
Contingent take-home incentive: Effects on drug use of methadone maintenance patients
8
Journal of Consulting and Clinical Psychology 1992, Vol. 60, No. 6,927-934 Copyright 1992 by the American Psychological Association, Inc. 0022-006X/92/S3.00 Contingent Take-Home Incentive: Effects on Drug Use of Methadone Maintenance Patients Maxine L. Stitzer Department of Psychiatry, Behavioral Pharmacology Research Johns Hopkins University School of Medicine . Francis Scott Key Medical Center Baltimore, Maryland Martin Y Iguchi Department of Mental Health Sciences Division of Addiction Research and Treatment Hahnemann University School of Medicine Linda J. Felch Department of Psychiatry Johns Hopkins University School of Medicine Francis Scott Key Medical Center Baltimore, Maryland This study examined contingent methadone take-home privileges for effectiveness in reducing on-going supplemental drug use of methadone maintenance patients. Fifty-three new intakes were randomly assigned to begin receiving take-home privileges after 2 consecutive weeks of drug-free urines or to a noncontingent procedure in which take-homes were delivered independently of urine test results. The contingent procedure produced more individuals with at least 4 consecutive weeks of abstinence (32% vs. 8%); 28% of noncontingent subjects also achieved abstinence after shifting to the contingent procedure. Lower baseline rate of drug-free urines was strongly associated with successful outcome, whereas the type of drug abused (cocaine vs. benzodiazepines) did not influ- ence outcomes. Findings support a recommendation for using contingent take-home incentives to motivate abstinence during methadone maintenance treatment. Methadone maintenance has been widely implemented for nearly 30 years as a treatment for opiate abuse. Methadone is an orally effective long-acting medication that can be a substitute for shorter acting opiate drugs typically taken intravenously (e.g., heroin) and that suppresses the use of these drugs through pharmacological satiation and cross tolerance. Treatment is as- sociated with reduced criminal activity and improved social productivity as well as reduced opiate use (Ball & Ross, 1991). However, pharmacological treatment with methadone does not directly address the full array of substance abuse or psychiatric and life-style problems that patients often bring to the treat- ment setting. One striking feature of contemporary drug abusers is their tendency to abuse multiple substances includ- ing alcohol, tobacco, and other illicit drugs besides heroin. Co- caine use during maintenance treatment is a notable feature of contemporary polydrug-abuse patterns (Condelli, Fairbank, Dennis, & Rachal, 1991; Hanbury, Sturiano, Cohen, Stimmel, & Aguillaume, 1986; Kosten, Gawin, Rounsaville, & Kleber, 1986), whereas illicit use of benzodiazepines continues to be a problem in a subgroup of maintenance patients (Iguchi et al., 1990; Stitzer, Bigelow, Liebson, & Hawthorne, 1982). Thus, the This research was supported by United States Public Health Service Research Grant DA04104 and Training Grant T32 DA07209 from the National Institute on Drug Abuse. Correspondence concerning this article should be addressed to Maxine L. Stitzer, Department of Psychiatry, Behavioral Pharmacol- ogy Research, Johns Hopkins University School of Medicine, Brands Scott Key Medical Center, 5510 Nathan Shock Drive, Suite 3000, Bal- timore, Maryland 21224. continuing use and abuse of supplemental drugs from non- opiate pharmacological classes is recognized as a significant clinical problem in methadone programs. From a pharmacolog- ical perspective, methadone treatment cannot be expected to influence the use of drugs other than opiates. However, from a behavioral perspective, methadone treatment brings polydrug- abusing patients into a therapeutic context that has the poten- tial to make a positive impact on the illicit use of nonopiate drugs. Therapeutic interventions chosen to influence supplemental drug use during treatment have two purposes. First, interven- tions must create or enhance motivation for cessation of illicit drug use, because drug abusers are generally reluctant to change their use patterns in the absence of external pressures or incentives. Second, interventions must be designed to reduce the likelihood of relapse once initial abstinence has been achieved. Contingency management techniques that make clinic privileges available pending objective evidence of absti- nence from illicit drugs are well suited to these purposes and are one of the only specific interventions for polydrug abuse to have been systematically evaluated for efficacy. One commonly used intervention that has received some evaluation is the con- tingent availability of further methadone treatment. This ap- proach constitutes a negative reinforcement or avoidance tech- nique whereby the patient must stop the use of supplemental drugs or face methadone dose reduction and eventual discharge from the treatment clinic. Evaluation studies have shown that contingent treatment delivery can be effective for some patients in motivating the elimination of supplemental drug use (Dolan, Black, Penk, Rabinowitz, & DeFord, 1985; McCarthy & 927
Transcript of Contingent take-home incentive: Effects on drug use of methadone maintenance patients

Journal of Consulting and Clinical Psychology1992, Vol. 60, No. 6,927-934
Copyright 1992 by the American Psychological Association, Inc.0022-006X/92/S3.00
Contingent Take-Home Incentive: Effects on Drug Useof Methadone Maintenance Patients
Maxine L. StitzerDepartment of Psychiatry, Behavioral Pharmacology Research
Johns Hopkins University School of Medicine. Francis Scott Key Medical Center
Baltimore, Maryland
Martin Y IguchiDepartment of Mental Health Sciences
Division of Addiction Research and TreatmentHahnemann University School of Medicine
Linda J. FelchDepartment of Psychiatry
Johns Hopkins University School of MedicineFrancis Scott Key Medical Center
Baltimore, Maryland
This study examined contingent methadone take-home privileges for effectiveness in reducingon-going supplemental drug use of methadone maintenance patients. Fifty-three new intakes wererandomly assigned to begin receiving take-home privileges after 2 consecutive weeks of drug-freeurines or to a noncontingent procedure in which take-homes were delivered independently of urinetest results. The contingent procedure produced more individuals with at least 4 consecutive weeksof abstinence (32% vs. 8%); 28% of noncontingent subjects also achieved abstinence after shifting tothe contingent procedure. Lower baseline rate of drug-free urines was strongly associated withsuccessful outcome, whereas the type of drug abused (cocaine vs. benzodiazepines) did not influ-ence outcomes. Findings support a recommendation for using contingent take-home incentives tomotivate abstinence during methadone maintenance treatment.
Methadone maintenance has been widely implemented fornearly 30 years as a treatment for opiate abuse. Methadone is anorally effective long-acting medication that can be a substitutefor shorter acting opiate drugs typically taken intravenously(e.g., heroin) and that suppresses the use of these drugs throughpharmacological satiation and cross tolerance. Treatment is as-sociated with reduced criminal activity and improved socialproductivity as well as reduced opiate use (Ball & Ross, 1991).However, pharmacological treatment with methadone does notdirectly address the full array of substance abuse or psychiatricand life-style problems that patients often bring to the treat-ment setting. One striking feature of contemporary drugabusers is their tendency to abuse multiple substances includ-ing alcohol, tobacco, and other illicit drugs besides heroin. Co-caine use during maintenance treatment is a notable feature ofcontemporary polydrug-abuse patterns (Condelli, Fairbank,Dennis, & Rachal, 1991; Hanbury, Sturiano, Cohen, Stimmel,& Aguillaume, 1986; Kosten, Gawin, Rounsaville, & Kleber,1986), whereas illicit use of benzodiazepines continues to be aproblem in a subgroup of maintenance patients (Iguchi et al.,1990; Stitzer, Bigelow, Liebson, & Hawthorne, 1982). Thus, the
This research was supported by United States Public Health ServiceResearch Grant DA04104 and Training Grant T32 DA07209 from theNational Institute on Drug Abuse.
Correspondence concerning this article should be addressed toMaxine L. Stitzer, Department of Psychiatry, Behavioral Pharmacol-ogy Research, Johns Hopkins University School of Medicine, BrandsScott Key Medical Center, 5510 Nathan Shock Drive, Suite 3000, Bal-timore, Maryland 21224.
continuing use and abuse of supplemental drugs from non-opiate pharmacological classes is recognized as a significantclinical problem in methadone programs. From a pharmacolog-ical perspective, methadone treatment cannot be expected toinfluence the use of drugs other than opiates. However, from abehavioral perspective, methadone treatment brings polydrug-abusing patients into a therapeutic context that has the poten-tial to make a positive impact on the illicit use of nonopiatedrugs.
Therapeutic interventions chosen to influence supplementaldrug use during treatment have two purposes. First, interven-tions must create or enhance motivation for cessation of illicitdrug use, because drug abusers are generally reluctant tochange their use patterns in the absence of external pressures orincentives. Second, interventions must be designed to reducethe likelihood of relapse once initial abstinence has beenachieved. Contingency management techniques that makeclinic privileges available pending objective evidence of absti-nence from illicit drugs are well suited to these purposes andare one of the only specific interventions for polydrug abuse tohave been systematically evaluated for efficacy. One commonlyused intervention that has received some evaluation is the con-tingent availability of further methadone treatment. This ap-proach constitutes a negative reinforcement or avoidance tech-nique whereby the patient must stop the use of supplementaldrugs or face methadone dose reduction and eventual dischargefrom the treatment clinic. Evaluation studies have shown thatcontingent treatment delivery can be effective for some patientsin motivating the elimination of supplemental drug use (Dolan,Black, Penk, Rabinowitz, & DeFord, 1985; McCarthy &
927

928 M. STITZER, M. IGUCHI, AND L. FELCH
Borders, 1985). However, aversive control techniques involvingreduction of methadone dose inevitably result in some patientsleaving treatment, specifically those who will not or can notconform to the demands of the contingent treatment contract(Iguchi, Stitzer, Bigelow, & Liebson, 1988; Stitzer, Bickel, Bige-low, & Liebson, 1986).
A second technique that has been evaluated involves theawarding of take-home privileges based on objective (i.e., urinal-ysis testing) evidence of abstinence from supplemental druguse. An early study by Stitzer and colleagues (Stitzer et al., 1982)and a more recent study by Iguchi et al. (1988) demonstratedthat about 50% of the benzodiazepine-abusing methadone pa-tients enrolled responded to a urinalysis-contingent take-homeintervention by reducing or eliminating their supplemental ben-zodiazepine use during intervention trials that lasted 12 to 20weeks. Magura and colleagues (Magura, Casriel, Goldsmith,Strug, & Lipton, 1988) found that 1-month contracting for con-tingent take-homes produced a favorable response (i.e., drugabstinence) in 34% of their polydrug-abusing subjects, whereasMilby and colleagues (Milby, Garrett, English, Fritschi, &Clarke, 1978) found a similar percentage of clients respondingto a take-home incentive program with increased numbers ofconsecutive drug-free urines, as required by the intervention.Most of these studies focused on selected groups of identifiedpolydrug-abusers and used within-subjects designs to evaluateeffectiveness of contingent take-home programs for improvingtreatment outcomes.
The purpose of the present study is to determine whethercontingent take-home privileges influence treatment outcomeswhen implemented as a general clinic policy with a group ofnewly admitted methadone maintenance patients. The study isof scientific importance because it improves on previous meth-odologies to provide a rigorous clinical-trials evaluation of thetherapeutic utility of contingent take-home procedures. Thestudy is of clinical importance because it emphasizes the use oftake-home privileges as a means to shape behavior with the goalof improving outcomes for polydrug abusing patients who havenot stopped their drug use on treatment entry. Thus, althoughmethadone clinics will often award take-home privileges topatients with long-standing histories of abstinence from all illi-cit drugs, few clinics use the take-home privilege in a flexibleand responsive contingency management program that pro-vides immediate rewards for behavior change (abstinence initia-tion) in patients who have habitually used supplemental illicitdrugs during treatment.
The study was conducted in a small (75 patients) treatmentresearch clinic. All newly admitted study patients could eitherearn take-home privileges under a urinalysis-contingent proce-dure (contingent take-home group) or receive take-home privi-leges independent of treatment performance (noncontingenttake-home group). The study improves on previous methodolo-gies by using a controlled experimental design with randomassignment. The study also features a quasi-experimentalwithin-subjects replication of contingent take-home effectsachieved by shifting noncontingent subjects to the contingentprotocol at a later point in their treatment participation. Fi-nally, we examined study results both for overall effects on per-formance of study groups and for evidence of clinically mean-ingful changes on an individual subject level.
Method
Subjects
Fifty-four patients admitted to methadone maintenance treatmentbetween July 1986 and February 1988 were enrolled in the study. Thisconstituted all patients applying to and eligible for methadone mainte-nance treatment during that time period. Subjects qualified for treat-ment admission by providing three consecutive opiate-positive urinesand by having physical evidence of recent intravenous drug use. Onesubject was subsequently excluded because of psychiatric and behav-ioral problems. All study participants provided written informed con-sent for participation in the study.
The average age of study subjects was 34 years (SD = 6.7 years) andthey reported on average a 15-year history of opiate use. At treatmententry 72% of study subjects were male, 66% were White, 34% wereemployed, and 23% were married, 40% were legally free, 38% were onprobation, and 22% were pending trial. Subjects did not receive formalpsychiatric assessment. There were no statistically significant differ-ences between the study groups on any of the demographic variables.
Procedure
Study setting. There were 40 patients enrolled in the treatment re-search clinic at the start of the study, and that number increased to 75patients during the study. Approximately 50% of clinic patients were onmethadone maintenance and the remaining were outpatient 90-daydetoxification patients. Maintenance patients entered treatment withthe understanding that they would be expected to participate in re-search related to their drug use and other behavior and that theirenrollment at the clinic was limited to 2 years, after which they wouldbe aided in finding alternative treatment at other clinic sites. Thus, thepresent study sample gradually replaced existing maintenance patientsas the study progressed, and soon constituted the entire clinic mainte-nance sample. Details of the random assignment study were explainedindividually and informed consent was obtained about 2 weeks beforethe random assignment point. Subjects were required to report to theclinic every day to ingest, under a nurse's supervision, their methadonedose in cherry syrup (unless they had previously been assigned to re-ceive a take-home dose of methadone for that day), and they wereterminated from treatment if they missed 3 consecutive days at theclinic. Average methadone dose was 51.4 mg per day (range = 30 to 60mg per day, mode = 50). On six holidays per year, the clinic was closedand all subjects received take-home doses. Subjects were also expectedto participate in a drug abuse counseling session once per weekthroughout treatment. Counseling focused on compliance with clinicregulations, crisis intervention, and lifestyle change as needed to pro-mote stability.
Urine sample collection and analysis. Urine samples were collectedevery Monday, Wednesday, and Friday from all subjects. Samples wereobtained under direct staff observation and the temperature of eachsample was tested as further verification of authenticity. All sampleswere tested using two methods: immediate testing on-site using En-zyme Multiplied Immunoassay Technique (EMIT) analysis, whichtested for methadone, opiates, cocaine, and benzodiazepines; andthin-layer chromatography (TLC) analysis conducted by an indepen-dent laboratory, which included tests for opiates (e.g., codeine, hydro-morphone, meperidine, or propoxyphene), stimulants (e.g., amphet-amine or methamphetamme), benzodiazepines (e.g., diazepam, lora-zepam, or oxazepam), sedatives (e.g., barbiturates or ethchlorvynol),phenothiazines, antidepressants, and phencyclidine.
Study time line. Subjects were stabilized for 12 weeks after treat-ment admission; this served as baseline for the random assignmentstudy. At this point, subjects were stratified on gender and race andrandomly assigned to one of two conditions: contingent (n = 26) or

METHADONE TAKE-HOME INCENTIVES 929
noncontingent (n = 27) opportunity to receive methadone take-homes.Subjects continued on the assigned protocol for 6 months. At thispoint, subjects who were originally assigned to the noncontingent con-dition and remained in treatment were eligible to be shifted to thecontingent protocol. This represents a quasi-experimental design (halfacross-over), because the contingent group was not also reversed. How-ever, several subjects were switched at a particular point in time, ratherthan in relation to their own study participation time line. Thus, dura-tion of participation in the noncontingent protocol varied across sub-jects. The 18 subjects who shifted protocols remained under the non-contingent protocol for an average of 46.3 days (range = 0 to 112 days)beyond the 6-month noncontingent protocol evaluation period beforeshifting to the contingent procedures. Data from the 12 weeks prior toprotocol change was used as a baseline.
Contingent protocol. Under the contingent protocol, subjects couldearn a maximum of three take-home doses per week (Tuesday, Thurs-day, and Saturday). The first (Tuesday) take-home privilege was as-signed after six consecutive drug-free urines (2 weeks) had been ob-served. An additional take-home day (Thursday and then Saturday)was authorized after each successive 2-week drug-free period. Thus, 6consecutive drug-free weeks (18 consecutive urines) were required toearn the maximum number of take-homes. Urinalysis results wereevaluated weekly for opportunities to initiate take-home privileges.Once take-homes had been assigned, urines were evaluated at 2-weekintervals for adjustment in the number assigned. One take-home dosewas forfeited for each drug positive urine sample that was detectedwithin a given 2-week block (detected either by EMIT or by TLC analy-ses). Following a reduction or cancellation of take-home privileges, 2full weeks of drug-free urinalysis results were required to earn backeach take-home day.
Subjects in the contingent condition could not receive previouslyauthorized take-home doses of methadone on days when their on-siteEMIT results were positive for illicit drugs. Thus, it is possible thatsome earned take-homes were never delivered because of subsequentdetection of positive urine test results. Because detection of drug posi-tive urines by either EMIT or TLC did not affect the assignment oftake-home privileges until the next assessment point, it is also possiblethat earned take-homes could occasionally be delivered after subjectshad resumed some level of drug use. In general, however, there werefew exceptions to protocol adherence.
When subjects were assigned a take-home dose of methadone ac-cording to the rules of the study protocol, they received the dose fromthe clinic in a sealed bottle and were expected to self-administer it athome the next day. Subjects were routinely required to return emptymethadone bottles to the clinic. To guard against take-home diversion,a random take-home recall procedure was instituted. Subjects wererequired to provide staff with a telephone number at which they couldbe reached on the morning that they had been assigned a take-homedose. Those who could not provide a telephone number were routinelyexpected to call the clinic in the morning on take-home days. During arecall, subjects who received take-homes were contacted in the morn-ing and asked to bring their take-home dose back to the clinic. Thefirst incidence of noncompliance could result in a 1-month suspensionof take-home privileges and the second incidence of noncompliance ina 3-month suspension. In all, four such recalls were conducted duringthe study (i.e., all take-homes that had been issued for a particular daywere recalled), with only 1 client failing to return the bottle and losingtake-home privileges for a 1-month period.
Noncontingent protocol. Subjects in the noncontingent conditionwere randomly assigned at the beginning of each calendar month toreceive either 0,1, 2, or 3 take-home doses of methadone per week forthe month. These take-home doses were delivered independent of ur-ine test results. The procedures for bottle return and take-home recalldescribed in the previous section also applied to noncontingent sub-jects.
Study measures. Demographic and drug history variables were as-sessed at intake. Measures included: age, years of education, race,gender, employment status, legal status, duration in months of currentepisode of regular daily opiate use, and duration in months of entirehistory of opiate use. A primary drug of abuse was assigned by apply-ing the following criteria to the subject's baseline drug use (a) The drugwith the highest frequency of urine positive tests was assigned as pri-mary providing it was detected in at least 20% of samples tested and (b)when two drugs appeared in more than 50% of urine tests, the subjectwas assigned to a dual-primary drug category. Outcome measures weresummarized from urinalysis results. A urine sample was counted aspositive for a particular drug category if a drug was detected usingeither EMIT or TLC analyses. Outcome measures included urine sam-ples positive for any illicit drug, urine samples positive for each of threedrug categories (i.e., benzodiazepines, opiates, and cocaine), and urinedays for which the subject did not give a sample.
Results
Contingent Versus Noncontingent Take-Homes
We performed separate analyses for the percentage of missedurine days, percentage of urines with any drug positive, percent-age of urines testing positive for cocaine, percentage of urinestesting positive for benzodiazepines, percentage of urines test-ing positive for opiates, and percentage of urines testing posi-tive for more than one drug. To account for dropout and includeall subjects in the analyses, we averaged urine data across base-line and intervention phases for each subject and analyzed thedata with a mixed-model analysis of variance (ANOVA) withTukey's post hoc tests conducted on the Group X Phase interac-tion. Treatment Weeks 13 and 14 were used to determine take-home privileges that could be received starting in Week 15;Weeks 13 and 14 were included in the intervention period foranalysis. All analyses were conducted using SPSS on a Macin-tosh computer; significance levels reported are for two-tailedtests.
Baseline drug use. Drug use was detected in 64% of urinescollected during the first 3 months after treatment enrollment,which constituted the baseline evaluation phase. Cocaine andbenzodiazepines were detected in urine testing with approxi-mately equal frequency (cocaine = 32% and benzodiazepines =38%). There were no significant differences between the groupsin rates or patterns of baseline drug use. Of the 53 subjectsincluded in the data analysis, urine testing indicated that 22subjects primarily used benzodiazepines alone or benzodiaze-pines and opiates, 20 subjects primarily used cocaine alone orcocaine and opiates, and 3 subjects primarily used opiatesalone. Four subjects had both cocaine and benzodiazepines inmore than 50% of their urines, and 4 subjects did not meet thecriteria for assignment of a primary drug of abuse during thebaseline period (i.e., no single drug was detected in at least 20%of urines).
Retention. Mean retention duration during the interventionperiod was 23.1 weeks (range = 7 to 28 weeks) for the contingentgroup and 22.8 weeks (range = 5 to 28 weeks) for the noncontin-gent group. These retention durations were not significantlydifferent, t(5l) = 0.13, ns. Final attrition included 10 subjects(38%) from the contingent group and 7 subjects (26%) from thenoncontingent group (z = 0.98, ns). The mean time in treatmentfor study dropouts was 14.8 weeks (range = 5 to 25 weeks). A

930 M. STITZER, M. IGUCHI, AND L. FELCH
comparison of early dropouts (n = 17) and subjects who stayedthrough the entire 28 weeks (« = 36) revealed that dropouts hadsignificantly more urines containing any drug positive duringbaseline (77% vs. 58%, p < .02), significantly more urines posi-tive for cocaine (45% vs. 26%, p < .05) and for opiates (30% vs.10%, p < .05), and significantly more urines containing multipledrugs (39% vs. 20%, p < .01). Treatment completers and drop-outs did not differ on any demographic factors.
Take-homes delivered. Subjects in the noncontingent groupreceived an average of 33.8 take-home doses (range = 2 to 52).Half of the subjects in the contingent group never earned atake-home dose of methadone; of the thirteen subjects who did,the mean number of take-homes received was 28.7 (range = 5to 71).
Urinalysis measures. Ninety-five percent of scheduled urinesamples were collected with no significant group differencesin the number of urines delivered. There was a significantGroup X Phase interaction on the percentage of urines positivefor any drug, F(l, 51) = 4.63, p < .04, but not on percentage ofurines positive for an individual drug (e.g., opiates, cocaine, orbenzodiazepines). Urines positive for any drug decreased from67.5% (baseline) to 64.3% (intervention) for the contingentgroup and increased from 60.8% (baseline) to 70.1% (interven-tion) for the noncontingent group. The increase in percentageof positive tests for the noncontingent group was not significantin post hoc testing. There was a similar nonsignificant trend forcocaine positive tests to decrease for the contingent group from41.2% during baseline to 35.9% during intervention and to in-crease for the noncontingent group from 35.4% during baselineto 42.0% during intervention (Group X Phase interaction), F(l,51) = 3.65, p < .10. Percent of urines positive for benzodiaze-pines ranged from 35% to 42% whereas percentage positive foropiates ranged from 14% to 22% with no systematic trendsnoted as a function of group assignment or time.
Conditional probabilities of change. Subjects who could im-prove (baseline rate of drug-free urines 90% or less) were classi-fied as improving if they showed an increase of 10% or more indrug-free urines during the intervention. Subjects who couldworsen (baseline drug-free urine rate of 10% or more) were clas-sified as worsening if they showed a decrease of 10% or more indrug-free urines during the intervention. Subjects whose urinepositive test rate for baseline versus intervention periods re-mained within ±10% were classified as unchanged. In the con-tingent group, 8 of 25 subjects who could improve did improvetheir percentage of drug-free urine tests by 10% or more (32% ofsubjects improving). In the noncontingent group, an improve-ment of 10% or more was seen in 3 of 25 subjects (12%) who wereable to improve. Although clearly a trend in the predicted direc-tion, a z test was not significant (z = 1.71, ns). In the contingentgroup, 7 of 20 subjects who could worsen did show a decrease inpercentage drug-free urines of 10% or more (35% of subjects). Inthe noncontingent group, 13 of 21 subjects who could worsen(62%) met the 10% criterion for worsening. Again, the trend wasapparent but the z test was not significant (z = 1.72, ns).
Clinical improvement. To assess the clinical importance ofchanges observed, only subjects who evidenced a 10% increasein percentage of drug-free urines submitted and who had atleast 4 consecutive weeks (12 consecutive samples) of drug-freeurines during the intervention period were classified as im-
proved. The 10% urine improvement criteria was selected toeliminate small changes based on chance fluctuations. The re-quirement for 4 consecutive drug-free weeks was based on crite-ria recently used for the evaluation of treatments for cocaineabuse (Carroll, Rounsaville, & Gawin, 1991; Gawin et al., 1989;Higgins et al., 1991).
As shown in Figure 1, 8 of the 25 subjects in the contingentgroup who were able to improve met the criteria (32%) versus 2of the 25 noncontingent subjects (8%; z = 2.12, p < .05). Onaverage, contingent subjects who met the criteria for clinicalimprovement increased their drug-free urine rates by 28 per-centage points (range = 13 to 52 percentage points), achieved anaverage rate of 70% drug-free urines during the intervention,and remained continuously abstinent for an average of 9.4weeks (range = 5.3 to 15.3 weeks). These subjects included bothprimary cocaine and primary benzodiazepine users. One ofthe noncontingent subjects who met criteria for clinical im-provement had given 80% drug-free urines during baseline; theother showed a substantial (46%) increase in percentage of drug-free urines and remained continuously drug-free for 5.3 weeks.
Within-Subjects Partial Crossover
Eighteen subjects who were originally assigned to the non-contingent group were shifted to the contingent protocol afterthe intervention period and 2 additional subjects dropped outafter the 6-month evaluation and before the protocol shift. Thissample represents subjects who were stabilized in the clinicenvironment and had been exposed to the reinforcer (take-home doses of methadone) during the previous phase of thestudy. Urine data was averaged across baseline and interventionphases for each subject and analyzed for pre-post changes usingpaired / tests.
Urinalysis measures. Drug use was detected in 65% of urinescollected during baseline (3 months before protocol shift) forthis subgroup. Cocaine and benzodiazepines were detected inurine testing with approximately equal frequency (cocaine =
Subjects Who Showed Clinical Improvement40 n
LU
LUQ.
30-
20-
10-
Contingent Non-contingent Switchers
Figure 1. The percentage of subjects who improved urine test resultsby 10% or more from baseline to intervention periods and submitted atleast 12 consecutive drug-free urines during the intervention period isshown for the original contingent (n = 26) and noncontingent (« = 27)take-home groups and also for the group of noncontingent subjectswho received delayed exposure to the contingent protocol later in treat-ment (n = 18).

METHADONE TAKE-HOME INCENTIVES 931
44% and benzodiazepines = 35%). Of the 18 subjects whoshifted protocols, 9 primarily used cocaine or cocaine andopiates and 4 primarily used benzodiazepines in the 12 weeksprior to the shift. Two subjects used both cocaine and benzodi-azepines frequently, as indicated by detection of both drugsin > 50% of urines; and for 1 subject, all three drugs (cocaine,benzodiazepines, and opiates) were detected in > 50% of ur-ines. Subjects who shifted protocols later in treatment showedimprovement in urinalysis results under the contingent proto-col. There was a significant decrease in urinalysis tests thatwere positive for any illicit drug from 65% to 55% positive tests,t(\ 7) = 2.65, p < .02. There was also a significant decrease in thepercentage of urines positive for cocaine from 44% to 32% posi-tive tests, t(\ 1) = 2.31, p < .04. The percentage of urines positivefor benzodiazepines was 35% and 29% and for opiates was 19%and 15% during baseline and intervention, respectively.
Conditional probabilities and clinical improvement. Of the 16subjects who could improve (baseline rates of drug-free urinesless than 90%), 7 (44%) showed increases of 10% or greater indrug-free urine tests during the intervention. Among subjectswho could worsen (subjects with at least 10% drug-free urinesduring baseline), 3 of 11 subjects (27%) had a decrease of 10% orgreater in drug-free urinalysis results. As shown in Figure 1, 5subjects (28%) in the crossover study met the stringent criteriafor clinical improvement applied to the original groups (10% orgreater increase in drug-free urines and at least 4 consecutiveweeks of drug-free urinalysis tests). These 5 subjects did notdiffer from the 11 other subjects who could have improved onnumber of days in treatment prior to the start of their contin-gent intervention (mean = 226 days for improvers and 216 daysfor nonimprovers). Average magnitude of improvement was33.5 percentage points (range = 21 to 49 percentage points). The5 patients who met the clinical improvement criteria achievedan average drug-free urine test rate of 82% during the interven-tion and were continuously abstinent for an average duration of15.5 weeks (range = 5.3 to 28.0 weeks). These values are allsimilar to those observed for improvers in the main study. Itshould be noted that this group of 5 improvers did not includethe 2 noncontingent subjects who had improved during theoriginal protocol; both of these subjects continued in treatmentwith high rates of drug-free urines.
Predictors of Improvement
Exploratory analyses were conducted using demographic,drug history, and baseline drug use measures to compare sub-jects who met stringent criteria for improvement with thosewho could have improved but did not. Subjects who had morethan 90% drug-free urines during the baseline period (and weretherefore unable to exhibit improvement) were excluded fromthese analyses (1 main study contingent subject and 2 delayedexposure subjects). Analyses were conducted separately formembers of the original contingent group and for members ofthe noncontingent group who participated in the within-sub-jects study because these individuals were exposed to the con-tingent intervention at different times in their treatment partici-pation and after different treatment histories.
Contingent group. Subjects who met the stringent criteria forclinically significant improvement (n = 8) were compared with
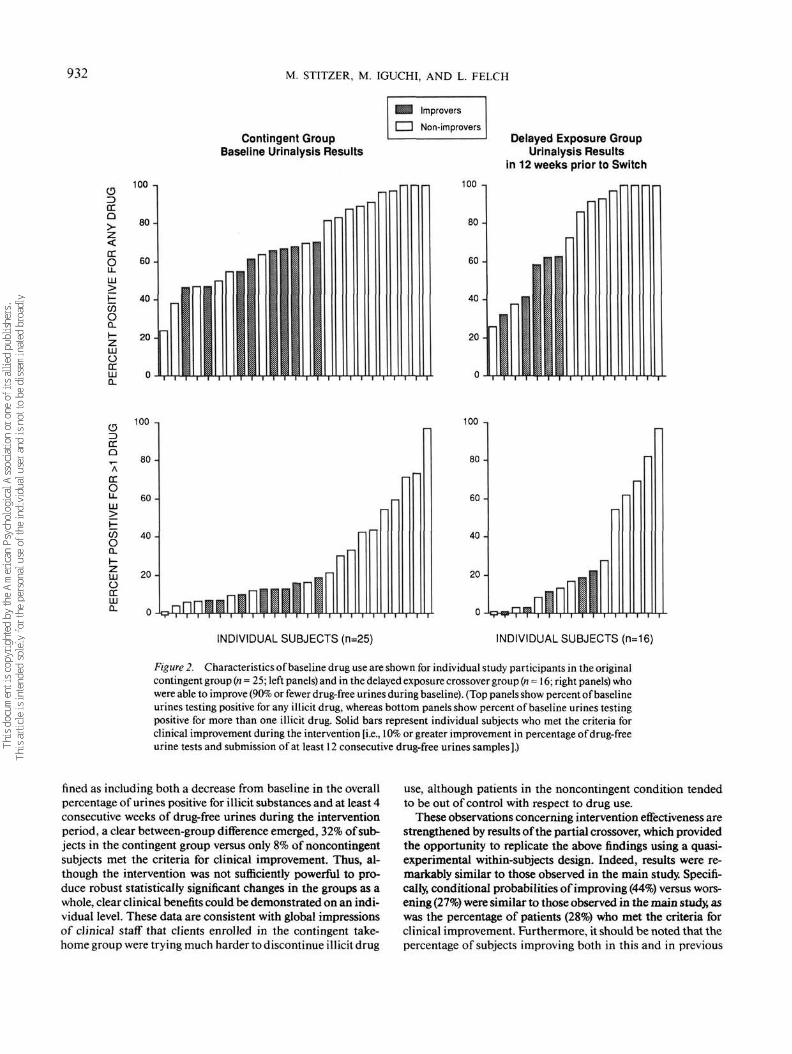
subjects who could have improved but either worsened or re-mained stable (n = 17). Improvers had a significantly smallerpercentage of urines that were positive for any drug during thebaseline period (Ms = 57% vs. 76%), t(23) =2.12, p= .045, thandid nonimprovers. Improvers also had significantly fewerurines that were positive for more than one drug (Ms =11% vs.35%), £(23) = 2.37, p = .026. Improvers and nonimprovers didnot differ significantly on any of the other variables compared.Figure 2 shows the percentage of baseline urines submitted byindividual improvers and nonimprovers that were positive forany illicit drug and for more than one drug simultaneously.
Partial crossover group. Subjects who demonstrated a clini-cally significant improvement (n = 5) were compared with sub-jects who could have improved but did not (n = 11). Improvershad fewer baseline urine samples that were positive for anyillicit drug (Ms = 5 1 % vs. 82%), t(l4) = 2.42, p = .03, fewersamples that were positive for opiate drugs (Ms = 5% vs. 29%),?(14) = 2.39, p = .034, and fewer samples positive simulta-neously for multiple drugs (Ms =11% vs. 39%), t(\ 4) = 2.52, p =.026, than those who did not improve. Improvers did not differsignificantly from nonimprovers on any of the demographic ordrug history variables. Individual data for drug positive andmultiple drug positives are shown in Figure 2.
Discussion
Previous studies have demonstrated that take-home medica-tions can be used as effective reinforcers to promote abstinencefrom illicit drugs in methadone maintenance patients (Iguchi etal., 1988; Magura et al., 1988; Milby et al, 1978; Stitzer et al.,1982). The design of these previous studies, however, does notrule out the possibility that the changes in behavior might bedue to the availability of take-home medications per se ratherthan their contingent delivery. The present study demonstratesthat take home medications, provided on a contingent basisafter 2 or more consecutive weeks of drug-free urines, are moreeffective for promoting drug-free urine submissions than aretake-home medications that are provided on a noncontingent,or random delivery schedule. This finding is generally consis-tent with previous studies in methadone programs that exam-ined changes in behavior during the contingent delivery ofother reinforcers including money (Hall, Bass, Hargreaves, &Loeb, 1979; Hall, Cooper, Burmaster, & Polk, 1977; McCaul,Stitzer, Bigelow, & Liebson, 1984; Stitzer, Bigelow, & Liebson,1980), take-home medications (Iguchi et al., 1988; Magura etal., 1988; Milby et al., 1978; Stitzer et al., 1982), and supple-mental methadone doses (Higgins, Stitzer, Bigelow, & Liebson,1986; Stitzer etal., 1986).
Although analyses of average urinalysis test results generallyfailed to support an intervention effect, a closer examination ofindividual urinalysis results provided ample support for effec-tiveness of the contingent take-home intervention on an individ-ual subject level. Conditional probabilities of improving versusworsening on urine test results were clearly in the expecteddirections, with more than twice as many contingent as non-contingent subjects improving (32% vs. 12%) and nearly twice asmany noncontingent as contingent subjects worsening (62% vs.35%). Furthermore, when clinically significant change was de-
932 M. STITZER, M. IGUCHI, AND L. FELCH
CDOCQ
oQ.
LUOtrLUCL
Contingent GroupBaseline Urinalysis Results
I Improvers
I I Non-improversDelayed Exposure Group
Urinalysis Resultsin 12 weeks prior to Switch
100 -.
80-
O 60LLLU
40-
20-
100 -,
80 -
60 -
40 -
20 -
cc° 8<HA
OCoLU
C/3OQ.
OOCLU
60 -
40 -
20 -
0 -
100 -,
80 -
60 -
40 -
20-
0 -V
INDIVIDUAL SUBJECTS (n=25) INDIVIDUAL SUBJECTS (n=16)
Figure 2. Characteristics of baseline drug use are shown for individual study participants in the originalcontingent group (n = 25; left panels) and in the delayed exposure crossover group (n = 16; right panels) whowere able to improve (90% or fewer drug-free urines during baseline). (Top panels show percent of baselineurines testing positive for any illicit drug, whereas bottom panels show percent of baseline urines testingpositive for more than one illicit drug. Solid bars represent individual subjects who met the criteria forclinical improvement during the intervention [i.e., 10% or greater improvement in percentage of drug-freeurine tests and submission of at least 12 consecutive drug-free urines samples].)
fined as including both a decrease from baseline in the overallpercentage of urines positive for illicit substances and at least 4consecutive weeks of drug-free urines during the interventionperiod, a clear between-group difference emerged, 32% of sub-jects in the contingent group versus only 8% of noncontingentsubjects met the criteria for clinical improvement. Thus, al-though the intervention was not sufficiently powerful to pro-duce robust statistically significant changes in the groups as awhole, clear clinical benefits could be demonstrated on an indi-vidual level. These data are consistent with global impressionsof clinical staff that clients enrolled in the contingent take-home group were trying much harder to discontinue illicit drug
use, although patients in the noncontingent condition tendedto be out of control with respect to drug use.
These observations concerning intervention effectiveness arestrengthened by results of the partial crossover, which providedthe opportunity to replicate the above findings using a quasi-experimental within-subjects design. Indeed, results were re-markably similar to those observed in the main study. Specifi-cally, conditional probabilities of improving (44%) versus wors-ening (27%) were similar to those observed in the main study, aswas the percentage of patients (28%) who met the criteria forclinical improvement. Furthermore, it should be noted that thepercentage of subjects improving both in this and in previous

METHADONE TAKE-HOME INCENTIVES 933
studies has been remarkably consistent at about 30% to 50%.For example, several studies from this and other laboratoriesthat tested a variety of contingent reinforcement interventionshave shown that 50% of subjects improved (Dolan et al., 1985;Iguchi et al, 1988; Stitzer et al, 1982,1986), whereas Magura etal. (1988) noted 34% improved in a contingent take-home study,which is quite consistent with the values reported here.
In addition to showing individual response variability, thestudy also provided important insights into predictors of suc-cess. Specifically, baseline levels and patterns of drug useemerged as a clear predictor of success on the contingent take-home program. Subjects who responded favorably to the inter-vention had lower baseline rates of drug-positive urine tests andengaged in less multiple drug use than nonresponding subjects.Thus, in both the main study and partial crossover, all subjectsdemonstrating clinical improvement during the interventionperiod had tested drug positive less than 70% of the time duringbaseline and had delivered relatively few urines (fewer than 25%of urines) containing multiple substances (see Figure 2). Thesefindings are consistent with observations reported by Dolan,Black, Penk, Rabinowitz, and DeFord (1986) who also foundthat lower baseline levels of drug use predicted response to atreatment termination contracting intervention.
Identification of predictor variables supplies important in-formation for clinicians who might want to target contingentreinforcement interventions to the most appropriate patients,in this case, those with less severe polydrug abuse. The analysisalso suggests that additional and more powerful interventionsare needed to address on-going supplemental drug use in moresevere cases. Alternative reinforcers or multiple reinforcermenus might be explored for patients who fail to respond totake-home incentives. Strategies for reducing the threshold forbehavior change might also be implemented, such as reinforc-ing smaller behavioral increments (e.g., reinforcing 1 week ofurine testing negative for illicit substances) or introducing nega-tive incentives such as dose reductions, the loss of programprivileges, or treatment discharge as a consequence of urinesthat tested positive for illicit substances. The latter solution,however, is not without a substantial risk of increasing patientdropout rates, which is problematic given the protectionagainst human immunodeficiency virus (HIV) exposure thatappears to be offered by methadone treatment (Abdul-Quaderet al, 1987; Hubbard, Marsden, Cavanaugh, Rachal, & Gins-berg, 1988). It might also be helpful to enhance treatment inter-ventions including more counseling and specialized skillstraining and to establish or to enhance nondrug sources of po-tential reinforcement such as employment, educational, social,and recreational activities.
The type of supplemental drug abused (cocaine vs. benzodi-azepines) did not appear to influence response to the contin-gent take-home intervention. This contrasts with observationsfrom a previous study by Magura et al. (1988), suggesting thatcocaine abusers were less likely to respond to a contingent rein-forcement intervention than benzodiazepine abusers. In thepresent study, baseline rates of drug abuse appeared to be muchmore important than the type of drug abused in determiningoutcomes. Overall, 54% of the subjects who demonstrated clini-cal improvement (main study and delayed exposure study com-bined) were primarily cocaine users or cocaine plus opiate
users, whereas 38% of the subjects were primarily benzodiaze-pine users or opiate and benzodiazepine users, and 1 subjectwas primarily an opiate user. It appears that users of both drugswere equally likely to respond to the intervention.
Although there were no significant differences betweentreatment groups on measures of retention, the survival analy-sis indicated a trend toward slightly greater dropout in the con-tingent condition. The data were examined for any relationbetween losing take-homes and treatment dropout, but no suchrelation could be found. Four subjects were identified in thecontingent take-home group who became drug-free for a periodof time during the intervention and began earning take-homes,but subsequently relapsed and lost their take-home privileges(none of these was among the group of patients classified asclinically improved). Only 1 of these relapsed patients termi-nated treatment during the remainder of the 6-month evalua-tion, and the drop-out occurred approximately 14 weeks afterthe relapse. Thus, the present study provided no evidence thatcontingent take-home procedures influenced treatment reten-tion or had any other unintended adverse effects.
A high overall rate of drug-positive urine samples was notedthroughout this study, ranging from 60% to 70% positives. Thispercentage is higher than generally reported by methadonetreatment clinics and probably reflects both a sampling bias inpatients admitted to treatment (based on the reputation of ourclinic for accepting polydrug abusers into treatment) and alsothe very intensive urinalysis testing schedule used, which wasdesigned to maximize detection of drug use. The possibilitythat the sample was biased toward inclusion of polydrug usersin no way compromises validity of the study results. If it hadany influence, this bias may have resulted in a relatively conser-vative estimate of treatment effects.
In summary, this study compares the contingent and non-contingent delivery of take-home medication privileges withrespect to the submission of urine samples free of illicit sub-stances. The outcome of the study clearly demonstrates that thecontingent delivery of the reinforcer resulted in significantlygreater changes in clinically relevant behaviors when comparedwith noncontingently delivered take-home medication. Approx-imately 30% of randomly assigned subjects showed a clinicallymeaningful improvement in urine test rates and patterns, andthis observation was replicated in a within-subjects quasi-ex-perimental crossover conducted with members of the originalnoncontingent group. Response to the contingent reinforce-ment intervention was strongly related to baseline levels of druguse, and successful cases showed less severe patterns of useduring baseline than did unsuccessful cases who submitted ahigher percentage of drug-positive urines and urines containingmultiple substances, indicating higher rates or amounts of use.Finally, it appeared that both cocaine and benzodiazepine sup-plementers were equally responsive to the reinforcement con-tingencies, and there are no data to suggest that cocaine is amore difficult drug to treat. On the basis of these findings,contingent take-home incentives are recommended as routineclinical practice in methadone clinics to encourage and sustainabstinence from supplemental drugs during treatment.
ReferencesAbdul-Quadar, A. S, Friedman, S. R, DesJarlias, D. C, Marmor,
M. M., Maslansky, R., & Bartelme, S. (1987). Methadone mainte-

934 M. STITZER, M. IGUCHI, AND L. FELCH
nance and behavior by intravenous drug users that can transmit HIVContemporary Drug Problems, 14, 425-434.
Ball, J. C, & Ross, A. (1991). The effectiveness ofmethadone mainte-nance treatment. New York: Springer-Verlag.
Carroll, K. M., Rounsaville, B. J., & Gawin, F. H. (1991). A compara-tive trial of psychotherapies for ambulatory cocaine abusers: Re-lapse prevention and interpersonal psychotherapy. American Jour-nal of Drug and Alcohol Abuse, 17, 229-247.
Condelli, W S., Fairbank, J. A., Dennis, M. L., & Rachal, J. V (1991).Cocaine use by clients in methadone programs: Significance, scope,and behavioral interventions. Journal oj'Substance Abuse Treatment,5,203-212.
Dolan, M. P., Black, J. L., Penk, W E., Rabinowitz, R., & DeFord, H. A.(1985). Contracting for treatment termination to reduce illicit druguse among methadone maintenance treatment failures. Journal ofConsulting and Clinical Psychology, 53, 549-551.
Dolan, M. P., Black, J. L., Penk, W E., Rabinowitz, R., & DeFord, H. A.(1986). Predicting the outcome of contingency contracting for drugabuse. Behavior Therapy, 17, 470-474.
Gawin, F. H., Kleber, H. D., Byck, R., Rounsaville, B. J., Kosten, T. R.,Jatlow, P. I., & Morgan, C. (1989). Desipramine facilitation of initialcocaine abstinence. Archives of General Psychiatry, 46, 117-121.
Hall, S. M., Bass, A., Hargreaves, W A., & Loeb, P. (1979). Contingencymanagement and information feedback in outpatient heroin detoxi-fication. Behavior Therapy, 10, 443-451.
Hall, S. M., Cooper, J. L., Burmaster, S., & Polk, A. (1977). Contin-gency contracting as a therapeutic tool with methadone mainte-nance clients: Six single subject studies. Behavior Research andTher-apy, 75,438-441.
Hanbury, R., Sturiano, V, Cohen, M., Stimmel, B., & Aguillaume, C.(1986). Cocaine use in persons on methadone maintenance. Ad-vances in Alcohol and Substance Abuse, 6, 97-106.
Higgins, S. T., Delaney, D. D, Budney, A. J., Bickel, W K., Hughes, J. R.,Foerg, F., & Fenwick, J. W (1991). A behavioral approach to achiev-ing initial cocaine abstinence. American Journal of Psychiatry, 148,1218-1224.
Higgins, S. T., Stitzer, M. L., Bigelow, G. E., & Liebson, I. A. (1986).Contingent methadone delivery: Effects on illicit-opiate use. Drugand Alcohol Dependence, 17,311-322.
Hubbard, R. C, Marsden, M. E., Cavanaugh, E., Rachal, J. V, & Gins-berg, H. M. (1988). Role of drug-abuse treatment in limiting thespread of AIDS. Reviews of Infectious Diseases, 10, 377-384.
Iguchi, M. Y, Griffiths, R. R., Bickel, W K., Handelsman, L., Chil-dress, A. R., & McLellan, A. T. (1990). Relative abuse liability ofbenzodiazepines in methadone maintenance populations in threecities. Problems of Drug Dependence, 1989 (Monograph No. 95; pp.364-365; No. ADM 90-1663). NIDA Research, Washington, DC:US. Government Printing Office.
Iguchi, M. Y, Stitzer, M. L., Bigelow, G. E., & Liebson, I. A. (1988).Contingency management in methadone maintenance: Effects ofreinforcing and aversive consequences on illicit polydrug use. Drugand Alcohol Dependence, 22,1-7.
Kosten, T. R., Gawin, F. H., Rounsaville, B. J., & Kleber, H. D. (1986).Cocaine abuse among opioid addicts: Demographic and diagnosticfactors in treatment. American Journal of Drug and Alcohol Abuse,12, 1-16.
Magura, S., Casriel, C., Goldsmith, D. S., Strug, D. L., & Lipton, D. S.(1988). Contingency contracting with polydrug-abusing methadonepatients. Addictive Behaviors, 13,113-118.
McCarthy, J. J., & Borders, O. T. (1985). Limit setting on drug abuse inmethadone maintenance patients. American Journal of Psychiatry,142, 1419-1423.
McCaul, M. E., Stitzer, M. L., Bigelow, G. E., & Liebson, I. A. (1984).Contingency management interventions: Effects on treatment out-come during methadone detoxification. Journal of Applied BehaviorAnalysis, 77,35-43.
Milby, J. B., Garrett, C., English, C., Fritschi, O., & Clarke, C. (1978).Take-home methadone: Contingency effects on drug-seeking andproductivity of narcotic addicts. Addictive Behaviors, 3, 215-220.
Stitzer, M. L., Bickel, W K., Bigelow, G. E., & Liebson, I. A. (1986).Effects ofmethadone dose contingencies on urinalysis test results ofpolydrug-abusing methadone-maintenance patients. Drugand Alco-hol Dependence, 18, 341-348.
Stitzer, M. L., Bigelow, G. E., & Liebson, I. A. (1980). Reducing druguse among methadone maintenance clients: Contingent reinforce-ment for morphine free urines. Addictive Behaviors, 5, 333-340.
Stitzer, M. L., Bigelow, G. E., Liebson, I. A., & Hawthorne, J. W (1982).Contingent reinforcement of benzodiazepine-free urines: Evalua-tion of a drug abuse treatment intervention. Journal of Applied Be-havior Analysis, 75, 493-503.
Received August 14,1991Revision received January 15,1992
Accepted January 24,1992 •




















