
Design of a Consensus-Derived Synoptic Operative Report for Lung Cancer Surgery
6
Design of a Consensus-Derived Synoptic Operative Report for Lung Cancer Surgery Laura Schneider, BS, Yaron Shargall, MD, Colin Schieman, MD, Andrew J. Seely, MD, PhD, Sadeesh Srinathan, MD, MS, Richard A. Malthaner, MD, MS, Andrew F. Pierre, MD, MS, Najib Safieddine, MD, Rosaire Vaillancourt, MD, Madelaine Plourde, MD, James Bond, MD, Scott Johnson, MD, MS, Shona E. Smith, MD, and Christian J. Finley, MD, MPH Department of Surgery, McMaster University, St. Joseph’s Healthcare Hamilton, Hamilton, Ontario; Department of Surgery, University of Ottawa, Ottawa Hospital General Campus, Ottawa, Ontario; Department of Surgery, University of Manitoba, Health Sciences Centre, Winnipeg, Manitoba; Departments of Surgery and Epidemiology and Biostatistics, University of Western Ontario, London Health Sciences Centre, London, Ontario; Department of Surgery, University of Toronto, Toronto General Hospital, Toronto, Ontario; Department of Surgery, Toronto East General Hospital, Toronto, Ontario; Department of Surgery, University of Laval, Quebec Heart and Lung Institute, Qu ebec, Quebec; Department of Surgery, Dalhousie University, Queen Elizabeth II Health Sciences Centre, Halifax, Nova Scotia; Department of Surgery, University of British Columbia, Surrey Memorial Hospital, Surrey, British Columbia; Department of Surgery, University of Alberta, Royal Alexandra Hospital, Edmonton, Alberta; and Department of Surgery, Northern Ontario School of Medicine, Sudbury, Ontario, Canada Background. For lung cancer surgery, a narrative operative report is the standard reporting procedure, whereas a synoptic-style report is increasingly utilized by healthcare professionals in various specialties with great success. A synoptic operative report more succinctly and accurately captures vital information and is rapidly generated with good intraobserver reliability. The objective of this study was to systematically develop a synoptic operative report for lung cancer surgery following a modified Delphi consensus model with the support of the Canadian thoracic surgery community. Methods. Using online survey software, thoracic sur- geons and related physicians were asked to suggest and rate data elements for a synoptic report following the modified Delphi consensus model. The consensus exercise-derived template was forwarded to a small working group, who further refined the definition and priority designation of elements until the working group had reached a satisfactory consensus. Results. In all, 139 physicians were invited to participate in the consensus exercise, with 36.7%, 44.6%, and 19.5% response rates, respectively, in the three rounds. Eighty-nine elements were agreed upon at the conclusion of the exercise, but 141 elements were for- warded to the working group. The working group agreed upon a final data set of 180 independently defined data elements, with 72 mandatory and 108 optional elements for implementation in the final report. Conclusions. This study demonstrates the process involved in developing a multidisciplinary, consensus- based synoptic lung cancer operative report. This novel report style is a quality improvement initiative to improve the capture, dissemination, readability, and potential utility of critical surgical information. (Ann Thorac Surg 2014;97:1163–8) Ó 2014 by The Society of Thoracic Surgeons O perative reporting is a necessary task after the completion of any surgical procedure. In lung can- cer surgery, the primary purpose of the operative report is to document and communicate information to other surgeons, physicians, and healthcare providers to ensure critical information is captured, findings are communi- cated, and care is well coordinated. Lung cancer represents a tremendous burden of dis- ease on Canadian and international healthcare systems. In Canada and the United States, lung cancer is the leading cause of cancer-related death, more than the combined annual totals of breast, colorectal, ovarian, liver, and prostate cancers [1]. Good communication be- tween healthcare practitioners is vital to the quality of care received by patients and as such, a recent focus on improving the quality of communication has occurred. The current standard practice for thoracic surgical reporting is to prepare a narrative operative report. This report is used to understand a patient’s operative proce- dure and to guide their subsequent treatment. This doc- ument’s ability to reliably convey the fundamental elements of the procedure are central in future treatments Accepted for publication Dec 18, 2013. Address correspondence to Dr Finley, St. Joseph’s Healthcare Hamilton, 50 Charlton Ave E, Juravinski Tower T-2105B, Hamilton, ON L8N 4A6, Canada; e-mail: fi[email protected]. The Appendices can be viewed in the online version of this article [http://dx.doi.org/10.1016/j.athoracsur.2013. 12.042] on http://www.annalsthoracicsurgery.org. Ó 2014 by The Society of Thoracic Surgeons 0003-4975/$36.00 Published by Elsevier Inc http://dx.doi.org/10.1016/j.athoracsur.2013.12.042 GENERAL THORACIC
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Design of a Consensus-Derived Synoptic Operative Report for Lung Cancer Surgery
THORACIC
GENERAL
Design of a Consensus-Derived Synoptic OperativeReport for Lung Cancer SurgeryLaura Schneider, BS, Yaron Shargall, MD, Colin Schieman, MD,Andrew J. Seely, MD, PhD, Sadeesh Srinathan, MD, MS, Richard A. Malthaner, MD, MS,Andrew F. Pierre, MD, MS, Najib Safieddine, MD, Rosaire Vaillancourt, MD,Madelaine Plourde, MD, James Bond, MD, Scott Johnson, MD, MS, Shona E. Smith, MD,and Christian J. Finley, MD, MPHDepartment of Surgery, McMaster University, St. Joseph’s Healthcare Hamilton, Hamilton, Ontario; Department of Surgery, Universityof Ottawa, Ottawa Hospital General Campus, Ottawa, Ontario; Department of Surgery, University of Manitoba, Health Sciences Centre,Winnipeg, Manitoba; Departments of Surgery and Epidemiology and Biostatistics, University of Western Ontario, London HealthSciences Centre, London, Ontario; Department of Surgery, University of Toronto, Toronto General Hospital, Toronto, Ontario;Department of Surgery, Toronto East General Hospital, Toronto, Ontario; Department of Surgery, University of Laval, Quebec Heartand Lung Institute, Qu�ebec, Quebec; Department of Surgery, Dalhousie University, Queen Elizabeth II Health Sciences Centre, Halifax,Nova Scotia; Department of Surgery, University of British Columbia, Surrey Memorial Hospital, Surrey, British Columbia; Departmentof Surgery, University of Alberta, Royal Alexandra Hospital, Edmonton, Alberta; and Department of Surgery, Northern Ontario Schoolof Medicine, Sudbury, Ontario, Canada
Background. For lung cancer surgery, a narrativeoperative report is the standard reporting procedure,whereas a synoptic-style report is increasingly utilized byhealthcare professionals in various specialties with greatsuccess. A synoptic operative report more succinctly andaccurately captures vital information and is rapidlygenerated with good intraobserver reliability. Theobjective of this study was to systematically develop asynoptic operative report for lung cancer surgeryfollowing a modified Delphi consensus model with thesupport of the Canadian thoracic surgery community.
Methods. Using online survey software, thoracic sur-geons and related physicians were asked to suggest andrate data elements for a synoptic report following themodified Delphi consensus model. The consensusexercise-derived template was forwarded to a smallworking group, who further refined the definition andpriority designation of elements until the working grouphad reached a satisfactory consensus.
Accepted for publication Dec 18, 2013.
Address correspondence to Dr Finley, St. Joseph’s Healthcare Hamilton,50 Charlton Ave E, Juravinski Tower T-2105B, Hamilton, ON L8N 4A6,Canada; e-mail: [email protected].
� 2014 by The Society of Thoracic SurgeonsPublished by Elsevier Inc
Results. In all, 139 physicians were invited toparticipate in the consensus exercise, with 36.7%, 44.6%,and 19.5% response rates, respectively, in the threerounds. Eighty-nine elements were agreed upon at theconclusion of the exercise, but 141 elements were for-warded to the working group. The working groupagreed upon a final data set of 180 independentlydefined data elements, with 72 mandatory and 108optional elements for implementation in the finalreport.Conclusions. This study demonstrates the process
involved in developing a multidisciplinary, consensus-based synoptic lung cancer operative report. This novelreport style is a quality improvement initiative toimprove the capture, dissemination, readability, andpotential utility of critical surgical information.
(Ann Thorac Surg 2014;97:1163–8)� 2014 by The Society of Thoracic Surgeons
perative reporting is a necessary task after the
Ocompletion of any surgical procedure. In lung can-cer surgery, the primary purpose of the operative reportis to document and communicate information to othersurgeons, physicians, and healthcare providers to ensurecritical information is captured, findings are communi-cated, and care is well coordinated.Lung cancer represents a tremendous burden of dis-ease on Canadian and international healthcare systems.In Canada and the United States, lung cancer is theleading cause of cancer-related death, more than the
combined annual totals of breast, colorectal, ovarian,liver, and prostate cancers [1]. Good communication be-tween healthcare practitioners is vital to the quality ofcare received by patients and as such, a recent focus onimproving the quality of communication has occurred.The current standard practice for thoracic surgical
reporting is to prepare a narrative operative report. Thisreport is used to understand a patient’s operative proce-dure and to guide their subsequent treatment. This doc-ument’s ability to reliably convey the fundamentalelements of the procedure are central in future treatments
The Appendices can be viewed in the online version ofthis article [http://dx.doi.org/10.1016/j.athoracsur.2013.12.042] on http://www.annalsthoracicsurgery.org.
0003-4975/$36.00http://dx.doi.org/10.1016/j.athoracsur.2013.12.042

1164 SCHNEIDER ET AL Ann Thorac SurgLUNG CANCER SYNOPTIC OPERATIVE REPORT DESIGN 2014;97:1163–8
GENERALTHORACIC
and in establishing the patient’s prognosis. However, theability to succinctly, accurately and reliably capture thisinformation varies widely [2]. Failure to adequatelyconvey the information critical to the prognosis andmanagement of this malignancy results in needlessincreased resource utilization and difficulty in treatmentdecisions [2].
Electronic synoptic reporting captures standardizedinformation at the point of care, and allows the informa-tion to be quickly transmitted to other members ofhealthcare teams. Starting in 2011, a Canadian Partner-ship Against Cancer pilot project tested an electronicsynoptic reporting system for breast, colorectal, ovarian,and head/neck surgeries. The study demonstratedimproved efficiency using synoptic reports rather thanthe currently used narrative reports. The report alsonoted an overall positive experience by surgeons, andthat reports were deemed to be more comprehensivethan narrative versions [3, 4]. Electronic synoptic reportscan also provide secondary gains through structured datafor streaming into databases available for policy makers,researchers, and clinicians in ways that narrative reportentries cannot, resulting in improved efficiencies forhealthcare organizations such as hospitals or cancerregistries [4]. A synoptic report also allows for the abilityto collect standardized data needed for multisite research,further broadening the utility and use of the data [3].Further additions can be made to templates to ensure thatthey include information to allow surgeons to assessadherence to clinical evidence, best practice, and safetyprocedures, actions that can benefit patients by promot-ing safer surgical care and more effective treatment.
Demonstrating the potential of synoptic reports, asynoptic pathology report is actively used across Canada,based on the American Pathologists Cancer Checklists,with good adoption and results [5]. Synoptic pathologyreporting showed great improvements in the quality andcompleteness of reporting. It also provides both commondata fields and elements that offer the ability to comparebetween institutions, facilitating more accurate researchactivities [6]. Synoptic pathology reporting has beenrecognized as an important quality improvement initia-tive and has subsequently gained widespread adoptionwith improvements in report clarity and consistency.
In short, we believe that synoptic operative reportingallows for rapid, complete, reproducible, and concisedocumentation of surgical findings [7], allows for the ac-curate collection and comparison of data affecting patientoutcomes [8], and improves patient safety by reducingcommunication errors [7]. They are rapidly generated andshow good intraobserver reliability [9, 10]. With thesegoals in mind, we created a national consensus-basedsynoptic operative report for lung cancer surgery.
Material and Methods
The creation of the base dataset of the synoptic operativereport for lung cancer surgery utilized an anonymousmodified Delphi method [11, 12] using three iterativerounds. This process was completed electronically using
an electronic survey tool (LimeSurvey) with two remindere-mails per iteration. This project was reviewed by theSt. Joseph’s Healthcare Research Ethics Board, andinformed consent was waived owing to implied consenton account of the study activities.In the initial round, a survey was provided to all
members of the Canadian Association of Thoracic Sur-geons (CATS) and opinion leaders in family medicine,pathology, diagnostic imaging, medical oncology, andradiation oncology requesting key items considered to beimportant in a lung cancer operative report. The firstround was an open-ended questionnaire asking partici-pants to list all parameters within a provided list ofheadings that they believe would be necessary to a lungcancer operative report. A priori, we intended to makethe lung cancer synoptic report compatible with The So-ciety of Thoracic Surgeons (STS) database; therefore,procedures were provided based on those listed in theSTS database [13] with the stipulation that some may beadded. A number of feasibility and uptake questions werealso asked of participants to gauge the utility of the effort.A further round was used to rate and evaluate the
generated information, allowing CATS members to rateeach variable on a 9-point Likert scale [12] and commentwith free text available if necessary. Consensus wasdefined as a mean score of 6.3 or greater (70th percentile)as significant for inclusion of an individual variable and amean score of 2.7 (30th percentile) or less signalingexclusion from the final data set. The third round wastriggered by an a priori protocol indicating that if 70% ormore of all variables reached consensus after the first tworounds, the process would be complete; otherwise, a thirdround was to be included [11, 12], with all results from therounds being forwarded to a small working group. Alldata elements with indeterminate responses that fellwithin the 30th and 70th percentiles were circulated toparticipants through online questionnaires for the thirdround. The same consensus definition was used from thesecond round. After each round, a deidentified summarywas provided to the group outlining the median andfrequency distribution on the Likert scale and qualitativecomments [11, 12]. Figure 1 summarizes the process un-dertaken to conceptualize and produce the resulting finaltemplate. The final, consensus-based dataset wascompleted and forwarded to the aforementioned smallworking group to form the data elements into a workablesynoptic operative report template.The development of the synoptic report template was
coordinated with representatives of the Canadian Part-nership Against Cancer. Following procedures completedfor other cancer disease sites, the results from Delphiconsensus work were refined by a working groupcomposed of national representatives in Canadianthoracic surgery. In the interest of promoting standardi-zation between disease sites, the elements confirmedthrough the Delphi consensus exercise were workedinto a generic template pioneered by the Canadian Part-nership Against Cancer using standardized headings.During four working group teleconferences, the groupwas tasked with making the final designations for the
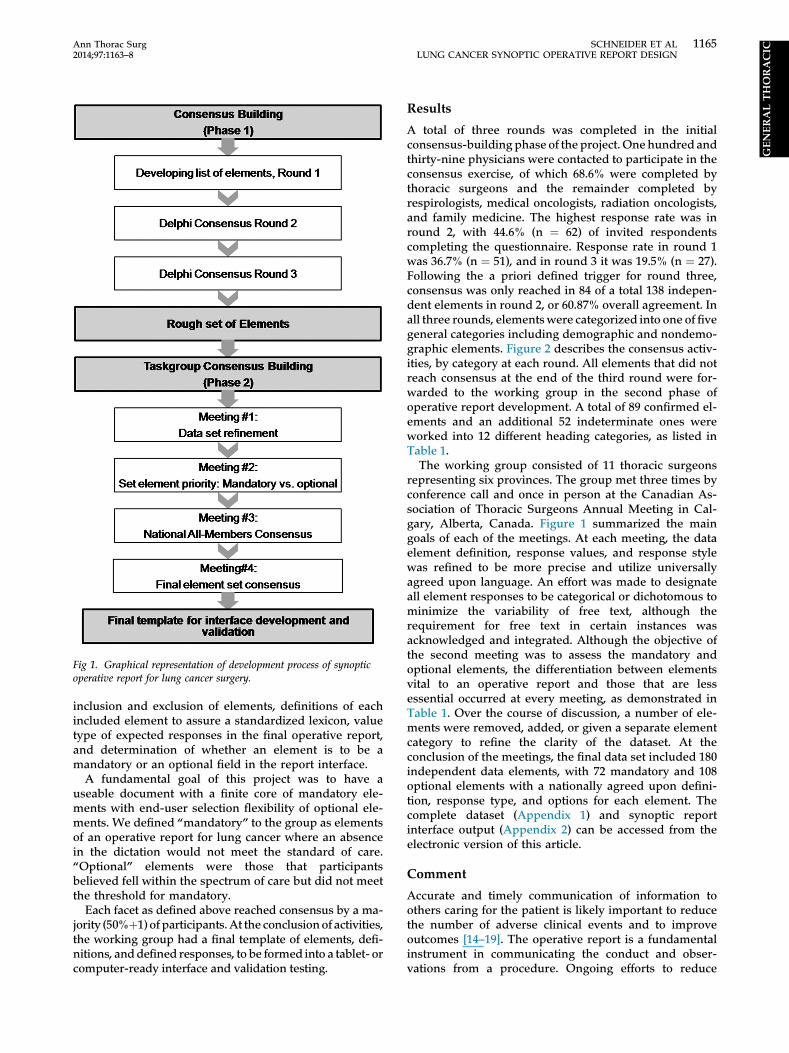
Fig 1. Graphical representation of development process of synopticoperative report for lung cancer surgery.
1165Ann Thorac Surg SCHNEIDER ET AL2014;97:1163–8 LUNG CANCER SYNOPTIC OPERATIVE REPORT DESIGN
GENERALTHORACIC
inclusion and exclusion of elements, definitions of eachincluded element to assure a standardized lexicon, valuetype of expected responses in the final operative report,and determination of whether an element is to be amandatory or an optional field in the report interface.
A fundamental goal of this project was to have auseable document with a finite core of mandatory ele-ments with end-user selection flexibility of optional ele-ments. We defined “mandatory” to the group as elementsof an operative report for lung cancer where an absencein the dictation would not meet the standard of care.“Optional” elements were those that participantsbelieved fell within the spectrum of care but did not meetthe threshold for mandatory.
Each facet as defined above reached consensus by a ma-jority (50%þ1) of participants.At the conclusionof activities,the working group had a final template of elements, defi-nitions, anddefined responses, to be formed into a tablet- orcomputer-ready interface and validation testing.
Results
A total of three rounds was completed in the initialconsensus-building phase of the project. Onehundred andthirty-nine physicians were contacted to participate in theconsensus exercise, of which 68.6% were completed bythoracic surgeons and the remainder completed byrespirologists, medical oncologists, radiation oncologists,and family medicine. The highest response rate was inround 2, with 44.6% (n ¼ 62) of invited respondentscompleting the questionnaire. Response rate in round 1was 36.7% (n ¼ 51), and in round 3 it was 19.5% (n ¼ 27).Following the a priori defined trigger for round three,consensus was only reached in 84 of a total 138 indepen-dent elements in round 2, or 60.87% overall agreement. Inall three rounds, elementswere categorized into one of fivegeneral categories including demographic and nondemo-graphic elements. Figure 2 describes the consensus activ-ities, by category at each round. All elements that did notreach consensus at the end of the third round were for-warded to the working group in the second phase ofoperative report development. A total of 89 confirmed el-ements and an additional 52 indeterminate ones wereworked into 12 different heading categories, as listed inTable 1.The working group consisted of 11 thoracic surgeons
representing six provinces. The group met three times byconference call and once in person at the Canadian As-sociation of Thoracic Surgeons Annual Meeting in Cal-gary, Alberta, Canada. Figure 1 summarized the maingoals of each of the meetings. At each meeting, the dataelement definition, response values, and response stylewas refined to be more precise and utilize universallyagreed upon language. An effort was made to designateall element responses to be categorical or dichotomous tominimize the variability of free text, although therequirement for free text in certain instances wasacknowledged and integrated. Although the objective ofthe second meeting was to assess the mandatory andoptional elements, the differentiation between elementsvital to an operative report and those that are lessessential occurred at every meeting, as demonstrated inTable 1. Over the course of discussion, a number of ele-ments were removed, added, or given a separate elementcategory to refine the clarity of the dataset. At theconclusion of the meetings, the final data set included 180independent data elements, with 72 mandatory and 108optional elements with a nationally agreed upon defini-tion, response type, and options for each element. Thecomplete dataset (Appendix 1) and synoptic reportinterface output (Appendix 2) can be accessed from theelectronic version of this article.
Comment
Accurate and timely communication of information toothers caring for the patient is likely important to reducethe number of adverse clinical events and to improveoutcomes [14–19]. The operative report is a fundamentalinstrument in communicating the conduct and obser-vations from a procedure. Ongoing efforts to reduce
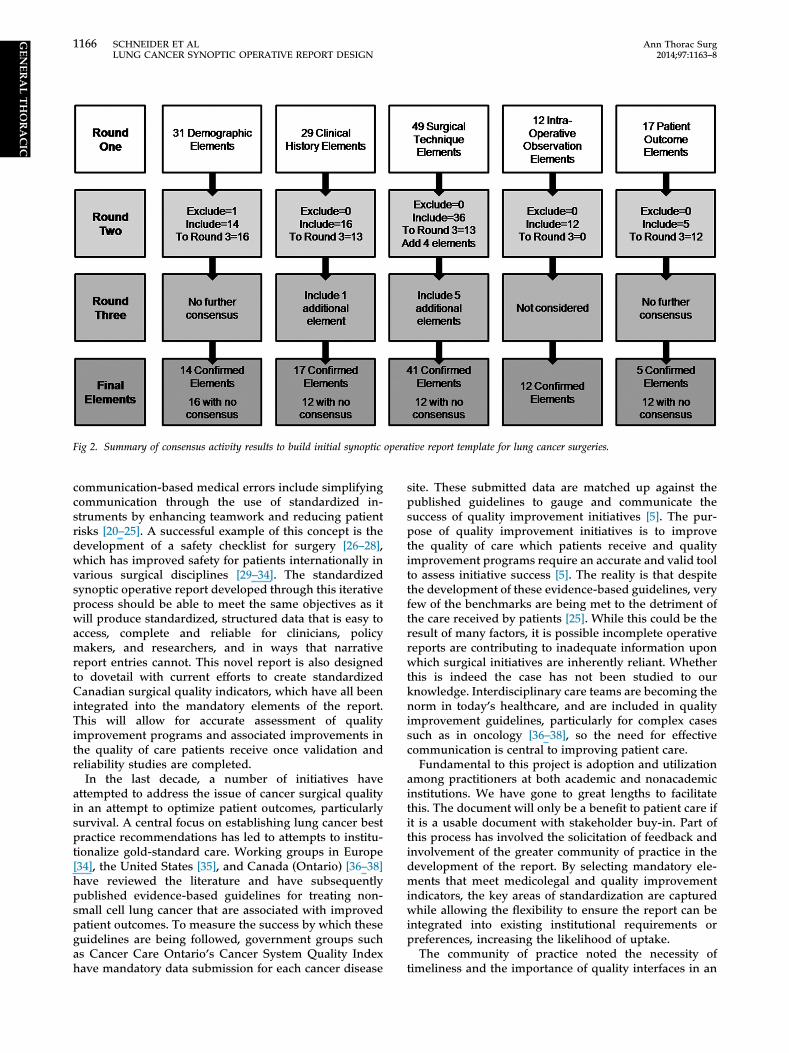
Fig 2. Summary of consensus activity results to build initial synoptic operative report template for lung cancer surgeries.
1166 SCHNEIDER ET AL Ann Thorac SurgLUNG CANCER SYNOPTIC OPERATIVE REPORT DESIGN 2014;97:1163–8
GENERALTHORACIC
communication-based medical errors include simplifyingcommunication through the use of standardized in-struments by enhancing teamwork and reducing patientrisks [20–25]. A successful example of this concept is thedevelopment of a safety checklist for surgery [26–28],which has improved safety for patients internationally invarious surgical disciplines [29–34]. The standardizedsynoptic operative report developed through this iterativeprocess should be able to meet the same objectives as itwill produce standardized, structured data that is easy toaccess, complete and reliable for clinicians, policymakers, and researchers, and in ways that narrativereport entries cannot. This novel report is also designedto dovetail with current efforts to create standardizedCanadian surgical quality indicators, which have all beenintegrated into the mandatory elements of the report.This will allow for accurate assessment of qualityimprovement programs and associated improvements inthe quality of care patients receive once validation andreliability studies are completed.
In the last decade, a number of initiatives haveattempted to address the issue of cancer surgical qualityin an attempt to optimize patient outcomes, particularlysurvival. A central focus on establishing lung cancer bestpractice recommendations has led to attempts to institu-tionalize gold-standard care. Working groups in Europe[34], the United States [35], and Canada (Ontario) [36–38]have reviewed the literature and have subsequentlypublished evidence-based guidelines for treating non-small cell lung cancer that are associated with improvedpatient outcomes. To measure the success by which theseguidelines are being followed, government groups suchas Cancer Care Ontario’s Cancer System Quality Indexhave mandatory data submission for each cancer disease
site. These submitted data are matched up against thepublished guidelines to gauge and communicate thesuccess of quality improvement initiatives [5]. The pur-pose of quality improvement initiatives is to improvethe quality of care which patients receive and qualityimprovement programs require an accurate and valid toolto assess initiative success [5]. The reality is that despitethe development of these evidence-based guidelines, veryfew of the benchmarks are being met to the detriment ofthe care received by patients [25]. While this could be theresult of many factors, it is possible incomplete operativereports are contributing to inadequate information uponwhich surgical initiatives are inherently reliant. Whetherthis is indeed the case has not been studied to ourknowledge. Interdisciplinary care teams are becoming thenorm in today’s healthcare, and are included in qualityimprovement guidelines, particularly for complex casessuch as in oncology [36–38], so the need for effectivecommunication is central to improving patient care.Fundamental to this project is adoption and utilization
among practitioners at both academic and nonacademicinstitutions. We have gone to great lengths to facilitatethis. The document will only be a benefit to patient care ifit is a usable document with stakeholder buy-in. Part ofthis process has involved the solicitation of feedback andinvolvement of the greater community of practice in thedevelopment of the report. By selecting mandatory ele-ments that meet medicolegal and quality improvementindicators, the key areas of standardization are capturedwhile allowing the flexibility to ensure the report can beintegrated into existing institutional requirements orpreferences, increasing the likelihood of uptake.The community of practice noted the necessity of
timeliness and the importance of quality interfaces in an
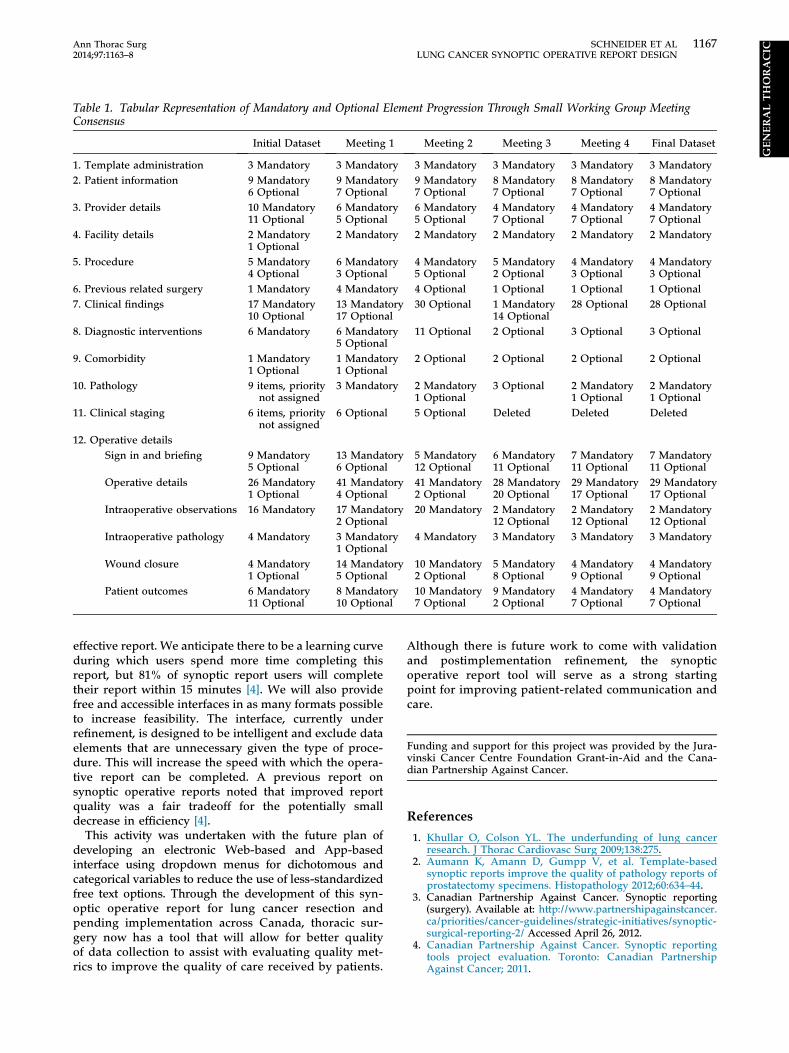
Table 1. Tabular Representation of Mandatory and Optional Element Progression Through Small Working Group MeetingConsensus
Initial Dataset Meeting 1 Meeting 2 Meeting 3 Meeting 4 Final Dataset
1. Template administration 3 Mandatory 3 Mandatory 3 Mandatory 3 Mandatory 3 Mandatory 3 Mandatory2. Patient information 9 Mandatory
6 Optional9 Mandatory7 Optional
9 Mandatory7 Optional
8 Mandatory7 Optional
8 Mandatory7 Optional
8 Mandatory7 Optional
3. Provider details 10 Mandatory11 Optional
6 Mandatory5 Optional
6 Mandatory5 Optional
4 Mandatory7 Optional
4 Mandatory7 Optional
4 Mandatory7 Optional
4. Facility details 2 Mandatory1 Optional
2 Mandatory 2 Mandatory 2 Mandatory 2 Mandatory 2 Mandatory
5. Procedure 5 Mandatory4 Optional
6 Mandatory3 Optional
4 Mandatory5 Optional
5 Mandatory2 Optional
4 Mandatory3 Optional
4 Mandatory3 Optional
6. Previous related surgery 1 Mandatory 4 Mandatory 4 Optional 1 Optional 1 Optional 1 Optional7. Clinical findings 17 Mandatory
10 Optional13 Mandatory17 Optional
30 Optional 1 Mandatory14 Optional
28 Optional 28 Optional
8. Diagnostic interventions 6 Mandatory 6 Mandatory5 Optional
11 Optional 2 Optional 3 Optional 3 Optional
9. Comorbidity 1 Mandatory1 Optional
1 Mandatory1 Optional
2 Optional 2 Optional 2 Optional 2 Optional
10. Pathology 9 items, prioritynot assigned
3 Mandatory 2 Mandatory1 Optional
3 Optional 2 Mandatory1 Optional
2 Mandatory1 Optional
11. Clinical staging 6 items, prioritynot assigned
6 Optional 5 Optional Deleted Deleted Deleted
12. Operative detailsSign in and briefing 9 Mandatory
5 Optional13 Mandatory6 Optional
5 Mandatory12 Optional
6 Mandatory11 Optional
7 Mandatory11 Optional
7 Mandatory11 Optional
Operative details 26 Mandatory1 Optional
41 Mandatory4 Optional
41 Mandatory2 Optional
28 Mandatory20 Optional
29 Mandatory17 Optional
29 Mandatory17 Optional
Intraoperative observations 16 Mandatory 17 Mandatory2 Optional
20 Mandatory 2 Mandatory12 Optional
2 Mandatory12 Optional
2 Mandatory12 Optional
Intraoperative pathology 4 Mandatory 3 Mandatory1 Optional
4 Mandatory 3 Mandatory 3 Mandatory 3 Mandatory
Wound closure 4 Mandatory1 Optional
14 Mandatory5 Optional
10 Mandatory2 Optional
5 Mandatory8 Optional
4 Mandatory9 Optional
4 Mandatory9 Optional
Patient outcomes 6 Mandatory11 Optional
8 Mandatory10 Optional
10 Mandatory7 Optional
9 Mandatory2 Optional
4 Mandatory7 Optional
4 Mandatory7 Optional
1167Ann Thorac Surg SCHNEIDER ET AL2014;97:1163–8 LUNG CANCER SYNOPTIC OPERATIVE REPORT DESIGN
GENERALTHORACIC
effective report. We anticipate there to be a learning curveduring which users spend more time completing thisreport, but 81% of synoptic report users will completetheir report within 15 minutes [4]. We will also providefree and accessible interfaces in as many formats possibleto increase feasibility. The interface, currently underrefinement, is designed to be intelligent and exclude dataelements that are unnecessary given the type of proce-dure. This will increase the speed with which the opera-tive report can be completed. A previous report onsynoptic operative reports noted that improved reportquality was a fair tradeoff for the potentially smalldecrease in efficiency [4].
This activity was undertaken with the future plan ofdeveloping an electronic Web-based and App-basedinterface using dropdown menus for dichotomous andcategorical variables to reduce the use of less-standardizedfree text options. Through the development of this syn-optic operative report for lung cancer resection andpending implementation across Canada, thoracic sur-gery now has a tool that will allow for better qualityof data collection to assist with evaluating quality met-rics to improve the quality of care received by patients.
Although there is future work to come with validationand postimplementation refinement, the synopticoperative report tool will serve as a strong startingpoint for improving patient-related communication andcare.
Funding and support for this project was provided by the Jura-vinski Cancer Centre Foundation Grant-in-Aid and the Cana-dian Partnership Against Cancer.
References
1. Khullar O, Colson YL. The underfunding of lung cancerresearch. J Thorac Cardiovasc Surg 2009;138:275.
2. Aumann K, Amann D, Gumpp V, et al. Template-basedsynoptic reports improve the quality of pathology reports ofprostatectomy specimens. Histopathology 2012;60:634–44.
3. Canadian Partnership Against Cancer. Synoptic reporting(surgery). Available at: http://www.partnershipagainstcancer.ca/priorities/cancer-guidelines/strategic-initiatives/synoptic-surgical-reporting-2/ Accessed April 26, 2012.
4. Canadian Partnership Against Cancer. Synoptic reportingtools project evaluation. Toronto: Canadian PartnershipAgainst Cancer; 2011.
1168 SCHNEIDER ET AL Ann Thorac SurgLUNG CANCER SYNOPTIC OPERATIVE REPORT DESIGN 2014;97:1163–8
GENERALTHORACIC
5. Srigley JR, McGowan T, Maclean A, et al. Standardizedsynoptic cancer pathology reporting: a population-basedapproach. J Surg Oncol 2009;99:517–24.
6. Harvey A, Zhang H, Nixon J, Brown CJ. Comparison of dataextraction from standardized versus traditional narrativeoperative reports for database-related research and qualitycontrol. Surgery 2007;141:708–14.
7. Hsu C, Sandford B. The Delphi technique: making sense ofconsensus. Practical assessment, research and evaluation2007;12(10). Available at: http://pareonline.net/getvn.asp?v¼12&n ¼ 10. Accessed April 26, 2012.
8. Synoptic reporting and structured data capture in healthcare.2012.Available at: http://www.scribd.com/doc/1036253/synoptic-reporting-and-structured-data-capturein-healthcare#download.Accessed April 26, 2012.
9. Hermensa RPMG, Ouwensa MMJT, Vonk-Okhuijsenb SY,et al. Development of quality indicators for diagnosis andtreatment of patients with non-small cell lung cancer: a firststep toward implementing a multidisciplinary, evidence-based guideline. Lung Cancer 2006;54:117–24.
10. Park J, Pillarisetty VG, Brennan MF, et al. Electronic synopticoperative reporting: assessing the reliability and complete-ness of synoptic reports for pancreatic resection. J Am CollSurg 2010;211:308–15.
11. Cantrill JA, Sibbald B, Buetow S. Indicators of the appro-priateness of long-term prescribing in general practice in theUnited Kingdom: consensus development, face and contentvalidity. Qual Health Care 1998;7:130–5.
12. Campbell SM, Cantrill JA, Roberts D. Prescribing indicatorsfor UK general practice: Delphi consultation study. BMJ2000;321:425–8.
13. Society of Thoracic Surgeons. Society of Thoracic Surgeonsgeneral thoracic surgery training manual version 2.2. 20Feb 2013. Available at: http://www.sts.org/quality-research-patient-safety/national-database/database-managers/general-thoracic-surgery-databa-1. Accessed May 21, 2013.
14. Murphy JG, Dunn WF. Medical errors and poor communi-cation. Chest 2010;138:1292–3.
15. Sutcliffe KM, Lewton E, Rosenthal MM. Communicationfailures: an insidious contributor to medical mishaps. AcadMed 2004;79:186–94.
16. Bernard M, Connelly R, Kuder LC, et al. Interdisciplinaryeducation. In: Klein S, ed. A national agenda for geriatriceducation: white papers. Rockville, MD: Bureau of HealthProfessions Health Resources and Services Administration;1995:57–80.
17. Flin R, Fletcher G, McGeorge P, et al. Anaesthetists’ attitudesto teamwork and safety. Anaesthesia 2003;58:233–42.
18. Gittell JH, Fairfield KM, Bierbaum B, et al. Impact of rela-tional coordination on quality of care, postoperative pain andfunctioning, and length of stay: a nine hospital study ofsurgical patients. Med Care 2000;38:807–19.
19. O’Daniel M, Rosenstein AH. Professional communicationand team collaboration. In: Hughes RG, ed. Patient safetyand quality: an evidence-based handbook for nurses. Vol 2.Rockville, MD: Agency for Healthcare Research and Quality(US), 2008;271–83.
20. de Vries EN, Prins HA, Crolla RMPH, et al. Effect of acomprehensive surgical safety system on patient outcomes.N Engl J Med 2010;363:1928–37.
21. Helmreich RL, Schaefer HG. Team performance in theoperating room. In: Bogner MS, ed. Human error in medi-cine. Hillside, NJ: Lawrence Erlbaum; 1998:225–53.
22. Leming-Lee S, France D, Feistritzer N, et al. Crew resourcemanagement in perioperative services: navigating theimplementation road map. J Clin Outcomes Manage 2005;12:353–8.
23. Leonard M, Graham S, Bonucom D. The human factor: thecritical importance of effective teamwork and communica-tion in providing safe care. Qual Saf Health Care2004;13(Suppl 1):185–90.
24. Darling G, Nenshi R, Schultz SE, et al. Chapter 5: surgery forlung cancer. In: Cancer surgery in Ontario. ICES Atlas.Toronto, ON: ICES; 2008:97–126.
25. Rosenstein A, O’Daniel M. Impact and implications ofdisruptive behavior in the perioperative arena. J Am CollSurg 2006;203:96–105.
26. Haynes AB, Weiser TG, Berry WR, et al. A surgical safetychecklist to reduce morbidity and mortality in a globalpopulation. N Engl J Med 2009;360:491–9.
27. Lingard L, Regehr G, Orser B, et al. Evaluation of a preop-erative checklist and team briefing among surgeons, nurses,and anesthesiologists to reduce failures in communication.Arch Surg 2008;143:12–8.
28. World Health Organization. Safe surgery saves lives.Geneva, Switzerland: World Health Organization; 2009.
29. Haynes AB, Weiser TG, Berry WR, et al. Changes in safetyattitude and relationship to decreased postoperativemorbidity and mortality following implementation of achecklist-based surgical safety intervention. BMJ Qual Saf2011;20:102–7.
30. Ministry of Health and Long-Term Care. Hospitals to usesurgical safety checklist. 2009. Toronto, ON: MOHLTC.Available at: http://www.health.gov.on.ca/en/news/release/2009/oct/patientsafety_1year_nr_20090922_2_.pdf. AccessedApril 26, 2012.
31. Ministry of Health and Long-Term Care. Patient safety indi-cator reporting: Ontario totals. 2011. Toronto, ON: MOHLTC.Available at: http://patientsafetyontario.net/reporting/en/psir_provincialindicatorreporting.aspx. Accessed April 26, 2012.
32. Neily J, Mills PD, Young-Xu Y, et al. Association betweenimplementation of a medical team training program andsurgical mortality. JAMA 2010;304:1693–700.
33. Askarian M, Kouchak F, Palenik CJ. Effect of surgical safetychecklists on postoperative morbidity and mortality rates,Shiraz, Faghihy Hospital, a 1-year study. Qual ManageHealth Care 2011;20:293–7.
34. Crino L, Weder W, van Meerbeeck J, Felip E. Early stage andlocally advanced (non-metastatic) non-small-cell lung can-cer: ESMO clinical practice guidelines for diagnosis, treat-ment and follow-up. Ann Oncol 2010;21(Suppl 5):103–15.
35. National Comprehensive Cancer Network. NCCN clinicalpractice guidelines in oncology (NCCN guidelines): nonsmall cell lung cancer. Version 3.2012. Available at: www.nccn.org. Accessed October 16, 2012.
36. Sundaresan S, Langer B, Oliver T, et al, for the Expert Panelon Thoracic Surgical Oncology. Thoracic surgical oncologystandards. Cancer Care Ontario. Released September 9, 2005.
37. Sundaresan S, Langer B, Oliver T, et alfor the Expert Panelon Thoracic Surgical Oncology. Standards for thoracic sur-gical oncology in a single-payer healthcare system. AnnThorac Surg 2007;84:693–701.
38. Cancer Quality Council of Ontario. Thoracic cancer surgerystandards and post-surgical mortality. Available at: http://www.csqi.on.ca/cms/One.aspx?portalId¼126935&pageId¼127980.Accessed October 12, 2012.




















