Copy of INTRODUCTIO1
18
INTRODUCTION Chronic Obstructive Pulmonary Disease (COPD), also known as chronic airflow limitation, is a group of disorders associated with persistent or recurrent obstruction of airflow, which include chronic bronchitis, emphysema. These conditions frequently overlap. Most commonly, bronchitis and emphysema occur together. The most common chronic lung disease, COPD affects an estimated 17 million persons in the United States. The incidence is rising. The most common cause is smoking cigarettes. COPD is a widespread disorder; 11.4 million U. S. adults (age 18 and over) are estimated to have the disease. However, close to 24 million have evidence of impaired lung function. It is the fourth leading cause of death in America. However, the burden of COPD is even greater from a global perspective, where it is projected to rank fifth in 2020 in burden of disease caused worldwide. Bronchiectasis - It is an extreme form of bronchitis, causes permanent, abnormal dilation and distortion of bronchi and bronchioles - It develops when bronchial walls are weakened by chronic inflammatory changes in the bronchial mucosa and occurs most often after recurrent inflammatory conditions - Any condition producing a narrowing of the lumen of the bronchioles, however, may result in bronchiectasis, including tuberculosis, adenoviral infections, and pneumonia - It is usually localized to a lung lobe or segment rather than generalize throughout the lungs Emphysema - Progressive destruction of alveoli related to chronic inflammation - Decreased surface area of respiratory bronchioles, alveoli, and alveolar ducts available for gas exchange - Airway collapse due to loss of elasticity in respiratory system tissues
-
Upload
independent -
Category
Documents
-
view
3 -
download
0
Transcript of Copy of INTRODUCTIO1
INTRODUCTION
Chronic Obstructive Pulmonary Disease (COPD), alsoknown as chronic airflow limitation, is a group of disordersassociated with persistent or recurrent obstruction ofairflow, which include chronic bronchitis, emphysema. Theseconditions frequently overlap. Most commonly, bronchitisand emphysema occur together.
The most common chronic lung disease, COPD affects anestimated 17 million persons in the United States. Theincidence is rising. The most common cause is smokingcigarettes.
COPD is a widespread disorder; 11.4 million U. S.adults (age 18 and over) are estimated to have the disease.However, close to 24 million have evidence of impaired lungfunction.
It is the fourth leading cause of death in America.However, the burden of COPD is even greater from a globalperspective, where it is projected to rank fifth in 2020 inburden of disease caused worldwide.
Bronchiectasis- It is an extreme form of bronchitis, causes
permanent, abnormal dilation and distortion ofbronchi and bronchioles
- It develops when bronchial walls are weakened bychronic inflammatory changes in the bronchial mucosaand occurs most often after recurrent inflammatoryconditions
- Any condition producing a narrowing of the lumen ofthe bronchioles, however, may result inbronchiectasis, including tuberculosis, adenoviralinfections, and pneumonia
- It is usually localized to a lung lobe or segmentrather than generalize throughout the lungs
Emphysema- Progressive destruction of alveoli related to
chronic inflammation- Decreased surface area of respiratory bronchioles,
alveoli, and alveolar ducts available for gasexchange
- Airway collapse due to loss of elasticity inrespiratory system tissues
- A chronic form of obstructive pulmonary disease(COPD)a) A group of diseases with the major characteristic
of airflow restrictionb) Common symptoms include difficulty with
exhalation caused by airways obstructed by edemaor excessive mucus production
c) Lung hyperinflation causes alveolar air trappingand leads to frequent pulmonary infections
d) Symptoms may be reversible in asthma, but aretypically progressive with emphysema, chronicbronchitis and cystic fibrosis
Etiology
Bronchiectasis Obstruction and infection are the major conditions
associated with bronchiectasis Primary ciliary dyskinesia, an autosomal recessive
syndrome with variable penetrance poorly functioningcilia contribute to the retention of secretions andrecurrent infections
Allergic bronchopulmonary aspergillosis is a condition thatresults from a hypersensitivity reaction to the fungusAspergillous fumigatus.
Emphysema Cigarette smoking is the primary etiology associated
with emphysema Contributing factors include chronic respiratory
inflammation from air pollution or occupationalsubstances such as coal, glass, and asbestos
Diagnosis in young and middle-aged adults may beassociated with hereditary deficiency of alpha1-antitrypsin, an enzyme that prevents breakdown of lungtissue protein.
Assessment findings
1. Clinical ManifestationsBronchiectasis
Cough and purulent sputum production in largequantities
Fever, hemoptysis, nasal stuffiness, and drainagefrom sinusitis
Fatigue and weakness Clubbing of the fingers (late in the disease)
Emphysema “Pink Puffer” is a classic clinical description
characterized by barrel chest, pursed lip breathing(caused by forced exhalation), obvious use ofaccessory muscles when breathing, and underweightappearance
Anorexia Lung auscultation yields overall diminished breath
sounds, and wheezes or crackles may be present Exertional dyspnea progresses with advancing disease Persistent tachycardia is related to inadequate
oxygenation Finger clubbing (late in the disease)
2. Laboratory and diagnostic study findings
Bronchiectasis Bronchoscopy helps to identify the source of
secretions or the bleeding sit in hemoptysis Chest X-rays show peribronchial thickening, areas of
atelectasis, and scattered cystic changes CBC detects anemia and leucocytosis PFTs detect decreased vital capacity, expiratory
flow, and hypoxemia Sputum culture and Gram stain identify predominant
organisms
Emphysema ABG studies show reduced PaO2 with normal PaCO2 until
late in the disease Chest X-ray in advanced disease reveal a flattened
diaphragm, reduced vascular marking in the lungperiphery, enlarged anteroposterior chest diameter,and a verticular heart
CBC shows increased Hb late in disease when clienthas severe persistent hypoxia
ECG shows tall, symmetrical P waves in leads II,III, and aVf, vertical QRS axis, and signs of rightventricular hypertrophy late in disease
PFTs show increase residual volume, total lungcapacity, diffusing capacity, and expiratory volumes
3. Therapeutic Managementa. Goals of therapy are to improve ventilation and
promote patent airway by removal of secretionsb. Remove environmental pollutants and encourage
smoking cessationc. Bronchodilator therapy
d. Beta adrenergic agonistse. Corticosteroid therapyf. Oxygen therapy and nebulization therapyg. Chest physiotherapyh. Intermittent positive pressure breathing (IPPB)i. Mechanical ventilationj. Surgical procedures include bullectomy, lung volume
reduction surgery and lung transplantation
4. Client educationa. Smoking cessationb. Teach clients how to avoid occupational or
environmental pollutantsc. Maintain adequate nutrition with emphasis on higher
calorie intake
Community-Acquired Pneumonia- It may be bacterial or viral infection; bacterial
infection often follows an upper respiratory tractviral infection.
Etiologic agent It may result from bacteria, viruses, mycoplasmas,
fungal agents, and protozoa Pneumonia may also result from aspiration from
aspiration of food, fluids, or vomitus or frominhalation of toxic or caustic chemicals, smoke,dusts, or gases
Major risk factors: 1) advanced age, 2) a history ofsmoking, 3) upper respiratory infection, 4) trachealintubation, 5) prolonged immobility, 6)immunosuppressive therapy, 7) a non-functional immunesystem, 8) malnutrition, 9) dehydration, and 10)chronic disease states, such as diabetes, heartdisease, chronic lung disease, renal disease, andcancer.
Additional risk factors are exposure to air pollution;altered consciousness (from alcoholism, drug overdose,general anesthesia, or a seizure disorder); inhalationof noxious substances; aspiration of food, liquid, orforeign or gastric material; and residence ininstitutional settings, where transmission of thedisease is more likely.
Assessment Finding Abrupt onset of high fever [greater than 100ºF
(37.8ºC)], shaking, chills, sweats, or pleuriticchest pain, and cough productive of mucopurulent
sputum occasionally patient may have hemoptysis,dyspnea, respiratory grunting and nasal flaring,flushed cheeks headache, and fatigue
Bronchial breath sounds ausculated over consolidatedlung fields; egophony “EE” to “AY”
Cyanotic lips and nail beds In elderly clients, the only signs may be mental
status change and dehydration
Laboratory Exam Chest radiograph shows density changes, primarily in
the lower lung fields Sputum culture and sensitivity are positive for a
specific causative organism White blood cell (WBC) count is elevated in
pneumonia of bacterial origin; WBC count isdepressed in pneumonia of mycoplasmal or viralorigin
PATIENT’S PFROFILE
NAME: BAB
AGE: 75 yrs old
ADDRESS: Solana, Cagayan
GENDER: Female
BIRTHDATE: June 05, 1937
HEIGHT: 5’2 / 157.4 cm
WEIGHT: 44 kg
BMI: 17.76
BIRTH PLACE: Santo Tomas, Isabela
CIVIL STATUS: Married
OCCUPATION: N/A (Retired Schoolteacher)
EDUCATIONAL ATTAINMENT: College Graduate
RELIGION: Roman Catholic
NATIONALITY: Filipino
ADMISSION:
Date: January 10, 2012
Time: 11:50 am
ADMITTING VITAL SIGNS:
RR: 24cpm PR: 105bpm
TEMP: 36.1 BP: 110/70 mmHg
ATTENDING PHYSICIAN: Dr. Rhoderick Ian Reyes
CHIEF COMPLAINT: Difficulty of Breathing
ADMITTING DIAGNOSIS: Pneumonia, Chronic Obstructed Pulmonary Disease (COPD) DM Type II
FINAL DIAGNOSIS: Community Acquired Pneumonia moderate risk, Bronchiectesis Cor Pulmonale
SOURCE OF INFORMATION: S.O, Patient BAB, and Chart
DATE HANDLED: January 13-14, 2013
DATE OF INTERVIEW: January 13-14, 2013
Table
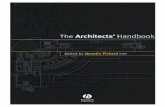
Figure 1. The graph shows the relationship between age andthe number of cases of lower respiratory infectionincluding COPD and Pneumonia among male and female in theyear 2011.
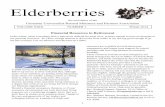
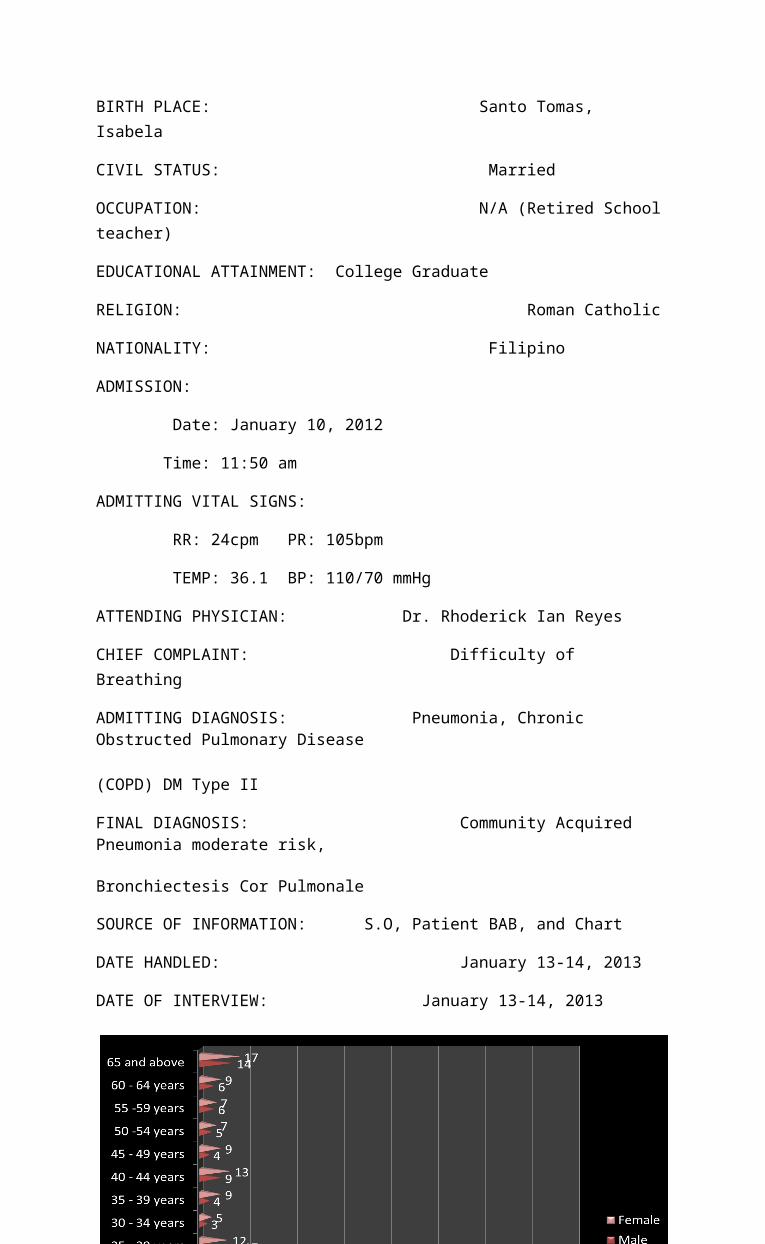
Figure 2. The graph shows the relationship between age andthe number of cases of lower respiratory infectionincluding COPD and Pneumonia among male and female in theyear 2012.
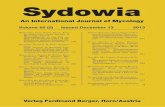
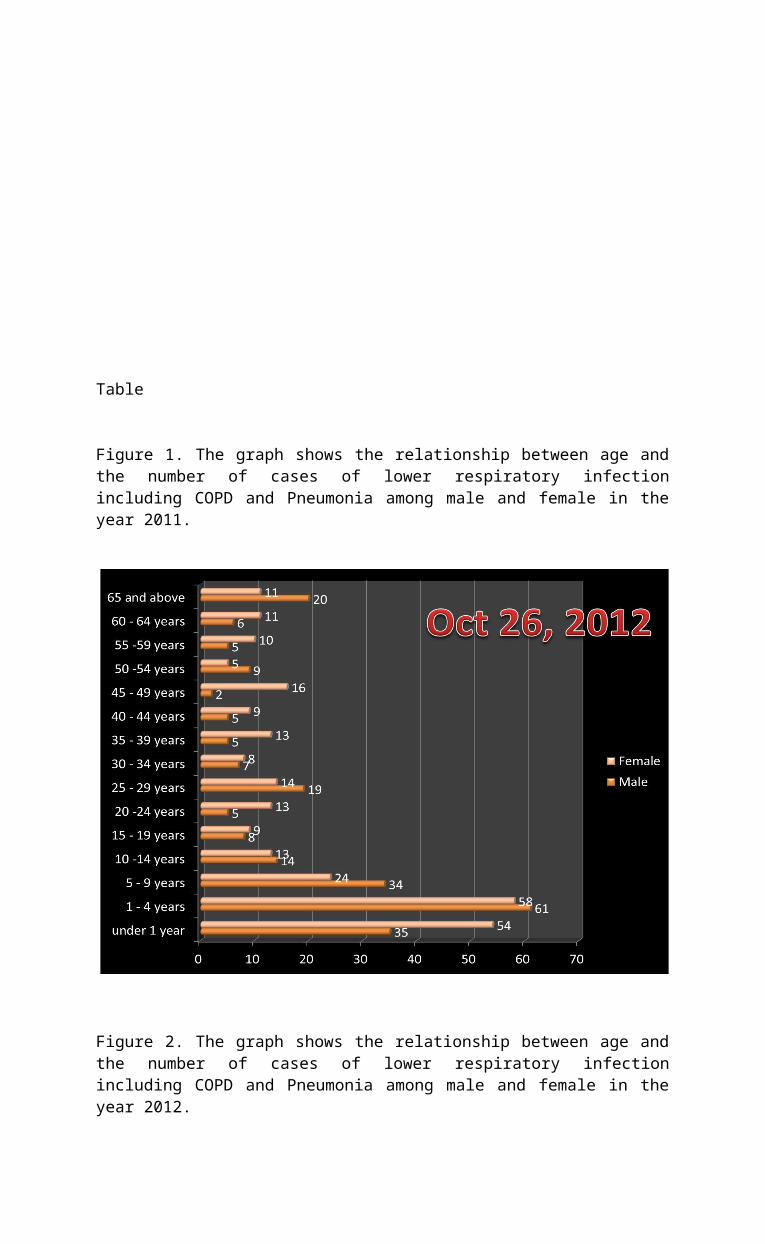
Figure 3. The graph shows the relationship between age andthe number of cases of lower respiratory infectionincluding COPD and Pneumonia among male and female in theyear 2011.
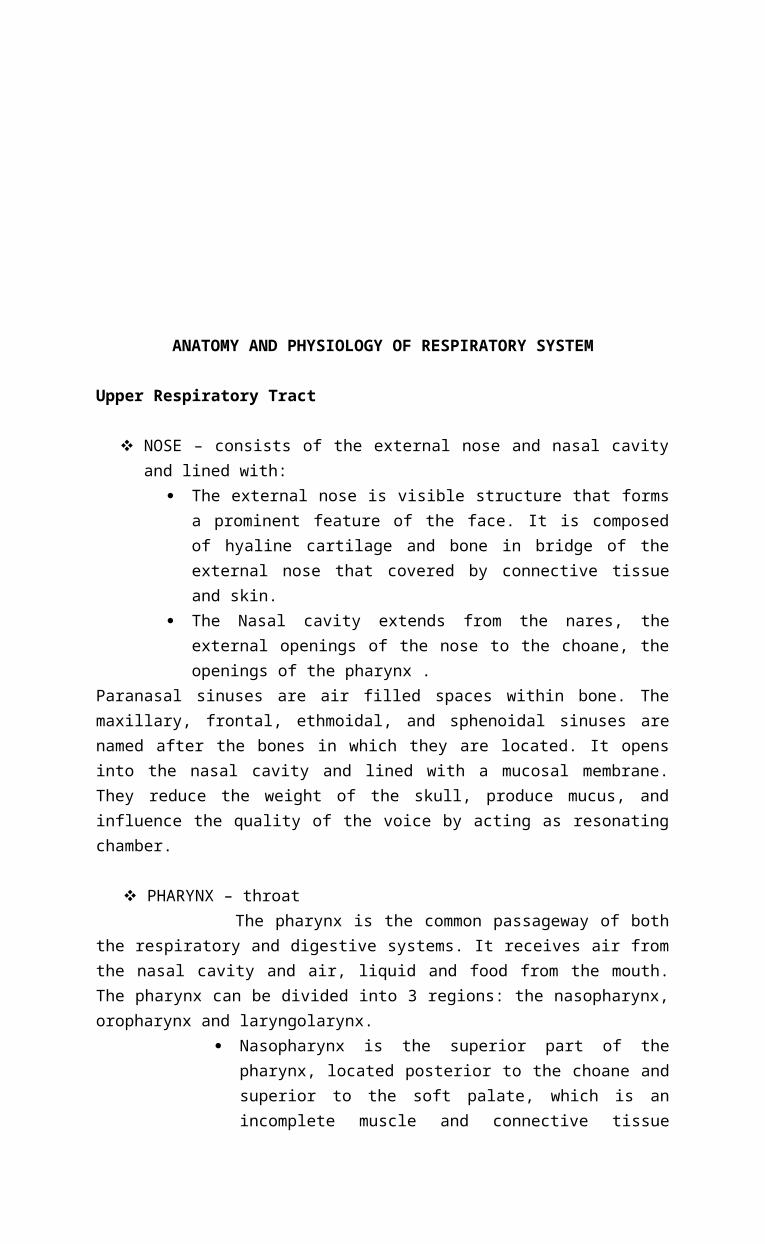
ANATOMY AND PHYSIOLOGY OF RESPIRATORY SYSTEM
Upper Respiratory Tract
NOSE – consists of the external nose and nasal cavityand lined with:
The external nose is visible structure that formsa prominent feature of the face. It is composedof hyaline cartilage and bone in bridge of theexternal nose that covered by connective tissueand skin.
The Nasal cavity extends from the nares, theexternal openings of the nose to the choane, theopenings of the pharynx .
Paranasal sinuses are air filled spaces within bone. Themaxillary, frontal, ethmoidal, and sphenoidal sinuses arenamed after the bones in which they are located. It opensinto the nasal cavity and lined with a mucosal membrane.They reduce the weight of the skull, produce mucus, andinfluence the quality of the voice by acting as resonatingchamber.
PHARYNX – throat The pharynx is the common passageway of both
the respiratory and digestive systems. It receives air fromthe nasal cavity and air, liquid and food from the mouth.The pharynx can be divided into 3 regions: the nasopharynx,oropharynx and laryngolarynx.
Nasopharynx is the superior part of thepharynx, located posterior to the choane andsuperior to the soft palate, which is anincomplete muscle and connective tissue
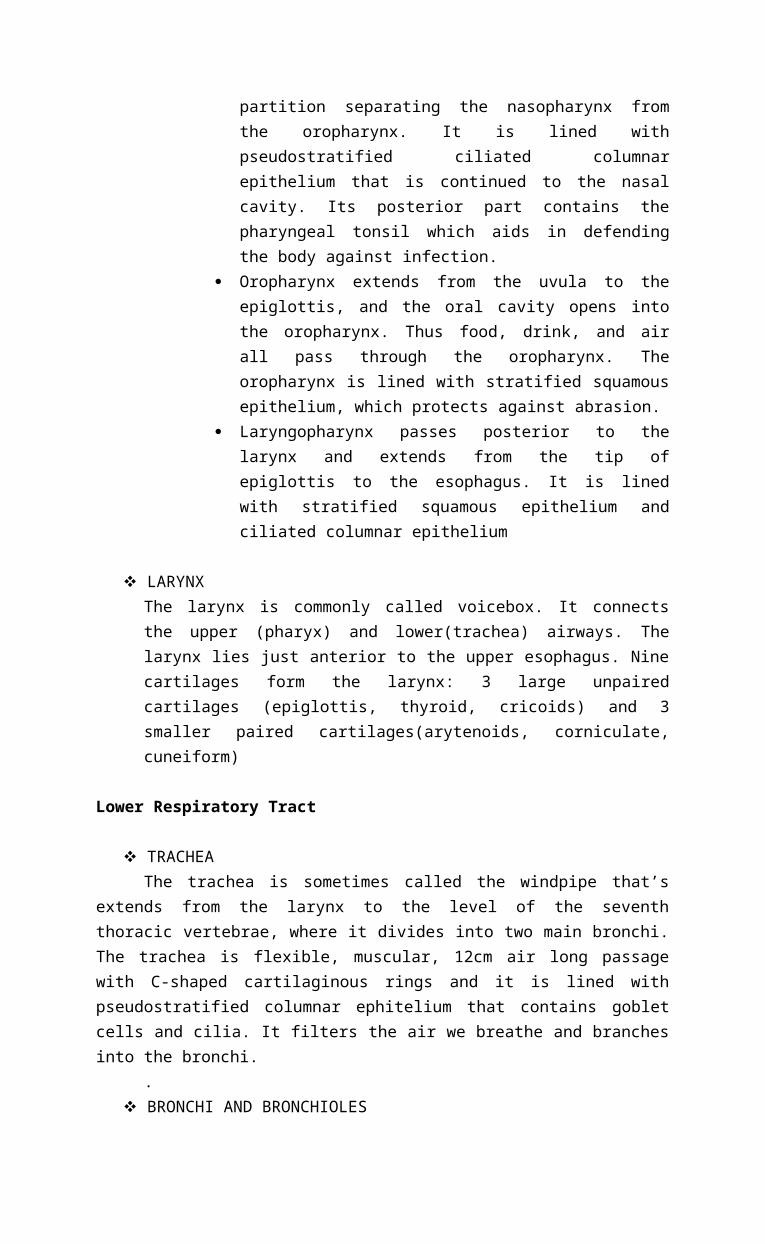
partition separating the nasopharynx fromthe oropharynx. It is lined withpseudostratified ciliated columnarepithelium that is continued to the nasalcavity. Its posterior part contains thepharyngeal tonsil which aids in defendingthe body against infection.
Oropharynx extends from the uvula to theepiglottis, and the oral cavity opens intothe oropharynx. Thus food, drink, and airall pass through the oropharynx. Theoropharynx is lined with stratified squamousepithelium, which protects against abrasion.
Laryngopharynx passes posterior to thelarynx and extends from the tip ofepiglottis to the esophagus. It is linedwith stratified squamous epithelium andciliated columnar epithelium
LARYNX The larynx is commonly called voicebox. It connectsthe upper (pharyx) and lower(trachea) airways. Thelarynx lies just anterior to the upper esophagus. Ninecartilages form the larynx: 3 large unpairedcartilages (epiglottis, thyroid, cricoids) and 3smaller paired cartilages(arytenoids, corniculate,cuneiform)
Lower Respiratory Tract
TRACHEAThe trachea is sometimes called the windpipe that’s
extends from the larynx to the level of the sevenththoracic vertebrae, where it divides into two main bronchi.The trachea is flexible, muscular, 12cm air long passagewith C-shaped cartilaginous rings and it is lined withpseudostratified columnar ephitelium that contains gobletcells and cilia. It filters the air we breathe and branchesinto the bronchi.
. BRONCHI AND BRONCHIOLES
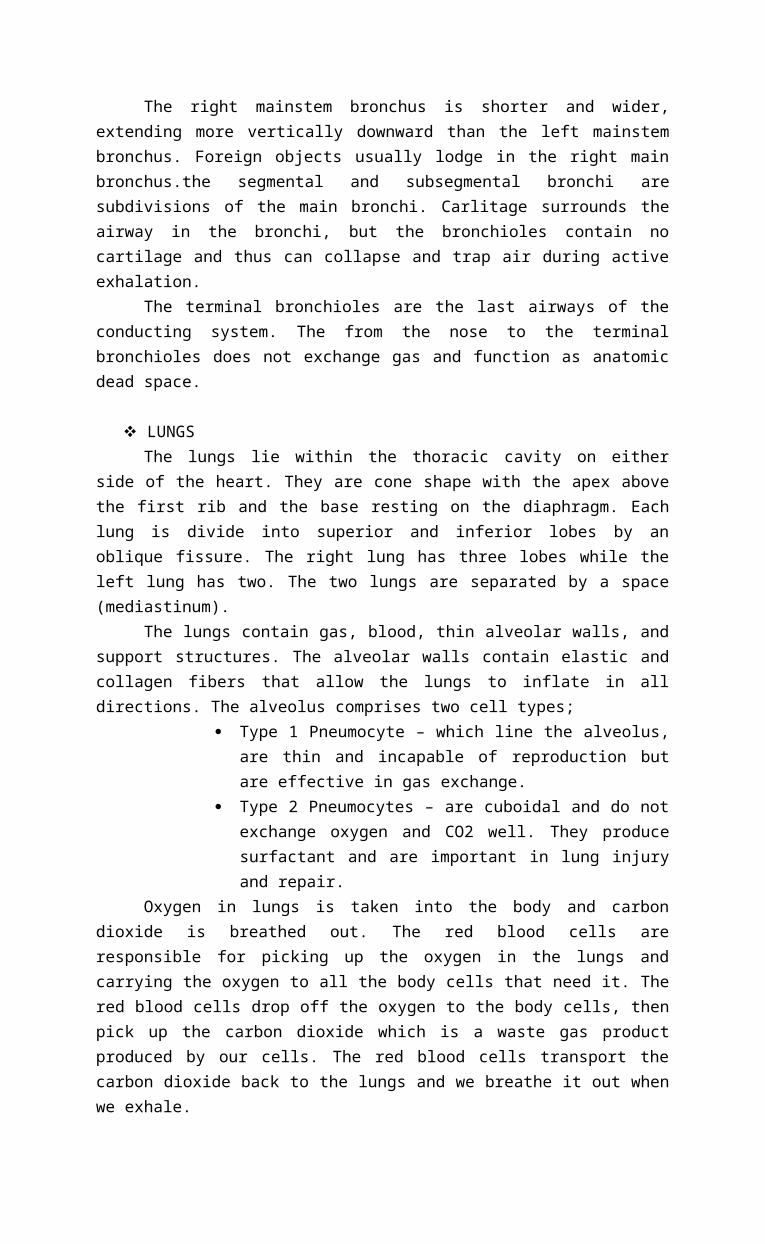
The right mainstem bronchus is shorter and wider,extending more vertically downward than the left mainstembronchus. Foreign objects usually lodge in the right mainbronchus.the segmental and subsegmental bronchi aresubdivisions of the main bronchi. Carlitage surrounds theairway in the bronchi, but the bronchioles contain nocartilage and thus can collapse and trap air during activeexhalation.
The terminal bronchioles are the last airways of theconducting system. The from the nose to the terminalbronchioles does not exchange gas and function as anatomicdead space.
LUNGSThe lungs lie within the thoracic cavity on either
side of the heart. They are cone shape with the apex abovethe first rib and the base resting on the diaphragm. Eachlung is divide into superior and inferior lobes by anoblique fissure. The right lung has three lobes while theleft lung has two. The two lungs are separated by a space(mediastinum).
The lungs contain gas, blood, thin alveolar walls, andsupport structures. The alveolar walls contain elastic andcollagen fibers that allow the lungs to inflate in alldirections. The alveolus comprises two cell types;
Type 1 Pneumocyte – which line the alveolus,are thin and incapable of reproduction butare effective in gas exchange.
Type 2 Pneumocytes – are cuboidal and do notexchange oxygen and CO2 well. They producesurfactant and are important in lung injuryand repair.
Oxygen in lungs is taken into the body and carbondioxide is breathed out. The red blood cells areresponsible for picking up the oxygen in the lungs andcarrying the oxygen to all the body cells that need it. Thered blood cells drop off the oxygen to the body cells, thenpick up the carbon dioxide which is a waste gas productproduced by our cells. The red blood cells transport thecarbon dioxide back to the lungs and we breathe it out whenwe exhale.
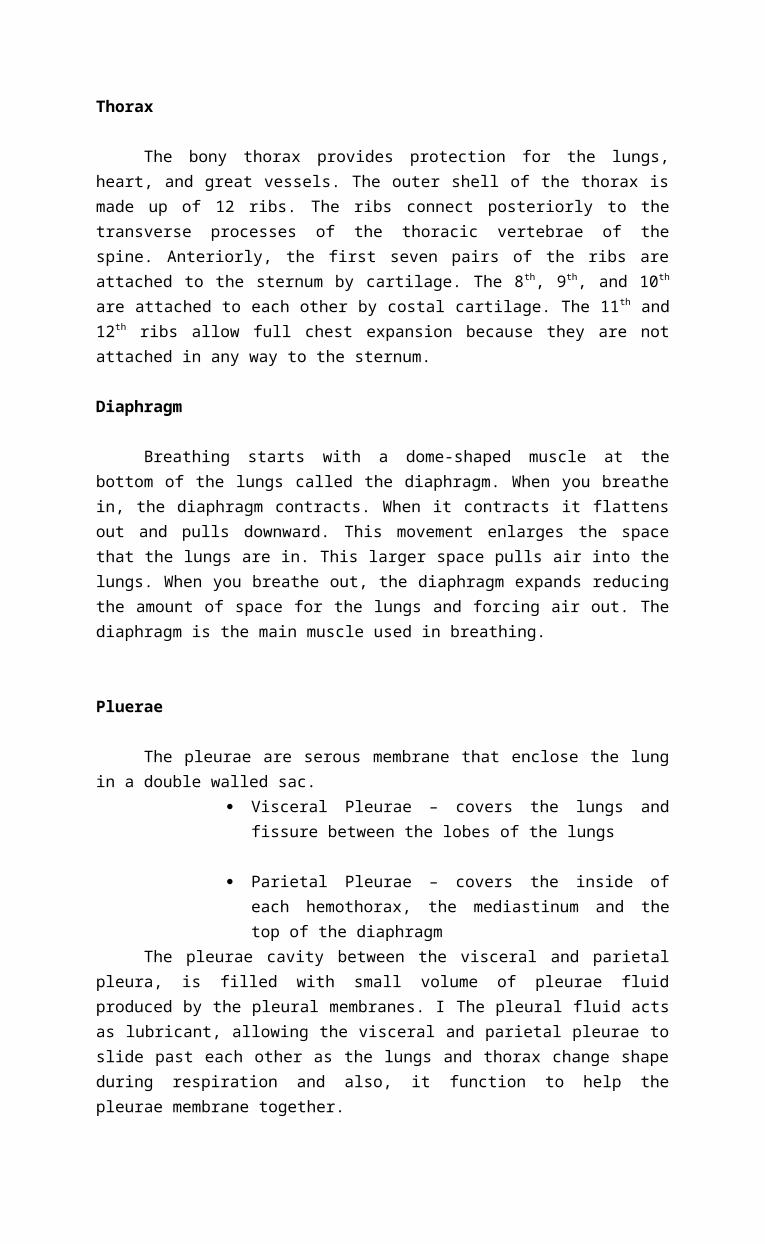
Thorax
The bony thorax provides protection for the lungs,heart, and great vessels. The outer shell of the thorax ismade up of 12 ribs. The ribs connect posteriorly to thetransverse processes of the thoracic vertebrae of thespine. Anteriorly, the first seven pairs of the ribs areattached to the sternum by cartilage. The 8th, 9th, and 10th
are attached to each other by costal cartilage. The 11th and12th ribs allow full chest expansion because they are notattached in any way to the sternum.
Diaphragm
Breathing starts with a dome-shaped muscle at thebottom of the lungs called the diaphragm. When you breathein, the diaphragm contracts. When it contracts it flattensout and pulls downward. This movement enlarges the spacethat the lungs are in. This larger space pulls air into thelungs. When you breathe out, the diaphragm expands reducingthe amount of space for the lungs and forcing air out. Thediaphragm is the main muscle used in breathing.
Pluerae
The pleurae are serous membrane that enclose the lungin a double walled sac.
Visceral Pleurae – covers the lungs andfissure between the lobes of the lungs
Parietal Pleurae – covers the inside ofeach hemothorax, the mediastinum and thetop of the diaphragm
The pleurae cavity between the visceral and parietalpleura, is filled with small volume of pleurae fluidproduced by the pleural membranes. I The pleural fluid actsas lubricant, allowing the visceral and parietal pleurae toslide past each other as the lungs and thorax change shapeduring respiration and also, it function to help thepleurae membrane together.
Function of the Respiratory System
VENTILATION
Ventilation, the movement of air in and out of thelungs, involves three forces;
Compliance – refer to the ease with whichthe lungs expands and indicates therelationship between the volume and thepressure of the lungs.
Surface tension – the result of the air-liquid interface to each alveolus, restrictsalveolar expansion on inspiration and aidsalveolar collapse collapse on expiration.
Muscular Effort – ventilation also requiresmuscular effort. For inspiration to occur,the pressure within the alveoli must be lessthan atmospheric pressure. Contraction ofthe diaphragm and the external intercostalsmuscle enlarge the size of the thorax. Twoaccessory muscle of inspiration are thescalene and sternocleidomastoid.
Gas Exchange and Transport
OXYGEN TRANSPORT
After diffusing into pulmonary the capillaries, oxygenis transported throughout the body by a circulatory system.The oxygen is dissolved in the plasma(3%) or bound in theferrous iron-containing protein hemoglobin(97%).
CARBON DIOXIDE TRANSPORT
CO2, the waste product of tissue metabolism, iscarried by the blood in the ff ways; combined with water ascarbonic acid(70%), coupled with hemoglobin(23%), dissolvedin plasma(7%).
Regulation of Acid - Base Balance
The lungs, through gas exchange, have a key role inregulating the acid-base balance in the body.
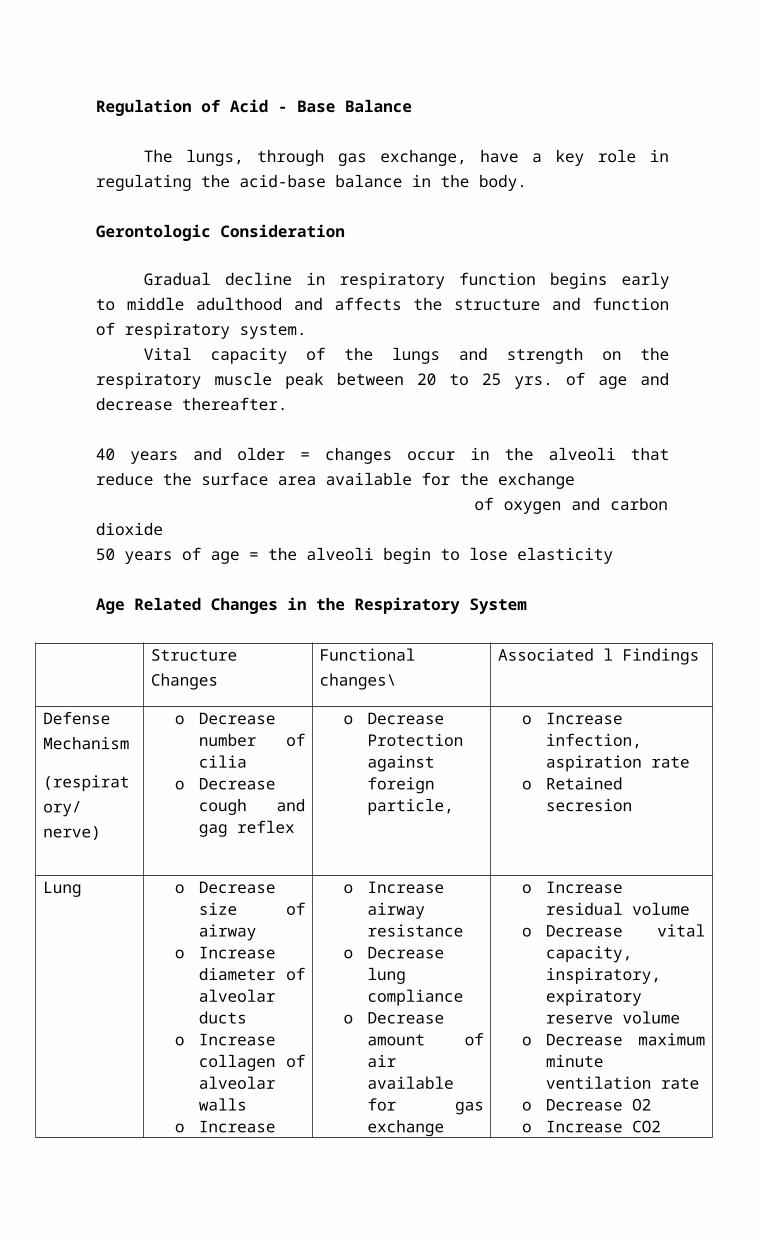
Gerontologic Consideration
Gradual decline in respiratory function begins earlyto middle adulthood and affects the structure and functionof respiratory system.
Vital capacity of the lungs and strength on therespiratory muscle peak between 20 to 25 yrs. of age anddecrease thereafter.
40 years and older = changes occur in the alveoli thatreduce the surface area available for the exchange of oxygen and carbondioxide50 years of age = the alveoli begin to lose elasticity
Age Related Changes in the Respiratory System
StructureChanges
Functionalchanges\
Associated l Findings
DefenseMechanism
(respiratory/nerve)
o Decreasenumber ofcilia
o Decreasecough andgag reflex
o DecreaseProtectionagainstforeignparticle,
o Increaseinfection,aspiration rate
o Retainedsecresion
Lung o Decreasesize ofairway
o Increasediameter ofalveolarducts
o Increasecollagen ofalveolarwalls
o Increase
o Increaseairwayresistance
o Decreaselungcompliance
o Decreaseamount ofairavailablefor gasexchange
o Increaseresidual volume
o Decrease vitalcapacity,inspiratory,expiratoryreserve volume
o Decrease maximumminuteventilation rate
o Decrease O2o Increase CO2
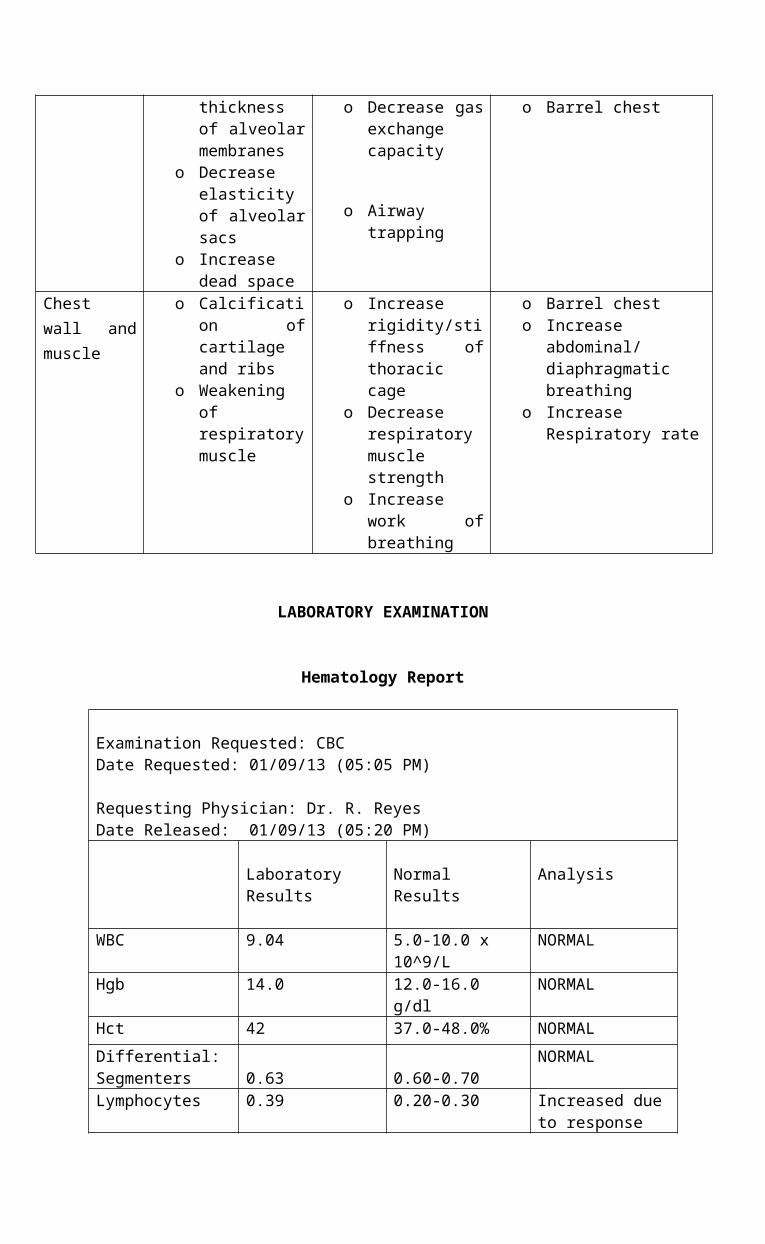
thicknessof alveolarmembranes
o Decreaseelasticityof alveolarsacs
o Increasedead space
o Decrease gasexchangecapacity
o Airwaytrapping
o Barrel chest
Chestwall andmuscle
o Calcification ofcartilageand ribs
o Weakeningofrespiratorymuscle
o Increaserigidity/stiffness ofthoraciccage
o Decreaserespiratorymusclestrength
o Increasework ofbreathing
o Barrel chesto Increase
abdominal/diaphragmaticbreathing
o IncreaseRespiratory rate
LABORATORY EXAMINATION
Hematology Report
Examination Requested: CBC Date Requested: 01/09/13 (05:05 PM)
Requesting Physician: Dr. R. Reyes Date Released: 01/09/13 (05:20 PM)
Laboratory Results
Normal Results
Analysis
WBC 9.04 5.0-10.0 x 10^9/L
NORMAL
Hgb 14.0 12.0-16.0 g/dl
NORMAL
Hct 42 37.0-48.0% NORMALDifferential:Segmenters 0.63 0.60-0.70
NORMAL
Lymphocytes 0.39 0.20-0.30 Increased dueto response
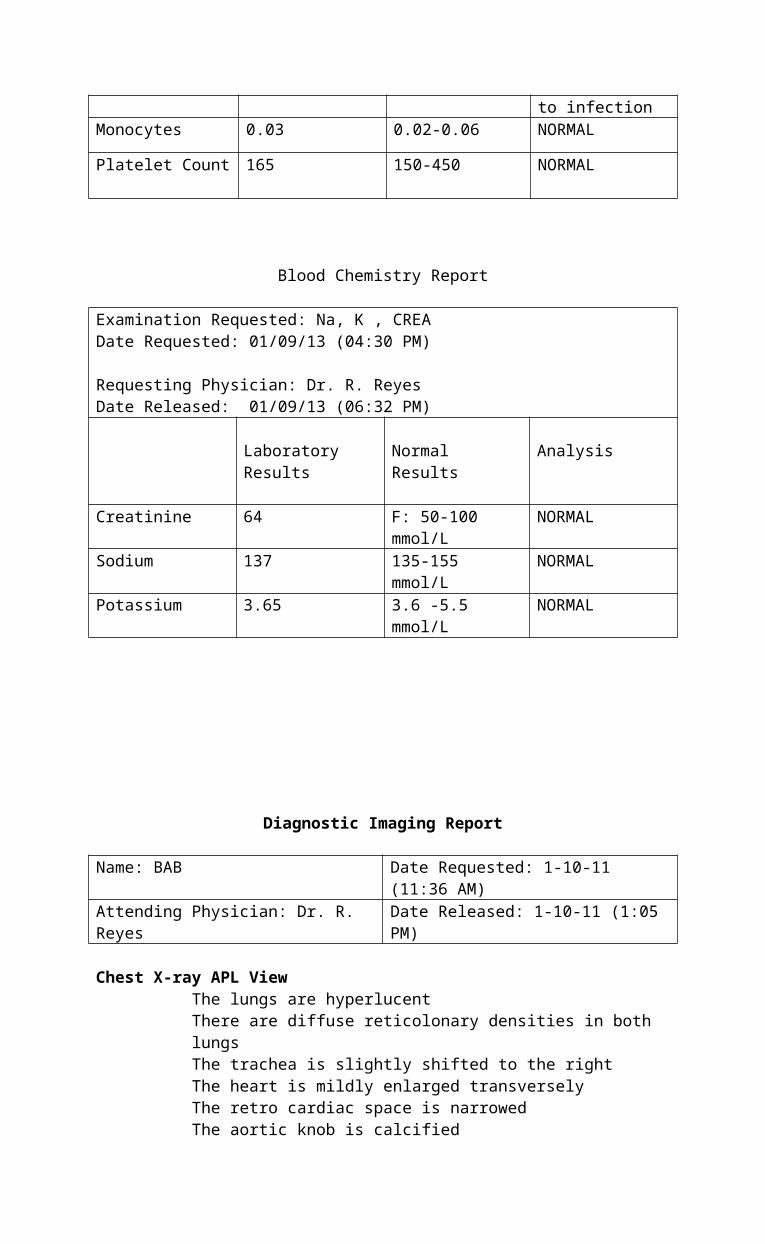
to infectionMonocytes 0.03 0.02-0.06 NORMAL
Platelet Count 165 150-450 NORMAL
Blood Chemistry Report
Examination Requested: Na, K , CREA Date Requested: 01/09/13 (04:30 PM)
Requesting Physician: Dr. R. Reyes Date Released: 01/09/13 (06:32 PM)
Laboratory Results
Normal Results
Analysis
Creatinine 64 F: 50-100 mmol/L
NORMAL
Sodium 137 135-155 mmol/L
NORMAL
Potassium 3.65 3.6 -5.5 mmol/L
NORMAL
Diagnostic Imaging Report
Name: BAB Date Requested: 1-10-11 (11:36 AM)
Attending Physician: Dr. R. Reyes
Date Released: 1-10-11 (1:05 PM)
Chest X-ray APL ViewThe lungs are hyperlucentThere are diffuse reticolonary densities in both lungsThe trachea is slightly shifted to the rightThe heart is mildly enlarged transverselyThe retro cardiac space is narrowedThe aortic knob is calcified
The hemidiaphragms are smoothThe costophrenic sulci are intactThere are spurs in the margins of the vertebral
bodiesThe rest of the visualized soft and osseous
structures are remarkable
Impression:
Pulmonary Emphysema and BronchiectasisInterstitial Pneumonia, BilateralMild CardiomegalyAtherosclerosis AortaDegenerative Osteophytes, Thoracic SpineSuggest follow up
References:
Black, J., and Hawks, J. (2005) Medical-Surgical Nursing:Clinical Management for Positive Outcomes, 7th Edition,Volume 2: Chapter 64 Oxygenation Disorders pp. 1830-1841
Kumar, V., Abbas, A. et al. (2010) Pathologic Basis of Disease 8th edition: Chapter 15 The Lung: pp. 692-693; 711-712
Seeley, R., Stephens, T. and Tate, P. (2008) Essentials ofAnatomy & Physiology 6th edition: Chapter 15 RespiratorySystem pp 416-446