Predictors of Response to Physical Therapy Intervention in Patients With Primary Hip Osteoarthritis
Upload
khangminh22Category
view
0download
0
Manual Therapy: Critical Assessment Profession of physical Therapy
Role the
Interest in manual therapy appears to continue to grow among physical therapy clinician$ and educators throughout the world even though the underlying con- cepts and techniques have not been justiJied by a knowledge base. The purposes of this article are to critically asress the role of manual therapy within the physical therapy p@eson and to provide an intduction to the other articles in this special issue, Eisner's model of explicit, implicit, and null curricula is used as a framework for our analysis and our discussion of manual therapy. The explicit area of manual therapy includes discusions of the deJinition and the role of manual therapy, the scientiJic rationale for manual therapy, and manual therapy in education and a comparison of manual therapy evaluative frameworks. The implicit area deals with the role of clinical decision making and critical thinking in manual therapy in education and rehabilitation. In the null (unaddressed) area of tnunual therapy, we suggest directions for future development and re- search. [FarrellJP, J m e n GM. Manual therapy: a critical assement of role in the profession of physical therapy. Phys Ther. 1992; 72:843-852. I
Key Words: Joint mobilization, Manual therapy, Orthopedics.
Mennell stated, Beyond all doubt the use of the human hand, as a method of reducing human suffering, is the oldest remedy known to man; historically no date can be given for its adoption.l@3)
The human hand continues to be an essential tool for physical therapists. Since the inception of physical ther- apy, manual treatment has been part of the identified knowledge base.2 How manual treatment (eg, massage, corrective exercise, muscle training): or the laying on of hands, has been used continues to evolve. Today, man- ual therapy is seen by many as an area of specialization within the pro-
fession. Manual therapists provide nonsurgical management of spinal and extremity dysfunction related to the neuromusculoskeletal system.3-5 We believe the role of the manual therapist in the rehabilitation process is to assess pain and function, detect movement abnormalities, test anatom- ical tissue structures, and design a treatment program that is related to realistic goals. The treatment should be continually reassessed and altered to optimize recovely to full function.6
Interest in manual therapy appears to continue to grow among physical therapists and educators throughout
JP Farrell, PT, is Senior Clinical Faculty, Kaiser-Hayward Physical Therapy Residency Program in Advanced Onhopedic Manual Therapy, Kaiser Permanente Medical Center, 27400 Hesperian Blvd, Hayward, CA 94541, and Private Practitioner, Redwood Onhopaedic Physical Therapy Inc, 20211 Patio Dr, Ste 205, Castro Valley, CA 94546 (USA). Address correspondence to Mr Farrell at the sec- ond address.
Joseph P Farrell Qall M Jensen
the world.7l8 Clinical interest and application in the manual therapy arena often exceed the current under- standing of the scientific rationale and basis for this form of treatment. The purposes of this article are to present a critical assessment of the role of manual therapy in the profession and to provide an introduction to the other articles in this special issue.
We will use a framework from the literature, Eisner's model9 of explicit, implicit, and null curricula, as a gen- eral framework for our analysis and discussion. In Eisner's framework, the explicit dimension refers to knowl- edge and ideas that are public, easily identified, and part of common prac- tice. Analysis of the explicit dimension of manual therapy will include discus- sions of the definition and the role of manual therapy, the scientific ratio- nale for manual therapy, the role of manual therapy in education, and a
GM Jensen, PhD, PT, is Associate Professor and Research Coordinator, Department of Physical Therapy, Samuel Merritt College, 370 Hawthorne Ave, Oakland, CA 94703. comparison of evaluative approaches
Physical Therapy/Volume 72, Number 12December 1992 843/ 11

in manual therapy. The implicit di- mension, often labeled as the most powerful dimension of the frame- work, includes the values and behav- iors that underlie that which we do explicitly (eg, the explicit focus is frequently on doing the evaluation, yet the clinician's analysis and inter- pretation of the clinical data are im- perative for a successful outcome). In the implicit dimension, our discussion will focus on the role of critical analy- sis in manual therapy (eg, systematic evaluation, critical thinking, clinical decision making). Our consideration of the null dimension, that which is unattended or forgotten, will include discussion of areas in need of further exploration and development.
Expllclt Dlmenslon
Defnltlon and Role
The practice of manual therapy has evolved from numerous clini- cians.MJo-13 The contributions of these clinicians has led to an eclectic set of evaluation and treatment proce- dures for musculoskeletal dysfunction.
I We believe that some experienced, skillful clinicians consider muscu- loskeletal conditions as complex as spinal dysfunction, as being multifac- torial and multistructural in effect.3 Consideration of these multiple fac- tors and structures is seen in the indications and procedures for man- ual therapy. Indications for manual treatment frequently evolve from clinical criteria rather than from de- scriptions of pathology (eg, asymme- try of position, altered joint range of motion, functional limitation, soft tissue texture abnormalities).6J4 As- sessment of soft tissue texture abnor- malities refers to the clinician's palpa- tion of the soft tissues (eg, skin, muscle, connective tissue structures), feeling for thickness, swelling, or tightnes6 A variety of physical ther- apy procedures frequently are re- quired to assist the patient in restor- ing function. These procedures may include soft tissue massage; various forms of traction; proprioceptive neu- romuscular facilitation; electrothera- peutic modalities, ergonomic analysis; exercise to improve strength, coordi-
nation, endurance, flexibility; stabiliza- tion and education; and specific man- ual therapy procedures.6.lo-13
In our view, manual therapy is not a specialty utilizing only passive move- ment techniques. Many manual thera- pists appear to agree that manual techniques include massage and mus- cle stretching of soft tissues, distrac- tion and traction techniques, specific (ie, specific to one vertebral motion segment such as L4-5) or general (ie, specific to a region of the spine such as L1-S1) high-velocity manipulation and joint mobilization, and what is called "adverse neural tissue mobiliza- ti0n."3,5,~.15 Butler defines adverse neural tissue mobilization as
. . . abnormal physiological and me- chanical responses produced from nervous system structures when their normal range of movement and stretch capabilities are tested.l5@55)
Manual techniques are one compo- nent part of nonsurgical management of the patient and are used to assist in elimination of pain and improve func- tion. A thorough examination per- formed by a skilled manual therapist should, however, govern the use of passive movement procedures as part of the treatment for the presenting clinical signs and symptoms.
The Practice Mairs Committee of the Orthopaedics Section of the American Physical Therapy Association (APTA), offered the following position:
Manipulative techniques by licensed physical therapists in evaluation and treatment of individuals with muscu- loskeletal dysfunction has [sic] always been an integral component within the scope of practice . . . . 1. Manipulation in all forms is within the scope of practice of the licensed physical thera- pist. 2. The force, amplitude, direction, duration, and frequency of manipula- tive treatment movements is a discre- tiona~y decision made by the physical therapist on the basis of education and clinical experience and on the patient's clinical profile. 3. Manipulation implies a variety of manual techniques which is not exclusive to any specific profe~sion.l6@~~)
There are multiple definitions of the terms "manipulation" and "mobiliza- tion." For example, Cyriaxlo defines manipulation as the use of hands to passively move a joint for a therapeu- tic purpose. Paris4 describes manipu- lation as the skillful application of a passive movement to a joint. Grieve defines manipulation as
. . . an accurately localized, single, quick and decisive movement of small amplitude, following careful position- ing of the patient. It is not necessarily energetic and is completed before the patient can stop it. The manipulation may have a regional or more localized effect, depending upon the technique or position of the patient.5@534)
The Orthopaedics Section of the APTA17 defines mobilization as the act of imparting movement, actively or passively, to a joint o r soft tissue. Maitland6 defines mobilization as the passive movement performed with a rhythm and grade ;o that the patient is able to prevent the technique from being performed. Paris18 suggests that the terms "mobilization" and "manip- ulation" are identical in meaning and thus can be used interchangeably.
Among some physical therapists in the United States, "mobilization" has probably evolved as a common term for two reasons: (1) Therapists may want to avoid the term "manipula- tion" because of its strong association with the chiropractic profession, and (2) "mobilization" is an accepted term in some physical therapy state prac- tice acts. Researchers have argued that there is recognition and acceptance for use of the term "manipulation" by physical therapists with training in this ~pecialty.'3-*~ Manipulation, in a gen- eral sense, means any manual proce- dure in which the hands or fingers are used to move a vertebral motion segment (ie, two adjacent vertebra and their interconnecting tissues),22 soft tissue structure, or a peripheral joint. We believe that the suitability of manipulation is dependent on precise clinical assessment and the patient's response to treatrt1ent.~J5 Various medical, chiropractic, osteopathic, and physical therapy clinicians use manip- ulative procedures and have many
Physical Therapy /Volume 72, Number 12December 1992

different terms to describe the techniques.
In summary, we believe manual ther- apy is more than the passive move- ment of joints. Manual therapy is not exclusive to any profession, and dif- ferent professionals use a variety of manual techniques. The practitioner should decide on the force, ampli- tude, direction, duration, and fre- quency of manual therapy techniques based on his or her educational back- ground and clinical experience to- gether with the patient's clinical profile.16
Sclentlflc Ratlonale
Professional interest in the application of manual therapy evaluation and treatment techniques appear to con- tinue to flourish,7,8,23 despite contin- ued slow development of a substan- tial, scientific rationale for manual therapy"23824 In addition, there appear to be no active investigative agendas among researchers and clinical ex- perts. In 1985, in the foreword of the second edition of Aspects of Manipu- lative Therapy, Maitland observed
None of us can aford to neglect the anatomical and physiological compo- nenw: of manipulative therapy, and it is essential that the clinician should try to bridge the gap between the practice and theory of how, when and why treatment should be administered and why it is su~cessful.~
Biomechanics, anatomy, and neuro- physiology are frequently the disci- plines used to provide rationales or theories for the use of manual thera- py,8,24-'6 although there are few stud- ies that have specifically examined whether and how these theoretical arguments provide a basis for prac- tice. In this issue, articles by Riddle, Di Fabio, Twomey, Threlkeld, and Walker critically assess what we know as well as what we need to know to provide a scientific basis for practice.
Research in manual therapy is compli- cated by the following factors: (1) Various clinicians and researchers disagree over the etiology of muscu- loskeletal pain; (2) indications for
manual therapy often revolve around criteria based on clinical findings rather than knowledge of the muscu- loskeletal pathology (eg, similar diag- noses can present different clinical findings); (3) musculoskeletal condi- tions often improve with time; and (4) the clinical application of manual therapy demands interaction of hu- man beings, and there is the effect of human beha~ior.6~14~16~27 The medical and physical therapy professions have examined the efficacy of manipulation in the treatment of patients who have low back ~ain.~%30 Some positive short-term effects have been found with application of manipulation or m0bilization.28~3~ The majority of re- search in manual therapy pertains to spinal conditions, particularly the lumbar In this issue, Di Fabio's article addresses the issue of efficacy in manual therapy.
Role of Manuai Therapy in Education
There is evidence that manual therapy has had an expanding role in physical therapy curricula. For example, in 1970, Stephens32 surveyed all physical therapy programs in the United States (N= 51) regarding the inclusion of manipulative therapy in entry-level curricula. In this survey, she used the term "manipulative therapy," not "manual therapy," and defined it as a system of manual therapeutic tech- niques for the restoration of the integ- rity of joints, including spinal articula- tions, by use of normal involuntary ranges of passive movement. Among the 40 programs (78%) that re- sponded to her survey, no programs offered separate courses in manipula- tive therapy, but 17% offered some instruction in manipulative therapy, with class time ranging from 3 to 20 hours. Thirty schools (59%) were not teaching manipulative techniques, and the most frequently cited reason was insufficient time because of cur- riculum priorities. Her initial defini- tion of manipulative therapy may have been somewhat restrictive, and she proposed an expanded definition of manipulative therapy at the comple- tion of her study. This expanded defi- nition included reference to restora-
tion of the normal anatomical and physiological relationships of the synovial joints and skilled, passive movements delivered to the relaxed joint within the normal joint ranges of voluntary and involuntary movement.
In 1988, a similar survey was done by Ben-Sorek and Davis,7 who inves- tigated the presence of joint mobili- zation in physical therapy curricula and compared their results with those of the 1970 survey by Ste~hens .3~ No operational defini- tion of joint mobilization was used in the survey. Only 50 physical ther- apy education programs were sur- veyed, and 38 (76%) of those pro- grams responded. Thirty-eight percent of the programs reported that mobilization was taught as a separate course, and 60% had mobi- lization as a subunit in another course. These data demonstrated significant increases in course offer- ings and content from the data gath- ered by Stephens in 1970. The most prevalent manual techniques used by programs were those of Paris,4 Mait- land,6 Cyriax,lo and Kaltenborn."
In January 1992, the Evaluative Crite- ria for Accreditation of Education Programs for the Preparation of Physi- cal Therapists went into effect.33 These criteria now include mobilization as one of the specific skills of the gradu- ate.33 The previous Standards and Criteria for Accreditation of Physical Therapy Educational Pr0grarns3~ had referred to the ability of the physical therapist to be able to perform defini- tive physical therapy testing of the musculoskeletal system with no spe- cific mention of mobilization skills. Physical therapy education has evolved considerably since 1970, when just a few programs included content and skills in "manipulative therapy." Currently, all entry-level education programs must have some content on mobilization. Tracking this process of curricular change for phys- ical therapy programs raises questions such as these for the profession: What elements are essential in our "opera- tional definitions" of certain clinical procedures (eg, mobilization, manual therapy)? and What forces drive deci-
Physical Therapy/Volume 72, Number

sion making for content in entry-level physical therapy cumcula?
Comparlson of Evaluatlve Approaches in Manual Therapy
The philosophical approach to eval- uation and treatment has been and continues to be the strongest point of identification and argument re- garding differences among the vari- ous approaches to manual therapy (Tabs. 1, 2). Our use of a "philo- sophical approach or basis" rather than a theoretical rationale for the manual therapy approach is purpose- ful. We believe that the basis for these manual therapy approaches is better described by using the term "philosophy" (ie, the general beliefs, concepts, and attitudes35 shared by those who practice) than by the term "theory." Our definition of theory is consistent with that of Kerlinger:
(A theory is] a set of interrelated con- structs (concepts), definitions, and propositions that present a systematic view of phenomena by specifying rela- tions among variables, with the pur- pose of explaining and predicting the phen0rncna.3~@9)
In 1979, Cookson and KenP7 and Cookson38 published review articles emphasizing the similarities and dif- ferences among the various ap- proaches commonly used in orthope- dic manual therapy. These articles provide an overview of the four major approaches in manual therapy as espoused by Maitland: Cyriax,Io Kal- tenborn,ll and MennelL13 A compari- son of the four evaluation approaches used in manual therapy, as reviewed by Cookson and Kent37 and Cook- son,38 as well as two other approaches frequently used by physical therapists (ie, McKenzie's approach to the spinel2 and the osteopathic approach to musculoskeletal dysfunction39~~) is presented in Tables 1 and 2. The selection of these six approaches is not meant to be exhaustive or com- prehensive, but it is representative of major approaches integrated into physical therapy practices today.
The philosophical basis presented for these evaluative approaches also ap-
pears to be a critical factor in under- standing how the evaluation will be structured and how the clinical find- ings will be interpreted. Table 1 pro- vides an overview of evaluation ap- proaches used in manual therapy that have been physician-generated (ie, Cyriax,lo Mennell,l3 and osteopath- i~39~40 approaches). Cyriax'slo contri- bution in devising a logical method for clinical examination of "soft tissue structures" or musculoskeletal prob- lems has been a component of many of the other evaluative frameworks in manual therapy.3 Common elements in these three approaches include gathering of patient data through taking of a history; active movement testing; palpation; and mobilization, manipulation, and patient education as treatment interventions. Again, the major differences appear in the philo- sophical basis for the approach, which in turn leads to a difference in inter- preting musculoskeletal signs and symptoms. For example, Cyriaxlo subscribes to an assessment system closely linked with his interpretation of applied anatomy (eg, differentiating contractile and noncontractile struc- tures). Mennell'sl3 primary focus is examination of synovial joints and treatment of joint dysfunction with joint-play techniques. Central to the osteopathic approach is the belief that the body is an integrated unit or total system; that is, the neuromusculoskel- eta1 system is connected with other systems of the body, and disease pro- cesses are frequently visible in the musculoskeletal system. A second belief is that structure governs func- tion and an abnormality in structure can lead to abnormal function. So- matic dysfunction is the impaired or altered function of the somatic system (skeletal, arthrodial, and myofascial structures and related vascular, lym- phatic, and neural elemer1ts).39,~~
The physical therapist-generated evaluative frameworks, like the physician-generated evaluative frameworks, subscribe to a philo- sophical basis. This philosophical basis often includes integration of other approaches, but with applica- tion of evaluation and treatment techniques done by the physical
therapist (Tab. 2). The evaluation frameworks for all three approaches (ie, Maitland,6 Kaltenborn," and McKenzieI2 approaches) have many elements similar to Cyriax'sl0 screening criteria. Each approach also includes examination proce- dures specific to the approach. For example, Maitland6 emphasizes the importance of continual assessment in developing working hypotheses based on evaluation. Kaltenborn" includes elements that represent his background as an osteopath (eg, reference to somatic dysfunction) as well as biomechanical assessments of joint motion. McKenzieIZ uses evaluation of repeated active move- ments and patient self-treatments as key elements in his assessment. Similarities among these three ap- proaches include the use of palpa- tion; testing of joint movements; and mobilization/manipulation, exercise, and patient education as treatment strategies.
As practitioners become more eclectic in their evaluation and management of patients, the lines between evalua- tive approaches are likely to continue to blur over time. A challenge for manual therapists will be to search for and identify the underlying theo- retical arguments for manual therapy evaluation and treatment procedures that cross the various "philosophical approaches" so that propositions can be derived from the theories and tested.
Implicit Dlmenslon
Musculoskeletal Evaluatlon: The Role of Critical Analysis
Even though we see that, explicitly, manual therapy approaches are based on somewhat different philosophies, they do share a common dimen- sion-there is always some form of systematic evaluation and treatment of patients with musculoskeletal dysfunc- tion. The implicit dimension, that is, the values and behaviors that are central to the work of the manual therapist, includes perhaps the most important contribution to the profes- sion made by manual therapy. This
Physical Therapy /Volume 72, Number 12December 1992

- Table 1. Comparisons of Physician-Generated Evaluative Approaches Used in Manual i'%erapy
Physical Therapy /Volume 72, Number 12December 1992
Philosophical basis
Key concepts
Evaluation framework History
Physical
Interpretation of evaluation
Treatment strategies
OsteopathlcN.4o Contentlons
1. The body is a total unit, and the neuromusculoskeletal system is connected with other systems; therefore, disease processes can be visible in the musculoskeletal system
2. The structure of the body governs function; an abnormality in structure can lead to abnormal function
3. Somatic dysfunction is the impaired function of related components of the somatic system (eg, skeletal, arthroidal, and myofascial structures and related vascular, lymphatic, and neural elements)
4. Manipulative therapy can restore and maintain normal structure and function relationships
Diagnosis of somatic dysfunction a Clinical examination focuses on the
presence of asymmetry, restriction of movement, and palpation of soft tissue texture changes (ie, palpation of skin, muscle, and other connective tissue for feeling of thickness, swelling, tightness, or temperature change)
History Knowledge of physical trauma, past visceral and soft tissue problems
Present complaint a Establish relationship behveen
adaptation, decornpensation, trauma. and time from patient's history
Physical examination Postural analysis
Regional screening functional units a Pelvic girdle
Foot Vertebral column Shoulder girdle Hand
Detailed evaluation of regions in dysfunction
Positional fault Restriction fault Segmental or multisegmental
Manipulation Mobilization Muscle energy Myofascial techniques Counterstrain Exercise therapy Patient education
Manual Therapy Approach
Cyrlaxlo (Orthopedic Medlclne) Contentlons
1. All pain has an anatomical source
2. All treatment must reach that anatomical source
3. If the diagnosis is correct, all treatment will benefit the source
Diagnosis of soft tissue lesions Categorization of referred pain Differentiation of contractile and noncontractile lesions
Observation, history Age and occupation Symptoms (site and spread, onset and duration, behavior) Medical considerations Inspection
Physical examination Active movements Passive movements Resisted movements Neurological examination Palpation
Identification of anatomical structure associated with lesion
Friction massage Injection Manipulation Mobilization Physical therapy (eg,
exercise, modalities) Patient education
Mennelll3 Contentlons
1 . Dysfunction is a sign of a serious pathological process or joint disease
2. Loss of normal joint movement or joint play can lead to dysfunction
3. Joint manipulation can restore normal joint-play movements
Assessment of joint play
Present complaint Onset Nature of pain Localization of pain Loss of movement
Past history Family history Medical systems review
Physical examination Inspection Palpation Examination of voluntary movements Muscle examination Special tests (eg. roentgenography)
a Examination of joint-play movements
Joint dysfunction
Manipulation Mobilization Physical therapy (eg, exercise,
modalities) Patient education
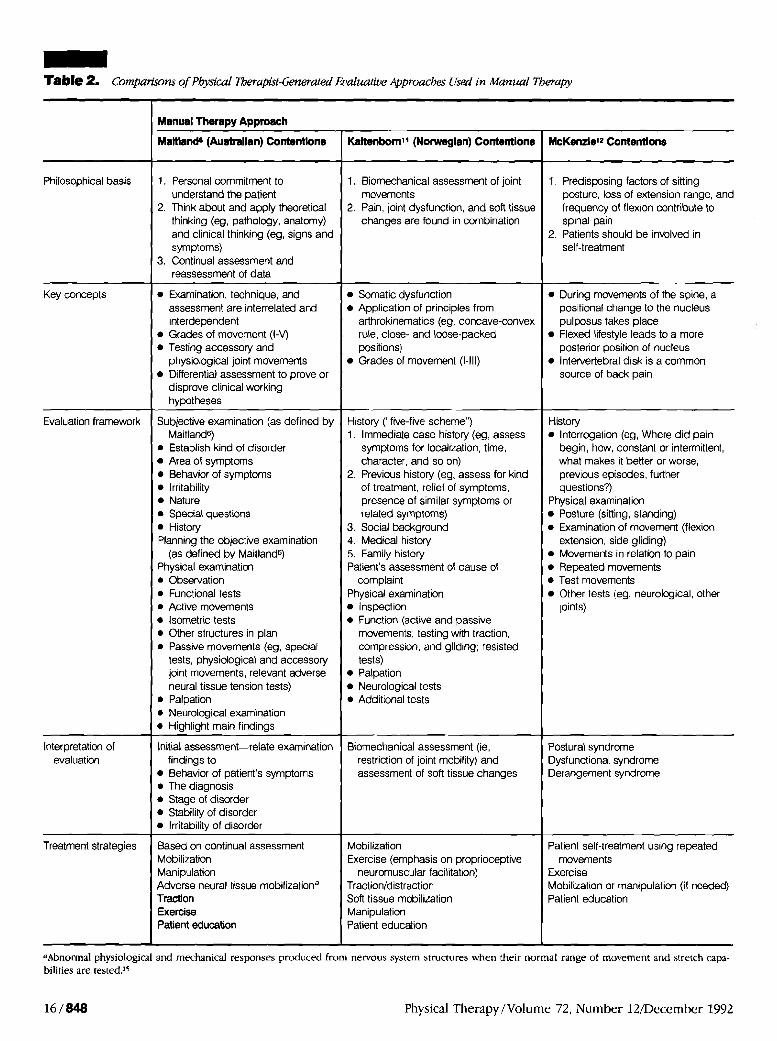
- Table 2. Comparisons of PLydca l~ap~-Genera ted Evaluative Approaches Used in Manual Therapy
aAbnormal physiological and mechanical responses produced from nervous system structures when their normal range of movement and stretch capa- bilities are tested.'5
16 / 848 Physical Therapy /Volume 72, Number 12/December 1992
Philosophical basis
Key concepts
Evaluation framework
Interpretation of evaluation
Treatment strategies
McKerulelz Contentions
1. Predisposing factors of sitting posture, loss of extension range, and frequency of flexion contribute to spinal pain
2. Patients should be involved in self-treatment
During movements of the spine, a positional change to the nucleus pulposus takes place Flexed lifestyle leads to a more posterior position of nucleus Intervertebral disk is a common source of back pain
History Interrogation (eg, Where did pain begin, how, constant or intermittent, what makes it better or worse, previous episodes, further questions?)
Physical examination Posture (sitting, standing) Examination of movement (flexion, extension, side gliding) Movements in relation to pain Repeated movements Test movements Other tests (eg, neurological, other joints)
Postural syndrome Dysfunctional syndrome Derangement syndrome
Patient self-treatment using repeated movements
Exercise Mobilization or manipulation (if needed) Patient education
Manual Therapy Approach
Maltland8 (Australian) Contentlons
1. Personal commitment to understand the patient
2. Think about and apply theoretical thinking (eg, pathology, anatomy) and clinical thinking (eg, signs and symptoms)
3. Continual assessment and reassessment of data
Examination, technique, and assessment are interrelated and interdependent Grades of movement (I-V) Testing accessory and physiological joint movements Differential assessment to prove or disprove clinical working hypotheses
Subjective examination (as defined by Maitlands) Establish kind of disorder Area of symptoms Behavior of symptoms Irritability Nature Special questions History
Planning the objective examination (as defined by Maitlands)
Physical examination Observation Functional tests Active movements Isometric tests Other structures in plan Passive movements (eg, special tests, physiological and accessory joint movements, relevant adverse neural tissue tension tests) Palpation Neurological examination Highlight main findings
Initial assessment-relate examination findings to Behavior of patient's symptoms The diagnosis Stage of disorder Stability of disorder Irritability of disorder
Based on continual assessment Mobilization Manipulation Adverse neural tissue mobilizationa Traction Exercise Patient education
Kaltenbornll (Norwegian) Contentlons
1. Biomechanical assessment of joint movements
2. Pain, joint dysfunction, and soft tissue changes are found in combination
Somatic dysfunction Application of principles from arthrokinematics (eg, concave-convex rule, close- and loose-packed positions) Grades of movement (1-111)
History ("five-five scheme") 1. Immediate case history (eg, assess
symptoms for localization, time, character, and so on)
2. Previous history (eg, assess for kind of treatment, relief of symptoms, presence of similar symptoms or related symptoms)
3. Social background 4. Medical history 5. Family history Patient's assessment of cause of
complaint Physical examination
Inspection Function (active and passive movements; testing with traction, compression, and gliding; resisted tests) Palpation Neurological tests Additional tests
Biornechanical assessment (ie, restriction of joint mobility) and assessment of soft tissue changes
Mobilization Exercise (emphasis on proprioceptive
neurornuscular facilitation) Tractionldistraction Soft tissue mobilization Manipulation Patient education

contribution is an emphasis on sys- tematic evaluation as well as analysis and interpretation of the clinical data.
We have seen increased integration of manual therapy in practice and educa- ti0n.7~23~32.33 Along with this growth has been an increased emphasis on the evaluative process as well as the thinking and reasoning behind clini- cal decision making. For example, Cookson and KenP7 argue that al- though therapeutic techniques ap- plied for a certain musculoskeletal condition may vary across the differ- ent philosophical approaches, evalua- tion of the patient to determine whether to treat or not to treat is essential. Over the last few years, several musculoskeletal texts have been written, not by physicians, but by physical therapists.5.6.41-'5 These texts focus on orthopedic assessment, including evaluation and treatment. The value of clinical reasoning and decision making in practice and edu- cation also is a theme in recent pro- fessional wr i t ing~.~69
In our view, this process of not only using a systematic evaluation scheme, but investigating the clinical reasoning and decision making that underlie the evaluation and the understanding and interpretation of findings is an ex- tremely important goal for the profes- sion. Professional expertise is de- scribed by many educators in the professions as not only the possession of technical skills, but also the use of analytical skills for critical analysis and deliberate action.sl-53 This critical analysis requires that the professional education process assist students in becoming critical analysts. This pro- cess must occur in the "context of action" or practice. For example, the practitioner must first make sense of a situation by imposing a structure or framework for analysis. This frame- work is used to help define a prob- lem and judge the potential conse- quences of action. Students and practitioners must think about what they will do and why and then take action. The initial emphasis for stu- dents should be on the thoughtful analysis of an experience rather than finding the correct procedure.52-5*
The importance of developing thera- pists' thinking and analytical skills, as well as their technical skills, raises important questions. Do entry-level degree programs promote critical analysis of technique and allow time for thoughtful analysis and reflection? Are these programs focused on cover- ing a given amount of material, con- sistent with trends in clinical prac- tice?54 Do we see in continuing education programs an equal empha- sis on critical analysis of scientific rationales or underlying theories as well as application and mastery of clinical techniques?
The Maitland, or Australian, approach includes an evaluative framework that is based on a conceptual model or framework.49jw We believe that the Australian evaluation framework is an example of how a clinician can facili- tate his or her clinical-reasoning pro- cess. What follows in this next section is an example of how the manual therapist uses the evaluation frame- work for organizing and interpreting clinical data.
The Australian Approach: An Example of a Framework for Critical Analysis
In the Australian approach, the evalua- tion process should begin when a patient walks into the treatment room. An interview process occurs in which the manual therapist guides the pa- tient's description of his or her symp- toms by defining the location and behavior of those symptoms, obtain- ing the patient history, and determin- ing any precautions that may preclude treatment. The interview (defined by Maitland6 as the subjective examina- tion) is vital as the first step in deter- mining the source of the patient's complaint. Maitland uses the term "subjective" here to represent the interactive portion of the examination, that is, the therapist's interview with the patient in which the therapist begins to interpret the patient's per- ceptions of his or her symptoms. The term "subjective" is not used in a scientific manner to represent a sub- jective measure o r test.55 The clinician makes an assessment or appraisal of
the interview data collected, which, in essence, is a clinical judgment or decision based on the experience, training, and skills of the clinician. A "working hypothesis" is formulated with the intent of identifying the po- tential musculoskeletal structures involved in the presenting pathology. The clinician uses his or her assess- ment skills and knowledge to rank the importance of each component of the working hypothesis according to the SINS algorithm. (S=severity, I= irritability, N = nature of the com- plaint, and S=stage of pathology).49.9
Severity is the term used to describe the clinician's assessment of the inten- sity of the patient's symptoms as they relate to a functional activity. For example, if the patient has ceased using his or her arm to dress and is unable to find a position to ease pain, then the symptoms are considered severe. Nonsevere symptoms are represented by the patient who is able to dress with arm or shoulder pain, yet the pain is not intense enough to stop the functional activity even though pain is experienced. Irritability is the term used to de- scribe the clinician's assessment based on (1) the amount of activity needed to bring on the patient's symptoms and (2) the amount of time before the patient's symptoms subside (dura- tion). For example, a shoulder pain that begins when the patient lifts an arm and that lasts for 4 hours means that the patient's condition is ex- tremely irritable (little activity causes considerable pain that lasts for a long period of time). Conversely, a shoul- der pain that is aggravated when the patient lifts his or her arm, but eases when the patient returns the arm to his or her side, would be considered a nonirritable condition.
The nature of the complaint is the term that represents the clinician's assessment of the patient's pain toler- ance, including consideration of cul- tural differences, stability of the condi- tion, type of pathology, and the physical therapist's hypothesis of the structures responsible for producing the pain complaint. The stage of the pathology is a term used to describe
Physical Therapy/Volume 72, Number 12December 1992

the clinician's assessment of what the progression of symptoms is for the patient. For example, if the patient reports that he or she had low back pain 2 days ago and now has lower- extremity pain radiating to the ankle, the clinician may suspect that the pathological condition is deteriorat- ing. The hypothesis would then be reranked accordingly.6~45
Clinical decisions that relate to inter- vention also revolve around assessing data during and at the conclusion of the physical examination, during the application of treatment techniques, and at the conclusion of the initial treatment.6150 From this form of analy- sis, treatment goals are established and a treatment strategy is formulated.
Throughout the course of treatment, the therapist continues to assess the effect of treatment on the patient's hnctional limitations that relate to his or her lifestyle and work environment and the active, passive, or functional movement signs and symptoms that relate to the clinical working hypothe- sis. Through continual assessment of each technique, exercise, or modality, the clinician progresses treatment and hypothesizes which structures or body regions most likely contribute to the patient's problem. For example, if a patient's active or passive movement signs, symptoms, and functional status are not changing at what the clinician believes is an appropriate rate, the clinician needs to reassess (ie, rerank, reject, or reformulate) the working hypothesis and alter the treatment accordingly.49
The clinician has a central role to play in collecting and interpreting clinical data for individual patients. We pro- pose that the clinician also has a cen- tral role to play in the generation of classification systems that identify commonalities and differences across patient cases. In 1989, Rose47 argued that therapists need to identify and characterize the relationships between clinical entities and specific treatments and management strategies. He ar- gued that clinicians need to use a process of rational practice and criti- cal thinking to achieve this goal. 0th-
e r~5~~57 have suggested that the use of established clinical classification sys- tems may assist physical therapists in this classification process. As the phys- ical therapy profession moves toward more systematic observation and classification of clinical phenomenon, the manual therapist could serve a critical role assisting with the develop ment of this process. In this special issue, the article by Jones provides further dialogue about the role of clinical reasoning in manual therapy.
Null Dlmenslon
We believe that there are other as- pects of manual therapy that are part of the null dimension, that is, aspects that are often ignored. Grieve de- scribes the present state of manual therapy well:
We continue to sound as though we know so much, when we know com- paratively little. It might be a good thing to admit this. We make much of clinical science, enthusiastically refer- ring to this or that part of the massive mountain of literature which best serves our particular interest . . . . Much of what we do is simply what has been proven on the clinical shop floor to be effective in getting our patients bet- ter-we do not always know ~ h y . ~ 3 ( p ~ )
One aspect of manual therapy that is frequently ignored is consistent dis- cussion and analysis of the identified theory or body of general principles underlying the knowledge base. We have noted that biomechanics, anat- omy, and neurophysiology are often discussed as providing an underlying rationale for manual therapy and are enthusiastically referred to as the elements that fit our applications.24 We need to ask ourselves, What are the sources of knowledge cited for manual therapy in either entry-level or continuing professional education? Is the knowledge base in manual therapy built on a model of tradition or authority or the scientific meth- od?58 A model of tradition refers to knowledge obtained from "truths" or beliefs that were accepted in the past and that continue to influence prac- tice. A model of authority is when knowledge is gained from experts
(authority figures) and that knowl- edge, like knowledge from tradition, has not been validated or verified through research.5B For example, the philosophical bases of the different approaches to manual therapy are generally well-known and central aspects of the written materials, yet there has been little focus on devel- oping and discussing application of theory to practice or generating test- able questions from identified key theories.
We cannot ignore that clinical prac- tice combines the elements of art and science. Clinical observation and manual technique are central components of the artistry of prac- tice in manual therapy. Feinstein59 suggests that clinical practice is nei- ther art nor science, but the most scientific art and the most humanis- tic science. Several articles in the July 1989 issue of Physical Therapy on clinical decision making focused on discussion and improvement of clinical mea~ures.47.55~60~61 Delitto60 suggests consideration of Feinstein's principles of clinimetric~6~ (eg, de- velopment of clinimetric indexes that address face validity and content validation and that have a formal expression of the index) as a way of expanding the scientific basis of clinical practice. Many of these prin- ciples have application for investiga- tions in manual therapy.
For example, palpation plays a central role in application of sevelal manual therapy techniques. Palpation is a practical skill that apparently requires many hours of training and practice to maste1-.~3 Many manual therapists believe that palpation of the spine and associated areas that contribute to the presenting symptoms may be the most informative aspect of the physi- cal examination." Sophisticated imag- ing techniques continue to serve as major tools in the diagnosis of muscu- loskeletal problems, with less reliance on palpation. The challenge for physi- cal therapists will be to integrate technology and manual skills so that both components can enhance thera- pists' understanding of musculoskele- tal problems. For example, Jull et a165
Physical Therapy / Volume 72, Number 12December 1992

studied 20 patients, all of whom had complained of chronic neck o r head- ache for at least 1 year, who under- went manual examination of the cer- vical zygapophyseal joints and radiographic assessment. In one group of patients (n = 11), the pres- ence or absence of symptoms associ- ated with a joint was established by radiographically controlled diagnostic nerve blocks. The manual therapist was unaware of the diagnosis and examined the patients 1 to 4 weeks after the nerve block. The order of events was reversed in the second group of patients (n=9); that is, the manual examination was first, fol- lowed by the diagnostic nerve blocks. Of the 20 patients studied, the manual therapist identified all 15 patients who had symptomatic zygapophyseal joints and also identified the 5 patients who did not have joint involvement. This study is an example of systematic investigation of the "an" of palpation and represents an initial step toward investigation of the validity of palpa- tion techniques.
Another area of manual therapy that is often ignored are investigations re- garding the effectiveness and efficacy of manual therapy. Several investiga- tions have examined the use of man- ual therapy for treating spinal condi- tions, particularly low back pain.1+2112+32 Di Fabio's article in this issue provides an analysis of this liter- ature. A related issue is exploration of the potential role of the placebo effect in manual therapy. Improvement of a patient's condition after physical ther- apy cannot be seen as evidence of the efficacy of manual techniques.
Gielen66 identifies two major ele- ments that contribute to the placebo effect: (1) the therapist-patient rela- tionship, which is influenced by the patient's perceptions of the therapist's expertise, trustworthiness, optimism, and enthusiasm, and (2) the use of other modalities. Patient education is also seen as a component of a manual therapy intervention (Tabs. 1, 2). In our theory development for manual therapy, we may need to consider a model that not only represents the dimensions we routinely think of as
underlying musculoskeletal evaluation and treatment (eg, anatomic, biome- chanical, neurophysiologic), but gives more purposeful consideration to aspects of human behavior. For exam- ple, theories regarding patient- provider interactions, health behavior, and cultural aspects of illness6- may also help clinicians develop a fuller understanding of the context of clini- cal practice.
This assessment of manual therapy has provided an introduction to the current role of manual therapy in the profession of physical therapy. Manual therapy represents more than just the application of passive movements, and the field continues to evolve as a subspecialty in physical therapy. The knowledge base and practice of man- ual therapy have strong ties to the philosophical approaches advocated by several clinicians. The scientific base of manual therapy is frequently tied to knowledge from other disci- plines (eg, anatomy, biomechanics, neurophysiology), with few or no investigations to substantiate the con- nections made between knowledge and practice, or the efficacy of prac- tice. Systematic and continual assess- ment is a central component of the clinical-reasoning process manual therapists use in confirming or dis- confirming a diagnosis. Investigations that focus on the clinical-reasoning and decision-making processes should be helpful initial steps in addressing questions such as, Why are patients getting better? and What kinds of patients get better with what treat- ments? Such investigations, ultimately, should be helpful in developing theo- ries of practice for the profession of physical therapy.
References
1 Mennell JM. Manual Therapy. Springfield, Ill: Charles C Thomas, Publishec 1951:3. 2 Grunewald L. A study of physiotherapy as a vocation Pbysiotherap.~ Review. 1928;8(4):37- 42. 3 Iamb D. A review of manual therapy for spinal pain: with reference to the lumbar spine. In: Grieve GP, ed. Modem Manual
Therapy. Ncw York, NY: Churchill Livingstone Inc; 1986:605421. 4 Paris SV. Mobilization of the spine. Phys Tbm 1979:59:98%995. 5 Grieve GP. Common Vertebral Joint Ptoh- l a . 2nd ed. New York, NY: Churchill Living- stone Inc; 1989:303-349, 534. 6 Maitland GD. Vertebral Manipulation. 5th ed. Boston, Mass: Butterwonh; 1986:l-13. 7 Ben-Sorek S, Davis CM. Joint mobilization education and clinical use in the United States. Phys Ther. 1988;68:1000-1004. 8 Glasgow E, Twomey LT, ed. Aspects of Ma- nipulatic~e Therapy. 2nd ed. New York, NY: Churchill Livingstone Inc; 1985. 9 Eisner E. The Educational Imagination: On Design and Evaluation of Educational Pro- grams. New York, IW MacMillan Publishing Co; 1979:74-92. 10 Cyriax JH. Textbook of Onhopaedic Medi- cine. Volume I: Diagnosis of Soj Tissue Le- sions. 8th cd. London, England: Bailliere Tin- dall; 1982. 11 Kaltenborn FM. Mobilization of the Ex- tremity Joints. 3rd ed. Oslo, Norway: Olaf Nor- lis Bokhandel Universitetsgaten; 1980. 12 McKenzie RA. The Lumbar Spine: Mechani- cal Diagnosis and Therapy. Waikanae, New Zealand: Spinal Publications; 1981. 1 3 Mennell JM. Back Pain: Diagnosis and Treatment Using Manipulative Techniques Boston, Mass: Little, Brown & Co Inc; 1960. 14 Haldeman S. Spinal manipulative therapy: a status repon. Clin Orthop. 1983;179:62-70. 15 Butler D. Mobilization of the Nervous Sys- tem. New York, NY: Churchill Livingstone Inc; 1991. 16 Nicholson G. Practice ABairs Committee repon: position statement on manipulation, orthopedic practice. Bulletin of the Ortho- paedics Section. American Physical Therapy Association. 1991;3(2):22-23. 17 Orthopaedic Physical Tberapj Tenninol- om. La Crosse, Wis: Onhopaedics Section Inc. 18 Paris SV. Spinal manipulative therapy. Clin Orthop. 1983;179:5541. 19 Farrell JP, Twomey LT. Acute low back pain: comparison of two conservative treat- ment approaches. Med J Amt. 1982;1:160-164. 20 Godfrey CM, Morgan PP, Schatzker J. A ran- domized trial of manipulation for low-back pain in a medical setting. Spine. 1984;9:301- 304. 21 Meade TW, Dyer S, Browne W, et al. Low back pain of mechanical origin: randomized comparison of chiropractic and hospital outpa- tient treatment. BMJ. 1990:300:1431-1437. 22 White AA, Panjabi MM. Clinical Biome- chanics of the Spine. 2nd ed. Philadelphia, Pa: JB Lippincott Co; 1990:45. 23 Grieve GP, ed. Modem Manual Tberapj of the Vertebral Column. New York, NY: Church- ill Livingstone Inc; 1986:v, 270-282. 24 Goldstein M, ed. The Research Statz~s of Spinal Manipulative Therapy. Bethesda, Md: Workshop for NIH; 1975. US Dept of Health, Education, and Welfare publication 76-998. 25 Kent B, ed. International Federation of Orthopaedic Manipulative Therapists Proceed- ings. Hayward, Calif: International Federation of Onhopaedic Manipulative Therapists; 1977. 26 Zusman M. Spinal manipulative therapy: review of some propose mechanisms, and a
Physical Therapy /Volume 72, Number 12December 1992

new hypothesis. AmtraIian Journal of Physio- therapy. 1986;32:89-99. 27 Hoehler FK, Tobis JS, Buerger AA. Spinal manipulation for low back pain. JAMA. 1981; 245:18351838. 28 Di Fabio RP. Clinical assessment of manip- ulation and mobilization of the lumbar spine: a critical review of the literature. Phys Ther. 1986;66:51-54. 29 Deyo a Conservative therapy for low back pain: distinguishing useful from useless treaunent. JAMA. 1983;250:1057-1062. 30 Grahm R. Clinical trials in low back pain. Clinics in Rheumatic Disease. 1980;6:143-157. 31 Ottenbacher K, Di Fabio RP. Efficacy of spinal manipulation/mobilization therapy: a meta-analysis. Spine 1985;10:833-?337. 32 Stephens E. Manipulative therapy in physi- cal therapy curricula. Phys Tbm 1973;53:4&50. 33 Evaluative Critena for Accreditation of Education Programs for the Preparation of Physical Therapists. Alexandria, Va: Commis- sion on Accreditation in Physical Therapy Edu- cation, American Physical Therapy Association; 1991. 34 Accreditation Handbook. Alexandria, Va: American Physical Therapy Association; 1985. 35 Webster's Ninth New Collegiate Dictionary. Springfield, Mass: Merriam-Webster Inc; 1991: 883. 36 Kerlinger FN. Foundations of Behavioral Research. 3rd ed. New York, NY: Holt, Rinehart & Winston Inc; 1986:9. 37 Cookson JC, Kent B. Orthopedic manual therapy-an overview, pan 1: the extremities. Phys Thw. 1979;59:136146. 38 Cookson JC. Orthopedic manual thera- py-an overview, pan 2: the spine. Phys Ther. 1973;59:259-267. 39 Stoddard h Manual of Osteopathic Prac- tice. London, England: Hutchinson & Co; 1969; 1-55. 40 DiGiovanna E, Schiowitz S. An Osteopathic Appmch to Diagnosis and Treatment. Phila- delphia, Pa: JB Lippincott Co; 1991:l-19.
41 Hertling D, Kessler RM. Management of Common Musculoskeletal Disorders. 2nd ed. Philadelphia, Pa: JB Lippincott Co; 1990. 42 Gould J, ed. Orthopaedic and Sports Physi- cal Therapy. 2nd ed. St Louis, Mo: CV Mosby Co; 1990. 43 Wadsworth CT. Manual Examination and Treatment of the Spine and Extremities. Balti- more, Md: Williams & Wilkins; 1988. 44 Magee D. Orthopedic Physical Arsessment. 2nd ed. Philadelphia, Pa: WB Saunders Co; 1992. 45 Maitland GD. Petipheral Manipulation. 3rd ed. Boston, Mass: Butterworth-Heinemann; 1991. 46 Magistro C. Clinical decision making in physical therapy: a practitioner's perspective. Phy~ Thw. 1989;69:525-534. 47 Rose SJ. Physical therapy diagnosis: role and function. Phys Ther. 1989;69:535-537. 48 Wolf S, ed. Clinical Decision Making in Physical Therapy. Philadelphia, Pa: FA Davis Co; 1986. 49 Grant R, Jones M, Maitland GD. Clinical decision making in upper quadrant dysfunc- tion. In: Grant R, ed. Physical Therapy of the Ceruical and Thoracic Spine. New York, NY: Churchill Livingstone Inc; 1988:51430. 50 Maitland GD. The Maitland concept: assess- ment, examination, and treatment by passive movement. In: Twomey LT, Taylor J, eds. Physi- cal Therapy of the Low Back. New York, NY: Churchill Livingstone Inc; 1987:135-156. 51 Kennedy M. Inexact sciences: professional education and the development of expertise. In: Rothkopf E, ed. Review of Research in Edu- cation. Washington, DC: American Educational Research Association; 1987:133-168. 52 Schon D. Educating the Reflective Practifio- ner. San Francisco, Calif: Jossey-Bass Publish- ers; 1987. 53 Cervero R. Effective Continuing Education
for Professionals. San Francisco, Calif: Jossey- Bass Publishers; 1988. 54 Shepard K, Jensen GM. Physical therapist curricula for the 1990s: educating the reflec- tive practitioner. Phys Ther 1990:70:566573.
55 Rothstein JM. On defining subjective and objective measurements. Phys Ther. 1989;69: 577-579. 56 Jette AM. Diagnosis and classification by physical therapists: a special communication. Phys the^ 1989;69:967-969. 57 Guccione AA. Physical therapy diagnosis and the relationship between impairments and function. Phys Tber. 1991;71:499-503. 58 Polit D, Hungler B. Nursing Research: Prin- ciples and Methods. 4th ed. Philadelphia, Pa: JB Lippincott Co; 1991:15-22. 59 Feinstein A. Clinical Judgment. Malabar, Fla: Roben E Krieger Publishing Co; 1967:291- 349. 60 Delitto A. Subjective measures and clinical decision making. Phys Ther. 1989;69:585589. 6 1 Jette AM. Measuring subjective clinical out- comes. Phys Ther. 1989;69:580-584. 62 Feinstein A. Clinimetrics. New Haven, Conn: Yale University Press; 1987. 63 Farrell JP. Cervical passive mobilization techniques: the ~ust ra l~an approach. Phyn'cal Medicine and Rehabilitation: State-of-the-An Reviews. 1990;4:309-334. 64 Maitland GD. Palpation examination of the posterior cervical spine: ideal, average, and normal. Australian Journal of Physiotherapy. 1982;28:3-12. 65 Jull G, Bodguk N, Marsland A. The accu- racy of manual diagnosis for cervical zygapo- physeal joint pain syndromes. Med J Aust. 1988;148:233-236. 66 Gielen F. Discussion of placebo effect in physiotherapy based on a noncritical review of the literature. Phyaothwapy Canada. 1989:41: 210-216. 6 7 Glanz K, Lewis F, Rimer B, eds. Health Be- havior and Health Education: Theoty, Re- search, and Practice. San Francisco, Calif: Jossey-Bass Publishers; 1990. 68 Dean E. Psychobiological adaptation model for physical therapy practice. Phys Tber. 1985; 65:1061-1068.
Physical Therapy /Volume 72, Number 12December 1992
Copyright © 2022 FDOKUMEN