Development and expression of neuropathic pain in CB1 knockout mice

European Journal of Pain 14 (2010) 670–681
Contents lists available at ScienceDirect
European Journal of Pain
journal homepage: www.EuropeanJournalPain.com
Review
Cognitive and behavioral interventions for the management of chronicneuropathic pain in adults – A systematic review
Elisabeth J. van de Wetering a,*, Karin M.M. Lemmens b, Anna P. Nieboer b, Robbert Huijsman b
a Erasmus MC, Erasmus University Rotterdam, Department of Health Policy and Management, P.O. Box 1738, 3000 DR Rotterdam, The Netherlandsb Erasmus University Rotterdam, Department of Health Policy and Management, The Netherlands
a r t i c l e i n f o
Article history:Received 13 May 2009Received in revised form 16 November 2009Accepted 27 November 2009Available online 21 January 2010
Keywords:Systematic reviewNeuropathic painCognitive techniquesBehavioral techniquesMind–body and relaxation techniques
1090-3801/$36.00 � 2009 European Federation of Intdoi:10.1016/j.ejpain.2009.11.010
* Corresponding author. Tel.: +31 10 408 2981; faxE-mail address: [email protected] (Elisab
a b s t r a c t
Background: Chronic neuropathic pain is often associated with conditions such as depression and anxietyand strongly affects daily functioning and overall quality of life. It is argued, therefore, that psychosocialinterventions should be added to traditional biomedical interventions. This systematic review evaluatesthe effectiveness of cognitive and behavioral interventions for the management of chronic neuropathicpain.Methods: Electronic databases were searched for all types of studies. Studies were selected by predefinedinclusion criteria. Methodological quality was assessed with the Health Technology Assessment-DiseaseManagement instrument. Furthermore, an explorative meta-analysis of four selected studies was per-formed.Results: Fourteen studies were assessed: three randomized controlled trials, three controlled before–afterstudies, seven uncontrolled before–after studies and one time series analysis. The findings of the meta-analysis were not consistent with a significant effect on pain intensity. Only one study had good meth-odological quality; it showed some significant effects of the interventions, but only in female participants.Other studies of limited methodological quality did report positive effects on pain and quality of life.Conclusions: This is the first systematic review that has evaluated the effectiveness of cognitive andbehavioral techniques for the management of chronic neuropathic pain. Given the limited methodolog-ical quality, no informative conclusions can be drawn with respect to the study objective. However, thisreview does provide insight into the difficulties of this specific area, the need for a clear and widelyaccepted definition of neuropathic pain and the need for standardized multidimensional measurementinstruments.
� 2009 European Federation of International Association for the Study of Pain Chapters. Published byElsevier Ltd. All rights reserved.
1. Introduction
Chronic neuropathic pain distinguishes itself from other typesof chronic (nociceptive) pain by signs and symptoms that arisefrom a primary lesion in the peripheral nerves and/or by dysfunc-tion in the central nervous system in the absence of nociceptorstimulation (Harden, 2005). Experts from the neurologic and paincommunities have defined neuropathic pain as ‘pain arising as a di-rect consequence of lesion or disease affecting the somatosensory sys-tem’ (Treede et al., 2008).
Neuropathic pain is a complex condition. The variety of causesand affected individuals form a very heterogeneous group andthe usual analgesics often fail to comprehensively achieve effectivepain relief. In addition, associated conditions such as depression,anxiety and sleeping disorders, often reinforce the adverse effects
ernational Association for the Stud
: +31 10 408 9094.eth J. van de Wetering).
of pain. Previous studies have shown that neuropathic pain inter-feres with psychological and social well being and strongly affectsdaily functioning and overall quality of life (Harden and Cohen,2003; Tölle et al., 2006).
Researchers have emphasized that a multidimensional ap-proach is needed to manage the entire spectrum of neuropathicpain, including comorbid conditions. The theoretical basis for suchan approach is a biopsychosocial model in which pain results froman interaction of physiologic, psychological and social factors thatinfluence perception of pain and response to pain (Gatchel,2004). Pain management should therefore include psychosocialinterventions in addition to the traditional biomedical interven-tions (Harden and Cohen, 2003).
Psychosocial interventions aim to modify patients’ thoughts,beliefs and behavioral responses to pain and thereby the painexperience (Turk et al., 2008; Scascighini and Sprott, 2008; Turkand Flor, 1984). The primary aim, however, is not reducing theintensity of pain but rather improving daily functioning, self
y of Pain Chapters. Published by Elsevier Ltd. All rights reserved.

Elisabeth J. van de Wetering et al. / European Journal of Pain 14 (2010) 670–681 671
efficacy and quality of life (Norrbrink Budh et al., 2006). In accor-dance with the biopsychosocial model of neuropathic pain, studiesdesigned to evaluate all kinds of pain treatment and interventionprograms should include effect measures in multiple outcome do-mains besides just pain severity.
Several studies have shown that cognitive behavioral therapycan be beneficial for chronic pain (Turk et al., 2008; Scascighiniand Sprott, 2008; Turk and Flor, 1984). However, evidence of theeffectiveness of cognitive behavior therapy with a focus on neuro-pathic pain syndromes is still lacking (Harden and Cohen, 2003).
Previous research demonstrated that patients with neuropathicpain differ from those with nociceptive pain in responses to andbeliefs about pain, major problems experienced and factorsincreasing pain. They therefore might respond differently to cogni-tive behavior therapy as well (Daniel et al., 2007). In the systematicreview presented here we evaluated the effectiveness of cognitiveand behavioral interventions for the management of chronic neu-ropathic pain.
2. Methods
2.1. Search strategy
Because neuropathic pain is traditionally classified by underly-ing causes (e.g. trigeminal neuralgia, painful diabetic neuropathy)this term is not often used as a keyword (Chong and Bajwa,2003). We therefore adopted a broad search strategy including re-ported conditions related to neuropathic pain (Dieleman et al.,2008; Harden, 2005). These conditions were combined with thekeywords ‘pain’, ‘neuralgia’ or neuralg�. Investigating interventionspresented a similar problem. The term ‘cognitive behavior therapy’is used for a variety of interventions, for example coping strategies,patient education, hypnosis, biofeedback, etc. For this reason, thesearch strategy included many keywords related to cognitive orbehavioral techniques retrieved from the literature (Turk et al.,2008; Morley et al., 1999) and from an explorative search of rele-vant Medical Subject Headings (MeSH) in the PubMed/MEDLINEdatabase. Both controlled vocabulary and free text terms wereused. The search strategy for the PubMed/MEDLINE database islisted in Appendix A. It was modified for other databases.
The first author (EW) performed an electronic search in August2008, covering the Cochrane Library (1800–2008), PubMed/MED-LINE (1966–2008), EMBASE (1994–2008), CINAHL (1982–2008)and PsycINFO (1970–2008). Moreover, references and citation listsfrom papers identified as meta-analyses, reviews or other studieswere searched for additional relevant studies.
2.2. Inclusion criteria
The titles and abstracts identified were screened on the follow-ing inclusion criteria: participants aged 18 years or older; chronicneuropathic pain or one of the listed conditions in combinationwith chronic pain or neuralgia; any type of cognitive or behavioraltechnique primarily aimed at modifying thoughts, emotions orbehavioral responses related to neuropathic pain. Unpublishedwork and studies in languages other than English were excluded.
Potentially relevant articles were obtained in full text. Two ofthe authors (EW and KL) independently assessed whether articlesindeed fulfilled the inclusion criteria and then compared the re-sults. Any disagreement was resolved by discussion and if neces-sary a third review author (AN) was consulted. The full textarticles that met the inclusion criteria were subjected to qualityassessment. Given the study objective, methodological qualitywas not an exclusion criterion for this review.
2.3. Assessment of methodological quality
Methodological quality was assessed with the Health Technol-ogy Assessment-Disease Management (HTA-DM) instrumentdeveloped by Steuten et al. (2004). This instrument was primarilydesigned for disease management programs.
Although cognitive or behavioral interventions by themselvesare not disease management programs, they are similarly complexinterventions that do not lend themselves well to blinding andwhich are evaluated by combinations of different designs. In addi-tion, the studies under review involve multiple outcome indicatorsand may have long follow-up periods.
It would follow that the HTA-DM instrument is suitable for thisreview, as it is applicable to a broad scope of studies including(quasi-)experimental studies as well as (un-)controlled and obser-vational studies. The assessment of methodological quality is basedon four components: study population; intervention; measure-ment of outcome; and data analysis and presentation (Steutenet al., 2004). The instrument contains 20 items to be scored as‘‘yes (1)/no (0)”.
2.4. Data analysis
Relevant data from the included studies were documented in astructured overview table. Additionally, an explorative meta-analysis of four studies was performed, using RevMan 5 (ReviewManager, 2008). Although the treatments differ on detail, thismeta-analysis was aimed at a more general level. This in line withthe current debate about the relevance of ‘common factors’ inpsychotherapy (Lampropoulos, 2000).
Data for pain intensity measured on a numeric scale from 0 to10 or a visual analogue scale (VAS) scale (0–100) were pooled, withVAS scores recoded on a scale of 0–10. Weighted mean differencesand 95% confidence intervals of the continuous variables were cal-culated by standard statistical techniques. The heterogeneity of thestudies was tested with the I2 statistical measure (Higgins et al.,2003).
3. Results
3.1. Description of studies
3.1.1. Literature searchThe initial comprehensive search identified 2271 references. As
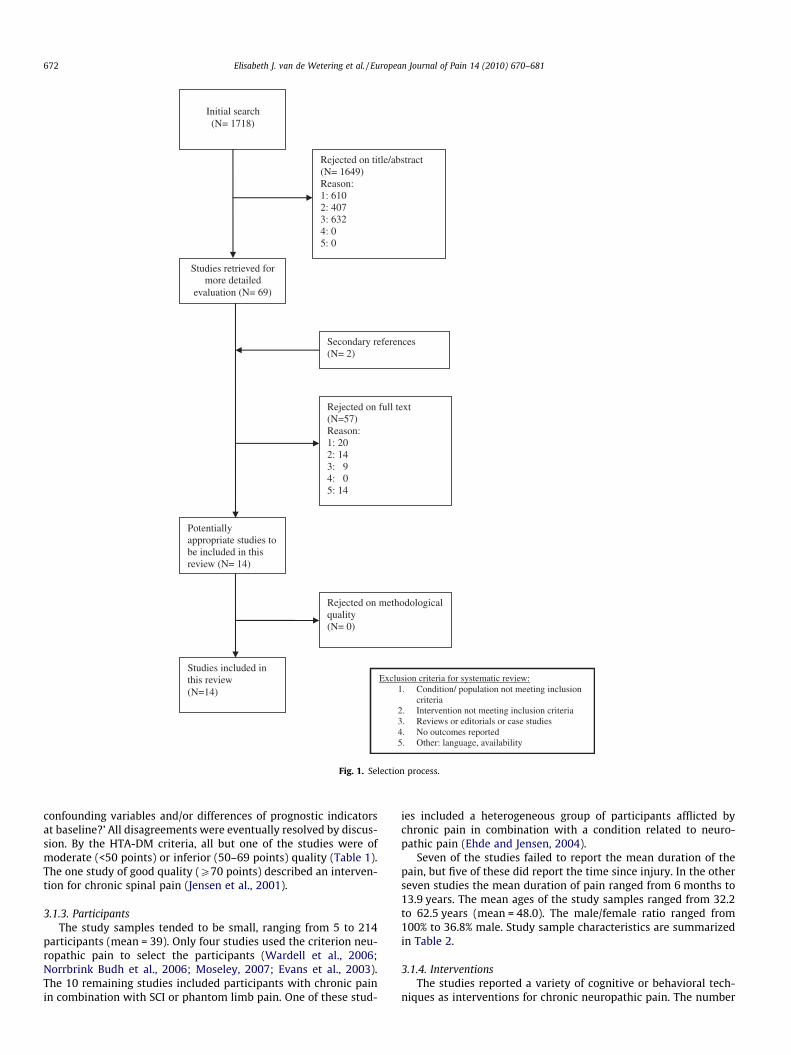
553 of these came from more than one database, only 1718 studiesentered the selection process. Applying the inclusion criteria to thearticle titles resulted in 1217 rejections. Subsequently, the ab-stracts of the 501 remaining studies were reviewed. This resultedin 432 rejections. The remaining 69 articles were screened basedon full text, which yielded two additional referenced studies. Only14 full text articles met all inclusion criteria. These included thetwo articles retrieved from secondary references (Fig. 1). Rejectionwas mostly based on the participants’ conditions not meeting theinclusion criteria.
3.1.2. Study qualityThree of the 14 studies were randomized controlled trials, three
were controlled before–after studies, seven were uncontrolled be-fore–after studies and one was a time series analysis. Only sevenstudies reported a follow-up time, ranging from 3 to 18 months.There was 85.7% agreement in scoring between the two assessors(EW and KL). Disagreements mainly concerned interpretation ofthe HTA-DM items – notably the items ‘Are the outcomes objec-tively assessed?’, ‘Is data-analysis performed according to theintention-to-treat principle?’ and ‘Are adjustments made for
Initial search (N= 1718)
Studies retrieved for more detailed
evaluation (N= 69)
Rejected on title/abstract (N= 1649) Reason: 1: 610 2: 407 3: 632 4: 0 5: 0
Rejected on full text (N=57) Reason: 1: 20 2: 14 3: 9 4: 0 5: 14
Potentially appropriate studies to be included in this review (N= 14)
Studies included in this review (N=14)
Rejected on methodological quality (N= 0)
Exclusion criteria for systematic review:1. Condition/ population not meeting inclusion
criteria 2. Intervention not meeting inclusion criteria 3. Reviews or editorials or case studies 4. No outcomes reported 5. Other: language, availability
Secondary references (N= 2)
Fig. 1. Selection process.
672 Elisabeth J. van de Wetering et al. / European Journal of Pain 14 (2010) 670–681
confounding variables and/or differences of prognostic indicatorsat baseline?’ All disagreements were eventually resolved by discus-sion. By the HTA-DM criteria, all but one of the studies were ofmoderate (<50 points) or inferior (50–69 points) quality (Table 1).The one study of good quality (P70 points) described an interven-tion for chronic spinal pain (Jensen et al., 2001).
3.1.3. ParticipantsThe study samples tended to be small, ranging from 5 to 214
participants (mean = 39). Only four studies used the criterion neu-ropathic pain to select the participants (Wardell et al., 2006;Norrbrink Budh et al., 2006; Moseley, 2007; Evans et al., 2003).The 10 remaining studies included participants with chronic painin combination with SCI or phantom limb pain. One of these stud-
ies included a heterogeneous group of participants afflicted bychronic pain in combination with a condition related to neuro-pathic pain (Ehde and Jensen, 2004).
Seven of the studies failed to report the mean duration of thepain, but five of these did report the time since injury. In the otherseven studies the mean duration of pain ranged from 6 months to13.9 years. The mean ages of the study samples ranged from 32.2to 62.5 years (mean = 48.0). The male/female ratio ranged from100% to 36.8% male. Study sample characteristics are summarizedin Table 2.
3.1.4. InterventionsThe studies reported a variety of cognitive or behavioral tech-
niques as interventions for chronic neuropathic pain. The number

Table 1Study quality using the Health Technology Assessment-Disease Management instrument (HTA_DM).
Bamford(2006)
Brodieet al.(2007)
BrownandLido(2008)
EhdeandJensen(2004)
Evanset al.(2003)
Hardenet al.(2005)
Jensenet al.(2001)
Jensen(2000)
Moseley(2007)
NorrbrinkBudhet al.(2006)
Shermanet al.(1979)
Sumitaniet al.(2008)
Wardellet al.(2006)
Zuckweilerand Kaas(2005)
Study population1 Are the criteria for selection clearly described? 0 1 1 1 1 1 1 0 0 1 1 1 1 02 Are the criteria for restriction clearly described? 0 0 1 0 0 0 1 0 0 0 0 0 0 03a Was the allocation concealed? 1 0 1 1 0 03b Is the intervention independent of other changes? 0 0 0 0 0 0 0 04a Are the relevant baseline characteristics comparable? 1 0 1 1 0 14b Are there sufficient data points? 1 1 1 1 0 0 0 05 Is there an accurate description of drop-outs? 0 0 1 0 1 0 1 0 0 1 0 0 0 0
Intervention6.1 Is the type of the intervention described? 1 1 1 1 1 1 1 1 1 1 1 1 1 16.2 Is the intensity/frequency of the intervention described? 1 1 1 1 1 1 1 1 1 1 1 1 1 16.3 Are characteristics of the region/institution in which the
intervention is implemented described?0 0 0 0 0 0 1 0 0 0 0 0 0 0
7 Are co-interventions avoided? 0 1 0 0 0 0 1 0 0 1 0 0 0 0
Measurement of outcome8.1 Results presented of clinical outcome measurements 1 1 1 1 1 1 0 1 1 1 1 1 1 18.2 Results presented of other than clinical outcomes 0 0 1 0 1 1 1 0 0 1 1 0 1 18.3 Results presented of process measures 1 0 0 1 0 0 1 1 0 0 0 0 0 08.4 Results presented of structure measures 0 0 0 0 0 0 0 0 0 0 0 0 0 09 Are the outcomes objectively assessed 0 1 1 0 1 1 1 1 1 1 0 0 1 010 Is the timing of measurement and follow-up period
adequate0 0 1 0 0 0 1 0 0 1 0 0 0 0
11 Adequate use of simulation techniques 0 0 0 0 0 0 0 0 0 0 0 0 0 0
Data analysis and presentation of data12a Is data-analysis performed according to the intention-to-
treat principle?1 0 1 1 0
12b Is data-analysis performed according to the intention-to-treat principle?
0 1 1 1 0 1 0 1 0
13 Is the presentation of data adequate? 1 1 1 1 1 1 1 1 1 1 1 1 1 114 Are adjustments made for confounding variables and/or
differences of prognostic indicators at baseline?1 0 0 0 0 0 0 0 0 0 1 1 0 0
15 Are the appropriate analytic techniques applied to theprimary outcome measures?
1 1 1 1 1 1 1 1 0 1 0 1 1 1
Tota score 8 11 13 8 11 10 16 8 6 12 7 8 9 6% 40 55 65 40 55 50 80 40 30 60 35 40 45 30
ElisabethJ.van
deW
eteringet
al./EuropeanJournal
ofPain
14(2010)
670–681
673

Table 2Study sample characteristics.
Study N Gender% (M;F) Mean age Duration episode (years)a
Bamford (2006) 25 60;40 57 7.1Brodie et al. (2007) 80 79;21 55 9
Since amputationBrown and Lido (2008) 10 70;30 62.5 13.9
Since amputationEhde and Jensen (2004) 18 67;33 46.4 >0.5Evans et al. (2003) 61 79;21 46.5 –Harden et al. (2005) 9 56;44 57.6 –Jensen et al. (2001) 214 45;55 43.3 2.6Jensen (2000) 22 64;36 45.7 13.9Moseley (2007) 5 100;0 32.2 4Norrbrink Budh et al. (2006) 38 37;63 52.2 1–>5Sherman et al. (1979) 16 100;0 – 12Sumitani et al. (2008) 22 73;27 48.4 4.8
Disease durationWardell et al. (2006) 12 100;0 54.7 I:3.9 C: 6.0
Since injuryZuckweiler and Kaas (2005) 14 71;29 Most > 50 9.9
Since amputation
a Years of pain duration unless reported otherwise, I: intervention group, C: control group.
674 Elisabeth J. van de Wetering et al. / European Journal of Pain 14 (2010) 670–681
of interventions varied from 1 session to 20 sessions within a per-iod ranging from 1 day to 30 weeks. Five studies concerned groupinterventions, five used individual interventions and four studiesfailed to report this information. Only four studies reported thata physician monitored the intervention or that a protocol was used.Six studies were controlled in some way; four studies arranged anactive control treatment for the duration of the intervention andtwo studies compared the intervention with usual care (Table 3).
3.1.5. MeasuresThe studies reported a large variety of outcome indicators and
measurement instruments. Pain was the only outcome indicatorreported by all studies. In some studies pain was the primary out-come indicator; in the study of Jensen et al. (2001) pain was justone dimension of the SF-36 quality of life questionnaire. Moststudies used the VAS or a numeric scale to quantify pain. Five stud-ies used a questionnaire which assessed pain in a multidimen-sional manner i.e. the West Haven-Yale Multidimensional PainInventory and the Brief Pain Inventory (Cleeland and Ryan, 1994;Kerns et al., 1985).
Seven studies included ‘quality of life’ (or mood) as an outcomeindicator, measured by 13 different instruments. Of these, the Hos-pital Anxiety and Depression Scale (Zigmond and Snaith, 1983) andthe Self-Report Beck depression inventory (Beck et al., 1961) wereeach used in two studies.
Other outcome indicators were performance, process measures,quality of sleep, use of health care system, sense of coherence andabsence from work (Table 3). Several studies used self-formulatedquestions or self-designed questionnaires.
3.2. Effectiveness of the interventions
Details of the studies evaluated in this review are presented inTable 3.
3.2.1. Randomized controlled trialsThe one study rated as good quality was a RCT with a follow-up
of 18 months (Jensen et al., 2001). The study included three typesof interventions with a variety of cognitive and behavioral tech-niques. Pain was assessed as one of the domains of the SF-36 butwas reported separately. In contrast to most of the other studiesno significant reduction in pain was found for the whole group.
The authors reported some positive significant effects on qualityof life and early retirement in the intervention groups comparedto the usual care group, but in female subjects only.
The other two RCTs, one with a virtual limb exercise interven-tion (Brodie et al., 2007) and one with a cognitive behavioral ther-apy intervention (Evans et al., 2003), reported significantreductions in pain in the intervention groups, but pain reductiondid not significantly differ between the intervention and treatmentcontrol groups. Still, Brodie et al. (2007) found a significant in-crease of phantom limb movement in the intervention group ascompared with the control group. A study by Evans et al. (2003) re-ported significant differences in quality of life between the inter-vention and control groups. Those who received cognitivebehavior therapy showed a significantly greater reduction indepressive symptoms, level of distress and interference than thecontrols who received supportive psychotherapy.
3.2.2. Controlled before–after studiesThree studies were not set up as a RCT but nevertheless in-
cluded control groups. A study by Norrbrink Budh et al. (2006)found some positive effects but no significant reduction of painas a result of the cognitive behavioral intervention. However, therewere significant differences between the intervention and controlgroup at the 12-month follow-up. In comparison with the usualcare group, the intervention group showed a significant improve-ment in sense of coherence and depression. Only the interventiongroup showed a significant decrease in levels of anxiety anddepression compared to baseline values. The intervention groupalso showed a significant decrease in the number of visits to thespinal cord unit and visits to physicians, whereas the control grouponly showed a significant decrease in the number of visits tophysicians.
Ehde and Jensen (2004) found a decrease in average pain inten-sity in both cognitive behavioral intervention groups but not in thecontrol group. Wardell et al. (2006) only reported a significantreduction of interference in the intervention group (healing touch)compared to the control group treated with guided progressiverelaxation.
Our meta-analysis of four studies – Brodie et al., 2007; Evanset al., 2003; Ehde and Jensen, 2004; Wardell et al., 2006 – didnot show a statistical effect of the intervention on pain intensity(Table 4).
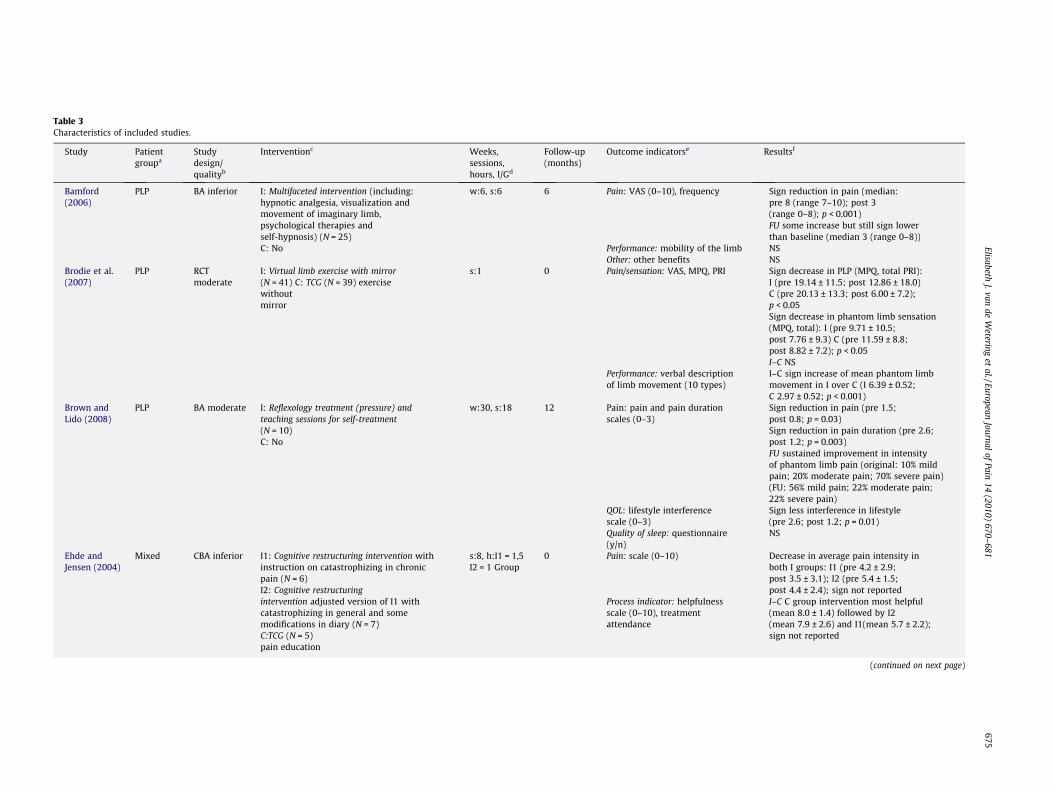
Table 3Characteristics of included studies.
Study Patientgroupa
Studydesign/qualityb
Interventionc Weeks,sessions,hours, I/Gd
Follow-up(months)
Outcome indicatorse Resultsf
Bamford(2006)
PLP BA inferior I: Multifaceted intervention (including:hypnotic analgesia, visualization andmovement of imaginary limb,psychological therapies andself-hypnosis) (N = 25)C: No
w:6, s:6 6 Pain: VAS (0–10), frequency � Sign reduction in pain (median:pre 8 (range 7–10); post 3(range 0–8); p < 0.001)� FU some increase but still sign lower
than baseline (median 3 (range 0–8))Performance: mobility of the limb � NSOther: other benefits � NS
Brodie et al.(2007)
PLP RCTmoderate
I: Virtual limb exercise with mirror(N = 41) C: TCG (N = 39) exercisewithoutmirror
s:1 0 Pain/sensation: VAS, MPQ, PRI � Sign decrease in PLP (MPQ, total PRI):I (pre 19.14 ± 11.5; post 12.86 ± 18.0)C (pre 20.13 ± 13.3; post 6.00 ± 7.2);p < 0.05� Sign decrease in phantom limb sensation
(MPQ, total): I (pre 9.71 ± 10.5;post 7.76 ± 9.3) C (pre 11.59 ± 8.8;post 8.82 ± 7.2); p < 0.05� I–C NS
Performance: verbal descriptionof limb movement (10 types)
� I–C sign increase of mean phantom limbmovement in I over C (I 6.39 ± 0.52;C 2.97 ± 0.52; p < 0.001)
Brown andLido (2008)
PLP BA moderate I: Reflexology treatment (pressure) andteaching sessions for self-treatment(N = 10)C: No
w:30, s:18 12 Pain: pain and pain durationscales (0–3)
� Sign reduction in pain (pre 1.5;post 0.8; p = 0.03)� Sign reduction in pain duration (pre 2.6;
post 1.2; p = 0.003)� FU sustained improvement in intensity
of phantom limb pain (original: 10% mildpain; 20% moderate pain; 70% severe pain)(FU: 56% mild pain; 22% moderate pain;22% severe pain)
QOL: lifestyle interferencescale (0–3)
� Sign less interference in lifestyle(pre 2.6; post 1.2; p = 0.01)
Quality of sleep: questionnaire(y/n)
� NS
Ehde andJensen (2004)
Mixed CBA inferior I1: Cognitive restructuring intervention withinstruction on catastrophizing in chronicpain (N = 6)I2: Cognitive restructuringintervention adjusted version of I1 withcatastrophizing in general and somemodifications in diary (N = 7)C:TCG (N = 5)pain education
s:8, h:I1 = 1,5I2 = 1 Group
0 Pain: scale (0–10) � Decrease in average pain intensity inboth I groups: I1 (pre 4.2 ± 2.9;post 3.5 ± 3.1); I2 (pre 5.4 ± 1.5;post 4.4 ± 2.4); sign not reported
Process indicator: helpfulnessscale (0–10), treatmentattendance
� I–C C group intervention most helpful(mean 8.0 ± 1.4) followed by I2(mean 7.9 ± 2.6) and I1(mean 5.7 ± 2.2);sign not reported
(continued on next page)
ElisabethJ.van
deW
eteringet
al./EuropeanJournal
ofPain
14(2010)
670–681
675

Study Patientgroupa
Studydesign/qualityb
Interventionc Weeks,sessions,hours, I/Gd
Follow-up(months)
Outcome indicatorse Resultsf
Table 3 (continued)
Study Patientgroupa
Studydesign/qualityb
Interventionc Weeks,sessions,hours, I/Gd
Follow-up(months)
Outcome indicatorse Resultsf
Evans et al.(2003)
Other RCTmoderate
I: Cognitive behavioral therapy (N = 28) cognitivebehavior therapy, study protocol was used andmonitored by psychologistC:TCG (N = 33) standard supportivepsychotherapy, study protocol was used and
w:6, s:6, h:1Group
0 Pain: BPI � Sign reduction in average level of painintensity in both groups: I: (pre 6.0 ± 2.2; post3.4 ± 2.5; p < 0.05); C: (pre 5.7 ± 1.8; post3.2 ± 2.4; p < 0.01)� I–C NS
monitored by psychologist QOL: BSI, BDI, HDRS, CSQ, INTRP � Significant differences for mean pain relatedinterference with functioning: Generalactivity I: (pre 6.1 ± 2.6; post 2.8 ± 2.7;p < 0.05) Mood I: (pre 5.3 ± 1.9; post 3.0 ± 2.3;p < 0.05) Walking I: (pre 6.3 ± 2.6; post3.6 ± 3.2; p < 0.05) Normal work I: (pre6.1 ± 3.0; post 2.8 ± 2.8; p < 0.05) C: (pre6.2 ± 2.8; post 4.9 ± 2.8; p < 0.05) Sleep I: (pre5.0 ± 2.7; post 2.1 ± 2.4; p < 0.01) C: (pre5.6 ± 2.9; post 4.0 ± 3.1; p < 0.05) Enjoymentof life I (pre 6.0 ± 1.8; post 2.7 ± 2.2; p < 0.01)C (pre 6.1 ± 2.6; post 4.6 ± 3.7; p < 0.05)� I–C I sign greater reduction in depressive
symptoms (mean change pre-post HDRS: I -1.7 ± 4.6; C 1.4 ± 5.7; p < 0.05)� I–C I sign greater reduction in level of distress
(mean change pre-post BSI: I: �0.32 ± 0.38; C0.02 ± 0.44; p < 0.05)
Performance: KPS � NSOther: analgesic medication diary,medical symptom checklist
� NS
Harden et al.(2005)
PLP TSAmoderate
I: Biofeedback (N = 9)C: No
s:7, h:30–140 min
0 Pain: VAS,MPQ � Sign decrease in mean daily pain (VAS) (pre38.2 ± 21.4; period 6: 20.5 ± 18.1; p < 0.01)
QOL: BDI, STAI � NSJensen et al.(2001)
SCI pain RCT good I1: Behavior-oriented physical therapy (N = 54)I2: Cognitive behavior therapy (N = 49)I3: Behavioral medicine rehabilitation (N = 63)FU: booster sessionsC: UC (N = 48) treatment as usual. Physicians,psychologists and physical therapists wereinvolved
w:4, h:I1 = 20I2 = 13,5I3 = full timeper week FU:s:6, h:1,5 persession Group
18 QOL: SF-36 (including pain) � I–C/FU Females in I groups sign improvementin mental health compared to C at 18-monthFU: I1 (B 13.5; CI95% 2.4–24.6; p < 0.05) I2 (B20.9; CI95% 8.4–33.4; p < 0.01) I3 (B 15.3;CI95% 3.8–26.9; p < 0.05)� I–C/ FU Females in I2 group sign improvement
in physical functioning (B13.3; CI95% 2.1–24.6; p < 0.05) and vitality (B 15.6; CI95% 2.1–29.1; p < 0.05) compared to C at 18-month FU� I–C/ FU Females in I3 group sign improvement
in general health compared to C at 18-monthFU (B13.9; CI95% 3.8–23.9; p < 0.01)� I-C/ FU Females in I2 and I3 group sign
improvement in social functioning comparedto C at 18-month FU: I2 (B 29.8; CI95% 14.0–45.6; p < 0.001) I3 (B 18.8 CI95% 4.1–33.5;p < 0.05)
Process indicator: relevance ofrehabilitation, adherence totreatment plan
� NS
Other: absence work, earlyretirement
� I–C/FU Females in I1 and I2 sign lower risk ofearly retirement during follow-up (I1 8%; I29%; C 35% granted full-time early retirement)
676Elisabeth
J.vande
Wetering
etal./European
Journalof
Pain14
(2010)670–
681

Jensen (2000) SCI pain BA inferior I: Hypnotic suggestion protocol andmonitored by clinicians (N = 22)C: No
s:1 Individual 0 Pain: intensity and unpleasantnessscale (0–10)
� Sign reduction in mean pain intensity (pre4.18 ± 2.44; post 2.48 ± 2.56; p < 0.05)� Sign reduction in mean unpleasantness (pre
4.00 ± 2.71; post 2.09 ± 2.19; p < 0.05)Process indicator: SHCS � NS
Moseley(2007)
SCI pain BA inferior I: Virtual walking, guided imagery (undertaken bypsychologist), watching an animated comedy film;FU virtual walk (N = 5)C: No
s:3, h:10 minFU: w:3, s:15,h:10 minIndividual
3 Pain: MPQ, VAS (100 mm) � NSProcess: vividness Illusion (VAS) � NSOther: body perception disturbance � NS
NorrbrinkBudh et al.(2006)
SCI pain CBAmoderate
I: Cognitive behavioral therapy combination ofeducation, behavioral therapy, relaxationtechniques, stretching and light exercise, bodyawareness training, treatment protocol (N = 27)C: UC (N = 11) followed up by post
w:10, s:20h:2,5Group
3, 6, 12 Pain: Borg CR 10scale, Pain Matcher � FU: NSQOL: NHP, LitSat-9 HAD SOC � I–C Sign improvement in sense of coherence (I
(median: pre 147 (range 115–183); FU 149.5(range 93–192)) C (median: pre 149 (range116–173); FU 124 (range 103–165); p < 0.05)and depression (data not reported) in the Igroup over C group� FU I group: sign reduction of anxiety (median
NHP scores) (pre 7 (range 0–16); 12- month 5(range 0–16); p < 0.05) & depression (pre 5(range 1–12); 12-month 4 (range 0–9);p < 0.05)
Quality of sleep: Akerstedtquestionnaire
� NS
Use healthcare system number ofvisits in year before the programand number of visits in yearfollowing the 12-months evaluation
� I group: sign decrease in median number ofvisits to health care personnel at spinal cordunit (pre 15; post 5; p = 0.03)� I group: sign decrease in median number of
visits to physicians (pre 3; post 1; p = 0.03)� C group: sign decrease in median number of
visits of physicians (pre 2; post 0; p = 0.02)Sherman et al.(1979)
PLP BA inferior I: Combination of progressive muscle relaxationexercise, feedback on stump and forehead muscletension, reassurance about normal phantomsensation and the relationship between anxiety andpain (N = 16)
s: average of 6Individual
0.5–3 Pain: scale (0–100) � FU Sign reduction of average pain levels (pre76 ± 13; FU 13 ± 19; p < 0.001)
C: No
QOL: anxiety scale (0–100) � FU Sign reduction of average anxiety levels(pre 72 ± 15; FU 24 ± 23; p < 0.001)
Sumitani et al.(2008)
Various BA inferior I: Mirror visual feedback (N = 22)C: No
w: mean 20, 4s: dailyh:10 minGroup
0 Pain: scale (0–10), pain quality � Sign reduction of average pain intensity (pre6.6 ± 1.7; post 4.2 ± 2.8; p < 0.002)� Sign decrease in deep pain item counts (pre
42; post 16; p < 0.005)
Wardell et al.(2006)
SCI pain Mixedinferior
I: Healing touch: individual sessions of energytherapy, provided by healing touch practitioners(N = 7)C: TCG (N = 5) guided progressive relaxation
w:6, s:6Individual
0 Other: awareness, motor imagery � Not reportedPain: BPI, VAS � NSQOL: PMS, DSLS, CES-10, coping VAS � I–C Sign less composite of interference in I
(t = �2.71, p = 0.035)Other: qualitative data � Sign variation in the experiences of the study
participants
(continued on next page)
ElisabethJ.van
deW
eteringet
al./EuropeanJournal
ofPain
14(2010)
670–681
677

Tabl
e3
(con
tinu
ed)
Stu
dyPa
tien
tgr
oupa
Stu
dyde
sign
/qu
alit
yb
Inte
rven
tion
cW
eeks
,se
ssio
ns,
hou
rs,I
/Gd
Foll
ow-u
p(m
onth
s)O
utc
ome
indi
cato
rse
Res
ult
sf
Zuck
wei
ler
and
Kaa
s(2
005)
PLP
BA
infe
rior
I:Zu
ckw
eile
r’s
Imag
eIm
prin
ting
:m
enta
lim
ager
yth
atre
prog
ram
sth
em
ind
toco
rrec
tth
edi
scre
pan
cybe
twee
nth
eol
dbo
dyim
age
and
the
chan
ged
body
form
(N=
14)
C:
No
s:pa
tien
tde
pen
den
th
:2�
1th
en30
min
Indi
vidu
al
6Pa
in:
freq
uen
cyof
pain
and
sen
sati
on(0
=n
ever
-6=
alw
ays)
�Si
gnre
duct
ion
infr
equ
ency
ofpa
in(m
ean
pre
3.93
;po
st1.
29;
p<
0.00
1)�
FUre
duct
ion
infr
equ
ency
ofpa
inst
ill
sign
afte
r6
mon
ths
(mea
n1.
43)
�Si
gnre
duct
ion
infr
equ
ency
ofse
nsa
tion
(mea
npr
e4.
71;
post
2.36
;p
<0.
001)
�FU
redu
ctio
nin
freq
uen
cyof
sen
sati
onst
ill
sign
afte
r6
mon
ths
(mea
n2.
21)
QO
L:di
stre
ssle
vel
(0–1
0)�
Sign
decr
ease
indi
stre
ssle
vels
abou
tpa
inan
dse
nsa
tion
(pai
n:m
ean
pre
7.23
;pos
t2.
46;
p<
0.00
1)(s
ensa
tion
:m
ean
pre
4.54
;po
st1.
31;
p<
0.00
2)�
FUde
crea
sein
dist
ress
leve
lsab
out
pain
and
sen
sati
on(m
ean
pain
1.85
;se
nsa
tion
1.15
)O
ther
:Ph
anto
mpa
intr
eatm
ent
outc
ome
ques
tion
nai
re�
NS
aPa
tien
tgr
oup:
PLP:
Phan
tom
lim
bpa
in,S
CI
pain
:sp
inal
cord
inju
rypa
in,M
ixed
:m
ixof
neu
ropa
thic
pain
con
diti
ons,
Oth
er:
oth
erco
ndi
tion
sre
late
dto
neu
ropa
thic
pain
.b
Res
earc
hD
esig
ns:
BA
:be
fore
–aft
erst
udy
,RC
T:ra
ndo
miz
edco
ntr
olle
dtr
ial,
CB
A:
con
trol
led
befo
re–a
fter
stu
dy,T
SA:
tim
ese
ries
anal
ysis
.c
Inte
rven
tion
:I:
inte
rven
tion
grou
p,C
:co
ntr
olgr
oup
(TCG
:tr
eatm
ent
con
trol
grou
p,U
C:
usu
alca
re,N
o:n
oco
ntr
olgr
oup)
,FU
:in
terv
enti
onin
foll
ow-u
ppe
riod
.d
Du
rati
onof
the
inte
rven
tion
inw
eeks
,am
oun
tof
sess
ion
san
dti
me
per
sess
ion
inh
ours
;I/
G:
Indi
vidu
alor
Gro
up
sess
ion
s.e
Out
com
ein
dica
tors
:M
PQ:
McG
ill
pain
ques
tion
nai
re,P
RI:
pain
ran
kin
gin
dex,
BPI
:B
rief
Pain
Inve
nto
ry,B
SI:
Bri
efSy
mpt
omIn
ven
tory
,BD
I:B
eck
Dep
ress
ion
Inve
nto
ry,H
DR
S:H
amil
ton
Dep
ress
ion
Rat
ing
Scal
e,C
SQ:
Cop
ing
Stra
tegi
esQ
ues
tion
nai
re,I
NTR
P:In
ven
tory
ofN
egat
ive
Thou
ghts
inR
espo
nse
toPa
in,K
PS:K
arn
ofsk
yPe
rfor
man
ceSc
ale,
STA
I:Tr
aitF
orm
ofth
eSt
ate-
Trai
tAn
xiet
yIn
ven
tory
,SH
CS:
Stan
ford
Hyp
not
icC
lin
ical
Scal
e,N
HP:
Not
tin
gham
Hea
lth
Profi
le,H
AD
:Hos
pita
lAn
xiet
yan
dD
epre
ssio
nsc
ale,
SOC
:Sen
seof
Coh
eren
ce,P
MS:
Profi
leof
Moo
dsSt
ates
,DSL
S:D
ien
erSa
tisf
acti
onw
ith
Life
Scal
e,C
ESD
-10:
Cen
ter
for
Epid
emio
logi
calS
tudi
es-D
epre
ssio
nsc
ale
shor
tfor
m.
fPr
e-po
st(d
irec
tly
afte
rth
ein
terv
enti
on)
resu
lts
are
pres
ente
du
nle
ssre
port
edot
herw
ise;
FU:
foll
ow-u
ppe
riod
com
pare
dto
base
lin
e;I–
C:
inte
rven
tion
grou
pve
rsu
sco
ntr
olgr
oup;
B:
para
met
eres
tim
ates
from
cova
rian
cean
alys
esfo
rdi
ffer
ence
sbe
twee
ntr
eatm
ent
grou
psve
rsu
sth
eco
ntr
olgr
oup
atth
e18
-mon
thfo
llow
-up.
678 Elisabeth J. van de Wetering et al. / European Journal of Pain 14 (2010) 670–681
3.2.3. Before–after studies and time series analysisThe remaining studies included a variety of therapies. Most
studies showed a significant decrease in pain intensity. Bamford(2006) reported a slight increase in pain during follow-up afterthe initial decrease, but pain intensity was still significantly lowerthan baseline values. In addition to pain reduction, Brown and Lido(2008) reported significantly less interference in lifestyle afterreflexology treatment, but no significant improvement in qualityof sleep. Sherman et al. (1979) and Zuckweiler and Kaas (2005)found significant reductions of average anxiety levels or distresslevels. The study of Moseley (2007) did not find any significant ef-fect of the intervention on the outcomes.
4. Discussion
Many articles have pointed out the merits of a biopsychosocialapproach to neuropathic pain. This is the first systematic reviewthat has evaluated the effectiveness of cognitive and behavioraltechniques for the management of chronic neuropathic pain. Theresults show that the evidence is still limited. This is not surprising,as most of the studies reviewed were pilot studies of recent date.Only one randomized controlled trial was judged to be of goodquality (Jensen et al., 2001).
Participants and interventions varied on detail but all partici-pants suffered from chronic neuropathic pain and all interventionswere based on cognitive or behavioral techniques. Although theinterventions may operate via very different mechanisms the dis-cussion of the ‘common factors’ in psychotherapy underlines theimportance of shared treatment similarities that are responsiblefor equivalent therapeutic outcomes (Lampropoulos, 2000). There-fore, we performed an explorative meta-analysis of four studies.This failed to show a significant effect of the interventions on painintensity. Still, the sample size was small and consequently therewas insufficient power to reject a false null hypothesis.
The strongest study, qualitatively speaking, did not report sig-nificant pain reduction for the whole group as a result of the inter-ventions. In the female subjects only, positive significant effectswere found on quality of life and early retirement in the interven-tion groups compared to the usual care group (Jensen et al., 2001).The other two randomized controlled trials did report significantreductions of pain. However, pain reduction did not differ betweenthe intervention and control groups. Again, additional positive ef-fects were found in the intervention groups compared to the con-trol groups.
Two of the controlled before–after studies did not find signifi-cant pain reduction in their intervention or control groups. Thethird study reported an average pain reduction in both interven-tion groups but not in the control group, though it was not clearwhether the effect was significant. Remarkably, all before–afterstudies reported positive effects on pain reduction. However, giventhe fact that these studies had an uncontrolled study design it isunclear whether the effects are a result of the interventions itselfor whether other, unobserved effects were involved.
A number of studies found significant positive effects of theintervention with regard to other outcome measures. This supportsthe relevance of the biopsychosocial approach of neuropathic pain,including multidimensional outcome measures. All included stud-ies reported additional outcome measures besides pain reduction;nine reported significant effects. Of these studies, five showed sig-nificant positive effects on psychological functioning. Without theadditional outcome measures these effects would simply not havebeen found.
A previous review of cognitive behavior therapy and behaviortherapy for chronic pain in adults found that active psychologicaltreatments based on the principle of cognitive behavioral therapy

Tabl
e4
Elisabeth J. van de Wetering et al. / European Journal of Pain 14 (2010) 670–681 679
are effective (Morley et al., 1999). The authors even found thatcompared to alternative active treatments, cognitive behavioraltreatments produced significantly greater reductions in pain. Thisfinding is in line with the positive, although still inconclusive, find-ings from this review.
4.1. Limitations
The definition of neuropathic pain is still a point of discussion;opinions may conflict on whether a certain pain condition is neu-ropathic or not. To cover this issue the search strategy included anumber of conditions related to neuropathic pain, derived fromthe literature.
In addition, there is the fact that neuropathic pain is a complexcondition with a variety of causes. Those afflicted therefore form avery heterogeneous group in which responsiveness to interven-tions may vary. This fact could explain the discrepancies in thefindings.
Furthermore, it should be noted that the methodological qualityof the included studies was very limited; consequently the resultsmay be biased by unobserved effects, often leading to false-posi-tive results. In addition, due to small sample sizes, the studies werestatistically insufficiently powerful to reject a false null hypothesis.
Nevertheless, the objective of this review was to assess theexisting evidence for cognitive and behavioral techniques as aneffective intervention for chronic neuropathic pain. The fact thatthere are only a few relevant studies of limited methodologicalquality is an important observation in itself.
4.2. Practice and research implications
Although we devised a very broad search strategy with anextensive list of conditions related to neuropathic pain, most ofthe studies retrieved concerned phantom limb pain or spinal cordinjury pain. Only four studies explicitly used the term neuropathicpain. We think this is due to the absence of a clear definition ofneuropathic pain, which makes it difficult to identify whetherchronic pain is neuropathic or not (Treede et al., 2008; Backonja,2003). Therefore, a clear definition of neuropathic pain, a goodscreening tool and a widely accepted list with conditions relatedto neuropathic pain would be very useful for future research.
Currently, a number of screening tools are available to identifyneuropathic pain, for instance, the Leeds Assessment of Neuro-pathic Symptoms and Signs (LANSS), the Neuropathic Pain Ques-tionnaire (NPQ) and painDETECT (Bennett et al., 2007). Fivescreening tools were found to be able to distinguish neuropathicpain from other types of chronic pain with up to 80% sensitivityand specificity. However, further validation is needed across cul-tures, languages and clinicians, and then, researchers must reachconsensus on which tool is most appropriate (Bennett et al., 2007).
As the included studies used a large variety of outcome indica-tors and outcome measures, it was not easy to compare and pooldata from the different studies. This shortcoming emphasizes theneed for standardized measurement instruments to evaluate neu-ropathic pain interventions. These should enable one to evaluateneuropathic pain interventions on a multidimensional level. Inthe studies included in this review, pain severity was often the pri-mary outcome measure. As mentioned earlier, however, chronicpain strongly interferes with psychological and social well beingand the biopsychosocial approach is not primarily aimed at painreduction. Therefore, the multidimensional approach to neuro-pathic pain should also be reflected in the outcome measures(Norrbrink Budh et al., 2006).
Additionally, the methodological quality of the included studieswas very low, with little follow-up data. Future research should

680 Elisabeth J. van de Wetering et al. / European Journal of Pain 14 (2010) 670–681
strive for stronger methodological quality and longer follow-upperiods.
Finally, since many researchers emphasize that a multidimen-sional approach to neuropathic pain is relevant, it would be inter-esting to investigate the effect of cognitive and behavioralinterventions implemented in combination with other neuropathicpain interventions.
4.3. Conclusions
Evidence of cognitive and behavioral techniques for the man-agement of neuropathic pain is still very limited. Therefore, noinformative conclusions can be drawn with respect to the studyobjective. However, we have provided insight into the difficultiesof this specific area of study. Future research will benefit from aclear and widely accepted definition of neuropathic pain, standard-ized multidimensional measurement instruments and the use ofimportant outcome domains other than pain severity alone.
More research with stronger methodological quality and longerfollow-up periods is needed in order to provide high quality evi-dence of the effectiveness of cognitive and behavioral techniquesfor the management of chronic neuropathic pain.
Acknowledgement
This article was supported by an unrestricted grant from DALIvoor PIJN (Dutch alliance for improvement of pain care), an initia-tive of Pfizer BV.
Appendix A. Search strategy
A.1. PubMed
1. peripheral nervous system diseases[mesh]2. neuropath*3. neurit*4. causalg*5. guillain–barre6. mononeuropath*7. ‘‘tunnel syndrome”8. neuralg*9. sciatica
10. polyneuropath*11. polyradiculo*12. radiculopath*13. ‘‘multiple sclerosis”14. multiple sclerosis[mesh]15. ‘‘nerve compression”16. spinal cord injuries[mesh]17. ‘‘spinal cord injuries”18. ‘‘spinal cord injury”19. ‘‘spinal cord compression”20. syringomyelia21. ‘‘spinal stenosis”22. ‘‘facial pain”23. Phantom24. OR/1-2325. Pain26. neuralgia OR neuralg*27. (#25 OR #26)28. behavior therapy[mesh]29. ‘‘behavior therapy” OR ‘‘behaviour therapy”30. ‘‘behavioral therapy” OR ‘‘behavioural therapy”31. hypnosis32. ‘‘cognitive therapy”
33. ‘‘aversive therapy”34. ‘‘aversion therapy”35. biofeedback36. ‘‘psychologic desensitization”37. ‘‘psychological desensitization”38. ‘‘relaxation techniques” OR ‘‘relaxation technique”39. ‘‘relaxation training”40. ‘‘guided imagery”41. ‘‘patient education”42. ‘‘self care”43. psychological adaptation[mesh]44. ‘‘rehabilitation”45. ‘‘behavior modification”46. ‘‘adaptive behavior”47. OR/28-4648. ‘‘randomized controlled trial” OR ‘‘randomized controlled
trials”49. ‘‘controlled clinical trial” OR ‘‘controlled clinical trials”50. ‘‘intervention study” OR ‘‘intervention studies”51. ‘‘time series”52. ‘‘time series analysis”53. pre-test OR post-test OR pre-test OR post-test54. ‘‘pre-test post-test design”55. ‘‘random allocation”56. impact57. ‘‘evaluation study” OR ‘‘evaluation studies”58. ‘‘comparative study” OR ‘‘comparative studies”59. random*[tw]60. ‘‘follow-up studies”61. ‘‘prospective studies”62. ‘‘quasi experimental design”63. OR/ 48–6264. animals[mesh]65. humans[mesh]66. (#64 NOT #65)67. ((#24 AND #27 AND #47 AND #63) NOT #66)
References
Backonja MM. Defining neuropathic pain. Anesth Analg 2003;97(3):785–90.Bamford C. A multifaceted approach to the treatment of phantom limb pain using
hypnosis. Contemp Hypn 2006;23(3):115–26.Beck AT, Ward CH, Mendelson M, Mock J, Erbaugh J. An inventory to measure
depression. Arch Gen Psychiatry 1961;4:561–71.Bennett MI, Attal N, Backonja MM, Baron R, Bouhassira D, Freynhagen R, et al. Using
screening tools to identify neuropathic pain. Pain 2007;127(3):199–203.Brodie EE, Whyte A, Niven CA. Analgesia through the looking-glass? A randomized
controlled trial investigating the effect of viewing a ‘virtual’ limb upon phantomlimb pain, sensation and movement. Eur J Pain 2007;11(4):428–36.
Brown CA, Lido C. Reflexology treatment for patients with lower limb amputationsand phantom limb pain – an exploratory pilot study. Complement Ther ClinPract 2008;14(2):124–31.
Chong MS, Bajwa ZH. Diagnosis and treatment of neuropathic pain. J Pain SymptomManage 2003;25(5):S4–S11.
Cleeland CS, Ryan KM. Pain assessment: global use of the brief pain inventory.Annals of the Academy of Medicine, Singapore 1994;23(2):129.
Daniel HC, Narewska J, Serpell M, Hoggart B, Johnson R, Rice ASC. Comparison ofpsychological and physical function in neuropathic pain and nociceptive pain:implications for cognitive behavioral pain management programs. Eur J Pain2007.
Dieleman JP, Kerklaan J, Huygen FJ, Bouma PA, Sturkenboom MC. Incidence ratesand treatment of neuropathic pain conditions in the general population. Pain2008.
Ehde DM, Jensen MP. Feasibility of a cognitive restructuring intervention fortreatment of chronic pain in persons with disabilities. Rehabil Psychol2004;49(3):254–8.
Evans S, Fishman B, Spielman L, Haley A. Randomized trial of cognitive behaviortherapy versus supportive psychotherapy for HIV-related peripheralneuropathic pain. Psychosomatics 2003;44(1):44.
Gatchel RJ. Comorbidity of chronic pain and mental health disorders: thebiopsychosocial perspective. Am Psychol 2004;59(8):795–805.
Harden N, Cohen M. Unmet needs in the management of neuropathic pain. J PainSymptom Manage 2003;25(5S):12–7.

Elisabeth J. van de Wetering et al. / European Journal of Pain 14 (2010) 670–681 681
Harden RN. Chronic neuropathic pain: mechanisms, diagnosis, and treatment. TheNeurologist 2005;11(2):111.
Harden RN, Houle TT, Green S, Remble TA, Weinland SR, Colio S, et al. Biofeedback inthe treatment of phantom limb pain: A time-series analysis. Appl PsychophysBiof 2005;30(1):83–93.
Higgins JPT, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ Publishing Group Ltd.; 2003. p. 557–60.
Jensen IB, Bergström G, Ljungquist T, Bodin L, Nygren AL. A randomized controlledcomponent analysis of a behavioral medicine rehabilitation program for chronicspinal pain: are the effects dependent on gender? Pain, Amsterdam 2001;91(1–2):65–78.
Jensen MP. The effect of hypnotic suggestion on spinal cord injury pain. J BackMusculoskeletal Rehab 2000;14(1):3–10.
Kerns RD, Turk DC, Rudy TE. The west haven-yale multidimensional pain inventory(WHYMPI). Pain 1985;23(4):345–56.
Lampropoulos GK. Definitional and research issues in the common factors approachto psychotherapy integration: misconceptions, clarifications, and proposals. JPsychother Integr 2000;10(4):415–38.
Morley S, Eccleston C, Williams A. Systematic review and meta-analysis ofrandomized controlled trials of cognitive behaviour therapy and behaviourtherapy for chronic pain in adults, excluding headache. Pain 1999;80(1–2):1–13.
Moseley GL. Using visual illusion to reduce at-level neuropathic pain in paraplegia.Pain 2007;130(3):294–8.
Norrbrink Budh C, Kowalski J, Lundeberg T. A comprehensive pain managementprogramme comprising educational, cognitive and behavioural interventions forneuropathic pain following spinal cord injury. J Rehab Med 2006;38(3):172–80.
Review Manager (RevMan). Version 5.0. Copenhagen: The Nordic Cochrane Centre.The Cochrane Collaboration; 2008 [computer program].
Scascighini L, Sprott H. Chronic nonmalignant pain: a challenge for patients andclinicians. Nat Clin Pract Rheumatol 2008;4(2):74–81.
Sherman RA, Gall N, Gormly J. Treatment of phantom limb pain with muscularrelaxation training to disrupt the pain–anxiety–tension cycle. Pain1979;6(1):47–55.
Steuten LM, Vrijhoef HJ, van Merode GG, Severens JL, Spreeuwenberg C. The healthtechnology assessment-disease management instrument reliably measuredmethodologic quality of health technology assessments of diseasemanagement. J Clin Epidemiol 2004;57(9):881–8.
Sumitani M, Miyauchi S, McCabe CS, Shibata M, Maeda L, Saitoh Y, et al. Mirrorvisual feedback alleviates deafferentation pain, depending on qualitativeaspects of the pain: a preliminary report. Rheumatology, Oxford2008;47(7):1038–43.
Tölle Thomas, Xu Xiao, Sadosky Alesia B. Painful diabetic neuropathy: a cross-sectional survey of health state impairment and treatment patterns. J DiabetesComplicat 2006;20(1):26–33.
Treede RD, Jensen TS, Campbell JN, Cruccu G, Dostrovsky JO, Griffin JW, et al.Neuropathic pain: redefinition and a grading system for clinical and researchpurposes. Neurology 2008;70:1630–5.
Turk DC, Swanson KS, Tunks ER. Psychological approaches in the treatment ofchronic pain patients – when pills, scalpels, and needles are not enough. Can JPsychiatry 2008;53(4):213–23.
Turk Dennis C, Flor Herta. Etiological theories and treatments for chronic back pain.II. Psychological models and interventions. Pain 1984;19(3):209–33.
Wardell DW, Rintala DH, Duan Z, Tan G. A pilot study of healing touch andprogressive relaxation for chronic neuropathic pain in persons with spinal cordinjury. J Holist Nurs 2006;24(4):231–40 [discussion 41-4].
Zigmond AS, Snaith RP. The hospital anxiety and depression scale. Acta PsychiatScand 1983;67(6):361–70.
Zuckweiler RL, Kaas MJ. Treating phantom pain and sensation with Zuckweiler’simage imprinting. J Prosthet Orthot 2005;17(4):103–12.
Copyright © 2022 FDOKUMEN