
Peptide Deformylase: A New Target in Antibacterial, Antimalarial and Anticancer Drug Discovery
Upload
independentCategory
view
0download
0
DISTRIBUTEDThe
forMODELPARTNERING
Drug Discovery and DevelopmentDuane Roth and
Pedro Cuatrecasas
From CONNECT, La Jolla, Calif. and the Departments of Pharmacology
and of Internal Medicine,
University of California, San Diego,
January 2010
©2010 by the Ewing Marion Kauffman Foundation. All rights reserved.
The DistributedPartnering Model forDrug Discovery and
Development
Duane Roth1 and Pedro Cuatrecasas2
From CONNECT1, La Jolla, Calif. and the Departments of Pharmacology and of Internal
Medicine, University of California2, San Diego,[email protected]
Corresponding author:Duane Roth
Address:8950 Villa La Jolla Drive,
Suite A-124, La Jolla, Calif. 92037
Phone: 858 964 1300 Fax: 858 964 1301
Email: [email protected]

A b s t r a c t
The Distributed Partnering Model for Drug Discovery and Development 1
Abstract: The major contributors to therapeutic
innovations in the 20th century have been the
pharmaceutical companies, with biotechnology
companies adding significantly over the last twenty-five
years. However, these models increasingly have failed
in translating the advances of biomedical sciences into
innovative products. We suggest a modern-day paradigm
for efficiently advancing new therapeutic products. This
"distributed partnering" approach would involve four
distinct, independent organizations to collaborate in a
risk-adjusted manner to discover, define, develop, and
deliver innovative products.
The new model would feature the formation of
companies called product definition companies (PDC),
which would focus solely on advancing innovation
through the initial definition research phase. PDCs would
consist of a team of experienced professionals who would
raise funds to manage several projects simultaneously.
PDCs would acquire early stage discoveries from research
institutions and invest in defining product applications
with a goal of selling the successful ones to
pharmaceutical companies for further development
and delivery.

T h e F u l l y I n t e g r a t e d P h a r m a c e u t i c a l C o . ( P h a r m a ) M o d e l
The Distributed Partnering Model for Drug Discovery and Development2
The Fully IntegratedPharmaceutical Co.(Pharma) Model
Once upon a time, the United Statespharmaceutical industry was prolific in developingnew and innovative medicines. One of this paper’sauthorsrecently described the conditions that madethis model so successful over many decades.Throughout the 1970s, most large pharmacompanies had a president of research or vicepresident of research and development, whooversaw basic research (i.e., discovery). This personwas given a budget and great freedom to pursuethe science wherever it might lead. Once a discoverywas made with the potential for becoming a newproduct, a development team was formed to betterdefine a product under the supervision of the vicepresident of research and development. Thedevelopment team had representation from allrelevant disciplines, including marketing. Theseteams focused on accomplishing all the stepsnecessary to bring the product to market.
As the product moved through early clinical trialsand the Food and Drug Administration process, thedelivery team developed the marketing plan for salesteams to launch the product around the world. Thismodel was productive by any measure and resultedin a steady stream of innovative products. However,this model, for many reasons, now is failing,resulting in a major threat to new drug innovation.3, 4
What went wrong?In the 1970s, industry leadership began to shift
toward an emphasis on strict business practices.3Many large pharmas began to borrow these newbusiness principles (e.g., management by objectives,etc.) from non-research-intensive corporations tomanage discovery, product definition, anddevelopment. These management tools includedrigid scrutiny and tight controls of research projectsthrough quarterly reviews, timelines, and Ganttcharts. However, this approach is inappropriate forbasic scientific research in the biomedical sciences.Pharmas truly are unique research-intensive matrixorganizations, ultimate adhocracies 6, that operatethrough complex collaborations betweenprofessionals from multiple and diverse disciplines,such as chemistry, biology, development, regulatoryaffairs, patenting, marketing, informationtechnology, statistics, manufacturing, finance, and
many others. Furthermore, these professionals mustfunction in dynamic, changing, and complexenvironments.
Proper functioning of the discovery/definition/development process requires that its managementreside within the scientific staff. However, theincreased dominance of the commercial side ofpharmas (which demanded impossible degrees ofpredictability, tight controls of science andtechnology, and changing “choices” of whichprojects to pursue) ultimately led to a shift of controlfrom research to marketing and commercialpersonnel. As suggested3, managing the researchand development process in this way iscounterproductive. Virtually every project is “killed”for one reason or another along the way, oftenrather arbitrarily. Thus, most pharmas essentiallyhave become development companies managed byunimaginative marketing departments. Today, fewwould make the argument that the current pharmamodel of drug discovery and development is aproductive model for advancing innovation. Despitebillions of dollars of investment and numerousattempts to institute systems to encourageinnovation, the current state of pharma discoverycontinues to decline (Figure 1).
The Biotech ModelBiotech began in the late 1970s when leading
scientists began to explore innovations in biology todevelop new therapeutics. The concept became areality with discoveries of the methods of producingproteins through genetic engineering (recombinantDNA) and of cloning antibodies (monoclonalantibodies).
In the early days, investments in biotech weremade almost instinctively, based on the excitement ofpotentially applying new biological methods toproduce therapeutics. Tom Perkins (founding partnerat Kleiner Perkins Caufield & Byers) described hisinvestment in Genentech Inc. as being based largelyon the enthusiasm of Bob Swanson, an excitedassociate partner. Swanson proposed to start a newventure in an entirely new industry based on thediscovery of Herb Boyer, a creative young academicscientist at the University of California, San Francisco.Perkins stated that after meeting with Swanson andBoyer, he and his partner, Eugene Kleiner, decided tofund a study to determine the feasibility of genesplicing (to produce proteins) and, if that worked, tofund Genentech. It did, and they did.
T h e B i o t e c h M o d e l
The Distributed Partnering Model for Drug Discovery and Development 3
An important concurrent development was thepassage of Bayh-Dole Act by the U.S. Congress in1980. This legislation allowed research institutes toown the intellectual property derived from federallyfunded research (e.g., National Institutes of Health(NIH), National Science Foundation (NSF), etc.). Thisaccelerated the formation of biotech startups toexploit the product definition anddevelopment of university-deriveddiscoveries. Further enthusiasm forfunding biotech startups was spurredby Genentech’s very successful initialpublic offering (IPO) in 1980.
The biotech model generallyoperated when entrepreneurs andventure capitalists organized to form anew company (i.e., a biotech) topursue commercialization of a licensedscientific discovery that arose frompublicly funded research. Much of theinitial funding was used to recruittechnical personnel and buildinfrastructure (i.e., laboratories,instrumentation, vivariums, pilotplants, etc.) similar to those existing inpharma, but on a smaller scale. These companiesinitially focused on product definition anddevelopment. As they advanced their lead product(s)
through development, they raised additional fundsfrom venture capitalists or sold equity in thecompany through IPOs. As the product developmentadvanced into late-stage clinical trials and theprospects of an FDA approval became realistic, mostbiotechs simply did not have the more extensiveinfrastructure or resources to conduct such studies
or to market the product. Thus, theearly biotechs partnered with largepharmas to advance the potential oftheir lead product(s). This modelbecame known as copartnering.
The goal of transitioning into anindependent, fully integrated pharmararely was achieved and copartneringwith—or acquisition by—pharmasbecame the prevalent outcome.
During the past twenty-five years,the biotech model produced a numberof successful products and companies.However, the evolution of biotech hasbeen so drastic that, as describedbelow, the existing model has becomeineffective and anachronistic in modern
times. More than half a trillion dollars have beeninvested in the biotech model over the past twenty-five years and, as detailed by Pisano, the overallreturn on investment has been negative.7
0
5
10
15
20
25
30
35
40
2004 2005 2006 2007 2008
36
2022
16
24
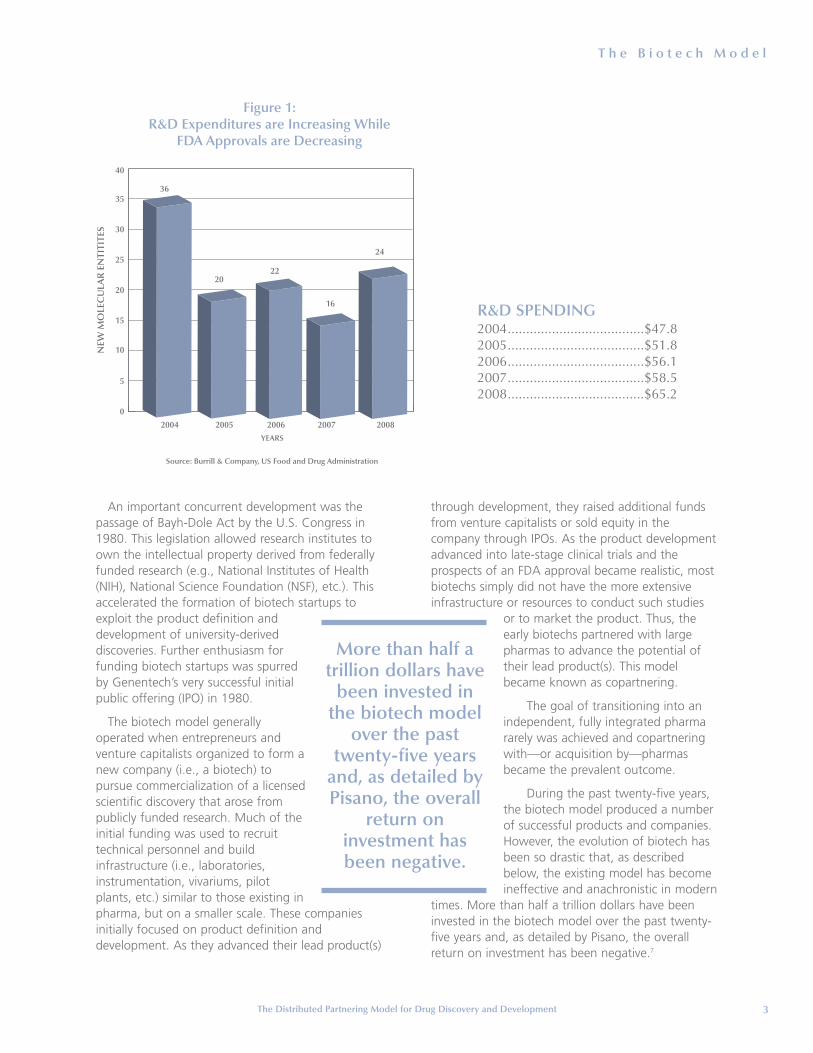
Figure 1: R&D Expenditures are Increasing While
FDA Approvals are Decreasing
Source: Burrill & Company, US Food and Drug Administration
YEARS
NEW
MO
LEC
ULA
R E
NTI
TITE
S
More than half atrillion dollars have
been invested inthe biotech model
over the pasttwenty-five years
and, as detailed byPisano, the overall
return oninvestment hasbeen negative.
R&D SPENDING2004.....................................$47.82005.....................................$51.82006.....................................$56.12007.....................................$58.52008.....................................$65.2

T h e B i o t e c h M o d e l
The Distributed Partnering Model for Drug Discovery and Development4
What went wrong?The very early product definition and development
success stories in biotech were nearly all based onthe recombinant DNA protein engineering andmonoclonal antibody technologies. In nearly allcases, the potential products were geneticallyengineered human proteins (some with slightvariation) of known function and role in thepathophysiology of diseases and all had highpotential for medical utility. The major challenge(other than intellectual property) was the large-scaleproduction of a highly purified human protein orantibody. Thus, the successes were known hormonesor growth factors, such as insulin, growth hormone,interferon, tissue plasminogen activator,erythropoietin and, later, monoclonal antibodies fortransplant rejection and cancer.
The early successes of these products andcompanies created much enthusiasm in theinvestment and academic communities, whichfueled hundreds of startup biotech companies. Overtime, the general definition of biotech evolved toinclude a broad scope of technologies involvingsmall molecules and diagnostics. The largerprofitable companies are referred to as “bigbiotechs” and function similarly to pharmas. Theterm “biotech” describes a small (usually a startup),innovative company focused on a single (or limited)biological or technology product.
In more recent times, the technologies,discoveries, and potential novel products have beenof a totally different nature in terms of “probabilityof success” when compared with the early biotechproducts. The projects have been highly innovativeand, thus, unpredictable, risky, and very likely toinvolve long-term commitments. Many of theprojects focus on small molecules, not proteins orantibodies. In effect, the research and developmentprojects have become similar to those with whichpharma deals. However, the small biotechs only cantackle one project (or a few) at a time and withinlimited time horizons. The venture capitalists andinvestors do not have the resources or patience forthese longer time horizons and the inevitablesetbacks and delays. Pharma, on the other hand,has, in principle, the capabilities and resources[although currently not the right organizationalprocedures or willingness 3] to handle many ofthese kinds of long-term projects simultaneously, topursue most things that look viable, and to re-workresearch when they experience impediments ordelays. Virtually every major successful product has
been afflicted with serious problems or setbacksduring development.3 The biotech model simplydoes not allow for such difficulties.
Today, even the most promising discoveries madein research institutes are seen by venture capitalistsas being too early and too risky for investing.Considerable efforts must be expended in analyticaland upscale chemistry, safety pharmacology,toxicology, formulations, metabolism, and manyother disciplines (preclinical development) before aspecific candidate can be deemed ready to proceedto human testing or to pharma licensing. Therefore,today’s venture capitalists prefer to invest intechnologies possessing well-identified leadcompounds with high probabilities of success thatare not far from entering clinical testing.Unfortunately, such opportunities almost never exist.
A New Model for“Distributed Partnering”in the 21st Century
The future of financing life science innovations willrequire new, more efficient, sustainable models thanthose of the current pharma and biotech models.2, 4
We propose a new model that involves theconcerted collaboration of multiple and variedorganizational partners. Here, the economic andtechnical risks along the discovery and developmentpaths are distributed and shared by independentpartners that contribute differing butcomplementary expertise, culture, and value in asequential process. The distributed partnering modelincludes four distinct, independent spheres thatcollaborate in a risk-adjusted manner to discover,define, develop, and deliver innovative products.
Discovery research As suggested by one of this paper’s authors and
recently documented by Block and Keller1, federaland state research funding have become the primarysources for discovery research. Fortunately, in theUnited States, the importance of funding suchresearch through federal agencies, such as the NIH,NSF, and Defense Advanced Research ProjectsAgency, now is accepted policy. In addition, manyinitiatives also are rising at the state level. Forexample, beginning in 2000, California was the firststate to fund basic discovery research with theestablishment of four publicly and privately financedinstitutes at the University of California and the

A N e w M o d e l f o r “ D i s t r i b u t e d P a r t n e r i n g ” i n t h e 2 1 s t C e n t u r y
The Distributed Partnering Model for Drug Discovery and Development 5
Governor Gray Davis Institutes for Science andInnovation. This investment was followed by voterapproval of Proposition 71 in 2004, a $3 billioneffort led by Robert Klein to establish the CaliforniaInstitute for Regenerative Medicine to fund stem cellresearch. Currently, more than a dozen states areinvesting in biomedical innovation andinfrastructure.
Numerous departments and centers oftranslational medicine and drug discovery now existthroughout the country. The nonprofit researchcommunity has responded with enthusiasm andenergy. The seeds for the future exploitation ofscientific advances for drug discovery already havebeen planted and the existing culture in academicsettings is perfect for this type of work3, althoughthe funding will have to be expandedsignificantly.
Once a grant has been awarded in agiven area of research, the recipientessentially is free to pursue the scienceregardless of where it leads, unlike thepharma and biotech models. The“management” of the science bynontechnical managers and theadministrative formalities are bothminimal. Instead, the scientists are incharge. Oversight occurs primarily, asit should, through peer review and thegranting agency. This culture cannotbe duplicated in pharma or biotech.The unrestricted pursuit of basicscience is essential to discovering theknowledge that can be the basis fornew product innovation.
Academic laboratories, successful in makingpotential new drug discoveries, eventually are facedwith technical and financial problems similar tothose in biotechs when proceeding to the nextstages of development, as described under “Whatwent wrong?” NIH translational grants have helped,but their scope is too limited, too focused, andthese grants rarely have extended to advancepreclinical development needs. As described, venturecapitalists simply will not fund this kind of earlystage work. Academic laboratories have limitedaccess to the funds or lack the expertise needed todo the advanced research and the early productdefinition required to move the project further. Inaddition, most academic researchers do not have theexperience, temperament, or even interest inundertaking most of this work. Unfortunately,
pharmas, like biotechs, usually are not a reasonableoption for handing off the work. They rarely areinterested in pursuing these early discoveries in theabsence of greater product definition. As a result,these potentially important early stage scientificdiscoveries are stifled by the absence of viablemechanisms for advancement.
Definition research Several approaches have been attempted to
address a means of providing product definition andearly development work (i.e., definition research) forinnovative academic discoveries. A recent reportfrom the Ewing Marion Kauffman Foundationdescribed two academic models that have beensuccessful in advancing early stage discoveries, the
Deshpande Center for TechnologicalInnovation at the MIT School ofEngineering and the William J. vonLiebig Center at the University ofCalifornia San Diego Jacobs School ofEngineering.5 Other approaches tofund early stage discoveries have beentried. They include incubators,accelerators, and virtual companies,most of which have the primary goalof starting new companies that facethe same challenges and funding risksdescribed above in the “What wentwrong?” biotech model.
Similar opportunity needs fordefinition research also occurfrequently in small biotechs. Here,potentially important discoveries are
abandoned because the biotech’s limited resourcesmust be focused on clinical-stage or other advancedprograms. Even in pharma, important discoveries areabandoned when they are not in sync with thecurrent strategic plan. To fulfill these unmet needsfor early product definition, we propose a new typeof innovation organization called a productdefinition company (PDC).
The PDC combines an experienced managementteam with investment capital to advance a portfolioof discoveries through the product definition stage.An ideal example of a PDC would be one involving asmall team of professionals highly experienced inareas, such as pharmaceutical research, clinicalsciences, regulatory affairs, operations, andmarketing. Some of these individuals would haveextensive contacts and knowledge of universities’early therapeutic discoveries for potential
The PDC combinesan experienced
management teamwith investment
capital to advance a portfolio ofdiscoveries through the
product definitionstage.

A N e w M o d e l f o r “ D i s t r i b u t e d P a r t n e r i n g ” i n t h e 2 1 s t C e n t u r y
The Distributed Partnering Model for Drug Discovery and Development6
acquisition. The combination of expert personnel,specific possible projects, and the unique businessmodel for the PDC would be the basis for raisingsufficient initial capital to launch the operation.Much of the work could be done on a virtual basis,contracting the development tasks to ProfessionalService Providers (PSP) to perform the key tasksrather than building new infrastructure. The use ofad hoc scientific experts and consultants would bestandard practice.
The PDC business model focuses on identifyingand licensing promising discoveries from researchinstitutes (and biotech/pharma). Licensees wouldreceive traditional up-front fees, milestones,royalties, and equity ownership. The PDC thenwould progress by undertaking (via PSPs) andsupervising the required productdefinition research for the acquiredprojects. The ultimate intention wouldbe to sell the risk-reduced “assetpackages” to third parties for furtherproduct development and delivery.Acquirers would include venturecapitalists, pharmas, and big biotechs.The venture capitalists most likelywould continue to fund advancedproduct development in a virtualmode, using PSPs rather than startingnew biotech companies as in theprevious model.
Typically, a PDC might investbetween $2 million and $10 million in a givenproject, depending on the cost required to achieveproof of relevancy8 for any given discovery within anaverage of three years. Proof of relevancy would bedefined on a case-by-case basis when third partiesjudge progress to be sufficiently attractive foracquisition. Given the early stage nature of mostdiscoveries under initial study, frequent technicalfailures during definition research would beexpected; many would probably occur early and,thus, be less costly. Even product definition failurescould create value through generation of valuableintellectual property.
The PDC would require initial investment fundssufficient to address multiple projects (i.e., ~ $50million to $100 million). Depending on the fundingand investment model selected, PDCs could beeither private or public companies. Potentialinvestors would include high net-worth individuals,hedge funds, strategic partners (includingpharma/big biotech, PSPs, etc.) and venture
capitalists. The investment basis would value theexpertise of the management team and its ability toevaluate and secure appropriate discoveries andtranslate them into potential products. The return onsuccessful projects could range from two times toten times that of invested funds upon completion ofadequate definition research, making this apotentially profitable model. (See appendix A).
PDCs certainly would locate in regions that havesignificant concentrations of biomedical researchinstitutions, such as San Diego, the San FranciscoBay area, and Boston, but they also could locatenear state universities and private institutes withmajor research efforts and funding. PDCs in theseregions could assist in advancing a culture that iscompatible with commercializing innovation. In the
recently published book, Start-UpNation, Dan Senor and Saul Singerdescribe Israel’s remarkable success intechnology innovation. They suggestthe creation of an innovative culture iskey to success on commercializingtechnology.9
Today, there are a multitude ofexcellent PSPs that can perform therequired technical work, as well as orbetter than biotechs and pharmas, atgreater efficiency and lower cost.Furthermore, many of these PSPs areso large, versatile, and experiencedthat they could tackle several different
aspects of the same project. Plus, all of the technicaland development work for the PDC projects wouldbe supervised and coordinated by experiencedproject managers.
Importantly, with the PSPs doing the development,technology transfer would occur in real-time as theknowledge would reside in the entities performingthe work. Thus, these technologies or productscould be even more valuable to those potentiallyinterested in acquiring the asset in the future. In thepharma and biotech models, the data for advancinga technology/product come primarily from thecompany’s assets (e.g., personnel, equipment, andfacilities), which are expensive and inefficient. Today,the data could come from anywhere in the world,and the costs are only for the required technicalwork. Lastly, many other PDC functions can beperformed on a virtual basis today, reducingunnecessary and expensive infrastructure andincreasing organizational nimbleness and flexibility.
The PDC businessmodel focuses
on identifying andlicensing promising
discoveries from researchinstitutes (and
biotech/pharma).

C o n c l u s i o n
The Distributed Partnering Model for Drug Discovery and Development 7
Development To complete the “development” of a new
product, delivery to the market still would require anumber of additional tasks before marketingapproval could be sought. Additional tasks includeformulation and dosage-form development,advanced clinical trials, upscale chemistry, long-termtoxicology, manufacturing technologies, andcomplex regulatory submissions, among otherrequirements. Venture capitalists could fund theseactivities either by forming a biotech, as in theexisting model, or by operating in a virtual mode byuse of PSPs as described above. For example, aventure capitalist may choose to fund advancedclinical trials (i.e., phase 2b, which is broadlydescribed in the industry as proof of concept) beforeselling the asset to pharma or big biotech for finalproduct development. Specialty funding companies,such as Symphony Capital, also could acquire PDCassets10 and would develop them in a manner similarto the venture capitalists. Alternatively, pharma andbig biotech would acquire the PDC asset at thisstage and, in a similar approach, fund the PSP to theproof of concept stage.
Delivery Subsequently, among the activities required are
marketing, manufacturing final product, distributionand sales, reimbursement arrangements, educationof medical and health professionals, consumers(patients) and payers (insurance companies andgovernment agencies), formulary registrations,global registrations, and post-marketing monitoringfor safety and efficacy. These tasks already areconducted effectively and managed by pharmas andbig biotechs. In fact, these tasks are the areas inwhich these corporations possess their greateststrengths.3, 4 The proposed model assumes that thesetypes of companies would acquire the potential newproducts arising from PDCs and introduce theproducts into their delivery pipelines.
ConclusionThe proposed new distributed partnering model
offers the potential for a more productive andefficient advancement of innovation and will beapplicable in any region with excellent research; itdoes not require legions of experiencedentrepreneurs or local established venture capitalistfirms to enact. The United States is well representedin each of the disciplines and cultures required in themodel:
• Discovery research (federal, state, andphilanthropic funding)
• Product definition and early development (large number of PSPs, vast industry experience,and entrepreneurial spirit)
• Advanced product development and delivery(extensive infrastructure, venture capitalistsinvestment funds, and some of the bestpharmas and big biotechs in the world)
This model focuses on advancing “products” asopposed to “companies” (i.e., we need thousandsof products not thousands of companies). Bycombining the expertise of these distinct culturesand organizations, innovative products could beadvanced efficiently, making the risks andinvestments more proportional to—and rationalfor—each partner. If successful, the United Statesmight continue, and even accelerate, its globaldominance in innovative medical products.
Finally, while this manuscript discusses theinnovative biomedical sector of innovation, themodel may well apply to other innovation sectors,including high-tech, information technology,cleantech, etc. As this early phase of innovationinvestment is crucial to the U.S. economy and toaddressing the nation’s most important challenges(e.g., higher quality, affordable healthcare; a cleanerenvironment; better security, etc.), the federalgovernment should consider a follow-on matchinginvestment to PDC private sector investors. Theprivate sector limited partners would set the termsand conditions with the federal government servingas an additional limited-partner investor. The federalinvestment covenants would be that the investmentsbe the first funding after seed, grants, etc. (i.e., pre-venture) in the technology and that a highpercentage of the investments (~80 percent) bemade in intellectual property technology that has afoundation in federal- or state-funded researchproject grants.
These investments will serve to grow our economyby immediately creating jobs in the crucialinnovation economy sector. Furthermore, whileinvestors may do well, society will be the greatestbeneficiary in terms of better health care, a cleanerenvironment, a more plentiful food supply, bettercommunications, and a safer world.
A p p e n d i x A
The Distributed Partnering Model for Drug Discovery and Development8
Year 1 Year 2 Year 3 Year 4 Year 5 Year 6 Year 7
Capital Related
GP $ 167 $ 167 $ 167 $ - $ - $ - $ -
Outside LPs 49,500 - - - - - -
Total Capital Related $ 49,667 $ 167 $ 167 $ - $ - $ - $ -
Fund Performance
LP Capital Invested $ (14,500) $ (14,500) $ (14,500) $ - $ - $ - $ -
LP Capital Returned - - - 8,250 16,500 16,500 8,250
LP Profit - - - 8,425 22,185 22,185 13,761
Total Capital Returned/ $ (14,500) $ (14,500) $ (14,500) $ 16, 675 $ 38,685 $ 38,685 $ 22,011
(Invested)
Management Fees (2,000) (2,000) (2,000) (2,000) (2,000) (400) (400)
GP Incentive Fees (1,685) (4,437) (4,437) (2,752)
Institution Incentive Fees (1,264) (3,328) (3,328) (2,064)
Total Fees $ (2,000) $ (2,000) $ (2,000) $ (4,949) $ (9,765) $ (8,165) $ (5,216)
Total Cash Inflow/(Outflow) $ (16,500) $ (16,500) $ (16,500) $ 11,726 $ 28,921 $ 30,521 $ 16,794
IRR 17%
Cash Inflow $ 38,462
Multiple of Capital Invested 1.8x
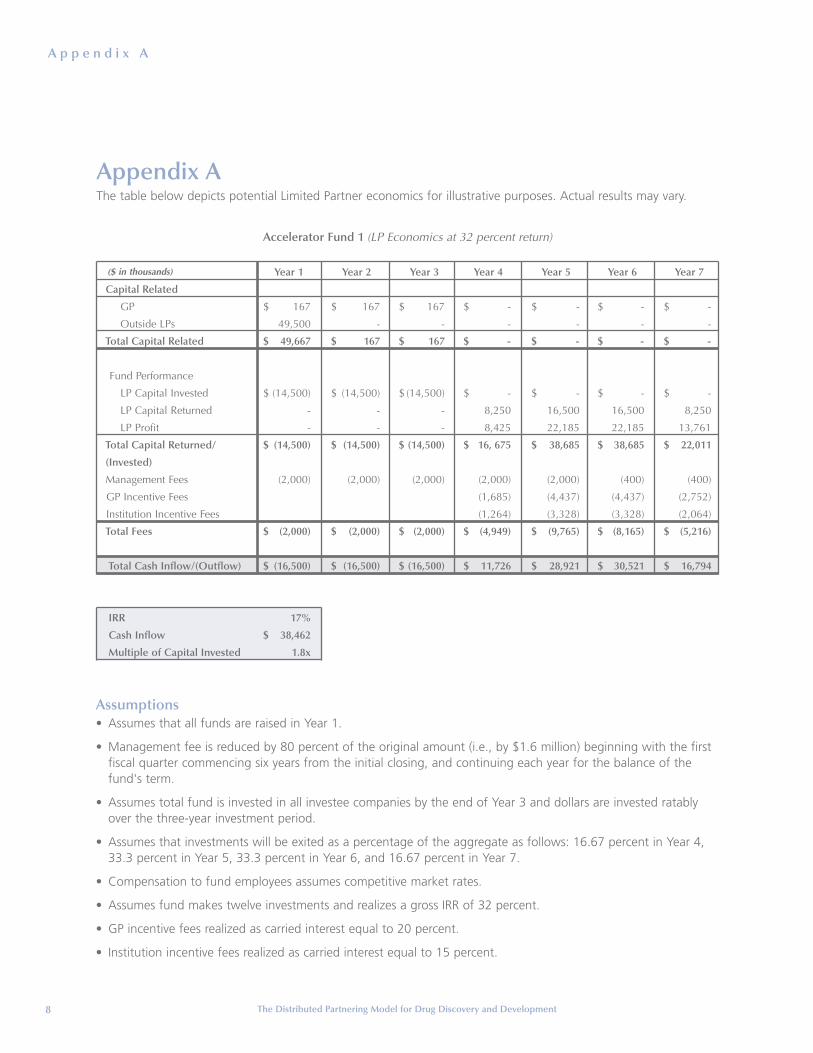
Accelerator Fund 1 (LP Economics at 32 percent return)
($ in thousands)
Appendix AThe table below depicts potential Limited Partner economics for illustrative purposes. Actual results may vary.
Assumptions• Assumes that all funds are raised in Year 1.
• Management fee is reduced by 80 percent of the original amount (i.e., by $1.6 million) beginning with the firstfiscal quarter commencing six years from the initial closing, and continuing each year for the balance of thefund's term.
• Assumes total fund is invested in all investee companies by the end of Year 3 and dollars are invested ratablyover the three-year investment period.
• Assumes that investments will be exited as a percentage of the aggregate as follows: 16.67 percent in Year 4,33.3 percent in Year 5, 33.3 percent in Year 6, and 16.67 percent in Year 7.
• Compensation to fund employees assumes competitive market rates.
• Assumes fund makes twelve investments and realizes a gross IRR of 32 percent.
• GP incentive fees realized as carried interest equal to 20 percent.
• Institution incentive fees realized as carried interest equal to 15 percent.
R e f e r e n c e s
The Distributed Partnering Model for Drug Discovery and Development 9
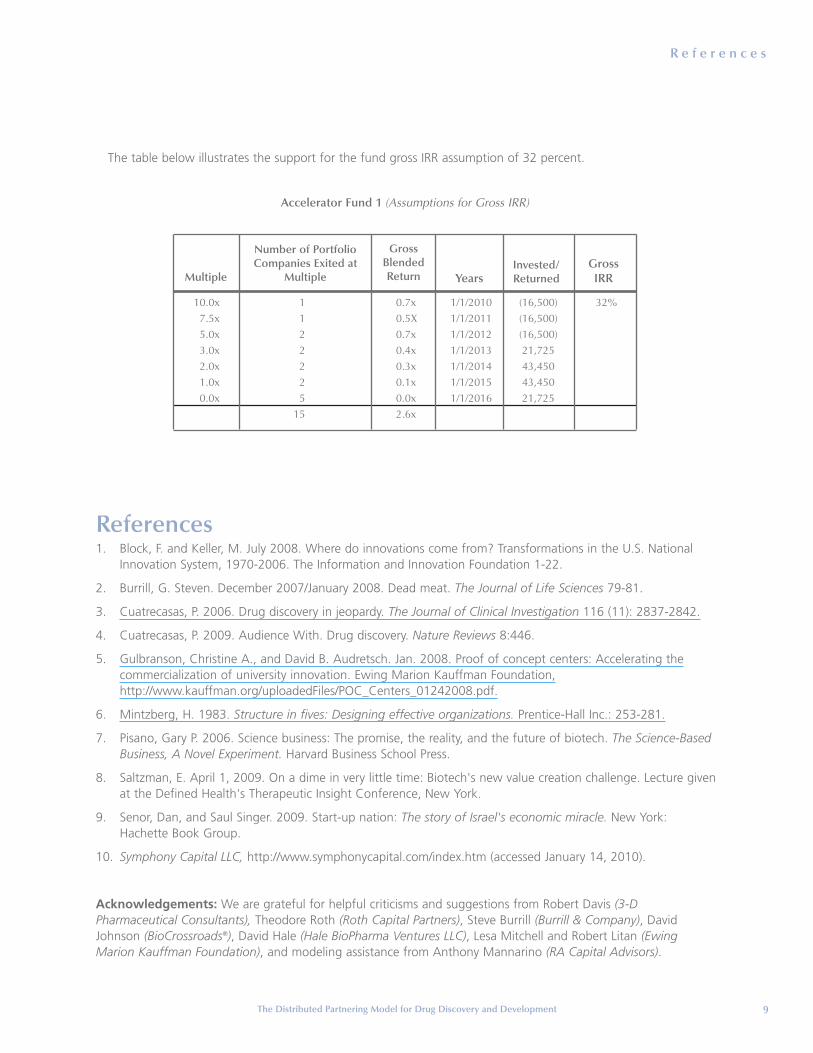
The table below illustrates the support for the fund gross IRR assumption of 32 percent.
Accelerator Fund 1 (Assumptions for Gross IRR)
10.0x 1 0.7x 1/1/2010 (16,500) 32%7.5x 1 0.5X 1/1/2011 (16,500)5.0x 2 0.7x 1/1/2012 (16,500)3.0x 2 0.4x 1/1/2013 21,7252.0x 2 0.3x 1/1/2014 43,4501.0x 2 0.1x 1/1/2015 43,4500.0x 5 0.0x 1/1/2016 21,725
15 2.6x
Multiple
Number of PortfolioCompanies Exited at
Multiple
GrossBlendedReturn Years
Invested/Returned
Gross IRR
References1. Block, F. and Keller, M. July 2008. Where do innovations come from? Transformations in the U.S. National
Innovation System, 1970-2006. The Information and Innovation Foundation 1-22.
2. Burrill, G. Steven. December 2007/January 2008. Dead meat. The Journal of Life Sciences 79-81.
3. Cuatrecasas, P. 2006. Drug discovery in jeopardy. The Journal of Clinical Investigation 116 (11): 2837-2842.
4. Cuatrecasas, P. 2009. Audience With. Drug discovery. Nature Reviews 8:446.
5. Gulbranson, Christine A., and David B. Audretsch. Jan. 2008. Proof of concept centers: Accelerating thecommercialization of university innovation. Ewing Marion Kauffman Foundation,http://www.kauffman.org/uploadedFiles/POC_Centers_01242008.pdf.
6. Mintzberg, H. 1983. Structure in fives: Designing effective organizations. Prentice-Hall Inc.: 253-281.
7. Pisano, Gary P. 2006. Science business: The promise, the reality, and the future of biotech. The Science-BasedBusiness, A Novel Experiment. Harvard Business School Press.
8. Saltzman, E. April 1, 2009. On a dime in very little time: Biotech's new value creation challenge. Lecture givenat the Defined Health's Therapeutic Insight Conference, New York.
9. Senor, Dan, and Saul Singer. 2009. Start-up nation: The story of Israel's economic miracle. New York:Hachette Book Group.
10. Symphony Capital LLC, http://www.symphonycapital.com/index.htm (accessed January 14, 2010).
Acknowledgements: We are grateful for helpful criticisms and suggestions from Robert Davis (3-DPharmaceutical Consultants), Theodore Roth (Roth Capital Partners), Steve Burrill (Burrill & Company), DavidJohnson (BioCrossroads®), David Hale (Hale BioPharma Ventures LLC), Lesa Mitchell and Robert Litan (EwingMarion Kauffman Foundation), and modeling assistance from Anthony Mannarino (RA Capital Advisors).
4801 ROCKHILL ROADKANSAS CITY, MISSOURI 64110
816-932-1000www.kauf fman.org
0110FP
Copyright © 2022 FDOKUMEN




















