CO and NO pulmonary diffusing capacity during pregnancy: Safety and diagnostic potential
12
This article appeared in a journal published by Elsevier. The attached copy is furnished to the author for internal non-commercial research and education use, including for instruction at the authors institution and sharing with colleagues. Other uses, including reproduction and distribution, or selling or licensing copies, or posting to personal, institutional or third party websites are prohibited. In most cases authors are permitted to post their version of the article (e.g. in Word or Tex form) to their personal website or institutional repository. Authors requiring further information regarding Elsevier’s archiving and manuscript policies are encouraged to visit: http://www.elsevier.com/copyright
Transcript of CO and NO pulmonary diffusing capacity during pregnancy: Safety and diagnostic potential
This article appeared in a journal published by Elsevier. The attachedcopy is furnished to the author for internal non-commercial researchand education use, including for instruction at the authors institution
and sharing with colleagues.
Other uses, including reproduction and distribution, or selling orlicensing copies, or posting to personal, institutional or third party
websites are prohibited.
In most cases authors are permitted to post their version of thearticle (e.g. in Word or Tex form) to their personal website orinstitutional repository. Authors requiring further information
regarding Elsevier’s archiving and manuscript policies areencouraged to visit:
http://www.elsevier.com/copyright

Author's personal copy
Respiratory Physiology & Neurobiology 170 (2010) 215–225
Contents lists available at ScienceDirect
Respiratory Physiology & Neurobiology
journa l homepage: www.e lsev ier .com/ locate / resphys io l
Frontiers review
CO and NO pulmonary diffusing capacity during pregnancy: Safety anddiagnostic potential
Gerald S. Zavorskya,b,∗, Arlin B. Bloodc,d, Gordon G. Powerd, Lawrence D. Longod,Raul Artal a, Emanuel J. Vlastosa
a Department of Obstetrics, Gynecology and Women’s Health, School of Medicine, Saint Louis University, Saint Mary’s Health Center, 6420 Clayton Road,Suite 290, Saint Louis, MO 63117, USAb Department of Pharmacological and Physiological Science, School of Medicine, Saint Louis University, 402 South Grand Blvd., Saint Louis, MO 63104, USAc Division of Neonatology, Department of Pediatrics, School of Medicine, Loma Linda University, Loma Linda, CA 92350, USAd Center for Perinatal Biology, School of Medicine, Loma Linda University, Loma Linda, CA 92350, USA
a r t i c l e i n f o
Article history:Accepted 3 February 2010
Keywords:Carbon monoxideNitric oxideGuidelinesRecommendationsPregnancy
a b s t r a c t
This paper reviews the scientific evidence for the safety of carbon monoxide (CO) and nitric oxide (NO)inhalation to measure pulmonary diffusing capacity (DLCO and DLNO) in pregnant women and their fetuses.In eight earlier studies, 650 pregnant women had DLCO measurements performed at various times duringpregnancy, with a minimum of two to four tests per session. Both pregnant subjects that were healthyand those with medical complications were tested. No study reported adverse maternal, fetal, or neonataloutcomes from the CO inhalation in association with measuring DLCO. Eleven pregnant women, chieflywith pulmonary hypertension, and 1105 pre-term neonates, mostly with respiratory failure, were admin-istered various dosages of NO (5–80 ppm for 4 weeks continuously in pregnant women, and 1–20 ppmfor 15 min to 3 weeks for the neonates). NO treatment was found to be an effective therapy for pregnantwomen with pulmonary hypertension. In neonates with respiratory failure and pulmonary hyperten-sion, NO therapy improved oxygenation and survival and has been associated with only minor, transientadverse effects. In conclusion, maternal carboxyhemoglobin ([HbCO]) levels can safely increase to 5% pertesting session when the dose-exposure limit is 0.3% CO inhalation for ≤3 min, and for NO, 80 ppm for≤3 min. The risk of late fetal or neonatal death from increased HbCO from diffusion testing is considerablyless than the risk of death from all causes reported by the Centers for Disease Control, and is thereforeconsidered “minimal risk”.
© 2010 Elsevier B.V. All rights reserved.
1. Introduction
The 2005 guidelines for standardizing pulmonary function testshave been jointly updated, approved, and published by the Amer-ican Thoracic Society (ATS) and the European Respiratory Society(ERS) (Macintyre et al., 2005; Miller et al., 2005a,b; Pellegrino etal., 2005; Wanger et al., 2005). These guidelines reflect the currentknowledge in the field, and establish measures of safe clinical prac-tice in quantifying pulmonary function. According to the ATS/ERSguidelines, only a few circumstances exist in which lung functiontesting is contraindicated (Miller et al., 2005b). For lung func-tion testing that includes measurements of pulmonary diffusingcapacity, there are only four contraindications: (1) chest or abdom-
∗ Corresponding author at: Department of Obstetrics, Gynecology and Women’sHealth, School of Medicine, Saint Louis University, Saint Mary’s Health Center, 6420Clayton Road, Suite 290, Saint Louis, MO 63117, USA. Tel.: +1 314 977 2574;fax: +1 314 977 2161.
E-mail address: [email protected] (G.S. Zavorsky).
inal pain, (2) oral or facial pain, (3) stress incontinence, (4) anddementia. Pregnancy is not considered a contraindication for themeasurement of pulmonary diffusing capacity (Miller et al., 2005b).
Despite the ATS/ERS guidelines, the question of whether mea-surement of pulmonary diffusing capacity in pregnant women is“safe” and “warranted” for themselves and their fetuses has notbeen studied adequately. Concern with performing diffusing capac-ity measurements during pregnancy stems from carbon monoxide(CO) exposure, resulting in increases in carboxyhemoglobin (HbCO)in the blood of the mother and fetus with each test. Accumula-tion of HbCO in excess can diminish the oxygen-carrying capacityof maternal and fetal blood to unsafe levels.
Nonetheless, determination of pulmonary diffusing capacitycan be an excellent prognostic indicator for maternal and fetaloutcomes, fitness, and mortality. Since impaired lung functionis associated with an increase and recurrence of cardiovasculardisease (Coburn et al., 1963), measuring pulmonary functionin a pregnant woman may be a valuable prognostic indicator ofadverse maternal (e.g. preeclampsia, gestational diabetes, cesareansection) and fetal outcomes (e.g. large for gestational age, small for
1569-9048/$ – see front matter © 2010 Elsevier B.V. All rights reserved.doi:10.1016/j.resp.2010.02.001

Author's personal copy
216 G.S. Zavorsky et al. / Respiratory Physiology & Neurobiology 170 (2010) 215–225
gestational age infants). In fact, a forced expiratory volume in 1 sthat is <80% of predicted in women who are pregnant is related tohigher incidence of pre-term births (<37 weeks gestation), a higherprevalence of gestational hypertension, and a higher risk for lowbirth weight babies (<2500 g) (Getahun et al., 2006, 2007; Schatz etal., 2006). Most recently, a low maternal hemoglobin concentration(<10 g/dl) has been related to a higher risk for stillbirths, pre-termbirths, and small for gestational age babies (Gonzales et al., 2009).Because hemoglobin concentration is a determinant of pulmonarydiffusing capacity, measurement of pulmonary diffusion may alsorelate to maternal and fetal outcomes, a possibility that has not yetbeen tested. Pulmonary diffusing capacity for carbon monoxide(DLCO) and nitric oxide (DLNO) at rest is also related to aerobiccapacity (Zavorsky et al., 2009), a strong independent predictor ofdeath in women (Gulati et al., 2003) and men (Myers et al., 2002).Thus, a measurement of pulmonary diffusion could be a prognosticmarker for mortality in pregnancy. Low pulmonary diffusion in apregnant woman may prompt a physician to recommend regularaerobic exercise to improve her fitness. Finally, DLCO and DLNO aresensitive indicators of the morphological changes assessed withcomputed tomography to detect emphysema and cystic fibrosis(Dressel et al., 2009; van der Lee et al., 2009).
What is the clinical significance of measuring alveolar mem-brane diffusing capacity (DM) in the pregnant female “diseased”lung? Well, the global measurement of DLCO only provides a globalindication of whether gas exchange is normal or not. It does notspecify where the abnormal physiology lies, whether the issueis low (or high) hemoglobin concentration, or low (or high) pul-monary capillary blood volume, or whether the problem lies solelywithin the alveolar-capillary membrane. A measurement of bothDLCO and DLNO together allows partitioning to obtain pulmonarycapillary blood volume (Vc) and DM (DM is essentially DLNO) so thatthere is a more precise determination of the location of the patho-physiology. Pregnant women who have a high DM/Vc ratio (whichis equal to the DLNO/DLCO ratio) should be evaluated for high pul-monary artery pressure compatible with pulmonary hypertension(Bonay et al., 2004; van der Lee et al., 2006). Therefore, a dispropor-tionate reduction in DM relative to Vc would decrease the DM/Vcratio (and thus decrease the DLNO/DLCO ratio), which is related toa wide spectrum of pulmonary vascular diseases (Oppenheimer etal., 2006) and could apply to pregnant women. Diabetes, which cancause pulmonary microangiopathy, lowers DLNO/DLCO compared tocontrols (Chance et al., 2008). Thus, a DLNO and DLCO measurementcould be a prognostic indicator for gestational diabetes.
Therefore, future direction of the measurements of DLCO andDLNO in pregnancy has promise as a screening tool for predictingaerobic capacity (as a determinant of mortality), and to help identifypulmonary hypertension, pulmonary vascular diseases, and gesta-tional diabetes (including type II and possibly type I diabetes). Withthe goals of advancing knowledge of alveolar gas exchange duringpregnancy and ensuring safe testing of lung function, the guide-lines proposed herein should help to facilitate the use of pulmonarydiffusing capacity measurement in the pregnant woman.
2. Carbon monoxide
Pulmonary diffusing capacity for carbon monoxide is a standardfunction test that measures alveolar-capillary diffusion. Becausethe measurement of oxygen transfer through the lung is technicallydifficult, and may be limited by blood flow and pulmonary tissue O2consumption, carbon monoxide (CO) has been used as an indirectindex of oxygen transfer, due to its high affinity to bonding withhemoglobin (Forster, 1957).
The standard DLCO protocol is to use the single-breath method.Following a few normal breaths, a subject first exhales to residualvolume, and then inhales a standard concentration of gases (0.3%
CO, 10% Helium, 21% O2, balance N2) to total lung capacity. As totallung capacity and vital capacity are minimally affected regardlessof the stage of pregnancy (Alaily and Carrol, 1978; Baldwin et al.,1977; McAuliffe et al., 2002; Milne, 1979) and regardless of obe-sity (Eng et al., 1975), inhalation to total lung capacity is possibleduring all three trimesters. After a 10-s breath-hold, the patient(subject) exhales in a smooth, unforced manner, without hesitationor interruption all the way to residual volume. The first 0.75–1.0 Lof expired air is discarded, and only the second liter of air (whichreflects alveolar gas) is analyzed. The remainder of the expired airis discarded as well. DLCO is calculated as the total CO uptake overtime divided by the alveolar partial pressure of CO (Macintyre etal., 2005).
DLCO can also be measured by rebreathing a standard concentra-tion of gases (0.3% CO, 10% Helium, 35% O2, balance N2), with a bagvolume that ranges from tidal volume (Snyder et al., 2006) to 60%of vital capacity (or 500 ml to 3.5 L) (Takahashi et al., 1995). Gasesare inhaled from a closed circuit anesthesia bag, and rebreathed for15 s at a frequency of about 30 breaths/min. The calculation of DLCOusing the rebreathing technique is essentially the same as that withbreath-holding. This method for DLCO is less commonly used, as itrequires more expensive equipment, such as a respiratory massspectrometer, and more complex calculations. However, becausewith rebreathing the CO gas is distributed in the lung more evenly,an advantage of this method, as opposed to the single-breath, is itsrelative insensitivity to unequal distribution of ventilation (Jansonset al., 1998; Roberts et al., 1990) and diffusion (Jansons et al., 1998;Kreukniet, 1970). Furthermore, rebreathing is preferred when sub-jects cannot hold their breath for long periods or, if for some reason,vital capacity is too small.
The primary safety concern with inhaling CO is the increasein fetal and maternal carboxyhemoglobin concentration ([HbCO])resulting in diminished blood oxygen-carrying capacity. Carbonmonoxide is a naturally occurring gas that is produced endoge-nously by catabolism of hemoglobin and other heme pigments,chiefly in the liver and spleen. Endogenous CO production isapproximately 0.001–0.007 ml/min (Coburn et al., 1963, 1965).In a non-smoking individual this results in a normal carboxy-hemoglobin level of about 0.7–1.1% (Coburn et al., 1965), whichincreases in pregnancy (Delivoria-Papadopoulos et al., 1974). Innon-smoking pregnant mothers, maternal [HbCO] is reported to be1.1 ± 0.2% (Longo, 1976), but the range is wide, at 0.4–2.6% (Longo,1977). Fetal [HbCO] is about 1.8 ± 0.3% (Longo, 1976), with a rangeof 0.4–2.8% (Longo, 1977).
Tests of pulmonary diffusing capacity increase [HbCO] byapproximately 0.7–0.8% per 10-s breath-hold maneuver (Forsteret al., 1954; Frey et al., 1987). The standard mixture of gases in amedical grade gas tank for testing is 0.3% CO, 10% He, 21% O2, with abalance of N2. Therefore, whether the diffusing capacity measure-ment involves single breath-hold or rebreathing maneuvers, theincrease in [HbCO] is about 0.7% per test. The ATS/ERS guidelinessuggest that no more than five measurements of diffusing capacitytests be performed in one testing session for all subjects, includingpregnant women (Macintyre et al., 2005). The limit of five diffusingcapacity tests is not related to safety concerns with [HbCO] accumu-lation, but rather because each maneuver increases [HbCO] by about0.7% and may reduce the DLCO measured in subsequent tests dueto a back pressure of CO in lung capillaries. Five diffusing capacitytests in a session reduces DLCO by 1.5 ml/min/Torr, which equatesto a reduction of about 5% from the first to the fifth determination(Zavorsky and Murias, 2006). These guidelines are based on DLCOmeasurement at rest, however. With exercise, additional testingmay be warranted to match the various levels of oxygen consump-tion to DLCO. In that manner, the slope of the relation betweenoxygen consumption and DLCO would provide an indication of pul-monary microvascular regulation.
Author's personal copy
G.S. Zavorsky et al. / Respiratory Physiology & Neurobiology 170 (2010) 215–225 217
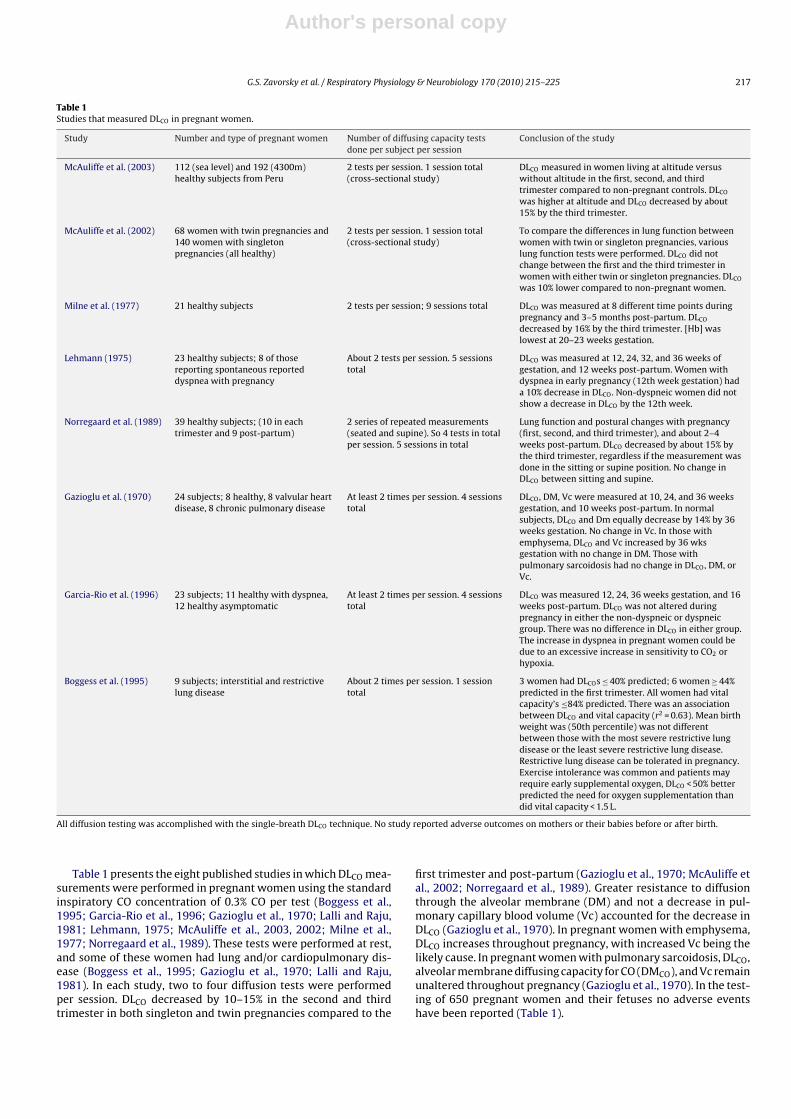
Table 1Studies that measured DLCO in pregnant women.
Study Number and type of pregnant women Number of diffusing capacity testsdone per subject per session
Conclusion of the study
McAuliffe et al. (2003) 112 (sea level) and 192 (4300m)healthy subjects from Peru
2 tests per session. 1 session total(cross-sectional study)
DLCO measured in women living at altitude versuswithout altitude in the first, second, and thirdtrimester compared to non-pregnant controls. DLCO
was higher at altitude and DLCO decreased by about15% by the third trimester.
McAuliffe et al. (2002) 68 women with twin pregnancies and140 women with singletonpregnancies (all healthy)
2 tests per session. 1 session total(cross-sectional study)
To compare the differences in lung function betweenwomen with twin or singleton pregnancies, variouslung function tests were performed. DLCO did notchange between the first and the third trimester inwomen with either twin or singleton pregnancies. DLCO
was 10% lower compared to non-pregnant women.
Milne et al. (1977) 21 healthy subjects 2 tests per session; 9 sessions total DLCO was measured at 8 different time points duringpregnancy and 3–5 months post-partum. DLCO
decreased by 16% by the third trimester. [Hb] waslowest at 20–23 weeks gestation.
Lehmann (1975) 23 healthy subjects; 8 of thosereporting spontaneous reporteddyspnea with pregnancy
About 2 tests per session. 5 sessionstotal
DLCO was measured at 12, 24, 32, and 36 weeks ofgestation, and 12 weeks post-partum. Women withdyspnea in early pregnancy (12th week gestation) hada 10% decrease in DLCO. Non-dyspneic women did notshow a decrease in DLCO by the 12th week.
Norregaard et al. (1989) 39 healthy subjects; (10 in eachtrimester and 9 post-partum)
2 series of repeated measurements(seated and supine). So 4 tests in totalper session. 5 sessions in total
Lung function and postural changes with pregnancy(first, second, and third trimester), and about 2–4weeks post-partum. DLCO decreased by about 15% bythe third trimester, regardless if the measurement wasdone in the sitting or supine position. No change inDLCO between sitting and supine.
Gazioglu et al. (1970) 24 subjects; 8 healthy, 8 valvular heartdisease, 8 chronic pulmonary disease
At least 2 times per session. 4 sessionstotal
DLCO, DM, Vc were measured at 10, 24, and 36 weeksgestation, and 10 weeks post-partum. In normalsubjects, DLCO and Dm equally decrease by 14% by 36weeks gestation. No change in Vc. In those withemphysema, DLCO and Vc increased by 36 wksgestation with no change in DM. Those withpulmonary sarcoidosis had no change in DLCO, DM, orVc.
Garcia-Rio et al. (1996) 23 subjects; 11 healthy with dyspnea,12 healthy asymptomatic
At least 2 times per session. 4 sessionstotal
DLCO was measured 12, 24, 36 weeks gestation, and 16weeks post-partum. DLCO was not altered duringpregnancy in either the non-dyspneic or dyspneicgroup. There was no difference in DLCO in either group.The increase in dyspnea in pregnant women could bedue to an excessive increase in sensitivity to CO2 orhypoxia.
Boggess et al. (1995) 9 subjects; interstitial and restrictivelung disease
About 2 times per session. 1 sessiontotal
3 women had DLCOs ≤ 40% predicted; 6 women ≥ 44%predicted in the first trimester. All women had vitalcapacity’s ≤84% predicted. There was an associationbetween DLCO and vital capacity (r2 = 0.63). Mean birthweight was (50th percentile) was not differentbetween those with the most severe restrictive lungdisease or the least severe restrictive lung disease.Restrictive lung disease can be tolerated in pregnancy.Exercise intolerance was common and patients mayrequire early supplemental oxygen, DLCO < 50% betterpredicted the need for oxygen supplementation thandid vital capacity < 1.5 L.
All diffusion testing was accomplished with the single-breath DLCO technique. No study reported adverse outcomes on mothers or their babies before or after birth.
Table 1 presents the eight published studies in which DLCO mea-surements were performed in pregnant women using the standardinspiratory CO concentration of 0.3% CO per test (Boggess et al.,1995; Garcia-Rio et al., 1996; Gazioglu et al., 1970; Lalli and Raju,1981; Lehmann, 1975; McAuliffe et al., 2003, 2002; Milne et al.,1977; Norregaard et al., 1989). These tests were performed at rest,and some of these women had lung and/or cardiopulmonary dis-ease (Boggess et al., 1995; Gazioglu et al., 1970; Lalli and Raju,1981). In each study, two to four diffusion tests were performedper session. DLCO decreased by 10–15% in the second and thirdtrimester in both singleton and twin pregnancies compared to the
first trimester and post-partum (Gazioglu et al., 1970; McAuliffe etal., 2002; Norregaard et al., 1989). Greater resistance to diffusionthrough the alveolar membrane (DM) and not a decrease in pul-monary capillary blood volume (Vc) accounted for the decrease inDLCO (Gazioglu et al., 1970). In pregnant women with emphysema,DLCO increases throughout pregnancy, with increased Vc being thelikely cause. In pregnant women with pulmonary sarcoidosis, DLCO,alveolar membrane diffusing capacity for CO (DMCO), and Vc remainunaltered throughout pregnancy (Gazioglu et al., 1970). In the test-ing of 650 pregnant women and their fetuses no adverse eventshave been reported (Table 1).

Author's personal copy
218 G.S. Zavorsky et al. / Respiratory Physiology & Neurobiology 170 (2010) 215–225
The current Occupational Safety and Health Administration(OSHA) permissible exposure limit (PEL) for carbon monoxide forall workers, including pregnant women, is 50 parts per million(ppm) (55 mg/m3) with an 8-h time-weighted average (TWA) con-centration (28,800 s) (National Institute for Occupational Safety andHealth, 2005). Thus, data presented in Table 1 demonstrate thatCO inhalation at concentrations recommended by the ATS/ERS forDLCO testing is within acceptable limits of the U.S. governmentregulations and has been demonstrated to be safe in a number ofpublished reports.
Overall pulmonary CO diffusion can be partitioned into the sub-components of alveolar DM and pulmonary capillary blood volume.The equation for DLCO has been described by Roughton and Forster(1957):
1DLCO
= 1DMCO
+ 1�CO · Vc
where DMCO is the alveolar membrane diffusing capacity for carbonmonoxide, �CO is the specific blood transfer conductance for CO,and Vc is the pulmonary capillary blood volume (Roughton andForster, 1957). To obtain DMCO and Vc, DLCO has been traditionallymeasured at two different levels of alveolar PO2 (PAO2
), e.g., at about100–120 mmHg and about 600 mmHg. For each alveolar PO2 level,1/DLCO is plotted on the y-axis and 1/�CO is plotted on the x-axis. Aline is drawn through the two points and the y-intercept (1/DMCO)and slope (1/Vc) can be solved.
3. Nitric oxide
During the past 15 years, the measurement of diffusion capac-ity of the lung using the transfer gases CO and nitric oxide (NO)together has been developed to obtain DMCO and Vc in a single-breath maneuver. The advantage of adding NO is that its rate ofcombination with hemoglobin is many-fold faster than that forCO (Meyer and Piiper, 1989), and the specific blood transfer con-ductance for NO (�NO) is so great that the red cell resistance toNO (1/�NO) approaches zero (Johnson et al., 1996; Manier et al.,1993, 1991; Phansalkar et al., 2004; Tamhane et al., 2001; Zavorskyand Lands, 2005; Zavorsky et al., 2004). Therefore, DLNO equalsmembrane diffusion capacity for NO (DMNO) and is independentof either pulmonary capillary blood volume or hemoglobin con-centration (van der Lee et al., 2005). The ratio of DLNO to DMCO isabout 2.4 (Phansalkar et al., 2004; Tamhane et al., 2001); there-fore, DMCO = DLNO/2.4. Because exposures of ≤60 ppm NO of a fewseconds to a few minutes do not interfere with various cardiopul-monary parameters or DLCO in adults (Brett et al., 1998; Phansalkaret al., 2004; Sheel et al., 2001; Tamhane et al., 2001; Zavorskyand Murias, 2006), it is useful to use NO along with CO to assessalveolar-membrane function and Vc.
The ability to estimate DMCO and pulmonary capillary blood vol-ume from the one-step simultaneous measurement of DLNO andDLCO has at least four advantages over the traditional two-stepmethod. (1) With the standard method, cardiac output may varybetween measurements of DLCO at different oxygen tensions, whichthen have to be interpolated to obtain DLCO at the two O2 ten-sions at the same cardiac output (Phansalkar et al., 2004). With theDLNO–DLCO method, all measurements are obtained at the samecardiac output and O2 tension, thus no interpolation is necessary.(2) With the traditional method, the CO gas distribution in the lungsmay be different at two different oxygen tensions, but with theDLNO–DLCO method only one inspiration is required which resultsin a similar distribution of NO and CO throughout the lung. (3) Withthe traditional two-step method, there is systematic underestima-tion of Vc and an overestimation of DMCO, as the inspiration attwo different oxygen tensions affects alveolar-capillary membranediffusion (Hsia et al., 1995). The DLNO–DLCO method avoids this
error and improves the accuracy of estimated DMCO and Vc. (4)The DLNO–DLCO method reduces the testing time and number ofmeasurements by half, allowing for easier data collection and halfthe CO exposure. This is a significant advantage for investigation aswell as patient care.
Like CO, NO is produced by the body and can be measured inexhaled breath. The amount of exhaled NO per breath is about2–22 parts per billion in women (Olivieri et al., 2006). As withCO, safety is a concern when using NO in pregnant women. Nitricoxide reacts at a nearly diffusion-limited rate with oxyhemoglobinto produce methemoglobin, and reacts with deoxyhemoglobin toproduce iron nitrosyl hemoglobin (HbNO). Because neither methe-moglobin nor HbNO can bind oxygen, accumulation of either speciescan become a safety concern if it occurs to an extent that itimpairs significantly the oxygen-carrying capacity of the blood.Small accumulations of methemoglobin and HbNO are of mini-mal safety concern, because methemoglobin (Fe3+) is reduced toferrous hemoglobin (Fe2+) by endogenous methemoglobin reduc-tase enzymes, with a methemoglobin half-life of 2–4 h (Blood andPower, 2007), and HbNO is eliminated with a half-life of 15–45 min(Takahashi et al., 1998). Due to the rapid reaction of NO with pul-monary capillary hemoglobin, no free NO reaches the fetus. In fact,the half-life of NO in blood is only milliseconds (Eich et al., 1996) andany free NO diffusing into pulmonary capillary blood is metabolizedbefore reaching the systemic circulation.
In the presence of oxygen, NO converts to nitrogen dioxide(NO2), a potent oxidant that can result in pulmonary edema andlung injury. However, with the addition of 60 ppm NO in the pres-ence of 35% oxygen in an anesthesia bag for 30 s, only about 1 ppmof NO2 will be produced (Fine, 1972; Sokol et al., 1999). Therefore,NO2 production is negligible provided care is taken to prevent themixture of NO with air until immediately prior to inhalation.
4. Evaluating the risk of CO and NO inhalation
In several research studies, [HbCO] has been increased experi-mentally, providing information regarding the toxicity of inhaledCO. One study increased [HbCO] in ten healthy subjects to 15% overa period of 30 min to test a new monitoring device (Barker et al.,2006). No adverse outcomes were reported. Despite a reduction inaerobic capacity (V̇O2 peak), which decreased by 6–9% when [HbCO]was 4–7% (Ekblom and Huot, 1972; Horvath et al., 1975; Ravenet al., 1974), and decreased by 15–24% when [HbCO] was 15–20%(Vogel and Gleser, 1972; Vogel et al., 1972), no adverse outcomeswere reported, and [HbCO] returned to normal within 24 h.
A reduction in arterial oxyhemoglobin concentration [HbO2 ](as from CO exposure) with reduction of arterial oxygen contentinduces systemic compensatory mechanisms. These include anincrease in the fraction of oxygen extracted by the tissues, andincreased blood flow, so that oxygen consumption is maintained(Vogel and Gleser, 1972). During moderate exercise, cardiac out-put increases (Pirnay et al., 1971; Vogel and Gleser, 1972; Vogel etal., 1972), while pH, arterial PCO2 and PO2 , the alveolar-to-arterialPO2 difference and the respiratory exchange ratio are not affected,even when [HbCO] equals 18–20% (Brody and Coburn, 1970; Vogeland Gleser, 1972). Thus, appropriate compensatory mechanismsare in place when [HbCO] is increased, as high as up to levels of 20%[HbCO].
When arterial PO2 is normal (95–100 Torr), as in breathing roomair, the increase in [HbCO] changes the shape of the oxyhemoglobindissociation curve similarly as if there were only a reduction inhemoglobin concentration (Brody and Coburn, 1969). For example,a [HbCO] of 10% reduces the arterial oxygen content by the sameamount as a reduction in hemoglobin concentration by 1.5 g/dl(Brody and Coburn, 1969). Therefore, a female with a hemoglobinconcentration of 10.5 g/dl and 98% arterial oxyhemoglobin satu-

Author's personal copy
G.S. Zavorsky et al. / Respiratory Physiology & Neurobiology 170 (2010) 215–225 219
Table 2Studies and case reports of inhaled NO use in pregnant women.
Study Number and type of pregnant women Concentration and length of timeNO was inhaled
Outcome
Robinson et al. (1999) (case report) 1 subject; 28 weeks gestation todelivery at 32 weeks and post-partum,with h/o HIV, pulmonary hypertension,peripartum cardiomyopathy
5–20 ppm, 4 weeks continuousinhaled NO with episodicmonitoring of methemoglobinlevels.
Inhaled NO reduced pulmonary arterypressure and right ventricular pressure,prolonged continuous inhaled NOtherapy may be an effective therapy inthe management of pulmonaryhypertension during pregnancy.
Lust et al. (1999) (case report) 1 subject; delivery and post-partum,Eisenmenger’s syndrome
Per nasal cannula during delivery,after delivery 10 ppm, ICU NO wasdelivered via transtrachealcatheter. 10 h.
Continuous inhaled NO reduced initialpulmonary arterial pressure andimproved oxygenation. Inhaled NO maybe used to improve oxygenation andantithrombotic effects of NO may limitthe increase in pulmonary arterialpressure expected with increasedcardiac output throughout labor amongpts with pulmonary vascular disease.
Goodwin et al. (1999) (case report) 1 subject; 36 weeks gestation withEisenmenger’s syndrome
20 ppm during labor. 80 ppmdecreased to 60 ppm by 3rd daypost-partum. Continuous duringsecond stage of labor (45 min) andpost-partum 3rd day, discontinuedafter 48 h.
Inhaled NO can be used to correct thehypoxemia of Eisenmenger’s syndrome.Administration of NO led to improvedoxygenation and lowered pulmonaryarterial pressures. Baby survived,woman died.
Decoene et al. (2001) (case report) 1 subject, unexpected pulmonaryhypertension that had an emergencyC-section
5 ppm 24 h continuous duringlabor, delivery and post-partum.
Administration of inhaled NO enabledoptimal control of pulmonaryhypertension. Use of inhaled NO canimprove the management of urgentC-section in women with unexpectedpulmonary hypertension.
Lam et al. (2001) (case report) 1 subject, primigravida with primarypulmonary hypertension
20 ppm, decreased to 10 ppm 8.5 hafter delivery, NO deliveredthrough an endotracheal tube (93 htotal).
NO can be used to successfully treatprimary pulmonary hypertension inpregnancy.
Bonnin et al. (2005) 15 subjects with severe pulmonaryhypertension, 3 were administered NO
50 ppm. In the 3 out of 15 subjects who wereadministered NO, 2 babies survivedafter delivery. The baby that died wasdelivered at 21 weeks gestation. Thebabies that survived at 32–34 weeksgestation. Maternal mortality was foundto be 36% with pulmonary arterialhypertension. Pregnancy should bediscouraged in patients with severepulmonary hypertension.
McMillan et al. (2002) 3 with pulmonary hypertensionsecondary to systemic lupuserythematosis (SLE) andanti-phospholipid syndrome
40 ppm during C-section (1st case).Second case, the amount of NO wasnot specified. NO inhalation did notoccur in third case.
1st case patient died post-C-section. 2ndcase patient died of severe heart failureafter C-section. 3rd case more mildPulmonary hypertension that wasdiagnosed earlier in pregnancy and hadmultidisciplinary management ofpregnancy which is necessary forpregnant women with pulmonaryhypertension.
Fig. 1. The predicted maternal and fetal [HbCO] when a mother breaths 50 ppm CO for 16 h, followed by an 8 h period in which no CO was inspired. The level of CO exposureis equivalent to smoking about 1–1.5 packs of cigarettes per day, followed by an 8 h sleep period. Figure modified by Longo (1977) based on the mathematical model by Hillet al. (1977).

Author's personal copy
220 G.S. Zavorsky et al. / Respiratory Physiology & Neurobiology 170 (2010) 215–225
ration [HbO2 ] would have the same arterial oxygen content as afemale with a hemoglobin concentration of 12 g/dl and an arterial[HbO2 ] of 88% (Brody and Coburn, 1969).
The use of inhaled NO gas has been routine in the treatment ofpulmonary hypertension in both newborn and adult patients formore than 10 years, providing useful information in evaluating thesafety of NO for diffusion testing in pregnant women. As detailed inTable 2, a number of reports have described the use of inhaled NO inpregnant women suffering from pulmonary hypertension (Bonninet al., 2005; Decoene et al., 2001; Goodwin et al., 1999; Lam et al.,2001; Lust et al., 1999; McMillan et al., 2002; Robinson et al., 1999).In these reports, NO was administered at delivery rates of 5–80 ppmfor minutes to hours, with no reported elevations of maternalmethemoglobin levels. In term and pre-term infants, inhaled NOhas been given at concentrations as high as 20 ppm and for up toa week at a time (Table 3). The administration of 1–20 ppm NO toinfants for days at a time was well-tolerated with the only notice-able effect being increased concentrations of methemoglobin. Evenso, the methemoglobin concentrations were not high enough towarrant discontinuation of inhaled NO treatment. The produc-tion of methemoglobin is a result of the direct reaction betweenNO and oxyhemoglobin in the lungs. Because NO in the blood ismetabolized too rapidly for it to travel from the maternal lung tothe fetal circulation, there should be no concern that inhaling NOwill result in fetal methemoglobinemia. Large multi-center studieswith thousands of enrolled patients have demonstrated no adverseeffects, including methemoglobinemia, of inhaled NO administeredfor days or even weeks at 20 ppm (Kinsella and Abman, 2007).
In fact, studies demonstrate that inhaled NO in pre-term infantsdecreases the risk of cognitive impairment and abnormal neu-rodevelopmental outcomes (i.e. cerebral palsy, bilateral blindness,bilateral hearing loss, or development delay) 2 years later by abouthalf, compared to a placebo group (Mestan et al., 2005). Other stud-ies have revealed no adverse NO attributable neurodevelopmentaloutcomes by 2 years of age (Hintz et al., 2007; Konduri et al., 2007)in NO-exposed infants.
To adequately assess the risks of CO and NO inhalation, it is use-ful to draw comparisons with exposure to these gases as a result ofsmoking tobacco. Each cigarette produces about 4% CO by volume(40,000 ppm), resulting in an average alveolar CO concentrationof about 450 ppm (Osborne et al., 1956). The NO concentration incigarette smoke is as much as 500 ppm (Eiserich et al., 1994; Pryorand Stone, 1993). Therefore, cigarette smoke contains many-foldhigher concentrations of CO and NO than employed in a diffusingcapacity test. Each cigarette smoked may increase the [HbCO] byabout 1% (Russell et al., 1973a,b). One pack per day smokers havean average [HbCO] of 5–6% (Hampson and Scott, 2006; Light et al.,2007; Reddy et al., 2007; Russell et al., 1973a), and for some 10%of smokers [HbCO] are ≥7.5% (Radford and Drizd, 1982). For thosethat regularly smoke about 20 cigarettes during the course of a day,mean [HbCO] levels are 8.2%, with some subjects as high as 14.2%and a day-to-day variation of 0.94% (Smith et al., 1998). Therefore,smokers have high levels of [HbCO] that persist day-to-day.
Maternal HbCO levels are 4–5% in pregnant mothers who smokeregularly (Cole et al., 1972; Davies et al., 1979) and [HbCO] is lin-early related to the number of cigarettes smoked per day (Cole et
Fig. 2. Changes in maternal and fetal [HbCO] during and after a 24 h exposure to 68 ppm CO and a 4 h exposure to 300 ppm CO. If the maternal value of 10% HbCO wereobtained at equilibrium (point A), the fetal [HbCO] would be equal to about 11%. If the sample was taken at point B during the washout phase, the fetal [HbCO] would be about14%. However, if the blood sample was taken during the uptake phase (point C), the fetal [HbCO] would be 2%. Not only is it impossible to predict fetal [HbCO] on the basisof a single maternal blood sample, but the length of time necessary to reduce the fetal [HbCO] depends on whether the concentration has already peaked or is still rising. Inthe case of lung diffusing testing, which could require up to about 3 min of 3000 ppm CO inhalation, the maternal [HbCO] may increase to 5%, but the fetal HbCO would hardlyincrease. This is typified by the enhanced “Detail” on the right panel in figure. Figures reproduced from Longo (1977).

Author's personal copy
G.S. Zavorsky et al. / Respiratory Physiology & Neurobiology 170 (2010) 215–225 221
Table 3Original studies of inhaled NO use in pre-term infants.
Study Number and gestational age of infants Concentration and length of timeNO was inhaled
Outcome
Chock et al. (2009) Infants with a gestational age of 27weeks with a history of prematurerupture of membranes 6 infantsreceived NO, 6 infants received placebo
5–10 ppm NO, duration of 30 minto 14 days.
Arterial PO2 increased by 40 mmHg in the NOgroup versus a decrease of 11 mmHg in theplacebo group. The mortality rate andincidence of bronchopulmonary dysplasiawere not different between the two groups.
Hintz et al. (2007) Infants < 34 weeks of age withrespiratory failure. 198 subjectsreceived NO and 200 received placebo
5–10 ppm NO for 76 + 73 h to 14days.
Inhaled NO did not reduce mortality orimprove neurodevelopment outcomes by18–22 months of age. However, inhaled NO didnot worsen neurodevelopmental outcomeseither.
Delsing et al. (2007) 4 sets of twins with twin-to-twintransfusion syndrome who had severepersistent pulmonary hypertension ofthe newborn
20 ppm for 2 days given to 4 sets oftwins (8 neonates).
All twin-to-twin transfusion syndrome infantswith severe persistent pulmonaryhypertension reacted promptly to inhaled NO.
Mestan et al. (2005) 70 infants at 27 weeks gestational agewere given inhaled NO. 80 infants weregiven placebo
10 ppm day 1. 5 ppm for the next 6days.
This was a follow-up study to examineneurodevelopmental outcomes of children at 2years of age who were given inhaled NO atbirth. Patients treated with inhaled NO hadapproximately half the risk of abnormalneurodevelopment compared to placebo. Therewas a 47% decrease in the risk of cognitiveimpairment compared to placebo group.
Konduri et al. (2004) Neonates born at ≥34 weeks gestationwith hypoxic respiratory failure. 150pre-term infants given NO and 149control subjects
5 ppm of NO which was increasedto 20 ppm for 57 ± 48 h.
Inhaled NO improves oxygenation but does notreduce the incidence of the use ofextracorporeal membrane oxygenation ormortality when initiated at an oxygen index of15–25 compared with > 25 in term andnear-term neonates with respiratory failure.
Konduri et al. (2007) 299 neonates born at ≥34 weeksgestation were randomized to receiveNO or placebo. A total 150 neonateswere given NO. 266 survived to age18–24 months
5 ppm of NO which was increasedto 20 ppm for 57 ± 48 h.
This was the follow-up study to the onepublished in 2004 (Konduri et al., 2004). Earlyinhaled NO therapy for hypoxic respiratoryfailure in term and near term infants is notassociated with an increase inneurodevelopmental impairment or hearingloss at 18–14 months postnatal.
Schreiber et al. (2003) 207 newborns, aged 34 weeks or lesswho were mechanically ventilatedwere randomized into NO or placebogroup. A total of 105 neonates receivedNO
Initial dose 10 ppm for 1 day, then5 ppm on days 2–6 (7 days total).
Significant reduction in death orbronchopulmonary dysplasia at 36 weeks ofage with inhaled NO compared to controls. Theuse of nitric oxide in premature infants withrespiratory distress syndrome decreases theincidence of chronic disease and death.
Kinsella and Abman (2007) 80 pre-term neonates, with gestationalage 34 weeks or less, 7 days age or less,and severe hypoxemia who were onmechanical ventilation
5 ppm or placebo, 7 days thenweaned. (40 neonates actuallyreceived NO).
Even though oxygenation improved 1 h afterinhaled NO, there was only a trend towarddecrease in bronchopulmonary dysplasia andno differences in rates of severe intracranialhemorrhage.
Kinsella et al. (2006) 793 newborns ≤34 weeks gestationwere randomly assigned to receive NOor placebo. A total of 395 neonatesreceived NO
Randomly assigned to receive5 ppm NO or placebo for 21 days.
No significant difference in the incidence ofdeath or bronchopulmonary dysplasia betweenpatients receiving NO or not. For infants with abirth weight of 1000–1250 g, inhaled NOreduced the incidence of bronchopulmonarydyplasia and overall brain injury. Inhaled NOdid not increase incidence of pulmonaryhemorrhage or other adverse events.
Clark et al. (2000) 248 neonates with pulmonaryhypertension enrolled ≥34 weeksgestation. Babies were 4 days old. 126randomly assigned to NO group, 122assigned to control group.
20 ppm for 24 h, then 5 ppm for96 h.
30-day mortality rate was the same in bothgroups (8%). Chronic lung disease developedless often in neonates treated with NO. InhaledNO reduced the extent to which extracorporealmembrane oxygenation is needed in neonateswith hypoxemic respiratory failure andpulmonary hypertension.
Van Meurs et al. (1997) 11 neonates, aged ≤ 34 weeksgestation with respiratory failure 4 h ormore after birth.
Four concentrations of inhaled NOwere used: 1, 5, 10, 20 ppm, andplacebo for 15 min.
No significant elevations of methemoglobinwere found with NO inhalation (0.6% beforeinhalation to 0.8% after 15 min of inhalation).NO inhalation improved the arterial PO2 toalveolar PO2 ratio in those with respiratoryfailure.

Author's personal copy
222 G.S. Zavorsky et al. / Respiratory Physiology & Neurobiology 170 (2010) 215–225
Table 4Recommendations for CO and NO inhalation at rest and during exercise in pregnant women and non-pregnant individuals per testing session.
Condition Recommended CO inhalation exposure time and dosage resulting in a recommendedacceptable [HbCO] concentration
Recommended NO inhalationexposure time and dosage
1. Men and non-pregnant women who are asymptomaticRest (AHA Class A1–3) [HbCO] = 10% when 0.3% CO is inhaled for ≤6 min after which breathing room air ensuesa 80 ppm over 6 minExercise (AHA Class A1–3) [HbCO] = 5% when 0.3% CO is inhaled for ≤3 min after which breathing room air ensues 80 ppm over 3 min
2. Men and non-pregnant women with cardiovascular diseaseRest (AHA Class B–D) [HbCO] = 5% when 0.3% CO is inhaled for ≤3 min after which breathing room air ensues 80 ppm over 3 minExercise (AHA class B and C) [HbCO] = 5% when 0.3% CO is inhaled for ≤3 min after which breathing room air ensues 80 ppm over 3 min
3. Asymptomatic pregnant womenb
Rest (AHA Class A1–3) [HbCO] = 5% when 0.3% CO is inhaled for ≤3 min after which breathing room air ensuesc 80 ppm over 3 minExercise (AHA Class A1–3) [HbCO] = 5% when 0.3% CO is inhaled for ≤3 min after which breathing room air ensuesc 80 ppm over 3 min
4. Pregnant women with cardiovascular diseaseb
Rest (AHA class B–D)* [HbCO] = 4% when 0.3% CO is inhaled for ≤3 min after which breathing room air ensuesc 80 ppm over 3 minExercise (AHA Class B and C) [HbCO] = 4% when 0.3% CO is inhaled for ≤3 min after which breathing room air ensuesc 80 ppm over 3 min
The American Heart Association (AHA) Risk Stratification Criteria (Fletcher et al., 2001; Fuster et al., 1996)Class A. Apparently Healthy
1. Children, adolescents, men < 45 years of age, and women < 55 years of age who have no symptoms or known presence of heart disease or major cardiovascular disease risk (CVD)factors.
2. Men ≥ 45 years of age or women ≥ 55 years who have no symptoms or known presence of heart disease with less than two major CVD risk factors.3. Men ≥ 45 years of age or women ≥ 55 years who have no symptoms or known presence of heart disease with more than two major CVD risk factors.
Class B. Presence of known, stable cardiovascular disease with low risk for complications. Includes individuals with any of the following diagnoses:
1. Coronary artery disease who condition is stable and who have the clinical characteristics described below.2. Valvular heart disease, excluding severe valvular stenosis or regurgitation.3. Congenital heart disease.4. Cardiomyopathy, ejection fraction ≤ 30%.5. Exercise test abnormalities that do not meet the criteria for Class C.
Clinical characteristics
a. New York Heart Association Class 1 or 2.b. Exercise capacity ≤ 6 METS.c. No evidence of congestive heart failure.d. No evidence of myocardial ischemia or angina at rest or on the exercise test at or below 6 METS.e. Appropriate rise in systolic blood pressure during exercise.f. Absence of sustained or non-sustained ventricular tachycardia at rest or with exercise.
Class C. Those at moderate to high risk for cardiac complications during exercise and/or unable to self-regulate activity or understand recommended activity level. Includes individualswith any of the following diagnoses:
1. Cardiovascular disease with the clinical characteristics outlined below.2. Valvular heart disease, excluding severe valvular stenosis or regurgitation.3. Congenital heart disease.4. Cardiomyopathy, ejection fraction ≤ 30%.5. Complex ventricular arrhythmias not well-controlled.
Clinical characteristics
a. New York Heart Association Class 3 or 4.b. Exercise capacity < 6 METS.c. Angina of ischemia ST depression at workload < 6 METS.d. Fall in systolic blood pressure below resting during exercise.e. Non-sustained ventricular tachycardia at rest or with exercise.f. Previous episode of primary cardiac arrest.g. A medical problem that the physician may be life threatening.
Class D. Unstable cardiovascular disease with activity restriction. Includes individuals with:
1. Unstable angina.2. Severe and symptomatic valvular stenosis or regurgitation.3. Congenital heart disease.4. Heart failure that is not compensated.5. Uncontrolled arrhythmias.6. Other medical condition that could be aggravated by exercise. No physical exercise is recommended.
CVD risk factors are:
1. Age: Men ≥ 45 years of age; women ≥ 55 years of age.2. Family history: Myocardial infarction, coronary revascularization, or sudden death before age 55 years in father or other first degree male relative, or before 65 years of age in mother
or other female first degree relative.3. Cigarette smoking: Current smoker or those who have quit within the past 6 months.4. Sedentary lifestyle: Not participating in a least 30 min of moderate intensity (40–60% of oxygen uptake reserve) on at least 3 days per week for at least 3 months.5. Obesity: Body mass index ≥ 30 kg/m2 or waist girth > 102 cm (40 in.) for men and >88 cm (35 in.) for women.6. Hypertension: Systolic blood pressure ≥ 140 mmHg and/or diastolic blood pressure ≥90 mmHg, confirmed by measurements on at least two separate occasions, or on anti-hypertensive
medication.7. Dylipidemia: Low density lipoprotein cholesterol ≥ 130 mg/dl (3.37 mmol/l) or high density lipoprotein cholesterol < 40 mg/dl (1.04 mmol/l) or on lipid lowering medication. If total
serum cholesterol is all that is available use ≥ 200 mg/dl (5.18 mmol/l).

Author's personal copy
G.S. Zavorsky et al. / Respiratory Physiology & Neurobiology 170 (2010) 215–225 223
Table 4 (Continued )
8. Prediabetes: Impaired fasting glucose ≥ 100 mg/dl (5.50 mmol/l) but <126 mg/dl (6.93 mmol/l) or impaired glucose tolerance from a 2 h oral glucose tolerancetest ≥ 140 mg/dl (7.70 mmol/l) confirmed by measurements on at least two separate occasions.
CVD risk factors are obtained from the American College of Sports Medicine Handbook (ACSM, 2009).a If neurophysiological skills are being tested in a research study (i.e. visuomotor coordination, visuospacial functioning, short and long term semantic memory) (Amitai et al., 1998),
HbCO levels are recommended not to exceed 5%.c Inhalation of 100% oxygen to reduce the half-life of CO to 74 min (Weaver et al., 2000) is not recommended because of the potential toxic effects of oxygen on the mother and fetus.
Tests of diffusing capacity (with 0.3% CO inhalation) increase HbCO by about 0.6–0.8% per 10 s breath-hold maneuver (Forster et al., 1954; Frey et al., 1987) or 15 s rebreathing maneuver.Therefore, one can use this as a template for estimating the [HbCO] when it is not measured (i.e. one diffusion test increases HbCO by 0.6–0.8%). Four rebreathing diffusion tests of 15 seach or 4 single-breath diffusion tests of 10 s each should be separated by 4 min between each test. The total CO exposure time in this example is therefore 40–60 s and is estimated toincrease HbCO by 2.4–3.2% (0.6% × 4 tests, or 0.8% × 4 tests).
b A maximum of 3 testing sessions per trimester is recommended during pregnancy in which maternal HbCO can increase up to 5% per session when 0.3% CO exposure is ≤ 3 min.Therefore, a maximum of 9 sessions in total throughout pregnancy are recommended, and sessions should be separated by 48 h. If only DLNO is measured during pregnancy, then amaximum of 5 testing sessions per trimester is thought permissible when ≤80 ppm NO is inhaled for ≤3 min per session (15 sessions in total throughout pregnancy). If testing pregnantsmokers, in which maternal levels are already 5%, and a measurement of diffusing capacity is needed, then CO exposure that is ≤1 min at a concentration of 0.3% (3000 ppm) can beallowed.The repeatability for DLNO (within session variability) is 17 ml/min/mmHg in non-pregnant women and men (Zavorsky and Murias, 2006). The reproducibility of DLNO (week to weekvariability) from these same subjects is 20 ml/min/mmHg (Murias and Zavorsky, 2007). Thus, we not expect the variability of DLNO to be different during pregnancy since DLNO isminimally affected by hemoglobin changes (van der Lee et al., 2005). Furthermore, as changes in hemoglobin concentration only vary by 1 g/dl throughout pregnancy or over a 28-daymenstrual cycle (McAuliffe et al., 2002; Vellar, 1974), the small 10–15% reduction in DLCO in the third trimester of pregnancy has little to do with maternal hemoglobin variability. Therepeatability and reproducibility of DLCO is 3 and 5 ml/min/mmHg, respectively in a non-pregnant state (Murias and Zavorsky, 2007; Zavorsky and Murias, 2006) and is not expected tovary during pregnancy.
al., 1972). It is not possible, however to estimate fetal [HbCO] onthe basis of a single maternal blood sample without knowledge ofexposure pattern. At steady state, fetal [HbCO] is higher than mater-nal due to a greater affinity of fetal hemoglobin for the CO andbecause average fetal oxygen saturations are less than maternal(Longo, 1977). The elimination half-life of CO from the fetal circula-tion is longer than from maternal circulation (Hill et al., 1977; Longoand Hill, 1977). When maternal and fetal [HbCO] levels are equili-brated, the mean fetal to maternal ratio for HbCO is 1.84 giving therelation: [Fetal [HbCO]% = 1.27 × maternal [HbCO]% + 0.76] (Cole etal., 1972). Fig. 1 shows the predicted maternal and fetal HbCO levelsequivalent to smoking 1–1.5 packs of cigarettes per day, followedby an 8-h sleep period. Note that peak fetal HbCO levels are higherthan maternal HbCO, and that, fetal HbCO lags substantially behindmaternal HbCO levels until 12 h into the day (Longo, 1977). Mathe-matical models predict a 4-h exposure to 300 ppm CO will producepeak maternal HbCO levels of about 25% after 4 h, while fetal [HbCO]will be only 12% (Longo, 1977) (Fig. 2). Thereafter maternal [HbCO]is predicted to fall, while fetal [HbCO] peaks at 15% (Longo, 1977)(Fig. 2). From this background it is concluded that a diffusing capac-ity test that lasts 10–15 s per test (with exposure to 3000 ppm CO)would not appreciably increase fetal [HbCO] levels, and maternallevels of [HbCO] would increase by about 0.7% per test (Forsteret al., 1954; Frey et al., 1987). Ten tests (100–150 s of total COexposure) would increase maternal [HbCO] to about 7%. Even withmore prolonged maternal exposures lasting up to 2 min fetal [HbCO]is anticipated to increase only slightly from pre-exposure levelsreaching a peak about 2 h after testing. It is concluded that rou-tine diffusing capacity testing at rest and during exercise would notincrease fetal [HbCO] appreciably or to a level that would adverselyaffect fetal physiology.
Given the NO and CO content in cigarettes, it may be useful toextrapolate available data regarding the effects of smoking on preg-nancy outcomes to evaluate the risks of inhaling NO and CO gasfor lung diffusing capacity testing in pregnancy. Pregnant smokershave a late fetal plus neonatal death rate that is higher by 10 per1000 births (to a 4.2% absolute death rate) compared to pregnantnon-smokers (3.2% absolute death rate) (Butler et al., 1972). Suchsmoking throughout pregnancy may be compared to a testing ses-sion in which maternal [HbCO] increases to 5% and persists for about4 h, or 0.12% of the last 20 weeks of pregnancy (4/3360 × 100 = 0.12%per testing session). Assuming a linear time dependency for adverseeffects, this would increase the death rate by about 0.0012%. TheCenters for Disease Control (CDC) death rate for accidental deathsis 0.04% and the death rate of all causes (accidents, homicides, sui-cides, diseases, cancer, infection, etc.) is about 0.8% (Kung et al.,
2008). Thus, by this comparison, the total CDC death rate is 667times more than the late fetal and neonatal death rate per testingsession in which pregnant mothers [HbCO] increase to 5%. This jus-tifies an IRB classification of the risk associated with DLCO testingin pregnant women and the resultant effects on their fetuses as“minimal risk.”
5. Conclusions
Based on the evidence provided in this review, we submit thatCO and NO inhalation for testing of pulmonary diffusing capac-ity is a safe procedure that may be justified by improved medicalcare. Given that the elimination half-life of [HbCO] in maternalblood is about 3.8–4 h (Lawther and Commins, 1970; Selvakumaret al., 1993), or 74 min when given 100% oxygen (Weaver et al.,2000), the following recommendations are provided in Table 4.We suggest different acceptable concentrations for pregnant andnon-pregnant women. When CO exposure in a pregnant woman is≤3 min at a concentration of 0.3% (3000 ppm), fetal [HbCO] will notrise appreciably post-testing. A maximum of 3 testing sessions pertrimester is recommended during pregnancy when DLCO is mea-sured (9 sessions in total throughout pregnancy, with a minimum of48 h between each session). Only if DLNO is measured, then a max-imum of 5 testing sessions per trimester is recommended duringpregnancy (15 sessions in total, with a minimum of 48 h betweeneach session). If testing pregnant smokers whose maternal [HbCO]is already at about 5%, then CO exposure that is ≤1 min at a con-centration of 0.3% (3000 ppm) can be allowed. Even though eachpulmonary diffusion test of 10–15 s in length is separated by 4 minof rest breathing room air, the exposure time within each test-ing session is suggested to be cumulative over a typical 30–45 minsession. Therefore, five 15 s DLCO tests (rebreathing), or four 10 ssingle-breath DLCO tests equates to 50–75 s of total CO exposuretime resulting in an increase of [HbCO] by 3–4%, since each DLCOtest increases [HbCO] by 0.6–0.8% per test.
Conflicts of interest
No author has any actual or potential conflicts of interest per-taining to this manuscript.
References
ACSM, 2009. ACSM’s Guidelines for Exercise Testing and Prescription, 8th ed. Lip-pincott Williams & Wilkins, Baltimore.

Author's personal copy
224 G.S. Zavorsky et al. / Respiratory Physiology & Neurobiology 170 (2010) 215–225
Alaily, A.B., Carrol, K.B., 1978. Pulmonary ventilation in pregnancy. Br. J. Obstet.Gynaecol. 85, 518–524.
Amitai, Y., Zlotogorski, Z., Golan-Katzav, V., Wexler, A., Gross, D., 1998. Neuropsy-chological impairment from acute low-level exposure to carbon monoxide. Arch.Neurol. 55, 845–848.
Baldwin, G.R., Moorthi, D.S., Whelton, J.A., MacDonnell, K.F., 1977. New lung func-tions and pregnancy. Am. J. Obstet. Gynecol. 127, 235–239.
Barker, S.J., Curry, J., Redford, D., Morgan, S., 2006. Measurement of carboxyhe-moglobin and methemoglobin by pulse oximetry: a human volunteer study.Anesthesiology 105, 892–897.
Blood, A.B., Power, G.G., 2007. In vitro and in vivo kinetic handling of nitrite inblood: effects of varying hemoglobin oxygen saturation. Am. J. Physiol. HeartCirc. Physiol. 293, H1508–H1517.
Boggess, K.A., Easterling, T.R., Raghu, G., 1995. Management and outcome of preg-nant women with interstitial and restrictive lung disease. Am. J. Obstet. Gynecol.173, 1007–1014.
Bonay, M., Bancal, C., de Zuttere, D., Arnoult, F., Saumon, G., Camus, F., 2004. Nor-mal pulmonary capillary blood volume in patients with chronic infiltrative lungdisease and high pulmonary artery pressure. Chest 126, 1460–1466.
Bonnin, M., Mercier, F.J., Sitbon, O., Roger-Christoph, S., Jais, X., Humbert, M., Audib-ert, F., Frydman, R., Simonneau, G., Benhamou, D., 2005. Severe pulmonaryhypertension during pregnancy: mode of delivery and anesthetic manage-ment of 15 consecutive cases. Anesthesiology 102, 1133–1137, discussion1135A–1136A.
Brett, S.J., Chambers, J., Bush, A., Rosenthal, M., Evans, T.W., 1998. Pulmonaryresponse of normal human subjects to inhaled vasodilator substances. Clin. Sci.(Lond.) 95, 621–627.
Brody, J.S., Coburn, R.F., 1969. Carbon monoxide-induced arterial hypoxemia. Sci-ence 164, 1297–1298.
Brody, J.S., Coburn, R.F., 1970. Effects of elevated carboxyhemoglobin on gasexchange in the lung. Ann. N. Y. Acad. Sci. 174, 255–260.
Butler, N.R., Goldstein, H., Ross, E.M., 1972. Cigarette smoking in pregnancy: itsinfluence on birth weight and perinatal mortality. Br. Med. J. 2, 127–130.
Chance, W.W., Rhee, C., Yilmaz, C., Dane, D.M., Pruneda, M.L., Raskin, P., Hsia, C.C.,2008. Diminished alveolar microvascular reserves in type-2 diabetes mellitusreflect systemic microangiopathy. Diabetes Care 31, 1596–1601.
Chock, V.Y., Van Meurs, K.P., Hintz, S.R., Ehrenkranz, R.A., Lemons, J.A., Kendrick,D.E., Stevenson, D.K., 2009. Inhaled nitric oxide for preterm premature ruptureof membranes, oligohydramnios, and pulmonary hypoplasia. Am. J. Perinatol.26, 317–322.
Clark, R.H., Kueser, T.J., Walker, M.W., Southgate, W.M., Huckaby, J.L., Perez, J.A., Roy,B.J., Keszler, M., Kinsella, J.P., 2000. Low-dose nitric oxide therapy for persistentpulmonary hypertension of the newborn. Clinical Inhaled Nitric Oxide ResearchGroup. N. Engl. J. Med. 342, 469–474.
Coburn, R.F., Blakemore, W.S., Forster, R.E., 1963. Endogenous carbon monoxideproduction in man. J. Clin. Invest. 42, 1172–1178.
Coburn, R.F., Forster, R.E., Kane, P.B., 1965. Considerations of the physiological vari-ables that determine the blood carboxyhemoglobin concentration in man. J. Clin.Invest. 44, 1899–1910.
Cole, P.V., Hawkins, L.H., Roberts, D., 1972. Smoking during pregnancy and its effectson the fetus. J. Obstet. Gynaecol. Br. Commonw. 79, 782–787.
Davies, J.M., Latto, I.P., Jones, J.G., Veale, A., Wardrop, C.A., 1979. Effects of stoppingsmoking for 48 hours on oxygen availability from the blood: a study on pregnantwomen. Br. Med. J. 2, 355–356.
Decoene, C., Bourzoufi, K., Moreau, D., Narducci, F., Crepin, F., Krivosic-Horber, R.,2001. Use of inhaled nitric oxide for emergency Cesarean section in a womanwith unexpected primary pulmonary hypertension. Can. J. Anaesth. 48, 584–587.
Delivoria-Papadopoulos, M., Coburn, R.F., Forster, R.E., 1974. Cyclic variation of rateof carbon monoxide production in normal women. J. Appl. Physiol. 36, 49–51.
Delsing, B., Lopriore, E., Blom, N., Te Pas, A.B., Vandenbussche, F.P., Walther, F.J.,2007. Risk of persistent pulmonary hypertension of the neonate in twin-to-twintransfusion syndrome. Neonatology 92, 134–138.
Dressel, H., Filser, L., Fischer, R., Marten, K., Muller-Lisse, U., de la Motte, D., Nowak,D., Huber, R.M., Jorres, R.A., 2009. Lung diffusing capacity for nitric oxide andcarbon monoxide in relation to morphological changes as assessed by computedtomography in patients with cystic fibrosis. BMC Pulm. Med. 9, 30.
Eich, R.F., Li, T., Lemon, D.D., Doherty, D.H., Curry, S.R., Aitken, J.F., Mathews, A.J.,Johnson, K.A., Smith, R.D., Phillips Jr., G.N., Olson, J.S., 1996. Mechanism of NO-induced oxidation of myoglobin and hemoglobin. Biochemistry 35, 6976–6983.
Eiserich, J.P., Vossen, V., O’Neill, C.A., Halliwell, B., Cross, C.E., van der Vliet, A., 1994.Molecular mechanisms of damage by excess nitrogen oxides: nitration of tyro-sine by gas-phase cigarette smoke. FEBS Lett. 353, 53–56.
Ekblom, B., Huot, R., 1972. Response to submaximal and maximal exercise at differ-ent levels of carboxyhemoglobin. Acta Physiol. Scand. 86, 474–482.
Eng, M., Butler, J., Bonica, J.J., 1975. Respiratory function in pregnant obese women.Am. J. Obstet. Gynecol. 123, 241–245.
Fine, D.H., 1972. Critical evaluation of Saltzman technique for NOx analysis in the0–100 ppm range. Environ. Sci. Technol. 6, 348–350.
Fletcher, G.F., Balady, G.J., Amsterdam, E.A., Chaitman, B., Eckel, R., Fleg, J., Froelicher,V.F., Leon, A.S., Pina, I.L., Rodney, R., Simons-Morton, D.A., Williams, M.A., Baz-zarre, T., 2001. Exercise standards for testing and training: a statement forhealthcare professionals from the American Heart Association. Circulation 104,1694–1740.
Forster, R.E., 1957. Exchange of gases between alveolar air and pulmonary capillaryblood: pulmonary diffusing capacity. Physiol. Rev. 37, 391–452.
Forster, R.E., Fowler, W.S., Bates, D.V., Van Lingen, B., 1954. The absorption of carbonmonoxide by the lungs during breath-holding. J. Clin. Invest. 33, 1135–1145.
Frey, T.M., Crapo, R.O., Jensen, R.L., Elliott, C.G., 1987. Diurnal variation of the diffus-ing capacity of the lung: is it real? Am. Rev. Respir. Dis. 136, 1381–1384.
Fuster, V., Gotto, A.M., Libby, P., Loscalzo, J., McGill, H.C., 1996. 27th Bethesda Con-ference: matching the intensity of risk factor management with the hazard forcoronary disease events. Task Force 1. Pathogenesis of coronary disease: thebiologic role of risk factors. J. Am. Coll. Cardiol. 27, 964–976.
Garcia-Rio, F., Pino, J.M., Gomez, L., Alvarez-Sala, R., Villasante, C., Villamor, J., 1996.Regulation of breathing and perception of dyspnea in healthy pregnant women.Chest 110, 446–453.
Gazioglu, K., Kaltreider, N.L., Rosen, M., Yu, P.N., 1970. Pulmonary function duringpregnancy in normal women and in patients with cardiopulmonary disease.Thorax 25, 445–450.
Getahun, D., Ananth, C.V., Peltier, M.R., Smulian, J.C., Vintzileos, A.M., 2006. Acute andchronic respiratory diseases in pregnancy: associations with placental abrup-tion. Am. J. Obstet. Gynecol. 195, 1180–1184.
Getahun, D., Ananth, C.V., Oyelese, Y., Peltier, M.R., Smulian, J.C., Vintzileos, A.M.,2007. Acute and chronic respiratory diseases in pregnancy: associations withspontaneous premature rupture of membranes. J. Matern. Fetal Neonatal Med.20, 669–675.
Gonzales, G.F., Steenland, K., Tapia, V., 2009. Maternal hemoglobin level and fetaloutcome at low and high altitudes. Am. J. Physiol. Regul. Integr. Comp. Physiol.297, R1477–R1485.
Goodwin, T.M., Gherman, R.B., Hameed, A., Elkayam, U., 1999. Favorable response ofEisenmenger syndrome to inhaled nitric oxide during pregnancy. Am. J. Obstet.Gynecol. 180, 64–67.
Gulati, M., Pandey, D.K., Arnsdorf, M.F., Lauderdale, D.S., Thisted, R.A., Wicklund, R.H.,Al-Hani, A.J., Black, H.R., 2003. Exercise capacity and the risk of death in women:the St James Women Take Heart Project. Circulation 108, 1554–1559.
Hampson, N.B., Scott, K.L., 2006. Use of a noninvasive pulse CO-oximeter to measureblood carboxyhemoglobin levels in bingo players. Respir. Care 51, 758–760.
Hill, E.P., Hill, J.R., Power, G.G., Longo, L.D., 1977. Carbon monoxide exchangesbetween the human fetus and mother: a mathematical model. Am. J. Physiol.232, H311–H323.
Hintz, S.R., Van Meurs, K.P., Perritt, R., Poole, W.K., Das, A., Stevenson, D.K.,Ehrenkranz, R.A., Lemons, J.A., Vohr, B.R., Heyne, R., Childers, D.O., Peralta-Carcelen, M., Dusick, A., Johnson, Y.R., Morris, B., Dillard, R., Vaucher, Y., Steichen,J., Adams-Chapman, I., Konduri, G., Myers, G.J., de Ungria, M., Tyson, J.E., Higgins,R.D., 2007. Neurodevelopmental outcomes of premature infants with severe res-piratory failure enrolled in a randomized controlled trial of inhaled nitric oxide.J. Pediatr. 151, 16–22, 22 e11–e13.
Horvath, S.M., Raven, P.B., Dahms, T.E., Gray, D.J., 1975. Maximal aerobic capacity atdifferent levels of carboxyhemoglobin. J. Appl. Physiol. 38, 300–303.
Hsia, C.C., Chuong, C.J., Johnson Jr., R.L., 1995. Critique of conceptual basis of diffusingcapacity estimates: a finite element analysis. J. Appl. Physiol. 79, 1039–1047.
Jansons, H., Fokkens, J.K., van der Tweel, I., Kreukniet, J., 1998. Re-breathing vs single-breath TLCO in patients with unequal ventilation and diffusion. Respir. Med. 92,18–24.
Johnson Jr., R.L., Heigenhauser, G.J.F., Hsia, C.C.W., Jones, N.L., Wagner, P.D., 1996.Determinants of gas exchange and acid-balance during exercise. In: Rowell, L.B.,Shepard, J.T. (Eds.), Handbook of Physiology. Section 12: Exercise: Regulationand Integration of Multiple Systems. Oxford University Press, New York, pp.515–584.
Kinsella, J.P., Abman, S.H., 2007. Inhaled nitric oxide in the premature newborn. J.Pediatr. 151, 10–15.
Kinsella, J.P., Cutter, G.R., Walsh, W.F., Gerstmann, D.R., Bose, C.L., Hart, C., Sekar, K.C.,Auten, R.L., Bhutani, V.K., Gerdes, J.S., George, T.N., Southgate, W.M., Carriedo,H., Couser, R.J., Mammel, M.C., Hall, D.C., Pappagallo, M., Sardesai, S., Strain, J.D.,Baier, M., Abman, S.H., 2006. Early inhaled nitric oxide therapy in prematurenewborns with respiratory failure. N. Engl. J. Med. 355, 354–364.
Konduri, G.G., Solimano, A., Sokol, G.M., Singer, J., Ehrenkranz, R.A., Singhal, N.,Wright, L.L., Van Meurs, K., Stork, E., Kirpalani, H., Peliowski, A., 2004. A ran-domized trial of early versus standard inhaled nitric oxide therapy in termand near-term newborn infants with hypoxic respiratory failure. Pediatrics 113,559–564.
Konduri, G.G., Vohr, B., Robertson, C., Sokol, G.M., Solimano, A., Singer, J., Ehrenkranz,R.A., Singhal, N., Wright, L.L., Van Meurs, K., Stork, E., Kirpalani, H., Peliowski, A.,Johnson, Y., 2007. Early inhaled nitric oxide therapy for term and near-termnewborn infants with hypoxic respiratory failure: neurodevelopmental follow-up. J. Pediatr. 150, 235–240, 240 e231.
Kreukniet, J., 1970. Relation between rebreathing CO-diffusing capacity of the lungand unequal ventilation. Scand. J. Respir. Dis. 51, 49–54.
Kung, H.C., Hoyert, D.L., Xu, J., Murphy, S.L., 2008. Deaths: final data for 2005. Natl.Vital Stat. Rep. 56, 1–120.
Lalli, C.M., Raju, L., 1981. Pregnancy and chronic obstructive pulmonary disease.Chest 80, 759–761.
Lam, G.K., Stafford, R.E., Thorp, J., Moise Jr., K.J., Cairns, B.A., 2001. Inhaled nitricoxide for primary pulmonary hypertension in pregnancy. Obstet. Gynecol. 98,895–898.
Lawther, P.J., Commins, B.T., 1970. Cigarette smoking and exposure to carbonmonoxide. Ann. N. Y. Acad. Sci. 174, 135–147.
Lehmann, V., 1975. Dyspnea in pregnancy. J. Perinat. Med. 3, 154–160.Light, A., Grass, C., Pursely, D., Krause, J., 2007. Carboxyhemoglobin levels in smok-
ers vs nonsmokers in a smoking environment. Presented at the 52nd AnnualMeeting of American Association for Respiratory Care (AARC), December 2006,

Author's personal copy
G.S. Zavorsky et al. / Respiratory Physiology & Neurobiology 170 (2010) 215–225 225
Las Vegas. Respir. Care, http://www.rcjournal.com/abstracts/2007/?id=aarc07111.
Longo, L.D., 1976. Carbon monoxide: effects on oxygenation of the fetus in utero.Science 194, 523–525.
Longo, L.D., 1977. The biological effects of carbon monoxide on the pregnant woman,fetus, and newborn infant. Am. J. Obstet. Gynecol. 129, 69–103.
Longo, L.D., Hill, E.P., 1977. Carbon monoxide uptake and elimination in fetal andmaternal sheep. Am. J. Physiol. 232, H324–H330.
Lust, K.M., Boots, R.J., Dooris, M., Wilson, J., 1999. Management of labor in Eisen-menger syndrome with inhaled nitric oxide. Am. J. Obstet. Gynecol. 181,419–423.
Macintyre, N., Crapo, R.O., Viegi, G., Johnson, D.C., van der Grinten, C.P., Brusasco, V.,Burgos, F., Casaburi, R., Coates, A., Enright, P., Gustafsson, P., Hankinson, J., Jensen,R., McKay, R., Miller, M.R., Navajas, D., Pedersen, O.F., Pellegrino, R., Wanger, J.,2005. Standardisation of the single-breath determination of carbon monoxideuptake in the lung. Eur. Respir. J. 26, 720–735.
Manier, G., Moinard, J., Stoicheff, H., 1993. Pulmonary diffusing capacity after max-imal exercise. J. Appl. Physiol. 75, 2580–2585.
Manier, G., Moinard, J., Techoueyres, P., Varene, N., Guenard, H., 1991. Pulmonarydiffusion limitation after prolonged strenuous exercise. Respir. Physiol. 83,143–153.
McAuliffe, F., Kametas, N., Rafferty, G.F., Greenough, A., Nicolaides, K., 2003. Pul-monary diffusing capacity in pregnancy at sea level and at high altitude. Respir.Physiol. Neurobiol. 134, 85–92.
McAuliffe, F., Kametas, N., Costello, J., Rafferty, G.F., Greenough, A., Nicolaides, K.,2002. Respiratory function in singleton and twin pregnancy. BJOG 109, 765–769.
McMillan, E., Martin, W.L., Waugh, J., Rushton, I., Lewis, M., Clutton-Brock, T., Tow-nend, J.N., Kilby, M.D., Gordon, C., 2002. Management of pregnancy in womenwith pulmonary hypertension secondary to SLE and anti-phospholipid syn-drome. Lupus 11, 392–398.
Mestan, K.K., Marks, J.D., Hecox, K., Huo, D., Schreiber, M.D., 2005. Neurodevelop-mental outcomes of premature infants treated with inhaled nitric oxide. N. Engl.J. Med. 353, 23–32.
Meyer, M., Piiper, J., 1989. Nitric oxide (NO), a new test gas for study of alveolar-capillary diffusion. Eur. Respir. J. 2, 494–496.
Miller, M.R., Hankinson, J., Brusasco, V., Burgos, F., Casaburi, R., Coates, A., Crapo, R.,Enright, P., van der Grinten, C.P., Gustafsson, P., Jensen, R., Johnson, D.C., MacIn-tyre, N., McKay, R., Navajas, D., Pedersen, O.F., Pellegrino, R., Viegi, G., Wanger,J., 2005a. Standardisation of spirometry. Eur. Respir. J. 26, 319–338.
Miller, M.R., Crapo, R., Hankinson, J., Brusasco, V., Burgos, F., Casaburi, R., Coates, A.,Enright, P., van der Grinten, C.P., Gustafsson, P., Jensen, R., Johnson, D.C., MacIn-tyre, N., McKay, R., Navajas, D., Pedersen, O.F., Pellegrino, R., Viegi, G., Wanger,J., 2005b. General considerations for lung function testing. Eur. Respir. J. 26,153–161.
Milne, J.A., 1979. The respiratory response to pregnancy. Postgrad. Med. J. 55,318–324.
Milne, J.A., Mills, R.J., Coutts, J.R., Macnaughton, M.C., Moran, F., Pack, A.I., 1977.The effect of human pregnancy on the pulmonary transfer factor for carbonmonoxide as measured by the single-breath method. Clin. Sci. Mol. Med. 53,271–276.
Murias, J.M., Zavorsky, G.S., 2007. Short-term variability of nitric oxide diffusingcapacity and its components. Respir. Physiol. Neurobiol. 157, 316–325.
Myers, J., Prakash, M., Froelicher, V., Do, D., Partington, S., Atwood, J.E., 2002. Exercisecapacity and mortality among men referred for exercise testing. N. Engl. J. Med.346, 793–801.
National Institute for Occupational Safety and Health, 2005. NIOSH Pocket Guide toChemical Hazards. NIOSH Publication 2005-149, Carbon Monoxide.
Norregaard, O., Schultz, P., Ostergaard, A., Dahl, R., 1989. Lung function and posturalchanges during pregnancy. Respir. Med. 83, 467–470.
Olivieri, M., Talamini, G., Corradi, M., Perbellini, L., Mutti, A., Tantucci, C., Malerba,M., 2006. Reference values for exhaled nitric oxide (reveno) study. Respir. Res.7, 94.
Oppenheimer, B.W., Berger, K.I., Hadjiangelis, N.P., Norman, R.G., Rapoport, D.M.,Goldring, R.M., 2006. Membrane diffusion in diseases of the pulmonary vascu-lature. Respir. Med. 100, 1247–1253.
Osborne, J.S., Adamek, S., Hobbs, M.E., 1956. Some components of gas phase ofcigarette smoke. Anal. Chem. 28, 211.
Pellegrino, R., Viegi, G., Brusasco, V., Crapo, R.O., Burgos, F., Casaburi, R., Coates, A.,van der Grinten, C.P., Gustafsson, P., Hankinson, J., Jensen, R., Johnson, D.C., Mac-Intyre, N., McKay, R., Miller, M.R., Navajas, D., Pedersen, O.F., Wanger, J., 2005.Interpretative strategies for lung function tests. Eur. Respir. J. 26, 948–968.
Phansalkar, A.R., Hanson, C.M., Shakir, A.R., Johnson Jr., R.L., Hsia, C.C., 2004. Nitricoxide diffusing capacity and alveolar microvascular recruitment in sarcoidosis.Am. J. Respir. Crit. Care Med. 169, 1034–1040.
Pirnay, F., Dujardin, J., Deroanne, R., Petit, J.M., 1971. Muscular exercise during intox-ication by carbon monoxide. J. Appl. Physiol. 31, 573–575.
Pryor, W.A., Stone, K., 1993. Oxidants in cigarette smoke. Radicals, hydrogen perox-ide, peroxynitrate, and peroxynitrite. Ann. N. Y. Acad. Sci. 686, 12–27, discussion27–18.
Radford, E.P., Drizd, T.A., 1982. Blood carbon monoxide levels in persons 3 to 74years of age, United States, 1976–1980. In: Advance Data from Vital and HealthStatistics. No. 76. PHS 82-1250, March 17th, 1982. U.S. Department of Healthand Human Services, Hyattsville, MD.
Raven, P.B., Drinkwater, B.L., Ruhling, R.O., Bolduan, N., Taguchi, S., Gliner, J., Hor-vath, S.M., 1974. Effect of carbon monoxide and peroxyacetyl nitrate on man’smaximal aerobic capacity. J. Appl. Physiol. 36, 288–293.
Reddy, A.P., Zaremba, M.L., Reddy, S.P., 2007. Noninvasive pulse co-oximetry as atool to detect smoking status in an outpatient setting. Chest 132, 490.
Roberts, C.M., MacRae, K.D., Seed, W.A., 1990. Multi-breath and single breath heliumdilution lung volumes as a test of airway obstruction. Eur. Respir. J. 3, 515–520.
Robinson, J.N., Banerjee, R., Landzberg, M.J., Thiet, M.P., 1999. Inhaled nitric oxidetherapy in pregnancy complicated by pulmonary hypertension. Am. J. Obstet.Gynecol. 180, 1045–1046.
Roughton, F.J.W., Forster, R.E., 1957. Relative importance of diffusion and chemicalreaction rates in determining rate of exchange of gases in the human lung, withspecial reference to true diffusing capacity of pulmonary membrane and volumeof blood in the lung capillaries. J. Appl. Physiol. 11, 290–302.
Russell, M.A., Cole, P.V., Brown, E., 1973a. Absorption by non-smokers of carbonmonoxide from room air polluted by tobacco smoke. Lancet 1, 576–579.
Russell, M.A., Wilson, C., Cole, P.V., Idle, M., Feyerabend, C., 1973b. Comparison ofincreases in carboxyhaemoglobin after smoking “extra-mild” and “non-mild”cigarettes. Lancet 2, 687–690.
Schatz, M., Dombrowski, M.P., Wise, R., Momirova, V., Landon, M., Mabie, W., New-man, R.B., Rouse, D.J., Lindheimer, M., Miodovnik, M., Caritis, S.N., Leveno, K.J.,Meis, P., Wapner, R.J., Paul, R.H., O’Sullivan, M.J., Varner, M.W., Thurnau, G.R.,Conway, D.L., 2006. Spirometry is related to perinatal outcomes in pregnantwomen with asthma. Am. J. Obstet. Gynecol. 194, 120–126.
Schreiber, M.D., Gin-Mestan, K., Marks, J.D., Huo, D., Lee, G., Srisuparp, P., 2003.Inhaled nitric oxide in premature infants with the respiratory distress syndrome.N. Engl. J. Med. 349, 2099–2107.
Selvakumar, S., Sharan, M., Singh, M.P., 1993. A mathematical model for the elimi-nation of carbon monoxide in humans. J. Theor. Biol. 162, 321–336.
Sheel, A.W., Edwards, M.R., Hunte, G.S., McKenzie, D.C., 2001. Influence of inhalednitric oxide on gas exchange during normoxic and hypoxic exercise in highlytrained cyclists. J. Appl. Physiol. 90, 926–932.
Smith, C.J., Guy, T.D., Stiles, M.F., Morton, M.J., Collie, B.B., Ingebrethsen, B.J., Robin-son, J.H., 1998. A repeatable method for determination of carboxyhemoglobinlevels in smokers. Hum. Exp. Toxicol. 17, 29–34.
Snyder, E.M., Beck, K.C., Hulsebus, M.L., Breen, J.F., Hoffman, E.A., Johnson, B.D., 2006.Short term hypoxic exposure at rest and during exercise reduces lung water inhealthy humans. J. Appl. Physiol. 101, 1623–1632.
Sokol, G.M., Van Meurs, K.P., Wright, L.L., Rivera, O., Thorn III, W.J., Chu, P.M., Sams,R.L., 1999. Nitrogen dioxide formation during inhaled nitric oxide therapy. Clin.Chem. 45, 382–387.
Takahashi, H., Iwabuchi, K., Kudo, Y., Tomoike, H., Niizeki, K., Uchida, K., Takahashi,K., 1995. Simultaneous measurement of pulmonary diffusing capacity for CO andcardiac output by a rebreathing method in patients with pulmonary diseases.Intern. Med. 34, 330–338.
Takahashi, Y., Kobayashi, H., Tanaka, N., Sato, T., Takizawa, N., Tomita, T., 1998. Nitro-syl hemoglobin in blood of normoxic and hypoxic sheep during nitric oxideinhalation. Am. J. Physiol. 274, H349–357.
Tamhane, R.M., Johnson Jr., R.L., Hsia, C.C., 2001. Pulmonary membrane diffusingcapacity and capillary blood volume measured during exercise from nitric oxideuptake. Chest 120, 1850–1856.
van der Lee, I., Zanen, P., Biesma, D.H., van den Bosch, J.M., 2005. The effect of redcell transfusion on nitric oxide diffusing capacity. Respiration 72, 512–516.
van der Lee, I., Zanen, P., Grutters, J.C., Snijder, R.J., van den Bosch, J.M., 2006. Dif-fusing capacity for nitric oxide and carbon monoxide in patients with diffuseparenchymal lung disease and pulmonary arterial hypertension. Chest 129,378–383.
van der Lee, I., Gietema, H.A., Zanen, P., van Klaveren, R.J., Prokop, M., Lammers, J.W.,van den Bosch, J.M., 2009. Nitric oxide diffusing capacity versus spirometry inthe early diagnosis of emphysema in smokers. Respir. Med. 103, 1892–1897.
Van Meurs, K.P., Rhine, W.D., Asselin, J.M., Durand, D.J., 1997. Response of prema-ture infants with severe respiratory failure to inhaled nitric oxide. Preemie NOCollaborative Group. Pediatr. Pulmonol. 24, 319–323.
Vellar, O.D., 1974. Changes in hemoglobin concentration and hematocrit duringthe menstrual cycle. I. A cross-sectional study. Acta Obstet. Gynecol. Scand. 53,243–246.
Vogel, J.A., Gleser, M.A., 1972. Effect of carbon monoxide on oxygen transport duringexercise. J. Appl. Physiol. 32, 234–239.
Vogel, J.A., Gleser, M.A., Wheeler, R.C., Whitten, B.K., 1972. Carbon monoxide andphysical work capacity. Arch Environ. Health 24, 198–203.
Wanger, J., Clausen, J.L., Coates, A., Pedersen, O.F., Brusasco, V., Burgos, F., Casaburi, R.,Crapo, R., Enright, P., van der Grinten, C.P., Gustafsson, P., Hankinson, J., Jensen,R., Johnson, D., Macintyre, N., McKay, R., Miller, M.R., Navajas, D., Pellegrino, R.,Viegi, G., 2005. Standardisation of the measurement of lung volumes. Eur. Respir.J. 26, 511–522.
Weaver, L.K., Howe, S., Hopkins, R., Chan, K.J., 2000. Carboxyhemoglobin half-life incarbon monoxide-poisoned patients treated with 100% oxygen at atmosphericpressure. Chest 117, 801–808.
Zavorsky, G.S., Lands, L.C., 2005. Lung diffusion capacity for nitric oxide and car-bon monoxide is impaired similarly following short-term graded exercise. NitricOxide 12, 31–38.
Zavorsky, G.S., Murias, J.M., 2006. A small amount of inhaled nitric oxide does notincrease lung diffusing capacity. Eur. Respir. J. 27, 1251–1257.
Zavorsky, G.S., Quiron, K.B., Massarelli, P.S., Lands, L.C., 2004. The relationshipbetween single-breath diffusion capacity of the lung for nitric oxide and carbonmonoxide during various exercise intensities. Chest 125, 1019–1027.
Zavorsky, G.S., Wilson, B., Harris, J.K., Kim, D.J., Carli, F., Mayo, N.E., 2009. Pulmonarydiffusion and aerobic capacity: is there a relation? Does obesity matter? ActaPhysiol. (Oxf.), doi:10.1111/j.1748-1716.2009.02059.x.