Clinical Pharmacology made Incredibly Easy!®, Third Edition
450
-
Upload
khangminh22 -
Category
Documents
-
view
5 -
download
0
Transcript of Clinical Pharmacology made Incredibly Easy!®, Third Edition

Rahimullah
Text Box
Download From: AghaLibrary.com


Clinical Pharmacology
made
IncrediblyEasy!IncrediblyEasy!
®
938900FM.qxd 08/26/2008 18:11 Page i
Rahimullah
Text Box
Download From: AghaLibrary.com

938900FM.qxd 08/26/2008 18:11 Page ii

Clinical Pharmacology
made
IncrediblyEasy!IncrediblyEasy!
®
938900FM.qxd 08/26/2008 18:11 Page iii

Staff
Executive Publisher
Judith A. Schilling McCann, RN, MSN
Editorial Director
David Moreau
Clinical Director
Joan M. Robinson, RN, MSN
Art Director
Mary Ludwicki
Clinical Project Manager
Jennifer Meyering, RN, BSN, MS, CCRN
Editors
Margaret Eckman, Diane Labus
Copy Editors
Kimberly Bilotta (supervisor), Jane Bradford,Shana Harrington, Lisa Stockslager, Dorothy P. Terry, Pamela Wingrod
Designer
Georg W. Purvis IV
Illustrator
Bot Roda
Digital Composition Services
Diane Paluba (manager), Joy Rossi Biletz, Donna S. Morris
Associate Manufacturing Manager
Beth J. Welsh
Editorial Assistants
Karen J. Kirk, Jeri O’Shea, Linda K. Ruhf
Indexer
Barbara Hodgson
The clinical treatments described and recommended in this
publication are based on research and consultation with nurs-
ing, medical, and legal authorities. To the best of our knowl-
edge, these procedures reflect currently accepted practice.
Nevertheless, they can’t be considered absolute and universal
recommendations. For individual applications, all recommen-
dations must be considered in light of the patient’s clinical
condition and, before administration of new or infrequently
used drugs, in light of the latest package-insert information.
The authors and publisher disclaim any responsibility for any
adverse effects resulting from the suggested procedures, from
any undetected errors, or from the reader’s misunderstanding
of the text.
© 2009 by Lippincott Williams & Wilkins. All rights reserved.
This book is protected by copyright. No part of it may be repro-
duced, stored in a retrieval system, or transmitted, in any form
or by any means—electronic, mechanical, photocopy, record-
ing, or otherwise—without prior written permission of the
publisher, except for brief quotations embodied in critical arti-
cles and reviews and testing and evaluation materials provid-
ed by publisher to instructors whose schools have adopted its
accompanying textbook. Printed in the United States of Ameri-
ca. For information, write Lippincott Williams & Wilkins, 323
Norristown Road, Suite 200, Ambler, PA 19002-2756.
CPIE3E—010608
Library of Congress Cataloging-in-Publication DataClinical pharmacology made incredibly easy!. — 3rd ed.
p. ; cm.Includes bibliographical references and index.1. Clinical pharmacology — Outlines, syllabi, etc. I. Lippincott Williams & Wilkins. [DNLM: 1. Pharmacology, Clinical — methods — Handbooks. 2. Drug Therapy — Handbooks. 3. PharmaceuticalPreparations — Handbooks. QV 39 C6417 2008]RM301.28.C556 2008
615'.1—dc22ISBN-13: 978-0-7817-8938-7 (alk. paper)ISBN-10: 0-7817-8938-9 (alk. paper) 2008009967
938900FM.qxd 08/26/2008 18:11 Page iv
Rahimullah
Text Box
Download From: AghaLibrary.com

v
ContentsContributors and consultants vii
Not another boring foreword ix
1 Fundamentals of clinical pharmacology 1
2 Autonomic nervous system drugs 21
3 Neurologic and neuromuscular drugs 49
4 Pain medications 93
5 Cardiovascular drugs 119
6 Hematologic drugs 155
7 Respiratory drugs 175
8 Gastrointestinal drugs 195
9 Genitourinary drugs 223
10 Anti-infective drugs 237
11 Anti-inflammatory, anti-allergy, andimmunosuppressant drugs 293
12 Psychotropic drugs 311
13 Endocrine drugs 339
14 Drugs for fluid and electrolyte balance 359
15 Antineoplastic drugs 371
Other major drugs 414
Vaccines and treatment for biological weapons exposure 421
Treatment and antidotes for chemical weapons exposure 422
Herbal drugs 423
Selected references 426
Index 427
Internet drug updates eDruginfo.com
938900FM.qxd 08/26/2008 18:11 Page v

938900FM.qxd 08/26/2008 18:11 Page vi

vii
Tricia M. Berry, PharmD, BCPS
Associate Professor of Pharmacy PracticeSt. Louis College of Pharmacy
Victor Cohen, BS, PharmD, BCPS
Assistant Professor of Pharmacy PracticeArnold & Marie Schwartz College of Pharmacy & Health
SciencesClinical Pharmacy Manager & Residency Program DirectorMaimonides Medical CenterBrooklyn, N.Y.
Jason C. Cooper, PharmD
Clinical Specialist, MUSC Drug Information CenterMedical University of South CarolinaCharleston
Michele A. Danish, PharmD, RPH
Pharmacy Clinical ManagerSt. Joseph Health ServicesNorth Providence, R.I.
Glen E. Farr, PharmD
Professor of Clinical Pharmacy & Associate DeanUniversity of Tennessee College of PharmacyKnoxville
Tatyana Gurvich, PharmD
Clinical PharmacologistGlendale (Calif.) Adventist Family Practice Residency Program
Catherine A. Heyneman, PharmD, MS, ANP
Associate Professor of Pharmacy PracticeIdaho State University College of PharmacyPocatello
Samantha P. Jellinek, PharmD, BCPS
Clinical Pharmacy Manager for Medication Reconciliation &Safety
Clinical Coordinator, Pharmacy Practice Residency ProgramMaimonides Medical CenterBrooklyn, N.Y.
Christine K. O’Neil, PharmD, BCPS, CGP, FCCP
Professor of Pharmacy PracticeDuquesne UniversityMylan School of PharmacyPittsburgh
Jean Scholtz, PharmD, BCPS, FASHP
Associate ProfessorDepartment of Pharmacy Practice and Pharmacy AdministrationUniversity of the Sciences in Philadelphia
Anthony P. Sorrentino, PharmD
Assistant Professor of Clinical PharmacyPhiladelphia College of PharmacyUniversity of the Sciences in Philadelphia
Suzzanne Tairu, PharmD
Clinical SpecialistThe Medical Affairs Company/Consultant for Pfizer Kennesaw, Calif.
Karen Jo Tietze, BS, PharmD
Professor of Clinical PharmacyPhiladelphia College of PharmacyUniversity of the Sciences in Philadelphia
Contributors and consultants
938900FM.qxd 08/26/2008 18:11 Page vii
Rahimullah
Text Box
Download From: AghaLibrary.com

938900FM.qxd 08/26/2008 18:11 Page viii

ixix
Not another boring foreword
If you’re like me, you’re too busy caring for your patients to wade through a foreword thatuses pretentious terms and umpteen dull paragraphs to get to the point. So let’s cut right tothe chase! Here’s why this book is so terrific:
It will teach you all the important things you need to know about clinicalpharmacology. (And it will leave out all the fluff that wastes your time.)
It will help you remember what you’ve learned.
It will make you smile as it enhances your knowledge and skills.
Don’t believe me? Try these recurring logos on for size:
Now I get it! illustrates normal physiology and the physiology of drug actions.
Warning! alerts you to potentially dangerous adverse reactions.
Yea or nay? sorts through current issues related to drug risks and benefits.
Safe and sound explains how to administer medications safely.
Memory jogger reinforces learning through easy-to-remember mnemonics.
938900FM.qxd 08/26/2008 18:11 Page ix
Rahimullah
Text Box
Download From: AghaLibrary.com

x
See? I told you! And that’s not all. Look for me and my friends in the marginsthroughout this book. We’ll be there to explain key concepts, provideimportant care reminders, and offer reassurance. Oh, and if you don’tmind, we’ll be spicing up the pages with a bit of humor along theway, to teach and entertain in a way that no other resource can.
I hope you find this book helpful. Best of luck throughoutyour career!
Joy
xNOT ANOTHER BORING FOREWORD
938900FM.qxd 08/26/2008 18:11 Page x

Pharmacology basicsThis chapter focuses on the fundamental principles of pharmacol-ogy. It discusses basic information, such as how drugs are namedand how they’re created. It also discusses the different routes bywhich drugs can be administered.
Kinetics, dynamics, therapeuticsThis chapter also discusses what happens when a drug enters thebody. This involves three main areas:
pharmacokinetics (the absorption, distribution,metabolism, and excretion of a drug)
pharmacodynamics (the biochemical and physi-cal effects of drugs and the mechanisms of drug ac-tions)
pharmacotherapeutics (the use of drugs to pre-vent and treat diseases).
1
Fundamentals of clinical pharmacology
Just the facts
In this chapter, you’ll learn:
♦ pharmacology basics
♦ routes by which drugs are administered
♦ key concepts of pharmacokinetics
♦ key concepts of pharmacodynamics
♦ key concepts of pharmacotherapeutics
♦ key types of drug interactions and adverse reactions.
Read on to findout what happenswhen a drug enters
the body.
938901.qxd 08/26/2008 14:30 Page 1

In addition, the chapter provides an introduction to drug inter-actions and adverse drug reactions.
What’s in a name?Drugs have a specific kind of nomenclature—that is, a drug can goby three different names:• The chemical name is a scientific name that precisely describesits atomic and molecular structure.• The generic, or nonproprietary, name is an abbreviation of thechemical name.• The trade name (also known as the brand name or proprietaryname) is selected by the drug company selling the product. Tradenames are protected by copyright. The symbol ® after the tradename indicates that the name is registered by and restricted to thedrug manufacturer.
To avoid confusion, it’s best to use a drug’s generic name be-cause any one drug can have a number of trade names.
In 1962, the federal government mandated the use of officialnames so that only one official name would represent each drug.The official names are listed in the United States Pharmacopeiaand National Formulary.
Family tiesDrugs that share similar characteristics are grouped together as apharmacologic class (or family). Beta-adrenergic blockers are anexample of a pharmacologic class.
The therapeutic class groups drugs by therapeutic use. Antihy-pertensives are an example of a therapeutic class.
Where drugs come fromTraditionally, drugs were derived from natural sources, such as:• plants• animals• minerals.
Today, however, laboratory researchers use traditional knowl-edge, along with chemical science, to develop synthetic drugsources. One advantage of chemically developed drugs is thatthey’re free from the impurities found in natural substances.
In addition, researchers and drug developers can manipulatethe molecular structure of substances such as antibiotics so that aslight change in the chemical structure makes the drug effectiveagainst different organisms. The first-, second-, third-, and fourth-generation cephalosporins are an example.
2FUNDAMENTALS OF CLINICAL PHARMACOLOGY
This is confusing!Each drug has at
least three names: achemical name, a
generic name, and atrade name.
938901.qxd 08/26/2008 14:30 Page 2

Old-fashioned medicineThe earliest drug concoctions from plants used everything: theleaves, roots, bulb, stem, seeds, buds, and blossoms. Subsequent-ly, harmful substances often found their way into the mixture.
As the understanding of plants as drug sources became moresophisticated, researchers sought to isolate and intensify activecomponents while avoiding harmful ones.
Power plantThe active components consist of several types and vary in char-acter and effect:• Alkaloids, the most active component in plants, react with acidsto form a salt that can dissolve more readily in body fluids. Thenames of alkaloids and their salts usually end in “-ine.” Examplesinclude atropine, caffeine, and nicotine.• Glycosides are also active components found in plants. Namesof glycosides usually end in “-in” such as digoxin.• Gums constitute another group of active components. Gumsgive products the ability to attract and hold water. Examples in-clude seaweed extractions and seeds with starch.• Resins, of which the chief source is pine tree sap, commonlyact as local irritants or as laxatives.• Oils, thick and sometimes greasy liquids, are classified asvolatile or fixed. Examples of volatile oils, which readily evapo-rate, include peppermint, spearmint, and juniper. Fixed oils, whicharen’t easily evaporated, include castor oil and olive oil.
Animal magnetismThe body fluids or glands of animals can also be drug sources. Thedrugs obtained from animal sources include:• hormones such as insulin• oils and fats (usually fixed) such as cod-liver oil• enzymes, which are produced by living cells and act as cata-lysts, such as pancreatin and pepsin• vaccines, which are suspensions of killed, modified, or attenuat-ed microorganisms. (See Old McDonald had a pharm, page 4.)
Mineral springsMetallic and nonmetallic minerals provide various inorganic mate-rials not available from plants or animals. The mineral sources areused as they occur in nature or are combined with other ingredi-ents. Examples of drugs that contain minerals are iron, iodine, andEpsom salts.
Down to DNAToday, most drugs are produced in laboratories and can be:
3PHARMACOLOGY BASICS
Drugs can bederived from just
about any substanceon earth.
938901.qxd 08/26/2008 14:30 Page 3

• natural (from animal, plant, or mineral sources)• synthetic.
Examples of drugs produced in the laboratory include thyroidhormone (natural) and ranitidine (synthetic).
Recombinant deoxyribonucleic acid research has led to otherchemical sources of organic compounds. For example, the re-ordering of genetic information has enabled scientists to developbacteria that produce insulin for humans.
How drugs are administeredA drug’s administration route influences the quantity given andthe rate at which the drug is absorbed and distributed. These vari-ables affect the drug’s action and the patient’s response.
Routes of administration include:• buccal, sublingual, translingual: certain drugs are given buc-cally (in the pouch between the cheek and gum), sublingually (un-der the tongue), or translingually (on the tongue) to speed theirabsorption or to prevent their destruction or transformation in thestomach or small intestine• gastric: this route allows direct instillation of medication intothe GI system of patients who can’t ingest the drug orally• intradermal: substances are injected into the skin (dermis);this route is used mainly for diagnostic purposes when testing forallergies or tuberculosis• intramuscular: this route allows drugs to be injected directlyinto various muscle groups at varying tissue depths; it’s used togive aqueous suspensions and solutions in oil, immunizations, andmedications that aren’t available in oral form
4FUNDAMENTALS OF CLINICAL PHARMACOLOGY
Hmm…farm freshpharmaceuticals?That’s an unusual
idea.
Old McDonald had a pharm
In the near future, traditional barnyard animals might also be small, or-ganic pharmaceutical factories. Some animals have already been ge-netically altered to produce pharmaceuticals, and their products arebeing tested by the Food and Drug Administration. Here are a few ex-amples of the possibilities:• a cow that produces milk containing lactoferrin, which can be used totreat human infections• a goat that produces milk containing antithrombin III, which can helpprevent blood clotting in humans• a sheep that produces milk containing alpha1-antitrypsin, which isused to treat cystic fibrosis.
938901.qxd 08/26/2008 14:30 Page 4

Streaming in• intravenous: the I.V. route allows injection of substances(drugs, fluids, blood or blood products, and diagnostic contrastagents) directly into the bloodstream through a vein; administra-tion can range from a single dose to an ongoing infusion deliveredwith great precision• oral: this is usually the safest, most convenient, and least expen-sive route; drugs are administered to patients who are consciousand can swallow• rectal and vaginal: suppositories, ointments, creams, gels, andtablets may be instilled into the rectum or vagina to treat local irri-tation or infection; some drugs applied to the mucosa of the rec-tum or vagina can be absorbed systemically• respiratory: drugs that are available as gases can be adminis-tered into the respiratory system; drugs given by inhalation arerapidly absorbed, and medications given by such devices as themetered-dose inhaler can be self-administered, or drugs can be ad-ministered directly into the lungs through an endotracheal tube inemergency situations• subcutaneous (subQ): with the subQ route, small amounts of adrug are injected beneath the dermis and into the subcutaneoustissue, usually in the patient’s upper arm, thigh, or abdomen• topical: this route is used to deliver a drug through the skin or amucous membrane; it’s used for most dermatologic, ophthalmic,otic, and nasal preparations.
Drugs may also be given as specialized infusions injected di-rectly into a specific site in the patient’s body, such as an epiduralinfusion (into the epidural space), intrathecal infusion (into thecerebrospinal fluid), intrapleural infusion (into the pleural cavity),intraperitoneal infusion (into the peritoneal cavity), intraosseousinfusion (into the rich vascular network of a long bone), and intra-articular infusion (into a joint).
New drug developmentIn the past, drugs were found by trial and error. Now they’re de-veloped primarily by systematic scientific research. The Food andDrug Administration (FDA) carefully monitors new drug develop-ment, which can take many years to complete.
Only after reviewing extensive animal studies and data on thesafety and effectiveness of the proposed drug will the FDA ap-prove an application for an investigational new drug (IND). (SeePhases of new drug development, page 6.)
5PHARMACOLOGY BASICS
938901.qxd 08/26/2008 14:30 Page 5

Exceptions to the ruleAlthough most INDs undergo all four phases of clinical evaluationmandated by the FDA, some can receive expedited approval. Forexample, because of the public health threat posed by acquiredimmunodeficiency syndrome (AIDS), the FDA and drug compa-nies have agreed to shorten the IND approval process for drugs totreat the disease. This allows doctors to give qualified AIDS pa-tients “treatment INDs,” which aren’t yet approved by the FDA.
Sponsors of drugs that reach phase II or III clinical trials canapply for FDA approval of treatment IND status. When the IND isapproved, the sponsor supplies the drug to doctors whose pa-tients meet appropriate criteria.
Despite the extensive testing and development that all drugsgo through, serious adverse reactions may occasionally occur,even though they weren’t discovered during clinical trials. It’s alsopossible that drug interactions aren’t discovered until after clinicaltrials have concluded and the drug has been approved. The FDAhas procedures in place for reporting adverse events and otherproblems to help track the safety of drugs. (See Reporting to theFDA.)
6FUNDAMENTALS OF CLINICAL PHARMACOLOGY
Phases of new drug development
When the Food and Drug Administration (FDA)approves the application for an investigationalnew drug, the drug must undergo clinical eval-uation involving human subjects. This clinicalevaluation is divided into four phases:
Phase I
The drug is tested on healthy volunteers inphase I.
Phase II
Phase II involves trials with people who havethe disease for which the drug is thought to beeffective.
Phase III
Large numbers of patients in medical researchcenters receive the drug in phase III. This larg-
er sampling provides information about infre-quent or rare adverse effects. The FDA will ap-prove a new drug application if phase III stud-ies are satisfactory.
Phase IV
Phase IV is voluntary and involves postmarketsurveillance of the drug’s therapeutic effects atthe completion of phase III. The pharmaceuti-cal company receives reports from doctorsand other health care professionals about thetherapeutic results and adverse effects of thedrug. Some medications, for example, havebeen found to be toxic and have been removedfrom the market after their initial release.
Reporting tothe FDA
The Food and Drug Ad-ministration (FDA) com-piles and tracks infor-mation related to prob-lems associated withdrugs under its regula-tion. Complete a Med-Watch form and send itto the FDA if you sus-pect an FDA-regulateddrug is responsible for apatient’s:• death• life-threatening illness• prolonged or initialhospitalization• disability• congenital anomaly• need for medical orsurgical intervention toprevent a permanent im-pairment.
Safe andsound
938901.qxd 08/26/2008 14:30 Page 6

PharmacokineticsKinetics refers to movement. Pharmacokinetics deals with adrug’s actions as it moves through the body. Therefore, pharmaco-kinetics discusses how a drug is:• absorbed (taken into the body)• distributed (moved into various tissues)• metabolized (changed into a form that can be excreted)• excreted (removed from the body).
This branch of pharmacology is also concerned with a drug’sonset of action, peak concentration level, and duration of action.
AbsorptionDrug absorption covers a drug’s progress from the time it’s admin-istered, through its passage to the tissues, until it reaches systemiccirculation.
On a cellular level, drugs are absorbed by several means—pri-marily through active or passive transport.
The lazy wayPassive transport requires no cellular energy becausediffusion allows the drug to move from an area of high-er concentration to one of lower concentration. Passivetransport occurs when small molecules diffuse acrossmembranes and stops when drug concentration on both sides ofthe membrane is equal.
Using muscleActive transport requires cellular energy to move the drug froman area of lower concentration to one of higher concentration. Ac-tive transport is used to absorb electrolytes, such as sodium andpotassium, as well as some drugs such as levodopa.
Taking a bitePinocytosis is a unique form of active transport that occurs whena cell engulfs a drug particle. Pinocytosis is commonly employedto transport fat-soluble vitamins (vitamins A, D, E, and K).
Watch the speed limit!If only a few cells separate the active drug from the systemic cir-culation, absorption will occur rapidly and the drug will quicklyreach therapeutic levels in the body. Typically, absorption occurswithin seconds or minutes when a drug is administered sublin-gually, I.V., or by inhalation.
7PHARMACOKINETICS
Ahhh. I justadore passivetransport. It
requires no energy.Ooops—time to flip
over!
Drugs given underthe tongue, I.V., or byinhalation are quickly
absorbed.
938901.qxd 08/26/2008 14:30 Page 7

Not so fastAbsorption occurs at a slower rate when drugs are administeredby the oral, I.M., or subQ routes because the complex membranesystems of GI mucosal layers, muscle, and skin delay drug pas-sage.
At a snail’s paceAt the slowest absorption rates, drugs can take several hours ordays to reach peak concentration levels. A slow rate usually oc-curs with rectally administered or sustained-release drugs.
Not enough timeOther factors can affect how quickly a drug is absorbed. For ex-ample, most absorption of oral drugs occurs in the small intestine.If a patient has had large sections of the small intestine surgicallyremoved, drug absorption decreases because of the reduced sur-face area and the reduced time that the drug is in the intestine.
Look to the liverDrugs absorbed by the small intestine are transported to the liverbefore being circulated to the rest of the body. The liver may me-tabolize much of the drug before it enters the circulation. Thismechanism is referred to as the first-pass effect. Liver metabolismmay inactivate the drug; if so, the first-pass effect lowers theamount of active drug released into the systemic circulation.Therefore, higher drug dosages must be administered to achievethe desired effect.
More blood, more absorptionIncreased blood flow to an absorption site improves drug absorp-tion, whereas reduced blood flow decreases absorption. Morerapid absorption leads to a quicker onset of drug action.
For example, the muscle area selected for I.M. administrationcan make a difference in the drug absorption rate. Blood flowsfaster through the deltoid muscle (in the upper arm) than throughthe gluteal muscle (in the buttocks). The gluteal muscle, however,can accommodate a larger volume of drug than the deltoid mus-cle.
Slowed by pain and stressPain and stress can decrease the amount of drug absorbed. Thismay be due to a change in blood flow, reduced movement throughthe GI tract, or gastric retention triggered by the autonomic ner-vous system response to pain.
8FUNDAMENTALS OF CLINICAL PHARMACOLOGY
A drug injectedinto muscle of the
buttocks is absorbedmore slowly andsometimes more
erratically than oneinjected into the
upper arm.
938901.qxd 08/26/2008 14:30 Page 8

High fat doesn’t helpHigh-fat meals and solid foods slow the rate at which contentsleave the stomach and enter the intestines, delaying intestinal ab-sorption of a drug.
Dosage form factorsDrug formulation (such as tablets, capsules, liquids, sustained-release formulas, inactive ingredients, and coatings) affects thedrug absorption rate and the time needed to reach peak bloodconcentration levels.
Absorption increase or decrease?Combining one drug with another drug, or with food, can cause in-teractions that increase or decrease drug absorption, dependingon the substances involved.
DistributionDrug distribution is the process by which the drug is deliveredfrom the systemic circulation to body tissues and fluids. Distribu-tion of an absorbed drug within the body depends on several fac-tors:• blood flow• solubility• protein binding.
Quick to the heartAfter a drug has reached the bloodstream, its distribution in thebody depends on blood flow. The drug is quickly distributed to or-gans with a large supply of blood. These organs include the:• heart• liver• kidneys.
Distribution to other internal organs, skin, fat, and muscle isslower.
Lucky lipidsThe ability of a drug to cross a cell membrane depends onwhether the drug is water or lipid (fat) soluble. Lipid-solubledrugs easily cross through cell membranes; water-soluble drugscan’t.
Lipid-soluble drugs can also cross the blood-brain barrier andenter the brain.
9PHARMACOKINETICS
938901.qxd 08/26/2008 14:30 Page 9

Free to workAs a drug travels through the body, it comes in contact with pro-teins such as the plasma protein albumin. The drug can remainfree or bind to the protein. The portion of a drug that’s bound to aprotein is inactive and can’t exert a therapeutic effect. Only thefree, or unbound, portion remains active.
A drug is said to be highly protein-bound if morethan 80% of the drug is bound to protein.
MetabolismDrug metabolism, or biotransformation, is the processby which the body changes a drug from its dosage formto a more water-soluble form that can then be excret-ed. Drugs can be metabolized in several ways:• Most drugs are metabolized into inactive metabolites(products of metabolism), which are then excreted.• Other drugs are converted to active metabolites,which are capable of exerting their own pharmacologicaction. Active metabolites may undergo further metabolism ormay be excreted from the body unchanged.• Some drugs can be administered as inactive drugs, called pro-drugs, which don’t become active until they’re metabolized.
Where metabolism happensThe majority of drugs are metabolized by enzymes in the liver;however, metabolism can also occur in the plasma, kidneys, andmembranes of the intestines. In contrast, some drugs inhibit orcompete for enzyme metabolism, which can cause the accumula-tion of drugs when they’re given together. This accumulation in-creases the potential for an adverse reaction or drug toxicity.
Conditional considerationsCertain diseases can reduce metabolism. These include liver dis-eases such as cirrhosis as well as heart failure, which reduces cir-culation to the liver.
Gene machineGenetics allows some people to metabolize drugs rapidly and oth-ers to metabolize them more slowly.
Stress testEnvironment, too, can alter drug metabolism. For example, ciga-rette smoke may affect the rate of metabolism of some drugs; astressful situation or event, such as prolonged illness, surgery, orinjury, can also change how a person metabolizes drugs.
10FUNDAMENTALS OF CLINICAL PHARMACOLOGY
If I’m notworking right, a
drug doesn’tget metabolized
normally.
Only free drugs,not those bound toprotein, can producea therapeutic effect.
938901.qxd 08/26/2008 14:31 Page 10

The age gameDevelopmental changes can also affect drug metabolism. For in-stance, infants have immature livers that reduce the rate of metab-olism, and elderly patients experience a decline in liver size, bloodflow, and enzyme production that also slows metabolism.
ExcretionDrug excretion refers to the elimination of drugs from the body.Most drugs are excreted by the kidneys and leave the bodythrough urine. Drugs can also be excreted through the lungs, ex-ocrine (sweat, salivary, or mammary) glands, skin, and intestinaltract.
Half-life = half the drugThe half-life of a drug is the time it takes for one-half of the drugto be eliminated by the body. Factors that affect a drug’s half-lifeinclude its rate of absorption, metabolism, and excretion. Know-ing how long a drug remains in the body helps determine how fre-quently it should be administered.
A drug that’s given only once is eliminated from the body al-most completely after four or five half-lives. A drug that’s adminis-tered at regular intervals, however, reaches a steady concentra-tion (or steady state) after about four or five half-lives. Steadystate occurs when the rate of drug administration equals the rateof drug excretion.
Onset, peak, and durationIn addition to absorption, distribution, metabolism, and excretion,three other factors play important roles in a drug’s pharmacoki-netics:• onset of action• peak concentration• duration of action.
Lights, camera… action!The onset of action refers to the time interval from when the drugis administered to when its therapeutic effect actually begins. Rateof onset varies depending on the route of administration and otherpharmacokinetic properties.
Peak performanceAs the body absorbs more drug, blood concentration levels rise.The peak concentration level is reached when the absorption rate
11PHARMACOKINETICS
Rememberthat drugs
can go throughme, too!
938901.qxd 08/26/2008 14:31 Page 11

equals the elimination rate. However, the time of peak concentra-tion isn’t always the time of peak response.
Sticking aroundThe duration of action is the length of time the drug produces itstherapeutic effect.
PharmacodynamicsPharmacodynamics is the study of the drug mechanisms that pro-duce biochemical or physiologic changes in the body. The inter-action at the cellular level between a drug and cellular compo-nents, such as the complex proteins that make up the cell mem-brane, enzymes, or target receptors, represents drug action. Theresponse resulting from this drug action is the drug effect.
It’s the cell that mattersA drug can modify cell function or rate of function, but it can’timpart a new function to a cell or to target tissue. Therefore, thedrug effect depends on what the cell is capable of accomplish-ing.
A drug can alter the target cell’s function by:• modifying the cell’s physical or chemical environment• interacting with a receptor (a specialized location on a cellmembrane or inside a cell).
Agonist drugsMany drugs work by stimulating or blocking drug receptors. Adrug attracted to a receptor displays an affinity for that receptor.When a drug displays an affinity for a receptor and stimulates it,the drug acts as an agonist. An agonist binds to the receptor andproduces a response. This ability to initiate a response after bind-ing with the receptor is referred to as intrinsic activity.
Antagonist drugsIf a drug has an affinity for a receptor but displays little or no in-trinsic activity, it’s called an antagonist. An antagonist prevents aresponse from occurring.
Reversible or irreversibleAntagonists can be competitive or noncompetitive.• A competitive antagonist competes with the agonist for recep-tor sites. Because this type of antagonist binds reversibly to the re-ceptor site, administering larger doses of an agonist can overcomethe antagonist’s effects.
12FUNDAMENTALS OF CLINICAL PHARMACOLOGY
Reachingthe peak of
concentrationcan be tough!
938901.qxd 08/26/2008 14:31 Page 12

• A noncompetitive antagonist binds to receptor sites and blocksthe effects of the agonist. Administering larger doses of the ago-nist can’t reverse the antagonist’s action.
Regarding receptorsIf a drug acts on a variety of receptors, it’s said to be nonselectiveand can cause multiple and widespread effects. In addition, somereceptors are classified further by their specific effects. For exam-ple, beta receptors typically produce increased heart rate andbronchial relaxation as well as other systemic effects.
Beta receptors, however, can be further divided into beta1 re-ceptors (which act primarily on the heart) and beta2 receptors(which act primarily on smooth muscles and gland cells).
Potent powerDrug potency refers to the relative amount of a drug required toproduce a desired response. Drug potency is also used to comparetwo drugs. If drug X produces the same response as drug Y but ata lower dose, then drug X is more potent than drug Y.
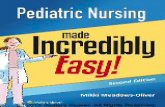
As its name implies, a dose-response curve is used to graphi-cally represent the relationship between the dose of a drug andthe response it produces. (See Dose-response curve, page 14.)
Maximum effectOn the dose-response curve, a low dose usually corresponds to alow response. At a low dose, a dosage increase produces only aslight increase in response. With further dosage increases, thedrug response rises markedly. After a certain point, however, anincrease in dose yields little or no increase in response. At thispoint, the drug is said to have reached maximum effectiveness.
Margin of safetyMost drugs produce multiple effects. The relationship between adrug’s desired therapeutic effects and its adverse effectsis called the drug’s therapeutic index. It’s also referredto as its margin of safety.
The therapeutic index usually measures the differ-ence between:• an effective dose for 50% of the patients treated• the minimal dose at which adverse reactions occur.
Narrow index = potential dangerDrugs with a narrow, or low, therapeutic index have anarrow margin of safety. This means that there’s a nar-row range of safety between an effective dose and alethal one. On the other hand, a drug with a high thera-peutic index has a wide margin of safety and poses lessrisk of toxic effects.
13PHARMACODYNAMICS
Stimulatebeta receptorsand I’m likely to
speed up.
I’d say thishas a narrow
margin of safety.Whoa!
938901.qxd 08/26/2008 14:31 Page 13

PharmacotherapeuticsPharmacotherapeutics is the use of drugs to treat disease. Whenchoosing a drug to treat a particular condition, health careproviders consider not only the drug’s effectiveness but also otherfactors such as the type of therapy the patient will receive.
Not all therapy is the sameThe type of therapy a patient receives depends on the severity, ur-gency, and prognosis of the patient’s condition and can include:• acute therapy, if the patient is critically ill and requires acute in-tensive therapy• empiric therapy, based on practical experience rather than onpure scientific data• maintenance therapy, for patients with chronic conditions thatdon’t resolve
14FUNDAMENTALS OF CLINICAL PHARMACOLOGY
This graph shows the dose-response curve for two differentdrugs. As you can see, at lowdoses of each drug, a dosageincrease results in only a smallincrease in drug response (forexample, from point A to point Bfor drug X). At higher doses, anincrease in dosage produces amuch greater response (frompoint B to point C). As thedosage continues to climb,however, an increase in dosageproduces very little increase inresponse (from point C to pointD).
This graph also shows thatdrug X is more potent than drugY because it produces the sameresponse, but at a lower dose(compare point A to point E).
Now I get it!
Dose-response curve
% o
f m
ax
ima
l re
spo
nse
0.0001 0.001 0.01 0.1 1.0
Dose
100
50
0
Drug X Drug Y
A
B
C D
E
938901.qxd 08/26/2008 14:31 Page 14

• supplemental or replacement therapy, to replenish or substi-tute for missing substances in the body• supportive therapy, which doesn’t treat the cause of the diseasebut maintains other threatened body systems until the patient’scondition resolves• palliative therapy, used for end-stage or terminal diseases tomake the patient as comfortable as possible.
I can only be myselfA patient’s overall health as well as other individual factors can al-ter that patient’s response to a drug. Coinciding medical condi-tions and personal lifestyle characteristics must be consideredwhen selecting drug therapy. (See Factors affecting a patient’s re-sponse to a drug.)
Decreased response…In addition, it’s important to remember that certain drugs have atendency to create drug tolerance and drug dependence in pa-tients. Drug tolerance occurs when a patient develops a decreasedresponse to a drug over time. The patient then requires larger dos-es to produce the same response.
…and increased desireTolerance differs from drug dependence, in which a patient dis-plays a physical or psychological need for the drug. Physical de-pendence produces withdrawal symptoms when the drug isstopped, whereas psychological dependence is based on a desireto continue taking the drug to relieve tension and avoid discom-fort.
Drug interactionsDrug interactions can occur between drugs or between drugs andfoods. They can interfere with the results of a laboratory test orproduce physical or chemical incompatibilities. The more drugs apatient receives, the greater the chances that a drug interactionwill occur.
Potential drug interactions include:• additive effects• potentiation• antagonistic effects• decreased or increased absorption• decreased or increased metabolism and excretion.
15DRUG INTERACTIONS
Factorsaffecting apatient’sresponse toa drug
Because no two peopleare alike physiologicallyor psychologically, pa-tient response to a drugcan vary greatly, de-pending upon such fac-tors as:• age• cardiovascularfunction• diet• disease• drug interactions• gender• GI function• hepatic function• infection• renal function.
Now I get it!
Memoryjogger
When a drugis said to be
potentiated by an-other drug, the re-sults are more po-tent—the drug goesbeyond its originalpotential.
938901.qxd 08/26/2008 14:31 Page 15

Adding it all upAdditive effects can occur when two drugs with similar actionsare administered to a patient. The effects are equivalent to thesum of either drug’s effects if it were administered alone in higherdoses.
Giving two drugs together, such as two analgesics (pain reliev-ers), has several potential advantages: lower doses of each drug,decreased probability of adverse reactions, and greater pain con-trol than from one drug given alone (most likely because of differ-ent mechanisms of action). There’s a decreased risk of adverse ef-fects when giving two drugs for the same condition because thepatient is given lower doses of each drug—the higher the dose,the greater the risk of adverse effects.
A synergistic situationA synergistic effect, also called potentiation, occurs when twodrugs that produce the same effect are given together and onedrug potentiates (enhances the effect of) the other drug. This pro-duces greater effects than when each drug is taken alone.
Fighting it outAn antagonistic effect occurs when the combined response of twodrugs is less than the response produced by either drug alone.
An absorbing problemTwo drugs given together can change the absorption of one orboth of the drugs:• Drugs that change the acidity of the stomach can affect the abil-ity of another drug to dissolve in the stomach.• Some drugs can interact and form an insoluble compound thatcan’t be absorbed.
Sometimes, an absorption-related drug interaction can beavoided by administering the drugs at least 2 hours apart.
Bound and determinedAfter a drug is absorbed, the blood distributes it throughout thebody as a free drug or one that’s bound to plasma protein.
When two drugs are given together, they can compete forprotein-binding sites, leading to an increase in the effects of onedrug as that drug is displaced from the protein and becomes afree, unbound drug.
Toxic wasteToxic drug levels can occur when a drug’s metabolism and excre-tion are inhibited by another drug. Some drug interactions affectexcretion only.
16FUNDAMENTALS OF CLINICAL PHARMACOLOGY
938901.qxd 08/26/2008 14:31 Page 16

Back to the labDrug interactions can also alter laboratory tests and can producechanges seen on a patient’s electrocardiogram.
Menu planningInteractions between drugs and food can alter the therapeutic ef-fects of the drug. Food can also alter the rate and amount of drugabsorbed from the GI tract, affecting bioavailability—the amountof a drug dose that’s made available to the systemic circulation.Drugs can also impair vitamin and mineral absorption.
Some drugs stimulate enzyme production, increasing metabol-ic rates and the demand for vitamins that are enzyme cofactors(which must unite with the enzyme in order for the enzyme tofunction). Dangerous interactions can also occur. For instance,when food that contains Vitamin K (such as green, leafy vegeta-bles) is eaten by a person taking warfarin, the drug’s anticoagula-tion properties are decreased and blood clots may form.
Grapefruit can inhibit the metabolism of certain medications,resulting in toxic blood levels; examples include fexofenadine,albendazole, and atorvastatin. Because of all the interactions foodcan have with drug metabolism, being aware of drug interactionsis essential.
Adverse drug reactionsA drug’s desired effect is called the expected therapeutic re-sponse. An adverse drug reaction (also called a side effect or ad-verse effect), on the other hand, is a harmful, undesirable re-sponse. Adverse drug reactions can range from mild ones that dis-appear when the drug is discontinued to debilitating diseases thatbecome chronic. Adverse reactions can appear shortly after start-ing a new medication but may become less severe with time.
Dosage dilemmaAdverse drug reactions can be classified as dose-related or patientsensitivity–related. Most adverse drug reactions result from theknown pharmacologic effects of a drug and are typically dose-related. These types of reactions can be predicted in most cases.
Dose-related reactions include:• secondary effects• hypersusceptibility• overdose• iatrogenic effects.
17ADVERSE DRUG REACTIONS
Review a patient’sdiet carefully—drug
interactions withfood can reduce
absorption or evenproduce dangerous
changes.
938901.qxd 08/26/2008 14:31 Page 17

Extra effectsA drug typically produces not only a major therapeutic effect butalso additional, secondary effects that can be harmful or benefi-cial. For example, morphine used for pain control can lead to twoundesirable secondary effects: constipation and respiratory de-pression. Diphenhydramine used as an antihistamine produces se-dation as a secondary effect and is sometimes used as a sleep aid.
Enhanced actionA patient can be hypersusceptible to the pharmacologic actions ofa drug. Such a patient experiences an excessive therapeutic re-sponse or secondary effects even when given the usual therapeu-tic dose.
Hypersusceptibility typically results from altered pharmacoki-netics (absorption, metabolism, and excretion), which leads tohigher-than-expected blood concentration levels. Increased recep-tor sensitivity also can increase the patient’s response to therapeu-tic or adverse effects.
Oh no—overdose!A toxic drug reaction can occur when an excessive dose is taken,either intentionally or by accident. The result is an exaggerated re-sponse to the drug that can lead to transient changes or more seri-ous reactions, such as respiratory depression, cardiovascular col-lapse, and even death. To avoid toxic reactions, chronically ill orelderly patients often receive lower drug doses.
Iatrogenic issuesSome adverse drug reactions, known as iatrogenic effects, canmimic pathologic disorders. For example, such drugs as antineo-plastics, aspirin, corticosteroids, and indomethacin commonlycause GI irritation and bleeding. Other examples of iatrogenic ef-fects include induced asthma with propranolol, induced nephritiswith methicillin, and induced deafness with gentamicin.
You’re so sensitivePatient sensitivity–related adverse reactions aren’t as common asdose-related reactions. Sensitivity-related reactions result from apatient’s unusual and extreme sensitivity to a drug. These adversereactions arise from a unique tissue response rather than from anexaggerated pharmacologic action. Extreme patient sensitivitycan occur as a drug allergy or an idiosyncratic response.
Friend or foe?A drug allergy occurs when a patient’s immune system identifies adrug, a drug metabolite, or a drug contaminant as a dangerous for-
18FUNDAMENTALS OF CLINICAL PHARMACOLOGY
Sensitivity-relatedadverse reactions arecaused by a patient’sextreme sensitivity to
a drug.
938901.qxd 08/26/2008 14:31 Page 18

eign substance that must be neutralized or destroyed. Previous ex-posure to the drug or to one with similar chemical characteristicssensitizes the patient’s immune system, and subsequent exposurecauses an allergic reaction (hypersensitivity).
An allergic reaction not only directly injures cells and tissuesbut also produces broader systemic damage by initiating cellularrelease of vasoactive and inflammatory substances.
The allergic reaction can vary in intensity from an immediate,life-threatening anaphylactic reaction with circulatory col-lapse and swelling of the larynx and bronchioles to a mildreaction with a rash and itching.
Idiosyncratic responseSome sensitivity-related adverse reactions don’t result frompharmacologic properties of a drug or from an allergy butare specific to the individual patient. These are called idio-syncratic responses. Some idiosyncratic responses have agenetic cause.
Quick quiz
1. While teaching a patient about drug therapy for diabetes, youreview the absorption, distribution, metabolism, and excretion ofinsulin and oral antidiabetic agents. Which principle of pharmacol-ogy are you describing?
A. PharmacokineticsB. PharmacodynamicsC. PharmacotherapeuticsD. Drug potency
Answer: A. Pharmacokinetics discusses the movement of drugsthrough the body and involves absorption, distribution, metabo-lism, and excretion.
2. Which type of drug therapy is used for a patient who has achronic condition that can’t be cured?
A. Empiric therapyB. Acute therapyC. Maintenance therapyD. Supplemental therapy
Answer: C. Maintenance therapy seeks to maintain a certain lev-el of health in patients who have chronic conditions.
19QUICK QUIZ
For an allergicreaction to occur, the
patient must havereceived the drug
before.
938901.qxd 08/26/2008 14:31 Page 19

3. Which branch of pharmacology studies the way drugs workin living organisms?
A. PharmacotherapeuticsB. PharmacokineticsC. Drug interactionsD. Pharmacodynamics
Answer: D. Pharmacodynamics studies the mechanisms of ac-tion of drugs and seeks to understand how drugs work in thebody.
ScoringIf you answered all three items correctly, excellent! You’ve ab-
sorbed this chapter in a hurry.If you answered two items correctly, terrific! You’ve reached ther-
apeutic levels of this chapter in a flash.If you answered fewer than two items correctly, no need for con-
cern. Sometimes food enhances absorption—so grab a quicksnack and come back for a review.
20FUNDAMENTALS OF CLINICAL PHARMACOLOGY
✰✰✰
✰✰
✰
938901.qxd 08/26/2008 14:31 Page 20

Cholinergic drugsCholinergic drugs promote the action of the neurotransmitteracetylcholine. These drugs are also called parasympathomimeticdrugs because they produce effects that imitate parasympatheticnerve stimulation.
Mimickers and inhibitorsThere are two major classes of cholinergic drugs:
Cholinergic agonists mimic the action of the neurotransmit-ter acetylcholine.
Anticholinesterase drugs work by inhibiting the destructionof acetylcholine at the cholinergic receptor sites. (See Howcholinergic drugs work, page 22.)
Cholinergic agonistsBy directly stimulating cholinergic receptors, cholinergic agonistsmimic the action of the neurotransmitter acetylcholine.
They include such drugs as:
2
Autonomic nervous system drugs
Just the facts
In this chapter, you’ll review:
♦ classes of drugs that affect the autonomic nervoussystem
♦ uses and varying actions of these drugs
♦ how these drugs are absorbed, distributed, metabolized,and excreted
♦ drug interactions and adverse effects of these drugs. Cholinergic drugsenhance the action of
acetylcholine,stimulating the
parasympatheticnervous system.
938902.qxd 08/26/2008 14:47 Page 21

• bethanechol• carbachol• cevimeline• pilocarpine.
Pharmacokinetics (how drugs circulate)The action and metabolism of cholinergic agonists vary widelyand depend on the affinity of the individual drug for muscarinic ornicotinic receptors.
No I.M. or I.V. injectionsCholinergic agonists rarely are administered by I.M. or I.V. injec-tion because they’re almost immediately broken down by cholin-esterases in the interstitial spaces between tissues and inside theblood vessels. Moreover, they begin to work rapidly and can cause
22AUTONOMIC NERVOUS SYSTEM DRUGS
Cholinergic drugs fall into one of two major classes: cholinergic agonists and anticholinesterase drugs. Here’s how these drugsachieve their effects.
Now I get it!
How cholinergic drugs work
Cholinergic agonists
When a neuron in the parasympathetic nervous system is stim-ulated, the neurotransmitter acetylcholine is released. Acetyl-choline crosses the synapse and interacts with receptors in anadjacent neuron. Cholinergic agonists stimulate cholinergic re-ceptors, mimicking the action of acetylcholine.
Anticholinesterase drugs
After acetylcholine stimulates the cholinergic receptor, it’s de-stroyed by the enzyme acetylcholinesterase. Anticholinester-ase drugs inhibit acetylcholinesterase. As a result, acetylcho-line isn’t broken down and begins to accumulate, leading toprolonged acetylcholine effects.
ACH
CAD
ACH
ACH
ACH
CADCAD
CAD
CAD
RECEPTOR
ACH
ACH
ACH
ACH
ACE
ACH
ACH
RECEPTOR
ACE
ACD
ACD
Key:
Acetylcholine Cholinergic agonist drug Acetylcholinesterase Anticholinesterase drugACH ACDACECAD
Neuron Neuron
938902.qxd 08/26/2008 14:47 Page 22

a cholinergic crisis (a drug overdose resulting in extreme muscleweakness and possibly paralysis of the muscles used in respira-tion).
Topically, orally, or under the skinCholinergic agonists are usually administered:• topically, with eye drops• orally• by subcutaneous (subQ) injection.
SubQ injections begin to work more rapidly than oral doses.
Metabolism and excretionAll cholinergic agonists are metabolized by cholinesterases:• at the muscarinic and nicotinic receptor sites• in the plasma (the liquid portion of the blood)• in the liver.
All drugs in this class are excreted by the kidneys.
Pharmacodynamics (how drugs act)Cholinergic agonists work by mimicking the action of acetylcho-line on the neurons in certain organs of the body called target or-gans. When they combine with receptors on the cell membranesof target organs, they stimulate the muscle and produce:• salivation• bradycardia (a slow heart rate)• dilation of blood vessels• constriction of the bronchioles• increased activity of the GI tract• increased tone and contraction of the bladder muscles• constriction of the pupils.
Pharmacotherapeutics (how drugs are used)Cholinergic agonists are used to:• treat atonic (weak) bladder conditions and postoperative andpostpartum urine retention• treat GI disorders, such as postoperative abdominal distentionand GI atony• reduce eye pressure in patients with glaucoma and during eyesurgery• treat salivary gland hypofunction caused by radiation therapy orSjögren’s syndrome.
23CHOLINERGIC DRUGS
Cholinergicagonists
administered byinjection are rapidly
broken down andcould cause a
cholinergic crisis.
938902.qxd 08/26/2008 14:47 Page 23

Drug interactionsCholinergic agonists have specific interactions with other drugs.Examples include the following:• Other cholinergic drugs, particularly anticholinesterase drugs(such as ambenonium, edrophonium, neostigmine, physostigmine,and pyridostigmine), boost the effects of cholinergic agonists andincrease the risk of toxicity.• Cholinergic blocking drugs (such as atropine, belladonna, ho-matropine, methantheline, methscopolamine, propantheline, andscopolamine) reduce the effects of cholinergic drugs.• Quinidine also reduces the effectiveness of cholinergic agonists.(See Adverse reactions to cholinergic agonists.)
Anticholinesterase drugsAnticholinesterase drugs block the action of the enzyme acetyl-cholinesterase (which breaks down the neurotransmitter acetyl-choline) at cholinergic receptor sites, preventing the breakdownof acetylcholine. As acetylcholine builds up, it continues to stimu-late the cholinergic receptors. (See One day at a time: Recogniz-ing a toxic response.)
Anticholinesterase drugs are divided into two categories—re-versible and irreversible.
24AUTONOMIC NERVOUS SYSTEM DRUGS
It’s difficult to predict adverse reactions to an-ticholinesterase drugs in a patient with myas-thenia gravis because the therapeutic dosevaries from day to day. Increased muscleweakness can result from:• resistance to the drug• receiving too little of the anticholinesterase• receiving too much of the anticholinesterase.
Enter edrophonium
Deciding whether a patient is experiencing atoxic drug response (too much drug) or a my-asthenic crisis (extreme muscle weakness andsevere respiratory difficulties) can be difficult.Edrophonium can be used to distinguish be-tween a toxic drug reaction and a myastheniccrisis. When edrophonium is used, suction,oxygen, mechanical ventilation, and emer-gency drugs, such as atropine, must be readilyavailable in case a cholinergic crisis occurs.
Yea or nay?
One day at a time: Recognizing a toxic response
Adversereactions tocholinergicagonists
Because they bind withreceptors in the para-sympathetic nervoussystem, cholinergic ago-nists can produce ad-verse effects in any or-gan innervated by theparasympathetic nerves.
These adverse ef-fects can include:• nausea and vomiting• cramps and diarrhea• blurred vision• decreased heart rateand low blood pressure• shortness of breath• urinary frequency• increased salivationand sweating.
Warning!
938902.qxd 08/26/2008 14:47 Page 24

These you can reverse…Reversible anticholinesterase drugs have a short duration of ac-tion and include:• ambenonium• demecarium• donepezil• edrophonium• galantamine• guanidine• neostigmine• physostigmine• pyridostigmine• rivastigmine• tacrine.
…these you can’tIrreversible anticholinesterase drugs have long-lasting effects andare used primarily as toxic insecticides and pesticides or as nervegas in chemical warfare. (Pyridostigmine enhances the effects ofantidotes used to counteract nerve agents.) Only one has thera-peutic usefulness: echothiophate.
PharmacokineticsHere’s a brief rundown of how anticholinesterase drugs movethrough the body.
Generally GIMany of the anticholinesterase drugs are readily absorbed fromthe GI tract, subcutaneous tissue, and mucous membranes.
Because neostigmine is poorly absorbed from the GI tract, thepatient needs a higher dose when taking this drug orally. Becausethe duration of action for an oral dose is longer, however, the pa-tient doesn’t need to take it as frequently. When a rapid effect isneeded, neostigmine should be given by the I.M. or I.V. route.
DistributionPhysostigmine can cross the blood-brain barrier (a protective bar-rier between the capillaries and brain tissue that prevents harmfulsubstances from entering the brain). Donepezil is highly bound toplasma proteins, tacrine is about 55% bound, rivastigmine is 40%bound, and galantamine is 18% bound.
25CHOLINERGIC DRUGS
Easy does it.Overstimulation
of theparasymphathetic
nervous systemcan send me intocardiac arrest!
938902.qxd 08/26/2008 14:47 Page 25

Metabolism and excretionMost anticholinesterase drugs are metabolized by enzymes in theplasma and excreted in urine. Donepezil, galantamine, rivastig-mine, and tacrine are metabolized in the liver.
PharmacodynamicsAnticholinesterase drugs promote the action of acetylcholine atreceptor sites. Depending on the site and the drug’s dose and du-ration of action, they can produce a stimulant or depressant effecton cholinergic receptors.
From minutes to weeksReversible anticholinesterase drugs block the breakdownof acetylcholine for minutes to hours; irreversible anti-cholinesterase drugs do so for days or weeks.
PharmacotherapeuticsAnticholinesterase drugs are used for a variety of therapeutic pur-poses, including:• to reduce eye pressure in patients with glaucoma and duringeye surgery• to increase bladder tone• to improve tone and peristalsis (movement) through the GI tractin patients with reduced motility or paralytic ileus (paralysis ofthe small intestine)• to promote muscle contractions in patients with myastheniagravis• to diagnose myasthenia gravis (neostigmine and edrophonium)• as an antidote to cholinergic blocking drugs (also called anti-cholinergic drugs), tricyclic antidepressants, belladonna alka-loids, and narcotics• to treat mild to moderate dementia and enhance cognition in pa-tients with Alzheimer’s disease (primarily donepezil, galantamine,rivastigmine, and tacrine).
Drug interactionsThese interactions can occur with anticholinesterase drugs:• Other cholinergic drugs, particularly cholinergic agonists (suchas bethanechol, carbachol, and pilocarpine), increase the risk of atoxic reaction when taken with anticholinesterase drugs.• Carbamazepine, dexamethasone, rifampin, phenytoin, and phe-nobarbital may increase donepezil’s rate of elimination.• Aminoglycoside antibiotics, anesthetics, cholinergic blockingdrugs (such as atropine, belladonna, propantheline, and scopol-amine), magnesium, corticosteroids, and antiarrhythmic drugs
26AUTONOMIC NERVOUS SYSTEM DRUGS
Depending on thedosage,
anticholinesterasedrugs can produce a
stimulant ordepressant effect on
receptors.
938902.qxd 08/26/2008 14:47 Page 26

(such as procainamide and quinidine) can reduce the effects ofanticholinesterase drugs and can mask early signs of a cholinergiccrisis. (See Adverse reactions to anticholinesterase drugs.)• Other medications with cholinergic-blocking properties, such astricyclic antidepressants, bladder relaxants, and antipsychotics,can also counteract the effects of anticholinesterase drugs.• The effects of tacrine, donepezil, and galantamine may be in-creased when these drugs are combined with known inhibitors ofcytochrome P-450 enzymes, such as cimetidine and erythromycin.• Cigarette use increases the clearance of rivastigmine.
Cholinergic blocking drugsCholinergic blocking drugs interrupt parasympathetic nerve im-pulses in the central and autonomic nervous systems. These drugsare also referred to as anticholinergic drugs because they preventacetylcholine from stimulating cholinergic receptors.
Not all receptors are receptiveCholinergic blocking drugs don’t block all cholinergic receptors,just the muscarinic receptor sites. Muscarinic receptors arecholinergic receptors that are stimulated by the alkaloid mus-carine and blocked by atropine.
First come the belladonna alkaloidsThe major cholinergic blocking drugs are the belladonna alka-loids:• atropine (the prototype cholinergic blocking drug)• belladonna• homatropine• hyoscyamine sulfate• methscopolamine• scopolamine.
Next come their synthetic sistersSynthetic derivatives of these drugs (the quaternary ammoniumdrugs) include:• glycopyrrolate• propantheline.
And finally the tertiary and quaternary aminesThe tertiary amines include:• benztropine• dicyclomine• oxybutynin
27CHOLINERGIC BLOCKING DRUGS
Adversereactions toanticholinester-ase drugs
Most of the adverse re-actions caused by anti-cholinesterase drugs re-sult from increased ac-tion of acetylcholine atreceptor sites.
Adverse reactionsassociated with thesedrugs include:• cardiac arrhythmias• nausea and vomiting• diarrhea• shortness of breath,wheezing, or tightness inthe chest• seizures• headache• anorexia• insomnia• pruritus• urinary frequency andnocturia.
Warning!
938902.qxd 08/26/2008 14:47 Page 27

• trihexyphenidyl• tolterodine.
Quaternary amines include one drug, trospium.Atropine may also be used as an antidote for nerve agents (See
the appendix, Vaccines and antidotes for biological and chemicalweapons.)
Let’s talk about it laterBecause benztropine and trihexyphenidyl are almost exclusivelytreatments for Parkinson’s disease, they’re discussed fully in chap-ter 3, Neurologic and neuromuscular drugs.
PharmacokineticsHere’s how cholinergic blockers move through the body.
AbsorptionThe belladonna alkaloids are absorbed from the:• eyes• GI tract• mucous membranes• skin.
The quaternary ammonium drugs and tertiary and quaternaryamines are absorbed primarily through the GI tract, although notas readily as the belladonna alkaloids.
If you want it fast, go I.V.When administered I.V., cholinergic blockers such as atropine be-gin to work immediately.
DistributionThe belladonna alkaloids are distributed more widely throughoutthe body than the quaternary ammonium derivatives or dicyclo-mine. The alkaloids readily cross the blood-brain barrier; the othercholinergic blockers don’t.
Metabolism and excretionThe belladonna alkaloids are only slightly to moderately protein-bound. This means that a moderate to high amount of the drug isactive and available to produce a therapeutic response. The bel-ladonna alkaloids are metabolized in the liver and excreted by thekidneys as unchanged drug and metabolites.
The quaternary ammonium drugs are a bit more complicated.Hydrolysis is a chemical process whereby a compound cleavedinto two or more simpler compounds occurs in the GI tract andthe liver; the drugs are excreted in feces and urine. Dicyclomine’s
28AUTONOMIC NERVOUS SYSTEM DRUGS
Belladonnaalkaloids are lesslikely to bind with
serum proteins, somore drug remains
available to produce atherapeutic effect.
938902.qxd 08/26/2008 14:47 Page 28

metabolism is unknown, but it’s excreted equally in feces andurine.
PharmacodynamicsCholinergic blockers can have paradoxical effects on the body, de-pending on the dosage and the condition being treated.
Dual dutyCholinergic blockers can produce a stimulating or depressing ef-fect, depending on the target organ. In the brain, they do both—low drug levels stimulate, and high drug levels depress.
Conditional considerationsThe effects of a drug on your patient are also determined by thepatient’s disorder. Parkinson’s disease, for example, is character-ized by low dopamine levels that intensify the stimulating effectsof acetylcholine. Cholinergic blockers depress this effect. In otherdisorders, however, they stimulate the central nervous system.
PharmacotherapeuticsCholinergic blockers are often used to treat GI disorders and com-plications.• All cholinergic blockers are used to treat spastic or hyperactiveconditions of the GI and urinary tracts because they relax musclesand decrease GI secretions. These drugs may be used to relax thebladder and to treat urinary incontinence. The quaternary ammo-nium and amine compounds such as propantheline are the drugsof choice for these conditions because they cause fewer adversereactions than belladonna alkaloids.• Belladonna alkaloids are used with morphine to treat biliary col-ic (pain caused by stones in the bile duct).• Cholinergic blocking drugs are given by injection before suchdiagnostic procedures as endoscopy and sigmoidoscopy to relaxthe GI smooth muscle.
Before surgeryCholinergic blockers such as atropine are given before surgery to:• reduce oral, gastric, and respiratory secretions• prevent a drop in heart rate caused by vagal nerve stimulationduring anesthesia.
Brainy belladonnaThe belladonna alkaloids can affect the brain. For example,scopolamine, given with the pain relievers morphine or meperi-
29CHOLINERGIC BLOCKING DRUGS
938902.qxd 08/26/2008 14:47 Page 29

dine, causes drowsiness and amnesia ina patient having surgery. It’s also used totreat motion sickness.
Belladonna alkaloids also have important therapeutic effectson the heart. Atropine is the drug of choice to treat:• symptomatic sinus bradycardia—when the heart beats too slow-ly, causing low blood pressure or dizziness (see How atropinespeeds the heart rate)• arrhythmias resulting from the use of anesthetics, choline es-ters, or succinylcholine.
30AUTONOMIC NERVOUS SYSTEM DRUGS
To understand how atropine affects the heart, first considerhow the heart’s electrical conduction system functions.
Without the drug
When the neurotransmitter acetylcholine is released, the va-gus nerve stimulates the sinoatrial (SA) node (the heart’s pace-maker) and the atrioventricular (AV) node, which controls con-duction between the atria and the ventricles of the heart. This
inhibits electrical conduction and causes the heart rate to slowdown.
With the drug
Atropine, a cholinergic blocking drug, competes with acetyl-choline for cholinergic receptor sites on the SA and AV nodes.By blocking acetylcholine, atropine speeds up the heart rate.
Now I get it!
How atropine speeds the heart rate
Atropine
Atropine occupying thecholinergic receptor siteand blocking acetylcholine
Parasympathetic impulsetraveling through thevagus nerve toward theSA and AV nodes
Terminal end of vagusnerve
Acetylcholine releasedinto the synapse
Receptor site occupiedby acetylcholine
Atropine andacetylcholine competingfor receptor site
Cholinergic blockingdrugs can help meregain my rhythm!
938902.qxd 08/26/2008 14:47 Page 30

An eye on the problemCholinergic blockers also are used as cycloplegics. That meansthat they:• paralyze the ciliary muscles of the eye (used for fine focusing)• alter the shape of the eye lens.
Moreover, cholinergic blockers act as mydriatics to dilate thepupils, making it easier to measure refractive errors during an eyeexamination or to perform eye surgery.
Punishing pesticidesThe belladonna alkaloids, particularly atropine and hyoscyamine,are effective antidotes to cholinergic and anticholinesterasedrugs. Atropine is the drug of choice to treat poisoning fromorganophosphate pesticides. Atropine and hyoscyamine alsocounteract the effects of the neuromuscular blocking drugs bycompeting for the same receptor sites.
Drug interactionsBecause cholinergic blockers slow the passage of food and drugsthrough the stomach, drugs remain in prolonged contact with themucous membranes of the GI tract. This increases the amount ofthe drug that’s absorbed and, therefore, increases the risk of ad-verse effects.
Increased effect…Drugs that increase the effects of cholinergic blockers include:• disopyramide• antidyskinetics such as amantadine• antiemetics and antivertigo drugs, such as buclizine, cyclizine,meclizine, and diphenhydramine• antipsychotics, such as haloperidol, phenothiazines, and thio-xanthenes• cyclobenzaprine• orphenadrine• tricyclic and tetracyclic antidepressants.
…or decreased effectDrugs that decrease the effects of cholinergic blockers include:• cholinergic agonists such as bethanechol• anticholinesterase drugs, such as neostigmine and pyridostig-mine.
Mixing it up some moreOther drug interactions can occur:• The risk of digoxin toxicity increases when digoxin is takenwith a cholinergic blocker.
31CHOLINERGIC BLOCKING DRUGS
938902.qxd 08/26/2008 14:47 Page 31

• Opiate-like analgesics further slow the movement of food anddrugs through the GI tract when taken with a cholinergic blocker.• The absorption of nitroglycerin tablets placed under the tongueis reduced when this drug is taken with a cholinergic blocker. (SeeAdverse reactions to cholinergic blockers.)
Adrenergic drugsAdrenergic drugs are also called sympathomimetic drugs be-cause they produce effects similar to those produced by the sym-pathetic nervous system.
Classified by chemical…Adrenergic drugs are classified into two groups based on theirchemical structure—catecholamines (naturally occurring as wellas synthetic) and noncatecholamines.
…or by actionAdrenergic drugs are also classified by how they act. They can be:• direct-acting, in which the drug acts directly on the organ or tis-sue innervated (supplied with nerves or nerve impulses) by thesympathetic nervous system• indirect-acting, in which the drug triggers the release of a neu-rotransmitter, usually norepinephrine• dual-acting, in which the drug has both direct and indirect ac-tions. (See Understanding adrenergics.)
Which receptor does it affect?The therapeutic uses of adrenergics—catecholamines as well asnoncatecholamines—depend on which receptors they stimulateand to what degree. Adrenergic drugs can affect:• alpha-adrenergic receptors• beta-adrenergic receptors• dopamine receptors.
Mimicking norepinephrine and epinephrineMost adrenergics produce their effects by stimulating alpha recep-tors and beta receptors. These drugs mimic the action of norepi-nephrine and epinephrine.
Doing it like dopamineDopaminergic drugs act primarily on receptors in the sympatheticnervous system stimulated by dopamine.
32AUTONOMIC NERVOUS SYSTEM DRUGS
Adversereactions tocholinergicblockers
Adverse reactions re-sulting from cholinergicblockers are closely re-lated to the drug dose.With these drugs, thedifference between atherapeutic dose and atoxic dose is small.
Adverse reactionsmay include:• dry mouth• reduced bronchial se-cretions• increased heart rate• decreased sweating.
Warning!
Memoryjogger
A direct-acting drug
has a direct effecton a target organ.
An indirect-actingdrug triggers a neu-rotransmitter thattakes over fromthere.
A dual-acting drugworks both ways.
938902.qxd 08/26/2008 14:47 Page 32

CatecholaminesBecause of their common basic chemical structure, all catechol-amines share certain properties—they stimulate the nervous sys-tem, constrict peripheral blood vessels, increase heart rate, and
33ADRENERGIC DRUGS
Adrenergicdrugs can bedirect-acting,
indirect-acting,or both.
Adrenergic drugs are distinguished by how they achieve their effect. The illustrations below showthe action of direct-, indirect-, and dual-acting adrenergics.
Now I get it!
Understanding adrenergics
Direct-acting adrenergic action
Direct-acting adrenergics directly stimulate adrener-gic receptors.
Indirect-acting adrenergic action
Indirect-acting adrenergics stimulate the release ofnorepinephrine from nerve endings into the synapse.
Dual-acting adrenergic action
Dual-acting adrenergics stimulate both adrenergicreceptor sites and the release of norepinephrinefrom nerve endings.
Key:Norepinephrine Adrenergic drug
N
D
N
N
N
D
D
D
RECEPTOR
N
D
N
N
DD
RECEPTOR
N
N
D
D
RECEPTOR
N
D
N
N
N
D
RECEPTOR
N
D
DN
938902.qxd 08/26/2008 14:47 Page 33

dilate the bronchi. They can be manufactured in the body or in alaboratory. Common catecholamines include:• dobutamine• dopamine• epinephrine, epinephrine bitartrate, and epinephrine hydrochlo-ride• norepinephrine (levarterenol)• isoproterenol hydrochloride and isoproterenol sulfate.
PharmacokineticsCatecholamines can’t be taken orally because they’re destroyed bydigestive enzymes. In contrast, when these drugs are given sublin-gually (under the tongue), they’re absorbed rapidly through themucous membranes. Any sublingual drug not completely ab-sorbed is rapidly metabolized by swallowed saliva.
Subcutaneously slowSubQ absorption is slowed because catecholamines cause theblood vessels around the injection site to constrict.
I.M. absorption is more rapid because there’s less constrictionof local blood vessels.
Distribution and metabolismCatecholamines are widely distributed in the body. They’re metab-olized and inactivated predominantly in the liver but can also bemetabolized in the:• GI tract• lungs• kidneys• plasma• other tissues.
ExcretionCatecholamines are excreted primarily in urine; however, a smallamount of isoproterenol is excreted in feces and some epineph-rine is excreted in breast milk.
PharmacodynamicsCatecholamines are primarily direct-acting. When catecholaminescombine with alpha receptors or beta receptors, they cause eitheran excitatory or an inhibitory effect. Typically, activation of alphareceptors generates an excitatory response, except for intestinalrelaxation. Activation of beta receptors typically produces an in-hibitory response, except in heart cells, where norepinephrineproduces excitatory effects.
34AUTONOMIC NERVOUS SYSTEM DRUGS
Catecholaminesare ineffective whentaken orally becausethey’re destroyed bydigestive enzymes.
Memoryjogger
To help youremember
the effects of cate-cholamines on alphaand beta receptors,remember that Astands for alpha(and activation, sug-gesting an excitatoryresponse), and Bstands for beta (orbanished, suggest-ing an inhibitory ef-fect).
938902.qxd 08/26/2008 14:47 Page 34

How hearteningThe clinical effects of catecholamines depend on the dosage andadministration route. Catecholamines are potent inotropes—theymake the heart contract more forcefully. As a result, the ventriclesempty more completely with each heartbeat, increasing the heart’sworkload and the amount of oxygen it needs to do this harderwork.
Rapid ratesCatecholamines also produce a positive chronotropiceffect, which means that they cause the heart to beatfaster. That happens because the pacemaker cells inthe heart’s sinoatrial (SA) node depolarize at a fasterrate. As catecholamines cause blood vessels to con-strict and blood pressure to rise, the heart rate canfall as the body tries to compensate for an excessiverise in blood pressure.
Fascinating rhythmCatecholamines can cause the Purkinje fibers (an intricate web offibers that carry electrical impulses into the ventricles) to firespontaneously, possibly producing abnormal heart rhythms, suchas premature ventricular contractions and fibrillation. Epineph-rine is more likely than norepinephrine to produce this sponta-neous firing.
PharmacotherapeuticsThe therapeutic uses of catecholamines depend on the particularreceptor that’s activated.• Norepinephrine stimulates alpha receptors almost exclusively.• Dobutamine and isoproterenol stimulate only beta receptors.• Epinephrine stimulates both alpha and beta receptors.• Dopamine activates primarily dopamine receptors.
Boosting blood pressureCatecholamines that stimulate alpha receptors are used to treatlow blood pressure (hypotension). They generally work best whenused to treat hypotension caused by:• relaxation of the blood vessel (also called a loss of vasomotortone)• blood loss (such as from hemorrhage).
Restoring rhythmCatecholamines that stimulate beta1 receptors are used to treat:• bradycardia
35ADRENERGIC DRUGS
Catecholaminesincrease my
workload.
938902.qxd 08/26/2008 14:47 Page 35

• heart block (a delay or interruption in the conduction of electri-cal impulses between the atria and ventricles)• low cardiac output.
It’s electricBecause they’re believed to make the heart more responsive to de-fibrillation (using an electrical current to terminate a deadly ar-rhythmia), beta1-adrenergic drugs are used to treat:• ventricular fibrillation (quivering of the ventricles, resulting inno pulse)• asystole (no electrical activity in theheart)• cardiac arrest.
Better breathingCatecholamines that exert beta2 activityare used to treat:• acute or chronic bronchial asthma• emphysema• bronchitis• acute hypersensitivity (allergic) reac-tions to drugs.
Kind to the kidneysDopamine, which stimulates the dopamine receptors, is used inlow doses to improve blood flow to the kidneys by dilating the re-nal blood vessels.
Synthetic vs. naturalThe effects of natural catecholamines (those produced by thebody) differ somewhat from the effects of manufactured cate-cholamines. Manufactured catecholamines have a short durationof action, which can limit their therapeutic usefulness.
Drug interactionsDrug interactions involving catecholamines can be serious, result-ing in hypotension, hypertension, arrhythmias, seizures, and highblood glucose levels in diabetic patients.• Alpha-adrenergic blockers, such as phentolamine, can producehypotension when taken with a catecholamine.• Beta-adrenergic blockers, such as propranolol, taken with a cat-echolamine can lead to bronchial constriction.• Epinephrine may cause hyperglycemia in diabetic patients re-ceiving the drug. These patients may require an increased dose ofinsulin or oral antidiabetic agents.
36AUTONOMIC NERVOUS SYSTEM DRUGS
Catecholamineshave a wide variety of
therapeutic uses.Almost all body
systems can feel theimpact!
938902.qxd 08/26/2008 14:47 Page 36

• Other adrenergics taken with a catecholamine can produce ad-ditive, or double, effects, such as hypertension and arrhythmias,as well as enhance other adverse effects. Increased risk of adverseeffects, such as hypertension, may occur when adrenergic drugsare given with other drugs that can cause hypertension.• Tricyclic antidepressants taken with a catecholamine can leadto hypertension. (See Adverse reactions to catecholamines.)
NoncatecholaminesNoncatecholamine adrenergic drugs have a variety of therapeuticuses because of the many effects they can have on the body, in-cluding:• local or systemic constriction of blood vessels (phenylephrine)• nasal and eye decongestion and dilation of the bronchioles (al-buterol, bitolterol, ephedrine, formoterol, isoetharine hydrochlo-ride, isoproterenol, levalbuterol, metaproterenol, pirbuterol, sal-meterol, and terbutaline)• smooth-muscle relaxation (terbutaline).
37ADRENERGIC DRUGS
Adverse reactions to catecholamines can include:• restlessness• asthmatic episode• dizziness• headache• palpitations• cardiac arrhythmias• hypotension• hypertension and hypertensive crisis• stroke• angina• increased blood glucose levels• tissue necrosis and sloughing (if a catecholamine given I.V. leaks intosurrounding tissue).
Warning!
Adverse reactions to catecholamines
938902.qxd 08/26/2008 14:47 Page 37

PharmacokineticsAlthough these drugs are all excreted in urine, they’re absorbed indifferent ways.
Absorption and distributionAbsorption of the noncatecholamines depends on the administra-tion route:• Inhaled drugs, such as albuterol, are absorbed gradually fromthe bronchi and result in lower drug levels in the body.• Oral drugs are absorbed well from the GI tract and are distrib-uted widely in body fluids and tissues.• Some noncatecholamines, such as ephedrine, cross the blood-brain barrier and can be found in high concentrations in the brainand cerebrospinal fluid (fluid that moves through and protects thebrain and spinal canal).
MetabolismNoncatecholamines are metabolized and inactivated primarily inthe liver but also in the lungs, GI tract, and other tissues.
ExcretionNoncatecholamines and their metabolites are excreted primarilyin urine. Some, such as inhaled albuterol, are excreted within 24hours; others, such as oral albuterol, within 3 days. Acidic urineincreases excretion of many noncatecholamines; alkaline urineslows excretion.
PharmacodynamicsNoncatecholamines can be direct-acting, indirect-acting, or dual-acting (unlike catecholamines, which are primarily direct-acting).• Direct-acting noncatecholamines that stimulate alpha receptorsinclude phenylephrine. Those that selectively stimulate beta2 re-ceptors include albuterol, isoetharine, metaproterenol, and terbu-taline.• Dual-acting noncatecholamines include ephedrine.
PharmacotherapeuticsNoncatecholamines stimulate the sympathetic nervous system,producing a variety of effects in the body. Phenylephrine, for ex-ample, causes vasoconstriction and is used to treat hypotension incases of severe shock. Terbutaline is used to stop preterm labor.
38AUTONOMIC NERVOUS SYSTEM DRUGS
938902.qxd 08/26/2008 14:47 Page 38

Drug interactionsHere are a few examples of drugs that interact with noncatechol-amines:• Anesthetics (general), cyclopropane, and halogenated hydrocar-bons can cause arrhythmias. Hypotension can also occur if thesedrugs are taken with noncatecholamines that exert predominantlybeta2 activity, such as terbutaline.• Monoamine oxidase inhibitors can cause severe hypertensionand even death.• Oxytocic drugs that stimulate the uterus to contract can be in-hibited when taken with terbutaline. When taken with other non-catecholamines, oxytocic drugs can cause hypertensive crisis or astroke.• Tricyclic antidepressants can cause hypertension and arrhyth-mias.• Urine alkalizers, such as acetazolamide and sodium bicarbon-ate, slow excretion of noncatecholamines, prolonging their dura-tion of action. (See Adverse reactions to noncatecholamines.)
39ADRENERGIC DRUGS
Monoamine oxidaseinhibitors interactdangerously with
noncatecholamines—possibly resulting in
death.
Adverse reactions to noncate-cholamine drugs may include:• headache• restlessness• anxiety or euphoria• irritability• trembling• drowsiness or insomnia• light-headedness• incoherence• seizures
• hypertension or hypotension• palpitations• bradycardia or tachycardia• irregular heart rhythm• cardiac arrest• cerebral hemorrhage• tingling or coldness in the armsor legs• pallor or flushing• angina.
Warning!
Adverse reactions tononcatecholamines
938902.qxd 08/26/2008 14:47 Page 39

Adrenergic blocking drugsAdrenergic blocking drugs, also called sympatholytic drugs, areused to disrupt sympathetic nervous system function. These drugswork by blocking impulse transmission (and thus sympatheticnervous system stimulation) at adrenergic neurons or adrenergicreceptor sites. Their action at these sites can be exerted by:• interrupting the action of adrenergic (sympathomimetic) drugs• reducing available norepinephrine• preventing the action of cholinergic drugs.
Classified informationAdrenergic blocking drugs are classified according to their site ofaction as:• alpha-adrenergic blockers (or alpha blockers)• beta-adrenergic blockers (or beta blockers).
Alpha-adrenergic blockersAlpha-adrenergic blockers work by interrupting the actions of thecatecholamines epinephrine and norepinephrine at alpha recep-tors. This results in:• relaxation of the smooth muscle in blood vessels• increased dilation of blood vessels• decreased blood pressure.
Drugs in this class include:• alfuzosin• ergoloid mesylates• phenoxybenzamine• phentolamine• prazosin, doxazosin, and terazosin• tamsulosin.
A mixed bagErgotamine is a mixed alpha agonist and antagonist; at high doses,it acts as an alpha-adrenergic blocker.
PharmacokineticsThe action of alpha-adrenergic blockers in the body isn’t well un-derstood. Most of these drugs are absorbed erratically when ad-ministered orally, and more rapidly and completely when adminis-tered sublingually. Alpha-adrenergic blockers vary considerably in
40AUTONOMIC NERVOUS SYSTEM DRUGS
Adrenergic blockingdrugs block
stimulation of thesympathetic nervous
system.
Let’s face it—theaction of alpha-
adrenergic blockers isa bit puzzling.
938902.qxd 08/26/2008 14:47 Page 40

their onset of action, peak concentration levels, and duration ofaction.
PharmacodynamicsAlpha-adrenergic blockers work in one of two ways:• They interfere with or block the synthesis, storage, release, andreuptake of norepinephrine by neurons.• They antagonize epinephrine, norepinephrine, or adrenergic(sympathomimetic) drugs at alpha receptor sites.
Not very discriminatingAlpha-adrenergic blockers include drugs that block stimulation ofalpha1 receptors and that may block alpha2 receptors.
Reducing resistanceAlpha-adrenergic blockers occupy alpha receptor sites on thesmooth muscle of blood vessels. (See How alpha-adrenergicblockers affect peripheral blood vessels.)
This prevents catecholamines from occupying and stimulatingthe receptor sites. As a result, blood vessels dilate, increasing lo-
41ADRENERGIC BLOCKING DRUGS
By occupying alpha receptor sites, alpha-adrenergic blockingdrugs cause the blood vessel walls to relax. This leads to dila-tion of the blood vessels and reduced peripheral vascular re-sistance (the pressure that blood must overcome as it flows ina vessel).
One result: Orthostatic hypotension
These effects can cause orthostatic hypotension, a drop inblood pressure that occurs when changing position from lyingdown to standing. Redistribution of blood to the dilated bloodvessels of the legs causes hypotension.
Now I get it!
How alpha-adrenergic blockers affect peripheral blood vessels
Vessel before drug’s effect Vessel dilated as a result of drug’s effect
Alpha-adrenergic blocker
Alpha receptor sites
Alpha-adrenergic blocker
Blood flowIncreasedblood flow
938902.qxd 08/26/2008 14:48 Page 41

cal blood flow to the skin and other organs. The decreased periph-eral vascular resistance (resistance to blood flow) helps to de-crease blood pressure.
Sympathetic response?The therapeutic effect of an alpha-adrenergic blocker depends onthe sympathetic tone (the state of partial constriction of bloodvessels) in the body before the drug is administered. For instance,when the drug is given with the patient lying down, only a smallchange in blood pressure occurs. In this position, the sympatheticnerves release very little norepinephrine.
Patient up, pressure downOn the other hand, when a patient stands up, norepinephrine is re-leased to constrict the veins and shoot blood back up to the heart.If the patient receives an alpha-adrenergic blocker, however, theveins can’t constrict and blood pools in the legs. Because blood re-turn to the heart is reduced, blood pressure drops. This drop inblood pressure that occurs when a person stands up is called or-thostatic hypotension.
PharmacotherapeuticsBecause alpha-adrenergic blockers cause smooth muscles to relaxand blood vessels to dilate, they increase local blood flow to theskin and other organs and reduce blood pressure. As a result,they’re used to treat:• benign prostatic hypertrophy• hypertension• peripheral vascular disorders (diseases of the blood vessels ofthe extremities), especially those in which blood vessel spasmcauses poor local blood flow, such as Raynaud’s disease (intermit-tent pallor, cyanosis, or redness of fingers), acrocyanosis (sym-metrical mottled cyanosis of the hands and feet), and frostbite• pheochromocytoma (a catecholamine-secreting tumor thatcauses severe hypertension).
Drug interactionsMany drugs interact with alpha-adrenergic blockers, producing asynergistic, or exaggerated, effect. The most serious interactionsare severe hypotension and vascular collapse.
These interactions can occur when these drugs are taken withergoloid mesylates and ergotamine:• Caffeine and macrolide antibiotics can increase the effects ofergotamine.• Dopamine increases the pressor (rising blood pressure) effect.
42AUTONOMIC NERVOUS SYSTEM DRUGS
Alpha-adrenergicblockers cause a
small change in bloodpressure if you’re lying
down…
…when you stand,the drug prevents
your veins fromconstricting.
938902.qxd 08/26/2008 14:48 Page 42

• Nitroglycerin can produce hypotension from excessive dilationof blood vessels.• Sympathomimetics, including many over-the-counter drugs, canincrease the stimulating effects on the heart, possibly resulting inhypotension with rebound hypertension. (See Adverse reactionsto alpha-adrenergic blockers.)
Beta-adrenergic blockersBeta-adrenergic blockers, the most widely used adrenergic block-ers, prevent stimulation of the sympathetic nervous system by in-hibiting the action of catecholamines at beta-adrenergic receptors.
From not so selective…Beta-adrenergic blockers can be selective or nonselective. Non-selective beta-adrenergic blockers affect:• beta1 receptor sites (located mainly in the heart)• beta2 receptor sites (located in the bronchi, blood vessels, anduterus).
Nonselective beta-adrenergic blockers include carteolol,carvedilol, labetalol, levobunolol, metipranolol, penbutolol, pin-dolol, sotalol, nadolol, propranolol, and timolol. (Carvedilol andlabetalol also block alpha1 receptors.)
43ADRENERGIC BLOCKING DRUGS
Most adverse reactions associated with alpha-adrenergic blockers arecaused primarily by dilation of the blood vessels. They include:• orthostatic hypotension or severe rebound hypertension• bradycardia or tachycardia• edema• difficulty breathing• light-headedness• flushing• arrhythmias• angina• heart attack• spasm of blood vessels in the brain• a shocklike state.
Warning!
Adverse reactions to alpha-adrenergic blockers
938902.qxd 08/26/2008 14:48 Page 43

…to highly discriminatingSelective beta-adrenergic blockers primarily affect beta1-adrenergic sites. They include acebutolol, atenolol, betaxolol,bisoprolol, esmolol, and metoprolol.
The not so beta blockersSome beta-adrenergic blockers, such as pindolol and acebutolol,have intrinsic sympathetic activity. This means that instead of at-taching to beta receptors and blocking them, these beta-adrenergic blockers attach to beta receptors and stimulate them.These drugs are sometimes classified as partial agonists.
PharmacokineticsBeta-adrenergic blockers are usually absorbed rapidly and wellfrom the GI tract and are somewhat protein-bound. Food doesn’tinhibit—and may even enhance—their absorption. Some beta-adrenergic blockers are absorbed more completely than others.
Peak by I.V.The onset of action of beta-adrenergic blockers is primarily dose-and drug-dependent. The time it takes to reach peak concentra-tion levels depends on the administration route. Beta-adrenergicblockers given I.V. reach peak levels much more rapidly thanthose taken by mouth.
DistributionBeta-adrenergic blockers are distributed widely in body tissues,with the highest concentrations found in the:• heart• liver• lungs• saliva.
Metabolism and excretionExcept for nadolol and atenolol, beta-adrenergic blockers are me-tabolized in the liver. They’re excreted primarily in urine, eitherunchanged or as metabolites, but can also be excreted in feces,bile and, to some degree, breast milk.
PharmacodynamicsBeta-adrenergic blockers have widespread effects in the body be-cause they produce their blocking action not only at adrenergicnerve endings but also in the adrenal medulla.
44AUTONOMIC NERVOUS SYSTEM DRUGS
The onset andpeak of beta-
adrenergic blockersvary widely,
depending on theadministration
route.
938902.qxd 08/26/2008 14:48 Page 44

A matter of the heartEffects on the heart include increased peripheral vascular resis-tance, decreased blood pressure, decreased force of the heart’scontractions, decreased oxygen consumption by the heart, slowedimpulse conduction between the atria and ventricles, and de-creased cardiac output (the amount of blood the heart pumpseach minute). (See How beta-adrenergic blockers work.)
Selective and nonselective effectsSome beta-adrenergic blocker effects depend on whether the drugis classified as selective or nonselective.
Selective beta-adrenergic blockers, which prefer to blockbeta1-receptor sites, reduce stimulation of the heart. They’re oftenreferred to as cardioselective beta-adrenergic blockers.
45ADRENERGIC BLOCKING DRUGS
By occupying beta receptor sites, beta-adrenergic blockers prevent catecholamines (norepi-nephrine and epinephrine) from occupying these sites and exerting their stimulating effects. Thisillustration shows the effects of beta-adrenergic blockers on the heart, lungs, and blood vessels.
Now I get it!
How beta-adrenergic blockers work
Reduced blood pressure
Reduced heart rate and reduced automaticity andexcitability (the ability to develop arrhythmias)
Slowed conduction of electrical impulses from theatria to the ventricles through the atrioventricularnode
Decreased force of the heart’s contractions
Constriction of bronchioles
Constriction of peripheral blood vessels (beta2receptors)
938902.qxd 08/26/2008 14:48 Page 45

Nonselective beta-adrenergic blockers, which block bothbeta1- and beta2-receptor sites, not only reduce stimulation of theheart but also cause the bronchioles of the lungs to constrict. Forinstance, nonselective beta-adrenergic blockers can cause bron-chospasm in patients with chronic obstructive lung disease. Thisadverse effect isn’t seen when cardioselective drugs are given atlower doses.
PharmacotherapeuticsBeta-adrenergic blockers are used to treat many conditions andare under investigation for use in many more. As mentioned previ-ously, their clinical usefulness is based largely (but not exclusive-ly) on how they affect the heart. (See Are beta-adrenergic block-ers underused in elderly patients?)
Helping the heartBeta-adrenergic blockers can be prescribed after a heart attack toprevent another heart attack or to treat:• angina• heart failure• hypertension• cardiomyopathy (a disease of the heart muscle)• supraventricular arrhythmias (irregular heartbeats that origi-nate in the atria, SA node, or atrioventricular node).
46AUTONOMIC NERVOUS SYSTEM DRUGS
Nonselectivebeta-adrenergic
blockers may causebronchospasm. Be
careful using them inpatients who have
respiratory disorders.
Research has clearly shown that use of beta-adrenergic blockers after a heart attack re-duces the risk of death and another heart at-tack. However, these drugs aren’t being pre-scribed for elderly patients.
Study findings
One study found that only 34% of patients wereprescribed a beta-adrenergic blocker after dis-charge from the hospital following a heart at-tack. Those least likely to receive a beta-adrenergic blocker included very sick patients,blacks, and the elderly.
Why?
The chief investigator of a study that looked atthe use of beta-adrenergic blockers in the el-derly believes that many doctors fear the ad-verse effects these drugs may produce in old-er patients. However, the study suggested thatbeta-adrenergic blockers are safe for elderlyheart attack patients if the lowest effectivedose of a selective beta-adrenergic blocker isprescribed.
Yea or nay?
Are beta-adrenergic blockers underused in elderlypatients?
938902.qxd 08/26/2008 14:48 Page 46

Jack of all tradesBeta-adrenergic blockers are also used to treat:• anxiety• cardiovascular symptoms associated with thyrotoxicosis (over-production of thyroid hormones)• essential tremor• migraine headaches• open-angle glaucoma• pheochromocytoma (tumor of the adrenal gland).
Drug interactionsMany drugs can interact with beta-adrenergic blockers to causepotentially dangerous effects. Some of the most serious effects in-clude cardiac or respiratory depression, arrhythmias, severebronchospasm, and severe hypotension that can lead to vascularcollapse. Other interactions can also occur:• Increased effects or toxicity can occur when cimetidine, digox-in, or calcium channel blockers (primarily verapamil) are takenwith beta-adrenergic blockers.• Decreased effects can occur when rifampin, antacids, calciumsalts, barbiturates, or anti-inflammatories, such as indomethacinand salicylates, are taken with beta-adrenergic blockers.• Lidocaine toxicity may occur when lidocaine is taken with beta-adrenergic blockers.• The requirements for insulin and oral antidiabetic drugs can bealtered when these drugs are taken with beta-adrenergic blockers.• The ability of theophylline to produce bronchodilation is im-paired by nonselective beta-adrenergic blockers.• Clonidine taken with a nonselective beta-adrenergic blocker cancause life-threatening hypertension during clonidine withdrawal.• Sympathomimetics taken with nonselective beta-adrenergicblockers can cause hypertension and reflex bradycardia. (See Ad-verse reactions to beta-adrenergic blockers.)
Quick quiz
1. During bethanechol therapy, which common adverse reac-tions should you expect to observe?
A. Dry mouth, flushed face, and constipationB. Fasciculations, dysphagia, and respiratory distressC. Nausea, vomiting, diarrhea, and intestinal crampsD. Anorexia, cardiac arrhythmias, fatigue, and broncho-
spasm
47QUICK QUIZ
Adversereactions tobeta-adrenergicblockers
Beta-adrenergic block-ers generally cause fewadverse reactions; thosethat do occur are drug-or dose-dependent andinclude:• hypotension• bradycardia• peripheral vascularinsufficiency• atrioventricular block• heart failure• fatigue• bronchospasm• diarrhea or constipa-tion• nausea and vomiting• abdominal discomfort• anorexia• flatulence• rash• fever with sore throat• spasm of the larynx• respiratory distress(allergic response).
Warning!
938902.qxd 08/26/2008 14:48 Page 47

Answer: C. Bethanechol is a cholinergic agonist. Common ad-verse effects of cholinergic agonists include such GI symptoms asnausea, vomiting, diarrhea, and intestinal cramps.
2. Catecholamines act as potent inotropes. That means thatthey:
A. cause the heart to contract forcefully.B. slow the heart rate.C. lower blood pressure.D. decrease urinary output.
Answer: A. Catecholamines cause the heart to contract forceful-ly, increasing the heart’s workload. They also cause the heart tobeat faster and raise blood pressure.
3. Noncatecholamines can interact with monoamine oxidase in-hibitors to cause:
A. arrhythmias.B. severe hypertension.C. seizures.D. tachycardia.
Answer: B. Noncatecholamines can interact very dangerouslywith monoamine oxidase inhibitors, causing severe hypertensionand even death.
4. Beta-adrenergic blockers have widespread effects becausethey produce their blocking action in the:
A. hypothalamus.B. anterior pituitary gland.C. pituitary gland.D. adrenal medulla.
Answer: D. Beta-adrenergic blockers have widespread effects inthe body because they produce their blocking action not only atadrenergic nerve endings but also in the adrenal medulla.
ScoringIf you answered all four items correctly, fabulous! You’re automat-
ic with the autonomic nervous system.If you answered three items correctly, great! You’ve had nothing
but positive interactions with these drugs.If you answered fewer than three items correctly, don’t worry.
Like the nervous system, you have a lot of information to co-ordinate. Just review the chapter and try again.
48AUTONOMIC NERVOUS SYSTEM DRUGS
✰✰✰
✰✰
✰
938902.qxd 08/26/2008 14:48 Page 48

Skeletal muscle relaxantsSkeletal muscle relaxants relieve musculoskeletal pain or spasmand severe musculoskeletal spasticity (stiff, awkward move-ments). They’re used to treat acute, painful musculoskeletal con-ditions and the muscle spasticity associated with multiple sclero-sis (MS) (a progressive demyelination of the white matter of thebrain and spinal cord that causes widespread neurologic dysfunc-tion), cerebral palsy (a motor function disorder caused by neuro-logic damage), stroke (reduced oxygen supply to the brain, result-ing in neurologic deficits), and spinal cord injuries that can resultin paralysis or death.
This chapter discusses the two main classes of skeletal musclerelaxants—centrally acting and direct-acting—as well as othermuscle relaxants.
Cycling problemsExposure to severe cold, lack of blood flow to a muscle, oroverexertion can send sensory impulses from the posterior senso-ry nerve fibers to the spinal cord and the higher levels of the cen-tral nervous system (CNS). These sensory impulses can cause areflex (involuntary) muscle contraction or spasm from trauma,epilepsy, hypocalcemia (low calcium levels), or muscle disorders.
3
Neurologic and neuromuscular drugs
Just the facts
In this chapter, you’ll review:
♦ classes of drugs used to treat neurologic and neuromus-cular disorders
♦ uses and varying actions of these drugs
♦ how these drugs are absorbed, distributed, metabolized,and excreted
♦ drug interactions and adverse effects of these drugs.
Ahhh. It’s sonice to be able
to relax!
938903.qxd 08/26/2008 14:58 Page 49

The muscle contraction further stimulates the sensory receptorsto a more intense contraction, establishing a cycle. Centrally act-ing muscle relaxants are believed to break this cycle by acting asCNS depressants.
Centrally acting skeletal muscle relaxantsCentrally acting skeletal muscle relaxants, which act on the CNS,are used to treat acute spasms caused by such conditions as:• anxiety• inflammation• pain• trauma.
For intermittent or chronic spasmsA patient with intermittent or chronic spasms may receive tizani-dine.
For acute spasmsA patient with acute muscle spasms may receive one of thesedrugs:• carisoprodol• chlorzoxazone• cyclobenzaprine• metaxalone• methocarbamol• orphenadrine• tizanidine.
Pharmacokinetics (how drugs circulate)There’s still a lot we don’t know about how centrally acting skele-tal muscle relaxants circulate within the body. In general, thesedrugs are absorbed from the GI tract, widely distributed in thebody, metabolized in the liver, and excreted by the kidneys.
Cyclobenzaprine sticks aroundWhen these drugs are administered orally, it can take from 30 min-utes to 1 hour for effects to be achieved. The duration of action ofmost of these drugs varies from 4 to 6 hours; cyclobenzaprine hasthe longest duration of action, at 12 to 25 hours.
50NEUROLOGIC AND NEUROMUSCULAR DRUGS
Spasticity canbe caused by a
cyclical pattern ofimpulses…
…andskeletal musclerelaxants helpto break the
pattern.
938903.qxd 08/26/2008 14:58 Page 50

Pharmacodynamics (how drugs act)The centrally acting drugs don’t relax skeletal muscles directly ordepress neuronal conduction, neuromuscular transmission, ormuscle excitability. Although their precise mechanism of action isunknown, these drugs are known to be CNS depressants. Theirmuscle relaxant effects may be related to their sedative effects.
Pharmacotherapeutics (how drugs are used)Patients receive centrally acting skeletal muscle relaxants to treatacute, painful musculoskeletal conditions. They’re usually pre-scribed along with rest and physical therapy.
Drug interactionsThe centrally acting skeletal muscle relaxants interact with otherCNS depressants (including alcohol, narcotics, barbiturates, anti-convulsants, tricyclic antidepressants, kava kava, and antianxietydrugs), causing increased sedation, impaired motor function, andrespiratory depression. In addition, some of these drugs have oth-er interactions:• Cyclobenzaprine interacts with monoamine oxidase inhibitors(MAOIs) and can result in a high body temperature, excitation,and seizures.• Cyclobenzaprine can decrease the antihypertensive effects ofthe blood pressure–lowering drugs guanethidine and clonidine.• Orphenadrine and cyclobenzaprine sometimes enhance the ef-fects of cholinergic-blocking drugs.• Methocarbamol can antagonize the cholinergic effects of the an-ticholinesterase drugs used to treat myasthenia gravis.• Orphenadrine can reduce the effects of phenothiazines.• Orphenadrine and propoxyphene taken together can cause addi-tive CNS effects, including mental confusion, anxiety, andtremors. (See Adverse reactions to centrally acting skeletal mus-cle relaxants, page 52.)• Tizanidine combined with diuretics, central alpha-adrenergic ag-onists, or antihypertensives may increase hypotensive drug ef-fects. Concurrent use of tizanidine with CNS depressants maycause additive CNS depression. Hormonal contraceptives may re-duce the clearance of tizanidine, necessitating a dosage reduction.
51SKELETAL MUSCLE RELAXANTS
Centrally actingskeletal muscle
relaxants (and plentyof rest) are used to
treat painfulmusculoskeletal
conditions.
938903.qxd 08/26/2008 14:58 Page 51

Direct-acting skeletal muscle relaxantsDantrolene is the most common direct-acting skeletal muscle re-laxant. Although dantrolene has a similar therapeutic effect to thecentrally acting drugs, it works through a different mechanism ofaction. Because its major effect is on the muscles, dantrolene hasa lower incidence of adverse CNS effects; high therapeutic doses,however, are toxic to the liver.
Common adverse effects of dantrolene include drowsiness,dizziness, malaise, fatigue, and weakness. More serious adverseeffects include seizures and hepatitis. (See Dantrolene.)
In the headDantrolene seems most effective for spasticity of cerebral origin.Because it produces muscle weakness, dantrolene is of question-able benefit in patients with borderline strength.
PharmacokineticsAlthough the peak drug concentration of dantrolene usually oc-curs within about 5 hours after it’s ingested, the patient may notnotice the therapeutic benefit for a week or more.
AbsorptionDantrolene is absorbed poorly from the GI tract and is highly plas-ma protein–bound. This means that only a small portion of thedrug is available to produce a therapeutic effect.
52NEUROLOGIC AND NEUROMUSCULAR DRUGS
A patient can develop physical and psychological dependenceafter long-term use of these drugs. Abruptly stopping any ofthese drugs can cause severe withdrawal symptoms. Other ad-verse reactions can also occur.
Common reactions
• Dizziness• Drowsiness
Occasional reactions
• Abdominal distress
• Ataxia• Constipation• Diarrhea• Heartburn• Nausea and vomiting
Severe reactions
• Allergic reactions• Arrhythmias• Bradycardia
Warning!
Adverse reactions to centrally acting skeletal muscle relaxants
Dantrolene
Because of the risk ofliver damage with long-term use of dantrolene,baseline liver functiontests should be obtainedand therapy should bediscontinued if benefitsaren’t seen in 45 days.
Safe andsound
938903.qxd 08/26/2008 14:58 Page 52

Metabolism and excretionDantrolene is metabolized by the liver and excreted in urine. Itselimination half-life in healthy adults is about 9 hours. Becausedantrolene is metabolized in the liver, its half-life may be pro-longed in patients with impaired liver function.
PharmacodynamicsDantrolene is chemically and pharmacologically unrelated to theother skeletal muscle relaxants.
Dantrolene works by acting on the muscle itself. It interfereswith calcium ion release from the sarcoplasmic reticulum andweakens the force of contractions. At therapeutic concentrations,dantrolene has little effect on cardiac or intestinal smooth muscle.
PharmacotherapeuticsDantrolene helps manage all types of spasticity but is most effec-tive in patients with:• cerebral palsy• MS• spinal cord injury• stroke.
Dantrolene is also used to treat and prevent malignant hyper-thermia. This rare but potentially fatal complication of anesthesiais characterized by skeletal muscle rigidity and high fever. (SeeHow dantrolene reduces muscle rigidity.)
Drug interactions• CNS depressants can increase the depressive effects of dantro-lene, resulting in sedation, lack of coordination, and respiratorydepression.• Estrogens, when given with dantrolene, can increase the risk ofliver toxicity.• I.V. verapamil, when given with dantrolene, may result in cardio-vascular collapse; these drugs shouldn’t be administered concur-rently.• Alcohol may increase CNS depression when given with dantro-lene.• Sun exposure may cause photosensitivity.
Other skeletal muscle relaxantsTwo other drugs used as skeletal muscle relaxants are baclofenand diazepam. Diazepam, however, is primarily an antianxietydrug. (See Diazepam as a skeletal muscle relaxant, page 54.)
53SKELETAL MUSCLE RELAXANTS
How dantrolenereduces musclerigidity
Dantrolene appears todecrease the number ofcalcium ions releasedfrom the sarcoplasmicreticulum (a structure inmuscle cells that plays arole in muscle contrac-tion and relaxation byreleasing and storingcalcium). The lower thecalcium level in the mus-cle plasma or myoplasm,the less energy pro-duced when calciumprompts the muscle’sactin and myosin fila-ments (responsible formuscle contraction) tointeract. Less energymeans a weaker musclecontraction.
Reducing rigidity,
halting hyperthermia
By promoting muscle re-laxation, dantrolene pre-vents or reduces therigidity that contributesto the life-threateningbody temperatures ofmalignant hyperthermia.
Now I get it!
938903.qxd 08/26/2008 14:58 Page 53

PharmacokineticsBaclofen and diazepam are absorbed rapidly from the GI tract. Ba-clofen is distributed widely (with only small amounts crossing theblood-brain barrier), undergoes minimal liver metabolism, and isexcreted primarily unchanged in urine.
Diazepam is metabolized in the liver and mostly excreted inthe urine, with a small amount excreted in the feces.
Slow to a stopIt can take from hours to weeks before the patient notices thebeneficial effects of baclofen. The elimination half-life of baclofenis 21⁄2 to 4 hours. Abrupt withdrawal of the drug can cause halluci-nations, seizures, and worsening of spasticity.
PharmacodynamicsIt isn’t known exactly how baclofen or diazepam works. Diazepamprobably depresses the CNS at the limbic and subcortical levels ofthe brain. It suppresses the spread of seizure activity in the cortex,thalamus, and limbic areas.
Baclofen is chemically similar to the neurotransmitter gamma-aminobutyric acid (GABA) and probably acts in the spinal cord. Itreduces nerve impulses from the spinal cord to skeletal muscle,decreasing the number and severity of muscle spasms and reduc-ing associated pain.
A choice drugBecause baclofen produces less sedation than diazepam and lessperipheral muscle weakness than dantrolene, it’s the drug ofchoice to treat spasticity.
54NEUROLOGIC AND NEUROMUSCULAR DRUGS
Stopping baclofentreatment abruptly
could result inseizures!
Diazepam as a skeletal muscle relaxant
Diazepam is a benzodiazepine drug that’s used to treat acute muscle spasms as well as spasticitycaused by chronic disorders. Other uses of diazepam include treating anxiety, alcohol withdraw-al, and seizures. It seems to work by promoting the inhibitory effect of the neurotransmittergamma-aminobutyric acid on muscle contraction.
The negatives: Sedation and tolerance
Diazepam can be used alone or with other drugs to treat spasticity, especially in patients withspinal cord lesions and, occasionally, in patients with cerebral palsy. It’s also helpful in patientswith painful, continuous muscle spasms who aren’t too susceptible to the drug’s sedative effects.Unfortunately, diazepam’s use is limited by its central nervous system effects and the tolerancethat develops with prolonged use.
938903.qxd 08/26/2008 14:58 Page 54

PharmacotherapeuticsBaclofen’s primary clinical use is for paraplegic or quadriplegicpatients with spinal cord lesions, most commonly caused by MSor trauma. For these patients, baclofen significantly reduces thenumber and severity of painful flexor spasms. However, it doesn’timprove stiff gait, manual dexterity, or residual muscle function.
Baclofen may be administered intrathecally for patients whoare unresponsive to oral baclofen or who experience intolerableadverse reactions. After a positive response to a bolus dose, animplantable port for chronic therapy is inserted.
Diazepam relieves anxiety, muscle spasms, and seizures, and itinduces calmness and sleep.
Drug interactionsBaclofen has few drug interactions:• The most significant drug interaction is an increase in CNS de-pression when baclofen is administered with other CNS depres-sants, including alcohol.• Analgesia can be prolonged when fentanyl and baclofen are ad-ministered together.• Lithium carbonate and baclofen taken together can aggravatehyperkinesia (an abnormal increase in motor function or activity).• Tricyclic antidepressants and baclofen taken together can in-crease muscle relaxation.• Baclofen may increase blood glucose levels, resulting in theneed for increased doses of oral antidiabetic agents and insulin.
Intrathecal baclofen shouldn’t be discontinued abruptly be-cause doing so has resulted in high fever, altered mental status,exaggerated rebound spasticity, and muscle rigidity that, in rarecases, has progressed to rhabdomyolysis, multiple organ systemfailure, and death. (See Adverse reactions to baclofen.)
Neuromuscular blocking drugsNeuromuscular blocking drugs relax skeletal muscles by disrupt-ing the transmission of nerve impulses at the motor end plate (thebranching terminals of a motor nerve axon). (See Motor end plate,page 56.)
Neuromuscular blockers have three major clinical indications:
to relax skeletal muscles during surgery
to reduce the intensity of muscle spasms in drug- or electri-cally induced seizures
55NEUROMUSCULAR BLOCKING DRUGS
Adversereactions tobaclofen
Most common
• Transient drowsiness
Less common
• Nausea• Fatigue• Vertigo• Hypotonia• Muscle weakness• Depression• Headache
Warning!
938903.qxd 08/26/2008 14:58 Page 55

to manage patients who are fighting the use of a ventilator tohelp with breathing.
Two main classificationsThere are two main classes of natural and synthetic drugs used asneuromuscular blockers—nondepolarizing and depolarizing.
Nondepolarizing blocking drugsNondepolarizing blocking drugs, also called competitive or stabi-lizing drugs, are derived from curare alkaloids and syntheticallysimilar compounds. They include:• atracurium• cisatracurium• pancuronium• rocuronium• vecuronium.
56NEUROLOGIC AND NEUROMUSCULAR DRUGS
The motor nerve axon divides toform branching terminals calledmotor end plates. These are en-folded in muscle fibers, but sep-arated from the fibers by thesynaptic cleft.
Competing with contraction
A stimulus to the nerve causesthe release of acetylcholine intothe synaptic cleft. There, acetyl-choline occupies receptor siteson the muscle cell membrane,depolarizing the membrane andcausing muscle contraction.Neuromuscular blocking agentsact at the motor end plate bycompeting with acetylcholinefor the receptor sites or byblocking depolarization.
Now I get it!
Motor end plate
Muscle cell membrane
Motor end plate
Axon
Synaptic cleft
Acetylcholine
Motor nerve Skeletal muscle fiber
938903.qxd 08/26/2008 14:58 Page 56

PharmacokineticsBecause nondepolarizing blockers are absorbed poorly from theGI tract, they’re administered parenterally. The I.V. route is pre-ferred because the action is more predictable.
DistributionThese drugs are distributed rapidly throughout the body.
Metabolism and excretionA variable but large proportion of the nondepolarizing drugs is ex-creted unchanged in urine. Some drugs, such as atracurium, pan-curonium, and vecuronium, are partially metabolized in the liver.
PharmacodynamicsNondepolarizing blockers compete with acetylcholine at thecholinergic receptor sites of the skeletal muscle membrane. Thisblocks acetylcholine’s neurotransmitter action, preventing themuscle from contracting.
The effect can be counteracted by anticholinesterase drugs,such as neostigmine and pyridostigmine, which inhibit the actionof acetylcholinesterase, the enzyme that destroys acetylcholine.
From weakness to paralysisThe initial muscle weakness produced by these drugs quicklychanges to a flaccid (loss of muscle tone) paralysis that affects themuscles in a specific sequence. The first muscles to exhibit flaccidparalysis are those of the eyes, face, and neck. Next, the limb, ab-domen, and trunk muscles become flaccid.Lastly, the intercostal muscles (between theribs) and diaphragm (the breathing muscle)are paralyzed. Recovery from the paralysisusually occurs in the reverse order.
Conscious and awareBecause these drugs don’t cross the blood-brain barrier, the patient remains consciousand can feel pain. Even though the patient isparalyzed, he’s aware of what’s happeningto him and can experience extreme anxi-ety but can’t communicate his feelings.For this reason, an analgesic or antianxi-ety drug should be administered alongwith a neuromuscular blocker. (See Us-ing a neuromuscular blocker safely.)
57NEUROMUSCULAR BLOCKING DRUGS
Paralysis fromneuromuscularblocking drugsproceeds in a
specific sequence.Recovery is allabout reverse!
Using aneuromuscularblocker safely
When using a neuro-muscular blocker, re-member these importantpoints to keep the pa-tient safe:• Emergency respiratorysupport equipment (en-dotracheal equipment,ventilator, oxygen, at-ropine, edrophonium,epinephrine, and neo-stigmine) should be im-mediately available.• Drug-induced neuro-muscular blockade maybe reversed with an an-ticholinesterase (suchas neostigmine or edro-phonium), which is usu-ally given with an anti-cholinergic, such as at-ropine.• Sedatives or generalanesthetics should beadministered beforeneuromuscular block-ers.
Safe andsound
938903.qxd 08/26/2008 14:58 Page 57

PharmacotherapeuticsNondepolarizing blockers are used for intermediate or prolongedmuscle relaxation to:• ease the passage of an endotracheal (ET) tube• decrease the amount of anesthetic required during surgery• facilitate realignment of broken bones and dislocated joints• paralyze patients who need ventilatory support but who fightthe ET tube and ventilation• prevent muscle injury during electroconvulsive therapy (ECT)(passing an electric current through the brain to treat depression)by reducing the intensity of muscle spasms.
Drug interactionsThese drugs alter the effects of nondepolarizing neuromuscularblockers:• Aminoglycoside antibiotics and anesthetics potentiate or exag-gerate the neuromuscular blockade.• Drugs that alter the serum levels of the electrolytes calcium,magnesium, or potassium also alter the effects of the nondepolar-izing blockers.• The anticholinesterases (neostigmine, pyridostigmine, and edro-phonium) antagonize nondepolarizing blockers and are used asantidotes to them.• Drugs that can increase the intensity and duration of paralysiswhen taken with a nondepolarizing blocker include inhalationanesthetics, aminoglycosides, clindamycin, polymyxin, verapamil,quinine derivatives, ketamine, lithium, nitrates, thiazide diuretics,tetracyclines, and magnesium salts.• Drugs that can cause decreased neuromuscular blockade whentaken with a nondepolarizing blocker include carbamazepine, hy-dantoins, ranitidine, and theophylline. (See Adverse reactions tonondepolarizing blockers.)• Concurrent use of corticosteroids may result in prolonged mus-cle weakness.
Depolarizing blocking drugsSuccinylcholine is the only therapeutic depolarizing blockingdrug. Although it’s similar to the nondepolarizing blockers in itstherapeutic effect, its mechanism of action differs. Succinyl-choline acts like acetylcholine, but it isn’t inactivated bycholinesterase. It’s the drug of choice when short-term muscle re-laxation is needed.
58NEUROLOGIC AND NEUROMUSCULAR DRUGS
Remember: theeffect of these drugscan be frightening for
the patient.
Adversereactions tonondepolarizingblockers
To all drugs in this
class
• Apnea• Hypotension• Skin reactions• Bronchospasm• Excessive bronchialand salivary secretions
To pancuronium
• Tachycardia• Cardiac arrhythmias• Hypertension
Warning!
938903.qxd 08/26/2008 14:58 Page 58

PharmacokineticsBecause succinylcholine is absorbed poorly from the GI tract, thepreferred administration route is I.V.; the I.M. route can be used, ifnecessary.
Metabolism and excretionSuccinylcholine is hydrolyzed in the liver and plasma by the en-zyme pseudocholinesterase, producing a metabolite with a nonde-polarizing blocking action. Succinylcholine is excreted by the kid-neys, with a small amount excreted unchanged.
PharmacodynamicsAfter administration, succinylcholine is rapidly metabolized, butat a slower rate than acetylcholine. As a result, succinylcholine re-mains attached to receptor sites on the skeletal muscle membranefor a longer period of time. This prevents repolarization of the mo-tor end plate and results in muscle paralysis.
PharmacotherapeuticsSuccinylcholine is the drug of choice for short-term muscle relax-ation, such as during intubation and ECT.
Drug interactionsThe action of succinylcholine is potentiated by a number of anes-thetics and antibiotics. In contrast to their interaction with nonde-polarizing blockers, anticholinesterases increase succinylcholineblockade. (See Adverse reactions to succinylcholine.)
Antiparkinsonian drugsDrug therapy is an important part of the treatment for Parkinson’sdisease, a progressive neurologic disorder characterized by fourcardinal features:• muscle rigidity (inflexibility)• akinesia (loss of muscle movement)• tremors at rest• disturbances of posture and balance.
A defect in the dopamine pathway…Parkinson’s disease affects the extrapyramidal system, which in-fluences movement. The extrapyramidal system includes the cor-pus striatum, globus pallidus, and substantia nigra of the brain.
59ANTIPARKINSONIAN DRUGS
Becausesuccinylcholine is
administered I.V. orI.M., it has a very fast
onset.
Adversereactions tosuccinylcholine
The primary adversedrug reactions to suc-cinylcholine are:• prolonged apnea• hypotension.
Genetics increases the
risk
The risks associatedwith succinylcholine in-crease with certain ge-netic predispositions,such as a low pseudo-cholinesterase level andthe tendency to developmalignant hyperthermia.
Warning!
938903.qxd 08/26/2008 14:58 Page 59

In Parkinson’s disease, a dopamine deficiency occurs in thebasal ganglia, the dopamine-releasing pathway that connects thesubstantia nigra to the corpus striatum.
…causes an imbalance of neurotransmittersReduction of dopamine in the corpus striatum upsets the normalbalance between two neurotransmitters, acetylcholine anddopamine. This results in a relative excess of acetylcholine. Theexcessive excitation caused by cholinergic activity creates themovement disorders that characterize Parkinson’s disease.
Other causesParkinson’s disease can also result from drugs, encephalitis, neu-rotoxins, trauma, arteriosclerosis, or other neurologic disordersand environmental factors.
Goals of drug therapyThe goals of drug therapy are to provide relief of symptoms and tomaintain the patient’s independence and mobility.
Drug therapy for Parkinson’s disease is aimed at correcting theimbalance of neurotransmitters by:• inhibiting cholinergic effects (with anticholinergic drugs)• enhancing the effects of dopamine (with dopaminergic drugs).
Anticholinergic drugsAnticholinergic drugs are sometimes called parasympatholyticdrugs because they inhibit the action of acetylcholine at specialreceptors in the parasympathetic nervous system.
Two classesAnticholinergics used to treat Parkinson’s disease are classified intwo chemical categories according to their chemical structure:• synthetic tertiary amines, such as benztropine, biperiden hy-drochloride, biperiden lactate, procyclidine, and trihexyphenidyl• antihistamines (such as diphenhydramine) that have anticholin-ergic properties, which are effective in treating the symptoms ofParkinson’s disease.
PharmacokineticsTypically, anticholinergic drugs are well absorbed from the GItract and cross the blood-brain barrier to their action site in thebrain. Most are metabolized in the liver, at least partially, and areexcreted by the kidneys as metabolites and unchanged drug. Theexact distribution of these drugs is unknown.
60NEUROLOGIC AND NEUROMUSCULAR DRUGS
A deficiency ofdopamine isn’t good
news... it prevents mefrom performing
normally.
938903.qxd 08/26/2008 14:58 Page 60

Up to 24 hoursBenztropine is a long-acting drug with a duration of up to 24 hoursin some patients. For most anticholinergics, half-life is undeter-mined. In addition to the oral route, some anticholinergics canalso be given I.M. or I.V.
PharmacodynamicsHigh acetylcholine levels produce an excitatory effect on the CNS,which can cause a parkinsonian tremor. Patients with Parkinson’sdisease take anticholinergic drugs to inhibit the action of acetyl-choline at receptor sites in the CNS and autonomic nervous sys-tem, thus reducing the tremor.
PharmacotherapeuticsAnticholinergics are used to treat all forms of Parkinson’s disease.They’re used most commonly in the early stages of Parkinson’sdisease when symptoms are mild and don’t have a major impacton the patient’s lifestyle. These drugs effectively control sialorrhea(excessive flow of saliva) and are about 20% effective in reducingthe incidence and severity of akinesia and rigidity.
Together or aloneAnticholinergics can be used alone or with amantadine in the ear-ly stages of Parkinson’s disease. In addition, anticholinergics canbe given with levodopa during the later stages to further relievesymptoms.
Drug interactionsInteractions can occur when certain medications are taken withanticholinergics:• Amantadine can cause increased anticholinergic adverse ef-fects.• Absorption of levodopa can be decreased, which could lead toworsening of parkinsonian signs and symptoms.• Antipsychotics taken with anticholinergics (such as pheno-thiazines, thiothixene, haloperidol, and loxapine) decrease the ef-fectiveness of both anticholinergics and antipsychotics. The inci-dence of anticholinergic adverse effects can also be increased.• Over-the-counter cough or cold preparations, diet aids, andanaleptics (drugs used to stay awake) increase anticholinergic ef-fects.• Alcohol increases CNS depression. (See Adverse reactions toanticholinergics, page 62.)
61ANTIPARKINSONIAN DRUGS
Anticholinergicdrugs can be used to
treat Parkinson’sdisease.
938903.qxd 08/26/2008 14:58 Page 61

Dopaminergic drugsDopaminergic drugs include several drugs that are chemically un-related:• levodopa, the metabolic precursor to dopamine• carbidopa-levodopa, a combination drug composed of car-bidopa and levodopa• amantadine, an antiviral drug with dopaminergic activity• bromocriptine, an ergot-type dopamine agonist• ropinirole and pramipexole, two non-ergot-type dopamine ago-nists• selegiline and rasagiline, type B MAOIs.
PharmacokineticsLike anticholinergic drugs, dopaminergic drugs are absorbed fromthe GI tract into the bloodstream and are delivered to their actionsite in the brain.
Slowing down with foodAbsorption of levodopa is slowed and reduced when it’s ingestedwith food. The body absorbs most levodopa, carbidopa-levodopa,pramipexole, or amantadine from the GI tract after oral adminis-tration, but only about 28% of bromocriptine. About 73% of an oraldose of selegiline is absorbed. Rasagiline is rapidly absorbed intothe bloodstream.
62NEUROLOGIC AND NEUROMUSCULAR DRUGS
Mild, dose-related adverse reactions are seenin 30% to 50% of patients who take anticholin-ergics. Dry mouth may be a dose-related reac-tion to trihexyphenidyl.
Common reactions
• Confusion• Restlessness• Agitation and excitement• Drowsiness or insomnia• Tachycardia and palpitations• Constipation
• Nausea and vomiting• Urine retention• Increased intraocular pressure, blurred vi-sion, pupil dilation, and photophobia
Sensitivity-related reactions
• Hives• Allergic rash
Reactions in patients older than age 60
• Increased sensitivity to anticholinergics, re-sulting in confusion, agitation, hallucinations,and possibly psychotic symptoms
Warning!
Adverse reactions to anticholinergics
938903.qxd 08/26/2008 14:58 Page 62

DistributionLevodopa is widely distributed in body tissues, including the GItract, liver, pancreas, kidneys, salivary glands, and skin.Carbidopa-levodopa and pramipexole are also widely distributed.Amantadine is distributed in saliva, nasal secretions, and breastmilk. Bromocriptine and rasagiline are highly protein-bound. Thedistribution of selegiline is unknown.
Metabolism and excretionDopaminergic drugs are metabolized extensively in various ar-eas of the body and eliminated by the liver, the kidneys, or both.• Large amounts of levodopa are metabolized in the stomachand during the first pass through the liver. The drug is metabo-lized extensively to various compounds that are excreted by thekidneys.• Carbidopa isn’t metabolized extensively. The kidneys excreteapproximately one-third of it as unchanged drug within 24hours.• Amantadine, ropinirole, and pramipexole are excreted mostlyunchanged by the kidneys.• Almost all of a bromocriptine or rasagiline dose is metabolizedby the liver to pharmacologically inactive compounds, which arethen eliminated primarily in feces, with only a small amount ex-creted in urine.• Selegiline is metabolized to L-amphetamine, L-methampheta-mine, and N-desmethyldeprenyl (the major metabolite), which areeliminated in urine.
PharmacodynamicsDopaminergic drugs act in the brain to improve motor function inone of two ways: by increasing the dopamine concentration or byenhancing neurotransmission of dopamine.
Getting the job doneLevodopa is inactive until it crosses the blood-brain barrier and isconverted to dopamine by enzymes in the brain, increasingdopamine concentrations in the basal ganglia. Carbidopa en-hances levodopa’s effectiveness by blocking the peripheral con-version of levodopa, thus permitting increased amounts of lev-odopa to be transported to the brain.
The other dopaminergic drugs have various mechanisms of ac-tion:• Amantadine’s mechanism of action isn’t clear. It’s thought to re-lease dopamine from intact neurons, but it may also have non-dopaminergic mechanisms.
63ANTIPARKINSONIAN DRUGS
Absorption oflevodopa is slowedand reduced whentaken with food.
938903.qxd 08/26/2008 14:58 Page 63

• Bromocriptine, ropinirole, and pramipexole stimulate dopaminereceptors in the brain, producing effects that are similar todopamine’s.• Rasagiline has an unknown mechanism of action.• Selegiline can increase dopaminergic activity by inhibiting typeB MAO activity or by other mechanisms.
PharmacotherapeuticsThe choice of therapy is highly individualized, depending on thepatient’s symptoms and extent of disability. Patients with mildParkinson’s disease whose main symptom is a tremor are com-monly given anticholinergics or amantadine. Selegiline is indicat-ed for extending the duration of levodopa by blocking its break-down; it has also been used in the early stages of Parkinson’s dis-ease because of its neuroprotective properties and potential toslow the progression of the disease.
Dopaminergic drugs are usually used to treat patients with se-vere Parkinson’s disease or those who don’t respond to anticholin-ergics alone. Levodopa is the most effective drug used to treatParkinson’s disease; however, it loses its effectiveness after 3 to 5years. (See Levodopa: Pros and cons.)
64NEUROLOGIC AND NEUROMUSCULAR DRUGS
Levodopa is commonly used to treat Parkin-son’s disease; however, its use isn’t withoutcontroversy. Initially, levodopa is very effectivein controlling symptoms. But after severalyears, the effects of the drug sometimes don’tlast as long (the wearing-off effect) or lead tosharp fluctuations in symptoms (the on-offphenomenon).
Early vs. late start
Some doctors feel that levodopa should bestarted early (when the diagnosis is made) in
low doses. Others believe it should be startedlater in the course of the disease (when symp-toms compromise function). Advocates of anearly start believe that fluctuations in the pa-tient’s response to levodopa stem from the pro-gression of Parkinson’s disease and not fromthe effects of levodopa.
Some doctors are concerned that levodopaaccelerates the progression of Parkinson’s dis-ease by providing a source of free radicals thatcontribute to the degeneration of dopaminer-gic neurons.
Yea or nay?
Levodopa: Pros and cons
938903.qxd 08/26/2008 14:58 Page 64

Flurry of fluctuationsWhen the patient’s response to levodopa fluctuates, dosage adjust-ments and increased frequency of administration may be tried.Alternatively, adjunctive therapy, such as dopamine agonists, se-legiline, amantadine, or catechol-O-methyltransferase (COMT) in-hibitors, may be added. Controlled-release forms of carbidopa-levodopa may be helpful in managing the wearing-off effect (whenlevodopa’s effects don’t last as long as they used to) or delayed-onset motor fluctuations.
Add carbidopa, reduce levodopaLevodopa is almost always combined with carbidopa as the stan-dard therapy for Parkinson’s disease. When these drugs are giventogether, the dosage of levodopa can be reduced, decreasing therisk of GI and cardiovascular adverse effects.
Tapered treatmentThe dosage of some dopaminergic drugs, such as amantadine, lev-odopa, pramipexole, and bromocriptine, must be gradually ta-pered to avoid precipitating parkinsonian crisis (sudden markedclinical deterioration) and possibly life-threatening complications,including muscle rigidity, elevated body temperature, tachycardia,mental changes, and increased serum creatine kinase (resemblingneuroleptic malignant syndrome).
Drug interactionsThere are a number of drug interactions related to dopaminergicdrugs, including some that are potentially fatal.• Levodopa’s effectiveness may be reduced when used concur-rently with pyridoxine (vitamin B6), phenytoin, benzodiazepines,reserpine, or papaverine.• MAOIs such as tranylcypromine increase the risk of hyperten-sive crisis.• Antipsychotics, such as phenothiazines, thiothixene, haloperi-dol, and loxapine, can reduce the effectiveness of levodopa.• Amantadine may potentiate the anticholinergic adverse effects,such as confusion and hallucinations, of anticholinergic drugs andreduce the absorption of levodopa.• Meperidine taken with selegiline at a higher-than-recommendeddose can cause a fatal reaction. (See Adverse reactions todopaminergic drugs, page 66.)
In some patients, levodopa can produce a significant interac-tion with foods. Dietary amino acids can decrease levodopa’s ef-fectiveness by competing with it for absorption from the intestineand slowing its transport to the brain.
65ANTIPARKINSONIAN DRUGS
938903.qxd 08/26/2008 14:58 Page 65

COMT inhibitorsCOMT inhibitors are used as adjuncts to levodopa-carbidopa ther-apy in managing patients with Parkinson’s disease who experi-ence the wearing-off effect at the end of a dosing interval.
Currently two COMT inhibitors are available:
tolcapone
entacapone.
PharmacokineticsTolcapone and entacapone are rapidly absorbed in the GI tractand have an absolute bioavailability of 65% and 35%, respectively.Both drugs are highly bound to albumin and therefore have limit-ed distribution to the tissues. They’re almost completely metabo-lized in the liver to inactive metabolites and are excreted in urine.
PharmacodynamicsTolcapone and entacapone are selective and reversible inhibitorsof COMT, the major metabolizing enzyme for levodopa, in thepresence of a decarboxylase inhibitor such as carbidopa. Inhibi-tion of COMT alters the pharmacokinetics of levodopa, leading tosustained plasma levels of this drug. This results in more sus-tained dopaminergic stimulation in the brain and improvement insigns and symptoms of Parkinson’s disease.
66NEUROLOGIC AND NEUROMUSCULAR DRUGS
My job is to almostcompletely metabolize
COMT inhibitors.Work, work, work!
Levodopa
• Nausea and vomiting• Orthostatic hypo-tension• Anorexia• Neuroleptic malig-nant syndrome• Arrhythmias• Irritability• Confusion
Amantadine
• Orthostatic hypo-tension• Constipation
Bromocriptine
• Persistent orthostatichypotension• Ventricular tachy-cardia• Bradycardia• Worsening angina
Rasagiline
• Hypertensive crisis(if taken with tyramine-containing foods)• Hallucinations• Flu syndrome• Arthralgia• Depression
Pramipexole,
ropinirole
• Orthostatic hypo-tension• Dizziness• Confusion• Insomnia
Warning!
Adverse reactions to dopaminergic drugs
938903.qxd 08/26/2008 14:58 Page 66

PharmacotherapeuticsEither tolcapone or entacapone may be added to the carbidopa-levodopa regimen of a patient who experiences wearing-off symp-toms at the end of a dosing interval or random “on-off” fluctua-tions in response to carbidopa-levodopa. COMT inhibitors have noantiparkinsonian effect when used alone and should always becombined with carbidopa-levodopa. The addition of a COMT in-hibitor often requires a decrease in the carbidopa-levodopadosage, particularly for patients receiving a levodopa dose ofmore than 800 mg.
Slow and steadyRapid withdrawal of a COMT inhibitor may lead to parkinsoniancrisis and may cause a syndrome of muscle rigidity, high fever,tachycardia, elevated serum creatine kinase, and confusion simi-lar to neuroleptic malignant syndrome. Although tapering sched-ules haven’t been evaluated, a slow tapering of the dosage is sug-gested.
Drug interactions• COMT inhibitors shouldn’t be used concurrently with Type AMAOIs but may be used with selegiline.• Because of MAO inhibition, COMT inhibitors shouldn’t be usedwith linezolid.• Significant cardiac effects or arrhythmias may result whenCOMT inhibitors are combined with catecholamine drugs(dopamine, dobutamine, epinephrine, methyldopa, or norepineph-rine).• Use of COMT inhibitors with CNS depressants (benzodi-azepines, tricyclic antidepressants, antipsychotics, ethanol, opioidanalgesics, and other sedative hypnotics) may cause additive CNSeffects.• Concurrent use of entacapone and bromocriptine may cause fi-brotic complications.
Calling an interference• Drugs that interfere with glucuronidation (erythromycin, ri-fampin, cholestyramine, and probenecid) may decrease enta-capone elimination.• Use of COMT inhibitors may increase the risk of orthostatic hy-potension in patients receiving dopaminergic therapy.• Tolcapone shouldn’t be initiated in patients with evidence of liv-er disease or alanine aminotransferase or aspartate aminotrans-ferase values greater than the upper limit of normal. In addition,the patient must be advised of the risks of liver injury and must
67ANTIPARKINSONIAN DRUGS
938903.qxd 08/26/2008 14:58 Page 67

give written informed consent before receiving tolcapone. (SeeAdverse reactions to COMT inhibitors.)
Anticonvulsant drugsAnticonvulsant drugs inhibit neuromuscular transmission and areprescribed for:• long-term management of chronic epilepsy (recurrent seizures)• short-term management of acute isolated seizures not caused byepilepsy, such as those occurring after trauma or brain surgery.
In addition, some anticonvulsants are used in the emergencytreatment of status epilepticus (a continuous seizure state).
Treatment of epilepsy should begin with a single drug whosedosage is increased until seizures are controlled or adverse reac-tions become problematic. Generally, a second alternative shouldbe tried as monotherapy before combination therapy is consid-ered. The choice of drug treatment depends on seizure type, drugcharacteristics, and patient preferences.
Major classesAnticonvulsants fall into several major classes:• hydantoins
68NEUROLOGIC AND NEUROMUSCULAR DRUGS
Catechol-O-methyltransferase (COMT)inhibitors may produce acute liver fail-ure, a life-threatening adverse reaction.Consequently, tolcapone should be usedonly in patients with Parkinson’s diseasewho are experiencing fluctuations in lev-odopa response and aren’t respondingto—or aren’t appropriate candidatesfor—other adjunctive therapies. Patientsshould be advised of the risks of liver in-jury and provide written informed con-sent before starting tolcapone.
Liver function tests should be ob-tained at the start of therapy to provide a
baseline and every 2 weeks for the firstyear of therapy, then every 4 weeks forthe next 3 months, and every 8 weeksthereafter.
COMT inhibitors can also producethese adverse reactions.
Common reactions
• Nausea• Dyskinesia• Diarrhea• Brown-orange urine discoloration (en-tacapone)• Hyperkinesia or hypokinesia
Less common reactions
• Orthostatic hypotension• Syncope• Dizziness• Fatigue• Abdominal pain• Constipation• Vomiting• Dry mouth• Back pain• Diaphoresis
Warning!
Adverse reactions to COMT inhibitors
938903.qxd 08/26/2008 14:58 Page 68

• barbiturates• iminostilbenes• benzodiazepines• carboxylic acid derivatives• 1-(aminomethyl) cyclohexane–acetic acid• phenyltriazines• carboxamides• sulfamate-substituted monosaccharides• succinimides• sulfonamides• pyrrolidines.
HydantoinsThe two most commonly prescribed anticonvulsants—phenytoinand phenytoin sodium—belong to the hydantoin class. Other hy-dantoins include fosphenytoin and ethotoin.
PharmacokineticsThe pharmacokinetics of hydantoins vary from drug to drug.
Phenytoin fits in slowlyPhenytoin is absorbed slowly after both oral and I.M. administra-tion. It’s distributed rapidly to all tissues and is highly (90%)protein-bound. Phenytoin is metabolized in the liver. Inactivemetabolites are excreted in bile and then reabsorbed from the GItract. Eventually, however, they’re excreted in urine.
Fosphenytoin for the short termFosphenytoin is indicated for short-term I.M. or I.V. administra-tion. It’s widely distributed throughout the body and is highly(90%) protein-bound. Fosphenytoin is metabolized by the liver andexcreted in urine.
Talkin’ ethotoinEthotoin is readily absorbed from the GI tract and is metabolizedby the liver. Extensively protein-bound, ethotoin is excreted inurine, primarily as metabolites.
PharmacodynamicsIn most cases, the hydantoin anticonvulsants stabilize nerve cellsto keep them from getting overexcited. Phenytoin appears towork in the motor cortex of the brain, where it stops the spread ofseizure activity. The pharmacodynamics of fosphenytoin and etho-toin are thought to mimic those of phenytoin. Phenytoin may also
69ANTICONVULSANT DRUGS
The mostcommonly prescribedanticonvulsant drugs
are phenytoin andphenytoin sodium.
938903.qxd 08/26/2008 14:58 Page 69

be used as an antiarrhythmic drug to control irregular heartrhythms, with properties similar to those of quinidine or pro-cainamide, although this use is decreasing.
PharmacotherapeuticsBecause of its effectiveness and relatively low toxicity, phenytoinis the most commonly prescribed anticonvulsant. It’s one of thedrugs of choice to treat:• complex partial seizures (also called psychomotor or temporallobe seizures)• tonic-clonic seizures.
Hydantoins (phenytoin and fosphenytoin) are the long-actinganticonvulsant of choice to treat status epilepticus after initial I.V.benzodiazepines.
Resistance is futileHealth care providers sometimes prescribe phenytoin and etho-toin in combination with other anticonvulsants for partial andtonic-clonic seizures in patients who are resistant to or intolerantof other anticonvulsants.
Drug interactionsHydantoins interact with a number of other drugs. Here are somedrug interactions of major to moderate clinical significance:• Phenytoin’s effect is decreased when it’s taken with phenobarbi-tal, diazoxide, theophylline, carbamazepine, rifampin, antacids, orsucralfate.• Phenytoin’s effect and potential for toxicity increase when it’staken with cimetidine, disulfiram, fluconazole, isoniazid, omepra-zole, sulfonamides, oral anticoagulants, chloramphenicol, valproicacid, or amiodarone.• Enteral tube feedings may interfere with the absorption of oralphenytoin. Stop feedings for 2 hours before and after phenytoinadministration.• The effect of these drugs is decreased when they’re taken with ahydantoin anticonvulsant: oral anticoagulants, antiretrovirals, lev-odopa, amiodarone, corticosteroids, doxycycline, methadone,metyrapone, quinidine, theophylline, thyroid hormone, hormonalcontraceptives, valproic acid, cyclosporine, and carbamazepine.(See Adverse reactions to hydantoins.)
BarbituratesThe long-acting barbiturate phenobarbital was formerly one of themost widely used anticonvulsants. It’s now used less frequently
70NEUROLOGIC AND NEUROMUSCULAR DRUGS
Adversereactions tohydantoins
Adverse reactions tohydantoins include:• drowsiness• ataxia• irritability• headache• restlessness• nystagmus• dizziness and vertigo• dysarthria• nausea and vomiting• abdominal pain• anorexia• depressed atrial andventricular conduction• ventricular fibrillation(in toxic states)• bradycardia, hypoten-sion, and cardiac arrest(with I.V. administration)• hypersensitivity reac-tions.
Warning!
938903.qxd 08/26/2008 14:59 Page 70

because of its sedative effects. Phenobarbital is sometimes usedfor long-term treatment of epilepsy and is prescribed selectively totreat status epilepticus if hydantoins are ineffective.
Other barbituratesMephobarbital, also a long-acting barbiturate, is sometimes usedas an anticonvulsant. Primidone, which is closely related chemi-cally to the barbiturates, is also used to treat chronic epilepsy.
PharmacokineticsEach barbiturate has a slightly different set of pharmacokineticproperties.
Phenobarbital for the long haulPhenobarbital is absorbed slowly but well from the GI tract. Peakplasma levels occur 8 to 12 hours after a single dose. The drug is20% to 45% bound to serum proteins and to a similar extent to oth-er tissues, including the brain. About 75% of a phenobarbital doseis metabolized by the liver, and 25% is excreted unchanged inurine.
Mephobarbital moves quicklyAlmost one-half of a mephobarbital dose is absorbed from the GItract and well distributed in body tissues. The drug is bound to tis-sue and plasma proteins. Mephobarbital undergoes extensive me-tabolism by the liver; only 1% to 2% is excreted unchanged inurine.
Primidone and proteinApproximately 60% to 80% of a primidone dose is absorbed fromthe GI tract and distributed evenly among body tissues. The drugis protein-bound to a small extent in the plasma. Primidone is me-tabolized by the liver to two active metabolites, phenobarbital andphenylethylmalonamide (PEMA). From 15% to 25% of primidone isexcreted unchanged in urine, 15% to 25% is metabolized to pheno-barbital, and 50% to 70% is excreted in urine as PEMA. Primidoneis also secreted in breast milk.
PharmacodynamicsBarbiturates exhibit anticonvulsant action at doses below thosethat produce hypnotic effects. For this reason, they usually don’tproduce addiction when used to treat epilepsy. Barbiturates ele-vate the seizure threshold by decreasing postsynaptic excitation.
PharmacotherapeuticsBarbiturates are an effective alternative therapy for:
71ANTICONVULSANT DRUGS
938903.qxd 08/26/2008 14:59 Page 71

• partial seizures• tonic-clonic seizures• febrile seizures.
Barbiturates can be used alone or with other anticonvulsants.I.V. phenobarbital is also used to treat status epilepticus. The ma-jor disadvantage of using phenobarbital for status epilepticus isthat it has a delayed onset of action when an immediate responseis needed. Barbiturates are ineffective in treating absenceseizures.
Consider thisMephobarbital has no advantage over phenobarbital and is usedwhen the patient can’t tolerate the adverse effects of phenobarbi-tal. Because of monitoring, costs, and dosing frequency, phenobar-bital is usually tried before primidone. Primidone may be effectivein patients who fail to respond to phenobarbital.
Drug interactionsThe effects of barbiturates can be reduced when they’re takenwith rifampin. Here are some other drug interactions:• The risk of toxicity increases when phenobarbital is taken withCNS depressants, valproic acid, chloramphenicol, felbamate,cimetidine, or phenytoin.• The metabolism of corticosteroids, digoxin, and estrogens maybe enhanced when these drugs are taken with phenobarbital, lead-ing to decreased effects.• Adverse effects of tricyclic antidepres-sants increase when they’re taken withbarbiturates.• Evening primrose oil may increase an-ticonvulsant dosage requirements. (SeeAdverse reactions to barbiturates.)
Reduced effectsBarbiturate use can decrease the effectsof many drugs, including beta-adrenergic blockers, corticos-teroids, digoxin, estrogens, doxy-cycline, oral anticoagulants, hor-monal contraceptives, quinidine,phenothiazine, metronidazole, tri-cyclic antidepressants, theo-phylline, cyclosporine, carba-mazepine, felodipine, and vera-pamil.
72NEUROLOGIC AND NEUROMUSCULAR DRUGS
Because ofmonitoring, costs,
and dosing frequency,phenobarbital is
usually tried beforeprimidone.
Adversereactions tobarbiturates
Adverse reactions tophenobarbital and me-phobarbital include:• drowsiness, lethargy,and dizziness• nystagmus, confusion,and ataxia (with largedoses)• laryngospasm, respira-tory depression, and hy-potension (when admin-istered I.V.).
The same, plus
psychoses
Primidone can causethe same central ner-vous system and GI ad-verse reactions as phe-nobarbital. It can alsocause acute psychosis,hair loss, impotence,and osteomalacia.
As a group
All three barbituratescan produce a hyper-sensitivity rash, otherrashes, lupus erythe-matosus–like syndrome(an inflammatory disor-der), and enlarged lymphnodes.
Warning!
938903.qxd 08/26/2008 14:59 Page 72

IminostilbenesCarbamazepine is the most commonly used iminostilbene anti-convulsant. It effectively treats:• partial and generalized tonic-clonic seizures• mixed seizure types• complex partial seizures (drug of choice).
PharmacokineticsCarbamazepine is absorbed slowly from the GI tract and is metab-olized in the liver by the cytochrome P-450 isoform 3A4 (CYP450)and is excreted in urine. Carbamazepine is distributed rapidly toall tissues; 75% to 90% is bound to plasma proteins. A smallamount crosses the placenta, and some is secreted in breast milk.The half-life varies greatly.
PharmacodynamicsCarbamazepine’s anticonvulsant effect is similar to that of pheny-toin. The drug’s anticonvulsant action can occur because of itsability to inhibit the spread of seizure activity or neuromusculartransmission in general.
PharmacotherapeuticsCarbamazepine is the drug of choice, in adults and children, fortreating:• generalized tonic-clonic seizures• simple and complex partial seizures.
Carbamazepine may worsen absence or myoclonic seizures.However, it relieves pain when used to treat trigeminal neuralgia(tic douloureux, characterized by excruciating facial pain alongthe trigeminal nerve) and may be useful in treating selective psy-chiatric disorders.
Drug interactionsCarbamazepine can reduce the effects of several drugs, includinghaloperidol, bupropion, lamotrigine, tricyclic antidepressants, oralanticoagulants, hormonal contraceptives, doxycycline, felbamate,theophylline, protease inhibitors, antipsychotics, and valproicacid. Other drug interactions can also occur:• Increased carbamazepine levels and toxicity can occur with theuse of cimetidine, danazol, diltiazem, erythromycin, isoniazid, se-lective serotonin reuptake inhibitors, propoxyphene, ketocona-zole, valproic acid, and verapamil.
73ANTICONVULSANT DRUGS
Be aware that(sniff!), even when
used as ananticonvulsant,
carbamazepine canaffect mood and
behavior.
938903.qxd 08/26/2008 14:59 Page 73

• Lithium and carbamazepine taken together increase the risk oftoxic neurologic effects.
Confusion alert!Don’t confuse Tegretol (a brand name for carbamazepine) withToradol (a brand name for ketorolac).• Carbamazepine levels may be decreased when taken with barbi-turates, felbamate, or phenytoin. (See Adverse reactions to carba-mazepine.)• The herbal remedy plantain may inhibit GI absorption of carba-mazepine.
BenzodiazepinesThe four benzodiazepine drugs that provide anticonvulsant ef-fects are:• clonazepam• clorazepate• diazepam (parenteral form)• lorazepam. (See Sound-alikes: Diazepam and lorazepam.)
Only one for ongoing treatmentOnly clonazepam is recommended for long-term treatment ofepilepsy. Diazepam may be used to treat status epilepticus or, inrectal form, repetitive seizures. Lorazepam I.V. is considered thedrug of choice for status epilepticus. Clorazepate is prescribed asan adjunct in treating partial seizures.
74NEUROLOGIC AND NEUROMUSCULAR DRUGS
Adversereactions tocarbamazepine
Occasionally, carba-mazepine can result inserious hematologic tox-icity. Because carba-mazepine is relatedstructurally to the tri-cyclic antidepressants,it can cause similar toxi-cities and affect behav-iors and emotions.
Hives and Stevens-Johnson syndrome (apotentially fatal inflam-matory disease) canalso occur. Rash is themost common hypersen-sitivity response.
Warning!
Be careful not to confuse the sound-alike drugs diazepam and lor-azepam. Both drugs are benzodiazepines that can be used to treat sta-tus epilepticus. Lorazepam I.V. is considered the drug of choice. Di-azepam provides only short-term effects and isn’t recommended forlong-term treatment because high serum concentrations are needed tocontrol seizures and long-term use can lead to addiction.
Safe and sound
Sound-alikes: Diazepam andlorazepam
938903.qxd 08/26/2008 14:59 Page 74

PharmacokineticsThe patient can receive benzodiazepines orally, parenterally or, inspecial situations, rectally (diazepam rectal gel).
Absorption and distributionBenzodiazepines are absorbed rapidly and almost completelyfrom the GI tract but are distributed at different rates. Proteinbinding of benzodiazepines ranges from 85% to 90%.
Metabolism and excretionBenzodiazepines are metabolized in the liver to multiple metabo-lites and are then excreted in urine. They readily cross the placen-ta and are secreted in breast milk.
PharmacodynamicsBenzodiazepines act as:• anticonvulsants• antianxiety agents• sedative-hypnotics• muscle relaxants.
Their mechanism of action is poorly understood.
PharmacotherapeuticsEach of the benzodiazepines can be used in slightly differentways.
Absence, atypical, and moreClonazepam is used to treat the following types of seizures:• absence (petit mal)• atypical absence (Lennox-Gastaut syndrome)• atonic• myoclonic.
I.V. or with othersDiazepam isn’t recommended for long-term treatment because ofits potential for addiction and the high serum concentra-tions required to control seizures.
I.V. lorazepam is currently considered the benzodi-azepine of choice for treating status epilepticus.
I.V. diazepam is used to control status epilepticus. Be-cause diazepam provides only short-term effects of lessthan 1 hour, the patient must also be given a long-actinganticonvulsant, such as phenytoin or phenobarbital, dur-ing diazepam therapy. Diazepam rectal gel is approved
75ANTICONVULSANT DRUGS
Diazepam can helpreduce the incidenceof recurrent seizuresin children. They can
get back to doingwhat they like to do!
938903.qxd 08/26/2008 14:59 Page 75

for treatment of repetitive seizures and has reduced the incidenceof recurrent seizures in children.
Clorazepate is used with other drugs to treat partial seizures.
Drug interactionsWhen benzodiazepines are taken with CNS depressants, sedatives,cimetidine, or hormonal contraceptives, depressant effects are en-hanced. This can cause motor skill impairment, respiratory de-pression, excessive sedation, CNS depression, and even death athigh doses. (See Adverse reactions to benzodiazepines.)
Carboxylic acid derivativesValproic acid, the most widely used carboxylic acid derivative, isunrelated structurally to the other anticonvulsants. Valproic acidis also available as:• valproate• divalproex.
PharmacokineticsValproate is converted rapidly to valproic acid in the stomach. Di-valproex is a precursor of valproic acid and separates into val-proic acid in the GI tract. Valproic acid is a hepatic enzyme in-hibitor; it’s absorbed well, is strongly protein-bound, and is metab-
76NEUROLOGIC AND NEUROMUSCULAR DRUGS
Most common
• Drowsiness• Confusion• Ataxia• Weakness• Dizziness• Nystagmus• Vertigo• Fainting• Dysarthria
• Headache• Tremor• Glassy-eyed appearance
Less common
• Depression of the heart andbreathing (with high doses andwith I.V. diazepam)• Rash and other acute hypersen-sitivity reactions
Warning!
Adverse reactions tobenzodiazepines
938903.qxd 08/26/2008 14:59 Page 76

olized in the liver. Metabolites and unchanged drug are excreted inurine.
Valproic acid readily crosses the placental barrier and also ap-pears in breast milk.
PharmacodynamicsThe mechanism of action for valproic acid remains unknown. Thedrug is thought to increase levels of GABA, an inhibitory neuro-transmitter, and to have a direct membrane-stabilizing effect.
PharmacotherapeuticsValproic acid is prescribed for long-term treatment of:• absence seizures• myoclonic seizures• tonic-clonic seizures• partial seizures.
Valproic acid may also be useful for neonatal seizures.
Drug interactionsValproic acid must be used cautiously in children under 2 yearsold, particularly those receiving multiple anticonvulsants andthose with congenital metabolic disorders, severe seizures withmental retardation, or organic brain disease. In these patients, val-proic acid carries a risk of potentially fatal liver toxicity (primarilyin the first 6 months of treatment).
This risk limits its use as a drug of choice for seizure disorders.However, while it’s a risk for all patients, the risk decreases withage. Caution should also be taken with patients with hepatic dis-ease.
Valproic warningsThese are the most significant drug interactions associated withvalproic acid:• Cimetidine, aspirin, erythromycin, and felbamate may increaselevels of valproic acid.• Carbamazepine, lamotrigine, phenobarbital, primidone, pheny-toin, and rifampin may decrease levels of valproic acid.• Valproic acid may decrease the effects of felbamate, phenobar-bital, primidone, benzodiazepines, CNS depressants, warfarin, andzidovudine. (See Adverse reactions to valproic acid, page 78.)
77ANTICONVULSANT DRUGS
Take cautionwhen giving
valproic acid topatients with
hepatic disease.
938903.qxd 08/26/2008 14:59 Page 77

1- (aminomethyl) cyclohexane–acetic acidThe 1- (aminomethyl) cyclohexane–acetic acid class includes thedrug gabapentin, which was designed to be a GABA agonist, al-though its exact mechanism of action is unknown.
Gabapentin is approved as adjunctive therapy for partialseizures in adults and in children ages 3 and older with epilepsy. Ithas also been used to treat pain, tremor associated with MS, bipo-lar disorder, and Parkinson’s disease as well as to prevent mi-graines.
PharmacokineticsGabapentin is readily absorbed in the GI tract. Because of thisactive-transport mechanism, the drug’s bioavailability may de-crease as the dosage increases. Gabapentin isn’t metabolized; it’sexcreted exclusively by the kidneys.
PharmacodynamicsGabapentin’s exact mechanism of action is unknown. The drugdoesn’t appear to act at the GABA receptor, affect GABA uptake,or interfere with GABA transaminase. Instead, gabapentin appearsto bind to a carrier protein and act at a unique receptor in thebrain, resulting in elevated GABA levels in the brain.
78NEUROLOGIC AND NEUROMUSCULAR DRUGS
Because rare, but deadly, livertoxicity has occurred with val-proic acid, it should be used withcaution in patients who have ahistory of hepatic disease. Chil-dren younger than age 2 have ahigh risk of developing hepatotox-icity.
Most other adverse reactionsare tolerable and dose-related.
These include:• nausea and vomiting• diarrhea• constipation• sedation• dizziness• ataxia• headache• muscle weakness• increased blood ammonia level.
Warning!
Adverse reactions to valproic acid
938903.qxd 08/26/2008 14:59 Page 78

PharmacotherapeuticsGabapentin is used as adjunctive therapy for partial and secondar-ily generalized seizures in adults and children ages 3 and older. Italso seems to be effective as monotherapy although it isn’t FDA-approved for that purpose.
Drug interactionsLike carbamazepine, gabapentin may worsen myoclonic seizures.
Gabapentin doesn’t induce or inhibit hepatic enzymes, so itcauses very few drug interactions and doesn’t affect the metabo-lism of other anticonvulsants. Antacids and cimetidine may affectgabapentin concentration.
Patients with renal impairment (creatinine clearance less than60 ml/minute) require a dosage reduction. (See Adverse reactionsto gabapentin.)
PhenyltriazinesThe phenyltriazine lamotrigine is chemically unrelated to otheranticonvulsants. This drug is FDA-approved as adjunctive therapyfor adults who have partial seizures and for children older thanage 2 who have generalized seizures or Lennox-Gastaut syndrome.It may also be used as monotherapy for partial seizures in adultsafter a hepatic enzyme–inducing anticonvulsant has been discon-tinued.
PharmacokineticsLamotrigine is rapidly and well absorbed.It’s metabolized by the liver and excretedby the kidneys. Clearance is increased inthe presence of other enzyme-inducing an-ticonvulsants. Lamotrigine isn’t significant-ly bound to plasma proteins.
PharmacodynamicsLamotrigine’s precise mechanism of action is unknown, but thedrug is thought to block voltage-sensitive sodium channels, thusinhibiting the release of the excitatory neurotransmitters gluta-mate and aspartate.
79ANTICONVULSANT DRUGS
Adversereactions togabapentin
Common adverse reac-tions to gabapentin in-clude:• fatigue• somnolence• dizziness• ataxia• leukopenia.
Less common ad-verse reactions include:• edema• weight gain• hostility• emotional lability• nausea and vomiting• bronchitis• viral infection• fever• nystagmus• rhinitis• diplopia• tremor.
Warning!
Lamotrigine israpidly and wellabsorbed in the
body. Wish I couldsay this spongewas as good at
absorption!
938903.qxd 08/26/2008 14:59 Page 79

PharmacotherapeuticsLamotrigine prevents partial seizure activity. In addition, lamotri-gine appears to be effective for many types of generalizedseizures. However it can worsen myoclonic seizures.
The drug may also lead to improvement in the patient’s mood.
Drug interactions• Lamotrigine’s effects may be decreased if the drug is given withcarbamazepine, phenytoin, phenobarbital, primidone, or aceta-minophen.• Lamotrigine may produce additive effects when combined withfolate inhibitors.• Valproic acid may decrease lamotrigine clearance and increasethe steady-state level and effects of lamotrigine. (See Adverse re-actions to lamotrigine.)
CarboxamidesOxcarbazepine, a carboxamide, is chemically similar to carba-mazepine but causes less induction of hepatic enzymes. Oxcar-bazepine is a prodrug. It’s useful as adjunctive therapy ormonotherapy for adults with partial seizures and as adjunctivetherapy for children with partial seizures.
PharmacokineticsOxcarbazepine is completely absorbed and extensively metabo-lized by hepatic enzymes to the 10-monohydroxy metabolite(MHD) that’s responsible for its pharmacologic activity. MHD isexcreted primarily by the kidneys.
9 hours in halfThe half-life of MHD is about 9 hours. Unlike carbamazepine, ox-carbazepine doesn’t induce its own metabolism.
PharmacodynamicsThe precise mechanism of action of oxcarbazepine and itsmetabolite MHD is unknown, but antiseizure activity is thought tooccur through blockade of sodium-sensitive channels, which pre-vents seizure spread in the brain.
80NEUROLOGIC AND NEUROMUSCULAR DRUGS
Adversereactions tolamotrigine
Adverse reactions tolamotrigine commonlyinclude:• dizziness• ataxia• somnolence• headache• diplopia• nausea• vomiting• rash.
Several types ofrash, including Stevens-Johnson syndrome, mayoccur with use of thisdrug. A generalized, ery-thematous, morbilliformrash may appear in thefirst 3 to 4 weeks of ther-apy; it’s usually mild tomoderate, but it may besevere.
Lamotrigine now car-ries a “black box” warn-ing regarding the rash,and the manufacturerrecommends discontin-uing the drug at the firstsign of rash. The risk ofrash may be increasedby starting at high dos-es, by rapidly increasingdoses, or by using val-proate concurrently.
Warning!
938903.qxd 08/26/2008 14:59 Page 80

PharmacotherapeuticsOxcarbazepine is FDA-approved as adjunctive therapy for partialseizures in adults and children older than age 4 and as monothera-py for adults.
As with carbamazepine, it’s also effective for generalizedseizures but may worsen myoclonic and absence seizures.
Drug interactions• Carbamazepine, phenytoin, phenobarbital, valproic acid, and ve-rapamil may decrease the levels of oxcarbazepine’s ac-tive metabolite MHD.
Pill worries• Oxcarbazepine may decrease the effectiveness ofhormonal contraceptives and felodipine.• Dosage reductions are necessary for patients withrenal impairment (creatinine clearance less than30 ml/minute) and those at risk for renal impairment,such as elderly patients. (See Adverse reactions to oxcar-bazepine.)
81ANTICONVULSANT DRUGS
Elderly patientsare at risk for renal
impairment, so makesure you reducethe dosage of
carboxamides in thispatient population.
About 20% to 30% of patientswho have had an allergic reactionto carbamazepine will experiencea hypersensitivity reaction tooxcarbazepine.
Common reactions
• Somnolence• Dizziness• Diplopia• Ataxia• Nausea and vomiting• Abnormal gait
• Tremor• Aggravated seizures• Rectal bleeding
Less common reactions
• Agitation• Confusion• Hypotension• Hyponatremia• Rhinitis• Speech disorder• Back pain• Upper respiratory tract infection
Warning!
Adverse reactions to oxcarbazepine
938903.qxd 08/26/2008 14:59 Page 81

Sulfamate-substituted monosaccharidesTopiramate, a sulfamate-substituted monosaccharide, is one of thenewer anticonvulsants available.
PharmacokineticsTopiramate is absorbed rapidly and is partially metabolized in theliver and excreted mostly unchanged in urine.
PharmacodynamicsTopiramate is believed to act by blocking voltage-dependent sodi-um channels, enhancing activity of the GABA receptors, and an-tagonizing glutamate receptors.
PharmacotherapeuticsTopiramate is approved as adjunctive therapy for partial and pri-mary generalized tonic-clonic seizures in adults and children olderthan age 2 and for children with Lennox-Gastaut syndrome. It mayalso prove beneficial for other types of seizures and as monother-apy.
Drug interactions• Carbamazepine, phenytoin, and valproic acid may cause de-creased topiramate levels.• Topiramate may decrease the effectiveness of hormonal contra-ceptives and decrease valproic acid levels.• CNS depressants may cause additive CNS effect when com-bined with topiramate.
50% off• For renally impaired patients (creatinine clearance less than70 ml/minute), the topiramate dosage should be reduced by 50%.(See Adverse reactions to topiramate.)
SuccinimidesThe succinimides, ethosuximide and methsuximide, are used tomanage absence seizures. Ethosuximide is considered the drug ofchoice for absence seizures.
PharmacokineticsThe succinimides are readily absorbed from the GI tract and me-tabolized in the liver and excreted in urine. Metabolites are be-
82NEUROLOGIC AND NEUROMUSCULAR DRUGS
Adversereactions totopiramate
Psychomotor slowing,word-finding difficulty,impaired concentration,and memory impairmentare common reactionsthat may require stop-ping topiramate. Lowstarting doses and slowdosage titration mayminimize these effects.
Other common ad-verse reactions include:• drowsiness• dizziness• headache• ataxia• nervousness• confusion• paresthesia• weight gain• diplopia.
Serious but infre-quent adverse reactionsinclude:• secondary angle-closure glaucoma• liver failure• decreased sweating• hyperthermia• heat stroke• renal calculi.
Warning!
938903.qxd 08/26/2008 14:59 Page 82

lieved to be inactive. The elimination half-life of ethosuximide isabout 60 hours in adults and 30 hours in children.
PharmacodynamicsEthosuximide’s exact mechanism of action is unknown. It’sthought to inhibit an enzyme necessary for the formation ofgamma-hydroxybutyrate, which has been associated with the in-duction of absence seizures.
PharmacotherapeuticsIn addition to being the drug of choice for treating absenceseizures, ethosuximide may also be used in combination with val-proic acid for hard-to-control absence seizures.
Drug interactionsEthosuximide isn’t protein-bound, so displacement reactions can’toccur. Carbamazepine may induce the metabolism of ethosux-imide. Valproic acid may inhibit the metabolism of ethosuximideonly if the metabolism is near saturation. (See Adverse reactionsto succinimides.)
SulfonamidesZonisamide, a sulfonamide, is approved as adjunctive treatmentfor partial seizures in adults.
PharmacokineticsZonisamide is absorbed relatively rapidly, with peak concentra-tions occurring in 2 to 6 hours. Zonisamide is widely distributedand is extensively bound to erythrocytes.
The drug is metabolized by the CYP3A4 enzyme in the liverand is excreted in urine, primarily as the parent drug and the glu-curonide metabolite.
PharmacodynamicsZonisamide’s precise mechanism of action is unknown, but it’s be-lieved to involve stabilization of neuronal membranes and sup-pression of neuronal hypersensitivity.
PharmacotherapeuticsZonisamide is approved only as adjunctive therapy for partialseizures in adults, but it appears to have a broad spectrum of ac-
83ANTICONVULSANT DRUGS
Adversereactions tosuccinimides
Ethosuximide is general-ly well tolerated. Themost common adverseeffects (occurring in upto 40% of patients) arenausea and vomiting.Other common adverseeffects include:• drowsiness and fa-tigue• lethargy• dizziness• hiccups• headaches• mood changes.
Rarely, blood dyscra-sias, rashes (includingStevens-Johnson syn-drome and erythemamultiforme), lupus-likesyndrome, and psychot-ic behaviors can occur.
Warning!
938903.qxd 08/26/2008 14:59 Page 83

tivity for other types of seizures (infantile spasms; myoclonic, gen-eralized, and atypical absence seizures).
Drug interactions• Drugs that induce liver enzymes, such as phenytoin, carba-mazepine, and phenobarbital, increase the metabolism and de-crease the half-life of zonisamide.
Serious serum• Concurrent use of zonisamide with drugs that inhibit or induceCYP3A4 may increase or decrease the serum concentration ofzonisamide. Zonisamide isn’t an inducer of CYP3A4, so it’s unlike-ly to affect other drugs metabolized by this system. (See Adversereactions to sulfonamides.)
PyrrolidinesLevetiracetam, a pyrrolidine derivative, is a newer antiseizuredrug that’s chemically unrelated to previously available antiepilep-tic drugs. It’s used as adjunctive therapy to treat certain types ofpartial and myoclonic seizures.
84NEUROLOGIC AND NEUROMUSCULAR DRUGS
Common adverse effects of zonisamide in-clude:• somnolence• dizziness• confusion• anorexia• nausea• diarrhea• weight loss• rash.
Slow titration of the dosage and adminis-tration with meals may decrease the incidenceof these adverse effects.
More serious adverse effects associatedwith zonisamide use include:• Stevens-Johnson syndrome• toxic epidermal necrolysis• psychosis• aplastic anemia• agranulocytosis.
Oligohydrosis, hyperthermia, and heatstroke have been reported in children. Zo-nisamide is contraindicated in patients with anallergy to sulfonamides. Low doses should beinitiated in elderly patients because of the pos-sibility of renal impairment in this population.
Warning!
Adverse reactions to sulfonamides
938903.qxd 08/26/2008 14:59 Page 84

PharmacokineticsLevetiracetam is administered orally or I.V. Oral administration re-sults in rapid and full absorption with a 100% bioavailability. Peakconcentrations occur in about 1 hour. Levetiracetam isn’t exten-sively metabolized; any metabolites that are produced aren’t ac-tive. The major metabolic pathway is enzymatic hydrolysis, andmetabolism doesn’t depend on any hepatic cytochrome P450isoenzymes. Levetiracetam is eliminated by renal excretion. Thehalf-life is about 8 hours and is unaffected by dose, route of ad-ministration, or repeated administration.
PharmacodynamicsThe precise mechanism of action isn’t known. The drug’santiepileptic effect doesn’t appear to involve known mechanismsrelating to inhibitory and excitatory neurotransmission.
PharmacotherapeuticsLevetiracetam has several indications for us, including:• adjunctive therapy for epilepsy in adults and children older thanage 4• adjunctive treatment for myoclonic seizures in adults and chil-dren older than age 12• adjunctive treatment for primary generalized tonic-clonicseizures in adults and children older than age 6.
Drug interactionsLevetiracetam has no known major drug interactions. (See Ad-verse reactions to levetiracetam.)
Antimigraine drugsMigraine is one of the most common primaryheadache disorders, affecting an estimated 24 millionpeople in the United States. An episodic disorder, mi-graine produces a unilateral pain that’s commonly de-scribed as pounding, pulsating, or throbbing. It maybe preceded by an aura. Other common symptomsare sensitivity to light or sound, nausea, vomiting,constipation, and diarrhea.
Researchers believe that migraine symptoms arecaused by cranial vasodilation or the release of va-soactive and proinflammatory substances fromnerves in an activated trigeminal system.
85ANTIMIGRAINE DRUGS
Adversereactions tolevetiracetam
Common adverse reac-tions to levetiracetam in-clude:• drowsiness• dizziness• fatigue• asthenia• headache• vomiting.
Less common ad-verse reactions include:• depression• pharyngitis• conjunctivitis• mood swings.
Warning!
Sensitivity tolight may be asymptom of a
migraine.
938903.qxd 08/26/2008 14:59 Page 85

Attacking achesTreatment of migraine aims to alter an attack once it’s under way(abortive or symptomatic treatment) or to prevent an attack.Choice of therapy depends on the severity, duration, and frequen-cy of the headaches; on the degree of disability that the headachecreates in the patient; and on patient characteristics.
Abortive treatments may include analgesics (aspirin and aceta-minophen), nonsteroidal anti-inflammatory drugs (NSAIDs), ergo-tamine, 5-hydroxytryptaminergic (5-HT1)-receptor agonists, andvarious miscellaneous drugs (such as isometheptene combina-tions, intranasal butorphanol, metoclopramide, and cortico-steroids). Prophylactic therapy includes beta-adrenergic blockers,tricyclic antidepressants, valproic acid, and NSAIDs, to name afew.
5-HT1- receptor agonists (triptans)The 5-HT1-receptor agonists, commonly knownas the triptans, are the treatment of choice formoderate to severe migraine. They include:• almotriptan• eletriptan• frovatriptan• naratriptan• rizatriptan• sumatriptan• zolmitriptan. (See Sound-alikes: Sumatriptan andzolmitriptan.)
PharmacokineticsWhen comparing the triptans, the key pharmacokinetic featuresare onset of action and duration of action. Rizatriptan, sumatrip-tan, and zolmitriptan have a half-life of approximately 2 hours; al-motriptan and eletriptan have a half-life of 3 to 4 hours; naratrip-tan has a half-life of about 6 hours; and frovatriptan has thelongest half-life (25 hours) and the most delayed onset of action.
Triptan tabletsAll of the triptans are available in an oral form. Rizatriptan andzolmitriptan are also available in rapid-dissolve tablets. Zolmitrip-tan and sumatriptan are available in intransal forms. Sumatriptanis also available as a subcutaneous injection. The injectable formof sumatriptan has the most rapid onset of action of all the trip-tans.
86NEUROLOGIC AND NEUROMUSCULAR DRUGS
Memoryjogger
How can youtell if it’s a
migraine or a head-ache? Look at themnemonic PAIN tosee if the patienthas these key symp-toms:
P—pain
A—aura
I—irritated by light
N—nausea.All the
triptans comein oral form.
Sound-alikes:Sumatriptanand zolmitriptan
Don’t confuse thesound-alike drugs suma-triptan and zolmitriptan.Both drugs are used totreat acute migraines,but recommended dos-es are significantly dif-ferent.
Safe andsound
938903.qxd 08/26/2008 14:59 Page 86

PharmacodynamicsTriptans are serotonin 5-HT1-receptor agonists, which constrictthe cranial vessels, inhibit neuropeptide release, and reduce theneurogenic inflammatory process transmission along the trigemi-nal pathway. These actions may abort or provide symptomatic re-lief for migraines. Aside from relieving pain, triptans are also ef-fective in controlling the nausea and vomiting associated with mi-graines.
PharmacotherapeuticsThe choice of a triptan depends on patient preferences for dosageform (if nausea and vomiting are present), presence of recurrentmigraines, and formulary restrictions. A patient experiencing nau-sea and vomiting may prefer injectable or intranasal sumatriptan.Recurrent migraines may respond to triptans with a longer half-life, such as frovatriptan and naratriptan. However, triptans with alonger half-life have a delayed onset of effect. Two newer triptans,almotriptan and eletriptan, have a rapid onset and an intermediatehalf-life.
Drug interactionsTriptans have many contraindications and aren’t for use in pa-tients with certain conditions. (See Triptans: Contraindicationsand cautions, page 88.)
The safety of treating more than three migraine attacks in a 30-day period with triptans hasn’t been es-tablished. (See Adverse reactions to 5-HT1-receptor agonists [triptans].)
In addition:• Triptans shouldn’t be administeredwithin 24 hours of another 5-HT1-receptor agonist.• Ergotamine-containing and ergot-typedrugs (such as dihydroergotamine andmethysergide) shouldn’t be given with-in 24 hours of a 5-HT1-receptor agonistbecause prolonged vasospastic reac-tions may occur.• Eletriptan shouldn’t be used withinat least 72 hours of these potentCYP3A4 inhibitors: ketoconazole, itra-conazole, nefazodone, clarithromycin,ritonavir, nelfinavir, and any other
87ANTIMIGRAINE DRUGS
It hasn’t beenproven yet whetherit’s safe to treatmore than three
migraines in a 30-dayperiod with triptans.
Adversereactions to5-HT1-receptoragonists(triptans)
Adverse effects of5-HT1-receptor agonistsinclude: • tingling, warm or hotsensation, or flushing• nasal and throat dis-comfort• vision disturbances• paresthesia• dizziness• fatigue or somnolence• chest pain or pressure;neck or throat pain; jawpain or pressure• weakness• dry mouth• indigestion, nausea,sweating• injection site reaction(sumatriptan subcuta-neously)• taste disturbances (in-tranasal sumatriptan).
Serious—but rare —cardiac events, includ-ing acute myocardial in-farction, arrhythmias,and death, have beenreported within a fewhours after use of 5-HT1-receptor agonists.
Warning!
938903.qxd 08/26/2008 14:59 Page 87

drugs that have demonstrated potent CYP3A4 inhibition, as de-scribed in their labeling.
Wait two weeks• Almotriptan, rizatriptan, sumatriptan, and zolmitriptan shouldnot be used with, or within 2 weeks of discontinuing, an MAOI.• Selective serotonin reuptake inhibitors (SSRIs), such as citalo-pram, fluoxetine, fluvoxamine, paroxetine, and sertraline, have, inrare cases, caused weakness, hyperreflexia, and incoordinationwhen administered with a triptan. (This reaction has also been re-ported when the appetite suppressant sibutramine is used with atriptan.) Monitor the patient closely if concomitant treatment witha triptan and an SSRI is clinically warranted.• The bioavailability of frovatriptan is 30% higher in patients tak-ing hormonal contraceptives.• Propranolol increases the bioavailability of zolmitriptan, riza-triptan, frovatriptan, and eletriptan.
88NEUROLOGIC AND NEUROMUSCULAR DRUGS
Incoordinationcan be an
adverse effectof mixing SSRIs
with triptan.
Triptans are contraindicated for patients withischemic heart disease (such as angina pec-toris, history of myocardial infarction, or docu-mented silent ischemia) and in patients whohave symptoms or findings consistent with is-chemic heart disease, coronary artery vaso-spasm (including Prinzmetal’s variant angina),or other significant underlying cardiovascularconditions.
Triptans shouldn’t be prescribed for pa-tients with cerebrovascular syndromes, suchas strokes or transient ischemic attacks, or forpatients with peripheral vascular disease, in-cluding—but not limited to—ischemic boweldisease. Triptans shouldn’t be given to patientswith uncontrolled hypertension or with hemi-plegic or basilar migraines.
In addition, triptans aren’t recommendedfor use in patients who have risk factors forunrecognized coronary artery disease (CAD)(such as hypertension, hypercholesterolemia,smoking, obesity, diabetes, strong family histo-ry of CAD, being a female with surgical orphysiologic menopause, or being a male overage 40) unless a cardiovascular evaluation in-dicates that the patient is reasonably free fromunderlying cardiovascular disease. If a triptanis used in this setting, the first dose should beadministered in a doctor’s office or other med-ically staffed and equipped facility.
Also, intermittent, long-term users of trip-tans and those who have risk factors shouldundergo periodic cardiac evaluation.
Safe and sound
Triptans: Contraindications and cautions
938903.qxd 08/26/2008 14:59 Page 88

Ergotamine preparationsErgotamine and its derivatives may be used as abortive or sympto-matic therapy for migraine.
Some common preparations used for migraine include:• ergotamine, available in sublingual and oral tablets and supposi-tories (combined with caffeine)• dihydroergotamine, available in injectable and intranasal forms.
PharmacokineticsErgotamine is incompletely absorbed from the GI tract. The in-tranasal form of dihydroergotamine is rapidly absorbed. Peakplasma concentration, following subcutaneous injection, is within45 minutes, and 90% of the dose is plasma protein-bound. Ergota-mine is metabolized in the liver, and 90% of the metabolites are ex-creted in bile; traces of unchanged drug are excreted in urine.
PharmacodynamicsErgotamine-derivative antimigraine effects are believed to be dueto blockade of neurogenic inflammation. They also act as partialagonists or antagonists at serotonin, dopaminergic, and alpha-adrenergic receptors depending on their site. Ergotamine prepara-tions often need to be prescribed with antiemetic preparationswhen used for migraine.
Dihydroergotamine, a hydrogenated form of ergotamine, dif-fers mainly in degree of activity. It has less vasoconstrictive actionthan ergotamine and much less emetic potential.
PharmacotherapeuticsErgotamine preparations are used to prevent or treat vascularheadaches, such as migraine, migraine variant, and clusterheadaches. Dihydroergotamine is used when rapid control of mi-graine is desired or when other routes are undesirable.
Drug interactions• Propranolol and other beta-adrenergic blocking drugs block thenatural pathway for vasodilation in patients receiving ergotaminepreparations, resulting in excessive vasoconstriction and cold ex-tremities.
89ANTIMIGRAINE DRUGS
938903.qxd 08/26/2008 14:59 Page 89

Steady, now…• There may be an increased risk of weakness, hyperflexion,and incoordination when using ergotamine preparations withSSRIs.• Sumatriptan may cause an additive effect, increasing therisk of coronary vasospasm. Don’t give any ergotamine prepa-rations and triptans within 24 hours of each other.• Drugs that inhibit the CYP3A4 enzyme (such as ery-thromycin, clarithromycin, ritonavir, nelfinavir, indinavir, andazole-derivative antifungal agents) may alter the metabolism ofergotamine, resulting in increased serum concentrations of er-gotamine. This increases the risk of vasospasm and cerebral orperipheral ischemia. These drugs shouldn’t be used together.• Vasoconstrictors may cause an additive effect when given withergotamine preparations, increasing the risk of high blood pres-sure. (See Adverse reactions to ergotamine derivatives.)
90NEUROLOGIC AND NEUROMUSCULAR DRUGS
Vasoconstrictorsmay increase therisk of high blood
pressure.
Adverse effects of ergotamine derivatives include:• nausea and vomiting• numbness• tingling• muscle pain• leg weakness• itching.
Prolonged administration of ergotamine derivatives may result ingangrene and rebound headaches. Contraindications to the use of er-gotamine preparations include coronary, cerebral, or peripheral vascu-lar disease; hypertension; and liver or kidney disease.
Warning!
Adverse reactions to ergotaminederivatives
938903.qxd 08/26/2008 14:59 Page 90

Quick quiz
1. A 15-year-old patient has a tonic-clonic seizure disorder andis prescribed phenytoin. Which term best describes the absorptionrate of oral phenytoin?
A. RapidB. IntermittentC. ErraticD. Slow
Answer: D. Phenytoin is absorbed slowly through the GI tract.It’s absorbed much more rapidly when administered I.V.
2. An 11-year-old patient develops myoclonic seizures. Whichpotential adverse reaction makes it unlikely that valproate will beprescribed for this patient?
A. Liver toxicityB. Central nervous system sedationC. Respiratory depressionD. Renal toxicity
Answer: A. When given to children and patients taking other an-ticonvulsants, valproate carries a risk of fatal liver toxicity.
3. A 48-year-old patient has been prescribed trihexyphenidyl forher Parkinson’s disease. Which adverse reaction is dose-related?
A. Excessive salivationB. Dry mouthC. BradycardiaD. Nausea
Answer: B. Dry mouth may be a dose-related adverse effect oftrihexyphenidyl therapy.
4. Which antiparkinsonian drug is associated with the on-offphenomenon and the wearing-off effect?
A. AmantadineB. BenztropineC. LevodopaD. Selegiline
Answer: C. Levodopa is associated with the on-off phenomenon(sharp fluctuations in symptoms) and the wearing-off effect(shorter duration of the drug’s effects) in patients who have takenthe drug for many years. Some doctors believe the drug should begiven in lower doses or started later in the course of the disorder.
91QUICK QUIZ
938903.qxd 08/26/2008 14:59 Page 91

ScoringIf you answered all four items correctly, marvelous! You’re mighty
fine with neuromusculars.If you answered three items correctly, congrats! Your knowledge
has a rapid onset and long duration.If you answered fewer than three items correctly, don’t worry.
Give yourself another dose of the chapter, and recheck theresults.
92NEUROLOGIC AND NEUROMUSCULAR DRUGS
✰✰✰
✰✰
✰
938903.qxd 08/26/2008 14:59 Page 92

Drugs and pain controlDrugs used to control pain range from mild, over-the-counter(OTC) preparations such as acetaminophen to potent generalanesthetics. They include:• nonopioid analgesics, antipyretics, and nonsteroidal anti-inflammatory drugs (NSAIDs)• opioid agonist and antagonist drugs• anesthetic drugs.
Nonopioid analgesics, antipyretics,and NSAIDs
Nonopioid analgesics, antipyretics, and NSAIDs are a broadgroup of pain medications. They’re discussed together because,in addition to pain control, they also produce antipyretic (fevercontrol) and anti-inflammatory effects. These drugs may be usedalone or in combination with other medications. They have aceiling effect (maximum dose above which there’s no addedbenefit) and don’t cause physical dependence.
The drug classes included in this group are:• salicylates (especially aspirin), which are widely used
4
Pain medications
Just the facts
In this chapter, you’ll learn:
♦ classes of drugs used to control pain
♦ uses and varying actions of these drugs
♦ how these drugs are absorbed, distributed, metabolized,and excreted
♦ drug interactions and adverse reactions to these drugs.
No pain, nogain? Not withme! You’ll feelbetter in no
time!
938904.qxd 08/26/2008 15:11 Page 93

• the para-aminophenol derivative acetaminophen• NSAIDs• the urinary tract analgesic phenazopyridine.
SalicylatesSalicylates are among the most commonly used pain medications.They’re used regularly to control pain and reduce fever and in-flammation.
Cheap, easy, and reliableSalicylates usually cost less than other analgesics and are readilyavailable without a prescription. Aspirin is the most commonlyused salicylate. Other common salicylates include:• choline magnesium trisalicylate• choline salicylate• diflunisal• salsalate• sodium salicylate.
Pharmacokinetics (how drugs circulate)Taken orally, salicylates are absorbed partly in the stomach, butprimarily in the upper part of the small intestine. The pure andbuffered forms of aspirin are absorbed readily, but sustained-release and enteric-coated salicylate preparations are absorbedmore slowly. Food or antacids in the stomach also delay absorp-tion. Salicylates given rectally have a slower, more erratic absorp-tion.
Distribution, metabolism, and excretionSalicylates are distributed widely throughout body tissues andfluids, including breast milk. In addition, they easily cross theplacental barrier.
The liver extensively metabolizes salicylates into severalmetabolites. The kidneys excrete the metabolites along withsome unchanged drug.
Pharmacodynamics (how drugs act)The different effects of salicylates stem from their separate mech-anisms of action. They relieve pain primarily by inhibiting the syn-thesis of prostaglandin. (Recall that prostaglandin is a chemicalmediator that sensitizes nerve cells to pain.) In addition, they mayalso reduce inflammation by inhibiting the prostaglandin synthesisand release that occurs during inflammation.
94PAIN MEDICATIONS
Salicylates arefound in many
OTC pain and coldpreparations.
Taking asalicylate withan antacid or
food slowsabsorption.
938904.qxd 08/26/2008 15:11 Page 94

Hot and botheredSalicylates reduce fever by stimulating the hy-pothalamus, producing dilation of the peripher-al blood vessels and increased sweating. Thispromotes heat loss through the skin and coolingby evaporation. Also, because prostaglandin E increases bodytemperature, inhibiting its production lowers a fever.
No clots allowedOne salicylate, aspirin, permanently inhibits platelet aggregation(the clumping of platelets to form a clot) by interfering with theproduction of a substance called thromboxane A2, necessary forplatelet aggregation. Not all salicylates have this effect. For exam-ple, choline magnesium doesn’t increase bleeding time.
Pharmacotherapeutics (how drugs are used)Salicylates are used primarily to relieve pain and reduce fever.However, they don’t effectively relieve visceral pain (pain from theorgans and smooth muscle) or severe pain from trauma.
You give me fever…Salicylates won’t reduce a normal body temperature. They can re-duce an elevated body temperature, and will relieve headache andmuscle ache at the same time.
What kind of joint is this?Salicylates can provide considerable relief in 24 hours whenthey’re used to reduce inflammation in rheumatic fever, rheuma-toid arthritis, and osteoarthritis.
Go with the flowAs a result of its anticlotting properties, aspirin can be used to en-hance blood flow during myocardial infarction (MI) and to pre-vent recurrence of MI.
How low can you go?No matter what the clinical indication, the main guideline of sali-cylate therapy is to use the lowest dose that provides relief. Thisreduces the likelihood of adverse reactions. (See Adverse reac-tions to salicylates.)
Drug interactionsBecause salicylates are highly protein-bound, they can interactwith many other protein-bound drugs by displacing those drugsfrom sites to which they normally bind. This increases the serum
95NONOPIOID ANALGESICS, ANTIPYRETICS, AND NSAIDS
Because they relievemuscle ache and reducetemperature, salicylateshelp treat symptoms of
colds and influenza.
Adversereactions tosalicylates
The most common ad-verse reactions to sali-cylates include gastricdistress, nausea, vomit-ing, and bleeding ten-dencies. Other adversereactions include:• hearing loss (whentaken for prolonged peri-ods)• diarrhea, thirst, sweat-ing, tinnitus, confusion,dizziness, impaired vi-sion, and hyperventila-tion (rapid breathing) • Reye’s syndrome(when given to childrenwith chickenpox or flu-like symptoms).
Warning!
938904.qxd 08/26/2008 15:11 Page 95

concentration of the unbound active drug, causing increased phar-macologic effects (the unbound drug is said to be potentiated).
The following drug interactions may occur:• Oral anticoagulants, heparin, methotrexate, oral antidiabeticagents, and insulin are among the drugs that have an increased ef-fect or risk of toxicity when taken with salicylates.• Probenecid, sulfinpyrazone, and spironolactone may have a de-creased effect when taken with salicylates.• Corticosteroids may decrease plasma salicylate levels and in-crease the risk of ulcers.• Alkalinizing drugs and antacids may reduce salicylate levels.• The antihypertensive effect of angiotensin-converting enzyme(ACE) inhibitors and beta-adrenergic blockers may be reducedwhen these drugs are combined with salicylates.• NSAIDs may have a reduced therapeutic effect and an increasedrisk of GI effects when taken with salicylates. (See Using salicy-lates safely.)
AcetaminophenAlthough the class of para-aminophenol derivatives includes twodrugs—phenacetin and acetaminophen—only acetaminophen isavailable in the United States. Acetaminophen is an OTC drug thatproduces analgesic and antipyretic effects. It appears in many
96PAIN MEDICATIONS
Before administering salicylates, be aware of these concerns regardingspecial populations:
Children and teenagers: Don’t use aspirin or salicylates to treat flu-like symptoms or chickenpox because of the risk of triggering Reye’ssyndrome.
Pregnant women: Aspirin is classified as pregnancy risk category D,and salicylates are classified as category C. Salicylates appear inbreast milk.
Surgical patients: Discontinue aspirin, if possible, 1 week beforesurgery because of the risk of postoperative bleeding.
Asthmatics: These patients have an increased risk of sensitivity toaspirin, leading to bronchospasm, urticaria, angioedema, or shock.
Safe and sound
Using salicylates safely
I feel an ulcercoming on… you
didn’t give mecorticosteroids,
did you?
938904.qxd 08/26/2008 15:11 Page 96

products designed to relieve the pain and symptoms associatedwith colds and influenza.
PharmacokineticsAcetaminophen is absorbed rapidly and completely from the GItract. It’s also absorbed well from the mucous membranes of therectum.
Distribution, metabolism, and excretionAcetaminophen is distributed widely in body fluids and readilycrosses the placental barrier. After acetaminophen is metabolizedby the liver, it’s excreted by the kidneys and, in small amounts, inbreast milk.
PharmacodynamicsAcetaminophen reduces pain and fever, but unlike salicylates, itdoesn’t affect inflammation or platelet function. It can cause anti-coagulation in the patient taking warfarin.
Mystery theaterThe pain-control effects of acetaminophen aren’t well understood.The drug may work in the central nervous system (CNS) by in-hibiting prostaglandin synthesis and in the peripheral nervous sys-tem in some unknown way. It reduces fever by acting directly onthe heat-regulating center in the hypothalamus.
PharmacotherapeuticsAcetaminophen is used to reduce fever and relieve headache,muscle ache, and general pain.
Child’s playAcetaminophen is the drug of choice to treat fever and flulikesymptoms in children. Additionally, the American Arthritis Associ-ation has indicated that acetaminophen is an effective pain reliev-er for some types of arthritis.
Drug interactionsAcetaminophen can produce the following drug interactions:• The effects of oral anticoagulants and thrombolytic drugs maybe slightly increased.• The risk of liver toxicity is increased when long-term alcoholuse, phenytoin, barbiturates, carbamazepine, and isoniazid arecombined with acetaminophen.
97NONOPIOID ANALGESICS, ANTIPYRETICS, AND NSAIDS
Acetaminophenis the drug of
choice to treatfever and flulikesymptoms in
children.
938904.qxd 08/26/2008 15:11 Page 97

• The effects of lamotrigine, loop diuretics, and zidovudine maybe reduced when these drugs are taken with acetaminophen. (SeeAdverse reactions to acetaminophen.)
Nonsteroidal anti-inflammatory drugsAs their name suggests, nonsteroidal anti-inflammatory drugs(NSAIDs), are typically used to combat inflammation. Their anti-inflammatory action equals that of aspirin. They also have anal-gesic and antipyretic effects. Unlike aspirin’s effects, the effects ofNSAIDs on platelet aggregation are temporary.
Picky, pickyThere are two types of NSAIDs: selective and nonselective. Thenonselective NSAIDs include diclofenac, etodolac, fenoprofen,flurbiprofen, ibuprofen, indomethacin, ketoprofen, ketorolac,meloxicam, nabumetone, naproxen, oxaprozin, piroxicam, andsulindac. The only selective NSAID available on today’s market iscelecoxib. (See Risks of using selective NSAIDs.)
PharmacokineticsAll NSAIDs (nonselective and selective) are absorbed in the GItract. They’re mostly metabolized in the liver and excreted primar-ily by the kidneys.
PharmacodynamicsTwo isoenzymes of cyclooxygenase, known as COX-1 and COX-2,convert arachidonic acid into prostaglandins. The nonselective
98PAIN MEDICATIONS
Adversereactions toacetaminophen
Most patients tolerateacetaminophen well.Unlike the salicylates,acetaminophen rarelycauses gastric irritationor bleeding tendencies.
Acetaminophen maycause severe liver toxic-ity, and the total dailydose should be moni-tored. (The total dailydose shouldn’t exceed4,000 mg/day.)
Other adverse reac-tions include:• skin rash• hypoglycemia• neutropenia.
Warning!
Two selective nonsteroidal anti-inflammatory drugs (NSAIDs) werepulled from the market after it was discovered they were associatedwith an increased risk of heart attack and stroke, leaving celecoxib asthe only available drug in its class. Patients considering the use of cele-coxib should be carefully screened for a history of cerebrovascular orcardiovascular disease and then closely monitored throughout treat-ment for signs or symptoms of developing problems.
Safe and sound
Risks of using selective NSAIDs
938904.qxd 08/26/2008 15:11 Page 98

NSAIDs block both COX-1 and COX-2. Selective NSAIDs blockonly the COX-2 enzyme.
Hard to stomachThe prostaglandins produced by COX-1 maintain the stomach lin-ing, while those produced by COX-2 cause inflammation. That’swhy the nonselective NSAIDs, which inhibit COX-1 along withCOX-2, commonly cause GI adverse effects. Selective NSAIDs,however, alleviate pain and inflammation without causing signifi-cant GI adverse effects because they inhibit only COX-2.
PharmacotherapeuticsNSAIDs are used primarily to decrease inflammation. They’re sec-ondarily used to relieve pain, but are seldom prescribed to reducefever. (See Using nonselective NSAIDs safely.)
COX-2 inhibitors are primarily used to relieve pain and to de-crease inflammation. These drugs are particularly useful in thetreatment of osteoarthritis, rheumatoid arthritis, acute pain, pri-mary dysmenorrhea, and familial adenomatous polyposis.
Call and responseThe following conditions respond favorably to treatment withNSAIDs:• ankylosing spondylitis (an inflammatory joint disease that firstaffects the spine)• moderate to severe rheumatoid arthritis (an inflammatory dis-ease of peripheral joints)
99NONOPIOID ANALGESICS, ANTIPYRETICS, AND NSAIDS
Before administering nonsteroidal anti-inflammatory drugs (NSAIDs),be aware of special population concerns.
Children: Some NSAIDs aren’t recommended for use in children.Elderly patients: The risk of ulcers increases with age.Pregnant women: Diclofenac, flurbiprofen, ketoprofen, and naprox-
en are pregnancy risk category B drugs. Etodolac, ketorolac, meloxi-cam, nabumetone, oxaprozin, and piroxicam are category C drugs. Be-cause most NSAIDs appear in breast milk, it’s best not to use thesedrugs in breast-feeding women.
Safe and sound
Using nonselective NSAIDs safely
938904.qxd 08/26/2008 15:11 Page 99

• osteoarthritis (a degenerative joint disease) in the hip, shoulder,or other large joints• osteoarthritis accompanied by inflammation• acute gouty arthritis (urate deposits in the joints)• dysmenorrhea (painful menstruation)• migraine headaches• bursitis and tendonitis• mild to moderate pain.
Drug interactionsA wide variety of drugs can interact with NSAIDs, especially withindomethacin, piroxicam, and sulindac. Because they’re highlyprotein-bound, NSAIDs are likely to interact with other protein-bound drugs. Such drugs as fluconazole, phenobarbital, rifampin,ritonavir, and salicylates affect absorption of NSAIDs, whereasNSAIDs affect the absorption of such drugs as oral anticoagulants,aminoglycosides, ACE inhibitors, beta-adrenergic blockers, digox-in, dilantin, and many others. (See Adverse reactions to nonselec-tive NSAIDs and Adverse reactions to COX-2 inhibitors.)
Because NSAIDs are metabolized by the liver, drug-drug inter-actions have been identified for all of them. For example, thesedrugs decrease the clearance of lithium, which can result in lithi-um toxicity. They also reduce the antihypertensive effects of ACEinhibitors and diuretics.
Phenazopyridine hydrochloridePhenazopyridine hydrochloride, an azo dye used in commercialcoloring, produces a local analgesic effect on the urinary tract.
100PAIN MEDICATIONS
Nonselective nonsteroidal anti-inflammatorydrugs (NSAIDs) produce similar adverse reac-tions, including:• abdominal pain, bleeding, anorexia, diarrhea,nausea, ulcers, and liver toxicity
• drowsiness, headache, dizziness, confusion,tinnitus, vertigo, and depression• bladder infection, blood in the urine, and kid-ney necrosis• hypertension, heart failure, and pedal edema.
Warning!
Adverse reactions to nonselective NSAIDs Adversereactions toCOX-2inhibitors
COX-2 inhibitors canhave the following ad-verse reactions:• dyspepsia, nausea,and vomiting• GI ulcers (to a lesserdegree than with nonse-lective NSAIDs)• hypertension, fluid re-tention, and peripheraledema• dizziness and head-ache.
COX-2 inhibitors areclassified as pregnancyrisk category C; most ap-pear in breast milk. As aprecaution, don’t use inbreast-feeding women.
Warning!
938904.qxd 08/26/2008 15:11 Page 100

PharmacokineticsWhen taken orally, the liver metabolizes 35% of phenazopyridine.The remainder is excreted unchanged in the urine, causing the pa-tient’s urine to turn an orange or red color.
PharmacodynamicsPhenazopyridine is taken orally and produces an analgesic effecton the urinary tract usually within 24 to 48 hours after therapy be-gins.
PhamacotherapeuticsThe drug is used to relieve such symptoms as pain, buring, ur-gency, and frequency associated with urinary tract infections.
Drug interactionsThere are no listed drug interactions with phenazopyridine. (SeeAdverse reactions to phenazopyridine hydrochloride.)
Opioid agonist and antagonist drugsThe word opioid refers to derivatives of the opium plant or to syn-thetic drugs that imitate natural narcotics. Opioid agonists (alsocalled narcotic agonists) include opium derivatives and syntheticdrugs with similar properties. They’re used to relieve or decreasepain without causing the person to lose consciousness.
Some opioid agonists may also have antitussive effects thatsuppress coughing and antidiarrheal actions that can control diar-rhea.
Anta-doteOpioid antagonists aren’t pain medications. Instead, they blockthe effects of opioid agonists and are used to reverse adverse drugreactions, such as respiratory and CNS depression, produced bythose drugs. Unfortunately, by reversing the analgesic effect, theyalso cause the patient’s pain to recur.
Having it both waysSome opioid analgesics, called mixed opioid agonist-antago-nists, have agonist and antagonist properties. The agonist compo-nent relieves pain, while the antagonist component decreases therisk of toxicity and drug dependence. These mixed opioid agonist-antagonists reduce the risk of respiratory depression and drugabuse.
101OPIOID AGONIST AND ANTAGONIST DRUGS
Adversereactionsto phenazo-pyridinehydrochloride
Phenazopyridine hydro-chloride can have cer-tain adverse reactions.• If the drug accumu-lates, the patient’s skinand sclera may assumea yellow tinge. If this oc-curs, the drug may needto be discontinued.• Acute renal or hepaticfailure may occur.
Warning!
Opioid refers toderivatives of theopium plant or tosynthetic drugsthat imitate theeffects of natural
narcotics.
938904.qxd 08/26/2008 15:11 Page 101

Opioid agonistsOpioid agonists include:• codeine• fentanyl• hydrocodone• hydromorphone• levorphanol• meperidine• methadone• morphine sulfate (including morphine sulfate sustained-releasetablets and intensified oral solution)• oxycodone• oxymorphone• propoxyphene• remifentanil• sufentanil.
Gold standardMorphine sulfate is the standard against which the effectivenessand adverse reactions of other pain medications are measured.(See Using opioid agonists safely.)
PharmacokineticsA person may receive an opioid agonist by any administrationroute, although inhalation administration is uncommon. Oral dos-es are absorbed readily from the GI tract; however, transmucosaland intrathecal opiates are faster-acting.
Speedy deliveryOpioid agonists administered I.V. provide the most rapid (almostimmediate) and reliable pain relief. The subcutaneous (subQ) andI.M. routes may result in delayed absorption, especially in patientswith poor circulation.
DistributionOpioid agonists are distributed widely throughout body tissues.They have a relatively low plasma protein-binding capacity (30%to 35%).
MetabolismOpioid agonists are metabolized extensively in the liver. For ex-ample, meperidine is metabolized to normeperidine, a toxicmetabolite with a longer half-life than meperidine. This metaboliteaccumulates in patients with renal failure and may lead to CNS ex-citation and seizures. Administration of meperidine for more than
102PAIN MEDICATIONS
Using opioidagonists safely
Be aware that morphinesulfate (MSO4) can beconfused with magne-sium sulfate (MgSO4). Toavoid confusing thedrugs, never use abbre-viations.
Safe andsound
938904.qxd 08/26/2008 15:11 Page 102

48 hours increases the risk of neurotoxicity and seizures frombuildup of normeperidine.
ExcretionMetabolites are excreted by the kidneys. A small amount is excret-ed in stool through the biliary tract.
PharmacodynamicsOpioid agonists reduce pain by binding to opiate receptor sites(mu receptors and N-methyl-D-aspartate receptors) in the periph-eral nervous system and the CNS. When these drugs stimulate theopiate receptors, they mimic the effects of endorphins (naturallyoccurring opiates that are part of the body’s own pain relief sys-tem). This receptor-site binding produces the therapeutic effectsof analgesia and cough suppression. It also produces adverse re-actions, such as respiratory depression and constipation.
Smooth operatorOpioid agonists, especially morphine, affect the smooth muscle ofthe GI and genitourinary tracts (the organs of the reproductiveand urinary systems). This causes contraction of the bladder andureters. It also slows intestinal peristalsis (rhythmic contractionsthat move food along the digestive tract), resulting in constipa-tion, a common adverse effect of opiates.
Too much of a good thingThese drugs also cause blood vessels to dilate, especially in theface, head, and neck. In addition, they suppress the cough centerin the brain, producing antitussive effects and causing constric-tion of the bronchial muscles. These effects can produce adversereactions if excessive. For example, if the blood vessels dilate toomuch, hypotension can occur.
PharmacotherapeuticsOpioid agonists are prescribed to relieve severe pain inacute, chronic, and terminal illnesses. They also reduceanxiety before a patient receives anesthesia and are some-times prescribed to control diarrhea and suppress cough-ing. (See How opioid agonists control pain, page 104.)
Methadone is used for temporary maintenance of nar-cotic addiction. Other opioids and remifentanil are usedfor the induction and maintenance of general anesthesia.
103OPIOID AGONIST AND ANTAGONIST DRUGS
Ahhh. I canbreathe easierwith morphine.
938904.qxd 08/26/2008 15:11 Page 103

Cardio-assistanceMorphine relieves shortness of breath in patients with pulmonaryedema (fluid in the lungs) and left-sided heart failure (inability ofthe heart to pump enough blood to meet the needs of the body). Itdoes this by dilating peripheral blood vessels, keeping more bloodin the periphery, and decreasing cardiac preload.
104PAIN MEDICATIONS
Opioid agonists, such as meperidine, inhibit pain transmission by mimicking the body’s natural pain control mechanisms.
Now I get it!
How opioid agonists control pain
Where neurons meet
In the dorsal horn of the spinal cord, pe-ripheral pain neurons meet central ner-vous system (CNS) neurons. At thesynapse, the pain neuron releases sub-stance P (a pain neurotransmitter). Thisagent helps transfer pain impulses to theCNS neurons that carry those impulsesto the brain.
Taking up space
In theory, the spinal interneurons re-spond to stimulation from the descendingneurons of the CNS by releasing endoge-nous opiates. These opiates bind to theperipheral pain neuron to inhibit releaseof substance P and to retard the trans-mission of pain impulses.
Stopping substance P
Synthetic opiates supplement this pain-blocking effect by binding with free opi-ate receptors to inhibit the release ofsubstance P. Opiates also alter con-sciousness of pain, but how this mecha-nism works remains unknown.
Peripheral pain neuron
Pain impulse
Spinal interneuron
Dorsal horn
CNS neuron
Substance P
Synapse
Pain impulse blocked
Opiate receptor
Endogenous opiate
Endogenousopiate
Meperidine(syntheticopiate)
Opiatereceptor
Substance Preleaseinhibited
938904.qxd 08/26/2008 15:11 Page 104

Drug interactions• The use of opioid agonists with other drugs that also decreaserespirations, such as alcohol, sedatives, hypnotics, and anesthet-ics, increases the patient’s risk of severe respiratory depression.• Taking tricyclic antidepressants, phenothiazines, or anticholin-ergics with opioid agonists may cause severe constipation andurine retention.• Drugs that may affect opioid analgesic activity includeamitriptyline, diazepam, phenytoin, protease inhibitors, and ri-fampin.• Drugs that may be affected by opioid analgesics include carba-mazepine, warfarin, beta-adrenergic blockers, and calcium chan-nel blockers. (See Adverse reactions to opioid agonists.)
Mixed opioid agonist-antagonistsMixed opioid agonist-antagonists attempt to relieve pain whilereducing toxic effects and dependency. The mixed opioid agonist-antagonists include:• buprenorphine• butorphanol• nalbuphine• pentazocine hydrochloride (combined with pentazocine lactate,naloxone, aspirin, or acetaminophen).
No free rideOriginally, mixed opioid agonist-antagonists appeared to have lessabuse potential than the pure opioid agonists. However, butor-phanol and pentazocine have reportedly caused dependence. Also,
105OPIOID AGONIST AND ANTAGONIST DRUGS
One of the most common adverse reactions toopioid agonists is decreased rate and depth ofbreathing that worsens as the dose of opioid isincreased. This may cause periodic, irregularbreathing or trigger asthmatic attacks in sus-ceptible patients.
Other adverse reactions include:• flushing
• orthostatic hypotension• pupil constriction.
Adverse reactions to meperidine include:• tremors• palpitations• tachycardia• delirium• seizures.
Warning!
Adverse reactions to opioid agonists
Mixed opioidagonist-antagonists
attempt to relievepain while reducingtoxic effects and
dependency.
938904.qxd 08/26/2008 15:11 Page 105

patients with chronic pain who are taking an opioid agonistshouldn’t take a mixed opioid agonist-antagonist with it becauseof the risk of withdrawal symptoms.
PharmacokineticsAbsorption of mixed opioid agonist-antagonists occurs rapidlyfrom parenteral sites. These drugs are distributed to most bodytissues and also cross the placental barrier. They’re metabolized inthe liver and excreted primarily by the kidneys, although morethan 10% of a butorphanol dose and a small amount of a penta-zocine dose are excreted in stool.
PharmacodynamicsThe exact mechanism of action of the mixed opioid agonist-antagonists isn’t known. However, researchers believe that thesedrugs weakly antagonize the effects of morphine, meperidine, andother opiates at one of the opioid receptor sites, while exerting ag-onistic effects at other opioid receptor sites.
No rush to goBuprenorphine binds with receptors in the CNS, altering percep-tion of and emotional response to pain through an unknownmechanism. It seems to release slowly from binding sites, produc-ing a longer duration of action than the other drugs in this class.
Don’t get emotionalThe site of action of butorphanol may be opiate receptors in thelimbic system (the part of the brain involved in emotion).
Like pentazocine, butorphanol also acts on pulmonary circula-tion, increasing pulmonary vascular resistance (the resistance inthe blood vessels of the lungs that the right ventricle must pumpagainst). Both drugs also increase blood pressure and the work-load of the heart.
PharmacotherapeuticsMixed opioid agonist-antagonists are used as analgesia duringchildbirth and are also administered postoperatively.
Independence dayMixed opioid agonist-antagonists are sometimes prescribed inplace of opioid agonists because they have a lower risk of drug de-pendence. Mixed opioid agonist-antagonists are also less likely tocause respiratory depression and constipation, although they can
106PAIN MEDICATIONS
Patients with ahistory of opioidabuse shouldn’t
receive mixedopioid agonist-antagonists.
938904.qxd 08/26/2008 15:11 Page 106

produce some adverse reactions. (See Adverse reactions to opioidagonist-antagonists.)
Drug interactionsIncreased CNS depression and an accompanying decrease in res-piratory rate and depth may result if mixed opioid agonist-antagonists are administered to patients taking other CNS depres-sants, such as barbiturates and alcohol.
Clean and sober?Patients who abuse opioids shouldn’t receive mixed opioidagonist-antagonists because these drugs can cause symptoms ofwithdrawal.
Mixed opioid agonist-antagonists are listed as pregnancy riskcategory C drugs; safety and use in breast-feeding women haven’tbeen established.
Opioid antagonistsOpioid antagonists have a greater attraction for opiate receptorsthan opioids do; however, they don’t stimulate those receptors. Asa result, opioid antagonists block the effects of opioid drugs,enkephalins, and endorphins.
Opioid antagonists include:• naloxone• naltrexone.
PharmacokineticsNaloxone is administered I.M., subQ, or I.V. Naltrexone is adminis-tered orally in tablet or liquid form. Both drugs are metabolized bythe liver and excreted by the kidneys.
PharmacodynamicsOpioid antagonists act by occupying opiate receptor sites, displac-ing opioids attached to opiate receptors, and preventing opioidsfrom binding at these sites. This process, known as competitiveinhibition, effectively blocks the effects of opioids.
PharmacotherapeuticsNaloxone is the drug of choice for managing an opioid overdose.It reverses respiratory depression and sedation and helps stabilizethe patient’s vital signs within seconds after administration.
107OPIOID AGONIST AND ANTAGONIST DRUGS
Adversereactions toopioid agonist-antagonists
The most common ad-verse reactions to opioidagonist-antagonists in-clude nausea, vomiting,light-headedness, seda-tion, and euphoria.
Warning!
938904.qxd 08/26/2008 15:11 Page 107

Naloxone also reverses the analgesic effects of opioids. There-fore, after naloxone administration, the patient may complain ofpain or even experience withdrawal symptoms.
Kicking the habitNaltrexone is used along with psychotherapy or counseling totreat drug abuse; however, the recipient must first have gonethrough a detoxification program. Otherwise, if the patient re-ceives naltrexone while he still has opioids in his body, acute with-drawal symptoms may occur. (See Managing naltrexone therapyfor drug addiction.)
Drug interactionsNaloxone produces no significant drug interactions. Naltrexonewill cause withdrawal symptoms if given to a patient receiving anopioid agonist or to an opioid addict. (See Adverse reactions tonaloxone and naltrexone.)
Anesthetic drugsAnesthetic drugs can be divided into three groups—general anes-thetics, local anesthetics, and topical anesthetics.
Inhale or inject?General anesthetic drugs are further subdivided into two maintypes: those given by inhalation and those given intravenously.
108PAIN MEDICATIONS
Managing naltrexone therapy for drug addiction
To prevent acute withdrawal during treatment for opioid addiction, plan to use naltrexone as partof a comprehensive rehabilitation program. Keep in mind the following guidelines:• Don’t give naltrexone until a negative naloxone challenge test is obtained. • Don’t give naltrexone to a patient who’s receiving an opioid agonist, addicted to an opioid ago-nist, or in the acute phase of opioid withdrawal because acute withdrawal symptoms may occuror worsen.• For a patient who’s addicted to a short-acting opioid, such as heroin or meperidine, wait at least7 days after the last opioid dose before starting naltrexone.• For a patient who’s addicted to a longer-acting opioid, such as methadone, wait at least 10 daysafter the last opioid dose before starting naltrexone.• During naltrexone therapy, be alert for signs of opioid withdrawal, such as drug craving, confu-sion, drowsiness, visual hallucinations, abdominal pain, vomiting, diarrhea, fever, chills, tachyp-nea, diaphoresis, salivation, lacrimation, runny nose, and mydriasis.
Adversereactions tonaloxone andnaltrexone
Naloxone and naltrex-one produce differentadverse reactions.
Naloxone
Naloxone may causenausea, vomiting and,occasionally, hyperten-sion and tachycardia. Anunconscious patient re-turned to consciousnessabruptly after naloxoneadministration may hy-perventilate and experi-ence tremors.
Naltrexone
Naltrexone can cause avariety of adverse reac-tions, including:• edema, hypertension,palpitations, phlebitis,and shortness of breath• anxiety, depression,disorientation, dizziness,headache, and nervous-ness• anorexia, diarrhea orconstipation, nausea,thirst, and vomiting• urinary frequency• liver toxicity.
Warning!
938904.qxd 08/26/2008 15:11 Page 108

Inhalation anestheticsCommonly used general anesthetics given by inhalation include:• desflurane• enflurane• halothane• isoflurane• nitrous oxide• sevoflurane.
PharmacokineticsThe absorption and elimination rates of an anesthetic are gov-erned by its solubility in blood. Inhalation anesthetics enter theblood from the lungs and are distributed to other tissues. Distribu-tion is most rapid to organs with high blood flow, such as thebrain, liver, kidneys, and heart. Inhalation anesthetics are elimi-nated primarily by the lungs; enflurane, halothane, and sevoflu-rane are also eliminated by the liver. Metabolites are excreted inthe urine.
PharmacodynamicsInhalation anesthetics work primarily by depressing the CNS, pro-ducing loss of consciousness, loss of responsiveness to sensorystimulation (including pain), and muscle relaxation. They also af-fect other organ systems.
PharmacotherapeuticsInhalation anesthetics are used for surgery because they offermore precise and rapid control of depth of anesthesia than injec-tion anesthetics do. These anesthetics, which are liquids at roomtemperature, require a vaporizer and special delivery system forsafe use.
Of the inhalation anesthetics available, desflurane, isoflurane,and nitrous oxide are the most commonly used.
Stop signsInhalation anesthetics are contraindicated in the patient withknown hypersensitivity to the drug, a liver disorder, or malignanthyperthermia (a potentially fatal complication of anesthesia char-acterized by skeletal muscle rigidity and high fever). (See Unusu-al but serious reaction and Adverse reactions to inhalation anes-thetics, page 110.)
109ANESTHETIC DRUGS
Anestheticdrugs can begeneral, local,
and topical. Somany choices!
Unusual butserious reaction
Malignant hyperthermia,characterized by a sud-den and often lethal in-crease in body tempera-ture, is a serious and un-common reaction toinhalation anesthetics. Itoccurs in geneticallysusceptible patients onlyand may result from afailure in calcium uptakeby muscle cells. Theskeletal muscle relaxantdantrolene is used totreat this condition.
Safe andsound
938904.qxd 08/26/2008 15:11 Page 109

Drug interactionsThe most important drug interactions involving inhalation anes-thetics occur with other CNS, cardiac, or respiratory-depressantdrugs. Inhalation anesthetics can cause CNS depression, cardiacarrhythmias, or depressed respirations, resulting in compromisedpatient status.
Intravenous anestheticsIntravenous anesthetics are typically used when the patient re-quires general anesthesia for just a short period such as duringoutpatient surgery. They’re also used to promote rapid inductionof anesthesia or to supplement inhalation anesthetics.
Main optionsThe drugs used as intravenous anesthetics are:• barbiturates (methohexital, thiopental)• benzodiazepines (midazolam)• dissociatives (ketamine)• hypnotics (etomidate, propofol)• opiates (fentanyl, sufentanil).
PharmacokineticsIntravenous anesthetics are lipid-soluble and well-distributedthroughout the body, crossing the placental barrier and enteringbreast milk. These drugs are metabolized in the liver and excretedin the urine.
110PAIN MEDICATIONS
The most common adverse reaction to inhala-tion anesthetics is an exaggerated patient re-sponse to a normal dose.
Waking up
After surgery, a patient may experience reac-tions similar to those seen with other centralnervous system depressants, including de-pression of breathing and circulation, confu-
sion, sedation, nausea, vomiting, ataxia, andhypothermia.
It happens with halothane
Rarely, liver necrosis develops several days af-ter halothane use and occurs most commonlywith multiple drug exposures. Symptoms in-clude rash, fever, jaundice, nausea, vomiting,eosinophilia, and alterations in liver function.
Warning!
Adverse reactions to inhalation anesthetics
938904.qxd 08/26/2008 15:11 Page 110

PharmacodynamicsOpiates work by occupying sites on specialized receptors scat-tered throughout the CNS and by modifying the release of neuro-transmitters from sensory nerves entering the CNS. Ketamine actsdirectly on the cortex and limbic system of the brain, producing aprofound sense of dissociation from the environment.
Getting sleepyBarbiturates, benzodiazepines, and etomidate seem to enhance re-sponses to the CNS neurotransmitter, gamma-aminobutyric acid.This inhibits the brain’s response to stimulation of the reticular ac-tivating system, the area of the brain stem that controls alertness.Barbiturates also depress the excitability of CNS neurons.
PharmacotherapeuticsBecause of the short duration of action of intravenous anesthet-ics, they’re used in brief surgical procedures such as outpatientsurgery.
Going soloBarbiturates are used alone in surgery that isn’t expected to bepainful and as adjuncts to other drugs in more extensive proce-dures. Benzodiazepines produce sedation and amnesia, but notpain relief.
Etomidate is used to induce anesthesia and to supplement low-potency inhalation anesthetics such as nitrous oxide. The opiatesprovide pain relief and supplement other anesthetics.
Drug interactionsI.V. anesthetics, particularly ketamine, can produce a variety ofdrug interactions.• Verapamil enhances the anesthetic effects of etomidate, causingrespiratory depression and apnea.• Administering ketamine together with halothane increases therisk of hypotension and reduces cardiac output (the amount ofblood pumped by the heart each minute).• Giving ketamine and nondepolarizing drugs together increasesneuromuscular effects, resulting in prolonged respiratory depres-sion.• Using barbiturates or opioids with ketamine may prolong recov-ery time after anesthesia.• Ketamine plus theophylline may promote seizures.
111ANESTHETIC DRUGS
938904.qxd 08/26/2008 15:11 Page 111

• Ketamine and thyroid hormones may cause hypertension andtachycardia (rapid heart rate). (See Adverse reactions to I.V. anes-thetics.)
Local anestheticsLocal anesthetics are administered to prevent or relieve pain in aspecific area of the body. In addition, these drugs are often usedas an alternative to general anesthesia for elderly or debilitatedpatients.
Chain gangLocal anesthetics may be:• “amide” drugs (with nitrogen in the molecular chain, such asbupivacaine, levobupivacaine, lidocaine, mepivacaine, prilocaine,and ropivacaine)• “ester” drugs (with oxygen in the molecular chain, such aschloroprocaine, cocaine, procaine, and tetracaine). (See Amidesand esters.)
PharmacokineticsAbsorption of local anesthetics varies widely, but distribution oc-curs throughout the body. Esters and amides undergo differenttypes of metabolism, but both yield metabolites that are excretedin the urine.
112PAIN MEDICATIONS
Amides andesters
Amide anesthetics arelocal anesthetics thathave nitrogen as part oftheir molecular makeup.They include:• bupivacaine• lidocaine• mepivacaine• prilocaine• ropivacaine.
Give them oxygen
Ester anesthetics haveoxygen, not nitrogen, aspart of their molecularmakeup. They include:• chloroprocaine• procaine• tetracaine.
Now I get it!
Ketamine
• Prolonged recovery• Irrational behavior• Excitement• Disorientation• Delirium, hallucinations• Increased heart rate• Hypertension
Propofol
• Respiratory depression• Hiccups, coughing, muscle-twitching
Thiopental
• Respiratory depression• Hiccups, coughing, muscle-twitching• Depressed cardiac functionand peripheral dilation
Etomidate
• Hiccups, coughing, muscle-twitching
Fentanyl
• Central nervous system(CNS) and respiratory depres-sion• Hypoventilation• Cardiac arrhythmias
Midazolam
• CNS and respiratory de-pression• Hypotension• Dizziness
Warning!
Adverse reactions to I.V. anesthetics
938904.qxd 08/26/2008 15:11 Page 112

PharmacodynamicsLocal anesthetics block nerve impulses at the point of contact inall kinds of nerves. They accumulate, causing the nerve cell mem-brane to expand. As the membrane expands, the cell loses its abil-ity to depolarize, which is necessary for impulse transmission.(See Blocking the pain pathways.)
PharmacotherapeuticsLocal anesthetics are used to prevent and relieve pain from med-ical procedures, disease, or injury. Local anesthetics may also beused for severe pain that topical anesthetics or analgesics can’t re-lieve.
Staying localLocal anesthetics are usually preferred to general anesthetics forsurgery in an elderly or debilitated patient or a patient with a dis-order that affects respiratory function, such as chronic obstruc-tive pulmonary disease and myasthenia gravis.
113ANESTHETIC DRUGS
Nerve endings transmit pain signals through the peripheral and centralnervous systems to the brain. Giving a central nerve block can block thesignal transmission and relieve pain. The illustration below shows twokey points where an anesthetic may be administered to produce a cen-tral nerve block
Now I get it!
Blocking the pain pathways
Lateral view
Vertebra
Spinal blockSpinal cord
Subarachnoid space
Epidural block
Epidural space
938904.qxd 08/26/2008 15:11 Page 113

Tighten upFor some procedures, a local anesthetic is combined with a drugthat constricts blood vessels, such as epinephrine. Vasoconstric-tion helps control local bleeding and reduces absorption of theanesthetic. Reduced absorption prolongs the anesthetic’s action atthe site and limits its distribution and CNS effects.
Drug interactionsLocal anesthetics produce few significant interactions with otherdrugs. They can, however, produce adverse reactions. (See Ad-verse reactions to local anesthetics.)
Topical anestheticsTopical anesthetics are applied directly to intact skin or mucousmembranes. All topical anesthetics are used to prevent or relieveminor pain.
All together nowSome injectable local anesthetics, such as lidocaine and tetra-caine, are also topically effective. In addition, some topical anes-thetics, such as lidocaine, are combined in other products.
PharmacokineticsTopical anesthetics produce little systemic absorption, except forthe application of cocaine to mucous membranes. However, sys-temic absorption may occur if the patient receives frequent orhigh-dose applications to the eye or large areas of burned or in-jured skin.
Tetracaine and other esters are metabolized extensively in theblood and to a lesser extent in the liver. Dibucaine, lidocaine, andother amides are metabolized primarily in the liver. Both types oftopical anesthetics are excreted in the urine.
PharmacodynamicsBenzocaine, butacaine, cocaine, dyclonine, and pramoxine pro-duce topical anesthesia by blocking nerve impulse transmission.They accumulate in the nerve cell membrane, causing it to expandand lose its ability to depolarize, thus blocking impulse transmis-sion. Dibucaine, lidocaine, and tetracaine may also block impulsetransmission across the nerve cell membranes.
114PAIN MEDICATIONS
Adversereactionsto localanesthetics
Dose-related centralnervous system (CNS)reactions include anxi-ety, apprehension, rest-lessness, nervousness,disorientation, confu-sion, dizziness, blurredvision, tremors, twitch-ing, shivering, andseizures. Dose-relatedcardiovascular reac-tions may include myo-cardial depression,bradycardia (slow heartrate), arrhythmias, hy-potension, cardiovascu-lar collapse, and cardiacarrest.
All the rest
Local anesthetic solu-tions that contain vaso-constrictors such asepinephrine can alsoproduce CNS and car-diovascular reactions,including anxiety, dizzi-ness, headache, rest-lessness, tremors, palpi-tations, tachycardia,angina, and hyperten-sion.
Warning!
938904.qxd 08/26/2008 15:11 Page 114

Sensory overloadThe aromatic compounds, such as benzyl alcohol and clove oil,appear to stimulate nerve endings. This stimulation causes coun-terirritation that interferes with pain perception.
A chilling endingEthyl chloride spray superficially freezes the tissue, stimulatingthe cold-sensation receptors and blocking the nerve endings in thefrozen area. Menthol selectively stimulates the sensory nerve end-ings for cold, causing a cool sensation and some local pain relief.
PharmacotherapeuticsTopical anesthetics are used to:• relieve or prevent pain, especially minor burn pain• relieve itching and irritation• anesthetize an area before an injection is given• numb mucosal surfaces before a tube, such as a urinarycatheter, is inserted• alleviate sore throat or mouth pain when used in a spray or so-lution.
All eyes and earsTetracaine is also used as a topical anesthetic for the eye. Benzo-caine is used with other drugs in several ear preparations.
Drug interactionsFew interactions with other drugs occur with topical anestheticsbecause they aren’t absorbed well into the systemic circulation.(See Adverse reactions to topical anesthetics.)
115ANESTHETIC DRUGS
Adversereactionsto topicalanesthetics
Topical anesthetics cancause several differentadverse reactions.• Benzyl alcohol cancause topical reactionssuch as skin irritation. • Refrigerants, such asethyl chloride, may pro-duce frostbite wherethey’ve been applied.• Topical anestheticscan cause a hypersensi-tivity reaction, includinga rash, itching, hives,swelling of the mouthand throat, and breath-ing difficulty.
Warning!
938904.qxd 08/26/2008 15:11 Page 115

Quick quiz
1. How does the topical anesthetic benzocaine relieve sunburnpain?
A. It numbs the skin surface, decreasing the perception ofpain.
B. It freezes the skin, which prevents nerve impulse trans-mission.
C. It blocks nerve impulse transmission by preventingnerve cell depolarization.
D. It stimulates nerve endings, interfering with the percep-tion of pain.
Answer: C. Benzocaine prevents nerve cell depolarization, thusblocking nerve impulse transmission and relieving pain.
2. Which adverse reaction is a patient most likely to experiencepostsurgery after receiving general anesthesia?
A. Nausea and vomitingB. SeizuresC. CyanosisD. Fever
Answer: A. After surgery involving general anesthesia, a patientis most likely to experience adverse reactions similar to those pro-duced by other CNS-depressant drugs, including nausea and vom-iting.
3. Before administering buprenorphine, the nurse asks the pa-tient if he has used opiates. That’s because administering a mixedopioid agonist-antagonist to a patient dependent on opioid ago-nists may cause which reaction?
A. Hypersensitivity reactionB. Withdrawal symptomsC. Urinary incontinenceD. Respiratory depression
Answer: B. Because they can counteract the effects of opioid ag-onists, mixed opioid agonist-antagonists can cause withdrawalsymptoms in patients dependent on opioid agonists.
116PAIN MEDICATIONS
938904.qxd 08/26/2008 15:11 Page 116

4. The drug commonly prescribed to treat an opioid overdose is:A. butorphanol.B. naloxone.C. pentazocine.D. ketamine.
Answer: B. Naloxone is the drug of choice for managing opioidoverdose.
5. What are the most common adverse reactions to aspirin?A. Increased rate and depth of respirationsB. Confusion, sedation, and hypothermiaC. Dizziness and vision changesD. Nausea, vomiting, and GI distress
Answer: D. Aspirin most commonly produces adverse GI reac-tions, such as nausea, vomiting, and GI distress.
6. Desflurane is which type of anesthetic?A. OpioidB. LocalC. TopicalD. General
Answer: D. Desflurane is a commonly used general anestheticthat’s administered by inhalation.
7. Topical anesthetics are used:A. as an alternative to general anesthesia for elderly or de-
bilitated patients.B. to numb mucosal surfaces before tube insertion.C. when anesthesia is needed for only a short period.D. to promote rapid induction of anesthesia.
Answer: B. Topical anesthetics are used to numb mucosal sur-faces as well as relieve or prevent pain, relieve itching and irrita-tion, anesthetize an area for an injection, and alleviate sore throator mouth pain.
117QUICK QUIZ
938904.qxd 08/26/2008 15:11 Page 117

ScoringIf you answered all seven items correctly, bravo! You’re a pain
medication powerhouse.If you answered five or six items correctly, fabulous! For you, this
chapter was painless.If you answered fewer than five items correctly, hey, don’t give
up! Remember: No pain, no gain.
118PAIN MEDICATIONS
✰✰✰
✰✰
✰
938904.qxd 08/26/2008 15:11 Page 118

Drugs and the cardiovascular systemThe heart, arteries, veins, and lymphatics make up the cardiovas-cular system. These structures transport life-supporting oxygenand nutrients to cells, remove metabolic waste products, and car-ry hormones from one part of the body to another. Because thissystem performs such vital functions, a problem with the heart orblood vessels can seriously affect a person’s health.
Types of drugs used to improve cardiovascularfunction include:• inotropic• antiarrhythmic• antianginal• antihypertensive• diuretic• antilipemic.
InotropicsInotropic drugs, such as cardiac glycosides and phosphodi-esterase (PDE) inhibitors, increase the force of the heart’s con-tractions. In other words, the drugs have what’s known as a posi-
5
Cardiovascular drugs
Just the facts
In this chapter, you’ll learn:
♦ classes of drugs used to treat cardiovascular disorders
♦ uses and varying actions of these drugs
♦ how these drugs are absorbed, distributed, metabolized,and excreted
♦ drug interactions and adverse reactions to these drugs.
Sometimesit seems likemy work isnever done!
938905.qxd 08/26/2008 15:21 Page 119

tive inotropic effect. (Inotropic means affecting the force or ener-gy of muscular contractions.)
Cardiac glycosides also slow the heart rate (called a negativechronotropic effect) and slow electrical impulse conductionthrough the atrioventricular (AV) node (called a negative dro-motropic effect).
Cardiac glycosidesCardiac glycosides are a group of drugs derived from digitalis, asubstance that occurs naturally in foxglove plants and in certaintoads. The most frequently used cardiac glycoside is digoxin.
Pharmacokinetics (how drugs circulate)The intestinal absorption of digoxin varies greatly; the capsulesare absorbed most efficiently, followed by the elixir form, andthen tablets. Digoxin is distributed widely throughout the body,with highest concentrations in the heart muscle, liver, and kid-neys. Digoxin binds poorly to plasma proteins.
In most patients, a small amount of digoxin is metabolized inthe liver and gut by bacteria. This effect varies and may be sub-stantial in some people. Most of the drug is excreted by the kid-neys as unchanged drug. (See Load that dose.)
Pharmacodynamics (how drugs act)Digoxin is used to treat heart failure because it strengthens thecontraction of the ventricles by boosting intracellular calcium atthe cell membrane, enabling stronger heart contractions.
Digoxin may also enhance the movement of calcium into themyocardial cells and stimulate the release, or block the reuptake,of norepinephrine at the adrenergic nerve terminal.
Stop that impulseDigoxin acts on the central nervous system (CNS) to slow theheart rate, thus making it useful for treating supraventricular ar-rhythmias (abnormal heart rhythms that originate above the bun-dle branches of the heart’s conduction system), such as atrial fib-rillation and atrial flutter. It also increases the refractory period(the period when the cells of the conduction system can’t conductan impulse).
Pharmacotherapeutics (how drugs are used)In addition to treating heart failure and supraventricular arrhyth-mias, digoxin is used to treat paroxysmal atrial tachycardia (an ar-
120CARDIOVASCULAR DRUGS
Digoxinpumpsme up!
Load that dose
Because digoxin has along half-life, a loadingdose must be given to apatient who requires im-mediate drug effects, asin supraventricular ar-rhythmia.
By giving a larger ini-tial dose, a minimum ef-fective concentration ofthe drug in the bloodmay be reached faster.
Note: Avoid giving aloading dose to a patientwith heart failure toavoid toxicity.
938905.qxd 08/26/2008 15:21 Page 120

rhythmia marked by brief periods of tachycardia that alternatewith brief periods of sinus rhythm).
Drug interactionsMany drugs can interact with digoxin.• Antacids, barbiturates, cholestyramine resin, kaolin and pectin,neomycin, metoclopramide, rifampin, and sulfasalazine reduce thetherapeutic effects of digoxin.• Calcium preparations, quinidine, verapamil, cyclosporine, tetra-cycline, clarithromycin, propafenone, amiodarone, spironolac-tone, hydroxychloroquine, erythromycin, itraconazole, andomeprazole increase the risk of digoxin toxicity.• Amphotericin B, potassium-wasting diuretics, and steroids tak-en with digoxin may cause hypokalemia (low potassium levels)and increase the risk of digoxin toxicity.• Beta-adrenergic blockers and calcium channel blockers takenwith digoxin may cause an excessively slow heart rate and ar-rhythmias.• Succinylcholine and thyroid preparations increase the risk of ar-rhythmias when they’re taken with digoxin.• St. John’s wort, an herbal preparation, can increase digoxin lev-els and risk of toxicity.
Digoxin can also produce adverse reactions, mostly involvingdigoxin toxicity. (See Recognizing signs and symptoms of digox-in toxicity, page 122, and Adverse reactions to cardiacglycosides.)
121INOTROPICS
Because cardiac glycosides have a narrow therapeutic index (marginof safety), they may produce digoxin toxicity. To prevent digoxin toxicity,the dosage should be individualized based on the patient’s serumdigoxin concentration.
Adverse reactions to digoxin include:• rash• fever• eosinophilia• arrhythmias.
Warning!
Adverse reactions to cardiacglycosides
938905.qxd 08/26/2008 15:21 Page 121

PDE inhibitorsPDE inhibitors are typically used for short-term management ofheart failure or long-term management in patients awaiting hearttransplant surgery. Specific PDE inhibitors are inamrinone andmilrinone.
PharmacokineticsAdministered I.V., inamrinone is distributed rapidly, metabolizedby the liver, and excreted by the kidneys. It’s rarely used becausesecondary thrombocytopenia may occur as an adverse reaction.
Ready for actionMilrinone is also administered I.V. It’s distributed rapidly and ex-creted by the kidneys, primarily as unchanged drug.
122CARDIOVASCULAR DRUGS
Digoxin toxicity usually produces cardiac, gastrointestinal, and neurologic signs and symptoms.To prevent severe or even life-threatening effects, be prepared to recognize the signs and symp-toms listed below. Also assess the patient for the most common early indicators of toxicity, whichare usually GI-related.
Safe and sound
Recognizing signs and symptoms of digoxin toxicity
Cardiac
• Accelerated junctional rhythms• Atrial tachycardia with atrioventricular (AV)block• Second-degree AV block (Wenckebach)• Sinoatrial arrest or block• Third-degree AV block (complete)• Ventricular arrhythmias
Gastrointestinal
• Abdominal pain• Anorexia• Diarrhea• Nausea• Vomiting
Neurologic
• Blue-yellow color blindness• Blurred vision• Colored dots in vision• Coma• Confusion• Depression• Disorientation• Flickering lights• Headache• Insomnia• Irritability• Lethargy• Personality changes• Psychosis • Restlessness• Seizures• White halos on dark objects
938905.qxd 08/26/2008 15:21 Page 122

PharmacodynamicsPDE inhibitors improve cardiac output by strengthening contrac-tions. These drugs are thought to help move calcium into the car-diac cell or to increase calcium storage in the sarcoplasmic reticu-lum. By directly relaxing vascular smooth muscle, they also de-crease peripheral vascular resistance (afterload) and the amountof blood returning to the heart (preload).
PharmacotherapeuticsInamrinone and milrinone are used to manage heart failure in pa-tients who haven’t responded adequately to treatment with car-diac glycosides, diuretics, or vasodilators. Prolonged use of thesedrugs may increase the patient’s risk of complications and death.(See Adverse reactions to PDE inhibitors.)
Drug interactions• PDE inhibitors may interact with disopyramide, causing hy-potension.• Because PDE inhibitors reduce serum potassium levels, takingthem with a potassium-wasting diuretic may lead to hypokalemia.
Antiarrhythmic drugsAntiarrhythmic drugs are used to treat arrhythmias, disturbancesof the normal heart rhythm.
123ANTIARRHYTHMIC DRUGS
Besidespumping iron,
cardiac outputcan be improved
with PDEinhibitors.
Adverse reactions to phosphodi-esterase (PDE) inhibitors are un-common, but the likelihood in-creases significantly when a pa-tient is on prolonged therapy.
Adverse reactions may in-clude:• arrhythmias
• nausea and vomiting• headache• fever• chest pain• hypokalemia• thrombocytopenia (especiallywith inamrinone)• mild increase in heart rate.
Warning!
Adverse reactions to PDE inhibitors
938905.qxd 08/26/2008 15:21 Page 123

TroublemakersUnfortunately, many antiarrhythmics are also capable of worsen-ing or causing the very arrhythmias they’re supposed to treat. Thebenefits need to be weighed carefully against the risks of antiar-rhythmic therapy.
A touch of classAntiarrhythmics are categorized into four classes:• I (which includes classes IA, IB, and IC)• II• III• IV.
Class I antiarrhythmics consist of sodium channel blockers.This is the largest group of antiarrhythmics. Class I agents are fre-quently subdivided into classes IA, IB, and IC. One drug, adeno-sine (an AV nodal blocking agent used to treat paroxysmal supra-ventricular tachycardia), doesn’t fall into any of these classes.
The mechanisms of action of antiarrhythmics vary widely, anda few drugs exhibit properties common to more than one class.
Class IA antiarrhythmicsClass IA antiarrhythmics are used to treat a wide variety of atrialand ventricular arrhythmias. Class IA antiarrhythmics include:• disopyramide• procainamide• quinidine (sulfate and gluconate).
PharmacokineticsWhen administered orally, class IA drugs are rapidly absorbed andmetabolized. Because they work so quickly, sustained-releaseforms of these drugs were developed to help maintain therapeuticlevels.
A shot to the headThese drugs are distributed through all body tissues. Quinidine,however, is the only one that crosses the blood-brain barrier.
All class IA antiarrhythmics are metabolized in the liver andare excreted unchanged by the kidneys. Acidic urine increases theexcretion of quinidine.
124CARDIOVASCULAR DRUGS
Because class IAantiarrhythmics workso quickly, sustained-release forms of thedrugs were created
to maintaintherapeutic levels.
938905.qxd 08/26/2008 15:22 Page 124

PharmacodynamicsClass IA antiarrhythmics control arrhythmias by altering the my-ocardial cell membrane and interfering with autonomic nervoussystem control of pacemaker cells.
No (para)sympathyClass IA antiarrhythmics also block parasympathetic stimulationof the sinoatrial (SA) and AV nodes. Because stimulation of theparasympathetic nervous system causes the heart rate to slowdown, drugs that block the parasympathetic nervous system in-crease the conduction rate of the AV node.
Rhythmic risksThis increase in the conduction rate can produce dangerous in-creases in the ventricular heart rate if rapid atrial activity is pre-sent, as in a patient with atrial fibrillation. In turn, the increasedventricular heart rate can offset the ability of the antiarrhythmicsto convert atrial arrhythmias to a regular rhythm.
PharmacotherapeuticsClass IA antiarrhythmics are prescribed to treat such arrhythmiasas premature ventricular contractions, ventricular tachycardia,atrial fibrillation, atrial flutter, and paroxysmal atrial tachycardia.
Drug interactionsClass IA antiarrhythmics can interact with other drugs:• Disopyramide taken with macrolide antibiotics, such as clar-ithromycin and erythromycin, increases the patient’s risk of devel-oping a prolonged QT interval. In turn, this may lead to an in-creased risk of arrhythmias, especially polymorphic ventriculartachycardia.• Disopyramide plus verapamil may increase myocardial depres-sion and should be avoided in patients with heart failure.• Other antiarrhythmics, such as beta-adrenergic blockers, in-crease the risk of arrhythmias.• Quinidine plus neuromuscular blockers may cause increasedskeletal muscle relaxation.• Quinidine increases the risk of digoxin toxicity.• Rifampin, phenytoin, and phenobarbital can reduce the effectsof quinidine and disopyramide.
GI symptoms are a common adverse reaction to class IA an-tiarrhythmics. (See Adverse reactions to class IA antiarrhyth-mics.)
125ANTIARRHYTHMIC DRUGS
Adversereactionsto class IAantiarrhythmics
Class IA antiarrhyth-mics, especially quini-dine, may produce GIsymptoms, such as diar-rhea, cramping, nausea,vomiting, anorexia, anda bitter taste.
Dramatic irony
Ironically, not only doclass IA antiarrhythmicstreat arrhythmias, butthey can also induce ar-rhythmias, especiallyconduction delays thatmay worsen existingheart blocks.
Warning!
938905.qxd 08/26/2008 15:22 Page 125

Class IB antiarrhythmicsClass IB antiarrhythmics are used for treating acute ventricular ar-rhythmias. They include:• lidocaine• mexiletine.
PharmacokineticsMexiletine is absorbed from the GI tract after oral administration.Lidocaine is administered I.V. to prevent rapid metabolism by theliver after it enters the hepatic portal circulation.
All bound up?Lidocaine is distributed widely throughout the body, including thebrain. Lidocaine and mexiletine are moderately bound to plasmaproteins. (Remember, only that portion of a drug that’s unboundcan produce a response.)
Class IB antiarrhythmics are metabolized in the liver and ex-creted in urine. Mexiletine also appears in breast milk.
PharmacodynamicsClass IB drugs work by blocking the rapid influx of sodium ionsduring the depolarization phase of the heart’s depolarization-repolarization cycle. This decreases the refractory period, whichreduces the risk of arrhythmia. (See How lidocaine works.)
Make a IB-line for the ventricleBecause class IB antiarrhythmics especial-ly affect the Purkinje fibers (fibers in theconducting system of the heart) and my-ocardial cells in the ventricles, they’re usedto treat only ventricular arrhythmias.
PharmacotherapeuticsClass IB antiarrhythmics are used to treat ventricular ectopicbeats, ventricular tachycardia, and ventricular fibrillation.
Class IB antiarrhythmics are usually the drug of choice inacute care because they don’t produce immediate serious adversereactions.
Drug interactionsClass IB antiarrhythmics may exhibit additive or antagonistic ef-fects when administered with other antiarrhythmics, such as
126CARDIOVASCULAR DRUGS
Adversereactions toclass IBantiarrhythmics
Adverse reactions toclass IB antiarrhythmicsinclude drowsiness,light-headedness,paresthesia, sensorydisturbances, hypoten-sion, and bradycardia.
Lidocaine toxicitycan cause seizures andrespiratory arrest.
Adverse reactions tomexiletine include hy-potension, atrioventricu-lar block, bradycardia,confusion, ataxia, anddouble vision. Mexiletinemay also produce nau-sea and vomiting.
Warning!
Think of class IBantiarrhythmicsas going straightto the bottom of
the heart.
938905.qxd 08/26/2008 15:22 Page 126

phenytoin, propranolol, procainamide, and quinidine. Other druginteractions include the following:• Rifampin may reduce the effects of mexiletine.• Theophylline levels increase when given with mexiletine.• Use of a beta-adrenergic blocker or disopyramide with mexile-tine may reduce the contractility of the heart. (See Adverse reac-tions to class IB antiarrhythmics.)
127ANTIARRHYTHMIC DRUGS
Lidocaine works in injured or ischemic myocardial cells to retard sodium influx and restore cardiac rhythm. Normally, the ventri-cles contract in response to impulses from the sinoatrial (SA) node. But when tissue damage occurs in the ventricles, ischemiccells can create an ectopic pacemaker, which can trigger ventricular arrhythmias. The illustrations below show how these ar-rhythmias develop at the cellular level—and how lidocaine suppresses them.
Now I get it!
How lidocaine works
Ischemic myocardial cell
Normal myocardial cells permit a limited amount of sodiumions to enter, which leads to controlled depolarization. Is-chemic myocardial cells allow a rapid infusion of sodium ions.This causes the cells to depolarize much more quickly thannormal and then begin firing spontaneously. The result: a ven-tricular arrhythmia.
Ischemic myocardial cell with lidocaine
By slowing sodium’s influx, lidocaine raises the cells’ electricalstimulation threshold (EST). The increased EST prolongs depo-larization in the ischemic cells and returns control to the SAnode, the heart’s main pacemaker.
Lidocaine
Sodium ion
Increased sodiuminflux
Sodium channel
Causes increaseddepolarization
Lidocaine
Slowed sodiuminflux
Lidocaine receptor
Causes decreaseddepolarization
938905.qxd 08/26/2008 15:22 Page 127

Class IC antiarrhythmicsClass IC antiarrhythmics are used to treat certain severe, refrac-tory (resistant) ventricular arrhythmias. Class IC antiarrhythmicsinclude:• flecainide• moricizine• propafenone.
PharmacokineticsAfter oral administration, class IC antiarrhythmics are absorbedwell, distributed in varying degrees, and probably metabolized bythe liver. They’re excreted primarily by the kidneys, except forpropafenone, which is excreted primarily in stool.
More about moricizineAfter oral administration, about 38% of moricizine is absorbed. Itundergoes extensive metabolism, with less than 1% of a dose ex-creted unchanged in the urine. Moricizine is highly protein-bound,leaving only a small portion of the drug free to produce its antiar-rhythmic effect.
PharmacodynamicsClass IC antiarrhythmics primarily slow conduction along theheart’s conduction system. Moricizine decreases the fast inwardcurrent of sodium ions of the action potential, depressing the de-polarization rate and the effective refractory period.
PharmacotherapeuticsLike class IB antiarrhythmics, class IC antiarrhythmics are used totreat and prevent life-threatening ventricular arrhythmias. They’realso used to treat supraventricular arrhythmias (abnormal heartrhythms that originate above the bundle branches of the heart’sconduction system).
Flecainide and propafenone may also be used to preventparoxysmal supraventricular tachycardia (PSVT) in patients with-out structural heart disease. Moricizine is used to manage life-threatening ventricular arrhythmias such as sustained ventriculartachycardia.
Drug interactionsClass IC antiarrhythmics may exhibit additive effects with otherantiarrhythmics. Other interactions include the following:
128CARDIOVASCULAR DRUGS
Memoryjogger
To rememberthe main
differences betweenwhat Class IA, ClassIB, and Class IC an-tiarrhythmics do,just think of theirnames:
Class IA: Alters themyocardial cell mem-brane
Class IB: Blocks therapid influx of sodiumions
Class IC: slows Con-duction
938905.qxd 08/26/2008 15:22 Page 128

• When used with digoxin, flecainide and propafenone increasethe risk of digoxin toxicity.• Propafenone increases plasma concentrations of warfarin andincreases prothrombin times.• Quinidine increases the effects of propafenone.• Cimetidine may increase the plasma level and the risk of toxici-ty of moricizine.• Propanolol or digoxin given with moricizine may increase thePR interval on the electrocardiogram.• Theophylline levels may be reduced in a patient receiving mori-cizine.• Ritonavir increases the plasma concentration and the effects ofpropafenone.• Propafenone increases the serum concentration and the effectsof metoprolol and propranolol. (See Adverse reactions to class ICantiarrhythmics.)
Class II antiarrhythmicsClass II antiarrhythmics are composed of beta-adrenergic antag-onists, or beta-adrenergic blockers. Beta-adrendergic blockersused as antiarrhythmics include:
129ANTIARRHYTHMIC DRUGS
Class IC antiarrhythmics can produce serious adverse reactions, in-cluding the development of new arrhythmias and aggravation of exist-ing arrhythmias. They’re avoided in patients with structural heart de-fects because of a high incidence of mortality.
Because propafenone has beta-blocking properties, it may causebronchospasm.
Adverse reactions to moricizine
The most serious adverse reaction is the appearance of new arrhyth-mias or the worsening of an existing arrhythmia.
Other cardiovascular adverse reactions include palpitations, short-ness of breath, chest pain, heart failure, and cardiac arrest.
GI adverse reactions include abdominal pain, heartburn, nausea,and vomiting.
Warning!
Adverse reactions to class ICantiarrhythmics
938905.qxd 08/26/2008 15:22 Page 129

• acebutolol (not used very often)• esmolol• propranolol.
PharmacokineticsAcebutolol and propranolol are absorbed almost entirely from theGI tract after an oral dose. Esmolol, which can be given only byI.V., is immediately available throughout the body.
Fat-headedAcebutolol and esmolol have low lipid solubility. That means thatthey can’t penetrate the highly fatty cells that act as barriers be-tween the blood and brain, called the blood-brain barrier.
Propranolol has high lipid solubility and readily crosses theblood-brain barrier.
No leftoversPropranolol undergoes significant first-pass effect, leaving only asmall portion of these drugs available to reach circulation and bedistributed to the body.
Esmolol is metabolized exclusively by red blood cells (RBCs),with only 1% excreted in urine. Propranolol’s metabolites are ex-creted in urine.
PharmacodynamicsClass II antiarrhythmics block beta-adrenergic receptor sites inthe conduction system of the heart. As a result, the ability of theSA node to fire spontaneously (automaticity) is slowed. The abili-ty of the AV node and other cells to receive and conduct an electri-cal impulse to nearby cells (conductivity) is also reduced.
Class II antiarrhythmics also reduce the strength of the heart’scontractions. When the heart beats less forcefully, it doesn’t re-quire as much oxygen to do its work.
PharmacotherapeuticsClass II antiarrhythmics slow ventricular rates in patients withatrial flutter, atrial fibrillation, and paroxysmal atrial tachycardia.
Drug interactionsClass II antiarrhythmics can cause a variety of drug interactions:• Administering these drugs with phenothiazines and other anti-hypertensives increases the antihypertensive effect.• When given with nonsteroidal anti-inflammatory agents, fluidand water retention may occur, decreasing the antihypertensiveeffect.
130CARDIOVASCULAR DRUGS
Class IIantiarrhythmics
can causehypotension
when taken withsome drugs.
938905.qxd 08/26/2008 15:22 Page 130

• The effects of sympathomimetics may be reduced when takenwith class II antiarrhythmics.• Beta-adrenergic blockers given with verapamil can depress theheart, causing hypotension, bradycardia, AV block, and asystole.• Beta-adrenergic blockers reduce the effects of sulfonylureas.• The risk of digoxin toxicity increases when digoxin is takenwith esmolol. (See Adverse reactions to class II antiarrhyth-mics.)
Class III antiarrhythmicsClass III antiarrhythmics are used to treat ventricular arrhyth-mias. The drugs in this class are amiodarone, dofetilide, ibutilide,and sotalol.
Which class are you in?Sotalol is a nonselective beta-adrenergic blocker (class II drug)that also has class III properties. Nonselective means that the drugdoesn’t have a specific affinity for a receptor. Although sotalol is aclass II drug, its class III antiarrhythmic effects are more predomi-nant, especially at higher doses. Therefore, it’s usually listed as aclass III antiarrhythmic.
PharmacokineticsThe absorption of these antiarrhythmics varies widely.
Slow goingAfter oral administration, amiodarone is absorbed slowly at wide-ly varying rates. The drug is distributed extensively and accumu-lates in many sites, especially in organs with a rich blood supplyand fatty tissue. It’s highly protein-bound in plasma, mainly to al-bumin.
Dofetilide is very well absorbed from the GI tract, with almost100% overall absorption. Of that, about 70% is bound to plasmaproteins. Ibutilide, which is administered only by I.V., has an ab-sorption of 100%. Sotalol’s absorption is slow and varies between60% and 100%, with minimal protein-binding.
PharmacodynamicsAlthough the exact mechanism of action isn’t known, class III an-tiarrhythmics are thought to suppress arrhythmias by converting aunidirectional block to a bidirectional block. Class III antiarrhyth-mics have little or no effect on depolarization. Rather, these drugsslow repolarization, prolonging the refractory period and durationof the action potential.
131ANTIARRHYTHMIC DRUGS
Adversereactionsto class IIantiarrhythmics
Common adverse reac-tions include:• arrhythmias• bradycardia• heart failure• hypotension• GI reactions, such asnausea, vomiting, anddiarrhea• bronchoconstriction.
Warning!
938905.qxd 08/26/2008 15:22 Page 131

PharmacotherapeuticsClass III antiarrhythmics are used for life-threatening arrhythmias.Amiodarone is the first-line drug of choice for ventricular tachy-cardia and ventricular fibrillation.
Drug interactions• Amiodarone increases phenytoin, procainamide, and quinidinelevels.• Amiodarone also increases the risk of digoxin toxicity.• Ibutilide shouldn’t be administered within 4 hours of class I orother class III antiarrhythmics because it increases the potentialfor a prolonged refractory period.• Dofetilide shouldn’t be administered with cimetidine, ketocona-zole, megestrol, prochlorperazine, sulfamethoxazole, trimetho-prim, or verapamil because of their potential to induce life-threatening arrhythmias.• Sotalol shouldn’t be administered with dolasetron or droperidolbecause of the increased risk of life-threatening arrhythmias.• Concomitant use of amiodarone and fluoroquinolones,macrolide antibiotics, and azole antifungals may cause prolonga-tion of the QTc interval, leading to cardiac arrhythmias, includingtorsades de pointes.
Pressure plungeSevere hypotension may develop from too-rapid I.V. administra-tion of amiodarone. (See Adverse reactions to class III antiar-rhythmics.)
132CARDIOVASCULAR DRUGS
Adverse reactions to class III antiarrhythmics, especially amio-darone, vary widely and commonly lead to drug discontinua-tion. A common adverse effect is aggravation of arrhythmias.
Adverse reactions to amiodarone...
Amiodarone may produce hypotension, nausea, and anorexia.Severe pulmonary toxicity occurs in 15% of patients and can befatal. Vision disturbances and corneal microdeposits may oc-cur.
... and ibultilide ...
Ibutilide may cause sustained ventricular tachycardia, prolon-gation of the QT interval, hypotension, nausea, and headache.
... and sotalol
Sotalol may cause atrioventricular block, bradycardia, ventric-ular arrhythmias, bronchospasm, and hypotension.
Warning!
Adverse reactions to class III antiarrhythmics
When a patienthas ventriculartachycardia, I
reach foramiodarone.
938905.qxd 08/26/2008 15:22 Page 132

Class IV antiarrhythmicsClass IV antiarrhythmics are composed of calcium channelblockers. The calcium channel blockers verapamil and diltiazemare used to treat supraventricular arrhythmias with a rapid ven-tricular response (rapid heart rate in which the rhythm originatesabove the ventricles).
For a thorough discussion of calcium channel blockers andhow they work, see “Calcium channel blockers,” page 138.
AdenosineAdenosine is an injectable antiarrhythmic indicated for acutetreatment of PSVT.
PharmacokineticsAfter I.V. administration, adenosine is probably distributed rapidlythroughout the body. It’s metabolized inside RBCs as well as invascular endothelial cells.
PharmacodynamicsAdenosine depresses the pacemaker activity of the SA node, re-ducing the heart rate and the ability of the AV node to conduct im-pulses from the atria to the ventricles.
PharmacotherapeuticsAdenosine is especially effective against reentry tachycardias(when an impulse depolarizes an area of heart muscle, then re-turns and repolarizes it) that involve the AV node.
No slouchAdenosine also effectively resolves PSVT in 90% of cases. It’s typi-cally used to treat arrhythmias associated with accessory bypasstracts, as in Wolff-Parkinson-White syndrome (brief periods ofrapid heart rate in which the rhythm originates above the ventri-cle).
Drug interactions• Methylxanthines antagonize the effects of adenosine, so largerdoses of adenosine may be necessary.• Dipyridamole and carbamazepine potentiate the effects ofadenosine, so smaller doses of adenosine may be necessary.
133ANTIARRHYTHMIC DRUGS
Remember, caffeineantagonizes the
effect of adenosine. Ifthe patient is a
coffee drinker, largerdoses of adenosinemay be necessary.
938905.qxd 08/26/2008 15:22 Page 133

• When adenosine is administered with carbamazepine, there’s anincreased risk of heart block. (See Adverse reactions to adeno-sine.)
Antianginal drugsAlthough angina’s cardinal symptom is chest pain, the drugs usedto treat angina aren’t typically analgesics.
Instead, antianginal drugs treat angina by reducing myocar-dial oxygen demand (reducing the amount of oxygen the heartneeds to do its work), by increasing the supply of oxygen to theheart, or both. (See How antianginal drugs work.)
The three classes of antianginal drugs discussed in this sectioninclude:• nitrates (for treating acute angina)• beta-adrenergic blockers (for long-term prevention of angina)
134CARDIOVASCULAR DRUGS
Angina occurs when the coro-nary arteries (the heart’s pri-mary source of oxygen) supplyinsufficient oxygen to the myo-cardium. This increases theheart’s workload, increasingheart rate, preload (blood vol-ume in the ventricle at the endof diastole), afterload (pres-sure in the arteries leadingfrom the ventricle), and forceof myocardial contractility.
Antianginal drugs (nitrates,beta-adreneric blockers, andcalcium channel blockers) re-lieve angina by decreasingone or more of these four fac-tors. This diagram summarizeshow antianginal drugs affectthe cardiovascular system.
Now I get it!
How antianginal drugs work
Adversereactions toadenosine
Common adverse reac-tions to adenosine in-clude:• facial flushing• shortness of breath• dyspnea• chest discomfort.
Warning!
AfterloadDecreased bycalcium channelblockers and nitrates
Heart rateDecreased by beta-adrenergic blockersand some calciumchannel blockers
PreloadDecreased bynitrates
ContractilityDecreased by beta-adrenergic blockersand calcium channelblockers
938905.qxd 08/26/2008 15:22 Page 134

• calcium channel blockers (used when other drugs fail to pre-vent angina).
NitratesNitrates are the drugs of choice for relieving acute angina. Ni-trates commonly prescribed to treat angina include:• amyl nitrite• isosorbide dinitrate• isosorbide mononitrate• nitroglycerin.
PharmacokineticsNitrates can be administered in a variety of ways.
All absorbed…Nitrates given sublingually (under the tongue), buccally (in thepocket of the cheek), as chewable tablets, as lingual aerosols(sprayed onto or under the tongue), or by inhalation (amyl nitrite)are absorbed almost completely because the mucous membranesof the mouth have a rich blood supply.
…Half-absorbed…Swallowed nitrate capsules are absorbed through the mucousmembranes of the GI tract, and only about one-half of the dose en-ters circulation.
Transdermal nitrates (a patch or ointment placed on the skin)are absorbed slowly and in varying amounts, depending on thequantity of drug applied, the location of its application, the sur-face area of skin used, and circulation to the skin.
…Or no absorption requiredI.V. nitroglycerin, which doesn’t need to be absorbed, goes directlyinto circulation.
PharmacodynamicsNitrates cause the smooth muscle of the veins and, to a lesser ex-tent, the arteries to relax and dilate. This is what happens:• When the veins dilate, less blood returns to the heart.• This, in turn, reduces the amount of blood in the ventricles atthe end of diastole, when the ventricles are full. (The volume ofblood in the ventricles just before contraction is called preload.)• By reducing preload, nitrates reduce ventricular size and ven-tricular wall tension (the left ventricle doesn’t have to stretch as
135ANTIANGINAL DRUGS
938905.qxd 08/26/2008 15:22 Page 135

much to pump blood). This, inturn, reduces the oxygen re-quirements of the heart.
Don’t fight itThe arterioles provide themost resistance to the bloodpumped by the left ventricle(called peripheral vascular re-sistance). Nitrates decrease af-terload by dilating the arteri-oles, reducing resistance, eas-ing the heart’s workload, andeasing the demand for oxygen.
PharmacotherapeuticsNitrates are used to relieveand prevent angina.
For speedy relief…The rapidly absorbed nitrates, such as nitroglycerin, are the drugsof choice for relief of acute angina because:• they have a rapid onset of action• they’re easy to take• they’re inexpensive.
…Or preventionLonger-acting nitrates, such as the daily nitroglycerin transdermalpatch, are convenient and can be used to prevent chronic angina.Oral nitrates are also used because they seldom produce seriousadverse reactions.
Drug interactions• Severe hypotension can result when nitrates interact with alco-hol.• Erectile dysfunction drugs shouldn’t be taken within 24 hours ofnitrate administration because of possible enhanced hypotensiveeffects.• Absorption of sublingual nitrates may be delayed when takenwith an anticholinergic drug.• Marked orthostatic hypotension (a drop in blood pressure whena person stands up) with light-headedness, fainting, or blurred vi-sion may occur when calcium channel blockers, antihyperten-sives, beta-adrenergic blockers, or phenothiazines and nitrates areused together. (See Adverse reactions to nitrates.)
136CARDIOVASCULAR DRUGS
The moreblood that fillsmy ventricles,the harder I
have to work…
…And the harder Iwork, the more oxygen
I need. By dilatingveins, nitrates reduce
the blood in myventricles—so I can
get some rest.
Adversereactionsto nitrates
Most adverse reactionsto nitrates result fromchanges in the cardio-vascular system. Thesereactions usually disap-pear when dosage is re-duced.
The three H’s
Headache is the mostcommon adverse reac-tion. Hypotension mayalso occur, accompa-nied by dizziness and in-creased heart rate.
Warning!
938905.qxd 08/26/2008 15:22 Page 136

Beta-adrenergic antagonistsBeta-adrenergic antagonists (also called beta blockers) are usedfor long-term prevention of angina and are one of the main typesof drugs used to treat hypertension. Beta-adrenergic blockers in-clude:• atenolol• metoprolol• nadolol• propranolol.
PharmacokineticsMetoprolol and propranolol are absorbed almost entirely from theGI tract, whereas less than one-half the dose of atenolol ornadolol is absorbed. These beta-adrenergic blockers are distrib-uted widely. Propranolol is highly protein-bound; the other beta-adrenergic blockers are poorly protein-bound.
Making an escapePropranolol and metoprolol are metabolized in the liver, and theirmetabolites are excreted in urine. Atenolol and nadolol aren’t me-tabolized and are excreted unchanged in urine and stool.
PharmacodynamicsBeta-adrenergic blockers decrease blood pressure and block beta-adrenergic receptor sites in the heart muscle and the conductionsystem. This decreases the heart rate and reduces the force of theheart’s contractions, resulting in a lower demand for oxygen.
PharmacotherapeuticsBeta-adrenergic blockers are indicated for long-term prevention ofangina. In acute coronary syndrome, metoprolol may be given ini-tially I.V., and then orally. Metoprolol may also be used for heartfailure.
Because of their ability to reduce blood pressure, beta-adren-ergic blockers are also first-line therapy for treating hypertension.
Drug interactionsA number of drugs interact with beta-adrenergic blockers.• Antacids reduce absorption of beta-adrenergic blockers.• Nonsteroidal anti-inflammatory drugs (NSAIDs) can decreasethe hypotensive effects of beta-adrenergic blockers.
137ANTIANGINAL DRUGS
We in the GItract are like
sponges when itcomes to
metoprolol andpropranolol!
938905.qxd 08/26/2008 15:22 Page 137

• Cardiac glycosides and calcium channel blockers can have neg-ative addictive effects on SA or AV node conduction when admin-istered with a beta-adrenergic blocker.• Diuretics or other hypotensive agents can potentiate the hy-potensive effects of beta-adrenergic blockers.• Lidocaine toxicity may occur when lidocaine is taken with beta-adrenergic blockers.• The requirements for insulin and oral antidiabetics can be al-tered by beta-adrenergic blockers.• The ability of theophylline to produce bronchodilation is im-paired by nonselective beta-adrenergic blockers. (See Adverse re-actions to beta-adrenergic blockers.)
Calcium channel blockersCalcium channel blockers are commonly used to prevent anginathat doesn’t respond to drugs in either of the other antianginalclasses. They’re the drug of choice to treat Prinzmetal’s angina. Asmentioned earlier, several of the calcium channel blockers arealso used as antiarrhythmics and to treat hypertension. Calciumchannel blockers used to treat angina include:• amlodipine• diltiazem• nicardipine• nifedipine• verapamil.
138CARDIOVASCULAR DRUGS
Beta-adrenergic blockers maycause:• bradycardia• angina• fluid retention• peripheral edema• heart failure• arrhythmias, especially atri-oventricular block• hypotension• dizziness
• nausea and vomiting• diarrhea• significant constriction of thebronchioles.
Quick stop causes concern
Suddenly stopping a beta-adrenergic blocker may trigger:• angina• hypertension• arrhythmias• acute myocardial infarction.
Warning!
Adverse reactions to beta-adrenergic blockers
938905.qxd 08/26/2008 15:22 Page 138

PharmacokineticsWhen administered orally, calcium channel blockers are absorbedquickly and almost completely. Because of the first-pass effect,however, the bioavailability of these drugs is much lower. The cal-cium channel blockers are highly bound to plasma proteins.
Gone without a traceAll calcium channel blockers are metabolized rapidly and almostcompletely in the liver.
PharmacodynamicsCalcium channel blockers prevent the passage of calcium ionsacross the myocardial cell membrane and vascular smooth-muscle
139ANTIANGINAL DRUGS
Calcium channel blockers in-crease the myocardial oxygensupply and slow the heartrate. Apparently, the drugsproduce these effects byblocking the slow calciumchannel. This action inhibitsthe influx of extracellular cal-cium ions across both myo-cardial and vascular smoothmuscle cell membranes. Cal-cium channel blockersachieve this blockade withoutchanging serum calcium con-centrations.
No calcium = dilation
This calcium blockade causesthe coronary arteries (and, toa lesser extent, the peripheralarteries and arterioles) to di-late, decreasing afterload andincreasing myocardial oxygensupply.
Now I get it!
How calcium channel blockers work
Some calciumchannel blockersslow the heartrate but don’t
change the levelof calcium in the
blood.
Calcium channelblocker
Cell membrane
Slow calciumchannel
Cell membrane
Calcium ion
938905.qxd 08/26/2008 15:22 Page 139

cells. This causes dilation of the coronary and peripheral arteries,which decreases the force of the heart’s contractions and reducesthe workload of the heart.
The relaxation responseAlso, by preventing arterioles from constricting, calcium channelblockers reduce afterload. Decreasing afterload further decreasesthe oxygen demands of the heart. (See How calcium channelblockers work, page 139.)
Rate reductionsSome calcium channel blockers (diltiazem and verapamil) also re-duce the heart rate by slowing conduction through the SA and AVnodes. A slower heart rate reduces the heart’s need for additionaloxygen.
PharmacotherapeuticsCalcium channel blockers are used for long-term prevention ofangina only, not short-term relief of chest pain. Calcium channelblockers are particularly effective for preventing Prinzmetal’sangina.
Drug interactions• Calcium salts and vitamin D reduce the effectiveness of calciumchannel blockers.• Nondepolarizing blocking drugs may have an enhanced muscle-relaxant effect when taken with calcium channel blockers.• Verapamil and diltiazem increase the risk of digoxin toxicity, en-hance the action of carbamazepine, and may cause myocardial de-pression. (See Adverse reactions to calcium channel blockers.)
Antihypertensive drugsAntihypertensive drugs, which act to reduce blood pressure, areused to treat hypertension, a disorder characterized by elevationin systolic blood pressure, diastolic blood pressure, or both.
Know the programTreatment for hypertension typically begins with a thiazide diuret-ic or a calcium channel blocker. (For more information, see “Cal-cium channel blockers,” page 138.) The patient may also receive abeta-adrenergic antagonist, angiotensin-converting enzyme (ACE)inhibitor, or an angiotensin II receptor blocker. The choice of
140CARDIOVASCULAR DRUGS
Adversereactions tocalciumchannelblockers
As with other antiangi-nal drugs, cardiovascu-lar reactions are themost common and seri-ous adverse reactions tocalcium channel block-ers. These include or-thostatic hypotension (adrop in blood pressurewhen a person standsup), heart failure, andhypotension. Diltiazemand verapamil cancause such arrhythmiasas bradycardia, sinusblock, and atrioventricu-lar block.
Others
Other possible adversereactions include dizzi-ness, headache, flush-ing, weakness, andpersistent peripheraledema.
Warning!
938905.qxd 08/26/2008 15:22 Page 140

these drugs depends on whether the patient has a compelling indi-cation, such as heart failure, history of an MI, high risk of coro-nary artery disease (CAD), diabetes, or chronic kidney disease.(See “Beta-adrenergic antagonists,” page 137.)
Other drugs used to treat hypertension include sympatholyticdrugs (other than beta-adrenergic blockers), and vasodilators. Attimes, a combination of drugs may be used.
Sympatholytic drugsSympatholytic drugs include several different types of drugs, butall reduce blood pressure by inhibiting or blocking the sympathet-ic nervous system. They’re classified by their site or mechanism ofaction and include:• central-acting sympathetic nervous system inhibitors (clonidineand methyldopa)• alpha-adrenergic blockers (doxazosin, phentolamine, prazosin,and terazosin)• mixed alpha- and beta-adrenergic blockers (carvedilol and la-betalol)• norepinephrine depletors (guanadrel, guanethidine, and reser-pine—these are rarely used).
PharmacokineticsMost sympatholytic drugs are absorbed well from the GI tract, dis-tributed widely, metabolized in the liver, and excreted primarily inurine.
PharmacodynamicsAll sympatholytic drugs inhibit stimulation of the sympathetic ner-vous system, causing dilation of the peripheral blood vessels ordecreased cardiac output, thereby reducing blood pressure.
PharmacotherapeuticsIf blood pressure fails to come under control with beta-adrenergicblockers and diuretics, an alpha-adrenergic blocker, such as pra-zosin, or a mixed alpha- and beta-adrenergic blocker, such as la-betalol, may be used. If the patient fails to achieve the desiredblood pressure, the physician may add a drug from a differentclass, substitute a drug in the same class, or increase the drugdosage.
141ANTIHYPERTENSIVE DRUGS
938905.qxd 08/26/2008 15:22 Page 141

Drug interactionsSympatholytic drugs can create these drug interactions:• Carvedilol taken with antidiabetics may result in increased hy-poglycemic effect.• Carvedilol taken with calcium channel blockers may result in in-creased conduction disturbances.• Carvedilol taken with digoxin may result in increased digoxinlevels.• Carvedilol taken with rifampin decreases carvedilol levels.• Clonidine plus tricyclic antidepressants may increase bloodpressure.• Clonidine taken with CNS depressants may worsen CNS depres-sion.• Reserpine taken with diuretics or other hypotensive agents canincrease the hypotensive effects of reserpine.• Reserpine taken with cardiac glycosides can lead to cardiac ar-rthymias.
Sympatholytic drugs can also produce significant adverse reac-tions. (See Adverse reactions to sympatholytics.)
Vasodilating drugsThere are two types of vasodilating drugs—direct vasodilatorsand calcium channel blockers. Both types decrease systolic anddiastolic blood pressure.
142CARDIOVASCULAR DRUGS
Alpha-adrenergic blockers
• Hypotension
Central-acting drugs
• Depression• Drowsiness• Edema• Liver dysfunction• Numbness, tingling• Vertigo
Guanadrel
• Difficulty breathing• Excessive urination• Fainting• Orthostatic hypotension
Guanethidine
• Decreased heart contrac-tility• Diarrhea• Fluid retention• Orthostatic hypotension
Reserpine
• Abdominal cramps, diarrhea• Angina• Blurred vision• Bradycardia• Bronchoconstriction• Decreased libido• Depression• Drowsiness• Weight gain• Fatigue• Hypotension
Warning!
Adverse reactions to sympatholytics
938905.qxd 08/26/2008 15:22 Page 142

Resistance is futileDirect vasodilators act on arteries, veins, or both. They include:• diazoxide• hydralazine• minoxidil• nitroprusside.
Hydralazine and minoxidil are usually used to treat resistant orrefractory hypertension. Diazoxide and nitroprusside are reservedfor use in hypertensive crisis.
No admittanceCalcium channel blockers produce arteriolar relaxation by pre-venting the entry of calcium into the cells. This prevents the con-traction of vascular smooth muscle. (See “Calcium channel block-ers,” page 138.)
PharmacokineticsMost of these drugs are absorbed rapidly and well-distributed.They’re all metabolized in the liver, and most are excreted by thekidneys.
PharmacodynamicsThe direct vasodilators relax peripheral vascular smooth muscle,causing the blood vessels to dilate. The increased diameter of theblood vessels reduces total peripheral resistance, which lowersblood pressure.
PharmacotherapeuticsVasodilating drugs are rarely used alone to treat hypertension.They’re usually combined with other drugs to treat the patientwith moderate to severe hypertension (hypertensive crisis).
Calcium channel blockers are occasionally used alone to treatmild to moderate hypertension.
Drug interactions• The antihypertensive effects of hydralazine and minoxidil areincreased when they’re given with other antihypertensive drugs,such as methyldopa or reserpine.• Vasodilating drugs may produce additive effects when givenwith nitrates, such as isosorbide dinitrate or nitroglycerin.• Few other drug interactions occur with vasodilating drugs. (SeeAdverse reactions to direct vasodilators.)
143ANTIHYPERTENSIVE DRUGS
Adversereactionsto directvasodilators
Direct vasodilators com-monly produce adversereactions related to re-flex activation of thesympathetic nervoussystem. As blood pres-sure falls, the sympa-thetic nervous system isstimulated, producingcompensatory mea-sures, such as vasocon-striction and tachy-cardia.
Other reactions tosympathetic stimulationinclude:• palpitations• angina• edema• breast tenderness• fatigue• headache• rash• severe pericardial ef-fusion.
Warning!
938905.qxd 08/26/2008 15:22 Page 143

ACE inhibitorsACE inhibitors are typically used when beta-adrenergic blockersor diuretics are ineffective. Commonly prescribed ACE inhibitorsinclude:• benazepril• captopril• enalapril• enalaprilat• fosinopril• lisinopril• moexipril• quinapril• ramipril• trandolapril.
PharmacokineticsACE inhibitors are absorbed from the GI tract, distributed to mostbody tissues, metabolized somewhat in the liver, and excreted bythe kidneys. Ramipril is also excreted in stool. Enalaprilat is theonly ACE inhibitor that’s administered I.V.
PharmacodynamicsACE inhibitors reduce blood pressure by interrupting the renin-angiotensin-aldosterone system. Normally, the kidneys maintainblood pressure by releasing the hormone renin. Renin acts on theplasma protein angiotensinogen to form angiotensin I. Angio-tensin I is then converted to angiotensin II. Angiotensin II, a po-tent vasoconstrictor, increases peripheral resistance and pro-motes the excretion of aldosterone. Aldosterone, in turn, pro-motes the retention of sodium and water, increasing the volume ofblood the heart needs to pump.
Conversion diversionACE inhibitors prevent the conversion of angiotensin I to an-giotensin II. As angiotensin II is reduced, arterioles dilate, reduc-ing peripheral vascular resistance.
Less water, less workBy reducing aldosterone secretion, ACE inhibitors promote theexcretion of sodium and water, which reduces the amount ofblood the heart needs to pump, thereby lowering blood pressure.
144CARDIOVASCULAR DRUGS
Enalaprilat is theonly one I deal with.And that’s the way,
uh-huh, uh-huhI like it,
uh-huh, uh-huh!
938905.qxd 08/26/2008 15:22 Page 144

PharmacotherapeuticsACE inhibitors may be used alone or with another drug, such as athiazide diuretic, to treat hypertension. Certain ACE inhibitors—such as captopril, enalapril, fosinopril, lisinopril, quinapril,ramipril, and trandolapril—may also be used to treat patients withheart failure or following MI. Such situations include:• left ventricular systolic failure (unless contraindicated or intol-erant)• left ventricular systolic dysfunction without symptoms of heartfailure• reducing mortality following acute MI (especially in patientswith prior myocardial injury)• preventing or delaying the development of left ventricular dila-tion and overt heart failure in patients with left ventricular dys-function (recent or remote)• possible production of complementary effects (combined withbeta-blockade)• history of or present fluid retention (combined with diuretics).
Ramipril is also indicated to prevent major cardiovascularevents in patients with a history of vascular disease or diabetes.It’s also used to reduce overall cardiovascular risk, includingdeath, nonfatal MI, nonfatal stroke, and complications of diabetes.Captopril is also indicated for the long-term treatment of diabeticneuropathy.
Drug interactionsACE inhibitors can cause several different types of interactionswith other cardiovascular drugs. All ACE inhibitors enhance thehypotensive effects of diuretics and other antihypertensives suchas beta-adrenergic blockers. They can also increase serum lithiumlevels, possibly resulting in lithium toxicity.
When ACE inhibitors are used with potassium-sparing diuret-ics, potassium supplements, or potassium-containing salt substi-tutes, hyperkalemia may occur.
Individual itemsACE inhibitors interact with many other medications, prescriptionas well as over-the-counter (OTC). For example, patients takingACE inhibitors should avoid taking all NSAIDs. Besides decreas-ing the antihypertensive effect of ACE inhibitors, NSAIDs may al-ter renal function. Also, antacids may impair the absorption of fos-inopril, and quinapril may reduce the absorption of tetracycline.
A patient taking ACE inhibitors shouldn’t take prescriptions orOTC medications or herbal products without first consulting hisphysician. (See Adverse reactions to ACE inhibitors.)
145ANTIHYPERTENSIVE DRUGS
Adversereactions toACE inhibitors
Angiotensin-convertingenzyme (ACE) inhibitorscan produce these ad-verse reactions:• headache and fatigue• dry, nonproductive,persistent cough• angioedema• GI reactions• increased serumpotassium concentra-tions• tickling in the throat• transient elevations ofblood urea nitrogen andserum creatinine levels(indicators of kidneyfunction).
Caused by captopril
Captopril may causeprotein in the urine, re-duced neutrophils andgranulocytes (a type ofwhite blood cells), rash,loss of taste, hypoten-sion, or a severe allergicreaction.
Warning!
938905.qxd 08/26/2008 15:22 Page 145

Angiotensin II receptor blockersAngiotensin II receptor blockers (ARBs) lower blood pressure byblocking the vasoconstrictive effects of angiotensin II. Specificdrugs include:• candesartan cilexetil• eprosartan• irbesartan• losartan• olmesartan• telmisartan• valsartan.
PharmacokineticsARBs have varying pharmacokinetic properties and all are highlybound to plasma proteins.
PharmacodynamicsARBs act by interfering with the renin-angiotensin-aldosteronesystem. Specifically, these drugs block the binding of angiotensinII to the AT1 receptor. This prevents angiotensin II from exertingits vasoconstricting properties and from promoting the excretionof aldosterone. Both of these actions result in lowered blood pres-sure.
ARBs don’t inhibit the conversion of angiotensin I to an-giotensin II, nor do they cause a breakdown in bradykinin (a va-sodilator).
PharmacotherapeuticsARBs may be used alone or in combination with other drugs suchas a diuretic. Valsartan may also be used as an alternative to anACE inhibitor or for the management of heart failure. Becauseirbesartan and losartan protect the renal system, they’re often pre-scribed for patients with type 2 diabetes. Losartan is also used toreduce the risk of stroke in high-risk patients with hypertensionand left ventricular hypertrophy. (See Adverse reactions to ARBs.)
Drug interactionsARBs can interact with other drugs in various ways.• When losartan is taken with fluconazole, an increased blood lev-el of losartan may result, leading to hypotension.• NSAIDs reduce the antihypertensive effects of ARBs.• Rifampin may increase metabolism of losartan and decrease itsantihypertensive effect.
146CARDIOVASCULAR DRUGS
Adversereactionsto ARBs
Adverse reactions toangiotensin II receptorblockers (ARBs) include:• headache and fatigue• cough and tickling inthe throat• angioedema• GI reactions• increased serumpotassium level• transient elevations ofblood urea nitrogen andserum creatinine levels.
Warning!
938905.qxd 08/26/2008 15:22 Page 146

• Candesartan may increase blood levels of lithium, leading tolithium toxicity.• When digoxin is taken with telmisartan, an increased blood lev-el of digoxin may occur, possibly leading to digoxin toxicity.• Potassium supplements may increase the risk of hyperkalemiawhen used with ARBs.
Antilipemic drugsAntilipemic drugs are used to lower abnormally high blood levelsof lipids, such as cholesterol, triglycerides, and phospholipids.The risk of developing CAD increases when serum lipid levels areelevated. Drugs are used in combination with lifestyle changes(such as proper diet, weight loss, and exercise) and treatment ofan underlying disorder causing the lipid abnormality to help lowerlipid levels.
The classes of antilipemic drugs include:• bile-sequestering drugs• fibric acid derivatives• 3-hydroxy-3-methylglutaryl coenzyme A (HMG-CoA) reductaseinhibitors• nicotinic acid• cholesterol absorption inhibitors.
Bile-sequestering drugsThe bile-sequestering drugs are cholestyramine, colestipol, andcolesevelam. These drugs are resins that remove excess bile acidsfrom the fat deposits under the skin.
PharmacokineticsBile-sequestering drugs aren’t absorbed from the GI tract. Instead,they remain in the intestine, where they combine with bile acidsfor about 5 hours. Eventually, they’re excreted in stool.
PharmacodynamicsThe bile-sequestering drugs lower blood levels of low-densitylipoproteins (LDLs). These drugs combine with bile acids in theintestines to form an insoluble compound that’s then excreted instool. The decreasing level of bile acid in the gallbladder triggersthe liver to synthesize more bile acids from their precursor, cho-lesterol.
147ANTILIPEMIC DRUGS
938905.qxd 08/26/2008 15:22 Page 147

Getting out of storageAs cholesterol leaves the bloodstream and other storage areas toreplace the lost bile acids, blood cholesterol levels decrease. Be-cause the small intestine needs bile acids to emulsify lipids andform chylomicrons, absorption of all lipids and lipid-soluble drugsdecreases until the bile acids are replaced.
PharmacotherapeuticsBile-sequestering drugs are the drugs of choice for treating typeIIa hyperlipoproteinemia (familial hypercholesterolemia) whenthe patient can’t lower his LDL levels through diet alone. Patientswhose blood cholesterol levels place them at a severe risk of CADwill most likely require one of these drugs in addition to dietarychanges.
Drug interactionsBile-sequestering drugs produce the following drug interactions:• They may bind with acidic drugs in the GI tract, decreasing theirabsorption and effectiveness. Acidic drugs likely to be affected in-clude barbiturates, phenytoin, penicillins, cephalosporins, thyroidhormones, thyroid derivatives, and digoxin.• Bile-sequestering drugs may decrease absorption of propra-nolol, tetracycline, furosemide, penicillin G, hydrochlorothiazideand gemfibrozil.• Bile-sequestering drugs may reduce absorption of lipid-solublevitamins, such as vitamins A, D, E, and K. Poor absorption of vita-min K can affect prothrombin times significantly, increasing therisk of bleeding. (See Adverse reactions to bile-sequesteringdrugs.)
Fibric acid derivativesFibric acid is produced by several fungi. Two derivatives of thisacid are fenofibrate and gemfibrozil. These drugs are used to re-duce high triglyceride levels and, to a lesser extent, high LDL lev-els.
PharmacokineticsFenofibrate and gemfibrozil are absorbed readily from theGI tract and are highly protein-bound. Fenofibrate is hy-drolyzed while gemfibrozil undergoes extensive metabo-lism in the liver. Both drugs are excreted in the urine.
148CARDIOVASCULAR DRUGS
Adversereactionsto bile-sequesteringdrugs
Short-term adverse re-actions to these drugsare relatively mild. Moresevere reactions can re-sult from long-term use.Adverse GI effects withlong-term therapy in-clude severe fecal im-paction, vomiting, diar-rhea, and hemorrhoid ir-ritation.
Rarely, peptic ulcersand bleeding, gallstones,and inflammation of thegallbladder may occur.
Warning!
Slow us down?Never! Just don’t
give us bile-sequestering
drugs!
938905.qxd 08/26/2008 15:22 Page 148

PharmacodynamicsAlthough the exact mechanism of action for these drugs isn’tknown, researchers believe that fibric acid derivatives may:• reduce cholesterol production early in its formation• mobilize cholesterol from the tissues• increase cholesterol excretion• decrease synthesis and secretion of lipoproteins• decrease synthesis of triglycerides.
Power in the bloodGemfibrozil produces two other effects:• It increases high-density lipoprotein (HDL) levels in the blood(remember, this is “good” cholesterol).• It increases the serum’s capacity to dissolve additional choles-terol.
PharmacotherapeuticsFibric acid drugs are used primarily to reduce triglyceride levels,especially very-low-density triglycerides, and secondarily to re-duce blood cholesterol levels. They’re typically used to treat pa-tients with types II, III, IV, and mild type V hyperlipoproteinemia.
Drug interactions• Fibric acid drugs may displace acidic drugs, such as barbitu-rates, phenytoin, thyroid derivatives, and cardiac glycosides.• The risk of bleeding increases when fibric acid derivatives aretaken with oral anticoagulants.• Fibric acid derivatives can lead to adverse GI effects.• The hypoglycemic effects of repaglinide may be increased andprolonged if taken with gemfibrozil.• Use of fibric acid derivatives and HMG-CoA reductase inhibitorsmay increase the risk of rhabdomyolysis.
HMG-CoA reductase inhibitorsHMG-CoA reductase inhibitors (also known as the statins) lowerlipid levels by interfering with cholesterol synthesis. These drugsinclude atorvastatin, fluvastatin, lovastatin, pravastatin, rosuvas-tatin, and simvastatin.
149ANTILIPEMIC DRUGS
Ah-ha! So,gemfibrozil not only
reduces triglyceridesbut also increases
high-densitylipoprotein levels andthe blood’s ability todissolve cholesterol.
938905.qxd 08/26/2008 15:22 Page 149

PharmacokineticsEach drug has slightly different pharmacokinetic properties. Withthe exception of pravastatin, all are highly bound to plasma pro-teins and undergo extensive first-pass metabolism. However, plas-ma levels don’t correlate with the drugs’ abilities to lower choles-terol.
PharmacodynamicsHMG-CoA reductase inhibitors inhibit the enzyme responsible forthe conversion of HMG-CoA to mevalonate, an early step in thesynthesis of cholesterol.
PharmacotherapeuticsStatins are used primarily to reduce LDL cholesterol and totalblood cholesterol levels. These agents also produce a mild in-crease in HDL cholesterol levels.
Statins are used to treat primary hypercholesterolemia (typesIIa and IIb). Because of their effect on LDL and total cholesterol,these drugs are also used to reduce the risk of CAD and to preventMI or stroke in patients with high cholesterol levels.
Drug interactions• Taking a statin drug with amiodarone, clarithromycin, cy-closporine, erythromycin, fluconazole, gemfibrozil, itraconazole,ketoconazole, or niacin increases the risk of myopathy or rhab-domyolysis (a potentially fatal breakdown of skeletal muscle,causing renal failure).• Lovastatin, rosuvastatin and simvastatin may increase the riskof bleeding when administered with warfarin.• All of these drugs should be administered 1 hour before or4 hours after the administration of bile-sequestering drugs(cholestyramine, colesevelam, and colestipol). (See Adverse reac-tions to HMG-CoA reductase inhibitors.)
Nicotinic acidAlso known as niacin, nicotinic acid is a water-soluble vitaminthat decreases cholesterol, triglyceride, and apolipoprotein B-100levels and increases the HDL level. The drug is available inimmediate-release and extended-release tablets.
150CARDIOVASCULAR DRUGS
Adversereactions toHMG-CoAreductaseinhibitors
HMG-CoA reductase in-hibitors may alter liverfunction studies, in-creasing aspartateaminotransferase, ala-nine aminotransferase,alkaline phosphatase,and bilirubin levels. Oth-er hepatic effects mayinclude pancreatitis,hepatitis, and cirrhosis.
Myalgia is the mostcommon musculoskele-tal effect, althougharthralgia and musclecramps may also occur.Myopathy and rhab-domyolysis are rare, butpotentially severe, reac-tions that may occurwith these drugs.
Possible adverse GIreactions include nau-sea, vomiting, diarrhea,abdominal pain, flatu-lence, and constipation.
Warning!
938905.qxd 08/26/2008 15:22 Page 150

PharmacokineticsNicotinic acid is rapidly and extensively absorbed following oraladministration. It’s moderately bound to plasma proteins; its over-all binding ranges from 60% to 70%. The drug undergoes rapid me-tabolism by the liver to active and inactive metabolites. About 75%of the drug is excreted in urine.
PharmacodynamicsThe mechanism of action by which nicotinic acid lowers triglyc-eride and apolipoprotein levels is unknown. However, it may workby inhibiting hepatic synthesis of lipoproteins that containapolipoprotein B-100, promoting lipoprotein lipase activity, reduc-ing free fatty acid mobilization from adipose tissue, and increasingfecal elimination of sterols.
PharmacotherapeuticsNicotinic acid is usually used in combination with other drugs tolower triglyceride levels in patients with type IV or V hyperlipi-demia who are at high risk for pancreatitis and to lower choles-terol and LDL levels in patients with hypercholesterolemia. It mayalso be used with other antilipemics to boost HDL levels.
Nicotinic acid is contraindicated in patients who are hypersen-sitive to nicotinic acid and in those with hepatic dysfunction, ac-tive peptic ulcer disease, or arterial bleeding.
Drug interactions• Together, nicotinic acid and an HMG-CoA reductase inhibitormay increase the risk of myopathy or rhabdomyolysis.• Bile-sequestering drugs (cholestyramine, colesevelam, andcolestipol) can bind with nicotinic acid and decrease its effective-ness.• When given with nicotinic acid, kava may increase the risk ofhepatotoxicity. (See Adverse reactions to nicotinic acid.)
151ANTILIPEMIC DRUGS
Adversereactions tonicotinic acid
High doses of nicotinicacid may produce va-sodilation and causeflushing. Extended-release forms tend toproduce less severevasodilation thanimmediate-releaseforms do. To help mini-mize flushing, administeraspirin 30 minutes be-fore nicotinic acid, orgive the extended-release form at night.
Nicotinic acid cancause hepatotoxicity;the risk of this adversereaction is greater withextended-release forms.
Other adverse reac-tions include nausea,vomiting, diarrhea, andepigastric or substernalpain.
Warning!
938905.qxd 08/26/2008 15:22 Page 151

Cholesterol absorption inhibitorsAs the name implies, cholesterol absorption inhibitors inhibit theabsorption of cholesterol and related phytosterols from the intes-tine. Ezetimibe is the drug in this class.
PharmacokineticsEzetimibe is rapidly and extensively absorbed following oral ad-ministration. It’s is readily absorbed and is highly bound to plasmaproteins. It’s primarily metabolized in the small intestine and ex-creted by the liver and kidneys.
PharmacodynamicsEzetimibe reduces blood cholesterol levels by inhibiting the ab-sorption of cholesterol by the small intestine. This leads to a de-crease in delivery of intestinal cholesterol to the liver, reducinghepatic cholesterol stores and increasing clearance from theblood.
PharmacotherapeuticsEzetimibe may be administered alone or with dietary changes totreat primary hypercholesterolemia and homozygous sitos-terolemia (hereditary hyperabsorption of cholesterol and plantsterols). The drug is also used in combination with HMG-CoA re-ductase inhibitors to treat primary hypercholesterolemia and ho-mozygous familial hypercholesterolemia.
Ezetimibe may also help lower total cholesterol and LDL cho-lesterol, and increase HDL cholesterol, when maximum-doseHMG-CoA reductase inhibitor therapy has been ineffective.
Drug interactions• Ezetimibe administered with cholestyramine may lead to de-creased effectiveness of ezetimibe.• Ezetimibe administered with cyclosporine, fenofibrate, or gem-fibrozil leads to increased levels of ezetimibe. (See Adverse reac-tions to cholesterol absorption inhibitors.)
152CARDIOVASCULAR DRUGS
Adversereactions tocholesterolabsorptioninhibitors
The most common ad-verse reactions include:• fatigue• abdominal pain and di-arrhea• pharyngitis and sinu-sitis• arthralgia• back pain• cough.
When these drugsare given with an HMG-CoA reductase inhibitor,the most common ad-verse reactions arechest pain, dizziness,headache, abdominalpain, diarrhea, pharyngi-tis, sinusitis, upper respi-ratory tract infection,arthralgia, back pain,and myalgia.
Warning!
938905.qxd 08/26/2008 15:22 Page 152

Quick quiz
1. Treatment with fenofibrate, a type of fibric acid derivative,would have to proceed cautiously if the patient is also receivingwhich drug?
A. PenicillinB. Thiazide diureticC. DigoxinD. Oral anticoagulant
Answer: D. Fibric acid derivatives cause an increased risk ofbleeding when given with an oral anticoagulant.
2. A patient is taking lovastatin, an HMG-CoA reductase in-hibitor. Which parameter should the patient monitor periodically?
A. Liver function test resultsB. Electrolyte levelsC. Vision testingD. Coagulation studies
Answer: A. Because increased liver enzyme levels may occur inpatients receiving long-term lovastatin therapy, liver function testresults should be monitored.
3. A patient diagnosed with hypertension is most likely to beprescribed which class of drugs first?
A. Angiotensin II receptor blockerB. Beta-adrenergic blockerC. Calcium channel blockerD. Angiotensin-converting enzyme inhibitor
Answer: C. Calcium channel blockers are typically the first treat-ment for hypertension.
4. Nitrates are the drug of choice for relieving acute angina. Ni-trates work by:
A. promoting vasodilation, reducing preload, and increas-ing afterload.
B. promoting vasodilation, reducing preload, and reducingafterload.
C. promoting vasodilation, increasing preload, and in-creasing afterload.
D. promoting vasodilation, increasing preload, and reduc-ing afterload.
Answer: B. Nitrates cause smooth muscle of the veins and arter-ies to relax and dilate. When veins dilate, less blood returns to theheart, thus reducing preload. Dilation of arterioles decreases re-sistance, thus decreasing afterload.
153QUICK QUIZ
938905.qxd 08/26/2008 15:22 Page 153

ScoringIf you answered all four items correctly, A+! You’re aces with ACE
inhibitors!If you answered three items correctly, cool! Cardiovascular drugs
aren’t giving you complications.If you answered fewer than three items correctly, stay mellow.
This is a complex chapter, and it might just take another go.
154CARDIOVASCULAR DRUGS
✰✰✰
✰✰
✰
Gimme five!Well, we made it this far.Now on to hematologic
drugs.
938905.qxd 08/26/2008 15:22 Page 154

Drugs and the hematologic systemThe hematologic system includes plasma (the liquid component ofblood) and blood cells, such as red blood cells (RBCs), whiteblood cells, and platelets. Types of drugs used to treat disorders ofthe hematologic system include:• hematinic• anticoagulant• thrombolytic.
Hematinic drugsHematinic drugs provide essential building blocks for RBC pro-duction. They do so by increasing hemoglobin, the necessaryelement for oxygen transportation.
Iron, vitamin B12, folic acidThis section discusses hematinic drugs used to treat micro-cytic and macrocytic anemia—iron, vitamin B12, and folicacid.
It also describes the use of erythropoietin agents to treatnormocytic anemia.
6
Hematologic drugs
Just the facts
In this chapter, you’ll learn:
♦ classes of drugs used to treat hematologic disorders
♦ uses and varying actions of these drugs
♦ how these drugs are absorbed, distributed, metabolized,and excreted
♦ drug interactions and adverse reactions to these drugs.
Need someRBCs built?
Turn tohematinic
drugs.
938906.qxd 08/26/2008 15:32 Page 155

IronIron preparations are used to treat the most common form of ane-mia—iron deficiency anemia. Iron preparations discussed in thissection include ferrous fumarate, ferrous gluconate, ferrous sul-fate, iron dextran, and sodium ferric gluconate complex.
Pharmacokinetics (how drugs circulate)Iron is absorbed primarily from the duodenum and upper jejunumof the intestine. Different iron formulations don’t vary in absorp-tion, but they do vary in the amount of elemental iron supplied.
Low iron increases absorptionThe amount of iron absorbed depends partially on the body’sstores of iron. When body stores are low or RBC production is ac-celerated, iron absorption may increase by 20% to 30%. On the oth-er hand, when total iron stores are large, the body absorbs onlyabout 5% to 10% of the iron available.
Enteric-coated preparations decrease iron absorption because,in that form, iron isn’t released until after it leaves the duodenum.The lymphatic system absorbs the parenteral form after I.M. injec-tions.
Hemoglobin has itIron is transported by the blood and bound to transferrin, its carri-er plasma protein. About 30% of the iron is stored primarily as he-mosiderin or ferritin in the reticuloendothelial cells of the liver,spleen, and bone marrow. About 66% of the total body iron iscontained in hemoglobin. Excess iron is excreted in urine, stool,sweat, and through intestinal cell-sloughing. It appears in breastmilk and crosses the placenta.
Pharmacodynamics (how drugs act)Although iron has other roles, its most important role is the pro-duction of hemoglobin. About 80% of iron in the plasma goes tothe bone marrow, where it’s used for erythropoiesis (productionof RBCs).
Pharmacotherapeutics (how drugs are used)Oral iron therapy is the preferred route for preventing or treatingiron deficiency anemia. It’s used to prevent anemias in childrenages 6 months to 2 years because this is a period of rapid growthand development. Pregnant women may need iron supplements toreplace the iron used by the developing fetus.
156HEMATOLOGIC DRUGS
It takes about6 months for
iron therapy tocorrect irondeficiencyanemia.
938906.qxd 08/26/2008 15:32 Page 156

Ironclad optionsParenteral iron therapy is used for patients who can’t absorb oralpreparations, aren’t compliant with oral therapy, or have boweldisorders (such as ulcerative colitis or Crohn’s disease). Patientswith end-stage renal disease who are receiving hemodialysis mayalso receive parenteral iron therapy at the end of their dialysis ses-sion. While parenteral iron therapy corrects the iron store defi-ciency quickly, it doesn’t correct the anemia any faster than oralpreparations would.
Iron preparations available for parenteral administration areiron dextran (given by I.M. injection or slow, continuous I.V. infu-sion) and iron sucrose. Iron sucrose is used for patients on he-modialysis. (See Testing for parenteral iron sen-sitivity.)
Drug interactionsIron absorption is reduced by antacids as wellas by such foods as coffee, tea, eggs, and milk.Other drug interactions involving iron include:• Absorption of tetracyclines (demeclocy-cline, doxycycline, minocycline, oxytetracy-cline, and tetracycline), methyldopa,quinolones (ciprofloxacin, levofloxacin, lome-floxacin, moxifloxacin, norfloxacin, ofloxacin,and sparfloxacin), levothyroxine, and penicil-lamine may be reduced when taken with oraliron preparations.• Cholestyramine, cimetidine, proton-pumpinhibitors, and colestipol may reduce iron ab-sorption in the GI tract. (See Adverse reac-tions to iron therapy.)
157HEMATINIC DRUGS
The most common adverse reactions to iron therapy are gastric irritation and constipation. Ironpreparations also darken stool, and liquid preparations can stain the teeth.
The most serious reaction is anaphylaxis, which may occur after administration of parenteraliron. To guard against such a reaction, administer an initial test dose before giving a full-dose in-fusion.
Warning!
Adverse reactions to iron therapy Testing forparenteral ironsensitivity
Parenteral iron cancause acute hypersensi-tivity reactions, includ-ing anaphylaxis, dysp-nea, urticaria, otherrashes, pruritus, arthral-gia, myalgia, fever,sweating, and allergicpurpura. To test for drugsensitivity and preventserious reactions, al-ways give a test dose ofiron dextran before be-ginning therapy.
Carefully assess thepatient’s response to thetest dose. If no adversereactions occur within 1hour, give the total dose.If adverse reactions oc-cur, notify the prescriberimmediately. To treatanaphylaxis, keep epi-nephrine and standardemergency equipmentreadily available.
Safe andsound
Ironabsorption
was reduced?Oops. Sorryabout that.
938906.qxd 08/26/2008 15:32 Page 157

Vitamin B12Vitamin B12 preparations are used to treat pernicious anemia.Common vitamin B12 preparations include cyanocobalamin andhydroxocobalamin.
PharmacokineticsVitamin B12 is available in parenteral, oral, and intranasal forms.For the body to absorb oral forms of vitamin B12, the gastric mu-cosa must secrete a substance called intrinsic factor. People whohave a deficiency of intrinsic factor develop a special type of ane-mia known as vitamin B12-deficiency pernicious anemia.
Parenteral possibilitiesWhen cyanocobalamin is injected by the I.M. or subcutaneous(subQ) route, it’s absorbed and bound to transcobalamin II fortransport to the tissues. It then travels via the bloodstream to theliver, where 90% of the body’s supply of vitamin B12 is stored.
Although hydroxocobalamin is absorbed more slowly from theinjection site, its uptake in the liver may be greater than that ofcyanocobalamin. Hydroxocobalamin is only administered I.M.
Most gets lostWith either drug, the liver slowly releases vitamin B12 as neededby the body. About 3 to 8 mcg of vitamin B12 are excreted in bileeach day and then reabsorbed in the ileum. It’s also secreted inbreast milk during lactation.
Within 48 hours after a vitamin B12 injection, 50% to 95% of thedose is excreted unchanged in urine.
PharmacodynamicsWhen vitamin B12 is administered, it replaces vitamin B12 that thebody would normally absorb from the diet. This vitamin is essen-tial for cell growth and replication and for the maintenance ofmyelin (nerve coverings) throughout the nervous system. VitaminB12 may also be involved in lipid and carbohydrate metabolism.
PharmacotherapeuticsCyanocobalamin and hydroxocobalamin are used to treat perni-cious anemia, a megaloblastic anemia characterized by decreasedgastric production of hydrochloric acid and intrinsic factor defi-ciency. Intrinsic factor, a substance normally secreted by the pari-etal cells of the gastric mucosa, is essential for vitamin B12 absorp-tion. Intrinsic factor deficiencies are common in patients whohave had total or partial gastrectomies or total ileal resection.
158HEMATOLOGIC DRUGS
Some patientslack a crucial
“intrinsic factor”that allowsvitamin B12absorption.
938906.qxd 08/26/2008 15:32 Page 158

Oral vitamin B12 preparations are used to supplement nutri-tional deficiencies of the vitamin. The parenteral and intranasalformulations are used to treat patients with pernicious anemia.
Drug interactionsAlcohol, aspirin, neomycin, chloramphenicol, and colchicine maydecrease the absorption of oral cyanocobalamin. (See Adverse re-actions to vitamin B12 therapy.)
Folic acidFolic acid is given to treat megaloblastic anemia due to folic aciddeficiency. This type of anemia usually occurs in patients whohave tropical or nontropical sprue, although it can also result frompoor nutritional intake during pregnancy, infancy, or childhood.
PharmacokineticsFolic acid is absorbed rapidly in the first third of the small intes-tine, distributed into all body tissues, and metabolized in the liver.Excess folate is excreted unchanged in urine, and small amountsof folic acid are excreted in stool. Folic acid also appears in breastmilk. Synthetic folic acid is readily absorbed, even in malabsorp-tion syndromes.
159HEMATINIC DRUGS
No dose-related adverse reactions occur with vitamin B12 therapy.However, some rare reactions may occur when vitamin B12 is adminis-tered parenterally.
Parenteral problems
Adverse reactions to parenteral administration can include hypersensi-tivity reactions that could result in anaphylaxis and death, pulmonaryedema, heart failure, peripheral vascular thrombosis, polycythemiavera, hypokalemia, itching, transient rash, hives, and mild diarrhea.
Warning!
Adverse reactions to vitamin B12therapy
938906.qxd 08/26/2008 15:32 Page 159

PharmacodynamicsFolic acid is an essential component for normal RBC productionand growth. A deficiency in folic acid results in megaloblastic ane-mia and low serum and RBC folate levels.
PharmacotherapeuticsFolic acid is used to treat folic acid deficiency. Patients who arepregnant or undergoing treatment for liver disease, hemolytic ane-mia, alcohol abuse, or skin or renal disorders typically need folicacid supplementation. Serum folic acid levels below 5 ng/ml indi-cate folic acid deficiency.
Leucovorin is a folic acid derivative used to treat folic acid de-ficiencies resulting from administration of methotrexate.
Drug interactions• Methotrexate, sulfasalazine, hormonal contraceptives, aspirin,triamterene, pentamidine, and trimethoprim reduce the effective-ness of folic acid.• In large doses, folic acid may counteract the effects of anticon-vulsants, such as phenytoin, potentially leading toseizures. (See Adverse reactions to folic acid.)
Erythropoietin agentsEpoetin alfa and darbepoetin alfa are glycopro-teins that stimulate RBC production (erythro-poiesis).
PharmacokineticsEpoetin alfa and darbepoetin alfa may be given subQ or I.V.After subQ administration, serum levels of epoetin alfa peakin 5 to 24 hours, while serum levels of darbepoetin alfa peakin 24 to 72 hours.
The circulating half-life of epoetin alfa is also shorter at 4to 13 hours, compared to 49 hours for darbepoetin alfa. Thetherapeutic effect of these agents lasts for several days after ad-ministration.
PharmacodynamicsEpoetin alfa and darbepoetin alfa boost the production of erythro-poietin, thus stimulating RBC production in bone marrow. Nor-mally, erythropoietin is formed in the kidneys in response to hy-poxia (reduced oxygen) and anemia.
160HEMATOLOGIC DRUGS
Adversereactions tofolic acid
Adverse reactions tofolic acid include:• erythema• itching• rash• anorexia and nausea• altered sleep patterns• difficulty concentrating• irritability• hyperactivity.
Warning!
It takes a lot tomake an RBC! Folic
acid, iron, vitamin B12,amino acids, copper,
and cobalt are allnecessary
components…
...Andhematinic
drugs usuallyreplace one ofthese missing
parts.
938906.qxd 08/26/2008 15:32 Page 160

Patients with conditions that decrease production of erythro-poietin typically develop normocytic anemia. This anemia canusually be corrected after 5 to 6 weeks of treatment with an ery-thropoietin agent.
PharmacotherapeuticsEpoetin alfa is used to:• treat patients with anemia associated with chronic renal failure• treat anemia associated with zidovudine therapy in patientswith human immunodeficiency virus infection• treat anemia in cancer patients receiving chemotherapy• reduce the need for allogenic blood transfusions in surgical pa-tients.
Darbepoetin alfa is used to treat anemia associated withchronic renal failure.
Drug interactionsNo known drug interactions exist with either drug, although theycan cause some adverse reactions. (See Adverse reactions to ery-thropoietin agents.)
Anticoagulant drugsAnticoagulant drugs are used to reduce the ability of the blood toclot. Major categories of anticoagulants include:• heparin and its derivatives• oral anticoagulants• antiplatelet drugs• direct thrombin inhibitors• factor Xa inhibitor drugs.
HeparinHeparin, prepared commercially from animal tissue, is an anti-thrombolytic agent used to treat and prevent clot formation. Be-cause it doesn’t affect the synthesis of clotting factors, heparincan’t dissolve already-formed clots.
Weighty wordsThe two types of heparin are unfractionated heparin (UFH) andlow-molecular-weight heparin (LMWH). LMWHs, such as dal-teparin, enoxaparin, and tinzaparin, were developed to prevent
161ANTICOAGULANT DRUGS
Heparin preventsclots from forming
but doesn’t dissolveexisting clots.
Adversereactions toerythropoietinagents
Hypertension is the mostcommon adverse reac-tion. Other adverse re-actions may include:• headache• joint pain• nausea• edema• fatigue• diarrhea• vomiting• chest pain• skin reactions at theinjection site• weakness• dizziness.
Warning!
938906.qxd 08/26/2008 15:32 Page 161

deep vein thrombosis (DVT) (a blood clot in the deep veins, usual-ly of the legs) in surgical patients.
PharmacokineticsBecause heparin isn’t absorbed well from the GI tract, it must beadministered parenterally. UFH is administered I.V. by continuousinfusion or by subQ injection. LMWHs, because of their prolongedcirculating half-life, can be administered once or twice daily bysubQ injection.
After I.V. administration, the distribution of heparin is immedi-ate; however, distribution isn’t as predictable following subQ in-jection.
I.M. is outHeparin isn’t given I.M. because of the risk of localized bleeding.Heparin is metabolized in the liver, and its metabolites are excret-ed in urine.
PharmacodynamicsHeparin prevents the formation of new thrombi.Here’s how it works:• Heparin inhibits the formation of thrombin andfibrin by activating antithrombin III.• Antithrombin III then inactivates factors IXa, Xa,XIa, and XIIa in the intrinsic and common pathways.The end result is prevention of a stable fibrin clot.• In low doses, heparin increases the activity of an-tithrombin III against factor Xa and thrombin and in-hibits clot formation.• Much larger doses are necessary to inhibit fibrinformation after a clot has been formed. This relationship betweendose and effect is the rationale for using low-dose heparin to pre-vent clotting.• Whole blood clotting time, thrombin time, and partial thrombo-plastin time (PTT) are prolonged during heparin therapy. Howev-er, these times may be only slightly prolonged with low or ultra-low preventive doses.
PharmacotherapeuticsHeparin may be used in a number of clinical situations to preventthe formation of new clots or the extension of existing clots.These situations include:• preventing or treating venous thromboemboli, characterized byinappropriate or excessive intravascular activation of blood clot-ting
162HEMATOLOGIC DRUGS
LMWHs helpprevent DVT in
surgicalpatients.
938906.qxd 08/26/2008 15:32 Page 162

• treating disseminated intravascular coagulation, a complicationof other diseases, resulting in accelerated clotting• treating arterial clotting and preventing embolus formation inpatients with atrial fibrillation, an arrhythmia in which ineffectiveatrial contractions cause blood to pool in the atria, increasing therisk of clot formation• preventing thrombus formation and promoting cardiac circula-tion in an acute myocardial infarction (MI) by preventing furtherclot formation at the site of the already formed clot.
Circulate freelyHeparin can be used to prevent clotting whenever the patient’sblood must circulate outside the body through a machine, such asthe cardiopulmonary bypass machine or hemodialysis machine,and during blood transfusions. (See Monitoring PTT in heparintherapy.)
You’re the oneHeparin is also useful for preventing clotting during intra-abdominal or orthopedic surgery. (These types of surgeries, inmany cases, activate the coagulation mechanisms excessively.) Infact, heparin is the drug of choice for orthopedic surgery.
163ANTICOAGULANT DRUGS
A patient receiving unfractionated heparin (UFH) therapy requires closemonitoring of his partial thromboplastin time (PTT). Dosage adjust-ments, based on the test results, are typically necessary to ensure ther-apeutic effectiveness without increased risk of bleeding.
Low-molecular-weight heparin (LMWH) therapy doesn’t require PTTmonitoring. Currently, no laboratory test exists to assess the effective-ness of LMWH therapy.
Heparin-induced thrombocytopenia
Platelet counts should be monitored in all patients receiving heparintherapy. A patient who develops heparin-induced thrombocytopenia(HIT) should be switched from anticoagulant therapy to argatroban, bi-valirudin, or lepirudin. These drugs are direct thrombin inhibitors indi-cated for use in the patient who needs anticoagulation therapy but hasHIT.
Safe and sound
Monitoring PTT in heparin therapy
938906.qxd 08/26/2008 15:32 Page 163

Drug interactions• Because heparin acts synergistically with all oral anticoagu-lants, the risk of bleeding increases when the patient takes bothdrugs together. The prothrombin time and International Normal-ized Ratio (INR), used to monitor the effects of oral anticoagu-lants, may also be prolonged.• The risk of bleeding increases when the patient takes nons-teroidal anti-inflammatory drugs (NSAIDs), iron dextran, cilosta-zol, or an antiplatelet drug, such as aspirin, clopidogrel, ticlopi-dine, or dipyridamole, while receiving heparin.
Another reason to quit• Drugs that antagonize or inactivate heparin include antihista-mines, cephalosporins, digoxin, neomycin, nicotine, nitroglycerin,penicillins, phenothiazines, quinidine, and tetracycline.• Nicotine may inactivate heparin; nitroglycerin may inhibit theeffects of heparin.• Administration of protamine sulfate and fresh frozen plasmacounteract the effects of heparin. (See Adverse reactions to he-parin.)
Oral anticoagulantsThe major oral anticoagulant used in the United States is thecoumarin compound warfarin.
164HEMATOLOGIC DRUGS
One advantage of heparin is that it produces relatively few adverse re-actions. Even so, these reactions can usually be prevented if the pa-tient’s partial thromboplastin time is maintained within the therapeuticrange.
Bleeding, the most common adverse reaction, can be reversed easi-ly by administering protamine sulfate, which binds to heparin to form astable salt.
Other adverse reactions include bruising, hematoma formation,necrosis of skin or other tissue, and thrombocytopenia.
Warning!
Adverse reactions to heparin
Heparin increasesthe effects of oral
anticoagulants. If apatient is also takingwarfarin, watch out
for bleeding.
938906.qxd 08/26/2008 15:32 Page 164

PharmacokineticsWarfarin is absorbed rapidly and almost completely when it’s tak-en orally. It binds extensively to plasma albumin and is metabo-lized in the liver and excreted in urine. Although warfarin is ab-sorbed quickly, its effects don’t occur for about 48 hours, with thefull effect taking 3 to 4 days.
Because warfarin is highly plasma-protein-bound and is metab-olized by the liver, administration of warfarin with other medica-tions may alter the amount of warfarin in the body. This may in-crease the risk of bleeding or clotting, depending upon the med-ications administered.
PharmacodynamicsOral anticoagulants alter the ability of the liver to synthesize vita-min K–dependent clotting factors, including prothrombin and fac-tors VII, IX, and X. However, clotting factors already in the blood-stream continue to coagulate blood until they become depleted,so anticoagulation doesn’t begin immediately. (See Monitoringwarfarin levels.)
PharmacotherapeuticsOral anticoagulants are prescribed to treat or prevent thromboem-bolism. Patients with this disorder begin taking the medicationwhile still receiving heparin. However, outpatients at high risk forthromboembolism may begin oral anticoagulants without first re-ceiving heparin.
Deep in the veinsOral anticoagulants are also the drugs of choice to prevent DVTand for patients with prosthetic heart valves or diseased mitralvalves. To decrease the risk of arterial clotting, oral anticoagulantsare sometimes combined with an antiplatelet drug, such as as-pirin, clopidogrel, or dipyridamole.
Drug interactionsMany patients who take oral anticoagulants also receive otherdrugs, placing them at risk for serious drug interactions.• Many drugs, such as highly protein-bound medications, increasethe effects of warfarin, resulting in an increased risk of bleeding.Examples include acetaminophen, allopurinol, amiodarone,cephalosporins, cimetidine, ciprofloxacin, clofibrate, danazol, dia-zoxide, disulfiram, erythromycin, fluoroquinolones, glucagon, he-parin, ibuprofen, isoniazid, ketoprofen, methylthiouracil, metron-idazole, miconazole, neomycin, propafenone, propylthiouracil,
165ANTICOAGULANT DRUGS
Although oralanticoagulants areabsorbed quickly, itcan take a couple of
days for their fulleffect to occur.
Monitoringwarfarin levels
Patients taking warfarinneed close monitoring ofprothrombin time and In-ternational NormalizedRatios to make sure theyare maintaining thera-peutic levels of the drug.If laboratory results falloutside the acceptedrange, warfarin dosageshould be adjusted.
938906.qxd 08/26/2008 15:32 Page 165

quinidine, streptokinase, sulfonamides, tamoxifen, tetracyclines,thiazides, thyroid drugs, tricyclic antidepressants, urokinase, andvitamin E.• Drugs metabolized by the liver may increase or decrease the ef-fectiveness of warfarin. Examples include barbiturates, carba-mazepine, corticosteroids, corticotropin, mercaptopurine, naf-cillin, hormonal contraceptives containing estrogen, rifampin,spironolactone, sucralfate, and trazodone.• The risk of phenytoin toxicity increases when phenytoin is tak-en with warfarin, and phenytoin may increase or decrease the ef-fects of warfarin.
Other interactions include the following:• A diet high in vitamin K reduces the effectiveness of warfarin.• Chronic alcohol abuse increases the patient’s risk of clottingwhile taking warfarin. Acute alcohol intoxication increases therisk of bleeding.• Vitamin K and fresh frozen plasma reduce the effects of war-farin. (See Adverse reactions to oral anticoagulants.)
Antiplatelet drugsAntiplatelet drugs are used to prevent arterial thromboembolism,particularly in patients at risk for MI, stroke, and arteriosclerosis(hardening of the arteries).
Aspirin, clopidogrel, dipyridamole, sulfinpyrazone, and ticlopi-dine are examples of oral antiplatelet drugs. Antiplatelet drugs ad-ministered I.V. include abciximab, eptifibatide, and tirofiban.
PharmacokineticsWhen taken orally, antiplatelet drugs are absorbed very quicklyand reach peak concentration in 1 to 2 hours. Aspirin maintains itsantiplatelet effect for about 10 days, or as long as platelets normal-ly survive. The effects of clopidogrel last about 5 days. Sulfinpyra-zone may require several days of administration before its anti-platelet effects occur.
After I.V. administration, antiplatelet drugs are quickly distrib-uted throughout the body. They’re minimally metabolized and ex-creted unchanged in urine. The effects of these drugs occur within15 to 20 minutes of administration and last about 6 to 8 hours.
Elderly patients and patients with renal failure may have de-creased clearance of antiplatelet drugs, which would prolong theantiplatelet effect.
166HEMATOLOGIC DRUGS
Adversereactionsto oralanticoagulants
The primary adverse re-action to oral anticoagu-lant therapy is minorbleeding. Severe bleed-ing can occur, however,with the most commonsite being the GI tract.Bleeding into the brainmay be fatal. Bruisesand hematomas mayform at arterial puncturesites (for example, aftera blood gas sample isdrawn). Necrosis organgrene of the skin andother tissues can occur.
Quick fix
The effects of oral anti-coagulants can be re-versed with phytona-dione (vitamin K1).
Warning!
938906.qxd 08/26/2008 15:32 Page 166

PharmacodynamicsAntiplatelet drugs interfere with platelet activity in different drug-specific and dose-related ways.• Low doses of aspirin inhibit clot formation by blocking the syn-thesis of prostaglandin, which in turn prevents formation of theplatelet-aggregating substance thromboxane A2.• Clopidogrel inhibits platelet aggregation by inhibiting platelet-fibrinogen binding.• I.V. antiplatelet drugs inhibit the glycoprotein IIa-IIIb receptor,which is the major receptor involved in platelet aggregation.• Dipyridamole may inhibit platelet aggregation because it in-creases adenosine, a coronary vasodilator and platelet aggrega-tion inhibitor.• Ticlopidine inhibits the binding of fibrinogen to platelets duringthe first stage of the clotting cascade.• Sulfinpyrazone inhibits several platelet functions. It lengthensplatelet survival and prolongs the patency of arteriovenous shuntsused for hemodialysis. A single dose rapidly inhibits platelet ag-gregation.
PharmacotherapeuticsAntiplatelet drugs have many different uses.
Managing MIsAspirin is used in patients who have had a previous MI orwho have unstable angina to reduce the risk of death in pa-tients at high risk for CAD. It’s also prescribed to reducethe risk of transient ischemic attacks (TIAs) (temporaryreduction in circulation to the brain).
Clopidogrel is used to reduce the risk of stroke or vas-cular death in patients with a history of a recent MI,stroke, or established peripheral artery disease. Clopido-grel is also used to help treat acute coronary syndromes,especially in patients undergoing percutaneous translumi-nal coronary angioplasty (PTCA) or coronary artery by-pass graft.
Eptifibatide may be used for patients with acute coronary syn-drome and for those undergoing percutaneous coronary interven-tion (PCI). Abciximab may also be used in combination with PCI.Tirofiban may be used to treat acute coronary syndrome.
Salve for surgeryDipyridamole is used with a coumarin compound to preventthrombus formation after cardiac valve replacement. Dipyri-damole may be administered with aspirin to prevent blood clots in
167ANTICOAGULANT DRUGS
Aspirin can helppatients who havehad an MI and can
also reduce therisk of stroke.
938906.qxd 08/26/2008 15:32 Page 167

patients who have had coronary artery bypass grafts (bypasssurgery) or prosthetic (artificial) heart valves.
Circumventing strokeTiclopidine is used to reduce the risk of thrombotic stroke in high-risk patients, such as those with a history of frequent TIAs or aprevious thrombotic stroke.
Drug interactions• Antiplatelet medications taken with NSAIDs, heparin, oral anti-coagulants, or another antiplatelet medication increase the risk ofbleeding.• Sulfinpyrazone taken with aspirin and oral anticoagulants in-creases the risk of bleeding.
Tales of toxicity• Aspirin increases the risk of toxicity of methotrexate and val-proic acid.• Aspirin and ticlopidine may reduce the effectiveness of sulfin-pyrazone to relieve signs and symptoms of gout.• Antacids may reduce the plasma levels of ticlopidine.
168HEMATOLOGIC DRUGS
Hypersensitivity reactions, particularly anaphylaxis, can occur. Bleeding is the most common ad-verse reaction when I.V. antiplatelet drugs are administered.
Warning!
Adverse reactions to antiplatelet drugs
Aspirin
• Stomach pain• Heartburn, nausea• Constipation• Blood in stool• Slight gastric blood loss
Clopidogrel
• Headache• Skin ulceration• Joint pain• Flulike symptoms• Upper respiratory tract in-fection
Sulfinpyrazone
• Abdominal discomfort
Ticlopidine
• Diarrhea• Nausea• Dyspepsia• Rash• Elevated liver function testresults• Neutropenia
Dipyridamole
• Headache• Dizziness• Nausea• Flushing• Weakness• Fainting• Mild GI distress
938906.qxd 08/26/2008 15:32 Page 168

• Cimetidine increases the risk of ticlopidine toxicity and bleed-ing.
You just don’t knowBecause guidelines haven’t been established for administratingticlopidine with heparin, oral anticoagulants, aspirin, or fibrinolyt-ic drugs, these drugs should be discontinued before ticlopidinetherapy begins. (See Adverse reactions to antiplatelet drugs.)
Direct thrombin inhibitorsThrombin inhibitors, including argatroban, bivalirudin, and lep-irudin, help prevent the formation of blood clots.
PharmacokineticsDirect thrombin inhibitors are typically administered by continu-ous I.V. infusion. They may also be given as an intra-coronary bo-lus during cardiac catheterization. In that case, the drug beginsacting in 2 minutes, with a peak response of 15 minutes and a du-ration of 2 hours. After subQ injection, plasma levels peak in 2hours; after I.V. administration, levels peak in less than 1 hour.
Effects on PTT become apparent within 4 to 5 hours of admin-istration. In patients with heparin-induced thrombocytopenia,platelet count recovery becomes apparent within 3 days.
Argatroban is metabolized by the liver and excreted primarilyin stool. Bivalirudin and lepirudin are metabolized by the liver andkidneys and excreted in urine
PharmacodynamicsDirect thrombin inhibitors interfere with blood clotting by directlyblocking all thrombin activity. These drugs offer several advan-tages over heparin: direct thrombin inhibitors act against solubleas well as clot-bound thrombin (thrombin in clots that have al-ready formed); their anticoagulant effects are more predictablethan those of heparin; and their actions aren’t inhibited by theplatelet release reaction.
The binding of the drug to thrombin is reversible.
PharmacotherapeuticsAdministered by I.V. infusion, argatroban and lepirudin are used totreat heparin-induced thrombocytopenia (HIT). Argatroban mayalso be given with aspirin to patients with HIT who are undergo-ing a cardiac procedure, such as PTCA, coronary stent placement,or atherectomy.
169ANTICOAGULANT DRUGS
938906.qxd 08/26/2008 15:32 Page 169

Bivalirudin has been approved for use in patients with unsta-ble angina undergoing PTCA, and should be used in conjunctionwith aspirin therapy.
Patients with liver dysfunction may require a reduced dose ofargatroban. Also, the dosage of bivalirudin and lepirudin may needto be reduced in patients with impaired renal function.
Use caution when administering a direct thrombin inhibitor toa patient who has an increased risk of bleeding. Patients at great-est risk for hemorrhage are those with severe hypertension, gas-tric ulcers, or hematologic disorders associated with increasedbleeding. Patients receiving spinal anesthesia or those undergoinga lumbar puncture or having major surgery (especially surgery ofthe brain, spinal cord, or the eye) also have an increased risk forbleeding.
Drug interactions• Hemorrhage can occur as an adverse reaction to direct throm-bin inhibitors, so avoid giving these drugs with another drug thatmay also increase the risk of bleeding.• Discontinue all parenteral anticoagulants before administeringargatroban.• Administration of argatroban along with warfarin increases theINR.• If the patient has received heparin, allow time for heparin’s ef-fect on PTT to decrease before administering argatroban. (SeeAdverse reactions to bivalirudin.)
Factor Xa inhibitor drugsFactor Xa inhibitor drugs are used to prevent DVT in patients un-dergoing total hip and knee replacement surgery or surgery to re-pair a hip fracture. The only factor Xa inhibitor drug used in theUnited States is fondaparinux.
PharmacokineticsAdministered subQ, fondaparinux is absorbed rapidly and com-pletely and is excreted primarily unchanged in urine. Its effectspeak within 2 hours of administration and last for about 17 to 24hours.
PharmacodynamicsFondaparinux binds to antithrombin III and greatly influences theneutralization of factor Xa by antithrombin III. Neutralization of
170HEMATOLOGIC DRUGS
Adversereactions tobivalirudin
The major adverse reac-tion to bivalirudin isbleeding; major hemor-rhage occurs infre-quently. Other adversereactions include:• intracranial hemor-rhage• retroperitoneal hemor-rhage• nausea, vomiting, ab-dominal cramps, and di-arrhea• headache• hematoma at I.V. infu-sion site.
Warning!
938906.qxd 08/26/2008 15:32 Page 170

factor Xa interrupts the coagulation cascade, thereby inhibitingclot formation.
PharmacotherapeuticsFondaparinux is used only to prevent the formation of blood clots.
Drug interactionsAvoid administering fondaparinux with another drug that may in-crease the risk of bleeding. (See Adverse reactions to factor Xainhibitors.)
Thrombolytic drugsThrombolytic drugs are used to dissolve a preexisting clot orthrombus, often in an acute or emergency situation. Some of thethrombolytic drugs currently used include alteplase, reteplase,streptokinase, tenecteplase, and urokinase.
PharmacokineticsAfter I.V. or intracoronary administration, thrombolytic drugs aredistributed immediately throughout the circulation, quickly acti-vating plasminogen (a precursor to plasmin, which dissolves fibrinclots).
Blood workAlteplase, reteplase, tenecteplase, and urokinase are cleared rap-idly from circulating plasma, primarily by the liver. Streptokinaseis removed rapidly from the circulation by antibodies and thereticuloendothelial system (a body system involved in defendingagainst infection and disposing of products of cell breakdown).These agents don’t appear to cross the placental barrier.
PharmacodynamicsThrombolytic drugs convert plasminogen to plasmin, which lyses(dissolves) thrombi, fibrinogen, and other plasma proteins. (SeeHow alteplase helps restore circulation, page 172.)
PharmacotherapeuticsThrombolytic drugs have a number of uses. They’re used to treatcertain thromboembolic disorders (such as acute MI, acute is-chemic stroke, and peripheral artery occlusion) and have also
171THROMBOLYTIC DRUGS
Adversereactions tofactor Xainhibitors
Adverse reactions thatcan occur with factor Xainhibitor therapy include:• bleeding• nausea• anemia• fever• rash• constipation• edema.
Warning!
Thrombolytic drugsdissolve clots or
thrombi in emergencysituations.
938906.qxd 08/26/2008 15:32 Page 171

been used to dissolve thrombi in arteriovenous cannulas (used indialysis) and I.V. catheters to reestablish blood flow.
The sooner the betterThrombolytic drugs are the drugs of choice to break down newlyformed thrombi. They seem most effective when administeredwithin 6 hours of the symptoms onset.
172HEMATOLOGIC DRUGS
When a thrombus forms in an artery, it obstructs the blood supply, causing ischemia and necrosis. Alteplase can dissolve a throm-bus in either the coronary or pulmonary artery, restoring the blood supply to the area beyond the blockage.
Obstructed artery
A thrombus blocks blood flowthrough the artery, causingdistal ischemia.
Inside the thrombus
Alteplase enters thethrombus, which consists ofplasminogen bound to fibrin.Alteplase binds to the fibrin-plasminogen complex, con-verting the inactive plasmino-gen into active plasmin. Thisactive plasmin digests the fib-rin, dissolving the thrombus.As the thrombus dissolves,blood flow resumes.
Now I get it!
How alteplase helps restore circulation
Thrombus
Bloodsupply
Arterywall
Ischemicarea
Alteplase
Plasminogen
Fibrin strand
Activeplasmin
Break infibrin strand
938906.qxd 08/26/2008 15:32 Page 172

Acute MI and othersIn addition, each drug has specific uses.• Alteplase is used to treat acute MI, pulmonary embolism, acuteischemic stroke, peripheral artery occlusion, and to restore paten-cy to clotted grafts and I.V. access devices.• Streptokinase is used to treat acute MI, pulmonary embolus,and DVT.• Reteplase and tenecteplase are used to treat acute MI.• Urokinase is used to treat pulmonary embolism and coronaryartery thrombosis and for catheter clearance.
Drug interactions• Thrombolytic drugs interact with heparin, oral anticoagulants,antiplatelet drugs, and NSAIDs to increase the patient’s risk ofbleeding.• Aminocaproic acid inhibits streptokinase and can be used to re-verse its fibrinolytic effects. (See Adverse reactions to throm-bolytic drugs.)
Quick quiz
1. A patient is given heparin to treat thrombophlebitis. If the pa-tient starts to bleed excessively during heparin therapy, whichdrug is likely to be prescribed to reverse its effects?
A. Vitamin KB. Factor VIIIC. ArgatrobanD. Protamine sulfate
Answer: D. Protamine sulfate reverses the effects of heparin.
2. Why is heparin administered concurrently with warfarin?A. Warfarin’s therapeutic effects don’t occur until clotting
factors are depleted.B. Heparin activates warfarin.C. Warfarin and heparin have a synergistic effect.D. Heparin helps the body absorb warfarin.
Answer: A. Heparin is administered concurrently with warfarinbecause warfarin is ineffective until clotting factors are depleted.
173QUICK QUIZ
Adversereactions tothrombolyticdrugs
The major reactions as-sociated with throm-bolytic drugs are bleed-ing and allergic respons-es, especially withstreptokinase.
Warning!
938906.qxd 08/26/2008 15:32 Page 173

3. How soon after cyanocobalamin (vitamin B12) therapy is be-gun can a patient expect to feel better?
A. 24 hoursB. 72 hoursC. 1 weekD. 2 weeks
Answer: A. The effects of cyanocobalamin can be felt 24 hoursafter initiation of treatment.
ScoringIf you answered all three items correctly, far out! You’re hip to
hematologic drugs.If you answered two items correctly, that’s great! You’ve caught
the wave of anticoagulants.If you answered fewer than two items correctly, play it cool. You
just might need some time to get the blood flowing.
174HEMATOLOGIC DRUGS
✰✰✰
✰✰
✰
That was reallyinformative. I
wonder what we’llread about next.
938906.qxd 08/26/2008 15:32 Page 174

Drugs and the respiratory systemThe respiratory system, extending from the nose to the pulmonarycapillaries, performs the essential function of gas exchange be-tween the body and its environment. In other words, it takes inoxygen and expels carbon dioxide.
Breathe easyDrugs used to improve respiratory symptoms are available in in-halation and systemic formulations. These drugs include:• beta2-adrenergic agonists• anticholinergics• corticosteroids• leukotriene modifiers• mast cell stabilizers• methylxanthines• monoclonal antibodies• expectorants• antitussives• mucolytics• decongestants.
7
Respiratory drugs
Just the facts
In this chapter, you’ll learn:
♦ classes of drugs used to treat respiratory disorders
♦ uses and varying actions of these drugs
♦ how these drugs are absorbed, distributed, metabolized,and excreted
♦ drug interactions and adverse reactions to these drugs.
I’ve got animportant job—gas
exchange—andsometimes I need a
little help fromrespiratory drugs to
get it done.
938907.qxd 08/26/2008 15:39 Page 175

Beta2-adrenergic agonistsBeta2-adrenergic agonists are used to treat symptoms associatedwith asthma and chronic obstructive pulmonary disease (COPD).Drugs in this class can be either short-acting or long-acting.
Short-acting beta2-adrenergic agonistsShort-acting beta2-adrenergic agonists include:• albuterol (systemic, inhalation)• levalbuterol (inhalation)• metaproterenol (inhalation)• pirbuterol (inhalation)• terbutaline (systemic).
Long-acting beta2-adrenergic agonistsLong-acting beta2-adrenergic agonists include:• formoterol (inhalation)• salmeterol (inhalation).
Pharmacokinetics (how drugs circulate)Beta2-adrenergic agonists are minimally absorbed from the GItract; inhaled forms exert their effects locally. After inhalation,beta2-adrenergic agonists appear to be absorbed over severalhours from the respiratory tract. These drugs don’t cross theblood-brain barrier; they’re extensively metabolized in the liver toinactive compounds and rapidly excreted in urine and stool.
Pharmacodynamics (how drugs act)Beta2-adrenergic agonists increase levels of cyclic adenosinemonophosphate by stimulating the beta2-adrenergic receptors inthe smooth muscle, resulting in bronchodilation. These drugs maylose their selectivity at higher doses, which can increase the riskof toxicity. Inhaled forms are preferred because they act locally inthe lungs, resulting in fewer adverse reactions than systemicallyabsorbed forms.
Pharmacotherapeutics (how drugs are used)Short-acting inhaled beta2-adrenergic agonists are the drugs ofchoice for fast relief of symptoms in the patient with asthma.They’re generally used as needed for asthma (includingexercise-induced asthma) and COPD. A patient with COPDmay use them around-the-clock on a specified schedule. How-ever, excessive use of a short-acting beta2-adrenergic agonist
176RESPIRATORY DRUGS
Short-actinginhaled beta2-
adrenergicagonists providerelief that’s fast!
938907.qxd 08/26/2008 15:39 Page 176

may indicate poor asthma control, requiring reassessment of thepatient’s therapeutic regimen.
A good combinationLong-acting beta2-adrenergic agonists tend to be used with anti-inflammatory agents, namely inhaled corticosteroids, to help con-trol asthma. (See Problems with long-acting beta2-adrenergic ag-onists.) They’re especially useful for the patient with nocturnalasthmatic symptoms. These drugs must be administered on aschedule. They aren’t used to relieve acute symptoms becausetheir onset of action isn’t fast enough. They also don’t affect thechronic inflammation associated with asthma.
Drug interactionsInteractions are uncommon when using the inhaled forms.Beta-adrenergic blockers decrease the bronchodilating effects ofbeta2-adrenergic agonists. They should be used together cautious-ly. (See Adverse reactions to beta2-adrenergic agonists.)
AnticholinergicsInhaled ipratropium, an anticholinergic, is a bronchodilator usedprimarily in the patient suffering from COPD, but it may also beused as an adjunct to beta2-adrenergic agonists.
Ipratropium Ipratropium is the most common anticholinergic used for respira-tory disorders.
177ANTICHOLINERGICS
If a patient is taking a long-acting beta2-adrenergic agonist, make sure that he’s using it only aspart of a combination therapy with other medications such as inhaled corticosteroids. Patientswho use long-acting beta2-adrenergic agonists as their only means of asthma control are at seri-ous risk for adverse effects, including death.
Safe and sound
Problems with long-acting beta2-adrenergic agonists Adversereactionsto beta2-adrenergicagonists
Adverse reactionsto short-acting beta2-adrenergic agonists in-clude:• paradoxical bron-chospasm• tachycardia• palpitations• tremors• dry mouth.
Adverse reactionsto long-acting beta2-adrenergic agonists in-clude:• bronchospasm• tachycardia• palpitations• hypertension• tremors.
Warning!
938907.qxd 08/26/2008 15:39 Page 177

PharmacokineticsAnticholinergics are minimally absorbed from the GI tract; theycome in inhaled forms that exert their effects locally.
PharmacodynamicsIpratropium inhibits muscarinic receptors, which results in bron-chodilation. This drug works by blocking the parasympathetic ner-vous system, rather than stimulating the sympathetic nervous sys-tem.
PharmacotherapeuticsAnticholinergics are used to relieve symptoms in the patient withCOPD. They’re less effective in long-term management of the pa-tient with asthma; however, they may be used as adjunctive thera-py (usually in combination with a short-acting beta2-adrenergic ag-onist on a scheduled basis).
Drug interactionsInteractions are uncommon when using the inhaled forms. Iprat-ropium should be used cautiously with antimuscarinic drugsand other anticholinergics. (See Adverse reactions to anticholin-ergics.)
CorticosteroidsCorticosteroids are anti-inflammatory drugs available in inhaledand systemic forms for the short- and long-term control of asthmasymptoms. Many products with differing potencies are available.
Inhaled corticosteroids include:• beclomethasone dipropionate• budesonide• flunisolide• fluticasone• triamcinolone acetonide.
Oral corticosteroids include:• prednisolone• prednisone.
I.V. corticosteroids include:• hydrocortisone sodium succinate• methylprednisolone sodium succinate.
178RESPIRATORY DRUGS
Adversereactions toanticholinergics
The most common ad-verse reactions to anti-cholinergics include:• nervousness• tachycardia• nausea and vomiting• paradoxical bron-chospasm (with exces-sive use)• dry mouth.
Warning!
938907.qxd 08/26/2008 15:39 Page 178

PharmacokineticsOral prednisone is readily absorbed and extensively metabolizedin the liver to the active metabolite prednisolone. The I.V. formhas a rapid onset. Inhaled drugs are minimally absorbed, althoughabsorption increases as the dosage is increased.
PharmacodynamicsCorticosteroids work by inhibiting the production of cytokines,leukotrienes, and prostaglandins; the recruitment of eosinophils;and the release of other inflammatory mediators. They also affectother areas in the body, which can cause long-term adverse reac-tions. (See Corticosteroids.)
PharmacotherapeuticsCorticosteroids are the most effective drugs available for the long-term treatment and prevention of acute asthma attacks.
Inhalation for preventionInhaled corticosteroids are the preferred drugs for preventing fu-ture attacks in the patient with mild to severe asthma. Use of in-haled corticosteroids reduces the need for systemic steroids inmany cases, thus reducing the patient’s risk of developing seriouslong-term adverse reactions.
Systemic for the seriousSystemic forms are usually reserved for moderate to severe at-tacks, but they’re also used in the patient with milder asthma that
179CORTICOSTEROIDS
Corticosteroidsare the most
effective drugs forthe long-termtreatment andprevention of
acute asthmaattacks.
These special populations may require special care when tak-ing corticosteroids:• Children: Growth should be monitored, especially whenthey’re taking systemic drugs or higher doses of inhaleddrugs.• Elderly patients: May benefit from receiving drugs that pre-vent osteoporosis, such as alendronate during therapy withcorticosteroids, especially if they’re taking higher doses ofinhaled or systemic steroids.
• Patients with diabetes: May require closer monitoring of theirblood glucose levels while on steroids.• Breast-feeding women: Corticosteroid levels are negligible inthe breast milk of mothers who take less than 20 mg/day of oralprednisone. The amount found in breast milk can be minimizedif the woman waits at least 4 hours after taking prednisone tobreast-feed her infant.
Safe and sound
Corticosteroids
938907.qxd 08/26/2008 15:39 Page 179

fails to respond to other measures. Systemic corticosteroidsshould be used at the lowest effective dosage and for the shortestperiod possible to avoid adverse reactions.
Drug interactionsInteractions are uncommon when using inhaled forms.• Hormonal contraceptives, ketoconazole, and macrolide antibi-otics may increase the activity of corticosteroids in general, result-ing in the need to decrease the steroid dosage.• Barbiturates, cholestyramine, rifampin, and phenytoin may de-crease the effectiveness of corticosteroids, resulting in the need toincrease the steroid dosage. (See Adverse reactions to inhaledcorticosteroids.)
Leukotriene modifiersLeukotriene modifiers are used for the prevention and long-termcontrol of mild asthma.
Leukotriene receptor antagonists include:• montelukast• zafirlukast.
Leukotriene formation inhibitors include:• zileuton.
PharmacokineticsMontelukast is rapidly absorbed. Zafirlukast’s absorption is de-creased by food, so it should be given 1 hour before or 2 hours af-ter meals.
All of the leukotriene modifiers are highly protein-bound(more than 90%).
Metabolism and excretionZafirlukast is extensively metabolized in the liver by the cy-tochrome P450 2C9 (CYP2C9) enzyme into inactive metabolitesand excreted primarily in stool. In general, this class of drugs ismetabolized, induced, or inhibited by the cytochrome P450 en-zyme system, which is important for establishing drug interac-tions.
Caution requiredZileuton is contraindicated in the patient with active liver disease.Closely monitor the patient with liver impairment who’s takingzafirlukast for adverse reactions; he may require a dosage adjust-ment. This doesn’t apply for montelukast.
180RESPIRATORY DRUGS
Adversereactionsto inhaledcorticosteroids
Adverse reactions to in-haled corticosteroidsmay include:• mouth irritation• oral candidiasis• upper respiratory tractinfection.
To reduce the risk ofadverse reactions frominhaled steroids, the pa-tient should use the low-est possible dosage tomaintain control, admin-ister doses using aspacer, and rinse out hismouth after administra-tion.
Warning!
938907.qxd 08/26/2008 15:39 Page 180

PharmacodynamicsLeukotrienes are substances released from mast cells, eosino-phils, and basophils that can cause smooth-muscle contraction ofthe airways, increased permeability of the vasculature, increasedsecretions, and activation of other inflammatory mediators.
Leukotrienes may be inhibited by two different mechanisms.The leukotriene receptor antagonists zafirlukast and montelukastprevent the D4 and E4 leukotrienes from interacting with their re-ceptors, thereby blocking their action. The leukotriene formationinhibitor zileuton inhibits the production of 5-lipoxygenase, there-by preventing the formation of leukotrienes.
PharmacotherapeuticsLeukotriene modifiers are primarily used to prevent and controlasthma attacks in the patient with mild to moderate disease. Mon-telukast is also indicated for the treatment of allergic rhinitis.
Drug interactions• Zafirlukast inhibits CYP2C9 and thus could increase the risk oftoxicity if used with phenytoin or warfarin.• Zafirlukast and zileuton inhibit CYP3A4 and thus could increasethe risk of toxicity if used with amlodipine, atorvastatin, carba-mazepine, clarithromycin, cyclosporine, erythromycin, hormonalcontraceptives, itraconazole, ketoconazole, lovastatin, nelfinavir,nifedipine, ritonavir, sertraline, simvastatin, or warfarin.• Zileuton inhibits CYP1A2 and thus could increase the risk oftoxicity if used with amitriptyline, clozapine, desipramine, fluvox-amine, imipramine, theophylline, or warfarin.
Talkin’ toxicity• Zafirlukast, zileuton, and montelukast are metabolized byCYP2C9 and thus could increase the risk of toxicity if used withamiodarone, cimetidine, fluconazole, fluoxetine, fluvoxamine, iso-niazid, metronidazole, or voriconazole. If carbamazepine, pheno-barbital, phenytoin, primidone, or rifampin is used with leuko-trienes, the effectiveness of the leukotrienes could be reduced.• Zileuton and montelukast are metabolized by CYP3A4 and thuscould increase the risk of toxicity if used with amiodarone, cimeti-dine, clarithromycin, cyclosporine, erythromycin, fluoxetine, flu-voxamine, grapefruit juice, itraconazole, ketoconazole, metronida-zole, or voriconazole and could result in decreased effectiveness ifused with carbamazepine, efavirenz, garlic supplements, modafi-nil, nevirapine, oxcarbazepine, phenobarbital, phenytoin, primi-done, rifabutin, rifampin, or St. John’s wort.
181LEUKOTRIENE MODIFIERS
Leukotrienes canbe very trying forasthma sufferers.
Montelukast,zafirlukast, and
zileuton help to inhibittheir action.
938907.qxd 08/26/2008 15:39 Page 181

• Zileuton is metabolized by CYP1A2 and thus could increase therisk of toxicity if used with cimetidine, clarithromycin, erythro-mycin, fluvoxamine, or isoniazid and could result in decreased ef-fectiveness if used with carbamazepine, phenobarbital, phenytoin,primidone, rifampin, ritonavir, or St. John’s wort or if used by asmoker. (See Adverse reactions to leukotriene modifiers.)
Mast cell stabilizersMast cell stabilizers are used to prevent asthma attacks, especial-ly in a child or a patient with mild disease. They’re also used in anadult or child with mild to moderate persistent asthma. Drugs inthis class include:• cromolyn• nedocromil.
PharmacokineticsMast cell stabilizers are minimally absorbed from the GI tract;they’re available in inhaled forms that exert their effects locally.
PharmacodynamicsThese drugs stabilize the mast cell membrane, possibly by inhibit-ing calcium channels, thus preventing the release of inflammatorymediators.
PharmacotherapeuticsMast cell stabilizers are used for the prevention and long-termcontrol of asthma symptoms. They do this by controlling the in-flammatory process.
Number 1 for childrenMast cell stabilizers are often used for children and patients withexercise-induced asthma.
Drug interactionsInteractions are uncommon when using inhaled forms. (See Ad-verse reactions to mast cell stabilizers.)
182RESPIRATORY DRUGS
Adversereactions toleukotrienemodifiers
Adverse reactions thatmay occur with leuko-triene modifiers include:• headache• dizziness• nausea and vomiting• myalgia.
Warning!
Adversereactions tomast cellstabilizers
Inhaled mast cell stabi-lizers may cause theseadverse reactions:• pharyngeal and tra-cheal irritation• cough• wheezing• bronchospasm• headache.
Warning!
938907.qxd 08/26/2008 15:39 Page 182

MethylxanthinesMethylxanthines, also called xanthines, are used to treat respira-tory disorders.
Types of methylxanthinesMethylxanthines include anhydrous theophylline and its deriva-tive salt aminophylline.
Theophylline is the most commonly prescribed oral methylx-anthine. Aminophylline is preferred when an I.V. methylxanthineis required. Caffeine is also a xanthine derivative.
PharmacokineticsThe pharmacokinetics of methylxanthines vary according towhich drug the patient is receiving, the dosage form, and the ad-ministration route.
AbsorptionWhen theophylline is given as an oral solution or a rapid-releasetablet, it’s absorbed rapidly and completely. High-fat meals can in-crease theophylline concentrations and the risk of toxicity.
Gastric measuresAbsorption of some of theophylline’s slow-release forms dependson the gastric pH. Food can alter absorption. When converting thepatient from I.V. aminophylline to oral theophylline, the dosage isdecreased by 20%.
DistributionTheophylline is approximately 56% protein-bound in adults and36% protein-bound in neonates. It readily crosses the placentalbarrier and is secreted in breast milk. Smokers and patients ondialysis may need higher doses.
Metabolism and excretionTheophylline is metabolized primarily in the liver by theCYP1A2 enzyme. In adults and children, about 10% of adose is excreted unchanged in urine; therefore, no dosageadjustment is required in patients with renal insufficiency.Elderly patients and those with liver dysfunction may re-quire a lower dose. Because an infant has an immature liv-er with reduced metabolic functioning, as much as one-half of a dose may be excreted unchanged in his urine.
183METHYLXANTHINES
High-fatmeals can
increase therisk of
theophyllinetoxicity.
Xanthinesstimulate my
medulla!
938907.qxd 08/26/2008 15:39 Page 183

Blood levels matterTheophylline levels must be measured to evaluate efficacyand avoid toxicity. The therapeutic serum concentration is10 to 20 mcg/ml (SI, 44 to 111 µmol/L). Levels must be assessedwhen drug therapy is initiated, when the dosage is changed, andwhen drugs are added or removed from the patient’s regimen.
PharmacodynamicsMethylxanthines act in many ways.
Relax and breathe deeplyMethylxanthines decrease airway reactivity and relieve bron-chospasm by relaxing bronchial smooth muscle. Theophylline isbelieved to inhibit phosphodiesterase, resulting in smooth-musclerelaxation, bronchodilation, and decreased inflammatory media-tors (namely mast cells, T cells, and eosinophils). Much of theo-phylline’s toxicity may be due to increased catecholamine release.
A stimulating conversationIn nonreversible obstructive airway disease (chronic bronchitis,emphysema, and apnea), methylxanthines appear to increase thesensitivity of the brain’s respiratory center to carbon dioxide andto stimulate the respiratory drive.
Pumping you upIn chronic bronchitis and emphysema, these drugs reduce fatigueof the diaphragm, the respiratory muscle that separates the ab-domen from the thoracic cavity. They also improve ventricularfunction and, therefore, the heart’s pumping action.
PharmacotherapeuticsTheophylline and its salts are used as second- or third-line therapyfor the long-term control and prevention of symptoms related to:• asthma• chronic bronchitis• emphysema.
Useful for neonates?Theophylline has been used to treat neonatal apnea (periods ofnot breathing in the neonate) and has been effective in reducingsevere bronchospasm in an infant with cystic fibrosis.
184RESPIRATORY DRUGS
Memoryjogger
How can you
remember what theo-
phylline and its salts
are used to treat?
Simple: Just remem-
ber that you really
need to “ACE” this
one! It’s used for
long-term control
and prevention of
symptoms related
to:
A— asthma
C—chronic bronchi-
tis
E—emphysema.
938907.qxd 08/26/2008 15:39 Page 184

Drug interactionsTheophylline drug interactions occur with substances that inhibitor induce the CYP1A2 enzyme. (See Adverse reactions tomethylxanthines.)• Inhibitors of the CYP1A2 enzyme (including cimetidine,ciprofloxacin, clarithromycin, erythromycin, fluvoxamine, hor-monal contraceptives, isoniazid, ketoconazole, ticlopidine, andzileuton) decrease theophylline metabolism, thus increasing itsserum level as well as the risk of adverse reactions and toxicity.The dosage of theophylline may need to be reduced.• Inducers of the CYP1A2 enzyme (including carbamazepine,phenobarbital, phenytoin, rifampin, St. John’s wort, and char-broiled meats) increase theophylline metabolism, thus de-creasing its serum level and possibly its effectiveness. Thedosage of theophylline may need to be increased.• Smoking cigarettes or marijuana increases theophyllineelimination, thus decreasing its serum level and effectiveness.• Taking adrenergic stimulants or drinking beverages thatcontain caffeine or caffeinelike substances may result in addi-tive adverse reactions to theophylline or signs and symptoms ofmethylxanthine toxicity.• Activated charcoal may decrease theophylline levels.• The use of enflurane or isoflurane with theophylline or theo-phylline derivatives increases the risk of cardiac toxicity.• Theophylline and its derivatives may reduce the effects of lithi-um by increasing its rate of excretion.• Thyroid hormones may reduce theophylline levels; antithyroiddrugs may increase theophylline levels.
185METHYLXANTHINES
Smokingincreases theelimination of
theophylline, whichreduces its
effectiveness.
Adverse reactions to methylxanthines may be transient or symptomatic of toxicity.
Warning!
Adverse reactions to methylxanthines
Gut reactions
Adverse GI system reactionsinclude:• nausea and vomiting• abdominal cramping• epigastric pain• anorexia• diarrhea.
Nerve racking
Adverse central nervous sys-tem reactions include:• headache• irritability• restlessness• anxiety• insomnia• dizziness.
Heart of the matter
Adverse cardiovascular reac-tions include:• tachycardia• palpitations• arrhythmias.
938907.qxd 08/26/2008 15:39 Page 185

Monoclonal antibodiesMonoclonal antibodies, particularly anti-immunoglobin (Ig) Emonoclonal antibodies, are used in patients with moderate-to-severe asthma with a positive skin test and who are inadequatelycontrolled with inhaled corticosteroids. Omalizumab is the onlydrug in this class.
Omalizumab
PharmacokineticsOmalizumab is slowly absorbed after subcutaneous injection. It’smetabolized by the liver, but the rate of metabolization dependson IgG clearance.
PharmacodynamicsOmalizumab inhibits the binding of IgE to its receptor on the mastcell and basophils. This in turns inhibits the release of allergicsubstances which potentiate asthma symptoms.
PharmacotherapeuticsOmalizumab is used in patients with moderate-to-severe asthmawith a positive skin test and insufficient control on inhaled corti-costeroids. Dosing for the drug is based on pretreatment serumIgE levels.
186RESPIRATORY DRUGS
When inhaledcorticosteroids
aren’t up to the task,monoclonal
antibodies may beused to control a
patient’s moderate-to-severe asthma.
Adverse reactions to monoclonal antibodiesinclude:• injection site reactions• upper respiratory tract infections• sinusitis• headache• pharyngitis
• allergic reaction.Allergic reactions may be severe enough to
be life-threatening and typically occur within2 hours of administration. However, in rarecases, delayed anaphylactic reactions (occur-ring more than 24 hours after administration)may occur.
Warning!
Adverse reactions to monoclonal antibodies
938907.qxd 08/26/2008 15:39 Page 186

Drug interactionsNo formal drug-interaction studies have been done. (See Adversereactions to monoclonal antibodies.)
ExpectorantsExpectorants thin mucus so it’s cleared more easily out of the air-ways. They also soothe mucous membranes in the respiratorytract. The result is a more productive cough.
GuaifenesinThe most commonly used expectorant is guaifenesin.
PharmacokineticsGuaifenesin is absorbed through the GI tract, metabolized by theliver, and excreted primarily by the kidneys.
PharmacodynamicsBy increasing production of respiratory tract fluids, expectorantsreduce the thickness, adhesiveness, and surface tension of mucus,making it easier to clear from the airways. Expectorants also pro-vide a soothing effect on the mucous membranes of the respirato-ry tract.
PharmacotherapeuticsGuaifenesin is used to relieve symptoms due to ineffective, pro-ductive coughs from many disorders, such as:• bronchial asthma• bronchitis• colds• emphysema• influenza• minor bronchial irritation• sinusitis.
Drug interactionsGuaifenesin isn’t known to have specific drug interactions; howev-er, it does cause some adverse reactions. (See Adverse reactionsto guaifenesin.)
187EXPECTORANTS
Expectorantsthin mucus,
helping me coughup clogging
secretions moreproductively.
Adversereactions toguaifenesin
Adverse reactions toguaifenesin include:• nausea• vomiting (if taken inlarge doses)• diarrhea• abdominal pain• drowsiness• headache• hives• rash.
Warning!
938907.qxd 08/26/2008 15:39 Page 187

AntitussivesAntitussive drugs suppress or inhibit coughing.
Types of antitussivesAntitussives are typically used to treat dry, nonproductive coughs.The major antitussives include:• benzonatate• codeine• dextromethorphan • hydrocodone bitartrate.
PharmacokineticsAntitussives are absorbed well through the GI tract, metabolizedin the liver, and excreted in urine.
PharmacodynamicsAntitussives act in slightly different ways.
Removing the sensationBenzonatate acts by anesthetizing stretch receptors throughoutthe bronchi, alveoli, and pleurae.
Taking direct actionCodeine, dextromethorphan, and hydrocodone suppress thecough reflex by direct action on the cough center in the medullaof the brain, thus lowering the cough threshold.
PharmacotherapeuticsThe uses of these drugs vary slightly, but each treats a serious,nonproductive cough that interferes with a patient’s ability to restor carry out activities of daily living.
Put it to the testBenzonatate relieves cough caused by pneumonia, bronchitis, thecommon cold, and chronic pulmonary diseases such as emphyse-ma. It can also be used during bronchial diagnostic tests, such asbronchoscopy, when the patient must avoid coughing.
Top of the chartsDextromethorphan is the most widely used cough suppressant inthe United States and may provide better antitussive effects thancodeine. Its popularity may stem from the fact that it isn’t associ-
188RESPIRATORY DRUGS
When a coughis dry, irritating,and exhausting,
antitussivesbring relief.
Benzonatatecan be useful
during diagnosticprocedures whenthe patient mustavoid coughing.
938907.qxd 08/26/2008 15:39 Page 188

ated with sedation, respiratory depression, or addiction at usualdoses.
For really tough coughsThe opioid antitussives (typically codeine and hydrocodone) arereserved for treating an intractable cough.
Drug interactionsAntitussives may interact with other drugs.• Codeine and hydrocodone may cause excitation, an extremelyelevated temperature, hypertension or hypotension, and comawhen taken with monoamine oxidase inhibitors (MAOIs).• Dextromethorphan use with MAOIs may produce excitation, anelevated body temperature, hypotension, and coma.• Codeine taken with other central nervous system (CNS) depres-sants, including alcohol, barbiturates, phenothiazines, and seda-tive-hypnotics, may increase CNS depression, resulting in drowsi-ness, lethargy, stupor, respiratory depression, coma, and evendeath. (See Adverse reactions to antitussives.)
MucolyticsMucolytics act directly on mucus, breaking down sticky, thick se-cretions so that they’re more easily eliminated.
189MUCOLYTICS
Benzonatate
Benzonatate needs to be swallowedwhole; chewing or crushing it can pro-duce a local anesthetic effect in themouth and throat, which can compro-mise the airway. These reactions canalso occur when taking benzonatate:• dizziness• sedation• headache• nasal congestion• burning in the eyes
• GI upset or nausea• constipation• rash, eruptions, or itching• chills• chest numbness.
Opioid antitussives
The most common reactions includenausea, vomiting, sedation, dizziness,and constipation. Other reactions in-clude:• pupil constriction
• bradycardia• tachycardia• hypotension• stupor• seizures• circulatory collapse• respiratory arrest.
Use opioid antitussives cautiously inthe patient with current or previous opi-oid addiction and in the patient with arespiratory disorder, such as asthma orchronic obstructive pulmonary disease.
Warning!
Adverse reactions to antitussives
938907.qxd 08/26/2008 15:39 Page 189

AcetylcysteineAcetylcysteine is the only mucolytic used clinically in the UnitedStates for the patient with abnormal or thick mucus.
PharmacokineticsInhaled acetylcysteine is absorbed from the pulmonary epitheli-um. When taken orally, the drug is absorbed from the GI tract.
Metabolism and excretionAcetylcysteine is metabolized in the liver; its excretion is un-known.
PharmacodynamicsAcetylcysteine decreases the thickness of respiratory tract secre-tions by altering the molecular composition of mucus. It also irri-tates the mucosa to stimulate clearance and restores glutathione,a substance that plays an important role in oxidation-reductionprocesses.
Liver cleanerGlutathione’s enzymatic action in the liver reduces acetaminophentoxicity from overdose.
PharmacotherapeuticsMucolytics are used with other therapies to treat the patient withabnormal or thick mucus secretions, such as the patient with:• atelectasis caused by mucus obstruction, as may occur in pneu-monia, bronchiectasis, or chronic bronchitis• bronchitis• pulmonary complications related to cystic fibrosis.
Patient preparationsMucolytics may also be used to prepare the patient for bronchog-raphy and other bronchial studies.
Overdose antidoteAcetylcysteine is the antidote for acetaminophen overdose. How-ever, it doesn’t fully protect against liver damage caused by aceta-minophen toxicity.
Drug interactionsActivated charcoal decreases acetylcysteine’s effectiveness. Whenusing acetylcysteine to treat an acetaminophen overdose, remove
190RESPIRATORY DRUGS
When thicksecretions
overwhelm me,mucolytics thin
mucus quickly so Ican breathe
better.
938907.qxd 08/26/2008 15:39 Page 190

activated charcoal from the stomach before administering. (SeeAdverse reactions to acetylcysteine.)
DecongestantsDecongestants may be classified as systemic or topical, dependingon how they’re administered.
Types of decongestantsAs sympathomimetic drugs, systemic decongestants stimulate thesympathetic nervous system to reduce swelling of the respiratorytract’s vascular network. Systemic decongestants include:• ephedrine• phenylephrine• pseudoephedrine.
Topical concernsTopical decongestants are also powerful vasoconstrictors. Whenapplied directly to swollen mucous membranes of the nose, theyprovide immediate relief from nasal congestion. These drugs in-clude:• ephedrine, epinephrine, and phenylephrine (sympathomimeticamines)• naphazoline and tetrahydrozoline (imidazoline derivatives ofsympathomimetic amines).
PharmacokineticsThe pharmacokinetic properties of decongestants vary.
Absorbed quickly…When taken orally, the systemic decongestants are absorbed read-ily from the GI tract and widely distributed throughout the bodyinto various tissues and fluids, including cerebrospinal fluid, theplacenta, and breast milk.
…metabolized slowlySystemic decongestants are slowly and incompletely metabolizedby the liver and excreted largely unchanged in urine within 24hours of oral administration.
Direct actionTopical decongestants act locally on the alpha receptors of thevascular smooth muscle in the nose, causing the arterioles to con-strict. As a result of this local action, absorption of the drug is neg-ligible.
191DECONGESTANTS
Adversereactions toacetylcysteine
During administration,acetylcysteine has a“rotten egg” odor thatmay cause nausea. Withprolonged or persistentuse, acetylcysteine mayproduce:• bronchospasm• drowsiness• nausea and vomiting• severe runny nose• stomatitis.
Acetylcysteine isn’trecommended for thepatient with asthma be-cause it may causebronchospasm.
Warning!
938907.qxd 08/26/2008 15:39 Page 191

PharmacodynamicsThe properties of systemic and topical decongestants vary slightly.
System(ic) analysisSystemic decongestants cause vasoconstriction by stimulatingalpha-adrenergic receptors in the blood vessels of the body. Thisreduces the blood supply to the nose, which decreases swelling ofthe nasal mucosa. They also cause contraction of urinary and GIsphincters, dilated pupils, and decreased insulin secretion.
Indirect hitThese drugs may also act indirectly, causing the release of norepi-nephrine from storage sites in the body, which results in peripher-al vasoconstriction.
On topic(al)Like systemic decongestants, topical decongestants stimulatealpha-adrenergic receptors in the smooth muscle of nasal bloodvessels, resulting in vasoconstriction. The combination of reducedblood flow to the nasal mucous membranes and decreased capil-lary permeability reduces swelling. This action improves respira-tion by helping to drain sinuses, clear nasal passages, and openeustachian tubes.
PharmacotherapeuticsSystemic and topical decongestants are used to relieve the symp-toms of swollen nasal membranes resulting from:• acute coryza (profuse discharge from the nose)• allergic rhinitis (hay fever)• the common cold• sinusitis• vasomotor rhinitis.
Team tacticsSystemic decongestants are commonly given with other drugs,such as antihistamines, antimuscarinics, antipyretic analgesics,and antitussives.
Advantage, topicalTopical decongestants provide two major advantages over sys-temics: minimal adverse reactions and rapid symptom relief.
Drug interactionsBecause they produce vasoconstriction, which reduces drug ab-sorption, topical decongestants seldom produce drug interactions.
192RESPIRATORY DRUGS
With sneezingusually comes
congestion.Better get a
decongestant!
938907.qxd 08/26/2008 15:39 Page 192

Systemic decongestants, however, may interact with other drugs.(See Adverse reactions to decongestants.)• Increased CNS stimulation may occur when systemic deconges-tants are taken with other sympathomimetic drugs, including epi-nephrine, norepinephrine, dopamine, dobutamine, isoproterenol,metaproterenol, terbutaline, and phenylephrine, and tyramine-containing foods.• Use of systemic decongestants with MAOIs may causesevere hypertension or a hypertensive crisis, which can be life-threatening. These drugs shouldn’t be used together.• Alkalinizing drugs may increase the effects of pseudoephedrineby reducing its urinary excretion.
Quick quiz
1. Which adverse reaction can occur if guaifenesin is taken inlarger doses than necessary?
A. ConstipationB. VomitingC. InsomniaD. Diarrhea
Answer: B. Vomiting can occur if guaifenesin is taken in abnor-mally large doses.
193QUICK QUIZ
Most adverse reactions to deconges-tants result from central nervous systemstimulation and include:• nervousness• restlessness• insomnia• nausea• palpitations• tachycardia• difficulty urinating• elevated blood pressure.
Systemic decongestants exacerbatehypertension, hyperthyroidism, diabetes,benign prostatic hypertrophy, glaucoma,and heart disease. They’re also secretedin breast milk in a breast-feedingwoman.
Topical decongestants
The most common adverse reaction as-sociated with prolonged use (more than5 days) of topical decongestants is re-bound nasal congestion.
Other reactions include:• burning and stinging of the nasal mu-cosa• sneezing• mucosal dryness or ulceration.
Issue of sensitivity
The patient who’s hypersensitive to othersympathomimetic amines may also behypersensitive to decongestants.
Warning!
Adverse reactions to decongestants
938907.qxd 08/26/2008 15:39 Page 193

2. Which medication should the patient avoid when taking dex-tromethorphan?
A. AcetaminophenB. GuaifenesinC. PhenelzineD. Famotidine
Answer: C. MAOIs, such as phenelzine, should be avoided by thepatient taking dextromethorphan; concurrent use may cause life-threatening reactions.
3. Besides bronchitis, acetylcysteine may also be used to treat:A. acetaminophen overdose.B. severe rhinorrhea.C. stomatitis.D. diarrhea.
Answer: A. Acetylcysteine is an effective antidote for aceta-minophen overdose.
4. Which adverse reaction most commonly occurs with a decon-gestant, such as tetrahydrozoline, especially if it’s taken more of-ten than recommended?
A. NauseaB. DizzinessC. DiarrheaD. Rebound nasal congestion
Answer: D. Rebound nasal congestion commonly occurs whentetrahydrozoline is taken more frequently than recommended.
ScoringIf you answered all four items correctly, you’re slicker than a mu-
colytic in action!If you answered three items correctly, you’re as relaxed as
bronchial smooth muscle on xanthines.If you answered fewer than three items correctly, you may need
to clear your head with a decongestant. Review the chapteronce more and try again!
194RESPIRATORY DRUGS
✰✰✰
✰✰
✰
Great job onrespiratory
drugs! Now let’sflip on over to
GI drugs.
938907.qxd 08/26/2008 15:39 Page 194

Drugs and the GI systemThe GI tract is basically a hollow, muscular tube that begins at themouth and ends at the anus; it encompasses the pharynx, esopha-gus, stomach, and the small and large intestines. Its primary func-tions are to digest food and absorb nutrients and fluids and ex-crete metabolic waste.
Getting on tractClasses of drugs used to improve GI function include:• peptic ulcer drugs• adsorbent, antiflatulent, and digestive drugs• obesity drugs• antidiarrheal and laxative drugs• antiemetic and emetic drugs.
Antiulcer drugsA peptic ulcer is a circumscribed lesion that develops in the mu-cous membranes of the lower esophagus, stomach, duodenum, orjejunum.
8
Gastrointestinal drugs
Just the facts
In this chapter, you’ll learn:
♦ classes of drugs used to improve GI function
♦ uses and varying actions of these drugs
♦ how these drugs are absorbed, distributed, metabolized,and excreted
♦ drug interactions and adverse reactions to these drugs.
I’m veryimportant to the
GI tract. I helpdigest food and
absorb nutrients!
938908.qxd 08/26/2008 15:49 Page 195

Counting causesThe five major causes of peptic ulcers are:
bacterial infection with Helicobacter pylori
the use of nonsteroidal anti-inflammatory drugs (NSAIDs)
hypersecretory states such as Zollinger-Ellison syndrome (acondition in which excessive secretion of gastric acid causes pep-tic ulcers)
cigarette smoking, which causes hypersecretion and impairsulcer healing
a genetic predisposition, which accounts for 20% to 50% ofpeptic ulcers.
Balancing actPeptic ulcer drugs are aimed at either eradicating H. pylori orrestoring the balance between acid and pepsin secretions and theGI mucosal defense. These drugs include:• systemic antibiotics• antacids• Histamine-2 (H2) receptor antagonists• proton pump inhibitors• other peptic ulcer drugs, such as misoprostol and sucralfate.
Systemic antibioticsH. pylori is a gram-negative bacterium that’s thought to be a ma-jor causative factor in the formation of peptic ulcers and gastritis(inflammation of the stomach lining). Eradication of the bacteriahelps to heal ulcers and decrease their recurrence.
Teamwork is a mustSuccessful treatment involves the use of two or more antibioticsin combination with other drugs such as acid suppressants. Sys-temic antibiotics used to treat H. pylori include:• amoxicillin• clarithromycin• metronidazole• tetracycline.
Pharmacokinetics (how drugs circulate)Systemic antibiotics are variably absorbed from the GI tract.
196GASTROINTESTINAL DRUGS
938908.qxd 08/26/2008 15:49 Page 196

Dairy delayFood, especially dairy products, decreases the absorption of tetra-cycline but doesn’t significantly delay the absorption of the otherantibiotics.
Distribution and excretionAll of these antibiotics are distributed widely and are excreted pri-marily in urine.
Pharmacodynamics (how drugs act)Antibiotics act by treating the H. pylori infection. They’re usuallycombined with an H2-receptor antagonist or a proton pump in-hibitor to decrease stomach acid and further promote healing.
Pharmacotherapeutics (how drugs are used)They are indicated for H. pylori eradication to reduce the risk of aduodenal ulcer. For this reason they may be used in conjunctionwith other medications such as proton pump inhibitors.
Successful strategySuccessful treatment plans use at least two antibiotics and a pro-ton pump inhibitor for 14 days and then use a proton pump in-hibitor for 6 more weeks to help reduce acid in patients with apeptic ulcer.
Drug interactionsTetracycline and metronidazole can interact with many other med-ications.• Tetracycline increases digoxin levels.• Metronidazole and tetracycline increase the risk of bleedingwhen taken with oral anticoagulants.• Metronidazole can cause a severe reaction when combined withalcohol. (See Adverse reactions to antibiotics.)
AntacidsAntacids are over-the-counter (OTC) medications that are used asadjunct therapy to treat peptic ulcers. They include:• aluminum carbonate gel• calcium carbonate• magaldrate (aluminum-magnesium complex)• magnesium hydroxide and aluminum hydroxide• simethicone.
197ANTIULCER DRUGS
Food decreasesthe absorption of
tetracycline.
Adversereactions toantibiotics
Antibiotics used to im-prove GI tract functionmay lead to adverse re-actions.• Metronidazole, clar-ithromycin, and tetracy-cline commonly causemild GI disturbances.• Clarithromycin andmetronidazole may alsoproduce abnormaltastes.• Amoxicillin may causediarrhea.
Warning!
938908.qxd 08/26/2008 15:49 Page 197

PharmacokineticsAntacids work locally in the stomach by neutralizing gastric acid.They don’t need to be absorbed to treat peptic ulcers.
Distribution and excretionAntacids are distributed throughout the GI tract and are eliminat-ed primarily in stool.
PharmacodynamicsThe acid-neutralizing action of antacids reduces the total amountof acid in the GI tract, allowing peptic ulcers to heal.
The more it works, the sooner it restsPepsin, one of the stomach secretions, acts more effectively whenthe stomach is highly acidic; therefore, as acidity drops, pepsin ac-tion is also reduced. Contrary to popular belief, antacids don’twork by coating peptic ulcers or the lining of the GI tract.
PharmacotherapeuticsAntacids are primarily prescribed to relieve pain and are used ad-junctively in peptic ulcer disease.
Settling the GI systemAntacids also relieve symptoms of acid indigestion, heartburn,dyspepsia (burning or indigestion), or gastroesophageal reflux dis-ease (GERD), in which the contents of the stomach and duode-num flow back into the esophagus.
Fighting phosphateAntacids may be used to control hyperphosphatemia (elevatedblood phosphate levels) in kidney failure. Because calcium bindswith phosphate in the GI tract, calcium carbonate antacids pre-vent phosphate absorption.
Drug interactionsAll antacids can interfere with the absorption of oral drugs givenat the same time. Absorption of digoxin, phenytoin, ketoconazole,iron salts, isoniazid, quinolones, and tetracyclines may be reducedif taken within 2 hours of antacids. (See Adverse reactions toantacids.)
198GASTROINTESTINAL DRUGS
Antacids caninterfere with the
absorption ofother orally
administereddrugs.
Adversereactions toantacids
All adverse reactions toantacids are dose relat-ed and include:• diarrhea• constipation• electrolyte imbalances• aluminum accumula-tion in serum.
Warning!
938908.qxd 08/26/2008 15:49 Page 198

H2-receptor antagonistsH2-receptor antagonists are commonly prescribed antiulcer drugsin the United States. They include:• cimetidine• famotidine• nizatidine• ranitidine.
PharmacokineticsCimetidine, nizatidine, and ranitidine are absorbed rapidlyand completely from the GI tract. Famotidine isn’t completely ab-sorbed. Antacids may reduce the absorption of H2-receptor antag-onists.
Distribution, metabolism, and excretionH2-receptor antagonists are distributed widely throughout thebody, metabolized by the liver, and excreted primarily in urine.
PharmacodynamicsH2-receptor antagonists block histamine from stimulating the acid-secreting parietal cells of the stomach.
The acid testAcid secretion in the stomach depends on the binding of gastrin,acetylcholine, and histamine to receptors on the parietal cells. Ifthe binding of one of these substances is blocked, acid secretionis reduced. The H2-receptor antagonists, by binding with H2 recep-tors, block the action of histamine in the stomach and reduce acidsecretion. (See How H2-receptor antagonists work, page 200.)
PharmacotherapeuticsH2-receptor antagonists are used therapeutically to:• promote healing of duodenal and gastric ulcers• provide long-term treatment of pathologic GI hypersecretoryconditions such as Zollinger-Ellison syndrome• reduce gastric acid production and prevent stress ulcers in theseverely ill patient and in the patient with reflux esophagitis or up-per GI bleeding.
Drug interactionsH2-receptor antagonists may interact with antacids and otherdrugs.
199ANTIULCER DRUGS
938908.qxd 08/26/2008 15:49 Page 199

200GASTROINTESTINAL DRUGS
These illustrations show how histamine-2 (H2) receptor antagonists reduce the release of gastric acid.
To stimulate gastric acid secretion, certain endogenous sub-stances—primarily histamine, but also acetylcholine and gas-trin—attach to receptors on the surface of parietal cells. Thesesubstances activate the enzyme adenyl cyclase, which con-verts adenosine triphosphate (ATP) to the intracellular catalystcyclic adenosine monophosphate (cAMP).
The cAMP ultimately stimulates proton-pump (H/K ATPase) ac-tivity. The pump catalyzes the exchange of extracellular potas-sium (K) ions for intracellular hydrogen (H) ions. When the H+
ions combine with extracellular chloride (Cl) ions excreted bygastric cells at a different site, the result is hydrochloric (HCl),or gastric, acid.
H2-receptor antagonists competitively bind to H2-receptor siteson the surface of parietal cells and inhibit the common pathwaythat histamine and the other substances must travel to stimu-late proton-pump activity and promote gastric acid secretion.
Now I get it!
How H2-receptor antagonists work
H2 receptor
Histamine
Parietal cell
H2 receptor
Histamine
H2 receptor
H2-receptorantagonist
Histamine
adenylcyclase
cAMP
cAMP
ATP
H/KATPase
H H
K
Cl
HCl
938908.qxd 08/26/2008 15:49 Page 200

• Antacids reduce the absorption of cimetidine, famotidine, nizati-dine, and ranitidine.• Cimetidine may increase the blood levels of oral anticoagulants,propranolol (and possibly other beta-adrenergic blockers), benzo-diazepines, tricyclic antidepressants, theophylline, procainamide,quinidine, lidocaine, phenytoin, calcium channel blockers, cyclo-sporine, carbamazepine, and opioid analgesics by reducing theirmetabolism in the liver and subsequent excretion.• Cimetidine taken with carmustine increases the risk of bonemarrow toxicity.• Cimetidine inhibits metabolism of ethyl alcohol in the stomach,resulting in higher blood alcohol levels. (See Adverse reactions toH2-receptor antagonists.)
Proton pump inhibitorsProton pump inhibitors disrupt chemical binding in stomachcells to reduce acid production, lessening irritation and allowingpeptic ulcers to better heal. They include:• esomeprazole• lansoprazole• omeprazole• pantoprazole• rabeprazole.
PharmacokineticsProton pump inhibitors are given orally in enteric-coated formulasto bypass the stomach because they’re highly unstable in acid.When in the small intestine, they dissolve and are absorbedrapidly.
Metabolism and excretionThese medications are highly protein-bound and are extensivelymetabolized by the liver to inactive compounds and then eliminat-ed in urine.
PharmacodynamicsProton pump inhibitors block the last step in the secretion of gas-tric acid by combining with hydrogen, potassium, and adenosinetriphosphate in the parietal cells of the stomach.
PharmacotherapeuticsProton pump inhibitors are indicated for:• short-term treatment of active gastric ulcers
201ANTIULCER DRUGS
Adversereactions toH2-receptorantagonists
The use of H2-receptorantagonists may lead toadverse reactions, espe-cially in the elderly pa-tient and the patient withaltered hepatic or renalfunction.• Cimetidine and raniti-dine may produceheadache, dizziness,malaise, muscle pain,nausea, diarrhea or con-stipation, rash, itching,loss of sexual desire, gy-necomastia (cimetidine),and impotence.• Famotidine and nizati-dine produce few ad-verse reactions; head-ache is the most com-mon, followed byconstipation or diarrheaand rash.
Warning!
938908.qxd 08/26/2008 15:49 Page 201

• active duodenal ulcers• erosive esophagitis• symptomatic GERD unresponsive to other therapies• active peptic ulcers associated with H. pylori infection, in com-bination with antibiotics• long-term treatment of hypersecretory states such as Zollinger-Ellison syndrome.
Drug interactionsProton pump inhibitors may interfere with the metabolism of di-azepam, phenytoin, and warfarin, causing increased half-life andelevated plasma levels of these drugs.
Absorbing talkProton pump inhibitors may also interfere with the absorption ofdrugs that depend on gastric pH for absorption, such as ketocona-zole, digoxin, ampicillin, and iron salts. (See Adverse reactions toproton pump inhibitors.)
Other antiulcer drugsResearch continues on the usefulness of other drugs in treatingpeptic ulcer disease. Two other drugs currently in use are:• misoprostol (a synthetic form of prostaglandin E1)• sucralfate.
PharmacokineticsEach drug has a slightly different pharmacokinetic property.
Absorption, metabolism, and excretionAfter an oral dose, misoprostol is absorbed extensively and rapid-ly. It’s metabolized to misoprostol acid, which is clinically active,meaning that it can produce a pharmacologic effect. Misoprostolacid is highly protein-bound and is excreted primarily in urine.
Sucralfate is minimally absorbed from the GI tract and is ex-creted in stool.
PharmacodynamicsThe actions of these drugs vary.
Nay-saying NSAIDsMisoprostol protects against peptic ulcers caused by NSAIDs byreducing the secretion of gastric acid and boosting the productionof gastric mucus, a natural defense against peptic ulcers.
202GASTROINTESTINAL DRUGS
That misoprostolis one active drug!
Adversereactions toproton pumpinhibitors
Adverse reactions toproton pump inhibitorsinclude:• abdominal pain• diarrhea• nausea and vomiting.
Warning!
938908.qxd 08/26/2008 15:49 Page 202

Protective pasteSucralfate works locally in the stomach, rapidly reacting with hy-drochloric acid to form a thick, pastelike substance that adheresto the gastric mucosa and, especially, to ulcers. By binding to theulcer site, sucralfate actually protects the ulcer from the damagingeffects of acid and pepsin to promote healing. This binding usuallylasts for 6 hours.
PharmacotherapeuticsEach of these drugs has its own therapeutic use.
Making it less complicatedMisoprostol prevents gastric ulcers caused by NSAIDs in the pa-tient at high risk for complications resulting from gastric ulcers.(See Dangers of misoprostol use during pregnancy.)
In the short runSucralfate is used for the short-term treatment (up to 8 weeks) ofduodenal or gastric ulcers and for the prevention of recurrent ul-cers or stress ulcers.
Drug interactionsMisoprostol and sucralfate may interact with other drugs.• Antacids may bind with misoprostol or decrease its absorption.However, this effect doesn’t appear to be clinically significant.• Antacids may reduce the binding of sucralfate to the gastric andduodenal mucosa, reducing its effectiveness.• Cimetidine, digoxin, norfloxacin, phenytoin, fluoroquinolones,ranitidine, tetracycline, and theophylline decrease the absorptionof sucralfate. (See Adverse reactions to other peptic ulcer drugs.)
203ANTIULCER DRUGS
Sucralfatereacts with
hydrochloric acidto form a
substance thatadheres to ulcer
sites.
Adversereactions toother pepticulcer drugs
Misoprostol
• Diarrhea (common andusually dose-related)• Abdominal pain• Gas• Indigestion• Nausea and vomiting
Sucralfate
• Constipation• Nausea and vomiting• Metallic taste
Warning!
Use of misoprostol during pregnancy can leadto premature birth, birth defects, or fetal abor-tion. When used after the 8th week of preg-nancy to induce labor or abortion, misoprostol
can cause uterine rupture as well. Misopros-tol-induced abortions may be incomplete. Forthese reasons, the drug is contraindicated forgastric ulcer prevention during pregnancy.
Safe and sound
Dangers of misoprostol use during pregnancy
938908.qxd 08/26/2008 15:49 Page 203

Adsorbent, antiflatulent, anddigestive drugs
Adsorbent, antiflatulent, and digestive drugs are used to fight un-desirable toxins, acids, and gases in the GI tract, aiding healthy GIfunction.
Adsorbent drugsNatural and synthetic adsorbents are prescribed as antidotes forthe ingestion of toxins, substances that can lead to poisoning oroverdose.
Charcoal sketchThe most commonly used clinical adsorbent is activated charcoal,a black powder residue obtained from the distillation of variousorganic materials.
PharmacokineticsActivated charcoal must be administered soon after toxic inges-tion because it can bind only with drugs or poisons that haven’tyet been absorbed from the GI tract.
Vicious cycleAfter initial absorption, some poisons move back into the in-testines, where they’re reabsorbed. Activated charcoal may be ad-ministered repeatedly to break this cycle.
Absorption, metabolism, and excretionActivated charcoal, which isn’t absorbed or metabolized by thebody, is excreted unchanged in stool.
PharmacodynamicsBecause adsorbents attract and bind to toxins in the intestine,they inhibit toxins from being absorbed by the GI tract. However,this binding doesn’t change toxic effects caused by earlier absorp-tion of the poison.
PharmacotherapeuticsActivated charcoal is a general-purpose antidote used for manytypes of acute oral poisoning. It isn’t indicated in acute poisoningfrom mineral acids, alkalines, cyanide, ethanol, methanol, iron,
204GASTROINTESTINAL DRUGS
Don’t worry. Weknow not to giveyou activatedcharcoal untilyou’re at least
1 year old.
938908.qxd 08/26/2008 15:49 Page 204

lithium, sodium chloride alkali, inorganic acids, or organic sol-vents. It also shouldn’t be used in a child who’s younger than age1 year. In addition, it shouldn’t be used in a patient who has a riskof GI obstruction, perforation, or hemorrhage or decreased or ab-sent bowel sounds, or who has had recent GI surgery.
Drug interactionsActivated charcoal can decrease absorption of oral medications;therefore, medications (other than those used to treat the ingestedtoxin) shouldn’t be taken orally within 2 hours of taking the acti-vated charcoal. The effectiveness of activated charcoal may be de-creased by vomiting induced by ipecac syrup. If both drugs areused to treat oral poisoning, activated charcoal should be used af-ter vomiting has ceased. (See Adverse reactions to activated char-coal.)
Antiflatulent drugsAntiflatulents disperse gas pockets in the GI tract. They’re avail-able alone or in combination with antacids. A major antiflatulentdrug currently in use is simethicone.
PharmacokineticsAntiflatulents aren’t absorbed from the GI tract. They’re distrib-uted only in the intestinal lumen and are eliminated intact in stool.
PharmacodynamicsAntiflatulents provide defoaming action in the GI tract. By produc-ing a film in the intestines, simethicone disperses mucus-enclosedgas pockets and helps prevent their formation.
PharmacotherapeuticsAntiflatulents are prescribed to treat conditions in which excessgas is a problem, such as:• functional gastric bloating• postoperative gaseous bloating• diverticular disease• spastic or irritable colon• air swallowing.
Drug interactionsSimethicone doesn’t interact significantly with other drugs anddoesn’t cause known adverse reactions.
205ADSORBENT, ANTIFLATULENT, AND DIGESTIVE DRUGS
Antiflatulentdrugs create a
film in theintestines thatcollapses anddisperses gas
bubbles.
Adversereactions toactivatedcharcoal
Activated charcoal turnsstools black and maycause constipation.
Teaming up
A laxative, such as sor-bitol, usually is givenwith activated charcoalto prevent constipationand improve taste.
Warning!
938908.qxd 08/26/2008 15:49 Page 205

Digestive drugsDigestive drugs (digestants) aid digestion in the patient who’smissing enzymes or other substances needed to digest food. Di-gestants that function in the GI tract, liver, and pancreas include:• pancreatin• pancrelipase• lipase• protease• amylase (pancreatic enzymes).
PharmacokineticsDigestants aren’t absorbed; they act locally in the GI tract and areexcreted in stool.
PharmacodynamicsThe action of digestants resembles the action of the body sub-stances they replace. Pancreatic enzymes replace normal pancre-atic enzymes. They exert their effect in the duodenum and upperjejunum of the upper GI tract.
Breaking it downThese drugs contain trypsin to digest proteins, amylase to digestcarbohydrates, and lipase to digest fats.
PharmacotherapeuticsBecause their action resembles the action of the body substancesthey replace, each digestant has its own indication.
Mirror imagesPancreatic enzymes are administered to the patient with insuffi-cient levels of pancreatic enzymes, such as the patient with pan-creatitis or cystic fibrosis. They may also be used to treat steator-rhea (disorder of fat metabolism characterized by fatty, foul-smelling stool).
Drug interactionsAntacids reduce the effects of pancreatic enzymes and shouldn’tbe given at the same time. Pancreatic enzymes may decrease theabsorption of folic acid and iron. (See Adverse reactions to diges-tive drugs.)
206GASTROINTESTINAL DRUGS
Adversereactions todigestive drugs
Pancreatic enzymes
• Abdominal cramping• Diarrhea• Nausea
Warning!
938908.qxd 08/26/2008 15:49 Page 206

Obesity drugsObesity drugs are used for patients who are morbidly obese andhave health problems that are likely to improve with weight loss.They’re used in combination with a weight management programthat includes diet, physical activity, and behavioral modification.Drug therapy should be used to improve health rather than pro-mote cosmetic weight loss.
Drugs for obesity fall into two categories:• appetite suppressants (phentermine and sibutramine)• fat blockers (orlistat).
PharmacokineticsSibutramine is rapidly absorbed from the intestines and rapidlydistributed to most body tissues. It’s metabolized in the liver andexcreted in the urine and feces. Orlistat isn’t absorbed systemical-ly; its action occurs in the GI tract. Orlistat is excreted in thefeces.
PharmacodynamicsAppetite suppressants increase the amount of norepinephrine anddopamine in the brain, thereby suppressing the appetite. The fat-blocking drug orlistat binds to gastric and pancreatic lipases inthe GI tract, making them unavailable to break down fats. Thisblocks absorption of 30% of the fat ingested in a meal.
PharmacotherapeuticsAppetite suppressants and fat blockers are used primarily forweight loss when losing weight will improve the patient’s healthand prevent death.
Drug interactionsObesity drugs interact with other drugs.• Appetite suppressants taken with cardiovascular stimulantsmay increase the risk of hypertension and arrhythmias. • Appetite suppressants taken with central nervous system (CNS)stimulants can cause increased anxiety and insomnia.• Appetite suppressants taken with serotonergic drugs (includingfluoxetine, sumatriptan, dextromethorphan, and lithium) cancause agitation, confusion, hypomania, impaired coordination,loss of consciousness, nausea, or tachycardia.
207ADSORBENT, ANTIFLATULENT, AND DIGESTIVE DRUGS
Obesity drugsshould only be usedfor morbidly obese
patients as part of acombined regimenthat includes diet,
physical activity, andbehavioral
modification.
938908.qxd 08/26/2008 15:49 Page 207

• Orlistat blocks the absorption of fat-soluble vitamins if taken to-gether. (See Adverse reactions to obesity drugs.)
Antidiarrheal and laxative drugsDiarrhea and constipation are the two major symptoms related todisturbances of the large intestine.
Is it local?Antidiarrheals act systemically or locally and include:• opioid-related drugs• kaolin and pectin• 5-HT3 receptor antagonists (alosetron).
Loosen up!Laxatives stimulate defecation and include:• hyperosmolar drugs• dietary fiber and related bulk-forming substances• emollients• stimulants• lubricants.
Opioid-related drugsOpioid-related drugs decrease peristalsis (involuntary, progres-sive, wavelike intestinal movement that pushes fecal matteralong) in the intestines and include:• diphenoxylate with atropine
208GASTROINTESTINAL DRUGS
Although manyover-the-counter
laxatives areavailable, diet andlifestyle changesare probably thebest first line ofdefense against
constipation.
Adverse reactions to obesity drugs include the following:• Phentermine can cause nervousness, dry mouth, constipation, andhypertension.• Sibutramine can cause dry mouth, headache, insomnia, nervousness,constipation, hypertension, tachycardia, and palpitations.• Orlistat causes abdominal pain, oily spotting, fecal urgency, flatulencewith discharge, fatty stools, fecal incontinence, and increased defeca-tion. These effects usually subside after a few weeks.
Warning!
Adverse reactions to obesity drugs
938908.qxd 08/26/2008 15:49 Page 208

• loperamide.
PharmacokineticsThe combination drug diphenoxylate with atropine is readily ab-sorbed from the GI tract. However, loperamide isn’t absorbed wellafter oral administration.
Distribution, metabolism, and excretionBoth drugs are distributed in serum, metabolized in the liver, andexcreted primarily in stool. Diphenoxylate with atropine is metab-olized to difenoxin, its biologically active major metabolite.
PharmacodynamicsDiphenoxylate with atropine and loperamide slow GI motility bydepressing peristalsis in the large and small intestines. Thesedrugs also decrease expulsive contractions throughout the colon.
PharmacotherapeuticsDiphenoxylate with atropine and loperamide are used to treatacute, nonspecific diarrhea. Loperamide is used to treat chronicdiarrhea.
Drug interactionsDiphenoxylate with atropine and loperamide may enhance the de-pressant effects of barbiturates, alcohol, opioids, tranquilizers,and sedatives. (See Adverse reactions to opioid-related drugs.)
Kaolin and pectinKaolin and pectin mixtures are locally acting OTC antidiarrheals.They work by adsorbing irritants and soothing the intestinal mu-cosa.
PharmacokineticsKaolin and pectin aren’t absorbed and, therefore, aren’t distrib-uted throughout the body. They’re excreted in stool.
PharmacodynamicsKaolin and pectin act as adsorbents, binding with bacteria, toxins,and other irritants in the intestinal mucosa. Pectin decreases thepH in the intestinal lumen and provides a soothing effect on the ir-ritated mucosa.
209ANTIDIARRHEAL AND LAXATIVE DRUGS
Kaolin andpectin give
diarrhea theone-two punch.
Adversereactions toopioid-relateddrugs
Adverse reactions todiphenoxylate with at-ropine and loperamideinclude:• nausea and vomiting• abdominal discomfortor distention• drowsiness• fatigue• central nervous sys-tem depression• tachycardia (fast heartrate)• paralytic ileus (re-duced or absent peri-stalsis in the intestines).
Warning!
938908.qxd 08/26/2008 15:50 Page 209

PharmacotherapeuticsKaolin and pectin are used to relieve mild to moderate acute diar-rhea. They may also be used to temporarily relieve chronic diar-rhea until the cause is determined and definitive treatment begun.
Drug interactionsThese antidiarrheals can interfere with the absorption of digoxinand other drugs by the intestinal mucosa if administered at thesame time. (See Adverse reactions to kaolin and pectin.)
5-HT3 receptor antagonistsAlosetron is a selective 5-HT3 receptor antagonist used for short-term treatment of women with irritable bowel syndrome (IBS)with severe diarrhea as the main symptom. This drug is availableonly through a restricted marketing program because of reportedserious GI adverse effects. Only prescribers enrolled in the pre-scribing program for alosetron may write a prescription for it.
PharmacokineticsAlosetron is rapidly absorbed after oral administration and is me-tabolized by the cytochrome P450 pathway.
PharmacodynamicsAlosetron is thought to block serotonin in the GI system, therebyreducing the abdominal cramping and discomfort, urgency, and di-arrhea commonly associated with IBS.
PharmacotherapeuticsAlosetron is used for the short-term treatment of a woman withIBS whose primary symptom is diarrhea. The drug shouldn’t betaken if the patient is constipated and should be stopped if consti-pation develops.
Drug interactionsAlosetron produces a 30% inhibition of N-acetyltransferase andCYP1A2. Although studies haven’t been done, the inhibition ofN-acetyltransferase may have clinical significance when alosetronis given with such drugs as isoniazid, procainamide, and hydral-azine. Alosetron given with other drugs that decrease GI motilitycould cause constipation. (See Adverse reactions to alosetron.)
210GASTROINTESTINAL DRUGS
Adversereactions tokaolin andpectin
Kaolin and pectin mix-tures cause few adversereactions. However,constipation may occur,especially in an elderlyor a debilitated patientand with overdose orprolonged use.
Warning!
Adversereactions toalosetron
Alosetron can cause se-rious and sometimes fa-tal adverse reactions,such as ischemic colitis,and complications ofconstipation, includingobstruction, perforation,and toxic megacolon.
Elderly patients
Older adults may haveincreased sensitivity toalosetron’s effects, thusincreasing their risk ofdeveloping serious con-stipation.
Warning!
938908.qxd 08/26/2008 15:50 Page 210

Hyperosmolar laxativesHyperosmolar laxatives work by drawing water into the intestine,thereby promoting bowel distention and peristalsis. They include:• glycerin• lactulose• saline compounds (magnesium salts, sodium biphosphate, sodi-um phosphate, polyethylene glycol [PEG], and electrolytes).
PharmacokineticsThe pharmacokinetic properties of hyperosmolar laxatives vary.
Direct placementGlycerin is placed directly into the colon by enema or suppositoryand isn’t absorbed systemically.
Minimal absorptionLactulose enters the GI tract orally and is minimally absorbed. Asa result, the drug is distributed only in the intestine. It’s metabo-lized by bacteria in the colon and excreted in stool.
Introducing ionsAfter saline compounds are introduced into the GI tract orally oras an enema, some of their ions are absorbed. Absorbed ions areexcreted in urine, the unabsorbed drug in stool.
Pegging PEGPEG is a nonabsorbable solution that acts as an osmotic drug, butdoesn’t alter electrolyte balance.
PharmacodynamicsHyperosmolar laxatives produce a bowel movement by drawingwater into the intestine. Fluid accumulation distends the boweland promotes peristalsis, resulting in a bowel movement.
PharmacotherapeuticsThe uses of hyperosmolar laxatives vary.• Glycerin is helpful in bowel retraining.• Lactulose is used to treat constipation and to reduce ammoniaproduction and absorption from the intestines in the patient withan elevated ammonia level, as occurs in cirrhosis and liver failure.• Saline compounds are used when prompt and complete bowelevacuation is required.
211ANTIDIARRHEAL AND LAXATIVE DRUGS
Hyperosmolarlaxatives help the
colon draw the waternecessary for
distention,peristalsis, andeventual bowel
movement.
938908.qxd 08/26/2008 15:50 Page 211

Drug interactionsHyperosmolar laxatives don’t interact significantly with otherdrugs. However, oral drugs given 1 hour before administering PEGhave significantly decreased absorption. (See Adverse reactions tohyperosmolar laxatives.)
Dietary fiber and related bulk-forming laxativesA high-fiber diet is the most natural way to prevent or treat consti-pation. Dietary fiber is the part of plants not digested in the smallintestine.
Bulking upBulk-forming laxatives, which resemble dietary fiber, containnatural and semisynthetic polysaccharides and cellulose. Theselaxatives include:• methylcellulose• polycarbophil• psyllium hydrophilic mucilloid.
PharmacokineticsDietary fiber and bulk-forming laxatives aren’t absorbed systemi-cally. The polysaccharides in these drugs are converted by intesti-nal bacterial flora into osmotically active metabolites that drawwater into the intestine.
212GASTROINTESTINAL DRUGS
A diet high infiber is the bestway to preventconstipation.
Adverse reactions to most hyperosmolar laxatives involve fluid and electrolyte imbalances.
Warning!
Adverse reactions to hyperosmolar laxatives
Glycerin
• Weakness• Fatigue
Lactulose
• Abdominal distention andcramps, gas• Nausea and vomiting• Diarrhea• Hypokalemia
• Hypovolemia• Increased blood glucoselevel
Saline compounds
• Weakness• Lethargy• Dehydration• Hypernatremia• Hypermagnesemia
• Hyperphosphatemia • Hypocalcemia• Cardiac arrhythmias • Shock
Polyethylene glycol
• Nausea• Explosive diarrhea• Bloating
938908.qxd 08/26/2008 15:50 Page 212

ExcretionDietary fiber and bulk-forming laxatives are excreted in stool.
PharmacodynamicsDietary fiber and bulk-forming laxatives increase stool mass andwater content, promoting peristalsis.
PharmacotherapeuticsBulk-forming laxatives are used to:• treat simple cases of constipation, especially constipation re-sulting from a low-fiber or low-fluid diet• aid patients recovering from acute myocardial infarction (MI) orcerebral aneurysms who need to avoid Valsalva’s maneuver(forced expiration against a closed airway) and maintain soft stool• manage patients with IBS and diverticulosis.
Drug interactionsDecreased absorption of digoxin, warfarin, and salicylates occursif these drugs are taken within 2 hours of taking fiber or bulk-forming laxatives. (See Adverse reactions to dietary fiber and re-lated bulk-forming laxatives.)
Emollient laxativesEmollients—also known as stool softeners—include the calcium,potassium, and sodium salts of docusate.
PharmacokineticsAdministered orally, emollients are absorbed and excretedthrough bile in stool.
PharmacodynamicsEmollients soften stool and make bowel movements easier byemulsifying the fat and water components of stool in the smalland large intestines. This detergent action allows water and fats topenetrate stool, making it softer and easier to eliminate.
Stimulating talkEmollients also stimulate electrolyte and fluid secretion from in-testinal mucosal cells.
213ANTIDIARRHEAL AND LAXATIVE DRUGS
Adversereactions todietary fiberand relatedbulk-forminglaxatives
Adverse reactions to di-etary fiber and relatedbulk-forming laxativesinclude: • gas• abdominal fullness• intestinal obstruction• fecal impaction (hardstool that can’t be re-moved from the rectum)• esophageal obstruc-tion (if sufficient liquidhasn’t been adminis-tered with the drug)• severe diarrhea.
Warning!
938908.qxd 08/26/2008 15:50 Page 213

PharmacotherapeuticsEmollients are the drugs of choice for softening stools in patientswho should avoid straining during a bowel movement, includingthose with:• recent MI or surgery• disease of the anus or rectum• increased intracranial pressure (ICP)• hernias.
Drug interactionsTaking oral doses of mineral oil with oral emollients increases thesystemic absorption of mineral oil and may result in tissue de-posits of the oil.
Proceed with cautionBecause emollients may enhance the ab-sorption of many oral drugs, drugs withlow margins of safety (narrow therapeu-tic index) should be administered cau-tiously with emollients. (See Adverse re-actions to emollient laxatives.)
Stimulant laxativesStimulant laxatives, also known as irritant cathartics, include:• bisacodyl• castor oil• senna.
PharmacokineticsStimulant laxatives are minimally absorbed and are metabolizedin the liver. The metabolites are excreted in urine and stool.
PharmacodynamicsStimulant laxatives promote peristalsis and produce a bowelmovement by irritating the intestinal mucosa or stimulating nerveendings of the intestinal smooth muscle.
No job is too smallCastor oil also increases peristalsis in the small intestine.
214GASTROINTESTINAL DRUGS
Emollients helpsoften the stool,
easing the strain ofdefecation.
Adversereactions toemollientlaxatives
Although adverse reac-tions to emollients sel-dom occur, they may in-clude:• bitter taste• diarrhea• throat irritation• mild, transient abdomi-nal cramping.
Warning!
938908.qxd 08/26/2008 15:50 Page 214

PharmacotherapeuticsStimulant laxatives are the preferred drugs for emptying the bow-el before general surgery, sigmoidoscopic or proctoscopic proce-dures, and radiologic procedures such as barium studies of the GItract.
They’re also used to treat constipation caused by prolongedbed rest, neurologic dysfunction of the colon, and constipatingdrugs such as opioids.
Drug interactionsNo significant drug interactions occur with the stimulant laxa-tives. However, because these laxatives produce increased intesti-nal motility, they reduce the absorption of other oral drugs admin-istered at the same time, especially sustained-release forms. (SeeAdverse reactions to stimulant laxatives.)
Lubricant laxativesMineral oil is the main lubricant laxative currently in clinical use.
PharmacokineticsIn its nonemulsified form, mineral oil is minimally absorbed; theemulsified form is about half absorbed. Absorbed mineral oil isdistributed to the mesenteric lymph nodes, intestinal mucosa, liv-er, and spleen.
Metabolism and excretionMineral oil is metabolized by the liver and excreted in stool.
PharmacodynamicsMineral oil lubricates stool and the intestinal mucosa and preventswater reabsorption from the bowel lumen. The increased fluidcontent of stool increases peristalsis. Administration by enemaalso produces distention.
PharmacotherapeuticsMineral oil is used to treat constipation and maintain soft stoolwhen straining is contraindicated, such as after a recent MI (toavoid Valsalva’s maneuver), eye surgery (to prevent increasedpressure in the eye), or cerebral aneurysm repair (to avoid in-creased ICP).
215ANTIDIARRHEAL AND LAXATIVE DRUGS
Adversereactions tostimulantlaxatives
Adverse reactions tostimulant laxatives in-clude: • weakness• nausea• abdominal cramps• mild inflammation ofthe rectum and anus• urine discoloration(with senna).
Warning!
938908.qxd 08/26/2008 15:50 Page 215

Impacting impactionAdministered orally or by enema, this lubricant laxative is alsoused to treat the patient with fecal impaction.
Drug interactionsMineral oil can interact with other drugs.• Mineral oil may impair the absorption of many oral drugs, in-cluding fat-soluble vitamins, hormonal contraceptives, and anti-coagulants.• Mineral oil may interfere with the antibacterial activity of non-absorbable sulfonamides. To minimize drug interactions, adminis-ter mineral oil at least 2 hours before these medications. (See Ad-verse reactions to mineral oil.)
Antiemetic and emetic drugsAntiemetics and emetics are two groups of drugs with opposingactions. Antiemetic drugs decrease nausea, reducing the urge tovomit. Emetic drugs, which are derived from plants, produce vom-iting.
AntiemeticsThe major antiemetics are:• antihistamines, including buclizine, cyclizine, dimenhydrinate,diphenhydramine, hydroxyzine hydrochloride, hydroxyzinepamoate, meclizine, and trimethobenzamide• phenothiazines, including chlorpromazine, perphenazine,prochlorperazine maleate, promethazine, and thiethylperazinemaleate
216GASTROINTESTINAL DRUGS
Mineral oilcan impair the
absorptionof some oral
drugs.
Adverse reactions to mineral oil include:• nausea and vomiting• diarrhea• abdominal cramping.
Warning!
Adverse reactions to mineral oil
938908.qxd 08/26/2008 15:50 Page 216

• serotonin 5-HT3 receptor antagonists, including dolasetron,granisetron, and ondansetron.
Top of the chartsOndansetron is currently the antiemetic of choice in the UnitedStates.
PharmacokineticsThe pharmacokinetic properties of antiemetics may vary slightly.
Absorption, metabolism, and excretionOral antihistamine antiemetics are absorbed well from the GI tractand are metabolized primarily by the liver. Their inactive metabo-lites are excreted in urine.
Phenothiazine antiemetics and serotonin 5-HT3 receptor antag-onists are absorbed well, extensively metabolized by the liver, andexcreted in urine and stool.
PharmacodynamicsThe action of antiemetics may vary.
What’s going on here?The mechanism of action that produces the antiemetic effect ofantihistamines is unclear.
Don’t pull the trigger!Phenothiazines produce their antiemetic effect by blocking thedopaminergic receptors in the chemoreceptor trigger zone in thebrain. (This area of the brain, near the medulla, stimulates thevomiting center in the medulla, causing vomiting.) These drugsmay also directly depress the vomiting center.
Stopping serotonin stimulationThe serotonin 5-HT3 receptor antagonists block serotonin stimula-tion centrally in the chemoreceptor trigger zone and peripherallyin the vagal nerve terminals, both of which stimulate vomiting.
PharmacotherapeuticsThe uses of antiemetics may vary.
Lend me your earAntihistamines are specifically used for nausea and vomitingcaused by inner ear stimulation. As a consequence, these drugsprevent or treat motion sickness. They usually prove most effec-
217ANTIEMETIC AND EMETIC DRUGS
Some antiemeticsblock the vomiting
center in my medullaor nearby areas thatstimulate vomiting.
938908.qxd 08/26/2008 15:50 Page 217

tive when given before activities that produce motion sicknessand are much less effective when nausea or vomiting has alreadybegun.
Severe casesPhenothiazine antiemetics and serotonin 5-HT3 receptor antago-nists control severe nausea and vomiting from various causes.They’re used when vomiting becomes severe and potentially haz-ardous, such as postsurgical or viral nausea and vomiting. Bothtypes of drugs are also prescribed to control the nausea and vom-iting resulting from chemotherapy and radiotherapy. (See Otherantiemetics.)
Drug interactionsAntiemetics may have many significant interactions.• Antihistamines and phenothiazines can produce additive CNSdepression and sedation when taken with CNS depressants, suchas barbiturates, tranquilizers, antidepressants, alcohol, and opi-oids.• Antihistamines can cause additive anticholinergic effects, suchas constipation, dry mouth, vision problems, and urine retention,when taken with anticholinergic drugs, including tricyclic antide-pressants, phenothiazines, and antiparkinsonian drugs.
218GASTROINTESTINAL DRUGS
When you’re notfeeling so hot, itmight be time for
an antiemetic.
Other antiemetics
Here are other antiemetics currently in use.
Scopolamine
Scopolamine prevents motion sickness, but itsuse is limited because of its sedative and anti-cholinergic effects. One transdermal prepara-tion, Transderm-Scop, is highly effective with-out producing the usual adverse effects.
Metoclopramide
Metoclopramide is used primarily to treat GImotility disorders including gastroparesis in di-abetic patients. It’s also used to preventchemotherapy-induced nausea and vomiting.
Diphenidol
Diphenidol is used to prevent vertigo (whirlingsensation) and to prevent or treat generalizednausea and vomiting. However, its use is limit-
ed because of the auditory and visual halluci-nations, confusion, and disorientation that mayoccur.
Dronabinol
Dronabinol, a purified derivative of cannabis, isa Schedule II drug (meaning it has a high po-tential for abuse) used to treat chemotherapy-induced nausea and vomiting in the patientwho doesn’t respond adequately to conven-tional antiemetics. It has also been used tostimulate appetite in the patient with acquiredimmunodeficiency syndrome. However, dron-abinol can accumulate in the body, and the pa-tient can develop tolerance or physical andpsychological dependence.
938908.qxd 08/26/2008 15:50 Page 218

• Phenothiazine antiemetics taken with anticholinergic drugs in-crease the anticholinergic effect and decrease the antiemetic ef-fects.• Droperidol used with phenothiazine antiemetics increases therisk of extrapyramidal (abnormal involuntary movements) effects.(See Adverse reactions to antiemetics.)
EmeticsEmetics are used to induce vomiting in a person who has ingestedtoxic substances. Ipecac syrup is used to induce vomiting in earlymanagement of oral poinsoning or drug overdose.
Controversy?The use of ipecac syrup has become controversial, however, be-cause it delays the use of activated charcoal. There’s a risk of po-tential abuse by individuals with eating disorders. The AmericanAcademy of Pediatrics no longer recommends the routine use ofipecac syrup. The first action parents or caregivers should take ifa child has ingested a poisonous substance is to call the poisoncontrol center and emergency medical services.
PharmacokineticsLittle information exists concerning the absorption, distribution,and excretion of ipecac syrup. After administration of ipecacsyrup, vomiting occurs within 10 to 30 minutes.
219ANTIEMETIC AND EMETIC DRUGS
Use of these antiemetic drugs may lead to ad-verse reactions:• Antihistamine and phenothiazine antiemeticsproduce drowsiness and sometimes paradoxi-cal central nervous system (CNS) stimulation.• CNS effects associated with phenothiazineand serotonin 5-HT3 receptor antagonistantiemetics include confusion, anxiety, eupho-ria, agitation, depression, headache, insomnia,restlessness, and weakness.
• The anticholinergic effect of antiemetics maycause constipation, dry mouth and throat,painful or difficult urination, urine retention, im-potence, and visual and auditory disturbances.• Phenothiazine antiemetics commonly causehypotension and orthostatic hypotension withan increased heart rate, fainting, and dizziness.
Warning!
Adverse reactions to antiemetics
938908.qxd 08/26/2008 15:50 Page 219

Measuring successThe success of treatment is directly linked to fluid intake withipecac administration.
PharmacodynamicsIpecac syrup induces vomiting by stimulating the vomiting centerlocated in the brain’s medulla.
PharmacotherapeuticsIpecac syrup is used to induce vomiting in the early managementof oral poisoning and drug overdose in individuals who are fullyconscious. It shouldn’t be used after ingestion of petroleum prod-ucts, volatile oils, or caustic substances, such as lye, because ofthe risk of additional esophageal injury or aspiration.
Drug interactionsBecause ipecac syrup is used only in acute situations, drug inter-actions rarely occur. If poisoning results from ingestion of a phe-nothiazine, the phenothiazine’s antiemetic effect may decrease theemetic effect of ipecac syrup. Ipecac syrup shouldn’t be adminis-tered concurrently with activated charcoal, which will absorb andinactivate it. (See Adverse reactions to ipecac syrup.)
220GASTROINTESTINAL DRUGS
Afteradministration of
ipecac syrup, vomitingoccurs within 10 to
30 minutes.
Adversereactions toipecac syrup
Ipecac syrup rarely pro-duces adverse reactionswhen used in the recom-mended dosages. How-ever, prolonged vomiting(for more than 1 hour) orrepeated vomiting (morethan six episodes in1 hour), lethargy, and di-arrhea may occur withregular dosage as well.Some people are verysensitive to ipecacsyrup.
Warning!
938908.qxd 08/26/2008 15:50 Page 220

Quick quiz
1. A patient is asked why he’s taking antibiotics for an ulcer.The practitioner explains that antibiotics will:
A. destroy the bacteria causing the ulcer.B. destroy the virus causing the ulcer.C. prevent infection from entering through open areas in
the gastric mucosa.D. prevent infection from occurring.
Answer: A. Antibiotics destroy bacteria responsible for ulcer for-mation.
2. What’s a common adverse reaction to misoprostol?A. IndigestionB. ConstipationC. HeadacheD. Diarrhea
Answer: D. Diarrhea is a common adverse reaction to misopros-tol.
3. How does simethicone relieve gas in the GI tract?A. It disperses and prevents gas pocket formation.B. It facilitates expulsion of gas pockets.C. It neutralizes gastric contents and reduces gas.D. It coats and protects the lining of the stomach.
Answer: A. Simethicone relieves gas in the GI tract by producinga film in the intestines that disperses mucus-enclosed gas pocketsand helps prevent their formation.
4. The antiemetic drug that would probably be best for a patientwho experiences motion sickness on an airplane is:
A. chlorpromazine.B. dronabinol.C. dimenhydrinate.D. dolasetron.
Answer: C. An antihistamine, such as dimenhydrinate, is themost effective antiemetic for a patient who experiences motionsickness during air travel.
5. To prevent a postsurgical patient from straining during abowel movement, the practitioner is most likely to prescribe:
A. docusate.B. magnesium citrate.C. bisacodyl.D. castor oil.
221QUICK QUIZ
938908.qxd 08/26/2008 15:50 Page 221

Answer: A. Docusate is commonly prescribed to prevent strain-ing during a bowel movement after surgery.
ScoringIf you answered all five items correctly, well done! You digested
this GI information admirably!If you answered four items correctly, keep up the good work
(preferably without emetics).If you answered fewer than four items correctly, you may need
extra stimulation. Reread this chapter and see what youcan do!
222GASTROINTESTINAL DRUGS
Boy, yourknowledge of clinical
pharmacology isreally taking off!
✰✰✰
✰✰
✰
938908.qxd 08/26/2008 15:50 Page 222

Drugs and the genitourinary systemThe GU system consists of the reproductive system (the sex or-gans) and the urinary system, which includes the kidneys, ureters,bladder, and urethra. The kidneys perform most of the work of theurinary system.
MultitalentedThe kidneys perform several vital tasks, including:• disposing of wastes and excess ions in the form of urine• filtering blood, which regulates its volume and chemical make-up• helping to maintain fluid, electrolyte, and acid-base balances• producing several hormones and enzymes• converting vitamin D to a more active form• helping to regulate blood pressure and volume by secretingrenin.
Helping handsTypes of drugs used to treat GU disorders include:• diuretics• urinary tract antispasmodics• erectile dysfunction therapy drugs• hormonal contraceptives.
9
Genitourinary drugs
Just the facts
In this chapter, you’ll learn:
♦ classes of drugs used to treat genitourinary (GU) disor-ders
♦ uses and varying actions of these drugs
♦ absorption, distribution, metabolization, and excretion ofthese drugs
♦ drug interactions and adverse reactions to these drugs.
I’m amaster at
multitasking!
938909.qxd 08/26/2008 15:56 Page 223

DiureticsDiuretics trigger the excretion of water and electrolytes from thekidneys, making these drugs a primary choice in the treatment ofrenal disease, edema, hypertension, and heart failure.
Thiazide and thiazide-like diureticsDerived from sulfonamides, thiazide and thiazide-like diuretics areused to treat edema and to prevent the development and recur-rence of renal calculi. They’re also used for such cardiovasculardiseases as hypertension and heart failure.
Thiazide diuretics include:• bendroflumethiazide• chlorothiazide• hydrochlorothiazide• hydroflumethiazide• methyclothiazide• polythiazide.
Thiazide-like diuretics include:• chlorthalidone• indapamide• metolazone.
Pharmacokinetics (how drugs circulate)Thiazide diuretics are absorbed rapidly but incompletely from theGI tract after oral administration. They cross the placenta and aresecreted in breast milk. These drugs differ in how well they’re me-tabolized, but all are excreted primarily in urine.
Thiazide-like diuretics are absorbed from the GI tract. Chlor-thalidone is 90% bound to erythrocytes; little is known about itsmetabolism. Indapamide is distributed widely into body tissuesand metabolized in the liver. Little is also known about the metab-olism of metolazone. All of these drugs are primarily excreted inurine.
Pharmacodynamics (how drugs act)Thiazide and thiazide-like diuretics promote the excretion of wa-ter by preventing the reabsorption of sodium in the kidneys. Asthe kidneys excrete the excess sodium, they excrete water alongwith it. These drugs also increase the excretion of chloride, potas-sium, and bicarbonate, which can result in electrolyte imbalances.With long-term use, thiazide diuretics also lower blood pressureby causing arteriolar vasodilation.
224GENITOURINARY DRUGS
938909.qxd 08/26/2008 15:56 Page 224

Turning down the volumeInitially, diuretic drugs decrease circulating blood volume, leadingto reduced cardiac output. However, if therapy is maintained, car-diac output stabilizes but plasma fluid volume decreases.
Pharmacotherapeutics (how drugs are used)Thiazides are used for the long-term treatment of hypertension;they’re also used to treat edema caused by kidney or liver disease,mild or moderate heart failure, and corticosteroid and estrogentherapy. Because these drugs decrease the level of calcium inurine, they may be used alone or with other drugs to prevent thedevelopment and recurrence of renal calculi.
Pointing out a paradoxIn patients with diabetes insipidus (a disorder characterized byexcessive urine production and excessive thirst resulting from re-duced secretion of antidiuretic hormone), thiazides paradoxicallydecrease urine volume, possibly through sodium depletion andplasma volume reduction.
Drug interactionsDrug interactions related to thiazide and thiazide-like diuretics re-sult in altered fluid volume, blood pressure, and serum electrolytelevels:• These drugs may decrease excretion of lithium, causing lithiumtoxicity.• Nonsteroidal anti-inflammatory drugs, including cyclooxyge-nase-2 (COX-2) inhibitors, may reduce the antihypertensive effectof these diuretics.• Use of these drugs with other potassium-depleting drugs anddigoxin may cause an additive effect, increasing the risk of digox-in toxicity.• These diuretics may increase the response to skeletalmuscle relaxants.• Use of these drugs may increase blood glucose levels, re-quiring higher doses of insulin or oral antidiabetic drugs.• These drugs may produce additive hypotension whenused with antihypertensives. (See Adverse reactions to thi-azide and thiazide-like diuretics.)
Loop diureticsLoop (high ceiling) diuretics are highly potent drugs. They includebumetanide, ethacrynic acid, and furosemide.
225DIURETICS
Administeringthiazide diuretics
along withantihypertensives can
result in additivehypotension. I don’tlike the way this is
adding up!
Adversereactions tothiazide andthiazide-likediuretics
The most common ad-verse reactions to thi-azide and thiazide-likediuretics include: • reduced blood volume• orthostatic hypoten-sion• hypokalemia• hyperglycemia• hyponatremia.
Warning!
938909.qxd 08/26/2008 15:56 Page 225

PharmacokineticsLoop diuretics are absorbed well in the GI tract and are rapidlydistributed. These diuretics are highly protein bound. They under-go partial or complete metabolism in the liver, except for furo-semide, which is excreted primarily unchanged. Loop diureticsare excreted primarily by the kidneys.
PharmacodynamicsLoop diuretics are the most potent diuretics available, producingthe greatest volume of diuresis (urine production). Bumetanide—which is 40 times more potent than furosemide—is the shortest-acting diuretic. Loop diuretics also have a high potential for caus-ing severe adverse reactions. (See Loop diuretics warning.)
The scoop on the loopLoop diuretics received their name because they act primarily onthe thick, ascending loop of Henle (the part of the nephron re-sponsible for concentrating urine) to increase the secretion ofsodium, chloride, and water. These drugs also inhibit sodium,chloride, and water reabsorption in the proximal tubule.
PharmacotherapeuticsLoop diuretics are used to treat edema associated with renal dis-ease, hepatic cirrhosis, and heart failure, as well as to treat hyper-tension (usually with a potassium-sparing diuretic or potassiumsupplement to prevent hypokalemia).
Ethacrynic acid may also be used for the short-term manage-ment of ascites due to malignancy, idiopathic edema, or lym-phedema. Furosemide may be used with mannitol to treat cere-bral edema.
Drug interactionsLoop diuretics produce a variety of drug interactions:• The risk of ototoxicity (damage to the organs of hearing) in-creases when aminoglycosides and cisplatin are taken with loopdiuretics (especially with high doses of furosemide). (See Adversereactions to loop diuretics.)• Loop diuretics reduce the hypoglycemic effects of oral antidia-betic drugs, possibly resulting in hyperglycemia.• These drugs may increase the risk of lithium toxicity.• The risk of electrolyte imbalances that can trigger arrhythmiasincreases when cardiac glycosides and loop diuretics are taken to-gether.
226GENITOURINARY DRUGS
Loop diureticswarning
Loop diuretics, with theexception of ethacrynicacid, contain sulfa. A pa-tient who has an allergyto sulfa may experiencean allergic reaction toloop diuretics. Use withcaution, and alert thepatient to this possibility.
Safe andsound
938909.qxd 08/26/2008 15:56 Page 226

• Use with digoxin may cause additive toxicity, increasing the riskof digoxin toxicity and arrhythmias.
Potassium-sparing diureticsPotassium-sparing diuretics have weaker diuretic and antihyper-tensive effects than other diuretics but provide the advantage ofconserving potassium. These drugs include amiloride, spironolac-tone, and triamterene.
PharmacokineticsPotassium-sparing diuretics are only available orally and are ab-sorbed in the GI tract. They’re metabolized by the liver (except foramiloride, which isn’t metabolized) and excreted primarily inurine.
PharmacodynamicsThe direct action of potassium-sparing diuretics on the distaltubule of the kidneys results in urinary excretion of sodium, wa-ter, bicarbonate, and calcium. The drug also decreases the excre-tion of potassium and hydrogen ions. These effects lead to re-duced blood pressure and increased serum potassium levels.
Compare and contrastStructurally similar to aldosterone, spironolactone acts as an al-dosterone antagonist. Aldosterone promotes the retention of sodi-um and water and the loss of potassium, whereas spironolactonecounteracts these effects by competing with aldosterone for re-ceptor sites. As a result, sodium, chloride, and water are excretedand potassium is retained.
PharmacotherapeuticsPotassium-sparing diuretics are used to treat:• edema• diuretic-induced hypokalemia in patients with heart failure• cirrhosis• nephrotic syndrome (abnormal condition of the kidneys)• heart failure• hypertension.
A hairy situationSpironolactone also is used to treat hyperaldosteronism (exces-sive secretion of aldosterone) and hirsutism (excessive hairgrowth), including hirsutism associated with Stein-Leventhal
227DIURETICS
Adversereactions toloop diuretics
The most common ad-verse reactions to loopdiuretics include: • fluid and electrolyteimbalances (includingmetabolic alkalosis, hy-povolemia, hypochlor-emia, hypochloremic al-kalosis, hyperglycemia,hyperuricemia, dehydra-tion, hyponatremia, hy-pokalemia, and hypo-magnesemia)• transient deafness• tinnitus• diarrhea• nausea• vomiting• abdominal pain• impaired glucose toler-ance• dermatitis• paresthesia• hepatic dysfunction• photosensitivity• orthostatic hypoten-sion.
Warning!
938909.qxd 08/26/2008 15:56 Page 227

(polycystic ovary) syndrome. Potassium-sparing diuretics arecommonly used with other diuretics to potentiate their action orcounteract their potassium-wasting effects.
Drug interactionsGiving potassium-sparing diuretics with potassium supplementsor angiotensin-converting enzyme inhibitors increases the risk ofhyperkalemia. Concurrent use of spironolactone and digoxin in-creases the risk of digoxin toxicity. (See Adverse reactions topotassium-sparing diuretics.)
Osmotic diureticsOsmotic diuretics cause diuresis through osmosis, moving fluidinto the extracellular spaces. They include mannitol and urea.
PharmacokineticsAdministered I.V. for rapid distribution, osmotic diuretics arefreely filtered by the glomeruli of the kidney—except for manni-tol, which is only slightly metabolized. Osmotic diuretics are ex-creted primarily in urine.
PharmacodynamicsOsmotic diuretics receive their name because they increase theosmotic pressure of the glomerular filtrate, which inhibits the re-absorption of sodium and water. They create an osmotic gradientin the glomerular filtrate and the blood. In the glomerular filtrate,the gradient prevents sodium and water reabsorption. In theblood, the gradient allows fluid to be drawn from the intracellularinto the intravascular spaces.
PharmacotherapeuticsOsmotic diuretics are used to treat acute renal failure and cere-bral edema and to reduce intracranial and intraocular pressure.Mannitol is used to promote diuresis in acute renal failure and topromote urinary excretion of toxic substances.
Drug interactionsTaking osmotic diuretics with lithium may increase renal excre-tion of lithium, which in turn decreases the effectiveness of lithi-um. Patients taking both drugs require lithium level monitoring.(See Adverse reactions to osmotic diuretics.)
228GENITOURINARY DRUGS
Adversereactions topotassium-sparingdiuretics
Few adverse drug reac-tions occur with potassi-um-sparing diuretics.However, their potassi-um-sparing effects canlead to hyperkalemia,especially if given with apotassium supplementor high-potassium diet.
Warning!
Adversereactions toosmoticdiuretics
Adverse reactions to os-motic diuretics include:• hyponatremia• dehydration• circulatory overload(from osmotic effects)• thrombophlebitis or lo-cal irritation at the infu-sion site.
Warning!
938909.qxd 08/26/2008 15:56 Page 228

Carbonic anhydrase inhibitorsCarbonic anhydrase inhibitors are diuretics that block the actionof carbonic anhydrase. They include acetazolamide and methazo-lamide.
PharmacokineticsCarbonic anhydrase inhibitors are absorbed through the GItract. Some systemic absorption also occurs after oph-thalmic administration. They’re distributed in tissues withhigh carbonic anhydrase content, such as erythrocytes, plas-ma, kidneys, eyes, liver, and muscle. Carbonic anhydrase in-hibitors are excreted by the kidneys in urine.
PharmacodynamicsIn the kidneys, carbonic anhydrase inhibitors decrease theavailability of hydrogen ions, which blocks the sodium-hydrogen exchange mechanisms. As a result, urinary excre-tion of sodium, potassium, bicarbonate, and water increases.
Don’t lose your sense of humorIn the eyes, carbonic anhydrase inhibition reduces aqueous humorproduction, which reduces intraocular pressure.
PharmacotherapeuticsCarbonic anhydrase inhibitors are used for diuresis and to treatglaucoma. Acetazolamide may also be used to treat epilepsy andacute mountain sickness.
Drug interactionsCarbonic anhydrase inhibitors produce a variety of drug interac-tions:• Salicylates may cause carbonic anhydrase inhibitor toxicity, in-cluding central nervous system depression and metabolic acido-sis.• Diflunisal may increase intraocular pressure when given with acarbonic anhydrase inhibitor.• Acetazolamide used concurrently with cyclosporine may in-crease cyclosporine levels and the risk of neurotoxicity.• Acetazolamide used concurrently with primidone may decreaseserum and urine levels of primidone. (See Adverse reactions tocarbonic anhydrase inhibitors.)
229DIURETICS
Acetazolamide…(huff)… may be
used… (puff)… totreat acutemountain
sickness…
Adversereactions tocarbonicanhydraseinhibitors
Adverse reactions tocarbonic anhydrase in-hibitors include:• hypokalemia• metabolic acidosis• electrolyte imbal-ances.
Warning!
938909.qxd 08/26/2008 15:56 Page 229

Urinary tract antispasmodicsUrinary tract antispasmodics help decrease urinary tract musclespasms. They include darifenacin, flavoxate, oxybutynin, solife-nacin, tolterodine, and trospium.
PharmacokineticsFlavoxate, oxybutynin, tolterodine, darifenacin, and solifenacinare most often administered orally and are rapidly absorbed. Tro-spium is administered orally but is poorly absorbed. Oxybutynin isalso available as a dermal patch. These drugs are all widely dis-tributed, metabolized in the liver, and excreted in urine. Urinarytract antispasmodics also cross the placenta and are excreted inbreast milk.
PharmacodynamicsUrinary tract antispasmodics relieve smooth muscle spasms by in-hibiting parasympathetic activity, which causes the detrusor andurinary muscles to relax. Flavoxate and oxybutynin also exhibitmany anticholinergic effects.
PharmacotherapeuticsUrinary tract antispasmodics are used for patients with overactivebladders who have symptoms of urinary frequency, urgency, or in-continence.
Urgent symptomsTrospium is also indicated for patients with overactive bladderswho have symptoms of urge urinary incontinence, and oxybutyninacts as an antispasmodic for uninhibited or reflex neurogenicbladder. (See How oxybutynin works.)
Drug interactionsUrinary tract antispasmodics have few drug interactions:• Use with anticholinergic agents may increase dry mouth, consti-pation, and other anticholinergic effects. (See Adverse reactionsto urinary tract antispasmodics.)• Urinary tract antispasmodics may decrease the effectiveness ofphenothiazines and haloperidol.• Trospium may interfere with the elimination of certain drugs ex-creted through the kidneys (such as digoxin, metformin, and van-comycin), resulting in increased blood levels of these drugs.
230GENITOURINARY DRUGS
How oxybutyninworks
When acetylcholine isreleased within the blad-der, it attaches to recep-tors on the surface ofsmooth muscle in thebladder, stimulatingbladder contractions.Oxybutynin suppressesthese involuntary con-tractions by blocking therelease of acetylcholine.This anticholinergic ef-fect is what makes oxy-butynin useful in thetreatment of overactivebladder.
Now I get it!
938909.qxd 08/26/2008 15:56 Page 230

Erectile dysfunction therapy drugsErectile dysfunction therapy drugs treat penile erectile dysfunc-tion that results from a lack of blood flowing through the corpuscavernosum. This type of erectile dysfunction usually stems fromvascular and neurologic conditions. Drugs used for erectile dys-function include alprostadil, sildenafil, tadalafil, and vardenafil.
PharmacokineticsErectile dysfunction drugs are well absorbed in the GI tract. Dis-tribution of these drugs isn’t known. The majority of thesedrugs—including sildenafil, tadalafil, and vardenafil—are givenorally, metabolized in the liver, and excreted in feces.
An exceptional drugAlprostadil is the exception: it’s administered directly into the cor-pus cavernosum, metabolized in the lungs, and excreted in urine.
PharmacodynamicsSildenafil, tadalafil, and vardenafil selectively inhibit the phospho-diesterase type 5 receptors, which causes an increase in blood lev-els of nitric oxide. This increase in nitric oxide levels activates thecGMP enzyme, which relaxes smooth muscles and allows blood toflow into the corpus cavernosum, causing an erection.
Alprostadil acts locally, promoting smooth muscle relaxation,which causes an increase in blood flow to the corpus cavernosumand produces an erection.
231ERECTILE DYSFUNCTION THERAPY DRUGS
Possible adverse reactions to urinary tractantispasmodics include:• blurred vision• headache• somnolence• urinary retention• dry mouth• dyspepsia
• constipation• nausea• vomiting• weight gain• pain• acute and secondary angle-closureglaucoma.
Warning!
Adverse reactions to urinary tract antispasmodics
938909.qxd 08/26/2008 15:56 Page 231

PharmacotherapeuticsAlprostadil, sildenafil, tadalafil, and vardenafil are all used in thetreatment of erectile dysfunction. Sildenafil is also indicated forthe treatment of pulmonary arterial hypertension.
Drug interactionsErectile dysfunction drugs may interact with other drugsin the following ways:• Nitrates and alpha-adrenergic blockers used in combi-nation with erectile dysfunction drugs may cause severehypotension and potentially serious cardiac events. (SeeAdverse reactions to erectile dysfunction drugs.)• Ketoconazole, itraconazole, and erythromycin may re-sult in increased levels of vardenafil or tadalafil.• Protease inhibitors, such as indinavir or ritonavir, maycause increased tadalafil or vardenafil levels.
232GENITOURINARY DRUGS
Sometimes we justcan’t get along:
Nitrates and alpha-adrenergic blockersused with erectiledysfunction drugscan cause severehypotension and
potentially seriouscardiac events.
Adverse reactions to erectile dysfunctiondrugs include:• decreased supine blood pressure and car-diac output • increased risk of cardiovascular events, in-cluding myocardial infarction, sudden cardiacdeath, ventricular arrhythmias, cerebrovascu-lar hemorrhage, transient ischemic attack, andhypertension
• headache• dizziness• flushing• dyspepsia• vision changes• prolonged erections (more than 4 hours),which can result in irreversible damage toerectile tissue• penile pain (with alprostadil).
Warning!
Adverse reactions to erectile dysfunction drugs
938909.qxd 08/26/2008 15:56 Page 232

Hormonal contraceptivesHormonal contraceptives inhibit ovulation. Contraceptives typi-cally contain a combination of hormones. For example, ethinylestradiol may be combined with desogestrel, drospirenone, lev-onorgestrel, norethindrone, norgestimate, or norgestrel. Also,mestranol may be combined with norethindrone. Ethinyl estradiolor ethynodiol diacetate may also be used alone as a contraceptive.
PharmacokineticsHormonal contraceptives are absorbed from the GI tract and arewidely distributed. They’re metabolized in the kidneys and excret-ed in urine and feces.
Patch powerSome forms of hormonal contraceptives are available in a trans-dermal patch form. These contraceptives are absorbed throughthe skin but have the same distribution, metabolism, and excre-tion as orally administered contraceptives.
PharmacodynamicsThe primary mechanism of action of combination hormonal con-traceptives (estrogen and progestin) is the suppression of go-nadotropins, which inhibits ovulation. Estrogen suppress-es secretion of follicle-stimulating hormone, which blocksfollicular development and ovulation. Progestin suppress-es the secretion of luteinizing hormone, which preventsovulation, even if the follicle develops. Progestin alsothickens the cervical mucus; this interferes with spermmigration and causes endometrial changes that preventimplantation of a fertilized ovum.
PharmacotherapeuticsThe primary purpose for taking hormonal contraceptives is theprevention of pregnancy in women. The combination of ethinylestradiol and norgestimate is also used to treat moderate acne infemales younger than age 15.
233HORMONAL CONTRACEPTIVES
It looks likewe’re not
welcome here,guys!
938909.qxd 08/26/2008 15:56 Page 233

Drug interactionsHormonal contraceptives can interact with other medications invarious ways:• Antibiotics, oxcarbazepine, phenobarbital, phenytoin, topira-mate, and modafinil may decrease the effectiveness of oral contra-ceptives. A patient taking these drugs with a hormonal contracep-tive needs to use a barrier contraceptive.• Atorvastatin may increase serum estrogen levels.• Cyclosporin and theophylline have an increased risk of toxicitywhen taken with hormonal contraceptives.• Prednisone increases the therapeutic and possibly toxic effectsof hormonal contraceptives. (See Adverse reactions to hormonalcontraceptives.)• Several herbal medications can affect serum levels of hormonalcontraceptives.
234GENITOURINARY DRUGS
Potentially serious adverse reactions to hormonal contraceptives in-clude arterial thrombosis, thrombophlebitis, pulmonary embolism, my-ocardial infarction, cerebral hemorrhage or thrombosis, hypertension,gallbladder disease, and hepatic adenomas.
Other adverse reactions include:• acne• bleeding or spotting between menstrual periods• bloating• breast tenderness or enlargement• changes in libido• diarrhea• difficulty wearing contact lenses• unusual hair growth• weight fluctuations• upset stomach• vomiting.
Warning!
Adverse reactions to hormonalcontraceptives
938909.qxd 08/26/2008 15:57 Page 234

Quick quiz
1. When caring for a patient taking a hydrochlorothiazide, youshould monitor the patient for:
A. hypertension.B. hypernatremia.C. hypokalemia.D. hypoglycemia.
Answer: C. Watch for signs of hypokalemia in a patient receivinghydrochlorothiazide.
2. When teaching a patient about diuretics, you should tell himto:
A. take the drug in the evening.B. call his practitioner if he loses more that 2 lb (0.9 kg)
per day.C. eat a high-sodium diet.D. avoid sun exposure for several hours after taking the
medication to prevent a photosensitivity reaction.
Answer: B. A weight loss of more that 2 lb per day indicates ex-cessive diuresis.
3. Urinary tract antispasmodics are used to treat:A. overactive bladder.B. erectile dysfunction.C. hypertension.D. seizures.
Answer: A. Urinary tract antispasmodics are used to treat anoveractive bladder.
4. Which drug necessitates use of an additional form of contra-ception for a patient taking hormonal contraceptives?
A. AtorvastatinB. TheophyllineC. CyclosporineD. Antibiotics
Answer: D. Advise the patient taking hormonal contraceptivesand an antibiotic to use additional form of birth control if she’salso taking certain antibiotics because antibiotics may decreasethe effectiveness of hormonal contraceptives.
235QUICK QUIZ
938909.qxd 08/26/2008 15:57 Page 235

ScoringIf you answered all four questions correctly, terrific! Everything’s
flowing smoothly for you when it comes to GU drugs.If you answered three questions correctly, super! Your stream of
knowledge about GU drugs is impressive.If you answered fewer than three questions correctly, don’t spaz
out! Relax, review the chapter, and try again.
236GENITOURINARY DRUGS
✰✰✰
✰✰
✰
938909.qxd 08/26/2008 15:57 Page 236

Selecting an antimicrobial drugSelecting an appropriate antimicrobial drug to treat a specific in-fection involves several important factors:• First, the microorganism must be isolated and identified—gen-erally through growing a culture.• Then its susceptibility to various drugs must be determined. Be-cause culture and sensitivity results take 48 hours, treatment usu-ally starts at assessment and then is reevaluated when test resultsare obtained.• The location of the infection must be considered. For therapy tobe effective, an adequate concentration of the antimicrobial mustbe delivered to the infection site.• Lastly, the cost of the drug must be considered as well as its po-tential adverse effects and the possibility of patient allergies.
Preventing pathogen resistanceThe usefulness of antimicrobial drugs is limited by pathogens thatmay develop resistance to a drug’s action.
Resistance is the ability of a microorganism to live and grow inthe presence of an antimicrobial drug that’s either bacteriostatic(inhibits the growth or multiplication of bacteria) or bactericidal
10
Anti-infective drugs
Just the facts
In this chapter, you’ll learn:
♦ classes of drugs that act as anti-infectives
♦ the uses and varying actions of these drugs
♦ how these drugs are absorbed, distributed, metabolized,and excreted
♦ drug interactions and adverse reactions to these drugs.
Because I’m asensitive guy, I’mresponsive only to
certain drugs.
938910.qxd 08/26/2008 16:35 Page 237

(kills bacteria). Resistance usually results from genetic mutationof the microorganism. (See The rise of the resistance movement.)
Antibacterial drugsAntibacterial drugs, also known as antibiotics (drugs that inhibitthe growth of bacteria), are used mainly to treat systemic (involv-ing the whole body rather than a localized area) bacterial infec-tions. The antibacterials include:• aminoglycosides• penicillins• cephalosporins• tetracyclines• lincomycin derivatives• macrolides• vancomycin• carbapenems• monobactams• fluoroquinolones• sulfonamides• nitrofurantoin (nitrofuran).
AminoglycosidesAminoglycosides provide effective bactericidal activity against:• gram-negative bacilli• some aerobic gram-positive bacteria• mycobacteria• some protozoa.
Common aminoglycosidesAminoglycosides currently in use include:• amikacin sulfate• gentamicin sulfate• kanamycin sulfate• neomycin sulfate• paromomycin sulfate• streptomycin sulfate• tobramycin sulfate.
Pharmacokinetics (how drugs circulate)Because aminoglycosides are absorbed poorly from the GI tract,they’re usually given parenterally. After I.V. or I.M. administration,aminoglycoside absorption is rapid and complete.
238ANTI-INFECTIVE DRUGS
The rise of theresistancemovement
Indiscriminate use of an-timicrobial drugs has se-rious consequences.Unnecessary exposureof organisms to thesedrugs encourages theemergence of resistantstrains, which are likelyto do far more damagethan their predecessors.
Make reservations
The use of antimicrobialdrugs should be re-served for patients withinfections caused bysusceptible organismsand should be used inhigh enough doses andfor an appropriate peri-od. New antimicrobialdrugs should be re-served for severely illpatients with serious in-fections that don’t re-spond to conventionaldrugs.
Yea or nay?
938910.qxd 08/26/2008 16:35 Page 238

DistributionAminoglycosides are distributed widely in extracellular fluid.They readily cross the placental barrier, but don’t cross the blood-brain barrier.
Metabolism and excretionAminoglycosides aren’t metabolized. They’re excreted primarilyunchanged by the kidneys.
Pharmacodynamics (how drugs act)Aminoglycosides act as bactericidal drugs (remember, this meansthey kill bacteria) against susceptible organisms by binding to thebacterium’s 30S subunit, a specific ribosome in the microorgan-ism, thereby interrupting protein synthesis and causing the bac-terium to die.
Rising resistanceBacterial resistance to aminoglycosides may be related to:• failure of the drug to cross the cell membrane• altered binding to ribosomes• destruction of the drug by bacterial enzymes.
One-two punchSome gram-positive enterococci resist aminoglycoside transportacross the cell membrane. When penicillin is used with aminogly-coside therapy, the cell wall is altered, allowing the aminoglyco-side to penetrate the bacterial cell.
Pharmacotherapeutics (how drugs are used)Aminoglycosides are most useful in treating:• infections caused by gram-negative bacilli• serious nosocomial (hospital-acquired) infections, such asgram-negative bacteremia (abnormal presence of microorganismsin the bloodstream), peritonitis (inflammation of the peritoneum,the membrane that lines the abdominal cavity), and pneumonia, incritically ill patients• urinary tract infections (UTIs) caused by enteric bacilli that areresistant to less toxic antibiotics, such as penicillins andcephalosporins• infections of the central nervous system (CNS) and the eye(treated with local instillation).
Works well with othersAminoglycosides are used in combination with penicillins to treatgram-positive organisms, such as staphylococcal or enterococcal
239ANTIBACTERIAL DRUGS
Aminoglycosidesare usually given
parenterallybecause they’repoorly absorbed
from the GI tract.
938910.qxd 08/26/2008 16:35 Page 239

infections. Combination therapy increases the drugs’ effective-ness.
Inactive dutyAminoglycosides are inactive against anaerobic bacteria.
Role callIndividual aminoglycosides may have their own particular useful-ness:• Streptomycin is active against many strains of mycobacteria, in-cluding Mycobacterium tuberculosis, and against the gram-posi-tive bacteria Nocardia and Erysipelothrix.• Amikacin, gentamicin, and tobramycin are active against Acine-tobacter, Citrobacter, Enterobacter, Klebsiella, Proteus (indole-positive and indole-negative), Providencia, Serratia, Escherichiacoli, and Pseudomonas aeruginosa.
Drug interactionsCarbenicillin and ticarcillin reduce the effects of amikacin, gen-tamicin, kanamycin, neomycin, streptomycin, and tobramycin.This is especially true if the penicillin and aminoglycoside aremixed in the same container or I.V. line.
Putting up a blockadeAmikacin, gentamicin, kanamycin, neomycin, streptomycin, andtobramycin administered with neuromuscular blockers increaseneuromuscular blockade, resulting in increased muscle relaxationand respiratory distress.
Kidney punchToxicity to the kidneys may result in renal failure; toxicity to theneurologic system results in peripheral neuropathy with numb-ness and tingling of the extremities. The risk of renal toxicity alsoincreases when amikacin, gentamicin, kanamycin, or tobramycinis taken with cyclosporine, amphotericin B, or acyclovir.
What? Say that again…The symptoms of ototoxicity (damage to the ear) caused byaminoglycosides may be masked by antiemetic drugs. Loop diuret-ics taken with aminoglycosides increase the risk of ototoxicity.Hearing loss may occur in varying degrees and may be irre-versible. (See Adverse reactions to aminoglycosides.)
240ANTI-INFECTIVE DRUGS
Adversereactions toaminoglyco-sides
Serious adverse reac-tions limit the use ofaminoglycosides. Theyinclude:• neuromuscular reac-tions, ranging from pe-ripheral nerve toxicity toneuromuscular block-ade• ototoxicity• renal toxicity.
Oral history
Adverse reactions tooral aminoglycosides in-clude:• nausea and vomiting• diarrhea.
Warning!
938910.qxd 08/26/2008 16:35 Page 240

PenicillinsPenicillins remain one of the most important and useful antibac-terials, despite the availability of numerous others. The penicillinscan be divided into four groups:• natural penicillins (penicillin G benzathine, penicillin G potassi-um, penicillin G procaine, penicillin G sodium, penicillin V potas-sium)• penicillinase-resistant penicillins (dicloxacillin, nafcillin,oxacillin)• aminopenicillins (amoxicillin, ampicillin)• extended-spectrum penicillins (carbenicillin, ticarcillin).
PharmacokineticsAfter oral administration, penicillins are absorbed mainly in theduodenum and the upper jejunum of the small intestine.
Absorb these factorsAbsorption of oral penicillin varies and depends on such factorsas the:• particular penicillin used• pH of the patient’s stomach and intestine• presence of food in the GI tract.
Most penicillins should be given on an empty stomach (1 hourbefore or 2 hours after a meal) to enhance absorption. Penicillinsthat can be given without regard to meals include amoxicillin,penicillin V, and amoxicillin/clavulanate potassium.
DistributionPenicillins are distributed widely to most areas of the body, in-cluding the lungs, liver, kidneys, muscle, bone, and placenta. Highconcentrations also appear in urine, making penicillins useful intreating UTIs.
Metabolism and excretionPenicillins are metabolized to a limited extent in the liver to inac-tive metabolites and are excreted 60% unchanged by the kidneys.Nafcillin and oxacillin are excreted in bile.
PharmacodynamicsPenicillins are usually bactericidal in action. They bind reversiblyto several enzymes outside the bacterial cytoplasmic membrane.
241ANTIBACTERIAL DRUGS
Despite thewide variety of
antibacterials inuse, penicillins are
still among themost useful.
938910.qxd 08/26/2008 16:35 Page 241

Playing with PBPsThese enzymes, known as penicillin-binding proteins (PBPs),are involved in cell-wall synthesis and cell division. Interferencewith these processes inhibits cell-wall synthesis, causing rapid de-struction of the cell.
PharmacotherapeuticsNo other class of antibacterial drugs provides as wide a spectrumof antimicrobial activity as the penicillins. As a class, they covergram-positive, gram-negative, and anaerobic organisms, althoughspecific penicillins are more effective against specific organisms.
Oral vs. I.M. routePenicillin is given by I.M. injection when oral administration is in-convenient or a patient’s compliance is questionable. Becauselong-acting preparations of penicillin G (penicillin G benzathineand penicillin G procaine) are relatively insoluble, they must beadministered by the I.M. route.
Drug interactionsPenicillins may interact with various drugs.• Probenecid increases the plasma concentration ofpenicillins.• Penicillins reduce tubular secretion of methotrex-ate in the kidney, increasing the risk of methotrexatetoxicity.• Tetracyclines and chloramphenicol reduce the bactericidal ac-tion of penicillins.• Neomycin decreases the absorption of penicillin V.• The effectiveness of hormonal contraceptives is reduced whenthey’re taken with penicillin V or ampicillin. Be sure to advise thepatient to use a reliable, alternative method of contraception inaddition to hormonal contraceptives during penicillin therapy.• Large doses of I.V. penicillins can increase the bleeding risk ofanticoagulants by prolonging bleeding time. Nafcillin and di-cloxacillin have been implicated in warfarin resistance.
Acting against aminoglycosidesHigh dosages of penicillin G and extended-spectrum penicillins(carbenicillin and ticarcillin) inactivate aminoglycosides. More-over, penicillins shouldn’t be mixed in the same I.V. solutions withaminoglycosides. (See Adverse reactions to penicillins.)
242ANTI-INFECTIVE DRUGS
Let’s move in.We’ll be just fineunless they bringon the penicillins!
938910.qxd 08/26/2008 16:35 Page 242

CephalosporinsMany antibacterial drugs introduced for clinical use in recentyears have been cephalosporins.
Through the generationsCephalosporins are grouped into generations according to theireffectiveness against different organisms, their characteristics,and their development.• First-generation cephalosporins include cefadroxil, cefazolinsodium, and cephalexin monohydrate.• Second-generation cephalosporins include cefaclor, cefprozil,cefoxitin, cefuroxime axetil, and cefuroxime sodium.• Third-generation cephalosporins include cefdinir, cefixime, ce-fotaxime sodium, cefpodoxime proxetil, ceftazidime, ceftibuten,and ceftriaxone sodium.• Fourth-generation cephalosporins include cefepime hydrochlo-ride.
A sensitive issueBecause penicillins and cephalosporins are chemically similar(they have what’s called a beta-lactam molecular structure),cross-sensitivity occurs in 10% to 15% of patients. This means thatsomeone who has had a reaction to penicillin is also at risk for areaction to cephalosporins.
243ANTIBACTERIAL DRUGS
Hypersensitivity reactions are the major ad-verse reactions to penicillins. They may in-clude:• anaphylactic reactions• serum sickness (a hypersensitivity reactionoccurring 1 to 2 weeks after injection of a for-eign serum)• drug fever• various rashes.
Oral penicillins
Adverse GI reactions associated with oralpenicillins include:
• tongue inflammation• nausea and vomiting• diarrhea.
Aminopenicillins and extended-spectrum
penicillins
The aminopenicillins and extended-spectrumpenicillins can produce pseudomembranouscolitis (diarrhea caused by a change in the flo-ra of the colon or an overgrowth of a toxinpro-ducing strain of Clostridium difficile).
Oxacillin
Oxacillin therapy may cause liver toxicity.
Warning!
Adverse reactions to penicillins
938910.qxd 08/26/2008 16:35 Page 243

PharmacokineticsMany cephalosporins are administered parenterally because theyaren’t absorbed from the GI tract. Some cephalosporins are ab-sorbed from the GI tract and can be administered orally, but foodusually decreases the absorption rate of these oral cephalospo-rins, though not the amount absorbed. Two cephalosporins (oralcefuroxime and cefpodoxime) actually have increased absorptionwhen given with food.
DistributionAfter absorption, cephalosporins are distributed widely and readi-ly cross the placenta.
Generational divideCefuroxime (second-generation) and the third-generation drugscefotaxime, ceftriaxone, and ceftazidime cross the blood-brainbarrier after I.V. or I.M. administration. Cefepime (fourth-genera-tion) also crosses the blood-brain barrier, but to what extent isn’tknown.
MetabolismMany cephalosporins aren’t metabolized at all. Cefotaxime sodiumis metabolized to the nonacetyl forms, which provide less antibac-terial activity than the parent compounds. To a small extent, cef-triaxone is metabolized in the intestines to inactive metabolites,which are excreted via the biliary system.
ExcretionAll cephalosporins are excreted primarily unchanged by the kid-neys with the exception of ceftriaxone, which is excreted in stoolvia bile.
PharmacodynamicsLike penicillins, cephalosporins inhibit cell-wall synthesis by bind-ing to the bacterial enzymes known as PBPs, located on the cellmembrane. After the drug damages the cell wall by binding withthe PBPs, the body’s natural defense mechanisms destroy the bac-teria. (See How cephalosporins attack bacteria.)
PharmacotherapeuticsThe four generations of cephalosporins have particular therapeu-tic uses.• First-generation cephalosporins, which act primarily againstgram-positive organisms, may be used as alternative therapy in
244ANTI-INFECTIVE DRUGS
Be careful! Aperson who has
had a reaction topenicillin may alsohave a reaction to
cephalosporins.
938910.qxd 08/26/2008 16:35 Page 244

the patient who’s allergic to penicillin, depending on how sensitiveto penicillin he is. They’re also used to treat staphylococcal andstreptococcal infections, including pneumonia, cellulitis (skin in-fection), and osteomyelitis (bone infection).• Second-generation cephalosporins act against gram-negativebacteria. Cefoxitin is the only cephalosporin effective againstanaerobes (organisms that live without oxygen).• Third-generation cephalosporins, which act primarily againstgram-negative organisms, are the drugs of choice for infectionscaused by Enterobacter, P. aeruginosa, and anaerobic organisms.• Fourth-generation cephalosporins are active against manygram-positive and gram-negative bacteria.
245ANTIBACTERIAL DRUGS
The antibacterial action of cephalosporins depends on their ability to penetrate the bacterial wall and bind with proteins on the cy-toplasmic membrane, as shown below.
Now I get it!
How cephalosporins attack bacteria
Mature bacterial cell Daughter cells after division
Capsule
Cytoplasmicmembrane
Chromosomes
Ribosome
Cephalosporinincorporates itselfinto the cell wall ofa susceptible,mature gram-positive or gram-negative bacterium.
Inclusion body
Inability ofthe cellwall tocloseleads tocell death.
Daughter cellsare unable toclose the cellwall as aresult ofeffects of thecephalosporin.
938910.qxd 08/26/2008 16:35 Page 245

Drug interactionsThe patient receiving cephalosporins who drinks alcoholic bever-ages with or up to 72 hours after taking a dose may experienceacute alcohol intolerance, with such signs and symptoms asheadache, flushing, dizziness, nausea, vomiting, or abdominalcramps within 30 minutes of alcohol ingestion. This re-action can occur up to 3 days after discontinuing theantibiotic. (See Adverse reactions to cephalosporins.)
In use with uricosuricsUricosurics (drugs to relieve gout), such as probenecidand sulfinpyrazone, can reduce kidney excretion ofsome cephalosporins. Probenecid is used therapeutical-ly to increase and prolong plasma cephalosporin con-centrations.
Cephalosporins may also decrease estrogen absorp-tion, leading to decreased efficacy of oral contracep-tives containing estrogen and progesterone.
246ANTI-INFECTIVE DRUGS
Cephalosporinspenetrate and
bind. That’s howthey wipe me out.
Adverse reactions to cephalosporins include:• confusion• seizures• bleeding• nausea• vomiting• diarrhea.
Ceftriaxone may be associated with a de-crease in prothrombin activity (prothrombintime and partial thromboplastin time), leadingto an increased risk of bleeding. Patients atrisk include those with renal impairment, liverdisease, or impaired vitamin K synthesis orstorage.
An issue of sensitivity
Hypersensitivity reactions are the most com-mon systemic adverse reactions tocephalosporins. They include:• hives• itching• measles-type rash• serum sickness (reaction after injection of aforeign serum characterized by edema, fever,hives, and inflammation of the blood vesselsand joints)• anaphylaxis (in rare cases).
Warning!
Adverse reactions to cephalosporins
938910.qxd 08/26/2008 16:35 Page 246

TetracyclinesTetracyclines are broad-spectrum antibiotics. They may be classi-fied as:• intermediate-acting compounds such as demeclocycline hy-drochloride• long-acting compounds, such as doxycycline hyclate andminocycline hydrochloride.
PharmacokineticsTetracyclines are absorbed from the stomach and small intestinewhen taken orally.
Distribution and excretionTetracyclines are distributed widely into body tissues and fluids,concentrated in bile, and excreted primarily by the kidneys. Doxy-cycline is also excreted in stool. Minocycline undergoes entero-hepatic recirculation.
PharmacodynamicsAll tetracyclines are primarily bacteriostatic, meaning they inhibitthe growth or multiplication of bacteria. They penetrate the bacte-rial cell by an energy-dependent process. Within the cell, they bindprimarily to a subunit of the ribosome, inhibiting the protein syn-thesis needed to maintain the bacterial cell.
PharmacotherapeuticsTetracyclines provide a broad spectrum of activity against:• gram-positive and gram-negative aerobic and anaerobic bacteria• spirochetes• mycoplasma• rickettsiae• chlamydiae• some protozoa.
Longer equals broaderThe long-acting compounds doxycycline and minocycline providemore action against various organisms than other tetracyclines.
Taking aimTetracyclines are used to treat Rocky Mountain spotted fever, Qfever, and Lyme disease. They’re the drugs of choice for treatingnongonococcal urethritis caused by Chlamydia and Ureaplasma.
247ANTIBACTERIAL DRUGS
938910.qxd 08/26/2008 16:35 Page 247

Combination therapy with a tetracycline and streptomycin is themost effective treatment for brucellosis.
Zit zapperTetracyclines in low dosages effectively treat acne because theycan decrease the fatty acid content of sebum.
Drug interactionsTetracyclines can reduce the effectiveness of hormonal contracep-tives, which may result in breakthrough bleeding or ineffectivecontraception. The patient taking hormonal contraceptives shoulduse a reliable, secondary method of contraception. Tetracyclinesmay also decrease the bactericidal action of penicillin.
Other interactions commonly affect the ability of tetracyclinesto move through the body.• Aluminum, calcium, and magnesium antacids reduce the ab-sorption of oral tetracyclines.• Iron salts, bismuth subsalicylate, and zinc sulfate reduce the ab-sorption of tetracyclines. Reduced absorption can be prevented byseparating doses of tetracyclines and these agents by 2 to 3 hours.• Barbiturates, carbamazepine, and phenytoin increase the me-tabolism and reduce the antibiotic effect of doxycycline.
Be wary of dairyThese drugs, with the exception of doxycycline and minocycline,may also interact with milk and milk products, which bind withthe drugs and prevent their absorption. To prevent decreased ab-sorption, administer the tetracycline 1 hour before or 2 hours aftermeals. (See Adverse reactions totetracyclines.)
Lincomycin derivativesBecause of its high potential forcausing serious adverse effects, clindamycin is an-other antibacterial prescribed only when there’s notherapeutic alternative. It’s used for many gram-pos-itive and anaerobic organisms.
Less from lincomycinLincomycin is less effective than clindamycin andis rarely used. Lincomycin shouldn’t be used in thetreatment of minor infections but would be used totreat serious respiratory or skin infections in the patient who’s al-lergic to other antibiotics indicated for the infection.
248ANTI-INFECTIVE DRUGS
It’s a good idea towait a few hours
after a meal to taketetracyclines.
Adversereactions totetracyclines
Tetracyclines producemany of the same ad-verse reactions as otherantibacterials, such as:• superinfection (over-growth of resistant or-ganisms)• nausea and vomiting• abdominal distressand distention• diarrhea.
Toxicities
Other adverse reactionsinclude:• photosensitivity reac-tions (red rash on areasexposed to sunlight)• liver toxicity• renal toxicity.
Warning!
938910.qxd 08/26/2008 16:35 Page 248

PharmacokineticsWhen taken orally, clindamycin is absorbed well and distributedwidely throughout the body. It’s metabolized by the liver and ex-creted by the kidneys and biliary pathways. About 20% to 30% oflincomycin, when taken orally, is absorbed from the GI tract; fooddelays its absorption. Lincomycin is partially metabolized in theliver and is excreted in the urine, stool, and bile.
PharmacodynamicsClindamycin and lincomycin inhibit bacterial protein synthesis byinhibiting the binding of bacterial ribosomes. At therapeutic con-centrations, clindamycin is primarily bacteriostatic against mostorganisms.
PharmacotherapeuticsBecause of their potential for causing serious toxicity andpseudomembranous colitis (characterized by severe diarrhea, ab-dominal pain, fever, and mucus and blood in stool), these drugsare limited to a few clinical situations in which safer alternativeantibacterials aren’t available.• Clindamycin is potent against most aerobic gram-positive organ-isms, including staphylococci, streptococci (except Enterococcusfaecalis), and pneumococci.• Clindamycin is effective against most clinically important anaer-obes and is used primarily to treat anaerobic intraabdominal,pleural, or pulmonary infections caused by Bacteroides fragilis.It’s also used as an alternative to penicillin in treating Clostridiumperfringens infections.• Clindamycin and lincomycin may be used as alternatives topenicillin in treating staphylococcal infections in a patient who’sallergic to penicillin.
Drug interactionsClindamycin and lincomycin have neuromuscular blocking prop-erties and may enhance the neuromuscular blocking action ofneuromuscular blockers. This can lead to profound respiratory de-pression. (See Adverse reactions to clindamycin.)
MacrolidesMacrolides are used to treat a number of common infections.They include erythromycin and its derivatives, such as:• erythromycin estolate• erythromycin ethylsuccinate
249ANTIBACTERIAL DRUGS
Adversereactions toclindamycin
Pseudomembranouscolitis may occur withclindamycin. This syn-drome can be fatal andrequires prompt discon-tinuation of the drug aswell as aggressive fluidand electrolyte manage-ment.
Although this is themost serious reaction toclindamycin and limitsits use, other reactionsmay also occur, such as:• diarrhea• stomatitis (mouth in-flammation)• nausea and vomiting• hypersensitivity reac-tions.
Warning!
938910.qxd 08/26/2008 16:35 Page 249

• erythromycin lactobionate• erythromycin stearate.
These aren’t derivativesOther macrolides include:• azithromycin• clarithromycin.
PharmacokineticsBecause erythromycin is acid-sensitive, it must be buffered orhave an enteric coating to prevent destruction by gastric acid. Ery-thromycin is absorbed in the duodenum. It’s distributed to mosttissues and body fluids except, in most cases, for cerebrospinalfluid (CSF). However, as a class, macrolides can enter the CSFwhen meninges are inflamed.
Metabolism and excretionErythromycin is metabolized by the liver and excreted in bile inhigh concentrations; small amounts are excreted in urine. It alsocrosses the placental barrier and is secreted in breast milk.
PharmacodynamicsMacrolides inhibit ribonucleic acid (RNA)–dependent protein syn-thesis by acting on a small portion of the ribosome, much like clin-damycin.
PharmacotherapeuticsErythromycin has a range of therapeutic uses.• It provides a broad spectrum of antimicrobial activity againstgram-positive and gram-negative bacteria, including Mycobacteri-um, Treponema, Mycoplasma, and Chlamydia.• It’s also effective against pneumococci and group A streptococ-ci. Staphylococcus aureus is sensitive to erythromycin; however,resistant strains may appear during therapy.• Erythromycin is the drug of choice for treating Mycoplasmapneumoniae infections as well as pneumonia caused by Legionel-la pneumophila.
An alternative to penicillinIn the patient who’s allergic to penicillin, erythromycin is effectivefor infections produced by group A beta-hemolytic streptococci orStreptococcus pneumoniae. It may also be used to treat gonor-rhea and syphilis in the patient who can’t tolerate penicillin G or
250ANTI-INFECTIVE DRUGS
Erythromycinneeds to be
buffered or coatedto prevent
destruction bygastric acid.
938910.qxd 08/26/2008 16:35 Page 250

the tetracyclines. Erythromycin may also be used to treat minorstaphylococcal infections of the skin.
Ranging far and wide…Azithromycin provides a broad spectrum of antimicrobial activityagainst gram-positive and gram-negative bacteria, including My-cobacterium, S. aureus, Haemophilus influenzae, Moraxella ca-tarrhalis, and Chlamydia. It’s also effective against pneumococciand groups C, F, and G streptococci.
Clarithromycin is a broad-spectrum antibacterial that’s activeagainst gram-positive aerobes, such as S. aureus, S. pneumoniae,and Streptococcus pyogenes; gram-negative aerobes, such asH. influenzae and M. catarrhalis; and other aerobes such asM. pneumoniae.
Clarithromycin has also been used in combination withantacids, histamine-2 blockers, and proton pump inhibitors totreat Helicobacter pylori–induced duodenal ulcer disease.
Drug interactionsMacrolides may interact with these drugs.• Erythromycin, azithromycin, and clarithromycin can increasetheophylline levels in the patient receiving high dosages of theo-phylline, increasing the risk of theophylline toxicity.• Clarithromycin may increase the concentration of carba-mazepine when used together. (See Adverse reactions tomacrolides.)
VancomycinVancomycin hydrochloride is used increasingly to treat methi-cillin-resistant S. aureus, which has become a major concern inthe United States and other parts of the world. Because of theemergence of vancomycin-resistant enterococci, vancomycinmust be used judiciously. As a rule of thumb, it should be usedonly when culture and sensitivity test results confirm the needfor it.
PharmacokineticsBecause vancomycin is absorbed poorly from the GI tract, it mustbe given I.V. to treat systemic infections. However, an oral form ofvancomycin is used to treat pseudomembranous colitis. Van-comycin diffuses well into pleural (around the lungs), pericardial(around the heart), synovial (joint), and ascitic (in the peritonealcavity) fluids.
251ANTIBACTERIAL DRUGS
Macrolides arebroad-spectrum
antibiotics used totreat a number of
common infections.
Adversereactions tomacrolides
Erythromycin producesfew adverse effects,which may include:• epigastric distress• nausea and vomiting• diarrhea (especiallywith large doses)• rash• fever• eosinophilia (an in-crease in the number ofeosinophils, a type ofwhite blood cell)• anaphylaxis.
Warning!
938910.qxd 08/26/2008 16:35 Page 251

No switching!Remember that I.V. vancomycin can’t be used in place of oral van-comycin and vice versa. The two forms aren’t interchangeable.
Metabolism and excretionThe metabolism of vancomycin is unknown. About 85% of thedose is excreted unchanged in urine within 24 hours. A smallamount may be eliminated through the liver and biliary tract.
PharmacodynamicsVancomycin inhibits bacterial cell-wall synthesis, damaging thebacterial plasma membrane. When the bacterial cell wall isdamaged, the body’s natural defenses can attack the organism.
PharmacotherapeuticsVancomycin is active against gram-positive organisms, such asS. aureus, S. epidermidis, S. pyogenes, Enterococcus, and S.pneumoniae.
In the I.V. leagueI.V. vancomycin is the therapy of choice for the patient with a seri-ous resistant staphylococcal infection who’s hypersensitive topenicillins.
Oral historyOral vancomycin is used for the patient with antibiotic-associatedClostridium difficile colitis who can’t take or has respondedpoorly to metronidazole.
The 1 in the 1-2 punchVancomycin, when used with an aminoglycoside, is also the treat-ment of choice for E. faecalis endocarditis in the patient who’s al-lergic to penicillin.
Drug interactionsVancomycin may increase the risk of toxicity when administeredwith other drugs toxic to the kidneys and organs of hearing, suchas aminoglycosides, amphotericin B, bacitracin, cisplatin, colistin,and polymyxin B. (See Adverse reactions to vancomycin.)
252ANTI-INFECTIVE DRUGS
Vancomycin mustbe used judiciously
because of theemergence of
vancomycin-resistantenterococci.
938910.qxd 08/26/2008 16:35 Page 252

CarbapenemsCarbapenems are a class of beta-lactam antibacterials that in-cludes:• ertapenem• imipenem-cilastatin sodium (a combination drug)• meropenem.
The Broadway of antibacterialsThe antibacterial spectrum of activity for imipenem-cilastatin isbroader than that of any other antibacterial studied to date. Be-cause of this broad spectrum of activity, it’s used for serious orlife-threatening infection, especially gram-positive and gram-negative health-care acquired infections. Broad-spectrum antibac-terials cover many organisms; narrow-spectrum antibacterials areeffective against a select few organisms.
PharmacokineticsThe pharmacokinetic properties of carbapenems vary slightly.
Distribution, metabolism, and excretionImipenem must be given with cilastatin because imipenem aloneis rapidly metabolized in the tubules of the kidneys, rendering itineffective. After parenteral administration, imipenem-cilastatin isdistributed widely. It’s metabolized by several mechanisms and ex-creted primarily in urine.
253ANTIBACTERIAL DRUGS
Adverse reactions to vancomycin, althoughrare, include:• hypersensitivity and anaphylactic reactions• drug fever• eosinophilia (an increased number ofeosinophils, a type of white blood cell [WBC])• neutropenia (a decreased number of neu-trophils, another type of WBC)• hearing loss (transient or permanent), espe-cially with excessive doses (as when it’s givenwith other ototoxic drugs).
Rash behavior
Severe hypotension may occur with rapid I.V.administration of vancomycin and may be ac-companied by a red rash with flat and raisedlesions on the face, neck, chest, and arms (redman’s syndrome).
Dosages of 1 g or less should be given over1 hour, and dosages of more than 1 g should begiven over 11⁄2 to 2 hours.
Warning!
Adverse reactions to vancomycin
938910.qxd 08/26/2008 16:35 Page 253

Ertapenem is completely absorbed after I.V. administrationand is more highly protein-bound than the other two carbapen-ems. It’s metabolized by hydrolysis and excreted mainly in urine.
Mostly unchangedAfter parenteral administration, meropenem is distributed widely,including to the CNS. Metabolism is insignificant; 70% of the drugis excreted unchanged in urine.
PharmacodynamicsImipenem-cilastatin, ertapenem, and meropenem are bactericidal.They exert antibacterial activity by inhibiting bacterial cell-wallsynthesis.
PharmacotherapeuticsImipenem has the broadest spectrum of activity of currently avail-able beta-lactam antibiotics.• It’s effective against aerobic gram-positive species, such asStreptococcus, S. aureus, and S. epidermidis.• It inhibits most Enterobacter species.• It also inhibits P. aeruginosa (including strains resistant topiperacillin and ceftazidime) and most anaerobic species, includ-ing B. fragilis.
Lone rangerImipenem may also be used alone to treat serious health-care ac-quired infections and infections in immunocompromised patientscaused by mixed aerobic and anaerobic organisms.
Don’t forget the other carbapenemsMeropenem is indicated for the treatment of intra-abdominal in-fections as well as for the management of bacterial meningitiscaused by susceptible organisms.
Ertapenem’s spectrum of activity includes intra-abdominal,skin, urinary tract, and gynecologic infections as well as commu-nity-acquired pneumonias caused by a variety of gram-positive,gram-negative, and anaerobic organisms.
Drug interactionsCarbapenems may interact with these drugs.• Taking probenecid with imipenem-cilastatin increases theserum level of cilastatin, but only slightly increases the serum lev-el of imipenem.• Probenecid may cause meropenem and ertapenem to accumu-late to toxic levels.
254ANTI-INFECTIVE DRUGS
938910.qxd 08/26/2008 16:35 Page 254

• The combination of imipenem-cilastatin and an aminoglycosideacts synergistically against E. faecalis, Staphylococcus aureusand Listeria monocytogenes. (See Adverse reactions to car-bapenems.)
MonobactamsAztreonam is the first member in the class of monobactam antibi-otics and the only one currently available. It’s a syntheticmonobactam with a narrow spectrum of activity that includesmany gram-negative aerobic bacteria.
PharmacokineticsAfter parenteral administration, aztreonam is rapidly and com-pletely absorbed and widely distributed throughout the body. It’smetabolized partially and excreted primarily in urine as un-changed drug.
PharmacodynamicsAztreonam’s bactericidal activity results from inhibition of bacteri-al cell-wall synthesis. It binds to the PBP-3 of susceptible gram-negative bacterial cells, inhibiting cell-wall division and resultingin lysis.
PharmacotherapeuticsAztreonam is indicated in a range of therapeutic situations.• It’s effective against a wide variety of gram-negative aerobic or-ganisms, including P. aeruginosa.• It’s effective against most strains of thefollowing organisms: E. coli, Enterobacter,Klebsiella pneumoniae, K. oxytoca, Pro-teus mirabilis, Serratia marcescens, H.influenzae, and Citrobacter.• It’s also used to treat complicated and un-complicated UTIs, septicemia, and lower respiratory tract, skinand skin-structure, intra-abdominal, and gynecologic infectionscaused by susceptible gram-negative aerobic bacteria.• It’s usually active against gram-negative aerobic organisms thatare resistant to antibiotics hydrolyzed by beta-lactamases. (Beta-lactamase is an enzyme that makes an antibiotic ineffective.)
It can need helpAztreonam shouldn’t be used alone as empiric therapy (treatmentbased on clinical experience rather than on medical data) in a se-
255ANTIBACTERIAL DRUGS
Aztreonaminhibits bacterial
cell-wallsynthesis.
Adversereactions tocarbapenems
Common adverse reac-tions to ertapenem,imipenem-cilastatin, andmeropenem include:• nausea and vomiting• diarrhea.
If you’re sensitive to
penicillin
Hypersensitivity reac-tions, such as rashes,may occur, particularlyin the patient with aknown hypersensitivityto penicillins.
Kidney conditions
In the patient with de-creased or impaired re-nal function, the dosagemay need to be adjust-ed.
Warning!
938910.qxd 08/26/2008 16:35 Page 255

riously ill patient who may have a gram-positive bacterial infec-tion or a mixed aerobic-anaerobic bacterial infection.
Drug interactionsAztreonam may interact with several other drugs.• Synergistic or additive effects occur when aztreonam is usedwith aminoglycosides or other antibiotics, such as cefoperazone,cefotaxime, clindamycin, and piperacillin.• Potent inducers of beta-lactamase production (cefoxitin,imipenem) may inactivate aztreonam. Concomitant use isn’t rec-ommended.• Taking aztreonam with clavulanic acid–containing antibioticsmay produce synergistic or antagonistic effects, depending on theorganism involved. (See Adverse reactions to aztreonam.)
FluoroquinolonesFluoroquinolones are structurally similar synthetic antibiotics.They are primarily administered to treat UTIs, upper respiratorytract infections, pneumonia, and gonorrhea and include:• ciprofloxacin• levofloxacin• moxifloxacin• norfloxacin• ofloxacin.
PharmacokineticsAfter oral administration, fluoroquinolones are absorbed well.
Metabolism and excretionFluoroquinolones aren’t highly protein-bound, are minimally me-tabolized in the liver, and are excreted primarily in urine.
PharmacodynamicsFluoroquinolones interrupt deoxyribonucleic acid (DNA) synthe-sis during bacterial replication by inhibiting DNA gyrase, an essen-tial enzyme of replicating DNA. As a result, the bacteria can’t re-produce.
PharmacotherapeuticsFluoroquinolones can be used to treat many UTIs. Each drug inthis class also has specific indications.
256ANTI-INFECTIVE DRUGS
Adversereactions toaztreonam
Aztreonam can causesome adverse reactions,including:• diarrhea• hypersensitivity andskin reactions• hypotension• nausea and vomiting• transient electrocar-diogram changes (in-cluding ventricular ar-rhythmias)• transient increases inserum liver enzymelevels.
Warning!
938910.qxd 08/26/2008 16:35 Page 256

• Ciprofloxacin is used to treat lower respiratory tract infections,infectious diarrhea, and skin, bone, and joint infections.• Levofloxacin is indicated for the treatment of lower respiratorytract infections, skin infections, and UTIs.• Moxifloxacin is used to treat acute bacterial sinusitis and mildto moderate community-acquired pneumonia.• Norfloxacin is used to treat UTIs and prostatitis.• Ofloxacin is used to treat selected sexually transmitted dis-eases, lower respiratory tract infections, skin and skin-structureinfections, and prostatitis (inflammation of the prostate gland).
Drug interactionsSeveral drug interactions may occur with the fluoroquinolones.• Administration with antacids that contain magnesium or alu-minum hydroxide results in decreased absorption of the fluoro-quinolone.• Some fluoroquinolones, such as ciprofloxacin, norfloxacin, andofloxacin, interact with xanthine derivatives, such as amino-phylline and theophylline, increasing the plasma theophylline lev-el and the risk of theophylline toxicity.• Giving ciprofloxacin or norfloxacin with probenecid results indecreased kidney elimination of these fluoroquinolones, increas-ing their serum levels and half-life.• Drugs that prolong the QT interval, such as antiarrhythmics,should be used cautiously during moxifloxacin therapy. (See Ad-verse reactions to fluoroquinolones.)
SulfonamidesSulfonamides were the first effective systemic antibacterialdrugs. They include:• co-trimoxazole (sulfamethoxazole and trimethoprim)• sulfadiazine.
PharmacokineticsMost sulfonamides are well absorbed and widely distributed in thebody. They’re metabolized in the liver to inactive metabolites andexcreted by the kidneys.
Lots and lots and lots of liquidBecause crystalluria and subsequent kidney stone formation mayoccur during the metabolic excretory phase, adequate fluid intakeis highly recommended during sulfonamide therapy. The patienttaking oral sulfonamides should take the medication with 8 oz of
257ANTIBACTERIAL DRUGS
Adversereactions tofluoroquino-lones
Fluoroquinolones arewell tolerated by mostpatients, but some seri-ous adverse effects mayoccur, including: • dizziness• nausea and vomiting• diarrhea• abdominal pain.
Serious reactions
Moderate to severe pho-totoxic reactions haveoccurred with direct andindirect sunlight andwith artificial ultravioletlights, with and withoutsunscreen. Light shouldbe avoided for severaldays after stopping fluo-roquinolone therapy.
Warning!
938910.qxd 08/26/2008 16:35 Page 257

water and should drink plenty of fluids throughout therapy (2 to 3L daily).
PharmacodynamicsSulfonamides are bacteriostatic drugs that prevent the growth ofmicroorganisms by inhibiting folic acid production. The decreasedfolic acid synthesis decreases the number of bacterial nucleotidesand inhibits bacterial growth.
PharmacotherapeuticsSulfonamides are commonly used to treat acute UTIs. With recur-rent or chronic UTIs, the infecting organism may not be suscepti-ble to sulfonamides. Therefore, the choice of therapy should bebased on bacteria susceptibility tests.
Infectious behaviorSulfonamides also are used to treat infections caused by Nocardiaasteroides and Toxoplasma gondii. Co-trimoxazole (a combina-tion of a sulfa drug and a folate antagonist) is used for a variety ofother infections, such as Pneumocystis carinii (Pneumocystisjiroveci) pneumonia, acute otitis media (due to H. influenzae andS. pneumoniae), and acute exacerbations of chronic bronchitis(due to H. influenzae and S. pneumoniae). Sulfonamides exhibita wide spectrum of activity against gram-positive and gram-nega-tive bacteria.
Drug interactionsSulfonamides have few significant interactions.• They increase the hypoglycemic effects of the sulfonylureas(oral antidiabetic drugs), which may decrease blood glucose lev-els.• When taken with methenamine, they may lead to the develop-ment of crystals in urine.• Co-trimoxazole may increase the anticoagulant effect ofcoumarin anticoagulants.• Co-timoxazole and methotrexate may cause increasedmethotrexate levels and increase the risk of toxicity.• Co-trimoxazole plus cyclosporine increases the risk of kidneytoxicity. (See Adverse reactions to sulfonamides.)
258ANTI-INFECTIVE DRUGS
If you’re takingsulfonamides,you’d better bedrinking lots of
fluids!
938910.qxd 08/26/2008 16:35 Page 258

NitrofurantoinNitrofurantoin is used to treat acute and chronic UTIs. It isn’tuseful in treating pyelonephritis or perinephric (around the kid-ney) diseases.
PharmacokineticsAfter oral administration, nitrofurantoin is absorbed rapidly andwell from the GI tract. Taking the drug with food enhances itsbioavailability. It’s available in a microcrystalline form and amacrocrystalline form. The microcrystalline form is absorbedmore slowly because of slower dissolution and thus causes less GIdistress.
DistributionThe drug is 20% to 60% protein-bound. Nitrofurantoin crosses theplacental barrier and is secreted in breast milk. It’s also distrib-uted in bile.
Metabolism and excretionNitrofurantoin is partially metabolized by the liver, and 30% to 50%is excreted unchanged in urine.
PharmacodynamicsUsually bacteriostatic, nitrofurantoin may become bactericidal,depending on its urinary concentration and the susceptibility ofthe infecting organism.
259ANTIBACTERIAL DRUGS
Excessively high doses of less water-solublesulfonamides can produce crystals in urineand deposits of sulfonamide crystals in the re-nal tubules. This complication isn’t a problemwith the newer water-soluble sulfonamides.Hypersensitivity reactions may occur and ap-pear to increase as the dosage increases.
Is it serum sickness?
A reaction that resembles serum sickness mayoccur, producing fever, joint pain, hives, bron-chospasm, and leukopenia (reduced whiteblood cell count).
Photo finish
Sulfonamides can also produce photosensitivi-ty reactions.
Warning!
Adverse reactions to sulfonamides
938910.qxd 08/26/2008 16:35 Page 259

Reduces power?Although its exact mechanism of action is unknown, nitrofuran-toin appears to inhibit formation of acetyl coenzyme A from pyru-vic acid, thereby inhibiting the energy production of the infectingorganism. Nitrofurantoin may also disrupt bacterial cell-wall for-mation.
PharmacotherapeuticsBecause the absorbed drug concentrates in urine, nitrofurantoin isused to treat UTIs. It has a higher antibacterial activity in acidurine. Nitrofurantoin isn’t effective against systemic bacterial in-fections.
Drug interactionsNitrofurantoin has few significant interactions.• Probenecid and sulfinpyrazone inhibit the excretion of nitrofu-rantoin by the kidneys, reducing its efficacy and increasing its tox-ic potential.• Magnesium salts and magnesium-containing antacids can de-crease the extent and rate of nitrofurantoin absorption.• Nitrofurantoin may decrease the antibacterial activity of nor-floxacin and nalidixic acid. (See Adverse reactions to nitrofuran-toin.)
Antiviral drugsAntiviral drugs are used to prevent or treat viral infections rang-ing from influenza to human immunodeficiency virus (HIV). Themajor antiviral drug classes used to treat systemic infections in-clude:• synthetic nucleosides• pyrophosphate analogues• influenza A and syncytial virus drugs• nucleoside analogue reverse transcriptase inhibitors (NRTIs)• non-nucleoside reverse transcriptase inhibitors (NNRTIs)• nucleotide analogue reverse transcriptase inhibitors• protease inhibitors.
Synthetic nucleosidesSynthetic nucleosides are a group of drugs used to treat many vi-ral syndromes that can occur in an immunocompromised patient,
260ANTI-INFECTIVE DRUGS
Antiviraldrugs keep
viruses frommultiplying.
Adversereactions tonitrofurantoin
Adverse reactions to ni-trofurantoin include:• GI irritation • anorexia• nausea and vomiting • diarrhea • dark yellow or brownurine• abdominal pain • chills• fever• joint pain• anaphylaxis• headache• hypersensitivity reac-tions involving the skin,lungs, blood, and liver.
Warning!
938910.qxd 08/26/2008 16:35 Page 260

including herpes simplex virus (HSV) and cytomegalovirus (CMV).Drugs in this class include:• acyclovir• famciclovir• ganciclovir• valacyclovir• valganciclovir.
Acyclovir sodium, used to treat HSV, is an effective antiviraldrug that causes minimal toxicity to cells. A derivative of acy-clovir, ganciclovir has potent antiviral activity against HSV andCMV.
A prodrug drugFamciclovir is used to treat acute herpes zoster, genital herpes,and recurrent HSV infections in the HIV-infected patient. Valacy-clovir is used to treat herpes zoster, genital herpes, and herpeslabialis. Valganciclovir is used to treat CMV retinitis in the patientwith acquired immunodeficiency syndrome (AIDS).
PharmacokineticsEach of these antiviral drugs travels its own route through thebody.
Slow by mouthWhen given orally, acyclovir absorption is slow and only 10% to30% complete. It’s distributed throughout the body and metabo-lized primarily inside the infected cells; the majority of the drug isexcreted in urine.
Bound? Not muchFamciclovir is less than 20% bound to plasma proteins. It’s exten-sively metabolized in the liver and excreted in urine.
I.V. onlyGanciclovir is administered I.V. because it’s absorbed poorly fromthe GI tract. More than 90% of ganciclovir isn’t metabolized and isexcreted unchanged by the kidneys.
Metabolic changesValacyclovir is converted to acyclovir during its metabolism andhas pharmacokinetic properties similar to those of acyclovir. Val-ganciclovir is metabolized in the intestinal wall and liver to ganci-clovir; however, interchanging the two drugs isn’t effective.
261ANTIVIRAL DRUGS
938910.qxd 08/26/2008 16:35 Page 261

PharmacodynamicsTo be effective, acyclovir, famciclovir, and ganciclovir must be me-tabolized to their active form in cells infected by HSV.
Presto change-oAcyclovir enters virus-infected cells, where it’s changed through aseries of steps to acyclovir triphosphate. Acyclovir triphosphateinhibits virus-specific DNA polymerase, an enzyme necessary forviral growth, thus disrupting viral replication.
On entry into CMV-infected cells, ganciclovir is converted toganciclovir triphosphate, which is thought to produce its antiviralactivity by inhibiting viral DNA synthesis.
Famciclovir enters viral cells (herpes simplex 1 and 2, varicellazoster), where it inhibits DNA polymerase, viral DNA synthesisand, thus, viral replication.
Valacyclovir rapidly converts to acyclovir; acyclovir then be-comes incorporated into viral DNA and inhibits viral DNA poly-merase, thus inhibiting viral multiplication.
Valganciclovir is converted to ganciclovir, which inhibits repli-cation of viral DNA synthesis of CMV.
PharmacotherapeuticsAcyclovir is used to treat infection caused by herpes viruses, in-cluding HSV types 1 and 2 and the varicella-zoster virus. Oral acy-clovir is used primarily to treat initial and recurrent HSV type 2 in-fections.
I.V. acyclovir is used to treat:• severe initial HSV type 2 infections in a patient with a normalimmune system• initial and recurrent skin and mucous membrane HSV type 1and 2 infections in an immunocompromised patient• herpes zoster infections (shingles) caused by the varicella-zoster virus in an immunocompromised patient• disseminated varicella-zoster virus in an immunocompromisedpatient• varicella infections (chickenpox) caused by the varicella-zostervirus in an immunocompromised patient.
RSVP for CMVGanciclovir is used to treat CMV retinitis in an immunocompro-mised patient, including a patient with AIDS or other CMV infec-tions such as encephalitis.
If it keeps coming backFamciclovir is used to treat acute herpes zoster, genital herpes,and recurrent HSV infections in a patient with HIV.
262ANTI-INFECTIVE DRUGS
I.V. acyclovir treatsshingles in an
immunocompromisedpatient.
938910.qxd 08/26/2008 16:35 Page 262

The valiant valsValganciclovir is used to treat CMV retinitis, and valacyclovir is ef-fective against herpes zoster, genital herpes, and herpes labialis.
Drug interactionsSynthetic nucleosides may interact with these drugs.• Probenecid reduces kidney excretion and increases blood levelsof ganciclovir, valganciclovir, valacyclovir, famciclovir, and acy-clovir, increasing the risk of toxicity.• Taking ganciclovir with drugs that are damaging to tissue cells,such as dapsone, pentamidine isethionate, flucytosine, vincristine,vinblastine, doxorubicin, amphotericin B, and co-trimoxazole, in-hibits replication of rapidly dividing cells in the bone marrow, GItract, skin, and sperm-producing cells.• Imipenem-cilastatin increases the risk of seizures when takenwith ganciclovir or valganciclovir.• Zidovudine increases the risk of granulocytopenia (reducednumber of granulocytes, a type of white blood cell) when takenwith ganciclovir. (See Adverse reactions to synthetic nucleo-sides.)
263ANTIVIRAL DRUGS
Treatment with these drugs may lead to particular adverse reactions.
Warning!
Adverse reactions to synthetic nucleosides
Acyclovir
Reversible kidney impairment may occur with rapid I.V. injec-tion (less than 10 minutes) or infusion of acyclovir.
Oral history
Common reactions to oral acyclovir include headache, nausea,vomiting, and diarrhea.
Issues of sensitivity
Hypersensitivity reactions may occur with acyclovir.
Ganciclovir
The most common adverse reactions to ganciclovir are granu-locytopenia and thrombocytopenia.
Famciclovir and valacyclovir
Common adverse reactions to famciclovir and valacyclovir in-clude headache, nausea, and vomiting.
Valganciclovir
Common adverse reactions to valganciclovir includeheadache, insomnia, seizures, retinal detachment, diarrhea,nausea, vomiting, abdominal pain, neutropenia, anemia, throm-bocytopenia, pancytopenia, bone marrow depression, aplasticanemia, sepsis, and hypersensitivity reactions.
938910.qxd 08/26/2008 16:35 Page 263

Pyrophosphate analoguesThe antiviral drug foscarnet is used to treat CMV retinitis in thepatient with AIDS. It’s also used to treat acyclovir-resistant HSVinfections in the immunocompromised patient.
PharmacokineticsFoscarnet is poorly bound to plasma proteins. In patients withnormal kidney function, the majority of foscarnet is excreted un-changed in urine.
PharmacodynamicsFoscarnet prevents viral replication by selectively inhibiting DNApolymerase.
PharmacotherapeuticsFoscarnet’s primary therapeutic use is treating CMV retinitis in thepatient with AIDS. It’s also used in combination therapy with gan-ciclovir for the patient who has relapsed with either drug.
Drug interactionsFoscarnet has few drug interactions.• Foscarnet and pentamidine together increase the risk ofhypocalcemia (low blood calcium levels) and toxicity to the kid-neys.• The use of foscarnet and other drugs that alter serum calciumlevels may result in hypocalcemia.• Foscarnet given with amiodarone increases the risk of car-diotoxicity and QT prolongation.• The risk of kidney impairment increases when drugs toxic tothe kidneys, such as amphotericin B and aminoglycosides, are tak-en with foscarnet. Because of the risk of kidney toxicity, the pa-tient should be aggressively hydrated during treatment. (See Ad-verse reactions to foscarnet.)
Influenza A and syncytial virus drugsAmantadine and its derivative, rimantadine hydrochloride, areused to prevent or treat influenza A infections. Ribavirin is usedto treat respiratory syncytial virus (RSV) infections in children.
264ANTI-INFECTIVE DRUGS
Adversereactions tofoscarnet
Adverse reactions tofoscarnet may include:• fatigue, depression,fever, confusion,headache, numbnessand tingling, dizziness,and seizures• nausea and vomiting,diarrhea, and abdominalpain • granulocytopenia,leukopenia, and anemia• involuntary musclecontractions and neu-ropathy• breathing difficultiesand coughing• rash• altered kidney function• electrolyte distur-bances.
Warning!
938910.qxd 08/26/2008 16:35 Page 264

Breathe inTo treat RSV, ribavirin is administered by aerosol inhalation, usinga small-particle aerosol generator.
PharmacokineticsAfter oral administration, amantadine and rimantadine are wellabsorbed in the GI tract and widely distributed throughout thebody. Ribavirin is administered by nasal or oral inhalation and iswell absorbed. It has a limited, specific distribution, with the high-est concentration found in the respiratory tract and in red bloodcells (RBCs). Ribavirin capsules are rapidly absorbed after admin-istration and are distributed in plasma.
Metabolism and excretionAmantadine is eliminated primarily in urine; rimantadine is exten-sively metabolized and then excreted in urine.
Ribavirin is metabolized in the liver and by RBCs. It’s excretedprimarily by the kidneys, with some excreted in stool.
PharmacodynamicsAlthough its exact mechanism of action is unknown, amantadineappears to inhibit an early stage of viral replication. Rimantadineinhibits viral RNA and protein synthesis.
The mechanism of action of ribavirin isn’t known completely,but the drug’s metabolites inhibit viral DNA and RNA synthesis,subsequently halting viral replication.
PharmacotherapeuticsAmantadine and rimantadine are used to prevent and treat respi-ratory tract infections caused by strains of the influenza A virus.They can reduce the severity and duration of fever and othersymptoms in patients already infected with influenza A.
Ribavirin, used to treat severe RSV infection in children, is alsoused in adults in combination with interferon alfa-2B for treat-ment of chronic hepatitic C.
In the meantimeThese drugs also protect the patient who has received the influen-za vaccine during the 2 weeks needed for immunity to develop aswell as the patient who can’t take the influenza vaccine because ofhypersensitivity.
265ANTIVIRAL DRUGS
Adversereactions toamantadine andrimantadine
Amantadine
Adverse reactions in-clude:• anorexia• anxiety• confusion• depression• dizziness• fatigue• forgetfulness• hallucinations• hypersensitivity reac-tions• insomnia• irritability• nausea• nervousness• psychosis.
Rimantadine
Adverse reactions to ri-mantadine are similar tothose for amantadine.However, they tend to beless severe.
Warning!
938910.qxd 08/26/2008 16:35 Page 265

Calming the shakesAmantadine is also used to treat parkinsonism and drug-inducedextrapyramidal reactions (abnormal involuntary movements).
Drug interactionsAmantadine may interact with some drugs. (See Adverse reac-tions to amantadine and rimantadine, page 265.)• Taking anticholinergics with amantadine increases adverse anti-cholinergic effects.• Amantadine given with the combination drug hydrochloroth-iazide and triamterene results in decreased urine excretion ofamantadine, causing increased amantadine levels.• Amantadine and co-trimoxazole levels are increased when usedtogether.
All quiet on the rimantadine frontNo clinically significant drug interactions have been documentedwith rimantadine.
Ribavirin has few interactions with other drugs.• Ribavirin reduces the antiviral activity of zidovudine, and con-comitant use of these drugs may cause blood toxicity.• Taking ribavirin and digoxin can cause digoxin toxicity, produc-ing such effects as GI distress, CNS abnormalities, and cardiac ar-rhythmias. (See Adverse reactions to ribavirin.)
Nucleoside analogue reverse transcriptase inhibitorsNRTIs are used to treat the patient with advanced HIV infection.Drugs in this class include:• abacavir• didanosine• emtricitabine• lamivudine• stavudine• zidovudine.
First in the fight against AIDSZidovudine was the first drug to receive Food and Drug Adminis-tration (FDA) approval for treating AIDS and AIDS-related com-plex.
PharmacokineticsEach of the NRTIs has its own pharmacokinetic properties.
266ANTI-INFECTIVE DRUGS
Adversereactions toribavirin
Adverse reactions to ri-bavirin include:• apnea (lack of breath-ing)• cardiac arrest• hypotension• nausea• pneumothorax (air inthe pleural space, caus-ing the lung to collapse)• worsening of respira-tory function.
Warning!
938910.qxd 08/26/2008 16:35 Page 266

Into spaceAbacavir is rapidly and extensively absorbed after oral administra-tion. It’s distributed in the extravascular space, and about 50%binds with plasma proteins. Abacavir is metabolized by the cy-tosolic enzymes and excreted primarily in urine with the remain-der excreted in stool.
Lamivudine and stavudine are rapidly absorbed after adminis-tration and are excreted by the kidneys.
Emtricitabine is rapidly and extensively absorbed after oral ad-ministration and is excreted by the kidneys.
Buffer neededBecause didanosine is degraded rapidly in gastric acid, didanosinetablets and powder contain a buffering drug to increase pH. Theexact route of metabolism isn’t fully understood. About one-halfof an absorbed dose is excreted in urine.
Well absorbed, widely distributedZidovudine is well absorbed from the GI tract, widely distributedthroughout the body, metabolized by the liver, and excreted by thekidneys. The dosage may need to be adjusted in the patient withkidney or liver disease, as is the case with most of the NRTIs.
PharmacodynamicsNRTIs must undergo conversion to their active metabolites to pro-duce their action.• Abacavir is converted to an active metabolite that inhibits theactivity of HIV-1 transcriptase by competing with a natural compo-nent and incorporating into viral DNA.• Didanosine undergoes cellular enzyme conversion to its activeantiviral metabolite to block HIV replication.• Emtricitabine inhibits the enzyme, reverse transcriptase, andthus inhibits viral DNA replication.• Lamivudine and stavudine are converted in the cells to their ac-tive metabolites, which inhibit viral DNA replication.• Zidovudine is converted by cellular enzymes to an active form,zidovudine triphosphate, which prevents viral DNA from replicat-ing. (See How zidovudine works, page 268.)
PharmacotherapeuticsNRTIs are used to treat HIV and AIDS.
267ANTIVIRAL DRUGS
Gastricacid rapidlydegrades
didanosine.
938910.qxd 08/26/2008 16:35 Page 267

268ANTI-INFECTIVE DRUGS
Zidovudine can inhibit replication of the human immunodeficiency virus (HIV). The first two illustrations show how HIV invadescells and then replicates itself. The bottom illustration shows how zidovudine blocks viral transformation.
Now I get it!
How zidovudine works
HIV particle enters cell.
HIV uses reverse transcriptase tochange its own ribonucleic acid(RNA) into deoxyribonucleic acid(DNA).
HIV particle
Host cell
DNA
Reverse transcriptase
RNA
Nucleus
Virus-constructed DNA takes overcellular genetic mechanism.
Messenger RNA (mRNA) and otherproteins form new HIV particle.
Host cell
Nucleus
DNA
mRNA
Proteins
New HIV particle
HIV particle enters cell.
Zidovudine mimics structure of re-verse transcriptase so it can blockviral transformation of RNA to DNA.
Host cell
RNA
Reverse transcriptase
Nucleus
938910.qxd 08/26/2008 16:35 Page 268

When you’re hospitalizedI.V. zidovudine is used for the hospitalized patient who can’t takeoral medication. It’s also used to prevent transmission of HIV fromthe mother to her fetus and to treat AIDS-related dementia.
Like all drugs for HIV infection, oral zidovudine is used as partof a multidrug regimen.
Getting a jump on HIVDidanosine, in combination with other antiretrovirals (antiviralsused to treat HIV infection), is an alternative initial treatment forHIV infection.
Part of the combo…Lamivudine, stavudine, and abacavir are used in combination withother antiretrovirals to treat HIV infection. Combivir is combina-tion therapy that includes lamivudine and zidovudine. Trizivir iscombination therapy that includes abacavir, lamivudine, and zi-dovudine; it was approved by the FDA in November 2000 to sim-plify dosing in the treatment of HIV.
Emtricitabine is used in combination with other antiretroviralsto treat HIV infection.
…but be careful hereBecause of inhibition of phosphorylation (the process needed toform the active DNA-inhibiting metabolite), stavudine shouldn’t begiven in combination with zidovudine.
Drug interactionsNRTIs may be responsible for many drug interactions.• Potentially fatal lactic acidosis and severe hepatomegaly withsteatosis have occurred in patients taking NRTIs alone or withother antiretrovirals such as tenofovir. The majority of patientswere women, and obesity and prolonged NRTI exposure may berisk factors.• An increased risk of cellular and kidney toxicity occurs when zi-dovudine is taken with such drugs as dapsone, pentamidineisethionate, flucytosine, vincristine, vinblastine, doxorubicin, in-terferon, and ganciclovir.• Taking zidovudine with probenecid, aspirin, acetaminophen, in-domethacin, cimetidine, or lorazepam increases the risk of toxici-ty of either drug.• Zidovudine plus acyclovir may produce profound lethargy anddrowsiness.• Didanosine may reduce the absorption of tetracyclines, delavir-dine, and fluoroquinolones.
269ANTIVIRAL DRUGS
938910.qxd 08/26/2008 16:35 Page 269

• Abacavir levels increase with alcohol consumption.• Emtricitabine has been studied in combination with indinavir,stavudine, famciclovir, and tenofovir; there were no clinically sig-nificant drug interactions. (See Adverse reactions to NRTIs.)
Non-nucleoside reverse transcriptase inhibitorsNNRTIs are used in combination with other antiretrovirals to treatHIV infection. The three agents in this class include:• delavirdine• efavirenz• nevirapine. (See Combining antiretroviral drugs.)
PharmacokineticsEfavirenz and delavirdine are highly protein-bound after absorp-tion and distribution, and nevirapine is widely distributed through-out the body. All three drugs are metabolized by the cytochromeP-450 liver enzyme system and excreted in urine and stool.
PharmacodynamicsNevirapine and delavirdine bind to the reverse transcriptase en-zyme, preventing it from exerting its effect, and thus preventingHIV replication. Efavirenz competes for the enzyme through non-competitive inhibition.
270ANTI-INFECTIVE DRUGS
Abacavirlevels increase
with alcoholconsumption.
Each of the nucleoside reverse transcriptase inhibitors (NRTIs) can cause adverse reactions.
Warning!
Adverse reactions to NRTIs
Zidovudine
• Blood-related reactions• Headache and dizziness• Muscle pain, fever, and rash• Nausea, vomiting, abdominal pain, diarrhea
Didanosine
• Diarrhea, nausea, vomiting, abdominal pain,constipation, stomatitis, unusual taste or lossof taste, dry mouth, pancreatitis
• Headache, peripheral neuropathy, dizziness• Muscle weakness, rash, itching, musclepain, hair loss
Abacavir
• Potentially fatal hypersensitivity reactions
Combiningantiretroviraldrugs
Monotherapy (usinga single drug) isn’t rec-ommended for humanimmunodeficiency virusinfection. For the bestresults, a combination ofantiretroviral agents isused.
938910.qxd 08/26/2008 16:35 Page 270

PharmacotherapeuticsNNRTIs are used in combination with other antiretrovirals in HIVtreatment; nevirapine is specifically indicated for the patientwhose clinical condition and immune status have deteriorated.
Drug interactionsNNRTIs may be responsible for many drug interactions.• Nevirapine may decrease the activity of protease inhibitors andhormonal contraceptives; these drugs shouldn’t be used together.• Delavirdine may increase levels of benzodiazepines, clar-ithromycin, rifabutin, saquinavir, and warfarin; it may also signifi-cantly increase concentrations of indinavir, requiring a decrease inthe indinavir dosage.• The indinavir dosage will need to be increased when given withefavirenz.• Nevirapine has been associated with a severe rash that may belife-threatening. If a rash occurs, discontinue the drug. (See Ad-verse reactions to NNRTIs.)
Nucleotide analogue reverse transcriptase inhibitorsNucleotide analogue reverse transcriptase inhibitors are used incombination with other antiretrovirals in the treatment of HIV.The only drug in this class to date is tenofovir, and it works muchlike the NRTIs.
PharmacokineticsTenofovir is absorbed much better after a high-fat meal. It’s thendistributed in small amounts into plasma and serum proteins. Me-tabolism isn’t thought to be mediated by cytochrome P-450 liverenzymes, and the drug is excreted by the kidneys.
PharmacodynamicsTenofovir competes with substrates and is subsequently incorpo-rated into the DNA chain, thus halting HIV replication.
PharmacotherapeuticsTenofovir is used in combination with other drugs to treat HIV in-fection.
Drug interactionsTenofovir may be responsible for some drug interactions.
271ANTIVIRAL DRUGS
Tenofovirworks like an
NRTI.
Adversereactions toNNRTIs
Adverse reactions tononnucleoside reversetranscriptase inhibitors(NNRTIs) include:• headache• dizziness• asthenia• nausea and vomiting• diarrhea• rash.
Warning!
938910.qxd 08/26/2008 16:35 Page 271

• Drugs that are eliminated through the kidneys or that decreasekidney function may increase levels of tenofovir when given con-currently.• Didanosine levels increase when it’s given with tenofovir; watchfor didanosine-based adverse effects.• Potentially fatal lactic acidosis and severe hepatomegaly withsteatosis have occurred in patients taking tenofovir alone or withother antiretrovirals. The majority of patients were women, andobesity and previous NRTI exposure may be risk factors. Patientswith preexisting liver disease should take this drug with caution.Suspend treatment if hepatotoxicity is suspected. (See Adverse re-actions to tenofovir.)
Protease inhibitorsProtease inhibitors are drugs that act against the enzyme HIV pro-tease, preventing it from dividing a larger viral precursor proteininto the active smaller enzymes that the HIV virus needs to fullymature. The result is an immature, noninfectious cell. Drugs inthis group include:• amprenavir• atazanavir• darunavir• fosamprenavir• indinavir sulfate• lopinavir and ritonavir• nelfinavir mesylate• ritonavir• saquinavir mesylate• tipranavir.
PharmacokineticsProtease inhibitors may have different pharmacokinetic proper-ties.
Active and inactiveAmprenavir is metabolized in the liver to active and inactivemetabolites and is minimally excreted in urine and stool.
Atazanavir is rapidly absorbed and is metabolized in the liverby the CYP3A. The drug is excreted mainly through stool andurine.
Darunavir is well absorbed when taken with food and highlyprotein-bound. It’s metabolized in the liver and excreted in stool.
Fosamprenavir is well absorbed and highly protein-bound. It’srapidly metabolized by CYP3A4 and it is unknown how it is ex-creted.
272ANTI-INFECTIVE DRUGS
Says here I do alot of absorbing and
metabolizing.Hmmm. No wonderI’m tired by the end
of the day!
Adversereactions totenofovir
Adverse reactions to thenucleotide analogue re-verse transcriptase in-hibitor tenofovir include:• nausea and vomiting• diarrhea• anorexia• abdominal pain• severe hepatomegaly(enlargement of theliver)• lactic acidosis (in-creased lactic acid pro-duction in the blood).
Warning!
938910.qxd 08/26/2008 16:35 Page 272

P-450 at it againLopinavir is extensively metabolized by the liver’s cytochromeP-450 system; ritonavir acts as an inhibitor of lopinavir. This com-bination drug’s antiviral activity is due to lopinavir.
Availability unknownNelfinavir’s bioavailability (the degree to which it becomes avail-able to target tissue after administration) isn’t determined. Foodincreases its absorption. It’s highly protein-bound, metabolized inthe liver, and excreted primarily in stool.
Broken into five…Ritonavir is well absorbed, metabolized by the liver, and brokendown into at least five metabolites. It’s mainly excreted in stool,with some elimination through the kidneys.
…and sevenIndinavir sulfate is rapidly absorbed and moderately bound toplasma proteins. It’s metabolized by the liver into seven metabo-lites. The drug is excreted mainly in stool.
Highly boundSaquinavir mesylate is poorly absorbed from the GI tract. It’swidely distributed, highly bound to plasma proteins, metabolizedby the liver, and excreted mainly by the kidneys.
Tipranavir has limited absorption, but its bioavailability in-creases when it’s taken with a high-fat meal. It’s metabolized bythe chromosome P-450 and excreted mostly unchanged in stool.
PharmacodynamicsAll of these drugs inhibit the activity of HIV protease and preventthe cleavage of viral polyproteins.
PharmacotherapeuticsProtease inhibitors are used in combination with other antiretrovi-ral agents for the treatment of HIV infection.
Drug interactionsProtease inhibitors may interact with many drugs. Here are somecommon interactions.• The action of saquinavir may be reduced by phenobarbital,phenytoin, dexamethasone, and carbamazepine.
273ANTIVIRAL DRUGS
938910.qxd 08/26/2008 16:35 Page 273

Blockers beware!• Ritonavir may increase the effects of alpha-adrenergic blockers,antiarrhythmics, antidepressants, antiemetics, antifungals, anti-lipemics, antimalarials, antineoplastics, beta-adrenergic blockers,calcium channel blockers, cimetidine, corticosteroids, erythro-mycin, immunosuppressants, methylphenidate, pentoxifylline,phenothiazines, and warfarin.• Indinavir sulfate inhibits the metabolism of midazolam and tria-zolam, increasing the risk of potentially fatal events such as car-diac arrhythmias.• Didanosine decreases gastric absorption of indinavir sulfate;these drugs should be administered at least 1 hour apart.• Rifampin markedly reduces plasma levels of most protease in-hibitors, including atazanavir.• Nelfinavir may greatly increase plasma levels of amiodarone, er-got derivatives, midazolam, rifabutin, quinidine, and triazolam.• Lopinavir and ritonavir are used in combination because of theirpositive effects on HIV RNA levels and CD4 counts. When giventogether, ritonavir inhibits the metabolism of lopinavir, leading toincreased plasma lopinavir levels.• Carbamazepine, phenobarbital, and phenytoin may reduce theeffectiveness of nelfinavir.• Protease inhibitors may increase sildenafil levels, resulting insildenafil-associated adverse reactions, including hypotension, vi-sion changes, and priapism.• Atazanavir shouldn’t be given with drugs also metabolized bythe CYPA3A pathway, such as HMG-CoA reductase inhibitors (in-cluding lovastatin, simvastatin, and atorvastatin). Concurrent usemay increase the risk of myopathy and rhabdomyolysis.
Interval issues• Drugs that prolong the PR interval, such as calcium channelblockers (including diltiazem) and beta-adrenergic blockers (in-cluding atenolol), should be used cautiously with atazanavir be-cause atazanavir may also prolong the PR interval.• Atazanavir shouldn’t be given with benzodiazepines, such as mi-dazolam and triazolam, because of the potential for increased se-dation or respiratory depression.• Atazanavir shouldn’t be given with ergot derivatives, such as er-gotamine and dihydroergotamine, because of the potential for life-threatening ergot toxicity resulting in peripheral vasospasm andischemia of the extremities.• St. John’s wort may reduce plasma levels of atazanavir anddarunavir.• Tipranavir and sulfonyureas administered together may result inhypoglycemia.
274ANTI-INFECTIVE DRUGS
Adversereactions to
protease inhibitorsinclude vision
changes.
938910.qxd 08/26/2008 16:35 Page 274

• Indinavir and ritonavir may increase plasma nelfinavir levels.(See Adverse reactions to protease inhibitors.)
Antitubercular drugsAntitubercular drugs are used to treat tuberculosis (TB), which iscaused by Mycobacterium tuberculosis. Not always curative,these drugs can halt the progression of a mycobacterial infection.
Myco-versatilityThese drugs also are effective against less common mycobacterialinfections caused by M. kansasii, M. avium-intracellulare,M. fortuitum, and related organisms.
Time consumingUnlike most antibiotics, antitubercular drugs may need to be ad-ministered over many months. This creates problems, such as pa-tient noncompliance, the development of bacterial resistance, anddrug toxicity. (See Directly observable therapy for TB, page 276.)
275ANTITUBERCULAR DRUGS
These common adverse reactions occur with protease inhibitors:
Warning!
Adverse reactions to protease inhibitors
• abdominal discomfort• abdominal pain• acid regurgitation• anorexia• back pain• deep vein thrombosis• depression• diarrhea• dizziness• dry mouth• encephalopathy• fatigue• flank pain• headache
• hemorrhagic colitis• hypercholesterolemia• hyperglycemia• hypertriglyceridemia• insomnia• leukopenia• muscle weakness• nausea and vomiting• neutropenia• pancreatitis• paresthesis• rash• Stevens-Johnson syndrome• taste perversion
938910.qxd 08/26/2008 16:35 Page 275

Drug regimens for treating TBTraditionally, isoniazid, rifampin, and ethambutol were the main-stays of multidrug TB therapy and successfully prevented theemergence of drug resistance.
A new regimen to combat resistanceBecause of the current incidence of drug-resistant TB strains, afour-drug regimen is now recommended for initial treatment:
isoniazid
rifampin
pyrazinamide
streptomycin or ethambutol.
One regimen may succeed anotherThe antitubercular regimen should be modified if local testingshows resistance to one or more of these drugs. If local outbreaksof TB resistant to isoniazid and rifampin are occurring in facilities(for example, health care or correctional facilities), then five- or
276ANTI-INFECTIVE DRUGS
Among infectious diseases, tuberculosis (TB)remains a frequent killer worldwide. Whatmakes treatment difficult is that it requireslong-term medical therapy—typically for aslong as 6 to 9 months. The long treatment peri-od commonly creates problems with patientcompliance (an inability or unwillingness to fol-low a treatment plan), and poor compliancecontributes to reactivation of the disease andthe development of drug-resistant TB.
DOT on the spot
Directly observable therapy (DOT) was devel-oped to combat these treatment issues. DOTrequires that a health care worker observe apatient take every dose of medication for the
duration of therapy. A controversy existsover whether every individual with TB shouldbe observed (universal DOT) or whether onlythe patient at risk for poor compliance shouldbe observed (selective DOT).
Who fails to comply?
The patient at risk for poor compliance in-cludes one with a history of poor complianceor drug or alcohol abuse, mental illness, home-lessness, incarceration, or residence in ahomeless shelter. Some areas, such as Missis-sippi and New York City, practice universalDOT; other areas, including Massachusetts,first evaluate a patient’s ability and willingnessto comply.
Yea or nay?
Directly observable therapy for TB
938910.qxd 08/26/2008 16:35 Page 276

six-drug regimens are recommended as initial therapy. (See Otherantitubercular drugs.)
PharmacokineticsMost antitubercular drugs are administered orally. When adminis-tered orally, these drugs are well absorbed from the GI tract andwidely distributed throughout the body. They’re metabolized pri-marily in the liver and excreted by the kidneys.
PharmacodynamicsAntitubercular drugs are specific for mycobacteria. At usual dos-es, ethambutol and isoniazid are tuberculostatic, meaning thatthey inhibit the growth of M. tuberculosis. In contrast, rifampin istuberculocidal, meaning that it destroys the mycobacteria. Be-cause bacterial resistance to isoniazid and rifampin can developrapidly, they should always be used with other antituberculardrugs.
Antireplication stationThe exact mechanism of action of ethambutol remains unclear,but it may be related to inhibition of cell metabolism, arrest ofmultiplication, and cell death. Ethambutol acts only against repli-cating bacteria.
277ANTITUBERCULAR DRUGS
Other antitubercular drugsSeveral other drugs are used as antituberculardrugs in combination with first-line drugs. Be-cause these drugs have a greater incidence oftoxicity, they’re used primarily for the patientwho’s resistant or allergic to less toxic drugs.
Fluoroquinolones
Fluoroquinolones, such as ciprofloxacin andofloxacin, are effective against Mycobacteri-um tuberculosis. Of these two drugs, ofloxacinis more potent and may be an initial choice inretreatment. These drugs are administeredorally and are generally well tolerated. GI ad-verse reactions are most commonly reported.However, resistance to fluoroquinolones devel-ops rapidly when these drugs are used aloneor in insufficient doses.
Streptomycin
Streptomycin was the first drug recognized aseffective in treating tuberculosis. Streptomycinis administered I.M. only. It appears to enhancethe activity of oral antitubercular drugs and isof greatest value in the early weeks to monthsof therapy. However, I.M. administration limitsits usefulness in long-term therapy. Rapidly ab-sorbed from the I.M. injection site, strepto-mycin is excreted primarily by the kidneys asunchanged drug. Most patients tolerate strep-tomycin well, but those receiving large dosesmay exhibit eighth cranial nerve toxicity (oto-toxicity).
938910.qxd 08/26/2008 16:35 Page 277

Breaking down wallsAlthough isoniazid’s exact mechanism of action isn’t known, thedrug is believed to inhibit the synthesis of mycolic acids, impor-tant components of the mycobacterium cell wall. This inhibitiondisrupts the cell wall. Only replicating, not resting, bacteria ap-pear to be inhibited.
Synthesis stopperRifampin inhibits RNA synthesis in susceptible organisms.The drug is effective primarily in replicating bacteria, butmay have some effect on resting bacteria as well.
Acid basedThe exact mechanism of action of pyrazinamide isn’tknown, but the antimycobacterial activity appears to belinked to the drug’s conversion to the active metabolitepyrazinoic acid. Pyrazinoic acid, in turn, creates an acidicenvironment where mycobacteria can’t replicate.
PharmacotherapeuticsIsoniazid usually is used with ethambutol, rifampin, or pyrazi-namide. This is because combination therapy for TB and othermycobacterial infections can prevent or delay the development ofresistance.
In uncomplicated casesEthambutol is used with isoniazid and rifampin to treat the patientwith uncomplicated pulmonary TB. It’s also used to treat infec-tions resulting from M. bovis and most strains of M. kansasii.
Isolating isoniazidAlthough isoniazid is the most important drug for treating TB, bac-terial resistance develops rapidly if it’s used alone. However, resis-tance doesn’t pose a problem when isoniazid is used alone to pre-vent TB in the patient who has been exposed to the disease, andno evidence exists of cross-resistance between isoniazid and oth-er antitubercular drugs. Isoniazid is typically given orally, but maybe given intravenously, if necessary.
Pulmonary powerRifampin is a first-line drug for treating pulmonary TB with otherantitubercular drugs. It combats many gram-positive and somegram-negative bacteria, but is seldom used for nonmycobacterialinfections because bacterial resistance develops rapidly. It’s usedto treat asymptomatic carriers of Neisseria meningitidis whenthe risk of meningitis is high, but it isn’t used to treat N. meningi-
278ANTI-INFECTIVE DRUGS
Bring it on! It cantake as many as fiveor six drugs to wipeme out, so you cells
are no problem!
938910.qxd 08/26/2008 16:35 Page 278

tidis infections because of the potential for bacte-rial resistance.
On the TB frontPyrazinamide is currently recommended as afirst-line TB drug in combination with ethambu-tol, rifampin, and isoniazid. Pyrazinamide is ahighly specific drug that’s active only againstM. tuberculosis. Resistance to pyrazinamide maydevelop rapidly when it’s used alone.
Drug interactionsAntitubercular drugs may interact with many other drugs. (SeeAdverse reactions to antitubercular drugs.)• Cycloserine and ethionamide may produce additive CNS effects,such as drowsiness, dizziness, headache, lethargy, depression,tremor, anxiety, confusion, and tinnitus (ringing in the ears), whenadministered with isoniazid.• Isoniazid may increase levels of phenytoin, carbamazepine, di-azepam, ethosuximide, primidone, theophylline, and warfarin.• When corticosteroids and isoniazid are taken together, the ef-fectiveness of isoniazid is reduced while the effects of corticos-teroids are increased.
279ANTITUBERCULAR DRUGS
Rifampin isyour first-line
defense againstpulmonary TB.
Here are common adverse reactions to antitubercular drugs.
Warning!
Adverse reactions to antitubercular drugs
Ethambutol
Itching, joint pain, GI distress, malaise,leukopenia, headache, dizziness, numbnessand tingling of the extremities, optic neuritis,and confusion may occur.
Although rare, hypersensitivity reactions toethambutol may produce rash and fever. Ana-phylaxis may also occur.
Isoniazid
Peripheral neuropathy is the most common ad-verse reaction. Severe and occasionally fatalhepatitis associated with isoniazid may occureven many months after treatment has
stopped. The patient must be monitored care-fully.
Rifampin
The most common adverse reactions includeepigastric pain, nausea, vomiting, abdominalcramps, flatulence, anorexia, and diarrhea.
Pyrazinamide
Liver toxicity is the major limiting adverse reac-tion. GI disturbances include nausea, vomiting,hyperuricemia, arthralgia, and anorexia.
938910.qxd 08/26/2008 16:35 Page 279

• Isoniazid may reduce the plasma levels of ketoconazole, itra-conazole, and oral antidiabetic agents.• Oral contraceptives and rifampin taken together may decreasethe effectiveness of the oral contraceptive.• When given together, rifampin, isoniazid, ethionamide, andpyrazinamide increase the risk of hepatotoxicity.• Pyrazinamide combined with phenytoin may increase phenytoinlevels.
Antimycotic drugsAntimycotic, or antifungal, drugs are used to treat fungal infec-tions. The major antifungal drug groups include:• polyenes• fluorinated pyrimidine• imidazole• synthetic triazoles• glucan synthesis inhibitors• synthetic allylamine derivatives. (See Other antimycoticdrugs.)
PolyenesThe polyenes include amphotericin B and nystatin. Ampho-tericin B’s potency has made it the most widely used antimycoticdrug for severe systemic fungal infections. It’s available in severalforms, including lipid-based preparations that may decrease renalor systemic toxicity. Nystatin is used only topically or orally totreat local fungal infections because it’s extremely toxic when ad-ministered parenterally.
PharmacokineticsAfter I.V. administration, amphotericin B is distributed throughoutthe body and excreted by the kidneys. Its metabolism isn’t well de-fined.
Oral nystatin undergoes little or no absorption, distribution, ormetabolism. It’s excreted unchanged in stool. Topical nystatin isn’tabsorbed through the skin or mucous membranes.
PharmacodynamicsAmphotericin B works by binding to sterol (a lipid) in the fungalcell membrane, altering cell permeability (ability to allow a sub-
280ANTI-INFECTIVE DRUGS
938910.qxd 08/26/2008 16:35 Page 280

stance to pass through) and allowing intracellular components toleak out.
A license to killAmphotericin B usually acts as a fungistatic drug (inhibiting fun-gal growth and multiplication), but can become fungicidal (de-stroying fungi) if it reaches high concentrations in the fungi.
Nystatin binds to sterols in fungal cell membranes and altersthe permeability of the membranes, leading to loss of cell compo-nents. Nystatin can act as a fungicidal or fungistatic drug, depend-ing on the organism present.
PharmacotherapeuticsAmphotericin B usually is administered to treat severe systemicfungal infections and meningitis caused by fungi sensitive to thedrug. It’s never used for noninvasive forms of fungal disease be-cause it’s highly toxic. It’s usually the drug of choice for severe in-fections caused by Candida, Paracoccidioides brasiliensis, Blas-tomyces dermatitidis, Coccidioides immitis, Cryptococcus neo-
281ANTIMYCOTIC DRUGS
Other antimycotic drugsSeveral other antimycotic drugs offer alternative forms of treat-ment for topical fungal infections.
Clotrimazole
An imidazole derivative, clotrimazole is used:• topically to treat dermatophyte and Candida albicans infec-tions • orally to treat oral candidiasis • vaginally to treat vaginal candidiasis.
Griseofulvin
Griseofulvin is used to treat fungal infections of the:• skin (tinea corporis)• feet (tinea pedis)• groin (tinea cruris) • beard area of the face and neck (tinea barbae) • nails (tinea unguium)• scalp (tinea capitis).
Long-term treatment
To prevent a relapse, griseofulvin therapy must continue untilthe fungus is eradicated and the infected skin or nails are re-placed.
Miconazole
Available as miconazole or miconazole nitrate, this imidazolederivative is used to treat local fungal infections, such as vagi-nal and vulvar candidiasis, and topical fungal infections such aschronic candidiasis of the skin and mucous membranes.
Delivery options
Miconazole may be administered: • I.V. or intrathecally (into the subarachnoid space) to treat fun-gal meningitis • I.V. or by bladder irrigation to treat fungal bladder infections • locally to treat vaginal infections • topically to treat topical infections.
Other topical antimycotic drugs
Ciclopirox olamine, econazole nitrate, haloprogin, butoconazolenitrate, naftifine, tioconazole, terconazole, tolnaftate, bute-nafine, terbinafine, sulconazole, oxiconazole, clioquinol, tri-acetin, and undecylenic acid are available only as topicaldrugs.
Memoryjogger
If a drug isfungicidal, it
destroys thefungus—cidus isa Latin term for“killing.” If it’sfungistatic, it pre-vents fungal growthand multiplication—stasis is a Greekterm for “halting.”
938910.qxd 08/26/2008 16:35 Page 281

formans, and Sporothrix schenckii. It’s also effective against As-pergillus fumigatus, Microsporum audouinii, Rhizopus, Candi-da glabrata, Trichophyton, and Rhodotorula.
Last-ditch effortBecause amphotericin B is highly toxic, its use is limited to the pa-tient who has a definitive diagnosis of life-threatening infectionand is under close medical supervision.
Topical concernsNystatin is used primarily to treat candidal skin infections. Differ-ent forms of nystatin are available for treating different types ofcandidal infections. Topical nystatin is used to treat candidal skinor mucous membrane infections, such as oral thrush, diaper rash,vaginal and vulvar candidiasis, and candidiasis between skinfolds.
Oral historyOral nystatin is used to treat GI infections.
Drug interactionsNystatin doesn’t interact significantly with other drugs, but am-photericin B may have significant interactions with many drugs.• Because of the synergistic effects between flucytosine and am-photericin B, these two drugs commonly are combined in therapyfor candidal or cryptococcal infections, especially for cryptococ-cal meningitis.• The risk of kidney toxicity increases when amphotericin B istaken with aminoglycosides, cyclosporine, or acyclovir.• Corticosteroids, extended-spectrum penicillins, and digoxinmay worsen the hypokalemia (low blood potassium levels) pro-duced by amphotericin B, possibly leading to heart problems.Moreover, the risk of digoxin toxicity is increased.• Amphotericin B plus nondepolarizing skeletal muscle relaxants(such as pancuronium bromide) increase muscle relaxation.• Electrolyte solutions may inactivate amphotericin B when dilut-ed in the same solution. Amphotericin B preparations must bemixed with dextrose 5% in water; they can’t be mixed with salinesolution.• Magnesium and potassium levels and kidney function must bemonitored frequently in patients receiving amphotericin. (See Ad-verse reactions to amphotericin B and Adverse reactions to nys-tatin.)
282ANTI-INFECTIVE DRUGS
Adversereactions tonystatin
Reactions to nystatinseldom occur, but highdosages may produce:• diarrhea• nausea and vomiting• abdominal pain• a bitter taste.
It can get under your
skin
Topical nystatin mayalso cause skin irritation,and a hypersensitivityreaction may occur withoral or topical adminis-tration.
Warning!
938910.qxd 08/26/2008 16:35 Page 282

FlucytosineFlucytosine is the only antimetabolite (a substance that closely re-sembles one required for normal physiologic functioning and thatexerts its effect by interfering with metabolism) that acts as an an-timycotic. It’s a purine and pyrimidine inhibitor that’s used primar-ily with another antimycotic drug, such as amphotericin B, to treatsystemic fungal infections.
PharmacokineticsAfter oral administration, flucytosine is well absorbed from the GItract and widely distributed. It undergoes little metabolism and isexcreted primarily by the kidneys.
PharmacodynamicsFlucytosine penetrates fungal cells, where it’s converted to its ac-tive metabolite fluorouracil. Fluorouracil then is incorporated intothe RNA of the fungal cells, altering their protein synthesis andcausing cell death.
PharmacotherapeuticsAlthough amphotericin B is effective in treating candidal and cryp-tococcal meningitis alone, flucytosine is given with it to reduce
283ANTIMYCOTIC DRUGS
Almost all patients receiving I.V. amphotericinB, particularly at the beginning of low-dosetherapy, experience: • chills• fever• nausea and vomiting• anorexia• muscle and joint pain• indigestion.
Anemia
Most patients also develop normochromic (ad-equate hemoglobin in each red blood cell[RBC]) or normocytic anemia (too few RBCs)that significantly decreases the hematocrit.Hypomagnesemia and hypokalemia may oc-cur, causing electrocardiographic changesand requiring replacement electrolyte therapy.
Kidney concerns
Up to 80% of patients may develop some de-gree of kidney toxicity, causing the kidneys tolose their ability to concentrate urine.
Warning!
Adverse reactions to amphotericin B
938910.qxd 08/26/2008 16:35 Page 283

the dosage and the risk of toxicity. This combination therapy isthe treatment of choice for cryptococcal meningitis.
Standing aloneFlucytosine can be used alone to treat candidal infections of thelower urinary tract because it reaches a high urinary concentra-tion. It’s also effective in treating infections caused by T. glabrata,Phialophora, Aspergillus, and Cladosporium.
Drug interactionsCytarabine may antagonize the antifungal activity of flucytosine,possibly by competitive inhibition. Hematologic, kidney, and liverfunction must be closely monitored during flucytosine therapy be-cause of the drug’s serious risk of toxicity. (See Adverse reactionsto flucytosine.)
ImidazoleKetoconazole, the most commonly used imidazole, is an effectiveoral antimycotic drug with a broad spectrum of activity.
PharmacokineticsWhen given orally, ketoconazole is absorbed variably and distrib-uted widely. It undergoes extensive liver metabolism and is ex-creted through bile and stool.
PharmacodynamicsWithin the fungal cells, ketoconazole interferes with sterol synthe-sis, damaging the cell membrane and increasing its permeability.This leads to a loss of essential intracellular elements and inhibi-tion of cell growth.
Can inhibit or killKetoconazole usually produces fungistatic effects, but can alsoproduce fungicidal effects under certain conditions.
PharmacotherapeuticsKetoconazole is used to treat topical and systemic infectionscaused by susceptible fungi, which include dermatophytes andmost other fungi.
Drug interactionsKetoconazole may have significant interactions with other drugs.
284ANTI-INFECTIVE DRUGS
Adversereactions toflucytosine
Flucytosine may pro-duce unpredictableadverse reactions,including:• confusion• headache• drowsiness• vertigo• hallucinations• difficulty breathing• respiratory arrest• rash• nausea and vomiting• abdominal distention• diarrhea• anorexia.
Warning!
938910.qxd 08/26/2008 16:35 Page 284

• Ketoconazole used with drugs that decrease gastric acidity,such as cimetidine, ranitidine, famotidine, nizatidine, antacids,and anticholinergic drugs, may decrease absorption of ketocona-zole and reduce its antimycotic effects. If the patient must takethese drugs, delay administration of ketoconazole by at least2 hours.• Taking ketoconazole with phenytoin may alter metabolism andincrease blood levels of both drugs.• When taken with theophylline, ketoconazole may decrease theserum theophylline level.• Using ketoconazole with other liver-toxic drugs may increasethe risk of liver disease.• Combined with cyclosporine therapy, ketoconazole may in-crease cyclosporine and serum creatinine levels.• Ketoconazole increases the effect of oral anticoagulants andcan cause hemorrhage.• Ketoconazole can inhibit the metabolism (and possibly increaselevels) of quinidine, sulfonylureas, carbamazepine, and proteaseinhibitors.• Ketoconazole shouldn’t be given with rifampin because serumketoconazole levels may decrease. (See Adverse reactions to keto-conazole.)
Synthetic triazolesThe synthetic triazoles include:• fluconazole• itraconazole• voriconazole.
Fluconazole belongs to a class of synthetic, broad-spectrumtriazoles and is also referred to as a bistriazole antimycotic drug.
Itraconazole and voriconazole also belong to the synthetic tri-azole class of drugs. They inhibit the synthesis of ergosterol, a vi-tal component of fungal cell membranes.
PharmacokineticsAfter oral administration, fluconazole is about 90% absorbed. It’sdistributed into all body fluids, and more than 80% of the drug isexcreted unchanged in urine.
Oral bioavailability is greatest when itraconazole is taken withfood; voriconazole is more effective if taken 1 hour before or aftera meal.
285ANTIMYCOTIC DRUGS
Adversereactions toketoconazole
The most common ad-verse reactions to keto-conazole are nauseaand vomiting. Less fre-quent reactions include: • anaphylaxis• joint pain• chills• fever• ringing in the ears• impotence• photophobia.
Toxic topics
Liver toxicity is rare andreversible when thedrug is stopped.
Warning!
938910.qxd 08/26/2008 16:35 Page 285

Bound and determinedItraconazole and voriconazole are bound to plasma proteins andextensively metabolized in the liver into a large number ofmetabolites. They’re minimally excreted in stool.
PharmacodynamicsFluconazole inhibits fungal cytochrome P-450, an enzyme respon-sible for fungal sterol synthesis, causing fungal cell walls to weak-en.
Itraconazole and voriconazole interfere with fungal cell-wallsynthesis by inhibiting the formation of ergosterol and increasingcell-wall permeability, making the fungus susceptible to osmoticinstability.
PharmacotherapeuticsFluconazole is used to treat mouth, throat, and esophageal can-didiasis and serious systemic candidal infections, including UTIs,peritonitis, and pneumonia. It’s also used to treat cryptococcalmeningitis.
Osis, smosisItraconazole is used to treat blastomycosis, nonmeningeal histo-plasmosis, candidiasis, aspergillosis, and fungal nail disease.Voriconazole is used to treat invasive aspergillosis and seriousfungal infections caused by Scedosporium apiospermum andFusarium species.
Drug interactionsFluconazole may have interactions with other drugs:• Using fluconazole with warfarin may increase the risk of bleed-ing.• It may increase levels of phenytoin and cyclosporine.• It may increase the plasma levels of oral antidiabetic drugs,such as glyburide, tolbutamide, and glipizide, increasing the riskof hypoglycemia.• Rifampin and cimetidine enhance the metabolism of flucona-zole, reducing its plasma level.• Fluconazole may increase the activity of zidovudine. (See Ad-verse reactions to synthetic triazoles.)
Itraconazole and voriconazole may have these interactions:• Both may increase the risk of bleeding when combined withoral anticoagulants.• Antacids, H2-receptor antagonists, phenytoin, and rifampin low-er plasma itraconazole levels.
286ANTI-INFECTIVE DRUGS
Itraconazoletreats fungal nail
disease.Hmm…might be
time for amanicure.
938910.qxd 08/26/2008 16:35 Page 286

• Voriconazole may inhibit the metabolism of phenytoin, benzodi-azepines, calcium channel blockers, sulfonylureas, andtacrolimus.• Voriconazole is contraindicated with sirolimus and ergot alka-loids because voriconazole may increase plasma levels ofsirolimus and ergots.• Voriconazole is contraindicated with quinidine and pimozide be-cause of the risk of prolonged QT interval and, rarely, torsades depointes.
Glucan synthesis inhibitorsCaspofungin is a drug in a new class of agents known as glucansynthesis inhibitors (also called echinocandins). Its major use isin the patient who hasn’t responded to other antifungal therapies,such as amphotericin B or itraconazole.
PharmacokineticsAfter being given intravenously, caspofungin is highly protein-bound, with little distribution into RBCs. The drug is slowly me-tabolized and is excreted in urine and stool.
PharmacodynamicsCaspofungin inhibits the synthesis of beta (1,3) D-glucan, an inte-gral component of the fungal cell wall.
287ANTIMYCOTIC DRUGS
Adverse reactions to flucona-zole include:• abdominal pain• diarrhea• dizziness• headache• elevated liver enzyme levels• nausea and vomiting• rash.
Adverse reactions to itracon-azole include:• dizziness• headache• hypertension• impaired liver function• nausea.
Adverse reactions to voricon-azole include:• vision disturbances• fever• chills• headache• tachycardia• nausea and vomiting• rash• elevated liver enzyme.
Warning!
Adverse reactions to synthetic triazoles
Caspofungin isused to treat invasive
aspergillosis in thepatient who hasn’tresponded to, or
can’t tolerate, otherantifungals.
938910.qxd 08/26/2008 16:35 Page 287

PharmacotherapeuticsCaspofungin is used to treat invasive aspergillosis in the patientwho hasn’t responded to, or can’t tolerate, other antifungals. Ithasn’t been studied as an initial treatment for invasive aspergillo-sis.
Drug interactions• Patients taking caspofungin and tacrolimus may need higherdoses of tacrolimus because caspofungin decreases the bloodtacrolimus level.• Inducers of drug clearance, such as phenytoin, carbamazepine,efavirenz, nevirapine, and nelfinavir, may lower caspofungin clear-ance.• Concurrent use of caspofungin and cyclosporine may result inelevated liver enzyme levels and decreased caspofungin clear-ance, so use together isn’t recommended. (See Adverse reactionsto caspofungin.)
Synthetic allylamine derivativesTerbinafine, the most commonly used synthetic allylamine deriva-tive, is an allylamine antifungal, which inhibits fungal cell growthby inhibiting an enzyme responsible for the manufacture of ergos-terol.
PharmacokineticsTerbinafine is well absorbed and distributed throughout the body,especially if taken with food. It’s extensively metabolized; morethan two-thirds of the drug is excreted in urine.
Risk to liverRare cases of liver failure have occurred with terbinafine use,even in the patient with no known history of liver disease. Avoidusing this drug if liver disease is suspected, and obtain baselineliver enzyme test results before use.
PharmacodynamicsTerbinafine is thought to inhibit squalene epoxidase, which blocksthe biosynthesis of ergosterol, an essential component of fungalcell membranes.
288ANTI-INFECTIVE DRUGS
Adversereactions tocaspofungin
Adverse reactions tocaspofungin include:• paresthesia (burningor prickling sensation)• tachycardia (exces-sively rapid heart beat)• tachypnea (excessive-ly rapid breathing)• nausea and vomiting• diarrhea• rash• facial swelling.
Warning!
938910.qxd 08/26/2008 16:35 Page 288

PharmacotherapeuticsThis drug is used to treat tinea unguium (fungal infections of thefingernail or toenail).
Drug interactions• Terbinafine clearance is decreased when it’s taken with cimeti-dine and increased when it’s taken with rifampin.• Terbinafine increases plasma levels of caffeine and dex-tromethorphan and decreases levels of cyclosporine. (See Adversereactions to terbinafine.)
Recombinant human activated protein C
Recombinant human activated protein C (rhAPC) is a relativelynew class of drug possessing antithrombotic, anti-inflammatory,and fibrinolytic properties. Although its mechanism of action isn’twell known, rhACP is used to treat patients with severe sepsiswhen the risk of death from acute organ dysfunction is extremelyhigh.
Drotrecogin alfaDrotrecogin alfa, the first FDA-approved rhACP drug, is used totreat severe sepsis in adult patients with acute organ dysfunctionwhen they are at risk for death.
PharmacokineticsAfter I.V. infusion, drotrecogin alfa achieves a median steady statelevel in 2 hours. Information about its distribution, metabolism,and excretion isn’t available.
PharmacodynamicsAlthough drotrecogin alfa’s anti-infective action isn’t known, itmay work by producing dose-dependent reductions in D-dimerand interleukin-6. Activated protein C exerts an antithrombotic ef-fect by inhibiting factors Va and VIIIa.
289RECOMBINANT HUMAN ACTIVATED PROTEIN C
Adversereactions toterbinafine
Adverse reactions toterbinafine include:• headache• visual disturbances• nausea• diarrhea• abdominal pain• neutropenia• Stevens-Johnson syn-drome.
Warning!
938910.qxd 08/26/2008 16:35 Page 289

PharmacotherapeuticsDrotrecogin alfa is used to treat adults who have severe sepsis as-sociated with acute organ dysfunction and who have a high risk ofdeath. The drug has antithrombotic, anti-inflammatory, and fibri-nolytic properties.
Drug interactionsDrotrecogin alfa may interact with another drug that affects he-mostasis, such as an anticoagulant, antiplatelet drug, or throm-bolytic, possibly increasing the risk of bleeding. (See Adverse re-actions to drotrecogin alfa and Contraindications for drotreco-gin alfa.)
290ANTI-INFECTIVE DRUGS
This drug is contraindicated in patients who are hypersensitive to the drug or any of its compo-nents. It’s also contraindicated in patients with active internal bleeding and those who have hadhemorrhagic stroke in the past 3 months or intracranial or intraspinal surgery in the past 2months. In addition, the drug is contraindicated in patients with severe head trauma, trauma withincreased risk of life-threatening bleeding, an epidural catheter, an intracranial neoplasm or masslesion, or cerebral herniation.
Safe and sound
Contraindications for drotrecogin alfa Adversereactions todrotrecogin alfa
The most common ad-verse reaction todrotrecogin alfa isbleeding. Bleeding seenwith this drug most oftenoccurs as ecchymosisor GI bleeding.
Warning!
938910.qxd 08/26/2008 16:35 Page 290

Quick quiz
1. Which rationale best justifies administering different antitu-bercular drugs concurrently in treating active tuberculosis?
A. They’re second-line drugs and effective only together.B. Rifampin increases the activity of isoniazid.C. Combination therapy can prevent or delay bacterial re-
sistance.D. Single therapy isn’t effective.
Answer: C. Combination therapy can prevent or delay bacterialresistance to antitubercular drugs.
2. Which adverse reaction do most patients experience when re-ceiving I.V. amphotericin B?
A. AnuriaB. Coagulation defectsC. Shortness of breathD. Normochromic or normocytic anemia
Answer: D. Normochromic or normocytic anemia is a commonadverse effect of I.V. amphotericin B.
3. What’s the I.V. drug of choice for serious resistant staphylo-coccal infections in the patient who’s allergic to penicillin?
A. VancomycinB. ErythromycinC. AzithromycinD. Streptomycin
Answer: A. Vancomycin is the I.V. drug of choice for methicillin-resistant S. aureus infections.
291QUICK QUIZ
938910.qxd 08/26/2008 16:35 Page 291

ScoringIf you answered all three items correctly, extraordinary! You’re
more than a match for unwanted microbes!If you answered two items correctly, congratulations. You’re win-
ning the battle against bacteria.If you answered fewer than two items correctly, dig in! The war
with drugs continues for five more chapters!
292ANTI-INFECTIVE DRUGS
Ten down,five chaptersto go. I think Imay need a
refill.
✰✰✰
✰✰
✰
938910.qxd 08/26/2008 16:35 Page 292

Drugs and the immune systemImmune and inflammatory responses protect the body from invad-ing foreign substances. These responses can be modified by cer-tain classes of drugs:• Antihistamines block the effects of histamine on target tissues.• Corticosteroids suppress immune responses and reduce inflam-mation.• Noncorticosteroid immunosuppres-sants prevent rejection of transplantedorgans and can be used to treat auto im-mune disease.• Uricosurics prevent or control the fre-quency of gouty arthritis attacks.
11
Anti-inflammatory, anti-allergy, andimmunosuppressant drugs
Just the facts
In this chapter, you’ll learn:
♦ classes of drugs that modify immune or inflammatory re-sponses
♦ uses and varying actions of these drugs
♦ how these drugs are absorbed, distributed, metabolized,and excreted
♦ drug interactions and adverse reactions to these drugs.
Quiet down, class!Today’s lesson
includes informationabout drug classes
that can modifyresponses.
938911.qxd 08/26/2008 16:33 Page 293

AntihistaminesAntihistamines primarily act to block histamine effects that oc-cur in an immediate (type I) hypersensitivity reaction, commonlycalled an allergic reaction. They’re available alone or in combina-tion products by prescription or over-the-counter.
Histamine-1 receptor antagonistsThe term antihistamine refers to drugs that act as histamine-1(H1) receptor antagonists; that is, they compete with histamine forbinding to H1-receptor sites throughout the body. However, theydon’t displace histamine already bound to the receptor.
It’s all about chemistryBased on chemical structure, antihistamines are categorized intofive major classes:• Ethanolamines include clemastine fumarate, dimenhydrinate,and diphenhydramine hydrochloride.• Alkylamines include brompheniramine maleate, chlorphenir-amine maleate, and dexchlorpheniramine maleate.• Phenothiazines include promethazine hydrochloride.• Piperidines include azatadine maleate, cetirizine hydrochloride,cyproheptadine hydrochloride, desloratadine, fexofenadine hy-drochloride, loratadine, and meclizine hydrochloride.• Miscellaneous drugs, such as hydroxyzine hydrochloride andhydroxyzine pamoate, also act as antihistamines.
Pharmacokinetics (how drugs circulate)H1-receptor antagonists are well absorbed after oral or parenteraladministration. Some can also be given rectally.
DistributionWith the exception of loratadine and desloratadine, antihistaminesare distributed widely throughout the body and central nervoussystem (CNS).
Less penetration, fewer effectsFexofenadine, desloratadine, and loratadine, which are nonsedat-ing antihistamines, minimally penetrate the blood-brain barrier sothat little of the drug is distributed in the CNS, producing fewer ef-fects there than other antihistamines.
294ANTI-INFLAMMATORY, ANTI-ALLERGY, AND IMMUNOSUPPRESSANT DRUGS
Antihistaminesrelieve symptoms ofan allergy; however,they don’t give the
body immunity to theallergen itself.
Memoryjogger
Anti- is afamiliar pre-
fix meaning “oppos-ing.” That’s exactlywhat antihistaminesdo: They oppose hist-amine effects (or al-lergic reactions).
938911.qxd 08/26/2008 16:33 Page 294

Metabolism and excretionAntihistamines are metabolized by liver enzymes and excreted inurine; small amounts appear in breast milk. Fexofenadine, mainlyexcreted in stool, is an exception. Cetirizine undergoes limited he-patic metabolism.
Pharmacodynamics (how drugs act)H1-receptor antagonists compete with histamine for H1 receptorson effector cells (the cells that cause allergic symptoms), blockinghistamine from producing its effects. (See How chlorpheniraminestops an allergic response, page 296.)
Antagonizing tacticsH1-receptor antagonists produce their effects by:• blocking the action of histamine on the small blood vessels• decreasing dilation of arterioles and engorgement of tissues• reducing the leakage of plasma proteins and fluids out of thecapillaries (capillary permeability), thereby lessening edema• inhibiting most smooth-muscle responses to histamine (in par-ticular, blocking the constriction of bronchial, GI, and vascularsmooth muscle)• relieving symptoms by acting on the terminal nerve endings inthe skin that flare and itch when stimulated by histamine• suppressing adrenal medulla stimulation, autonomic gangliastimulation, and exocrine gland secretion, such as lacrimal andsalivary secretion.
Straight to the headSeveral antihistamines have a high affinity for H1 receptors in thebrain and are used for their CNS effects. These drugs includediphenhydramine, dimenhydrinate, promethazine, and variouspiperidine derivatives.
No stomach for thisH1-receptor antagonists don’t affect parietal cell secretion in thestomach because their receptors are H2 receptors, not H1.
Pharmacotherapeutics (how drugs are used)Antihistamines are used to treat the symptoms of type I hypersen-sitivity reactions, such as:• allergic rhinitis (runny nose and itchy eyes caused by a localsensitivity reaction)• vasomotor rhinitis (rhinitis not caused by allergy or infection)• allergic conjunctivitis (inflammation of the membranes of theeye)
295ANTIHISTAMINES
Keep in mindthat although
histamine bindingis blocked, the
overall release ofhistaminecontinues.
938911.qxd 08/26/2008 16:33 Page 295

296ANTI-INFLAMMATORY, ANTI-ALLERGY, AND IMMUNOSUPPRESSANT DRUGS
Although chlorpheniramine can’t reverse symptoms of an aller-gic response, it can stop the progression of the response.Here’s what happens.
Release the mediators
When sensitized to an antigen, a mast cell reacts to repeatedantigen exposure by releasing chemical mediators. One ofthese mediators, histamine, binds to histamine-1 (H1) receptorsfound on effector cells (the cells responsible for allergic symp-toms). This initiates the allergic response that affects the respi-
ratory, cardiovascular, GI, endocrine, and integumentary sys-tems.
The first one there wins
Chlorpheniramine competes with histamine for H1-receptorsites on the effector cells. By attaching to these sites first, thedrug prevents more histamine from binding to the effector cells.
Now I get it!
How chlorpheniramine stops an allergic response
Effector cells
Respiratory
responses
• Bronchialconstriction andbronchospasm• Decreased vitalcapacity• Itchy nose andthroat• Rhinorrhea (runnynose)• Sneezing
Cardiovascular
responses
• Decreased bloodpressure• Elevated heart rate• Increasedvasodilation• More capillary per-meability
GI
responses
• Increased parietalcell secretion• Increased smooth-muscle contraction
Endocrine
responses
• Increased releaseof epinephrine andnorepinephrine
Integumentary
responses
• Angioedema (hivesand swelling of skin,mucous membranes,or internal organs)• Flushing• Itching
Systemic allergic responses stopped
Antigen
Chlorpheniramine
Histamine
H1-receptor sites
Chemical mediators
Sensitized mast cell
938911.qxd 08/26/2008 16:33 Page 296

• urticaria (hives)• angioedema (submucosal swelling in the hands, face, and feet).
Not just for allergiesAntihistamines can have other therapeutic uses:• Many are used primarily as antiemetics (to control nausea andvomiting).• They can also be used as adjunctive therapy to treat an anaphy-lactic reaction after the serious symptoms are controlled.• Diphenhydramine can help treat Parkinson’s disease and drug-induced extrapyramidal reactions (abnormal involuntary move-ments).• Because of its antiserotonin qualities, cyproheptadine may beused to treat Cushing’s disease, serotonin-associated diarrhea,vascular cluster headaches, and anorexia nervosa.
Drug interactionsAntihistamines may interact with many drugs, sometimes withlife-threatening consequences:• They may block or reverse the vasopressor effects of epineph-rine, producing vasodilation, increased heart rate, and very lowblood pressure.• They may mask the toxic signs and symptoms of ototoxicity (adetrimental effect on hearing) associated with aminoglycosides orlarge dosages of salicylates.• They may increase the sedative and respiratory depressant ef-fects of CNS depressants, such as tranquilizers or alcohol.• Loratadine may cause serious cardiac effects when taken withmacrolide antibiotics (such as erythromycin), fluconazole, keto-conazole, itraconazole, miconazole, cimetidine, ciprofloxacin, andclarithromycin. (See Adverse reactions to antihistamines.)
CorticosteroidsCorticosteroids suppress immune responses and reduce inflam-mation. They’re available as natural or synthetic steroids.
There’s no improving on natureNatural corticosteroids are hormones produced by the adrenalcortex; most corticosteroids are synthetic forms of these hor-mones. Natural and synthetic corticosteroids are classified ac-cording to their biological activities:• Glucocorticoids, such as cortisone acetate and dexamethasone,affect carbohydrate and protein metabolism.
297CORTICOSTEROIDS
Adversereactions toantihistamines
The most common ad-verse reaction to anti-histamines (with the ex-ceptions of fexofenadineand loratadine) is cen-tral nervous system(CNS) depression. OtherCNS reactions include:• dizziness• lassitude and fatigue• disturbed coordination• muscle weakness.
Gut reactions
GI reactions may in-clude:• epigastric distress• loss of appetite• nausea and vomiting• constipation• diarrhea• dryness of the mouth,nose, and throat.
They can get the heart
racing
Cardiovascular reac-tions may include:• hypotension• hypertension• rapid heart rate• arrhythmias.
A sensitive issue
Sensitivity reactions canalso occur.
Warning!
938911.qxd 08/26/2008 16:33 Page 297

• Mineralocorticoids, such as aldosterone and fludrocortisone ac-etate, regulate electrolyte and water balance.
GlucocorticoidsMost glucocorticoids are synthetic analogues of hormones secret-ed by the adrenal cortex. They exert anti-inflammatory, metabolic,and immunosuppressant effects. Drugs in this class include:• beclomethasone• betamethasone• cortisone• dexamethasone• hydrocortisone• methylprednisolone• prednisolone• prednisone• triamcinolone.
PharmacokineticsGlucocorticoids are well absorbed when administered orally. AfterI.M. administration, they’re absorbed completely.
DistributionGlucocorticoids are bound to plasma proteins and distributedthrough the blood.
Metabolism and excretionGlucocorticoids are metabolized in the liver and excreted by thekidneys.
PharmacodynamicsGlucocorticoids suppress hypersensitivity and immune responsesthrough a process that isn’t entirely understood. Researchers be-lieve that glucocorticoids inhibit immune responses by:• suppressing or preventing cell-mediated immune reactions• reducing levels of leukocytes, monocytes, and eosinophils• decreasing the binding of immunoglobulins to cell surface re-ceptors• inhibiting interleukin synthesis.
Taking the red (and more) outGlucocorticoids suppress the redness, edema, heat, and tender-ness associated with the inflammatory response. They start on thecellular level by stabilizing the lysosomal membrane (a structure
298ANTI-INFLAMMATORY, ANTI-ALLERGY, AND IMMUNOSUPPRESSANT DRUGS
Unfortunately,when glucocorticoidsinhibit the immuneresponse they mayalso simultaneouslymask the signs and
symptoms of seriousinfections.
938911.qxd 08/26/2008 16:33 Page 298

within the cell that contains digestive enzymes) so that it doesn’trelease its store of hydrolytic enzymes into the cells.
No leaks, no dripsAs corticosteroids, glucocorticoids prevent the leakage of plasmafrom capillaries, suppress the migration of polymorphonuclearleukocytes (cells that kill and digest microorganisms), and inhibitphagocytosis (ingestion and destruction).
To ensure a job well done, glucocorticoids decrease antibodyformation in injured or infected tissues and disrupt histamine syn-thesis, fibroblast development, collagen deposition, capillary dila-tion, and capillary permeability. (See How methylprednisoloneworks.)
299CORTICOSTEROIDS
Tissue trauma normally leads to tissue irritation, edema, inflammation, and production of scar tissue. Methylprednisolone counter-acts the initial effects of tissue trauma, promoting healing.
Now I get it!
How methylprednisolone works
Tissueirritation
Unstable white blood cell(WBC) membranes release
acid hydrolases.
Methylprednisolone not administered Methylprednisolone administered
Healing
Tissue trauma
Capillary permeabilityincreases.
WBC adhesions form oncapillary membrane.
EdemaInflammation
and scartissue
StabilizedWBC
membranes
Reducedcapillary
permeability
DiminishedWBC
adhesions
Inhibitedmacrophageaccumulation
Macrophages accumulate intraumatized tissue.
938911.qxd 08/26/2008 16:33 Page 299

PharmacotherapeuticsBesides their use as replacement therapy for patients with adreno-cortical insufficiency, glucocorticoids are prescribed for immuno-suppression and reduction of inflammation and for their effectson the blood and lymphatic systems.
Drug interactionsMany drugs interact with corticosteroids:• Aminoglutethimide, barbiturates, phenytoin, and rifampin mayreduce the effects of corticosteroids.• Their potassium-wasting effects may be enhanced by ampho-tericin B, chlorthalidone, ethacrynic acid, furosemide, and thi-azide diuretics.• Erythromycin and troleandomycin may increase their effects byreducing their metabolism.• They reduce the serum concentration and effects of salicylates.• The risk of peptic ulcers associated with nonsteroidal anti-inflammatory drugs and salicylates increases when these agentsare taken with corticosteroids.• The response to vaccines and toxoids may be reduced in a pa-tient taking corticosteroids.• Estrogen and hormonal contraceptives that contain estrogen in-crease the effects of corticosteroids.• The effects of antidiabetic drugs may be reduced, resulting in in-creased blood glucose levels. (See Adverse reactions to cortico-steroids.)
300ANTI-INFLAMMATORY, ANTI-ALLERGY, AND IMMUNOSUPPRESSANT DRUGS
Corticosteroids affect almostall body systems. Their wide-spread adverse effects in-clude:• insomnia• increased sodium and wa-ter retention• increased potassium excre-tion
• suppressed immune and in-flammatory responses• osteoporosis• intestinal perforation• peptic ulcers• impaired wound healing.
Diabetes and more
Endocrine system reactionsmay include:
• diabetes mellitus• hyperlipidemia• adrenal atrophy• hypothalamic-pituitary axissuppression• cushingoid signs and symp-toms (such as buffalo hump,moon face, and elevatedblood glucose levels).
Warning!
Adverse reactions to corticosteroids
938911.qxd 08/26/2008 16:33 Page 300

MineralocorticoidsMineralocorticoids affect electrolyte and water balance. Thesedrugs include:• fludrocortisone acetate, a synthetic analogue of hormones se-creted by the adrenal cortex• aldosterone, a natural mineralocorticoid (the use of which hasbeen curtailed by high cost and limited availability).
PharmacokineticsFludrocortisone acetate is absorbed well and distributed to allparts of the body.
Metabolism and excretionFludrocortisone acetate is metabolized in the liver to inactivemetabolites. The drug is excreted by the kidneys, primarily as in-active metabolites.
PharmacodynamicsFludrocortisone acetate affects fluid and electrolyte balance byacting on the distal renal tubule to increase sodium reabsorptionand potassium and hydrogen secretion.
PharmacotherapeuticsFludrocortisone acetate is used as replacement therapy for pa-tients with adrenocortical insufficiency (reduced secretion of glu-cocorticoids, mineralocorticoids, and androgens).
Seasoning reasoningFludrocortisone acetate may also be used to treat salt-losing con-genital adrenogenital syndrome (characterized by a lack of corti-sol and deficient aldosterone production) after the patient’s elec-trolyte balance has been restored.
Drug interactionsAs is the case with adverse reactions, the drug interactions associ-ated with mineralocorticoids are similar to those associated withglucocorticoids.
301CORTICOSTEROIDS
Fludrocortisoneacetate gets meworking harder toincrease sodiumreabsorption andpotassium and
hydrogen secretion.
938911.qxd 08/26/2008 16:33 Page 301

Other immunosuppressantsSeveral drugs used for their immunosuppressant effects in pa-tients undergoing allograft transplantation (transplantation be-tween two people who aren’t identical twins) are also used experi-mentally to treat autoimmune diseases (diseases resulting from aninappropriate immune response directed against the self). They in-clude:• azathioprine• basiliximab• cyclosporine• daclizumab• lymphocyte immune globulin (ATG [equine])• muromonab-CD3• mycophenolate mofetil• sirolimus• tacrolimus• thymoglobulin (antithymocyte globulin [rabbit]).
Also theseCyclophosphamide, classified as an alkylating drug, is also used asan immunosuppressant; however, it’s primarily used to treat can-cer.
Anakinra is an immunosuppressant used to treat adults withmoderate to severe active rheumatoid arthritis who haven’t re-sponded to at least one disease-modifying antirheumatic drug.
PharmacokineticsImmunosuppressants take different paths through the body.
AbsorptionWhen administered orally, azathioprine and mycophenolate arereadily absorbed from the GI tract, whereas absorption of cy-closporine, tacrolimus, and sirolimus is varied and incomplete.
Only I.V.Anakinra, ATG, basiliximab, daclizumab, muromonab-CD3, andthymoglobulin are administered only by I.V. injection.
DistributionThe distribution of azathioprine, basiliximab, and daclizumab isn’tfully understood. Cyclosporine and muromonab-CD3 are distrib-uted widely throughout the body. Azathioprine and cyclosporinecross the placental barrier. The distribution of ATG isn’t clear, but
302ANTI-INFLAMMATORY, ANTI-ALLERGY, AND IMMUNOSUPPRESSANT DRUGS
938911.qxd 08/26/2008 16:33 Page 302

it may appear in breast milk. Distribution of tacrolimus dependson several factors; 75% to 99% is protein-bound. Sirolimus is 97%protein-bound.
Metabolism and excretionAzathioprine and cyclosporine are metabolized in the liver.Muromonab-CD3 is consumed by T cells circulating in the blood.The metabolism of ATG is unknown.
Mycophenolate is metabolized in the liver to mycophenolateacid, an active metabolite, and then further metabolized to an in-active metabolite, which is excreted in urine and bile. Concentra-tions of mycophenolate and acyclovir may increase in the pres-ence of nephrotoxicity.
Azathioprine, anakinra, and ATG are excreted in urine; cy-closporine is excreted principally in bile. It’s unknown howmuromonab-CD3 is excreted.
Tacrolimus is extensively metabolized and excreted primarilyin bile; less than 1% is excreted unchanged in urine. Sirolimus ismetabolized by the mixed function oxidase system, primarily cy-tochrome P-450 (CYP3A4); 91% is excreted in stool and 2.2% inurine. Metabolism and excretion of basiliximab and daclizumabaren’t understood.
PharmacodynamicsHow certain immunosuppressants achieve their desired effectshas yet to be determined.
What’s going on here?The exact mechanism of action of azathioprine, cyclosporine, andATG is unknown, but may be explained by these theories:• Azathioprine antagonizes metabolism of the amino acid purineand, therefore, may inhibit ribonucleic acid and deoxyribonucleicacid structure and synthesis. It also may inhibit coenzyme forma-tion and function.• Cyclosporine is thought to inhibit helper T cells and suppressorT cells.• ATG may eliminate antigen-reactive T cells in the blood, alterT-cell function, or both.
They do know this much…In patients receiving kidney allografts, azathioprine suppressescell-mediated hypersensitivity reactions and produces various al-terations in antibody production. Muromonab-CD3, a monoclonalantibody, is understood to block the function of T cells.
Anakinra, basiliximab, and daclizumab block the activity of in-terleukin. Mycophenolate inhibits responses of T and B lympho-
303OTHER IMMUNOSUPPRESSANTS
Cyclosporine mayinhibit helper T
cells, but we aren’treally sure.
938911.qxd 08/26/2008 16:33 Page 303

cytes, suppresses antibody formation by B lymphocytes, and mayinhibit recruitment of leukocytes into sites of inflammation andgraft rejection.
Sirolimus is an immunosuppressant that inhibits T-lymphocyteactivation and proliferation that occur in response to antigenicand cytokine stimulation; it also inhibits antibody formation.
PharmacotherapeuticsImmunosuppressants are used mainly to prevent rejection in pa-tients who undergo organ transplantation. (See Cyclosporine:Miracle drug or death sentence?)
Drug interactionsMost drug interactions with this class of drugs involve other im-munosuppressant and anti-inflammatory drugs and various antibi-otic and antimicrobial drugs. (See Adverse reactions to noncorti-costeroid immunosuppressants.)• Allopurinol increases the blood levels of azathioprine.• Verapamil increases blood levels of sirolimus.• Voriconazole shouldn’t be given with sirolimus because thecombination inhibits CYP3A4 enzymes, resulting in increasedsirolimus levels.• When mycophenolate is taken with antacids or cholestyramine,mycophenolate levels decrease.
304ANTI-INFLAMMATORY, ANTI-ALLERGY, AND IMMUNOSUPPRESSANT DRUGS
Organ transplantation can save a life. Howev-er, cyclosporine, an immunosuppressant usedto reduce the risk of organ rejection, may alsocause cancer.
Does cyclosporine encourage cells to
become cancerous?
It has long been believed that when the im-mune system is weakened by immunosuppres-sants, it loses its ability to fight and kill cancer-ous cells. Recent research suggests that cy-closporine may also encourage abnormal cells
to become cancerous and perhaps even growaggressively. This research has raised con-cern about the use of cyclosporine in organtransplantation.
A double-edged sword
However, this concern needs to be balancedagainst the life-threatening risk of organ rejec-tion. Scientists are now looking for ways toblock this tumor-promoting effect of cyclo-sporine.
Yea or nay?
Cyclosporine: Miracle drug or death sentence?
938911.qxd 08/26/2008 16:33 Page 304

• Coadministration of mycophenolate with acyclovir, especially inpatients with renal impairment, may increase concentrations ofboth drugs.• Cyclosporine levels may increase if cyclosporine is taken withketoconazole, calcium channel blockers, cimetidine, anabolicsteroids, hormonal contraceptives, erythromycin, or metoclo-pramide.• The risk of toxicity to the kidneys increases when cyclosporineor sirolimus is taken with acyclovir, aminoglycosides, or ampho-tericin B.• Taking anakinra, ATG, basiliximab, cyclosporine, daclizumab,muromonab-CD3, sirolimus, or thymoglobulin with other immuno-suppressants (except corticosteroids) increases the risk of infec-tion and lymphoma (neoplasm of the lymph tissue; typically malig-nant).• Barbiturates, rifampin, phenytoin, sulfonamides, and trimetho-prim decrease plasma cyclosporine and sirolimus levels.
305OTHER IMMUNOSUPPRESSANTS
All noncorticosteroid immunosuppressants can cause hypersensitivity reactions. Here are adverse reactions to individual drugs.
Warning!
Adverse reactions to noncorticosteroid immunosuppressants
Azathioprine
• Bone marrow suppression• Nausea and vomiting• Liver toxicity
Cyclosporine
• Kidney toxicity• Hyperkalemia• Infection• Liver toxicity• Nausea and vomiting
Daclizumab
• GI disorders• Hypertension• Hypotension• Chest pain• Tachycardia• Edema• Dyspnea
• Pulmonary edema• Thrombosis• Bleeding• Renal tubular necrosis
Lymphocyte immune
globulin
• Fever and chills• Reduced white blood cell(WBC) or platelet count• Infection• Nausea and vomiting
Muromonab-CD3
• Fever and chills• Nausea and vomiting• Tremor• Pulmonary edema• Infection
Mycophenolate mofetil
• Nausea• Diarrhea• Leukopenia• Headache• Weakness• Urinary frequency• Leg cramps or pain• Liver function test result ab-normalities• Rash
Sirolimus
• Anemia• Thrombocytopenia• Hyperlipidemia• Hypertension
Tacrolimus
• Nausea and vomiting
• Diarrhea• Constipation• Tremor• Leukopenia• Hypertension• Nephrotoxicity• Hepatotoxicity
Thymoglobulin
• Abdominal pain• Diarrhea• Dyspnea• Fever and chills• Headache• Infection• Nausea and vomiting• Reduced WBC or plateletcount• Systemic infections• Dizziness
938911.qxd 08/26/2008 16:33 Page 305

• Serum digoxin levels may increase when cyclosporine is takenwith digoxin.• Anakinra shouldn’t be given to patients with active infections orneutropenia.
Uricosurics and other antigout drugsUricosurics, along with other antigout drugs, exert their effectsthrough their anti-inflammatory actions.
UricosuricsThe two major uricosurics are:
probenecid
sulfinpyrazone.
Getting the gout outUricosurics act by increasing uric acid excretion in urine. The pri-mary goal in using uricosurics is to prevent or control the frequen-cy of gouty arthritis attacks.
PharmacokineticsUricosurics are absorbed from the GI tract.
DistributionDistribution of the two drugs is similar, with 75% to 95% ofprobenecid and 98% of sulfinpyrazone being protein-bound.
Metabolism and excretionMetabolism of the drugs occurs in the liver, and excretion is pri-marily by the kidneys. Only small amounts of these drugs are ex-creted in stool.
PharmacodynamicsProbenecid and sulfinpyrazone reduce the reabsorption of uricacid at the proximal convoluted tubules of the kidneys. This re-sults in excretion of uric acid in urine, reducing serum urate lev-els.
PharmacotherapeuticsProbenecid and sulfinpyrazone are indicated for the treatment of:
306ANTI-INFLAMMATORY, ANTI-ALLERGY, AND IMMUNOSUPPRESSANT DRUGS
938911.qxd 08/26/2008 16:34 Page 306

• chronic gouty arthritis• tophaceous gout (the deposition of tophi or urate crystals underthe skin and into joints).
A part-time promoterProbenecid is also used to promote uric acid excretion in patientsexperiencing hyperuricemia.
Substitute when acuteProbenecid and sulfinpyrazone shouldn’t be given during an acutegouty attack. If taken at that time, these drugs prolong inflamma-tion. Because these drugs may increase the chance of an acutegouty attack when therapy begins and whenever the serum uratelevel changes rapidly, colchicine is administered during the first3 to 6 months of probenecid or sulfinpyrazone therapy.
Drug interactionsMany drug interactions, some potentially serious, can occur withuricosuric drugs:• Probenecid significantly increases or prolongs the effects ofcephalosporins, penicillins, and sulfonamides.• Serum urate levels may increase when probenecid is taken withantineoplastic drugs.• Probenecid increases the serum concentration of dapsone,aminosalicylic acid, and methotrexate, causing toxic reactions.• Sulfinpyrazone increases the effectiveness of warfarin, increas-ing the risk of bleeding.• Salicylates reduce the effects of sulfinpyrazone.• Sulfinpyrazone may potentiate the effects of oral antidiabeticdrugs, increasing the risk of hypoglycemia. (See Adverse reac-tions to uricosurics.)
Other antigout drugsAllopurinol is used to reduce production of uric acid, preventinggouty attacks, and colchicine is used to treat acute gouty attacks.
PharmacokineticsAllopurinol and colchicine take somewhat different paths throughthe body.
All aboard allopurinolWhen given orally, allopurinol is absorbed from the GI tract. Allo-purinol and its metabolite oxypurinol are distributed throughoutthe body except in the brain, where drug concentrations are 50%
307URICOSURICS AND OTHER ANTIGOUT DRUGS
Probenecid andsulfinpyrazone
shouldn’t be used totreat an acute gouty
attack.
Adversereactions touricosurics
Adverse reactions to uri-cosurics include uricacid stone formation andblood abnormalities.
Probenecid
• Headache• Anorexia• Nausea and vomiting• Hypersensitivity reac-tions
Sulfinpyrazone
• Nausea• Indigestion• GI pain• GI blood loss
Warning!
938911.qxd 08/26/2008 16:34 Page 307

of those found in the rest of the body. It’s metabolized by the liverand excreted in urine.
Following colchicine’s courseColchicine is absorbed from the GI tract and is partially metabo-lized in the liver. The drug and its metabolites then reenter the in-testinal tract through biliary secretions. After reabsorption fromthe intestines, colchicine is distributed to various tissues. It’s ex-creted primarily in stool and to a lesser degree in urine.
PharmacodynamicsAllopurinol and its metabolite oxypurinol inhibit xanthine oxi-dase, the enzyme responsible for the production of uric acid. Byreducing uric acid formation, allopurinol eliminates the hazardsof hyperuricuria.
Migration controlColchicine appears to reduce the inflammatory response to mono-sodium urate crystals deposited in joint tissues. Colchicine mayproduce its effects by inhibiting migration of white blood cells(WBCs) to the inflamed joint. This reduces phagocytosis and lac-tic acid production by WBCs, decreasing urate crystal depositsand reducing inflammation.
PharmacotherapeuticsAllopurinol treats primary gout, hopefully preventing acute goutyattacks. It can be prescribed with uricosurics when smallerdosages of each drug are directed. It’s used to treat:• gout or hyperuricemia that may occur with blood abnormalitiesand during treatment of tumors or leukemia• primary or secondary uric acid nephropathy (with or withoutthe accompanying symptoms of gout)• patients who respond poorly to maximum dosages of urico-surics or who have allergic reactions or intolerance to uricosuricdrugs (it’s also used to prevent recurrent uric acid stone forma-tion).
Acute alertColchicine is used to relieve the inflammation of acute goutyarthritis attacks. If given promptly, it’s especially effective in re-lieving pain. In addition, giving colchicine during the first severalmonths of allopurinol, probenecid, or sulfinpyrazone therapy mayprevent the acute gouty attacks that sometimes accompany theuse of these drugs.
308ANTI-INFLAMMATORY, ANTI-ALLERGY, AND IMMUNOSUPPRESSANT DRUGS
Colchicinerelieves a painfulgouty attack by
going to work rightin the joint. It canhave you runningsmoothly again.
938911.qxd 08/26/2008 16:34 Page 308

Drug interactionsColchicine doesn’t interact significantly with other drugs. Whenallopurinol is used with other drugs, the resulting interactions canbe serious:• Allopurinol potentiates the effect of oral anticoagulants.• Allopurinol increases the serum concentrations of mercapto-purine and azathioprine, increasing the risk of toxicity.• Angiotensin-converting enzyme inhibitors increase the risk ofhypersensitivity reactions to allopurinol.• Allopurinol increases serum theophylline levels.• The risk of bone marrow depression increases when cyclophos-phamide is taken with allopurinol. (See Adverse reactions to otherantigout drugs.)
Quick quiz
1. How does diphenhydramine work?A. It blocks production of histamine.B. It prevents binding of histamine to receptors.C. It reverses the effects of histamine.D. It increases levels of histamine.
Answer: B. Diphenhydramine prevents binding of histamine toreceptors.
2. What’s the most common adverse reaction for most antihista-mines, with the exceptions of fexofenadine and loratadine?
A. Drug feverB. GI distressC. Respiratory distressD. Sedation
Answer: D. Sedation, or CNS depression, is the most commonadverse reaction to most antihistamines.
3. Which signs and symptoms suggest that a patient is experi-encing Cushing’s syndrome?
A. Buffalo hump, elevated blood glucose levels, and moonface
B. Low blood pressure, rapid heart rate, and difficultybreathing
C. Low blood glucose levels and reduced platelet countD. Increased thirst, increased urination, and increased ap-
petite
309QUICK QUIZ
Adversereactions toother antigoutdrugs
Allopurinol and colchi-cine commonly causenausea, vomiting, diar-rhea, and intermittentabdominal pain.
Allopurinol
The most common ad-verse reaction to allo-purinol is a rash.
Colchicine
Prolonged administra-tion of colchicine maycause bone marrowsuppression.
Warning!
938911.qxd 08/26/2008 16:34 Page 309

Answer: A. Buffalo hump, elevated blood glucose levels, andmoon face are all signs and symptoms of Cushing’s syndrome.This condition can occur as an adverse reaction to corticoste-roids.
4. Which condition indicates that a patient is experiencing anadverse reaction to azathioprine?
A. Kidney failureB. Peptic ulcerC. Bone marrow suppressionD. Heart failure
Answer: C. Bone marrow suppression indicates that a patient isexperiencing an adverse reaction to azathioprine.
5. Which sign is an adverse reaction to probenecid?A. EdemaB. VomitingC. VertigoD. Decreased urine output
Answer: B. Vomiting is an adverse reaction to probenecid.
ScoringIf you answered all five items correctly, extraordinary! You cer-
tainly aren’t allergic to smarts!If you answered three or four items correctly, congratulations!
You’re taking the sting out of learning!If you answered fewer than three items correctly, keep trying!
With continued improvement, the next chapter should haveyou feeling better!
310ANTI-INFLAMMATORY, ANTI-ALLERGY, AND IMMUNOSUPPRESSANT DRUGS
✰✰✰
✰✰
✰
938911.qxd 08/26/2008 16:34 Page 310

Drugs and psychiatric disordersThis chapter presents drugs that are used to treat various sleepand psychogenic disorders, such as anxiety, depression, and psy-chotic disorders.
Sedative and hypnotic drugsSedatives reduce anxiety, tension, or excitement. Some degree ofdrowsiness commonly accompanies sedative use.
You’re getting very sleepy…When given in large doses, sedatives are considered hypnotics,which induce a state resembling natural sleep. The three mainclasses of synthetic drugs used as sedatives and hypnotics are:
benzodiazepines
barbiturates
nonbenzodiazepine-nonbarbiturate drugs.
12
Psychotropic drugs
Just the facts
In this chapter, you’ll learn:
♦ classes of drugs that alter psychogenic behavior andpromote sleep
♦ uses and varying actions of these drugs
♦ how these drugs are absorbed, distributed, metabolized,and excreted
♦ drug interactions and adverse reactions to these drugs.
Justtalking about
hypnoticsmakes me
sleepy.
938912.qxd 08/26/2008 16:46 Page 311

And if that doesn’t put you to sleep…Other sedatives may include sedating antidepressants, such as tra-zodone, and over-the-counter sleep aids.
BenzodiazepinesBenzodiazepines produce many therapeutic effects, including:• sedation before anesthesia• sleep inducement• relief of anxiety and tension• skeletal muscle relaxation• anticonvulsant activity.
Keep your eye on the hypnotic onesBenzodiazepines are used in various clinical situations and exerteither a primary or a secondary sedative or hypnotic effect. Ben-zodiazepines used primarily for their sedative or hypnotic effectsinclude:• estazolam• flurazepam• lorazepam• quazepam• temazepam• triazolam.
When some calm is neededBenzodiazepines used primarily for the treatment of anxiety in-clude:• alprazolam• chlordiazepoxide• clonazepam• clorazepate• diazepam• lorazepam• oxazepam.
Pharmacokinetics (how drugs circulate)Benzodiazepines are absorbed rapidly and completely from the GItract and are distributed widely in the body. Penetration into thebrain also occurs rapidly. Some benzodiazepines, such as diaze-pam and lorazepam, may also be given parenterally.
How fast?The rate of absorption determines how quickly the drug will work;flurazepam and triazolam have the fastest onset.
312PSYCHOTROPIC DRUGS
938912.qxd 08/26/2008 16:46 Page 312

How long?The duration of effect is determined by the extent of distribution.Triazolam binds quickly to fat and is widely distributed; therefore,it has a short duration of action.
Metabolism and excretionAll benzodiazepines are metabolized in the liver and excreted pri-marily in urine. Some benzodiazepines have active metabolites,which may give these drugs a longer period of action.
Pharmacodynamics (how drugs act)Researchers believe that benzodiazepines work by stimulatinggamma-aminobutyric acid (GABA) receptors in the ascendingreticular activating system (RAS) of the brain. The RAS is associ-ated with wakefulness and attention and includes the cerebralcortex and limbic, thalamic, and hypothalamic levels of the cen-tral nervous system (CNS). (See How benzodiazepines work,page 314.)
Low will ease your mindAt low dosages, benzodiazepines decrease anxiety by acting onthe limbic system and other areas of the brain that help regulateemotional activity. The drugs can usually calm or sedate the pa-tient without causing drowsiness.
High will ease you into sleepAt higher dosages, benzodiazepines induce sleep, probably be-cause they depress the RAS of the brain.
Zzzzzzzzzzzz…Benzodiazepines increase total sleep time and reduce the numberof awakenings. In most cases, benzodiazepines don’t decrease thetime spent in rapid-eye-movement (REM) sleep, the state of sleepin which brain activity resembles the activity it shows whenawake; the body’s muscles relax, and the eyes move rapidly. Be-cause benzodiazepines don’t decrease the duration of REM sleep,they have a significant advantage over barbiturates.
During each sleep cycle the sleeping person progresses fromstage 1, which is drowsiness, to stages 3 and 4, which are deep-sleep stages. Benzodiazepines reduce the amount of time spent instages 3 and 4. The decrease in stage 4 sleep is accompanied by areduction in nightmares.
Pharmacotherapeutics (how drugs are used)Clinical indications for benzodiazepines include:
313SEDATIVE AND HYPNOTIC DRUGS
At low dosages,benzodiazepinesdecrease anxietywithout causing
drowsiness.
938912.qxd 08/26/2008 16:46 Page 313

314PSYCHOTROPIC DRUGS
These illustrations show how benzodiazepines work at the cellular level.
Speed and passage
The speed of impulses from apresynaptic neuron across asynapse is influenced by thenumber of chloride ions in thepostsynaptic neuron. The pas-sage of chloride ions into thepostsynaptic neuron dependson the inhibitory neurotransmit-ter called gamma-aminobutyricacid, or GABA.
It binds
When GABA is released fromthe presynaptic neuron, it trav-els across the synapse andbinds to GABA receptors on thepostsynaptic neuron. This bind-ing opens the chloride chan-nels, allowing chloride ions toflow into the postsynaptic neu-ron and causing the nerve im-pulses to slow down.
The result is another kind of
depression
Benzodiazepines bind to recep-tors on or near the GABA recep-tor, enhancing the effect ofGABA and allowing more chlo-ride ions to flow into the post-synaptic neuron. This depressesthe nerve impulses, causingthem to slow down or stop.
Now I get it!
How benzodiazepines work
GABA
Presynapticneuron
Impulses
Synapse
GABA
GABA receptor
Impulses slowdown
Enhancedeffectallowsgreater flowof chlorideions
Impulsesslow or stop
Chloride ion
Postsynapticneuron
Chloride ions
Benzodiazepine
Cl
Cl
Cl
Cl
Cl
Cl
Cl
Cl
Cl
Cl
Cl
ClClCl
ClCl Cl
938912.qxd 08/26/2008 16:46 Page 314

• relaxing the patient during the day of or before surgery• treating insomnia• producing I.V. anesthesia• treating alcohol withdrawal symptoms• treating anxiety and seizure disorders• producing skeletal muscle relaxation.
Drug interactionsExcept for other CNS depressants such as alcohol, few drugs in-teract with benzodiazepines.
Deep sleepWhen benzodiazepines are taken with other CNS depressants (in-cluding alcohol and anticonvulsants), the result is enhanced seda-tive and CNS depressant effects, including reduced level of con-sciousness, reduced muscle coordination, respiratory depression,and death.
Possible problems with the pillHormonal contraceptives may reduce the metabolism of flurazepam hydrochloride, increasing the risk of toxicity.
Triazolam may be affected by inhibitors of the CYP3A system(such as erythromycin and ketoconazole). (See Adverse reactionsto benzodiazepines.)
315SEDATIVE AND HYPNOTIC DRUGS
Benzodiazepines may cause:• amnesia• fatigue• muscle weakness• mouth dryness• nausea and vomiting• dizziness• ataxia (impaired ability to coordinate move-ment).
Getting groggy
Unintentional daytime sedation, hangover ef-fect (residual drowsiness and impaired reac-
tion time on awakening), and rebound insom-nia may also occur.
One more may be one too many
These drugs have a potential for abuse, toler-ance, and physical dependence. Benzodi-azepines with a long half-life or active metabo-lites may accumulate and cause adverse ef-fects in elderly patients. In general, lowerstarting doses, with gradual dosage increases,should be used in elderly patients who are tak-ing benzodiazepines.
Warning!
Adverse reactions to benzodiazepines
938912.qxd 08/26/2008 16:46 Page 315

BarbituratesThe major pharmacologic action of barbiturates is to reduce over-all CNS alertness. Barbiturates used primarily as sedatives andhypnotics include:• amobarbital• butabarbital• mephobarbital• pentobarbital• phenobarbital• secobarbital.
On the doseLow doses of barbiturates depress the sensory and motor cortexin the brain, causing drowsiness. High doses may cause respirato-ry depression and death because of their ability to depress all lev-els of the CNS.
PharmacokineticsBarbiturates are well absorbed from the GI tract, distributedrapidly, metabolized by the liver, and excreted in urine.
PharmacodynamicsAs sedative-hypnotics, barbiturates depress the sensory cortex ofthe brain, decrease motor activity, alter cerebral function, and pro-duce drowsiness, sedation, and hypnosis.
We interrupt this transmission…These drugs appear to act throughout the CNS; however, the RASof the brain, which is responsible for wakefulness, is a particularlysensitive site.
PharmacotherapeuticsBarbiturates have many clinical indications, including:• daytime sedation (for short periods only, typically less than2 weeks)• hypnotic effects for patients with insomnia• preoperative sedation and anesthesia• relief of anxiety• anticonvulsant effects.
Popularity plungePatients develop tolerance to barbiturates more quickly thanto benzodiazepines, and physical dependence on barbiturates
316PSYCHOTROPIC DRUGS
Low doses ofbarbiturates depress
parts of the brain.High doses cause
respiratorydepression.
938912.qxd 08/26/2008 16:46 Page 316

may occur even with a small daily dosage. In comparison, benzo-diazepines are relatively effective and safe and, for these reasons,have replaced barbiturates as the sedatives and hypnotics ofchoice.
Drug interactionsBarbiturates may interact with many other drugs:• They may reduce the effects of beta-adrenergic blockers (meto-prolol, propranolol), chloramphenicol, corticosteroids, doxycy-cline, oral anticoagulants, hormonal contraceptives, quinidine, tri-cyclic antidepressants (TCAs), metronidazole, theophylline,and cyclosporine.• Hydantoins, such as phenytoin, reduce the metabolism of phe-nobarbital, resulting in increased toxic effects.• Their use with methoxyflurane may stimulate production ofmetabolites that are toxic to the kidneys.• Their use with other CNS depressants (especially alcohol) maycause excessive CNS depression.• Valproic acid may increase barbiturate levels.• Monoamine oxidase inhibitors (MAOIs) inhibit the metabolismof barbiturates, increasing their sedative effects.• When barbiturates are taken with acetaminophen, the risk ofliver toxicity increases. (See Adverse reactions to barbiturates.)
Nonbenzodiazepines-nonbarbituratesNonbenzodiazepine-nonbarbiturates act as hypnotics for treat-ment of simple insomnia. These drugs, which offer no special ad-vantages over other sedatives, include:• chloral hydrate• eszopiclone• ramelton• zaleplon• zolpidem.
Diminishing returnsChloral hydrate and zaleplon lose their effectiveness by the end ofthe second week. Zolpidem is usually effective for up to 35 days.Eszopiclone and ramelton are approved for long-term treatmentof insomnia.
PharmacokineticsNonbenzodiazepines-nonbarbiturates are absorbed rapidly fromthe GI tract, metabolized in the liver, and excreted in urine.
317SEDATIVE AND HYPNOTIC DRUGS
Adversereactions tobarbiturates
Barbiturates may havewidespread adverse ef-fects.
S.O.S. for CNS
Central nervous system(CNS) reactions include:• drowsiness• lethargy• headache• depression.
Heart of the matter
Cardiovascular and res-piratory effects include:• mild bradycardia• hypotension• hypoventilation• spasm of the larynx(voice box) and bronchi• reduced rate ofbreathing• severe respiratory de-pression.
All the rest
Other reactions include:• vertigo• nausea and vomiting• diarrhea• epigastric pain• allergic reactions.
Warning!
938912.qxd 08/26/2008 16:46 Page 317

PharmacodynamicsThe mechanism of action for nonbenzodiazepines-nonbarbituratesisn’t fully known; however, they produce depressant effects simi-lar to barbiturates.
PharmacotherapeuticsNonbenzodiazepines-nonbarbiturates are typically used for:• treatment of simple insomnia• sedation before surgery• sedation before EEG studies.
Drug interactionsWhen nonbenzodiazepines-nonbarbiturates are used with otherCNS depressants, additive CNS depression occurs, resulting indrowsiness, respiratory depression, stupor, coma, or death. (SeeWarning about sleep agents.)
A chlorus of interactionsChloral hydrate may increase the risk of bleeding in patients tak-ing oral anticoagulants. Use with I.V. furosemide may producesweating, flushing, variable blood pressure, and uneasiness. (SeeAdverse reactions to nonbenzodiazepines-nonbarbiturates.)
Antianxiety drugsAntianxiety drugs, also called anxiolytics, include some of themost commonly prescribed drugs in the United States. They areused primarily to treat anxiety disorders. The three main types ofantianxiety drugs are benzodiazepines (discussed in a previoussection), barbiturates (also discussed in a previous section), andbuspirone.
318PSYCHOTROPIC DRUGS
Adversereactions tononbenzo-diazepines-nonbarbiturates
The most common dose-related adverse reac-tions involving nonben-zodiazepines-nonbarbi-turates include:• nausea and vomiting• gastric irritation• hangover effects (pos-sibly leading to respira-tory depression or evenrespiratory failure).
Warning!
The U.S. Food and Drug Administration requires that all sedative-hypnotic drugs include a warn-ing on the drug label about the risk of complex sleep-related behaviors. Complex sleep-relatedbehaviors include preparing and eating food, making phone calls, and even driving when not fullyawake, while having no memory of the event.
Safe and sound
Warning about sleep agents
938912.qxd 08/26/2008 16:46 Page 318

BuspironeBuspirone is the first antianxiety drug in a class of drugs knownas azaspirodecanedione derivatives. This drug’s structure andmechanism of action differ from those of other antianxiety drugs.
Advantage, buspironeBuspirone has several advantages, including:• less sedation• no increase in CNS depressant effects when taken with alcoholor sedative-hypnotics• lower abuse potential.
PharmacokineticsBuspirone is absorbed rapidly, undergoes extensive first-pass ef-fect, and is metabolized in the liver to at least one active metabo-lite. The drug is eliminated in urine and stool.
PharmacodynamicsAlthough the mechanism of action of buspirone isn’t known, it’sknown that buspirone doesn’t affect GABA receptors like the ben-zodiazepines do.
Midbrain modulatorBuspirone seems to produce various effects in the midbrain andacts as a midbrain modulator, possibly due to its high affinity forserotonin receptors.
PharmacotherapeuticsBuspirone is used to treat generalized anxiety states. Patients whohaven’t received benzodiazepines seem to respond better to bu-spirone.
In case of panicBecause of its slow onset of action, buspirone is ineffective whenquick relief from anxiety is needed.
Drug interactionsUnlike other antianxiety drugs, buspirone doesn’t interact with al-cohol or other CNS depressants. When buspirone is given withMAOIs, hypertensive reactions may occur. (See Adverse reactionsto buspirone.)
319ANTIANXIETY DRUGS
Buspirone hasa slow onset, so it
isn’t useful forpanic attacks.
Adversereactions tobuspirone
The most common reac-tions to buspirone in-clude:• dizziness• light-headedness• insomnia• rapid heart rate• palpitations• headache.
Warning!
938912.qxd 08/26/2008 16:46 Page 319

Antidepressant and mood stabilizerdrugs
Antidepressant and mood stabilizer drugs are used to treat affec-tive disorders—disturbances in mood, characterized by depres-sion or elation.
Pole positionsUnipolar disorders, characterized by periods of clinical depres-sion, are treated with:• selective serotonin reuptake inhibitors (SSRIs)• MAOIs• TCAs• miscellaneous antidepressants.
Bipolar disorders, characterized by alternating periods of man-ic behavior and clinical depression, are treated with lithium andanticonvulsant drugs.
Other mood stabilizers include divalproex, carbamazepine, andolanzapine.
Selective serotonin reuptake inhibitorsDeveloped to treat depression with fewer adverse reactions,SSRIs, are chemically different from MAOIs and TCAs. (SeePutting a new stress on SSRIs.)
Some of the SSRIs currently available are:• citalopram• duloxetine• escitalopram• fluoxetine• fluvoxamine• paroxetine• sertraline• venlafaxine. (See Stopping SSRIs.)
PharmacokineticsSSRIs are absorbed almost completely after oral administrationand are highly protein-bound.
Metabolism and excretionSSRIs are primarily metabolized in the liver and are excreted inurine.
320PSYCHOTROPIC DRUGS
Putting a newstress on SSRIs
The Food and Drug Ad-ministration approvedsertraline (Zoloft) andparoxetine (Paxil) as thedrugs of choice for treat-ing posttraumatic stressdisorder. In order forthese drugs to be used,the patient must havesymptoms, such as in-tense fear, helplessness,and horror that exist forat least 1 month andcause significant im-paired functioning.
938912.qxd 08/26/2008 16:46 Page 320

PharmacodynamicsSSRIs inhibit the neuronal reuptake of the neurotransmitter sero-tonin.
PharmacotherapeuticsSSRIs are used to treat the same major depressive episodes asTCAs and have the same degree of effectiveness. Fluvoxamine,fluoxetine, sertraline, and paroxetine are also used to treat obses-sive-compulsive disorder. Fluoxetine has also been approved forthe treatment of bulimia. Paroxetine is also indicated for socialanxiety disorder.
Venlafaxine is an antidepressant drug that’s chemically differ-ent from other antidepressants and has unique properties in termsof absorption and mechanism of action. It has been particularly ef-fective in patients with very severe depression.
Don’t panic, but there’s more…SSRIs may also be useful in treating panic disorders, eating disor-ders, personality disorders, impulse control disorders, and anxietydisorders. Several SSRIs are approved for premenstrual (dysphor-ic) disorder.
Drug interactionsDrug interactions associated with SSRIs involve their ability tocompetitively inhibit a liver enzyme that’s responsible for oxida-tion of numerous drugs, including TCAs, carbamazepine, meto-
321ANTIDEPRESSANT AND MOOD STABILIZER DRUGS
Abruptly stopping selective serotonin reuptakeinhibitor (SSRI) therapy may result in SSRI dis-continuation syndrome, with dizziness, vertigo,ataxia, nausea, vomiting, muscle pains, fatigue,tremor, and headache. Psychological symp-toms, such as anxiety, crying spells, irritability,feeling sad, memory problems, and vividdreams, may also occur.
This syndrome is more common in SSRIswith a shorter half-life, such as paroxetine and
venlafaxine, and occurs in up to one-third ofpatients receiving SSRI therapy.
Go slow
Tapering the dosage of the drug slowly overseveral weeks can prevent SSRI discontinua-tion syndrome. Fluoxetine is the least likely tocause this problem because of its extremelylong half-life. The syndrome is self-limiting(over 2 to 3 weeks with treatment).
Safe and sound
Stopping SSRIs
938912.qxd 08/26/2008 16:46 Page 321

prolol, flecainide, encainide, and antipsychotics, such as clozapineand thioridazine.
They don’t mix with MAOIsThe use of SSRIs with MAOIs can cause serious, potentially fatalreactions. Individual SSRIs also have their own particular interac-tions. (See Adverse reactions to SSRIs.)• Use of citalopram and paroxetine with warfarin may lead to in-creased bleeding.• Carbamazepine may increase clearance of citalopram.• Fluoxetine increases the half-life of diazepam and displaceshighly protein-bound drugs, leading to toxicity.• Fluvoxamine use with diltiazem hydrochloride may causebradycardia.• Paroxetine shouldn’t be used with tryptophan because this com-bination can cause headache, nausea, sweating, and dizziness.• Paroxetine may increase procyclidine levels, causing increasedanticholinergic effects.• Cimetidine, phenobarbital, and phenytoin may reduce paroxe-tine metabolism by the liver, increasing the risk of toxicity.• Paroxetine and sertraline may interact with other highly pro-tein-bound drugs, causing adverse reactions to either drug. (SeeRisks of antidepressants.)
Tricyclic antidepressantsTCAs are used to treat depression. They include:• amitriptyline• amoxapine• clomipramine• desipramine• doxepin
322PSYCHOTROPIC DRUGS
Adversereactionsto SSRIs
Anxiety, insomnia, som-nolence, palpitations,various rashes, and sex-ual dysfunction (anor-gasmia and delayedejaculation) may occurwith the use of serotoninselective reuptake in-hibitors (SSRIs).
Other reactions
Decreased plasma glu-cose levels can occurwith fluoxetine. Ortho-static hypotension mayoccur with citalopramand paroxetine.
Warning!
Studies have shown a correlation between taking an antidepressant and the increased risk ofsuicidal behavior in young adults ages 18 to 24. Because of this risk, the FDA has mandated ablack-box warning (the strongest warning possible) to be added to the labels of all antidepres-sants, warning practitioners to evaluate the need for the antidepressant with the increased risk itpresents.
Safe and sound
Risks of antidepressants
938912.qxd 08/26/2008 16:46 Page 322

• imipramine• nortriptyline• protriptyline• trimipramine.
PharmacokineticsAll of the TCAs are active pharmacologically, and some of theirmetabolites are also active. They’re absorbed completely whentaken orally but undergo first-pass effect.
Distribution, metabolism, and excretionWith first-pass effect, a drug passes from the GI tract to the liver,where it’s partially metabolized before entering the circulation.TCAs are metabolized extensively in the liver and eventually ex-creted as inactive compounds (only small amounts of active drugare excreted) in urine.
They just melt in fatThe extreme fat solubility of these drugs accounts for their widedistribution throughout the body, slow excretion, and long half-lives.
PharmacodynamicsResearchers believe that TCAs increase the amount of norepi-nephrine, serotonin, or both in the CNS by preventing their reup-take into the storage granules in the presynaptic nerves. They alsoblock acetylcholine and histamine receptors.
The upside to preventing reuptakeAfter a neurotransmitter has performed its job, several fates arepossible, including rapidly reentering the neuron from which itwas released (or reuptake). Preventing reuptake results in in-creased levels of these neurotransmitters in the synapses, reliev-ing depression.
PharmacotherapeuticsTCAs are used to treat episodes of major depression. They’re es-pecially effective in treating depression of insidious onset accom-panied by weight loss, anorexia, or insomnia. Physical signs andsymptoms may respond after 1 to 2 weeks of therapy; psychologi-cal symptoms, after 2 to 4 weeks.
323ANTIDEPRESSANT AND MOOD STABILIZER DRUGS
938912.qxd 08/26/2008 16:46 Page 323

Problem patientsTCAs are much less effective in patients with hypochondriasis,atypical depression, or depression accompanied by delusions.When given with a mood stabilizer, they may be helpful in treatingacute episodes of depression in bipolar I disorder.
Migraines and moreTCAs are also used for preventing migraine headaches and intreating phobias (panic disorder with agoraphobia), urinary incon-tinence, attention deficit disorder, obsessive-compulsive disorder,neuropathic pain (chronic pain that can occur with peripheralneuropathies, herpes zoster infections, traumatic nerve injuries,and some types of cancer or cancer treatments), diabetic neuropa-thy, and enuresis.
Drug interactionsTCAs interact with several commonly used drugs:• They increase the catecholamine effects of amphetamines andsympathomimetics, leading to hypertension.• Barbiturates increase the metabolism of TCAs and decreasetheir blood levels.
324PSYCHOTROPIC DRUGS
Adverse reactions to TCAs include:• orthostatic hypotension (a drop in bloodpressure on standing)• sedation• jaundice• rashes• photosensitivity reactions• a fine resting tremor• decreased sexual desire• inhibited ejaculation• transient eosinophilia• reduced white blood cell count• manic episodes (in patients with or withoutbipolar disorder)
• exacerbation of psychotic symptoms in sus-ceptible patients.
Special effects
Although rare, TCA therapy may also lead to:• granulocytopenia• palpitations• conduction delays• rapid heartbeat• impaired cognition, cardiovascular adversereactions (in elderly patients).
Sudden death has occurred in children andadolescents taking desipramine. For this rea-son a baseline electrocardiogram is recom-mended before giving a TCA to patients in thisage-group.
Warning!
Adverse reactions to TCAs
938912.qxd 08/26/2008 16:46 Page 324

• Cimetidine impairs metabolism of TCAs by the liver, increasingthe risk of toxicity.• Concurrent use of TCAs with MAOIs may cause an extremely el-evated body temperature, excitation, and seizures.• An increased anticholinergic effect, such as dry mouth, urine re-tention, and constipation, is seen when anticholinergic drugs aretaken with TCAs.• TCAs reduce the antihypertensive effects of clonidine andguanethidine. (See Adverse reactions to TCAs.)
Monoamine oxidase inhibitorsMAOIs are divided into two classifications based on chemicalstructure:• hydrazines, which include phenelzine sulfate• nonhydrazines, consisting of a single drug, tranylcypromine sul-fate.
PharmacokineticsMAOIs are absorbed rapidly and completely from the GI tract andare metabolized in the liver to inactive metabolites. These metabo-lites are excreted mainly by the GI tract and, to a lesser degree, bythe kidneys.
PharmacodynamicsMAOIs appear to work by inhibiting MAO, an enzyme that’s widelydistributed throughout the body and that normally metabolizesmany neurotransmitters, including norepinephrine, dopamine, andserotonin. This leaves more norepinephrine, dopamine, and sero-tonin available to the receptors, thereby relieving the symptoms ofdepression.
PharmacotherapeuticsThe indications for MAOIs are similar to those for other antide-pressants. MAOIs are particularly effective for treating panic dis-order with agoraphobia, eating disorders, posttraumatic stress dis-order, and pain disorders.
MAOIs may be more effective than other antidepressants in thetreatment of atypical depression. Atypical depression producessigns opposite to those of typical depression. For example, the pa-tient gains weight, sleeps more, and has a higher susceptibility torejection.
325ANTIDEPRESSANT AND MOOD STABILIZER DRUGS
938912.qxd 08/26/2008 16:46 Page 325

It tackles typical depression, tooMAOIs may be used to treat typical depression resistant to othertherapies or when other therapies are contraindicated. For exam-ple, tranylcypromine is the preferred MAOI for patients with de-pression who have liver disease. Other uses include treatment for:• phobic anxieties• neurodermatitis (an itchy skin disorder seen in anxious, ner-vous people)• hypochondriasis (abnormal concern about health)• refractory narcolepsy (sudden sleep attacks).
Drug interactionsMAOIs interact with a wide variety of drugs:• Taking MAOIs with amphetamines, methylphenidate, levodopa,sympathomimetics, and nonamphetamine appetite suppressantsmay increase catecholamine release, causing hypertensive crisis.• Using them with fluoxetine, TCAs, citalopram, clomipramine,trazodone, sertraline, paroxetine, and fluvoxamine may result inan elevated body temperature, excitation, and seizures.• When taken with doxapram, MAOIs may cause hypertensionand arrhythmias and may increase the adverse reactions todoxapram.• MAOIs may enhance the hypoglycemic effects of antidiabeticdrugs.• Administering MAOIs with meperidine may result in excitation,hypertension or hypotension, extremely elevated body tempera-ture, and coma. (See Moving from MAOIs.)
326PSYCHOTROPIC DRUGS
If othertherapies don’t
work, MAOIs maybe prescribed.
Moving fromMAOIs
Monoamine oxidase in-hibitors (MAOIs) shouldbe discontinued 2 weeksbefore starting an alter-native antidepressant. A2-week waiting period(5 weeks for fluoxetine)should also elapse whendiscontinuing an anti-depressant and startingan MAOI.
Adverse reactions to mono-amine oxidase inhibitors(MAOIs) include:• hypertensive crisis (whentaken with tyramine-richfoods)• orthostatic hypotension• restlessness• drowsiness• dizziness
• headache• insomnia• constipation• anorexia• nausea and vomiting• weakness• joint pain• dry mouth• blurred vision• peripheral edema
• urine retention• transient impotence• rash• skin and mucous membranehemorrhage.
Reaction relief
Adverse reactions may beavoided by giving the drug insmall divided doses.
Warning!
Adverse reactions to MAOIs
938912.qxd 08/26/2008 16:46 Page 326

Forbidden fruit (and other foods)Certain foods can interact with MAOIs and produce severe reac-tions. The most serious reactions involve tyramine-rich foods,such as red wines, aged cheese, and fava beans. Foods with mod-erate tyramine contents—for example, yogurt and ripe bananas—may be eaten occasionally, but with care. (See Adverse reactionsto MAOIs.)
Miscellaneous antidepressantsOther antidepressants in use today include:• maprotiline and mirtazapine, tetracyclic antidepressants• bupropion, a dopamine reuptake blocking agent• venlafaxine, a serotonin-norepinephrine reuptake inhibitor• trazodone, a triazolopyridine agent• nefazodone, a phenylpiperazine agent.
PharmacokineticsThe paths these antidepressants take through the body may vary:• Maprotiline and mirtazapine are absorbed from the GI tract, dis-tributed widely in the body, metabolized by the liver, and excretedby the kidneys.• Bupropion is well absorbed from the GI tract and metabolizedby the liver. Its metabolites are excreted by the kidneys. It appearsto be highly bound to plasma proteins.• Venlafaxine is rapidly absorbed after oral administration, par-tially bound to plasma proteins, metabolized in the liver, and ex-creted in urine.• Trazodone is well absorbed from the GI tract, distributed widelyin the body, and metabolized by the liver. About 75% is excreted inurine; the remainder is excreted in stool.• Nefazodone is rapidly and completely absorbed but, because ofextensive metabolism, only about 20% of the drug is available. Thedrug is almost completely bound to plasma proteins and is excret-ed in urine.
PharmacodynamicsMuch about how these drugs work has yet to be fully understood:• Maprotiline and mirtazapine probably increase the amount ofnorepinephrine, serotonin, or both in the CNS by blocking theirreuptake by presynaptic neurons (nerve terminals).
327ANTIDEPRESSANT AND MOOD STABILIZER DRUGS
Tyramine-richfoods, such as redwine, can producesevere reactions iftaken with MAOIs.
938912.qxd 08/26/2008 16:46 Page 327

• Bupropion was once thought to inhibit the reuptake of the neu-rotransmitter dopamine; however, it more likely acts on nonadren-ergic receptors.• Venlafaxine is thought to potentiate neurotransmitter activity inthe CNS by inhibiting the neural reuptake of serotonin and norepi-nephrine.• Trazodone, although its action is unknown, is thought to exertantidepressant effects by inhibiting the reuptake of norepineph-rine and serotonin in the presynaptic neurons.• Nefazodone’s action isn’t precisely defined. It inhibits neuronaluptake of serotonin and norepinephrine. It’s also a serotonin an-tagonist, which explains its effectiveness in treating anxiety.
PharmacotherapeuticsThese miscellaneous drugs are all used to treat depression. Tra-zodone may also be effective in treating aggressive behavior andpanic disorder.
Drug interactionsAll of these antidepressants may have serious, potentially fatal, ef-fects when combined with MAOIs. Each of these drugs also car-ries its own specific risks when used with other drugs:• Maprotiline and mirtazapine interact with CNS depressants tocause an additive effect.• Bupropion combined with levodopa, phenothiazines, or TCAsincreases the risk of adverse reactions, including seizures.
328PSYCHOTROPIC DRUGS
These antidepressants may produce various adverse reactions.
Warning!
Adverse reactions to miscellaneous antidepressants
Maprotiline
• Seizures• Orthostatic hypoten-sion• Tachycardia• Electrocardiographicchanges
Mirtazapine
• Tremors• Confusion• Nausea• Constipation
Bupropion
• Headache• Confusion• Tremor• Agitation• Tachycardia• Anorexia• Nausea and vomiting
Venlafaxine and
nefazodone
• Headache• Somnolence• Dizziness• Nausea
Trazodone
• Drowsiness• Dizziness
938912.qxd 08/26/2008 16:46 Page 328

• Trazodone may increase serum levels of digoxin and phenytoin.Its use with antihypertensive agents may increase hypotensive ef-fects. CNS depression may be enhanced if trazodone is adminis-tered with other CNS depressants.• Nefazodone may increase the digoxin level if administered withdigoxin. It increases CNS depression when combined with CNSdepressants. (See Adverse reactions to miscellaneous antidepres-sants.)
LithiumLithium carbonate and lithium citrate are used to prevent ortreat mania. The discovery of lithium was a milestone in treatingmania and bipolar disorders.
PharmacokineticsWhen taken orally, lithium is absorbed rapidly and completely andis distributed to body tissues.
Metabolism and excretionAn active drug, lithium isn’t metabolized and is excreted from thebody unchanged.
PharmacodynamicsIt’s theorized that in mania, the patient experiences excessive cat-echolamine stimulation. In bipolar disorder, the patient is affectedby swings between the excessive catecholamine stimulation ofmania and the diminished catecholamine stimulation of depres-sion.
Returning to normalLithium’s exact mechanism of action is unknown. It may regulatecatecholamine release in the CNS by:• increasing norepinephrine and serotonin uptake• reducing the release of norepinephrine from the synaptic vesi-cles (where neurotransmitters are stored) in the presynaptic neu-ron• inhibiting norepinephrine’s action in the postsynaptic neuron.
Getting more of the messageResearchers are also examining lithium’s effects on electrolyteand ion transport. Lithium may also modify the actions of secondmessengers such as cyclic adenosine monophosphate.
329ANTIDEPRESSANT AND MOOD STABILIZER DRUGS
938912.qxd 08/26/2008 16:46 Page 329

PharmacotherapeuticsLithium is used primarily to treat acute episodes of mania and toprevent relapses of bipolar disorders.
Under investigationOther uses of lithium being researched include preventing unipo-lar depression and migraine headaches and treating depression,alcohol dependence, anorexia nervosa, syndrome of inappropriateantidiuretic hormone, and neutropenia.
No margin for errorLithium has a narrow therapeutic margin of safety. A blood levelthat is even slightly higher than the therapeutic level can be dan-gerous.
Drug interactionsSerious interactions with other drugs can occur because of lithi-um’s narrow therapeutic range:• The risk of lithium toxicity increases when lithium is taken withthiazide and loop diuretics and nonsteroidal anti-inflammatorydrugs.• Administration of lithium with haloperidol, phenothiazines, orcarbamazepine may increase the risk of neurotoxicity.• Lithium may increase the hypothyroid effects of potassium io-dide.• Sodium bicarbonate may increase lithium excretion, reducingits effects.• Lithium’s effects are reduced when lithium is taken with the-ophylline.
Take this with a grain (or more) of saltA patient on a severe salt-restricted diet is sus-ceptible to lithium toxicity. On the other hand,an increased intake of sodium may reduce thetherapeutic effects of lithium. (See Adverse re-actions to lithium.)
Antipsychotic drugsAntipsychotic drugs can control psychotic symptoms,such as delusions and hallucinations, and thought disor-ders that can occur with schizophrenia, mania, and otherpsychoses.
330PSYCHOTROPIC DRUGS
A regular saltintake helps to
maintain steadylithium levels.
Adversereactionsto lithium
Common adverse reac-tions to lithium include:• reversible electrocar-diogram changes• thirst• polyuria• elevated white bloodcell count.
A flood in the blood
Elevated toxic blood lev-els of lithium may pro-duce:• confusion• lethargy• slurred speech• increased reflex reac-tions• seizures.
Warning!
938912.qxd 08/26/2008 16:46 Page 330

By any other nameDrugs used to treat psychoses have several different names, in-cluding:• antipsychotic, because they can eliminate signs and symptomsof psychoses• major tranquilizer, because they can calm an agitated patient• neuroleptic, because they have an adverse neurobiologic effectthat causes abnormal body movements.
Two major groupsRegardless of what they’re called, all antipsychotic drugs belongto one of two major groups:
atypical antipsychotics, which include aripiprazole, cloza-pine, olanzapine, paliperidone, quetiapine, risperidone, andziprasidone
typical antipsychotics, which include phenothiazines andnonphenothiazines.
Atypical antipsychoticsAtypical antipsychotic drugs are agents designed to treat schizo-phrenia. They include aripiprazole, clozapine, olanzapine, paliperi-done, quetiapine, risperidone, and ziprasidone.
PharmacokineticsAtypical antipsychotics are absorbed after oral administration.
Metabolism and excretionAtypical antipsychotics are metabolized by the liver. Metabolitesof clozapine, olanzapine, quetiapine, and ziprasidone are inactive,whereas risperidone and paliperidone have active metabolites.They’re highly plasma protein-bound and eliminated in urine, witha small portion eliminated in stool.
PharmacodynamicsAtypical antipsychotics typically block the dopamine receptors,but to a lesser extent than the typical antipsychotics, resulting infar fewer extrapyramidal adverse effects. Additionally, atypical an-tipsychotics block serotonin receptor activity.
331ANTIPSYCHOTIC DRUGS
938912.qxd 08/26/2008 16:46 Page 331

Putting it togetherThese combined actions account for their effectiveness againstthe positive and negative symptoms of schizophrenia with mini-mal extrapyramidal effects.
PharmacotherapeuticsAtypical antipsychotics are considered the first line of treatmentfor patients with schizophrenia because of equal or improved ef-fectiveness combined with improved tolerability.
Lower doses do for dementiaAtypical antipsychotics are commonly used to treat behavioraland psychotic symptoms in patients with dementia. Dosages aresignificantly lower for these patients than for patients with schizo-phrenia.
Drug interactionsDrugs that alter the P-450 enzyme system alter the metabolism ofsome atypical antipsychotics.
The straight “dopa”Atypical antipsychotics counteract the effects of levodopa andother dopamine agonists. (See Adverse reactions to atypical an-tipsychotics.)
332PSYCHOTROPIC DRUGS
Atypical antipsychotics have fewer ex-trapyramidal effects than typical anti-psychotics and carry a minimal risk forseizures (except for clozapine).
Aripiprazole
Aripiprazole is a newer atypical antipsy-chotic and may produce mild sedation.
Clozapine
Clozapine is associated with agranulo-cytosis (an abnormal decrease in white
blood cells). Weight gain is common, andseizures may also occur.
Olanzapine
Olanzapine places the patient at minimalrisk for extrapyramidal effects. Weightgain is common.
Quetiapine
Quetiapine is associated with sedation.
Risperidone and paliperidone
Risperidone and paliperidone have ahigher risk of extrapyramidal effects than
other atypical antipsychotics, especiallywhen prescribed at doses at the higherrange of normal.
Ziprasidone
Because ziprasidone may cause electro-cardiogram changes, it’s usually recom-mended as an alternative therapy onlyafter the patient has failed to respond toother atypical antipsychotics.
Warning!
Adverse reactions to atypical antipsychotics
938912.qxd 08/26/2008 16:47 Page 332

Typical antipsychoticsTypical antipsychotics, which include phenothiazines and non-phenothiazines, can be broken down into smaller classifications.
Different adverse reactionsMany clinicians believe that the phenothiazines should be treatedas three distinct drug classes because of the differences in the ad-verse reactions they cause:• Aliphatics primarily cause sedation and anticholinergic effects.They’re low potency drugs that include chlorpromazine.• Piperazines primarily cause extrapyramidal reactions and in-clude fluphenazine decanoate, fluphenazine enanthate, fluphena-zine hydrochloride, perphenazine, and trifluoperazine.• Piperidines primarily cause sedation and anticholinergic andcardiac effects; they include mesoridazine and thioridazine.
Different chemical structureBased on their chemical structure, nonphenothiazine antipsy-chotics can be divided into several drug classes, including:• butyrophenones, such as haloperidol and haloperidol decanoate• dibenzoxazepines such as loxapine• dihydroindolones such as molindone• diphenylbutylpiperidines such as pimozide• thioxanthenes, such as thiothixene and thiothixene hydro-chloride.
PharmacokineticsAlthough phenothiazines are absorbed erratically, they’re verylipid-soluble and highly protein-bound. Therefore, they’re distrib-uted to many tissues and are highly concentrated in the brain.
Like phenothiazines, nonphenothiazines are absorbed errati-cally, are lipid-soluble, and are highly protein-bound. They’re alsodistributed throughout the tissues and are highly concentrated inthe brain.
Metabolism and excretionAll phenothiazines are metabolized in the liver and excreted inurine and bile. Because fatty tissues slowly release accumulatedphenothiazine metabolites into the plasma, phenothiazines mayproduce effects up to 3 months after they’re stopped.
Nonphenothiazines are also metabolized in the liver and ex-creted in urine and bile.
333ANTIPSYCHOTIC DRUGS
938912.qxd 08/26/2008 16:47 Page 333

PharmacodynamicsAlthough the mechanism of action of phenothiazines isn’t fully un-derstood, researchers believe that these drugs work by blockingpostsynaptic dopaminergic receptors in the brain.
The mechanism of action of nonphenothiazines resembles thatof phenothiazines.
Erecting a blockadeThe antipsychotic effect of phenothiazines is due to receptorblockade in the limbic system. Their antiemetic effect is due to re-ceptor blockade in the chemoreceptor trigger zone located in thebrain’s medulla.
Sending a chargePhenothiazines also stimulate the extrapyramidal system (motorpathways that connect the cerebral cortex with the spinal nervepathways).
PharmacotherapeuticsPhenothiazines are used primarily to:• treat schizophrenia• calm anxious or agitated patients• improve a patient’s thought processes• alleviate delusions and hallucinations.
Working overtimeOther therapeutic uses have been found for phenothiazines:• They’re administered to treat other psychiatric disorders, suchas brief reactive psychosis, atypical psychosis, schizoaffectivepsychosis, autism, and major depression with psychosis.• In combination with lithium, they’re used in the treatment of pa-tients with bipolar disorder, until the slower-acting lithium pro-duces its therapeutic effect.• They’re prescribed to quiet mentally challenged children and ag-itated geriatric patients, particularly those with dementia.• The preoperative effects of analgesics may be boosted withtheir addition.• They’re helpful in the management of pain, anxiety, and nauseain patients with cancer.
Solo solutionsAs a group, nonphenothiazines are used to treat psychotic disor-ders. Thiothixene is also used to control acute agitation. Haloperi-dol and pimozide may also be used to treat Tourette syndrome.
334PSYCHOTROPIC DRUGS
Phenothiazinesmay produceeffects up to
3 months afterthey’re stopped.
Phenothiazines aresometimes prescribed
to quiet mentallychallenged children
and agitatedgeriatric patients.
938912.qxd 08/26/2008 16:47 Page 334

Drug interactionsPhenothiazines interact with many different types of drugs andmay have serious effects:• Increased CNS depressant effects, such as stupor, may occurwhen phenothiazines are taken with CNS depressants.• CNS depressants may reduce phenothiazine effectiveness, re-sulting in increased psychotic behavior or agitation.• Taking anticholinergic drugs with phenothiazines may result inincreased anticholinergic effects, such as dry mouth and constipa-tion. By increasing phenothiazine metabolism, anticholinergicdrugs may also reduce the antipsychotic effects of phenothiazines.• Phenothiazines may reduce the antiparkinsonian effects of lev-odopa.• Concurrent use with lithium increases the risk of neurotoxicity.• Concurrent use with droperidol increases the risk of extrapyra-midal effects.• The threshold for seizures is lowered when phenothiazines areused with anticonvulsants.• Phenothiazines may increase the serum levels of TCAs and beta-adrenergic blockers. Thioridazine can cause serious, even fatal,cardiac arrhythmias when combined with such drugs as fluvoxam-ine, propranolol, pindolol, and fluoxetine that inhibit the cyto-chrome P-450 2D6 isoenzyme, or drugs known to prolong the QTcinterval. (See Adverse reactions to typical antipsychotics.)
335ANTIPSYCHOTIC DRUGS
Neurologic reactions are the most commonand serious adverse reactions associated withphenothiazines.
Extrapyramidal symptoms
Extrapyramidal symptoms (EPS) may appearafter the first few days of therapy; tardivedyskinesia may occur after several years oftreatment.
S.O.S.! Extreme EPS!
Neuroleptic malignant syndrome is a potential-ly fatal condition that produces muscle rigidity,
extreme EPS, severely elevated body tempera-ture, hypertension, and rapid heart rate. If leftuntreated, it can result in respiratory failureand cardiovascular collapse.
Little difference
Most nonphenothiazines cause the same ad-verse reactions as phenothiazines.
Special caution
Antipsychotics with anticholinergic propertiesshould be avoided in elderly patients.
Warning!
Adverse reactions to typical antipsychotics
938912.qxd 08/26/2008 16:47 Page 335

Fewer interactionsNonphenothiazines interact with fewer drugs than phenothiazines.Their dopamine-blocking activity can inhibit levodopa and maycause disorientation in patients receiving both medications. Halo-peridol may boost the effects of lithium, producing encephalopa-thy (brain dysfunction).
StimulantsStimulants are used to treat attention deficit hyperactivity disor-der (ADHD), a condition characterized by inattention, impulsivity,and hyperactivity. They include:• dextroamphetamine• lisdexamfetamine• methylphenidate• mixed amphetamine salts• modafinil.
PharmacokineticsStimulants are well absorbed from the GI tract and are distributedwidely in the body. Methylphenidate undergoes significant firstpass effect.
Metabolism and excretionStimulants are metabolized in the liver and excreted primarily inurine.
PharmacodynamicsThese drugs are believed to work by increasing levels of dopa-mine and norepinephrine in one of three ways: by blocking thereuptake of dopamine and norepinephrine, by enhancing thepresynaptic release, or by inhibiting MAO.
PharmacotherapeuticsStimulants are the treatment of choice for ADHD. They’re help-ful in improving attention, leading to improved school or workperformance, and decreasing impulsivity and hyperactivity, ifpresent. Pemoline, however, is no longer a first line choice fortreatment of ADHD because it can cause hepatotoxicity.
Dextroamphetamine and methylphenidate are also used inthe treatment of narcolepsy.
336PSYCHOTROPIC DRUGS
Stimulants areused to help patientswith ADHD improve
school and workperformance.
938912.qxd 08/26/2008 16:47 Page 336

Drug interactions• Methylphenidate may decrease the effect of guanethidine andmay increase the effects of TCAs, warfarin, and some anticonvul-sant drugs.• Stimulants shouldn’t be used within 14 days of discontinuingtherapy with an MAOI.• Stimulants are highly abused substances, and close monitoringis required. (See Adverse reactions to stimulants.)
Quick quiz
1. What’s the difference between a sedative and a hypnotic?A. Sedatives produce physical dependence; hypnotics
don’t.B. Sedatives reduce anxiety or excitement; hypnotics in-
duce sleep.C. Sedatives require larger doses than hypnotics to pro-
duce desired effects.D. Sedatives increase anxiety; hypnotics reduce anxiety.
Answer: B. Sedatives reduce anxiety or excitement; hypnoticsinduce sleep.
337QUICK QUIZ
Adverse reactions to stimulants are listed below.
Warning!
Adverse reactions to stimulants
Dextroamphetamine and
lisdexamfetamine
• Restlessness• Tremor• Insomnia• Tachycardia• Palpitations• Arrhythmias• Dry mouth• Unpleasant taste• Diarrhea
Methylphenidate
• Dizziness• Insomnia• Seizures• Palpitations• Arrhythmias• Abdominal pain• Rash• Thrombocytopenia
Mixed amphetamine salts
• Restlessness• Insomnia• Hyperexcitability• Palpitations• Arrhythmias• Tremor• Abdominal pain• Dry mouth• Unpleasant taste
Measure up
Stimulants may affect growth;children should be monitoredclosely for height and weightchanges.
Take a holiday
Drug holidays are recom-mended every year to assessthe continued need for a stim-ulant.
938912.qxd 08/26/2008 16:47 Page 337

2. With the use of the nonbenzodiazepine-nonbarbiturate chlo-ral hydrate, what adverse reactions are most likely?
A. Severe withdrawal symptomsB. Hypersensitivity reactionsC. Cardiac adverse effectsD. GI symptoms and hangover effects
Answer: D. GI symptoms and hangover effects are common ad-verse reactions to chloral hydrate.
3. Which medication should a patient treated with lithiumavoid?
A. Hormonal contraceptivesB. Loop diureticsC. Oral antidiabetic drugsD. Antihypertensive drugs
Answer: B. Lithium shouldn’t be prescribed with loop diuretics.
ScoringIf you answered all three items correctly, extraordinary! You defi-
nitely aren’t psyched out by pharmacology!If you answered two items correctly, congratulations! Your knowl-
edge should have you feeling elated!If you answered fewer than two items correctly, there’s no need
for anxiety! By the end of the next chapter, you’ll probablyhave your head on straight!
338PSYCHOTROPIC DRUGS
All this talkabout sedativesand hypnoticshas made me
sleepy!
✰✰✰
✰✰
✰
938912.qxd 08/26/2008 16:47 Page 338

Drugs and the endocrine systemThe endocrine system consists of glands, which are specializedcell clusters, and hormones, the chemical transmitters secreted bythe glands in response to stimulation.
Keeping well balancedTogether with the central nervous system, the endocrine sys-tem regulates and integrates the body’s metabolic activitiesand maintains homeostasis (the body’s internal equilibrium).The drug classes that treat endocrine system disorders in-clude:• natural hormones and their synthetic analogues• hormonelike substances• drugs that stimulate or suppress hormone secretion.
Antidiabetic drugs and glucagonInsulin, a pancreatic hormone, and oral antidiabetic drugs areclassified as hypoglycemic drugs because they lower blood glu-cose levels. Glucagon, another pancreatic hormone, is classifiedas a hyperglycemic drug because it raises blood glucose levels.
13
Endocrine drugs
Just the facts
In this chapter, you’ll learn:
♦ classes of drugs that affect the endocrine system
♦ uses and varying actions of these drugs
♦ how these drugs are absorbed, distributed, metabolized,and excreted
♦ drug interactions and adverse reactions to these drugs.
We’re special. Wehelp make up glands,which are a part of
the endocrinesystem.
938913.qxd 08/26/2008 16:55 Page 339

Sugar surplusDiabetes mellitus, or simply diabetes, is a chronic disease of in-sulin deficiency or resistance. It’s characterized by disturbances incarbohydrate, protein, and fat metabolism. This leads to elevatedlevels of the sugar glucose in the body. The disease appears in twoprimary forms:
type 1, previously referred to as insulin-dependent diabetesmellitus
type 2, previously referred to as non-insulin-dependent dia-betes mellitus.
InsulinPatients with type 1 diabetes require an external source of insulinto control blood glucose levels. Insulin may also be given to pa-tients with type 2 diabetes.
Types of insulin include:• rapid-acting: lispro• short-acting: regular• intermediate-acting: NPH• long-acting: Ultralente.
Pharmacokinetics (how drugs circulate)Insulin isn’t effective when taken orally because the GI tractbreaks down the protein molecule before it reaches the blood-stream.
Under the skinAll insulins, however, may be given by subcutaneous (subQ) injec-tion. Absorption of subQ insulin varies according to the injectionsite, the blood supply, and degree of tissue hypertrophy at the in-jection site.
In the I.V. leagueRegular insulin may also be given by I.V. infusion as well as indialysate fluid infused into the peritoneal cavity for patients onperitoneal dialysis therapy.
Distribution, metabolism, and excretionAfter absorption into the bloodstream, insulin is distributedthroughout the body. Insulin-responsive tissues are located in theliver, adipose tissue, and muscle. Insulin is metabolized primarilyin the liver and to a lesser extent in the kidneys and muscle, andit’s excreted in stool and urine.
340ENDOCRINE DRUGS
938913.qxd 08/26/2008 16:55 Page 340

Pharmacodynamics (how drugs act)Insulin is an anabolic, or building, hormone that helps:• promote storage of glucose as glycogen• increase protein and fat synthesis• slow the breakdown of glycogen, protein, and fat• balance fluids and electrolytes.
Insulin’s special effectsAlthough it has no antidiuretic effect, insulin can correct the poly-uria (excessive urination) and polydipsia (excessive thirst) associ-ated with the osmotic diuresis that occurs in hyperglycemia by de-creasing the blood glucose level. Insulin also facilitates the move-ment of potassium from the extracellular fluid into the cell. (SeeHow insulin aids glucose uptake.)
341ANTIDIABETIC DRUGS AND GLUCAGON
These illustrations show how insulin allows a cell to use glucose for energy.
Now I get it!
How insulin aids glucose uptake
Insulin canhelp balancefluids and
electrolytes!
Glucose can’t enter the cell withoutthe aid of insulin.
Normally produced by the beta cellsof the pancreas, insulin binds to the re-ceptors on the surface of the target cell.Insulin and its receptor first move to theinside of the cell, which activates glu-cose transporter channels to move to thesurface of the cell.
These channels allow glucose toenter the cell. The cell can then use theglucose for metabolism.
Insulinreceptor
Glucosetransportchannel
Glucose
Insulin
Glucoseavailableformetabolism
938913.qxd 08/26/2008 16:55 Page 341

Pharmacotherapeutics (how drugs are used)Insulin is indicated for:• type 1 diabetes• type 2 diabetes when other methods of controlling blood glu-cose levels have failed or are contraindicated• type 2 diabetes when blood glucose levels are elevated duringperiods of emotional or physical stress (such as infection andsurgery)• type 2 diabetes when oral antidiabetic drugs are contraindicatedbecause of pregnancy or hypersensitivity• gestational diabetes.
When things get complicatedInsulin is also used to treat two complications of diabetes: diabet-ic ketoacidosis, more common with type 1 diabetes, and hyperos-molar hyperglycemic nonketotic syndrome, which is more com-mon with type 2 diabetes.
What? But I don’t have diabetes…Insulin is also used to treat severe hyperkalemia (elevated serumpotassium levels) in patients without diabetes. Potassium moveswith glucose from the bloodstream into the cell, lowering serumpotassium levels.
Drug interactionsSome drugs interact with insulin, altering its ability to decreasethe blood glucose level; other drugs directly affect glucose levels:• Anabolic steroids, salicylates, alcohol, and monoamine oxidaseinhibitors (MAOIs) may increase the hypoglycemic effect of in-sulin.• Corticosteroids, sympathomimetic drugs, thiazide diuretics, anddextrothyroxine sodium may reduce the effects of insulin, result-ing in hyperglycemia.• Beta-adrenergic blockers may prolong the hypoglycemic effectof insulin and may mask signs and symptoms of hypoglycemia.(See Adverse reactions to insulin.)
Oral antidiabetic drugsMany types of oral antidiabetic drugs are approved for use in theUnited States. Types of available oral antidiabetic drugs include:• first-generation sulfonylureas, which include acetohexamide,chlorpropamide, tolazamide, and tolbutamide• second-generation sulfonylureas, which include gliclazide, glip-izide, glimepiride, and glyburide.
342ENDOCRINE DRUGS
Adversereactionsto insulin
Adverse reactions to in-sulin include:• hypoglycemia (below-normal blood glucoselevels)• Somogyi effect (hypo-glycemia followed by re-bound hyperglycemia)• hypersensitivity reac-tions• lipodystrophy (distur-bance in fat deposition)• insulin resistance.
Warning!
938913.qxd 08/26/2008 16:55 Page 342

• thiazolidinediones, which include pioglitazone and rosiglitazone• a biguanide drug, metformin• alpha-glucosidase inhibitors, which include acarbose andmiglitol• a meglitinide drug, repaglinide• an amino acid derivative, nateglinide• combination therapies, which include glipizide and metformin,glyburide and metformin, and rosiglitazone and metformin.
PharmacokineticsOral antidiabetic drugs are well absorbed from the GI tract anddistributed via the bloodstream throughout the body. Becauserepaglinide has a short duration of action, it’s given before meals.
Metabolism and excretionOral antidiabetic drugs are metabolized primarily in the liver andare excreted mostly in urine, with some excreted in bile. Gly-buride is excreted equally in urine and stool; rosiglitazone and pi-oglitazone are largely excreted in both.
PharmacodynamicsIt’s believed that oral antidiabetic drugs produce actions bothwithin and outside the pancreas (extrapancreatic) to regulateblood glucose.
Pancreas partnersOral antidiabetic drugs probably stimulate pancreatic beta cells torelease insulin in a patient with a minimally functioning pancreas.Within a few weeks to a few months of starting sulfonylureas, pan-creatic insulin secretion drops to pretreatment levels, but bloodglucose levels remain normal or near-normal. Most likely, it’s theactions of the oral antidiabetic agents outside of the pancreas thatmaintain this glucose control.
Working beyond the pancreasOral antidiabetic drugs provide several extrapancreatic actions todecrease and control blood glucose. They can go to work in theliver and decrease glucose production (gluconeogenesis) there.Also, by increasing the number of insulin receptors in the periph-eral tissues, they provide more opportunities for the cells tobind sufficiently with insulin, initiating the process of glucosemetabolism.
343ANTIDIABETIC DRUGS AND GLUCAGON
What’s that?Aha! Oral
antidiabetic drugswork in and out ofthe pancreas toregulate glucose
levels.
938913.qxd 08/26/2008 16:55 Page 343

Cautionarytales
To maintain blood glu-cose levels as close tonormal as possible,pregnant women shouldavoid oral antidiabeticagents. Insulin therapyis recommended in-stead.
Because aging iscommonly associatedwith a decline in kidneyfunction, and becausethe kidneys substantiallyexcrete metformin, met-formin should be usedwith caution in elderlypatients. Patients withrenal and hepatic im-pairment should alsoavoid metformin.
Getting in on the actionOther oral antidiabetic agents produce specific ac-tions:• Pioglitazone and rosiglitazone improve insulinsensitivity and lower glucose production by theliver.• Metformin decreases liver production and intestinal absorptionof glucose and improves insulin sensitivity.• Acarbose and miglitol inhibit enzymes, delaying glucose absorp-tion.• Repaglinide and nateglinide increase insulin secretion.
PharmacotherapeuticsOral antidiabetic drugs are indicated for patients with type 2 dia-betes if diet and exercise can’t control blood glucose levels. Thesedrugs aren’t effective in patients with type 1 diabetes because thepatients’ pancreatic beta cells aren’t functioning at a minimallevel.
The old 1-2 punchCombinations of multiple oral antidiabetic drugs or an oral anti-diabetic drug with insulin therapy may be indicated for some pa-tients who don’t respond to either therapy alone. (See Cautionarytales.)
Drug interactionsHypoglycemia and hyperglycemia are the main risks when oral an-tidiabetic drugs interact with other drugs.
Getting too lowHypoglycemia may occur when sulfonylureas are combined withalcohol, anabolic steroids, chloramphenicol, cimetidine, clofi-brate, coumadin, fluconazole, gemfibrozil, MAOIs, phenylbuta-zone, ranitidine, salicylates, or sulfonamides. It may also occurwhen metformin is combined with cimetidine, nifedipine, pro-cainamide, ranitidine, or vancomycin. Hypoglycemia is less likelyto occur when metformin is used as a single agent.
Going too highHyperglycemia may occur when sulfonylureas are taken with cor-ticosteroids, dextrothyroxine, rifampin, sympathomimetics, andthiazide diuretics.
Because metformin given with iodinated contrast dyes cancause acute renal failure, metformin doses should be withheld inpatients undergoing procedures that require I.V. contrast dye and
344ENDOCRINE DRUGS
If diet and exercisedon’t work, it might
be time for oralantidiabetic drugs.
Safe andsound
938913.qxd 08/26/2008 16:55 Page 344

not restarted for at least 48 hours after the procedure. (See Ad-verse reactions to oral antidiabetic drugs.)
GlucagonGlucagon, a hyperglycemic drug that raises blood glucose levels,is a hormone normally produced by the alpha cells of the islets ofLangerhans in the pancreas. (See How glucagon raises glucoselevels, page 346.)
PharmacokineticsAfter subQ, I.M., or I.V. injection, glucagon is absorbed rapidly.Glucagon is distributed throughout the body, although its effectoccurs primarily in the liver.
Metabolism and excretionGlucagon is degraded extensively by the liver, kidneys, and plas-ma, and at its tissue receptor sites in plasma membranes. It’s re-moved from the body by the liver and the kidneys.
PharmacodynamicsGlucagon regulates the rate of glucose production through:• glycogenolysis, the conversion of glycogen back into glucose bythe liver• gluconeogenesis, the formation of glucose from free fatty acidsand proteins• lipolysis, the release of fatty acids from adipose tissue for con-version to glucose.
PharmacotherapeuticsGlucagon is used for emergency treatment of severe hypoglyce-mia. It’s also used during radiologic examination of the GI tract toreduce GI motility.
Drug interactionsGlucagon interacts adversely only with oral anticoagulants, in-creasing the tendency to bleed. Adverse reactions to glucagon arerare.
345ANTIDIABETIC DRUGS AND GLUCAGON
Adversereactionsto oralantidiabeticdrugs
Hypoglycemia is a majoradverse reaction to oralantidiabetic drugs, espe-cially when combinationtherapy is used. Hereare some common ad-verse reactions to indi-vidual oral antidiabeticdrugs.
Sulfonylureas
• Nausea• Epigastric fullness• Blood abnormalities• Water retention• Rash• Hyponatremia• Photosensitivity
Metformin
• Metallic taste• Nausea and vomiting• Abdominal discomfort
Acarbose
• Abdominal pain• Diarrhea• Flatulence
Thiazolidinediones
• Weight gain• Swelling
Warning!
938913.qxd 08/26/2008 16:55 Page 345

346ENDOCRINE DRUGS
When adequate stores of glycogen are present, glucagon canraise glucose levels in patients with severe hypoglycemia.What happens is easy to follow:• Initially, glucagon stimulates the formation of adenylate cy-clase in the liver cell.• Adenylate cyclase then converts adenosine triphosphate(ATP) to cyclic adenosine monophosphate (cAMP).
• This product initiates a series of reactions that result in anactive phosphorylated glucose molecule.• In this phosphorylated form, the large glucose molecule can’tpass through the cell membrane.• Through glycogenolysis (the breakdown of glycogen, thestored form of glucose), the liver removes the phosphate groupand allows the glucose to enter the bloodstream, raising bloodglucose levels for short-term energy needs.
Now I get it!
How glucagon raises glucose levels
Glucagon
Glucagon receptor
ATP
Inactive kinase
Inactive phosphorylase
Adenylate cyclase
cAMP
Active kinase
Active phosphorylase
Liver cell Glycogenolysis
Serum glucose
Glucose
Glucose-6-phosphatase
Glucose-6-phosphate
Phosphoglucomutase
Glucose-1-phosphate
Glycogen
938913.qxd 08/26/2008 16:55 Page 346

EstrogensEstrogens mimic the physiologic effects of naturally occurring fe-male sex hormones.
To serve and protectEstrogens are used to correct estrogen-deficient states and, alongwith hormonal contraceptives, prevent pregnancy.
Natural and synthetic estrogenEstrogens that treat endocrine system disorders include:• natural products, such as conjugated estrogenic sub-stances, estradiol, and estropipate• synthetic estrogens, such as esterified estrogens,estradiol cypionate, estradiol valerate, and ethinylestradiol.
PharmacokineticsEstrogens are well absorbed and distributed throughoutthe body. Metabolism occurs in the liver, and themetabolites are excreted primarily by the kidneys.
PharmacodynamicsThe exact mechanism of action of estrogen isn’t clearly under-stood, but it’s believed to increase synthesis of deoxyribonucleicacid, ribonucleic acid, and protein in estrogen-responsive tissuesin the female breast, urinary tract, and genital organs.
PharmacotherapeuticsEstrogens are prescribed:• primarily for hormone replacement therapy in postmenopausalwomen to relieve symptoms caused by loss of ovarian function(see Hormone replacement therapy and heart disease, page 348)• less commonly for hormonal replacement therapy in womenwith primary ovarian failure or female hypogonadism (reducedhormonal secretion by the ovaries), for prevention and treatmentof osteoporosis in postmenopausal women, and in patients whohave undergone surgical castration• palliatively to treat advanced, inoperable breast cancer in post-menopausal women and prostate cancer in men.
347ESTROGENS
I takecare of
excretion…
…and I’min charge ofmetabolism.
938913.qxd 08/26/2008 16:55 Page 347

Drug interactionsRelatively few drugs interact with estrogens:• Estrogens may decrease the effects of anticoagulants, increas-ing the risk of blood clots.• Antibiotics, barbiturates, carbamazepine, phenytoin, primidone,and rifampin reduce estrogen effectiveness.• Estrogens interfere with the absorption of dietary folic acid,which may result in a folic acid deficiency. (See Adverse reactionsto estrogens.)
Pituitary drugsPituitary drugs are natural or synthetic hormones that mimic thehormones produced by the pituitary gland. The pituitary drugsconsist of two groups:• Anterior pituitary drugs may be used diagnostically or therapeu-tically to control the function of other endocrine glands, such asthe thyroid gland, adrenals, ovaries, and testes.• Posterior pituitary drugs may be used to regulate fluid volumeand stimulate smooth-muscle contraction in selected clinical situ-ations.
348ENDOCRINE DRUGS
Estrogenscan be used totreat prostatecancer in men.
Following a 5-year study, the Women’s Health Initiative reported increased risks of myocardial in-farction, stroke, breast cancer, pulmonary emboli, and deep vein thrombosis in women beingtreated with conjugated equine estrogens and progesterone as compared to those taking aplacebo.
The U.S. Preventive Services Task Force recommends against the use of estrogen and pro-gestin to prevent coronary heart disease in healthy women.
What to do?
Because the long-term safety of short-term therapy has yet to be determined, the Food and DrugAdministration and American College of Obstetricians and Gynecologists recommend thatwomen who choose to take hormone replacement therapy for menopausal symptoms use thesedrugs for the shortest duration possible and in the lowest possible dosages.
Yea or nay?
Hormone replacement therapy and heart disease Adversereactions toestrogens
Adverse reactions to es-trogens include:• hypertension• thromboembolism(blood vessel blockagecaused by a blood clot)• thrombophlebitis (veininflammation associatedwith clot formation).
Warning!
938913.qxd 08/26/2008 16:55 Page 348

Anterior pituitary drugsThe protein hormones produced in the anterior pituitary glandregulate growth, development, and sexual characteristics by stim-ulating the actions of other endocrine glands. Anterior pituitarydrugs include:• adrenocorticotropics, which include corticotropin, corticotro-pin repository, corticotropin zinc hydroxide, and cosyntropin• somatrem and somatropin, growth hormones• gonadotropics, which include chorionic gonadotropin andmenotropins• thyrotropics, which include thyroid-stimulating hormone, thy-rotropin, and protirelin.
PharmacokineticsAnterior pituitary drugs aren’t given orally because they’re de-stroyed in the GI tract. Some of these hormones can be adminis-tered topically, but most require injection.
Absorption, distribution, and metabolismUsually, natural hormones are absorbed, distributed, and metab-olized rapidly. Some analogues, however, are absorbed and me-tabolized more slowly. Anterior pituitary hormone drugs aremetabolized at the receptor site and in the liver and kidneys. Thehormones are excreted primarily in urine.
PharmacodynamicsAnterior pituitary drugs exert a profound effect on the body’sgrowth and development. The hypothalamus controls secretionsof the pituitary gland. In turn, the pituitary gland secretes hor-mones that regulate secretions or functions of other glands.
Concentrate on this formulaThe concentration of hormones in the blood helps determine hor-mone production rate. Increased hormone levels inhibit hormoneproduction; decreased levels raise production and secretion.
PharmacotherapeuticsAnterior pituitary hormone drugs are used for diagnostic and ther-apeutic purposes:• Corticotropin and cosyntropin are used diagnostically to differ-entiate between primary and secondary failure of the adrenalcortex.• Corticotropin is also used to treat adrenal insufficiency.• Somatrem is used to treat growth hormone deficiency.
349PITUITARY DRUGS
Anteriorpituitary drugs act
on endocrineglands to controltheir functions.
938913.qxd 08/26/2008 16:55 Page 349

Drug interactionsAnterior pituitary drugs interact with several types of drugs:• Administering immunizations to a person receiving cortico-tropin increases the risk of neurologic complications and may re-duce the antibody response.• Corticotropin reduces salicylate levels.• Enhanced potassium loss may occur when diuretics are takenwith corticotropins.• Barbiturates, phenytoin, and rifampin increase the metabolismof corticotropin, reducing its effects.
Estrogen effects• Estrogen increases the effect of corticotropin.• Taking estrogens, amphetamines, and lithium with cosyntropincan alter results of adrenal function tests.• Concurrent use of amphetamines and androgens with somatremmay promote epiphyseal closure (closure of the cartilaginousbone growth plate).• Concurrent use of somatrem and corticosteroids inhibits thegrowth-promoting action of somatrem. (See Adverse reactions toanterior pituitary drugs.)
Posterior pituitary drugsPosterior pituitary hormones are synthesized in the hypothala-mus and stored in the posterior pituitary, which, in turn, secretesthe hormones into the blood. These drugs include:• all forms of antidiuretic hormone (ADH), such as desmopressinacetate and vasopressin• the oxytocic drug oxytocin.
PharmacokineticsBecause enzymes in the GI tract can destroy all protein hormones,these drugs can’t be given orally. Posterior pituitary drugs may begiven by injection or intranasal spray.
Absorption, distribution, and metabolismLike other natural hormones, oxytocic drugs are usually absorbed,distributed, and metabolized rapidly. Parenterally administeredoxytocin is absorbed rapidly; however, when it’s administered in-tranasally, absorption is erratic.
350ENDOCRINE DRUGS
When givingcertain drugs,you need to becareful to avoidsome diuretics.
Adversereactionsto anteriorpituitary drugs
The major adverse reac-tions to pituitary drugsare hypersensitivity re-actions.
Over the long haul
Long-term use of corti-cotropin can causeCushing’s syndrome.
Warning!
938913.qxd 08/26/2008 16:55 Page 350

PharmacodynamicsUnder neural control, posterior pituitary hormones affect:• smooth-muscle contraction in the uterus, bladder, and GI tract• fluid balance through kidney reabsorption of water• blood pressure through stimulation of the arterial wall muscles.
Going to cAMPADH increases cyclic adenosine monophosphate (cAMP), whichincreases the permeability of the tubular epithelium in the kid-neys, promoting reabsorption of water. High dosages of ADH stim-ulate contraction of blood vessels, increasing the blood pressure.
Desmopressin reduces diuresis and promotes clotting by in-creasing the plasma level of factor VIII (antihemophilic factor).
Baby talkIn pregnant women, oxytocin may stimulate uterine contractionsby increasing the permeability of uterine cell membranes to sodi-um ions. It also can stimulate lactation through its effect on mam-mary glands.
PharmacotherapeuticsADH is prescribed for hormone replacement therapy in patientswith neurogenic diabetes insipidus (an excessive loss of urinecaused by a brain lesion or injury that interferes with ADH synthe-sis or release). However, it doesn’t effectively treat nephrogenicdiabetes insipidus (caused by renal tubular resistance to ADH).
The ABC’s of ADH treatmentDesmopressin is the drug of choice for chronic ADH deficiencyand is administered intranasally. It’s also indicated for primarynocturnal enuresis. Desmopressin has a long duration of actionand relatively few adverse effects.
Short-term ADH treatment is indicated for patients with tran-sient diabetes insipidus after head injury or surgery; therapy maybe lifelong for patients with idiopathic hormone deficiencies.Used for short-term therapy, vasopressin elevates blood pressurein patients with hypotension caused by lack of vascular tone. Italso relieves postoperative gaseous distention.
They help with deliveries (before, during, and after)Oxytocics are used to:• induce labor and complete incomplete abortions• treat preeclampsia, eclampsia, and premature rupture of mem-branes• control bleeding and uterine relaxation after delivery• hasten uterine shrinking after delivery• stimulate lactation.
351PITUITARY DRUGS
WithoutADH, I can’t
reabsorbfluid.
938913.qxd 08/26/2008 16:55 Page 351

Drug interactionsA variety of drugs can cause interactions with posterior pituitarydrugs:• Alcohol, demeclocycline, epinephrine, and lithium may de-crease the ADH activity of desmopressin and vasopressin.• Chlorpropamide, clofibrate, carbamazepine, and cyclophos-phamide increase ADH activity.• Synergistic effects may occur when barbiturates or cyclo-propane anesthetics are used concurrently with ADH, leading tocoronary insufficiency or arrhythmias.• Cyclophosphamide may increase the effect of oxytocin.• Concurrent use of vasopressors (anesthetics, ephedrine,methoxamine) and oxytocin increases the risk of hypertensive cri-sis and postpartum rupture of cerebral blood vessels. (See Ad-verse reactions to posterior pituitary drugs.)
Thyroid and antithyroid drugsThyroid and antithyroid drugs function to correct thyroid hor-mone deficiency (hypothyroidism) and thyroid hormone excess(hyperthyroidism).
Thyroid drugsThyroid drugs can be natural or synthetic hormones and maycontain triiodothyronine (T3), thyroxine (T4), or both.
352ENDOCRINE DRUGS
Oxytocin is usedto induce labor
and can also helpwith postdelivery
problems.
Hypersensitivity reactions are the most com-mon adverse reactions to posterior pituitarydrugs.
Natural ADH
Anaphylaxis may occur after injection. Naturalantidiuretic hormone (ADH) can also cause:• ringing in the ears• anxiety
• hyponatremia (low serum sodium levels)• proteins in urine• eclamptic attacks• pupil dilation• transient edema.
Synthetic ADH
Adverse reactions to synthetic ADH are rare.
Warning!
Adverse reactions to posterior pituitary drugs
938913.qxd 08/26/2008 16:55 Page 352

All naturalNatural thyroid drugs are made from animal thyroid and include:• thyroid USP (desiccated), which contains both T3 and T4• thyroglobulin, which also contains both T3 and T4.
Man-madeSynthetic thyroid drugs are actually the sodium salts of theL-isomers of the hormones. These synthetic hormones include:• levothyroxine sodium, which contains T4• liothyronine sodium, which contains T3• liotrix, which contains both T3 and T4.
PharmacokineticsThyroid hormones are absorbed variably from the GI tract, distrib-uted in plasma, and bound to serum proteins.
Metabolism and excretionThyroid drugs are metabolized through deiodination, primarily inthe liver, and excreted unchanged in stool.
PharmacodynamicsThe principal pharmacologic effect is an increased metabolic ratein body tissues. Thyroid hormones affect protein and carbohy-drate metabolism and stimulate protein synthesis. They promotegluconeogenesis (the formation of glucose from free fatty acidsand proteins) and increase the use of glycogen stores.
They get the heart pumping…Thyroid hormones increase heart rate and cardiac output (theamount of blood pumped by the heart each minute). They mayeven increase the heart’s sensitivity to catecholamines and in-crease the number of beta-adrenergic receptors in the heart(stimulation of beta receptors in the heart increases heartrate and contractility).
…and the blood flowingThyroid hormones may increase blood flow to the kidneysand increase the glomerular filtration rate (the amount ofplasma filtered through the kidney each minute) in hypothy-roid patients, producing diuresis.
PharmacotherapeuticsThyroid drugs act as replacement or substitute hormones in thesesituations:
353THYROID AND ANTITHYROID DRUGS
I can pumpmore and more
with thyroidhormones.
938913.qxd 08/26/2008 16:55 Page 353

• to treat the many forms of hypothyroidism• with antithyroid drugs to prevent goiter formation (an enlargedthyroid gland) and hypothyroidism• to differentiate between primary and secondary hypothyroidismduring diagnostic testing• to treat papillary or follicular thyroid carcinoma.
The drug of choiceLevothyroxine is the drug of choice for thyroid hormone replace-ment and thyroid-stimulating hormone suppression therapy.
Drug interactionsThyroid drugs interact with several common medications. (SeeAdverse reactions to thyroid drugs.)• They increase the effects of oral anticoagulants, increasing thetendency to bleed.• Cholestyramine and colestipol reduce the absorption of thyroidhormones.• Phenytoin may displace thyroxine from plasma-binding sites,temporarily increasing levels of free thyroxine.• Taking thyroid drugs with digoxin may reduce serum digoxinlevels, increasing the risk of arrhythmias or heart failure.• Carbamazepine, phenytoin, phenobarbital, and rifampin in-crease metabolism of thyroid hormones, reducing their effective-ness.• Serum theophylline levels may increase when theophylline isadministered with thyroid drugs.
354ENDOCRINE DRUGS
Most adverse reactions tothyroid drugs result fromtoxicity.
GI impact
Adverse reactions in the GIsystem include:• diarrhea• abdominal cramps• weight loss• increased appetite.
Heart of the matter
Adverse reactions in the car-diovascular system include:• palpitations• sweating• rapid heart rate• increased blood pressure• angina• arrhythmias.
Toxic topics
General manifestations of tox-ic doses include:• headache• tremor• insomnia• nervousness• fever• heat intolerance• menstrual irregularities.
Warning!
Adverse reactions to thyroid drugs
938913.qxd 08/26/2008 16:55 Page 354

Antithyroid drugsA number of drugs act as antithyroid drugs, or thyroid antago-nists. Used for patients with hyperthyroidism (thyrotoxicosis),these drugs include:• thioamides, which include propylthiouracil and methimazole• iodides, which include stable iodine and radioactive iodine.
PharmacokineticsThioamides and iodides are absorbed through the GI tract, con-centrated in the thyroid, metabolized by conjugation, and excret-ed in urine.
PharmacodynamicsDrugs used to treat hyperthyroidism work in different ways.
The antithesis to synthesisThioamides block iodine’s ability to combine with tyrosine, there-by preventing thyroid hormone synthesis.
In Wolff (-Chaikoff)’s clothingStable iodine inhibits hormone synthesis through the Wolff-Chaikoff effect, in which excess iodine decreases the formationand release of thyroid hormone.
Warning: Radioactive materialRadioactive iodine reduces hormone secre-tion by destroying thyroid tissue through in-duction of acute radiation thyroiditis (inflam-mation of the thyroid gland) and chronicgradual thyroid atrophy. Acute radiation thy-roiditis usually occurs 3 to 10 days after ad-ministering radioactive iodine. Chronic thyroidatrophy may take several years to appear.
PharmacotherapeuticsAntithyroid drugs are commonly used to treat hyperthyroidism,especially in the form of Graves’ disease (hyperthyroidism causedby autoimmunity), which accounts for 85% of all cases.
In case of removalTo treat hyperthyroidism, the thyroid gland may be removed bysurgery or destroyed by radiation. Before surgery, stable iodine is
355THYROID AND ANTITHYROID DRUGS
In the Wolff-Chaikoff effect,excess iodinedecreases theformation and
release of thyroidhormone.
938913.qxd 08/26/2008 16:55 Page 355

used to prepare the gland for surgical removal by firming it anddecreasing its vascularity.
Stable iodine is also used after radioactive iodine therapy tocontrol symptoms of hyperthyroidism while the radiation takeseffect.
If it gets too severePropylthiouracil, which lowers serum T3 levels faster than methi-mazole, is usually used for rapid improvement of severe hyperthy-roidism.
When taking them for twoPropylthiouracil is preferred over methimazole in pregnantwomen because its rapid action reduces transfer across the pla-cental barrier and it doesn’t cause aplasia cutis (a severe skin dis-order) in the fetus.
Propylthiouracil and methimazole appear in breast milk, so it’srecommended that mothers taking these drugs shouldn’t breast-feed. If a breast-feeding woman must take one of these drugs,propylthiouracil is the preferred drug.
One a day keeps the trouble awayBecause methimazole blocks thyroid hormone formation for alonger time, it’s better suited for administration once per day topatients with mild to moderate hyperthyroidism. Therapy maycontinue for 12 to 24 months before remission occurs.
Drug interactionsIodide preparations may react synergistically with lithium, caus-ing hypothyroidism. Other interactions aren’t clinically significant.(See Adverse reactions to antithyroid drugs.)
356ENDOCRINE DRUGS
Adversereactions toantithyroiddrugs
The most serious ad-verse reaction tothioamide therapy isgranulocytopenia. Hy-persensitivity reactionsmay also occur.
In bad taste
The iodides can causean unpleasant brassytaste and burning sensa-tion in the mouth, in-creased salivation, andpainful swelling of theparotid glands.
Too sensitive
Rarely, I.V. iodine admin-istration can cause anacute hypersensitivityreaction. Radioactive io-dine also can cause arare—but acute—reac-tion 3 to 14 days afteradministration.
Warning!
938913.qxd 08/26/2008 16:55 Page 356

Quick quiz
1. How does insulin lower the blood glucose level?A. It prevents glucose absorption from the GI tract.B. It increases glucose excretion from the GI tract.C. It increases glucose absorption.D. It promotes the transport of glucose into cells.
Answer: D. Insulin promotes the transport of glucose into cells.
2. Why can’t glucagon be given orally?A. It works too slowly when given orally.B. It’s destroyed by the GI tract.C. It’s absorbed unpredictably.D. It’s too caustic to the GI tract.
Answer: B. Glucagon is destroyed by the GI tract.
3. Which signs indicate that a patient taking levothyroxine is ex-periencing thyroid toxicity?
A. Diarrhea and weight lossB. Weight gain and constipationC. Slow heart rate and low blood pressureD. Irregular heart rate and low blood pressure
Answer: A. Diarrhea and weight loss are signs of thyroid toxicityin a patient taking levothyroxine.
4. The posterior pituitary drug used to stimulate uterine con-tractions is:
A. vasopressin.B. oxytocin.C. desmopressin.D. estrogen.
Answer: B. Oxytocin stimulates uterine contractions by increas-ing permeability of uterine cell membranes to sodium ions. It canalso stimulate lactation.
5. Estrogens are sometimes prescribed to treat which conditionin men?
A. Renal cancerB. Testicular cancerC. Colorectal cancerD. Prostate cancer
Answer: D. Estrogens are sometimes prescribed for palliativetreatment of prostate cancer.
357QUICK QUIZ
938913.qxd 08/26/2008 16:55 Page 357

ScoringIf you answered all five items correctly, extraordinary! You’re hy-
per-knowledgeable about hyperglycemic drugs and more!If you answered four items correctly, congratulations! You have a
well-balanced understanding of pharmacology!If you answered fewer than four items correctly, keep trying! You
have two more Quick quizzes to go!
358ENDOCRINE DRUGS
We sure are gettingto know our drugs.
Now, on to fluids andelectrolytes!
✰✰✰
✰✰
✰
938913.qxd 08/26/2008 16:55 Page 358

Drugs and homeostasisIllness can easily disturb the homeostatic mechanisms that helpmaintain normal fluid and electrolyte balance. Such occurrencesas loss of appetite, medication administration, vomiting, diarrhea,surgery, and diagnostic tests can also alter this delicate balance.Fortunately, numerous drugs can be used to correct these imbal-ances and help bring the body back to homeostasis.
Electrolyte replacement drugsAn electrolyte is a compound or element that carries an electricalcharge when dissolved in water. Electrolyte replacement drugsare inorganic or organic salts that increase depleted or deficientelectrolyte levels, helping to maintain homeostasis, the stabilityof body fluid composition and volume. They include:• potassium, the primary intracellular fluid (ICF) electrolyte• calcium, a major extracellular fluid (ECF) electrolyte• magnesium, an electrolyte essential for homeostasis foundin ICF• sodium, the principal electrolyte in ECF necessary for homeo-stasis.
14
Drugs for fluid and electrolyte balance
Just the facts
In this chapter, you’ll learn:
♦ classes of drugs that affect fluid and electrolyte balance
♦ uses and varying actions of these drugs
♦ how these drugs are absorbed, distributed, metabolized,and excreted
♦ drug interactions and adverse reactions to these drugs.
Look out! Anelectrolyte carries
an electricalcharge when it’s
dissolved in water.
938914.qxd 08/26/2008 17:00 Page 359

PotassiumPotassium is the major positively charged ion (cation) in ICF. Be-cause the body can’t store potassium, adequate amounts must beingested daily. If this isn’t possible, potassium replacement can beaccomplished orally or I.V. with potassium salts, such as:• potassium acetate• potassium bicarbonate• potassium chloride• potassium gluconate• potassium phosphate.
Pharmacokinetics (how drugs circulate)Oral potassium is absorbed readily from the GI tract.
Absorption, metabolism, and excretionAfter absorption into the ECF, almost all of the potassium passesinto the ICF. There, the enzyme adenosinetriphosphatase main-tains the concentration of potassium by pumping sodium out ofthe cell in exchange for potassium.
Normal serum levels of potassium are maintained by the kid-neys, which excrete most excess potassium intake. The rest is ex-creted in stool and sweat.
Pharmacodynamics (how drugs act)Potassium moves quickly into ICF to restore depleted potassiumlevels and reestablish balance. It’s an essential element in deter-mining cell membrane potential and excitability.
Feel nervous about potassium?Potassium is necessary for proper functioning of all nerve andmuscle cells and for nerve impulse transmission. It’s also essentialfor tissue growth and repair and for maintenance of acid-basebalance.
Pharmacotherapeutics (how drugs are used)Potassium replacement therapy corrects hypokalemia, low levelsof potassium in the blood. Hypokalemia is a common occurrencein conditions that increase potassium excretion or depletion,such as:• vomiting, diarrhea, or nasogastric suction• excessive urination• some kidney diseases• cystic fibrosis• burns
360DRUGS FOR FLUID AND ELECTROLYTE BALANCE
Because the bodycan’t store
potassium, I makesure I eat adequateamounts every day.
This banana is a goodsource of potassium.
938914.qxd 08/26/2008 17:00 Page 360

• excess of antidiuretic hormone or therapy with a potassium-depleting diuretic• laxative abuse• alkalosis• insufficient potassium intake from starvation, anorexia nervosa,alcoholism, or clay ingestion• administration of a glucocorticoid, I.V. amphotericin B, vitaminB12, folic acid, granulocyte-macrophage colony–stimulating factor,or I.V. solutions that contain insufficient potassium.
Be still my heartPotassium decreases the toxic effects of digoxin. Because potassi-um inhibits the excitability of the heart, normal potassium levelsmoderate the action of digoxin, reducing the chances of toxicity.
Drug interactionsPotassium should be used cautiously in patients receivingpotassium-sparing diuretics (such as amiloride, spironolactone,and triamterene) or angiotensin-converting enzyme inhibitors(such as captopril, enalapril, and lisinopril) to avoid hyperkal-emia. (See Adverse reactions to potassium.)
CalciumCalcium is a major cation in ECF. Almost all of the calcium in thebody (99%) is stored in bone, where it can be mobilized, if neces-sary. When dietary intake isn’t enough to meet metabolic needs,calcium stores in bone are reduced.
Bound, complexed, ionizedExtracellular calcium exists in three forms—it’s bound to plasmaprotein (mainly albumin); complexed with such substances asphosphate, citrate, or sulfate; and ionized. Ionized calcium is thephysiologically active form and plays a role in cellular functions.
Salting the bodyChronic insufficient calcium intake can result in bone demineral-ization. Calcium is replaced orally or I.V. with calcium salts,such as:• calcium carbonate• calcium chloride• calcium citrate• calcium glubionate• calcium gluceptate• calcium gluconate• calcium lactate.
361ELECTROLYTE REPLACEMENT DRUGS
Adversereactions topotassium
Most adverse reactionsto potassium are relatedto the method of admin-istration.
Oral history
Oral potassium some-times causes nausea,vomiting, abdominalpain, and diarrhea.Enteric-coated tabletsmay cause small-bowelulceration, stenosis, he-morrhage, and obstruc-tion.
I.V. issues
I.V. infusion of potassiumpreparations can causepain at the injection siteand phlebitis (vein in-flammation). Givenrapidly, I.V. administra-tion may cause cardiacarrest. Infusion of potas-sium in patients with de-creased urine produc-tion increases the risk ofhyperkalemia.
Warning!
938914.qxd 08/26/2008 17:00 Page 361

PharmacokineticsOral calcium is absorbed readily from the duodenum and proxi-mal jejunum. A pH of 5 to 7, parathyroid hormone, and vitamin Dall aid calcium absorption.
Absorbed with absorptionAbsorption also depends on dietary factors, such as calcium bind-ing to fiber, phytates, and oxalates, and on fatty acids, with whichcalcium salts form insoluble soaps.
Distribution and excretionCalcium is distributed primarily in bone. Calcium salts are elimi-nated unchanged primarily in stool; the remainder is excreted inurine.
PharmacodynamicsCalcium moves quickly into ECF to restore calcium levels andreestablish balance. Calcium has several important roles in thebody:• Extracellular ionized calcium plays an essential role in normalnerve and muscle excitability.• Calcium is integral to normal functioning of the heart, kidneys,and lungs, and it affects the blood coagulation rate as well as cellmembrane and capillary permeability.• Calcium is a factor in neurotransmitter and hormone activity,amino acid metabolism, vitamin B12 absorption, and gastrinsecretion.• Calcium plays a major role in normal bone and tooth formation.
PharmacotherapeuticsCalcium is helpful in treating magnesium intoxication. It alsohelps strengthen myocardial tissue after defibrillation (electricshock to restore normal heart rhythm) or a poor response to epi-nephrine during resuscitation. Pregnancy and breast-feeding in-crease calcium requirements, as do periods of bone growth duringchildhood and adolescence.
In the I.V. leagueThe major clinical indication for I.V. calcium is acute hypocal-cemia (low serum calcium levels), which necessitates a rapid in-crease in serum calcium levels, as in tetany, cardiac arrest, vita-min D deficiency, parathyroid surgery, and alkalosis. I.V. calciumis also used to prevent a hypocalcemic reaction during exchangetransfusions.
362DRUGS FOR FLUID AND ELECTROLYTE BALANCE
Just aboutall the calciumin the body canbe found in the
bones.
938914.qxd 08/26/2008 17:00 Page 362

Oral historyOral calcium is commonly used to supplement a calcium-deficientdiet and prevent osteoporosis. Chronic hypocalcemia from suchconditions as chronic hypoparathyroidism (a deficiency ofparathyroid hormones), osteomalacia (softening of bones), long-term glucocorticoid therapy, and plicamycin and vitamin D defi-ciency is also treated with oral calcium.
Drug interactionsCalcium has few significant interactions with other drugs.• Preparations administered with digoxin may cause cardiac ar-rhythmias.• Calcium replacement drugs may reduce the response to calciumchannel blockers.• Calcium replacements may inactivate tetracyclines.• Calcium supplements may decrease the amount of atenololavailable to the tissues, resulting in decreased effectiveness of thedrug.• When given in total parenteral nutrition, calcium may react withphosphorus present in the solution to form insoluble calciumphosphate granules, which may find their way into pulmonary ar-terioles, causing emboli and possibly death. (See Adverse reac-tions to calcium.)
MagnesiumMagnesium is the most abundant cation in ICF after potassium.It’s essential in transmitting nerve impulses to muscle and activat-ing enzymes necessary for carbohydrate and protein metabolism.About 65% of all magnesium is in bone, and 20% is in muscle.
Officiating in the ICFMagnesium stimulates parathyroid hormone secretion, thus regu-lating ICF calcium levels.
Traffic controlMagnesium also aids in cell metabolism and the movement ofsodium and potassium across cell membranes.
A run on magnesiumMagnesium stores may be depleted by:• malabsorption• chronic diarrhea• prolonged treatment with diuretics
363ELECTROLYTE REPLACEMENT DRUGS
Always oil theol’ bones withsome calcium!
Adversereactionsto calcium
Calcium preparationsmay produce hypercal-cemia (elevated serumcalcium levels). Earlysigns include:• drowsiness• lethargy• muscle weakness• headache• constipation• metallic taste.
Take this to heart
Electrocardiogramchanges that occur withelevated serum calciumlevels include a short-ened QT interval andheart block. Severehypercalcemia cancause cardiac arrhyth-mias, cardiac arrest, andcoma.
Warning!
938914.qxd 08/26/2008 17:00 Page 363

• nasogastric suctioning• prolonged therapy with parenteral fluids not containing magne-sium• hyperaldosteronism• hypoparathyroidism or hyperparathyroidism• excessive release of adrenocortical hormones• acute and chronic alcohol consumption• drugs, such as cisplatin, aminoglycosides, cyclosporine, and am-photericin B.
Restocking the mineral storesMagnesium is typically replaced in the form of magnesium sulfatewhen administered I.V. or in the form of magnesium oxide if givenorally.
PharmacokineticsMagnesium sulfate is distributed widely throughout the body.I.V. magnesium sulfate acts immediately, whereas the drug actswithin 30 minutes after I.M. administration. However, I.M. injec-tions can be painful, can induce sclerosis, and need to be repeatedfrequently.
Metabolism and excretionMagnesium sulfate isn’t metabolized and is excreted unchanged inurine and stool; some appears in breast milk.
PharmacodynamicsMagnesium sulfate replenishes and prevents magnesium deficien-cies. It also prevents or controls seizures by blocking neuromus-cular transmission.
PharmacotherapeuticsI.V. magnesium sulfate is the drug of choice for replacement thera-py in symptomatic magnesium deficiency (hypomagnesemia). It’swidely used to treat or prevent preeclamptic and eclamptic sei-zure activity and is used to treat ventricular arrhythmias such astorsades de pointes. It’s also used to treat seizures, severe toxe-mia, and acute nephritis in children.
Drug interactionsMagnesium has few significant interactions with other drugs.• Magnesium used with digoxin may lead to heart block.• Magnesium sulfate combined with alcohol, narcotics, antianxi-ety drugs, barbiturates, antidepressants, hypnotics, antipsychotic
364DRUGS FOR FLUID AND ELECTROLYTE BALANCE
I.V. magnesiumsulfate is the
drug of choice forhypomagnesemia.
938914.qxd 08/26/2008 17:00 Page 364

drugs, or general anesthetics may increase central nervous systemdepressant effects.• Magnesium sulfate combined with succinylcholine or tubocu-rarine potentiates and prolongs the neuromuscular blocking ac-tion of these drugs. (See Adverse reactions to magnesium.)
SodiumSodium is the major cation in ECF. Sodium performs many func-tions:• It maintains the osmotic pressure and concentration of ECF,acid-base balance, and water balance.• It contributes to nerve conduction and neuromuscular function.• It plays a role in glandular secretion.
Don’t sweat itSodium replacement is necessary in conditions that rapidly de-plete sodium, such as anorexia, excessive loss of GI fluids, and ex-cessive perspiration. Diuretics and tap water enemas can also de-plete sodium, particularly when fluids are replaced by plain water.
The salt flatsSodium also can be lost in trauma or wound drainage, adrenalgland insufficiency, cirrhosis of the liver with ascites, syndrome ofinappropriate antidiuretic hormone, and prolonged I.V. infusion ofdextrose in water without other solutes.
Calling all chloridesSodium is typically replaced in the form of sodium chloride.
PharmacokineticsOral and parenteral sodium chloride are quickly absorbedand distributed widely throughout the body.
Metabolism and excretionSodium chloride isn’t significantly metabolized. It’s elimi-nated primarily in urine but also in sweat, tears, and saliva.
PharmacodynamicsSodium chloride solution replaces deficiencies of the sodi-um and chloride ions in the blood plasma.
365ELECTROLYTE REPLACEMENT DRUGS
When I’m outjogging, I lose
important fluids.Sodium can help me
replace depletedfluids and maintain
water balance.
Adversereactions tomagnesium
Adverse reactions tomagnesium sulfate,which can be life-threatening, include:• hypotension• circulatory collapse• flushing• depressed reflexes• respiratory paralysis• cardiac arrest.
Warning!
938914.qxd 08/26/2008 17:00 Page 365

PharmacotherapeuticsSodium chloride is used for water and electrolyte replacement inpatients with hyponatremia from electrolyte loss or severe sodiumchloride depletion.
A welcome infusionSevere symptomatic sodium deficiency may be treated by I.V. infu-sion of a solution containing sodium chloride.
Drug interactionsNo significant drug interactions have been reported with sodiumchloride. (See Adverse reactions to sodium.)
Alkalinizing and acidifying drugsAlkalinizing and acidifying drugs act to correct acid-base imbal-ances in the blood. These acid-base imbalances include:• metabolic acidosis, a decreased serum pH caused by excess hy-drogen ions in the ECF, which is treated with alkalinizing drugs• metabolic alkalosis, an increased serum pH caused by excessbicarbonate in the ECF, which is treated with acidifying drugs.
Odd coupleAlkalinizing and acidifying drugs have opposite effects:• An alkalinizing drug will increase the pH of the blood and de-crease the concentration of hydrogen ions.• An acidifying drug will decrease the pH of the blood and in-crease the concentration of hydrogen ions.
Rx for o.d.Some of these drugs also alter urine pH, making them useful intreating some urinary tract infections and drug overdoses.
Alkalinizing drugsAlkalinizing drugs are used to treat metabolic acidosis and to in-crease blood pH. These include:• sodium bicarbonate• sodium citrate• sodium lactate• tromethamine.
366DRUGS FOR FLUID AND ELECTROLYTE BALANCE
Adversereactionsto sodium
Adverse reactions tosodium include:• pulmonary edema (ifgiven too rapidly or inexcess)• hypernatremia• potassium loss.
Warning!
938914.qxd 08/26/2008 17:00 Page 366

Increasing another pHSodium bicarbonate is also used to increase urine pH.
PharmacokineticsAll of the alkalinizing drugs are absorbed well when given orally.
Metabolism and excretionSodium citrate and sodium lactate are metabolized to the activeingredient, bicarbonate. Sodium bicarbonate isn’t metabolized.Tromethamine undergoes little or no metabolism and is excretedunchanged in urine.
PharmacodynamicsSodium bicarbonate separates in the blood, providing bicarbonateions that are used in the blood buffer system to decrease the hy-drogen ion concentration and raise blood pH. (Buffers prevent ex-treme changes in pH by taking or giving up hydrogen ions to neu-tralize acids or bases.) As the bicarbonate ions are excreted inurine, urine pH rises. Sodium citrate and lactate, after conversionto bicarbonate, alkalinize the blood and urine in the same way.
Hitching up with hydrogenTromethamine acts by combining with hydrogen ions to alkalinizethe blood; the resulting tromethamine–hydrogen ion complex isexcreted in urine.
PharmacotherapeuticsAlkalinizing drugs are commonly used to treat metabolic acidosis.Other uses include raising urine pH to help remove certain sub-stances, such as phenobarbital, after an overdose.
Drug interactionsThe alkalinizing drugs sodium bicarbonate, sodium citrate, andsodium lactate can interact with a wide range of drugs to increaseor decrease their pharmacologic effects.• They may increase excretion and reduce the effects of chlor-propamide, ketoconazole, lithium, and salicylates.• They may reduce the excretion and increase the effects of am-phetamines, flecainide, quinidine, and pseudoephedrine.• The antibacterial effects of methenamine are reduced when tak-en with alkalinizing drugs. (See Adverse reactions to alkalinizingdrugs, page 368.)
367ALKALINIZING AND ACIDIFYING DRUGS
Alkalinizingdrugs treatmetabolic
acidosis byincreasingblood pH.
Memoryjogger
Remember:A low pH
means a solution isacidic, and a high pHmeans it’s alkaline.Therefore, to raisethe pH, you use analkalinizing drug and,likewise, to lower thepH, you use an acidi-fying drug.
938914.qxd 08/26/2008 17:00 Page 367

Acidifying drugsAcidifying drugs are used to correct metabolic alkalosis. Theseinclude:• acetazolamide (used in treatment of acute mountain sickness)• ammonium chloride.
Ascorbic acid, along with ammonium chloride, serves as a uri-nary acidifier.
PharmacokineticsThe action of most acidifying drugs is immediate.
Absorption, metabolism, and excretionOrally administered ammonium chloride is absorbed completelyin 3 to 6 hours. It’s metabolized in the liver to form urea, which isexcreted by the kidneys.
Break it downAcetazolamide inhibits the enzyme carbonic anhydrase, whichblocks hydrogen ion secretion in the renal tubule, resulting in in-creased excretion of bicarbonate and a lower pH. Acetazolamidealso acidifies urine but may produce metabolic acidosis in normalpatients.
368DRUGS FOR FLUID AND ELECTROLYTE BALANCE
When yourstomach
doesn’t feelquite right, you
might needsome acidifying
drugs!
Adverse reactions to alkalinizing drugs vary.
Sodium bicarbonate
• Bicarbonate overdose• Cerebral dysfunction, tissue hypoxia, andlactic acidosis (with rapid administration fordiabetic ketoacidosis)• Water retention and edema
Sodium citrate
• Metabolic alkalosis, tetany, or aggravation ofexisting heart disease (with overdose)• Laxative effect (with oral administration)
Sodium lactate
• Metabolic alkalosis (with overdose)• Extravasation• Water retention or edema (in patient withkidney disease or heart failure)
Tromethamine
• Hypoglycemia• Respiratory depression• Extravasation• Hyperkalemia• Toxic drug levels (if given for more than24 hours)
Warning!
Adverse reactions to alkalinizing drugs
938914.qxd 08/26/2008 17:00 Page 368

PharmacodynamicsAcidifying drugs have several actions:• Ammonium chloride lowers the blood pH after being metabo-lized to urea and to hydrochloric acid, which provides hydrogenions to acidify the blood or urine.• Ascorbic acid directly acidifies urine, providing hydrogen ionsand lowering urine pH.• Acetazolamide increases the excretion of bicarbonate, loweringblood pH.
PharmacotherapeuticsA patient with metabolic alkalosis requires therapy with an acidi-fying drug that provides hydrogen ions; such a patient may needchloride ion therapy as well.
Safe and easyMost patients receive both types of ions in oral or parenteral dos-es of ammonium chloride, a safer drug that’s easy to prepare.
Kidney concernsIn patients with renal dysfunction, acetazolamide may be ineffec-tive and cause loss of potassium in urine.
Drug interactionsAcidifying drugs don’t cause clinically signifi-cant drug interactions. However, concurrentuse of ammonium chloride and spironolac-tone may cause increased systemic acidosis.(See Adverse reactions to acidifying drugs.)
369ALKALINIZING AND ACIDIFYING DRUGS
Oral forms ofammoniumchloride aresafer andeasier toprepare.
Adversereactions toacidifying drugs
Adverse reactions toacidifying drugs are usu-ally mild, such as GI dis-tress. Overdose maylead to acidosis.
Acetazolamide
• Drowsiness• Seizures• Anorexia• Nausea and vomiting• Diarrhea• Altered taste• Aplastic anemia
Ammonium chloride
• Metabolic acidosisand loss of electrolytes,especially potassium(with large doses)
Ascorbic acid
• GI distress (with highdoses)• Hemolytic anemia(in a patient withglucose-6-phosphatedehydrogenase defi-ciency)
Warning!
938914.qxd 08/26/2008 17:00 Page 369

Quick quiz
1. Which drug can cause hypokalemia?A. DigoxinB. Amphotericin BC. SpironolactoneD. Lansoprazole
Answer: B. Hypokalemia is a common occurrence in conditionsthat increase potassium excretion or depletion, such as adminis-tration of glucocorticoid, I.V. amphotericin B, vitamin B12, folicacid, granulocyte-macrophage colony–stimulating factor, or I.V.solutions that contain insufficient potassium.
2. Potassium should be used cautiously in patients receiving:A. amiloride.B. furosemide.C. digoxin.D. cetirizine.
Answer: A. Potassium should be used cautiously in patients re-ceiving potassium-sparing diuretics, such as amiloride, to avoidhyperkalemia.
3. How does sodium bicarbonate correct metabolic acidosis?A. By lowering blood pH after being metabolizedB. By increasing hydrogen ion concentrationC. By combining with hydrogen ions to alkalinize the
bloodD. By decreasing hydrogen ion concentration
Answer: D. Sodium bicarbonate corrects acidosis by decreasinghydrogen ion concentration.
ScoringIf you answered all three items correctly, extraordinary! You’re
one well-balanced individual!If you answered two items correctly, congratulations! You’re mov-
ing closer to complete harmony!If you answered fewer than two items correctly, keep trying! By
the end of the book, you’re sure to have all your levels up!
370DRUGS FOR FLUID AND ELECTROLYTE BALANCE
✰✰✰
✰✰
✰
938914.qxd 08/26/2008 17:00 Page 370

Drugs and cancerIn the 1940s, antineoplastic (chemotherapeutic) drugs were de-veloped to treat cancer. However, these agents commonly had se-rious adverse effects.
A brighter futureToday, many of these toxicities can be lessened so they aren’t asdevastating to the patient. With modern chemotherapy, childhoodmalignancies, such as acute lymphoblastic leukemia, and adultcancers, such as testicular cancer, are curable in most patients.New therapeutic strategies, such as using monoclonal antibodiesor targeting specific proteins, are further improving the time that apatient’s cancer can remain in remission. In addition, drugs suchas interferons are being used to treat patients with cancer.
Alkylating drugsAlkylating drugs, given alone or with other drugs, effectively actagainst various malignant neoplasms. These drugs fall into one ofsix classes:• nitrogen mustards• alkyl sulfonates
15
Antineoplastic drugs
Just the facts
In this chapter, you’ll learn:
♦ classes of drugs used to treat cancer
♦ uses and varying actions of these drugs
♦ how these drugs are absorbed, distributed, metabolized,and excreted
♦ drug interactions and adverse reactions to these drugs. The 1940s saw thedevelopment of
chemotherapeuticdrugs.
938915.qxd 08/26/2008 17:12 Page 371

• nitrosoureas• triazenes• ethylenimines• alkylating-like drugs.
Unfazed at any phaseAll of these drugs produce their antineoplastic effects by damag-ing deoxyribonucleic acid (DNA). They halt DNA’s replicationprocess by cross-linking its strands so that amino acids don’t pairup correctly. Alkylating drugs are cell cycle–phase nonspecific.This means that their alkylating actions may take place at anyphase of the cell cycle.
Nitrogen mustardsNitrogen mustards represent the largest group of alkylatingdrugs. They include:• chlorambucil• cyclophosphamide• estramustine• ifosfamide• mechlorethamine hydrochloride• melphalan.
First and fastMechlorethamine hydrochloride was the first nitrogen mustard in-troduced and is rapid-acting.
Pharmacokinetics (how drugs circulate)The absorption and distribution of nitrogen mustards, as withmost alkylating drugs, vary widely.
Metabolism and excretionNitrogen mustards are metabolized in the liver and excreted bythe kidneys. Mechlorethamine undergoes metabolism so rapidlythat no active drug remains after a few minutes. Most nitrogenmustards possess more intermediate half-lives than mechloreth-amine.
Pharmacodynamics (how drugs act)Nitrogen mustards form covalent bonds with DNA molecules in achemical reaction known as alkylation. Alkylated DNA can’t repli-cate properly, thereby resulting in cell death. Unfortunately, cells
372ANTINEOPLASTIC DRUGS
Alkylatingdrugs deactivatemy DNA, cutting
short my life.
I see somenitrogen mustards
headed my way.Time to get to
work!
938915.qxd 08/26/2008 17:12 Page 372

may develop resistance to the cytotoxic effects of nitrogen mus-tards. (See How alkylating drugs work.)
Pharmacotherapeutics (how drugs are used)Because they produce leukopenia (reduced number of whiteblood cells [WBCs]), the nitrogen mustards are effective in treat-ing malignant neoplasms, such as Hodgkin’s disease (cancer caus-ing painless enlargement of the lymph nodes, spleen, and lym-phoid tissues) and leukemia (cancer of the blood-forming tissues),that can have an associated elevated WBC count.
Nitrogen bombNitrogen mustards also prove effective against malignant lym-phoma (cancer of the lymphoid tissue), multiple myeloma (cancerof the marrow plasma cells), melanoma (malignancy that arises
373ALKYLATING DRUGS
Alkylating drugs can attack deoxyribonucleic acid (DNA) in two ways, as shown in these illustrations.
Now I get it!
How alkylating drugs work
Bifunctional alkylation
Some drugs become inserted between two base pairs in theDNA chain, forming an irreversible bond between them. This iscalled bifunctional alkylation; it causes cytotoxic effects capa-ble of destroying or poisoning cells.
Monofunctional alkylation
Other drugs react with just one part of a pair, separating it fromits partner and eventually causing it and its attached sugarto break away from the DNA molecule. This is called mono-functional alkylation; it eventually may cause permanent celldamage.
Drug
C G
C G
C G
C G
A
AT
G C
C G
C G
C G
C G
A
AT
G C
TT
938915.qxd 08/26/2008 17:12 Page 373

from melanocytes), and cancers of the breast, ovaries, uterus,lung, brain, testes, bladder, prostate, and stomach.
Drug interactionsNitrogen mustards interact with a wide variety of other drugs:• Calcium-containing drugs and foods, such as antacids and dairyproducts, reduce absorption of estramustine.• Cyclophosphamide taken with cardiotoxic drugs producesadditive cardiac effects.• Cyclophosphamide may reduce serum digoxin levels.• An increased risk of ifosfamide toxicity exists when thedrug is taken with allopurinol, barbiturates, chloral hydrate, orphenytoin.• Corticosteroids reduce the effects of ifosfamide.• The lung toxicity threshold of carmustine may be reducedwhen taken with melphalan.• Interferon alpha may reduce serum concentration of mel-phalan. (See Adverse reactions to nitrogen mustards.)
Alkyl sulfonatesBusulfan, an alkyl sulfonate, has historically been used to treatchronic myelogenous leukemia, polycythemia vera (increased redblood cell mass and increased number of WBCs and platelets),and other myeloproliferative (pertaining to an overactive bonemarrow) disorders. It’s also used for treatment of leukemia duringbone marrow transplant procedures.
PharmacokineticsBusulfan is rapidly well absorbed from the GI tract. Little isknown about its distribution.
Metabolism and excretionBusulfan is extensively metabolized in the liver before urinary ex-cretion. Its half-life is 2 to 3 hours.
PharmacodynamicsAs an alkyl sulfonate, busulfan forms covalent bonds with theDNA molecules in alkylation.
PharmacotherapeuticsBusulfan primarily affects granulocytes (a type of WBC) and, to alesser degree, platelets. Because of its action on granulocytes, it
374ANTINEOPLASTIC DRUGS
The calcium indairy products
reduces theabsorption ofestramustine.
Adversereactionsto nitrogenmustards
Many patients experi-ence fatigue during ni-trogen mustard therapy.Other adverse reactionsinclude:• severe leukopenia andthrombocytopenia• nausea and vomiting• stomatitis• reversible hair loss• severe skin reactionswith direct contact• severe tissue damage,if extravasation occurs.
Warning!
938915.qxd 08/26/2008 17:12 Page 374

has been used for treating chronic myelogenous leukemia and asadjunct therapy before and after bone marrow transplantation.
A backup optionBusulfan is also effective in treating polycythemia vera, althoughother drugs are usually used to treat it because busulfan can causesevere myelosuppression (halting of bone marrow function).
Drug interactionsThere’s an increased risk of bleeding when busulfan is takenwith anticoagulants or aspirin. Concurrent use of busulfan andthioguanine may cause liver toxicity, esophageal varices (en-larged, swollen veins in the esophagus), or portal hypertension(increased pressure in the portal vein of the liver). (See Adversereactions to busulfan.)
NitrosoureasNitrosoureas are alkylating agents that work by halting cancercell reproduction. They include:• carmustine• lomustine• streptozocin.
PharmacokineticsWhen administered topically to treat mycosis fungoides (a rareskin malignancy), carmustine is 5% to 28% systemically absorbed.After oral administration, lomustine is absorbed adequately,though incompletely.
I.V. is the wayStreptozocin and carmustine are administered I.V. because they’repoorly absorbed orally.
Metabolism and excretionNitrosoureas are lipophilic (attracted to fat), distributing to fattytissues and cerebrospinal fluid. They’re metabolized extensivelybefore urine excretion.
PharmacodynamicsDuring a process called bifunctional alkylation, nitrosoureas in-terfere with amino acids, purines, and DNA needed for cancercells to divide, thus halting their reproduction.
375ALKYLATING DRUGS
Adversereactionsto busulfan
The major adverse reac-tion to busulfan is bonemarrow suppression,producing severeleukopenia, anemia, andthrombocytopenia (re-duced white blood cells,red blood cells, andplatelets, respectively).This reaction is usuallydose-related and re-versible.
Warning!
938915.qxd 08/26/2008 17:12 Page 375

PharmacotherapeuticsThe nitrosoureas are highly lipid (fat) soluble, which allows themor their metabolites to easily cross the blood-brain barrier. Be-cause of this ability, nitrosoureas are used to treat brain tumorsand meningeal leukemias.
Drug interactionsEach of the nitrosoureas has its own interactions with otherdrugs. Cimetidine may increase carmustine’s bone marrow toxici-ty. Streptozocin prolongs the elimination half-life of doxorubicin,prolonging the leukopenia and thrombocytopenia. (See Adversereactions to nitrosoureas.)
TriazenesDacarbazine, a triazene, functions as an alkylating drug after be-ing activated by the liver.
PharmacokineticsAfter I.V. injection, dacarbazine is distributed throughout the bodyand metabolized in the liver. Within 6 hours, 30% to 46% of a doseis excreted by the kidneys (half is excreted unchanged, and half isexcreted as one of the metabolites).
Dysfunction junctionIn patients with kidney or liver dysfunction, dacarbazine’s half-lifemay increase to 7 hours.
PharmacodynamicsDacarbazine must first be metabolized in the liver to become anactive drug. It seems to inhibit ribonucleic acid (RNA) and proteinsynthesis. Like other alkylating drugs, dacarbazine is cell cycle–nonspecific.
PharmacotherapeuticsDacarbazine is used primarily to treat patients with malignantmelanoma but is also used with other drugs to treat patients withHodgkin’s disease.
376ANTINEOPLASTIC DRUGS
Adversereactions tonitrosoureas
All of the nitrosoureascan produce severenausea and vomiting.
Down to the bone
Carmustine and lomus-tine produce bone mar-row suppression thatbegins 4 to 6 weeks aftertreatment and lasts 1 to2 weeks.
Kidney concerns
Kidney toxicity and kid-ney failure may also oc-cur with patients takingnitrosoureas. High-dosecarmustine may pro-duce reversible liver tox-icity.
Pulmonary problems
Carmustine may causelung toxicity character-ized by lung infiltrates orfibrosis (scarring).
Warning!
938915.qxd 08/26/2008 17:12 Page 376

Drug interactionsNo significant drug interactions have been reported with dacar-bazine. (See Adverse reactions to triazenes.)
EthyleniminesThiotepa, an ethylenimine derivative, is a multifunctional alkylat-ing drug.
PharmacokineticsAfter I.V. administration, thiotepa is 100% bioavailable. Significantsystemic absorption may occur when thiotepa is administeredinto pleural (around the lungs) or peritoneal (abdominal) spacesto treat malignant effusions or is instilled into the bladder.
Metabolism and excretionThiotepa crosses the blood-brain barrier and is metabolized exten-sively in the liver. Thiotepa and its metabolites are excreted inurine.
PharmacodynamicsThiotepa exerts its cytotoxic activity by interfering with DNAreplication and RNA transcription. Ultimately, it disrupts nucleicacid function and causes cell death.
PharmacotherapeuticsThiotepa is used to treat bladder cancer. This alkylating drug isalso prescribed for palliative (symptom-relief) treatment of lym-phomas and ovarian or breast cancers.
Wait! There’s moreThiotepa is used for the treatment of intracavitary effusions (accu-mulation of fluid in a body cavity). It may also prove useful in thetreatment of lung cancer.
Drug interactionsThiotepa may interact with other drugs.• Concurrent use of thiotepa, anticoagulants, and aspirin may in-crease the risk of bleeding.• Taking thiotepa with neuromuscular blocking drugs may pro-long muscular paralysis.
377ALKYLATING DRUGS
Adversereactionsto triazenes
Dacarbazine use maycause some adverse re-actions, including:• leukopenia• thrombocytopenia• nausea and vomiting(which begin within 1 to3 hours after administra-tion in most patients andmay last up to 48 hours)• phototoxicity• flulike symptoms• hair loss.
Warning!
938915.qxd 08/26/2008 17:12 Page 377

• Concurrent use of thiotepa and other alkylating drugs or radia-tion therapy may intensify toxicity rather than enhance the thera-peutic response.
It’ll take your breath awayWhen used with succinylcholine, thiotepa may cause prolongedrespirations and apnea (periods of not breathing). Thiotepa ap-pears to inhibit the activity of cholinesterase, the enzyme that de-activates succinylcholine. (See Adverse reactions to thiotepa.)
Alkylating-like drugsCarboplatin, cisplatin, and oxaliplatin are heavy metal complex-es that contain platinum. Because their action resembles that of abifunctional alkylating drug, they are referred to as alkylating-likedrugs.
PharmacokineticsThe distribution and metabolism of carboplatin aren’t definedclearly. After I.V. administration, carboplatin is eliminated primari-ly by the kidneys. The elimination of carboplatin is biphasic. Ithas an initial half-life of 1 to 2 hours and a terminal half-life of21⁄2 to 6 hours. In patients with decreased renal function, the ter-minal half-life of carboplatin may last from 30 to 300 hours.Oxali-platin is 70% to 90% bound to plasma proteins, and the protein-binding increases over time. It’s widely distributed into most bodytissues and is eliminated in phases.
Into the lungs and peritoneumWhen administered intrapleurally (into the pleural space aroundthe lung) or intraperitoneally (into the peritoneum), cisplatin mayexhibit significant systemic absorption. Highly protein bound, cis-platin reaches high concentrations in the kidneys, liver, intestines,and testes but has poor central nervous system (CNS) penetra-tion. The drug undergoes some liver metabolism, followed by ex-cretion through the kidney.
Going platinumPlatinum is detectable in tissue for at least 4 months after admin-istration.
PharmacodynamicsLike alkylating drugs, carboplatin, cisplatin, and oxaliplatin arecell cycle–nonspecific and inhibit DNA synthesis. They act like
378ANTINEOPLASTIC DRUGS
Adversereactionsto thiotepa
The major adverse reac-tions to thiotepaare blood-related and in-clude leukopenia, ane-mia, thrombocytopenia,and pancytopenia (defi-ciency of all cellular ele-ments of the blood),which may be fatal.
Other adverse reac-tions include:• nausea and vomiting(commonly)• stomatitis and ulcera-tion of the intestinal mu-cosa (especially at bonemarrow transplantationdoses)• hives, rash, and pruri-tus (occasionally).
Warning!
938915.qxd 08/26/2008 17:12 Page 378

bifunctional alkylating drugs by cross-linking strands of DNA andinhibiting DNA synthesis.
PharmacotherapeuticsThese alkylating-like drugs are used in the treatment of severalcancers.• Carboplatin is used primarily to treat ovarian and lung cancer.• Cisplatin is prescribed to treat bladder and metastatic ovariancancer.• Cisplatin is the drug of choice to treat metastatic testicular can-cers.• Cisplatin may also be used to treat head, neck, and lung cancer(although these indications are clinically accepted, they’re cur-rently unlabeled uses).• Oxaliplatin is used in combination with other agents to treatcolorectal cancer.
Drug interactionsAlkylating-like drugs interact with a few other drugs:• When carboplatin, oxaliplatin, or cisplatin is administered withan aminoglycoside, the risk of toxicity to the kidney increases.• Carboplatin or cisplatin taken with bumetanide, ethacrynic acid,or furosemide increases the risk of ototoxicity (damaging the or-gans of hearing and balance).• Cisplatin may reduce serum phenytoin levels. (See Adverse re-actions to alkylating-like drugs.)
Antimetabolite drugsBecause antimetabolite drugs structurally resemble DNA basepairs, they can become involved in processes associated withDNA base pairs—that is, the synthesis of nucleic acids and pro-teins.
Getting specificAntimetabolites differ sufficiently from DNA base pairs in howthey interfere with this synthesis. Because the antimetabolites arecell cycle–specific and primarily affect cells that actively synthe-size DNA, they’re referred to as S phase–specific. Normal cellsthat are reproducing actively, as well as the cancer cells, are af-fected by the antimetabolites.
379ANTIMETABOLITE DRUGS
Adversereactions toalkylating-likedrugs
Alkylating-like drugsproduce many of thesame adverse reactionsas the alkylating drugs.• Carboplatin can pro-duce bone marrow sup-pression.• Kidney toxicity may oc-cur with cisplatin, usual-ly after multiple coursesof therapy. Carboplatin isless toxic to the kidneys.• Cisplatin producesmarked nausea andvomiting. With long-termcisplatin therapy, neuro-toxicity can occur. Neu-rotoxicity is less com-mon with carboplatin.• Tinnitus and hearingloss may occur with cis-platin and, less com-monly, with carboplatin.• Oxaliplatin may causeanaphylaxis, anemia, orincreased risk of bleed-ing or infection.
Warning!
938915.qxd 08/26/2008 17:12 Page 379

Each according to its metaboliteThese drugs are subclassified according to the metabolite affectedand include:• folic acid analogues• pyrimidine analogues• purine analogues.
Folic acid analoguesAlthough researchers have developed many folic acid analogues,the early compound methotrexate remains the most commonlyused.
PharmacokineticsMethotrexate is well absorbed and distributed throughout thebody. It can accumulate in any fluid collection, such as ascites orpleural or pericardial effusion, possibly resulting in prolongedelimination and higher than expected toxicity, especially myelo-suppression. At usual dosages, it doesn’t enter the CNS readily.
Metabolism and excretionAlthough methotrexate is metabolized partially, it’s excreted pri-marily unchanged in urine.
A disappearing actMethotrexate exhibits a three-part disappearance from plasma;the rapid distributive phase is followed by a second phase, whichreflects kidney clearance. The last phase, the terminal half-life, is3 to 10 hours for a low dose and 8 to 15 hours for a high dose.
PharmacodynamicsMethotrexate reversibly inhibits the action of the enzyme dihydro-folate reductase, thereby blocking normal folic acid processingand thus inhibiting DNA and RNA synthesis. The result is celldeath. Folinic acid is used in high-dose methotrexate therapy tohelp prevent cell death.
PharmacotherapeuticsMethotrexate is especially useful in treating:• acute lymphoblastic leukemia (abnormal growth of lympho-cyte precursors, the lymphoblasts), the most commonleukemia in children
380ANTINEOPLASTIC DRUGS
Methotrexate isespecially useful intreating the mostcommon childhood
leukemia.
938915.qxd 08/26/2008 17:12 Page 380

• acute lymphocytic leukemia (abnormal growth of lymphocytes);methotrexate may be given as treatment or prophylaxis formeningeal leukemia• CNS diseases (given intrathecally, or through the spinal cordinto the subarachnoid space)• choriocarcinoma (cancer that develops from the chorionic por-tions of the products of conception)• osteogenic sarcoma (bone cancer)• malignant lymphomas• cancers of the head, neck, bladder, testis, and breast.
Unconventional treatmentThe drug is also prescribed in low doses to treat such disorders assevere psoriasis, graft versus host disease, and rheumatoid arthri-tis that don’t respond to conventional therapy.
Drug interactionsMethotrexate interacts with several other drugs:• Probenecid decreases methotrexate excretion, increasing therisk of methotrexate toxicity, including fatigue, bone marrow sup-pression, and stomatitis (mouth inflammation).• Salicylates and nonsteroidal anti-inflammatory drugs, especiallydiclofenac, ketoprofen, indomethacin, and naproxen, also in-crease methotrexate toxicity.• Cholestyramine reduces absorption of methotrexate from theGI tract.• Concurrent use of alcohol and methotrexate increases the riskof liver toxicity.• Taking co-trimoxazole with methotrexate may produce bloodcell abnormalities.• Penicillin decreases renal tubular secretion of methotrexate, in-creasing the risk of methotrexate toxicity. (See Adverse reactionsto methotrexate.)
Pyrimidine analoguesPyrimidine analogues are a diverse group of drugs that inhibitproduction of pyrimidine nucleotides necessary for DNA synthe-sis. They include:• capecitabine• cytarabine• floxuridine• fluorouracil• gemcitabine.
381ANTIMETABOLITE DRUGS
Adversereactions tomethotrexate
Adverse reactions tomethotrexate include:• bone marrow suppres-sion• stomatitis• pulmonary toxicity, ex-hibited as pneumonitisor pulmonary fibrosis• skin reactions, such asphotosensitivity and hairloss.
Kidney concerns
With high doses, kidneytoxicity can also occurwith methotrexate use.During high-dose thera-py, leucovorin (folinicacid) may be used in atechnique known asleucovorin rescue tominimize adverse reac-tions.
The spine of the matter
Adverse reactions to in-trathecal administration(through the dura intothe subarachnoidspace) of methotrexatemay include seizures,paralysis, and death.Other less severe ad-verse reactions mayalso occur, includingheadaches, fever, neckstiffness, confusion, andirritability.
Warning!
938915.qxd 08/26/2008 17:12 Page 381

PharmacokineticsBecause pyrimidine analogues are poorly absorbed when they’regiven orally, they’re usually administered by other routes.
Distribution, metabolism, and excretionWith the exception of cytarabine, pyrimidine analogues are welldistributed throughout the body, including in cerebrospinal fluid(CSF). They’re metabolized extensively in the liver and are excret-ed in urine. Intrathecal cytarabine may be given with or withoutcranial radiation to treat CNS leukemia.
PharmacodynamicsPyrimidine analogues kill cancer cells by interfering with the nat-ural function of pyrimidine nucleotides. (See How pyrimidineanalogues work.)
PharmacotherapeuticsPyrimidine analogues may be used to treat many tumors. Howev-er, they’re primarily indicated in the treatment of:• acute leukemias• GI tract adenocarcinomas, such as colorectal, pancreatic,esophageal, and stomach adenocarcinomas
382ANTINEOPLASTIC DRUGS
To understand how pyrimidine analogueswork, it helps to consider the basic structure ofdeoxyribonucleic acid (DNA).
Climbing the ladder to understanding
DNA resembles a ladder that has been twist-ed. The rungs of the ladder consist of pairs ofnitrogenous bases: adenine always pairs withthymine, and guanine always pairs with cyto-sine. Cytosine and thymine are pyrimidines;adenine and guanine are purines.
One part sugar…
The basic unit of DNA is the nucleotide. A nu-cleotide is the building block of nucleic acids.It consists of a sugar, a nitrogen-containingbase, and a phosphate group. It’s on thesecomponents that pyrimidine analogues do theirwork.
In the guise of a nucleotide
After pyrimidine analogues are converted intonucleotides, they’re incorporated into DNA,where they may inhibit DNA and ribonucleicacid synthesis as well as other metabolic reac-tions necessary for proper cell growth.
Now I get it!
How pyrimidine analogues work
938915.qxd 08/26/2008 17:12 Page 382

• cancers of the breast and ovaries• malignant lymphomas.
Drug interactionsNo significant drug interactions occur with most of thepyrimidine analogues; however, several drug interactionsare possible with capecitabine.• Antacids, when given with capecitabine, may increaseabsorption of capecitabine.• Capecitabine can increase the pharmacodynamic ef-fects of warfarin, thereby increasing the risk of bleeding.• Capecitabine may increase serum phenytoin levels.(See Adverse reactions to pyrimidine analogues.)
Purine analoguesPurine analogues are incorporated into DNA and RNA, interfer-ing with nucleic acid synthesis and replication. They include:• fludarabine phosphate• cladribine• mercaptopurine• pentostatin• thioguanine.
383ANTIMETABOLITE DRUGS
Withpyrimidine
analogues, wemay all win!
Like most antineoplastic drugs, pyrimidine ana-logues can cause:• fatigue and lack of energy• inflammation of the mouth, esophagus, andthroat• bone marrow suppression• nausea and anorexia.
Cytarabine
• Severe cerebellar neurotoxicity• Chemical conjunctivitis
• Diarrhea• Fever• Hand-foot syndrome• Crab erythema (when high-dose cytarabineis combined with continuous infusions of fluo-rouracil)
Fluorouracil
• Diarrhea• Hair loss• Mucositis (when combined with folinic acid)
Warning!
Adverse reactions to pyrimidine analogues
938915.qxd 08/26/2008 17:12 Page 383

PharmacokineticsThe pharmacokinetics of purine analogues aren’t clearly defined.They’re largely metabolized in the liver and excreted in urine.
PharmacodynamicsAs with the other antimetabolites, fludarabine, mercaptopurine,and thioguanine first must be converted via phosphorylation (in-troduction to a phosphate) to the nucleotide level to be active.The resulting nucleotides are then incorporated into DNA, wherethey may inhibit DNA and RNA synthesis as well as other metabol-ic reactions necessary for proper cell growth. Cladribine respondsin a similar fashion.
Analogous to pyrimide analoguesThis conversion to nucleotides is the same process that pyrimi-dine analogues go through but, in this case, it’s purine nucleotidesthat are affected. Purine analogues are cell cycle–specific as well,exerting their effect during that same S phase.
Death to T cellsPentostatin inhibits adenosine deaminase (ADA), causing an in-crease in intracellular levels of deoxyadenosine triphosphate. Thisleads to cell damage and death. The greatest activity of ADA is incells of the lymphoid system, especially malignant T cells.
PharmacotherapeuticsPurine analogues are used to treat acute and chronic leukemiasand may be useful in the treatment of lymphomas.
Drug interactionsNo significant interactions occur with cladribine or thioguanine.
A serious flub with fludarabine• Taking fludarabine with pentostatin may cause severe pulmo-nary toxicity, which can be fatal.• Taking pentostatin with allopurinol may increase the risk ofrash.• Taking pentostatin with vidarabine may enhance the effect of vi-darabine and increase the risk of toxicity.
Down to the bone• Concomitant administration of mercaptopurine and allopurinolmay increase bone marrow suppression by decreasing mercapto-purine metabolism. (See Adverse reactions to purine analogues.)
384ANTINEOPLASTIC DRUGS
Adversereactionsto purineanalogues
Purine analogues cancause:• bone marrow suppres-sion• nausea and vomiting• anorexia• mild diarrhea• stomatitis• a rise in uric acidlevels.
High-dose horrors
Fludarabine, when usedat high doses, maycause severe neurologiceffects, including blind-ness, coma, and death.
Warning!
938915.qxd 08/26/2008 17:12 Page 384

Antibiotic antineoplastic drugsAntibiotic antineoplastic drugs are antimicrobial products thatproduce tumoricidal (tumor-destroying) effects by binding withDNA. These drugs inhibit the cellular processes of normal and ma-lignant cells. They include:• anthracyclines (daunorubicin, doxorubicin, idarubicin)• bleomycin• dactinomycin• mitomycin• mitoxantrone.
PharmacokineticsAntibiotic antineoplastic drugs are usually administered I.V.
Direct deliveriesSome drugs are also administered directly into the body cavity be-ing treated. Bleomycin, doxorubicin, and mitomycin are some-times given as topical bladder instillations, resulting in minimalsystemic absorption. When bleomycin is injected into the pleuralspace for malignant effusions, up to one-half of the dose is ab-sorbed systemically.
Distribution, metabolism, and excretionDistribution of antibiotic antineoplastic drugs throughout thebody varies; their metabolism and elimination also vary.
PharmacodynamicsWith the exception of mitomycin, antibiotic antineoplastic drugsintercalate, or insert themselves, between adjacent base pairs of aDNA molecule, physically separating them.
Taking the extra baseRemember, DNA looks like a twisted ladder with the rungs madeup of pairs of nitrogenous bases. These drugs insert themselvesbetween those nitrogenous bases. Then, when the DNA chainreplicates, an extra base is inserted opposite the intercalated an-tibiotic, resulting in a mutant DNA molecule. The overall effect iscell death.
Clean breakMitomycin is activated inside the cell to a bifunctional or even tri-functional alkylating drug. Mitomycin produces single-strand
385ANTIBIOTIC ANTINEOPLASTIC DRUGS
938915.qxd 08/26/2008 17:12 Page 385

breakage of DNA. It also cross-links DNA and inhibits DNA syn-thesis.
PharmacotherapeuticsAntibiotic antineoplastic drugs act against many cancers, includ-ing:• acute leukemia• breast, ovarian, bladder, and lung cancer• cancers of the GI tract• choriocarcinoma• Ewing’s sarcoma (a malignant tumor that originates in bonemarrow, typically in long bones or the pelvis) and other soft-tissuesarcomas• Hodgkin’s disease and malignant lymphomas• melanoma• osteogenic sarcoma and rhabdomyosarcoma (malignant neo-plasm composed of striated muscle cells)• squamous cell carcinoma of the head, neck, and cervix• testicular cancer• Wilms’ tumor (a malignant neoplasm of the kidney, occurring inyoung children).
Drug interactionsAntibiotic antineoplastic drugs interact with many other drugs.(See Adverse reactions to antibiotic antineoplastic drugs.)• Concurrent therapy with fludarabine and idarubicin isn’t recom-mended because of the risk of fatal lung toxicity.• Bleomycin may decrease serum digoxin and serum phenytoinlevels.• Doxorubicin may reduce serum digoxin levels.• Combination chemotherapies enhance leukopenia and thrombo-cytopenia (reduced number of platelets).• Mitomycin plus vinca alkaloids may cause acute respiratory dis-tress.
Hormonal antineoplastic drugsand hormone modulators
Hormonal antineoplastic drugs and hormone modulators areprescribed to alter the growth of malignant neoplasms or to man-age and treat their physiologic effects.
386ANTINEOPLASTIC DRUGS
Adversereactionsto antibioticantineoplasticdrugs
The primary adverse re-action to antibiotic anti-neoplastic drugs is bonemarrow suppression. Ir-reversible cardiomyopa-thy and acute electro-cardiogram changescan also occur as wellas nausea and vomiting.
Extra steps
An antihistamine and anantipyretic should begiven before bleomycinto prevent fever andchills. Anaphylactic re-actions can occur in pa-tients receiving bleo-mycin for lymphoma, sotest doses should be giv-en first.
Seeing colors
Doxorubicin may colorurine red; mitoxantronemay color it blue-green.
Warning!
938915.qxd 08/26/2008 17:12 Page 386

Hitting them where it hurtsHormonal therapies and hormone modulators prove effectiveagainst hormone-dependent tumors, such as cancers of the pros-tate, breast, and endometrium. Lymphomas and leukemias areusually treated with therapies that include corticosteroids be-cause of their potential for affecting lymphocytes.
Aromatase inhibitorsIn postmenopausal women, estrogen is produced througharomatase, an enzyme that converts hormone precursorsinto estrogen. Aromatase inhibitors prevent androgenfrom being converted into estrogen in postmenopausalwomen, thereby blocking estrogen’s ability to activate can-cer cells; limiting the amount of estrogen means that lessestrogen is available to reach cancer cells and make themgrow.
Two typesThere are two types of aromatase inhibitors. Type 1, or steroidal,inhibitors include exemestane; type 2, or nonsteroidal, inhibitorsinclude anastrozole and letrozole.
PharmacokineticsAromatase inhibitors are taken orally (in pill form) and are usuallywell tolerated. Steady-state plasma levels after daily doses arereached in 2 to 6 weeks. Inactive metabolites are excreted inurine.
PharmacodynamicsAromatase inhibitors work by lowering the body’s production ofestrogen. In about one-half of all patients with breast cancer, thetumors depend on estrogen to grow. Aromatase inhibitors areused only in postmenopausal women because they lower theamount of estrogen that’s produced outside the ovaries, such as inmuscle and fat tissue. Because these drugs induce estrogen depri-vation, bone thinning and osteoporosis may develop over time.
To reverse or not to reverse: That is the questionType 1 inhibitors, such as exemestane, irreversibly inhibit the aro-matase enzyme, whereas type 2 inhibitors, such as anastrozole, re-versibly inhibit it. Type 1 aromatase inhibitors may still be effec-tive after a type 2 aromatase inhibitor has failed.
387HORMONAL ANTINEOPLASTIC DRUGS AND HORMONE MODULATORS
In postmenopausalwomen, estrogen isproduced through
aromatase.
Memoryjogger
Remember:Hormonal-
dependent (genderspecific) tumors aretreated with hormon-al therapies; tumorscommon to both gen-ders are treated withcorticosteroids.
938915.qxd 08/26/2008 17:12 Page 387

Competitive advantageAnastrozale and letrozole work by competitively binding to hemeof the cytochrome P450 subunit of aromatase, leading to de-creased levels of estrogen in all tissues; they don’t affect synthesisof adrenocorticosteroids, aldosterone, or thyroid hormones.
PharmacotherapeuticsAromatase inhibitors are primarily used to treat postmenopausalwomen with metastatic breast cancer. They may be administeredalone or with other agents such as tamoxifen.
Drug interactionsCertain drugs may decrease the effectiveness of anastrozole, in-cluding tamoxifen and estrogen-containing drugs. (See Adversereactions to aromatase inhibitors.)
AntiestrogensAntiestrogens bind to estrogen receptors and block estrogen ac-tion. The antiestrogens include tamoxifen citrate, toremifene cit-rate, and fulvestrant. Tamoxifen and toremifene are nonsteroidalestrogen agonist-antagonists, and fulvestrant is a pure estrogenantagonist.
PharmacokineticsAfter oral administration, tamoxifen is well absorbed and under-goes extensive metabolism in the liver before being excreted instool. Serum levels of fulvestrant, when given I.M., peak in 7 to 9days. Its half-life is 40 days. Toremifene is well absorbed, and ab-sorption isn’t influencd by food.
PharmacodynamicsThe exact antineoplastic action of these agents isn’t known. How-ever, they’re known to act as estrogen antagonists. Estrogen re-ceptors, found in the cancer cells of one-half of premenopausaland three-fourths of postmenopausal women with breast cancer,respond to estrogen to induce tumor growth.
It’s bound to inhibit growthThe antiestrogens fulvestrant, tamoxifen, and toremifene bind tothe estrogen receptors and inhibit estrogen-mediated tumorgrowth in breast tissue. Tamoxifen may be able to do this becauseit binds to receptors at the nuclear level or because the binding re-
388ANTINEOPLASTIC DRUGS
Aromataseinhibitors help treatmetastatic breastcancer that occursafter menopause.
Adversereactions toaromataseinhibitors
Adverse reactions toaromatase inhibitors arerare. They may includedizziness, mild nausea,mild muscle and jointaches, and hot flashes.
Occasionally, aro-matase inhibitors canalso affect cholesterollevels; anastrazolemay elevate both high-density and low-densitylipoprotein levels.
Warning!
938915.qxd 08/26/2008 17:12 Page 388

duces the number of free receptors in the cytoplasm. Ul-timately, DNA synthesis and cell growth are inhibited.
PharmacotherapeuticsTamoxifen is used alone and as adjuvant treatment with radi-ation therapy and surgery in women with negative axillarylymph nodes and in postmenopausal women with positiveaxillary nodes. It’s used for advanced breast cancer involv-ing estrogen receptor–positive tumors in postmenopausalwomen and may be used in palliative treatment of advancedor metastatic breast cancer that’s estrogen receptor–positive.Tumors in postmenopausal women are more responsive totamoxifen than those in premenopausal women. Tamoxifen
389HORMONAL ANTINEOPLASTIC DRUGS AND HORMONE MODULATORS
The current indication for the use of tamoxifen is based on the1998 results of the “Breast Cancer Prevention Trial,” sponsoredby the National Cancer Institute. Results indicated that tamox-ifen reduced the rate of breast cancer in healthy high-riskwomen by one-half. However, tamoxifen has serious adverseeffects that include potentially fatal blood clots and uterinecancer. The question is whether these risks are worth the ben-efits in healthy women.
The National Cancer Institute’s report
To help answer this question, the National Cancer Institutepublished a report in November of 1999. They concluded thatmost women older than age 60 would receive more harm thanbenefit from tamoxifen. Even though women younger than age60 could benefit from taking tamoxifen, they were still at riskunless they had a hysterectomy, which eliminated the risk ofuterine cancer or were in the very high-risk group for develop-ing breast cancer.
Breaking it down further
The report also concluded that the risks of tamoxifen weregreater than the benefits for black women older than age 60and almost all other women older than age 60 who still had a
uterus. But for older women without a uterus and with a 3.5%chance of developing breast cancer over the next 5 years, thebenefits may outweigh the risks.
NSABP studies update
A report from the 2000 annual meeting of the American Societyof Clinical Oncology, presented an analysis of data gatheredfrom the National Surgical Adjuvant Breast and Bowel Project’s(NSABP’s) nine studies of adjuvant tamoxifen for breast cancer.The data analysis indicates that tamoxifen is as effective inBlack women as in White women in reducing the occurrenceof contralateral breast cancer (breast cancer that develops inthe healthy breast after treatment in the opposite breast).
Future findings
The Study of Tamoxifen and Raloxifene (STAR), is a clinical trialthat was conducted to determine whether raloxifene can pre-vent breast cancer better and with fewer adverse effects thantamoxifen. The study began in 1999 and recently concluded.The results showed that the raloxifem-treated group had a low-er incidence of uterine cancer and clotting events than the ta-moxifen group.
Yea or nay?
Who benefits from tamoxifen?
I can see that the fates ofsome tumors are linked with the
hormones they depend on. Ipredict hormonal therapies will
put them in grave danger.
938915.qxd 08/26/2008 17:12 Page 389

may also be used to reduce the incidence of breast cancer inwomen at high risk.
Toremifene is used to treat metastatic breast cancer in post-menopausal women with estrogen receptor–positive tumors.
Fulvestrant is used in postmenopausal women with receptor-positive metastatic breast cancer with disease progression aftertreatment with tamoxifen. (See Who benefits from tamoxifen?page 389.)
Drug interactionsThere are no known drug interactions for fulvestrant. However,these reactions may occur with other antiestrogens:• Tamoxifen and toremifene increase the effects of warfarin, in-creasing the risk of bleeding.• Bromocriptine increases the effects of tamoxifen.• Drugs that induce certain liver enzymes, such as phenytoin, ri-fampin, and carbamazepine, may increase tamoxifen metabolism,causing decreased serum levels. (See Adverse reactions to anti-estrogens.)
AndrogensThe therapeutically useful androgens are synthetic derivatives ofnaturally occurring testosterone. They include:• fluoxymesterone• testolactone• testosterone enanthate• testosterone propionate.
PharmacokineticsThe pharmacokinetic properties of therapeutic androgens resem-ble those of naturally occurring testosterone.
AbsorptionThe oral androgens—fluoxymesterone and testolactone—are wellabsorbed. The parenteral ones—testosterone enanthate andtestosterone propionate—are designed specifically for slow ab-sorption after I.M. injection.
Distribution, metabolism, and excretionAndrogens are well distributed throughout the body, metabolizedextensively in the liver, and excreted in urine.
390ANTINEOPLASTIC DRUGS
Adversereactions toantiestrogens
The most common ad-verse reactions to anti-estrogens, such astamoxifen, toremifene,and fulvestrant, include:• hot flashes• nausea• vomiting.
Tamoxifen
• Diarrhea• Fluid retention• Vaginal bleeding
Toremifene
• Vaginal discharge orbleeding• Edema
Fulvestrant
• Diarrhea• Constipation• Abdominal pain• Headache• Backache• Pharyngitis
Warning!
938915.qxd 08/26/2008 17:12 Page 390

Checking the suspensionThe duration of the parenteral forms is longer because the oil sus-pension is absorbed slowly. Parenteral androgens are adminis-tered one to three times per week.
PharmacodynamicsAndrogens probably act by one or more mechanisms. They mayreduce the number of prolactin receptors or may bind competi-tively to those that are available.
Keeping its sister hormone in checkAndrogens may inhibit estrogen synthesis or competitively bindat estrogen receptors. These actions prevent estrogen from affect-ing estrogen-sensitive tumors.
PharmacotherapeuticsAndrogens are indicated for the palliative treatment of advancedbreast cancer, particularly in postmenopausal women with bonemetastasis.
Drug interactionsAndrogens may alter dose requirement in patients receiving in-sulin, oral antidiabetic drugs, or oral anticoagulants. Taking themwith drugs that are toxic to the liver increases the risk of liver tox-icity. (See Adverse reactions to androgens.)
AntiandrogensAntiandrogens are used as an adjunct therapy with gonadotropin-releasing hormone analogues in treating advanced prostate can-cer. These drugs include:• flutamide• nilutamide• bicalutamide.
PharmacokineticsAfter oral administration, antiandrogens are absorbed rapidly andcompletely.
Metabolism and excretionAntiandrogens are metabolized rapidly and extensively and ex-creted primarily in urine.
391HORMONAL ANTINEOPLASTIC DRUGS AND HORMONE MODULATORS
Adversereactions toandrogens
Nausea and vomitingare the most commonadverse reactions to an-drogens. Fluid retentioncaused by sodium reten-tion may also occur.
Just for women
Women may develop:• acne• clitoral hypertrophy• deeper voice• increased facial andbody hair• increased sexualdesire• menstrual irregularity.
Just for men
Men may experiencethese effects as a resultof conversion of steroidsto female sex hormonemetabolites:• gynecomastia• prostatic hyperplasia• testicular atrophy.
Just for kids
Children may develop:• premature epiphysealclosure• secondary sex charac-teristic developments(especially in boys).
Warning!
938915.qxd 08/26/2008 17:12 Page 391

PharmacodynamicsFlutamide, nilutamide, and bicalutamide exert theirantiandrogenic action by inhibiting androgen up-take or preventing androgen binding in cell nucleiin target tissues.
PharmacotherapeuticsAntiandrogens are used with a gonadotropin-releasing hor-mone analogue, such as leuprolide, to treat metastaticprostate cancer.
Special feature: no flareupConcomitant administration of antiandrogens and a gonadotropin-releasing hormone analogue may help prevent the disease flarethat occurs when the gonadotropin-releasing hormone analogue isused alone.
Drug interactionsAntiandrogens don’t interact significantly with other drugs. How-ever, flutamide and bicalutamide may affect prothrombin time (atest to measure clotting factors) in a patient receiving warfarin.(See Adverse reactions to antiandrogens.)
ProgestinsProgestins are hormones used to treat various forms of cancer.These drugs include:• hydroxyprogesterone caproate• medroxyprogesterone acetate• megestrol acetate.
PharmacokineticsWhen taken orally, megestrol acetate is well absorbed. After I.M.injection in an aqueous or oil suspension, hydroxyprogesteronecaproate and medroxyprogesterone are absorbed slowly fromtheir deposit sites.
Distribution, metabolism, and excretionThese drugs are well distributed throughout the body and may se-quester in fatty tissue. Progestins are metabolized in the liver andexcreted as metabolites in urine.
392ANTINEOPLASTIC DRUGS
Antiandrogenshelp treat
metastaticprostatecancer.
Adversereactions toantiandrogens
When antiandro-gens are used withgonadotropin-releasinghormone analogues, themost common adversereactions are:• hot flashes• decreased sexualdesire• impotence• diarrhea• nausea• vomiting• breast enlargement.
Warning!
938915.qxd 08/26/2008 17:12 Page 392

PharmacodynamicsThe mechanism of action of progestins in treating tumors isn’tcompletely understood. Researchers believe the drugs bind to aspecific receptor to act on hormonally sensitive cells.
They aren’t exhibitionistsBecause progestins don’t exhibit a cytotoxic activity (destroyingor poisoning cells), they’re considered cytostatic (they keep thecells from multiplying).
PharmacotherapeuticsProgestins are used for the palliative treatment of advanced en-dometrial, breast, prostate, and renal cancers. Of these drugs,megestrol is used most commonly.
Drug interactionsNo drug interactions have been identified for megestrol. However,other progestins do have significant interactions with other drugs.• Barbiturates, carbamazepine, and rifampin reduce the progestineffects of hydroxyprogesterone.• Hydroxyprogesterone and medroxyprogesterone may interferewith bromocriptine’s effects, causing menstruation to stop.• Hydroxyprogesterone taken with dantrolene and other liver-toxic drugs increases the risk of liver toxicity.• Dose adjustments in oral anticoagulants may be needed whenthey’re taken with hydroxyprogesterone.• Aminoglutethimide and rifampin may reduce the progestin ef-fects of medroxyprogesterone. (See Adverse reactions to pro-gestins.)
Gonadotropin-releasing hormone analoguesGonadotropin-releasing hormone analogues are used for treat-ment of advanced prostate cancer. They include:• goserelin• leuprolide• triptorelin.
PharmacokineticsGoserelin is absorbed slowly for the first 8 days of therapy andrapidly and continuously thereafter. After subcutaneous injection,leuprolide is well absorbed. Neither drug’s distribution, metabo-lism, or excretion is defined clearly.
393HORMONAL ANTINEOPLASTIC DRUGS AND HORMONE MODULATORS
Adversereactions toprogestins
Mild fluid retention isprobably the most com-mon reaction to prog-estins. Other adverse re-actions include:• thromboemboli• breakthrough bleed-ing, spotting, andchanges in menstrualflow• breast tenderness• liver function abnor-malities.
Oil issues
Patients who are hyper-sensitive to the oil carri-er used for injection(usually sesame or cas-tor oil) may experience alocal or systemic hyper-sensitivity reaction.
Warning!
938915.qxd 08/26/2008 17:12 Page 393

Triptorelin serum levels peak within 1 week ofI.M. injection; the drug remains detectable in serumfor 4 weeks.
PharmacodynamicsGoserelin and leuprolide act on the male’s pituitarygland to increase luteinizing hormone (LH) secre-tion, which stimulates testosterone production. Thepeak testosterone level is reached about 72 hoursafter daily administration.
Running the reverseWith long-term administration, however, goserelin and leuprolideinhibit LH release from the pituitary and subsequently inhibit tes-ticular release of testosterone. Because prostate tumor cells arestimulated by testosterone, the reduced testosterone level inhibitstumor growth.
Then there’s triptorelinTriptorelin is a potent inhibitor of gonadotropin secretion. Afterthe first dose, levels of LH, follicle-stimulating hormone (FSH),testosterone, and estradiol surge transiently. After long-term con-tinuous administration, LH and FSH secretion steadily declinesand testicular and ovarian steroid production decreases. In men,testosterone declines to a level typically seen in surgically castrat-ed men. As a result, tissues and functions that depend on thesehormones become inactive.
394ANTINEOPLASTIC DRUGS
Goserelin andleuprolide reducethe testosterone
level, which canhelp inhibit tumor
growth.
Hot flashes, impotence, and decreased sexualdesire are commonly reported reactions togonadotropin-releasing hormone analogues.Other adverse reactions include:• peripheral edema• nausea and vomiting• constipation• anorexia.
Flares and flashes
Disease symptoms and pain may worsen orflare during the first 2 weeks of goserelin orleuprolide therapy. The flare can be fatal in pa-tients with bony vertebral metastasis.
Triptorelin may cause hot flashes andskeletal pain. Less commonly, it may cause hy-pertension, diarrhea, vomiting, urine retention,and impotence.
Warning!
Adverse reactions to gonadotropin-releasinghormone analogues
938915.qxd 08/26/2008 17:12 Page 394

PharmacotherapeuticsGoserelin, leuprolide, and triptorelin are used for the palliativetreatment of metastatic prostate cancer. The drugs lower thetestosterone level without the adverse psychological effects ofcastration or the adverse cardiovascular effects of diethylstilbe-strol.
Drug interactionsNo drug interactions have been identified with goserelin, leupro-lide, or triptorelin. (See Adverse reactions to gonadotropin-releasing hormone analogues.)
Natural antineoplastic drugsA subclass of antineoplastic drugs known as natural products in-cludes:• vinca alkaloids• podophyllotoxins.
Vinca alkaloidsVinca alkaloids are nitrogenous bases derived from the periwin-kle plant. These drugs are cell cycle–specific for the M phase andinclude:• vinblastine• vincristine• vinorelbine.
PharmacokineticsAfter I.V. administration, the vinca alkaloids are well distributedthroughout the body.
Metabolism and excretionVinca alkaloids undergo moderate liver metabolism before beingeliminated through different phases, primarily in stool with asmall percentage eliminated in urine.
PharmacodynamicsVinca alkaloids may disrupt the normal function of the microtu-bules (structures within cells that are associated with the move-ment of DNA) by binding to the protein tubulin in the microtu-bules.
395NATURAL ANTINEOPLASTIC DRUGS
The vinca alkaloidsare cell cycle–specific.
They do their workduring the M phase,which is the phase of
mitosis, or celldivision.
938915.qxd 08/26/2008 17:12 Page 395

Separation anxietyWith the microtubules unable to separate chromosomes properly,the chromosomes are dispersed throughout the cytoplasm orarranged in unusual groupings. As a result, formation of the mitot-ic spindle is prevented, and the cells can’t complete mitosis (celldivision).
Under arrestCell division is arrested in metaphase, causing cell death. There-fore, vinca alkaloids are cell cycle–specific for the M phase. Inter-ruption of the microtubule function may also impair some types ofcellular movement, phagocytosis (engulfing and destroying micro-organisms and cellular debris), and CNS functions.
PharmacotherapeuticsVinca alkaloids are used in several therapeutic situations:• Vinblastine is used to treat metastatic testicular cancer, lym-phomas, Kaposi’s sarcoma (the most common acquired immuno-deficiency syndrome [AIDS]–related cancer), neuroblastoma (ahighly malignant tumor originating in the sympathetic nervoussystem), breast cancer, and choriocarcinoma.• Vincristine is used in combination therapy to treat Hodgkin’sdisease, non-Hodgkin’s lymphoma, Wilms’ tumor, rhabdomyosar-coma, and acute lymphocytic leukemia.• Vinorelbine is used to treat non–small-cell lung cancer. Itmay also be used in the treatment of metastatic breast cancer,cisplatin-resistant ovarian cancer, and Hodgkin’s disease.
Drug interactionsVinca alkaloids can interact with other drugs.• Erythromycin may increase the toxicity of vinblastine.• Vinblastine decreases the plasma levels of phenytoin.• Vincristine reduces the effects of digoxin.• Asparaginase decreases liver metabolism of vincristine, increas-ing the risk of toxicity.• Calcium channel blockers enhance vincristine accumulation, in-creasing the tendency for toxicity. (See Adverse reactions to vin-ca alkaloids.)
PodophyllotoxinsPodophyllotoxins are semisynthetic glycosides that are cell cycle–specific and act during the G2 and late S phases of the cell cycle.They include:
396ANTINEOPLASTIC DRUGS
Adversereactions tovinca alkaloids
Nausea, vomiting, consti-pation, and stomatitismay occur in patientstaking vinca alkaloids.Tissue necrosis may alsooccur with extravasation.
Toxic topics
Vinblastine and vinorel-bine toxicities occur pri-marily as bone marrowsuppression.
Muscle matters
Neuromuscular abnor-malities commonly occurwith vincristine andvinorelbine and, occa-sionally, with vinblastinetherapy.
Tumor trouble
Vinblastine may producetumor pain described asan intense stinging orburning in the tumor bed,with an abrupt onset 1 to3 minutes after drug ad-ministration. The painusually lasts 20 minutesto 3 hours.
Less hair there
Reversible alopecia oc-curs in up to one-half ofpatients receiving vincaalkaloids; it’s more likelyto occur with vincristinethan with vinblastine.
Warning!
938915.qxd 08/26/2008 17:12 Page 396

• etoposide• teniposide.
Outside activitiesEtoposide is effective in the treatment of testicular cancer, non-Hodgkin’s lymphoma, lung cancer, and acute leukemia. Teniposidehas demonstrated some activity in treating Hodgkin’s disease, lym-phomas, and brain tumors.
PharmacokineticsWhen taken orally, podophyllotoxins are only moderately ab-sorbed. Although the drugs are widely distributed throughout thebody, they achieve poor CSF levels.
Metabolism and excretionPodophyllotoxins undergo liver metabolism and are excreted pri-marily in urine.
PharmacodynamicsAlthough their mechanism of action isn’t completely understood,podophyllotoxins produce several biochemical changes in tumorcells.
Arresting developmentAt low concentrations, these drugs block cells at the late S orG2 phase. At higher concentrations, they arrest the cells inthe G2 phase.
Breaking a rung on the ladderPodophyllotoxins can also break one of the strands of the DNAmolecule and can inhibit nucleotide transport and incorporationinto nucleic acids.
PharmacotherapeuticsEtoposide is used to treat testicular cancer lymphomas, prostatecancer, and small-cell lung cancer. Teniposide is used to treatacute lymphoblastic leukemia.
Drug interactionsPodophyllotoxins have few significant interactions with otherdrugs.• Etoposide may increase the risk of bleeding in a patient takingwarfarin.• Teniposide may increase the clearance and intracellular levelsof methotrexate. (See Adverse reactions to podophyllotoxins.)
397NATURAL ANTINEOPLASTIC DRUGS
I may have areason tocelebrate!
Teniposide showssome activity intreating brain
tumors!
Adversereactions topodophyllo-toxins
The majority of patientsreceiving podophyllotox-ins experience hair loss.Other adverse reactionsinclude:• nausea and vomiting• anorexia• stomatitis• bone marrow suppres-sion, causing leukopeniaand, less commonly,thrombocytopenia• acute hypotension (if apodophyllotoxin is in-fused too rapidly I.V.).
Warning!
938915.qxd 08/26/2008 17:12 Page 397

Monoclonal antibodiesRecombinant DNA technology has allowed for the development ofmonoclonal antibodies directed at such targets as other immunecells or cancer cells. Monoclonal antibodies include:• alemtuzumab• gemtuzumab ozogamicin• ibritumomab tiuxetan• rituximab• trastuzumab.
PharmacokineticsBecause of their large protein molecule structure, monoclonal an-tibodies aren’t absorbed orally. They may have a limited distribu-tion as well as a long half-life, sometimes measured in weeks.
PharmacodynamicsMonoclonal antibodies bind to target receptors or cancer cells andcause tumor death via several mechanisms: They may induce pro-grammed cell death; they may recruit other elements of the im-mune system to attack the cancer cell; or they may deliver a doseof a toxic chemotherapy drug (gemtuzumab) or radiation (ibritu-momab) to the tumor site.
PharmacotherapeuticsMonoclonal antibodies have demonstrated activity in both solidtumors and hematologic malignancies, such as:• non-Hodgkin’s lymphoma—rituximab and ibritumomab (targetCD20 or malignant B lymphocytes)• chronic lymphocytic leukemia—alemtuzumab (target CD52antigen or B cells)• acute myeloid leukemia—gemtuzumab (target CD33 antigen inmyeloid leukemic cells)• breast cancer—trastuzumab (target HER-2 protein in breastcancer cells).
Drug interactionsAlthough no interactions have been noted with alemtuzumab, mul-tiple drug interactions are associated with other monoclonal anti-bodies.
398ANTINEOPLASTIC DRUGS
These drugssometimes work by
recruiting the immunesystem to attack a
cancer cell.
938915.qxd 08/26/2008 17:12 Page 398

• Ibritumomab may interfere with the actions of such drugs aswarfarin, aspirin, clopidogrel, ticlopidine, nonsteroidal anti-inflammatory drugs, azathioprine, cyclosporine, and corticoste-roids.• Trastuzumab increases the cardiac toxicity associated with an-thracycline administration. (See Adverse reactions to monoclonalantibodies.)
Topoisomerase I inhibitorsTopoisomerase I inhibitors are derivatives of camptothecin andinhibit the enzyme topoisomerase I. These agents are derived froma naturally occurring alkaloid from the Chinese tree Camptothecaacuminata. Currently available topoisomerase I inhibitors in-clude:• irinotecan• topotecan.
PharmacokineticsBoth irinotecan and topotecan are minimally absorbed andmust be given I.V. Irinotecan undergoes metabolic changes to be-come the active metabolite SN-38. The half-life of SN-38 is about10 hours; SN-38 is eliminated through biliary excretion. Topotecanis metabolized by the liver, although renal excretion is a signifi-cant path for elimination.
PharmacodynamicsTopoisomerase I inhibitors exert their cytotoxic effect by inhibit-ing topoisomerase I enzyme, an essential enzyme that mediatesthe relaxation of supercoiled DNA.
It’s all about that DNATopoisomerase inhibitors bind to the DNA topoisomerase I com-plex and prevent resealing, thereby causing DNA strand breaks.This results in impaired DNA synthesis.
PharmacotherapeuticsTopoisomerase I inhibitors act against both solid tumors andhematologic malignancies:• Irinotecan is used to treat colorectal cancer and small-cell lungcancer.
399TOPOISOMERASE I INHIBITORS
Adversereactions tomonoclonalantibodies
All monoclonal antibod-ies are associated withinfusion-related reac-tions that have occa-sionally been fatal.These include fever,chills, shortness ofbreath, low blood pres-sure, and anaphylaxis.
In addition, the fol-lowing adverse reac-tions can occur:• Alemtuzumab is asso-ciated with myelosup-pression and an in-creased risk of oppor-tunistic infections, suchas pneumocystitis,pneumonia, and fungaland viral infections.• Gemtuzumab ozogam-icin is associated withsignificant myelosup-pression and liver tox-icity.• Ibritumomab tiuxetanis associated with in-creased myelosuppres-sion to rituximab.
Warning!
938915.qxd 08/26/2008 17:12 Page 399

• Topotecan is used to treat ovarian cancer, small-cell lung can-cer, and acute myeloid leukemia.
Drug interactionsTopoisomerase I inhibitors, particularly irinotecan, can interactwith other drugs.• Ketoconazole significantly increases SN-38 serum levels, there-by increasing the risk of irinotecan-associated toxicities.• Irinotecan when taken with diuretics may exacerbate dehydra-tion caused by irinotecan-induced diarrhea.• Laxatives taken with irinotecan can induce diarrhea.• Prochlorperazine administered with irinotecan can increase theincidence of extrapyramidal toxicities. (See Adverse reactions totopoisomerase I inhibitors.)
Targeted therapiesA groundbreaking approach to anticancer therapies involves tar-geting proteins associated with the growth patterns of specifictypes of cancer. Drugs used for this new approach to cancer treat-ment include:• bortezomib• gefitinib• imatinib.
PharmacokineticsBortezomib isn’t absorbed orally and must be given I.V. It’s exten-sively distributed into body tissues and metabolized by the liver.
Gefitinib is available in an oral form, and about half of thedose is absorbed. The drug is widely distributed in tissues. It un-dergoes hepatic metabolism with minimal urinary excretion.
Imatinib is also available in an oral form and is almost com-pletely absorbed. It’s 95% bound to plasma proteins and is exten-sively metabolized by the liver. The half-life of imatinib is about15 hours.
PharmacodynamicsBortezomib inhibits proteosomes, which are involved in integralcell-cycle function and promote tumor growth. Proteolysis bybortezomib results in disruption of the normal homeostatic mech-anisms and leads to cell death.
400ANTINEOPLASTIC DRUGS
Adversereactions totopoisomerase Iinhibitors
Common reactions
The more common ad-verse reactions to topo-isomerase I inhibitors,particularly irinotecan,include:• diarrhea (possiblysevere)• abdominal cramps• hair loss or thinning• increased sweatingand production of saliva• nausea, vomiting, andloss of appetite• tiredness• watery eyes.
Additional reactions
Occasionally, these re-actions may occur:• mouth sores andulcers• muscle cramps• rashes, which may beitchy• significant myelosup-pression, especially withtopotecan (rare)• temporary effects onliver function test re-sults.
Warning!
938915.qxd 08/26/2008 17:13 Page 400

Too much of this…Gefitinib inhibits the epidermal growth factor receptor-1 tyrosinekinase, which is overexpressed in such cancers as non–small-celllung cancer. This inhibition blocks signaling pathways for growth,survival, and metastasis of cancer.
…too many of thoseIn patients with chronic myeloid leukemia, the BCR-ABL proteinstimulates other tyrosine kinase proteins, causing an abnormallyhigh production of WBCs. Imatinib binds to the adenosine triphos-phate–binding domain of the BCR-ABL protein, effectively shut-ting down the abnormal WBC production.
PharmacotherapeuticsBortezomib is used to treat multiple myeloma that has relapsed af-ter standard chemotherapy.
Gefitinib is used as a single agent for patients with non–small-cell lung cancer that hasn’t responded to two standard chemother-apy regimens.
Imatinib is used to treat chronic myeloid leukemia, acute lym-phoid leukemia, and GI stomal tumors.
Drug interactionsBortezomib, gefitinib, and imatinib have been associated withsome drug interactions.• Bortezomib when taken with drugs that inhibit cytochromeCYP3A4 (such as amiodarone, cimetidine, erythromycin, dilti-azem, fluoxetine, verapamil, zafirlukast, and zileuton) or inducecytochrome CYP3A4 (such as amiodarone, carbamazepine, nevir-apine, phenobarbital, phenytoin, and rifampin), could cause eithertoxicities or reduced efficacy of these drugs.• Bortezomib when taken with oral hypoglycemics could causehypoglycemia and hyperglycemia in patients with diabetes.• Plasma levels of gefitinib and imatinib are reduced, sometimessubstantially, when these drugs are given with carbamazepine,dexamethasone, phenobarbital, phenytoin, rifampin, or St. John’swort.• High doses of ranitidine with sodium bicarbonate when takenwith gefitinib reduce gefitinib levels.• Administration of gefitinib or imatinib with warfarin causes ele-vations in the International Normalized Ratio, increasing the riskof bleeding.• Clarithromycin, erythromycin, itraconazole, and ketoconazole,when taken with imatinibor may increase imatinib plasma levels.
401TARGETED THERAPIES
A new approach totreating cancer
involves targeting theproteins that causethe growth of certain
cancer types.
938915.qxd 08/26/2008 17:13 Page 401

• Carbamazepine, dexamethasone, phenobarbital, phenytoin, orrifampin given with imatinib may increase metabolism of imatiniband decrease imatinib level.• Imatinib given with simvastatin increases simvastatin levelsabout threefold.• Imatinib increases plasma levels of other CYP3A4-metabolizeddrugs, such as triazolo-benzodiazepines, calcium channel block-ers, and certain HMG-CoA reductase inhibitors. (See Adverse re-actions to targeted therapies.)
Unclassifiable antineoplastic drugsMany other antineoplastic drugs can’t be included in existing clas-sifications. These drugs include:• arsenic trioxide• asparaginases• procarbazine• hydroxyurea• interferon• aldesleukin• altretamine• paclitaxel (taxane)• docetaxel (taxane).
402ANTINEOPLASTIC DRUGS
Patients should avoid becoming pregnant while taking borte-zomib, gefitinib, or imatinib because in animal studies thesedrugs crossed the placental barrier, causing fetal harm anddeath.
There are also adverse reactions specific to each therapy.
Bortezomib
• Fatigue, malaise, weakness, nausea, diarrhea, appetite loss,constipation, pyrexia, and vomiting (most common reactions)• Peripheral neuropathy, headache, low blood pressure, livertoxicity, thrombocytopenia, renal toxicity, and cardiac toxicity,such as arrhythmias, heart failure, myocardial ischemia and in-
farction, pulmonary edema, and pericardial effusion (less com-mon reactions)
Gefitinib
• Rash, diarrhea, and abnormal eyelash growth• Lung and liver damage
Imatinib
• Periorbital and lower limb edema, possibly resulting in pul-monary edema, effusions, and heart or renal failure• Nausea, vomiting, liver function abnormalities, and myelosup-pression (especially neutropenia and thrombocytopenia)
Warning!
Adverse reactions to targeted therapies
938915.qxd 08/26/2008 17:13 Page 402

Arsenic trioxideArsenic trioxide is a commercially available treatment for pa-tients with acute promyelocytic leukemia (a rare form of acutemyeloid leukemia). It’s indicated when standard therapy hasfailed.
PharmacokineticsArsenic trioxide is administered I.V. because it’s inadequately ab-sorbed orally. The metabolism of arsenic trioxide involves reduc-tion via arsenate reductase, with subsequent methylation to inac-tive metabolites in urine. Arsenic is distributed in the heart, liver,kidney, lung, hair, and nails. (See Preventng the fatal effects of ar-senic.)
PharmacodynamicsArsenic trioxide causes DNA fragmentation.
PharmacotherapeuticsArsenic trioxide is used to treat acute promyelocytic leukemiathat has relapsed after standard chemotherapy. It’s also being in-vestigated for treatment of multiple myeloma.
Drug interactionsGiving arsenic trioxide with other drugs known to prolong theQT interval may increase the risk of cardiac arrhythmias. (See Ad-verse reactions to arsenic trioxide.)
403UNCLASSIFIABLE ANTINEOPLASTIC DRUGS
Arsenic trioxide has been linked to acute promyelocytic leukemia (APL) differentiation syndrome.To prevent its life-threatening effects, follow these guidelines:• Monitor the patient for signs and symptoms of APL differentiation syndrome, including dyspnea,weight gain, pulmonary infiltrates, and pleural or pericardial effusion with or without leukocytosis.• If you detect any of these signs or symptoms, notify the prescriber immediately.• Expect to treat the syndrome with high doses of corticosteroids.
Safe and sound
Preventing the fatal effects of arsenic
Adversereactions toarsenic trioxide
Arsenic trioxide cancause electrocardio-gram abnormalities,which could progress tolife-threatening cardiacarrhythmias. Other ad-verse reactions include:• anxiety• dizziness• headache• hypocalcemia• insomnia• liver damage• muscle and boneaches• nausea and vomiting• rash• tremor.
Warning!
938915.qxd 08/26/2008 17:13 Page 403

AsparaginasesAsparaginases are cell cycle–specific and act during the G1phase. They include:• asparaginase• pegaspargase.
PharmacokineticsAsparaginase is administered parenterally. It’s considered 100%bioavailable when administered I.V. and about 50% bioavailablewhen administered I.M.
Distribution and metabolismAfter administration, asparaginase remains inside the blood ves-sels, with minimal distribution elsewhere. The metabolism of as-paraginase is unknown; only trace amounts appear in urine.
PharmacodynamicsAsparaginase and pegaspargase capitalize on the biochemical dif-ferences between normal cells and tumor cells.
Tumor cells—eat your asparagine or elseMost normal cells can synthesize asparagine, but some tumor cellsdepend on other sources of asparagine for survival. Asparaginaseand pegaspargase help to degrade asparagine to aspartic acidand ammonia. Deprived of their supply of asparagine, the tumorcells die.
PharmacotherapeuticsAsparaginase is used primarily in combination with standardchemotherapy to induce remission in patients with acute lympho-cytic leukemia.
If allergic…Pegaspargase is used to treat acute lymphocytic leukemia in pa-tients who are allergic to the native form of asparaginase.
Drug interactionsAsparaginase drugs may interact with other drugs. Asparaginaseand pegaspargase may reduce the effectiveness of methotrexate.Concurrent use of asparaginase with prednisone or vincristine in-creases the risk of toxicity. (See Adverse reactions to asparagi-nase drugs.)
404ANTINEOPLASTIC DRUGS
Adversereactions toasparaginasedrugs
Many patients receivingasparaginase and peg-aspargase develop nau-sea and vomiting. Fever,headache, abdominalpain, pancreatitis, coag-ulopathy, and liver tox-icity may also occur.
Rising risk
Asparaginase and peg-aspargase can causeanaphylaxis, which ismore likely to occur withintermittent I.V. dosingthan with daily I.V. dos-ing or I.M. injections.The risk of a reaction ris-es with each successivetreatment.
Hypersensitivity re-actions may also occur.
Warning!
Withoutasparaginase,I’m finished!
938915.qxd 08/26/2008 17:13 Page 404

ProcarbazineProcarbazine hydrochloride, a methylhydrazine derivative withmonoamine oxidase inhibitor (MAOI) properties, is used to treatHodgkin’s disease and primary and metastatic brain tumors.
PharmacokineticsAfter oral administration, procarbazine is well absorbed. It readilycrosses the blood-brain barrier and is well distributed into CSF.
Metabolism and excretionProcarbazine is metabolized rapidly in the liver and must be acti-vated metabolically by microsomal enzymes. It’s excreted in urine,primarily as metabolites. Respiratory excretion of the drug occursas methane and carbon dioxide gas.
PharmacodynamicsAn inert drug, procarbazine must be activated metabolically in theliver before it can produce various cell changes. It can cause chro-mosomal damage, suppress mitosis, and inhibit DNA, RNA, andprotein synthesis. Cancer cells can quickly develop resistance toprocarbazine.
PharmacotherapeuticsProcarbazine is used in the treatment of Hodgkin’s disease, lym-phoma, and brain cancer.
Drug interactionsInteractions with procarbazine can be significant.• It produces an additive effect when administered with CNS de-pressants.• Taken with meperidine, it may result in severe hypotension anddeath.
Mirroring MAOBecause of procarbazine’s MAOI properties, hypertensive reac-tions may occur when it’s administered concurrently with sympa-thomimetics, antidepressants, and tyramine-rich foods. (See Ad-verse reactions to procarbazine.)
405UNCLASSIFIABLE ANTINEOPLASTIC DRUGS
Procarbazine hasMAOI properties. So
watch out fortyramine-rich foods!
Adversereactions toprocarbazine
Late-onset bone marrowsuppression is the mostcommon dose-limitingtoxicity associated withprocarbazine. Interstitialpneumonitis (lung in-flammation) and pul-monary fibrosis (scar-ring) may also occur.
A bad start
Initial procarbazine ther-apy may induce flulikesymptoms, includingfever, chills, sweating,lethargy, and musclepain.
Gut reactions
GI reactions includenausea, vomiting, stom-atitis, and diarrhea.
Warning!
938915.qxd 08/26/2008 17:13 Page 405

HydroxyureaHydroxyurea is used most commonly for patients with chronicmyelogenous leukemia.
When your neck is on the lineHydroxyurea is also used for solid tumors and head and neckcancer.
PharmacokineticsHydroxyurea is readily absorbed and well distributed into CSF af-ter oral administration. It reaches a peak serum level 2 hours afteradministration.
Metabolism and excretionAbout one-half of the dose is metabolized by the liver to carbondioxide, which is excreted by the lungs, or to urea, which is ex-creted by the kidneys. The remaining one-half is excreted un-changed in urine.
PharmacodynamicsHydroxyurea exerts its effect by inhibiting the enzyme ribonu-cleotide reductase, which is necessary for DNA synthesis.
Divide and conquerHydroxyurea kills cells in the S phase of the cell cycle and holdsother cells in the G1 phase, where they’re most susceptible to irra-diation.
PharmacotherapeuticsHydroxyurea is used to treat selected myeloproliferative disor-ders. It may produce temporary remissions in some patients withmetastatic malignant melanomas as well.
Working with radiationHydroxyurea is also used in combination therapy with radiation totreat cancers of the head, neck, and lungs.
Drug interactionsCytotoxic drugs and radiation therapy enhance the toxicity of hy-droxyurea. (See Adverse reactions to hydroxyurea.)
406ANTINEOPLASTIC DRUGS
Fortunately,hydroxyurea can
treat lungcancers!
Adversereactions tohydroxyurea
Treatment with hydroxy-urea leads to few ad-verse reactions. Thosethat do occur include:• bone marrow suppres-sion• drowsiness• headache• nausea and vomiting• skin rash• anorexia• elevated uric acid lev-els, which require somepatients to take allopuri-nol to prevent kidneydamage.
Warning!
938915.qxd 08/26/2008 17:13 Page 406

InterferonsA family of naturally occurring glycoproteins, interferons are sonamed because of their ability to interfere with viral replication.These drugs exhibit anticancer activity as well as activity againstcondylomata acuminata (soft, wartlike growths on the skin andmucous membrane of the genitalia caused by a virus). The threetypes of interferons are:
alfa interferons derived from leukocytes
beta interferons derived from fibroblasts (connective tissuecells)
gamma interferons derived from fibroblasts and lympho-cytes.
PharmacokineticsAfter I.M. or subcutaneous administration, interferons are usuallywell absorbed. Information about their distribution is unavailable.
Metabolism and excretionAlfa interferons are filtered by the kidneys, where they’re degrad-ed. Liver metabolism and biliary excretion of interferons are negli-gible.
PharmacodynamicsAlthough their exact mechanism of action is unknown, interferonsappear to bind to specific membrane receptors on the cell surface.When bound, they initiate a sequence of intracellular events thatincludes the induction of certain enzymes.
Running interferenceThis process may account for the ability of interferons to:• inhibit viral replication• suppress cell proliferation• enhance macrophage activity (engulfing and destroying mi-croorganisms and other debris)• increase cytotoxicity of lymphocytes for target cells.
PharmacotherapeuticsAlfa interferons have shown their most promising activity in treat-ing blood malignancies, especially hairy cell leukemia. Their ap-proved indications currently include:• hairy cell leukemia
407UNCLASSIFIABLE ANTINEOPLASTIC DRUGS
Interferonscan put a stop
to viralreplication.
938915.qxd 08/26/2008 17:13 Page 407

• AIDS-related Kaposi’s sarcoma• condylomata acuminata.
Interfering in these areas as well…Alfa interferons also demonstrate some activity against chronicmyelogenous leukemia, malignant lymphoma, multiple myeloma,melanoma, and renal cell carcinoma.
Drug interactionsInterferons interact with other drugs:• They may enhance the CNS effects of CNS depressants and sub-stantially increase the half-life of methylxanthines (including theo-phylline and aminophylline).• Concurrent use with a live virus vaccine may potentiate replica-tion of the virus, increasing the adverse effects of the vaccine anddecreasing the patient’s antibody response.• Bone marrow suppression may be increased when an interferonis used with radiation therapy or a drug that causes blood abnor-malities or bone marrow suppression.• Alfa interferons increase the risk of kidney failure frominterleukin-2. (See Adverse reactions to interferons.)
AldesleukinAldesleukin is a human recombinant interleukin-2 derivative that’sused to treat metastatic renal cell carcinoma.
PharmacokineticsAfter I.V. administration of aldesleukin, about 30% is absorbed intoplasma and about 70% is absorbed rapidly by the liver, kidneys,and lungs. The drug is excreted primarily by the kidneys.
PharmacodynamicsThe exact antitumor mechanism of action of aldesleukin is un-known. The drug may stimulate an immunologic reaction againstthe tumor.
PharmacotherapeuticsAldesleukin is used to treat metastatic renal cell carcinoma. Itmay also be used in the treatment of Kaposi’s sarcoma andmetastatic melanoma.
408ANTINEOPLASTIC DRUGS
Adversereactions tointerferons
Blood toxicity occurs inup to one-half of pa-tients taking interferonsand may produceleukopenia, neutropenia,thrombocytopenia, andanemia. Adverse GI re-actions include anorex-ia, nausea, and diarrhea.
Alfa concerns
The most common ad-verse reaction to alfa in-terferons is the develop-ment of flulike symp-toms, which mayproduce fever, fatigue,muscle pain, headache,chills, and joint pain.
It catches your breath
Coughing, difficultybreathing, hypotension,edema, chest pain, andheart failure have alsobeen associated with in-terferon therapy.
Warning!
938915.qxd 08/26/2008 17:13 Page 408

Drug interactionsAldesleukin will interact with other drugs.• Concomitant administration of aldesleukin and drugs with psy-chotropic properties (such as opioids, analgesics, antiemetics,sedatives, and tranquilizers) may produce additive CNS effects.• Glucocorticoids may reduce aldesleukin’s antitumor effects.• Antihypertensive drugs may potentiate aldesleukin’s hypoten-sive effects.• Concurrent therapy with drugs that are toxic to the kidneys(such as aminoglycosides), bone marrow (such as cytotoxicchemotherapy drugs), heart (such as doxorubicin), or liver (suchas methotrexate or asparaginase) may increase toxicity to theseorgans. (See Adverse reactions to aldesleukin.)
AltretamineAltretamine is a synthetic cytotoxic antineoplastic drug that’sused as palliative treatment for patients with ovarian cancer.
PharmacokineticsAltretamine is well absorbed after oral administration.
Metabolism and excretionAltretamine is metabolized extensively in the liver and excretedby the liver and kidneys. The parent compound is poorly bound toplasma proteins.
PharmacodynamicsThe exact mechanism of action of altretamine is unknown. How-ever, its metabolites are alkylating drugs.
PharmacotherapeuticsAltretamine is used as palliative treatment of persistent or recur-ring ovarian cancer after first-line therapy with cisplatin or analkylating drug-based combination.
Drug interactionsAltretamine has a few significant interactions with other drugs.Concomitant therapy with cimetidine may increase altretamine’shalf-life, increasing the risk of altretamine toxicity.
409UNCLASSIFIABLE ANTINEOPLASTIC DRUGS
Adversereactions toaldesleukin
During clinical trials,more than 15% of pa-tients developed ad-verse reactions toaldesleukin. These in-clude:• pulmonary congestionand difficulty breathing• anemia, thrombocy-topenia, and leukopenia• elevated bilirubin,transaminase, and alka-line phosphate levels• hypomagnesemia andacidosis• reduced or absent uri-nary output• elevated serum creati-nine level• stomatitis• nausea and vomiting.
Warning!
938915.qxd 08/26/2008 17:13 Page 409

Don’t mix with MAOIUse with an MAOI may cause severe orthostatic hypotension (adrop in blood pressure upon rising). (See Adverse reactions to al-tretamine.)
Paclitaxel and docetaxelAntineoplastic drugs are used to treat metastatic ovarian andbreast cancer after chemotherapy has failed. They include:• paclitaxel• docetaxel.
PharmacokineticsAfter I.V. administration, paclitaxel is highly bound to plasma pro-teins. Docetaxel is administered I.V. with a rapid onset of action.
Metabolism and excretionPaclitaxel is metabolized primarily in the liver with a smallamount excreted unchanged in urine. Docetaxel is excreted pri-marily in stool.
PharmacodynamicsPaclitaxel and docetaxel exert their chemotherapeutic effect bydisrupting the microtubule network essential for mitosis and oth-er vital cellular functions.
PharmacotherapeuticsPaclitaxel is used when first-line or subsequent chemotherapy hasfailed in treating metastatic ovarian cancer as well as metastaticbreast cancer.
Head, neck, and belowThe taxanes may also be used for treating head and neck cancer,prostate cancer, and non–small-cell lung cancer. (See Culturalconsiderations with docetaxel use.)
Drug interactionsTaxanes may interact with other drugs.• Concomitant use of paclitaxel and cisplatin may cause additivemyelosuppressive effects.• Cyclosporine, ketoconazole, erythromycin, and troleandomycinmay modify the metabolism of docetaxel.
410ANTINEOPLASTIC DRUGS
Adversereactions toaltretamine
More than 10% of pa-tients using altretaminein clinical trials experi-enced adverse reac-tions, such as:• nausea and vomiting• neurotoxicity• peripheral neuropathy• anemia.
Bone marrowsuppression is alsocommon.
Warning!
When othertreatments fail, don’tgive up! Try paclitaxelto treat metastaticovarian cancer and
breast cancer.
938915.qxd 08/26/2008 17:13 Page 410

• Phenytoin may decrease paclitaxel serum level, leading to a lossof efficacy.• Quinupristin/dalfopristin may increase paclitaxel serum levels,increasing the risk of toxicity. (See Adverse reactions to paclitax-el and docetaxel.)
Quick quiz
1. What’s the major adverse reaction that’s common to all alky-lating drugs?
A. PhotosensitivityB. Nerve toxicityC. Cardiac toxicityD. Bone marrow suppression
Answer: D. Bone marrow suppression is a common adverse re-action to all alkylating drugs.
411QUICK QUIZ
Clinical trials of docetaxel in Japanese andAmerican patients with breast cancer re-vealed significant differences in the incidenceof adverse effects between the two cultures.
The results
Japanese women were more likely to developthrombocytopenia—14.4% versus 5.5%. How-ever, the Japanese women in this study wereless likely than the American patients (6% ver-sus 29.1%) to develop many of the other ad-verse reactions such as hypersensitivity reac-tions.
Other results showed fewer incidences offluid retention, neurosensory effects, musclepain, infection, and development of anemia inthe Japanese patients. The study also indicat-ed that Japanese patients are more likely todevelop fatigue and weakness than are Ameri-can women.
Putting it into a plan
These results are important to consider whencaring for patients receiving docetaxel andcan provide clues for developing a care planand for knowing what adverse reactions to ex-pect.
Yea or nay?
Cultural considerations with docetaxel use Adversereactions topaclitaxel anddocetaxel
During clinical trials,25% or higher of patientsexperienced these ad-verse reactions to pacli-taxel:• bone marrow suppres-sion• hypersensitivity reac-tions• abnormal EEG tracings• peripheral neuropathy• muscle pain and jointpain• nausea, vomiting, anddiarrhea• mucous membrane in-flammation• hair loss.
Docetaxel
Adverse reactions to do-cetaxel include:• hypersensitivity reac-tions• fluid retention• leukopenia, neutro-penia, or thrombocy-topenia• hair loss• stomatitis• numbness and tingling• pain• weakness and fatigue.
Warning!
938915.qxd 08/26/2008 17:13 Page 411

2. The drug likely to be administered with methotrexate to mini-mize its adverse effects is:
A. fluorouracil.B. leucovorin.C. cladribine.D. trastuzumab.
Answer: B. Leucovorin is typically administered in conjunctionwith methotrexate to minimize adverse effects.
3. Before administering bleomycin to a patient, why should youadminister an antihistamine and an antipyretic?
A. To prevent fever and chillsB. To prevent anaphylactic shockC. To prevent bone marrow suppressionD. To prevent hypertension
Answer: A. An antihistamine and an antipyretic may be adminis-tered before bleomycin to prevent fever and chills.
ScoringIf you answered all three items correctly, extraordinary! You real-
ly mowed down the malignant neoplasms!If you answered two items correctly, congratulations! You’re more
than competent to combat cancer!If you answered fewer than two items correctly, give it another
shot! Remember, this is your last crack at a quick quiz!
412ANTINEOPLASTIC DRUGS
Hip HipHooray! You
made it.Way to go!
✰✰✰
✰✰
✰
938915.qxd 08/26/2008 17:13 Page 412

Other major drugs 414
Vaccines and treatment forbiological weapons exposure 421
Treatment and antidotes forchemical weapons exposure 422
Herbal drugs 423
Selected references 426
Index 427
Appendices, references, and index
938916BM.qxd 08/26/2008 17:17 Page 413

Other major drugs
414
OPHTHALMIC DRUGS
Drug
Antiallergic agents
AzelastineCromolynEmedastineKetotifenLodoxamideOlopatadine
Anesthetics
ProparacaineTetracaine
Anti-infectives
CiprofloxacinErythromycinGentamicinLevofloxacinNatamycinNorfloxacinOfloxacinSulfacetamideSulfisoxazoleTobramycinTrifluridine
Action
• Decrease irritation
• Prevent the initiation andtransmission of nerve im-pulses
• Kill bacteria or inhibitgrowth of bacteria orviruses
Treatment uses
• To treat allergic conjunctivitis• To treat seasonal conjunctivitis• To treat keratitis
• To anesthetize the cornea, allowingapplication of instruments for mea-suring intraocular pressure (IOP) orremoving foreign bodies• To prepare for suture removal, con-junctival or corneal scraping, andtear duct manipulation
• To treat corneal ulcers or conjunc-tivitis caused by bacteria, fungus, orvirus (each drug is specific to particu-lar organisms)
Adverse reactions
• Tearing
• Corneal inflammation• Corneal opacities• Delayed corneal healing• Eye pain and redness• Loss of visual acuity• Scarring
• Secondary eye infections (withprolonged use)• Severe hypersensitivity reac-tions
938916BM.qxd 08/26/2008 17:17 Page 414

415OTHER MAJOR DRUGS
OPHTHALMIC DRUGS (continued)
Drug
Anti-inflammatories
Steroidal anti-inflammatoriesDexamethasoneFluorometholoneLoteprednolPrednisoloneRimexolone
Nonsteroidal anti-inflammatoriesDiclofenacFlurbiprofenKetorolacSuprofen
Lubricants
MethylcellulosePolyvinyl alcohol
Miotics
CarbacholPilocarpine
Mydriatics
DipivefrinEpinephrineHydroxyamphetaminePhenylephrine
Action
• Decrease leukocyte infil-tration at inflammationsites, causing reduced ooz-ing of fluids and reducededema, redness, and scar-ring
• Decrease inflammationand itching
• Act as artificial tears• Moisten cornea
• Stimulate and contractthe sphincter muscle of theiris, constricting the pupil• Improve aqueous outflow
• Act on the iris to dilatethe pupil• Lower IOP
Treatment uses
• To treat inflammatory disorders andhypersensitivity-related conditions ofthe cornea, iris, conjunctiva, sclera,and anterior uvea
• To inhibit pupil constriction duringsurgery (flurbiprofen and suprofen)• To reduce itching due to seasonalallergies (ketorolac)• To treat inflammation after surgery
• To protect cornea during diagnosticprocedures• To moisten contact lenses
• To treat open-angle glaucoma,acute and chronic angle-closureglaucoma, and certain cases of sec-ondary glaucoma resulting from in-creased IOP
• To dilate the pupils for intraocularexaminations• To lower IOP in patients with glau-coma
Adverse reactions
• Corneal ulceration• Delayed corneal healing• Increased susceptibility to viralor fungal corneal infection
• Tearing, discomfort
• None
• Blurred vision• Bronchospasm• Cataract formation• Eye pain• Photosensitivity• Reversible iris cysts
• Blurred vision• Confusion• Dry skin• Flushing• Impaired ability to coordinatemovement• Irritation• Rapid heart rate• Transient burning sensations
938916BM.qxd 08/26/2008 17:17 Page 415

416 OTHER MAJOR DRUGS
OPHTHALMIC DRUGS (continued)
Drug
Atropine sulfateCyclopentolate
hydrochlorideHomatropine
hydrobromideTropicamide
Adrenergic blockers(topical)ApraclonidineBetaxololBrimonidineCarteololLevobunololMetipranololTimolol maleate
Carbonic anhydraseinhibitorsAcetazolamideBrinzolamideDorzolamide
Osmotic agentsGlycerinIsosorbideMannitol
Prostaglandin analoguesBimatoprostLatanoprostTravoprostUnoprostone
Action
• Act on the ciliary body ofthe eye to paralyze thefine-focusing muscles(thereby preventing ac-commodation for near vi-sion)
• May reduce aqueous hu-mor formation and slightlyincrease aqueous humoroutflow
• Inhibit action of carbonicanhydrase, thus decreas-ing aqueous humor pro-duction
• Reduce volume of vitre-ous humor• Decrease IOP
• Decrease IOP
Treatment uses
• To perform refractive eye examina-tions in children before and after oph-thalmic surgery• To treat conditions involving the iris
• To prevent and control elevated IOP,chronic open-angle glaucoma, andsecondary glaucoma
• To treat chronic open-angle glauco-ma, acute angle-closure episodes,and secondary glaucoma
• To prepare for intraocular surgery• To treat acute glaucoma
• To treat glaucoma
Adverse reactions
• Same as for mydriatics
• Bronchospasm• Fatigue• Headaches• Slow heart rate
• Hemolytic or aplastic anemia• Hypokalemia• Leukopenia• Nausea and vomiting
• Hypokalemia• Diuresis
• Irritation• Tearing
Mydriatics and cycloplegics
Other drugs to lower IOP
938916BM.qxd 08/26/2008 17:17 Page 416

417OTHER MAJOR DRUGS
OTIC DRUGS
Drug
Anesthetics (local)
Benzocaine
Anti-infectives
Acetic acidBoric acidChloramphenicolColistin sulfateNeomycin sulfatePolymyxin B sulfate
Anti-inflammatories
HydrocortisoneDexamethasone-
sodium phosphate
Cerumenolytics
Carbamide peroxideTriethanolamine
polypeptide
Action
• Temporarily interrupt theconduction of nerve im-pulses
• Kill bacteria or inhibitbacterial growth• Inhibit fungal growth(acetic acid and boric acid)
• Inhibit edema, capillarydilation, fibrin deposition,and phagocyte and leuko-cyte migration• Reduce capillary and fi-broblast proliferation, col-lagen deposition, and scarformation
• Reduce hardened ceru-men by emulsifying andmechanically loosening it
Treatment uses
• To temporarily relieve ear pain
• To treat otitis externa• To treat otitis media (colistin andpolymyxin B sulfate)
• To treat inflammatory conditions ofthe external ear canal
• To loosen and remove cerumenfrom the ear canal
Adverse reactions
• Ear irritation or itching• Edema• Hives• Masking of the symptoms of afulminating middle ear infection
• Burning• Dermatitis• Ear itching• Hives
• Masking or exacerbation ofunderlying otic infection• Transient local stinging orburning sensations
• Mild, localized redness anditching
938916BM.qxd 08/26/2008 17:17 Page 417

418 OTHER MAJOR DRUGS
DERMATOLOGIC DRUGS
Drug
Anti-infectives
AntibacterialsAzelaic acidBacitracinClindamycinErythromycinGentamicinMafenideMetronidazoleMupirocinNeomycinSilver sulfadiazineSulfacetamide
sodiumTetracycline
AntifungalsAmphotericin BButenafineCiclopiroxClotrimazoleEconazoleKetoconazoleMiconazoleNaftifineNystatinOxiconazoleSulconazoleTerbinafine
AntiviralsAcyclovirPenciclovir
Action
• Kill or inhibit the growthof bacteria
• Kill or inhibit the growthof fungi
• Inhibit the growth ofherpes virus
Treatment uses
• To treat infections caused by bacte-ria (each drug is specific to particularorganisms; combination productsmay also be used)
• To treat infections caused by fungi(each drug is specific to particular or-ganisms)
• To treat herpes genitalis or herpeslabialis
Adverse reactions
• Contact dermatitis• Rash• Skin burning, itching, and red-ness• Skin dryness• Stinging
• Same as for antibacterials
• Same as for antibacterials
938916BM.qxd 08/26/2008 17:17 Page 418

419OTHER MAJOR DRUGS
DERMATOLOGIC DRUGS (continued)
Drug
Anti-inflammatories
AlclometasoneBetamethasone
dipropionateClobetasolClocortoloneDesonideDesoximetasoneDexamethasoneDiflorasone diacetateFluocinoloneFluocinonideFlurandrenolideFluticasoneHalcinonideHalobetasolHydrocortisoneMometasoneTriamcinolone
acetonide
Minoxidil
KeratolyticsAcitretinAdapaleneIsotretinoinTazaroteneTretinoin
Action
• Suppress inflammationby binding to intracellularcorticosteroid receptors,initiating a cascade of anti-inflammatory mediators• Cause vasoconstrictionin inflamed tissue and pre-vent macrophages andleukocytes from movinginto the area
• Stimulate hair growth bycausing vasodilation,which increases blood flowto the skin (exact mecha-nism of action is unknown)
• Produce antibacterial ef-fects• Reduce inflammation
Treatment uses
• To relieve inflammation and itchingin topical steroid-responsive disor-ders, such as eczema, psoriasis, an-gioedema, contact dermatitis, sebor-rheic dermatitis, atopic dermatitis,and hives
• To treat male and female patternbaldness
• To treat mild acne, oily skin, andacne vulgaris (oral antibiotic therapyused as needed for deep acne)
Adverse reactions
• Adrenal hormone suppression• Stretch marks and epidermalatrophy (after 3 to 4 weeks ofuse)
• Fluid retention• Rapid heart rate• Weight gain
• Burning• Hives• Rash• Scaling, blistering, and peeling• Skin dryness• Skin irritation• Superinfection (with prolongeduse)
Hair growth stimulants
Topical antiacne drugs
938916BM.qxd 08/26/2008 17:17 Page 419

420 OTHER MAJOR DRUGS
DERMATOLOGIC DRUGS (continued)
Drug
CounterirritantsBenzoyl peroxide
AntimicrobialsClindamycinDoxycyclineErythromycinMinocyclineTetracycline
Gamma benzenehexachloride
LindaneMalathionPermethrin
Action
• Produce antibacterial ef-fects• Reduce inflammation
• Produce antibacterial ef-fects• Reduce inflammation
• Act on parasite nerve cellmembranes to disrupt thesodium channel current,causing paralysis (someare also ovicidal)
Treatment uses
• To treat mild acne, oily skin, andacne vulgaris (oral antibiotic therapyused as needed for deep acne)
• To treat mild acne, oily skin, andacne vulgaris (oral antibiotic therapyused as needed for deep acne)
• To treat scabies and lice
Adverse reactions
• Same as for keratolytics
• Same as for keratolytics• Hypersensitivity reactions(oral)• Candidal vaginitis (oral)• Gram-negative pustular folli-culitis (oral)
• Contact dermatitis• Hypersensitivity reactions• Respiratory allergy symptoms
Topical antiacne drugs (continued)
Scabicides and pediculicides
938916BM.qxd 08/26/2008 17:17 Page 420

Listed here are potentially threatening biological (bacterial and viral) agents as well as treatments and vaccines currently avail-able for conditions caused by biological agents.
Implement standard precautions for all cases of suspected exposure. For cases of smallpox, institute airborne precautions forthe duration of the illness and until all scabs fall off. For pneumonic plague cases, institute droplet precautions for 72 hours afterinitiation of effective therapy.
421
Biological agent (condition)
Bacillus anthracis (anthrax)
Clostridium botulinum (botulism)—Not contagious
Francisella tularensis (tularemia)—Not contagious
Variola major (smallpox)—Transmit-ted by inhalation of air droplets oraerosols; patient most infectiousfrom onset of maculopapular rashthrough first 7 to 10 days
Yersinia pestis (plague)—Transmit-ted person to person via aerosol(pneumonic plague)
Treatment
• Ciprofloxacin, doxycycline, penicillin
• Supportive; may require endotrachealintubation and mechanical ventilation• Passive immunization with equine an-titoxin to lessen nerve damage
• Gentamicin or streptomycin; alterna-tively, doxycycline, chloramphenicol,and ciprofloxacin
• No FDA-approved antiviral available;cidofovir may be therapeutic if adminis-tered 1 to 2 days after exposure
• Streptomycin or gentamicin; alterna-tively, doxycycline, ciprofloxacin, orchloramphenicol
Vaccine
• Limited supply of an inactivated cell-freeproduct available; when used, shortens peri-od of antimicrobial prophylaxis• Not recommended in absence of exposureto anthrax
• Postexposure prophylaxis with equine bot-ulinum antitoxin• Botulinum toxoid available from the Cen-ters for Disease Control and Prevention; re-combinant vaccine under development
• Vaccination with live, attenuated vaccinecurrently under investigation and review bythe Food and Drug Administration (FDA)
• Vaccine available as prophylaxis within3 to 4 days of exposure
• Vaccination no longer available; didn’t pro-tect against primary pneumonic plague
Vaccines and treatment for biological weapons exposure
938916BM.qxd 08/26/2008 17:17 Page 421

Listed here are potentially threatening chemical agents, treatments currently available, and antidotes.In the event of chemical agent exposure, follow standard precautions and decontamination protocols, such as removing cloth-
ing and sealing it in plastic bags, irrigating the eyes, washing skin and hair using copious water, treating waste water as needed,and decontaminating the health care facility according to the specific agent involved.
422
Chemical agent
Nerve agents
SarinSomanTabunVX
Cyanides
Cyanogen chlorideHydrogen cyanide
Vesicants or blister
agents
LewisiteMustard lewisiteNitrogen mustardPhosgene oximeSulfur mustard
Treatment
• Supportivecare• Diazepam orlorazepam toprevent sei-zures
• Supportivecare• 100% oxygenby face mask;may need en-dotracheal (ET)intubation with100% FIO2
• Activatedcharcoal forconscious pa-tient
• Thermal burntherapy• Respiratorysupport andeye care
Antidote
• Atropine I.M. orI.V.• Pralidoximechloride I.M. orI.V.
• Amyl nitrite viainhalation• Sodium nitriteI.V. and sodiumthiosulfate I.V.;dosage based onpatient’s weightand hemoglobinlevel
• No antidoteavailable for mus-tards or phos-gene oxime• For lewisite andlewisite mustardmixtures: BritishAnti-Lewisite I.M.(rarely available)
Chemical agent
Pulmonary or
choking agents
ChlorineDiphosgenePhosgeneSulfur dioxide
Ricin (biotoxin iso-lated from castorbean oil extract)
T-2 mycotoxins (tox-ic compounds pro-duced by fungi)FusariumMyroteciumStachybotrysTrichodermaVerticimonosporium
Treatment
• Supportivecare• Oxygen thera-py; possible ETintubation andmechanicalventilation withpositive-endexpiratorypressure
• Supportivecare• For ingestion,activated char-coal
• Supportivecare• For ingestion,activated char-coal• Possible high-dose steroids
Antidote
• None
• None
• None
Treatment and antidotes for chemical weapons exposure
938916BM.qxd 08/26/2008 17:17 Page 422

Herbal drugs
Herbal medicine
Aloe
Chamomile
Cranberry
Echinacea
Feverfew
Common uses
Oral
• Constipation• Bowel evacuationTopical
• Minor burns• Skin irritation
Oral
• Anxiety or restlessness• Diarrhea• Motion sickness• IndigestionTopical
• Inflammation• Wound healing• Cutaneous burnsTeas
• Sedation• Relaxation
• Prophylaxis for urinary tractinfection (UTI)• Treatment of UTI• Prevention of renal calculi
• Supportive therapy to preventand treat common cold andacute and chronic infections ofthe upper respiratory tract
• Prevention and treatment ofmigraines and headaches• Hot flashes• Rheumatoid arthritis• Asthma• Menstrual problems
Special considerations
• The laxative actions of aloe may take up to 10 hours after ingestion tobe effective.• Monitor the patient for signs of dehydration; geriatric patients are par-ticularly at risk.
• People sensitive to ragweed and chrysanthemums or others in theCompositae family may be more susceptible to contact allergies andanaphylaxis.• Patients with hay fever or bronchial asthma caused by pollens aremore susceptible to anaphylactic reactions.• Pregnant women shouldn’t use chamomile.• Chamomile may enhance anticoagulant’s effect.
• Only the unsweetened form of cranberry prevents bacteria from ad-hering to the bladder wall and preventing or treating UTIs
• Echinacea is considered supportive therapy and shouldn’t be used inplace of antibiotic therapy.
• Avoid using in pregnant patients because feverfew is also an abortifa-cient.• Feverfew may increase the risk of abnormal bleeding when combinedwith an anticoagulant or antiplatelet.• Abruptly stopping feverfew may cause “postfeverfew syndrome” in-volving tension headaches, insomnia, joint stiffness and pain, andlethargy.
423
The following table lists some common herbal drugs, their uses, and considerations to know when caring for patients taking thesedrugs.
938916BM.qxd 08/26/2008 17:17 Page 423

424 HERBAL DRUGS
Herbal medicine
Garlic
Ginger
Ginkgo biloba
Ginseng
Green tea
Common uses
• Decrease cholesterol andtriglyceride levels• Prevent atherosclerosis• Age-related vascular changes• Prevent GI cancer• Coughs, colds, fevers, andsore throats
• Nausea (antiemetic)• Motion sickness• Morning sickness• GI upset (colic, flatulence, in-digestion)• Hypercholesteremia• Liver toxicity• Burns• Ulcers• Depression
• “Memory” agent• Alzheimer’s disease• Multi-infarct dementia• Cerebral insufficiency• Intermittent claudication• Tinnitus• Headache
• Fatigue• Improve concentration• Treat atherosclerosis• Also believed to strengthenthe body and increase resis-tance to disease after sicknessor weakness
• Prevent cancer• Hyperlipidemia• Atherosclerosis• Dental caries• Headaches• Central nervous system (CNS)stimulant• Mild diuretic
Special considerations
• Odor of garlic may be apparent on breath and skin.• Garlic may prolong bleeding time in patients receiving anticoagulants.• Excess raw garlic intake may increase the risk of adverse reactions.• Garlic shouldn’t be used in patients with diabetes, insomnia, pemphi-gus, organ transplants, or rheumatoid arthritis or in those who have re-cently undergone surgery.
• Ginger may increase the risk of bleeding, bruising, or nosebleeds.• Pregnant women should obtain medical advice before using gingermedicinally.• Ginger may interfere with the intended therapeutic effects of certainconventional drugs.
• Adverse effects occur in less than 1% of patients; the most common isGI upset.• Ginkgo biloba may potentiate anticoagulants and increase the risk ofbleeding.• Ginkgo extracts are considered standardized if they contain 24%flavonoid glycosides and 6% terpene lactones.• Seizures have been reported in children after ingestion of more then50 seeds.• Treatment should continue for 6 to 8 weeks but for no more than 3months.
• Ginseng may cause severe adverse reactions when taken in largedoses (more than 3 g per day for 2 years), such as increased motor andcognitive activity with significant diarrhea, nervousness, insomnia, hy-pertension, edema, and skin eruptions.• Ginseng may potentiate anticoagulants and increase the risk of bleed-ing.
• Green tea contains caffeine.• Avoid prolonged and high caffeine intake, which may cause restless-ness, irritability, insomnia, palpitations, vertigo, headache, and adverseGI effects.• Adding milk may decrease adverse GI effects of green tea.• Green tea may potentiate anticoagulants and increase the risk ofbleeding.
938916BM.qxd 08/26/2008 17:17 Page 424

425HERBAL DRUGS
Herbal medicine
Kava
St. John’s wort
Vitex
Yohimbine
Common uses
• Antianxiety• Stress• Restlessness• Sedation• Promote wound healing• Headache• Seizure disorders• Common cold• Respiratory infections
• Mild to moderate depression• Anxiety• Psychovegetative disorders• Sciatica• Viral infections
• Premenstrual syndrome
• Impotence (works as anaphrodisiac)
Special considerations
• Kava is contraindicated in pregnancy and lactation.• Kava shouldn’t be used in combination with St. John’s wort.• Kava shouldn’t be taken with other CNS depressants, monoamine oxidase inhibitors, levodopa, antiplatelets, alcohol, or anxiolytics.• Kava can cause drowsiness and may impair motor reflexes and men-tal acuity; advise the patient to avoid hazardous activities.• Effects should appear within 2 days of initiation of therapy.
• Effects may take several weeks; however, if no improvement occursafter 4 to 6 weeks, consider alternative therapy.• St. John’s wort interacts with many different types of drugs.• St. John’s wort shouldn’t be used in combination with prescriptionantidepressants or antianxiety medications.
• Vitex should be taken in the morning with water.• Vitex is a very slow acting substance; it may take several cycles to see an effect.
• Yohimbine may cause CNS excitation, including tremor, sleeplessness,anxiety, increased blood pressure, and tachycardia.• Don’t use in patients with renal or hepatic insufficiency.
938916BM.qxd 08/26/2008 17:17 Page 425

Selected references
426
American Drug Index, 50th ed. Philadelphia: Facts andComparisons, 2006.
American Hospital Formulary Service. AHFS Drug Infor-mation 2008. Bethesda, Md.: American Society ofHospital Pharmacists, 2008.
Arana, G.W., et al. Handbook of Psychiatric Drug Therapy.Philadelphia: Lippincott Williams and Wilkins, 2006.
Bisno, A.L. “Practice Guidelines for the Diagnosis and Man-agement of Skin and Soft-tissue Infections,” ClinicalInfectious Disease 41:1174-78, 2005.
Burke, M.B., and Wilkes, G.M. 2006 Oncology NursingDrug Handbook. Sudbury, Mass.: Jones & BartlettPubs., Inc., 2006.
Centers for Disease Control and Prevention. www.cdc.gov
Chong, O.T. “An Integrative Approach to Addressing Clini-cal Issues in Complementary and Alternative Medi-cine in an Outpatient Oncology Center,” ClinicalJournal of Oncology Nursing 10(1):83-88, February2006.
Chu, E. Physicians’ Cancer Chemotherapy Drug Manual2006. Sudbury, Mass.: Jones & Bartlett Pubs., Inc.,2008.
Gensure, R., and Jüppner, H. “Parathyroid Hormone with-out Parathyroid Glands,” Endocrinology 146(2):544-46, February 2005.
Golan, D., et al. Principles of Pharmacology: The Patho-physiologic Basis of Drug Therapy, 2nd ed. Philadel-phia: Lippincott Williams & Wilkins, 2007.
Gutierrez, K. Pharmacotherapeutics: Clinical Reasoningin Primary Care, 2nd ed. Philadelphia: W.B. Saun-ders Co., 2008.
Houck, P.M., and Bratzler, D.W. “Administration of FirstHospital Antibiotics for Community-Acquired Pneu-monia: Does Timeliness Affect Outcomes?” CurrentOpinion in Infectious Diseases 18(2):151-56, April2005.
Kanner, E.M., and Tsai, J.C. “Current and Emerging MedicalTherapies for Glaucoma,” Expert Opinion on Emerg-ing Drugs 10(1):109-18 February 2005.
Lippincott’s Nursing Drug Guide 2008. Philadelphia: Lip-pincott Williams & Wilkins, 2008.
Nolan, C.R.“Strategies for Improving Long-Term Survival inPatients with ESRD,” Journal of the American Soci-ety of Nephrology 16(Suppl 2): S120-S127, November2005.
Nursing I.V. Drug Handbook, 9th ed. Philadelphia: Lippin-cott Williams & Wilkins, 2006.
Nursing2008 Drug Handbook, 28th ed. Philadelphia: Lip-pincott Williams & Wilkins, 2008.
Physician’s Desk Reference, 58th ed. Montvale, Md.: Thom-son PDR, 2004.
Professional Guide to Pathophysiology, 2nd ed. Philadel-phia: Lippincott Williams & Wilkins, 2007.
Psychopharmacology, 2nd ed. Arlington, Va.: AmericanPsychiatric Publishing, Incorporated, 2006.
Roach, S., and Zorko, B.S. Pharmacology for Health Pro-fessionals. Philadelphia: Lippincott Williams &Wilkins, 2006.
Roach, S., and Ford, S.M. Introductory Clinical Pharma-cology, 8th ed. Philadelphia: Lippincott Williams &Wilkins, 2007.
Salzman, C. Clinical Geriatric Psychopharmacology, 4thed. Philadelphia: Lippincott Williams & Wilkins, 2005.
Sande, M.A., and Eliopoulos, G. The Sanford Guide toHIV/AIDS Therapy, 14th ed. Hyde Park, Vt.: Antimi-crobial Therapy, Inc., 2005.
U.S. Food and Drug Administration: www.fda.gov
938916BM.qxd 08/26/2008 17:17 Page 426

i refers to an illustration; t refers to a table.
Index
A Abacavir, 266-270Abciximab, 165-169Absorption, 7-9
drug interactions and, 16Acarbose, 342-345Acebutolol, 43-47, 129-131Acetaminophen, 96-98
nonselective, safe use of, 99selective, risks of using, 98
Acetazolamide, 229, 368-369, 416tAcetic acid, 417tAcetohexamide, 342-345Acetylcholine, 21, 22i, 23, 24, 26,
27, 60, 61Acetylcysteine, 190-191Acidifying drugs, 368-369Acitretin, 419tActivated charcoal, 204-205, 422tActive transport, 7Acute therapy, 14Acyclovir, 260-263, 418tAdapalene, 419tAdditive effects, 16Adenosine, 133-134Adrenergic blocking drugs, 40-47
topical, 416tAdrenergic drugs, 32-39
classifying, 32mechanism of action of, 33i
Adsorbent drugs, 204-205Adverse drug reactions, 17-19
dose-related, 17-18patient sensitivity–related, 18-19
Agonist, 12Albuterol, 37-39, 176-177Alclometasone, 419tAldesleukin, 408-409Aldosterone, 301Alemtuzumab, 398-399Alfuzosin, 40-43Alkalinizing drugs, 366-368Alkylating drugs, 371-379
mechanism of action of, 373i
Alkylating-like drugs, 378-379Alkyl sulfonates, 374-375Allopurinol, 307-309Allylamine derivatives, synthetic,
288-289Almotriptan, 86-88Aloe, 423tAlosetron, 210Alpha-adrenergic blockers, 40-43,
141-142mechanism of action of, 41i
Alprazolam, 312-313, 314i, 315Alprostadil, 231-232Alteplase, 171-173, 172iAltretamine, 409-410Aluminum carbonate gel, 197-198Aluminum-magnesium complex,
197-198Amantadine, 62-66, 264-266Ambenonium, 24-27Amikacin, 238-240Amiloride, 227-228Aminoglycosides, 238-2401-(aminomethyl) cyclohexane–acetic
acid, 78-79Aminophylline, 183-185Amiodarone, 131-132Amitriptyline, 322-325Amlodipine, 138-140Ammonium chloride, 368-369Amobarbital, 316-317Amoxapine, 322-325Amoxicillin, 196-197, 241-243Amphetamine salts, mixed, 336-337Amphotericin B, 280-283, 418tAmpicillin, 241-243Amprenavir, 272-275Amylase, 206Amyl nitrite, 135-136Anakinra, 302-306Anastrozole, 387-388Androgens, 390-391Anesthetic drugs, 108-115
ophthalmic, 414totic, 417t
Angiotensin-converting enzymeinhibitors, 144-145
Angiotensin II receptor blockers,146-147
Animals as drug sources, 3, 4Antacids, 197-198Antagonist, 12
types of, 12-13Antagonistic effect, 16Anterior pituitary drugs, 349-350Antiacne drugs, topical, 419-420tAntiallergic agents as ophthalmic
drugs, 414tAntiandrogens, 391-392Antianginal drugs, 134-140
mechanism of action of, 134iAntianxiety drugs, 318-319Antiarrhythmic drugs, 123-134Antibacterial drugs, 238-260
dermatologic, 418tAntibiotic antineoplastic drugs,
385-386Antibiotics, systemic, as gastrointesti-
nal drugs, 196-197. See also An-tibacterial drugs.
Anticholinergic drugs, 27-32, 60-62,177-178
Anticholinesterase drugs, 24-27differentiating toxic response to,
from myasthenic crisis, 24mechanism of action of, 22i
Anticoagulant drugs, 161-171Anticonvulsant drugs, 68-85Antidepressants, 320-329
risks of, 322Antidiabetic drugs, 339-345Antidiarrheal drugs, 208-210Antidiuretic hormone, 350-352Antiemetics, 216-219Antiestrogens, 388-390Antiflatulent drugs, 205Antifungal drugs, 280-289
dermatologic, 418tAntigout drugs, 306-309Antihistamines, 216-219, 294-297
9389INDEXqxd 08/26/2008 17:20 Page 427

428INDEX
i refers to an illustration; t refers to a table.
Antihypertensive drugs, 140-147Anti-infective drugs, 237-290
dermatologic, 418tophthalmic, 414totic, 417t
Anti-inflammatoriesdermatologic, 419tophthalmic, 415totic, 417t
Antilipemic drugs, 147-152Antimetabolite drugs, 379-384Antimicrobial drug, selecting, 237Antimigraine drugs, 85-90Antimycotic drugs, 280-289Antineoplastic drugs, 371-411
unclassifiable, 402-411Antiparkinsonian drugs, 59-68Antiplatelet drugs, 165-169Antipsychotic drugs, 330-336Antipyretics, 93-101Antiretroviral drugs, 266-275Antithymocyte globulin, 302-306Antithyroid drugs, 355-356Antitubercular drugs, 275-280Antitussives, 188-189Antiulcer drugs, 195-203Antiviral drugs, 260-275
dermatologic, 418tAnxiolytics, 318-319Apraclonidine, 416tArgatroban, 169-170Aripiprazole, 331-332Aromatase inhibitors, 387-388Arsenic trioxide, 403Ascorbic acid, 368-369Asparaginases, 404Aspirin, 94-96, 166-169Atazanavir, 272-275Atenolol, 43-47, 137-138Atorvastatin, 149-150Atracurium, 56-58Atropine, 27-32, 30i, 416tAtypical antipsychotics, 331-332Autonomic nervous system drugs,
21-47Azaspirodecanedione derivatives, 319Azatadine, 294-295, 297Azathioprine, 302-306
Azelaic acid, 418tAzelastine, 414tAzithromycin, 249-251Aztreonam, 255-256
B Bacitracin, 418tBaclofen, 53-55Barbiturates, 70-72, 110-112, 316-317Basiliximab, 302-306Beclomethasone, 178-180, 298-300Belladonna, 27-32Benazepril, 144-145Bendroflumethiazide, 224-225Benzocaine, 114-115, 417tBenzodiazepines, 74-76, 110-112,
312-313, 315mechanism of action of, 314i
Benzonatate, 188-189Benzoyl peroxide, 420tBenztropine, 27-32, 60-62Benzyl alcohol, 114-115Beta-adrenergic blockers, 43-47,
129-131, 137-138cardioselective, 45mechanism of action of, 45iunderuse of, in elderly patients, 46
Beta2-adrenergic agonists, 176-177Betamethasone, 298-300Betaxolol, 43-47, 416tBethanechol, 21-24Bicalutamide, 391-392Bile-sequestering drugs, 147-148Bimatoprost, 416tBiological weapons exposure, vac-
cines and treatment for, 421tBiotransformation. See Metabolism.Biperiden, 60-62Bisacodyl, 214-215Bisoprolol, 43-47Bistriazole antimycotic drug, 285-287Bitolterol, 37-39Bivalirudin, 169-170Bleomycin, 385-386Boric acid, 417tBortezomib, 400-402Brimonidine, 416tBrinzolamide, 416t
Bromocriptine, 62-66Brompheniramine, 294-295, 297Buccal route of administration, 4Buclizine, 216-219Budesonide, 178-180Bulk-forming laxatives, 212-213Bumetanide, 225-227Bupivacaine, 112-114Buprenorphine, 105-107Bupropion, 327-329Buspirone, 319Busulfan, 374-375Butabarbital, 316-317Butacaine, 114-115Butenafine, 281, 418tButoconazole, 281Butorphanol, 105-107
C Calcium carbonate, 197-198Calcium channel blockers, 138-140,
142-143mechanism of action of, 139i
Calcium replacement, 361-363Cancer, drugs and, 371Candesartan cilexetil, 146-147Capecitabine, 381-383Captopril, 144-145Carbachol, 21-24, 415tCarbamazepine, 73-74Carbamide peroxide, 417tCarbapenems, 253-255Carbenicillin, 241-243Carbidopa-levodopa, 62-66Carbonic anhydrase inhibitors,
229, 416tCarboplatin, 378-379Carboxamides, 80-81Carboxylic acid derivatives, 76-78Cardiac glycosides, 120-122Cardiovascular drugs, 119-152Carisoprodol, 50-52Carmustine, 375-376Carteolol, 43-47, 416tCarvedilol, 43-47, 141-142Caspofungin, 287-288Castor oil, 214-215Catecholamines, 33-37
9389INDEXqxd 08/26/2008 17:20 Page 428

429INDEX
i refers to an illustration; t refers to a table.
Catechol-O-methyltransferaseinhibitors, 66-68
Cefaclor, 243-246Cefadroxil, 243-246Cefazolin, 243-246Cefdinir, 243-246Cefepime, 243-246Cefixime, 243-246Cefotaxime, 243-246Cefoxitin, 243-246Cefpodoxime, 243-246Cefprozil, 243-246Ceftazidime, 243-246Ceftibuten, 243-246Ceftriaxone, 243-246Cefuroxime, 243-246Celecoxib, 98-100Central-acting sympathetic nervous
system inhibitors, 141-142Centrally acting skeletal muscle relax-
ants, 50-52Central nerve block, 113iCephalexin, 243-246Cephalosporins, 243-246
mechanism of action of, 245iCerumenolytics, 417tCetirizine, 294-295, 297Cevimeline, 21-24Chamomile, 423tChemical weapons exposure, treat-
ment and antidotes for, 422tChloral hydrate, 317-318Chlorambucil, 372-374Chloramphenicol, 417t, 421tChlordiazepoxide, 312-313, 314i, 315Chloroprocaine, 112-114Chlorothiazide, 224-225Chlorpheniramine, 294-295, 296i, 297Chlorpromazine, 216-219, 333-336Chlorpropamide, 342-345Chlorthalidone, 224-225Chlorzoxazone, 50-52Cholesterol absorption inhibitors, 152Cholestyramine, 147-148Choline magnesium trisalicylate, 94-96Cholinergic agonists, 21-24
mechanism of action of, 22iCholinergic blocking drugs, 27-32,
60-62, 177-178
Cholinergic drugs, 21-27mechanism of action of, 22i
Choline salicylate, 94-96Chorionic gonadotropin, 349-350Ciclopirox, 281, 418tCidofovir, 421tCimetidine, 199, 200i, 201Ciprofloxacin, 256-257, 277, 414t, 421tCisatracurium, 56-58Cisplatin, 378-379Citalopram, 320-322Cladribine, 383-384Clarithromycin, 196-197, 249-251Class IA antiarrhythmics, 124-125Class IB antiarrhythmics, 126-127Class IC antiarrhythmics, 128-129Class II antiarrhythmics, 129-131Class III antiarrhythmics, 131-132Class IV antiarrhythmics, 133-134. See
also Calcium channel blockers.Clemastine, 294-295, 297Clindamycin, 248-249, 418t, 420tClioquinol, 281Clobetasol, 419tClocortolone, 419tClomipramine, 322-325Clonazepam, 74-76, 312-313, 314i, 315Clonidine, 141-142Clopidogrel, 165-169Clorazepate, 74-76, 312-313, 314i, 315Clotrimazole, 281, 418tClove oil, 114-115Clozapine, 331-332Cocaine, 112-115Codeine, 102-105, 188-189Colchicine, 307-309Colesevelam, 147-148Colestipol, 147-148Colistin sulfate, 417tCompetitive drugs, 56-58Competitive inhibition, 107Corticosteroids, 178-180, 297-301
special population concernsand, 179
Corticotropin, 349-350Corticotropin repository, 349-350Cortisone, 298-300Cosyntropin, 349-350Co-trimoxazole, 257-259
COX-2 inhibitors, 98-99, 100. See alsoNonsteroidal anti-inflammatorydrugs.
Cranberry, 423tCromolyn, 182, 414tCyanocobalamin, 158-159Cyclizine, 216-219Cyclobenzaprine, 50-52Cyclopentolate, 416tCyclophosphamide, 302-306, 372-374Cycloplegics, 416tCyclosporine, 302-306Cyproheptadine, 294-295, 297Cytarabine, 381-383
D Dacarbazine, 376-377Daclizumab, 302-306Dactinomycin, 385-386Dalteparin, 161-164Dantrolene, 52-53Darbepoetin alfa, 160-161Darifenacin, 230-231Darunavir, 272-275Daunorubicin, 385-386Decongestants, 191-193Delavirdine, 270-271Demecarium, 24-27Demeclocycline, 247-248Depolarizing blocking drugs, 58-59Dermatologic drugs, 418-420tDesflurane, 109-110Desipramine, 322-325Desloratadine, 294-295, 297Desmopressin, 350-352Desonide, 419tDesoximetasone, 419tDexamethasone, 298-300, 415t,
417t, 419tDexchlorpheniramine, 294-295, 297Dextroamphetamine, 336-337Dextromethorphan, 188-189Diazepam, 53-55, 74-76, 312-313, 314i,
315, 422tDiazoxide, 142-143Dibucaine, 114-115Diclofenac, 98-100, 415tDicloxacillin, 241-243Dicyclomine, 27-32
9389INDEXqxd 08/26/2008 17:20 Page 429

430INDEX
i refers to an illustration; t refers to a table.
Didanosine, 266-270Dietary fiber, 212-213Diflorasone, 419tDiflunisal, 94-96Digestive drugs, 206Digoxin, 120-122Digoxin toxicity, signs and symptoms
of, 122Dihydroergotamine, 89-90Diltiazem, 133-134, 138-140Dimenhydrinate, 216-219, 294-295, 297Diphenhydramine, 60-62, 216-219,
294-295, 297Diphenidol, 218Diphenoxylate with atropine, 208-209Dipivefrin, 415tDipyridamole, 165-169Direct-acting skeletal muscle relax-
ants, 52-53Directly observable therapy, 276Direct thrombin inhibitors, 169-170Direct vasodilators, 142-143Disopyramide, 124-125Distribution, 9-10
drug interactions and, 16Diuretics, 224-229Divalproex, 76-78Dobutamine, 33-37Docetaxel, 410-411Docusate salts, 213-214Dofetilide, 131-132Dolasetron, 216-219Donepezil, 24-27Dopamine, 33-37Dopaminergic drugs, 62-66Dorzolamide, 416tDose-response curve, 13, 14iDoxazosin, 40-43, 141-142Doxepin, 322-325Doxorubicin, 385-386Doxycycline, 247-248, 420t, 421tDronabinol, 218Drotrecogin alfa, 289-290Drug administration routes, 4-5
effect of, on absorption, 7-8Drug allergy, 18-19Drug dependence, 15
Drug effect, 12Drug interactions, 15-17Drug nomenclature, 2Drug potency, 13Drug sources, 2-4Drug tolerance, 15Duloxetine, 320-322Duration of action, 12Dyclonine, 114-115
E Echinacea, 423tEchinocandins, 287-288Echothiophate, 24-27Econazole, 281, 418tEdrophonium, 24-27
toxic drug response versus myas-thenic crisis and, 24
Efavirenz, 270-271Electrolyte replacement drugs, 359-366Eletriptan, 86-88Emedastine, 414tEmetics, 219-220Emollient laxatives, 213-214Empiric therapy, 14Emtricitabine, 266-270Enalapril, 144-145Enalaprilat, 144-145Endocrine drugs, 339-356Enflurane, 109-110Enoxaparin, 161-164Entacapone, 66-68Ephedrine, 37-39, 191-193Epidural infusion, 5Epinephrine, 33-37, 415tEpoetin alfa, 160-161Eprosartan, 146-147Eptifibatide, 165-169Erectile dysfunction therapy drugs,
231-232Ergoloid mesylates, 40-43Ergotamine, 40-43Ergotamine preparations, 89-90Ertapenem, 253-255Erythromycin, 249-251, 414t, 418t, 420tErythropoietin agents, 160-161Escitalopram, 320-322Esmolol, 43-47, 129-131Esomeprazole, 201-202
Estazolam, 312-313, 314i, 315Estradiol, 347-348Estramustine, 372-374Estrogenic substances, conjugated,
347-348Estrogens, 347-348
esterified, 347-348Estropipate, 347-348Eszopiclone, 317-318Ethacrynic acid, 225-227Ethambutol, 276-280Ethinyl estradiol, 233-234, 347-348Ethosuximide, 82-83Ethotoin, 69-70Ethyl chloride, 114-115Ethylenimines, 377-378Ethynodiol diacetate, 233-234Etodolac, 98-100Etomidate, 110-112Etoposide, 396-397Excretion, 11
drug interactions and, 16Exemestane, 387-388Expected therapeutic response, 17Expectorants, 187Ezetimibe, 152
F Factor Xa inhibitor drugs, 170-171Famciclovir, 260-263Famotidine, 199, 200i, 201Fenofibrate, 148-149Fenoprofen, 98-100Fentanyl, 102-105, 110-112Ferrous fumarate, 156-157Ferrous gluconate, 156-157Ferrous sulfate, 156-157Feverfew, 423tFexofenadine, 294-295, 297Fibric acid derivatives, 148-149First-pass effect, 8Flavoxate, 230-231Flecainide, 128-129Floxuridine, 381-383Fluconazole, 285-287Flucytosine, 283-284Fludarabine, 383-384
9389INDEXqxd 08/26/2008 17:20 Page 430

Fludrocortisone, 301Flunisolide, 178-180Fluocinolone, 419tFluocinonide, 419tFluorometholone, 415tFluoroquinolones, 256-257, 277Fluorouracil, 381-383Fluoxetine, 320-322Fluoxymesterone, 390-391Fluphenazine, 333-336Flurandrenolide, 419tFlurazepam, 312-313, 314i, 315Flurbiprofen, 98-100, 415tFlutamide, 391-392Fluticasone, 178-180Fluvastatin, 149-150Fluvoxamine, 320-322Folic acid, 159-160Folic acid analogues, 380-381Fondaparinux, 170-171Food, drug interactions and, 17Food and Drug Administration, new
drug development and, 5-6Formoterol, 37-39, 176-177Fosamprenavir, 272-275Foscarnet, 264Fosinopril, 144-145Fosphenytoin, 69-70Frovatriptan, 86-88Fulvestrant, 388-390Furosemide, 225-227
G Gabapentin, 78-79Galantamine, 24-27Gamma benzene hydrochloride, 420tGanciclovir, 260-263Garlic, 423tGastric route of administration, 4Gastrointestinal drugs, 195-220Gefitinib, 400-402Gemcitabine, 381-383Gemfibrozil, 148-149Gemtuzumab ozogamicin, 398-399Genitourinary drugs, 223-234Gentamicin, 238-240, 414t, 418t, 421tGinger, 423-424tGinkgo biloba, 424t
Ginseng, 424tGliclazide, 342-345Glimepiride, 342-345Glipizide, 342-345Glucagon, 345, 346iGlucan synthesis inhibitors, 287-288Glucocorticoids, 298-300Glyburide, 342-345Glycerin, 211-212, 416tGlycopyrrolate, 27-32Gonadotropin-releasing hormone
analogues, 393-395Goserelin, 393-395Granisetron, 216-219Green tea, 424tGriseofulvin, 281Guaifenesin, 187Guanadrel, 141-142Guanethidine, 141-142Guanidine, 24-27
H Hair growth stimulants, 419tHalcinonide, 419tHalf-life, 11Halobetasol, 419tHaloperidol, 333-336Haloprogin, 281Halothane, 109-110Hematinic drugs, 155-161Hematologic drugs, 155-173Heparin, 161-164
partial thromboplastin time monitor-ing and, 163
Herbal drugs, 423-424tHistamine-1 receptor antagonists,
294--297Histamine-2 receptor antagonists,
199, 201mechanism of action of, 200i
HMG-CoA reductase inhibitors,149-150
Homatropine, 27-32, 416tHomeostasis, drugs and, 359Hormonal antineoplastic drugs,
386-395Hormonal contraceptives, 233-234Hormone modulators, 386-395
Hormone replacement therapy, heartdisease and, 348
5-HT1-receptor agonists, 86-88contraindications to, 88
5-HT3 receptor antagonists, 210Hydantoins, 69-70Hydralazine, 142-143Hydrochlorothiazide, 224-225Hydrocodone, 102-105, 188-189Hydrocortisone, 178-180, 298-300,
417t, 419tHydroflumethiazide, 224-225Hydromorphone, 102-105Hydroxocobalamin, 158-159Hydroxyamphetamine, 415t5-Hydroxy-3-methylglutaryl coenzyme
A reductase inhibitors, 149-150Hydroxyprogesterone, 392-393Hydroxyurea, 406Hydroxyzine, 216-219, 294-295, 297Hyoscyamine sulfate, 27-32Hyperglycemic drug, 345, 346iHyperosmolar laxatives, 211-212Hypersusceptibility, 18Hypoglycemic drugs, 339-345
IJ Iatrogenic effects, 18Ibritumomab tiuxetan, 398-399Ibuprofen, 98-100Ibutilide, 131-132Idarubicin, 385-386Idiosyncratic response, 19Ifosfamide, 372-374Imatinib, 400-402Imidazole, 284-285Iminostilbenes, 73-74Imipenem-cilastatin, 253-255Imipramine, 322-325Immune system drugs, 293-309Immunosuppressants, 302-306Inamrinone, 122-123Indapamide, 224-225Indinavir, 272-275Indomethacin, 98-100Influenza A drugs, 264-266Inhalation anesthetics, 109-110Inotropics, 119-123
431INDEX
i refers to an illustration; t refers to a table.
9389INDEXqxd 08/26/2008 17:20 Page 431

Insulin, 340-342, 341iInterferons, 407-408Intra-articular infusion, 5Intradermal route of administration, 4Intramuscular route of administration,
4, 8Intraocular pressure, drugs to lower,
416tIntraosseous infusion, 5Intraperitoneal infusion, 5Intrapleural infusion, 5Intrathecal infusion, 5Intravenous anesthetics, 110-112Intravenous route of administration,
5, 7Intrinsic activity, 12Investigational new drug, approval
process for, 5-6Ipecac syrup, 219-220Ipratropium, 176-177Irbesartan, 146-147Irinotecan, 399-400Iron, 156-157
parenteral, testing for sensitivityto, 157
Iron dextran, 156-157Irritant cathartics, 214-215Isoetharine, 37-39Isoflurane, 109-110Isoniazid, 276-280Isoproterenol, 33-39Isosorbide, 135-136, 416tIsotretinoin, 419tItraconazole, 285-287
K Kanamycin, 238-240Kaolin and pectin, 209-210Kava, 424tKetamine, 110-112Ketoconazole, 284-285, 418tKetoprofen, 98-100Ketorolac, 98-100, 415tKetotifen, 414t
L Labetalol, 43-47, 141-142Lactulose, 211-212
Lamivudine, 266-270Lamotrigine, 79-80Lansoprazole, 201-202Latanoprost, 416tLaxatives, 211-216Lepirudin, 169-170Letrozole, 387-388Leucovorin, 160Leukotriene modifiers, 180-182Leuprolide, 393-395Levalbuterol, 37-39, 176-177Levarterenol, 33-37Levetiracetam, 84-85Levobunolol, 43-47, 416tLevobupivacaine, 112-114Levodopa, 62-66
pros and cons of, 64Levofloxacin, 256-257, 414tLevorphanol, 102-105Levothyroxine, 352-354Lidocaine, 112-115, 126-127
mechanism of action of, 127iLincomycin derivatives, 248-249Lindane, 420tLiothyronine, 352-354Liotrix, 352-354Lipase, 206Lisdexamfetamine, 336-337Lisinopril, 144-145Lithium, 329-330Local anesthetics, 112-114Lodoxamide, 414tLomustine, 375-376Loop diuretics, 225-227Loperamide, 208-209Lopinavir, 272-275Loratadine, 294-295, 297Lorazepam, 74-76, 312-313, 314i,
315, 422tLosartan, 146-147Loteprednol, 415tLovastatin, 149-150Loxapine, 333-336Lubricant laxatives, 215-216Lubricants, ophthalmic, 415tLymphocyte immune globulin, 302-306
M Macrolides, 249-251Mafenide, 418tMagaldrate, 197-198Magnesium hydroxide and aluminum
hydroxide, 197-198Magnesium replacement, 363-365Magnesium salts, 211-212Maintenance therapy, 14Malathion, 420tMannitol, 228, 416tMaprotiline, 327-329Margin of safety, 13Mast cell stabilizers, 182Mechlorethamine, 372-374Meclizine, 216-219, 294-295, 297Medroxyprogesterone, 392-393Megestrol, 392-393Meloxicam, 98-100Melphalan, 372-374Menotropins, 349-350Menthol, 114-115Meperidine, 102-105Mephobarbital, 70-72, 316-317Mepivacaine, 112-114Mercaptopurine, 383-384Meropenem, 253-255Mesoridazine, 333-336Mestranol, 233-234Metabolism, 10-11
drug interactions and, 16, 17Metaproterenol, 37-39, 176-177Metaxalone, 50-52Metformin, 342-345Methadone, 102-105Methazolamide, 229Methimazole, 355-356Methocarbamol, 50-52Methohexital, 110-112Methotrexate, 380-381Methscopolamine, 27-32Methsuximide, 82-83Methyclothiazide, 224-225Methylcellulose, 212-213, 415tMethyldopa, 141-142Methylphenidate, 336-337Methylprednisolone, 178-180,
298-300, 299i
432INDEX
i refers to an illustration; t refers to a table.
9389INDEXqxd 08/26/2008 17:20 Page 432

Methylxanthines, 183-185Metipranolol, 43-47, 416tMetoclopramide, 218Metolazone, 224-225Metoprolol, 43-47, 137-138Metronidazole, 196-197, 418tMexiletine, 126-127Miconazole, 281, 418tMidazolam, 110-112Miglitol, 342-345Milrinone, 122-123Mineralocorticoids, 301Mineral oil, 215-216Minerals as drug sources, 3Minocycline, 247-248, 420tMinoxidil, 142-143, 419tMiotics, 415tMirtazapine, 327-329Misoprostol, 202-203
dangers of using, during preg-nancy, 203
Mitomycin 385-386Mitoxantrone, 385-386Mixed alpha- and beta-adrenergic
blockers, 141-142Mixed opioid agonist-antagonists,
101, 105-107Modafinil, 336-337Moexipril, 144-145Molindone, 333-336Mometasone, 419tMonoamine oxidase inhibitors,
325-327Monobactams, 255-256Monoclonal antibodies, 186-187,
398-399Montelukast, 180-182Mood stabilizer drugs, 329-330Moricizine, 128-129Morphine sulfate, 102-105Motor end plate, neuromuscular
blocking drugs and, 56iMoxifloxacin, 256-257Mucolytics, 189-191Mupirocin, 418tMuromonab-CD3, 302-306Mycophenolate mofetil, 302-306Mydriatics, 415-416t
N Nabumetone, 98-100Nadolol, 43-47, 137-138Nafcillin, 241-243Naftifine, 281, 418tNalbuphine, 105-107Naloxone, 107-108Naltrexone, 107-108
for drug addiction, 108Naproxen, 98-100Naratriptan, 86-88Narcotic agonists. See Opioid
agonists.Natamycin, 414tNateglinide, 342-345Natural antineoplastic drugs, 395-397Nedocromil, 182Nefazodone, 327-329Negative chronotropic effect, 120Negative dromotropic effect, 120Nelfinavir, 272-275Neomycin, 238-240, 417t, 418tNeostigmine, 24-27Neuromuscular blocking drugs, 55-59
motor end plate and, 56isafe use of, 57
Nevirapine, 270-271New drug development, 5-6Niacin, 150-151Nicardipine, 138-140Nicotinic acid, 150-151Nifedipine, 138-140Nilutamide, 391-392Nitrates, 135-136Nitrofurantoin, 259-260Nitrogen mustards, 372-374Nitroglycerin, 135-136Nitroprusside, 142-143Nitrosoureas, 375-376Nitrous oxide, 109-110Nizatidine, 199, 200i, 201Nonbenzodiazepines-nonbarbiturates,
317-318Noncatecholamines, 37-39Nondepolarizing blocking drugs, 56-58Non-nucleoside reverse transcriptase
inhibitors, 270-271Nonopioid analgesics, 93-101
Nonselective drug, 13Nonsteroidal anti-inflammatory drugs,
98-100risks of using, 98
Norepinephrine, 33-37Norepinephrine depletors, 141-142Norfloxacin, 256-257, 414tNortriptyline, 322-325Nucleoside analogue reverse tran-
scriptase inhibitors, 266-270Nucleosides, synthetic, 260-263Nucleotide analogue reverse tran-
scriptase inhibitors, 271-272Nystatin, 280-282, 418t
O Obesity drugs, 207-208Ofloxacin, 256-257, 277, 414tOlanzapine, 331-332Olmesartan, 146-147Olopatadine, 414tOmalizumab, 186-187Omeprazole, 201-202Ondansetron, 216-219Onset of action, 11Ophthalmic drugs, 414-416tOpioid agonists, 101, 102-105
pain control and, 104isafe use of, 102
Opioid antagonists, 101, 107-108Opioid-related drugs as antidiarrheals,
208-209Oral anticoagulants, 164-166Oral antidiabetic drugs, 342-345Oral route of administration, 5, 8Orlistat, 207-208Orphenadrine, 50-52Osmotic agents, 416tOsmotic diuretics, 228Otic drugs, 417tOverdose, 18Oxacillin, 241-243Oxaliplatin, 378-379Oxaprozin, 98-100Oxazepam, 312-313, 314i, 315Oxcarbazepine, 80-81Oxiconazole, 281, 418tOxybutynin, 27-32, 230-231
433INDEX
i refers to an illustration; t refers to a table.
9389INDEXqxd 08/26/2008 17:20 Page 433

Oxycodone, 102-105Oxymorphone, 102-105Oxytocin, 350-352
P Paclitaxel, 410-411Pain medications, 93-115Paliperidone, 331-332Palliative therapy, 15Pancreatic enzymes, 206Pancreatin, 206Pancrelipase, 206Pancuronium, 56-58Pantoprazole, 201-202Parasympatholytic drugs, 60-62Parasympathomimetic drugs. See
Cholinergic drugs.Paromomycin, 238-240Paroxetine, 320-322Partial agonists, 44Passive transport, 7Pathogen resistance, preventing,
237-238Patient sensitivity–related reactions,
18-19Patient’s response to drug, factors that
affect, 15Peak concentration, 11-12Pediculicides, 420tPegaspargase, 404Penbutolol, 43-47Penciclovir, 418tPenicillin-binding proteins, 241-242Penicillins, 241-243, 421tPentazocine, 105-107Pentobarbital, 316-317Pentostatin, 383-384Peptic ulcer drugs, 195-203Peripheral vascular resistance, 136Permethrin, 420tPerphenazine, 216-219, 333-336Pharmacodynamics, 12-13, 14iPharmacokinetics, 7-12Pharmacologic class, 2Pharmacotherapeutics, 14-15Phenazopyridine hydrochloride,
100-101
Phenelzine, 325-327Phenobarbital, 70-72, 316-317Phenothiazines, 216-219Phenoxybenzamine, 40-43Phentermine, 207-208Phentolamine, 40-43, 141-142Phenylephrine, 37-39, 191-193, 415tPhenyltriazines, 79-80Phenytoin, 69-70Phosphodiesterase inhibitors, 122-123Physostigmine, 24-27Pilocarpine, 21-24, 415tPimozide, 333-336Pindolol, 43-47Pinocytosis, 7Pioglitazone, 342-345Pirbuterol, 37-39, 176-177Piroxicam, 98-100Pituitary drugs, 348-352Plants as drug sources, 3Podophyllotoxins, 396-397Polycarbophil, 212-213Polyenes, 280-283Polyethylene glycol, 211-212Polymyxin B sulfate, 417tPolythiazide, 224-225Polyvinyl alcohol, 415tPositive inotropic effect, 119-120Posterior pituitary drugs, 350-352Potassium replacement, 360-361Potassium-sparing diuretics, 227-228Potentiation, 16Pramipexole, 62-66Pramoxine, 114-115Pravastatin, 149-150Prazosin, 40-43, 141-142Prednisolone, 178-180, 298-300, 415tPrednisone, 178-180, 298-300Prilocaine, 112-114Primidone, 70-72Probenecid, 306-307Procainamide, 124-125Procaine, 112-114Procarbazine, 405Prochlorperazine, 216-219Procyclidine, 60-62Prodrug, 10Progestins, 392-393
Promethazine, 216-219, 294-295, 297Propafenone, 128-129Propantheline, 27-32Proparacaine, 414tPropofol, 110-112Propoxyphene, 102-105Propranolol, 43-47, 129-131, 137-138Propylthiouracil, 355-356Prostaglandin analogues, 416tProtease, 206Protease inhibitors, 272-275Protirelin, 349-350Proton pump inhibitors, 201-202Protriptyline, 322-325Pseudoephedrine, 191-193Psychotropic drugs, 311-337Psyllium hydrophilic mucilloid, 212-213Purine analogues, 383-384Pyrazinamide, 276-280Pyridostigmine, 24-27Pyrimidine analogues, 381-383
mechanism of action of, 382Pyrophosphate analogues, 264Pyrrolidines, 84-85
Q Quazepam, 312-313, 314i, 315Quetiapine, 331-332Quinapril, 144-145Quinidine, 124-125
R Rabeprazole, 201-202Radioactive iodine, 355-356Ramelton, 317-318Ramipril, 144-145Ranitidine, 199, 200i, 201Rasagiline, 62-66Recombinant human activated protein
C, 289-290Rectal route of administration, 5Remifentanil, 102-105Repaglinide, 342-345Replacement therapy, 15Reserpine, 141-142Respiratory drugs, 175-193Respiratory route of administration, 5
434INDEX
i refers to an illustration; t refers to a table.
9389INDEXqxd 08/26/2008 17:20 Page 434

Reteplase, 171-173Ribavirin, 264-266Rifampin, 276-280Rimantadine, 264-266Rimexolone, 415tRisperidone, 331-332Ritonavir, 272-275Rituximab, 398-399Rivastigmine, 24-27Rizatriptan, 86-88Rocuronium, 56-58Ropinirole, 62-66Ropivacaine, 112-114Rosiglitazone, 342-345Rosuvastatin, 149-150
S Salicylates, 94-96
safe use of, 96Saline compounds, 211-212Salmeterol, 37-39, 176-177Salsalate, 94-96Saquinavir, 272-275Scabicides, 420tScopolamine, 27-32, 218Secobarbital, 316-317Secondary effects, 18Sedative-hypnotic drugs, 311-318Selective serotonin reuptake in-
hibitors, 320-322discontinuation syndrome and, 321
Selegiline, 62-66Senna, 214-215Serotonin 5-HT3 receptor antagonists,
216-219Sertraline, 320-322Sevoflurane, 109-110Sibutramine, 207-208Side effects, 17-19Sildenafil, 231-232Silver sulfadiazine, 418tSimethicone, 197-198, 205Simvastatin, 149-150Sirolimus, 302-306Skeletal muscle relaxants, 49-55Sleep agents, warning about, 318Sodium bicarbonate, 366-368Sodium biphosphate, 211-212
Sodium citrate, 366-368Sodium ferric gluconate complex,
156-157Sodium lactate, 366-368Sodium phosphate, 211-212Sodium replacement, 365-366Sodium salicylate, 94-96Solifenacin, 230-231Somatrem, 349-350Somatropin, 349-350Sotalol, 43-47, 131-132Spironolactone, 227-228St. John’s wort, 424tStabilizing drugs, 56-58Stable iodine, 355-356Statins, 149-150Stavudine, 266-270Stimulant laxatives, 214-215Stimulants, 336-337Stool softeners, 213-214Streptokinase, 171-173Streptomycin, 238-240, 276-280, 421tStreptozocin, 375-376Subcutaneous route of administration,
5, 8Sublingual route of administration, 4, 7Succinimides, 82-83Succinylcholine, 58-59Sucralfate, 202-203Sufentanil, 102-105, 110-112Sulconazole, 281, 418tSulfacetamide, 414t, 418tSulfadiazine, 257-259Sulfamate-substituted monosaccha-
rides, 82Sulfamethoxazole and trimethoprim,
257-259Sulfinpyrazone, 165-169, 306-307Sulfisoxazole, 414tSulfonamides, 83-84, 257-259Sulindac, 98-100Sumatriptan, 86-88Supplemental therapy, 15Supportive therapy, 15Suprofen, 415tSympatholytic drugs, 40-47, 141-142Sympathomimetic drugs. See Adren-
ergic drugs.
Syncytial virus drugs, 264-266Synthetic drug sources, 2, 3-4
T Tacrine, 24-27Tacrolimus, 302-306Tadalafil, 231-232Tamoxifen, 388-390
risks versus benefits of, 389Tamsulosin, 40-43Targeted therapies, 400-402Target organs, 23Tazarotene, 419tTelmisartan, 146-147Temazepam, 312-313, 314i, 315Tenecteplase, 171-173Teniposide, 396-397Tenofovir, 271-272Terazosin, 40-43, 141-142Terbinafine, 281, 288-289, 418tTerbutaline, 37-39, 176-177Terconazole, 281Testolactone, 390-391Testosterone, 390-391Tetracaine, 112-115, 414tTetracycline, 196-197, 418t, 420tTetracyclines, 247-248Theophylline, 183-185Therapeutic class, 2Therapeutic index, 13Thiazide and thiazide-like diuretics,
224-225Thiethylperazine, 216-219Thioguanine, 383-384Thiopental, 110-112Thioridazine, 333-336Thiotepa, 377-378Thiothixene, 333-336Thrombolytic drugs, 171-173Thymoglobulin, 302-306Thyroglobulin, 352-354Thyroid antagonists, 355-356Thyroid drugs, 352-354Thyroid-stimulating hormone, 349-350Thyroid USP (desiccated), 352-354Thyrotropin, 349-350Ticarcillin, 241-243Ticlopidine, 165-169
435INDEX
i refers to an illustration; t refers to a table.
9389INDEXqxd 08/26/2008 17:20 Page 435
Rahimullah
Text Box
Download From: AghaLibrary.com

Timolol, 43-47, 416tTinzaparin, 161-164Tioconazole, 281Tipranavir, 272-275Tirofiban, 165-169Tizanidine, 50-52Tobramycin, 238-240, 414tTolazamide, 342-345Tolbutamide, 342-345Tolcapone, 66-68Tolnaftate, 281Tolterodine, 27-32, 230-231Topical anesthetics, 114-115Topical route of administration, 5Topiramate, 82Topoisomerase I inhibitors, 399-400Topotecan, 399-400Toremifene, 388-390Trandolapril, 144-145Translingual route of administration, 4Tranylcypromine, 325-327Trastuzumab, 398-399Travoprost, 416tTrazodone, 327-329Tretinoin, 419tTriacetin, 281Triamcinolone, 178-180, 298-300, 419tTriamterene, 227-228Triazenes, 376-377Triazolam, 312-313, 314i, 315Triazoles, synthetic, 285-287Tricyclic antidepressants, 322-325Triethanolamine polypeptide, 417tTrifluoperazine, 333-336Trifluridine, 414tTrihexyphenidyl, 27-32, 60-62Trimethobenzamide, 216-219Trimipramine, 322-325Triptans. See 5-HT1-receptor agonists.Triptorelin, 393-395Tromethamine, 366-368Tropicamide, 416tTrospium, 230-231Tuberculosis
directly observable therapy for, 276drug regimens for treating, 276-280
Typical antipsychotics, 333-336
U Undecylenic acid, 281Unfractionated heparin, 161-164Unoprostone, 416tUrea, 228Uricosurics, 306-307Urinary tract antispasmodics, 230-231Urokinase, 171-173
V Vaginal route of administration, 5Valacyclovir, 260-263Valganciclovir, 260-263Valproate, 76-78Valproic acid, 76-78Valsartan, 146-147Vancomycin, 251-253Vardenafil, 231-232Vasodilating drugs, 142-143Vasopressin, 350-352Vecuronium, 56-58Venlafaxine, 320-322, 327-329Verapamil, 133-134, 138-140Vinblastine, 395-396Vinca alkaloids, 395-396Vincristine, 395-396Vinorelbine, 395-396Vitamin B12, 158-159Vitex, 424tVoriconazole, 285-287
W Warfarin, 164-166
monitoring levels of, 165
X Xanthines, 183-185
Y Yohimbine, 424t
Z Zafirlukast, 180-182Zaleplon, 317-318Zidovudine, 266-270, 268iZileuton, 180-182Ziprasidone, 331-332Zolmitriptan, 86-88
Zolpidem, 317-318Zonisamide, 83-84
436INDEX
i refers to an illustration; t refers to a table.
9389INDEXqxd 08/26/2008 17:20 Page 436
Rahimullah
Text Box
Download From: AghaLibrary.com

Notes
9389INDEXqxd 08/26/2008 17:20 Page 437

Notes
9389INDEXqxd 08/26/2008 17:20 Page 438
Rahimullah
Text Box
Download From: AghaLibrary.com