Cholera in the Caribbean - PAHO
42
Cholera in the Caribbean Dr. James Dobbins, PAHO/CPC/PED PAHO PAHO
-
Upload
khangminh22 -
Category
Documents
-
view
4 -
download
0
Transcript of Cholera in the Caribbean - PAHO

Cholera in the Caribbean
Dr. James Dobbins, PAHO/CPC/PED
PAHOPAHO


Major Perspectives on Cholera
• Description of cholera (with video)
• Background on cholera in the Caribbean
• Update on current cholera outbreak
• Prevention of cholera outbreaks
• Planning for cholera outbreaks
Additional Aspects of Cholera
• Detection of cholera – Priya Bagwandin
– Leslie Edwards
• Management of cholera outbreaks
– Community management – Sally Edwards– Emergency management – Robert Lee
• Planning for cholera – Terese Maitland

Description of Cholera
• Video of cholera patient
• Spectrum of disease
• Signs and symptoms
• Agent
• Transmission
• Treatment

Video of Cholera Patient
Caution!: this is an extremely graphic video of a cholera patient excreting large quantities of bodily fluid.

Spectrum of Disease
• Up to 90% of infections are asymptomatic
• Asymptomatic individuals still shed bacteria
• 20% of symptomatic patients have severe
disease
• Onset of severe disease can be < 6 hours
• Patients with severe disease can die within hours
if not rapidly rehydrated
• Type ‘O’ blood risk factor for severe illness
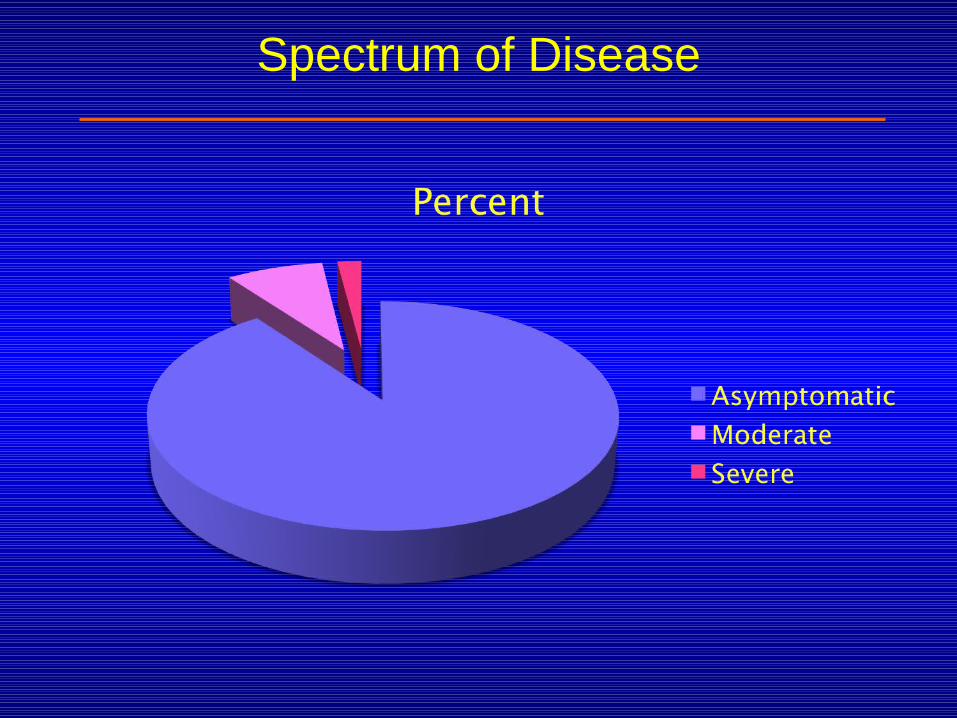
Spectrum of Disease
Signs and Symptoms of Cholera
• Abrupt onset of watery diarrhea
• Rapid loss of up to 10 to 20 liters of fluid
• Vomiting is common in severe cases• • Usually without fever
• Low blood pressure

Cholera Agent: Vibrio cholerae
• One of 70 species of Vibrio bacteria
• Only some strains of V. cholerae are toxigenic
• Disease caused by toxin when bacterium attaches to the wall of the small intestine
• Production of toxin requires presence of two plasmids, CTX and TCP

Cholera Agent: (continued)
• Classification of V. cholerae:
– Toxigenicity: Toxigenic and non-toxigenic– ‘O’ protein type: 1 and 139 (75)– Two biotypes: Classical and El Tor– Two serotypes: Inaba and Ogawa
• Can survive, grow, and persist in both salt water and fresh water
• Can attach to zooplankton and move with water or shellfish (not killed by boiling shellfish)
• Very easy to kill with chlorine and by boiling water

Transmission of Cholera
• Fecal contamination of water and food– Primarily water-borne for lower-income
populations– Primarily food-borne for upper-income
populations
• Also from aquatic environment
• Infective dose is approximately 1 million organisms

Treatment of Cholera
• Oral rehydration salts (ORS) for all cases if tolerated
• IV infusion with lactated ringer’s solution for severe cases [multiple lines if needed]
• Antibiotics in severe cases (depending on resistance)– Doxycycline– Azithromycin– Erythromycin– Ciprofloxacin

Treatment of Cholera
SEVERITY PERCENT LOCATION TREATMENT
Mild 13% Home ORS
Moderate 5% CTU/CTC ORS
Severe 2% CTU/CTCORS
IV LRSANTIBIOT

Initial Outbreak of Cholera in the Caribbean, 1849 - 1854
• Began in Cartegena, 1849
• Spread next to:– Jamaica (1850)– Nevis (1853)
• From Nevis, it spread to:– St. Kitts (1854)– Barbados (1854)– Trinidad (1854)
1854 Trinidad Cholera Outbreak
• Outbreak lasted for 19 weeks
• Out of a total population of 77,000:
– Approximately 20% were symptomatic
– Almost 100% infected
– 6% of the population died
– Case-fatality ratio of 30%
– More severe for African population

Trinidad Control Measures in 1854
• Prevention: burned barrels of pitch on all street corners
• Treatment: ingested oil of camphor that had been infused into lumps of sugar
• Result: 100% attack rate
30% case-fatality ratio

Trinidad Control Measures in 1854
• Prevention: burned barrels of pitch on all street corners
• Treatment: ingested oil of camphor that had been infused into lumps of sugar
• Result: 100% attack rate
30% case-fatality ratio
Update on Cholera in the Caribbean
• 1991agent in Peru:– Toxigenic O1– El Tor– Inaba
• 2010 agent in Haiti and DOR: – toxigenic O1– El Tor– Ogawa
Update on the Caribbean
Countries Affected Confirmed Cases / Deaths• Haiti 285,931 / 4,870• Dom. Republic 918 / 12
- - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - -• Venezuela 278 / 0• Canada 1 0• United States 10 0• Martinique 7 0• (Mexico) 1 0

Update on Haiti
• Overall, new cases per week are declining
• Haiti is divided into 10 Departments
• Each has its own outbreak depending the timing
of introduction and local conditions
• New cases are declining or stable in 8 depts.
• New cases rising only in South and Southeast
departments
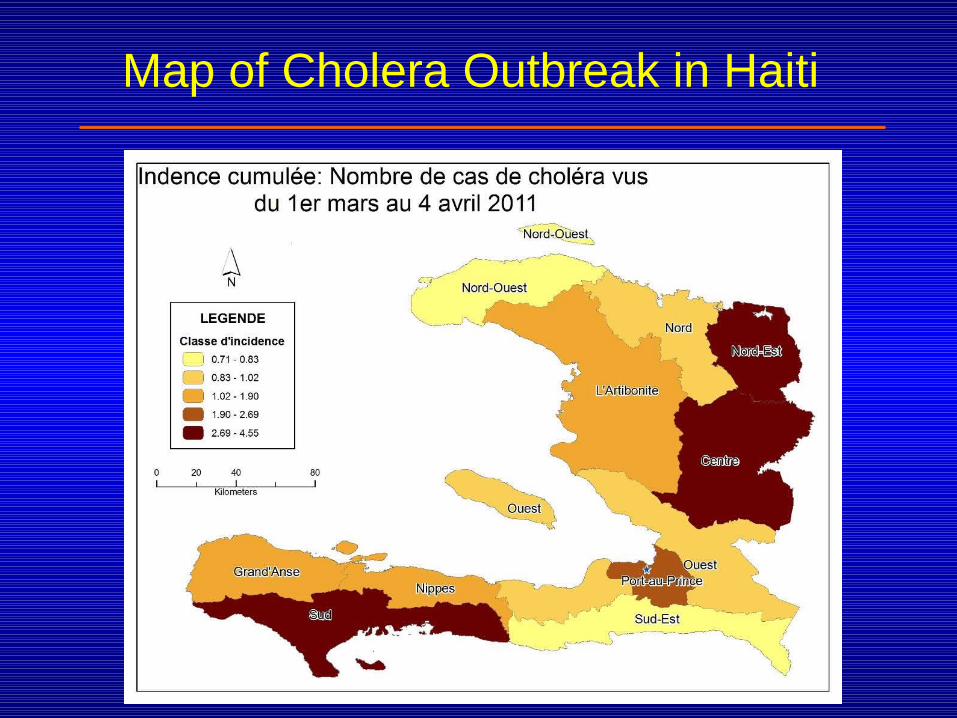
Map of Cholera Outbreak in Haiti

Epidemic Curves by Department
Artibonite
0
1,000
2,000
3,000
4,000
5,000
6,000
7,000
8,000
08/1
1/10
15/1
1/10
22/1
1/10
29/1
1/10
06/1
2/10
13/1
2/10
20/1
2/10
27/1
2/10
03/0
1/11
10/0
1/11
17/01/1
1
24/0
1/11
31/0
1/11
07/0
2/11
14/0
2/11
21/02/1
1
28/0
2/11
07/0
3/11
14/0
3/11
21/0
3/11
28/0
3/11
04/0
4/11
Week of reporting
Nb
ho
spit
aliz
atio
ns
Port au Prince
0
1,000
2,000
3,000
4,000
5,000
6,000
08/11/
2010
15/11/
2010
22/11/
2010
29/11/
2010
06/12/
2010
13/12/
2010
20/12/
2010
27/12/
2010
03/01/
2011
10/01/
2011
17/01/
2011
24/01/
2011
31/01/
2011
07/02/
2011
14/02/
2011
21/02/
2011
28/02/
2011
07/03/
2011
14/03/
2011
21/03/
2011
28/03/
2011
04/04/
2011
Week of reporting
Nb ho
spita
lizat
ions
South East
0
100
200
300
400
500
08/1
1/20
10
15/1
1/20
10
22/1
1/20
10
29/1
1/20
10
06/1
2/20
10
13/1
2/20
10
20/1
2/20
10
27/1
2/20
10
03/0
1/20
11
10/0
1/20
11
17/0
1/20
11
24/0
1/20
11
31/0
1/20
11
07/0
2/20
11
14/0
2/20
11
21/0
2/20
11
28/0
2/20
11
07/0
3/20
11
14/0
3/20
11
21/0
3/20
11
28/0
3/20
11
04/0
4/20
11
Week of reporting
Nb
hosp
ital
izat
ions
Grande Anse
0
500
1,000
1,500
2,000
2,500
08/1
1/20
10
15/1
1/20
10
22/1
1/20
10
29/1
1/20
10
06/1
2/20
10
13/1
2/20
10
20/1
2/20
10
27/1
2/20
10
03/0
1/20
11
10/0
1/20
11
17/0
1/20
11
24/0
1/20
11
31/0
1/20
11
07/0
2/20
11
14/0
2/20
11
21/0
2/20
11
28/0
2/20
11
07/0
3/20
11
14/0
3/20
11
21/0
3/20
11
28/0
3/20
11
04/0
4/20
11
Week of reporting
Nb
hosp
ital
izat
ions

Update on the Dominican Republic
1 0 1 2 11 13 13
58 50 4019
35 35
7153
2955 46 43
6288
3918 27 19 110 5 5 6
66
92 95
73102
104
61
7189
131
108
104
111101
9179
80
61
4751
4646
2
32
0
50
100
150
200
250
42 43 44 45 46 47 48 49 50 51 52 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16
Confirmados Sospechosos
República Dominicana: Distribución de casos sospechosos y confirmados por SE
Acumulado al 23 abril 2011 (SE 16)
Sala de situación de cólera. Dirección General de Epidemiología (DIGEPI). Ministerio de Salud Pública. República Dominicana
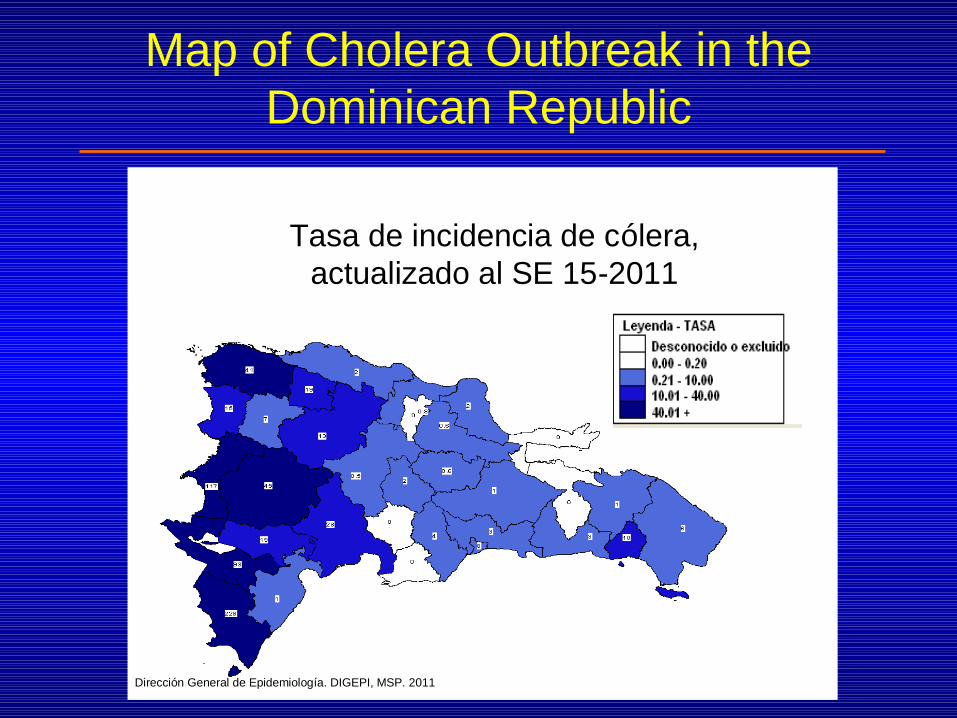
Map of Cholera Outbreak in the Dominican Republic
Tasa de incidencia de cólera, actualizado al SE 15-2011
Dirección General de Epidemiología. DIGEPI, MSP. 2011

Prevention of Cholera - 1
• Personal hygiene:
– Purify drinking and cooking water
– Wash all food
– Wash hands before cooking or eating
– Use sanitation facilities for defecation

Prevention of Cholera - 2
• Environmental control:
– Provide clean water for populations
– Provide sanitary facilities for populations
– Food safety
• Social gatherings
• Market places
– Target high-risk populations

Prevention of Cholera - 3
• Vaccination against Cholera
– There is an approved vaccine but it is not very efficacious
– A new vaccine performs somewhat better but has not been approved by WHO
– Not a viable option for the Caribbean

Prevention of Cholera - 4
• Prophylactic use of antibiotics
– Clearly defined population
– High risk of infection
– Used successfully during a cholera outbreak in a prison in DOR

Planning for Cholera Outbreaks
• One component of overall planning for disaster management
• Part of the Health Emergency component
• Cholera-specific activities need to be addressed

Planning for a Cholera Outbreak
• Adapt national health disaster plan to accommodate cholera
• Designate specific rehydration centers
• Order supplies and equipment for centers
• Train hospital staff in clinical management
• Communicate risk to public• Increase coordination among all disaster
management partners
Planning for a Cholera Outbreak
• Adapt national health disaster plan to accommodate cholera
• Designate specific rehydration centers
• Order supplies and equipment for centers
• Train hospital staff in clinical management
• Communicate risk to public• Increase coordination among all disaster
management partners

Remaining Steps for Planning
• Complete identifying and supplying main rehydration centers in all countries
• Complete training of hospital staff for the rehydration centers
• Evaluate completeness of national health disaster plans through needs assessment and simulation exercises

Response to a Cholera Outbreak
• Enhance surveillance for early detection
• Follow up contacts of confirmed cases
• Ensure proper clinical management of patients
• Ensure proper environmental controls
– Disinfection of hospital waste
– Disinfection of dead bodies
• Promptly manage the health emergency
• Communicate information to the public

Risk Factors for Introduction and Spread of Cholera
• Legal and illegal immigrants living precariously
• Focal points for air and sea transportation
• Limited access to clean water and safe sanitation
• Long referral time to health facilities
• Overcrowding as in slums and institutions
• Under-supervised food markets
• Places recently affected by natural disasters
• Remote indigenous and rural populations

0%
100% DOR
TCI
BAH SLU DOM JAM
SXM ANU TRT ANG CUR
BAR CAY GRE MON SVG
BVI GUY SKN
ARU BZE SUR
BON STE
BDA SAB
75%
50%
25%
Risk of Introduction of Cholera

0%
100% DOR
TCI
GUY
SVG SUR
SXM
SLU DOM
MON
JAM ANG
BAH ANU CRE SKN STE CUR
TRT BZE BVI
ARU BAR BON
BDA CAY SAB
75%
50%
25%
Risk of Spread of Cholera

Risk of Cholera in the Caribbean
0
25
50
75
100
0 25 50 75 100
Risk of Introduction of Cholera
Ris
k o
f S
pre
ad
of
Ch
ole
ra

Risk of Cholera in the Caribbean
0
25
50
75
100
0 25 50 75 100
Risk of Introduction of Cholera
Ris
k o
f S
pre
ad
of
Ch
ole
raDOR
TCI
JAM
BAH
SLUSXM
ANU
TRT
GUY
SUR SVG
MON
ANG
SKN
GRECUR
CAY
BAR
BVI
STE
BER
BONARU
BZE
DOM
SAB
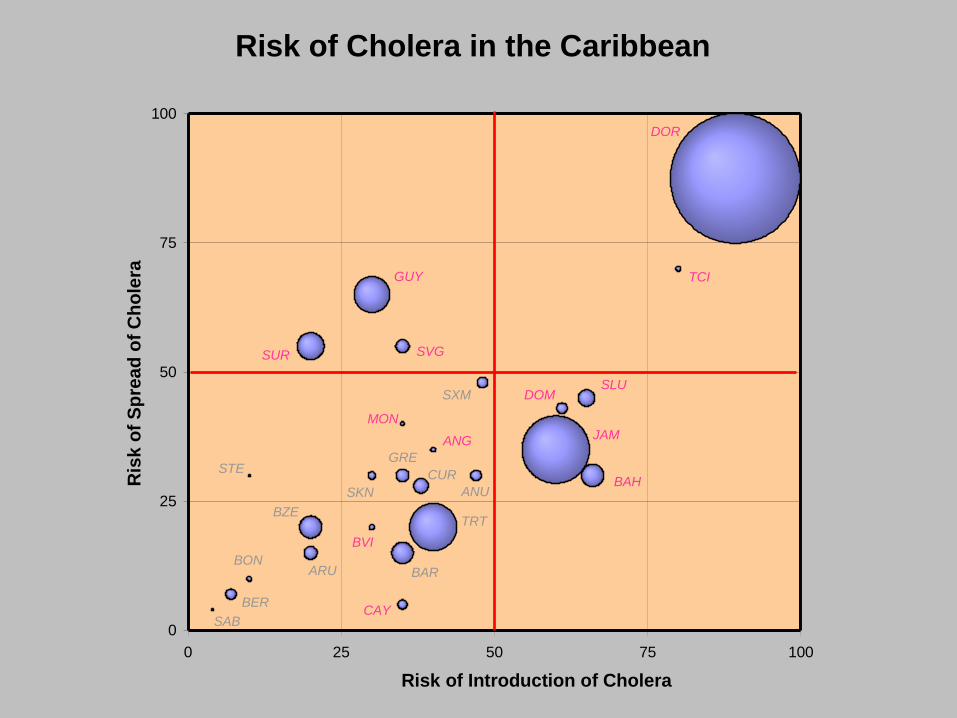
Risk of Cholera in the Caribbean
0
25
50
75
100
0 25 50 75 100
Risk of Introduction of Cholera
Ris
k o
f S
pre
ad
of
Ch
ole
raDOR
TCI
JAM
BAH
SLUSXM
ANU
TRT
GUY
SUR SVG
MON
ANG
SKN
GRECUR
CAY
BAR
BVI
STE
BER
BONARU
BZE
DOM
SAB

Cholera Outbreak Vulnerability
Most vulnerable groups
PAHO & CAREC active preparations
PAHO outbreak response

Thank You