Core Review
22
Copyright © 2012 International Anethesia Research Society. Unauthorized reproduction of this article is prohibited. XXX 2012 • Volume X • Number X www.anesthesia-analgesia.org 1 Author affiliations are provided at the end of the article. Accepted for publication July 3, 2012. Supplemental digital content is available for this article. Direct URL citations appear in the printed text and are provided in the HTML and PDF versions of this article on the journal’s Web site (www.anesthesia-analgesia.org). See Disclosures at end of article for Author Conflicts of Interest. Reprints will not be available from the authors. Address correspondence to Colin F. Royse, MBBS, MD, FANZCA, Department of Surgery, The University of Melbourne, 245 Cardigan St., Carlton, Victoria, Australia, 3053. Address e-mail to [email protected]. Copyright © 2012 International Anesthesia Research Society DOI: 10.1213/ANE.0b013e31826a79c1 “An invasion of armies can be resisted, but not an idea whose time has come.” —Victor Hugo REVIEW STRUCTURE In this review, we describe the evolution of physician- performed ultrasound in anesthesia and critical care medi- cine, including the relevance of developments in technology. The concept of an expertise pyramid and levels of proficiency are discussed. Uses of point-of-care ultrasound are detailed for transesophageal echocardiography (TEE), transthoracic echocardiography (TTE), lung ultrasound, vascular access, regional anesthesia, and goal-focused TTE. The final section addresses training and future directions. ULTRASOUND FOR NONCARDIOLOGISTS—WHERE DID IT START? The first ultrasound machines were developed in the 1950s, based on sonar technology developed in World War II. 1 Over the next 3 decades, this technology was developed commercially and became widely adopted by cardiologists, radiologists, and obstetric physicians. The equipment was bulky and very expensive, and the imaging was of relatively poor quality compared with today’s standards. This limited the technology to major facilities such as diagnostic labo- ratories or the cardiac surgery operating room. Ultrasound entered anesthesiology practice in the late 1980s with the introduction of intraoperative TEE for cardiac surgery. 2 Paradoxically, this delayed the widespread adoption of ultrasound into anesthesiology practice because of the inva- sive nature of TEE and its complications. 3,4 The requirement for sedation or anesthesia, and the need for a high level of diagnostic knowledge by the cardiac anesthesiologists 5,6 equivalent to cardiologists tended to exclude physicians who wished to use ultrasound at a more qualitative level. Those unable to perform a full cardiologist level diagnostic study were considered inadequately trained and therefore should be prevented from accessing the technology. Thus, perioperative echocardiography was seen as the domain of the expert, who generally was the cardiac anesthesiologist. Smaller, robust, less-expensive, yet high-quality ultra- sound machines were a necessary precursor to greater use of ultrasound, but equally important was a mindset change to consider surface ultrasound applications, including TTE and ultrasound-guided procedures, as important areas for noncardiac anesthesiologists. In parallel, but somewhat delayed in time, other acute care specialties adopted similar changes in view and ultrasound usage. The changing role of ultrasound can be viewed in evolu- tionary terms. The early stage is when discreet ultrasound examinations are performed by diagnostic laboratories, usually by technologists and reported by cardiologists or radiologists, and the treating clinician subsequently reviews a written report. These tend to be comprehen- sive examinations that are interpreted in-depth by highly trained physicians, but with often considerable delay in delivery of the information to the treating physician. The middle stage is the current practice of point-of-care ultra- sound examination. The big transition has been the use of ultrasound at the point-of-care by the treating physician Core Review: Physician-Performed Ultrasound: The Time Has Come for Routine Use in Acute Care Medicine Colin F. Royse, MBBS, MD, FANZCA,*† David J. Canty, MBBS, FANZCA, PGDipEcho,*‡§|| John Faris, MBChB, DAvMed, FAFOM, FFOM, FANZCA, BA, ASCeXAM, PGDipClinUs,¶#**†† Darsim L. Haji, MBChB, FACEM, PGDipEcho,‡‡ Michael Veltman, MBBS, FANZCA, ASCExam, FASE,¶#**§§ and Alistair Royse, MBBS, MD, FRACS, FCSANZ|||| The use of ultrasound in the acute care specialties of anesthesiology, intensive care, emer- gency medicine, and surgery has evolved from discrete, office-based echocardiographic examinations to the real-time or point-of-care clinical assessment and interventions. “Goal- focused” transthoracic echocardiography is a limited scope (as compared with comprehen- sive examination) echocardiographic examination, performed by the treating clinician in acute care medical practice, and is aimed at addressing specific clinical concerns. In the future, the practice of surface ultrasound will be integrated into the everyday clinical practice as ultrasound-assisted examination and ultrasound-guided procedures. This evolution should start at the medical student level and be reinforced throughout specialist training. The key to making ultrasound available to every physician is through education programs designed to facili- tate uptake, rather than to prevent access to this technology and education by specialist craft groups. There is evidence that diagnosis is improved with ultrasound examination, yet data showing change in management and improvement in patient outcome are few and an impor- tant area for future research. (Anesth Analg 2012;X:•••–•••) E CORE REVIEW ARTICLE
Transcript of Core Review

Copyright © 2012 International Anethesia Research Society. Unauthorized reproduction of this article is prohibited.Copyright © 2012 International Anethesia Research Society. Unauthorized reproduction of this article is prohibited.XXX 2012 • Volume X • Number X www.anesthesia-analgesia.org 1
Author affiliations are provided at the end of the article.
Accepted for publication July 3, 2012.
Supplemental digital content is available for this article. Direct URL citations appear in the printed text and are provided in the HTML and PDF versions of this article on the journal’s Web site (www. anesthesia- analgesia.org).
See Disclosures at end of article for Author Conflicts of Interest.
Reprints will not be available from the authors.
Address correspondence to Colin F. Royse, MBBS, MD, FANZCA, Department of Surgery, The University of Melbourne, 245 Cardigan St., Carlton, Victoria, Australia, 3053. Address e- mail to [email protected].
Copyright © 2012 International Anesthesia Research SocietyDOI: 10.1213/ANE.0b013e31826a79c1
“An invasion of armies can be resisted, but not an idea whose time has come.”
—Victor Hugo
REVIEW STRUCTUREIn this review, we describe the evolution of physician- performed ultrasound in anesthesia and critical care medi-cine, including the relevance of developments in technology. The concept of an expertise pyramid and levels of proficiency are discussed. Uses of point- of- care ultrasound are detailed for transesophageal echocardiography (TEE), transthoracic echocardiography (TTE), lung ultrasound, vascular access, regional anesthesia, and goal- focused TTE. The final section addresses training and future directions.
ULTRASOUND FOR NONCARDIOLOGISTS—WHERE DID IT START?The first ultrasound machines were developed in the 1950s, based on sonar technology developed in World War II.1 Over the next 3 decades, this technology was developed commercially and became widely adopted by cardiologists, radiologists, and obstetric physicians. The equipment was bulky and very expensive, and the imaging was of relatively poor quality compared with today’s standards. This limited
the technology to major facilities such as diagnostic labo-ratories or the cardiac surgery operating room. Ultrasound entered anesthesiology practice in the late 1980s with the introduction of intraoperative TEE for cardiac surgery.2 Paradoxically, this delayed the widespread adoption of ultrasound into anesthesiology practice because of the inva-sive nature of TEE and its complications.3,4 The requirement for sedation or anesthesia, and the need for a high level of diagnostic knowledge by the cardiac anesthesiologists5,6 equivalent to cardiologists tended to exclude physicians who wished to use ultrasound at a more qualitative level. Those unable to perform a full cardiologist level diagnostic study were considered inadequately trained and therefore should be prevented from accessing the technology. Thus, perioperative echocardiography was seen as the domain of the expert, who generally was the cardiac anesthesiologist.
Smaller, robust, less- expensive, yet high- quality ultra-sound machines were a necessary precursor to greater use of ultrasound, but equally important was a mindset change to consider surface ultrasound applications, including TTE and ultrasound- guided procedures, as important areas for noncardiac anesthesiologists. In parallel, but somewhat delayed in time, other acute care specialties adopted similar changes in view and ultrasound usage.
The changing role of ultrasound can be viewed in evolu-tionary terms. The early stage is when discreet ultrasound examinations are performed by diagnostic laboratories, usually by technologists and reported by cardiologists or radiologists, and the treating clinician subsequently reviews a written report. These tend to be comprehen-sive examinations that are interpreted in- depth by highly trained physicians, but with often considerable delay in delivery of the information to the treating physician. The middle stage is the current practice of point- of- care ultra-sound examination. The big transition has been the use of ultrasound at the point- of- care by the treating physician
Core Review: Physician- Performed Ultrasound: The Time Has Come for Routine Use in Acute Care MedicineColin F. Royse, MBBS, MD, FANZCA,*† David J. Canty, MBBS, FANZCA, PGDipEcho,*‡§|| John Faris, MBChB, DAvMed, FAFOM, FFOM, FANZCA, BA, ASCeXAM, PGDipClinUs,¶#**†† Darsim L. Haji, MBChB, FACEM, PGDipEcho,‡‡ Michael Veltman, MBBS, FANZCA, ASCExam, FASE,¶#**§§ and Alistair Royse, MBBS, MD, FRACS, FCSANZ||||
The use of ultrasound in the acute care specialties of anesthesiology, intensive care, emer-gency medicine, and surgery has evolved from discrete, office- based echocardiographic examinations to the real- time or point- of- care clinical assessment and interventions. “Goal-focused” transthoracic echocardiography is a limited scope (as compared with comprehen-sive examination) echocardiographic examination, performed by the treating clinician in acute care medical practice, and is aimed at addressing specific clinical concerns. In the future, the practice of surface ultrasound will be integrated into the everyday clinical practice as ultrasound- assisted examination and ultrasound- guided procedures. This evolution should start at the medical student level and be reinforced throughout specialist training. The key to making ultrasound available to every physician is through education programs designed to facili-tate uptake, rather than to prevent access to this technology and education by specialist craft groups. There is evidence that diagnosis is improved with ultrasound examination, yet data showing change in management and improvement in patient outcome are few and an impor-tant area for future research. (Anesth Analg 2012;X:•••–•••)
E CORE REVIEW ARTICLE

Copyright © 2012 International Anethesia Research Society. Unauthorized reproduction of this article is prohibited.
E CORE REVIEW ARTICLE
2 www.anesthesia-analgesia.org ANESTHESIA & ANALGESIA
rather than by a cardiology or radiology service. In car-diac anesthesiology, this involves comprehensive TEE during the operation by the anesthesiologist. For the acute care specialties, this includes goal- focused TTE7 and TEE, ultrasound- guided regional anesthesia8 (including neuraxial9,10 and truncal11 blocks), vascular access,12 and lung13 and pleural scans.14 For the emergency physician, this could also include the FAST abdominal scan (Focused Assessment with Sonography for Trauma).15 The next stage of evolution will be when we incorporate ultrasound into everyday practice rather than performing separate ultra-sound examinations, i.e., ultrasound- assisted examina-tion and ultrasound- guided procedures. Consequently, goal- focused TTE becomes “ ultrasound- assisted examina-tion of the heart,” a lung scan becomes “ ultrasound- assisted examination of the chest,” whereas nerve blocks, vascular access, and pleural drainage become “ ultrasound- guided procedures.” With this evolution, the range and uses of ultrasound will expand dramatically to improve exami-nation of the abdomen, joints, legs (for deep vein throm-bosis), airway, and examinations to help guide physicians during resuscitation and trauma. Expertise in ultrasound by the anesthesiologist may also be useful in assisting the surgeon intraoperatively for direct organ imaging such as of the aorta, liver, kidneys, and lymph nodes, because the skill set of ultrasound use and knowledge is transferable to examination of other body areas. Equally, the surgeon may use the same skill set preoperatively when assessing the patient, or transfer these techniques for direct imaging of internal organs during the operation by placing the probe in a sterile sheath.
THE ROLE OF TECHNOLOGY IN THE EVOLUTION OF ULTRASOUND USEThere is little doubt that advances in ultrasound technol-ogy including reduced equipment size and price have had a major role in the expansion of its use outside of cardiology or radiology. The concept of limited training and the “ultra-sound stethoscope” is not new, but required small, portable technology with adequate image fidelity.
The first generation of portable devices (large desktop computer–sized machines built into a console with wheels) were used principally for TTE and general ultrasound in patients in intensive care, who were too sick to transport to other departments. Inferior imaging ability made more difficult by mechanical ventilation mostly limited their use to abdominal, pelvic, and vascular ultrasound or to office- based TTE. The second generation mobile machines were smaller (laptop computer sized and detachable from a trolley) and had improved imaging capability, nota-bly harmonic imaging, which was a key step forward in mobile TTE. Unfortunately, further miniaturization into hand- carried ultrasound (HCU) systems weighing typi-cally <6 pounds had inferior image quality and lacked echocardiographic modalities used for quantification (par-ticularly spectral pulsed and continuous wave Doppler). There was a greater risk of missing clinically important pathology than by cart- based systems, and this raised con-cern that the use of this technology could lead to patient harm. A position paper was released by the American
Society of Echocardiography in 2002, cautioning practi-tioners to restrict the level of interpretation to the ability of the HCU device.16 This position statement was remark-able in that it predicted many developments that have occurred since then. Importantly, the American Society of Echocardiography task force endorsed the concept of ultrasound- assisted examination stating that it “believes that this technology will extend the concept of the ‘com-plete physical examination,’ allowing more rapid assess-ment of cardiovascular anatomy, function, and physiology.” Furthermore, the evolution of portable ultrasound systems was predicted: “Because the small HCU device may evolve into a full diagnostic device, its use and dissemination will not rest simply on the size of the instrument but on the indi-vidual user and his or her understanding of and response to the information imparted.” In a more recent position paper on focused cardiac ultrasound in the emergent set-ting,17 the American Society of Echocardiography acknowl-edged the use of HCU in ultrasound- assisted examination by noncardiologists. The consensus group recommended choice of ultrasound platform to be “scaled” to the exper-tise of the operator and intended uses, including noncar-diac (e.g., vascular, abdominal, pelvic), which may not be available yet in the HCU devices. The predictions in 2002 have largely been correct with regard to the enormous tech-nological advancement, such that the portable machines of today are fully capable echocardiography systems capable of multiple imaging applications. The limitations imposed by technology in 2002 are largely irrelevant in 2012. In very recent times, however, there has been introduction of even smaller ultrasound systems, capable of fitting into a coat pocket or palm. This latest evolution holds the greatest promise for integration of ultrasound into bedside exami-nation, because of the enhanced portability. However, as in 2002, these HCU devices have limited abilities and the evidence of their utility is still emerging.
THE EXPERTISE PYRAMIDThe concept of an expertise pyramid is shown in Figure 1. Ultrasound- assisted examination is at the broad base of the pyramid, and it is envisaged that the majority of acute care specialists should be able to obtain this level of exper-tise. At the top of the pyramid are the highly trained and qualified experts in ultrasound. It is likely that high- level expertise will be restricted to one specific area, such as echo-cardiography (TTE or TEE), abdominal ultrasound, or chest ultrasound, and will include specialists from acute care disciplines as well as radiologists and cardiologists. The achievement of high- level expertise will be dependent on the level of ultrasound training rather than traditional spe-cialist craft groups. The middle of the pyramid is a space where physicians may develop moderately advanced skill and knowledge in a specific area (such as TTE) with good general knowledge and skills in ultrasound. It is also a tran-sition zone, as practitioners start at the ultrasound- assisted examination level, increase the expertise to become a “good basic sonographer” before ultimately becoming “an expert.” It is envisaged that supervision and mentorship will be pro-vided by practitioners who are at one level higher in experi-ence than the trainee.
Copyright © 2012 International Anethesia Research Society. Unauthorized reproduction of this article is prohibited.Copyright © 2012 International Anethesia Research Society. Unauthorized reproduction of this article is prohibited.
Routine Physician- Performed Ultrasound
XXX 2012 • Volume X • Number X www.anesthesia-analgesia.org 3
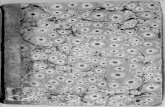
Video 1. Parasternal long- axis view showing a normal heart.
Video 2. Parasternal short- axis view showing a normal heart.
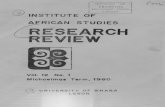
Video 3. Parasternal long- axis view showing aortic stenosis.
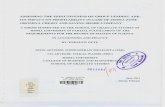
Video 4. Parasternal short- axis view showing aortic stenosis.
Video 5. Parasternal long- axis view showing right ventricular failure.
Video 6. Parasternal short- axis view showing right ventricular (RV) failure. Note the appearance of the RV and left ventricle (LV) as “a pair of eyes” looking at you, and indicating a large RV. Note also the “D” shape of the LV.
The concept of an expertise pyramid is widely incor-porated into recommendations by learned societies and accreditation bodies on what is required to achieve com-petency. A summary of these recommendations is shown in Table 1. The majority of published recommendations are heavily focused on number of cases performed and various levels of supervision, and requirement for examinations. There are some recommendations in which knowledge and practical skills are separated, for example, the diploma
of diagnostic ultrasound by the Australian Institute of Ultrasound. Achieving competency in knowledge (as dis-tinct from practical skill) is tested either via an examina-tion process or via completion of approved short courses. The Australian and New Zealand College of Anaesthetists’ recommendation, PS46 for TEE competency, is an example

Copyright © 2012 International Anethesia Research Society. Unauthorized reproduction of this article is prohibited.
E CORE REVIEW ARTICLE
4 www.anesthesia-analgesia.org ANESTHESIA & ANALGESIA
of this for which there are multiple pathways available for achieving the knowledge base.a These include recognized fellowships, the University of Melbourne Postgraduate Diploma course, or completion of the NBE PTEeXAM.
Intensive CareRecently, several roundtable consensus statements have been published on recommendations for ultrasound use by intensive care physicians, which define competencies and support the concept of the expertise pyramid. Mayo et al.18 report on consensus definitions for general and cardiac ultrasound, including basic and advanced applications, and the competencies required to achieve each level. The International Expert Statement on training standards for critical care ultrasonography19 was a consensus of 29 societ-ies, and recommended categories of general ultrasound and basic and advanced cardiac ultrasound. There was com-plete agreement among the participants that general critical care ultrasound and “basic” critical care echocardiogra-phy should be mandatory in the curriculum of intensive care unit (ICU) physicians. Volpicelli et al.20 reported on a consensus agreement on the implementation of lung ultra-sound. The ideal training pathway for physician- performed ultrasound, irrespective of the modality and scope of prac-tice, would include supervised acquisition and assess-ment of knowledge base, practical skill, and interpretation of images. Ultimately, the specific pathways for achiev-ing competence will be determined by specialist societies and credentialing requirements for practice at individual institutions.
AnesthesiologyFor anesthesiology, the historical development of ultra-sound use excluded the majority of practitioners. The major problem with the expertise pyramid is that echocardiogra-phy started with TEE for cardiac surgery, which required a full diagnostic level of knowledge and expertise to be gained in the first instance. Essentially, the pyramid was turned upside down so that one had to be at the top of the pyramid in expertise to commence using the technology. This had the
profound effect of limiting opportunity for noncardiac anes-thesiologists to adopt the technology, because the time and effort to achieve competency was well beyond their clinical scope or opportunity. Furthermore, in the operating room, TEE rapidly became “the domain of the cardiac anesthesiol-ogist,” whereas TTE and other surface ultrasound applica-tions remained the domain of cardiologists and radiologists.
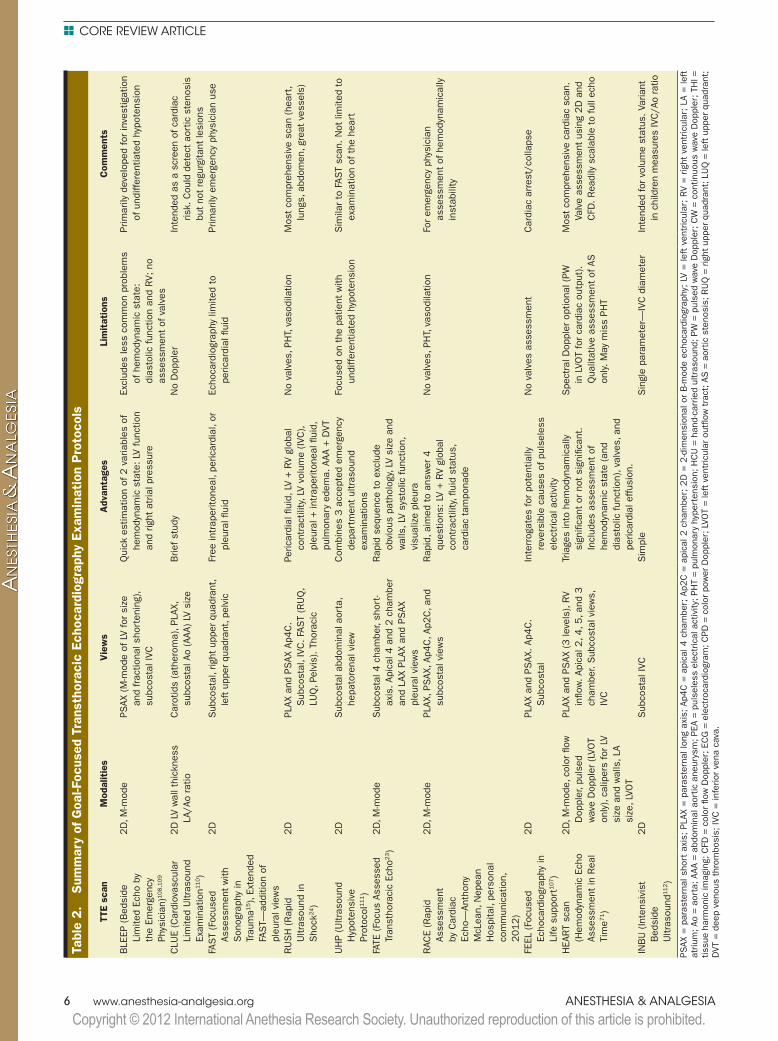
This paradigm, however, is changing with the incor-poration of point- of- care ultrasound use.21 In this middle stage of evolution, point- of- care applications that are well established include ultrasound- guided regional anesthesia, goal- focused TTE (e.g., Hemodynamic Echocardiography Assessment in Real Time [HEART] scan22 or Focused Assessed Transthoracic Echocardiography [FATE]23), and abdominal scanning for trauma (e.g., Focused Assessment with Sonography in Trauma [FAST]15 or Rapid Ultrasound in Shock [RUSH]24) with other uses, such as lung imaging,25 deep vein thrombosis assessment,26 and soft tissue injury27 assessment, developing as the emerging uses. A summary of named goal- focused studies is shown in (Table 2). Importantly, there is a change in emphasis toward accept-ing a limited knowledge base and use of pattern recog-nition of pathology, and a reduced number of cases in training to achieve competence for goal- focused examina-tion. This has facilitated the uptake of ultrasound technol-ogy at a basic level by a much wider group of acute care specialists. Goal- focused echocardiography, however, is not intended to be a state- of- the- art, comprehensive echo-cardiography assessment, but is about identifying clini-cally important cardiac pathology to determine whether patients are at risk for hemodynamic compromise and to guide specific hemodynamic treatment.
Ultimately, broad- base integration of ultrasound technology into clinical practice requires teaching and acceptance at a medical school level, and this is gain-ing popularity. An ultrasound curriculum was success-fully implemented across all 4 years of medical school at the University of South Carolina School of Medicine in 2006.28 The curriculum was based on a point- of- care pro-gram that was developed for emergency medicine physi-cians with a broad coverage of ultrasound specialties. It was well received by the students and teachers, and simi-lar programs have since been increasingly implemented at other institutions from the entire curriculum29 to shorter
Figure 1. The “expertise pyramid.” Four lev-els of expertise are shown, starting with ultrasound- assisted examination, suitable for all physicians, and the “star” at the top of the pyra-mid representing teachers, supervisors of train-ing, or heads of echocardiography laboratories. TEE = transesophageal echocardiography; TTE = transthoracic echocardiography.
a ANZCA Professional Document PS46 Recommendations for Training and Practice of Diagnostic Perioperative Transoesophageal Echocardiography in Adults, 2004.

Copyright © 2012 International Anethesia Research Society. Unauthorized reproduction of this article is prohibited.Copyright © 2012 International Anethesia Research Society. Unauthorized reproduction of this article is prohibited.
Routine Physician- Performed Ultrasound
XXX 2012 • Volume X • Number X www.anesthesia-analgesia.org 5
Table 1. Society- Defined Guidelines for Training and Achieving Competence in Echocardiography
Country–organization Level of training Scope Studies performed/reviewed
Assessment
Anesthesiology (intraoperative TEE)
USA–NBA/SCA Basic Monitoring 50/100 TEE Basic PTEeXAM
Advanced Diagnostic +150 TEE Advanced PTEeXAM
UK/Europe–ACTA/EACTA Advanced Comprehensive and perioperative TEE
125 TEE75 TEE if already accredited
for TTE
125 reports + 5 with images, supervisor reports and exam
Australia/NZ–ANZCA Advanced Diagnostic 100/100 TEE initial+30/50 per year to maintain
competency
One of the following:• Diploma of Clinical
Ultrasound• Advanced PTEeXAM• Diploma of Diagnostic
Ultrasound• Recognized fellowship
in TEE
Cardiology (TTE + TEE), not intraoperative TEE
USA–ASE TTELevel 1 – 3 monthsLevel 2 – 3 monthsLevel 3 – 6 months
Intraoperative TEE as per NBE
Basic TTEComprehensive TTEAble to direct an echo
laboratory
75/75+75/75+150/300
Maintain signed logbookMaintain signed logbookExam—ASCeXAM
UK–BSE TTETEE
250 TTEAs per ACTA above
250 reports, 5 full cases, supervisor reports, and exam
Australia/NZ–Cardiac Society
Acquired during cardiology training
TTETEE
300/300 (50 TEE)+200 per year
Maintain signed logbook No formal assessment
Advanced training (fellowship)
100/100+25 per year
Maintain signed logbook No formal assessment
Radiology
Australia–ASUM DDU – Part 1DDU – Part 2
Specialty specificSpecialty specific
Not specifiedNot specified
Written examWritten + oral exam +5 full case studies
Emergency and intensive care medicine (TEE, TTE + surface ultrasound)
UK–emergency medicine Level 1 Cardiac arrest/shock FAST107/vascular access
50 Maintain signed logbook, competency based assessment
Level 2 (draft) Multiple organ systems 3–5 per week Level 2 not yet established
UK–intensive care General Abdominal, pleural lung, vascular
Not specified For general, basic and advanced echo: logbook with reports verified by a qualified supervisor
Expert round table19,20 Basic echo Basic TTE 30 Certification not mandatory
Advanced echo Fully supervised TTE and fully supervised TEE
150 TTE, 50 TEE
SCA = Society of Cardiovascular Anesthesiologists; NBE = National Board of Echocardiography; TEE = transesophageal echocardiography; PTEeXAM = examination of special competence in advanced perioperative transesophageal echocardiography; ACTA = Association of Cardiothoracic Anaesthetists of Great Britain; EACTA = European Association of Cardiothoracic Anaesthetists; ANZCA = Australian and New Zealand College of Anaesthetists; ASE = American Society of Echocardiography; ASCeXAM = examination of special competence in adult echocardiography; TTE = transthoracic echocardiography; BSE = British Society of Echocardiography; ASUM = Australian Society of Ultrasound Medicine; DDU = Diploma of Diagnostic Ultrasound; FAST = Focused Assessment with Sonography in Trauma.
teaching programs.30–35 The rapid, widespread uptake of ultrasound into undergraduate teaching was presented at the inaugural world congress on ultrasound in medical education in 2011.36
IS USING ULTRASOUND EFFECTIVE?Point- of- care ultrasound examination provides diagnostic information to the clinician, which may aid clinical assess-ment and decision- making, hence ultrasound machines are
Copyright © 2012 International Anethesia Research Society. Unauthorized reproduction of this article is prohibited.
E CORE REVIEW ARTICLE
6 www.anesthesia-analgesia.org ANESTHESIA & ANALGESIA
Tabl
e 2.
Sum
mar
y of
Goa
l- Foc
used
Tra
nsth
orac
ic E
choc
ardi
ogra
phy
Exam
inat
ion
Pro
toco
ls
TTE
scan
Mod
alit
ies
Vie
ws
Adv
anta
ges
Lim
itat
ions
Com
men
ts
BLE
EP (B
edsi
de
Lim
ited
Echo
by
the
Emer
genc
y Ph
ysic
ian)
108,1
09
2D
, M-m
ode
PSAX
( M
- mod
e of
LV
for
size
an
d fr
actio
nal s
hort
enin
g),
subc
osta
l IVC
Qui
ck e
stim
atio
n of
2 v
aria
bles
of
hem
odyn
amic
sta
te: LV
fun
ctio
n an
d rig
ht a
tria
l pre
ssur
e
Excl
udes
less
com
mon
pro
blem
s of
hem
odyn
amic
sta
te:
dias
tolic
fun
ctio
n an
d RV;
no
asse
ssm
ent
of v
alve
s
Prim
arily
dev
elop
ed for
inve
stig
atio
n of
und
iffer
entia
ted
hypo
tens
ion
CLU
E (C
ardi
ovas
cula
r Li
mite
d U
ltras
ound
Ex
amin
atio
n110)
2D
LV
wal
l thi
ckne
ss
LA/A
o ra
tioC
arot
ids
(ath
erom
a), P
LAX,
su
bcos
tal A
o (A
AA) LV
siz
eB
rief st
udy
No
Dop
pler
Inte
nded
as
a sc
reen
of ca
rdia
c ris
k. C
ould
det
ect
aort
ic s
teno
sis
but
not
regu
rgita
nt le
sion
sFA
ST
(Foc
used
As
sess
men
t w
ith
Son
ogra
phy
in
Trau
ma1
5),
Exte
nded
FA
ST—
addi
tion
of
pleu
ral v
iew
s
2D
Sub
cost
al, r
ight
upp
er q
uadr
ant,
left
upp
er q
uadr
ant,
pelv
icFr
ee in
trap
erito
neal
, per
icar
dial
, or
pleu
ral fl
uid
Echo
card
iogr
aphy
lim
ited
to
peric
ardi
al fl
uid
Prim
arily
em
erge
ncy
phys
icia
n us
e
RU
SH
(R
apid
U
ltras
ound
in
Sho
ck24)
2D
PLAX
and
PS
AX A
p4C
. S
ubco
stal
, IVC
. FA
ST
(RU
Q,
LUQ
, Pel
vis)
. Th
orac
ic
Peric
ardi
al fl
uid,
LV
+ R
V gl
obal
co
ntra
ctili
ty, L
V vo
lum
e (IV
C),
pleu
ral +
intr
aper
itone
al fl
uid,
pu
lmon
ary
edem
a. A
AA +
DVT
No
valv
es, P
HT, v
asod
ilatio
nM
ost
com
preh
ensi
ve s
can
(hea
rt,
lung
s, a
bdom
en, g
reat
ves
sels
)
UH
P (U
ltras
ound
H
ypot
ensi
ve
Prot
ocol
111)
2D
Sub
cost
al a
bdom
inal
aor
ta,
hepa
tore
nal v
iew
Com
bine
s 3 a
ccep
ted
emer
genc
y de
part
men
t ul
tras
ound
ex
amin
atio
ns
Focu
sed
on t
he p
atie
nt w
ith
undi
ffer
entia
ted
hypo
tens
ion
Sim
ilar
to F
AST
scan
. N
ot li
mite
d to
ex
amin
atio
n of
the
hea
rt
FATE
(Fo
cus
Asse
ssed
Tr
anst
hora
cic
Echo
23)
2D
, M-m
ode
Sub
cost
al 4
cha
mbe
r, sh
ort-
axis
. Ap
ical
4 a
nd 2
cha
mbe
r an
d LA
X PL
AX a
nd P
SAX
pl
eura
l vie
ws
Rap
id s
eque
nce
to e
xclu
de
obvi
ous
path
olog
y, L
V si
ze a
nd
wal
ls, L
V sy
stol
ic fun
ctio
n,
visu
aliz
e pl
eura
RAC
E (R
apid
As
sess
men
t by
Car
diac
Ec
ho—
Anth
ony
McL
ean,
Nep
ean
Hos
pita
l, pe
rson
al
com
mun
icat
ion,
2012)
2D
, M-m
ode
PLAX
, PS
AX, A
p4C
, Ap2
C, a
nd
subc
osta
l vie
ws
Rap
id, a
imed
to
answ
er 4
qu
estio
ns: LV
+ R
V gl
obal
co
ntra
ctili
ty, fl
uid
stat
us,
card
iac
tam
pona
de
No
valv
es, P
HT, v
asod
ilatio
nFo
r em
erge
ncy
phys
icia
n as
sess
men
t of
hem
odyn
amic
ally
in
stab
ility
FEEL
(Fo
cuse
d Ec
hoca
rdio
grap
hy in
Li
fe s
uppo
rt107)
2D
PLAX
and
PS
AX. Ap
4C
. S
ubco
stal
Inte
rrog
ates
for
pot
entia
lly
reve
rsib
le c
ause
s of
pul
sele
ss
elec
tric
al a
ctiv
ity
No
valv
es a
sses
smen
tC
ardi
ac a
rres
t/co
llaps
e
HEA
RT
scan
(H
emod
ynam
ic E
cho
Asse
ssm
ent
in R
eal
Tim
e71)
2D
, M- m
ode,
col
or fl
ow
Dop
pler
, pul
sed
wav
e D
oppl
er (LV
OT
only
), ca
liper
s fo
r LV
si
ze a
nd w
alls
, LA
size
, LVO
T
PLAX
and
PS
AX (3 le
vels
), RV
inflo
w. Ap
ical
2, 4
, 5, a
nd 3
ch
ambe
r. S
ubco
stal
vie
ws,
IV
C
Tria
ges
into
hem
odyn
amic
ally
si
gnifi
cant
or
not
sign
ifica
nt.
Incl
udes
ass
essm
ent
of
hem
odyn
amic
sta
te (an
d di
asto
lic fun
ctio
n), v
alve
s, a
nd
peric
ardi
al e
ffus
ion.
Spe
ctra
l Dop
pler
opt
iona
l (PW
in
LVO
T fo
r ca
rdia
c ou
tput
).
Qua
litat
ive
asse
ssm
ent
of A
S
only.
May
mis
s PH
T
Mos
t co
mpr
ehen
sive
car
diac
sca
n.
Valv
e as
sess
men
t us
ing
2D
and
C
FD. R
eadi
ly s
cala
ble
to ful
l ech
o
INB
U (In
tens
ivis
t B
edsi
de
Ultr
asou
nd112)
2D
Sub
cost
al IV
CS
impl
eS
ingl
e pa
ram
eter
—IV
C d
iam
eter
Inte
nded
for
vol
ume
stat
us. Va
riant
in
chi
ldre
n m
easu
res
IVC
/Ao
ratio
PSAX
= p
aras
tern
al s
hort
axi
s; P
LAX
= p
aras
tern
al lo
ng a
xis;
Ap4
C =
api
cal 4
cha
mbe
r; A
p2C
= a
pica
l 2 c
ham
ber;
2D
= 2
-dim
ensi
onal
or
B- m
ode
echo
card
iogr
aphy
; LV
= le
ft v
entr
icul
ar;
RV
= r
ight
ven
tric
ular
; LA
= le
ft
atriu
m; A
o = a
orta
; AAA
= a
bdom
inal
aor
tic a
neur
ysm
; PEA
= p
ulse
less
ele
ctric
al a
ctiv
ity; P
HT
= p
ulm
onar
y hy
pert
ensi
on; H
CU
= h
and-
carr
ied
ultr
asou
nd; P
W =
pul
sed
wav
e D
oppl
er; C
W =
con
tinuo
us w
ave
Dop
pler
; TH
I =
tissu
e ha
rmon
ic im
agin
g; C
FD =
col
or fl
ow D
oppl
er; E
CG
= e
lect
roca
rdio
gram
; CPD
= c
olor
pow
er D
oppl
er; L
VOT
= le
ft v
entr
icul
ar o
utflo
w tra
ct; A
S =
aor
tic s
teno
sis;
RU
Q =
rig
ht u
pper
qua
dran
t; L
UQ
= le
ft u
pper
qua
dran
t;
DVT
= d
eep
veno
us t
hrom
bosi
s; IV
C =
infe
rior
vena
cav
a.

Copyright © 2012 International Anethesia Research Society. Unauthorized reproduction of this article is prohibited.Copyright © 2012 International Anethesia Research Society. Unauthorized reproduction of this article is prohibited.
Routine Physician- Performed Ultrasound
XXX 2012 • Volume X • Number X www.anesthesia-analgesia.org 7
Tabl
e 3.
Sum
mar
y of
Stu
dies
on
the
Impa
ct o
f Tr
anse
soph
agea
l Ech
ocar
diog
raph
y on
Dec
isio
n- M
akin
g in
Sur
gery
and
Int
ensi
ve C
are
Stu
dyM
etho
dolo
gyIn
fluen
ce o
f TE
E on
man
agem
ent
Com
men
ts
Ane
sthe
siol
ogis
t in
trao
pera
tive
TEE
in a
dult
car
diac
sur
gery
Mis
hra
1998
113
Pros
pect
ive
obse
rvat
iona
l stu
dy in
5016 c
ardi
ac
oper
atio
nsN
ew in
form
atio
n 11.7
% r
esul
ting
in a
cha
nge
in m
anag
emen
t in
25.8
% in
clud
ing
surg
ery
in 1
1.7
% (ne
ed for
gra
ft
revi
sion
0.8
%, I
ABP
0.8
%, o
r in
adeq
uate
val
ve r
epai
r 2.0
8%
)
No
maj
or T
EE- re
late
d G
I com
plic
atio
ns
Sut
ton
1998
114
Pros
pect
ive
obse
rvat
iona
l stu
dy in
233 c
ardi
ac
oper
atio
nsN
ew in
form
atio
n in
21%
res
ultin
g in
a c
hang
e in
sur
gery
in
10%
Sur
gery
cha
nge
in 6
% o
f pa
tient
s w
here
the
TEE
w
as r
outin
e an
d 22%
whe
n re
ques
ted
by t
he
surg
eon
Clic
k 2000
40
Pros
pect
ive
obse
rvat
iona
l stu
dy in
3245 c
ardi
ac
oper
atio
nsPr
ebyp
ass:
new
info
rmat
ion
in 1
5%
, cha
nged
sur
gery
in 1
4%
; po
stby
pass
: ne
w in
form
atio
n in
6%
, cha
nged
sur
gery
in
4%
Mos
t su
rgic
al c
hang
es w
ere
clos
ure
of p
aten
t fo
ram
en o
vale
. N
o m
ajor
TEE
- rela
ted
GI
com
plic
atio
nsC
outu
re 2
000
42
Pros
pect
ive
obse
rvat
iona
l stu
dy in
851 c
ardi
ac
oper
atio
nsC
hang
e in
man
agem
ent
in 1
4.6
%C
hang
es in
clud
ed m
odifi
catio
n of
med
ical
th
erap
y (5
3%
), su
rgic
al o
pera
tion
(30%
), an
d co
nfirm
atio
n of
dia
gnos
is (27%
).N
owra
ngi 2
001
41
Pros
pect
ive
obse
rvat
iona
l stu
dy in
3245 a
ortic
va
lve
repl
acem
ents
Cha
nge
in s
urge
ry in
14.6
%Ao
rtic
val
ve r
epla
cem
ent
patie
nts
only
Fans
haw
e 2002
37
Ret
rosp
ectiv
e ob
serv
atio
nal s
tudy
in 4
30 c
ardi
ac
oper
atio
nsC
hang
e in
sur
gery
(al
l ope
ratio
ns) in
5.6
% a
nd in
ele
ctiv
e C
ABG
cha
nge
3.5
%Fo
rres
t 2002
38
Ret
rosp
ectiv
e ob
serv
atio
nal s
tudy
in 2
343 C
ABG
op
erat
ions
Cha
nge
in s
urge
ry in
4.5
%O
nly
CAB
G p
atie
nts
wer
e st
udie
d. T
he G
I co
mpl
icat
ion
rate
att
ribut
able
to
TEE
was
0.0
9%
.Q
addo
ura
2004
39
Pros
pect
ive
obse
rvat
iona
l stu
dy in
474 C
ABG
op
erat
ions
Preb
ypas
s: n
ew in
form
atio
n in
10%
, cha
nged
sur
gery
in
3.4
%; po
stby
pass
: ne
w in
form
atio
n in
3.2
%, c
hang
ed
surg
ery
in 2
%
Onl
y C
ABG
pat
ient
s w
ere
stud
ied.
Eltz
schi
g 2008
115
Ret
rosp
ectiv
e ob
serv
atio
nal s
tudy
in 1
2,5
66
card
iac
oper
atio
nsS
urge
ry w
as c
hang
ed in
7%
(pr
ebyp
ass
) an
d 2.2
%
(pos
tbyp
ass)
in a
ll pa
tient
s.A
high
er im
pact
occ
urre
d in
com
bine
d C
ABG
/va
lve
proc
edur
es (12.3
% p
reby
pass
and
2.2
% p
ostb
ypas
s), t
han
isol
ated
val
ve
proc
edur
es (6.3
% p
reby
pass
and
3.3
%
post
bypa
ss) or
CAB
G (5.4
% p
reby
pass
and
1.5
% p
ostb
ypas
s).
Kle
in 2
009
116
Pros
pect
ive
obse
rvat
iona
l stu
dy in
2473 c
ardi
ac
oper
atio
nsC
hang
e in
sur
gery
in 1
5%
Two
serio
us e
soph
agea
l inj
urie
s (1
fat
al) w
ere
due
to T
EE in
sert
ion.
(con
tinue
d)

Copyright © 2012 International Anethesia Research Society. Unauthorized reproduction of this article is prohibited.
E CORE REVIEW ARTICLE
8 www.anesthesia-analgesia.org ANESTHESIA & ANALGESIA
Stu
dyM
etho
dolo
gyIn
fluen
ce o
f TE
E on
man
agem
ent
Com
men
ts
Ane
sthe
siol
ogis
t in
trao
pera
tive
TEE
in p
edia
tric
car
diac
sur
gery
Kau
shal
1998
117
Obs
erva
tion
stud
y in
300 c
onge
nita
l car
diac
su
rger
y op
erat
ions
Preb
ypas
s: n
ew in
form
atio
n in
5.6
%, c
hang
ed s
urge
ry 3
%;
post
bypa
ss: ch
ange
in s
urge
ry 6
.6%
Use
d to
ass
ess
succ
ess
of s
urgi
cal r
epai
r w
ith
70%
hav
ing
succ
essf
ul r
epai
r, 23.3
% h
avin
g ac
cept
able
res
idua
l def
ects
, and
6.6
% h
ad
mor
e se
vere
def
ects
with
sur
gica
l rev
isio
n re
quire
d in
0.0
3%
. N
o m
ajor
TEE
- rela
ted
GI
com
plic
atio
nsR
ando
lph
2002
118
Pros
pect
ive
obse
rvat
iona
l stu
dy in
1002
cong
enita
l hea
rt s
urge
ry o
pera
tions
Cha
nge
in s
urge
ry 1
3.8
%C
hang
es w
ere
mor
e fr
eque
nt d
urin
g re
oper
atio
ns, v
alve
rep
airs
(ao
rtic
or
atrio
vent
ricul
ar),
and
com
plex
out
flow
tra
ct
reco
nstr
uctio
ns. N
o m
ajor
TEE
- rela
ted
GI
com
plic
atio
nsB
ette
x 2003
119
Pros
pect
ive
obse
rvat
iona
l stu
dy a
t 2 c
ente
rs in
865 c
onge
nita
l car
diac
sur
gery
ope
ratio
nsTE
E le
d to
cha
nge
in d
iagn
osis
in 1
3.8
%, c
hang
ed m
edic
al
ther
apy
in 1
9.4
% a
nd s
urge
ry in
12.7
%M
edic
al c
hang
es in
clud
ed p
harm
acol
ogic
al (1
5.6%
) an
d flu
id m
anag
emen
t (3.
8%).
TEE
findi
ngs
pred
icte
d po
stop
erat
ive
diffi
culti
es in
4.0
%.
Ma
2007
120
Pros
pect
ive
obse
rvat
iona
l stu
dy in
350
cong
enita
l car
diac
sur
gery
ope
ratio
nsPr
ebyp
ass:
new
info
rmat
ion
in 9
.4%
, cha
nged
sur
gery
in
6.6
%; po
stby
pass
: ne
w in
form
atio
n in
16.3
%, c
hang
ed
surg
ery
in 3
.7%
No
maj
or T
EE- re
late
d G
I com
plic
atio
ns
Ane
sthe
siol
ogis
t in
trao
pera
tive
TEE
in a
dult
non
card
iac
surg
ery
Bra
ndt
1998
121
Pros
pect
ive
obse
rvat
iona
l stu
dy in
66 n
onca
rdia
c op
erat
ions
. In
dica
tions
: he
mod
ynam
ic
inst
abili
ty, p
reop
erat
ive
eval
uatio
n, t
raum
a,
and
hypo
xem
ia
New
find
ings
in 8
0%
lead
ing
to a
cha
nge
in s
urge
ry in
23%
No
maj
or T
EE- re
late
d G
I com
plic
atio
ns
Kol
ev 1
998
122
Pros
pect
ive
obse
rvat
iona
l stu
dy a
t 7 c
ente
rs in
224 c
ardi
ac a
nd n
onca
rdia
c op
erat
ions
Cha
nge
in m
edic
al m
anag
emen
t in
25%
and
sur
gery
in 4
%Al
l pat
ient
s ha
d pu
lmon
ary
arte
ry c
athe
ter
mon
itorin
g. M
edic
al c
hang
es in
clud
ed fl
uid
ther
apy, v
asoa
ctiv
e in
fusi
ons,
and
dep
th o
f an
esth
esia
.S
uria
ni 1
998
123
Ret
rosp
ectiv
e ob
serv
atio
nal s
tudy
in 1
23
nonc
ardi
ac o
pera
tions
Maj
or im
pact
in 1
5%
incl
udin
g a
chan
ge in
tre
atm
ent
of
life-
thre
aten
ing
even
t 7%
, cha
nged
sur
gery
1.6
%, c
hang
ed
intr
aope
rativ
e or
pos
tope
rativ
e m
anag
emen
t 3.2
%
No
maj
or T
EE- re
late
d G
I com
plic
atio
ns
Den
ault
2002
124
Pros
pect
ive
obse
rvat
iona
l stu
dy in
214
nonc
ardi
ac o
pera
tions
(du
ring
surg
ery
in 1
55
patie
nts,
aft
er s
urge
ry in
PAC
U in
4, a
fter
su
rger
y in
ICU
in 5
5)
Intr
aope
rativ
e ch
ange
s oc
curr
ed in
med
ical
man
agem
ent
in
40%
, and
sur
gery
in 1
8%
.C
hang
es w
ere
intr
aope
rativ
e (2
0%
), in
PAC
U
(1.4
%),
and
in IC
U (18.7
%)
Hof
er 2
004
125
Pros
pect
ive
obse
rvat
iona
l stu
dy in
99 n
onca
rdia
c op
erat
ions
Cha
nge
drug
the
rapy
in 4
7%
and
flui
d th
erap
y in
24%
Hig
her
influ
ence
in fl
uid
ther
apy
for
liver
and
lu
ng t
rans
plan
tatio
n (5
0%
) th
an o
ther
sur
gery
ty
pes
(24%
)S
chul
mey
er
2006
126
Pros
pect
ive
obse
rvat
iona
l stu
dy in
98 n
onca
rdia
c op
erat
ions
Use
ful i
n 98%
of pa
tient
s. In
trao
pera
tive
chan
ges
occu
rred
in
48%
, pos
tope
rativ
e ch
ange
s 25%
, sub
stitu
te for
pu
lmon
ary
arte
ry c
athe
ter
mon
itorin
g 24%
Mos
t fr
eque
nt in
trao
pera
tive
chan
ges
wer
e in
m
edic
atio
n an
d flu
id t
hera
py.
Tabl
e 3.
(Con
tinue
d)
(con
tinue
d)

Copyright © 2012 International Anethesia Research Society. Unauthorized reproduction of this article is prohibited.Copyright © 2012 International Anethesia Research Society. Unauthorized reproduction of this article is prohibited.
Routine Physician- Performed Ultrasound
XXX 2012 • Volume X • Number X www.anesthesia-analgesia.org 9
Stu
dyM
etho
dolo
gyIn
fluen
ce o
f TE
E on
man
agem
ent
Com
men
ts
TEE
in in
tens
ive
care
Oh
1990
127
Pros
pect
ive
obse
rvat
iona
l stu
dy in
49 p
atie
nts
(car
diac
sur
gery
and
non
card
iac)
. In
dica
tions
in
clud
ed a
ortic
pat
holo
gy, e
mbo
lus,
pos
t- AM
I, en
doca
rditi
s.
New
find
ings
in 5
9%
lead
ing
to s
urge
ry in
24%
(fin
ding
s co
nfirm
ed a
t op
erat
ion
in a
ll)N
o m
ajor
TEE
- rela
ted
GI c
ompl
icat
ions
Pear
son
1990
43
Pros
pect
ive
obse
rvat
iona
l stu
dy in
61 p
atie
nts.
In
dica
tions
incl
uded
hem
odyn
amic
inst
abili
ty,
MR
, val
vula
r dy
sfun
ctio
n, e
ndoc
ardi
tis, a
ortic
di
ssec
tion,
and
org
an d
onat
ion.
Cha
nged
man
agem
ent
in 4
4%
lead
ing
to s
urge
ry in
8%
(fi
ndin
gs c
onfir
med
at
oper
atio
n in
all)
No
maj
or T
EE- re
late
d G
I com
plic
atio
ns
Font
1991
128
Ret
rosp
ectiv
e ob
serv
atio
nal s
tudy
in 1
12
patie
nts
(aft
er c
ardi
ac s
urge
ry)
Cha
nged
man
agem
ent
in 1
6%
lead
ing
to c
hang
es in
med
ical
th
erap
y in
4%
and
sur
gery
in 1
2%
(fin
ding
s co
nfirm
ed a
t op
erat
ion
in a
ll)
No
maj
or T
EE- re
late
d G
I com
plic
atio
ns
Fost
er 1
992
129
Pros
pect
ive
obse
rvat
iona
l stu
dy in
61 p
atie
nts
(car
diac
and
non
card
iac)
. In
dica
tions
: en
doca
rditi
s, e
mbo
lus,
hyp
oten
sion
, MR
, LV
func
tion,
aor
tic d
isse
ctio
n, v
alve
dys
func
tion,
an
d m
isce
llane
ous
Cha
nged
man
agem
ent
in 2
2%
lead
ing
to s
urge
ry in
19%
(fi
ndin
gs c
onfir
med
at
oper
atio
n in
all)
No
maj
or T
EE- re
late
d G
I com
plic
atio
ns
Rei
cher
t 1992
44
Pros
pect
ive
obse
rvat
iona
l stu
dy in
60 p
atie
nts
in
the
ICU
aft
er c
ardi
ac s
urge
ry w
ith p
ersi
sten
t hy
pote
nsio
n de
spite
PAC
use
New
find
ings
on
TEE
in 5
0%
lead
ing
to a
cha
nge
in
man
agem
ent
incl
udin
g flu
id r
esus
cita
tion
(10%
), su
rger
y fo
r ta
mpo
nade
(2.3
%),
and
no s
urge
ry b
ecau
se o
f ex
clus
ion
of t
ampo
nade
(8.3
%)
Echo
card
iogr
aphy
als
o id
entifi
ed s
ubca
tego
ries
of p
atie
nts
at h
igh
risk
of d
eath
(th
ose
with
si
gns
of r
ight
ven
tric
ular
and
biv
entr
icul
ar
failu
re).
Kho
ury
1993
45
Pros
pect
ive
obse
rvat
iona
l stu
dy in
77 p
atie
nts
(car
diac
and
non
card
iac)
. In
dica
tions
: he
mod
ynam
ic in
stab
ility
, end
ocar
ditis
, em
bolu
s, a
nd a
ortic
dis
sect
ion
Cha
nged
man
agem
ent
in 4
8%
lead
ing
to c
hang
es in
med
ical
th
erap
y in
19%
and
sur
gery
in 2
9%
No
maj
or T
EE- re
late
d G
I com
plic
atio
ns
Hw
ang
1993
46
Inde
term
inat
e ob
serv
atio
nal s
tudy
in 8
0 c
ritic
ally
ill
pat
ient
s in
the
ICU
(48) an
d em
erge
ncy
depa
rtm
ent
(32). In
dica
tions
incl
uded
ao
rtic
dis
sect
ion,
hem
odyn
amic
inst
abili
ty,
embo
lism
, MR
, and
end
ocar
ditis
.
New
find
ings
in 5
0%
res
ultin
g in
car
diac
sur
gery
in 1
8%
with
co
nfirm
atio
n of
find
ings
at
surg
ery
No
maj
or T
EE- re
late
d G
I com
plic
atio
ns
Che
nzbr
aun
1994
130
Pros
pect
ive
obse
rvat
iona
l stu
dy in
100 p
atie
nts
afte
r ca
rdia
c su
rger
y. In
dica
tions
incl
uded
ao
rtic
dis
sect
ion,
end
ocar
ditis
, em
bolu
s,
hem
odyn
amic
inst
abili
ty, a
nd m
isce
llane
ous.
Cha
nged
man
agem
ent
in 3
3%
lead
ing
to c
hang
es in
sur
gery
in
16%
No
maj
or T
EE- re
late
d G
I com
plic
atio
ns
Vig
non
1994
131
Pros
pect
ive
obse
rvat
iona
l stu
dy in
2 c
ente
rs o
n 111 p
atie
nts
in IC
U (m
ixed
pop
ulat
ion)
Ove
rall
chan
ge in
man
agem
ent
due
to T
EE in
36%
incl
udin
g su
rger
y in
8%
. C
hang
e in
man
agem
ent
of 6
6%
in s
hock
ed
patie
nts
No
TEE-
rela
ted
com
plic
atio
ns w
ere
reco
rded
.
Hei
denr
eich
1995
47
Pros
pect
ive
obse
rvat
iona
l stu
dy in
61 p
atie
nts
in
the
ICU
with
hyp
oten
sion
New
find
ings
in 2
8%
(co
mpa
red
with
TEE
) le
d to
sur
gery
in
20%
.N
o m
ajor
TEE
- rela
ted
GI c
ompl
icat
ions
Poel
aert
1995
48
Ret
rosp
ectiv
e ob
serv
atio
nal s
tudy
in 1
08
patie
nts
in IC
U (no
car
diac
sur
gery
pat
ient
s).
Indi
catio
ns: he
mod
ynam
ic in
stab
ility
fro
m
card
iac
failu
re o
r se
psis
Of 64%
of pa
tient
s w
ith a
PAC
, 44%
und
erw
ent
ther
apy
chan
ges
afte
r TE
E: 4
1%
in t
he c
ardi
ac a
nd 5
4%
in t
he
sept
ic s
ubgr
oup.
In 4
1%
of pa
tient
s w
ithou
t a
PAC
, TEE
le
d to
a c
hang
e in
the
rapy
.
No
maj
or T
EE- re
late
d G
I com
plic
atio
ns
Soh
n 1995
49
Pros
pect
ive
obse
rvat
iona
l stu
dy in
127 c
ardi
ac
and
nonc
ardi
ac p
atie
nts
with
hem
odyn
amic
in
stab
ility
Cha
nged
man
agem
ent
in 5
2%
lead
ing
to c
hang
es in
sur
gery
in
21%
No
maj
or T
EE- re
late
d G
I com
plic
atio
ns
(con
tinue
d)
Tabl
e 3.
(Con
tinue
d)

Copyright © 2012 International Anethesia Research Society. Unauthorized reproduction of this article is prohibited.
E CORE REVIEW ARTICLE
10 www.anesthesia-analgesia.org ANESTHESIA & ANALGESIA
Stu
dyM
etho
dolo
gyIn
fluen
ce o
f TE
E on
man
agem
ent
Com
men
ts
Alam
1996
50
Pros
pect
ive
obse
rvat
iona
l stu
dy in
121 p
atie
nts
in t
he IC
U w
ith h
ypot
ensi
onN
ew fi
ndin
gs in
32%
lead
ing
to s
urge
ry in
18%
Sla
ma
1996
132
Pros
pect
ive
obse
rvat
iona
l stu
dy in
61 p
atie
nts
in
a m
edic
al IC
U. In
dica
tions
: sh
ock,
hyp
oxem
ia,
and
endo
card
itis
Cha
nged
man
agem
ent
in 2
1%
lead
ing
to c
hang
es in
med
ical
th
erap
y in
11%
and
sur
gery
in 8
%N
o m
ajor
TEE
- rela
ted
GI c
ompl
icat
ions
McL
ean
1998
133
Pros
pect
ive
obse
rvat
iona
l stu
dy in
53 p
atie
nts
(non
card
iac)
. In
dica
tions
: em
bolu
s, a
orta
, ve
ntric
ular
fun
ctio
n, e
ndoc
ardi
tis, a
nd s
urgi
cal
inve
stig
atio
n
New
find
ings
in 1
1%
, sup
port
ive
findi
ngs
in 3
4%
No
serio
us T
EE c
ompl
icat
ions
wer
e re
cord
ed.
Har
ris 1
999
51
Ret
rosp
ectiv
e ob
serv
atio
nal s
tudy
in 2
06
patie
nts
(aft
er c
ardi
ac s
urge
ry) in
whi
ch
the
prin
cipa
l ind
icat
ion
was
hem
odyn
amic
in
stab
ility
New
find
ings
in 4
7%
lead
ing
to c
hang
ed m
anag
emen
t in
32%
in
clud
ing
med
ical
the
rapy
in 1
9%
and
sur
gery
in 3
3%
Wak
e 2001
52
Ret
rosp
ectiv
e ob
serv
atio
nal s
tudy
in 1
30
patie
nts
afte
r ca
rdia
c su
rger
y. In
dica
tions
: he
mod
ynam
ic in
stab
ility
, car
diac
thr
ombu
s, o
r ve
geta
tion
Tota
l cha
nge
in 5
8.5
% o
f pa
tient
s; d
rug
ther
apy
in 4
3.3
% a
nd
surg
ery
in 1
5.3
%Th
e TE
E di
agno
sis
supp
orte
d th
e cl
inic
al
diag
nosi
s in
41.5
% o
f pa
tient
s.
Col
reav
y 2002
53
Ret
rosp
ectiv
e ob
serv
atio
nal s
tudy
in 2
55
patie
nts
afte
r ca
rdia
c su
rger
y. In
dica
tions
in
clud
ed in
stab
ility
, end
ocar
ditis
, em
bolu
s,
aort
a, a
nd m
isce
llane
ous.
New
find
ings
in 6
7%
of pa
tient
s w
ith h
ypot
ensi
on a
nd c
hang
e in
med
ical
man
agem
ent
and
resu
lting
nor
mot
ensi
on
in 3
1%
, inc
ludi
ng s
urge
ry in
22%
. O
vera
ll m
anag
emen
t ch
ange
in 3
2%
TEE
GI- r
elat
ed c
ompl
icat
ions
incl
uded
or
opha
ryng
eal b
leed
ing
in 1
pat
ient
.
Bru
ch 2
003
54
Pros
pect
ive
obse
rvat
iona
l stu
dy in
115 p
atie
nts
(car
diac
and
non
card
iac)
for
hem
odyn
amic
in
stab
ility
, em
bolu
s, e
ndoc
ardi
tis, v
alve
dy
sfun
ctio
n, a
ortic
dis
sect
ion,
and
tra
uma
Tota
l cha
nge
in 4
3%
of pa
tient
s; m
edic
al t
hera
py in
33%
(m
edic
atio
n an
d flu
id c
hang
es) an
d su
rger
y in
10
% (TE
E fin
ding
s co
nfirm
ed a
t op
erat
ion
in a
ll)
No
maj
or T
EE- re
late
d G
I com
plic
atio
ns.
Hut
tem
ann
2004
55
Ret
rosp
ectiv
e ob
serv
atio
nal s
tudy
in 2
16
patie
nts
in IC
U (no
t ca
rdia
c su
rger
y) for
he
mod
ynam
ic in
stab
ility
New
find
ings
in 8
8.4
% le
d to
a c
hang
e in
med
ical
m
anag
emen
t in
68.5
% a
nd s
urge
ry in
5.6
%TE
E G
I com
plic
atio
ns in
clud
ed s
elf- l
imiti
ng
orop
hary
ngea
l ble
edin
g (1
.4%
).
Sch
mid
lin 2
001
56
Ret
rosp
ectiv
e ob
serv
atio
nal s
tudy
in 3
01
patie
nts
afte
r ca
rdia
c su
rger
y. In
dica
tions
in
clud
ed h
emod
ynam
ic in
stab
ility
, sus
pici
on o
f ca
rdia
c ta
mpo
nade
, and
mis
cella
neou
s.
45%
new
find
ings
or
impo
rtan
t fin
ding
exc
lude
d. T
ampo
nade
w
as d
iagn
osed
in 1
1%
and
exc
lude
d in
12%
. C
hang
e in
m
anag
emen
t 73%
ove
rall,
incl
udin
g ph
arm
acol
ogy
and
fluid
s in
40%
, res
tern
otom
y in
14%
, no
rest
erno
tom
y in
13%
, and
mis
cella
neou
s ch
ange
s in
7%
No
maj
or T
EE- re
late
d G
I com
plic
atio
ns
Bre
derla
u 2006
57
Pros
pect
ive
obse
rvat
iona
l stu
dy in
339 p
atie
nts
in IC
U (no
t ca
rdia
c su
rger
y) for
hem
odyn
amic
in
stab
ility
New
find
ings
in 5
6%
led
to a
cha
nge
in m
anag
emen
t in
45%
. N
ew fi
ndin
gs in
clud
ed v
olum
e de
plet
ion
(47%
) an
d re
gion
al w
all m
otio
n ab
norm
aliti
es (27%
) an
d gl
obal
left
ve
ntric
ular
dys
func
tion
(22%
).O
rme
2009
58
Pros
pect
ive
obse
rvat
iona
l stu
dy in
71 p
atie
nts
in IC
U (no
t ca
rdia
c su
rger
y) for
hem
odyn
amic
in
stab
ility
Cha
nge
in m
anag
emen
t in
51.2
% o
f st
udie
s, in
clud
ing
fluid
ad
min
istr
atio
n, in
otro
pe o
r dr
ug t
hera
py, a
nd t
reat
men
t lim
itatio
n
Rep
orte
d co
mpl
icat
ions
are
res
tric
ted
to s
igni
fican
t ga
stro
inte
stin
al (
GI)
trau
ma.
TEE
= t
rans
esop
hage
al e
choc
ardi
ogra
phy;
IAB
P = i
ntra
aort
ic b
allo
on p
ump;
CAB
G =
cor
onar
y ar
teria
l by
pass
gra
ftin
g; I
CU
= i
nten
sive
car
e un
it; P
ACU
= p
osta
nest
hesi
a ca
re u
nit;
MR
= m
itral
reg
urgi
tatio
n; P
AC =
pu
lmon
ary
arte
ry c
athe
ter;
AM
I = a
cute
myo
card
ial i
nfar
ctio
n.
Tabl
e 3.
(Con
tinue
d)

Copyright © 2012 International Anethesia Research Society. Unauthorized reproduction of this article is prohibited.Copyright © 2012 International Anethesia Research Society. Unauthorized reproduction of this article is prohibited.
Routine Physician- Performed Ultrasound
XXX 2012 • Volume X • Number X www.anesthesia-analgesia.org 11
Tabl
e 4.
Sum
mar
y of
Stu
dies
on
the
Impa
ct o
f Tr
anst
hora
cic
Echo
card
iogr
aphy
on
Hem
odyn
amic
Man
agem
ent
and
Dec
isio
n- M
akin
g in
Ane
sthe
sia,
Em
erge
ncy
Med
icin
e, a
nd Int
ensi
ve C
are
Stu
dyM
etho
dolo
gyIn
fluen
ce o
f TT
E on
man
agem
ent
Com
men
ts
Ane
sthe
siol
ogis
t pe
riop
erat
ive
TTE
in n
onca
rdia
c su
rger
yC
anty
2009
74
Pros
pect
ive
obse
rvat
iona
l stu
dy in
87 n
onca
rdia
c su
rger
y pa
tient
s w
here
TTE
was
req
uest
ed b
y th
e tr
eatin
g an
esth
esio
logi
st.
Cha
nges
in m
edic
al m
anag
emen
t in
34%
(h
emod
ynam
ic m
anag
emen
t, an
esth
etic
te
chni
que,
and
pos
tope
rativ
e ca
re) an
d su
rgic
al
man
agem
ent
in 7
% (su
rger
y al
tere
d in
2%
and
de
ferr
ed in
5%
)
TTE
perf
orm
ed b
y si
ngle
ane
sthe
siol
ogis
t (H
EAR
T sc
an). C
hang
es o
ccur
red
in t
he p
reop
erat
ive
asse
ssm
ent
clin
ic (9%
), pr
eope
rativ
e in
ope
ratin
g ro
om (25%
), in
trao
pera
tive
(10%
), an
d PA
CU
(2%
).
Cow
ie 2
011
75
Pros
pect
ive
obse
rvat
iona
l stu
dy in
170
nonc
ardi
ac s
urge
ry p
atie
nts.
Indi
catio
ns
incl
uded
mur
mur
(58%
), he
mod
ynam
ic
inst
abili
ty, v
entr
icul
ar fun
ctio
n, d
yspn
ea, a
nd
poor
fun
ctio
nal c
apac
ity.
Cha
nge
in m
anag
emen
t in
82%
incl
udin
g po
stpo
ned
surg
ery
for
card
iolo
gy T
TE (20%
),
canc
eled
sur
gery
(4%
), pe
riope
rativ
e he
mod
ynam
ic c
hang
es (51%
), an
d le
vel o
f po
stop
erat
ive
care
(7%
)
TTE
perf
orm
ed b
y ca
rdio
vasc
ular
ane
sthe
siol
ogis
ts.
Dia
gnos
tic im
ages
obt
aine
d in
98%
. Ao
rtic
ste
nosi
s in
26%
, pul
mon
ary
hype
rten
sion
in 1
4%
. Fi
ndin
gs
confi
rmed
by
a ca
rdio
logi
sts
in 9
2%
Can
ty 2
012
72
Pros
pect
ive
obse
rvat
iona
l stu
dy in
100
nonc
ardi
ac s
urge
ry p
atie
nts
seen
in t
he
preo
pera
tive
clin
ic. In
dica
tions
incl
uded
su
spec
ted
card
iac
dise
ase
or a
ge >
65 y
.
Cha
nge
in m
anag
emen
t in
54%
incl
udin
g ch
ange
d su
rger
y in
2%
. C
hang
es in
clud
ed a
ste
p up
in
trea
tmen
t in
36%
and
a s
tep
dow
n in
tre
atm
ent
in 8
%.
TTE
perf
orm
ed b
y si
ngle
ane
sthe
siol
ogis
t (H
EAR
T sc
an). H
emod
ynam
ic m
anag
emen
t ch
ange
s in
clud
ed a
nest
hetic
tec
hniq
ue, i
nvas
ive
mon
itorin
g,
and
vaso
pres
sor
infu
sion
. Fi
ndin
gs c
onfir
med
by
a ca
rdio
logi
st in
92%
but
diff
eren
ces
wer
e no
t cl
inic
ally
sig
nific
ant
Can
ty 2
012
73
Pros
pect
ive
obse
rvat
iona
l stu
dy in
99 e
mer
genc
y no
ncar
diac
sur
gery
pat
ient
s. In
dica
tions
in
clud
ed s
uspe
cted
car
diac
dis
ease
or
age
>65 y
.
New
find
ings
in 6
7%
and
cha
nge
in m
anag
emen
t in
44%
incl
udin
g ch
ange
d su
rger
y in
2%
. C
hang
es
incl
uded
a s
tep
up in
tre
atm
ent
in 2
0%
and
a
step
dow
n in
tre
atm
ent
in 3
4%
.
TTE
perf
orm
ed b
y ca
rdio
vasc
ular
ane
sthe
siol
ogis
ts
(HEA
RT
scan
). C
hang
es w
ere
proc
edur
al in
14%
(p
reop
erat
ive
refe
rral
, sur
gery
typ
e, o
r le
vel o
f po
stop
erat
ive
care
) an
d he
mod
ynam
ic m
anag
emen
t ch
ange
s in
30%
(in
vasi
ve m
onito
ring,
flui
d an
d va
sopr
esso
r, an
d an
esth
etic
tec
hniq
ue)
Inte
nsiv
e ca
re
Vig
non
1994
131
Pros
pect
ive
obse
rvat
iona
l stu
dy in
40 n
onca
rdia
c su
rger
y pa
tient
s. In
dica
tions
incl
uded
LV
dysf
unct
ion,
PH
T, R
A th
rom
bus,
per
icar
dial
ef
fusi
on, v
alve
and
pos
tcar
diac
arr
est
LV
asse
ssm
ent.
Cha
nged
man
agem
ent
in 1
6%
. TT
E w
as in
fluen
tial
in p
atie
nts
with
per
icar
dial
effus
ion
(100%
), LV
dy
sfun
ctio
n (7
7.5
%),
and
hypo
tens
ion
(24%
).
TTE
perf
orm
ed b
y in
tens
ivis
ts
Jens
en 2
004
23
Pros
pect
ive
obse
rvat
iona
l stu
dy in
227
nonc
ardi
ac s
urge
ry p
atie
nts
not
mak
ing
clin
ical
pro
gres
s. 6
6%
wer
e m
echa
nica
lly
vent
ilate
d.
New
find
ings
wer
e de
cisi
ve in
24.5
%, s
uppl
emen
tal
in 3
7.3
%, a
nd s
uppo
rtiv
e in
35.6
%.
TTE
was
per
form
ed b
y in
tens
ivis
ts (FA
TE p
roto
col).
D
iagn
ostic
imag
es o
btai
ned
incl
uded
api
cal (
80%
), le
ft p
aras
tern
al (69%
), an
d su
bcos
tal (
58.4
%).
Jose
ph 2
004
66
Pros
pect
ive
obse
rvat
iona
l stu
dy in
100 p
atie
nts
with
sho
ck w
hen
an e
choc
ardi
ogra
m (TE
E) w
as
requ
este
d
TTE
reve
aled
a c
ardi
ac c
ause
of sh
ock
in 6
3%
. S
ensi
tivity
of TT
E fo
r ca
rdia
c ca
use
of s
hock
was
100%
, spe
cific
ity 9
5%
, pos
itive
pre
dict
ive
valu
e 97%
, and
neg
ativ
e pr
edic
tive
valu
e 100%
. Th
ere
wer
e re
lativ
e co
ntra
indi
catio
ns t
o TE
E in
15%
of
case
s.
TTE
was
per
form
ed b
y ca
rdia
c so
nogr
aphe
rs
(com
preh
ensi
ve T
TE). Im
agin
g w
as d
iagn
ostic
in
99%
.
Man
asia
2005
134
Pros
pect
ive
obse
rvat
iona
l stu
dy in
90 c
ardi
ac
and
nonc
ardi
ac s
urge
ry p
atie
nts
New
find
ings
occ
urre
d in
84%
of pa
tient
s le
adin
g to
ch
ange
d m
anag
emen
t in
37%
.TT
E w
as p
erfo
rmed
by
inte
nsiv
ists
with
brie
f tr
aini
ng
(10 h
) in
TTE
, whi
ch w
as c
heck
ed b
y ca
rdia
c so
nogr
aphe
rs. TT
E im
agin
g w
as d
iagn
ostic
in 9
4%
an
d in
terp
rete
d co
rrec
tly in
84%
.
(con
tinue
d)

Copyright © 2012 International Anethesia Research Society. Unauthorized reproduction of this article is prohibited.
E CORE REVIEW ARTICLE
12 www.anesthesia-analgesia.org ANESTHESIA & ANALGESIA
Stu
dyM
etho
dolo
gyIn
fluen
ce o
f TT
E on
man
agem
ent
Com
men
ts
Sta
nko
2005
135
Pros
pect
ive
obse
rvat
iona
l stu
dy in
126 c
ardi
ac
and
nonc
ardi
ac s
urge
ry p
atie
nts
New
find
ings
led
to c
hang
ed m
anag
emen
t in
41%
of
pat
ient
s. M
ajor
cha
nges
occ
urre
d in
8%
(s
urge
ry c
hang
es o
r ot
her
new
act
ive
trea
tmen
t)
and
min
or c
hang
es in
92%
(m
edic
atio
n ch
ange
s or
ref
erra
l).
TTE
was
per
form
ed b
y ca
rdia
c so
nogr
aphe
rs
(com
preh
ensi
ve T
TE).
Orm
e 2009
58
Pros
pect
ive
obse
rvat
iona
l stu
dy in
187
nonc
ardi
ac s
urge
ry p
atie
nts.
Indi
catio
ns
incl
uded
LV
and
RV
asse
ssm
ent,
infe
ctiv
e en
doca
rditi
s, p
eric
ardi
al e
ffus
ion,
and
pu
lmon
ary
edem
a.
Man
agem
ent
was
cha
nged
in 5
1.2
% o
f pa
tient
s an
d in
clud
ed c
hang
es t
o flu
id
adm
inis
trat
ion,
inot
rope
or
drug
the
rapy
, and
tr
eatm
ent
limita
tion.
The
mai
n im
pact
was
in
hem
odyn
amic
ally
uns
tabl
e pa
tient
s.
TTE
was
per
form
ed b
y in
tens
ivis
ts. D
iagn
ostic
imag
es
wer
e ob
tain
ed in
91.3
% o
f sp
onta
neou
sly
brea
thin
g an
d 84.2
% o
f m
echa
nica
lly v
entil
ated
pat
ient
s.
Emer
genc
y de
part
men
t TT
EJo
nes
2004
136
Ran
dom
ized
con
trol
led
tria
l of ea
rly v
ersu
s de
laye
d TT
E in
214 p
atie
nts
with
non
trau
mat
ic
hypo
tens
ion
and
sym
ptom
s of
sho
ck (e.
g.,
sync
ope,
dys
pnea
, unr
espo
nsiv
enes
s, fat
igue
)
Early
TTE
incr
ease
d th
e lik
elih
ood
of d
etec
ting
the
corr
ect
diag
nosi
s of
hyp
oten
sion
fro
m 5
0%
to
80%
.
TTE
perf
orm
ed b
y a
third
- yea
r em
erge
ncy
med
icin
e re
side
nt o
r bo
ard-
cert
ified
em
erge
ncy
phys
icia
n
Hau
ser
1989
137
Pros
pect
ive
obse
rvat
iona
l stu
dy in
81 p
atie
nts
with
che
st p
ain
and
nond
iagn
ostic
EC
G
chan
ges
New
find
ings
in 1
6%
led
to a
cha
nge
in d
ispo
sitio
n pl
an in
19%
.TT
E w
as p
erfo
rmed
by
card
iolo
gist
s.
Atar
2004
138
Pros
pect
ive
obse
rvat
iona
l stu
dy in
70 p
atie
nts
with
che
st p
ain
and
nond
iagn
ostic
EC
G
chan
ges
TTE
dete
cted
acu
te c
oron
ary
synd
rom
e w
ith a
se
nsiti
vity
of 100%
, spe
cific
ity o
f 93%
, and
ne
gativ
e an
d po
sitiv
e pr
edic
tive
valu
es o
f 71%
an
d 100%
.
TTE
diag
nosi
s of
acu
te c
oron
ary
synd
rom
e w
as
com
pare
d w
ith d
isch
arge
dia
gnos
is in
clud
ing
trop
onin
T m
easu
rem
ents
.
Bla
iva
2001
139
Pros
pect
ive
obse
rvat
iona
l stu
dy in
169 p
atie
nts
in c
ardi
ac a
rres
t re
ceiv
ing
CPR
No
patie
nt w
ith s
onog
raph
ical
ly id
entifi
ed c
ardi
ac
stan
dstil
l sur
vive
d to
leav
e th
e em
erge
ncy
depa
rtm
ent
rega
rdle
ss o
f th
e in
itial
ele
ctric
al
rhyt
hm.
TTE
was
per
form
ed b
y em
erge
ncy
phys
icia
ns a
nd
trai
nees
. Th
is fi
ndin
g w
as u
nifo
rm r
egar
dles
s of
do
wnt
ime.
Sal
en 2
005
140
Pros
pect
ive
obse
rvat
iona
l stu
dy a
t 4 c
ente
rs in
70 p
atie
nts
with
car
diac
arr
est
rece
ivin
g C
PRPa
tient
s pr
esen
ting
vent
ricul
ar a
kine
sis
did
not
have
ret
urn
of s
pont
aneo
us c
ircul
atio
n re
gard
less
of th
eir
card
iac
rhyt
hm, a
syst
ole,
or
PEA.
TTE
was
per
form
ed b
y em
erge
ncy
phys
icia
ns.
Taya
l 2003
141
Pros
pect
ive
obse
rvat
iona
l stu
dy in
20 p
atie
nts
who
had
PEA
or
near
PEA
Eigh
t pa
tient
s w
ith v
entr
icul
ar a
kine
sis
on T
TE
did
not
reco
ver;
12 p
atie
nts
with
ven
tric
ular
ak
ines
is a
nd 7
with
per
icar
dial
effus
ion
all
surv
ived
to
hosp
ital d
isch
arge
.
TTE
was
per
form
ed b
y em
erge
ncy
phys
icia
ns.
Bla
ivas
2001
142
Pros
pect
ive
obse
rvat
iona
l stu
dy in
103 p
atie
nts
with
dys
pnea
(un
expl
aine
d an
d ne
w o
nset
)Pe
ricar
dial
effus
ion
(13.6
%) an
d pa
tient
dis
posi
tion
wer
e ac
cura
tely
det
erm
ined
by
TTE.
TTE
was
per
form
ed b
y em
erge
ncy
phys
icia
ns.
Liu
2005
108
Pros
pect
ive
obse
rvat
iona
l stu
dy in
103 p
atie
nts
with
car
diom
egal
yTT
E in
crea
sed
diag
nost
ic a
ccur
acy
from
62%
(c
linic
al e
xam
inat
ion)
to
83%
. M
isse
d ca
rdia
c di
agno
ses
wer
e re
duce
d by
60%
.
TTE
was
per
form
ed b
y em
erge
ncy
phys
icia
ns.
Jone
s 2005
143
Pros
pect
ive
obse
rvat
iona
l stu
dy in
103
patie
nts
with
non
trau
mat
ic h
ypot
ensi
on
with
hyp
oten
sion
and
clin
ical
evi
denc
e of
ci
rcul
ator
y sh
ock
TTE
dete
ctio
n of
hyp
erdy
nam
ic L
V fu
nctio
n ha
d a
high
spe
cific
ity (93%
) of
sep
tic s
hock
.TT
E w
as p
erfo
rmed
by
emer
genc
y ph
ysic
ians
and
tr
aine
es.
TTE
= tr
anst
hora
cic
echo
card
iogr
aphy
; HEA
RT
= H
emod
ynam
ic E
choc
ardi
ogra
phic
Ass
essm
ent i
n R
eal T
ime;
PAC
U =
pos
tane
sthe
sia
care
uni
t; F
ATE
= F
ocus
ed A
sses
sed
Tran
stho
raci
c Ec
hoca
rdio
grap
hy; P
HT
= p
ulm
onar
y hy
pert
ensi
on; R
A = r
ight
atr
ial;
LV =
left
ven
tric
ular
; RV
= r
ight
ven
tric
ular
; EC
G =
ele
ctro
card
iogr
am;
CPR
= c
ardi
opul
mon
ary
resu
scita
tion;
PEA
= p
ulse
less
ele
ctric
al a
ctiv
ity.
Tabl
e 4.
(Con
tinue
d)

Copyright © 2012 International Anethesia Research Society. Unauthorized reproduction of this article is prohibited.Copyright © 2012 International Anethesia Research Society. Unauthorized reproduction of this article is prohibited.
Routine Physician- Performed Ultrasound
XXX 2012 • Volume X • Number X www.anesthesia-analgesia.org 13
not considered a therapeutic device. In terms of efficacy, there are 3 aspects to consider: is diagnosis improved, does improved diagnosis lead to change in decision- making, and do changes in decision- making lead to better patient outcome? The controversy starts earlier: even if diagnosis is improved, it is up to the user to decide on subsequent changes, if any, to management.
The last aspect is the most controversial, because even with correct knowledge, the practitioner may not initi-ate appropriate or best therapy. In the literature, there are very few randomized studies or outcome data investi-gating the use of ultrasound in critical care applications. Therefore, in this review, we focus on diagnostic accuracy and decision- making.
TRANSESOPHAGEAL ECHOCARDIOGRAPHYMost of the literature aims to identify the incidence of new findings that were not detected by either clinical or other cardiac tests. There are 2 focus areas: elective use in cardiac surgery, and use in the ICU for hemodynamically compromised patients. A summary of findings is shown in Table 3, consistently reporting the high rate of influences of TEE on diagnosis and management. In cardiac surgery, the use of routine TEE leads to identification of new find-ings sufficient to change the operation in approximately 5% of patients.37–39 Most of these changes relate to a clini-cally relevant difference from preoperative assessment of anatomical abnormalities, such as moderate or severe valve disease. In studies in which TEE was used in selected patients, such as in patients at increased risk or enduring hemodynamic instability, the frequency of change is much higher (14%–21%).40–42
In the ICU, where the principal indication for TEE was hemodynamic compromise, the TEE led to a change in diag-nosis and management in 40% of cases.43–58 The majority of changes were in hemodynamic treatment (vasopressor, inotrope infusions, and fluid management) but a signifi-cant proportion relate to surgical decision- making (such as diagnosis or exclusion of pericardial tamponade and aortic dissection).
On the basis of these observational, and largely proof- of- concept studies, TEE has become incorporated into routine practice in cardiac surgery and postoperative care. Given the potential serious complications of esophageal injury, however, the decision to use TEE must be justified, and approved indications are published by governing bod-ies.59,60 There are, however, no outcome studies in which TEE has been randomized as an intervention to assess patient outcome.
TRANSTHORACIC ECHOCARDIOGRAPHYMost of the literature on the use of TTE outside of cardi-ology laboratories relates to the diagnostic superiority of TTE over clinical examination, especially when performed by novices and with handheld ultrasound technology.61–65 Initially, the literature compared the image quality of held echocardiography with comprehensive systems, and sub-sequently reported its clinical applications. It is this litera-ture that best supports the concept of “ ultrasound- assisted examination.” A common finding was the influence on
clinical management of the new cardiac diagnoses revealed by echocardiography.
A summary of publications in critical care is shown in Table 4. With the recent and considerable improvements in technology, TTE now rivals TEE as the investigation of choice for hemodynamic instability,66 because adequate imaging is now feasible in most mechanically ventilated patients (95%–98%)23,67,68 and is noninvasive. The summa-rized data show frequent changes in diagnosis and man-agement with TTE in patients requiring noncardiac surgery, admission to the ICU, and the emergency department. Taken together, it is apparent that a junior doctor equipped with minimal training in echocardiography and a por-table ultrasound machine will outperform an experienced cardiologist with a stethoscope.69 Vignon et al.70 recently investigated the efficacy of a brief echocardiography train-ing program (12 hours) for intensive care residents, who subsequently demonstrated a high level of competence in diagnosis of basic hemodynamic disorders using TTE. Royse et al.71 evaluated the training course used to teach the HEART scan goal- focused TTE study on interpretation of pathology using recorded videos and found a high agree-ment with course students and experts. Importantly, there are no studies in which clinical examination outperformed echocardiography.
In anesthesiology, there are few data evaluat-ing the effect of echocardiography diagnosis on clini-cal decision- making, and these are mostly series of case reports or proof- of- concept observational studies. However, in patients who have or are at risk of cardiac disease, the detection rate of clinically significant pathol-ogy is in the order of 25% of patients, which leads to changes in perioperative management.72,73 In prospec-tive observational studies by Canty et al.72–74 and Cowie,75 the therapeutic impact from focused TTE was 39% to 82%, which was principally before anesthesia (90%) for noncardiac surgery, but also during and after surgery in mechanically ventilated patients. Important management changes were identification of high cardiac risk patients and alteration in preoperative assessment and level of postoperative care (10%–15%), but surgery was changed for a small proportion of patients (2%) as a result of the new information from TTE. The majority of changes were in hemodynamic management (30%–40%), including more rational use of invasive monitoring and fluid and vaso-pressor use. In a study by Canty et al.,72 during which goal- focused TTE was used in the preadmission clinic setting, the overall effect was to step down planned treat-ment (based on a reassurance from normal TTE findings) in more patients than to step up treatment based on clini-cally significant pathology. The effect on workflow was to reduce the intensity of treatment and resource use. This, however, has not been subjected to economic or outcomes analysis.
These publications mirror the earlier work with TEE, showing strong proof of concept that either goal- focused or comprehensive TTE may change our practice in the pre-admission clinic in a large proportion of patients. The inci-dence of abnormal findings by limited echocardiography is similar to that of comprehensive echocardiography studies in the preadmission setting. Faris et al.76 investigated the

Copyright © 2012 International Anethesia Research Society. Unauthorized reproduction of this article is prohibited.
E CORE REVIEW ARTICLE
14 www.anesthesia-analgesia.org ANESTHESIA & ANALGESIA
incidence of cardiovascular pathology in patients attend-ing a preadmission clinic, where the indication for TTE was based on appropriate use criteria guidelines issued by the American Society of Echocardiography. They reported that 27.6% of patients considered appropriate for TTE had at least moderate or severe cardiac pathology. However, many of these studies are “proof of concept,” and the clinical use of the new information was determined by the treating cli-nician. Further research is required to determine whether the change in diagnosis or management leads to improve-ment in outcomes.
LUNG ULTRASOUNDLung ultrasound imaging is an emerging discipline that has widespread application to surgery, anesthesiology, and intensive care and has been incorporated into the focused TTE protocols FATE23 and RUSH.24 Certain diagnoses, such as detection of pneumothorax and pleural effusion are widely recognized and easy to obtain.13,25 Pleural effu-sion size is reasonably accurately assessed by measuring pleural fluid dimensions with ultrasound when compared with drainage volume.77,78 The size of pneumothorax can be estimated by measuring the “contact point” where the
probe is moved around the chest to see where the lung joins the pleural space.79 Despite demonstration of improved safety of pleural drainage with point- of- care ultrasound,14,80 uptake into clinical use has been slow.14,81,82 The emerg-ing areas of interest, however, are to correlate lung imag-ing with patterns of pathology such as alveolar- interstitial syndrome83 (including pulmonary edema), consolidation and collapse,84 abscess, emphysema, and even pulmonary embolus.85 Lichtenstein and Meziere13 reported effective and rapid diagnosis of these disorders in critically ill patients with acute respiratory failure using lung ultrasound, dem-onstrating a very high sensitivity and specificity compared with computed tomography. The routine use of lung ultra-sound in critical care has the potential to substitute for com-puted tomography and chest radiography, particularly for repeated examinations, and thus reduce radiation exposure to patients and staff.86
ULTRASOUND- GUIDED VASCULAR ACCESS Real- time use of ultrasound to guide vascular access is well established as a point- of- care application of ultrasound. This is the one area in which there is high- level evidence of benefit, but mostly for internal jugular vein cannulation.
Figure 2. Composite diagram of 3 patients presenting for fractured neck of femur surgery with systolic murmur. Images are from transtho-racic studies performed before anesthesia. The “good case” shows an unrestricted aortic valve (AV) in panel A, and normal left ventricular (LV) size and function in panel B. The murmur is from a sclerotic AV (not shown was absence of mitral regurgitation). The “bad case” shows a severely calcified and restricted AV in panel C but normal LV size and function in panel D. The “ugly case” shows an unrestricted AV, but dilated right ven-tricle (RV) and LV is in panel E, and a dilated RV and D- shaped interventricular septum in panel F, consistent with having severe pulmonary hyper-tension and biventricular failure. The systolic murmur was due to tricuspid regurgitation. The first patient proceeded with no change to man-agement; the second proceeded with arterial line monitoring, vasopressor infusion, and post-operative high- dependency unit; and the third patient had palliative care instead of surgery.

Copyright © 2012 International Anethesia Research Society. Unauthorized reproduction of this article is prohibited.Copyright © 2012 International Anethesia Research Society. Unauthorized reproduction of this article is prohibited.
Routine Physician- Performed Ultrasound
XXX 2012 • Volume X • Number X www.anesthesia-analgesia.org 15
In 2011, a combined task force of the American Society of Echocardiography and the Society of Cardiovascular Anesthesiologists published recommendations supporting the routine use of ultrasound- guided internal jugular vas-cular access “whenever possible,” which was based on 30 level 1 studies supporting its use.87 The National Institute for Clinical Excellenceb (United Kingdom) published similar rec-ommendations in 2002 and a subsequent audit demonstrated reduced central venous catheter–related complications in 284 patients since its implementation at a single institution.88
ULTRASOUND- GUIDED REGIONAL ANESTHESIAThe use of ultrasound to guide regional blockade is now widely accepted throughout the world. The literature cov-ers 3 phases: the first was to describe how to perform the block and to describe the sonographic anatomy; the second was to show performance advantage such as faster onset of block, less local anesthetic used, or high rate of efficacy; and the third phase was to identify whether it makes a clinical difference such as improved success, longer dura-tion, and reduced morbidity compared with the anatomical landmark or nerve stimulator- guided techniques. Soeding et al.92 demonstrated faster onset and more complete onset of brachial plexus blocks with an ultrasound-guided tech-nique compared with blind technique. Improved analgesia was reported with ultrasound- guided regional anesthesia in 2 recent meta- analyses.89,90 There was insufficient evi-dence to draw conclusions on improved outcome, but a reduction in surrogate morbidity including vascular punc-ture and diaphragmatic paralysis was demonstrated in the meta- analysis by Neal et al.90 Importantly, there are no reports showing that ultrasound is inferior to blind tech-niques, and significant morbidity from peripheral nerve blockade is very rare.91 Adoption of ultrasound has without doubt led to a rapid expansion in regional blockade in acute and chronic pain medicine and to new techniques including a variety of vertebral (neuraxial),9,10 paravertebral, and trun-cal (e.g., transverses abdominus plane11,93) blocks.
GOAL- FOCUSED TTE: SEPARATING “THE GOOD, THE BAD, AND THE UGLY”The incorporation of goal- focused TTE is perhaps the great-est challenge for anesthesiologists and critical care physi-cians in the next few years. It is also a necessary step in the evolution of clinical ultrasound before it evolves to “ ultrasound- assisted examination.” There are several para-digm shifts that are necessary for widespread adoption of goal- focused TTE. We must accept that novices can perform goal- focused TTE.94 A further paradigm shift is that diag-nosis of pathology is largely based on pattern recognition rather than detailed knowledge base and formal quantifica-tion. This is not full diagnosis, but rather answering clini-cal questions in real time, with referral to more experienced practitioners for full diagnosis at a later stage. An example is the identification of aortic stenosis, whereby pattern recognition can be used to determine clinically important
stenosis, whereas formal quantification to assess the sever-ity requires the use of spectral Doppler particularly. The presence of heavily calcified and restricted aortic valve leaf-lets is one pattern that rapidly identifies potentially clini-cally significant aortic stenosis.
In a study of interpretative ability of novices after a train-ing course to teach the HEART scan, novices reported on 5 videotaped echocardiography cases in which only 2-dimen-sional (2D) and color flow Doppler images were available.71 The agreement between novice and expert was very high for hemodynamic state and valve severity. In particular, few clinically important valve lesions were misdiagnosed, whereas there was a tendency to overcall the severity of mild valve lesions. Using continuous wave Doppler, Cowie and Kluger95 studied the ability of novices to measure peak aortic gradients from the apical 5-chamber view and compared it with that of expert cardiac anesthesiologists. There was very high agreement of significant aortic stenosis (based on valve morphology) and good agreement (based on peak velocity alone (κ 0.8–1), reinforcing the importance of pattern recognition of aortic stenosis on 2D imaging.
In recent years, the concept of portable ultrasound is less relevant because most portable echocardiography systems had all basic echocardiographic modalities and approached cart- based machines in image quality. However, this is not true of the palm- sized echocardiography machines and these may have limitations in their ability to perform goal- focused studies. Furthermore, one must overcome the fear that the clinician may “miss something important” when doing a limited versus comprehensive study, that is, the notion that a missed diagnosis outweighs any positive prospect of new or correct diagnoses. There are 2 polar opinions to this state-ment. One view is that misdiagnosis by ultrasound could lead to patient harm, and the best way to avoid that is to ensure that only practitioners who are expert in perform-ing and interpreting echocardiography are given access to high- level equipment and allowed to perform echocardiog-raphy. The alternative view is that clinical diagnosis is fre-quently incorrect compared with echocardiography, and even accepting that practitioners with limited training and experi-ence will miss or misdiagnose pathology on occasions, that ultrasound- assisted examination will reduce the incidence of incorrect diagnosis compared with physical examination alone,22,65 and that there could be a clinical consequence to not performing echocardiography. Practice is likely to lie between the 2 poles and should be directed by evidence.
The Australian experience may provide insights into the likely mode of adoption and education in ultrasound in acute care medicine. In 2004, the University of Melbourne Postgraduate Diploma of Perioperative and Critical Care Echocardiography was released with the predominant focus on TEE for cardiac anesthesiology, and the major-ity of students had no interest in TTE. In 2012, the course is now in 2 levels: the first level concentrates more on TTE and surface ultrasound but with basic TEE, and the second level is devoted to diagnostic knowledge base and empha-sis on both TTE and TEE. The distribution by specialty is now overwhelmingly in favor of noncardiac acute care specialties, with fewer than 25% of students being cardiac anesthesiologists (personal communication, University of Melbourne Ultrasound Education Group, 2012). The
b NICE. Guidance on the Use of Ultrasound Locating Devices for Placing Central Venous Catheters. Technology Appraisal Guidance No. 49. Avai-lable at: http://www.nice.org.uk/nicemedia/live/11474/32461/32461.pdf. Accessed February 22, 2012.

Copyright © 2012 International Anethesia Research Society. Unauthorized reproduction of this article is prohibited.
E CORE REVIEW ARTICLE
16 www.anesthesia-analgesia.org ANESTHESIA & ANALGESIA
majority of noncardiac anesthesiologists do not perform TEE and have no interest in it. In North America, the move toward limited echocardiography has been in the form of “basic TEE,” although it is likely that a paradigm shift toward limited TTE will occur given the noninvasive nature of this technology and removal of the need for sedation or anesthe-sia to perform the study.
In general, normal or mild pathology is unlikely to lead to hemodynamic compromise under anesthesia. Examples of “good, bad, and ugly” are shown in Figure 2. Acute care physicians will be reassured if the ejection systolic murmur they heard on auscultation is only aortic sclerosis. However, they will be alerted if it is moderate or severe aortic stenosis, and alarmed if a patient who is short of breath has severe pul-monary hypertension and right heart failure. See online sup-plemental digital content for examples of normal (Video 1, see Supplemental Digital Content 1, http://links.lww.com/AA/A451, and Video 2, see Supplemental Digital Content 2, http://links.lww.com/AA/A452), aortic stenosis (Video 3, see Supplemental Digital Content 3, http://links.lww.com/AA/A453, and Video 4, see Supplemental Digital Content 4, http://links.lww.com/AA/A454), and right ventricular failure (Video 5, see Supplemental Digital Content 5, http://links.lww.com/AA/A455, and Video 6, see Supplemental Digital Content 6, http://links.lww.com/AA/A456).
There are many published goal- focused studies, and each has a catchy acronym. They range in scope from very simple (2D only) studies to assess ventricular function in a peri- arrest situation (Table 4), to more extensive yet still lim-ited studies incorporating 2D and color flow Doppler to eval-uate valve and ventricular function (HEART scan22,71). The common feature is to concentrate on either 2D only, or 2D and color flow Doppler analysis, and to avoid formal quan-tification using pulsed wave or continuous wave Doppler. Another common feature is an emphasis on pattern recogni-tion of pathology rather than extensive quantification. The scanning ability and level of knowledge required to be pro-ficient in quantification and spectral Doppler is much higher than that required to view 2D imaging, or with color flow Doppler. Removing spectral Doppler also reduces the time
taken to perform the study, such that a goal- focused study can be performed and reported in 10 minutes or less. The ability to discriminate hemodynamically significant from nonsignificant aortic stenosis is important, because it is a significant risk factor for postoperative mortality,96 is poorly assessed clinically,97,98 and may be asymptomatic even if severe.99 This has been achieved by focused TTE performed by anesthesiologists72–74 and others100–102 using 2D assess-ment of valve cusp separation without the use of quantita-tive spectral Doppler (standard with comprehensive TTE).
Although acronym, goal- focused examinations define a particular sequence of study views, the point- of- care physi-cian must ultimately determine what structures to look at first, according to clinical requirement. For example, the subcostal view is most appropriate during an arrest situation because images can be obtained without interrupting chest compression.
HOW DO WE ACHIEVE ULTRASOUND FOR EVERYONE?To achieve full evolution, training in ultrasound should be incorporated into medical school teaching. It should be viewed as part of clinical assessment and examination. There are some centers already adopting this approach.
Within acute care medical disciplines, the logical approach is to start with limited TTE and surface ultra-sound applications, and then to progress up the pyramid of expertise. Learned societies and credentialing organizations should produce guidelines to identify what knowledge is required and how many studies should be performed to ensure competency.18,19 Such recommendations should seek to be consistent across specialty craft groups.
The barriers to adoption of ultrasound for everyone revolve in part around education and equipment. In the past decade, there has been a major shift in focus from static and large cart- based ultrasound machines to portable, yet high- quality, ultrasound systems. Although the cart- based machines are the most sophisticated and provide the best image quality, they are not well suited to many areas of critical care practice. The smaller, portable machines are
Table 5. Examples of iPhone/Android Apps and Educational Websites
Name Type Focus Comment
iASE iPhone/Android Guidelines and normal values Pocket guide. Distributed by American Society of Echocardiography
EchoCalc iPhone/Android Reference values and calculator for quantification
Distributed by the British Society of Echocardiography
Echocardiography i-pocketcards iPhone/Android Atlas and reference guideFocus Pocket Guide iPhone/iPad Aide- memoire for the FOCUS study Describes views and sequenceFate Card iPhone/Android Aide- memoire for the FATE study Describes views, values, and sequencePocketGuide iPhone Ultrasound- guided regional anesthesia Pocket book style, release 2012iHeartScan iPhone/iPad Report form database for the HEART
scanEnter data real time to produce
written report, release 2012e-Echocardiography Website Echocardiography and ultrasound
learning resourceMuch more extensive than iPhone
apps. Offers CME accreditationEcho University Online Website Education to prepare for examinations Target cardiologists and sonographersSociety Websites Websites Many society websites offer
echocardiography educationExamples include SCA and ASE
ASE = American Society of Echocardiography; FOCUS = Focused Cardiac Ultrasound Study; FATE = Focused Assessed Transthoracic Echo; HEART scan = Haemodynamic Echocardiography Assessment in Real Time; CME = Continuing Medical Education; SCA = Society of Cardiovascular Anesthesiologists.

Copyright © 2012 International Anethesia Research Society. Unauthorized reproduction of this article is prohibited.Copyright © 2012 International Anethesia Research Society. Unauthorized reproduction of this article is prohibited.
Routine Physician- Performed Ultrasound
XXX 2012 • Volume X • Number X www.anesthesia-analgesia.org 17
easier to move and position next to patients, whether in the ICU, the anesthesia induction room, or in the preadmission clinic. The cost is also reduced considerably, such that an echocardiogram machine in 1995 was the cost of a house ($250,000), whereas today a very capable portable machine is the cost of a car ($30,000–$60,000). This has allowed provid-ers to increase the number of machines available. However the “silo” mentality between medical specialty craft groups has limited cross- discipline training opportunities.
Australia is a good model for how education can lead a change in practice. The adoption of TEE in cardiac sur-gery in the mid-1990s was relatively slow and ad hoc, with the early adopters going overseas or getting limited training within Australia. There was a deficiency of train-ing courses and even textbooks on TEE. Those wishing to adopt the technology had to work very hard to obtain the knowledge and practice to become proficient. This produced a need for a high- quality and extensive knowl-edge to cater to the diagnostic- level interpretive skills required in cardiac surgery. This led to the production of the University of Melbourne distance education courses. These courses provided access to knowledge for those wishing to become skilled in TEE, with the consequence that many Australian anesthesiology or cardiothoracic surgery depart-ments insisted that cardiac anesthesiologists complete the Postgraduate Diploma or an equivalent fellowship or exam-ination such as the NBE PTEeXAM. This approach was endorsed by the Australian and New Zealand College of Anaesthetists. However, this approach limited the echocar-diography knowledge to cardiac anesthesiologists perform-ing TEE. In response to demand, the TEE- based course split into 2 parts in 2009, with the first half aimed at the noncar-diac anesthesiologist, emergency, and intensive care physi-cians, where TTE would be the first and most frequently used echocardiography modality, complemented by a basic level of TEE. Clinicians can limit their echocardiography training and graduate with a postgraduate certificate or continue to the level of diploma where the focus is TEE and diagnostic- level knowledge. The delivery of these courses is entirely via distance education, which allows clinicians to study in their own time and place, thereby facilitating access to information. In addition, formalized training workshops were established to teach the HEART scan goal- focused study. The impact on clinical practice has been dramatic. In Australia and New Zealand, where there are approximately 5000 anesthesiologists or critical care physicians, 1375 have completed the workshops, more than 400 have completed the certificate level, and more than 500 have completed the diploma level. The predominant use of echocardiography among anesthesiologists and critical care physicians is now goal- focused TTE, with TEE remaining predominantly the domain of the cardiac anesthesiologist (personal commu-nication, University of Melbourne Ultrasound Education Group, 2012). The importance of distance- based education is to make it easy for clinicians to work through a process to acquire the knowledge in a structured and graded manner. These courses are now run as professional development pro-grams for the Society of Cardiovascular Anesthesiologists (SCA ON- CUE levels 1 and 2), increasing availability to North American and worldwide practice.
It is likely that education platforms that are tailored to physician needs and practice environments will facilitate a high rate of adoption of ultrasound into clinical prac-tice. There are already many short courses, workshops, texts, and electronic material to aid learning. A selection of iPhone apps and websites are shown in Table 5, which will aid the practitioner as reference guides, aide- memoires, pocket books, or calculators and report forms as well as platforms for e- learning. However, integration of ultra-sound into everyday practice (ultrasound for everyone) will only be accomplished when it is part of the curricula of medical schools and specialist training organizations. A recent expert panel on intensive care training36 recom-mended unanimously that general critical care ultrasound and basic echocardiography should be a core part of the ICU curriculum. Other societies, boards, and colleges will produce training and practice guidelines to help steer the path of education, practice guidelines, and competency assessment.
IS THERE A DANGER IN WIDESPREAD ADOPTION OF ULTRASOUND?There is certainly widespread consensus from noncardiol-ogy specialties that ultrasound should be an integral part of their practice.19 There is, however, a paucity of outcome data on the use of routine ultrasound in anesthesiology, intensive care, or emergency medicine. As a comparative example, it took 15 to 20 years after widespread adoption of the pulmo-nary artery catheter before research questioned whether the balance was harm or benefit.103,104 Research is likely to direct appropriate use, and better define clinical situations in which benefit clearly outweighs risk of harm. This research, combined with expert consensus leads to recommendations for the performance and appropriate use of echocardiogra-phy.105,106 Education, definition of competency, and quality assurance programs are likely to evolve to reduce the risk of harm. This is a dynamic topic, which is likely to change as we move toward widespread adoption of ultrasound into everyday practice.
SUMMARYUltrasound is becoming an integral part of anesthesiol-ogy and acute care medical practice. What started out as TEE for cardiac surgery has spread to ultrasound- guided regional anesthesia and vascular access, goal- focused TTE, and emerging use of lung, abdominal, vascular, and soft tis-sue imaging. The multiple roles of ultrasound have many complementary components, and the future direction is to consider ultrasound as simply part of clinical assessment and an aid to guide procedures. E
AUTHOR AFFILIATIONSFrom the *Anesthesia and Pain Management Unit, Department of Surgery, The University of Melbourne, Carlton, Victoria, Australia; †Department of Anesthesia and Pain Management, The Royal Melbourne Hospital, Parkville, Victoria, Australia; ‡Department of Anaesthesia and Pain Management, The Royal Hobart Hospital, The Royal Melbourne Hospital, Parkville, Victoria, Australia; §Department of Anaesthesia, Monash Medical Centre, Melbourne, Victoria, Australia; ‖Department of Medicine, The University of Tasmania, Hobart,

Copyright © 2012 International Anethesia Research Society. Unauthorized reproduction of this article is prohibited.
E CORE REVIEW ARTICLE
18 www.anesthesia-analgesia.org ANESTHESIA & ANALGESIA
Australia; ¶Department of Anaesthesia, Sir Charles Gairdner, Perth, Australia; #Department of Anaesthesia, Joondalup Hospital, Perth, Australia; **Echocardiography Group, Department of Surgery, The University of Melbourne, Carlton, Victoria, Australia; ††Fremantle School of Medicine, University of Notre Dame, Perth, Australia; ‡‡Emergency Department, Frankston Hospital, Peninsula Health, Frankston, Australia; §§Department of Anaesthesia, Royal Perth Hospital, Perth, Australia; and ‖‖Department of Surgery, The University of Melbourne, Carlton, Victoria, Australia.
DISCLOSURESName: Colin F. Royse, MBBS, MD, FANZCA.Contribution: This author helped prepare the manuscript.Conflicts of Interest: Employee of University of Melbourne; involved in the development of course materials described (Postgraduate Certificate and Diploma of Clinical Ultrasound and HEART scan), Director of Heartweb, which conducts the SCA ON- CUE courses.Name: David J. Canty, MBBS, FANZCA, PGDipEcho.Contribution: This author helped prepare the manuscript.Conflicts of Interest: Employee of University of Melbourne; involved in the development of course materials described in the text (Postgraduate Certificate and Diploma of Clinical Ultrasound and HEART scan).Name: John Faris, MBChB, DAvMed, FAFOM, FFOM, FANZCA, BA, ASCeXAM, PGDipClinUs.Contribution: This author helped prepare the manuscript.Conflicts of Interest: Involved in the development of course materials described in the text (Postgraduate Certificate and Diploma of Clinical Ultrasound and HEART scan).Name: Darsim L. Haji, MBChB, FACEM, PGDipEcho.Contribution: This author helped prepare the manuscript.Conflicts of Interest: Involved in the development of course materials described in the text (Postgraduate Certificate and Diploma of Clinical Ultrasound and HEART scan).Name: Michael Veltman, MBBS, FANZCA, ASCExam, FASE.Contribution: This author helped prepare the manuscript.Conflicts of Interest: Involved in the development of course materials described in the text (Postgraduate Certificate and Diploma of Clinical Ultrasound and HEART scan).Name: Alistair Royse, MBBS, MD, FRACS, FCSANZ.Contribution: This author helped prepare the manuscript.Conflicts of Interest: Employee of University of Melbourne; involved in the development of course materials described in the text (Postgraduate Certificate and Diploma of Clinical Ultrasound and HEART scan), Director of Heartweb, which conducts the SCA ON- CUE courses.This manuscript was handled by: Martin J. London, MD.
REFERENCES 1. Edler I, Lindstrom K. The history of echocardiography. Ultra-
sound Med Biol 2004;30:1565–644 2. Kneeshaw JD. Transoesophageal echocardiography (TOE) in
the operating room. Br J Anaesth 2006;97:77–84 3. Kallmeyer IJ, Collard CD, Fox JA, Body SC, Shernan SK. The
safety of intraoperative transesophageal echocardiography: a case series of 7200 cardiac surgical patients. Anesth Analg 2001;92:1126–30
4. Huang CH, Lu CW, Lin TY, Cheng YJ, Wang MJ. Complications of intraoperative transesophageal echocardiography in adult cardiac surgical patients: experience of two institutions in Tai-wan. J Formos Med Assoc 2007;106:92–5
5. Shanewise JS, Cheung AT, Aronson S, Stewart WJ, Weiss RL, Mark JB, Savage RM, Sears- Rogan P, Mathew JP, Quinones MA,
Cahalan MK, Savino JS. ASE/SCA guidelines for performing a comprehensive intraoperative multiplane transesophageal echocardiography examination: recommendations of the American Society of Echocardiography Council for Intra-operative Echocardiography and the Society of Cardiovascular Anesthesiologists Task Force for Certification in Perioperative Transesophageal Echocardiography. Anesth Analg 1999;89: 870–84
6. Cahalan MK, Abel M, Goldman M, Pearlman A, Sears- Rogan P, Russell I, Shanewise J, Stewart W, Troianos C. American Society of Echocardiography and Society of Cardiovascu-lar Anesthesiologists task force guidelines for training in perioperative echocardiography. Anesth Analg 2002;94: 1384–8
7. Beaulieu Y. Bedside echocardiography in the assessment of the critically ill. Crit Care Med 2007;35:S235–49
8. Marhofer P, Chan VW. Ultrasound- guided regional anesthesia: current concepts and future trends. Anesth Analg 2007;104: 1265–9
9. Rapp HJ, Folger A, Grau T. Ultrasound- guided epidural cath-eter insertion in children. Anesth Analg 2005;101:333–9
10. Chin KJ, Perlas A, Chan V, Brown- Shreves D, Koshkin A, Vaishnav V. Ultrasound imaging facilitates spinal anesthesia in adults with difficult surface anatomic landmarks. Anesthesiology 2011;115:94–101
11. Abrahams MS, Horn JL, Noles LM, Aziz MF. Evidence- based medicine: ultrasound guidance for truncal blocks. Reg Anesth Pain Med 2010;35:S36–42
12. Maecken T, Grau T. Ultrasound imaging in vascular access. Crit Care Med 2007;35:S178–85
13. Lichtenstein DA, Meziere GA. Relevance of lung ultrasound in the diagnosis of acute respiratory failure: the BLUE protocol. Chest 2008;134:117–25
14. Havelock T, Teoh R, Laws D, Gleeson F. Pleural procedures and thoracic ultrasound: British Thoracic Society Pleural Disease Guideline 2010. Thorax 2010;65:ii61–76
15. Scalea TM, Rodriguez A, Chiu WC, Brenneman FD, Fallon WF Jr, Kato K, McKenney MG, Nerlich ML, Ochsner MG, Yoshii H. Focused Assessment with Sonography for Trauma (FAST): results from an international consensus conference. J Trauma 1999;46:466–72
16. Seward JB, Douglas PS, Erbel R, Kerber RE, Kronzon I, Rakowski H, Sahn LD, Sisk EJ, Tajik AJ, Wann S. Hand- carried cardiac ultrasound (HCU) device: recommendations regard-ing new technology. A report from the Echocardiography Task Force on New Technology of the Nomenclature and Standards Committee of the American Society of Echocardiography. J Am Soc Echocardiogr 2002;15:369–73
17. Labovitz AJ, Noble VE, Bierig M, Goldstein SA, Jones R, Kort S, Porter TR, Spencer KT, Tayal VS, Wei K. Focused cardiac ultrasound in the emergent setting: a consensus statement of the American Society of Echocardiography and American College of Emergency Physicians. J Am Soc Echocardiogr 2010;23:1225–30
18. Mayo PH, Beaulieu Y, Doelken P, Feller- Kopman D, Harrod C, Kaplan A, Oropello J, Vieillard- Baron A, Axler O, Lichtenstein D, Maury E, Slama M, Vignon P. American College of Chest Physicians/La Societe de Reanimation de Langue Francaise statement on competence in critical care ultrasonography. Chest 2009;135:1050–60
19. Expert Round Table on Ultrasound in ICU. International expert statement on training standards for critical care ultrasonogra-phy. Intensive Care Med 2011;37:1077–83
20. Volpicelli G, Elbarbary M, Blaivas M, Lichtenstein DA, Mathis G, Kirkpatrick AW, Melniker L, Gargani L, Noble VE, Via G, Dean A, Tsung JW, Soldati G, Copetti R, Bouhemad B, Reis-sig A, Agricola E, Rouby JJ, Arbelot C, Liteplo A, Sargsyan A, Silva F, Hoppmann R, Breitkreutz R, Seibel A, Neri L, Storti E, Petrovic T. International evidence- based recommenda-tions for point- of- care lung ultrasound. Intensive Care Med 2012;38:577–91
21. Moore CL, Copel JA. Point- of- care ultrasonography. N Engl J Med 2011;364:749–57
Copyright © 2012 International Anethesia Research Society. Unauthorized reproduction of this article is prohibited.Copyright © 2012 International Anethesia Research Society. Unauthorized reproduction of this article is prohibited.
Routine Physician- Performed Ultrasound
XXX 2012 • Volume X • Number X www.anesthesia-analgesia.org 19
22. Faris JG, Veltman MG, Royse CF. Limited transthoracic echo-cardiography assessment in anaesthesia and critical care. Best Pract Res Clin Anaesthesiol 2009;23:285–98
23. Jensen MB, Sloth E, Larsen KM, Schmidt MB. Transthoracic echocardiography for cardiopulmonary monitoring in inten-sive care. Eur J Anaesthesiol 2004;21:700–7
24. Perera P, Mailhot T, Riley D, Mandavia D. The RUSH exam: Rapid Ultrasound in SHock in the evaluation of the critically ill. Emerg Med Clin North Am 2010;28:29–56, vii
25. Bouhemad B, Zhang M, Lu Q, Rouby JJ. Clinical review: bed-side lung ultrasound in critical care practice. Crit Care 2007; 11:205
26. Kory PD, Pellecchia CM, Shiloh AL, Mayo PH, DiBello C, Koenig S. Accuracy of ultrasonography performed by criti-cal care physicians for the diagnosis of DVT. Chest 2011;139: 538–42
27. Nazarian LN. The top 10 reasons musculoskeletal sonography is an important complementary or alternative technique to MRI. AJR Am J Roentgenol 2008;190:1621–6
28. Hoppmann RA, Rao VV, Poston MB, Howe DB, Hunt PS, Fowler SD, Paulman LE, Wells JR, Richeson NA, Catalana PV, Thomas LK, Britt Wilson L, Cook T, Riffle S, Neuffer FH, McCallum JB, Keisler BD, Brown RS, Gregg AR, Sims KM, Pow-ell CK, Garber MD, Morrison JE, Owens WB, Carnevale KA, Jennings WR, Fletcher S. An integrated ultrasound curriculum (iUSC) for medical students: 4-year experience. Crit Ultrasound J 2011;3:1–12
29. Rao S, van Holsbeeck L, Musial JL, Parker A, Bouffard JA, Bridge P, Jackson M, Dulchavsky SA. A pilot study of comprehensive ultrasound education at the Wayne State University School of Medicine: a pioneer year review. J Ultrasound Med 2008; 27:745–9
30. Angtuaco TL, Hopkins RH, DuBose TJ, Bursac Z, Angtuaco MJ, Ferris EJ. Sonographic physical diagnosis 101: teach-ing senior medical students basic ultrasound scanning skills using a compact ultrasound system. Ultrasound Q 2007;23: 157–60
31. Fernandez- Frackelton M, Peterson M, Lewis RJ, Perez JE, Coates WC. A bedside ultrasound curriculum for medical stu-dents: prospective evaluation of skill acquisition. Teach Learn Med 2007;19:14–9
32. Tshibwabwa ET, Groves HM, Levine MA. Teaching musculo-skeletal ultrasound in the undergraduate medical curriculum. Med Educ 2007;41:517–8
33. Syperda VA, Trivedi PN, Melo LC, Freeman ML, Ledermann EJ, Smith TM, Alben JO. Ultrasonography in preclinical education: a pilot study. J Am Osteopath Assoc 2008;108: 601–5
34. Wright SA, Bell AL. Enhancement of undergraduate rheuma-tology teaching through the use of musculoskeletal ultrasound. Rheumatology (Oxford) 2008;47:1564–6
35. Gogalniceanu P, Sheena Y, Kashef E, Purkayastha S, Darzi A, Paraskeva P. Is basic emergency ultrasound training feasible as part of standard undergraduate medical education? J Surg Educ 2010;67:152–6
36. Hoppmann RA, Riley R, Fletcher S, Howe D, Poston MB, Rao V, Harris S. First World Congress on ultrasound in medical educa-tion hosted by the University of South Carolina School of Medi-cine. J S C Med Assoc 2011;107:189–90
37. Fanshawe M, Ellis C, Habib S, Konstadt SN, Reich DL. A retrospective analysis of the costs and benefits related to alterations in cardiac surgery from routine intraoperative transesophageal echocardiography. Anesth Analg 2002;95: 824–7
38. Forrest AP, Lovelock ND, Hu JM, Fletcher SN. The impact of intraoperative transoesophageal echocardiography on an unselected cardiac surgical population: a review of 2343 cases. Anaesth Intensive Care 2002;30:734–41
39. Qaddoura FE, Abel MD, Mecklenburg KL, Chandrasekaran K, Schaff HV, Zehr KJ, Sundt TM, Click RL. Role of intraopera-tive transesophageal echocardiography in patients having coro-nary artery bypass graft surgery. Ann Thorac Surg 2004;78: 1586–90
40. Click RL, Abel MD, Schaff HV. Intraoperative transesophageal echocardiography: 5-year prospective review of impact on sur-gical management. Mayo Clin Proc 2000;75:241–7
41. Nowrangi SK, Connolly HM, Freeman WK, Click RL. Impact of intraoperative transesophageal echocardiography among patients undergoing aortic valve replacement for aortic steno-sis. J Am Soc Echocardiogr 2001;14:863–6
42. Couture P, Denault AY, McKenty S, Boudreault D, Plante F, Per-ron R, Babin D, Normandin L, Poirier N. Impact of routine use of intraoperative transesophageal echocardiography during cardiac surgery. Can J Anaesth 2000;47:20–6
43. Pearson AC, Castello R, Labovitz AJ. Safety and utility of trans-esophageal echocardiography in the critically ill patient. Am Heart J 1990;119:1083–9
44. Reichert CL, Visser CA, Koolen JJ, vd Brink RB, van Wezel HB, Meyne NG, Dunning AJ. Transesophageal echocardiography in hypotensive patients after cardiac operations. Comparison with hemodynamic parameters. J Thorac Cardiovasc Surg 1992;104:321–6
45. Khoury AF, Afridi I, Quinones MA, Zoghbi WA. Transesopha-geal echocardiography in critically ill patients: feasibility, safety, and impact on management. Am Heart J 1994;127:1363–71
46. Hwang JJ, Shyu KG, Chen JJ, Tseng YZ, Kuan P, Lien WP. Use-fulness of transesophageal echocardiography in the treatment of critically ill patients. Chest 1993;104:861–6
47. Heidenreich PA, Stainback RF, Redberg RF, Schiller NB, Cohen NH, Foster E. Transesophageal echocardiography predicts mortality in critically ill patients with unexplained hypoten-sion. J Am Coll Cardiol 1995;26:152–8
48. Poelaert JI, Trouerbach J, De Buyzere M, Everaert J, Colardyn FA. Evaluation of transesophageal echocardiography as a diagnostic and therapeutic aid in a critical care setting. Chest 1995;107:774–9
49. Sohn DW, Shin GJ, Oh JK, Tajik AJ, Click RL, Miller FA Jr, Seward JB. Role of transesophageal echocardiography in hemody-namically unstable patients. Mayo Clin Proc 1995;70:925–31
50. Alam M. Transesophageal echocardiography in critical care units: Henry Ford Hospital experience and review of the litera-ture. Prog Cardiovasc Dis 1996;38:315–28
51. Harris KM, Petrovic O, Davila- Roman VG, Yusen RD, Litten-berg B, Barzilai B. Changing patterns of transesophageal echo-cardiography use in the intensive care unit. Echocardiography 1999;16:559–65
52. Wake PJ, Ali M, Carroll J, Siu SC, Cheng DC. Clinical and echo-cardiographic diagnoses disagree in patients with unexplained hemodynamic instability after cardiac surgery. Can J Anaesth 2001;48:778–83
53. Colreavy FB, Donovan K, Lee KY, Weekes J. Transesopha-geal echocardiography in critically ill patients. Crit Care Med 2002;30:989–96
54. Bruch C, Comber M, Schmermund A, Eggebrecht H, Bartel T, Erbel R. Diagnostic usefulness and impact on management of transesophageal echocardiography in surgical intensive care units. Am J Cardiol 2003;91:510–3
55. Huttemann E, Schelenz C, Kara F, Chatzinikolaou K, Reinhart K. The use and safety of transoesophageal echocardiography in the general ICU: a minireview. Acta Anaesthesiol Scand 2004;48:827–36
56. Schmidlin D, Schuepbach R, Bernard E, Ecknauer E, Jenni R, Schmid ER. Indications and impact of postoperative trans-esophageal echocardiography in cardiac surgical patients. Crit Care Med 2001;29:2143–8
57. Brederlau J, Kredel M, Wurmb T, Dirks J, Schwemmer U, Broscheit J, Roewer N, Greim CA. Transesophageal echo-cardiography for non- cardiac surgery patients: superfluous luxury or essential diagnostic tool? [in German]. Anaesthesist 2006;55:937–40, 942–3
58. Orme RM, Oram MP, McKinstry CE. Impact of echocardiogra-phy on patient management in the intensive care unit: an audit of district general hospital practice. Br J Anaesth 2009;102:340–4
59. Cheitlin MD, Armstrong WF, Aurigemma GP, Beller GA, Bierman FZ, Davis JL, Douglas PS, Faxon DP, Gillam LD, Kimball TR, Kussmaul WG, Pearlman AS, Philbrick JT, Rakowski H, Thys DM, Antman EM, Smith SC Jr, Alpert JS,
Copyright © 2012 International Anethesia Research Society. Unauthorized reproduction of this article is prohibited.
E CORE REVIEW ARTICLE
20 www.anesthesia-analgesia.org ANESTHESIA & ANALGESIA
Gregoratos G, Anderson JL, Hiratzka LF, Hunt SA, Fuster V, Jacobs AK, Gibbons RJ, Russell RO. ACC/AHA/ASE 2003 guideline update for the clinical application of echocardiog-raphy: summary article—a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (ACC/AHA/ASE Committee to Update the 1997 Guidelines for the Clinical Application of Echocar-diography). Circulation 2003;108:1146–62
60. Douglas PS, Khandheria B, Stainback RF, Weissman NJ, Brin-dis RG, Patel MR, Alpert JS, Fitzgerald D, Heidenreich P, Mar-tin ET, Messer JV, Miller AB, Picard MH, Raggi P, Reed KD, Rumsfeld JS, Steimle AE, Tonkovic R, Vijayaraghavan K, Yeon SB, Hendel RC, Peterson E, Wolk MJ, Allen JM. ACCF/ASE/ACEP/ASNC/SCAI/SCCT/SCMR 2007 appropriateness cri-teria for transthoracic and transesophageal echocardiography: a report of the American College of Cardiology Foundation Quality Strategic Directions Committee Appropriateness Cri-teria Working Group, American Society of Echocardiography, American College of Emergency Physicians, American Society of Nuclear Cardiology, Society for Cardiovascular Angiogra-phy and Interventions, Society of Cardiovascular Computed Tomography, and the Society for Cardiovascular Mag-netic Resonance endorsed by the American College of Chest Physicians and the Society of Critical Care Medicine. J Am Coll Cardiol 2007;50:187–204
61. Fedson S, Neithardt G, Thomas P, Lickerman A, Radzienda M, DeCara JM, Lang RM, Spencer KT. Unsuspected clinically important findings detected with a small portable ultrasound device in patients admitted to a general medicine service. J Am Soc Echocardiogr 2003;16:901–5
62. Scholten C, Rosenhek R, Binder T, Zehetgruber M, Maurer G, Baumgartner H. Hand- held miniaturized cardiac ultrasound instruments for rapid and effective bedside diagnosis and patient screening. J Eval Clin Pract 2005;11:67–72
63. de Groot- de Laat LE, ten Cate FJ, Vourvouri EC, van Domburg RT, Roelandt JR. Impact of hand- carried cardiac ultrasound on diagnosis and management during cardiac consultation rounds. Eur J Echocardiogr 2005;6:196–201
64. Rugolotto M, Hu BS, Liang DH, Schnittger I. Rapid assessment of cardiac anatomy and function with a new hand- carried ultra-sound device (OptiGo): a comparison with standard echocar-diography. Eur J Echocardiogr 2001;2:262–9
65. Rugolotto M, Chang CP, Hu B, Schnittger I, Liang DH. Clini-cal use of cardiac ultrasound performed with a hand- carried device in patients admitted for acute cardiac care. Am J Cardiol 2002;90:1040–2
66. Joseph MX, Disney PJ, Da Costa R, Hutchison SJ. Transthoracic echocardiography to identify or exclude cardiac cause of shock. Chest 2004;126:1592–7
67. Marcelino PA, Marum SM, Fernandes AP, Germano N, Lopes MG. Routine transthoracic echocardiography in a general intensive care unit: an 18 month survey in 704 patients. Eur J Intern Med 2009;20:e37–42
68. Jakobsen CJ, Torp P, Sloth E. Perioperative feasibility of imag-ing the heart and pleura in patients with aortic stenosis under-going aortic valve replacement. Eur J Anaesthesiol 2007;24: 589–95
69. Kobal SL, Trento L, Baharami S, Tolstrup K, Naqvi TZ, Cercek B, Neuman Y, Mirocha J, Kar S, Forrester JS, Siegel RJ. Compari-son of effectiveness of hand- carried ultrasound to bedside car-diovascular physical examination. Am J Cardiol 2005;96:1002–6
70. Vignon P, Dugard A, Abraham J, Belcour D, Gondran G, Pepino F, Marin B, Francois B, Gastinne H. Focused training for goal-oriented hand-held echocardiography performed by noncardi-ologist residents in the intensive care unit. Intensive Care Med 2007;33:1795–9
71. Royse CF, Haji DL, Faris JG, Veltman MG, Kumar A, Royse AG. Evaluation of the interpretative skills of participants of a limited transthoracic echocardiography training course (H.A.R.T.scan course). Anaesth Intensive Care 2012;40:498–504
72. Canty DJ, Royse CF, Kilpatrick D, Bowman L, Royse AG. The impact of focused transthoracic echocardiography in the pre- operative clinic. Anaesthesia 2012;67:618–25
73. Canty DJ, Royse CF, Kilpatrick D, Williams DL, Royse AG. The impact of pre- operative focused transthoracic echocardiogra-phy in emergency non- cardiac surgery patients with known or risk of cardiac disease. Anaesthesia 2012;67:714–20
74. Canty DJ, Royse CF. Audit of anaesthetist- performed echo-cardiography on perioperative management decisions for non- cardiac surgery. Br J Anaesth 2009;103:352–8
75. Cowie B. Three years’ experience of focused cardiovascular ultrasound in the peri- operative period. Anaesthesia 2011;66: 268–73
76. Faris J, Hartley K, Fuller C, Langston R, Royse C, Veltman M. Audit of cardiac pathology detection using a criteria- based perioperative echocardiography service. Anaesth Intensive Care 2012;40:702–9
77. Vignon P, Chastagner C, Berkane V, Chardac E, Francois B, Nor-mand S, Bonnivard M, Clavel M, Pichon N, Preux PM, Maubon A, Gastinne H. Quantitative assessment of pleural effusion in critically ill patients by means of ultrasonography. Crit Care Med 2005;33:1757–63
78. Balik M, Plasil P, Waldauf P, Pazout J, Fric M, Otahal M, Pachl J. Ultrasound estimation of volume of pleural fluid in mechani-cally ventilated patients. Intensive Care Med 2006;32:318–21
79. Lichtenstein D, Meziere G, Biderman P, Gepner A. The “lung point”: an ultrasound sign specific to pneumothorax. Intensive Care Med 2000;26:1434–40
80. Diacon AH, Brutsche MH, Soler M. Accuracy of pleural punc-ture sites: a prospective comparison of clinical examination with ultrasound. Chest 2003;123:436–41
81. Akram A, Hartung T. Intercostal chest drains: a wake- up call from the National Patient Safety Agency rapid response report. J R Coll Physicians Edinb 2009;39:117–20
82. Harris A, O’Driscoll BR, Turkington PM. Survey of major com-plications of intercostal chest drain insertion in the UK. Post-grad Med J 2010;86:68–72
83. Lichtenstein D, Meziere G, Biderman P, Gepner A, Barre O. The comet- tail artifact: an ultrasound sign of alveolar- interstitial syndrome. Am J Respir Crit Care Med 1997;156:1640–6
84. Cortellaro F, Colombo S, Coen D, Duca PG. Lung ultrasound is an accurate diagnostic tool for the diagnosis of pneumonia in the emergency department. Emerg Med J 2012;29:19–23
85. Mathis G, Blank W, Reissig A, Lechleitner P, Reuss J, Schuler A, Beckh S. Thoracic ultrasound for diagnosing pulmonary embo-lism: a prospective multicenter study of 352 patients. Chest 2005;128:1531–8
86. Peris A, Tutino L, Zagli G, Batacchi S, Cianchi G, Spina R, Bon-izzoli M, Migliaccio L, Perretta L, Bartolini M, Ban K, Balik M. The use of point- of- care bedside lung ultrasound significantly reduces the number of radiographs and computed tomography scans in critically ill patients. Anesth Analg 2010;111:687–92
87. Troianos CA, Hartman GS, Glas KE, Skubas NJ, Eberhardt RT, Walker JD, Reeves ST. Guidelines for performing ultra-sound guided vascular cannulation: recommendations of the American Society of Echocardiography and the Society of Cardiovascular Anesthesiologists. J Am Soc Echocardiogr 2011;24:1291–318
88. Wigmore TJ, Smythe JF, Hacking MB, Raobaikady R, Mac-Callum NS. Effect of the implementation of NICE guidelines for ultrasound guidance on the complication rates associated with central venous catheter placement in patients presenting for routine surgery in a tertiary referral centre. Br J Anaesth 2007;99:662–5
89. Choi S, Brull R. Is ultrasound guidance advantageous for inter-ventional pain management? A review of acute pain outcomes. Anesth Analg 2011;113:596–604
90. Neal JM, Brull R, Chan VW, Grant SA, Horn JL, Liu SS, McCartney CJ, Narouze SN, Perlas A, Salinas FV, Sites BD, Tsui BC. The ASRA evidence- based medicine assessment of ultrasound- guided regional anesthesia and pain medicine: executive summary. Reg Anesth Pain Med 2010;35:S1–9
91. Barrington MJ, Watts SA, Gledhill SR, Thomas RD, Said SA, Sny-der GL, Tay VS, Jamrozik K. Preliminary results of the Austral-asian Regional Anaesthesia Collaboration: a prospective audit of more than 7000 peripheral nerve and plexus blocks for neurologic and other complications. Reg Anesth Pain Med 2009;34:534–41

Copyright © 2012 International Anethesia Research Society. Unauthorized reproduction of this article is prohibited.Copyright © 2012 International Anethesia Research Society. Unauthorized reproduction of this article is prohibited.
Routine Physician- Performed Ultrasound
XXX 2012 • Volume X • Number X www.anesthesia-analgesia.org 21
92. Soeding PE, Sha S, Royse CE, Marks P, Hoy G, Royse AG. A ran-domized trial of ultrasound- guided brachial plexus anaesthesia in upper limb surgery. Anaesth Intensive Care 2005;33:719–25
93. Hebbard PD, Barrington MJ, Vasey C. Ultrasound-guided continuous oblique subcostal transversus abdominis plane blockade: description of anatomy and clinical technique. Reg Anesth Pain Med 2010;35:436-41
94. Royse CF, Seah JL, Donelan L, Royse AG. Point of care ultra-sound for basic haemodynamic assessment: novice compared with an expert operator. Anaesthesia 2006;61:849–55
95. Cowie B, Kluger R. Evaluation of systolic murmurs using transthoracic echocardiography by anaesthetic trainees. Anaesthesia 2011;66:785–90
96. Kertai MD, Bountioukos M, Boersma E, Bax JJ, Thomson IR, Sozzi F, Klein J, Roelandt JR, Poldermans D. Aortic stenosis: an under-estimated risk factor for perioperative complications in patients undergoing noncardiac surgery. Am J Med 2004;116:8–13
97. Das P, Pocock C, Chambers J. The patient with a systolic mur-mur: severe aortic stenosis may be missed during cardiovascu-lar examination. QJM 2000;93:685–8
98. van Klei WA, Kalkman CJ, Tolsma M, Rutten CL, Moons KG. Pre- operative detection of valvular heart disease by anaesthe-tists. Anaesthesia 2006;61:127–32
99. Dal- Bianco JP, Sengupta PP, Khandheria BK. Role of echocar-diography in the diagnosis and management of asymptomatic severe aortic stenosis. Expert Rev Cardiovasc Ther 2008;6:223–33
100. Weyman AE, Feigebaum H, Dillon JC, Chang S. Cross- sectional echocardiography in assessing the severity of valvular aortic stenosis. Circulation 1975;52:828–34
101. Godley RW, Green D, Dillon JC, Rogers EW, Feigenbaum H, Weyman AE. Reliability of two- dimensional echocardiogra-phy in assessing the severity of valvular aortic stenosis. Chest 1981;79:657–62
102. Chang S, Clements S, Chang J. Aortic stenosis: echocardio-graphic cusp separation and surgical description of aortic valve in 22 patients. Am J Cardiol 1977;39:499–504
103. Robin ED. Death by pulmonary artery flow- directed catheter: time for a moratorium? Chest 1987;92:727–31
104. Connors AF Jr, Speroff T, Dawson NV, Thomas C, Harrell FE Jr, Wagner D, Desbiens N, Goldman L, Wu AW, Califf RM, Fulk-erson WJ Jr, Vidaillet H, Broste S, Bellamy P, Lynn J, Knaus WA. The effectiveness of right heart catheterization in the initial care of critically ill patients. SUPPORT Investigators. JAMA 1996;276:889–97
105. Douglas PS, Garcia MJ, Haines DE, Lai WW, Manning WJ, Patel AR, Picard MH, Polk DM, Ragosta M, Ward RP, Weiner RB. ACCF/ASE/AHA/ASNC/HFSA/HRS/SCAI/SCCM/SCCT/SCMR 2011 Appropriate Use Criteria for Echocar-diography. A Report of the American College of Cardiology Foundation Appropriate Use Criteria Task Force, American Society of Echocardiography, American Heart Association, American Society of Nuclear Cardiology, Heart Failure Society of America, Heart Rhythm Society, Society for Cardiovascular Angiography and Interventions, Society of Critical Care Medi-cine, Society of Cardiovascular Computed Tomography, and Society for Cardiovascular Magnetic Resonance Endorsed by the American College of Chest Physicians. J Am Coll Cardiol 2011;57:1126–66
106. American Society of Anesthesiologists and Society of Car-diovascular Anesthesiologists Task Force on Transesopha-geal Echocardiography. Practice guidelines for perioperative transesophageal echocardiography. An updated report by the American Society of Anesthesiologists and the Society of Car-diovascular Anesthesiologists Task Force on Transesoph ageal Echocardiography. Anesthesiology 2010;112:1084–96
107. Breitkreutz R, Walcher F, Seeger FH. Focused echocardio-graphic evaluation in resuscitation management: concept of an advanced life support- conformed algorithm. Crit Care Med 2007;35:S150–61
108. Liu SC, Chang WT, Huang CH, Weng TI, Ma Matthew HM, Chen WJ. The value of portable ultrasound for evaluation of cardiomegaly patients presenting at the emergency depart-ment. Resuscitation 2005;64:327–31
109. Pershad J, Myers S, Plouman C, Rosson C, Elam K, Wan J, Chin T. Bedside limited echocardiography by the emergency physi-cian is accurate during evaluation of the critically ill patient. Pediatrics 2004;114:e667–71
110. Kimura BJ, Shaw DJ, Agan DL, Amundson SA, Ping AC, DeMaria AN. Value of a cardiovascular limited ultrasound examination using a hand- carried ultrasound device on clini-cal management in an outpatient medical clinic. Am J Cardiol 2007;100:321–5
111. Rose JS, Bair AE, Mandavia D, Kinser DJ. The UHP ultrasound protocol: a novel ultrasound approach to the empiric evalua-tion of the undifferentiated hypotensive patient. Am J Emerg Med 2001;19:299–302
112. Carr BG, Dean AJ, Everett WW, Ku BS, Mark DG, Okusanya O, Horan AD, Gracias VH. Intensivist bedside ultrasound (INBU) for volume assessment in the intensive care unit: a pilot study. J Trauma 2007;63:495–500
113. Mishra M, Chauhan R, Sharma KK, Dhar A, Bhise M, Dhole S, Omar A, Kasliwal RR, Trehan N. Real- time intraoperative transesophageal echocardiography—how useful? Experience of 5,016 cases. J Cardiothorac Vasc Anesth 1998;12:625–32
114. Sutton DC, Kluger R. Intraoperative transoesophageal echo-cardiography: impact on adult cardiac surgery. Anaesth Inten-sive Care 1998;26:287–93
115. Eltzschig HK, Rosenberger P, Loffler M, Fox JA, Aranki SF, Shernan SK. Impact of intraoperative transesophageal echo-cardiography on surgical decisions in 12,566 patients under-going cardiac surgery. Ann Thorac Surg 2008;85:845–52
116. Klein AA, Snell A, Nashef SA, Hall RM, Kneeshaw JD, Arrow-smith JE. The impact of intra- operative transoesophageal echocardiography on cardiac surgical practice. Anaesthesia 2009;64:947–52
117. Kaushal SK, Dagar KS, Singh A, Kumar K, Radhakrishnan S, Girotra S, Shrivastava S, Iyer KS. Intraoperative echocardiog-raphy as a routine adjunct in assessing repair of congenital heart defects: experience with 300 cases. Ann Card Anaesth 1998;1:36–45
118. Randolph GR, Hagler DJ, Connolly HM, Dearani JA, Puga FJ, Danielson GK, Abel MD, Pankratz VS, O’Leary PW. Intraopera-tive transesophageal echocardiography during surgery for con-genital heart defects. J Cardiothorac Vasc Surg 2002;124:1176–82
119. Bettex DA, Schmidlin D, Bernath MA, Pretre R, Hurni M, Jenni R, Chassot PG, Schmid ER. Intraoperative transesopha-geal echocardiography in pediatric congenital cardiac sur-gery: a two- center observational study. Anesth Analg 2003; 97:1275–82
120. Ma XJ, Huang GY, Liang XC, Chen ZG, Jia B, Li X, Ye M. Tran-soesophageal echocardiography in monitoring, guiding, and evaluating surgical repair of congenital cardiac malformations in children. Cardiol Young 2007;17:301–6
121. Brandt RR, Oh JK, Abel MD, Click RL, Orszulak TA, Seward JB. Role of emergency intraoperative transesophageal echocar-diography. J Am Soc Echocardiogr 1998;11:972–7
122. Kolev N, Brase R, Swanevelder J, Oppizzi M, Riesgo MJ, van der Maaten JM, Abiad MG, Guarracino F, Zimpfer M. The influence of transoesophageal echocardiography on intra-operative decision making: a European multicentre study. European Perioperative TOE Research Group. Anaesthesia 1998;53:767–73
123. Suriani RJ, Neustein S, Shore- Lesserson L, Konstadt S. Intraop-erative transesophageal echocardiography during noncardiac surgery. J Cardiothorac Vasc Anesth 1998;12:274–80
124. Denault AY, Couture P, McKenty S, Boudreault D, Plante F, Perron R, Babin D, Buithieu J. Perioperative use of transesoph-ageal echocardiography by anesthesiologists: impact in non-cardiac surgery and in the intensive care unit. Can J Anaesth 2002;49:287–93
125. Hofer CK, Zollinger A, Rak M, Matter- Ensner S, Klaghofer R, Pasch T, Zalunardo MP. Therapeutic impact of intra- operative transoesophageal echocardiography during noncardiac sur-gery. Anaesthesia 2004;59:3–9
126. Schulmeyer MC, Santelices E, Vega R, Schmied S. Impact of intraoperative transesophageal echocardiography during non-cardiac surgery. J Cardiothorac Vasc Anesth 2006;20:768–71

Copyright © 2012 International Anethesia Research Society. Unauthorized reproduction of this article is prohibited.
E CORE REVIEW ARTICLE
22 www.anesthesia-analgesia.org ANESTHESIA & ANALGESIA
127. Oh JK, Seward JB, Khandheria BK, Gersh BJ, McGregor CG, Freeman WK, Sinak LJ, Tajik AJ. Transesophageal echo-cardiography in critically ill patients. Am J Cardiol 1990; 66:1492–5
128. Font VE, Obarski TP, Klein AL, Bartlett JC, Nemec JJ, Stew-art WJ, Salcedo EE. Transesophageal echocardiography in the critical care unit. Cleve Clin J Med 1991;58:315–22
129. Foster E, Schiller NB. The role of transesophageal echocardiog-raphy in critical care: UCSF experience. J Am Soc Echocardiogr 1992;5:368–74
130. Chenzbraun A, Pinto FJ, Schnittger I. Transesophageal echo-cardiography in the intensive care unit: impact on diagnosis and decision- making. Clin Cardiol 1994;17:438–44
131. Vignon P, Mentec H, Terre S, Gastinne H, Gueret P, Lemaire F. Diagnostic accuracy and therapeutic impact of transthoracic and transesophageal echocardiography in mechanically venti-lated patients in the ICU. Chest 1994;106:1829–34
132. Slama MA, Novara A, Van de Putte P, Diebold B, Safavian A, Safar M, Ossart M, Fagon JY. Diagnostic and therapeutic impli-cations of transesophageal echocardiography in medical ICU patients with unexplained shock, hypoxemia, or suspected endocarditis. Intensive Care Med 1996;22:916–22
133. McLean AS. Transoesophageal echocardiography in the inten-sive care unit. Anaesth Intensive Care 1998;26:22–5
134. Manasia AR, Nagaraj HM, Kodali RB, Croft LB, Oropello JM, Kohli- Seth R, Leibowitz AB, DelGiudice R, Hufanda JF, Benja-min E, Goldman ME. Feasibility and potential clinical utility of goal- directed transthoracic echocardiography performed by noncardiologist intensivists using a small hand- carried device (SonoHeart) in critically ill patients. J Cardiothorac Vasc Anesth 2005;19:155–9
135. Stanko LK, Jacobsohn E, Tam JW, De Wet CJ, Avidan M. Trans-thoracic echocardiography: impact on diagnosis and manage-ment in tertiary care intensive care units. Anaesth Intensive Care 2005;33:492–6
136. Jones AE, Tayal VS, Sullivan DM, Kline JA. Randomized, con-trolled trial of immediate versus delayed goal- directed ultra-sound to identify the cause of nontraumatic hypotension in emergency department patients. Crit Care Med 2004;32:1703–8
137. Hauser AM. The emerging role of echocardiography in the emergency department. Ann Emerg Med 1989;18:1298–303
138. Atar S, Feldman A, Darawshe A, Siegel RJ, Rosenfeld T. Util-ity and diagnostic accuracy of hand- carried ultrasound for emergency room evaluation of chest pain. Am J Cardiol 2004;94:408–9
139. Blaivas M, Fox JC. Outcome in cardiac arrest patients found to have cardiac standstill on the bedside emergency department echocardiogram. Acad Emerg Med 2001;8:616–21
140. Salen P, Melniker L, Chooljian C, Rose JS, Alteveer J, Reed J, Heller M. Does the presence or absence of sonographically identified cardiac activity predict resuscitation outcomes of cardiac arrest patients? Am J Emerg Med 2005;23:459–62
141. Tayal VS, Kline JA. Emergency echocardiography to detect pericardial effusion in patients in PEA and near- PEA states. Resuscitation 2003;59:315–8
142. Blaivas M. Incidence of pericardial effusion in patients pre-senting to the emergency department with unexplained dys-pnea. Acad Emerg Med 2001;8:1143–6
143. Jones AE, Craddock PA, Tayal VS, Kline JA. Diagnostic accuracy of left ventricular function for identifying sepsis among emer-gency department patients with nontraumatic symptomatic undifferentiated hypotension. Shock 2005;24:513–7