Doctor–Patient Communication, Health-Related Beliefs, and Adherence in Glaucoma
11
Doctor–Patient Communication, Health-Related Beliefs, and Adherence in Glaucoma Results from the Glaucoma Adherence and Persistency Study David S. Friedman, MD, PhD, 1,2 Steven R. Hahn, MD, 3,4 Laurie Gelb, MPH, 5 Jason Tan, MS, 6 Sonali N. Shah, RPh, MPH, 7 Elizabeth E. Kim, MD, 7 Thom J. Zimmerman, MD, PhD, 8 Harry A. Quigley, MD 1 Objective: To use multiple data sources to determine drivers of patient adherence to topical ocular hypotensive therapy. Design: Retrospective database and chart reviews in combination with prospective patient surveys. Diverse medical environments where insured patients in the research database seek care. Participants: Three hundred patients with a new claim diagnosis for open-angle glaucoma who initially were prescribed one of three prostaglandins and 103 physicians participating in the same medical plans. Methods: A structured interview addressing self-reported adherence, experiences with medication, com- munication with the physician, and health-related beliefs associated with adherence behavior was administered to surveyed patients. Phone interviews were conducted with participating ophthalmologists. Main Outcome Measure: Of adherence, medication possession ratio. Results: Eight variables were associated independently with a lower medication possession ratio: (1) hearing all of what you know about glaucoma from your doctor (compared with some or nothing); (2) not believing that reduced vision is a risk of not taking medication as recommended; (3) having a problem paying for medications; (4) difficulty while traveling or away from home; (5) not acknowledging stinging and burning; (6) being nonwhite; (7) receiving samples; and (8) not receiving a phone call visit reminder. The multivariate model explained 21% of the variance. Conclusions: These findings indicate that doctor–patient communications and health-related beliefs of patients contribute to patient adherence. Patient learning styles that are associated with less concern about the future effects of glaucoma and the risks of not taking medications are associated with lower adherence. Specifically, knowledge about potential vision loss from glaucoma is a critical element that tends to be missed by more passive doctor-dependent patients who tend to be poorly adherent. These findings suggest that educational efforts in the office may improve patient adherence to medical therapies. Ophthalmology 2008;115: 1320 –1327 © 2008 by the American Academy of Ophthalmology. On average, patients with chronic medical conditions take from 30% to 70% of prescribed medication doses, and 30% to 50% discontinue medications in the first months of ther- apy. 1–7 The ophthalmic literature shows similarly low rates of adherence to treatment. 8 –11 Theoretical constructs of adherence propose that patient behavior is determined by Originally received: May 30, 2007. Final revision: November 1, 2007. Accepted: November 15, 2007. Available online: March 5, 2008. Manuscript no. 2007-728. 1 Wilmer Eye Institute, Baltimore, Maryland. 2 Department of International Health, Johns Hopkins Bloomberg School of Public Health, Baltimore, Maryland. 3 Departments of Medicine and Psychiatry, Albert Einstein College of Medicine, Bronx, New York. 4 Medintel On-Call, Pleasantville, New York. 5 Wilmington, Delaware. 6 HealthCore, Inc., Wilmington, Delaware. 7 Pfizer Inc, New York, New York. 8 Department of Ophthalmology & Visual Sciences, University of Louis- ville School of Medicine, Louisville, Kentucky. Supported by an unrestricted grant from Pfizer. The funding organization participated in the design of the study; conducting the study; data collec- tion; data management; data analysis; interpretation of the data; and prep- aration, review, and approval of the manuscript. Drs Friedman, Quigley, and Hahn are paid consultants to PACE, Inc. on behalf of Pfizer. This relationship is managed on behalf of Drs Friedman and Quigley by the Johns Hopkins Committee on Conflict of Interest. Dr Kim and Ms Shah are employees of Pfizer. At the time the research was conducted, both Mr Tan and Ms Gelb were employed by HealthCore, where Mr Tan remains employed. HealthCore is a consultancy whose activ- ities on the project were funded by Pfizer, as are Ms Gelb’s at present. Dr Zimmerman is a consultant to PACE and Pfizer. Correspondence to David S. Friedman, MD, PhD, 600 North Wolfe Street, Wilmer 120, Johns Hopkins Hospital, Baltimore, MD 21287. E-mail: [email protected]. 1320 © 2008 by the American Academy of Ophthalmology ISSN 0161-6420/08/$–see front matter Published by Elsevier Inc. doi:10.1016/j.ophtha.2007.11.023
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Doctor–Patient Communication, Health-Related Beliefs, and Adherence in Glaucoma

Doctor–Patient Communication, Health-RelatedBeliefs, and Adherence in GlaucomaResults from the Glaucoma Adherence andPersistency Study
David S. Friedman, MD, PhD,1,2 Steven R. Hahn, MD,3,4 Laurie Gelb, MPH,5 Jason Tan, MS,6
Sonali N. Shah, RPh, MPH,7 Elizabeth E. Kim, MD,7 Thom J. Zimmerman, MD, PhD,8 Harry A. Quigley, MD1
Objective: To use multiple data sources to determine drivers of patient adherence to topical ocularhypotensive therapy.
Design: Retrospective database and chart reviews in combination with prospective patient surveys. Diversemedical environments where insured patients in the research database seek care.
Participants: Three hundred patients with a new claim diagnosis for open-angle glaucoma who initially wereprescribed one of three prostaglandins and 103 physicians participating in the same medical plans.
Methods: A structured interview addressing self-reported adherence, experiences with medication, com-munication with the physician, and health-related beliefs associated with adherence behavior was administeredto surveyed patients. Phone interviews were conducted with participating ophthalmologists.
Main Outcome Measure: Of adherence, medication possession ratio.Results: Eight variables were associated independently with a lower medication possession ratio: (1) hearing all
of what you know about glaucoma from your doctor (compared with some or nothing); (2) not believing that reducedvision is a risk of not taking medication as recommended; (3) having a problem paying for medications; (4) difficultywhile traveling or away from home; (5) not acknowledging stinging and burning; (6) being nonwhite; (7) receivingsamples; and (8) not receiving a phone call visit reminder. The multivariate model explained 21% of the variance.
Conclusions: These findings indicate that doctor–patient communications and health-related beliefs ofpatients contribute to patient adherence. Patient learning styles that are associated with less concern about thefuture effects of glaucoma and the risks of not taking medications are associated with lower adherence.Specifically, knowledge about potential vision loss from glaucoma is a critical element that tends to be missedby more passive doctor-dependent patients who tend to be poorly adherent. These findings suggest thateducational efforts in the office may improve patient adherence to medical therapies. Ophthalmology 2008;115:1320 –1327 © 2008 by the American Academy of Ophthalmology.
On average, patients with chronic medical conditions takefrom 30% to 70% of prescribed medication doses, and 30%to 50% discontinue medications in the first months of ther-
Originally received: May 30, 2007.Final revision: November 1, 2007.Accepted: November 15, 2007.Available online: March 5, 2008. Manuscript no. 2007-728.1 Wilmer Eye Institute, Baltimore, Maryland.2 Department of International Health, Johns Hopkins Bloomberg School ofPublic Health, Baltimore, Maryland.3 Departments of Medicine and Psychiatry, Albert Einstein College ofMedicine, Bronx, New York.4 Medintel On-Call, Pleasantville, New York.5 Wilmington, Delaware.6 HealthCore, Inc., Wilmington, Delaware.7 Pfizer Inc, New York, New York.8 Department of Ophthalmology & Visual Sciences, University of Louis-
ville School of Medicine, Louisville, Kentucky.1320 © 2008 by the American Academy of OphthalmologyPublished by Elsevier Inc.
apy.1–7 The ophthalmic literature shows similarly low ratesof adherence to treatment.8 –11 Theoretical constructs ofadherence propose that patient behavior is determined by
Supported by an unrestricted grant from Pfizer. The funding organizationparticipated in the design of the study; conducting the study; data collec-tion; data management; data analysis; interpretation of the data; and prep-aration, review, and approval of the manuscript.
Drs Friedman, Quigley, and Hahn are paid consultants to PACE, Inc.on behalf of Pfizer. This relationship is managed on behalf ofDrs Friedman and Quigley by the Johns Hopkins Committee on Conflict ofInterest. Dr Kim and Ms Shah are employees of Pfizer. At the time the researchwas conducted, both Mr Tan and Ms Gelb were employed by HealthCore,where Mr Tan remains employed. HealthCore is a consultancy whose activ-ities on the project were funded by Pfizer, as are Ms Gelb’s at present. DrZimmerman is a consultant to PACE and Pfizer.
Correspondence to David S. Friedman, MD, PhD, 600 North Wolfe Street,Wilmer 120, Johns Hopkins Hospital, Baltimore, MD 21287. E-mail:
[email protected].ISSN 0161-6420/08/$–see front matterdoi:10.1016/j.ophtha.2007.11.023

Friedman et al � Doctor–Patient Communication and Health-Related Beliefs
the balance between beliefs about the threat of the diseaseand the benefits and burdens of treatment.1,12–18 Multiplefactors such as economic status,1,15,19–22 education, cogni-tive ability,23,24 family support,1,24–28 cost of and access tocare,22,29–34 drug side effects,2,15,19,21,35,36 and comorbidillnesses37,38 affect these domains of patient beliefs. Health-related beliefs are of particular interest because they are akey component of doctor-patient communication and areamenable to change.39–52 However, evidence demonstratingthe impact of health-related beliefs on adherence is sparse.
Studies of adherence in glaucoma using administrativeclaims data have confirmed poor adherence9,53–56 but shedlittle light on its causes. Studies using self-reported adher-ence to glaucoma medication regimens have shown thatpatient characteristics including lack of knowledge aboutglaucoma, male gender, cost of medicines, poor patient–doctor relationships, forgetfulness, and complicated regi-mens adversely affect adherence.11,57–61 However, the va-lidity of self-reported adherence is suspect. Surreptitiouselectronic monitoring has demonstrated that patients withglaucoma overreport medication adherence, for example,administering 76% of pilocarpine doses while reporting thatthey took 97%.62 Previously published data from the presentstudy and in other diseases also support this finding.63–66
The Glaucoma Adherence and Persistency Study (GAPS)was designed to examine adherence by combining admin-istrative claims database measures with information frompatient interviews to assess patient characteristics, includinghealth-related beliefs and patients’ experience with theirphysicians and data from medical records, to assess actualpatterns of care. Results from GAPS, presented in thisreport, focus on the effect of patients’ beliefs about glau-coma, self-reported role in learning about the disease, andexperiences communicating with doctors on adherence withglaucoma medication. These observations should be appli-cable to other chronic diseases such as hypercholesterol-emia that are treated with daily medication, are asymptom-atic for most of their course, are associated with seriousoutcomes, and require monitoring technology that usually isaccessible only in the doctor’s office.
Patients and Methods
A detailed description of the GAPS methodology has been pub-lished previously.67 The protocol, including the survey research, iscompliant with the Health Insurance Portability and Accountabil-ity Act and was approved by the Johns Hopkins University andQuorum Review Institutional Review Boards, and verbal authori-zation was obtained from all survey subjects. Subjects were se-lected from a research database that provides information from ageographically diverse sample of medical claims data and accessto physicians, patients, and their charts for research. The studycohort was drawn from claims made from January 1, 1999,through August 31, 2005.
Data were derived from four sources: (1) retrospective analysisof the research database; (2) phone interviews with 103 participat-ing ophthalmologists; (3) phone interviews with 300 patients, 115of whom were patients of the surveyed physicians; and (4) chartreviews of 300 patients, including the charts of 225 of the 300
surveyed patients, 74 patients who were not surveyed but werepatients of surveyed physicians, and one patient who was neithersurveyed nor a patient of the surveyed physicians.67
Subject Selection
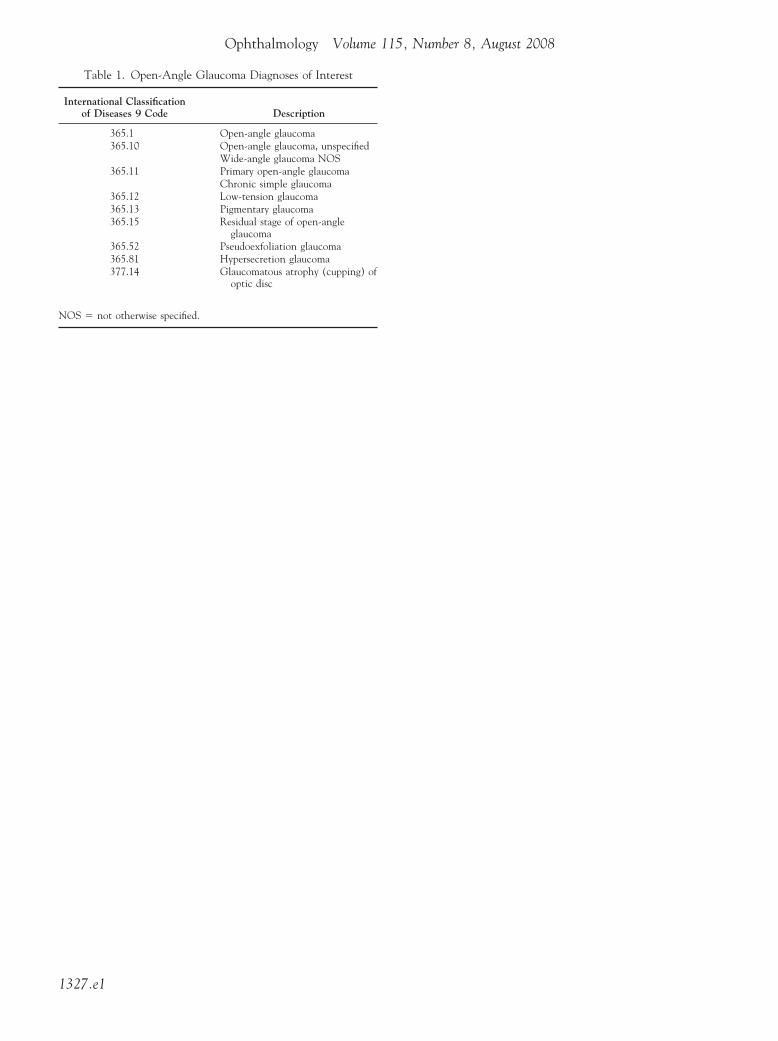
Beginning with patients of surveyed physicians, we recruited sub-jects who received a topical ocular prostaglandin as their firstglaucoma medication (the index prescription) and no other glau-coma medication within 30 days of the index prescription.67 Sub-jects had to have a claim diagnosis consistent with open-angleglaucoma (Table 1 [available at http://aaojournal.org]) 6 monthsbefore to 12 months after their index prescription. Subjects were atleast 40 years old and were enrolled for at least 6 months in theirplan before the index prescription. Most subjects (236/300) wereenrolled for 12 months or more after the index prescription, and theremainder were enrolled for at least 3 months.
Medication Possession Ratio
Medication possession ratio (MPR) was the primary measure ofadherence used in this study. MPR is the ratio of the days of supplyof medication dispensed divided by the days between pharmacyfulfillments.68,69 The days of supply of medication was based onthe actual number of drops per bottle.70 It was assumed thatmedications were taken once daily for prostaglandins and timololgel-forming solution and twice daily for all other medications.
Patient Survey
A structured interview addressing self-reported adherence, ex-periences with medication, communication with the physician,and health-related beliefs associated with adherence behaviorwas administered to surveyed patients. All questions used nat-uralistic and nontechnical language; terms such as compliance,persistency, and adherence were not used. Responses to severalgroups of similar items were combined into scores that thenwere stratified as categorical variables after inspecting scoredistributions. Calculated variables included: difficulty takingmedications while traveling and away from home, computedfrom two variables and scored dichotomously; confidence inknowledge of glaucoma, computed from three variables andscored in three categories; and information provided and ques-tions answered by the physician, computed from eight variablesand scored in three categories. The prevalence of glaucoma isknown to vary by patient race,71,72 and race and ethnicity havebeen associated with different adherence behaviors.61,73 Wetherefore collected information about race and ethnicity byasking participants to choose from categories presented by theinvestigator. Subjects were given the option to add a newclassification if the predefined categories did not apply.
Data Analysis
The association between patients’ responses to survey items andMPR as a continuous variable was assessed using the Wilcoxonrank-sum test, Kruskal-Wallis test, and Spearman correlation.MPR also was analyzed as a categorical variable stratified as lowadherence for the lowest quartile of MPR distribution (range,0–0.36), moderate adherence for the second and third quartiles ofMPR distribution (range, 0.37–0.88), and high adherence for thehighest MPR quartile (range, 0.89–2.18). Relationships betweenindependent variables and MPR as a categorical variable wereassessed with the chi-square test, Wilcoxon rank-sum test, andKruskal-Wallis test. Parameters associated with adherence then
were assessed in a multivariate analysis that included the 297 of1321
Ophthalmology Volume 115, Number 8, August 2008
300 surveyed patients for whom complete survey data were avail-able. Demographic characteristics included in the model were:gender, age, self-reported time from diagnosis, and educationalattainment. Income was correlated closely with educational attain-ment and therefore was not included in the model.
Results
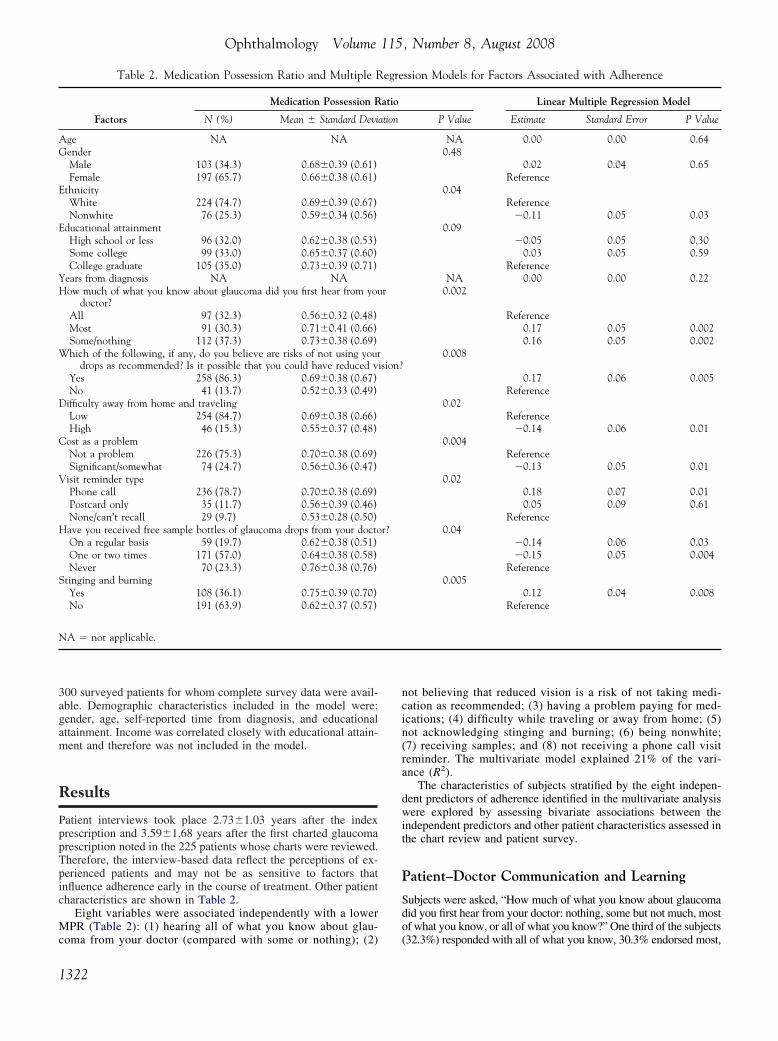
Patient interviews took place 2.73�1.03 years after the indexprescription and 3.59�1.68 years after the first charted glaucomaprescription noted in the 225 patients whose charts were reviewed.Therefore, the interview-based data reflect the perceptions of ex-perienced patients and may not be as sensitive to factors thatinfluence adherence early in the course of treatment. Other patientcharacteristics are shown in Table 2.
Eight variables were associated independently with a lowerMPR (Table 2): (1) hearing all of what you know about glau-
Table 2. Medication Possession Ratio and Multiple R
Factors
Medication Possession R
N (%) Mean � Standard Devi
Age NA NAGender
Male 103 (34.3) 0.68�0.39 (0.61)Female 197 (65.7) 0.66�0.38 (0.61)
EthnicityWhite 224 (74.7) 0.69�0.39 (0.67)Nonwhite 76 (25.3) 0.59�0.34 (0.56)
Educational attainmentHigh school or less 96 (32.0) 0.62�0.38 (0.53)Some college 99 (33.0) 0.65�0.37 (0.60)College graduate 105 (35.0) 0.73�0.39 (0.71)
Years from diagnosis NA NAHow much of what you know about glaucoma did you first hear from you
doctor?All 97 (32.3) 0.56�0.32 (0.48)Most 91 (30.3) 0.71�0.41 (0.66)Some/nothing 112 (37.3) 0.73�0.38 (0.69)
Which of the following, if any, do you believe are risks of not using yourdrops as recommended? Is it possible that you could have reduced v
Yes 258 (86.3) 0.69�0.38 (0.67)No 41 (13.7) 0.52�0.33 (0.49)
Difficulty away from home and travelingLow 254 (84.7) 0.69�0.38 (0.66)High 46 (15.3) 0.55�0.37 (0.48)
Cost as a problemNot a problem 226 (75.3) 0.70�0.38 (0.69)Significant/somewhat 74 (24.7) 0.56�0.36 (0.47)
Visit reminder typePhone call 236 (78.7) 0.70�0.38 (0.69)Postcard only 35 (11.7) 0.56�0.39 (0.46)None/can’t recall 29 (9.7) 0.53�0.28 (0.50)
Have you received free sample bottles of glaucoma drops from your doctoOn a regular basis 59 (19.7) 0.62�0.38 (0.51)One or two times 171 (57.0) 0.64�0.38 (0.58)Never 70 (23.3) 0.76�0.38 (0.76)
Stinging and burningYes 108 (36.1) 0.75�0.39 (0.70)No 191 (63.9) 0.62�0.37 (0.57)
NA � not applicable.
coma from your doctor (compared with some or nothing); (2)
1322
not believing that reduced vision is a risk of not taking medi-cation as recommended; (3) having a problem paying for med-ications; (4) difficulty while traveling or away from home; (5)not acknowledging stinging and burning; (6) being nonwhite;(7) receiving samples; and (8) not receiving a phone call visitreminder. The multivariate model explained 21% of the vari-ance (R2).
The characteristics of subjects stratified by the eight indepen-dent predictors of adherence identified in the multivariate analysiswere explored by assessing bivariate associations between theindependent predictors and other patient characteristics assessed inthe chart review and patient survey.
Patient–Doctor Communication and Learning
Subjects were asked, “How much of what you know about glaucomadid you first hear from your doctor: nothing, some but not much, mostof what you know, or all of what you know?” One third of the subjects
ssion Models for Factors Associated with Adherence
Linear Multiple Regression Model
P Value Estimate Standard Error P Value
NA 0.00 0.00 0.640.48
0.02 0.04 0.65Reference
0.04Reference
�0.11 0.05 0.030.09
�0.05 0.05 0.300.03 0.05 0.59
ReferenceNA 0.00 0.00 0.22
0.002
Reference0.17 0.05 0.0020.16 0.05 0.002
0.008
0.17 0.06 0.005Reference
0.02Reference
�0.14 0.06 0.010.004
Reference�0.13 0.05 0.01
0.020.18 0.07 0.010.05 0.09 0.61
Reference0.04
�0.14 0.06 0.03�0.15 0.05 0.004
Reference0.005
0.12 0.04 0.008Reference
egre
atio
ation
r
ision?
r?
(32.3%) responded with all of what you know, 30.3% endorsed most,

Friedman et al � Doctor–Patient Communication and Health-Related Beliefs
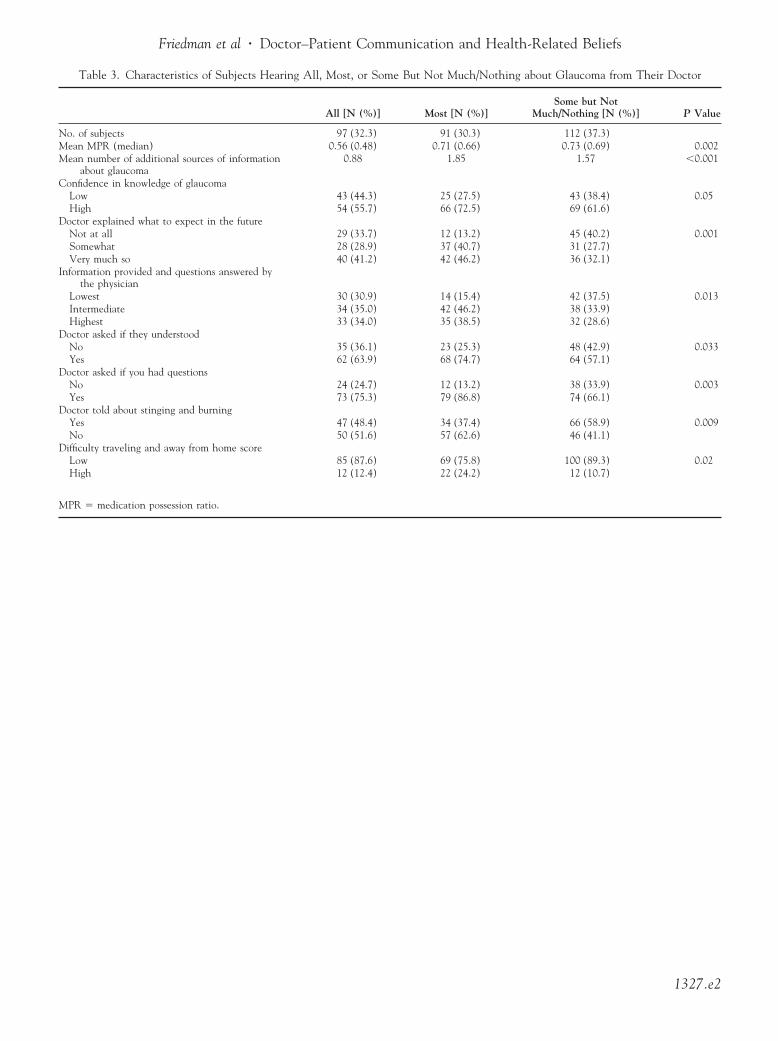
32.0% endorsed some but not much, and 5.3% endorsed nothing.Subjects choosing nothing and some but not much were combined foranalysis (Table 3 [available at http://aaojournal.org], Fig 1). The threegroups had similar age, gender, ethnicity, education, income, anddisease severity (P�0.05 for all). As described below, the surveyresponses of those who learned all they know from their physiciancharacterize them as doctor-dependent learners. Those who learnedmost but not all were described as collaborative learners. Finally,those who learned not much or nothing from their physicians werecharacterized as independent learners.
Doctor-dependent learners had poorer adherence than the othertwo groups; their median MPR was 0.48 compared with 0.66 forthe collaborative learners and 0.69 for the independent learners(P�0.05). In the multivariate analysis, controlling for the contri-bution of all the other variables in the model, the adjusted meanMPR for doctor-dependent learners was 0.16 lower than the col-laborative learners and 0.17 lower than the independent learners(P�0.05; Table 2).
Doctor-dependent learners were less likely to report that theirphysician asked if they had any questions or if they understoodwhat they had been told. Collaborative learners reported receivingmore information from their doctor than either of the other twocategories. One third (35%) of doctor-dependent patients usedadditional sources of information to learn about glaucoma, versus55% of collaborative learners and 54% of independent learners.Consistent with all of these findings, collaborative learners werethe most confident in their knowledge of glaucoma, followed byindependent learners, whereas doctor-dependent patients had thelowest confidence.
Concern about Vision Loss
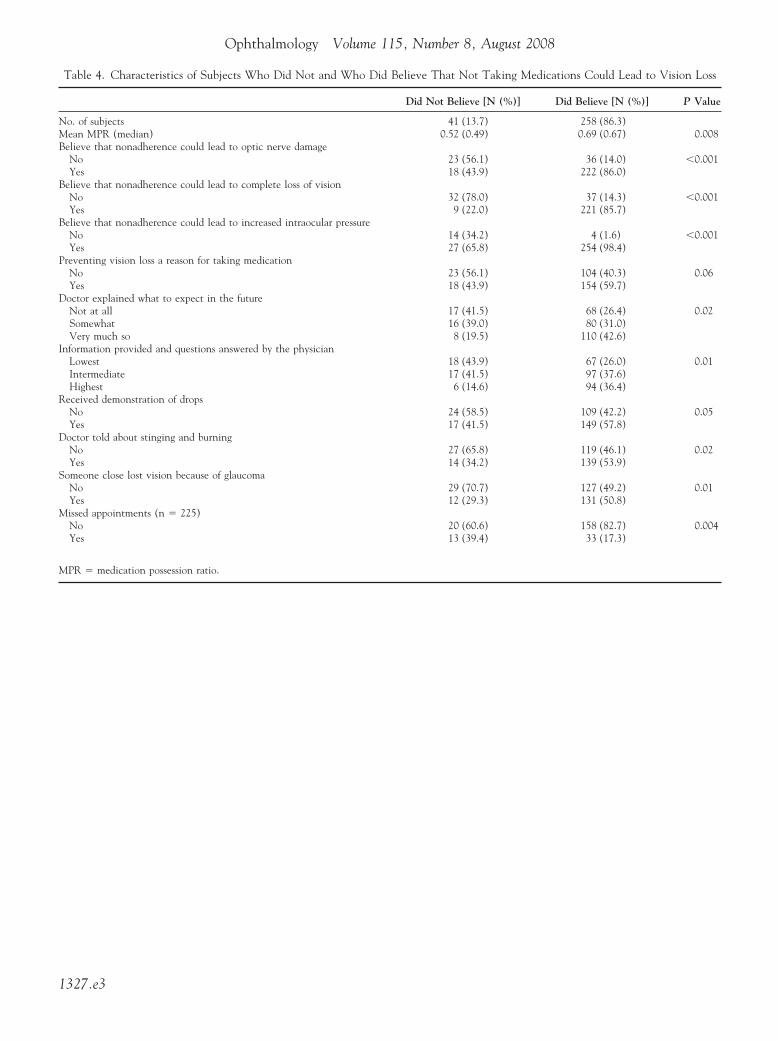
Most patients (86%) believed that not taking glaucoma medi-cations as recommended would risk loss of vision. Adherencewas significantly lower (unadjusted mean MPR, 0.52 vs. 0.69)in the 14% who stated that they did not believe that nonadher-ence to glaucoma medication put them at risk for reduced vision(Table 2). This association was sustained in the multivariateanalysis (Table 2, Fig 2).
Subjects who were not concerned that nonadherence put them
Figure 1. Bar graph demonstrating adherence (medication possessionratio [MPR]) and amount initially learned about glaucoma from doctor.Question regarding amount initially learned from doctor: How much ofwhat you know about glaucoma did you first hear from your doctor? P �0.009 (chi-square test) for relationship between MPR and amount initiallylearned about glaucoma from doctor.
at risk for vision loss also did not believe they would be at risk for
optic nerve damage, increased intraocular pressure, or completevision loss (P�0.05 for all, unadjusted analyses; Table 4 [availableat http://aaojournal.org]). Unconcerned patients were less likely toreport that someone close to them had lost vision because of eyedisease. Significantly, the unconcerned were more likely to reportthat their doctor did not tell them what to expect from the futureregarding their glaucoma, a characteristic they have in commonwith doctor-dependent learners (Fig 3). They reported receivingless information and fewer answers to questions from their physi-cians and were less likely to report receiving a demonstration onusing drops or being told by their physician about stinging andburning as a possible side effect. Finally, the unconcerned weremore than twice as likely to have a charted notation of a missedappointment.
Other Barriers to Adherence
Most patients (84.7%) denied difficulty taking medications whentraveling or away from home (Table 2). Unsurprisingly, patientswho did report this barrier had lower adherence (adjusted meanMPR, 0.14 lower; Table 2). They were more likely to run out ofdrops and to forget to take medication.
The one quarter (24.7%) of patients who stated that paying fordrops was somewhat of or a significant problem had an adjustedmean MPR that was 0.13 lower than those without difficultypaying (Table 2). These patients were more likely to have lowerincomes and educational attainment and were more likely to beblack and female. Patients who had difficulty paying were morelikely to run out of drops and to agree strongly that they do not likethinking about their glaucoma.
Patient Perception of Physician Practices: VisitReminders and Free Samples
Patients who reported receiving phone call visit reminders (with orwithout a postcard reminder) had better adherence than those whoreceived only postcards, received no reminders, or could not recall(Table 2). The adjusted decrement in MPR associated with noreminder or could not remember compared with phone reminderwas 0.18. The MPR was significantly lower in those who received
Figure 2. Bar graph demonstrating adherence (medication possessionratio [MPR]) and belief that reduced vision is a risk of nonadherence.Question regarding impact of nonadherence: Which of the following, ifany, do you believe are risks of not using your drops as recommended: Is itpossible that you could have reduced vision? P � 0.019 (chi-square test)for relationship between MPR and belief that reduced vision is a risk of not
using drops.1323

Ophthalmology Volume 115, Number 8, August 2008
samples regularly (decrement of 0.15) and in those who receivedsamples one or two times (decrement of 0.14) compared with thosewho received no samples (Table 2).
Stinging and Burning and HyperemiaTwo adverse effects played a role in medication-related behavior.Stinging and burning seemed to indicate that medication actuallywas being taken: the 36% of subjects who acknowledged thisadverse effect had a higher MPR than those who did not (Table 2).However, hyperemia was the most common adverse effect noted:135 of the 195 subjects with at least one charted adverse event hadhyperemia as one of them. In patient charts, hyperemia was notedin 12% of all patients and was associated with stopping or switch-ing medication, or both, in 37% of those experiencing it. It was thesymptom responsible for stopping or switching medication in 63%of those who did so because of an adverse effect.
Ethnicity, Educational Attainment, and IncomeThree quarters (74.7%) of the study sample were white, 14.7%were black, and 10.7% were neither. In the multivariate analyseswhen dichotomized as white versus nonwhite and adjusted forincome or educational attainment, MPR was higher in whites(P�0.05; Table 2). Educational attainment showed a positivelinear association with MPR in bivariate analysis but was notassociated significantly with adherence in the multivariate model.
Discussion
The GAPS study identified several barriers to adherencethat are potentially amenable to intervention, including lackof concern about the risk of vision loss, passive dependenceon the doctor for information about glaucoma, failure toreceive a phone call visit reminder, and difficulty takingmedication while away from home or while traveling. Twofactors, the provision of samples and acknowledging sting-ing and burning, are associated with adherence for reasonsthat include both patient behavior and measurement artifact.GAPS also identified factors that clinicians cannot influenceeasily: the cost of medication and effects of ethnicity orunmeasured factors that are associated with ethnicity.
Theoretical models of health-related behavior proposethat concern about the threat of the illness, belief in theeffectiveness of treatment, and the perceived burden oftreatment are critical determinants of adherence.* Health-related attitudes and beliefs are influenced by many factors,including personal experience with the illness, knowledgegained from other sufferers, information available in thecommunity, and clinicians’ influence on patients’ under-standing and concerns. The GAPS data document the im-portance of specific beliefs about glaucoma and its treat-ment and the influence of doctor–patient communication onthose beliefs and adherence behavior.
Doctor–Patient Relationship, Communication, andHealth-Related BeliefsA substantial minority of subjects (14%) reported not beingconcerned that they could lose vision if they did not take
*Refs. 1–4, 7, 12, 13, 16, 23, 29, 50, 74–76.
1324
their eye drops, and these individuals were less adherent totreatment and doctor’s visits than those who were con-cerned. Lack of concern about reduced vision was associ-ated with an array of similar beliefs about total loss ofvision, increased intraocular pressure, and optic nerve dam-age. Similarly, there was a trend for the unconcerned to beless likely to endorse prevention of vision loss as a reasonfor taking medication.
The GAPS data suggest that doctor–patient communica-tion plays a role in patient concern about glaucoma. Uncon-cerned patients reported receiving less information and hav-ing fewer questions answered by physicians. They were lesslikely to report receiving instructions about drops or hearingabout stinging and burning. Most importantly, they wereless likely to report hearing about what to expect in thefuture from glaucoma, a characteristic that the unconcernedshare with patients who had a passive doctor-dependentlearning style.
Doctor-dependent learners who depended exclusively ontheir physician to learn about the disease had poorer adher-ence than collaborative learners, that is, those who learnedmost but not all they know from their doctors, or indepen-dent learners, who learned not much or nothing from theirdoctors. Doctor-dependent learners reported that their doc-tors were less likely to ask if they have questions or if theyunderstand what they have been told. They received feweranswers to their questions and less information from theirdoctors and consequently were less confident in their knowl-edge of glaucoma. Collaborative learners learned most of whatthey know from their physicians, but they also used additionalsources of information and had the highest confidence in theirknowledge of glaucoma. Independent learners adhered as wellas collaborative learners despite learning less from their phy-sicians. It is possible that the difference between collaborativelearners and independent learners lies more with their doctors’patient education practices than in the patient’s ability or in-terest in learning. The passivity of doctor-dependent learnersmay extend to other aspects of their health-related behaviorbesides communication with physicians. Identifying these sub-jects, ensuring that they do understand the future consequencesof glaucoma even if they do not ask, and empowering them totake more control over their health may contribute to improvedadherence.
Cost of Medication and Taking Medication WhileAway from Home or Traveling
The cost of medication22,32,34 and difficulty taking medica-tion while away from home or traveling77 are previouslyidentified remediable barriers to adherence that are impor-tant to identify. Patients with difficulty away from home areyounger, report forgetting to take medications more often,and are more concerned about side effects and the stigma ofothers knowing that they take drops. These characteristicssuggest a more active individual with a more complicatedlifestyle who may benefit from physician-initiated problemsolving. In addition, physicians can identify less costlyregimens or can assist patients in participating in reduced-
fee plans when cost is identified as a barrier.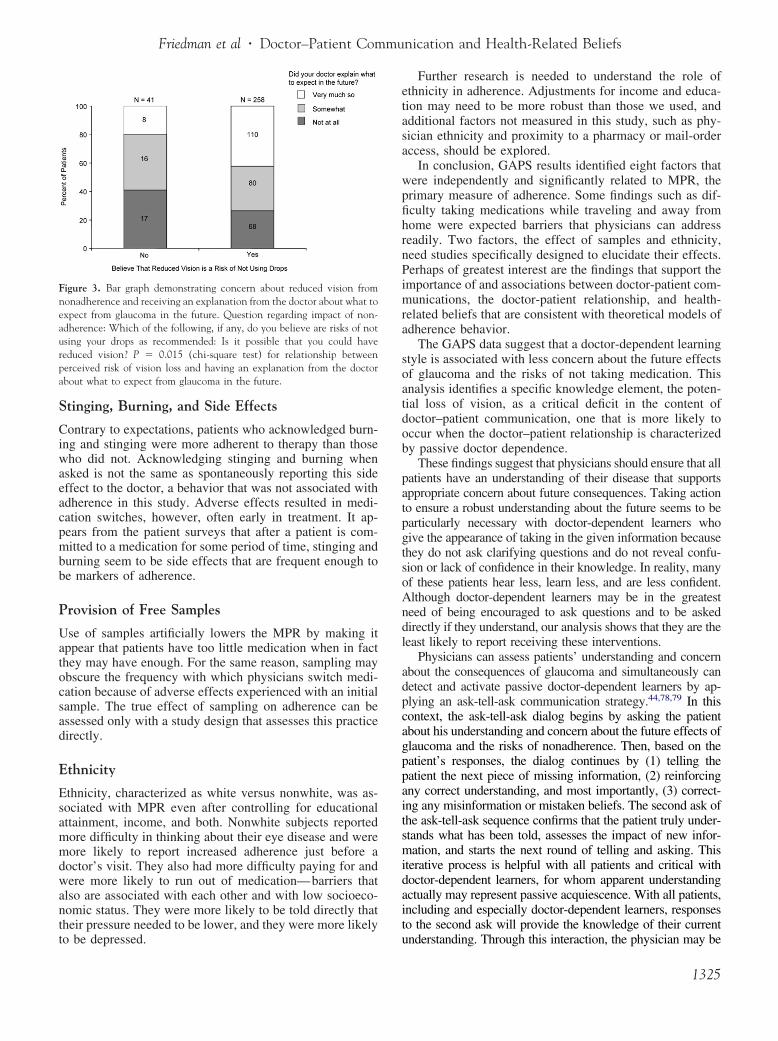
Friedman et al � Doctor–Patient Communication and Health-Related Beliefs
Stinging, Burning, and Side Effects
Contrary to expectations, patients who acknowledged burn-ing and stinging were more adherent to therapy than thosewho did not. Acknowledging stinging and burning whenasked is not the same as spontaneously reporting this sideeffect to the doctor, a behavior that was not associated withadherence in this study. Adverse effects resulted in medi-cation switches, however, often early in treatment. It ap-pears from the patient surveys that after a patient is com-mitted to a medication for some period of time, stinging andburning seem to be side effects that are frequent enough tobe markers of adherence.
Provision of Free Samples
Use of samples artificially lowers the MPR by making itappear that patients have too little medication when in factthey may have enough. For the same reason, sampling mayobscure the frequency with which physicians switch medi-cation because of adverse effects experienced with an initialsample. The true effect of sampling on adherence can beassessed only with a study design that assesses this practicedirectly.
Ethnicity
Ethnicity, characterized as white versus nonwhite, was as-sociated with MPR even after controlling for educationalattainment, income, and both. Nonwhite subjects reportedmore difficulty in thinking about their eye disease and weremore likely to report increased adherence just before adoctor’s visit. They also had more difficulty paying for andwere more likely to run out of medication—barriers thatalso are associated with each other and with low socioeco-nomic status. They were more likely to be told directly thattheir pressure needed to be lower, and they were more likely
Figure 3. Bar graph demonstrating concern about reduced vision fromnonadherence and receiving an explanation from the doctor about what toexpect from glaucoma in the future. Question regarding impact of non-adherence: Which of the following, if any, do you believe are risks of notusing your drops as recommended: Is it possible that you could havereduced vision? P � 0.015 (chi-square test) for relationship betweenperceived risk of vision loss and having an explanation from the doctorabout what to expect from glaucoma in the future.
to be depressed.
Further research is needed to understand the role ofethnicity in adherence. Adjustments for income and educa-tion may need to be more robust than those we used, andadditional factors not measured in this study, such as phy-sician ethnicity and proximity to a pharmacy or mail-orderaccess, should be explored.
In conclusion, GAPS results identified eight factors thatwere independently and significantly related to MPR, theprimary measure of adherence. Some findings such as dif-ficulty taking medications while traveling and away fromhome were expected barriers that physicians can addressreadily. Two factors, the effect of samples and ethnicity,need studies specifically designed to elucidate their effects.Perhaps of greatest interest are the findings that support theimportance of and associations between doctor-patient com-munications, the doctor-patient relationship, and health-related beliefs that are consistent with theoretical models ofadherence behavior.
The GAPS data suggest that a doctor-dependent learningstyle is associated with less concern about the future effectsof glaucoma and the risks of not taking medication. Thisanalysis identifies a specific knowledge element, the poten-tial loss of vision, as a critical deficit in the content ofdoctor–patient communication, one that is more likely tooccur when the doctor–patient relationship is characterizedby passive doctor dependence.
These findings suggest that physicians should ensure that allpatients have an understanding of their disease that supportsappropriate concern about future consequences. Taking actionto ensure a robust understanding about the future seems to beparticularly necessary with doctor-dependent learners whogive the appearance of taking in the given information becausethey do not ask clarifying questions and do not reveal confu-sion or lack of confidence in their knowledge. In reality, manyof these patients hear less, learn less, and are less confident.Although doctor-dependent learners may be in the greatestneed of being encouraged to ask questions and to be askeddirectly if they understand, our analysis shows that they are theleast likely to report receiving these interventions.
Physicians can assess patients’ understanding and concernabout the consequences of glaucoma and simultaneously candetect and activate passive doctor-dependent learners by ap-plying an ask-tell-ask communication strategy.44,78,79 In thiscontext, the ask-tell-ask dialog begins by asking the patientabout his understanding and concern about the future effects ofglaucoma and the risks of nonadherence. Then, based on thepatient’s responses, the dialog continues by (1) telling thepatient the next piece of missing information, (2) reinforcingany correct understanding, and most importantly, (3) correct-ing any misinformation or mistaken beliefs. The second ask ofthe ask-tell-ask sequence confirms that the patient truly under-stands what has been told, assesses the impact of new infor-mation, and starts the next round of telling and asking. Thisiterative process is helpful with all patients and critical withdoctor-dependent learners, for whom apparent understandingactually may represent passive acquiescence. With all patients,including and especially doctor-dependent learners, responsesto the second ask will provide the knowledge of their current
understanding. Through this interaction, the physician may be1325

Ophthalmology Volume 115, Number 8, August 2008
able to help overcome some of the barriers to adherenceidentified in the GAPS.
References
1. Haynes RB, McDonald HP, Garg AX. Helping patients followprescribed treatment: clinical applications. JAMA 2002;288:2880–3.
2. Haynes RB, Yao X, Degani A, et al. Interventions to enhancemedication adherence. Cochrane Database Syst Rev 2005;(4):CD000011.
3. Haynes RB, McDonald H, Garg AX, Montague P. Interven-tions for helping patients to follow prescriptions for medica-tions. Cochrane Database Syst Rev 2002;(2):CD000011.
4. DiMatteo MR, Giordani PJ, Lepper HS, Croghan TW. Patientadherence and medical treatment outcomes: a meta-analysis.Med Care 2002;40:794–811.
5. DiMatteo MR. Variations in patients’ adherence to medicalrecommendations: a quantitative review of 50 years of re-search. Med Care 2004;42:200–9.
6. Knight KM, McGowan L, Dickens C, Bundy C. A systematicreview of motivational interviewing in physical health caresettings. Br J Health Psychol 2006;11:319–32.
7. Sabate E, ed. Adherence to long-term therapies: evidence foraction. Geneva: World Health Organization; 2003:7, 48–49,61, 66, 73–75, 88–89. Available at: http://whqlibdoc.who.int/publications/2003/9241545992.pdf. Accessed September 3,2007.
8. Olthoff CM, Schouten JS, van de Borne BW, Webers CA.Noncompliance with ocular hypotensive treatment in patientswith glaucoma or ocular hypertension: an evidence-basedreview. Ophthalmology 2005;112:953–61.
9. Nordstrom BL, Friedman DS, Mozaffari E, et al. Persistenceand adherence with topical glaucoma therapy. Am J Ophthal-mol 2005;140:598–606.
10. Schwartz GF. Compliance and persistency in glaucoma fol-low-up treatment. Curr Opin Ophthalmol 2005;16:114–21.
11. Bour T, Blanchard F, Segal A. Therapeutic observance andlife of patients with primary open-angle glaucoma: apropos of341 cases in the department of Marne [in French]. J FrOphtalmol 1993;16:380–91.
12. Starace F, Massa A, Amico KR, Fisher JD. Adherence to anti-retroviral therapy: an empirical test of the information-motiva-tion-behavioral skills model. Health Psychol 2006;25:153–62.
13. Amico KR, Toro-Alfonso J, Fisher JD. An empirical test ofthe information, motivation and behavioral skills model ofantiretroviral therapy adherence. AIDS Care 2005;17:661–73.
14. Schultz JS, O’Donnell JC, McDonough KL, et al. Determi-nants of compliance with statin therapy and low-density li-poprotein cholesterol goal attainment in a managed care pop-ulation. Am J Manag Care 2005;11:306–12.
15. Bender BG. Overcoming barriers to nonadherence in asthmatreatment. J Allergy Clin Immunol 2002;109(suppl):S554–9.
16. Goldring AB, Taylor SE, Kemeny ME, Anton PA. Impact ofhealth beliefs, quality of life, and the physician-patient rela-tionship on the treatment intentions of inflammatory boweldisease patients. Health Psychol 2002;21:219–28.
17. McDonald HP, Garg AX, Haynes RB. Interventions to en-hance patient adherence to medication prescriptions: scientificreview. JAMA 2002;288:2868–79.
18. Brawley LR, Culos-Reed SN. Studying adherence to thera-peutic regimens: overview, theories, recommendations. Con-trol Clin Trials 2000;21(suppl):156S–63S.
19. Delgado PL. Approaches to the enhancement of patient ad-
1326
herence to antidepressant medication treatment. J ClinPsychiatry 2000;61(suppl):6–9.
20. Ellis S, Shumaker S, Sieber W, et al. Adherence to pharma-cological interventions: current trends and future directions.Control Clin Trials 2000;21(suppl):218S–25S.
21. Krueger KP, Berger BA, Felkey B. Medication adherence andpersistence: a comprehensive review. Adv Ther 2005;22:313–56.
22. Kennedy J, Coyne J, Sclar D. Drug affordability and prescrip-tion noncompliance in the United States: 1997–2002. ClinTher 2004;26:607–14.
23. Johnson MJ. The Medication Adherence Model: a guide forassessing medication taking. Res Theory Nurs Pract 2002;16:179–92.
24. van Vliet MJ, Schuurmans MJ, Grypdonck MH, DuijnsteeMS. Improper intake of medication by elders—insights oncontributing factors: a review of the literature. Res TheoryNurs Pract 2006;20:79–93.
25. Godin G, Cote J, Naccache H, et al. Prediction of adherence toantiretroviral therapy: a one-year longitudinal study. AIDSCare 2005;17:493–504.
26. Kyngas H. Predictors of good compliance in adolescents withepilepsy. Seizure 2001;10:549–53.
27. Loghman-Adham M. Medication noncompliance in patientswith chronic disease: issues in dialysis and renal transplanta-tion. Am J Manag Care 2003;9:155–71.
28. Nischal KC, Khopkar U, Saple DG. Improving adherence toantiretroviral therapy. Indian J Dermatol Venereol Leprol2005;71:316–20.
29. Roter DL, Hall JA, Merisca R, et al. Effectiveness of inter-ventions to improve patient compliance: a meta-analysis. MedCare 1998;36:1138–61.
30. Doran E, Robertson J, Rolfe I, Henry D. Patient co-paymentsand use of prescription medicines. Aust N Z J Public Health2004;28:62–7.
31. Littenberg B, Strauss K, MacLean CD, Troy AR. The use ofinsulin declines as patients live farther from their source ofcare: results of a survey of adults with type 2 diabetes. BMCPublic Health [serial online] 2006;6:198. Available at: http://www.biomedcentral.com/1471-2458/6/198. Accessed Septem-ber 3, 2007.
32. Schafheutle EI, Hassell K, Noyce PR, Weiss MC. Access tomedicines: cost as an influence on the views and behaviour ofpatients. Health Soc Care Community 2002;10:187–95.
33. Strauss K, MacLean C, Troy A, Littenberg B. Driving distanceas a barrier to glycemic control in diabetes. J Gen Intern Med2006;21:378–80.
34. Sharkey JR, Ory MG, Browne BA. Determinants of self-management strategies to reduce out-of-pocket prescriptionmedication expense in homebound older people. J Am GeriatrSoc 2005;53:666–74.
35. Horne R. Compliance, adherence, and concordance: implica-tions for asthma treatment. Chest 2006;130(suppl):65S–72S.
36. Nordqvist O, Sodergard B, Tully MP, et al. Assessing andachieving readiness to initiate HIV medication. Patient EducCouns 2006;62:21–30.
37. Hays RD, Kravitz RL, Mazel RM, et al. The impact of patientadherence on health outcomes for patients with chronic disease inthe Medical Outcomes Study. J Behav Med 1994;17:347–60.
38. Rose M, Fliege H, Hildebrandt M, et al. The network ofpsychological variables in patients with diabetes and theirimportance for quality of life and metabolic control. DiabetesCare 2002;25:35–42.
39. Bultman DC, Svarstad BL. Effects of physician communicationstyle on client medication beliefs and adherence with antidepres-
sant treatment. Patient Educ Couns 2000;40:173–85.
Friedman et al � Doctor–Patient Communication and Health-Related Beliefs
40. Chapman KR, Walker L, Cluley S, Fabbri L. Improving patientcompliance with asthma therapy. Respir Med 2000;94:2–9.
41. DiMatteo MR. Future directions in research on consumer-provider communication and adherence to cancer preventionand treatment. Patient Educ Couns 2003;50:23–6.
42. DiMatteo MR. Patient adherence to pharmacotherapy: theimportance of effective communication. Formulary 1995;30:596–8, 601–2, 605.
43. DiMatteo MR. The role of effective communication withchildren and their families in fostering adherence to pediatricregimens. Patient Educ Couns 2004;55:339–44.
44. Evans WG, Tulsky JA, Back AL, Arnold RM. Communica-tion at times of transitions: how to help patients cope with lossand re-define hope. Cancer J 2006;12:417–24.
45. Golin C, DiMatteo MR, Duan N, et al. Impoverished diabeticpatients whose doctors facilitate their participation in medicaldecision making are more satisfied with their care. J GenIntern Med 2002;17:857–66.
46. Hall JA, Roter DL, Katz NR. Meta-analysis of correlates ofprovider behavior in medical encounters. Med Care 1988;26:657–75.
47. Klingle RS, Burgoon M. Patient compliance and satisfactionwith physician influence attempts: a reinforcement expectancyapproach to compliance-gaining over time. Communic Res1995;22:148–87.
48. Martin LR, DiMatteo MR, Lepper HS. Facilitation of patientinvolvement in care: development and validation of a scale.Behav Med 2001;27:111–20.
49. Stewart M, Brown JB, Boon H, et al. Evidence on patient-doctor communication. Cancer Prev Control 1999;3:25–30.
50. Stewart M, Brown JB, Donner A, et al. The impact of patient-centered care on outcomes. J Fam Pract 2000;49:796–804.
51. Loh A, Leonhart R, Wills CE, et al. The impact of patientparticipation on adherence and clinical outcome in primarycare of depression. Patient Educ Couns 2007;65:69–78.
52. Mishra P, Hansen EH, Sabroe S, Kafle KK. Adherence isassociated with the quality of professional-patient interactionin Directly Observed Treatment Short-Course, DOTS. PatientEduc Couns 2006;63:29–37.
53. Dasgupta S, Oates V, Bookhart BK, et al. Population-basedpersistency rates for topical glaucoma medications measuredwith pharmacy claims data. Am J Manag Care 2002;8(suppl):S255–61.
54. Reardon G, Schwartz GF, Mozaffari E. Patient persistencywith topical ocular hypotensive therapy in a managed carepopulation. Am J Ophthalmol 2004;137(suppl):S3–12.
55. Shaya FT, Mullins CD, Wong W, Cho J. Discontinuation ratesof topical glaucoma medications in a managed care popula-tion. Am J Manag Care 2002;8(suppl):S271–7.
56. Spooner JJ, Bullano MF, Ikeda LI, et al. Rates of discontin-uation and change of glaucoma therapy in a managed caresetting. Am J Manag Care 2002;8(suppl):S262–70.
57. Spaeth GL. Visual loss in a glaucoma clinic. I. Sociologicalconsiderations. Invest Ophthalmol 1970;9:73–82.
58. Bloch S, Rosenthal AR, Friedman L, Caldarolla P. Patientcompliance in glaucoma. Br J Ophthalmol 1977;61:531–4.
59. MacKean JM, Elkington AR. Compliance with treatment ofpatients with chronic open-angle glaucoma. Br J Ophthalmol1983;67:46–9.
60. Konstas AG, Maskaleris G, Gratsonidis S, Sardelli C. Com-
pliance and viewpoint of glaucoma patients in Greece. Eye2000;14:752–6.
61. Patel SC, Spaeth GL. Compliance in patients prescribed eye-drops for glaucoma. Ophthalmic Surg 1995;26:233–6.
62. Kass MA, Meltzer DW, Gordon M, et al. Compliance withtopical pilocarpine treatment. Am J Ophthalmol 1986;101:515–23.
63. Mazze RS, Shamoon H, Pasmantier R, et al. Reliability ofblood glucose monitoring by patients with diabetes mellitus.Am J Med 1984;77:211–7.
64. Clowes JA, Peel NF, Eastell R. The impact of monitoring onadherence and persistence with antiresorptive treatment forpostmenopausal osteoporosis: a randomized controlled trial.J Clin Endocrinol Metab 2004;89:1117–23.
65. Burnier M, Schneider MP, Chiolero A, et al. Electronic com-pliance monitoring in resistant hypertension: the basis forrational therapeutic decisions. J Hypertens 2001;19:335–41.
66. Simmons MS, Nides MA, Rand CS, et al. Unpredictability ofdeception in compliance with physician-prescribed broncho-dilator inhaler use in a clinical trial. Chest 2000;118:290–5.
67. Friedman DS, Quigley HA, Hahn SR, et al. Using pharmacyclaims data to study adherence to glaucoma medications:methodology of the Glaucoma Adherence and PersistencyStudy (GAPS). Invest Ophthalmol Vis Sci 2007;48:5052–7.
68. Sikka R, Xia F, Aubert RE. Estimating medication persistencyusing administrative claims data. Am J Manag Care 2005;11:449–57.
69. Hess LM, Raebel MA, Conner DA, Malone DC. Measurementof adherence in pharmacy administrative databases: a proposalfor standard definitions and preferred measures. Ann Pharma-cother 2006;40:1280–8.
70. Fiscella RG, Green A, Patuszynski DH, Wilensky J. Medicaltherapy cost considerations for glaucoma. Am J Ophthalmol2003;136:18–25.
71. Sommer A, Tielsch JM, Katz J, et al. Racial differences in thecause-specific prevalence of blindness in east Baltimore.N Engl J Med 1991;325:1412–7.
72. Javitt JC, McBean AM, Nicholson GA, et al. Undertreatmentof glaucoma among black Americans. N Engl J Med 1991;325:1418–22.
73. Curtin RB, Svarstad BL, Keller TH. Hemodialysis patients’ non-compliance with oral medications. ANNA J 1999;26:307–16.
74. DiMatteo MR, Haskard KB. Further challenges in adherenceresearch: measurements, methodologies, and mental healthcare. Med Care 2006;44:297–9.
75. Drieschner KH, Lammers SM, van der Staak CP. Treatmentmotivation: an attempt for clarification of an ambiguous con-cept. Clin Psychol Rev 2004;23:1115–37.
76. Wilkinson J. Understanding motivation to enhance patientcompliance. Br J Nurs 1997;6:879–84.
77. Smith JD, Oakley D. Why do women miss oral contraceptivepills? An analysis of women’s self-described reasons for missedpills. J Midwifery Womens Health 2005;50:380–5.
78. Back AL, Arnold RM, Baile WF, et al. Approaching difficultcommunication tasks in oncology. CA Cancer J Clin 2005;55:164–77.
79. Boyle D, Dwinnell B, Platt F. Invite, listen, and summarize: apatient-centered communication technique. Acad Med 2005;
80:29–32.1327
Ophthalmology Volume 115, Number 8, August 2008
Table 1. Open-Angle Glaucoma Diagnoses of Interest
International Classificationof Diseases 9 Code Description
365.1 Open-angle glaucoma365.10 Open-angle glaucoma, unspecified
Wide-angle glaucoma NOS365.11 Primary open-angle glaucoma
Chronic simple glaucoma365.12 Low-tension glaucoma365.13 Pigmentary glaucoma365.15 Residual stage of open-angle
glaucoma365.52 Pseudoexfoliation glaucoma365.81 Hypersecretion glaucoma377.14 Glaucomatous atrophy (cupping) of
optic disc
NOS � not otherwise specified.
1327.e1
Friedman et al � Doctor–Patient Communication and Health-Related Beliefs
Table 3. Characteristics of Subjects Hearing All, Most, or Some But Not Much/Nothing about Glaucoma from Their Doctor
All [N (%)] Most [N (%)]Some but Not
Much/Nothing [N (%)] P Value
No. of subjects 97 (32.3) 91 (30.3) 112 (37.3)Mean MPR (median) 0.56 (0.48) 0.71 (0.66) 0.73 (0.69) 0.002Mean number of additional sources of information
about glaucoma0.88 1.85 1.57 �0.001
Confidence in knowledge of glaucomaLow 43 (44.3) 25 (27.5) 43 (38.4) 0.05High 54 (55.7) 66 (72.5) 69 (61.6)
Doctor explained what to expect in the futureNot at all 29 (33.7) 12 (13.2) 45 (40.2) 0.001Somewhat 28 (28.9) 37 (40.7) 31 (27.7)Very much so 40 (41.2) 42 (46.2) 36 (32.1)
Information provided and questions answered bythe physician
Lowest 30 (30.9) 14 (15.4) 42 (37.5) 0.013Intermediate 34 (35.0) 42 (46.2) 38 (33.9)Highest 33 (34.0) 35 (38.5) 32 (28.6)
Doctor asked if they understoodNo 35 (36.1) 23 (25.3) 48 (42.9) 0.033Yes 62 (63.9) 68 (74.7) 64 (57.1)
Doctor asked if you had questionsNo 24 (24.7) 12 (13.2) 38 (33.9) 0.003Yes 73 (75.3) 79 (86.8) 74 (66.1)
Doctor told about stinging and burningYes 47 (48.4) 34 (37.4) 66 (58.9) 0.009No 50 (51.6) 57 (62.6) 46 (41.1)
Difficulty traveling and away from home scoreLow 85 (87.6) 69 (75.8) 100 (89.3) 0.02High 12 (12.4) 22 (24.2) 12 (10.7)
MPR � medication possession ratio.
1327.e2
Ophthalmology Volume 115, Number 8, August 2008
Table 4. Characteristics of Subjects Who Did Not and Who Did Believe That Not Taking Medications Could Lead to Vision Loss
Did Not Believe [N (%)] Did Believe [N (%)] P Value
No. of subjects 41 (13.7) 258 (86.3)Mean MPR (median) 0.52 (0.49) 0.69 (0.67) 0.008Believe that nonadherence could lead to optic nerve damage
No 23 (56.1) 36 (14.0) �0.001Yes 18 (43.9) 222 (86.0)
Believe that nonadherence could lead to complete loss of visionNo 32 (78.0) 37 (14.3) �0.001Yes 9 (22.0) 221 (85.7)
Believe that nonadherence could lead to increased intraocular pressureNo 14 (34.2) 4 (1.6) �0.001Yes 27 (65.8) 254 (98.4)
Preventing vision loss a reason for taking medicationNo 23 (56.1) 104 (40.3) 0.06Yes 18 (43.9) 154 (59.7)
Doctor explained what to expect in the futureNot at all 17 (41.5) 68 (26.4) 0.02Somewhat 16 (39.0) 80 (31.0)Very much so 8 (19.5) 110 (42.6)
Information provided and questions answered by the physicianLowest 18 (43.9) 67 (26.0) 0.01Intermediate 17 (41.5) 97 (37.6)Highest 6 (14.6) 94 (36.4)
Received demonstration of dropsNo 24 (58.5) 109 (42.2) 0.05Yes 17 (41.5) 149 (57.8)
Doctor told about stinging and burningNo 27 (65.8) 119 (46.1) 0.02Yes 14 (34.2) 139 (53.9)
Someone close lost vision because of glaucomaNo 29 (70.7) 127 (49.2) 0.01Yes 12 (29.3) 131 (50.8)
Missed appointments (n � 225)No 20 (60.6) 158 (82.7) 0.004Yes 13 (39.4) 33 (17.3)
MPR � medication possession ratio.
1327.e3