Costs of congenital rubella syndrome (CRS) in Oman: Evidence based on long-term follow-up of 43...
9
Vaccine 24 (2006) 6437–6445 Costs of congenital rubella syndrome (CRS) in Oman: Evidence based on long-term follow-up of 43 children Salah Al-Awaidy a,∗ , Ulla K. Griffiths b , Hosammudin Mohammed Nwar a , Shyam Bawikar a , Masoud Salim Al-Aisiri c , Rajiv Khandekar d , Ali Jaffer Mohammad e , Susan E. Robertson f a Department of Communicable Disease Surveillance and Control, Directorate General of Health Affairs, Ministry of Health, Muscat, Sultanate of Oman b Health Policy Unit, London School of Hygiene and Tropical Medicine, Keppel Street, London WC1E 7HT, UK c Department of Financial Planning, Directorate General of Health Affairs, Ministry of Health, Muscat, Sultanate of Oman d Eye and Ear Health Care, Department of Noncommunicable Diseases, Directorate General of Health Affairs, Ministry of Health, Muscat, Sultanate of Oman e Ministry of Health, Muscat, Sultanate of Oman f Department of Immunization, Vaccines and Biologicals, World Health Organization, Geneva 27, CH-1211 Switzerland Received 14 December 2005; received in revised form 22 May 2006; accepted 23 May 2006 Available online 13 June 2006 Abstract As part of the national plan for elimination of rubella and congenital rubella syndrome (CRS), Oman established a national registry of CRS cases. As of May 2005, the registry included 43 surviving CRS cases, with a mean age of 11.9 years. Clinical examinations found that 84% had ocular defects, 84% had auditory/speech defects, 70% had neurological manifestations, and 42% had cardiac defects. Lifetime medical, special education, and rehabilitation costs were assessed. Using a discount rate of 3%, the average direct lifetime cost per surviving CRS patient was estimated at US$ 18,644. When including predicted lost productivity due to CRS, the average discounted direct and indirect lifetime costs per surviving CRS patient amounted to US$ 98,734. © 2006 Elsevier Ltd. All rights reserved. Keywords: Congenital rubella syndrome; Cost study; Disability 1. Introduction WHO estimates indicate that there are still more than 100,000 new cases of congenital rubella syndrome (CRS) occurring each year [1]. Children with CRS suffer from multiple birth defects, including deafness, blindness, con- genital heart disease, and mental retardation. While some CRS defects are readily identified in infants, others are hard to diagnose until older ages (i.e. deafness) and some of the problems associated with CRS are known to have late onset (i.e. diabetes, thyroid disorders). A global review of stud- ∗ Corresponding author. Tel.: +96 82 460 1921; fax: +96 82 460 1832. E-mail addresses: [email protected] (S. Al-Awaidy), [email protected] (S.E. Robertson). ies assessing the costs of CRS was published in 2002 [2]. Altogether 22 studies were identified, including 10 from developing countries. The review concluded that more CRS costing studies from developing countries should be encour- aged, and that such studies should use standardized economic methods. The need for standardised methods was emphasized in an accompanying editorial [3]. Oman experienced large rubella epidemics in 1987–1989 [4] and 1992–1994 [5]. Since then there has been a dramatic decline in the incidence of rubella following widespread use of rubella vaccine. In March 1994, there was a national campaign to deliver measles–rubella (MR) vaccine to the target group aged 15 months–18 years. Some 700,000 per- sons received MR vaccine during the campaign, with 94% coverage of the target age group. At the same time as the cam- 0264-410X/$ – see front matter © 2006 Elsevier Ltd. All rights reserved. doi:10.1016/j.vaccine.2006.05.089
Transcript of Costs of congenital rubella syndrome (CRS) in Oman: Evidence based on long-term follow-up of 43...
A
CtmCl©
K
1
1omgCtp(
r
0d
Vaccine 24 (2006) 6437–6445
Costs of congenital rubella syndrome (CRS) in Oman: Evidencebased on long-term follow-up of 43 children
Salah Al-Awaidy a,∗, Ulla K. Griffiths b, Hosammudin Mohammed Nwar a,Shyam Bawikar a, Masoud Salim Al-Aisiri c, Rajiv Khandekar d,
Ali Jaffer Mohammad e, Susan E. Robertson f
a Department of Communicable Disease Surveillance and Control, Directorate General of Health Affairs,Ministry of Health, Muscat, Sultanate of Oman
b Health Policy Unit, London School of Hygiene and Tropical Medicine, Keppel Street, London WC1E 7HT, UKc Department of Financial Planning, Directorate General of Health Affairs, Ministry of Health, Muscat, Sultanate of Oman
d Eye and Ear Health Care, Department of Noncommunicable Diseases, Directorate General of Health Affairs,Ministry of Health, Muscat, Sultanate of Oman
e Ministry of Health, Muscat, Sultanate of Omanf Department of Immunization, Vaccines and Biologicals, World Health Organization, Geneva 27, CH-1211 Switzerland
Received 14 December 2005; received in revised form 22 May 2006; accepted 23 May 2006Available online 13 June 2006
bstract
As part of the national plan for elimination of rubella and congenital rubella syndrome (CRS), Oman established a national registry ofRS cases. As of May 2005, the registry included 43 surviving CRS cases, with a mean age of 11.9 years. Clinical examinations found
hat 84% had ocular defects, 84% had auditory/speech defects, 70% had neurological manifestations, and 42% had cardiac defects. Lifetime
edical, special education, and rehabilitation costs were assessed. Using a discount rate of 3%, the average direct lifetime cost per survivingRS patient was estimated at US$ 18,644. When including predicted lost productivity due to CRS, the average discounted direct and indirectifetime costs per surviving CRS patient amounted to US$ 98,734.2006 Elsevier Ltd. All rights reserved.
iAdcami
eywords: Congenital rubella syndrome; Cost study; Disability
. Introduction
WHO estimates indicate that there are still more than00,000 new cases of congenital rubella syndrome (CRS)ccurring each year [1]. Children with CRS suffer fromultiple birth defects, including deafness, blindness, con-
enital heart disease, and mental retardation. While someRS defects are readily identified in infants, others are hard
o diagnose until older ages (i.e. deafness) and some of theroblems associated with CRS are known to have late onseti.e. diabetes, thyroid disorders). A global review of stud-
∗ Corresponding author. Tel.: +96 82 460 1921; fax: +96 82 460 1832.E-mail addresses: [email protected] (S. Al-Awaidy),
[email protected] (S.E. Robertson).
[ductsc
264-410X/$ – see front matter © 2006 Elsevier Ltd. All rights reserved.oi:10.1016/j.vaccine.2006.05.089
es assessing the costs of CRS was published in 2002 [2].ltogether 22 studies were identified, including 10 fromeveloping countries. The review concluded that more CRSosting studies from developing countries should be encour-ged, and that such studies should use standardized economicethods. The need for standardised methods was emphasized
n an accompanying editorial [3].Oman experienced large rubella epidemics in 1987–1989
4] and 1992–1994 [5]. Since then there has been a dramaticecline in the incidence of rubella following widespreadse of rubella vaccine. In March 1994, there was a national
ampaign to deliver measles–rubella (MR) vaccine to thearget group aged 15 months–18 years. Some 700,000 per-ons received MR vaccine during the campaign, with 94%overage of the target age group. At the same time as the cam-
6 accine 2
pidiO1(hra9[
2nbaantoia1Cai
2
2e
Ctthac[ssiarotu
2c
w
iafct
2
sftsnn
2
WdtwwufiCrdfi
2
etmTaa6atasews
2
cAhp
438 S. Al-Awaidy et al. / V
aign, a dose of MR vaccine was introduced into the routinemmunization schedule for children at age 15 months. Thisecision was based on the results of a clinical trial conductedn 1992–1993, which showed excellent seroconversion ofmani children to rubella vaccine at age 15 months [6]. In997, MR vaccine was changed to measles–mumps–rubellaMMR) vaccine. Coverage with the 15 month vaccine doseas been 97% or higher since 1994. In addition, postpartumubella vaccination has been a national policy since 2001nd a nationwide coverage survey in 2004 demonstrated that9.5% of postpartum women had received rubella vaccine7].
Oman has a target for elimination of rubella and CRS in005 [7,8]. In April 1996, Oman initiated a fever and rash ill-ess surveillance system. Since 1997, blood specimens haveeen collected from >95% of suspected patients with rashnd fever. The specimens are first tested for measles IgMntibody and, if negative, for rubella IgM antibody by theational measles/rubella laboratory. There have been fewerhan 10 confirmed rubella cases each year since 1997. As partf the national plan for rubella and CRS elimination, a reg-stry of CRS cases was established in 2000, which includesll children with CRS reported to the Ministry of Health since988 [8]. This paper reports on data collected in the nationalRS registry as of May 2005, findings of follow-up clinicalssessments of the CRS cases, and estimates of the direct andndirect costs of CRS in Oman.
. Methods
.1. Registration of CRS cases and follow-upxaminations
In Oman, the Ministry of Health set up a registry forRS cases in 2000. CRS cases that have been reported to
he national surveillance system since 1988 are included inhe registry. At the start of 2000, a total of 79 CRS casesad been reported, but more cases were identified followingNational Workshop on Rubella and CRS held for medi-
al officers from all regions of the country in October 20008]. Since 2001, surviving children with CRS have beencheduled for biannual detailed clinical assessments usingtandardized forms. The assessments include a general phys-cal examination, as well as examinations by ophthalmology,udiology, otorhinolaryngology, pediatrics, cardiology, neu-ology, and endocrinology specialists. We analysed the resultsf the follow-up examinations and used these to estimate life-ime treatment and rehabilitation costs. The cost analysis wasndertaken from a societal viewpoint.
.2. Medical resources used during treatment of CRS
asesInpatient hospital resources used to treat CRS casesere identified from patient medical records. Major resource
schw
4 (2006) 6437–6445
tems, such as the number of days in hospital, type of surgery,nd type of laboratory tests, were recorded. Resource userom neonatal hospital stay, outpatient visits and special edu-ation were estimated by interviewing medical and educa-ional staff caring for children with CRS.
.2.1. Newborn evaluationFor each child with CRS the local birth registry was con-
ulted for information on birth weight and neonatal riskactors. Hospital neonatologists and paediatricians estimatedhat each newborn with low birth weight (<2500 g) or othererious risks would have spent an average of 14 days in theeonatal intensive care unit, with one follow-up visit to aeonatologist.
.2.2. Eye diseaseAn ophthalmologist examined each child with CRS.
here feasible, a complete eye examination, includingilated retinal assessment, was carried out. Available inpa-ient medical records for CRS patients who had eye surgeryere reviewed. An ophthalmologist estimated that all patientsith eye surgery or serious eye disease would require follow-p consultation with an ophthalmologist once a year for therst 15 years after the surgery and every 3 years thereafter.hildren with visual impairment (as assessed at the most
ecent examination) were assumed to require a new low visionevice (spectacles, magnifying lens, etc.) once a year for therst 15 years of life and every 3 years thereafter.
.2.3. Hearing loss/speech defectsAn otorhinolaryngologist and an audiologist examined
ach child with CRS. Where the child was cooperative, pureone audiometric testing was carried out. Hearing impair-
ents were classified as sensorineural, conductive, or mixed.he average age at detection of hearing impairment wasssumed to be 2 years. Children with hearing aids weressumed to require check ups at the ear clinic once every
months for the first 15 years and every 5 years there-fter; they were assumed to receive eight hearing aids duringheir lifetime. Speech was also assessed, noting impairmentsnd delays. Optimal treatment of speech impairment involvespeech therapy for approximately 45 min once a week; how-ver, as there are only two speech therapists working in thehole of Oman, it was assumed that children would receive
peech therapy once a month for a period of 3 years.
.2.4. Congenital heart diseaseEach child with CRS was assessed by a paediatrician or
ardiologist for cardiac history and current cardiac status.vailable inpatient medical records for CRS patients whoave had cardiac surgery were reviewed. It was assumed thatatients who had surgical correction of patent ductus arterio-
us alone would require one follow-up consultation with aardiologist, whereas patients with other types of congenitaleart disease would require annual follow-up consultationsith a cardiologist.
accine 24 (2006) 6437–6445 6439
2
adTrtcfidgit
2
ds
2o
pstniecaastbDrbUa
tHMolfaffpiors
Table 1Unit cost estimates most frequently used in the analysis, in US$ 2001 values
Type Cost item Unit cost (US$)
Surgery Cardiac surgery 1111Eye surgery 498
Hospital cost per bed day Neonatal intensive caredepartment
208
Pediatric surgerydepartment
167
Eye surgery department 103
Diagnostic procedure Magnetic resonanceimaging scan
312
Electroencephalogram 44Rubella IgM ELISA test 11
Outpatient visit Neonatology clinic 154Paediatric surgery clinic 151Ophthalmology clinic 112Physical therapy clinic 105Paediatrics clinic 60Orthopedics clinic 37Audiology clinic 21Speech therapy clinic 21
Drugs Thyroxine (per day) 0.021Tegretol (per day) 2.09
E
Tf1
2
afcCv“[hdwfptttaar
S. Al-Awaidy et al. / V
.2.5. Neurological diseaseEach child with CRS was assessed by a paediatrician or
neurologist for microcephaly, cerebral palsy, seizure disor-er, mental impairment, and any other neurological disease.he assessment included information on whether the child
equired special schooling. For cerebral palsy, it was assumedhat either the patient would attend a special rehabilitationentre for cerebral palsy or the patient would require 40 visitsor rehabilitation therapy, 4 visits to an orthopaedics special-st, and annual follow-up visits to a neurologist. For seizureisorder, diagnostic procedures include an electroencephalo-ram and a magnetic resonance imaging scan. Drug therapys required lifelong and there are annual follow-up visits tohe neurologist.
.2.6. Other manifestationsEach child with CRS was assessed by a paediatrician for
iabetes, other endocrine disorders, and any other medical orurgical disorders.
.3. Unit costs of health resource items and discountingf future costs
The unit costs of the resource items identified from theatient records were retrieved from a detailed cost-accountingystem maintained at the Ministry of Health. For health cen-res, the average costs per visit are reported. For regional andational hospitals the costs per bed-day are specified accord-ng to cost centre, e.g. general surgery, neurology, paediatrics,tc. Moreover, the cost-accounting system provides the unitost of various surgical procedures. The unit cost measuresccount for all expenses, including staff time, drugs, food,dministration, etc. The annual cost of attendance at a specialchool was obtained from the Ministry of Education [9] andhe annual cost of attendance at a community-based reha-ilitation centre was obtained from the Ministry of Socialevelopment. All unit cost data were in Omani rials and
eported for the year 2001. We converted the cost data to US$y using the average 2001 exchange rate of 0.385 rials perS$ [10]. The unit costs most frequently used in the analysis
re summarised in Table 1.We chose the year 2001 as the base year, as this was the la-
est year with final cost data from the cost-accounting system.owever, very few of the costs were actually incurred in 2001.ost of the children received surgery during the first 5 years
f life and the follow-up visits take place for their remainingifetime. Hence, the resource use is a mixture of past anduture costs. We estimated all costs in 2001 values withoutttempting to predict changes in real unit costs over time. Alluture costs were discounted by 3% per year. A picture of theuture stream of costs after year 2001 was established from theatient records review, the follow-up examinations and from
nterviews with specialists. We assumed a life expectancyf 50 years for the CRS patients with cerebral palsy. For theemaining patients, we assumed a life expectancy of 74 years;imilar to the rest of the Omani population in year 2002 [11].viwc
quipment Low vision aid (includingglasses)
52
Hearing aid, both ears 532
he results are presented with and without discounting ofuture costs, and we undertook a sensitivity analysis using a0% discount rate per annum.
.4. Indirect costs of CRS
Indirect costs of CRS include the time lost from productivectivities of the patient as well as time lost by parents to careor their child. In light of the severity of the cases, indirectosts are undoubtedly high for the families of children withRS. There are three recognised methods for quantifying thealue of productivity costs: “the human capital approach”,the friction cost approach” and the “US Panel approach”12]. The human capital approach focuses on the impact ofealth care on lost work time, whether through illness oreath, and is the most commonly used method. Normally,ork time is valued according to the gross wage rate. In the
riction cost approach, the existence of involuntary unem-loyment limits production losses due to death and illnesso the period required to replace the deceased worker fromhe ranks of the unemployed. This approach arose as a cri-ique to the human capital approach, as it is argued that thispproach provides an estimate of potential lost production asresult of disease, rather than the loss that would be expe-
ienced in practice. In the US Panel approach health state
alues, such as the Quality Adjusted Life Year, are used tomplicitly incorporate the impact of illness on the ability toork and financial loss [13]. As there are recognized short-omings to all the methods used for attaching an economic
6 accine 2
vwcictdpf
3
3
nt(caCiHpprprMcc
ft
rioafiC
my4aituaBRNtstmoa
3
3
a
440 S. Al-Awaidy et al. / V
alue to a life, we present the total cost estimates with andithout inclusion of productivity costs. We used the human
apital method for estimating lost productivity and we onlyncluded the loss to the CRS case and not to the parents of thehild. The average market wage in Oman in 2001 was usedo approximate the value of an individual’s productive outputuring their working years. This was estimated as US$ 6464er capita per year [14]. We assumed that a person worksrom age 20 to 60 years.
. Results
.1. Patient registration and follow-up
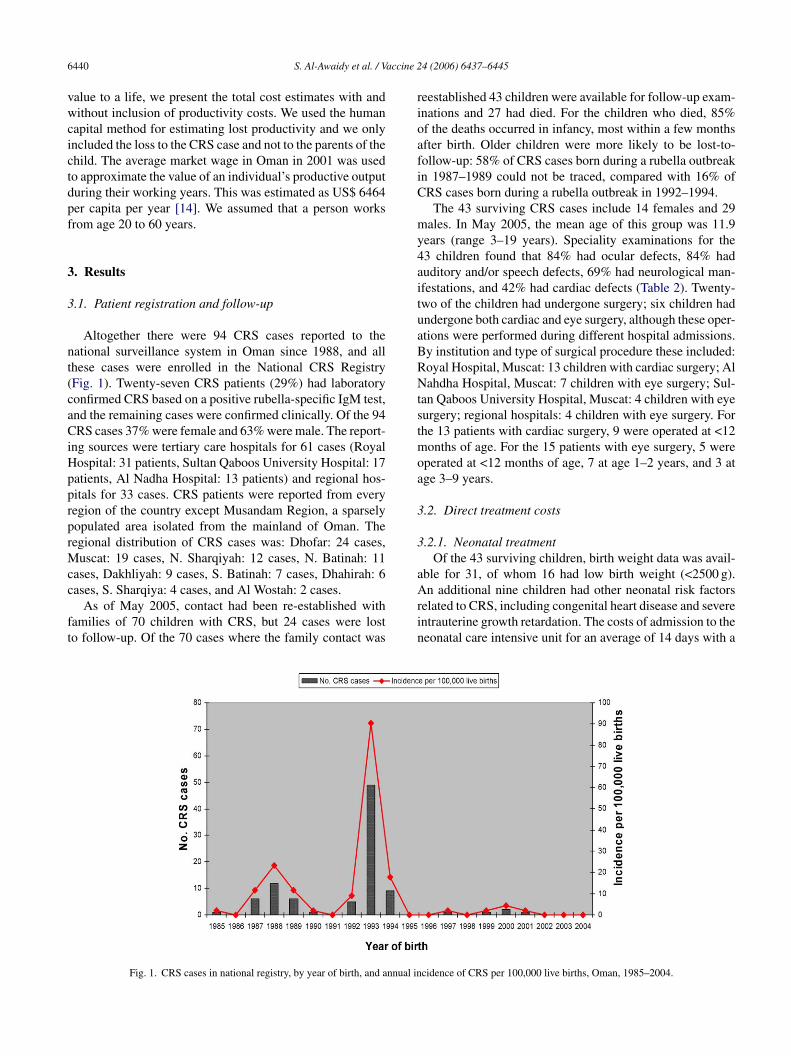
Altogether there were 94 CRS cases reported to theational surveillance system in Oman since 1988, and allhese cases were enrolled in the National CRS RegistryFig. 1). Twenty-seven CRS patients (29%) had laboratoryonfirmed CRS based on a positive rubella-specific IgM test,nd the remaining cases were confirmed clinically. Of the 94RS cases 37% were female and 63% were male. The report-
ng sources were tertiary care hospitals for 61 cases (Royalospital: 31 patients, Sultan Qaboos University Hospital: 17atients, Al Nadha Hospital: 13 patients) and regional hos-itals for 33 cases. CRS patients were reported from everyegion of the country except Musandam Region, a sparselyopulated area isolated from the mainland of Oman. Theegional distribution of CRS cases was: Dhofar: 24 cases,
uscat: 19 cases, N. Sharqiyah: 12 cases, N. Batinah: 11ases, Dakhliyah: 9 cases, S. Batinah: 7 cases, Dhahirah: 6
ases, S. Sharqiya: 4 cases, and Al Wostah: 2 cases.As of May 2005, contact had been re-established withamilies of 70 children with CRS, but 24 cases were losto follow-up. Of the 70 cases where the family contact was
Arin
Fig. 1. CRS cases in national registry, by year of birth, and annual in
4 (2006) 6437–6445
eestablished 43 children were available for follow-up exam-nations and 27 had died. For the children who died, 85%f the deaths occurred in infancy, most within a few monthsfter birth. Older children were more likely to be lost-to-ollow-up: 58% of CRS cases born during a rubella outbreakn 1987–1989 could not be traced, compared with 16% ofRS cases born during a rubella outbreak in 1992–1994.
The 43 surviving CRS cases include 14 females and 29ales. In May 2005, the mean age of this group was 11.9
ears (range 3–19 years). Speciality examinations for the3 children found that 84% had ocular defects, 84% haduditory and/or speech defects, 69% had neurological man-festations, and 42% had cardiac defects (Table 2). Twenty-wo of the children had undergone surgery; six children hadndergone both cardiac and eye surgery, although these oper-tions were performed during different hospital admissions.y institution and type of surgical procedure these included:oyal Hospital, Muscat: 13 children with cardiac surgery; Alahdha Hospital, Muscat: 7 children with eye surgery; Sul-
an Qaboos University Hospital, Muscat: 4 children with eyeurgery; regional hospitals: 4 children with eye surgery. Forhe 13 patients with cardiac surgery, 9 were operated at <12
onths of age. For the 15 patients with eye surgery, 5 wereperated at <12 months of age, 7 at age 1–2 years, and 3 atge 3–9 years.
.2. Direct treatment costs
.2.1. Neonatal treatmentOf the 43 surviving children, birth weight data was avail-
ble for 31, of whom 16 had low birth weight (<2500 g).
n additional nine children had other neonatal risk factorselated to CRS, including congenital heart disease and severentrauterine growth retardation. The costs of admission to theeonatal care intensive unit for an average of 14 days with a
cidence of CRS per 100,000 live births, Oman, 1985–2004.
S. Al-Awaidy et al. / Vaccine 24 (2006) 6437–6445 6441
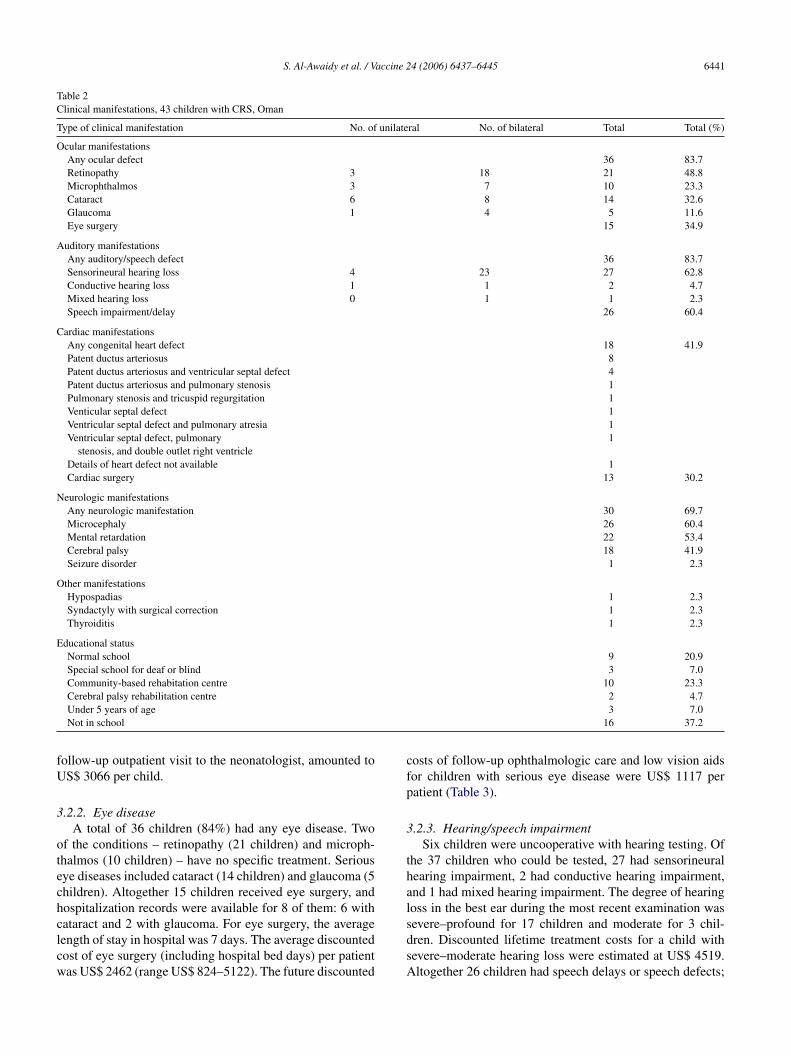
Table 2Clinical manifestations, 43 children with CRS, Oman
Type of clinical manifestation No. of unilateral No. of bilateral Total Total (%)
Ocular manifestationsAny ocular defect 36 83.7Retinopathy 3 18 21 48.8Microphthalmos 3 7 10 23.3Cataract 6 8 14 32.6Glaucoma 1 4 5 11.6Eye surgery 15 34.9
Auditory manifestationsAny auditory/speech defect 36 83.7Sensorineural hearing loss 4 23 27 62.8Conductive hearing loss 1 1 2 4.7Mixed hearing loss 0 1 1 2.3Speech impairment/delay 26 60.4
Cardiac manifestationsAny congenital heart defect 18 41.9Patent ductus arteriosus 8Patent ductus arteriosus and ventricular septal defect 4Patent ductus arteriosus and pulmonary stenosis 1Pulmonary stenosis and tricuspid regurgitation 1Venticular septal defect 1Ventricular septal defect and pulmonary atresia 1Ventricular septal defect, pulmonary
stenosis, and double outlet right ventricle1
Details of heart defect not available 1Cardiac surgery 13 30.2
Neurologic manifestationsAny neurologic manifestation 30 69.7Microcephaly 26 60.4Mental retardation 22 53.4Cerebral palsy 18 41.9Seizure disorder 1 2.3
Other manifestationsHypospadias 1 2.3Syndactyly with surgical correction 1 2.3Thyroiditis 1 2.3
Educational statusNormal school 9 20.9Special school for deaf or blind 3 7.0Community-based rehabitation centre 10 23.3
fU
3
otechclcw
cfp
3
thal
Cerebral palsy rehabilitation centreUnder 5 years of ageNot in school
ollow-up outpatient visit to the neonatologist, amounted toS$ 3066 per child.
.2.2. Eye diseaseA total of 36 children (84%) had any eye disease. Two
f the conditions – retinopathy (21 children) and microph-halmos (10 children) – have no specific treatment. Seriousye diseases included cataract (14 children) and glaucoma (5hildren). Altogether 15 children received eye surgery, andospitalization records were available for 8 of them: 6 with
ataract and 2 with glaucoma. For eye surgery, the averageength of stay in hospital was 7 days. The average discountedost of eye surgery (including hospital bed days) per patientas US$ 2462 (range US$ 824–5122). The future discountedsdsA
2 4.73 7.0
16 37.2
osts of follow-up ophthalmologic care and low vision aidsor children with serious eye disease were US$ 1117 peratient (Table 3).
.2.3. Hearing/speech impairmentSix children were uncooperative with hearing testing. Of
he 37 children who could be tested, 27 had sensorineuralearing impairment, 2 had conductive hearing impairment,nd 1 had mixed hearing impairment. The degree of hearingoss in the best ear during the most recent examination was
evere–profound for 17 children and moderate for 3 chil-ren. Discounted lifetime treatment costs for a child withevere–moderate hearing loss were estimated at US$ 4519.ltogether 26 children had speech delays or speech defects;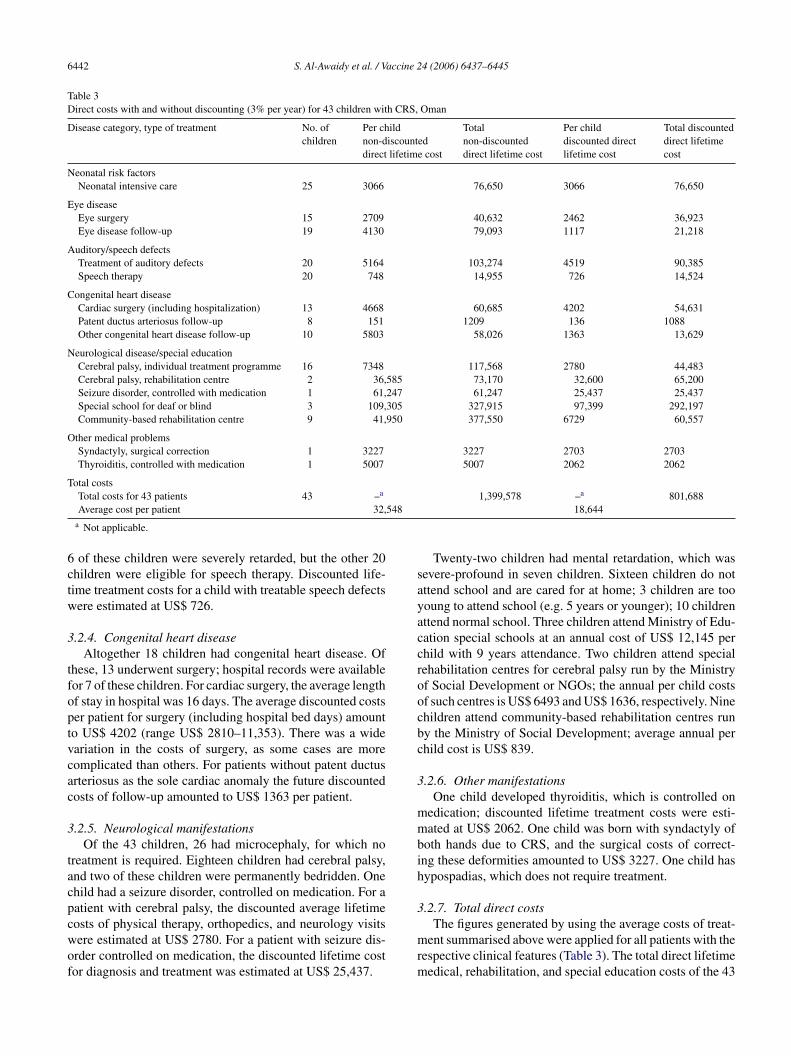
6442 S. Al-Awaidy et al. / Vaccine 24 (2006) 6437–6445
Table 3Direct costs with and without discounting (3% per year) for 43 children with CRS, Oman
Disease category, type of treatment No. ofchildren
Per childnon-discounteddirect lifetime cost
Totalnon-discounteddirect lifetime cost
Per childdiscounted directlifetime cost
Total discounteddirect lifetimecost
Neonatal risk factorsNeonatal intensive care 25 3066 76,650 3066 76,650
Eye diseaseEye surgery 15 2709 40,632 2462 36,923Eye disease follow-up 19 4130 79,093 1117 21,218
Auditory/speech defectsTreatment of auditory defects 20 5164 103,274 4519 90,385Speech therapy 20 748 14,955 726 14,524
Congenital heart diseaseCardiac surgery (including hospitalization) 13 4668 60,685 4202 54,631Patent ductus arteriosus follow-up 8 151 1209 136 1088Other congenital heart disease follow-up 10 5803 58,026 1363 13,629
Neurological disease/special educationCerebral palsy, individual treatment programme 16 7348 117,568 2780 44,483Cerebral palsy, rehabilitation centre 2 36,585 73,170 32,600 65,200Seizure disorder, controlled with medication 1 61,247 61,247 25,437 25,437Special school for deaf or blind 3 109,305 327,915 97,399 292,197Community-based rehabilitation centre 9 41,950 377,550 6729 60,557
Other medical problemsSyndactyly, surgical correction 1 3227 3227 2703 2703Thyroiditis, controlled with medication 1 5007 5007 2062 2062
Total costs
548
6ctw
3
tfoptvcac
3
tacpcwof
sayaccroocbc
3
mmbih
3
Total costs for 43 patients 43 –a
Average cost per patient 32,a Not applicable.
of these children were severely retarded, but the other 20hildren were eligible for speech therapy. Discounted life-ime treatment costs for a child with treatable speech defectsere estimated at US$ 726.
.2.4. Congenital heart diseaseAltogether 18 children had congenital heart disease. Of
hese, 13 underwent surgery; hospital records were availableor 7 of these children. For cardiac surgery, the average lengthf stay in hospital was 16 days. The average discounted costser patient for surgery (including hospital bed days) amounto US$ 4202 (range US$ 2810–11,353). There was a wideariation in the costs of surgery, as some cases are moreomplicated than others. For patients without patent ductusrteriosus as the sole cardiac anomaly the future discountedosts of follow-up amounted to US$ 1363 per patient.
.2.5. Neurological manifestationsOf the 43 children, 26 had microcephaly, for which no
reatment is required. Eighteen children had cerebral palsy,nd two of these children were permanently bedridden. Onehild had a seizure disorder, controlled on medication. For aatient with cerebral palsy, the discounted average lifetime
osts of physical therapy, orthopedics, and neurology visitsere estimated at US$ 2780. For a patient with seizure dis-rder controlled on medication, the discounted lifetime costor diagnosis and treatment was estimated at US$ 25,437.mrm
1,399,578 –a 801,68818,644
Twenty-two children had mental retardation, which wasevere-profound in seven children. Sixteen children do notttend school and are cared for at home; 3 children are toooung to attend school (e.g. 5 years or younger); 10 childrenttend normal school. Three children attend Ministry of Edu-ation special schools at an annual cost of US$ 12,145 perhild with 9 years attendance. Two children attend specialehabilitation centres for cerebral palsy run by the Ministryf Social Development or NGOs; the annual per child costsf such centres is US$ 6493 and US$ 1636, respectively. Ninehildren attend community-based rehabilitation centres runy the Ministry of Social Development; average annual perhild cost is US$ 839.
.2.6. Other manifestationsOne child developed thyroiditis, which is controlled on
edication; discounted lifetime treatment costs were esti-ated at US$ 2062. One child was born with syndactyly of
oth hands due to CRS, and the surgical costs of correct-ng these deformities amounted to US$ 3227. One child hasypospadias, which does not require treatment.
.2.7. Total direct costs
The figures generated by using the average costs of treat-ent summarised above were applied for all patients with theespective clinical features (Table 3). The total direct lifetimeedical, rehabilitation, and special education costs of the 43
accine 2
sdTw
3
avAjnjoUwp
C3
3
tpUaw
4
r
snftdtwUAtpU
tathottyoaadpbdfC
i
TE
C
BB
G
J
O
P
S. Al-Awaidy et al. / V
urviving CRS patients amounted to US$ 1,399,578 withoutiscounting and US$ 801,688 with discounting at a 3% rate.he average direct lifetime cost per surviving CRS patientas US$ 18,644 using a 3% discount rate.
.3. Indirect costs of CRS
The lifetime productivity loss of a patient with 100% dis-bility amounted to US$ 265,000 without discounting futurealues and to US$ 109,330 discounting at 3% per year.mong the 43 children in the surviving cohort, 24 were
udged to have multiple handicaps so severe that they wouldot be able to work at all (100% disability), and 15 wereudged to have 50% disability. Thus, for the entire cohortf 43 survivors the discounted indirect lifetime costs wereS$ 3,443,883. In addition there were 27 children with CRSho died, discounted indirect costs due to their lost lifetimeroductivity amounted to US$ 2,951,910.
The average, lifetime productivity costs lost per survivingRS patient amounted to US$ 80,090 with a discount rate of% per year.
.4. Sensitivity analysis
Using a 10% annual discount rate, the average direct life-ime treatment cost was US$ 14,365 and the average lifetimeroductivity cost lost per surviving CRS patient amounted toS$ 16,263. Thus the senitivity analysis found that the total
verage direct and indirect costs for a surviving CRS patientere US$ 30,628 with a 10% discount rate.
. Discussion
There has been great progress toward elimination ofubella and CRS in Oman, with no CRS cases identified
tvc[
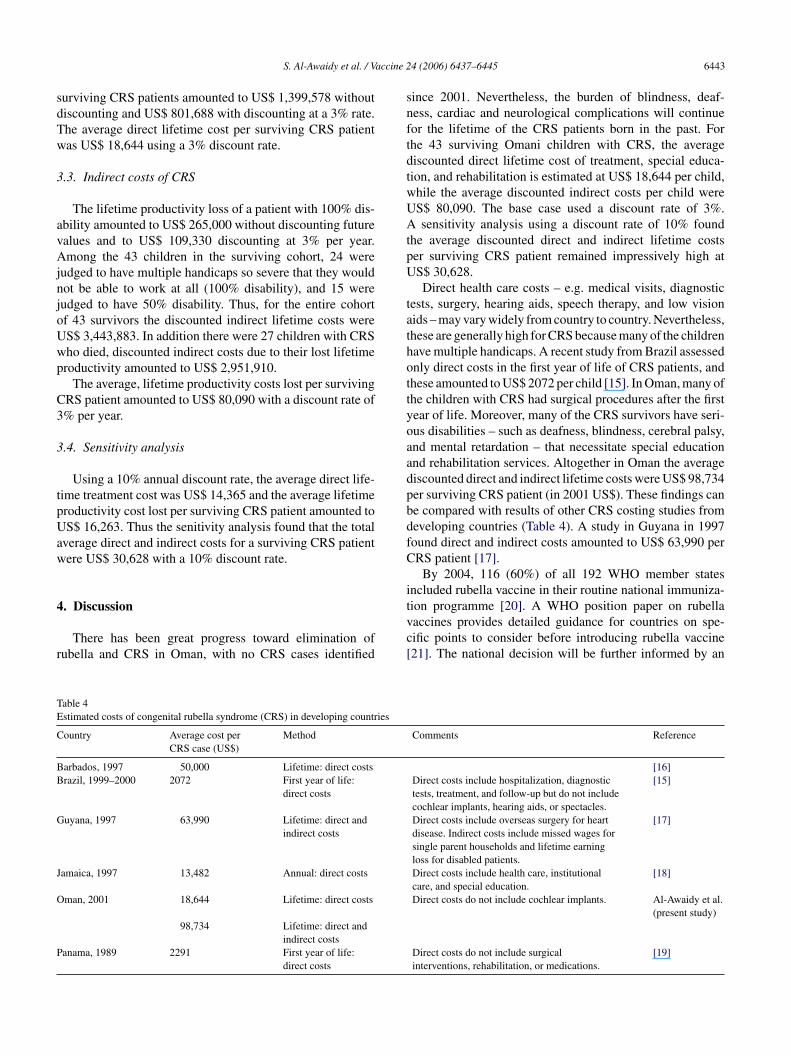
able 4stimated costs of congenital rubella syndrome (CRS) in developing countries
ountry Average cost perCRS case (US$)
Method
arbados, 1997 50,000 Lifetime: direct costsrazil, 1999–2000 2072 First year of life:
direct costs
uyana, 1997 63,990 Lifetime: direct andindirect costs
amaica, 1997 13,482 Annual: direct costs
man, 2001 18,644 Lifetime: direct costs
98,734 Lifetime: direct andindirect costs
anama, 1989 2291 First year of life:direct costs
4 (2006) 6437–6445 6443
ince 2001. Nevertheless, the burden of blindness, deaf-ess, cardiac and neurological complications will continueor the lifetime of the CRS patients born in the past. Forhe 43 surviving Omani children with CRS, the averageiscounted direct lifetime cost of treatment, special educa-ion, and rehabilitation is estimated at US$ 18,644 per child,hile the average discounted indirect costs per child wereS$ 80,090. The base case used a discount rate of 3%.sensitivity analysis using a discount rate of 10% found
he average discounted direct and indirect lifetime costser surviving CRS patient remained impressively high atS$ 30,628.Direct health care costs – e.g. medical visits, diagnostic
ests, surgery, hearing aids, speech therapy, and low visionids – may vary widely from country to country. Nevertheless,hese are generally high for CRS because many of the childrenave multiple handicaps. A recent study from Brazil assessednly direct costs in the first year of life of CRS patients, andhese amounted to US$ 2072 per child [15]. In Oman, many ofhe children with CRS had surgical procedures after the firstear of life. Moreover, many of the CRS survivors have seri-us disabilities – such as deafness, blindness, cerebral palsy,nd mental retardation – that necessitate special educationnd rehabilitation services. Altogether in Oman the averageiscounted direct and indirect lifetime costs were US$ 98,734er surviving CRS patient (in 2001 US$). These findings cane compared with results of other CRS costing studies fromeveloping countries (Table 4). A study in Guyana in 1997ound direct and indirect costs amounted to US$ 63,990 perRS patient [17].
By 2004, 116 (60%) of all 192 WHO member statesncluded rubella vaccine in their routine national immuniza-
ion programme [20]. A WHO position paper on rubellaaccines provides detailed guidance for countries on spe-ific points to consider before introducing rubella vaccine21]. The national decision will be further informed by anComments Reference
[16]Direct costs include hospitalization, diagnostictests, treatment, and follow-up but do not includecochlear implants, hearing aids, or spectacles.
[15]
Direct costs include overseas surgery for heartdisease. Indirect costs include missed wages forsingle parent households and lifetime earningloss for disabled patients.
[17]
Direct costs include health care, institutionalcare, and special education.
[18]
Direct costs do not include cochlear implants. Al-Awaidy et al.(present study)
Direct costs do not include surgicalinterventions, rehabilitation, or medications.
[19]

6 accine 2
acctsmcO
parTCsfooOimfidc[
1aprtUhincdrawdcdice1[
litgeI
waftso
tahtci–iicndO
hdaocst1ttefaOttvitOmiop
A
do
444 S. Al-Awaidy et al. / V
ssessment of the cost-effectiveness of rubella vaccinationompared to other health interventions [2,3]. In a conciseost-effectiveness analysis of rubella vaccine an estimate ofhe economic burden of CRS, as presented in the presenttudy from Oman, should be included. Although such esti-ates need to take into account country-specific health care
osts and the local costs of lost work time, the example ofman should prove useful.In industrialized countries there are a number of CRS
atient registries, including Australia [22–24], Canada [25],nd the United Kingdom [26]. To our knowledge, the Omanegistry is the only one located in a developing country.he Oman CRS registry includes a substantial cohort ofRS survivors with long-term follow-up and comprehen-
ive clinical assessments. Previous papers based on datarom the Oman CRS registry have documented the devel-pment of the registry [7] and explored the ophthalmologicutcomes of CRS patients [27]. The Ministry of Health ofman intends to continue medical follow-up of this cohort
n future years. Further late onset manifestations of CRSay be expected in some children. In Canada, long-term
ollow-up of 100 CRS survivors for a mean of 34 years hasdentified the following late manifestations, all of which wereetected after 5 years of age: 23% seizure disorder, 21% glau-oma, 12% diabetes mellitus, and 10% thyroid dysfunction25].
Of the entire group of 94 Omani children reported since988 with CRS, there were 27 children (28.7%) who diednd 24 children (25.5%) lost to follow-up. While these pro-ortions seem high, a number of previous studies have alsoeported high mortality with CRS and high attrition in long-erm follow-up of CRS survivors. Early studies from theSA during the 1969 pandemic include several reports ofigh mortality. Cooper et al. reported 35% mortality dur-ng the first year of life in one group of 58 infants witheonatal thrombocytopenic purpura due to CRS [28]. Amonghildren reported to a USA national surveillance systemuring 1969–1973, 18% had died by the time their caseeports were submitted, most within the first few monthsfter birth [29]. O’Neill followed a group of CRS patientsith eye disease and 26% died, with two-thirds of theeaths before 16 months of age [30]. In Panama, among aohort of 54 infants with CRS born in 1986–1987, 14 (26%)ied with 11 deaths in the neonatal period and the remain-ng 3 deaths within the first 4 months [19]. A prospectiveohort study at Johns Hopkins University during 1963–1964nrolled 328 children with CRS; at follow-up 7 years later,5 (5%) were dead, and 70 (21%) were lost to follow-up31].
The 94 patients reported to the Oman CRS registry mostikely represent only the “tip of the iceberg” of all individualsn the country with CRS. First, there is a striking dispropor-
ion by sex, with only one-third of CRS cases reported inirls. Other data from Oman show that among 697 studentsnrolled in special schools in 2004, only 37% were girls [9].t is thought that in more rural areas of the country, familiesEoFm
4 (2006) 6437–6445
orry that identification of a daughter as “disabled” throughttendance at a special school may detract from her chancesor a good marriage. In addition, the majority of patients inhe Oman registry have severe presentations of CRS, and iteems likely that many children with milder manifestationsf CRS were not detected.
A limitation in our cost estimates is that we assumehat treatment practices and services for people with dis-bilities will remain at a 2001 level in future years. Weave not taken into account a likely increase in costs dueo improved services. In particular, we did not include theosts of cochlear implants, which are now widely used inndustrialized countries, where an estimated 50,000 patientsincluding children with congenital deafness – have received
mplants [32]. Cochlear implants have begun to be carried outn Oman, at a price of US$ 23,000–26,000 per ear; however,urrently this procedure is reserved for patients who haveo neurological problems. To date, cochlear implant proce-ures have not been carried out for any of the CRS cases inman.A large proportion of the Omani cohort of CRS survivors
ad central nervous system defects, including mental retar-ation. Children with blindness alone or deafness alone mayttend special schools, but children who are deaf and blindr deaf–blind and mentally retarded may require specialare during their entire lifetime [33]. In Western countriesuch children typically receive long-term care in institu-ions, which is extremely expensive with costs exceeding US$00,000 per year [34]. In Oman, family-based care remainshe norm for severely disabled persons. In keeping with thisradition, the Omani Ministry of Social Development hasstablished 19 community-based rehabilitation centres in dif-erent regions of the country, which offer day-care servicesnd outreach services to some 1500 disabled individuals. Anmani nongovernmental organization, the Association for
he Welfare of Handicapped Children, has established 6 cen-res that offer day-care services for some 300 disabled indi-iduals. Of the cohort of 43 child-survivors of CRS describedn this paper, about one-quarter participate in governmen-al or nongovernmental community-based rehabilitation. Themani system is much less costly than institutionalization. Itay offer a culturally appropriate model for other countries
n the Middle East, Africa, and Asia which place a high valuen family centered support systems for multiply handicappedersons.
cknowledgements
The authors are grateful to the families of the Omani chil-ren with CRS for their cooperation. This project was carriedut with scientific oversight from the Steering Committee on
pidemiology and Field Research of the WHO Departmentf Immunization, Vaccines and Biologicals. Thanks to Dr.Z. El Samani and Dr J. Vandelaer for critical review of theanuscript.
accine 2
R
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
S. Al-Awaidy et al. / V
eferences
[1] Robertson SE, Featherstone DA, Gacic-Dobo M, Hersh BS. Rubellaand congenital rubella syndrome: global update. Pan Am J PublicHealth 2003;14(5):306–15.
[2] Hinman AR, Irons B, Lewis M, Kandola K. Economic analyses ofrubella and rubella vaccines: a global review. Bull World Health Org2002;80(4):264–70.
[3] Kou UK. More vaccines? Using economic analysis to decide. BullWorld Health Org 2002;80(4):263.
[4] Juma AH. Infantile “rubella” cataract in Oman. Oman Med Newsletter1989;6(1):27–8.
[5] World Health Organization, Expanded Programme on Immunization.Rubella outbreak, Oman. Wkly Epidemiol Rec 1994;69(45):333–7.
[6] Kohler KA, Suleiman AJM, Robertson SE, Malankar P, Al-KhusaibyS, Helfand RF, et al. Immunogenicity of measles and rubella vaccinesin Oman: a prospective clinical trial. J Infect Dis 2003;187(Suppl.1):S177–85.
[7] Ministry of Health, Sultanate of Oman. Elimination of congenitalrubella syndrome: progress towards the goal of elimination by 2005in Oman. Commun Health Dis Surveil Newsletter 2004;13(1):1–4.
[8] Ministry of Health, Sultanate of Oman. Elimination of rubella andCRS in Oman by 2005. Commun Health Dis Surveil Newsletter2000;9(3):1–3.
[9] Ministry of Education, Sultanate of Oman. Educational Statistical Year-book, 35th issue, Academic Year 2004–2005. Muscat: Ministry ofEducation; 2005.
10] OANDA. FXHistory: historical currency exchange rates. Accessed on1 March 2005 at http://www.oanda.com/convert/fxhistory.
11] World Bank. World development indicators database. Accessed on 30September 2005 at http://devdata.worldbank.org/data-query.
12] Pritchard C, Schulpher M. Productivity costs: principles and practicein economic evaluation. London: Office of Health Economics; 2000.
13] Gold MR, Siegel JE, Russell LB, Weinstein MC. Cost-effectiveness inhealth and medicine. New York: Oxford University Press; 1996.
14] United Nations Industrial Development Organization. Employment,wages and related indictors by industry. Accessed on 1 March 2005at http://www.unido.org/data/country/stats.
15] Lanzieri TM, Parise MS, Siqueira MM, Fortaleza BM, Segatto TC,Prevots DR. Incidence, clinical features and estimated costs of congen-ital rubella syndrome after a large rubella outbreak in Recife, Brazil,1999–2000. Pediatr Infect Dis J 2004;23(12):1116–22.
16] Kommu R, Chase H. Follow-up of rubella issues and costing of CRSin Barbados. In: Final report, 14th meeting of the English-speaking
Caribbean EPI managers. Washington, DC: Pan American Health Orga-nization; 1998.17] Kandola K. CRS cost burden analysis for Guyana. In: Final report, 14thmeeting of the English-speaking Caribbean EPI managers. Washington,DC: Pan American Health Organization; 1998.
4 (2006) 6437–6445 6445
18] Robinson M. CRS unit costing in Jamaica. In: Final Report, 14th meet-ing of the English-speaking Caribbean EPI managers. Washington, DC:Pan American Health Organization; 1998.
19] Saad de Owens C, Tristan de Espino R. Rubella in Panama: still aproblem. Pediatr Infect Dis J 1989;8:110–5.
20] World Health Organization. Immunization schedule by anti-gen. Accessed on 15 November 2005 at http://www.who.int/immunization monitoring/en/globalsummary/scheduleselect.cfm.
21] World Health Organization. Rubella vaccines: WHO position paper.Wkly Epidemiol Rec 2000;75(20):181–9.
22] Menser MA, Dods L, Harley JD. A twenty-five year follow-up of con-genital rubella. Lancet 1967;ii:1347–50.
23] McIntosh EDG, Menser MA. A fifty-year follow-up of congenitalrubella. Lancet 1992;340:414–5.
24] Forrest JM, Turnbull FM, Sholler GF, Hawker RE, Martin FJ, DoranTT, et al. Gregg’s congenital rubella patients 60 years later. Med J Aust2002;177(11–12):664–7.
25] Munroe S. A survey of late emerging manifestations of congenitalrubella in Canada. Brantford, Ontario: Canadian Deafblind and RubellaAssociation; 1999.
26] Tookey PA, Peckham CS. Surveillance of congenital rubella in GreatBritain, 1971–96. BMJ 1999;318:769–70.
27] Khandekar R, Al-Awaidy S, Ganesh A, Bawikar S. An epidemi-ological and clinical study of ocular manifestations of congenitalrubella syndrome in Omani children. Arch Ophthalmol 2004;122(4):541–4.
28] Cooper LZ, Green RH, Krugman S, Giles JP, Mirick GS. Neonatalthrombocytopenic purpura and other manifestations of rubella con-tracted in utero. Am J Dis Child 1965;110:416–27.
29] Modlin JF, Brandling Bennett AD. Surveillance of congenital rubellasyndrome 1969–1973. J Infect Dis 1974;130(3):316–8.
30] O’Neill JF. The ocular manifestations of congenital infection: a studyof the early effect and long-term outcome of maternally transmit-ted rubella and toxoplasmosis. Tr Am Ophth Soc 1998;96:813–79.
31] Wolff SM. The ocular manifestations of congenital rubella: a prospec-tive study of 328 cases of congenital rubella. J Pediatr Ophthalmol1973;10(2):101–41.
32] Ramsden RT. Prognosis after cochlear implantation. BMJ2004;328:419–20.
33] Kahndekar R, Al-Khabori M. Double disability: the hearing-impairedblind in the Sultanate of Oman. Int J Audiol 2004;43:1–5.
34] Coucouvanis K, Prouty RW, Bruininks RH, Lakin KC. Current popula-tions and longitudinal trends of state residential settings (1950–2004).
In: Prouty RW, Smith G, Lakin KC, editors. Residential services forpersons with developmental disabilities: status and trends through2004. Minneapolis: University of Minnesota, Research and TrainingCenter on Community Living, Institute on Community Integration;2005.