Cognitive Behavioral Therapy With a Paranoid Schizophrenic ...
17
Clinical Case Studies 9(5) 311–327 © The Author(s) 2010 Reprints and permission: http://www. sagepub.com/journalsPermissions.nav DOI: 10.1177/1534650110383009 http://ccs.sagepub.com Cognitive Behavioral Therapy With a Paranoid Schizophrenic Patient Andrew M. Kuller 1 and Thröstur Björgvinsson 1 Abstract This case study describes the cognitive-behavioral therapy (CBT) of a married adult male diagnosed with paranoid schizophrenia. “Michael” was initially oriented to CBT for psychosis (CBTp) in a partial hospital program at McLean Hospital in Belmont, Massachusetts. Michael was then followed as an outpatient over 30 weekly sessions of CBTp. Over the course of treatment, Michael remained paranoid. However, his self-reported levels of conviction and preoccupation decreased measurably, and he experienced improvements in mood and psychosocial functioning. These results support a growing body of research demonstrating effectiveness of CBTp with schizophrenia and have implications for solo practitioners facing pressure to utilize evidence- based treatments. Further research is needed on the effectiveness of CBTp in outpatient settings. Keywords cognitive-behavioral therapy, schizophrenia, paranoid, psychosis 1 Theoretical and Research Basis In 1952, Beck delivered successful outpatient psychotherapy to a patient with paranoid schizophrenia. The patient, a 28-year-old veteran of World War II, was convinced that he was under surveillance by the FBI. Comorbidly, he was depressed and anxious and no longer able to function at work. Beck’s treatment included discussion of the content of the patient’s delusions and collaboration with the patient in implementing cognitive-behavioral change strategies. Over the course of 30 weekly outpatient sessions, the patient’s level of conviction in his delusional beliefs receded, and as his insight improved, he experienced improvements in mood and psycho- social functioning. With this seminal case study, Beck laid important groundwork for both the generic cognitive model (Beck, 1976) and cognitive-behavioral therapy for psychosis (CBTp; Kingdon & Turkington, 2005). Unfortunately, although CBT has now been applied extensively to most mood and anxiety disorders and has a robust research base (Barlow, 2005; Beck, 2005), clini- cians have been slow to adapt CBT for patients with schizophrenia and other psychotic disorders. One conceptual barrier has been greater understanding of the role of pathophysiology. As 1 McLean Hospital/Harvard Medical School, Belmont, MA Corresponding Author: Andrew M. Kuller, PsyD, Department of Psychology, McLean Hospital/Harvard Medical School, 115 Mill Street, Belmont, MA 02478 Email: [email protected] at PENNSYLVANIA STATE UNIV on September 16, 2016 ccs.sagepub.com Downloaded from
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Cognitive Behavioral Therapy With a Paranoid Schizophrenic ...

Clinical Case Studies9(5) 311 –327
© The Author(s) 2010Reprints and permission: http://www. sagepub.com/journalsPermissions.nav
DOI: 10.1177/1534650110383009http://ccs.sagepub.com
Cognitive Behavioral Therapy With a Paranoid Schizophrenic Patient
Andrew M. Kuller1 and Thröstur Björgvinsson1
Abstract
This case study describes the cognitive-behavioral therapy (CBT) of a married adult male diagnosed with paranoid schizophrenia. “Michael” was initially oriented to CBT for psychosis (CBTp) in a partial hospital program at McLean Hospital in Belmont, Massachusetts. Michael was then followed as an outpatient over 30 weekly sessions of CBTp. Over the course of treatment, Michael remained paranoid. However, his self-reported levels of conviction and preoccupation decreased measurably, and he experienced improvements in mood and psychosocial functioning. These results support a growing body of research demonstrating effectiveness of CBTp with schizophrenia and have implications for solo practitioners facing pressure to utilize evidence-based treatments. Further research is needed on the effectiveness of CBTp in outpatient settings.
Keywords
cognitive-behavioral therapy, schizophrenia, paranoid, psychosis
1 Theoretical and Research BasisIn 1952, Beck delivered successful outpatient psychotherapy to a patient with paranoid schizophrenia. The patient, a 28-year-old veteran of World War II, was convinced that he was under surveillance by the FBI. Comorbidly, he was depressed and anxious and no longer able to function at work. Beck’s treatment included discussion of the content of the patient’s delusions and collaboration with the patient in implementing cognitive-behavioral change strategies. Over the course of 30 weekly outpatient sessions, the patient’s level of conviction in his delusional beliefs receded, and as his insight improved, he experienced improvements in mood and psycho-social functioning.
With this seminal case study, Beck laid important groundwork for both the generic cognitive model (Beck, 1976) and cognitive-behavioral therapy for psychosis (CBTp; Kingdon & Turkington, 2005). Unfortunately, although CBT has now been applied extensively to most mood and anxiety disorders and has a robust research base (Barlow, 2005; Beck, 2005), clini-cians have been slow to adapt CBT for patients with schizophrenia and other psychotic disorders. One conceptual barrier has been greater understanding of the role of pathophysiology. As
1McLean Hospital/Harvard Medical School, Belmont, MA
Corresponding Author:Andrew M. Kuller, PsyD, Department of Psychology, McLean Hospital/Harvard Medical School, 115 Mill Street, Belmont, MA 02478Email: [email protected]
at PENNSYLVANIA STATE UNIV on September 16, 2016ccs.sagepub.comDownloaded from

312 Clinical Case Studies 9(5)
etiological models such as the diathesis-stress hypothesis do emphasize the relationship between psychological factors and genetic vulnerabilities (e.g., Strauss & Carpenter, 1981), psychosis has been perceived primarily as a neurobiological phenomenon qualitatively outside the realm of normal human experience (Johns & van Os, 2001). Therefore, clinicians treating psychosis have been unlikely to deliver psychological treatments of any kind (Mojtabai, Nicholson, & Carpenter, 1998), and the front-line treatment for schizophrenia has been antipsychotic medication and case management (Tarrier & Wykes, 2005).
However, in recent years there has been renewed interest in psychological approaches, par-ticularly as initial optimism about efficacy of atypical antipsychotics has been tempered with poor adherence rates and disappointing side effect profiles (Lieberman et al., 2005). CBTs in particular have generated significant clinical and research activity (Tarrier, 2008), as clinicians who were already using CBT and behavioral analysis to treat other psychiatric conditions adapted CBT to address psychosis (Chadwick, Birchwood, & Trower, 1996; Fowler, Garety, & Kuipers, 1995; Kingdon & Turkington, 1994) and initiated randomized controlled trials (RCTs) to dem-onstrate the effectiveness of these techniques (Turkington, Kingdon, & Weiden, 2006).
Addition of CBT as an adjunctive treatment to medication and case management is now sup-ported by a growing body of research evidence. RCT’s have demonstrated efficacy with positive symptoms (Tarrier & Wykes, 2005; Turkington et al., 2008), negative symptoms (Perivoliotis & Cather, 2009; Turkington, Kingdon, & Weiden, 2006), and secondary morbidity such as depres-sion, anxiety, and impairments in social/occupational functioning (Granholm et al., 2005; Wykes, Steel, Everitt, & Tarrier, 2008). There have been methodological limitations across stud-ies, such as lack of blind assessors or active control groups (Dickerson, 2000). Still, meta-analy-ses suggest modest effect sizes, with a global mean weighted average of 0.37 (Zimmermann, Favrod, Trieu, & Pomini, 2005) and effect sizes as high as 0.40 (95% confidence interval [CI] = 0.252, 0.548) when CBTp is applied to a specific target symptom (Wykes et al., 2008).
In the United Kingdom, treatment guidelines established by the National Health Service sup-port the research findings, as British clinicians are required to offer at least 16 sessions of weekly CBT to all patients with treatment refractory positive symptoms (National Institute for Clinical Excellence [NICE], 2009). In the United States, clinicians are less likely to practice CBT than their British counterparts (Kuller, Ott, Goisman, Wainwright, & Rabin, 2010), as U.S. programs have been slow to adapt CBT as a treatment for psychosis despite the evidence of its efficacy (Lehman et al., 1998; Mojtabai et al., 2009). The Schizophrenia Patient Out-comes Research Team (PORT), an American team funded by the National Institute of Mental Health and the Agency for Health Care Policy and Research, recently found that few patients with schizophrenia have access to evidence-based psychological treatments of any kind (Dixon et al., 2009). It is estimated that 95% of U.S. patients with a diagnosis of schizophrenia receive either no care or less-than-optimal (i.e., evidence-based) care (Drake, Bond, & Essock, 2009).
To address this problem, U.S. clinicians and researchers are rapidly developing CBTp with approaches tailored for specific clinical problems or presentations. At the Massachusetts General Hospital, Cather and colleagues (2005) designed the first treatment outcome study of CBTp for negative symptoms with a manualized, active comparison condition. At the University of North Carolina, the Graduated Recovery Intervention Program (GRIP) is a CBTp pilot program devel-oped for first episode psychosis (Waldheter et al., 2008). CBTp for patients with chronic symp-toms is in development at both the veterans’ affairs (VA) Medical Center in Philadelphia and at the Massachusetts Mental Health Center at Harvard Medical School.
As hospital-based programs continue to adapt cognitive-behavioral approaches to the treat-ment of psychotic populations, outpatient clinicians will need familiarity with CBTp to effectively bridge the gap for patients as they transition from institution to mental health center (and often back again). Dissemination of CBTp treatment guidelines is vital to increase clinicians’ skill base
at PENNSYLVANIA STATE UNIV on September 16, 2016ccs.sagepub.comDownloaded from

Kuller and Björgvinsson 313
and therapeutic optimism. Case study reports can help advance this process by providing examples of how CBTp can be transported effectively from day treatment to outpatient settings.
The current article is a case study of a patient introduced to CBTp while receiving treatment at McLean Hospital in a partial hospital program that recently installed a CBTp track. The patient is followed from discharge at the partial hospital through 30 sessions of weekly outpatient CBTp.
CBTpPsychosis is an extraordinary condition of the mind. By definition, psychotic individuals have lost contact with reality and are subject to delusions, hallucinations, profound personality changes, and formal thought disorder (American Psychiatric Association [APA], 2000). In the cognitive-behavioral approach, normalization of these symptoms is the central assumption (Morrison & Barratt, 2009). Rather than conceptualizing psychotic symptoms outside the realm of normal human experiences, delusions and hallucinations are arranged along a continuum of normality ranging from functional to dysfunctional (Fowler, Garety, & Kuipers, 1998). Psycho-sis is described in the same general terms as the experiences of individuals who are not mentally ill (Kingdon & Turkington, 2005).
Although normalization can be counterintuitive, the rationale is fairly straightforward. As an example, paranoid delusions are a defining characteristic of schizophrenia and are typically per-ceived strictly as a psychotic phenomenon. However, most people have had the experience of coming late to a business meeting or dinner party and feeling that others might have been talking about them. In CBTp, these common experiences would be viewed on the same continuum as a more extreme delusion that the government has hidden microphones in the ceiling tiles; the dif-ference is conceptualized as quantitative and not qualitative.
Because the development of CBTp has occurred in multiple settings internationally, treatment delivery is heterogeneous. However, there are probably more similarities across treatments than there are differences. As the PORT team points out, the current lack of a standardized method to organize treatments can lead to confusion and mask the fact that many treatments share a few basic elements—collaborative identification of target problems or symptoms and the develop-ment of cognitive and behavioral strategies to cope with those problems or symptoms (Dixon et al., 2009). In a recent study, Morrison and Barratt (2009) identified aspects of CBTp consistent across treatments, including the provision of a normalizing rationale, the establishment of a solid therapeutic alliance, collaborative agenda setting with regular homework assignments, and the exploration of psychotic experiences through the process of guided discovery.
Case formulation is essential to the practice of CBTp. It is uncommon for a psychotic patient to provide a comprehensive personal narrative during the initial sessions. Therefore, the clinician gathers information flexibly throughout the course of treatment, identifying new treatment tar-gets as relevant clinical data are revealed. Important factors to identify include early formative experiences, the onset of current problems (including vulnerabilities and precipitants), and per-petuating factors (Pain, Chadwick, & Abba, 2008). As with most forms of CBT, the patient learns to identify automatic thoughts, core beliefs, and behaviors related to those thoughts and beliefs. The treatment process is collaborative; the clinician neither challenges nor colludes with the patient’s beliefs. In fact, it is not always necessary to convince the patient that they have a mental illness (Turkington, Kingdon et al., 2006). The treatment emphasis is reduction of emotional distress and improved psychosocial functioning.
Typically, CBTp is organized around the four basic symptom clusters in schizophrenia: delusions, hallucinations, negative symptoms, and formal thought disorder. General approaches to each are outlined below:
at PENNSYLVANIA STATE UNIV on September 16, 2016ccs.sagepub.comDownloaded from

314 Clinical Case Studies 9(5)
Delusions. Many clinicians are reluctant to address delusions in psychotherapy. Often, unwillingness to apply cognitive-behavioral strategies is based on the premise that delusions are fixed ideas that are completely resistant to change. In CBTp, the clinician assumes that any false belief has the potential to be affected by reality testing, regardless of how rigidly the belief is held. Simultaneously, the clinician maintains the perspective that it is unnecessary for a delusion to be completely abandoned before there is attenuated symptomatology. Urgency of attending to a delusion is dependent on the patient’s concomitant level of emotional distress and/or functional impairment. When the belief causes significant distress or dysfunction, then it is reasonable to address the belief as one would have any problematic belief in a standard cognitive-behavioral intervention.
Delusions are usually assessed along multiple dimensions. According to Chadwick et al. (1996), the two most clinically relevant dimensions are level of conviction (how certain a client is of a belief) and preoccupation (the amount of time spent thinking about the belief). Delusions generally cause greater negative emotional or behavioral consequences when firmly held or when they occupy more of a person’s consciousness. Therefore, the goal in CBTp is to reduce the levels of conviction and preoccupation.
When exploring a delusion, the clinician avoids judgment, instead attempting to convey uncertainty about the truth. An open-minded, inquisitive stance invites the patient to engage in the process of guided discovery. Together with the clinician, the patient examines when the belief originated, the evidence for and against the belief, and the effect of the belief on current level of functioning (Beck, Rector, Stolar, & Grant, 2009). Beliefs are formulated as hypotheses that can be explored through peripheral questioning and inference chaining (Turkington, Kingdon et al., 2006).
Hallucinations. Auditory hallucinations are reported by 60% to 80% of schizophrenic patients during an acute episode (Hoffman, 2008). However, as auditory hallucinations are a defining characteristic of schizophrenia, the CBTp clinician explains to the patient that people can also experience auditory hallucinations in a variety of other psychiatric conditions (e.g., posttrau-matic stress disorder, affective disorders) and in extreme situations involving deprivation, isola-tion, fatigue, intoxication, or trauma. In fact, probably anyone can experience hallucinations given the right conditions (Strauss, 1969). Treatment includes psychoeducation on the stress-vulnerability model. The clinician explains that hallucinations (e.g., hearing voices) may be a symptom related to stress and genetic vulnerability.
Beck and colleagues (2009) suggested that the treatment of hearing voices starts with an assessment of the frequency, severity, and physical properties of the voices; the identification of triggers to and consequences of the voices; and discussion of beliefs about voices. The patient is then socialized to the cognitive model and introduced to cognitive-behavioral strategies.
Voices are often conceptualized as the activating event (the “A”) in Ellis’ A-B-C formulation, with the “B” being the individual’s beliefs about the voices and the “C” being the emotional and behavioral consequences of the belief (Chadwick et al., 1996). An important clarification in this model is that beliefs about the voices are not necessarily direct interpretations of the voice. In fact, the level of dysfunction is likely more related to beliefs about the voice than the voice itself. Thought records can be used to explore alternative explanations, which in turn often results in reduced emotional distress and dysfunctional behaviors. Behavioral strategies include reducing stress/arousal (e.g., taking a bath), distraction such as listening to music, wearing earplugs, and dedicating some time each day to listening to the voices.
Negative symptoms. Negative symptoms include affective flattening and an overall reduction in verbal expressivity, self-directed activity, and pleasure or interest in formerly pleasurable activities. These symptoms can be quite alienating for the clinician trying to understand the inner experience of a psychotic patient (Karon, 1992). However, negative symptoms are important to
at PENNSYLVANIA STATE UNIV on September 16, 2016ccs.sagepub.comDownloaded from

Kuller and Björgvinsson 315
address, as there is some evidence that they are primarily responsible for the socio-occupational dysfunction in schizophrenia (Perivoliotis & Cather, 2009).
As with positive symptomatology, normalization is critical. Negative symptoms are concep-tualized as the consequence of stress overload. It is common for people who are feeling over-whelmed to experience lower levels of motivation and activity and to withdraw from connection with others. From a stress-vulnerability perspective, patients with pronounced negative symp-tomatology may have a greater natural tendency to withdraw under periods of stress. Although the patient convalesces, the clinician should avoid pushing the patient out of negative symptoms (Kingdon & Turkington, 2005).
In treatment, cognitive-behavioral strategies are applied to identify dysfunctional automatic thoughts and behaviors associated with the negative symptoms. Often, reduced activity is the result of negative self-appraisals, self-stigmatizing illness beliefs, social avoidance behaviors, and negative expectancies regarding pleasure and success (Beck et al., 2009). Some negative symptoms are secondary to positive symptoms; for example, a patient might reduce social activ-ity in response to voices telling her that she is evil. In cases such as these, the voices would likely be the first treatment target.
Formal thought disorder. Positive formal thought disorder includes loosening of associations, idiosyncratic language use, and use of words in novel ways, whereas negative formal thought disorder can include thought blocking, impoverishment of speech, and thought content (Beck et al., 2009). According to the CBTp formulation, thought becomes more disordered in the pres-ence of stress. Therefore, the treatment involves psychoeducation on the relationship between stress and communication problems, stress reduction/relaxation strategies, and communications skills practice. Often, anxiety is attenuated as the patient discovers that they can be understood.
2 Case PresentationThe following case study describes the practice of CBTp as it occurred in a naturalistic setting. Identifying information has been altered to preserve the patient’s anonymity. The patient, Michael, a 33-year-old married White man with paranoid schizophrenia, was originally introduced to CBTp in the Behavioral Health Partial treatment program at McLean Hospital. On discharge from the partial hospital program, Michael continued individual treatment as an outpatient with a licensed clinical psychologist (first author of this article).
3 Presenting ComplaintsMichael’s chief complaint was “anxiety.” He also presented with fixed paranoid delusions that he was under surveillance by the Mafia and that they intended to murder him. He reported that the FBI was protecting him and sending him messages to alert him to this danger. He suspected, although with less conviction, that his wife may be involved with the Mafia. In addition to his paranoia, Michael evidenced auditory hallucinations, somatic hallucinations, and negative symp-toms, including impoverished speech, affective flattening, and decreased self-initiated activity.
4 HistoryThe current situation began several months before the treatment. At the time, Michael was suc-cessful in work and his marriage was healthy. He was enjoying a good overall adjustment despite becoming seriously ill in his late 20’s. He earned a comfortable living as a web designer and lived with his wife and two young sons in a house in the city. He had been hospitalized twice previously for acute psychosis. Each time, he had compensated with the help of a supportive
at PENNSYLVANIA STATE UNIV on September 16, 2016ccs.sagepub.comDownloaded from

316 Clinical Case Studies 9(5)
family, adequate financial resources, and inpatient hospitalization. His medication regimen consisted of aripiprazole 30mg.
Michael’s most recent decompensation occurred in the context of financial problems and occupa-tional stress. His family had recently acquired a new, larger home with a higher mortgage. At the same time, Michael’s work responsibilities had increased substantially, such that he was expected to quickly master new tasks well beyond his established skill set. He sensed that his job performance was inadequate and he lived in heightened fear of a negative evaluation. Desperate to keep pace, he often stayed working at his computer until early morning, sacrificing sleep for increased productivity.
As Michael’s illness progressed, his interpretations of the external world became distorted. Suddenly, the Internet blog of his favorite newspaper columnist appeared to contain coded mes-sages identifying members of the Mafia. Michael hypothesized that he was meant to receive these messages so that he might notify the authorities. Everyday occurrences acquired special significance related to this delusion. For example, in the whistle of a passing stranger Michael translated a veiled accusation that he was planning to “sing like a canary.” Faint whistles, anony-mous and menacing, appeared to haunt him from a distance. Michael also experienced bizarre somatic sensations: the top of his head seemed to “vibrate” when he was anxious, leading Michael to believe that the FBI had implanted a sophisticated electronic device wired to warn him of danger. At the height of his paranoia, Michael was no longer able to work. He spent his days and nights at home with the doors locked and the shades drawn.
Michael was finally hospitalized following an incident that occurred while he and his family were eating a meal at a local restaurant. Suddenly, believing that the waiter had poisoned his food, and suspecting that his wife was an accomplice, Michael slipped out of the restaurant and ran to a nearby fire station, where he begged the firemen to rush him to the hospital for medical treatment. Instead, Michael was brought to an inpatient unit at McLean Hospital, where he was admitted. Although Michael adamantly rejected any suggestion that he might be delusional, he agreed to the hospitalization as he felt he might be “safer” on the inpatient unit. In fact, he was unwilling to return home, as he believed that his wife was part of the conspiracy.
Following discharge from the inpatient unit, Michael initiated partial hospital treatment in the McLean Behavioral Health Partial Program, a 5-day-a-week program that lasted from 9:00 a.m. to 3:00 p.m. His treatment team there consisted of a psychologist, psychiatrist, vocational coun-selor, occupational therapist, and mental health counselors as well as psychology interns and practicum students. As in this program, aripiprazole was discontinued and risperidone 5 mg and molindone 75 mg were added. Michael was also oriented to the CBTp treatment model. Clinicians provided a normalizing rationale and began the process of guided discovery, so that Michael could identify and make sense of his psychiatric symptomatology.
5 AssessmentObtaining a comprehensive case history from a patient with psychosis can be a challenge in an outpatient setting. People with psychosis often present with considerable psychological limitations and are typically unable to provide extensive information regarding illness course, precipitating factors, and so on. Further complicating the psychodiagnostic process is the fact that psychotic patients usually present to outpatient clinics from inpatient or partial-hospital settings, where time constraints preclude the possibility of a thorough record review. However, a limited initial case history does not prevent effective clinical work. Additional background information is typically obtained and assimilated throughout the course of outpatient treatment. For Michael, some initial assessment data were obtained through clinical interviews, family meetings, contacts with outpa-tient providers, and record review. The preliminary results suggested that Michael met criteria for Schizophrenia, paranoid type, chronic, based on parameters set forth in the Diagnostic and Statis-tical Manual of Mental Disorders—Fourth Edition, Text Revision (DSM-IV-TR; APA, 2000).
at PENNSYLVANIA STATE UNIV on September 16, 2016ccs.sagepub.comDownloaded from

Kuller and Björgvinsson 317
6 Case Conceptualization
Michael was a good candidate for CBTp. He was aware in a general way that he was ill, and there is evidence that CBTp is more likely to work with patients who have some insight about their illness or an awareness of their symptoms (Naeem, Kingdon, & Turkington, 2008). Michael evidenced late illness onset, a positive indicator of response to treatment (Crow, 1980). He also appeared to have a favorable introduction to CBTp in the partial hospital specialty track. When asked to choose an aftercare plan, Michael requested outpatient therapy with the psychologist from the CBTp program.
Because Michael and the therapist had a previous working relationship, the therapist had a working case conceptualization before the initial session. His formulation, based on the diathesis-stress hypothesis, addressed the four basic areas suggested by Kingdon and Turkington (2005): predisposing factors (i.e., psychological and genetic vulnerabilities), precipitating factors, per-petuating factors, and protective factors (see Figure 1). The therapist’s initial treatment plan was based on the problem list generated by this case formulation.
As often occurs, Michael’s initial problem list did not match the therapist’s list of problems to tackle. Though the therapist conceptualized Michael’s paranoid delusions as an early treatment target, Michael was primarily concerned with his physical safety. In fact, Michael had moved in with his sister in a neighboring city. He refused to live with his wife because he suspected that she was connected to the Mafia. He was adherent to his medication regimen; however, he believed that his antipsychotic medications were prescribed solely for anxiety. Rather than challenging Michael on these issues, the therapist planned to engage Michael around issues that were pertinent to him, including his personal safety and deciding whether to divorce his wife (to ensure his safety).
It is important to note that the therapist remained open to the possibility that Michael was in fact in some kind of danger. The objective data did not appear to support actual Mafia or FBI involvement. However, conflict within the marital relationship did appear to be a source of ongo-ing stress, and it was not unreasonable to imagine that Michael’s wife posed a threat to his emo-tional or physical well-being. The therapist explored this hypothesis with the patient and simultaneously maintained the basic formulation that Michael’s beliefs about his wife were dis-torted. The therapist supported Michael making an informed, reality-based decision about his marriage. To this end, the therapist engaged Michael in guided discovery, so that Michael could examine his beliefs about his wife at his own pace.
When asked about his chief complaint, Michael did report severe anxiety that was both dis-tressing and debilitating. The therapist addressed this anxiety with Michael explicitly. The thera-pist provided psychoeducation on the cognitive-behavioral treatment of anxiety, including the relationship between anxiety and associated thoughts, feelings, and behaviors. The therapist explained that whether Michael’s life was in danger or not, it may be possible to use cognitive-behavioral strategies to lower his overall anxiety level and to improve his general functioning. The treatment involved standard CBT interventions (e.g., thought records, behavioral schedules, etc.). Between sessions, Michael completed homework assignments with hypothesis testing and reduc-tion of avoidance behaviors.
7 Course of Treatment and Assessment of ProgressSessions 1 and 2
As suggested by Beck et al. (2009), the focus of the initial outpatient sessions was rapport build-ing and the collaborative assessment of emotional and functional impairments. The therapist attempted to fill in informational gaps in Michael’s personal history. However, Michael’s height-ened preoccupation with his paranoid delusions limited the scope of the therapist’s inquiries.
at PENNSYLVANIA STATE UNIV on September 16, 2016ccs.sagepub.comDownloaded from

318 Clinical Case Studies 9(5)
When Michael appeared to become agitated or anxious about a particular issue or theme, the therapist changed topics flexibly to preserve the therapeutic alliance. For example, when the therapist asked Michael to talk about his marital history, Michael appeared to become imme-diately defensive, as though the therapist were challenging Michael’s beliefs about his wife’s role in the alleged Mafia conspiracy. The therapist moved flexibly to another topic.
Michael was asked what he knew about his problems and whether he preferred to know his diagnosis. Many patients with psychosis prefer not to know their formal diagnosis; in fact, there is an association between disclosure of psychiatric diagnosis and increased risk of suicide (Kingdon & Turkington, 2005). Michael preferred to speak about his psychiatric symptomatol-ogy as an “illness.” Using Michael’s preferred terminology, the therapist provided psychoedu-cation on the diathesis-stress model. The therapist explained that Michael may have become “ill” as the result of genetic vulnerability and the accumulation of life stress.
Predisposing Factors
Precipitating Factors
Perpetuating Factors
Protective Factors
Current Concerns1. Physical safety 2. What to do about wife 3. Anxiety
THOUGHTS
The Mafia is going tomurder me
My wife is in on theconspiracy.
FEELINGS
Anxiety
Depression
ACTIONS
Social isolation
Shutting down (reducedemotional responsivity)
Avoiding wife
SOCIALAvoiding contact with wifeNot in touch with friends outside ofthe family
PHYSICALPoor sleep hygiene and eating habitsNo physical exercise
UNDERLYING CONCERNSFear of losing house and not being able to support family
Family historyof mentalillness
Psychologicalvulnerabilities
FinancialProblemsOccupationalstressMarital conflict
Wife can becritical andunsympathetic
Few friends
Above averageintelligence
Supportivefamily
Figure 1. Case formulation
at PENNSYLVANIA STATE UNIV on September 16, 2016ccs.sagepub.comDownloaded from

Kuller and Björgvinsson 319
As with many patients with a diagnosis of schizophrenia, Michael’s functional problems included inconsistent medication adherence, problems with sleep, lack of structure, and poor self-care. As these activities of daily living were targeted in the therapist’s initial treatment plan, in the early going Michael demonstrated little motivation to address basic skills deficits. In fact, while recognizing that he was “ill,” he appeared genuinely unconcerned about the effect of his illness on his life. When asked in the first session what he might like to work on in therapy, Michael’s only self-motivated goal was to “guarantee my safety.” The therapist, honing in on the anxiety underlying Michael’s concern, countered by asking Michael what his life might look like when he felt safe. In other words, what would Michael be doing differently if he were “well”? The therapist’s intention was to begin the process of collaboratively identifying specific skills deficits that could then become treatment targets.
Sessions 3 to 30Outpatient sessions followed a typical CBTp format. Each session opened with collaborative agenda-setting followed by a review of homework from the previous session. The therapist then engaged Michael in guided discovery to promote insight. Additional issues were added to the problem list as they materialized through the course of psychotherapy, and the problem list was reviewed toward the end of each session. Finally, Michael and the therapist agreed on homework to complete for the following session.
Treatment of each of the four CBTp symptom clusters proceeded as follows:Delusions. Michael presented with fixed paranoid delusions involving the Mafia. His beliefs
were assessed along two dimensions: level of conviction and level of preoccupation. At intake to outpatient treatment, Michael rated his level of conviction as “98” on a scale ranging from 0 to 100 (with 100 conveying absolute certainty). His level of preoccupation was “90.” Michael also suspected that his wife may have been involved with the Mafia conspiracy. He interpreted her lack of apparent concern about the Mafia as evidence that she might be complicit in the con-spiracy. His levels of conviction and preoccupation about his wife’s involvement were both “80 out of 100.”
Treatment began with normalization and psychoeducation. The therapist explained to Michael that given his concerns about the Mafia, it was understandable that he was feeling overwhelmed and was unable to function normally. In other words, regardless of whether the Mafia threat was real, Michael’s obsessive worrying about the Mafia was an additional source of problems. The therapist took care to validate the patient’s affective experience whereas care-fully avoiding collusion (e.g., “no wonder you are scared, the Mafia is after you!”) or confronta-tion (e.g., “you are paranoid, the Mafia has no reason to be after you!”). The therapist suggested that Michael might experience improvements in mood and functioning if he found better ways to manage his thoughts about the Mafia. The therapist also proposed that Michael’s overall anxi-ety level may be exacerbated by other worries, such as problems with personal relationships or finances.
Starting in Session 3, Michael’s beliefs were explored collaboratively with an initial focus on the onset of problems. Michael’s ability to place events chronologically was somewhat limited. However, a timeline did gradually emerge. Michael recalled that earlier to his hospitalization there had been a tremendous build up of work stress. He was “struggling” to keep pace and was “living in constant fear” that he was going to be asked to leave his position. As pressure accumu-lated, Michael reportedly received his first coded message from the FBI. He said that the mes-sage appeared in an online blog and was written in such a way that only he was able to decipher its true meaning. Michael reported that the message contained the names of members of the Mafia and that he was meant to identify them to local authorities.
at PENNSYLVANIA STATE UNIV on September 16, 2016ccs.sagepub.comDownloaded from

320 Clinical Case Studies 9(5)
The therapist chose this moment in the interview to engage Michael in peripheral questioning. Rather than trying to persuade Michael that his beliefs about the blog were delusional, the therapist investigated Michael’s belief system with a series of questions related indirectly to the delusional content. The therapist’s goal was to try to understand how Michael had arrived at his conclusions.
Therapist: “So, help me to understand. How does one post a coded message onto a blog?”Michael: “That’s easy. Just post a message under a fake name.”Therapist: “And how would you make sure that the message reaches the right person?”Michael: “You figure out what blog the person reads, and post it there.”Therapist: “I see. So, once the message it posted, how do you know the right person will
understand the code? Why wouldn’t other people be able to understand the code, too?”Michael: “I don’t know. The FBI has their ways. I know what really happened.”
At this point, Michael appeared to become agitated at the implausibility of his argument. The therapist did not press Michael on his logic at this early point in the treatment. Any gains in reality testing achieved through confrontation would have been overshadowed by a rupture to the therapeutic alliance. The therapist’s goal at this stage was not to convince Michael that he was delusional. Instead, the instillation of doubt was intended to reduce intensity of Michael’s beliefs and emotional distress related to those beliefs.
Slowly, Michael cobbled together a coherent narrative about his experiences. In Session 15, Michael reported that simply talking about what had happened was “healing,” as “no one listens to me.” The therapist asked Michael why he believed the FBI would chose a civilian for a life-threatening assignment. Michael admitted that he was “surprised” that the FBI had chosen him to “bring down the Mafia,” but he began to feel “excited” as he suddenly became “important.” The therapist, alert to Michael’s emotional experience, noted privately that Michael might have been feeling insignificant earlier to the onset of his paranoid delusions—particularly given Michael’s struggles to keep pace at his place of employment. The therapist asked Michael whether there might be a connection between “feeling unimportant” and his thoughts about the FBI. Although Michael denied any relationship between the emotional experience and the delusion, he was able to identify a core belief: “I don’t matter.” The therapist helped Michael to identify the cognitive distortions underlying this depressogenic core belief.
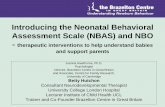
The therapist maintained a collaborative stance, providing Michael with opportunities to examine his beliefs reflectively. Over time, Michael’s certainty about the reality of the Mafia threat decreased, and he was thinking about the Mafia much less frequently (see Figure 2). For example, in Session 21, when asked how often he was thinking about the Mafia Michael said,
0
20
40
60
80
100
1 6 11 16 21 26Therapy Session
Lev
els
of
C/P
Conviction Preoccupation
Figure 2. Levels of conviction and preoccupation
at PENNSYLVANIA STATE UNIV on September 16, 2016ccs.sagepub.comDownloaded from

Kuller and Björgvinsson 321
“Hardly ever. Five out of 100,” and when asked how sure he was about the threat Michael reported, “5 out of 100.” It is important to note that Michael’s levels of conviction and preoc-cupation fluctuated from week to week; however, the overall trends were toward reduction in psychotic symptomatology. To reiterate a crucial point, as the authors see it, this reduction was facilitated by nonjudgmental, guided discovery of Michael’s beliefs.
As the severity of Michael’s paranoia diminished, concomitantly he gained the capacity to recognize secondary morbidity such as agoraphobia and isolation. Psychosocial issues were added to the problem list and treatment plan as they materialized in session. For example, in Session 8 Michael reported distress over his inability to dine in restaurants due to his fear that he was “vulnerable” in public places. The therapist asked Michael whether he would be willing to attempt a series of graded exposures, or “experiments,” to determine whether he could ultimately tolerate his anxiety long enough to enjoy a meal at a favorite restaurant. In Session 14, Michael accomplished this goal despite mild anxiety, and by Session 21 he reported that he was “rarely” anxious while eating out.
Michael’s paranoia concerning his wife was a primary source of material throughout the first 10 sessions. As his level of conviction decreased, Michael became willing to attempt homework assignments in which he spent increasing amounts of time with his wife and sons. These behav-ioral experiments likely facilitated Michael’s gradual realization that his wife likely had no con-nection to organized crime. By Session 6, Michael had moved back home with his family, and in Session 12 he reported that he had “stopped worrying” about his wife.
Hallucinations. Michael reported both auditory and somatic hallucinations. When asked whether he ever heard things that others were not able to hear, Michael said that he frequently heard people whistling but was unable to locate the source. These anonymous “whistles,” or voices, were directly connected to Michael’s paranoid beliefs regarding Mafia persecution. Michael also reported somatic hallucinations involving physical sensations on the top of his head. His belief was that the FBI had surgically implanted a sophisticated electronic device there to warn him of danger from the environment; he could feel the device “vibrating” in times of danger. When the therapist suggested that perhaps the physical sensations were a common physi-ological manifestation of anxiety, Michael quickly and adamantly maintained his position that the FBI “must be involved somehow.”
When multiple hallucinations are present, it can be challenging for the therapist to prioritize. Kingdon and Turkington (2005) suggested initially addressing symptoms that are less firmly held. For Michael, both auditory and somatic hallucinations were responsible for significant functional impairments, as he avoided any situation associated with whistling or unusual somatic sensations. However, as the therapist collected frequency and severity data, it became evident that the vibrating sensations occurred more infrequently and with less overall effect. Furthermore, the auditory hallucinations were more closely connected with Michael’s central beliefs concerning the Mafia and were therefore likely to prove resistant to hypothesis testing. Therefore, the therapist decided to prioritize somatic hallucinations as an early treatment target.
In guided discovery, therapist used peripheral questioning to elicit beliefs that were indi-rectly related to the somatic hallucination. For example, in the following exchange the therapist questioned Michael on his beliefs about the technological aspects of the “device.” The purpose of this line of inquiry was to instill doubt in Michael about the certainty of this somatic hallucination.
Therapist: “So, you believe that a device in your head vibrates when you’re in danger.”Michael: “That’s right. There are vibrations. My head feels tight.”Therapist: “I see. And how does the device determine whether or not you’re in danger?”Michael: “I don’t know. I think it’s electronic. Maybe it’s a computer.”
at PENNSYLVANIA STATE UNIV on September 16, 2016ccs.sagepub.comDownloaded from

322 Clinical Case Studies 9(5)
Therapist: “I see. Well, there could be a computer in your head. But I’m still not sure I understand how a computer would analyze the environment and determine that you’re in danger. How do you think it would do that?”
Michael: “I think it’s like an alarm on a house.”Therapist: “I see. And how does that kind of alarm work?”Michael: “It tells you if there’s an intruder. It has sensors.”Therapist: “So, you believe there is a device in your head that has sensors?”Michael: “Yes. It knows when I shouldn’t trust people. All I know is what I feel.”Therapist: “Well, I’m confused. I can imagine a device that senses movement or sounds,
but I’m not sure I understand how it would sort out when a situation is dangerous or not. Do you think this is something we could explore a little further? Maybe for homework you could look into different kinds of alarm systems to see how they operate. Would you be willing to do that?”
Without ever directly challenging Michael’s beliefs directly, the therapist stimulated doubt in Michael’s mind. The therapist also explored alternative explanations, providing psychoeducation on the physiology of anxiety and how it is often experienced in the body (e.g., tension headaches). By Session 8, Michael warmed to an alternative explanation that eventually became his primary assumption—that the “vibrations” in his head were symptoms of anxiety. With this new, more functional belief in place, Michael was less likely to avoid people just because his head throbbed. Despite lingering doubts, the reduction in the level of conviction promoted attenuated symptomatology.
Michael’s beliefs about his auditory hallucinations were investigated when appropriate in the context of exploration of his paranoid delusions. As Michael’s insight improved, he became less concerned about the whistles he had heard while acutely ill. However, he maintained his beliefs that the whistles “almost definitely” came from members of the Mafia. Fortunately, Michael experienced a significant reduction in the frequency of his auditory hallucinations shortly after initiating outpatient treatment and clozapine pharmacotherapy.
Negative symptoms. Premorbidly, Michael was a social and engaging young man, deeply con-nected to his family and well liked at work. In the aftermath of his current decompensation, Michael struggled with even the most basic communication skills. He reported that his wife often appeared frustrated with his apparent “lack of focus” or “emotional connection.” In therapy ses-sions, Michael presented with a flat affect and impoverished speech; the majority of his state-ments provided only minimal information and were often delivered with little affective valence. At home, Michael’s motivation and interest in usual activities was low. He spent most of his waking hours on the couch, watching television, napping, or “staring into space.” Michael did not appear particularly distressed about his limitations. In fact, he indicated that the pressure to reconstitute was largely external (i.e., coming from his family).
The therapist identified numerous possible treatment targets. However, he also kept in mind the importance of pacing, as pressure applied prematurely would raise Michael’s stress level and delay progress. In Session 3, the therapist commented that Michael’s activity level was much lower than it had been before he became ill. The therapist then explained that generally when people feel overwhelmed, they tend to withdraw or shut down. Perhaps, as Michael recovered, he might resume former activities or cultivate new interests. The therapist was careful to validate Michael’s current position while introducing the idea that change might be possible down the road. The therapist then asked Michael if there were any concrete behaviors he might like to work on in therapy. Michael’s initial list included “getting off the couch,” helping with the dishes, and talking with his wife.
Regular homework assignments were pivotal in Michael’s recovery. Each session included collaborative identification of at least one concrete problem to tackle between sessions. For
at PENNSYLVANIA STATE UNIV on September 16, 2016ccs.sagepub.comDownloaded from

Kuller and Björgvinsson 323
example, Michael had become quite socially isolated since his most recent hospitalization. His awareness of this problem emerged gradually as his paranoia decreased. In Session 16, Michael expressed an interest in reaching out to a former coworker. However, he felt “embarrassed” about his illness and worried that he “wouldn’t know what to say.” The therapist helped Michael to identify negative automatic thoughts (e.g., people with mental illness are scary) and core beliefs (e.g., I am not worthy of people’s time). Michael’s homework assignment following Session 17 was to compose a practice email. After reviewing this email with the therapist in Session 18, Michael sent the email. In Session 20, Michael reported happily that he had “gotten the nerve” to have coffee with the coworker. Subsequently, he was more optimistic about his chances for returning to work.
Formal Thought DisorderMichael did not present with signs of formal thought disorder.
SummaryMichael, a 33-year-old married White man with a diagnosis of chronic paranoid schizophrenia, presented to outpatient treatment with paranoid delusions, auditory and somatic hallucinations, and pervasive negative symptomatology. Michael received 30 weekly sessions of outpatient CBTp and improved significantly over the course of treatment. Most notably, there was a dra-matic reduction in the frequency and severity of his paranoid thoughts. As the result of this improvement, Michael was able to trust his wife again and moved back home. He also experi-enced a significant reduction in hallucinations. From a functional perspective, he was better able to accomplish activities of daily living, such as leaving the house, performing chores in the home, and becoming more actively engaged with his family.
8 Complicating Factors (Including Medical Management)There were no complicating factors in this case study.
9 Managed Care ConsiderationsMichael’s treatment was not limited by managed care. CBTp is an empirically validated treatment and the insurance company readily authorized all 30 sessions. Michael had the financial resources to pay the copayments for each session.
10 Follow-UpAlthough Michael’s acute episode resolved, he continued to evidence residual psychotic symp-tomatology. He would continue to benefit from interventions that address reality testing, mood/anxiety issues, and functional impairments. As CBTp is a collaborative treatment that utilizes guided discovery and other interactive processes, Michael would benefit from long-term outpatient treatment.
11 Treatment Implications of the CaseThis case study has important implications in the treatment of schizophrenia. First, it demonstrates that CBTp can be transported effectively from institution to outpatient setting. The effectiveness of CBTp in outpatient settings is good news, particularly as more American institutions embrace
at PENNSYLVANIA STATE UNIV on September 16, 2016ccs.sagepub.comDownloaded from

324 Clinical Case Studies 9(5)
CBTp as the treatment of choice for psychotic populations (Dixon et al., 2009) and are more likely to discharge patients from CBTp programs back into the community. To ensure continuity of care, solo practitioners will need to acquire competencies in the delivery of CBTp if they are to meet the rapidly changing needs of their patients.
A second implication of this case study concerns managed care. As the U.S. health care crisis continues, pressure mounts for clinicians to deliver evidence-based treatments (EBTs; Barlow, 2005). In the treatment of schizophrenia, it is crucial for mental health professionals to deliver EBTs, as a prolonged duration of untreated psychosis is associated with worse outcome (Norman & Malla, 2001) and elevated treatment costs (Moscarelli, Capri, & Neri, 1991). CBTp is supported by a robust research base and, as this case study demonstrates, the delivery of CBTp can occur in an outpatient setting. Health insurance companies, both privately and publicly owned, should support the delivery of CBTp to psychiatric outpatients as a cost-saving measure.
A third implication of this case study is that further research is needed on the effectiveness of outpatient CBTp. Although the subject of this case study did improve, there is no external validity with a sample size of 1. U.S. researchers should develop randomized, controlled trials of out-patient CBTp. It would be useful to compare the effectiveness of CBTp with active controls (e.g., psychotic outpatients treated with supportive therapy), particularly if the empirical findings supported evidence-based decommissioning of ineffective treatments.
12 Recommendations to Clinicians and StudentsAt this juncture, most U.S. clinicians and students do not use CBTp in the treatment of patients with schizophrenia. In fact, despite the empirical research findings, many clinicians are unaware of basic CBTp principles. This disparity between the research findings and real-world clinical practices is at least partially rooted in the educational infrastructure. For example, psychologists educated in the United States do not necessarily receive comprehensive training in evidence-based practices during graduate school, in predoctoral internships, or through continuing educa-tion courses (Beck, 2005). Therefore, there is no guarantee that a U.S. psychologist will ever be exposed to CBTp at any point in their training or professional development. This is a sobering fact given the APA’s endorsement of evidence-based practices in psychology (EBPP; APA Presidential Task Force, 2006).
In the future, widespread dissemination of CBTp’s general principles and practical applica-tions would improve the quality of care for individuals with schizophrenia. To this end, graduate school faculty members and predoctoral internship training committees should receive instruc-tion and supervision on the theory and practice of CBTp. Similarly, senior clinicians across other clinical disciplines (e.g., psychiatry and social work) should receive formal instruction and clini-cal supervision. Ultimately, this will lead to a new generation of U.S. clinicians who understand the goals of CBTp and can choose whether to adhere to CBTp principles in their work with schizophrenic patients.
Another recommendation for clinicians and students alike is to maintain a realistic mindset when treating patients with schizophrenia. Although some patients will experience complete symptom remission, an all-or-none mentality is often inappropriate. For example, in this case study, the patient remained paranoid but still experienced reductions in conviction and preoccu-pation. As this case study demonstrates, if patients can achieve a partial reduction in positive or negative symptoms, they often experience concomitant attenuation of secondary mood/anxiety problems and psychosocial impairments. Clinicians and students should set multiple concrete treatment goals covering the full range of clinical problems. Noticing the small improvements promotes therapeutic optimism, for both patient and clinician.
at PENNSYLVANIA STATE UNIV on September 16, 2016ccs.sagepub.comDownloaded from

Kuller and Björgvinsson 325
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research and/or authorship of this article.
References
American Psychiatric Association. (2000). Diagnostic and statistical manual of mental disorders (4th ed., text rev.). Washington, DC: Author.
American Psychological Association Presidential Task Force on Evidence-Based Practice. (2006). Evidence-based practice in psychology. American Psychologist, 61, 271-285.
Barlow, D. H. (2005). What’s new about evidence-based assessment? Psychological Assessment, 17, 308-311.Beck, A. T. (1952). Successful outpatient psychotherapy of a chronic schizophrenic with a delusion based
on borrowed built. Psychiatry: Interpersonal and Biological Processes, 15, 305-312.Beck, A. T. (1976). Cognitive therapy and the emotional disorders. New York, NY: International Universities
Press.Beck, A. T. (2005). The current state of cognitive therapy. Archives of General Psychiatry, 62, 953-959.Beck, A. T., Rector, N. A., Stolar, N., & Grant, P. (2009). Schizophrenia: Cognitive theory, research, and
therapy. New York, NY: Guilford.Cather, C., Penn, D., Otto, M., Yovek, I., Mueser, K., & Goff, D. (2005). A pilot study of functional cognitive
behavioral therapy (fCBT) for schizophrenia. Schizophrenia Research, 74, 201-209.Chadwick, P. D., Birchwood, M. J., & Trower, P. (1996). Cognitive therapy for delusions, voices and
paranoia. Chichester, UK: Wiley.Crow, T. J., (1980). Molecular pathology of schizophrenia: More than one disease process. British Medical
Journal, 280, 66-68.Dickerson, F. B. (2000). Cognitive behavioral psychotherapy for schizophrenia: A review of recent empirical
studies. Schizophrenia Research, 43, 71-90.Dixon, L. B., Dickerson, F., Bellack, A. S., Bennett, M., Dickinson, D., Goldberg, R. W., . . . Kreyenbuhl, J.
(2009). The 2009 schizophrenia PORT psychosocial treatment recommendations and summary state-ments. Schizophrenia Bulletin, 36, 48-70.
Drake, R. E., Bond, G. R., & Essock, S. M. (2009). Implementing evidence based practices for people with schizophrenia. Schizophrenia Bulletin, 35, 704-713.
Fowler, D., Garety, P., & Kuipers, E. (1995). Cognitive-behaviour therapy for psychosis: Theory and practice. Chichester, UK: Wiley.
Fowler, D., Garety, P., & Kuipers, E. (1998). Cognitive therapy for psychosis: Formulation, treatment, effects and service implications. Journal of Mental Health, 7, 123-134.
Granholm, E., McQuaid, J. R., McClure, F. S., Auslander, L. A., Perivoliotis, D., Pedrelli, P., . . . Jeste, D. V. (2005). A randomized, controlled trial of cognitive behavioral social skills training for middle-aged and older outpatients with chronic schizophrenia. American Journal of Psychiatry, 162, 520-529.
Hoffman, R. E. (2008). Auditory/visual hallucinations, speech perceptions neurocircuitry, and the social deafferentation hypothesis. Clinical Electroencephalography and Neuroscience Journal, 39, 87-90.
Johns, L. C., & van Os, J. (2001). The continuity of psychotic experiences in the general population. Clinical Psychology Review, 21, 1125-1141.
Karon, B. P. (1992). The fear of understanding schizophrenia. Psychoanalytic Psychology, 9, 191-211.Kingdon, D., & Turkington, D. (1994). Cognitive-behavioral therapy of schizophrenia. New York, NY:
Guilford Press.
at PENNSYLVANIA STATE UNIV on September 16, 2016ccs.sagepub.comDownloaded from

326 Clinical Case Studies 9(5)
Kingdon, D., & Turkington, D. (2005). Cognitive therapy of schizophrenia. New York, NY: Guilford.Kuller, A. M., Ott, B. D., Goisman, R. M., Wainwright, L. D., & Rabin, R. J. (2010). Cognitive behavioral
therapy and schizophrenia: A survey of clinical practices and views on efficacy in the United States and United Kingdom. Community Mental Health Journal, 46, 2-9.
Lehman, A. F., Steinwachs, D. M., Dixon, L. B., Postrado, L., Scott, J. E., Fahey, M., . . . & Skinner, E. A. (1998). Patterns of usual care for schizophrenia: Initial results from the schizophrenia patient outcomes research team (PORT) client survey. Schizophrenia Bulletin, 24, 11-23.
Lieberman, J. A., Stroup, T. S., McEvoy, J. P., Swartz, M. S., Rosenheck, R. A., Perkins, D. O., . . . Hsaio, J. K. (2005). Effectiveness of antipsychotic drugs in patients with chronic schizophrenia. New England Journal of Medicine, 353, 1209-1223.
Mojtabai, R., Fochtman, L., Chang, S., Kotov, R., Craig, T. J., & Bromet, E. (2009). Unmet need for care in schizophrenia. Schizophrenia Bulletin, 35, 679-695.
Mojtabai, R., Nicholson, R. A., & Carpenter, B. N. (1998). Role of psychosocial treatments in management of schizophrenia: A meta-analytic review of controlled outcome studies. Schizophrenia Bulletin, 24, 569-587.
Morrison, A. P., & Barratt, S. (2009). What are the components of CBT for psychosis? A delphi study. Schizophrenia Bulletin, 36, 136-142.
Moscarelli, M., Capri, S., & Neri, L. (1991). Cost evaluation of chronic schizophrenic patients during the first three years after the first contact. Schizophrenia Bulletin, 17, 421-426.
Naeem, F., Kingdon, D., & Turkington, D. (2008). Predictors of response to cognitive behaviour therapy in the treatment of schizophrenia: A comparison of brief and standard interventions. Cognitive Therapy and Research, 32, 651-656.
National Institute for Clinical Excellence. (2009). Schizophrenia: Core interventions in the treatment and management of schizophrenia in primary and secondary care (update). Retrieved January 1, 2010, from http://www.nice.org.uk/Guidance/CG82/NiceGuidance/pdf/English
Norman, R. M. G., & Malla, A. K. (2001). Duration of untreated psychosis: A critical examination of the concept and its importance. Psychological Medicine, 31, 381-400.
Pain, C. M., Chadwick, P., & Abba, N. (2008). Clients’ experience of case formulation in cognitive behaviour therapy for psychosis. British Journal of Clinical Psychology, 47, 127-138.
Perivoliotis, D., & Cather, C. (2009). Cognitive behavioral therapy of negative symptoms. Journal of Clinical Psychology, 65, 815-830.
Strauss, J. S. (1969). Hallucinations and delusions as points on continua function: Rating scale evidence. Archives of General Psychiatry, 21, 581-586.
Strauss, J. S., & Carpenter, W. T. (1981). Schizophrenia. New York, NY: Plenum.Tarrier, N. (2008). Schizophrenia and other psychotic disorders. In D. H. Barlow (Ed.), Clinical handbook
of psychological disorders: A step-by-step treatment manual (4th ed., pp. 463-491). New York, NY: Guilford.
Tarrier, N., & Wykes, T. (2005). Is there evidence that cognitive therapy is an effective treatment for schizophrenia? A cautious or cautionary tale? Behaviour, Research and Therapy, 42, 1377-1401.
Turkington, D., Kingdon, D., Rathod, S., Hammond, K., Pelton, J., & Mehta, R. (2006). Outcomes of an effectiveness trial of cognitive-behavioural intervention by mental health nurses in schizophrenia. British Journal of Psychiatry, 189, 36-40.
Turkington, D., Kingdon, D., & Weiden, P. J. (2006). Cognitive behavior therapy for schizophrenia. American Journal of Psychiatry, 163, 365-373.
Turkington, D., Sensky, T., Scott, J., Barnes, T., Nur, U., Siddle, R., . . . Kingdon, D. (2008). A randomized controlled trial of cognitive-behavior therapy for persistent symptoms in schizophrenia: A five-year follow-up. Schizophrenia Research, 98, 1-7.
at PENNSYLVANIA STATE UNIV on September 16, 2016ccs.sagepub.comDownloaded from

Kuller and Björgvinsson 327
Waldheter, E. J., Penn, D. L., Perkins, D. O., Mueser, K. T., Owens, L. W., & Cook, E. (2008). The graduated recovery intervention program for first episode psychosis: Treatment development and preliminary data. Community Mental Health Journal, 44, 443-455.
Wykes, T., Steel, C., Everitt, B., & Tarrier, N. (2008). Cognitive behavior therapy for schizophrenia: Effect sizes, clinical models, and methodological rigor. Schizophrenia Bulletin, 34, 523-537.
Zimmermann, G., Favrod, J., Trieu, V. H., & Pomini, V. (2005). The effect of cognitive behavioral treat-ment on the positive symptoms of schizophrenia spectrum disorders: A meta-analysis. Schizophrenia Research, 77, 1-9.
Bios
Andrew M. Kuller, PsyD, is a clinical team manager in the Behavioral Health Partial Hospital Program at McLean Hospital, faculty in the Psychology Internship Program at McLean Hospital/Harvard Medical School, and an instructor in psychology in the Department of Psychiatry at Harvard Medical School.
Thröstur Björgvinsson, PhD, ABPP, is the director of the Behavioral Health Partial Hospital Program at McLean Hospital and the codirector of the psychology internship program at McLean Hospital/Harvard Medical School. He is also the founder and director of the Houston Obsessive-Compulsive Disorder (OCD) Program that provides intensive specialized treatment for severe OCD.
at PENNSYLVANIA STATE UNIV on September 16, 2016ccs.sagepub.comDownloaded from