Devices and systems targeted towards augmented robotic radical prostatectomy
9
Our reference: IRBM 252 P-authorquery-v9 AUTHOR QUERY FORM Journal: IRBM Please e-mail or fax your responses and any corrections to: E-mail: [email protected] Article Number: 252 Fax: +33 (0) 1 71 16 51 88 Dear Author, Please check your proof carefully and mark all corrections at the appropriate place in the proof (e.g., by using on-screen annotation in the PDF file) or compile them in a separate list. Note: if you opt to annotate the file with software other than Adobe Reader then please also highlight the appropriate place in the PDF file. To ensure fast publication of your paper please return your corrections within 48 hours. For correction or revision of any artwork, please consult http://www.elsevier.com/artworkinstructions. Any queries or remarks that have arisen during the processing of your manuscript are listed below and highlighted by flags in the proof. Click on the ‘Q ’ link to go to the location in the proof. Location in Query / Remark: click on the Q link to go article Please insert your reply or correction at the corresponding line in the proof Q1 Please confirm that given names and surnames have been identified correctly. Q2 Please supply the names of the cities and countries for affiliations “e” and “f”. Q3 Please provide the volume numbers and page range for the bibliography in references [1, 9]. Please check this box or indicate your approval if you have no corrections to make to the PDF file Thank you for your assistance.
Transcript of Devices and systems targeted towards augmented robotic radical prostatectomy
Our reference IRBM 252 P-authorquery-v9
AUTHOR QUERY FORM
Journal IRBM Please e-mail or fax your responses and any corrections to
E-mail correctionsesmeelsevierthomsondigitalcom
Article Number 252 Fax +33 (0) 1 71 16 51 88
Dear Author
Please check your proof carefully and mark all corrections at the appropriate place in the proof (eg by using on-screenannotation in the PDF file) or compile them in a separate list Note if you opt to annotate the file with software other thanAdobe Reader then please also highlight the appropriate place in the PDF file To ensure fast publication of your paper pleasereturn your corrections within 48 hours
For correction or revision of any artwork please consulthttpwwwelseviercomartworkinstructions
Any queries or remarks that have arisen during the processing of your manuscript are listed below and highlighted by flags inthe proof Click on the lsquoQrsquo link to go to the location in the proof
Location in Query Remark click on the Q link to go
article Please insert your reply or correction at the corresponding line in the proof
Q1 Please confirm that given names and surnames have been identified correctlyQ2 Please supply the names of the cities and countries for affiliations ldquoerdquo and ldquofrdquoQ3 Please provide the volume numbers and page range for the bibliography in references [1 9]
Please check this box or indicate your approval ifyou have no corrections to make to the PDF file
Thank you for your assistance
Please cite this article in press as Voros S et al Devices and systems targeted towards augmented robotic radical prostatectomy IRBM (2013)
httpdxdoiorg101016jirbm201301014
ARTICLE IN PRESS+ModelIRBM 252 1ndash8
Disponible en ligne sur
wwwsciencedirectcom
IRBM xxx (2013) xxxndashxxx
Original article
Devices and systems targeted towards augmented robotic radicalprostatectomy
1
2
S Voros alowast A Moreau-Gaudry b B Tamadazte a G Custillon b R Heus a M-P Montmasson aQ1
F Giroud a O Gaiffe c C Pieralli c G Fiard d J-A Long d J-L Descotes d C Vidal eA Nguyen-Dinh f P Cinquin g
3
4
5
a UJF-Grenoble 1 CNRS INSERM TIMC-IMAG UMR 5525 38041 Grenoble France6
b Centre drsquoInvestigation Clinique Innovation Technologique INSERM CHU de Grenoble UJF-Grenoble 1 CIT803 38041 Grenoble France7
c FEMTO-ST UMR CNRS 6174 Universiteacute de Franche-Comteacute 25030 Besancon cedex France8
d Urology Department Grenoble University Hospital Grenoble France9
e Endocontrol-Medical SA10
f VERMON SAQ211
g UJF-Grenoble 1 CNRS TIMC-IMAG UMR 5525 Centre drsquoInvestigation Clinique Innovation Technologique INSERM CHU de Grenoble CIT803 38041
Grenoble France
12
13
Received 11 January 2013 received in revised form 11 January 2013 accepted 15 January 2013
14
Abstract15
Prostate cancer is the most frequent male cancer and the second cause of male cancer mortality in developed countries Therefore it represents
a major public health issue Health problem and the development of new therapeutic strategies to address this issue is essential During a prosta-
tectomy the surgeon looks for a compromise between an exhaustive removal of pathologic tissue (to achieve the best carcinogenic prognosis) and
the functional consequences linked to a wide excision (ie avoid as much as possible urinary incontinence and sexual dysfunction) In this con-
text the ANR TecSan DEPORRA project regroups French research laboratories (TIMC-IMAG FEMTO-ST) companies (Endocontrol-Medical
VERMON) and hospital departments (CIC-IT Urologyamp pathology Department of the Grenoble University Hospital) to bring innovative tools
for radical prostatectomy These tools will provide to the surgeon new information from several imaging modalities (video fluorescence and US
imaging) and combine them in an augmented environment We believe that this augmented environment will ultimately help the surgeon to perform
his surgical gesture ldquooptimallyrdquo and will improve the patientrsquos carcinogenic and functional prognosis
16
17
18
19
20
21
22
23
24
copy 2013 Published by Elsevier Masson SAS25
26
1 Introduction27
Prostate cancer is the most frequent male cancer and the sec-28
ond cause of male cancer mortality in developed countries with29
643000 cases and 20 new cases in 2008 according to the 200830
World Cancer Report of the International Agency for Research31
Cancer Its incidence has never stopped increasing in the past 2532
years because of the population ageing and individual screening33
In 75 of the cases it is diagnosed at a localized stage within the34
prostate (T1 or T2) At this localized stage different treatments35
lowast Corresponding author
E-mail address SandrineVorosimagfr (S Voros)
are available among which surgery radical prostatectomy (or 36
surgical ablation of the prostate) is often considered as the 37
ldquogold standardrdquo to treat prostate cancer in precise indications 38
Several approaches are in competition open surgery laparo- 39
scopic surgery or robotic surgery The laparoscopic approach 40
will probably replace open surgery in the future years notably 41
because it reduces perioperative morbidity Robotic surgery (the 42
reference robot for this approach being Intuitive Surgicalrsquos da 43
Vincireg robot) offers the surgeons a comfort close to open surgery 44
in a mini-invasive environment This comfort allows for the 45
reduction of the ldquolearning curverdquo However concerning the ben- 46
efits for the patient according to the European Association of 47
Urology (EAU) guidelines [1] ldquoit is not clear which technique 48
1959-0318$ ndash see front matter copy 2013 Published by Elsevier Masson SAS
httpdxdoiorg101016jirbm201301014
Please cite this article in press as Voros S et al Devices and systems targeted towards augmented robotic radical prostatectomy IRBM (2013)
httpdxdoiorg101016jirbm201301014
ARTICLE IN PRESS+ModelIRBM 252 1ndash8
2 S Voros et al IRBM xxx (2013) xxxndashxxx
is superior in terms of oncological and functional results and49
cost-effectiveness Prospective trials are urgently neededrdquo an50
argument also shared in two recent Health Technology Assess-51
ments on robot assisted surgery (Belgian HTA 2009 Irish HTA52
2012)53
In the current surgical practice the surgeon must determine54
the best compromise between a complete removal of the prostate55
gland and morbidity The ideal removal consists in removing56
completely the prostate within its capsule a non complete57
removal may lead to positive surgical margins which are associ-58
ated to a higher risk of biochemical recurrence [2] (15ndash20 of59
the patients) Lesions of the urethral sphincter situated under the60
prostate can lead to incontinence (7 of the patients) Lesions61
of the neurovascular bundles (immediately in contact with the62
posterior side of the prostate) may lead to erectile problems of63
varying intensity The surgeon can try to spare more or less these64
organs depending on the preoperative staging completed by65
magnetic resonance imaging (MRI) The quality of the prostate66
removal (absence of positive surgical margins) is determined67
postoperatively thanks to a histopathology exam at the anato-68
mopathology laboratory Thus the surgeon cannot adapt his69
surgical strategy peroperatively70
2 Objectives71
In this controversial context regarding robotically assisted72
prostatectomy we propose a new robotic navigation concept73
guided by some of the principal complications of a radical pros-74
tatectomy (cancer relapse incontinence and impotence) based75
on peroperative multimodal imaging Surgical navigation sys-76
tems allow for the combination of several imaging modalities in77
a common environment thus providing more useful information78
to the surgeon during a surgery than a single imaging modality79
In most of the existing systems information from preoperative80
imaging modalities is combined with the peroperative imaging81
modality However in the case of laparoscopic surgery (soft tis-82
sue surgery) the registration of preoperative images with the83
laparoscopic images is very challenging because the organs can84
move and deform To our knowledge there are only a few navi-85
gation systems for laparoscopic navigation [3] none of which86
are used clinically87
Our proposed navigation concept is based on three coupled88
components that will ultimately ldquoaugmentrdquo the laparoscopic89
images and allow the surgeon to see beyond the visible and90
adapt his surgical strategy peroperatively91
bull an augmented laparoscope allowing the surgeon to navigate92
more harmoniously inside the abdominal cavity as he would93
do in open surgery and potentially to provide three dimen-94
sional information95
bull peroperative visualization technologies allowing the surgeon96
to visualize the important anatomical structures for radical97
prostatectomy98
visualization of the prostate and surrounding organs thanks99
to an innovative transurethral ultrasound probe100
identification and visualization of the tumor and prostatic 101
cells thanks to bimodal fluorescence probe 102
bull integration of the multimodal information to navigation 103
systems thanks to the registration of the different imaging 104
modalities when required 105
3 Material amp methods 106
31 Augmented laparoscopy thanks to an innovative video 107
device 108
Laparoscopic surgery in general can be challenging for a sur- 109
geon for several reasons among which the limited field of view 110
of the endoscope (ldquokeyholerdquo surgery) In consequence whether 111
it is displaced by a human assistant or a robotic endoscope holder 112
the endoscope is mobilized a lot since it is used to see precisely 113
the operating field but also to monitor the instruments introduc- 114
tion and displacement inside the abdominal cavity Movements 115
of the endoscope increase the risk of staining of the lens which 116
leads to a removal of the endoscope from the patient to clean the 117
lens increasing the surgery duration and discomfort 118
To provide a solution to this difficulty we have developed 119
an innovative vision system that can be used in combination 120
with a traditional endoscope thanks to an encapsulation in a 121
traditional trocar Our system is composed of two miniature 122
cameras that are positioned like a pair of glasses around the 123
endoscope (Fig 1) and provide a panoramic view of the abdom- 124
inal cavity These cameras are similar to those present on cell 125
phones and cost only a few US$ in large scale diffusion The 126
system has been designed for an easy insertion deployment and 127
removal of the cameras and has been patented [4] Since it is 128
positioned around the endoscope it provides roughly the same 129
view direction as the endoscope and a registration between the 130
laparoscopic image and the vision system images is unneces- 131
sary The cameras of the innovative vision system are mounted 132
in stereoscopic conditions which could allow for a local 3D 133
reconstruction of the scene Our preclinical evaluation of the 134
potential expected medical service of this device is presented in 135
section 4 136
32 Augmented laparoscopy thanks to an innovative 137
ultrasound system 138
Previous work [5] has already shown that the use of tran- 139
srectal ultrasound during laparoscopic radical prostatectomies 140
could assist the surgeons in the visualization of specific prostate 141
contour anatomy and of the neurovascular bundles and in 142
the bladder neck dissection According to the authors the use 143
of transrectal ultrasound in laparoscopic prostatectomy com- 144
pensated for the lack of tactile feedback compared to open 145
surgery achieved significant decrease in the incidence of posi- 146
tive surgical margins and achieved quicker and superior potency 147
recovery In this work the ultrasound images were not fused 148
with the laparoscopic images and the surgeon had to perform 149
a challenging mental registration of the two imaging modali- 150
ties Long et al [6] also showed the potential of a guidance of 151
a transrectal ultrasound probe with a robotic endoscope holder 152
Please cite this article in press as Voros S et al Devices and systems targeted towards augmented robotic radical prostatectomy IRBM (2013)
httpdxdoiorg101016jirbm201301014
ARTICLE IN PRESS+ModelIRBM 252 1ndash8
S Voros et al IRBM xxx (2013) xxxndashxxx 3
Fig 1 The proposed global vision system a) the mini-cameras used for the vision system b) CAD drawing of the augmented endoscope concept the mini-cameras
are inserted into a modified trocar When the endoscope is inserted the vision system is deployed like glasses around the endoscope c) and d) rapid prototyping
realization
(Endocontrolrsquos ViKY system) Holmes et al [7] have developed153
a 2D transurethral ultrasound probe for brachytherapy that is154
manually rotated around its axis to provide 3D imaging They155
affirm that the endourethral approach permits a better resolu-156
tion than the transrectal approach for the visualization of the157
prostate The transurethral approach also allows avoiding some158
of the intrinsic limitations of transrectal ultrasound imaging (a159
layer of air forms between the prostate and the rectum during160
the prostate dissection making the ultrasound visualization of161
the prostate impossible after this surgical phase)162
In light of these previous works we have developed two163
transurethral ultrasound probe prototypes (one for 2D imaging164
and a motorized version where the probe rotates around its axis165
to provide 3D images) (Fig 2) The 2D probe is composed of166
64 piezoelectric elements with a frequency of 10 MHz and a167
3 mm diameter semi-rigid catheter for an easy introduction The168
3D probe has the same central frequency but it is composed of169
128 piezoelements and has a 6 mm diameter catheter They are170
Fig 2 The innovative intraurethral ultrasound probe Top the 3D transurethral
probe able to rotate around its axis Bottom the 2D transurethral probe
connected to an Ultrasonix ultrasound machine allowing us to 171
control all the piezoelectric elements 172
In parallel we have also developed an endoscopicultrasound 173
fusion demonstrator The registration is based on the POSIT 174
algorithm [8] and is based on the manual localization in both 175
imaging modalities of artificial landmarks In the frame of this 176
project two complementary approaches have been investigated 177
passive landmarks (laparoscopic needles planted in the prostate) 178
and innovative active ultrasound landmarks that emit an ultra- 179
sound signal that can be detected by the transurethral probe 180
allowing for their precise localization in the ultrasound referen- 181
tial [9] (Fig 3) 182
Our preliminary results for the registration of ultrasound and 183
laparoscopic images using passive landmarks and for the precise 184
3D localization of the ultrasound ldquoactiverdquo markers are described 185
in section 4 186
33 Augmented laparoscopy thanks to fluorescence 187
imaging 188
During a radical prostatectomy the ability to visualize bio- 189
logical characteristics of tissue (prostatic vs non-prostatic on 190
the one hand normal vs malignant on the other hand) could help 191
the surgeon to respectively determine precisely the location of 192
the prostate capsule and assess the extent of the cancer and thus 193
allow him or her to adapt his surgical strategy peroperatively 194
Based on these observations we have developed a bimodal 195
fluorescence fibered probe for the peroperative characterization 196
of tissue for radical prostatectomy 197
Please cite this article in press as Voros S et al Devices and systems targeted towards augmented robotic radical prostatectomy IRBM (2013)
httpdxdoiorg101016jirbm201301014
ARTICLE IN PRESS+ModelIRBM 252 1ndash8
4 S Voros et al IRBM xxx (2013) xxxndashxxx
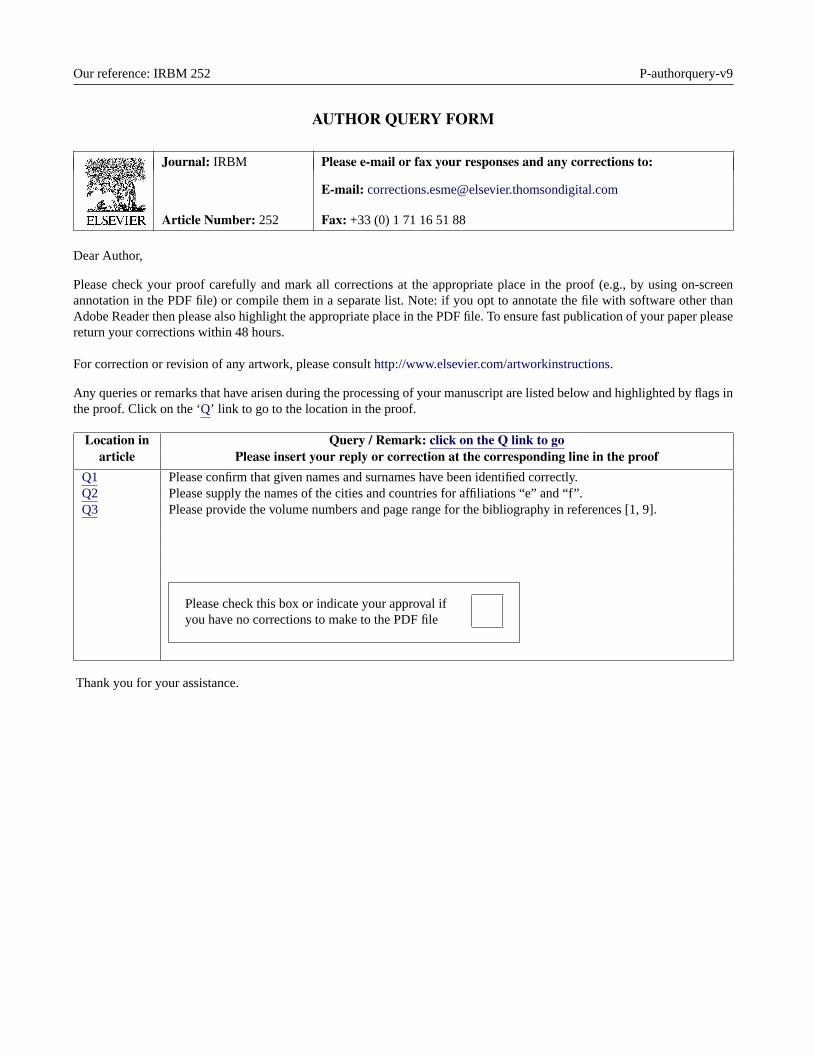
Fig 3 The proposed markers for the registration of ultrasound and endoscopic
images Top ldquoactiverdquo landmark (laparoscopic ultrasound emitter) Bottom ldquopas-
siverdquo landmark (laparoscopic needle) used for the registration of ultrasound and
laparoscopic images
bull the normalmalignant characterization of the tissues is based198
on the detection of the autofluorescence of the Protopor-199
phyrin IX (PpIX) protein which accumulates in malignant200
cells Indeed the elimination cycle of Protorphyrin is per-201
turbed in case of malignant cells It causes thus an increase202
of Protoporphyrin concentration A first prototype (already203
available see Fig 4 left) comes in the form of a testbench204
equipped with a laser source emitting at 405 nm (excitation 205
wavelength for the PpIX protein) and with optical fibers and 206
a spectrometer allowing the collection of a fluorescence spec- 207
trum of 3648 points in the range 345ndash1040 mm (the testbench 208
can image a 25 times 25 mm2 area with a spatial resolution of 209
100 m and a penetration depth of roughly 300 m) Using 210
this spectrum an intensity image can be created (Fig 4 211
right) The analysis of prostate tissue samples gathered in 212
the frame of a biomedical protocol (section 4) will allow us 213
to determine the optimal parameters for the acquisition of 214
the fluorescence spectrum and build discrimination criteria 215
from the measurements between malignanthealthy tissue and 216
prostaticnon-prostatic tissue 217
bull the prostaticnon-prostatic characterization of the tissues is 218
based on the detection of the prostate-specific membrane anti- 219
gen (PSMA) which is specific of the prostatic membrane 220
This detection is made possible by the immunofluorescence 221
tagging of the PSMA using a specific anti-PSMA antibody 222
labelled with a fluorescent tracer When excited by light at 223
a characteristic absorption wavelength the fluorescent tracer 224
emits light at a characteristic emission wavelength Two flu- 225
orescent tracers are investigated in the DEPORRA project 226
Fluorescein IsoThioCyanate (FITC) and Cyanine 5 Both 227
FITC and Cyanine 5 have a characteristic emission wave- 228
length different from the autofluorescence wavelength of the 229
Protoporpphyrin IX protein allowing for the characterization 230
of the tissue type (prostatic vs non-prostatic) and the tissue 231
status (healthy vs malignant) with the same testbench (Fig 5) 232
The testbench presented on Fig 4 has also been equipped 233
with two laser sources emitting at 488 nm and 642 nm exci- 234
tation wavelengths respectively for FITC and Cyanine 5 for 235
recognizing prostate tissue from those environing 236
A bimodal laparoscopic-compliant fluorescence probe based 237
on the miniaturization of the fluorescence testbench will be avail- 238
able in 2013 (Fig 6 top) Preliminary results based on the 239
analysis of histopathologic slices will be presented in section 240
4 In order to overlay the probersquos fluorescence measurement on 241
the laparoscopic images we plan on detecting automatically the 242
position of the tip of the laparoscopic probe using a real-time 243
Fig 4 Experimental fluorescence design and results Left experimental optical device Right typical intensity image obtained
Please cite this article in press as Voros S et al Devices and systems targeted towards augmented robotic radical prostatectomy IRBM (2013)
httpdxdoiorg101016jirbm201301014
ARTICLE IN PRESS+ModelIRBM 252 1ndash8
S Voros et al IRBM xxx (2013) xxxndashxxx 5
Perc
ent
of
maxim
a
Wavelength (nm)
PpIX emission
FITC excitation
FITC emission
PpIX excitation
350 400 450 500 550 600 650 700 750
Perc
ent
of
maxim
a
10
00
08
06
04
02
Wavelength (nm)
PpIX emission
Cy5 excitation
Cy5 emission
PpIX excitation
BA
350 400 450 500 550 600 650 700 750
10
00
08
06
04
02
Fig 5 Excitation and emission spectra of Protoporphyrin IX Fluorescein IsoThioCyanate and Cyanine 5 (Cy5) fluorochromes A Overlay of the excitation (blue
dashed line) and emission (orange solid line) spectra of Protoporphyrin IX with excitation (green dashed line) and emission (emission spectrum) of Fluorescein
IsoThioCyanate B Overlay of the excitation (blue dashed line) and emission (orange solid line) spectra of Protoporphyrin IX with excitation (red dashed line) and
emission (red solid line) of Cy5
Fig 6 The bimodal fluorescence laparoscopic probe and the image-based anal-
ysis approach to localize it in laparoscopic images Top the CAD drawing
of the bimodal fluorescence laparoscopic probe Bottom automatic detection
of a laparoscopic instrument which will be used to overlay the probersquos tissue
characterization measurements on the laparoscopic images
image analysis approach that we have developed [10] (Fig 6244
bottom)245
34 Preclinical and clinical evaluation246
Preliminary evaluation of the devices and the software devel-247
oped in the frame of this project has already been performed on248
laboratory testbenchs and during three cadaver experiments at249
the anatomy laboratory (section 4) However in order to acquire250
the qualitative and quantitative proofs necessary to perform the251
fist clinical evaluations of our innovative medical devices on 252
patients we have submitted two biomedical research protocols 253
bull the first one called ldquofusion of echographic (ultrasound) and 254
endoscopic imagesrdquo (FEE) is a pilot monocentric study on a 255
cohort of 15 patients and is currently running It aims at val- 256
idating our ultrasound approach and evaluating its expected 257
medical benefit during radical prostatectomies the surgeons 258
will insert surgical needles in the prostate and endorectal 259
ultrasound images and laparoscopic images will be recorded 260
The data will be processed offline in the laboratory to assess 261
quantitatively the feasibility of the registration of ultrasound 262
and laparoscopic images using passive markers This proto- 263
col already accepted by the ethical instances will be a pilot 264
monocentric study with 15 patients 265
bull the second protocol called COPROST will allow us to obtain 266
fresh prostate chips during transurethral resections in the 267
frame of a pilot monocentric prospective non-randomized 268
open and controlled clinical trial The protocol with an 269
inclusion period of 24 months is already defined and writ- 270
ten following the French Regulation on Biomedical Research 271
and biological tissue collection It is being submitted to the 272
ethical committee ldquocomiteacute de protection des personnesrdquo and 273
the ldquoagence nationale de seacutecuriteacute du meacutedicament et des pro- 274
duits de santeacuterdquo (ANSM) The prostate chips will be on one 275
hand characterized by anatomopathologists to determine their 276
nature (pathologic vs healthy prostatic vs non-prostatic) and 277
will allow us to validate our immunofluorescence protocol and 278
fine-tune our auto and immunofluorescence measurements 279
protocols on fresh tissue samples 280
4 Results 281
In this section we present our preclinical evaluation of the 282
different prototypes and software presented in the previous sec- 283
tion 284
41 Augmented laparoscopy thanks to an innovative video 285
device 286
In order to evaluate the potential benefits of the pro- 287
posed vision system we asked a surgeon to perform a simple 288
Please cite this article in press as Voros S et al Devices and systems targeted towards augmented robotic radical prostatectomy IRBM (2013)
httpdxdoiorg101016jirbm201301014
ARTICLE IN PRESS+ModelIRBM 252 1ndash8
6 S Voros et al IRBM xxx (2013) xxxndashxxx
Fig 7 Ultrasound image of a prostate acquired with our innovative transurethral
ultrasound probe during a cadaver experiment The image was acquired with our
first prototype (64 piezoelectric elements)
surgical task once with the traditional endoscope alone and289
once with the proposed system alone (although in practice they290
can be combined to associate local and global views) The tasks291
consisted in localizing a suture needle and bringing it to a fixed292
target point The experiment was performed on porcine organs293
placed in a training box and repeated six times by the surgeon294
At each realization the needlersquos initial position was repositioned295
randomly at a distance equivalent to its initial position and the296
surgeon started randomly with the traditional endoscope or the297
proposed system In both cases a robotic endoscope holder was298
used to mobilize the endoscope and the vision system allowing299
us to record the displacements of the vision systems300
The full methodology and results are currently under sub-301
mission but to summarize the mean time required to perform302
the six experiments with the traditional endoscope was of 190 s303
compared to 245 s with the proposed system Moreover the sur-304
geon needed to give an average of 232 commands to the robotic305
scope holder to perform one stitch with the endoscope alone306
compared to 46 commands with the proposed system These307
preliminary results suggest that the proposed system could sig-308
nificantly reduce the laparoscopic surgery time and the cognitive309
load required for the control of the endoscope We now plan on310
performing cadaver experiments to evaluate the deployment of311
the vision system in conditions close to the clinical reality and312
to evaluate the system with several surgeons313
42 Augmented laparoscopy thanks to an innovative314
ultrasound system315
We performed two cadaver experiments which allowed us316
to determine the optimal characteristics for the realization of317
the intraurethral ultrasound probe During these experiments318
we evaluated the (difficult) insertion of the catheter through319
the urethra and the prostate visualization It must be noted that320
our clinicians partners stressed that the rigor mortis made this321
insertion harder These experiments allowed us to find the best322
rigidity for the catheter of the probe it must be flexible enough323
Fig 8 Demonstration of the fusion of ultrasound and laparoscopic images using
passive landmarks on chicken breasts Top-left the ultrasound image top-right
the laparoscopic image The passive landmarks are indicated with the green
arrows in the laparoscopic image They are selected manually in both modalities
to perform the registration Bottom the fusion of the two imaging modalities
to be introduced in the urethra but rigid enough to avoid the 324
distortions of the catheter 325
The first ultrasound probe (2D) was designed with 64 326
piezoelements It appeared that it was not enough On the one 327
hand the probe imaged a too small part of the prostate so that 328
it was difficult to identify what was represented on the ultra- 329
sound image (Fig 7) Furthermore it was impossible to know 330
in which direction the probe was oriented On the other hand 331
we demonstrated [9] that a longer probe increases the precision 332
of the localization of the active ultrasound transducers That is 333
why the second probe designed for the project (3D) has 128 334
piezoelements This second probe has graduations located on 335
its catheter visible on Fig 2 They allow the surgeon to know 336
the probersquos insertion depth in the urethra and a line along the 337
catheter allows appreciating the torsion applied to the catheter 338
The localization of the active transducers is currently under 339
submission It is based on a global positioning system (GPS) 340
method We made some experiments on a testbench making 341
localization in water to have ideal homogeneous conditions and 342
Please cite this article in press as Voros S et al Devices and systems targeted towards augmented robotic radical prostatectomy IRBM (2013)
httpdxdoiorg101016jirbm201301014
ARTICLE IN PRESS+ModelIRBM 252 1ndash8
S Voros et al IRBM xxx (2013) xxxndashxxx 7
Fig 9 Preliminary experiments of the autofluorescence detection with our testbench The autofluorescence of chlorophyll which has optical properties very similar
to Protoporphyrin IX was observed on our testbench Left direct image of a leaf right fluorescence image of the leaf at 680 nm As expected chlorophyll seems
absent in the veins
Fig 10 Specific fluorescence signal of anti-prostate-specific membrane antigen marker A Nuclear counter-staining of prostatic tissue with Hoechst (blue DNA
marker) We observe the nuclei of prostate cells regularly organized in the glandular epithelium Prostatic glands are separated by stroma B Fluorescence emission
of anti-prostate-specific membrane antigen-Fluorescein IsoThioCyanate on cellular membranes of prostatic cells C Overlay of the A and B images This figure
demonstrates the specificity on fixed prostatic tissue of a specific anti-PSMA antibody labelled with Fluorescein IsoThioCyanate We can also detect the contribution
of non-specific autofluorescence of prostatic concretions (Fig 11) (times20 magnification)
localization on a chicken breast to have more realistic condi-343
tions In both cases we were able to localize the active transducer344
with a precision less than 625 m Moreover the computation345
time is a few hundred milliseconds for a 2D localization These346
results demonstrate that the localization is fast enough to be347
implemented for a prostatectomy For the moment only a 2D 348
localization has been made with the active landmarks and the 349
3D localization is in progress Then we will be able to per- 350
form a registration with laparoscopic images using ldquoactiverdquo 351
markers 352
Fig 11 Non-specific autofluorescence observed in the prostate fixed tissues This figure shows the benefits of a near infrared marker like Cyanine 5 (excited at
633 nm) compared to Fluorescein IsoThioCyanate (excited at 488 nm) A Auto fluorescence under laser excitation at 488 nm We observe that prostate concretions
(calcified material) respond to this excitation by a strong fluorescence signal B Auto fluorescence under laser excitation at 633 nm The use of Cyanine 5 reduces
widely autofluorescence of some structures such as prostate concretions (times20 magnification)
Please cite this article in press as Voros S et al Devices and systems targeted towards augmented robotic radical prostatectomy IRBM (2013)
httpdxdoiorg101016jirbm201301014
ARTICLE IN PRESS+ModelIRBM 252 1ndash8
8 S Voros et al IRBM xxx (2013) xxxndashxxx
Concerning the registration between laparoscopic and ultra-353
sound images we performed several testbench evaluations of354
the registration algorithm on chicken breasts The result of such355
a registration obtained by manually pairing passive markers356
visible on both the laparoscopic and ultrasound imaging modal-357
ities are presented on Fig 8 In this example we obtained a358
registration root mean square error (RMS) of 038 mm359
43 Augmented laparoscopy thanks to fluorescence360
imaging361
First experiments were performed on leaves to demonstrate362
the feasibility of the detection of chlorophyll autofluorescence363
which has optical properties very similar to PpIX (absorption at364
405 nm and emission at 680 nm) as described on Fig 9 Then365
experiments were conducted on histology slices of the human366
prostate with as we anticipated inconclusive results because367
of the expected low signal-to-noise ratio caused by the insuffi-368
cient thickness of a histology slice (3 m thickness) compared to369
the optimal use of the device (300 m thickness) These results370
motivated our biomedical research COPROST on macroscopic371
fresh prostate samples372
Concerning the immunofluorescence protocol we were able373
to demonstrate the specificity of the anti-PSMA antibody on374
fixed tissue samples labelled with FITC as illustrated by Fig 10375
We observed higher autofluorescence problems when excit-376
ing the sample at the FITC specific wavelength compared to377
an excitation at the Cyanine 5 specific wavelength (Fig 11)378
These results motivated the inclusion of both fluorophores in our379
biomedical research COPROST on macroscopic fresh prostate380
samples FITC because it was already used to demonstrate speci-381
ficity of anti-PSMA antibody and Cyanine 5 because its near382
infra-red characteristics make it a better candidate on fresh mate-383
rial (higher penetration in tissue) and will improve signalnoise384
ratio as previously demonstrated385
To our knowledge most of the optical biopsy approaches as386
previously defined have been validated either on histologic slices387
or on ratmice prostate models However these approaches have388
limitations prostatic tissue is impaired by the chemical treat-389
ment required for histologic preparation and animal models do390
not directly mimic all aspects of human prostate cancer [11] In391
short it has not been proved yet that a successful detection with392
the investigated devices on histopathology slices or on animal393
models is sufficient to guarantee a successful detection on fresh394
human tissues The experiments that will be performed in the395
frame of the COPROST protocol in 2013 will be determinant to396
confirm the feasibility of our approach on fresh tissue samples397
5 DiscussionConclusion398
The DEPORRA project allowed for the development of inno-399
vative devices and navigation prototypes in the objective of400
allowing the surgeon to see ldquobeyond the visiblerdquo during a radi-401
cal prostatectomy First evaluations of the devices and methods402
have been performed preclinically and are very encouraging for403
the development of innovative approaches to assist the surgeon
during such a complex surgery Our preliminary results have also 404
shown the limits of preclinical validation and have convinced us 405
of the necessity to launch biomedical researches that will allow 406
us to validate further the devices This process required a con- 407
sequent amount of effort and time but is mandatory for the 408
fine-tuning of our tissue characterization tools and to obtain the 409
first clinical proofs of the relevance of the developed medical 410
devices which are mandatory to perform clinical evaluations of 411
the complete navigation systems 412
We now need to push further the integration of the devices 413
into such navigation systems in order to exploit at best the infor- 414
mation provided by each modality and to determine the optimal 415
approach for displaying the relevant information to the surgeon 416
in a clinical environment This will imply a conception and 417
development effort a definition of qualitative and quantitative 418
parameters for the first assessment of the delivered medical ben- 419
efit of our developments risks analysis and biomedical research 420
preparations in order to meet the ethical instances requirements 421
Acknowledgments 422
This work has been supported by French National Research 423
Agency (ANR) through TecSan program (project DEPORRA 424
no ANR-09-TECS-006) 425
References 426
[1] Heidenreich A Bolla M Joniau S Mason MD Matveev V Mottet N et al 427
Guidelines on prostate cancer Eur Assoc Urol 2011 [www uroweb org] 428
[2] Pfitzenmaier J Pahernik S Tremmel T Haferkamp A Buse S Hohen- 429
fellner M Positive surgical margins after radical prostatectomy do 430
they have an impact on biochemical or clinical progression BJU Int 431
2008102(10)1413ndash8 432
[3] Soler L Nicolau S Schmid J Koehl C Marescaux J et al Virtual reality 433
and augmented reality in digestive surgery In Third IEEE and ACM Inter- 434
national Symposium on Mixed and Augmented Reality (ISMAR) 2004 435
p 278ndash9 436
[4] S Voros B Tamadazte P Cinquin C Fouard Systegraveme drsquoimagerie multi- 437
vision pour chirurgie laparoscopique demande de deacutepocirct de brevet FR 438
1259489 102012 439
[5] Ukimura O Ahlering TE Gill IS Transrectal ultrasound-guided 440
energy-free nerve-sparing laparoscopic radical prostatectomy J Endourol 441
200822(9)1993ndash5 442
[6] Long JA Lee BH Guillotreau J Autorino R Laydner H Yakoubi R et al 443
Real-time robotic transrectal ultrasound navigation during robotic radical 444
prostatectomy initial clinical experience Urology 201280(3)608ndash13 445
[7] Holmes III DR Davis BJ Bruce CJ Robb RA 3D visualization analysis 446
and treatment of the prostate using trans-urethral ultrasound Comput Med 447
Imaging Graph 200327339ndash49 [2003] 448
[8] Dementhon D Model-based object pose in 25 lines of code Int J Comput 449
Vis 199515(1ndash2)123ndash41 450
[9] Custillon G Voros S Cinquin P Nguyen-Dinh A Moreau-Gaudry A 451
Bidimensional localization of active ultrasound transducers for use in 452
laparoscopic prostate surgery IEEE Trans Med Imaging 2012 Q3 453
[10] Wolf R Duchateau J Cinquin P Voros S 3D tracking of laparoscopic 454
instruments using statistical and geometric modeling Med Image Com- 455
put Comput Assist Interv 20116891203ndash10 [Lecture notes in computer 456
science] 457
[11] Valkenburg KC Williams BO ldquoMouse models of prostate cancerrdquo Prostate 458
Cancer 2011201122 httpdxdoiorg1011552011895238 [Article ID 459
895238] 460

Please cite this article in press as Voros S et al Devices and systems targeted towards augmented robotic radical prostatectomy IRBM (2013)
httpdxdoiorg101016jirbm201301014
ARTICLE IN PRESS+ModelIRBM 252 1ndash8
Disponible en ligne sur
wwwsciencedirectcom
IRBM xxx (2013) xxxndashxxx
Original article
Devices and systems targeted towards augmented robotic radicalprostatectomy
1
2
S Voros alowast A Moreau-Gaudry b B Tamadazte a G Custillon b R Heus a M-P Montmasson aQ1
F Giroud a O Gaiffe c C Pieralli c G Fiard d J-A Long d J-L Descotes d C Vidal eA Nguyen-Dinh f P Cinquin g
3
4
5
a UJF-Grenoble 1 CNRS INSERM TIMC-IMAG UMR 5525 38041 Grenoble France6
b Centre drsquoInvestigation Clinique Innovation Technologique INSERM CHU de Grenoble UJF-Grenoble 1 CIT803 38041 Grenoble France7
c FEMTO-ST UMR CNRS 6174 Universiteacute de Franche-Comteacute 25030 Besancon cedex France8
d Urology Department Grenoble University Hospital Grenoble France9
e Endocontrol-Medical SA10
f VERMON SAQ211
g UJF-Grenoble 1 CNRS TIMC-IMAG UMR 5525 Centre drsquoInvestigation Clinique Innovation Technologique INSERM CHU de Grenoble CIT803 38041
Grenoble France
12
13
Received 11 January 2013 received in revised form 11 January 2013 accepted 15 January 2013
14
Abstract15
Prostate cancer is the most frequent male cancer and the second cause of male cancer mortality in developed countries Therefore it represents
a major public health issue Health problem and the development of new therapeutic strategies to address this issue is essential During a prosta-
tectomy the surgeon looks for a compromise between an exhaustive removal of pathologic tissue (to achieve the best carcinogenic prognosis) and
the functional consequences linked to a wide excision (ie avoid as much as possible urinary incontinence and sexual dysfunction) In this con-
text the ANR TecSan DEPORRA project regroups French research laboratories (TIMC-IMAG FEMTO-ST) companies (Endocontrol-Medical
VERMON) and hospital departments (CIC-IT Urologyamp pathology Department of the Grenoble University Hospital) to bring innovative tools
for radical prostatectomy These tools will provide to the surgeon new information from several imaging modalities (video fluorescence and US
imaging) and combine them in an augmented environment We believe that this augmented environment will ultimately help the surgeon to perform
his surgical gesture ldquooptimallyrdquo and will improve the patientrsquos carcinogenic and functional prognosis
16
17
18
19
20
21
22
23
24
copy 2013 Published by Elsevier Masson SAS25
26
1 Introduction27
Prostate cancer is the most frequent male cancer and the sec-28
ond cause of male cancer mortality in developed countries with29
643000 cases and 20 new cases in 2008 according to the 200830
World Cancer Report of the International Agency for Research31
Cancer Its incidence has never stopped increasing in the past 2532
years because of the population ageing and individual screening33
In 75 of the cases it is diagnosed at a localized stage within the34
prostate (T1 or T2) At this localized stage different treatments35
lowast Corresponding author
E-mail address SandrineVorosimagfr (S Voros)
are available among which surgery radical prostatectomy (or 36
surgical ablation of the prostate) is often considered as the 37
ldquogold standardrdquo to treat prostate cancer in precise indications 38
Several approaches are in competition open surgery laparo- 39
scopic surgery or robotic surgery The laparoscopic approach 40
will probably replace open surgery in the future years notably 41
because it reduces perioperative morbidity Robotic surgery (the 42
reference robot for this approach being Intuitive Surgicalrsquos da 43
Vincireg robot) offers the surgeons a comfort close to open surgery 44
in a mini-invasive environment This comfort allows for the 45
reduction of the ldquolearning curverdquo However concerning the ben- 46
efits for the patient according to the European Association of 47
Urology (EAU) guidelines [1] ldquoit is not clear which technique 48
1959-0318$ ndash see front matter copy 2013 Published by Elsevier Masson SAS
httpdxdoiorg101016jirbm201301014
Please cite this article in press as Voros S et al Devices and systems targeted towards augmented robotic radical prostatectomy IRBM (2013)
httpdxdoiorg101016jirbm201301014
ARTICLE IN PRESS+ModelIRBM 252 1ndash8
2 S Voros et al IRBM xxx (2013) xxxndashxxx
is superior in terms of oncological and functional results and49
cost-effectiveness Prospective trials are urgently neededrdquo an50
argument also shared in two recent Health Technology Assess-51
ments on robot assisted surgery (Belgian HTA 2009 Irish HTA52
2012)53
In the current surgical practice the surgeon must determine54
the best compromise between a complete removal of the prostate55
gland and morbidity The ideal removal consists in removing56
completely the prostate within its capsule a non complete57
removal may lead to positive surgical margins which are associ-58
ated to a higher risk of biochemical recurrence [2] (15ndash20 of59
the patients) Lesions of the urethral sphincter situated under the60
prostate can lead to incontinence (7 of the patients) Lesions61
of the neurovascular bundles (immediately in contact with the62
posterior side of the prostate) may lead to erectile problems of63
varying intensity The surgeon can try to spare more or less these64
organs depending on the preoperative staging completed by65
magnetic resonance imaging (MRI) The quality of the prostate66
removal (absence of positive surgical margins) is determined67
postoperatively thanks to a histopathology exam at the anato-68
mopathology laboratory Thus the surgeon cannot adapt his69
surgical strategy peroperatively70
2 Objectives71
In this controversial context regarding robotically assisted72
prostatectomy we propose a new robotic navigation concept73
guided by some of the principal complications of a radical pros-74
tatectomy (cancer relapse incontinence and impotence) based75
on peroperative multimodal imaging Surgical navigation sys-76
tems allow for the combination of several imaging modalities in77
a common environment thus providing more useful information78
to the surgeon during a surgery than a single imaging modality79
In most of the existing systems information from preoperative80
imaging modalities is combined with the peroperative imaging81
modality However in the case of laparoscopic surgery (soft tis-82
sue surgery) the registration of preoperative images with the83
laparoscopic images is very challenging because the organs can84
move and deform To our knowledge there are only a few navi-85
gation systems for laparoscopic navigation [3] none of which86
are used clinically87
Our proposed navigation concept is based on three coupled88
components that will ultimately ldquoaugmentrdquo the laparoscopic89
images and allow the surgeon to see beyond the visible and90
adapt his surgical strategy peroperatively91
bull an augmented laparoscope allowing the surgeon to navigate92
more harmoniously inside the abdominal cavity as he would93
do in open surgery and potentially to provide three dimen-94
sional information95
bull peroperative visualization technologies allowing the surgeon96
to visualize the important anatomical structures for radical97
prostatectomy98
visualization of the prostate and surrounding organs thanks99
to an innovative transurethral ultrasound probe100
identification and visualization of the tumor and prostatic 101
cells thanks to bimodal fluorescence probe 102
bull integration of the multimodal information to navigation 103
systems thanks to the registration of the different imaging 104
modalities when required 105
3 Material amp methods 106
31 Augmented laparoscopy thanks to an innovative video 107
device 108
Laparoscopic surgery in general can be challenging for a sur- 109
geon for several reasons among which the limited field of view 110
of the endoscope (ldquokeyholerdquo surgery) In consequence whether 111
it is displaced by a human assistant or a robotic endoscope holder 112
the endoscope is mobilized a lot since it is used to see precisely 113
the operating field but also to monitor the instruments introduc- 114
tion and displacement inside the abdominal cavity Movements 115
of the endoscope increase the risk of staining of the lens which 116
leads to a removal of the endoscope from the patient to clean the 117
lens increasing the surgery duration and discomfort 118
To provide a solution to this difficulty we have developed 119
an innovative vision system that can be used in combination 120
with a traditional endoscope thanks to an encapsulation in a 121
traditional trocar Our system is composed of two miniature 122
cameras that are positioned like a pair of glasses around the 123
endoscope (Fig 1) and provide a panoramic view of the abdom- 124
inal cavity These cameras are similar to those present on cell 125
phones and cost only a few US$ in large scale diffusion The 126
system has been designed for an easy insertion deployment and 127
removal of the cameras and has been patented [4] Since it is 128
positioned around the endoscope it provides roughly the same 129
view direction as the endoscope and a registration between the 130
laparoscopic image and the vision system images is unneces- 131
sary The cameras of the innovative vision system are mounted 132
in stereoscopic conditions which could allow for a local 3D 133
reconstruction of the scene Our preclinical evaluation of the 134
potential expected medical service of this device is presented in 135
section 4 136
32 Augmented laparoscopy thanks to an innovative 137
ultrasound system 138
Previous work [5] has already shown that the use of tran- 139
srectal ultrasound during laparoscopic radical prostatectomies 140
could assist the surgeons in the visualization of specific prostate 141
contour anatomy and of the neurovascular bundles and in 142
the bladder neck dissection According to the authors the use 143
of transrectal ultrasound in laparoscopic prostatectomy com- 144
pensated for the lack of tactile feedback compared to open 145
surgery achieved significant decrease in the incidence of posi- 146
tive surgical margins and achieved quicker and superior potency 147
recovery In this work the ultrasound images were not fused 148
with the laparoscopic images and the surgeon had to perform 149
a challenging mental registration of the two imaging modali- 150
ties Long et al [6] also showed the potential of a guidance of 151
a transrectal ultrasound probe with a robotic endoscope holder 152
Please cite this article in press as Voros S et al Devices and systems targeted towards augmented robotic radical prostatectomy IRBM (2013)
httpdxdoiorg101016jirbm201301014
ARTICLE IN PRESS+ModelIRBM 252 1ndash8
S Voros et al IRBM xxx (2013) xxxndashxxx 3
Fig 1 The proposed global vision system a) the mini-cameras used for the vision system b) CAD drawing of the augmented endoscope concept the mini-cameras
are inserted into a modified trocar When the endoscope is inserted the vision system is deployed like glasses around the endoscope c) and d) rapid prototyping
realization
(Endocontrolrsquos ViKY system) Holmes et al [7] have developed153
a 2D transurethral ultrasound probe for brachytherapy that is154
manually rotated around its axis to provide 3D imaging They155
affirm that the endourethral approach permits a better resolu-156
tion than the transrectal approach for the visualization of the157
prostate The transurethral approach also allows avoiding some158
of the intrinsic limitations of transrectal ultrasound imaging (a159
layer of air forms between the prostate and the rectum during160
the prostate dissection making the ultrasound visualization of161
the prostate impossible after this surgical phase)162
In light of these previous works we have developed two163
transurethral ultrasound probe prototypes (one for 2D imaging164
and a motorized version where the probe rotates around its axis165
to provide 3D images) (Fig 2) The 2D probe is composed of166
64 piezoelectric elements with a frequency of 10 MHz and a167
3 mm diameter semi-rigid catheter for an easy introduction The168
3D probe has the same central frequency but it is composed of169
128 piezoelements and has a 6 mm diameter catheter They are170
Fig 2 The innovative intraurethral ultrasound probe Top the 3D transurethral
probe able to rotate around its axis Bottom the 2D transurethral probe
connected to an Ultrasonix ultrasound machine allowing us to 171
control all the piezoelectric elements 172
In parallel we have also developed an endoscopicultrasound 173
fusion demonstrator The registration is based on the POSIT 174
algorithm [8] and is based on the manual localization in both 175
imaging modalities of artificial landmarks In the frame of this 176
project two complementary approaches have been investigated 177
passive landmarks (laparoscopic needles planted in the prostate) 178
and innovative active ultrasound landmarks that emit an ultra- 179
sound signal that can be detected by the transurethral probe 180
allowing for their precise localization in the ultrasound referen- 181
tial [9] (Fig 3) 182
Our preliminary results for the registration of ultrasound and 183
laparoscopic images using passive landmarks and for the precise 184
3D localization of the ultrasound ldquoactiverdquo markers are described 185
in section 4 186
33 Augmented laparoscopy thanks to fluorescence 187
imaging 188
During a radical prostatectomy the ability to visualize bio- 189
logical characteristics of tissue (prostatic vs non-prostatic on 190
the one hand normal vs malignant on the other hand) could help 191
the surgeon to respectively determine precisely the location of 192
the prostate capsule and assess the extent of the cancer and thus 193
allow him or her to adapt his surgical strategy peroperatively 194
Based on these observations we have developed a bimodal 195
fluorescence fibered probe for the peroperative characterization 196
of tissue for radical prostatectomy 197
Please cite this article in press as Voros S et al Devices and systems targeted towards augmented robotic radical prostatectomy IRBM (2013)
httpdxdoiorg101016jirbm201301014
ARTICLE IN PRESS+ModelIRBM 252 1ndash8
4 S Voros et al IRBM xxx (2013) xxxndashxxx
Fig 3 The proposed markers for the registration of ultrasound and endoscopic
images Top ldquoactiverdquo landmark (laparoscopic ultrasound emitter) Bottom ldquopas-
siverdquo landmark (laparoscopic needle) used for the registration of ultrasound and
laparoscopic images
bull the normalmalignant characterization of the tissues is based198
on the detection of the autofluorescence of the Protopor-199
phyrin IX (PpIX) protein which accumulates in malignant200
cells Indeed the elimination cycle of Protorphyrin is per-201
turbed in case of malignant cells It causes thus an increase202
of Protoporphyrin concentration A first prototype (already203
available see Fig 4 left) comes in the form of a testbench204
equipped with a laser source emitting at 405 nm (excitation 205
wavelength for the PpIX protein) and with optical fibers and 206
a spectrometer allowing the collection of a fluorescence spec- 207
trum of 3648 points in the range 345ndash1040 mm (the testbench 208
can image a 25 times 25 mm2 area with a spatial resolution of 209
100 m and a penetration depth of roughly 300 m) Using 210
this spectrum an intensity image can be created (Fig 4 211
right) The analysis of prostate tissue samples gathered in 212
the frame of a biomedical protocol (section 4) will allow us 213
to determine the optimal parameters for the acquisition of 214
the fluorescence spectrum and build discrimination criteria 215
from the measurements between malignanthealthy tissue and 216
prostaticnon-prostatic tissue 217
bull the prostaticnon-prostatic characterization of the tissues is 218
based on the detection of the prostate-specific membrane anti- 219
gen (PSMA) which is specific of the prostatic membrane 220
This detection is made possible by the immunofluorescence 221
tagging of the PSMA using a specific anti-PSMA antibody 222
labelled with a fluorescent tracer When excited by light at 223
a characteristic absorption wavelength the fluorescent tracer 224
emits light at a characteristic emission wavelength Two flu- 225
orescent tracers are investigated in the DEPORRA project 226
Fluorescein IsoThioCyanate (FITC) and Cyanine 5 Both 227
FITC and Cyanine 5 have a characteristic emission wave- 228
length different from the autofluorescence wavelength of the 229
Protoporpphyrin IX protein allowing for the characterization 230
of the tissue type (prostatic vs non-prostatic) and the tissue 231
status (healthy vs malignant) with the same testbench (Fig 5) 232
The testbench presented on Fig 4 has also been equipped 233
with two laser sources emitting at 488 nm and 642 nm exci- 234
tation wavelengths respectively for FITC and Cyanine 5 for 235
recognizing prostate tissue from those environing 236
A bimodal laparoscopic-compliant fluorescence probe based 237
on the miniaturization of the fluorescence testbench will be avail- 238
able in 2013 (Fig 6 top) Preliminary results based on the 239
analysis of histopathologic slices will be presented in section 240
4 In order to overlay the probersquos fluorescence measurement on 241
the laparoscopic images we plan on detecting automatically the 242
position of the tip of the laparoscopic probe using a real-time 243
Fig 4 Experimental fluorescence design and results Left experimental optical device Right typical intensity image obtained
Please cite this article in press as Voros S et al Devices and systems targeted towards augmented robotic radical prostatectomy IRBM (2013)
httpdxdoiorg101016jirbm201301014
ARTICLE IN PRESS+ModelIRBM 252 1ndash8
S Voros et al IRBM xxx (2013) xxxndashxxx 5
Perc
ent
of
maxim
a
Wavelength (nm)
PpIX emission
FITC excitation
FITC emission
PpIX excitation
350 400 450 500 550 600 650 700 750
Perc
ent
of
maxim
a
10
00
08
06
04
02
Wavelength (nm)
PpIX emission
Cy5 excitation
Cy5 emission
PpIX excitation
BA
350 400 450 500 550 600 650 700 750
10
00
08
06
04
02
Fig 5 Excitation and emission spectra of Protoporphyrin IX Fluorescein IsoThioCyanate and Cyanine 5 (Cy5) fluorochromes A Overlay of the excitation (blue
dashed line) and emission (orange solid line) spectra of Protoporphyrin IX with excitation (green dashed line) and emission (emission spectrum) of Fluorescein
IsoThioCyanate B Overlay of the excitation (blue dashed line) and emission (orange solid line) spectra of Protoporphyrin IX with excitation (red dashed line) and
emission (red solid line) of Cy5
Fig 6 The bimodal fluorescence laparoscopic probe and the image-based anal-
ysis approach to localize it in laparoscopic images Top the CAD drawing
of the bimodal fluorescence laparoscopic probe Bottom automatic detection
of a laparoscopic instrument which will be used to overlay the probersquos tissue
characterization measurements on the laparoscopic images
image analysis approach that we have developed [10] (Fig 6244
bottom)245
34 Preclinical and clinical evaluation246
Preliminary evaluation of the devices and the software devel-247
oped in the frame of this project has already been performed on248
laboratory testbenchs and during three cadaver experiments at249
the anatomy laboratory (section 4) However in order to acquire250
the qualitative and quantitative proofs necessary to perform the251
fist clinical evaluations of our innovative medical devices on 252
patients we have submitted two biomedical research protocols 253
bull the first one called ldquofusion of echographic (ultrasound) and 254
endoscopic imagesrdquo (FEE) is a pilot monocentric study on a 255
cohort of 15 patients and is currently running It aims at val- 256
idating our ultrasound approach and evaluating its expected 257
medical benefit during radical prostatectomies the surgeons 258
will insert surgical needles in the prostate and endorectal 259
ultrasound images and laparoscopic images will be recorded 260
The data will be processed offline in the laboratory to assess 261
quantitatively the feasibility of the registration of ultrasound 262
and laparoscopic images using passive markers This proto- 263
col already accepted by the ethical instances will be a pilot 264
monocentric study with 15 patients 265
bull the second protocol called COPROST will allow us to obtain 266
fresh prostate chips during transurethral resections in the 267
frame of a pilot monocentric prospective non-randomized 268
open and controlled clinical trial The protocol with an 269
inclusion period of 24 months is already defined and writ- 270
ten following the French Regulation on Biomedical Research 271
and biological tissue collection It is being submitted to the 272
ethical committee ldquocomiteacute de protection des personnesrdquo and 273
the ldquoagence nationale de seacutecuriteacute du meacutedicament et des pro- 274
duits de santeacuterdquo (ANSM) The prostate chips will be on one 275
hand characterized by anatomopathologists to determine their 276
nature (pathologic vs healthy prostatic vs non-prostatic) and 277
will allow us to validate our immunofluorescence protocol and 278
fine-tune our auto and immunofluorescence measurements 279
protocols on fresh tissue samples 280
4 Results 281
In this section we present our preclinical evaluation of the 282
different prototypes and software presented in the previous sec- 283
tion 284
41 Augmented laparoscopy thanks to an innovative video 285
device 286
In order to evaluate the potential benefits of the pro- 287
posed vision system we asked a surgeon to perform a simple 288
Please cite this article in press as Voros S et al Devices and systems targeted towards augmented robotic radical prostatectomy IRBM (2013)
httpdxdoiorg101016jirbm201301014
ARTICLE IN PRESS+ModelIRBM 252 1ndash8
6 S Voros et al IRBM xxx (2013) xxxndashxxx
Fig 7 Ultrasound image of a prostate acquired with our innovative transurethral
ultrasound probe during a cadaver experiment The image was acquired with our
first prototype (64 piezoelectric elements)
surgical task once with the traditional endoscope alone and289
once with the proposed system alone (although in practice they290
can be combined to associate local and global views) The tasks291
consisted in localizing a suture needle and bringing it to a fixed292
target point The experiment was performed on porcine organs293
placed in a training box and repeated six times by the surgeon294
At each realization the needlersquos initial position was repositioned295
randomly at a distance equivalent to its initial position and the296
surgeon started randomly with the traditional endoscope or the297
proposed system In both cases a robotic endoscope holder was298
used to mobilize the endoscope and the vision system allowing299
us to record the displacements of the vision systems300
The full methodology and results are currently under sub-301
mission but to summarize the mean time required to perform302
the six experiments with the traditional endoscope was of 190 s303
compared to 245 s with the proposed system Moreover the sur-304
geon needed to give an average of 232 commands to the robotic305
scope holder to perform one stitch with the endoscope alone306
compared to 46 commands with the proposed system These307
preliminary results suggest that the proposed system could sig-308
nificantly reduce the laparoscopic surgery time and the cognitive309
load required for the control of the endoscope We now plan on310
performing cadaver experiments to evaluate the deployment of311
the vision system in conditions close to the clinical reality and312
to evaluate the system with several surgeons313
42 Augmented laparoscopy thanks to an innovative314
ultrasound system315
We performed two cadaver experiments which allowed us316
to determine the optimal characteristics for the realization of317
the intraurethral ultrasound probe During these experiments318
we evaluated the (difficult) insertion of the catheter through319
the urethra and the prostate visualization It must be noted that320
our clinicians partners stressed that the rigor mortis made this321
insertion harder These experiments allowed us to find the best322
rigidity for the catheter of the probe it must be flexible enough323
Fig 8 Demonstration of the fusion of ultrasound and laparoscopic images using
passive landmarks on chicken breasts Top-left the ultrasound image top-right
the laparoscopic image The passive landmarks are indicated with the green
arrows in the laparoscopic image They are selected manually in both modalities
to perform the registration Bottom the fusion of the two imaging modalities
to be introduced in the urethra but rigid enough to avoid the 324
distortions of the catheter 325
The first ultrasound probe (2D) was designed with 64 326
piezoelements It appeared that it was not enough On the one 327
hand the probe imaged a too small part of the prostate so that 328
it was difficult to identify what was represented on the ultra- 329
sound image (Fig 7) Furthermore it was impossible to know 330
in which direction the probe was oriented On the other hand 331
we demonstrated [9] that a longer probe increases the precision 332
of the localization of the active ultrasound transducers That is 333
why the second probe designed for the project (3D) has 128 334
piezoelements This second probe has graduations located on 335
its catheter visible on Fig 2 They allow the surgeon to know 336
the probersquos insertion depth in the urethra and a line along the 337
catheter allows appreciating the torsion applied to the catheter 338
The localization of the active transducers is currently under 339
submission It is based on a global positioning system (GPS) 340
method We made some experiments on a testbench making 341
localization in water to have ideal homogeneous conditions and 342
Please cite this article in press as Voros S et al Devices and systems targeted towards augmented robotic radical prostatectomy IRBM (2013)
httpdxdoiorg101016jirbm201301014
ARTICLE IN PRESS+ModelIRBM 252 1ndash8
S Voros et al IRBM xxx (2013) xxxndashxxx 7
Fig 9 Preliminary experiments of the autofluorescence detection with our testbench The autofluorescence of chlorophyll which has optical properties very similar
to Protoporphyrin IX was observed on our testbench Left direct image of a leaf right fluorescence image of the leaf at 680 nm As expected chlorophyll seems
absent in the veins
Fig 10 Specific fluorescence signal of anti-prostate-specific membrane antigen marker A Nuclear counter-staining of prostatic tissue with Hoechst (blue DNA
marker) We observe the nuclei of prostate cells regularly organized in the glandular epithelium Prostatic glands are separated by stroma B Fluorescence emission
of anti-prostate-specific membrane antigen-Fluorescein IsoThioCyanate on cellular membranes of prostatic cells C Overlay of the A and B images This figure
demonstrates the specificity on fixed prostatic tissue of a specific anti-PSMA antibody labelled with Fluorescein IsoThioCyanate We can also detect the contribution
of non-specific autofluorescence of prostatic concretions (Fig 11) (times20 magnification)
localization on a chicken breast to have more realistic condi-343
tions In both cases we were able to localize the active transducer344
with a precision less than 625 m Moreover the computation345
time is a few hundred milliseconds for a 2D localization These346
results demonstrate that the localization is fast enough to be347
implemented for a prostatectomy For the moment only a 2D 348
localization has been made with the active landmarks and the 349
3D localization is in progress Then we will be able to per- 350
form a registration with laparoscopic images using ldquoactiverdquo 351
markers 352
Fig 11 Non-specific autofluorescence observed in the prostate fixed tissues This figure shows the benefits of a near infrared marker like Cyanine 5 (excited at
633 nm) compared to Fluorescein IsoThioCyanate (excited at 488 nm) A Auto fluorescence under laser excitation at 488 nm We observe that prostate concretions
(calcified material) respond to this excitation by a strong fluorescence signal B Auto fluorescence under laser excitation at 633 nm The use of Cyanine 5 reduces
widely autofluorescence of some structures such as prostate concretions (times20 magnification)
Please cite this article in press as Voros S et al Devices and systems targeted towards augmented robotic radical prostatectomy IRBM (2013)
httpdxdoiorg101016jirbm201301014
ARTICLE IN PRESS+ModelIRBM 252 1ndash8
8 S Voros et al IRBM xxx (2013) xxxndashxxx
Concerning the registration between laparoscopic and ultra-353
sound images we performed several testbench evaluations of354
the registration algorithm on chicken breasts The result of such355
a registration obtained by manually pairing passive markers356
visible on both the laparoscopic and ultrasound imaging modal-357
ities are presented on Fig 8 In this example we obtained a358
registration root mean square error (RMS) of 038 mm359
43 Augmented laparoscopy thanks to fluorescence360
imaging361
First experiments were performed on leaves to demonstrate362
the feasibility of the detection of chlorophyll autofluorescence363
which has optical properties very similar to PpIX (absorption at364
405 nm and emission at 680 nm) as described on Fig 9 Then365
experiments were conducted on histology slices of the human366
prostate with as we anticipated inconclusive results because367
of the expected low signal-to-noise ratio caused by the insuffi-368
cient thickness of a histology slice (3 m thickness) compared to369
the optimal use of the device (300 m thickness) These results370
motivated our biomedical research COPROST on macroscopic371
fresh prostate samples372
Concerning the immunofluorescence protocol we were able373
to demonstrate the specificity of the anti-PSMA antibody on374
fixed tissue samples labelled with FITC as illustrated by Fig 10375
We observed higher autofluorescence problems when excit-376
ing the sample at the FITC specific wavelength compared to377
an excitation at the Cyanine 5 specific wavelength (Fig 11)378
These results motivated the inclusion of both fluorophores in our379
biomedical research COPROST on macroscopic fresh prostate380
samples FITC because it was already used to demonstrate speci-381
ficity of anti-PSMA antibody and Cyanine 5 because its near382
infra-red characteristics make it a better candidate on fresh mate-383
rial (higher penetration in tissue) and will improve signalnoise384
ratio as previously demonstrated385
To our knowledge most of the optical biopsy approaches as386
previously defined have been validated either on histologic slices387
or on ratmice prostate models However these approaches have388
limitations prostatic tissue is impaired by the chemical treat-389
ment required for histologic preparation and animal models do390
not directly mimic all aspects of human prostate cancer [11] In391
short it has not been proved yet that a successful detection with392
the investigated devices on histopathology slices or on animal393
models is sufficient to guarantee a successful detection on fresh394
human tissues The experiments that will be performed in the395
frame of the COPROST protocol in 2013 will be determinant to396
confirm the feasibility of our approach on fresh tissue samples397
5 DiscussionConclusion398
The DEPORRA project allowed for the development of inno-399
vative devices and navigation prototypes in the objective of400
allowing the surgeon to see ldquobeyond the visiblerdquo during a radi-401
cal prostatectomy First evaluations of the devices and methods402
have been performed preclinically and are very encouraging for403
the development of innovative approaches to assist the surgeon
during such a complex surgery Our preliminary results have also 404
shown the limits of preclinical validation and have convinced us 405
of the necessity to launch biomedical researches that will allow 406
us to validate further the devices This process required a con- 407
sequent amount of effort and time but is mandatory for the 408
fine-tuning of our tissue characterization tools and to obtain the 409
first clinical proofs of the relevance of the developed medical 410
devices which are mandatory to perform clinical evaluations of 411
the complete navigation systems 412
We now need to push further the integration of the devices 413
into such navigation systems in order to exploit at best the infor- 414
mation provided by each modality and to determine the optimal 415
approach for displaying the relevant information to the surgeon 416
in a clinical environment This will imply a conception and 417
development effort a definition of qualitative and quantitative 418
parameters for the first assessment of the delivered medical ben- 419
efit of our developments risks analysis and biomedical research 420
preparations in order to meet the ethical instances requirements 421
Acknowledgments 422
This work has been supported by French National Research 423
Agency (ANR) through TecSan program (project DEPORRA 424
no ANR-09-TECS-006) 425
References 426
[1] Heidenreich A Bolla M Joniau S Mason MD Matveev V Mottet N et al 427
Guidelines on prostate cancer Eur Assoc Urol 2011 [www uroweb org] 428
[2] Pfitzenmaier J Pahernik S Tremmel T Haferkamp A Buse S Hohen- 429
fellner M Positive surgical margins after radical prostatectomy do 430
they have an impact on biochemical or clinical progression BJU Int 431
2008102(10)1413ndash8 432
[3] Soler L Nicolau S Schmid J Koehl C Marescaux J et al Virtual reality 433
and augmented reality in digestive surgery In Third IEEE and ACM Inter- 434
national Symposium on Mixed and Augmented Reality (ISMAR) 2004 435
p 278ndash9 436
[4] S Voros B Tamadazte P Cinquin C Fouard Systegraveme drsquoimagerie multi- 437
vision pour chirurgie laparoscopique demande de deacutepocirct de brevet FR 438
1259489 102012 439
[5] Ukimura O Ahlering TE Gill IS Transrectal ultrasound-guided 440
energy-free nerve-sparing laparoscopic radical prostatectomy J Endourol 441
200822(9)1993ndash5 442
[6] Long JA Lee BH Guillotreau J Autorino R Laydner H Yakoubi R et al 443
Real-time robotic transrectal ultrasound navigation during robotic radical 444
prostatectomy initial clinical experience Urology 201280(3)608ndash13 445
[7] Holmes III DR Davis BJ Bruce CJ Robb RA 3D visualization analysis 446
and treatment of the prostate using trans-urethral ultrasound Comput Med 447
Imaging Graph 200327339ndash49 [2003] 448
[8] Dementhon D Model-based object pose in 25 lines of code Int J Comput 449
Vis 199515(1ndash2)123ndash41 450
[9] Custillon G Voros S Cinquin P Nguyen-Dinh A Moreau-Gaudry A 451
Bidimensional localization of active ultrasound transducers for use in 452
laparoscopic prostate surgery IEEE Trans Med Imaging 2012 Q3 453
[10] Wolf R Duchateau J Cinquin P Voros S 3D tracking of laparoscopic 454
instruments using statistical and geometric modeling Med Image Com- 455
put Comput Assist Interv 20116891203ndash10 [Lecture notes in computer 456
science] 457
[11] Valkenburg KC Williams BO ldquoMouse models of prostate cancerrdquo Prostate 458
Cancer 2011201122 httpdxdoiorg1011552011895238 [Article ID 459
895238] 460

Please cite this article in press as Voros S et al Devices and systems targeted towards augmented robotic radical prostatectomy IRBM (2013)
httpdxdoiorg101016jirbm201301014
ARTICLE IN PRESS+ModelIRBM 252 1ndash8
2 S Voros et al IRBM xxx (2013) xxxndashxxx
is superior in terms of oncological and functional results and49
cost-effectiveness Prospective trials are urgently neededrdquo an50
argument also shared in two recent Health Technology Assess-51
ments on robot assisted surgery (Belgian HTA 2009 Irish HTA52
2012)53
In the current surgical practice the surgeon must determine54
the best compromise between a complete removal of the prostate55
gland and morbidity The ideal removal consists in removing56
completely the prostate within its capsule a non complete57
removal may lead to positive surgical margins which are associ-58
ated to a higher risk of biochemical recurrence [2] (15ndash20 of59
the patients) Lesions of the urethral sphincter situated under the60
prostate can lead to incontinence (7 of the patients) Lesions61
of the neurovascular bundles (immediately in contact with the62
posterior side of the prostate) may lead to erectile problems of63
varying intensity The surgeon can try to spare more or less these64
organs depending on the preoperative staging completed by65
magnetic resonance imaging (MRI) The quality of the prostate66
removal (absence of positive surgical margins) is determined67
postoperatively thanks to a histopathology exam at the anato-68
mopathology laboratory Thus the surgeon cannot adapt his69
surgical strategy peroperatively70
2 Objectives71
In this controversial context regarding robotically assisted72
prostatectomy we propose a new robotic navigation concept73
guided by some of the principal complications of a radical pros-74
tatectomy (cancer relapse incontinence and impotence) based75
on peroperative multimodal imaging Surgical navigation sys-76
tems allow for the combination of several imaging modalities in77
a common environment thus providing more useful information78
to the surgeon during a surgery than a single imaging modality79
In most of the existing systems information from preoperative80
imaging modalities is combined with the peroperative imaging81
modality However in the case of laparoscopic surgery (soft tis-82
sue surgery) the registration of preoperative images with the83
laparoscopic images is very challenging because the organs can84
move and deform To our knowledge there are only a few navi-85
gation systems for laparoscopic navigation [3] none of which86
are used clinically87
Our proposed navigation concept is based on three coupled88
components that will ultimately ldquoaugmentrdquo the laparoscopic89
images and allow the surgeon to see beyond the visible and90
adapt his surgical strategy peroperatively91
bull an augmented laparoscope allowing the surgeon to navigate92
more harmoniously inside the abdominal cavity as he would93
do in open surgery and potentially to provide three dimen-94
sional information95
bull peroperative visualization technologies allowing the surgeon96
to visualize the important anatomical structures for radical97
prostatectomy98
visualization of the prostate and surrounding organs thanks99
to an innovative transurethral ultrasound probe100
identification and visualization of the tumor and prostatic 101
cells thanks to bimodal fluorescence probe 102
bull integration of the multimodal information to navigation 103
systems thanks to the registration of the different imaging 104
modalities when required 105
3 Material amp methods 106
31 Augmented laparoscopy thanks to an innovative video 107
device 108
Laparoscopic surgery in general can be challenging for a sur- 109
geon for several reasons among which the limited field of view 110
of the endoscope (ldquokeyholerdquo surgery) In consequence whether 111
it is displaced by a human assistant or a robotic endoscope holder 112
the endoscope is mobilized a lot since it is used to see precisely 113
the operating field but also to monitor the instruments introduc- 114
tion and displacement inside the abdominal cavity Movements 115
of the endoscope increase the risk of staining of the lens which 116
leads to a removal of the endoscope from the patient to clean the 117
lens increasing the surgery duration and discomfort 118
To provide a solution to this difficulty we have developed 119
an innovative vision system that can be used in combination 120
with a traditional endoscope thanks to an encapsulation in a 121
traditional trocar Our system is composed of two miniature 122
cameras that are positioned like a pair of glasses around the 123
endoscope (Fig 1) and provide a panoramic view of the abdom- 124
inal cavity These cameras are similar to those present on cell 125
phones and cost only a few US$ in large scale diffusion The 126
system has been designed for an easy insertion deployment and 127
removal of the cameras and has been patented [4] Since it is 128
positioned around the endoscope it provides roughly the same 129
view direction as the endoscope and a registration between the 130
laparoscopic image and the vision system images is unneces- 131
sary The cameras of the innovative vision system are mounted 132
in stereoscopic conditions which could allow for a local 3D 133
reconstruction of the scene Our preclinical evaluation of the 134
potential expected medical service of this device is presented in 135
section 4 136
32 Augmented laparoscopy thanks to an innovative 137
ultrasound system 138
Previous work [5] has already shown that the use of tran- 139
srectal ultrasound during laparoscopic radical prostatectomies 140
could assist the surgeons in the visualization of specific prostate 141
contour anatomy and of the neurovascular bundles and in 142
the bladder neck dissection According to the authors the use 143
of transrectal ultrasound in laparoscopic prostatectomy com- 144
pensated for the lack of tactile feedback compared to open 145
surgery achieved significant decrease in the incidence of posi- 146
tive surgical margins and achieved quicker and superior potency 147
recovery In this work the ultrasound images were not fused 148
with the laparoscopic images and the surgeon had to perform 149
a challenging mental registration of the two imaging modali- 150
ties Long et al [6] also showed the potential of a guidance of 151
a transrectal ultrasound probe with a robotic endoscope holder 152
Please cite this article in press as Voros S et al Devices and systems targeted towards augmented robotic radical prostatectomy IRBM (2013)
httpdxdoiorg101016jirbm201301014
ARTICLE IN PRESS+ModelIRBM 252 1ndash8
S Voros et al IRBM xxx (2013) xxxndashxxx 3
Fig 1 The proposed global vision system a) the mini-cameras used for the vision system b) CAD drawing of the augmented endoscope concept the mini-cameras
are inserted into a modified trocar When the endoscope is inserted the vision system is deployed like glasses around the endoscope c) and d) rapid prototyping
realization
(Endocontrolrsquos ViKY system) Holmes et al [7] have developed153
a 2D transurethral ultrasound probe for brachytherapy that is154
manually rotated around its axis to provide 3D imaging They155
affirm that the endourethral approach permits a better resolu-156
tion than the transrectal approach for the visualization of the157
prostate The transurethral approach also allows avoiding some158
of the intrinsic limitations of transrectal ultrasound imaging (a159
layer of air forms between the prostate and the rectum during160
the prostate dissection making the ultrasound visualization of161
the prostate impossible after this surgical phase)162
In light of these previous works we have developed two163
transurethral ultrasound probe prototypes (one for 2D imaging164
and a motorized version where the probe rotates around its axis165
to provide 3D images) (Fig 2) The 2D probe is composed of166
64 piezoelectric elements with a frequency of 10 MHz and a167
3 mm diameter semi-rigid catheter for an easy introduction The168
3D probe has the same central frequency but it is composed of169
128 piezoelements and has a 6 mm diameter catheter They are170
Fig 2 The innovative intraurethral ultrasound probe Top the 3D transurethral
probe able to rotate around its axis Bottom the 2D transurethral probe
connected to an Ultrasonix ultrasound machine allowing us to 171
control all the piezoelectric elements 172
In parallel we have also developed an endoscopicultrasound 173
fusion demonstrator The registration is based on the POSIT 174
algorithm [8] and is based on the manual localization in both 175
imaging modalities of artificial landmarks In the frame of this 176
project two complementary approaches have been investigated 177
passive landmarks (laparoscopic needles planted in the prostate) 178
and innovative active ultrasound landmarks that emit an ultra- 179
sound signal that can be detected by the transurethral probe 180
allowing for their precise localization in the ultrasound referen- 181
tial [9] (Fig 3) 182
Our preliminary results for the registration of ultrasound and 183
laparoscopic images using passive landmarks and for the precise 184
3D localization of the ultrasound ldquoactiverdquo markers are described 185
in section 4 186
33 Augmented laparoscopy thanks to fluorescence 187
imaging 188
During a radical prostatectomy the ability to visualize bio- 189
logical characteristics of tissue (prostatic vs non-prostatic on 190
the one hand normal vs malignant on the other hand) could help 191
the surgeon to respectively determine precisely the location of 192
the prostate capsule and assess the extent of the cancer and thus 193
allow him or her to adapt his surgical strategy peroperatively 194
Based on these observations we have developed a bimodal 195
fluorescence fibered probe for the peroperative characterization 196
of tissue for radical prostatectomy 197
Please cite this article in press as Voros S et al Devices and systems targeted towards augmented robotic radical prostatectomy IRBM (2013)
httpdxdoiorg101016jirbm201301014
ARTICLE IN PRESS+ModelIRBM 252 1ndash8
4 S Voros et al IRBM xxx (2013) xxxndashxxx
Fig 3 The proposed markers for the registration of ultrasound and endoscopic
images Top ldquoactiverdquo landmark (laparoscopic ultrasound emitter) Bottom ldquopas-
siverdquo landmark (laparoscopic needle) used for the registration of ultrasound and
laparoscopic images
bull the normalmalignant characterization of the tissues is based198
on the detection of the autofluorescence of the Protopor-199
phyrin IX (PpIX) protein which accumulates in malignant200
cells Indeed the elimination cycle of Protorphyrin is per-201
turbed in case of malignant cells It causes thus an increase202
of Protoporphyrin concentration A first prototype (already203
available see Fig 4 left) comes in the form of a testbench204
equipped with a laser source emitting at 405 nm (excitation 205
wavelength for the PpIX protein) and with optical fibers and 206
a spectrometer allowing the collection of a fluorescence spec- 207
trum of 3648 points in the range 345ndash1040 mm (the testbench 208
can image a 25 times 25 mm2 area with a spatial resolution of 209
100 m and a penetration depth of roughly 300 m) Using 210
this spectrum an intensity image can be created (Fig 4 211
right) The analysis of prostate tissue samples gathered in 212
the frame of a biomedical protocol (section 4) will allow us 213
to determine the optimal parameters for the acquisition of 214
the fluorescence spectrum and build discrimination criteria 215
from the measurements between malignanthealthy tissue and 216
prostaticnon-prostatic tissue 217
bull the prostaticnon-prostatic characterization of the tissues is 218
based on the detection of the prostate-specific membrane anti- 219
gen (PSMA) which is specific of the prostatic membrane 220
This detection is made possible by the immunofluorescence 221
tagging of the PSMA using a specific anti-PSMA antibody 222
labelled with a fluorescent tracer When excited by light at 223
a characteristic absorption wavelength the fluorescent tracer 224
emits light at a characteristic emission wavelength Two flu- 225
orescent tracers are investigated in the DEPORRA project 226
Fluorescein IsoThioCyanate (FITC) and Cyanine 5 Both 227
FITC and Cyanine 5 have a characteristic emission wave- 228
length different from the autofluorescence wavelength of the 229
Protoporpphyrin IX protein allowing for the characterization 230
of the tissue type (prostatic vs non-prostatic) and the tissue 231
status (healthy vs malignant) with the same testbench (Fig 5) 232
The testbench presented on Fig 4 has also been equipped 233
with two laser sources emitting at 488 nm and 642 nm exci- 234
tation wavelengths respectively for FITC and Cyanine 5 for 235
recognizing prostate tissue from those environing 236
A bimodal laparoscopic-compliant fluorescence probe based 237
on the miniaturization of the fluorescence testbench will be avail- 238
able in 2013 (Fig 6 top) Preliminary results based on the 239
analysis of histopathologic slices will be presented in section 240
4 In order to overlay the probersquos fluorescence measurement on 241
the laparoscopic images we plan on detecting automatically the 242
position of the tip of the laparoscopic probe using a real-time 243
Fig 4 Experimental fluorescence design and results Left experimental optical device Right typical intensity image obtained
Please cite this article in press as Voros S et al Devices and systems targeted towards augmented robotic radical prostatectomy IRBM (2013)
httpdxdoiorg101016jirbm201301014
ARTICLE IN PRESS+ModelIRBM 252 1ndash8
S Voros et al IRBM xxx (2013) xxxndashxxx 5
Perc
ent
of
maxim
a
Wavelength (nm)
PpIX emission
FITC excitation
FITC emission
PpIX excitation
350 400 450 500 550 600 650 700 750
Perc
ent
of
maxim
a
10
00
08
06
04
02
Wavelength (nm)
PpIX emission
Cy5 excitation
Cy5 emission
PpIX excitation
BA
350 400 450 500 550 600 650 700 750
10
00
08
06
04
02
Fig 5 Excitation and emission spectra of Protoporphyrin IX Fluorescein IsoThioCyanate and Cyanine 5 (Cy5) fluorochromes A Overlay of the excitation (blue
dashed line) and emission (orange solid line) spectra of Protoporphyrin IX with excitation (green dashed line) and emission (emission spectrum) of Fluorescein
IsoThioCyanate B Overlay of the excitation (blue dashed line) and emission (orange solid line) spectra of Protoporphyrin IX with excitation (red dashed line) and
emission (red solid line) of Cy5
Fig 6 The bimodal fluorescence laparoscopic probe and the image-based anal-
ysis approach to localize it in laparoscopic images Top the CAD drawing
of the bimodal fluorescence laparoscopic probe Bottom automatic detection
of a laparoscopic instrument which will be used to overlay the probersquos tissue
characterization measurements on the laparoscopic images
image analysis approach that we have developed [10] (Fig 6244
bottom)245
34 Preclinical and clinical evaluation246
Preliminary evaluation of the devices and the software devel-247
oped in the frame of this project has already been performed on248
laboratory testbenchs and during three cadaver experiments at249
the anatomy laboratory (section 4) However in order to acquire250
the qualitative and quantitative proofs necessary to perform the251
fist clinical evaluations of our innovative medical devices on 252
patients we have submitted two biomedical research protocols 253
bull the first one called ldquofusion of echographic (ultrasound) and 254
endoscopic imagesrdquo (FEE) is a pilot monocentric study on a 255
cohort of 15 patients and is currently running It aims at val- 256
idating our ultrasound approach and evaluating its expected 257
medical benefit during radical prostatectomies the surgeons 258
will insert surgical needles in the prostate and endorectal 259
ultrasound images and laparoscopic images will be recorded 260
The data will be processed offline in the laboratory to assess 261
quantitatively the feasibility of the registration of ultrasound 262
and laparoscopic images using passive markers This proto- 263
col already accepted by the ethical instances will be a pilot 264
monocentric study with 15 patients 265
bull the second protocol called COPROST will allow us to obtain 266
fresh prostate chips during transurethral resections in the 267
frame of a pilot monocentric prospective non-randomized 268
open and controlled clinical trial The protocol with an 269
inclusion period of 24 months is already defined and writ- 270
ten following the French Regulation on Biomedical Research 271
and biological tissue collection It is being submitted to the 272
ethical committee ldquocomiteacute de protection des personnesrdquo and 273
the ldquoagence nationale de seacutecuriteacute du meacutedicament et des pro- 274
duits de santeacuterdquo (ANSM) The prostate chips will be on one 275
hand characterized by anatomopathologists to determine their 276
nature (pathologic vs healthy prostatic vs non-prostatic) and 277
will allow us to validate our immunofluorescence protocol and 278
fine-tune our auto and immunofluorescence measurements 279
protocols on fresh tissue samples 280
4 Results 281
In this section we present our preclinical evaluation of the 282
different prototypes and software presented in the previous sec- 283
tion 284
41 Augmented laparoscopy thanks to an innovative video 285
device 286
In order to evaluate the potential benefits of the pro- 287
posed vision system we asked a surgeon to perform a simple 288
Please cite this article in press as Voros S et al Devices and systems targeted towards augmented robotic radical prostatectomy IRBM (2013)
httpdxdoiorg101016jirbm201301014
ARTICLE IN PRESS+ModelIRBM 252 1ndash8
6 S Voros et al IRBM xxx (2013) xxxndashxxx
Fig 7 Ultrasound image of a prostate acquired with our innovative transurethral
ultrasound probe during a cadaver experiment The image was acquired with our
first prototype (64 piezoelectric elements)
surgical task once with the traditional endoscope alone and289
once with the proposed system alone (although in practice they290
can be combined to associate local and global views) The tasks291
consisted in localizing a suture needle and bringing it to a fixed292
target point The experiment was performed on porcine organs293
placed in a training box and repeated six times by the surgeon294
At each realization the needlersquos initial position was repositioned295
randomly at a distance equivalent to its initial position and the296
surgeon started randomly with the traditional endoscope or the297
proposed system In both cases a robotic endoscope holder was298
used to mobilize the endoscope and the vision system allowing299
us to record the displacements of the vision systems300
The full methodology and results are currently under sub-301
mission but to summarize the mean time required to perform302
the six experiments with the traditional endoscope was of 190 s303
compared to 245 s with the proposed system Moreover the sur-304
geon needed to give an average of 232 commands to the robotic305
scope holder to perform one stitch with the endoscope alone306
compared to 46 commands with the proposed system These307
preliminary results suggest that the proposed system could sig-308
nificantly reduce the laparoscopic surgery time and the cognitive309
load required for the control of the endoscope We now plan on310
performing cadaver experiments to evaluate the deployment of311
the vision system in conditions close to the clinical reality and312
to evaluate the system with several surgeons313
42 Augmented laparoscopy thanks to an innovative314
ultrasound system315
We performed two cadaver experiments which allowed us316
to determine the optimal characteristics for the realization of317
the intraurethral ultrasound probe During these experiments318
we evaluated the (difficult) insertion of the catheter through319
the urethra and the prostate visualization It must be noted that320
our clinicians partners stressed that the rigor mortis made this321
insertion harder These experiments allowed us to find the best322
rigidity for the catheter of the probe it must be flexible enough323
Fig 8 Demonstration of the fusion of ultrasound and laparoscopic images using
passive landmarks on chicken breasts Top-left the ultrasound image top-right
the laparoscopic image The passive landmarks are indicated with the green
arrows in the laparoscopic image They are selected manually in both modalities
to perform the registration Bottom the fusion of the two imaging modalities
to be introduced in the urethra but rigid enough to avoid the 324
distortions of the catheter 325
The first ultrasound probe (2D) was designed with 64 326
piezoelements It appeared that it was not enough On the one 327
hand the probe imaged a too small part of the prostate so that 328
it was difficult to identify what was represented on the ultra- 329
sound image (Fig 7) Furthermore it was impossible to know 330
in which direction the probe was oriented On the other hand 331
we demonstrated [9] that a longer probe increases the precision 332
of the localization of the active ultrasound transducers That is 333
why the second probe designed for the project (3D) has 128 334
piezoelements This second probe has graduations located on 335
its catheter visible on Fig 2 They allow the surgeon to know 336
the probersquos insertion depth in the urethra and a line along the 337
catheter allows appreciating the torsion applied to the catheter 338
The localization of the active transducers is currently under 339
submission It is based on a global positioning system (GPS) 340
method We made some experiments on a testbench making 341
localization in water to have ideal homogeneous conditions and 342
Please cite this article in press as Voros S et al Devices and systems targeted towards augmented robotic radical prostatectomy IRBM (2013)
httpdxdoiorg101016jirbm201301014
ARTICLE IN PRESS+ModelIRBM 252 1ndash8
S Voros et al IRBM xxx (2013) xxxndashxxx 7
Fig 9 Preliminary experiments of the autofluorescence detection with our testbench The autofluorescence of chlorophyll which has optical properties very similar
to Protoporphyrin IX was observed on our testbench Left direct image of a leaf right fluorescence image of the leaf at 680 nm As expected chlorophyll seems
absent in the veins
Fig 10 Specific fluorescence signal of anti-prostate-specific membrane antigen marker A Nuclear counter-staining of prostatic tissue with Hoechst (blue DNA
marker) We observe the nuclei of prostate cells regularly organized in the glandular epithelium Prostatic glands are separated by stroma B Fluorescence emission
of anti-prostate-specific membrane antigen-Fluorescein IsoThioCyanate on cellular membranes of prostatic cells C Overlay of the A and B images This figure
demonstrates the specificity on fixed prostatic tissue of a specific anti-PSMA antibody labelled with Fluorescein IsoThioCyanate We can also detect the contribution
of non-specific autofluorescence of prostatic concretions (Fig 11) (times20 magnification)
localization on a chicken breast to have more realistic condi-343
tions In both cases we were able to localize the active transducer344
with a precision less than 625 m Moreover the computation345
time is a few hundred milliseconds for a 2D localization These346
results demonstrate that the localization is fast enough to be347
implemented for a prostatectomy For the moment only a 2D 348
localization has been made with the active landmarks and the 349
3D localization is in progress Then we will be able to per- 350
form a registration with laparoscopic images using ldquoactiverdquo 351
markers 352
Fig 11 Non-specific autofluorescence observed in the prostate fixed tissues This figure shows the benefits of a near infrared marker like Cyanine 5 (excited at
633 nm) compared to Fluorescein IsoThioCyanate (excited at 488 nm) A Auto fluorescence under laser excitation at 488 nm We observe that prostate concretions
(calcified material) respond to this excitation by a strong fluorescence signal B Auto fluorescence under laser excitation at 633 nm The use of Cyanine 5 reduces
widely autofluorescence of some structures such as prostate concretions (times20 magnification)
Please cite this article in press as Voros S et al Devices and systems targeted towards augmented robotic radical prostatectomy IRBM (2013)
httpdxdoiorg101016jirbm201301014
ARTICLE IN PRESS+ModelIRBM 252 1ndash8
8 S Voros et al IRBM xxx (2013) xxxndashxxx
Concerning the registration between laparoscopic and ultra-353
sound images we performed several testbench evaluations of354
the registration algorithm on chicken breasts The result of such355
a registration obtained by manually pairing passive markers356
visible on both the laparoscopic and ultrasound imaging modal-357
ities are presented on Fig 8 In this example we obtained a358
registration root mean square error (RMS) of 038 mm359
43 Augmented laparoscopy thanks to fluorescence360
imaging361
First experiments were performed on leaves to demonstrate362
the feasibility of the detection of chlorophyll autofluorescence363
which has optical properties very similar to PpIX (absorption at364
405 nm and emission at 680 nm) as described on Fig 9 Then365
experiments were conducted on histology slices of the human366
prostate with as we anticipated inconclusive results because367
of the expected low signal-to-noise ratio caused by the insuffi-368
cient thickness of a histology slice (3 m thickness) compared to369
the optimal use of the device (300 m thickness) These results370
motivated our biomedical research COPROST on macroscopic371
fresh prostate samples372
Concerning the immunofluorescence protocol we were able373
to demonstrate the specificity of the anti-PSMA antibody on374
fixed tissue samples labelled with FITC as illustrated by Fig 10375
We observed higher autofluorescence problems when excit-376
ing the sample at the FITC specific wavelength compared to377
an excitation at the Cyanine 5 specific wavelength (Fig 11)378
These results motivated the inclusion of both fluorophores in our379
biomedical research COPROST on macroscopic fresh prostate380
samples FITC because it was already used to demonstrate speci-381
ficity of anti-PSMA antibody and Cyanine 5 because its near382
infra-red characteristics make it a better candidate on fresh mate-383
rial (higher penetration in tissue) and will improve signalnoise384
ratio as previously demonstrated385
To our knowledge most of the optical biopsy approaches as386
previously defined have been validated either on histologic slices387
or on ratmice prostate models However these approaches have388
limitations prostatic tissue is impaired by the chemical treat-389
ment required for histologic preparation and animal models do390
not directly mimic all aspects of human prostate cancer [11] In391
short it has not been proved yet that a successful detection with392
the investigated devices on histopathology slices or on animal393
models is sufficient to guarantee a successful detection on fresh394
human tissues The experiments that will be performed in the395
frame of the COPROST protocol in 2013 will be determinant to396
confirm the feasibility of our approach on fresh tissue samples397
5 DiscussionConclusion398
The DEPORRA project allowed for the development of inno-399
vative devices and navigation prototypes in the objective of400
allowing the surgeon to see ldquobeyond the visiblerdquo during a radi-401
cal prostatectomy First evaluations of the devices and methods402
have been performed preclinically and are very encouraging for403
the development of innovative approaches to assist the surgeon
during such a complex surgery Our preliminary results have also 404
shown the limits of preclinical validation and have convinced us 405
of the necessity to launch biomedical researches that will allow 406
us to validate further the devices This process required a con- 407
sequent amount of effort and time but is mandatory for the 408
fine-tuning of our tissue characterization tools and to obtain the 409
first clinical proofs of the relevance of the developed medical 410
devices which are mandatory to perform clinical evaluations of 411
the complete navigation systems 412
We now need to push further the integration of the devices 413
into such navigation systems in order to exploit at best the infor- 414
mation provided by each modality and to determine the optimal 415
approach for displaying the relevant information to the surgeon 416
in a clinical environment This will imply a conception and 417
development effort a definition of qualitative and quantitative 418
parameters for the first assessment of the delivered medical ben- 419
efit of our developments risks analysis and biomedical research 420
preparations in order to meet the ethical instances requirements 421
Acknowledgments 422
This work has been supported by French National Research 423
Agency (ANR) through TecSan program (project DEPORRA 424
no ANR-09-TECS-006) 425
References 426
[1] Heidenreich A Bolla M Joniau S Mason MD Matveev V Mottet N et al 427
Guidelines on prostate cancer Eur Assoc Urol 2011 [www uroweb org] 428
[2] Pfitzenmaier J Pahernik S Tremmel T Haferkamp A Buse S Hohen- 429
fellner M Positive surgical margins after radical prostatectomy do 430
they have an impact on biochemical or clinical progression BJU Int 431
2008102(10)1413ndash8 432
[3] Soler L Nicolau S Schmid J Koehl C Marescaux J et al Virtual reality 433
and augmented reality in digestive surgery In Third IEEE and ACM Inter- 434
national Symposium on Mixed and Augmented Reality (ISMAR) 2004 435
p 278ndash9 436
[4] S Voros B Tamadazte P Cinquin C Fouard Systegraveme drsquoimagerie multi- 437
vision pour chirurgie laparoscopique demande de deacutepocirct de brevet FR 438
1259489 102012 439
[5] Ukimura O Ahlering TE Gill IS Transrectal ultrasound-guided 440
energy-free nerve-sparing laparoscopic radical prostatectomy J Endourol 441
200822(9)1993ndash5 442
[6] Long JA Lee BH Guillotreau J Autorino R Laydner H Yakoubi R et al 443
Real-time robotic transrectal ultrasound navigation during robotic radical 444
prostatectomy initial clinical experience Urology 201280(3)608ndash13 445
[7] Holmes III DR Davis BJ Bruce CJ Robb RA 3D visualization analysis 446
and treatment of the prostate using trans-urethral ultrasound Comput Med 447
Imaging Graph 200327339ndash49 [2003] 448
[8] Dementhon D Model-based object pose in 25 lines of code Int J Comput 449
Vis 199515(1ndash2)123ndash41 450
[9] Custillon G Voros S Cinquin P Nguyen-Dinh A Moreau-Gaudry A 451
Bidimensional localization of active ultrasound transducers for use in 452
laparoscopic prostate surgery IEEE Trans Med Imaging 2012 Q3 453
[10] Wolf R Duchateau J Cinquin P Voros S 3D tracking of laparoscopic 454
instruments using statistical and geometric modeling Med Image Com- 455
put Comput Assist Interv 20116891203ndash10 [Lecture notes in computer 456
science] 457
[11] Valkenburg KC Williams BO ldquoMouse models of prostate cancerrdquo Prostate 458
Cancer 2011201122 httpdxdoiorg1011552011895238 [Article ID 459
895238] 460

Please cite this article in press as Voros S et al Devices and systems targeted towards augmented robotic radical prostatectomy IRBM (2013)
httpdxdoiorg101016jirbm201301014
ARTICLE IN PRESS+ModelIRBM 252 1ndash8
S Voros et al IRBM xxx (2013) xxxndashxxx 3
Fig 1 The proposed global vision system a) the mini-cameras used for the vision system b) CAD drawing of the augmented endoscope concept the mini-cameras
are inserted into a modified trocar When the endoscope is inserted the vision system is deployed like glasses around the endoscope c) and d) rapid prototyping
realization
(Endocontrolrsquos ViKY system) Holmes et al [7] have developed153
a 2D transurethral ultrasound probe for brachytherapy that is154
manually rotated around its axis to provide 3D imaging They155
affirm that the endourethral approach permits a better resolu-156
tion than the transrectal approach for the visualization of the157
prostate The transurethral approach also allows avoiding some158
of the intrinsic limitations of transrectal ultrasound imaging (a159
layer of air forms between the prostate and the rectum during160
the prostate dissection making the ultrasound visualization of161
the prostate impossible after this surgical phase)162
In light of these previous works we have developed two163
transurethral ultrasound probe prototypes (one for 2D imaging164
and a motorized version where the probe rotates around its axis165
to provide 3D images) (Fig 2) The 2D probe is composed of166
64 piezoelectric elements with a frequency of 10 MHz and a167
3 mm diameter semi-rigid catheter for an easy introduction The168
3D probe has the same central frequency but it is composed of169
128 piezoelements and has a 6 mm diameter catheter They are170
Fig 2 The innovative intraurethral ultrasound probe Top the 3D transurethral
probe able to rotate around its axis Bottom the 2D transurethral probe
connected to an Ultrasonix ultrasound machine allowing us to 171
control all the piezoelectric elements 172
In parallel we have also developed an endoscopicultrasound 173
fusion demonstrator The registration is based on the POSIT 174
algorithm [8] and is based on the manual localization in both 175
imaging modalities of artificial landmarks In the frame of this 176
project two complementary approaches have been investigated 177
passive landmarks (laparoscopic needles planted in the prostate) 178
and innovative active ultrasound landmarks that emit an ultra- 179
sound signal that can be detected by the transurethral probe 180
allowing for their precise localization in the ultrasound referen- 181
tial [9] (Fig 3) 182
Our preliminary results for the registration of ultrasound and 183
laparoscopic images using passive landmarks and for the precise 184
3D localization of the ultrasound ldquoactiverdquo markers are described 185
in section 4 186
33 Augmented laparoscopy thanks to fluorescence 187
imaging 188
During a radical prostatectomy the ability to visualize bio- 189
logical characteristics of tissue (prostatic vs non-prostatic on 190
the one hand normal vs malignant on the other hand) could help 191
the surgeon to respectively determine precisely the location of 192
the prostate capsule and assess the extent of the cancer and thus 193
allow him or her to adapt his surgical strategy peroperatively 194
Based on these observations we have developed a bimodal 195
fluorescence fibered probe for the peroperative characterization 196
of tissue for radical prostatectomy 197
Please cite this article in press as Voros S et al Devices and systems targeted towards augmented robotic radical prostatectomy IRBM (2013)
httpdxdoiorg101016jirbm201301014
ARTICLE IN PRESS+ModelIRBM 252 1ndash8
4 S Voros et al IRBM xxx (2013) xxxndashxxx
Fig 3 The proposed markers for the registration of ultrasound and endoscopic
images Top ldquoactiverdquo landmark (laparoscopic ultrasound emitter) Bottom ldquopas-
siverdquo landmark (laparoscopic needle) used for the registration of ultrasound and
laparoscopic images
bull the normalmalignant characterization of the tissues is based198
on the detection of the autofluorescence of the Protopor-199
phyrin IX (PpIX) protein which accumulates in malignant200
cells Indeed the elimination cycle of Protorphyrin is per-201
turbed in case of malignant cells It causes thus an increase202
of Protoporphyrin concentration A first prototype (already203
available see Fig 4 left) comes in the form of a testbench204
equipped with a laser source emitting at 405 nm (excitation 205
wavelength for the PpIX protein) and with optical fibers and 206
a spectrometer allowing the collection of a fluorescence spec- 207
trum of 3648 points in the range 345ndash1040 mm (the testbench 208
can image a 25 times 25 mm2 area with a spatial resolution of 209
100 m and a penetration depth of roughly 300 m) Using 210
this spectrum an intensity image can be created (Fig 4 211
right) The analysis of prostate tissue samples gathered in 212
the frame of a biomedical protocol (section 4) will allow us 213
to determine the optimal parameters for the acquisition of 214
the fluorescence spectrum and build discrimination criteria 215
from the measurements between malignanthealthy tissue and 216
prostaticnon-prostatic tissue 217
bull the prostaticnon-prostatic characterization of the tissues is 218
based on the detection of the prostate-specific membrane anti- 219
gen (PSMA) which is specific of the prostatic membrane 220
This detection is made possible by the immunofluorescence 221
tagging of the PSMA using a specific anti-PSMA antibody 222
labelled with a fluorescent tracer When excited by light at 223
a characteristic absorption wavelength the fluorescent tracer 224
emits light at a characteristic emission wavelength Two flu- 225
orescent tracers are investigated in the DEPORRA project 226
Fluorescein IsoThioCyanate (FITC) and Cyanine 5 Both 227
FITC and Cyanine 5 have a characteristic emission wave- 228
length different from the autofluorescence wavelength of the 229
Protoporpphyrin IX protein allowing for the characterization 230
of the tissue type (prostatic vs non-prostatic) and the tissue 231
status (healthy vs malignant) with the same testbench (Fig 5) 232
The testbench presented on Fig 4 has also been equipped 233
with two laser sources emitting at 488 nm and 642 nm exci- 234
tation wavelengths respectively for FITC and Cyanine 5 for 235
recognizing prostate tissue from those environing 236
A bimodal laparoscopic-compliant fluorescence probe based 237
on the miniaturization of the fluorescence testbench will be avail- 238
able in 2013 (Fig 6 top) Preliminary results based on the 239
analysis of histopathologic slices will be presented in section 240
4 In order to overlay the probersquos fluorescence measurement on 241
the laparoscopic images we plan on detecting automatically the 242
position of the tip of the laparoscopic probe using a real-time 243
Fig 4 Experimental fluorescence design and results Left experimental optical device Right typical intensity image obtained
Please cite this article in press as Voros S et al Devices and systems targeted towards augmented robotic radical prostatectomy IRBM (2013)
httpdxdoiorg101016jirbm201301014
ARTICLE IN PRESS+ModelIRBM 252 1ndash8
S Voros et al IRBM xxx (2013) xxxndashxxx 5
Perc
ent
of
maxim
a
Wavelength (nm)
PpIX emission
FITC excitation
FITC emission
PpIX excitation
350 400 450 500 550 600 650 700 750
Perc
ent
of
maxim
a
10
00
08
06
04
02
Wavelength (nm)
PpIX emission
Cy5 excitation
Cy5 emission
PpIX excitation
BA
350 400 450 500 550 600 650 700 750
10
00
08
06
04
02
Fig 5 Excitation and emission spectra of Protoporphyrin IX Fluorescein IsoThioCyanate and Cyanine 5 (Cy5) fluorochromes A Overlay of the excitation (blue
dashed line) and emission (orange solid line) spectra of Protoporphyrin IX with excitation (green dashed line) and emission (emission spectrum) of Fluorescein
IsoThioCyanate B Overlay of the excitation (blue dashed line) and emission (orange solid line) spectra of Protoporphyrin IX with excitation (red dashed line) and
emission (red solid line) of Cy5
Fig 6 The bimodal fluorescence laparoscopic probe and the image-based anal-
ysis approach to localize it in laparoscopic images Top the CAD drawing
of the bimodal fluorescence laparoscopic probe Bottom automatic detection
of a laparoscopic instrument which will be used to overlay the probersquos tissue
characterization measurements on the laparoscopic images
image analysis approach that we have developed [10] (Fig 6244
bottom)245
34 Preclinical and clinical evaluation246
Preliminary evaluation of the devices and the software devel-247
oped in the frame of this project has already been performed on248
laboratory testbenchs and during three cadaver experiments at249
the anatomy laboratory (section 4) However in order to acquire250
the qualitative and quantitative proofs necessary to perform the251
fist clinical evaluations of our innovative medical devices on 252
patients we have submitted two biomedical research protocols 253
bull the first one called ldquofusion of echographic (ultrasound) and 254
endoscopic imagesrdquo (FEE) is a pilot monocentric study on a 255
cohort of 15 patients and is currently running It aims at val- 256
idating our ultrasound approach and evaluating its expected 257
medical benefit during radical prostatectomies the surgeons 258
will insert surgical needles in the prostate and endorectal 259
ultrasound images and laparoscopic images will be recorded 260
The data will be processed offline in the laboratory to assess 261
quantitatively the feasibility of the registration of ultrasound 262
and laparoscopic images using passive markers This proto- 263
col already accepted by the ethical instances will be a pilot 264
monocentric study with 15 patients 265
bull the second protocol called COPROST will allow us to obtain 266
fresh prostate chips during transurethral resections in the 267
frame of a pilot monocentric prospective non-randomized 268
open and controlled clinical trial The protocol with an 269
inclusion period of 24 months is already defined and writ- 270
ten following the French Regulation on Biomedical Research 271
and biological tissue collection It is being submitted to the 272
ethical committee ldquocomiteacute de protection des personnesrdquo and 273
the ldquoagence nationale de seacutecuriteacute du meacutedicament et des pro- 274
duits de santeacuterdquo (ANSM) The prostate chips will be on one 275
hand characterized by anatomopathologists to determine their 276
nature (pathologic vs healthy prostatic vs non-prostatic) and 277
will allow us to validate our immunofluorescence protocol and 278
fine-tune our auto and immunofluorescence measurements 279
protocols on fresh tissue samples 280
4 Results 281
In this section we present our preclinical evaluation of the 282
different prototypes and software presented in the previous sec- 283
tion 284
41 Augmented laparoscopy thanks to an innovative video 285
device 286
In order to evaluate the potential benefits of the pro- 287
posed vision system we asked a surgeon to perform a simple 288
Please cite this article in press as Voros S et al Devices and systems targeted towards augmented robotic radical prostatectomy IRBM (2013)
httpdxdoiorg101016jirbm201301014
ARTICLE IN PRESS+ModelIRBM 252 1ndash8
6 S Voros et al IRBM xxx (2013) xxxndashxxx
Fig 7 Ultrasound image of a prostate acquired with our innovative transurethral
ultrasound probe during a cadaver experiment The image was acquired with our
first prototype (64 piezoelectric elements)
surgical task once with the traditional endoscope alone and289
once with the proposed system alone (although in practice they290
can be combined to associate local and global views) The tasks291
consisted in localizing a suture needle and bringing it to a fixed292
target point The experiment was performed on porcine organs293
placed in a training box and repeated six times by the surgeon294
At each realization the needlersquos initial position was repositioned295
randomly at a distance equivalent to its initial position and the296
surgeon started randomly with the traditional endoscope or the297
proposed system In both cases a robotic endoscope holder was298
used to mobilize the endoscope and the vision system allowing299
us to record the displacements of the vision systems300
The full methodology and results are currently under sub-301
mission but to summarize the mean time required to perform302
the six experiments with the traditional endoscope was of 190 s303
compared to 245 s with the proposed system Moreover the sur-304
geon needed to give an average of 232 commands to the robotic305
scope holder to perform one stitch with the endoscope alone306
compared to 46 commands with the proposed system These307
preliminary results suggest that the proposed system could sig-308
nificantly reduce the laparoscopic surgery time and the cognitive309
load required for the control of the endoscope We now plan on310
performing cadaver experiments to evaluate the deployment of311
the vision system in conditions close to the clinical reality and312
to evaluate the system with several surgeons313
42 Augmented laparoscopy thanks to an innovative314
ultrasound system315
We performed two cadaver experiments which allowed us316
to determine the optimal characteristics for the realization of317
the intraurethral ultrasound probe During these experiments318
we evaluated the (difficult) insertion of the catheter through319
the urethra and the prostate visualization It must be noted that320
our clinicians partners stressed that the rigor mortis made this321
insertion harder These experiments allowed us to find the best322
rigidity for the catheter of the probe it must be flexible enough323
Fig 8 Demonstration of the fusion of ultrasound and laparoscopic images using
passive landmarks on chicken breasts Top-left the ultrasound image top-right
the laparoscopic image The passive landmarks are indicated with the green
arrows in the laparoscopic image They are selected manually in both modalities
to perform the registration Bottom the fusion of the two imaging modalities
to be introduced in the urethra but rigid enough to avoid the 324
distortions of the catheter 325
The first ultrasound probe (2D) was designed with 64 326
piezoelements It appeared that it was not enough On the one 327
hand the probe imaged a too small part of the prostate so that 328
it was difficult to identify what was represented on the ultra- 329
sound image (Fig 7) Furthermore it was impossible to know 330
in which direction the probe was oriented On the other hand 331
we demonstrated [9] that a longer probe increases the precision 332
of the localization of the active ultrasound transducers That is 333
why the second probe designed for the project (3D) has 128 334
piezoelements This second probe has graduations located on 335
its catheter visible on Fig 2 They allow the surgeon to know 336
the probersquos insertion depth in the urethra and a line along the 337
catheter allows appreciating the torsion applied to the catheter 338
The localization of the active transducers is currently under 339
submission It is based on a global positioning system (GPS) 340
method We made some experiments on a testbench making 341
localization in water to have ideal homogeneous conditions and 342
Please cite this article in press as Voros S et al Devices and systems targeted towards augmented robotic radical prostatectomy IRBM (2013)
httpdxdoiorg101016jirbm201301014
ARTICLE IN PRESS+ModelIRBM 252 1ndash8
S Voros et al IRBM xxx (2013) xxxndashxxx 7
Fig 9 Preliminary experiments of the autofluorescence detection with our testbench The autofluorescence of chlorophyll which has optical properties very similar
to Protoporphyrin IX was observed on our testbench Left direct image of a leaf right fluorescence image of the leaf at 680 nm As expected chlorophyll seems
absent in the veins
Fig 10 Specific fluorescence signal of anti-prostate-specific membrane antigen marker A Nuclear counter-staining of prostatic tissue with Hoechst (blue DNA
marker) We observe the nuclei of prostate cells regularly organized in the glandular epithelium Prostatic glands are separated by stroma B Fluorescence emission
of anti-prostate-specific membrane antigen-Fluorescein IsoThioCyanate on cellular membranes of prostatic cells C Overlay of the A and B images This figure
demonstrates the specificity on fixed prostatic tissue of a specific anti-PSMA antibody labelled with Fluorescein IsoThioCyanate We can also detect the contribution
of non-specific autofluorescence of prostatic concretions (Fig 11) (times20 magnification)
localization on a chicken breast to have more realistic condi-343
tions In both cases we were able to localize the active transducer344
with a precision less than 625 m Moreover the computation345
time is a few hundred milliseconds for a 2D localization These346
results demonstrate that the localization is fast enough to be347
implemented for a prostatectomy For the moment only a 2D 348
localization has been made with the active landmarks and the 349
3D localization is in progress Then we will be able to per- 350
form a registration with laparoscopic images using ldquoactiverdquo 351
markers 352
Fig 11 Non-specific autofluorescence observed in the prostate fixed tissues This figure shows the benefits of a near infrared marker like Cyanine 5 (excited at
633 nm) compared to Fluorescein IsoThioCyanate (excited at 488 nm) A Auto fluorescence under laser excitation at 488 nm We observe that prostate concretions
(calcified material) respond to this excitation by a strong fluorescence signal B Auto fluorescence under laser excitation at 633 nm The use of Cyanine 5 reduces
widely autofluorescence of some structures such as prostate concretions (times20 magnification)
Please cite this article in press as Voros S et al Devices and systems targeted towards augmented robotic radical prostatectomy IRBM (2013)
httpdxdoiorg101016jirbm201301014
ARTICLE IN PRESS+ModelIRBM 252 1ndash8
8 S Voros et al IRBM xxx (2013) xxxndashxxx
Concerning the registration between laparoscopic and ultra-353
sound images we performed several testbench evaluations of354
the registration algorithm on chicken breasts The result of such355
a registration obtained by manually pairing passive markers356
visible on both the laparoscopic and ultrasound imaging modal-357
ities are presented on Fig 8 In this example we obtained a358
registration root mean square error (RMS) of 038 mm359
43 Augmented laparoscopy thanks to fluorescence360
imaging361
First experiments were performed on leaves to demonstrate362
the feasibility of the detection of chlorophyll autofluorescence363
which has optical properties very similar to PpIX (absorption at364
405 nm and emission at 680 nm) as described on Fig 9 Then365
experiments were conducted on histology slices of the human366
prostate with as we anticipated inconclusive results because367
of the expected low signal-to-noise ratio caused by the insuffi-368
cient thickness of a histology slice (3 m thickness) compared to369
the optimal use of the device (300 m thickness) These results370
motivated our biomedical research COPROST on macroscopic371
fresh prostate samples372
Concerning the immunofluorescence protocol we were able373
to demonstrate the specificity of the anti-PSMA antibody on374
fixed tissue samples labelled with FITC as illustrated by Fig 10375
We observed higher autofluorescence problems when excit-376
ing the sample at the FITC specific wavelength compared to377
an excitation at the Cyanine 5 specific wavelength (Fig 11)378
These results motivated the inclusion of both fluorophores in our379
biomedical research COPROST on macroscopic fresh prostate380
samples FITC because it was already used to demonstrate speci-381
ficity of anti-PSMA antibody and Cyanine 5 because its near382
infra-red characteristics make it a better candidate on fresh mate-383
rial (higher penetration in tissue) and will improve signalnoise384
ratio as previously demonstrated385
To our knowledge most of the optical biopsy approaches as386
previously defined have been validated either on histologic slices387
or on ratmice prostate models However these approaches have388
limitations prostatic tissue is impaired by the chemical treat-389
ment required for histologic preparation and animal models do390
not directly mimic all aspects of human prostate cancer [11] In391
short it has not been proved yet that a successful detection with392
the investigated devices on histopathology slices or on animal393
models is sufficient to guarantee a successful detection on fresh394
human tissues The experiments that will be performed in the395
frame of the COPROST protocol in 2013 will be determinant to396
confirm the feasibility of our approach on fresh tissue samples397
5 DiscussionConclusion398
The DEPORRA project allowed for the development of inno-399
vative devices and navigation prototypes in the objective of400
allowing the surgeon to see ldquobeyond the visiblerdquo during a radi-401
cal prostatectomy First evaluations of the devices and methods402
have been performed preclinically and are very encouraging for403
the development of innovative approaches to assist the surgeon
during such a complex surgery Our preliminary results have also 404
shown the limits of preclinical validation and have convinced us 405
of the necessity to launch biomedical researches that will allow 406
us to validate further the devices This process required a con- 407
sequent amount of effort and time but is mandatory for the 408
fine-tuning of our tissue characterization tools and to obtain the 409
first clinical proofs of the relevance of the developed medical 410
devices which are mandatory to perform clinical evaluations of 411
the complete navigation systems 412
We now need to push further the integration of the devices 413
into such navigation systems in order to exploit at best the infor- 414
mation provided by each modality and to determine the optimal 415
approach for displaying the relevant information to the surgeon 416
in a clinical environment This will imply a conception and 417
development effort a definition of qualitative and quantitative 418
parameters for the first assessment of the delivered medical ben- 419
efit of our developments risks analysis and biomedical research 420
preparations in order to meet the ethical instances requirements 421
Acknowledgments 422
This work has been supported by French National Research 423
Agency (ANR) through TecSan program (project DEPORRA 424
no ANR-09-TECS-006) 425
References 426
[1] Heidenreich A Bolla M Joniau S Mason MD Matveev V Mottet N et al 427
Guidelines on prostate cancer Eur Assoc Urol 2011 [www uroweb org] 428
[2] Pfitzenmaier J Pahernik S Tremmel T Haferkamp A Buse S Hohen- 429
fellner M Positive surgical margins after radical prostatectomy do 430
they have an impact on biochemical or clinical progression BJU Int 431
2008102(10)1413ndash8 432
[3] Soler L Nicolau S Schmid J Koehl C Marescaux J et al Virtual reality 433
and augmented reality in digestive surgery In Third IEEE and ACM Inter- 434
national Symposium on Mixed and Augmented Reality (ISMAR) 2004 435
p 278ndash9 436
[4] S Voros B Tamadazte P Cinquin C Fouard Systegraveme drsquoimagerie multi- 437
vision pour chirurgie laparoscopique demande de deacutepocirct de brevet FR 438
1259489 102012 439
[5] Ukimura O Ahlering TE Gill IS Transrectal ultrasound-guided 440
energy-free nerve-sparing laparoscopic radical prostatectomy J Endourol 441
200822(9)1993ndash5 442
[6] Long JA Lee BH Guillotreau J Autorino R Laydner H Yakoubi R et al 443
Real-time robotic transrectal ultrasound navigation during robotic radical 444
prostatectomy initial clinical experience Urology 201280(3)608ndash13 445
[7] Holmes III DR Davis BJ Bruce CJ Robb RA 3D visualization analysis 446
and treatment of the prostate using trans-urethral ultrasound Comput Med 447
Imaging Graph 200327339ndash49 [2003] 448
[8] Dementhon D Model-based object pose in 25 lines of code Int J Comput 449
Vis 199515(1ndash2)123ndash41 450
[9] Custillon G Voros S Cinquin P Nguyen-Dinh A Moreau-Gaudry A 451
Bidimensional localization of active ultrasound transducers for use in 452
laparoscopic prostate surgery IEEE Trans Med Imaging 2012 Q3 453
[10] Wolf R Duchateau J Cinquin P Voros S 3D tracking of laparoscopic 454
instruments using statistical and geometric modeling Med Image Com- 455
put Comput Assist Interv 20116891203ndash10 [Lecture notes in computer 456
science] 457
[11] Valkenburg KC Williams BO ldquoMouse models of prostate cancerrdquo Prostate 458
Cancer 2011201122 httpdxdoiorg1011552011895238 [Article ID 459
895238] 460
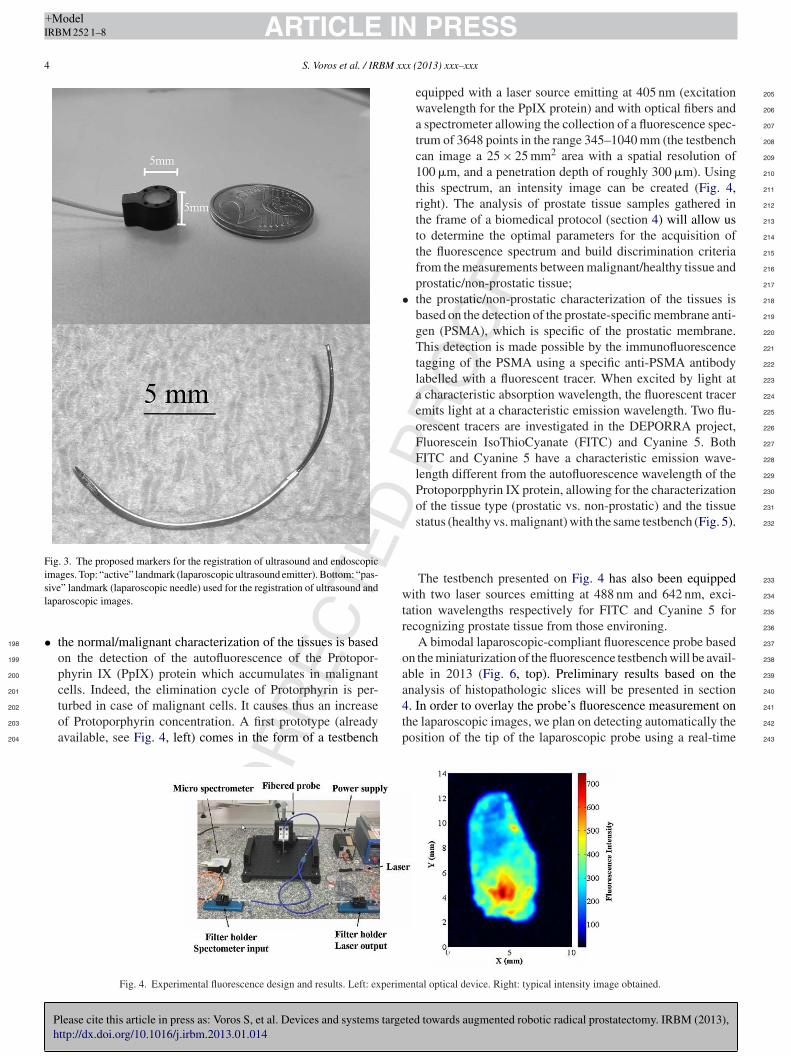
Please cite this article in press as Voros S et al Devices and systems targeted towards augmented robotic radical prostatectomy IRBM (2013)
httpdxdoiorg101016jirbm201301014
ARTICLE IN PRESS+ModelIRBM 252 1ndash8
4 S Voros et al IRBM xxx (2013) xxxndashxxx
Fig 3 The proposed markers for the registration of ultrasound and endoscopic
images Top ldquoactiverdquo landmark (laparoscopic ultrasound emitter) Bottom ldquopas-
siverdquo landmark (laparoscopic needle) used for the registration of ultrasound and
laparoscopic images
bull the normalmalignant characterization of the tissues is based198
on the detection of the autofluorescence of the Protopor-199
phyrin IX (PpIX) protein which accumulates in malignant200
cells Indeed the elimination cycle of Protorphyrin is per-201
turbed in case of malignant cells It causes thus an increase202
of Protoporphyrin concentration A first prototype (already203
available see Fig 4 left) comes in the form of a testbench204
equipped with a laser source emitting at 405 nm (excitation 205
wavelength for the PpIX protein) and with optical fibers and 206
a spectrometer allowing the collection of a fluorescence spec- 207
trum of 3648 points in the range 345ndash1040 mm (the testbench 208
can image a 25 times 25 mm2 area with a spatial resolution of 209
100 m and a penetration depth of roughly 300 m) Using 210
this spectrum an intensity image can be created (Fig 4 211
right) The analysis of prostate tissue samples gathered in 212
the frame of a biomedical protocol (section 4) will allow us 213
to determine the optimal parameters for the acquisition of 214
the fluorescence spectrum and build discrimination criteria 215
from the measurements between malignanthealthy tissue and 216
prostaticnon-prostatic tissue 217
bull the prostaticnon-prostatic characterization of the tissues is 218
based on the detection of the prostate-specific membrane anti- 219
gen (PSMA) which is specific of the prostatic membrane 220
This detection is made possible by the immunofluorescence 221
tagging of the PSMA using a specific anti-PSMA antibody 222
labelled with a fluorescent tracer When excited by light at 223
a characteristic absorption wavelength the fluorescent tracer 224
emits light at a characteristic emission wavelength Two flu- 225
orescent tracers are investigated in the DEPORRA project 226
Fluorescein IsoThioCyanate (FITC) and Cyanine 5 Both 227
FITC and Cyanine 5 have a characteristic emission wave- 228
length different from the autofluorescence wavelength of the 229
Protoporpphyrin IX protein allowing for the characterization 230
of the tissue type (prostatic vs non-prostatic) and the tissue 231
status (healthy vs malignant) with the same testbench (Fig 5) 232
The testbench presented on Fig 4 has also been equipped 233
with two laser sources emitting at 488 nm and 642 nm exci- 234
tation wavelengths respectively for FITC and Cyanine 5 for 235
recognizing prostate tissue from those environing 236
A bimodal laparoscopic-compliant fluorescence probe based 237
on the miniaturization of the fluorescence testbench will be avail- 238
able in 2013 (Fig 6 top) Preliminary results based on the 239
analysis of histopathologic slices will be presented in section 240
4 In order to overlay the probersquos fluorescence measurement on 241
the laparoscopic images we plan on detecting automatically the 242
position of the tip of the laparoscopic probe using a real-time 243
Fig 4 Experimental fluorescence design and results Left experimental optical device Right typical intensity image obtained
Please cite this article in press as Voros S et al Devices and systems targeted towards augmented robotic radical prostatectomy IRBM (2013)
httpdxdoiorg101016jirbm201301014
ARTICLE IN PRESS+ModelIRBM 252 1ndash8
S Voros et al IRBM xxx (2013) xxxndashxxx 5
Perc
ent
of
maxim
a
Wavelength (nm)
PpIX emission
FITC excitation
FITC emission
PpIX excitation
350 400 450 500 550 600 650 700 750
Perc
ent
of
maxim
a
10
00
08
06
04
02
Wavelength (nm)
PpIX emission
Cy5 excitation
Cy5 emission
PpIX excitation
BA
350 400 450 500 550 600 650 700 750
10
00
08
06
04
02
Fig 5 Excitation and emission spectra of Protoporphyrin IX Fluorescein IsoThioCyanate and Cyanine 5 (Cy5) fluorochromes A Overlay of the excitation (blue
dashed line) and emission (orange solid line) spectra of Protoporphyrin IX with excitation (green dashed line) and emission (emission spectrum) of Fluorescein
IsoThioCyanate B Overlay of the excitation (blue dashed line) and emission (orange solid line) spectra of Protoporphyrin IX with excitation (red dashed line) and
emission (red solid line) of Cy5
Fig 6 The bimodal fluorescence laparoscopic probe and the image-based anal-
ysis approach to localize it in laparoscopic images Top the CAD drawing
of the bimodal fluorescence laparoscopic probe Bottom automatic detection
of a laparoscopic instrument which will be used to overlay the probersquos tissue
characterization measurements on the laparoscopic images
image analysis approach that we have developed [10] (Fig 6244
bottom)245
34 Preclinical and clinical evaluation246
Preliminary evaluation of the devices and the software devel-247
oped in the frame of this project has already been performed on248
laboratory testbenchs and during three cadaver experiments at249
the anatomy laboratory (section 4) However in order to acquire250
the qualitative and quantitative proofs necessary to perform the251
fist clinical evaluations of our innovative medical devices on 252
patients we have submitted two biomedical research protocols 253
bull the first one called ldquofusion of echographic (ultrasound) and 254
endoscopic imagesrdquo (FEE) is a pilot monocentric study on a 255
cohort of 15 patients and is currently running It aims at val- 256
idating our ultrasound approach and evaluating its expected 257
medical benefit during radical prostatectomies the surgeons 258
will insert surgical needles in the prostate and endorectal 259
ultrasound images and laparoscopic images will be recorded 260
The data will be processed offline in the laboratory to assess 261
quantitatively the feasibility of the registration of ultrasound 262
and laparoscopic images using passive markers This proto- 263
col already accepted by the ethical instances will be a pilot 264
monocentric study with 15 patients 265
bull the second protocol called COPROST will allow us to obtain 266
fresh prostate chips during transurethral resections in the 267
frame of a pilot monocentric prospective non-randomized 268
open and controlled clinical trial The protocol with an 269
inclusion period of 24 months is already defined and writ- 270
ten following the French Regulation on Biomedical Research 271
and biological tissue collection It is being submitted to the 272
ethical committee ldquocomiteacute de protection des personnesrdquo and 273
the ldquoagence nationale de seacutecuriteacute du meacutedicament et des pro- 274
duits de santeacuterdquo (ANSM) The prostate chips will be on one 275
hand characterized by anatomopathologists to determine their 276
nature (pathologic vs healthy prostatic vs non-prostatic) and 277
will allow us to validate our immunofluorescence protocol and 278
fine-tune our auto and immunofluorescence measurements 279
protocols on fresh tissue samples 280
4 Results 281
In this section we present our preclinical evaluation of the 282
different prototypes and software presented in the previous sec- 283
tion 284
41 Augmented laparoscopy thanks to an innovative video 285
device 286
In order to evaluate the potential benefits of the pro- 287
posed vision system we asked a surgeon to perform a simple 288
Please cite this article in press as Voros S et al Devices and systems targeted towards augmented robotic radical prostatectomy IRBM (2013)
httpdxdoiorg101016jirbm201301014
ARTICLE IN PRESS+ModelIRBM 252 1ndash8
6 S Voros et al IRBM xxx (2013) xxxndashxxx
Fig 7 Ultrasound image of a prostate acquired with our innovative transurethral
ultrasound probe during a cadaver experiment The image was acquired with our
first prototype (64 piezoelectric elements)
surgical task once with the traditional endoscope alone and289
once with the proposed system alone (although in practice they290
can be combined to associate local and global views) The tasks291
consisted in localizing a suture needle and bringing it to a fixed292
target point The experiment was performed on porcine organs293
placed in a training box and repeated six times by the surgeon294
At each realization the needlersquos initial position was repositioned295
randomly at a distance equivalent to its initial position and the296
surgeon started randomly with the traditional endoscope or the297
proposed system In both cases a robotic endoscope holder was298
used to mobilize the endoscope and the vision system allowing299
us to record the displacements of the vision systems300
The full methodology and results are currently under sub-301
mission but to summarize the mean time required to perform302
the six experiments with the traditional endoscope was of 190 s303
compared to 245 s with the proposed system Moreover the sur-304
geon needed to give an average of 232 commands to the robotic305
scope holder to perform one stitch with the endoscope alone306
compared to 46 commands with the proposed system These307
preliminary results suggest that the proposed system could sig-308
nificantly reduce the laparoscopic surgery time and the cognitive309
load required for the control of the endoscope We now plan on310
performing cadaver experiments to evaluate the deployment of311
the vision system in conditions close to the clinical reality and312
to evaluate the system with several surgeons313
42 Augmented laparoscopy thanks to an innovative314
ultrasound system315
We performed two cadaver experiments which allowed us316
to determine the optimal characteristics for the realization of317
the intraurethral ultrasound probe During these experiments318
we evaluated the (difficult) insertion of the catheter through319
the urethra and the prostate visualization It must be noted that320
our clinicians partners stressed that the rigor mortis made this321
insertion harder These experiments allowed us to find the best322
rigidity for the catheter of the probe it must be flexible enough323
Fig 8 Demonstration of the fusion of ultrasound and laparoscopic images using
passive landmarks on chicken breasts Top-left the ultrasound image top-right
the laparoscopic image The passive landmarks are indicated with the green
arrows in the laparoscopic image They are selected manually in both modalities
to perform the registration Bottom the fusion of the two imaging modalities
to be introduced in the urethra but rigid enough to avoid the 324
distortions of the catheter 325
The first ultrasound probe (2D) was designed with 64 326
piezoelements It appeared that it was not enough On the one 327
hand the probe imaged a too small part of the prostate so that 328
it was difficult to identify what was represented on the ultra- 329
sound image (Fig 7) Furthermore it was impossible to know 330
in which direction the probe was oriented On the other hand 331
we demonstrated [9] that a longer probe increases the precision 332
of the localization of the active ultrasound transducers That is 333
why the second probe designed for the project (3D) has 128 334
piezoelements This second probe has graduations located on 335
its catheter visible on Fig 2 They allow the surgeon to know 336
the probersquos insertion depth in the urethra and a line along the 337
catheter allows appreciating the torsion applied to the catheter 338
The localization of the active transducers is currently under 339
submission It is based on a global positioning system (GPS) 340
method We made some experiments on a testbench making 341
localization in water to have ideal homogeneous conditions and 342
Please cite this article in press as Voros S et al Devices and systems targeted towards augmented robotic radical prostatectomy IRBM (2013)
httpdxdoiorg101016jirbm201301014
ARTICLE IN PRESS+ModelIRBM 252 1ndash8
S Voros et al IRBM xxx (2013) xxxndashxxx 7
Fig 9 Preliminary experiments of the autofluorescence detection with our testbench The autofluorescence of chlorophyll which has optical properties very similar
to Protoporphyrin IX was observed on our testbench Left direct image of a leaf right fluorescence image of the leaf at 680 nm As expected chlorophyll seems
absent in the veins
Fig 10 Specific fluorescence signal of anti-prostate-specific membrane antigen marker A Nuclear counter-staining of prostatic tissue with Hoechst (blue DNA
marker) We observe the nuclei of prostate cells regularly organized in the glandular epithelium Prostatic glands are separated by stroma B Fluorescence emission
of anti-prostate-specific membrane antigen-Fluorescein IsoThioCyanate on cellular membranes of prostatic cells C Overlay of the A and B images This figure
demonstrates the specificity on fixed prostatic tissue of a specific anti-PSMA antibody labelled with Fluorescein IsoThioCyanate We can also detect the contribution
of non-specific autofluorescence of prostatic concretions (Fig 11) (times20 magnification)
localization on a chicken breast to have more realistic condi-343
tions In both cases we were able to localize the active transducer344
with a precision less than 625 m Moreover the computation345
time is a few hundred milliseconds for a 2D localization These346
results demonstrate that the localization is fast enough to be347
implemented for a prostatectomy For the moment only a 2D 348
localization has been made with the active landmarks and the 349
3D localization is in progress Then we will be able to per- 350
form a registration with laparoscopic images using ldquoactiverdquo 351
markers 352
Fig 11 Non-specific autofluorescence observed in the prostate fixed tissues This figure shows the benefits of a near infrared marker like Cyanine 5 (excited at
633 nm) compared to Fluorescein IsoThioCyanate (excited at 488 nm) A Auto fluorescence under laser excitation at 488 nm We observe that prostate concretions
(calcified material) respond to this excitation by a strong fluorescence signal B Auto fluorescence under laser excitation at 633 nm The use of Cyanine 5 reduces
widely autofluorescence of some structures such as prostate concretions (times20 magnification)
Please cite this article in press as Voros S et al Devices and systems targeted towards augmented robotic radical prostatectomy IRBM (2013)
httpdxdoiorg101016jirbm201301014
ARTICLE IN PRESS+ModelIRBM 252 1ndash8
8 S Voros et al IRBM xxx (2013) xxxndashxxx
Concerning the registration between laparoscopic and ultra-353
sound images we performed several testbench evaluations of354
the registration algorithm on chicken breasts The result of such355
a registration obtained by manually pairing passive markers356
visible on both the laparoscopic and ultrasound imaging modal-357
ities are presented on Fig 8 In this example we obtained a358
registration root mean square error (RMS) of 038 mm359
43 Augmented laparoscopy thanks to fluorescence360
imaging361
First experiments were performed on leaves to demonstrate362
the feasibility of the detection of chlorophyll autofluorescence363
which has optical properties very similar to PpIX (absorption at364
405 nm and emission at 680 nm) as described on Fig 9 Then365
experiments were conducted on histology slices of the human366
prostate with as we anticipated inconclusive results because367
of the expected low signal-to-noise ratio caused by the insuffi-368
cient thickness of a histology slice (3 m thickness) compared to369
the optimal use of the device (300 m thickness) These results370
motivated our biomedical research COPROST on macroscopic371
fresh prostate samples372
Concerning the immunofluorescence protocol we were able373
to demonstrate the specificity of the anti-PSMA antibody on374
fixed tissue samples labelled with FITC as illustrated by Fig 10375
We observed higher autofluorescence problems when excit-376
ing the sample at the FITC specific wavelength compared to377
an excitation at the Cyanine 5 specific wavelength (Fig 11)378
These results motivated the inclusion of both fluorophores in our379
biomedical research COPROST on macroscopic fresh prostate380
samples FITC because it was already used to demonstrate speci-381
ficity of anti-PSMA antibody and Cyanine 5 because its near382
infra-red characteristics make it a better candidate on fresh mate-383
rial (higher penetration in tissue) and will improve signalnoise384
ratio as previously demonstrated385
To our knowledge most of the optical biopsy approaches as386
previously defined have been validated either on histologic slices387
or on ratmice prostate models However these approaches have388
limitations prostatic tissue is impaired by the chemical treat-389
ment required for histologic preparation and animal models do390
not directly mimic all aspects of human prostate cancer [11] In391
short it has not been proved yet that a successful detection with392
the investigated devices on histopathology slices or on animal393
models is sufficient to guarantee a successful detection on fresh394
human tissues The experiments that will be performed in the395
frame of the COPROST protocol in 2013 will be determinant to396
confirm the feasibility of our approach on fresh tissue samples397
5 DiscussionConclusion398
The DEPORRA project allowed for the development of inno-399
vative devices and navigation prototypes in the objective of400
allowing the surgeon to see ldquobeyond the visiblerdquo during a radi-401
cal prostatectomy First evaluations of the devices and methods402
have been performed preclinically and are very encouraging for403
the development of innovative approaches to assist the surgeon
during such a complex surgery Our preliminary results have also 404
shown the limits of preclinical validation and have convinced us 405
of the necessity to launch biomedical researches that will allow 406
us to validate further the devices This process required a con- 407
sequent amount of effort and time but is mandatory for the 408
fine-tuning of our tissue characterization tools and to obtain the 409
first clinical proofs of the relevance of the developed medical 410
devices which are mandatory to perform clinical evaluations of 411
the complete navigation systems 412
We now need to push further the integration of the devices 413
into such navigation systems in order to exploit at best the infor- 414
mation provided by each modality and to determine the optimal 415
approach for displaying the relevant information to the surgeon 416
in a clinical environment This will imply a conception and 417
development effort a definition of qualitative and quantitative 418
parameters for the first assessment of the delivered medical ben- 419
efit of our developments risks analysis and biomedical research 420
preparations in order to meet the ethical instances requirements 421
Acknowledgments 422
This work has been supported by French National Research 423
Agency (ANR) through TecSan program (project DEPORRA 424
no ANR-09-TECS-006) 425
References 426
[1] Heidenreich A Bolla M Joniau S Mason MD Matveev V Mottet N et al 427
Guidelines on prostate cancer Eur Assoc Urol 2011 [www uroweb org] 428
[2] Pfitzenmaier J Pahernik S Tremmel T Haferkamp A Buse S Hohen- 429
fellner M Positive surgical margins after radical prostatectomy do 430
they have an impact on biochemical or clinical progression BJU Int 431
2008102(10)1413ndash8 432
[3] Soler L Nicolau S Schmid J Koehl C Marescaux J et al Virtual reality 433
and augmented reality in digestive surgery In Third IEEE and ACM Inter- 434
national Symposium on Mixed and Augmented Reality (ISMAR) 2004 435
p 278ndash9 436
[4] S Voros B Tamadazte P Cinquin C Fouard Systegraveme drsquoimagerie multi- 437
vision pour chirurgie laparoscopique demande de deacutepocirct de brevet FR 438
1259489 102012 439
[5] Ukimura O Ahlering TE Gill IS Transrectal ultrasound-guided 440
energy-free nerve-sparing laparoscopic radical prostatectomy J Endourol 441
200822(9)1993ndash5 442
[6] Long JA Lee BH Guillotreau J Autorino R Laydner H Yakoubi R et al 443
Real-time robotic transrectal ultrasound navigation during robotic radical 444
prostatectomy initial clinical experience Urology 201280(3)608ndash13 445
[7] Holmes III DR Davis BJ Bruce CJ Robb RA 3D visualization analysis 446
and treatment of the prostate using trans-urethral ultrasound Comput Med 447
Imaging Graph 200327339ndash49 [2003] 448
[8] Dementhon D Model-based object pose in 25 lines of code Int J Comput 449
Vis 199515(1ndash2)123ndash41 450
[9] Custillon G Voros S Cinquin P Nguyen-Dinh A Moreau-Gaudry A 451
Bidimensional localization of active ultrasound transducers for use in 452
laparoscopic prostate surgery IEEE Trans Med Imaging 2012 Q3 453
[10] Wolf R Duchateau J Cinquin P Voros S 3D tracking of laparoscopic 454
instruments using statistical and geometric modeling Med Image Com- 455
put Comput Assist Interv 20116891203ndash10 [Lecture notes in computer 456
science] 457
[11] Valkenburg KC Williams BO ldquoMouse models of prostate cancerrdquo Prostate 458
Cancer 2011201122 httpdxdoiorg1011552011895238 [Article ID 459
895238] 460

Please cite this article in press as Voros S et al Devices and systems targeted towards augmented robotic radical prostatectomy IRBM (2013)
httpdxdoiorg101016jirbm201301014
ARTICLE IN PRESS+ModelIRBM 252 1ndash8
S Voros et al IRBM xxx (2013) xxxndashxxx 5
Perc
ent
of
maxim
a
Wavelength (nm)
PpIX emission
FITC excitation
FITC emission
PpIX excitation
350 400 450 500 550 600 650 700 750
Perc
ent
of
maxim
a
10
00
08
06
04
02
Wavelength (nm)
PpIX emission
Cy5 excitation
Cy5 emission
PpIX excitation
BA
350 400 450 500 550 600 650 700 750
10
00
08
06
04
02
Fig 5 Excitation and emission spectra of Protoporphyrin IX Fluorescein IsoThioCyanate and Cyanine 5 (Cy5) fluorochromes A Overlay of the excitation (blue
dashed line) and emission (orange solid line) spectra of Protoporphyrin IX with excitation (green dashed line) and emission (emission spectrum) of Fluorescein
IsoThioCyanate B Overlay of the excitation (blue dashed line) and emission (orange solid line) spectra of Protoporphyrin IX with excitation (red dashed line) and
emission (red solid line) of Cy5
Fig 6 The bimodal fluorescence laparoscopic probe and the image-based anal-
ysis approach to localize it in laparoscopic images Top the CAD drawing
of the bimodal fluorescence laparoscopic probe Bottom automatic detection
of a laparoscopic instrument which will be used to overlay the probersquos tissue
characterization measurements on the laparoscopic images
image analysis approach that we have developed [10] (Fig 6244
bottom)245
34 Preclinical and clinical evaluation246
Preliminary evaluation of the devices and the software devel-247
oped in the frame of this project has already been performed on248
laboratory testbenchs and during three cadaver experiments at249
the anatomy laboratory (section 4) However in order to acquire250
the qualitative and quantitative proofs necessary to perform the251
fist clinical evaluations of our innovative medical devices on 252
patients we have submitted two biomedical research protocols 253
bull the first one called ldquofusion of echographic (ultrasound) and 254
endoscopic imagesrdquo (FEE) is a pilot monocentric study on a 255
cohort of 15 patients and is currently running It aims at val- 256
idating our ultrasound approach and evaluating its expected 257
medical benefit during radical prostatectomies the surgeons 258
will insert surgical needles in the prostate and endorectal 259
ultrasound images and laparoscopic images will be recorded 260
The data will be processed offline in the laboratory to assess 261
quantitatively the feasibility of the registration of ultrasound 262
and laparoscopic images using passive markers This proto- 263
col already accepted by the ethical instances will be a pilot 264
monocentric study with 15 patients 265
bull the second protocol called COPROST will allow us to obtain 266
fresh prostate chips during transurethral resections in the 267
frame of a pilot monocentric prospective non-randomized 268
open and controlled clinical trial The protocol with an 269
inclusion period of 24 months is already defined and writ- 270
ten following the French Regulation on Biomedical Research 271
and biological tissue collection It is being submitted to the 272
ethical committee ldquocomiteacute de protection des personnesrdquo and 273
the ldquoagence nationale de seacutecuriteacute du meacutedicament et des pro- 274
duits de santeacuterdquo (ANSM) The prostate chips will be on one 275
hand characterized by anatomopathologists to determine their 276
nature (pathologic vs healthy prostatic vs non-prostatic) and 277
will allow us to validate our immunofluorescence protocol and 278
fine-tune our auto and immunofluorescence measurements 279
protocols on fresh tissue samples 280
4 Results 281
In this section we present our preclinical evaluation of the 282
different prototypes and software presented in the previous sec- 283
tion 284
41 Augmented laparoscopy thanks to an innovative video 285
device 286
In order to evaluate the potential benefits of the pro- 287
posed vision system we asked a surgeon to perform a simple 288
Please cite this article in press as Voros S et al Devices and systems targeted towards augmented robotic radical prostatectomy IRBM (2013)
httpdxdoiorg101016jirbm201301014
ARTICLE IN PRESS+ModelIRBM 252 1ndash8
6 S Voros et al IRBM xxx (2013) xxxndashxxx
Fig 7 Ultrasound image of a prostate acquired with our innovative transurethral
ultrasound probe during a cadaver experiment The image was acquired with our
first prototype (64 piezoelectric elements)
surgical task once with the traditional endoscope alone and289
once with the proposed system alone (although in practice they290
can be combined to associate local and global views) The tasks291
consisted in localizing a suture needle and bringing it to a fixed292
target point The experiment was performed on porcine organs293
placed in a training box and repeated six times by the surgeon294
At each realization the needlersquos initial position was repositioned295
randomly at a distance equivalent to its initial position and the296
surgeon started randomly with the traditional endoscope or the297
proposed system In both cases a robotic endoscope holder was298
used to mobilize the endoscope and the vision system allowing299
us to record the displacements of the vision systems300
The full methodology and results are currently under sub-301
mission but to summarize the mean time required to perform302
the six experiments with the traditional endoscope was of 190 s303
compared to 245 s with the proposed system Moreover the sur-304
geon needed to give an average of 232 commands to the robotic305
scope holder to perform one stitch with the endoscope alone306
compared to 46 commands with the proposed system These307
preliminary results suggest that the proposed system could sig-308
nificantly reduce the laparoscopic surgery time and the cognitive309
load required for the control of the endoscope We now plan on310
performing cadaver experiments to evaluate the deployment of311
the vision system in conditions close to the clinical reality and312
to evaluate the system with several surgeons313
42 Augmented laparoscopy thanks to an innovative314
ultrasound system315
We performed two cadaver experiments which allowed us316
to determine the optimal characteristics for the realization of317
the intraurethral ultrasound probe During these experiments318
we evaluated the (difficult) insertion of the catheter through319
the urethra and the prostate visualization It must be noted that320
our clinicians partners stressed that the rigor mortis made this321
insertion harder These experiments allowed us to find the best322
rigidity for the catheter of the probe it must be flexible enough323
Fig 8 Demonstration of the fusion of ultrasound and laparoscopic images using
passive landmarks on chicken breasts Top-left the ultrasound image top-right
the laparoscopic image The passive landmarks are indicated with the green
arrows in the laparoscopic image They are selected manually in both modalities
to perform the registration Bottom the fusion of the two imaging modalities
to be introduced in the urethra but rigid enough to avoid the 324
distortions of the catheter 325
The first ultrasound probe (2D) was designed with 64 326
piezoelements It appeared that it was not enough On the one 327
hand the probe imaged a too small part of the prostate so that 328
it was difficult to identify what was represented on the ultra- 329
sound image (Fig 7) Furthermore it was impossible to know 330
in which direction the probe was oriented On the other hand 331
we demonstrated [9] that a longer probe increases the precision 332
of the localization of the active ultrasound transducers That is 333
why the second probe designed for the project (3D) has 128 334
piezoelements This second probe has graduations located on 335
its catheter visible on Fig 2 They allow the surgeon to know 336
the probersquos insertion depth in the urethra and a line along the 337
catheter allows appreciating the torsion applied to the catheter 338
The localization of the active transducers is currently under 339
submission It is based on a global positioning system (GPS) 340
method We made some experiments on a testbench making 341
localization in water to have ideal homogeneous conditions and 342
Please cite this article in press as Voros S et al Devices and systems targeted towards augmented robotic radical prostatectomy IRBM (2013)
httpdxdoiorg101016jirbm201301014
ARTICLE IN PRESS+ModelIRBM 252 1ndash8
S Voros et al IRBM xxx (2013) xxxndashxxx 7
Fig 9 Preliminary experiments of the autofluorescence detection with our testbench The autofluorescence of chlorophyll which has optical properties very similar
to Protoporphyrin IX was observed on our testbench Left direct image of a leaf right fluorescence image of the leaf at 680 nm As expected chlorophyll seems
absent in the veins
Fig 10 Specific fluorescence signal of anti-prostate-specific membrane antigen marker A Nuclear counter-staining of prostatic tissue with Hoechst (blue DNA
marker) We observe the nuclei of prostate cells regularly organized in the glandular epithelium Prostatic glands are separated by stroma B Fluorescence emission
of anti-prostate-specific membrane antigen-Fluorescein IsoThioCyanate on cellular membranes of prostatic cells C Overlay of the A and B images This figure
demonstrates the specificity on fixed prostatic tissue of a specific anti-PSMA antibody labelled with Fluorescein IsoThioCyanate We can also detect the contribution
of non-specific autofluorescence of prostatic concretions (Fig 11) (times20 magnification)
localization on a chicken breast to have more realistic condi-343
tions In both cases we were able to localize the active transducer344
with a precision less than 625 m Moreover the computation345
time is a few hundred milliseconds for a 2D localization These346
results demonstrate that the localization is fast enough to be347
implemented for a prostatectomy For the moment only a 2D 348
localization has been made with the active landmarks and the 349
3D localization is in progress Then we will be able to per- 350
form a registration with laparoscopic images using ldquoactiverdquo 351
markers 352
Fig 11 Non-specific autofluorescence observed in the prostate fixed tissues This figure shows the benefits of a near infrared marker like Cyanine 5 (excited at
633 nm) compared to Fluorescein IsoThioCyanate (excited at 488 nm) A Auto fluorescence under laser excitation at 488 nm We observe that prostate concretions
(calcified material) respond to this excitation by a strong fluorescence signal B Auto fluorescence under laser excitation at 633 nm The use of Cyanine 5 reduces
widely autofluorescence of some structures such as prostate concretions (times20 magnification)
Please cite this article in press as Voros S et al Devices and systems targeted towards augmented robotic radical prostatectomy IRBM (2013)
httpdxdoiorg101016jirbm201301014
ARTICLE IN PRESS+ModelIRBM 252 1ndash8
8 S Voros et al IRBM xxx (2013) xxxndashxxx
Concerning the registration between laparoscopic and ultra-353
sound images we performed several testbench evaluations of354
the registration algorithm on chicken breasts The result of such355
a registration obtained by manually pairing passive markers356
visible on both the laparoscopic and ultrasound imaging modal-357
ities are presented on Fig 8 In this example we obtained a358
registration root mean square error (RMS) of 038 mm359
43 Augmented laparoscopy thanks to fluorescence360
imaging361
First experiments were performed on leaves to demonstrate362
the feasibility of the detection of chlorophyll autofluorescence363
which has optical properties very similar to PpIX (absorption at364
405 nm and emission at 680 nm) as described on Fig 9 Then365
experiments were conducted on histology slices of the human366
prostate with as we anticipated inconclusive results because367
of the expected low signal-to-noise ratio caused by the insuffi-368
cient thickness of a histology slice (3 m thickness) compared to369
the optimal use of the device (300 m thickness) These results370
motivated our biomedical research COPROST on macroscopic371
fresh prostate samples372
Concerning the immunofluorescence protocol we were able373
to demonstrate the specificity of the anti-PSMA antibody on374
fixed tissue samples labelled with FITC as illustrated by Fig 10375
We observed higher autofluorescence problems when excit-376
ing the sample at the FITC specific wavelength compared to377
an excitation at the Cyanine 5 specific wavelength (Fig 11)378
These results motivated the inclusion of both fluorophores in our379
biomedical research COPROST on macroscopic fresh prostate380
samples FITC because it was already used to demonstrate speci-381
ficity of anti-PSMA antibody and Cyanine 5 because its near382
infra-red characteristics make it a better candidate on fresh mate-383
rial (higher penetration in tissue) and will improve signalnoise384
ratio as previously demonstrated385
To our knowledge most of the optical biopsy approaches as386
previously defined have been validated either on histologic slices387
or on ratmice prostate models However these approaches have388
limitations prostatic tissue is impaired by the chemical treat-389
ment required for histologic preparation and animal models do390
not directly mimic all aspects of human prostate cancer [11] In391
short it has not been proved yet that a successful detection with392
the investigated devices on histopathology slices or on animal393
models is sufficient to guarantee a successful detection on fresh394
human tissues The experiments that will be performed in the395
frame of the COPROST protocol in 2013 will be determinant to396
confirm the feasibility of our approach on fresh tissue samples397
5 DiscussionConclusion398
The DEPORRA project allowed for the development of inno-399
vative devices and navigation prototypes in the objective of400
allowing the surgeon to see ldquobeyond the visiblerdquo during a radi-401
cal prostatectomy First evaluations of the devices and methods402
have been performed preclinically and are very encouraging for403
the development of innovative approaches to assist the surgeon
during such a complex surgery Our preliminary results have also 404
shown the limits of preclinical validation and have convinced us 405
of the necessity to launch biomedical researches that will allow 406
us to validate further the devices This process required a con- 407
sequent amount of effort and time but is mandatory for the 408
fine-tuning of our tissue characterization tools and to obtain the 409
first clinical proofs of the relevance of the developed medical 410
devices which are mandatory to perform clinical evaluations of 411
the complete navigation systems 412
We now need to push further the integration of the devices 413
into such navigation systems in order to exploit at best the infor- 414
mation provided by each modality and to determine the optimal 415
approach for displaying the relevant information to the surgeon 416
in a clinical environment This will imply a conception and 417
development effort a definition of qualitative and quantitative 418
parameters for the first assessment of the delivered medical ben- 419
efit of our developments risks analysis and biomedical research 420
preparations in order to meet the ethical instances requirements 421
Acknowledgments 422
This work has been supported by French National Research 423
Agency (ANR) through TecSan program (project DEPORRA 424
no ANR-09-TECS-006) 425
References 426
[1] Heidenreich A Bolla M Joniau S Mason MD Matveev V Mottet N et al 427
Guidelines on prostate cancer Eur Assoc Urol 2011 [www uroweb org] 428
[2] Pfitzenmaier J Pahernik S Tremmel T Haferkamp A Buse S Hohen- 429
fellner M Positive surgical margins after radical prostatectomy do 430
they have an impact on biochemical or clinical progression BJU Int 431
2008102(10)1413ndash8 432
[3] Soler L Nicolau S Schmid J Koehl C Marescaux J et al Virtual reality 433
and augmented reality in digestive surgery In Third IEEE and ACM Inter- 434
national Symposium on Mixed and Augmented Reality (ISMAR) 2004 435
p 278ndash9 436
[4] S Voros B Tamadazte P Cinquin C Fouard Systegraveme drsquoimagerie multi- 437
vision pour chirurgie laparoscopique demande de deacutepocirct de brevet FR 438
1259489 102012 439
[5] Ukimura O Ahlering TE Gill IS Transrectal ultrasound-guided 440
energy-free nerve-sparing laparoscopic radical prostatectomy J Endourol 441
200822(9)1993ndash5 442
[6] Long JA Lee BH Guillotreau J Autorino R Laydner H Yakoubi R et al 443
Real-time robotic transrectal ultrasound navigation during robotic radical 444
prostatectomy initial clinical experience Urology 201280(3)608ndash13 445
[7] Holmes III DR Davis BJ Bruce CJ Robb RA 3D visualization analysis 446
and treatment of the prostate using trans-urethral ultrasound Comput Med 447
Imaging Graph 200327339ndash49 [2003] 448
[8] Dementhon D Model-based object pose in 25 lines of code Int J Comput 449
Vis 199515(1ndash2)123ndash41 450
[9] Custillon G Voros S Cinquin P Nguyen-Dinh A Moreau-Gaudry A 451
Bidimensional localization of active ultrasound transducers for use in 452
laparoscopic prostate surgery IEEE Trans Med Imaging 2012 Q3 453
[10] Wolf R Duchateau J Cinquin P Voros S 3D tracking of laparoscopic 454
instruments using statistical and geometric modeling Med Image Com- 455
put Comput Assist Interv 20116891203ndash10 [Lecture notes in computer 456
science] 457
[11] Valkenburg KC Williams BO ldquoMouse models of prostate cancerrdquo Prostate 458
Cancer 2011201122 httpdxdoiorg1011552011895238 [Article ID 459
895238] 460

Please cite this article in press as Voros S et al Devices and systems targeted towards augmented robotic radical prostatectomy IRBM (2013)
httpdxdoiorg101016jirbm201301014
ARTICLE IN PRESS+ModelIRBM 252 1ndash8
6 S Voros et al IRBM xxx (2013) xxxndashxxx
Fig 7 Ultrasound image of a prostate acquired with our innovative transurethral
ultrasound probe during a cadaver experiment The image was acquired with our
first prototype (64 piezoelectric elements)
surgical task once with the traditional endoscope alone and289
once with the proposed system alone (although in practice they290
can be combined to associate local and global views) The tasks291
consisted in localizing a suture needle and bringing it to a fixed292
target point The experiment was performed on porcine organs293
placed in a training box and repeated six times by the surgeon294
At each realization the needlersquos initial position was repositioned295
randomly at a distance equivalent to its initial position and the296
surgeon started randomly with the traditional endoscope or the297
proposed system In both cases a robotic endoscope holder was298
used to mobilize the endoscope and the vision system allowing299
us to record the displacements of the vision systems300
The full methodology and results are currently under sub-301
mission but to summarize the mean time required to perform302
the six experiments with the traditional endoscope was of 190 s303
compared to 245 s with the proposed system Moreover the sur-304
geon needed to give an average of 232 commands to the robotic305
scope holder to perform one stitch with the endoscope alone306
compared to 46 commands with the proposed system These307
preliminary results suggest that the proposed system could sig-308
nificantly reduce the laparoscopic surgery time and the cognitive309
load required for the control of the endoscope We now plan on310
performing cadaver experiments to evaluate the deployment of311
the vision system in conditions close to the clinical reality and312
to evaluate the system with several surgeons313
42 Augmented laparoscopy thanks to an innovative314
ultrasound system315
We performed two cadaver experiments which allowed us316
to determine the optimal characteristics for the realization of317
the intraurethral ultrasound probe During these experiments318
we evaluated the (difficult) insertion of the catheter through319
the urethra and the prostate visualization It must be noted that320
our clinicians partners stressed that the rigor mortis made this321
insertion harder These experiments allowed us to find the best322
rigidity for the catheter of the probe it must be flexible enough323
Fig 8 Demonstration of the fusion of ultrasound and laparoscopic images using
passive landmarks on chicken breasts Top-left the ultrasound image top-right
the laparoscopic image The passive landmarks are indicated with the green
arrows in the laparoscopic image They are selected manually in both modalities
to perform the registration Bottom the fusion of the two imaging modalities
to be introduced in the urethra but rigid enough to avoid the 324
distortions of the catheter 325
The first ultrasound probe (2D) was designed with 64 326
piezoelements It appeared that it was not enough On the one 327
hand the probe imaged a too small part of the prostate so that 328
it was difficult to identify what was represented on the ultra- 329
sound image (Fig 7) Furthermore it was impossible to know 330
in which direction the probe was oriented On the other hand 331
we demonstrated [9] that a longer probe increases the precision 332
of the localization of the active ultrasound transducers That is 333
why the second probe designed for the project (3D) has 128 334
piezoelements This second probe has graduations located on 335
its catheter visible on Fig 2 They allow the surgeon to know 336
the probersquos insertion depth in the urethra and a line along the 337
catheter allows appreciating the torsion applied to the catheter 338
The localization of the active transducers is currently under 339
submission It is based on a global positioning system (GPS) 340
method We made some experiments on a testbench making 341
localization in water to have ideal homogeneous conditions and 342
Please cite this article in press as Voros S et al Devices and systems targeted towards augmented robotic radical prostatectomy IRBM (2013)
httpdxdoiorg101016jirbm201301014
ARTICLE IN PRESS+ModelIRBM 252 1ndash8
S Voros et al IRBM xxx (2013) xxxndashxxx 7
Fig 9 Preliminary experiments of the autofluorescence detection with our testbench The autofluorescence of chlorophyll which has optical properties very similar
to Protoporphyrin IX was observed on our testbench Left direct image of a leaf right fluorescence image of the leaf at 680 nm As expected chlorophyll seems
absent in the veins
Fig 10 Specific fluorescence signal of anti-prostate-specific membrane antigen marker A Nuclear counter-staining of prostatic tissue with Hoechst (blue DNA
marker) We observe the nuclei of prostate cells regularly organized in the glandular epithelium Prostatic glands are separated by stroma B Fluorescence emission
of anti-prostate-specific membrane antigen-Fluorescein IsoThioCyanate on cellular membranes of prostatic cells C Overlay of the A and B images This figure
demonstrates the specificity on fixed prostatic tissue of a specific anti-PSMA antibody labelled with Fluorescein IsoThioCyanate We can also detect the contribution
of non-specific autofluorescence of prostatic concretions (Fig 11) (times20 magnification)
localization on a chicken breast to have more realistic condi-343
tions In both cases we were able to localize the active transducer344
with a precision less than 625 m Moreover the computation345
time is a few hundred milliseconds for a 2D localization These346
results demonstrate that the localization is fast enough to be347
implemented for a prostatectomy For the moment only a 2D 348
localization has been made with the active landmarks and the 349
3D localization is in progress Then we will be able to per- 350
form a registration with laparoscopic images using ldquoactiverdquo 351
markers 352
Fig 11 Non-specific autofluorescence observed in the prostate fixed tissues This figure shows the benefits of a near infrared marker like Cyanine 5 (excited at
633 nm) compared to Fluorescein IsoThioCyanate (excited at 488 nm) A Auto fluorescence under laser excitation at 488 nm We observe that prostate concretions
(calcified material) respond to this excitation by a strong fluorescence signal B Auto fluorescence under laser excitation at 633 nm The use of Cyanine 5 reduces
widely autofluorescence of some structures such as prostate concretions (times20 magnification)
Please cite this article in press as Voros S et al Devices and systems targeted towards augmented robotic radical prostatectomy IRBM (2013)
httpdxdoiorg101016jirbm201301014
ARTICLE IN PRESS+ModelIRBM 252 1ndash8
8 S Voros et al IRBM xxx (2013) xxxndashxxx
Concerning the registration between laparoscopic and ultra-353
sound images we performed several testbench evaluations of354
the registration algorithm on chicken breasts The result of such355
a registration obtained by manually pairing passive markers356
visible on both the laparoscopic and ultrasound imaging modal-357
ities are presented on Fig 8 In this example we obtained a358
registration root mean square error (RMS) of 038 mm359
43 Augmented laparoscopy thanks to fluorescence360
imaging361
First experiments were performed on leaves to demonstrate362
the feasibility of the detection of chlorophyll autofluorescence363
which has optical properties very similar to PpIX (absorption at364
405 nm and emission at 680 nm) as described on Fig 9 Then365
experiments were conducted on histology slices of the human366
prostate with as we anticipated inconclusive results because367
of the expected low signal-to-noise ratio caused by the insuffi-368
cient thickness of a histology slice (3 m thickness) compared to369
the optimal use of the device (300 m thickness) These results370
motivated our biomedical research COPROST on macroscopic371
fresh prostate samples372
Concerning the immunofluorescence protocol we were able373
to demonstrate the specificity of the anti-PSMA antibody on374
fixed tissue samples labelled with FITC as illustrated by Fig 10375
We observed higher autofluorescence problems when excit-376
ing the sample at the FITC specific wavelength compared to377
an excitation at the Cyanine 5 specific wavelength (Fig 11)378
These results motivated the inclusion of both fluorophores in our379
biomedical research COPROST on macroscopic fresh prostate380
samples FITC because it was already used to demonstrate speci-381
ficity of anti-PSMA antibody and Cyanine 5 because its near382
infra-red characteristics make it a better candidate on fresh mate-383
rial (higher penetration in tissue) and will improve signalnoise384
ratio as previously demonstrated385
To our knowledge most of the optical biopsy approaches as386
previously defined have been validated either on histologic slices387
or on ratmice prostate models However these approaches have388
limitations prostatic tissue is impaired by the chemical treat-389
ment required for histologic preparation and animal models do390
not directly mimic all aspects of human prostate cancer [11] In391
short it has not been proved yet that a successful detection with392
the investigated devices on histopathology slices or on animal393
models is sufficient to guarantee a successful detection on fresh394
human tissues The experiments that will be performed in the395
frame of the COPROST protocol in 2013 will be determinant to396
confirm the feasibility of our approach on fresh tissue samples397
5 DiscussionConclusion398
The DEPORRA project allowed for the development of inno-399
vative devices and navigation prototypes in the objective of400
allowing the surgeon to see ldquobeyond the visiblerdquo during a radi-401
cal prostatectomy First evaluations of the devices and methods402
have been performed preclinically and are very encouraging for403
the development of innovative approaches to assist the surgeon
during such a complex surgery Our preliminary results have also 404
shown the limits of preclinical validation and have convinced us 405
of the necessity to launch biomedical researches that will allow 406
us to validate further the devices This process required a con- 407
sequent amount of effort and time but is mandatory for the 408
fine-tuning of our tissue characterization tools and to obtain the 409
first clinical proofs of the relevance of the developed medical 410
devices which are mandatory to perform clinical evaluations of 411
the complete navigation systems 412
We now need to push further the integration of the devices 413
into such navigation systems in order to exploit at best the infor- 414
mation provided by each modality and to determine the optimal 415
approach for displaying the relevant information to the surgeon 416
in a clinical environment This will imply a conception and 417
development effort a definition of qualitative and quantitative 418
parameters for the first assessment of the delivered medical ben- 419
efit of our developments risks analysis and biomedical research 420
preparations in order to meet the ethical instances requirements 421
Acknowledgments 422
This work has been supported by French National Research 423
Agency (ANR) through TecSan program (project DEPORRA 424
no ANR-09-TECS-006) 425
References 426
[1] Heidenreich A Bolla M Joniau S Mason MD Matveev V Mottet N et al 427
Guidelines on prostate cancer Eur Assoc Urol 2011 [www uroweb org] 428
[2] Pfitzenmaier J Pahernik S Tremmel T Haferkamp A Buse S Hohen- 429
fellner M Positive surgical margins after radical prostatectomy do 430
they have an impact on biochemical or clinical progression BJU Int 431
2008102(10)1413ndash8 432
[3] Soler L Nicolau S Schmid J Koehl C Marescaux J et al Virtual reality 433
and augmented reality in digestive surgery In Third IEEE and ACM Inter- 434
national Symposium on Mixed and Augmented Reality (ISMAR) 2004 435
p 278ndash9 436
[4] S Voros B Tamadazte P Cinquin C Fouard Systegraveme drsquoimagerie multi- 437
vision pour chirurgie laparoscopique demande de deacutepocirct de brevet FR 438
1259489 102012 439
[5] Ukimura O Ahlering TE Gill IS Transrectal ultrasound-guided 440
energy-free nerve-sparing laparoscopic radical prostatectomy J Endourol 441
200822(9)1993ndash5 442
[6] Long JA Lee BH Guillotreau J Autorino R Laydner H Yakoubi R et al 443
Real-time robotic transrectal ultrasound navigation during robotic radical 444
prostatectomy initial clinical experience Urology 201280(3)608ndash13 445
[7] Holmes III DR Davis BJ Bruce CJ Robb RA 3D visualization analysis 446
and treatment of the prostate using trans-urethral ultrasound Comput Med 447
Imaging Graph 200327339ndash49 [2003] 448
[8] Dementhon D Model-based object pose in 25 lines of code Int J Comput 449
Vis 199515(1ndash2)123ndash41 450
[9] Custillon G Voros S Cinquin P Nguyen-Dinh A Moreau-Gaudry A 451
Bidimensional localization of active ultrasound transducers for use in 452
laparoscopic prostate surgery IEEE Trans Med Imaging 2012 Q3 453
[10] Wolf R Duchateau J Cinquin P Voros S 3D tracking of laparoscopic 454
instruments using statistical and geometric modeling Med Image Com- 455
put Comput Assist Interv 20116891203ndash10 [Lecture notes in computer 456
science] 457
[11] Valkenburg KC Williams BO ldquoMouse models of prostate cancerrdquo Prostate 458
Cancer 2011201122 httpdxdoiorg1011552011895238 [Article ID 459
895238] 460
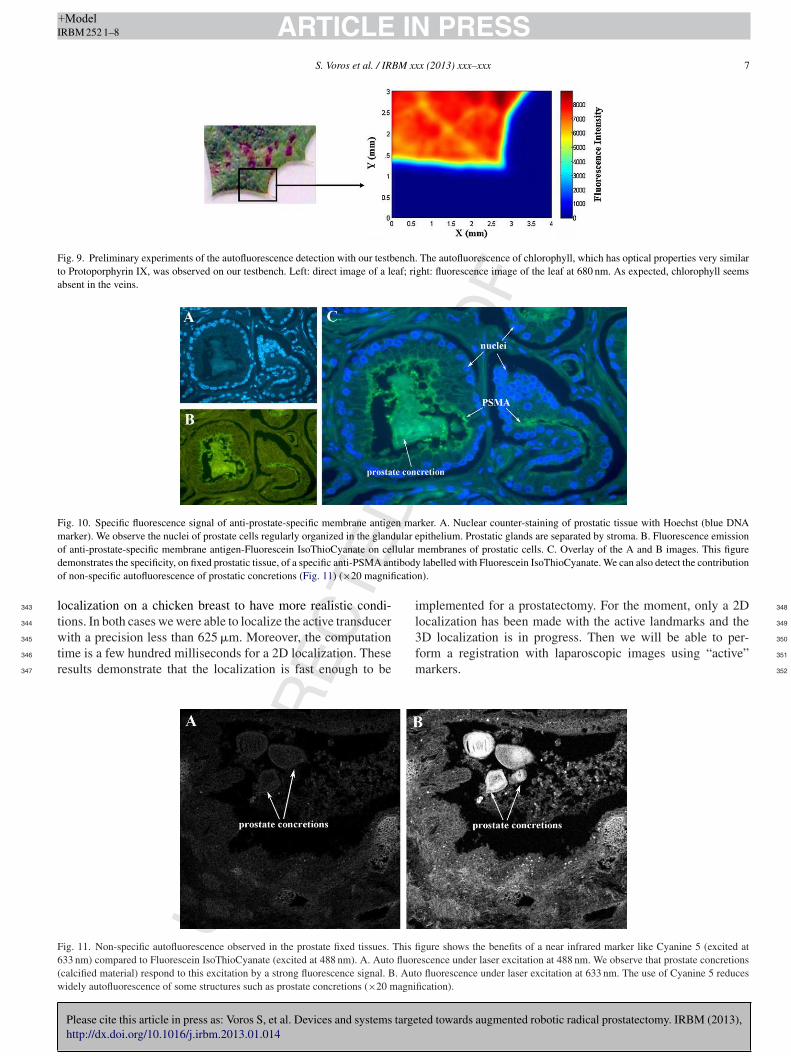
Please cite this article in press as Voros S et al Devices and systems targeted towards augmented robotic radical prostatectomy IRBM (2013)
httpdxdoiorg101016jirbm201301014
ARTICLE IN PRESS+ModelIRBM 252 1ndash8
S Voros et al IRBM xxx (2013) xxxndashxxx 7
Fig 9 Preliminary experiments of the autofluorescence detection with our testbench The autofluorescence of chlorophyll which has optical properties very similar
to Protoporphyrin IX was observed on our testbench Left direct image of a leaf right fluorescence image of the leaf at 680 nm As expected chlorophyll seems
absent in the veins
Fig 10 Specific fluorescence signal of anti-prostate-specific membrane antigen marker A Nuclear counter-staining of prostatic tissue with Hoechst (blue DNA
marker) We observe the nuclei of prostate cells regularly organized in the glandular epithelium Prostatic glands are separated by stroma B Fluorescence emission
of anti-prostate-specific membrane antigen-Fluorescein IsoThioCyanate on cellular membranes of prostatic cells C Overlay of the A and B images This figure
demonstrates the specificity on fixed prostatic tissue of a specific anti-PSMA antibody labelled with Fluorescein IsoThioCyanate We can also detect the contribution
of non-specific autofluorescence of prostatic concretions (Fig 11) (times20 magnification)
localization on a chicken breast to have more realistic condi-343
tions In both cases we were able to localize the active transducer344
with a precision less than 625 m Moreover the computation345
time is a few hundred milliseconds for a 2D localization These346
results demonstrate that the localization is fast enough to be347
implemented for a prostatectomy For the moment only a 2D 348
localization has been made with the active landmarks and the 349
3D localization is in progress Then we will be able to per- 350
form a registration with laparoscopic images using ldquoactiverdquo 351
markers 352
Fig 11 Non-specific autofluorescence observed in the prostate fixed tissues This figure shows the benefits of a near infrared marker like Cyanine 5 (excited at
633 nm) compared to Fluorescein IsoThioCyanate (excited at 488 nm) A Auto fluorescence under laser excitation at 488 nm We observe that prostate concretions
(calcified material) respond to this excitation by a strong fluorescence signal B Auto fluorescence under laser excitation at 633 nm The use of Cyanine 5 reduces
widely autofluorescence of some structures such as prostate concretions (times20 magnification)
Please cite this article in press as Voros S et al Devices and systems targeted towards augmented robotic radical prostatectomy IRBM (2013)
httpdxdoiorg101016jirbm201301014
ARTICLE IN PRESS+ModelIRBM 252 1ndash8
8 S Voros et al IRBM xxx (2013) xxxndashxxx
Concerning the registration between laparoscopic and ultra-353
sound images we performed several testbench evaluations of354
the registration algorithm on chicken breasts The result of such355
a registration obtained by manually pairing passive markers356
visible on both the laparoscopic and ultrasound imaging modal-357
ities are presented on Fig 8 In this example we obtained a358
registration root mean square error (RMS) of 038 mm359
43 Augmented laparoscopy thanks to fluorescence360
imaging361
First experiments were performed on leaves to demonstrate362
the feasibility of the detection of chlorophyll autofluorescence363
which has optical properties very similar to PpIX (absorption at364
405 nm and emission at 680 nm) as described on Fig 9 Then365
experiments were conducted on histology slices of the human366
prostate with as we anticipated inconclusive results because367
of the expected low signal-to-noise ratio caused by the insuffi-368
cient thickness of a histology slice (3 m thickness) compared to369
the optimal use of the device (300 m thickness) These results370
motivated our biomedical research COPROST on macroscopic371
fresh prostate samples372
Concerning the immunofluorescence protocol we were able373
to demonstrate the specificity of the anti-PSMA antibody on374
fixed tissue samples labelled with FITC as illustrated by Fig 10375
We observed higher autofluorescence problems when excit-376
ing the sample at the FITC specific wavelength compared to377
an excitation at the Cyanine 5 specific wavelength (Fig 11)378
These results motivated the inclusion of both fluorophores in our379
biomedical research COPROST on macroscopic fresh prostate380
samples FITC because it was already used to demonstrate speci-381
ficity of anti-PSMA antibody and Cyanine 5 because its near382
infra-red characteristics make it a better candidate on fresh mate-383
rial (higher penetration in tissue) and will improve signalnoise384
ratio as previously demonstrated385
To our knowledge most of the optical biopsy approaches as386
previously defined have been validated either on histologic slices387
or on ratmice prostate models However these approaches have388
limitations prostatic tissue is impaired by the chemical treat-389
ment required for histologic preparation and animal models do390
not directly mimic all aspects of human prostate cancer [11] In391
short it has not been proved yet that a successful detection with392
the investigated devices on histopathology slices or on animal393
models is sufficient to guarantee a successful detection on fresh394
human tissues The experiments that will be performed in the395
frame of the COPROST protocol in 2013 will be determinant to396
confirm the feasibility of our approach on fresh tissue samples397
5 DiscussionConclusion398
The DEPORRA project allowed for the development of inno-399
vative devices and navigation prototypes in the objective of400
allowing the surgeon to see ldquobeyond the visiblerdquo during a radi-401
cal prostatectomy First evaluations of the devices and methods402
have been performed preclinically and are very encouraging for403
the development of innovative approaches to assist the surgeon
during such a complex surgery Our preliminary results have also 404
shown the limits of preclinical validation and have convinced us 405
of the necessity to launch biomedical researches that will allow 406
us to validate further the devices This process required a con- 407
sequent amount of effort and time but is mandatory for the 408
fine-tuning of our tissue characterization tools and to obtain the 409
first clinical proofs of the relevance of the developed medical 410
devices which are mandatory to perform clinical evaluations of 411
the complete navigation systems 412
We now need to push further the integration of the devices 413
into such navigation systems in order to exploit at best the infor- 414
mation provided by each modality and to determine the optimal 415
approach for displaying the relevant information to the surgeon 416
in a clinical environment This will imply a conception and 417
development effort a definition of qualitative and quantitative 418
parameters for the first assessment of the delivered medical ben- 419
efit of our developments risks analysis and biomedical research 420
preparations in order to meet the ethical instances requirements 421
Acknowledgments 422
This work has been supported by French National Research 423
Agency (ANR) through TecSan program (project DEPORRA 424
no ANR-09-TECS-006) 425
References 426
[1] Heidenreich A Bolla M Joniau S Mason MD Matveev V Mottet N et al 427
Guidelines on prostate cancer Eur Assoc Urol 2011 [www uroweb org] 428
[2] Pfitzenmaier J Pahernik S Tremmel T Haferkamp A Buse S Hohen- 429
fellner M Positive surgical margins after radical prostatectomy do 430
they have an impact on biochemical or clinical progression BJU Int 431
2008102(10)1413ndash8 432
[3] Soler L Nicolau S Schmid J Koehl C Marescaux J et al Virtual reality 433
and augmented reality in digestive surgery In Third IEEE and ACM Inter- 434
national Symposium on Mixed and Augmented Reality (ISMAR) 2004 435
p 278ndash9 436
[4] S Voros B Tamadazte P Cinquin C Fouard Systegraveme drsquoimagerie multi- 437
vision pour chirurgie laparoscopique demande de deacutepocirct de brevet FR 438
1259489 102012 439
[5] Ukimura O Ahlering TE Gill IS Transrectal ultrasound-guided 440
energy-free nerve-sparing laparoscopic radical prostatectomy J Endourol 441
200822(9)1993ndash5 442
[6] Long JA Lee BH Guillotreau J Autorino R Laydner H Yakoubi R et al 443
Real-time robotic transrectal ultrasound navigation during robotic radical 444
prostatectomy initial clinical experience Urology 201280(3)608ndash13 445
[7] Holmes III DR Davis BJ Bruce CJ Robb RA 3D visualization analysis 446
and treatment of the prostate using trans-urethral ultrasound Comput Med 447
Imaging Graph 200327339ndash49 [2003] 448
[8] Dementhon D Model-based object pose in 25 lines of code Int J Comput 449
Vis 199515(1ndash2)123ndash41 450
[9] Custillon G Voros S Cinquin P Nguyen-Dinh A Moreau-Gaudry A 451
Bidimensional localization of active ultrasound transducers for use in 452
laparoscopic prostate surgery IEEE Trans Med Imaging 2012 Q3 453
[10] Wolf R Duchateau J Cinquin P Voros S 3D tracking of laparoscopic 454
instruments using statistical and geometric modeling Med Image Com- 455
put Comput Assist Interv 20116891203ndash10 [Lecture notes in computer 456
science] 457
[11] Valkenburg KC Williams BO ldquoMouse models of prostate cancerrdquo Prostate 458
Cancer 2011201122 httpdxdoiorg1011552011895238 [Article ID 459
895238] 460

Please cite this article in press as Voros S et al Devices and systems targeted towards augmented robotic radical prostatectomy IRBM (2013)
httpdxdoiorg101016jirbm201301014
ARTICLE IN PRESS+ModelIRBM 252 1ndash8
8 S Voros et al IRBM xxx (2013) xxxndashxxx
Concerning the registration between laparoscopic and ultra-353
sound images we performed several testbench evaluations of354
the registration algorithm on chicken breasts The result of such355
a registration obtained by manually pairing passive markers356
visible on both the laparoscopic and ultrasound imaging modal-357
ities are presented on Fig 8 In this example we obtained a358
registration root mean square error (RMS) of 038 mm359
43 Augmented laparoscopy thanks to fluorescence360
imaging361
First experiments were performed on leaves to demonstrate362
the feasibility of the detection of chlorophyll autofluorescence363
which has optical properties very similar to PpIX (absorption at364
405 nm and emission at 680 nm) as described on Fig 9 Then365
experiments were conducted on histology slices of the human366
prostate with as we anticipated inconclusive results because367
of the expected low signal-to-noise ratio caused by the insuffi-368
cient thickness of a histology slice (3 m thickness) compared to369
the optimal use of the device (300 m thickness) These results370
motivated our biomedical research COPROST on macroscopic371
fresh prostate samples372
Concerning the immunofluorescence protocol we were able373
to demonstrate the specificity of the anti-PSMA antibody on374
fixed tissue samples labelled with FITC as illustrated by Fig 10375
We observed higher autofluorescence problems when excit-376
ing the sample at the FITC specific wavelength compared to377
an excitation at the Cyanine 5 specific wavelength (Fig 11)378
These results motivated the inclusion of both fluorophores in our379
biomedical research COPROST on macroscopic fresh prostate380
samples FITC because it was already used to demonstrate speci-381
ficity of anti-PSMA antibody and Cyanine 5 because its near382
infra-red characteristics make it a better candidate on fresh mate-383
rial (higher penetration in tissue) and will improve signalnoise384
ratio as previously demonstrated385
To our knowledge most of the optical biopsy approaches as386
previously defined have been validated either on histologic slices387
or on ratmice prostate models However these approaches have388
limitations prostatic tissue is impaired by the chemical treat-389
ment required for histologic preparation and animal models do390
not directly mimic all aspects of human prostate cancer [11] In391
short it has not been proved yet that a successful detection with392
the investigated devices on histopathology slices or on animal393
models is sufficient to guarantee a successful detection on fresh394
human tissues The experiments that will be performed in the395
frame of the COPROST protocol in 2013 will be determinant to396
confirm the feasibility of our approach on fresh tissue samples397
5 DiscussionConclusion398
The DEPORRA project allowed for the development of inno-399
vative devices and navigation prototypes in the objective of400
allowing the surgeon to see ldquobeyond the visiblerdquo during a radi-401
cal prostatectomy First evaluations of the devices and methods402
have been performed preclinically and are very encouraging for403
the development of innovative approaches to assist the surgeon
during such a complex surgery Our preliminary results have also 404
shown the limits of preclinical validation and have convinced us 405
of the necessity to launch biomedical researches that will allow 406
us to validate further the devices This process required a con- 407
sequent amount of effort and time but is mandatory for the 408
fine-tuning of our tissue characterization tools and to obtain the 409
first clinical proofs of the relevance of the developed medical 410
devices which are mandatory to perform clinical evaluations of 411
the complete navigation systems 412
We now need to push further the integration of the devices 413
into such navigation systems in order to exploit at best the infor- 414
mation provided by each modality and to determine the optimal 415
approach for displaying the relevant information to the surgeon 416
in a clinical environment This will imply a conception and 417
development effort a definition of qualitative and quantitative 418
parameters for the first assessment of the delivered medical ben- 419
efit of our developments risks analysis and biomedical research 420
preparations in order to meet the ethical instances requirements 421
Acknowledgments 422
This work has been supported by French National Research 423
Agency (ANR) through TecSan program (project DEPORRA 424
no ANR-09-TECS-006) 425
References 426
[1] Heidenreich A Bolla M Joniau S Mason MD Matveev V Mottet N et al 427
Guidelines on prostate cancer Eur Assoc Urol 2011 [www uroweb org] 428
[2] Pfitzenmaier J Pahernik S Tremmel T Haferkamp A Buse S Hohen- 429
fellner M Positive surgical margins after radical prostatectomy do 430
they have an impact on biochemical or clinical progression BJU Int 431
2008102(10)1413ndash8 432
[3] Soler L Nicolau S Schmid J Koehl C Marescaux J et al Virtual reality 433
and augmented reality in digestive surgery In Third IEEE and ACM Inter- 434
national Symposium on Mixed and Augmented Reality (ISMAR) 2004 435
p 278ndash9 436
[4] S Voros B Tamadazte P Cinquin C Fouard Systegraveme drsquoimagerie multi- 437
vision pour chirurgie laparoscopique demande de deacutepocirct de brevet FR 438
1259489 102012 439
[5] Ukimura O Ahlering TE Gill IS Transrectal ultrasound-guided 440
energy-free nerve-sparing laparoscopic radical prostatectomy J Endourol 441
200822(9)1993ndash5 442
[6] Long JA Lee BH Guillotreau J Autorino R Laydner H Yakoubi R et al 443
Real-time robotic transrectal ultrasound navigation during robotic radical 444
prostatectomy initial clinical experience Urology 201280(3)608ndash13 445
[7] Holmes III DR Davis BJ Bruce CJ Robb RA 3D visualization analysis 446
and treatment of the prostate using trans-urethral ultrasound Comput Med 447
Imaging Graph 200327339ndash49 [2003] 448
[8] Dementhon D Model-based object pose in 25 lines of code Int J Comput 449
Vis 199515(1ndash2)123ndash41 450
[9] Custillon G Voros S Cinquin P Nguyen-Dinh A Moreau-Gaudry A 451
Bidimensional localization of active ultrasound transducers for use in 452
laparoscopic prostate surgery IEEE Trans Med Imaging 2012 Q3 453
[10] Wolf R Duchateau J Cinquin P Voros S 3D tracking of laparoscopic 454
instruments using statistical and geometric modeling Med Image Com- 455
put Comput Assist Interv 20116891203ndash10 [Lecture notes in computer 456
science] 457
[11] Valkenburg KC Williams BO ldquoMouse models of prostate cancerrdquo Prostate 458
Cancer 2011201122 httpdxdoiorg1011552011895238 [Article ID 459
895238] 460