High-Density Lipoprotein Subfractions - What the Clinicians Need to Know

CLIN. CHEM. 31/2, 217-222 (1985)
CLINICALCHEMISTRY, Vol. 31, No. 2, 1985 217
Comparison of Improved Precipitation Methods for Quantification of High-Density Lipoprotein CholesterolG. Russell Warnicl#{231}Thuy Nguyen, and Alegrla A. Albers
We compared the standard Lipid Research Clinics heparin-Mn2 (46 mmol/L) method and five improved precipitationmethods for quantification of high-density lipoprotein (HOL)cholesterol. Three of these methods-a dextran sulfate-Mg2 procedure,reportedas a Selected Method, a modifiedheparin-Mn2 (92 mmol/L) method, and a modified phos-photungstate-Mg2 procedure-all gave similar results.Three other methods-the standard heparin-Mn2’ (46mmol/L) method and two polyethyleneglycolmethods (75g/L or pH 10 reagent at 100 g/L final concentrations)-gaveslightlyhighervaluesforHDL cholesterol.Additionof NaCI orglucose to specimens did not significantly change proteinprecipitation. In terms of sedimentation effectiveness withhypertriglyceridemicspecimens,themethods were rankedinthe following order: polyethylene glycol (pH 10, 100 gIL) >dextran sulfate-Mg2 > heparin-Mn2 (92mmol/L) = poly-ethylene glycol (75 g/L) > phosphotungstate-Mg2 > hepa-rin-Mn2 (46 mmol/L).
Additional Keyphrases: hypertriglyceridemia variation, sourceof
The differential association of the lipoproteins with risk ofcoronary artery disease necessitates quantification of theindividual lipoprotein classes. Recent studies (1-3) haveemphasized the importance of lipoprotein measurement,especially that of the high-density lipoprotein (HDL) class.’Low-density lipoprotein (LDL) concentrations are often esti-mated in the routine laboratory (4). The many reports ofmethods, modifications, and evaluations in the recent litera-ture signal not only the high interest in HDL measurementbut also the difficulty of performing this measurement.Recent proficiency surveys demonstrate the magnitude ofthe problem (5-7).
HDL generally is quantified as the cholesterol remainingin the supernate afterchemical precipitation and sedimen-tation of other lipoproteins. The earliest commonly usedmethod involved precipitation with heparin and manga-nese. The original method, described by Burstein and Sa-maille (8) for serum specimens, was adapted for use withEDTA-treated plasma (9, 10) without adjusting the manga-nese concentration. Although the method was reasonablyaccurate, the manganese concentration was shown in sever-al studies (11-13) to be borderline for use with plasma,perhaps because of manganese binding by EDTA, and anincrease in manganese concentration was recommended.Doubling the manganese concentration reportedly (11) notonly improved precipitation of the non-HDL apoB-associat-ed lipoproteins but also improved sedimentation of the
Northwest Lipid Research Clinic, Harborview Medical Center,Seattle, WA 98104; and the Department of Medicine, University ofWashington, Seattle, WA.
‘Nonstandard abbreviations: HDL, LDL, VLDL, high-, low-,andvery-low-density lipoproteins, respectively; apo, apolipoprotein;EDTA, disodium ethylenediaminetetracetate.
Received May 8, 1984; accepted September 17, 1984.
insoluble lipoproteins in the presence of high concentrationsof triglyceride. However, in this combination the manganesecan interfere with some of the common enzymic cholesterolmethods (14).
In an alternative method (15) dextran sulfate and magne-sium are used. This method, published as a Selected Method(16) for HDL, was designed to optimize the conditions forremoving LDL and VLDL, the apoB-associated lipoproteins,without excessive HDL precipitation. Previous similarmethods (17, 18) had involved use of a dextran sulfate of Mr500 000 and a magnesium concentration that reportedly(19) precipitatedsome of the HDL fraction, thereby causingunderestimation of the HDL cholesterol.
A third precipitation method, with sodium phosphotung-state and magnesium, was originally described by Bursteinet al. (20) and subsequently reported (21) for routine quanti-fication of HDL cholesterol. However, the recommendedconcentrations were later reported (19) to precipitate someH])L and underestimate the HDL concentration. A subse-quent modification (22) with less phosphotungstate andmagnesium reportedly had improved accuracy. Polyethyl-ene glycol (Mr 6000) was used at 120 g/L to precipitate thelipoproteins (23), but this concentration was reported toprecipitate significant quantities of HDL (19). In subsequentmodifications 100 g per liter of polyethylene glycol was used(24) and then 75 g/L (25). In another modification (26), thefinal polyethylene glycol concentration was 100 g/L, withthe pH of the reagent adjusted to 10.
Our evaluation of improved or “second-generation” HDLmethods was undertaken to assess their agreement onnormolipidemic specimens and on specimens with high andlow concentrations of cholesterol, triglyceride, and HDL.Therefore, the methods were compared on specimens with arange of total cholesterol, triglyceride, and HDL cholesterolvalues. We also tested specimens to which we added eithersodium chloride, to increase the ionic strength, or glucose, toapproximate a specimen from a diabetic patient-factorsthat reportedly affect lipoprotein precipitation (27). Methodswere compared for effectiveness of lipoprotein sedimenta-tion, by checking the proportion of specimens with turbidsupernates. Cholesterol was measured in all supernates. Wemeasured total protein in a subset of supernates and precipi-tates to determine whether the effectiveness of sedimenta-
tion of hypertriglyceridemic specimens might be due tocoprecipitation of other plasma proteins.
Materials and Methods
Specimens
Blood samples were collected between June 1981 and May1983 at the Northwest Lipid Research Clinic from malesand females, ages 6 to 75 years, according to establishedprotocol (10). A combination of apparently healthy volun-teers and hyperlipidemic referral patients provided speci-mens with a broad range of values for cholesterol, triglycer-ide, and HDL cholesterol. Plasma total cholesterol rangedfrom 1.42 to 10.35 g/L and total triglyceride from a low of
218 CLINICALCHEMISTRY, Vol. 31, No. 2, 1985
0.33 g/L to a high of 77.60 g/L. All subjects reported in themorning alter a 12- to 14-h fast. Blood from the antecubi-tal vein was collected into 15-mL Vacutainer Tubes contain-ing 22.5 mg of EDTA, mixed thoroughly, and cooled mime-diately at 4 #{176}C.
Within 3 h we removed blood cells by centrifugation at1500 x g for 20 mm. Plasma specimens were then stored at4#{176}Cfor lipoprotein separation by the various precipitationmethods. This was done the day of sample collection or, atthe latest, the following day.
Separation of Lipoproteinsby PrecipitationThe indicated precipitation methods were applied concur-
rently to aliquots from each specimen. In some cases,specimen volume was insufficient to perform all precipita-tion methods and some methods were deleted. Precipitatingreagents at concentrations described below were added andvortex-mixed to samples that were either equilibrated toroom temperature (23-27 #{176}C)or kept at 4 #{176}Cas indicated.The temperature and duration of incubation varied asindicated below. All sedimentation of insoluble lipoproteinaggregates was done by centrifugation at 4#{176}C,but the g-force and duration used were specific for each method.
Dextran sulfate (50)-Mg2 (15): We prepared a 20 g/Lsolution of dextran sulfate (Dextralip 50, 5 x iO D, lot no.251-118A; Sochibo S.A., 92100 Boulogne, France), to whichwas added a sodium azide-chloramphenicol-gentamicin so-lution (15) as preservative, and a 1.0 mol/L solution ofMgCl2 . 61120 (lot no. 946-7510; J. T. Baker Co., Phillips-burg, NJ 08865), adjusted to pH 7.0. Both were stored inglass-stoppered vials at 4 #{176}C.The working reagent wasprepared freshly each week by mixing equal volumes of theabove two solutions.
To 2.0 mL of plasma we added 200 1zL of the dextransulfate-Mg2+ combined solution, mixed thoroughly for 8-10s, and incubated at room temperature for 15 mm beforecentrifuging at 1500 x g for 30 win.
Heparin-Mn2: We evaluated two methods involvingone at a final concentration of 46 mmol/L and the
second at 92 mmolIL. The final concentration of heparin was1.3 g/L in both cases.
Heparin-Mn2 (46 mmol/L) (10): The heparin reagent,stored at 4#{176}C,contained 5 x i03 USP units/L, prepared bydiluting one part of sodium heparin (Liquaemin sodium, 4 xio USP unitsfL; Organon Co., West Orange, NJ 07052) withseven parts 0.15 mol/L NaCl solution. A 1.0 mol/L solutionof MnCl2 . 4H0 (reagent grade, J. T. Baker Co.) was alsoprepared.
To 2.0 mL of each specimen we added sequentially (withthorough mixing after each addition) 80 pL of the aboveheparin reagent and 100 pL of 1.0 moWL MnCl2 solution.This mixture was incubated at 4#{176}Cfor 30 win, thencentrifuged at 1500 x g for 30 win.
Heparin-Mn2 (92 inolIL) (11): For this method, theworking reagent was a heparin-Mn2 combined solutionobtained by mixing 0.6 mL of the above heparin stock (4 xi07 USP units/L) with 10 mL of 1.06 mol/L MnC12 solution.
To 2.0 mL of plasma we added 200 L of the heparin-Mn2 combined reagent, mixed, and incubated the solutionfor 10 mm at room temperature before centrifugation as inthe other heparin-Mn2 method.
Phosphotungstate-Mg2 (22): We prepared a 40 g/L sodi-um phosphotungstate solution by dissolving 4 g ofphosphotungstate acid (lot no. 68C-0366; Sigma ChemicalCo., St. Louis, MO 63178) in approximately 50 mL of de-ionized water, adding 16 mL of 1.0 mol/L NaOH (reagentgrade; Mallinckrodt, Inc., St. Louis, MO 63147) adjustingthe pH of the solution to 7.4 with NaOH, and diluting to 100
mL with de-ionized water. The concentration of the MgCl2solution was 2.0 mol/L. For the combined working reagentwe mixed four volumes of the sodium phosphotungstatesolution with one volume of the MgCl2 solution.
Lipoproteins were precipitated from 2-mL aliquots ofspecimens by adding, with thorough mixing, 200 L of thecombined phosphotungstate-Mg2 reagent. After incuba-tion for 5 win at room temperature, the samples werepromptly centrifuged at 5000 x g for 10 win.
Polyethylene glycol 6000 (100 gIL final concentration, pH10) (26): The reagent solution was prepared by dissolving 20g of polyethylene glycol 6000 (lot no. 81260; Fluka AGChemische Fabrik, CH-9470 Buchs SG, F.R.G.) and 1.50 g(20 mmol) of glycine (lot no. 003362; J. .T. Baker Co.) inabout 60 mL of de-ionized water. We then adjusted the pH ofthe solution to pH 10 with 1.0 mol/L NaOH before diluting itto 100 mL with de-ionized water.
To 1.0 mL of specimen we added an equal volume of thepolyethylene glycol solution, mixed thoroughly for 8-10 s,and then incubated the mixture at room temperature for 10rein before centrifugation at 1500 x g for 30 mm.
Polyethylene glycol 6000(75 gIL final concentration) (25):This reagent was prepared by dissolving 45 g of polyethyl-ene glycol 6000 in 100 mL of de-ionized water. We added 400iL of the reagent to a 2.0-mL aliquot of plasma. Becausethis polyethylene glycol solution was viscous, we were verycareful to transfer the indicated volume. We mixed thesample thoroughly, incubated it at room temperature for 15mm, and then centrifuged it at 1500 x g for 30 mm.
Lipid AnalysisCholesterol and triglycerides were quantified by Lipid
Research Clinic procedures (10) for continuous-flow analysis(AutoAnalyzer II). Supernates were mixed thoroughly toresuspend any precipitates before extraction into isopro-panol in the presence of a zeolite mixture. We determinedcholesterol by a method involving the Liebermann-Bur-chard reagent (10) and triglyceride by a fluorometric proce-dure involving 2,4-pentanedione (10). Standard solutionsand quality-control samples were provided by the ClinicalChemistry Standardization Laboratory, Centers for DiseaseControl, Atlanta, GA 30333; moreover, our own analyticalprocedures met their standardization requirements. Preci-sion was excellent, with CVs of <1.0% for cholesterolmeasurement, including the HDL cholesterol range. For theprecipitation step and HDL cholesterol measurement, theCVs were approximately 3%.Analysis conditions were also designed to maximize the
measurement precision in the supernates that have low
HDL concentrations. To eliminate between-run and be-tween-tray variation, comparison samples from each subjectwere analyzed consecutively in one tray. Systentatic biaseffects of within-tray baseline drift and scaleexpansion wereminimized by randomizing the order of the comparisonsamples for each subject. The precipitating reagents did notinterfere with this cholesterol procedure.
Ultrafiltration
The incomplete sedimentation of lipoprotemn aggregatesthat may occur in hypertriglyceridemic specimens results inturbid or cloudy supernates and overestimation of HDL. Inthis study we wiped tubes free of condensate and carefullyinspected for turbidity immediately after their removal fromthe centrifuge. Any turbid supernates were clarified byultrafiltration (28) through 25-mm Millipore filters(0.22-p.m pore size; Millipore Co., Bedford, MA 01730), protectedby two prefilters. Turbid supernates (volume must be 1.5mL or greater) were transferred by pipetting into a Luer-tip
C
o.
/,1
//‘
‘I
2
2
2
5LFATE SOI-L2. C51STER
//
/
V..t.
/
//0(0500 SULFaTE SOT-FIG?. CHOLESTEROL IflO’LI
CLINICAL CHEMISTRY, Vol. 31, No. 2, 1985 219
syringebarrel attached to the Swinnex upper part and wereforced through the filter with moderate pressure from theplunger. The clear ifitrates were collected for analysis.
Matrix EffectsWe pipetted 9.0-mL aliquots of each plasma pool into each
of three 10-mL volumetric flasks, to compare the methodsfor specimens to which either sodium chloride or glucosewas added to approximate extreme specimens that might beencountered. To one flask we added 8.77 mg of NaC1(approximately 10% increase in final concentration); to thesecond flask we added 40 mg of glucose. All three flaskswere carefully adjusted to 10-mL final volume with 0.15moIJL NaCl solution. We then precipitated duplicate ali-quota from each flask, applying each, separation method.
Protein MeasurementWe prepared standards of bovine serum albumin (Cohn
Fraction V, fatty acid free; Sigma Chemical Co.) in salinesolution. Aliquots of the supernates obtained from thevarious I{DL precipitation methods were diluted with 0.15mol/L NaCl. The corresponding precipitates were resolubi-lized in 0.15 mo)JL NaCl solution, and the final volumeaccurately measured. To aliquots (in triplicate) of the dilut-ed supernate and precipitate solutions we added 25 p.L ofsodium deoxycholate (Sigma) 20 g/L, and the appropriatevolume of saline to give a final volume of 1.5 mL. Afterthorough vortex-mixing and standing for about 15 rein, 0.5mL of trichloroacetic acid (24%) was added, and the mixture
was then centrifuged at 1500 x g for 30 mm. The trichloro-acetic acid supernates were aspirated carefully, and theprotein in the remaining pellet was assayed by use of amodified Lowry procedure (29). Protein concentrations werereported in terms of the original specimen volume.
Results and DiscussionThe dextran sulfate-Mg’ method was selected as the
comparison method for this report because previous studies(15, 16) demonstrated good specificity for HDL separation.
In the earlier work (15, 16) dextran sulfate-Mg super-nates of EDTA-treated plasma contained virtually no apoB,indicating specific separation of LDL. On the other hand,the dextran sulfate-Mg precipitate fractions containedlittle apoA-I, suggesting that precipitation of HDL was notexcessive.
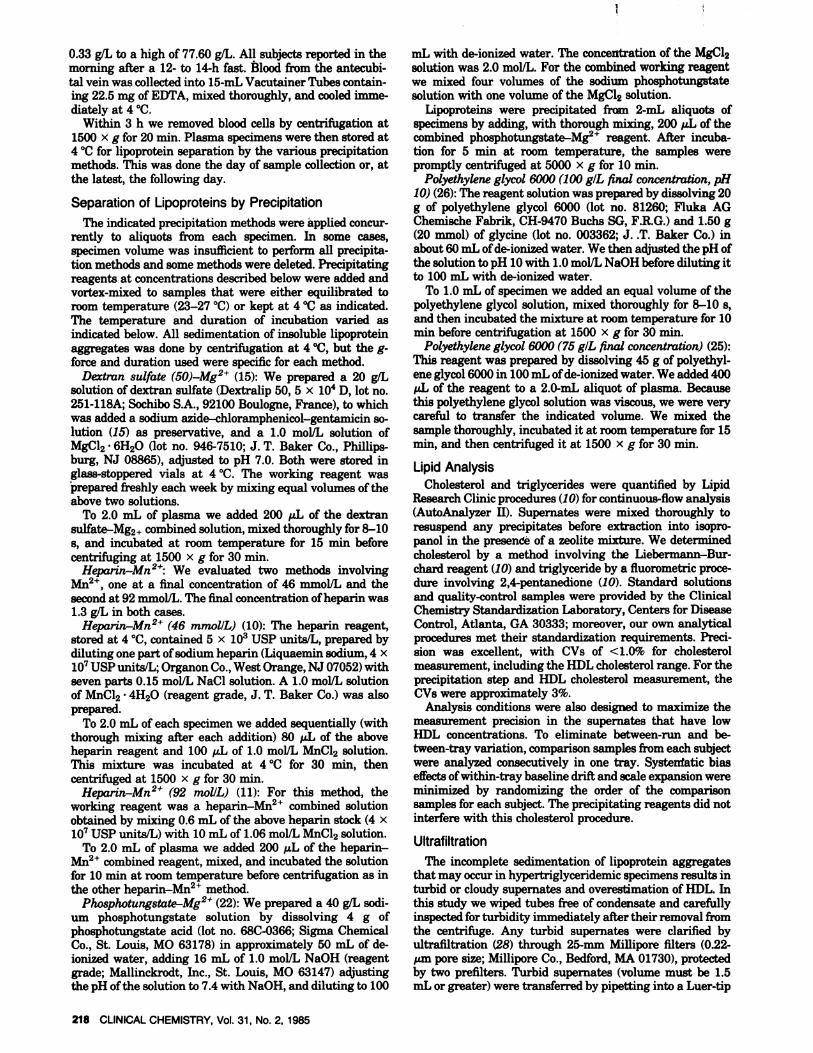
The agreement of each precipitation method with thedextran sulfate-Mg comparison method is illustrated inFigure 1. Results by the heparin-Mn2 (46 mmol/L) methodwere highly correlated (0.995) and in reasonably goodagreement with those by the dextran sulfate method, asshown by a slope of 1.05 and a y-intercept of -21 mgfL(Figure la). Although heparin-Mn2” (46 mmol/L) valueswere generally somewhat higher at higher HDL, thiswascompensated by a slight tendency for underestimation atlow HDL levels, and the overall difference in this set ofspecimens was small and not statistically significant.
The modified heparin-Mn2 (92 mmol/L) method gave
slightly lower values. The agreement with the dextransulfate method was excellent, with a correlation coefficientof 0.997, slope of 1.01, andy-intercept of -10.4 mg/L (Figurelb). Even though the heparin-Mn2 results averaged only 6mg/L lower (464 vs 470 mgfL) the small difference wasconsistent throughout the range and statistically significant(p sO.005).
These relationships are consistent with previous reports.
The standard heparin-Mn2 (46 mmol/L) method has beenreported (11-13, 15, 16) to slightly overestimate HDL inEDTA-treated plasma specimens, owing to incomplete pre-cipitation of the apoB-associated lipoproteins (VLDL and/orLDL). At 46 mmol/L the 2+ concentration reportedly wasmarginal for complete precipitation of LDL, and a higher2+ concentration was recommended (11, 13, 30).
More than 10 years of experience with the standardheparmn-Mn2 (46 mmolJL) method in this laboratory sup-port these conclusions and suggest that in inexperiencedhands the overestimation by this method might be largerthan that observed here. From 1976 to 1980 we quantifiedapoB-associated lipoproteins by a radial immunodiffusionassay in our routine heparin-Mn2 (46 mmolJL) supernates.
I,
/DrxrRwSuLERrE SQl-M02. COLE5TER& I IL I
5IRrE so -G2. COOI#{128}5tEROl GIL
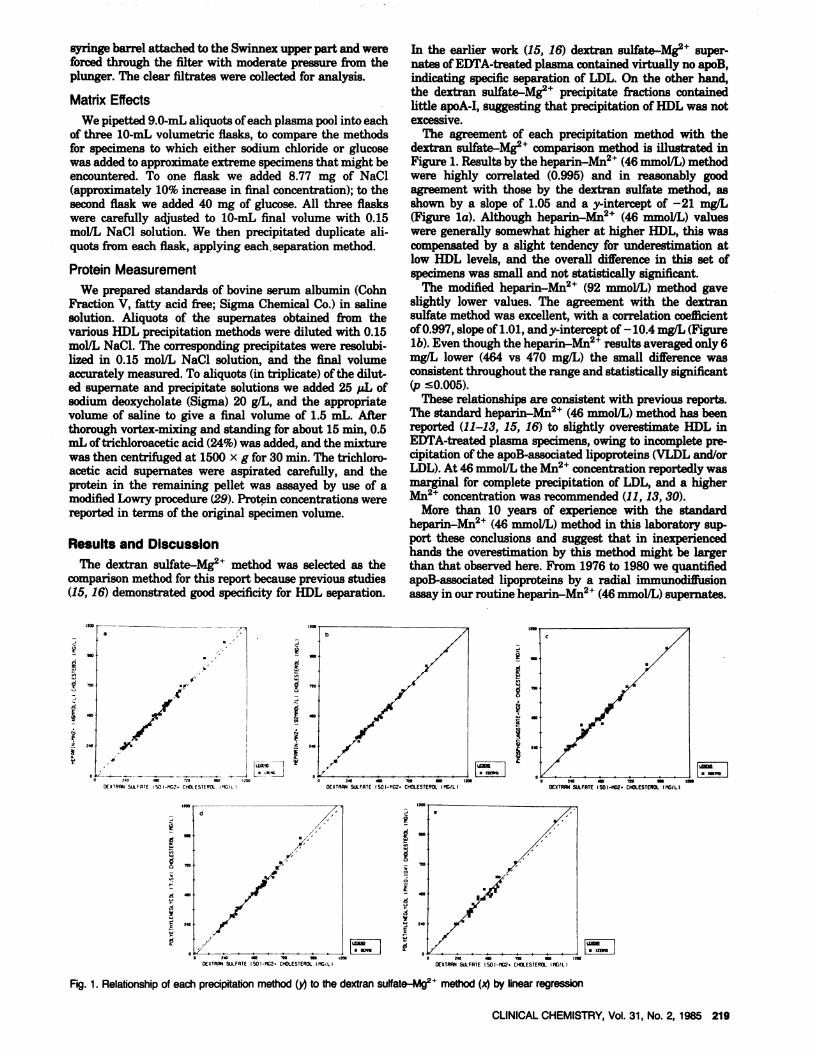
Fig. 1. Relationship of each precipitationmethod (.) to the dextran sulfate-Mg2 method (x) by linear regression
220 CLINICAL CHEMISTRY, Vol. 31, No. 2, 1985
With this feedback on the specificity of the separation, theamount of apoB-associated lipoprotein in supernates de-creased, probably because of improvements in technique.Greater care was taken in preparing the reagents to ensurethat the critical Mn2 concentration was exact and not low.In addition, technologists became increasingly aware thateven slightly turbid supernates contained significant apoB,because of incomplete LDL/VLDL sedimentation, and morecare was given to detect turbid supernates that were subject-ed to dilution or ultrafiltration. Without this experience andcare, overestimation by the standard heparin-Mn2 proce-dure could likely be greater.
Results by the modified phosphotungstate method werealso in excellent agreement with those by the dextransulfate method (Figure ic). The correlation coefficient was0.993, with slope of 0.998 andy-intercept of 2 mg/L. For 59specimens the means for the phosphotungstate method andfor the dextran sulfate method were 470 mg/L and 469 mgIL, respectively, not statistically significantly different. Notethat the final concentrations of phosphotungstate and Mg2we used in this comparison were lower than in mostprevious studies. Because the higher concentrations usedpreviously resultedin underestimated HDL cholesterol (19),this modification appears to improve the accuracy of thephosphotungstate-Mg method.
On the other hand, the polyethylene glycol method with afinal reagent concentration of 75 g/L gave slightly higherresults(492 vs 484 mg/L), but again the difference was notstatistically significant in this set. Figure id illustrates thatthe tendency for positive bias is especially apparent onspecimens with high HDL concentrations, as evidenced bythe slope of 1.06 partly compensated by a negative y-intercept. Clearly, the final concentration of 75 g/L usedhere improved the accuracy of HDL measurement as com-pared with previous versions in which higher polyethyleneglycol concentrations were used. However, a 75 g/L finalconcentration of polyethylene glycol may be slightly low. Adisadvantage of this particular polyethene glycol method isthe viscosity of the concentrated polyethylene glycol solu-tion, which necessitates considerable care to transfer the fullvolume of reagent.
The final method, in which we used polyethylene glycoladjusted to pH 10 at a final concentration of 100 g/L, gave asimilar pattern (Figure le) with slope of 1.05, y-intercept of-13, but slightly more scatter (r = 0.985). Adjustment of thepH to 10 apparently inhibits lipoprotein precipitation andcompensates for the higher reagent concentration as com-pared with the previous methods.
This comparison demonstrates that these modifications ofthe precipitation methods improve their accuracy. Theagreement observed here is much betterthan that observedwith earlier versions of the same methods (19). Further-more, the small between-method differences observed hereresultprimarily from specimens with high HDL concentra-tions. Considering only the subset of specimens with highHDL (�500 mgIL by dextran sulfate-Mg), we observedthe following positive or negative differences in comparisonwith dextran sulfate-Mg values: + 10 mg/L (for heparin-Mg2, 46 mmol/L), -6 mg/L (heparin-Mn2, 92 mmolJL),-3 mg/L (phosphotungstate-Mg), + 13 mg/L (polyethyl-ene glycol, 7.5%), and + 10 mg/L (polyethylene glycol, pH 10,10%). The differences for heparin-Mn2 (46 mrnol/L) andpolyethylene glycol (7.5%) were statistically significant (p0.05).
The Lipid Research Clinics’ cholesterol method used forthis evaluation was not subject to interference by any of theprecipitation reagents. Therefore, the comparison resultswere not confounded by the interference effects that have
been reported for enzymic cholesterol methods. The interfer-ence of Mn2’4’ with enzymic cholesterol analyses is wellknown (14). Dextran sulfate of Mr 500000 reportedly (31)interferes negatively with enzymic assay. The 50 000-Dadextran sulfate used here was demonstrated not to interferewith some enzymic methods (15). Sodium phosphotungstatereportedly(32) may interfere with some methods.
The ionic strength of the sample has been reported (27) toaffect lipoprotein precipitation by some methods. In ourstudy, addition of sodium chloride to plasma pools to in-crease the ionic strength by about 10% did not significantlychange the mean values for cholesterol in the supernate inany of the precipitation methods: for each of the variousprecipitation methods on four pools to which sodium chlo-ride was added these values were all within 10 mgIL of thosefor the unaltered control pools by each precipitation method.The differences between the various precipitation methodson the pools with and without added sodium chloride weresimilar to those illustrated in Figure 1. These resultssuggest that even though ionic strength has been reportedto affect lipoprotein precipitation, variations within theexpected physiological range are unlikely to have a signifi-cant effect on HDL cholesterol as measured by any of thesemethods. Similarly, the addition of approximately 500mg ofglucose per deciliter to pools, to approximate a diabeticspecimen, also did not significantlychange values forsuper-natant cholesterol by any of the precipitation methods:mean values for glucose treated and control pools differed byless than 10 mg/L for each of the precipitation methods.
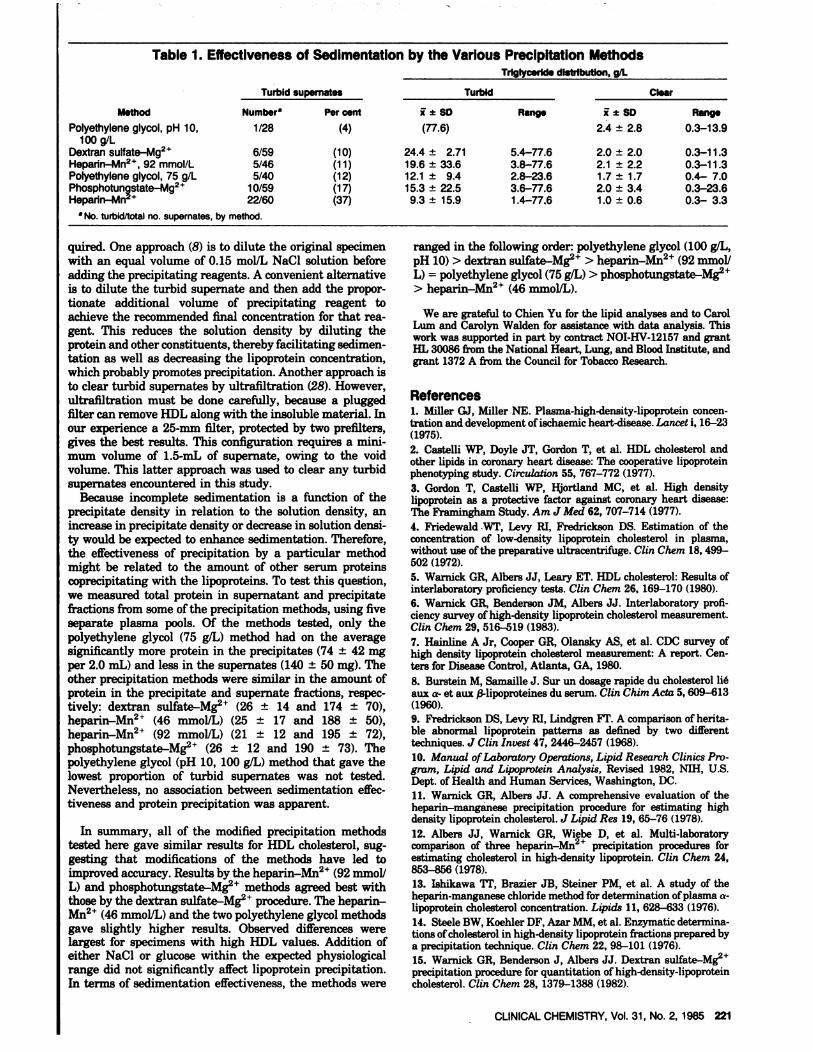
The next problem to be considered is that of turbidity orcloudiness seen in supernates immediately after centrifuga-tion, a problem usually associated with incomplete sedimen-tation of the insoluble VLDLILDL aggregates. This oftenoccurs with hypertriglyceridemic specimens, because thetriglycerides make the overall density of the aggregateabout the same as that of the solution. In this instance, theinsoluble lipoproteins are not sedimented by low-speedcentrifugation. In our study, some precipitation methodsproduced better sedimentation than others. The polyethyl-ene glycol method (pH 10-100 g/L) had 4% (one of 28) turbidsupernates (Table 1). Only one specimen, with triglyceridesof 77.6 g/L, did not give a clear supernate, and specimenswith triglycerides up to 13.9 g/L separated well. The dextransulfate method had 10% (sixof 59) turbidsupernatesandspecimens with triglycerides up to 11.3 g/L gave clearsupernates, while specimens with triglyceride concentra-tions as low as 5.4 g/L gave turbid supernates. The heparin-Mn2 (92 mmol/L) method and the polyethylene glycol (75 gIL) methods were similar, with 11% and 12% turbid super-nates, respectively. The heparin-Mn2’4 method appeared tobe slightly better overall, because the range of triglyceridesin specimens with both clear and turbid supernates washigher. This version of the phosphotungstate-Mg methodhad 17% turbid supernates. The range of triglyceride valuesfor this method was somewhat unusual. Some high-triglyc-eride specimens gave clear supernates, but some specimenswith low triglycerides gave turbid supernates. The heparin-Mn2 (46 mmolIL) method gave the highest proportion ofturbid supernates, 37%.
Turbidity of the supernate generally is the result ofincomplete sedimentation of the insoluble lipoproteins-inour experience one of the major sources of error in HDLcholesterol quantitation. In proficiency surveys (5, 6) theinter-laboratory variation was generally highest for hyper-triglyceridemic specimens. Measurement of cholesterol in aturbid supernate overestimates HDL cholesterol, in somecases substantially.
To avoid this overestimation, further treatment is re-
CLINICAL CHEMISTRY, Vol. 31, No. 2, 1985 221
Table 1.
Method
Effectiveness of Sedimentation
Turbid supernates
by the Various PrecipitatiTriglyceride di
on Methodsstrlbutlon, g/L
Turbid Clear
Number Per cent i a SD Range i a SD RangePolyethylene glycol, pH 10,
100 g/LDextran sulfate-Mg2Heparin_Mn2*, 92 mmol/LPolyethylene glycol, 75 g/LPhosphotungstate-Mg2Heparin-Mn
a No. turbid/total no. supernate
1/28 (4)
6/59 (10)5/46 (11)5/40 (12)
10/59 (17)22/60 (37)
S. by method.
(77.6)
24.4 ± 2.7119.6 ± 33.612.1 ± 9.415.3 ± 22.59.3 ± 15.9
5.4-77.63.8-77.62.8-23.63.6-77.61.4-77.6
2.4 ± 2.8
2.0 ± 2.02.1 ± 2.21.7 ± 1.72.0 ± 3.41.0 ± 0.6
0.3-13.9
0.3-11.30.3-11.30.4-7.00.3-23.60.3- 3.3
quired. One approach (8) is to dilute the original specimenwith an equal volume of 0.15 mol/L NaC1 solution beforeadding the precipitating reagents. A convenient alternativeis to dilute the turbid supernate and then add the propor-tionate additional volume of precipitating reagent toachieve the recommended final concentration for that rea-gent. This reduces the solution density by diluting theprotein and other constituents, thereby facilitating sedimen-tation as well as decreasing the lipoprotein concentration,which probably promotes precipitation. Another approach isto clear turbid supernates by ultrafiltration (28). However,ultrafiltration must be done carefully, because a pluggedifiter can remove HDL along with the insoluble material. Inour experience a 25-mm ifiter, protected by two prefilters,gives the best results. This configuration requires a mini-mum volume of 1.5-mL of supernate, owing to the voidvolume. This latter approach was used to clear any turbidsupernates encountered in this study.
Because incomplete sedimentation is a function of theprecipitatedensity in relation to the solution density, anincreasein precipitatedensity or decrease in solution densi-ty would be expected to enhance sedimentation. Therefore,the effectiveness of precipitation by a particular methodmight be related to the amount of other serum proteinscoprecipitating with the lipoproteins. To test this question,we measured total protein in supernatant and precipitatefractions from some of the precipitation methods, using fiveseparate plasma pools. Of the methods tested, only thepolyethylene glycol (75 g/L) method had on the averagesignificantly more protein in the precipitates (74 ± 42 mgper 2.0 mL) and less in the supernates (140 ± 50 mg). Theother precipitation methods were similar in the amount ofprotein in the precipitate and supernate fractions, respec-tively: dextran sulfate-Mg (26 ± 14 and 174 ± 70),heparin-Mn24’ (46 mmolJL) (25 ± 17 and 188 ± 50),heparin-Mn2 (92 mmol/L) (21 ± 12 and 195 ± 72),phosphotungstate-Mg2 (26 ± 12 and 190 ± 73). Thepolyethylene glycol (pH 10, 100 g/L) method that gave thelowest proportion of turbid supernates was not tested.Nevertheless, no association between sedimentation effec-tiveness and protein precipitation was apparent.
In summary, all of the modified precipitation methodstested here gave similar results for HDL cholesterol, sug-gesting that modifications of the methods have led toimproved accuracy. Results by the heparin-Mn2 (92 mmolJL) and phosphotungstate-Mg2 methods agreed best withthose by the dextran sulfate-Mg procedure. The heparin-Mn2’ (46 mmol/L) and the two polyethylene glycol methodsgave slightly higher results. Observed differences werelargest for specimens with high HDL values. Addition ofeither NaC1 or glucose within the expected physiologicalrange did not significantly affect lipoprotein precipitation.In terms of sedimentation effectiveness, the methods were
ranged in the following order: polyethylene glycol (100 gIL,pH 10) > dextran sulfate-Mg2 > heparin-Mn2’4’ (92 mmollL) = polyethylene glycol (75 g/L) > phosphotungstate-Mg> heparin-Mn” (46 mmol/L).
We are grateful to Chien Yu for the lipid analyses and to CarolLum and Carolyn Walden for assistance with data analysis.Thiswork was supported in part by contract NOI-HV-12 157 and grantHL 30086 from the National Heart, Lung, and Blood Institute, andgrant1372 A from the Council for Tobacco Research.
References1. Miller GJ, Miller NE. Plasma-high-density-lipoprotein concen-tration and developmentofischaemic heart-disease. Lancet i, 16-23(1975).2. Castelli WP, Doyle JT, Gordon T, et al. HDL cholesterol andother lipids in coronaryheart disease: The cooperative lipoproteinphenotyping study. Circulation 55,767-772 (1977).
3. Gordon T, Castelli WP, Hjortland MC, et al. High densitylipoprotein as a protective factor against coronary heart disease:The Framinghain Study. Am J Med 62, 707-714 (1977).
4. Friedewald WT, Levy RI, Fredrickson DS. Estimation of theconcentration of low-density lipoprotein cholesterol in plasma,without use of the preparative ultracentrifuge. Clin Clam 18,499-502 (1972).
5. Warnick GR, Albers JJ, Leary ET. HDL cholesterol: Results ofinterlaboratory proficiency tests. Clin Clam 26, 169-170 (1980).6. Warnick GR, Benderson JM, Albers JJ. Interlaboratory profi-ciency survey of high-density lipoprotein cholesterol measurement.Clin Clam 29, 516-519 (1983).7. Hainline A Jr,Cooper GR, Olansky AS, et al. CDC survey ofhigh density lipoprotein cholesterol measurement: A report.Cen-ters for Disease Control, Atlanta, GA, 1980.8. Burstein M, Samaille J. Sur un dosage rapide du cholesterol lieaux a- etaux /3-lipoproteines du serum. Clin Chim Acta 5,609-613(1960).9. Fredrickson DS, Levy RI, Lindgren yr. A comparison of herita-ble abnormal lipoprotein patterns as defined by two differenttechniques. J Clin Invest 47,2446-2457 (1968).10. Manual of Laboratoiy Operations, Lipid Research Clinics Pro-gram, Lipid and Lipoprotein Analysis, Revised 1982, NIH, U.S.Dept. of Health and Human Services,Washington, DC.11.Warnick GR, Albers JJ. A comprehensive evaluation of theheparin-manganese precipitation procedure for estimating highdensity lipoprotein cholesterol. J Lipid Res 19,65-76 (1978).
12. Albers JJ, Warnick GR, Wiebe D, et al. Multi-laboratorycomparison of three heparin-Mn2’ precipitation procedures forestimating cholesterol in high-density lipoprotein. Clin Clam 24,853-856 (1978).13. IshikawaTI’, Brazier JB, Steiner PM, et al. A study of theheparin-manganese chloride method fordeterminationofplasma a-lipoprotein cholesterol concentration. Lipids 11, 628-633 (1976).14. Steele BW, Koehler DF, Azar MM, et al. Enzymatic determina-tions of cholesterol in high-density lipoprotein fractions prepared bya precipitation technique. Clin Clam 22,98-101 (1976).
15. Warnick GR, Benderson J, Albers JJ. Dextran sulfate-Mg2precipitation procedure for quantitation of high-density-lipoproteincholesterol. Clin Clam 28, 1379-1388 (1982).

222 CLINICAL CHEMISTRY, Vol. 31, No. 2, 1985
16. Warnick GR, Benderson J, Albers JJ. Dextran sulfate-Mgprecipitation procedure for quantitation of high.density-lipoproteincholesterol. Selected Methods Clin Clam 10,91-99 (1983).
17. Kostner GM. Enzymatic determination of cholesterol in high-density lipoprotein fractions prepared by polyanionprecipitation.Clin Clam 22,695 (1976). Letter.
18. Finley PR, Schifman RB, Williams RJ, Lichti DA. Cholesterolin high-density lipoprotein: Use of Mg7dextran sulfate in itsenzymic measurement. Clin Clam 24, 931-933 (1978).
19.Warnick GR, Cheung MC, Albers JJ. Comparison of currentmethods forhigh-densitylipoproteincholesterolquantitation.ClinClam 25,596-604 (1979).
20. Burstein M, Scholnick HE, Morfin R. Rapid method fortheisolation of lipoproteins from human serum by precipitation withpolyanions. J Lipid Res 11, 583-595 (1970).
21. Lopes-Virella MI, Stone P, Ellis 5, Colwell JA. Cholesteroldetermination in high-density lipoproteins separated by three dif.ferent methods. Clin Clam 23, 882-884 (1977).
22. Kostner GM, Avogaro P, Bittolo Bon G, et al. Determination ofhigh-density lipoproteins: Screening methods compared. Clin Clam25, 939-942 (1979).
23. Vikari J. Precipitation of plasma lipoproteins by PEG-6000 andits evaluation with electrophoresis and ultracentrifugation. ScandJ Clin Lab Invest 36, 265-268 (1976).
24. Allen JK, HensleyWJ, Nicholls AV, Whitfield JB. An enzymicand centrifugal method for estimating high-density lipoproteincholesterol. Clin Clam 25, 325-327 (1979).
25. Demacker PNM, Humans AGM, Vos-Janasen HE, et al.Astudyoftheuse ofpolyethyleneglycolinestimatingcholesterol inhighdensitylipoprotein.Clin C/tern 26,1775-1779 (1980).
26. law C, Grub F, Murador E. Improved method for determina-tion of high-density-lipoprotein cholesterol. I. Isolation of high-density lipoproteins by use ofpolyethyleneglycol6000.Clin Clam27, 371-374 (1981).27. Burstein M, Legmann P. Lipoprotein Precipitation, S. Karger,Basel, Switzerland, 1982.28. Warnick GR, Albers JJ. Heparin/Mn2 quantitation of high-density lipoprotein cholesterol: An ultrafiltration procedure forlipemic samples. Clin Clam 24, 900-904 (1978).29. Bensadown A, Weinstein D. Assay of proteins in the presence ofinterfering materials. Anal Biochem 70, 241-250 (1976).30. Mao SJT, Kottke BA. Determination of high-density lipopro-tein cholesterolby heparin-MnCl2 precipitation. Clin Clam 26,1369 (1980).31. Henderson LO, LaGarde E, Herbert PN. Artifactual reductionof high-density lipoprotein cholesterol estimates after dextran sul-fate-Mg precipitation. Am J Clin Pathol, 664-668 (1980).32. Niedmann PD, Luthe H, Wieland H, et al. Richtigkeit derHDL-Cholesterinmessung. Kim Woclanschr 61, 133-138 (1983).
Copyright © 2022 FDOKUMEN