week 6 between 83and 90% of intranasal users were still in the study compared to52–61% of smokers (Log-Rank(3)10.19, .02).
3.3. Cocaine use outcome
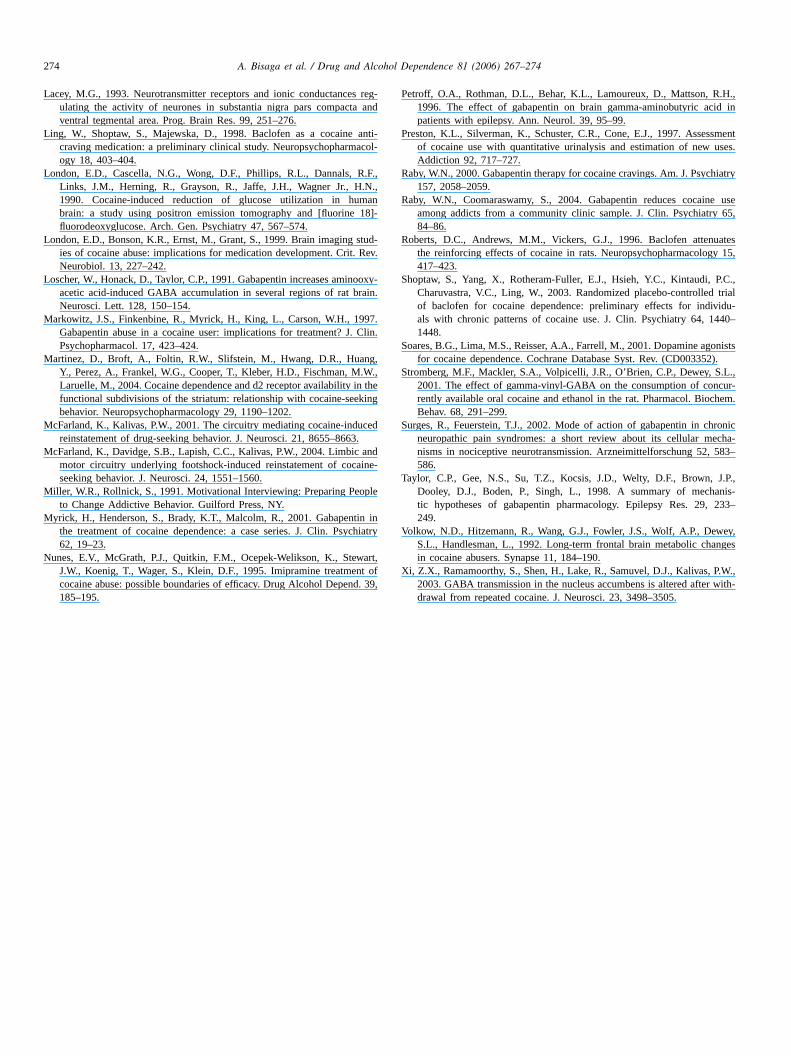
The average percentages of days with new cocaine use we27 and 24% for the gabapentin and placebo group, respectivel36, 15, 28 and 18% for the gabapentin groups (high and lowand the placebo groups (high and low). Time-course analyseof cocaine use during the study are presented inTable 2andFig. 1. When the subjects were pooled across the four stratification groups, gabapentin and placebo treatment groups dinot significantly differ with respect to their odds of cocaine useover the course of the study (z =−1.25, .22).Table 2presentsthe results of the model with level of use during the 2-weeklead-in, in addition to treatment condition and time, as factorsin the model. There was a significant difference in the slopes folow- and high-use groups over time (z = 2.67, .007). As can beseen inFig. 1, the high-use groups decrease their use over time
F rse ot durint
by 30%, while the low-use groups maintain their frequency ofuse. Furthermore, there was a non-significant trend suggestingthat the low-use group treated with gabapentin maintained theirlikelihood of cocaine use, while the low-use group assigned toplacebo increased their likelihood of use over time (z =−1.49,.14). To further investigate the effect of lead-in level of use overtime, we fitted a model with level and days as factors. The oddsratio of the low-use group compared to the high-use group gradu-ally increases over the course of the study (due to the decrease incocaine use within the high-use group) such that by the end of thestudy low and high users are nearly equally likely to use cocaine.Parallel analyses were performed for the craving outcome mea-sure (Table 2). Over the course of the study, all participantsobserved a decrease in craving frequency (z =−2.09, .04), butthere were no significant effects of treatment or level of use.Primary analyses were repeated for the minimum adequate trialsample (patients remaining in the trial for at least 4 weeks) andfor trial completers. The results from these analyses were con-sistent with the results obtained from the intent-to-treat samplepresented above.
3.4. Abstinence
Abstinence was defined as 3 consecutive weeks of no useat any time during the trial. The two treatment groups did notdiffer in the rate of subjects attaining abstinence (33% in bothg usersd encet ersus4 in-i te ofa 36%f
3
iness( roup)a ose ofg werer tion,s ffectsw withg herew thiss ntin.T werer andc ssionw o ber
eeks4 t least1 ppedo hadg dur-i eek
ig. 1. Predicted probabilities of frequency of cocaine use during the couhe study by treatment group (gabapentin vs. placebo) and level of usehe lead-in (high vs. low).
rey,)s
-d
r
fg
abapentin and placebo groups). Subjects classified as highuring the 2-week lead-in were less likely to achieve abstin
han low users (16% versus 52% for gabapentin, 24% v5% for placebo PBO;X(3) = 9.10, .03). Route of cocaine adm
stration (intranasal versus smoked) did not influence the rabstinence (30% versus 35% for gabapentin, 20% versus
or placebo;X(3) = .29, .96).
.5. Adverse events and medication compliance
The most frequently reported adverse effects were dizz10% of gabapentin-treated patients versus 0% in placebo gnd tiredness/sedation (8% versus 4%). In response, the dabapentin was reduced in three patients and side-effectsesolved. Other side-effects included constipation, indigesore throat, insomnia, diarrhea and dysuria. These side-eere reported sporadically by 12% of the patients treatedabapentin and 4% of the patients treated with placebo. Tere five serious adverse events (SAE) that occurred intudy, four occurring in patients randomized to gabapehree of the SAEs in the gabapentin group were mild andesolved without hospitalization (chest pain, bloody stoolsalf pain) and one warranted removal from the study (depreith suicidal tendencies). None of the SAEs were judged t
elated to the gabapentin.Blood samples for gabapentin levels were collected at w
, 8 and 12. Of the 51 subjects randomized to gabapentin, asample was obtained from 41 patients (10 subjects dro
ut prior to week 4). Eighty three percent of those patientsabapentin levels detectable in their blood at some point
ng the trial (86% at week 4, 88% at week 8 and 82% at w

272 A. Bisaga et al. / Drug and Alcohol Dependence 81 (2006) 267–274
12). Mean gabapentin blood level across all three measurementsfor the group was 2.60 mcg/ml (S.D. 2.34, range 0.0–8.8); 2.66(S.D. 2.32) mcg/ml at week 4, 2.75 (S.D. 2.06) mcg/ml at week8 and 3.01 (S.D. 1.776) mcg/ml at week 12). These averagedlevels are less than half of what would be expected with chronicmaintenance on gabapentin (Kuzniecky et al., 2002) suggestingmoderate levels of medication compliance in this study.
We examined whether compliance with medication inpatients treated with gabapentin was related to outcome. Using amedian split on mean gabapentin levels we classified those sub-jects at or above the median (1.87 mcg/ml) as medication com-pliant and those below the median as medication non-compliant.There was no significant difference between compliant and non-compliant subjects in the proportion of days with new cocaineuse [compliant .30 (.21), non-compliant .26 (.22),p = .53]. Wealso correlated mean gabapentin levels with the number of daysof new use and number of weeks in treatment and found nosignificant correlation between either (p > .30). Self-reportedcompliance was also examined. Subjects reported compliancethree times per week. There was no significant correlation of self-reported compliance with the days of new cocaine use outcomefor the whole sample (r =−.04,p = .73) or for the gabapentin orplacebo treatment groups (r = .08,p = .65 andr =−.18,p = .30,respectively).
4. Discussion
sug-g indi-v ento encb e rato ainec trial.
eriest nt oc 1;R nt lts au de-q entsH foret ed tp pham trialt ugho tivem limi ns.
withg s og pentv oseo tudyw al tri-a withn show
to be more effective than lower doses in blunting cocaine’s sub-jective effects (Hart et al., 2004).
Compared to low-level users, participants classified as highlevel users during the 2-week lead-in were less likely to achieveabstinence during the trial. There was a 30% reduction inthe frequency of cocaine use in the high-level use groups,while no further reduction was observed in the low-use groups.Both gabapentin and placebo-treated high-use patients grad-ually reduced the frequency of cocaine use as the treatmentprogressed, but by the end of the study low and high users wereequally likely to use cocaine. This suggests that that the clas-sification of cocaine users into low and high-use groups duringthe 2-week lead-in may be useful for predicting outcome duringthe study, as it has been shown previously (Bisaga et al., 2005),but may not be indicative of longer term drug use (as the mea-surements over time appear to be subject to regression to themean).
Route of cocaine administration was a significant predictor ofearly retention, with smokers dropping out of treatment at a fasterrate than intranasal users. This has been found previously andhighlights the difficulty studying treatments in cocaine-smokers(Agosti et al., 1996). Self-reports showed that cocaine cravinggenerally decreased over time in all patients, but there was nostatistically significant effect of treatment, level of use or routeof administration on the craving.
Among participants with low level of cocaine use during the2 stingt tcomec eivedg dur-i rad-u tmentp . Thefi denti tudyr ial oft i-c oddso reas-i ffecto inedw rgicm ablet lapsep ayb e att witha ot tivem dencet t alsos ationsa es ofc eitherp par-t ly tot
The results of this randomized, placebo-controlled trialest that gabapentin (3200 mg/day) combined with weeklyidual psychotherapy, is not broadly effective for the treatmf cocaine dependence. There was no significant differetween the gabapentin and placebo treatment groups in thf achieving abstinence, retention in treatment, level of cocraving or the likelihood of cocaine use during the 12-week
Our finding is in contrast to previous reports of case shat have found gabapentin to be useful in the treatmeocaine dependence (Markowitz et al., 1997; Myrick et al., 200aby, 2000; Raby and Coomaraswamy, 2004). Generally, whe
here is no difference between treatment groups, the resusually more difficult to interpret (e.g. study might have inauate power to detect smaller differences between treatmowever, the present study is well-controlled, and there
he findings can be considered more conclusive comparrevious studies. In previous trials of cocaine dependenceacotherapies, positive findings were often seen in open
hat were later not confirmed with controlled trials. Even thopen label trials may be useful for ruling out clearly ineffecedications, the present study provides an example of the
ted use of open label trials in detecting effective medicatioOther differences between this and previous studies
abapentin include the use of different target doseabapentin. Prior studies have used daily doses of gabaarying from 800 to 2400 mg, while we have tested a daily df 3200 mg. It could be that a higher dose, as used in our sould be less effective than lower doses used in other clinicls. However, this seems unlikely since in laboratory studieson-treatment seekers higher doses of gabapentin were
ees
f
re
).,or-s
-
fin
,
n
-week lead-in, there was a non-significant trend suggehat gabapentin-treated subjects had a more favorable ouompared to placebo-treated individuals. Patients that recabapentin continued to maintain low levels of use achieved
ng the lead-in period, while patients treated with placebo gally increased their frequency of cocaine use as the trearogressed. No such effect was seen in the high-use groupnding of a differential treatment effect in cocaine-depenndividuals that have a low baseline level of cocaine use at sandomization has been seen previously in a treatment tropiramate (Kampman et al., 2004), another GABA-ergic antonvulsant medication. Over the 13 weeks of this trial, thef use decreased in the topiramate-treated group, while inc
ng in the placebo-treated group, although in this study, the ef topiramate in higher level users was not evaluated. Combith our results, these findings might suggest that GABA-eedication may be more effective in patients that were
o achieve initial abstinence, and therefore, may have a rereventive effect. This is different from medication that me more effective in patients who continue with active us
rial outset (i.e. abstinence–induction effect) as is the casemantadine (Kampman et al., 2000). These findings point t
he importance of distinguishing between the effect of putaedication on the two separate phases of cocaine depen
reatment: abstinence–induction and relapse-prevention. Iuggests that a treatment approach that combines medics well as psychosocial interventions aimed at both phasocaine dependence treatment could be more effective byroviding a broader, and therefore, stronger effect for each
icipant or by targeting patients that may respond selectivereatments directed at either one of these phases (seeCarroll et

A. Bisaga et al. / Drug and Alcohol Dependence 81 (2006) 267–274 273
al., 2004for a discussion on strategies for combining medicationand therapy in medication development trials).
Finally, the detected serum gabapentin levels were relativelylow suggesting that many patients were not compliant withmedication. This may further confound conclusions about theeffectiveness of gabapentin although the level of medicationcompliance did not seem to be related to treatment outcome.
Among the strengths of this study are frequent quantita-tive and qualitative measures of drug-use behavior and theimplementation of a lead-in period to reduce the number ofnon-compliant patients from the randomized trial. There were,however, several weaknesses of the present study that may limitits generalizability. The population of patients selected for thisstudy might not have been representative of the general pop-ulation applying for cocaine dependence treatment. Candidateswith several psychiatric comorbidities as well as those who wereunable to complete study screening or commit to required inten-sity of study visits were excluded from participation. Patientswho did not complete lead-in period were also excluded, furtherrarefying the sample. On the other hand, the study populationwas still heterogenous in terms of the key variables of routeand level of cocaine use (four strata). Another limitation ofthe present design is that sample size and power to test addi-tional hypotheses regarding the effect of medication in thesesubgroups was low. In future medication-screening trials, a morehomogenous population, where medication effect might be morer studa tronp d oa ilinge nenw thee not mons mmaf
n ofc chi-a more ntiot t waa ouga ilarf outs ertr hieva ishefia ctedw romp rgica ndei bstn hod( ina-t cinge
Acknowledgments
This work was supported by NIDA Center Grant DA09236and Grants: K23 DA00429 (Dr. Bisaga), K23 DA16743 (Dr.Aharonovich), K02 DA00288 (Dr. Nunes) and K02 DA00465(Dr. Levin). We wish to thank Marianne Awad, Ivana Huang,Erica Almquist, pharmacy staff, as well as Drs. Jami Rothenberg,David McDowell and the staff of STARS treatment program fortheir contribution to this project.
References
Agosti, V., Nunes, E., Ocepeck-Welikson, K., 1996. Patient factors relatedto early attrition from an outpatient cocaine research clinic. Am. J. DrugAlcohol Abuse 22, 29–39.
Alterman, A.I., Kampman, K., Boardman, C.R., Cacciola, J.S., Rutherford,M.J., McKay, J.R., Maany, I., 1997. A cocaine-positive baseline urine pre-dicts outpatient treatment attrition and failure to attain initial abstinence.Drug Alcohol Depend. 46, 79–85.
Bisaga, A., Aharonovich, E., Garawi, F., Levin, F.R., Rubin, E., Raby, W.N.,Vosburg, S.K., Nunes, E.V., 2005. Utility of lead-in period in cocainedependence pharmacotherapy trials. Drug Alcohol Depend. 77, 7–11.
Campbell, U.C., Lac, S.T., Carroll, M.E., 1999. Effects of baclofen on main-tenance and reinstatement of intravenous cocaine self-administration inrats. Psychopharmacology (Berlin) 143, 209–214.
Carroll, K.M., Rounsaville, B.J., Gordon, L.T., Nich, C., Jatlow, P., Bisigh-ini, R.M., Gawin, F.H., 1994. Psychotherapy and pharmacotherapy forambulatory cocaine abusers. Arch. Gen. Psychiatry 51, 177–187.
C ioralcohol
E urinepend.
F olve-ns in. Psy-
G neu-the
G i, K.,urines
omized
H 04.bjectiveend.
K .P.,with
K ei-ent
K depo-.
K f the
K ma-BA290,
K ring-ine,
elevant, should be studied to increase the efficacy of thend to reduce type II error. In our study, the presence of a ssychosocial treatment component may also have reducebility to detect the effectiveness of gabapentin (i.e. a ceffect). On the other hand, weakening the therapy compoould likely have resulted in a higher attrition rate, limitingfficacy of the trial. Further, the rates of abstinence were
hat high, suggesting there was room for medication to detrate an effect. Balancing such limitations remains a dileor clinical trials of this type (Carroll et al., 2004).
In summary, we have shown that in a sample populatioocaine-dependent individuals without comorbid major psytric disorders, gabapentin was well tolerated but was noffective than placebo when added to weekly relapse-preve
herapy. Level of cocaine use in the first 2 weeks of treatmengood predictor of cocaine use during the treatment, alth
t the completion of the trial, the likelihood of use was simor all subjects, regardless of the level of use at treatmentet. A non-significant trend suggests gabapentin might exelapse preventive effect in patients who were able to acbstinence at the outset of treatment, reminiscent of publndings with other anticonvulsants (Kampman et al., 2004),lthough this effect, if real at all, was too small to be deteith the limited sample size. Taken together with findings freclinical and other clinical studies, this suggests GABA-enticonvulsants may deserve further study in cocaine-depe
ndividuals and that designs should be considered in which aence is induced at the outset either with behavioral mete.g. voucher incentives or brief hospitalization) or a combion with other medications that might exert abstinence-induffects.
ygur
t
t-
ensh
-aed
nti-s
arroll, K.M., Kosten, T.R., Rounsaville, B.J., 2004. Choosing a behavtherapy platform for pharmacotherapy of substance users. Drug AlDepend. 75, 123–134.
hrman, R.N., Robbins, S.J., Cornish, J.W., 2001. Results of a baselinetest predict levels of cocaine use during treatment. Drug Alcohol De62, 1–7.
uchs, R.A., Evans, K.A., Parker, M.C., See, R.E., 2004. Differential invment of the core and shell subregions of the nucleus accumbeconditioned cue-induced reinstatement of cocaine seeking in ratschopharmacology (Berlin) 176, 459–465.
oldstein, R.Z., Volkow, N.D., 2002. Drug addiction and its underlyingrobiological basis: neuroimaging evidence for the involvement offrontal cortex. Am. J. Psychiatry 159, 1642–1652.
onzalez, G., Sevarino, K., Sofuoglu, M., Poling, J., Oliveto, A., GonsaGeorge, T.P., Kosten, T.R., 2003. Tiagabine increases cocaine-freein cocaine-dependent methadone-treated patients: results of a randpilot study. Addiction 98, 1625–1632.
art, C.L., Ward, A.S., Collins, E.D., Haney, M., Foltin, R.W., 20Gabapentin maintenance decreases smoked cocaine-related sueffects, but not self-administration by humans. Drug Alcohol Dep73, 279–287.
ampman, K.M., Volpicelli, J.R., Alterman, A.I., Cornish, J., O’Brien, C2000. Amantadine in the treatment of cocaine-dependent patientssevere withdrawal symptoms. Am. J. Psychiatry 157, 2052–2054.
ampman, K.M., Pettinati, H., Lynch, K.G., Dackis, C., Sparkman, T., Wgley, C., O’Brien, C.P., 2004. A pilot trial of topiramate for the treatmof cocaine dependence. Drug Alcohol Depend. 75, 233–240.
ocsis, J.D., Honmou, O., 1994. Gabapentin increases GABA-inducedlarization in rat neonatal optic nerve. Neurosci. Lett. 169, 181–184
uhar, M.J., Ritz, M.C., Boja, J.W., 1991. The dopamine hypothesis oreinforcing properties of cocaine. Trends Neurosci. 14, 299–302.
ushner, S.A., Dewey, S.L., Kornetsky, C., 1999. The irreversible gamaminobutyric acid (GABA) transaminase inhibitor gamma-vinyl-GAblocks cocaine self-administration in rats. J. Pharmacol. Exp. Ther.797–802.
uzniecky, R., Ho, S., Pan, J., Martin, R., Gilliam, F., Faught, E., Hetheton, H., 2002. Modulation of cerebral GABA by topiramate, lamotrigand gabapentin in healthy adults. Neurology 58, 368–372.
274 A. Bisaga et al. / Drug and Alcohol Dependence 81 (2006) 267–274
Lacey, M.G., 1993. Neurotransmitter receptors and ionic conductances reg-ulating the activity of neurones in substantia nigra pars compacta andventral tegmental area. Prog. Brain Res. 99, 251–276.
Ling, W., Shoptaw, S., Majewska, D., 1998. Baclofen as a cocaine anti-craving medication: a preliminary clinical study. Neuropsychopharmacol-ogy 18, 403–404.
London, E.D., Cascella, N.G., Wong, D.F., Phillips, R.L., Dannals, R.F.,Links, J.M., Herning, R., Grayson, R., Jaffe, J.H., Wagner Jr., H.N.,1990. Cocaine-induced reduction of glucose utilization in humanbrain: a study using positron emission tomography and [fluorine 18]-fluorodeoxyglucose. Arch. Gen. Psychiatry 47, 567–574.
London, E.D., Bonson, K.R., Ernst, M., Grant, S., 1999. Brain imaging stud-ies of cocaine abuse: implications for medication development. Crit. Rev.Neurobiol. 13, 227–242.
Loscher, W., Honack, D., Taylor, C.P., 1991. Gabapentin increases aminooxy-acetic acid-induced GABA accumulation in several regions of rat brain.Neurosci. Lett. 128, 150–154.
Markowitz, J.S., Finkenbine, R., Myrick, H., King, L., Carson, W.H., 1997.Gabapentin abuse in a cocaine user: implications for treatment? J. Clin.Psychopharmacol. 17, 423–424.
Martinez, D., Broft, A., Foltin, R.W., Slifstein, M., Hwang, D.R., Huang,Y., Perez, A., Frankel, W.G., Cooper, T., Kleber, H.D., Fischman, M.W.,Laruelle, M., 2004. Cocaine dependence and d2 receptor availability in thefunctional subdivisions of the striatum: relationship with cocaine-seekingbehavior. Neuropsychopharmacology 29, 1190–1202.
McFarland, K., Kalivas, P.W., 2001. The circuitry mediating cocaine-inducedreinstatement of drug-seeking behavior. J. Neurosci. 21, 8655–8663.
McFarland, K., Davidge, S.B., Lapish, C.C., Kalivas, P.W., 2004. Limbic andmotor circuitry underlying footshock-induced reinstatement of cocaine-seeking behavior. J. Neurosci. 24, 1551–1560.
Miller, W.R., Rollnick, S., 1991. Motivational Interviewing: Preparing People
M in inchiat
N wart,t of
d. 39
Petroff, O.A., Rothman, D.L., Behar, K.L., Lamoureux, D., Mattson, R.H.,1996. The effect of gabapentin on brain gamma-aminobutyric acid inpatients with epilepsy. Ann. Neurol. 39, 95–99.
Preston, K.L., Silverman, K., Schuster, C.R., Cone, E.J., 1997. Assessmentof cocaine use with quantitative urinalysis and estimation of new uses.Addiction 92, 717–727.
Raby, W.N., 2000. Gabapentin therapy for cocaine cravings. Am. J. Psychiatry157, 2058–2059.
Raby, W.N., Coomaraswamy, S., 2004. Gabapentin reduces cocaine useamong addicts from a community clinic sample. J. Clin. Psychiatry 65,84–86.
Roberts, D.C., Andrews, M.M., Vickers, G.J., 1996. Baclofen attenuatesthe reinforcing effects of cocaine in rats. Neuropsychopharmacology 15,417–423.
Shoptaw, S., Yang, X., Rotheram-Fuller, E.J., Hsieh, Y.C., Kintaudi, P.C.,Charuvastra, V.C., Ling, W., 2003. Randomized placebo-controlled trialof baclofen for cocaine dependence: preliminary effects for individu-als with chronic patterns of cocaine use. J. Clin. Psychiatry 64, 1440–1448.
Soares, B.G., Lima, M.S., Reisser, A.A., Farrell, M., 2001. Dopamine agonistsfor cocaine dependence. Cochrane Database Syst. Rev. (CD003352).
Stromberg, M.F., Mackler, S.A., Volpicelli, J.R., O’Brien, C.P., Dewey, S.L.,2001. The effect of gamma-vinyl-GABA on the consumption of concur-rently available oral cocaine and ethanol in the rat. Pharmacol. Biochem.Behav. 68, 291–299.
Surges, R., Feuerstein, T.J., 2002. Mode of action of gabapentin in chronicneuropathic pain syndromes: a short review about its cellular mecha-nisms in nociceptive neurotransmission. Arzneimittelforschung 52, 583–586.
Taylor, C.P., Gee, N.S., Su, T.Z., Kocsis, J.D., Welty, D.F., Brown, J.P.,Dooley, D.J., Boden, P., Singh, L., 1998. A summary of mechanis-
233–
V wey,nges
X P.W.,with-
to Change Addictive Behavior. Guilford Press, NY.yrick, H., Henderson, S., Brady, K.T., Malcolm, R., 2001. Gabapent
the treatment of cocaine dependence: a case series. J. Clin. Psy62, 19–23.
unes, E.V., McGrath, P.J., Quitkin, F.M., Ocepek-Welikson, K., SteJ.W., Koenig, T., Wager, S., Klein, D.F., 1995. Imipramine treatmencocaine abuse: possible boundaries of efficacy. Drug Alcohol Depen185–195.
ry
,
tic hypotheses of gabapentin pharmacology. Epilepsy Res. 29,249.
olkow, N.D., Hitzemann, R., Wang, G.J., Fowler, J.S., Wolf, A.P., DeS.L., Handlesman, L., 1992. Long-term frontal brain metabolic chain cocaine abusers. Synapse 11, 184–190.
i, Z.X., Ramamoorthy, S., Shen, H., Lake, R., Samuvel, D.J., Kalivas,2003. GABA transmission in the nucleus accumbens is altered afterdrawal from repeated cocaine. J. Neurosci. 23, 3498–3505.




















