
Home-Based Preoperative Chlorhexidine Bathing Cloths to Prevent Surgical Site Infection

Correlation Between Preoperative Magnetic ResonanceImaging and Surgical Margins with Modified Mohs forDermatofibrosarcoma Protuberans
CARLOS SERRA-GUILLEN, MD,� ONOFRE SANMARTIN, MD,� BEATRIZ LLOMBART, MD,�
EDUARDO NAGORE, MD,� CARLOS DELTORO, MD,y ISABEL MARTIN, MD,y
RAFAEL BORELLA-ESTRADA, MD,� CELIA REQUENA, MD,� ANTONIO MARTORELL-CALATAYUD, MD,�
JOSE CERVERA, MD,y AND CARLOS GUILLEN, MD�
BACKGROUND Dermatofibrosarcoma protuberans (DFSP) is characterized by asymmetrical and poorlydefined growth. Magnetic resonance imaging (MRI) has been proposed for the delimitation of thistumor.
OBJECTIVES To study the utility of MRI in evaluating the depth of infiltration in DFSP and to comparethe efficiency of clinical palpation with that of MRI in delimiting the invasiveness of DFSP.
METHODS Observational, prospective study of DFSP cases. The MRI scans for all cases were comparedwith the exact histological infiltration plane obtained using modified Mohs micrographic surgery (MMS).
RESULTS Forty-three DFSPs were included: 22 primary, nine recurrent, and 12 extirpated with positive mar-gins. Sensitivity for detecting deep invasion was 58% on examination using palpation and 67% using MRI.
CONCLUSIONS We present the largest series of DFSP cases studied using MRI published to date. Inprimary cases, MRI has greater sensitivity than palpation for detecting depth of infiltration (67% vs 58%).MRI seems to be useful in primary DFSP in locations other than the head, neck, and upper part of thethorax. MRI is not useful for confirming tumor persistence in extirpated DFSP with positive margins orfor studying lateral extension in primary DFSP.
The authors have indicated no significant interest with commercial supporters.
Dermatofibrosarcoma protuberans (DFSP) is an
infrequent cutaneous tumor, fibrohistiocytic
in nature, slow growing, and infiltrative.1 Clinically,
it appears as a skin-coloured plaque or tumor,
frequently located on the trunk, that may go unno-
ticed because of its indolent nature. As the tumor
grows, lateral and deep infiltration begins, and
protuberant nodules develop on the surface.2,3
Histologically, it is characterized by a uniform pro-
liferation of fusiform cells arranged in an irregular
intertwined fascicle, creating a storiform2–5 pattern.
The cellular density is much greater at the center of
the tumor than around the edges, where digitiform
projections begin to appear in the form of fibrous
tracts containing a small number of tumor cells that
can infiltrate subcutaneous cellular tissue (SCT),
muscular fascia, muscle, and even bone.2–5 These
tentacle-like tumor prolongations can extend far
from the central area; this means that DFSP has an
unpredictable subclinical extension, which in turn
means a high rate of recurrence even after broad
surgical excision.6–9 Mohs micrographic surgery
(MMS), which allows the entire margins of surgically
removed tissue to be studied histologically, is the
treatment of choice for DFSP. This surgical technique
provides much lower recurrence rates than conven-
tional surgery because it allows the morphology of
the tumor to be delimited much more precisely while
sparing much healthy peritumoral tissue.6–9
The use of imaging techniques in the study of soft
tissue tumors is a common and necessary practice in
most cases, because they provide information in
addition to that gathered in the clinical examination.
& 2011 by the American Society for Dermatologic Surgery, Inc. � Published by Wiley Periodicals, Inc. �ISSN: 1076-0512 � Dermatol Surg 2011;37:1–8 � DOI: 10.1111/j.1524-4725.2011.02077.x
1
Departments of �Dermatology and yRadiology, Instituto Valenciano de Oncologıa, Valencia, Spain

More specifically, the use of ultrasound, computed
tomography, and magnetic resonance imaging (MRI)
is standard practice for the precise diagnosis of soft
tissue tumors or for specifying their location.10
Given the characteristic clinical appearance of DFSP,
it is usually easy to diagnose using biopsy alone, and
imaging techniques are not routinely used in the
diagnostic process, but because of its infiltrative
nature, in certain cases, it may be useful to include
some sort of imaging technique to ascertain the lat-
eral extension and particularly the level of infiltra-
tion because simple clinical palpation, although
convenient, is not entirely reliable.
In 1994, Kransdorf and Meis-Kindblom11 published
the first study on the use of MRI in DFSP. In their
series of 11 people with DFSP, MRI was used in four,
in which a well-delimited, yet unspecific image of the
tumor was obtained. Various cases have subse-
quently been published in which MRI was used
preoperatively, demonstrating a certain efficacy,
particularly in cases of large DFSP tumors.12–17 The
largest series is that of Torreggiani and colleagues,17
who studied 10 cases of DFSP with MRI but were
able to distinguish only between superficial and deep
and between clearly and poorly delimited. Therefore,
there is no series of cases extensive enough to extract
valid conclusions regarding the use of MRI with
DFSP. In this sense, as Riggs and colleagues indi-
cate,12 to determine the utility of MRI in DFSP, it is
necessary to compare the MRI with the exact depth
of the tumor removed using MMS, because the de-
finitive surgical defect after MMS provides the exact
level of infiltration and an approximate silhouette of
the tumor morphology.
We present an observational and prospective study
comparing MRI and palpation of DFSP cases that
were subsequently extirpated with MMS.
Objectives
The main objective of the study was to ascertain the
reliability of MRI in cases of primary DFSP, to
evaluate its ability to specify the exact level of infil-
tration and lateral extension, and to determine
whether it provides more information than clinical
palpation of the tumor. The study also sought to
deduce the usefulness of MRI in determining the
depth of infiltration in cases of recurrent DFSP and
in establishing tumor persistence in cases of extir-
pated DFSP with affected margins.
Patients and Methods
The study included all people with DFSP seen in the
Dermatology Department at the Instituto Valenciano
de Oncologıa between July 2004 and December
2009. The study included primary tumors, recurrent
tumors, and recently extirpated tumors with positive
margins that had been referred for MMS. All cases
were diagnosed using conventional histologic anal-
ysis with hematoxylin and eosin staining, immuno-
histochemical analysis with CD 34, and positive
expression of translocation COL1A1-PDGFB on
reverse transcription and polymerase chain reaction.
Patients who had received neoadjuvant treatment
with imatinib and those who had not undergone
MMS were excluded. On the first visit, the clinical
information compiled for the study in the case of
primary DFSP included location, largest diameter,
smallest diameter, and depth of infiltration by pal-
pation. First, at least two clinicians (C.S.G., O.S.,
B.L.L.) palpated all tumors. Tumors were considered
not to be deeply infiltrated when they were mobile or
could be moved easily in a direction parallel to that
of the surface of the tumor and when, on palpation,
they seemed to be limited to the SCT. Tumors were
considered to be deeply infiltrated when they were
stationary or could not be moved easily in a direction
parallel to the surface of the tumor or when, on
palpation, they seemed to be adhered to the under-
lying muscular plane. For recurrent cases, the infor-
mation collected included the location of the tumor
and the number of previous treatments. For cases of
excised DFSP and affected margins, only clinical
data regarding location of the tumor were collected.
The MRI was done after the first visit and before
MMS using a Siemens Magnetom Symphony
D E R M AT O L O G I C S U R G E RY2
C O R R E L AT I O N B E T W E E N M R I A N D S U R G I C A L M A R G I N S I N D F S P

Maestro Class, 1.5 T with a Flex Large surface coil.
The study protocol used empty sequences followed
by injection of Prohance or Multihance paramag-
netic contrast agent in volumes that varied according
to the weight of each patient. After establishing a
localizer, sagittal T1-TSE and coronal STIR se-
quences were taken without intravenous contrast,
both with a frequency of 256, and T1-TSE and
T1-STIR axial sequences with a frequency of 516.
After injection of the intravenous contrast agent,
T1-TSE sequences were taken with axial, coronal, or
sagittal fat saturation. On the images obtained after
injection of the contrast agent, the diameters of the
lesion on the cutaneous plane were measured, and
the effect on deep structures was evaluated. Two
radiologists with expertise in soft tissue tumors
without any clinical information studied all cases
independently. The two observers jointly evaluated
uncertain cases or those with conflicting opinions.
The information gathered from the MRI in primary
DFSP cases included the largest diameter, the
smallest diameter, and the exact plane of the DFSP
infiltration, which could be SCT, muscular fascia,
muscle, periosteum, or bone. In cases of recurring
DFSP, MRI was used to determine the plane of
tumor infiltration. In patients who had recently un-
dergone surgery with affected margins, MRI was
used only to determine the persistence or absence of
the tumor.
Modified MMS18 was performed using formalin-
fixed, paraffin-embedded, horizontal sections. First,
the tumors, or the scar tissue in the case of extirpated
tumors with affected margins, were debulked, after
which the first stage of 1 cm of clinically healthy skin
was taken, reaching depths down to the totality of
the SCT. The Mohs specimen was oriented using silk
suture thread and photographed. The tissue was
divided into multiple specimens, mapped for precise
anatomic orientation, and sent to the Mohs histo-
technician for formalin fixation and paraffin em-
bedding before horizontal sections were taken. The
sections were stained with hematoxylin and eosin
and confirmed using CD34 immunostaining. Within
48 hours, the results were relayed to the dermatol-
ogist, who then marked the Mohs map. In patients
with positive margin(s), the residual tumor was
excised with additional 0.5- to 1-cm margins. The
process of excision continued until negative margins
were achieved. The skin defects were temporarily
covered with synthetic wound dressings until com-
plete excision was proven. The information gathered
from MMS included the number of stages, the largest
diameter of the final surgical defect, the smallest di-
ameter of the final surgical defect, and the micro-
scopic infiltration plane most seriously affected (SCT,
muscular fascia, muscle, periosteum, or bone). In
primary DFSP cases and recurrent cases with doubtful
interpretation of the level of microscopic infiltration,
a histologic study of all of the debulked tumor or
the entire piece of the Mohs stage was conducted to
determine the exact plane of tumor invasion. In re-
cently extirpated DFSP with affected margins, it was
also necessary to confirm whether any residual tumor
remained after the initial excision using a conven-
tional histologic study of the scar debulking.
For the MRI and the histologic infiltration, the DFSP
was considered superficial if the tumor was limited
to the SCT and deep if the tumor had reached the
muscular fascia or beyond.
The sensitivity, specificity, positive predictive value
(PPV), and negative predictive value (NPV) of clin-
ical palpation were calculated as a method for
ascertaining the depth of the primary DFSP and in
the case of MRI as a method for ascertaining the
depth of primary DFSP and the depth of recurrent
DFSP. Spearman correlation was used to determine
the correlation between clinical palpation and the
level of histologic invasion and to determine the
correlation grade between the level of depth reported
by the MRI and the level of histological invasion in
primary and recurrent DFSP.
Results
Forty-three people with DFSP were included in the
study: 22 primary cases, nine with recurrent tumors,
and 12 with recently extirpated tumors with affected
3 7 :* * : 2 0 1 1 3
S E R R A - G U I L L E N E T A L

margins. None of the 43 DFSPs in the study recurred
within a mean follow-up period of 35.8 months
(median 33 months, range 9–109 months).
Primary DFSP
Table 1 shows the clinical characteristics, the MRI
findings, and the MMS results of the 22 primary
cases (Figures 1 and 2). In 19 of the 22 primary cases
of DFSP, the size provided by the MRI image was
smaller than the clinically measured size of the
tumor. In two cases, the size of the tumor with the
clinical measurement coincided with that of the MRI
image. Only in one case did the size provided by
the MRI image exceed the clinical size. The number
of Mohs stages needed to obtain negative margins
TABLE 1. Primary Cases
Case Location
Tumor
Size,
cm
Infiltration
According
to Clinical
Palpation
MRI
Size,
cm
Infiltration
Plane in
MRI
Mohs
Stages,
n
Surgical
Defect,
cm
Histologic
Infiltration
Plane
1 Thorax 6� 3 Yes 6� 3 Fascia 2 9� 6 Muscle
2 Scapular 5� 4 No 3.8� 3 Fascia 1 6.5� 5 Fascia
3 Groin 5.5� 3 No 3.5� 3.5 SCT 1 7� 5 SCT
4 Shoulder 5� 4 No 4.2� 3.8 SCT 1 6� 5 SCT
5 Shoulder 4.5� 3 No 3.5� 2.7 SCT 1 6.5� 5 SCT
6 Scalp 5.5� 2.5 No 5� 2.8 SCT 3 12� 5.5 Periosteum
7 Shoulder 3.5� 1.5 No 2� 0.7 SCT 1 5.5� 5 Fascia
8 Lumbar 1.8� 1.5 No 1.7� 1.2 SCT 1 4� 3.5 SCT
9 Scapular 6.5� 4 No 3� 0.8 SCT 1 9� 6.5 SCT
10 Scapular 5� 2.5 No 4.6� 4.2 SCT 1 7� 4.5 SCT
11 Supraclavicular 4� 3.5 Yes 3.1� 1.2 Fascia 2 7� 4 Muscle
12 Lumbar 6.5� 4 No 5� 2.5 SCT 1 8.5� 6 SCT
13 Clavicular 2.5� 2 Yes 2.7� 1.5 Fascia 2 5.5� 4 Muscle
14 Neck 2.5� 2 Yes 1.7� 1.7 Fascia 3 7.5� 5 Muscle
15 Arm 6� 5.5 Yes 3.7� 2.7 SCT 3 8� 8 Muscle
16 Forehead 4� 3 No 3� 2 SCT 2 5.5� 5 Muscle
17 Scapular 6� 5 No 6� 3.8 Fascia 1 8� 7 Fascia
18 Thorax 8� 3.5 Yes 7.5� 3 SCT 1 11� 6 SCT
19 Scapular 2� 2 No 2� 2 SCT 1 4� 4 SCT
20 Shoulder 4.5� 4 Yes 4� 2.3 Fascia 2 7.5� 7.5 Fascia
21 Thorax 5.5� 3.5 Yes 3.9� 3.1 Fascia 2 8.5� 6 Muscle
22 Leg 3� 2 No 3.3� 3.3 SCT 1 5� 4 SCT
MRI = magnetic resonance imaging; SCT = subcutaneous cellular tissue.
Figure 1. Primary dermatofibrosarcoma protuberans (case 9). (A) Not infiltrated, 6.5-� 4-cm tumor located on the back.(B) Magnetic resonance image of a dermatofibrosarcoma protuberans limited to the subcutaneous tissue.
D E R M AT O L O G I C S U R G E RY4
C O R R E L AT I O N B E T W E E N M R I A N D S U R G I C A L M A R G I N S I N D F S P
was one in 13 cases, two in six cases, and three in
three cases. In all cases, the size of the defect created
after MMS was larger than the size of the tumor
shown by the MRI. Clinical palpation correctly de-
tected depth of infiltration in the primary DFSP cases
with a sensitivity of 58%, specificity of 90%, PPV of
87.5%, and NPV of 64.3%. The Spearman rho
correlation coefficient between clinical palpation
and histologic infiltration was 0.54 (p = .009) and
between the MRI image and the level of histologic
infiltration was 0.56 (p = .006). MRI was capable of
detecting the infiltration depth in primary DFSP
cases with a sensitivity of 67%, specificity of 100%,
PPV of 100%, and NPV of 71.4%. The results of the
clinical exploration and MRI in primary DFSP cases
are shown on Table 2.
Recurrent DFSP
Table 3 shows the location and level of infiltration
provided by the MRI and the level of histological
infiltration for the nine cases of recurrent DFSP. Of
the nine cases, three had previously undergone just
one surgical procedure, whereas in six cases, the
tumor had recurred on two or more occasions after
surgical excision (3 cases with 2 previous extirpa-
tions and 3 cases with 3 previous extirpations).
The results of the MRI as a test for detecting infil-
tration depth in recurrent DFSP were as follows:
sensitivity 60%, specificity 100%, PPV 100%, and
NPV 67% (Table 4). The Spearman rho correlation
coefficient between the infiltration depth studied
using MRI and the level of histologic infiltration was
0.51 (p = .16).
Extirpated DFSP with Positive Margins
Of the 12 recently extirpated cases of DFSP with
affected margins, the MRI reported tumor persis-
tence in five cases, tumor absence in two cases,
and uncertain interpretation in five cases. The
histologic study of these 12 cases showed tumor
persistence in 10 cases and only two cases in which
there were no tumors remain. The results of the
12 recently extirpated cases of DFSP with affected
margins and their locations are shown in Table 5.
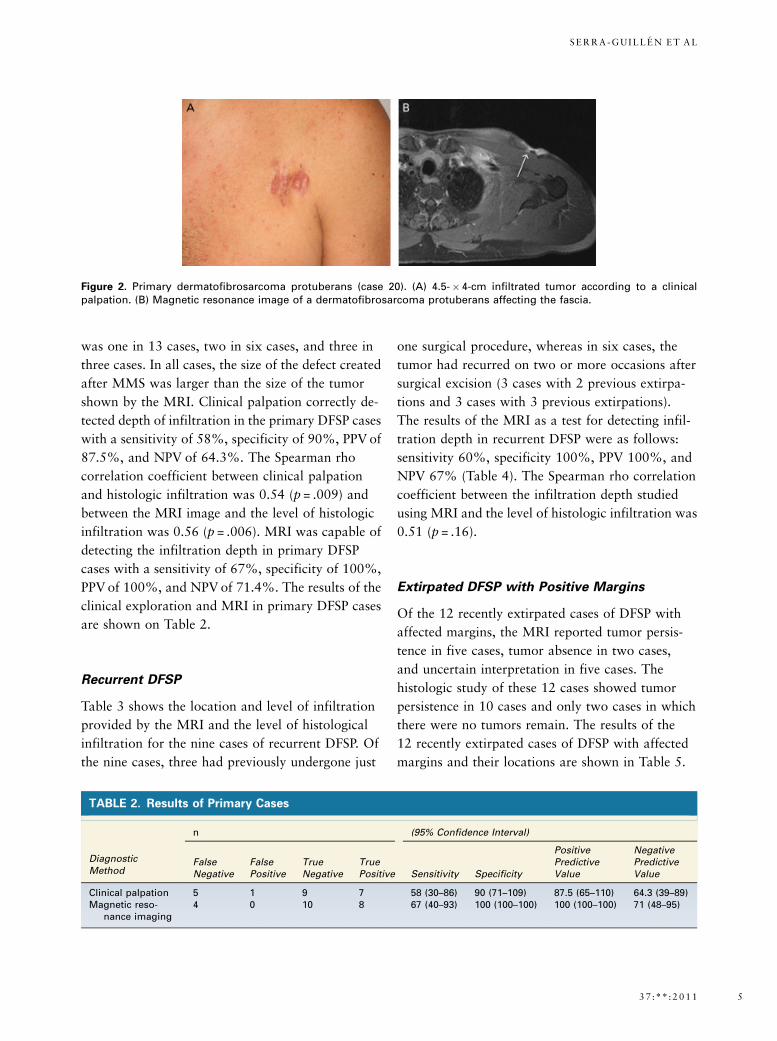
Figure 2. Primary dermatofibrosarcoma protuberans (case 20). (A) 4.5-�4-cm infiltrated tumor according to a clinicalpalpation. (B) Magnetic resonance image of a dermatofibrosarcoma protuberans affecting the fascia.
TABLE 2. Results of Primary Cases
DiagnosticMethod
n (95% Confidence Interval)
FalseNegative
FalsePositive
TrueNegative
TruePositive Sensitivity Specificity
PositivePredictiveValue
NegativePredictiveValue
Clinical palpation 5 1 9 7 58 (30–86) 90 (71–109) 87.5 (65–110) 64.3 (39–89)Magnetic reso-
nance imaging4 0 10 8 67 (40–93) 100 (100–100) 100 (100–100) 71 (48–95)
3 7 :* * : 2 0 1 1 5
S E R R A - G U I L L E N E T A L

Discussion
Clinical Palpation
Palpation is a routine exploratory technique used in
most cutaneous tumors; it offers information on the
consistency, extension, and infiltration depth. Be-
cause of the type of infiltrative growth of DFSP, it is
particularly important to determine the value of
palpation as a method for routine examination. Ac-
cording to our study, clinical palpation has limited
value for determining infiltration depth in primary
DFSP cases. We found that palpation had a sensi-
tivity of 58% for detecting in-depth invasion; this
may be considered low, because a high percentage of
cases (42%) were deemed superficial when in fact
they were deep. Moreover, the probability that a
tumor is superficial, when using palpation and being
diagnosed as such, is 64.3% (NPV). Nevertheless,
most of the deep DFSPs were identified correctly as
deeply infiltrated by clinical examination (PPV of
87.5%). In conclusion, clinical palpation is recom-
mended as a routine and accessible exploratory
method because it provides reliable information in
the majority of cases, even though it is important
to take into account the limitations due to the in-
filtrative nature of this tumor.
Magnetic Resonance Imaging
Although MRI is the imaging test most commonly
used in soft tissue tumors,10 little is known about its
value in the study of DFSP because there have been
few studies and publications addressing this.
Delimitation of Depth: According to our results,
MRI is of greater value than clinical palpation in
detecting depth of infiltration in primary DFSP cases
(sensitivity 58% for clinical palpation vs 67% for
MRI). MRI correctly reported all cases of DFSP
limited to the SCT as superficial (100% specificity),
and all the cases reported by MRI as deeply infil-
trated were also correctly identified (8 cases, PPV
100%). We found no relationship between tumor
size and accuracy of MRI in detecting depth of in-
filtration. Although MRI lost precision in determin-
ing depth of infiltration in tumors located in the
TABLE 3. Recurrent Cases
Case Location
Infiltration Plane in Magnetic
Resonance Imaging
Histologic Infiltration
Plane
Previous
Treatments
1 Suprascapular SCT Muscle 3
2 Shoulder Muscle Muscle 1
3 Back SCT SCT 3
4 Arm SCT SCT 1
5 Buttock Lack of tumor SCT 1
6 Foot SCT Muscle 2
7 Foot SCT SCT 2
8 Scapular Fascia Fascia 3
9 Scapular Fascia Fascia 2
SCT = subcutaneous cellular tissue.
TABLE 4. Results of Recurrent Cases
Diagnostic
Method
n (95% Confidence Interval)
False
Negative
False
Positive
True
Negative
True
Positive Sensitivity Specificity
Positive
Predictive
Value
Negative
Predictive
Value
Magnetic
resonance
imaging
2 0 4 3 60 (17–103) 100 (100–100) 100 (100–100) 67 (29–104)
D E R M AT O L O G I C S U R G E RY6
C O R R E L AT I O N B E T W E E N M R I A N D S U R G I C A L M A R G I N S I N D F S P

head, neck, and upper thorax, in seven of the eight
cases in these locations (cases 1, 6, 11, 13, 14, 16, 18,
and 21), MRI reported the affected plane to be more
superficial than it was. In this regard, as various
studies have shown,19–22 DFSPs on the head and neck
are particularly susceptible to a higher rate of recur-
rence than on the rest of the body. The fact that these
locations have the anatomic peculiarity that the mus-
cular plane is located close to the cutaneous surface,
where the skin is not as thick as in other locations,
may explain the poor prognosis for DFSP on the head
and neck to a certain extent. Furthermore, DFSP
spreads microscopically through the SCT septa to the
fascia and the muscle in a less obvious way than in
other locations and therefore goes unnoticed in con-
ventional histologic studies and apparently also on
MRI. Therefore, MRI seems to be useful and reliable
in primary DFSP when the tumor is located some-
where other than the head, neck, and upper thorax.
As for the utility of MRI in cases of recurrent DFSP,
our results show that it has a value similar to that
of primary cases, although with only nine cases, no
definitive conclusions can be drawn. There appears
to be no relationship between the number of previ-
ous treatments received by each person with DFSP
and better or poorer precision in detecting infiltra-
tion by MRI. Nevertheless, in all three cases with
only one recurrence of DFSP, MRI diagnosed the
exact plane of infiltration (2 in SCT and 1 in muscle),
unlike cases with two or more recurrences, in which
MRI was accurate in four cases but diagnosed the
infiltration in a plane less than the true depth in two
cases. In any event, more cases are needed to confirm
this trend.
Detection of Tumor Persistence in DFSP Excision
with Affected Margins: In five of the 12 DFSP cases
studied, MRI provided an uncertain image and was
therefore not considered useful for scheduling a re-
exeresis of the scar tissue. In the two cases in which
MRI showed tumor absence, DFSP remains were
found in the histologic study that would certainly
have resulted in a recurrence had they not been re-
moved. Therefore, MRI is not useful for detecting
tumor persistence in cases of recent incompletely
extirpated tumors.
Lateral Delimitation: Although imaging techniques
are generally considered unnecessary for delimiting
the lateral margins of DFSP, this study shows that, in
a majority of primary cases (19/22), MRI indicated a
smaller tumor size than clinical examination deter-
mined, and a smaller defect was created after exci-
sion by MMS. Therefore, considering that the lateral
limits of DFSP can extend microscopically as far as
12 cm from the macroscopic edge of the tumor,9
MRI is not recommended for determining lateral
extension in DFSP.
The fact that this series of DFSP contains a large
number of cases in which the histologic infiltration
goes beyond the SCT (12/22 primary DFSP cases and
TABLE 5. Extirpated DFSP with Positive Margins
Case Location
Tumoral Persistence in Magnetic
Resonance Imaging
Histologic Tumor
Persistence
1 Scalp Uncertain Persistence
2 Scapular Uncertain Persistence
3 Arm Persistence Persistence
4 Thorax Uncertain Persistence
5 Scalp Persistence Persistence
6 Thorax Persistence Absence
7 Supraclavicular Absence Persistence
8 Scalp Persistence Persistence
9 Shoulder Absence Persistence
10 Infraclavicular Uncertain Persistence
11 Cheek Persistence Persistence
12 Arm Uncertain Absence
3 7 :* * : 2 0 1 1 7
S E R R A - G U I L L E N E T A L

5/9 recurrent cases) could be perceived as a non-
representative sample because the DFSP usually is
limited to the SCT in most cases.2,23 This possible
bias is probably because the cases referred to our
department were particularly complex because of the
location or size of the tumor, and therefore the
possibility of deeper infiltration was greater.
In conclusion, to the best of our knowledge, we
present the largest series to date of DFSP cases
studied using MRI. According to our results, MRI is
superior to clinical palpation in detecting depth of
infiltration of DFSP. Although the best method for
determining depth of infiltration and lateral exten-
sion of DFSP is histologic analysis using MMS, MRI
can be useful as a preoperative study in primary
cases situated in locations other than the head, neck,
and upper thorax. In DFSPs in which the tumor
has been excised with positive margins, MRI is
not useful for determining the persistence of the
tumor. MRI does not appear to be useful for
determining the lateral limits of DFSP.
References
1. LeBoit P, Burg G, Weedon D, Sarasin A. Soft tissue tumors. In:
LeBoit P, Burg G, Weedon D, et al., editors. World Health Or-
ganization Classification of Tumors. Pathology and Genetics. Skin
Tumors. Lyon: IARC; 2006. p. 229–62.
2. Gloster HM Jr. Dermatofibrosarcoma protuberans. J Am Acad
Dermatol 1996;35:355–74.
3. Sanmartin O, Llombart B, Lopez-Guerrero JA, Serra C, et al.
Dermatofibrosarcoma protuberans. Actas Dermosifiliogr
2007;98:77–87.
4. Taylor HB, Helwig EB. Dermatofibrosarcoma protuberans. A
study of 115 cases. Cancer 1962;15:717–25.
5. McPeak CJ, Cruz T, Nicastri AD. Dermatofibrosarcoma protu-
berans: an analysis of 86 casesFfive with metastasis. Ann Surg
1967;166:803–16.
6. Hobbs ER, Wheeland RG, Bailin PL, Ratz JL, et al. Treatment of
dermatofibrosarcoma protuberans with Mohs micrographic sur-
gery. Ann Surg 1988;207:102–7.
7. Gloster HM Jr., Harris KR, Roenigk RK. A comparison between
Mohs micrographic surgery and wide surgical excision for the
treatment of dermatofibrosarcoma protuberans. J Am Acad
Dermatol 1996;35:82–7.
8. Dawes KW, Hanke CW. Dermatofibrosarcoma protuberans
treated with Mohs micrographic surgery: cure rates and surgical
margins. Dermatol Surg 1996;22:530–4.
9. Ratner D, Thomas CO, Johnson TM, Sondak VK, et al. Mohs
micrographic surgery for the treatment of dermatofibrosarcoma
protuberans. Results of a multiinstitutional series with an analysis
of the extent of microscopic spread. J Am Acad Dermatol
1997;37:600–13.
10. Murphey M, Kransdorf M. Radiologic evaluation of soft tissue
tumors. In: Weiss S, Goldblum JR, editors. Enzinger and Weiss’s
Soft Tissue Tumors. 5th ed. Philadelphia: Mosby; 2008. p. 33–71.
11. Kransdorf MJ, Meis-Kindblom JM. Dermatofibrosarcoma pro-
tuberans: radiologic appearance. Am J Roentgenol 1994;
163:391–4.
12. Riggs K, McGuigan KL, Morrison WB, Samie FH, et al. Role of
magnetic resonance imaging in perioperative assessment of dermato-
fibrosarcoma protuberans. Dermatol Surg 2009;35:2036–41.
13. Chen X, Chen YH, Zhang YL, Guo YM, et al. Magnetic reso-
nance imaging and mammographic appearance of dermatofibro-
sarcoma protuberans in a male breast: a case report and literature
review. J Med Case Reports 2009;3:8246–9.
14. Laffan EE, Ngan BY, Navarro OM. Pediatric soft-tissue tumors
and pseudotumors: MRI imaging features with pathologic corre-
lation: part 2. Tumors of fibroblastic/myofibroblastic, so-called
fibrohistiocytic, muscular, lymphomatous, neurogenic, hair ma-
trix, and uncertain origin. Radiographics 2009;29:e36.
15. Bergin P, Rezaei S, Lau Q, Coucher J. Dermatofibrosarcoma
protuberans, magnetic resonance imaging and pathological cor-
relation. Australas Radiol 2007;51Spec No.:B64–6.
16. Thornton SL, Reid J, Papay FA, Vidimos AT. Childhood
dermatofibrosarcoma protuberans: role of preoperative imaging.
J Am Acad Dermatol 2005;53:76–83.
17. Torreggiani WC, Al-Ismail K, Munk PL, Nicolaou S, et al.
Dermatofibrosarcoma protuberans: MRI imaging features. Am J
Roentgenol 2002;178:989–93.
18. Hafner J, Schutz K, Morgenthaler W, Steiger E, et al. Micro-
graphic surgery (‘slow Mohs’) in cutaneous sarcomas. Dermatol-
ogy 1999;198:37–43.
19. Paradisi A, Abeni D, Rusciani A, Cigna E, et al. Dermatofibro-
sarcoma protuberans: wide local excision vs. Mohs micrographic
surgery. Cancer Treat Rev 2008;34:728–36.
20. Gayner SM, Lewis JE, McCaffrey TV. Effect of resection margins
on dermatofibrosarcoma protuberans of the head and neck. Arch
Otolaryngol Head Neck Surg 1997;123:430–3.
21. Tom WD, Hybarger CP, Rasgon BM. Dermatofibrosarcoma pro-
tuberans of the head and neck: treatment with Mohs surgery using
inverted horizontal paraffin sections. Laryngoscope
2003;113:1289–93.
22. Loss L, Zeitouni NC. Management of scalp dermatofibrosarcoma
protuberans. Dermatol Surg 2005;31:1428–33.
23. Bowne WB, Antonescu CR, Leung DH, Katz SC, et al. Dermato-
fibrosarcoma protuberans: a clinicopathologic analysis of patients
treated and followed at a single institution. Cancer 2000;88:2711–20.
Address correspondence and reprint requests to: CarlosSerra-Guillen, MD, Department of Dermatology, InstitutoValenciano de Oncologıa, C/Beltran Baguena 4, 46009Valencia, Spain, or e-mail: [email protected]
D E R M AT O L O G I C S U R G E RY8
C O R R E L AT I O N B E T W E E N M R I A N D S U R G I C A L M A R G I N S I N D F S P
Copyright © 2022 FDOKUMEN




















