Dispensing and Community Pharmacy Exam Date
28
Exam: F. Y. B. Pharm (Sem I – CBCS) Subject: Dispensing and Community Pharmacy Exam Date: 12.12.17 Q. P. Code: 05093 Answer Key Q.1.a) Classify dosage forms (2) Q.1.b) Define i) Compounding and ii) Dispensing (2) Compounding: The preparation, mixing, assembling, packaging, or labeling of a drug or device as a result of a practitioner’s prescription Dispensing: It involves supplying already available packed medicine/drug manufactured by pharmaceutical manufacturers to patient or patient’s caretaker by evaluation of prescription. Q.1.c) Write in brief about dispensing of proprietary medicines. (2) A proprietary medicine in a non-secret compound which is marketed under the maker’s name (i.e. medicines having a brand name). These can be dispensed in 2 ways: 1. From a manufacturer’s bulk container This includes: a) Pouring the prescribed volume of liquid from a bottle usually holding 500 ml to 2 litres into a container of appropriate size b) Counting out the required number of a unit dosage form like tablets or capsules from a tin or bottle usually holding from 100 – 1000 units and packing them into a container of appropriate size. Exceptions: some medicines cannot be repacked if they fall under the following 2 categories: i. Proprietary preparations requiring addition of a vehicle during dispensing ii. Proprietary medicines in special container: eg aerosol cans Dosage Form Solids Unit eg. tablets, capsules Bulk eg. powders, granules Liquids Monophasic eg. solutions Biphasic eg. suspensions, emulsions Semi Solids eg. ointments, pastes, creams, gels
-
Upload
khangminh22 -
Category
Documents
-
view
3 -
download
0
Transcript of Dispensing and Community Pharmacy Exam Date

Exam: F. Y. B. Pharm (Sem I – CBCS) Subject: Dispensing and Community Pharmacy Exam Date: 12.12.17 Q. P. Code: 05093
Answer Key Q.1.a) Classify dosage forms (2)
Q.1.b) Define i) Compounding and ii) Dispensing (2) Compounding: The preparation, mixing, assembling, packaging, or labeling of a drug or device as a result of a practitioner’s prescription Dispensing: It involves supplying already available packed medicine/drug manufactured by pharmaceutical manufacturers to patient or patient’s caretaker by evaluation of prescription. Q.1.c) Write in brief about dispensing of proprietary medicines. (2) A proprietary medicine in a non-secret compound which is marketed under the maker’s name (i.e. medicines having a brand name). These can be dispensed in 2 ways: 1. From a manufacturer’s bulk container
This includes: a) Pouring the prescribed volume of liquid from a bottle usually holding 500 ml to 2
litres into a container of appropriate size b) Counting out the required number of a unit dosage form like tablets or capsules
from a tin or bottle usually holding from 100 – 1000 units and packing them into a container of appropriate size. Exceptions: some medicines cannot be repacked if they fall under the following 2 categories:
i. Proprietary preparations requiring addition of a vehicle during dispensing ii. Proprietary medicines in special container: eg aerosol cans
Dosage Form
Solids
Unit eg. tablets, capsules
Bulk eg. powders, granules
Liquids
Monophasic eg. solutions
Biphasic eg. suspensions, emulsions
Semi Solids eg. ointments, pastes, creams, gels

2. In manufacturer’s original pack Many medicines are issued in small individual packs coinciding with the most popular quantities ordered on prescription. Eg aerosols, ointments etc Some key points to be considered while dispensing in the original pack include:
i. All literature eg leaflets should be removed unless clearly intended for the patient
ii. A dispensing label should be attached without hiding the manufacturer’s label
Q.1.d) Calculate the dose for a 8 year old patient if the adult dose of the same drug is 250 mg (2) Solution: 100 mg Q.1.e) Define emulsion. Classify emulsifying agents. (2) Definition: An emulsion is essentially a liquid preparation containing 2 immiscible liquids, one of which is distributed throughout the other as minute globules
Q.1.f) Enlist the advantages and disadvantages of powders as a dosage form (2) Advantages (Any 2)
i. Materials which are insoluble and susceptible to microbial attack can be dispensed in powder form.
ii. Convenient to dispense a drug that has large dose – powders for indigestion, constipation and diarrhoea. Dose is taken by mixing it with water or by placing it on tongue and swallowing it with a drink of water.
iii. Small children and elderly patients cannot swallow tablets and capsules – drug can be dispensed in powdered form.
Emulsifying agents
Natural
Plant source eg. acacia
Animal source eg. wool fat
Semi synthetic polysaccharides
eg NaCMC Synthetic
Anionic eg SLS
Cationic eg cetrimide
Nonionic eg. Tweens
Inorganic eg. bentonite
Alcohols eg. lecithin

iv. Faster absorption as compared to tablets and capsules. v. Divided powders provides a convenient means of dispensing correct quantities of
powder where the ingredients are mixed and taken. Disadvantages (Any 2)
i. Drugs having bitter and unpleasant taste cannot be dispensed satisfactorily in powdered dosage form – taken with honey or jam.
ii. Not the ideal form to dispense volatile, deliquescent, hygroscopic or oxygen sensitive drug.
iii. Dispensing of powder is a time consuming process – dispensing of potent drug. iv. Bulk powders – 5gm assumed to be equivalent to 5ml – labelled in terms of 5ml
spoon. Same weight of various medicaments often produce different volumes so this method of dosage is in accurate
Q.1.g) Enumerate the advantages and disadvantages of pills (2) Advantages (Any 2)
i. Easy to formulate ii. Compact in size hence swallowing is easy
iii. Masks unpleasant taste and odour iv. Stable for a long period of time
Disadvantages (Any 2)
i. Bioavailability is low ii. They pass through the GIT unaltered i.e. disintegration is variable
iii. Maintenance of shape is difficult iv. Dose uniformity is low
Q.1.h) Give anyone example of chemical incompatibility. How would you overcome the same? (2) Any 1 example – 1 mark Solution for the same – 1 mark Eg. 1 Incompatibility: Potassium chlorate + charcoal/ sugar/ sulphur/ organic compounds etc leads to explosion if trituration or heating is done Solution: Such compounds should be powdered separately and mixed lightly without any friction Eg. 2 Incompatibility: Carbon dioxide is evolved if a carbonate or bicarbonate is dispensed in a liquid medicine containing an acidic drug. To prevent leakage or explosion, the reaction must be completes before the preparation is bottled. Eg. Borax + sodium bicarbonate and glycerine Solution: Boric acid produced from the hydrolysis of borax, reacts with glycerol to form monobasic glycerol-boric acid which liberates carbon dioxide from the bicarbonate. Hot water is added to hasten the reaction

Q.1.i) Enlist the principles of pharmaceutical care (2) 1. Data collection 2. Information evaluation 3. Formulating a plan 4. Implementing the plan 5. Monitoring and modifying the plan assuring positive outcomes
Q.1.j) Give any 4 examples of OTC products (2) Any 4 products for 0.5 mark each

Q.2.a) Enlist the various routes of administration. Explain the oral route in detail (4) Marking scheme: enlisting – 2 marks Advantages of oral route – 1 mark Disadvantages of oral route – 1 mark Routes of drug administration:
1. Enteral a. Oral b. Sublingual c. Rectal
2. Parenteral a. Intravenous b. Intramuscular c. Subcutaneous d. Intradermal e. Intrathecal f. Intraosseous g. Intra-arterial
3. Others a. Topical b. Inhalational c. Ocular d. Nasal e. Otic
Oral route: Giving a drug by mouth is the most common route of administration but it is also the most variable, and requires the most complicated pathway to the tissues. Advantages:
1. Convenient - can be self- administered, pain free, easy to take 2. Absorption - takes place along the whole length of the GI tract 3. Cheap - compared to most other parenteral routes
Disadvantages:
1. Sometimes inefficient - only part of the drug may be absorbed 2. First-pass effect - drugs absorbed orally are initially transported to the liver via the
portal vein eg. Propranolol, lidocaine 3. Irritation to gastric mucosa - nausea and vomiting 4. Destruction of drugs by gastric acid and digestive juices eg. Penicillin, proteins and
peptides 5. Effect too slow for emergencies 6. Unpleasant taste of some drugs 7. Unable to use in unconscious patient

Q.2.b) Highlight the container-closure and labelling directions for (any TWO). (4) Container closure – 1 Any 2 labelling directions – 1 Emulsion Storage: Amber coloured narrow mouth bottles with a plastic screw closure Labelling directions:
a. Discard if two layers separate b. Shake well before use c. Store in a cool place away from sunlight d. Do not freeze
Suppository Storage: Rigid paperboard boxes or Flat box with a lid Labelling directions:
a. Store in a cool place b. For rectal use only c. Not to be taken orally d. Moisten before use (for macrogol suppositories)
Lozenge Storage: Air tight container or strip packing Labelling directions:
a. To be sucked slowly b. Do not drink water immediately after consumption
Q.2.c) Comment on the following prescription. (4) Rx Calciferol solution - 0.15 ml Glycerin - 0.3 ml Water (q.s.) to - 5 ml Label: 5 ml to be taken daily Calculation and formula table – 2 Procedure – 1 Label – 1
Sr. no. Ingredient Quantity given
1 Calciferol solution 0.15 ml
2 Glycerin 0.3 ml
3 Water q.s. to 5 ml
Formula for primary emulsion As the oil is less than 20%, bland oil is added to make up the internal phase. Total quantity
of oil required is
Oil (4) Water (2) Acacia (1) Tragacanth (1/10)

Calciferol solution
Arachis oil
0.15 ml 0.85 ml 0.5 ml 0.25 g 0.025 g
Procedure:
1. Measure out calciferol solution and Arachis oil and transfer them to a clean and dry mortar
2. Lightly disperse acacia and tragacanth in the oil mixture 3. Add the water required for primary emulsion at once and triturate vigorously till a
clicking sound is distinctly heard. 4. Add glycerine and small quantity of water to make pourable. 5. Transfer to a pre-tared container. 6. Make up the volume with water. 7. Label appropriately.
Label
5 ml
The Emulsion
Rx, Miss XYZ
Direction: 5 ml to be taken daily Shake well before use Discard if two layers separate
Storage: Store in a cool place away from sunlight Do not freeze
Dispensed by: Checked by: Dispensing date: Expiry date:
Name and address of the pharmacy

Q.3.a) Define a prescription and explain its various parts (4) Definition - Prescription is an order from a physician, dentist or any other registered medical practitioner to a pharmacist for the supply of medicine, dressing or appliance for the patient. Its parts:
1. Date - Date must be written on the prescription by the prescriber at the same time when it is written. The date on the prescription helps a pharmacist to find out the cases where prescription is brought for dispensing long time after its issue. Prescriptions containing narcotic or other habit-forming drugs must bear the date.
2. Patient information - Name, age, sex and address of the patient must be written on the prescription. If it is not written then, the pharmacist himself should ask the patient about these particulars and put down at the top of the prescription. This avoids the possibility of giving the finished product to a person other than the one it is meant for. Patient's full name must be written instead of surname or the family name. Age and sex of the patient especially in the case of children helps the pharmacist in checking the medication and the dose. Therefore, there will be less danger of its being administered to the wrong member of the family or the hospital ward having similar names. The address of the patient is recorded to help for any reference at a later stage, to contact the patient or to deliver the medication personally.
3. Rx symbol or Superscription - The superscription is represented by a symbol, Rx, which is always written at the beginning of the prescription. In the days of mythology and superstition the symbol was considered as a prayer to Jupiter, the God of healing, for quick recovery of the patient but now this symbol is understood as an abbreviation of the Latin word recipe, meaning "take thou" or "you take".
4. Medication prescribed or Inscription - This is the main part of the prescription. It contains the names and quantities of the prescribed ingredients. The names of the ingredients are written each on a separate line, followed by the quantity ordered and the last item written is generally the vehicle or diluent. In complex prescriptions containing several ingredients the inscription is divided into three parts:
i. The base or the active medicament which is intended to produce the therapeutic effect;
ii. The adjuvant which is included either to enhance the action of the medicament or to make the product more palatable;
iii. The vehicle which is either used to dissolve the solid substances and/or to increase the volume of the preparation for ease of administration.
5. Dispensing directions to the pharmacist or Subscription - This part of the prescription contains prescriber's directions to the pharmacist regarding the dosage form to be prepared and number of doses to be dispensed. Since, nowadays only a few prescriptions are compounded therefore such directions are less frequent.
6. Direction for patient or Signatura - - It is usually abbreviated as "Sig" on the prescriptions and consists of the directions to be given to the patient regarding the administration of the drug. It usually indicates the quantity of medicament or number or dosage units to be taken, how many times in a day or at what time it should be taken and the manner in which it is to be administered or applied.

7. Refill, special labelling, and /or other instructions – The number of authorised refills should be indicated on each prescription by the prescriber to avoid unwarranted refills especially for habit forming drugs.
8. Signature and registration number of prescriber - All other parts of the prescription may be printed or type-written but the prescriber's name must be hand-written and should be signed with ink. This eliminates the danger of dispensing medicament on a spurious order and it authenticates the prescription. The prescriptions containing narcotic or other habit-forming drugs must bear the address and registration number of the prescriber. This identifies the special license which a prescriber must have to prescribe the narcotic and other habit-forming drugs
Q.3.b) Classify ointment bases. Describe any ONE base in detail (4) Classification – 1 mark Description of base – 3 marks
1) Oleaginous base: These are the oldest ointment bases but are slowly losing their importance because:
• They are greasy • They are sticky and are difficult to remove both from skin and clothing. • They retain body heat which may produce uncomfortable feeling of warmth. • They do not help in the absorption of medicaments.
Examples: Petrolatum (white paraffin and soft paraffin)
• It is a purified mixture of semi-solid hydrocarbons obtained from petroleum. • Two type – Yellow and white • Both the paraffins have M.P of 38°C to 56°C. • White soft paraffin is prepared by bleaching yellow paraffin. • White soft paraffin is used when the medicament is white or colourless. • White soft paraffin is never used in the preparation of ophthalmic ointments
because white soft paraffin may contain traces of bleaching agents which are left over after bleaching the yellow soft paraffin and hence it may cause irritation to eye.
Ointment bases
Oleoginous bases eg. paraffin
Absorption Bases
Non-emulsified bases eg. wool fat
Water in oil bases eg. hydrous wool fat Water miscible bases eg.
emulsifying ointment
Water soluble bases eg. macrogol

Hard paraffin • It is a purified mixture of solid hydrocarbons obtained from petrolatum. • It is colourless or white translucent, odourless, tasteless wax like substance. • It is used to harden the ointment base.
Liquid Paraffin • It consists of mixture of liquid hydrocarbons and obtained from petroleum by
distillation. • It is also known as white mineral oil or liquid petroleum. • It is colourless, odourless, tasteless and transparent oily liquid. • It is soluble in ether and chloroform but insoluble in water and alcohol. • It is used along with hard paraffin and soft paraffin to get a desired consistency of
the ointment 2) Absorption bases
• They are generally anhydorus substances • They have the property of absorbing water but still retain their ointment like
consistency. • Non-emulsified bases absorb water and aqueous solutions producing w/o emulsions. • Water in oil emulsions are capable of absorbing more water.
Advantages: • Compatible with large number of medicaments. • Absorb a large quantity of water or aqueous substances. • Heat stable. • May be used in their anhydrous form or in emulsified form. • They are quite greasy, but these can be easily removed from the skin
A] Non-emulsified bases: They absorb water and aqueous solution producing w/o emulsions They consists of mixture of a sterol type emulgent with one or more paraffins As compared to hydrocarbon bases:
Less occlusive Good emollients Assist oil soluble medicaments to penetrate the skin Easier to spread and wash
Examples: i) Wool fat
• It is purified fat like substance obtained from the wool of sheep. • It is also known as anhydrous lanolin. • It can absorb about 50% of its weight of water. • So it is used in ointments where the proportion of water or aqueous liquids to be
incorporated in hydrocarbon base is too large. • It is an important constituent of simple ointment base and eye ointment base.
ii) Wool alcohol • It is obtained from wool fat by treating with alkali and separating the fraction
containing cholesterol and other alcohols. • It contains not less than 30% of cholesterol. • It used as an emulsifying agent for the preparation of w/o emulsion.
• It is also used to improve the texture, stability and emollient properties of o/w emulsions.
iii) Beeswax • It is purified wax obtained from honey comb of bees. • It is available as yellow beeswax and white beeswax. • White beeswax is obtained by bleaching the yellow beeswax. • It is used as a stiffening agent in pastes and ointments.
iv) Cholesterol • Hydrophilic petroleum USP is an absorption base. • It contains 3% cholsterol, 3% stearyl alcohol, 8% white beeswax and 86% white soft
paraffin • Cholesterol confers water absorbing power
B] Emulsion bases • These bases are semi-solid or have a cream like consistency. • Both o/w and w/o emulsions are used as ointment base. • The o/w type of emulsion bases are more popular because these can be easily
removed from the skin or clothes by washing with water. • The w/o type of bases are greasy and sticky. • The emulsifying ointment is prepared from emulsifying wax, white soft paraffin and
liquid paraffin. Example: Hydrous wool fat
• It is the purified fat like substance obtained from wool of sheep. • It is also known as lanolin. • It is insoluble in water but soluble in ether and chloroform. • Hydrous wool fat is a mixture of 70% w/w wool fat and 30% w/w purified water. • It is used alone as emollient and as an ingredient of several other ointments.
3) Water Miscible Bases Advantages:
1. Even easier to wash off than absorption bases 2. Miscibility with exudates from lesions 3. Reduced interference with skin functions 4. Good contact with skin because of their surfactant content 5. High cosmetic acceptability 6. Greater patient compliance 7. Easy removal from hair.
Examples of bases: Emulsifying ointment BP (anionic), cetrimide emulsifying ointment BP (cationic) and cetomacrogol emulsifying ointment BP (non-ionic). They contain paraffins and o/w emulgent General formula
Ingredient Quantity
Anionin/ cationin/ non-ionic emulsifying wax 30 %
White soft paraffin 50 %
Liquid paraffin 20 %

Official examples: Compound benzoic acid ointment BPC (Whitfield’s ointment), zinc undecenoate ointment BPC 4) Water soluble bases
• These are commonly known as “greaseless ointment bases”. • The water soluble bases consist of water soluble ingredients such as polyethylene
glycol polymers which are popularly known as “carbowaxes” or “Macrogol” • The carbowaxes are water soluble, non-volatile and inert substances. • Depending upon the molecular weight, carbowaxes are available in different
consistencies i.e. liquids, semisolids and solids. Their molecular weight varies from 200 to 6000.
• 200 – 400: viscous liquid, 1500: greasy semisolid, 1540 – 6000: waxy solids • By mixing different carbowaxes, ointments of varying consistencies can be obtained. Advantages
• Easy removal from skin • Good absorption by skin • Good solvent properties • Freedom from greasiness • Satisfactory aging properties • Compatibility with many dermatological medicaments
Disadvantages • Limited uptake of water • More hygroscopic than paraffins • Reduction in activity of certain antibacterial agents like phenols,
hydroxybenzoates and quarternary ammonium compounds • Solvent action on polythene
Q.3.b) Describe in detail the disadvantages of cocoa butter as a suppository base (4) Disadvantages of cocoa butter: 1. Polymorphism:
Polymorphism in cocoa butter is observed due to high proportion of unsaturated triglycerides. The formation of various forms of cocoa butter depends on the degree of heating, on the cooling process and on the conditions during this process. Each form of cocoa butter has different melting point and drug release rates. Cocoa butter exists in 4 crystalline forms: • α form
• Melts at 24oC • Obtained by suddenly cooling melted cocoa butter to 0oC.
• ß form • Crystallizes out of the liquefied cocoa butter with stirring at 18 to 23oC. • Its melting point lies between 28 and 31oC.
• ß` form • Changes slowly into the stable ß form. • Melts between 34 and 35oC. • Change is accompanied by volume contraction.

• γ form • Melts at 18oC • Obtained by pouring a cool cocoa butter, before it solidifies, into a container
which is cooled at deep freeze temperature
Cocoa butter when heated to temperature above 36°C with slow cooling leads to the
formation of stable ß crystals with normal melting point. But if it is heated to above
36°C, unstable α crystals are formed which melt at about 20°C. Even if the cocoa
butter is heated to below 36°C but rapidly cooled leads to the formation of unstable
γ crystals which melt at about 15°C. Unstable forms return to stable form after
several days & may not set at room temp. Or if set by cooling may remelt in warm
conditions
2. Adherence to mould - Cocoa butter does not contract sufficiently on cooling to loosen the suppositories in the mould. Sticking may be overcome by adequate lubrication.
3. Low softening point - To raise the softening point, white bees wax may be added to
theobroma oil suppositories intended for use in tropical and subtropical countries
4. Melting point reduction - Phenol and chloral hydrate have a tendency to lower the melting point of cocoa butter. So, solidifying agents like beeswax (4%) may be incorporated to compensate for the softening effect of the added substance.
5. Rancidity during storage - Due to the oxidation of unsaturated glycerides
6. Poor water absorbing capacity - Improved by the addition of emulsifying agents.
7. Leakage from the body - Sometimes the melted base escapes from the rectum or vagina,
so, it is rarely used as a pessary base
8. Expensive - Relatively high cost
Q.3.c) Discuss compounding and dispensing of effervescent granules in detail (4) Effervescent granules are uncoated granules generally containing acid substances and carbonates or hydrogen carbonates which react rapidly in the presence of water to release carbon dioxide. They are intended to be dissolved or dispersed in water before administration. Excipients: Drug, citric acid, tartaric acid and sodium bicarbonate. A sweetener like saccharin or sucrose can be added. In water, acid and bicarbonate react and release CO2. This carbonated water masks bitter and saline taste of drug. They could be prepared by 2 methods: 1) Heat method Procedure:
• Heat evaporating dish on a water bath to 60°C • Add previously sieved drug and effervescent mixture • Mix when the powder becomes moist • Damp mass (dough) • Passed through sieve of suitable size (# 8-10) • Dried in oven at temperature not exceeding 54°C • Passed through sieve of suitable size (# 16-22 superimposed on # 36-44) • Packed in air tight container
Water needed for granulation is provided from 2 sources: 1. From water of crystallization of citric acid – it contain one molecule of water which is released on heating
Citric Acid 2. Water produced from reaction of citric acid and tartaric acid with sodium bicarbonate
Loss of weight occurs due to loss of water and carbon dioxide. Approximately 1/7th of the powder weight is lost (must be taken into consideration while calculating the quantity of granules to be prepared) 2) Wet granulation Procedure:
Drug and excipients are sieved and weighed
A damp mass is made with the aid of a non-aqueous solvent like alcohol
Passed through sieve of suitable size (# 8-10)
Dried in oven at temperature not exceeding 54°C
Passed through sieve of suitable size (# 16-22 superimposed on # 36-44)
Packed in air tight container Packaging: They are packaged in air tight container or tightly closed aluminum sachets Labelling directions: To be dissolved in water and to be consumed while effervescing.

Q.4.a) How would you formulate a suspension containing an indiffusible solid? (4) Suspensions containing indiffusible substance do not remain evenly distributed for long time, leading to non-uniformity of dosage. Eg. Calamine, chalk etc General method of preparation 1. Finely powder all the ingredients 2. Mix them in mortar and add compound tragacanth powder 3. Measure3/4th of the vehicle and triturate to form a smooth cream 4. Examine the suspension for foreign particles 5. Pour into a tared bottle 6. Rinse the mortar with small quantity of the vehicle 7. Transfer the rinsings to the bottle 8. Add any liquid ingredient 9. Add more of the vehicle to produce the required volume Q.4.a) Classify solutions. Describe in brief any TWO solutions meant for oral use (4) Classification of solution 1. Taken orally
a. Mixtures b. Elixirs c. Linctuses d. Draughts e. Syrups f. Drops
2. Used in mouth and throat a. Mouthwashes b. Gargles c. Throat paints d. Throat sprays
3. Instilled in body cavities a. Douches b. Enemas c. Ear drops d. Nasal drops e. Nasal sprays
4. Applied to body surfaces a. Collodions b. Liniments c. Lotions d. Paints

Solutions taken orally: 1) Mixtures: Prescribed for acute conditions like cough, indigestion, diarrhoea, constipation and rheumatism Short shelf life i.e. generally one month If dose is less or not a multiple of 5, the mixture must be diluted to be able to be taken as 5ml spoonful. Dilution may affect stability hence must be done just before administration Excipients: Medicaments: Infusions Vehicle with definite therapeutic activity. 1 part of concentrate & 9 parts of water. Should be used within 12 hours. Eg: Compound Gentian Infusion (appetizer) & Senega Infusion (Expectorant) Water made from essential oil Oil dissolved in high concentration of alcohol. Part of oil is precipitated – fine dispersion. Shake well before use. Eg: Anise oil, Cinnamon oil etc. Vehicle: Potable water Should be supplied from mains. Avoid local storage tank water as contaminated with micro-organisms. Freshly Boiled and cooled water BP Used when the source is local storage tank. Potable water is unsuitable – for ferrous sulphate preparations. Aromatic Waters Flavouring/ therapeutic/ preservative action Prepared by diluting a concentrated preparation. Concentrate : water – 1: 39 except for chloroform water (1:1) Sometimes reduction of preservative activity due to dilution. Adjuncts Antioxidants & reducing agents: Ascorbic acid – prevents oxidation of ferrous to ferric ion Sodium metabisulphite – prevents oxidation of sodium salicylate. Colouring agents: No special colouring agents are added. Sometimes medicaments are coloured. Flavouring agents:
Aromatic waters - Anise water Syrup and/or glycerol - Sweetening children's preparations. Liquorice liquid extract - Disguising the taste of saline ingredients Lemon Spirit - Cover the taste of alkaline citrates. Orange syrup & compound orange spirit - Disguise the metallic and astringent taste of iron salts
Preservatives:
Chloroform (0.25% v/v) Double strength chloroform water. Preservatives in products of vegetable extracts. Sweetening properties. Benzoic acid (0.1% w/v) Main activity – undissociated acid Effective in acid preparations of pH 5 or below. Not effective in neutral & alkaline solutions. 2) Elixirs Elixirs are aromatic, sweetened hydro-alcoholic solutions containing medicinal substances. They are liquids having an aromatic odor and a pleasant taste. The color of elixirs varies according to the nature of the ingredients; some are artificially colored. Containers: dispensed in well filled, well closed, air tight glass bottles having screw caps. Storage: Stored in cool place protected from light. Excipients: Alcohol, glycerol and propylene glycol Required for:
Production of clear solution
Solubilise the potent medicaments of low solubility. Chemical stabilizers - e.g. Disodium edetate is incorporated to sequester heavy metals that catalyse decomposition of antibiotic. Colouring agents - e.g. Amaranth Magenta red, Tartrazine Saffron, Green S Green Sweetening agents - e.g. Sucrose syrups, glycerol, sorbitol solution, invert syrup and saccharin sodium are used. Flavours - e.g. Blackcurrant Syrup in Chloral Elixir, Concentrated Raspberry Juice with invert syrup, Lemon spirit with syrup and invert syrup, Compound Orange Syrup Preservatives - 20% alcohol, propylene glycol or glycerol are preservative.
Syrup is self-preservative due to high osmotic pressure.
Chloroform; it is used in the form of double strength water.
Benzoic acid and methyl paraben 3) Linctus Viscous liquid oral preparations used for the treatment of cough. Ingredients – demulcent, sedative and expectorant. Usual vehicle used is syrup – soothing effect on sore mucous membrane. Taken in small doses – usual dose is 5ml. Sipped and swallowed slowly without diluting to have maximum and prolonged effect. Containers: dispensed in well filled, well closed, air tight glass bottles having screw caps. Storage: Stored in cool place protected from light. Excipients Vehicles
Syrup BP and Tolu syrup
Tolu syrup – mild expectorant action

Syrup – should be stored at constant temperature - Fluctuations in temp encourage crystallisation.
Well closed container – prevents the entry of moisture Flavouring Agents Vehicle itself Fruit flavoured syrup – lemon & blackcurrant Oxymel – acidic honey sweet taste. Benzaldehyde spirit – almond flavour. Preservatives Plain syrup - High osmotic pressure. Tolu syrup – bacterial action of benzoic acid & cinnamic acid. Linctus made from Sorbitol solution – chloroform spirit and/or benzoic acid Chemical stabilizers Most linctuses are stable. Invert sugar – reducing action. Prevents degradation of colouring & flavouring agents. Colouring Agents Coal tar dyes. Compound Tartrazine solution. 4) Draughts
Liquid preparation taken as single dose.
Usual Volume is 50ml.
Examples of draught preparations 1. Ipecacuanha Emetic Draught BPC
Used in emergency treatment of poisoning in children.
So the dose varies with the age of the child.
Either a single small dose can be used or more than one dose may be required to induce vomiting.
So may be supplied in multiple dose container.
2. Paraldehyde Draught BPC Paraldehyde 4 ml Syrup 8 ml Liquorice liquid extract 3 ml Water to 50 ml. Paraldehyde on storage oxidises to acetic acid which can be fatal. Hence the product should be used within 24 hours of opening. Paraldehyde is a GI irritant and has a disagreeable taste, thus when shaken with water and if left undissolved maybe mistaken for air bubbles. It is more soluble in cold water. Hence cold water should be used in its preparation
5) Pediatric drops If the dose is small and cannot be diluted due to stability issues then the preparation has to be given as drops. Eg. Indomethacin mixture, nitrofurantoin mixture, nystatin mixture, digoxin elixir.
These preparations consists of potent medicaments so the dose must be measured precisely. Personal variations may occur in using the dropper. There are 2 types of dropper that can be used:
• Graduated dropper – fractions of millilitre • Pre-calibrated dropper – Number of drops equivalent to prescribed dose.
The size of the drops from a medicine dropper depends on:
Surface tension
Viscosity
Density
Temperature of the liquid
External diameter of the tip
Rate of dropping 6) Syrups Syrup is a concentrated or nearly saturated solution of sucrose in purified water. Concentration of sugar is 66.7% w/w. Syrups containing medicinal substances are called ‘medicated syrups’. Syrups containing aromatic or flavoured substances are known as ‘flavoured syrups’. Advantages: Retards oxidation - Partly hydrolysed into reducing sugars such as levulose and dextrose Prevents Decomposition -Due to high osmotic pressure prevents growth of bacteria, fungi and moulds Palatability - Valuable vehicle for nauseous and bitter substances Preparation Methods - Depends on types of ingredients
Simple solution method eg. Ginger syrup
Extraction Method eg. Tolu syrup
Chemical Interaction Method eg. Ferrous sulphate syrup Excipients:
• Vehicles • Freshly boiled and cooled purified water • Do not use potable water
• Chemical stabilizers • Glycerol, sorbitol & propylene glycol • Prevents crystallization
• Colouring Agents • Coal tar dyes - Amaranth • Compound tartrazine
• Flavouring Agents • Tinctures – Lemon & ginger tincture • Fruit Juices – Raspberry juice & wild cherry. • Essence – vanilla & orange
• Preservatives • Benzoic acid, sodium benzoate & methyl paraben

Storage of syrups:
The should be stored in well dried well stoppered bottles in a cool dark place.
The syrup should be stored at a temperature not exceeding 25°C. The glass bottles fitted with white polypropylene moulded or black thermosetting plastic screw closures are commonly used for the storage of bottles. These bottles may be colourless or amber coloured.
Q.4.b) Discuss the compounding and dispensing of cocoa butter suppositories (4) Steps involved in compounding of coca butter suppositories are: 1. Check the displacement values of medicaments 2. Calculate the quantity of medicaments 3. Excess quantity is weighed – unavoidable wastage
Major loss due to sticking of the material to the sides of the dish So the smallest dish should be selected.
4. Initially weigh the quantity for 4 extra suppositories After experience weigh the quantity for 2 extra suppositories
5. Weigh the required amount of fat in a porcelain dish Avoid metal dishes due to overheating problem
6. Finely powder the medicaments and pass it through sieve no. 180 and weigh the required quantities 7. Heat a tile on water bath and mix the powder on a tile with a flexible spatula 8. Place the base on water bath until 2/3rd contents are melted and then remove it.
Overheating may occur if the base is allowed to melt completely. 9. Rest of the base is melted with continuous stirring with spatula and avoid glass rod for stirring 10. Pour about half of the base on to the mixed medicaments 11. Prepare a smooth dispersion as quickly as possible by levigating with spatula 12. To prevent excessive cooling use small tile and this will also avoid loss on the edge of the tile 13. If the base is solidified hold the tile on water bath for few seconds 14. Transfer the dispersion to the dish and stir to form homogenous mixture 15. Continue stirring until the mixture begins to thicken 16. Then fill each cavity of the mould to overflowing
Cavities are overfilled to prevent depressions in the tops of the suppositories due to the contraction of the base during cooling If there is delay to pour the mass into cavities then continue the stirring because setting of the mass will take place before filling This also prevents the sedimentation of insoluble solids
17. There may be solidification of mass during pouring so reheat the mass and make it pourable
The base of the dish should be wiped to prevent contamination of mass with water 18. Leave in a cool place until the mass is set and remove the excess with a sharp knife or razor blade or warm spatula

19. Put the knife or blade or spatula at an angle of about 30°C and draw it from left to right pressing down at the same time 20. Open the mould and remove the suppositories. If difficult to open, tap the mould and remove it. Q.4.c) Discuss the responsibilities of a community pharmacist (4) The responsibilities of a community pharmacist include:
1. Processing of prescription 2. Drug information about their action 3. Drug utilization 4. Drug distribution 5. Drug selection 6. Patient counselling and evaluating 7. Ensuring better healthcare
• Nutrition Counselling • Women Welfare-Pregnancy and Infant Care • Rational Use of Drugs • Sexually Transmitted Diseases-AIDS • Alcohols, Drug Abuse and Smoking Cessation • Family Planning
8. Individualization of Drug Therapy 9. Extemporaneous preparation 10. Traditional and alternative medicines 11. Responding to symptoms of minor ailments 12. Domiciliary services 13. Agricultural and veterinary practice 14. Maintain records

Q.5.a) Define "health" as per WHO. Discuss the areas in which a pharmacist can get involved to promote health of a community (4) World Health Organization defines “Health” as a state of complete, physical, mental and social well-being and not merely as absence of disease or infirmity Health promotion is the process of enabling people to increase control over, and to
improve, their health. It moves beyond a focus on individual behaviour towards a wide
range of social and environmental interventions.
1. Nutrition Counselling Community pharmacist can make, significant contributions in:
a. Assuring adequate nutrition by advising his patients about basic food needs b. Keeping to correct improper food habits in children c. Advising on special requirements d. Suggesting special diet instructions for diabetic patients and people with food
allergy e. Participating in school lunch programs and schemes like mid-day meals etc. in
rural areas. 2. Women Welfare-Pregnancy and Infant Care
A woman goes through different stages throughout her life, each of which has specific need and the presence of a counselor is needed in each one of them.
The pharmacist who understands the normal course of pregnancy and infancy is at a distinct advantage as he or she can guide the mother in simple matters of hygiene and management.
The community pharmacist can encourage breastfeeding and can play a major role by guiding the mother for the protection of the child by following proper immunization schedule.
3. Rational Use of Drugs
A community pharmacist can also advise on the administration of the medication, provide information on the storage of the medication and wherever necessary he can counsel the patient.
Education regarding the disadvantage of polypharmacy can also be given to the patient.
Drug information system should be set up and access to adverse drug reaction system should be made.
A community pharmacist should do therapeutic drug monitoring and he should have a sound knowledge of genotype reporting i.e. predictive pharmacology.
Drug information awareness programmes should be conducted to make people
aware of side effects of certain OTC drugs e.g. Aspirin - a wonder drug also has
many side effects like gastric ulceration; asthma and large doses may cause
tinnitus. Regular use of paracetamol can cause harm to the liver. Drugs such as
Action 500, Coldarin can increase blood pressure in patients having
hypertension.
Community pharmacist can provide counselling to common people unaware of
these side effects
4. Sexually Transmitted Diseases-AIDS
India has 3.5 million HIV positive cases, which is about 10% of the global HIV cases and barely second to South Africa.
HIV drugs are expensive and beyond the reach of common man.
Huge resource of community pharmacist can educate people in the prevention and information of HIV/AIDS.
For this, Federation of Indian Pharmacists project in India on involvement of pharmacist in fight against AIDS is very relevant.
Another sensitive issue is the increasing number of women patients suffering from AIDS. Their number rose from 7% in 1985 to 18% in 1995.
Explaining to people what HIV is, its transmission, risk reduction, patient counselling are a few things that a community pharmacist can provide.
5. Alcohols, Drug Abuse and Smoking Cessation
The pharmacist has a key role to help individuals who become dependent upon alcohol.
Drug abuse is similar to alcoholism yet different because it has been gaining more acceptances among young people.
Annual mortality from tobacco use exceeds that from all other causes combined.
Smoking is the greatest single preventable cause of morbidity and mortality in India.
It is the responsibility of a community pharmacist to take an active role in helping the smokers to stop smoking.
Following a number of smoking policies through out the pharmacy, by written information and posters, can do this.
The pharmacist can advise on the products available to assist the patient in giving up smoking.
Counselling sessions can be made by the community pharmacist to stop smoking 6. Family Planning
One of the greatest needs of the hour is to control the tremendously increasing population in India.
A community pharmacist is the one who can control this rising population by counselling with people and doing programmes which exhibit the problems related with large families.
He can tell the various families planning measures that are available in the market at affordable prices.
He can educate the people and convince them about the advantages of having small families
Q.5.b) What is patient counselling? Give its significance. Describe in brief the steps involved in patient counselling (4) Patient counselling refers to the process of providing information, advice and assistance to help patients use their medications appropriately
Its significance: 1. Better patient understanding of their illness and the role of medication in its
treatment 2. Improved medication adherence 3. More effective drug treatment 4. Reduced incidences of medication errors, adverse effects and unnecessary
healthcare costs 5. Improved quality of life for the patient. 6. Better coping strategies to deal with medication related adverse effects. 7. Improved professional rapport between the patient and the pharmacist.
Steps involved in patient counselling
1. Preparing for the session
Success of counselling depends on the knowledge and skill of the counsellor
The pharmacist should know as much as possible about the patient and his/ her treatment details
Source of information: o Patient o Their prescription o Previous records
The patient needs to be in the right frame of body and mind to be counseled.
He should not be in: o Hurry o Pain o Non-communicative
2. Opening of the session
a. Establish caring relationships with patients as appropriate to the practice setting and stage in the patient’s health care management.
b. Assess the patient’s knowledge about his or her health problems and medications, physical and mental capability to use the medications appropriately and attitude toward the health problems and medications.
c. Provide information orally and use visual aids or demonstrations to fill patients’ gaps in knowledge and understanding.
d. If a patient is experiencing problems with his or her medications, gather appropriate data and assess the problems
e. Verify patients’ knowledge and understanding of medication use. Ask patients to describe or show how they will use their medications and identify their effects.
f. Handle distressed or disturbed patients
3. Counselling content
This is the heart of the session
During this step the pharmacist explains to the patient about his/ her medication and treatment regimen.
Lifestyle changes may also be discussed.
The information to be given includes:
i. Name and strength of the medication ii. The reason why it has been prescribed or how it works
iii. How much and how often to take the medication iv. Expected duration of treatment v. Expected benefits of treatment
vi. Possible adverse effects vii. Possible medication or dietary interactions
viii. Advice on correct storage ix. Minimum duration required to show therapeutic benefits x. What to do if a dose is missed
xi. Special monitoring required eg blood tests xii. Arrangement for obtaining further supplies
4. Closing the session
Always check the patient’s understanding
They may always have new questions
Always end the session by asking “Do you have any further questions?”
Summarise the main points in a logical order
Encourage the patients to encourage the patient to make contact if they need further advice or information
After the patient leaves, document the session o Write note or use counseling sticker in progress note o Include assessment of patient and/or care giver understanding
Q.5.c) Paraphrase the code of ethics for a pharmacist in relation to his trade as laid down by the Pharmacy Council of India (4) 1. Price Structure
• Prices of drugs and medicinal preparations charged from the customers should be fair and including dispensing and compounding charges without unduly taxing the purchaser
2. Fair Trade Practice • A pharmacist should not make any attempts to capture the business of fellow
pharmacist by unhealthy competition or cut-throat competitions, that is by offering reduced prices, gifts, prizes etc
• Trade marks, labels, symbols or any other signs of other pharmacists should not be copied or imitated
• Drugs or other ingredients required, should always be purchased from reputable sources
3. Hawking of Drugs • Hawking of drugs or medicines should not be practised and any attempt should not
be made to collect orders from door-to-door • Self servicing method in the pharmacy or drug stores should not be allowed as it
would encourage self-medication which is undesirable and dangerous 4. Advertising and Display
• There should not be any display or advertisement on premises, in the newspaper or elsewhere regarding the abilities and services provided by the pharmacy.
• The pharmacist should not make such advertisements which contain: • Misleading or exaggerated statements or claims • A guarantee of therapeutic efficacy • An offer to refund paid money • An appeal to fear • The word “cure” in reference to an ailment or symptoms of ill-health
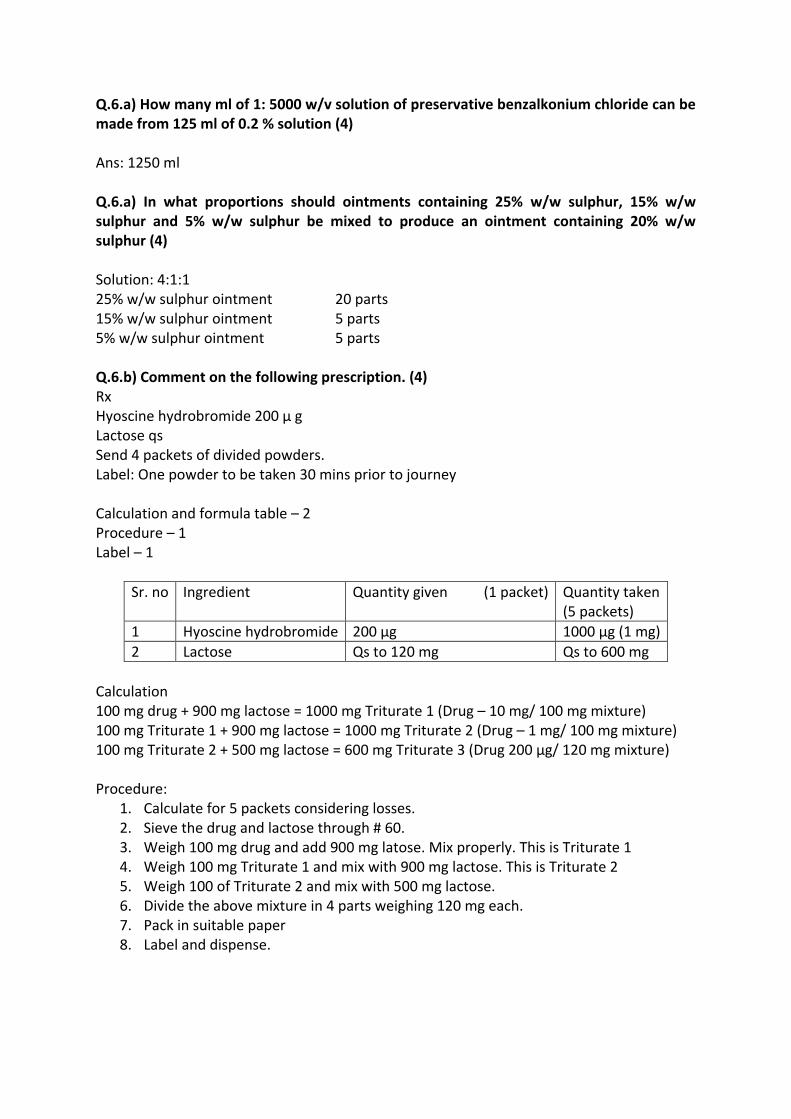
Q.6.a) How many ml of 1: 5000 w/v solution of preservative benzalkonium chloride can be made from 125 ml of 0.2 % solution (4) Ans: 1250 ml Q.6.a) In what proportions should ointments containing 25% w/w sulphur, 15% w/w sulphur and 5% w/w sulphur be mixed to produce an ointment containing 20% w/w sulphur (4) Solution: 4:1:1 25% w/w sulphur ointment 20 parts 15% w/w sulphur ointment 5 parts 5% w/w sulphur ointment 5 parts Q.6.b) Comment on the following prescription. (4) Rx Hyoscine hydrobromide 200 μ g Lactose qs Send 4 packets of divided powders. Label: One powder to be taken 30 mins prior to journey Calculation and formula table – 2 Procedure – 1 Label – 1
Sr. no Ingredient Quantity given (1 packet) Quantity taken (5 packets)
1 Hyoscine hydrobromide 200 μg 1000 μg (1 mg)
2 Lactose Qs to 120 mg Qs to 600 mg
Calculation 100 mg drug + 900 mg lactose = 1000 mg Triturate 1 (Drug – 10 mg/ 100 mg mixture) 100 mg Triturate 1 + 900 mg lactose = 1000 mg Triturate 2 (Drug – 1 mg/ 100 mg mixture) 100 mg Triturate 2 + 500 mg lactose = 600 mg Triturate 3 (Drug 200 µg/ 120 mg mixture) Procedure:
1. Calculate for 5 packets considering losses. 2. Sieve the drug and lactose through # 60. 3. Weigh 100 mg drug and add 900 mg latose. Mix properly. This is Triturate 1 4. Weigh 100 mg Triturate 1 and mix with 900 mg lactose. This is Triturate 2 5. Weigh 100 of Triturate 2 and mix with 500 mg lactose. 6. Divide the above mixture in 4 parts weighing 120 mg each. 7. Pack in suitable paper 8. Label and dispense.

Label
4 packets
The Powder
Rx, Mr. XYZ
Direction: One powder to be taken 30 mins prior to journey
Storage: Store in a cool and dry place
Dispensed by: Checked by: Dispensing date: Expiry date
Pharmacy name and address.
Q.6.c.i) What is a balanced diet? Give its significance (2) A balanced diet is one that gives your body the nutrients it needs to function correctly Its significance:
1. A balanced diet is important because your organs and tissues need proper nutrition to work effectively.
2. Without good nutrition, your body is more prone to disease, infection, fatigue, and poor performance.
3. Children with a poor diet run the risk of growth and developmental problems and poor academic performance.
4. Bad eating habits can persist for the rest of their lives. 5. Rising levels of obesity and diabetes in India are prime examples of the effects of a
poor diet and a lack of exercise. Q.6.c.ii) Give the causative agents for the following diseases (2)
i. Diphtheria - Corynebacterium diphtheriae ii. Typhoid - Salmonella typhi
iii. Scabies - Sarcoptes scabei iv. Tetanus - Clostridium tetani
______________________________