CHW Annual Report 2001/2002 (Low Quality) - OpenGov NSW
75
-
Upload
khangminh22 -
Category
Documents
-
view
3 -
download
0
Transcript of CHW Annual Report 2001/2002 (Low Quality) - OpenGov NSW




1
Contents122nd Annual Report of the Board of Directorsof the Royal Alexandra Hospital for Children(The Children’s Hospital at Westmead)for the year ending 30 June 2002
Highlights 2 Committees 12
Philosophy of Care 3 Overview of Divisional Achievements 14
President and Chief Executive Report 4 Patient Care Statistics 24
Our Mission Vision and Values 4 Freedom of Information 24
Activity and Finances 4 Risk Management and 25 Insurance Activities
Our Patron 5 Service Improvement 28
Our Board 5 Cultural Diversity 29
Our Staff 5 Disability Action Plan 29
Our Supporters 5 Engaging the Community 30
The Future 5 Human Resources 31
Board and Management 6 Benefactors and Donors 33
Board Meeting Attendances 6 Roll of Honour 37
Profiles – Board of Directors 7 Certification of Accounts 38
Profiles – Executive Staff 9 Independent Audit Report 39
Lines of Management Responsibility 10 Financial Overview 41
Corporate Governance Statement 11 Financial Statements 42
Cover: Mason Dixon with dad James. Dad’s liver saved Mason’s life.Photograph courtesy of Vicki Leopold / Who Weekly.

2
Highlights 2001/2002
The following is a snapshot of the many successes achieved this year at TheChildren’s Hospital at Westmead. These highlights demonstrate the dedicationand commitment of our team to making this a great Hospital.
• The Gene Therapy ResearchUnit treated an infant with X-linked severe combinedimmunodeficiency (SCID-X1)by gene therapy. The firstAustralian group to achievethis major biomedicalmilestone and one of only fourgroups in the world.
• CHW led the development ofthree paediatric clinicalpractice guidelines for NSWHealth: fever, croup andbronchiolitis. CHW staffchaired multidisciplinaryworking parties, withrepresentation from all threeNSW specialist children'shospitals, general hospitals inmetro and rural areas,Emergency Departmentclinicians, GPs andconsumers.
• Established the Cystic FibrosisTreatment Centre providingroutine visits, specimencollection, home IV antibioticconsultations and educationalsupport for newly diagnosedpatients. The number ofEmergency Departmentpresentations in the last sixmonths has decreasedsignificantly.
• Molecular PathologyLaboratory now operational,providing quick and efficientdiagnostic results from tinyamounts of specimenmaterial. Allows rapiddiagnosis of viral, bacterialand fungal infection resultingin early appropriate treatment.
• Established a weeklymultidisciplinary paediatricchronic pain clinic. Chronicpain is prevalent in thepaediatric population andneeds a specialised service forits management.
• Set up a neurogenetics serviceoffering patients with a varietyof inherited disorders, acoordinated approach to theirclinical care and a direct linkto our integrated local andinternational researchprograms.
• Developed an adverse eventsdatabase, coordinated by theService Improvement Unitsafety program, enhancingpatient safety and providingbetter risk management.
• Established a Congenital andPerinatal Infection Clinic, thefirst such service in Australia.
• Adolescent Medicine Unitestablished Teen Link, a pilotservice for adolescents andparents on methadoneprograms in Western Sydney.
• Introduced ‘Bear Permit’, aninitiative of the FamilyFocused Care Committee tostreamline processes forchildren with chronic illness,who require frequent visits oradmissions.
• Created the PaediatricPalliative Care Passport, whichfacilitates easy and fair accessto palliative care throughoutthe health care system.
• Opened dialogue with NSWFire Brigades to set upscheme to treat juvenile fire-setters, particularly withreference to familiesvoluntarily seeking help beforemajor incident occurs.
• Telemedicine Project hascommenced for the NSWHeart Service.
• Adolph Basser CardiacInstitute replaced and
installed new PaediatricCardiac Catheter Laboratoryfor NSW, resulting in improvedimage quality, laboratoryergonomics, reliability, andpatient flow.
• Celebrated the 25th
Anniversary of AdolescentMedicine at CHW with areception at GovernmentHouse and gala dinner,recognising CHW's leadershiprole in adolescent health bothin Australia andinternationally.
• Child Protection Unit jointlyhosted the first internationalShaken Baby SyndromeConference in September2001 and hosted the JIRTForum in March 2002.
• Participated in the first LinenNumerical Profile auditachieving a score of 96%.
• Child Development Unitinitiated an Early InterventionService for Autism incollaboration with the AutisticAssociation.
• Established the Chair ofPaediatric Allergy and ClinicalImmunology. An Australianfirst which will provide thehighest standard of clinicalservices in paediatric allergyand promote research into theallergic diseases in childhood.
• As part of the state-widenetworking initiative,expanded the Greater WesternSydney Child Health Networkfrom four to ten partners -Greater Western Child HealthNetwork. This will allowincreased collaborationbetween CHW and other metroand rural Area Health Servicesto improve services forchildren closer to home.

Philosophy of Care
The Children’s Hospital at Westmead is a free-standing children’s hospitaldedicated to the care of children from all over New South Wales, from otherStates of Australia and from other countries.
Purpose built to meet the needs ofchildren and their families, theHospital has a bed capacity of339; comprising 290 overnightbeds and 49 for same daytreatment. For many children, ourHospital is the only place they canreceive the unique treatment theyneed.
A teaching hospital of theUniversity of Sydney and theUniversity of Western Sydney, ourHospital is also a leadinginstitution in children’s clinicalresearch focusing on effectivelyturning research into medicine.
The Children’s Hospital atWestmead is a Body Corporateestablished pursuant to the HealthServices Act of 1997.
Our Vision• Better Health for Children• Excellence in Child Health Care
Our MissionThe Children’s Hospital atWestmead will constantlychallenge the existing boundariesin paediatrics and child health byleading change and striving forexcellence in clinical care,research, teaching and advocacy.
• Hospital services – to provide atotal healing environment forchildren and their families. We dothis by combining the best ofscience with the technical andcaring skills of our staff in abuilding which blends innovativedesign with art and gardens.
• Community – to expandcommunity and outreach activitieswhich offer appropriate care in theappropriate place.
• Advocacy – to promote theinterests and needs of all children.
• Teaching – to place a highpriority on excellence andleadership in education andtraining to support our staff and toshare our knowledge with others.
• Research – to place a highpriority on research to improve thelives of our present and futurepatients.
Principles guiding ourWork
• Health gain – to ensure thatimproving children’s health andquality of life are the focus of ourefforts.
• Concern for people – to carefor our patients, their families, ourstaff and our supporters asindividual people with their ownneeds.
• Doing it better – to provide thebest possible patient care by theeffective use of resources,recognising the need tocontinuously review and improveprocedures and processes.
• A hub of paediatrics – to play apivotal role in establishing withothers a network to share ourknowledge and skills in paediatricsfor the health of children.
• Making the future better – toinvest in and facilitate researchthat improves our understandingof how to prevent or treat diseasesin children and to work withgovernment and communityagencies to promote the healthand well-being of all children.
Values• Commitment• Accountability• Respect• Excellence• Service
3

4
President and Chief Executive ReportOur Annual Report is different this year. Although the content is much the same,it is published on the Hospital’s website, with only a small number being printedto meet statutory requirements. The report will be widely available, but at amuch reduced cost, so that our funds can be used where they are most needed– for the care of sick children.
Rather than review all of our achievements, we urge you to look at the Highlightsof the Year (page 2) and the Overview of Divisional Achievements (pages 14-23).Much has been achieved in the past year, from cutting edge research to newtreatments for disabled children, but there is still much to do. We are continuingthe evolving process of being more outward looking, working with otherhealthcare providers, listening and responding to the families we treat andbuilding cross-disciplinary teams where the focus is on the child and family.
We are aware that a child’sadmission to hospital is just oneincident in the child’s life, eventhough it may be an extremelyimportant one. We recognisethat the child and family are ourguests, that it is a privilege tocare for them and that werespect them as individuals, aswell as respecting their opinionsand culture. We also know thatthe care we provide is oftenenhanced when we work withother services within andbeyond the Hospital.
Examples of working with otherservices include the PaediatricNetwork, a concept establishedby this Hospital and which hasnow been taken up state-wide;the establishment of regularmeetings with Sydney Children’sHospital to look at areas of co-operation and sharing; theWestmead Research Hubcomprising our own ResearchDivision, the Children’s MedicalResearch Institute, theWestmead Hospital ResearchGroup and the MillenniumInstitute; and the WesternSydney Quadrangle which is aforum designed to facilitate co-operative working relationshipsbetween the main fourneighbouring Health Services inthe Greater West of Sydney.
We continue discussions withthe Children’s Medical ResearchInstitute about how we can worktogether more closely. Althoughthe proposal for a merger of our
research activities has been setaside for the time being, thereare many other avenues toextend collaboration. Our newresearch building, which willoccupy an area between theCMRI and the Hospital’s currentresearch block, will be animportant catalyst for this.
Our Mission, Visionand Values
We are consciously ‘walking thetalk’, particularly with regard toour five Values: C.A.R.E.S. –Commitment, Accountability,Respect, Excellence, Service. Toensure that the public knowwhat we stand for, our Visionand Values have been placed onthe twin pillars at the Hospitalentrance. This is more thandecoration. It is to proclaimwhat we stand for and whatpeople can expect from us. It isalso a reminder to all of us whowork in this Hospital that this isthe expectation that the publicshould have of us.
These Values fit with ourevolving culture of continuousimprovement at every level ofthe Hospital. The Team at theService Improvement Unit isleading the way in helping us touse data to look at what we aredoing, so that we can find waysof doing it better. The focus ison improving the system so thatcommunication is open andhonest and the environment is
safe for our patients, our staffand others who use ourservices. We believe that withthis focus, financialimprovement will also follow.It was pleasing then, that therecent periodic EQuIP review bythe Australian Council onHealthcare Standardscommented on the extent andbreadth of quality initiativesright across the Hospital and onthe commitment from all levelsof staff to quality improvement.
Activity and Finances
We treated more children thanlast year. Due to the continuingchange in patterns of care,many children with cancer,leukaemia, diabetes, cysticfibrosis and those needing sleepinvestigations can now bemanaged as day patients oroutpatients. This trend willcontinue, with inpatientnumbers falling and outpatientcare increasing as we find newways of reducing the time achild needs to stay in hospital.
The Hospital’s financial resultwas within 0.06% of theincreased government budgetallocation received. This goodresult was largely due to ourability to raise more revenuefrom our Bandaged BearOutpatient Clinics and ourprivately insured patients,although 87% of our patients donot carry, or declare, privateinsurance.

5
A recent Australian studyconfirmed the American datathat it is more expensive to treatchildren in hospital than to treatadults, particularly for childrenunder 3 years, the predominantage group we admit. Comparedwith other children’s hospitals inAustralia, we perform veryfavourably.
Although we have significantdonated funds, there is ashortage of uncommitted fundsto support clinical activities andequipment because most of thefunds are given to us tagged forspecific purposes such as ournew research facility, BearCottage and specific items ofequipment. Now that we havebeen on the Westmead site forseven years, there is a need formore maintenance of the fabricof the building, as well as formaintaining and renewing ourstate of the art equipment, mostof which was purchased at thetime we moved to Westmead.This brings the challenge ofmaintaining the Hospital in anexcellent state, when the greatmajority of our budget is neededfor maintaining day-to-dayservices.
Our Patron
Queen Elizabeth, the QueenMother, had been the Hospital’sPatron for 77 years. In ourentire history we have only hadtwo Patrons, Queen Alexandraand Queen Elizabeth, the QueenMother. The Board felt that withthe passing of our incomparablePatron, we should acknowledgethe end of such an era by notseeking a successor.
Our Board
Val Street, a distinguishedBoard member since 1989retired because of ill health andGabrielle Kibble, who served onthe Board since 2000, stooddown due to othercommitments. We weredelighted that Joanna Caponwas awarded an OAM in theAustralia Day Honours List. TheBoard welcomes Mr. JohnChoueifate as a new member.
Our Staff
Every year our staff receive arange of national andinternational awards. Some ofthese in the last 12 monthshave included: Dr Martin Silinkand Dr Bridget Wilcken wereawarded AM in the Order ofAustralia; Greg McCauley wasawarded the Australian ServiceMedal from the AustralianDefence Forces; David Littlereceived the prestigiousAmerican, British, CanadianTravelling Fellowship inOrthopaedics; John Collins wasawarded the Cottrell TravellingFellowship; Nadia Letts won aChurchill Scholarship to look atmyoelectric prostheses in theUSA; Helen Gosby becameAustralia’s first NursePractitioner in PaediatricEmergency; David Fitzsimmonswas elected President of theAustralian Cleft Lip Association;Bronwyn Thomas and JanHancock won the prize for thebest presentation at theNational PaediatricPhysiotherapy Conference;Wolfgang Hoelger was YoungInvestigator of the Year at theChildren and Bone Conferencein the UK and Jacqui Dalby-Payne won the Young ClinicianAward at the Australian PacificDigestive Diseases Week.
Many other staff served beyondthe Hospital as senior officers innational and internationalorganisations, on journaleditorial boards, as Governmentadvisors, as international guestspeakers or by contributing tochild health through theirresearch and publications.
During the year we weresaddened to hear of the deathof Dr. Reuben Hertzberg, whohad played an important part inthe development of paediatricophthalmology.
Our Supporters
We continue to haveoutstanding support fromcommunity groups, individualsupporters and corporations.
They make the differencebetween us being just a verygood Children’s Hospital andone of the world’s greatChildren’s Hospitals. This is atrue partnership in working withus to improve the lives of sickchildren.
The Future
What will the Hospital be like10, 15, 20 or 30 years fromnow? The pattern of paediatriccare is likely to be very different,with much more emphasis onsophisticated ambulatory care,with only the extremely illneeding hospital admission.The molecular biology revolutionwill bring treatments we canonly dream of, but the family,social and emotional problemswhich impact on many of ouryoung patients are likely toremain. To help plan the futurewe have established a FuturesCommittee made up of some ofour talented young staff. Theirjob is to help plan for thisexciting future. Theirsuggestions and research willhelp our current planning, aswell as preparing them for whenthey become the nextgeneration of health careleaders.
John A. Dunlop, AMPresident
Kim Oates, AMChief Executive

6
Board and ManagementPatron
Her Majesty Queen Elizabeth, TheQueen Mother (to 31 March 2002)
Board of Directors
President:John Dunlop, AM (appointed 1983,Board Director since 1973)
Vice-President:Val Street, MEd (Hon), MSc, MACE(appointed 1998, Board Directorsince 1989)
Honorary Treasurer:David Say, CA, FCA, DipBA, MBCS(appointed 1993, Board Directorsince 1989)
Directors:Graham Lawrence, MSM (1993)
Kim Oates, AM, MD, MHP, FRCP,FRACP, FRACMA, FAFPHM, DCH(1990)
John Pascoe, AO, BA, LLB (1986)
John Young, AO, MD, DSc, FAA,FRACP (1989)
Gabrielle Kibble, AO, BA, DTCP(Syd.), FRAPI (2000)
The Hon. Peter Anderson, AM, BA(Pol Stud) (2000)
Joanna Capon, MA (2000)
Kevin Doyle, (2000)
Staff Elected Member:W. Hawker, DipPhys (1998)
Honorary Solicitor:Gadens Ridgeway
Consultant Legal Advisor:Murray Tobias AM QC
Executive Management
Chief Executive:Kim Oates, AM, MD, MHP, FRCP,FRACP, FRACMA, FAFPHM, DCH
Executive Director (Clinical Services)and Deputy Chief Executive:Peter Procopis, MB, BS, FRACP
Director of Clinical Services -Nursing:Jenni Jarvis
Director of Corporate Services:Russell Smith, BBus, GradDipBA,AFCHSE, CHE,
Acting Director of Finance:Rosemary Chung, FCPA
Director of Community Relationsand Marketing:David Jackett, ACMA
Director of Information ServicesRalph Hanson, BSc (Med), MBBCH,MPH, MRACMA, FRACP, FACEM
Medical Staff CouncilRepresentatives attending Board:Paul Knight, MB, BS, FRACP (1998)
John Donnelly, MB, BS, FFARACS,FANZCA (2001)
Postal AddressLocked Bag 4001Westmead NSW 2145Sydney AustraliaTelephone (02) 9845 0000Facsimile (02) 9845 3489www.chw.edu.au
Board MeetingAttendances1/7/01 - 30/6/02
NamePossibleMeetings*
MeetingsAttended
J A Dunlop
V Street
D G A Say
G Lawrence
R K Oates
J H Pascoe
G Kibble
J A Young
P Anderson
K Doyle
J Capon
W Hawker
10
2
10
10
9
8
11
8
10
9
10
9
10
2
10
10
9
4
7
5
6
8
10
8
* If a Board member has been grantedleave, meetings held during that leave arenot considered as possible meetings.

7
Profiles – Board of DirectorsJohn Dunlop
John Dunlop was elected Presidentin January 1983. He became amember of the Board in 1973 andhas served the Hospital as HonoraryTreasurer (1978-1981) and Vice-President (1981-1983). He is aDirector of the Children's MedicalResearch Institute, The HospitalsContribution Fund of AustraliaLimited and Health Super Pty Ltd.
He is President of the HealthServices Association of New SouthWales and a Councillor of theAustralian Healthcare Association.John Dunlop was formerly ManagingDirector of Edwards Dunlop & CoLtd. He was appointed a Member inthe Order of Australia in 1987 inrecognition of his work for children'shealth.
Val Street
Val Street is a Tertiary EducationConsultant and was formerlyPrincipal of the Women's College.She was a Fellow of the Senate ofthe University of Sydney and is nowa Fellow of the University of WesternSydney. She is also on the board ofthe Philharmonic Choirs.
She was elected to the HospitalBoard in December 1989 andappointed a Vice-President in 1998.
David Say
David Say is a non-executiveDirector of a number of companiesincluding HSBC Bank Australia(Chairman) Australian Centre forLanguages (Chairman), SouthernStar Group, Timwin Group andSydney West International College(Director). A Chartered Accountant,he holds a Diploma of BusinessStudies from IMI, Geneva.
He was elected to the Board in April1989 and appointed HonoraryTreasurer in 1993. He is acommitted supporter of theChildren's Hospital Fund.
Gabrielle Kibble
Gabrielle Kibble has a Bachelor ofArts and also a Diploma of Townand Country Planning from theUniversity of Sydney. She is aFellow of the Royal AustralianPlanning Institute, is an AdjunctProfessor in the Faculty of the BuiltEnvironment at the University ofNSW and holds an HonoraryDoctor of Science from thatUniversity.
She has extensive experience inthe public sector, particularly inurban planning and infrastructuredevelopment as a former CEO ofthe Department of Urban Affairsand Planning and Director-Generalof the NSW Department ofHousing. She has been Chair ofSydney Water since 1998; Chair ofthe University of Western SydneyNepean Council, DeputyChancellor of that University,Deputy Chair of the MinisterialCouncil to advise the Minister ofHealth in NSW on reform of thehealth system. She Chairs theExternal Review and EvaluationGroup to monitor implementationof the Government Action Plan forHealth. She sits on the Board ofWestern Sydney and WentworthArea Health Services and wasappointed to the Board of thishospital in 2000.
Graham LawrenceGraham Lawrence joined theBoard in 1993 and was Chairmanof the Marketing Committee forthe New Children’s Hospital CaringCampaign and more recently amember of The Appeal PlanningCommittee for the Cure for KidsCampaign. He has a 35-yearcareer in advertising andpublishing. Graham has held thepositions of CEO of NewsMagazine Pty Ltd, GroupAdvertising Sales Director of NewsLtd, Deputy Publisher and Directorof Australian Consolidated PressLtd. He holds a Master ofStrategic Marketing and is anHonorary Fellow of theInternational Marketing Institute ofAustralia.
Kim Oates
(see profile: Executive Staff)
John Pascoe
John Pascoe is a graduate of theAustralian National University and,after admission as a solicitor,became a partner in the legal firm,Stephen Jaques & Stephen in1977. He joined the Board ofGeorge Weston Foods Limited in1981 and is now Chairman of thatCompany. He is Chairman of theBoard of Management ofCentrelink and Chairman ofSealcorp Holdings Limited. He isManaging Director for theInsurance & Financial Servicesdivision at Phillips Fox lawyers,Director of Aristocrat TechnologiesAustralia Pty Limited and AgedCare Standards & AccreditationAgency Limited. He is NationalChairman of The Duke ofEdinburgh’s Award Scheme inAustralia and a Member of theBoard of Trustees of the Duke ofEdinburgh’s Award InternationalFoundation (UK), Royal AlexandraHospital for Children and theAdvisory Council to AustralianGraduate School of Management.He is the Deputy Chair of theInstitute of Early ChildhoodFoundation. He was appointed anOfficer in the General Division ofthe Order of the Australia in 2002.
John Pascoe was an AssociateMember of the Trade PracticesCommission from 1983 to 1989;Chairman of Commsecure Limitedand Objective Corporation Limitedfrom 2000 to 2002; a Director ofCambooya Limited from 1993 to2002; a part-time member of theBoard of Tourism of New SouthWales from 1997 to 2002; aDirector of Qantas Airways Limitedfrom 1991 to 1993; a Member ofthe Australian ManufacturingCouncil from 1993 to 19975;Chairman of Airservices Australiafrom 1995 to 1996; a Trustee ofthe Sydney Opera House from1988 to 1997; and President ofthe Corporations and SecuritiesPanel from 1994 – 1998.

8
John Young
John Young is Professor ofPhysiology and Pro-Vice-Chancellor(Health Sciences) in the Universityof Sydney. He is a prominentPhysiologist who has played animportant role in international andnational physiological societies. Heis Field Editor of the EuropeanJournal of Physiology, a Fellow ofthe Australian Academy of Science,a member of both the British andthe American Physiology Societiesand a corresponding member of theGerman Physiological Society.Currently, he is President of theFederation of Asian and OceanianPhysiological Societies. He has justretired as Vice-President andSecretary (Biological) of theAustralian Academy of Science. Heis also a member of the MedicalBoard of NSW and of the NationalHealth and Medical ResearchCouncil of Australia. John Youngwas appointed an Officer in theOrder of Australia in 1994.
The Hon Peter Anderson
The Hon Peter Anderson, AM hashad a successful career in bothpublic and private life. A former longtime member of the NSWParliament, he held a number ofsenior ministries. These includedPolice and Emergency Services,Health, Youth and CommunityServices and Minister Assisting thePremier. Mr Anderson was anAlderman on Penrith City Councilfrom 1977 to 1983 and onProspect County Council from 1977to 1980 (Chair 1977-1978).Mr Anderson is also Chair of AustralMalaysian Mining Ltd, Pulai MiningSdn Berhad, Australian Traders Ltdand also the NSW Tow TruckAuthority. He is a Director of theCancer Surgery ResearchFoundation Ltd. He is also Chair ofthe Committee of Management ofthe Penrith Regional Gallery and theLewers Bequest and Deputy Chairof the Joan Sutherland PerformingArts Centre. He is also a member ofthe Board of Wentworth Area HealthService
Joanna Capon
Joanna Capon was appointed to theBoard in 2000. She has been theHospital’s honorary art curator since1995. She is the Chair of Operation
Art from 1996, A member of TheChildren’s Hospital Council, theChair of the Quality Council, theChair of the Australian Centre forPhotography and a member of theNSW Visual Arts and CraftsCommittee.
She has an MA in historicalarchaeology from Sydney Universityand is an art historian, historicalarchaeologist, author and lecturer.
Kevin Doyle
Kevin Doyle joined the HospitalBoard in 2000. He was until March2002 Chair of Vivendi WaterAustralia Pty Limited and Director oftheir affiliated companies inAustralia. He has a degree inEngineering from the University ofSydney and Finance from HECFrance and New York University.Having worked for 22 years inFrance and the USA he returned toAustralia in 1991 to establish theAustralian operation of the VivendiGroup.
Wendy Hawker
Wendy Hawker was elected to theBoard as Staff Member in 1998.She is currently employed at theHospital as Executive SupportManager, having been the HeadPhysiotherapist from 1980 to 2000.She served as Chair of the Divisionof Allied Health Professionals from1993-2001 and Chair of theCombined Divisions of Allied Healthand Standards from1999-2001.She served on the Council of theAustralian PhysiotherapyAssociation, was an active memberof the founding committee of thePhysiotherapists in ManagementGroup and served as a member ofthe Physiotherapists VocationalBranch of the Public ServiceAssociation.
She developed strong workingrelationships throughout theHospital through her secondmentsto the Commissioning Team, whichorganised the move of the Hospitalfrom Camperdown to Westmead,and to the Implementation Team ofthe Human Resources InformationSystem.

9
Profiles – Executive StaffKim Oates
Kim Oates was appointed as ChiefExecutive in December 1997.Apart from several years workingin the UK and the USA, he has hada continuous association with theHospital since starting as aPaediatric Resident in 1969. Forthe 12 years prior to his currentappointment he was the DouglasBurrows Professor of Paediatrics &Child Health in the University ofSydney, a Member of thehospital’s Board of Directors andChairman of the hospital’s Divisionof Medicine. He has receivedseveral international awards forhis research and advocacy forabused and neglected children.
Peter Procopis
A/Prof Peter Procopis joined theHospital staff in the Neurology Clinicin 1969. After a period of furthertraining in the USA he returned in1973 as a Visiting Neurologist. Hewas appointed Staff Neurologist in1979, Director of Medical Servicesin 1985 and Executive Director in1990. He is active in College affairsbeing the inaugural Chairman of theAustralian Board of PaediatricCensors and was Chairman of theCommittee for Examinations of theRoyal Australasian College ofPhysicians until 1996 and Councilmember from 1997 to 2001. He isnow Chairman of the RACP Board ofContinuing Education. He wasPresident of the Australian Collegeof Paediatrics from 1993 - 1995. In1999 he was appointed as theRACP nominee to the Medical Boardof NSW. His interests inpostgraduate medical education ledto his appointment to thePostgraduate Medical Council ofNSW from 1994 to 2000. He wasDeputy Chair in 2000.
Jennifer Jarvis
Jenni is a paediatric nurse whojoined the CHW in February 2000.She previously worked in severalpositions of clinical leadership at
the Women’s & Children’sHospital, Adelaide, SA. Jenni is apassionate advocate of inquiry,clinical practice improvement,professional nursing practice,leadership and continuousimprovement. Jenni’s focus inrecent roles has been thedevelopment of family focusedand partnership based models ofcare delivery, patient safetyprograms and serviceimprovement. Jenni is an activemember of the Children’sHospitals of Australasia,particularly in relation to thedevelopment of paediatric costinginformation, clinical practiceimprovement and benchmarking.
Russell Smith
Russell Smith joined the Hospital inAugust 1991 as Deputy Director ofAdministrative Services. Hepreviously worked at St Vincent's(Private) Hospital in Toowoomba,Queensland, as Executive Officer.He held management committeepositions on the Private Hospital'sAssociation, Queensland and theAustralian Catholic Health CareAssociation. He holds a Bachelor ofBusiness (Health Administration)from Queensland University ofTechnology, a Graduate Diploma inBusiness Administration from theUniversity of Sydney and is anAssociate Fellow of the AustralianCollege of Health ServiceExecutives. He was appointedDirector of Corporate Services inApril 1993.
David Jackett
David Jackett joined the Hospital asDirector of Community Relationsand Marketing in 1994. He is aChartered Management Accountantby profession, having qualified inEngland in 1982. He has worked inmarketing having held brandmanagement roles with WilkinsonSword, Cerebos and Johnson andJohnson. In the four years prior tojoining the Hospital, he wasMarketing Manager at Air NewZealand.
Ralph Hanson
Dr Ralph Hanson joined theHospital in 1982. After successfullycompleting his training inpaediatrics, he was appointed asStaff Specialist and subsequentlyHead of the Emergency Departmentand Outpatients. In 1997 he wasseconded to the position ofManager, Clinical Services NetworkTaskforce and subsequentlyappointed Chair of InformationServices in 1998 and Director ofInformation Services in February2000. He has extensive experiencein health informatics andinformation management. He isboth a Fellow of the AustralasianCollege of Physicians and theAustralasian College of EmergencyMedicine and has a Masters inPublic Health.
Rosemary Chung
Rosemary Chung commencedservice with the Hospital inFebruary, 1994. She is a graduateof the University of New SouthWales, with a Bachelor ofCommerce, majoring in Accounting,Management and InformationSystems. Rosemary is a qualifiedFCPA. Since May 2001 Rosemaryhas been in the role of ActingDirector of Finance. Rosemarydraws on twenty years experiencewithin the financial industry, bothwithin Australia and Malaysia.

10
Lines of Management ResponsibilityBoard of Directors
DirectorInformation
Services
Dr RalphHanson
DirectorCorporatServices
Mr RusselSmith
ResearchProf Peter Gunning
DevelopmentMedicine
PsychologicalHealth and
RehabilitationProf Ken Nunn
LaboratoService
Dr Susan Arb
Chief Executive OfficerProf Kim Oates
Internal AuditMr Alan Ching
e
l
rs
uc
Deputy Chief Executive Officerand Executive Director
A/Prof Peter Procopis
Divisional Chairs
DirectorFinance
Ms RosemaryChung (Acting)
DirectorClinical
Services –Nursing
Ms JenniferJarvis
DirectorCommunity
Relations andMarketing
Mr David Jackett
ServiceImprovement
Unit
SurgeryDr John Pitkin
Allied HealthMs Alison Jones
EducationProf David Isaacs
y
kle
SpecialtyMedicine
A/Prof PeterVan Asperen
Critical Careand
Diagnostics
Dr Jonathan Gillis
AcademicDivision of
GeneralMedicine
A/Prof HenryKilham

11
Corporate Governance StatementThe Board is responsible for the corporate governance practices of TheChildren’s Hospital at Westmead. This statement sets out the main corporategovernance practices in operation throughout the financial year, except whereindicated.
The Children’s Hospitalat Westmead Board
The Board carries out all itsfunctions, responsibilities andobligations in accordance with theHealth ServicesAct of 1997.
The Board is committed to betterpractices contained in the Guideon Corporate Governance, issuedjointly by the Health ServicesAssociation and the NSW HealthDepartment.
Board membership consists of aChair, nine other members, a staffelected member, and the ChiefExecutive Officer, as an ‘ex-officio’member.
The Board has in place practicesthat ensure that the primarygoverning responsibilities of theBoard are fulfilledin relation to:
• Setting strategic direction
• Ensuring compliance withstatutory requirements
• Monitoring organisationalperformance
• Monitoring quality of healthservices
• Board appraisal
• Community consultation
• Professional development
This Report contains informationregarding the identity of eachBoard member noting the i)qualifications, specific skills andexperience they bring to the Board;ii) term of appointment of Boardmembers; iii) frequency of Boardmeetings and members’attendance at meetings.
Resources Available tothe Board
The Board and its members hasavailable to it various sources ofindependent advice. This includesadvice of the external auditor (theAuditor General or the nominee ofthat office), the internal auditorwho is free to give advice direct tothe Board, and professionaladvice.
The engagement of independentprofessional advice to the Boardshall be subject to the approval ofthe Board or of a committee of theBoard.
Strategic Direction
The Board has in place processesfor the effective planning anddelivery of health services to thecommunities and patients servicedby the Area Health Service. Thisprocess includes the setting of astrategic direction for both theorganisation and for the healthservice it provides.
Code of EthicalBehaviour
As part of the Board’s commitmentto the highest standard of conduct,the Board has adopted a Code ofEthical Behaviour to guide Boardmembers in carrying out theirduties and responsibilities. TheCode covers such matters as:responsibilities to the community,compliance with laws andregulations, and ethicalresponsibilities.
The Board has also endorsed theCode of Conduct, which applies tothe management and otheremployees of the Area HealthService. A copy of this Code ofConduct, following review in
August 1999, was distributed to allstaff members and is available onthe Hospital’s Intranet.
Performance Appraisal
The Board has ensured that thereare processes in place to:
• monitor progress of thematters contained within thePerformance Agreementbetween the Board and theDirector General of the NSWHealth Department.
• regularly review theperformance of the Boardthrough a process of Board selfappraisal.
Risk Management
The Board is responsible forsupervising and monitoring riskmanagement by The Children’sHospital at Westmead, includingthe Service’s system of internalcontrols. The Board hasmechanisms for monitoring theoperations and financialperformance of the Service.
The Board receives and considersall reports of the Service’s externaland internal auditors and, throughthe Audit Committee, ensures thataudit recommendations areimplemented.
Committee Structure
The Board meets at regularintervals and has in placemechanisms for the conduct ofspecial meetings. The Board has acommittee structure in place toenhance its corporate governancerole. These committees meetregularly.

12
Committees
Quality CouncilThe Board has in place systems andactivities for measuring androutinely reporting on the safety andquality of care provided to thecommunity. These systems andactivities reflect the principles,performance and reportingguidelines as detailed in theFramework for Managing the Qualityof Health Services in NSWdocumentation.
Role: The Quality Council has beenestablished to provide leadership incontinuous service improvementthroughout the Hospital. Thecommittee reports to the Board on allareas of quality of service, particularlyin relation to the six dimensions ofquality contained in the NSW HealthQuality Framework document.
MembershipBoard Representatives- Ms Joanna Capon (Chair)Chief ExecutiveExecutive DirectorDirector, Clinical Services - NursingDirector, Division of Information
ServicesManager, Service Improvement UnitChair, Clinical Review CommitteeClinical Practice Improvement
CoordinatorThree Medical cliniciansRepresentatives, Nursing (two)Representative, Allied HealthRepresentative, Risk ManagementRepresentative, Information
ServicesRepresentative, EducationRepresentative, Ambulatory
Services
Representative, Patients’ OfficeGP representativeConsumer representative
Finance CommitteeThe Board has established aFinance Committee, chaired by thePresident, which meets monthly.The Board complies with theprovisions of the Accounts andAudit Determination for AreaHealth Services.
Role: The Finance Committeeexamines budget allocations,monitors the financial performanceof the Hospital in relation to itsbudget, ensures appropriatedelegated financial controls andreports to the Board on theeffectiveness of the Hospital’sfinancial management and theregulations under which it operates.
MembershipBoard Representatives- Mr J A Dunlop (Chair)- Mr D G A Say-- Ms V Street- Mr Kevin DoyleChief ExecutiveExecutive DirectorDirector, FinanceDirector, Corporate ServicesDirector, Community Relations and
MarketingDirector, Clinical Services - NursingDirector, Information Services
Audit CommitteeThe Board has established anAudit Committee, chaired by amember of the Board, whichmeets quarterly.
Role: The Audit Committee acts asan advisory body to the Board ofDirectors in discharging the Board’sresponsibilities for issues relating tointernal and external audits,Management and internal controls,financial reporting and accountingpolicies.
MembershipBoard Representatives- Mr D G A Say (Chair)- Mr J A Dunlop- Ms V Street- Mr Kevin DoyleIn attendance:Chief ExecutiveExecutive DirectorDirector, FinanceDirector, Corporate ServicesDirector, Community Relations and
MarketingDirector, Clinical Services - NursingInternal Audit ManagerA partner, Deloitte Touche
TohmatsuExternal Audit Representatives- A partner, Ernst and YoungDirector of Audit, Auditor General’s
Office of NSW
Corporate GovernanceCommittee
Role: The primary objective of theCorporate Governance Committee isto assist the Board to achievestrategic leadership and overallgood governance of the Hospital andto ensure the proper management ofthe Board’s responsibilities.
Board of DirectorsAudit
Committee
EthicsCommittee
MedicalAdvisory
Committee
ResearchCommitteeQuality Council
FinanceCommittee
EducationCommittee

13
MembershipBoard Representatives- Mr J Dunlop (Chair)- Ms G Kibble- Mr J Pascoe- Ms W HawkerChief Executive
Medical AdvisoryCommittee
Role: The Medical AdvisoryCommittee advises the Board andClinical Executive about all mattersrelating to the medical care ofchildren. It also recommends tothe Board appointments of seniormedical practitioners and visitingmedical officers and recommendsto the Board credentialling ofsenior medical practitioners andvisiting medical officers.
MembershipBoard Representative- Mr J A Dunlop (Chair)Chief ExecutiveExecutive DirectorDirector, Clinical Services - NursingDouglas Burrows Professor of
Paediatrics and Child HealthChairman, Division of SurgeryChairman, Medical Staff CouncilChairman, Division of Critical Care
and Diagnostic ServicesChairman, Division of Laboratory
ServicesChairman, Division of
Developmental MedicinePsychological Health andRehabilitation
Chairman, Academic Division ofGeneral Medicine
Chairman, Division of SpecialtyMedicine
Chief Resident Medical Officer
Ethics CommitteeMembership
Role: This Committee safeguardsthe rights of infants, children andyoung people who seek the help ofthe Hospital, or who are brought tothe Hospital or its outreachservices. The Committee hasparticular concern that newprotocols, treatment and researchare properly reviewed andmaintained.
MembershipProf Peter Rowe (Chair)Anne O’Neill (Secretary)
Board Representative- Prof R.K OatesCommunity Members not affiliated
with the institutionMrs Ruth BurleighMr Rod YoungMr Ian Butcher (Lawyer)Ms Helen Maguire (Chaplain)Prof Sue Nagy (Nursing Research)Ms Helen Slayter (Allied Health
Research)Dr Peter Cooper (Professional
Care)
Education Committee
Role: The Education Committeecoordinates education initiatives forboth professional and non-professional staff within theHospital and community.
MembershipChairman, Division of Education
(Chair)Head, Education CentreChief ExecutiveExecutive DirectorDirector, Corporate ServicesRepresentative, Other Professions
Education CommitteeRepresentative, University
Department of Paediatrics andChild Health
Representative, UniversityDepartment of PaediatricNursing
Representative, Medical EducationCommittee
Representative, Nursing EducationCommittee
Representative, Allied Health andTechnical Education Committee(2)
Joint ConsultativeCommittee
Role: Provides a forum forconsultation and discussionbetween the Children’s Hospital,Unions and specified staffrepresentatives.
MembershipChief Executive Officer (Chair)Executive DirectorDirector, Clinical Services - NursingDirector, FinanceDirector, Corporate ServicesManager, Staff Services
DepartmentChief Resident Medical OfficerElected Staff Member of the Board
Representative, Medical StaffCouncil
Minute SecretaryRepresentatives, Australian Salaried
Medical Officers’ Federation:Head Office official, one localbranch representative
Representatives, Health andResearch EmployeesAssociation:- Head Office official, one localbranch representative from eachof the following:- General Sub Branch- Allied Sub Branch- Hospital Managers Sub Branch- Junior Doctors Sub Branch
Representatives, NSW NursesAssociation:- Head Office official, two localbranch representatives
Representatives, Trade Staff Union:- Head Office official, one localbranch representative
Spokeswomen’s Representative
Research Committee
Role: To encourage and promotean inquiring approach to healthproblems in children and to advisethe Board on use of researchfunds.
MembershipBoard Representative- Mr J Dunlop (Chair)Chief ExecutiveExecutive DirectorProfessor of Paediatrics and Child
HealthRepresentative, Nursing/Allied
Health ResearchRepresentative, Scientific Advisory
CommitteeRepresentative, Research and
Development AdvisoryCommittee
Director, Children’s MedicalResearch Institute
Representative, Public HealthResearch
Representative, LaboratoryResearch
Representative, Surgical/MedicalResearch

14
Overview of Divisional AchievementsThis year’s report of divisional achievements includes examples of workperformed across all Hospital divisions. These specific examples illustrate ourvision for excellence in child health care and highlight our commitment toconstantly challenging boundaries. Reported against our Strategic Goals andPerformance Agreement with NSW Health, these achievements have made asignificant contribution to improving child health in Australia.
Goal: Healthier ChildrenAchievements relevant to the NSW Health Performance AgreementMental Health• There have been more than 500 telepsychiatry contacts and 50 outreach visits through the CAPTOS (Child &
Adolescent Psychiatry Telemedicine Outreach Service) program.• Mental Health projects have targeted teen parenting, chronic self-mutilation, prevention of psychological
problems in children with chronic illness, and preventing eating disorders.
Chronic and Complex and Other Care• In the area of Chronic and Complex care, the Hospital has reduced bed days for children with cystic fibrosis,
diabetes and eczema by setting up ambulatory services and a home intravenous therapy program.• A treatment protocol for the state-wide study of Acute Lymphoblastic Leukaemia has been approved by the
Ethics Committees of both SCH and CHW.• A Telemedicine Project has been commenced for the NSW Heart Service.
Public Health Protection and Health Promotion• Fact sheet on passive smoking was developed, as well as ads in ‘Sydney’s Child’ to encourage no smoking
around children.• A Poisons Prevention package was distributed to 1258 child care providers across the state, the ‘Kids and
Poisons’ brochure reached approximately 70,000 parents/carers.
What we Achieved Significance for CHW / Child HealthIncreased Day of Surgery admission rate (DOSA), andmaximised the number of procedures that can bedone as day only cases
Decreased hospital admission for the child and theirfamily.
Evaluated the best use of new and existing vaccines inthe Australian context.
Provided recommendations appropriate for Australianchildren
Established free replacement service for Gastrostomyfeeding devices.
Improved care for patients with gastrostomies.
Adolph Basser Cardiac Institute conducted a full-dayprogram on congenital heart disease for PaediatricCardiologists as part of the 2002 Sydney WorldCongress of Cardiology.
Adolph Basser Cardiac Institute and CHW recognisedas a centre of clinical expertise in the management ofchildren with Congenital heart disease.
Developed a ‘Kids and Poisons’ Package incollaboration with the Poisons Information Centre.
State-wide distribution has increased awareness ofprecautions that parents/carers/child care providerscan take in the home/carer environment to preventchildhood poisonings.
Measured anthropometry of 245 inpatients and 272outpatients to improve knowledge on nutritionintervention.
Increased awareness of the need for accurateanthropometric measurement for nutritionalassessments. 22% of inpatients and 32% outpatientswere overweight or obese, 6% of inpatients andoutpatients were underweight.
Secured Government Action Plan funding to establishauditory screening in the Newborn Intensive Care Unit.
Hearing impairment diagnosed in the first few weeksof life, directly and positively influencing speech andlanguage outcomes.

15
What we Achieved Significance for CHW / Child HealthThe Children's Cochlear Implant Centre received$500K enhancement funding from NSW Health andimplanted 60 children. The Centre also embarked oneight outreach visits to regional NSW.
Increased number of children receiving Cochlearimplants and improved services and training for localstaff in regional NSW.
Physiotherapy produced a general paediatricinformation package used by physiotherapists fromrural NSW on clinical visits.
Improved quality of service and care to children inrural NSW. Decreased anxiety for physiotherapists inrural NSW.
Camperdown Ward initiated a parent forum thatresulted in adoption of a child and family centredmodel of care. Also initiated a doctor group to developinformation for consumers.
Improved consumer communication eg. newsuggestion box format, parent information board andnewsletter feedback page. Parents also invited, aspart of the ethics approval process, to discussproposed protocols and risks.
Introduced a nurse-initiated Discharge Program for shortstay patients in Faithfull Ward, supported by TodmanRecovery staff.
Decreased length of stay post operatively for patientsand their families and increased appropriate bedutilisation.
Improved methods of identifying pain in neonates. Improved neonatal pain management.Identified incidence of bladder spasm - and methodsof prevention - in children following ureteric surgery.
Improved pain management of children followingureteric surgery.
Established a Congenital and Perinatal Infection Clinic- the first such service in Australia.
Links with neonatal services in Western Sydney toensure hepatitis C infected infants have appropriatefollow up.
Undertook the largest trial in renal health in children. Better outcomes for children with urine infection.Identified the issues which hinder optimal care forchildren hospitalised for extended periods of time.
Improved partnerships between nurses and parents ofchildren who are hospitalised for extended periods.
Developed a compendium of all trials in renalmedicine.
Better access to best available research data.
Initiated several new translational research projectswhich aim to:a) improve the prediction of Childhood AcuteLymphoblastic Leukaemia Outcome using Geneexpression;b) examine prognostic indicators of cell types withinneuroblastoma tumours;c) investigate the role of structural proteins inchemoresistance of neuroblastoma.
Improved cancer treatments including:a) reliably identifying, at diagnosis, patients at greaterrisk of relapse, who could undergo more stringenttherapy;b) optimising the therapeutic approach by identifyingtumours of more aggressive nature to predict patientoutcome; andc) aiding diagnosis and therapy.
Established the use of ‘microarray’ technology throughvarious research projects.
This new technology offers a huge diagnostic potentialto analyse the gene expression pattern of thousands ofgenes in a single experiment.
Used new therapeutics, biologic response modifiers, ina group of eight children; the first in Australia, withexcellent improvement in arthritis control in sixchildren.
Major improvement in treatment of juvenile arthritis.
Improved early diagnosis of coeliac disease. Decreased hospitalisation and prevention ofmalnutrition.
Established a dysphagia clinic and increasedgastrostomy feeding for children with cerebral palsy.
Reduced hospitalisation and improved nutrition inchildren with cerebral palsy.
Established a clinical service in sports medicine for allchildren including those with sports related injuriesand those with chronic diseases who may benefit fromexercise programs.
A unique child health service in Australia,consolidating the Hospital’s leadership role in thearea of Paediatric Sports Medicine.
Established the Urgent Paediatric Neurology Clinic runby the Neurology Fellow.
Faster access to specialised evaluation &investigation for children with neurological conditions.
Established a Movement Disorder Clinic. A specialised service and opportunity for research intochildhood movement disorders.
Collaborated in research with Project LEAP for GPtraining and family based weight managementpractices in Melbourne.
Complements existing excellence in family basedpractices for child health.
Developed a ‘parent-held’ manual for CF patients. Increased family involvement in CF management.

16
What we Achieved Significance for CHW / Child HealthDeveloped and trialed a family-based Active Kidsphysical activity intervention in association with localcommunity resources.
Innovative program which could be modelled acrossNSW.
Commenced review clinics for patients who havewaited more than 9 months, to ascertain whethersurgery still required.
Confirmation of procedure requirement and reduceHospital waiting list numbers.
Volunteers Dept introduced a morning ‘snack trolley’service on the wards for parents and carers.
Accommodates parents and carers who do not want toleave the bedside to purchase food and beverages.
Introduced a new Day-of-Surgery Admission (DOSA)booklet to allow selected patients to be admittedwithout attending a pre-admission clinic.
Streamlined admissions process reduces length ofstay for children in hospital andbetter utilises Hospital resources.
Parents’ Hostel provided free bedside accommodationfor one Parent/Carer.
Financially challenged families can stay with child.Child happier.
In conjunction with the Deafness Centre, PsychologicalMedicine established a specialist clinic for the mentalhealth needs of deaf children and adolescents.
A first time service for NSW for children andadolescents with special communication needs anddisability.
In collaboration with the Dept of Surgery, DeafnessCentre established a multidisciplinary Microtia Clinic.
Assists in identifying, treating and preventinglanguage and communication problems.
Expanded newborn screening techniques detected 11babies with life threatening inborn errors ofmetabolism, before they developed symptoms.
The early introduction of appropriate treatment hasled to a significantly improved prognosis for thebabies.
Introduced diagnostic testing for Marfan syndrome. Establishes the need for life long monitoring ofchildren born in families with a history of Marfansyndrome.
Introduction of diagnostic testing for TNFR AssociatedPeriodic Syndrome (TRAPS - a genetic disorder thatcauses a periodic fever, associated with arthritis).TRAPS testing complements our existing testing forfamilial Mediterranean fever.
Aids diagnosis, particularly in the expanding ethnicgroups where these disorders are common.
Introduction of sub-telomere FISH array testing to aiddiagnosis of mild/moderate mental retardation.
Improved diagnostic service in Cytogenetics. Crypticdeletion of sub-telomeric genes is thought to accountfor 5-10% of currently undiagnosed cases ofmild/moderate mental retardation.
Successfully attracted paediatric network funding for aGreater Western Sydney asthma education project.Multidisciplinary working party, including GPs,commenced work on improving asthma action plansand teaching use of inhalational devices.
Children in Greater Western Sydney suffer highmorbidity from asthma and this project is expected toreduce the impact of asthma on children and theirfamilies and, in the longer term, reduce presentationsto EDs across Greater Western Sydney.
Received $20 million from donations of cash andshares, sales of merchandise and bequests. Thisexceeds the previous year’s figure by $3 million.
Used to supplement income received from the StateGovernment, grants and private patient revenue toprovide a service equal to the world’s best.
Purchased an autorefractor for the eye clinic. Improved accuracy and ease of refraction of childrenseen in the eye clinic. Also can be used as a screeningtool to detect refractive errors in children.
Evaluated the Diabetes Day Care Program. Provides greater family access to paediatric diabetesmanagement.
Rehabilitation completed the pilot study of BotulinumToxin for children with cerebral palsy. A separatestudy showed problems of obesity in children andadolescents with acquired brain injury.
Reduces spasticity and improves quality of life forchildren with cerebral palsy.
Families of every child admitted to Burns Unit are nowassessed by a Social Worker and a long termengagement is entered into regarding emotional andsocial problems.
Early intervention by Social Work is more likely to havelong term benefit than at any other time.
Evaluated the implementation of a transition programfor adolescents with chronic endocrine conditions.
Better coordinated care leads to fewer patientsdropping out of the system or having ‘crisisadmissions’.
Diabetes Day Care Program provided a 7-daypaediatric diabetes management service wherechildren and families attend during the day but sleepat home.
Successfully managed 80 children with newlydiagnosed diabetes.

17
What we Achieved Significance for CHW / Child HealthRecognition of the Growth/Endocrine service as acentre for state-wide referrals for the management ofgrowth hormone therapy attracted enhancementfunding from DOH of a full time equivalent clinicalnurse specialist to support the service.
The service has been able to meet increasing referrals(>50%) for management of children on growthhormone therapy.
Microbiology laboratory is now the reference centre inNSW for pneumococcal serotyping.
Monitors all serotyping of pneumococcal diseases.
Goal: Fair AccessAchievements relevant to the NSW Health Performance agreementAcute Service Access• There was increased pressure on beds in the last two months of the financial year, due to the higher number of
presentations to the Emergency Department (1370 more than the same period last year). This led to anincrease in the number of children experiencing delays in admission, and therefore the Hospital did notreached the targets for either the Overdue Urgent Patients waiting longer than 3 months, or the Extended waitpatients, those who have waited longer than 12 months.
• The Hospital did, however, better the benchmarks relating to multiple delays and Day-only surgery, and thetarget for the number of children who are currently waiting.
• The strategies used to increase the DOSA’s rate were successful and the Hospital reached a peak in May of78.4%. Although the Hospital did not meet the target set for June 2002, it has improved its position almost10% since June 2001.
What we Achieved Significance for CHW / Child HealthCreated palliative care links with Sydney Children’sHospital and John Hunter Hospital.
Integrated Paediatric Palliative Care - Statewideservice.
National Centre for Immunisation Research andSurveillance liaised with the NSW Child Health Survey.
Improved quality of data collection and interpretationin our specialist area.
Established a new Heart Clinic every four weeks in theGosford area.
Improved access for children in Central Coast areas.
Expanded Child Development Unit specialistconsultations to Broken Hill and Alice Springs.
Improved access to services for children in remoteareas.
Telemedicine Project commenced for the NSW HeartService.
Quality case reviews achieved through VideoConference links between Sydney Children’s Hospitaland CHW.
Introduction of an ambulatory eczema service forpatients has freed ward beds for other medicalpatients.
Some reduction in pressure for beds. Improvededucation of parents and children in the nature andmanagement of eczema.
Seconded Advanced Trainee Paediatric Registrars tothe newly developed Community Paediatric Services atMt Druitt and Liverpool Hospitals.
Training of future Paediatricians and significantcontribution to the development of appropriatePaediatric Services in the Community.
Seven Hospital Factsheets translated intoVietnamese, Chinese and Arabic, and available fromour website.
Improved access to health information for people fromculturally diverse communities.
Developed and implemented a late effects transfersystem in Oncology to ensure appropriate follow up oflong term survivors by GPs, not tertiary centres.
Handbook distributed to all GPs. Patients carry arecord of their treatment and co-risk factors.
Provided a support service to smaller centres caringfor oncology patients through less acute periods ofcare.
Visits to CHW and work opportunities serve toconsolidate skills.
Introduced a Surgical Cancellations working party. Prevention of surgical cancellations.Enhanced the profile of the Tumour Bank throughproduction of quarterly newsletter and improvedwebsite.
Facilitated research in major international centres.
Established the use of gene knock-out technology on theWestmead Campus.
This technology gives us the ability to make animalmodels of human diseases. It is also part of ourcontribution to the greater Westmead ResearchCampus.
Maintained the surgical outreach clinic in Orange. Fewer attendances to CHW. Less family dislocation.

18
What we Achieved Significance for CHW / Child HealthPromoted the Oncology Confocal Microscope Facilityacross the Westmead research campus (all CHWresearchers, CMRI, Westmead Millennium Instituteand Westmead Hospital researchers).
Provides fair access to a wide range of researchers tohelp improve outcomes of research and furtherdevelop research culture.
Established paediatric gastroenterological services inNorthern and South Western Area Health Services.
Improved health care access for children withgastroenterological problems living in these Areas.
Established education and training networks toenhance safe participation of children in sport andphysical activity.
Effective partnerships have ensured strongeradvocacy for child health issues.
Provided Clinical Placements for four Nurses fromrural NSW under the funding of Greater WestPaediatric Information Network.
Improved service for children and families at PortMacquarie, Lithgow and Bathurst.
Adolescent Medicine Unit completed Access StudyPhase 1 which involved networking with divisions ofgeneral practice, schools, community health centres,youth health centres throughout NSW.
Better understanding of the obstacles to care and thehealth needs of adolescents and their families.Funding for Phase II granted.
The Brain Injury Service broadened the intake criteriato include children with tumours of the centralnervous system or post epilepsy surgery.
Improved access to coordinated rehabilitation care.
Initiated the Child Mental Health Project in conjunctionwith the Transcultural Mental Health Centre.
Improved mental health of children and their familiesfrom non-English speaking backgrounds in NSW.
Expanded CAPTOS (Child & Adolescent PsychiatryTelemedicine Outreach Service) to eight regional areahealth services with video conferencing and regularvisits to 40 rural areas.
Provides tertiary child mental health services toregional young people.
Radiology and Anaesthesia Departments developed ageneral anaesthetic MRI List for outpatients.
Improved access to MRI, resulting in decreasedwaiting times.
Developed a Paediatric Information Network (PIN) aspart of the CHW website.
Provides access to Divisions of General Practice andother Area Health Services to a clearing house of ChildHealth Resources developed at CHW.
In collaboration with Children’s Hospitals Australasia,contributed to ‘Costing Kid’s Care’ a research initiativeundertaken into the true costs of treating children.
Moving towards appropriate funding for specialistpaediatric teaching hospitals.
Goal: Quality ServiceAchievements relevant to the NSW Health Performance AgreementInitiatives in Quality Management• CHW now has an excellent system for reporting, investigating and managing incidents and near misses. This
data is used to identify opportunities for improvements to care and drives learning and system wideimprovements at CHW. Our strategy is called the ‘patient safety program’.
• The Clinicians Toolkit has been widely disseminated and utilised. Regular promotion of the tools, plus supportand education for clinicians in their improvement activities and initiatives is offered by the ServiceImprovement Unit.
Equal Employment Opportunity• We have increased the number of staff with a disability employed in our Hospital from 3% to 7%. Several
programs are now in place and the Hospital was nominated in 2002 by two separate disability agencies for thePrime Minister’s Employer of the Year award.
Nursing Recruitment and Retention• A significant number of strategies to help retain nursing staff have been developed and implemented. These
include the introduction of vacation care; dedicated funding for study and conference leave; increased newgraduate intake; implementation of recruitment and retention programs.
Community Engagement and Working in Partnerships• The Family Focused Care Committee has set up a number of groups to advise on issues identified by families
such as parent administered medication, improving facilities for people with a disability, development of the‘Bear Permit’ for children who have frequent admissions.

19
What we Achieved Significance for CHW / Child HealthCommenced a collaborative study in chronic pain withRoyal Children’s Hospital Melbourne.
Improved quality of care to children with chronic painand their families.
Implemented an electronic Discharge Summarysystem.
Ensures that all patients are provided with a timelydischarge summary to ensure the continuity of care.
Laser Doppler Imager now used for earlier distinctionbetween deep & superficial burns.
Improved identification means more appropriatedressings are applied to superficial burns resulting inless frequent changing, less pain, less familydisruption and earlier discharge. Deep burns haveearlier operation, so earlier discharge and better longterm result.
Liver transplant procedures performed with little or noblood products.
Improved recovery and shorter hospital stay.
Conducted a study into changes in body waterfollowing paediatric Heart Surgery.
Results of this study will help better manage fluidsgiven to children around the time of heart operations.
Adolph Basser Cardiac Institute devised a detaileddepartmental protocol for the assessment ofPotassium levels in Cardioplegia Solution.
Improved Quality Assurance. All Cardioplegia solutionis checked before use.
Psychology Department developed and successfullycompleted treatment programs for specific visualprocessing and reading disorders in children.
Improved care.
Physiotherapy – with Occupational Therapy, the CysticFibrosis Team and Wade ward staff – developed abooklet for adolescent CF patients, about hospitaladmission.
Helps alleviate misunderstanding and prevent fearabout hospital admission.
Evaluated eligibility criteria for pneumococcalconjugate vaccine.
Reduced hospitalisations and deaths frompneumococcal disease.
Implemented salary packaging scheme for all the staffof the Hospital.
Benefits offered will assist staff retention and thescheme expands service provisions for staff.
Implemented Electronic Fund Transfer (EFT) forpayments to staff and small suppliers.
Improved service and efficiency and reducedstationery costs.
Improved service in the Fracture Clinic including theintroduction of a hand trauma clinic; clown doctorvisits; distribution of discharge information to patients;and increased medical coverage for all clinics.
Reduced waiting times; smoother flow of patientsthrough clinic, increased knowledge and awarenessfor patients and their families; plus parent, patientand staff satisfaction.
Introduced innovative recruitment strategies fornursing, including the integration of third yearundergraduate pool nurses with several returning ontoour New Graduate Program.
These nurses have helped expand our currentworkforce and contribute to the future of nursing atCHW.
Developed wound care tables for the threeNeurosurgeons in Commercial Travellers Ward.
Prominent display ensures appropriate care given toall patients.
Pilot study undertaken of treatment outcomes forchildren having a Caecostomy procedure for thedelivery of Antegrade Enema.
Results ensured that appropriate protocols includepre-operative preparation and ongoing follow-up.
Developed research-based protocol for care ofchildren with Thomas splints.
Improved ability to reduce skin ulceration in childrenwith Thomas splints.
Developed the Orthopaedic Pin site care continuousimprovement program.
Dramatically decreased pin site infections andcomplications.
Completed a systematic review of the optimal timingof intravenous line changes.
Reduced costs of unnecessary intravenous linechanges.
Developed and implemented a course for nursing staffon finding evidence on which to base practice.
Nursing staff can access the best evidence on whichto base practice.
Awarded a Wellcome Trust (UK) Equipment Grant for$184,000 to aid in the acquisition of a Laser CaptureMicro-dissection Microscope.
Establishment of this technology and facility at CHW andacross the Westmead Campus will help advancemedical research in many areas.
Provided an education and training program toenhance greater participation in physical activity forchildren with chronic illness and disabilities.
Improved quality of life for children with chronic illnessand disabilities.
Monitored children with epilepsy at home byAmbulatory Monitor.
Maintains quality studies on children with epilepsywith minimal family disruption.

20
What we Achieved Significance for CHW / Child HealthDeveloped a Linen Policy to encourage responsiblelinen management and provision of a high level ofservice.
Improved access to clean linen and cost reductions.
Education Centre produced and distributed a brochurepromoting our videoconference facilities.
Increased use of facilities by outside groups hasincreased revenue.
As part of NHMRC program grant, developed a trialdecision support system for children presenting to theEmergency Department with fever.
Potential to improve outcomes of children with fever.
Adolescent Medicine Unit and Psychological Medicineestablished an Eating Disorders Unit with assessment,admission, treatment and research protocols.
These protocols are being adopted by other units andwill result in improved quality and efficiency oftreatment of eating disorders in NSW.
Centre for the Prevention of Psychological Problems inChildren completed research on 1500 emergencymental health attendances by young people in fiveEmergency Departments in Western Sydney.
Recommendations reported to DOH and servicestakeholders of Western Sydney will enhance serviceprovision and development of publications.
Published the Cochrane Review of the Prevention ofEating Disorders and developed a treatment trainingmanual for young people in preventing eatingdisorders.
Assists prevention of eating disorders in young people.
Pain Team introduced new pain managementprescription charts, with refined database andassessment protocols.
Greater safety in the prescription of opioid infusions,improved information flow between all individualsinvolved in pain management.
Adolph Basser Cardiac Institute developed aDischarge Information Pack for parents of childrenwho have recently had heart surgery.
Improved post-discharge care by parents.
Implemented a model of better practice review tosupport the implementation of Clinical IT Systems.
Improved business practices and effective changemanagement with large IT system implementations.
Improved the transcription services available toambulatory services.
Reduced the turn around time for clinical letters from1-3 weeks to 24 hours leading to better continuity ofcare.
Successfully implemented the Health InformationExchange and Business Objects reporting.
Improved access to management information for CHWmanagers.
Goal: ValueAchievements relevant to the NSW Health Performance AgreementService Development• With GAP funding, the Hospital set up new services in neurogenetics and molecular pathology and a newborn
auditory screening project is ready to begin in the second half of 2002.
What we Achieved Significance for CHW / Child HealthPresented important research findings at the 27thInternational Herpesvirus Workshop.
Increased knowledge about the immunological basisfor the newborn's susceptibility to neonatal HSVdisease.
In conjunction with Wentworth AHS and NSW Health,reviewed the results of NSW Health 'Paediatric CostsStudy 2000' and made recommendations regardingidentification of high cost complex cases andpaediatric cost weights for NSW
Developing costs for paediatric activity in specialistchildren's hospitals and general hospitals is animportant step towards improved management ofpaediatric resources.
Established the weekly Outpatient Respiratory SupportService Nurse Clinic.
Providing families with education, training andassistance in all aspects of home management.
Completed Randomised Controlled Trial to determineefficacy of antibiotic prophylaxis in preventing urinarytract infection and new kidney damage in children withureteric reflux but no urinary tract infection.
Provides evidence to support not using antibiotics toprevent UTI in children with ureteric reflux who havenot had UTI.
Contributed to paediatric section of NHMRC guidelinesfor treatment of non-Hodgkin’s lymphoma.
Benchmark guidelines established for the treatmentof this disease in Australia.
Major publication on energy metabolism in CysticFibrosis accepted by Journal of Pediatrics.
Increased focus on nutritional care in CF females.

21
What we Achieved Significance for CHW / Child HealthChild Protection Unit trained 800 staff in newChildren's and Young Persons (Care and Protection)Act 1998.
Awareness raising in child protection.
Children’s Hospital Education Research Instituteestablished a weekly Educational clinic for childrenand their families suffering from a chronic illness orgenetic disorder.
Clinics are tailored specifically to each child, and arefollowed up by detailed reports with practicalrecommendations for home and school.
Attracted funding from the International HerpesvirusMedical Forum Glaxo Smith Kline Elion ResearchAward.
Increased research opportunities to investigate waysto prevent or treat neonatal herpes simplex virusdisease.
Implemented Managed Print Services. Rationalised the print services throughout the Hospitalto minimise waste.
Enhanced the process of benchmarking internally andwith peer hospitals.
Provides meaningful information across CHW to helpdrive service improvement.
Developed a model for Clinical Budgeting in Wards. Supports the implementation of Clinical Budgetingthat reflects clinical activity.
The Alice Campbell Eczema and Psoriasis Educationand Treatment Centre within Turner Ward nowproviding an ambulatory service for the treatment ofchildren with chronic skin conditions.
A clear focus on education for parents and carerswhilst keeping these children out of hospital.
Participated in the development of StatewideGuidelines for the management of Asthma, Croup &Bronchiolitis.
Provides a uniform approach to the management ofthese conditions in children in NSW.
Co-ordinated the Greater Western Sydney Child HealthNetwork (GWSCHN) Asthma Project.
Provides a uniform approach to asthma managementand asthma education within the Greater West.
Goal: Advocacy
What we Achieved Significance for CHW / Child HealthCreated new protocols to improve pain managementduring procedures and established pain assessmenttools for all children - including pre-verbal child andthe cognitively impaired.
Equality of care for all children regardless ofimpairment.
As a founding participant in the AustralasianBiospecimens Network (ABN), established nationalguidelines for the legal and ethical collection ofBiospecimens for research.
Better outcomes from research endeavours throughgreater access to larger numbers of patient samples.
Orthopaedic Dept received funding to performpharmacokinetic trial of Zoledronate in children.
Currently no proper data on this drug in children.
Developed a Cystic Fibrosis Parent Newsletter. Improved communication with parents about newtreatments and research studies.
Established SAT (School Aged Therapy) WEST, whereservice providers for students with physical disabilityand their families meet and work collaboratively,share information and encourage professionaldevelopment.
Improved continuum of therapy care for school agedchildren with physical disability in the Greater WesternSydney area.
Child Care Centre Director involved in a NSW Healthreview of current child care provisions in workplacecentres.
Provided recommendations for improved service andmore flexibility for staff.

22
What we Achieved Significance for CHW / Child HealthThe Hospital’s Advocacy Group has:• increased community awareness of childhood
obesity• created Australia’s first charter for children’s sport• promoted greater vigilance in swimming pool safety• advocated for health warnings to appear on high
caffeine soft drinks• lobbied for hot water temperature regulating in new
homes• promoted dangers of reversing in driveways• campaigned to warn motorists and parents about
the dangers of children running out from behindschool buses.
Improved health and welfare of children and youngpeople.
Goal: Partnerships
What we Achieved Significance for CHW / Child HealthReleased the pilot of PIN (Paediatric InformationNetwork) - a password protected part of the CHWInternet - allowing NSW Health staff and GPs access toCHW resources and shared information across thechild health network.
The expertise of CHW and other paediatric and childhealth services will be shared across all serviceproviders.
Received funding from NSW Health, via the GreaterWestern Child Health Network, to pilot 'Grand Rounds'via the internet and distribution on CD-ROM.
Significantly improves access to excellent educationalresources for doctors, nurses and allied health staff inmetro, rural and remote locations.
Signed a Memorandum of Understanding with Co-operative Research Centre for Vaccine Technology.
Partnership with a major basic research organisationwill help to accelerate pace of early clinical trials ofnew vaccines
Developed an outline for the implementation of aChild Health Information Network as part of the NSWElectronic Health Record net strategy in partnershipwith WSAHS, SWSAHS, WAHS and DOH.
Improved delivery of health care services to childrenand their families in the Greater Western Sydneythrough better access to clinical information.
With the help of SBS Radio, conducted a series ofradiothons, targeting nine different language groups.
Provided unique access to multicultural audiencesacross Australia to raise awareness of child healthneeds. Raised $250,000 and provided a platform forgreater involvement with multicultural communities inthe future.
Commissioned research to determine publicawareness of our services and how well they aredelivered which revealed that over 90% of thepopulation is aware of the Hospital and generallypleased with services provided.
Enhanced understanding of community needs andhow best to meet those needs. Results also providedguidance on ways to improve our communicationstrategies.
Speech Pathology developed parent informationsheets in voice, preschool language and feeding, inpartnership with the University of Sydney'.
Improved parental understanding of speech pathologyproblems will lead to greater partnerships inintervention.
Amalgamated the Home Ventilation/ Oxygen Programand the David Read Sleep Unit to become theRespiratory Support Service (RSS).
Provides a coordinated approach to treatment,discharge planning and community support for themanagement of infants and children requiringrespiratory support.
In collaboration with the NSW Department ofEducation and Training, developed the TracheostomyCare Training Program.
Assists teachers’ aides, respite/ residential carers andchild care centres to competently manage a child witha tracheostomy.
Partnership with Sydney/Queensland Universities ledto successful NHMRC Program Grant.
Increased research into febrile illnesses in children.
Systematic reviews registered by CREBN (Centre forResearch and Evidence-Based Nursing) with sevenCochrane Review Groups.
Ensures high quality systemic reviews of nursing care.
What we Achieved Significance for CHW / Child HealthIncreased parent involvement in the Pain and PalliativeCare Unit, eg participation in staff selection, consumersurvey audits and Grand Rounds.
Active consumer participation in service delivery.
CREBN established research partnerships withpaediatric centres in Brisbane, Perth, Melbourne andSydney to apply a multi-centre focus to nursingresearch.
Nursing research now being conducted with a multi-centre focus.
Established collaborative research with the Centre forViral Research, Millennium Institute.
Led to a joint NH&MRC project grant submission.
Collaboration established with the University ofMelbourne to investigate mechanisms of newborn'ssusceptibility to neonatal herpes simplex disease.
Facilitates supply of transgenic mice and also led toan invitation to submit joint grant proposal to March ofDimes (USA).
Participated in a network of paediatric surgeonsthroughout NSW.
Promotes new developments in Paediatric Surgeryand improved surgical care.
Partnership established between Orthopaedics andGeneral Surgery for vascular tumour cases.
Provides coordinated trauma service.
Improved liaison between Orthopaedics andNeurosurgery.
Enhanced partnership led to development of acervical trauma service
50 patients transferred from Oncology Late EffectsClinic to the care of their GPs.
Facilitated on-going care of long-term Oncologysurvivors by their GPs.
Involved in the ‘Critical Windows’ project on healthrelated behaviour in children.
Improved understanding of physical activity, inactivityand nutrition in school aged children.
Developed and launched a Hospital Security WatchProgram with Chubb Australia.
Provides a safer environment and better protectionagainst theft and/or damage of Hospital property.
The Developmental Psychiatry Clinic developed aservice link with the Behavioural Intervention andSupport Service.
Shared skills and resources with DADAHC to supportyoung people with intellectual disability.
Children’s Hospital Education Research Institute(CHERI) established research partnerships with:• Curtin University about maths for boys with AD/HD;• University of Western Sydney about eating disorders;• University of Sydney about Anorexia Nervosa; and
with• University of Sydney and local schools about
supporting children’s cognitive, social and physicaldevelopment.
Collaborative partnerships helping to address health,education and psychology concerns for children.
Collaborated with WSAHS, SWSAHS and WAHS todevelop a strategy for rationalising IT data centresacross the four Area Health Services.
Enhanced management of the high cost ofInformation Technology.
“Our position as one of the leading children’s hospitals in the world depends onour ability to understand and apply the new biomedical research. Our immediategoal is to focus our energies on solving substantial medical problems. Research isnot an interesting diversion, it is about improving the quality of clinical treatmentand contributing to the future of medicine.”
Professor Peter GunningChair, Division of Research
23
Reports on specific research activities are available on our website at www.chw.edu.au/research/report/

24
Patient Care StatisticsSummary of Key Statistics
2001/02 2000/01 1999/2000 1998/99
Bed CapacityTotal Beds at 30 JuneAverage number of beds available during year
339239
339242
350247
350248
Patient DetailsInpatientsNumber in hospital at 1 JulyAdmissions during yearTotal patients treatedNumber in hospital at 30 JuneBed days of inpatients treatedNumber of operationsOutpatientsTotal occasions of service
20326,22226,425
21181,71013,210
525,631
21825,49725,715
20383,52513,162
507,475
23026,15126,381
21875,96913,647
526,135
24529,12029,365
23086,55013,601
534,784
AverageDaily average of inpatientsAdjustment for outpatientsAdjusted daily average (ADA)Average stay of inpatients (days)Bed occupancy rate (%) (after adjustment for weekday beds)
223.9144.0367.9
3.1293.8
228.8139.0367.8
3.2793.4
207.6143.8351.4
3.1892.1
237.1146.5383.6
2.9795.8
Inpatient activity for the year2001/2002 was 0.4% belowtarget for separations and 3.7%below target for case weightedseparations.
Despite not reaching activitytargets, activity was higher
than the two previous years butremained below that of 1998/99due to the shift from same day tooutpatient care that occurred inthat year. The average length ofstay has decreased relative to200/01 and is reflected in thedecreased bed days despite the
increased activity.
The number of operationsincreased and outpatient activityincreased by 3.6% relative to lastyear.
Freedom of InformationThe provisions of Freedom ofInformation Act (FOI) state thatunder Section 25 (1b), if copies ofdocuments can be released underalternative legislation or policy, afacility is able to refuseapplications under FOI and grantaccess under these alternatepolicies.
As a matter of NSW Department ofHealth policy, clients/patients areguaranteed a right of access toinformation held in their personalhealth record – Patient Access toMedical Records.
Inspection is free of charge andthere is a fee for copies, notexceeding FOI fees. All FOIrequests are forwarded to theFreedom of Information Officer,Medical Records Department forattention.
In 2001/2002 there were 210applications for access to medicalrecords by clients/patients.A list of The Children’s Hospital atWestmead policy documents thatare available for inspection,purchase or free of charge, isincorporated in the Summary of
Affairs published in theGovernment Gazette every 6months. The Summary lists allpolicy documents held by theagency and explains how to accessthe documents.
For further information relating toFreedom of Information, contactthe Freedom of Information Officeron (02) 9845 2849 or by post:
Medical Records Department,The Children’s Hospital at
Westmead,Locked Bag 4001,
Westmead NSW 2145.

25
Risk Management and Insurance ActivitiesThe Hospital continues to pursue the integration of risk management into theBusiness Planning and Reporting cycle with the aim of risk managementbecoming part of day-to-day activities. Work is ongoing to develop andimplement a suitable framework that supports this objective and which includesthe coordination of existing risk management initiatives.
During the year Deloitte ToucheTohmatsu conducted a BusinessRisk Assessment Review of theHospital and its activities. Thereview assessed risk by way of thefollowing categories:
Strategic Risk – external factordriven and/or that may impact onthe Hospital’s ability to perform itsactivities in the medium to longterm.
Operational Risk – day to day riskssuch as patient care management.
Existing risk managementprocesses were identified and withmanagement’s input anassessment of the remainingresidual risk (current/net exposurefaced by the Hospital) was derived.Strategic risk areas which had ahigh net exposure includedfunding, staff availability, clinicalrisk management and privacymanagement. At an operationallevel some of the key risksidentified include patient caremanagement, maintenance ofmedical records, employee safetyand integrity of financial data. Thereview findings have beencompiled into an action plan thatidentifies risk category, riskexposure, principal riskmanagement activities and thelevel of residual risk.
The development andimplementation of an enhancedrisk management framework, incombination with the business riskassessment action plan, will formthe basis for ongoing managementof the Hospital’s risk exposure.
Chain of Responsibility
Risk management is supported atBoard level and through Executiveendorsement of related policiesand procedures. All Hospitalemployees are encouraged to
recognise and acceptresponsibility for riskmanagement. Departmentmanagers and supervisors arerequired to assess their activitiesin terms of existing or potentialrisk and where necessaryimplement appropriate risktreatment measures. A RiskManagement Coordinator, anOccupational Health, Safety andRehabilitation Coordinator and aRisk Management EducationOfficer provide specialist supportand there are a number of riskmanagement related committeeseg. Disaster Planning,Occupational Health & Safety,Quality Council, Clinical Reviewand Product Review. In addition,the roles of the ServiceImprovement Unit and the ClinicalReview Committee are an integralcomponent of the Hospital’s riskmanagement strategies.
Occupational Health,Safety andRehabilitation
• 362 work accidents and 22incidents were reported
• 79 Workers’ Compensationclaims were lodged. Totalhours paid: 6180 hours.
• Mean time lost per claim: 78hours or 2.05 weeks.
• 56 staff participated inRehabilitation this year and 20of these were for non-workrelated conditions. 19programs are still current andof the others there has been a90% success rate in returningstaff to pre-injury positions.
Staff Vaccinations
636 staff vaccinations were givenin 2001/2002. This consisted ofstaff receiving vaccinations for:hepatitis B (99); hepatitis A (10);combined hepatitis A&B (Twinrix:
2); Influenza (501); ADT: (7),Varicella zoster (11), meningitis(Mencevax 3) and typhoid (3).
Distribution ofWorkplaceIncidents/Accidents
Reported from July 2001 – June2002
Type Number
Blood Exposure 73Manual Handling 51Slip/Fall 64No lost time injuries 99Time lost injuries 16Journey Injuries 36Visitors* 23Incidents 22
Total 384
*Other than Slip/Fall or Blood Exposure
Workplace Claims –Main Occupation Groups
Main OccupationGroups
TotalClaims2000/2001
TotalClaims2001/2002
NursingGeneralAdministrationMedical/MedicalSupportHotel ServicesGeneralMaintenance
19
20
1526
3
25
16
1225
1
Totals 83 79
Note: The above claim numbers aresubmitted claims and so this data mayconflict with previous report information.Claim numbers for a particular Fund Yearcan vary from year to year. The above datais at 30 June 2002.

26
Risk Minimisation
Strategies employed during theyear to eliminate or reduce injuryrisk include:
• Policy review and developmentto reflect changes in the newOH&S Legislation. Inconsultation with staffreviewed policies to facilitatecompliance.
• Risk Management EducationOfficer employed in April2002. Employed to support arange of workplace safetyinitiatives but in particularongoing development of aManual Handling TrainingProgram.
• A comprehensive review,update and enhancement ofthe Hazardous SubstanceDatabase to include allchemicals used in the Hospitaland also Risk Assessmentsand MSDS.
• OH&S elections conducted inMay 2002. All committeemembers to be trained inaccordance with the newOH&S Legislation.
• A comprehensive OH&SCommittee inspectionprogram developed.
• Ongoing extensive ergonomicsurveys, workplace andequipment modificationsand/or designs to promote asafe working environment.
Treasury Managed Fund Detail
Motor vehicle 2001/2002 (as at 30 June 2002)
Benchmark premium(budget allocation)$22,839
Deposit premium(amount paid into fund)$20,809
Surplus
$2,030
Claims total: 14 Incurred cost $6,334
Note: A defensive driver training program has been introduced to try to address anincreasing number of vehicle claims.
Worker’s Compensation
Benchmark premium(budget allocation)$3,457,741
Deposit premium(amount paid into fund)$1,468,014
Surplus
$1,989,727
Claims detail as at 30 June 2002Claims total: 75Incurred cost: $300,000Incurred cost per employee: $157.8 (Health average $426.8)Claims per 100 employees: 3.96 (Health average 8.06)
Note: Claim numbers have remained consistent with the previous two years. TheHospital’s performance is favourable when compared to the Health average.
Public Liability Claim Detail as at 30 June 2002
Type of claim Number of claims Total incurred2000/2001
2001/2002
2000/2001
2001/2002
Treatment non-surgicalTreatment surgicalTripping/slippingAccidental damageLiftingLibel/slander
821-11
73-1--
$
3,083,910 781,626
11,880-
106,064 36,230
$
1,139,721 251,072
- 3,000
--
Totals 13 11 4,019,710 1,393,793
Note: Non-surgical and surgical remain high risk exposures but on-going riskminimisation strategies are being developed through a clinical review process.
Property Claim Detail as at 30 June 2002
Type of claim Number of claims Total incurred2000/2001
2001/2002
2000/2001
2001/2002
Storm & TempestTheft/BurglaryAccidental DamageMisplaced/Lost
1312
-1--
$
29,31013,071
583 6,181
$
-422
--
Totals 7 1 49,145 422

27
Annual Report of theRadiation Safety Officer
The Radiation Safety Committeemet in February, May, August andNovember, and its membershipcontinues to include broadrepresentation from across theHospital.
The role of the Radiation SafetyCommittee is to provide adviceand support to the HospitalExecutive in achieving compliancewith laws and regulations, and toassist the Radiation Safety Officerin ensuring that the use ofradiation at this Hospital occurs ina safe and controlled fashion.
At times when the Radiation SafetyOfficer is on leave, other membersof the Radiation Safety Committeeprovide cover. Leanne Mills(Manager, Clinical SciencesLaboratories) and the staff of theNuclear Medicine Departmentdeserve particular thanks for theirhelp.
A successful initiative of theRadiation Safety Committee thisyear has been the production of aTraining Video, aimed at nursingstaff and parents who encounterpatients undergoing NuclearMedicine scans. Congratulationsto cinematographer CatherineUren, and thank you to the staffwho allowed her to videotape theirprocedures. A second trainingvideo is in preparation.
The Radiation Safety Officersubmitted a detailed RadiationSafety for Laboratory Personnelcourse syllabus to the EPA, withthe intent of having the courseaccredited for local use. If thecourse is approved, this will savethe Hospital a considerabletraining expenditure.
A regular task for the RadiationSafety Committee and RadiationSafety Officer is the review ofEthics Applications, to ensure thatradiation used in research projectsdoes not unjustifiably exposepatients, or staff, and does notlead to accumulation ofradioactive waste.
Among several documentsreviewed this year is a DraftGuideline for Radiation Safety
Committees and Radiation SafetyOfficers, issued by theEnvironment Protection Authority(EPA) for public comment. TheHospital was thanked for acomprehensive submission.
Both the State regulatory body, theEPA, and the Federal regulatorybody, the Australian RadiationProtection and Nuclear SafetyAuthority, have excellentWebpages that have beenimproved in the last year. Thesecan be a resource for usefulinformation for both staff andmembers of the public.
The focus of the Radiation SafetyCommittee, as in the past, hasbeen on issues related to training,waste management, andlegislative compliance. TheCommittee is encouraging the useof non-radioactive techniques inthe laboratories, and will continueto promote the safe use ofradiation in the Hospital.
Fraud Control
The Hospital’s Fraud Control Policyincluding Code of Conduct isissued to all staff members and isavailable on the Hospital’s Intranetand Website.
All staff members are expected toobserve this policy bydemonstrating honest, ethical andprofessional behaviour.
Staff and any others who deal withthe Hospital are expected topromptly bring any instance ofsuspected internal or externalfraud to the attention ofmanagement. This will result in theprocess of investigation as set outin the Hospital’s Fraud Controlpolicy.
Internal Audit usually conductsinvestigations on suspected fraud.This may involve investigations incooperation with the Police andthe Independent CommissionAgainst Corruption.
The Chief Executive has anobligation to report criminaloffences to the Police as well asactual or suspected corruption tothe Independent CommissionAgainst Corruption.

28
Service ImprovementThe Service Improvement Unit (SIU) was established over 12 months ago tointegrate the core components of the Hospital’s approach to ContinuousImprovement. In the last 12 months the Hospital has further strengthened itscommitment to a culture of Improving Performance and ConsumerParticipation. We now have growing expectations of what it means to provide asafe, high quality and ever improving service to all.
The SIU has as its vision "toestablish a culture of seekingexcellence through continuousimprovement at CHW" and itsmission is "to provide leadershipin, and education and support for,continuous improvement, for allstaff at the Hospital and tofacilitate the pursuit of excellencein Child Health Care".
The major roles of the SIU are asfollows:• Patient safety• Service improvement• Review of Hospital systems
operation• Education and support for
continuous improvement• Clinical review• Clinical practice improvement• Consumer participation• Patient liaison, advocacy and
troubleshooting• Project management, strategic
and operational planning• Complaint management and
feedback coordination• Accreditation coordination• Resource development• Benchmarking activities
In summary, the SIU’s role is tocoordinate improvement effortsacross all areas of the Hospital toensure that we are providing thehighest quality and safety of carepossible.
Just some of the initiatives that theSIU team have been involved inare:
• The development of the PatientSafety Program (PSP) whichincludes the creation of a newelectronic database to captureall patient related incidents andnear misses. This system wentlive on 15 April 2002 following acomprehensive educationprogram. The PSP replaces a
paper-based system, which washistorically used by nursing toidentify incidents. Initialcomparisons between the twosystems have revealed that thereare now more reports being filedand there is superior dataquality. The reporting of ‘near-miss’ events (that is reportingwhen errors are prevented) ishighly prized and acknowledgingand celebrating these reportswith staff further enhances oursystematic approach to ensuringpatient safety is anorganisational priority. Trendedreports from the PSP can bereviewed locally (in the wardsand departments) and centrallyand improvement opportunitiesidentified and supported atvarious departmental andorganisational improvementmeetings. The PSP hasheightened awareness of patientsafety at CHW and is ensuring asystems approach to improvinghealth care delivery.
• The Clinical Review Committee(CRC) is a multi-disciplinarycommittee which meets underqualified privilege granted by theNSW Health Minister. It meetsmonthly to review clinical cases.Recommendations forImprovement in Patient Care aresent from the Committee to theQuality Council and to theClinical Executive. The CRCcontinues to have major successin identifying opportunities forimprovement in clinical care andHospital processes. Most casesreviewed come from specificreferral rather than chart audit.
• Accreditation - CHW underwent aperiodic review by the AustralianCouncil of Health Care Standardsin late June and we are awaitingcomprehensive feedback.Preliminary feedback has been
very positive about the culture ofcontinuous improvement that isbeing developed at CHW.
• Complaint Management - Withthe implementation of anupgraded Complaints Database,trending of complaints eachquarter by issue and departmentis being performed to identifyareas of possible improvement.Several improvement initiativeshave occurred for which thealerting incidents were primarilyor partly recognised through thecomplaint mechanism. Onseveral occasions adverseevents were referred by both thecomplaints process and theclinical review process, allowinga smooth investigation of theincident, suggestions forimprovement and timelyfeedback to the families. It hasbeen a busy year for medico-legal matters because of a newState law on limited liability,which came into effect into themiddle of 2001. The ComplaintsManager and Patients' Friendwork in partnership to ensure allfeedback is utilised forimprovement and that staff andfamilies are supported throughthis process.
• Partnerships - The facilitationand encouragement of CHWconsumers to actively participatein service planning and decisionmaking, is fundamental to thedevelopment of an environmentfor continuous improvement.Partnerships have beenestablished between staff andfamilies and this teamwork isdriving many serviceimprovement initiatives. Just afew examples of projects include:a project looking at improvedinformation about admission andlife on the wards for families; theBear Permit for families whosechildren attend CHW regularly;

29
improved facilities and waitingareas for families; improvedamenities and services forpeople with a disability whoattend CHW; and thedevelopment of a toolkit tosupport staff and consumers towork together to improve theservices we provide.
• The function of the QualityCouncil has been reviewed andas a result the CHW Board hasendorsed new Terms ofReference for the QC. The QC iscurrently developing an ActionPlan for the coming 12 monthsand now has an Intranet site.
• A new Report Format forImprovement Projects waslaunched in June 2002. Thereport will help to standardiseand facilitate the sharing ofimprovement information acrossCHW. A central collection pointhas been established, allowingbetter access for all staff at CHWto all the great things happeningwithin the Hospital.
• The current Strategic Plan iscurrent until 2003 and a teamhas just started to meet torecommend the process bywhich our new Strategic Planshould be developed with aneven stronger focus on improvingperformance, measurement andconsumer participation.
Cultural DiversityThe Hospital’s commitment toequity of access is highlighted in aspecial ‘Ethnic Access Statement’and the Strategic Plan. TheHospital’s ‘Ethnic Access Policy’enshrines the right of equality ofaccess to health servicesregardless of ethnic origin orlinguistic skills and theresponsibility of the health systemto respond appropriately to theneeds of our culturally andlinguistically diverse population.We recognise that language andcultural barriers can make itdifficult for some children toreceive appropriate health care orincrease the stress associatedwith medical treatments andhospitalisation. Many of thefamilies who attend this Hospitalspeak a community languageother than English at home.
Families also vary in their attitudesto, and beliefs and experience ofchildhood illness.
The Hospital’s Ethnic AccessCommittee (EAC) has grown inenthusiasm and commitment overthe past year. The EAC hasrepresentation from the HealthCare Interpreter Service (HCIS), theTranscultural Mental HealthCentre, Adolescent Medicine,Community Paediatrics, Nursing,Social Work, Chaplaincy, PublicRelations, junior and seniormedical staff, and has continuedto seek ways to improve theaccess to hospital services. TheEAC is chaired by Dr ShantiRaman, Area Child Health Advisorto Western Sydney Area HealthService, thus maintaining stronglinks with community health andother services in the Area. The EAChas liaised with key organisationsproviding health services tovulnerable culturally andlinguistically diverse communities,including refugees, minoritycommunities and the indigenouscommunity. The EAC through itsmembership has maintained astrong focus on advocacy,particularly for vulnerable groups.
Following the success ofMulticultural Week in 2001, theEAC organised a bigger and bettercelebration of cultural diversitywithin the Hospital community in2002. The CHW MulticulturalWeek coincided with the NSWHealth Department designatedweek, and was held in the week ofJuly 22nd. Our purpose this yearwas not just to promote awarenessand understanding of the culturaldiversity of our population, but toalso focus on the needs of some ofthe newly emerging communitiesin Western Sydney. We focused onfour distinct population groups thisyear; they were the Pacific Islandercommunity, the Filipinocommunity, the Afghan communityand the East Timorese community.The community groups organised avariety of cultural displays andentertainment, provided food, andinvolved children and parentsusing the Hospital. The success ofMulticultural Week was veryevident in the high level of interestand participation in these eventsby staff and patients.The importance of ensuring
cultural sensitivity and goodcommunication with children andparents from diverse backgroundswas again recognised through thehigh utilisation of the WesternSydney Health Care InterpreterService. During the past year morethan 5,000 occasions of servicewere provided to patients andfamilies through the InterpreterService. Regular staff training isundertaken to enhance culturalawareness and the effective use ofinterpreters. The use of thetelephone interpreter service (TIS)has also been promoted amongstaff when the HCIS is notavailable.
Disability Action Plan
In 2001/2002, the DisabilityAction Planning Group, which is asub-committee of the FamilyFocused Care Committee, has runa series of focus groups forfamilies to identify the issuessurrounding service provision atCHW for this group of consumers.The group has four parentrepresentatives and its majorachievements have been:• A disability information site on
the Intranet (to be expanded tothe Internet by July 2002).
• The Education Centre’scommunication programs haveincorporated case exampleshighlighting parent issues.
• The trialing of a communicationboard that is easy to generateand widely available in clinicalareas.
• Improved signage around theHospital to assist all families andvisitors in finding their wayaround the Hospital, in particularamenities.
• A large change table catering forolder children and adolescentswith disability has been installedon the Galleria level.
• A trialing of a snack trolley forparents who find it difficult toleave their child’s bedside.
• Improved awareness of disabilityand communication with staffabout specialised needs.
The disability action plan surveywill be conducted again later thisyear to ascertain the effectivenessof improvements made.

30
Engaging the CommunityChaplains
The six members of theecumenical chaplaincy team havebeen appointed and financed bytheir churches and accredited bythe Hospital. As part of holisticcare to patients, families andHospital staff, they provide regularward visits, respond to specificdenomination requests andmaintain a network for referrals.
Baptisms, funerals and memorialservices are provided as requestedas well as weekday prayer timeand Hospital Bible Fellowship. Allare involved in either wardmeetings or Hospital committees,including the Service ofRemembrance. The chaplainscarry the trauma page duringworking hours and also provide a24 hour On Call service.
One of our greatest strengths isthat pastoral care is offered topeople of any denomination, faithor no religion. The book forprayers and the Quiet Room reflectthe inclusive nature of chaplaincyat the CHW with scripturetranslations in many languagesand the Koran available. StaffCarols, a service at Christmas andweekly Catholic Mass areprovided.
Volunteer Services
Our Volunteers continue to providea valuable service to the Hospitalin a strong supportive role.Volunteers can be found helpingwith patients, internal transport,supporting parents, in factcontributing to the extras that goto make our Hospital a familycentred environment.
The 350 Volunteers who offeredtheir time to the Hospital this yearcommitted 1800 hours each week.
Volunteer Donations for 2001 toThe Children’s Hospital atWestmead will allocated asfollows:
• $100,00 to the Burns Unit forLaser Doppler Imagery.
• $78,500 to the Audiology forthe ALGO 2e Screener($34,000) and the SynergyPortable Diagnostic ABR($44,500) for screeningnewborns hearing.
• $39,625 to the Vacation CareUnit to start functioning as aseparate identity.
• $52,000 to be donated foreither Anaesthetic Trolleys orLaparoscopic Instrumentsincluding telescopes,handpieces and camera headsfor use in General, Urologic andENT Surgery ($40,000) orRhyton Instruments for NeureaSurgery and a TibialComponent for Orthopaedics($12,000).
Volunteers now also supportparents, in the evenings and onweekends, in the EmergencyDepartment. They offer assistancein caring for the other children,providing a listening ear, theoccasional cup of tea andgenerally helping the departmentmaintain a friendly environment.The weekend opening of thesibling care area has proved verysuccessful and is appreciated byparents who are able to relax whilevisiting their sick child, knowingtheir other children are being welllooked after. In 2001 Sibling carecentre accommodated 2002children.
The Volunteers continued tooperate the Volunteers Shop andTrash & Treasure Stall andprovided regular staff barbeques.
The Volunteers not only sell raffletickets in house for the Hospital,but help raise a lot of money inexternal raffles.
The Volunteers also spend manyhours giving their service toexternal activities such as theTeddy Bear’s Picnic and BearCottage.

31
Overseas TravelA summary of conference leave(domestic and overseas) undertakenover the year is provided below. Themajority of travel was for attendance orpresentation at a Conference.
Type ofTravel
Funding No. ofApplications
Overseas $1,339,505 234
Domestic/Other
$612,921 1080
Totals $1,952,426 1314
Funding source Fundingamount
Bulkeley fund $134,101
Staff Specialists (Level 1general fund & PPT)
$1,392,807
Other funding (Generalfunds & SPT)
$425,518
Total Funding $1,952,426
Human ResourcesThe Children’s Hospital at Westmead maintains Human Resource and IndustrialRelations policies and procedures that support the vision and strategic goals ofthe Hospital. All policies comply with NSW Health requirements, relevantlegislation and awards.
What we Achieved Significant Outcomes of theProject for CHW
Various Human Resourcesrelated policies andprocedures were updated in auser-friendly format.
Policies and Procedures aremore accessible, simple to useand are supplemented bytraining and educationprograms.
A creative recruitment projectfor nurses was conductedbetween January and March2002. This project was acollaboration betweenNursing, Staff Services andPublic Relations.
The Hospital reduced its nursingvacancies from 80FTE to 9 FTEover this period.
A 360-degree performancemanagement system wasdeveloped and piloted inNursing during 2001/2002.
An executive performancemanagement system based onthe NSW Public SectorExecutive Capabilities iscurrently in first draft and willbe implemented later thisyear.
Provides a sophisticated meansfor evaluation of service plansand individual performance,within a developmentframework.
EEO Management Plan 2000-2003.The Hospital has introduced astrategy of affirmative action inemployment for persons with adisability and for Aboriginaland Torres Strait Islanders.Traineeships havecommenced in these two EEOgroups and have proven highlysuccessful.
Demonstrated leadership inacceptance of difference to ourcommunity, which led tonomination for the PrimeMinister’s Employer of the YearAward.
Improved Aboriginalemployment percentage from.08 to 1% over the period.
Recognition AwardsThe following list of employees received awards for service excellence nominated and determined by their peers.
Month Employee ofthe Month
Department Month Employee of theMonth
Department
Jul-01 Joy Lee Western Sydney Genetics Feb-02 Nuala Harkin EndocrinologyAug-01 Sally Wharton Anaesthesia Mar-02 Andrew Cole Adolph Basser Cardiac InstituteSep-01 Lisa Folkes Fundraising Apr-02 Tracey Ferguson RehabilitationOct-01 Lenka Bararon Computer Services May-02 Mabel Harrison Nuclear MedicineNov-01 Len Cross Maintenance Jun-02 Mark Hanlon ImmunologyJan-02 Alison Jones Occupational Therapy

32
Actual and Estimated Staff Numbers by LevelLevel TOTAL
STAFF(Number)
Respondents Men Women AboriginalPeople &Torres StraitIslanders
People fromRacial, Ethnic,Ethno-ReligiousMinority Groups
People WhoseLanguage FirstSpoken as aChild was notEnglish
People witha Disability
People witha DisabilityRequiringWork-relatedAdjustment
<$27,606 30 26 5 25 0 5 5 6 3
$27,606 - $36,258 710 670 142 568 10 199 236 39 8
$36,259 - $40,535 177 169 25 152 1 30 37 5 0
$40,536 - $51,293 750 680 84 666 5 139 129 45 8
$51,294 - $66,332 432 401 77 355 3 82 66 29 6
$66,333 - $82,914 213 142 102 111 0 51 39 4 0
>$82,914 (non SES) 161 151 93 68 0 27 19 15 6
>$82,914 (SES)
TOTAL 2,473 2,239 528 1,945 19 533 531 143 31
Staff Employed at 30 June 2002Full Time Equivalent 2001/2002 2000/2001 1999/2000 1998/1999
Administrative and Clerical 319 318 306 291Nursing 611 556 587 621Medical 250 241 243 239Medical Support Services 429 409 395 385Hotel Services 187 194 174 178Maintenance 16 16 15 15Special Purpose and Trust Fund 182 184 161 166
Total 1,994 1,918 1,881 1,895
Equal Employment OpportunityLevel TOTAL
STAFF(Number)
Respondents Men Women AboriginalPeople &Torres StraitIslanders
People fromRacial, Ethnic,Ethno-ReligiousMinority Groups
People WhoseLanguage FirstSpoken as aChild was notEnglish
People witha Disability
People witha DisabilityRequiringWork-relatedAdjustment
Permanent Full-time 1,285 94% 25% 75% 0.7% 25% 25% 7% 1.2%
Permanent Part-time 656 94% 7% 93% 0.7% 20% 21% 7% 2.0%
Temporary Full-time 416 75% 33% 67% 1.3% 26% 24% 4% 1.0%
Temporary Part-time 116 84% 20% 80% 3.1% 23% 26% 4% 1.0%
Casual 253 47% 10% 90% 2.5% 17% 14% 5% 0.8%
TOTAL 2,726 86% 20% 80% 1.0% 23% 23% 6% 1.3%

33
Benefactors and DonorsAlthough we are funded by the NSW State Government, each year we turn to thecommunity for additional financial support to allow us to transform TheChildren’s Hospital at Westmead from a very good hospital to one whichprovides excellence in care for sick children, equal to the world’s best.
Again we extend a very specialthank you to all our donors andsupporters who have given sogenerously this year.
FounderMr Frank Lowy AC
BenefactorsMrs Edith BeatonMrs Ruth BurleighMr John DouglassMr James & Mrs Helen GrahamCr Jean Hay AMMs Gabrielle Kibble AOMr John O'Toole MBE OAMA/Prof John Overton OAMMiss Val StreetMrs Joan WoodCityRailMarkson Sparks! Pty LtdParramatta Leagues ClubEstate Late Noni Dora AudetteEstate Late Nina Maud E
BeveridgeEstate Late Mavis Sarah DarbonEstate Late Bessie Jean
FaulknerEstate Late Phyllis Lillian RoseEstate Late Olive Joan May
RudderEstate Late Enid Joyce Tamblyn
Groups and CorporateDonors over $5000A & D Koureas Pty LtdA53 Inner Wheel DistrictACCO AustraliaAdshelAdvend Australia Pty LtdAGC Pty Ltd - Charity Auction
NightAirport GroundforceAlcon AustraliaAMA Charitable FoundationAmcalAmgen Australia Pty LtdANA Harbour Grand Hotel
SydneyApex Clubs of NSWAPI - New York City Marathon
FundraiserAPI Industries LimitedAshleigh Thornhill Appeal Trust
Associazione Arenese (CZ)Associazione Bagnara CalabraAustralasian Order of Old
BastardsAustralian Jockey ClubAustralian Kidney FoundationAustralian Lebanese Ladies
Fund IncAustralian Regional Wholesalers
Pty LtdAuto One Australia Golf DayBain International Payroll
Contribution Scheme -Accounts Payable
Balgowlah RSL Memorial ClubBalmain Shores Construction
TeamBandaged Bear Celebrity Benefit
NightBankstown Caring for KidsBasellBayerBechara & CompanyBeronia Investments Pty LtdBlacktown Workers ClubBlood Sweat & TearsBluey Day NSWBowlers Club of NSW LtdBREIF Club of SydneyBridgestar Pty LtdBrightwater BathwareBT Financial GroupBuchanan Jazz NightBulldogs Leagues ClubCabra Vale Ex-Active
Serviceman's ClubCabramatta Rugby League ClubCamden Haven Community
Church of Christ Op ShopCamden High SchoolCantarella Bros Pty LtdCentury 21 AustraliaCGE Utilities Aust Pty LtdChannel SevenChiarello Family FundraisingChildren's Cancer Welfare
ServicesChinese Australian Services
Society LtdChubb Security AustraliaCinderella Debutant BallCitrix Systems Asia PacificCity Tattersalls ClubClubs NSW Eastern Zone Race
Day CommitteeCoal Operations Aust Limited
Commonwealth Bank ofAustralia
ConnecTeD FundraisingConroys Trade Supplies - Golf
DayConvoy for Kids SydneyCoptic Orthodox ChurchCornucopia Committee IncCospak PlasticsCranbrook SchoolCredit Suisse First BostonCumberland Community Club
LtdDaily Telegraph / Sunday
TelegraphDeutsche BankE.T Dragracers ClubElectronics For Imaging Pty Ltd -
Oncology FundraiserElite Property BrokersEventide Homes (NSW)Fairfield RSL Memorial ClubFive Dock RSL Club LimitedFlame Opals (Australia) Pty LtdFootwear Leather And Allied
TradesFRF Taxi Trucks & CouriersFriends For KidsFun Enterprises Pty LtdGenzyme Australasia Pty LtdGenzyme TherapeuticsGillette Australia Pty LtdGolfers Charity Bash CommitteeGoodman FielderGregala Pty LtdGresham Partners LimitedGrosvenor Club LimitedHandyland Pty LtdHappy Ever After BallHarbord Diggers Memorial ClubHarrington Park FoundationHarte International Pty LtdHCF Australia LtdHeart Kids NSW IncHellenic Society of The Golden
WestHenry H Roth Charitable
Foundation (Holocaust) Pty LtdHills District Cancer &
Leukaemia CommitteeHumour FoundationIGA DistributionsInflatable ImageInghams Enterprises Pty LtdInner Wheel Club of GuildfordIOOF Cot Fund of NSW

34
Italian Affair Committee LtdJames Bennett Pty LimitedJB Were & Son Charitable FundJoan CottrellJoanna Capon & AssociatesJohn R Turk FundKayaking for Kemo KidsKel Geddes ManagementKids with Cancer FoundationKindifarmKmart - Head OfficeLabor Council of NSWLiangrove Group Pty LtdLions Club of Manly Inc.Macquarie Bank FoundationMalouf Real EstateMandarin ClubManildra Group of CompaniesManly District Support
Committee LtdMarissa Buzzai FundraisingMedtronic Australasia Pty LtdMix 106.5Mobius Marketing DesignMucopolysaccharide & Related
Diseases Society Aust LtdMums on a MissionMustang Owners Club of AustNabiac Charity Fun Run IncNational Australia Bank Limited
Lending Services NSWNestle Australia LimitedNewington CollegeNorth Sydney Harbourview HotelNova 969NRMA Road ServiceNSW Fire Brigade - Katoomba
Fire StationNSW Fire Brigade - NewtownNSW Fire Brigade - Payroll
DeductionsNSW Fire Brigades State
Training CollegeNSW Food & Allied Trades Golf
AssocNSW Leagues Club LimitedNSW Police Hurstville Local Area
CommandNSW Rural Fire ServiceOgnis Pty LtdOncology Childrens FoundationOsteogenesis Imperfecta
Society of AustraliaOur Lady of Mercy CollegePangalloParadises InkParramatta Leagues Club LtdParramatta RSL Social Dart ClubPayless ShoesPermanent Trustee FoundationPerpetual John Bedwell FundPremier Warehousing and
DistributionPrinceton Publishing Pty LtdProspect Electrical Wholesalers
Pty LtdProtrust Pty Ltd
Pymble Pub PensionersRachel Parkinson Hospital
Equipment FundRadio 2UERAHC - Fundraising DepartmentRAHC - Public RelationsRainbow Home and Respite
ServicesReal Estate Institute of NSW
Northern DivisionRett Syndrome Association of
NSW IncRett Syndrome Australian
Research FundRita Cinema RandwickRiteman Pty LtdRossfreight Charity TrustRotary Club of ChatswoodRotary Club of Ku-ring-gaiRotary Club of WarringahSchering-Plough Pty LtdSelect Appointments Pty LtdSellers Holdings Pty LtdSeven Network Social Club
FundraisingShell Refining Australia Pty LtdShipping Industry Golf ChallengeShop Distributive & Allied
Employees' AssociationSir Robert & Lady Askin
Charities TrustSmith & Nephew Surgical Pty
LtdSouth Sydney Junior Rugby
LeagueSovereign Order of Saint John of
Jerusalem Knights HospitallerSovereign Order of St John of
JerusalemSt Patrick's Day Ball CommitteeStarlight FoundationStud & Track Manufacturing Pty
LtdSupersix EventsSusan Kaltman Chinese Opera
GroupSydney's ChildSydney Sae Soon Presbyterian
Church IncSydney Water CorporationThe Crows Nest ClubThe Lebanese Moslem
AssociationThe National Coursing
AssociationThe Orange Grove HotelThe Petre FoundationThe Promotional ShopThe Travellers Cot FundThiess Services Staff
FundraisingTony Di Marti's Charity Dinner
DanceToy Charity Foundation of
AustraliaTrivia NightTrudeau & Associates Pty Ltd
United Grand Lodge of NSWMasons
United in HopeVabat IncorporatedVariety Club of NSWWarringah CouncilWatermark Property ConsultantsWD-40 Company (Australia) Pty
LtdWest Ryde Hotel - Charity EventsWestern Earthmoving Pty LtdWestminster Financial GroupWestpac Banking CorporationWestpac Financial Markets
FundraisingWhitehall Property HoldingsWoolworths LimitedWoolworths SupermarketsWT PartnershipWyndlorn Pastoral Company Pty
LtdXSI Technology Pty Ltd
Private Donor giftsover $1000Adams, Mr DavidAdams, Mr WCAdams, Mr & Mrs WF & KHAdamsas, Mr & Mrs DAdamson, Mr CRAlbert, Mrs AntoinetteAlbert, Mr & Mrs P & HAlbert AO, Mr RobertAmedee, Mrs Gloria JAngus, Mr IAquilina, Mr BTArnott, Mr WRAssaf, Mr JosephAyles, Mr KABadawi, Dr NadiaBaines, Reverend PeterBallieu Myer, MrBalnaves, Mr NeilBarnes, Mr & Mrs PBashir AC, Her Excellency MarieBateman, Ms LeanneBega, Mr PeterBeirne, Mr & Ms G & JBergin, Justice PABirkin, Mrs AnitaBirmingham, Mr & Mrs WRBisley, Mrs HMBlackler, Dr SMBlazevic, Mrs SueBleasel, Dr AndrewBleasel, Mr & Mrs L & VBoffo, Mr LBooth, Dr MichaelBorda, Mr KenBotros, Mr HarryBourke, Mrs TMBrown, Mr IanBrown, Mr & Mrs SS & PABrown, Mr CraigBrunsdon, Mr NKBurdack, Ms Deborah

35
Burgess, Mr Cliff ABurrows, Mrs ValmaButson, Miss JEByrne, Mr Arthur WByrnes, Mr & Mrs JCahill, Mr MJCairns, Mr GordonCaldwell, Ms IreneCampese OAM, Mr DavidCapon OAM, Mrs JCarmichael AO CBE, Mr ACarter, Mrs VECassagne, Ms CathleenChambers, Dr MichaelChauhan, Mr AmratCheung, Ms JennyChilton, Mr FredChin, Miss TChiu, Mr PaulClarke, Mr KCBClarke-Bruce, Mr MatthewClift, Mr & Mrs MJClifton, Mr VClinton, Mr SCohen, Mr RogerColeridge, Mr MCollins, Miss MConde, Mr & Mrs JCCondon, Mr SchonCondon, Mr PatrickCook, Mrs RMCorrigan, Mrs JCowin, Ms SharonCrawley, Mrs MICrowe, Mr & Mrs R & MCudlipp, Mr WOCurtis, Mr NicholasDalla-Pozza, Dr LucianoD'Amico, Mrs LoretaDavidson, Dr JADavis, Mr EJDavis, Mr & Mrs Roger &
PamelaDawes, Mrs MDawson, Mr CMDawson, Mr & Mrs SDeck, Mr StuartDedda, Mr AnthonyDempster, Mr HJDeveson, Mrs Ivy LDolbel, Mrs PDone, Mr KenDonnelly, Ms MelissaDouglas, Mr KDouglas, Mr MDouglas, Miss LDouglass, Mr JWDoyle, Mr KevinDuffy, Mr ATDuffy, Ms PatriciaDumbrell, Mr & Mrs StanleyDuncan, Mrs JoyceDunlop AM, Mr JohnDurney, Mr & Mrs LesterEconomus, Miss HMEconomus, Miss JMEfthymiou, Mr & Mrs
El Rassi, Ms MichelleElias, Mr BenElsarky, Mr MohamedFairfax, Lady VincentFairfax AM, Mr JBFairfax AO, Mr JOFeltrin, Ms BarbaraFerguson, Mr RobertFerguson, Mrs JennyFerres, Mr John AFinkelsen, Mr & Mrs JohnForrest, Dr JFreedman AM, Mr LawrenceFyfe, Mrs SGilmartin, Mr & Mrs NP & SCGlasson, Dr MartinGlennie, Miss PTGlenny, Mrs JodieGoh, Mr TYGoldsmith, Mr & Mrs Max &
PamGoldston-Morris, Dr MaurineGonski, Mr DavidGorman, Mr & Mrs TGottlieb, Mr MelGoundrie, Mr GaryGowing, Mrs BGGrace, Mrs BAGraham, Mr & Mrs JPGraham, Mrs MavisGreig, Miss EGreiner AO, Cr KathrynGrimes, Mr StaffordGunning, Mr & Mrs PJ & LJHakim, Mrs NHampe, Mrs NHannah, Mr MikeHargraves, Mrs JHarris, Mr & Mrs CGHarris, Mrs CatherineHatton, Mr & Mrs Ken & PaddyHazelhurst, Ms NoniHellicar, Ms MeredithHendler, Mr/Ms SHenry, Mr ColinHevesi-Nagy, Mr/Ms SJHexton, Mr JohnHickey, Mrs BarbaraHicks, Mr IanHiggins, Mr & Mrs Terry & JennyHilmer AO, Mr Fred GHoffman, Mr BMHogan, Mr WarrenHoulton, Mrs RonaHowarth, Mr FrankHowarth, Mr JohnHughes, Mr/Ms PHunt, Mr PeterHutchinson, Mr JIvison, Mr GeorgeJackaman, Mrs CherryJackson, Mr & Mrs David &
LorraineJackson, Mr & Mrs S & JJaundrell, Mr & Mrs Malcom &
AngellinaJeffress, Mr Neville
Johnson, Mr BenJohnson, Mrs JZJuanas, Mr & Mrs EKallas, Mrs KayKelly, Ms SusanKendall, Mrs LynKernaghan, Mr LeeKhattar, Ms LauraKibble AO, Ms GabrielleKiraly, Mr AndrewKnoblanche, Mrs AnneLa Manna, Ms CathyLai, Mr VincentLam, Mrs NancyLanda, Mrs AnneLangley, Ms TLarkin, Mr EdmundLawrence, Mr GrahamLawrie, Mr/Ms RRLeatch, Mr& Mrs Robert & PamLee, Mr & Mrs RJLeece, Mr JohnLew, Dr William GLim, Mrs Ooi-FahLin, Dr DanielLinnell, Mrs BALondish, Mr IanLowy, Mr DavidLoxton, Dr SusanLuu, Ms AnnaLuu, Mr QuangMacadie, Mrs IreneMacFarlane, Mr & Mrs IanMacintosh, Mr DavidMackay, Mr HughMackisack, Mrs JMMagid, Mr LMManichanh, the FamilyMaple-Brown, Mr & MrsMapp, Mr GrahameMapp AM, Mr GEMartin, Mrs AlexandraMartin, Mrs DMMartin AM, Dr FrankMattick, Mr & Mrs PW & PCMcBride, Ms Caroline FayeMcClure, Mr SteveMcCormick, Dr RGMcCowage, Dr GeoffreyMcFadyen, Mr & Mrs BJMcintosh, Mr SimonMcIntyre, Mr AnthonyMcIntyre, Mr MDMcKay, Dr KarenMcNiven, Mr JohnMekker, Mr AmosMelvaine, Mr/Ms DMerchant OAM, Mr & Mrs
Dennis & GayMezrani, Mr MarkMiller, Mr & Ms John & SuzanneMoore, Mr AlexMoraitis, Mr NicholasMorgan, Mr GKMoujalli, Mr JPMudaliar, Mr Anil KrishnaMurphy, Mr James P

36
Murray, Mr DavidMustica, Mr CANash, Mr WTNasso, Mr TonyNicolaou, Mr & Mrs PaulOates OAM, Mrs FOates AM, Prof KimO'Brien, Mr WarrenO'Connor, Mr John RPacker, Mr JamesPark, Reverend Chong SukPascoe AO, Mr JohnPaterson, Mrs LMPennycuick, Mr RonaldPerkins, Mr RussellPetre, Mr DanielPhillips, Mr M JohnPhuah, Mr & Mrs HB & NSHPodda, Mr EfisioPollock, Dr & Mrs RPontifex, Mr GaryPoon, Dr & Mrs ChrisPotter, Ms RobinPotts, Mr & Mrs BrentPowell, Mr RPretty, Mr TedPrice, Ms AngelaPrice, Mr JPriestley, The Hon LJPuxley, Mr/Ms ARagg, Mr WRaine, Mr MSRamsden, Mrs EJIRanogajec, Mr ZeljkoRaven, Mr RERe, Mr JosephRead, Mr ChrisReid, Ms JennyRendle, Mr & Mrs J & CReoch, Mr AndrewRich, Ms ChristinaRitchie, Mr PeterRitchie, Mr & Mrs PDRoberts, Mr & Mrs BRoss, Ms JuliaRossi Harris, Mrs CatherineRossiter, Mrs SylviaRothery, Mr DJSampson, Mrs RuthSavage, Ms HelenSay, Mr DGASaywell, Mr Preston GScaravilli, Mr Joe & GuyScarlett, Mrs MScheinberg, Dr & Mrs AdamScheinberg, Mr JustinScotford, Mrs DScott, Mr ERSelim, Mr & Mrs JSergi OAM, Mr PatrickSevern, Mr RodneySewell, Mr RogerSheridan, Mr KenSherman, Mr BrianSherwood, MrsSilk, Mr & Mrs C & MSillence, Mr Tom
Singleton, Mrs JulieSingleton AM, Mr JohnSkarratt, Mr GraemeSlee, Mr GHSmith, Mr DickSneddon, Mr TomSomers, Mrs JStephen, Mr/Ms AMStephens, Mr MalcolmSteward, Miss ValStoker, Mr ErnieStrange, Mr BrianStuckey, Mr & Mrs JAStyles, Mrs MerrySutherland, Ms Marni YSwirsky, Mr PaulSymond AM, Mr JohnTertini , Mr & Mrs JThorpe, Mr IanTobias, Mr & Mrs MurrayTosson, Dr GTouma, Mr RaymondTowers, Ms VickiTrapaga, Ms MonicaTriguboff, Mr MichaelTurik, Ms TaniaTurk, Mrs Lois ATurnbull, Mr BradUrand, Ms KathrynVeitch, Mrs MargaretVella, Mr StephenVernon, Mr Brian TWain, Mr BarryWalker, Mr DWarburton, Mr JohnWard, Mr & Mrs Karen & MalWatson, Mr & Mrs Bill & GraceWebster, The Honourable
RobertWehby, Mr & Mrs AS & RAWeldon, Mr KevinWestgate, Mr David SWeston, Mr & Mrs Craig & ChrisWhite, Ms JulieWhittemore JP, Mr Charles HJWilliams, Mr & Mrs C & CWilson, Mrs AdrienneWood, Mr MichaelWooster, Mr CPWynn, Mr RichardYip, Mr NYoung, Mrs Laurie MYoung, Mrs LOYoung AO, Prof JohnYu AC, Dr JohnZammit, Mr Gerard

37
Roll of HonourWe were again honoured this year by a number of very special people whoremembered The Children’s Hospital at Westmead in their Wills. Each bequest isa precious gift, promising better health for children now and in futuregenerations. We extend our condolences to their families, and with gratitudeand respect, honour their memories.Legacies and Bequests – excluding Trusts
Noni Dora AudetteAlan BatkinNancy Jean BertramNina Maud E BeveridgeAmelia Mary BrownMaurice J BrunellEffie Jane BrunetJoseph Hilton BryantFreda Elizabeth O CannockJohn Leonard ClarkeStella Martha CohenMuriel Alice CookeThelma Vera CoxFrancis DalyMavis Sarah DarbonLionel E F DegeFrancis John DelpradoIvy DevesonTrevor W DewsburyFlorence Gertrude DownesGordon William DukesJames DuncanBessie Jean Faulkner
Gloria F FlanaganKeith Stobo FlemingMarion FordHelga GalibardovEdna Jane GambellRobert Thomas GortonSirima Joyce GunasekaraGrace Muriel HallAlice P HutchinsonLeslie B IsmayFrances Maud KearyMary KennyGrace Elizabeth LangfordHilda May MacFarlaneDaphne MasonHilda Florence McColeKenneth McMahonJoyce MillerMargaret MontgomeryGeorge Arthur Henry MountyJohn Noel MurleyLaura Elsie NordheimGeorge Albert Edward Nye
Jean Birkett PeeblesMrs E K RamshawPhyllis Lillian RoseCharlotte RossOlive Joan May RudderHazel May SavageEileen Florence SchmeisingJoyce Mary SettreeBeryl Ada SmithVeronica Josephine SpillaneDavid Phillip StokesIvor C R TaconEnid Joyce TamblynGesiena Johanna TemminkVelma May ThomasMary Ellen ValentineWallace Russell WallerJosephine E WhiteGeorge John WhittyMuriel E WilkinsonBeryl Martha WilliamsAlison E WithersWaclaw WitkowskiWalter Charles Wright Philip

38
Financial OverviewExecutive Summary
The Royal Alexandra Hospital for Children received its Budget Allocation forthe 2001/02 financial year on 31 August 2001. The allocation letter alsoprovided advice on budgets (including growth funding) up to 2003/04, suchforward notice enabling the Service to better plan its service delivery.
The agreed 2001/02 Net Cost of Services budget for the Health Service was$71.9 million against which the audited actual of $70.6 million representeda variation of $1.3 million or 1.8%.
The reported variation can be attributed to the larger than planned donationsand grants received for the research, clinical and community child healthservices. The Hospital has been able to cover all the increased cost ofoperations through donations and additional revenue raised from chargeableservices.
In achieving the above result the Hospital is satisfied that it has operatedwithin the advised level of Government Cash Payments and restrictedoperating costs to the budget available. Further, it has ensured that nogeneral creditors over 45 days exist at the end of any month.
Significant Budget Increases 2001/2002Some of the major increases in budget allocations that occurred during2001/2002 are as follows:
Use of $3M General Growth enhancements for such services as metabolicbone disorders, auditory (hearing), Newborn Screening, Cardiology, MolecularPathology, Haematologist, Bone Marrow Transplant, Eczema and PsoriasisServices, High Dependency Units, Audiometric Assessment of Patients PostGrommets, General Medicine and Surgery.
During the year award increases of 3% occurred, thereby increasing salarycosts by $2.8 million.
Program ReportingThe amount spent on each program depends on the use of the donatedfunds and the enhancement received by the Hospital during the year.Comparing to the previous year, the Hospital had increased its spending onthe following program by more than $1 million.
Program $’M % Explanation
1.1 Primary and Community Based Services
1.2 32 Enhancement and increasedexpenditure from donated fundsfor specific primary andcommunity child health services
1.3 Outpatient Services
6.3 22 A shift in ambulatory care fromsame day care for diabetes andoncology patients
2.2 Overnight Acute Inpatient Services
(4.6) (54)Increase of revenue by $12.9million compared to theprevious year resulted in thereduction in the net cost ofservices for the program
2.3 Same Day Acute Inpatient Services
4.6 878 Enhancement from GeneralGrowth and increase use inspecial and trust funds inproviding the services
6.1 Teaching and Research
5.0 2128 The variation is a result of a one-off donation and Grant of $15million received for researchbuilding last year.
Directions in FinancingAs part of the initiatives detailedin the Health Council Report,Episodic Funding has beenintroduced as a means ofdistributing funds to hospitals forsome acute services, EmergencyDepartments and Intensive CareUnits. These services will beincreasingly funded inaccordance with plannedactivities as opposed to thetraditional method of providingbudgets based on prior yearevents.
The Hospital recognises the needto update its administrativebases in order to provide theoptimum support for the manyclinical advances affected inrecent years. The Hospital hadplanned the upgrades of systemsto support the clinical services in2002/2003:For example; Radiology ImagingSystems, Document ImagingSystems and Hospas Systems
The 2002/2003 BudgetThe 2002/2003 Budget wasreceived on 13 September 2002and provides for an increase of$3 million in growth funding,bringing the total growth fundingprovided since 1 July 2000 to$6.7 million on an ongoingannual basis.
The $3 million has been providedto undertake initiatives which willimprove the quality of care andincrease or enhance the range ofservices offered by the Children’sHospital, eg Cardiac Surgery,Emergency Department,Community Outreach, Laboratoryand Diagnostic Services, Pain andPalliative Care Unit, PamidronateProgram, Respiratory SupportServices, Diabetes, DysphagiaClinic, Neurology Services; Qualityof Care Unit, Surgical Services,Obesity Management.

39

40

41

42
Financial StatementsFor the 122nd Annual Report ofThe Royal Alexandra Hospital for Children(The Children’s Hospital at Westmead)for the year ending 30 June 2002

43
Royal Alexandra Hospital for ChildrenStatement of Financial Performance for the year ended 30 June 2002
Notes Actual Budget Actual2002 2002 2001$000 $000 $000
EXPENSES
Operating Expenses Employee Related 3 131,469 128,707 123,380 Visiting Medical Officers 3,978 4,091 3,889 Goods and Services 4 39,734 36,281 35,211Maintenance 5 6,023 4,650 5,498Depreciation and Amortisation 2(k), 6 17,447 17,712 17,832Grants and Subsidies 7 280 280 -
Total Expenses 198,931 191,721 185,810
REVENUES
Sale of Goods and Services 8 95,445 92,082 84,855Investment Income 9 1,819 1,887 4,250Grants and Contributions 10 26,019 22,200 35,423Other Revenue 11 5,576 4,164 3,812
Total Revenues 128,859 120,333 128,340
Loss on Disposal of Non Current Assets 12 (511) (518) (365)
Net Cost Of Services 31,34 70,583 71,906 57,835
GOVERNMENT CONTRIBUTIONS
NSW Health DepartmentRecurrent Allocations 2(a) 45,885 45,885 48,755NSW Health DepartmentCapital Allocations 2(a) 4,053 4,053 274Acceptance by the Crown Entityof Superannuation Liability 2(c) 9,246 9,249 8,649
Total Government Contributions 59,184 59,187 57,678
RESULT FOR THE YEAR 25 (11,399) (12,719) (157)
Net Increase in Asset Revaluation Reserve 62,865 - 76
Total Revenues, Expenses and ValuationAdjustments Recognised Directly in Equity 62,865 - 76
TOTAL CHANGES IN EQUITY OTHER THANTHOSE RESULTING FROM TRANSACTIONSWITH OWNERS AS OWNERS 51,466 (12,719) (81)
The accompanying notes form part of these Financial Statements

44
Royal Alexandra Hospital for ChildrenStatement of Financial Position as at 30 June 2002
Notes Actual Budget Actual2002 2002 2001$000 $000 $000
ASSETS
Current Assets
Cash 15 28,819 23,498 8,010Receivables 16 5,369 6,222 6,552Inventories 17 2,864 2,950 2,895Other Financial Assets 18 - - 23,698
Total Current Assets 37,052 32,670 41,155
Non-Current Assets
Receivables 16 215 - 213Other Financial Assets 18 40,031 38,345 29,507 Property, Plant and Equipment Land and Buildings 19 310,248 249,113 253,855 Plant and Equipment 19 37,396 37,185 44,216 Other 19 2,719 2,719 3,266
Total Property, Plant and Equipment 350,363 289,017 301,337
Total Non-Current Assets 390,609 327,362 331,057
Total Assets 427,661 360,032 372,212
LIABILITIES
Current Liabilities
Payables 22 7,240 6,522 6,303Interest Bearing Liabilities 23 - - 1,359Employee Entitlements and Other Provisions 24 15,295 17,794 17,419
Total Current Liabilities 22,535 24,316 25,081
Non-Current Liabilities
Employee Entitlements and Other Provisions 24 22,699 17,473 16,170
Total Non-Current Liabilities 22,699 17,473 16,170
Total Liabilities 45,234 41,789 41,251
Net Assets 382,427 318,243 330,961
EQUITYReserves 25 123,286 60,422 60,421Accumulated Funds 25 259,141 257,821 270,540
Total Equity 382,427 318,243 330,961
The accompanying notes form part of these Financial Statements

45
Royal Alexandra Hospital for ChildrenStatement of Cash Flow for the year ended 30 June 2002
Notes Actual Budget Actual2002 2002 2001$000 $000 $000
CASH FLOWS FROM OPERATING ACTIVITIES
Payments
Employee Related (118,505) (118,465) (112,417)Grants and Subsidies (280) (280) -Other (48,460) (44,436) (44,703)
Total Payments (167,245) (163,181) (157,120)
Receipts
Sale of Goods and Services 18,686 12,798 13,860Interest Received 1,806 1,887 4,261Grants and Contributions 26,018 23,931 34,772Other 5,776 4,165 4,165
Total Receipts 52,286 42,781 57,058
CASH FLOWS FROM GOVERNMENT
NSW Health Department Recurrent Allocations 123,445 123,445 117,674NSW Health Department Capital Allocations 4,053 4,053 274Cash Reimbursements from the Crown Entity 828 828 562
Net Cash Flows from Government 128,326 128,326 118,510
NET CASH FLOWS FROM OPERATINGACTIVITIES 31 13,367 7,926 18,448
CASH FLOWS FROM INVESTING ACTIVITIES
Proceeds from Sale, Land and Buildings, Plant andEquipment and Infrastructure Systems 256 230 550Proceeds from Sale of Investments 42,072 15,210 105,017Purchases of Lands and Buildings, Plant andEquipment and Infrastructure System (4,377) (6,519) (7,196)Purchase of Investments (29,150) - (114,354)
NET CASH FLOWS FROM INVESTINGACTIVITIES 8,801 8,921 (15,983)
NET INCREASE IN CASH 22,168 16,847 2,465
Opening Cash and Cash Equivalents 6,651 6,651 4,186
CLOSING CASH AND CASH EQUIVALENTS 15 28,819 23,498 6,651
The accompanying notes form part of these Financial Statements

46
Royal Alexandra Hospital for ChildrenProgram Statement – Expenses and Revenues for the year ended 30 June 2002
Service’s Expensesand Revenues Program Program Program Program Program
1.1* 1.2* 1.3* 2.1* 2.2*
2002 2001 2002 2001 2002 2001 2002 2001 2002 2001$000 $000 $000 $000 $000 $000 $000 $000 $000 $000
ExpensesOperating Expenses Employee Related 4,192 4,069 118 70 22,719 19,144 7,446 7,685 66,109 61,308 Visiting Medical Officers - - - - 2,335 2,188 - - 1,570 1,582 Goods and Services 675 939 12 5 10,327 7,101 1,126 1,568 20,933 17,501 Maintenance 222 164 - 2 1,709 1,440 266 271 2,422 2,179 Depreciation and Amortisation
447 447 - 7 5,111 4,687 590 1,131 7,777 8,110
Grants and Subsidies 280 - - - - - - - - -
Total Expenses 5,816 5,619 130 84 42,201 34,560 9,428 10,655 98,811 90,680
Revenues Sale of Goods and Services
413 307 - 5 2,959 2,070 760 795 87,725 72,353
Investment Income 39 150 - 1 284 345 64 109 1,043 921 Grants and Contributions 394 1,279 - 7 3,086 2,847 587 897 5,110 7,607 Other Revenue 124 225 - 2 1,000 657 180 204 1,205 1,316
Total Revenue 970 1,961 - 15 7,329 5,919 1,591 2,005 95,083 82,197
Loss on Sale of NonCurrent Assets (14) (24) - - (108) (33) (24) (11) (239) (91)NET COST OFSERVICES 4,860 3,682 130 69 34,980 28,674 7,861 8,661 3,967 8,574
The preparation of each year’s program statement is based on statistical data for the previous year, together withany known program enhancements or definitional changes that have been advised by NSW Health. Using thismethodology for 2001/02, no material variations have occurred, with the movements largely representing theeffects of cost escalation, revenue increases and specific enhancement funding.
The accompanying notes form part of these Financial Statements

47
Program Program Program Program Program Grand2.3* 3.1* 4.1* 5.1* 6.1* Total
2002 2001 2002 2001 2002 2001 2002 2001 2002 2001 2002 2001$000 $000 $000 $000 $000 $000 $000 $000 $000 $000 $000 $000
5,533 5,046 1,422 1,144 1,835 1,597 4,834 4,080 17,261 19,237 131,469 123,38073 71 - - - - - - - 48 3,978 3,889
1,975 2,872 75 296 484 135 1,323 1,072 2,804 3,722 39,734 35,211323 277 - 49 65 40 302 188 714 888 6,023 5,498
1,096 1,085 111 70 152 146 680 591 1,483 1,558 17,447 17,832
- - - - - - - - - - 280 -
9,000 9,351 1,608 1,559 2,536 1,918 7,139 5,931 22,262 25,453 198,931 185,810
3,012 7,807 - 25 187 112 - 350 389 1,031 95,445 84,855
60 92 4 12 17 21 48 61 260 2,538 1,819 4,250646 762 33 95 168 173 1,278 501 14,717 21,255 26,019 35,423200 177 12 28 47 37 626 113 2,182 1,053 5,576 3,812
3,918 8,838 49 160 419 343 1,952 1,025 17,548 25,877 128,859 128,340
(23) (9) (2) - (6) (2) (23) (7) (72) (188) (511) (365)
5,105 522 1,561 1,399 2,123 1,577 5,210 4,913 4,786 (236) 70,583 57,835
*The name and purpose of each program is summarised in Note 13.

48
Royal Alexandra Hospital for ChildrenNotes to and forming part of the Financial Statements for the year ended 30 June 2002
1. The Hospital Reporting Entity
The Royal Alexandra Hospital for Children ‘the Hospital’, trading as The Children’s Hospital at Westmead,comprises all the operating activities of the Hospital facilities under the control of the Hospital. It alsoencompasses the Special Purposes and Trust Funds which, while containing assets which are restricted forspecified uses by the grantor or the donor, are nevertheless controlled by the Hospital.
The reporting entity is consolidated as part of the NSW Total State Sector and as part of the NSW PublicAccounts.
2. Summary of Significant Accounting Policies
The Hospital’s Financial Statements are a general purpose financial report which has been prepared on anaccrual basis and in accordance with applicable Australian Accounting Standards, other authoritativepronouncements of the Australian Accounting Standards Board (AASB), Urgent Issues Group (UIG) ConsensusViews and the requirements of the Health Services Act 1997 and its regulations including observation of theAccounts and Audit Determination for Area Health Services and Public Hospitals.
Where there are inconsistencies between the above requirements, the legislative provisions have prevailed.
In the absence of a specific Accounting Standard, other authoritative pronouncements of the AASB or UIGConsensus View, the hierarchy of other pronouncements as outlined in AAS6 ‘Accounting Policies’ isconsidered.
Statements of Accounting Concepts are used as guidance in the absence of applicable Accounting Standards,other mandatory professional requirements and legislative requirements.
Except for certain investments and land and buildings, plant and equipment and infrastructure systems, whichare recorded at valuation, the financial statements are prepared in accordance with the historical costconvention. All amounts are rounded to the nearest one thousand dollars and are expressed in Australiancurrency.
Other significant accounting policies used in the preparation of these financial statements are as follows:
a) NSW Health Department AllocationsPayments are made by the NSW Health Department on the basis of the net allocation for the Hospital asadjusted for approved supplementations mostly for salary agreements, patient flows between the Hospital andother States and approved enhancement projects. This allocation is included in the Statement of FinancialPerformance before arriving at the ‘Result for the Year’ on the basis that the allocation is earned in return forthe health services provided in 2001/2002 on behalf of the Department. Allocations are normally recognisedupon the receipt of Cash.
b) Employee EntitlementsWages and Salaries, Annual Leave, Long Service Leave, Sick Leave and On-Costs
Liabilities for wages and salaries, annual leave, and vesting sick leave and related on-costs are recognisedand measured as the amount unpaid at the reporting date at current pay rates in respect of employees’services up to that date.
Long service leave is measured on a nominal basis and is based on the remuneration rates at year-end for allemployees with five or more years of service. It is considered that this measurement technique producesresults not materially different from the estimate determined by using the present value basis ofmeasurement.
The Hospital had increased its provision by $1,907,000 to provide for the accumulated public holidays leaveand extra leave that is now accurately accrued in the payroll system.
Employee leave entitlements are dissected between the ‘Current’ and ‘Non Current’ components on the basisof anticipated payments for the next twelve months. This in turn is based on past trends and knownresignations and retirements. The result is that the current liability for Long Service Leave is stated as$2,395,000. The full liability for employees with greater than 10 years’ service amounts to $14,850,878.

49
Royal Alexandra Hospital for ChildrenNotes to and forming part of the Financial Statements for the year ended 30 June 2002
Unused non-vesting sick leave does not give rise to a liability as it is not considered probable that sick leavetaken in the future will be greater than the entitlements accrued in the future.
The outstanding amounts of workers’ compensation insurance premiums and fringe benefits tax, which areconsequential to employment, are recognised as liabilities and expenses where the employee entitlements towhich they relate have been recognised.
c) SuperannuationThe Hospital's liability for superannuation is assumed by the Crown Entity. The Hospital accounts for theliability as having been extinguished resulting in the amount assumed being shown as part of the non-monetary revenue item described as ‘Acceptance by the Crown Entity of Superannuation Liability’.
The superannuation expense for the financial year is determined by using the formulae specified by the NSWHealth Department. The expense for Basic Benefit and First State Super schemes is calculated as apercentage of the employees' salaries. For State Superannuation Scheme and State AuthoritiesSuperannuation Scheme, the expense is calculated as a multiple of the employees' superannuationcontributions.
d) InsuranceThe Hospital's insurance activities are conducted through the NSW Treasury Managed Fund Scheme of self-insurance for Government agencies. The premium is determined by the Fund Manager based on pastexperience.
e) Revenue RecognitionRevenue is recognised when the Hospital has control of the good or right to receive, it is probable that theeconomic benefits will flow to the Hospital and the amounts of revenue can be measured reliably. Additionalcomments regarding the accounting policies for the recognition of revenue are discussed below.
Sale of Goods and ServicesRevenue from the sale of goods and services comprises revenue from the provision of products or services, ieuser charges. User charges are recognised as revenue when the Hospital obtains control of the assets thatresult from them.
Patient FeesPatient Fees are derived from chargeable inpatients and non-inpatients on the basis of rates specified by theNSW Health Department from time to time.
Investment IncomeInterest revenue is recognised as it accrues. Rent revenue is recognised in accordance with AAS17‘Accounting for Leases’. Dividend revenue is recognised when the Hospital’s right to receive payment isestablished.
Debt ForgivenessIn accordance with the provisions of Australian Accounting Standard AAS23, debts are accounted for asextinguished when and only when settlement occurs through repayment or replacement by another liability orthe debt is subject to a legal defeasance.
Use of Hospital FacilitiesSpecialist doctors with rights of private practice are charged for the use of Hospital facilities at ratesdetermined by the NSW Health Department and are based on fees collected.
f) Use of Outside FacilitiesThe Hospital uses a number of facilities owned and maintained by third parties, mainly local authorities, todeliver community health services. No charges are raised by the authorities.

50
Royal Alexandra Hospital for ChildrenNotes to and forming part of the Financial Statements for the year ended 30 June 2002
g) Goods and Services Tax (GST)Revenues, expenses and assets are recognised net of the amount of GST, except:
• the amount of GST incurred by the Hospital as a purchaser that is not recoverable from the AustralianTaxation Office is recognised as part of the cost of acquisition of an asset or as part of an item of expense;
• receivables and payables are stated with the amount of GST included.
h) Inter Area and Interstate Patient FlowsThe Hospital recognises the flow of acute inpatients from the area in which they are resident to other areaswithin the State and across Australia. The expense and revenue values reported within the financialstatements have been based on 2000/2001 activity data using standard cost weighted separation values toreflect estimated costs in 2001/02 for acute weighted inpatient separations. The Hospital is treating patientsfrom all Area Health Services and is therefore being reimbursed by the benefiting Area based on thecalculations provided by NSW Health Department.
The reporting adopted also aims to provide a greater accuracy of the cost of the Hospital’s statewide serviceprovisions and disclose the extent to which service is provided to residents of other NSW Area Health Servicesand other Australian States and Territories.
The adjustments have no effect on equity values as the movement in Net Cost of Services is matched by acorresponding adjustment to the value of the NSW Health Recurrent Allocation.
The composition of patient flow revenue is disclosed in Notes 8.
i) Acquisition of AssetsThe cost method of accounting is used for the initial recording of all acquisitions of assets controlled by theHospital. Cost is determined as the fair value of the assets given as consideration plus the costs incidental tothe acquisition.
Assets acquired at no cost, or for nominal consideration, are initially recognised as assets at their fair value atthe date of acquisition except for assets transferred as a result of an administrative restructure.
Fair value means the amount for which an asset could be charged between a knowledgeable, willing buyerand a knowledgeable, willing seller in an arm’s length transaction.
Land and Buildings that are owned by the Health Administration Corporation or the State and administered bythe Hospital are deemed to be controlled by the Hospital and are reflected as such in the financial statements.
j) Plant and EquipmentIndividual items of plant and equipment costing $5,000 and above are capitalised.
k) DepreciationDepreciation is provided for on a straightline basis for all depreciable assets so as to write off the depreciableamount of each asset as it is consumed over its useful life to the Hospital. Land is not a depreciable asset.
Details of depreciation rates for major asset categories are as follows:
Buildings 2.3% 2.5%Leasehold Property 2.5%Electro Medical Equipment- Costing less than $200,000 10.0%- Costing more than or equal to $200,000 12.5%Computer Equipment 20.0%Computer Software 20.0%Office Equipment 10.0%Plant and Machinery 10.0%Furniture, Fittings and Furnishings 5.0%

51
Royal Alexandra Hospital for ChildrenNotes to and forming part of the Financial Statements for the year ended 30 June 2002
During the year, the estimated useful life of buildings was revised upwards from 40 years to 50 years. Foreach of the remaining 43 years of the asset’s lives, including the current financial year, the depreciationexpense will reduce by $279,000 from the original estimate of $6,911,000.
l) Revaluation of Physical Non-Current AssetsBuildings and improvements, plant and equipment and infrastructure assets (excluding land) are valuedbased on the estimated written down replacement cost of the most appropriate modern equivalentreplacement facility having a similar service potential to the existing asset. Land is valued on an existing usebasis, subject to any restrictions or enhancements since acquisition.
In accordance with Treasury policy, the Hospital has applied the AASB1041 ‘Revaluation of Non-CurrentAssets’ transitional provisions for the public sector and has elected to continue to apply the existingrevaluation basis, while Treasury’s policy on fair value is finalised. It is expected, however, that in mostinstances the current valuation methodology will approximate fair value.
Revaluations are made at least every 5 years and with sufficient regularity to ensure that the carrying amountof each asset in the class does not differ materially from its fair value at reporting date. Valuations of landand building are determined in accordance with an independent valuation. The last of such revaluations wascompleted in April 2002.
Where assets are revalued upward or downward as a result of a revaluation of a class of non-current physicalassets, the Hospital restates separately the gross amount and the related accumulated depreciation of thatclass of assets.
The recoverable amount test has not been applied as the Hospital is a not-for-profit entity whose servicepotential is not related to the ability to generate net cash inflows.
Revaluation increments are credited directly to the Asset Revaluation Reserve except when, to the extent thatan increment reverses a revaluation decrement in respect of that class of asset previously recognised as anexpense in the ‘result for the year from ordinary activities’, the increment is recognised immediately asrevenue in the ‘result for the year from ordinary activities’.
Revaluation decrements are recognised immediately as expenses in the ‘movement in accumulated fundsfrom ordinary activities’ except that, to the extent that a credit balance exists in the asset revaluation reservein respect of the same class of assets, they are debited directly to the Asset Revaluation Reserve.
Revaluation increments and decrements are offset against one another within a class of non-current assets,but not otherwise.
m) Maintenance and repairsRepairs and maintenance cost and minor replacements (items less than $5,000) are expenses as incurredexcept where they relate to the replacement of a component of an asset in which case the costs arecapitalised and depreciated.
n) Leased AssetsA distinction is made between finance leases, which effectively transfer from the lessor to the lesseesubstantially all the risks and benefits incidental to ownership of the leased assets, and operating leasesunder which the lessor effectively retains all such risks and benefits.
Where a non-current asset is acquired by means of a finance lease, the asset is recognised at its fair value atthe inception of the lease. The corresponding liability is established at the same amount. Lease paymentsare allocated between the principal component and the interest expense.
Operating lease payments are charged to the Statement of Financial Performance in the periods in which theyare incurred.
o) InventoriesInventories are stated at the lower of cost and net realisable value. Costs are assigned to individual items ofstock mainly on the basis of weighted average costs.
Obsolete items are disposed of in accordance with instructions issued by the NSW Health Department.

52
Royal Alexandra Hospital for ChildrenNotes to and forming part of the Financial Statements for the year ended 30 June 2002
p) Other Financial Assets‘Other financial assets’ are generally recognised at cost, with the exception of Treasury Corporation (TCorp)Hour Glass Facilities and Managed Fund Investments, which are measured at market value.
For non-current ‘other financial assets’, revaluation increments and decrements are recognised in the samemanner as physical non-current assets (see para m).
For current ‘other financial assets’, revaluation increments and decrements are recognised in the Statementof Financial Performance.
Donated value is equivalent to the market value at the date of receipt since 30 June 2000. The equityinvestment is valued at its market value.
For current investments, revaluation increments and decrements are recognised in the Statement of FinancialPerformance.
Interest revenues are recognised as they accrue.
q) Financial InstrumentsFinancial instruments give rise to positions that are a financial asset of either the Hospital or its counter partyand a financial liability (or equity instrument) of the other party. For the Hospital, these include cash at bank,receivables, other financial assets and payables.
In accordance with Australian Accounting Standard AAS33, ‘Presentation and Disclosure of FinancialInstruments’, information is disclosed in Note 21 in respect of the credit risk and interest rate risk of financialinstruments. All such amounts are carried in the accounts at net fair value.
The specific accounting policy in respect of each class of such financial instrument is stated hereunder.
Classes of instruments recorded at cost and their terms and conditions at balance date are as follows:
Cash
Accounting Policies - Cash is carried at nominal values reconcilable to monies on hand and independent bankstatements.
Terms and Conditions - Monies on deposit attract an effective interest rate of approximately 4.7 % per annum.
Receivables
Accounting Policies - Receivables are recognised and carried at cost, based on the original invoice amountless a provision for any uncollectable debts. An estimate for doubtful debts is made when collection of the fullamount is no longer probable. Bad debts are written-off as incurred. No interest is earned on trade debtors.Accounts are issued on 30-day terms.
Investments
Accounting Policies - Investments reported at cost and net realisable value include both short term and fixedterm deposits, exclusive of Hour Glass Funds invested with Treasury Corporation. Interest is recognised in theStatement of Financial Performance when earned. Shares are carried at revalued carrying amount [Note 2(p)]with dividend income recognised when the dividends are declared by the investee.
Terms and Conditions – Short term deposits have an average maturity of 90 days and effective interest rate of4% to 6% as compared to 4.7% and 5.9% per annum in the previous year. Fixed term deposits have anaverage maturity of 1,460 days (1,825 days in 2000/01) and effective interest rates of -1% to 5% ascompared to 6% and 7.94% in the previous year.
Classes of instruments recorded at market value comprise:
Shares quoted on the Australian Stock Exchange.

53
Royal Alexandra Hospital for ChildrenNotes to and forming part of the Financial Statements for the year ended 30 June 2002
Treasury Corporation’s Hour Glass Investment Facilities
The Hospital has investments in TCorp’s Hour Glass Investment facilities. The Hospital’s investments arerepresented by a number of units in managed investments within the facilities. Each facility has differentinvestment horizons and comprises a mix of asset classes appropriate to that investment horizon. TCorpappoints and monitors fund managers and establishes and monitors the application of appropriateinvestment guidelines.
The Hospital’s investments are:
2002 2001
Cash Facility - 23,653Long Term Growth Facility 23,635 21,271
23,635 44,924
These investments can generally be redeemed with five business days’ notice (depending on the facility). Thevalue of the investments held could decrease as well as increase, depending upon market conditions. Thevalue that best represents the maximum credit risk exposure is the net fair value. The value of the aboveinvestments represents the Hospital’s share of the value of the underlying assets of the facility and is statedat net fair value.
There are no classes of instruments that are recorded at other than cost or market valuation.
All financial instruments, including revenue, expenses and other cash flows arising from instruments, arerecognised on an accruals basis.
Payables
These amounts represent liabilities for goods and services provided to the Hospital and other amounts,including interest. Interest is accrued over the period it becomes due.
r) Trust FundsThe Hospital receives monies in a trustee capacity for various trusts as set out in Note 27. As the Hospitalperforms only a custodial role in respect of these monies, and because the monies cannot be used for theachievement of the Hospital’s own objectives, they are not brought to account in the financial statements.
s) Reclassification of Financial Information‘Lease and Rental Income’ was recognised in prior year statements as Sale of Goods and Services, whereas,from 2001/02, the Hospital’s reporting has been amended to comply with ‘Whole of Government’ reportingand brings the revenue to account under Investment Income.
Intra Area Patient Flows / Inter State Patient Flows were recognised as payments within the Statement of CashFlows in 2000/01, consistent with the treatment required across all of NSW Health’s controlled entities.
As a result of these changes, the amounts for 2000/01 have been reclassified to ensure comparability.
t) Budgeted AmountsThe budgeted amounts are drawn from the budgets as formulated at the beginning of the financial year andwith any adjustments for the effects of additional supplementation provided.
u) Changes in Accounting PolicyFrom 2001/02 all Health Services have been provided with adjustments that recognise the flow of acuteinpatients to/from other Australian States and Territories. To the extent that services are provided to personsfrom outside of New South Wales, revenues are recognised. To the extent that services are provided to anArea’s residents outside of New South Wales an expense is recorded. The adjustments have no effect on theequity values as the movement in Net Cost of Services is matched by a corresponding adjustment to the valueof the NSW Health Recurrent Allocation.
The composition of patient flow revenue is disclosed in Note 8(b) and Note 8(c).

54
Royal Alexandra Hospital for ChildrenNotes to and forming part of the Financial Statements for the year ended 30 June 2002
2002 2001$000 $000
3. Employee Related Expenses
Employee related expenses comprise the following:
Salaries and Wages 106,009 100,096Long Service Leave [Note 2(b)] 3,035 3,191Annual Leave [Note 2(b)] 11,293 9,490Nursing Agency Payments 345 546Other Agency Payments 73 146Workers Compensation Insurance 1,468 1,262Superannuation [Note 2(c)] 9,246 8,649
131,469 123,380
Salaries and Wages includes $145,000 paid to members of the Health Services Board consistent with theStatutory Determination by the Minister for Health, which provided remuneration effective from 1 July 2000.
The Payments have been made with the following bands:
$ Range Number Paid
$0 to $15,000 10 $15,000 to $30,000 1
No other fees or benefits were paid by the Hospital to its Board Members.

55
Royal Alexandra Hospital for ChildrenNotes to and forming part of the Financial Statements for the year ended 30 June 2002
2002 2001$000 $000
4. Goods and Services
(a) Expenses on Goods and Services comprise the following:
Computer Related Expenses 306 359Domestic Charges 2,326 2,155Drug Supplies 8,950 7,483Food Supplies 2,240 2,230Fuel, Light and Power 1,546 1,216General Expenses 6,312 5,639Hospital Ambulance Transport Costs 400 432Insurance 60 16Medical and Surgical Supplies 8,078 7,495Postal and Telephone Costs 1,235 1,242Printing and Stationery 1,575 1,038Rates and Charges 275 214Special Service Departments 4,620 4,481Staff Related Costs 883 522Travel Related Costs 928 689
39,734 35,211
(b) General expenses include:
Advertising 460 415Books and Magazines 349 241Consultancies
Operating Activities 252 541 Capital Works 40 -
Courier and Freight 233 182Auditor’s Remuneration – Audit of Financial Reports 56 82Auditor’s Remuneration – Other Services - 17Legal Expenses 342 71Membership / Professional Fees 276 146Other Operating Lease Expense 1,479 1,342Provision for Bad and Doubtful Debts 491 214
5. Maintenance
Repairs and Routine Maintenance 4,946 4,202 Replacements and Additional Equipment less
than $5,000 1,077 1,296
6,023 5,498
6. Depreciation and Amortisation
Depreciation – Buildings 6,619 6,512Depreciation – Plant and Equipment 10,181 10,886Depreciation – Other 647 434
17,447 17,832

56
Royal Alexandra Hospital for ChildrenNotes to and forming part of the Financial Statements for the year ended 30 June 2002
2002 2001$000 $000
7. Grants and Subsidies
Voluntary Organisation 280 -
8. Sale of Goods and Services
(a) Sale of Goods and Services comprise the following:
Patient Fees [Note 2(e)] 6,013 5,112Staff Meals and Accommodation 16 20Infrastructure Charge – Facility Fees [Note 2 (e)] 5,858 5,077Car Parking 1,139 863Child Care Fees 407 382Fees for Medical Records 25 21Non-Staff Meals 2,113 2,129Sale of Prostheses 625 393Patient Inflows from Interstate 1,731 1,458Inter Area Patient Inflows, NSW 75,829 67,461Pharmacy 304 343Other 1,385 1,596
95,445 84,855
(b) Revenues from Inter-Area Patient Inflowson an Area basis as follows:
Central Sydney 5,067 4,948Northern Sydney 7,522 7,368Western Sydney 24,510 21,864Wentworth 6,672 5,771South West Sydney 13,862 12,072Central Coast 3,279 3,360Hunter 1,443 988Illawarra 2,411 1,830South Eastern Sydney 2,211 1,864Northern Rivers 364 554Mid North Coast 1,985 1,591New England 1,391 840Macquarie 1,250 711Mid Western 1,856 2,052Far West 104 52Greater Murray 840 747Southern NSW 1,062 849
75,829 67,461
(c) Revenues from Patient Inflowsfrom Interstate are as follows:
Australian Capital Territory 1,184 919Northern Territory 27 27Queensland 270 189South Australia 135 206Tasmania 38 46Victoria 42 52Western Australia 35 19
1,731 1,458
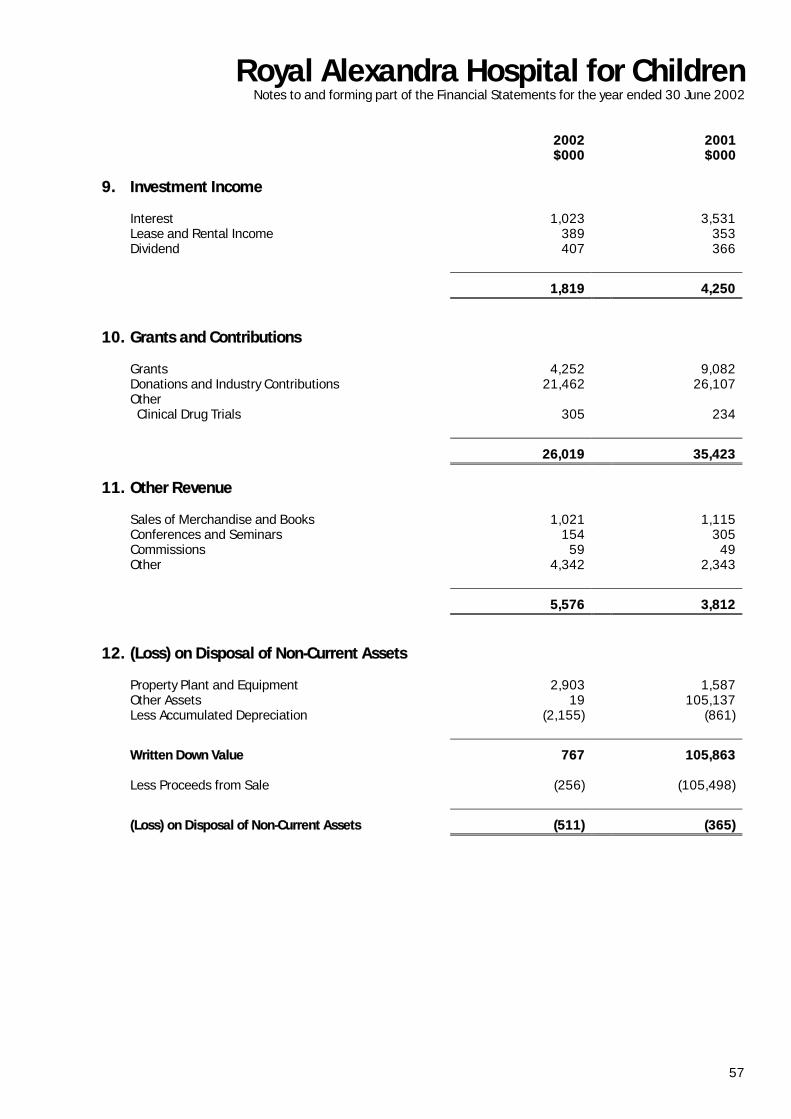
57
Royal Alexandra Hospital for ChildrenNotes to and forming part of the Financial Statements for the year ended 30 June 2002
2002 2001$000 $000
9. Investment Income
Interest 1,023 3,531Lease and Rental Income 389 353Dividend 407 366
1,819 4,250
10. Grants and Contributions
Grants 4,252 9,082Donations and Industry Contributions 21,462 26,107Other
Clinical Drug Trials 305 234
26,019 35,423
11. Other Revenue
Sales of Merchandise and Books 1,021 1,115Conferences and Seminars 154 305Commissions 59 49Other 4,342 2,343
5,576 3,812
12. (Loss) on Disposal of Non-Current Assets
Property Plant and Equipment 2,903 1,587Other Assets 19 105,137Less Accumulated Depreciation (2,155) (861)
Written Down Value 767 105,863
Less Proceeds from Sale (256) (105,498)
(Loss) on Disposal of Non-Current Assets (511) (365)

58
Royal Alexandra Hospital for ChildrenNotes to and forming part of the Financial Statements for the year ended 30 June 2002
13. Programs/Activities of the Health Service
Program 1. - Primary and Community Based ServicesObjective: To improve, maintain or restore health through health promotion, early intervention,
assessment, therapy and treatment services for clients in a home or community setting.
Program 1.2 - Aboriginal Health ServicesObjective: To raise the health status of Aborigines and to promote a healthy life style.
Program 1.3 - Outpatient ServicesObjective: To improve, maintain or restore health through diagnosis, therapy, education and treatment
services for ambulant patients in a hospital setting.
Program 2.1 - Emergency ServicesObjective: To reduce the risk of premature death and disability for people suffering injury or acute
illness by providing timely emergency diagnostic, treatment and transport services.
Program 2.2 - Overnight Acute Inpatient ServicesObjective: To restore or improve health and manage risks of illness, injury and childbirth through
diagnosis and treatment for people intended to be admitted to hospital on an overnightbasis.
Program 2.3 - Same Day Acute Inpatient ServicesObjective: To restore or improve health and manage risks of illness, injury and childbirth through
diagnosis and treatment for people intended to be admitted to hospital and discharged onthe same day.
Program 3.1 - Mental Health ServicesObjective: To improve the health, well being and social functioning of people with disabling mental
disorders and to reduce the incidence of suicide, mental health problems and mentaldisorders in the community.
Program 4.1 - Rehabilitation and Extended Care ServicesObjective: To improve or maintain the well being and independent functioning of people with
disabilities or chronic conditions, the frail aged and the terminally ill.
Program 5.1 - Population Health ServicesObjective: To promote health and reduce the incidence of preventable disease and disability by
improving access to opportunities and prerequisites for good health.
Program 6.1 - Teaching and ResearchObjective: To develop the skills and knowledge of the health workforce to support patient care and
population health. To extend knowledge through scientific enquiry and applied researchaimed at improving the health and well being of the people of New South Wales.

59
Royal Alexandra Hospital for ChildrenNotes to and forming part of the Financial Statements for the year ended 30 June 2002
Purchase ofAssets
HealthPromotion,
Education andResearch Total
$000 $000 $000
14. Conditions on ContributionsContributions recognised as revenues during current year for which expenditure in manner specified had not occurred as at balance date 992 18,123 19,115
Contributions recognised in previous years which were not expended in the current financial year 20,991 18,788 39,779
Total amount of unexpended contributions as at balance date 21,983 36,911 58,894
Comment on restricted assets appears in Note 20
2002 2001$000 $000
15. Current Assets – CashCash at Bank on hand 3,791 8,010Deposits at Call 25,028 -
28,819 8,010
Cash assets recognised in the Statement of Financial Position are reconciled to cash at the end of the financial year as shown in the Statement of Cash Flows as follows:
Cash (per Statement of Financial Position) 28,819 8,010Bank Overdraft - (1,359)
Closing cash and Cash Equivalents(per Statement of Cash Flows) 28,819 6,651
16. Current / Non - Current ReceivablesCurrent
(a) Sales of Goods and Services 3,532 2,410 Other Debtors Non - Operating Debtors - 420 Other Debtors 2,391 4,006 Prepayments 301 250 Interest Receivable 37 7
Sub Total 6,261 7,093
Less Provision for Doubtful Debts (892) (541)
5,369 6,552
(b) Bad debts written off during the yearCurrent Receivables
Sale of Goods and Services 140 36

60
Royal Alexandra Hospital for ChildrenNotes to and forming part of the Financial Statements for the year ended 30 June 2002
2002 2001$000 $000
16. Current/Non - Current ReceivablesNon Current
(a) Sales of Goods and Services 215 213
(b) Bad debts written-off during the year:
Non-Current Receivables Sales of Goods and Services - 220
(c) Sales of Goods and Services Includes:
Patient Fees – Compensable 224 569Patient Fees – Ineligible 885 733Patient Fees – Other 2,638 1,321
3,747 2,623
17. InventoriesCurrent - At Cost
Drugs 542 434Medical and Surgical Supplies 1,410 1,520Food and Hotel Supplies 34 53Engineering Supplies 100 178Fundraising Merchandise 124 143Other including Goods in Transit 654 567
2,864 2,895
18. Current / Non - Current Other Financial AssetsCurrent
Treasury Corporation – Hour Glass Facility - 23,653Other Loans and Deposits - 45
- 23,698
Non - Current
Treasury Corporation - Hour Glass Facility 23,635 21,271Other Loans and Deposits 8,000 21Shares 8,396 8,215
40,031 29,507
The Hospital had transferred its current investment from Treasury Corporation to a newly appointed FundManager, HSBC Asset Management (Australia) Limited. The amount of $21,289,000 is reported under Cash inaccordance with NSW Health Guidelines for investment at call.

61
Royal Alexandra Hospital for ChildrenNotes to and forming part of the Financial Statements for the year ended 30 June 2002
Land LeaseholdLand
Buildings Constructionin Progress
Plant andEquipment
Other Total
$000 $000 $000 $000 $000 $000 $000
19. Property, Plant and Equipment
Balance at 1 July 2001At Valuation date 30 June 1995 544 - - - - - 544At Valuation date 30 June 1997 14,600 - 256,400 - - - 271,000At Cost - 750 7,298 - 120,980 5,488 134,516Total Balance 1 July 2001 15,144 750 263,698 - 120,980 5,488 406,060
Revaluation Adjustment[see Note 2(I)]
1,650 - 61,207 - - - 62,857
Capital Expenditure & Donations[see Note 2(j)] - - 76 93 4,109 99 4,377Disposals - - - - (2,903) - (2,903)
16,794 750 324,981 93 122,186 5,587 470,391
Balance at 30 June 2002At Valuation Date 30 June 1995 544 - - - - - 544At Valuation Date 30 June 2002 16,250 - 324,981 - - - 341,231At Cost - 750 - 93 122,186 5,587 128,616Total Balance at 30 June 2002
16,794 750 324,981 93 122,186 5,587 470,391
DepreciationValuation Depreciation Balance - - 25,728 - - - 25,728Cost Depreciation Balance - 9 - - 76,764 2,221 78,994Total Balance at 1 July 2001 - 9 25,728 - 76,764 2,221 104,722
Charge for the year[see Note 2(k)]
- 19 6,600 - 10,181 647 17,447
Disposals - - - - (2,155) - (2,155)Revaluation Adjustment[see Note 2(l)] - - 14 - - - 14
- 28 32,342 - 84,790 2,868 120,028
Balance at 30 June 2002At Valuation Date 30 June 2002 - - 32,342 - - - 32,342At Cost Balance - 28 - - 84,790 2,868 87,686Total Balance at 30 June 2002
- 28 32,342 - 84,790 2,868 120,028
Carrying Amount at 30 June 2002At Valuation date 30 June 2002 16,794 - 292,639 - - - 309,433Cost Carrying Amount - 722 - 93 37,396 2,719 40,930Carrying Amount at 30 June 2002
16,794 722 292,639 93 37,396 2,719 350,363
i) Land and Buildings include land owned by the NSW Health Department and administered by the Hospital [Notes2(j) and 2(l)].
(ii) Land and buildings at Westmead were valued by Mr J Carr APPI (Certified Practising Valuer) Registered ValuerNo 1699 from the State Valuation Office on 26 April 2002 [Notes 2 (j) and 2(l)] as part of the normal requirementto provide valuations at five yearly intervals.
Land was valued at $16,250,000 (cost $14,600,000). It did not include the leasehold land at Manly, on whichBear Cottage Hospice is located. The term of the lease is 20 years with an option to renew for a further 20 years.The rent payable is $1 per annum.

62
Royal Alexandra Hospital for ChildrenNotes to and forming part of the Financial Statements for the year ended 30 June 2002
Buildings were valued at $324,981,000 (cost $221,275,000).
(iii) The proposal to sell the property at Camperdown (to another Government Agency) is currently with NSW Healthfor approval. This property was valued in 1995 and the Hospital does not expect to receive more than its currentvalue from the transaction.
(iv) Plant and Equipment, other than motor vehicles, are valued at cost less accumulated depreciation.
20. Restricted Assets
The Hospital’s Financial Statements include the following assets which are restricted by externally imposedconditions, for example, donor requirements. The assets are only available for application in accordance with theterms of the donor restrictions.
Major Category Brief Details of Externally Imposed Conditions 2002 2001$000 $000
Children’s Hospital Fund Donations and fundraisings held for the purchase ofspecific equipment and/or services. 1,351 1,695
Special Purposes TrustFunds
Donations, contributions and fundraisings held intrust for the benefit of specific patient, departmentand/or staff groups. 21,720 18,275
Perpetually InvestedTrust Funds
Funds invested in perpetuity. The income therefromis used in accordance with donors’ or trustees’instructions for the benefit of patients and/or insupport of Hospital services. 5,649 5,736
Research Funds Funds to be used for research on child health andother related research carried out by the Hospital. 7,289 6,456
Coffee Shop Trust Accumulated funds distributed from the Coffee ShopTrust to be used for the purposes specified by theTrust which includes Clinical Fellowships andequipment. 247 289
Bear Cottage Hospice Donations, contributions and fundraisings heldtowards the cost of setting up Bear Cottage Hospice,a home for chronically ill children and their families,to provide them with palliative care in a homeenvironment. 2,006 2,282
Research Capital Campaign Donations, contributions and fundraisings heldtowards the building of the Clinical ResearchBuilding, to provide infrastructure and facilities tomeet the growing needs of the research on diseaseand children’s health. 20,632 19,296
58,894 54,029

21. Financial Instruments
a) Interest Rate Risk
Interest rate risk, is the risk that the value of the financial instrument will fluctuate due to changes in market interest rates.The Hospital’s exposure to interest rate risks and the effective interest rates of financial assets and liabilities, both recognised and unrecognised, at theStatement of Financial Position date are as follows:
Fixed Interest Rate Maturing in:Financial Instruments Floating InterestRate
I year or less Over 1 to 5 years More than5 years
Non-interestbearing
Total CarryingAmount as per
the Statement ofFinancial Position
WeightedaverageEffective
Interest Rate *
2002 2001 2002 2001 2002 2001 2002 2001 2002 2001 2002 2001 2002 2001$000 $000 $000 $000 $000 $000 $000 $000 $000 $000 $000 $000 % %
Financial Assets
Cash 12,509 7,999 16,299 - - - - - 11 11 28,819 8,010 5 4Receivables - - - - - - - - 5,584 6,765 5,584 6,765 N/A N/AShares - - - - 8,396 8,215 8,396 8,215 N/A N/ATreasury CorporationInvestments - - - - - - - - 23,635 44,924 23,635 44,924 N/A 7Other Loans and Deposits - - - 45 5,343 21 2,657 - - - 8,000 66 5 5
Total Financial Assets 12,509 7,999 16,299 45 5,343 21 2,657 - 37,626 59,915 74,434 67,980
Financial Liabilities
Borrowings – Bank Overdraft - 1,359 - - - - - - - - - 1,359 - -Payables - - - - - - - - 7,240 6,303 7,240 6,303 - -
Total Financial Liabilities - 1,359 - - - - - - 7,240 6,303 7,240 7,662
Weighted Average effective interest rate was computed on a semi annual basis.It is not applicable for non-interest bearing financial instruments.
Royal Alexandra H
ospital for ChildrenN
otes to and forming part of the Financial Statem
ents for the year ended 30 June 2002

(b) Credit Risk
Credit risk is the risk of financial loss arising from another party to a contract or financial position failing to discharge a financial obligation thereunder.
The Hospital’s maximum exposure to credit risk is represented by the carrying amounts of the financial assets included in the Statement of Financial Position.
Governments Banks Patients Other Total2002 2001 2002 2001 2002 2001 2002 2001 2002 2001$000 $000 $000 $000 $000 $000 $000 $000 $000 $000
Financial Assets
Cash 6,388 - 623 7,999 - - 21,808 11 28,819 8,010Receivables - 814 - 7 2,011 2,087 3,573 3,857 5,584 6.765Shares - - - - - - 8,396 8,215 8,396 8,215Treasury Corporation Investments 23,635 44,924 - - - - - - 23,635 44,924Other Loans and Deposits 21 21 - 45 - - 7,979 - 8,000 66
Total Financial Assets 30,044 45,759 623 8,051 2,011 2,087 41,756 12,083 74,434 67,980
The only significant concentration of credit risk arises in respect of patients ineligible for free treatment under the Medicare provisions.
Receivables due from these entities totalled $885,000 at 30 June 2002 (2000/01: $733,000).
c) Net Fair Value
As stated in Note 2(q), all financial instruments are carried at Net Fair Value, the values of which are reported in the Statement of Financial Position.
The Hospital holds no Derivative Financial Instruments.
Royal Alexandra H
ospital for ChildrenN
otes to and forming part of the Financial Statem
ents for the year ended 30 June 2002

65
Royal Alexandra Hospital for ChildrenNotes to and forming part of the Financial Statements for the year ended 30 June 2002
22. Payables 2002 2001$000 $000
CurrentCreditors 7,101 6,090
Other Creditors 139 213
7.240 6,303
23. Other
Bank Overdraft - 1,359
Repayment of Borrowings
Not later than one year - 1,359
24. Current / Non - Current Liabilities –Employee Entitlements and Other Provisions
Current
Employee Annual Leave 8,777 7,875Employee Long Service Leave 2,395 6,179Accrued Salaries and Wages 2,859 2,144Taxation and Other Payroll Deductions 1,264 1,221
Aggregate Employee Entitlements / Other Provisions 15,295 17,419
Non - Current
Employee Annual Leave 5,408 4,043Employee Long Service Leave 17,291 12,127
Aggregate Employee Entitlements / Other Provisions 22,699 16,170

Royal Alexandra Hospital for ChildrenNotes to and forming part of the Financial Statements for the year ended 30 June 2002
25. EquityAccumulated Funds Asset Revaluation
ReserveTotal Equity
2002 2001 2002 2001 2002 2001$000 $000 $000 $000 $000 $000
Balance at the beginning of theFinancial year 270,540 270,027 60,421 60,345 330,961 330,372
Changes in equity – other thantransactions with owners asowners
Result for the year (11,399) (157) - - (11,399) (157)
Increment on Revaluation of:Investment Revaluation - - 21 746 21 746Land and Buildings - - 62,844 - 62,844 -
Transfers to / (from)Revaluation Reserves
- 670 - (670) - -
Balance at the end of thefinancial year 259,141 270,540 123,286 60,421 382,427 330,961
26. Commitments for Expenditure 2002 2001$000 $000
(a) Capital Commitments
Aggregate expenditure contracted for at balance date, butnot provided for in the accounts:
Not later than one year 1,514 -Later than one year, but not later than five 500 -
Total Capital Expenditure Commitments (including GST)2,014 -
(b) Operating Lease Commitments
Commitments in relation to non-cancellable operating leasesare payable as follows:
Not later than one year 1,977 1,373Later than one year, but not later than five 2,816 1,399
Total Operating Lease Commitments (including GST)4,792 2,772
These operating leases are not recognised in the financial statements as liabilities.Operating Leases represent Rental of Premises, Vehicles and Plant and Equipment
(c) Contingent Asset Related to Commitment for Expenditure
The total ‘Operating Lease Commitments’ above includes input tax credits of $433,611 that are expected tobe recoverable from the Australian Taxation Office.

67
Royal Alexandra Hospital for ChildrenNotes to and forming part of the Financial Statements for the year ended 30 June 2002
27. Trust Funds
The Hospital holds Trust Fund monies of $833,047 that are used for the safe keeping of patients’ monies,deposits on hired items of equipment and Private Practice Trusts. These monies are excluded from the financialstatements, as the Hospital cannot use them for the achievement of its objectives. The following is a summary ofthe transactions in the trust accounts:
2002 2001$000 $000
Cash Balance at the beginning of the financial year 628 246
Receipts 772 795
Expenditure (517) (413)
Cash Balance at the end of the financial year 883 628
28. Contingent Liabilities
(a) Claims on Managed Fund
Since 1 July 1989, the Hospital has been a member of the NSW Treasury Managed Fund. The Fund willpay to or on behalf of the Hospital all sums which it shall become legally liable to pay by way ofcompensation or legal liability if sued except for employment related, discrimination and harassmentclaims that do not have Statewide implications. The costs relating to such exceptions are to be absorbedby the Hospital. As such, since 1 July 1989, apart from the exceptions noted above, no contingentliabilities exist in respect of liability claims against the Hospital. A Solvency Fund (now called Pre-Managed Fund Reserve) was established to deal with the insurance matters incurred before 1 July 1989that were above the limit of insurance held or for matters that were incurred prior to 1 July 1989 andwould have become verdicts against the State. That Solvency Fund will likewise respond to all claimsagainst the Hospital.
(b) Workers’ Compensation Hindsight Adjustment
When the New Start (to the) Treasury Managed Fund was introduced in 1995/96, hindsight adjustmentsin respect of Workers’ Compensation (three years from commencement of Fund Year) and Motor Vehicle(18 months from commencement of Fund Year) became operative.
The calculation of hindsight adjustments has been reviewed in 2001/02 to provide an interim adjustmentafter three years with a final adjustment at the end of year five.
The interim hindsight adjustment has now been effected for the 1998/99 year and resulted in a decreasein expenses of $1,639,042.
A contingent liability/asset may now exist in respect of the 1999/2000, 2000/01 and 2001/02Compensation Fund years.
The Treasury Managed Fund provides estimates as at 30 June each year and the latest available, vizthose advised as at 30 June 2002 estimates that and asset of $59,394 is applicable.
This estimate, however, is subject to further actuarial calculation and a better indication of quantum willnot be available until the last quarter of 2002.

Royal Alexandra Hospital for ChildrenNotes to and forming part of the Financial Statements for the year ended 30 June 2002
29. Charitable Fundraising Activities
Fundraising Activities
The Hospital conducts direct fundraising.All revenue and expenses have been recognised in the financial statements of the Hospital.Fundraising activities are dissected as follows:
Income Raised DirectExpenditure*
IndirectExpenditure+
Net Proceeds
$000 $000 $000 $000
Appeals(In House) 10,059 604 1,690 7,765
Events 3,277 52 - 3,225
Legacies 8,125 - - 8,125
21,461 656 1,690 19,115
Percentage of Income 100% 3% 8% 89%
* Direct Expenditure includes printing, postage, raffle prizes, consulting fees and other related direct costs.
+ Indirect Expenditure includes direct overheads such as office staff administrative costs, cost apportionment oflight, power and other overheads.
The net proceeds were used for the following purposes: 2002$000
Purchase of Equipment 14,322
Research 2,031
Other Expenses 1,199
Held in Special Purpose and Trust Funds Pending Purchase 1,563
19,115
The provisions of the Charitable Fundraising Act 1991 and the regulations under that Act have been compliedwith and internal controls exercised by the Hospital are considered appropriate and effective in accounting for allthe income received in all material respects.

69
Royal Alexandra Hospital for ChildrenNotes to and forming part of the Financial Statements for the year ended 30 June 2002
30. 2001/02 Voluntary Services
It is considered impracticable to quantify the monetary value of the invaluable voluntary services provided to theHospital. Services provided include:
FundraisingProvision of relief staff to administration areasSibling Child Care CentreAssistance in the wards with inpatient careAssistance with child care for the Adolescent, Deafness Centre, Spina Bifida and Limb Deficiency ClinicsHospital Granny ServiceVolunteers, Gift ShopVolunteers, White Elephant StallRadio Bed RockStarlight RoomBook Bunker
2002 2001$000 $000
31. Reconciliation of Net Cost of Services to Net CashFlows from Operating Activities
Net Cash Flows from Operating Activities 13,367 18,448Depreciation (17,447) (17,832)Inter Area / Interstate Patient Inflows 77,560 68,919Provision for Doubtful Debts (337) 37Acceptance by the Crown Entity of Superannuation Liability (9,246) (8,649)Increase in Provisions (3,647) (3,247)(Increase)/Decrease in Prepayments and Other Assets (1,218) 3,717Increase in Creditors (778) (353)Loss on Sale of Property, Plant and Equipment (511) (365)NSW Health Department Recurrent Allocations (123,445) (117,674)NSW Health Department Capital Allocations (4,053) (274)Cash Reimbursements from the Crown Entity (828) (562)
Net Cost of Services (70,583) (57,835)
32. Non Cash Financing and Investing Activities
Assets Received by Donation - 38

Royal Alexandra Hospital for ChildrenNotes to and forming part of the Financial Statements for the year ended 30 June 2002
33. Unclaimed Moneys
Unclaimed salaries and wages are paid to the credit of the Department of Industrial Relations and Employment inaccordance with the provisions of the Industrial Arbitration Act, 1940, as amended.
All money and personal effects of patients which are left in the custody of the Hospital by any patient who isdischarged or dies in the Hospital and which are not claimed by the person lawfully entitled thereto within a periodof twelve months are recognised as the property of the Hospital.
All such money and the proceeds of the realisation of any personal effects are lodged to the credit of theSamaritan Fund, which is used specifically for the benefit of necessitous patients or necessitous outgoing patients.
34. Budget Review
Net Cost of Services
The actual net cost of services was lower than budget by $1,323,000. This was primarily owing to additionaldonations received in excess of budget during the year for the research building, research and services.
Result for the Year from Ordinary Activities
The Hospital had operated its core activities within the funds allocated from NSW Health. This is mainly used topay for the salary and wages and general goods and services for the Hospital. The Hospital had relied greatly on itsdonations and grants to support most of its research activities, specialised services and equipment.
Movement in Accumulated Funds
The movement in Accumulated Funds included the increment in Revaluation of Asset Reserves for Land andBuildings by $62,844,000 to a value of $341,231,000 in April 2002.
Assets and Liabilities
Total Net Assets are $64,184,000 higher than budget primarily owing to the revaluation of land and buildingwhere no budget was provided and an increase in funds available for research and other services.
Cash Flows
Movements in the level of the NSW Health Department Recurrent Allocation that have occurred since the time ofthe initial allocation on 31 August 2001 are as follows: -
$000
Initial Allocation, 31 August 2001 42,216
Award Increases 1,039
Special Projects;Examples: Program of Aids for Disabled People, Mental Health Plan 313
Other;Examples: Cochlear Implant, Paediatric Network,National Immunisation Program, VMOs Award Increases 2,317
Balance as per Statement of Financial Performance 45,885
35. Post Balance Date Events
No significant events occur after the balance date is reported that will significantly affect the financial result of theHospital.
End of Financial Statements.


hours of operation• The Emergency Department at The Children’s Hospital at Westmead is open 24 hours a day.
• Outpatients Clinics are staffed from 8am to 5pm Monday to Friday.
Cnr Hawkesbury Road andHainsworth Street, WestmeadLocked Bag 4001Westmead NSW 2145
Telephone: (02) 9845 0000Fax: (02) 9845 3489Website: www.chw.edu.au
Copyright 2002 The Children’s Hospital at Westmead. 150 copies of this report were produced at a cost of $7per copy. (Improved distribution strategies decreased production from 1,500 copies, resulting in an increase in theaverage price per copy but an overall cost reduction.)