
CONDUCTING THE EMERGENCY TEAM - Beier & Larsen
129
FACULTY OF HEALTH AND MEDICAL SCIENCES UNIVERSITY OF COPENHAGEN PHDTHESIS Ture Larsen CONDUCTING THE EMERGENCY TEAM Focus on leadership Academic advisors: Randi Beier-Holgersen, Peter Dieckmann, Doris Østergaard This thesis has been submitted to the Graduate School of the Faculty of Health and Medical Sciences, University of Copenhagen Submitted 02.01.18
-
Upload
khangminh22 -
Category
Documents
-
view
2 -
download
0
Transcript of CONDUCTING THE EMERGENCY TEAM - Beier & Larsen

F A C U L T Y O F H E A L T H A N D M E D I C A L S C I E N C E S U N I V E R S I T Y O F C O P E N H A G E N
PHDTHESISTureLarsen
CONDUCTINGTHEEMERGENCYTEAMFocusonleadership
Academicadvisors:RandiBeier-Holgersen,PeterDieckmann,DorisØstergaard
ThisthesishasbeensubmittedtotheGraduateSchooloftheFacultyofHealthandMedical
Sciences,UniversityofCopenhagen
Submitted02.01.18

2

3
ThestudiesinthisPhDthesiswereconductedbetween2015and2017atSimNord,Nordsjællands
Hospital,UniversityofCopenhagenandtheCapitalRegionofDenmark
Forfurtherinformation,contact
TureLarsen
Oldfuxvej20
2400NV
Denmark
Mail:[email protected]
Phone:+4531127281
Website:http://turelarsen.dk/phd.html
ORCID:http://orcid.org/0000-0002-5410-6340
Front-pageillustration:
Aquicklydrawnsketchoftheparallelbetweentheconductorandtheclinicalteamleader(byTL)

4
ACADEMICADVISORS
RandiBeier-Holgersen,AssociateProfessor,MD,MHPE.SeniorSurgeon,Departmentof
GastrointestinalSurgery,NordsjællandsHospital,Denmark
PeterDieckmann,PhD,Dipl.-Psych.Psychologist,SeniorScientist,CopenhagenAcademyfor
MedicalEducationandSimulation(CAMES),CapitalRegionofDenmarkandUniversityof
Copenhagen,Copenhagen,Denmark
DorisØstergaard,MD,DMSc,Professor,MHPE.HeadofInstitute,CopenhagenAcademyfor
MedicalEducationandSimulation(CAMES),CapitalRegionofDenmarkandUniversityof
Copenhagen,Copenhagen,Denmark
ASSESSMENTCOMMITTEE
JacobRosenberg,MD,DMSc,Professor,chiefsurgeon,Dept.ofSurgery,HerlevandGentofte
Hospitals,UniversityofCopenhagen,Denmark.
NielsQvist,MD,DMSc,Professor,chiefsurgeon,Dept.A.ofSurgery,OdenseUniversitetshospital,
Denmark
PeterEttrupLarsen,Dr.ofMusicalArts(DMA),Conductor,MAinMusicologyandRhetoric,
AssociateProfessorofDigitalConductingStudies,TheUniversityinStavanger,Norway
FUNDING
ThePhDprojecthasbeensupportedbyTrygFoundation,LaerdalFoundationandNordsjællands
Hospital,Denmark.
5
ACKNOWLEDGEMENTS
ThankstoRandi.Thankyouforcreatingthiscrazyandinnovativeidea.Allideas,theories,views,
anddecisionswerecreatedjointlyinourresearchpartnership.Noideashaveeverbeenrejected
andallthoughtsandassociationshavebeenfollowed,understoodanddiscussedindepth,
thoroughly,seriouslyandwithlotsoflaughs.Ithasbeenagreatprivilegeandexperiencetopresent
theprojectonourmanytripsfromSingaporeoverIstanbul,andGlasgowtoToronto,Quebecand
Vancouver.
ThankyoutomycolleaguesatSimNord.ThankstoSusannetorealisethepotentialandpossibilities
inRandi’sidea.ThankstoRikkeandGitteformanydiscussions,supportandengagement.Thanksto
Lindaforalwaysbeingreadytohelp.ThankstoErikandCasperforlistening,discussingand
supporting.IhavebeenwellreceivedandfeltlikepartofSimNord.
ThanktoHRandtheResearchdepartmentatNOHforhelpingrealizingtheprojectandforfinancial
support.
ThankstoPeterforaswellsupportfortheideaaswellascriticismofmethods,methodology,
ontology,epistemology,conclusionsandwriting.Thishasonlyintensifiedmydesiretosharpenmy
workandmypoints.
ThankstoDorisforparticipatingintheprojectgroup,itishighlyappreciatedthatyouchoosetoadd
yournameandknowledgetothisdifferentresearchproject.
ThankstoJetteforhelpingwiththechallengingsearchintheliteratureaswellassupportand
inspiringdiscussions.
ThankstoSusanLaubeforproofreadingonthearticles.ThankstoNigelBarnardforproofreading
onThesis.

6
TABLEOFCONTENTS
PAPERSINCLUDEDINTHETHESIS................................................................................................8
ABBREVIATIONSANDDEFINITIONS.............................................................................................9
SUMMARYOFTHETHESIS.........................................................................................................11
SAMMENFATNINGPÅDANSK....................................................................................................13
STRUCTUREOFTHETHESIS........................................................................................................15
BACKGROUND...........................................................................................................................16TheConductor..................................................................................................................................17
Emergencyinhealthcare..................................................................................................................17
AIMS.........................................................................................................................................18
CONCEPTUALFRAMEWORK.......................................................................................................18Differentontologies.........................................................................................................................18
Qualitativemethodologyconsiderations.........................................................................................19
LEARNINGTHEORYCONSIDERATIONS.......................................................................................21Theoriessupportingconceptualchangeortransformation.............................................................21
EmbodiedCognition.........................................................................................................................21
TransformativeLearningTheory......................................................................................................21
Apprenticeship.................................................................................................................................21
Flowtheory–apedagogicideal.......................................................................................................22
Anxietycounteractslearning............................................................................................................22
Thinking,fastandslow.....................................................................................................................23
Learningpyramid,NTL......................................................................................................................24
ANALYSISCONSIDERATIONSONEXTRALINGUISTICDATA.........................................................24Incongruencebetweenoralandextralinguisticcommunication....................................................24
Semiotics..........................................................................................................................................25
Multimodality(extralinguisticcommunication)..............................................................................25
Videoanalysis...................................................................................................................................26
Conductorsandvideo.......................................................................................................................26
Videoandsimulationinhealthcare..................................................................................................27
PRE-UNDERSTANDING...............................................................................................................27

7
METHOD...................................................................................................................................28SystematicReview............................................................................................................................28
Qualitativecontentanalysisasamethod........................................................................................28
Video................................................................................................................................................30
Transcriptions...................................................................................................................................30
Evaluations.......................................................................................................................................30
ETHICALCONSIDERATIONS........................................................................................................31
PRESENTATIONOFTHEINCLUDEDPAPERS................................................................................32Study1..............................................................................................................................................32
Study2..............................................................................................................................................34
Study3..............................................................................................................................................36
DISCUSSION..............................................................................................................................39Developmentandconductionofacourseaddressingleadership...............................................41Feedback.......................................................................................................................................43Faculty..........................................................................................................................................44Assessmentoftheimpactofthecourse......................................................................................46
STRENGTHSANDLIMITATIONS..................................................................................................46
CONCLUSION.............................................................................................................................50
PERSPECTIVES...........................................................................................................................51
TRAININGRESIDENTSTOLEADEMERGENCYTEAMS[PARTONE]:ASYSTEMATICREVIEW........53
TRAININGRESIDENTSTOLEADEMERGENCYTEAMS[PARTTWO]..............................................79
CONDUCTINGTHEEMERGENCYTEAM:ANOVELWAYTOTRAINTHETEAM-LEADERFOREMERGENCIES...........................................................................................................................93
APPENDIX................................................................................................................................122
ONLINEAPPENDIX...................................................................................................................122
REFERENCES............................................................................................................................124

8
PAPERSINCLUDEDINTHETHESIS
Paper1
TureLarsen,RandiBeier-Holgersen,JetteMeelby,PeterDieckmann,DorisØstergaard.
Trainingresidentstoleademergencyteams[PartOne]:ASystematicReview
SubmittedtoAnnalsofSurgery(December2017)
Paper2
TureLarsen,RandiBeier-Holgersen,DorisØstergaard,PeterDieckmann.
Trainingresidentstoleademergencyteams[PartTwo]:Barriers,ChallengesandLearningGoals
concerningtrainingresidentstoleademergencies:aQualitativeReview
SubmittedtoAnnalsofSurgery(December2017)
Paper3
TureLarsen,RandiBeier-Holgersen,PeterDieckmann,DorisØstergaard.
Conductingtheemergencyteam:Anovelwaytotraintheteam-leaderforemergencies
SubmittedtoLancet(December2017)

9
ABBREVIATIONSANDDEFINITIONS
LBDQ LeadershipBehaviourDescriptionQuestionnaire1
NOTECHS NonTechnicalSkillsbehaviouralmarkersystem.Amethodfor
assessinganindividualpilot’snontechnicalskills(e.g.leadership,
decisionmaking,teamworking,situationawareness).2
NTL TheNationalTrainingLaboratories’averageretentionratesfor
differenttrainingandteachingmethods
PRISMA PreferredReportingItemsforSystematicReviewsandMeta-
Analyses.PRISMAisanevidence-basedminimumsetofitemsfor
reportinginsystematicreviewsandmeta-analyses3
GRADE GradingofRecommendationsAssessment,Developmentand
Evaluation.TheGRADEprocessdevelopsrecommendations,the
evidenceprofile,andSummaryofFindingstable.Gradedescribes
theprocessforframingquestionsandidentifyingoutcomes4
CASP CriticalAppraisalSkillsProgramme4
Abduction TheoryàDataßàDataàTheoryàAnalysisàConclusion
Deduction TheoryàDataàAnalysisàConclusion
Induction DataàTheoryàAnalysisàConclusion
QCA QualitativeContentAnalysis
GT GroundedTheory
Ontology Knowledgeaboutbeing(thenatureofbeing)5
Epistemology Knowledgeaboutknowledge(science/knowledge)5
Positivist:
Positivist’sontology Believesthereisonesinglerealityandbelievesinuniversal
concepts6
Positivist’sepistemology Empiricist:collecting–hypothesis–testhypothesisobjectively
usingstatistical.Nointerpretation.
Positivist’smethodology Theorydeveloping:Hypotheticdeductivemethod
Constructivist
Constructivist’sontology There’snosinglereality,realityisconstructedinthecontext7
10
Constructivist’sepistemology Interpretreality(putsoneselfintheproject)
Constructivist’smethodology Inductive(lookatsinglecasesstudies)
Writtencommunication Linguisticisbasedonwordsandsentences.Thevalueofawordis
rarelycompletelyneutral,astherearetypicallyconnotationstoa
word.Furthermore,itispossibletotalkaboutthesurfacecontent
ofthetextaswellasinterpretationsoftheunderlyingmeaning8
Extralinguistics Non-verbalcommunication,pictures,videos,allmeansof
multimodalcommunication9
Oralcommunication Speaking,lectures,andpresentations:Linguistics,includingthe
possibilityofaddingextralinguistics
Facetofacecommunication Interpersonalcommunication:allcommunicatorsactively
participateandareresponsibleforitscreation.Linguistics,
includingextralinguistics
Semiotics Therangeofdifferentkindsofsignsthatcanbefoundascompared
tolanguagethatcomprisesabstractsymbols.10CharlesSanders
Peirce(1839-1914)describedthoughtsnotas’ideas’butas’signs,’
externaltotheselfandwithoutmeaningunlessinterpretedbya
subsequentthought.Hisgeneraltheoryofsigns–orsemiotic–is
especiallypertinenttomethodologiescurrentlybeingdebated11
Multimodality Describingothermeaningsthanbasedonlanguageandlinguistics.
Thereisvisuallanguage,gesturallanguage,andsoforth.Itis
sociallyproduced,culturalresourcesformakingmeaning.
Situationsaregivenwheretextonlygivesapartialaccountofwhat
isgoingon12

11
SUMMARYOFTHETHESIS
Thespecificapproachtothisthesisistoexploreadifferentapproachtotraintheemergencyteam
leaderwithhelpfromanotherprofession.Furthermoreinvestigateexistingaspectsoftrainingof
theteamleaderinemergenciesinhealthcare.
Thisthesisisbasedonanabductiveapproach.Themainideaisconceivedincollaborationbetween
asurgeonandanorchestralconductorwhorealisedaparallelbetweenleadingamedicalteamand
leadinganorchestraintermsofthenon-verbalcommunicationthatdemonstratesthattheleader
hasassumedleadership.
Ithasbeendescribedintheliteratureforthelast30yearsthatthereisanurgentneedtotrain
residentsandmedicalstudentsinleadershipinacutemedicalsituations.Theliteraturedescribes
theneedfortheteamleadertorisetotheoccasionwhencalledupontoactasleadersof
emergencyteams:manyresidents/rescuersfeelunpreparedtoadopttheleadershiprolein
emergencies.Itisimportanttoassumeleadershipduringtheteamworkthattakesplaceinthe
criticalsituation,aslackofleadershipisconcludedtobeoneofthecausesofpooroutcomesfor
thecriticallyillpatient.
Theconclusionofasystematicreviewthatincludedalltheinterventionstudiesfound,focusingon
whetherornotfoundadequatetrainingintheteamleadershiproleamongresidents,is
unfortunatelythatnofocusedleadershiptraininghastakenplace.
Instead,literaturerevealedalargenumberoftaxonomiesaimingatmeasuringtheabilityof
residentstoimplementvariousprofessionalalgorithmswithoutspecificfocusontheleadership
role.Theliteraturehasdevotedtimetodevelopingmeasuringinstrumentsintheformof
taxonomiesandhasnotfocusedonthedevelopmentofleadership.Itispossibletoconcludethat
focushassubstitutedfromhowtotrainleadershiptomeasureleadership.
Inaqualitativecontentanalysisofthefoundliterature,itwasconcludedthatleadershiptrainingis
anecessitywhichisneededtobeaddressed,buteffortshassofarbeenfocusedelsewhereanda
usefulleadershiptraininginemergenciesitisstillindemand.
Byfurtherreviewandqualitativecontentanalysisoftheliterature,includingalltheopinionsand
reviewsfound,itwasidentifiedthatacrucialfactortoaddressistheanxietyresidentscan
experiencewhentheyaretotakeonleadershipinacutecriticalsituations.Theliteratureitself

12
describeshowtheresidentsshouldbetrainedinmentallyassumingleadership,radiatingcalmness
andcredibilityanddemonstratingauthorityinthecriticalandchaoticsituation.Byreviewingthe
literature,learninggoalsthatshouldbethefocusofanupcomingtrainingwereidentified.Those
shouldaddresstheactualneedstheresidenthasinthesituation.
Thecoursewasdevelopedinanon-medicalchallengingcontext,butcloselyrelatedtotheclinic.
Musicalexerciseswereused,whichmadethecourseharmlesstotheindividualmedicalparticipant
whowasnotexpectedtobeabletohandlethechallengesand‘obstacles’intheexercises.
However,themusical‘obstacles’broughttheparticipantintothementallychallengingstate,
resultingthatalloftheparticipant’spersonalinappropriatenon-verbalexpressionswererevealed
inthesituation.Thisenabledtheorchestralconductortoaddressthese,givepersonalanddirect
feedbacktoparticipant,andthustheparticipantwasenabledtorecogniseownweaknessesand
guidedbytheconductorwasgivenopportunitytostrengthentheseexpressions.Inaddition,the
musicalexercisesgavetheparticipantanexperienceofflowwhenconducting,andtheindividual
participantexperiencedtheintensefeelingwhenallcommunicationtakesplacethroughtheleader.
Thecourseswereevaluatedusingvideorecordings,transcriptionsofthese,evaluationsfromthe
courseparticipants,aswellaswrittencommentsfromtwostudentswhohelpedtotranscribethe
transcriptions.Thelatterdidnotattendthecoursesandwereblindedtotheideaofthecourse.
Again,aqualitativecontentanalysiswasconductedandtheconclusionisthatthecourseisableto
supporttheindividualparticipant’sabilitytogaininsightintohis/herownleadershipchallenges
andtoprovideadviceandassistanceindevelopinghisnon-verbalappearanceandexpression.
Ingeneral,thisthesishasdescribedhowcollaborationbetweentwoverydifferentprofessionshas
managedtoexploitthevariousontologicalapproachestotheexperienceoftheworldinapositive
andconstructiveway.Itpointsoutthatitisbeneficialtoallowtoseebeyondowndomainor
profession.
13
SAMMENFATNINGPÅDANSK
Formåletmeddenneafhandlingeratundersøgeomdetermuligtatbrugeenandenprofessiontil
attræneteamlederrolleniakuttemedicinsketeams.Derudoverundersøgeomderfindesandre
holdningerelleraspektervedrørendetræningafteamlederrolleniakuttesituationeriklinikken.
Denneteseerbaseretpåenabduktivtilgang.Ideenerundfangetietsamarbejdemellemenkirurg
samtenorkesterdirigent,dersåenparallelmellemdetatledeetmedicinskteamogetorkester
mht.bl.a.dennon-verbalekommunikation,derviser,atlederenharpåtagetsiglederskabet.
Detergennemdesidste30årbeskrevetilitteraturenatdereretbehovforattræneyngrelæger
ogmedicinskestudenterilederskabiakuttemedicinskesituationer.Litteraturenbeskriveretbehov
foratteamlederentræderikarakterogpåtagersiglederskabetunderdetteamsamarbejdeder
foregåridenkritiskesituation,idetmanglendelederskabkonkluderesatværeenafårsagernetil
dårligtoutcomefordenkritisksygepatient.
Konklusionenpåetsystematiskreviewmedinklusionafallefundneinterventionsstudiermedfokus
påomderfindesellerharfundetfokuseretoplæringiteam-lederrollenblandtyngrelægerer
desværre,atderikkeharfundetfokuseretledelsestræningsted.Istedetfindesilitteraturenet
stortantaltaxonomiertilmålingafyngrelægersevnetilgennemførelseafforskelligefaglige
algoritmerudenspecifiktfokuspålederrollen.Litteraturenharfokuseretpåatudvikle
måleinstrumenteriformaftaxonomierogharikkefokuseretpåudviklingafoplæringssituationeri
lederrollen.Mankankonkludereatfokusersubstitueretfrahvordantrænermanlederskabtil
hvordanmanmålerlederskab.
Vedenkvalitativindholdsanalyseafdenfundnelitteraturerkonklusionenatlederskabstræninger
etnødvendigtbehov,derskaldækkes,menatindsatsenindtilvidereharværetfokuseret
andetstedsogatdenfortsatefterspørges.
Vedyderligereengennemgang/kvalitativindholdsanalyseaflitteraturen,hvorogsåallefundne
opinionsogreviewsmedtages,findes,atdenafgørendefaktor,derskaladressereserdenangst
somyngrelægeroplever,nårdeskalpåtagesiglederskabetiakuttekritiskesituationer.Der
beskrives,hvordandeyngrelægerskaltrænesiatmentaltpåtagesiglederskabet,udstråleroog
autoritetidenkritiske/kaotiskesituation.Vedgennemgangenaflitteraturenfindeshermedde

14
læringsmål,sombørværefokusienkommendetræning,hvistræningskalfokuserepådebehov
denyngrelægeharisituationen.
Kursetblevudvikletienikkemedicinskfagligkontekst,menmedtætrelationtildenmedicinske
verden.Derbenyttesmusikalskeøvelser,hvilketgørkursetufarligtfordenenkeltemedicinsk
fagligekursist,derikkeforventesatkunnehåndterede”benspænd”dereriøvelserne.Demusiske
benspændformåededogatbringekursisterneidenmentaltudfordrendetilstand,dermedførteat
alledeuhensigtsmæssigenon-verbaleudtryk,somerenudfordringvedrørendelederskabi
teamledelsen,komtiludtryk.Dettegavorkesterdirigentenmulighedforathjælpedenenkelte
kursisttilaterkende,hvoregnesvaghederfandtessamtmulighedforatarbejdemeddisse.
Derudovergavdemusiskeøvelserenoplevelseafflowiledelsessituationen,hvordenenkelte
kursistoplevededenfølelsedeter,nåralledelseforegårgennemlederen.
Kurserneblevevalueredevedhjælpafvideooptagelser,transskriptionerafdisse,evalueringerfra
kursisternesamtkommentarerfratostudenterderhjalptilmedatfortagetransskriptionerne.
Sidstnævntedeltogikkepåkurserneogvarblindedefortankernebagkurset.Igenblevgennemført
enkvalitativindholdsanalyse,ogkonklusionenpådenneer,atkursetformåratunderstøtteden
enkeltekursistsmulighedforatfåindsigtiegneudfordringerilederrollensamtatgiverådoghjælp
tilatudviklesitnon-verbaleudtryk.
Overordnethardennetesebeskrevethvordansamarbejdemellemtomegetforskellige
professionerharformåetatudnyttedeforskelligeontologisketilgangetiloplevelsenafverdenpå
enpositivogkonstruktivmåde.Denpåpegerdetfrugtbareiattilladesigatseudoveregen
faggruppe/profession.

15
STRUCTUREOFTHETHESIS
Thefirstchapterpresentsthebackground.Thesecondchapterpresentstheconceptualframework;
theontologyandthemethodologyofthethesis.Furthermorethischapterpresentstheories
consideredrelevanttothethesis;learningtheories,discussiononanxietyandlearning,theintuitive
andtherationalwayofthinking,andanassessmentmodeloftheimpactoflearning.Finally,the
chapterpresentsseveralapproachestonon-linguisticorextralinguisticlanguage.Thethirdchapter
presentsthemethodsusedanddataacquisitionandanalysis.Thefourthchapterprovidesabrief
descriptionofthethreestudies.Chapterfivepresentsadiscussionoftheimplicationofthefindings
inthethesis.Chaptersixdiscussesthelimitationsinthethreestudies,andfinallyconcludesonthe
threestudies,highlightsimplicationsforpracticeandsuggestsfutureresearch.
Studyoneexaminesthemedical,pedagogicalandpsychologicaldatabasesifthereisawell-
functioningtrainingoftheclinicalteamleaderinemergencies,27articleswererelevant.In
addition,itexaminesbyaqualitativecontentanalysiswhetherthereisconsensusonthe
importanceofleadership.
Studytwoexaminesthe27articlesfoundplusadditional13articlesifitispossibletoidentify
challengesandlearninggoalsconcerningleadershiptraininginemergencies.
Studythreepresentstheinterventionofthethesis,acourseconductedanddesignedbya
conductorandaconsultantforresidents,medicalstudentsandseniornursesattheemergency
room.
Atthebackofthedissertationanonlineappendixthatpresentsthecomprehensiveresultsofthe
qualitativecontentanalysesissituated.Inaddition,alogfromthecoursecontainingfieldnotes,
transcribeddialogues,andevaluations.Finally,linkstotwodocumentspresentingvideosfromthe
courseispresent.

16
BACKGROUND
Teamleadershipinemergenciesisreportedasbeingimportantforthequalityoftheperformance
ofteams13-24,forpatientoutcome,patientsafetyandpatientcare22,23,25-35.Thequalityofteam
leadershipmayeveninfluencepatientmortalityandsurvivalrates19,23,27,32.
However,manystudiesidentifythatleadershiptraininghasbeeninadequate1,16,17,23,27,29,36-39,and
arecurrentcallforaworkableleadershiptrainingprogrammehasbeenexpressedexplicitly
1,14,16,17,21-23,26,27,29,34,36-43.Thisneedhasprevailedthroughoutthe30-yearperiodaddressedinour
investigation.
Theliteratureaffirmedthattargetedleadershiptrainingisveryimportant.Itisnecessaryfor
residentstoaddressandhandleanxiety16,23,27,32,44andpanic32instressful20,22,25,27,31,32,34,41,45and
complex19-22,35,39,41situations.Therefore,inordertoprovidegoodandconvincingleadership,
residentsmustlearntobeconfident1,16,23,27,32,36,37,39,41,42,44,46,47andcalm16,30,32,44whenassuming
theleadershipinemergencies.
However,‘something’isapparentlystillmissing,andthereasonwhy‘residentsfeelunpreparedand
unsupervisedasleaders’27shouldbeexplored.
Theparallelbetweentheconductorandtheteamleaderinemergenciesinthiscontextisthehighly
intensesituationstheyworkin:bothsituationsrequireclearandconvincingleadershipandthereis
notimeorroomfordiscussions.Neithertheconcertnorthecardiacarrestcanbeinterrupted.The
leader’sguidanceandinstructionsmustbecarriedoutimmediately.
OneyearpriortothestartofthePhDstudy,apilotprojectwasconducted.Aconsultantwhoalso
wasanamateurtromboneplayerrealizedtheparallelbetweentheteamleaderandtheconductor
whenherconcertbandreceivedanewskilledconductor.Theconsultantandtheconductor
designedacourseformedicalstudentswhoparticipatedinaprogramintroducingnon-verbal
communicationandteamleadership.Theresultsfromthecourseisdescribedinthearticle“Team
Management-Canmusiccontributetobetterunderstanding?”48.(Abstractispresentedinthe
appendixsection).
Manyinitiativeshavesoughttoaddressleadershiptraininginemergencies:inparticularleadership
ispartoftheScottishinitiativeAnaesthetists’NontechnicalSkills(ANTS)49,adaptedto‘Non-
TechnicalSkillsforSurgeons’(NOTSS)38,andto‘ScrubPractitioners’ListofIntra-operativeNon-

17
TechnicalSkills’(SPLINTS)50.ThelatterreplacedNOTECHSfornurses51–whichwasalsomodified
to:OxfordNOTECHS52andamongotherthings:T-NOTECHS53,aswellastheSwissleadership
trainingprogrammebasedontheLeadershipBehaviourDescriptionQuestionnaire(LBDQ)1.These
programmesfocusondevelopingformativeassessmenttools54,behaviouralmarkers55and
taxonomiesinordertomeasure15,22,33,38leadershipskills.Since2015theliteraturehasbegunto
questionthenumberoftools–andmethodsused–inthetaxonomies34.
Handlingnegativefeelingsisnotapartofexistingprogrammes.Leadershipduringanemergency
situationinvolvesknowledgeandskills,butalsoimpliesdealingwiththepressure16,25,28,34,38,56of
beingthedecision-makerandtakingtheultimateresponsibilityforwhathappens(ordoesnot).
THECONDUCTOR
Theconductorworkspurposefullywithhispostureandappearanceinordertoeliminateanything
thatcouldpossiblypreventthemessagefrombeinginterpretedasintended.Theconductors’main
focustoachievetheauthoritytoleadanorchestra,itisimportanttoappearcalm,balanced,
competent,authentic,andcredible.Thisisthebasicstartingpointfortheconductor,when
recognised,heisablebegintoworkandchoosehisstyleofleadership57.
Thisviewsexpressingtheconductor’sreflectionsonhisworkwiththeorchestra’smusiciansare
generalanddonotreflecttheopinionsofasingleconductor.Theabovedescriptionofthe
conductorsfocusisreadbytwosymphonicconductors,anddiscussedthoroughly.Bothconductors
couldendorsethereflectionsandopinionsthatwerepresented.
Noliteratureaddressesthesecompetenciesequallyinhealthcare.
EMERGENCYINHEALTHCARE
“Emergencymedicalcareteamshave[…]littletimefordeliberateplanningandelaborate
communicationwhileprovidingcare.Second,suchteamsaregenerallyadhoc,thatis,assignedto
worktogetherineverchangingcompositions”40.‘Adhoc’teamsarealsoreferredtoas‘crash’
teams23.
Thissituationiscomplex16,19-22,24,25,29,30,33,35,39,41,44,56,58andstressful16,20,22,23,25,27,29-34,41,45,47,59and
hasbeenreferredtoasachaoticsituation1,32,34,41,44,46,60perceivedaswithanxiety1,14,16,23,27,32,36,44.
Inthisframework,theemergencyteamleadershouldrisetotheoccasionwhencalledupon,mark

18
leadershipandidentifycompetenciesandresourcesoftheteamforthepurposeofensuringthe
besttreatmentofthepatient.
Theproblemhasbeentodefinetheseissuesandsubsequentlyfindawaytotraintheseobjectives
inhealthcare.
AIMS
Theoverallobjectiveofthisthesiswastoexploreadifferentapproachtotraintheleaderofthe
emergencyteamwithhelpfromanotherdomain.Furthermoretoinvestigateexistingaspectsof
trainingoftheteamleaderinemergenciesinhealthcareusingdifferentmethodsinthreestudies
withthefollowingaims:
Study1:Todescribehowliteratureaddressesworkableandoperationalleadershiptrainingforthe
emergencymedicalteam-leaderandtoenhanceunderstandingofleadershiptraininginthe
medicalenvironment.
Study2:Aninvestigationtodetermineanyconsensusinopinionsandviewsaboutchallengesor
barriersintrainingleadershipinemergencies.
Study3:Theoverallaimofthecourseistoinvestigatewhether,inanemergency,aclinicalteam
leadercouldapplyaconductor’sleadershipskills.Adescriptionofacourseheldforresidents,
medicalstudentsandemergencyroomnurses.
CONCEPTUALFRAMEWORK
DIFFERENTONTOLOGIES
Ontology:OntosisGreekforbeing,logosmeansstudyi.e.‘thestudyofbeing’.Whatcanbesaidto
reallybe,orexist?Epistemology:Epistememeansknowledgeandlogosstudyi.e.‘thestudyof
knowledge’.Evenifsomethingreallyexists,howcanIknow?
Theresearcher,whoisaconductor,isinfluencedbyaconstructivist’sontology,statingthatreality
isasocialconstructionandmustbeseeninthecontextofindividuals,andthereforemany
(interpretedandconstructed)realitiesarepresent.Hisepistemologyisinductiveandinterpretative.
19
Qualitativeresearchmethodsare“usedintheexplorationofmeaningsofsocialphenomenaas
experiencedbyindividualsthemselves,intheirnaturalcontext”7.
Atypicalsurgeonisworkinginapositivisticresearchtradition,believingthattheworldisobjective
andcanbemeasured,thatthereareuniversalconcepts,andthatthesecanbeobjectivelyverified
bystatisticalmanoeuvres.Thereisonlyonereality.Hisepistemologyisasanempiricist,thatis,he
istesting.“Medicaldoctorsbelievethattheirfieldisfoundedonscientificknowledge;where
knowledgeisdefinedasfactsthatcanbeempiricallyverifiedbythebiomedicalmethod”,asstated
byMalterud6.
QUALITATIVEMETHODOLOGYCONSIDERATIONS
Thefollowingresearchapproacheshaveservedassourcesofinspirationinthisthesis:Grounded
theory(GT)61,62,qualitativecontentanalysis(QCA)8,63,andhermeneutics5.Centraltothese
approachesisthattheyallrelyonacontinuousmovementbetweenpre-understandingand
analysis,‘movingtoandfrom’64.
ThefollowingfeaturesarecommontoGTandQCA:Theresearcherlooksatphenomenawithfresh
eyesandfromnewperspectiveswithoutrestrictionwithinalreadyexistinghypotheses–andbased
onthefindings,ideasaredeveloped–andtheresearcherstakesanotherlookatthephenomena
8,63.Inhermeneuticsitisstatedthattounderstandapartofatext,onemustunderstandthe
whole.Atthesametime,however,onecanonlyunderstandthewholewhenunderstandingthe
individualparts5.Allthreeapproachestointerpretationbringtheimportanceoftheinterpreter
intofocus.Hans-GeorgGadamerarguedthatknowledgeisnotsomethingthatweacquireand
controlasapossession.Ratherknowledgeistobeunderstoodassomethinginwhichwearealways
alreadysituated.Thereasonweunderstandanythingatallisbecausewealreadystandinit65.It
hasbeenarguedinhermeneuticsthatpuredescriptionisimpossiblebecausedescriptionalways
involvesinterpretation5.Datacanbecollectedfrommultiplechannelsinallthreemethods,such
asinterviews,observations,documents,andvisualmaterials5.
OriginallyQCAwasdevelopedwithinthefieldofcommunicationandlinguisticsasameansto
understandthemeaningoftextandcontext8inordertochallenge/supplementatendencyto
focusonthequantitativecontent.GTmethodologyemergedfromthefieldofsociology66.GTisa
reactiontopositivisticperspectivesonscience8.Hermeneuticsisamethodologyworkingwith
semiotics,presumptions,andpre-understandings5.

20
MajorCodingDifferencesAmongThreeApproachestoContentAnalysis
TypeofContentAnalysis
StudyStartsWith
TimingofDefiningCodesorKeywords
SourcesofCodesorKeywords
Conventionalcontentanalysis Observation Codesaredefinedduringdataanalysis
Codesarederivedfromdata
Directedcontentanalysis Theory Codesaredefinedbeforeandduringdataanalysis
Codesarederivedfromtheoryorrelevantresearchfindings
Summativecontentanalysis Keywords Keywordsareidentifiedbeforeandduringdataanalysis
KeywordsarederivedfrominterestofresearchersorreviewofLiterature
Table1.Hsieh:ThreeApproachestoQualitativeContentAnalysis63.
AspresentedinTable1,aninductiveapproach(conventional63)isappropriatewhenprior
knowledgeregardingthephenomenonunderinvestigationislimitedorfragmented8.Inan
inductiveapproach,codes,categories,orthemesaredirectlydrawnfromthedata8.Adeductive
approach(directed63)startswithpreconceivedcodesorcategoriesderivedfrompriorrelevant
theory,research,orliterature8.Asummativeapproachidentifiesandquantifiescertainwordsin
anattemptnottoinfermeaningbut,rather,toexploretheextenttowhichacertainwordisbeing
used,thusitisaquantitativeanalysis:theresearchercodesthevisibleandsurfacecontentoftext
(manifestcontent8)andcountwords.Butiftheresearchercodestheunderlyingmeaningofthe
text(latentcontentanalysis8)itisasummativeapproachtoQCA63.
Inqualitativestudiestheresearcherbringshimselfintotheinvestigation,andconsequently
attentionshouldbedrawntotheobjectivityandscientificqualityofthestudy.‘Subjectivity’arises
whentheeffectoftheresearcherisignored7.
However,theeffectoftheresearcherishighlyimplementedintheseapproaches.InGTandQCA
thefindingscaninfluencedatacollection,thatis,aninterpretationistakingplacebeforeexamining
thefindingssecondtime.Inhermeneuticsitisarguedthatunderstandingandpre-understanding
arefundamentalconditionstoeachother.
Theoriginoftheseapproachesisrelatedto’abduction’asdefinedbyCharlesSandersPeirce
(1839–1914).Anabductiveapproachtoresearchmakesitpossiblefortheresearchertopresenta
qualifiedpresumption(educatedguessorinference)67whencommencinghisinvestigation.Based
onhisfindings,heacquiresnewknowledge,hemightalter/adaptthisnewknowledgetothe
presumptionandtheprocessstartsover.

21
LEARNINGTHEORYCONSIDERATIONS
THEORIESSUPPORTINGCONCEPTUALCHANGEORTRANSFORMATION
Thissectionexplainshowthelearningenvironmentcansupportconceptualchangeand
transformation.
EMBODIEDCOGNITION
“Cognitionisembodiedwhenitisdeeplydependentuponfeaturesofthephysicalbodyofan
agent,thatis,whenaspectsoftheagent’sbodybeyondthebrainplayasignificantcausalor
physicallyconstitutiveroleincognitiveprocessing”68.Thetheorymightbeusedinthedesignof
effectivelearningenvironments,especiallythosetargetingconceptualchange69.Thecourse
describedinthisthesisassumesthatonehastoexperiencethepressureasaconductorbypractice
tounderstanditasdescribedinEmbodiedCognition.
TRANSFORMATIVELEARNINGTHEORY
InTransformativeLearningTheory70itisstatedthatoneprerequisiteforcreatingareal
transformationisbeingfacedwitha‘disorientingdilemma’definedasanacutepersonalorsocial
crisisandthrough10phases(Table2)of‘perspectivetransformation’leadingto‘areintegration
intoone’slifeonthebasisofconditionsdictatedbyone’snewperspective’71.
1 Adisorientingdilemma2 Self-examinationwithfeelingsofguiltorshame3 Acriticalassessmentofassumptions4 Recognitionthatone’sdiscontentandprocessoftransformationaresharedandthatothershavenegotiatedasimilar
change5 Explorationofoptionsfornewroles,relationships,andactions6 Planningofacourseofaction7 Acquisitionofknowledgeandskillsforimplementingone’splans8 Provisionallytryingoutnewroles9 Buildingofcompetenceandself-confidenceinnewrolesandrelationships10 Areintegrationintoone’slifeonthebasisofconditionsdictatedbyone’snewperspective
Table2.10phasesofperspectivetransformation,TransformativeLearningTheory70
Inthecoursementioned,participantswerepresentedfora‘DisorientingDilemma’atapersonal
levelasinthiscourse:theparticipantsweregivenassignmentsalmostimpossibletosolve.
APPRENTICESHIP
Apprenticeshipispractice,thestudentlearnsfromseniormasterwhoactsasrolemodel.The
masterfurthermoreallowshimselftobesubjectiveandbasesfeedbackonhisownexperiences

22
fromhisprofession.Inshort,thelearningmechanismsandprocessesaredefinedas:Imitation,
identificationwithrolemodels,feedbackonspecificworksolutions,indepthprofessionalfocusand
peer-to-peerlearning72(TL’stranslationfromDanish).
Inaddition,regardingapprenticeshipandleadership,itisstatedbyMintzbergthatleadership“isa
practice.Itisnotaprofession,notascience.Youcan’tlearnitthewayyoulearnsurgeryor
engineering”73.Thisisrelevanttothecoursedescribedinthisthesis,becausetheconductorhas
acquiredhisskillsmainlythroughpracticingleadership.
FLOWTHEORY–APEDAGOGICIDEAL
Thissectionexplainshowalearningenvironmentcansupporttheintensityinastudent’sfocusina
learningsituation.
“Flow”isdefinedbythepsychologistCsikszentmihályias:“thecreativemomentwhenapersonis
completelyinvolvedinanactivityforitsownsake.Theegofallsaway.Timeflies.Everyaction,
movement,andthoughtfollowsinevitablyfromthepreviousone…”74.“Theflowstatemustbea
generalpedagogicalidealbecauseitisoftenextremelygoodlearning,asyouareoptimally
challenged,fullyfocusedandemotionallyinvolvedsoyoutendtorememberverymuchofwhat
youaredealingwith”75(TL’stranslationfromDanish).Theconductorknowsthatwhen
collaborationworksoptimallywiththeorchestra,astatecanoccurwheretimeandplaceis
dissolvedasdescribedinFlow-Psychology76,andwantstogivetheparticipantsanopportunityto
experiencethefeelingofflowatthecoursedescribed.
ANXIETYCOUNTERACTSLEARNING
Anxietycausesthebodytoprepareitselfforfightorflight.ChrisWilliams,professorofpsychosocial
psychiatrystates“Ifyouareinasituationofimminentactualthreat,thentheincreasedalertness
andbodyresponsecanbelifesaving,[…]butifitoccurswhentryingtorevise,orpresentatalk,or
atsuchahighlevelthatitparalysesorcauseserrors,itcaninterferewithwhatwewanttodo.”[…]
ConsultantpsychiatristRajeevKrishnadasstates:“Undernormalcircumstancestheamygdalais
undertightcontrolfromtheprefrontalcortex,whichevaluatesthethreatassociatedwiththe
stimulus.[…]Ifitisthreatening,theamygdalafearresponseismaintained.” Thisisclearlynota
stateconducivetolearningorconcentratinginaseminar,saysclinicalpsychologistDrAngharad
Rudkin.“Evenifyoumanagetotakeinwhatisbeingsaid,theinformationislikelytobounce
around[inyourbrain],notbeingprocessedproperlyorstoredinyourlong-termmemory”77.
23
Itisimportanttoaddressfear;aconductorwhoisafraidinfrontofanorchestrahasbeendeprived
oftheopportunitytowork.However,anxietyisusedasafoundationforcreatingthedisorienting
dilemmadescribedabove.
THINKING,FASTANDSLOW
PsychologistDanielKahnemandiscussesthreetopicsrelevanttothisthesis:System1andsystem2,
theintuitiveexpert,andsubstitution.
System1andsystem2
Kahnemandescribestwowaysofthinking.System1isfastandintuitiveandautomatic:associative
memorycontinuallyconstructsacoherentinterpretationofwhatisgoingoninourworldatany
instant.System2isslower,deliberateandlogical:consistingofcontrolledoperationsrepresenting
aneffortfulmentalactivity.ThehighlydiverseoperationsofSystem2haveonefeatureincommon:
theyrequireattentionandaredisruptedwhenattentionisdrawnaway.Intensefocusingonatask
insystem2canmakepeopleeffectivelyblind,eventostimulithatnormallyattractattention.
System1runsautomaticallyandSystem2isnormallyinacomfortablelow-effortmode,inwhich
onlyafractionofitscapacityisengaged.System1continuouslygeneratessuggestionsforSystem2:
impressions,intuitions,intentions,andfeelings.IfendorsedbySystem2,impressionsandintuitions
turnintobeliefs,andimpulsesturnintovoluntaryactions78.
Theintuitiveexpert
TheintuitiveexpertisatermintroducedbyKahneman,andheexplains:“Thechessmasterwho
walkspastastreetgameandannounces“whitematesinthree”withoutstopping,orthephysician
whomakesacomplexdiagnosisafterasingleglanceatapatient.Expertintuitionstrikesusas
magical,butitisnot.”Italsooccursinourdailylives:“Mostofusarepitch-perfectindetecting
angerinthefirstwordofaphonecall,recognizingasweenteraroomthatwewerethesubjectof
theconversation,andquicklyrespondedtosubtlesignsthatthedriverofthecarinthenextlaneis
dangerous.Oureverydayintuitiveabilitiesarenolessmarvellousthanthestrikinginsightsofan
experiencedfirefighterorphysician–onlymorecommon”78.
Substitution
Themechanismofreplacingadifficultquestionwithasimpleroneisextensivelydescribedby
Kahneman:“whenfacedwithadifficultquestion,weoftenansweraneasieroneinstead,usually
withoutnoticingthesubstitution[…]Thetargetquestionistheassessmentyouintendtoproduce.

24
Theheuristicquestionisthesimplerquestionthatyouanswerinstead.Thetechnicaldefinitionof
heuristicisasimpleprocedurethathelpsfindadequate,thoughoftenimperfect,answersto
difficultquestions”78.
Kahnemansobjectiveshaveanimpactontheexistingtaxonomybasedtrainingaswellasthe
substitutionfoundintheliterature,but,furthermore,atthecoursedescribedinthethesis;the
master/apprenticeshiprelationshipandachievementoflearninggoalsfortheparticipants.
LEARNINGPYRAMID,NTL
TheNationalTrainingLaboratorieshasfoundthefollowingaverageretentionratesfordifferent
trainingandteachingmethods.Thisisincludedinthethesisinordertodiscussatwhichlevelthe
learninginthedescribedcourseis,accordingtoNTL.
Figure1.TheLearningPyramid
ANALYSISCONSIDERATIONSONEXTRALINGUISTICDATA
Whentwopeoplearepresent,communicationwillalwaystakeplace.Itisimpossiblenotto
communicate79.
Thisthesisaimsatinvestigatingandexploringtheconductor’snon-verbalskills.Therefore,the
followingtheoriesandmethodsofanalysisareincludedtoillustrateevidenceonnon-linguistic
communication,includingtheuseofvideoforresearchpurposes.
INCONGRUENCEBETWEENORALANDEXTRALINGUISTICCOMMUNICATION
Inthe1960s,Mehrabianbecameawarethattherewereotherfactorsthanlinguisticsthatwere
importantinfacetofacecommunication.Mehrabianperformedsimpleinterventionswherehe

25
demonstratedhisfindingsoninconsistentmessagesoffeelingsandattitudes(andtherelative
importanceofwordsvs.nonverbalcues).Whenthereisincongruencebetweenwords,voiceand
facialexpressionincommunication,ourattentionwillbedrawnfromthewordsandtheirmeaning
tonon-verbalcommunication.Thatis,wherethewordsdidnotmatchthefacialexpression
specificallyinMehrabian’sresearchpeopletendedtobelievetheexpressiontheysaw,notthe
wordsspoken80,81.
SEMIOTICS
ApioneerinsemioticswasCharlesSandersPeirce(1839-1914)andtodayhisthoughtsareamong
thefoundationsforMultimodalAnalysis.Atthecentreofhisphilosophywasamodeloftheway
humanbeingsthink,hechallengedtraditionalmodelsbydescribingthoughtsnotas’ideas’butas
’signs,’externaltotheselfandwithoutmeaningunlessinterpretedbyasubsequentthought.His
generaltheoryofsigns–orsemiotic–isespeciallypertinenttomethodologiescurrentlybeing
debated11.Hepioneeredapproachestostudyingvisualsemiotics,andwasinterestedintherange
ofdifferentkindsofsignsthatcanbefoundascomparedtolanguagethatcomprisesabstract
symbols10.
Pierce’sworkaboutsymbolizationandtotheconsciouscontrolandawarenessofsignsbecame
knowntoSusannKLanger(1895-1985).Langerisimportantforthisthesiswhenshestates:“The
limitsoflanguagearenotthelastlimitsofexperience,andthingsinaccessibletolanguagemay
havetheirownformsofconception,thatistosay,theirownsymbolicdevices”82.
MULTIMODALITY(EXTRALINGUISTICCOMMUNICATION)
GuntherKress(ProfessorofSemiotics)emphasisesthatinlinguisticsthereisalwayssomethingthat
isparalinguisticorextralinguisticexistingtogether9.Multimodalityisdescribingothermeanings
thanbasedonlanguageandlinguistics.Thereisvisuallanguage,gesturallanguage,andsoforth.It
issociallyproduced,culturalresourcesformakingmeaning.Situationsaregivenwheretextonly
givesapartialaccountofwhatisgoingon12.Thoughitisimportantweshouldnotthrow
knowledgeoverboard:linguisticshasshownushowlanguageworksandsociolinguisticsshowshow
itisused9.Multimodaldiscourseanalysisopensthepossibilityofmovingagainstthe
“reductivenessoftwentieth-centurygeneralizationsandabstractions[…]andtowardafullaccount
[…]oftheimpactofthefactthat,ashumans,wearephysical,materialbodiesandthatmeaning
cannotbeunderstoodoutsidetherecognitionofthismateriality”83.“Gaze,gestureandposture,

26
forinstance,tendtobeconsideredasupporttospeech;reinforcingorotherwisemodifyingspeech
butnotprovidingcommunicationinitsownright,andimageisoftenthoughttobeinasupportive
relationtowriting.Multimodalresearchacrossarangeofsocialsettingscastdoubtsonthis
assumption”84.
VIDEOANALYSIS
Itwasstatedin2000thatwhentranscribing‘visualphenomena’weareonlyatthebeginningofthis
process85.Anditwasconsideredachallengeassociatedwithenormousmethodologicaland
theoreticalproblems85.Furthermore,videoasdatacollectionwasextensivelydiscussedby
researchers86.
Xiaoetal.statedin2004thatvideorecordingsarearichsourceofdataforsuchresearchbecause,
incomparisontoobservationalnotesandaudiorecording,videorecordingscapturemuchofthe
richnessofhumaninteractionsandofthecontextinwhichactivitiesarestudied66.However,Xiao
doesnottaketheconsequencewhenhedecidestolimittheuseofvideostoverbalanalysisof
what’sgoingoninhisstudy.OnepossibleexplanationcouldbethatXiaodidnothavemethodsor
toolkitstodescribe/analysethis“richnessofhumaninteraction”whichheemphasizes.In2010
Raudaskoskistatedthatvisualdatamaterialhasnoestablishedtranscriptionstandards87.
Theavailabilityanduseofvideohasevolvedexponentiallyoverthelastdecade,andproductionof
HighDefinitionvideoisnowavailabletoeverybodyattheirdailylifeespeciallyviamobilephones
camcorder.Itistodayanaturalmeanofcommunicationandvideosaresharedonallsocialmedia.
Itmightbearguedthatvideohasevolvedintobeinganindependentformofcommunicationonits
own.AccordingtoStatisticBrainResearchInstituteitisinterestingtoascertainthatin2016300
hoursofvideowasuploadedtoYouTubeeveryminute,totalnumberofpeoplewhouseYoutube
1.325.000.000,andthenumberofvideosviewedeverydaywas4.950.000.000.
CONDUCTORSANDVIDEO
Inrecentyears,theuseofvideorecordingshasbeenanaturalandintegralpartofconductor
teachingattheconservatoriesaroundtheworld.Forexample,attheSibeliusAcademyinHelsinki,
Finland,acameraismountedintherehearsalroomforthepurposeofrecordingtheconductorin
close-upasheconductstheorchestra.Avideoroomhasbeenbuiltwherestudentsreceiveand
providefeedbackontheperformancetogetherwiththelectureraftertherehearsalwiththe
orchestra.

27
VIDEOANDSIMULATIONINHEALTHCARE
Videoiswidelyusedinsimulationtraininginhealthcare,hencethestudentsarehighlyaccustomed
tothepresenceofacameraduringthetraining.Videorecordingsintheemergencydepartmentare
usedinUSAandareregardedasaneffectivetoolforimprovingtraumateamperformanceby
educatingclinicalstaffregardingrolesandresponsibilities88.Theuseofasurgicalblackbox
[integratingvideorecordings]hasbeenresearched89.Deliverysituations,thatrepresent
complications,arevideorecordedatAarhusUniversityHospitalinDenmarkinaPhDresearch
projectin2017managedbyLiseBrogaard,PhD-student.
PRE-UNDERSTANDING
Inaccordancewithqualitativeresearchtraditions,thePhDstudent’spreconceptionsareaccounted
for.Beinganorchestralconductor,Ifindthesocialmechanismsthattakeplaceintheinteraction
betweenconductorandmusiciansextremelyinteresting,bothtoobserveaswellastoinfluencein
mypositionasconductor.Furthermore,Ihavebeenaprofessionalmusicianandhavethusthe
otherperspectiveonthiscooperationseenfromtheteam’spointofview,andhavethus
experiencedthehugedistancebetweenthosehighlydifferentviewpoints.InadditionIama
composerandassuchIhavecreatedandhavedetailedorchestratedcomplexactionsandeventsat
alongtimedistance,asallcomposersdo.Thosearethepre-understandingsIbringintothisproject.

28
METHOD
SYSTEMATICREVIEW
Inthefirststudy,wesystematicallyreviewedtheliterature.Quantitativestudieswereclassed
accordingtoPRISMA3,Cochrane90,andGRADE91.PRISMAfocusesonthereportingofreviews
evaluatingrandomizedtrials,butcanalsobeusedasabasisforreportingsystematicreviewsof
othertypesofresearch,particularlyevaluationsofinterventions.GRADE’sapproachtoratingthe
qualityofevidenceisusedinthisstudy.WithGRADE,thequalityofevidencewasassessed,aswell
studydesign/methodasriskofbias,inconsistency,indirectness,imprecisionandpublicationbias.
InadditionCochrane’srecommendationsfortheriskofspecificbiashavebeenassessed:selection,
performance,attrition,detectionandreportingbias.Therehasbeenattentiontointernalvalidity
andexternalvalidityintheassessments.QualitativestudieswereclassedaccordingtoCASP(Critical
AppraisalSkillsProgramme)4.
Anumberofpresumptionswereincludedinthesearchinthesystematicreviewforthepurposeof
narrowingthenumberofarticlesinthissearch.Onepresumptionwasthatoperationalleadership
trainingisrelatedtonon-verbalcommunication.AnotherpresumptionwasthatNTSorNOTSS
mightturnouttoaddressthetopic.Athirdpresumptionwasthatspecificwordsaboutleadership
werenecessary(authority,respect,management,leader,lead,etc.).Theliteraturewassearched
forthewordsdescribingtheconductor’scompetencies(conductor,orchestra,symphon*).
Educationwasaddedinthesearch(teach,educa*,train*,learn*).Variousemergencies(CPR,
intensive,acuteetc.)wereadded.‘Meshterms’wassearchedinthePubmeddatabase:‘leadership’
and‘education,medical’.Combinationsoftheaboveweretestedtofindtheconnectionwiththe
clinicalteamleader.SupplementarysearchwasinspiredbyarticlesfoundinPubmed’s‘similar
articles’.Inspiredbythenewarticlesnewkeywordsemerged(trainingleaders,teamlearning,
urgency,situation,taskperformance,resuscitation,cardiacarrest,humanfactors,performance,
advancedlifesupport,etc.)combinationsofthesewereaddedtothesearch.
QUALITATIVECONTENTANALYSISASAMETHOD
Afterconductingtheconventionalsystematicreviewitwasdecidedtoexaminethearticlesin
anotherperspectiveabductive-inductiveQCA.

29
Strategyforqualitativecontentanalysis
Inthesystematicreview,allarticlesincludedweregroupedtogetherinasinglePDFdocumentand
searchedseveraltimesforkeywords,theirsynonymsand,ifavailable,theirmeaningfulsimilar
positiveandnegativeanalogies,phrasesandsentences.Thequotesweregroupedintothemesin
aniterativeprocess,andsortedchronologically.Themostimportant/significantquoteschosenon
basisoftheauthors’interpretationarepresentedinthisthesis.
AtthebeginningoftheQCAthemethodwas‘conventional’,abductive–inductive.Whencodes
becameestablished,thesearchandanalysisbecamedirectedbythosefindings.Byusinga
directed,summativeapproachon‘quantitativemanifestcontentanalysis’63inordertoexplore
usageofthevisibleandsurfacecontentofthetextitwaspossibletoidentifyconsensusonselected
wordsfromaquantitativeapproach.Byusing‘qualitativelatentcontentanalysis’8itispossibleto
interprettheunderlyingmeaningofthewordsandthus,rather,interpretaqualitativeapproach.
Thepreconceivedcategoriesinthesearchconductedinthesecondpaperwereguidedbythe
contentofanarticle44.Directed(deductive)qualitativecontentanalysisstartswithpreconceived
codesorcategoriesderivedfrompriorrelevanttheory,research,orliterature63.Introducinga
differentperspectiveonthearticlesfoundinthesystematicreview,theinclusioncriteriawere
expandedtocoverexperience,perceptionsandemotionsrelatingtoleadershiptrainingin
emergencysituations,andthereforeprimaryaswellassecondaryarticlesbecamerelevant.
QCAwasfinallyusedtoanalyseacourseforresidents,3rdsemestermedicalstudentsandnurses,as
presentedinthethirdpaperaswell:Alltext-baseddataweregatheredintoonesinglePDF
documentandsearchedforkeywordsandsentencesdescribingthecontentofthecourse,andthe
wordswereinterpretedinameaningfulcontext.ThemethodwasQualitativeContentAnalysis,
conventional,andinductive:Themesemergedinandabductive–inductiveprocess,abductive
becausetheconductorhadhispresumptionsforthecourse–inductivebecausethefindings
adjustedthepresumptions.Whenthemesbasedonkeywordswereestablished,theprocess
becamedirectedbythethemes,thustheprocessbecamedeductive.Threekeywordswerepresent
atthecoursethoughrarelyverbalized,butshoweduponthevideofootage.Thewordswere
groupedintothreethemesaccordingtothepresumptionsaswellasthefindingsinthedataset.

30
VIDEO
Videofootagewasreviewedseveraltimes,andeditedwiththeaimofexemplifyingthethemes
describedabove.Integratedvideoandaudiorecordingsrepresenting22:12hoursofobservationof
allthecoursesfortheresidentsandstudentsweremade.Onecamerafocusedonthe‘leader’and
anotheronthe‘team’.ThefirstfourcoursedayswererecordedontheGoProSilveredition,and
thesecameraswerereplacedbytheGoProHERO4Blackedition,whichhashighdefinition
resolution(4K),allowingzoominginonthedetailsofthefootageintheeditingprocess.TheHD
footagewaseditedonaMacBookProwithtwoexternaltwoTBharddrives(oneforbackup).
Recordingsfromasinglecoursedaytookupbetween40and60GBofdiskspace:all22:12hoursof
recordingsfilledapproximatelyoneTBofharddrivespace.ThevideoswereeditedinAdobe
PremiereProCC,release2017.1.2.
TRANSCRIPTIONS
Writtenfieldnoteswerecompiledforallthecourses.Completedialoguesweretranscribedfromsix
courses(thefinalcoursedesign).TranscriptionmadepartlybyTLandpartlybytwomedical
studentswhowerenotattendingorinformedaboutthecourse(‘blinded’astothebackground,
methodandassumptionsforthecourse).Throughouttheproject,TLkeptaresearchdiary,where
observationsandthoughtsdeemedtoberelevantfortheprojectwererecorded(Onlinelog
availableinAppendix).
EVALUATIONS
Alltheparticipants(students,residentsandnurses)evaluatedthecourseimmediatelyafter.They
gavewrittenquantitativeevaluationsandrespondedtoashortsurveyoffourquantitative
questionsplusanoptionforafreeassessmentcomment(Appendix).Thestudentsandresidents
wereencouragedtoreflectonthecourseinwrittenevaluationsafterthecourse.Afterreceiving
editedvideoclipsshowingtheirpersonalperformanceduringthetwocoursedays,thestudents
andresidentsweresentasurveywith14questions.The‘blinded’studentswroteaqualitativenon-
guidedreflectionfromthevideostranscribed.

31
ETHICALCONSIDERATIONS
TheCommitteesonHealthResearchEthicsfortheCapitalRegionofDenmarkwasaskedtogive
ethicalapprovalbutaformalreviewwaswaivedforthisstudy(H-4-2015-FSP).Allparticipantsgave
writtenconsentfortheirvideostobedisplayed/publishedhere.

32
PRESENTATIONOFTHEINCLUDEDPAPERS
STUDY1
Trainingresidentstoleademergencyteams:ASystematicReview
Aim:Todescribehowliteratureaddressesworkableandoperationalleadershiptrainingforthe
emergencymedicalteam-leaderandtoenhanceunderstandingofleadershiptraininginthe
medicalenvironment
Results
Twenty-sevenarticleswereidentified.Onesinglestudyaddressingworkableandtargeted
leadershiptrainingwasidentified41.Mostofthearticlesdiscussedseveraldifferenttypesof
behaviouralmarkersandtaxonomies.Leadershiptrainingwasforthemostpartcombinedwiththe
trainingofalgorithmsincludingmedicalcompetencies.Ninestudieswerebasedoninterviewsor
questionnaires.
Atotalof20taxonomiesaddressingleadership,teamwork,andcommunicationwerementionedin
thearticles.Twentyfiveofthetwentysevenarticleswereinfluencedbyoneorbothoftwo
frequentlymentionedtaxonomies:1)TheLeadershipBehaviorDescriptionQuestionnaire,LBDQ
(adaptedfrommilitary)(ninearticles).2)TheNon-technicalskillstaxonomy,NOTECHS(adapted
fromaviation)(sevenarticles).Theabovementionedstudiesdidnotrefertoeachother.Nineother
articles,however,referredtobothtaxonomies.
Resultofcontentanalysis
Threekeythemeswereevolved:1)Leadership2)Taxonomies3)Trainingleadershipandmedical
competence.
Leadership
Eightdifferentdefinitionsofleadershipwereidentified.Fourarticlesstatedinthebackgroundto
theirstudythatleadershipislacking,andfivearticlesdiscussedorconcludedexplicitlythat
leadershipwaslacking.Threearticlesmentionedthatleadershiptrainingwasimportantand
appearedtoimprovebehaviour.Nineconcludedthatleadershiptrainingwouldhaveapositive
impact.Thatleadershiptraininghasbeenignoredwasstatedinthebackgroundforthreestudies.
Ninearticlesdiscussedorconcludedthatleadershiptraininghasbeenignored.18ofthe25authors
(20/27articles)identifiedarecurringneedforexplicittargetedteamleadershiptrainingin

33
healthcare,7articlesmentionedthisinthebackground/introductionand13articlesasafindingor
aconclusion.Ninearticlesproposeddifferentapproachesorfocusareastoimproveleadershipin
emergencies.(Aviation,NTS,Gender,Ethnicity,Non-Verbalcommunicationetc.)
Taxonomies
Fourarticlesagreedthattheideaofusingbehaviouralmarkersystemswastoidentifyexplicitlythe
neededskillswiththepurposeofteaching,observingandmeasuring.Twoarticlesfinda
comprehensivetaxonomyadvantageous;twostatedthattaxonomiesshouldbesimple.Fivearticles
statedthatmeasurementtoolswerelacking.Sevenarticlesannouncedthedevelopmentofanew
oradaptedtool.Threearticlesstatedinthebackgroundthatitcouldbedifficulttokeeptrackof
theactualcontentofthevarietyoftoolsandmethods.Onestatedexplicitly(in2015)thatthetime
hadcometostopdevelopingnewtoolsandbeginfocussingonworkableinterventionsinthisarea.
Trainingleadershipandmedicalcompetencesimultaneously
Onearticlestatedthatreducingthecognitiveworkloadbeforehandbyseparatingroleinstructions
wouldhaveapositiveimpactontheCPRperformanceandonthetrainees.Sixarticlesexplicitly
statedthatleadershiptrainingdifferedfrommedicalknowledgetraining.Onearticlestatedthatit
wasimportanttofocusonleadershipseparatedfrommedicalknowledge.
Conclusion
Notargetedtrainingprogrammeswerefound.Theliteraturehasfocusedondevelopingleadership
measurementtools.Aprevailingneedforexplicittargetedteamleadershiptraininginhealthcare
wasidentifiedinmostarticlesfound.

34
STUDY2
Trainingresidentstoleademergencyteams:Barriers,ChallengesandLearningGoalsconcerningtrainingresidentstoleademergencies:aQualitativeReview
Aim:Aninvestigationtodetermineanyconsensusinopinionsandviewsaboutchallenges,barriers
orlearninggoalsintrainingleadershipinemergencies
Results
Fortyarticleswereincluded.Ninethemesemerged1)Residentsfeelunsupervisedandunprepared
2)Acomplex,stressful,unpredictableandchaoticexperience3)Anunpleasant,disturbing,
frighteningandpanickedperception4)Loweredstress5)Confidence6)Howaleaderisperceived
7)Ashortcuttoperceptionofauthority8)AssumingLeadership9)Borntolead–orlearntolead
ResidentsfeelunsupervisedandunpreparedTenarticlesconcludedthatresidentsfeltunpreparedasleadersofcardiacarrestteams.
Acomplex,stressful,unpredictableandchaoticexperience
Abroadconsensuswereidentifiedthatleadershipinemergenciesisexperiencedasacomplex
issue,aswellintermsofstressfulsituationsdemandingimportantdecisionsforthebenefitofthe
patient,asofmanagingtheteamitself.Ninearticles,inthebackgroundforthestudies,mentioned
complexity,sevenstatedcomplexityinthediscussion/conclusionsection.Theterm:copingwith
pressurewasmentionedbysixarticles,andthreeusedasimilartermcopingwithstress.The
stressfulworkingconditionswereemphasizedinthebackgroundsectionofeightarticlesandten
articleshighlightedtheseconditionsinthediscussion/conclusionsection.Threearticlesdescribed
theperformanceinemergenciesasunpredictableorunanticipated.Thewordchaoswasusedby
sevenarticles,astheydescribedthesituation.
Anunpleasant,disturbing,frighteningandpanickedperception
Theemergencysituationswerecharacterizedbyvariousformsofdiscomfort:theconcerned
traineeswerementionedbysevenarticles,eightarticlesmentionedanxiety.Onearticlementioned
panic.
Loweredstress
Fourarticlesclaimedthatagoodleaderwasabletocreate“loweredstress”orto“calmother
peopledown”.Twoarticlesmentionednoiseandcrowdcontrol.32

35
Confidence
Threearticlesstatedthatconfidencewasimportantinthebackgroundsection.13articles
concludedthatadegreeofself-confidenceiscrucialforthequalityoftheleadership.
Howaleaderisperceived
Eightarticlesdiscussedtheteam’sperceptionoftheleader.Toestablishacomfortableandsafe
environmentfortheteam,teammembersmustbeabletoperceivetheirleaderastrustworthy16,47.
Jacobssonetal.emphasizesthatitwasimportancethattheleader“hadastrongethosand
expressedcompetence”30.
Ashortcuttoperceptionofauthority
Threearticlesstatethattheleadershouldtakecareofhis/herappearance“especiallyforfirst
meetings”andinthiscontextthat:“Theclinicianwillworkonwaystodevelophis/herown
charisma”46.Itisimportanttoadopt“apowerfulposture”32,and“Teammemberswhoareaware
ofhowtheyusetheirbodiestocommunicatewillbeabletofacilitateandimprovetheir
performance”35.Anotherissueemphasizedasimportantbyeightarticlesishowtheleaderuses
his/hervoice.
AssumingLeadership
Tobecomeagoodleaderitisimportanttoassumetheleadershipwithallitsimplicationsincluding
risksandfailure.Fivearticlesstatethisviewintheintroduction/backgroundsections.Sixarticles
elaboratethisviewintheirdiscussion/conclusionsections.Whenassumingleadershiponecan
benefitfrom‘introspection’46,‘psychologicalself-care’60,or‘self-management’47.
Borntolead–orlearntolead
Sevenarticlesmentionthatsomeareborntoleadwhileothershavetolearn.
Conclusion
Barriersforacquiringleadershipcompetenciesrequiredwhenmanagingemergencyteamswere
identified.Learninggoalswereidentified.Strongnegativeemotionssuchasstress,anxietyand
panicwerefoundwhenworkinginemergencies.

36
STUDY3
Conductingtheemergencyteam:Anovelwaytotraintheteam-leaderforemergencies
Aim:Theoverallaimofthecourseistoinvestigatewhether,inanemergency,aclinicalteamleader
couldapplyaconductor’sleadershipskills.Adescriptionofacourseheldforresidents,medical
studentsandnurses.
Methods
Wedevelopedacourseforresidentsand3rdsemestermedicalstudents.Inordertosimulatean
emergencysituationandtooptimizeleadershiptrainingthecoursecreatesaframeworkwith
stress,anxiety,anddiscomfortinaharmless,non-clinical,andsafesetting.Theparticipantswere
challengedtoactasconductorsinmusicalexercises.Aconsultantandanorchestralconductor
werethefacultyforthecourse.Oneadditionalcoursedaywasheldforemergencyroomnurses.
Dataacquisitionandanalysis
Alltheparticipantsmadeevaluationsimmediatelyafterthecourses,n=61.Theygavewritten
quantitativeevaluationsandrespondedtoashortsurveyoffourquantitativequestionsplusan
optionforafreeassessmentcomment.Thestudentsandresidents,n=38,wereencouragedto
reflectonthecourseinwrittenevaluationsafterthecourse,thosequalitativeevaluationswere
receivedfrom20participants(53%).Thecourseswererecordedontwovideocameras.After
receivingeditedvideoclipsshowingtheirpersonalperformanceduringthetwocoursedays,the
studentsandresidentsweresentasurveywith14question,thosewerereceivedfrom10
participants(26%).Writtencommentsreceived24monthsafterthecoursefrom4participants
(10%).SelectedcoursesweretranscribedverbatimbyTLandbytwo‘blinded’students
respectively.The‘blinded’studentswroteaqualitativenon-guidedreflectionfromthevideos
transcribed.Participantsevaluatedandcommentedoneachother’sdevelopmentatthecourse.
Analysis
QualitativeContentanalysis
Alltext-baseddatawasgatheredintoonesinglepdf-documentandsearchedforkeywordsand
sentencesdescribingthecontentofthecourse,andthewordswereinterpretedinameaningful
context.ThemethodwasQualitativeContentAnalysis.Themesemergedinanabductive–
inductiveprocess.Whenthemeswereestablishedtheprocessbecamedirectedbythethemes,
thustheprocessbecamedeductive.Threekeywordswerepresentatthecoursethoughrarely

37
verbalized,butshoweduponthevideofootage.Videofootagewasreviewedseveraltimes,and
editedwiththeaimofexemplifyingthethemesdescribedabove.
Results
20three-hourcoursedayswerecompleted.
Threekeythemesemerged:1)Learningenvironment.2)Pedagogics.3)Learninggoals–the
conductor’sfocus.
Learningenvironment
Safe,enjoyablelaughterhadasignificantimpactonthecourseindicatingthattheparticipantsfelt
safeandenjoyedparticipating.15/38participantsstatedthattheyfeltthatthefacultyfully
understoodthechallengestheyfaced(‘gotundertheirskin’).17/38participantsstatedthatthey
greatlyappreciatedthispersonaland‘straighton’feedback.15/38participantsduringthecourse
and21/38participantsafterthecoursestatedthatthisfeedbackhascausedasignificant
developmentintheindividualparticipant’sbehaviour.Theparticipantsobserved,notedand
commentedfrequentlyoneachother’sperformanceanddevelopmentinthedialoguesrecordedat
thecourse.
Pedagogics
Itwasimportanttogivetheparticipantsafeelingoftheintensecommunicationwhenleadingan
orchestranon-verbally.Itwasobservedthatatrance-likestatefrequentlyoccurredbetweenthe
leaderandtheteamduringtheexercises.
Partofthelearningprocessthroughapprenticeshipistheverydirectpersonalfeed-back.As
presentedonthevideos,theparticipantswerechangingtheirbehaviourduringthecourse.
Learninggoals–theconductor’sfocus
Atotalof47/61(students,residentsandnurses)expressedthattheyhadbecomeawareofthe
importanceofbodylanguage.17/38(studentsandresidents)specificallystatedthattheyhad
achievedinteractionbetweenbodylanguage,appearanceandauthority–andunderstoodwhythis
leadstocalmnessandconfidence.Eighteenparticipantsstatedthattheyhadlearnedthateye-
contactisapowerfultoolforensuringthatdecisionsarecommunicated,receivedandunderstood.
Theparticipantslearnedthatinthiscoursecontextitwasvalidtotalkaboutandexpresssubjective
perceptions.15participantsstatedthattheywerepushedoutoftheircomfortzone,however19

38
participantsacknowledgedthattheenvironmentwasneverthelesssafe.Participantsweresurprised
andimpressedtoseehowmuchtheycouldcommunicateandhowexplicitandnuancedtheycould
maketheirdemandswithoutspeaking.
Additionalfindings
Oneblindedstudentandfourparticipantsstatedthattheyforgotthenewlylearnedlessonswhen
challengedonclinicalknowledge.Threeofthoseplusadditionalanotherfourstudentsand
residentsstatedthatitwasadvantageoustotrainleadershipseparatelyfrommedicalcompetence.
Theexperiencednursesrespondedmostpositivelytothecourse.Theaverageageinthisgroupwas
over50years,whichindicatesthatafteryearsofexperiencethisgroupwasawareofhowfatalit
couldbewhentheteamleaderfailed.35oftheparticipantsagreedthatthecoursewashighly
relevantfortheirclinicalpractice.Twoyearsafterthecourse,fourparticipantsstatedthatithad
changedtheirprofessionalbehaviour.11participantsstatedthatthecontentofthecoursehadan
importantobjective,whichwaslackinginteachingattheuniversity.13participantsstatedthatthe
subjectwasrelevanttoeducationalcontexts,totheclinic,whencollaboratingingeneral,daytoday
work,doctors’work,instructingcross-fit,swimminglessons,publicspeakingandattendingoral
exams.
Conclusion
Theparticipantsnotedandcommentedoneachother’sdevelopmentonthecourse.Accordingto
theirself-reportingafterthecoursethetransferofaconductor’sskillschangedtheparticipating
students’,nurses’andresidents’behaviour,andintroducedamethodtohandleanxietyandshow
calmnessandauthority.Thiscourseclearlyseemstoaccommodatetheneedforanoperationaland
targetedtrainingoftheteamleaderinemergencies,addressingawaytoachieveconfidenceina
stressful,butsafelearningenvironment.

39
DISCUSSION
Theoverallobjectiveofthisthesiswastoexploreadifferentapproachtotraintheemergencyteam
leaderwithhelpfromanotherprofession.Furthermore,toinvestigateexistingaspectsoftrainingof
theteamleaderinemergenciesinhealthcare.Thischapterwillsummarizethemainfindingsand
discussthestrengthandweaknessesofthestudies.
Nodefinedandworkableleadershiptrainingwasidentifiedinthesystematicreviewandnoclear
definitionofleadershiphasbeenfound.Inadditiontheliteratureonthissubjectaredominatedby
‘significantvariabilityinterminology,trainingmodalitiesandevaluation’inthisfield15,41,43.
Nevertheless,scientistsagreethatleadershiptraininghasanimpact,improvesbehaviourand
changesclinicaloutcome.Despitethis,theliteraturedemonstratedthatformalleadershiptraining
hasbeeninadequateorthateducationisinsufficient.Thisthesisdemonstratedagap–oratleast
lackofconsequence–inbetweenwhatmedicaleducatorsknowsandwhatactiontheydotake.
Anexplanationcouldbethatresearchinhealthcarehasatraditionforapplyingthepositivistic
clinicalresearchtradition,theneedtomeasure.Inaccordancewiththisexplanation:mostofthe
articlesfoundinthesystematicreviewinthisthesis(23of27)revealedapositivisticontology
aimingtomakequalitativefindingsquantitativeandmeasurable–andusedstatisticstoprovethe
result1,13-15,17,21-23,26,27,29,33-37,39-43,56,59.Theenthusiasmoftheresearchersisnoticeablewhenthey
considersolvingtheproblemasstatedbyProf.Yulein2006“thisstudyhastakentheadditional
stepofidentifyingexplicitlytheparticularnon-technicalskillswhichmightbebothtaughtand
observed–andthereforemeasured”38.Hereitseemstobecomeagoalinitselftobeableto
measure.
Butwhennodefinitionofleadershipisfound,asstatedabove,itwillsubsequentlynotbepossible
totrytomeasureanythingconcerningleadership.Anexplanationtothisdilemmacouldbethatthe
socialandcommunicativequalitiestheteamleaderneedsisnotmeasurable,butnevertheless
representsveryrealinterpretationsandconstructionsofrealityinbetweenhumans.Thisisin
accordancewiththeontologyofaconstructivistapproachandnottheontologyofapositivistic
approach.
Anotherexplanationtothischangeoffocuscouldalsobeexplainedby‘substitution’.The
mechanismofreplacingadifficultquestionwithasimpleroneisextensivelydescribedby
psychologistDanielKahneman:“whenfacedwithadifficultquestion,weoftenansweraneasier

40
oneinstead,usuallywithoutnoticingthesubstitution[…]Thetargetquestionistheassessmentyou
intendtoproduce.Theheuristicquestionisthesimplerquestionthatyouanswerinstead”78.
Thepredominanttrainingfoundinvolvestaxonomiesandalgorithmtrainingasdemonstratedinthe
SystematicReview.Thisisdominatedbytwoschoolsofmedicaleducationalresearch,oneinspired
bythemilitary,theLBDQ,andtheotheroneinspiredbyaviation,NOTECHS.Itisnotwithinthe
scopeofthisthesistodiscusswhythereisverysparsecommunicationbetweenthetworesearch
groups,butitisasurprisingfindingthatmaybeimportant.Theweaknessofusingmilitaryand
aviationmodelsisthattheyareaimedatpeoplewhohaveleadershipasafull-timeemployment,
whiledoctorsalsohavetocopewithseveralotherrolesintheirprofession,inaccordancewith
CanMEDSdefinitionofthesevenrolesofthedoctor92.
Asdescribedabove,literaturerevealedalargenumberoftaxonomiesaimingatmeasuringthe
abilityofresidentstoimplementvariousprofessionalalgorithmswithoutspecificfocusonthe
leadershiprole.Itcanbearguedthatthisrelationshipexpressesmoreaboutanactualclinicalskill
andbasicallynothingaboutthequalityofleadership.Again,inaccordancewithKahneman78,itis
possibletoarguethattraininginclinicalskillsandmemorizingalgorithmsaddressestheeffortful,
slowandrationaloperationsofsystem2whileinteractionbetweenpeople(leadership)takesplace
intheautomatic,fastandintuitivesystem1.Itisdifficulttooperateinbothsystemssimultaneously
anderrorscanoccurifthetwosystemsconflictwitheachother.
Thisthesisdescribesthatitisappropriatetotrainclinicalknowledgeandleadershipseparately.
Evidencefromevaluationsandvideosinthisstudydemonstratesthattheparticipantsarevery
excitedtohavetheopportunitytofocusexplicitlyontheirpersonalleadershipskillsaswellas
statedintheliterature14,17,23,27,33,36,41.
Instudy2,ithasbeendescribedthatthereisaneedtoaddresstheyoungphysician’sstrong
negativefeelingsassociatedwiththeleadershiprole.Anxietycanblocklearning(amygdalahijack)
andanxietycanblockperformance,‘paralysesorcauseserrors,itcaninterferewithwhatwewant
todo’asstatedbyProf.Williams77.Itisnotfoundintheexistingtrainingthattheresearchershave
considered–orevenmanaged–toaddressthefearthatyoungdoctorscanexperienceina
stressfulsituation.

41
Developmentandconductionofacourseaddressingleadership
Thisprojectdevelopedanunconventionalcoursefocusingontrainingleadershipfortheclinical
teamleaderinemergenciesinaneffectivewaythatseemstoaddresswhattheliteraturehas
soughtfor30years.
Inthisregard,itisimportantnottothreatentheyoungdoctorsprofessionally.Onthiscoursethey
arenotassessedonclinicalcompetencies,participantsdonotcompetewiththeirprofessional
knowledge.Thefocusissolelyontheleadershipaspectinthemusicalexercisesthataddressthe
intuitivesystem1,inaccordancewithKahneman,addressescreativityalsoand,infact,arefun
challengesasevidencedbythedata.Commontoallparticipants,however,isthetotallackof
knowledgeandprerequisitesforsolvingtheexercises.Allparticipants,inthisregardstartsona
sharedbaselineclosetozero.Thisisanimportantpointthatisinlinewiththephasesof
transformationallearningtheory70,71.Participantsaregivenanimpossibletasktobeperformedin
astressfulsituationwheretheyarehighlyvulnerableinfrontofeveryone.Thisisdescribedas‘a
disorientingdilemma’,whichprovidesanexcellentstartingpointforlatertransformationin
accordancewithtransformationallearningtheory.Asdescribedinthedata,aswellasclearlyvisible
onthevideos,cohesioniscreatedwhentheparticipantsdiscoverthatthisrecognitionof
inadequacyissharedbyall.Thisphaseisalsoexpressedasanimportantpartofthetransformative
learningprocess,whichdescribesaphasefour,whereitispronouncedasfollows:’Recognition
thatone’sdiscontentandprocessoftransformationaresharedandthatothershavenegotiateda
similarchange’70,71.Manyparticipantsexpressedthattheydiscoverednewcharacteristicsof
themselvesfromthecourse.
Previouslyithasbeenclaimedthatanxietycanblocklearning.Nevertheless,asdemonstrated,itis
possibletoprocesstheanxietycreatedonthiscoursebecausethechallengeisalmostimpossible
andthereforeridiculouslyunfair,creatingcohesionamongtheparticipantsandlotsoflaughter.
Furthermore,theexercisesarefunitselfwhendealingwithmusicandcreativity,notalgorithmsand
clinicalknowledge.
Itwasanimportantobjectivetogivetheparticipantsafeelingoftheintensecommunicationwhen
leadinganorchestranon-verbally.Thiswasasmuch‘learningbyfeeling’as‘learningbydoing’.
Withtheintentionofgivingtheparticipantsthisdeepunderstandingandexperienceofbeingin
control,creatingconfidenceintheleadership,focusontheworkathandandcreatingcalmnessin
theteam,itwasconsidereddesirablethattheparticipantsintheirownbodyexperiencedthatit
42
waspossibleinpractice.Thefeedbackwasdependentuponfeaturesofthephysicalbodyofthe
participant,thatis,aspectsofthebodybeyondthebrainandthereforethecognitionofthe
participantisembodied,asdescribedinembodiedcognition68.Thisphenomenaisdescribedas
importantforeffectivelearningespeciallypromotinglearningtargetingconceptualchange,in
accordancewithembodiedcognition69.
Itisdescribedintheliteraturethatthereisaneedtoaddressthestrongnegativefeelingsofyoung
doctorsassociatedwiththerole.Therefore,consciousworkistointegratethefearintothedesign
ofthecourse.Itmayseemparadoxicalthatitshouldbepossibletocreateasafelearning
environmentwhileintroducinganxiety-inducingexercises,butitisneverthelesswhathappensand
thisparadoxisemphasizedbytheparticipants’evaluations.Everybodylaughsveryoftenand
everyoneisspeakingfreely,asisevidentfromtranscriptionsofthecourseandofthevideos.
Discussionsamongthestudentspromoteahighleveloflearning,witharetentionrateof50%,
accordingtoNTL’saverageretentionratesfordifferenttrainingandteachingmethods.
Forashortwhile,theparticipantgetstheopportunitytoworkasaconductorandactuallyinfluence
otherstoactandrespondtotheirintuition–noquestionsareasked–andespeciallywhen
conductingtheGhettoBlastersessionastatecanoccurwheretimeandplaceisdissolved,the
participantsareoptimallychallenged,fullyfocusedandemotionallyinvolved–describedas
learningbyfeeling–ascanbeobservedatthevideos(youtu.be/KcyZf3_QfMk).Thisconditionis
describedinFlow-Psychologyasageneralpedagogicideal74-76.Furthermore,thisisalso‘learning
bydoing’(bypractice),whichpromotesahigherleveloflearning,witharetentionrateat75%,
accordingtoNTL.
Theteachingmethodatthecourseisapprenticeship.Theconductoractsasarolemodeland
providesfeedback.Theparticipantsimitatetheconductorandreceivefeedbackontheirown
performance,whichguaranteesindepthprofessionalfocusaccordingtothequalitiesof
apprenticeship72.Participantschosetocallthisfeedback‘straighton’,andthisgavethemthe
opportunitytogaindirectinsightintotheirownweaknessesasexperiencedbytheconductor.
Onefactorthatisunusualinrelationtomedicaleducationisthattheconductorallowshimselfto
haveanopinionandbesubjectivewhengivingfeedback.Inaccordancewiththeprinciplesof
hermeneutics,itispossibletorecognizeandobserverealitywhenpresentinitandbeingableto
interpretonthebasisofpresumptions5,65.Theconductoriscapablebecauseheisan‘intuitive
expert’,accordingtoKahneman78.

43
Abenefitofthismethodisthattheparticipantsrealisethatitisacceptabletotrustanintuitionand
besubjectiveintheirinterpretationastheconductordoes.Thisisemphasizedonthejoint
discussionsandreflectionswhereparticipantsdiscoverthatthisabilityisnotatalentora
competencereservedtotheconductor.Thesepersonalsubjectiveinterpretationsaresharedby
everyoneandthusgenerallyapplicable.Itshouldbeemphasisedthattheparticipantsdonotlearn
tointerpretatthiscourse,theyalreadyknow;webelieveitisdeepwithinustoseektounderstand
andfindexplanations,thatis,tointerpret.Thecourseteachestheparticipantstotrusttheirown
intuitive,subjectiveinterpretationandconsequently;thatitispossibletobeinterpretedor‘read’
asdesired.Therefore,realityisanon-measurableconstruction,butneverthelessrealconstruction
ofwhattakesplaceinpeople’smindswhentheyaretogether.Realitybecomesasocial
constructionof(intuitive)interpretationsandmustbeseeninthecontextofindividualsinteracting,
asalsodescribedinconstructivism.
Thestudyistobeseeninacontextofallowingexperiencesandperceptionstoexistbeyondthe
limitsoflanguage,accordingtosemioticsandmultimodality9-12,83,84,86,93.Thecoursedealswith
non-verbalcommunicationonmultiplelevels.1)Oneleveldealswithbodilyexpressionand
gesture.2)Anothermoreintangible,butstillshared,recognisedleveldealingwith’presencetothe
moment’,’credibility’,’responsiveness’and’authority’.3)Finallythere’smusic,which,accordingto
Langer,dealswithexperiencesinaccessibletolanguage82.EspeciallyintheGhetto-Blaster
exercises,theparticipantgetsacquaintedwithanexerciseinwhichtheyareplayingcreativelywith
amusic-aesthetictheyhavenotexperiencedbefore.The(spoken)focusattheabovementioned
level1and2,butthelanguageintheexercisesisthemusic–level3.Themusicandthe
interpretationofthemusicisatopicthatisrarelymentionedinthetextmaterialrepresentingdata
fromthecourse,butitmaybeimportantforanon-verbalcoursetoworkwiththiscreativeand
wordlesscommunicativemediawheretheoutcomeonlyexistsinthemomentitiscreated–and
onlyinthecognitionandinterpretationinthemindsoftheparticipants.
Feedback
Asdocumentedintheevaluationsandinthevideofootage,theparticipantsaremostexcitedabout
thepersonalandclearfeedback.Thisisconsidered–bytheparticipants–asaveryusefuland
completelyuniquestrengthofthecourseasdescribedintheevaluationsafterthecourses.
Obviously,thisisnotasurprisingreaction,it’shighlyunusualforadultstocommentoneachother’s
appearanceandnon-verbalcommunication,butthisishighlyappreciatedinthiscontext.

44
Itisadelicatebalanceforthefacultywhenfeedbackisgiventotheparticipant;itisimportantto
‘getundertheskin’oftheparticipant,butcrucialthatthefeedbackissafe;thisisthedecisive
challengeforthecourse.Participantsstatedthattheyfeltthatthefacultyfullyunderstoodthe
challengestheyfaced.
Animportantfactoristhatfeedbackisgivenimmediatelythemomentaproblemarises.Common
practiceinsimulationtrainingistoprovidefeedbackafterthesimulationiscompleted;i.e.witha
certaindistanceoftime.Asdemonstratedonthevideos,theconductorimmediatelypinpointsan
inappropriatebehaviour,isabletoimitateitandtherebydemonstratethedisadvantageofthis
behaviourandheisabletodemonstratewhatamoreappropriatebehaviourwouldlooklikeinthe
situation,inaccordancewithapprenticeship72.
Initially,itistheconductorwhogivesfeedback,thenitistheclinicalteacherforclinicalrelevance
butsoonduringthecoursethefeedbackishandedtothecourseparticipants.Thereareon-going
discussionsandreflectionsonthelessonslearnedandabouttheinterpretationofthenon-verbal
expressionsthatarethesubjectsofthecourse,andequippedwiththisnewawarenessand
vocabulary,theparticipantsgraduallygiveeachotherfeedbackoneachother’sbehaviourand
appearanceasleaders.Whentheparticipantscommentoneachother’sdevelopment,itis
consideredasthemostoptimallearningsetting,witharetentionrateat90%,accordingtoNTL.
Anotherimportantlearningtakesplacewhenparticipantsobservehowandwhypersonalfeedback
isgiven,andexperiencehowthisfeedbackimmediatelyinfluences,transformsandstrengthensthe
‘leader’s’credibilityinfrontoftheteam.
Faculty
Theparticipantslearnfromtheconductor,whoisamasterinnon-verbalcommunicationand
leadershipoftheorchestra.Hehimselfhasacquiredhisleadershipcompetenciesthrough
apprenticeship,andtheseskillshaveevolvednotthroughtheoreticallearning,but,inaccordance
withMintzbergthroughmanyyearsofpractise73.Thisgiveshimahighlevelofcredibilityamong
theparticipants.
Asdemonstratedinthedata,thecourseworksexplicitlyandishighlytargetedwithintangible
topicssuchasnon-verbalcommunication,appearance,presenceandauthority.Itispossibleto
workwiththesesubjectsbecausethecoursedrawsontheexperienceofaconductorwhoworks

45
consciously(deliberately)withthesesubjectsinhisprofessionwhenhestandsinfrontofthe
orchestra.
Onecansaythattheentireargumentforthisthesisabouttheconductor’scommunicationisthat
theconductorcanworktobeinterpretedunambiguously–withoutusingwords,andthisskillis
valuableknowledgefortheclinicalteamleader.
Participantsacknowledgehisexpertiseandexperiencehowmuchhecan‘speak’withoutwordsand
acquireaclearunderstandingofthispossibilityofcommunication,which,accordingtoMehrabian’s
research,isaverystrongelementin‘facetoface’communication;peopletendstobelievethe
expressiontheysee80,81.
Thisconductorseemstoclaimthatthereisonlyonewayofconductinganorchestra:keepcalm,
raisedsternum,incontrolofarmsandbody.Butthereareevidentlymany,differentandoften
extremelypassionateandexpressiveconductors,andfurthermoretheirleadershipstyleisvery
differentaswell.RiccardoMuti=commandingstylecentredaround‘I,theconductor’.Richard
Strauss=onlyexecutionofthewrittenmusic–nointerpretation.HerbertvonKarajan=closedeyes
andnoclearinstructions,allaboutinterpretationandlistening.CarlosKleiber=createsconditions,
motivationandpartnership–butauthoritativeleadership.LeonardBernstein=demonstratingthe
feelingsofthemusic57.Whatisthesameforallconductorsisthatthebasicknowledgeandability
areshared.Onlywhenthisisacquireditispossibletoaddpersonalitytotheleadershipstyle.
However,itwasimportantthattheotherteacheronthecourseisclinicallecturerandconsultant
andsettheframeworkforthecourse.Byconsultantspresence,theclinicalrelevanceisvisualized
andguaranteedinthedialoguesanddiscussionsonthecourse.Thelecturerdrawsparallelsfrom
thelearnedtotheclinicandtheclinicalteamleader.
Itisinterestingtoascertainthattheskillsandcompetencesaddressedinthecoursearesituatedon
ameta-levelandareaprerequisitefortheteaching:thefacultyhastobeabletoassumethe
leadershiproleaseducatorswhoareabletoimprovisewhenteaching,whichisaskillrequiringa
highlevelofexperienceandknowledgeaccordingtoKoivunenandBarrett94,95.Itisveryimportant
forthefacultytobeabletodemonstrate‘presenceatthemoment’and‘responsiveness’inorderto
appearcredibleasteachersandrolemodels.Iftheteachinginleadershipwasbasedontheories
andtheteacherwasunabletodemonstrateleadership,theteachingwouldnothavetheimpactit
had.Itwouldnotbeexperiencedasauthenticbutratherasanassertionoranabstraction.

46
Assessmentoftheimpactofthecourse
Accordingtotheresultsofthecourse,participantsreportedtogainself-confidence,calmnessand
overviewwhencalledupontoactasconductors.Videorecordingsfromthecoursehaveshown
thatthecoursestrengthenedtheparticipant’scredibility,andtheparticipantsreceivedtoolsfor
dealingwithpersonalanxietyasdemonstratedinthequalitativecontentanalysisofthe
transcriptionsfromthecourse,theevaluationsaswellasshowninthevideofootage.
TheKirkpatrickModelisahighlyrecognizedwayofassessinglearning96.Onaquestionnaire
designedaccordingtothismodel,theparticipantsthemselvesassessedhowthelearningwill
changetheirbehaviorandhowtheywillimplementthelearnedintheirprofessionalwork.The
qualityofthisassessmentmaybechallenged.Itwouldhavebeenbetterifathirdparthad
evaluatedthechangeinbehaviour.Thisisnotanoptioninthisthesis.However,manyevaluations,
afterthecourse,describedthatthecoursehadanimpactontheirprofessionalactivitiesaswellas
intheirdailylives.
Onevideosequencesummarizesinaveryconvincingwayoneofthecoreobjectivesofthecourse
anddocumentsthetransformationofaparticipant.Thisvideodemonstrateshowthetrainers‘gets
undertheskin’oftheparticipants,showsthereflectiononthelearningandthesupportfromthe
otherparticipants.Theparticipantinfocusgoesfromsaying“Mypalmsaretotallysweaty”and“I
thinkit’shorrible”tosay:“Iwisheveryonecouldtrythis”and“Itismostimpressive”.
youtu.be/GW7XPdnf-EU.
Weallowourselvestointerpretthatwechangetheparticipants’behaviorasteamleaders,
measuredbytheirownexperienceontheirownbodyaswellasbyobservingtheotherparticipants
inthesituation.However,wethinkitisnecessarytointerpretbecausewearediscussingthingsthat
havenodefinitedefinition.Thereisnofixeddefinitionofthequalityofleadershipanditisnot
possibletoassess‘charisma’orassessthequalityofnon-verbalcommunicationandleadership,
onlyqualitativeandinterpretativeapproachesexist.
STRENGTHSANDLIMITATIONS
Thesearchinthesystematicreviewhasbeensystematic,objectiveandreproducible.Butthe
searchstringproducedcanbecriticizedforinvolvingnon-verbalcommunicationinthesearch.Itis
theresearchers’convictionthatitisnecessarytoaddressthistopicinthetraining.Thesearchcan

47
becriticizedfornotincorporatingthetheoreticalaspectofleadership,butithasnotbeenthe
purposeofthestudy,whichhasexplicitlyfocusedonfindinganoperationalandworkabletraining.
Itcouldbealimitationthatthesearchstringusedfocusedonleadershiptraininginavarietyof
emergencies.Itcouldbearguedthatotherleaderdevelopmentprogrammesmighthavebeen
ignored,bydoingso.
Itcanbediscussedwhetheritisreasonabletoexaminetextsinarticleswritteninpositivist
ontologywithaninterpretativeepistemology.Itcouldbearguedthatitisirrelevanttoemphasize
andinterpretwhatthearticlestatesbasedonexperienceinascientificstudy.Thescientificpremise
fortheirstudymustbediscussedonthebasisoftheirscientificapproach,design,method,and
analysis.Itcanbeconsideredinappropriatetomakethearticlesaccountableforstatementsasitis
expressedinthearticles.However,thisinterpretativemethodtellswherethefocushasbeen.The
methodrevealswhetherleadershipisneededandthatleadershipisimportant.Theinterpretative
methodmakesuslookthroughtheliterature,intermsofconsensusonopinionsaswellasbehind
theaimsofthearticles.
Astrengthofthisthesisisthelatentcontentanalysisbywhichitispossibletoincludethe
underlyingmeaningofatext,andthestudyaswellsearchedsynonymsand,ifavailable,meaningful
similarpositiveandnegativeanalogies,phrasesandsentences.Thisanalysisisbroaderthan
Isersonswords,whichwasusedastheobjectivesintheQCA.
Itcanbediscussedifthepopulationwhoattendedthecoursewasrepresentative,iftherewasany
selectionbias.Theresidentsandthemedicalstudentswereofferedacourseinleadershiptraining,
andmaybethosewhoenrolledinthecoursewereparticipantswhohaddifficultytakingthe
authorityinthisrole.Iftherehadbeenmoreattendeeswhoalreadyhadhighself-confidenceas
leaders,therewouldnotbesomuchimprovementoftheparticipants,andeventually,the
evaluationswouldhavebeenmoremoderate.Nursesparticipatedinotherterms,theywerenot
offeredacoursebutweretoldtoattend.Theyfoundthecoursemostvaluable.
Ithasbeeninaccordancewiththisgeneralpracticeinconductorteachingtointegratevideoatthe
course.Onebasicideafortheprojectistoplaceaparticipantinastressfulandvulnerablesituation
infrontoftheotherparticipants,givinghimdifficulttaskstosolveinthesituationforthepurpose
ofprovokingdiscomfortandanxiety.Ifthecameraisexperiencedasanadditionalstressfactor,it
willonlyaddbeneficialchallengestotheideaoftheinterventionitself.

48
Ithasbeenrepeatedlyshownthattherearecommunicativetermswhicharenotverbalin
accordancewithMehrabian,Peirce,MultimodalAnalysisandLanger11,67,80,82,83,97.Ithasbeen
demonstratedthatvideohasevolvedtoanindependentcommunicationtoolsuitableforshowing
thediversityofsocialinteractioninaccordancewithXiao66.Ithasbeendemonstratedseveral
timesinthisstudythatinterpretationandintuitioncanbeshared,andthusgeneral.Insome
situations,werecognisethatthereisonlyonereality,themeasurablereality.Inothersituations,
andespeciallyinthecontextofhumaninteraction,wemustacknowledgethatthereareseveral
realities,andtheseareconstructedandinterpretedamongpeoplewhointeract.Inaccordance
withthis,weallowourselvestopresenttheeditedvideosthatarenotinterpretedwithwordsas
evidence.Itshouldbementionedthatallthevideospresentedintheappendixareinfactmore
explanatorywhendocumentingthediversityandnuancesinthecontentofthecourse.
Inordertounderlinewhichobjectiveswereaddressedduringthecourse,thisisdemonstrated
primarilybywordsintheformofquotes.Itisstatedthatthemoreparticipantswhosaythesame
independentlyofeachother,thegreaterthepossibilitythatthestatementisgenerallyapplicable.
Thiscanbecriticizedforusingpositiviststatisticsinastudybasedonaninterpretativeapproach.
Thechallengeinherentinthisthesisistodocumenttheconductor’shighlyqualitativeapproach
whenintroducingnon-verbalcommunicationinaclinicalresearchtradition.Moreover,itisnot
consideredthatoneontologyexcludetheother.
Whatcanbedocumentedcanbeseenfromtheavailabledata:Itisestimatedthat1)the
participants’reflectionsatthecoursereflecttheirimmediateexperience.2)Theirevaluationsafter
thecoursereflectwhattheytookhomefromthecourse.Theseanswersareavailableoneweek
after,tenmonthsafteranduptotwoyearsafterthecoursewasconducted.3)Thetwo‘blinded’
studentscommentedthecourseimpactoncourseparticipantsindependently,basedontheirown
interpretationofthevideos.4)Videosareeditedandcategorizedaccordingtotheencoded
themes.Thecontentofthisdatapresentsatriangulationofthecourse’simpact.
Astrengthforthecoursewasthediverseontologiesrepresentedbytheresearchersinthestudy.
ThePhDstudent,theconductor,andthemainsupervisor,theconsultant,constitutedaunique
researchteamintheconstellationbetweentwoverydifferentontologiesacquiredthroughtheir
verydifferentprofessions.Thisrepresentedadifferentapproachinrelationtotheconventional
approachinmedical-pedagogicalresearchinthisfield.Theylookedatthephenomenawithfresh
eyesandfromnewperspectiveswithoutrestrictionwithinalreadyexistinghypotheses,buthadan

49
ideabasedonintuition.Fromthefindings,newknowledgewasacquired,thisnewknowledgewas
adaptedtotheoriginalideaandtheprocesswasrestarted,accordingtotheabductive-inductive
methodologyintroducedbyPierce67,andfoundinthehermeneutics5,GT62,63,andQCA8,63.
Throughthosevariousontologiesandthusthefollowingdiscussionsonepistemology,thesubject
hasbeenstudiedandelucidatedfromseveralangles.Consequentlythisledtonewfindingson
leadershipintheclinicthroughunderstandingofwhataconductordoesinfrontoftheorchestra.

50
CONCLUSION
Noconsistentandtargetedleadershiptrainingfortheemergencymedicalteamleaderwas
identified.Formanyyearsmultipletaxonomiesandassessmenttoolshavebeendevelopedbut
failedtocometoaddressleadershiptraining.Aneedforexplicittargetedteamleadershiptraining
inhealthcarewasidentified.Theauthorsrecommendtrainingofleadershiptakeanotherturnto
investigateifitispossibletofindotherandmoreefficientwaystotraintheteamleaderin
emergencies.
Barriersforacquiringleadershipcompetenciesrequiredwhenmanagingemergencyteamswere
identified.Learninggoalswereidentified.Strongnegativeemotionssuchasstress,anxietyand
panicwerefoundwhenworkinginemergencies.Wedevelopedacoursethataddressedthose
barriers.
Theparticipantsnotedandcommentedoneachother’sdevelopmentonthecourse.Accordingto
theirself-reportingafterthecoursethetransferofaconductor’sskillschangedtheparticipating
students’,nurses’andresidents’behaviour,andintroducedamethodtohandleanxietyandshow
calmnessandauthority.Thiscourseclearlyseemstoaccommodatetheneedforanoperationaland
targetedtrainingoftheteamleaderinemergencies,addressingawaytoachieveconfidenceina
stressful,butsafelearningenvironment.Inadditiontheoutcometurnedouttobeaprofound
transformationofparticipants’self-understanding.
Thethesisillustratedthatitwasbeneficialtoinvolveanotherprofessiontohealthcare.Thisthesis
demonstratedagap–oratleastlackofconsequence–inbetweenwhatisknownandwhataction
istaken.

51
PERSPECTIVES
Implicationsforfuturepractice
Thethesisdescribeshowitispossibletoachieveleadershipskillsbyusingmusicalexercises.Itis
thereforerecommendedtocontinuethedevelopmentofcoursesinmedicalunchallenging,
harmlessenvironmentsthatalloweachresident/studenttogaininsightintotheirownpersonal
challengesandguidanceinhowtoworkwiththese.Thisthesishasshownacontextwherethisis
possible.
Educationalimplications
Werecommend:Ifthiscourseistobeintroducedasacompulsorypartoftheeducatingofdoctors,
theidealtimewouldbeafterclinicalskillshavebeenacquired,experiencegainedandroutines
understoodintheclinic.Thecoursewillbeanimportantsupplementtoexistingeducational
programsforresidents.
Furtherresearch
Itisrecommendedtoevaluatewhetherthelearningcanbetransferredtoclinicalpracticeand
whethertheyhaveapositiveimpactonthetreatmentofpatients.
Researchisneededtoexamineifitispossibletotraintheseskillsinmixedclinicalteams.
Researchisneededtodevelopandvalidateascoretoassessthequalityofnon-verbal
communicationandleadership.Thiscouldbemeasuredatconductorstudentsataconservatory.
Inthisconnection,anotherstudycouldbeconductedtoinvestigatetheemotionalresponseof
conductorstudentswhenconducting.Measuredonpulse,orhormonalchangesinnorepinephrine
orcortisollevelifpossible.
Itisrecommendedtodevelopa‘trainthetrainer’programmeaimingtoeducatemoretrainersand
involvetheminthefurtherdevelopmentofthecourse.Inthiscontext,itisrecommendedto
developacertificationmethodfora‘trainthetrainer’educationprogramme.

52

53
TRAININGRESIDENTSTOLEADEMERGENCYTEAMS[PARTONE]:ASYSTEMATIC
REVIEW
TureLarsen,RandiBeier-Holgersen,JetteMeelby,PeterDieckmann,DorisØstergaard
TureLarsen,PhDStudent,SimulationUnit(SimNord),DepartmentofAdministration,Nordsjællands
Hospital,Denmark
RandiBeier-Holgersen,MD,MHPE,DepartmentofGastrointestinalSurgery,Nordsjællands
Hospital,Denmark
JetteMeelby,MLS,DepartmentofClinicalResearch,NordsjællandsHospital,Denmark
PeterDieckmann,PhD,Dipl.-Psych.CopenhagenAcademyforMedicalEducationandSimulation
(CAMES),CapitalRegionofDenmarkandUniversityofCopenhagen,Copenhagen,Denmark
DorisØstergaard,MD,DMSc,Professor,DiplomaHPE,CopenhagenAcademyforMedicalEducation
andSimulation(CAMES),CapitalRegionofDenmarkandUniversityofCopenhagen,Copenhagen,
Denmark
Correspondingauthor:TureLarsen,SimNord,Kvalitetsafdelingen,NordsjællandsHospital,
Dyrehavevej29,3400Hillerød,Denmark.Phone:+4531127281,Mail:[email protected]
RandiBeier-Holgersen,DorisØstergaard,andPeterDieckmann:reprintswillnotbeavailablefrom
theauthors
Funding:TrygFoundation,LaerdalFoundationandNordsjællandsHospital,Denmark.
Disclosure:T.L.receivedgrantsfromTrygFoundation,LaerdalFoundationandNordsjællands
Hospital,Denmark.R.B.H,D.Ø.andP.D.havenoconflictsofinteresttodeclare.Thesponsorsofthe
studyhadnoroleinthestudydesign,datacollection,dataanalysis,datainterpretation,orinthe
writingofthereport.

54
Abstract
Objective:Todescribehowliteratureaddressesworkableandoperationalleadershiptrainingfor
theemergencymedicalteam-leaderandtoenhanceunderstandingofleadershiptraininginthe
medicalenvironment
SummaryBackgroundData:Worldwide,medicalsupervisorsfinditdifficulttogetstudentstorise
totheoccasionasleadersofemergencyteams:manyresidents/rescuersfeelunpreparedtoadopt
theleadershiproleinemergencies.Itappearsthatmanyresidents/rescuersfeelunpreparedto
adopttheroleasleaderinemergencies.Inspiteoftheknowledgeacquiredin30yearsofresearch,
scientistsarestillseekingasolutionastohowtoteachworkableleadershipinhealthcare.
Method:Asystematicreviewwasconducted(May-December2016inaccordancewiththePRISMA
2009Checklist).Aqualitativecontentanalysiswasadded.
Results:27articles,by25singlecorrespondingauthors,wereconsideredprimaryandcoveredthe
period1986-2016.Notargetedleadershiptrainingfordoctorswasfound.Themajorityofthe
researchprojectsdescribeddifferenttypesofbehaviouralmarkers,taxonomiesandchecklists.A
needforexplicittargetedteamleadershiptraininginhealthcarewasidentifiedin20/27articles.
Conclusions:Noconsistentandtargetedleadershiptrainingfortheemergencymedicalteamleader
wasidentified.Overtheyears,multipletaxonomiesandassessmenttoolshavebeendevelopedbut
failedtoaddressleadershiptraining.Theauthorsrecommendtrainingofleadershiptakeanother
turntoinvestigateifitispossibletofindotherandmoreefficientwaystotraintheteamleaderin
emergencies.
Introduction
Worldwidemedicalsupervisorsfinditdifficulttogetstudentstorisetotheoccasionwhencalled
upontoactasleadersofemergencyteams:manyresidents/rescuersfeelunpreparedtoadoptthe
leadershiproleinemergencies.16,17,23,26,27,32,37,39
Theaimofthissystematicreviewistoinvestigatehowliteraturedescribesworkableand
operationalleadershiptrainingfortheemergencymedicalteam-leader.Thescholarlyfieldof
leadershipandgeneralhealthcare-leadershipisrich,butthisstudyisnotaimedatdiscussing
differentiatedleadershipbehaviouratatheoreticallevel.

55
Thecorrespondingauthorinthissystematicreviewrepresentsanotherprofession.But,
nevertheless,hasaclearsenseofpracticalandoperationalleadershipacquiredfromaprofession
ofbeinganorchestralconductor.Thestudycouldbeconsideredasafreshlookathowthe
literatureandteachersapproachleadershiptraininginemergencies.
Thisstudywilldescribeissuesrelatedtotheeducationandtrainingoftheclinicalteamleaderin
emergencies.
Background
In1986Isersonstated:“Mostpeoplearenotbornleaders;theymustbetaughtleadership
techniques”44.In2016Robinsonandcolleaguesasserted:“Inthefieldofcardiacarrestleadership,
anincreasingweightofevidencesupportsthenotionthatindividualscanbetrainedtolead”23.
Forthelastthreedecades,leadershiphasbeendescribedasanimportantissueinhealthcare.But
inspiteoftheknowledgeacquiredin30yearsofresearch,scientistsarestilllookingforasolution
astohowtoteachworkableleadershipinhealthcare1,16,17,21-23,25-29,34,36-39,41,42,44,46,47,58-60.This
studyindicatesthatitisseemsnecessarytoacknowledgethat‘practicalguidanceneededforthe
deliberatepracticeofleadershipskills’22insteadoffocusingondevelopingneworadapting
existingleadershipmeasuringinstruments.
Thereappearstobealackofclarityontheperceptionof“goodteamleadership”intheliterature.
In2010Yukl98cited:“therearealmostasmanydefinitionsofleadershipastherearepersonswho
haveattemptedtodefinetheconcept”(Stogdill(1974,p.259).AndYuklcontinues:“Thestreamof
newdefinitionshascontinuedunabatedsinceStogdillmadehisobservation,Leadershiphasbeen
definedintermsoftraits,behaviors,influence,interactionpatterns,rolerelationships,and
occupationofanadministrativeposition”.
Method
ThesystematicreviewwasconductedinaccordancewiththePreferredReportingItemsfor
SystematicreviewandMeta-Analysis2009(PRISMA)Checklist.Asearchofthedatabasesof
Pubmed,Psycinfo(viaOvid),andERICwascarriedoutinJune-December2016withtheaidofa
researchlibrarian.AppendixIshowsthesearchtermsandstrategy,towhichnotimelimitor
languagerestrictionswereapplied.Thesearchstrategywasnotlimitedbydesignormethodology.
Alltypesofpapersconcerningleadershiptrainingandeducationinemergencymedicalscenarios
wereincluded.Technicalskillstraining,organizationalleadershipandteamworktrainingwithout

56
explicitfocusonleadershipwereexcluded.Duringtheearlystagesofthesearch,systematic
reviewsidentifyingrelevantoriginalarticleswereusedassources.
TheCommitteesonHealthResearchEthicsfortheCapitalRegionofDenmarkwasaskedtogive
ethicalapprovalbutaformalreviewwaswaivedforthisstudy(H-4-2015-FSP).
Screeningarticles
Oneauthor(TL)searchedPubMedandscreenedtitlesincluding820eligiblearticles.Pubmed´s
feature‘similararticles’wasusedandafurther226articleswereidentified.Afurthersearchwas
conductedinspiredbythenewkeywordsfoundinthearticles,andanother131articleswerefound.
ThesearchstrategywasappliedtoasearchinthedatabasesofPsycinfo(viaOVID)andEric
resultingin1.177articlesfromPubmed,82fromPsycinfo,and242fromERIC.Afterremoving
duplicates,twoauthors(TLandRBH)screened1.405titlesandabstractsapplyingtheabove
mentionedinclusionandexclusioncriteria.Onearticlewasaddedonthebasisofthereferences
(Yule,2006)38.Thetwoauthorsthenreadthefulltextofthe53potentialarticlesapplying
inclusionandexclusioncriteria.39articleswereselected.Therewasahighdegreeofoverall
agreementbetweenthetworaters(94.45%).Interraterreliabilitywasverygood(Cohen’sκ
coefficient=0,852).Differencesofopinionaboutinclusionorexclusionwereresolvedbydiscussion
betweenTLandRBH.13articleswereexcludedbecausetheircontentdidnotmeettheinclusion
criteriaandonearticlewasincompletebecauseofmissingreferences.Towardstheendofthe
reviewprocessonefurtherarticle,foundinanadditionalmanualsearchinGoogle(Ford2016)was
added24.40articlesandreportswereidentified.Ofthese27wereconsideredprimaryasthey
wereoriginalarticleswithinterventionsandnewfindings/evidence.13articleswereconsidered
secondary:10reviewsand3opinions.Fig.1(Flowchart)
Qualityofbodyofevidence
Areviewofqualitativeaswellasquantitativeresearchpaperswasconducted.Quantitativearticles
wereclassedaccordingtoPRISMA,CochraneandGRADE.Qualitativearticleswereclassed
accordingtoCASP(CriticalAppraisalSkillsProgramme).Theywereconsideredprimaryifthey
reportedempiricaldataaboutleadershiptrainingorbehaviour(i.e.,specificreportsabout
leadershiptaxonomiesandfindingsinquestionnaires).Onlyprimarystudiesareincludedinthis
SystematicReview.(Table1)

57
Abductionasamethod
Anabductiveapproachtoresearchmakesitpossiblefortheresearchertopresentaqualified
presumption(educatedguessorinference)67whencommencinghisinvestigation.Basedonhis
findings,heacquiresnewknowledge,hemightalter/adaptthisnewknowledgetothe
presumptionandtheprocessstartsover.Thisprincipleisthefoundationofmorecontemporary
methodse.g.GroundedTheoryorQualitativeContentAnalysis.
QualitativeContentAnalysis
Aninductiveapproach(conventional,inductive63)toQualitativeContentAnalysis(QCA)is
appropriatewhenpriorknowledgeregardingthephenomenonunderinvestigationislimitedor
fragmented.8Inaninductiveapproach,codes,categories,orthemesaredirectlydrawnfromthe
data8withoutimposingpreconceivedcategoriesortheoreticalperspectives.63Byadding‘latent
contentanalysis’8itispossibletointerprettheunderlyingmeaningofthewords.
QualitativeContentAnalysisinthisstudy
Afterconductingtheconventionalsystematicreviewnofocusedtrainingofteamleadershipwas
revealedandinsteadmanyleadershipmeasurementtoolswerefound.Itwasdecidedtoexamine
the27primaryarticlesinanabductive-inductiveQCA.Thisinvestigationwasconductedwiththe
purposetoidentifyopinionsaboutleadershipinemergenciesandviewsontheidentified
leadershipmeasurementtools.
Strategyforqualitativecontentanalysis
AllarticlesweregroupedtogetherinasinglePDFdocumentandsearchedseveraltimesfor
keywords,theirsynonymsand,ifavailable,theirmeaningfulsimilarpositiveandnegativeanalogies,
phrasesandsentences.Thequotesweregroupedintothemesinaniterativeprocess,andsorted
chronologicallyinappendixII.Whenthoughttopossiblyinfluencetheinterpretation,theywere
sortedaccordingtowheretheyappearedinthearticles:beforeorafterthemethodologysection,
i.e.expressingeitherapre-conditioninthebackgroundforthestudyorafindingoraconclusionas
aresultofthestudy.Apre-conditionforaninterventionmaychangewhentheinvestigationis
completedandaconclusionmaycontradictthepre-condition.Therefore,itisassumedthata
conclusioncanbestrongerthanapre-condition.Themostimportant/significantquoteschosenon
basisoftheauthors’interpretationarepresentedinthisarticle.AllquotesareavailableinAppendix
II.

58
Results
27originalarticles,coveringtheperiodfrom1986to2016wereincludedinthereview.Two
authorswereresponsibleformorethanonearticle:Yule34,38andCooper1,42.Ofthe27articles
fivewereRandomizedControlledTrials,sixCaseControls,tenCaseStudies,andsixQualitative
Studies.
Onesolestudyaddressingworkableandtargetedleadershiptrainingwasfound41.Thisstudy
focusesonleadershiptrainingseparatefrommedicalcompetence.Onearticlecoveringnon-verbal
communicationandpositioningaroundthepatientsimulatorwasidentified35.Onearticle
investigatedwhetherexternaldistractorsinfluencedperformanceduringaCPRscenario59.Eleven
studiesonresuscitation,eightontrauma,fouronsurgeons,twoonALSwerefound(acutedyspnea
43andburns56)andfinallyoneonleadershipstyleinhealthcareteams“asperceivedbynurses”
36.Themajorityofthearticlesdescribedanddiscusseddifferenttypesofbehaviouralmarkersand
taxonomies.Leadershiptrainingwasmostlycombinedwiththetrainingofmedicalcompetencies
includingalgorithms.Fourstudiesusedaquestionnaireaftertraining.Onestudyconductedafocus
groupinterviewaftertraining.Ninestudieswerebasedonquestionnairesorinterviews.Asummary
ofthearticlesisdisplayedinTable1.
LBDQorNOTECHSmeasurementtools:25ofthe27articlesweretosomeextentinfluencedbyone
orbothofthemostfrequentlymentionedtaxonomies,onedevelopedoriginallyforthemilitary
andtheotherfortheaviationindustry.1)TheLeadershipBehaviorDescriptionQuestionnaire,LBDQ
(military,1945)(Fig.2)(ninearticles,eightauthors1,14,17,23,27,32,33,42,59mainlysituatedin
Switzerland).2)TheNon-technicalskillstaxonomy,NOTECHS(aviation,thenineties)Adaptedto
healthcarein2003:Anaesthetist’snontechnicalSkills(ANTS)andadaptedtosurgeonsin2006:Non-
TechnicalSkillsforSurgeons(NOTSS)(Fig.3)(sevenarticles,sixauthors15,21,34,38,39,43,56mainly
situatedinScotland).Theabovementionedresearchers(LBDQorNOTECHS)didnotrefertoeach
other.However,nineauthors13,16,22,26,29,30,35,40,41referredtobothtaxonomies.Researchinto
leadershipisstronglydominatedbythetwodifferentconceptsandtheirprerequisiteswhichhave
influenced93%ofthearticlesinthisstudy.Twoarticlesfoundinthisreviewdonotreferto
NOTECHSorLBDQbuthaveuniquereferences.36,37
14articlescoveredtrainingtosomeextent(trainingalgorithmsanddebriefing).13articlesfocused
onotheraspects(surveys,questionnairesetc.).(Table2)
59
Resultofcontentanalysis
Threekeythemesemerged:Leadership,taxonomies,andtrainingleadershipandmedical
competencesimultaneously.Thequotesarecollectedinthethemesandtheirsubgroups,andare
representativeforsubgroups(pre-conditionorconclusion).
Leadership
Definitions:LeadershipisimplicitlydefinedintheLeadershipBehaviorDescriptionQuestionnaire
(LBDQ)taxonomy(Fig.2)aswellasintheNon-TechnicalSkillsforSurgeons(NOTSS)taxonomy(Fig.
3).Inaddition,sixotherdefinitionswerefound1,16,36,37,41,56.Manthaandcolleaguesrefersto
Heifetz(2009)in2016:
“…leadershipinvolvesanalyzingcomplexsituations,identifyingavailableresourcesandrequiredexpertise,
formulatingastrategyinreal-time,andcoordinatingmultiplestakeholders”41.
Leadershipislacking:Fourarticles16,23,38,40statedinthebackgroundtotheirstudythatleadership
islacking.
Fivearticles14,16,17,21,23discussedorconcludedexplicitlythatleadershipwaslacking.
“Ourstudysuggeststhatparticipantsdidnothaveagenerallackofleadershipskills,buttheymaynothave
linkedthenecessityofleadingandstructuringateamtotheresuscitationsituation”17.
Hunzikerandcolleagues,2010
Leadershiptrainingisimportant–leadershipchangesbehaviour
Gilfoyleandcolleaguesstatedinthebackgroundtotheirarticlein2007:
“Teamleadershiphasbeenrecognizedasveryimportantformanyyears,inareassuchasbusiness,the
military,andaviation”26.
Three1,26,39articlesdiscussedthatleadershiptrainingwasimportantandappearedtoimprove
behaviour.Nine13,15,17,23,27,33-35,42studiesconcludedthatleadershiptrainingwouldhaveapositive
impact.
“OuraimwastofocusontheleadershipaspectofCPR,asithasbeenwidelyrecognizedasbeinglinkedtothe
adherencetoestablishprotocols,fewererrors,andmorefavorablepatientoutcome”33.
Castelaoandcolleagues,2015

60
Leadershiptraininghasbeenignored:Despiterecognitionthatleadershiptrainingappearsto
changeandimprovebehaviour,itseemsthatleadershiptraininghasbeenignored,asstatedinthe
backgroundforthreestudies37-39.
“Traditionally,developmentofphysicianleadershiphasoccurredatrandominsurgicaltraining.Onepossible
reasonisthatsurgicaleducatorshavefocusedondetailedinstructiononcriticalpatientsituations,
resuscitation,andtechnicalskills,buttheyhaveprovidedlittleformaltrainingintheessentialleadershipskills”
37.
Itaniandcolleagues,2004
Ninearticles1,16,17,22,23,27,29,36,39discussedorconcludedthatleadershiptraininghasbeenignored.
“Traditionally,surgicaleducationhasnotformallytaughtleadershipskills…”39.
Nicksaandcolleagues,2015
Leadershiptrainingisrequired:18ofthe25authors(20/27articles)identifiedarecurringneedfor
explicittargetedteamleadershiptraininginhealthcare,7articles17,22,34,36,38,39,43mentionedthisin
thebackground/introductionand13articles1,14-16,23,26,27,29,34,37,39,41,42asafindingoraconclusion.
Amongthelatter,Marschandcolleagues,2004:
“Absenceofleadershipbehavior[…]wereassociatedwithpoorteamperformance…thisfindingcouldhave
importantimplicationsfortheteachingofmedicalemergencies”14.
“Werecommendthattraininginandassessmentofleadershipskillsinemergencyscenariosshouldbean
integralcomponentofpostgraduatemedicaltraining”23.
Robinsonandcolleagues,2016
Ninearticles13,21,30,32,33,35,40,56,59proposeddifferentapproachesorfocusareastoimprove
leadershipinemergencies.(Aviation,NTS,Gender,Ethnicity,Non-Verbalcommunicationetc.)
Taxonomies
Atotalof20taxonomiesaddressingleadership,teamwork,andcommunicationwerementionedin
thearticles.(Table3)
Thepurposeoftaxonomies:TheideaofusingbehaviouralmarkersystemswasexplainedbyYule
andcolleaguesin2006:
“TheprototypeNOTSSbehaviouralmarkersystemwasdesignedtoallowstructuredobservationandfeedback
totraineeandconsultantsurgeonsonobservablenon-technicalskills[…]thisstudyhastakentheadditional
61
stepofidentifyingexplicitlytheparticularnon-technicalskillswhichmightbebothtaughtandobserved–and
thereforemeasured”38.
Thisviewissharedbythreearticles15,22,33.
Comprehensiveorsimple:Somearticles22,36findacomprehensivetaxonomyadvantageous:
Leenstraandcolleagues,2016:
“TheTTLSdetails5skillcategories[…]and37skillelements.Theskillelementsarecapturedby67behavioral
markers”22.
Somepreferasimpletool43,59:Carlsonandcolleagues,2009:
“Onebarriermaybethatmanyreportedinstrumentsmaybetoocomplex”43.
Measurementtoolslacking:Fourarticles15,21,29,43pointedoutintheintroduction/backgroundthat
measurementtoolswerelacking.
“AlthoughtheimportanceofteamNTSscontinuestobeatopicofinvestigation,theroleoftheteamleader
hasnotbeenevaluatedinpreviousstudies”21.
Briggsandcolleagues,2015
AndKrageandcolleaguesconcludedin2014:
“However,toourknowledgenostandardscoringprotocolsareavailabletoassessoverallindividualhuman
performanceoftheresuscitationteamleaderduringCPR”59.
Newtooldeveloped:Twoarticles22,38statedintheaim/backgroundthatnewtoolshadbeen
developed:Leenstraandcolleagues,2016:
“Toaddresstheneedforataxonomyofleadershipskillsthatspecifiestheskillcomponentstobelearnedand
thebehaviorsbywhichtheycanbeassessedacrossthefivephasesoftraumacare,theauthorsdevelopedthe
TaxonomyofTraumaLeadershipSkills”22.
Fivearticles26,33,36,39,43announcedthedevelopmentofaneworadaptedtoolinthe
discussion/conclusionsectionoftheirarticles:Nicksaandcolleaguesusedapreviouslyadapted
NOTECHStaxonomy,2015:
“AmodifiedOxfordNon-TechnicalSkills(NOTECHS)scale[…]wasusedtoassesssurgicalresidentnontechnical
performance”39.

62
Threearticles15,41,43statedinthebackgroundtotheirstudythatitcouldbedifficulttokeeptrack
oftheactualcontentofthevarietyoftoolsandmethodsdeveloped.
“WhileNTShavebeenshowntocorrelatewithtechnicalproficiency,thereissignificantvariabilityin
terminology,trainingmodalities,andevaluationofNTS”41.
Manthaandcolleagues,2016
Yuleandcolleaguesindicatedin2015thatthefocusmightadvantageouslybechangedawayfrom
thedevelopmentofnewmeasuringtools:
“Therateofdevelopingassessmenttoolsinthisareahasoutpaceddevelopmentofworkableinterventionsto
improvenon-technicalskillsinsurgicaltrainingandbeyond”34.
Trainingleadershipandmedicalcompetencesimultaneously
Itmaybeadvantageoustoseparateleadershiptrainingfromtraininginmedicalcompetencies,
Castelaoandcolleaguesstatesinthebackground:
“…thecomplexityofsuchamultifactorialstructureincreases,creatingthepotentialforanincomplete
understandingofthewholeprocess.[…]Thus,reducingthecognitiveworkloadbeforehandbyseparatingrole
instructionscanhaveapositiveimpactontheCPRperformanceandonthetrainees’individuallearning
process”33.
Sixarticles14,17,23,27,36,41concludedthatleadershiptrainingdifferedfrommedicalknowledge
training.
“…thetrainingprovidedthroughtheALSqualificationisnotsufficienttodevelopthenecessarylevelof
leadershipskillsforacardiacarrestteamleader”23.
Robinsonandcolleagues,2016
AndManthaandcolleaguesconcludedin2016inthestudyfocusingexplicitlyonleadershiptraining
separatefrommedicalknowledge:
“Short-termoutcomesofthisleadershipcurriculumdemonstrateasignificantincreaseinparamedictrainees’
self-perceivedconfidence,communication,andleadershipskills”41.
Discussion
Oneoftheobjectivesofthissystematicreviewwastosearchforaworkablemethodtotrain
physiciansforleadershipinemergencies.Forthelastthreedecades,leadershiphasbeendescribed
asanimportantissueinhealthcare.Wefoundsixdefinitionsofleadership,whichcentredmostly
onachievingcommonaimsthroughcollaborationbetweenleaderandteam.Somearticles

63
describedleadershipasamorecomplexprocessinwhichtheleaderhadtoanalysethesituation
andhandlemultiplestakeholders.Wedidnotfindacleardefinitionandmustconclude,likeStogdill
in1974,that“therearealmostasmanydefinitionsofleadershipastherearepersonswhohave
attemptedtodefinetheconcept”.
Despitetherebeingnocleardefinition,theliteraturedescribeslackofleadershipashighly
prejudicialtoperformanceduringacritical,clinicalsituationandperformanceasveryvariable.The
literaturesoughthelpoutsidethemedicalworldfromthemilitary(LBDQ)andfromaviation
(NOTECHS),adaptedtaxonomiestothebehaviouroftheleaderandteamandcustomizedthemto
medicalemergencies.TheLBDQandNOTECHStaxonomieswereoriginallydevelopedtoassess
officersandpilotsincommandofaircrafts–leadersintheirprofessions.Peopleselectedand
educatedtobeleadersinprofessionalemergencies.Itcouldbesaidthatthisstartingpointis
essentiallydifferentforthatofnewlyqualifiedyoungdoctorswhohavenotyetbeenintroducedto
leadership.Inmedicinethetaxonomies(i.e.LBDQformXII,NOTSS)seemtohavebeendeveloped
andadaptedtoassessmedicalalgorithms(i.e.ALS)orprocedures(i.e.surgery)inordertooptimize
patientoutcomebychanging/improvingthebehaviouroftheteam-leaderandhisteam.Butmany
articlesconcludedthatleadershipisstilllacking.
Overtheyearstheresearchhastriedtodefineanappropriatetaxonomytomeasureandimprove
doctors’abilitytoactasleaders.Itisveryinterestingthat2/3oftheresearchintotaxonomieshas
beenconductedbytwocompletelyseparateresearchgroupsinspiredbyeitherthemilitaryorthe
aviationindustryalmostwithoutreferringtoeachother.Theother1/3ofresearcherswasinspired
bybothtaxonomies.Thetaxonomiesmostlyassessedhowwellthealgorithmhadbeencompleted,
nottheactualqualityofleadership.Onecouldassertthattheythereforemeasuredhowwellthe
doctorsknewhowtotreatthepatient.Onecouldconcludethatleadershiptrainingactuallytakes
placeinaclinicalcontextwhichiscomplexitself–focusingsimultaneouslyon‘taskdistribution’,
‘humanfactors’or‘initiatingstructure’(LBDQ)or‘taskmanagement’,‘non-technicalskills’or
‘situationawareness’(NOTECHS)aswellasonmedicalknowledgeandcreatingstructureswhile
implementingalgorithmsandmaintainingstandards.Butthissettingcoulddiminishtheactual
focusontargetedleadershiptraining.
Theuseoftaxonomiesandassessmenttoolsinmedicinecouldbeexplainedbythewishtoproduce
evidencefortheactionsandchangesintreatment/behaviour.Wediscoveredseveraltaxonomies
andassessmenttoolsintheliterature;somecomprehensive,someverysimple.Howeverthe
64
literaturestillaffirmsthatstandardperformancemeasurementtoolsarelackingandthereforea
constantlyincreasingnumberofnewtoolshavebeendeveloped.Inaddition,itshouldbe
mentionedthatsignificantdiversitywasrevealedintermsofterminology,trainingmethods,
evaluationsandconclusionsintheinterventionsfound.Itcouldbeconcludedthatthedefinitionof
leadershipisunclearandthereforeconsensusisimpossible.Theliteraturebeginstoquestionthe
numberoftools–andmethodsused–inthetaxonomies.
Asdemonstratedintheresultssection,scientistsagreethatleadershiptraininghasanimpact,
improvesbehaviourandchangesclinicaloutcome.Despitethis,theliteraturedemonstratedthat
formalleadershiptraininghasbeenneglectedorthateducationisinsufficient.Itstillappearstobe
askillthatistraditionallyacquiredby‘learningbydoing’.Neverthelesstheliteratureaffirmedthat
targetedleadershiptrainingisveryimportant.Morethanhalfofthe27articlesexamined
concludedthattherewasanurgentneedtodevelopaworkablemethodtoprovideresidentswith
specificandtargetedleadershiptraining.
Severalarticlesstateditmaybeanadvantagetoseparateleadershiptrainingfrommedical
competenciestraining.Medicalandbehaviouraltrainingareverydifferenttopics,andtraining
simultaneouslycouldevenworkbecounter-productivebecauseofthehugecognitiveworkload.To
ourknowledgenobodyhasaddressedworkabletargetedteamleadertrainingfordoctorsin
emergencies.Taxonomiesmightdetail‘whattodo’,butapparentlydonotaddresstheactualneeds
oftheteam-leaderinemergenciesinordertoassumeleadershipinasatisfactorymanner.
Itispossibletoarguethatthis–asthisstudyalsoreveals–obviouslyisnotnewknowledge,the
importanceofthishasbeenemphasizedandsoughtafterfor30years.Theresultofthissystematic
reviewisthusnegativeandconsequently,itispossibletoarguethatthestudyisunsuccessful.One
canalso,astheauthorsofthestudy,arguethattheresultisalarmingandrevealsthedeficiencyof
researchinthisareainthelast30years.Thiscanbeconsideredasasubstantialcontributionadding
constructiveandimportantknowledge.
Conclusion:Noconsistentandtargetedleadershiptrainingfortheemergencymedicalteamleader
wasidentified.Formanyyearsmultipletaxonomiesandassessmenttoolshavebeendevelopedbut
failedtocometotermswithleadershiptraining.Yuleandcolleaguesbacktrackedin2015:
“Therateofdevelopingassessmenttoolsinthisareahasoutpaceddevelopmentofworkableinterventionsto
improvenon-technicalskillsinsurgicaltrainingandbeyond”34.

65
Aneedforexplicittargetedteamleadershiptraininginhealthcarewasidentifiedin20/27articles.
Theauthorsrecommendtrainingofleadershiptakeanotherturntoinvestigateifitispossibleto
findotherandmoreefficientwaystotraintheteamleaderinemergencies.
Furtherresearchrecommendations
Doestheliteratureidentifyareastobeaddressedinthetrainingofleadershipforresidentswhen
actingasteamleadersinemergencies?
Contributors
TLarsenhadfullaccesstoallthedatainthestudyandhadfinalresponsibilityforthedecisionto
submitforpublication.TLundertookthesearchformaterial,extractedandcollecteddata,
developedtheanalysisstrategy,andwroteuptheresults.TL&RBeier-Holgersen,conceivedand
designedtheproject,reviewedthescientificreports,madequalityassessmentsandinterpretation
oftheresults.JMeelbyassistedintheliteraturesearchandprovidedadvice.PDieckmannandD
Østergaardprovidedadviceandcriticallyrevisedthemanuscript.

66
AppendixI,AsearchforLeadershipTraininginHealthcare–SearchstrategySearchinPubmed
#1((((gestureORmimicOReye-contactOReyecontactOReyebrowORsmile))OR(((NTSSkillsOR"non-technicalskills"ORnotss))OR((communicat*)AND("nonverbal"OR"nonverbal"OR"non-verbal"ORvisual)))))=99.119entries
#1b((gestureOR"bodylanguage"ORmimicOR"eye-contact"OR"eyecontact"OReyebrowORsmile))OR(((NTSSkillsOR"non-technicalskills"OR"nontechnicalskills"ORnotss))OR((communicat*)AND("nonverbal"OR"nonverbal"OR"non-verbal"ORvisual)))NOT(autismORpregnancyORpainORAlzheimer*ORvertebralORdrawing*ORchildren)=69.150entries
#2(taskmanagementORauthorityORdisciplineORrespect)OR(leadsORleadingORleadORteamleaderOR"teamleader"ORteamleader)=1.465.692entries
#2c((taskmanagementORauthorityORdisciplineORrespect))OR(leadsORleadingORleadORteamleaderOR"teamleader"ORteamleader)NOT(“leadto”or“leadsto”or“leadingto”)=824.514entries
#1AND#2limitedtoSystematicrev.=138entries
#3:(conductor*ORorchestra*ORsymphon*)=22.335
#1AND#2AND#3=29entries
#4:(teach*OReducat*ORtrain*ORlearn*)=1.684.125
#1bAND#2cAND#4=432entries
#5(((("advancedlifesupport")OR("cardiopulmonaryresuscitation"[MeSHTerms]OR("cardiopulmonary"[AllFields]AND"resuscitation"[AllFields])OR"cardiopulmonaryresuscitation"[AllFields]))OR((Acute*ORintensiveORemergencyORtraumaORtraumaticORresuscitat*OR"cardiacarrestsimulation"))))=2.501.517
#8(("leadership"[Mesh])AND"Education,Medical"[Mesh])=1.262
#5AND#8=114entries
#9“bodylanguage”=354
#10communicat*ORleadershipORleadingorleadsorleadORteamleaderOR"teamleader"ORteam-leader=1.476.894entries

67
#9AND#10(NOT(autismORpregnancyORpainORAlzheimer*ORvertebralORdrawing*ORchildrenorconsultationorhypno*))=107entries
Total=820
SupplementarysearchinspiredbyarticlesfoundinPubmed’s‘similararticles’=226entries
Total=1046
Newkeywordsemergedinspiredbythenewarticles:
“trainingleaders”OR(“teamlearning”AND“interprofessionalteams”)OR(urgencyANDsituationandleadersandgoal)OR(leadershipand“resuscitationteams”andtaskandperformance)OR(Leadershipandmanagementandeducationandtrain*andhealthcareanddoctors)OR(leadershipand“cardiacarrest”andtask)OR(Leadershipandcardiopulmonaryresuscitationandskills)OR(leadershipand(“cardiacarrest”ORcardiopulmonary)andresuscitationandhumanfactors)OR((“cardiacarrest”ORcardiopulmonary)and"resuscitationperformance"andtraining)OR(leadershipandteamand(“cardiacarrest”ORcardiopulmonary)andperformanceandcommunication)OR(leadand"advancedlifesupport"andperformanceandtraining)OR(leadsand"advancedlifesupport"andperformanceandtraining)OR(leadingand"advancedlifesupport"andperformanceandtraining)OR(leadershipand"advancedlifesupport"andperformanceandtraining)
134entries

68
Fig.1

69
Studytype Objective Contentofintervention Outcome/Conclusions RiskofbiasValidityofevidence
RCT
YULE,S.etal.2015
Demonstratetheeffectofnon-technicalskillscoachingonintraoperativebehaviorsandclinicallysignificantdecisionsduringsimulatedoperations.
16surgeons,twogroups.Fiveoperationseachsurgeon.CasegroupreceivedcoachingonNTSaftereachoperation-controlnot.Operationoneandfivewasvideorecorded.Blindedassesors
Coachingimprovedresidents’non-technicalskillsinthesimulatedORcomparedwiththoseinthecontrolgroup
Performancebias:participantsnotblinded.Smallsamplesize.Nobaselineforparticipantswererecorded.Externvalidityunclear.
LowbodyofevidenceaccordingtoGRADE.++
FERNANDEZCASTELAOetal.2015
ThisstudyassessedtheimpactoftheCRMteamleadertrainingonCPRperformanceandteamleaderverbalization
Forty-fiveteamsoffourmembersreceivedALStraining.OneineachteamassignedtoteamleaderinaCPRsimulation.Teamleadersingrouponeattended90min.CRMtraining.Allothers90min.ALStraining.Videorecorded.Check-listbasedtooldevelopedbyexperts.Authorsassesorsblindedtotheexperimentalallocation
TrainingonlythedesignatedteamleadersinCRMimprovesperformanceoftheentireteam,inparticularguidelineadherenceandteamleaderbehavior.(Emphasisontrainingofteamleaderbehaviorappearstobebeneficialinresuscitationandemergencymedicalcourseperformance.)
Selectionbias:Randomization1alphabetically.Randomization2unclear.Randomization3unclear.Performancebias:participantsnotblinded.Statisticalmethodquestionable(studycalledformediannotmean).Nobaselineforparticipantswererecorded.
LowbodyofevidenceaccordingtoGRADE.++
KRAGE,R.etal.2014
ToinvestwhetherexternaldistractorsinfluenceperformanceduringastandardizedsimulatedCPRscenarioingeneralandwhetherlevelofexperiencehasanimpact
30physisicians,twosimulatedCPR.Cross-overstudy:1:distractors(radionoise70dB,scriptedfamilymember,talkingatcrucialmoments)2:not.Videorecorded.Scoringprotocoldeveloped.Twoassesorsratedindependently
Nointeractionwasobservedbetweenadditionaldistractorsandexperiencelevel.Externaldistractorsmarkedlyreducethequalityofcardiopulmonaryresuscitation.
Performancebias:participantsnotblinded.Smallsamplesize(N=10ineachgroup).
ModeratebodyofevidenceaccordingtoGRADE.+++
HUNZIKER,S.etal.2010
TheaimofthisstudywastocompareleadershipinstructionwithageneraltechnicalinstructioninsimulatedCPRscenario
237(280)medicalstud.inteamsofthree.CPRsimulation,pre-video.Basicinstruction20min.Twogroups.Case:Leadershiptraining.Control:Technicaltraining.CPRsimulation,2post-video,n=96andn=93.Followupafter4Mo.Videotapescodedbytwoindependentblindedresearchers
Causalrelationshipbetweenleadershipandperformancewasproven:Leadershipinstructionsweresuperiortotechnicalinstructions,withmoreleadershiputterancesandbetteroverallcardiopulmonaryresuscitationperformance.
Performancebias:participantsnotblinded.
HighbodyofevidenceaccordingtoGRADE.++++
COOPER,S.etal.2001
Developacoursetrainingleaderswiththeaimofchangingbehaviorandperformance
ThreedayALScourse.N=68.Threecourses.DayoneALStraining.DaytwoandthreeallactedasteamleaderinaCPRsimulation.Afterdaytwocasegroupattendedaleadershipseminar.Controlnot.Fiveindependentassesors,blinded
Theleadershiptrainingprogrammesignificantlyimprovedcandidatesleadershipperformanceinthetrainingsituation
Performancebias:participantsnotblinded.Unclearassessmentprocedure.
ModeratebodyofevidenceaccordingtoGRADE.+++
Case-Control
MANTHA,A.etal.2016
NTScurriculumforIndianparamedictraineesfocusedonstrengtheningon-sceneleadership,teamwork,andpublicspeakingskills
40paramedictrainees.Six-daycourse.Traineescompletedself-assessmentsanddeliveredtwobriefvideo-recordedpresentationsbeforeandaftercompletionofthecurriculum.Independentblindedobserversscored10randomlyselectedtrainees.
Outcomesofthisleadershipcurriculumdemonstrateasignificantincreaseinparamedictrainees’self-perceivedconfidence,communication,andleadershipskills
Performancebias.
LowbodyofevidenceaccordingtoGRADE
NICKSA,G.A.etal.2015
Toeducatesurgicalresidentsinleadership,teamwork,effectivecommunication,andinfrequentlyperformedemergencysurgicalprocedureswiththeuseofinterprofessionalsimulations.
43surgicalresidentsPGYs1and2.Interdisciplinaryhigh-riskclinicalscenarios.Pre(control)and6MoafterPost(case)37respondedtoasurvey.Authorassesor
ThePGY2residentsimprovedtheirskills,butthePGY1residentsdidnot.Atotalof89%oftheresidentsfeltthesessionswereofgreatbenefit.
Educationallevelcouldbeaconfounder
VerylowbodyofevidenceaccordingtoGRADE
ROBERTS, Toinvestigateifbrief 57medicalstaffmembers.Pretest Participantschangedteamwork Moderate

70
N.K.etal.2014
trainingwouldhaveasustainedeffectonindividualacquisitionandretentionofknowledgeandteampracticebehaviorsandonteambehaviorsofhealthcareprofessionalsinmedicalemergencysituations…
simulatedCPRsessions.Thentrainingconcludingwithapostsimulation.Debriefing.Threeweekslaterthirdsimulation.Videorecordings.Twoblindedraters.Questionnaire
andcommunicationbehaviorontheposttest,andchangesweresustainedaftera3-weekinterval,thoughtherewassomelossofretention.Brieftrainingexercisescanchangeteamworkandcommunicationbehaviorsonadhoctraumateams.
bodyofevidenceaccordingtoGRADE
MAKINEN,M.etal.2007
Thepurposeofthisstudywastoassesstheresuscitationskillsofnursestofacilitateconstructionofaneducationalprogramme
FromFinland:110,Sweden:40nurses.Case,leadershiptraining(S),controlnot(F).Subjectstestedinpairs.Achecklistusedtograde.5assesorsindependently,notblinded
Definingandteachingleadershipseemstoimproveresuscitationperformance.
Notblindedassesors
VerylowbodyofevidenceaccordingtoGRADE
GILFOYLE,E.etal.2007
Educationalintervention.evaluateimmediateandlongtermlearningoutcomesinordertodeterminewhetherresidentscouldacquireandretainteamleadershipskillsinpediatricadvancedresuscitation.
Case15paediatricresidents2leaderskillstraining,simulatedresuscitationscenarios.Evaluatedagain6monthslater.ControlN=7notraining.Ratingbychecklistandself-reportedquestionnaire
Residentsacquiredresuscitationteamleadershipskillsfollowinganeducationalintervention.Six-monthfollow-updemonstratedskillretentionbeyondtheinitialintervention.Controlgroupsuggestedthatthiswasbecauseparticipantshadattendedthefirstworkshop.
Verysmallsamplesize.Inkonsistencyingroups.DoubtfuluseofstudentsT-test
VerylowbodyofevidenceaccordingtoGRADE
MCCUE,J.D.etal.1986
Toassesstheresidents'leadershipstyleandthenurses'perceptionsoftheeffectivenessofthosestyles.
17residents.Aself-administered,self-ratingleadershipstyleindicator,LSI.SelfReportsandNursesReports.Questionnaire.Computerizedscale.Notblindedassesors
Thepresentstudysuggeststhatfemaleresidentsmaybemorelikelytousehighrelationshipleadershipstylesintheirinteractionwithnurses…analysisofleadershipstyleisapotentiallyusefulwayofhelpingresidentsassumeleadershipmoreeffectively.
Onlywomennurses.Sexbias.Onlyresidentsknowntonurseswasallowed=notblindedassessors
VerylowbodyofevidenceaccordingtoGRADE
CaseStudy
ROBINSON,P.S.etal.2016
Toassesstheperceptionsofleadershipandteamworkingamongmembersofacardiacarrestteamandtoevaluatefuturetrainingneeds
102membersofacardiacarrestteam.Survey.Responsessoughtfromdoctors,nursesandhealthcareassistants
Werecommendthattraininginandassessmentofleadershipskillsinemergencyscenariosshouldbeanintegralcomponentofpostgraduatemedicaltraining
Notrelevant
HARGESTAM,M.etal.2016
Investigatehowtraumateammembersarepositionedintheemergencyroom.Howleaderscommunicateintermsofgazedirection,vocalnuances,andgesturesduringtraumateamtraining.
108participants.Eighteentraumateamswereaudioandvideorecordedduringtraumateamtraining.Focusisonteamleaders’communication,analysisisperformedinrelationtobothverbalandnon-verbalcommunication.
Non-verbalcommunicationreinforcedtheteam-leaders’communication.Team-memberswhoareawareoftheirnon-verbalcommunicationcanimprovetheirperformance.Vaguenon-verbalcommunicationreinforcesambiguityandcanleadtoerrors
Notrelevant
BRIGGS,A.etal.2015
Doesteam’sandteamleader’sNTSscorrelatewithtechnicalperformanceofclinicaltasks?
20teams.Twoseparate,high-fidelity,simulatedtraumascenarios.Video,dividedinto4consecutivesections.TeamleaderassessmentusingNOTSS.Entireteam2additionalratersusedT-NOTECHS
TheNTSsoftraumateamsandteamleadersdeteriorateasclinicalscenariosprogress,andtheperformanceofteamleadersandteamsishighlycorrelated.CognitiveNTSscorescorrelatewithcriticaltaskperformance.
Notrelevant
RINGEN,A.H.etal.2011
ToassesstheexperienceandeducationofNorwegiantraumateamleaders,andallowthemtodescribetheirperceivededucationalneeds
Writtenquestionnaires.All45hospitalsinNorwayreceivingseverelyinjuredtraumavictimswerecontacted,randomlyselectedweeknight.Teamleadersaskedtospecifywhattraumarelatedtrainingprogramstheyhadparticipatedin,howmuchexperiencetheyhad,andwhatfurthertrainingtheywished,ifany.
Levelofexperienceamongteamleaderswashighlyvariableandtheireducationalbackgroundinsufficientaccordingtointernationalandproposednationalstandards.Teamleadersstatedthatmoreexperienceandbettertrainingareimportanttotheminordertobecomebetterleaders
Notrelevant

71
CARLSON,J.etal.2009
Todevelopameasurementtoolreliableatcapturingteambehaviorduringahigh-fidelitysimulationwhenusedbymultipleraters.Usethetooltoexploretherelationshipbetweentheteambehaviorsmeasuredandthestandardoftechnicalmedicalcaredeliveredspecifictotheneedsofthecase.
Studyparticipants(n=113),44teams(2or3teammembers)Duringtheworkshop,everyteamparticipatedinthesamescriptedcasescenariofacilitatedbythesametraininginstructor.Ratersusingtheteambehaviormeasurementtoolwereunawareoftheteams’globalassessmentoftechnicalstandardofmedicalcaredelivered
Themethodsusedprovideapossiblemethodfortrainingandassessingteamperformanceduringsimulation.Theinstrumentpresentedinthisstudyoffersapossibletemplateforfuturework
Notrelevant
HAYES,C.W.etal.2007
Determineinternalmedicineresidents’perceptionsoftheadequacyoftheirtrainingtoserveasinhospitalcardiacarrestteamleaders
654residentsweresentasurvey,289residents(44.2%)responded.Subjects:adequacyoftraining,perceptionofpreparedness,adequacyofsupervisionandfeedback,andeffectivenessofadditionaltrainingtools
Asignificantnumberofinternalmedicineresidentsfeelinadequatelytrained,unprepared,andunsupervisedtoleadcardiacarrestteamsinteachinghospitals.
Notrelevant
ITANI,K.M.etal.2004
Assesstheperceptionofsurgicalresidentsinleadershipskills.
Questionnairewasadministeredto43residents.1)theresidentsranked18leadershipskillsonascaleof1to4inimportanceforcareerdevelopment.2)asimilarscalewithregardtotheirpersonalconfidenceandcompetenceinthesesameareas.3)toevaluatethemselveswithregardtofiveleadershiptraits.
Traditionally,developmentofphysicianleadershiphasoccurredatrandominsurgicaltraining.Itisourjobassurgicaleducatorstoprovidethisopportunitytoourresidents.Ethicswastheonlyareainwhich75%oftheresidentsbelievedthemselvestobemorethanminimallycompetent
Notrelevant
MARSCH,S.C.etal.2004
Howhumanfactorsaffecttheteamperformanceduringasimulatedcardiacarrest.Andshowcorrelationbetweenleadershipbehaviourandoutcome
16teams,eachthreehealth-careworkers.Simulator.Video.Dataanalysiswasperformedindependentlybytwooftheauthorsusingachecklist.
Twothirdsofteamscomposedofqualifiedhealth-careworkersfailedtoprovidebasiclifesupportand/ordefibrillationwithinanappropriatetimewindow.
Notrelevant
WISBORG,T.etal.2003
Doesthetrainingofmultiprofessionaltraumateamsandresusciationteamsfornewbornsvary?
Atelephonesurveyoftrainingpractices.Theheadnurseateachemergencydepartment(n=50)andneonatalward(n=16)wasinterviewedinastructuredfashion.Theywereaskediftheiremergencyteampersonnelhadparticipatedinpracticalmultiprofessionaltrainingduringtheprevious6or12months.
Regularteamtrainingrepresentsanunderusedpotentialtoimprovehandlingoflow-frequencyemergencies.
Notrelevant
COOPER,S.etal.1999
Determinetherelationshipbetweenleadershipbehaviour,teamdynamicsandtaskperformance
20resuscitationattemptswereobserved(19onvideo).Allteamsmorethanfivemembers.Atotalof18leaders.LBDQ:measurelevelofstructure.Interpersonalbehaviourandtasksofresuscitationwithateamdynamicsandataskperformancescale.Observers:anALSinstructorandavideorater
Leaderswhoinitiatedastructure,distributedtasks,andremained“handsoff”improvedteamperformance.Anemergencyleadershiptrainingprogrammeisessentialtoenhancetheperformanceofleadersandtheirteams.
Notrelevant
QualitativeStudies
SADIDEEN,H.etal.2016
VideoanalysisofleadershipbehaviorswithinTheBurnsSuite(asimulationtooltodeliverinterprofessionalandteamworktraining).ExplorewhetherSimulation-basedteamtrainingwithinTBScanelaborateonkeyleadershiptheories.WhichleadershipmodelsappearedpredominantwithinTBS.
N=12,3simulations,eachteam4members.Video.Focusgroupinterviewsafterdebriefing.Objectivetoidentifyleadershipskillsmappingthemontoleadershiptheory.2authorsand2otherauthorsindependentlyassesors
Effectiveleadershipisessentialforsuccessfulfunctioningofworkteamsandaccomplishmentoftaskgoals.Leadershipinateam-basedresuscitationscenariocanbeconsideredasdistributed,ratherthancontinuouslybeingassociatedwithaspecificleader.
“Therewasadifficultyinblindingauthorsduringcodingofparticipantleadershipbehaviors,whichmayhaveintroducedanelementofdetectionbias,althoughcarewasexercisedtoavoidthis”
AccordingtoCASPthereisaclearstatementsoffindingsandtheresearchisvaluable

72
LEENSTRA,N.F.etal.2016
Toaddresstheneedforataxonomyofleadershipskillsthatspecifiestheskillcomponentstobelearnedandthebehaviorsbywhichtheycanbeassessedacrossthefivephasesoftraumacare,theauthorsdevelopedtheTaxonomyofTraumaLeadershipSkills,TTLS
28interviewsw.traumaleadersand14raters.Skillelementscapturedby67behavioralmarkers.Categorizedusingmultipleraters
TheTTLSprovidesaframeworkforteaching,learning,andassessingteamleadershipskillsintraumacareandothercomplex,acutecaresituations
AccordingtoCASPthereisaclearstatementsoffindingsandtheresearchisvaluable
KOLEH-MAINEN,C.etal.2014
Investigatingcodeleadershipasperceivedbyresidentsinfourareas:(1)learningtobeacodeleader(2)leadershipdefinescodesuccess(3)idealcodeleadershipbehaviors(4)leadershipandgender
25residents,semi-structuredtelephoneorin-personinterviews.Recordedandtransscribed.Threeauthorsanalyzedthreeinterviewsfocusingoncontentareas.Fourauthorsreadalltranscripstinfull
Leadershipdefinescodesuccess.Poorleadershipwascitedasthemajorfactortoachaoticcode.Participantsreportedthatitwasimportanttobe“authoritative”;tohavea“strongpresence”bybeingbothseenandheard.Femaleparticipantsdescribedfeelingstressfromhavingtoviolategenderbehavioralnormsintheroleofcodeleader.
AccordingtoCASPthereisaclearstatementsoffindingsandtheresearchisvaluable
JACOBSSON,M.etal.2012
Analyzehowformalleaderscommunicateknowledge,createconsensus,andpositionthemselvesinrelationtoothersintheteam
Sixteentraumateams,sixmembersoneachteam.Highfidelitytraininginanemergencydepartment.Video.
Thisstudyindicatesthatcommunicationintraumateamsiscomplexandconsistsofmorethanjusttransferringmessagesquickly.Italsoconcernswhattheleadersexpress,andevenmoreimportantly,howtheyspeaktoandinvolveotherteammembers
AccordingtoCASPthereisaclearstatementsoffindingsandtheresearchisvaluable
HJORTDAHL,M.etal.2009
Toobtainadeeperunderstandingofwhichnon-technicalskillsareimportanttomembersofthetraumateamduringinitialexaminationandtreatmentoftraumapatients.
Twelvesemi-structuredinterviews.2authorsparticipatedinall12.
Leadershipwasperceivedasanessentialcomponentintraumamanagement.Theidealleadershouldbeanexperiencedsurgeon,haveextensiveknowledgeoftraumacare,communicateclearlyandradiateconfidence.Lackofleadershipwasoftengivenasareasonfordysfunctionalteamwork.
AccordingtoCASPthereisaclearstatementsoffindingsandtheresearchisvaluable
YuleSetal.2006aDeveloping
Describethemethodusedtoidentifysurgeons’non-technicalskills,andthedevelopmentofaskillstaxonomyandbehaviouralratingsystemtostructureobservationandfeedbackinsurgicaltraining
27consultantsurgeons.Interview.Identifykeynon-technicalskillsandinterpersonalskills.Multidisciplinarygroupdevelopedtheinterviewscedule(psycologists,surgeonsandananaesthetist).Interviewsrecorded,transscribedandanalysedbytheepairsofpsycologistsindependently.
TheNOTSSskillstaxonomyandmarkersystempresentedherehasbeengroundedempiricallyinsurgery,andwasdevelopedwithdomainexperts(consultantsurgeons)ateverystagetoensurethatthesystemisexplicit,transparentandhasanacceptabledegreeofconstructvalidity.
AccordingtoCASPthereisaclearstatementsoffindingsandtheresearchisvaluable
Table1:Primarystudies

73
Studytype Leadershipisimportantfortheoutcome
Educationalneeds/recommendations Measure/Aim Teaching?
RCT
YULE,S.etal.2015 "…Non-technicalskillsmatteratcriticalstagesofsurgicalcare"
"Importantnextstepsaretoimplementnon-technicalskillscoachingintherealOR"
Measure,NOTSS Non-technicalskillscoaching +
FERNANDEZCASTELAOetal.2015
"InCPR,effectiveleadershipispositivelyassociatedwithpatientoutcome"
"…leaderstrainedinaseparateexplicitstepappearstobeanefficientwaytofosterteamprocessesandoutcomesasawhole"
Measure(LBDQinspired)
CRMteamleadertrainingandadditionalALS-training.TeamleadersoftheCRM-TLgroupsattendeda90-minCRM-TLtraining
+
KRAGE,R.etal.2014"...stresscaninterferewiththeperformanceoftechnicalskillsincriticalsituations"
"…moreeffortintotrainingthenon-technicalskillsofindividualsandteamswhoareworkinginahighstressenvironment"
Measure,protocolERCguidelines Notteaching -
HUNZIKER,S.etal.2010Briefleadershipinstructions
"…strongleadershipmaypositivelyinfluenceteamperformance"
"However,becauseinexperiencedrescuersareofteninvolvedearlyinsituationsofcardiacarrest,theirtrainingisofoutmostimportance"
Measure,prespecifiedchecklist(LBDQinspired)
Leadershipinstructionwithprespecifiedchecklists-LBDQinspired +
COOPER,2001
"…aleadershipdevelopmentprogrammesignificantlychangesbehaviourandincreasesperformance"
Itisrecommendedthata"formalleadershipdevelopmentprogrammeshouldbeintroducedintoadvancedlifesupportcourses".
Measure(LBDQinspired)
Theexperimentalgroupthenattendeda75-minleadershipdevelopmentseminar
+Case-Control MANTHA,A.etal.2016
"...wedesignedanNTScurriculumforIndianparamedictraineesfocusedonstrengtheningon-sceneleadership,teamwork,andpublicspeakingskills"
"focusedNTSdevelopmentcurriculumintoIndianparamediceducationandfurtherevaluationofthelongtermimpactsofthisadaptiveleadershiptraining".
PersonaltrainingANDmeasuringposture,gesture,eye-contactemotions,confidence-etc.
6-dayseminar.Presentationofanonprofessionaltopictoclassmates.
+
NICKSA,G.A.etal.2015
"Simulation-basededucationhasbeenshowntodirectlyimpactphysicians’clinicalbehaviorandchangeoutcomes"
"Traditionally,surgicaleducationhasnotformallytaughtleadershipskills,effectivecommunication,professionalism,orteammanagement"
Measure,NOTECHS
Teaching:"feedback,facilitateddiscussion,instructedonareasofknowledgeasneeded,providedinsight,andencouragedparticipantself-reflection"
+
ROBERTS,N.K.etal.2014
"...themajorityofparticipantsstronglyagreedthatthetraininghadthepotentialtoimprovepatientsafety"
"…thereisagreatdealoftalkaboutthedesirabilityofmultiprofessionalteamtraining,butthenumberofexamplesofsuchtraininginhospitalsettingsislimited".
Measure(LBDQ-inspired,TeamSTEPPSinspired,Kilpatrick)
Simulation-videoanalysis-simulation-debriefing.3weekslater:simulationandquestionnaire
*
MAKINEN,M.etal.2007
"Definingandteachingleadershipseemstoimproveresuscitationperformance"
"InpreviousanalysesmadethemajorityofphysiciansandnursesfeltthattraininginCPRwasinsufficientatvariouslevelsofcare"
Measure-compareSwedenandFinland
Notteaching -
GILFOYLE,E.etal.2007
"Teamswhofunctionwithaneffectiveteamleader[…]haveamorefavourableoutcomefortheirpatients,bothsimulatedandreal"
"...itisourhopethatlearningleadershipskillsspecifictoresuscitationwillcarryovertootherareasofprofessionalpracticeofpaediatricmedicine"
Measure,checklistandquestionnaire.CRM
Half-dayworkshop:Basedontheneedsassessmentlearningobjectivesweredeveloped.2simulations-debfiefing
*

74
MCCUE,J.D.etal.1986
"…increasedemphasisontheimportanceofdoctors'noncognitiveskillsinmedicalpractice…"
"Althoughphysiciansarerequiredtoactasleadersinavarietyofsituations,leadershipabilityandleadershiptraininghavebeenlargelyignoredbymedicaleducators…"
Nurses'perceptions.Measuring.Tool:LSI
Two-hourdiscussionaboutleadership. *
CaseStudy ROBINSON,P.S.etal.2016
"LeadershipskillsdirectlycorrelatewiththequalityoftechnicalperformanceofCPRandclinicaloutcomes"
"…traininginandassessmentofleadershipskillsinemergencyscenariosshouldbeanintegralcomponentofpostgraduatemedicaltraining"
Measure.Survey,12ratedstatementsand4dichotomousquestions-LikertScale
Notteaching -
HARGESTAM,M.etal.2016
"...understanding…non-verbalcommunicationcouldnotonlyimproveteamworkbutalsoincreasepatientsafety..."
"Communicationcannotbetakenforgranted;itneedstobepracticedregularlyjustastechnicalskillsneedtobetrained".
Measure.Non-verbalfocus.
Teamtraining,CRM +
BRIGGS,A.etal.2015
…theperformanceofteamleadersandteamsishighlycorrelated...teamworkandNTSperformancedocorrelatewithclinicaloutcomesintraumaresuscitation
"IncreasedattentiontoNTSsduringtraumateamtrainingmayleadtosustainedperformancethroughouttraumascenarios"
Measure.NOTSS,T-NOTECHS
Simulations-briefCRMtraining.FocusonMeasuring *
RINGEN,A.H.etal.2011
"Thismightleadtonegativeconsequencesnotonlyfortheteamleaderandmembers,butmayalsoaffectpatientoutcomes"
"Proposednationalstandardsshouldbeurgentlyimplementedtoensureequalaccesstohighqualitytraumacare"
Measure.Questionnaire.NTS
Notteaching -
CARLSON,J.etal.2009
"…cognitiveorsocialskillsthatplayanimportantroleinpromotingsafetyandsuccessfulproblemmanagement"
"Theoveralltoolshouldcontainasfewitemsaspossibletoeffectivelyyetreliablycaptureleadershipstyleandkeyteambehaviors".
Measure.Developmentofatool
Simulation-facilitator-debriefing *
HAYES,C.W.etal.2007
"…thequalityofcardiopulmonaryresuscitationprovidedinteachinghospitalsissuboptimalsuggestthatinadequateresidenttrainingmaycontributetopoorpatientoutcomes".
"Theperceivedlackofadequatetrainingseemedtoberesponsible,atleastinpart,tofeelingsofbeingunprepared,overwhelmed,andofworryingaboutcommittingerrorsduringcardiacarrests"
Measure.Survey.Likert-Scale.
Notteaching -
ITANI,K.M.etal.2004 NA
"…developmentofphysicianleadershiphasoccurredatrandominsurgicaltraining...theyhaveprovidedlittleformaltrainingintheessentialleadershipskills"
Measure.Questionnaire,measuring18leadershipskills
Notteaching -
MARSCH,S.C.etal.2004
"Inthepresentstudy,theabsenceofstructuredleadershipbehaviourwasassociatedwithunfavourableoutcome"
Absenceofleadershipbehaviourwas"associatedwithpoorteamperformance…thisfindingcouldhaveimportantimplicationsfortheteachingofmedicalemergencies"
Measure.StrongLBDQinspired
Simulation-video-debriefing *
WISBORG,T.etal.2003
"…trainingofmultiprofessionalteamswillimprovepatienttreatment...asubstantialproportionofdeathsoccurringaftertraumaareavoidable"
"Leadershiptrainingalsoseemstoimproveleadershipperformanceduringcardiacarrest"
Measure.Survey.Prevalence Notteaching -

75
COOPER,S.etal.1999
…astudywhichdemonstratedthat"leaderswhoinitiatedastructure,distributedtasks,andremained“handsoff”improvedteamperformance"
"…withoutperformancefeedback,leaderswillnothaveamodeltopositivelyinfluencetheirbehaviourandperformancewillbedependentonpersonality"
Measure.StrongLBDQinspired Notteaching -
QualitativeStudies SADIDEEN,H.etal.2016
"Effectiveleadershipisessentialforsuccessfulfunctioningofworkteamsandaccomplishmentoftaskgoals"
"Understandingleadershipbehaviors[…]canidentifyimportantbehaviorsrequiredtooptimizenontechnicalskillsinamajorresuscitation"
Measure Simulation-video-debriefing. *
LEENSTRA,N.F.etal.2016
"poorleadershiphasbeenidentifiedasapotentialthreattopatientsafety"
"Goodleadershipisessentialforoptimaltraumateamperformance,andtargetedtrainingofleadershipskillsisnecessarytoachievesuchleadershipproficiency"
Measure.Needforataxonomy.TTLS.67behaviouralMarkers
Notteaching -
KOLEHMAINEN,C.etal.2014
Effectiveleadershipiscritical....Poorleadershipwasconsistentlycitedasthemajorcontributingfactortoachaoticcode:“ifyou’requietandwishy-washy,itjustgoeshorrifically"
"practicalguidanceneededforthedeliberatepracticeofleadershipskills…targetedtrainingofleadershipskillsisnecessarytoachievesuchleadershipproficiency"
Measure.Survey.Gender.
Notteaching -
JACOBSSON,M.etal.2012
"itisachallengefortheformalleadertocoordinateteammembers’tasksinordertooptimizeteamworktoobtainasuccessfuloutcome"
NA MeasuringLeadershipStyles Notteaching -
HJORTDAHL,M.etal.2009
"Betterteamfunctioncouldimprovepatientoutcome.[…]Lackofleadershipwasoftengivenasareasonfordysfunctionalteamwork"
"Theneedforbettertrainingoftraumateamsandespeciallyteamleadersrequiresfurtherinvestigationandaction"
Measure.Survey.Gender. Notteaching -
YuleSetal.2006a(Development)
"Futureresearchwillestablishthecriterionvalidityofnon-technicalskillsratingsonperformanceintheoperatingtheatreandonpatientsafetyoutcomes"
"Todate,theformaltrainingofsurgeonshasfocusedondevelopingtechnicalskills...leadershiphavebeendevelopedinaninformalandtacitmanner"
Measure.Developmentofataxonomy
Notteaching -
Table2.Symbols:+=actualteaching.*=debriefing,discussion.-=noteaching/training

76
AdaptedLBDQ(FormXII):LBDQ(initiatingstructure)
1 Lettheteamknowwhatwasexpectedofthem2 Useofuniformguidelines3 Positiveattitude4 Whatshouldbedone5 Howthingsshouldbedone6 Allocatetasks7 Makesurethathispartintheteamwasunderstood8 Plantheworktobedone9 Maintaindefinitestandards10 Remain‘handsoff’
Fig.2.Abridgedbytheauthor(TL)(Cooper,2001)
NOTSSskillstaxonomy(V1.1)2006
Category Element
Situationawareness GatheringinformationUnderstandinginformationProjectingandanticipatingfuturestate
Decisionmaking ConsideringoptionsSelectingandcommunicatingoptionImplementingandreviewingdecisions
Taskmanagement PlanningandpreparationFlexibility⁄respondingtochange
Leadership SettingandmaintainingstandardsSupportingothersCopingwithpressure
Communicationandteamwork
ExchanginginformationEstablishingasharedunderstandingCoordinatingteamactivities
Fig.3.AspresentedbySYule38

77
Taxonomiesdiscoveredinthisreview:leadership,teamwork,andcommunication
Type1945:LDBQ LeadershipBehaviourDescriptionQuestionnaire-military
1978:CRM Crewresourcemanagement-aviation.Lateradaptedtohealthcare
1980:LSI LeadershipStyleIndicator(48adjectives)1998:CRM CRMcurriculumvalidatedbyGaba
1999:LDBQ(FormXII) Adaptedfrom1790originalstatementstotendimensionsofbehaviour2000:Jartel(JARTEL) JointAviationRequirements:TranslationandElaborationofLegislation
2002:NOTECHS(NTS) Non-TechnicalSkillsforAirlinePilots
2003:ANTS Anaesthetists’Non-TechnicalSkills2005:ACGME AccreditationCouncilforGraduateMedicalEducationhasestablished6
competenciesforresidentandfellowdevelopment
2006:NOTSS Non-TechnicalSkillsforSurgeons
2007:MayoHighPerformanceTeamworkScale
Ratesteamperformanceontheconsistencyof16differentcriteria
2007:GILFOYLE Checklist(adaptedfromGaba1998)
2009:JimCarlson Areliableteambehaviourmeasurementtool
2009:OxfordNOTECHS Measuringteamworkbehaviourintheoperatingtheatre2010:SMARTT Algorithm:SituationManagementActivityRapidityTroubleshootTalktome
2011:OttawaGlobalRatingScale
OttawaCrisisResourceManagementGlobalRatingScale.Evaluatestheperformanceoftheteamleader
2012:T-NOTECHS TheModifiedNon-TechnicalSkillsScaleforTraumasystem
2013:SLI Surgeons’LeadershipInventory,Taxonomy2015:OxfordNOTECHS AmodifiedOxfordNOTECHSScale(Nicksa)
2016:TTLS TaxonomyofTraumaLeadershipSkills.5skillcategories,and37skillelements.Theskillelementsarecoveredby67behaviouralmarkers
Table3

78

79
TRAININGRESIDENTSTOLEADEMERGENCYTEAMS[PARTTWO]
Barriers,ChallengesandLearningGoals:aQualitativeReview
TureLarsen,RandiBeier-Holgersen,DorisØstergaard,PeterDieckmann
TureLarsen,PhDStudent,SimulationUnit(SimNord),DepartmentofAdministration,NordsjællandsHospital,Denmark
RandiBeier-Holgersen,MD,MHPE,DepartmentofGastrointestinalSurgery,NordsjællandsHospital,Denmark
DorisØstergaard,MD,DMSc,Professor,DiplomaHPE,CopenhagenAcademyforMedicalEducationandSimulation(CAMES),CapitalRegionofDenmarkandUniversityofCopenhagen,Copenhagen,Denmark
PeterDieckmann,PhD,Dipl.-Psych.CopenhagenAcademyforMedicalEducationandSimulation(CAMES),CapitalRegionofDenmarkandUniversityofCopenhagen,Copenhagen,Denmark
Correspondingauthor:TureLarsen,SimNord,Kvalitetsafdelingen,NordsjællandsHospital,Dyrehavevej29,3400Hillerød,Denmark.Phone:+4531127281,Mail:[email protected]
RandiBeier-Holgersen,DorisØstergaard,andPeterDieckmann:reprintswillnotbeavailablefromtheauthors
Funding:TrygFoundation,LaerdalFoundationandNordsjællandsHospital,Denmark.
Disclosure:T.L.receivedgrantsfromTrygFoundation,LaerdalFoundationandNordsjællands
Hospital,Denmark.R.B.H,D.Ø.andP.D.havenoconflictsofinteresttodeclare.Thesponsorsofthe
studyhadnoroleinthestudydesign,datacollection,dataanalysis,datainterpretation,orinthe
writingofthereport.

80
Abstract:
Objective:Aninvestigationtodetermineanyconsensusinopinionsandviewsaboutchallengesor
barriersintrainingleadershipinemergencies.
SummaryofBackgroundData:Leadershipinemergenciesisreportedasbeingveryimportantfor
thepatientoutcome.Asystematicreviewfailedin2016tofindanyfocusedtrainingofthis
function.Theresearchhasfocusedondevelopingtaxonomiesandtoolstomeasuringleadership.
Anexplicitneedforworkableleadershiptrainingofteamleadersinemergencieswasidentified.
Method:Articlesfoundinthesystematicreview,otherreviewsandopinionswereincludedto
incorporateexperiences,perceptionsandemotionsconnectedwithleadershiptrainingin
emergencysituations.Onthebasisofanarticlewrittenin1986,statementsaboutchallenges
regardingleadershiptrainingwereidentifiedandallarticlesweresearchedforthese.Themethod
wasdirectedsummarizedqualitativecontentanalysis.
Findings:Intotal40articlescoveringtheyears1986-2016wereanalysed.Mainfindings:23articles
describedthesituationasstressful,18describedtheimportanceofself-confidenceand16
describedthesituationascomplexorcomplicated,12describedthesituationwasperceivedwith
concern,anxietyorpanic.
Conclusions:Theliteraturerecommendsfindingasolutiontoteachresidentstogainconfidencein
stressfulsurroundings.Theliteraturerecommendsfindingawaytoworkwithbodylanguage,non-
verbalcommunication,attitudeandappearanceinordertoradiatecredibilityinasettingseparated
frommedicalknowledge.
Background
Teamleadershipinemergenciesisreportedasbeingimportantforthequalityofthetechnical
performanceofteams,13-24forpatientoutcome,patientsafetyandpatientcare.22,23,25-35The
qualityofteamleadershipmayeveninfluencepatientmortalityandsurvivalrates.19,23,27,32
However,manystudiesrecognisethatleadershiptraininghasbeenneglected,1,16,17,23,27,29,36-39and
arecurrentcallforaworkableleadershiptrainingprogrammehasbeenexpressedexplicitly.
1,14,16,17,21-23,26,27,29,34,36-43Thisneedhasprevailedthroughoutthe31-yearperiodaddressedinour
investigation.

81
Asystematicreviewoftheliteratureonleadershiptrainingforresidentsrevealednofocused
trainingofthisfunctionin27eitherqualitativeorquantitativeinterventionstudies(describedin
PartOneofthisarticle:Larsen,Tetal:Trainingresidentstoleademergencyteams:ASystematic
Review(underreview)).
Manyinitiativeshavesoughttoaddresstheproblems:inparticularitcanbeemphasizedthat
leadershipispartoftheScottishinitiativeAnaesthetists’NontechnicalSkills(ANTS)49,adaptedto
‘Non-TechnicalSkillsforSurgeons’(NOTSS)38andto‘ScrubPractitioners’ListofIntra-operative
Non-TechnicalSkills’(SPLINTS).50ThelatterreplacedNOTECHSfornurses51–whichwasalso
modifiedto:OxfordNOTECHS52andamongotherthings:T-NOTECHS53,aswellastheSwiss
leadershiptrainingprogrammebasedontheLeadershipBehaviourDescriptionQuestionnaire
(LBDQ)1.Theseprogrammesfocusondeveloping‘formativeassessmenttools’,54behavioural
markers55andtaxonomiesinordertomeasure15,22,33,38leadershipskills.Thecontent,qualityand
complexity22,36,43,59ofthesetoolshavebeendiscussedextensively;existingtoolshavebeen
adapted/modifiedornewtoolshavebeendeveloped22,26,33,36,38,39,43andthoseinvolvedhavespent
yearsdiscussing,inpapers,the‘significantvariabilityinterminology,trainingmodalitiesand
evaluation’41inthisfield.15,43
However,‘something’isapparentlystillmissing,andthereasonwhy‘residentsfeelunpreparedand
unsupervisedasleaders’27shouldbeexplored.Oneexplanationcouldbethatthereisalackof
clarityabouttheperceptionanddefinitionofgoodleadership,asdescribedbyStogdill(1974),who
wrote:“[Thereare]almostasmanydefinitionsofleadershipastherearepersonswhohave
attemptedtodefinetheconcept”.99Anotherexplanationcouldbethattheexistingprogrammes
havefailedtolocatetheactualchallengesintheefforttodevelopassessmenttools.
Theaimofthisarticleisdeterminewhethertheliteraturerevealsanyopinions,attitudes,
experiencesorviewstoidentifyanyactual,butperhapsoverlookedchallengesorbarrierswhich
leadershiptrainingforresidentsinemergenciesneedstoaddress.Similarly,thestudywill
investigatewhetheritispossibletoidentifyconsensusonwhatcharacterizesagoodclinicalteam
leader,thusidentifyingspecificlearninggoals.Finally,thearticlewillexaminetheliteratureto
determinewhetherthereisconsensusaboutthosechallenges,barriers,andgoals.Inaddition,this
resultwouldrevealwhethertherehavebeenanydevelopmentsoverthelast31yearsinrelationto
thesefindingsregardingleadershiptraining.Dowefindthesameneedstodaythathaveidentified
overthepastthreedecadesorhasasolutionbeenfound?

82
Method
Duringthesystematicsearchincludingtheearliermentionedsystematicreview,40articleswere
foundrelevant,coveringtheperiod1986-2016.Adetailedreviewofsearchstrategyandquality
assessmentisdescribedindetailinthearticle:Larsen,Tetal:Trainingresidentstoleademergency
teams:ASystematicReview(underreview).Thereviewsandopinionpieceswereincludedinour
review,astheycontainedconceptsthatwererelevantforsystematizingthecurrentdiscussion.
TheCommitteesonHealthResearchEthicsfortheCapitalRegionofDenmarkwasaskedtogive
ethicalapprovalbutaformalreviewwaswaivedforthisstudy(H-4-2015-FSP).
Byusingadirected,summativeapproachon‘quantitativemanifestcontentanalysis’63inorderto
exploreusageofthevisibleandsurfacecontentofthetextitispossibletoidentifyconsensuson
selectedwordsfromaquantitativeapproach.Byusing‘qualitativelatentcontentanalysis’8itis
possibletointerprettheunderlyingmeaningofthewordsandthus,rather,interpretaqualitative
approach.Directed(deductive)qualitativecontentanalysisstartswithpreconceivedcodesor
categoriesderivedfrompriorrelevanttheory,research,orliterature.63Introducingadifferent
perspectiveonthearticlesfoundintheabove-mentionedsystematicreview,theinclusioncriteria
wereexpandedtocoverexperience,perceptionsandemotionsrelatingtoleadershiptrainingin
emergencysituations,andthereforeprimaryaswellassecondaryarticlesbecamerelevant.
Thepreconceivedcategoriesinthesearchwasguidedbythecontentofanarticlepublishedin
1986,31yearsagoandwrittenbyKennethIserson.44Thearticlewasidentifiedasveryrelevantin
thatitfocusedontheactualexperienceofphysicianswhenperformingasteamleaderinan
emergency.Modernsafetyconceptsemphasizetheneedtotaketheactualworkingconditionsinto
accountandnot(only)howworkshouldbeperformed.Isersonstatesinthisarticle:“Incritical
clinicalsituationsleadershipisoftenlacking”.Thisisbecause“physiciansarenevertaughtclinical
leadership”.Isersonemphasizestheneedwhenhestates:“Especiallyinemergencycare,
developmentofclinicalleadershipisvitalandmustbeintegratedintooureducationsystematall
levels.”Finallytheauthorconcludes:“Thisisaseriousdeficiencyinmedicaltraining.”Thearticle
providedkeyconceptsthatarestilltobefoundincontemporarypapers,22,23,31,39,41,46formulated
theissuesveryclearlyandthusservedtoguideourfurthersearch.
KeywordswereselectedinIserson’sarticle.Hestronglyemphasizesthatphysiciansare1)
unsupervisedandunpreparedtorisetotheoccasionasteamleadersinemergencies.Hedescribes
2)thesituationitself,whichmaybe“stressful”,“chaotic”and“confusing”,andthereforeteam

83
leadersoftenexperiencethesituationwith3)negativefeelings,suchasbeing“uncomfortable”,as
an“overwhelmingburden”,andperceiveitwith“fear”and“anxiety”.Inorderto“restoreorder”in
achaoticsituationitisnecessarythattheleadercreates4)calmnessfortheteamandtherefore5)
self-confidenceisprerequisiteforgoodleadership.AccordingtoIerson,agoodleaderis6)
perceivedthroughhis“forceofpersonality”and“dominance”,andtheleaderdemonstrates7)
capacityasleader/appearsasauthoritativeifheisabletoshow“responsibility”,“knowledge”,
“powerandauthority”.Heemphasizesthenecessityof8)assumingleadership,whichinvolvesthe
mentaldecisiontoassume“themantleofthegroup’spossiblefailure”.Hefinallystatesthatitis
possibleto9)“learntolead”.Thoseninekeyissuesconstitutethethemestobeexaminedinthis
article.
All40articleswerecollectedinasinglePDFdocumentandsearchedforwordstoinvestigatein
ordertoestablishwhethertheabovekeyissuesidentifiedbyIsersonarestillrelevanttodayinthe
abovethemes.Acomprehensiveexaminationofthedocumentwasconductedsearchingforkey
words,theirsynonymsand,ifavailable,meaningfulpositiveandnegativeanalogies,associations,
metaphors,andsentencesusingthesearchfunctioninAdobeAcrobatReaderDC,version
2017.012.20093.Wordsweresearchedinthedocument,andsentencesbasedonthesewords
werescreenedinrelationtotheirrelevanceforthecontentofthisstudy.Sentenceswereincluded
iftheycontainedanythingaboutteamleadership,teamwork,orpersonalchallengesandfeelings
relatedtothis.ThewordswereselectedbyTL,andrelevancetoinclusionandexclusionwas
discusseduntilTLandRBHreachedagreementonthedecision.
Thekeywordsweregroupedintheabove-mentionedninethemes,andthethemesandquotes
containingthewordsweresortedchronologicallyandpresentedinAppendixI.
Themostimportant/significantquoteschosenonthebasisofthearticlesexaminedarepresented
inthisarticle.Whenconsideredtohaveapossibleinfluenceoninterpretation,quotesweresorted
accordingtowheretheyappearedinthearticles:beforeorafterthemethodologysection,i.e.,
whethertheyformedapre-conditioninthebackgroundforthearticleorafindingorconclusion.
Weassumedthataconclusioncanbestrongerthanapre-condition;apre-conditionforan
interventionorareviewmaybechangedwhentheinvestigationiscompletedandaconclusionmay
contradictthepre-condition.
Referencesmentionedinthebackgroundsectionplusallquotesmentionedintheresultsectionare
availableinappendixI.

84
Results
Thekeywordsweregroupedintoninekeythemes(Table1).Thestudyrevealedsentencesthat
arguedorexpressedattitudesdescribingwhatsubjectswererelevantchallengesinteamleadership
training.Therewasanemphasisonshowingdiversityinthestatementspresented.Originalquotes
arepresentedaswellasotherarticles’referencestothem.
Residentsfeelunsupervisedandunprepared:Tenarticles16,17,23,26,27,31,37,39,44,46concludedthat
residentsfeltunpreparedasleadersofcardiacarrestteams.
“Nevertheless,ourdatasupportpublishedfindingsthattraineeswouldlikefurtherleadershiptraining.”
Robinsonetal.,201623
Acomplex,stressful,unpredictableandchaoticexperience:Therewasbroadconsensusthat
leadershipinemergenciesisperceivedasacomplexissue,bothintermsofstressfulsituations
demandingmanydecisionsforthebenefitofthepatient,aswellasofmanagingrelationswithin
theteamitself.
Ninearticles16,24,25,29,30,33,44,56,58mentionedcomplexityintheirintroduction/backgroundsections.
”Leadershipisacomplexconcept,andthetoolsusedtoassessthequalityofleadershiparepoorlydescribed,
inadequatelyvalidated,andinfrequentlyused.”
Fordetal.,201624
Inthediscussion/conclusionsections,sevenarticles19-22,35,39,41stressedcomplexity.
“Sincemanysituationscannotberesolvedbytechnicalmasteryalone,adaptiveleadershipinvolvesanalyzing
complexsituations,identifyingavailableresourcesandrequiredexpertise,formulatingastrategyinreal-time,
andcoordinatingmultiplestakeholders.”
Manthaetal.,2016.41
Sixarticles16,25,28,34,38,56usedthephrase“Copingwithpressure”asapre-definedterminthe
originalNOTSS-taxonomy(Non-TechnicalSkillsforSurgeons)asdevelopedbyYuleetal.in200625,38
andpresentedbyFlinetal.in2007.28Threeotherarticles21,24,40usedasimilarphrase:“Coping
withstress”.
Eightarticles16,23,27,29,30,33,47,59emphasizedthestressfulworkingconditionsintheir
introduction/backgroundsections.
“Cardiopulmonaryresuscitation(CPR)isperceivedasastressfultaskbymedicalteams.”

85
Krageetal.,201459
Tenarticles20,22,25,27,31,32,34,41,44,45highlightedtheseconditionsinthediscussion/conclusionsection.
“Cardiopulmonaryresuscitationcanproduceconsiderablestress,andtheexperienceofstressandoverload
mayimpairPerformance.”
Hunzikeretal.,201331
Performanceinanemergencywasdescribedas“unpredictable”23,30or“unanticipated”.25
Jacobssonetal.,2012:“Thetaskscarriedoutbyemergencyinterdisciplinaryteamsarecomplex,
unpredictable,andurgent.”30
“Inhospitalcardiacarrestsarechallenging,stressfulandunpredictable.Theycancomewithoutwarning,often
inunfamiliarclinicalenvironments,withlimitedordifficultaccesstoequipment.Furthermore,theirsuccess
dependsonthecoordinatedperformanceofanoftenad-hoccardiacarrest(‘crash’)team.”
Robinsonetal.,201623
Sevenarticles1,32,34,41,44,46,60usedtheword‘chaos’whendescribingthesituation.Chaoswhenno
leaderrisestotheoccasion.44Chaoswhenleadershipisnotclear46intheenvironmentforIndian
ParamedicswasdescribedbyManthaetal.,2016:
“…facecomplexandchaoticclinicalenvironmentsthatdemandeffectiveleadership,communication,and
teamwork.”41
Anunpleasant,disturbing,frighteningandpanickedperception:Theemergencysituationwas
characterizedbyvariousformsofdiscomfort.
“Theleaderneedstodisplayapositiveattitude,motivateandencouragetheteam,inasituationthatisoften
unpleasantanddisturbing.”
Cooperetal.,19991
Notsurprisinglythisledtoconcernedtrainees.1,16,23,27,32,37,39
“Theperceivedlackofadequatetrainingseemedtoberesponsible,atleastinpart,tofeelingsofbeing
unprepared,overwhelmed,andofworryingaboutcommittingerrorsduringcardiacarrestsinasignificant
numberofresidents.”
Hayeset.al,2007.27
Eightarticles1,14,16,23,27,32,36,44mentionedanxiety.
“Severaloftheinexperiencedteamleadersmentionedthattheyfeltanxiouswhentheywerethesolesurgeon
intheemergencyroom”

86
Hjortdahletal.,2009.16
Asinglearticlementionedpanic.
“Theyalsodescribedoftenbeing“panicked”buttryingtoappearasthe“calmestpersonintheroom”.“One
likenedhisbehaviortoaduck,saying:“Ifyou’veeverwatchedaduckonapond,itlooksasthoughit’sfloating
effortlesslyacrossthelake.Butifyou’veeverlookedunderneathataduck’sfeet,they’repaddlingfeverishly.”
Kolehmainenetal.,201432
Loweredstress:Fourarticles16,30,32,44claimedthatagoodleaderwasabletocreate“lowered
stress”44andto“calmotherpeopledown”32
Twoarticles32,58mentionednoiseandcrowdcontrol.
“…theteamleaderhasanimportantroleinnoiseandcrowdcontrol.”
Merceretal.,201458
Confidence:Threearticles1,29,39usedthewordconfidenceintheirbackgroundsection:theteam
should“demonstrateconfidenceintheirleader”,1theleadershould“radiateconfidence”,29and
theleadershouldhave“confidenceinperformingemergencyprocedures.”39
13articles1,16,23,27,32,36,37,39,41,42,44,46,47concludedthatthedegreeofself-confidenceiscrucialforthe
qualityoftheleadership.Thiswillproduce“moreeffectiveleaders”,36“savethesituation”,44
make“trainingforleadershipmucheasier”,1and“improvepatientcareandcardiacarrest
outcomes”23.
“…residentsoftentakeyearstogaintheconfidenceandexpertisetomasterthenon-technicalandtechnical
skillsneededtoaddresshigh-riskclinicalemergencies.”
Nicksaetal.,201539
Howaleaderisperceived:Eightarticles13,16,29-31,44,47discussedtheteam’sperceptionoftheleader.
Toestablishacomfortableandsafeenvironmentfortheteam,teammembersmustbeableto
perceivetheirleaderastrustworthy.16,47Stolleretal.,2013:“Theteammembershadtobeableto
trusttheirleader.”47Hjortdahletal.,2009:“Onenursesaidthatiftheleaderseemsconfidentshe
feelsconfidenttoo.”16Jacobssonetal.emphasizesthatitwasimportancethattheleader“hada
strongethosandexpressedcompetence.”30

87
Ashortcuttoperceptionofauthority:Threearticles32,35,46statethattheleadershouldtakecareof
his/herappearance“especiallyforfirstmeetings”andinthiscontextthat:“Theclinicianwillwork
onwaystodevelophis/herowncharisma.”46Itisimportanttoadopt“apowerfulposture”32and
“Teammemberswhoareawareofhowtheyusetheirbodiestocommunicatewillbeableto
facilitateandimprovetheirperformance.”35
“…participantswhoassumedapowerfulversusanon-powerfulposturefeltmoreconfidentandweremore
likelytotakeaction.”
Kolehmainenetal.,2014.32
Anotherissueemphasizedasimportantbyeightarticles16,26,29,30,32,35,41,44ishowtheleaderuses
his/hervoice.
“Anyonewhotellsyouthatbeingawhitemalewithadeepvoiceandwho’salittlebittallerisnotan
advantagetobeingperceivedpositively,orperceivedasincontrol,wouldbelying,inreallyanysituationnot
justacode.”
Kolehmainenetal.,2014.32
AssumingLeadership:Tobecomeagoodleaderitisimportanttoassumetheleadershipwithallits
implicationsincludingrisksandfailure.Fivearticles1,18,24,26,32statethisviewinthe
introduction/backgroundsections.
Sixarticles16,20,32,36,44,46elaboratethisviewintheirdiscussion/conclusionsections.
“…recentAdvancedTraumaLifeSupport(ATLS)guidelineshavecodifiedleadership’simportanceby
emphasizingthatforateamto“performeffectivelyoneteammembershouldassumetheroleoftheteam
leader.”
Fordetal.,2016.24
Whenassumingleadershiponecanbenefitfrom‘introspection’46,‘psychologicalself-care’,60or
‘self-management.’47
”…theabilitytounderstandandmanageoneselfandtounderstandothersandmanagerelationships–has
beenshowntodifferentiatebetweengreatandaverageleaders.”
Stolleretal.,2013.47
Borntolead–orlearntolead:Sevenarticles1,16,23,26,32,42,44mentionthatsomeareborntolead
whileothershavetolearn.
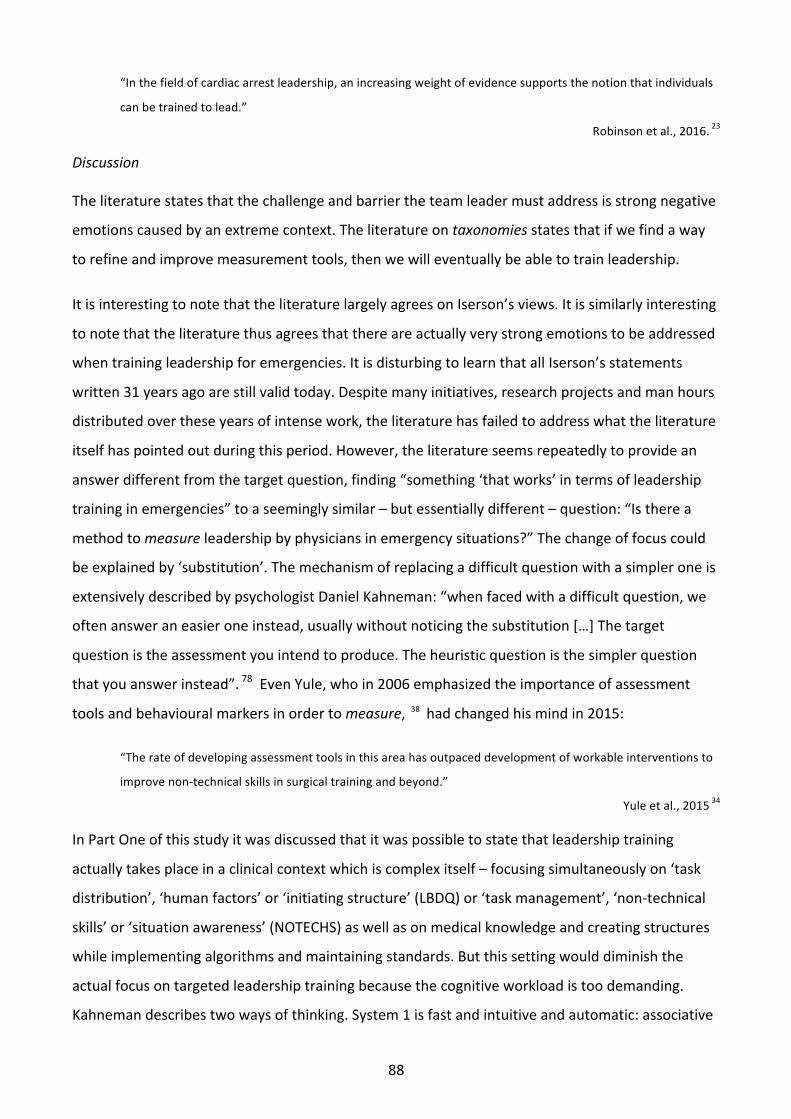
88
“Inthefieldofcardiacarrestleadership,anincreasingweightofevidencesupportsthenotionthatindividuals
canbetrainedtolead.”
Robinsonetal.,2016.23
Discussion
Theliteraturestatesthatthechallengeandbarriertheteamleadermustaddressisstrongnegative
emotionscausedbyanextremecontext.Theliteratureontaxonomiesstatesthatifwefindaway
torefineandimprovemeasurementtools,thenwewilleventuallybeabletotrainleadership.
ItisinterestingtonotethattheliteraturelargelyagreesonIserson’sviews.Itissimilarlyinteresting
tonotethattheliteraturethusagreesthatthereareactuallyverystrongemotionstobeaddressed
whentrainingleadershipforemergencies.ItisdisturbingtolearnthatallIserson’sstatements
written31yearsagoarestillvalidtoday.Despitemanyinitiatives,researchprojectsandmanhours
distributedovertheseyearsofintensework,theliteraturehasfailedtoaddresswhattheliterature
itselfhaspointedoutduringthisperiod.However,theliteratureseemsrepeatedlytoprovidean
answerdifferentfromthetargetquestion,finding“something‘thatworks’intermsofleadership
traininginemergencies”toaseeminglysimilar–butessentiallydifferent–question:“Istherea
methodtomeasureleadershipbyphysiciansinemergencysituations?”Thechangeoffocuscould
beexplainedby‘substitution’.Themechanismofreplacingadifficultquestionwithasimpleroneis
extensivelydescribedbypsychologistDanielKahneman:“whenfacedwithadifficultquestion,we
oftenansweraneasieroneinstead,usuallywithoutnoticingthesubstitution[…]Thetarget
questionistheassessmentyouintendtoproduce.Theheuristicquestionisthesimplerquestion
thatyouanswerinstead”.78EvenYule,whoin2006emphasizedtheimportanceofassessment
toolsandbehaviouralmarkersinordertomeasure,38hadchangedhismindin2015:
“Therateofdevelopingassessmenttoolsinthisareahasoutpaceddevelopmentofworkableinterventionsto
improvenon-technicalskillsinsurgicaltrainingandbeyond.”
Yuleetal.,201534
InPartOneofthisstudyitwasdiscussedthatitwaspossibletostatethatleadershiptraining
actuallytakesplaceinaclinicalcontextwhichiscomplexitself–focusingsimultaneouslyon‘task
distribution’,‘humanfactors’or‘initiatingstructure’(LBDQ)or‘taskmanagement’,‘non-technical
skills’or‘situationawareness’(NOTECHS)aswellasonmedicalknowledgeandcreatingstructures
whileimplementingalgorithmsandmaintainingstandards.Butthissettingwoulddiminishthe
actualfocusontargetedleadershiptrainingbecausethecognitiveworkloadistoodemanding.
Kahnemandescribestwowaysofthinking.System1isfastandintuitiveandautomatic:associative

89
memorycontinuallyconstructsacoherentinterpretationofwhatisgoingon.System2isslower,
deliberateandlogical:consistingofcontrolledoperationsrepresentinganeffortfulmentalactivity.
78Accordingtothis:whentrainingsituationawarenessandleadershipincombinationwithmedical
knowledgeandalgorithmswechallengetheresidenttoworkbothinsystem1and2
simultaneously.Thisisaverydifficulttrainingsetting.
Themostimportantsubjecttotheauthorsofthispaperisthefoundationfortheleadershiprole:
theprimarydeliberatedecisiontoassumeleadershipasdescribedintenoffortyarticles.To
‘assumeleadership’isamental,deliberatedecision,andimportantchoicetobemadebeforehand.
Thisshouldbepartoftheeducation.Thebasicfoundationforbeingabletotaketheleadership.
Intheliteraturewefoundaconsensusontheactualchallengethatneedstobetakeninto
consideration.Overthepast31yearstheliteraturehasstatedthatthesenegativeemotions,
feelingsandperceptionsarehighlyinvolvedwhenateamleaderneedstorisetotheoccasionin
frontofanemergencyteam,buttheliteraturehasnotasyetdescribedamethodtoaccommodate
this.Thishasbeenthecasewhetherthereasonhasbeenlackofknowledge,lackofleadership
definition,lackoffocusorlackofabilitytohandlethesimplebutdifficultquestion:tofind
“something‘thatworks’intermsofleadershiptraininginemergencies”inordertoprepare
residentsforthis.
Asstatedbysixarticlesagoodleadershouldcreatecalmnessintheextremesituation.13articles
concludedthattheteamleader’sdegreeofself-confidenceiscrucialforthequalityofthe
leadership.Twospecificlearninggoalstobeaddressedintheteachingofteamleadershiptraining
wereexpressed.
Anotherfindingis,thatitisimportantthattheleaderhascharisma,istrustworthyandexpress
competence.Elevenarticlesrecognisethatnon-verbalcommunicationisimportant;threearticles
mentionbodypostureandeightarticlesstresstheimportanceofhowtospeakanduseofthe
voice.Obviously,itshouldbeinvestigatedhowtooptimisetheleaderscharismaaswellasradiating
credibilityandcompetenceincludingnon-verbalcommunication.
“Inacceptingtheleadershiprole,theindividualassumesthemantleofthegroup’spossiblefailure.Any
individual’sfalteringcanbelaidattheleader’sfeet.Thisisthelawoftotalresponsibility.”
Iserson,198644

90
Limitations
Whenconsideredtohaveapossiblerelevancetotheaimofthisarticle,quotesweresorted
accordingtowheretheyappearedinthearticles:beforeorafterthemethodologysection,i.e.
whethertheyexpressedapre-conditioninthebackgroundforthearticleorafinding/conclusion
asaresultofaninvestigation.Itisassumedthataconclusionmaybestrongerthanapre-condition;
apre-conditionforaninterventionorareviewmaychangewhentheinvestigationhasbeen
completedandaconclusionmaycontradictthepre-condition.Itturnedoutthatwhetherthewords
werementionedasapre-conditionoraconclusionhadnoeffectontheoutcome.Areasonforthis
couldbethatthewordshadbeninheritedandrecycledthroughouttheliterature.Ontheother
hand,itmaybearguedthatitisnotcrucialwhetherthewordsappearasaconclusionontheaimof
aninterventioninaresearchproject.Whatisimportanttoourstudyisthefactthatthearticles
consideritnecessarytoemphasizethewordsintheirarticlesatanystagewhatsoever.
Conclusions
Assumingleadershipisanindividualandpersonalmatterandanimportantanddeliberatechoice.
Theliteraturerecommendsthatamethodshouldbefoundwhichteachesresidentshowtoachieve
calmnessandconfidenceinastressfulandthreateningcontext.Tothisenditisrecommendedto
findawaytoworkwithbodylanguage,non-verbalcommunication,attitudeandappearancein
ordertoaddressemotionsandradiateauthorityandcredibilityinasettingseparatedfrommedical
knowledge.
Contributors
T.Larsenhadfullaccesstoallthedatainthestudyandhadfinalresponsibilityforthedecisionto
submitforpublication.TLundertookthesearchformaterial,extractedandcollecteddata,
developedtheanalysisstrategy,andwroteuptheresults.TL&RBeier-Holgersenconceivedand
designedtheproject,reviewedthescientificreportsandperformedqualityassessmentsand
interpretationoftheresults.P.DieckmannandD.Østergaardprovidedadviceandcriticallyrevised
themanuscript.

91
Themesdescribingwhatproblemstheliteraturerefertoasissuesateamleadercanexperienceinfrontofanemergencyteam
Whenanarticlemakesastatementbothinthebackgroundandconclusionsectionsonlyoneref.islisted.
No.ofstatements
Physiciansfeelunsupervisedandunprepared
Residentsfeelunprepared/lackofcompetence/needfurthertraining16,17,23,26,27,31,37,39,46
10
Theexperienceoftheemergencysituation
Acomplex/complicatedsituation16,19-22,24,25,29,30,33,35,39,41,44,56,58 16
Astressfulsituation/pressure16,20,22,23,25,27,29-34,41,45,47,59Inadditionstress/pressureisimplicitlypartofNOTECHS21,24,28,40,56
185
Anunpredictable/unanticipatedsituation23,25,30 3
Achaoticsituation1,32,34,41,44,46,60 7
Anoverwhelmingexperience
Anunpleasant/disturbingsituation1,32 2
Perceivedwithanxiety/asathreat/‘alosingbattle’/fail1,14,16,23,27,32,36,44 8
Perceivedwithpanic32 1
Perceivedwithconcern/doubt/isoverwhelming/isworrying/isstressed1,14,27 3
Theleaderisablecreatecalmness
Goodleadershipcreatescalmnessandloweredstress16,30,32,44,58 5
Self-confidenceisimportant
Self-confidenceisanimportantelementinleadership1,16,23,27,29,32,36,37,39,41,42,44,46,47 18
Theteam’sperceptionoftheleader
Individualleadershipbehaviourwillhaveanimpactontheteam’sperception(radiateconfidence,overallorganization,clearlydefined,trustworthy,mostimportanthumanfactor,communicatesclearly,strongethosetc.)13,16,29-31,44,47
8
Theleader’sappearance:short-cuttoauthority
Bodyposture,appearance,non-verbalcommunication32,35,46 3
Voice(calm,clear,distinct,deep,fluentetc.)16,26,29,30,32,35,41,44 8
Assumingleadership–adeliberatedecision
Assumingleadership/risks/responsibility1,16,18,20,24,26,32,36,44,46 11
Managingoneself/introspection/psychologicalself-care46,47,60 3
Mentallyprepare/rehearse/mentalstrain/mentalmodels25,32,56,58 4
Itispossibletolearntolead
Leadershipcomesnaturallytosome/isaproblemforothers1,16,23,26,32,42,44 7
Table1

92

93
CONDUCTINGTHEEMERGENCYTEAM:ANOVELWAYTOTRAINTHETEAM-LEADERFOR
EMERGENCIES
TureLarsen,RandiBeier-Holgersen,PeterDieckmann,DorisØstergaard
TureLarsen,PhDStudent,SimulationUnit(SimNord),DepartmentofAdministration,Nordsjællands
Hospital,Denmark
RandiBeier-Holgersen,MD,MHPE,DepartmentofGastrointestinalSurgery,Nordsjællands
Hospital,Denmark
DorisØstergaard,MD,DMSc,Professor,DiplomaHPE,CopenhagenAcademyforMedicalEducation
andSimulation(CAMES),CapitalRegionofDenmarkandUniversityofCopenhagen,Copenhagen,
Denmark
PeterDieckmann,PhD,Dipl.-Psych.CopenhagenAcademyforMedicalEducationandSimulation
(CAMES),CapitalRegionofDenmarkandUniversityofCopenhagen,Copenhagen,Denmark
Correspondingauthor:TureLarsen,SimNord,Kvalitetsafdelingen,NordsjællandsHospital,
Dyrehavevej29,3400Hillerød,Denmark.Phone:+4531127281,Mail:[email protected]
RandiBeier-Holgersen,DorisØstergaard,andPeterDieckmann:reprintswillnotbeavailablefrom
theauthors
Funding:TrygFoundation,LaerdalFoundationandNordsjællandsHospital,Denmark.
Disclosure:T.L.receivedgrantsfromTrygFoundation,LaerdalFoundationandNordsjællands
Hospital,Denmark.R.B.H,D.Ø.andP.D.havenoconflictsofinteresttodeclare.Thesponsorsofthe
studyhadnoroleinthestudydesign,datacollection,dataanalysis,datainterpretation,orinthe
writingofthereport.

94
Abstract
Introduction:Worldwide,medicalsupervisorsfinditdifficulttogetstudentstorisetotheoccasion
whencalledupontoactasleadersofemergencyteams:manyresidents/rescuersfeelunprepared
toadopttheleadershiprole.Thechallengeistoaddresstheresidentsverystrongemotionscaused
bytheextremelystressfulcontext.Nosystematicleadershiptrainingtakesthisaspectintoaccount.
Aim:Theoverallaimofthecourseistoinvestigatewhether,inanemergency,aclinicalteamleader
couldapplyaconductor’sleadershipskills.
Background:Anorchestralconductorisaspecialistinpracticingleadershipfocusingonnon-verbal
communication.Theconductorworkswithhighlytrainedspecialistsandmustleadthemto
cooperateandputhisinterpretationintoeffect.Theconductorworkspurposefullyinorderto
appearcalm,genuineandgainauthority.
Method:Aconductorandaconsultantpreparedacourseforresidents,medicalstudentsand
nurses,n=61.Tenxtwocoursedayswerecompleted.Theexercisesweremusicalandthussafefor
thestudentsastherewerenoclinicalskillsatstake.Theprogrammeaimedtocreatestressand
anxietyinasafelearningenvironment.
Conclusion:Thetransferofaconductor’sskillsimprovedandprofoundlychangedtheparticipating
students’,nurses’andresidents’behaviourandintroducedamethodtohandleanxietyandshow
calmnessandauthority.
Perspectives:Ifthiscourseinleadershipistobeintroducedasacompulsorypartoftheeducating
ofdoctors,theidealtimewouldbeafterclinicalskillshavebeenacquired,experiencegainedand
routinesunderstoodintheclinic.
Funding:TrygFoundation,LaerdalFoundationandNordsjællandsHospital,Denmark.
Introduction
Worldwide,medicalsupervisorsfinditdifficulttogetstudentstorisetotheoccasionwhencalled
upontoactasleadersofemergencyteams100:manyresidentsfeelunpreparedfortheleadership
roleinemergencies16,17,23,26,27,32,37,39.However,leadershipinemergenciesisconsideredvery
importantforpatientsafety1,13,14,16,17,19-23,26,27,29-33andcanaffectmortality.19,23,27,32

95
Itisnecessaryforresidentstoaddressandhandleanxiety16,23,27,32,44andpanic32instressful
20,22,25,27,31,32,34,41,45andcomplex19-22,35,39,41situations.100Therefore,inordertoprovidegoodand
convincingleadership,residentsmustlearntobeconfident1,16,23,27,32,36,37,39,41,42,44,46,47andcalm
16,30,32,44whenassumingtheroleofteamleader.100
Thereisnosystematicleadershiptrainingthattakesthisaspectintoaccount.Handlingnegative
feelingsisnotpartofexistingprogrammes.101Leadershipduringanemergencysituationinvolves
knowledgeandskills,butalsoimpliesdealingwiththepressure16,25,28,34,38,56ofbeingthedecision-
makerandthepressureofbearingtheultimateresponsibilityforwhathappens(ordoesnot).101
Thisarticledescribesacoursethatsupplementsexistingprogrammesbyaddressingtheemotional
challengesforthoseleaders.
Background
Leadershipanditsrelationtohealthcare
Itisimportanttofullyunderstandthatleadershipandassumingleadershipisanindividualand
personalmatterandadeliberatechoice.101Itisnecessarythatthepersonwhostepsforwardas
teamleaderfullyunderstandstherisksandresponsibilitiesoftheleadershiprole1,20,32,44,47–also
referredtoastheleaders’introspection,46psycologicalself-care,60mentalreadiness20,25or
havingtheabilitytounderstandandmanageoneself.47“Inacceptingtheleadershiprole,the
individualassumesthemantleofthegroup’spossiblefailure.Anyindividual’sfalteringcanbelaid
attheleader’sfeet.Thisisthelawoftotalresponsibility”,44statedbyIsersonin1986.
Theconductor’sroleanditsrelationtoleadershipinhealthcare
Anorchestralconductorisaspecialistinpracticingleadershipfocusingonnon-verbal
communication.Theconductor’sgoalistointerpretandrealizethecomposer’sintentionsandto
conveythisinterpretationtotheorchestratoensurethemusiccomesaliveinanartistically
satisfactoryway.Theconductorworkswithhighlytrainedspecialistsandmustleadthemto
cooperateandputhisinterpretationintoeffect.
Inordertoachievetherespectandauthoritytoleadanorchestra,itisimportanttoappearcalm,
balanced,competent,authentic,andcredible.Theleaderworkspurposefullywithhispostureand
appearanceinordertoeliminateanythingthatcouldpossiblypreventthemessagefrombeing
interpretedasintended.

96
Itisnecessaryfortheconductortolisten,sense,andobservewhatactuallytakesplaceintheroom
anddemonstratea‘presencetothemoment’,whichwillgivehimtheabilitytoconstantlyadapt
andadjusttochangesandembracetheunexpected.Thispresenceshouldalsoreflecthis
‘responsiveness’,definedbytheabilitytosense,notice,recognize,feel,andexperiencethe
emotionsofanotherpersonorgroupofpersonssubjectively.
Thisabilitytogainanoverviewofthesituationinallitscomplexityandfindsolutionsbasedon
technicalaswellashumanresourceswillbeperceivedbytheteamassignsofcompetence.When
theleaderaddsthecourageto‘improvise’onthebasisofagivensituation,hewillnotonly
demonstratecompetence,butmakehispresencefelt.Insodoing,hewillbeperceivedaseven
moregenuinebytheteams.
“Improvisationrequiresalotofexperienceanddisciplineandcannotbeexecutedbybeginners,
neitherisitsomethingtobepulledoutwheneverythingelsefails”.94Theimportanceofskilled
professionalsbeingabletoimproviseintheirleadershiprolesisalsodiscussedandemphasizedby
jazz-pianistandProfessorofManagement,FrankJ.Barrett.95
Byworkingwiththeseobjectives,theconductorortheteamleader’scredibilitywillbeenhanced.
Conductorsknowthatonlywhenthiscredibilityisestablishedistheconductorabletoleadthe
orchestra,andtoprovidetheappropriatelevelofencouragementorcriticismconsidered
appropriatewithoutupsettinganyone.
Table2showstherelationbetweenthefunctionsofaconductorandateamleader.Basedonthese
similarities,weconsiderthattraininginthenon-clinicalcontextofconductingmusicmighthelp
residentstotakeintoaccount,face,anddealwiththeemotionalchallengesofbeingaleader.The
conductor’sfocusandobjectivesduringthecoursearepresentedintable3.
Theoverallaimofthecourseistoinvestigatewhether,inanemergency,aclinicalteamleader
couldapplyaconductor’sleadershipskills.
Method
Thissectioncoversseveralaspects.Firstly,pedagogicconsiderationsandassumptions,thenthe
developmentofthecourseandhowitwasconducted,andfinallytheevaluation.
Pedagogicconsiderations
Anxietyandsafety

97
Inordertosimulateanemergencysituationandtooptimizeleadershiptrainingthecoursecreates
aframeworkwithstress,anxiety,anddiscomfortinaharmless,non-clinical,andsafesetting.Itis
importanttoprovidepsychologicalsafety102wheretheparticipantsfeelabletoacceptbeing
uncomfortableandfeelthattheywillbeviewedpositivelyeveniftheymakemistakes.103
Transformativelearningperspective
Thecourseassumesthatparticipantshavetoexperienceandobtaina‘bodilyfeel’ofthepressure
ofbeingaconductorinordertoreallyunderstandit,asdescribedinEmbodiedCognition.68This
theoryisusedinthedesignofeffectivelearningenvironments,especiallythosetargeting
conceptualchange.69AccordingtoTransformativeLearningTheory70oneprerequisitefor
ensuringarealtransformationistobefacedwitha‘disorientingdilemma’71.A‘Disorienting
Dilemma’isdefinedasanacutepersonalorsocialcrisisor,atanotherlevellikeonthiscourse:the
participantsweregivenassignmentswhichwerealmostimpossibletosolve.
Changeofsetting
Thecoursebuildsonachangeofteachingstrategytoimplementanelementofsurprise,whichis
alsoneededtocreatethedilemmathatisusedastriggerfortransformativelearningprocess.There
isaradicalchangeofsettingwiththeshiftfromatraditionalclass-roomset-uptoamusicalset-up
inanotherroom;thischangeofsettingemphasizesthegreatimportancethattheinstructorsattach
tothissurprisingexercise.
Apprenticeship
Traditionally,aconductorhimselfistrainedviaanapprenticeshipandthismethodwouldbe
appliedtothecourse.Individual‘straighton’feedback,offeredwiththeutmostcareand
sensitivity,isacornerstonewhendoingtheexercises:theparticipantsmustnotfeelconcernedat
thispoint.Theconductorhasexperiencedthatlearningispromotedbygettingclosetothislimit
whengivingthisverypersonalfeedback.
Developmentofthecourse
Asdescribedintheliterature,theconsultanthadexperiencedthelackofleadershipandanxietyin
simulationtrainingofresidentsandthemissingfocusonleadership.Asanamateurtrombone
playersherealizedtheparallelbetweentheteamleaderandtheconductorwhenherconcertband
receivedanewskilledconductor.Thedevelopmentofthecoursewasbasedonaconductor’sskills

98
inordertogivemedicalstudents,nurses,andresidentsthetoolsrequiredtoappearcalmand
credibleintotheemergencyteam.
Theconductofthecourse
Aconsultantandanorchestralconductorwerethefacultyforthecourse.
Theconsultantwasfamiliarwiththestudentsandresidentsassheisresponsiblefortheir
educationatthehospital.Inaddition,herpresenceguaranteedtheclinicalrelevanceofthecourse.
Thepresenceoftheconductorwasanewelementintheclinicalcontextandthereforethe
participantsweremoreattentive.
Classrooms:Teachingtookplaceinthreedifferentrooms.Roomonewasanordinaryclassroom
setup.Thefacultystoodinfrontoftheboard.Thissituationwasaknownandsafeframeworkfora
courseformedicalstudentsanddoctors.Inroomtwo,amusicstandwasplacedinfrontofasemi-
circlewithchairsfortheparticipants.Behindthesemi-circlewasapiano.Thismusicalsetupwasa
‘changeasetting’fortheparticipants.Roomthreecontainedafullyequippedsimulationroomwith
aSimMan2Gpatientsimulator,againfamiliartoeverybody.
Primarily,theconsultantexplainedthebackgroundofthecourse,andbasedonherownexperience
describedacasewheretheteamleaderfailedwithunfortunateconsequences.Thesimilarity
betweenateamleaderinanemergencyandaconductorataconcertwasdescribed:twohighly
tensesituationsdemandingfirmleadershipinwhichdecisionsmustbeobeyedandthereisn’t
muchroomfordiscussion.Then,theConductorbrieflydescribedhisthoughtsonleadershipas
describedinthebackgroundsectionandintable3.Theconductorpromotedachangeofsettingby
explainingthatteachingwouldcontinueintheadjoiningroom,andthecourseparticipants
themselveswouldhavetheopportunitytoactasconductorsandsingersinachoir.
AchronologicalreviewofthecontentofthecoursedaysispresentedinTable4.
Participants
AllparticipantswererecruitedfromNordsjællandsHospital,Denmark:Residentsstartingworkin
spring2015werecontactedbymailandofferedacourseonteamleadershipandnon-verbal
communication.Theresidentswereappointedandparticipatedinthecourseonemonthpriorto
thebeginningoftheirfirstclinicalperiodasadoctor.Inautumn2014,3rdsemestergraduate

99
studentswereofferedcoursesstartinginJanuary2015.Thestudentsenrolled.Asanexperiment,
anadditionaltrainingdaywasaddedfortwodifferentteams.Toinvestigatewhetherthecourse
wasapplicabletootherages,groupsandhealth-careprofessionalsorwasrelevantinteamwork
withnurses,acoursedaywasheldforemergencyroomnurses.
TheCommitteesonHealthResearchEthicsfortheCapitalRegionofDenmarkwasaskedtogive
ethicalapprovalbutaformalreviewwaswaivedforthisstudy(H-4-2015-FSP).Allparticipantsgave
writtenconsentfortheirvideostobedisplayed/publishedhere.
Evaluationmethods
Dataacquisitionandanalysis
Integratedvideoandaudiorecordingsrepresenting22:12hoursofobservationofallthecourses
fortheresidentsandstudentsweremade.Onecamerafocusedonthe‘leader’andanotheronthe
‘team’.ThefirstfourcoursedayswererecordedontheGoProSilveredition,andthesecameras
werereplacedbytheGoProHERO4Blackedition,whichhashighdefinitionresolution(4K),
allowingzoominginonthedetailsofthefootageintheeditingprocess.TheHDfootagewasedited
onaMacBookProwithtwoexternaltwoTBharddrives(oneforbackup).Recordingsfromasingle
coursedaytookupbetween40and60GBofdiskspace:all22:12hoursofrecordingsfilled
approximatelyoneTBofharddrivespace.ThevideoswereeditedinAdobePremiereProCC,
release2017.1.2.
Dialoguesfromselectedcoursesweretranscribedverbatim(includingshortdescriptionsof
importantevents,e.g.‘laughter’).Writtenfieldnoteswerecompiledforallthecourses.Complete
dialoguesweretranscribedfromsixcourses(thefinalcoursedesign)–atotalof160pages.
TranscriptionmadepartlybyTLandpartlybytwomedicalstudentswhowerenotattendingor
informedaboutthecourse(‘blinded’astothebackground,methodandassumptionsforthe
course).Throughouttheproject,TLkeptaresearchdiary,whereobservationsandthoughts
deemedtoberelevantfortheprojectwererecorded(OnlinelogavailableinAppendixtoarticle
three).
Commentsandevaluations
Alltheparticipantsmadeevaluationsimmediatelyafterthecourses,n=61.Theygavewritten
quantitativeevaluationsandrespondedtoashortsurveyoffourquantitativequestionsplusan
optionforafreeassessmentcomment(Appendix1).Thestudentsandresidentswereencouraged

100
toreflectonthecourseinwrittenevaluationsafterthecourse.Afterreceivingeditedvideoclips
showingtheirpersonalperformanceduringthetwocoursedays,thestudentsandresidentswere
sentasurveywith14questions(AppendixII).
Analysis
Abductionasamethod
Anabductiveapproachtoresearchmakesitpossiblefortheresearchertopresentaqualified
presumption(educatedguessorinference)67whencommencinghisinvestigation.Basedonhis
findings,heacquiresnewknowledge,hemightalter/adaptthisnewknowledgetothe
presumptionandtheprocessstartsover.Thisprincipleisthefoundationofmorecontemporary
methodse.g.GroundedTheoryorQualitativeContentAnalysis.
QualitativeContentAnalysis
Alltext-baseddataweregatheredintoonesinglepdf-documentandsearchedforkeywordsand
sentencesdescribingthecontentofthecourse,andthewordswereinterpretedinameaningful
context.ThemethodwasQualitativeContentAnalysis,conventional,andinductive:Themes
emergedinandabductive–inductiveprocess,abductivebecausetheconductorhadhis
presumptionsforthecourse–inductivebecausethefindingsadjustedthepresumptions.When
themeswereestablishedtheprocessbecamedirectedbythethemes,thustheprocessbecame
deductive.Thewordsweregroupedintothreethemes(table5,6,and7)accordingtothe
assumptions(asdescribedinthebackgroundsectionandintable3)andfindingsinthedataset.
Thewordswereinterpretedinameaningfulcontext.
Threekeywordswereimportantforthecoursethoughrarelyverbalized:videofootagewas
searchedforTrance,ApprenticeshipandTransformationbasedontheconductor’sassumptionsfor
thecourse.‘Trance’isanexperience,‘apprenticeship’isanoverallimportantteachingconcept,
‘transformation’isanaim,butnoneofthosekeywordswereexplicitlyverbalizedduringthecourse
(table5).
Videofootagewasreviewedseveraltimes,andeditedwiththeaimofexemplifyingthethemes
describedabove.

101
Results
20three-hourcoursedayswerecompletedintheperiodJanuary–May2015,threecoursedays
werecancelledbecauseoflackofparticipation.Sevenparticipantswerenotabletoattendcourse
daytwobecauseoftimepressurefromotheractivities(table1).
Writtenqualitativeevaluationswerereceivedonedaytofivemonthsafterthecoursefrom20of
38participants(53%).Thevideomaterialwaseditedto332smallvideoclipsandeachparticipant
wassenttheirpersonalvideostogetherwithanewsurvey.Thesesurveyswerereceived2·5–10
monthsafterthecourse,14e-mailremindersweresentandtenofthe38participantsresponded
(26%).Unsolicitedcommentsreceived24monthsafterthecoursefromfourofthe38participants
(10%).Inaddition,two‘blinded’studentswrotenon-guidedreflectiononthecoursebasedonthe
contentoftheirtranscriptionsoffourcoursedays.Theseconsiderationsareincludedinthedata
set.
Threethemesemerged:Table5,Learningenvironment.Table6,Pedagogics.Table7,Learninggoals
–theconductor’sfocus.
Allthemesarehighlightedwithquotesaccordingtowhethertheyweremadeduringthecourses
illustratingwhattookplaceduringthecourses(table9)(comprehensiveinappendixIII)orwere
providedinevaluationsafterthecourses,reflectingthoughtsfromthecourseuptotwoyearslater
(table10and11)(comprehensiveinappendixIV).
Tenshortvideoswereeditedaccordingtothethemesandproducedfromthe22:12hoursof
footagefromthecourses.Thevideosallgiveanimpressionofthelearningenvironmentand
includelaughter.Thevideosandthethemestheyareillustratingarepresentedintable12.
Table12,Video1showsa‘changeofsetting’fortheresidentsandtheimpactofbeingchallengedto
conductasimplechildren’ssong.Giventhedifficultchallengeofbeatinga‘basicfour-beatpattern’
(ill.1andtable12,video1)theparticipantsbecamemorestressedinanalreadystressfulsituation,
andthisrevealedpersonalphysicalchallengesandinterference–theycouldthenbeassessedby
theconductor.
Thevideo(video1)showclearsignsofparticipantsfeelinginsecure:twistingtheirhands,scratching
theirneck,shakingtheirshouldersorhead,laughing–mouthwideopen,hidingtheirhandsintheir

102
lapsandshowinganxietywhilelaughingwasinterpretedasparticipantsfeelingstressed,findingthe
taskverydifficultandstrugglingtosolvethechallenge.
Theparticipants’discomfortanduncertaintyledthemtopaymoreattentiontotheconductor–
andstrengthenedthecohesionamongtheparticipantswhenlaughingateachother.
Learningenvironment
Selectedcommentsareshownbelowinthethemes.Alldataaredescribedintable5and6,quotes
arepresentedintable9and10aswellasAppendixIIIandIV.
Learningenvironment
‘Manypointsandalotoflearningarereceivedbestinasafeenvironmentandwhenplaying,whichonemust
saythatthecoursefulfils’.
[S13],twomonthsafter
Safe,enjoyablelaughterhadasignificantimpactonthecourseindicatingthattheparticipantsfelt
safeandenjoyedparticipating.
Reflectionsaboutthelearningprocesswerefound.Thisfurtherconfirmsthattheparticipantsfelt
safetospeakupandsharereflectionsaboutthecontentofthecourse.
Trance
Itwasobservedthatatrance-likestatefrequentlyoccurredbetweentheleaderandtheteam
duringtheexercises,asshowninvideo6,7and9andtable8and9,aswellasAppendixIIIandIV.
Apprenticeship/‘Straighton’feedback
Participantsrecognizedthattheconductorwasaspecialistwho,throughhisprofession,had
acquiredtheabilitytofocusonnon-verballanguage(Table6).Partofthelearningprocessthrough
apprenticeshipistheverydirectpersonalfeed-back(Table12,Video3).Theconductorworkedwith
theparticipants’bodypostureandaddressedsimplephysicalelements:hands,neck,chin,back,
chestetc.Thiswasdoneinordertoemphasizedifferentpersonalphysicalissueswhileexplainingto
theteamtheirimpactandimportance.Furthermore,participantsobservedhowpersonal
instructionmadeabigimpactonthepersonwhoreceivedtheinstruction,andexperiencedhow
individualfeedbackimmediatelyinfluences,transformsandstrengthenstheleader’scredibilityin
frontoftheteam.15participantsstatedthattheyfeltthatthefacultyfullyunderstoodthe

103
challengestheyfaced(‘gotundertheirskin’)(Table7:Stressandobstacles).17participantsstated
thattheygreatlyappreciatedthispersonaland‘straighton’feedback(Table9and9:
Apprenticeship).
Transformation
15participantsduringthecourseand21participantsafterthecoursestatedthattherehadbeen
significantdevelopmentintheindividualparticipant’sbehaviour.(Table5:Transformationand
appendixIIIandIV).
Learninggoals–theconductor’sfocus
Describedintable7.
Physics
‘Itwasalsoveryclearthattheparticipantsgainedamuchgreaterbodyawareness.Theybecameawareofhow
theycommunicate,whattheysignalwiththeirbodylanguageandwhatallthisdoeswiththemessagetheyare
goingtoconvey’
‘Blinded’student2
47participantsexpressedthattheyhadbecomeawareoftheimportanceofbodylanguagewhen
communicating.
Authority
‘Thegoodthingaboutpracticingnon-verbalcommunicationwastoexperiencecalmness,whichcouldalsobe
createdinanemergency.Therewasnotsomuchnoiseintheformofpeoplespeakingallatonce,butIalso
experiencedaninnercalmnessincommunicatingmymessageclearlyandwaswellawarethattherecipient
hadunderstoodtheorder,andIwasabletoconcentrateonthenextpartofthetreatmentalgorithm.’
[R8],fourmonthsafter
17participantsspecificallystatedthattheyhaveachievedinteractionbetweenbodylanguage,
appearanceandauthority–andunderstoodwhythisleadstocalmnessandself-confidence–
confidencefortheleaderaswellforthemembersoftheteam.
‘SowhenIfeelthatI’mcalm–youcanseeittoo.’
[S5]dialoguefromacourse
Eye-contact

104
‘Especiallyasadoctorandateamleaderinanemergencysituationwherethereisagreattendencyforthings
togetmessyandcommunicationisnotefficient,youcanpassordersandcommunicatethroughmimics,body
languageandyoureyes.'’
[S3],onemonthafter
Eightparticipantsduringthecourseandtenparticipantsafterthecoursestatedthattheyhad
learnedthateye-contactisapowerfultoolforensuringthatdecisionsarecommunicated,received
andunderstood.
Presenceatthespecificmoment
‘Wearenotgoodatbeingpresent…Iamnot.Butitisimportanttobepresentwhenleadingalargegroupof
people…Presencecanbeusedinalotofcontexts!’
[S4],dialoguefromthecourse
Theimportanceoflistening,beingattentiveanddemonstratingawarenesswasatopicintroduced
repeatedlybythefacultyduringthecourses.Theparticipantunderstandstheimportanceof
presenceinpromotingthequalityofcooperationwiththeteamandeightparticipantsstatedthis
explicitly.
Responsiveness
’Yes,IfeltthatIgotthemmore...undercontrol.Becausewhenyoulookatpeople–you’llknowexactlywhere
theyare–andwhereIammyself’
[R7],dialoguefromacourse
Theparticipantslearnedthatinthiscoursecontextitwasvalidtotalkaboutandexpresssubjective
perceptions(Ifeel,Icansee,itseemslike,Icansense,Icantell).Sentientperceptionswerestated
by11participants.
Stressandobstacles
’IwaspushedtothelimitatthesametimeasIneededtousewhatwasnewlylearned,whichwasaproductive
challenge’
[S21],threemonthsafter
15participantsstatedthattheywerepushedoutoftheircomfortzone,however19participants
acknowledgedthattheenvironmentwasneverthelesssafe.Afewscepticalcommentsfromone
participantandone‘blinded’studentwereidentified(presentedintable11):independentlyof
eachother,theyfoundittoocomplicatedand,intermsoftheclinic,irrelevantfordoctorstolearn
conductingtechniques.

105
Communication
‘…Impressivetoseehowmuchyoucansaywithoutwords,justbodylanguageandmimic.’
[S10],fivemonthsafter.
Participantsweresurprisedandimpressedtoseehowmuchtheycouldcommunicateandhow
explicitandnuancedtheycouldmaketheirdemandswithoutspeaking.
‘Unbelievablehowmuchyoucansayandaskforwithoutusingwords’
[S3]dayone
Non-verbal,Smile/Grin
Conductor:Theverybest:that’syoursmilewhenitsucceeded!Whenyousucceed,youlooksoproudand
happy!Andwearesohappytobepartofyourprideandyourproject.[S7]agrees:Whenyougivethatsmile,
wegetsucha‘Yes!Ididitright!’
Dialoguefromacourse
Non-verbal,Smile/Grin:Thewords‘smile’and’grin’wasfoundinthreecontexts:Safelearning
environment:Itwasfrequentlyobservedandregisteredthattheparticipantsactuallylaughedand
smiledduringthecoursewhentheywereenjoyingthemselves.Anxietyandstress:Itwasalso
observedandrecordedthatduringthecoursetheparticipantslaughedandsmiledasan
involuntaryandnervousreactiontostress.Non-verbalcommunication:Asmileespeciallycan
expressverynuancedanddifferentemotions:kindness,pride,appreciation,embarrassment,
compassion,sillinessandconfusionetc.Assuch,howandwhentouseasmilewhen
communicatingasaleaderwasdiscussedindepth–i.e.whenitpromotesandwhenitinterferes
withtheleadership.
Engagement
...IfeltlikeIwasapartofyour[project].Youwereengaged!Becauseifyouwerenot,you’djusthave
proceeded,andthenI’djustgo:‘Well,whocaresanyway’
[S5]dialoguefromacourse
Participantsexperiencedthat,inordertodemonstrateauthorityandleadershipinaconvincing
manner,itwasnecessaryfortheleadertoshowhewasfullyabsorbedintheproject.
Additionalfindings
(Presentedintable9,aswellasAppendixIV)

106
Theadditionalfindingsweremainlyguidedbyonesurprisingfactor;formostoftheparticipants
transferringthenewlyacquiredleadershipcompetenciesfromamusicalsettingtoafullscaleCPR
simulationturnedouttobeaproblem(Table11,video10,andtable9,aswellasAppendixIV).A
reasonableexplanationwasthat,whenchallengedontheirclinicalknowledge,theparticipants
forgotaboutnon-verbalcommunicationandleadership(thereforeanewthemewasintroduced:
Trainingalgorithmsandleadership).However,theparticipantswereexcitedaboutthecontentof
thecourseandconsideredthecompetenciestobeimportantfortheirfutureworkasdoctors(new
theme:Relevance).Thisproblemledtodiscussionsaboutwhenineducationwouldbetheideal
timetolearntheseskills(Whentolearn).Thesediscussionsandthewrittenevaluationsconfirmed
thatthecourseaddressedimportanttopicswhichwerenotcoveredinformaleducation(Missing
angleattheuniversity).Aninterestingfindingwasthatthecourseparticipantsconsideredthatthe
coursecouldbeusedinmanyothercontextsbesidesthemusicalandclinical(Generallyapplicable).
Thesethemesconcernedtheperspectiveofthelessonslearnedfromthecourses,andtheyare
presentedintable8.
Trainingalgorithmsandleadership
14oftheparticipantsstatedthattheyhadbenefitedfromtheCPRexercise,butthemajority
showedtheyforgotthenewlylearnedlessonswhenchallengedonclinicalknowledge(oneexample
intable12,Video10).Fourparticipantsstatedthatitwasadvantageoustotrainleadership
separatelyfrommedicalcompetence.
Whentolearn
Thenursesrespondedmostpositivelytothecourse(figure1).Theaverageageinthisgroupwas
over50,approximately20yearsolderthanthetwoothergroups,whichindicatesthatafteryears
ofexperiencethisgroupwasawareofhowfatalitcouldbewhentheteamleaderfailed.Thisview
wasconfirmedbythreeparticipantswhopointedoutthattheidealtimetoattendthiscoursein
relationtothemedicaleducationprogrammewouldbeafterclinicalknowledgeandclinicalroutine
/experiencehadbeenacquired.
Relevance
’…withouttheabilitytocommunicate,sixyearsofstudyaretosomeextentalmostuseless’
[S7],dayone
35oftheparticipantsagreedthatthecoursewashighlyrelevantfortheirclinicalpractice.

107
’Anyonecouldneeditinthedailywork’
Nurse1,dayone
Twoyearsafterthecourse,fourparticipantsstatedthatithadchangedtheirprofessional
behaviour.
“Ipersonallythinkthecoursehasbeenagoodfoundation,nowthatI’vestartedasaresident.”
[S14],unsolicitedcomment,24monthsafter(bye-mail)
MissingangleattheUniversity
11participantsstatedthatthecontentofthecoursehadanimportantobjectivewhichwaslacking
inteachingattheuniversity.
Generallyapplicable
‘IfeltabigimprovementwhenattendinganoralexaminationlastMonday...Igotridoftheworstofmybad
habits!Socool!’
[S5]daytwo
13participantsstatedthatthesubjectwasrelevanttoeducationalcontexts,clinics,when
collaboratingingeneral,daytodaywork,doctors’work,instructingcross-fit,swimminglessons,
publicspeakingandattendingoralexams.
’ThinkIwillbenefitfromthisbothprofessionallyandprivately…’
[S11],dayone
Newknowledge
Asshowninfigures1and2,allcourseparticipantsrespondedpositivelytothecourse.80·4%stated
thattheyacquirednewideas.Nursesyieldedthehighestresult,95·7%reportedthattheyacquired
agreatdealofnewknowledge.
Discussion
Summaryofmainfindings
Thetransferofaconductor’sskillsimprovedandprofoundlychangedtheparticipatingstudents’,
nurses’andresidents’behaviourandintroducedamethodtohandleanxietyanddemonstrate
calmnessandauthority.

108
Webelievethatthiscourserepresentsthemissinglinkbetweenwhattheresearchershavedone
andwhattheresearchershaveknownandsoughtformorethanthreedecades.
Thecourseworksinanareathatgoesbeyondlanguage,demonstratingasharedperceptionin
collaborationwhencreatingmusictogether.ThephilosopherSusanKLangermadethisa
prerequisiteandexplaineditwhenshestated:‘thelimitsoflanguagearenotthelastlimitsof
experience,andthingsinaccessibletolanguagemayhavetheirownformsofconception’.82This
leadstotheconceptdescribedas‘trance’inthisarticlewheretimeandplacedissolve.
Whencollaborationisoptimalwhenworkingwithanorchestra,astatecanoccurwheretimeand
placearedissolvedasdescribedinflow-psychology.“Flow”isdefinedbythepsychologist
Csikszentmihályias:“thecreativemomentwhenapersoniscompletelyinvolvedinanactivityfor
itsownsake.Theegofallsaway.Timeflies.Everyaction,movement,andthoughtfollowsinevitably
fromthepreviousone…”(Interview,Wiredmagazine,September2006issue,p.21.)…“Theflow
statemustbeageneralpedagogicalidealbecauseitisoftenextremelygoodlearning,asyouare
optimallychallenged,fullyfocusedandemotionallyinvolvedsoyoutendtorememberverymuch
ofwhatyouaredealingwith”(TL’stranslation).75
Animportantpartofthereflectiontakesplaceduringdialoguesduringthecourse.Atthebeginning
ofthefirstday,theconductoruseswordsheconsidersimportantinrelationtoteaching.He
introducesconceptssuchas‘assumingleadership’,‘radiateauthority’,‘presenceatthespecific
moment’andshowing‘engagement’.Gradually,reflectionandfeedbackarelefttothestudents
who,equippedwiththeseobjectivesandvocabulary,assesseachother’sperformances.Itshould
bementionedthatthereisadelicatebalancebetweencourseparticipantsactuallyacquiringthis
newknowledgeandsimplyrepeatingthewordsoftheconductor.
Expressingsafetyorsheeravoidancemanoeuvre?(Table12,video5)Whentheparticipantsare
dancing,makingcaricatures,andflirtingwiththemembersofteamasdemonstratedinthisvideo,
itisdebatablewhethertheyaredoingsoasanexpressionofwell-beingandsecurityorinorderto
drawattentionawayfromtheirpersonalsenseofinsecurityinthespecificsituation.Thisisa
recurringtopicforthecourse:stressandobstaclesgohandinhandwithsafetyandhappiness.
Itisinterestingtoascertainthattheskillsandcompetencesaddressedinthecoursearesituatedon
ameta-levelandareaprerequisitefortheteaching:thefacultyhastobeabletoassumethe
leadershiproleaseducatorswhoareabletoimprovisewhenteaching.Everyparticipantbringsin

109
hisownexperiences,perceptionsandemotions(table12,video11).Itisveryimportantforthe
facultytobeabletodemonstrate‘presenceatthespecificmoment’and‘responsiveness’inorder
toappearcredibleasteachersandrolemodels.
Itispossibletouseexistinglearningtheoriestodefineandexplainwhythecoursehasahuge
impactontheparticipants,buttheprojecthascreatednewlearninggoalsandamethodologyofits
own.
‘Ithinkthecourseisagreatopportunitytoworkwithyourselfinasafebutchallengingway,andthereisa
greatdealofpraisefortheinstructorstoensuringagoodframework’
[S10],videosurvey,fivemonthsafter
Limitations
Itispossibletoarguethatthecoursewasaclinicalchallengeandsettingwhileaconsultantand
fellowstudentswerepresent,andthattheparticipants’professionalknowledgewastherefore
challengedandtheywereincompetitionwitheachother.Butastheresultsinthevideosandthe
text-analysisshow,themajoritystatedthattheyperceivedthelearningenvironmentassafe.
Beyondlimitsoflanguage:wordscannotexpresssubstantialpartsofhumanperceptionand
experience.However,inordertounderlinewhichobjectiveswereaddressedduringthecourse,this
isdemonstratedprimarilybywordsintheformofquotes.Thechallengeinherentinthisarticleisto
documenttheconductor’shighlyqualitativeapproachinintroducingnon-verbalcommunicationin
aclinicalresearchtradition.Itshouldbementionedthatallthevideospresentedintable12arein
factmoreexplanatorywhendocumentingthenuancesinthecontentofthecourse.
Perspectives
Ifthiscourseinleadershipistobeintroducedasacompulsorypartoftheeducatingofdoctors,
considerationshouldbegiventowhenitistobeimplemented.Ourresultsindicatetheidealtime
wouldbeafterclinicalskillshavebeenacquired,experiencegainedandroutinesunderstoodinthe
clinic.
Conclusion
Theaimofthisprojectwastotransferthecompetenciesfromanorchestralconductortoresidents
inhealthcareinemergencies.Thefocuswasonappearance,authorityandnon-verbal
communication.Thetransferofaconductor’sskillsimprovedandprofoundlychangedthe

110
participatingstudents’,nurses’andresidents’behaviourandintroducedamethodtohandle
anxietyandshowcalmnessandauthority.Thiscourseseemstoaccommodatetheneedforan
operationalandtargetedtrainingoftheteamleaderinemergencies,addressingawaytoachieve
confidenceinastressful,butsafelearningenvironment.Inadditiontheoutcometurnedouttobea
profoundtransformationofparticipants’self-understanding.
Contributors
TLarsenhadfullaccesstoallthedatainthestudyandhadfinalresponsibilityforthedecisionto
submitforpublication.TLundertookthecollectionofdata,developedtheanalysisstrategy,and
wroteuptheresults.TL&RBeier-Holgersen,conceivedanddesignedtheprojectand
interpretationoftheresults.PDieckmannandDØstergaardprovidedadviseandcriticallyrevised
themanuscript.
Declarationofinterests
Wedeclarenocompetinginterests.
Roleofthefundingsource
ThisprojectwassupportedbyagrantfromTrygFoundation,TheResearchCouncilandtheHR
DepartmentatNordsjællandsHospital,andtheLaerdalFoundation.Theopinionsexpressedinthis
Reviewdonotnecessarilyreflectthoseofthefunders.

111
Population Participationincourse.January–May2015 Day1(3hours) Day2(3hours) Day(3hours) (11coursedays) (7coursedays) (2coursedays)Residents 15 11 0Medicalstudents 23 20 4Nurses 23 0 0Total 61 31 4
Table1.Populationandparticipationincourse
TheConductor TheTeamLeader1 Hastheprofessionalcompetencetocontrolthe
processHastheprofessionalcompetencetocontroltheprocess
2 Themusicianshaveclearlydefinedtasksintheteam
Thespecialistshaveclearlydefinedtasksintheteam
3 Worksinaprocessthattakesplaceovertime.Aprocessthatcannotbeinterrupted
Worksinaprocessthattakesplaceovertime.Aprocessthatshouldnotbeinterrupted
4 Theindividualmusiciansmustbeledtostepforwardandperformtheirtasksandstepbacktoletothersperformtheirroleintheprocess
Theindividualteammembersmustbeledtostepforwardandperformtheirtasksandstepbacktoletothersperformtheirroleintheprocess
5 Hashisscorebutisopentosoloist’sinput(musicalinterpretation)
Hashisalgorithmbutisopentoinputfromtheteammembers
6 Mustcontinuouslyadjustandadapttheworkintermsofhowtheconcertisevolvingandrespondingtothemusicians’efforts
Mustcontinuouslyadjustandadapttheworkintermsofhowtheprocessisevolvingandrespondingtothemembers’efforts
7 Mustbeabletoreadtheorchestraasagroupaswellastheindividualmusicians,andtorespondtopeopleandshowempathy
Mustbeabletoreadtheteamasagroupaswellastheindividualmembersandtorespondtopeopleandshowempathy
8 Mustbepreparedtohandlecrisesandconflictsintheorchestraandtosolveproblemsinstantly
Mustbepreparedtohandlecrisesandconflictsattheteamandtosolveproblemsinstantly
9 Top-downmanagement/authoritativeleadership Top-downmanagement/authoritativeleadership10 Managesateamofprofessional,highlytrained
musicianswhoseskillsdefinetheirrolesManagesateamofprofessionalhighlyskilledspecialistsandisawareofwhatskillsexistintheteamandhowthesearebestused
11 Providesnothinginitself,nohands-on.Thetaskisdefinedasoverview,communicationandleadership
Cancontributeactivelyintheteambutshouldbeawareoftheriskofhead-down.Thetaskisdefinedasoverview,communicationandleadership
12
Workinginaculturewhereallmusicianslookattentivelyatthehead,focusontheirowntask,respondtotheother’sefforts,andtrustinhisresponsibilityandoverview
Workinginaculturewhereeyecontactandnonverbalcommunicationarenotrecognizedtools13 Workinginaculturewheregestures,eyecontact,
facialexpressionsandbodylanguageisdefinedastheonlytoolincommunication.Used,sentandreceivedinstantly
14 Keeptheleadershipfromstarttotheveryend.Butthemusiciansisinsomeextentabletooverruletheconductoriftheydon’tfindhimcapableatconductingtheconcert
Anotherteammembermayclaimtheleadershipintheprocess
15 Cannotuseverbalcommunicationattheconcert Verbalprescriptionsarestandardincommunication
Table2:Aparallelizationbetweentheconductorandteamleader’sfunction

112
TheconductorsfocusAppearanceimmediate,intuitivedecodingAppearsconfidentAppearseasilyreadableAppearscomfortableProfessionallyfocused(Authority,engaged)Leadership–ShowsPowerLeadership–Isdemanding(oppositecaring)Presencetothemoment(Intense)Presencetothemoment(listening)Presencetothemoment(payingattention)AbsorbedinhisprojectPhysique,exactobservations:controlofbodyAppearscalmAppearsrelaxedSeekingeyecontactRelaxeduseoffacialexpressionsRelaxeduseofEyesRelaxeduseofEyebrowsRelaxeduseofsmilesShouldersbackRaisedchinIncontrolofhandsIncontroloflegsDisturbingelements,exactobservationsVeryindividualcharacteristics.Examples:Fixedgrin.Unintendedsmile.Lickingtheirlips.Veryraisedeyebrows.Awkwardlocationofhand.Noddinghishead.Leaningviolentlyforward.Touchinghisface.Scratchesontheneck,showingstressanddiscomfort,etc.
Table3

113
Musicalexercises,course-dayoneExercise Content Objectives CommentInitiateasound(classandsimulationroom)
Traineesmustinturngettheotherstosing‘ah’initiatedbyasimpleConductinggesture
Calmness,authorityandrequireanaction.
Thisexercisewasreplacedbyconducting‘FrereJacques’aftertwocourses
Beatingabasic4/4pattern(musicroom)
Asimpleconductingexercisethatfocusesonthecorrectmovementsofhands
Necessarypreparationforthefollowingexercise.Anapparentlysimplebutinfactdifficultobstacle
Abigobstacle,requiresagreatattention
‘FrereJaques’(musicroom)
Conductingachoir Authority,presencetothemoment,‘firstmeeting’andnon-verbalcommunication
Obstacles,disorientingdilemma,discomfort,stressandanxiety
GhettoBlasterorchestra,(classroom)
ConductaGhettoBlasterorchestra,improvisingw.threesounds
Leadingamultidisciplinaryteam.Authority,presencetothemoment,appearanceandcommunicatingwithoutwords.
Experiencetheintensityinthecommunicationwhenconductinganorchestra‘achievingastateoftrance’
Musicalexercises,course-daytwoGhettoBlasterorchestra,(classroom)
ConductaGhettoBlasterorchestra,improvisingwithtensounds
Leadingamultidisciplinaryteam.Authority,presencetothemoment,appearanceandcommunicatingwithoutwords.
Experiencetheintensityinthecommunicationwhenconductinganorchestra‘achievingastateoftrance’
Mastery,(classroom))
Theconductortellsandshows
Experiencethestrongauthority,presencetothemoment,appearanceandnonverbalcommunicationfromaprofessionalconductor.
Thepowerofeye-contactanduseofempathy
GhettoBlasterorchestra(classroom)
ConductaGhettoBlasterorchestra:followascore
Leadingacomplexsituationfollowingacomposedscore.Aparalleltoaclinicalalgorithm.Adifficultobstacle
Obstacle,disorientingdilemma,discomfort.Leadershipinanextremelycomplicatedexercise.
CPRalgorithmwithsoundsonGhettoBlasters(classroom)
SoundswerecomposedtoillustratethedifferenttaskstobeperformedataCPRemergency.TheyweretobeperformedaccordingtotheCPRalgorithm
Transfertotheclinic
Thisexercisewasremovedfromthecourseaftertwocourse-days.
CPRsimulation(Simulationroom)
PerformafullCPRsimulationasteamleaderwithamedicalteam
Transferofthelearnedleadershipcompetenciestotheclinic
Itwasaproblemtrainingleadershipandmedicalalgorithmssimultaneously
Emergency,course-daythreePersonalvideos Watchingvideosfromthe
firstcourse-dayReflectingonthecourseandthetopicsandownperformance
Majorimpactontheparticipants
Emergencysimulation(Simulationroom)
Performafullemergencysimulationasteamleader
Incl.todiagnose.Apossibilityforcalling‘time-out’ifproblemsoccur
Mostparticipantsexperiencedthissimulationasregularacutetraining
Table4

114
Illustration1.Beatingtimelikeaconductor:abasicfour-beatpattern
Learningenvironment Video:Table12 QuoteLaughter Theparticipantisenjoyingthe
course:laughing,dancing,playing,actingsillyetc.
Video1,3&5 Table10:‘Learningenvironment’and‘Non-verbal,grin/smile
Reflection Inordertoaddressanxietyitisessentialtocreateasafelearningenvironment.
Table9and9:Allcommentsexpressareflection.Bothduringthecoursesandafterthecourses
Table5
Pedagogics Video:Table12 QuoteTrance
Itwasimportanttogivetheparticipantsafeelingoftheintensecommunicationwhenleadinganorchestranon-verbally.
Video6,7,and9 Table9:TranceTable10:Trance
Apprenticeship/’Straighton’feedback
Aconductorisusuallytrainedthroughapprenticeshipanditisthereforenaturalthatthislearningmethodisappliedtothiscourse.
Video1,2,3,and8 Table9:ApprenticeshipTable10:Apprenticeship
Transformation Thepurposeofthecourseistoprovideparticipantswithtoolstoactconvincinglyandcalminstressfulandunpredictablesituations,thatis:apossibilitytobeabletochangeofbehaviour.
Video8,plusprogressanddevelopmentfromvideo4to9
Table9:TransformationTable10:Transformation
Table6
Learninggoals–theconductor’sfocus Video:Table12 QuotePhysics
Appear/look/stand,arm,back,body–posture/body–language/body–position,chest,chin,ear,face/mimic,hands,head,mouth,shoulder,straight,upright
Video3 Table9:PhysicsTable10:Apprenticeship/Non-verbalcommunicationandPhysicsTable11:Physics
Authority Authority,calm,command,confident,control,credible,decisive,demand,determines,issuingorders,leadership,manage,overview,power,
Video9 Table9:AuthorityTable10:Authority

115
relaxed,safe,super,sureEye-contact Eyecontact,eyebrows,eye,gaze,
lookVideo2,6,7,8,and9 Table9:Eyecontact
Table10:EyecontactPresencetothemoment
Attentive,concentrated,conscious,empathy,focus,hear,informed,listening,present
Video6,7and9 Table9:PresencetothemomentTable10:Presencetothemoment
Responsiveness Feel,look/see,perceive,seem,sense/tell
Video6,7and9 Table9:Responsiveness
Stress&obstacles
Chaos,difficult,disturb,doubt,personallimits,nervous,panic,pressure,pulse,stress,tense/strain,uncertain
Video1,4and8 Table9:Stress&obstaclesTable10:Stress&obstaclesTable11:Stress&obstacles
Communication Clear,communication,contact,message,react,respond,signal,vague
Video6,7and9 Table9:CommunicationTable10:Communication
Non-Verbal:Grin/Smile
Smile/Grinexpressing:nervousreaction,kindness,proudness,appreciation,embarrassment,compassion,sillinessorconfusion
Video1,3,4,5and6 Table9:Non-Verbal:Grin/SmileTable10:Non-Verbal:Grin/Smile
Engagement Absorbed,busy,engaged/enthusiastic,excited,happy/lookingforwardto.Intense,shine,thrilled
Video1,6,7,and9 Table9:Engagement
Table7
Additionalfindingsrevealedbyanalysingthedata.Lessonslearnedfromthecourse
Video/figure Quote
Trainingalgorithmsandleadership
Trainingalgorithmsisaboutacquiringknowledgeinastrained,‘slower,moredeliberateandeffortfulformofthinking’whichrequiresallattentionandfocus.
Table12:video10 Table10:Trainingalgorithmsandleadership
Whentolearn Threeparticipantsstatedthatonlywhenmedicalknowledgeandknowledgeofalgorithmshavebeenacquireditispossibletodealwithleadership.
Table10:Whentolearn
Relevance Morethan80%oftheparticipantsstatedthattheywouldimplementthenewideasintheirdailyworktoahighextent.Therestoftheparticipantsstatedthattheywouldimplementthenewideasintheirdailyworktosomeextent.
Figure1and2 Table10:Relevance
Missingangleattheuniversity
Severalparticipantsmentionedthatthecontentofthecoursehadanimportantobjectivewhichwaslackinginteachingattheuniversity.
Table10:Missingangleattheuniversity
Generallyapplicable Itwasmentionedthatthesubjectisrelevanttoeducationalcontexts,clinics,collaborationingeneral,daytodaywork,doctorswork,instructcross-fit,swimminglessons,publicspeakingandattendingoralexam.
Table10:Generallyapplicable
Table8

116
Table9Thetablecontainsselectedcitationsfromparticipantsduringthecourse.Intheleftcolumnkeythemesisgiven,intherightcolumncitationsfromtheparticipantsisgiven.S=Student,R=Resident,BS=‘Blinded’Student,CS=Consultant,C=ConductorLearningenvironment[Video1,2,3and5]
Laughterisnotaspokenword,butaregisteredanddescribedeventthatoccursfrequentlyonthecoursedays.(Laugh,grin,fun,smile)Thisindicatesthatthecourseparticipantsfeelcomfortableandsafeatthecourses.Reflectionisfrequentlytakingplaceatthecourse–whichindicatesthatparticipantsfeelcomfortabletospeakupandsharethoughtsonthelearning.
Trance[Video6,7,and9]
[S1]:...Ialsofeltcompletelyinmyownworld.Itwasareallyamazingfeeling.[S1]:It’sjustreallycoolwhenyougetthatfeeling.Thatkindof‘flow’whereyoucanmanageeverything.
Apprentice-ship/RoleModel
[S7]toConductor:Youarecompletelyoffthescale…ifthisisakindofscatterplotthenwearehere–andyouareallthewayuphere.It’samazing![S13]toConductor:Well,therearelotsofthingsIcan’tsee.Withoutfindingitoutfromyou…Ireckon…
Transfor-mation[Video8,plusdevelop-mentfromvideo4to9]
[S10]:Yes,it’scrazy![CS]:It’sreallyamazingwhathashappenedsincewhenyoufirstwalkedthroughthatdoor,whenwestarted[S10]:Yeah...(scrunchinghereyebrowsandshakinghishead)...two[CS]and[S10]together:...hoursago![CS]:Yeah![R3]:Ijustthink,youknow,itwasjustsogreattoseeyouguys,or–IsupposeIhavetriedmyselfaswell–butanyway,justtobeabletosee!Howmuchyouhaveallprogressedwiththiscourse.I’mjustsatherethinkingshit,wow!
Physics[Video3]
[R3]:YoucanreallytellthedifferencewhenyoustraightenyourselfupConductor:I’mtryingtofind…howaboutthisword?Tryingtogiveyouakindofbodily”pointzero”…Imeanwhereyouareinbalance.Andafteryouhavethis”pointzero”–that’swhenyoucanstarttoaddasmileor…angerorempathyorwhatever,butwithabodyyouareabletocontrol.
Authority[Video9]
[S5]to[S10]:Itreallylookedlikeyouwereincontrolandyouweretotallyconfident…[C]:Youwereinthemomentnow.[CS]:Anditwasyouthatledmealltheway.[S1]:Ialsothinkitwas…itwasreallycool!You
findthiskindofcalmness.Thatyoucanjustbepresent,youknow?That’swhatithastobelikewhenyoubecomeadoctor.
Eyecontact[Video2,6,7,8,and9]
[S5]:(makesatunnelshapewithherhandsbetweenConductor’sfaceandher’s)Youalmostfeltthatyougotkindofa…tunnel(mimesthe”tunnel”eagerly)andthatyoulookandhavethis”connection”.[C]:We’reBOTHgonnafigurethisout…‘YouandI’[S1].Thereisnodoubtaboutit.Youmakeeyecontact[S1]:Iagree.Iwasinnodoubtthatyouwereincontrolofus.Youlookedreallyintenselyatus![R3]:Yeah,itwasasifbefore,peoplewerejustlookingforthesakeoflooking.Butnow!(Pointsathereyes)You’relookingatus!
Presencetothemoment[Video6,7,and9]
[S1]:ThatwasalsowhyIjustwantedtolistentohowitsounded.Youknow,juststandingtherelisteningtoallthedifferentpartscomingtogether.[R1]to[R2]:Youwerereally”likethis”,”likethis”…everytimeyoumadeachangeyoujustdidthis…withalittlenodwithyourheadlikethis…andthen,”wow,NOWitsoundsgood!”
Responsive-ness[Video6,7,and9]
[R5]:IthinkIgotalotoutofit,inthesensethatitwasclearthatitwasyoumakingthedecisions,butyouwerealsoveryempathetic.[R4]to[R3]:youreyeswereveryintense…so…therewasnodoubtingwhatyouwanted…[S1]:ButIcanreallysenseyourenergy,especiallyyou(Conductor).Itwasawesome!
Stress&challenges[Video1,4,and8]
[R7]:It’schaotic,Ican’tfindmywayandthenIgetstressed.Thenitbecomesevenmorechaotic![S10]:It’sacrazychallenge!
Communi-cation[Video6,7,and9]
[S3]:YeahwellIfeltthatwhenItookyouingroupsoftwo,therewasn’tanydoubtwhatyoutwowantedand…[CS]:Inrealityyoucommunicatedagreatdealwithoutsayingaword.
Non-VerbalGrin/Smile[video1,3,4,5,and6
[C]:Soifyoushowasillylaugh,they’llthink:”Well,whythatsillylaugh?”[S3]:Phew!Idon’thaverhythm!(grinning,wavingherhands)
Engagement[Video1,6,7,and9]
[C]:Yougiveoutthisamazingpresenceand:nowlet’sdothis!![R6]overjoyed:Ican’twait![C]:Yes,andwhathappensisyoureyesjustclosedown.Youarenotpresentatall[S1]:Yes,Icanfeelithappening[C]:Youarenotinthisroomatall

117
Table10Thetablecontainsselectedcitationsfromparticipantsafterthecourse.Intheleftcolumnkeythemesisgiven,intherightcolumncitationsfromtheparticipantsisgiven.S=Student,D=Resident,BS=‘Blinded’Student,CS=Consultant,C=ConductorLearningenvironment[Video2][Video5]
[S6],14daysafter:FrereJacqueswasagreatwaytostartthecourse,anditwascarriedoutinawaythatmadeito.k.tolaughatourselvesandateachother.Atthesametimeyoumanagedtokeepitseriousenoughthatitdidn’tbecomenonsensical.Wecoulduselaughtertomakeiteasiertogetoutsideourcomfortzones,butwithoutaclearpurposethewholethingwouldhavecollapsed.Idon’tknowhowyoudidit,butyoudeservecreditforit.[S9],onemonthafter:…creatingasafeandsecurelearningenvironmentinthespaceofafewminutes,whichmakesforasteeplearningcurve.Especiallywhenthefirsttaskissomethingasoutoftheordinaryasconductingachoir.[S11],threemonthsafter:Youwereallowedto“failinYourappearance”.[BS1]:Itwasreallygreatthatyouaskedthestudentswhattheywereexperiencingandletothersgivecritique.Tureissometimesabitquickoffthemarktosaywhathethinksandexperiences.Thissometimesaffectswhattheotherssayandsometimesitfeelslikethestudentsjustagreewithhiminsteadofsayingwhattheythink.
Trance[Video6,7,and9]
[BS2]:[S5]lookswithhermouthwideopen,impressed.Theothersaredeepinfocus…Thelightsgoout,nobodyreactsThemusicintensifies,[S5]smiles,[S10]looksquicklytooneside…Everyoneisfullyfocused–trance-like.Conductorendsthesession:Isn’tthisfun?
Apprentice-ship/’Straighton’feedback[Video1,2,3and8]
[S11],threemonthsafter:Unbelievablygoodteaching!ReallygreatthatTuresaidwhathethoughtyoucoulddobetter,straighttothepointwithoutbeatingaboutthebush.Solid,clearandgoodteaching![S12],sixmonthsafter:[wasfeedbackfromtheinstructoranyhelp?]Yestoagreatextent.Especiallywhenyoufeltthatthefeedbackfromtheinstructorwasspot-onandIthinkthiswasthecasetoaverylargedegree.[S9],twomonthsafter:Solidlearning!Wewerereallyallowedtoworkwithourexpressiveness.
Apprentice-ship/Non-verbalCommuni-cation[Video1,2,3,and8]
[S13],twomonthsafter:Duringtheconductingexercisesitwasreallyusefultogetfeedbackonourposture,mimicandgesture.Tobemadeawareofwhatsignalsyousendnon-stop,whetheryouwanttoornot.[S9],twomonthsafter:Therewaslotsoflearninghere.Especiallyasyouweregoodtocatchthesmalldetailsthattheuntrainedeye
doesn’tsee,butreactstoanyway.”Trans-formation[Video8,plusprogressfromvideo4to9]
[S10],fivemonthsafter:Allthreeofusprogressedagreatdealinashortspaceoftime,anditwasincrediblyfascinating.[S6],dayone:Ilearnedsomegeneralthingsandthingsaboutmyself.[S20],onemonthafter:…it’sinterestingthattheskillswelearnfromyouarealreadyinthebackofourmindreadytouseonlyafterashorttime
Physics[Video3]
[S11]threemonthsafter:IthinkIhavegoodcontroloverhowIstandandmovemyarms,butmyfacegoesamokwithoutmenoticingit;itclearlymakesmeappearveryuncertain..
Authority[Video9]
[S19],sixmonthsafter:Yourexpressionbecomesmoreauthoritativeafteryougetfeedbackandyougiveoffmore”leader-charisma”.[Nurse2],dayone:Itisagoodthingtobeabletoappearauthoritative.Beawareofthis
Eyecontact[Video2,6,7,8,and9]
[S8],dayone:Eyecontactisimportant,therebygivingpossibilityfornon-verbalorders[S18],dagone:Ibecameveryawareofeyecontactandrelaxedbodylanguage
Presencetothemoment[Video6,7and9]
[S7],threemonthsafter:Iwasquiteexcitedabouttrainingwhatitistorelaxandrestwithinyourselfandyourbodywhenyouarestandinginfrontofagroupofhighlyqualifiedstrangers.Keepingcalm,leadershipandtheupperhandmentally,andlettingitshowinyourbodylanguage.Itreallycrossedmypersonalboundariesbutitwasveryuseful!
Stress&challenges[Video1,4,and8]
[BS2]:Myexperiencewasthatitwasareallygoodenvironmenttolearnin.Theywereforcedcompletelyoutoftheircomfortzoneandwere”brokendown”,inthesensethattheywereinasituationtheyhadneverbeeninbefore,andhadthereforenoestablishedstrategiestheycouldusetodealwiththechallenge.[S6],fivemonthsafter:Inanycase,itfeltabitliketurningpartofyourselfinsideout,standinginfrontofallofyou.
Communi-cation[Video6,7,and9]
[S10],fivemonthsafter:Itwasveryimpressivetoexperiencehowmuchyoucansaywithoutwords,justwithbodylanguageandmimics.[NURSE2],dayone:Incrediblewhatyoucanmanagewithoutlanguage
Non-VerbalGrin/Smile[video1,3,4,5,and6
[S6],14daysafter:Wecoulduselaughtertomakeiteasiertogetoutsideourcomfortzones
Training
[S14],sixmonthsafter:Maybetojumpfromthe

118
algorithmsandleadership[Video10]
exercisestothecardiacarrestscenariowasalittlesudden…?Inanycaseyouforgeteverythingyouhavelearnedwhenyouarestandinginfrontofthatbed.[S12],sixmonthsafter:Butabitdifficulttotransfersomeofthesmalldetailswhenyouarenot100percentcertainofthecardiacarrestalgorithm.
Whentolearn
[S9],twomonthsafter:Istillthinkthatitshouldbecombinedwithin-depthknowledgeofthecardiacarrestalgorithm,aspartofadoctor’sconfidenceandbodylanguageisconnectedwithhavingtheirknowledgeinplace.However,whenthisknowledgeisacquired,thereisalottobegainedfromthistypeofmusictraining,asyouarestrippingthedoctorofhisorherknowledgeandputtinghiminanenvironmentwhereonlytheirbodylanguagecounts.[S3],onemonthafter:Myonlycriticismwouldbethatasayoungerdoctor/medicinestudent,youhavetoomuchfocusonyourprofessionalknowledgeandofcourseyouprioritisethiswhenyouareinanemergencysituation,andunfortunatelyyoudon’thaveenoughresourcestothinkaboutandmakeuseofthenon-verbalcommunicationtraining.Ontheotherhand,itcouldbeanappropriatecourseformoreexperienceddoctorsthathavetheirknowledgeandexperienceinplace-theywouldhavetheresourcesneededtomakeuseofthenon-verbalcommunicationtraining.
Relevance
[BS2]:Anotherimportantthingisthatyoucanbeverybrightintermsofyourmedicalknowledge,butifyoudon’tmanagetocommunicateinawaythatgetsthroughtopeople,yourknowledgeiseffectivelyreducedtonothing.Inotherwords,beingadoctorisaboutalotmorethanbeingabletorememberwhatisinthetextbooks.[S6],dayone:ItwasmuchbetterthanwhatIexpected.Averypositiveexperience.Beatsothercommunicationcoursesmanytimesover[S13],twomonthsafter:Trainingintakingdecisionswhileeverybody’seyesareonyouishighlyrelevantfordoctorsandmedicalstudents.[S5],fourmonthsafter:…thenervousnessandmyreactionwerecompletelythesame.AndthewayIhavetolearntotackleitisalsothesame,regardlessofwhetherIamwithapatientinaward,orinaclassroomwithmedicalstudents.
Missingangleattheuniversity
[S7],dayone:Crazilyimportantaspectofadoctor’swork,whichIneverrealizedwasmissingfromourexistingeducationbeforetoday.[S3]dayone:Veryimportantlearningaroundwhatitistobeateamleader,whichyouneverthinkaboutonadailybasisorreceiveinstructioninitwhilsttraining.[S15]dayone:Superexcitingandveryrelevantinrelationtothefuturejob.Asubjectthatismissinginourtraining.[R1],twomonthsafter:Atthesametimeitisaroleinwhichyourarelyreceiveformalteachingduringtraining.[S16],onemonthafter:IngeneralareallygreatcoursewhichIhopebecomesanobligatorypartofthetraining.Ithinkeveryonecouldbenefitfromit!
Generallyapplicable
[NURSE1]:’Everybodycouldneeditintheirday-to-daywork’[S17]dayone:Canbeusedinateachingcontext,inaclinic,andmanymoresituations[S7],threemonthsafter:Unfortunately,Ihaven’thadtheopportunitytotryoutthesenewlylearnedskillsintheclinicyet.ButIinstructalittlecross-fitteam,andIcanreallyuseitthere![S4]oneweekafter:Also,haveyouplannedanymorecoursesformedicinestudents?Ihaveamateortwowhothinkthatsoundsinteresting.’
Table11Scepticism.D=Resident,BS=‘Blinded’StudentStressandobstacles
[BS1]:ThefirstgamewithFrereJaquesfocusesonsomethingthatistootechnicallycomplicatedinrelationtoamedicalbenefit[R2],twomonthsafter:IsometimesfeltYoufocusedonsomedetailsthatwereindifferenttousasdoctors.I.e.IthinktoomuchtimewasspentonthecorrectfactortoconductFrereJaques
Physics
[R2],twomonthsafter:Istillthinkthattoomuchemphasiswasplacedonnothavingtosmile/shouldlookveryserious.

119
11videos(hyperlinks).Allvideosgivesanimpressionofasafelearningenvironmentandshowsenjoyinglaughter1.Trainingbeatingafourbeatpatternyoutu.be/WW898db57Zw
Duration:0:38.Achangeofsetting:fourmaleandfourfemaleparticipantsaretrainingbeatingabasicfour-beatscheme.Focusedattention,handlingadifficultobstacle.Cohesionontheteam.Theme:Stressandobstacles
2.Apprenticeshipyoutu.be/EnHlustj3F0
Duration:1:50.Theconductorexplainsandshowscarefornineparticipantsinordertomaketheindividualparticipantsobtainafeelofcalmnesswhenperformingasaleader.Theconductorstandsasarolemodel.Themes:Apprenticeship,Eye-contact,Presencetothemoment,Responsiveness,Communication,Non-verbal,Engagement.
3.‘Straighton’Feedbackyoutu.be/fwbgfTNf_e8
Duration:2:04.13participantsreceivevery’Straighton’personalfeedbackfromtheconductorwhogoestothelimit.Themes:Apprenticeship/‘Straighton’feedback,Physics,Authority,Stressandobstacles,Communication,Non-verbal.
4.Discomfort&Obstaclesyoutu.be/UmIFk9VXuCQ
Duration:2:12.21participantsshowdiscomfort:shaketheirheads,laughnervously,scratchtheirneck,showrollingeyes,hidethefaceintheirhands,smileapologeticetc.Themes:Stressandobstacles,non-verbal
5.Asafeenvironmentyoutu.be/_ZmUYjI-T4E
Duration:2:24.19participantsshowtheyfeelsafe,foolaroundandlaugh.Femaleparticipantoftendoesthe‘shimmy’,smalldancemovements,playswithahatetc.Themes:Safelearningenvironment
6.Theintensityincommunicationwhenconductingyoutu.be/3sPmMQCne_E
Duration:0:29.Fourparticipantsconductteam.Theyareshowingexcellentleadershipandareina‘stateofTrance’withtheirteam.Themes:Trance,Authority,Eye-contact,Presencetothemoment,Responsiveness,Communication,Non-verbal,Engagement.
7.Achievingastateofflowyoutu.be/KcyZf3_QfMk
Duration:1:12.Oneparticipantconductscompletelyabsorbedformorethantenminutes.Theteam(orchestra)isn’tmoving,fullyfocusedontheconductor.Lightgoesoutat0:20(2:37)butnobodypaysattentiontothis.Themes:Trance,Authority,Eye-contact,Presencetothemoment,Responsiveness,Communication,Non-verbal,Engagement
8.ATransformationyoutu.be/GW7XPdnf-EU
Duration:6:54.Arealtransformation(Englishsubtitles).Showshowthetrainers‘getsundertheskin’oftheparticipants.Showsthereflectiononthelearningandthesupportfromtheotherparticipants.Theparticipantinfocusgoesfromsaying“Mypalmsaretotallysweaty”and“Ithinkit’shorrible”tosay:“Iwisheveryonecouldtrythis”and“Itisveryimpressive”.Themes:Trance,Transformation,Authority,Eye-contact,Presencetothemoment,Responsiveness,Stressandobstacles,Communication,Non-verbal,Engagement
9.EndPointyoutu.be/IQtMa0VJgjw
Duration:1:55.16participantsshowingexcellentleadershipwhenconducting.Incontroloftheirbody,attentivetotheproject,confident,absorbedandinfullcontrolofthesituation.Themes:Trance,Authority,Eye-contact,Presencetothemoment,Responsiveness,Communication,Non-verbal,Engagement
10.ABreakdownyoutu.be/f5BiNFL_zDU
Duration:1:21.Aparticipantbreakdown.Afterattendingthetwocourse-daysconcerningleadershipshetriestotransferthelearnedskillstotheclinicinamedicalacutesimulation.Whenconfrontedwithherlackofmedicalknowledgesheforgetsalltrainedleadershipskillsandlosescontrolofthesituation.Themes:Physics,Stressandobstacles,Non-verbal,Trainingalgorithmsandleadership.
11.Uniqueindividualsyoutu.be/Bdok4ArYXcM
Everyparticipantbringsintheirownexperiences,perceptionsandemotions
Table12

120
Figure2.DidIgetnewideas?n=61participants.Answersfromcoursedays1and2,atotalofn=96answers
Figure3.WillIapplyinformationandideas?n=61participants.Answersfromcoursedays1and2,atotalofn=96answers
0
20
40
60
80
100
Very high
Some A little None
Perc
ent
New knowledge and ideas
All participants Students
Young Doctors Nurses
0
20
40
60
80
100
Very high
Some A little None
Perc
ent
Influence on behaviour
All participants Students
Young Doctors Nurses
121
AppendixI:
AppendixII:
Videosurveysenttothestudentsalongwithfour-eightvideoclipsshowingtheindividualparticipant’sperformanceasteamleaderatthetwocoursedaysAboutthevideosusabilityasalearninginstrumentWhichofthevideosmadeanimpressiononyouandwhy?Doyouhavecommentsontheindividualvideos?Doyouwanttoreturnandgobacktothevideos?Aboutthelearningmethod,whendidyouexperiencelearningInthemoreclassicalteachingsituations?Whenyouwereinstructedyourself?Whenyouobservedothersbeinginstructed?Intheimmediatereactionsoftheotherswhenyoureceivedinstruction?Wasthepersonalfeedbackfromtheinstructorapplicable?Wastheconversationsbetweenthecourseparticipantsrewarding?Wasitusefulthattheinstructorscameclosetoyou?Wasthereasafeenvironmentontheteam?Wasiteasytobeheard?Weretheexercisesrelevanttoyourperformanceasteamleaderinthecardiacarrestscenario?Doyouhavefurthercommentsaboutyourfirstreviewafterwatchingthevideos?

122
APPENDIX
Abstractto“TeamManagement-Canmusiccontributetobetterunderstanding?”
AIM:totrainmedicalstudentstousenon-verbalcommunicationliketheconductorofanorchestra.
Theoverallgoalwastoimprovecommunicationinmedicalteams.
METHOD:inordertoexplaintothestudentshowtotakecontrolasateamleader,communicate
moreeffectivelyandworkwellinateam,theconductordescribedtheskillsrequiredtoconductan
orchestra.Heexplainedhowtouseeyecontact,bodylanguageandgesturesandsetthestudents
twomusicalexercisestoperformandthengaveindividualfeedbackontheirperformance.These
skillswerethentransferredtoasimulatedmedicalemergencysituationinwhicheverystudentwas
giventheopportunitytoplaytheteamleader.
RESULTS:thestudentsfoundtheexperienceunexpectedlyusefulasitenabledthemtofocusonthe
skillsrequiredofaleaderandthisresultedingreaterself-awareness,enhancedself-confidenceand
bettercommunication.
CONCLUSION:medicalstudentscanbenefitgreatlyfromapplyingaconductor'sskillstoamedical
situation:theirleadershipability,degreeofcooperationandprofessionalcompetenceare
considerablyenhanced48
ONLINEAPPENDIX
Articleone
AppendixII:Foundopinionsaboutleadershipinemergenciesandviewsontheidentifiedleadership
measurementtoolsinthesystematicreview.Comprehensiveresultofqualitativecontentanalysis
(conventional):turelarsen.dk/Appendix/TER-AppendixII.pdf
Articletwo
AppendixI:Opinions,attitudes,experiencesorviewstoidentifyanychallengesorbarrierswhich
leadershiptrainingforresidentsinemergenciesneedstoaddress.Identifiedconsensusonwhat
characterizesagoodclinicalteamleader:learninggoals.Comprehensiveresultofqualitative
contentanalysis(directed):turelarsen.dk/Appendix/B-AppendixI.pdf

123
Articlethree
AppendixIII:Commentsmadebytheparticipantsduringthecoursesillustratingthethemesfound.
Comprehensiveresultofqualitativecontentanalysis:turelarsen.dk/Appendix/CET-AppendixIII.pdf
AppendixIV:Commentsmadebytheparticipantsafterthecoursesillustratingthethemesfound.
Comprehensiveresultofqualitativecontentanalysis:turelarsen.dk/Appendix/CET-AppendixIV.pdf
11editedvideosshowingresultsfromqualitativecontentanalysis:
turelarsen.dk/Appendix/11videos.pdf
Logfromthecourse:turelarsen.dk/Appendix/Log2015.pdf
Supplementarymaterial
Beforeandaftervideos:turelarsen.dk/Appendix/BA-videos.pdf

124
REFERENCES
1.CooperS,WakelamA.Leadershipofresuscitationteams:"Lighthouseleadership'.Resuscitation.1999;42(1):27-45.
2.FlinR,MaranN.Identifyingandtrainingnon-technicalskillsforteamsinacutemedicine.QualSafHealthCare.2004;13(suppl1):i80-i84.doi:10.1136/qshc.2004.009993.
3.PRISMA(preferredreportingitemsforsystematicreviewsandmeta-analyses).prisma-statement.org/.Updated2015.
4.SinghJ.Criticalappraisalskillsprogramme.JournalofPharmacologyandPharmacotherapeutics.2013;4(1):76-77.
5.RennieDL.Qualitativeresearchasmethodicalhermeneutics.PsycholMethods.2012;17(3):385-398.
6.MalterudK.Theartandscienceofclinicalknowledge:Evidencebeyondmeasuresandnumbers.TheLancet.2001;358(9279):397.
7.MalterudK.Qualitativeresearch:Standards,challenges,andguidelines.Lancet.2001;358(9280):483-488.
8.ChoJ,LeeE.Reducingconfusionaboutgroundedtheoryandqualitativecontentanalysis:Similaritiesanddifferences.TheQualitativeReport.2014;19(32):1-20.
9.KressG.Multimodality:Keyconcepts.conversationwithguntherkress..2012-https://youtu.be/rZ4rMVCWkQs;MODE,InstitutionofEducation,UniversityofLondon.
10.JewittC.Theroutledgehandbookofmultimodalanalysis.In:JewittC,ed.2.ed.ed.MiltonPark,Abingdon,Oxon:Routledge;2014:468.
11.PeirceCS.Peirceonsigns-writingsonsemioticbycharlessanderspeirce.ChapelHill;London:TheUniversityofNorthCarolinaPress;2014.
12.BezemerJ,DiamantopoulouS,JewittC,KressG,MaversD.Usingasocialsemioticapproachtomultimodality:Researchinglearninginschools,museumsandhospitals..2012,March;01NationalCentreforResearchMethods.
13.WisborgT,RonningTH,BeckVB,BratteboG.Preparingteamsforlow-frequencyemergenciesinnorwegianhospitals.ActaAnaesthesiolScand.2003;47(10):1248-1250.
14.MarschSC,MullerC,MarquardtK,ConradG,TschanF,HunzikerPR.Humanfactorsaffectthequalityofcardiopulmonaryresuscitationinsimulatedcardiacarrests.Resuscitation.2004;60(1):51-56.
15.MakinenM,AuneS,Niemi-MurolaL,etal.AssessmentofCPR-Dskillsofnursesingoteborg,swedenandespoo,finland:Teachingleadershipmakesadifference.Resuscitation.2007;72(2):264-269.
16.HjortdahlM,RingenAH,NaessAC,WisborgT.Leadershipistheessentialnon-technicalskillinthetraumateam--resultsofaqualitativestudy.ScandJTraumaResuscEmergMed.2009;17:48-7241-17-48.
17.HunzikerS,BuhlmannC,TschanF,etal.Briefleadershipinstructionsimprovecardiopulmonaryresuscitationinahigh-fidelitysimulation:Arandomizedcontrolledtrial.CritCareMed.2010;38(4):1086-1091.

125
18.GeorgiouA,LockeyDJ.Theperformanceandassessmentofhospitaltraumateams.ScandJTraumaResuscEmergMed.2010;18:66-7241-18-66.
19.HunzikerS,TschanF,SemmerNK,HowellMD,MarschS.Humanfactorsinresuscitation:Lessonslearnedfromsimulatorstudies.JEmergTraumaShock.2010;3(4):389-394.
20.HunzikerS,JohanssonAC,TschanF,etal.Teamworkandleadershipincardiopulmonaryresuscitation.JAmCollCardiol.2011;57(24):2381-2388.
21.BriggsA,RajaAS,JoyceMF,etal.Theroleofnontechnicalskillsinsimulatedtraumaresuscitation.JSurgEduc.2015;72(4):732-739.
22.LeenstraNF,JungOC,JohnsonA,WendtKW,TullekenJE.Taxonomyoftraumaleadershipskills:Aframeworkforleadershiptrainingandassessment.AcadMed.2016;91(2):272-281.
23.RobinsonPS,ShallE,RakhitR.Cardiacarrestleadership:Inneedofresuscitation?PostgradMedJ.2016.
24.FordK,MenchineM,BurnerE,etal.Leadershipandteamworkintraumaandresuscitation.WestJEmergMed.2016;17(5):549-556.
25.YuleS,FlinR,Paterson-BrownS,MaranN.Non-technicalskillsforsurgeonsintheoperatingroom:Areviewoftheliterature.Surgery.2006;139(2):140-149.
26.GilfoyleE,GottesmanR,RazackS.Developmentofaleadershipskillsworkshopinpaediatricadvancedresuscitation.MedTeach.2007;29(9):e276-83.
27.HayesCW,RheeA,DetskyME,LeblancVR,WaxRS.Residentsfeelunpreparedandunsupervisedasleadersofcardiacarrestteamsinteachinghospitals:Asurveyofinternalmedicineresidents.CritCareMed.2007;35(7):1668-1672.
28.FlinR,YuleS,Paterson-BrownS,MaranN,RowleyD,YoungsonG.Teachingsurgeonsaboutnon-technicalskills.Surgeon.2007;5(2):86-89.
29.RingenAH,HjortdahlM,WisborgT.Norwegiantraumateamleaders--trainingandexperience:Anationalpointprevalencestudy.ScandJTraumaResuscEmergMed.2011;19:54-7241-19-54.
30.JacobssonM,HargestamM,HultinM,BrulinC.Flexibleknowledgerepertoires:Communicationbyleadersintraumateams.ScandJTraumaResuscEmergMed.2012;20:44-7241-20-44.
31.HunzikerS,TschanF,SemmerNK,MarschS.Importanceofleadershipincardiacarrestsituations:Fromsimulationtoreallifeandback.SwissMedWkly.2013;143:w13774.
32.KolehmainenC,BrennanM,FilutA,IsaacC,CarnesM.Afraidofbeing"witchywitha'b'":Aqualitativestudyofhowgenderinfluencesresidents'experiencesleadingcardiopulmonaryresuscitation.AcadMed.2014;89(9):1276-1281.
33.FernandezCastelaoE,BoosM,RingerC,EichC,RussoSG.EffectofCRMteamleadertrainingonteamperformanceandleadershipbehaviorinsimulatedcardiacarrestscenarios:Aprospective,randomized,controlledstudy.BMCMedEduc.2015;15:116-015-0389-z.
34.YuleS,ParkerSH,WilkinsonJ,etal.Coachingnon-technicalskillsimprovessurgicalresidents'performanceinasimulatedoperatingroom.JSurgEduc.2015;72(6):1124-1130.

126
35.HargestamM,HultinM,BrulinC,JacobssonM.Traumateamleaders'non-verbalcommunication:Videoregistrationduringtraumateamtraining.ScandJTraumaResuscEmergMed.2016;24:37-016-0230-7.
36.McCueJD,MagrinatG,HansenCJ,BaileyRS.Residents'leadershipstylesandeffectivenessasperceivedbynurses.JMedEduc.Jan1986;61(1):53-58.
37.ItaniKM,LiscumK,BrunicardiFC.Physicianleadershipisanewmandateinsurgicaltraining.AmJSurg.2004;187(3):328-331.
38.YuleS,FlinR,Paterson-BrownS,MaranN,RowleyD.Developmentofaratingsystemforsurgeons'non-technicalskills.MedEduc.2006;40(11):1098-1104.
39.NicksaGA,AndersonC,FidlerR,StewartL.Innovativeapproachusinginterprofessionalsimulationtoeducatesurgicalresidentsintechnicalandnontechnicalskillsinhigh-riskclinicalscenarios.JAMASurg.2015;150(3):201-207.
40.RobertsNK,WilliamsRG,SchwindCJ,etal.Theimpactofbriefteamcommunication,leadershipandteambehaviortrainingonadhocteamperformanceintraumacaresettings.AmJSurg.2014;207(2):170-178.
41.ManthaA,CogginsNL,MahadevanA,StrehlowRN,StrehlowMC,MahadevanSV.Adaptiveleadershipcurriculumforindianparamedictrainees.IntJEmergMed.2016;9(1):9-016-0103-x.Epub2016Feb20.
42.CooperS.Developingleadersforadvancedlifesupport:Evaluationofatrainingprogramme.Resuscitation.2001;49(1):33-38.
43.CarlsonJ,MinE,BridgesD.Theimpactofleadershipandteambehavioronstandardofcaredeliveredduringhumanpatientsimulation:Apilotstudyforundergraduatemedicalstudents.TeachLearnMed.2009;21(1):24-32.
44.IsersonKV.Criticalleadership.JEmergMed.1986;4(4):335-340.
45.SommerKJ.Pilottraining:Whatcansurgeonslearnfromit?ArabJUrol.2014;12(1):32-35.
46.FondG,DucasseD,AttalJ,etal.Charismaandleadership:Newchallengesforpsychiatry.Encephale.2013;39(6):445-451.
47.StollerJK,TaylorCA,FarverCF.Emotionalintelligencecompetenciesprovideadevelopmentalcurriculumformedicaltraining.MedTeach.2013;35(3):243-247.
48.LarsenT,Beier-HolgersenR.Teammanagement-canmusiccontributetobetterunderstanding?.MedEdPublish.2014.
49.FletcherG,FlinR,McGeorgeP,GlavinR,MaranN,PateyR.Anaesthetists'non-technicalskills(ANTS):Evaluationofabehaviouralmarkersystem.BrJAnaesth.2003;90(5):580-588.
50.MitchellL,FlinR,YuleS,MitchellJ,CouttsK,YoungsonG.Developmentofabehaviouralmarkersystemforscrubpractitioners'non-technicalskills(SPLINTSsystem).JEvalClinPract.2013;19(2):317-323.
51.FlinRH,MitchellL.Safersurgery:Analysingbehaviourintheoperatingtheatre.Farnham:Ashgate;2009:xxvi,456s.,illustreret.
127
52.MishraA,CatchpoleK,McCullochP.TheoxfordNOTECHSsystem:Reliabilityandvalidityofatoolformeasuringteamworkbehaviourintheoperatingtheatre.QualSafHealthCare.2009;18(2):104-108.
53.SteinemannS,BergB,DiTullioA,etal.Assessingteamworkinthetraumabay:Introductionofamodified"NOTECHS"scalefortrauma.AmJSurg.2012;203(1):69-75.
54.SpanagerL,KongeL,DieckmannP,Beier-HolgersenR,RosenbergJ,OestergaardD.Assessingtraineesurgeons'nontechnicalskills:Fivecasesaresufficientforreliableassessments.JSurgEduc.2015;72(1):16-22.
55.KlampferB,FlinR,HelmreichR,etal.Groupinteractioninhighriskenvironments:Enhancingperformanceinhighriskenvironments,recommendationsfortheuseofbehaviouralmarkers..2001.
56.SadideenH,WeldonSM,SaadeddinM,LoonM,KneeboneR.Avideoanalysisofintra-andinterprofessionalleadershipbehaviorswithin"theburnssuite":Identifyingkeyleadershipmodels.JSurgEduc.2016;73(1):31-39.
57.TalgamI.Leadlikethegreatconductors:ATED-talk.youtube.com/watch?v=R9g3Q-qvtss.Updated2009.
58.MercerS,ArulGS,PughHE.Performanceimprovementthroughbestpracticeteammanagement:Humanfactorsincomplextrauma.JRArmyMedCorps.2014;160(2):105-108.
59.KrageR,TjonSoeiLenL,SchoberP,etal.Doesindividualexperienceaffectperformanceduringcardiopulmonaryresuscitationwithadditionalexternaldistractors?Anaesthesia.2014;69(9):983-989.
60.WillemsA,WaxmanB,BaconAK,SmithJ,KittoS.Interprofessionalnon-technicalskillsforsurgeonsindisasterresponse:Aliteraturereview.JInterprofCare.2013;27(5):380-386.
61.StraussA,CorbinJ.Basicsofqualitativeresearch:Groundedtheory,procedures,andtechniques.NewburyPark:SagePublications;1990.
62.GlaserBG,StraussAL.Thediscoveryofgroundedtheory,strategiesforqualitativeresearch.NewYork:AldinedeGruyter;1967.
63.HsiehHF,ShannonSE.Threeapproachestoqualitativecontentanalysis.QualHealthRes.2005;15(9):1277-1288.
64.ReichertzJ.Abduction:Thelogicofdiscoveryofgroundedtheory.Forum:QualitativeSocialResearch.2009;11(1).
65.ZimmermanJ.Hermeneutics:Averyshortintroduction.OxfordUniversityPress;2015.10.1093/actrade/9780199685356.001.0001.
66.XiaoY,SeagullFJ,MackenzieCF,KleinK.Adaptiveleadershipintraumaresuscitationteams:Agroundedtheoryapproachtovideoanalysis.Cognition,Technology&Work.2004;6(3):158-164.
67.BurchR.Charlessanderspeirce.https://plato.stanford.edu/entries/peirce/.UpdatedWedNov12,2014.
68.WilsonRA,FogliaL.Embodiedcognition.In:EdwardN.Zalta,ed.Thestanfordencyclopediaofphilosophy.Spring2017ed.MetaphysicsResearchLab,StanfordUniversity;2017.
69.HoltonDL.Constructivism+embodiedcognition=enactivism:Theoreticalandpracticalimplicationsforconceptualchange..AERA2010Conference.

128
70.JonesLC.Youlearnitinyourheart:Transformativelearningtheoryandclinicalpastoraleducation.JPastoralCareCounsel.2010;64(4):7.1-10.
71.MezirowJ.Transformationtheoryofadultlearning.In:WeltonM,R.,ed.Indefenseofthelifeworld.criticalperspectivesonadultlearning.StateUniversityofNewYorkPress;1995:39-50.
72.NielsenK.Mesterlære.læringsomsocialpraksis.Kbh:HansRitzelsForlag;1999.
73.MintzbergH.RethinkingtheMBA.https://hbr.org/2009/03/rethinking-the-mba.html.UpdatedVisitedNov.2017.
74.CsikszentmihályiM.Interview.Wiredmagazine.2006:p.21.
75.KnoppHH.Omkunstenatfindeflowienverden,derofteforhindrerdet.KognitionogPædagogik-tidsskriftomtænkningoglæring.2004;14(52):66-82.
76.CsikszentmihályiM,NakamuraJ.Flowtheoryandresearch.In:SnyderCR,ShaneJL,eds.OxfordhandbookofPOSITIVEPSYCHOLOGY.SecondEditioned.NewYork:OxfordUniversityPress;2009:195.
77.RixJ.Howanxietyscramblesyourbrainandmakesithardtolearn.theguardian.com/education/2015/nov/21/how-anxiety-scrambles-your-brain-and-makes-it-hard-to-learn.Updated21Nov.2015.
78.KahnemanD.Thinking,fastandslow.(2011).Thinking,fastandslow.499pp.NewYork,NY,US:Farrar,StrausandGiroux.US.
79.WatzlawickP.Pragmaticsofhumancommunication,astudyofinteractionalpatterns,pathologies,andparadoxes.[1.Nortonpaperbacked.]ed.NewYork:W.W.Norton;2011.
80.MehrabianA,FerrisSR.Inferenceofattitudesfromnonverbalcommunicationintwochannels.JConsultPsychol.1967;31(3):248-252.
81.MehrabianA.Silentmessages.In:Belmont:Wadsworth;1971:75-80.
82.LangerSK.Philosophyinanewkey,astudyinthesymbolismofreason,rite,andart.Cambridge,Mass.;1942.
83.KressG.Multimodaldiscourseanalysis.In:GeeJ,P.,HandfordM,eds.Theroutledgehandbookofdiscourseanalyses.London:Routledge;2012:35.
84.JewittC.Anintroductiontomultimodality.In:JewittC,ed.Theroutledgehandbookofmultimodalanalysis.2.ed.ed.London:Routledge;2014:15-30.
85.GoodwinC.Thehandbookofvisualanalysis;pages157-182.In:London:SAGEPublicationsLtd;2017.http://methods.sagepub.com/book/the-handbook-of-visual-analysis.10.4135/9780857020062.
86.JewittC.Anintroductiontousingvideoforresearch..2012,March;03NationalCentreforResearchMethodsWorkingPaper.
87.RaudaskoskiPL.Observationsmetoder(herundervideoobservation).In:Kvalitativemetoder.HansReitzel;2015:97-112.

129
88.BrownDM.Videorecordingofemergencydepartmenttraumaresuscitations.JTraumaNurs.2003;10(3):79-80.
89.MoultonD.Surgicalblackboxmaysewupmalpracticecases.CMAJ:CanadianMedicalAssociationJournal.2015;187(11):794-794.
90.RosenbergJ.Systematiskreviewogmeta-analyse.2.udg.ed.S.l.:CreateSpaceIndependentPublishingPlatform;2016.
91.BalshemH,HelfandM,SchunemannHJ,etal.GRADEguidelines:3.ratingthequalityofevidence.JClinEpidemiol.2011;64(4):401-406.
92.CanMEDSflower.http://canmeds.royalcollege.ca/en/about.Updated2017.
93.BezemerJ,KressG,CopeA,KneeboneR.Learningintheoperatingtheatre:Asocialsemioticperspective.In:CookC,NewmanM,eds.Work--basedlearninginclinicalsettings:Insightsfromsocio--culturalperspectives.Abingdon:Radcliffe;2012:125.
94.KoivunenN,WennesG.Showusthesound!aestheticleadershipofsymphonyorchestraconductors.Leadership.2011;7(1):51-71.
95.BarrettF.Yestothemess:Surprisingleadershiplessonsfromjazz.Boston,MA:HarvardBusinessPress;2012:2002pages.
96.Theofficialsiteofthekirkpatrickmodel.kirkpatrickpartners.com/Our-Philosophy/The-Kirkpatrick-Model.UpdatedNov.30,2017.
97.MaJ.Thesynergyofpeirceandvygotskyasananalyticalapproachtothemultimodalityofsemioticmediation.Mind,Culture,andActivity.2014;21(4).
98.YuklG.Leadershipinorganizations.SeventhEditioned.NewJersey:Pearson;2010.
99.StogdillRM.Handbookofleadership:Asurveyoftheoryandresearch.In:NewYork-London:;1974:259.
100.LarsenT,Beier-HolgersenR,DieckmannP,ØstergaardD.Trainingresidentstoleademergencyteams:Asystematicreview[partone].Underreview.2018.
101.LarsenT,Beier-HolgersenR,ØstergaardD,DieckmannP.Trainingresidentstoleademergencyteams[parttwo].barriers,challengesandlearninggoals:Aqualitativereview.Underreview.2018.
102.Edmondson,Amy.Psychologicalsafetyandlearningbehaviorinworkteams.AdmSciQ.1999;44:350-383.
103.RudolphJW,RaemerDB,SimonR.Establishingasafecontainerforlearninginsimulation:Theroleofthepresimulationbriefing.SimulHealthc.2014;9(6):339-349.




















