
Delayed thrombin-induced platelet–fibrin clot generation by clopidogrel: A new dose-related effect...
8
ARTICLE IN PRESS REGULAR ARTICLE Delayed thrombin-induced platelet fibrin clot generation by clopidogrel: A new dose-related effect demonstrated by thrombelastography in patients undergoing coronary artery stenting Paul A. Gurbel a, * , Kevin P. Bliden a , Kirk Guyer b , Nikhil Aggarwal a , Udaya S. Tantry a a Sinai Center for Thrombosis Research, Hoffberger Building, Suite 56, 2401 W. Belvedere Ave, Baltimore, MD 21215, USA b Department of Chemistry, Indiana University, South Bend, IN, USA Received 25 January 2006; received in revised form 3 May 2006; accepted 9 May 2006 Abstract Background: We have previously demonstrated that clopidogrel reduces platelet activation and aggregation in patients undergoing stenting. However, the effect of the clopidogrel loading dose on the rate of thrombin-induced platelet—fibrin clot formation is unknown in this patient population. Methods and results: Using thrombelastography (TEGR) we measured the time to platelet—fibrin clot formation (R), a marker of the speed of thrombin generation, in 120 patients undergoing elective coronary artery stenting treated with standard and high loading doses of clopidogrel. Platelet reactivity to adenosine diphosphate (ADP) by light transmittance aggregometry (LTA) was determined simultaneously. Measure- ments were made immediately before and at 24 h after clopidogrel treatment. Clopidogrel produced a prolongation in R (4.4 F 1.4 min pre vs. 5.4 F 1.7 min post, p b 0.001) that directly correlated with the change in platelet aggregation (r = 0.65, p b 0.0001). Prolongation in R was greatest in patients treated with a high loading dose ( p = 0.004). Conclusions: Delayed thrombin-induced platelet—fibrin clot formation as measured by TEG is a newly reported dose-related effect of clopidogrel that may contribute to the overall antithrombotic properties of the drug in patients undergoing stenting. This effect was more marked in patients loaded with 600 mg, lending further mechanistic 0049-3848/$ - see front matter D 2006 Elsevier Ltd. All rights reserved. doi:10.1016/j.thromres.2006.05.006 * Corresponding author. Tel.: +1 410 601 9600; fax: +1 410 601 9601. E-mail address: [email protected] (P.A. Gurbel). KEYWORDS Platelets; Clopidogrel; Thrombin; Clot; Aggregation Thrombosis Research (2006) xx, xxx—xxx intl.elsevierhealth.com/journals/thre TR-02978; No of Pages 8 DTD 5
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Delayed thrombin-induced platelet–fibrin clot generation by clopidogrel: A new dose-related effect...
intl.elsevierhealth.com/journals/thre
DTD 5
REGULAR ARTICLE
Delayed thrombin-induced platelet�fibrin clotgeneration by clopidogrel: A new dose-relatedeffect demonstrated by thrombelastography inpatients undergoing coronary artery stenting
Paul A. Gurbel a,*, Kevin P. Bliden a, Kirk Guyer b, Nikhil Aggarwal a,Udaya S. Tantry a
a Sinai Center for Thrombosis Research, Hoffberger Building, Suite 56, 2401 W. Belvedere Ave,Baltimore, MD 21215, USAb Department of Chemistry, Indiana University, South Bend, IN, USA
Received 25 January 2006; received in revised form 3 May 2006; accepted 9 May 2006
0049-3848/$ - see front matter D 200doi:10.1016/j.thromres.2006.05.006
* Corresponding author. Tel.: +1 410E-mail address: PGURBEL@LIFEBRID
KEYWORDSPlatelets;Clopidogrel;Thrombin;Clot;Aggregation
Abstract
Background: We have previously demonstrated that clopidogrel reduces plateletactivation and aggregation in patients undergoing stenting. However, the effect ofthe clopidogrel loading dose on the rate of thrombin-induced platelet—fibrin clotformation is unknown in this patient population.Methods and results: Using thrombelastography (TEGR) we measured the time toplatelet—fibrin clot formation (R), a marker of the speed of thrombin generation, in120 patients undergoing elective coronary artery stenting treated with standard andhigh loading doses of clopidogrel. Platelet reactivity to adenosine diphosphate (ADP)by light transmittance aggregometry (LTA) was determined simultaneously. Measure-ments were made immediately before and at 24 h after clopidogrel treatment.Clopidogrel produced a prolongation in R (4.4F1.4 min pre vs. 5.4F1.7 min post,p b0.001) that directly correlated with the change in platelet aggregation (r =0.65,p b0.0001). Prolongation in R was greatest in patients treated with a high loadingdose ( p =0.004).Conclusions: Delayed thrombin-induced platelet—fibrin clot formation as measuredby TEG is a newly reported dose-related effect of clopidogrel that may contribute tothe overall antithrombotic properties of the drug in patients undergoing stenting. Thiseffect was more marked in patients loaded with 600 mg, lending further mechanistic
ARTICLE IN PRESSThrombosis Research (2006) xx, xxx—xxx
6 Elsevier Ltd. All rights reserved.
601 9600; fax: +1 410 601 9601.GEHEALTH.ORG (P.A. Gurbel).
TR-02978; No of Pages 8

ARTICLE IN PRESSP.A. Gurbel et al.2
support for this dose of clopidogrel as a more effective antithrombotic regimen thanthe standard 300 mg dose. Measurement of R may serve as a new indicator ofclopidogrel responsiveness.D 2006 Elsevier Ltd. All rights reserved.
Introduction
Clopidogrel is a thienopyridine that selectivelyinhibits the platelet P2Y12 receptor and reducesischemic complications in patients with unstablecoronary syndrome. Thienopyridines also reducethe incidence of stent thrombosis [1—5]. Theprimary mechanism proposed for the beneficialeffects of clopidogrel is inhibition of ADP-inducedaggregation. The results of several studies havealso suggested that clopidogrel treatment may haveanti-inflammatory effects [6—8].
Our group and others have demonstrated thatclopidogrel attenuates platelet activation followingcoronary stenting andwe have also shown that a highloading dose produces greater platelet inhibition asmeasured by conventional light transmittanceaggregometry [9—11]. Since thrombin generationoccurs mainly on the surface of activated plateletsand platelet—monocyte aggregates, clopidogreltherapy may exert an antithrombotic effect throughattenuation of platelet activation with a resultantdecline in surface-generated thrombin and throm-bin-induced platelet—fibrin clot formation. Howev-er, the latter effect of clopidogrel has not beenextensively studied in patients following coronarystenting. Moreover, the effect of various clopidogrelloading doses on the rate of thrombin-induced clotformation is entirely unknown. Therefore, the aimsof our investigation were to measure the onset ofthrombin induced platelet—fibrin clot formation bythrombelastography, a marker of the speed ofthrombin generation, in patients undergoing coro-nary stenting treated with clopidogrel and analyzethe relation to clopidogrel loading dose and extentof platelet inhibition.
Methods
Patients
One hundred and twenty consecutive patientsundergoing non-emergent coronary stenting provid-ed informed consent prior to the procedure. TheInvestigational Review Board at Sinai Hospital ofBaltimore approved this study. All patients were N18years old and had to have been treated with a 81—325 mg daily dose of aspirin for at least 5 days prior
to the procedure. Exclusion criteria were a history ofbleeding diathesis, acute myocardial infarctionwithin 48 h, elevated cardiac markers (above upperlimits normal for the respective assay), cerebrovas-cular eventwithin 3months, chronic vessel occlusionor angiographically visible thrombus, illicit drug oralcohol abuse, prothrombin time greater than 1.5times control, platelet count b100,000/mm3, he-matocrit b30%, creatinine N4.0 mg/dl, glycoprotein(GP) IIb/IIIa inhibitor use, and thienopyridine useprior to the procedure. Patients treatedwith heparinor lowmolecular weight heparin prior to or after thecompletion of the procedure were also excluded.
Of the 120 patients, 73 were treated with astandard (300 mg) loading dose of clopidogrel and47 were treated with a high loading dose (600 mg)at discretion of the treating physician. Clopidogrelwas administered in the catheterization laborato-ry immediately after successful stent implanta-tion. All patients received unfractionated heparinas an intravenous bolus to achieve an activatedclotting time z300 s in the catheterizationlaboratory. Aspirin was administered at 325 mgon the day of the procedure and daily thereafter.The maintenance dose of clopidogrel was 75 mgdaily. Patients treated with a GPIIb/IIIa inhibitorin the catheterization laboratory were excludedfrom the analysis.
Blood sampling
Pre-treatment blood samples were obtained in thecatheterization laboratory before heparin adminis-tration through the indwelling femoral vesselsheath. The blood samples were transferred tovacutainer blood collecting tubes (Becton — Dick-inson) containing 3.8% trisodium citrate for lighttransmittance aggregation studies or 40 USP lithi-um heparin for TEG studies after discarding thefirst 2—3 ml of free flowing blood. Blood sampleswere also collected at 24 h post-stenting. Thevacutainer tubes were filled to capacity and gentlyinverted 3 to 5 times to ensure complete mixing ofthe anticoagulant.
Light transmittance aggregometry
Platelet aggregation was assessed as previouslydescribed [9—11]. Briefly, the blood-citrate tubes
ARTICLE IN PRESS
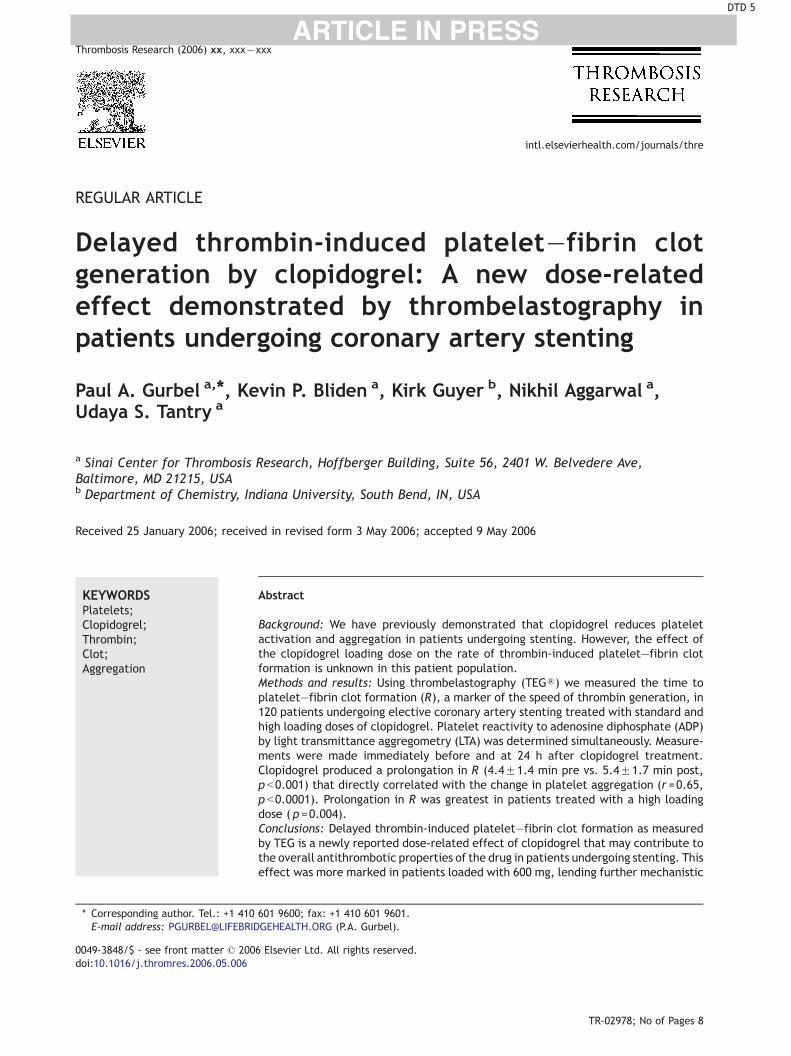
Figure 1 Schematic of TEG system. A torsion wire suspending a pin is immersed in blood. As the clot forms whilethe cup is rotated 458, the pin will rotate depending on the strength of the fibrin—platelet bonds. A signal isdischarged continuously that reflects the onset of clotting (reaction time, R) and the clot strength (MA).
Table 1 Patient demographics
300 mgclopidogrel(n =73)
600 mgclopidogrel(n =47)
p
Age (years) 66F12 67F12 NSRace (Caucasian) (%) 66 73 NSGender (male) (%) 61 70 NSBMI 30F8 28F5 NSRisk factors/past
medical history (%)Smoking 46 60 0.068Family history of CAD 40 48 NSHypertension 53 69 0.042Hyperlipidemia 65 77 0.082Diabetes 45 36 NSPrior myocardialinfarction
27 28 NS
Prior CABG 26 24 NSPrior PTCA 36 41 NS
Pretreatmentmedications (%)Beta blockers 72 86 0.037ACE inhibitors 56 59 NSCalcium blockers 20 27 NSLipid lowering agents
3A4 pathwaymetabolized 71 76 NS
Non 3A4 pathwaymetabolized 6 9 NS
Laboratory dataWBC (�1000/mm3) 7.8F2.6 7.3F2.1 NSPlatelets(�1000/mm3)
237F36 220F30 NS
Hemoglobin (g/dl) 15.4F2 18.4F2 NSCreatinine (g/dl) 1.1F0.8 1.2F0.4 NS
Data reported as meanFS.D.
ACE=angiotensin converting enzyme. BMI=body mass index.CABG=coronary artery bypass graft surgery. CAD=coronaryartery disease. PTCA=percutaneous coronary angioplasty.WBC=white blood cells. 3A4=hepatic cytochrome P 450 3A4.
Thrombelastography and platelet�fibrin clot generation by clopidogrel 3
were centrifuged at 120�g for 5 min to recoverplatelet rich plasma (PRP) and further centrifugedat 850�g for 10 min to recover platelet poorplasma (PPP). Platelets were stimulated with 5AM and 20 AM ADP and the aggregation was assessedusing a Chronolog Lumi-Aggregometer (Model 490-4D) with the Aggrolink software package (Chrono-log, Havertown, PA). Aggregation was expressed asthe maximum percent change in light transmit-tance from baseline using PPP as a reference.
Clot strength and fibrin generation time
The TEG Hemostasis System (Haemoscope Corpora-tion, Niles, IL, USA) with automated analyticalsoftware provides quantitative and qualitativemeasurements of the physical properties of a clot[12—14]. In essence, the TEG is a viscoelasticmonitor that measures the degree of platelet—fibrin mediated clot strength. The platelet—fibrinnetwork in the blood sample links a rotating samplecup with a stationary pin suspended by a torsionwire (Fig. 1). The torque of the rotating cup istransmitted to the immersed pin. Pin movement isconverted to an electrical signal by a transducerand is interpreted by the computer to create atracing. The degree of platelet contribution to theclot strength through platelet—fibrin bonding di-rectly influences the magnitude of pin movementand ultimately the amplitude of the tracing. In thepresent study, the time from the start of thesample run to the first significant levels of clotformation [reaction time (R) (min)] was measured(Fig. 1). The R parameter, a measure of time toinitial thrombin induced platelet—fibrin clot for-mation, has been correlated with the velocity ofthrombin generation [12].
About 1 mL of heparinized blood was transferredto a vial containing kaolin and mixed by inversion.500 AL of the activated blood were then transferred
to a vial containing heparinase and mixed toneutralize the heparin effect. The neutralizedblood (360 AL) was immediately added to a heparin-ase-coated cup and assayed in the TEG analyzer
ARTICLE IN PRESS
Table 2 Procedural characteristics
300 mgclopidogrel(n =73)
600 mgclopidogrel(n =47)
p
Length of procedure(min)
69F28 58F26 NS
Ejection fraction (%) 50F10 52F8 NSNumber of vesselstreated
1.2F0.5 1.3F0.6 NS
Lesion morphologyDe novo (%) 91 86 NS
Lesion location (%)LAD 39 29 NSCX 26 23 NSRCA 27 40 0.07SVG 8 8 NS
Stent types (%)Drug eluting 64 75 NSBare metal 27 23 NSPTCA only 9 2 NSReference vesseldiameter (mm)
3F0.5 3.1F0.4 NS
Total lesionlength (mm)
21F16 18F12 NS
Pre-stenosis (%) 86 85 NSPost-stenosis (%) 6 5 NSProcedural success(%)
96 95 NS
Data reported as meanFS.D.
CX=circumflex artery. LAD=left anterior descending artery.RCA=right coronary artery.
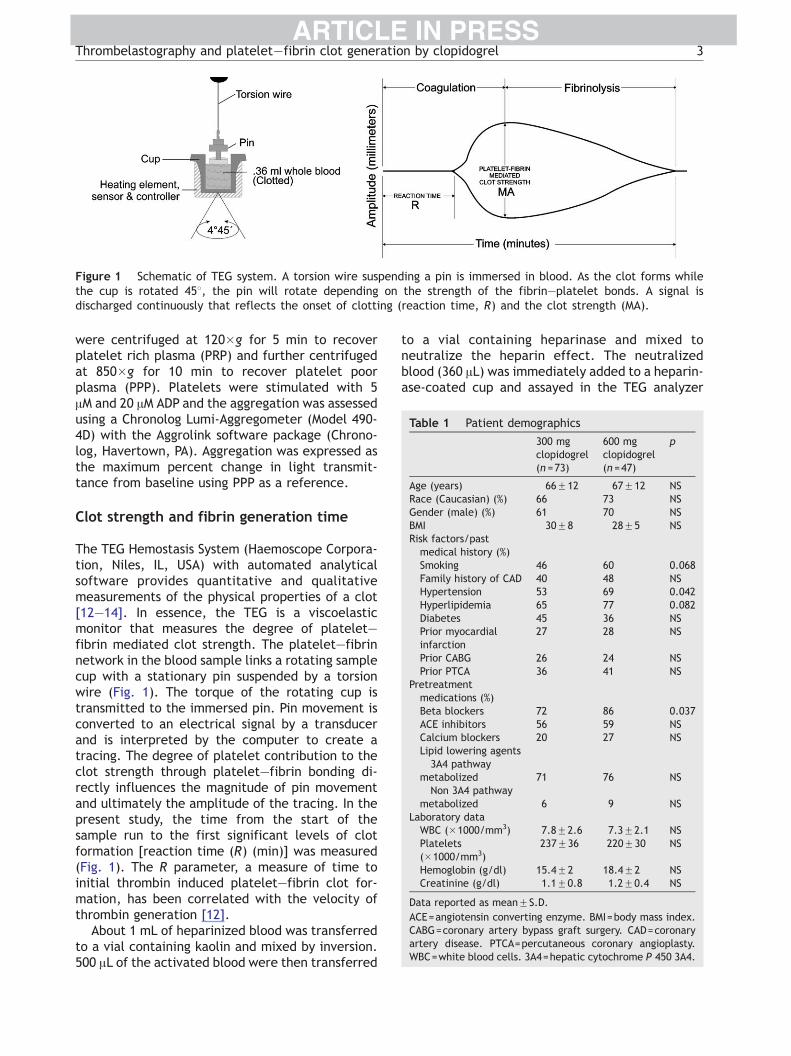
Figure 2 (A) Distribution of the absolute change inplatelet aggregation (5 AM ADP). The curve indicates thebest fit for a normal distribution as generated by theStatistica software. (B) Distribution of the absolutechange in platelet aggregation (20 AM ADP). The curveindicates the best fit for a normal distribution asgenerated by the Statistica software.
P.A. Gurbel et al.4
according to the manufacturer’s instructions toobtain the thrombin-induced clot.
Definitions
Absolute change in platelet aggregation
¼ Baseline platelet aggregation
� Post�treatment platelet aggregation:
Absolute change in R ¼ Baseline R
� Post�treatment R:
Statistical analysis
Comparisons were made between baseline andpost-clopidogrel measurements, and betweenpatients receiving 300 mg and 600 mg clopidogrelby t-tests (Statistica software). Based on thenormal distribution of data the meanFS.E.M. isreported. Pearson’s correlation coefficient wascalculated to describe the relation between theabsolute change in platelet aggregation at 24 hpost-stenting to the absolute change in R (Statisticasoftware).
Results
Patients and clinical outcomes
One hundred and twenty patients underwentcoronary stenting and had blood samples analyzed.The analyses were 100% complete for all measure-ments. The demographics and procedural charac-teristics of patients treated with 300 mg and600 mg clopidogrel are shown in Tables 1 and 2,respectively. There were no major differencesbetween the two groups except more patients in600 mg group were hypertensive (p =0.042) andreceiving beta blockers (p =0.037).
Platelet aggregation
5 and 20 AM ADP-induced aggregation were signif-icantly reduced by clopidogrel therapy in theoverall group (p b0.001 for both agonist concen-trations, Table 4). There was a wide variability in
ARTICLE IN PRESS
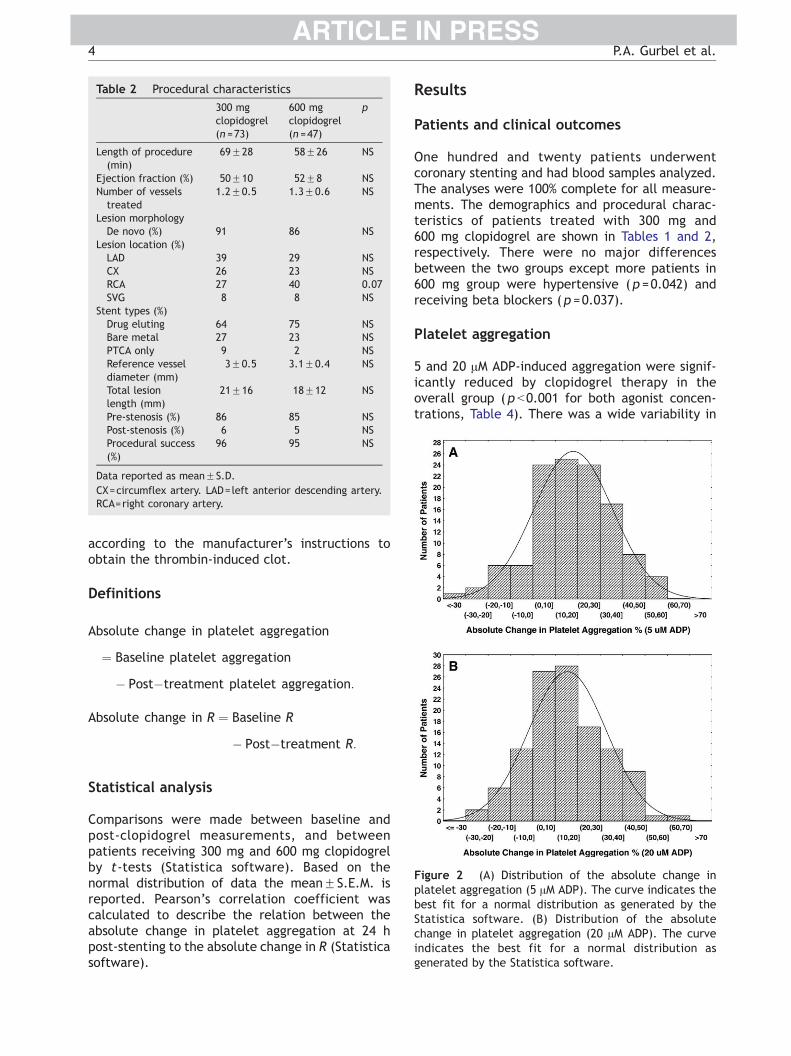
Figure 3 (A) Distribution of post-treatment plateletaggregation as measured by 5 AM ADP-induced aggrega-tion. The curve indicates the best fit for a normaldistribution as generated by the Statistica software. (B)Distribution of post-treatment platelet aggregation asmeasured by 20 AM ADP-induced aggregation. The curveindicates the best fit for a normal distribution asgenerated by the Statistica software.
Thrombelastography and platelet�fibrin clot generation by clopidogrel 5
the extent of the absolute change in aggregationand post-treatment aggregation as measured by 5AM and 20 AM platelet aggregation (Figs. 2A and Band 3A and B, respectively). The higher loadingdose produced lower post-treatment aggregation(p =0.03 for 5 AM ADP and p =0.009 for 20 AM ADP,Table 4) and greater absolute inhibition (p =0.002for 5 AM ADP and p =0.003 for 20 AM ADP, Table 3).
Reaction time
Clopidogrel therapy significantly prolonged R in theoverall group (p b0.001, Table 4) and the effect
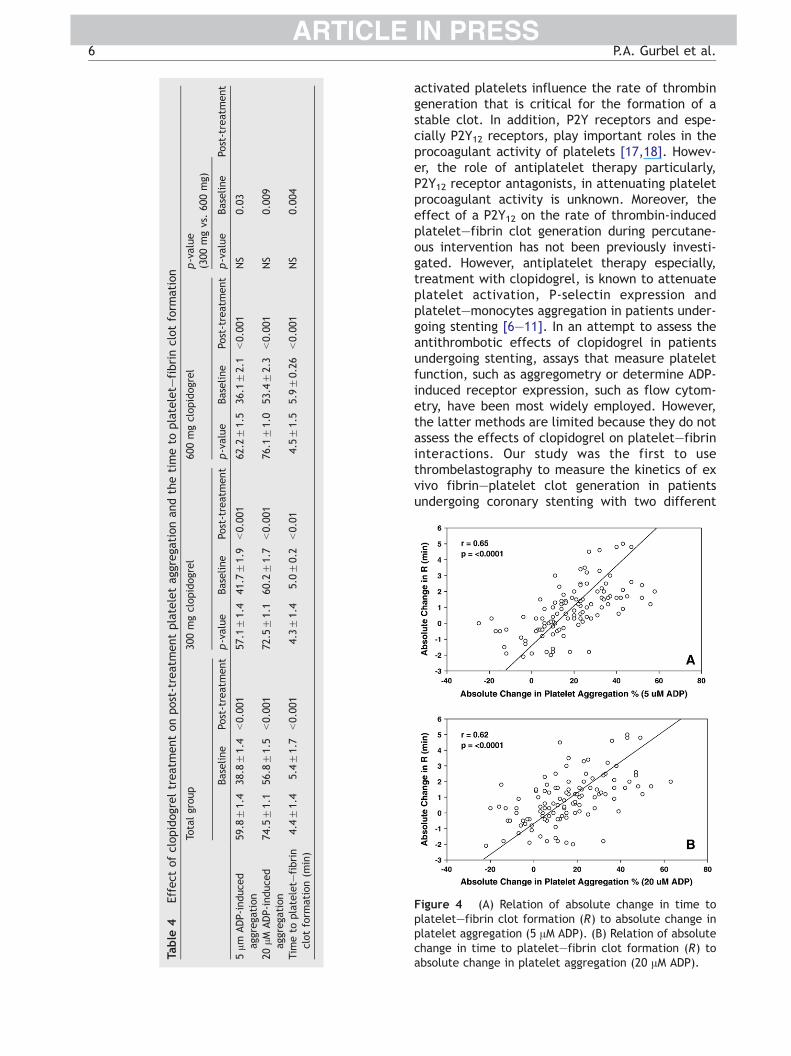
Table 3 Effect of clopidogrel on absolute change in ADP-fibrin clot formation
Absolute change in platelet aggregation (5 AM ADP)Absolute change in platelet aggregation (20 AM ADP)Absolute change in time to platelet—fibrin clot formation (min)
was greater in patients treated with a 600 mgloading dose (p =0.004, Table 4). The absolutechange in R was also more pronounced in patientstreated with 600 mg clopidogrel (p =0.01, Table 3).
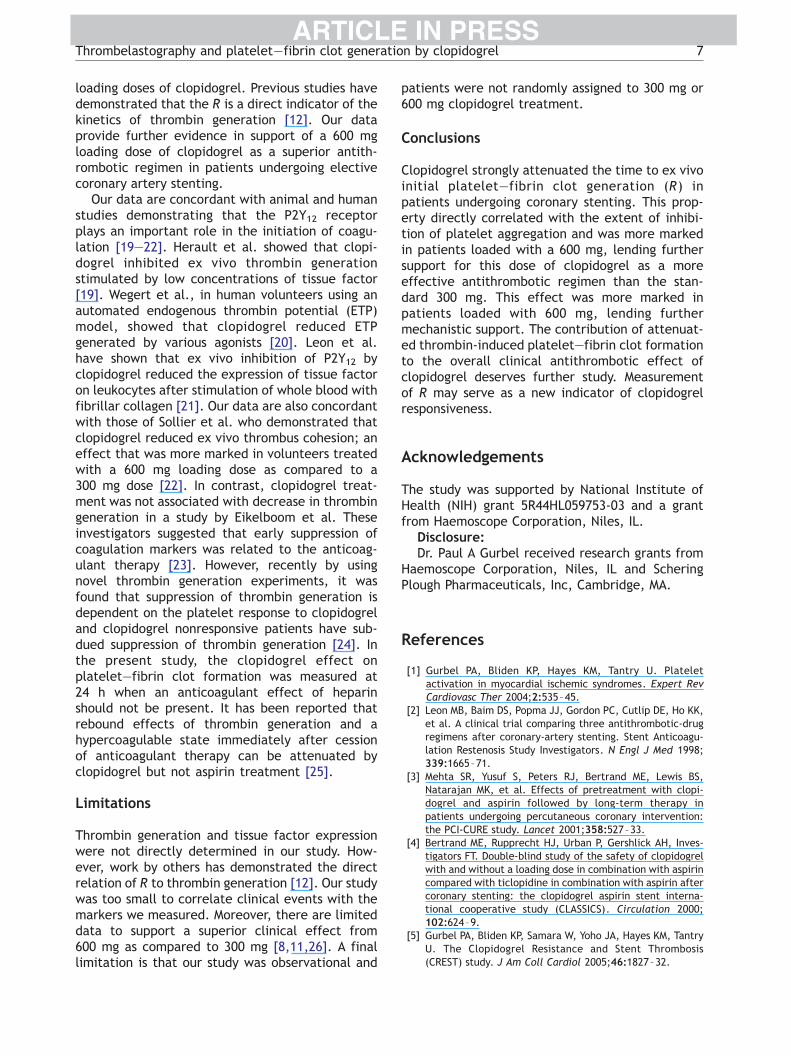
Relation of platelet aggregation to timeto platelet�fibrin clot formation
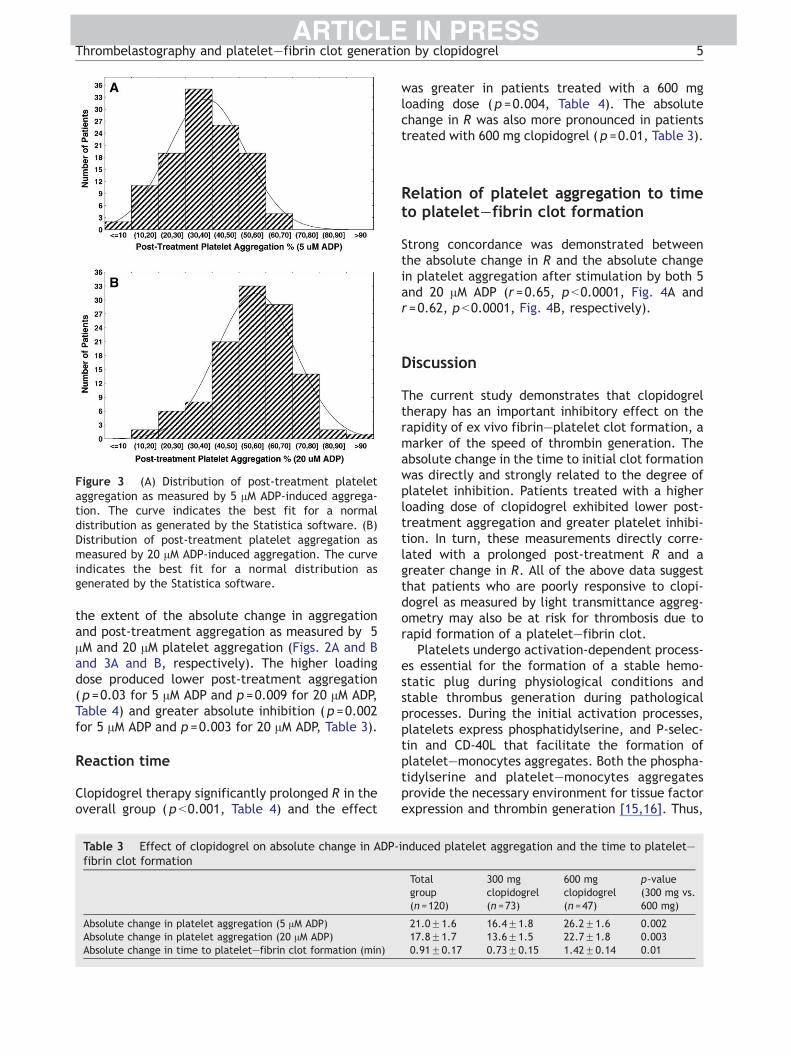
Strong concordance was demonstrated betweenthe absolute change in R and the absolute changein platelet aggregation after stimulation by both 5and 20 AM ADP (r =0.65, p b0.0001, Fig. 4A andr =0.62, p b0.0001, Fig. 4B, respectively).
Discussion
The current study demonstrates that clopidogreltherapy has an important inhibitory effect on therapidity of ex vivo fibrin—platelet clot formation, amarker of the speed of thrombin generation. Theabsolute change in the time to initial clot formationwas directly and strongly related to the degree ofplatelet inhibition. Patients treated with a higherloading dose of clopidogrel exhibited lower post-treatment aggregation and greater platelet inhibi-tion. In turn, these measurements directly corre-lated with a prolonged post-treatment R and agreater change in R. All of the above data suggestthat patients who are poorly responsive to clopi-dogrel as measured by light transmittance aggreg-ometry may also be at risk for thrombosis due torapid formation of a platelet—fibrin clot.
Platelets undergo activation-dependent process-es essential for the formation of a stable hemo-static plug during physiological conditions andstable thrombus generation during pathologicalprocesses. During the initial activation processes,platelets express phosphatidylserine, and P-selec-tin and CD-40L that facilitate the formation ofplatelet—monocytes aggregates. Both the phospha-tidylserine and platelet—monocytes aggregatesprovide the necessary environment for tissue factorexpression and thrombin generation [15,16]. Thus,
induced platelet aggregation and the time to platelet—
Totalgroup(n =120)
300 mgclopidogrel(n =73)
600 mgclopidogrel(n =47)
p-value(300 mg vs.600 mg)
21.0F1.6 16.4F1.8 26.2F1.6 0.00217.8F1.7 13.6F1.5 22.7F1.8 0.0030.91F0.17 0.73F0.15 1.42F0.14 0.01
ARTICLE IN PRESS
Table
4Effect
ofclopidogreltreatmentonpost-treatmentplateletag
grega
tionan
dthetimeto
platelet—
fibrinclotform
ation
Totalgroup
300mgclopidogrel
600mgclopidogrel
p-value
(300mgvs.600mg)
Baseline
Post-treatment
p-value
Baseline
Post-treatment
p-value
Baseline
Post-treatment
p-value
Baseline
Post-treatm
ent
5Am
ADP-induce
dag
grega
tion
59.8
F1.4
38.8
F1.4
b0.00
157
.1F1.4
41.7
F1.9
b0.00
162
.2F1.5
36.1
F2.1
b0.001
NS
0.03
20AM
ADP-induce
dag
grega
tion
74.5
F1.1
56.8
F1.5
b0.00
172
.5F1.1
60.2
F1.7
b0.00
176
.1F1.0
53.4
F2.3
b0.001
NS
0.009
Tim
eto
platelet—
fibrin
clotform
ation(m
in)
4.4F1.4
5.4F1.7
b0.00
14.3F1.4
5.0F0.2
b0.01
4.5F1.5
5.9F0.26
b0.001
NS
0.004
Figure 4 (A) Relation of absolute change in time toplatelet—fibrin clot formation (R) to absolute change inplatelet aggregation (5 AM ADP). (B) Relation of absolutechange in time to platelet—fibrin clot formation (R) toabsolute change in platelet aggregation (20 AM ADP).
P.A. Gurbel et al.6
activated platelets influence the rate of thrombingeneration that is critical for the formation of astable clot. In addition, P2Y receptors and espe-cially P2Y12 receptors, play important roles in theprocoagulant activity of platelets [17,18]. Howev-er, the role of antiplatelet therapy particularly,P2Y12 receptor antagonists, in attenuating plateletprocoagulant activity is unknown. Moreover, theeffect of a P2Y12 on the rate of thrombin-inducedplatelet—fibrin clot generation during percutane-ous intervention has not been previously investi-gated. However, antiplatelet therapy especially,treatment with clopidogrel, is known to attenuateplatelet activation, P-selectin expression andplatelet—monocytes aggregation in patients under-going stenting [6—11]. In an attempt to assess theantithrombotic effects of clopidogrel in patientsundergoing stenting, assays that measure plateletfunction, such as aggregometry or determine ADP-induced receptor expression, such as flow cytom-etry, have been most widely employed. However,the latter methods are limited because they do notassess the effects of clopidogrel on platelet—fibrininteractions. Our study was the first to usethrombelastography to measure the kinetics of exvivo fibrin—platelet clot generation in patientsundergoing coronary stenting with two different
ARTICLE IN PRESSThrombelastography and platelet�fibrin clot generation by clopidogrel 7
loading doses of clopidogrel. Previous studies havedemonstrated that the R is a direct indicator of thekinetics of thrombin generation [12]. Our dataprovide further evidence in support of a 600 mgloading dose of clopidogrel as a superior antith-rombotic regimen in patients undergoing electivecoronary artery stenting.
Our data are concordant with animal and humanstudies demonstrating that the P2Y12 receptorplays an important role in the initiation of coagu-lation [19—22]. Herault et al. showed that clopi-dogrel inhibited ex vivo thrombin generationstimulated by low concentrations of tissue factor[19]. Wegert et al., in human volunteers using anautomated endogenous thrombin potential (ETP)model, showed that clopidogrel reduced ETPgenerated by various agonists [20]. Leon et al.have shown that ex vivo inhibition of P2Y12 byclopidogrel reduced the expression of tissue factoron leukocytes after stimulation of whole blood withfibrillar collagen [21]. Our data are also concordantwith those of Sollier et al. who demonstrated thatclopidogrel reduced ex vivo thrombus cohesion; aneffect that was more marked in volunteers treatedwith a 600 mg loading dose as compared to a300 mg dose [22]. In contrast, clopidogrel treat-ment was not associated with decrease in thrombingeneration in a study by Eikelboom et al. Theseinvestigators suggested that early suppression ofcoagulation markers was related to the anticoag-ulant therapy [23]. However, recently by usingnovel thrombin generation experiments, it wasfound that suppression of thrombin generation isdependent on the platelet response to clopidogreland clopidogrel nonresponsive patients have sub-dued suppression of thrombin generation [24]. Inthe present study, the clopidogrel effect onplatelet—fibrin clot formation was measured at24 h when an anticoagulant effect of heparinshould not be present. It has been reported thatrebound effects of thrombin generation and ahypercoagulable state immediately after cessionof anticoagulant therapy can be attenuated byclopidogrel but not aspirin treatment [25].
Limitations
Thrombin generation and tissue factor expressionwere not directly determined in our study. How-ever, work by others has demonstrated the directrelation of R to thrombin generation [12]. Our studywas too small to correlate clinical events with themarkers we measured. Moreover, there are limiteddata to support a superior clinical effect from600 mg as compared to 300 mg [8,11,26]. A finallimitation is that our study was observational and
patients were not randomly assigned to 300 mg or600 mg clopidogrel treatment.
Conclusions
Clopidogrel strongly attenuated the time to ex vivoinitial platelet—fibrin clot generation (R) inpatients undergoing coronary stenting. This prop-erty directly correlated with the extent of inhibi-tion of platelet aggregation and was more markedin patients loaded with a 600 mg, lending furthersupport for this dose of clopidogrel as a moreeffective antithrombotic regimen than the stan-dard 300 mg. This effect was more marked inpatients loaded with 600 mg, lending furthermechanistic support. The contribution of attenuat-ed thrombin-induced platelet—fibrin clot formationto the overall clinical antithrombotic effect ofclopidogrel deserves further study. Measurementof R may serve as a new indicator of clopidogrelresponsiveness.
Acknowledgements
The study was supported by National Institute ofHealth (NIH) grant 5R44HL059753-03 and a grantfrom Haemoscope Corporation, Niles, IL.
Disclosure:Dr. Paul A Gurbel received research grants from
Haemoscope Corporation, Niles, IL and ScheringPlough Pharmaceuticals, Inc, Cambridge, MA.
References
[1] Gurbel PA, Bliden KP, Hayes KM, Tantry U. Plateletactivation in myocardial ischemic syndromes. Expert RevCardiovasc Ther 2004;2:535–45.
[2] Leon MB, Baim DS, Popma JJ, Gordon PC, Cutlip DE, Ho KK,et al. A clinical trial comparing three antithrombotic-drugregimens after coronary-artery stenting. Stent Anticoagu-lation Restenosis Study Investigators. N Engl J Med 1998;339:1665–71.
[3] Mehta SR, Yusuf S, Peters RJ, Bertrand ME, Lewis BS,Natarajan MK, et al. Effects of pretreatment with clopi-dogrel and aspirin followed by long-term therapy inpatients undergoing percutaneous coronary intervention:the PCI-CURE study. Lancet 2001;358:527–33.
[4] Bertrand ME, Rupprecht HJ, Urban P, Gershlick AH, Inves-tigators FT. Double-blind study of the safety of clopidogrelwith and without a loading dose in combination with aspirincompared with ticlopidine in combination with aspirin aftercoronary stenting: the clopidogrel aspirin stent interna-tional cooperative study (CLASSICS). Circulation 2000;102:624–9.
[5] Gurbel PA, Bliden KP, Samara W, Yoho JA, Hayes KM, TantryU. The Clopidogrel Resistance and Stent Thrombosis(CREST) study. J Am Coll Cardiol 2005;46:1827–32.
ARTICLE IN PRESSP.A. Gurbel et al.8
[6] Xiao Z, Theroux P. Clopidogrel inhibits platelet—leukocyteinteractions and thrombin receptor agonist peptide-in-duced platelet activation in patients with an acutecoronary syndrome. J Am Coll Cardiol 2004;43:1982–8.
[7] Aggarwal A, Blum A, Schneider DJ, Sobel BE, Daverman HL.Soluble CD40 ligand is an early initiator of inflammationafter coronary intervention. Coron Artery Dis 2004;15:471–5.
[8] Gurbel PA, Yoho J, Bliden KP, Zaman K, Kreutz RP, Tantry US.The effects of high vs. standard clopidogrel loading dosewith and without eptifibatide on markers of inflammation:results from the CLEAR PLATELETS-1b Study. Circulation inpress.
[9] Gurbel PA, Bliden KP, Hiatt BL, O’Connor CM. Clopidogrelfor coronary stenting: response variability, drug resistance,and the effect of pretreatment platelet reactivity. Circu-lation 2003;107:2908–13.
[10] Gurbel PA, Bliden KP, Hayes KM, Yoho JA, Herzog WR, TantryUS. The relation of dosing to clopidogrel responsiveness andthe incidence of high post-treatment platelet aggregationin patients undergoing coronary stenting. J Am Coll Cardiol2005;45:1392–6.
[11] Gurbel PA, Bliden KP, Zaman KA, Yoho JA, Hayes KM, TantryUS. Clopidogrel loading with eptifibatide to arrest thereactivity of platelets: results of the Clopidogrel LoadingWith Eptifibatide to Arrest the Reactivity of Platelets(CLEAR PLATELETS) study. Circulation 2005;111:1153–9.
[12] Rivard GE, Brummel K, Mann KG, Hofer A, Fan L, Cohen E.Evaluation of the profile of thrombin generation during theprocess of whole blood clotting as assessed by thromboe-lastography. J Thromb Haemost 2005;3:2039–43.
[13] Khurana S, Mattson JC, Westley S, O’Neill WW, Timmis GC,Safian RD. Monitoring platelet glycoprotein IIb/IIIa—fibrininteraction with tissue factor-activated thromboelastogra-phy. J Lab Clin Med 1997;130:401–11.
[14] McCrath DJ, Cerboni E, Frumento RJ, Hirsh AL, Bennett-Guerrero E. Thromboelastography maximum amplitudepredicts postoperative thrombotic complications includingmyocardial infarction. Anesth Analg 2005;100:1576–83.
[15] Monroe DM, Hoffman M, Roberts HR. Platelets andthrombin generation. Arterioscler Thromb Vasc Biol2002;22:1381–9.
[16] Celi A, Pelligrini G, Lorenzet R, De Blasi A, Ready N, FurieBC, et al. P-selectin induces the expression of tissue factoron monocytes. Proc Natl Acad Sci U S A 1994;91:8767–71.
[17] Leon C, Alex M, Klocke A, Morgenstern E, Moosbauer C,Eckly A, et al. Platelet ADP receptors contribute to the
initiation of intravascular coagulation. Blood 2004;103:594–600.
[18] Leon C, Ravanat C, Freund M, Cazenave JP, Gachet C.Differential involvement of the P2Y1 and P2Y12 receptors inplatelet procoagulant activity. Arterioscler Thromb VascBiol 2003;23:1941–7.
[19] Herault JP, Dol F, Gaich C, Bernat A, Herbert JM. Effect ofclopidogrel on thrombin generation in platelet-rich plasmain the rat. Thromb Haemost 1999;81:957–60.
[20] Wegert W, Graff J, Kaiser D, Breddin HK, Klinkhardt U,Harder S. Effects of antiplatelet agents on platelet-inducedthrombin generation. Int J Clin Pharmacol Ther 2002;40:135–41.
[21] Leon C, Alex M, Klocke A, Morgenstern E, Moosbauer C,Eckly A, et al. Platelet ADP receptors contribute to theinhibition of intravascular coagulation. Blood 2004;103:594–600.
[22] Bal dit Sollier C, Mahe I, Berge N, Simoneau G, Bergmann JF,Drouet L. Reduced thrombus cohesion in an ex vivo humanmodel of arterial thrombosis induced by clopidogreltreatment: kinetics of the effect and influence of singleand double loading-dose regimens. Thromb Res 2003;111:19–27.
[23] Eikelboom JW, Weitz JI, Budaj A, Zhao F, Copland I,Maciejewski P, et al. Clopidogrel does not suppress bloodmarkers of coagulation activation in aspirin-treatedpatients with non-ST-elevation acute coronary syndromes.Eur J Heart 2002;23:1771–9.
[24] van der Meijden PE, Feijge MA, Giesen PL, Huijberts M, vanRaak LP, Heemskerk JW. Platelet P2Y12 receptors enhancesignalling towards procoagulant activity and thrombingeneration. A study with healthy subjects and patients atthrombotic risk. Thromb Haemost 2005;93:1128–36.
[25] Di Nisio M, Bijsterveld NR, Meijers JC, Levi M, Buller HR,Peters RJ. Effects of clopidogrel on the rebound hyperco-agulable state after heparin discontinuation in patientswith acute coronary syndromes. J Am Coll Cardiol 2005;46:1582–3.
[26] Patti G, Colonna G, Pasceri V, Pepe LL, Montinaro A, DiSciascio G. Randomized trial of high loading dose ofclopidogrel for reduction of periprocedural myocardialinfarction in patients undergoing coronary intervention:results from the ARMYDA-2 (Antiplatelet therapy forReduction of MYocardial Damage during Angioplasty) study.Circulation 2005;111:2099–106.




















