
The Synergistic Relationship between Painting and Poetry in ...
Upload
independentCategory
view
2download
0
Development of a low-dose anti-resorptive drug regimen reveals synergisticsuppression of bone formation when coupled with disuse
Shane A.J. Lloyd,1,2 Neil D. Travis,2 Teng Lu,2 and Ted A. Bateman2
1Department of Anesthesiology, Pharmacology and Therapeutics, University of British Columbia, Vancouver, BritishColumbia, Canada; and 2Department of Bioengineering, Clemson University, Clemson, South Carolina
Submitted 12 June 2007; accepted in final form 2 January 2008
Lloyd SAJ, Travis ND, Lu T, Bateman TA. Development ofa low-dose anti-resorptive drug regimen reveals synergistic sup-pression of bone formation when coupled with disuse. J ApplPhysiol 104: 729–738, 2008. First published January 3, 2007;doi:10.1152/japplphysiol.00632.2007.—Safe and effective counter-measures to spaceflight-induced osteoporosis are required to mitigatethe potential for mission-critical fractures and ensure long-term bonehealth in astronauts. Two anti-resorptive drugs, the bisphosphonatezoledronic acid (ZOL) and the anti-receptor activator of NF-�B ligandprotein osteoprotegerin (OPG), were investigated to find the mini-mum, comparable doses that yield a maximal increase in bone quality,while minimizing deleterious effects on turnover and mineralization.Through a series of five trials in normally loaded female mice (n �56/trial), analysis of trabecular volume fraction and connectivity usingmicrocomputed tomography, along with biomechanical testing, quan-titative histomorphometry, and compositional analysis, was used toselect 45 �g/kg ZOL and 500 �g/kg OPG as doses that satisfy thesecriteria. These doses were then examined for their ability to mitigatebone loss following short-term unloading through hindlimb suspen-sion (HLS). Seventy-two mice were prophylactically administeredZOL, OPG, or PBS and assigned to loaded control or 2-wk HLSgroups (n � 12 for each of 6 groups). Both anti-resorptives were ableto preserve trabecular microarchitecture and femoral elastic and max-imum force in HLS mice (�30–40% ZOL/OPG vs. PBS). In HLSmice, anti-resorptive dosing reduced resorption perimeter at the fem-oral endocortical surface by 30% vs. PBS. In loaded control mice,anti-resorptives produced no change in bone formation rate; however,reductions in bone formation rate brought about by HLS were exac-erbated by anti-resorptive treatment, suggesting synergistic inhibitionof osteoblasts during disuse. Refined anti-resorptive dosing will tendto target countermeasures to the period of disuse, resulting in fasterrecovery and less adverse effects for astronauts.
spaceflight; osteoprotegerin; zoledronic acid; osteoporosis; bone loss;microcomputed tomography
THE “VISION FOR SPACE exploration” has directed the NationalAeronautics and Space Administration (NASA) toward humanexploration of the Moon and Mars within the next 30 years(22). In addition to the many engineering challenges associatedwith such an undertaking, there are important biomedicalissues that result from extended exposure to the space envi-ronment, including muscle atrophy (35), altered immune func-tion (39), and metabolic disruptions (24). The risk of bone lossis also a major obstacle for the future of long-durationspaceflight (34, 36).
In microgravity, skeletal unloading causes increased boneresorption, which leads to long-term demineralization of load-
bearing bones (34). Astronauts experience an average net lossof �230 mg calcium/day (33). Bone loss at a rate of 0.5–2.0%/mo in load-bearing bones creates a risk of fracturesduring the mission and in the months following return to Earth(20). With a Mars mission lasting up to 3 yr, the prospect ofmission-critical fractures is not trivial. The consequences ofsuch an event so far from Earth could be extremely hazardousto all crewmembers. Moreover, postflight bone recovery timeis two to three times longer than the period of microgravityexposure (19). A study by Lang and colleagues (21) revealedthat, 1 yr after a 4- to 6-mo stay on the International SpaceStation, astronauts� femoral bone mineral density had madeonly a partial recovery. To minimize these deleterious effectsand ensure astronaut health pre- and postflight, a robust systemof countermeasures must be developed.
Spaceflight countermeasures currently employed, such asexercise and resistance training, have been shown to effec-tively prevent muscle atrophy, but they have not translatedsuccessfully to the prevention of bone loss (38). Bisphospho-nates were the first class of drugs approved for the treatment ofosteoporosis. To exert their pharmacological effect, these drugsare thought to act as analogs to pyrophosphate and are incor-porated into bone following their addition to adenine nucleo-tides (30). Bisphosphonates help maintain bone mass, inhibitosteoclast-mediated bone resorption, and reduce the risk ofboth vertebral and nonvertebral fractures (13). Although theuse of bisphosphonates as a countermeasure is under consid-eration by NASA, the etiology of spaceflight-induced osteopo-rosis is fundamentally different from the osteoporosis com-monly found in the postmenopausal women for whom thesedrugs were originally developed (14).
Bone remodeling is a continual process that includes boththe resorption and formation of bone. This homeostatic processallows for maintenance of normal bone mass and quality, thusensuring skeletal competence under dynamic loading condi-tions. In a phenomenon referred to as “coupling”, the activitiesof bone-building osteoblasts and bone-resorbing osteoclasts areintimately linked and balanced (17, 25). During spaceflight,osteoclast-mediated bone resorption has been shown to in-crease dramatically, and the resultant bone loss is compoundedby the effects of reduced calcium consumption, reduced intes-tinal calcium absorption, and increased calcium excretion (33).In microgravity, there is an uncoupling of bone resorption andformation that is not seen in postmenopausal osteoporosis (34).Analysis of specific alkaline phosphates and osteocalcin hasshown that, during spaceflight, bone formation actually re-
Address for reprint requests and other correspondence: T. A. Bateman, 501Rhodes Engineering Research Center, Clemson Univ., Clemson, SC 29634(e-mail: [email protected]).
The costs of publication of this article were defrayed in part by the paymentof page charges. The article must therefore be hereby marked “advertisement”in accordance with 18 U.S.C. Section 1734 solely to indicate this fact.
J Appl Physiol 104: 729–738, 2008.First published January 3, 2007; doi:10.1152/japplphysiol.00632.2007.
8750-7587/08 $8.00 Copyright © 2008 the American Physiological Societyhttp://www. jap.org 729

mains steady or declines slightly instead of moving in parallelwith resorption (33). Through coupling, bisphosphonates andother anti-resorptive therapies will tend to suppress both boneresorption and formation (16). However, suppression of boneturnover postflight, which can be exacerbated by the longhalf-life of bisphosphonates following incorporation into bone,could adversely affect astronaut recovery. Of course, recoveryfollowing spaceflight may not follow the coupling mecha-nism seen during normal remodeling and may instead resemblethat observed during pathological conditions, such as fracturerepair, where formation increases independent of resorption(27). Furthermore, clinical studies have demonstrated thatbisphosphonates are capable of blunting the anabolic effect ofparathyroid hormone (PTH) (4, 12). Analogous postflight an-abolic suppression would not be favorable, given that thisresponse is required to recover bone mass lost during space-flight unloading.
As countermeasures to the consequences of spaceflight,NASA and the National Space Biomedical Research Institutehave proposed the use of alendronate and two other anti-resorptives (23): zoledronic acid (ZOL) (Reclast, NovartisPharmaceuticals, Basel, Switzerland) and the osteoprotegerin(OPG) analog AMG 162 (Denosumab, Amgen, ThousandOaks, CA) (2, 26). Endogenous OPG is a novel, secreted, TNFreceptor-related protein that acts as a decoy receptor for recep-tor activator of NF-�B ligand, a cytokine required for osteo-clast activation (6). ZOL is a bisphosphonate that is Food andDrug Administration (FDA) approved for use in treating hy-percalcemia of malignancy (5) and postmenopausal osteopo-rosis (3). However, these drugs and their recommended ther-apeutic doses are not optimized for microgravity-associatedbone loss in astronauts. Regardless of the agent selected, theformulation of specific countermeasures is critical to optimiz-ing recovery by expeditiously returning bone turnover to pre-flight levels.
Administration of supramaximal doses of anti-resorptiveagents can lead to unnecessary inhibition of bone formationpostflight, while the use of subtle dosing can target the therapyto a desired timeframe (i.e., during the mission) and can ensurethat a maximal effect is achieved with the administration of aminimal dose. For osteoporosis, this approach will limit sup-pression of osteoblast activity and bone turnover. This isparticularly relevant given the pharmacokinetics of a protein-based treatment such as Denosumab, which is not incorporatedinto bone like bisphosphonates and is metabolized in a rela-tively short duration. Denosumab is a fully human, monoclonalantibody that mimics the action of the naturally occurringprotein OPG; however, it should be noted that Denosumabcould not be used in the present animal studies because it isspecific to the human receptor activator of NF-�B ligand.
We propose that it is advantageous and medically beneficialto determine the minimum, comparable, efficacious doses ofZOL and OPG in mice. In this paper, the regimen-developmentprocess is presented as a series of iterative studies in a murinemodel that gradually refines the target dose for each drug as a“proof-of-concept”. Microcomputed tomography (microCT),compositional analysis, and quantitative histomorphometrywere used to evaluate bone quality and indicators of boneresorption and formation. In later iterations of this dose-development phase, the range of bone assays was expanded,and the target doses were more precisely refined.
These doses were then tested for their ability to maintainskeletal competence during limited periods of disuse, whileminimizing the aforementioned effects on bone formation.ZOL and OPG were administered prophylactically to micebefore unloading through hindlimb suspension (HLS), theaccepted ground-based model for simulating the adverse ef-fects of microgravity on bone and muscle in both rats (15) andmice (1, 31, 32). By placing the animal at an incline, itshindlimbs are free of mechanical loading, and a cephalic fluidshift occurs. Although not without its limitations, HLS doessufficiently simulate two of the most important physiologicaleffects of microgravity.
This paper represents the first in a series of investigations,with the ultimate aim being to establish an anti-resorptivetreatment plan that is effective in preventing bone loss incombination with other anabolic countermeasures, such thatbone turnover may be returned to normal levels as soon aspossible after the mission. Given the uncoupling of boneturnover that occurs during spaceflight, it is hypothesized thatthe development of subtle, refined, anti-resorptive dosing willallow bone resorption to be effectively inhibited, independentof bone formation. Such an approach would tend to target thecountermeasure to the period of disuse and lead to less adverseeffects on the skeletal health of astronauts.
MATERIALS AND METHODS
Animals
Female C57BL/6J mice (Jackson Laboratories, Bar Harbor, ME)with identical, exact date of birth (6 or 12 wk, depending on trial)were utilized. Animals were weighed and divided into groups toachieve an approximately equivalent mean mass (15.3 � 0.1 g) andminimally equivalent standard deviation. Animals were group housed(3 mice/cage), given food and water ad libitum, and allowed a 1-wkacclimatization period before the start of a study. Each treatmentgroup was composed of 8–12 animals, depending on the trial. Thebiotechnology company Amgen (Thousand Oaks, CA) provided all ofthe drugs utilized in these studies. It should be noted that, primarilydue to concerns regarding the development of an immunogenicresponse to human OPG in mice, all studies were limited to 2 wk induration. All animal protocols were approved by the Animal Care andUse Committee at Clemson University and were carried out under thesupervision of certified veterinary and veterinary-assistant staff.
Maximal Dose Study
To establish the maximal anti-resorptive response, a preliminarystudy was conducted with the relatively large doses of 10 mg/kg ZOLand 20 mg/kg OPG. On day 0, mice were subcutaneously (SC)injected with phosphate-buffered saline (PBS) or one of the anti-resorptives.
Dose Development Study
The process for determining the minimum, comparable, efficaciousdose of ZOL and OPG involved a series of five iterative trials. In theearly phases, a limited number of assays were applied to each trial;principally, trabecular microarchitecture through microCT was em-ployed. At this stage, it was critical to establish a range of efficaciousdoses rather than to concentrate on analysis of a large number of boneassays. In each iteration, mice were administered a SC injection ofPBS, ZOL, or OPG. Three doses of each anti-resorptive were chosen:low (0.1�), medium (1�), and high (10�). For the first iteration,Trial I, doses of ZOL (0.3, 3, 30 �g/kg) and OPG (1, 10, 100 �g/kg)were administered.
730 COMPARABLE ANTI-RESORPTIVE DOSING
J Appl Physiol • VOL 104 • MARCH 2008 • www.jap.org

Trabecular bone parameters were examined with microCT, and theminimum dose to produce maximal response vs. PBS (i.e., 30 �g/kgZOL and 100 �g/kg OPG) was set as the median dose for the nextiteration, Trial II.
The procedure for Trial II was identical, with treatment groups(n � 8/group) of PBS, ZOL (15, 30, 100 �g/kg), and OPG (50, 100,1,000 �g/kg). MicroCT analysis of tibial trabecular bone propertiesrevealed that �30 �g/kg ZOL and 100 �g/kg OPG produced anoptimal response. This process continued with each iteration, narrow-ing the range of the bracketing doses as outlined in Table 1. As theoptimal dose became more refined, assays were expanded frommicroCT to include compositional analysis, quantitative histomor-phometry, and biomechanical testing. This allowed for comparison ofthe various aspects of bone formation and resorption.
HLS Study
Following the dose-development process, optimal doses of 45�g/kg ZOL and 500 �g/kg OPG were selected for evaluation in amodel of simulated microgravity called HLS. Animals were randomlyassigned to one of six treatment groups (n � 12/group): loaded control(LC; PBS, 45 �g/kg ZOL or 500 �g/kg OPG) or HLS (PBS, 45 �g/kgZOL or 500 �g/kg OPG). LC mice were housed in groups of threewithin standard vivarium cages, whereas HLS mice were maintainedin individual cages. On day 0, all animals were weighed and given aSC injection of PBS, ZOL, or OPG.
The HLS apparatus is composed of a 2-cm plastic dowel andattached swivel hook that was attached to the animal’s tail withhypoallergenic tape, such that when the hook was attached to thecage’s guide wire, the animal was suspended at a 30° angle with itsforelimbs reaching the wire mesh floor. The condition of all animalsand their weight was recorded daily.
Study End Point
On day 14 of the maximal, dose-development, and HLS experi-ments, all mice were anesthetized with 2% isoflurane and killed bycardiac puncture and cervical dislocation. Hindlimbs were removed,and both tibiae and femora were cleaned of nonosseous tissue. The leftfemur of each animal, required for mechanical testing and composi-tional analysis, was allowed to air-dry for 48 h. The right femur andtibia, required for histomorphometry and microCT assays, respec-tively, were fixed in a 10% neutral buffered formalin solution for 48 h,rinsed with distilled water, and stored in 70% ethanol.
MicroCT
Tibiae were randomized and loaded four at a time into a sampletube filled with 70% ethanol. MicroCT analysis (�CT20, ScancoMedical, Bassersdorf, Switzerland) with a voxel size of 9 �m (15-�mresolution) in all three spatial directions was conducted. Trabecular
bone parameters were obtained with scans of 0.9-mm trabecular bonesections at the proximal end of the tibia, immediately distal to theepiphyseal plate. Examined parameters included trabecular bone vol-ume (BV), total volume (TV), and connectivity density (Conn.Dens)of trabecular struts. Trabecular volume fraction was calculated fromBV/TV. These parameters have been established as being critical tobone quality (18).
Biomechanical Testing
For biomechanical testing of the femora, bones were rehydrated inPBS for 90 min before evaluation to simulate in vivo properties (7).Three-point bending tests were performed using an Instron 5582(BlueHill 2 software, Instron, Norwood, MA). Femora were tested tofailure with an 8-mm span length and a deflection rate of 5 mm/min.The maximal force (Pe, N) and deflection (e, mm) were measured forall mechanically tested bones. These two properties were also deter-mined at the elastic limit and the failure point. Stiffness (N/mm) wascalculated from Pe/e.
Quantitative Histomorphometry
Fixed femora were allowed to air-dry and then were embeddedwith non-infiltrating Epo-Kwick epoxy (Buehler, Lake Bluff, IL). Theformed disks were sectioned with a low-speed saw (Buehler, 12.7cm � 0.5 mm diamond blade) at the mid-diaphysis of the femur.These sections were wheel-polished to a flat, smooth surface using600-, 800-, and 1,200-grit carbide paper, followed by polishing witha cloth impregnated with 6-�m diamond paste. This allowed micro-graphs at �50 magnification to be taken of the bone cross sectionsunder UV light (400 nm) with an FS filter. All animals in dose-development Trial V and in the HLS study had been given a SCinjection of calcein bone label (10 mg/kg) on day 7, which produceda visible green label, indicating the bone formation sites during theperiod of the study. Quantitative histomorphometric analysis wasperformed using these photographs and SigmaScan Pro software(SPSS, San Rafael, CA).
Measurements of bone morphology (29) included total bone areaenclosed by periosteal perimeter and endocortical area. Cortical area(Ct.Ar) was calculated as total bone area enclosed by periostealperimeter minus endocortical area. The area between the calcein labeland the cortical perimeter was measured as bone formation area, andlinear content of the labeled perimeter was defined as active miner-alizing perimeter (AMPm). Bone formation rate (BFR � bone for-mation area/7 days) and mineral apposition rate (MAR � BFR/AMPm) were calculated separately in the periosteal and endocorticalareas. The proportional endocortical eroded surface (Ec.ES) wasmeasured by quantifying the portion of the nonlabeled surface with arough/ruffled border and dividing it by the length of the endocorticalperimeter.
Compositional Analysis
For both maximal and dose-development studies, mineral-contentanalysis was performed on whole fractured femurs (37). For the HLSstudy, analysis of the diaphysis, epiphysis, and whole femur wasperformed separately. A properly calibrated analytic scale was usedfor all measurements. Dry mass (Dry-M) was measured after heatingthe bones to 105°C for 24 h. Mineral mass (Min-M) was measuredafter the bones had been ashed by baking at 800°C for another 24 h.Percent mineralization (%Min) was calculated by the formula%Min � Min-M/Dry-M � 100%.
Statistics
Statistical analysis of results was completed using SigmaStat soft-ware version 8.2 (Systat Software, San Jose, CA). For the maximaland dose-development studies, comparisons were made using a one-way ANOVA with a Student-Newman-Keuls post hoc test to reveal
Table 1. Dose development study: Summary of the dosesadministered in the five iterative trials used to determine thecomparable, efficacious doses of ZOL and OPG
ZOL Dose OPG Dose
Trial Low Medium High Low Medium High
I 0.3 3 30 1 10 100II 15 30 100 50 100 1000
III 6 30 300 100 500 2500IV 10 30 45 100 250 500V 10 30 45 100 250 500
Doses are in �g/kg. Analysis of trabecular architecture, mineral composi-tion, mechanical testing, and histomorphometry was used to select the brack-eting doses for each subsequent trial. ZOL, zoledronic acid; OPG, osteopro-tegerin.
731COMPARABLE ANTI-RESORPTIVE DOSING
J Appl Physiol • VOL 104 • MARCH 2008 • www.jap.org
significance between groups. A 95% level of significance (type Ierror) was utilized for each of these tests. For the HLS study, atwo-way ANOVA, with a Tukey test for follow-up comparisons, wasused to pool the data appropriately and to determine the overall effectsof anti-resorptive treatment and HLS. Differences for the HLS studywere determined with a P 0.05. Trends were used to evaluate highthroughput dose-development data and represent a P 0.1. Data arepresented as means � SE.
RESULTS
MicroCT: Maximal Dose Study
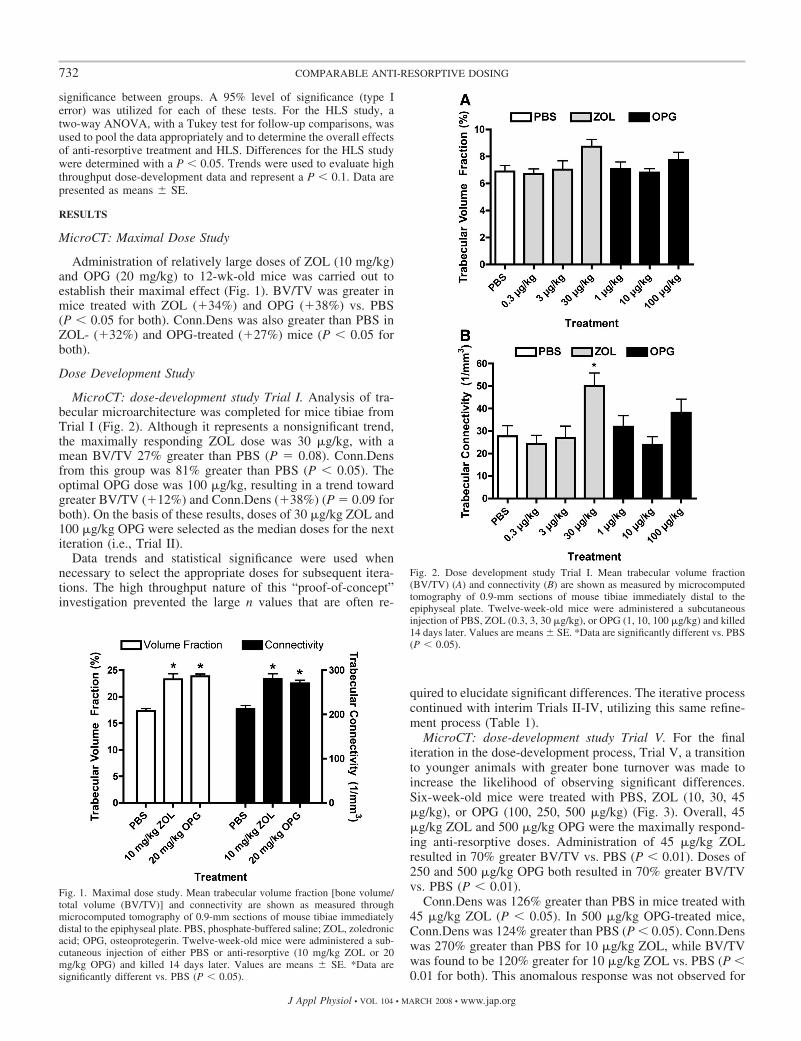
Administration of relatively large doses of ZOL (10 mg/kg)and OPG (20 mg/kg) to 12-wk-old mice was carried out toestablish their maximal effect (Fig. 1). BV/TV was greater inmice treated with ZOL (�34%) and OPG (�38%) vs. PBS(P 0.05 for both). Conn.Dens was also greater than PBS inZOL- (�32%) and OPG-treated (�27%) mice (P 0.05 forboth).
Dose Development Study
MicroCT: dose-development study Trial I. Analysis of tra-becular microarchitecture was completed for mice tibiae fromTrial I (Fig. 2). Although it represents a nonsignificant trend,the maximally responding ZOL dose was 30 �g/kg, with amean BV/TV 27% greater than PBS (P � 0.08). Conn.Densfrom this group was 81% greater than PBS (P 0.05). Theoptimal OPG dose was 100 �g/kg, resulting in a trend towardgreater BV/TV (�12%) and Conn.Dens (�38%) (P � 0.09 forboth). On the basis of these results, doses of 30 �g/kg ZOL and100 �g/kg OPG were selected as the median doses for the nextiteration (i.e., Trial II).
Data trends and statistical significance were used whennecessary to select the appropriate doses for subsequent itera-tions. The high throughput nature of this “proof-of-concept”investigation prevented the large n values that are often re-
quired to elucidate significant differences. The iterative processcontinued with interim Trials II-IV, utilizing this same refine-ment process (Table 1).
MicroCT: dose-development study Trial V. For the finaliteration in the dose-development process, Trial V, a transitionto younger animals with greater bone turnover was made toincrease the likelihood of observing significant differences.Six-week-old mice were treated with PBS, ZOL (10, 30, 45�g/kg), or OPG (100, 250, 500 �g/kg) (Fig. 3). Overall, 45�g/kg ZOL and 500 �g/kg OPG were the maximally respond-ing anti-resorptive doses. Administration of 45 �g/kg ZOLresulted in 70% greater BV/TV vs. PBS (P 0.01). Doses of250 and 500 �g/kg OPG both resulted in 70% greater BV/TVvs. PBS (P 0.01).
Conn.Dens was 126% greater than PBS in mice treated with45 �g/kg ZOL (P 0.05). In 500 �g/kg OPG-treated mice,Conn.Dens was 124% greater than PBS (P 0.05). Conn.Denswas 270% greater than PBS for 10 �g/kg ZOL, while BV/TVwas found to be 120% greater for 10 �g/kg ZOL vs. PBS (P 0.01 for both). This anomalous response was not observed for
Fig. 1. Maximal dose study. Mean trabecular volume fraction [bone volume/total volume (BV/TV)] and connectivity are shown as measured throughmicrocomputed tomography of 0.9-mm sections of mouse tibiae immediatelydistal to the epiphyseal plate. PBS, phosphate-buffered saline; ZOL, zoledronicacid; OPG, osteoprotegerin. Twelve-week-old mice were administered a sub-cutaneous injection of either PBS or anti-resorptive (10 mg/kg ZOL or 20mg/kg OPG) and killed 14 days later. Values are means � SE. *Data aresignificantly different vs. PBS (P 0.05).
Fig. 2. Dose development study Trial I. Mean trabecular volume fraction(BV/TV) (A) and connectivity (B) are shown as measured by microcomputedtomography of 0.9-mm sections of mouse tibiae immediately distal to theepiphyseal plate. Twelve-week-old mice were administered a subcutaneousinjection of PBS, ZOL (0.3, 3, 30 �g/kg), or OPG (1, 10, 100 �g/kg) and killed14 days later. Values are means � SE. *Data are significantly different vs. PBS(P 0.05).
732 COMPARABLE ANTI-RESORPTIVE DOSING
J Appl Physiol • VOL 104 • MARCH 2008 • www.jap.org
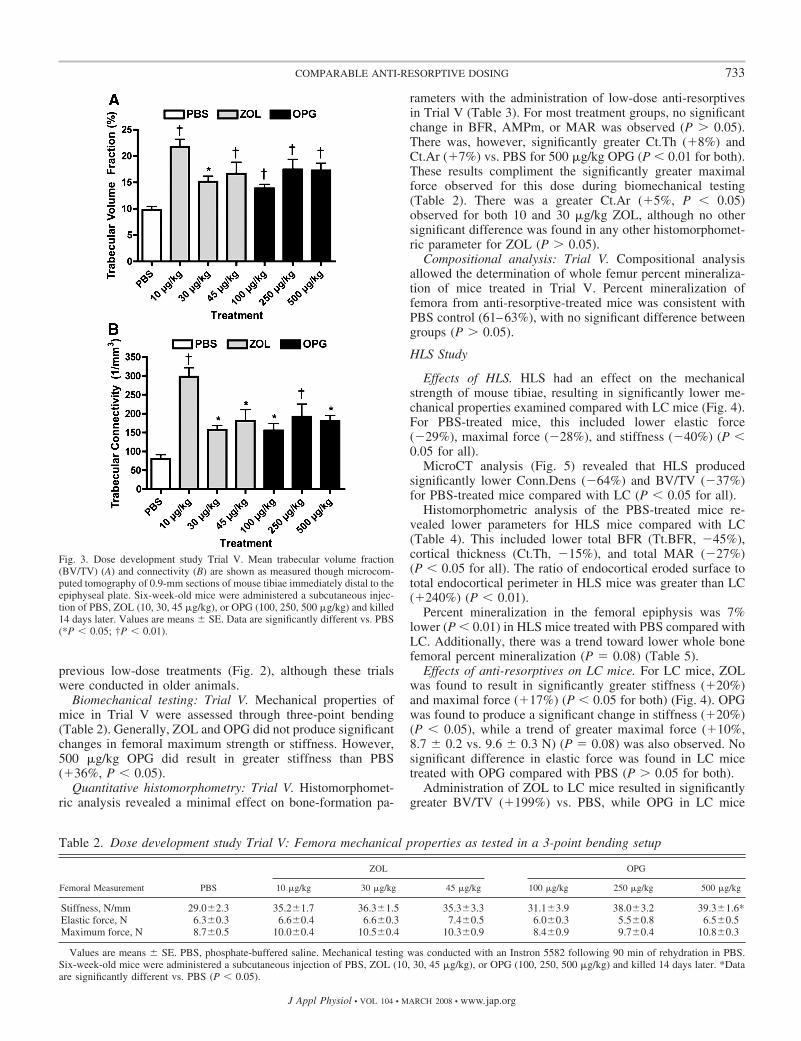
previous low-dose treatments (Fig. 2), although these trialswere conducted in older animals.
Biomechanical testing: Trial V. Mechanical properties ofmice in Trial V were assessed through three-point bending(Table 2). Generally, ZOL and OPG did not produce significantchanges in femoral maximum strength or stiffness. However,500 �g/kg OPG did result in greater stiffness than PBS(�36%, P 0.05).
Quantitative histomorphometry: Trial V. Histomorphomet-ric analysis revealed a minimal effect on bone-formation pa-
rameters with the administration of low-dose anti-resorptivesin Trial V (Table 3). For most treatment groups, no significantchange in BFR, AMPm, or MAR was observed (P � 0.05).There was, however, significantly greater Ct.Th (�8%) andCt.Ar (�7%) vs. PBS for 500 �g/kg OPG (P 0.01 for both).These results compliment the significantly greater maximalforce observed for this dose during biomechanical testing(Table 2). There was a greater Ct.Ar (�5%, P 0.05)observed for both 10 and 30 �g/kg ZOL, although no othersignificant difference was found in any other histomorphomet-ric parameter for ZOL (P � 0.05).
Compositional analysis: Trial V. Compositional analysisallowed the determination of whole femur percent mineraliza-tion of mice treated in Trial V. Percent mineralization offemora from anti-resorptive-treated mice was consistent withPBS control (61–63%), with no significant difference betweengroups (P � 0.05).
HLS Study
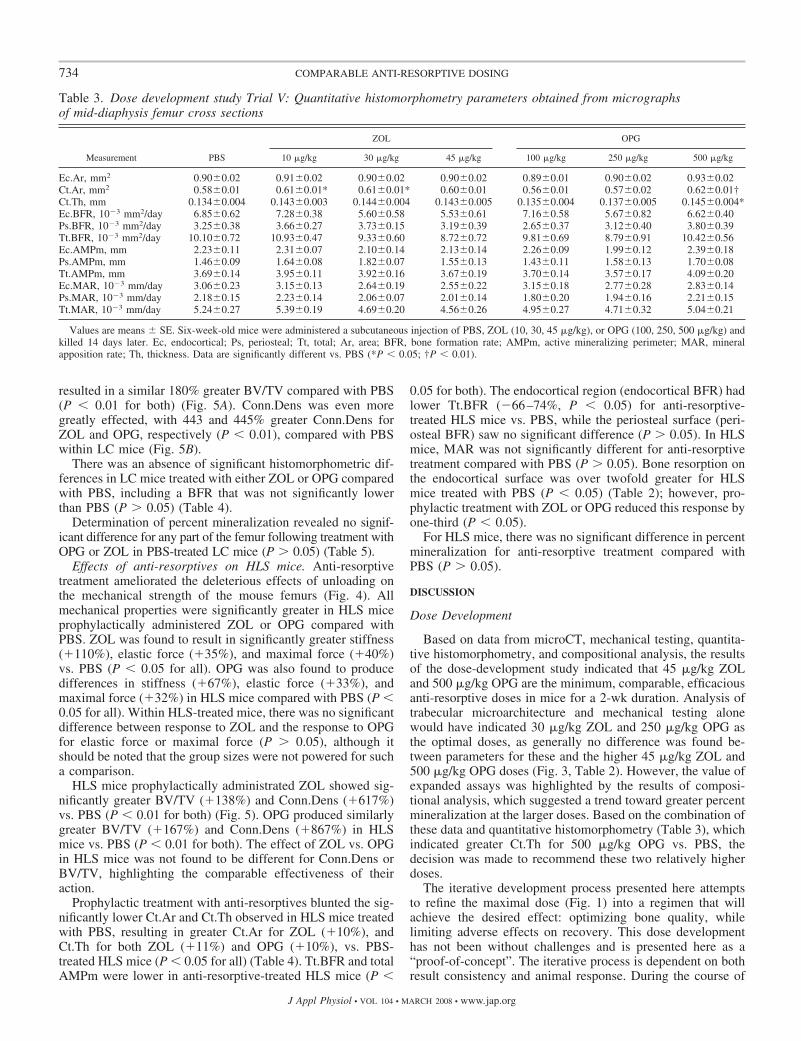
Effects of HLS. HLS had an effect on the mechanicalstrength of mouse tibiae, resulting in significantly lower me-chanical properties examined compared with LC mice (Fig. 4).For PBS-treated mice, this included lower elastic force(�29%), maximal force (�28%), and stiffness (�40%) (P 0.05 for all).
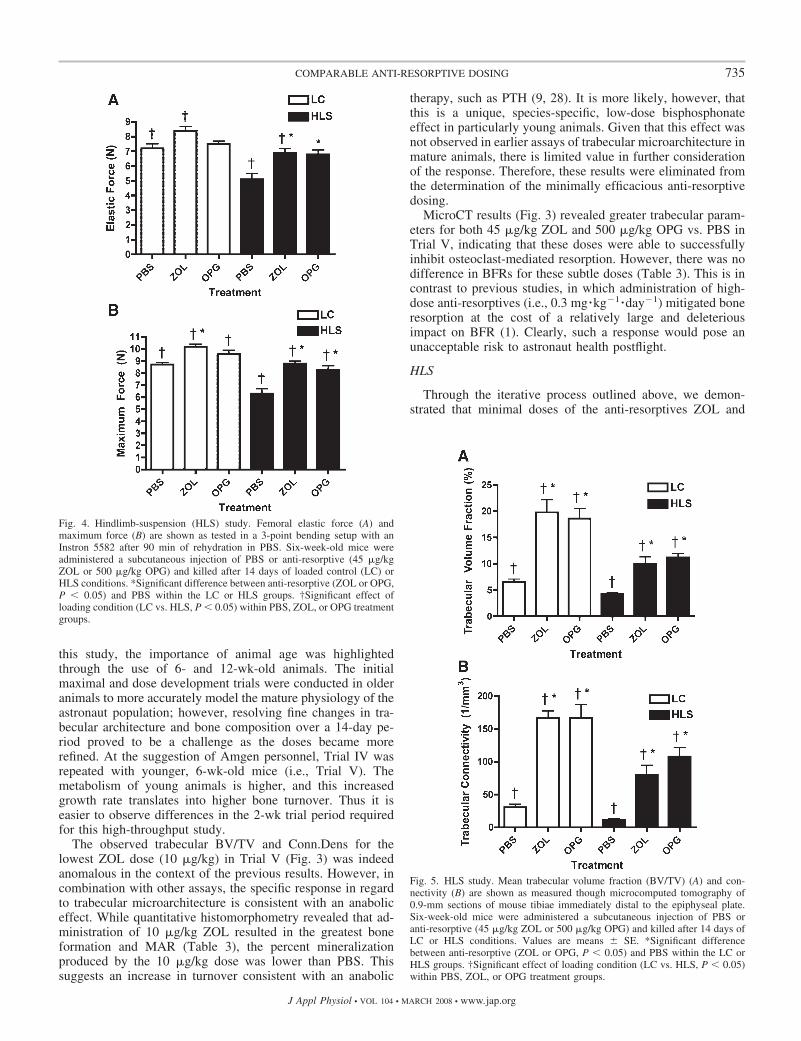
MicroCT analysis (Fig. 5) revealed that HLS producedsignificantly lower Conn.Dens (�64%) and BV/TV (�37%)for PBS-treated mice compared with LC (P 0.05 for all).
Histomorphometric analysis of the PBS-treated mice re-vealed lower parameters for HLS mice compared with LC(Table 4). This included lower total BFR (Tt.BFR, �45%),cortical thickness (Ct.Th, �15%), and total MAR (�27%)(P 0.05 for all). The ratio of endocortical eroded surface tototal endocortical perimeter in HLS mice was greater than LC(�240%) (P 0.01).
Percent mineralization in the femoral epiphysis was 7%lower (P 0.01) in HLS mice treated with PBS compared withLC. Additionally, there was a trend toward lower whole bonefemoral percent mineralization (P � 0.08) (Table 5).
Effects of anti-resorptives on LC mice. For LC mice, ZOLwas found to result in significantly greater stiffness (�20%)and maximal force (�17%) (P 0.05 for both) (Fig. 4). OPGwas found to produce a significant change in stiffness (�20%)(P 0.05), while a trend of greater maximal force (�10%,8.7 � 0.2 vs. 9.6 � 0.3 N) (P � 0.08) was also observed. Nosignificant difference in elastic force was found in LC micetreated with OPG compared with PBS (P � 0.05 for both).
Administration of ZOL to LC mice resulted in significantlygreater BV/TV (�199%) vs. PBS, while OPG in LC mice
Fig. 3. Dose development study Trial V. Mean trabecular volume fraction(BV/TV) (A) and connectivity (B) are shown as measured though microcom-puted tomography of 0.9-mm sections of mouse tibiae immediately distal to theepiphyseal plate. Six-week-old mice were administered a subcutaneous injec-tion of PBS, ZOL (10, 30, 45 �g/kg), or OPG (100, 250, 500 �g/kg) and killed14 days later. Values are means � SE. Data are significantly different vs. PBS(*P 0.05; †P 0.01).
Table 2. Dose development study Trial V: Femora mechanical properties as tested in a 3-point bending setup
ZOL OPG
Femoral Measurement PBS 10 �g/kg 30 �g/kg 45 �g/kg 100 �g/kg 250 �g/kg 500 �g/kg
Stiffness, N/mm 29.0�2.3 35.2�1.7 36.3�1.5 35.3�3.3 31.1�3.9 38.0�3.2 39.3�1.6*Elastic force, N 6.3�0.3 6.6�0.4 6.6�0.3 7.4�0.5 6.0�0.3 5.5�0.8 6.5�0.5Maximum force, N 8.7�0.5 10.0�0.4 10.5�0.4 10.3�0.9 8.4�0.9 9.7�0.4 10.8�0.3
Values are means � SE. PBS, phosphate-buffered saline. Mechanical testing was conducted with an Instron 5582 following 90 min of rehydration in PBS.Six-week-old mice were administered a subcutaneous injection of PBS, ZOL (10, 30, 45 �g/kg), or OPG (100, 250, 500 �g/kg) and killed 14 days later. *Dataare significantly different vs. PBS (P 0.05).
733COMPARABLE ANTI-RESORPTIVE DOSING
J Appl Physiol • VOL 104 • MARCH 2008 • www.jap.org
resulted in a similar 180% greater BV/TV compared with PBS(P 0.01 for both) (Fig. 5A). Conn.Dens was even moregreatly effected, with 443 and 445% greater Conn.Dens forZOL and OPG, respectively (P 0.01), compared with PBSwithin LC mice (Fig. 5B).
There was an absence of significant histomorphometric dif-ferences in LC mice treated with either ZOL or OPG comparedwith PBS, including a BFR that was not significantly lowerthan PBS (P � 0.05) (Table 4).
Determination of percent mineralization revealed no signif-icant difference for any part of the femur following treatment withOPG or ZOL in PBS-treated LC mice (P � 0.05) (Table 5).
Effects of anti-resorptives on HLS mice. Anti-resorptivetreatment ameliorated the deleterious effects of unloading onthe mechanical strength of the mouse femurs (Fig. 4). Allmechanical properties were significantly greater in HLS miceprophylactically administered ZOL or OPG compared withPBS. ZOL was found to result in significantly greater stiffness(�110%), elastic force (�35%), and maximal force (�40%)vs. PBS (P 0.05 for all). OPG was also found to producedifferences in stiffness (�67%), elastic force (�33%), andmaximal force (�32%) in HLS mice compared with PBS (P 0.05 for all). Within HLS-treated mice, there was no significantdifference between response to ZOL and the response to OPGfor elastic force or maximal force (P � 0.05), although itshould be noted that the group sizes were not powered for sucha comparison.
HLS mice prophylactically administrated ZOL showed sig-nificantly greater BV/TV (�138%) and Conn.Dens (�617%)vs. PBS (P 0.01 for both) (Fig. 5). OPG produced similarlygreater BV/TV (�167%) and Conn.Dens (�867%) in HLSmice vs. PBS (P 0.01 for both). The effect of ZOL vs. OPGin HLS mice was not found to be different for Conn.Dens orBV/TV, highlighting the comparable effectiveness of theiraction.
Prophylactic treatment with anti-resorptives blunted the sig-nificantly lower Ct.Ar and Ct.Th observed in HLS mice treatedwith PBS, resulting in greater Ct.Ar for ZOL (�10%), andCt.Th for both ZOL (�11%) and OPG (�10%), vs. PBS-treated HLS mice (P 0.05 for all) (Table 4). Tt.BFR and totalAMPm were lower in anti-resorptive-treated HLS mice (P
0.05 for both). The endocortical region (endocortical BFR) hadlower Tt.BFR (�66–74%, P 0.05) for anti-resorptive-treated HLS mice vs. PBS, while the periosteal surface (peri-osteal BFR) saw no significant difference (P � 0.05). In HLSmice, MAR was not significantly different for anti-resorptivetreatment compared with PBS (P � 0.05). Bone resorption onthe endocortical surface was over twofold greater for HLSmice treated with PBS (P 0.05) (Table 2); however, pro-phylactic treatment with ZOL or OPG reduced this response byone-third (P 0.05).
For HLS mice, there was no significant difference in percentmineralization for anti-resorptive treatment compared withPBS (P � 0.05).
DISCUSSION
Dose Development
Based on data from microCT, mechanical testing, quantita-tive histomorphometry, and compositional analysis, the resultsof the dose-development study indicated that 45 �g/kg ZOLand 500 �g/kg OPG are the minimum, comparable, efficaciousanti-resorptive doses in mice for a 2-wk duration. Analysis oftrabecular microarchitecture and mechanical testing alonewould have indicated 30 �g/kg ZOL and 250 �g/kg OPG asthe optimal doses, as generally no difference was found be-tween parameters for these and the higher 45 �g/kg ZOL and500 �g/kg OPG doses (Fig. 3, Table 2). However, the value ofexpanded assays was highlighted by the results of composi-tional analysis, which suggested a trend toward greater percentmineralization at the larger doses. Based on the combination ofthese data and quantitative histomorphometry (Table 3), whichindicated greater Ct.Th for 500 �g/kg OPG vs. PBS, thedecision was made to recommend these two relatively higherdoses.
The iterative development process presented here attemptsto refine the maximal dose (Fig. 1) into a regimen that willachieve the desired effect: optimizing bone quality, whilelimiting adverse effects on recovery. This dose developmenthas not been without challenges and is presented here as a“proof-of-concept”. The iterative process is dependent on bothresult consistency and animal response. During the course of
Table 3. Dose development study Trial V: Quantitative histomorphometry parameters obtained from micrographsof mid-diaphysis femur cross sections
ZOL OPG
Measurement PBS 10 �g/kg 30 �g/kg 45 �g/kg 100 �g/kg 250 �g/kg 500 �g/kg
Ec.Ar, mm2 0.90�0.02 0.91�0.02 0.90�0.02 0.90�0.02 0.89�0.01 0.90�0.02 0.93�0.02Ct.Ar, mm2 0.58�0.01 0.61�0.01* 0.61�0.01* 0.60�0.01 0.56�0.01 0.57�0.02 0.62�0.01†Ct.Th, mm 0.134�0.004 0.143�0.003 0.144�0.004 0.143�0.005 0.135�0.004 0.137�0.005 0.145�0.004*Ec.BFR, 10�3 mm2/day 6.85�0.62 7.28�0.38 5.60�0.58 5.53�0.61 7.16�0.58 5.67�0.82 6.62�0.40Ps.BFR, 10�3 mm2/day 3.25�0.38 3.66�0.27 3.73�0.15 3.19�0.39 2.65�0.37 3.12�0.40 3.80�0.39Tt.BFR, 10�3 mm2/day 10.10�0.72 10.93�0.47 9.33�0.60 8.72�0.72 9.81�0.69 8.79�0.91 10.42�0.56Ec.AMPm, mm 2.23�0.11 2.31�0.07 2.10�0.14 2.13�0.14 2.26�0.09 1.99�0.12 2.39�0.18Ps.AMPm, mm 1.46�0.09 1.64�0.08 1.82�0.07 1.55�0.13 1.43�0.11 1.58�0.13 1.70�0.08Tt.AMPm, mm 3.69�0.14 3.95�0.11 3.92�0.16 3.67�0.19 3.70�0.14 3.57�0.17 4.09�0.20Ec.MAR, 10�3 mm/day 3.06�0.23 3.15�0.13 2.64�0.19 2.55�0.22 3.15�0.18 2.77�0.28 2.83�0.14Ps.MAR, 10�3 mm/day 2.18�0.15 2.23�0.14 2.06�0.07 2.01�0.14 1.80�0.20 1.94�0.16 2.21�0.15Tt.MAR, 10�3 mm/day 5.24�0.27 5.39�0.19 4.69�0.20 4.56�0.26 4.95�0.27 4.71�0.32 5.04�0.21
Values are means � SE. Six-week-old mice were administered a subcutaneous injection of PBS, ZOL (10, 30, 45 �g/kg), or OPG (100, 250, 500 �g/kg) andkilled 14 days later. Ec, endocortical; Ps, periosteal; Tt, total; Ar, area; BFR, bone formation rate; AMPm, active mineralizing perimeter; MAR, mineralapposition rate; Th, thickness. Data are significantly different vs. PBS (*P 0.05; †P 0.01).
734 COMPARABLE ANTI-RESORPTIVE DOSING
J Appl Physiol • VOL 104 • MARCH 2008 • www.jap.org
this study, the importance of animal age was highlightedthrough the use of 6- and 12-wk-old animals. The initialmaximal and dose development trials were conducted in olderanimals to more accurately model the mature physiology of theastronaut population; however, resolving fine changes in tra-becular architecture and bone composition over a 14-day pe-riod proved to be a challenge as the doses became morerefined. At the suggestion of Amgen personnel, Trial IV wasrepeated with younger, 6-wk-old mice (i.e., Trial V). Themetabolism of young animals is higher, and this increasedgrowth rate translates into higher bone turnover. Thus it iseasier to observe differences in the 2-wk trial period requiredfor this high-throughput study.
The observed trabecular BV/TV and Conn.Dens for thelowest ZOL dose (10 �g/kg) in Trial V (Fig. 3) was indeedanomalous in the context of the previous results. However, incombination with other assays, the specific response in regardto trabecular microarchitecture is consistent with an anaboliceffect. While quantitative histomorphometry revealed that ad-ministration of 10 �g/kg ZOL resulted in the greatest boneformation and MAR (Table 3), the percent mineralizationproduced by the 10 �g/kg dose was lower than PBS. Thissuggests an increase in turnover consistent with an anabolic
therapy, such as PTH (9, 28). It is more likely, however, thatthis is a unique, species-specific, low-dose bisphosphonateeffect in particularly young animals. Given that this effect wasnot observed in earlier assays of trabecular microarchitecture inmature animals, there is limited value in further considerationof the response. Therefore, these results were eliminated fromthe determination of the minimally efficacious anti-resorptivedosing.
MicroCT results (Fig. 3) revealed greater trabecular param-eters for both 45 �g/kg ZOL and 500 �g/kg OPG vs. PBS inTrial V, indicating that these doses were able to successfullyinhibit osteoclast-mediated resorption. However, there was nodifference in BFRs for these subtle doses (Table 3). This is incontrast to previous studies, in which administration of high-dose anti-resorptives (i.e., 0.3 mg �kg�1 �day�1) mitigated boneresorption at the cost of a relatively large and deleteriousimpact on BFR (1). Clearly, such a response would pose anunacceptable risk to astronaut health postflight.
HLS
Through the iterative process outlined above, we demon-strated that minimal doses of the anti-resorptives ZOL and
Fig. 4. Hindlimb-suspension (HLS) study. Femoral elastic force (A) andmaximum force (B) are shown as tested in a 3-point bending setup with anInstron 5582 after 90 min of rehydration in PBS. Six-week-old mice wereadministered a subcutaneous injection of PBS or anti-resorptive (45 �g/kgZOL or 500 �g/kg OPG) and killed after 14 days of loaded control (LC) orHLS conditions. *Significant difference between anti-resorptive (ZOL or OPG,P 0.05) and PBS within the LC or HLS groups. †Significant effect ofloading condition (LC vs. HLS, P 0.05) within PBS, ZOL, or OPG treatmentgroups.
Fig. 5. HLS study. Mean trabecular volume fraction (BV/TV) (A) and con-nectivity (B) are shown as measured though microcomputed tomography of0.9-mm sections of mouse tibiae immediately distal to the epiphyseal plate.Six-week-old mice were administered a subcutaneous injection of PBS oranti-resorptive (45 �g/kg ZOL or 500 �g/kg OPG) and killed after 14 days ofLC or HLS conditions. Values are means � SE. *Significant differencebetween anti-resorptive (ZOL or OPG, P 0.05) and PBS within the LC orHLS groups. †Significant effect of loading condition (LC vs. HLS, P 0.05)within PBS, ZOL, or OPG treatment groups.
735COMPARABLE ANTI-RESORPTIVE DOSING
J Appl Physiol • VOL 104 • MARCH 2008 • www.jap.org

OPG are able to result in greater trabecular bone parameters inhealthy, normally loaded mice compared with control. Thesubsequent HLS study confirmed these findings. Analysis oftrabecular connectivity and volume fraction revealed a two- tofourfold increases in both microCT parameters (Fig. 5). Moreapplicable to therapeutic spaceflight use, however, is our find-ing that prophylactic administration of these minimal doseswas able to prevent the deleterious effects of simulated micro-gravity on the trabecular microarchitecture of young mice. Infact, both trabecular connectivity and BV fraction of suspendedmice pretreated with ZOL and OPG were restored to levelssimilar to that of normal LC mice. This is in contrast toPBS-treated HLS mice, which showed significant reductions of37–64% in both BV/TV and Conn.Dens (P 0.01). Thesefindings suggest that the administration of relatively largedoses of anti-resorptive may not be necessary to maintain theintegrity of trabecular bone during extended microgravity ex-posure.
As mentioned previously, the ability of anti-resorptives toeffectively inhibit bone resorption is ideal, but the concomitantinhibition of bone formation is of special concern, particularlyat high doses. This concept can be seen in our analysis of bonehistomorphometry parameters for loaded and unloaded mice(Table 4). Although anti-resorptive treatment was able toreduce osteoclast-mediated endocortical resorption broughtabout by HLS, it also further potentiated the suppression ofendocortical bone formation rate. Of course, it is important to
note that treatment with OPG and ZOL in LC mice did notresult in suppression of bone formation, Ct.Th, or AMPm.Despite their different mechanisms of action, there was nodifference between the suppressing effects of ZOL and OPG.These findings highlight the uncoupling of bone formation andresorption that occurs during unloading (34) and the fact thatunloading may act cooperatively with anti-resorptive treatments topotentiate inhibition of osteoblasts via coupling. Alternatively, theobserved response may be a form of mechanical adaptation,whereby anti-resorptive-induced decreases in bone resorptionmaintain bone strength during unloading, thereby resulting in adecrease in osteoblast-mediated bone formation. Future studiesmight investigate multiple time points in animal recovery toconfirm these findings and elucidate the mechanism behind theresponse. Although not investigated in the present study, itwould be reasonable to hypothesize that the magnitude andduration of the suppression of bone-formation rate followingreloading would be reduced compared with higher doses.Furthermore, the 2-wk duration of the studies outlined pres-ently is an important limitation, especially considering thevarying mechanisms of action of the two anti-resorptivesinvestigated and their rise to maximal efficacy. Considerations,including the development of an immunogenic response tohuman OPG in mice and previous data from 2-wk shuttlemissions, were our guiding motivation for selecting this dura-tion. Despite this, both the consistency and significance of the
Table 4. Hindlimb suspension study: Quantitative histomorphometry parameters from hindlimb-suspendedand loaded-control mice obtained from micrographs of mid-diaphysis femur cross sections
Loaded Controls Hindlimb Suspended
Measurement PBS ZOL OPG PBS ZOL OPG
Ec.Ar, mm2 0.88�0.01† 0.90�0.01 0.91�0.01 0.97�0.03† 0.91�0.01 0.92�0.02Ct.Ar, mm2 0.60�0.01† 0.64�0.01† 0.64�0.01† 0.52�0.04† 0.57�0.01*† 0.56�0.01†Ct.Th, mm 0.143�0.003† 0.150�0.002† 0.149�0.002† 0.121�0.009† 0.134�0.003*† 0.133�0.003*†Ec.BFR, 10�3 mm2/day 6.77�0.66† 5.41�0.41† 6.97�0.35† 3.51�0.81† 0.91�0.37*† 1.20�0.42*†Ps.BFR, 10�3 mm2/day 6.16�0.41† 6.47�0.43† 5.29�0.41† 3.56�0.56† 3.17�0.37† 2.75�0.26†Tt.BFR, 10�3 mm2/day 12.93�0.77† 11.88�0.62† 12.26�0.54† 7.07�1.19† 4.08�0.57*† 3.95�0.52*†Ec.AMPm, mm 2.39�0.12† 2.42�0.15† 2.49�0.11† 1.45�0.32† 0.61�0.21*† 0.76�0.22*†Ps.AMPm, mm 2.11�0.07† 2.09�0.12† 1.94�0.08† 1.43�0.07† 1.48�0.07† 1.38�0.07†Tt.AMPm, mm 4.50�0.11† 4.51�0.18† 4.43�0.13† 2.88�0.39† 2.09�0.21*† 2.14�0.24*†Ec.MAR, 10�3 mm/day 2.82�0.22† 2.24�0.10† 2.80�0.10† 1.83�0.32† 1.19�0.23† 1.22�0.21†Ps.MAR, 10�3 mm/day 2.89�0.12† 3.09�0.15† 2.69�0.11† 2.35�0.20† 2.10�0.19† 1.96�0.12†Tt.MAR, 10�3 mm/day 5.71�0.27† 5.33�0.20† 5.49�0.17† 4.18�0.48† 3.30�0.35† 3.18�0.28†Ec.ES 0.14�0.02† 0.11�0.02† 0.14�0.02† 0.33�0.04† 0.20�0.03*† 0.23�0.03*†
Values are means � SE. Six-week-old mice were administered a subcutaneous injection of PBS or anti-resorptive (45 �g/kg ZOL or 500 �g/kg OPG) andkilled after 14 days of loaded-control or hindlimb-suspension conditions. Ec.ES, endocortical eroded surface. *Significant difference between anti-resorptive(ZOL or OPG, P 0.05) and PBS within the loaded-control or hindlimb-suspended groups. †Significant effect of loading condition (loaded vs. hindlimbsuspended, P 0.05) within PBS, ZOL, or OPG treatment groups.
Table 5. Hindlimb suspension study: Percent mineralization of diaphysis, epiphysis, and whole mouse femurs fromhindlimb-suspended and loaded-control mice
Loaded Controls Hindlimb Suspended
Femur Component PBS ZOL OPG PBS ZOL OPG
Whole bone 58.4�0.3 60.1�0.1 60.1�0.2* 56.4�0.3 58.4�0.3 57.6�0.2*Epiphysis 56.8�0.2* 58.0�0.1* 57.5�0.2* 52.8�0.3* 55.2�0.9* 54.8�0.2*Diaphysis 62.7�0.3 63.8�0.1 62.8�0.1 61.7�0.2 63.3�0.7 62.3�0.1
Values are means � SE in %mineralization. Six-week-old mice were administered a subcutaneous injection of PBS or anti-resorptive (45 �g/kg ZOL or 500�g/kg OPG) and killed after 14 days of loaded-control or hindlimb-suspension conditions. *Significant effect of loading condition (loaded vs. hindlimbsuspended, P 0.05) within PBS, ZOL, or OPG treatment groups.
736 COMPARABLE ANTI-RESORPTIVE DOSING
J Appl Physiol • VOL 104 • MARCH 2008 • www.jap.org

results throughout this “proof-of-concept” study highlight theapplicability of the results.
Therapeutic Translation
The development of an effective therapeutic countermeasureto spaceflight-induced osteoporosis should not be undertakenwithout regard for the long-term health of the astronaut popu-lation. Excessive anti-resorptive treatment and severe inhibi-tion of bone resorption may not be necessary to protect anastronaut’s skeletal system from the temporary stress of thespace environment. Compared with PBS control, administra-tion of high-dose anti-resorptives (i.e., 10 mg/kg ZOL, 20mg/kg OPG) in the present study was found to result in greatertrabecular volume fraction and connectivity, which both in-creased by one-third compared with PBS (Fig. 1). One of themost important properties of a protein-based treatment, such asDenosumab or the PTH analog Teriparatide (Forteo, Eli Lilly,Indianapolis, IN), is that they do not become incorporated intobone like bisphosphonates. These drugs are also cleared fromthe body more quickly and are less likely to adversely suppressbone turnover postflight. Despite these beneficial properties,the concomitant issue of bone turnover inhibition with eitherOPG or ZOL is important to consider.
One could administer an arbitrarily high dose of ZOL, OPG,or another anti-resorptive and effectively inhibit bone resorp-tion and minimize bone loss in microgravity. However, theserious effects on bone turnover and detrimental long-termeffects on recovery could result in a net negative balance forthe astronaut. Previous studies have highlighted the bluntedanabolic response to agents such as PTH when given followinganti-resorptive therapies (3, 11). These postflight recoveryconsiderations are especially important considering the relativeyouth of astronauts, who would be expected to have at least 40more productive years of life following their mission. A refineddosing regimen that incorporates the desirable response inregard to bone microarchitecture, with minimal adverse effectson turnover, is clearly required.
Although ZOL has the potential to be administered intrave-nously as infrequently as once a year (3), the relative ease andsafety of a SC Denosumab injection in microgravity is aconsideration. Alternatively, oral bisphosphonates, such asalendronate, may prove to be the most convenient option, asthey have fewer risks of complication during administration(8). Furthermore, it would not be prudent to discount otherFDA approved bisphosphonates, such as ibandronate andrisedronate. In particular, risedronate has a less profound effecton bone turnover than other agents in this class (10).
The refinement of this minimally efficacious dosing regimenclearly has application only to the specific animal model forwhich it was developed. Ultimately, a human clinical trial, withan objective similar to the present study, would need to beconducted in normally loaded patients. The relative dosingratios recommended here (�1:10 for ZOL/OPG) would be areasonable starting point for administration. Such a studywould utilize dual-energy X-ray absorptiometry, peripheralquantitative computed tomography, serum markers, and ideallya bone biopsy to evaluate outcomes and combined effects ontrabecular microarchitecture, cortical strength, and bone for-mation. The next logical step would be a follow-up bed-reststudy to evaluate the ability of the minimally efficacious
anti-resorptive dosing to ameliorate the effects of prolongeddisuse in humans.
Conclusion
The determination of 45 �g/kg ZOL and 500 �g/kg OPG asthe minimum, comparable, efficacious, anti-resorptive regimendemonstrates that bone quality can be preserved with low-doseanti-resorptive therapy. The fact that significant increases inbone microarchitecture can be achieved without reducingBFRs alludes to the potential of this type of regimen toameliorate the effects of long-duration spaceflight withoutinhibiting bone turnover postflight. Such countermeasurescould help to ensure astronaut health, mission safety, and thesuccess of future long-duration space exploration.
ACKNOWLEDGMENTS
The authors thank all members of the Godley-Snell Animal ResearchFacility and the Osteoporosis Biomechanics Laboratory (http://www.batemanlab.com) for assistance. We also thank Jenny Bourne for reviewing, editing, andformatting support.
GRANTS
This work is funded by the National Space Biomedical Research Institutethrough NASA NCC 9-58.
DISCLOSURES
Amgen Inc. provided the zoledronic acid and osteoprotegerin that wasutilized in this study. T. Bateman is the recipient of a monetary gift fromAmgen Inc.
REFERENCES
1. Bateman TA, Dunstan CR, Ferguson VL, Lacey DL, Ayers RA,Simske SJ. Osteoprotegerin mitigates tail suspension-induced osteopenia.Bone 26: 443–449, 2000.
2. Bekker PJ, Holloway DL, Rasmussen AS, Murphy R, Martin SW,Leese PT, Holmes GB, Dunstan CR, DePaoli AM. A single-doseplacebo-controlled study of AMG 162, a fully human monoclonal anti-body to RANKL, in postmenopausal women. J Bone Miner Res 19:1059–1066, 2004.
3. Black DM, Delmas PD, Eastell R, Reid IR, Boonen S, Cauley JA,Cosman F, Lakatos P, Leung PC, Man Z, Mautalen C, Mesenbrink P,Hu H, Caminis J, Tong K, Rosario-Jansen T, Krasnow J, Hue TF,Sellmeyer D, Eriksen EF, Cummings SR. Once-yearly zoledronic acidfor treatment of postmenopausal osteoporosis. N Engl J Med 356: 1809–1822, 2007.
4. Black DM, Greenspan SL, Ensrud KE, Palermo L, McGowan JA,Lang TF, Garnero P, Bouxsein ML, Bilezikian JP, Rosen CJ. Theeffects of parathyroid hormone and alendronate alone or in combination inpostmenopausal osteoporosis. N Engl J Med 349: 1207–1215, 2003.
5. Body JJ, Lortholary A, Romieu G, Vigneron AM, Ford J. A dose-finding study of zoledronate in hypercalcemic cancer patients. J BoneMiner Res 14: 1557–1561, 1999.
6. Boyle WJ, Simonet WS, Lacey DL. Osteoclast differentiation andactivation. Nature 423: 337–342, 2003.
7. Broz JJ, Simske SJ, Greenberg AR, Luttges MW. Effects of rehydra-tion state on the flexural properties of whole mouse long bones. J BiomechEng 115: 447–449, 1993.
8. Cryer B, Binkley N, Simonelli C, Lewiecki EM, Lanza F, Chen E,Petruschke RA, Mullen C, de Papp AE. A randomized, placebo-controlled, 6-month study of once-weekly alendronate oral solution forpostmenopausal osteoporosis. Am J Geriatr Pharmacother 3: 127–136,2005.
9. Dempster DW, Cosman F, Kurland ES, Zhou H, Nieves J, Woelfert L,Shane E, Plavetic K, Muller R, Bilezikian J, Lindsay R. Effects of dailytreatment with parathyroid hormone on bone microarchitecture and turn-over in patients with osteoporosis: a paired biopsy study. J Bone MinerRes 16: 1846–1853, 2001.
737COMPARABLE ANTI-RESORPTIVE DOSING
J Appl Physiol • VOL 104 • MARCH 2008 • www.jap.org

10. Ding M, Day JS, Burr DB, Mashiba T, Hirano T, Weinans H, SumnerDR, Hvid I. Canine cancellous bone microarchitecture after one year ofhigh-dose bisphosphonates. Calcif Tissue Int 72: 737–744, 2003.
11. Finkelstein JS, Hayes A, Hunzelman JL, Wyland JJ, Lee H, Neer RM.The effects of parathyroid hormone, alendronate, or both in men withosteoporosis. N Engl J Med 349: 1216–1226, 2003.
12. Finkelstein JS, Leder BZ, Burnett SM, Wyland JJ, Lee H, de la PazAV, Gibson K, Neer RM. Effects of teriparatide, alendronate, or both onbone turnover in osteoporotic men. J Clin Endocrinol Metab 91: 2882–2887, 2006.
13. Fleisch HA. Bisphosphonates: preclinical aspects and use in osteoporosis.Ann Med 29: 55–62, 1997.
14. Gallagher JC. Role of estrogens in the management of postmenopausalbone loss. Rheum Dis Clin North Am 27: 143–162, 2001.
15. Globus RK, Bikle DD, Morey-Holton E. The temporal response of boneto unloading. Endocrinology 118: 733–742, 1986.
16. Greenspan SL, Harris ST, Bone H, Miller PD, Orwoll ES, Watts NB,Rosen CJ. Bisphosphonates: safety and efficacy in the treatment andprevention of osteoporosis. Am Fam Physician 61: 2731–2736, 2000.
17. Howard GA, Bottemiller BL, Turner RT, Rader JI, Baylink DJ.Parathyroid hormone stimulates bone formation and resorption in organculture: evidence for a coupling mechanism. Proc Natl Acad Sci USA 78:3204–3208, 1981.
18. Judex S, Boyd S, Qin YX, Miller L, Muller R, Rubin C. Combininghigh-resolution micro-computed tomography with material composition todefine the quality of bone tissue. Curr Osteoporos Rep 1: 11–19, 2003.
19. Lane HW, Smith SM. Physiological adaptations to space flight. LifeSupport Biosph Sci 6: 13–18, 1999.
20. Lang T, LeBlanc A, Evans H, Lu Y, Genant H, Yu A. Cortical andtrabecular bone mineral loss from the spine and hip in long-durationspaceflight. J Bone Miner Res 19: 1006–1012, 2004.
21. Lang TF, Leblanc AD, Evans HJ, Lu Y. Adaptation of the proximalfemur to skeletal reloading after long-duration spaceflight. J Bone MinerRes 21: 1224–1230, 2006.
22. Lawler A. Space exploration. Scientists add up gains, losses in Bush’snew vision for NASA. Science 303: 444–445, 2004.
23. LeBlanc AD, Driscol TB, Shackelford LC, Evans HJ, Rianon NJ,Smith SM, Feeback DL, Lai D. Alendronate as an effective countermea-sure to disuse induced bone loss. J Musculoskelet Neuronal Interact 2:335–343, 2002.
24. Markin AA, Zhuravleva OA, Morukov BV, Vostrikova LV, Zabolots-kaia IV, Poluektova VP. [Characteristics of cosmonauts’ metabolismafter extended missions on the international space station]. AviakosmEkolog Med 39: 36–41, 2005.
25. Martin TJ. Hormones in the coupling of bone resorption and formation.Osteoporos Int 3, Suppl 1: 121–125, 1993.
26. McClung MR, Lewiecki EM, Cohen SB, Bolognese MA, WoodsonGC, Moffett AH, Peacock M, Miller PD, Lederman SN, Chesnut CH,
Lain D, Kivitz AJ, Holloway DL, Zhang C, Peterson MC, Bekker PJ.Denosumab in postmenopausal women with low bone mineral density.N Engl J Med 354: 821–831, 2006.
27. Midura RJ, Su X, Androjna C. A simulated weightlessness state dimin-ishes cortical bone healing responses. J Musculoskelet Neuronal Interact6: 327–328, 2006.
28. Neer RM, Arnaud CD, Zanchetta JR, Prince R, Gaich GA, ReginsterJY, Hodsman AB, Eriksen EF, Ish-Shalom S, Genant HK, Wang O,Mitlak BH. Effect of parathyroid hormone (1–34) on fractures and bonemineral density in postmenopausal women with osteoporosis. N EnglJ Med 344: 1434–1441, 2001.
29. Parfitt AM, Drezner MK, Glorieux FH, Kanis JA, Malluche H,Meunier PJ, Ott SM, Recker RR. Bone histomorphometry: standardiza-tion of nomenclature, symbols, and units. Report of the ASBMR Histo-morphometry Nomenclature Committee. J Bone Miner Res 2: 595–610,1987.
30. Rodan GA, Fleisch HA. Bisphosphonates: mechanisms of action. J ClinInvest 97: 2692–2696, 1996.
31. Simske SJ, Greenberg AR, Luttges MW. Effects of suspension-inducedosteopenia on the mechanical behaviour of mouse long bones. J Mater SciMater Med 2: 43–50, 1991.
32. Simske SJ, Guerra KM, Greenberg AR, Luttges MW. The physical andmechanical effects of suspension-induced osteopenia on mouse longbones. J Biomech 25: 489–499, 1992.
33. Smith SM, Wastney ME, Morukov BV, Larina IM, Nyquist LE,Abrams SA, Taran EN, Shih CY, Nillen JL, Davis-Street JE, Rice BL,Lane HW. Calcium metabolism before, during, and after a 3-mo space-flight: kinetic and biochemical changes. Am J Physiol Regul Integr CompPhysiol 277: R1–R10, 1999.
34. Smith SM, Wastney ME, O’Brien KO, Morukov BV, Larina IM,Abrams SA, Davis-Street JE, Oganov V, Shackelford LC. Bone mark-ers, calcium metabolism, and calcium kinetics during extended-durationspace flight on the mir space station. J Bone Miner Res 20: 208–218, 2005.
35. Tesch PA, Berg HE, Bring D, Evans HJ, LeBlanc AD. Effects of 17-dayspaceflight on knee extensor muscle function and size. Eur J Appl Physiol93: 463–468, 2005.
36. Tilton FE, Degioanni JJ, Schneider VS. Long-term follow-up of Skylabbone demineralization. Aviat Space Environ Med 51: 1209–1213, 1980.
37. Tommasini SM, Nasser P, Schaffler MB, Jepsen KJ. Relationshipbetween bone morphology and bone quality in male tibias: implicationsfor stress fracture risk. J Bone Miner Res 20: 1372–1380, 2005.
38. Vico L, Collet P, Guignandon A, Lafage-Proust MH, Thomas T,Rehaillia M, Alexandre C. Effects of long-term microgravity exposureon cancellous and cortical weight-bearing bones of cosmonauts. Lancet355: 1607–1611, 2000.
39. Zayzafoon M, Meyers VE, McDonald JM. Microgravity: the immuneresponse and bone. Immunol Rev 208: 267–280, 2005.
738 COMPARABLE ANTI-RESORPTIVE DOSING
J Appl Physiol • VOL 104 • MARCH 2008 • www.jap.org
Copyright © 2022 FDOKUMEN




















