37 Linguistic deviation and the rhetoric figures in ... - XLinguae
Upload
independentCategory
view
3download
0
Major Articles
Dissociated Vertical Deviation and Head Tilts
Alvina Pau l ine Sant iago, M D , and A r t h u r L. R o s e n b a u m , M D
Introduction. The association of anomalous head posture and dissociated vertical deviation does not seem to be appreciated, as evidenced bythe paucity of literature linking these two conditions. Method:The series describes 14 patients who had an anomalous head posture and dissociated vertical deviation. The assumed head tilts appeared to decrease the magnitude and improve the motor control of dissociated vertical deviation. Results:Twelve of 14 patients tilted their heads contralateral to the eye with the dissociated vertical deviation, or away from the eye with a larger amount of dissociated vertical deviation if the disorder was bilateral. Two patients tilted their heads to the same side as the eye with the dissociated vertical deviation. Forced head tilt testing in the opposite direction showed an increase in the magnitude of the dissociated vertical deviation or poorer control of the deviation. Dissociated 'vertical deviation was not related to oblique muscle dysfunction. Peripheral fusion was demonstrated in 10 patients, as evidenced by low-grade stereopsis or Worth 4 dot fusion at near. One patient did not show any demonstrable fusion with conventional tests. Another did not show evidence of stereopsis, but Worth 4 dot testing was not performed. Two other patients were too young to cooperate with sensory testing. Anomalous head posture was controlled or minimized after the control ofthe dissociated vertical deviation by surgery in four patients. Two patients showed improved stereopsis after surgery for dissociated vertical deviation. Conclusion: Dissociated vertical deviation should be included in the differential diagnosis of an ocular cause of head tilts. Forced contralateral head tilt testing will confirm whether dissociated vertical deviation is the cause if motor control of the dissociated vertical deviation worsens or becomes manifest rather than latent. The presence of an anomalous head posture in patients 'with dissociated vertical deviation can be improved with strabismus surgery. (J AAPOS 1998;2:5-11)
D issociated vertical deviation is an intermittent vertical deviation usually seen in patients when fusion is disrupted) It is commonly found in
patients with infantile esotropia, even after surgical correction of the horizontal deviation has been successful, regardless of timing of surgery. ~, 2 In addition to the vertical component, excycloduction and horizontal move- ments are observed. 3
Crone 4 first reported on alternating hyperphoria (an earlier synonym for dissociated vertical deviation) and head tilt. He described a constellation of findings consisting of esotropia, hypertropia in lateral gaze, nystagmus, alternating hyperphoria with excycloduction of the eye under cover and incycloduction of the fixing
From the Division of Pediatric Ophthalmology and Strabismus, Department of Ophthalmology, aVules Steiu Eye Institute, University of California, Los Angeles. Supported in part by the Kimmel Research Fund. Reprint requests: A*~:hur L. Rosenbaum, MD, Division of Pediatric Ophthalmology and Sls'abismus, 2%les Stein Eye Institute, University of California Center for Health Sciences, 1 O0 Stein Plaza, Universi{y of California, Los Angeles, Los Angeles, CA 90095. Copyright © 1998 by the American Assodation for Pediatric Ophthalmology and Strabismus. 2091-8531/985Y.00 + 0 7Y/1/8YI60
eye, and torticollis. The latter was found in 23 % of 113 in this series, with the head tilt more commonly found toward the fixing eye. M1 patients who had torticollis had underlying esotropia. This finding was reiterated by other authors from that era. s, 6 Since that period the association of torticollis with dissociated vertical devia- tion has been largely underreported. Head tilts ipsilat- eral 7, * or contralateral 4-7 to the eye with the dissociated vertical deviation were both observed. Only one study implicated dissociated vertical deviation definitively as a cause of a manifest head tilt with confirmation by forced contralateral head tilt testing. 7
Common ocular etiologies for abnormal head postures include incomitant strabismus (both horizontal and vertical), nystagmus (including spasmus nutans), visual field cuts, cosmetic reasons, oculomotor apraxia, refractive error, and ptosis. 7, 9-11 In one series as many as 63 % of cases with abnormal head postures had incomitant squints. 7 Vertical incomitance was due to cyclovertical muscle palsy, double elevator palsy, Brown syndrome, and blow-out fracture. Horizontal incomitance was found in patients with Duane syndrome and sixth nerve palsy. Dissociated vertical deviation as a reason for manifest head tilts has
~ournal of AAPOS February 1998

Journal of AAPOS 6 Santiago and Rosenbaum Volume 2 Number I Februacv 1998
TABLE I. Patient profile: dissociated vertical deviation with head tilts
Patient Age at first No. visit (yr) Sex Previous ocular surgery Age at surgery (yr) DVD onset (yr) Diagnosis
1 1 M MR recession OU 0.7 0.8 Infantile esotropia
LR resection, SR recession OU 1.5
SR rerecession OS* 2.0
SR rerecession OU* 5.5
2 3 M MR recession OU 1 1 Infantile esotropia
I0 recession OD 2
3 27 F MR recession OU? 16 ? Infantile esotropia?
4 12.3 M MR recession OU 0.5 2 Infantile esotropia
Anterior transposition I00U 53
LR resection OU 8.3
SO tuck OU 11
LR recession OU* 13
5 0.04 F MR recession OU* 0.4 1.5 Infantile esotropia
6 1.3 F MR recession OU 1.1 1.8 Infantile esotrepia
Failed recovery slipped MR OD 1.2
Recovery slipped MR OD* 1.7
SR recession OU* 4
7 6 F I0 recession with anterior 4.5 4.8 Accommodative esotropia transposition OU
8 22 F MR recession, LR resection OD? 0.5 ? Infantile esotropia?
9 0.6 F MR recession OU* 0.8 2.3 Infantile esotropia
LR resection, SR recession OU* 10
SR rerecession OU* 14.3
I0 recession OU* 15
10 0.7 M None - - 1.8 Accommodative esotropia
11 0.6 M MR recession OU* 0.7 0.9 Infantile esotropia
LR resection, I0 recession OU* 1.5
Rerecession with anterior I00U* 2 transposition
I0 myectomy OS* 3.1
12 3.5 M MR recession OU 0.8 3.5 Infantile esotropia
13 0.5 M MR recession OU* 0.5 2 Infantile esotropia
I0 recession OS* 3
SR recession OU 4
14 4.3 M MR recession OU 1 4 Infantile esotropia
LR resection, I0 recession OS 4
DVO, Dissociated vertical deviation; M, male; MR, medial rectus; OU, both eyes; LR, lateral rectus; SR, superior rectus; I0, inferior oblique; F, female; SO, superior oblique.
*Surgeries performed by senior author.

Santiago and Rosenbaum 7 Journal of AAPOS Volume 2 Number I February 1998
El6.1. Patient 13 showing dissociated vertical deviation OD in primary position that increases when Spielmann 22 occluder is used. Left head tilt shows control of dissociated vertical deviation OD. Right head tilt shows manifest (tropic) large dissociated vertical deviation OD. Figure also shows inferior oblique overaction of right eye. Absence of true hypertropia was ruled out by absence of hypotropia in contralateral eye by alternate prism cover testing.
recently been reported in 9% of patients with anomalous head postures. 7
The aim of this article is to increase awareness that dissociated vertical deviation may be a cause of head tilt. We describe a series of patients who developed an anomalous head posture to eliminate or control the dissociated vertical deviation. This cognizance gives us a new perspective in analyzing the dissociated vertical deviation phenomenon and a new insight in the manage- ment of patients with head tilts.
P A T I E N T S A N D M E T H O D S
The first case we recognized with dissociated vertical deviation and a manifest head tilt was in patient 1 in 1993. Since then, we prospectively collected similar consecutive cases until December 1996. Patients who have true hyperdeviation that occurred with dissociated vertical deviation were excluded. A total of 14 patients with dissociated vertical deviation and anomalous head postures from the consultation practice of the senior author were reviewed. Eight males and six females were included in this series. The patient profile before the development of head tilt is summarized in Table 1. This table lists age at first consultation, diagnosis, past ocular surgeries, and age when surgery was performed, as well as the age at which dissociated vertical deviation was noted or documented. Of the 14 patients, 2 were diagnosed with accommodative esotropia and the rest with infantile esotropia. Of the patients with infantile esou'opia, initial surgeries were done between the ages of 0.4 to 1.1 years, with a mean of 0.7 year.
Strabismus measurements were obtained in the pri- mary position, right and left gaze, 25 to 30 degrees upgaze and downgaze, and with manifest head tilt and forced contralateral head tilt testing. Dissociated vertical devia- tion was measured by prism undercover test whenever possible, u Dissociated vertical deviation was differenti-
ated from a true vertical deviation by the presence of hy-potropia in the contralateral eye in true hypertropias. 13 Ocular rotations were evaluated with use of a 9-point scale with 4 representing severe underaction, 0 as normal, and +4 as maximum overaction) 4, is Inferior oblique function was evaluated with ocular rotations in elevation and adduction, whereas superior oblique function was evalu- ated in depression and adduction. Quantitative measure- ments in the oblique gaze fields were not obtained. The amount of head tilt was measured with a goniometer whenever possible while the patient fixated on an accommodative target at 6 m and at 33 cm. Stereopsis was measured with a Titmus stereoacuity test at 33 cm. For patients without stereopsis of at least 3000 sec of arc, fusion at near was assessed with the Wor th 4 dot test.
In cases where the inferior oblique was recessed, pure recession was performed without anterior transposition. Our technique of inferior oblique recession places the anterior fibers of the inferior oblique 5 mm posterior to the lateral border of the inferior rectus insertion for a 14 mm recession. The posterior fibers are placed parallel to the long axis of the inferior rectus. For each millimeter less of a recession, the anterior fibers of the inferior oblique are moved 1 mm temporal to the lateral border of the inferior rectus (e.g., a 12 mm recession is 5 mm posterior and 2 mm temporal to the lateral border of the inferior rectus insertion).
R E S U L T S
Twelve of 14 patients assumed a head tilt away from the eye with the manifest dissociated vertical deviation or away from the eye with a larger amount of dissociated vertical deviation if the condition was bilateral (Figure 1). Two patients adopted an ipsilateral head tilt. A summary of representative clinical findings are shown in Table 2. Patients 6, 7, and 11 did not have complete measurements
Journal of AAPOS 8 Santiago and Rosenbaum Volume 2 Number 1 February 1998
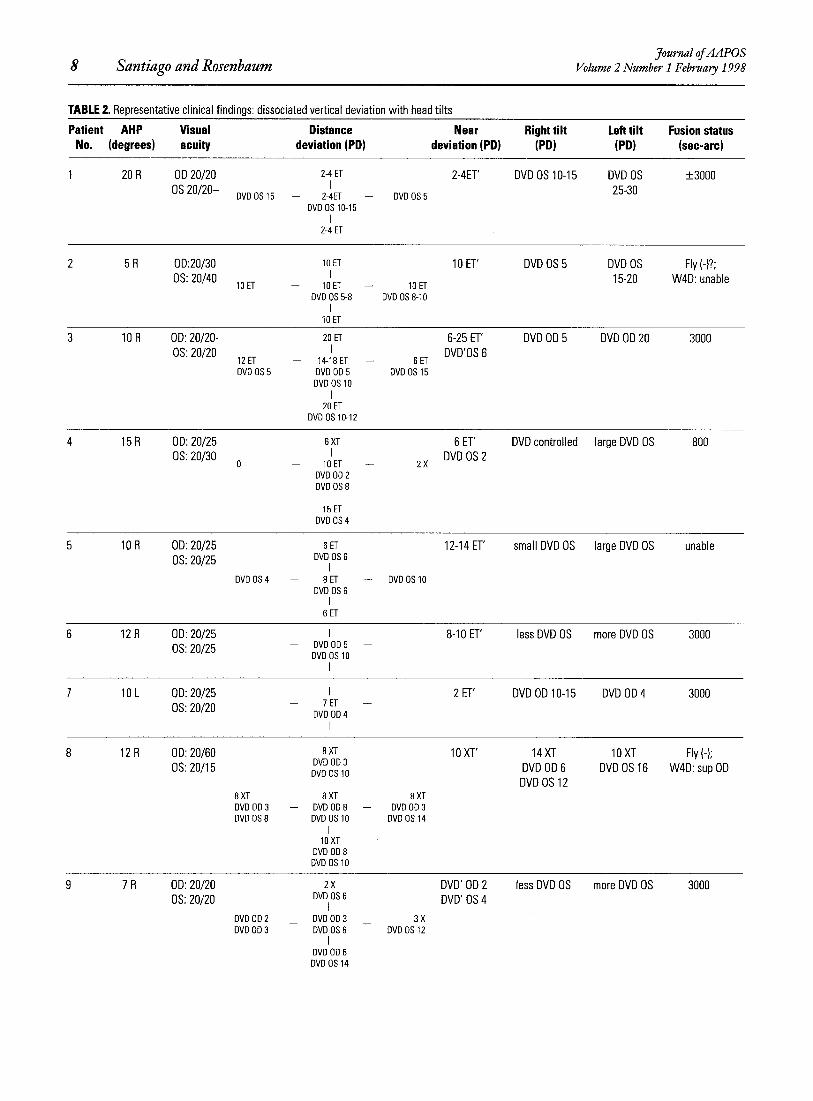
TABLE 2. Representative clinical findings: dissociated vertical deviation with head tilts
Patient AHP Visual Distance Near Right tilt Left tilt Fusion status No. (degrees) acuity deviat ion(PD) deviat ion(PD) (PD) (PD) (sec-arc)
1 20 R OD 20/20 2-4 ET 2-4ET' DVD OS 10-15 DVD OS + 3000 I 25-30 OS 20/20- DVD OS 15 -- 2-4ET -- DVD OS 5
DVD OS 10-15 I
2-4 ET
2 5 R 0D:20/30 lO ET 10 ET' DVD OS 5 DVD OS Fly (-)?; OS: 20/40 I 15-20 W4D: unable
1gET -- IOET -- IOET DVD OS 5-8 DVD OS 8-10
I 10 ET
3 10 R OD: 20/20- 20 ET 6-25 ET' DVD OD 5 DVD OD 20 3000 OS: 20/20 I DVD'OS 6
12 ET -- 14-18 ET -- 6 ET DVD OS 5 DVD OD 5 DVD OS 15
DVD OS 10 I
20 ET DVD OS 10-12
4 15 R OD: 20/25 6XT 6 ET' DVD controlled large DVD OS 800 OS: 20/30 I DVD OS 2
o - IOET -- 2X DVD OD 2 DVD OS 8
I 15 ET
DVD OS 4
5 10 R OD: 20/25 8 ET 12-14 ET' small DVD OS large DVD OS unable OS: 20/25 DVD OS 6
I DVD OS 4 -- 8 ET -- DVD OS 10
DVD OS 6 I
6 ET
6 12 R OD: 20/25 I 8-10 ET' less DVD OS more DVD OS 3000 0S:20/25 - DVDOD5 --
DVD OS 10 I
7 10 L OD: 20/25 I 2 ET' DVD OD 10-15 DVD OD 4 3000 OS: 20/20 - 7 ET --
DVD OD 4 I
8 12R OD: 20/60 8XT IOXT' 14XT IOXT Fly(-); OS: 20/15 DVD OD 3 DVD OD 6 DVD OS 16 W4D: sup OD DVD OS 10
I DVD OS 12 8 XT 8 XT 8 XT DVD OD 3 -- DVD OD 8 -- DVD OD 3 DVD OS 8 DVD OS 10 DVD OS 14
I 18 XT
DVD OD 8 DVD OS 10
9 7 R OD: 20/20 2 x DVD' OD 2 less DVD OS more DVD OS 3000 OS: 20/20 DVD OS 8 DVD' OS 4
DVD OD 2 DVD OD 3 3 X DVD OD 3 DVD OS 6 DVD OS 12
I DVD OD 6 DVD OS 14
Journal of AAPOS Volume 2 Number I February 1998 Santiago and Rosenbaum 9
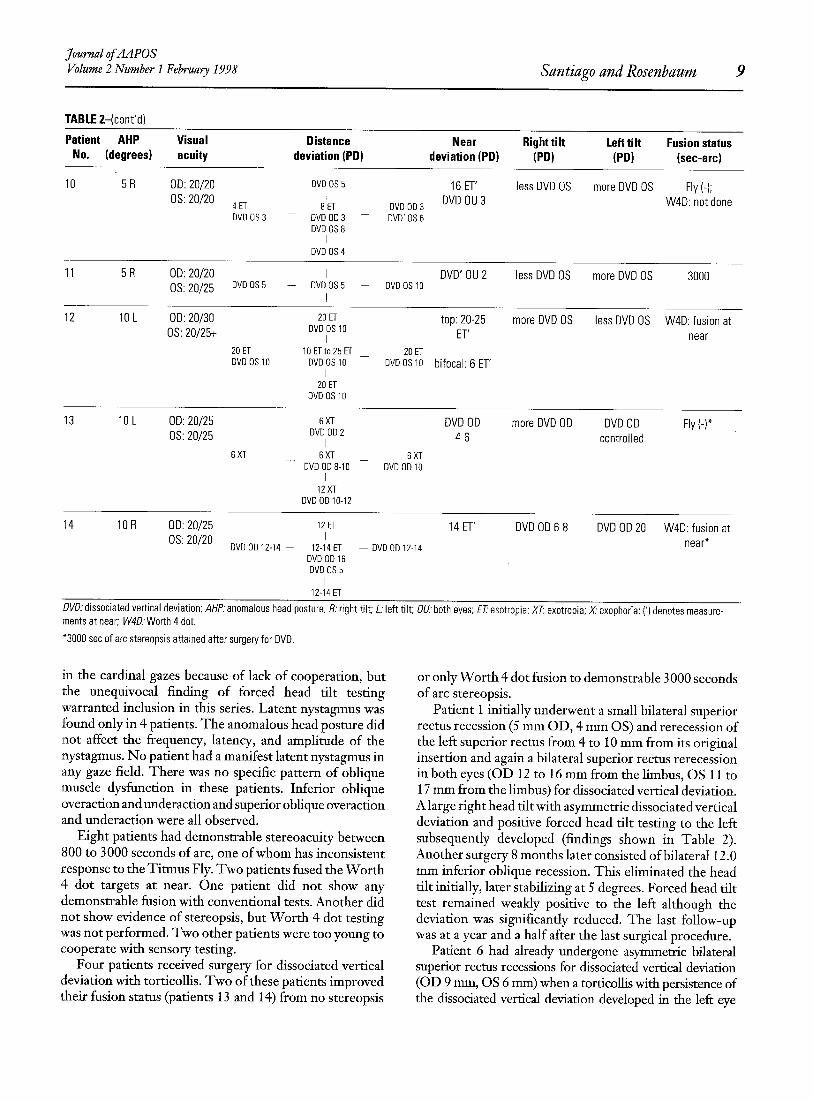
TABLE 2-(cont'd)
Patient AHP Visual Distance Near Rioht tilt Left tilt Fusion status No. (deorees) acuity deviation(PD) deviation(PD) (PD) (PD) (sec-arc)
10 5 R OD: 20/20 DVD OS 5 16 ET' less DVD OS more DVD OS Fly (-); I DVD OU 3 W4D: not done OS: 20/20 4 ET 8 ET DVD OD 3
DVD OS 3 -- DVD OD 3 - - DVD' OS 6 DV130S 8
I DVD OS 4
11 5 R OD: 20/20 I DVD' OU 2 less DVD OS more DVD OS OS: 20/25 13VD OS 5 -- DVD OS 5 -- DVD OS 10
P
3000
12 10 L OD: 20/30 20 ET top: 20-25 more DVD OS less DVD OS OS: 20/25+ DVD OS lO j ET
20 ET 10 ETto 25 ET 20 ET DVD OS 10 DVD OS 10 13VD OS 10 bifocal: 6 ET'
I 20 ET
DVD OS 10
W4D: fusion at near
13 10 L OD: 20/25 6XT DVD OD more DVD OD DVD OD OS: 20/25 DV13 013 2 4-6 controlled [
6 XT 6 XT 6 XT DVD OD 8-10 DVD OD 10
I 12XT
13VD OD 10-12
Fly (-)*
14 10 R OD: 20/25 12 ET 14 ET' BVD OD 6-8 DVD OD 20 OS: 20/20 I
DVD 0D12-14 -- 12-14ET - - DVO OD 12-14 DVD OD 16 DVD OS 5
I 12-14 ET
W4D: fusion at near*
DVD: dissociated vertical deviation; AHP: anomalous head posture; R.' right tilt; L: left tilt; OU: both eyes; ET~ esotropia; XT~ exotropia; X' exophoria; (') denotes measure- ments at near; W4D:Worth 4 dot.
*3000 sec of arc stereopsis attained after surgery for DVD.
in the cardinal gazes because of lack of cooperation, but the unequivocal finding of forced head tilt testing "warranted inclusion in this series. Latent nystagmus was :found only in 4 patients. The anomalous head posture did not affect the frequency, latency, and amplitude of the nystagmus. No patient had a manifest latent nystagmus in any gaze field. There was no specific pattern of oblique muscle dysfunction in these patients. Inferior oblique overaction and underaction and superior oblique overaction and underaction were all observed.
Eight patients had demonstrable stereoacuity between 800 to 3000 seconds of arc, one of whom has inconsistent response to the Titmus Fly. Two patients fused the Worth 4 dot targets at near. One patient did not show any demonstrable fusion with conventional tests. Another did not show evidence of stereopsis, but Worth 4 dot testing was not performed. Two other patients were too young to cooperate with sensory testing.
Four patients received surgery for dissociated vertical deviation with torticollis. Two of these patients improved their fusion status (patients 13 and 14) from no stereopsis
or only Worth 4 dot fusion to demonstrable 3000 seconds of arc stereopsis.
Patient 1 initially underwent a small bilateral superior rectus recession (5 mm OD, 4 mm OS) and rerecession of the left superior rectus from 4 to 10 mm from its original insertion and again a bilateral superior rectus rerecession in both eyes (OD 12 to 16 mm from the limbus, OS 11 to 17 mm from the limbus) for dissociated vertical deviation. A large right head tilt with asymmetric dissociated vertical deviation and positive forced head tilt testing to the left subsequently developed (findings shown in Table 2). Another surgery 8 months later consisted of bilateral 12.0 mm inferior oblique recession. This eliminated the head tilt initially, later stabilizing at 5 degrees. Forced head tilt test remained weakly positive to the left although the deviation was significantly reduced. The last follow-up was at a year and a half after the last surgical procedure.
Patient 6 had already undergone asymmetric bilateral superior rectus recessions for dissociated vertical deviation (OD 9 mm, OS 6 ram) when a torticollis with persistence of the dissociated vertical deviation developed in the left eye

10 Santiago and Rosenbaum Journal of AAPOS
Volume 2 Number I February 1998
(see representative findings in Table 2). The left superior rectus was recessed further from 12 mm to 17 mm from the limbus. Although both head tilt and dissociated vertical deviation improved, the patient had a moderate right inferior oblique overaction with incomitant dissociated vertical deviation. She underwent a 12.0 mm recession of the right inferior oblique. Her anomalous head posture was corrected, and the dissociated vertical deviation was markedly improved. Only a flick of dissociated vertical deviation was observed with the cover test. It has been a year since her last surgery.
By the time patient 13 was seen for an anomalous head posture, he had undergone two prior surgeries on the cyclovertical muscles. His left inferior oblique muscle had been recessed 11.5 mm for unilateral inferior oblique overaction, and both superior rectus muscles had been recessed for dissociated vertical deviation (OD 5 ram, OS 9 ram). Findings 5 months after the last surgery are summarized in Table 2. The patient's incomitant dissoci- ated vertical deviation associated with unilateral right inferior oblique overaction (resulting from fixation duress after weakening of both superior rectus) was treated with 12.0 mm right inferior oblique recession. Stereopsis improved to 3000 seconds of arc when none could be demonstrated preoperatively. Head tilt was corrected. A small dissociated vertical deviation (+_2 PD) remained in primary position. These findings have been stable at the time of his last follow-up (4 months after surgery).
Patient 14 had esotropia and bilateral dissociated vertical deviation that was larger in the right eye. His ipsilateral head tilt seemed to control the magnitude of the dissociated vertical deviation of the right eye (see summary of findings, Table 2). He subsequently underwent bilateral superior rectus recessions (OD 9 ram, OS 8 ram) and bilateral lateral rectus resection. After surgery, fusion at near improved to 3000 seconds of arc stereopsis. At the time of the last follow-up (8.5 months), the patient did not show any head tilting. Primary position measurements were 6 PD of esotropia, and dissociated vertical deviation of the left eye measured +_ 4 to 6 PD.
D I S C U S S I O N
Dissociated vertical deviation is most commonly associ- ated with congenital esotropia) During the manifest or tropic phase of dissociated vertical deviation, the patient is asymptomatic because of suppression. When the motor alignment is optimal, or when peripheral binocular vision is maintained, the deviation remains latent and is controlled as a phoria. With fatigue, illness, or emotional disturbance, dissociated vertical deviation may lapse into a manifest tropia. 2
Our series revealed that a head tilt away from the dissociated eye (or the eye with the larger dissociated vertical deviation if the disorder was bilateral) was more commonly adopted by patients in an attempt to control the dissociated vertical deviation. The four patients who underwent surgery for dissociated vertical deviation had
improvement in their head posture (by 10 to 15 degrees) after reduction of the size of the dissociated vertical deviation in the forced primary.
The patients in this series assumed a head posture to reduce the size of the dissociated vertical deviation or control it as a phoria. M1 patients had an initial diagnosis of esotropia. Two patients were diagnosed with accommoda- tive esotropia, and the rest with infantile esotropia.
The reason contralateral head tilt was assumed more commonly than ipsilateral head tilt remains perplexing. This is in sharp contrast to a recent series that found the reverse trend.: In both studies, however, anomalous head posture was assumed to control dissociated vertical deviation and was confirmed by contralateral forced head tilt testing, which revealed either an increase in the magnitude of dissociated vertical deviation or worsening of control of the dissociated vertical deviation.
Dissociated vertical deviation has been theorized to be the result of a supranudear dysfunction, whereas others have implicated several of the cyclovertical muscles either singly or in combination, z, 16-2, The laws of Sherrington and Hering may not be tmiversally applicable to all patients with dissociated vertical deviation. Jampolsky 19 has postulated that the normal vestibuloocular mechanisms may not be function- ing in dissociated vertical deviation.
The mechanism for head tilting in dissociated vertical deviation is not well understood. The stimulus to maintain fusion or at least optimal motor control appears to cause some patients with dissociated vertical deviation to have a head tilt. More than half our patients showed demon- strable peripheral fusion as evidenced by low-grade stereopsis or Worth 4 dot fusion. This level of fusion disappears when testing is performed in contralateral head tilt position. The inconsistent response of one patient to the fly vectograph may be related to the phoric and tropic phases of dissociated vertical deviation. The dissociative Worth 4 dot test used to test fusion patients may not be optimal in patients with possible borderline fusion capabilities. In all patients who were unable to cooperate with testing for fusion or stereopsis, anomalous head posture was adopted to minimize the magnitude or enhance the control of the dissociated vertical deviation (motor control). In all patients, including those in whom we failed to document peripheral fusion, no to minimal shift by prism undercover test was seen with their preferred head flits. M1 four patients that underwent surgery for dissociated vertical deviation had improved head postures after reduction of the size of dissociated vertical deviation in primary gaze. Two patients even showed improved fusion status after surgery.
Anomalous head posture may also be due to a superior rectus contracture that can occur after prolonged dissoci- ated vertical deviation. 19 This may explain the observation that patients with dissociated vertical deviation may assume a head posture similar to that of patients with cyclovertical muscle palsy. 2° A right superior rectus

Journal of AAPOS Volume 2 Number 1 February 1998 Santiago and Rosenbaurn I 1
contracture, for example, is associated with increased vertical deviation on ipsilateral head tilt (so patients assume a contralateral head tilt). This may be true in patients who did not have any cyclovertical muscle surgery and patients who had weakening procedures of the inferior oblique muscle without accompanying superior rectus procedures. In all patients, however, no hypertropic deviation was found on alternate cover testing in the
vertical muscle imbalance. In these patients the dissoci- ated vertical deviation is not manifest because of its control by the compensatory head flit. T h e confirmation is easy with attention to dissociated vertical deviation measurements in the different cardinal positions of gaze, as well as forced head tilt testing to the opposite side, which usually reveals a larger dissociated vertical deviation by prism undercover test.
cardinal positions of gaze or on forced head tilt testing. I t remains possible that patients may be tilting their
heads for other reasons, such as unrecognized nystagmus or idiopathic causes. T h e unequivocal findings of a larger dissociated vertical deviation on forced contralateral head tilt testing argue against these possibilities. All patients controlled the dissociated vertical deviation f rom a motor stand point when using their preferred head posture.
Another interesting observation is that head tilting did not occur in our patients until strabismus surgery (either for horizontal deviation or dissociated vertical deviation) has been successful in correcting or improving the deviation in primary gaze. It may be theorized that before surgery the magnitude of the strabismus interfered with fusional mechanisms. With improved alignment in the primary position, the pauent's fusional mechanisms are allowed to function. In some patients the optimal control of alignment is accomplished with an anomalous head posture.
Lang 2I described a syndrome consisting of congenital esotropia with ocular posture. T h e patient often had nystagmus with a latent component , dissociated vertical deviation, and a head tilt not related to a null zone for nystagmus. T h e head posture was often variable in direction and the correction of even a mild refractive error improved the head posture. Our patients were all given optimal spectacle correction when necessary and yet still manifested a head tilt.
Anomalous head posture can interfere with a child's education, physical and psychosocial functions, and appear- ance. Reduction of head tilt can be accomplished by successful surgical reduction of the amplitude of dissociated vertical deviation. A recent series reported that 9% of head tilts are caused by dissociated vertical deviation and that a manifest head tilt was present in 35% of patients with an ocular fixation preference. 7 With the way our database is constructed, it is very difficult to determine our incidence of anomalous head postures in patients with dissociated vertical deviation. W e see many patients with dissociated vertical deviation, but since we started this study we have only seen 14 such cases in a 3-year observation period.
This unusual cause of an anomalous head posture should be included in the differential diagnosis of a child with a head tilt. Unless the physician is aware of this association, the presence of dissociated vertical deviation may be overlooked. Head tilting may be improved after surgical correction of dissociated vertical deviation. In many cases the parent 's concern in seeking medical attention was the observation of a head posture and not a
References
1. Helveston EM. Dissociated vertical deviation--a clinical and laboratory study. Trans Am Ophthalmol Soc 1980;78:734-79.
2. Parks MM. Dissociated hyperdeviations. In: Ocular motility and strabismus. Hagerstown (MD): Harper & Row; 1975. p. 149-52.
3. Wilson ME, McClatchey SK. Dissociated horizontal deviation. J Pediatr Ophthalmol Strabismus 1991;28:90-5.
4. Crone RA. Alternating hyperphoria. Br J Ophthalmol 1954; 38:591-604.
5. Lyle TK, Bridgeman GJO. The binocular reflexes and the treatment of strabismus. In: Worth and Chavasse's squint. London: Balliere, Tindall & Cox; 1959. p. 345-55.
6. Anderson JR. Ocular vertical deviations and the treatment of strabismus. 2nd edition. London: British Medical Association; 1959.
7. Bechtel RT, Kushner BJ, Morton GV. The relationship between dissociated vertical divergence (DVD) and head tilts. J Pediatr Ophthalmol Strabismus 1996;33:303-6.
8. Cibis GW. Dissociated vertical deviation. In: Cibis GW, Tongue AC, Stass-Isern ML, editors. Decision making in pediatric ophthalmology. St. Louis: BC Becker; 1993. p. 234-5.
9. Hiatt RL, Cope-Troupe C. Abnormal head positions due to ocular problems. Ann Ophthalmol 1978;10:881-92.
10. Kushner BJ. Ocular causes of abnormal head postures. Ophthalmology 1979;86:2115-25.
11. Rubin SE, Wagner RS. Ocular torticollis. Surv Ophthalmol 1986;30:366-76.
12. Schwartz T, Scott W. Unilateralsuperior rectus recession for the treatment of dissociated vertical deviation. J Pediatr Ophthalmol Strabismus 1991;28:219-22.
13. Wesson ME. The ocular significance of abnormal head postures. Br Orthopt J 1964;21:14-28.
14. Scott WE, Kraft SP. Classification and Surgical treatment of superior oblique palsies, I: unilateral superior oblique palsies. Trans New Orleans Acad Ophthalmol 1986;34:15-38.
15. Doughty DD, Lennarson LW, Scott WE. A graphic portrayal of versions. Perspect Ophthalmol 1978;2:55-9.
16. Verhoeff FH. Occlusion hypertropia. Arch Ophthalmol 1941;25:780-95.
17. Brown HW. Dissociated vertical anomalies. In: Arruga A, editor. International Strabismus Symposium. New York: S Karger; 1966. p. 337-42.
18. Stegall FW. Dissociated vertical deviations: current research. Am Orthopt J 1981 ;31:40-6.
19. Jampotsky A. Management of vertical strabismus. Trans New Orleans Acad Ophthalmol 1986;34:141-71.
20. Clark JT. Approach to patient with abnormal head posture. Am Orthopt J 1995;45:2-6.
21. Lang J. Der kongenitale oder fruhkindliche Strabismus [Congenital or infantile strabismus]. Ophthalmologica 1967;154:201-8.
22. Spielmann A. Adduction, latent nystagmus, infantile strabismus and the optomotor syndrome of congenital uniocular organic amblyopia. In: Kaufman H, editor. Transactions of the sixteenth meeting of the European Strabismological Association. Giessen: The Association; 1987. p. 291.
Copyright © 2022 FDOKUMEN