Clinical study of craniospinal compliance non-invasive monitoring method
11
A e-/'s, /Aur-O/r4r- Jr-1?/ CLINICAL STUDY OF CRANIOSPINAL COMPLIANCE NON.INVASIVL.ZAO V' MONITORING METHOD A. Ragauskast, G. Daubarisl, V. Petkus2, R. Sliteris2, R. Raisutis2, I. pip.r3, S.Rockaa, E. Jarzemskasa, V. Matijosaitiss t Kaunas University of Technology, Lithuania 2 Vittamedtechnologijos, Lithuania, 3 Southern General Hospital, Glasgow, U.K., a Viltti.tr University EmergencyHospital, Lithuania, s Hospital of KaunasUniversity of Medicine, Lithuania Contact person: Arminas Ragauskas, University Professor, DSc, FBC, FLSHD Head of Telematics Sc. Lab. Kaunas University of Technology, Lithuania Studentu 50-451a, LT-3031, Kaunas, Lithuania Tel:+370 686 20084 Fax: +370 37 736897 E-mail: [email protected]
Transcript of Clinical study of craniospinal compliance non-invasive monitoring method

A e-/'s, /Aur-O/r4r- Jr-1?/
CLINICAL STUDY OF CRANIOSPINAL COMPLIANCE NON.INVASIVL.ZAO V'
MONITORING METHOD
A. Ragauskast, G. Daubarisl, V. Petkus2, R. Sliteris2, R. Raisutis2, I. pip.r3, S. Rockaa,
E. Jarzemskasa, V. Matijosaitiss
t Kaunas University of Technology, Lithuania
2 Vittamed technologijos, Lithuania,
3 Southern General Hospital, Glasgow, U.K.,
a Viltti.tr University Emergency Hospital, Lithuania,
s Hospital of Kaunas University of Medicine, Lithuania
Contact person:
Arminas Ragauskas, University Professor, DSc, FBC, FLSHD
Head of Telematics Sc. Lab.
Kaunas University of Technology, Lithuania
Studentu 50-451a, LT-3031, Kaunas, Lithuania
Tel: +370 686 20084
Fax: +370 37 736897
E-mail: [email protected]
Summary
The ability to quantify non-invasively the effect of posture on intracranial physiology by using cine
phase-contrast MRI may lead to the development of new diagnostic tests to evaluate such functions
as regulation of CBF and ICP, and the effect of pathologies on these functions. Results similar to
MRI technology can be obtained using non-invasive ultrasonic method (Vittamed) for intracranial
blood volume pulse wave (IBVPW) measurement and intracraniospinal compliance (ICC)
monitoring.
IBVPW have been investigated in supine and urpright positions of healthy volunteers using
Vittamed technology. A group of 13 healthy volunteers (9F, 4M, mean age25.I+l-3.4) was studied.
More than 3000 IBVPW were analysed in order to show the difference of shape and amplitude in
supine and upright positions. Averaged shape of ten IBVPW waves was presented in the
normalized window with dimensions 1.0x1.0.
The results show significant difference between averaged IBVPW shapes in upright (highest
intracraniospinal compliance) and supine (lower intracraniospinal compliance) body positions.
Body posture caused IBVPW subwave P2 and P3 changes LP2:l9o/o and AP3:IIyo .
Amplitude of IBVPW in upright body position was significantly higher than in the supine one. The
value of IBVPW amplitude's ratio in supine and upright positions was 1.55+/-0.61.
Keywords: Body posture, ICP, intracranial blood volume pulse waves, cerebral hemodynamics,
non-invasive monitoring, craniospinal compliance
Introduction
Body posture strongly affects intracranial hydrodynamics and cerebral hemodynamics. The link
between posture-related changes in cerebral hemodynamics, intracranial hydrodynamics, and
paterns of venous drainage can be quantified by cine phase-contrast MRI [1 ,2] . The ability to non-
invasively quantify the effect of posture on intracranial physiology may lead to the development of
new diagnostic tests to evaluate such functions as regulation of CBF and ICP, and the effect of
pathologies on these functions. It has been shown that in the posture change of healthy volunteers
from supine to upright postures the intracraniospinal compliance changes up to 2.8 times when ICPL

changes from 10.6+/-3.6mmHg to 4.5+l-L 82 mmHg [2]. The study [2] showed that posture-related
changes in ICC and ICP have a great impact on cerebral blood as well as on CSF circulation. It also
has been shown in the original MRI study that the shape of IBV pulse waves is strongly related to
the intracraniospinal compliance [2].
In our study we found that similar to MRI technology results can be obtained using non-invasive
ultrasonic method (Vittamed) for intracranial blood volume pulse wave (IBVPW) measurement [3-
14]. The method has been tested using simultaneous invasive ICP and non-invasive IBV wave
monitoring of TBI patients. A study on piglets also has been performed, and body posture effect on
ICP and IBV pulse wave shape has been investigated [7]. 13 patients with TBI were monitored
following Clinical Research Protocol No.99124006, AIBS No.990135, HSSRB log No.A-9676.87
hours of simultaneous monitoring of invasive and non-invasive data were analyzed [3,9].
Diagnostic value of IBV pulse waves has been investigated in our previous studies [4, 8, 10, i 1,14].
A total of 75 patients were examined using Vittamed technology and these included cases of acute,
chronic and stabilized hydrocephalus, spinal cord injury and terminal blood flow [3,8,10]. These
were compared to a control group of 53 healthy volunteers. A detectable change in IBV pulse
waveform shape was observed in situations when disturbance in intracranial hydrodynamics was
present, e.g., during hypoventilation tests, in cases of terminal blood flow and hydrocephaly,
depicting the level of hydrocephalus activity and the patient's compensatory capabilities as well as
the effect of treatment [3,8,10].
The objective of the present study was to investigate changes in IBV pulse wave shape of healthy
volunteers in supine and upright body positions using new ultrasonic Vittamed monitor 105.
Materials and Methods
A non-invasive method of intracranial blood volume measurement using ultrasound is based upon
the transmission of short ultrasonic pulses from one side of the skull to the other and dynamic
measurements of the time-of-flight of ultrasonie pulses. The time-of-flight depends on the acoustic
properties of intracranial blood, brain tissue and cerebrospinal fluid. Changes in any of these
components' volume will change the time-of-flight [6]. 3

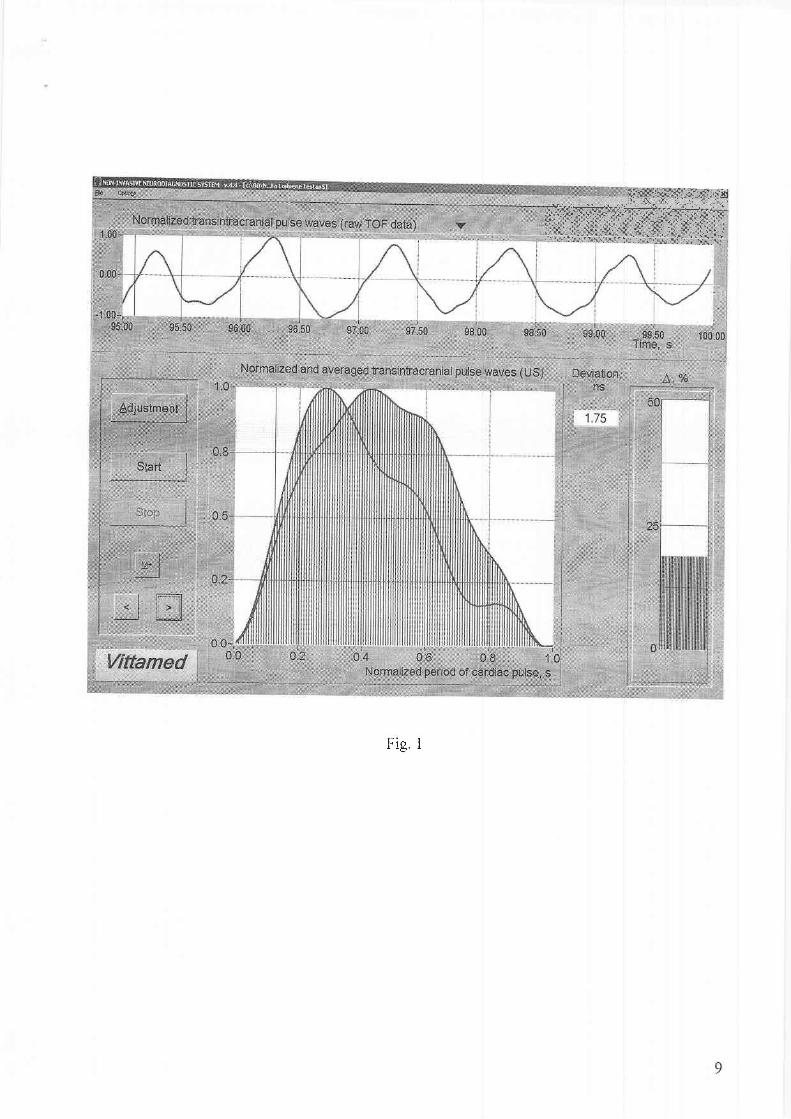
Following previous clinicai studies new Vittamed monitor model 105 has been created (Fig. 1). It
has been used to measure and record waveforms at a sampling frequency of 25 Hz.In order to
decrease the influence of heart rate changes and respiratory modulation on the measured
waveforms, the measured IBV pulse waves were averaged over at least three respiratory cycles and
normalized to the peak value. What we have termed the normahzation window in a 1.0x1.0
dimensionless grid, is shown in Fig. 1 and readily allows comparison of different IBV pulse wave
recordings.
A group of 13 healthy volunteers ((9F" 4M, mean age 25.1+/-3.4) were studied in supine and
upright body positions. They had no history of headaches, neuroinfections, head trauma,
neurosurgical operations or any other symptoms of elevated ICP. Volunteers were investigateci.
following the protocol beginning in upright (standing) position with 3 minutes data recording test.
A three-minutes resting time interval was used after taking supine body position. After that. a
three-minutes recording was performed.
Before the recording, a mechanical frame with ultrasonic transducers and sonopads has been fixed
on the human head in the intraventricular acoustic path position. An electrocardiographic 3-lead
channel was used for synchronization of each IBV pulse wave recording. Pulse waves which were
distorted by artefacts have been automatically excluded from further waveform analvsis bv
software of Vittamed 105 monitor.
Arterial blood pressure was measured in upright and supine positions. More than 3000 IBV pulse
waves were analyzed in order to show the difference of IBV pulse wave shape and amplitude in
supine and upright positions.
Results and Discussion
The results of comparison of simultaneous invasive and non-invasive (after linear conversion) ICp
pulse waves monitoring in ICU are shown in Fig. 2. As follows from Fig.2 correlation factor range
is from r:0.973, p:0.00000025 (ICP:80mmHg) to r:0.706, p:0.000001 (ICP:20mmHg). The
possibility to obtain information about pulse wave shape non-invasively is evident.

The difference of averaged IBV pulse wave shape and its amplitude of the group of 13 healthy
volunteers in supine and upright body positions is shown in Fig. 3 a) and b). Arterial blood pressure
in the group of healthy volunteers was measured in both body positions. It was llg+l-g mmHg and
74+l- 7mmHginsupineposit ion and,I22+/- 10mmHg /78+/-8mmHginuprightposit ion.
Results show significant difference of IBV pulse wave shapes in upright (highest intracraniospinal
compliance) and supine (lower intracraniospinal compliance) body positions. Body posture caused
IBV pulse waves subwaves P2 and, P3 changes LP2:18%o and,AP3:l Iyofor the group of healthy
volunteers (Fig' 3 a)). The differences are statistically signifrcant with a p value of 0.00001 or
smaller.
The amplitude of IBV pulse wave shape in upright body position was significantly higher than in
supine body position (the averaged value of the amplitude's ratio was 1.55+/-0.61). Such
differences in IBV pulse wave shapes (Fig. 3 a)) and amplitudes (Fig. 3 b)) can be expla.ined by
physiological changes of arterial / venous blood and CSF volumetric waves in different body
positions. It has been discovered in previous studies that total venous outflow in upright position is
lower comparing to that of supine position [2]. Slightly lower total cerebral blood flow and smaller
CSF volume were found to be in the sitting position [2].
The effect of posture on intracraniospinal physiology can be quantified by ultrasonic Vittamed IBV
pulse wave measurement method. It has shown that ultrasonically measured IBV pulse wave shape
and amplitude depend on the body posture and intracraniospinal compliance changes.
Ultrasonically measured posture-related changes of IBV pulse wave shape reflect the
intracraniospinal hydrodynamics and cerebral hemodynamics.
Acknowledgements
The research was supported by the US Dept. of Defence (Agreement DAMD17-00-2-0065) and EU
Structural Funds (Proj ect BPD04-ERPF-3 . 1 . 7-03 - 0 5/0020).

References
1' Raksin P B, Alperin N, et al. Noninvasive intracranial compliance and pressure based on
dynamic MRI of blood flow and CSF flow. Neurosurg Focus ra@);Article 4,2003
2. Alperin N, et al. Quantifying the Effect of Posture on Intracranial Physiology in Humans by MRI
Flow Studies. J Magn Reson Imaging 2005;22:591-596
3. Chambers I R, Daubaris G, Jarzemskas E, Fountas K, Kvascevicius R, Ragauskas A, Rocka S,
Robinson J S, Sitkauskas A. The clinical application of non-invasive intracranial blood volume
pulse wave monitoring. Physiological Measurements 2005,yo1.26, no. 6, p. 1019-1032
4' Fountas KN, Sitkauskas A, Feltes CH, Kapsalaki EZ, Dimopoulos VG, Kassam M, Grigorian
AA, Robinson JS, Ragauskas A. Is non-invasive monitoring of intracranial pressure waveform
analysis possible? Preliminary results of a comparative study of non-invasive vs. invasive
inttactanial slow-wave waveform analysis monitoring in patients with traumatic brain iniurv. Med
Sci Monit 2005: 1l(2): 58-63
5. Ragauskas A, Daubaris G. US Patents 5,388,583, 1995,6,387.051,2002
6. Ragauskas A, Daubaris G, Ragaisis V, Petkus V. Implementation of non-invasive brain
physiological monitoring concepts. Medical Engineering and Physics 2003;25:667-678
7. Ragauskas A, Kanapienis A. Simultaneous invasive and noninvasive ICP waves study on
animals. Medical & Biological Engineering & Computing: proceedings of the l lth Nordic-Baltic
Conference on Biomedical Engineering, June 6-10, 7999, Tallin, Estonia. Herts. UK : peter
Peregrinus Ltd. ISSN 0140-01 18. 1999, Vol. 37, S. 1, p. 330-331
8. Rocka S. Hydrodynamic peculiarities of the non-invasively acquired ultrasonic intracranial pulse
waves. Doctoral thesis of Biomedical Sciences, Vilnius University Emergency Hospital, 2003
9. Ragaisis V. Non-invasive optimised monitoring of cerebrovascular autoregulation in patients
after severe head injury. Doctoral thesis of Biomedical Sciences, Hospital of Kaunas University of
Medicine.2003

10' Kvascevicius R' Transintracranial ultrasonic diagnostics in hydrocephalus. Doctoral thesis of
Biomedical Sciences, vilnius university Emergency Hospital, 2003
l1' Kalasauskas L. Diagnosis and treatment of traumatic subdural hygromas, possibility of using
the new noninvasive ultrasonographic method. Doctoral thesis of Biomedical Sciences, Hospital of
Kaunas University of Medicine, 2003
12. Matukevicius A' Testing of intracranial medium volume dynamics by using new sonographic
technology. Doctoral thesis of Biomedical Sciences, Hospital of Kaunas University of Medicine,
2000
13' Deltuva V. Intracranial pressue measuring by using non-invasive sonographic technology.
Doctoral thesis of Biomedical Sciences, Hospital of Kaunas University of Medicin e, 1999
14. Ragauskas A et al. Cerebrovasc Dis 1999;9 (suppl 2):31,46; 2000;10 (suppl l):34; 2001;
1 1(suppl 3):44;2002;13 (suppl 4,25); 2003;16 (suppl 4): I 8, 2004;17 (suppl 4):04

Figure legends
Fig. 1. The display panel of the non-invasive Vittarned monitor for intracranial blood volume pulsewave shape comparison. Two IBV pulse waves are shown in normalised window with dimensions1.0x1.0: reference wave (left wave) in upright bocly position, the wave under comparison (rightwave) in supine body posture,ruhen ICp has been elevated
Fig. 2' Simultaneous invasive and non-invasive records of ICP pulse waves when ICp : g0 mmHg(a), ICP:60 mmHg (b), ICP :40 mmHg (c) and ICp:20 mmHg (d) applying invasive caminJand non-invasive Vittamed mo,nitors (TBI patient in coma)
Fig. 3. iBV pulse wave averaged shapes of the group of 13 healthy volunteers in upright andsupine body positions: a) with marked P1, P2 and P3 subwaves and their differences Ap2=7gyo andAP3:710/o which were cause<l by body posture. Vertical bars show physiological fluctuations ofpulse wave shape expressed a.s +/-SD for all the group of healthy volunteersib) non_normalizedIBV pulse waves in upright and supine body postures
*ff.S;r *{.tr +!
trtrry#ry
F io 1

Pulse waves (lGP=80mmHg)
1 08o
C"- 4
a ' 0
f , -z4-o
-8
1 0Io
P 4l zd 0
! - z4-6-n
1
Time, s
a)
1 0R
6E tT , 4
E 2I L Uo
4-6-8
1 0Io
C"I 4E ^E zd 0oa - z
4-o
{
Fig.2
Pulse waves (lGP=40rnmHg)
d)
1 0

i ,i '
l :o 0_61 ;v
rooN n r
I
EL
oz
U)
a,(s7ou)o_
co
0.3 a.4 0.5 0.6 0
Normalized cardiac cycle,
Normalized cardiac cycld, s
b)
Fig. 3
0 . 2 0 3 0 4 0 5 0 . 6 0 . 7 0 B 0 . 9
l 1