
Cost-Effectiveness of Optimal Use of Acute Myocardial Infarction Treatments and Impact on Coronary...
21
78 A cute myocardial infarction (AMI) is an increasing cause of death in China. 1 Most Chinese patients with AMI die within the acute stage (30 days after onset), and of those who die, 75% die within the first 24 hours. 2 Although reperfusion therapy and several standard oral medications (antiplatelet drugs, β-blockers, statins, and angiotensin-converting enzyme inhibitors) reduce AMI case fatality and are recommended by international and Chinese AMI management guidelines, 3–6 nationwide Chinese hospital registries have found that at least half of eligible patients with AMI do not receive all stan- dard oral medications. Fewer than 50% of patients with ST-segment–elevation myocardial infarction (STEMI) receive reperfusion therapy. 7–9 Improved utilization of these acute treatment strategies is needed to reduce AMI deaths, but China’s limited healthcare resources require a careful estimate of their comparative effectiveness and cost-effectiveness in the Chinese population. Furthermore, because ≈62% of Chinese AMI deaths occur before hos- pital arrival, 10 the potential impact of hospital-based AMI treatments on total coronary heart disease (CHD) mor- tality may be limited. This study aimed to estimate the effectiveness and cost-effectiveness of optimal use of key hospital-based AMI treatments, including their impact on total CHD deaths, using a computer-simulated, state-tran- sition (Markov) model of CHD in China. Editorial see p 8 Background—The cost-effectiveness of the optimal use of hospital-based acute myocardial infarction (AMI) treatments and their potential impact on coronary heart disease (CHD) mortality in China is not well known. Methods and Results—The effectiveness and costs of optimal use of hospital-based AMI treatments were estimated by the CHD Policy Model-China, a Markov-style computer simulation model. Changes in simulated AMI, CHD mortality, quality-adjusted life years, and total healthcare costs were the outcomes. The incremental cost-effectiveness ratio was used to assess projected cost-effectiveness. Optimal use of 4 oral drugs (aspirin, β-blockers, statins, and angiotensin- converting enzyme inhibitors) in all eligible patients with AMI or unfractionated heparin in non–ST-segment–elevation myocardial infarction was a highly cost-effective strategy (incremental cost-effectiveness ratios approximately US $3100 or less). Optimal use of reperfusion therapies in eligible patients with ST-segment–elevation myocardial infarction was moderately cost effective (incremental cost-effectiveness ratio ≤$10 700). Optimal use of clopidogrel for all eligible patients with AMI or primary percutaneous coronary intervention among high-risk patients with non–ST-segment– elevation myocardial infarction in tertiary hospitals alone was less cost effective. Use of all the selected hospital-based AMI treatment strategies together would be cost-effective and reduce the total CHD mortality rate in China by ≈9.6%. Conclusions—Optimal use of most standard hospital-based AMI treatment strategies, especially combined strategies, would be cost effective in China. However, because so many AMI deaths occur outside of the hospital in China, the overall impact on preventing CHD deaths was projected to be modest. (Circ Cardiovasc Qual Outcomes. 2014;7:78-85.) Key Words: cost-benefit analysis ◼ myocardial infarction ◼ quality-adjusted life years ◼ therapy © 2014 American Heart Association, Inc. Circ Cardiovasc Qual Outcomes is available at http://circoutcomes.ahajournals.org DOI: 10.1161/CIRCOUTCOMES.113.000674 Received May 22, 2013; accepted November 15, 2013. From the Department of Epidemiology, Beijing Anzhen Hospital, Capital Medical University, Beijing Institute of Heart, Lung and Blood Vessel Diseases, Beijing, China (M.W., J.L., D.Z.); Division of General Medicine, Department of Medicine, Columbia University, New York, NY (A.E.M.); Department of Medicine, San Francisco General Hospital and the University of California at San Francisco (P.G.C.); Veteran’s Administration Palo Alto Health Care System and Stanford University School of Medicine, Palo Alto, CA (P.A.H.); Department of Epidemiology and Population Genetics, Cardiovascular Institute and Fu Wai Hospital, Beijing, China (D.G.); Department of Epidemiology, Tulane University, School of Public Health and Tropical Medicine, New Orleans, LA (J.H.); and Faculties of Health Sciences and Medicine, Columbia University Medical Center, New York, NY (L.G.). The Data Supplement is available at http://circoutcomes.ahajournals.org/lookup/suppl/doi:10.1161/CIRCOUTCOMES.113.000674/-/DC1. Correspondence to Dong Zhao, MD, PhD, Department of Epidemiology, Beijing Anzhen Hospital, Capital Medical University, Beijing Institute of Heart, Lung and Blood Vessel Diseases, No. 2 Anzhen Rd, Chaoyang District, Beijing 100029, China. E-mail [email protected] Cost-Effectiveness of Optimal Use of Acute Myocardial Infarction Treatments and Impact on Coronary Heart Disease Mortality in China Miao Wang, MD, MPH; Andrew E. Moran, MD, MPH; Jing Liu, MD, PhD; Pamela G. Coxson, PhD; Paul A. Heidenreich, MD, MS; Dongfeng Gu, MD, PhD; Jiang He, MD, PhD; Lee Goldman, MD, MPH; Dong Zhao, MD, PhD Original Article by guest on June 14, 2016 http://circoutcomes.ahajournals.org/ Downloaded from by guest on June 14, 2016 http://circoutcomes.ahajournals.org/ Downloaded from by guest on June 14, 2016 http://circoutcomes.ahajournals.org/ Downloaded from by guest on June 14, 2016 http://circoutcomes.ahajournals.org/ Downloaded from by guest on June 14, 2016 http://circoutcomes.ahajournals.org/ Downloaded from by guest on June 14, 2016 http://circoutcomes.ahajournals.org/ Downloaded from by guest on June 14, 2016 http://circoutcomes.ahajournals.org/ Downloaded from by guest on June 14, 2016 http://circoutcomes.ahajournals.org/ Downloaded from by guest on June 14, 2016 http://circoutcomes.ahajournals.org/ Downloaded from by guest on June 14, 2016 http://circoutcomes.ahajournals.org/ Downloaded from by guest on June 14, 2016 http://circoutcomes.ahajournals.org/ Downloaded from by guest on June 14, 2016 http://circoutcomes.ahajournals.org/ Downloaded from by guest on June 14, 2016 http://circoutcomes.ahajournals.org/ Downloaded from by guest on June 14, 2016 http://circoutcomes.ahajournals.org/ Downloaded from
-
Upload
independent -
Category
Documents
-
view
2 -
download
0
Transcript of Cost-Effectiveness of Optimal Use of Acute Myocardial Infarction Treatments and Impact on Coronary...
78
Acute myocardial infarction (AMI) is an increasing cause of death in China.1 Most Chinese patients
with AMI die within the acute stage (30 days after onset), and of those who die, 75% die within the first 24 hours.2 Although reperfusion therapy and several standard oral medications (antiplatelet drugs, β-blockers, statins, and angiotensin-converting enzyme inhibitors) reduce AMI case fatality and are recommended by international and Chinese AMI management guidelines,3–6 nationwide Chinese hospital registries have found that at least half of eligible patients with AMI do not receive all stan-dard oral medications. Fewer than 50% of patients with ST-segment–elevation myocardial infarction (STEMI) receive reperfusion therapy.7–9 Improved utilization of
these acute treatment strategies is needed to reduce AMI deaths, but China’s limited healthcare resources require a careful estimate of their comparative effectiveness and cost-effectiveness in the Chinese population. Furthermore, because ≈62% of Chinese AMI deaths occur before hos-pital arrival,10 the potential impact of hospital-based AMI treatments on total coronary heart disease (CHD) mor-tality may be limited. This study aimed to estimate the effectiveness and cost-effectiveness of optimal use of key hospital-based AMI treatments, including their impact on total CHD deaths, using a computer-simulated, state-tran-sition (Markov) model of CHD in China.
Editorial see p 8
Background—The cost-effectiveness of the optimal use of hospital-based acute myocardial infarction (AMI) treatments and their potential impact on coronary heart disease (CHD) mortality in China is not well known.
Methods and Results—The effectiveness and costs of optimal use of hospital-based AMI treatments were estimated by the CHD Policy Model-China, a Markov-style computer simulation model. Changes in simulated AMI, CHD mortality, quality-adjusted life years, and total healthcare costs were the outcomes. The incremental cost-effectiveness ratio was used to assess projected cost-effectiveness. Optimal use of 4 oral drugs (aspirin, β-blockers, statins, and angiotensin-converting enzyme inhibitors) in all eligible patients with AMI or unfractionated heparin in non–ST-segment–elevation myocardial infarction was a highly cost-effective strategy (incremental cost-effectiveness ratios approximately US $3100 or less). Optimal use of reperfusion therapies in eligible patients with ST-segment–elevation myocardial infarction was moderately cost effective (incremental cost-effectiveness ratio ≤$10 700). Optimal use of clopidogrel for all eligible patients with AMI or primary percutaneous coronary intervention among high-risk patients with non–ST-segment–elevation myocardial infarction in tertiary hospitals alone was less cost effective. Use of all the selected hospital-based AMI treatment strategies together would be cost-effective and reduce the total CHD mortality rate in China by ≈9.6%.
Conclusions—Optimal use of most standard hospital-based AMI treatment strategies, especially combined strategies, would be cost effective in China. However, because so many AMI deaths occur outside of the hospital in China, the overall impact on preventing CHD deaths was projected to be modest. (Circ Cardiovasc Qual Outcomes. 2014;7:78-85.)
Key Words: cost-benefit analysis ◼ myocardial infarction ◼ quality-adjusted life years ◼ therapy
© 2014 American Heart Association, Inc.
Circ Cardiovasc Qual Outcomes is available at http://circoutcomes.ahajournals.org DOI: 10.1161/CIRCOUTCOMES.113.000674
Received May 22, 2013; accepted November 15, 2013.From the Department of Epidemiology, Beijing Anzhen Hospital, Capital Medical University, Beijing Institute of Heart, Lung and Blood Vessel Diseases,
Beijing, China (M.W., J.L., D.Z.); Division of General Medicine, Department of Medicine, Columbia University, New York, NY (A.E.M.); Department of Medicine, San Francisco General Hospital and the University of California at San Francisco (P.G.C.); Veteran’s Administration Palo Alto Health Care System and Stanford University School of Medicine, Palo Alto, CA (P.A.H.); Department of Epidemiology and Population Genetics, Cardiovascular Institute and Fu Wai Hospital, Beijing, China (D.G.); Department of Epidemiology, Tulane University, School of Public Health and Tropical Medicine, New Orleans, LA (J.H.); and Faculties of Health Sciences and Medicine, Columbia University Medical Center, New York, NY (L.G.).
The Data Supplement is available at http://circoutcomes.ahajournals.org/lookup/suppl/doi:10.1161/CIRCOUTCOMES.113.000674/-/DC1.Correspondence to Dong Zhao, MD, PhD, Department of Epidemiology, Beijing Anzhen Hospital, Capital Medical University, Beijing Institute of Heart,
Lung and Blood Vessel Diseases, No. 2 Anzhen Rd, Chaoyang District, Beijing 100029, China. E-mail [email protected]
Cost-Effectiveness of Optimal Use of Acute Myocardial Infarction Treatments and Impact on Coronary Heart
Disease Mortality in ChinaMiao Wang, MD, MPH; Andrew E. Moran, MD, MPH; Jing Liu, MD, PhD;
Pamela G. Coxson, PhD; Paul A. Heidenreich, MD, MS; Dongfeng Gu, MD, PhD; Jiang He, MD, PhD; Lee Goldman, MD, MPH; Dong Zhao, MD, PhD
Original Article
by guest on June 14, 2016http://circoutcomes.ahajournals.org/Downloaded from by guest on June 14, 2016http://circoutcomes.ahajournals.org/Downloaded from by guest on June 14, 2016http://circoutcomes.ahajournals.org/Downloaded from by guest on June 14, 2016http://circoutcomes.ahajournals.org/Downloaded from by guest on June 14, 2016http://circoutcomes.ahajournals.org/Downloaded from by guest on June 14, 2016http://circoutcomes.ahajournals.org/Downloaded from by guest on June 14, 2016http://circoutcomes.ahajournals.org/Downloaded from by guest on June 14, 2016http://circoutcomes.ahajournals.org/Downloaded from by guest on June 14, 2016http://circoutcomes.ahajournals.org/Downloaded from by guest on June 14, 2016http://circoutcomes.ahajournals.org/Downloaded from by guest on June 14, 2016http://circoutcomes.ahajournals.org/Downloaded from by guest on June 14, 2016http://circoutcomes.ahajournals.org/Downloaded from by guest on June 14, 2016http://circoutcomes.ahajournals.org/Downloaded from by guest on June 14, 2016http://circoutcomes.ahajournals.org/Downloaded from

Wang et al Optimal Use of AMI Treatments 79
MethodsCHD Policy Model-China and Its ParametersThe total number of hospitalized patients with AMI, deaths in hospi-talized patients with AMI, and CHD deaths in 2013 based on the cur-rent AMI treatment status were estimated. Changes in total healthcare costs, quality-adjusted life years (QALYs), 30-day deaths of hospital-ized patients with AMI, and yearly CHD deaths attributable to the optimal use of each treatment strategy were projected using the CHD Policy Model-China (Appendix Figure I in the Data Supplement).11 The Ethics Committees of both Beijing Anzhen Hospital (Beijing, China) and Columbia University Medical Center (New York, NY) in-formed that this simulation study need not get approval because no identifiable individual data were used.
The annual probability of first-ever hospitalized or out-of-hospital AMI, including sudden cardiac deaths, in the population without prior CHD was estimated from the China Multi-Provincial Cohort Study conditioned on the prevalence of major risk factors and relative risk of CHD associated with these risk factors.11 The yearly probability of re-peat acute coronary events in patients with chronic CHD was estimated based on the prevalence of CHD and the risk of acute coronary events in patients with chronic CHD.12,13 Thirty-day deaths in hospitalized patients with AMI were projected based on the number of hospitalized patients with AMI and the 30-day case fatality rate observed in a study of AMI in Beijing.2 Total CHD deaths in 2013 comprised AMI deaths, sudden cardiac deaths, and chronic CHD deaths. To test the accuracy of model prediction over time, we used the model to compare predicted CHD mor-tality rates with the real mortality rates from 2000 to 2010 based on data from the World Health Organization (WHO) and National Health and Family Planning Commission of China (Appendix Figure II in the Data Supplement). A complete list of input parameter assumptions is listed in Appendix Table I in the Data Supplement.
Selection of Key Treatment Strategies and Estimation of Current UtilizationSelected key hospital-based treatments recommended by both the Chinese and international guidelines for STEMI and non– STEMI (NSTEMI)3–6 were classified as follows: A1, optimal use of aspirin, β-blockers, statins, and angiotensin-converting enzyme inhibitors in patients with AMI during the first 30 days after onset; A2, optimal use of clopidogrel in patients with AMI during the first 30 days af-ter onset; B, optimal use of unfractionated heparin in patients with NSTEMI; C1, optimal use of primary percutaneous coronary inter-vention (PCI) in tertiary hospitals and thrombolysis in secondary hos-pitals in patients with STEMI (with a consideration of the availability of PCI technology); C2, optimal use of primary PCI in all patients with STEMI; and C3, optimal use of primary PCI in high-risk pa-tients with NSTEMI in tertiary hospitals. Only strategies C1 and C2 are mutually exclusive and cannot be combined for implementation. For each treatment strategy, model simulation assumed improvement from the current utilization level (base case) to optimal utilization; that is, utilization of the treatment in 100% of eligible patients with-out known contraindications to the treatment (100%–current utiliza-tion rate–contraindication rate). Patients with contraindications to one treatment could be eligible for other treatments.
The current utilization of the standard AMI treatments—alone or in combination with other treatments—was based on the Bridging the Gap in Coronary Heart Disease Secondary Prevention in China (BRIG) project.7 The BRIG project treatment utilization estimates were similar to those in the Clinical Pathways in Acute Coronary Syndromes in China (CPACS) study8 and the Chinese Registry of Acute Coronary Events (CRACE)9 (Appendix Table II in the Data Supplement). The prevalence of contraindications to treatments was obtained from clinical trials (Table 1).15,18–22,24,25,27,33,35
Treatment Cost EstimationIncreased costs attributable to the optimization of acute treatment were calculated by multiplying the number of additional patients resulting from optimal utilization by the mean cost of the treatment. Total health-care costs comprised acute treatment costs plus age- and sex-specific yearly per capita background healthcare costs as estimated from the Chinese National Health Services Survey38 and the China World Health Survey.39 All costs were estimated from a societal perspective and were inflated to 2013 using the average rate of inflation in China from 2008 to 2013 published by Trading Economics and then converted into US dollars ($) according to the exchange rate published by the Bank of China (1 Chinese yuan=$0.1611; accessed May 15, 2013).
Drug costs were obtained from the essential medicines maximum retail price list updated by the Evaluation Center of Drug Pricing, National Development and Reform Commission. The costs of reper-fusion therapies were estimated by the data from the China Health Statistics Yearbook, the Beijing Public Health Information Center, and health economics research.1,32 Detailed costs are listed in Table 1.
Effectiveness EstimationEffectiveness of optimal use of the key AMI treatments was projected based on changes in QALYs gained, 30-day in-hospital AMI deaths prevented, and change in total CHD deaths. Patients with AMI who survived because of increased utilization of 1 of the treatment strate-gies would still be at risk for a chronic CHD death during the re-mainder of the year. The increased number of patients with AMI who survived to the end of the year because of optimized treatment utiliza-tion was equal to the total number of prevented CHD deaths.
The number of QALYs saved by optimal use of acute treatments was calculated by multiplying the number of life years gained from AMI survivors by the QALY weights of health states in both the first 30 days after AMI onset and AMI survivors in the chronic CHD state. QALY weights were calculated as 1−disability-adjusted life year weights esti-mated in the Global Burden of Disease 2010 Study.40 A QALY weight of 0.44 was applied for the first 30 days after a nonfatal AMI. The
WHAT IS KNOWN
• Acute myocardial infarction (AMI) is an increasing cause of death in China. Several nationwide registry studies found low utilization of key AMI acute treat-ments recommended by the guidelines in most Chi-nese hospitals.
• Improved utilization of the hospital-based acute treatment strategies is needed to reduce AMI deaths, but China’s limited healthcare resources require rational optimization of limited medical resources.
• Because about two thirds of Chinese AMI deaths occur before hospital arrival, the potential impact of hospital-based AMI treatments on total coronary heart disease mortality is not known.
WHAT THE STUDY ADDS
• Most hospital-based AMI treatment strategies rec-ommended by the guidelines would be highly or moderately cost effective in China.
• Full and simultaneous improvements of all standard hospital-based AMI treatment strategies assessed in this study would only attribute to 9.6% reduction in the coronary heart disease mortality rate.
• Given the trend toward higher absolute numbers and rates of coronary heart disease in China, prehospital emergency care, public education on symptoms of AMI, and available treatments for AMI should be improved.
by guest on June 14, 2016http://circoutcomes.ahajournals.org/Downloaded from
80 Circ Cardiovasc Qual Outcomes January 2014
QALY weight for chronic AMI survivors was 0.90, considering that a proportion of survivors had symptoms of angina or heart failure.
The 30-day all-cause mortality benefits of selected treatments were mainly derived from the results of large meta-analyses or systematic reviews of randomized controlled clinical trials (Table 1).14,16,23,28,37 When multiple treatments were applied in combination, it was as-sumed that the effects were independent (Table 2).41,42
For the proportion of treated patients estimated to experience treatment-related major adverse events during the first 30 days after AMI onset, QALY penalties were applied for the entire 30 days (0.39 for intracranial hemorrhage, 0.80 for extracranial bleeding, 0.91 for rhabdomyolysis, and 0.67 for transient liver failure).40,43,44 The inci-dence of treatment-related major severe adverse events was obtained from clinical trials (Table 1).16,17,22,26,29–31,34,36
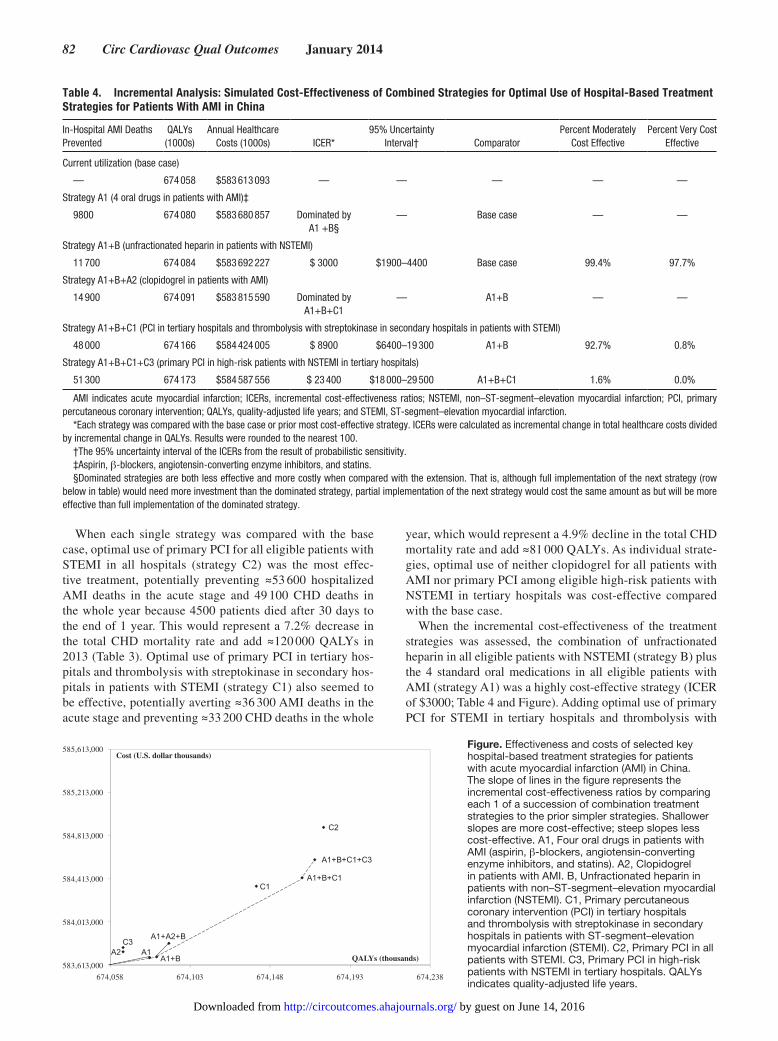
Cost-Effectiveness AnalysisIncremental cost-effectiveness ratios (ICERs) were used to evaluate the cost-effectiveness of optimal use of the key treatments. ICERs were calculated by dividing the incremental change in total health-care costs by the incremental change in QALYs.45 Cost-effectiveness was assessed both by comparing each individual or combined strat-egy with the current utilization (Table 3 and Appendix Table III in the Data Supplement, comparison with the base case) and by com-paring each one of a succession of combination treatment strategies with prior simpler-to-implement strategies (incremental analysis,
Table 4 and Figure). The metric recommended by WHO Choosing Interventions That Are Cost Effective (WHO-CHOICE) was used to assess the degree of cost-effectiveness (highly cost-effective, ICER less than the gross domestic product [GDP] per capita; moderately cost-effective, ICER of 1–3×GDP per capita; and not cost-effective, ICER of >3×GDP per capita).46 The GDP per capita of China in 2013 was estimated to be $5721 by the GDP per capita of China ($5445 in 2011) published by the World Bank, which was adjusted upward by the inflation rates in 2012 and 2013 published by Trading Economics.
Sensitivity AnalysesOne-way sensitivity analyses were performed to explore the impact of assuming upper- or lower-limit bounds for the main analysis ef-fectiveness and cost inputs on the results (ranges shown in Table 1). Monte Carlo probabilistic sensitivity analysis was used to simul-taneously explore the uncertainty distributions of 2 key input as-sumptions: relative risk for all-cause mortality related to treatments compared with no treatment and treatment costs. Effectiveness and costs of each strategy were randomly drawn 1000 times from the ef-fectiveness and cost uncertainty distributions and entered into simula-tions. The resulting 1000 pairs of total costs and QALYs were used to calculate the upper and lower 95% bounds of their ICERs and the proportion of ICERs under the predetermined thresholds for moder-ately cost-effective and very cost-effective.
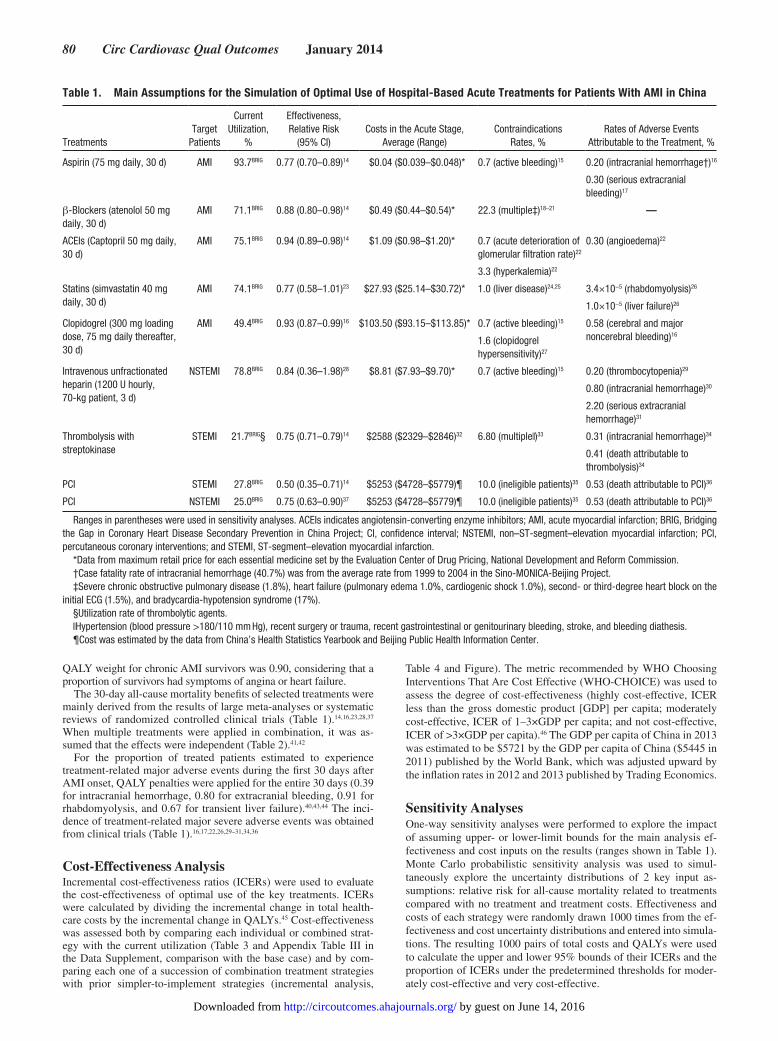
Table 1. Main Assumptions for the Simulation of Optimal Use of Hospital-Based Acute Treatments for Patients With AMI in China
TreatmentsTarget
Patients
Current Utilization,
%
Effectiveness, Relative Risk
(95% CI)Costs in the Acute Stage,
Average (Range)Contraindications
Rates, %Rates of Adverse Events
Attributable to the Treatment, %
Aspirin (75 mg daily, 30 d) AMI 93.7BRIG 0.77 (0.70–0.89)14 $0.04 ($0.039–$0.048)* 0.7 (active bleeding)15 0.20 (intracranial hemorrhage†)16
0.30 (serious extracranial bleeding)17
β-Blockers (atenolol 50 mg daily, 30 d)
AMI 71.1BRIG 0.88 (0.80–0.98)14 $0.49 ($0.44–$0.54)* 22.3 (multiple‡)18–21 —
ACEIs (Captopril 50 mg daily, 30 d)
AMI 75.1BRIG 0.94 (0.89–0.98)14 $1.09 ($0.98–$1.20)* 0.7 (acute deterioration of glomerular filtration rate)22
0.30 (angioedema)22
3.3 (hyperkalemia)22
Statins (simvastatin 40 mg daily, 30 d)
AMI 74.1BRIG 0.77 (0.58–1.01)23 $27.93 ($25.14–$30.72)* 1.0 (liver disease)24,25 3.4×10−5 (rhabdomyolysis)26
1.0×10−5 (liver failure)26
Clopidogrel (300 mg loading dose, 75 mg daily thereafter, 30 d)
AMI 49.4BRIG 0.93 (0.87–0.99)16 $103.50 ($93.15–$113.85)* 0.7 (active bleeding)15 0.58 (cerebral and major noncerebral bleeding)16
1.6 (clopidogrel hypersensitivity)27
Intravenous unfractionated heparin (1200 U hourly, 70-kg patient, 3 d)
NSTEMI 78.8BRIG 0.84 (0.36–1.98)28 $8.81 ($7.93–$9.70)* 0.7 (active bleeding)15 0.20 (thrombocytopenia)29
0.80 (intracranial hemorrhage)30
2.20 (serious extracranial hemorrhage)31
Thrombolysis with streptokinase
STEMI 21.7BRIG§ 0.75 (0.71–0.79)14 $2588 ($2329–$2846)32 6.80 (multiple‖)33 0.31 (intracranial hemorrhage)34
0.41 (death attributable to thrombolysis)34
PCI STEMI 27.8BRIG 0.50 (0.35–0.71)14 $5253 ($4728–$5779)¶ 10.0 (ineligible patients)35 0.53 (death attributable to PCI)36
PCI NSTEMI 25.0BRIG 0.75 (0.63–0.90)37 $5253 ($4728–$5779)¶ 10.0 (ineligible patients)35 0.53 (death attributable to PCI)36
Ranges in parentheses were used in sensitivity analyses. ACEIs indicates angiotensin-converting enzyme inhibitors; AMI, acute myocardial infarction; BRIG, Bridging the Gap in Coronary Heart Disease Secondary Prevention in China Project; CI, confidence interval; NSTEMI, non–ST-segment–elevation myocardial infarction; PCI, percutaneous coronary interventions; and STEMI, ST-segment–elevation myocardial infarction.
*Data from maximum retail price for each essential medicine set by the Evaluation Center of Drug Pricing, National Development and Reform Commission.†Case fatality rate of intracranial hemorrhage (40.7%) was from the average rate from 1999 to 2004 in the Sino-MONICA-Beijing Project.‡Severe chronic obstructive pulmonary disease (1.8%), heart failure (pulmonary edema 1.0%, cardiogenic shock 1.0%), second- or third-degree heart block on the
initial ECG (1.5%), and bradycardia-hypotension syndrome (17%).§Utilization rate of thrombolytic agents.‖Hypertension (blood pressure >180/110 mm Hg), recent surgery or trauma, recent gastrointestinal or genitourinary bleeding, stroke, and bleeding diathesis.¶Cost was estimated by the data from China’s Health Statistics Yearbook and Beijing Public Health Information Center.
by guest on June 14, 2016http://circoutcomes.ahajournals.org/Downloaded from
Wang et al Optimal Use of AMI Treatments 81
Results
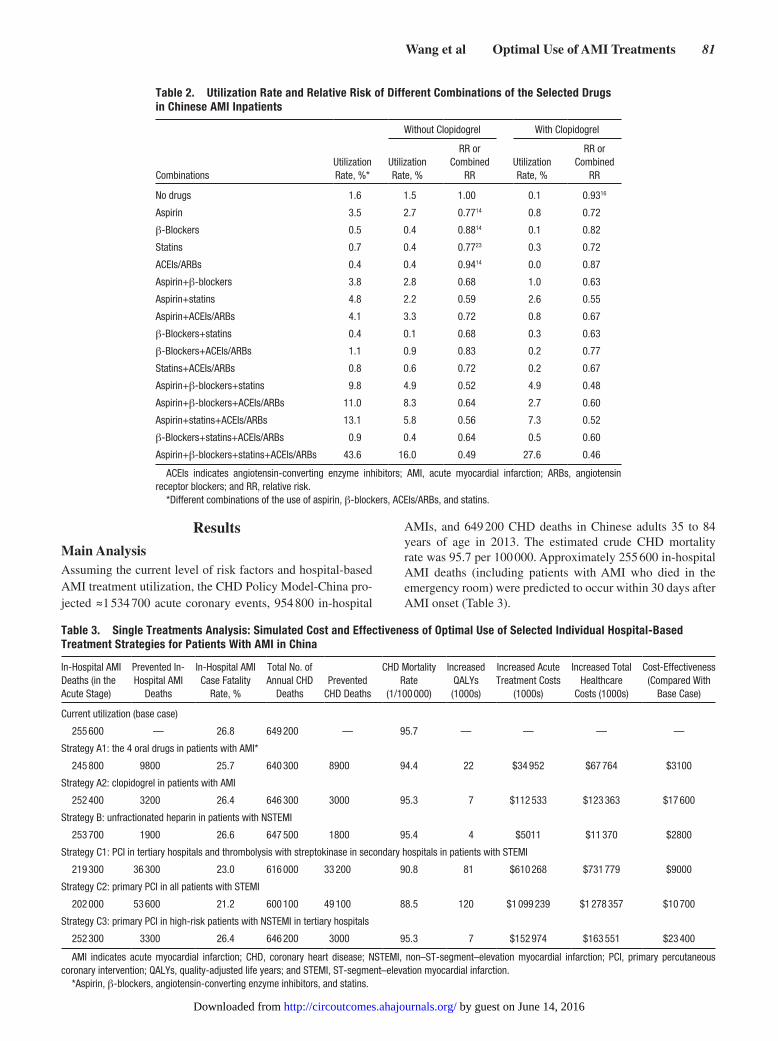
Main AnalysisAssuming the current level of risk factors and hospital-based AMI treatment utilization, the CHD Policy Model-China pro-jected ≈1 534 700 acute coronary events, 954 800 in-hospital
AMIs, and 649 200 CHD deaths in Chinese adults 35 to 84 years of age in 2013. The estimated crude CHD mortality rate was 95.7 per 100 000. Approximately 255 600 in-hospital AMI deaths (including patients with AMI who died in the emergency room) were predicted to occur within 30 days after AMI onset (Table 3).
Table 3. Single Treatments Analysis: Simulated Cost and Effectiveness of Optimal Use of Selected Individual Hospital-Based Treatment Strategies for Patients With AMI in China
In-Hospital AMI Deaths (in the Acute Stage)
Prevented In- Hospital AMI
Deaths
In-Hospital AMI Case Fatality
Rate, %
Total No. of Annual CHD
DeathsPrevented
CHD Deaths
CHD Mortality Rate
(1/100 000)
Increased QALYs (1000s)
Increased Acute Treatment Costs
(1000s)
Increased Total Healthcare
Costs (1000s)
Cost-Effectiveness (Compared With
Base Case)
Current utilization (base case)
255 600 — 26.8 649 200 — 95.7 — — — —
Strategy A1: the 4 oral drugs in patients with AMI*
245 800 9800 25.7 640 300 8900 94.4 22 $34 952 $67 764 $3100
Strategy A2: clopidogrel in patients with AMI
252 400 3200 26.4 646 300 3000 95.3 7 $112 533 $123 363 $17 600
Strategy B: unfractionated heparin in patients with NSTEMI
253 700 1900 26.6 647 500 1800 95.4 4 $5011 $11 370 $2800
Strategy C1: PCI in tertiary hospitals and thrombolysis with streptokinase in secondary hospitals in patients with STEMI
219 300 36 300 23.0 616 000 33 200 90.8 81 $610 268 $731 779 $9000
Strategy C2: primary PCI in all patients with STEMI
202 000 53 600 21.2 600 100 49 100 88.5 120 $1 099 239 $1 278 357 $10 700
Strategy C3: primary PCI in high-risk patients with NSTEMI in tertiary hospitals
252 300 3300 26.4 646 200 3000 95.3 7 $152 974 $163 551 $23 400
AMI indicates acute myocardial infarction; CHD, coronary heart disease; NSTEMI, non–ST-segment–elevation myocardial infarction; PCI, primary percutaneous coronary intervention; QALYs, quality-adjusted life years; and STEMI, ST-segment–elevation myocardial infarction.
*Aspirin, β-blockers, angiotensin-converting enzyme inhibitors, and statins.
Table 2. Utilization Rate and Relative Risk of Different Combinations of the Selected Drugs in Chinese AMI Inpatients
CombinationsUtilization Rate, %*
Without Clopidogrel With Clopidogrel
Utilization Rate, %
RR or Combined
RRUtilization Rate, %
RR or Combined
RR
No drugs 1.6 1.5 1.00 0.1 0.9316
Aspirin 3.5 2.7 0.7714 0.8 0.72
β-Blockers 0.5 0.4 0.8814 0.1 0.82
Statins 0.7 0.4 0.7723 0.3 0.72
ACEIs/ARBs 0.4 0.4 0.9414 0.0 0.87
Aspirin+β-blockers 3.8 2.8 0.68 1.0 0.63
Aspirin+statins 4.8 2.2 0.59 2.6 0.55
Aspirin+ACEIs/ARBs 4.1 3.3 0.72 0.8 0.67
β-Blockers+statins 0.4 0.1 0.68 0.3 0.63
β-Blockers+ACEIs/ARBs 1.1 0.9 0.83 0.2 0.77
Statins+ACEIs/ARBs 0.8 0.6 0.72 0.2 0.67
Aspirin+β-blockers+statins 9.8 4.9 0.52 4.9 0.48
Aspirin+β-blockers+ACEIs/ARBs 11.0 8.3 0.64 2.7 0.60
Aspirin+statins+ACEIs/ARBs 13.1 5.8 0.56 7.3 0.52
β-Blockers+statins+ACEIs/ARBs 0.9 0.4 0.64 0.5 0.60
Aspirin+β-blockers+statins+ACEIs/ARBs 43.6 16.0 0.49 27.6 0.46
ACEIs indicates angiotensin-converting enzyme inhibitors; AMI, acute myocardial infarction; ARBs, angiotensin receptor blockers; and RR, relative risk.
*Different combinations of the use of aspirin, β-blockers, ACEIs/ARBs, and statins.
by guest on June 14, 2016http://circoutcomes.ahajournals.org/Downloaded from
82 Circ Cardiovasc Qual Outcomes January 2014
When each single strategy was compared with the base case, optimal use of primary PCI for all eligible patients with STEMI in all hospitals (strategy C2) was the most effec-tive treatment, potentially preventing ≈53 600 hospitalized AMI deaths in the acute stage and 49 100 CHD deaths in the whole year because 4500 patients died after 30 days to the end of 1 year. This would represent a 7.2% decrease in the total CHD mortality rate and add ≈120 000 QALYs in 2013 (Table 3). Optimal use of primary PCI in tertiary hos-pitals and thrombolysis with streptokinase in secondary hos-pitals in patients with STEMI (strategy C1) also seemed to be effective, potentially averting ≈36 300 AMI deaths in the acute stage and preventing ≈33 200 CHD deaths in the whole
year, which would represent a 4.9% decline in the total CHD mortality rate and add ≈81 000 QALYs. As individual strate-gies, optimal use of neither clopidogrel for all patients with AMI nor primary PCI among eligible high-risk patients with NSTEMI in tertiary hospitals was cost-effective compared with the base case.
When the incremental cost-effectiveness of the treatment strategies was assessed, the combination of unfractionated heparin in all eligible patients with NSTEMI (strategy B) plus the 4 standard oral medications in all eligible patients with AMI (strategy A1) was a highly cost-effective strategy (ICER of $3000; Table 4 and Figure). Adding optimal use of primary PCI for STEMI in tertiary hospitals and thrombolysis with
Table 4. Incremental Analysis: Simulated Cost-Effectiveness of Combined Strategies for Optimal Use of Hospital-Based Treatment Strategies for Patients With AMI in China
In-Hospital AMI Deaths Prevented
QALYs (1000s)
Annual Healthcare Costs (1000s) ICER*
95% Uncertainty Interval† Comparator
Percent Moderately Cost Effective
Percent Very Cost Effective
Current utilization (base case)
— 674 058 $583 613 093 — — — — —
Strategy A1 (4 oral drugs in patients with AMI)‡
9800 674 080 $583 680 857 Dominated by A1 +B§
— Base case — —
Strategy A1+B (unfractionated heparin in patients with NSTEMI)
11 700 674 084 $583 692 227 $ 3000 $1900–4400 Base case 99.4% 97.7%
Strategy A1+B+A2 (clopidogrel in patients with AMI)
14 900 674 091 $583 815 590 Dominated by A1+B+C1
— A1+B — —
Strategy A1+B+C1 (PCI in tertiary hospitals and thrombolysis with streptokinase in secondary hospitals in patients with STEMI)
48 000 674 166 $584 424 005 $ 8900 $6400–19 300 A1+B 92.7% 0.8%
Strategy A1+B+C1+C3 (primary PCI in high-risk patients with NSTEMI in tertiary hospitals)
51 300 674 173 $584 587 556 $ 23 400 $18 000–29 500 A1+B+C1 1.6% 0.0%
AMI indicates acute myocardial infarction; ICERs, incremental cost-effectiveness ratios; NSTEMI, non–ST-segment–elevation myocardial infarction; PCI, primary percutaneous coronary intervention; QALYs, quality-adjusted life years; and STEMI, ST-segment–elevation myocardial infarction.
*Each strategy was compared with the base case or prior most cost-effective strategy. ICERs were calculated as incremental change in total healthcare costs divided by incremental change in QALYs. Results were rounded to the nearest 100.
†The 95% uncertainty interval of the ICERs from the result of probabilistic sensitivity.‡Aspirin, β-blockers, angiotensin-converting enzyme inhibitors, and statins.§Dominated strategies are both less effective and more costly when compared with the extension. That is, although full implementation of the next strategy (row
below in table) would need more investment than the dominated strategy, partial implementation of the next strategy would cost the same amount as but will be more effective than full implementation of the dominated strategy.
A1A2
C1
C2
C3
A1+B
A1+A2+B
A1+B+C1
A1+B+C1+C3
583,613,000
584,013,000
584,413,000
584,813,000
585,213,000
585,613,000
674,058 674,103 674,148 674,193 674,238
Cost (U.S. dollar thousands)
QALYs (thousands)
Figure. Effectiveness and costs of selected key hospital-based treatment strategies for patients with acute myocardial infarction (AMI) in China. The slope of lines in the figure represents the incremental cost-effectiveness ratios by comparing each 1 of a succession of combination treatment strategies to the prior simpler strategies. Shallower slopes are more cost-effective; steep slopes less cost-effective. A1, Four oral drugs in patients with AMI (aspirin, β-blockers, angiotensin-converting enzyme inhibitors, and statins). A2, Clopidogrel in patients with AMI. B, Unfractionated heparin in patients with non–ST-segment–elevation myocardial infarction (NSTEMI). C1, Primary percutaneous coronary intervention (PCI) in tertiary hospitals and thrombolysis with streptokinase in secondary hospitals in patients with ST-segment–elevation myocardial infarction (STEMI). C2, Primary PCI in all patients with STEMI. C3, Primary PCI in high-risk patients with NSTEMI in tertiary hospitals. QALYs indicates quality-adjusted life years.
by guest on June 14, 2016http://circoutcomes.ahajournals.org/Downloaded from

Wang et al Optimal Use of AMI Treatments 83
streptokinase for STEMI in secondary hospitals or primary PCI for patients with STEMI in all hospitals was moderately cost-effective (ICER of <$10 700; in the range of 1–3×GDP per capita). Strategies including clopidogrel for all AMI (strat-egy A1+A2+B) and adding primary PCI for NSTEMI (strat-egy A1+A2+B+C1+C3, data not shown) were both dominated by more cost-effective combination strategies that did not include these 2 treatments (Table 4).
Optimal use of each individual treatment was estimated to prevent 1800 to 49 100 CHD deaths, which would represent a 0.3% to 7.2% reduction in the CHD mortality rate. Optimal use of the 4 standard oral medications in all eligible hospitalized patients with AMI (strategy A1), which is the easiest strategy to implement rapidly, would reduce the total CHD mortality rate by only 1.3%. Implementing all strategies in combination (strategy A1+A2+B+C2+C3), regardless of cost-effectiveness, would decrease the CHD mortality rate by 9.6% at most.
Sensitivity AnalysesVarying cost inputs in 1-way sensitivity analyses led to little change in the ICERs (Appendix Table III in the Data Supple-ment), even at their extreme ranges. For example, compared with the base case, assuming higher costs of the 4 oral medica-tions and heparin would lead to only a slightly higher ICER ($3100 per QALY gained), as would the upper range of the PCI cost for patients with STEMI (ICER of $11 500). Assuming a lower PCI cost did not substantially improve the cost-effective-ness of primary PCI for high-risk patients with NSTEMI (ICER of $21 300). In probabilistic sensitivity analyses, the strategy combining 4 standard oral medications for all AMI and heparin for NSTEMI was very cost-effective in 97.7% of simulations. The strategy that added PCI for STEMI in tertiary hospitals and thrombolysis in secondary hospitals was moderately cost-effective in 92.7% of simulations and rarely very cost-effective (0.8%). Adding primary PCI for NSTEMI to these strategies was moderately cost-effective in only 1.6% of simulations and never very cost-effective (Table 4).
DiscussionThis study evaluated the cost-effectiveness of several AMI treat-ment strategies and their impact on total CHD mortality using the CHD Policy Model-China. The results suggest that optimal use of the 4 standard oral medications in all eligible patients with AMI , unfractionated heparin in patients with NSTEMI, or any of the STEMI reperfusion strategies (primary PCI alone or in combination with thrombolysis using streptokinase) would be cost-effective treatment strategies in China. Solely improv-ing use of clopidogrel for patients with AMI or primary PCI among high-risk patients with NSTEMI in tertiary hospitals did not seem to be cost-effective strategies, at least according to the WHO-CHOICE standard.46 However, we also estimated that optimal use of all hospital-based AMI treatments in this study would decrease China’s total CHD mortality (inclusive of acute in- and out-of-hospital deaths) by 9.6% at most.
Our results suggest that several hospital-based AMI treatment strategies were effective and very cost-effective and should be promoted. However, full implementation of even the most cost-effective treatment strategies would face big challenges in China. First, some low-income patients with AMI cannot
afford the high out-of-pocket payments required for some treat-ments. The CPACS study showed that 69% of patients were nonadherent to statins treatment because of high out-of-pocket costs.8 China’s basic medical insurance coverage had increased to 95% in 2011, and China’s 12th Five-Year Plan set a goal of lowering individual out-of-pocket payments to <30% of the share of total health expenditures.47 These 2 changes may lower the current obstacle of high out-of-pocket costs for individual patients with AMI. Second, there is currently no systematic program for overseeing the implementation of clinical practice guidelines in China. The American Heart Association Get With The Guidelines program has succeeded in lowering AMI case fatality by promoting and implementing practice guidelines, providing a blueprint for other countries.48
A nationwide investigation of 728 PCI-capable hospitals showed that the average numbers of PCI-capable hospitals were 40.1, 25.5, and 20.1 per 10 million of the population in the cities of Beijing, Tianjin, and Shanghai, respectively. In contrast, the national average was 8.1 per 10 million.49 The results show the geographic disparities in PCI capabili-ties in China. Improvements in PCI capabilities would require large investments: building catheterization laboratories, add-ing equipment, and training qualified medical personnel—none of which could be achieved in the short term. The National Health and Family Planning Commission enacted Cardiovascular Interventional Technology Practice Standards aimed at improving the quality of medical care, but these standards had a limited impact on the development of PCI, especially in secondary hospitals. These practical limitations led us to simulate a strategy to improve the use of primary PCI for STEMI in tertiary hospitals combined with thrombol-ysis for STEMI in secondary hospitals. This strategy seems to be moderately cost-effective, potentially preventing 36 300 AMI deaths, which would represent a 5.1% reduction in the CHD mortality rate. For all Chinese patients with STEMI, the logistical challenge of decreasing the door-to-balloon and door-to-needle time for reperfusion therapy must be urgently addressed. In a recent study of patients admitted to Beijing ter-tiary hospitals in which cardiac catheterization was available 24 hours a day, only 7% of patients treated with thrombolysis met the guidelines’ goal of a door-to-needle time of <30 min-utes; 22% of patients underwent PCI in <90 minutes.50
Simultaneous and optimal use of all treatment strategies selected by this study was estimated to decrease the total CHD mortality by 9.6%, an impact that was limited by the large proportion of prehospital AMI deaths in China. A surveil-lance study covering the entire Beijing area showed that 62% of acute coronary events deaths occurred before arriving at the hospital in 2009.10 Meanwhile, 79% of prehospital deaths of acute coronary events occurred at home.10 One reason for this high out-of-hospital fraction may be a low awareness of the importance of obtaining timely medical care. A study in Beijing tertiary hospitals showed that the median time from symptom onset to admission of the patients with STEMI was 140 minutes.50 Another investigation showed that only 7.1% of patients with AMI called the emergency number immediately at the time of symptoms onset.51 The increasing trend in inci-dence of acute coronary events is yet another challenge for the ability of China’s healthcare system to reduce CHD deaths.52
by guest on June 14, 2016http://circoutcomes.ahajournals.org/Downloaded from

84 Circ Cardiovasc Qual Outcomes January 2014
Limitations of the AnalysisSimilar to any computer simulation-based comparative effectiveness analysis, this study was limited by reliance on multiple assumptions and data inputs from diverse studies. We chose high-quality epidemiological data and China-spe-cific, nationally representative data to construct the model. The medication use rates of BRIG participants used in this study were similar to those measured in the CPACS8 and the CRACE study.9 Twenty-four parameters involving treatment effectiveness, contraindications, and major severe adverse event rates in our model were based on American or Euro-pean studies or large international meta-analyses, systematic reviews, or randomized controlled trials because no qualified parameters were available from studies conducted in China or among Chinese patients. However, we did not find enough evidence to indicate ethnic differences between Chinese patients with AMI and patients of other ethnicities among the parameters we used. As our sensitivity analyses suggested, our results were consistent across a range of all key model inputs. Urokinase is most widely used in fibrinolytic therapy for patients with STEMI in China, but few data on the clini-cal effectiveness of this medication have been published (ie, data on changes in 30-day all-cause mortality related to treat-ment). Assuming that the 2 thrombolytic agents have a simi-lar effect on reducing 30-day all-cause mortality and similar adverse event profiles, the cost-effectiveness of a reperfusion strategy using urokinase for patients with STEMI would be similar to that of streptokinase (Appendix Table III in the Data Supplement).
This study evaluated the cost-effectiveness of optimiz-ing the use of several hospital-based AMI treatment strate-gies. However, the evaluation did not include specific costs of system-level changes that might be required to achieve the assumed utilization rates (eg, infrastructure and workforce expansion, physician training, or quality improvement), so the costs may be underestimated. In this study, we assumed that the effectiveness of each treatment had an independent effect among the combinations of treatment strategies.
ConclusionsUsing the WHO-CHOICE standard, most treatment strategies recommended by guidelines would be highly or moderately cost-effective in China. Improved primary PCI for patients with STEMI would prevent the largest number of hospitalized AMI deaths. Because so many AMI deaths occur outside of the hospital in China, full and simultaneous improvements of all standard hospital-based AMI treatment strategies assessed in this study would decrease CHD mortality by <10%. Improve-ment of the capacity of prehospital care for patients with AMI is urgently needed in China.
Sources of FundingThis research was supported by grants from the National Program on Key Basic Research Project of China (contract No. 2012CB517806), the National Science & Technology Pillar Program during the 12th Five-Year Plan Period (contract Nos. 2011BAI09B01 and 2011BAI11B03), and the Capital Health Research and Development of Special (contract No. 2011-1005-01) to Drs Zhao and Liu and the Mentored Career Development Award (contract No. K08HL089675) from the National Heart, Lung, and Blood Institute of the U.S.
National Institutes of Health to Dr Moran. These funding bodies had no role in the study design, data analysis, data interpretation, or writ-ing of the manuscript.
DisclosuresNone.
References 1. Ministry of Health. China Health Statistics Yearbook in 2011. Beijing,
China: China Union Medical University Press; 2011. 2. Wang W, Zhao D, Yao L, Zhou M, Wu Z. Population-based epidemio-
logical study for case fatality of acute coronary events in Beijing. Chin J Cardiol. 2000;28:228–230.
3. O’Gara PT, Kushner FG, Ascheim DD, Casey DE Jr, Chung MK, de Lemos JA, Ettinger SM, Fang JC, Fesmire FM, Franklin BA, Granger CB, Krumholz HM, Linderbaum JA, Morrow DA, Newby LK, Ornato JP, Ou N, Radford MJ, Tamis-Holland JE, Tommaso CL, Tracy CM, Woo YJ, Zhao DX, Anderson JL, Jacobs AK, Halperin JL, Albert NM, Brindis RG, Creager MA, DeMets D, Guyton RA, Hochman JS, Kovacs RJ, Kushner FG, Ohman EM, Stevenson WG, Yancy CW; American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. 2013;127:e362–e425.
4. Jneid H, Anderson JL, Wright RS, Adams CD, Bridges CR, Casey DE Jr, Ettinger SM, Fesmire FM, Ganiats TG, Lincoff AM, Peterson ED, Philippides GJ, Theroux P, Wenger NK, Zidar JP. 2012 ACCF/AHA fo-cused update of the guideline for the management of patients with un-stable angina/non-ST-elevation myocardial infarction (updating the 2007 guideline and replacing the 2011 focused update): a report of the American College of Cardiology Foundation/American Heart Association Task Force on practice guidelines. Circulation. 2012;126:875–910.
5. Cardiology Branch of Chinese Medical Association, Editor Committee of Chinese Journal of Cardiology. Guidelines for the diagnosis and manage-ment of acute ST-segment elevation myocardial infarction. Chin J Cardiol. 2010;38:675–690.
6. Chinese Society of Cardiology of Chinese Medical Association Editorial Board of Chinese Journal of Cardiology. Guideline for diagnosis and treat-ment of patients with chronic stable angina (no abstract). Chin J Cardiol. 2007;35:195–206.
7. Liu Q, Zhao D, Liu J, Wang W. Current clinical practice patterns and out-come for acute coronary syndromes in China: results of BRIG project. Chin J Cardiol. 2009;37:213–217.
8. Bi Y, Gao R, Patel A, Su S, Gao W, Hu D, Huang D, Kong L, Qi W, Wu Y, Yang Y, Turnbull F; CPACS Investigators. Evidence-based medica-tion use among Chinese patients with acute coronary syndromes at the time of hospital discharge and 1 year after hospitalization: results from the Clinical Pathways for Acute Coronary Syndromes in China (CPACS) study. Am Heart J. 2009;157:509–516.e1.
9. Song XT, Chen YD, Pan WQ, Lü SZ; CRACE investigators. Gender based differences in patients with acute coronary syndrome: findings from Chinese Registry of Acute Coronary Events (CRACE). Chin Med J (Engl). 2007;120:1063–1067.
10. Gao YL, Su JT, Wei ZH, Liu JL, Wang J. Characteristics of out-of-hospital acute coronary heart disease deaths of Beijing permanent residents at the age of 25 or more from 2007 to 2009. Chin J Cardiol. 2012;40:199–203.
11. Moran A, Gu D, Zhao D, Coxson P, Wang YC, Chen CS, Liu J, Cheng J, Bibbins-Domingo K, Shen YM, He J, Goldman L. Future cardiovascular disease in China: Markov model and risk factor scenario projections from the coronary heart disease policy model-China. Circ Cardiovasc Qual Outcomes. 2010;3:243–252.
12. Rosengren A, Wilhelmsen L, Hagman M, Wedel H. Natural history of myocardial infarction and angina pectoris in a general population sample of middle-aged men: a 16-year follow-up of the Primary Prevention Study, Göteborg, Sweden. J Intern Med. 1998;244:495–505.
13. Lampe FC, Whincup PH, Wannamethee SG, Shaper AG, Walker M, Ebrahim S. The natural history of prevalent ischaemic heart disease in middle-aged men. Eur Heart J. 2000;21:1052–1062.
14. Heidenreich PA, McClellan M. Trends in treatment and outcomes for acute myocardial infarction: 1975-1995. Am J Med. 2001;110:165–174.
15. Frilling B, Schiele R, Gitt AK, Zahn R, Schneider S, Glunz HG, Gieseler U, Baumgärtel B, Asbeck F, Senges J; Maximum Individual Therapy in
by guest on June 14, 2016http://circoutcomes.ahajournals.org/Downloaded from
Wang et al Optimal Use of AMI Treatments 85
Acute Myocardial Infarction (MITRA); Myocardial Infarction Registry (MIR) Study Groups. Characterization and clinical course of patients not receiving aspirin for acute myocardial infarction: results from the MITRA and MIR studies. Am Heart J. 2001;141:200–205.
16. Chen ZM, Jiang LX, Chen YP, Xie JX, Pan HC, Peto R, Collins R, Liu LS; COMMIT (Clopidogrel and Metoprolol in Myocardial Infarction Trial) collaborative group. Addition of clopidogrel to aspirin in 45,852 patients with acute myocardial infarction: randomised placebo-controlled trial. Lancet. 2005;366:1607–1621.
17. Baigent C, Blackwell L, Collins R, Emberson J, Godwin J, Peto R, Buring J, Hennekens C, Kearney P, Meade T, Patrono C, Roncaglioni MC, Zanchetti A. Aspirin in the primary and secondary prevention of vascular disease: collaborative meta-analysis of individual participant data from randomised trials. Lancet. 2009;373:1849–1860.
18. de Graaf FR, Schuijf JD, van Velzen JE, Kroft LJ, de Roos A, Sieders A, Jukema JW, Schalij MJ, van der Wall EE, Bax JJ. Evaluation of contrain-dications and efficacy of oral Beta blockade before computed tomographic coronary angiography. Am J Cardiol. 2010;105:767–772.
19. Killip T III, Kimball JT. Treatment of myocardial infarction in a coronary care unit. A two year experience with 250 patients. Am J Cardiol. 1967;20:457–464.
20. Rathore SS, Gersh BJ, Berger PB, Weinfurt KP, Oetgen WJ, Schulman KA, Solomon AJ. Acute myocardial infarction complicated by heart block in the elderly: prevalence and outcomes. Am Heart J. 2001;141:47–54.
21. Chadda KD, Lichstein E, Gupta PK, Choy R. Bradycardia-hypotension syndrome in acute myocardial infarction: reappraisal of the overdrive ef-fects of atropine. Am J Med. 1975;59:158–164.
22. Yusuf S, Teo KK, Pogue J, Dyal L, Copland I, Schumacher H, Dagenais G, Sleight P, Anderson C. Telmisartan, ramipril, or both in patients at high risk for vascular events. N Engl J Med. 2008;358:1547–1559.
23. Briel M, Schwartz GG, Thompson PL, de Lemos JA, Blazing MA, van Es GA, Kayikçioglu M, Arntz HR, den Hartog FR, Veeger NJ, Colivicchi F, Dupuis J, Okazaki S, Wright RS, Bucher HC, Nordmann AJ. Effects of early treatment with statins on short-term clinical outcomes in acute coro-nary syndromes: a meta-analysis of randomized controlled trials. JAMA. 2006;295:2046–2056.
24. Sandler RS, Everhart JE, Donowitz M, Adams E, Cronin K, Goodman C, Gemmen E, Shah S, Avdic A, Rubin R. The burden of selected digestive diseases in the United States. Gastroenterology. 2002;122:1500–1511.
25. Cohen DE, Anania FA, Chalasani N; National Lipid Association Statin Safety Task Force Liver Expert Panel. An assessment of statin safety by hepatologists. Am J Cardiol. 2006;97:77C–81C.
26. Law M, Rudnicka AR. Statin safety: a systematic review. Am J Cardiol. 2006;97:52C–60C.
27. Cheema AN, Mohammad A, Hong T, Jakubovic HR, Parmar GS, Sharieff W, Garvey MB, Kutryk MJ, Fam NP, Graham JJ, Chisholm RJ. Characterization of clopidogrel hypersensitivity reactions and manage-ment with oral steroids without clopidogrel discontinuation. J Am Coll Cardiol. 2011;58:1445–1454.
28. Magee KD, Campbell SG, Moher D, Rowe BH. Heparin versus placebo for acute coronary syndromes. Cochrane Database Syst Rev. 2008:CD003462.
29. Warkentin TE, Eikelboom JW. Who is (still) getting HIT? Chest. 2007;131:1620–1622.
30. Sabatine MS, Morrow DA, Dalby A, Pfisterer M, Duris T, Lopez-Sendon J, Murphy SA, Gao R, Antman EM, Braunwald E; ExTRACT-TIMI 25 Investigators. Efficacy and safety of enoxaparin versus unfractionated heparin in patients with ST-segment elevation myocardial infarction also treated with clopidogrel. J Am Coll Cardiol. 2007;49:2256–2263.
31. Blazing MA, de Lemos JA, White HD, Fox KA, Verheugt FW, Ardissino D, DiBattiste PM, Palmisano J, Bilheimer DW, Snapinn SM, Ramsey KE, Gardner LH, Hasselblad V, Pfeffer MA, Lewis EF, Braunwald E, Califf RM; “A to Z” Investigators. Safety and efficacy of enoxaparin vs unfrac-tionated heparin in patients with non-ST-segment elevation acute coronary syndromes who receive tirofiban and aspirin: a randomized controlled trial. JAMA. 2004;292:55–64.
32. Jiang L. An economic evaluation of thrombolysis in myocardial infarction. China Prac Med. 2008;3:101–103.
33. French JK, Williams BF, Hart HH, Wyatt S, Poole JE, Ingram C, Ellis CJ, Williams MG, White HD. Prospective evaluation of eligibility for thrombo-lytic therapy in acute myocardial infarction. BMJ. 1996;312:1637–1641.
34. TERIMA Group of Investigators. TERIMA-2: national extension of thrombolytic treatment with recombinant streptokinase in acute myocar-dial infarct in Cuba. Thromb Haemost. 2000;84:949–954.
35. King SB III, Yeh W, Holubkov R, Baim DS, Sopko G, Desvigne-Nickens P, Holmes DR Jr, Cowley MJ, Bourassa MG, Margolis J, Detre KM. Balloon angioplasty versus new device intervention: clinical outcomes. A comparison of the NHLBI PTCA and NACI registries. J Am Coll Cardiol. 1998;31:558–566.
36. Malenka DJ, O’Rourke D, Miller MA, Hearne MJ, Shubrooks S, Kellett MA Jr, Robb JF, O’Meara JR, VerLee P, Bradley WA, Wennberg D, Ryan T Jr, Vaitkus PT, Hettleman B, Watkins MW, McGrath PD, O’Connor GT; The Northern New England Cardiovascular Disease Study Group. Cause of in-hospital death in 12,232 consecutive patients undergoing per-cutaneous transluminal coronary angioplasty. Am Heart J. 1999;137(4 pt 1):632–638.
37. Sarkees ML, Bavry AA. Acute coronary syndrome (unstable angina and non-ST elevation MI). Clin Evid (Online). 2009;1:209.
38. Centre for Health Statistics and Information, Ministry of Health. An Analysis Report of National Health Services Survey in 2003. Beijing, China: Peking Union Medical College Press; 2004.
39. World Health Organization. China World Health Survey 2002. Geneva, Switzerland: World Health Organization; 2005.
40. Moran AE, Forouzanfar MH, Roth G, Mensah GA, Ezzati M, Flaxman A, Murray CJL, Naghavi M. The global burden of ischemic heart disease in 1990 and 2010: The Global Burden of Disease 2010 study. Circulation. In press.
41. Wald NJ, Law MR. A strategy to reduce cardiovascular disease by more than 80%. BMJ. 2003;326:1419.
42. Hippisley-Cox J, Coupland C. Effect of combinations of drugs on all cause mortality in patients with ischaemic heart disease: nested case-control analysis. BMJ. 2005;330:1059–1063.
43. O’Brien CL, Gage BF. Costs and effectiveness of ximelagatran for stroke prophylaxis in chronic atrial fibrillation. JAMA. 2005;293:699–706.
44. Mathers CD, Lopez AD, Murray CJL. The burden of disease and mor-tality by condition: data, methods, and results for 2001. In: Lopez AD, Mathers CD, Ezzati M, Jamison DT, Murray CJL, eds. Global Burden of Disease and Risk Factors. Washington, DC: World Bank; 2006:45–240.
45. Weinstein MC, Siegel JE, Gold MR, Kamlet MS, Russell LB. Recommendations of the Panel on Cost-effectiveness in Health and Medicine. JAMA. 1996;276:1253–1258.
46. Baltussen RM AT, Tan Torres T, Hutubessy RC, Acharya A, Evans DB, Murray CJ. Generalized Cost-Effectiveness Analysis: A Guide. Geneva, Switzerland: World Health Organization; 2003.
47. Zhang L, Liu N. Health reform and out-of-pocket payments: lessons from China. Health Policy Plan. 2013. Published ahead of print February 21, 2013.
48. Eagle KA, Montoye CK, Riba AL, DeFranco AC, Parrish R, Skorcz S, Baker PL, Faul J, Jani SM, Chen B, Roychoudhury C, Elma MA, Mitchell KR, Mehta RH; American College of Cardiology’s Guidelines Applied in Practice (GAP) Projects in Michigan; American College of Cardiology Foundation (Bethesda, MD) Guidelines Applied in Practice Steering committee. Guideline-based standardized care is associated with substantially lower mortality in medicare patients with acute myo-cardial infarction: the American College of Cardiology’s Guidelines Applied in Practice (GAP) Projects in Michigan. J Am Coll Cardiol. 2005;46:1242–1248.
49. Yuan F, Song XT, Lu SZ. Percutaneous coronary intervention in mainland China in 2008: register results. Chin J Cardiol. 2010;38:629–632.
50. Zhang SY, Hu DY, Sun YH, Yang JG. Current management of patients with ST elevation myocardial infarction in metropolitan Beijing, China. Clin Invest Med. 2008;31:E189–E197.
51. Yan L. The influence on medicine - taking behavior of patients with AMI by their relatives. J Commun Med. 2012;10:20–22.
52. Sun JY, Liu J, Xie XQ, Wei ZH, Wang W, Wang M, Qi Y, Guo MN, Zhang XY, Wan H, Zhao D. Surveillance on the incidence of acute coronary events in the permanent residents of Beijing aged 25 years and more from 2007 to 2009. Chin J Cardiol. 2012;40:194–198.
by guest on June 14, 2016http://circoutcomes.ahajournals.org/Downloaded from
Gu, Jiang He, Lee Goldman and Dong ZhaoMiao Wang, Andrew E. Moran, Jing Liu, Pamela G. Coxson, Paul A. Heidenreich, Dongfeng
on Coronary Heart Disease Mortality in ChinaCost-Effectiveness of Optimal Use of Acute Myocardial Infarction Treatments and Impact
Print ISSN: 1941-7705. Online ISSN: 1941-7713 Copyright © 2014 American Heart Association, Inc. All rights reserved.
Greenville Avenue, Dallas, TX 75231is published by the American Heart Association, 7272Circulation: Cardiovascular Quality and Outcomes
doi: 10.1161/CIRCOUTCOMES.113.0006742014;7:78-85; originally published online January 14, 2014;Circ Cardiovasc Qual Outcomes.
http://circoutcomes.ahajournals.org/content/7/1/78World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://circoutcomes.ahajournals.org/content/suppl/2014/02/12/CIRCOUTCOMES.113.000674.DC1.htmlData Supplement (unedited) at:
http://circoutcomes.ahajournals.org//subscriptions/
at: is onlineCirculation: Cardiovascular Quality and Outcomes Information about subscribing to Subscriptions:
http://www.lww.com/reprints
Information about reprints can be found online at: Reprints:
document. Question and AnswerPermissions and Rightspage under Services. Further information about this process is available in the
which permission is being requested is located, click Request Permissions in the middle column of the WebCopyright Clearance Center, not the Editorial Office. Once the online version of the published article for
can be obtained via RightsLink, a service of theCirculation: Cardiovascular Quality and Outcomesin Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
by guest on June 14, 2016http://circoutcomes.ahajournals.org/Downloaded from

SUPPLEMENTAL MATERIAL
Model Calibration Model calibration: comparison with mortality rate targets for China
The Coronary Heart Disease(CHD) Policy Model-China defined CHD as myocardial
infarction (International Classification of Diseases, Ninth Revision(ICD-9) 410, 412 or
ICD-10 I21, I22), angina and other CHD (ICD-9 411, 413 and 414, or ICD-10 I20,
I23-I25), and a fixed proportion of “ill-defined” cardiovascular disease coded events
and deaths (ICD-9 codes 427.1, 427.4, 427.5, 428, 429.0, 429.1, 429.2, 429.9, 440.9 or
ICD-10 I47.2, I49.0, I46, I50, I51.4, I51.5, I51.9, and I70.9).1 Target total mortality for
the Chinese adults aged 35-84 years in the year 2002 were obtained from the World
Health Organization (WHO). Age and sex-specific CHD, stroke, and non-CHD
mortality rates estimated from the Chinese National Hypertension Epidemiology
Follow-up Survey (CHEFS) and then inflated rates by 30% to fit the ‘envelope’ of the
WHO mortality estimates for 2002. In a calibration procedure, incidence was adjusted
to match with age- and sex-specific mortality targets within one percent in the base
year. In order to evaluate the accuracy of CHD Policy Model(CHDPM) predictions
over time, China CHD mortality for ages 35-84 years over 1987-2010 were obtained
from the Ministry of Health (MOH, renamed as National Health and Family Planning
Commission in 2013) of China and the WHO. The Appendix Figure 2 below
demonstrates that CHDPM predictions are reasonably close to MOH and WHO
estimates over time, though the model does not reproduce year-to-year fluctuations that
may be artifactual.
Incidence of CHD in persons with no prior diagnosis of cardiovascular disease
1
CHD incidence in men and women aged 35-84 years with no prior CHD diagnosis was
based on 10-year incidence rates from the the CHEFS.2 and calibrated to fit with CHD
mortality and case-fatality assumptions.
CHD case-fatality rate assumptions Main CHDPM 28-day case-fatality assumptions were estimated from pooled Beijing
Sino-MONICA Study data from 1993-2004 (personal communication, Dong Zhao,
MD, PhD, 2006) and the main age-specific CHD case-fatality rate assumptions were
estimated from the overall rates (Appendix Table 4).
Source of CHD Incidence Estimates: Description of the CHEFS: Study Design: A multi-stage, random clustering design was used to identify a
nationally representative sample of Chinese men and women >= age 15 years
beginning in 1991 living in 30 provinces of China. In 1999, investitgators from each
province were invited to participate in a the CHEFS.3, 4 Seventeen provinces
participated in the follow up study. 83,533 men and 86,338 women older than age 40
at the time of the 1991 baseline examination were eligible for follow-up. Follow up
disease event data were gathered from 158,666 participants or proxies by interview in
1999-2000 (93.4 percent follow-up rate). Urban and rural status was determined
according to China census designations, and North and South China were divided by
the Yangtze river.
Follow up and ascertainment of cardiovascular disease events: In follow up
examinations during 1999 and 2000, participants or their proxies were tracked to a
current address and in-depth interviews were conducted in order to obtain information
on history of disease, hospitalizations, or deaths. For deaths, death certificates were
2
obtained from local public health or police departments. For hospitalized deaths,
hospital records were obtained, including physical examination, laboratory findings,
electrocardiograph records, brain imaging, and autopsy findings were included in the
evaluation of cases. An end-point assessment committee in each province reviewed
and confirmed (or rejected the hospital discharge diagnosis or cause of death on the
basis of abstracted information, using prespecified criteria). A study-wide endpoint
assessment committee at the Chinese Academy of Medical Sciences in Beijing,
consisting of cardiologists, neurologists, and a clinical epidemiologist reviewed all
diagnostic and cause of death information and determined the final diagnosis or cause
of death. Two committee members independently verified diagnosis or cause of death
and disagreements were adjudicated after discussion by other committee members.
Cases were also classified according to the ICD-9 or ICD-101, 5, 6.
3
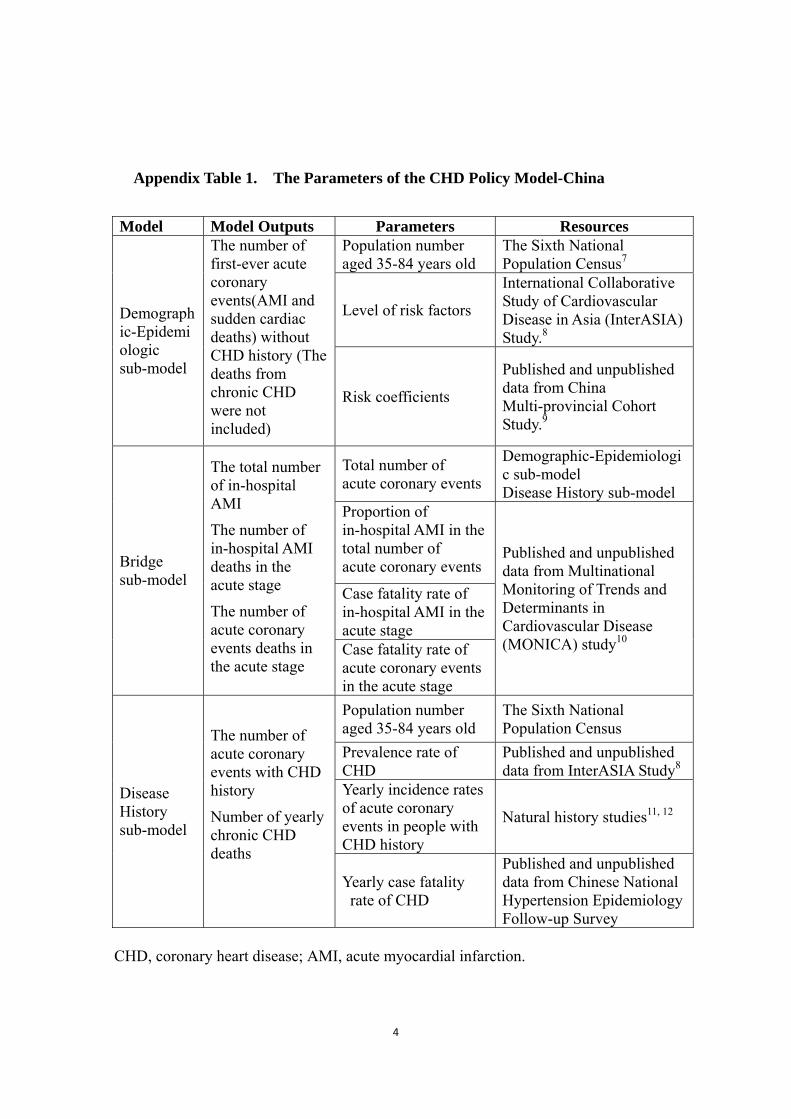
Appendix Table 1. The Parameters of the CHD Policy Model-China
Model Model Outputs Parameters Resources Population number aged 35-84 years old
The Sixth National Population Census7
Level of risk factors
International Collaborative Study of Cardiovascular Disease in Asia (InterASIA) Study.8
Demographic-Epidemiologic sub-model
The number of first-ever acute coronary events(AMI and sudden cardiac deaths) without CHD history (The deaths from chronic CHD were not included)
Risk coefficients
Published and unpublished data from China Multi-provincial Cohort Study.9
Total number of acute coronary events
Demographic-Epidemiologic sub-model Disease History sub-model
Proportion of in-hospital AMI in the total number of acute coronary events
Case fatality rate of in-hospital AMI in the acute stage
Bridge sub-model
The total number of in-hospital AMI
The number of in-hospital AMI deaths in the acute stage
The number of acute coronary events deaths in the acute stage
Case fatality rate of acute coronary events in the acute stage
Published and unpublished data from Multinational Monitoring of Trends and Determinants in Cardiovascular Disease (MONICA) study10
Population number aged 35-84 years old
The Sixth National Population Census
Prevalence rate of CHD
Published and unpublished data from InterASIA Study8
Yearly incidence rates of acute coronary events in people with CHD history
Natural history studies11, 12
Disease History sub-model
The number of acute coronary events with CHD history
Number of yearly chronic CHD deaths
Yearly case fatality rate of CHD
Published and unpublished data from Chinese National Hypertension Epidemiology Follow-up Survey
CHD, coronary heart disease; AMI, acute myocardial infarction.
4
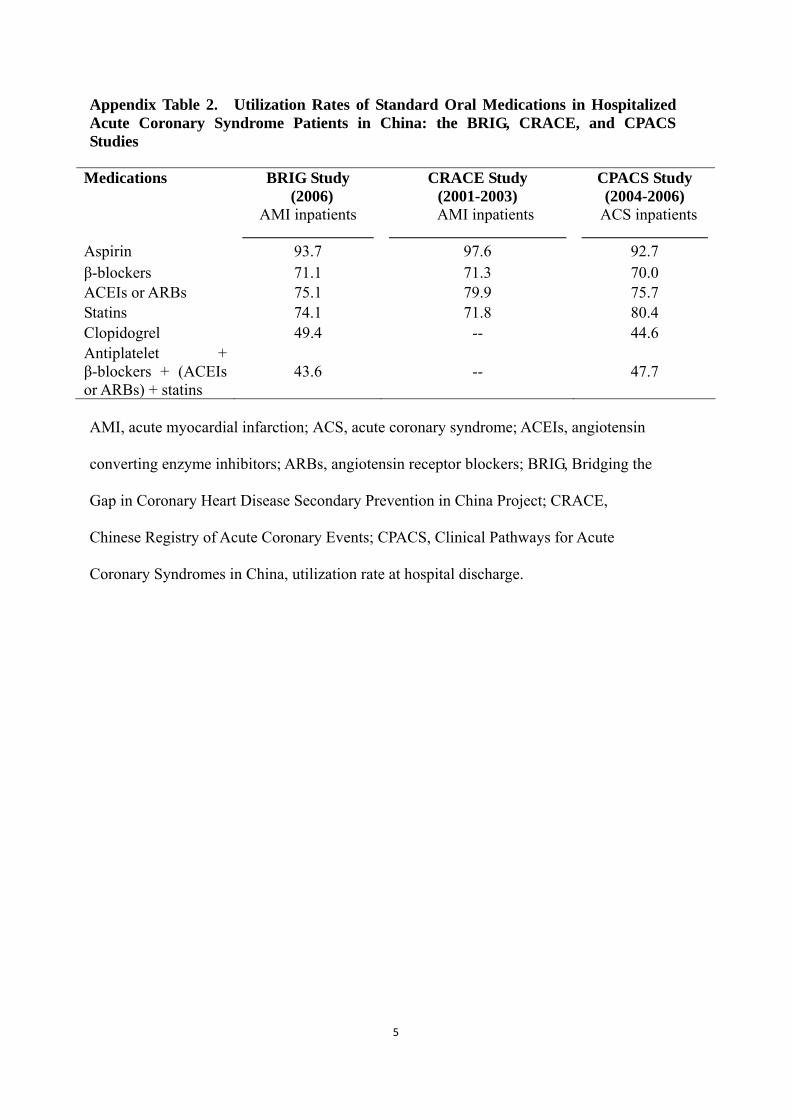
Appendix Table 2. Utilization Rates of Standard Oral Medications in Hospitalized Acute Coronary Syndrome Patients in China: the BRIG, CRACE, and CPACS Studies
Medications BRIG Study (2006)
AMI inpatients
CRACE Study (2001-2003)
AMI inpatients
CPACS Study (2004-2006)
ACS inpatients
Aspirin 93.7 97.6 92.7 β-blockers 71.1 71.3 70.0 ACEIs or ARBs 75.1 79.9 75.7 Statins 74.1 71.8 80.4 Clopidogrel 49.4 -- 44.6 Antiplatelet + β-blockers + (ACEIs or ARBs) + statins
43.6 -- 47.7
AMI, acute myocardial infarction; ACS, acute coronary syndrome; ACEIs, angiotensin
converting enzyme inhibitors; ARBs, angiotensin receptor blockers; BRIG, Bridging the
Gap in Coronary Heart Disease Secondary Prevention in China Project; CRACE,
Chinese Registry of Acute Coronary Events; CPACS, Clinical Pathways for Acute
Coronary Syndromes in China, utilization rate at hospital discharge.
5
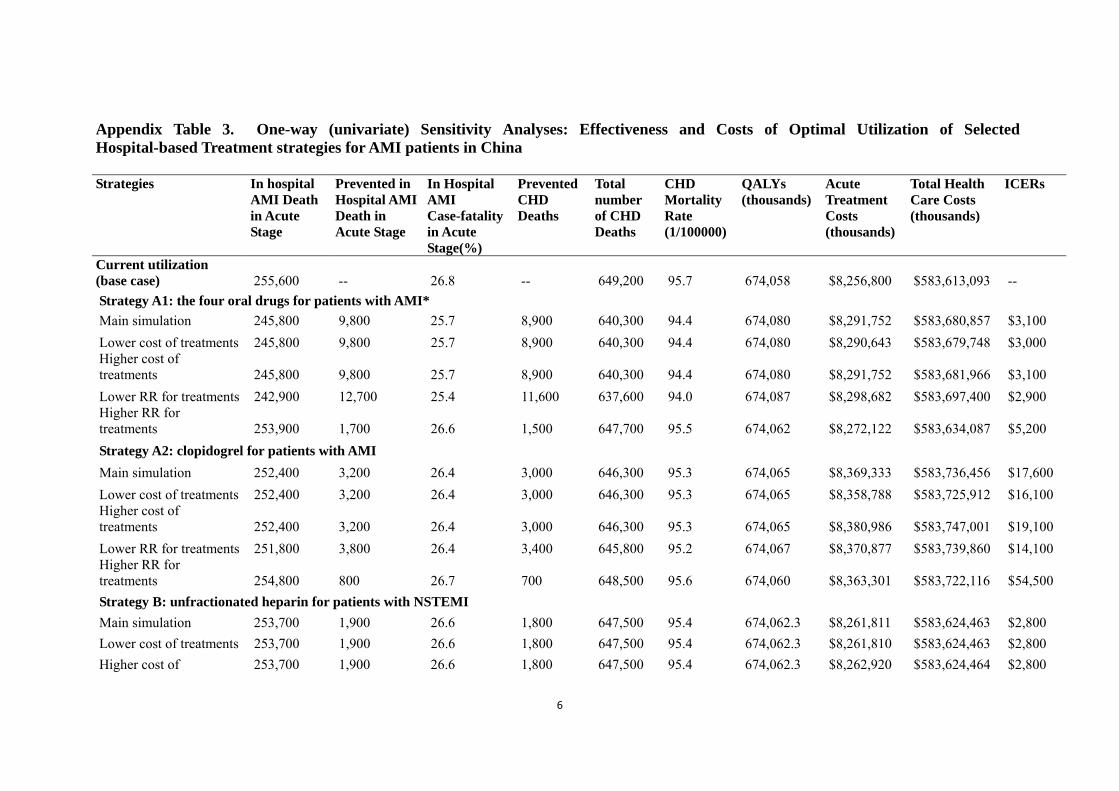
Appendix Table 3. One-way (univariate) Sensitivity Analyses: Effectiveness and Costs of Optimal Utilization of Selected Hospital-based Treatment strategies for AMI patients in China Strategies In hospital
AMI Death in Acute Stage
Prevented in Hospital AMI Death in Acute Stage
In Hospital AMI Case-fatality in Acute Stage(%)
Prevented CHD Deaths
Total number of CHD Deaths
CHD Mortality Rate (1/100000)
QALYs (thousands)
Acute Treatment Costs (thousands)
Total Health Care Costs (thousands)
ICERs
Current utilization (base case) 255,600 -- 26.8 -- 649,200 95.7 674,058 $8,256,800 $583,613,093 --
Strategy A1: the four oral drugs for patients with AMI*
Main simulation 245,800 9,800 25.7 8,900 640,300 94.4 674,080 $8,291,752 $583,680,857 $3,100
Lower cost of treatments 245,800 9,800 25.7 8,900 640,300 94.4 674,080 $8,290,643 $583,679,748 $3,000 Higher cost of treatments 245,800 9,800 25.7 8,900 640,300 94.4 674,080 $8,291,752 $583,681,966 $3,100
Lower RR for treatments 242,900 12,700 25.4 11,600 637,600 94.0 674,087 $8,298,682 $583,697,400 $2,900 Higher RR for treatments 253,900 1,700 26.6 1,500 647,700 95.5 674,062 $8,272,122 $583,634,087 $5,200
Strategy A2: clopidogrel for patients with AMI
Main simulation 252,400 3,200 26.4 3,000 646,300 95.3 674,065 $8,369,333 $583,736,456 $17,600
Lower cost of treatments 252,400 3,200 26.4 3,000 646,300 95.3 674,065 $8,358,788 $583,725,912 $16,100 Higher cost of treatments 252,400 3,200 26.4 3,000 646,300 95.3 674,065 $8,380,986 $583,747,001 $19,100
Lower RR for treatments 251,800 3,800 26.4 3,400 645,800 95.2 674,067 $8,370,877 $583,739,860 $14,100 Higher RR for treatments 254,800 800 26.7 700 648,500 95.6 674,060 $8,363,301 $583,722,116 $54,500
Strategy B: unfractionated heparin for patients with NSTEMI
Main simulation 253,700 1,900 26.6 1,800 647,500 95.4 674,062.3 $8,261,811 $583,624,463 $2,800
Lower cost of treatments 253,700 1,900 26.6 1,800 647,500 95.4 674,062.3 $8,261,810 $583,624,463 $2,800
Higher cost of 253,700 1,900 26.6 1,800 647,500 95.4 674,062.3 $8,262,920 $583,624,464 $2,800
6

treatments
Lower RR for treatments 248,000 7,600 26.0 6,900 642,200 94.7 674,075.2 $8,275,523 $583,657,318 $2,600 Higher RR for treatments 267,600 -12,000 28.0 -11,000 660,200 97.3 674,031.0 $8,227,843 $583,543,822 Harmful
Strategy C1: PCI in tertiary hospitals and thrombolysis (streptokinase) in secondary hospitals for patients with STEMI
Main simulation 219,300 36,300 23.0 33,200 616,000 90.8 674,140 $8,867,068 $584,344,872 $8,900
Lower cost of treatments 219,300 36,300 23.0 33,200 616,000 90.8 674,140 $8,814,558 $584,292,363 $8,300 Higher cost of treatments 219,300 36,300 23.0 33,200 616,000 90.8 674,140 $8,919,577 $584,397,381 $9,600
Lower RR for treatments 212,300 43,300 22.2 39,700 609,500 89.8 674,155 $8,884,219 $584,385,232 $8,000 Higher RR for treatments 227,800 27,800 23.9 25,500 623,700 91.9 674,121 $8,845,410 $584,295,079 $10,800
Strategy C2: PCI for all STEMI
Main simulation 202,000 53,600 21.2 49,100 600,100 88.5 674,178 $9,356,039 $584,891,450 $10,700
Lower cost of treatments 202,000 53,600 21.2 49,100 600,100 88.5 674,178 $9,258,674 $584,794,085 $9,800 Higher cost of treatments 202,000 53,600 21.2 49,100 600,100 88.5 674,178 $9,453,404 $584,988,815 $11,500
Lower RR for treatments 190,900 64,700 20.0 59,300 589,900 87.0 674,203 $9,383,846 $584,956,226 $9,300 Higher RR for treatments 226,600 29,000 23.7 26,600 622,700 91.8 674,123 $9,291,640 $584,745,259 $17,400
Strategy C3: PCI for high risk patients with NSTEMI in tertiary hospitals Main simulation 252,300 3,300 26.4 3,000 646,200 95.3 674,065 $8,409,774 $583,776,644 $23,400 Lower cost of treatments 252,300 3,300 26.4 3,000 646,200 95.3 674,065 $8,395,353 $583,762,222 $21,300 Higher cost of treatments 252,300 3,300 26.4 3,000 646,200 95.3 674,065 $8,424,196 $583,791,066 $25,400 Lower RR for treatments 251,100 4,500 26.3 4,100 645,100 95.1 674,068 $8,413,130 $583,784,090 $17,100 Higher RR for treatments 254,200 1,400 26.6 1,300 647,900 95.5 674,061 $8,404,573 $583,765,554 $50,800
7
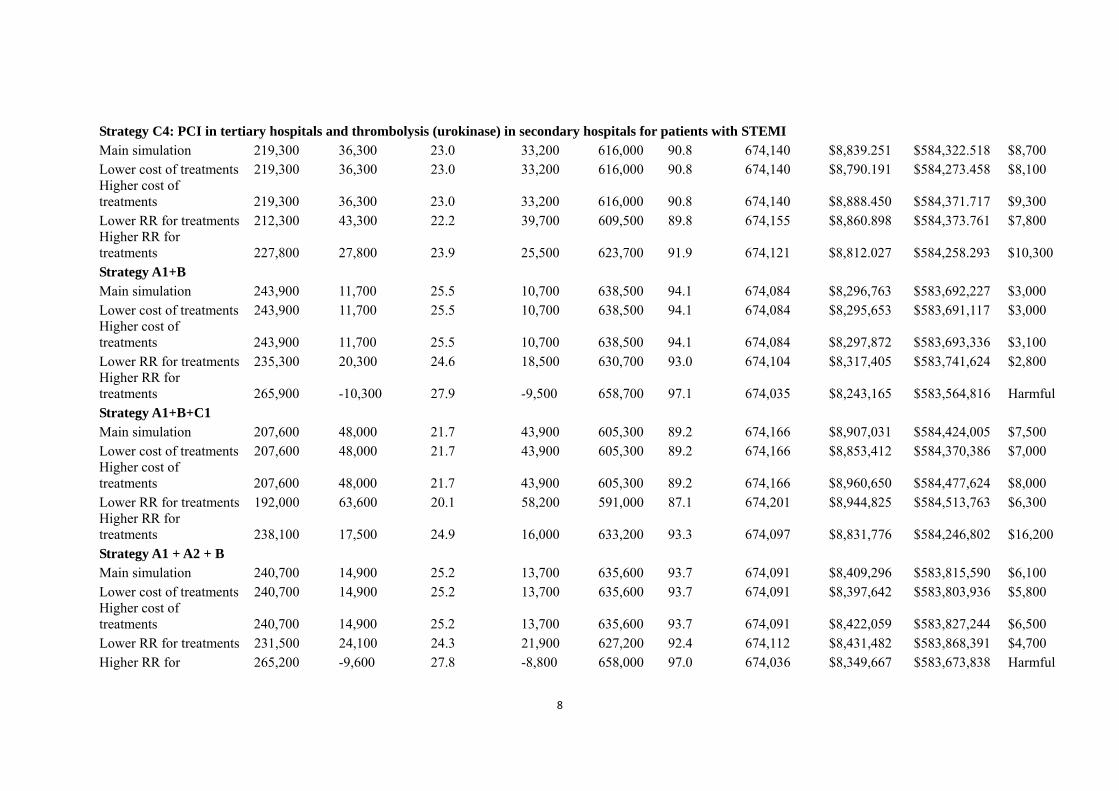
Strategy C4: PCI in tertiary hospitals and thrombolysis (urokinase) in secondary hospitals for patients with STEMI Main simulation 219,300 36,300 23.0 33,200 616,000 90.8 674,140 $8,839.251 $584,322.518 $8,700 Lower cost of treatments 219,300 36,300 23.0 33,200 616,000 90.8 674,140 $8,790.191 $584,273.458 $8,100 Higher cost of treatments 219,300 36,300 23.0 33,200 616,000 90.8 674,140 $8,888.450 $584,371.717 $9,300 Lower RR for treatments 212,300 43,300 22.2 39,700 609,500 89.8 674,155 $8,860.898 $584,373.761 $7,800 Higher RR for treatments 227,800 27,800 23.9 25,500 623,700 91.9 674,121 $8,812.027 $584,258.293 $10,300 Strategy A1+B Main simulation 243,900 11,700 25.5 10,700 638,500 94.1 674,084 $8,296,763 $583,692,227 $3,000 Lower cost of treatments 243,900 11,700 25.5 10,700 638,500 94.1 674,084 $8,295,653 $583,691,117 $3,000 Higher cost of treatments 243,900 11,700 25.5 10,700 638,500 94.1 674,084 $8,297,872 $583,693,336 $3,100 Lower RR for treatments 235,300 20,300 24.6 18,500 630,700 93.0 674,104 $8,317,405 $583,741,624 $2,800 Higher RR for treatments 265,900 -10,300 27.9 -9,500 658,700 97.1 674,035 $8,243,165 $583,564,816 Harmful Strategy A1+B+C1 Main simulation 207,600 48,000 21.7 43,900 605,300 89.2 674,166 $8,907,031 $584,424,005 $7,500 Lower cost of treatments 207,600 48,000 21.7 43,900 605,300 89.2 674,166 $8,853,412 $584,370,386 $7,000 Higher cost of treatments 207,600 48,000 21.7 43,900 605,300 89.2 674,166 $8,960,650 $584,477,624 $8,000 Lower RR for treatments 192,000 63,600 20.1 58,200 591,000 87.1 674,201 $8,944,825 $584,513,763 $6,300 Higher RR for treatments 238,100 17,500 24.9 16,000 633,200 93.3 674,097 $8,831,776 $584,246,802 $16,200 Strategy A1 + A2 + B Main simulation 240,700 14,900 25.2 13,700 635,600 93.7 674,091 $8,409,296 $583,815,590 $6,100 Lower cost of treatments 240,700 14,900 25.2 13,700 635,600 93.7 674,091 $8,397,642 $583,803,936 $5,800 Higher cost of treatments 240,700 14,900 25.2 13,700 635,600 93.7 674,091 $8,422,059 $583,827,244 $6,500 Lower RR for treatments 231,500 24,100 24.3 21,900 627,200 92.4 674,112 $8,431,482 $583,868,391 $4,700 Higher RR for 265,200 -9,600 27.8 -8,800 658,000 97.0 674,036 $8,349,667 $583,673,838 Harmful
8

9
treatments
Strategy A1+B+C1+C3 Main simulation 204,300 51,300 21.4 46,900 602,300 88.8 674,173 $9,060,006 $584,587,556 $8,500 Lower cost of treatments 204,300 51,300 21.4 46,900 602,300 88.8 674,173 $8,991,965 $584,519,515 $7,900 Higher cost of treatments 204,300 51,300 21.4 46,900 602,300 88.8 674,173 $9,128,047 $584,655,597 $9,100 Lower RR for treatments 187,500 68,100 19.6 62,300 586,900 86.5 674,211 $9,101,155 $584,684,760 $7,000 Higher RR for treatments 236,600 19,000 24.8 17,300 631,900 93.1 674,101 $8,979,549 $584,399,262 $18,300 Strategy A1+A2+B+C1+C3 Main simulation 201,100 54,500 21.1 49,900 599,400 88.3 674,180 $9,172,539 $584,710,919 $9,000 Lower cost of treatments 201,100 54,500 21.1 49,900 599,400 88.3 674,180 $9,093,953 $584,632,334 $8,400 Higher cost of treatments 201,100 54,500 21.1 49,900 599,400 88.3 674,180 $9,252,233 $584,789,504 $9,600 Lower RR for treatments 183,700 71,900 19.2 65,700 583,400 86.0 674,219 $9,215,232 $584,811,526 $7,400 Higher RR for treatments 235,900 19,700 24.7 18,000 631,200 93.0 674,102 $9,086,051 $584,508,284 $20,300 Strategy A1+ A2+B+C2+C3 Main simulation 183,900 71,700 19.3 65,800 583,500 86.0 674,219 $9,661,510 $585,257,497 $10,200 Lower cost of treatments 183,900 71,700 19.3 65,800 583,500 86.0 674,219 $9,538,070 $585,134,057 $9,400 Higher cost of treatments 183,900 71,700 19.3 65,800 583,500 86.0 674,219 $9,786,060 $585,380,938 $11,000 Lower RR for treatments 162,300 93,300 17.0 85,300 563,800 83.1 674,267 $9,714,859 $585,382,520 $8,500 Higher RR for treatments 234,700 20,900 24.6 19,100 630,100 92.9 674,105 $9,532,281 $584,958,464 $28,600 ICERs, incremental cost-effectiveness ratios (compared with the base case); AMI, acute myocardial infarction; CHD, coronary heart
disease; QALYs, quality-adjusted life years; STEMI, ST-elevation myocardial infarction; NSTEMI, Non-ST-elevation myocardial infarction; and PCI, percutaneous coronary intervention. * Aspirin, β-blockers, angiotensin converting enzyme inhibitors, and statins.
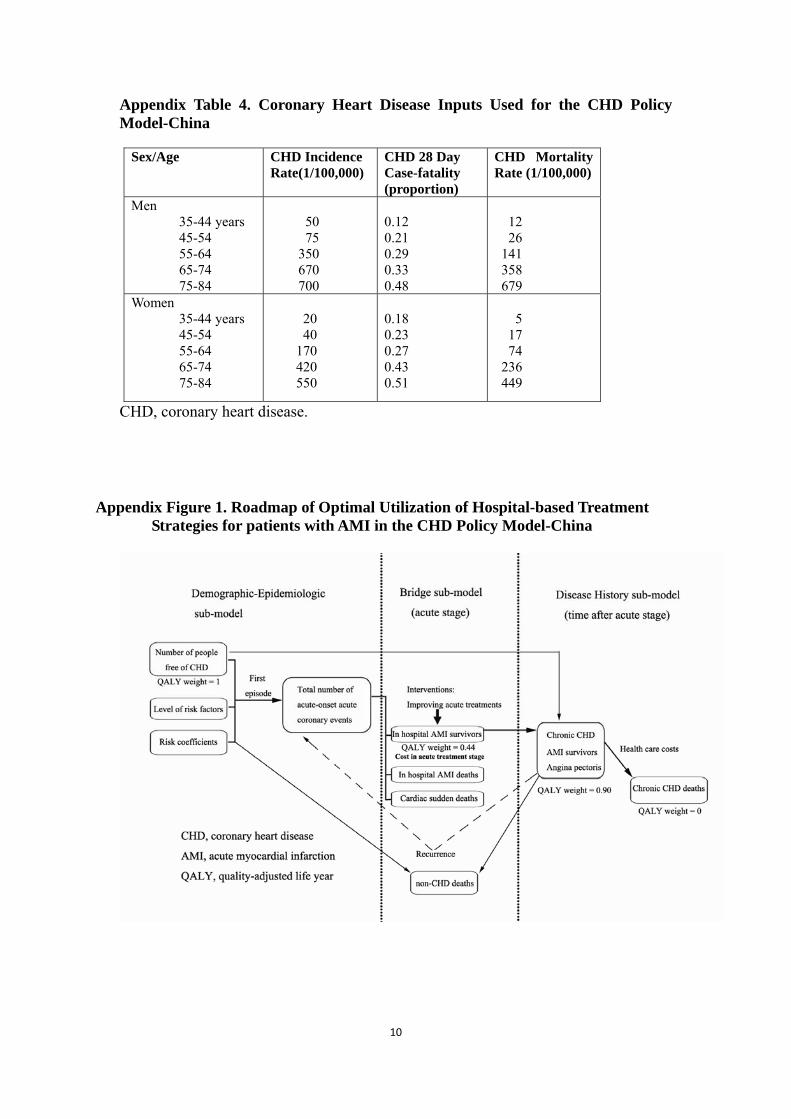
Appendix Table 4. Coronary Heart Disease Inputs Used for the CHD Policy Model-China
Sex/Age CHD Incidence Rate(1/100,000)
CHD 28 Day Case-fatality (proportion)
CHD Mortality Rate (1/100,000)
Men 35-44 years 45-54 55-64 65-74 75-84
50 75 350 670 700
0.12 0.21 0.29 0.33 0.48
12 26 141 358 679
Women 35-44 years 45-54 55-64 65-74 75-84
20 40 170 420 550
0.18 0.23 0.27 0.43 0.51
5 17 74 236 449
CHD, coronary heart disease.
Appendix Figure 1. Roadmap of Optimal Utilization of Hospital-based Treatment
Strategies for patients with AMI in the CHD Policy Model-China
10
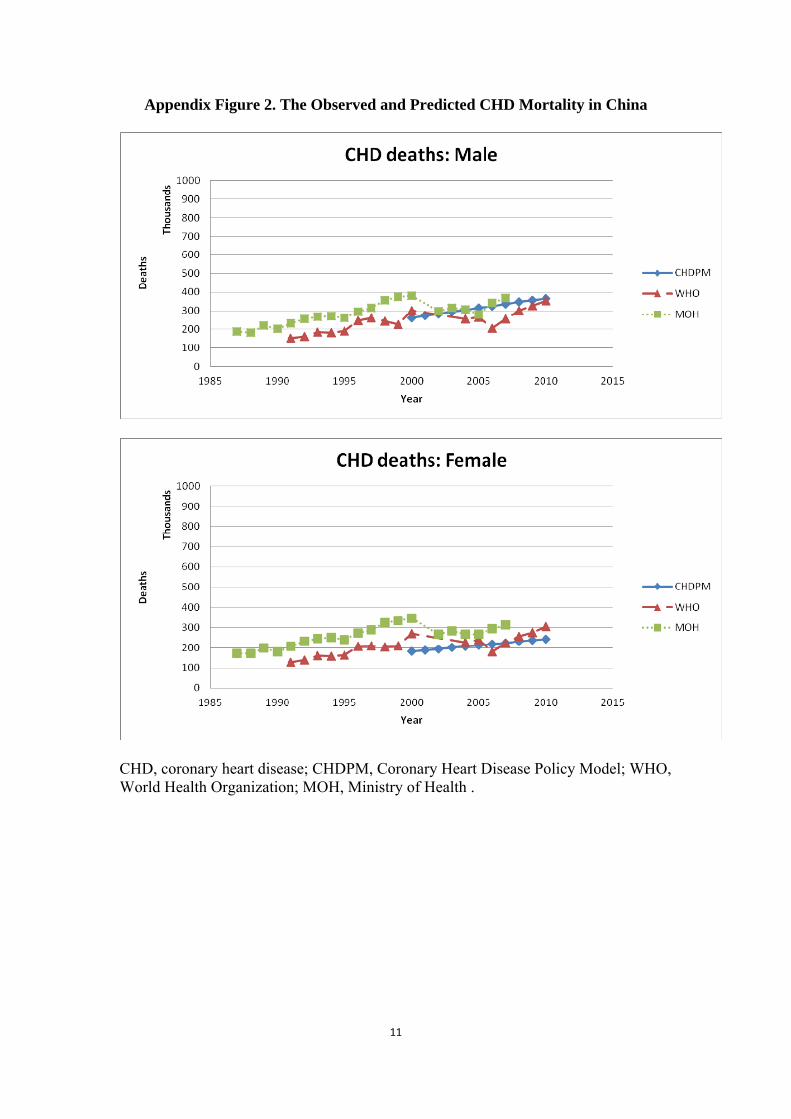
Appendix Figure 2. The Observed and Predicted CHD Mortality in China
CHD, coronary heart disease; CHDPM, Coronary Heart Disease Policy Model; WHO, World Health Organization; MOH, Ministry of Health .
11

References 1. Lozano R, Murray C.J.L., Lopez, A.D., and Satoh, T. Miscoding and misclassification of
ischaemic heart disease mortality. Global Programme on Evidence for Health Policy Working Paper No. 12. Geneva, World Health Organization. 2001.
2. Gu D, Kelly TN, Wu X, Chen J, Duan X, Huang JF, Chen JC, Whelton PK and He J. Blood pressure and risk of cardiovascular disease in Chinese men and women. Am J Hypertens. 2008;21:265-72.
3. Kelly TN, Gu D, Chen J, Huang JF, Chen JC, Duan X, Wu X, Yau CL, Whelton PK and He J. Hypertension subtype and risk of cardiovascular disease in Chinese adults. Circulation. 2008;118:1558-66.
4. He J, Gu D, Wu X, Reynolds K, Duan X, Yao C, Wang J, Chen CS, Chen J, Wildman RP, Klag MJ and Whelton PK. Major causes of death among men and women in China. The New England journal of medicine. 2005;353:1124-34.
5. Moran A, Zhao D, Gu D, Coxson P, Chen CS, Cheng J, Liu J, He J and Goldman L. The future impact of population growth and aging on coronary heart disease in China: projections from the Coronary Heart Disease Policy Model-China. BMC public health. 2008;8:394.
6. Moran A, Gu D, Zhao D, Coxson P, Wang YC, Chen CS, Liu J, Cheng J, Bibbins-Domingo K, Shen YM, He J and Goldman L. Future cardiovascular disease in China: markov model and risk factor scenario projections from the coronary heart disease policy model-China. Circ Cardiovasc Qual Outcomes. 2010;3:243-52.
7. 2010 Population Census of China. Beijing: China Statistical Press; 2012. 8. He J, Neal B, Gu D, Suriyawongpaisal P, Xin X, Reynolds R, MacMahon S and Whelton PK.
International collaborative study of cardiovascular disease in Asia: design, rationale, and preliminary results. Ethn Dis. 2004;14:260-8.
9. Liu J, Hong Y, D'Agostino RB, Sr., Wu Z, Wang W, Sun J, Wilson PW, Kannel WB and Zhao D. Predictive value for the Chinese population of the Framingham CHD risk assessment tool compared with the Chinese Multi-Provincial Cohort Study. JAMA. 2004;291:2591-9.
10. Wang W, Zhao D, Yao L, Zhou M and Wu Z. Population-based epidemiological study for case fatality of acute coronary events in Beijing. Chinese Journal of Cardiology. 2000;28:228-230.
11. Rosengren A, Wilhelmsen L, Hagman M and Wedel H. Natural history of myocardial infarction and angina pectoris in a general population sample of middle-aged men: a 16-year follow-up of the Primary Prevention Study, Goteborg, Sweden. J Intern Med. 1998;244:495-505.
12. Lampe FC, Whincup PH, Wannamethee SG, Shaper AG, Walker M and Ebrahim S. The natural history of prevalent ischaemic heart disease in middle-aged men. Eur Heart J. 2000;21:1052-62.
12




















