Cognitive Neurolinguistics
16
Dr. Apoorva Pauranik MGM Medical College & M.Y. Hospital Professor, Department of Neurology Indore Cognitive Neurolinguistics Introduction : People are more than curious about language. They are passionate, because it is the most accessible part of the mind. It is expected that study of language will lead to insight about human nature. Neurologists should also be interested in cognitive neurolinguistics because aphasia and related disorders of speech, communication, reading and writing are major and important component of their clinical workload. Post stroke aphasia is commonest. It occurs in 21- 38% of stroke survivors as a chronic disability. Community incidence is 43/100,000/year and prevalence about 3000 per million. 1 It is more common than many other neurological diseases like Parkinsonism or multiple sclerosis or motor neuron disease. Head injury, brain tumors, encephalitis also aid to number of cases with aphasia. Dementia is an impending epidemic with increasing average age. Defects in language function are an important component of dementia. Learning disability particularly dyslexia (prevalence 5%) is a major community problem whose assessment and therapeutic rehabilitation is also guided by neurolinguistics principles. Unfortunately there is a huge treatment gap for children and adults suffering from dyslexia, aphasia and related disorders. There is paucity of neurologists, speech pathologists and clinical psychologists, both in absolute and relative terms. Departments are not well equipped for methods of speech therapy. Most saddeningly there is lack of motivation amongst all concerned specialists who share a therapeutic nihilism 2 . The later feeds to and its fed by a similar attitude in patients and caregivers. The irony becomes stark when we realize that so much can be done, now particularly with the development and refinement of cognitive neuro (and psycho) linguistics models, theories and practices which can be further amplified by new tools and technologies from computers and communication. 3 What is Cognitive Neurolinguistics?
Transcript of Cognitive Neurolinguistics

Dr. Apoorva Pauranik MGM Medical College & M.Y. Hospital
Professor, Department of Neurology Indore
Cognitive NeurolinguisticsIntroduction :
People are more than curious about language. They are passionate,because it is the most accessible part of the mind. It is expectedthat study of language will lead to insight about human nature.
Neurologists should also be interested in cognitive neurolinguisticsbecause aphasia and related disorders of speech, communication,reading and writing are major and important component of theirclinical workload. Post stroke aphasia is commonest. It occurs in 21-38% of stroke survivors as a chronic disability. Community incidenceis 43/100,000/year and prevalence about 3000 per million.1 It is morecommon than many other neurological diseases like Parkinsonism ormultiple sclerosis or motor neuron disease. Head injury, brain tumors,encephalitis also aid to number of cases with aphasia. Dementia is animpending epidemic with increasing average age. Defects in languagefunction are an important component of dementia. Learning disabilityparticularly dyslexia (prevalence 5%) is a major community problemwhose assessment and therapeutic rehabilitation is also guided byneurolinguistics principles.
Unfortunately there is a huge treatment gap for children and adultssuffering from dyslexia, aphasia and related disorders. There ispaucity of neurologists, speech pathologists and clinicalpsychologists, both in absolute and relative terms. Departments arenot well equipped for methods of speech therapy. Most saddeninglythere is lack of motivation amongst all concerned specialists whoshare a therapeutic nihilism2. The later feeds to and its fed by asimilar attitude in patients and caregivers. The irony becomes starkwhen we realize that so much can be done, now particularly with thedevelopment and refinement of cognitive neuro (and psycho) linguisticsmodels, theories and practices which can be further amplified by newtools and technologies from computers and communication. 3
What is Cognitive Neurolinguistics?

Dr. Apoorva Pauranik MGM Medical College & M.Y. Hospital
Professor, Department of Neurology IndoreCognitive Neurolinguistics studies the relation of language andcommunication to different aspects of brain function, i.e. it tries toexplore how the brain understands and produces language andcommunication. This involves attempting to combine theory fromneurology/neurophysiology (how the brain is structured and how itfunctions) with linguistic theory (how language is structured and howit functions). Structure (Hardware) and function (Software) areintricately interdependent and of equal theoretical and practicalimportance.
Cognitive Neurolinguistics is an example of interdisciplinaryenterprise par excellence in which humanities as well as medical,natural and social sciences along with technology are represented.
Cognitive neurolinguistics is a part of spectrum of fields includingneurology, speech pathology, psychology, linguistics, imaging,neurobiology and physiology and genetics. The boundaries are fuzzy andthere is significant overlap and interaction.
Evolution of Neurolinguistics
The thought about thought and about other mental process (includinglanguage) took a longtime to be clearly posed as pertaining to themind body relationship. While Hippocrates (400 b.c.) describedaccounts on infirmities that produced lack of language, the quest forunderstanding healthy faculty of language was not pursued till laterpart of 20th century. The anatomy and cognition came together for thefirst time in 19th century with Broca’s and Wernicke’s models for thelanguage faculty, followed by Lichthiem.
A cognition revolution occurred in 1960s with Noam Chomskey’sgenerative grammar and Steven Pinker’s “Language Instinct’. In latesixties the scientific environment was ripe to instill biolinguisticsinvestigations. Norman Geshwind reintroduced connectionist model withmore anatomic details and defended that any cognitive output had to be
Dr. Apoorva Pauranik MGM Medical College & M.Y. Hospital
Professor, Department of Neurology Indoreanalyzed in terms of explicit hypothesis as to their underlying neuralmechanisms. The 70s and 80s witnessed the introduction of non invasiveor minimally invasive assessment techniques in the study of thehealthy faculty of language. The number of neurolinguisticslaboratories in the best universities in the world has grownexponentially since 1990s . Cognitive neurolinguistics has a strongclinical tradition by now.
The first application of experimental psycholinguistic methods andtheory in studies of aphasic language appeared in early 1960s.Thousands of studies based on the perspective of cognitive psychology,linguistics and clinical science have been done to explain thephenomenology of apahsia. In 1990s the pendulum swang in oppositedirection. Aphasiological phenomenon now became part of ‘data’ to testlinguistic or cognitive theories. William Milberg and SheilaBlumstein(2000)4 lamented that the clinical and biological context ofaphasic symptoms became an epistemological orphan and emphasized theneed for reclamation of the clinical details of aphasic deficits as afocus of aphasic research.
The clinical data or observations which constitute the substrate of CNcome from patients suffering from acquired or developmental disordersof brain. Practicing neurologists, unfortunately do not explore orutilize or contribute to the field. It need not be so. There are manyputative advantages of interaction for all stake holders, includingneurolinguists and clinicians on one hand and theoretical linguisticsand cognitive scientists on the other and above all to the patients.
The central questions of neurolinguistics are many, including: Whathappens to language and communication after brain damage of differenttypes? How did the ability to communicate and the ability to uselanguage develop in the evolution of the species? How can we relatethis development to the evolution of the brain? How do children learnto communicate and use language? How can we relate their acquisitionof language to the development of their brains? How can we measure andvisualize processes in the brain that are involved in language and

Dr. Apoorva Pauranik MGM Medical College & M.Y. Hospital
Professor, Department of Neurology Indorecommunication? How can we make good models of language andcommunication processes that will help us to explain the linguisticphenomena that we study? How can we make computer simulations oflanguage processing, language development and language loss? How canwe make experiments that will allow us to test our models andhypotheses about language processing? How can neurolinguistics dataand theory guide us in planning speech therapy and otherrehabilitative measures in a given patient with aphasia?
When neurolinguistics is approached as part of psycholinguistics,localization does not matter. Neural activity is used like behavioralreaction time so as to determine the ‘when’ aspect (time course) ofprocesses. Neurolinguistics can also be approached as part ofneurobiology. Then the goal becomes to articulate a theory of languagein terms of structure of brain. ‘Where’ and ‘how’ questions are justas important as ‘when’ questions. The scope of neurolinguistics ismuch more specifically defined than that of general cognitive sciencesbecause it is based on linguistic theory. (Caplan 1992)5.
As a result of advances in cognitive neurologistics the traditionalmodel of language organization in brain (figure1) is being refined toinclude new areas and new roles (figure 2). Many box and arrow modelshave evolved to explain word processing and sentence construction(figure 3). (Hillis 2007)6.
Focal neurodegenerative disease like Primary Progressive Aphasia leadto different constellation of language deficits than those encounteredin stroke because left anterior and inferior temporal cortex is nottypically damaged in CVA. Semantic dementia is characterized byprogressive dissolution of modality independent semantics or meaningof words and objects.
Gradually a theory of speech therapy is emerging which includes amodel of cognitive process (to be treated). Hypotheses are in placeabout the functional damages which could be amenable to amelioration.Plasticity and neural mechanism of recovery are better understood.Other extraneous factors having a bearing upon recovery are well

Dr. Apoorva Pauranik MGM Medical College & M.Y. Hospital
Professor, Department of Neurology Indorerecognized. The more often a patient produces a particular correctresponse (with as much facilitation as needed), the more often thatperson will be able to produce the same correct response independentlyin future.
New tools of Study :
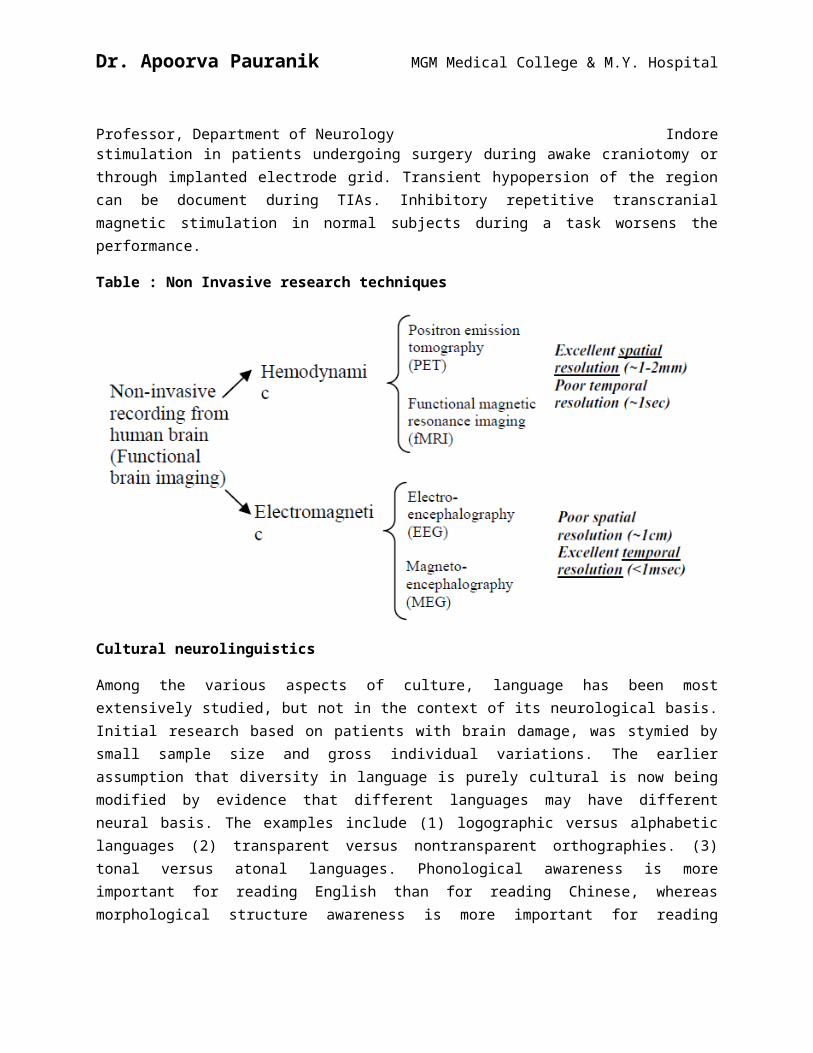
Two types of neurophysiological techniques are applied to languageassessment: hemodynamic and electromagnetic. As shown in Table, thehemodynamic techniques – PET (positron emission tomography) and fMRI(functional magnetic resonance imaging) – have excellent spatialresolution (~1-2mm). Contrastingly, they offer a poor temporalresolution (~1sec), which does not conform to the temporal window oflanguage cognition. Both PET and fMRI are efficient methods inlocalizing specific brain functions. The electromagnetic techniques –EEG (electroencephalography), evoked potentials and MEG(magnetoencephalography) – provide excellent temporal resolution,which lies on the order of milliseconds. This is an accountablestrength when assessing the brain in the execution of linguistic taskswhose time window is also on the order of milliseconds. However, theEEG does not offer good spatial resolution (~1cm). Even the MEG, whichoffers improved localization in relation to the EEG, sometimesreaching the resolution of a few millimeters, cannot match the spatialprecision of PET and fMRI.
One of the common methods in neurolinguistics is to surprise the brainin various ways, so as to get some sort of robust response. What thebrain is surprised by can be useful way to find out what the brainknows. There is a surprise response called the ‘mismatch negativity’.That is elicited when you habituate the listener to one sound categoryand then suddenly cross a perceptual boundary. The brain responds toimplausibility (the shirt was ironed, the thunderstorm was ironed) andungrammatically (the shirt was ironed, the bow was on ironed) in arobust manner.
Midfusiform gyrus shows activation on fMRI during reading tasks. Tovalidate the observation one now can inhibit this region with cortical
Dr. Apoorva Pauranik MGM Medical College & M.Y. Hospital
Professor, Department of Neurology Indorestimulation in patients undergoing surgery during awake craniotomy orthrough implanted electrode grid. Transient hypopersion of the regioncan be document during TIAs. Inhibitory repetitive transcranialmagnetic stimulation in normal subjects during a task worsens theperformance.
Table : Non Invasive research techniques
Cultural neurolinguistics
Among the various aspects of culture, language has been mostextensively studied, but not in the context of its neurological basis.Initial research based on patients with brain damage, was stymied bysmall sample size and gross individual variations. The earlierassumption that diversity in language is purely cultural is now beingmodified by evidence that different languages may have differentneural basis. The examples include (1) logographic versus alphabeticlanguages (2) transparent versus nontransparent orthographies. (3)tonal versus atonal languages. Phonological awareness is moreimportant for reading English than for reading Chinese, whereasmorphological structure awareness is more important for reading

Dr. Apoorva Pauranik MGM Medical College & M.Y. Hospital
Professor, Department of Neurology IndoreChinese. Hindi and other semi-syllablic Indian scripts fall inbetween. 7
In a recent meta-analysis of neural bases of reading , Bolger et al(2005)8 quantitatively compared the findings of 43 studies of differentlanguages (25 with alphabetic languages, 9 with Chinese, 5 withJapanese Kana, and 4 with Japanese Kanji). They found that activationsin the frontotemporal, occipitotemporal and occipital regions wereshared across languages. Important cross-language differences werefound in the left middle frontal gyrus (MFG), temporoparietal region,and right fusiform cortex. Nouns and verbs in Chinese activate a widerange of overlapping brain areas in distributed networks in both theleft and the right hemisphere. In Indo-European languages they arerepresented discretely-verbs in left frontal cortex, nouns inposterior temporal-occipital regions.
Two neuro-biological principles have been recognized – (i) Neuralplasticity-which allows culture to have an imprint on the brain and(ii) Neural specialization which sustains cross cultural differences.At birth infants are universally capable of differentiating phoneticcontrasts in all languages as a result of native language experience(or ‘tunning’). However, the ability to distinguish nonnative phoneticcontrasts dramatically declines as early as 6 months. English speakerscannot identify Hindi phonetic contrasts that differ in voice onsettime from -90 to 0 ms (Sharma and Dorman, 2000)9. In fact, evidence isaccumulating that language learning can change brain functions andeven anatomy due to neural plasticity. Bilinguals have been found toshow increased gray matter density in the left inferior parietalregion as compared to monolinguals.10
For the study of aphasia to become a truly universal science,description of aphasic deficits from limited variety of languages inclearly inadequate, as are the explanatory theories and thetherapeutics approaches based on these theories. Structural variationsof individual languages constitutes an important variable exertingdifferential effects upon the patterns of aphasic symptoms.

Dr. Apoorva Pauranik MGM Medical College & M.Y. Hospital
Professor, Department of Neurology IndoreA case of point is the aphasic syndrome called Agrammatism. A crosslanguage comparative study of agrammatic aphasic narratives in itslanguages had been conducted over past many hears (Menn and Obler)11.Some of the results indicated that so called representative featuresof agrammatic speech such as the omission of grammatical morphemes andthe use of infinitive verb from are not as representative as hard beenthought and in fact vary with structural variations of individuallanguages. A symptoms such as word other difficulties has much moreimportance for languages with little morphology and where word otheris important to convey thematic roles, than in languages wherethematic roles are encoded via grammatical morphemes (imagine a nativespeaker of Sanskrit developing nonfluent aphasia and so calledagrammatism).
The Indian Scene ;
Neurolingusitic research in Indian languages has not taken off. Therehave been a few sporadic attempts here and there but no concerted andcoordinated planning of visionary nature. As a part of PL-480 grantDr. S. Janki collected lot of data from large number of aphasicpatients at New Delhi. Dr. V.Virmani had published some papers inclinical aphasiology and bilingualism. Dr. Pratibha Karanth at AllIndia Institute of Speech and Hearing, Mysore can be credited withdeveloping a using a comprehensive neurolingiuistic text battery foraphasia in Kannada. She has seminal contribution in alexia inDravidian languages and currently engaged in childhood acquisition oflanguages and semantic disorders in aphasia. Dr. Subhash Bhatnagar canbe cited as a successful example of a pure linguist who subsequentlycarved an academic career as a neurolinguist. He has developed a Hindiversion of Boston Diagnostic Aphasia Examination and validation. Hewas also part of Cross Language Agrammatism study. Dr. Jyotsana Vaid,a psychologist has important publications on bilingualism. Dr. SudhirBhan was awarded PhD from Osmania University on a specific aspect oflexicon. i.e. kinship terms in aphasic patients. The present author(A. Pauranik) has independently developed a Hindi version of BDAEsomewhat similar to Dr. Subhash Bhatnagar’s, which has been validated

Dr. Apoorva Pauranik MGM Medical College & M.Y. Hospital
Professor, Department of Neurology Indoreon 200 patients and 50 controls subjects. He has presented works on‘Interaction between literacy and aphasia’, ‘Clinico-anatomicalcorrelation of lesions in Brain with type of aphasic deficit’s, Alexiaand Agraphia in Hindi English Bilinguals’, ‘A neurolinguisticsanalysis of paraphasic errors, ‘Analysis of narrative discourse inbilingual aphasia’ and ‘Language impairment in dementia’. He has alsodeveloped material for assessment of reading and writing based oncognitive neuropsychological model and hence having subtests fornonwords, transcription across Devnagri, Roman and others.
There has been no true reciprocation by linguists towards the fewneurologists active in this field. Many other languages spoken byrelatively fewer people and not having as rich a tradition inlinguistics, as most Indian Languages, have much more literature.
Cognitive neurolinguists have not been able to share their findingswith those of other related fields. They have also not been able tobuild a common language that may integrate the different disciplines,particularly relevant for clinical neurologists like me. For complexepistemologic reasons, linguistics has never been readily absorbedinto other scientific fields. Take a look on any neuroscience book. Achapter on vision seamlessly uses the physical terms from optics, andsimilarly the ones on metabolic disorders from chemistry and audiologyfrom acoustics. Unfortunately linguists have not managed yet to maketerms like morphology, syntax and phonology, vocabulary items for myfellow clinical neurologists.
The Tasks ahead
Some of the tasks before us in India are to have comprehensive goodquality studies for language use patterns, state of art laboratoriesfor phonetic research in Indian languages, electronic resources tosupport applied linguistic research, creation of various spoken andwritten language database and semester level course on ‘structure ofan Indian language for clinicians.’

Dr. Apoorva Pauranik MGM Medical College & M.Y. Hospital
Professor, Department of Neurology IndoreSimilarly Indian Academy of Neurology and Neurological society ofIndia will be doing good if they encourage and support orientation andtraining programs in aphasiology. It may be worthwhile for some of usto join projects like Aphasia Bank (Brian Mckwhinny) 12 However, Itwill require lot of ground work before doing so, particularlydevelopment of MOR grammar for Hindi and other Indian language. DiptiMishra and her team at Indian Institute of Information Technology atHyderabad are engaged in task of developing software for taggingspeech samples with reference to parts of speech and morphologicalmarkers.
Cognitive neurolinguistics based aphasia assessment and therapy may beaccomplished even with limited resources. Group therapies may havelimitations because of lack of one to one interaction and individualdifferences, yet are useful, effective and motivating. We have beenfailing to use family members as therapists by way of home basedexercises which have been shown to be as effective.
Many computerized devices are being invented and improvised to augmentthe communication. Web based software and programs are available forpractice at home. The same can be delivered on CDs or flash drives,where the internet is not available. Teletherapy is not a rocketscience and nor very expensive. Patient’s and caregivers can be sparedthe time and costs incurred in travelling, improving compliance.
I am glad to announce a CME cum workshop on aphasia on 16, 17, 18 or17,18, 19 August 2012 at Indore. Dr. David Calplan (neurologists,Bostan), Dr. Gloria Waters (speech therapists, Boston), Dr. AndrewKertesz (neurologists, Ontario, Canada) and Dr. Chris Code (clinicalpsychologists, Exter, UK) have consented to be the faculty.

Dr. Apoorva Pauranik MGM Medical College & M.Y. Hospital
Professor, Department of Neurology IndoreFigure : 1 – The classical model
Figure :2 - The new revised model

Dr. Apoorva Pauranik MGM Medical College & M.Y. Hospital
Professor, Department of Neurology Indore

Dr. Apoorva Pauranik MGM Medical College & M.Y. Hospital
Professor, Department of Neurology IndoreFigure : 3

Dr. Apoorva Pauranik MGM Medical College & M.Y. Hospital
Professor, Department of Neurology Indore

Dr. Apoorva Pauranik MGM Medical College & M.Y. Hospital
Professor, Department of Neurology IndoreReference :
1. Engelter ST, Gostynski M, Papa S, Frei M, Born C, Adjacic GrossV, et al. Epidemiology of aphasia attribute to first ischaemicstroke : Incidence, severity, fluency, etiology and thrombolysis.Stroke 2006;37:1379-84
2. Basso A, Aphasia and its therapy, Oxford University Press,Newyork 2003, page 262
3. Whitworth A, Webster J, Howard D, A cognitive neuropsychologicalapproach to assessment and Intervention in Aphasia. A cliniciansguide. Psychology Press, Hove and Newyork 2005, page 258-264
4. Millberg W, Blumstein S. Back to the future: reclaiming aphasiafrom Cognitive neurolinguistics, Brain Lang.2000;Jan:71(1):160-163.
5. Calplan D, Neurolinguistics and linguistic aphasiology, CambridgeCambridge University Press, 1992.
6. Hillis AE, Aphasia : Progress in the last quartger of a century,Neurology 2007; 69-200
7. Chen C, Xue G, Mei L, Chen C, and Dong Q, CulturalNeurolinguistics, J.Y. Chiao (Ed.) Progress in Brain Research,Vol 178, 159-171
8. Bolger, D.Jl, Perfetti C.A., & Schneider W. (2005). Cross-cultural effect on the brain revisited; Universal structures pluswriting system variation. Human Brain Mapping. 25, 92-104.
9. Sharma A, & Dorman M.F. (2000). Neurophysiologic correlates ofcross-language phonetic perception. The journal of the AcousticalSociety of America, 107, 2697-2703
10. Mechelli, A., Crinion J.T., Noppeney U, O’Doherty JAshburner J, Frackowiak R.S. et al 2004. Neurolinguistics:Structural plasticity in the bilingual brain. Nature 431, 757.
11. Menn , L. Obler, L.K. (1990), Agrammatic aphasia : A Crosslanguage narrative source book (Vols, 1,2,3,). Philadelphia, PA.John Benjamins Publishing Company
12. MacWhinney B. The Talkbank project (2007), Department ofpsychology, paper 174 http://repository.cmu.edu/psychology/174/

Dr. Apoorva Pauranik MGM Medical College & M.Y. Hospital
Professor, Department of Neurology Indore