Comprehensive examination of the trans-diagnostic cognitive behavioral model of eating disorders in...
6
AUTHOR QUERY FORM Journal: EATBEH Please e-mail or fax your responses and any corrections to: Aravind, Poornima E-mail: [email protected] Fax: +1 619 699 6721 Article Number: 729 Dear Author, Please check your proof carefully and mark all corrections at the appropriate place in the proof (e.g., by using on-screen annotation in the PDF file) or compile them in a separate list. Note: if you opt to annotate the file with software other than Adobe Reader then please also highlight the appropriate place in the PDF file. To ensure fast publication of your paper please return your corrections within 48 hours. For correction or revision of any artwork, please consult http://www.elsevier.com/artworkinstructions. Any queries or remarks that have arisen during the processing of your manuscript are listed below and highlighted by flags in the proof. Click on the ‘Q’ link to go to the location in the proof. Location in article Query / Remark: click on the Q link to go Please insert your reply or correction at the corresponding line in the proof Q1 Please confirm that given names and surnames have been identified correctly. Q2 The “Applied Technology for Neuro-Psychology Laboratory” and the “Istituto Auxologico Italiano” in affiliation address d have been assumed to be part of the “Catholic University of Milan”. Thus, “Faculty of Psychology, Catholic University of Milan & Applied Technology for Neuro-Psychology Laboratory, Istituto Auxologico Italiano, Milan, Italy” has been changed to “Faculty of Psychology, Applied Technology for Neuro-Psychology Laboratory, Istituto Auxologico Italiano, Catholic University of Milan, Milan, Italy”. Please check, and correct if necessary. Q3 Highlights should consist of only 85 characters per bullet point, including spaces. However, the highlights provided for this item exceed the maximum requirement; thus, they were not captured. Kindly provide the replacement highlights that conform to the requirement for us to proceed. For more information, please see the Guide for Authors. Q4 Please provide an update for reference “Dakanalis, Timko, et al., in press”. Q5 Please provide an update for reference “Dakanalis, Zanetti, et al., in press”. Q6 Please provide an update for reference “Dakanalis, Zanetti, Riva, et al., in press”. Please check this box if you have no corrections to make to the PDF file. □ Thank you for your assistance. Our reference: EATBEH 729 P-authorquery-v11 Page 1 of 1
Transcript of Comprehensive examination of the trans-diagnostic cognitive behavioral model of eating disorders in...

AUTHOR QUERY FORM
Journal: EATBEH Please e-mail or fax your responses and any corrections to:Aravind, PoornimaE-mail: [email protected]: +1 619 699 6721
Article Number: 729
Dear Author,
Please check your proof carefully and mark all corrections at the appropriate place in the proof (e.g., by using on-screen annotationin the PDF file) or compile them in a separate list. Note: if you opt to annotate the file with software other than Adobe Reader thenplease also highlight the appropriate place in the PDF file. To ensure fast publication of your paper please return your correctionswithin 48 hours.
For correction or revision of any artwork, please consult http://www.elsevier.com/artworkinstructions.
Any queries or remarks that have arisen during the processing of your manuscript are listed below and highlighted by flags in theproof. Click on the ‘Q’ link to go to the location in the proof.
Location in article Query / Remark: click on the Q link to goPlease insert your reply or correction at the corresponding line in the proof
Q1 Please confirm that given names and surnames have been identified correctly.
Q2 The “Applied Technology for Neuro-Psychology Laboratory” and the “Istituto Auxologico Italiano” inaffiliation address d have been assumed to be part of the “Catholic University of Milan”. Thus,“Faculty of Psychology, Catholic University of Milan & Applied Technology for Neuro-PsychologyLaboratory, Istituto Auxologico Italiano, Milan, Italy” has been changed to “Faculty of Psychology,Applied Technology for Neuro-Psychology Laboratory, Istituto Auxologico Italiano, CatholicUniversity of Milan, Milan, Italy”. Please check, and correct if necessary.
Q3 Highlights should consist of only 85 characters per bullet point, including spaces. However, thehighlights provided for this item exceed the maximum requirement; thus, they were not captured.Kindly provide the replacement highlights that conform to the requirement for us to proceed. For moreinformation, please see the Guide for Authors.
Q4 Please provide an update for reference “Dakanalis, Timko, et al., in press”.
Q5 Please provide an update for reference “Dakanalis, Zanetti, et al., in press”.
Q6 Please provide an update for reference “Dakanalis, Zanetti, Riva, et al., in press”.
Please check this box if you have nocorrections to make to the PDF file. □
Thank you for your assistance.
Our reference: EATBEH 729 P-authorquery-v11
Page 1 of 1

1Q3
2
3Q1
4567Q2
8
91011121314151617181920212223
42
43
44
45
46
47
48
49
50
51
52
53
54
55
56
57
58
59
60
61
Eating Behaviors xxx (2013) xxx–xxx
EATBEH-00729; No of Pages 5
Contents lists available at ScienceDirect
Eating Behaviors
Comprehensive examination of the trans-diagnostic cognitive behavioralmodel of eating disorders in males
OFAntonios Dakanalis a,⁎, C. Alix Timko b, Massimo Clerici c, M. Assunta Zanetti a, Giuseppe Riva d
a Department of Brain and Behavioural Sciences, University of Pavia, Italyb Behavioral and Social Sciences Department, University of the Sciences, Philadelphia, PA, USAc Department of Neurosciences and Biomedical Technologies, University of Milano-Bicocca, Italyd Faculty of Psychology, Applied Technology for Neuro-Psychology Laboratory, Istituto Auxologico Italiano, Catholic University of Milan, Milan, Italy
O
⁎ Corresponding author at: Department of Brain and BehPavia, P.za Botta 11, 27100, Pavia, Italy.
E-mail address: [email protected] (A. Dakan
1471-0153/$ – see front matter © 2013 Published by Elsehttp://dx.doi.org/10.1016/j.eatbeh.2013.10.003
Please cite this article as: Dakanalis, A., et al.,in males, Eating Behaviors (2013), http://dx.d
Ra b s t r a c t
a r t i c l e i n f o24
25
26
27
28
29
30
31
32
33
34
Article history:Received 19 December 2012Received in revised form 19 August 2013Accepted 9 October 2013Available online xxxx
Keywords:Cognitive–behavioralTrans-diagnostic ModelEating disordersMenStructural equation modeling
35
36
37
38
39
CTED P
The Trans-diagnostic Model (TM) of eating pathology describes how one or more of four hypothesizedmechanisms (i.e., mood intolerance, core low self-esteem, clinical perfectionism and interpersonal difficulties)may interrelate with each other and with the core psychopathology of eating disorders (i.e., over-evaluation ofweight and shape) to maintain the disordered behaviors. Although a cognitive behavioral treatment based onthe TMhas shown to be effective in treating eating disorders, themodel itself has undergone only limited testing.This is the first study to both elaborate and test the validity of the TM in a large sample (N = 605) ofundergraduate men. Body mass index was controlled within structural equation modeling analyses. Althoughnot all expected associations for the maintenance variables were significant, overall the validity of the modelwas supported. Concern about shape and weight directly led to exercise behaviors. There was a direct pathfrom binge eating to exercise and other forms of compensatory behaviors (i.e., purging); but no significantpath from restriction to binge eating. Of the maintaining factors, mood intolerance was the only maintainingvariable directly linked to men's eating disorder symptoms. The other three maintaining factors of the TMindirectly impacted restriction through concerns about shape andweight, whereas only interpersonal difficultiespredicted low self-esteem and binge eating. Potential implications for understanding and targeting eatingdisturbances in men are discussed.
© 2013 Published by Elsevier Ltd.
4041
E
62
63
64
65
66
67
68
69
70
71
72
73
74
75
76
77
78
UNCO
RR1. Introduction
The Trans-diagnosticModel (TM; Fairburn, Cooper, & Shafran, 2003)of eating pathology was developed in order to recognize the commonfeatures of all eating disorders (EDs) and the high rate of diagnosticcrossover (Fairburn & Cooper, 2011). At its core is an over-evaluationof weight and shape and attempts to control them. The attempts atcontrol manifest as severe restriction, which in turn exacerbates shapeand weight concerns (SWCs) and can lead to further restriction or abinge/purge cycle. What is unique about the TM is that it posits thatsome individuals may struggle in one of four areas hypothesized tomaintain EDs: clinical perfectionism, core low self-esteem, moodintolerance, and/or interpersonal difficulties (Cooper & Fairburn, 2011).
Although randomized controlled trials (Fairburn et al., 2009)provide preliminary support for the efficacy of the Cognitive BehavioralTherapy—Enhanced (CBT-E; Fairburn, 2008), good treatment outcomedoes not necessarily constitute evidence for the adequacy of the TMon which the treatment is based. Recently, there has been increasedfocus on testing the validity of the conceptual relationship of the TM
79
80
81
82
avioural Sciences, University of
alis).
vier Ltd.
Comprehensive examinationoi.org/10.1016/j.eatbeh.2013
in both clinical and non-clinical female samples (e.g., Hoiles, Egan, &Kane, 2012; Lampard, Byrne, McLean, & Fursland, 2011; Schnitzler,von Ranson, & Wallace, 2012; Tasca et al., 2011). Overall data fromthese studies tended to support the validity of the TM in women.
1.1. Rationale and aims
The lack of a direct comprehensive evaluation of the TM of EDs inmen is somewhat surprising, given that men and women are moresimilar than dissimilar in terms of core ED behaviors (i.e., comparablerestriction and binge eating rates), though they differ in the frequencyof certain compensatory behaviors (Hudson, Hiripi, Pope, & Kessler,2007; Lavender, De Young, & Anderson, 2010). There is a comparablerate of excessive exercise between young men and women, but lowerlevels of purging among men (Lavender et al., 2010; Striegel-Mooreet al., 2009). Although the main purpose of compensatory behaviors isto counteract the effects of eating in order to avoid weight gain, inmen, who tend to be more preoccupied with enhancing musculature(Dakanalis & Riva, 2013), exercise is not exclusively in the serviceweight reduction, but may also be utilized for the purpose of musclemass gain (Anderson & Bulik, 2004). According to the TM, all formsof EDs should represent varying behavioral expressions of SWCs(Fairburn et al., 2003). However, given the different nature of SWCs in
of the trans-diagnostic cognitive behavioral model of eating disorders.10.003
Original text:
Inserted Text
"givenname"
Original text:
Inserted Text
"givenname"
Original text:
Inserted Text
"givenname"
Original text:
Inserted Text
"givenname"
Original text:
Inserted Text
"givenname"
Original text:
Inserted Text
"surname"
Original text:
Inserted Text
"surname"
Original text:
Inserted Text
"surname"
Original text:
Inserted Text
"surname"
Original text:
Inserted Text
"surname"
Original text:
Inserted Text
"with "
Original text:
Inserted Text
"givenname"
Original text:
Inserted Text
"is "
Original text:
Inserted Text
"with "
Original text:
Inserted Text
"with "
Original text:
Inserted Text
"with "
Original text:
Inserted Text
"with "
Original text:
Inserted Text
"with "
Original text:
Inserted Text
"with "
Original text:
Inserted Text
"with "
Original text:
Inserted Text
"with "
Original text:
Inserted Text
"with "
Original text:
Inserted Text
"with "
Original text:
Inserted Text
"with "
Original text:
Inserted Text
"with "
Original text:
Inserted Text
"with "
Original text:
Inserted Text
"with "
Original text:
Inserted Text
"with "
Original text:
Inserted Text
"with "
Original text:
Inserted Text
"with "
Original text:
Inserted Text
"with "
Original text:
Inserted Text
"with "
Original text:
Inserted Text
"with "
Original text:
Inserted Text
"with "
Original text:
Inserted Text
"with "
Original text:
Inserted Text
"with "
Original text:
Inserted Text
"with "
Original text:
Inserted Text
"with "
Original text:
Inserted Text
"with "
Original text:
Inserted Text
"with "
Original text:
Inserted Text
"with "
Original text:
Inserted Text
"with "
Original text:
Inserted Text
"with "
Original text:
Inserted Text
"with "
Original text:
Inserted Text
"with "
Original text:
Inserted Text
"with "
Original text:
Inserted Text
"with "
Original text:
Inserted Text
"with "
Original text:
Inserted Text
"with "
Original text:
Inserted Text
"with "
Original text:
Inserted Text
"with "
Original text:
Inserted Text
"with "
Original text:
Inserted Text
"with "
Original text:
Inserted Text
"with "
Original text:
Inserted Text
"’"
Original text:
Inserted Text
"-"
Original text:
Inserted Text
"-"
Original text:
Inserted Text
"-"
Original text:
Inserted Text
"st"
Original text:
Inserted Text
"st"

83
84
85
86
87
88
89
90
91
92
93
94
95
96
97
98
99
100
101
2 A. Dakanalis et al. / Eating Behaviors xxx (2013) xxx–xxx
men, the dual function of exercise behavior, and the different ratesof certain compensatory behaviors, it is unclear if and how the TMfits men.
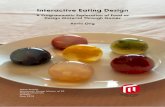
The goals of the current studywere to (a) test the TM among collegemen, who are recognized as a “high” risk group for the onset of harmfuleating and body-related disordered behaviors (Hudson et al., 2007),and (b) consider exercise and other forms of compensatory behaviors(i.e., purging, fasting) separately in the evaluation of the model, asrecommended (Anderson & Bulik, 2004). Our hypothesized model,depicted in Fig. 1A was analyzed using a structural equation modelingin which the specification of the structural relationships was based on
UNCO
RRECT
Fig. 1. This figure represents the hypothesized Trans-diagnostic Model of eating disorders in mpaths added (B). Singe-headed and double-headed arrows represent the impact of one variabthe structural model are presented. *p b .05.
Please cite this article as: Dakanalis, A., et al., Comprehensive examinationin males, Eating Behaviors (2013), http://dx.doi.org/10.1016/j.eatbeh.2013
the illustrations of the TM model and men's ED literature (Dakanalis &Riva, 2013; Fairburn et al., 2003).
2. Methods
2.1. Participants
Participants were 613 men ranging in age from 18 to 30 (M=20.64,SD=4.3) recruited from four large universities in Italy. The majority ofthe sample (95%) is identified asWhite/European (95%) andheterosexual(93%). Average body mass index (BMI=kg/m2), was 23.90 (SD=4.2).
ED P
RO
OF
en (A) and the final structural model with non-significant paths trimmed and significantle on other and correlations between pairs of variables, respectively. Path coefficients for
of the trans-diagnostic cognitive behavioral model of eating disorders.10.003
Original text:
Inserted Text
"st"
Original text:
Inserted Text
"s"
Original text:
Inserted Text
"’"
Original text:
Inserted Text
"st"

T
102
103
104
105
106
107
108
109
110
111
112
113
114
115
116
117
118
119
120
121
122
123
124
125
126
127
128
129
130
131
132
133
134
135
136
137
138
139
140
141
142
143
144
145
146
147
148
149
150
151
152
153
154
155
156
157
158
159
160
161
162
163
164
165
166
167
168
169
170
171
172
173
174
175
176
177
178
179
180
181
182
183
184
185
186
187
188
189
190
191
192
193
194
195
196
197
198
199
200
201
202
203
204
205
206
207
208
209
210
211
212
213
214
215
216
217
218
219
220
221
222
1 The results of bootstrapping (available from the authors upon request) indicated thatall indirect effects of the final structural model were significant.
3A. Dakanalis et al. / Eating Behaviors xxx (2013) xxx–xxx
UNCO
RREC
2.2. Instruments
Thirteen selective scales or subscales of the Italian validated versionsof seven instruments with well-established psychometric proprietiesamong college-aged men were used in the current study. Their singleitems or a combination of scales or subscales were used as indicatorvariables (Byrne, 2011) of nine latent variables (Fig. 1A).
Scales of the Eating Disorder Inventory—3 (Garner, 2008) were usedto measure mood intolerance (via the eight items of the emotionaldysregulation scale), low self-esteem (via the six items of self-esteemscale), binge eating (via the eight items of the bulimia scale) andinterpersonal difficulties (via the 7-item interpersonal insecurity scaleand the 7-item interpersonal alienation scale).
The 9-item Male Body Dissatisfaction Scale (Dakanalis, Timko et al.,in press) and the 4-item appearance intolerance subscale of the MuscleDysmorphia Disorder Inventory (Santarnecchi & Dèttore, 2012) wereused to measure male SWCs.
The six exercise strategies subscale items of the Body ChangeInventory (Bastianelli, Vicentini, Spoto, & Vidotto, 2007), which assessthe frequency of exercise to reduce fat/weight and increasemuscularity,were used to measure exercise behavior.
Three subscales of the Frost Multidimensional PerfectionismScale (Lombardo, 2008) were used to measure clinical perfectionism —
personal standards (7 items), concern over mistakes (9 items), anddoubts about action (4 items).
The five restraint subscale items of the Eating Disorder ExaminationQuestionnaire — Version 6 (Fairburn, 2010) were used to measuredietary restriction.
The five compensatory behavior subscale items of the BulimicInvestigatory Test, Edinburgh — Severity Index (Orlandi, Mannucci, &Cuzzolaro, 2005), which assess the frequency/severity of methods forcounteract the effects of bing eating (i.e., fasting, purging), were usedto measure other forms of compensatory behaviors.
2.3. Procedure
Participants were recruited via advertisements posted in academicdepartments in four large universities in Italy. The research advertise-ments directed interested participants to a web page that provideddetails about the study. After indicating their consent, participantscompleted the study's measures, which were presented in a counter-balanced order and formatted so that participants could not skipindividual items (Dakanalis, Zanetti, Rival et al., in press). Severalstrategies were used to reduce the likelihood of erroneous dataincluding the insertion of a validity question in each measure,checking the IP address of all participants, and evaluating forthe presence of outliers. After these procedures, data from 605 menremained for analysis. All procedures were approved by theappropriate ethics board.
2.4. Statistics
The “measurement model” was first tested for acceptable fit to thedata using confirmatory factor analysis (CFA) and then the “structuralmodel” (Fig. 1A) was tested (Byrne, 2011); BMI was a covariate inthis model (Stice, 2002). Both models were examined using themaximum-likelihood method (as pre-analysis did not revealed anyevidence for non-normality) in Mplus 5.1 (Muthén & Muthén,1998–2007). Criteria for good model fit were a comparative fit index(CFI) and a Tucker–Lewis index (TLI) of .95 or greater, a standardizedrootmean square residual (SRMR) of .08 or less, and a rootmean squareerror of approximation (RMSEA) of .06 or less (Byrne, 2011). Weplanned to trim non-significant structural paths and to add paths notoriginally specified but that impacted the fit of the model to the databased on the modification index values (MIs N 5.0); the chi-squaredifference (Δχ2) was used to compare nested models (Byrne, 2011).
Please cite this article as: Dakanalis, A., et al., Comprehensive examinationin males, Eating Behaviors (2013), http://dx.doi.org/10.1016/j.eatbeh.2013
ED P
RO
OF
3. Results
Descriptive statistics, internal reliability estimates of each measureand partial correlations (holding BMI as a covariate) are shown inTable 1.
A CFA testing the relationships between the measured and latentvariables indicated a good model fit: CFI= .97, TLI= .96, SRMR= .06,RMSEA= .04. All loadings (ranging from .80 to .93) were significant at.001 level; therefore, all latent factors were adequately operationalizedthrough their respective indicators.
The structural model fit the data well: CFI= .95, TLI= .95, SRMR=.07, RMSEA = .05. However, restriction did not predict binge eating,while all other specified paths were statistically significant (Fig. 1B).The trimmed model, in which the non-significant path was deleted,did not result in decreased model fit [CFI= .95, TLI= .95, SRMR= .07,RMSEA=.05; Δχ2 (1, N=605)= .99, pN .05] and thus was retained.
Three un-estimated paths with a value N5.0 were noted in thetrimmed model: the paths frommood intolerance to dietary restrictionand exercise behavior and the path from interpersonal difficulties tobinge eating. The revised model, in which these paths were added(CFI=.96, TLI=.96, SRMR=.06, RMSEA=.04), provided a significantlybetter fit than the trimmed model, Δχ2 (3, N=605)=37.09, p b .001,and consequently was retained. The significant structural coefficientsfrom this final structural model1 are presented in Fig. 1B.
Interpersonal difficulties, core low self-esteem, and clinical perfect-ionism predicted 52.8% of the variance in SWCs. Mood intolerance andSWCs accounted for 35.3% of the variance in restriction. Binge eating,SWCs, and mood intolerance contributed 29.1% of the variance inexercise behavior. Binge eating and mood intolerance predicted 14.9%of the variance in other forms of compensatory behaviors. Finally,mood intolerance and interpersonal difficulties predicted 41.6% of thevariance in binge eating.
4. Discussion
Consistent with previous studies that examined the validity of TM ofEDs in female clinical and community samples (Hoiles et al., 2012;Lampard et al., 2011; Schnitzler et al., 2012; Tasca et al., 2011), wefound that (a) interpersonal difficulties were directly linked to lowself-esteem, (b) there is a direct path frombinge eating to compensatorybehaviors and (c) clinical perfectionism, low self-esteem and inter-personal difficulties only indirectly influence restriction through SWCs,highlighting the importance of over-evaluation with one's appearance.The results of this study indicate that men differ from women in termsof the TM due to the direct impact that SWCs have on the likelihood ofexercising. This is in-line with literature indicating that men are morelikely to use exercise to reduce subcutaneous fat and increase muscledefinition (Dakanalis & Riva, 2013).
Mood intolerance was the only maintaining variable directly linkedto restriction. The significant relationships between binge eating, otherforms of compensatory behaviors, and mood intolerance are in-linewith TM. These behaviors are believed to have an emotional regulatoryfunction and to occur in attempt to reduce negative affect (Gross, 2007).Although the direct paths between mood intolerance, restriction, andexercise support this hypothesis, replication of these findings is needed.
Surprisingly, there was no direct relationship between restrictionand binge eating. Although this goes against a central assumption ofthe TM, there is increasing evidence that restriction does not alwayslead to binge eating (e.g., Dakanalis, Zanetti, Clerici et al., in press;Lampard et al., 2011; Spoor et al., 2006). The direct paths from inter-personal difficulties and mood intolerance to binge eating, as well asevidence that healthy-weight treatment programs for EDs and inter-ventions that do not focus on reducing restriction (i.e., interpersonal
of the trans-diagnostic cognitive behavioral model of eating disorders.10.003
Original text:
Inserted Text
"st"
Original text:
Inserted Text
"r"
Original text:
Inserted Text
"me"
Original text:
Inserted Text
"-"
Original text:
Inserted Text
" - "
Original text:
Inserted Text
" - "
Original text:
Inserted Text
" -"
Original text:
Inserted Text
" –"
Original text:
Inserted Text
"’"
Original text:
Inserted Text
"indices "
Original text:
Inserted Text
"r"
Original text:
Inserted Text
"me"
Original text:
Inserted Text
"me"
Original text:
Inserted Text
"me"
Original text:
Inserted Text
"me"
Original text:
Inserted Text
"me"

T
PRO
OF
223
224
225
226
227
228
229
230
231
232
233
234
235
236
237
238
239
240
241
242
243
244
245
246
247
248
249
250
251
252253
254255256
257258259
260261
262263264
265
266267268269270271272273274275276277278279280281282283284285286287288289 Q4290291292293 Q5294295296 Q6297298299300301
Table 1t1:1
t1:2 Means, standard deviations (SDs), Cronbach's alpha coefficients, and partial correlations (with body mass index controlled).
t1:3 Measures 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. 13.
t1:4 1. EDI3-II –
t1:5 2. EDI3-IA .64⁎ –
t1:6 3. EDI3-LSE .23⁎ .19⁎⁎ –
t1:7 4. MPS-CM .18⁎⁎ .17⁎⁎ .20⁎ –
t1:8 5. MPS-PS .20⁎ .18⁎⁎ .30⁎ .59⁎ –
t1:9 6. MPS-DA .24⁎ .26⁎ .31⁎ .56⁎ .67⁎ –
t1:10 7. EDI3-ED .22⁎ .23⁎ .32⁎ .28⁎ .10 .09 –
t1:11 8. MBDS .47⁎ .46⁎ .51⁎ .54⁎ .55⁎ .56⁎ .08 –
t1:12 9. MMDI-AI .45⁎ .44⁎ .50⁎ .55⁎ .60⁎ .49⁎ .06 .74⁎ –
t1:13 10. EDEQ-R .14⁎⁎⁎ .13⁎⁎⁎ .09 .17⁎⁎⁎ .15⁎⁎⁎ .14⁎⁎⁎ .28⁎ .68⁎ .75⁎ –
t1:14 11. EDI3-BL .54⁎ .46⁎ .10 .05 .04 .03 .64⁎ .03 .05 .23⁎⁎ –
t1:15 12. BCI-ES .12⁎⁎⁎ .14⁎⁎⁎ .14⁎⁎⁎ .18⁎⁎⁎ .17⁎⁎⁎ .15⁎⁎⁎ .24⁎ .33⁎ .30⁎ .09 .33⁎⁎ –
t1:16 13. BITE-CB .03 .02 .06 .03 .05 .04 .29⁎ .08 .09 .10 .30⁎⁎ .09 –
t1:17 α .90 .94 .91 .90 .93 .90 .92 .90 .89 .90 .92 .92 .87t1:18 M 27.80 25.10 21.89 21.20 19.80 10.02 36.05 40.94 14.77 20.18 33.11 16.99 9.10t1:19 SD 19.13 17.90 15.74 6.12 6.76 3.77 15.01 16.86 6.06 14.30 21.55 5.89 4.40t1:20 Scale range 7–42 7–42 6–36 9–45 7–35 4–20 8–48 9–54 4–20 0–30 8–48 6–30 0–35
t1:21 Note. N=605. EDI3-II, IA, LSE, ED, and BL=Eating Disorder Inventory—3, Interpersonal Insecurity scale, Interpersonal Alienation scale, Low Self-Esteem scale, Emotional Dysregulationt1:22 scale, and Bulimia scale, respectively;MPS-CM, PS andDA=Multidimensional PerfectionismScale, Concern overMistakes subscale, Personal Standards subscale, andDoubts aboutActionst1:23 subscale, respectively; MBDS = Male Body Dissatisfaction Scale; MMDI-AI = Muscle Dysmorphia Disorder Inventory, Appearance Intolerance subscale; EDEQ-R = Eating Disordert1:24 Examination Questionnaire—Version 6, Restraint subscale; BCI-ES = Body Change Inventory, Exercise Strategies subscale; BITE-CB = Bulimic Investigatory Test Edinburgh—Severityt1:25 Index, Compensatory Behaviour subscale.
⁎ p b .001.t1:26⁎⁎ p b .01.t1:27⁎⁎⁎ p b .05.t1:28
4 A. Dakanalis et al. / Eating Behaviors xxx (2013) xxx–xxx
UNCO
RREC
psychotherapy) also decrease binge eating relative to assessment-onlycontrol conditions (e.g., Agras, Walsh, Fairburn, Wilson, & Kraemer,2000; Burton & Stice, 2006) lend credence to the hypothesis that factorsother than restrictionmay play a critical role in the devolvement and/ormaintenance of binge eating (e.g., Hopwood, Clarke, & Perez, 2007;Lampard et al., 2011).
Menwith clinical or subclinical levels of EDsmay benefit from CBT-E(Fairburn, 2008), which targets the maintenance variables relevant toeach individual in addition to SWCs. If our results are confirmed infuture studies, men's ED prevention programs could be designed totarget male body concerns and mood intolerance in order to indirectlyand directly reduce men's eating disordered behaviors (Dakanalis &Riva, 2013).
4.1. Limitations
The sample mainly consisted of white heterosexual college-agedmen; potentially impacting generalizability. Future research shouldascertain whether these results could be replicated in a male clinicalsample and in men of different sexual orientation and of variousethnicities (Dakanalis et al., 2012). The cross-sectional design of thisstudy does not permit examination of causal relationships and feedbackmaintenance loops within the model (i.e., if the use of compensatorybehaviors encourage further binge eating) and therefore, enhancedexperimental and longitudinal design are needed.
4.2. Conclusions
Although the predicted relationship between restriction andbinge eating was not supported, the TM appears to fit male EDsymptomatology. Data from this study highlight the possibilitythat difficulties in emotional regulation may play a role in all formsof men's disordered eating behaviors.
Role of funding sourcesThere were no funding sources for this study and/or preparation of the manuscript.
ContributorsAuthors A.D., M.C., and A.M.Z., designed the study. Authors C.A.T., A.D. and G.R. wrote
the manuscript. Authors A.D. and G.R. conducted the statistical analysis. Authors M.C.,
Please cite this article as: Dakanalis, A., et al., Comprehensive examinationin males, Eating Behaviors (2013), http://dx.doi.org/10.1016/j.eatbeh.2013
ED C.A.T., and A.M.Z., conducted literature searches to provide background literature and
situate the study within the current state of the field. All authors have approved thisfinal version of the manuscript.
Conflict of interestAll authors declare that they have no conflicts of interest.
AcknowledgmentsThe authors would like to thank Laura Favagrossa, Valentina E. Di Mattei, Fabio
Madeddu and Lucio Sarno, and Kelly Cuccolo for their help with this manuscript.
References
Agras, W. S., Walsh, T., Fairburn, C. G., Wilson, G. T., & Kraemer, H. C. (2000). Amulticentercomparison of cognitive–behavioral therapy and interpersonal psychotherapy forbulimia nervosa. Archives of General Psychiatry, 57, 459–466.
Anderson, C. B., & Bulik, C. M. (2004). Gender differences in compensatory behaviors,weight and shape salience, and drive for thinness. Eating Behaviors, 5, 1–11.
Bastianelli, A., Vicentini, M., Spoto, A., & Vidotto, G. (2007). Risk factors for eatingdisturbances. Italian Journal of Occupational Medicine and Ergonomics: Suppl B Psychology,29, 50–55.
Burton, E., & Stice, E. (2006). Evaluation of a healthy-weight treatment program forbulimia nervosa: A preliminary randomized trial. Behaviour Research and Therapy,44, 1727–1738.
Byrne, B. (2011). Structural equation modeling with Mplus. Basic concepts, application andprogramming. New York: Routledge.
Cooper, Z., & Fairburn, C. G. (2011). The evolution of “enhanced” cognitive behaviortherapy for eating disorders: Learning from treatment nonresponse. Cognitive andBehavioral Practice, 18, 394–402.
Dakanalis, A., Di Mattei, V. E., Pagani Bagliacca, E., Prunas, A., Sarno, L., Riva, G., et al.(2012). Disordered eating behaviors among Italian men: Objectifying media andsexual orientation differences. Eating Disorders, 20(5), 356–367.
Dakanalis, A., & Riva, G. (2013). Current considerations for eating and body-relateddisorders among men. In L. B. Sams, & J. A. Keels (Eds.), Body image: Genderdifferences, sociocultural influences and health implications (pp. 195–216). New York:Nova Science Publishers.
Dakanalis, A., Timko, A., Madeddu, F., Volpato, C., Clerici, M., Riva, G., et al. (in press). Arethe male body dissatisfaction and drive for muscularity scales reliable andvalid instruments? Journal of Health Psychology. http://dx.doi.org/10.1177/1359105313498108 (in press).
Dakanalis, A., Zanetti, A.M., Clerici, M., Madeddu, F., Riva, G., & Caccialanza, R. (in press).Italian version of the Dutch Eating Behavior Questionnaire: Psychometric proprietiesand measurement invariance across sex, BMI-status and age. Appetite (in press).
Dakanalis, A., Zanetti, A.M., Riva, G., Colmegna, F., Volpato, C., Madeddu, F., et al. (in press).Male body dissatisfaction and eating disorder symptomatology: Moderating variablesamongmen. Journal ofHealth Psychology. http://dx.doi.org/10.1177/1359105313499198(in press).
Fairburn, C. G. (2008). Cognitive behaviour therapy and eating disorders. New York, US:Guildford Press.
of the trans-diagnostic cognitive behavioral model of eating disorders.10.003
Original text:
Inserted Text
"of "
Original text:
Inserted Text
"e"
Original text:
Inserted Text
"’"
Original text:
Inserted Text
"’"
Original text:
Inserted Text
"’"
Original text:
Inserted Text
"’"
Original text:
Inserted Text
","
Original text:
Inserted Text
"-"
Original text:
Inserted Text
"A. M."
Original text:
Inserted Text
"A. M."
Original text:
Inserted Text
"A. M."

302303304305306307308309310311312313314315316317318319320321322323324325326327
328329330331332333334335336337338339340341342343344345346347348349350351352353
355
5A. Dakanalis et al. / Eating Behaviors xxx (2013) xxx–xxx
Fairburn, C. G. (2010). Cognitive behavior therapy and eating disorders. Florence, IT: Eclipsidi Ipsico.
Fairburn, C. G., & Cooper, Z. (2011). Eating disorders, DMS-V, and clinical reality. TheBritish Journal of Psychiatry, 198, 8–10.
Fairburn, C. G., Cooper, Z., Doll, H. A., O'Connor, M. E., Bohn, K., Hawker, D.M., et al.(2009). Transdiagnostic cognitive–behavioral therapy for patients with eatingdisorders: A two-site trial with 60-week follow-up. American Journal ofPsychiatry, 166, 311–319.
Fairburn, C. G., Cooper, Z., & Shafran, R. (2003). Cognitive behaviour therapy foreatingdisorders: A transdiagnostic theory and treatment. Behaviour Research and Therapy,41, 509–528.
Garner, D.M. (2008). Eating Disorder Inventory—3. Florence, IT: Organizzazioni Speciali.Gross, J. J. (2007). Handbook of emotion regulation. New York, NY: Guilford Press.Hoiles, K. J., Egan, S. J., & Kane, R. T. (2012). The validity of the transdiagnostic cognitive
behavioural model of eating disorders in predicting dietary restraint. EatingBehaviors, 13, 123–126.
Hopwood, C. J., Clarke, A. N., & Perez, M. (2007). Pathoplasticity of bulimic features andinterpersonal problems. International Journal of Eating Disorders, 40, 652–658.
Hudson, J. I., Hiripi, E., Pope, H. G., & Kessler, R. C. (2007). The prevalence and correlates ofeating disorders in the national comorbidity survey replication. Biological Psychiatry,61, 348–358.
Lampard, A.M., Byrne, S. M., McLean, N., & Fursland, A. (2011). An evaluation of theenhanced cognitive–behavioral model of bulimia nervosa. Behaviour Research andTherapy, 49, 529–535.
Lavender, J. M., De Young, K. P., & Anderson, D. A. (2010). Eating Disorder ExaminationQuestionnaire (EDE-Q): Norms for undergraduatemen. Eating Behaviors, 11, 119–121.
UNCO
RRECT
354
Please cite this article as: Dakanalis, A., et al., Comprehensive examinationin males, Eating Behaviors (2013), http://dx.doi.org/10.1016/j.eatbeh.2013
OF
Lombardo, C. (2008). Italian adaptation of the Multidimensional Perfection Scale (MPS).Psicoterapia Cognitiva e Comportamentale, 14, 31–46.
Muthén, L. K., & Muthén, B. O. (1998–2007). Mplus user's guide (5th ed.)Los Angeles, CA:Muthén & Muthén.
Orlandi, E., Mannucci, E., & Cuzzolaro, M. (2005). Bulimic Investigatory Test, Edinburgh(BITE). A validation study of the Italian version. Eating Weight and Disorders, 10,14–20.
Santarnecchi, E., & Dèttore, D. (2012). Muscle dysmorphia in different degrees ofbodybuilding activities: Validation of the Italian version of Muscle DysmorphiaDisorder Inventory and Bodybuilder Image Grid. Body Image, 9, 396–403.
Schnitzler, C. E., von Ranson, K. M., & Wallace, L. M. (2012). Adding thin-idealinternalization and impulsiveness to the cognitive–behavioral model of bulimicsymptoms. Eating Behaviors, 13, 219–225.
Spoor, S. T. P., Stice, E., Bekker, M. H. J., van Stien, T., Croon, M.A., & van Heck, G. L.(2006). Relations between dietary restraint, depressive symptoms, and bingeeating: A longitudinal study. International Journal of Eating Disorders, 39,700–707.
Stice, E. (2002). Risk and maintenance factors for eating pathology: A meta-analyticreview. Psychological Bulletin, 128, 825–848.
Striegel-Moore, R. H., Rosselli, F., Perrin, N., DeBar, L., Wilson, G. T., May, A., et al. (2009).Gender difference in the prevalence of eating disorder symptoms. InternationalJournal of Eating Disorders, 42, 471–474.
Tasca, G. A., Presniak, M.D., Demidenko, N., Balfour, L., Krysanski, V., Trinneer, A., et al.(2011). Testing a maintenance model for eating disorders in a sample seekingtreatment at a tertiary care center: A structural equation modeling approach.Comprehensive Psychiatry, 52, 678–687.
OED P
R
of the trans-diagnostic cognitive behavioral model of eating disorders.10.003
Original text:
Inserted Text
"C. G."
Original text:
Inserted Text
"H. A."
Original text:
Inserted Text
"M. E."
Original text:
Inserted Text
"D. M."
Original text:
Inserted Text
"-"
Original text:
Inserted Text
"-"
Original text:
Inserted Text
"L. K."
Original text:
Inserted Text
"L. K."
Original text:
Inserted Text
"B. O."
Original text:
Inserted Text
"’"
Original text:
Inserted Text
"-"