ECG delineation techniques and applications in Cobra venom interacted patients

Delineation of myocardial stunning and hibernation by positron emission tomography in advanced coronary artery disease
Andrea Conversano, MD, a John F. Walsh, MD, a Edward M. Geltman, MD, a,b Julio E. Perez, MD, b Steven R. Bergmann, MD, PhD, a,b and Robert J. Gropler, MD a,b St. Louis, Me.
With positron emission tomography, the resting flow abnor- malities underlying reversible left ventricular dysfunction in 17 patients with chronic coronary artery disease were delin- eated. The level of flow in reversibly dysfunctional segments (i.e., those demonstrating improvement after revasculari- zation) was markedly variable, ranging from 0.32 to 1.25 ml/ gm/min, in 20 of these segments, flow was preserved, whereas in 12 segments, flow was reduced, when compared with that in, age-matched controls. Preservation of flow was associated with preservation of myocardial oxygen con- sumption and no alterations in myocardial substrate use. In contrast, a reduction in flow resulted in a decrease myocar- dial oxygen consumption and an increase in myocardial glucose use. Thus resting reversible left ventricular dys- function in patients with chronic coronary artery disease can reflect a diversity of resting flow abnormalities. Moreover, myocardial perfusion at rest is frequently within normal lim- its, suggesting that the reversible mechanical dysfunction in these patients is attributable to intermittent myocardial stunning and not hibernation. (AM HEART J 1996;131:440-50.)
Left ventricular dysfunction is the primary clinical manifestation for a significant proportion of patients with chronic coronary artery disease. In spite of rec- ognition that in many of these patients, left ventric- ular function will improve either spontaneously or after successful coronary revascularization, the spe- cific derangements in myocardial perfusion underly- ing reversible resting systolic dysfunction are not
From the ~Division of Nuclear Medicine, Edward Mallinckrodt Institute of Radiology, and the bCardiovascular Division, Department of Internal Med- icine, Washington University School of Medicine. Supported in part by a grant from the Edward Mallinckrodt, Jr., Founda- tion, St. Louis, Missouri, and by NIH grants HL17646 (SCOR in Coronary and Vascular Diseases) and HL13851. The study was performed during Dr. Gropler's tenure as a Clinician-Scientist Awardee from the American Heart Association. Received for publication June 30, 1995; accepted Aug. 21, 1995.
Reprint requests: Robert J. Gropler, MD, Division of Nuclear Medicine, Mallinckrodt Institute of Radiology, 510 South Kingshighway Boulevard, St. Louis, Me. 63110. Copyright © 1996 by Mosby-Year Book, Inc. 0002-8703/96/$5.00 + 0 4/1/69511
well characterized. Accurate delineation of the un- derlying flow disturbance and it s impact on recovery of myocardium in response to specific modes of cor- onary artery recanalization is necessary to delineate mechanisms responsible for the impairment in per- fusion, to provide a basis for the accurate interpreta- tion of diagnostic studies designed to identify pa- tients likely to derive benefit from mechanical re- vascularization procedures, and to facilitate the development and evaluation of novel therapies (both pharmacologic and mechanical) designed to restore or preserve nutritive perfusion.
Recognition of improved systolic function after coronary revascularization in patients with chronic coronary artery disease has led to the concept that in response to a persistent reduction in myocardial blood flow, function is depressed to maintain the balance between oxygen supply and demand and, as a consequence, to prevent or delay the onset of my- ocardial necrosis. This adaptive state has been termed myocardial hibernation. 1, 2 Moderate reduc- tions in myocardial blood flow lead to concomitant and reversible reductions in function without necro- sis in dog hearts; however, such conditions have been demonstrated in only brief intervals of a few hours. 3 However, because a reduction in resting flow, in ab- solute terms, has not been demonstrated in patients with reversible resting left ventricular dysfunction attributable to chronic coronary artery disease, de- finitive evidence for the presence of myocardial hibernation in human beings is still lacking.
Reversible mechanical dysfunction can also be a manifestation of myocardial stunning: prolonged re- versible systolic dysfunction after successful reper- fusion. 4 In contrast to myocardial hibernation, a wealth of experimental evidence supports the exist- ence of myocardial stunning. 5, 6 In human beings, this phenomenon has been thought to occur prima- rily in patients with acute myocardial infarction treated successfully with either thrombolytic agents
440

Volume 131, Number 3
American Heart Journal Conversano et al. 441
or p r ima ry coronary angioplasty. 7, s Recent ly we demons t ra t ed t ha t in pa t ien ts wi th chronic coronary a r t e r y disease, myocardia l oxygen consumpt ion in revers ibly dysfunct ional myocard ium, as m e a s u r e d by posi tron emission tomography (PET) and car- bon- 11 acetate , was on average comparable with tha t exhibi ted by myocard ium with normal function. Given the close coupling be tween myocardia l blood flow and oxygen consumption, this f inding suggested tha t perfusion (in milliliters/gram/minute) was within normal limits for many of these patients. 9 Vanover- schelde et al.10 confirmed this hypothesis by demon- s t ra t ing in a similar group of pat ients tha t in reversibly dysfunctional myocardial segments, resting myocar- dial perfusion (quantified by P E T and nitrogen-13 am- monia), was on average, within normal limits and comparable with tha t in segments exhibiting normal mechanical function. However, the proportion of re- versibly dysfunctional segznents where resting myo- cardial blood flow was reduced or preserved and thus ma y have represented myocardial hibernation or in- te rmi t ten t stunning, respectively, was not reported.
Accordingly, in this study, flow was del ineated in regions of rest ing, revers ible left ven t r icu la r dys- funct ion in pa t ien ts wi th chronic coronary a r t e ry disease. In addition, the ex ten t to which the abnor- mali t ies in res t ing flow were associated wi th per tur - bat ions in myocardia l metabol i sm was defined. To achieve these aims, in pa t ien ts with res t ing left yen- t r icular dysfunct ion as a resu l t of chronic coronary a r t e r y disease, regional myocardia l perfusion, oxy- gen consumpt ion and glucose metabol i sm u n d e r res t ing conditions were quant i f ied by P E T before coronary revascular iza t ion in myocard ium t h a t ex- hibi ted improvemen t in mechanica l funct ion in re- sponse to revascular izat ion.
METHODS Patients. The protocol was approved by the Human
Studies Committee and the Radioactive Drug Research Committee of Washington University School of Medicine, and written informed consent was obtained from each pa- tient. Seventeen patients (14 men and 3 women; mean age = 57 years; age range = 30 to 69 years) who had left ventricular wall-motion abnormalities as a result of an- giographically documented coronary artery disease were studied. The clinical characteristics of these patients are summarized in Table I. Eleven had sustained at least one myocardial infarction from 2 months to 18 years before enrollment in the study. Three patients had undergone coronary artery bypass surgery 18, 6, and 4 years earlier. Six patients exhibited symptoms consistent with chronic stable ang4na, whereas an unstable anginal pattern was present in 5 patients. In 6 patients, symptoms of left yen- tricular dysfunction predominated.
Cardiac catheterization and selective coronary angiog- raphy followed by coronary revascularization (coronary artery bypass surgery or coronary artery angioplasty) were performed in all patients. Most patients had angiograph- ically defined lesions in at least two vessels and thus un- derwent coronary artery bypass grafting (Table I). The ad- equacy of the revascularization procedure was verified by review of the operative reports documenting the success- ful placement of bypass grafts and, in the case of coronary angioplasty, by angiographic documentation of successful balloon dilation. None of the patients exhibited signs or symptoms of acute myocardial infarction during the inter- val between the performance of the initial PET and wall- motion studies and performance of the follow-up wall-me- tion study.
Assessment of ventricular function. For each patient, regional systolic function was assessed before (mean = 21 -+ 21 days) and after (mean = 2.9 + 1.1 months) coronary re- vascularization. In 14 patients, regional systolic function was assessed before and after revascularization by two-di- mensional echocardiography. In 3 patients, radionuclide ventriculography was performed before and after coronary revascularization.
Regional systolic function was quantified as recently de- scribed.9,11 For the purposes of analysis, the left ventric- ular myocardium was segmented into seven regions (sep- tal, anterobasal, anterior, apical, lateral, posterolateral, and inferior). With both methods, (echocardiography and radionuclide ventriculography), regional systolic function was graded according to the scoring system recommended by the American Society for Echocardiography (1, normal; 2, hypokinetic; 3, akinetic; 4, dyskinetic; and 5, aneurys- mal). 12 The wall-motion analyses were performed by two observers blinded to both PET and clinical data. The average wall-motion score reflecting values assigned by both observers was tabulated for each segment in each study.
Abnormal systolic function was defined as an average wall-motion score ---2. Reversibly dysfunctional myocar- dial segments were defined as those exhibiting either nor- real systolic function or an improvement in average wall- motion score of at least two full grades after revascular- ization. Initially dysfunctional segments that exhibited improvement in average wall-motion score more than one full grade were classified as irreversibly injured. Initially dysfunctional segments in which systolic function did not normalize or exhibited improvement of one or more but fewer than two full grades were not included in the primary analysis, as they most likely reflect significant admixtures of reversible and irreversible dysfunctional tissue. These fairly strict criteria were also applied to re- duce the likelihood of confounding by altered loading con- ditions. In patients who underwent coronary artery bypass surgery, the interventricular septum was excluded from analysis because abnormalities in contractile performance independent ofischemia occur frequently in this region af- ter bypass surgery.
Tomographic assessment of perfusion and metabo- lism. Tomographic assessments of perfusion and metabo-

March 1996 4 4 2 Conversano et al. American Heart Journal
T a b l e I. Cl in ica l c h a r a c t e r i s t i c s
Age (yr) / Previous MI Angiographic Medications Revascularization Subject Gender (time since MI) findings (at enrollment) procedure
1 50/M No 90% LAD Nitrates CABG 90% CFX Calcium blockers 100% RCA
2 68/F No 80% LAD Nitrates CABG 80% CFX Calcium blockers 80% RCA Digoxin
3 30/M No 100% LAD Calcium blockers CABG B-Blockers
4 69/F Yes (4 yr) Nitrates PTCA B-Blockers
5 65/F Yes (20 yr) Nitrates CABG B-Blockers
6 68/M No Nitrates CABG Calcium-blockers Diuretics
7 68/F Yes (1 yr) Nitrates CABG B-Blockers
8 47/M Yes (5 yr) Nitrates CABG Calcium-blockers ~-blockers
9 52/M Yes (1 yr) Nitrates CABG Digoxin Diuretics
10 64/M Yes (18 yr) Nitrates CABG ACE inhibitors
11 65/M Yes (2 too) Nitrates CABG B-Blockers ACE inhibitors
12 49/M No Nitrates CABG B-Blockers
13 48/M Yes (24 mo) Nitrates CABG Digoxin Diuretics ACE inhibitors
14 64/M No 100% LAD Nitrates CABG 80% CFX Digoxin 100% RCA Diuretics (SVG patent) ACE inhibitors
15 57/M Yes (1 yr) 50% L Main Nitrates CABG 100% LAD Digoxin 40% CFX Diuretics 100% RCA ACE inhibiters
16 60/F Yes (16 yr) 100% LAD Nitrates CABG (SVG occluded) Calcium blockers 100% CFX Diuretics (SVG patent) ACE inhibiters 100% RCA (SVG occluded)
17 44/M Yes (11 yr) 100% LAD' 9O% CFX 100% RCA
90% LAD 80% CFX (patent SVG) 70% RCA (patent SVG) 60% L main 100% LAD 60% CFX 100% RCA 70% LAD 80% CFX 90% RCA 100% LAD 100% CFX 75% RCA 70% LAD 100% CFX 100% RCA 100% LAD 100% CFX 90% RCA 100% LAD 90% CFX 8O% RCA 100% LAD 75% CFX 75% RCA 80% LAD 8O% CFX 100% RCA 100% LAD 90% CFX 90% RCA
B-Blocker C A B G
L main, Left main artery; LAD, left anterior descending artery; CFX, circumflex artery; RCA, right coronary artery; SVG, saphenous vein graft; MI, my- ocardial infarction; ACE, angiotensin-converting enzyme; CABG, coronary artery bypass grafting; PTCA, percutaneous transluminal coronary angioplasty.

Volume 131, Number 3 American Heart Journal Conversano et al. 443
lism were performed in all patients before coronary revas- cularization (mean = 22 + 23 days). PET studies were performed on average within 6 _+ 7 days of the assess- ments of systolic function. The methods used to measure regional myocardial perfusion, oxygen consumption, and glucose metabolism have been reported previously in detail.9, 13-15 In brief, PET studies were performed on standard positron emission tomographic instrumentation available at Washington University. All subjects were studied in the postprandial state supplemented with an oral glucose solution before the administration of fluo- rine-18 fluorodeoxyghicose (see the following). An initial transmission scan was performed to correct subsequent emission scans for attenuation. After the transmission scan, oxygen-15 water (0.30 to 0.40 mCi/kg) was adminis- tered as a bolus intravenously with the immediate initia- tion of a list-mode data collection for 150 sec. After allow- ing for decay of 1SO-water, 40 mCi of C150 was adminis- tered by inhalation with a subsequent 300-second list- mode data collection. Next, 11C-acetate (0.25 to 0.30 mCi/ kg) was administered intravenously, followed by an 1800- second list-mode data collection. Subsequently, lSF-fluor- rodeoxyglucose (9 to 10 mCi) was administered intraven- ously, with an 1800-second list-mode data collection per- formed 45 min later. To ensure that each patient was po- sitioned consistently within the PET system for all data collections, position was checked with the use of a low-en- ergy laser, and indelible marks were placed on the torso. None of the patients exhibited clinical findings or electro- cardiographic evidence (which was monitored continu- ously) of myocardial ischemia during the tomographic studies.
Regional myocardial blood flow was quantified using the parameter optimization developed and validated previ- ously at our institution. 1315 However, to permit better quantification at very low flow rates, the partial volume correction factor within this algorithm was fixed to a value calculated independently from the transmission and 150- carbon-monoxide scans, as previously described by Iida et al. 16 We recently demonstrated in experimental animals that transmural myocardial flow rates to as low as 0.20 ml/gm/ml could be quantified accurately with this meth- od. 17 Myocardial oxygen consumption was quantified by determining the myocardial turnover rate constant of ac- etate, kl, which reflects the rate of clearance of 11C activ- ity from myocardium after the administration of 11C ace- tate and which correlates closely with myocardial oxygen consumption measured directly, is, 19 Analysis of clearance kinetics of 11C activity obviates corrections for partial-vol- ume effects (because such effects should be stable over the brief time course of the dynamic data collection). Regional myocardial glucose metabolism was assessed from com- posite images of relative lSF-fluorodeoxyglucose activity. Because uptake was assessed on an image representing one point in time, correction for decreased count recovery caused by partial-volume effects must be performed. Ac- cordingly, the same partial-volume correction factor used for the blood-flow calculation within a given segment was used to correct segmental values of 18F-fluorodeoxyghicose activity. For the purposes of measuring the level of myo-
cardial glucose metabolism normalized to blood flow within each segment, 18F-fluorodeoxyglucose activity normalized to the average myocardial activity in segments exhibiting normal function was divided by the myocardial blood flow normalized to the average myocardial blood flow in seg- ments with normal function. Average values for myocar- dial blood flow, kl, and 18F-fluorodeoxyglucose activity normalized to blood flow were calculated for each of the seven segments per patient. Tomographic measurements of perfusion and metabolism have been reported previ- ously in seven of the patients. 9,2° However, in those studies, the ability of measurements of myocardial oxida- tive metabolism and glucose metabolism to identify viable myocardium was examined. Measurements of myocardial blood flow in absolute terms was not performed.
Classification of myocardial segments from flow val- ues. To determine whether the level of resting perfusion was associated with changes in myocardial metabolism, values for myocardial blood flow in the reversibly dysfunc- tional segments were referenced to mean values obtained in age-matched control subjects for the purposes of defin- ing preserved or reduced flow levels. The control group consisted of 19 healthy normal volunteers (12 men and seven women; mean age 55 -+ 8 years) with no history and a low likelihood of coronary artery disease. Regional flow values within this group averaged 1.02 _+ 0.26 ml/gm/min. In reversibly dysfunctional segments, resting flow was classified as preserved (and thus suggestive of intermit- tent stunning) when values for flow were ~0.50 ml/gm/min (within two standard deviations of the mean value for my- ocardial blood flow in the control group). Conversely, a re- duction in resting flow (suggestive of myocardial hiberna- tion) was defined as a flow value of <0.50 ml/gm/min (that is, a value lower than the mean value minus two standard deviations of flow measured in the control group). Subse- quently, values for myocardial oxygen consumption and glucose metabolism normalized to flow were characterized before coronary revascularization in reversibly dysfunc- tional segments the level of flow. For comparison purposes, myocardial blood flow, oxygen consumption, and glucose metabolism normalized to flow were characterized before coronary revascularization in normal and irreversibly damaged myocardial segments as well.
Statistics. Results for continuous variables are pre- sented as mean values -+ the standard deviation. Indepen- dent sample values were subjected to analysis of variance and by the t test, corrected for the number of comparisons with the Bonferroni method, p Values <0.05 were consid- ered significant.
RESULTS Measurements of myocardial blood flow in relation to
systolic function. As judged from the analyses of wall motion, 32 segments were identified as normal, and 87 segments were identified as dysfunctional. Thir- ty-nine of the segments were excluded from fur ther analysis because of ei ther technical considerations (e.g., location in in tervent r icular sep tum in pat ients undergoing coronary a r te ry bypass surgery, incom-

March 1996 444 Conversano et al. American Heart Journal
Fig. 1. Images of myocardial perfusion and metabolism in patients with diverse perfusion and reversibly dysfunctional segments. Relative perfusion (left) with l~O-water; parametric displays (middle) of regional values of myocardial clearance of 11C activity after the administration of 11C-acetate and reflect regional oxidative metabolism; regional glucose metabolism (right) with lSF-fluorodeoxyglucose. Color bars repre- sent activity in all images. Orientation is septum to left and anterior wall on top. Reversible dysfunction was present in anterior wall (upper), yet myocardial blood flow was normal at 1.2 ml/gm/min. Both oxi- dative metabolism and glucose metabolism were comparable to values in normally functioning lateral wall. These findings are consistent with stunned myocardium. Reversible dysfunction (lower) is present in the anteroapical wall. Perfusion was reduced at 0.50 ml/gm/min. Oxidative metabolism was reduced relative to that in normally functioning posterolateral wall. Glucose metabolism was increased relative to flow. These findings likely reflect myocardial hibernation.
plete revascularization, or inability to quantify my- ocardial blood flow because of inadequate counting statistics; n = 31), or because of an intermediate im- provement in regional function after revasculariza- tion, as described previously; n = 8. Of the 80 seg- ments submitted for further analysis, 25 were clas- sifted as normal, 32 as reversibly dysfunctional, and 23 as irreversibly dysfunctional.
In segments with reversible dysfunction, resting flow values averaged 0.65 _+ 0.28 ml/gndmin, which was less than the average flow value exhibited by segments with normal function (0.85 _+ 0.36 ml/gm/ min; p < 0.02) but was higher than resting flow val- ues exhibited by irreversibly dysfunctional segments (average, 0.35 _+ 0.14 ml/gm/min; p < 0.0001). How- ever, the level of resting myocardial perfusion in the
reversibly dysfunctional segments was markedly variable, ranging from 0.32 to 1.25 ml/gm/min (Figs. 1 and 2). From the cut-off value of 0.50 ml/gm/min, 20 segments were classified as having preserved flow with an average value of 0.80 _+ 0.25 ml/gm/min, comparable with flow values exhibited by normal segments in patients, but less than that observed in normal volunteers (p < 0.0004). In 12 reversibly dys- functional segments, flow was reduced, averaging 0.39 +_ 0.05 ml/gndmin. This level of flow was com- parable with that exhibited by irreversibly dysfunc- tional segments (p = NS). This suggests that mea- surements of myocardial blood flow, even in absolute terms, will not accurately distinguish dysfunctional myocardium that retains the capacity to recover from dysfunctional myocardium that does not, par-

Volume 131, Number 3 American Heart Journal Conversano et al. 445
2.00
1.50
1.00
0.50
0.00
A
B!, 81.
........ i,: t ...... NL. VOL. NL. FXN. REVER. IRREV.
Fig. 2. Individual and average values (and i SD) for myocardial blood flow in myocardial se~aents ex- hibiting normal function (A; n = 25), reversible dysfunction (O; n -- 32), and irreversible dysfunction ( O ; n = 23) from assessments of systolic function in response to coronary revascularization. Segmental values for 19 normal volunteers are shown as well (average = 1.02 _+ 0.26 ml/mg/min). Dotted line at 0.50 ml/gm/ min, two standard deviations below mean for controls and was used as a cut-offto define abnormally low values in patients. The range of flow in reversibly dysfunctional segments is wide. Twenty segments ex- hibited values within the normal range; 12 exhibited flow values >2 standard deviations below mean for controls. *p < 0.0001 compared with irreversibly dysfunctional segments; **p < 0.0004 compared with normal volunteers.
0.100
0.080
0.060
0.040
0.020
0.000
[]
T 8 T [] ~ T
o,
8 T ~ 0
NL. FXN. REVER. REVER. IRREV. (NL. MBF) (Low MBF)
Fig. 3. Average values and SDs for measurements of myocardial oxygen consumption in reversibly dys- functional segments that exhibited normal or reduced blood flow. Measurements in segments exhibiting normal contractile function (NL FXN) or irreversible dysfunction (IRREV) are included for comparison. In reversibly dysfunctional segments (REVER) with preserved perfusion, oxygen consumption was compa- rable with that measured in segments with normal function. In contrast, in reversibly dysfunctional seg- ments with reduced perfusion (i.e., hibernating), oxygen consumption was reduced compared with that ob- served in reversibly dysfunctional segments with maintained perfusion. *p < 0.03 compared with normal or reversibly dysfunctional segments with normal flow; **p < 0.0001 compared with normal segments or reversibly dysfunctional segments with preserved flow and ##p < 0.001 compared with reversibly dysfunc- tional segments with reduced flow.
t icular ly w h e n the level of r e s t ing flow is reduced. In seven pa t ien ts , r evers ib ly dysfunct ional s egmen t s wi th p re se rved or reduced flow coexisted.
Measurements of myocardial oxygen consumption and glucose metabolism. To determine the metabolic
consequences of the a l te ra t ions in res t ing perfusion, as well as to provide an indirect conf i rmat ion of the accuracy of the res t ing flow values, both myocard ia l oxygen consumpt ion and glucose me tabo l i sm were assessed (Figs. 1, 3, and 4). In revers ib ly dysfunc-

March 1996 446 Conversano et al. American Heart Journal
2.50
2.00
1.S0
1.00
0.50
0.00
0
0
8! l ! T o , •
8 I o I
REVER. REVER. IRREV. (NL. MBF) (Low MBF)
Fig. 4. Average values and SDs for measurements of myocardial glucose metabolism normalized to flow in reversibly dysfunctional segments (REVER) that exhibited normal (NL MBF) or reduced (Low MBF) blood flow. Measurements in segments with irreversible dysfunction (IRREV) are included for compari- son. By definition, measurements in segments exhibiting normal contractile function exhibited value of one. In reversibly dysfunctional segments with preserved perfusion, glucose metabolism normalized to flow was comparable with that measured in segments with normal function. In contrast, in reversibly dysfunc- tional segments with reduced perfusion, glucose metabolism was increased relative to flow compared with that observed in reversibly dysfunctional segments with maintained perfusion. *p < 0.02 compared with normal segments or reversibly dysfunctional segments with preserved flow.
tional segments with preserved resting flow, the turnover rate constant, which reflects myocardial oxygen consumption (average k1=0.051 +- 0.012 min-Z), was comparable to that observed in segments exhibiting normal function (average kz = 0.049 +- 0.010 min-1; p = NS). Commensurate with the re- duction in resting myocardial blood flow, oxygen consumption as reflected by the turnover rate con- stant was reduced (average kl = 0.045 _+ 0.08 min -1) in reversibly dysfunctional segments in which flow values were below the 0.50 ml/gm/min cut-off (p < 0.03) compared with that exhibited by normal segments or reversibly dysfunctional segments with preserved flow. However, the level of myocardial ox- ygen consumption in these low-flow segments was still higher than that observed in the irreversibly in- jured segments (average kl = 0.032 +- 0.05 min-1; p < 0.001), in spite of the similar levels of flow.
In two patients, measurements of glucose metab- olism could not be performed because of the lack of differential uptake of the tracer by myocardium with respect to the blood pool. In the other 15 patients, reversibly dysfunctional segments with preserved flow exhibited levels of glucose metabolism normal- ized to flow (average ratio, 1.01 +- 0.29) comparable to that observed in normal segments (ratio = 1 by definition; p = NS). In contrast, when myocardial perfusion was reduced, glucose metabolism in rela- tion to flow was elevated (average ratio = 1.28 +- 0.36; p < 0.02 compared with normal segments or revers-
ibly dysfunctional segments with preserved flow). However, the level of glucose metabolism normalized to flow was comparable to that in irreversibly dys- functional segments (average ratio = 1.26 + _ 0.34; p = NS).
Flow and metabolic findings in partially reversibly dysfunctional segments. In the eight dysfunctional segments that exhibited intermediate improvement in systolic function after revascularization, resting myocardial perfusion averaged 0.52 +_ 0.28 ml/gm/ min. Six of the segments had flow values that were <0.50 ml/gm/min. Myocardial oxygen consumption tended to be reduced (kl = 0.043 _+ 0.005 min-1)i and glucose metabolism normalized to flow tended to be increased at (ratio = 1.17 _+ 0.28) in these segments, suggesting alterations in myocardial metabolism. However, the sample size was too small to achieve statistical significance. It is unclear if the reduction in perfusion was reflective primarily of myocardial hibernation (with incomplete recovery of function) or of admixture with significant amounts of irreversibly damaged tissue.
DISCUSSION
Reversible left ventricular dysfunction present under resting conditions in patients with chronic coronary artery disease has been generally believed to be the mechanical manifestation of chronic hy- poperfusion leading to hibernating myocardium. However, the results of this study demonstrate that

Volume 131, Number 3
American Heart Journal Conversano et al. 447
the pattern of abnormalities in resting perfusion is more complex. Although hypoperfusion is observed in a large proportion of reversibly dysfunctional seg- ments, perfusion at rest is frequently within normal limits, suggesting that the reversible mechanical dysfunction in these patients is attributable to in- termittent myocardial stunning and not to hiberna- tion. Furthermore, the metabolic consequences of these diverse flow abnormalities differ, which has important implications with respect to the interpre- tation of diagnostic studies designed to identify dys- functional but still viable myocardium by specific metabolic patterns.
Comparison with results of previous studies. We demonstrated previously that, in patients with chronic coronary artery disease, the level ofmyocar- dial oxygen consumption in reversibly dysfunctional myocardium was on average comparable to that ex- hibited by myocardium with normal function. This finding suggested that perfusion was within normal limits for many of these patients, given the close coupling between myocardial blood flow and oxygen consumption. 9 Recently, Vanoverschelde et a l ) ° demonstrated that, in reversibly dysfunctional myo- cardial segments, resting myocardial perfusion (quantified by PET and 13N-ammonia) was, on aver- age, within normal limits and comparable to that measured in segments exhibiting normal mechani- cal function. These data, taken together, provide strong evidence that the resting reversible left ven- tricular dysfunction observed in patients with chronic coronary artery disease reflected myocardial stun- ning.
The results of this study demonstrate that resting myocardial perfusion is markedly variable in myo- cardium exhibiting reversible systolic dysfunction. Resting myocardial perfusion can be either pre- served or reduced in such tissue, reflecting the pres- ence of either myocardial stunning or hibernation, respectively. Moreover, the wide of spectrum of flow values suggests that admixture of tissues with dif- fering levels of perfusion is likely. Furthermore, markedly different levels of myocardial oxygen con- sumption and patterns of myocardial substrate use were present based on the level ofperfusion (Figs. 1, 3, and 4). In reversibly dysfunctional segments with preserved flow, myocardial oxygen consumption was maintained, and there was no evidence of altered substrate use as the level of glucose metabolism tel- ative to the level of flow was not enhanced, a meta- bolic pattern consistent with myocardial stunning. In contrast, areas with reduced flow had perturba- tions in myocardial metabolism; myocardial oxygen consumption was reduced, and glucose metabolism
relative to the level of flow was increased. In these segments, the level of flow was comparable with that observed in the irreversibly dysfunctional segments. These data suggest that the level of flow alone, even when measured in absolute terms, will not accu- rately differentiate dysfunctional myocardium capa- ble of improving systolic function after revascular- ization from dysfunctional myocardium that cannot. Thus measurement of myocardial metabolism will likely be necessary to differentiate these two types of tissue.
Potential mechanisms. Several mechanisms may induce ischemia in these patients. A pattern sugges- tive of intermittent stunning by definition must rep- resent a dynamic process, as intermittent ischemia must occur. Thus intermittent stunning may be at- tributable to unrecognized, repetitive, transitory oc- clusion and spontaneous reperfusion caused by cy- cles of thrombosis and lysis. Indeed, in >50% of pa- tients with chronic coronary artery disease, both urinary and plasma levels of fibrinopeptide-A are el- evated, consistent with occult thrombosis. 22, 23 In addition, both spontaneous coronary vasospasm and persistent mechanical dysfunction after exercise-in- duced ischemia have been demonstrated in these patients. 24,25 Consequently, the extent to which procoagulant activity (and its potential interaction with the spontaneous, episodic aggregation and dis- aggregation ofplatelets), coronary vasospasm (either primary or secondary), or demand ischemia are causative is unknown.
The extent to which the angiographic severity of coronary artery disease is related to patterns of flow abnormalities observed is unknown. The anglo- graphic severity of coronary artery disease might be more pronounced in arteries subtended by myocar- dium in which resting flow was reduced compared with that in coronary arteries subtended by myocar- dium in which flow was preserved. To delineate whether these diverse flow abnormalities underlying resting mechanical dysfunction are indeed related to the angiographic severity of coronary artery disease will require quantitative angiographic measure- ments or estimates of their physiologic severity (i.e., measurements of vasodilator reserve) to be per- formed.
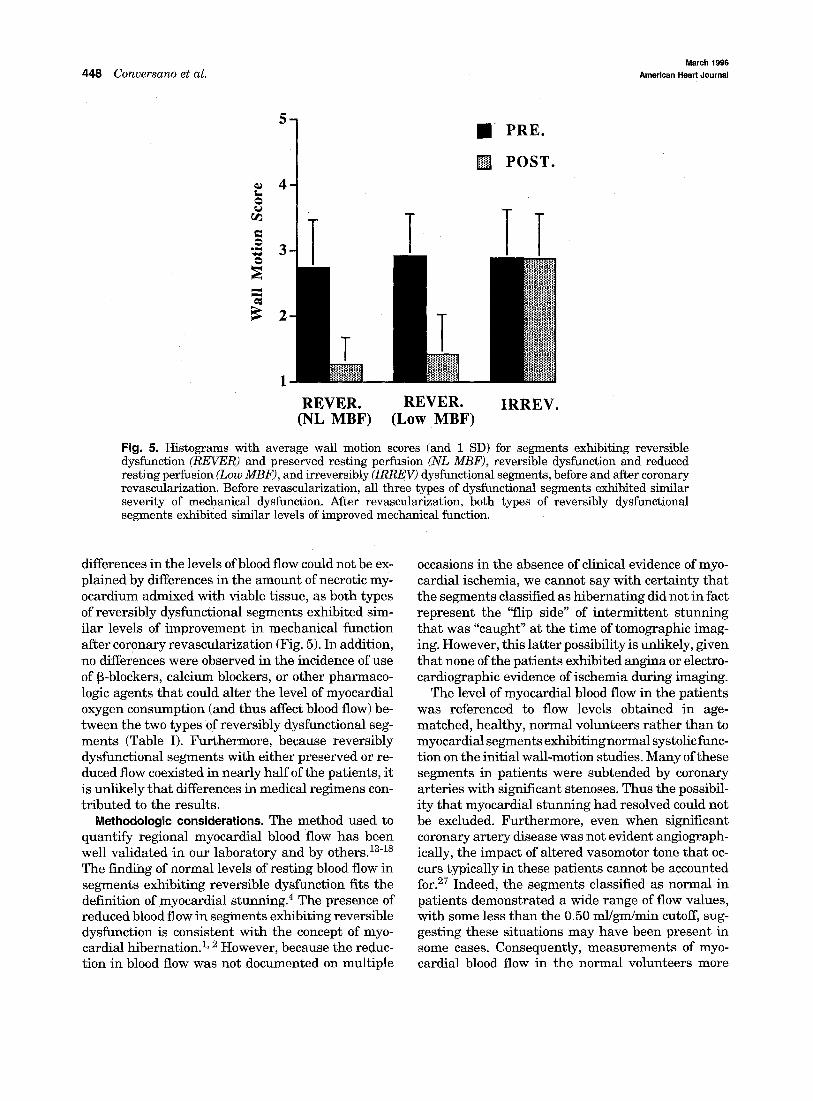
Because of the close coupling between myocardial oxygen demand and blood flow, differences in the levels of mechanical dysfunction present initially could lead to difference s in levels of resting perfusion. However, this explanation was unlikely in our study, as both types of reversibly dysfunctional segments exhibited similar levels of mechanical dysfunction before revascularization (Fig. 5). Furthermore, the
March 1996
448 Conversano et al. American Heart Journal
O
. m r
O
.
.
.
2
• P R E .
[ ] P O S T .
T l TT
1
REVER. R E V E R . IRREV. (NL MBF) (Low MBF)
Fig. 5. Histograms with average wall motion scores (and 1 SD) for segments exhibiting reversible dysfunction (REVER) and preserved resting perfusion (NL MBF), reversible dysfunction and reduced resting perfusion (Low MBF), and irreversibly (IRREV) dysfunctional segments, before and after coronary revascularization. Before revascularization, all three types of dysfunctional segments exhibited similar severity of mechanical dysfunction. After revascularization, both types of reversibly dysfunctional segments exhibited similar levels of improved mechanical function.
differences in the levels of blood flow could not be ex- plained by differences in the amount of necrotic my- ocardium admixed with viable tissue, as both types of reversibly dysfunctional segments exhibited sim- ilar levels of improvement in mechanical function after coronary revascularization (Fig. 5). In addition, no differences were observed in the incidence of use of ~-blockers, calcium blockers, or other pharmaco- logic agents that could alter the level of myocardial oxygen consumption (and thus affect blood flow) be- tween the two types of reversibly dysfunctional seg- ments (Table I). Furthermore, because reversibly dysfunctional segments with either preserved or re- duced flow coexisted in nearly half of the patients, it is unlikely that differences in medical regimens con- tr ibuted to the results.
Methodologic considerations. The method used to quantify regional myocardial blood flow has been well validated in our laboratory and by others. 13-1s The finding of normal levels of resting blood flow in segments exhibiting reversible dysfunction fits the definition of myocardial stunning. 4 The presence of reduced blood flow in segments exhibiting reversible dysfunction is consistent with the concept of myo- cardial hibernation. 1, 2 However, because the reduc- tion in blood flow was not documented on multiple
occasions in the absence of clinical evidence of myo- cardial ischemia, we cannot say with certainty that the segments classified as hibernating did not in fact represent the "flip side" of intermittent stunning that was "caught" at the time of tomographic imag- ing. However, this latter possibility is unlikely, given that none of the patients exhibited angina or electro- cardiographic evidence of ischemia during imaging.
The level of myocardial blood flow in the patients was referenced to flow levels obtained in age- matched, healthy, normal volunteers rather than to myocardial segments exhibiting normal systolic func- tion on the initial wall-motion studies. Many of these segments in patients were subtended by coronary arteries with significant stenoses. Thus the possibil- ity that myocardial stunning had resolved could not be excluded. Furthermore, even when significant coronary artery disease was not evident angiograph- ically, the impact of altered vasomotor tone that oc- curs typically in these patients cannot be accounted for. 27 Indeed, the segments classified as normal in patients demonstrated a wide range of flow values, with some less than the 0.50 ml/gm/min cutoff, sug- gesting these situations may have been present in some cases. Consequently, measurements of myo- cardial blood flow in the normal volunteers more

Volume 131, Number 3 American Heart Journal Conversano et al. 4 4 9
likely represent flow values exhibited by normal myocardium.
At first blush, the finding of similar levels of glu- cose metabolism normalized to flow exhibited by re- versibly dysfunctional segments with low flow and irreversibly dysfunctional segments would appear at odds with results of previous studies demonstrating the presence of increased metabolism with glucose normalized to flow, a metabolic pattern more typical of dysfunctional but viable myocardium than of irre- versibly damaged myocardium. 28,29 However, in studies documenting this observation, the number of dysfunctional segments demonstrating this meta- bolic pattern was reported rather than the magni- tude of the mismatch between glucose metabolism and flow, as was performed in our study.
Implications. Although there is a wide range in resting flow in myocardial segments with reversible dysfunction, the importance of accurate delineation of the underlying flow disturbance and its impact on recovery ofmyocardium in response to specific modes of recanalization is great. Accurate identification of these flow abnormalities and the extent to which they may reflect myocardial stunning or hibernation provides the basis for delineating the molecular and biochemical mechanisms responsible for these phe- nomena. Characterization of these underlying flow abnormalities will provide a framework for the accu- rate interpretation of diagnostic studies designed to identify patients likely to derive benefit from me- chanical revascularization procedures. In patients with predominantly myocardial hibernation, me- chanical revascularization may be the only option, as medical therapies designed to decrease oxygen sup- ply might in theory be less useful. Even in patients with predominantly myocardial stunning, signifi- cant and severe occlusive coronary artery disease is typically present, blunting myocardial perfusion re- serve. 1° Thus mechanical revascularization would still be necessary in these patients. Delineation of the flow abnormalities responsible for the mechanical dysfunction will facilitate the development and eval- uation of novel pharmacologic and mechanical ther- apeutic strategies designed to maintain nutritive perfusion in patients with coronary disease. For ex- ample, in patients in whom coronary revasculariza- tion was not an option but yet substantial left ventricular dysfunction caused by myocardial stun- ning was present, novel antithrombotics or coronary vasolytics to improve oxygen supply or aggressive medical therapy to reduce oxygen demand might re- sult in improved left ventricular function. Thus it is anticipated that accurate characterization of the flow abnormalities underlying reversible mechanical
dysfunction will result in improved care of these pa- tients.
The a u t h o r s t h a n k Ms. P i la r Herrero, MS, for h e r work in op- t imiz ing the m a t h e m a t i c a l model u sed to quan t i fy myocardia l blood flow by P E T a n d 1SO-water u sed in the study.
REFERENCES
1. Braunwald E, Rutherford JD. Reversible ischemic left ventricular dys- function: evidence for the "hibernating myecardium." J Am Cell Car- diol 1986;8:1467-70,
2. Rahimtoola SH. The hibernating myocardium. A~I HEART J 1989; 117: 211-21.
3. Fedele FA, Gewirtz H, Capone P~J, Sharaf B, Most AS. Metabolic response to prolonged reduction of myocardial blood flow distal to a se- vere coronary artery stenosis. Circulation 1988;78:729-35.
4. Bolli R. Myocardial "stunning ~' in man. Circulation 1992;86:1671-9L 5. Lavallee M, Cox D, Patrick TA, Vatner SF. Salvage of myocardial oc-
clusion by coronary artery reperfusion 1, 2 and 3 hours after occlusion in conscious dogs. Circ Res 1983;53:235-47.
6. Bush LR, Buja LM, Samowitz W, Rude RE, Watben M, Tilton GD, Willerson JT. Recovery of left ventricular segmental function after long-term reperfusion following temporary coronary occlusion in con- scious dogs: comparison of 2- and 4-hour occlusions. Circ Res 1983; 53: 248-63.
7. Topol EJ, Weiss JL, Brinker JA, Brin KP, Gottlieb SO, Becker LC, Bulkley BH, Chandra N, Flaherty JT, Gerstenblith G, Gottlieb SH, Guerci AD, Ouyang P, Llewellyn MP, Weisfeldt ML, Shapiro SP. Re- gional wall motion improvement after coronary thrombolysis with re- combinant tissue plasminogen activator: importance of coronary angi- oplasty. J Am Cell Cardiol 1985;6:426-33.
8. Serruys PW, Simoons ML, Suryapranata H, Vermeer F, Wijns W, van den Brand M, Bar F, Zwaan C, Krauss H, Remme WJ, Res J, Verheught FWA, van Domburg R, Lubsen J, Hugenholtz PG. Preservation of glo- bal and regional left ventricular function after early thrombolysis in acute myocardial infarction. J Am Cell Cardiol 1986;7:729-42.
9. Gropler RJ, Geltman EM, Sampathkumaran KS, Perez JE, Sobel BE, Bergmann SR, Siegel BA. Functional recovery after revascularization for chronic coronary artery disease is dependent on maintenance of ox- idative metabolism. J Am Cell Cardiol 1992;20:569-77.
10. Vanoverschelde JLJ, Wijns W, Depr~ C, Essamri B, Heyndrickx GR, Borgers M, Bol A, Melin JA. Mechanisms of chronic regional postis- chemic dysfunction in humans: new insights from the study of nonin- farcted collateral-dependent myocardium. Circulation 1993;87:1513- 23.
11. Gropler RJ, Siegel BA, Sampathkumaran K, Perez JE, Sobel BE, Bergmann SR, Geltman EM. Dependence of recovery of contractile function on maintenance of oxidative metabolism after myocardial in- farction. J Am Cell Cardiol 1992;19:989-97.
12. Schiller NB, Shan PM, Crawfor M, DeMaria A, Devereau R, Feigen- baum H, Gutgesell H, Reichek N, Sahn D, Schnittger I, Silverman NH, Tajik AJ. Recommendations for quantitation of the left ventricle by two-dimensional echocardiography. JAm SocEchocardiogr 1989;2:358- 67.
13. Herrero P, Hartmann J J, Senneff MJ, Bergmann SR. Effects of time discrepancies between input and myocardial time-activity curves on estimates of regional myocardial perfusion with PET. J Nucl Med 1994; 35:558-66.
14. Bergmann SR, Herrero P, Markham J, Weinheimer CJ, Walsh MN. Noninvasive quantitation of myocardial blood flow in human subjects with oxygen- 15-Iabeled water and positron emission tomography. J Am Cell Cardiol 1989;14:639-52.
15. Herrero P, Markham J, Bergmann SR. Quantitation of myocardial blood flow with H2150 and positron emission tomography: assessment and error analysis of a mathematical approach. J Comput Assist Tomogr 1989;13:862-73.
16. Iida I, Rhodes CG, de Silva R, Yamamoto Y, Araugo LI, MaseriA, Jones T. Myocardial tissue fraction: correction for partial volume effects and measure of tissue viability. J Nucl Med 1991;32:2169-75.
17. Herrere P, Weinheimer CJ, Toeniskoetter PD, Staudenherz A, Walsh

March 1996
450 Conversano et al. American Heart Journal
JF, Gropler RJ, Bergmann SR. Quantification of regional myocardial perfusion in low flow regions using positron emission temography and oxygen-15 water [Abstract]. Circulation 1993;88:I-274.
18. Brown MA, Marshall DR, Sebel BE, Bergmann SR. Delineation of my- ocardial oxygen utilization with carbon-ll-acetate. Circulation 1987; 76:687-96.
19. Ambrecht JJ, Buxton DB, Schelbert HR. Validation of [1-nc] acetate as a tracer for noninvasive assessment of oxidative metabolism with positron emission tomography in normal, ischemic, postischemic, and hyperemic canine myocardium. Circulation 1989;81:1594-605.
20. Gropler RJ, Geltman EM, Sampathkumaran KS, Perez JE, Schecht- man KB, Conversano A, Sobel BE, Bergmann SR, Siegel BA. Compar- ison of C-11 acetate and F-18 fluorodeoxyglucose for delineating viable myocardium by positron emission tomography. J Am Call Cardiol 1993;22:1587-97.
21. Neri N, Seraeri GG, Gensini GF, Abbate R, Mugnaini C, Favilla S, Brunelli C, Chierchia S, Parodi O. Increased fibrinopeptide A formation and thromboxane A2 production in patients with ischemic heart disease: relationships to coronary pathoanatomy, risk factors, and clinical manifestations. AM HEART J 1981;101:185-94.
22. Ardissino D, Gamba MG, Merlini PA, RoUa A, Barberis P, Demicheli G, Testa S, Bruno N, Specchia G. Fibrinopeptide A excretion in urine: a marker of the cumulative thrombin activity in stable versus unstable angina patients. Am J Cardiol 1991;68:58B-63B.
23. Takatsu F, Suzuki A, Nagaya T. Variant angina peetoris with pro- longed electrical and mechanical stunning. Am J Cardio11986;58:647-9.
24. Mathias P, Kerin NZ, Blevisn RD, Cascase P, Rubenfire M. Coronary vasospasm as a cause of stunned myocardium. AM HEART J 1987; 113: 383-5.
25. Homans DC, Sublett E, Dai XZ, Bache RJ. Persistence of regional left ventricular dysfunction after exercise-induced myocardial ischemia. J Clin Invest 1986;77:66-73.
26. Kloner RA, Allen J, Cox TA, Zheng Y, Ruiz CE. Stunned lei~ ventric- ular myocardium after exercise treadmill testing in coronary artery disease. Am J Cardiol 1991;68:329-34.
27. Uren NG, Marraccini P, Gistri R, De Silva R, Camici PG. Altered cor- onary vasodilater reserve and metabolism in myocardium subtended by normal arteries in patients with coronary artery disease. J Am Cell Cardiol 1993;22:650-8.
28. TiUisch J, Brunker R, Marshall R, Schwaiger M, Mandelkern M, Phelps M, Schelbert HC. Reversibility of cardiac wall-motion abnormalities predicted by positron tomography. N Engl J Med 1986;314:884-8.
29. Tamaki N, Yonekura Y, Yamashita K, Saji H, Magata Y, Senda M, Konishi Y, Hirata K, Ban T, Konishi J. Positron emission tomography using fluorine- 18-deoxyglucose in evaluation of coronary artery bypass grafting. Am J Cardiol 1989;64:860-5.
Copyright © 2022 FDOKUMEN