Developing advanced rural nursing practice: A whole new scope of responsibility
6
Collegian (2011) 18, 177—182 av ailab le at www.sciencedirect.com jo ur nal homep age: www.elsevier.com/locate/coll Developing advanced rural nursing practice: A whole new scope of responsibility Robyn Cant, PhD, MHlthSc, GradDipHEd a , Melanie Birks, PhD, MEd, BN; DipAppSci(Nsg), RN, FRCNA b , Joanne Porter, MN, GradDipCritCare, BN, RN a , Elisabeth Jacob, MEd, GradDipCritCare, DipAppSc(Nsg), RN a , Simon Cooper, PhD, MEd, BA, RGN a,∗ a School of Nursing and Midwifery, Monash University, Churchill, Vic 3842, Australia b Central Queensland University, Noosa Campus, PO Box 1128, Noosaville, QLD 4566, Australia Received 17 May 2011; received in revised form 28 July 2011; accepted 2 August 2011 KEYWORDS Advanced nursing; Autonomy; Rural nursing; Scope of practice Summary Rural registered nurses’ experiences of advanced clinical nursing practice were explored whilst they were enrolled in an advanced primary care course of study. Thirty-two nurses employed in rural health services in Victoria, Australia, studied advanced practice nurs- ing by distance education with a clinical component. At course conclusion, focus groups and a quantitative on-line survey were conducted to explore outcomes. Nurses reported positive self- perceptions of their educational preparation with scores of >7/10 for competence, confidence, preparedness for advanced practice and job satisfaction. Focus group discussions concurred with positive survey results. The course was valuable in developing skills and knowledge, enabling more holistic patient care. The main themes that emerged related to the advancement of the nurse as a professional, and enhancement of patient care. Within their scope of practice, nurses assessed, diagnosed and treated minor patient illness presentations either independently or collaboratively with medical advice. The context of rural health services dictated practice and levels of autonomy. Nurses perceived the new role reduced an overload of medical work, whilst increasing patients’ access to care. As a result of the course 24% of participants reported a change in their work role. Nurses employed in rural health services reported positive potential for advanced collaborative practice in rural health care, in association with medical profession- als. Defined role boundaries, role responsibilities and dedicated advanced practice positions will be required to achieve implementation of the role. © 2011 Royal College of Nursing, Australia. Published by Elsevier Australia (a division of Reed International Books Australia Pty Ltd). All rights reserved. ∗ Corresponding author. Tel.: +61 3 99026627; fax: +61 3 99026527. E-mail addresses: [email protected] (R. Cant), [email protected] (S. Cooper). 1322-7696/$ — see front matter © 2011 Royal College of Nursing, Australia. Published by Elsevier Australia (a division of Reed International Books Australia Pty Ltd). All rights reserved. doi:10.1016/j.colegn.2011.08.001
-
Upload
independent -
Category
Documents
-
view
5 -
download
0
Transcript of Developing advanced rural nursing practice: A whole new scope of responsibility

Collegian (2011) 18, 177—182
av ai lab le at www.sc iencedi rec t .com
jo ur nal homep age: www.elsev ier .com/ locate /co l l
Developing advanced rural nursing practice:A whole new scope of responsibility
Robyn Cant, PhD, MHlthSc, GradDipHEda,Melanie Birks, PhD, MEd, BN; DipAppSci(Nsg), RN, FRCNAb,Joanne Porter, MN, GradDipCritCare, BN, RNa,Elisabeth Jacob, MEd, GradDipCritCare, DipAppSc(Nsg), RNa,Simon Cooper, PhD, MEd, BA, RGNa,∗
a School of Nursing and Midwifery, Monash University, Churchill, Vic 3842, Australiab Central Queensland University, Noosa Campus, PO Box 1128, Noosaville, QLD 4566, Australia
Received 17 May 2011; received in revised form 28 July 2011; accepted 2 August 2011
KEYWORDSAdvanced nursing;Autonomy;Rural nursing;Scope of practice
Summary Rural registered nurses’ experiences of advanced clinical nursing practice wereexplored whilst they were enrolled in an advanced primary care course of study. Thirty-twonurses employed in rural health services in Victoria, Australia, studied advanced practice nurs-ing by distance education with a clinical component. At course conclusion, focus groups and aquantitative on-line survey were conducted to explore outcomes. Nurses reported positive self-perceptions of their educational preparation with scores of >7/10 for competence, confidence,preparedness for advanced practice and job satisfaction. Focus group discussions concurred withpositive survey results. The course was valuable in developing skills and knowledge, enablingmore holistic patient care. The main themes that emerged related to the advancement ofthe nurse as a professional, and enhancement of patient care. Within their scope of practice,nurses assessed, diagnosed and treated minor patient illness presentations either independentlyor collaboratively with medical advice. The context of rural health services dictated practiceand levels of autonomy. Nurses perceived the new role reduced an overload of medical work,whilst increasing patients’ access to care. As a result of the course 24% of participants reporteda change in their work role. Nurses employed in rural health services reported positive potential
for advanced collaborative practice in rural health care, in association with medical profession-als. Defined role boundaries, role responsibilities and dedicated advanced practice positions willbe required to achieve implementation of the role.© 2011 Royal College of NursingInternational Books Australia Pt∗ Corresponding author. Tel.: +61 3 99026627; fax: +61 3 99026527.E-mail addresses: [email protected] (R. Cant), simon.j.cooper
1322-7696/$ — see front matter © 2011 Royal College of Nursing, Australia. Published by Elsevie
doi:10.1016/j.colegn.2011.08.001
, Australia. Published by Elsevier Australia (a division of Reed
y Ltd). All rights reserved.@monash.edu (S. Cooper).
r Australia (a division of Reed International Books Australia Pty Ltd). All rights reserved.

1
I
TbuhobfitMete
nCtitiar(otssrt2
gcoiKAtitpt2(dvra
ttnsaPTtari
atac
M
Qs(luws
dttbnvuwic
ulcoAealiawaims
R
Oattended one of the four focus groups. Thirty-two of thecourse participants (84%) responded to an on-line question-naire.
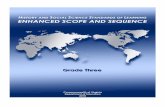
1. QUALITATIVE PHASE
Focus group s
2. QUANITITATIVE PHASE
INTERPRE TATION :Qualitati ve + quantitati ve resultsComparis onData re ductionStatist ica l inference
78
ntroduction
he discipline of nursing continues to grow and developoth in terms of the breadth and scope of the workndertaken by professional nurses, and the impact thisas on the status of nursing as a profession. In the facef an increasingly complex health care system impactedy social, economic and technological factors, the needor nurses to practice beyond their traditional scope isncreasing. This is particularly the case in rural loca-ions and in non-traditional health care settings (Francis &ills, 2010). Although the scope of practice and associatedducational opportunities continue to grow, the nomencla-ure used to describe advanced practice roles is yet tovolve.
In some countries, the terms advanced practice nurse andurse practitioner are used interchangeably (Internationalouncil of Nurses, 2010) however in Australia they meanwo different things. The role of ‘nurse practitioner’ (NP)n an advanced nursing position are recognized and creden-ialed. However, the role of ‘advanced practice’ (AP) nursess as yet undetermined. Nurses qualified to practice at andvanced level are fulfilling expanded roles in Australianural health services in response to workforce demandsCooper, Birks, Porter, & Cant, 2010). The Royal Collegef Nursing Australia (2006) describes this role as regis-ered nursing practice ‘that utilises extended and expandedkills, experience and knowledge in assessment, diagno-is, planning, implementation and evaluation of the careequired’ for a patient. The roles are dependent on the con-ext of the health service (International Council of Nurses,010).
Advanced roles usually require education at a post-raduate level, with expectations of a higher level ofompetence than for a registered nurse (RN) (Royal Collegef Nursing Australia, 2006). Whilst acknowledging thencreased knowledge, skills and functioning of AP nurses,ucera, Higgins, & McMillan (2010) suggest that what setsP nursing apart from other roles is the primary focus ofhe nurse on the patient. The AP nurse can start patientnvestigations to determine a provisional diagnosis andhen begin treatment (Francis & Mills, 2010). Advancedractice competencies have been linked with a more holis-ic model of patient care (Daly & Carnwell, 2003; Por,008). However, Duffield, Gardner, Chang, Fry, and Stasa2011) suggest that in Australia, an ad hoc approach toeveloping these new nursing practice roles based uponarious specific demands has led to a blurring of theoles and responsibilities; a factor that now needs to beddressed.
As there is no consensus description of advanced prac-ice, we set out to explore the views of nurses who enacthese roles. The current paper reports on rural registeredurses’ experiences of clinical nursing having undertakentudies in advanced nursing practice. The nurses completed
Post Graduate Certificate of Rural and Remote Advancedrimary Health Care by flexible study mode over 12 months.his aimed to enable AP nurses to work collaboratively,
o conduct comprehensive health assessments and to plannd articulate care based on clinical evidence. Nurses wereequired to conduct assessments and undertake the AP rolen their workplaces. The course prepares nurses to practice FR. Cant et al.
t advanced nurse level but not as accredited nurse prac-itioners. An evaluation of participants’ study experiencend clinical practice component was conducted at courseonclusion in May 2010.
ethods
ualitative and quantitative research techniques were cho-en to access the nurses’ views, using a convergence designCreswell & Plano Clark, 2007) (Fig. 1). Prior to data col-ection, the project received ethics approval from theniversity’s human research ethics committee. Consistentith this approval, all participants provided written con-
ent.Initially, a convenience sample of 25 postgraduate stu-
ents participated in one of four focus groups convened byhe researchers in the last week of their study course. Par-icipants were asked how clinical practice was influencedy the training course and about their perceptions of APursing roles. Audio-recorded narratives were transcribederbatim and then open-coded thematically to develop annderstanding of patterns of response. Coding and analysisas conducted by a researcher independent of the teach-
ng staff (RC) with agreement upon identified themes beingonfirmed by two of the authors (RC; JP).
Subsequently, a purposely developed questionnaire wassed to collect data with content and face validity estab-ished through stakeholder review. Thirty-six open andlosed questions asked about knowledge and skills devel-pment, knowledge translation and collaborative practice.nswers were either dichotomous (Yes/No), rated on a Lik-rt scale of 1—5 or 1—10, or asked for open text. Thenonymized survey was administered electronically (on-ine) one week after the focus groups were conducted,nitially by e-mailed invitation to participate (with a link toccess the survey) from the course convenor. Collated dataas downloaded from the Internet for analysis using SPSSs a database and analysis was conducted by a researcherndependent of the teaching staff. As the survey was anony-ous, no tracking of participant responses over the two
tudy phases was possible.
esults
f 38 nurses who completed the course curriculum, 25
Self-reporte d questi onnaire
igure 1 Research design: convergence triangulation model.

ope
hapafib
mtto
f
aNtsitpr
nf
iciraf
Developing advanced rural nursing practice: A whole new sc
Characteristics of participating nurses
Questionnaire responders were predominantly female (97%)with a median year of first nurse registration 1989 (range1976—2005). Nearly all described their current clinical roleas being in a rural hospital in the state of Victoria. Theiremployment was predominately in senior nursing roles suchas a nurse unit manager or associate nurse unit manager ina medical, surgical or emergency ward.
Themes from focus groups and survey results
The survey results concurred with focus group themes. Dis-cussions about nursing roles centred on the high value ofthe course in developing the nurses’ skills and knowledge,enabling more holistic patient care. The main themes iden-tified from the analysis were developing skills for advancedpractice and enhancing patient care. These are explored inthe following discussion, with illustrative quotations.
Developing skills for advanced practice
In the survey, nurses were asked whether they had all theessential knowledge required for the current role; 28 of 32(88%) were in agreement. When asked whether they had allthe essential clinical skills required for the advanced role, 23of 32 (72%) agreed. In the survey (questionnaire) and in focusgroup discussions, nurses described numerous ways in whichtheir clinical knowledge and skills had improved. Some ofthese topics were: local anaesthetic infiltration, suturingand plastering, ECG recognition, heart and breath soundsand ear and eye examinations. They frequently mentionedtheir enhanced ability to conduct detailed patient assess-ments and viewed this as a great benefit to their nursingpractice. Fourteen of 31 nurses (45%) claimed that prior tothe course they were able to conduct comprehensive healthassessments and to plan and articulate care requirements.with all (100%) agreeing that the course had enhanced thisability. Nurses were working at a higher level in a moreautonomous role.
More decision-making, more autonomy and taking a bitmore accountability with your decisions and actions.(Focus group 1)
. . .when a patient comes in, you look at the differentaspects now, whereas I would have just concentrated onwhat they were complaining about. (Focus group 3)
[You’re] The person making the judgment calls. (Focusgroup 2)
Skills enhancement resulted in a change of practice; theynow considered the ‘whole picture’ compared to previouslyconducting a nursing admission assessment and handing thecase over to a doctor for diagnosis and management. Prac-tice was based on evidence, commonly with utilization ofclinical resource manuals. Furthermore, respondents arguedthat they could now identify gaps in their knowledge and
had gained the confidence to ask for information from otherhealth professionals when necessary.Participants perceived an improvement in their phar-macology knowledge, with more in-depth understanding of
of responsibility 179
ow, as well as why, medications were prescribed. Most wereble to prescribe some drugs when this was within the unit’sractice protocol, or else they utilized telephoned medicalpproval. With new skills nurses reported feeling more con-dent, able to perform complex health assessments and toegin a patient’s treatment.
[I’m] a lot more confident in what my clinical skills are,and that’s because I am constantly analyzing, [thinking]- how could I have missed that? (Focus group 4)
Advanced practice experience during the course includedanaging patients in emergency departments. Nurses found
hemselves practicing systematically with use of criticalhinking skills in an effort to resolve the broader aspectsf a patient’s medical condition.
People who haven’t done this course . . .they’re just inthis square box and they don’t look for - more lateralthinking. (Focus group 2)
They also reported that advanced nursing skills allowedor earlier intervention with a patient.
I notice that we pick up on things a lot earlier. . . Yeh, soyou pick up on the signs that this patient, even in theward and not necessarily in the ED- but, you pick up thatthey are not well and you are able to quickly get ontothat. (Focus group 2)
Participants were asked about inter-professional workingnd collaborative practice in the survey and in focus groups.early all nurses had collaborated inter-professionally inhe last 12 months with medical staff, allied health profes-ionals (physiotherapists, podiatrists, etc.), and paramedicsn situations which included referrals to emergency, men-al health, palliative care, diabetes educators, speechathologists and various social services. Survey participantseported positive relationships with their colleagues.
I feel comfortable and confident in reporting my assess-ment and findings for patients and I have no problemswith reiterating my opinions and questioning their treat-ment if I am unsure of the reason for their decisions.The GPs are always very open for discussion and I findthis works very well for the care of each patient. (Surveyrespondent)
There was respect for these enhanced skills with recog-ition by colleagues (both nursing and medical) of the needor autonomous practice in rural primary health care.
When it comes to working with the doctors, its enhancedteam work much, much better. (Focus group 4)
However, barriers to collaborative practice were alsodentified; for example differences in opinion over medi-ation management including ‘blocking’ of standing orders;nformation sharing failures; referral restrictions (e.g. someeferrals made only through GPs); lack of acknowledgmentnd respect for advanced nursing skills by the medical pro-ession, and change management issues, for example:
. . .doctors not having time to discuss issues. Doctorsnot wanting to collaborate, as they wish to act alone.Inadequate systems in place to make collaboration user-friendly. (Survey respondent)

1
crrn
hafA
E
Riabie
pearra
nf
mmnlp
lwctut
D
AfiefsdnihPrtiKajiifyoceh1
re(teNa
80
Other senior nurses are threatened by this new pro-cess. (Survey respondent)
Respondents resolved some of these issues with improvedommunication techniques, education, and building aespectful relationship, but as one indicated, financialeward systems restrict the development of autonomousursing practice.
Why would they (want to overcome collaborative barri-ers)? The GP might need to see the patient to check meds,etc. But for some patients it’s a barrier as they don’t needto see the GP, but are told no review unless they do. Thiscan be a cost of $30 for 1 minute. (Survey respondent)
For three-quarters of the nurses (76%) the course of studyad positively impacted on workload and there was 100%greement that the course had increased their work satis-action. However there were still identified challenges forP nurses working in rural locations.
The distance study has in many ways prepared us for thatlonely role that we do every day: to work independentlyand autonomously. (Survey respondent)
nhancing patients’ access to care
espondents also suggested that their learning resultedn a considerable impact on patients, including improvedssessment leading to enhanced treatment decisions, triageenefits, quicker access to treatment (e.g. suturing), andmproved medication management and safety netting, forxample:
A patient presenting with anaphylaxis was quickly andthoroughly assessed, managed and supported in returninghome. I didn’t have to wait for the MO to come before Iwas able to implement appropriate management. (Surveyrespondent)
I am able to complete a comprehensive assessment, reacha definitive diagnosis and initiate care appropriate to thepatient’s needs. When legislation is passed, I will be ableto minimise time for the patients in the A&E by elimi-nating the need to contact the GP to order treatment.(Survey respondent)
Most nurses reported spending increased time with eachatient. They were better able to provide patients withducation about their presenting condition/s; perceiveds empowering a patient towards self-care and possiblyeducing their need for re-presentation. Patients would beeferred on to other services as needed. AP roles were seens improving care pathways:
. . . if we are able to take those triage 4’s and 5’s and stopringing the doctor in the middle of the night, the reten-tion in our area of medical services is going to be higher. . .
Because, advance care practice will allow us to do that;it comes with a whole new scope of responsibility. (Focusgroup 3)
There was respect for these enhanced skills with recog-ition by colleagues (both nursing and medical) of the needor autonomous practice in rural primary health care.
C
oe
R. Cant et al.
..one of our doctors when they saw the depth that I hadbeen working at to do this course, they actually had a lotmore respect for me as a nurse and had discussed thingsreally openly.. I think it’s more of a team collaborationthing, for the patient. (Focus group 1)
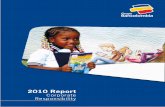
Themes from focus groups related to knowledge enhance-ent and practice development are illustrated in a conceptodel showing the transition from registered nurse to AP
urse (Fig. 2). Learning outcomes resulted in improved col-aborative team work and perceptions of positive impact onatient care.
In spite of these positive perceptions, there were majorimitations to the success of the AP role because the roleas experimental and unfunded. Frustrations were voicedoncerning hospital organisational structures and expecta-ions that nurses would undertake AP roles in addition to thesual senior management positions—–as was the case duringhe nurses’ study experience.
‘I found it really difficult to run the ED and do that role.’(Focus group 1)
iscussion
dvanced clinical nursing roles are as yet embryonic. Thesendings indicate that advanced nursing practice was deliv-red in various ways in rural health services. Feedbackrom this group of nurses is of value to inform the profes-ion about current practice issues and to forecast strategicirections for training and role development. The move toational registration of the nursing profession in Australian 2010 (Commonwealth of Australian Governments, 2008)ighlights the fact that, unlike Registered Nurse or Nurseractitioners, advanced practice nursing has no nationalecognition nor agreed role definition. It is evident thathis is a dilemma because different jurisdictions have differ-ng rules and authorizations for advanced practice (Turner,eyzer, & Rudge, 2007). Some authors (Duffield et al., 2011)rgue that it is time for standardization of nursing roles,ob titles and responsibilities throughout the country. Thiss confirmed in the current study, where nurses were pos-tive about the potential for AP nursing in rural centres,elt well equipped for the new role following their studies,et found significant practice barriers due to industrial andrganisational structures. Other studies in Australia haveoncluded that rural nurses already work in advanced gen-ralist roles due to the lack of on-site medical and alliedealth staff (Hegney, 1997; Hegney, McCarthy, & Pearson,999).
Advanced practice roles need to be formalized by policy,egulation and pay structures to avoid the role delin-ation difficulties experienced by NPs in rural AustraliaTurner et al., 2007). The development of specific compe-ency standards for AP roles, such as those that currentlyxist to ensure consistency of standards for Registeredurses (Australian Nursing and Midwifery Council, 2006b),nd Nurse Practitioners (Australian Nursing and Midwifery
ouncil, 2006a) will aid in this formalisation process.The AP roles described by participants concur with previ-us studies that describe AP as both role expansion and rolextension (Daly & Carnwell, 2003). Nurses conducted full

Developing advanced rural nursing practice: A whole new scope of responsibility 181
Depth of cri tic al thinking
Pharmac ology knowledge
DEVELOPING AP SKILLS
Deeper knowle dge
Assessment
IMPROVED PAT IENT ACCESS TO CARE
PATIENT ED UCATI ON AN D EMPOWER MENT
COMMUNITY EN GAGEMEN T & PRE VEN TIVE HEAL TH PROMOTI ON
Team collaboration & Mutual r espect
ENHANCING PATIENT CARE
Increa sed confidence Lea der in evidence based prac tice
Holisti c patient ca re Greater re sponsibility
to d
ae(nsehif
bp2wcw(mtW
Figure 2 Concept model of nurses’ engagement with learning
assessments of patients presenting to emergency depart-ments who sat at the lower end of the triage scale (category4 or 5) with minor conditions. For some diagnoses, they wereable to treat the patient according to the local practicepolicies and in so doing, might relieve some of the treat-ment burdens for doctors- whether or not medical staffwere on duty. The new skills/knowledge enabled expan-sion of the nurses’ clinical roles to include diagnosing,suturing or plastering and limited medication supply. Roleextension included education of patients, referral to otherservices and conducting followup. There was greater col-laboration with medical team members such as a generalpractitioner. In these respects, the role did not differ signif-icantly from expectations of the fully autonomous practiceof a more qualified nurse practitioner (Australian Nursingand Midwifery Council, 2006a). It should be noted, however,that the NP role extends beyond autonomous clinical nursingto include higher level clinical leadership with ‘‘a readinessand an obligation to advocate for their client base and theirprofession at the systems level of health care’’ (Carryer,Gardner, Dunn, & Gardner, 2007:1818). There has been ques-
tioning of the definition of autonomous practice when nurseswork not independently, but within a team of health profes-sionals (Turner et al., 2007). From our results, it is apparentthat this question is largely unresolved.omnD
evelop skills for advanced practice and the perceived impact.
Advanced practice that requires role extension withcceptance of greater responsibility is consistent withxpectations of career advancement that Francis and Mills2010) describe as necessary to arrest staff attrition in theursing workforce. Our participants reported greater jobatisfaction, which is in keeping with a staff retention strat-gy. Furthermore, and as suggested by the previous authors,ealth services will need to change to accept responsibil-ty for a higher level of nursing continuing education in theuture to maintain this extended scope of nursing practice.
This study has raised issues of role classification and roleoundaries. Nurses were fully focused on the needs of theatient as described in the defining literature (Kucera et al.,010) and aimed to provide holistic care (Por, 2008). Thereas agreement, however, that they were unable to performomprehensive patient assessments and treat new patientshilst simultaneously maintaining their substantive role
such as Nurse Unit Manager). Whilst advanced nursing rolesay assist rural and remote health services to better meet
he needs of patients and to fill a practice gap (Williamson,ebb, Abelson-Mitchell, & Cooper, 2006), further study
f workforce allocation is required to establish realisticodels for AP that are economic and meet health serviceseeds over a number of roster shifts. Bryant-Lukosius andiCenso (2004), for example, describe a framework for

1
itAaGmmorrao
iACddi
C
Naaaiahstwi
C
StE
A
TSt
R
A
A
B
C
C
C
C
C
D
D
F
H
H
I
K
P
R
T
82
mplementing AP nursing roles in Canada. They suggest thathe implementation process itself improves recognition ofP nurses’ skills and knowledge, with greater collaborationnd integration into health care systems. Further, Chang,ardner, Duffield, and Ramis (2010) developed a consensusodel for role delineation of AP nurses versus NP thatight assist the implementation process. Clear articulation
f how AP nurses function within the health care team inelationship with NPs and RNs is also necessary to avoidole confusion and ambiguity. This development might bessisted by trialing of fulltime AP roles in rural sites whereur AP nurses reported positive experiences.
This study is limited by a number of design issues includ-ng self-reports from a small sample of nurses in one state ofustralia. This introduces potential for bias in the reporting.onsequently, the results may not translate into other workomains. Further work is needed to fully understand theevelopment and maintenance of advanced practice nursingn primary care settings.
onclusion
urses employed in rural health services reported theirdvanced practice training equipped them to work moreutonomously, to undertake detailed patient assessmentsnd begin or else manage treatment in the context ofnter-professional care. The AP nurse role was perceiveds impacting positively upon patients’ access to timelyealth care, especially in services without available medicaltaff. More defined role boundaries and role responsibilities,ogether with the establishment of dedicated AP positionsill be required to achieve routine advanced practice nurs-
ng in the rural health care environment.
ontributors
C, MB, JP contributed to the study design and data collec-ion. RC and JP conducted data analysis. MB, RC, JP, SC andJ drafted the paper.
cknowledgements
his study was funded by the Victorian Department of Humanervices. We wish to also acknowledge the nurses who con-ributed their views for this study.
eferences
ustralian Nursing and Midwifery Council. (2006). National com-petency standards for the nurse practitioner. Retrieved from.http://www.anmc.org.au
ustralian and Nursing Midwifery Council. (2006). Nationalcompetency standards for the registered nurse. Retrievedfrom. http://www.nursingmidwiferyboard.gov.au/Codes-and-Guidelines.aspx#competencystandards
W
R. Cant et al.
ryant-Lukosius, D., & DiCenso, A. (2004). A framework for theintroduction and evaluation of advanced practice nursing roles.Journal of Advanced Nursing, 48(5), 530—540.
arryer, J., Gardner, G., Dunn, S., & Gardner, A. (2007). Thecore role of the nurse practitioner: Practice, professionalismand clinical leadership. Journal of Clinical Nursing, 16(10),1818—1825.
hang, A. M., Gardner, G. E., Duffield, C., & Ramis, M. (2010). A Del-phi study to validate an advanced practice nursing tool. Journalof Advanced Nursing, 66(10), 2320—2330. doi:10.1111/j.1365-2648.2010.05367.x
ommonwealth of Australian Governments (COAG). (2008). Inter-governmental agreement for a national registration andaccreditation scheme for the health professions. Canberra:COAG.
ooper, S., Birks, M., Porter, J., & Cant, R. (2010). Evaluation ofthe rural and remote advanced primary care certificate course:A report prepared by Monash University for the Department ofHealth Victoria. Churchill, Victoria, Australia: Monash Univer-sity.
reswell, J., & Plano Clark, V. (2007). Designing and conductingmixed methods research. Thousand Oaks, California: Sage Pub-lications.
aly, W., & Carnwell, R. (2003). Nursing roles and levels of practice:A framework for differentiating between elementary, special-ist and advancing nursing practice. Journal of Clinical Nursing,12(2), 158—167. doi:10.1046/j.1365-2702.2003.00690.x
uffield, C., Gardner, G., Chang, A., Fry, M., & Stasa, H. (2011).National regulation in Australia: A time for standardisation inroles and titles. Collegian, 18(2), 45—49.
rancis, K. L., & Mills, J. (2010). Sustaining and growing therural nursing and midwifery workforce: Understanding theissues and isolating directions for the future. Collegian, 18(2),55—60.
egney, D. (1997). Extended, expanded, multi-skilled or advancedpractice?—–Rural nurses in Australia, 1991—1994. Collegian, 4(4),22—27.
egney, D., McCarthy, A., & Pearson, A. (1999). Effects of size ofhealth service on scope of rural nursing practice. Collegian, 6(4),21—26.
nternational Council of Nurses. (2010). International nursepractitioner—–Advance practice nursing network; practiceissues, definition and characteristics of the role. Retrievedfrom. http://icn-apnetwork.org/
ucera, K., Higgins, I., & McMillan, M. (2010). Advanced nursingpractice: A futures model derived from narrative analysis ofnurses’ stories. Australian Journal of Advanced Nursing, 27(4),43—53.
or, J. (2008). A critical engagement with the concept of advancingnursing practice. Journal of Nursing Management, 16(1), 84—90.
oyal College of Nursing Australia. (2006). Position statement:Advanced practice nursing. Retrieved from. http://www.rcna.org.au
urner, C., Keyzer, D., & Rudge, T. (2007). Spheres of influenceor autonomy? A discourse analysis of the introduction of nursepractitioners in rural and remote Australia. Journal of AdvancedNursing, 59(1), 38—46. doi:10.1111/j.1365-2648.2007.04275.x
illiamson, G. R., Webb, C., Abelson-Mitchell, N., & Cooper, S.(2006). Change on the horizon: Issues and concerns of neophyteadvanced health care practitioners. Journal of Clinical Nursing,15(9), 1091—1098. doi:10.1111/j.1365-2702.2005.01462.x