
Clonal spread of CTX-M-15-producing Klebsiella pneumoniae in a Croatian hospital
10
Clonal spread of CTX-M-15-producing Klebsiella pneumoniae in a Croatian hospital Mirna Vranic-Ladavac, 1 Zrinka Bosnjak, 2 Natasa Beader, 2,3 Nada Barisic, 1 Smilja Kalenic 2,3 and Branka Bedenic 2,3 Correspondence Branka Bedenic [email protected] Received 22 February 2010 Accepted 19 June 2010 1 County of Istria Public Health Institute, Nazorova 23, Pula, Croatia 2 Clinical Hospital Center Zagreb, Kispatic Street 12, Zagreb, Croatia 3 School of Medicine, University of Zagreb, Salata 3, Zagreb, Croatia This study was conducted to detect and analyse the presence of extended-spectrum b-lactamase (ESBL)-producing Klebsiella pneumoniae associated with a nosocomial outbreak at a Croatian hospital. During 2007, 162 K. pneumoniae isolates with reduced susceptibility to third-generation cephalosporins were collected from various hospital units and patient specimens. Most of the strains were isolated from urine (61 %), followed by blood cultures (13 %), wound swabs (13 %), tracheal aspirates (5 %), intra-abdominal abscess aspirates (4 %), intravascular catheters (3 %) and cerebrospinal fluid (1 %). Medical wards were the most important source of the isolates (46 %); 21 % of the isolates originated from surgical intensive-care units. All patients had infections acquired during their stay in hospital. No community-acquired infections were reported. Sixty of these isolates were chosen for further analysis. A double-disc synergy test (DDST) was used to detect ESBLs. MICs were determined by the broth microdilution method according to CLSI guidelines. The transferability of ceftazidime resistance was tested by conjugation (broth mating method). PCR was used to detect alleles encoding ESBL enzymes. Plasmids encoding ESBLs were extracted with the Macherey Nagel Mini kit according to the manufacturer’s recommendations. The genotypes of the strains were compared by analysis of banding patterns generated by PFGE of XbaI-digested genomic DNA. ESBLs were found by DDST in all isolates. All strains were resistant to cefuroxime, ceftazidime, cefotaxime, ceftriaxone, aztreonam, piperacillin/tazobactam and ciprofloxacin. There was variable susceptibility/resistance to cefepime and gentamicin. No resistance to ceftazidime/clavulanate and carbapenems was observed. Only six strains transferred resistance to an Escherichia coli recipient strain, with low frequency. All isolates yielded an amplicon of 545 bp with consensus MA primers. Multiplex PCR was positive for group 1 CTX-M b-lactamases. Sequencing of selected amplicons revealed the presence of bla CTX-M-15 , with coding regions containing identical nucleotide sequences. Similarly to isolates from India, our isolates contained the ISEcpI insertion sequence located upstream of the bla CTX-M- 15 gene, which has recently been demonstrated to mobilize 39-adjacent genes to transfer between DNA replicons. The isolates contained a large plasmid of approximately 150 kb. The isolates were assigned to five clusters (.85 % similarity), which contained subclusters. The results of this work provided insights into the molecular epidemiology of the spread of ESBLs in K. pneumoniae involved in an outbreak at a Croatian hospital. The hospital antibiotic policy resulted in ceftriaxone being the most heavily prescribed third-generation cephalosporin, which might be expected to select for cefotaximases such as CTX-M-15. INTRODUCTION Since plasmid-mediated extended-spectrum b-lactamases (ESBLs) were first detected in a Klebsiella oxytoca isolate in Germany in 1983 (Kliebe et al., 1985), they have been reported increasingly worldwide. Production of ESBLs is the major mechanism of resistance to oxymino-cephalos- porins and aztreonam in Gram-negative bacteria (Bradford, 2001; Jacoby & Munoz-Price, 2005). ESBLs are predominantly derivatives of plasmid-mediated TEM or SHV b-lactamases, and arise through mutations that alter the configuration of the active site, thereby expanding the hydrolytic spectrum of the enzyme (Jacoby & Munoz- Abbreviations: DDD, defined daily dosis; DDST, double-disc synergy test; ESBL, extended-spectrum b-lactamase. Journal of Medical Microbiology (2010), 59, 1069–1078 DOI 10.1099/jmm.0.019778-0 019778 G 2010 SGM Printed in Great Britain 1069
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Clonal spread of CTX-M-15-producing Klebsiella pneumoniae in a Croatian hospital

Clonal spread of CTX-M-15-producing Klebsiellapneumoniae in a Croatian hospital
Mirna Vranic-Ladavac,1 Zrinka Bosnjak,2 Natasa Beader,2,3 Nada Barisic,1
Smilja Kalenic2,3 and Branka Bedenic2,3
Correspondence
Branka Bedenic
Received 22 February 2010
Accepted 19 June 2010
1County of Istria Public Health Institute, Nazorova 23, Pula, Croatia
2Clinical Hospital Center Zagreb, Kispatic Street 12, Zagreb, Croatia
3School of Medicine, University of Zagreb, Salata 3, Zagreb, Croatia
This study was conducted to detect and analyse the presence of extended-spectrum b-lactamase
(ESBL)-producing Klebsiella pneumoniae associated with a nosocomial outbreak at a Croatian
hospital. During 2007, 162 K. pneumoniae isolates with reduced susceptibility to third-generation
cephalosporins were collected from various hospital units and patient specimens. Most of the
strains were isolated from urine (61 %), followed by blood cultures (13 %), wound swabs (13 %),
tracheal aspirates (5 %), intra-abdominal abscess aspirates (4 %), intravascular catheters (3 %)
and cerebrospinal fluid (1 %). Medical wards were the most important source of the isolates
(46 %); 21 % of the isolates originated from surgical intensive-care units. All patients had
infections acquired during their stay in hospital. No community-acquired infections were reported.
Sixty of these isolates were chosen for further analysis. A double-disc synergy test (DDST) was
used to detect ESBLs. MICs were determined by the broth microdilution method according to
CLSI guidelines. The transferability of ceftazidime resistance was tested by conjugation (broth
mating method). PCR was used to detect alleles encoding ESBL enzymes. Plasmids encoding
ESBLs were extracted with the Macherey Nagel Mini kit according to the manufacturer’s
recommendations. The genotypes of the strains were compared by analysis of banding patterns
generated by PFGE of XbaI-digested genomic DNA. ESBLs were found by DDST in all isolates.
All strains were resistant to cefuroxime, ceftazidime, cefotaxime, ceftriaxone, aztreonam,
piperacillin/tazobactam and ciprofloxacin. There was variable susceptibility/resistance to cefepime
and gentamicin. No resistance to ceftazidime/clavulanate and carbapenems was observed. Only
six strains transferred resistance to an Escherichia coli recipient strain, with low frequency. All
isolates yielded an amplicon of 545 bp with consensus MA primers. Multiplex PCR was positive
for group 1 CTX-M b-lactamases. Sequencing of selected amplicons revealed the presence of
blaCTX-M-15, with coding regions containing identical nucleotide sequences. Similarly to isolates
from India, our isolates contained the ISEcpI insertion sequence located upstream of the blaCTX-M-
15 gene, which has recently been demonstrated to mobilize 39-adjacent genes to transfer between
DNA replicons. The isolates contained a large plasmid of approximately 150 kb. The isolates were
assigned to five clusters (.85 % similarity), which contained subclusters. The results of this work
provided insights into the molecular epidemiology of the spread of ESBLs in K. pneumoniae
involved in an outbreak at a Croatian hospital. The hospital antibiotic policy resulted in ceftriaxone
being the most heavily prescribed third-generation cephalosporin, which might be expected to
select for cefotaximases such as CTX-M-15.
INTRODUCTION
Since plasmid-mediated extended-spectrum b-lactamases(ESBLs) were first detected in a Klebsiella oxytoca isolate inGermany in 1983 (Kliebe et al., 1985), they have been
reported increasingly worldwide. Production of ESBLs isthe major mechanism of resistance to oxymino-cephalos-porins and aztreonam in Gram-negative bacteria(Bradford, 2001; Jacoby & Munoz-Price, 2005). ESBLsare predominantly derivatives of plasmid-mediated TEMor SHV b-lactamases, and arise through mutations thatalter the configuration of the active site, thereby expandingthe hydrolytic spectrum of the enzyme (Jacoby & Munoz-
Abbreviations: DDD, defined daily dosis; DDST, double-disc synergytest; ESBL, extended-spectrum b-lactamase.
Journal of Medical Microbiology (2010), 59, 1069–1078 DOI 10.1099/jmm.0.019778-0
019778 G 2010 SGM Printed in Great Britain 1069

Price, 2005). The CTX-M family of b-lactamases includesevolutionarily related ESBLs with a much higher level ofactivity against cefotaxime than against ceftazidime, andtheir similarity to some species-specific b-lactamases, suchas those of Klebsiella oxytoca and Citrobacter diversus, hasbeen known for some time (Pitout et al., 2005; Bonnet,2004). The recent finding of 99 % sequence similaritybetween the CTX-M-2 enzyme and the b-lactamase ofKluyvera ascorbata has indicated the origins of at least afraction of the CTM variants (Baraniak et al., 2002). Incontrast to TEM and SHV ESBLs, which rely on pointmutations in the blaTEM and blaSHV genes to expand theirsubstrate profiles, CTX-M ESBLs have an intrinsicextended-spectrum profile. Whereas only four enzymes ofthis family (CTX-M-1, MEN-1, CTX-M-2 and Toho-1)were described between 1990 and 1995, the list hasincreased rapidly in recent years (Baraniak et al., 2002).In some countries, CTX-M b-lactamases are the mostprevalent types of ESBL, for instance in Switzerland(Lartigue et al., 2007), Russia (Edelstein et al., 2003),Greece (Pournaras et al., 2004), Spain (Canton et al., 2002),Japan (Yamasaki et al., 2003), Taiwan (Yu et al., 2002),China (Chanawong et al., 2002) and Argentina (Quinteroset al., 2003).
Since the first isolation of ESBL-producing Klebsiellapneumoniae in Croatia (Bedenic & Zagar, 1998), a growingvariety of ESBL enzymes have been detected from membersof the Enterobacteriaceae (Bedenic et al., 2001, 2005). InCroatia, the first isolates found to produce CTX-M b-lactamases were Escherichia coli from the UniversityHospital in Split (Tonkic et al., 2007). Very soon afterthe first report, CTX-M-producing E. coli were reportedfrom other centres in Croatia (Literacka et al., 2009).
Recently, a significant increase in the prevalence of ESBL-producing K. pneumoniae was observed in the hospital inPula, Croatia. The strains were associated with a hospitaloutbreak. The majority of strains showed higher levels ofresistance to cefotaxime compared with ceftazidime,consistent with the production of CTX-M b-lactamases.The aim of this study was an epidemiological description ofan outbreak of infections caused by ESBL-positive K.pneumoniae within the hospital with molecular character-ization. We aimed to study the evolution of an outbreakassociated with ESBL-producing klebsiellae in a healthcareinstitution.
METHODS
Bacterial isolates. During 2007, 162 K. pneumoniae isolates withreduced susceptibility to third-generation cephalosporins werecollected from various hospital units and patient specimens in theGeneral Hospital in Pula, Croatia. This represents 60 % (162/270) ofthe total number of K. pneumoniae isolates. The General Hospital atPula is a 506-bed tertiary hospital and serves a population of 214 000people. The mean age of the patients was 64.5 years (range 16–95).Most of the isolates were from urine (61 %), followed by bloodcultures (13 %), wound swabs (13 %), tracheal aspirates (5 %), intra-abdominal abscess aspirates (4 %), intravascular catheters (3 %) and
cerebrospinal fluid (1 %) (Table 1). Medical wards were the most
important source of the isolates (46 %); 21 % of the isolates originatedfrom surgical intensive-care units (Table 1). All patients had
infections acquired during their hospital stay. The type of hospital
infection was defined in accordance with Centers for Disease Control
and Prevention criteria. No community-acquired infections werereported.
The strains were identified by conventional biochemical testing.ESBLs are routinely detected in the hospital laboratory by a double-
disc synergy test (DDST) performed on all K. pneumoniae isolates
with reduced inhibition zones around ceftazidime and cefotaxime
discs. Production of ESBLs was confirmed by E-test (AB Biodisk) andby the Vitek automated system (bioMerieux).
Sixty of the isolates were chosen for further analysis (Table 1). The
isolate selection criterion was the availability of the strains for furtheranalysis. Only 60 isolates had been inoculated in deep agar cultures to
be preserved for future studies. Laboratory staff do not routinely keep
all isolates, and the isolates that appeared at the beginning of theoutbreak were not kept because the laboratory staff were not yet
aware of the outbreak.
Antibiotic consumption. Consumption of antibiotics was measured
in DDD (defined daily dosis).
Detection of ESBL by DDST. ESBL production was determined by
DDST and confirmed by a reduction of at least threefold in the
ceftazidime MIC by clavulanate (Jarlier et al., 1988).
Antibiotic susceptibility testing. Susceptibilities to a wide range ofantibiotics were determined by disc-diffusion and broth microdilu-
tion methods. MICs were determined in microtitre plates and
Mueller–Hinton broth according to CLSI guidelines (CLSI, 2007). E.coli ATCC 25922 was used for quality control.
A phenotype consistent with production of a CTX-M-type b-
lactamase was defined by a cefotaxime MIC ¢8-fold higher thanthe ceftazidime MIC, with the MICs of both agents being reduced
significantly (¢8-fold) in the presence of 4 mg clavulanic acid l21
(CLSI, 2007).
Transfer of resistance determinants. K. pneumoniae isolates wereinvestigated for the transferability of their resistance determinants.
Conjugation experiments were set up employing E. coli A15R2 strain,
which is free of plasmids and resistant to rifampicin (Elwell & Falkow,1986). Transconjugants were selected on combined plates containing
cefotaxime (1 mg l21) and rifampicin (256 mg l21). The frequency of
conjugation was expressed relative to the number of donor cells.
Characterization of ESBLs. The presence of blaESBL genes wasdetermined by PCR using primers targeting blaTEM, blaSHV, blaCTX-M
and blaPER genes and conditions described previously (Nuesch-
Inderbinen et al., 1996; Arlet et al., 1995; Woodford et al., 2004).
Bacterial DNA was extracted by the boiling method. Primers used inthis study were MN-1 and MN-2 (Nuesch-Inderbinen et al., 1996) for
detection of SHV b-lactamases, OT-3 and OT-4 (Arlet et al., 1995) for
detection of TEM b-lactamases, MA-1 and MA-2 (Woodford et al.,
2004) for detection of CTX-M b-lactamases and PER-1F and PER-1R(Pagani et al., 2004) for detection of PER b-lactamases (Table 2).
blaOXA-1 genes were amplified with primers OXA-1F and OXA-1R.
Strains were further tested by multiplex PCR with primers specific forCTX-M groups 1, 2, 8, 9 and 25 (Woodford et al., 2006). Since the
above primers do not amplify the whole coding sequence of the
blaCTX-M gene, we used additional primers to distinguish between
CTX-M-15 and CTX-M-28. The sequences of these primers werekindly provided by Professor L. Martinez (Santander, Spain)
(personal communication).
M. Vranic-Ladavac and others
1070 Journal of Medical Microbiology 59
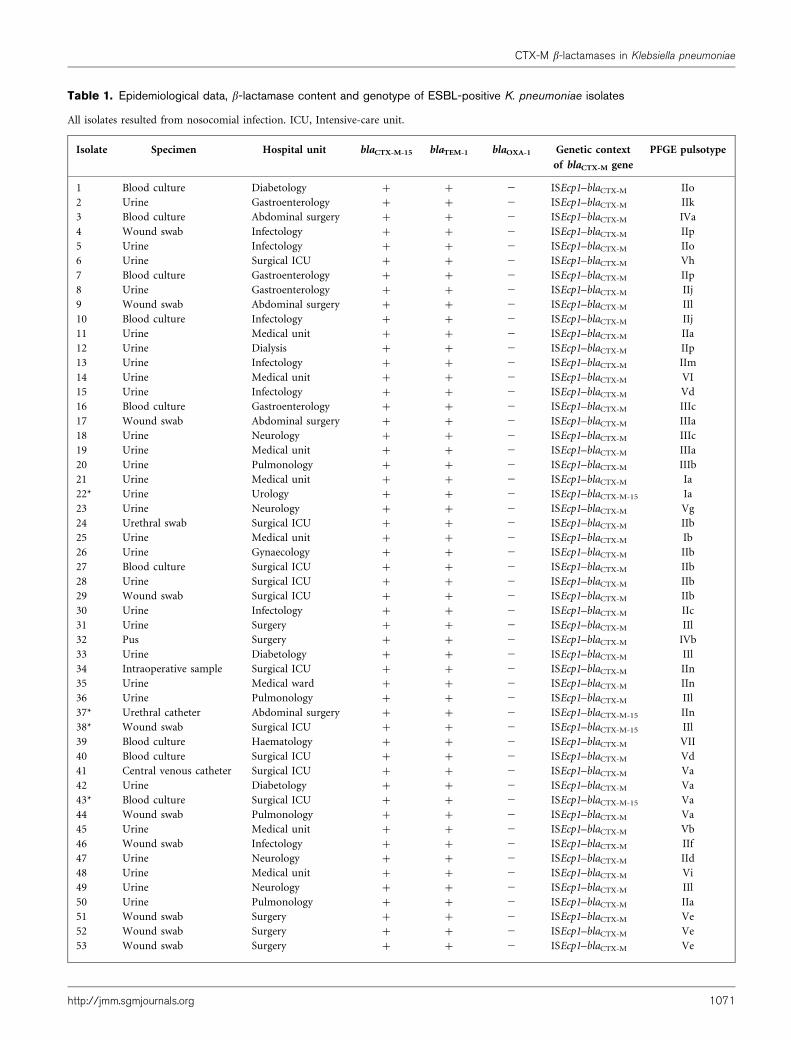
Table 1. Epidemiological data, b-lactamase content and genotype of ESBL-positive K. pneumoniae isolates
All isolates resulted from nosocomial infection. ICU, Intensive-care unit.
Isolate Specimen Hospital unit blaCTX-M-15 blaTEM-1 blaOXA-1 Genetic context
of blaCTX-M gene
PFGE pulsotype
1 Blood culture Diabetology + + 2 ISEcp1–blaCTX-M IIo
2 Urine Gastroenterology + + 2 ISEcp1–blaCTX-M IIk
3 Blood culture Abdominal surgery + + 2 ISEcp1–blaCTX-M IVa
4 Wound swab Infectology + + 2 ISEcp1–blaCTX-M IIp
5 Urine Infectology + + 2 ISEcp1–blaCTX-M IIo
6 Urine Surgical ICU + + 2 ISEcp1–blaCTX-M Vh
7 Blood culture Gastroenterology + + 2 ISEcp1–blaCTX-M IIp
8 Urine Gastroenterology + + 2 ISEcp1–blaCTX-M IIj
9 Wound swab Abdominal surgery + + 2 ISEcp1–blaCTX-M IIl
10 Blood culture Infectology + + 2 ISEcp1–blaCTX-M IIj
11 Urine Medical unit + + 2 ISEcp1–blaCTX-M IIa
12 Urine Dialysis + + 2 ISEcp1–blaCTX-M IIp
13 Urine Infectology + + 2 ISEcp1–blaCTX-M IIm
14 Urine Medical unit + + 2 ISEcp1–blaCTX-M VI
15 Urine Infectology + + 2 ISEcp1–blaCTX-M Vd
16 Blood culture Gastroenterology + + 2 ISEcp1–blaCTX-M IIIc
17 Wound swab Abdominal surgery + + 2 ISEcp1–blaCTX-M IIIa
18 Urine Neurology + + 2 ISEcp1–blaCTX-M IIIc
19 Urine Medical unit + + 2 ISEcp1–blaCTX-M IIIa
20 Urine Pulmonology + + 2 ISEcp1–blaCTX-M IIIb
21 Urine Medical unit + + 2 ISEcp1–blaCTX-M Ia
22* Urine Urology + + 2 ISEcp1–blaCTX-M-15 Ia
23 Urine Neurology + + 2 ISEcp1–blaCTX-M Vg
24 Urethral swab Surgical ICU + + 2 ISEcp1–blaCTX-M IIb
25 Urine Medical unit + + 2 ISEcp1–blaCTX-M Ib
26 Urine Gynaecology + + 2 ISEcp1–blaCTX-M IIb
27 Blood culture Surgical ICU + + 2 ISEcp1–blaCTX-M IIb
28 Urine Surgical ICU + + 2 ISEcp1–blaCTX-M IIb
29 Wound swab Surgical ICU + + 2 ISEcp1–blaCTX-M IIb
30 Urine Infectology + + 2 ISEcp1–blaCTX-M IIc
31 Urine Surgery + + 2 ISEcp1–blaCTX-M IIl
32 Pus Surgery + + 2 ISEcp1–blaCTX-M IVb
33 Urine Diabetology + + 2 ISEcp1–blaCTX-M IIl
34 Intraoperative sample Surgical ICU + + 2 ISEcp1–blaCTX-M IIn
35 Urine Medical ward + + 2 ISEcp1–blaCTX-M IIn
36 Urine Pulmonology + + 2 ISEcp1–blaCTX-M IIl
37* Urethral catheter Abdominal surgery + + 2 ISEcp1–blaCTX-M-15 IIn
38* Wound swab Surgical ICU + + 2 ISEcp1–blaCTX-M-15 IIl
39 Blood culture Haematology + + 2 ISEcp1–blaCTX-M VII
40 Blood culture Surgical ICU + + 2 ISEcp1–blaCTX-M Vd
41 Central venous catheter Surgical ICU + + 2 ISEcp1–blaCTX-M Va
42 Urine Diabetology + + 2 ISEcp1–blaCTX-M Va
43* Blood culture Surgical ICU + + 2 ISEcp1–blaCTX-M-15 Va
44 Wound swab Pulmonology + + 2 ISEcp1–blaCTX-M Va
45 Urine Medical unit + + 2 ISEcp1–blaCTX-M Vb
46 Wound swab Infectology + + 2 ISEcp1–blaCTX-M IIf
47 Urine Neurology + + 2 ISEcp1–blaCTX-M IId
48 Urine Medical unit + + 2 ISEcp1–blaCTX-M Vi
49 Urine Neurology + + 2 ISEcp1–blaCTX-M IIl
50 Urine Pulmonology + + 2 ISEcp1–blaCTX-M IIa
51 Wound swab Surgery + + 2 ISEcp1–blaCTX-M Ve
52 Wound swab Surgery + + 2 ISEcp1–blaCTX-M Ve
53 Wound swab Surgery + + 2 ISEcp1–blaCTX-M Ve
CTX-M b-lactamases in Klebsiella pneumoniae
http://jmm.sgmjournals.org 1071

Primers IS26F and IS26R were used to amplify a 400 bp fragment
spanning the link between the IS26 insertion sequence and the blaCTX-M
gene in CTX-M-producing isolates (Woodford et al., 2004). Primers
ISEcp1L1 and ALA-5 were applied to amplify the ISEcpI insertion
sequence (Literacka et al., 2009).
In order to determine the genetic context of blaCTX-M genes, PCR
mapping was performed using primers for IS26 and ISEcpI combined
with forward and reverse primers for blaCTX-M genes (Saladin et al.,
2002). PCR products were visualized by agarose gel electrophoresis
after staining with ethidium bromide. Amplicons from selected
Table 1. cont.
Isolate Specimen Hospital unit blaCTX-M-15 blaTEM-1 blaOXA-1 Genetic context
of blaCTX-M gene
PFGE pulsotype
54 Urine Nephrology + + 2 ISEcp1–blaCTX-M Vg
55* Blood culture Medical unit + + 2 ISEcp1–blaCTX-M-15 Vi
56 Urethral catheter Neurology + + 2 ISEcp1–blaCTX-M IIg
57 Urine Medical unit + + 2 ISEcp1–blaCTX-M IId
58 Wound swab Infectology + + 2 ISEcp1–blaCTX-M IId
59 Urine Neurosurgery + + 2 ISEcp1–blaCTX-M IId
60 Wound swab Surgical ICU + + 2 ISEcp1–blaCTX-M IIg
*Strains with sequenced blaCTX-M genes and blaTEM genes (selected amplicons contained blaCTX-M-15 and blaTEM-1).
Table 2. Selected primers used in the study
Primer Sequence (5§–3§) Orientation Target sequence Reference
MN-1 CGCCGGGTTATTCTTATTTGTCGC Forward blaSHV Nuesch-Inderbinen et al. (1996)
MN-2 TCTTTCCGATGCCGCCGCCAGTCA Reverse blaSHV Nuesch-Inderbinen et al. (1996)
OT-3 ATGAGTATTCAACATTTCCG Forward blaTEM Arlet et al. (1995)
OT-4 CCAATGCTTAATCAGTGAGG Reverse blaTEM Arlet et al. (1995)
MA-1 SCSATGTGCAGYACCAGTAA3 Forward blaCTX-M Woodford et al. (2004)
MA-2 CGCCRATATGRTTGGTGGTG Reverse blaCTX-M Woodford et al. (2004)
PER-1F GGGACA(A/G)TC(G/C)(G/T)ATGAATGTCA Forward blaPER-1 Pagani et al. (2004)
PER-1R GG(C/T)(G/C)GCTTAGATAGTGCTGAT Reverse blaPER-1 Pagani et al. (2004)
OXA-1F ACACAATACATATCAACTTCGC Forward blaOXA-1 Literacka et al. (2009)
OXA-1R AGTGTGTTTAGAATGGTGATC Reverse blaOXA-1 Literacka et al. (2009)
CTX-M gr.1 AAAAATCACTGCGCCAGTTC Forward blaCTX-M-1 Woodford et al. (2006)
CTX-M gr.1 AGCTTATTCATCGCCACGTT Reverse blaCTX-M-1 Woodford et al. (2006)
CTX-M gr.2 GGACGCTACCCCTGCTATT Forward blaCTX-M-2 Woodford et al. (2006)
CTX-M gr.2 CCAGCGTCAGATTTTTCAGG Reverse blaCTX-M-2 Woodford et al. (2006)
CTX-M-8-FOR TCGCGTTAAGCGGATGATGC Forward blaCTX-M-8 Woodford et al. (2006)
CTX-M-8-REV AACCCACGATGTGGGTAGC Reverse blaCTX-M-8 Woodford et al. (2006)
CTX-M-9-FOR CAAAGAGAGTGCAACGGATG Forward blaCTX-M-9 Woodford et al. (2006)
CTX-M-9-REV ATTGGAAAGCGTTCATCACC Reverse blaCTX-M-9 Woodford et al. (2006)
CTX-M-25 GCACGATGACATTCGGG Forward blaCTX-M-25 Woodford et al. (2006)
CTX-M-F1 ATAAAACCGGCAGCGGTG Forward blaCTX-M-15/28 L. Martinez (personal communication)
CTX-M-R2 GAATTTTGACGATCGGGG Reverse blaCTX-M-15/28 L. Martinez (personal communication)
IS26F GCGGTAAATCGTGGAGTGAT Forward IS26 Woodford et al. (2004)
IS26R ATTCGGCAAGTTTTTGCTGT3 Reverse IS26 Woodford et al. (2004)
ISEcp1L1 CAGCTTTTATGACTCG Forward ISEcp1 Literacka et al. (2009)
ALA-5 CCTAAATTCCACGTGTGG Reverse ISEcp1 Literacka et al. (2009)
qnrAF ATTTCTCACGCCAGGATTTG Forward qnrA Robicsek et al. (2006b)
qnrAR GATCGGCAAAGGTTAGGTCA Reverse qnrA Robicsek et al. (2006b)
qnrBF GATCGTGAAAGCCAGAAAGG Forward qnrB Robicsek et al. (2006b)
qnrBR ACGATGCCTGGTAGTTGTCC Reverse qnrB Robicsek et al. (2006b)
qnrSF ACGACATTCGTCAACTGCAA Forward qnrS Robicsek et al. (2006b)
qnrSR TAAATTGGCACCCTGTAGGC Reverse qnrS Robicsek et al. (2006b)
M. Vranic-Ladavac and others
1072 Journal of Medical Microbiology 59

strains were then column-purified (Qiagen DNA purification kit) and
sequenced directly using an ABI PRISM 377 Genetic Analyzer
(Applied Biosystems). After sequencing the PCR products, we used
the BLAST program to look for sequence similarity to other blaESBL
genes. Reference strains producing CTX-M-15 and CTX-M-2 b-
lactamases were provided by Neil Woodford (Health Protection
Agency, London, UK), and reference strains producing TEM-1, TEM-
2 and SHV-1 b-lactamases were kindly provided by Professor A.
Bauernfeind (Microer, Munich, Germany).
PCR Nhe test. A PCR Nhe test was performed to distinguish between
SHV-1 and SHV-ESBL (Nuesch-Inderbinen et al., 1996).
Detection of quinolone resistance determinants. Plasmid-borne
quinolone resistance genes qnrA, qnrB and qnrS were detected by PCR
as described previously (Robicsek et al., 2006a, b).
Characterization of plasmids encoding ESBLs. Plasmids were
extracted with the Macherey Nagel Mini kit according to the
manufacturer’s instructions from 20 representative strains. The sizes of
plasmids were estimated from a standard curve of the logarithm of
molecular size of four plasmids of 148, 64, 36 and 7 kb, respectively, from
E. coli NTCC 50192 against the logarithm of relative mobility. Plasmid
extractions were subjected to PCR with primers specific for ESBLs.
Molecular typing by PFGE of bacterial DNA. PFGE genotyping of
XbaI-digested genomic DNA was performed with a CHEF-DRIII
system (Bio-Rad); the images were processed using the GelCompar
software and a dendrogram was computed after band intensity
correlation using global alignment with 2 % optimization and
UPGMA (unweighted pair-group method using arithmetical averages)
clustering. The isolates were considered to be clonally related if they
showed more than 80 % similarity (or differed by fewer than three
bands) in their PFGE patterns (Kaufman, 1998; Tenover et al., 1995).
RESULTS AND DISCUSSION
Antibiotic consumption
Ceftriaxone was the most prescribed extended-spectrumcephalosporin during 2004–2007 in the hospital, as shownin Table 3. The consumption of ceftriaxone increased from1496 DDD in 2004 to 3657 in 2007, in contrast toceftazidime, which decreased from 340 DDD in 2004 to236 DDD in 2007. Cefepime was not prescribed at all andcefotaxime was only administered in a few cases. The
consumption of meropenem increased from 681 DDD in2004 to 1231 DDD in 2007. Imipenem is administered lessfrequently than meropenem. Consumption of gentamicinand ciprofloxacin exceeded b-lactams in all tested years(Table 3).
Detection of ESBLs
All strains resistant to third-generation cephalosporinswere found by DDST to produce ESBLs. The prevalence ofESBLs in 2007 was 60 %, showing significant increasescompared with 2006 (27 %), 2005 (17 %) and 2004 (14 %).
Antibiotic susceptibilities
All strains were uniformly resistant to cefuroxime, ceftazi-dime and ciprofloxacin and almost all to cefotaxime (98 %),ceftriaxone (98 %), cefepime (97 %), aztreonam (96 %) andpiperacillin/tazobactam (98 %). There was variable suscept-ibility/resistance to cefoxitin (43 % resistance) and genta-micin (83 % resistance). No resistance to ceftazidime/clavulanate or carbapenems was observed (Table 4). Theaddition of clavulanic acid reduced the MICs of ceftazidimeby more than three dilutions. The MIC90 of cefuroxime andcefotaxime exceeded 512 mg l21 and those of ceftazidimeand ceftriaxone exceeded 256 mg l21 (Table 4). The mostpotent antibiotics were ceftazidime combined with clavula-nate and carbapenems, with MIC90 of 0.25 and 0.5 mg l21,respectively (Table 4).
Conjugation
Only ten strains transferred resistance to the E. coli recipientstrain, with low frequency. Resistance to tetracycline wascotransferred to the recipient strain with cefotaxime resistancefrom ten strains and sulfamethoxazole resistance from ninestrains. Resistance to cefoxitin and ciprofloxacin was nottransferable.
Characterization of b-lactamases
The b-lactamase contents of the isolates are shown in Table 1.All isolates yielded an amplicon of 545 bp with consensusMA primers. Donor strains were also positive for SHV b-lactamases. No PCR products were obtained in transconju-gants with primers specific for blaSHV. Transconjugantstrains possessed only the CTX-M b-lactamases of group 1.Multiplex PCR was positive for group 1 of CTX-M b-lactamases. Sequencing of selected amplicons revealed thepresence of blaCTX-M-15, with coding regions containingidentical nucleotide sequences. The DNA sequence of thePCR products exhibited 98 % similarity to blaCTX-M-15 fromGenBank. The PCR Nhe test was negative for all SHV-PCRproducts, indicating the presence of the intrinsic SHV-1 b-lactamase of K. pneumoniae. The clinical isolates alsopossessed TEM-1 b-lactamase, which is not an ESBL, butthe gene encoding this enzyme was not transferable to arecipient strain in the conjugation experiment. Sequencing of
Table 3. Consumption of antibiotics (DDD) in the hospitalover time
Antibiotic 2004 2005 2006 2007
Ceftriaxone 1496 2381.5 3098.5 3657
Ceftazidime 340.5 269.4 261.3 236.3
Cefotaxime 5 0 0 5
Cefepime 0 0 0 0
Gentamicin 4409.2 4290.8 3289.2 4440.8
Ciprofloxacin 3795.7 5938.3 7682 8140.8
Imipenem 63 100 102.5 212.5
Meropenem 681.5 597.3 4990 1231
Total 74511.1 80039.6 95965.3 109851.4
CTX-M b-lactamases in Klebsiella pneumoniae
http://jmm.sgmjournals.org 1073

selected TEM amplicons revealed the presence of TEM-1 b-lactamase. PER-1 and OXA-1 b-lactamases were not found.
PCR mapping
The IS26 insertion sequence was not found. ISEcpI wasfound upstream of the blaCTX-M-15 gene.
Characterization of fluoroquinolone resistancedeterminants
PCRs with primers specific for qnrA, qnrB and qnrS geneswere negative.
Characterization of plasmids encodingESBLs
A large plasmid of approximately 150 kb was isolated fromall 20 tested strains. The strains also possessed one or twosmaller plasmids of less than 36 kb. Five different plasmidprofiles were observed. In a future study, we will digest theplasmids with EcoRI restriction endonuclease to determinewhether they are related. Plasmid extractions were positivefor CTX-M and TEM b-lactamases but negative for SHV b-lactamases.
Genotyping of the isolates
The isolates were assigned to five clusters (.85 %similarity) which contained subclusters, as shown inTable 1 and Fig. 1. The subclusters differed from eachother in two to three bands, which is consistent with asingle genetic event (point mutation or insertion ordeletion of DNA). Cluster 2 was predominant among theisolates and contained 34 isolates. Two strains weresporadic and showed distinct PFGE fingerprints (differedin .50 % of the well-resolved fragments). There wereseveral breakouts caused by genetically identical strains.
Subcluster 2b included three strains from surgical intens-ive-care units collected between August and October 2007.Subcluster 5a contained four strains from different clinicalwards and from various specimens collected in July andAugust 2007. Strains in subcluster 2d originated fromvarious hospital wards and specimens and were obtained atdifferent times.
The results of this work provide insights into the molecularepidemiology of the spread of ESBLs in K. pneumoniaeinvolved in an outbreak at a Croatian hospital. Asignificant increase in the prevalence of ESBL-producingK. pneumoniae in 2007 (60 %) indicated a hospitaloutbreak. Our study found CTX-M-15 b-lactamase to bethe most prevalent among isolates of K. pneumoniae. Thistype of CTX-M b-lactamase is the most prevalent aroundthe world, and was previously reported in nearby countriessuch as Hungary (Livermore et al., 2007), Austria (Eisneret al., 2006), Slovenia (Mesko Meglic et al., 2009) and Italy(Mugnaioli et al., 2006). It was first described in NewDelhi, India, in 1999 (Karim et al., 2001). CTX-M-15 isalso predominant in other European countries such asSwitzerland (Lartigue et al., 2007), Bulgaria (Markovskaet al., 2004), France (Lavigne et al., 2006) and Spain (Oteoet al., 2009). Previous studies also found CTX-M-15 amonghospital isolates of E. coli from Croatia (Literacka et al.,2009). CTX-M-15 differs from CTX-M-3 b-lactamase by asingle amino acid change (Asp-240AGly). In this study, wetested isolates for TEM, SHV, CTX-M and PER b-lactamases. Whereas these genes were found in all isolates,other rare types of ESBLs such as WEB or IBC cannot beexcluded without further testing, but were beyond thescope of this study.
Clustering of K. pneumoniae isolates sustains the hypo-thesis of either patient-to-patient transmission or commonsource acquisition (e.g. contaminated equipment formechanical ventilation). It is interesting that geneticallyidentical organisms appeared in different time periods, in
Table 4. Antibiotic susceptibilities of CTX-M b-lactamase-producing K. pneumoniae isolates
Antibiotic (CLSI breakpoint) MIC range MIC50 MIC90 Resistant strains (%)
Cefuroxime (¢32) 256–¢512 ¢512 ¢512 100
Ceftazidime (¢32) 32–.256 ¢256 ¢256 100
Ceftazidime/clavulanic acid* ¡0.03–2 0.12 0.25 0
Cefotaxime (¢64) 32–¢512 128 ¢¢512 98
Ceftriaxone (¢64) 32–¢256 ¢256 ¢256 98
Cefepime (¢32) 16–¢256 64 256 95
Cefoxitin (¢32) 0.5–256 16 128 43
Aztreonam (¢32) 16–128 64 128 96
Piperacillin/tazobactam (¢128/4) 64–¢128 ¢128 ¢128 98
Imipenem (¢16) ¡0.03–1 0.12 0.5 0
Meropenem (¢16) ¡0.03–4 0.12 0.5 0
Gentamicin (¢8) 0.12–¢256 64 128 83
Ciprofloxacin (¢4) 16–¢128 64 128 100
*Breakpoint for ceftazidime combined with clavulanic acid is not given by CLSI (2007).
M. Vranic-Ladavac and others
1074 Journal of Medical Microbiology 59
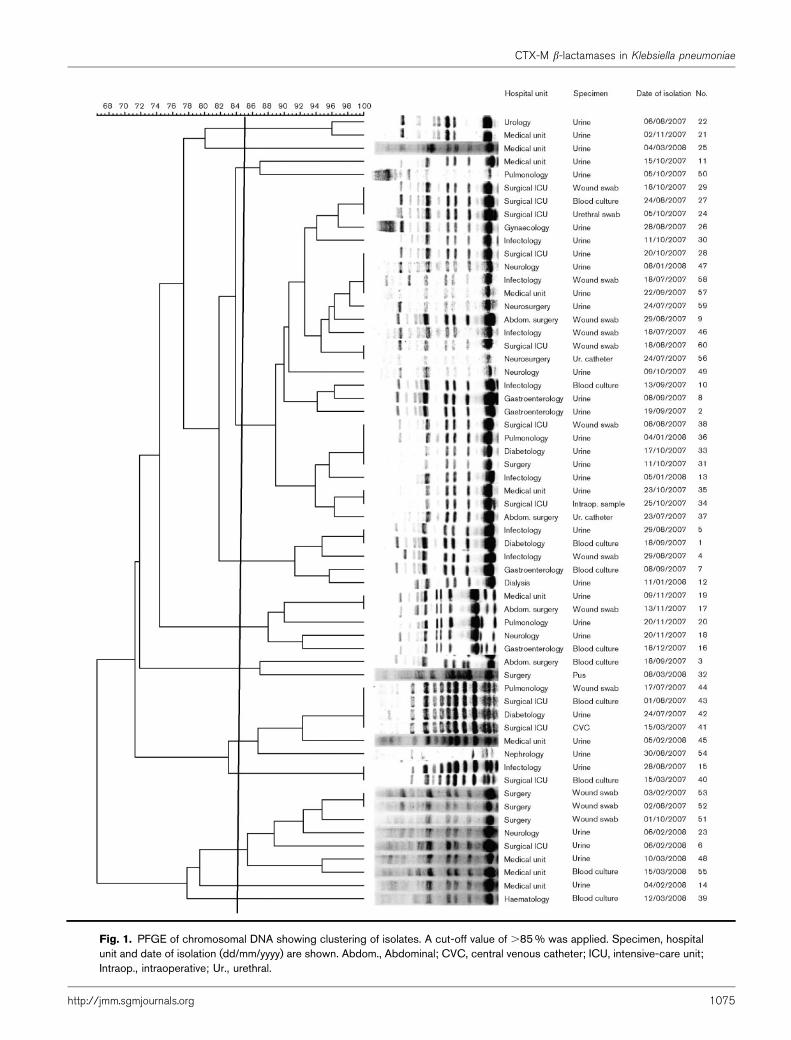
Fig. 1. PFGE of chromosomal DNA showing clustering of isolates. A cut-off value of .85 % was applied. Specimen, hospitalunit and date of isolation (dd/mm/yyyy) are shown. Abdom., Abdominal; CVC, central venous catheter; ICU, intensive-care unit;Intraop., intraoperative; Ur., urethral.
CTX-M b-lactamases in Klebsiella pneumoniae
http://jmm.sgmjournals.org 1075

different wards and patient specimens. Carbapenems arefrequently the only therapeutic option available fortreatment of hospital-acquired severe infections caused bymultiresistant ESBL-producing K. pneumoniae isolates.Nevertheless, universal susceptibility to these last-lineantimicrobials is no longer guaranteed. Resistance toceftazidime observed in all strains is consistent with theproduction of CTX-M-15 b-lactamase, which hydrolysesceftazidime efficiently, as do CTX-M-16 and CTX-M-28.These data suggest that the phenotypic approach based oncomparison of cefotaxime and ceftazidime MICs haslimited value in predicting the presence of CTX-M ESBLsin clinical isolates. The efficacy of b-lactam/inhibitorcombinations depends on the amount of enzyme. Strainsthat hyperproduce CTX-M b-lactamases usually developresistance to b-lactam/inhibitor combinations. That couldexplain the resistance to extended-spectrum cephalosporinsobserved in our strains.
Associated aminoglycoside and fluoroquinolone resistanceis frequent in ESBL-producing bacteria. Some of the strainswere resistant to cefoxitin, but resistance was nottransferable to an E. coli recipient, indicating a chro-mosomal origin of the resistance gene. Concerning non-b-lactam susceptibilities of CTX-M producers, all strainswere resistant to ciprofloxacin. High rates of resistance tociprofloxacin in CTX-M producers have also been reportedfrom Austria (Eisner et al., 2006), Canada (Pitout et al.,2005), Italy (Mugnaioli et al., 2006) and Hungary(Damjanova et al., 2008). Similar to the situation inCroatia, ciprofoxacin-resistant K. pneumoniae isolates fromHungary were associated with epidemic clones(Damjanova et al., 2008). PCRs with primers specific forqnr genes were negative. However, the fluoroquinoloneresistance in our strains was probably due to mutations ingenes coding for chromosomally encoded type II topo-isomerases, efflux pumps or porin-related proteins; deter-mination of the exact mechanism of resistance was beyondthe scope of this study. Since fluoroquinolones are oftenused to treat urinary tract infections, and the urinary tractwas the most important source of CTX-M-15-producingisolates, it is possible that fluoroquinolones exertedselection pressure that favoured survival of isolates thatpossessed quinolone resistance determinants. Coresistanceto non-b-lactam antibiotics is also frequent, either bycotransfer of the resistance determinants in the samegenetic elements (such as aminoglycoside resistance) orsimply by coselection of the two resistance mechanisms, asoccurs with fluoroquinolones.
Since plasmids encoding ESBLs also contain resistancegenes for aminoglycosides, it is possible that consumptionof these antibiotics could exert selection pressure thatfavours the spread of plasmids with ESBL genes. In thisstudy, only 10 of 60 strains possessed conjugative plasmids.Other mating methods should be tested, such as the filtermating method, to determine whether they would yieldmore transconjugants, but this was not feasible in ourlaboratory. The hospital antibiotic policy results in
ceftriaxone being the most heavily prescribed third-generation cephalosporin, which might be expected toselect for cefotaximases such as CTX-M-15. Substitution ofpiperacillin/tazobactam for extended-spectrum cephalos-porins has been shown to decrease the prevalence of ESBLsin K. pneumoniae and E. coli (Lee et al., 2007). There are nopublished reports on the correlation between antibio-tic usage and the increased prevalence of CTX-M b-lactamases, but there are bibliographic data that show thatchanges in antibiotic policy have resulted in decreases inESBL production in E. coli and K. pneumoniae (Lee et al.,2007).
Several reports have suggested that the ability of the ISEcpIelement to mobilize and promote expression of CTX-M-15is a significant factor in rapid spread of the blaCTX-M-15
gene (Markovska et al., 2004), and this could be themechanism that underlies the spread of the CTX-M-15enzyme in Croatia. However, the spread of blaCTX-M genesis largely due to the overall genetic background of thestrain and plasmid.
PFGE analysis showed that the outbreak of CTX-M-producing K. pneumoniae was caused by isolates that werehighly related, in contrast to several studies that have foundthe spread of single clones (Eckert et al., 2004; Oteo et al.,2006).
Regular evaluation of isolate characteristics and monitor-ing the spread of the more virulent isolates within inpatientpopulation are essential for timely identification andefficient management of nosocomial outbreaks. All patientswere treated with meropenem. Heightened infectioncontrol measures and discouraged use of third-generationcephalosporin antibiotics led to effective control of theoutbreak, which had ceased by the end of 2007.
The emergence of CTX-M enzymes in Croatia and elsewherehighlights the importance of using either both ceftazidimeand cefotaxime or cefpodoxime to detect possible ESBLproduction prior to performing cephalosporin–clavulanatesynergy tests for confirmation (Winstanley et al., 2004).
Outbreaks caused by CTX-M-producing organisms are stillvery rare and have been reported only sporadically(Bradford et al., 1998; Palucha et al., 1999; Kiratisin et al.,2007; Mena et al., 2006). The rapid spread of CTX-M-15 b-lactamase between different wards was attributable toclonal dissemination of related strains and horizontaltransfer of multiresistant plasmids carrying blaCTX-M-15
genes between isolates. CTX-M-15 producers constantlyevolve in the hospital, acquiring other mechanisms ofresistance to b-lactams, which is probably driven by thehigh-level use of newer b-lactam antibiotics.
Finally, the spread of CTX-M-producing members of theEnterobacteriaceae in Croatia in a manner similar to thatobserved in neighbouring countries may indicate difficult-ies in controlling this emerging resistance determinantirrespective of the antibiotic policy. This demonstrates theneed to monitor both hospitalized and general practice
M. Vranic-Ladavac and others
1076 Journal of Medical Microbiology 59

patients for the further emergence of transferable resistanceto extended-spectrum cephalosporins. Continuous surveil-lance in tracking CTX-M-producing K. pneumoniae in thehospital is necessary to prevent their influx into thecommunity.
ACKNOWLEDGEMENTS
The study was supported by the Croatian Ministry of Science,
Education and Sport, grant no. 108-1080-0015.
REFERENCES
Arlet, G., Brami, G., Decre, D., Flippo, A., Gaillot, O., Lagrange, P. H. &Philippon, A. (1995). Molecular characterization by PCR-restriction
fragment polymorphism of TEM beta-lactamases. FEMS Microbiol
Lett 134, 203–208.
Baraniak, A., Fiett, J., Sulikowska, A., Hryniewicz, W. & Gniadkowski, M.(2002). Countrywide spread of CTX-M-3 extended-spectrum beta-
lactamase-producing microorganisms of the family Enterobacteriaceae
in Poland. Antimicrob Agents Chemother 46, 151–159.
Bedenic, B. & Zagar, Z. (1998). Extended-spectrum beta-lactamases
in clinical isolates of Klebsiella pneumoniae from Zagreb, Croatia.
J Chemother 10, 449–459.
Bedenic, B., Randegger, C., Stobberingh, E. & Hachler, H. (2001).
Molecular epidemiology of extended-spectrum beta-lactamases from
Klebsiella pneumoniae strains isolated in Zagreb, Croatia. Eur J Clin
Microbiol Infect Dis 20, 505–508.
Bedenic, B., Schmidt, H., Herold, S., Monaco, M., Plecko, V., Kalenic, S.,Katic, S. & Skrlin-Subic, J. (2005). Epidemic and endemic spread of
Klebsiella pneumoniae producing SHV-5 beta-lactamase in Dubrava
University Hospital, Zagreb. J Chemother 17, 367–375.
Bonnet, R. (2004). Growing group of extended-spectrum beta-
lactamases: the CTX-M enzymes. Antimicrob Agents Chemother 48, 1–
14.
Bradford, P. A. (2001). Extended-spectrum beta-lactamases in the
21st century: characterization, epidemiology, and detection of this
important resistance threat. Clin Microbiol Rev 14, 933–951.
Bradford, P. A., Yang, Y., Sahm, D., Grope, I., Gardovska, D. &Storch, D. (1998). CTX-M-5, a novel cefotaxime-hydrolyzing beta-
lactamase from an outbreak of Salmonella typhimurim in Latvia.
Antimicrob Agents Chemother 42, 1980–1984.
Canton, R., Oliver, A., Coque, T. M., Varela,, M. del C., Perez-Dıaz, J. C.& Baquero, F. (2002). Epidemiology of extended-spectrum b-
lactamase-producing Enterobacter isolates in a Spanish hospital
during a 12-year period. J Clin Microbiol 40, 1237–1243.
Chanawong, A., M’Zali, F. H., Heritage, J., Xiong, J. H. & Hawkey, P. M.(2002). Three cefotaximases, CTX-M-9, CTX-M-13, and CTX-M-14
among Enterobacteriaceae in the People’s Republic of China.
Antimicrob Agents Chemother 46, 630–637.
CLSI (2007). Performance standards for antimicrobial susceptibility
testing, 17th informational supplement. CLSI/NCCLS document
M100-S17. Wayne, PA: Clinical and Laboratory Standards Institute.
Damjanova, I., Toth, A., Paszti, J., Hajbel-Vekony, G., Jakab, M.,
Berta, J., Milich, H. & Fuzi, M. (2008). Expansion and countrywide
dissemination of ST11, ST15, and ST147 ciprofloxacin-resistant CTX-
M-15-type b-lactamase-producing Klebsiella pneumoniae epidemic
clones in Hungary in 2005 – the new ‘MRSAs’? J Antimicrob
Chemother 62, 978–985.
Eckert, C., Gautier, V., Saladin-Allard, M., Hidri, N., Verdet, C., Ould-Hocine, Z., Barnaud, G., Delisle, F., Rossier, A. & other authors(2004). Dissemination of CTX-M-type beta-lactamases among clinical
isolates of Enterobacteriaceae in Paris, France. Antimicrob Agents
Chemother 48, 1249–1255.
Edelstein, M., Pimkin, M., Palagin, I., Edelstein, I. & Stratchounski, L.(2003). Prevalence and molecular epidemiology of CTX-M extendedspectrum beta-lactamase-producing Escherichia coli and Klebsiella
pneumoniae in Russian hospitals. Antimicrob Agents Chemother 47,
3724–3732.
Eisner, A., Fagan, E. J., Feierl, G., Kessler, H. H., Marth, E., Livermore,D. M. & Woodford, N. (2006). Emergence of Enterobacteriaceae
isolates producing CTX-M extended-spectrum beta-lactamase inAustria. Antimicrob Agents Chemother 50, 785–787.
Elwell, L. P. & Falkow, S. (1986). The characterization of R plasmids
and the detection of plasmid-specified genes. In Antibiotics inLaboratory Medicine, 2nd edn, pp. 683–721. Edited by V. Lorian.
Baltimore: Williams & Wilkins.
Jacoby, G. A. & Munoz-Price, L. S. (2005). The new beta-lactamases.
N Engl J Med 352, 380–391.
Jarlier, V., Nicolas, M. H., Fournier, G. & Philippon, A. (1988).Extended broad-spectrum beta-lactamases conferring transferable
resistance to newer beta-lactam agents in Enterobacteriaceae: hospitalprevalence and susceptibility patterns. Rev Infect Dis 10, 867–878.
Karim, A., Poirel, L., Nagarajan, S. & Nordmann, P. (2001). Plasmid-
mediated extended-spectrum beta-lactamase (CTX-M-3 like) fromIndia and gene association with insertion sequence ISEcp1. FEMS
Microbiol Lett 201, 237–241.
Kaufman, M. E. (1998). Pulsed-field gel electrophoresis. In MolecularBacteriology. Protocols and Clinical Applications, pp. 33–51. Edited
by N. Woodford & A. Johnson. Totowa, NJ: Humana Press.
Kiratisin, P., Apisarnthanarak, A., Saifon, P., Laesripa, C., Kitphati, R.& Mundy, L. M. (2007). The emergence of a novel ceftazidime-resistant
CTX-M extended-spectrum beta-lactamase, CTX-M-15, in bothcommunity-onset and hospital-acquired infections in Thailand.
Diagn Microbiol Infect Dis 58, 349–355.
Kliebe, C., Nies, B. A., Meyer, J. F., Toixdorf-Neutzling, R. M. &Wiedemann, B. (1985). Evolution of plasmid-coded resistance to
broad-spectrum cephalosporins. Antimicrob Agents Chemother 28,302–307.
Lartigue, M. F., Zinsius, C., Wenger, A., Bille, J., Poirel, L. &Nordmann, P. (2007). Extended-spectrum beta-lactamases of theCTX-M type now in Switzerland. Antimicrob Agents Chemother 51,
2855–2860.
Lavigne, J. P., Marchandin, H., Delmas, J., Bouziges, N., Lecaillon, E.,Cavalie, L., Jean-Pierre, H., Bonnet, R. & Sotto, A. (2006). qnrA in
CTX-M producing Escherichia coli isolates from France. AntimicrobAgents Chemother 50, 4224–4228.
Lee, J., Pai, H., Kim, N. H., Eun, B. W., Kang, H. J. K., Park, K. H., Choi,E. H., Shin, H. Y., Kim, E. C. & other authors (2007). Control ofextended-spectrum b-lactamase-producing Escherichia coli and
Klebsiella pneumoniae in a children’s hospital by changing anti-
microbial agent usage policy. J Antimicrob Chemother 60, 629–637.
Literacka, E., Bedenic, B., Baraniak, A., Fiett, J., Tonkic, M., Jajic-Bencic, I. & Gniadkowski, M. (2009). blaCTX-M genes in Escherichia
coli from Croatian hospitals are located in new (blaCTX-M-3a) andwidely spread (blaCTX-M-3a and blaCTX-M-15) genetic structures.
Antimicrob Agents Chemother 53, 1630–1635.
Livermore, D. M., Canton, R., Gniadkowski, M., Nordmann, P.,Rossolini, G. M., Arlet, G., Ayala, J., Coque, T. M., Kern-Zdanowicz, I.& other authors (2007). CTX-M: changing the face of ESBLs inEurope. J Antimicrob Chemother 59, 165–174.
CTX-M b-lactamases in Klebsiella pneumoniae
http://jmm.sgmjournals.org 1077

Markovska, R., Schneider, I., Keuleyan, E. & Bauernfeind, A. (2004).Extended-spectrum beta-lactamase (ESBL) CTX-M-15-producingEscherichia coli and Klebsiella pneumoniae in Sofia, Bulgaria. ClinMicrobiol Infect 10, 752–755.
Mena, A., Plascencia, V., Garcia, L., Hidalgo, O., Ayestaran, J. I.,Alberti, S., Borrell, N., Perez, J. L. & Oliver, A. (2006). Characterizationof a large outbreak by CTX-M-1-producing Klebsiella pneumoniaeand mechanisms leading to in vivo carbapenem resistance devel-opment. J Clin Microbiol 44, 2831–2837.
Mesko Meglic, K., Koren, S., Palepou, M. F. I., Karisik, E., Livermore,D. M., Pike, R., Andolovic, A., Jeverica, S., Krizan-Hergouth, V. &other authors (2009). Nationwide survey of CTX-M-type extended-spectrum b-lactamases among Klebsiella pneumoniae isolates inSlovenian hospitals. Antimicrob Agents Chemother 53, 287–291.
Mugnaioli, C., Luzzaro, F., De Luca, F., Brigante, G., Perilli, M.,Amicosante, G., Stefani, S., Toniolo, A. & Rossolini, G. M. (2006).CTX-M-type extended-spectrum beta-lactamases in Italy: molecularepidemiology of an emerging countrywide problem. AntimicrobAgents Chemother 50, 2700–2706.
Nuesch-Inderbinen, M. T., Hachler, H. & Kayser, F. H. (1996).Detection of genes coding for extended-spectrum SHV beta-lactamases in clinical isolates by a molecular genetic method, andcomparison with the E test. Eur J Clin Microbiol Infect Dis 15, 398–402.
Oteo, J., Navarro, C., Cercenado, E., Delgrado-Iribarren, A., Wilhelmi, I.,Orden, B., Garcıa, C., Miguelanez, S., Perez-Vazquez, M. & otherauthors (2006). Spread of Escherichia coli strains with high-levelcefotaxime and ceftazidime resistance between the community, long-term facilities, and hospital institutions. J Clin Microbiol 44, 2359–2366.
Oteo, J., Cuevas, O., Lopez-Rodrıgez, I., Banderas-Florido, A.,Vindel, A., Perez-Vazquez, M., Bautista, V., Arroyo, M., Garcıa-Cabellero, J. & other authors (2009). Emergence of CTX-M-15-producing Klebsiella pneumoniae of multilocus sequence types 1, 11,14, 17, 20, 35 and 36 as pathogens and colonizers in newborns andadults. J Antimicrob Chemother 64, 524–528.
Pagani, L., Mantengoli, E., Migliavacca, R., Nucleo, E., Pollini, S.,Spalla, M., Daturi, R., Romero, E. & Rossolini, G. M. (2004).Multifocal detection of multidrug-resistant Pseudomonas aeruginosaproducing PER-1 extended-spectrum beta-lactamase in NorthernItaly. J Clin Microbiol 42, 2523–2529.
Palucha, A., Mikiewicz, B., Hryniewicz, W. & Gniadkowski, M. (1999).Concurrent outbreaks of extended-spectrum beta-lactamase-pro-ducing organisms of the family Enterobacteriaceae in a Warsawhospital. J Antimicrob Chemother 44, 489–499.
Pitout, J. D., Nordmann, P., Laupland, K. B. & Poirel, L. (2005).Emergence of Enterobacteriaceae producing extended-spectrum beta-lactamases in the community. J Antimicrob Chemother 56, 52–59.
Pournaras, S., Ikonomidis, A., Kristo, I., Tsakris, A. & Maniatis, A. N.(2004). CTX-M enzymes are the most common extended-spectrum
beta-lactamases among Escherichia coli in a tertiary Greek hospital.J Antimicrob Chemother 54, 574–575.
Quinteros, M., Radice, M., Gardella, N., Rodriguez, M. M., Costa, N.,Korbenfeld, D., Couto, E., Gutkind, G. & Microbiology Study Group(2003). Extended-spectrum beta-lactamases in Buenos Aires,Argentina, public hospitals. Antimicrob Agents Chemother 47, 2864–2867.
Robicsek, A., Jacoby, G. A. & Hooper, D. C. (2006a). The worldwideemergence of plasmid-mediated quinolone resistance. Lancet InfectDis 6, 629–640.
Robicsek, A., Strahilevitz, J., Sahm, D. F., Jacoby, G. A. & Hooper, D. C.(2006b). qnr prevalence in ceftazidime-resistant Enterobacteriaceaeisolates from the United States. Antimicrob Agents Chemother 50, 2872–2874.
Saladin, M., Cao, V. T., Lambert, T., Donay, J. L., Herrmann, J. L.,Ould-Hocine, Z., Verdet, C., Delisle, F., Philippon, A. & Arlet, G.(2002). Diversity of CTX-M beta-lactamases and their promoterregions from Enterobacteriaceae isolated in three Parisian hospitals.FEMS Microbiol Lett 209, 161–168.
Tenover, F. C., Arbeit, R. D., Goering, R. V., Mickelsen, P. A., Murray,B. E., Persing, D. H. & Swaminathan, B. (1995). Interprintingchromosomal DNA restriction patterns produced by pulsed-field gelelectrophoresis: criteria for bacterial strain typing. J Clin Microbiol 33,2233–2239.
Tonkic, M., Bedenic, B., Goic-Barisic, I., Katic, S., Kalenic, S.,Kaufmann, M. E., Woodford, N. & Punda-Polic, V. (2007). First reportof CTX-M producing isolates from Croatia. J Chemother 19, 97–100.
Winstanley, T. G., Ridgway, E. J., Parys, B. T., Woodford, N., Ward, E.& Livermore, D. M. (2004). First isolation of CTX-M-3 beta-lactamaseproducer in the United Kingdom. Int J Antimicrob Agents 24, 625–627.
Woodford, N., Ward, M. E., Kaufmann, M. E., Turton, J., Fagan, E. J.,James, D., Johnson, A. P., Pike, R., Warner, M. & other authors(2004). Community and hospital spread of Escherichia coli producingCTX-M extended-spectrum beta-lactamases in the UK. J AntimicrobChemother 54, 735–743.
Woodford, N., Ellington, M. J., Coelho, J., Turton, J., Ward, M. E.,Brown, S., Amyes, S. G. B. & Livermore, D. M. (2006). Multiplex PCRfor genes encoding prevalent OXA carbapenemases. Int J AntimicrobAgents 27, 351–353.
Yamasaki, K., Komatsu, M., Yamashita, T., Shimakawa, K., Ura, T.,Nishio, H., Satoh, K., Washidu, R., Kinoshita, S. & Aihara, M. (2003).Production of CTX-M-3 extended-spectrum beta-lactamase andIMP-1 metallo-b-lactamase by five Gram-negative bacilli: survey ofclinical isolates from seven laboratories collected in 1998 and 2000, inthe Kinki region of Japan. J Antimicrob Chemother 51, 631–638.
Yu, W. L., Winokur, P. & Von Stein, D. L. (2002). First description ofKlebsiella pneumoniae harboring CTX-M-b-lactamases (CTX-M-14and CTX-M-3) in Taiwan. Antimicrob Agents Chemother 46, 1098–1100.
M. Vranic-Ladavac and others
1078 Journal of Medical Microbiology 59




















