Optical Spectroscopy for Noninvasive Monitoring of Stem Cell Differentiation

970
.i ® 111 us Wave Doppler Echocardilography for Noninvasives~
t
Ventricular /
Relaxation Timer
'tr
a lr .tant Spectra In PatientsCHUNGUANG CHEN, MD,* LEON
ROD GUEZ, MD, JEAN-PAUL LET O , MD,ROBERT A. LEVINE, MD, MARC S . SE IG N, MD, MICHAEL A. FIF R, MD,ARTHUR E. WEY AN, MD, JAMES 1). THOMAS, MDBoston, Massachusetts ; Hamburg, Germany; and Cleveland, Ohio
vasl method for estimating maxim dP/dt and therela tie constant. This study wale designed to test thismethod In patients .
Background. The mwdmW first derivative of left ventricularre (dP/dt) and the
constant of left veotri
isovolu-(1) are Important variables of left ventricular
but t
for involve measurement with high fidelitycatheters has limited their we In dialcal cardiology .M s . a patients with taw[ agitation were stud-
ied. The Do m1tral urgitsant velocity spectrum was re-corded
with
r left ventricularin all patients .
rgi t velocity prowere digilized
con
to veu is oat
(VA) pressuret carves
the
pi
Bernoulli equation and dif-f
dP/dt. The re lion time constant(r) w calculated
m
a zero pressure asymptotecatheter left ventricular pressure decay (r,) and Orom the Doppler.
v VA gradient curve with cor =teas . Two methods were
e noninvasive evaluation of left ventricular systolic anddiastolic function remains an important goal in cardiology(1-9) . According to the Bernoulli equation, analysis of theDoppler mitral regurgitant velocity profile allows accuratecalculation of the left ventriculoatrial (VA) pressure difer-ence throughout systole and early diastole before mitralvalve opening (2,3) . Differentiation of this pressure differ-ence then yields the rate of change in the left ventricular
From the Cardiac Unit, Massachusetts General Hospital . Harvard Med-ical School. Boston, Massachusetts ; Department of Cardiology, UniversityHospital Hamburg, Hamburg, Germany ; and the Department of Cardiology,Cleveland Clinic Foundation, Cleveland, Ohio . This study was presented inpart at the bath Annual Scientific Sessions of the American Heart Association,Anaheim, California, November 1991 .
Manuscript received April 26, 1993 ; revised manuscript received July 23,1993, accepted August 4, 1993 .
*Present Address and address for orresngndence : Dr. Chunguang Chen,Division of Cardiology, Hartford Hospital, 80 Seymour Street, Hartford,Connecticut 06115 .
01994 by the American College of Cardiology
used to correct the Doppler gradient curve to better approximatethe left ventricular pressure d y before calculating the relax-ation tart constants 1) adding arbitrary 10 urns Hg (rro), d2) adding the actual mean pulmonary capillary pressure (TLA) .
Res . The Doppler-derived maximal positive dP/dt (1,39402 mm Hgis [mean ± 51)1) correlated well (r ® 0.91) with thecatheter-derived m dP/dt (1,449 307 mm H s). Although
Doppler-derived negative dP/dt differ slightly fromcatheter measurement (1,014 289 vs. 1,195± 3 m Hg/s, p <0.01), the correlation between Doppler and catheter measure-ments was similarly g (r ® 0.09, p < 0.0001) . The correlationbetween rap and r,: was excellent (r ® 0 .93, p < 0.01), but theDoppler-derived rao (50.0 ± 11 .0 ins) slightly underestimated thecatheter-derived rs (55.5 ± 12.8 ms, p < 0.01) . This slightunderestimation could corrected by adding the actual pulmo-nary cap wedge pressure to the Doppler gradient curve .
Conclusions . Doppler ech rdlography provides an accurateand reliable meth for estimating left ventricular maximalpositive dP/dt, negative maximal dP/dt and the relaxation timeconstant (i) in patients with odiral regurgitation .
(J Am Coil C iol 1994,23 :970- 6)
JACC Vol. 23, No, 4March 15,1994:970-6
pressure (dP/dt).in particular, peak positive dP/dt duringisovolumetric contraction and peak negative dP/dt duringventricular relaxation (3) . Furthermore, analysis of thispressure difference during isovolumetric relaxation can yieldthe relaxation time constant (4). We previously hypothesizedthat if changes in left atrial pressure during isovolumetricsystole and diastole are negligible in relation to changes inleft ventricular pressure, 1) the mitral regurgitant velocityupslope should predict the left ventricular pressure increaseduring isovolumetric systole, and, thus, peak dP/dt ; and 2)the mitral regurgitant velocity downslope should predict thedecay in left ventricular pressure during isovolumetric relax-ation and thus yield peak negative dP/dt and the relaxationtime constant . This hypothesis was examined in a caninemodel, and the results have been published elsewhere (3,4) .However, such a detailed analysis has not been performed inhumans. Therefore, the purpose of this study was to test theaccuracy of Doppler-derived dP/dt and the reliability of the
0735-10971941$7 .00
objective W y d nstrsted experimentally thatthe mi t v , lty n m can be used to esdinaleleft vet r pressure raft t systole and way provide a

JACC VU 23, No. 4March 15, 1994 :970-6
Doppler-derived relaxation time constant in patients withmitral regurgitation.
MethodsThis study was conducted in 12 patients with rnitral
regurgitation who underwent routine cardiac catheterizationat Massachusetts General Hospital (9 patients) or HamburgUniversity Hospital (3 patients) . There were eight men andfour women, with a mean age of 47 ± 18 years (range 21 to72). Semiquantitative severity of mitral regurgitation was Ito 2+ in 10 of 12 patients ; I patient had 3+ ; and I had 4+regurgitation by angiography (9) . The etiology of mitralregurgitation was coronary artery disease in seven patients,cardiomyopathy in three and rheumatic mitral regurgitationin two. Ten patients were in sinus rhythm, and two had asIalfibrillation . In all patients, high fidelity left ventricular pres-sures were obtained during cardiac catheterization withmicromanometer catheters and recorded simultaneouslywith continuous wave Doppler nutral regurgitant spectra .
Data acquisition . Doppler echocardiography . Two-dimensional echocardiographic images and continuous waveand color Doppler data were acquired using a Hewlett-Packard 72020 ultrasound imaging system . The presence ofmitral regurgitation was defined by color Doppler flowmapping. The mitral regurgitant velocity curves were ob-tained from an apical approach by using either a nonimagingDoppler transducer or a combined imaging and Dopplertransducer. In each case, the continuous wave Dopplerultrasound beam was aligned as parallel as possible to thecolor Doppler mitral regurgitant jets . If a blind continuouswave Doppler transducer was used, then the maximal andmost clearly delineated velocity envelopes were recorded(3,4) . All Doppler spectral velocity profiles and two-dimensional images were recorded at a speed of 100 mm/s on0.5 in . (1 .27 cm) videotape for further analysis .
Cardiac catheterization . Left heart catheterization wasperformed by way of the right femoral artery. Amicromanometer-tipped catheter (Millar Mikro-tip, MillarInstruments) was inserted over a guide wire into the leftventricle to record ventricular pressure . Pulmonary capil-lary wedge pressures were recorded by using a Swan-Ganzflow-directed catheter . Great care was taken to ensure theaccuracy of the pressure measurements . Fluid-filledtransducers were balanced at atmospheric pressure andcalibrated. All pressure measurements and a single electro-cardiographic lead were continuously recorded on an eight-channel strip chart recorder. Paper speed was increased to100 mm/s when recording was simultaneous with Dopplerrecording .
Data analysis . Doppler-derived dPIdt . The data wereprocessed in the following manner : The continuous waveDoppler mitral regurgitant profile was traced manually-beginning at the initial part of the QRS wave and ending atthe zero crossover polo-and was digitized at 5-ms intervalsby using a Bitpad (Summagraphics, Inc .) interfaced with a
CHEN ET AL .
971DOPPLER-DERIVED dPldt AND r IN MITRAL REGURGITATION
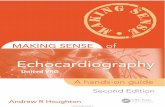
customized program written in the Asyst prog,-a,,,pruipg en-virunment (Macmillan, Inc .) (3,4) . The instantaneous pres-sure decrease between the ventricle and atrium was calcu-lated from the modified Bernoulli equation : AP = 4v2 , whereAP is the pressure gradient (mm Hg), and v is the instanta-neous regurg'tant jet velocity (m/s) . The pressure gradientcurve was then reconstructed for each traced heartbeat (Fig .IA). The instantaneous left ventricular dP/dt throughoutsystole and early diastole (isovolumetric relaxation period)was determined from this reconstructed pressure curve bydifferentiating the data at 5-ms intervals (Fig . IA). Themaximal dP/dt during the early systoi_2p phase and thenegative maximal dP/dt at the early diastolic phase wereobtained from the instantaneous dP/dt curve (3) . For eachpatient, three cardiac cycles were analyzed and the valuesaveraged for further comparison .
Doppler-derived relaxation time constant . The left ven-tricular relaxation time constant (0 was calculated assumi,kga zero pressure asymptote (6) : P(t) = Poe"/), where P0 isleft ventricular pressure at the time of maximal negativedP/dt, at which point time t = 0, and r was calculated byexponential regression (Fig . IB) . The natural logarithm of Pwas fitted to the line Bt + A, and r was defined as ®1/B, thenegative reciprocal of the regression slope . Because thelogarithm of left ventricular pressure minus atria] pressure isnot equal to the logarithm of left ventricular pressure, anestimated atria] pressure was added to adjust the Doppler-derived pressure gradient curve to approximate left ventricularpressure (P) from which to calculate the Doppler-derived r (4) .On the basis of our earlier animal investigations (4), a fixed10 mm Hg was added to the Doppler-derived VA pressuregradient curve for calculating the relaxation time constant( ,rlo ) . Alternatively, we also used the actual pulmonarycapillary wedge pressure added to the atrioventricular (AV)pressure gradient for calculation of the relaxation timeconstant (TLA) . For each hemodynamic stage, three cardiaccycles were analyzed and the values averaged for furthercomparison .
Catheter measurements . Simultaneous Millar catheter-recorded left ventricular pressures were manually traced anddigitized at 5-ms intervals beginning at the initial part of theQRS wave and ending when the ventricular pressure wasequal to the end-diastolic pressure . Instantaneous left ven-tricular dP/dt was determined from the ventricular pressurecurve by numeric differentiation at 5-ms intervals . MaximaldP/dt at the early systolic phase and the negative maximaldP/dt at the early diastolic phase were obtained from theinstantaneous dP/dt curve . Likewise, the left ventricularrelaxation time constant was calculated using the zero as-ymptote, as proposed by Weiss et al . (6) . For each patient,three cardiac cycles were analyzed and the values averagedfor further comparison .
Statistical analysis . Data are expressed as mean valueSD. Comparisons of maximal positive dP/dt, maximal nega-tive dP/dt, and the relaxation time constant between Dopplerand catheterization measurements were performed using

972
A
5
4
3
2
0
0
Log P
CHEN ET AL .
JACC Vol . 23, No. 4
DOPPLER-DERIVED dP/dt AND T IN MITRAL REGURGITATION
March 15,1994 :970-6
~aenlfW d~P/W &,W4YO/5,a41
&V
so _---".. goo
4002"0
200-400
-400no
300
W kaooMe (met
0
10
20
30
40
50 80
70
00
B 7110 (1) IN= negative MaL dp/dt (mus)
Figure 1. Example of Doppler measurements of the first derivativeof left ventricular pressure (00) and the relaxation time constant(* A, Doppler mitral regurgitant velocity spectrum (top) andventriculoatrial (VA) pressure gradient curve and its first derivativederived from the Doppler velocity spectrum (bottom) . Arrows indi-cate the beginning and end of the segment from the Doppler-reconstructed VA pressure gradient curve that was iater log trans-formed and used for calculation of the relaxation time constant (r) .B, Linear regression plot of log transformation of Doppler approx-imate left ventricular pressure IP(t)) during isovolumetric relaxation(N,= in A) and time starting from tht, maximal negative dP/dt . Theapproximation of left ventricular pressure was made by adding10 mm Hg to the Doppler-derived VA gradient curve. The relaxationtime constant W was the reciprocal of the regression slope, whichwas 54 ms in this case by the Doppler method .
univariate linear regression analysis and paired Student ttest. Standard deviation of regression was calculated . Accu-racy was assessed by calculating the mean and standard
Y 0.18X + 3.99r 0.99T = 54 ms
deviation of the difference between Doppler- and catheter-based measurements (10). A p value :r= 0 .05 was consideredstatistically significant .
Results
Peak left ventricular systolic pressure was 123 t22 min Hg, with an end-diastolic left ventricular pressure of18 ± 4 mm Hg. The pulmonary capillary wedge pressurer.-cording was obtained in only eight patients, demonstratinga mean pulmonary capillary pressure of 19 ± 5 mm Hg and asystolic (v) wave of 23 ± 7 mni Hg . The left ventricular ejectionfraction measured by echocardiography was 56 ± 7% .
hive dP/dt . For the 12 patients analyzed, thepeak positive dP/dt derived from the Doppler mitral regur-gitant velocity profiles (1,394 ± 302 mm Hg1s) was slightlylower than that derived from the Millar catheter recordings(1,449 ± 307 mm Hg/s), but the difference was not statisti-cally significant (QdAilt = -55 ± 126 mm Hg/s, p = NS) .Overall correlation was excellent (r = 0.91, standard devia-tion of regression 131 mm Hg/s), and the two data sets layclose to the line of identity (Fig. 2) .
five PC Similarly, Doppler estimation ofpeak negative dP/dt correlated well with the hemodynamicassessment (Fig. 3) bet with a somewhat more prominentunderestimation than that seen with peak positive dP/dt .There was a significant difference (p < 0 .05) between Dop-pler peak negative dP/dt (1,014 ± 289 min Hg/s) and the peaknegative dP/dt from catheterization data (1,195 ± 154 mmHg1s), with A(-dP/dt) = -182 ± 145 mm lies .
UR ventricular relaxation time constant (T) . Figure 4compares measurements of the relaxation time constant (T),with the hemodynamic assessment along the xx axis (T,, =55.5 12.8 ms) and Doppler measurement along the y axis(no 510 ± 11.0 ms). There was a slight underestimation ofthe relaxation time constant by the Doppler method (AT =--5 .5 ± 4.9 ms, p < 0 .01) when the VA gradient was adjustedby adding an assumed left atrial pressure of 10 mm Hg, butoverall there was excellent correlation across the data range .When the VA gradient was corrected by the mean pulmo-nary capillary wedge pressure (n 8), the correlationbetween the Doppler-derived (rLA 57.3 ± 14.5 ms) andcatheter-derived (T, = 58 .5 ± 14.7 ms) relaxation timeconstants improved (Fig. 5), and no significant differencewas found between the Doppler and catheter measurements(AT = 1 .9 ± 7,6 ins, n = 8, p = NS) .
Discussion
Widespread use of isovolumetric variables of left ventric-ular systolic and diastolic function is limited in large part bythe need for invasive, high fidelity pressure measurements atcardiac catheterization . The present study has demonstratedthat these important indexes of ventricular function can bequantified noninvasively by using Doppler echocardiographyin patients with mitral regurgitation. Peak left ventricular

JACC Vol . 23, No. 4March 15,1994 :970-6
200
Peak IMMIlPe LV4011
Y WK +r 0 .91P < 0 .01SDR = 131
Catheter measurement
Error in peak -Ijkli
Adp1da m -55± 126 unnfflWs
800 1000 1200 1400 1600 1800 2000 2200
Catheter measureirent
Figure 2 . Top, Correlation between the maximal positive first de-rivative of left ventricular (LV) pressure (dP/dt) determined by theDoppler method and by Millar catheter.-recorded left ventricularpressure . Bottom, Agreement plot of the difference between Dopplerand catheter measurements of the maximal dP/dt . Note that therewas no significant systematic underestimation or overestimation .SDR = standard deviation of regression .
dP/dt can be accurately determined from the upslope of themitral regurgitant velocity profile, whereas the velocitydownslope closely correlates with the peak negative dP/dt .Furthermore, the time constant of left ventricular relaxation(r) can be calculated from the Doppler VA gradient curve inisovolumetric diastole after correction for estimated leftatrial pressure. Because some degree of mitral regurgitationis commonly observed in patients with heart disease, theseresults may prove widely applicable in the routine evaluationof ventricular systolic and diastolic function by Dopplerechocardiography if left atrial pressure is estimated by usingDoppler echocardiography or pulmonary capillary wedgepressure simultaneously .
Accuracy of ventricular dP/dt. Accurate estimation of leftventricular dP/dt from the Doppler-derived VA gradientcurve depends on several factors . First, the pressure gradi-ent must be accurately calculated using the simplified Ber-noulli equation. For the peak pressure difference acrossrestrictive orifices typical of valvular regurgitation, thisaccuracy has been demonstrated both in experimental andclinical studies (2,3,7) . However, when considering theinstantaneous pressure difference, one cannot neglect a
DOPPLER-DERIVED dPldt AN
1800
1400
- 1600y 0.67K + 231
1280
100004 800
I
600 l - '600
8oo 1030 1209 140o 160o
Catheter measurement
600
200
eu _MO
ft. .400
I
Peak negative LVdp!dt [rnmHg1sj,-'
CHEN ET AL,FIN MITRAL REGUEGITATIO N
a
Error in -dp/dt measurement
&4WA = -182±145 MMHWG
0
0 0
0
0
a
0
00
-600 '-600
800 1000 1200 1400 1600 18
Catheter Fnewweraent
Figure 3. Top, Correlation between the maximal negative dP/dtdetermined by the Doppler method and by pillar catheter-recordedleft ventricular pressure . Bottom, Agreement plot of the differencebetween Doppler and catheter measurements of the maximal nega-tive dP/dt . Note that there was a systematic underestimation byDoppler method . Abbreviations as in Figure 2 .
priori the inertial term in the complete Bernoulli equation,which has its largest magnitude at times of rapid velocitychanges. Furthermore, there is concern that the finite tem-poral resolution of contemporary continuous wave Dopplerequipment, which gathers data for 5 to 10 ms betweenFourier transform velocity estimates, may limit the accuracyof tracking rapidly changing velocity (8) . Fortunately, it haspreviously been shown in a canine medel of mitral regurgi-tation that the instantaneous pressure gradient and its firstderivative can be accurately measured throughout systoleand isovolumetric diastole by applying the simplified Ber-noulli equation to the Doppler mitral regurgitant velocityprofile (3), supporting its use in human mitral regurgitation .
Second, one must consider the impact of atrial pressureon these calculations because we measure the VA pressuredifference AP but use it as a surrogate for ventricularpressure itself. For dP/dt calculations, the rate of change ofatrial pressure is of critical concern . If atrial pressure wereconstant, regardless of its absolute magnitude, then d AP/dtwould precisely equal ventricular dP/dt . We have showndirectly in the previous canine study (3) and by inference inthe current study that at the time of peak positive ventricular
1800
973

974 CHEN ET AL.DO"LERWERIVED dP/dt AND T FN MITRAL REGURGITATION
AT a .5JA 4.9 08
0
Figum 4. Top, Correlation between the relaxation time constant(710)determined by the Doppler method with correction of left atria[(LA) pressure by adding 10 mm Hg to the Doppler gradient curveand that recorded by Millar catheter-recorded left ventricularpressure (re ). Bottom, Agreement plot of the difference betweenDoppler and catheter measurements of r. Note that there was asystemic underestimation of T, by 710. SDR = standard deviation ofregression .
dP/dt, the change in atrial pressure is negligible, leading tothe accurate results shown in Figure .2; .
For the maximal negative dP/dt, the decrease in atrialpressure associated with the downslope of the v wave duringisovolumetric ventricular relaxation has a more adverseimpact on the Doppler estimation. Both the previous canineinvestigation (3) and the current study show that the Dopplermethod tended to underestimate the catheter-derived peaknegative dP/dt . Nevertheless, despite an average 15% under-estimation, a very strong correlation was noted betweenthese measurements (Fig. 3) .
Doppler estinsation of tion time constant (7) . Where-as Doppler-derived dP/dt is affected only by changes in atrialpressure, prediction of the exponential time constant ofventricular relaxation must also consider the absolute levelof atrial pressure . This is due to fixed shifts in ventricularpressure that profoundly affect the results of exponentialregression because of the nonlinear nature of the logarithmictransformation. Therefore, to obtain an accurate measure-ment of relaxation time constant, some estimate of atrial
DkCCVol. 2jNY4March 15,1994 :970-6
Figure 5 . Top, Correlation between the relaxation time constantO, A) determined by the Doppler method with correction of left atrialpressure by adding actual left atrial pressure to the Doppler gradientcurve and that determined by Millar catheter-recorded left ventric-ular pressure (7,) . Bottom, Agreement plot of the difference betweenDoppler and catheter measurements of r.
pressure must be added to the VA gradient . Ideally, thisshould be based on actual measured atrial pressure . Anestimate of left atrial pressure from a pulmonary arteryballoon catheter or from the difference between the systolicarterial pressure and the peak Dopplet VA gradient shouldbe available in most patients with mitral regurgitation (7) .Alternatively, from our animal experiments, it appears thatadding a fixed 10 mm Hg to the Doppler gradient yields anaccurate estimation of relaxation time constant across a widerange of actual left atrial pressures (4) . In the current humanstudy, the Doppler-derived relaxation time constant calcu-lated using a 10-mm Hg correction for mean atrial pressurealso correlated well with the hemodynamic relaxation timeconstant. However, relaxation time constant was slightly(5 .5 ms, 10A of the mean value) but significantly underesti-mated (Fig. 4), perhaps reflecting the higher pulmonarycapillary pressure actually observed in these patients, whichaveraged 19 mm Hg. Correction using actual pulmonarycapillary wedge pressure yielded better agreement (Fig . 5) .Significant overestimation of relaxation time constant couldresult if a large atrial v wave (e.g ., from acute severe mitralregurgitation) decreased rapidly during isovolumetric relax-

JACC Vol. 23, No. 4
CHEN ET AL .March 13, 094 :970-6
DOPKERTERIVED Mldt AND r IN MITRAL REGURGITATION
ation, leading to a flattening of the reconstructed ventricularpressure curve . Therefore, accuracy of relaxation time cen-stant measurement based on the Doppler mitral velocityprofile is adversely affected by an extremely elevated leftatrial pressure and v wave, and correction by adding anestimated left atrial pressure to the Doppler data should besought under these situations . Fortunately, in many patientsan estimate of left atrial pressure may be available frompulmonary artery monitoring or from noninvasive measure-ment either by Doppler mitral inflow velocity profile or bysubtracting the peak Doppler VA pressure gradient frosystolic arterial blood pressure . Such estimates need not beprecise because we have shown that adding an arbitrarvalue of 10 mm Hg to VA gradient data yielded accurateestimates of relaxation time constant in a wide range ofactual left atrial pressures (4) .
Several approaches have been proposed for calculatingthe exponential time constant of ventricular relaxation(9-14), assuming decay to a zero or nonzero pressureasymptote . Previous animal studies have shown relaxationtime constant calculated using a zero asymptote to be anaccurate approach in most cases (6,13,16,17), with lesssensitivity to random noise in the data . Yellin et al . (13) haveevaluated the accuracy of relaxation time constant calcu-lated using a zero asymptote compared with the true relax-ation time constant calculated using the actual asymptote ina nonfilling dog ventricle model by totally occluding themitral annulus during one cardiac cycle, which allowed theventricle to relax to its minimal pressure (P.) of -7.3 ±3.3 mm 1Ig (13) . In that model, they demonstiated thatrelaxation time constant calculated using a zero asymptote isnot different from the true relaxation time constant based onthe nonfilling cycle . However, the zero asymptote may leadto significant error if the minimal pressure (P .) is extremelynegative, as suggested by Ohtani et al . (16) . There have beenvery limited data with regard to left ventricular minimalpressure in the human nonfilling ventricle . Paulus et al . (17)recorded a left ventricular minimal I ressure ranging from --3to 7 mm Hg during balloon occlusion of the mitral orifice inpatients with mitral stenosis undergoing mitral balloon val-vuloplasty . The zero asymptote was demonstrated to yieldmore accurate estimates of actual relaxation time constantthan the nonzero asymptote approach in their study (17) . Inour previous animal study (3), we showed that the Doppler-derived relaxation time constant calculated using a zeroasymptote accurately predicted the catheter-derived relax-ation time constant using the same calculation (4) . This,therefore, was the approach used in the current study .
An alternative method for calculating relaxation timeconstant (7) is to allow the pressure to decay to an arbitraryasymptote PB : PV(t) = POe-" + PB . The variables P B and P 0and r can be estimated by either linear regression of -dP/dtagainst P or by nonlinear least-squares techniques (11,14-16). A potential advantage of this approach is that relaxation
time constant defined it this way is independent of left atrialpressure, which is subsumed in the adjustable P E . Urafertu-nately, relaxation time constant defined with an arbitrarya Vmyow has been shown to have much greater beat to beatvariability than the zero asymptote relaxation time constantand to deviate significantly from the zero asymptote relax-ation time constant (13,17) . This is probably due to the factthat allowing the nonzero asymp ote involves a third degreeof freedom in the variable estimation, resulting in increasingthe correlation of the fit but only at the expense of widenedvariable confidence intervals .
Study limitations. The major limitation of this Dopplerethod is the requirement that patients have mitral re-
gurgitation detectable by continuous wave Doppler echo-cardiography. Fortunately, mitral regurgitation is commonlyobserved in normal patients and is usually present in con-gestive, ischemic and hypertrophic cardiomyopathies (18-23). A further difficulty is to obtain a complete, well delin-eated regurgitant spectral envelope in patients with tracemitral regurgitation and eccentrically directed mitral regur-gitant jets. In the current study we were able to record clear,complete velocity curves from eccentric regurgitant jetsusing apical views without significantly off-angle Dopplermitral velocity profile recording. As with any Doppler ve-locity measurement, the ultrasound beam must be alignedparallel to the velocity vectors at the regurgitant orifice toprevent underestimation of the pressure gradients . Underes-timation of the VA gradient by a significantly off-anglerecorded Doppler velocity profile could lead to underestima-tion of relaxation time constant . Thus, careful scanning isnecessary to obtain maximal velocity spectra by blind Dop-pler transducer using auditory monitoring or by image-directed continuous wave Doppler transducers . However, alarge scale prospectrie study is necessary to evaluate thefeasibility and reproducibility of this method in unselectedpatients .
Current implementation of this instantaneous Dopplermethod demands careful hand digitization of the mitralregurgitant velocity profile . It is possible that if this methodwere integrated into the imaging software of an echocardio-graph, an automated determination of isovolumetric vari-ables might be easily accomplished .
Summary. In patients with mitral regurgitation, an iso-volumetric variable of systolic left ventricular function, themaximal positive dP/dt, can be accurately estimated by usingthe upslope of the Doppler regurgitant velocity spectrum .The downslope of the Doppler spectrum allows calculationof indexes of left ventricular relaxation, such as maximalnegative dP/dt and the relaxation time constant ( ,r), but thelatter measurement requires an estimate of left atrial pres-sure. The Doppler-derived peak negative d1r,'dt and relax-ation time constant are slightly underestimated, a problemanticipated to be more prominent in patients with high leftatrial v wave pressure .
I
975

976
References1 . DeMaria AN, Wisenbaugh T. Identification and treatment of diastolic
dysfunction: role of transmittal Doppler recordings. I Am Coll Cardiol19670:1106-7.
2 . Nishimura RA, Tajik AL Determination of left-sided pressure gradientsby utilizing Doppler aortic and mitral regurgitant signals : validation bySNOW= dual catheter and Doppler studies . J Am Coll Cardial1988 :11 .317-21 .
3. Clan C, Rodriguez L . Guerrero JL, et aJ. Noninvasive estimation of theAMOneous first derivative of left ventricular pressure using continuous-wave Doppler echocardiography . Circulation 1991-,83 :2101-10 .
4. Chen C, Rodriguez L, Levine RA, Weyman AE, Thomas JD . Noninva-sive measurement of the time constant of left ventricular relaxation usingthe continuous-wave Doppler velocity profile of mitral regurgitation .Circulation 1492 ;86:27"2 .8 .
S . BortucciC, RecusaniF .etal . A -ew method for estimating1 .,~4 wi,itkular dpldt by continuous wave Doppler-echocardiography :vldf(i,~Iiofi studies at catheterization . Circulation 1989 ,,80,1287-.91
6. Wei" JL, Frederiksen JW, Weisfeldt ML . Hemodynamic determinants ofthe time-course of fall in canine left ventricular pressure . I Clin Invest191659 :751-60 .
7, Hatle L . Ange(san B . Doppler Ultrasound in Cardiology : Physical Prin-ciples and Clinical Application . Philadelphia : Lea & Febiger, 1984 :1-238 .
8 . Lee R. Waveform analysis and technical considerations in Dopplerinstrumentation . In : Sutton MS, Oldershaw PJ, editors . Textbook ofAdult and Pediatric Echocardiography and Doppler . Boston : BlackwellScientific, 1989 :19-76 .
9, Grossman W. Cardiac Catheterization and Angiography . 3rd ed . Phila-delphia : Lea & Febiger, 1986 :302-6,
10. Bland 3M, Altman DG . Statistical methods for assessing ag&arientbetween two methods of clinical measurement . Lancet 1986 ;1 :307-10.
11 . Mirsky I . Assessment of diastolic function: suggested methods and futureconsiderations . Circulation 1984 ;69:836-41 .
CHEN ET AL .
JACC Vol. 23, No. 4DOPPLER-DERIVED Oldt AND -r IN MITRAL REGURWATION
March 15. 1994:970-6
12 . Zile MR, Gaasch WH . Mechanical loads and the isovolumic and fillingindices of left vev : .,,cular relaxation . Prog Cardiovasc Dis 1990:32 :33:L46.
13 . Yellin EL, Hori M, Yoran C, Sonnenblick Ell, Gabbay S . Frater RWM.Left ventricular relaxation in the filling and non-filling intact canine heart .Am J Physiol 1986 ;250:H620-9 .
14. Murgo JP, Zile MR, Blaustein AS, Bing OSHL . Evaluation of time courseof left ventricular isovolumic relaxation in man . in : Grossman W, LorellBH, editors. Diastolic Relaxation of the Heart . Boston: Martinus Nijhoff,1988:125-32 .
15 . Carroll JD, Hess OM, Krayenbuehl HP. Diastolic function duringexercise-induced iscliernia in man : In ref 14-.217-30 .
16 . Ohtani M, Nikolic SD, Glantz SA . A new approach to in situ leftventricular volume clamping in dogs . Am J Physiol 1991 ;261 :141335-41
17 . Paulus WJ, Vantrimpont PJ, Rousseau MF . Diastolic function of thenon-filling human kit ventricle. I Am Coll Cardiol 1992 ;20:1524-32
18. Berger PB, Ruocco NA, Ryan TJ, et al. Incidence and significance ofmitral regurgitation following first myocardial infarction treated withti-PA : results from TIMI It (abstracti. J Am Coll Caidiol 1991 :17 :247A.
19. Boltwood CM. Tei C, Wong M, Shah PM . Quantitative echocardiographyof the mitral complex in dilated cardiomyepathy : the mechanism offunctional mitral regurgitation . Circulation 1983,68:4984K
20. Gahl K . Sutton R, Pearson M, Caspari P, Lairet A . McDonald L. Mitralregurgitation in coronary heart disease . Br Heart J 1977,39 :13-8,
21 . Loperfldo F . Biasucci LM, Pennestri F, et al . Pulsed Doppler echocar-diographic analysis of mitral regurgitation after myocardial infarction . AsnJ Cardiol 19m,58:692-7,
22 . Izumi S, Miyatake K, Beppu S . et al. Mechanism of mitral regurgitationin patients with myocardial infarction : a study using real-time two-dimensional Doppler flow imaging and echocardiography . Circulation1987;76 :777-83.
23. Strauss RH, Stevenson LW, Dadourian BA, Child JS . Predictability ofinitial regurgitation detected by Doppler echocardiography in patientsreferred for cardiac lraraAantation. Am J Cardiol 1987-,59 :892-4 .
Copyright © 2022 FDOKUMEN