
corticost engl
35
ACTH, Corticosteroi ds, antagonists
Transcript of corticost engl
ACTH, Corticosteroi
ds, antagonists

MECHANISM OF ACTION
Peptide hormones : receptors at cell membrane, second messengers
Steroid hormones : receptors in cytoplasm and nucleus. Steroid enters all cells but bind to receptors in cytosol in target cell only transformation and translocation of the H-R complex to DNA and enhance transcription

ADRENOCORTICOSTEROIDSRole of ACTHGlucocorticoids (nat.: cortisol,corticosteron)
Mineralocorticoids (aldosteron)Physiological & pharmacological effects:
---related to survival / coping stress / sometimes life saving
-antiinflammation, immunosuppressant, metabolic, water retention & electrolyte balance, “risk- benefit ratio” assessment

Dosage
A given dose maybe physiological or pharmacological, depend on the condition of the organism (environment & activities).
in adrenalectomized animal: a small dose is physiological under favorable condition, but a large dose is also physiological if the condition is stressful. In normal animal similar large dose is pharmacological, given repetitiously induces hypercorticism
Endogenous: daily fluctuation, diurnal variation, highest in the morning in normal condition. Exogenous: mimicking a natural one 1 dd in the morning, short half-life

Relative potency of corticosteroid
Potency as anti- inflammatory parallel those on carbohydrate metabolism, but not with Na & water retention capacity,
Potency as life saver parallel Na retention

PharmacokineticsAbsorption per oral is good (lipophilic)Topical application may cause systemic effect if large area or prolonged, absorbed from conjunctiva, synovial; and slowly through skin
Aerosol for respiratory is absorbed equivalent oral, long-term nasal spray can lead to atrophy briefly
Changes in chemical structure may change rate of absorption, time of onset of effects, duration of action
in plasma 90% is bound to CBG and albuminEstrogen increase biosynthesis of CBG in the liver
Major sites of inactivation: liver ,kidneyHypothyroidismmetabolism of steroid decrease
PharmacodynamicsAct via controlling the rate of synthesis of protein inside the target cell
Decreased production of PG, cytokines, interleukins
Inhibits the release of cytokines,Decreased proliferation and migration of lymphocites & macrophagessuppress phagocytic, antigen processing activity
Thus inhibits the manifestation of inflammation
And inhibiting immune responsepredispose patient to infections
Permissive effect: acting in concert with other regulatory forces: eg sympatomimetic amine

Pharmacodynamic
Increased glycogenolysis & gluconeogenesis
Increased protein catabolism & decreased synthesis
Decreased osteoblast formation & activityDecreased Ca absorption from the GI tractDecreased TSH secretionNa & water retention

ANTIINFLAMMATION
INFLAMMATION:Early: Rubor, calor, dolor, tumor, functio laesa
Late: wound contraction & healing
ANTIINFLAMMATION:WBC accumulation Macrophages activity (TB bacillus multiply) Fibroblasts, collagen formation, cicatrix
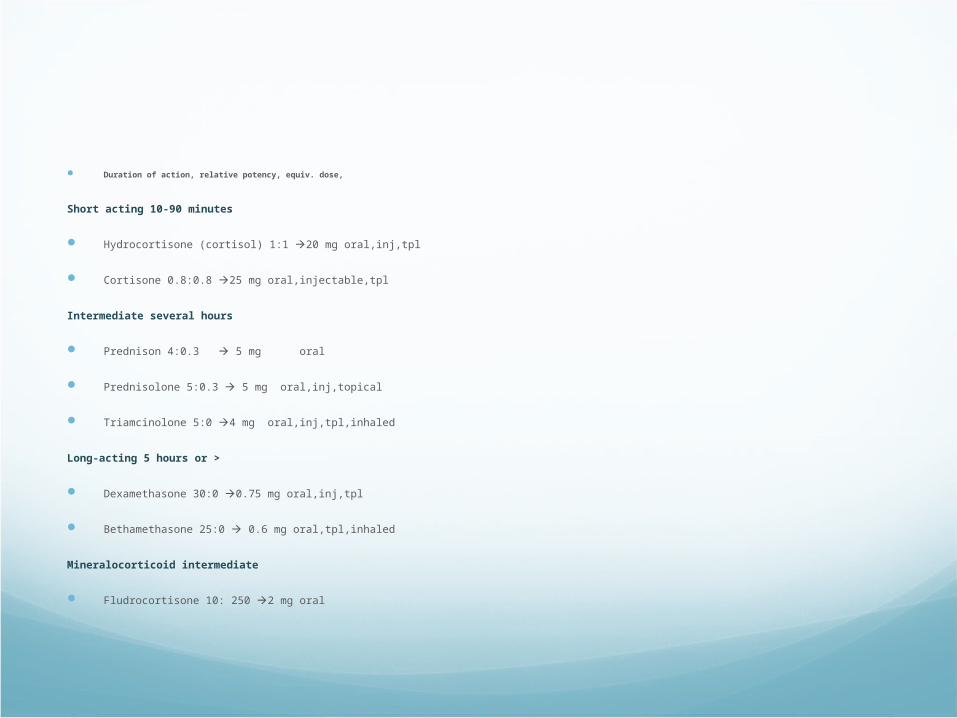
Duration of action, relative potency, equiv. dose,
Short acting 10-90 minutes
Hydrocortisone (cortisol) 1:1 20 mg oral,inj,tpl
Cortisone 0.8:0.8 25 mg oral,injectable,tpl
Intermediate several hours
Prednison 4:0.3 5 mg oral
Prednisolone 5:0.3 5 mg oral,inj,topical
Triamcinolone 5:0 4 mg oral,inj,tpl,inhaled
Long-acting 5 hours or >
Dexamethasone 30:0 0.75 mg oral,inj,tpl
Bethamethasone 25:0 0.6 mg oral,tpl,inhaled
Mineralocorticoid intermediate
Fludrocortisone 10: 250 2 mg oral

RISKS:
Masking effectMissuse : sense of well-being, expected weight gain, fast relieve of symptoms
Deficiency in abrupt discontinuation of longterm treatment tappering- off

Side Effects:
OedemaHyperglycemia, exacerbation of DMSuppression of the immune syst. vulnerable to common & opportunistic infections, herpes, fungal infection
Buffalo hump, moon face, less fat in the extremities (limb & arms), hypertension iatrogenic Cushing’s Syndrome
Skin striae, thinningOsteoporosis (vulnerable to fracture)Growth suppression in childrenAcute adrenal insufficiency fatal

Side effectsBehavioral problemProlonged suppression of the H-P-Adrenal axis after drug discontinuation
Peptic ulcers (bleeding, perforation)

Contraindication (relative):
Ulcus pepticumHeart failureGlaucomaHerpes simplexDiabetes mellitusPsychosisMild, moderate infections

Toxicity [1]
Two categories: 1.Results from withdrawal therapy2.Results from continued use at supraphysiological doses
The major undesirable effects: results from their hormonal actions iatrogenic Cushing’s syndromeGlucocorticoid used < 2 weeks serious AEs unusual; insomnia, behavioral changes, acute peptic ulcers

Withdrawal of Therapyo acute adrenal insufficiency (severe complications) – prolonged therapy with corticosteroids suppressed the HPA axis (recover several weeks to months or years)o corticosteroids > 2 weeks adrenal suppressiono flare-up of the underlying disease (most frequent complications) – anorexia, nausea/vomiting, weight loss, lethargy, headache, fever, joint of mucle pain, postural hypotensiono pseudotumor cerebri
Toxicity [2]

Toxicity [3] Continued use of supraphysiological glucocorticoid dosesa.Fluid and Electrolyte abnormalities – hypokalemic alkalosis & hypertensionb.Metabolic changes – hyperglycemia with glycosuriac.Immune response – ↑ susceptibility to infection & a risk for reactivation of latent tuberculosisd.Possible risk of peptic ulcers – hemorrhage & perforation of ulcers (also receive NSAIDS)e.Myopathy – weakness of proximal limb muscle, respiratory muscles (recovery slow and incomplete)f.Behavioral changes – nervousness, insomnia, changes in mood or psyche, & overt psychosis

Toxicity [4] Continued use of supraphysiological glucocorticoid doses (cont.)g. Cataracts – well-established, related to dosage &
duration of therapy, resolution of opacities not complete, may progress, prednisone ≥ 10-15 mg/day should receive periodic slit-lamp examinations
h. Osteoporosis – frequent serious (30-50%), all ages, related to dosage & duration of therapy, prednisone ≥ 5 mg/day for ≥ 3 months bone densitometryMechanisms of osteoporosis:
• inhibition of gonadal steroid hormone• diminished gastrointestinal absorption of Ca2+ • inhibition of bone formation – suppressive effects on osteoblasts & stimulation of resorption by osteoclasts• inhibition of intestinal Ca2+ uptake secondary ↑ parathyroid hormone ↑ bone resorption

Toxicity [5] Maintaining of glucocorticoid-induced osteoporosis:• Ca2+ intake 1500 mg/day + Ca2+ supplement + vitamin D intake 800 IU/day• gonadal hormone replacement therapy• recombinant parathyroid hormone 1-34 (teriparatide, FORTEO)• bisphosphonate
i. Osteonecrosis – relative common, related to duration and doses, high dose short periods of time, generally progress, require joint replacement therapyj. Regulation of growth and development – growth retardation in children

Inflammation Mediators affected
Interferon, interleukin-1Interleukin-2Prostaglandin,Leukotrien,Bradikinin,histamin

PreparationOralInjectablesTopical for skin, eye, mucosal,Inhalation

Therapeutic uses [major principles] Empirical and palliative, except for deficiency states relative risks and benefits the appropriate dose – trial and error, reevaluated periodically, lowest dose as the duration of glucocorticoid therapy is > 1 week ↑ time- and dose-related increases in the incidence of disabling and potentially lethal effects abrupt cessation of glucocorticoids after prolonged therapy - ↑ risk of adrenal insufficiency general rule: long courses of therapy at high doses SHOULD BE reserved for life-threatening disease

Therapeutic overview
Replacement therapy in adrenal insufficiencyAntiinflammatory & immunosuppressiveRheumatic diseasesHepatic diseasesAnemia/ bone marrow suppressionAutoimmune disease e.g. Lupus erythematosus,
glomerulonephritis, Nephrotic syndrome, Crohn’s disease (colitis)
Asthma bronchiale, COPDFetus: induction of surfactant in the lung
before birth
Therapeutic overview
Cortisol & cortison only for replacement th/ because high mineralocorticoid ( but related to survival !)
Intermed.(e.g.prednison) is used for long-term usage, and asthma br.
Dexa & beta- methasone are highly antiinflam. but long acting and growth suppression, bone demineralization not for longterm use. Best for acute short term max antiinfl. e.g septic shock,brain edema

Therapeutic overview
Alternate day administrationHigh dose shot once only life savingStart with high dose than go lowerStart with low dose than go higherMaintenance doseTappering offInfection during usage increase dose

INHIBITORS/BLOCKERSSteroid synthesis inhibitor : adrenocortex hyperfunction metyrapone,ketokonazole,aminogluthetimide
Steroid receptor blockers: glucocorticoid excess RU 486; mineralocorticoid excessspironolactone
Antagonists of adrenocortical agents [1]
Hypercortisolism – surgery [treatment of choice] + adjuvant with inhibitors of steroidogenesis ketoconazole, metyrapone, etomidate, & mitotanePrecipitate acute adrenal
insufficiency
Used in appropriate dosescheck the status of HPA axis’ pts

Antagonists of adrenocortical agents [2]
Ketoconazole – antifungal, inhibitor of adrenal and gonadal steroidogenesis [doses ↑, inhibit the activity of CYP17; doses ↑↑, inhibit CYP11A1] dosage: 600-1200 mg/day BID or TID SE: hepatic dysfunction, potential drug-drug interactions
Metyrapone - selective inhibitor of CYP11B1 (11β-hydroxylase) used as a diagnostic test for HPA axis – metyrapone 30 mg/kg po midnight, next morning 8 AM measured 11-deoxycortisol: - plasma cortisol <8 μg/dL adequate inhibition of CYP11B1 - 11-deoxycortisol <7 μg/dL impaired HPA axis treating hypercorticism: metyrapone 4 g/day SE: hirsutism, hypertension, nausea, headache, sedation, rash

Antagonists of adrenocortical agents [3]
Etomidate – anesthetic agent and sedative, inhibits cortisol secretion at subhypnotic doses, inhibits CYP11B1 dosage: bolus 0.03 mg/kg IV, followed by infusion of 0.1-0.3 mg/kg/hour
Mitotane - adrenocorticolytic agent, for long-term control of hypercortisolismDosage: 0.5-3 g TID, onset of action takes weeks to months SE: GI disturbances and ataxia
Mifepristone - progesterone receptor antagonist antiprogesterone, terminate early pregnancy higher doses – inhibits GR currently, investigational & restricted to inoperable pts

Thank you
Have a nice day

PITUITARY HORMONESAnd their synthetic analogsControl of metabolism, growth, reproduction
Pharmacologic use :1.Replacement th/2.Drug therapy3.Diagnostics tools (stimulation tests)

GHRH=GRF & GHRP (synthetic eg. Sermorelin)
Diagnostic: GHRH or sermorelin in GH def. to test pituitary function. GH response is blunted in hypothyroidism, obesity, adults > 40 yr
Synthetic human GH for th/ of GH def. sermorelin & GHRH analog subcutan for def children w/ short stature less than 7.5-8 yr up to optimal height (close monitoring) no response = + hypothyroidism GH th/
S.e: inj.site rx, headache,hyperactivity, somnolence etc.

GH (Somatotropin) & rhGHStimulates growth at open epiphysis via
insulin-like growth factor (somatomedin), lipolysis at adipose tissue, growth of skeletal muscle
Piptuitary derived GH is no longer usedAnimal GH cant be used because does-not
resemble human’s ineffectiveRecombinant human GH widely used SOMATROPIN
& SOMATREM equipotent w/ naturalIndication: GH def, GH responsive stateNot indicated for aging (to delay or reverse)

Somatostatin (GH-inhibitingH, Somatotropin Release – inhibiting H)
Found in hypothalamus, CNS, pancreas, GI tr.Synthetic available, very short act T1/2 1-3 min
Inhibit release of GH, glucagon, insulin, gastrin
Analog: OCREOTIDE T1/2 80 min, 45x potent inhibit GH ,only 2x potent inhibit insulin secretion reduce sympt of hormone secreting tumors, bleeding from esophageal varices
A lot of s.e.

Pegvisomant (GH receptor antagonist)
Th/ acromegalyA derivative of a mutant GH: increased affinity in one binding site, decreased in other binding site with slower clearance














