COMPARISON OF VARIOUS EYE PROTECTION METHODS ...
93
COMPARISON OF VARIOUS EYE PROTECTION METHODS UNDER GENERAL ANESTHESIA BY Dr. Nikhil George Dissertation Submitted to the Rajiv Gandhi University Of Health Sciences, Karnataka, Bangalore In partial fulfillment Of the requirements for the degree of Doctor of Medicine in Anaesthesiology Under the guidance of Dr. SAVITHA K.S. Department of Anesthesiology St. John’s national academy of health sciences Bangalore 2009
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of COMPARISON OF VARIOUS EYE PROTECTION METHODS ...

COMPARISON OF VARIOUS EYE PROTECTION METHODS UNDER GENERAL ANESTHESIA
BY
Dr. Nikhil George
Dissertation Submitted to the Rajiv Gandhi University Of Health Sciences, Karnataka, Bangalore
In partial fulfillment Of the requirements for the degree of
Doctor of Medicine
in
Anaesthesiology
Under the guidance of Dr. SAVITHA K.S.
Department of Anesthesiology St. John’s national academy of health sciences
Bangalore
2009

DECLARATION BY THE CANDIDATE
I hereby declare that this dissertation/thesis entitled” A Comparison of Various Eye
Protection Methods Under General Anesthesia ” is a bonafide and genuine research work
carried out by me under the guidance of Dr. Savitha K.S., Professor, Department of
Anaesthesiology.
Dr. Nikhil George
15/10/2009
Bangalore

CERTIFICATE BY THE GUIDE
This is to certify that the dissertation entitled “ A Comparison of Various Eye Protection
Methods Under General Anesthesia” is a bonafide research work done by Dr. Nikhil George
in partial fulfilment of the requirement for the degree of Doctor of medicine in
Anaesthesiology.
Dr. Savitha K.S.
15/10/2009 Professor,
Department of Anaesthesiology,

ENDORSEMENT BY THE HEAD OF THE DEPARTMENT
This is to certify that the dissertation entitled “A Comparison of Various Eye Protection
Methods Under General Anesthesia ” is a bonafide research work done by Dr.Nikhil
George under the guidance of Dr. Savitha K.S., Professor , Department of Anaesthesiology.
15/10/2009
Bangalore
Dr. Radhika Dhanpal
Head of Department
Department of Anaesthesiology

ENDORSEMENT BY THE DEAN
This is to certify that the dissertation entitled “A Comparison of Various Eye Protection Methods
Under General Anesthesia” is a bonafide research work done by Dr. Nikhil George under the
guidance of DR.Savitha K.S., Professor , Department of Anaesthesiology.
Dr. Prem Pias,
Dean,
St. John’s National academy of health sciences
15/10/2009
Bangalore

COPYRIGHT
Declaration by the Candidate I hereby declare that the Rajiv Gandhi University of Health Sciences, Karnataka shall
have the rights to preserve, use and disseminate this dissertation / thesis in print or electronic
format for academic / research purpose.
© Rajiv Gandhi University of Health Sciences, Karnataka
15/10/2009
Bangalore
Dr. Nikhil George

TABLE OF CONTENTS
1. Introduction Page No.1
2. Objectives Page No.3
3. Review of Literature Page No.5
4. Methodology Page No.32
5. Results Page No.37
6. Discussion Page No.51
7. Conclusion Page No.63
8. Summary Page No.65
9. Bibliography Page No.68
10. Annexures Page No.73

LIST OF ABBREVIATIONS
ASA American Society of Anesthesiology
ATP Adenosine Tri Phosphate
ECG Electrocardiogram
Ig Immunoglobulin
GA General Anesthesia
HPMC Hydroxy Propyl Methyl Cellulose
mm Millimeters
Mcg Micrograms
Mosm Milliosmolarity
NIBP Non Invasive Blood Pressure
SpO2 Oxygen saturation
ACKNOWLEDGMENT
I take pleasant opportunity to express my profound sense of gratitude,
respect and sincere thanks to my ever inspiring professor and guide DR.Savitha
K.S.,Professor , Department of Anaesthesiology, SJMCH for her constant support and
guidance. Without her initiative, constant advice and continuous guidance , this
work would not have been possible.
I am highly indebted to Dr. Radhika Dhanpal, professor and head of
department, department of anaesthesiology, SJMCH, for her expert guidance,
encouragement, support throughout my course and dissertation.
I thank Dr. Lalitha Talwalkar,Dr. Kshama Kilpadi, Dr. Latha John, Dr.
Satyanarayana, Dr. Vasudeva Upadhaya, Dr. Bindu, Dr.
Reena,Professors of anaesthesiology for their support, guidance and
encouragement during the clinical work of the study.I am grateful to my teachers
Dr. Sarojini Thomas, Dr. Elavarasi, Dr. Jui, Dr.Sunanda, Dr. Dominic, for their practical
tips, guidance and support during the course of the study.
I thank my lecturers Dr. Pradeep, Dr. Prasanna, Dr. Ramaprasad, Dr. Sachin for their
help in conducting my study.

My sincere thanks to the OT staff for their help and co-operation during this study.
My sincere thanks to my colleagues.
I am greatly indebted to my family for their constant support and encouragement.
Last but not the least , I am very much grateful to all my patients for their kind co-
operation without whom this study would not have been possible.
15/10/2009
Bangalore Dr. Nikhil George

ABSTRACT
Patients undergoing prolonged non ocular surgery with general anaesthesia may develop
ocular complication. The ocular complication can be due to injury by surgical drapes,
anaesthetic or surgical equipment or inadequate lid closure. Under general anaesthesia there
is an abolition of protective corneal reflex. Basal tear production is also reduced during
general anaesthesia which leads to drying of the cornea. Absent pain perception under general
anaesthesia can also contribute to ocular complications during general anaesthesia.
To compare and assess the efficacy of hypo allergic adhesive tape, paraffin based
lubricant eye ointment and hydroxyl propyl methyl cellulose tear substitute ointment as eye
protection methods under general anaesthesia.
MATERIALS AND METHODS
The study was conducted in St. John’s Medical College during the period of September
2007 to September 2009. 200 patients (400 eyes) undergoing general anaesthesia for non
ophthalmological procedures were selected for the study. They were subdivided into four
groups of fifty patients each using a randomisation chart after obtaining written informed
consent. Institutional ethics review board approval was obtained for the study.
Each group was again divided into 2 equal subgroups for eye protection methods.

RIGHT LEFT
A Tape Paraffin
B Paraffin Tape
C Tape Hydroxypropyl
Methylcellulose
D Hydroxypropyl Tape
Methylcellulose
E Tape Tape+ Paraffin
F Tape+ Paraffin Tape
G T ape Tape+Hydroxypropyl
methylcellulose
H Tape+Hydroxypropyl Tape
methylcellulose
Inclusion criteria
ASA 1 and ASA 2 patients coming for non ocular surgeries under general anaesthesia
for more than 45 minutes in St.John’s Medical College Hospital during the period of
September 2007 to September 2009 between age 12 years and 60 years.

Exclusion criteria
The following groups of patients were excluded from the study
-patients with known dry eye syndrome
-patients with corneal diseases
-patients on ocular medications
-patients with connective tissue disorders
-patients with thyroid ophthalmopathy
-patients in prone or lateral positions
-patients with cranial nerve palsies
-patients with Horner’s syndrome
-pregnant patients
-patients not willing to give consent.
Eye protection methods were instituted after an eye examination during which cornea
was examined with vital staining with fluorescein and any prior lesions were ruled out.
Schirmer test was performed prior to induction of general anaesthesia for assessment of basal
tear production. General anaesthesia was instituted according to institutional protocol. Post
operatively Schirmer test was repeated 30 minutes after the end of general anaesthesia by an
observer blinded to the study. Post operative basal tear production was assessed with
Schirmer test. Vital staining with fluorescein was also done in the post operative period, to

assess any corneal abnormalities. If any abnormalities were detected the patient was sent for
an ophthalmological consultation.
DISCUSSION
The most commonly reported ophthalmological complication under general anaesthesia
in literature is corneal abrasion. Other reported injuries include injuries from toxic chemicals,
injuries from surgical drapes and equipments. Various degrees of vision loss related to
pressure on eye or optic nerves retinal ischemia have also been reported.
Grover et al. compared the efficacy of eye ointment and adhesive tape with control
untapped for protection of eyes under general anaesthesia. They found that basal tear
production was reduced in all groups and the maximum reduction was seen in unprotected
eyes. The study also found an incidence of corneal epithelial defect in unprotected eyes was
10%.Eyes with multiple corneal epithelial defects occurred only in control untapped group.
Corneal injuries were more common in the lower zone and the middle zone.
Batra and Bali studied the incidence of corneal abrasion during general anaesthesia in 200
patients. Eyes were left uncovered in one group while in the other group eyes were closed
with adhesive tape. None of the patients whose eyes were closed showed positive staining
with fluorescein for corneal abnormalities. In the uncovered eye an incidence 44 percent was
found for corneal abrasion. It was observed that in all positive cases the staining was present
in the inferior third of cornea.
STUDY DESIGN
A multiple cross over designs with four groups each divided into two sub
groups and subjects were allotted in the cross over design was undertaken to study the

efficacy of various eye protection methods and basal tear production under general
anaesthesia.
RESULTS
The median age for the study group was found to be 37 yrs.
Basal tear production was found to be reduced in all groups with maximum reduction
under taped group,39.19% reduction. Minimum reduction in basal tear production was found
in eyes protected with Hydroxypropyl methylcellulose ointment.
No incidence of positive staining with fluorescein staining was found in any of the
groups.
CONCLUSION
To conclude
- Eye protection is mandatory in all cases under general anaesthesia
-Eye protection methods including taping of eye with hypo allergic adhesive tape ,instilling
hydroxypropyl methyl cellulose based tear substitutes or instilling paraffin based ocular
lubricant protect the eye from injuries equally efficiently
- Basal tear production is reduced under standardised general anaesthesia techniques.
Key words- eye protection taping of eye, paraffin ointment, HPMC ointment, basal tear
secretion, fluorescein staining

LIST OF TABLES
No Tables Page no.
1 Randomization chart 33 2 Age distribution 35 3 Gender Distribution 40 4 Comparison of Tape with Paraffin 41 5 Comparison of Tape with HPMC 42 6 Comparison of Tape with Tape +paraffin 43 7 Comparison of Tape with Tape +HPMC 45
8 Fluorescein staining with Tape and Paraffin 47
9 Fluorescein staining with Tape and HPMC 48
10 Fluorescein staining with Tape and Tape +Paraffin 49
11 Fluorescein staining with Tape and Tape +HPMC 50

LIST OF FIGURES
No Figures Page no.
1 Anatomy of Lacrimal Apparatus 7 2 Layers of ear film 11 3 Layers of Cornea 15 4 Cross section of cornea 15 5 Corneal Epithelial erosions 17 6 Layers of Tear Film 19 7 Structure of Fluorescein 20 8 Punctate epithelial erosions 21 9 Fluorescein Strips 22 10 Fluorescein staining 23 11 Structure of HPMC 24 12 Distribution of age 39 13 Distribution of gender 40
14 Effect of Tape against Paraffin based on Schirmer test score 41
15 Effect of Tape against HPMC on Schirmer test score 42
16 Comparison of Schirmer test score in Tape and Tape + Paraffin group 44
17 Comparison of Schirmer test score in Tape and Tape + HPMC group 45
18 Comparison of fluorescein test in Tape and Paraffin 47 19 Comparison of fluorescein test in Tapeand HPMC 48
20 Comparison of fluorescein test in Tape and tape with Paraffin 49
21 Comparison of fluorescein test in Tape and tape with HPMC 50

INTRODUCTION

INTRODUCTION
When a patient comes to the surgical suite for anesthesia, either general anesthesia or local
anesthesia with varying degrees of sedation; care must be exercised by anesthesiologist to prevent
unnecessary and untoward complications.
Patients undergoing prolonged non ocular surgery with general anesthesia may develop ocular
complications1, 2. The risk of ocular complications can be due to multiple factors, firstly because there
is an abolition of protective corneal reflex under general anaesthesia3. There is also a decreased basal
tear production during general anesthesia leading to drying of the cornea2. Pain perceptions are also
absent under general anesthesia which can contribute to ocular complications1, 3,.
Corneal abrasion has been mentioned as the most frequent ophthalmic complication
following general anesthesia4 .Corneal abrasion has been found mostly due to drying of the cornea. It
may also be due to direct trauma to cornea. Other types of reported eye injuries have included injuries
from toxic chemicals allowed to contact the eyes during induction of anesthesia and various degrees
of visual loss, possibly due to pressure on eye or optic nerve4,5,6.The eyes can be protected during
general anesthesia by taping the eyes closed with a hypoallergenic adhesive tape2, with paraffin based
ointment7,8or with tear substitute hydroxyl propyl methyl cellulose ointment1,9,10. The purpose of the
present study was to determine the efficacy of various eye protection methods.

OBJECTIVE OF THE STUDY

OBJECTIVE OF THE STUDY
• To compare and assess the efficacy of different eye protection methods.
Lid taping with hypoallergic tape.
Instilling of paraffin based ointment.
Instilling of 2% hydroxyl methyl cellulose.
• To assess basal tear production under general anesthesia.
• To find an ideal regime for eye protection under general anesthesia.

REVIEW OF LITERATURE

REVIEW OF LITERATURE
Lacrimal Apparatus
Lacrimal drainage system consists of the following structures
1. The puncta are located at the posterior edge of lid margin at the junction of lash-bearing
lateral five sixths and the medial non-ciliated one sixth. Normally they face slightly posteriorly and
can be inspected by averting the medial aspect of lids.
2. The canaliculi pass vertically from the lid margin for about 2mm. They then turn medially
and run horizontally for about 8mm to reach lacrimal sac. The superior and inferior canaliculi most
often unite to form the common canaliculus which opens into the lateral wall of the lacrimal sac. In
some individuals each canaliculus opens separately. A small flap of mucosa, the valve of
Rosenmuller, overhangs the junction of common canaliculus and the lacrimal sac, and prevents reflux
of tear into canaliculi.
3. The lacrimal sac is about 10mm long and lies in the lacrimal fossa between the anterior and
the posterior lacrimal crests. The lacrimal bone and the frontal process of the maxilla separate the
lacrimal sac from the middle meatus of the nasal cavity.
4. The nasolacrimal duct is about 12mm long and is the continuation of lacrimal sac. It
descends and angles slightly laterally and posteriorly to open into the inferior nasal meatus, lateral to
and below the inferior turbinate. Opening of the duct is partially covered by a mucosal fold, the valve
of Hasner11.
Fig 1. Anatomy of Lacrimal Apparatus


Tear film
Tear film is that surface of the eye which remains in direct contact with the environment. Tear
film is critically important for protecting the eye from external influences and for maintaining the
health of the underlying cornea and conjunctiva. The optical stability and normal function of the eye
depends on an adequate supply of fluid covering its surface9,12.
Tear film serves
1. An optical function by maintaining an optically uniform corneal surface.
2. Mechanical function of flushing cellular debris, foreign matter from the cornea and
conjunctival sac and by lubricating the surface.
3. Corneal nutritional function.
4. An antibacterial function.
Abnormalities of the tear film affecting its constituents or volume leads to serious dysfunction
of the eyelids and conjunctiva with concomitant loss of corneal transparency. A thin tear film is
uniformly spread over the cornea by blinking and ocular movements.
The volume of tear fluids is about 5-10μl with normal secretion rate of about 1-
2μl/min13. About 95% of tear production is by lacrimal gland and lesser amounts are produced by
goblet cells and the accessory lacrimal glands of the conjunctiva12,13.
The tear film is composed of three layers:
• Superficial Lipid Layer
• Middle Aqueous layer
• Posterior Mucin Layer

Superficial Lipid Layer
The superficial layer at the air tear interface is formed over the aqueous part of the tear film
from the oily secretions of Meibomian glands and the accessory sebaceous glands of Zeis and Moll.
Meibomian gland openings are distributed along the eye lid margin immediately behind the last
follicles.
The thickness of this layer varies with the width of the palpebral fissure and is between 0.1
and 0.2 mcm. Being oily in nature it forms a barrier along the lid margins that retain the lid margin
tear strip and prevents its overflow on to skin.
This outer lipid layer has the following main function.
• It reduces the rate of evaporation of the underlying aqueous tear layer.
• It increases surface tension and assists in the vertical stability of the tear film so that tears do
not overflow the lid margin.
• It lubricates the eye lid as they pass over the surface of the globe.
Middle aqueous layer
This intermediate layer of the tear film is the aqueous phase which is secreted by the main
lacrimal gland and the accessory glands of Krause and Wolfring.
This layer constitutes almost the total thickness of tear film, 6.5 – 10 μm. This layer contains
two phases, a more concentrated and a highly dilute one.

This layer contains inorganic salts, water, proteins enzymes, glucose, urea, metabolites,
electrolytes, glycoprotein and surface active biopolymers. Uptake of oxygen through this layer is
essential to normal corneal metabolism.
This layer has four main functions
• It supplies atmospheric oxygen to the corneal epithelium.
• It has antibacterial substances like lactoferrin and lysozyme.
• It provides smooth optical surface by removing any minute irregularities of the cornea.
• It washes away debris from cornea and conjunctiva.

Posterior Mucin layer
The innermost layer of the tear film is a thin mucoid layer elaborated by goblet cells of
conjunctiva and also by the glands of Henle and glands of Manz. It is the deepest stratum of the
precorneal tear film. This layer is 0.02 to 0.4μm thick. This adsorbs on the epithelial surface of the
cornea and conjunctiva, rendering them hydrophilic. This surface is dependent upon a constant supply
of mucus which must be of proper chemical and physical nature to maintain corneal and conjunctival
surfaces in the proper state of hydration.
Fig. 2 Layers of Tear Film
Tear film formation dynamics
During closure of the eyelids the superficial lipid layer of the tear film is compressed by the
eyelid edges because it is energetically unfavorable for the lipid to penetrate under the lids into the
fornix. The thickness of lipid layer increases. The aqueous layer of tear film remains uniform under
the lids and acts as a lubricant between the eyelids and the globe. In a complete blink the two tear
menisci join and most of their bulk is held at their junction to fill the slight bridge formed by the
meeting eyelids and at the canthus. When the eyelids open first they form an aqueous tear surface on
which the compressed lipid spreads rapidly14. A deficiency of conjunctival secretions can lead to dry
eye symptoms even in the presence of an adequate aqueous tear component. Generally there is a
balance between the secretion and the excretion of tears and the rate of drainage increases with
increased tear volume11.

Tear Drainage
Normally about 10-25% of the total tears secreted are lost by evaporation. Evaporation rate is
low because of the protective oily surface. In the absence of protective oily layer the rate of
evaporation is increased 10-20 times. Normally tear flows along the upper and lower marginal strips
and enters the upper and lower canaliculi by capillarity and possibly by suction.Also with each blink a
negative suction is created which sucks the tears from the canaliculi. Gravity also plays a part in
drainage12.

Tear composition
Tear contains 98.2% water and 1.8% solids
Physical properties
• pH 7.2 - 7.7
• Osmotic pressure 305 mosm/Kg
• Volume 0.50-0.67 g / 16hr waking
Chemical properties
• Water 98.2g/100ml
• Solids 1.8g/100ml
Electrolytes16
• Sodium 120-170mmol/l
• Potassium 26- 42mmol/l
Hormonal control of tear production
Androgens play an important role in regulating tear film secretion on the ocular surface15,17.
Androgen deficiency plays and important role in pathogenesis of evaporative dry eye in
women with Sjogrens disease. It contributes to the Meibomian gland dysfunction, tear film instability
and evaporative dry eye which are the characteristics of this auto immune disorder12,18.
Neural controls of tear production
The cornea, lacrimal gland, mucous cells and meibomian glands are all richly innervated.
Parasympathetic, sympathetic and sensory inervation play complex stimulatory or inhibiting role.
Abnormalities of any of these pathways can cause overall dysregulation of lacrimal function.
The lacrimal gland is innervated by parasympathetic, sympathetic and sensory nerves.
Parasympathetic innervation predominates with a network of fibers surrounding most of the acini.
Even though each acinar cell is not innervated, cells within an acinus are electrically and chemically
connected by gap junctions. Activation of one cell is communicated to other cells within acinus so

than even non innervated cells can be activated. Sympathetic nerves are also found in the lacrimal
gland with fewer sympathetic than parasympathetic nerves. These nerves innervate acinar ducts and
also the vascular cells20.
The primary function of the lacrimal gland is to secrete proteins, electrolytes and water on to
the ocular surface. Nerves and hormones play an important role in the regulation of lacrimal gland
secretion. Neural reflexes, initiated by afferent sensory nerves in the cornea, conjunctiva and nasal
mucosa responding to mechanical, thermal or chemical stimulation or by the optic nerve responding
to light, activate the efferent parasympathetic and sympathetic nerves of the lacrimal gland. These
nerves release their neurotransmitters to interact with specific receptors on the basolateral membranes
of acinar and duct cells. These activate signal transduction pathways causing appropriate changes in
the tear production mechanism13,21.

CORNEA
Cornea is the most densely innervated tissue in the body. The sensory supply is via the first
division of trigeminal nerve. There is a sub-epithelial and stromal plexus of nerves13.
The average corneal diameter is 11.5mm vertical and 12mm horizontal
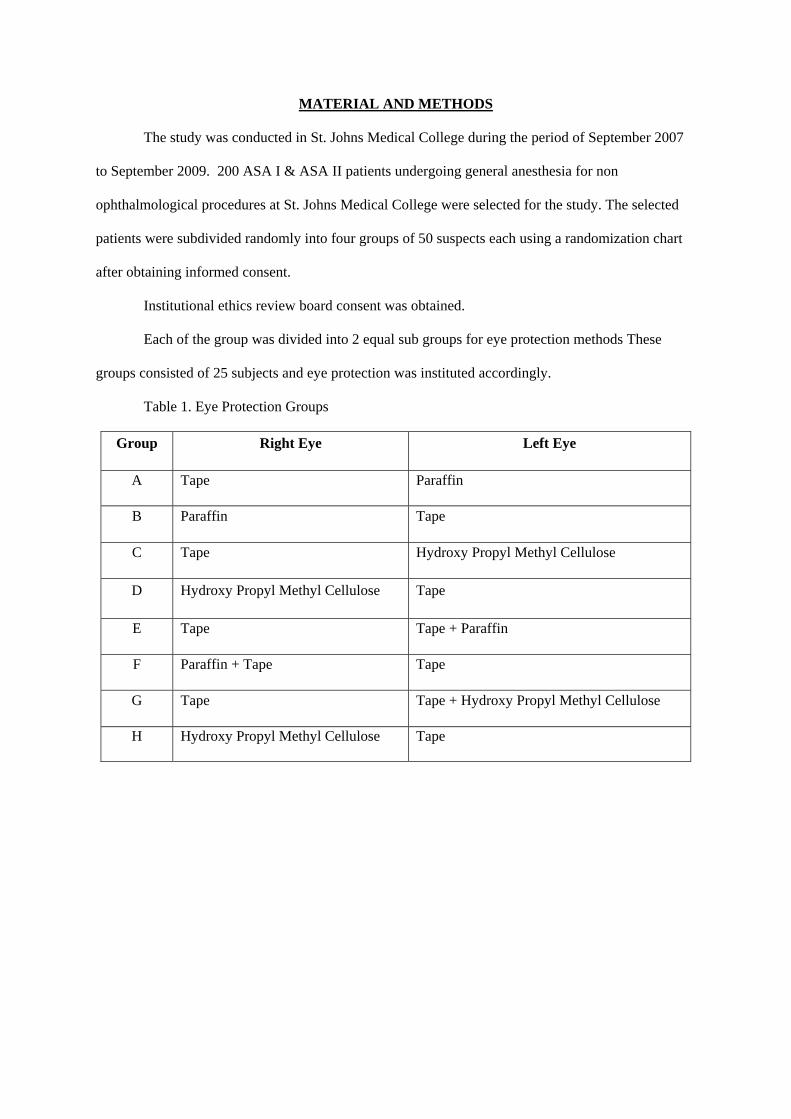
The cornea consists of the following layers
1. Epithelium is stratified squamous and non keratinized tissue and comprises.
• A single layer of basal columnar cells attached by hemidesmosomes to the underlying
basement membrane.
• Two to three layers of airy cells
• Two layers of squamous surface cell
The surface area of the outermost cells is increased by microvilli that facilitate the attachments
of mucin and the teen film .After a life span of a few days the superficial cell are regenerated16.
2. Bowman layer is the acellular superficial layers of the stroma. It is a tough layer that protects the
corneal stroma, consisting of a similar irregularly-arranged collagen fibers
3. Stroma makes upto 90% of corneal thickness. It is principally composed of regularly oriented layers
of collagen fibrils whose spacing is maintained by proteoglycan ground substance with interspersed
modified fibroblasts.
4.Descemet membrane is composed of the lattice work of collagen fibrils
5.Endothelium consists of a single layer of hexagonal cells that cannot regenerate.
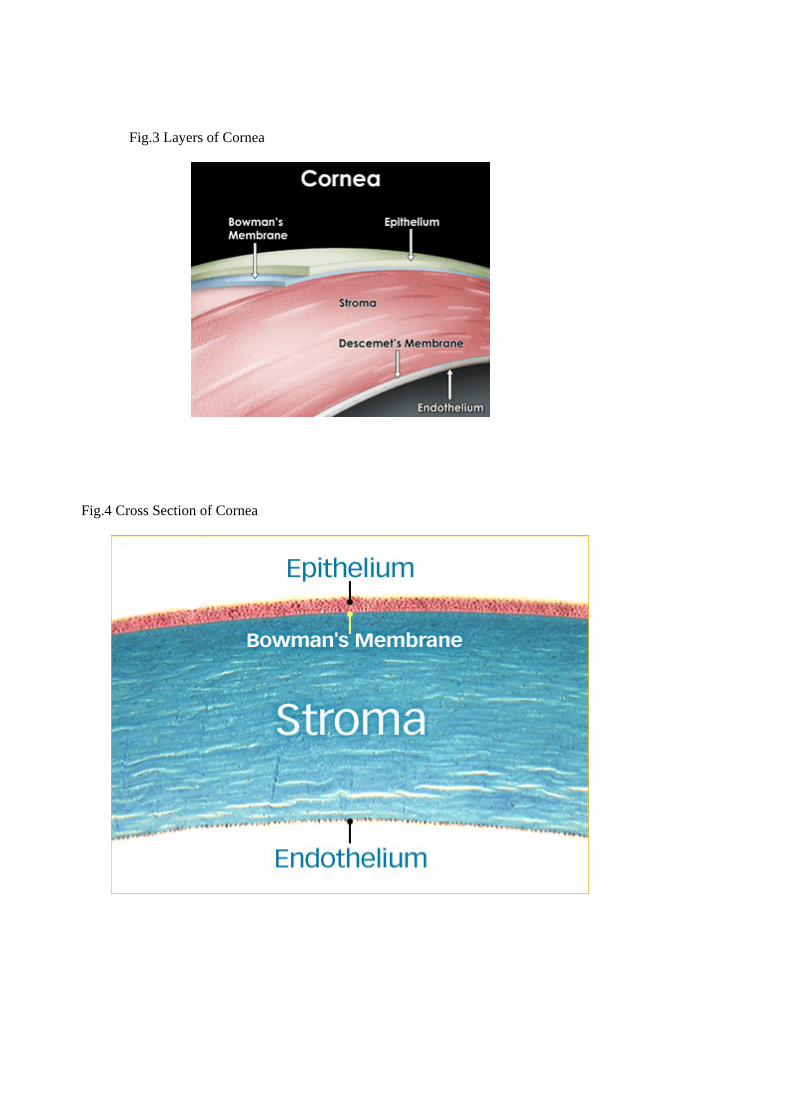
Fig.3 Layers of Cornea
Fig.4 Cross Section of Cornea

Corneal changes in dry eye
In moderate to severe cases of dry eye the following corneal changes may be present16,.
Punctate epithelial erosions involving the inferior cornea which are best seen by instillation of
fluorescein into inferior conjunctival fornix22.
Fig.5 Punctate corneal erosions
Filaments appearing as small comma shaped opacities with free end hanging over cornea and
moving with each blink. These filaments are composed of central mucous core encased by
epithelial cells and are best shown on Rose Bengal staining.
Mucous plaques appear as semi translucent whitish grey, slightly elevated lesions of varying size
and shape23. They consist of mucus, epithelial cells and proteinaceous lipoid material. These
plaques are commonly seen associated with corneal filaments22.

Schirmer test
Clinical measurement of tear film volume and tear flow rates would help the clinician
quantify the severity of aqueous deficiency. Although sophisticated methods of obtaining these data
are available24 (Flurophotometry), they are not useful in daily clinical practice. The Schirmer’s test,
although crude by comparison remains the only practical clinical measurement of tear production.
The Schirmer’s test25 measures the volume of tears produced during a fixed time period. It is
performed by placing the folded 5mm wide end of a standard 41 Whatman filter paper over the lower
lid between its middle and lateral thirds. The patient, in a dimly lit room, looks straight ahead and
blinks normally. After 5 minutes the strip is removed and the amount of wetting is measured from the
fold. Jones modified the test by instilling a topical anesthetic agent, being careful to remove excess
fluid before inserting the filter paper He reasoned that this technique would eliminate the reflux
tearing produced by irritation from the filter paper and that the resultant wetting would then represent
basic tear production from the glands of Krause and Wolfring26. The clinical value of these two
techniques is still debated.
Although Schirmer reported 15mm of wetting as the lower limit of normal, lower values are
common in asymptomatic subjects27. According to one report, even if 5.5 mm of wetting was used as
the lower limit of normal, one of every six asymptomatic individuals would be misclassified as having
a tear deficiency. An individual when tested on multiple occasions may have extremely variable
Schirmer test results. Perhaps a part of variability in Schirmer results may be due to a lack of careful
attention to such variables as lid margin stimulation and time after drop instillation28. Despite its
imprecision, the Schirmer test is simple inexpensive readily available, easily performed and without
side effects29,30. As such it remains one of the most common clinical techniques for measuring
aqueous tear production.

Fig.6 Measured Schirmer Strips

Fluorescein staining
Fluorescein is a vital dye. It lacks intrinsic toxicity and is used to detect epithelial defects and
surface irregularities of the cornea. It is a diagnostic corneal test for the same. It is commercially
available impregnated in filter paper strips and also as a sterile 0.25% or 2% solution. Because of the
ease and frequency with which the solution form of this stain can be contaminated, the strips are
preferred.
Synthesis
Fluorescein was first synthesized by Adolf von Baeyer in 1871. It can be prepared from
phthalic anhydride and resorcinol in the presence of zinc chloride via the Friedel-Crafts reaction.
Fig.7 Structure of Fluorescein
Fluorescence occurs when a substance emits light of a given wavelength after it is excited by
light of a different wavelength .Sodium fluorescein emits light of 520 mm (green) after it is excited by
light of approximately 490mm(blue).
Fluorescein is applied by wetting the strip and touching it to the inferior bulbar or palpebral
conjunctival surface, the patient blinks several times, caressing the dye to dissolve in the pre corneal
tear film and to be distributed over the ocular surface. Staining is manifest whenever there is
disruption of cell-cell junctions, which allows the material to diffuse rapidly into the corneal stroma.
Full thickness defects in the corneal epithelium expose the stroma and stain a brilliant, fluorescent
green when observed with cobalt blue light. Initially the pattern does not change upon repeated
blinking. However the dye diffuses into the stroma in short order causing the area of staining to

expand and the brilliance of staining to diminish. These changes occur in minutes and require that the
staining pattern to be examined immediately after stain is applied. Partial thickness epithelial defects
stain less prominently than full thickness defects31.
Fig.8 Punctate Erosions In The Cornea
Fluorescein staining must be distinguished from fluorescein pooling. Fluorescein stain
collects and pools in depressions and over irregularities of the corneal surface despite the presence of
an intact epithelium. Irrigation with a sterile ophthalmic solution clears fluorescein if the epithelium
is intact and allows pooling to be distinguished from staining.

Fig. 9 Commercially available Fluorescein strips
Fig.10 Fluorescein staining of cornea showing punctuate epithelial erosions

White Soft paraffin
White soft paraffin is a semisolid mixture of hydrocarbons obtained from petroleum and then
bleached.
Properties
It is a white translucent soft mass, and retaining the characteristics on storage and when
melted and allowed to cool without stirring, odourless when rubbed on skin7.
Solubility Insoluble in water and in alcohol (95%).
Soluble in chloroform, solvent ether and light petroleum
Boiling range 400-600 c
Melting Point 380-560c
pH : Neutral
Main constituents of paraffin ointment
White beeswax 20g
Hard paraffin 30g
Cetostearyl alcohol 50g
White soft paraffin 900g
melted together and stirred until cold

Hydroxypropyl methyl cellulose
Pharmacology - Hydroxypropyl methyl cellulose is an isotonic, non-pyrogenic viscoelastic
solution with a high molecular weight (>80,000 Daltons). It prevents trauma to corneal epithelium and
other ocular structures. It is also used as a demulcent agent. It is also used in anterior segment
surgeries to maintain a deep chamber3.
Indication
• Surgical aid
• Tear substitute
Fig.11 Structure of HPMC

LITERATURE REVIEW
Grover, Kumar, Sharma, Sethi, Grewal et al compared and assessed the efficacy of eye ointment and
adhesive tape for protection of eyes under general anesthesia.
One hundred and fifty patients, (300 eyes) undergoing general anesthesia for > 90 minutes for
non-ophthalmic procedures were dividend randomly into three groups (C, T & O). Eyes in group C
were left as control, in group T, hypo allergen tape was applied and in group O ,ointment was used. In
all eyes basal tear production and visceral activity was assessed and corneal examination was carried
out after fluorescein staining both before and after surgery. All patients were subjected to
conventional general anesthesia technique.
General anesthesia reduced basal teal production irrespective of method of eye protection
used. They found that the overall incidence of corneal epithelial defect was 10% of which 90%
occurred in control groups, 6.6% in tape 3.3% ointment group. They also found that incidence of
corneal epithelial defects did not alter with increase in duration of surgery. They concluded that
during general anesthesia eyes need protection either by tape or ointment as incidence of corneal
injury is greater in unprotected eyes.
Boggild-Madsen, Bundgarrd N, Hammer U, Jakobsen B, did a study on 120 patients who
were anesthetized for more than 90 minutes. They were given eye protection with paraffin based
occulentum simplex in one eye and water based 4% methyl cellulose in the other. Anesthesia was
conducted with halothane or thiopentone and pethidine or by a neurolept technique. Periocular edema
and reaction in the conjunctiva resembling conjunctivitis was less pronounced after methyl cellulose.
When both paraffin based ointment and halothane anesthesia were used, there were signs of drug
interactions as patient conjunctiva were now distinctly red. In all three types of anesthesia, methyl
cellulose produces a firm gluing of the eye lids with the result that eye is not dried out and the eye is
protected mechanically so that foreign bodies and corneal abrasions are avoided. There were no

untoward effects of methyl cellulose. It is concluded that methyl cellulose 4 % provides better eye
protection than paraffin during general anesthesia1.
Cross DA, Krupin T, et al. conducted a study on the implications of the effects of general
anesthesia on basal tear production. During their study ophthalmic preparations were frequently
instilled topically to protect the eye during general anesthesia. The purpose of their study was to
determine if such prophylactic precautions are warranted, as determined by the effect of general
anesthesia on basal tear production by Schirmer’s test. As general surgical anesthesia produced a
marked depression of basal tear production, both mechanical protection and topical medication were
recommended for the ocular care of patients undergoing general surgical anesthesia8.
Batra YK, Bali IM conducted a study on the eyes of 200 healthy adult patients undergoing
general anesthesia. The eyes were stained with fluorescein strips for detection of corneal abrasion in
the immediate postoperative period. Twenty six of fifty nine patients in whom the eyes remained
partly open showed positive staining. The remaining 141 patients in whom the eyes were naturally
closed or protected with adhesive tape or vase line gauze, did not develop exposure keratitis. It was
suggested that covering of eyes is necessary in all cases undergoing general anesthesia so as to avoid
these frequent complications of anesthesia10.
Cuchiara RT and Black S conducted a study on corneal abrasion during neurosurgical
procedure under anesthesia over a period of 13 months. All patients had their eyes closed during
procedure. One group had ointment; the other group received no eye ointment. The ointment group
was compared with non-ointment group. Four thousand six hundred and fifty two patients were
evaluated in this study. The incidence of corneal abrasion in this patient population was found to be
0.17%. Eight patients were suspected of having corneal abrasion based on their symptoms. When
corneal abrasion was suspected, an ophthalmology consultation was sought and the diagnosis
confirmed by fluorescein staining. Four of the abrasions were in patients who received no ointment
and four were in patients who received ointment. They suggested taping the eye immediately after

induction of anesthesia and leaving their eyes taped until the end of procedure. They also
recommended that the use of eye ointment is optional4.
Schmidt P, Bogglild Madsen NB, conducted a double blind study with 47 anesthetized
patients. They were given eye protection with paraffin based neutral eye ointment in one eye and
water based methyl cellulose 4% in the other. Twenty four hours later the eyes were stained with Rose
Bengal/fluorescein. No unintended effects of the ointment were found and no injury to the eyes was
seen. Compared with the paraffin based ointment the methyl cellulose ointment produced a more firm
adhesion of the eye lids. They concluded that a water based 4% methyl cellulose ointment is an
alternative to neutral eye ointment7.
Cross DA, Krupin T conducted a study on the implications of the effects of general anesthesia
on basal tear production. The purpose of study was to determine the prophylactic precautions are
warranted, as determined by the effect of general surgical anesthesia on basal tear production by the
Schirmer I test. As general surgical anesthesia produced a marked depression of basal tear production,
both mechanical protection and topical medication are recommended for the ocular case of patients
undergoing general surgical anesthesia2.
Marquard R et al studied effects of adhesive artificial tear solution and an ointment basing on
tear production and tear film stability on patients in the intensive care units and during surgery. In 10
relaxed and ventilated patients of the ICU there was no change in the tear production after application
of either therapy. In 30 patients, undergoing surgery in endotracheal anesthesia, the break-up time and
the test according to Schirmer were measured pre and post operatively. Like in the ICU patients no
difference in tear production could be found. Artificial tear solutions were found to be better than
ointment base regarding stability and tear film. In addition patients felt more comfortable with
artificial tear solution.

Smolle M, Keller C et al conducted a study comparing the effect of clear hydrogel and
ointment in providing eye comfort after brief surgery. Ninety-two patients undergoing total
intravenous general anesthesia were randomly allocated to receive either ocular ointment or clear
hydrogel after induction of anesthesia. Subjects were assessed one hour following termination of
anesthesia. They found that there was an increased incidence of foreign body sensation, adherent eye
lashes and disturbances elicited by blurred vision in the ointment group as compared to clear
hydrogel.
Siffring PA , Poulton TJ compared the efficacy of conventional eye protection strategies in
preventing corneal abrasions and assessed the frequency and duration of various ocular complaints
associated with each technique. One hundred and twenty seven adult patients for elective surgery
under general anesthesia were part of the study. They found that during general anesthesia of short
duration for procedures away from the head and neck in supine position, closure of the eyelids with
tape with or without methyl cellulose drops are effective and sufficient for most patients undergoing
anesthesia.
Roth S, Thisted RA, et al surveyed 60,965 patients who underwent anesthesia for a non-
ocular surgery at our institution from January 1988 to July 1992. Eye injuries were identified by
examining several sources of information, including date, form, quality improvement, postoperative
visits or telephone calls, and examination of medical records and postoperative patients who required
an ophthalmology consultation. Records were reviewed to determine the types and cause of eye
injuries. Of 34 patients who sustained eye injuries (0.056%), the most common was corneal abrasion
(n=21). Other injuries were conjunctivitis, blurred vision, red eye, chemical injury, direct trauma and
blinders. Other factors associated with higher relative risk of eye injury were long surgical duration,
prone or lateral positioning during surgery, operation on the head and neck region. In only 21% of
cases was a specific cause of injury identified.
Gild W, Posner K, et al. analyzed claims against anesthesiologist for eye injuries as part of the
ASA closed claims project. Eye injuries occurred in 3% of all claims in database (71 of 2046). Two

distinct subsets were identified. First was characterized by corneal abrasion during general anesthesia.
The second subset of eye injuries was characterized by patient movement during ophthalmologist
surgery. The analysis found that corneal abrasions produced fewer permanent injuries than either
patient movement related injuries or other eye injury claims.
Orlin SE, Kurata FK, Krupin T ,et al. compared taping of eye lid with instillation of
lubricating ointment as a prophylactic measure against corneal injury during general anesthesia.
Seventy six patients undergoing general anesthesia for non-ocular surgery were studied prospectively.
Preoperative examination included visual acuity, slit lamp examination using portable slit lamp,
staining of cornea with fluorescein and Rose Bengal dye, and determination of basal tear secretory
rate. Three to five hours postoperatively, the patients were examined at bedside. Visual activity was
measured and the conjunctiva and cornea were examined with a portable slit lamp with fluorescein
and Rose Bengal dye9.
The patient received a follow up examination at 24 hours if any abnormalities were noted on
the first postoperative examination. One patient showed minimal staining of the conjunctiva in the
inferior cul-de-sac with both fluorescein and Rose Bengal dye in the eye that received no ointment;
this resolved by 24 hours. The fellow eye of this patient that received lubricating ointment did not
have staining with either eye. The remaining 75 patients had no evidence of postoperative corneal or
conjunctival change in either eye.
Terry HR Jr. Kearus TP et al analyzed untoward ophthalmic and neurologic events of
anesthesia. They found that the most frequent ophthalmic complication following general anesthesia
is corneal abrasion. Most corneal abrasions are due to drying of the corneal epithelium. The corneal
epithelium of an eye that is open and exposed to the air dries very quickly, and an abrasion develops.
The best prophylaxis against such corneal abrasions is to keep the eyelid closed during operative
procedure3.

Roth S studied the effect of halothane on retinal and choroidal blood flow in cats, using
radioactively labeled Ce 141, Sn 113 and Nb 95. It was found that the halothane anesthetic produces a
significant dose dependent increase in retinal and a decrease in choroidal blood flow in cats.

MATERIAL AND METHODS
MATERIAL AND METHODS
The study was conducted in St. Johns Medical College during the period of September 2007
to September 2009. 200 ASA I & ASA II patients undergoing general anesthesia for non
ophthalmological procedures at St. Johns Medical College were selected for the study. The selected
patients were subdivided randomly into four groups of 50 suspects each using a randomization chart
after obtaining informed consent.
Institutional ethics review board consent was obtained.
Each of the group was divided into 2 equal sub groups for eye protection methods These
groups consisted of 25 subjects and eye protection was instituted accordingly.
Table 1. Eye Protection Groups
Group Right Eye Left Eye
A Tape Paraffin
B Paraffin Tape
C Tape Hydroxy Propyl Methyl Cellulose
D Hydroxy Propyl Methyl Cellulose Tape
E Tape Tape + Paraffin
F Paraffin + Tape Tape
G Tape Tape + Hydroxy Propyl Methyl Cellulose
H Hydroxy Propyl Methyl Cellulose Tape

Inclusion Criteria
All ASA I and ASA II patients coming for non ocular surgery in supine position under
general anesthesia lasting for more than 45 minutes in St. Johns Medical College Hospital during the
period of September 2007 to September 2009 in the age group between 12yrs to 60 years.
Exclusion Criteria
The following groups of patients were excluded from this study
• Patients with known dry eye syndrome as it will interfere with the study
• Patients with ocular diseases or disorders
• Patients on ocular medication as it will interfere with the study
• Patients with connective tissue disorders like Sjogrens disease, rheumatoid arthritis etc, as
they are prone for dry eye
• Patients with thyroid ophthalmopathy
• Patients in prone or lateral position as assessment may not be proper in these groups
• Patients with Facial nerve palsy
• Patients with Horner’s syndrome
• Patients not willing to give consent
• Pregnant patients
Method of collection of Data
The 200 patients selected with the help of inclusion and exclusion criteria were allocated to
four groups using a randomization chart.
Each group was subdivided into two groups each for eye protection methods.

Eye protection methods were instituted after an eye examination. Cornea was
examined.Fluorescein staining was done and any prior lesions were ruled out Schirmer’s test was
performed for assessment of basal tear production.
All patients were given general anesthesia according to institutional protocol. An IV cannula
was secured preoperatively. Preoperative monitoring in the form of electrocardiogram, heart rate,
systolic and diastolic blood pressure, mean arterial blood pressure, oxygen saturation and end tidal
carbon dioxide monitoring were instituted.
Patients were induced with general anesthesia using Glycopyrollate, Ondansetron, Fentanyl 2-
3 mg/kg, Propofol 2-3 mg / kg or Thiopentone sodium 3-5 mg/kg, Vecuronium – 0.1 mg/kg or
Atracurium 0.5mg/kg and inhalational agents N2O + isoflurane + O2.
Eye protection methods were started after induction of anesthesia according to randomization
chart by an anesthesiologist who was blinded to the study.
Anesthesia was maintained using inhalation anesthesia isoflurane + N2O with bolus doses of
fentanyl with muscle relaxants.
After evidence of spontaneous recovery appears viz. patient has started spontaneous
respiration,the patients were given cholinesterase inhibitor with anticholinergic for reversal of
neuromuscular blockade.
Eye was examined after the procedure. Basal tear production was measured using Schirmer’s test.
Cornea was examined with fluorescein for evidence of any lesion.
If any significant eye findings were present a repeat examination was done after 30 minutes
and an ophthalmological consultation was done to check for consistent findings.

Statistical Methods: Descriptive statistical analysis has been carried out in the present
study. Results on continuous measurements are presented on Mean ± SD (Min-Max) and
results on categorical measurements are presented in Number (%). Significance is assessed at
5 % level of significance. Student t test (two tailed, dependent) has been used to find the
significance of study parameters (Schirmer test score) on continuous scale within each group.
Student t test has been used to find the homogeneity of parameters on continuous scale and
Chi-square /Fisher exact test has been used to find the homogeneity of samples on categorical
scale38,39.
1. Chi-Square Test
EiEiOi∑ −
=2
2 )(χ , Where Oi is Observed frequency and Ei is Expected frequency
2.Fisher Exact Test
Class1 Class2 Total
Sample1 a b a+b
Sample2 c d c+d
Total a+c b+d n
2x2.Fisher Exact Test statistic= ∑∑ ++++
=!!!!
1!
)!()!()!()!(dcban
dbcadcbap
3. Student t-test for paired comparisons
Objective: To investigate the significance of the difference between single population means. No
assumption is made about the population variances39.
nsxxt
/)21( −
=

where ∑ −−= 1/)( 2 nddis
and di is the difference formed for each pair of observations
4.Significant figures
* Moderately significant ( P value:0.01<P ≤ 0.05)
** Strongly significant (P value : P≤0.01)
Statistical software: The Statistical software namely SPSS 15.0, Stata 8.0, MedCalc 9.0.1
and Systat 11.0 were used for the analysis of the data and Microsoft word and Excel have
been used to generate graphs, tables etc.

Results

Results
Table 2 Demographic Data
MeanSD37.98±13.62
Fig.12 Distribution of Age
Age in years Number %
11-20 15 7.5
21-30 61 30.5
31-40 36 18.0
41-50 43 21.5
51-60 41 20.5
>60 4 2.0
Total 200 100.0


Table 3 Gender Distribution
Gender Number %
Male 105 52.5
Female 95 47.5
Total 200 100.0
Fig.13 Distribution of Gender

Table 4: Effect of Tape against Paraffin based on Schirmer test score
Schirmer test
score Group A Group B P value
Pre-op 15.66±2.15 14.96±2.25 0.092
Post-op 10.12±1.57 9.72±1.01 0.074
% Change 35.40% 35.02% -
Significance t=17.612;
P<0.001**
t=17.850;
P<0.001** -
Fig.14
0
2
4
6
8
10
12
14
16
18
20
Pre-op Post-op
Schi
rmer
test
sco
re
Group AGroup B
In our study of comparison of tape against paraffin based ointment with Schirmer’s test, post-
operatively Schirmer’s value decreased to 10.12+_1.57mm in taped group while the post operative
Schirmer’s reduced to 9.72+_1.01 mm in the group with paraffin based ointment applied.
Table 5: Effect of Tape against HPMC on Schirmer test score

Schirmer test
score Group C Group D P value
Pre-op 16.38±1.75
(12-19)
15.62±1.54
(12-19) 0.027*
Post-op 9.96±1.32
(7-12)
10.04±1.51
(7-14) 0.779
% Change 39.19% 35.72% -
Significance t=20.766;
P<0.001**
t=17.392;
P<0.001** -
Fig.15 Effect of Tape against HPMC on Schirmer score
0
2
4
6
8
10
12
14
16
18
20
Pre-op Post-op
Schi
rmer
test
sco
re
Group CGroup D
Study of comparison of tape with hydroxyl propyl methyl cellulose based ointment for assessing basal
tear production was done and it was found that pre-operative basal tear production was
16.38+_1.75mm for tape as compared to 9.96+_1.32mm post operatively. Pre operative basal tear
production assessed with Schirmer’s test for group with eye protection with hydroxyl propyl methyl

cellulose based ointment was found to be 15.62+_1.54 while postoperatively if decreased to
9.72+_1.01.
Table 6: Comparison of Schirmer test score in Tape and Tape + Paraffin group
Schirmer test
score Group E Group F P value
Pre-op 15.94±1.33
(13-19)
16.60±1.25
(13-19) 0.005**
Post-op 10.56±1.01
(8-13)
10.58±1.14
(8-13) 0.925
% Change 33.75% 36.26% -
Significance t=22.055;
P<0.001**
t=24.413;
P<0.001** -
Fig.16Comparison of Tape with Tape and Paraffin

0
2
4
6
8
10
12
14
16
18
20
Pre-op Post-op
Schi
rmer
test
sco
re
Group EGroup F
Preoperative Schirmer’s was found to be 15.94+_1.33 mms. in the group which had tape alone as eye
protection while it reduced to 10.56+_1.01 mms. postoperatively in the same group. Schirmer’s test
score was found to be 16.60+_1.25 mms. preoperatively in the group which had tape with paraffin as
eye protection method.The basal tear production reduced post operatively to 10.58+_1.14 mms. in this
group.

Table 7: Comparison of Schirmer test score in Tape and Tape + HPMC group
Schirmer
test score Group G Group H P value
Pre-op 15.64±1.21
(13-18)
16.30±1.59
(12-19) 0.022*
Post-op 10.62±1.35
(8-15)
10.68±1.09
(8-13) 0.726
% Change 32.09% 34.48% -
Significance t=20.495;
P<0.001**
t=20.632;
P<0.001** -
Results are presented as Mean ± SD (Min-Max)
Fig.17 Comparison of Tape with Tape with HPMC
0
2
4
6
8
10
12
14
16
18
20
Pre-op Post-op
Schi
rmer
test
sco
re
Group GGroup H

Basal tear production in patients protected with tape alone in pre operative period was
15.64+_1.21 while post operatively it reduced to 20.62+_1.35.In patients who had their eyes
protected with tape and hydroxyl propyl methyl cellulose preoperative basal tear production was
found to be 16.30+_1.59 while post operatively it reduced to 10.68+_1.09

Comparison of fluorescein test-to check for corneal abrasion
Table 8: Comparison of fluorescein test-to check for corneal abrasion
corneal abrasion Group A Group B P value
Normal 50(100.0%) 50(100.0%) -
Positive - - -
Significance - - -
Fig.18 Comparison of fluorescein test-to check for corneal abrasion Tape with Paraffin

Table 9: Comparison of fluorescein test-to check for corneal abrasion
corneal abrasion Group C Group D P value
Normal 50(100.0%) 50(100.0%) -
Present - - -
Significance - - -
Fig.19 Comparison of fluorescein test-to check for corneal abrasion Tape with HPMC
Table 10: Comparison of fluorescein test-to check for corneal abrasion
corneal abrasion Group E Group F P value
Normal 50(100.0%) 50(100.0%) -
Present - - -
Significance - - -
Fig.20 Comparison of fluorescein test-to check for corneal abrasion Tape with Tape and
Paraffin

Table 11: Comparison of fluorescein test-to check for corneal abrasion
corneal abrasion Group G Group H P value
Normal 50(100.0%) 50(100.0%) -
Present - - -
Significance - - -
Fig.21Comparison of fluorescein test-to check for corneal abrasion Tape with Tape and
HPMC
The patients were checked postoperatively for corneal abrasions with fluorescein staining.
None of the patients in the study developed corneal abrasion postoperatively.

DISCUSSION

DISCUSSION
When a patient comes to the surgical suite for anaesthesia, either general anaesthesia or local
anaesthesia with varying degrees of sedation, care must be exercised by anesthesiologist as well as the
surgical teams to prevent untoward events3. Ophthalmic complications following general anaesthesia
are not uncommon.
The most common reported ophthalmologic complication during general anesthesia for non
ocular surgery in literature is corneal abrasion4. Other reported eye injuries are injuries from toxic
chemicals allowed to contact eyes during general anaesthesia. Various degrees of vision loss related to
pressure on eye or optic nerve, retinal ischaemia, acute angle closure glaucoma due to atropine.
Blindness occurs rarely due to ophthalmological injuries to eye especially during
ophthalmologic surgeries. Position of the patient may also play a significant role in the incidence of
ophthalmological complications during anaesthesia. In patients undergoing surgery in the lateral
posture, the dependent eye is more prone to develop corneal epithelial defects3.
Ophthalmic injuries result from direct trauma or decreased basal tear production due to
general anaesthesia. The most frequent ophthalmological complications following general anesthesia
is corneal abrasion. Fortunately few corneal abrasions lead to any permanent ocular injuries. Most
corneal abrasions however are not due to trauma but instead due to drying of corneal epithelium.
The best prophylaxis against corneal abrasion is to keep the eyelid closed during operative procedure5.
Another serious complications occurring during anaesthesia is retinal infarction produced by
pressure on the globe. Care must be exercised that no undue pressure on the eye lids occurs during
any surgical procedure. The risk of pressure on the eye increases during various procedures performed
when the patient is in face down position or when horse shoe face piece is used. Blindness resulting
from pressure is generally permanent3.
Acute glaucoma occurring during perioperative period is not uncommon. An episode of acute
glaucoma is probably initiated by the worry and anxiety of the patient and may even occur in the
perioperative period before any premedication has been given or procedure performed3.
With the increased frequency of cardiac and vascular surgical procedures the incidence of
embolic closure of retinal artery has increased in recent years. Awareness of these complications by
the anesthesiologist and the use of proper techniques to prevent them when possible can lower their
incident. The close cooperation of the anesthesiologist, the surgeon, and the ophthalmologist often
will prevent serious sequelae arising from these complications. When they do occur, if a patient
complains of eye pain or visual abnormality on awakening from anesthetic, prompt examination and
treatment is indicated. An ophthalmological consultation should be scheduled as early as possible3.
Siffring PA & Poulton TJ studied 127 adult patients scheduled for elective surgery under
general anaesthesia. Subjects were randomly dividend into four groups of equal size. Group A
received intraocular Lacritube ointment and tape closure. Group B, Dura tears ointment and tape, and
Group C methyl cellulose drops and tape; and Group D, hypoallergenic tape alone as eye protection.
Postoperatively the eyes were examined for evidence of corneal abrasion using fluorescein and
ultraviolet light. No evidence of corneal abrasion was detected in any of the 127 patients studied.
Patient age, duration of procedures and time of post operative evaluation were not significantly
different among groups.
Grover et al compared the efficacy of eye ointment and adhesive tape for protection of eyes
under general anesthetic. One hundred and fifty patients, 300 eyes undergoing general anesthesia for
non-ophthalmic procedures were divided into three groups. Eye in one group was left as control,
second group had hypoallergenic tape applied and third group had ointment used. In all eyes basal tear
production and visual acuity was assessed and corneal examination was carried out after fluorescein
staining both before and after surgery. They found that basal tear production was reduced in all groups
postoperatively as compared to preoperative values. Although basal tear production was reduced in
three groups postoperatively, the maximum reduction was seen in unprotected eyes followed by tape
and ointment group.

The overall incidence of corneal epithelial defect in this study was 10%. Eyes with multiple
corneal epithelial defects occurred only in control group. This suggests that during GA, protection of
the eyes is mandatory either by tape or ointment. Corneal injuries were more common in the
dependent eye in the lateral position. Of the 33 corneal epithelial defects, 23 were noted in the lower
zone and 10 in the middle zone.
Cross and Krupin studied the effects of general anaesthesia on basal tear production. Basal
tear production in 16 patients undergoing general surgical anaesthesia was measured using Schirmer I
test. Baseline tear measurement was made before premedication. Repeat Schirmer determination,
were made at 10, 30 and 60 minutes after induction, the eye lid being taped closed between
measurements. The average basal tear production in patients undergoing general surgical anaesthesia
was found to be severely inhibited. The inhibition of both reflex and basal tear production creates a
potentially injurious corneal environment.
The loss of protective eye lid closure under general anesthetic further increases the risk of
corneal exposure. Taping the eye lids closed to prevent exposure may not be sufficient protection
because of marked depression of tear production. The basal tear film is primarily responsible for
adequate hydration and nutrition of the cornea. This occurs in all the patients and is not related to the
inhalation agent used; nitrous oxide-oxygen, halothane or isoflurane.
They suggested that prophylactic ocular care with patient should include prevention of
mechanical exposure of cornea and replacement of deficient tear.
Batra and Bali studied the incidence of corneal abrasion during general
anesthesia.Investigation was done with 200 adult patients scheduled for elective surgery under general
anesthesia. In 100 patients the eyes were left uncovered while in the other 100 eyes were deliberately
closed with simple adhesive tape. The eyes were examined for corneal abrasion at the end of the
anesthetic period in the recovery room. This study showed an incidence of 44 patients for positive
staining with fluorescein. It was observed that maximum incidence of corneal abrasion was seen when
the duration of anesthetic was between 90-150 minutes. In all positive eases the staining was present
in the inferior third of cornea. None of the patients were the eyes were closed showed positive
staining.
Gild WM, et al studied eye injuries as part of ASA Closed Claims Analysis Project. Total database
of 2046 cases were studied during 1974 and 1987 .Eye injuries occurred in 3% of all claims in the
database (71 of 2046).Two distinct subsets were identified. The first was characterized by corneal
abrasion during general anesthesia (25% of 71 claims; 35%) the second subset was characterized by
patient movement during ophthalmological surgery (21 of 71; 30%) Although the study was not an
incidence study, it supported other studies showing that corneal abrasions constitute the single largest
ophthalmic complication following general anesthesia. They found that corneal abrasions produced
fewer permanent injuries than other eye injuries.
Roth S, Thistead RA et al surveyed 60,965 patients who underwent anesthesia for non ocular
surgeries from January 1988 to July 1992 who sustained eye injuries after anesthesia and non ocular
surgeries. Records were reviewed to determine the types and cause of eye injuries. They found that
the overall incidence of eye injury was 0.056 %( 34 patients). Duration of anesthesia was an
independent risk factor for eye injury; per hour of anesthetic time, risk was increased for patients
undergoing lengthier procedure. Use of general anesthesia was an independent risk factor associated
with eye injury. The risk of injury was greater in patient whose surgery involved the head or neck .A
specific cause could be discerned in only 21% of the cases. In most cases a specific cause could not be
determined
Our study assessed the basal tear film production preoperatively and postoperatively. 200
patients (400eyes) selected with the help of inclusion and exclusion criteria were allocated to four
groups using a randomization chart by an observer blinded to the study. Basal tear production was
measured using Schirmer’s test preoperatively. Eye protection methods were instituted as per
randomization chart by an anesthesiologist blinded to the study. Anesthesia was instituted as per
hospital protocol. Schirmer’s test repeated was postoperatively. If any significant eye finding were
present a repeat examination was done after 30 minutes. An ophthalmological consultation was done
to check for consistent findings.

In our study of comparison of tape against paraffin based ointment with Schirmer’s test, mean pre-op
Schirmer was found to be 15.66+_ 2.15 mm for taped group while mean pre-op Schirmer was
14.96+_2.25 mm for paraffin based ointment group. Post-operatively Schirmer’s value decreased to
10.12+_1.57mm in taped group while the post operative Schirmer’s reduced to 9.72+_1.01 mm in the
group with paraffin based ointment applied. The percentage change was found to be 35.40% for eye
protection with tape alone group. While the group with eye protection with paraffin based ointment
the decrease in basal tear production under general anesthesia was found consistent with prior studies
using tape and paraffin based eye ointment as eye protection methods.
In our study of comparison of tape with hydroxyl propyl methyl cellulose based ointment for
assessing basal tear production ,it was found that pre-operative basal tear production was
16.38+_1.75mm for tape as compared to 9.96+_1.32mm post operatively. Pre operative basal tear
production assessed with Schirmer’s test for group with eye protection with hydroxyl propyl methyl
cellulose based ointment was found to be 15.62+_1.54 while postoperatively if decreased to
9.72+_1.01
We also compared basal tear production of tape and tape with paraffin under standardized general
anaesthesia care.
Preoperative Schirmer’s was found to be 15.94+_1.33 mms. in the group which had tape alone as eye
protection while it reduced to 10.56+_1.01 mms. postoperatively in the same group. Schirmer’s test
score was found to be 16.60+_1.25 mms. preoperatively in the group which had tape with paraffin as
eye protection method.The basal tear production reduced post operatively to 10.58+_1.14 mms. in this
group.
Comparison of basal tear production under general anaesthesia in patient who had eye protected with
tape to patient who had eye protection done with tape and hydroxyl propyl methyl cellulose was also
studied.
It was found that basal tear production in patients with tape alone in pre operative period was
15.64+_1.21 while post operatively it reduced to 20.62+_1.35.In patients who had their eyes protected

with tape and hydroxyl propyl methyl cellulose preoperative basal tear production was found to be
16.30+_1.59 while post operatively it reduced to 10.68+_1.09
In our study basal tear production pre operatively was compared with postoperatively after
standardized general anesthesia technique. It was found that basal tear production was reduced post
operatively with various eye protection methods. The maximum reduction was seen in eyes protected
perioperatively with adhesive taping. These results confirm the study done by Grover et al which
compared basal tear production reduced under general anesthesia.
Grover et al compared the efficacy of eye ointment and adhesive tape for protection of eyes under
general anesthetic. One hundred and fifty patients, 300 eyes undergoing general anesthesia for non-
ophthalmic procedures were divided into three groups. Eye in one group was left as control, second
group had hypoallergenic tape applied and third group had ointment used. In all eyes basal tear
production and visual acuity was assessed and corneal examination was carried out after fluorescein
staining both before and after surgery .They found that the overall incidence of corneal epithelial
defect was 10% of which 90% occurred in control groups, 6.6% in tape 3.3% ointment group. They
also found that incidence of corneal epithelial defects did not alter with increase in duration of
surgery. The concluded that during general anesthesia eyes needs protection either by tape or ointment
as incidence of corneal injury is greater in unprotected eyes.
. Batra YK, Bali IM conducted a study on the eyes of 200 healthy adult patients undergoing general
anesthesia. The eyes were stained with fluorescein strips for detection of corneal abrasion in the
immediate postoperative period. Twenty six of fifty nine patients in whom the eyes remained partly
open showed positive staining. The remaining 141 patients in whom the eyes were naturally closed or
protected with adhesive tape or vase line gauze, did not develop exposure keratitis. It was suggested
that covering of eyes is necessary in all cases undergoing general anesthesia so as to avoid these
frequent complications of anesthesia. 00 patients (400 eyes) were also examined for corneal
abnormalities pre operative end post operative as part of the study
The eyes were protected with either tape, paraffin based ointment, hydroxyl propyl methyl cellulose,
tape with paraffin or tape with hydroxyl propyl methyl cellulose. None of the eyes were left

unprotected as Grover et al had studied and found that eye protection is mandatory under general
anesthesia.
Pre-op none of the subjects had any corneal abnormalities. Eyes were protected as per randomization
chart. After general anesthesia technique and various eye protection maneuvers in supine position,
eyes were again examined with vital staining. Fluorescein dye was used in the study for vital staining.
Post operatively none of the eyes developed any corneal pathology.
This confirmed the studies of Grover et al and Batra that eye protection techniques are mandatory in
all cases of general anaesthesia and any one technique ie use of hypoallergic tapes alone or paraffin
based ocular lubricant or hydroxyl propyl methyl cellulose is sufficient. It is also concluded that basal
tear production is decreased in all cases of general anaesthesia under standard anaesthesia technique
irrespective of eye protection methods used.
Draw backs of study
-sample size of less 200 patients (400eyes).
Gild WM, et al studied ASA Closed Claims Analysis Project. Total database of 2046 cases
were studied during 1974 and 1987 .Eye injuries occurred in 3% of all claims in the database (71 of
2046).Two distinct subsets were identified. The first was characterized by corneal abrasion during
general anesthesia (25% of 71 claims; 35%) the second subset was characterized by patient movement
during ophthalmological surgery (21 of 71; 30%)
-ophthalmological review was not taken preoperatively
-observer variability
Conclusion

Conclusion
To conclude
- eye protection is mandatory in all cases under general anesthesia technique
- eye protection methods including taping the eyes with hypoallergenic tape,
instilling paraffin based ocular lubricant or instilling hydroxyl propyl methyl
cellulose based tear substitute are equally efficacious in protecting the eye from
untoward ophthalmological injuries.
- Basal tear protection is reduced under standardized general anesthesia technique.

Summary
Summary
- Patients undergoing prolonged non ocular surgery with general anesthesia may
develop ocular complications. The risk of ocular complications can be due to
multiple factors, firstly because there is an abolition of protective corned reflex
under general anesthesia. There is also a decreased basal tear production during
general anesthesia leading to drying of the cornea. Pain perceptions are also
absent under general anesthesia which can contribute to ocular complication The
most common reported ophthalmologic complication during general anesthesia
for non ocular surgery in literature is corneal abrasion .The eyes can be protected
during general anesthesia by taping the eyes closed with a hypoallergenic
adhesive tape, with paraffin based ointment or with tear substitute hydroxyl
propyl methyl cellulose ointment. The purpose of the present study was to
determine the efficacy of various eye protection methods. Our study assessed the
basal tear film production preoperatively and postoperatively using Schirmer’s
test. The eyes were protected with either tape, paraffin based ointment, hydroxyl
propyl methyl cellulose, tape with paraffin or tape with hydroxyl propyl methyl
cellulose. None of the eyes were left unprotected. It was found that basal tear
production was reduced post operatively with various eye protection methods.
The maximum reduction was seen in eyes protected perioperatively with adhesive
taping. 200 patients (400 eyes) selected for the study were also examined for
corneal abnormalities pre operative end post operative as part of the study using
vital staining technique with fluorescein dye. Basal tear production is decreased
in all cases of general anesthesia under standard anesthesia technique irrespective
of eye protection methods used. Eye protection is mandatory in all cases under
general anesthesia technique


BIBLIOGRAPHY

BIBLIOGRAPHY
1.Boggild Madson NB, Bundgarrd-Neilsen P, Hammer U: Comparison of eye protection with methyl
cellulose and paraffin ointments during general anesthesia. Can Anesth Soc J 1981;28:575-8
2.Krupin T, Cross DA, Becker B: Decreased basal tear production associated with general anesthesia.
Arch Ophthalmol 1997;95:107-8
3.Terry HR Jr, KearnsTP, LoveJG, OrwellG: Untoward ophthalmic and neurologic events of
anaesthesia. Surg Clin North Am 1965;45;927-9
4.Cucchiara RF, Black S:Corneal abrasion during anesthesia and surgery. Anesthesiology
1988;69:978-9
5.Snow JC, Kripke BJ, Chandra P, Norton ML, Woodcome HA: Corneal injuries during general
anesthesia. Anesth Analg 1975;54:465-7
6.Orlin FK, Cooperman LH: Complications in anesthesiology. Philadelphia,JB
Lippincott’1983pp345-346.
7.SchimdtP, Boggild Madsen NB: Protection of the eyes with ophthalmic ointments during general
anesthesia. Acta Ophthalmol 1981;59;422-7
8.Cross DA, Krupin T: Implications of the effects of general anesthesia on basal tear production.
Anesth Anal 1977;56:35-37
9.Orlin SE, Kurata FK, Krupin T, Schnieder M: ocular lubricants and corneal injury
during anaesthesia .Anaesth Anal 1989,69:384-5
10.Batra YK, Bali IM: Corneal abrasion during general anaesthesia.Anaesth Analg 1977;56:363-55.
11.Walcott B: Anatomy and innervations of human lacrimal gland.In Albert DM, Jakobei
FA(eds.):Principles and Practice of Ophthalmology: Basic sciences. Philadelphia, WB Saunders
1994,p454

12.Dartt DA: Physiology of tear production, In Lemp MA(ed):The Dry Eye, Berlin, Springer-
Verlag,1992,p65
13..Lamberts DW; Physiology of tear film In Smolin G,Thoft RA(eds)
The Cornea 3rd edition, Boston.
14.Dartt DA: Regulation of tear secretion. Adv Exp Med BIOL 350:1994
15.Sullivan DA, Block L, Pena JDO: Influence of androgens and pituitary hormones on the structural
profile and secretory activity of the lacrimal gland
16. Mircheff AK: Lacrimal fluid and electrolyte secretion a review. Curr Eye Res 1989;8:607-609
17. Sullivan DA, Allansmith MR: Hormonal regulation of the secretory immune system in the
eye:androgen modulation of the IgA levels in the tears of the rats. J Immunolo 1985;134:2978-2982
18. Hann LE, Allansmith MR,Sullivan DA: Impact of ageing and gender on the Ig containing cell
profile of the lacrimal gland. Acta Ophthalmol 1988;66:87-92
19. Sullivan DA,Bloch KJ, Allansmith MR: Hormonal influence on the secretory immune system of
the eye: androgen regulation of the secretory component levels in rat tears. J Immunol
1984;132:1130-1135
20. Thaysen JH: The lacrimal gland In:Andreoli TE, Hoffman JF,Fanestil DD,eds.Physiology of
membrane disorders. New York :Plenum,1978:415.
21. Bachman WG, Wilson GS:Essential ions in the maintanence of corneal epithelial surface. Inv
Ophthalmol Vis Sci 1985;26:1484-1487
22. SterneME ,Gao J: The Role of the lacrimal functional unit in the pathology of dry eye. Ann NY
Acad Sci 02966:211-22
23. Tsubota K : Tear dynamics and dry eye. Preg Retin Eye Res1998;17(4);565-96

24. Van Bysterveld OP:Diagnostic test in the sicca syndrome. Arch Ophthalmology 82:10,1969
25. Schirmer O. Studien zur physiologie und pathologie der tranenabsonderung und tranenabfuhr.
Graefes Arch Clin Exp Ophthalmol1903:56:197-291
26. JonesLT: The lacrimal secretory system and its treatment
27.Sterne ME, Beuerma RW, Fox RI,Gao J: The Pathology of dry eye. The interaction between ocular
surface and lacrimal glands.Cornea1998:17(6):584-89
28. Clinch TE ,Benedetto DA, Felberg NT ,Laibson PR: Scirmers test a closer look. Arch Ophthalmol
1983;101:1382-1385
29. Wright JC, Meger GE: A review of the Schirmer’s test for tear production .Arch Ophthalmol
67:564,1962
30. Pin Schmidt NW:Evaluation of Schirmer tear test. South Med J 63:1256 1962
31. Fenstra RPG, Tseng SCG: Comparison of Fluorescein and Rose Bengal staining.
Ophthalmology 99:605,1992
32.Grover VK, Kumar KVM, Sharma S:Comparison of methods of eye protection under general
anesthesia.Can J Anesth 1998;45:575-77
33.Marquardt R,Christ T. Gelatinous Tear substitutes in the critical care unit (German).Anesth
Notfallmed 1987;22:235-8
34.Siffring PA,Poulton TJ;prevention of of phthalmologic complications in general
anesthesia.ANESTHESIOLOGY 1987;66:440
35.Roth S ,RoizenMF Optic nerve injury:role of anesthesiologist Anesth Analg 1996:82;435-437
36.Gild WM,Posner MR:Eye injuries associated with anesthesia, a closed claims
analysis.ANESTHESIOLOGY 1992;76:204-8

37.Bernard Rosner (2000), Fundamentals of Biostatistics, 5th Edition, Duxbury, page 80-240
38.M. Venkataswamy Reddy (2002), Statistics for Mental Health Care Research, NIMHANS
publication, INDIA, page 108-144
39.Sunder Rao P S S , Richard J : An Introduction to Biostatistics, A manual for students in health
sciences , New Delhi: Prentice hall of India. 86-160

Annexure

PROFORMA
EYE PROTECTION DURING GENERAL ANAESTHESIA
-A Comparison of different methods
Serial no Group 1 A B
2 A B
3 A B
4 A B
Patient Name: Age Sex
OP/MRD no :
Diagnosis :
Operative procedure:
ASA Grading 1 2 3 4 5
Premedication- glycopyrrolate/atropine
Induction->Inhalational/Intravenous/inhalational +intravenous
Maintenance->
Recovery->
PRE-OPERATIVE OPHTHALMOLOGICAL ASSESSMENT
Rt Eye Lt Eye

Flourescein staining +/_ +/_
Schirmer test mm mm
POST-OPERATIVE
Flourescein stain +/_ +/_
upper upper
middle middle
lower lower
Schirmer test mm mm

ASA pre.op
S. No Group Name Age Sex Hospital ID R.schirmer L.schirmer
1 A Salomi 32 f 2355012 1 16 15 2 A Shamin 52 f 2452882 2 17 14 3 A Bibi 21 f 2371548 1 16 19 4 A Susan 22 f 2426700 1 17 12 5 A Tejaswini 22 f 2373493 1 15 14 6 A Chitra 38 f 1694469 1 16 13 7 A Sarojamma 55 f 2456903 1 17 16 8 A Prapti 46 f 2399630 1 18 13 9 A Gangamma 40 f 2456941 1 18 17 10 A Venkatesh 35 m 2352428 1 19 19 11 A Nandakumar 30 m 2447871 1 15 14 12 A Srinivas 35 m 2453428 1 17 15 13 A Arun Kumar 18 m 2980793 1 19 13 14 A Neelamma 49 f 984112 1 12 11 15 A Ratnavati 54 f 2456810 2 16 15 16 A Subrmani 20 m 2217647 2 14 18 17 A Madhesh 40 m 2454135 1 19 12 18 A Narayan 27 m 2449940 1 14 16 19 A Lakshmi 26 f 2452671 1 17 14 20 A Joseph 29 m 2473621 1 17 18 21 A Pawan 19 f 2456064 1 13 13 22 A Joyce 25 m 2455874 1 19 16 23 A Harsha 27 m 2455891 1 16 13 24 A Harini 31 f 2452172 1 16 12 25 A Mahalakshmi 22 m 2431379 1 15 14 26 B Sai 24 f 2456621 1 16 12 27 B Panchali 30 f 2456623 1 14 16 28 B Deepa 33 f 2901871 1 12 14 29 B Usha 22 f 2453363 1 14 13 30 B Chinnajamma 52 f 2421601 2 18 14 31 B Gangadharappa 52 m 2435340 2 13 15 32 B Rajappa 26 m 2455408 1 19 18 33 B Venkataraju 25 m 2453107 1 13 13 34 B Neal 15 m 1934787 1 14 16 35 B Sujana 26 f 2448361 1 12 13 36 B Bhandari 52 m 248378 2 15 19 37 B Muniraj 29 m 2441374 1 16 12 38 B Prajesh 26 m 2242587 1 14 16 39 B Meera 49 f 2411374 1 17 14 40 B Meenakshi 29 f 2451333 1 19 13 41 B Ramesh 45 m 2444075 1 19 14 42 B Maniama 56 f 2364882 1 14 15

43 B Ramesh 54 m 1439573 2 15 16 44 B Shivaram 47 m 2389295 2 17 18 45 B shobha 56 f 2450864 2 15 13 46 B christy 26 m 2373792 1 15 13 47 B sarvesh 45 m 2376798 1 19 18 48 B regina 36 f 2455716 1 12 14 49 B mary 32 f 2471384 1 15 17 50 B varghese 59 m 345509 2 15 19 51 C Joseph 25 m 2455712 1 16 15 52 C thomas 56 m 2253781 1 15 15 53 C chinna 60 m 2454674 2 15 17 54 C laila 54 f 2455967 1 18 12 55 C bhushan 52 m 2467882 18 16 56 C shiek 39 m 2461686 1 19 15 57 C dawood 52 m 2678172 1 13 14 58 C falguni 28 f 2458762 1 14 19 59 C seit 52 m 2123751 1 18 14 60 C vijaya 17 f 2381632 2 15 16 61 C aiyappa 27 m 2460933 1 16 17 62 C malini 22 f 2329576 1 19 15 63 C merlin 22 m 1324720 1 15 15 64 C sharada 57 f 2107040 2 16 17 65 C krishnana 42 m 2327927 1 16 15 66 C navven 24 m 2331721 1 19 14 67 C kumar 22 m 2381445 1 18 17 68 C karthick 22 m 2457692 1 12 15 69 C vijaya 45 f 2461591 1 19 16 70 C lakshmi 22 f 1889254 1 17 16 71 C udaya 22 m 2462008 1 15 15 72 C anupama 60 f 2317619 1 16 19 73 C savithri 50 f 2416105 2 19 16 74 C waheeda 48 f 2461793 1 18 15 75 C shiva 31 m 2456267 1 16 17 76 D kupparaj 39 m 2461694 1 17 18 77 D sonu 19 m 2459233 1 17 19 78 D navven 22 m 2352291 1 13 15 79 D sidarth 29 m 2285340 1 15 15 80 D sridhar 39 m 2343985 1 14 17 81 D muddamaa 17 f 795835 1 16 17 82 D selina 42 f 1785321 1 16 18 83 D uma 33 f 2457809 1 15 18 84 D joythim 30 m 2457933 1 17 13 85 D bhaskar 21 m 2446947 1 19 16 86 D john 28 m 2458539 1 15 15 87 D moksha 41 f 2458321 1 17 16 88 D kalyan 25 m 2444910 1 16 16

89 D shiva 39 m 2366742 1 16 15 90 D azhar 21 m 2458796 1 15 14 91 D hussien 49 m 2206028 1 15 18 92 D ramu 60 m 2455948 2 12 17 93 D chardrasekhar 27 m 2453796 1 17 18 94 D archana 17 f 2162587 1 16 16 95 D shubha 27 f 2267784 1 16 18 96 D hammed 38 m 2461577 1 15 16 97 D dinesh 21 m 1800851 1 17 17 98 D kurain 43 m 1302985 1 13 15 99 D alagappa 43 m 1800840 1 14 15 100 D ananthmma 60 f 1879044 2 16 15 101 E sara 32 f 2319878 1 17 16 102 E thomas 29 m 1884002 1 17 16 103 E prasanna 41 m 1884263 1 16 18 104 E radha 50 f 16499894 1 16 18 105 E rajgopal 32 m 1884201 1 17 17 106 E abhishek 19 m 1779300 1 17 17 107 E savithramma 53 f 1883296 1 14 15 108 E thyagaraj 51 m 1869190 2 15 18 109 E ramesh 36 m 2378196 1 15 16 110 E george 58 m 1877884 2 14 16 111 E suman 13 m 1875529 1 14 17 112 E baby 30 f 2480883 1 18 18 113 E dhanalakshmi 13 f 2483756 1 17 16 114 E bahskar 26 m 2481538 1 16 16 115 E thimmaraya 35 m 2479774 1 15 17 116 E jolly 34 f 2478152 1 16 15 117 E venkitesh 22 m 2030212 1 16 15 118 E manjunath 45 m 2480418 1 14 18 119 E rathna 54 f 2460349 1 15 18 120 E rajkumari 42 f 2483442 1 16 16 121 E rajitha 40 f 2431938 1 16 16 122 E bhagyawathi 41 f 2481648 1 15 17 123 E pushpa 23 f 2469666 1 15 16 124 E mary 45 f 2483150 1 14 13 125 E lucy 54 f 2478277 2 16 18 126 F dilshad 45 f 2468675 1 16 15 127 F murugan 14 m 2479409 1 18 15 128 F vishnuprasad 50 m 2477239 2 17 17 129 F sampamal 60 f 2456064 2 16 17 130 F saroj 35 f 2477116 1 18 16 131 F mary 35 f 2483367 2 18 15 132 F ansar 60 m 2476359 1 17 15 133 F sattar 45 m 2325628 1 16 18 134 F Arun Kumar 29 m 2480293 1 15 16

135 F prashanth 50 m 26780 1 16 13 136 F radha 29 f 2483494 1 19 18 137 F mohan 23 m 2484170 1 16 15 138 F vijay 32 m 2215259 1 18 14 139 F narendra 50 m 2485326 1 17 18 140 F dinakaran 34 m 2475632 1 17 17 141 F anandan 45 m 2479532 1 14 15 142 F pramod 20 m 2452696 1 15 17 143 F murugeshan 40 m 2482265 1 16 16 144 F krishnana 60 m 2479203 2 16 17 145 F bhayva 22 f 2119915 1 15 15 146 F regina 60 f 2311188 1 18 18 147 F padma 47 f 2493855 1 18 19 148 F gouramma 45 f 2503886 1 17 16 149 F giriamma 60 m 2475985 1 16 17 150 F venkatta 45 m 2497424 1 18 17 151 G rakesh 22 m 2288281 1 16 18 152 G babu 34 m 2498141 1 15 17 153 G savithri 56 f 1446244 2 17 17 154 G malik 45 m 2498369 1 15 16 155 G sathyaraj 36 m 698092 1 15 15 156 G pillama 56 f 2438811 1 16 15 157 G alice 49 f 2190953 1 16 16 158 G muniyamma 56 f 2471212 2 17 16 159 G nirmala 42 f 2499665 1 14 13 160 G lakshmi 60 f 2451490 2 16 17 161 G sunanada 35 f 2498910 1 15 18 162 G sr.mary 63 f 2504727 2 17 16 163 G sriramulu 45 m 2499172 1 16 12 164 G latha 39 f 2404797 1 16 16 165 G saibunnissa 34 f 2098688 1 17 17 166 G govindaraj 45 m 2504163 1 13 17 167 G jayamma 56 f 2502879 1 13 18 168 G sandhya 45 f 2499009 1 18 16 169 G githiya 29 f 2488786 1 14 18 170 G akrinissa 69 f 2500343 2 16 15 171 G shivamurali 34 m 2496016 1 17 14 172 G asma 21 f 2502759 1 16 18 173 G angela 30 f 2500089 1 15 16 174 G lakshmamma 46 f 2468714 1 17 16 175 G sajith 28 m 2500180 1 14 15 176 H sandeep 21 m 2494289 1 16 15 177 H preetha 27 f 2494852 1 15 17 178 H narayanappa 60 m 2497731 2 18 15 179 H parvathamma 62 f 2476501 2 16 15 180 H suresh 23 m 2446069 1 17 15

181 H panchanam 45 m 1136652 1 14 16 182 H indrareddy 62 f 2484751 2 18 14 183 H nasreen 50 f 2500952 1 17 15 184 H sandeep 19 m 2486555 1 16 16 185 H narasimharaj 59 m 2495945 2 15 16 186 H sr.prathima 34 f 1735256 1 16 15 187 H ranjini 18 f 2503048 1 16 17 188 H madadmal 51 f 2487877 1 17 17 189 H kullayappa 45 m 2504409 1 16 13 190 H venkithesh 26 m 2231168 1 18 15 191 H jolly 56 f 685638 2 18 17 192 H lohitha 34 f 2501302 1 19 16 193 H vasudeva 47 m 2428660 2 14 15 194 H sathya 45 m 2493839 2 16 15 195 H radhika 54 f 2462953 1 13 14 196 H lalitha 58 f 2414306 2 18 17 197 H latha 49 f 250083 2 19 16 198 H pradeep 30 m 801826 1 19 17 199 H ravi 26 m 2423368 1 17 16 200 H shilpa 25 f 2128265 1 15 17