
Deliberative curriculum inquiry for integration in an MD curriculum: Dalhousie University's...
9
2012; 34: e785–e793 WEB PAPER Deliberative curriculum inquiry for integration in an MD curriculum: Dalhousie University’s curriculum renewal process LYNETTE REID, ANNA MACLEOD, DAVID BYERS, DIANNE DELVA, TIM FEDAK, KAREN MANN, TOM MARRIE, BRENDA MERRITT & CHRISTY SIMPSON Dalhousie University, Canada Abstract Background: Dalhousie University’s MD Programme faced a one-year timeline for renewal of its undergraduate curriculum. Aim: Key goals were renewed faculty engagement for ongoing quality improvement and increased collaboration across disciplines for an integrated curriculum, with the goal of preparing physicians for practice in the twenty-first century. Methods: We engaged approximately 600 faculty members, students, staff and stakeholders external to the faculty of medicine in a process described by Harris (1993) as ‘deliberative curriculum inquiry’. Temporally overlapping and networked intraprofessional and interprofessional teams developed programme outcomes, completed environment scans of emerging content and best practices, and designed curricular units. Results: The resulting curriculum is the product of new collaborations among faculty and exemplifies distinct forms of integration. Innovations include content and cases shared by concurrent units, foundations courses at the beginning of each year and integrative experiences at the end, and an interprofessional community health mentors programme. Conclusion: The use of deliberative inquiry for pre-med curriculum renewal on a one-year time frame is feasible, in part through the use of technology. Ongoing structures for integration remain challenging. Although faculty collaboration fosters integration, a learner-centred lens must guide its design. Introduction Curricular integration is ‘the interweaving of disciplines to teach a subject from multiple perspectives’ (Muller et al. 2008). At the content level, it requires a framework shared across disciplines. At the institution level, it requires culture change: faculty must design and teach across traditional departmental and course boundaries. As Harris describes in her classic analysis, curriculum design is more than a technical task: it is an institutional process (Harris 1993). We describe here our rapid pre-clerkship curriculum renewal, which engaged a broad range of faculty members, students, staff, and stake- holders in a process described by Harris as ‘deliberative curriculum inquiry’ (Harris 1993). In the course of deliberative curriculum inquiry, multiple models of integration (Harden 2000) for the resulting curriculum emerged. Medical schools struggle with curriculum mapping. Mapping is considered essential to curriculum planning and oversight, but by the mid-2000s, only 20% of surveyed medical schools in the United Kingdom and Canada had completed curriculum maps (Harden 2001; Willett 2008). The process of designing a curriculum via objectives is both ‘top-down’ and learner-centred, as described in Wiggins and McTighe’s ‘understanding by design’ framework (2001). Educators focus on student outcomes of learning, asking: what lasting under- standings do learners need to develop? Objectives and learning occasions are then ‘constructively aligned’ (Biggs 1996) to enable students to achieve specific knowledge, skills and attitudes, and integrate these for successful participation in the practice environment, while mapping assessment to objectives enables the programme to monitor learner achieve- ment in relation to programme goals. The resulting ‘map’ of a curriculum, typically housed in a database, enables everyone involved in the curriculum to learn and teach more effectively. Curriculum planners can monitor content for its staging, and identify gaps and redundancies; individual faculty can see their contributions in relation to the whole and identify relevant skills and content students learn elsewhere in the curriculum. Students similarly have a ‘map’ of where the curriculum is Practice points: . Deliberative curriculum inquiry is feasible for forging a shared curriculum vision. . Deliberative inquiry facilitates the development of an integrated curriculum. . Deliberative curriculum inquiry is feasible for rapid curriculum renewal. . Content integration is facilitated by faculty collaboration, but its implementation must remain student-centred. . Appropriate supports must be in place for technologies, like wikis that can facilitate curriculum renewal. Correspondence: L. Reid, Department of Bioethics, Dalhousie University, PO Box 15000, Halifax NS B3H 4R2, Canada. Tel: 902-494-1842; fax: 902- 494-3865; email: [email protected] ISSN 0142–159X print/ISSN 1466–187X online/12/O120785–9 ß 2012 Informa UK Ltd. e785 DOI: 10.3109/0142159X.2012.687479 Med Teach Downloaded from informahealthcare.com by 117.171.236.219 on 05/20/14 For personal use only.
Transcript of Deliberative curriculum inquiry for integration in an MD curriculum: Dalhousie University's...

2012; 34: e785–e793
WEB PAPER
Deliberative curriculum inquiry for integration inan MD curriculum: Dalhousie University’scurriculum renewal process
LYNETTE REID, ANNA MACLEOD, DAVID BYERS, DIANNE DELVA, TIM FEDAK, KAREN MANN,TOM MARRIE, BRENDA MERRITT & CHRISTY SIMPSON
Dalhousie University, Canada
Abstract
Background: Dalhousie University’s MD Programme faced a one-year timeline for renewal of its undergraduate curriculum.
Aim: Key goals were renewed faculty engagement for ongoing quality improvement and increased collaboration across
disciplines for an integrated curriculum, with the goal of preparing physicians for practice in the twenty-first century.
Methods: We engaged approximately 600 faculty members, students, staff and stakeholders external to the faculty of medicine in
a process described by Harris (1993) as ‘deliberative curriculum inquiry’. Temporally overlapping and networked intraprofessional
and interprofessional teams developed programme outcomes, completed environment scans of emerging content and best
practices, and designed curricular units.
Results: The resulting curriculum is the product of new collaborations among faculty and exemplifies distinct forms of integration.
Innovations include content and cases shared by concurrent units, foundations courses at the beginning of each year and
integrative experiences at the end, and an interprofessional community health mentors programme.
Conclusion: The use of deliberative inquiry for pre-med curriculum renewal on a one-year time frame is feasible, in part through
the use of technology. Ongoing structures for integration remain challenging. Although faculty collaboration fosters integration, a
learner-centred lens must guide its design.
Introduction
Curricular integration is ‘the interweaving of disciplines to
teach a subject from multiple perspectives’ (Muller et al. 2008).
At the content level, it requires a framework shared across
disciplines. At the institution level, it requires culture change:
faculty must design and teach across traditional departmental
and course boundaries. As Harris describes in her classic
analysis, curriculum design is more than a technical task: it is
an institutional process (Harris 1993). We describe here our
rapid pre-clerkship curriculum renewal, which engaged a
broad range of faculty members, students, staff, and stake-
holders in a process described by Harris as ‘deliberative
curriculum inquiry’ (Harris 1993). In the course of deliberative
curriculum inquiry, multiple models of integration (Harden
2000) for the resulting curriculum emerged.
Medical schools struggle with curriculum mapping.
Mapping is considered essential to curriculum planning and
oversight, but by the mid-2000s, only 20% of surveyed medical
schools in the United Kingdom and Canada had completed
curriculum maps (Harden 2001; Willett 2008). The process of
designing a curriculum via objectives is both ‘top-down’ and
learner-centred, as described in Wiggins and McTighe’s
‘understanding by design’ framework (2001). Educators focus
on student outcomes of learning, asking: what lasting under-
standings do learners need to develop? Objectives and
learning occasions are then ‘constructively aligned’ (Biggs
1996) to enable students to achieve specific knowledge, skills
and attitudes, and integrate these for successful participation in
the practice environment, while mapping assessment to
objectives enables the programme to monitor learner achieve-
ment in relation to programme goals. The resulting ‘map’ of a
curriculum, typically housed in a database, enables everyone
involved in the curriculum to learn and teach more effectively.
Curriculum planners can monitor content for its staging, and
identify gaps and redundancies; individual faculty can see their
contributions in relation to the whole and identify relevant
skills and content students learn elsewhere in the curriculum.
Students similarly have a ‘map’ of where the curriculum is
Practice points:
. Deliberative curriculum inquiry is feasible for forging a
shared curriculum vision.
. Deliberative inquiry facilitates the development of an
integrated curriculum.
. Deliberative curriculum inquiry is feasible for rapid
curriculum renewal.
. Content integration is facilitated by faculty collaboration,
but its implementation must remain student-centred.
. Appropriate supports must be in place for technologies,
like wikis that can facilitate curriculum renewal.
Correspondence: L. Reid, Department of Bioethics, Dalhousie University, PO Box 15000, Halifax NS B3H 4R2, Canada. Tel: 902-494-1842; fax: 902-
494-3865; email: [email protected]
ISSN 0142–159X print/ISSN 1466–187X online/12/O120785–9 � 2012 Informa UK Ltd. e785DOI: 10.3109/0142159X.2012.687479
Med
Tea
ch D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y 11
7.17
1.23
6.21
9 on
05/
20/1
4Fo
r pe
rson
al u
se o
nly.

taking them, and a mechanism for readily finding and relating
materials via objectives. They are also introduced to the
process of reflecting on their learning in relation to goals, an
element of lifelong learning.
Harris (1993) describes the structural challenges that medical
schools encounter when this approach, which she calls the
‘empirical analytical tradition’, meets the competing pressures of
institutional life. Medical school faculty are responsible to
clinical as well as research priorities; each individual may feel
little ownership of the curriculum, given their small role in a
complex and integrated enterprise. They may be particularly
reluctant to engage in work perceived as unnecessary
(Davenport et al. 2009). Mapping may be seen as a technical
process of database design; the human question of aligning
intraprofessional and interprofessional collaboration for
common educational goals may be forgotten. As Harris
describes, the institutional setting of practice, intraprofessional
and interprofessional culture(s), the missions of research,
patient care and policy, and departmental ownership of
educational content must be negotiated and brought into
‘alignment’. Beyond the institution, the education of future
physicians must prepare them to be full participants in a
changing world, not only with respect to the ever-accelerating
pace of scientific knowledge production, but also with respect to
transformations in the physician–patient relationship fostered
by the internet, calls for physician leadership within healthcare
systems, the changing demographic profile and health needs of
the community, rapid technological advances, and economic
pressures that threaten equitable and accessible healthcare.
In 2009–2010, Dalhousie University’s Faculty of Medicine
faced the task of rapid renewal of a two-year case-oriented
problem-stimulated problem-based learning (PBL) pre-clerk-
ship curriculum that had not been significantly revised since its
implementation 16 years earlier. The timeline was determined
by accreditation results, and by plans for a distant campus. We
benefited from the experience of our institution’s School of
Occupational Therapy in their design of a new MSc-level
curriculum on an outcomes-oriented model. Their example of
defining and aligning shared outcome-based learning objec-
tives, values and beliefs to develop a framework for individual
course objectives and design, and for creating an appropriate
learning environment supported the model of deliberative
curriculum inquiry. The School of Occupational Therapy
enjoys a small, cohesive faculty and benefited from faculty
release time; the Faculty of Medicine is a large, diverse
community with competing priorities, and faced its task with
no teaching release, though with some funding to facilitate
retreats, team meetings and engagement of educational
specialists.
Aims
Our aims for curriculum renewal included meeting the one-
year timeline for launching a distributed programme, fulfilling
accreditation standards, particularly around mapping, achiev-
ing better integration of basic, clinical and social/humanistic
sciences, and re-engaging faculty for ongoing curriculum
collaboration and quality improvement. Given that we were
both clarifying responsibilities for oversight of the
programme, and fostering more interprofessional and
intraprofessional collaboration in the resulting integrated
units, a central challenge was to be broadly inclusive while
avoiding chaos.
Methods
Drawing on Schwab’s work at the University of Chicago in the
1970s, Harris recommends deliberative curriculum inquiry to
address such institutional challenges. In deliberative curricu-
lum inquiry, members of purposefully constituted groups
reach curriculum decisions through processes of deliberation.
Deliberative inquiry has several strengths that foster effective
curriculum development (Prideaux 2003). It enables a broad
group to bring diverse perspectives to consider curriculum
needs and how they can best be addressed, providing
justification for decisions and fostering the commitment of
participants. It provides a structure within which integration
can be accomplished across disciplinary and professional
boundaries. It allows for the explicit inclusion of the values,
resources, goals and context. It can enhance the effectiveness
of more linear, stepped approaches to curriculum develop-
ment (e.g., Kern et al. 2009). Perhaps most significantly, it
reflects the complex environment of medical education (Harris
1993).
Such a complex process also brings challenges. Diverse
groups with different perspectives may need time (a rare
commodity) to reach common understanding of curriculum
needs. Distributed ownership of curriculum can also challenge
the development of integrated curricula. Differences of
approaches to methods of teaching and learning, appropriate
learning environments and understanding of curriculum goals
can create confusion for faculty and learners.
Our process of deliberative curriculum inquiry largely
involved re-prioritization of existing resources, with the
exception of an education specialist hired to support faculty
in translating their commitment to outcomes-oriented design
into practice. We engaged in four parallel and networked
processes of overall curriculum planning (Figure 1) during the
fall of 2009 and a subsequent unit design process in the
winter/spring of 2010. Approximately 600 faculty, students and
stakeholders participated in the renewal efforts, broadly
transforming institutional culture and preparing educators to
collaborate for integration. Technology was essential to
facilitating collaboration and enabling rapid connection with
stakeholders.
To design programme outcomes, we held a retreat of 100
faculty members, researchers and community stakeholders
who deliberated on the local context and national and
international competency profiles (RCPSC 2005; GMC 2009).
A small group synthesized the results of the retreat. The
process of designing programme-level outcomes was docu-
mented and shared on a blog, which served as a conduit for
rapid stakeholder input. The results of this process served as a
touchstone for subsequent decisions.1
In a second parallel process, 20 curriculum scan groups
(comprising approximately 220 members; some served on
more than one group) searched the literature and networked
L. Reid et al.
e786
Med
Tea
ch D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y 11
7.17
1.23
6.21
9 on
05/
20/1
4Fo
r pe
rson
al u
se o
nly.

nationally and internationally to present best practices for both
content and educational approaches in important areas.2 Each
group was deliberatively constructed, with a focus on
integrating the necessary faculty expertise and interprofes-
sional collaboration, including specialist and generalist physi-
cians, other health professionals, scientists, education
specialists and students.
These results fed into a Curriculum Symposium organized
by a third group, where several hundred participants discussed
the scan groups reports and learned about recent develop-
ments in learning theory and in the organization of clerkship.
On the basis of the Curriculum Symposium, the scan group
reports and ongoing appraisal of the literature, the undergrad-
uate associate dean and educational specialists proposed the
following principles as guidance: (1) a patient-centred focus
that (2) supports life-long learning and (3) is learner-centred,
offering (4) integrated learning experiences, (5) clearly linked
to objectives/outcomes and with a (6) menu of learning
formats, with (7) assessment tied to student outcomes. These
guiding principles informed our unit design process and
served as a checkpoint in reviewing proposed unit plans and
curricular materials.
This first phase of the process ended in a smaller,
deliberative curriculum retreat consisting of the core curricu-
lum committee and a group of teaching faculty, students and
stakeholders. This group of 30 participants weighed and
prioritized the resulting recommendations, in light of the
guiding principles and the educational outcomes, reaching
agreement on core strategic decisions and prioritized recom-
mendations by voting.3
Networking parallel processes enabled us to compress the
first stage of renewal into 4 months: the retreat in early
September, scan group reports completed by mid-November,
the Symposium in late November and the final deliberative
retreat in mid-December. This process might easily have
stretched over two years or more if completed sequentially by
a single group (Wiener et al. 2010). Horizontal communication
between these processes and engagement of participants
across multiple working groups ensured that emerging results
from each process informed the other.
The shortened timeline challenged our efforts to obtain
formal, systematic public input. The CanMEDS competency
framework results from broad, inclusive consultation and lent
legitimacy via its inclusion. Nonetheless, we wanted to build
relationships with stakeholders and our local community. We
engaged the public in two ways: via print and radio media, the
dean solicited on-line input on the question, ‘what makes a
good doctor?’. Meanwhile, we carried out a series of
Community Conversations across the Maritime provinces.
These served as a stakeholder check as results were emerging
from our working groups.
New, topic-specific unit design teams were formed in
January 2010, with approximately 100 members. These were
again deliberatively formulated, including specialist and gen-
eralist physicians, clinicians and basic scientists, specialists in
medical education and link persons for crosscutting subjects
(anatomy, pathology, physiology and pharmacology). Some
participants had already taken part in earlier stages of renewal;
some were new at this point. Each unit had at least one
interprofessional collaborator and a link to the Professional
Figure 1. Parallel and networked processes.
Deliberative curriculum inquiry at Dalhousie
e787
Med
Tea
ch D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y 11
7.17
1.23
6.21
9 on
05/
20/1
4Fo
r pe
rson
al u
se o
nly.
Competencies (ProComp) Unit for integration with the con-
current longitudinal unit in social and behavioural sciences,
ethics, law and health policy. Mapping to the four programme-
level educational outcomes, the groups developed learning
objectives at three levels: unit (highest-level, to be attained
upon completion of the unit), component (mid-level, repre-
senting the major aspects of the unit) and learning occasion
levels (lectures, laboratories and tutorials). In reality, this
process is iterative and ongoing, with objectives refined and
clarified as learning and assessment activities are designed and
revised.
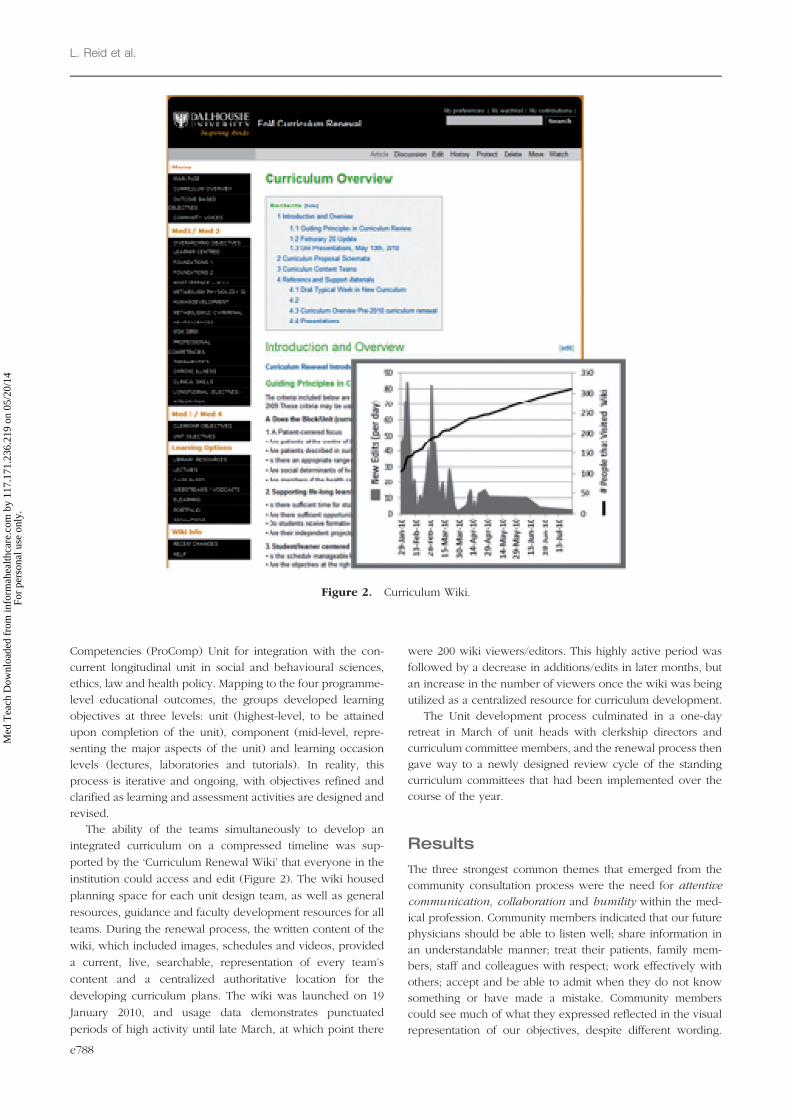
The ability of the teams simultaneously to develop an
integrated curriculum on a compressed timeline was sup-
ported by the ‘Curriculum Renewal Wiki’ that everyone in the
institution could access and edit (Figure 2). The wiki housed
planning space for each unit design team, as well as general
resources, guidance and faculty development resources for all
teams. During the renewal process, the written content of the
wiki, which included images, schedules and videos, provided
a current, live, searchable, representation of every team’s
content and a centralized authoritative location for the
developing curriculum plans. The wiki was launched on 19
January 2010, and usage data demonstrates punctuated
periods of high activity until late March, at which point there
were 200 wiki viewers/editors. This highly active period was
followed by a decrease in additions/edits in later months, but
an increase in the number of viewers once the wiki was being
utilized as a centralized resource for curriculum development.
The Unit development process culminated in a one-day
retreat in March of unit heads with clerkship directors and
curriculum committee members, and the renewal process then
gave way to a newly designed review cycle of the standing
curriculum committees that had been implemented over the
course of the year.
Results
The three strongest common themes that emerged from the
community consultation process were the need for attentive
communication, collaboration and humility within the med-
ical profession. Community members indicated that our future
physicians should be able to listen well; share information in
an understandable manner; treat their patients, family mem-
bers, staff and colleagues with respect; work effectively with
others; accept and be able to admit when they do not know
something or have made a mistake. Community members
could see much of what they expressed reflected in the visual
representation of our objectives, despite different wording.
Figure 2. Curriculum Wiki.
L. Reid et al.
e788
Med
Tea
ch D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y 11
7.17
1.23
6.21
9 on
05/
20/1
4Fo
r pe
rson
al u
se o
nly.

Ultimately, our community members challenged us to ensure
that we continue to ‘personalize the profession of medicine’
throughout and beyond our curriculum renewal process.
Along with a patient-centred approach, the renewed pre-
clerkship curriculum is case-based, with a high degree of
integration among the relevant biomedical, clinical and social/
humanistic sciences. The major systems-based units range
from a half to a full semester in length and occupy three half-
days of classroom (lecture, laboratory and tutorial) time per
week. These occur alongside two longitudinal 2-year Units,
Clinical Skills and ProComp, which focus respectively on
clinical and communication skills and the social, behavioural,
ethical, legal and organizational aspects of medicine, each
occupying roughly a half-day per week. The remainder of the
schedule is reserved for electives and other self-directed
learning.4
Case-based and patient-centred learning, withstrengthened integration
Muller et al. argue that, ‘an integrated approach to education
may have important benefits for learning and retention
because it facilitates contextual and applied learning, and
can promote the development of the well-organized knowl-
edge structures that underlie effective clinical reasoning’
(Muller et al. 2008). The PBL of our previous curriculum was
intended as a high-level approach to integration, described by
Harden’s integration ladder model as the ‘top rung’ (Harden
2000): ideally, the paper patient’s presenting problem frames
learning in the context of an authentic practice challenge for
students, who draw on any and all disciplines needed to
reason to diagnosis and to propose management options. In
our experience, however, the ‘PBL detective game’ detracted
from attempts at patient-centredness in cases (Macleod 2011).
Furthermore, PBL is known to limit transfer of knowledge
because of its focus on single index cases (Eva et al. 1998).
Curriculum redesign included a shift from a traditional PBL
approach to case-based learning (CBL; Srinivasan et al. 2007).
While CBL and PBL are informed by the same principles of
discovery learning, learners in CBL have access to case
narratives and learning objectives in advance of the tutorial;
in tutorial, they integrate new and existing knowledge and
engage in discussion to co-construct knowledge and learn
deeply. They may be exposed in some weeks to multiple
vignettes in a given area. A deliberate focus on the patient
within a bio-psychosocial framework is achieved by cases that
are detailed and authentic, in terms of content, educational
resources and social perspectives, and by addressing, wher-
ever possible, the same or closely related cases in the
concurrent biomedical and the longitudinal ProComp units.
Other innovations included adding overlooked topics such
as oral health, nutrition, sports and occupational medicine.
Integration is supported by the ‘Foundations’ units at the
beginning of each year, and integrative experiences (a Rural
Week community placement in year 1 and an Integration Unit
including geriatrics, oncology, and palliative care in year 2) at
the end. To provide an early interprofessional experience, we
implemented a community-based health mentors programme
in year 1, based on the model of the Jefferson mentors (Collins
et al. 2009). Interprofessional student teams interview patients
in the community and learn about the experience of chronic
disease and its management from the patient’s perspective.
We describe below in more detail three results that
demonstrate the strengths of deliberative curriculum inquiry
to create shared frameworks and foster collaboration: the
programme-level framework and educational approach, and
two specific integrative units, the Foundations Unit, which
remediates background basic science understanding and
prepares students for integrated learning of basic and clinical
sciences, and the longitudinal ProComp Unit, which introduces
students to challenges in the practice of medicine for which we
integrate ethics, law, population health, evidence-based
practice, health policy, practice organization and quality
improvement in the spirit of reflective practice and lifelong
learning.
Programme-level educational outcomes andeducational approach
The Educational Outcomes group produced a concept map
diagram (Figure 3) representing programme outcomes.
Consistent with Epstein and Hundert’s (2002) vision of
professional competence as integrative, our diagram repre-
sents the integration for professional practice of knowledge,
technical skills, cognitive/reflective skills and attitudes.
Visually, our concept map depicts four domains around the
outside of a square: the ‘roles’ of professional, community
contributor, life-long learner, and skilled clinician. Within the
square are the knowledge (four overlapping scientific
domains: biomedical, humanistic; epidemiological and
social), skills (communication, collaboration, problem-solving,
critical thinking and advocacy) and attitudinal attributes
(compassionate, conscientious, reflective, curious, innovative,
accountable, ethical, socially responsible and collegial) to be
‘habitually and judiciously used’ for the benefit of the patient,
who stands at the centre of the diagram. The idea of the
‘square’ and its ‘sides’ quickly became a touchstone in
planning.
The writing group used the concept of ‘entrustable profes-
sional activities’ (EPA) to link programme outcomes to
concrete and readily grasped activities. An EPA is ‘a critical
part of professional work that can be identified as a unit to be
entrusted to a trainee once sufficient competence has been
reached’ (ten Cate & Scheele 2007). We asked the
Figure 3. Curriculum outcomes: the ‘square’.
Deliberative curriculum inquiry at Dalhousie
e789
Med
Tea
ch D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y 11
7.17
1.23
6.21
9 on
05/
20/1
4Fo
r pe
rson
al u
se o
nly.

question: ‘What should a program director be able to trust that
a graduate of our program will be able to do on entering
postgraduate training?’ (ten Cate et al. 2010). In our view, EPAs
extend beyond narrow, delegated clinical skills, such as
‘perform an accurate history and physical’, to broad entrus-
table activities, such as ‘demonstrate appropriate professional
attitudes and ethical commitments’. Students develop their
professional behaviours as they progress through medical
school, and are assessed on their behaviours as outlined in the
objectives. Students must remediate breaches of professional
behaviour, just as they must remediate inability to perform an
accurate history. The EPAs are commitments to programme
directors and patients that our graduates are ready to assume
these responsibilities.
Integration: Foundations for integrating clinical andbiomedical sciences
The renewed curriculum integrates the basic and clinical
sciences from the beginning. This involves the longitudinal
nesting or ‘infusion’ (Harden’s step 4 integration) of basic
sciences content (anatomy, pathology, microbiology, pharma-
cology and therapeutics) that was previously the focus of
discipline-based units. Physicians require a strong foundation
of basic science knowledge to support scientific reasoning in
clinical practice, and as a framework for the assimilation of
new discoveries (AAMC & HHMC 2009). One of our goals is to
nurture our students’ interest and capacity to participate
actively in research.
Despite recommendations that incoming students should
be more evenly prepared to study medicine, Dalhousie has no
course pre-requisites for admission. The 6-week Foundations
Unit at the beginning of year 1 prepares students for the
integration of clinical and basic science learning in the
curriculum, and provides support for students to achieve
core pre-medical science competencies. This unit focuses on
cell and molecular biology, through lectures, case-based
tutorials and electronic and self-directed learning resources
to facilitate and help integrate student understanding of key
concepts and principles in genomes and gene expression,
proteins and enzymes, cell structure and dynamics, signal
transduction and cellular fate. This is framed to prepare
students for more advanced concepts in the longitudinally
integrated basic science themes, providing them with an
introduction to the language and central concepts of these
traditional biomedical disciplines, and resources. It provides a
‘roadmap’ of how they will assimilate knowledge in the
various systems units across the curriculum and
prepares students for developments that are coming at an
astounding pace, with an ever-increasing impact on medical
practice.
Concurrently, evidence-based practice is introduced to
assist students to begin to frame questions, search the
literature, critically appraise retrieved information and apply
their findings to patient care in conjunction with patient values
and wishes. This thread continues throughout the ProComp
Unit. Challenges in the evidence base, regulatory processes
and resource allocation (e.g. as exemplified by the real world
issues of cox-2 inhibitors, public attitudes towards vaccines,
the controversy over screening mammography and the role of
PSA testing for the detection of prostate cancer) are the subject
of cases integrating epidemiology, ethics and health systems,
in the context of physicians’ interprofessional collaboration in
clinical practice.
Integration: The ProComp Unit
Ethics, law, population health and evidence-based practice
had been added to the former curriculum as medical practice
changed and expectations for social accountability evolved.
Through the processes of deliberative curriculum inquiry,
academic and clinical faculty forged new working relation-
ships to integrate their disciplines from a practice perspective.
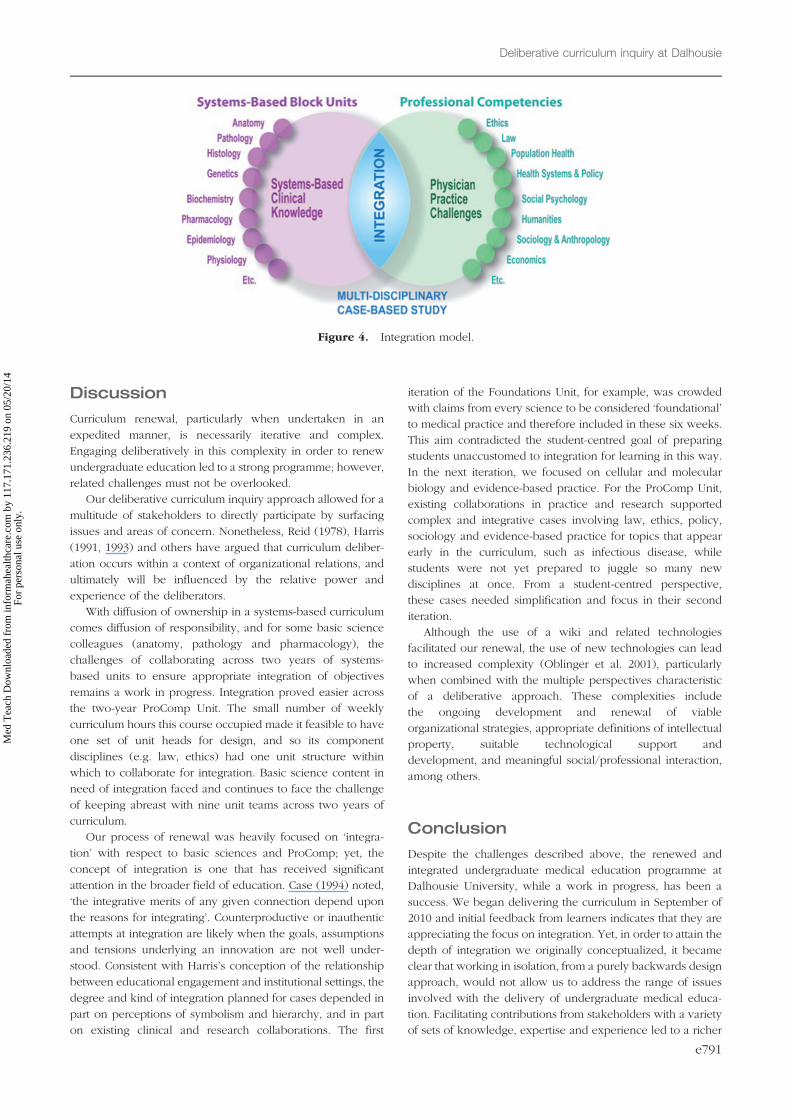
In our systems-based biomedical units, students learn the
various biomedical sciences together towards the goals of
identifying and managing clinical conditions, while preparing
for life-long learning and future scientific developments.
Equally, we reasoned, students should approach the ethical,
social, epidemiological and behavioural sciences together in
the service of meeting patient needs in social context, while
preparing students for life-long learning in the changing
landscape of practice challenges, such as patient safety,
health technology assessment, chronic disease management
and end of life care. (Figure 4)
The development of the ProComp Unit involved establish-
ing many new interdisciplinary collaborative relationships for
case-writing, as well as new practices of collaboration in
tutoring. Each student group has co-tutors, a physician and
someone from another healthcare profession, or a non-clinical
faculty member with expertise in epidemiology, population
health, ethics or law. Higher education literature supports the
potential of co-teaching/team-teaching in small group and
other settings (Murata 2002): it provides opportunities for
professional development and the establishment of a sense
of community (Murata 2002), addresses higher order
learning objectives (Wenger & Hornyak 1999), supports
a constructivist learning environment (Anderson & Speck
1998) and allows faculty to role model collaborative
relationships.
Integration of curricular content depends in part on the
degree of collaboration in professional practice, and this varies
between practice areas. Accordingly, in the ProComp Unit, the
model of integration varies from case to case, as the following
examples illustrate. ProComp focuses on diabetes in a chronic
disease management framework, while the concurrent endo-
crinology component of the Metabolism 1 Unit focuses on
acute care episodes – an example of ‘temporal coordination’,
or Harden’s Step 5. During an HIV/AIDS case in the Host
Defense Unit, in which a university student develops AIDS
while in Canada on a student visa, students learn in the block
Unit about immunology and infectious disease, and in
ProComp about global health and the concept of burden of
disease, while revisiting and applying public health responsi-
bilities, and being introduced to the rights of temporary
residents and immigrants as patients – an example of
‘correlation’, or Harden’s Step 7.
L. Reid et al.
e790
Med
Tea
ch D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y 11
7.17
1.23
6.21
9 on
05/
20/1
4Fo
r pe
rson
al u
se o
nly.
Discussion
Curriculum renewal, particularly when undertaken in an
expedited manner, is necessarily iterative and complex.
Engaging deliberatively in this complexity in order to renew
undergraduate education led to a strong programme; however,
related challenges must not be overlooked.
Our deliberative curriculum inquiry approach allowed for a
multitude of stakeholders to directly participate by surfacing
issues and areas of concern. Nonetheless, Reid (1978), Harris
(1991, 1993) and others have argued that curriculum deliber-
ation occurs within a context of organizational relations, and
ultimately will be influenced by the relative power and
experience of the deliberators.
With diffusion of ownership in a systems-based curriculum
comes diffusion of responsibility, and for some basic science
colleagues (anatomy, pathology and pharmacology), the
challenges of collaborating across two years of systems-
based units to ensure appropriate integration of objectives
remains a work in progress. Integration proved easier across
the two-year ProComp Unit. The small number of weekly
curriculum hours this course occupied made it feasible to have
one set of unit heads for design, and so its component
disciplines (e.g. law, ethics) had one unit structure within
which to collaborate for integration. Basic science content in
need of integration faced and continues to face the challenge
of keeping abreast with nine unit teams across two years of
curriculum.
Our process of renewal was heavily focused on ‘integra-
tion’ with respect to basic sciences and ProComp; yet, the
concept of integration is one that has received significant
attention in the broader field of education. Case (1994) noted,
‘the integrative merits of any given connection depend upon
the reasons for integrating’. Counterproductive or inauthentic
attempts at integration are likely when the goals, assumptions
and tensions underlying an innovation are not well under-
stood. Consistent with Harris’s conception of the relationship
between educational engagement and institutional settings, the
degree and kind of integration planned for cases depended in
part on perceptions of symbolism and hierarchy, and in part
on existing clinical and research collaborations. The first
iteration of the Foundations Unit, for example, was crowded
with claims from every science to be considered ‘foundational’
to medical practice and therefore included in these six weeks.
This aim contradicted the student-centred goal of preparing
students unaccustomed to integration for learning in this way.
In the next iteration, we focused on cellular and molecular
biology and evidence-based practice. For the ProComp Unit,
existing collaborations in practice and research supported
complex and integrative cases involving law, ethics, policy,
sociology and evidence-based practice for topics that appear
early in the curriculum, such as infectious disease, while
students were not yet prepared to juggle so many new
disciplines at once. From a student-centred perspective,
these cases needed simplification and focus in their second
iteration.
Although the use of a wiki and related technologies
facilitated our renewal, the use of new technologies can lead
to increased complexity (Oblinger et al. 2001), particularly
when combined with the multiple perspectives characteristic
of a deliberative approach. These complexities include
the ongoing development and renewal of viable
organizational strategies, appropriate definitions of intellectual
property, suitable technological support and
development, and meaningful social/professional interaction,
among others.
Conclusion
Despite the challenges described above, the renewed and
integrated undergraduate medical education programme at
Dalhousie University, while a work in progress, has been a
success. We began delivering the curriculum in September of
2010 and initial feedback from learners indicates that they are
appreciating the focus on integration. Yet, in order to attain the
depth of integration we originally conceptualized, it became
clear that working in isolation, from a purely backwards design
approach, would not allow us to address the range of issues
involved with the delivery of undergraduate medical educa-
tion. Facilitating contributions from stakeholders with a variety
of sets of knowledge, expertise and experience led to a richer
Figure 4. Integration model.
Deliberative curriculum inquiry at Dalhousie
e791
Med
Tea
ch D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y 11
7.17
1.23
6.21
9 on
05/
20/1
4Fo
r pe
rson
al u
se o
nly.

and more integrated approach. Refinement of our integration
models and team approaches, and research into their
effectiveness, are ongoing.
Declaration of interest: The authors report no conflicts of
interest. The authors alone are responsible for the content and
writing of this article.
Notes on contributors
DAVID BYERS, PhD, is a Professor in the Departments of Biochemistry &
Molecular Biology and Pediatrics at Dalhousie University, with research
interests in the discovery of novel antibiotics targeting microbial lipid
metabolism. His educational focus is the teaching of biochemistry to
medical and science students, and he was a co-developer and initial Unit
Head of the Foundations Unit.
DIANNE DELVA, MD, is a Professor of Family Medicine and was the
Associate Dean of Undergraduate Medical Education at the time of the
renewal. She contributed to the development of the curriculum.
TIM FEDAK, PhD, Director of Distributed Education and Assistant
Professor in the Division of Medical Education, seeks to enhance the use
of new media and education technologies for the support of medical
education.
ANNA MACLEOD, PhD, is an Assistant Professor and the Education
Specialist, Division of Medical Education and chairs the Undergraduate
Medical Education Assessment and the Objectives and Case Review
Committees. She is an educational researcher interested in medical
education curriculum and pedagogy.
KAREN MANN, PhD, is a Professor Emeritus in the Division of Medical
Education at Dalhousie University in Halifax, Canada. She is also a
Professor and holds a part-time Chair in Medical Education, Manchester
Medical School in Manchester, United Kingdom.
THOMAS J. MARRIE, MD, is Dean, Faculty of Medicine, Dalhousie
University, and past Dean, Faculty of Medicine and Dentistry, University
of Alberta. He is an Infectious Diseases Physician, with a research focus on
community acquired pneumonia and spans the spectrum from basic to
applied science.
BRENDA MERRITT, PhD, is a faculty member within the Dalhousie School
of Occupational Therapy. Her primary research interests include investi-
gating the impact that chronic health conditions have on daily life
performance and evaluating the quality of curricula within health profes-
sion programmes.
LYNETTE REID, PhD, is an Assistant Professor in the Department of
Bioethics, Dalhousie University, with a research and teaching interest in the
social dimension of professional ethics. She led, with colleagues, the
curriculum outcomes process, and is co-developer and co-Unit Head of the
Professional Competencies Unit.
CHRISTY SIMPSON, PhD, is Head and Associate Professor, Department of
Bioethics, Dalhousie University. She, with other colleagues, facilitated the
community conversations for the Faculty of Medicine.
Notes1. Curriculum goals and outcomes available online at: http://
undergraduate.medicine.dal.ca/curriculum/goals.htm
2. Topics and reports are available online at: http://curriculum.
medicine.dal.ca/practices.htm
3. Reported at http://news.medicine.dal.ca/CMTretreat.htm
and http://news.medicine.dal.ca/CMTTodolist.htm
4. Diagrams representing the units and schedule are available
at http://undergraduate.medicine.dal.ca/curriculum/med1.htm
and http://undergraduate.medicine.dal.ca/curriculum/
med2.htm
References
AAMC, HHMC (Association of American Medical Colleges & Howard
Hughes Medical Institute). 2009. Scientific Foundations for Future
Physicians: Report of the AAMC-HHMI Committee. Washington DC:
AAMC. [Accessed 27 July 2011] Available from http://www.hhmi.org/
grants/pdf/08-209_AAMC-HHMI_report.pdf
Anderson RS, Speck BW. 1998. ‘‘Oh what a difference a team makes’’:
Why team teaching makes a difference. Teach Teach Educ
14(7):671–686.
Biggs J. 1996. Enhancing teaching through constructive alignment. High
Educ 32(3):347–364.
Case R. 1994. Our crude handling of educational reforms: The case of
curricular integration. Canadian J Educ 19(1):80–93.
Collins L, Arenson CA, Jerback C, Dressel R, Kane P, Antony R, Necky J,
Oduneye A. 2009. Chronic Illness Care Education: Reflections on a
Longitudinal Interprofessional Mentorship Experience. Health Policy
Newslett 21(4):3.
Davenport NC, Spath ML, Blauvelt MJ. 2009. A step-by-step approach to
curriculum review. Nurse Educ 34(4):181–185.
Epstein RM, Hundert EM. 2002. Defining and assessing professional
competence. JAMA 287(2):226–235.
Eva KW, Neville AJ, Norman GR. 1998. Exploring the aetiology of content
specificity: Factors influencing analogic transfer and problem solving.
Acad Med 73(Suppl.):1–5.
GMC (General Medical Council). 2009. Tomorrow’s Doctors: Outcomes
and standards for undergraduate medical education. London:
General Medical Council. [Accessed 27 July 2011] Available from
http://www.gmc-uk.org/education/undergraduate/tomorrows_doctors_
2009.asp
Harden RM. 2000. The integration ladder: A tool for curriculum planning
and evaluation. Med Educ 34(7):551–557.
Harden RM. 2001. AMEE Guide No. 21: Curriculum mapping: A tool for
transparent and authentic teaching and learning. Med Teach
23(2):123–137.
Harris IB. 1991. Deliberative Inquiry: The Arts of Planning. In: Short E, editor.
Forms of curriculum inquiry. New York: SUNY Press. pp 285–308.
Harris IB. 1993. Perspectives for curriculum renewal in medical education.
Acad Med 68(6):484–486.
Kern DE. 2009. Curriculum development in medical education: A
six-step approach. 2nd ed. Baltimore, MD: Johns Hopkins University
Press.
MacLeod A. 2011. Six ways problem-based learning cases
can sabotage patient-centered medical education. Acad Med
86(7):818–825.
Muller JH, Jain S, Loeser H, Irby DM. 2008. Lessons learned about
integrating a medical school curriculum: Perceptions of students,
faculty and curriculum leaders. Med Educ 42(8):778–785.
Murata R. 2002. What does team teaching mean? A case study of
interdisciplinary teaming. J Educ Res 96(2):67–77.
Oblinger DG, Barone CA, Hawkins BL. 2001. Distributed education and its
challenges: An overview. Washington, DC: American Council on
Education and EDUCAUSE. [Accessed 20 September 2011] Available
from http://www.acenet.edu/bookstore/pdf/distributed-learning/dis-
tributed-learning-01.pdf
Prideaux D. 2003. Curriculum design. BMJ 326:268–270.
RCPSC (Royal College of Physicians and Surgeons of Canada). 2005. The
CanMEDS 2005 physician competency framework: Better standards,
better physicians, better care. Frank JR, editor. Ottawa: Royal College of
Physicians and Surgeons of Canada. [Accessed 27 July 2011] Available
from http://rcpsc.medical.org/canmeds/CanMEDS2005/CanMEDS
2005_e.pdf
Reid WA. 1978. Thinking about the curriculum: The nature and treatment of
curriculum problems. London: Routledge & Kegan Paul. p84.
L. Reid et al.
e792
Med
Tea
ch D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y 11
7.17
1.23
6.21
9 on
05/
20/1
4Fo
r pe
rson
al u
se o
nly.

Srinivasan M, Wilkes M, Stevenson F, Nguyen T, Slavin S. 2007.
Comparing problem-based learning with case-based learning:
Effects of a major curricular shift at two institutions. Acad Med
82(1):74–82.
ten Cate O, Scheele F. 2007. Competency-based postgraduate training: Can
we bridge the gap between theory and clinical practice? Acad Med
82(6):542–547.
ten Cate O, Snell L, Carraccio C. 2010. Medical competence: The interplay
between individual ability and the health care environment. Med Teach
32(8):669–675.
Wenger MS, Hornyak MJ. 1999. Team teaching for higher level learning: A
framework of professional collaboration. J Manage Educ 23(3):311.
Wiener CM, Thomas PA, Goodspeed E, Valle D, Nichols DG. 2010.
‘‘Genes to Society’’—The logic and process of the new curriculum for
the Johns Hopkins University School of Medicine. Acad Med
85:498–506.
Wiggins GP, McTighe J. 2001. Understanding by Design. Upper Saddle
River, NJ: Merrill/Prentice Hall.
Willett TG. 2008. Current status of curriculum mapping in Canada and the
UK. Med Educ 42(8):786–793.
Deliberative curriculum inquiry at Dalhousie
e793
Med
Tea
ch D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y 11
7.17
1.23
6.21
9 on
05/
20/1
4Fo
r pe
rson
al u
se o
nly.




















