
ANNUAL REPORT - PAHO
417
2008 ANNUAL REPORT Emergency Preparedness and Disaster Relief Emergency Preparedness and Disaster Relief
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of ANNUAL REPORT - PAHO
2008ANNUAL REPORTEmergency Preparedness and Disaster ReliefEmergency Preparedness and Disaster Relief

2008ANNUAL REPORT
Area on Emergency Preparednessand Disaster Relief
Presented to the Members of the Partnership for Health Preparedness
Canadian International Development Agency
Office of U.S. Foreign Disaster Assistance (USAID)
II
A n n u a l R e p o r t 2 0 0 8
III
Introduction .......................................................................................................................................................1
Chapter 1. Improving Disaster Preparedness in the Health Sector ..............................3
Chapter 2. Protecting Health Services from the Impact of Disasters .......................13
Chapter 3. Supporting Countries to Respond to Disaster Events
in the Health Sector ........................................................................................................21
Chapter 4. Forging Stronger Partnerships at National, Regional
and Global Levels .............................................................................................................33
Annexes .....................................................................................................................................................39
Acronyms .....................................................................................................................................................41
Table of Contents

IV

1
This is the 2008 Annual Report of the Pan American Health Or-
ganization’s Area on Emergency Preparedness and Disaster Relief
(PED). It is presented to the Office of U.S. Foreign Disaster Assis-
tance of the U.S. Agency for International Development (OFDA/
USAID) and to the International Humanitarian Assistance Directorate of the
Canadian International Development Agency (IHA/CIDA). This report covers
calendar year 2008 (January – December).
In 2008, the Pan American Health Organization prepared and approved a
new strategic plan for disaster preparedness, risk reduction and response in Latin
America and the Caribbean. This plan is entitled Strategic Plan for a Secure and
Disaster-resilient Health Sector in the Americas, 2008-2012.
The Strategic Plan includes five strategic lines of action: improving disaster
preparedness capacity in the health sector; protecting health services from the
risk of disasters; supporting countries to respond to disaster events in the health
sector; forging stronger partnerships with national, regional and global partners;
and mainstreaming health disaster risk reduction across sectors. For purposes
of reporting in this annual report, activities related to forging partnerships and
mainstreaming health disaster risk reduction have been combined into one
chapter.
Introduction
2
A n n u a l R e p o r t 2 0 0 8
3
Chapter 1
Support to Health Disaster Programs in the Ministries of Health
For more than three decades, the formal es-tablishment of a disaster management unit or office in each Ministry of Health in Latin America and the Caribbean has been a pri-
mary objective and an indicator of success of PAHO/WHO’s technical cooperation. The capacity of the program to effect change in the health sector, its hu-man resources and budget and the program’s impor-tance within the hierarchy of the Ministry varies from country to country, but several indicators are viewed as indispensable: an ‘all-hazards’ approach to the co-ordination of disaster response; a professional staff and a budget line; direct access and lines of reporting to the policy level of the Ministry; and broad cross-sector outreach. In 2006, PAHO/WHO surveyed its member countries to set a baseline against which to measure progress toward formalizing such a program (see box at right).
The results of this first survey led PAHO/WHO to target, in its biennial workplan (2008-09), seven countries for strengthening: Bolivia, Costa Rica,
A health sector disaster program with the leadership, credibility and coordinating authority within the national context, which also integrates the participation of a wide range of actors, including NGOs and private sector operators.
Improving Disaster Preparedness in the Health Sector
In 2006, PAHO/WHO completed a major survey of its Member States that looked at many issues related to disaster preparedness, mitigation and
response. At the time, the survey revealed that 26 (79%) of the 33 countries in the Region had formally institutionalized a health disaster reduction program or office. Only one country lacked either a focal point or some other ad hoc arrangement. Although most offices or units were shown to be modestly staffed, only 15 of the 33 countries said they had a specific budget line for disaster health preparedness.
WHO will initiate a global survey in 2009, which will provide an opportunity to update and track progress in this important area.
Ministry of Health Disaster Programs Show Room for Improvement

4
A n n u a l R e p o r t 2 0 0 8
Guyana, Panama, Paraguay, Suriname and Uruguay. The case of Costa Rica offers an example of support. As a result of health sector reforms, the disaster office, along with other units and programs in the Ministry of Health, lost its place in the organizational chart. However, recent floods and an earthquake in Costa Rica demonstrated that the ministry of health did in-deed need a disaster management mechanism to co-ordinate with public and private health providers, the National Emergency Commission and other sectors. The new health authorities, who initially were reluc-tant to maintain a disaster office in the organizational structure, asked PAHO to help solve this issue and a formal process is now underway to create a new disas-ter program that will best fit within the framework of Costa Rica’s health sector reform.
Improving health disaster preparedness regionwide is not accomplished by simply creating a health sec-tor emergency program. Once the program has been established in the Ministry of Health, it must receive continuous support: from advocacy at the highest decision making levels, to modest funding in some cases, to providing opportunities for capacity build-ing and the provision of technical documents and tools. The health disaster coordinators that lead these ministry units are equal partners in crafting a plan of action. For example, in the Caribbean, health disas-ter coordinators from 22 countries met to examine a number of issues, including the impact of climate change on health, disease surveillance in disaster situ-ations, and coordination mechanisms for health and pandemic preparedness. They agreed to a one-year common work plan that follows the lines of PAHO/WHO’s strategic plan for disaster risk reduction. It in-cludes the review and updating of national health sec-tor disaster plans, the formation of outbreak contain-ment teams, strengthening of the regional emergency response team, carrying out simulation exercises and formalizing agreements and partnerships for disaster risk reduction. The report of this meeting is available through the URL in Annex 1. One of the most im-portant results of this meeting was that work began on the development of a health sector disaster man-agement self-assessment tool. PAHO/WHO worked with national health disaster professionals to develop draft benchmarks against which countries will dem-onstrate institutional commitment to disaster risk re-duction. This tool is available in draft form (Annex 2), and after follow up with the countries, will be applied in 2009.
In recent years, many health professionals in mem-ber countries have found themselves under increas-
ing pressure to expand their knowledge and skills in an ever-wider range of issues related to disasters, and PAHO/WHO has invested time and resources to en-sure they are as up-to-date as possible. Climate change is one such issue. During 2008, PAHO/WHO held several subregional meetings on climate change and its effects on health in the Americas. Based on these meetings and on consultations with member coun-tries, PAHO developed a white paper (Annex 3) to present evidence that climate change is a phenomenon that increasingly affects human health and to describe what action must be taken to protect people from cur-rent and expected climate related health impacts. This paper was the subject of debate at the September 2008 Directing Coun-cil meeting of the Pan American Health Organi-zation, where a panel of experts discussed the pro-posed plan of ac-tion to strengthen the capacity of health systems lo-cally and nation-ally to assess and protect human health from risks related to climate change. One pri-ority stemming from this plan was the creation of an “observatory” or space in which the health sector could collect and discuss ev idence-based data on the topic. This plan will be implemented in 2009.
Much like disaster preparedness and risk reduc-tion, climate change is a crosscutting issue in PAHO and one that requires harnessing the expertise of many public health experts to work with member countries. In 2008, the Area on Emergency Preparedness and Disaster Relief formed part of an Organization-wide steering committee and encouraged health disaster programs throughout the Region to take up this issue in light of the 2008 World Health Day, which focused on climate change. To support Member States to keep
The adverse health impact of climate change can be both direct and indirect. Di-
rect impacts result in heat waves, floods and storms and other extreme weather events. The indirect impact of climate change influences the transmission of vector-borne, water-borne and food-borne diseases, the avail-ability of water and agricultural production. These are not minor issues. Diseases that are sensitive to climate include some of our biggest killers, such as malaria and diarrhea, and climate change increases risk factors for other conditions such as malnutrition, the single largest contributor to the global burden of disease.
An excerpt from remarks by the Director of PAHO at the
2008 World Health Day on Climate Change and Health

5
abreast of the latest information and technical resourc-es, the Regional Disaster Information Center (CRID) began production of a specialized bibliographic CD with full-text documents on climate change, health and disasters. This information tool will be ready in 2009 on CD and the Internet.
Strengthening health sector disaster offices means providing their human resources with professional de-velopment opportunities. PAHO’s subregional disas-ter office for South America (based in Ecuador) host-ed a rotation for health disaster focal points from four provinces in that country. They were selected based on the type of natural hazards their region faces and on the focal point’s potential to grow in his/her job and assume more substantive responsibilities, includ-ing at the international level. Each focal point spent two months with PAHO/WHO disaster professionals at the Country Representation in Quito to improve their skills and readiness for disaster response and to review and make improvements to his/her municipal disaster preparedness plan of action. They reviewed existing technical information and capacity build-ing materials as well as other available sources of in-formation that could be used to improve local level planning. Each was given a chance to participate in workshops and seminars on a variety of issues related to disaster management. The net effect was the same as a two-month training course. PAHO/WHO’s sup-port to this rotation was matched by a commitment on the part of the Ministry of Health, who continued to pay the focal points’ salaries and benefits during this period. Based on the availability of funds and interest expressed by other countries, this opportunity may be replicated in 2009, with the ultimate goal of expanding our regional Roster of experienced health disaster experts.
A similar process took place in Central America. Given their capacity and experience, the heads of disaster offices in three ministries of health served as evaluators for a drill on pandemic preparedness in El Salvador. This type of exchange among experts within a region that shares similar vulnerabilities has proven to be good for sustainability.
Several PAHO/WHO programs—emergency preparedness, communicable diseases and health ser-vices—have collaborated to develop a set of tools to assess national preparedness for pandemic influenza. Using a tabletop exercise and an approach similar to that used to assess the safety of hospitals, the tools measure the three principal components of the health response to pandemic influenza: multisectoral readi-
ness, outbreak alert and control, and health services’ response capacity. Each component has a set of critical actions. These are weighted according to their impor-tance to the success of the overall response. The ability to fulfill each critical action is assessed as high, inter-mediate or poor, according to established standards. These tools are an important step toward an objective and comparable assessment and will be used in Cen-tral America and South America in 2009.
Coordination at the National Level
The leadership role of the Ministries of Health in the area of disaster preparedness, risk reduction and response is enhanced when coordination is improved within the health sector and among other sectors. In most countries, national coordination mechanisms exist for issues related to disaster preparedness and re-sponse, although the health sector is usually not the lead agency. In 2008, several initiatives provided an opportunity to reinforce the health sector’s leadership role in multisectoral risk reduction and preparedness.
Several courses on pre-paredness for emergencies involving hazardous chemi-cals and radioactive material provided an excellent oppor-tunity for intersectoral coor-dination and preparedness for a hazard that is becoming increasingly more frequent in the developing world. CET-ESB is the WHO Collaborating Center for Preven-tion, Preparedness and Response to Chemical Emer-gencies, and in previous years, they had worked with PAHO/WHO to design and carry out a comprehen-sive course on chemical accidents at their institution in Sao Paulo, Brazil. However, annually, only about 30 participants could be reached. In 2008, the course was decentralized and experts from CETESB were de-ployed to Peru, enabling a much greater number of nationals to attend (some participants from Uruguay also attended, as it will be the venue of the next course in 2009). As countries improve their capacity in this field, PAHO will support the active participation of the health sector in national committees on hazard-ous materials.
A similar course was held in Honduras. Prior to the start, CETESB worked with national authorities to conduct a diagnosis of Honduras’ vulnerability to
C h a p t e r 1 - I m p r o v i n g D i s a s t e r P r e p a r e d n e s s i n t h e H e a l t h S e c t o r

6
A n n u a l R e p o r t 2 0 0 8
accidents involving hazardous materials. Although the course was primarily national in scope, representa-tives of institutions including health, civil protection, ministry of environment, firefighters and universities from other Central American countries were invited. After discussions on preparedness, prevention and re-sponse to emergencies involving hazardous chemicals, the course concluded with a drill to put into practice the knowledge acquired. An important outcome of this training exercise was the creation of a national intersectoral group in Honduras that would continue to work on this issue, within the context of national disaster plans.
The response by countries in the Americas to their own disasters and to those in other countries has high-lighted certain gaps in emergency preparedness. One is the ability to set up and make operational health situation rooms and emergency operations centers, which are important hubs of coordination and which, in theory, should make it possible to make decisions and generate timely and accurate information. Con-ducting a rapid evaluation of damage and needs in the health sector and analyzing information are skills that
are critical to the success of health situation rooms or EOCs. Therefore, in 2008, PAHO/WHO deployed specialized public health staff and set up health EOCs in several disaster situations. Basic equipment was provided to health emergency operations centers in El Salvador, Ecuador, Colombia and Peru to support their coordination role both as the national link to the PAHO EOC and with their counterparts at national level. Despite these positive experiences, much work remains to be done.
In addition, to further address this gap, PAHO/WHO began work to strengthen capacity in five countries in Central America and the Dominican Re-public and Haiti to manage information and to im-prove communications and decision making through health emergency operations centers. The central pil-lar of this initiative is the national disaster response team, which is at the forefront of information collec-tion that can be used for decision making within and outside the health sector. Existing manuals for evalu-ating health sector damage and needs will be reviewed and guidelines will be developed for the national level, similar to those that currently exist for the regional Health Emergency Response Team.
Other emergency preparedness initiatives also pro-vided important coordination opportunities in the Caribbean. PAHO’s increased focus on the elderly in disaster situations is one such example. A work-shop (Annex 4) on this topic improved partnerships for disaster preparedness, thanks to broad participa-tion, including policy makers, nursing home manag-ers, international and local NGOs such as HelpAge International and VOICE, and re-gional organizations such as CDERA and the CARICOM Secretariat. Partici-pants reviewed the challenges involved in providing care for the elderly before, during and after a disaster, and identi-fied potential strate-gies to address these challenges. Com-munity leadership and capacity build-ing were considered critical in moving forward. Key short-
The elderly are dispro-portionately affected by disasters due to a variety
of factors including increased vulnerability from physical causes, chronic diseases and dis-ability, and multiple social factors. Globally, the proportion of older people is growing faster than any other age group. In the Carib-bean, the UN estimates that the over-60 population will increase from 11.1% (4,500,000) in 2005 to 24.6% (12,400,000) in 2050.
Vulnerable Groups in Disasters: The Elderly
Early in 2008, 13 of Ecuador’s 24 provinces were seriously im-pacted by floods, which claimed 54 lives and forced some 10,000 persons into temporary shelters. PAHO and the Ministry of Health
conducted a post-disaster assessment and one key was the need for a health sector plan to deal with the annual recurring problems related to the rains and floods
Later in 2008, regional health authorities in Ecuador convened a co-
ordination meeting of health institutions involved in response and as a
result, a plan was developed to prepare for the next (2009) winter flood
along the coastal region of Ecuador (copies of the documents available
on request). The plan addresses health concerns such as respiratory and
diarrheal diseases and vector-borne diseases such as dengue, as well as
population displacement and crowding in shelters, which also contrib-
ute to an increased incidence of disease.
The Plan advances a number of strategies including training for the
diagnosis and medical care of diseases that surge during the winter pe-
riod (mass media campaigns on prevention of communicable diseases;
development of community risk maps; updating current knowledge on
epidemiological surveillance and the identification and control of out-
breaks). Each strategic line has activities corresponding to preparedness
and response. The plan will be activated during the next cycle of flood-
ing, giving Ecuador the chance to evaluate improved and coordinated
preparedness and response.
Preparing for recurring floods offers important opportunity for coordination in Ecuador

7
term initiatives included the development of pre-paredness plans for nursing homes; inclusion of elder-ly considerations in vulnerability assessments before a disaster and in needs assessments in the aftermath of a disaster; training in managing the elderly and making shelters ‘elderly friendly.’
Some countries that attended the workshop have begun implementation of the recommenda-tions. In Belize, the National Council on Ageing (NCA) spear-headed a study of the vulnerability of the elderly in emergency situations and they will host a meeting in early 2009, with stake-holder agencies that include the Red Cross, National Association of Village Councils, the Ministry of Hu-man Development and service organizations including HelpAge In-ternational. The NCA is also working to raise
awareness of the impact of disasters on the elderly and has made emergency management and older persons a priority area.
Training and Capacity BuildingOne sign of progress and improvement in the Min-
istry of Health disaster offices is the type of training and capacity building being requested from PAHO/WHO. No longer are countries asking PAHO to de-sign, organize and carry out traditional disaster pre-paredness training. They themselves have assumed much of the responsibility for topics such as hospital planning or evaluation of health sector needs in the aftermath of a disaster. Countries are looking for sup-port in newer, more sophisticated areas such as pan-demic influenza; distance learning and virtual courses; or the organization and deployment of national rapid response teams.
Pandemic Influenza
PAHO/WHO has been working on a number of activities to prepare the countries for an influenza pan-
demic. The main thrust has been to assist in the prepa-ration, development and testing of a national influen-za pandemic plan, advocacy for the non-health sector participation in preparedness —particularly with na-tional disaster agencies and uniformed forces— and strengthening health institution readiness by develop-ing and training on various protocols designed to pro-mote hospital and health center capacity to respond to emergencies. A toolkit is being developed, aimed at mayors or civic leaders who may find they have to deal with a panicked community and with little addi-tional help from outside. This collection of guidelines gives the non-technical reader enough information to prepare a small community for the pandemic. It is designed to complement national pandemic plans, and while it does not include hospital or health center arrangements that are covered in the national plan, it does have information for the householder on how to prepare for a pandemic, including what to do with a sick person at home. All English and Dutch-speak-ing Caribbean countries have developed a national plan for pandemic and most have trained outbreak response teams to investigate suspected human cases of avian or pandemic influenza. At present, countries are looking to strengthen their hospital safety plans by including provisions for a pandemic.
Simulations and Drills
Simulation exercises and drills were used to con-duct training and capacity building exercises. At glob-al level, PAHO/WHO completed a two-day interna-tional emergency response exercise entitled ConvEx-3 Emergency Radiation Simulation Exercise. While the actual simu-lation took place over the course of two days, planning for the ex-ercise took two years. This lengthy planning time was necessary to coordinate the many agencies involved: nine international organiza-tions and 74 countries participated in the simulation. The simulation was coordinated by the International Atomic Energy Agency (IAEA), within the frame-work of the Inter-Agency Committee on Response to Nuclear Accidents (IACRNA). All levels of the WHO system took part in the exercise. In the Americas, PA-HO’s Emergency Operations Center remained open and on high alert over a 36-hour period, as was the case with the EOC at WHO Headquarters in Geneva
C h a p t e r 1 - I m p r o v i n g D i s a s t e r P r e p a r e d n e s s i n t h e H e a l t h S e c t o r
As Jamaica prepared for Tropical Storm Gustav in August 2008, it imple-
mented some measures which were presented in the work-shop on the Elderly in Disaster Situations. One main issue that authorities tried to tackle was making the shelters ‘age friendly’ for seniors, this having been a long standing issue. A basic yet pertinent intervention was the provision of cots of the correct height and size in some shelters.
Transferring Disaster Preparedness Knowledge
into Action

8
A n n u a l R e p o r t 2 0 0 8
and at the International Atomic Energy Agency in Vienna. The EOC staff monitored messages sent by email and fax, scanned the IAEA website and hosted periodic teleconferences, while assisting the technical leads to prepare reports.
PAHO/WHO’s Country Office in Mexico played a key role in the exercise, with messages being ex-changed throughout the first night. This spirit and enthusiasm gave the exercise its life and served as a real learning opportunity. WHO Collaborating Cen-ters also participated in the exercise. PAHO/WHO’s Emergency Operations Center, led by the Organiza-tion’s radiological health expert, called meetings with 31 members of the headquarters Disaster Task Force and worked closely with the International Health Regulations (IHR) team, as the simulation developed and the simulated situation at Laguna Verde became more serious. During the meetings, input was sought from all parties, decisions were made, and PAHO was able to respond to the requests from Mexico and the IAEA. The entire exercise was formally monitored and evaluated so that lessons from the exercise can be used to improve future response operations.
PAHO/WHO also continued to provide support to Caribbean countries to conduct drills and simula-tions and improve response to mass casualty events. Training and capacity building of national level part-ners focused on mass casualty management and inci-dent command systems, ECAT (Emergency Care and Treatment) and LSS/SUMA. In Grenada, PAHO/WHO worked with national authorities to conduct a full-scale fire simulation exercise in the General Hos-pital, the country’s only referral hospital. The exercise achieved its objectives and had the full support of the Ministry of Health, the National Disaster Manage-ment Agency and the Fire Department. There was also political backing, evidenced by the participation of both the Minister of Health and the Junior Minis-ter of Health in the exercise and the debriefing. Sub-
sequently, the Minister also stated his commit-ment to addressing the weaknesses identified during the exercise. The exercise generated much interest in the media, and the government has since announced that it will be looking for a new site for a hos-pital. It also provided an opportunity for the Ministry of Health to improve inter- and in-tra-coordination and to focus on preparedness for hazards other than natural hazards. An ed-ucational video was pre-pared from the exercise for wider distribution in the Caribbean and is available on request.
The Princess Alexan-dra Hospital in Anguilla
• TheexerciseallowedPAHOofficestotestitsemergencymanagementplans.
• Technicalexpertsanalyzedandsynthesizedinformation,addingvaluetothetechnicalreportsthatwerepro-
duced.
• Theexerciseillustratedhowavarietyoftehnicalprogamscancollaborateduringanemergency,inthiscase,IHR,
emergencies and disasters and radiological health.
• Communicationatalllevelsneedstobeimproved,includingovercomingbasicbutimportanttechnicalglitches
that can impact the success of the exercise: the website, the telephone switchboard at country level, and confer-
ence call connections.
• Technicalcapacityforradiologicalhealthislimited.
Observations from the Simulation Exercise
Like many other hospitals, the
staff of Grenada’s General Hospital
had never participated in an in-
ternal disaster simulation exercise
(the exception to this was staff
from the Accident and Emer-
gency Department). Although
many hospitals in the Caribbean
have a wealth of experience with
simulation exercises, for the most
part, these have been limited to
external exercises used to test ar-
eas such as the response to mass
casualties.
However, when the Grenada
General Hospital finished applying
the Safe Hospitals Checklist, one
of the areas found to be at high
risk for fire was the facility’s
oxygen bank. The Hospital Safety
Index was applied as part of a
project to strengthen communi-
ties through safer health facilities
in the Caribbean.

9
also tested its readiness to respond to emergencies, via a hurricane tabletop simulation exercise. The exercise was conducted using the actual public advisories is-sued by the Department of Disaster Management during Hurricane Omar, which struck the island in October 2008. The hospital disaster preparedness plan was updated using the lessons learned from the exercise. Similarly, in Dominica, the Red Cross was supported to implement a national simulation exer-cise. The support focused primarily on the Princess Margaret Hospital’s response in the exercise.
Training for Mass Casualty Events
In 2008, the Ca-ribbean initiated a Training of Trainers (TOT) program in mass casualty man-agement. Three courses were held to lay the ground-work for countries to assume responsi-bility for delivery of the MCM courses presently offered by PAHO/WHO, thus ensuring their sustainability and satisfying the need for more instruc-tors in the Region. The newly trained and updated in-structors will plan and conduct train-ing sessions in their various orga-nizations and col-laborate with other instructors to con-duct inter-sectoral training sessions locally and possi-
bly regionally. They will also assist other countries in planning, training and, where possible, responding to mass casualty incidents. Nine countries now have a cadre of instructors. Of these, instructors in Jamaica, Belize, Suriname and Guyana already taught MCM courses in their country in 2008. PAHO will con-tinue this program through the end of 2010, at which time the Organizations’ role will then become one of quality assurance —updating and maintaining the
quality of training materials— while exploring new approaches to improve the efficiency and effectiveness of delivering the course.
Health Disaster Management Basics
In 2000, PAHO/WHO developed the LEAD-ERS course—a two-week intensive capacity-building course for professional development in the disaster risk reduction field. The LEADERS course offers a balance between the development process, wide-rang-ing mitigation issues, effective preparedness and effi-cient response. It is geared toward participants who are stakeholders in risk reduction issues, including but not limited to Health Disaster Coordinators, Nation-al Disaster Coordinators, public sector managers and other counterparts who deal with mitigation issues, as well as academics who work in disaster mitigation topics. The LEADERS course (the Spanish-language version is called LIDERES) has been offered almost 20 times since 2000 and has reached approximately 450 individuals. However, after almost 10 years, a critical mass has been established, and an NGO, FUNDALIDERES, has taken over the management of the course. Increasingly, and particularly in the larger countries in the Region, a ‘national’ version of the LEADERS course is being held. Brazil is one example. Since 2003, the country has taken over the annual LEADERS courses in Portuguese and the gov-ernment of Brazil has earmarked its own budget fund-ing for the courses. The Ministry of Health consid-ers LEADERS an important training tool and at the most recent course, Brazil hosted participants from other countries in the Americas and candidates from Portuguese-speaking countries in Africa. The future of the LEADERS Course will have to follow the Bra-zilian model.
The future for comprehensive health disaster man-agement training lies with a new online course in public health. Several years ago, PAHO took initial steps to use distance learning methodologies for ca-pacity building. Partnering with FLACSO, the Latin American Faculty of Social Sciences, PAHO/WHO developed several modules on health and disaster policies, as part of a broader FLACSO distance learn-ing program. Substantial interest was generated as a result of this initial experience, and during 2008, the planning process began for a comprehensive course on all aspects of public health and disasters, including epidemiology, safe hospitals, partnerships, risk man-agement and more. This new distance learning course, will be hosted by PAHO on the Organization’s virtual campus for public health, a platform to provide con-
C h a p t e r 1 - I m p r o v i n g D i s a s t e r P r e p a r e d n e s s i n t h e H e a l t h S e c t o r
Belize was affected by a
tropical storm in 2008,
which caused widespread
rainfall that resulted in life-threat-
ening floods in communities
along the Mopan, Macal and up-
per Belize Rivers. 50,450 persons
were estimated to be affected
and up to one month after the
event, over 700 persons were still
staying in shelters or with rela-
tives and friends.
Less than a month earlier,
PAHO/WHO had supported a
mass casualty course in Belize.
This course proved timely, as
participants were able to imple-
ment what was learned. Special
mention was made of the orga-
nized response in San Ignacio,
where the District Coordinator for
the National Disaster Office had
participated in the course.
Mass Casualty Training Pays Off
10
A n n u a l R e p o r t 2 0 0 8
tinuing education to the public health community. This new course will begin in 2009 and will be be-come a prerequisite for attending future LEADERS courses in the Region.
New Outreach
Finally, for training efforts to have an impact on the health sector, it is not always necessary to directly target only health professionals. In the Caribbean, PAHO/WHO collaborated with UNICEF and other stakeholders to plan and deliver a workshop on “Ca-ribbean Media and Emergencies —responding to our reality from a rights-based perspective.” The work-shop resulted in PAHO reaching beyond its core con-stituency of the Ministries of Health to engage and support media and broadcast practitioners, providing them with training and technical information materi-als on disaster risk reduction. The 30 participants rep-resented 23 radio and TV stations from 18 countries.
PAHO/WHO capitalized on this workshop to ele-vate the issue of emergency preparedness as an impor-tant prerequisite for effective emergency response. It presented a channel through which the general public can be educated and empowered and thus demand greater accountability of public officials in disaster risk reduction. Within one week of the session, the national TV station in Barbados asked PAHO/WHO to appear on its ‘Morning Time’ program to speak about the myths and realities of natural disasters. This was well received and the initially pre-arranged 15 minute-appearance was complimented by a second eight-minute show.
Publications and Information Management
Over a period of 30 years, PAHO/WHO has made a significant contribution to the development of a knowledge base on public health and disasters. This information takes many forms: technical and scien-tific publications, advocacy and promotional mate-rial, databases and multimedia products. The output has evolved along with changes in technology and access, particularly in Latin America and the Carib-bean. Following the roadmap set forth in PAHO’s new disaster preparedness and risk reduction Strategic Plan 2008-2012, this year special attention was paid to this programmatic component. These materials and information resources enrich the entire scope of PAHO’s work: some consist of tools to improve disas-ter preparedness, others help to reduce risk in health
facilities or support countries in the health response to disasters. In their design, production and use, al-liances with national, regional and/or global partners are sought and built.
Information Networks
The Regional Disaster Information Center (CRID) is now almost two decades old. Originally created by PAHO/WHO, it has evolved into a multiagency cen-ter of excellence that works with countries in the Re-gion to set standards and guidelines for organization and dissemination of information and to strengthen the capacity of countries themselves to manage these activities. In 2008, CRID developed a plan to broad-en its information management support to regional ministries of health. For example, El Salvador has a large volume of documents on all aspects of disaster management, many of which are actual hospital di-saster plans. With a view toward organizing this infor-mation and making it widely available to health cen-ters, other hospitals and the public in general, CRID develops and uses specialized products and services to make it possible to consult and gain access online to this material. In addition to supporting individual countries, CRID also supported regional information networks, including:
• (BiVa-PaD), a network of disaster preparednessand response information centers which CRID helped to establish in the Civil Defense/Protection agencies in Bolivia, Colombia, Ecuador and Peru. A modest amount of equipment was provided, staff was trained to use information management tools and processes were developed to set up da-tabases and web pages in each Center. The most important outcome was a DVD containing 493

11
full-text documents of regional interest related to risk management. The outreach to Civil Protection agencies was an important step, as their focus tra-ditionally has been on response. One member of this network, Ecuador’s Virtual Library for Disas-ter Prevention and Response, has provided excel-lent support to national risk reduction institutions, despite having to build their Center from scratch and ‘survive’ a transfer of supervision from the Civil Defense to another national risk reduction department.
• TheinformationcentersthatmakeuptheCAN-DHI network in Central America are gaining im-portance as providers of risk reduction information and builders of regional capacity. The CANDHI Network is a joint initiative of PAHO/WHO, the U.S. National Library of Medicine and the CRID, together with four Central American countries. The CANDHI Center in Honduras, at the national Medical Library, has engaged in a program to build awareness—at the library’s directorate level—of di-saster issues, thus contributing to the sustainability of the project. Another approach was taken with Honduras’ national disaster agency (COPECO) to develop information management skills and strate-gies in the use of new bibliographic reference tools. In Nicaragua, the CANDHI Center forms part of the national Risk Management Commission, which raises the Center’s visibility and leadership and confers importance on their work.
Much of CRID’s success has been achieved through partnerships they have developed. PAHO/WHO and the UNISDR are the principal financing entities and form part of the Center’s steering committee. The U.S. National Library of Medicine (NLM) has been an important partner for more than five years and is a co-developer of the CANDHI Network in Cen-tral America. NLM is now working with CRID to develop a toolkit (resources, practical recommenda-tions and methodologies) that will aid risk reduction organizations and agencies to manage disaster infor-mation. During 2008, CRID solidified ties through collaborative ventures with the IFRC, UNICEF, and the Center for the Prevention of Natural Disasters in Central America (CEPREDENAC).
In summary, in 2008, the CRID’s principal achievements included:
• An improvement in thequalityof theirproductsand services, with a focus on the health aspects of disaster risk reduction;
• Improved technical assistance to countries tode-velop their capacity to manage disaster informa-tion;
• Opening of avenues of collaboration with otherregional and global entities;
• StrengtheningoftheLatinAmericanNetworkofRisk Management Information Centers.
Publications and Training Material
New material on public health and disasters for
managers
Professional mobility and changes in government at the national level have always generated a need to ensure continuous access to training opportunities, materials and information resources that will main-tain new leaders and managers who take decisions in health sector disaster programs up-to-date. To this end, PAHO developed a body of training materi-als that are presented in a systematic, practical, and summarized fashion, available online. Review of these materials and completion of exercises are now a pre-requisite for attendance at the new LEADERS course or similar workshops for managers. They will also be incorporated into a standalone course on PAHO’s Virtual Public Health Campus.
Guide for simulations and drills
In 2008, a practical guide was prepared to design and evaluate simulation exercises and drills in dif-ferent emergency and disaster scenarios. This guide makes it easier for countries to develop actual exer-cises, to organize training sessions around this topic and to understand the differences, similarities and benefits of designing and carrying out either simula-tions or drills.
Materials to support countries during response
The development and strengthening of national and regional response capacity requires guidelines and technical documents. In 2008, an updated version of the Field Guide for the PAHO Regional Health Emer-gency Response Team was produced. It offers practi-cal guidance on setting up and activating the regional team; the mobilization of resources; and an explana-tion of the concept, coordination and responsibilities of the UN Cluster mechanism. Twenty-four annexes contain additional operational information for the members of the team.
C h a p t e r 1 - I m p r o v i n g D i s a s t e r P r e p a r e d n e s s i n t h e H e a l t h S e c t o r

12
A n n u a l R e p o r t 2 0 0 8
In addition, a Guide for Managing Information and Communications in Disaster Situations was de-veloped to guide the generation and dissemination of information and to facilitate work with the media dur-ing emergencies. Several training activities, including practical exercises based on the content of this guide, are scheduled for 2009.
In 2008, several important decisions were taken concerning other information vehicles. After more than 30 years of uninterrupted publication, the news-letter Disasters: Preparedness and Mitigation in the
Americas reduced the frequency of publication and in-creased in size. Published four times a year since 1979, it is now be published twice a year, but has increased from 8 to 12 pages. The changes to the print newslet-ter allow for a more in-depth treatment of issues that are not time sensitive. As a complement, a monthly Bulletin entitled Briefly Noted is being published in electronic format only. Its content is much shorter and much more time sensitive. While the print news-letter reaches 26,000 subscribers worldwide, Briefly Noted has a distribution of 8,000 e-mail readers.

13
Protecting Health Services from the Impact of Disasters
Chapter 2
Protecting health facilities and health services from the impact of disasters and in emer-gency situations requires taking into ac-count several factors. The first is protection
of the physical structure itself. Evidence has shown that the cost of building a new disaster-safe hospital is negligible when measures are included in early design considerations. Building new health facilities that are disaster-resilient is a global commitment and a goal set forth in the Hyogo Framework for Action 2005-2015.1 Reaching this goal is as much about having vision and commitment as it is about actual resources and the knowledge exists to make this happen.
However, rather than the complete structural col-lapse of a hospital, it is much more common that a hospital simply cannot function. The building itself may appear to be sound, but equipment and lifelines are so seriously damaged that health services cannot be provided. The health workforce must also be trained to deal with these special situations.
All hospitals belong to a health services network. Therefore, for a hospital to remain fully operational in disaster situations, the network that it is a part of also must be operating at optimum capac-ity. PAHO/WHO defines an integrat-ed health services system as: “A net-work of organiza-tions that provides, or is organized to provide, ongoing services, based on primary health care and coordinated from the first level, to a particular population in a particular territory, and that is accountable for the clinical and financial results
Better protected health services —including staff, management systems, equipment, assets and physical infrastructure— that are safe and remain functional during and after a disaster.
A safe hospital is a facility whose services
remain accessible and functional, at
maximum capacity and within the same
infrastructure, immediately following a disaster.
The term ‘safe hospital’ encompasses all health
facilities, regardless of their level of complexity. A
hospital is ‘safe’ when it enjoys the highest level
of protection possible, when access routes to the
health facility are open and critical lifelines con-
tinue to supply the health facility, guaranteeing
continuity of operations and the ability to absorb
the additional demand for medical care.
What is a Safe Hospital?
1 The World Conference on Disaster Reduction, held in Kobe, Japan in 2005, set the goal of building all new hospitals to withstand the impact of disasters as a priority to be reached 2015. Building on this momentum, the UN International Strategy for Disaster Reduction (ISDR) launched the World Disaster Reduction Campaign for 2008-2009, with the global theme ‘hospitals safe from disasters.’ Read more about this campaign in chapter 4.

14
A n n u a l R e p o r t 2 0 0 8
and the health status of the population it serves. These systems, widely participatory, vertically integrated, and horizontally coordinated, offer a wide range of services to address the ongoing needs of their users, from promotion and prevention to outpatient and in-patient services, care for acute and chronic illnesses, home care, rehabilitation, palliative care, and public health services.”
Technical Support to Member Countries
The 45th Directing Council of the Pan American Health Organization (2004) approved a resolution urging Member States to adopt “Hospitals Safe from Disasters” as a national risk reduction policy. Several years later, the 27th Pan American Sanitary Conference (2007), the highest health body in the Americas, urged Member States to take additional steps, including devel-oping tools to assess the likelihood that a health facility would remain functional during and after a disaster (read the full resolutions in Annex 5). If the 2004 resolution provided a united call for reducing risk in hospitals at the global level , the 2007 resolution set forth a clear man-date, one that PAHO/WHO has taken seriously and around which it has designed strategic lines of action to protect health facilities and health services from the im-pact of disasters.
In the Caribbean, PAHO/WHO focused support on ensuring the safety of health facilities and health services. Aiding countries to apply the Hospital Safety Index and develop safety improvement plans for targeted health
facilities were the key areas of this line of work. PAHO worked directly with eight countries (St. Vincent and the Grenadines, St. Kitts, Nevis, Gre-nada, Anguilla, Bar-bados, Dominica, Montserrat) to apply the Hospital Safety In-dex in one hospital in each country (unlike extremely large coun-tries such as Brazil or
Mexico, these eight Eastern Caribbean countries each have only one major hospital).
The Safe Hospitals Checklist (one component of the Hospital Safety Index—see next section) was used to as-sess the level of safety in 145 areas of the hospital. Once
the Checklist was completed, the score for each compo-nent is weighted according to its relative importance to a hospital’s ability to withstand a disaster and continue functioning. The final Safety Index score places a health facility into one of three categories of safety (A, B or C), helping authorities determine which facilities most ur-gently need interventions (see Annex 6).
In the case of the Eastern Caribbean countries, seven of the eight hospitals received a score in category B, which indicated that the facility’s current safety levels could po-tentially put patients and staff at risk. The eighth hospi-tal fell into Category C, indicating that its current safety level was unsatisfactory, putting patients and staff at risk. If the recommendations stemming from the evaluations were addressed, all eight hospitals would see significant improvements in their safety levels. However, the hos-pital that ranked in category C (the lowest) would see the greatest improvement, moving from category C to A. By the end of 2008, five of the eight countries had developed safety improvement plans.
In South America, activities focused on setting up local ‘safe hospitals’ programs, including designing and implementing risk-reduction actions and establishing multidisciplinary teams that were trained to carry this work forth. In Ecuador, the Minister of Health launched a national Safe Hospitals Policy and Program, thus posi-tioning this as a national priority. In Peru, the Regional Health Council created and approved a regional (Are-quipa) ‘safe hospitals’ program and a multidisciplinary committee was set up to prepare the policy. Finally, in Bolivia, where health services are a municipal respon-sibility, efforts focused on developing a municipal pro-gram. Thanks to local collaboration and participation, the municipality of Sipe Sipe now has a safe hospitals program. In addition to the safe hospitals programs, all three countries created multidisciplinary assessment teams and these individuals were trained to evaluate hospitals and replicate assessments for future interven-tions.
The Hospital Safety Index was applied in 12 selected health facilities in Ecuador, Bolivia and Peru. However, local authorities realized they also needed to assess the safety level of smaller facilities as well as to use the results of these assessments to develop or update contingency plans for continuity of health care services during and after emergencies. Therefore, many health authorities contributed their own local resources to carry out assess-ments in additional health facilities. Because of this vis-ible and essential display of political will and ownership, more than 260 health facilities were assessed in these three countries alone.

15
C h a p t e r 2 - P r o t e c t i n g H e a l t h S e r v i c e s f r o m t h e I m p a c t o f D i s a s t e r s
Ministries of Health in several counties in Central America—El Salvador, Nicaragua, Panama—passed norms mandating that health facilities at all levels take steps to ensure they can continue to function in disaster situations. These steps call for a hospital disaster plan that is updated annually. The disaster offices of the Ministries of Health are charged with overseeing the technical qual-ity of these plans. During the widespread flooding in Central America in the second half of 2008, these plans were set in motion. According to reports from disaster coordinators in the ministries of health, the response had improved over previous years.
Central American countries were in the initial stage of consolidating a safe hospitals program in 2008, with sup-port from PAHO/WHO. A work plan was devised with a number of countries: El Salvador, Honduras, Guate-mala and Nicaragua to identify and correct vulnerabil-ity in health facilities in selected municipalities of these countries. Emphasis was on the entire network of health services. The Hospital Safety Index will be the princi-pal tool used to identify vulnerability in existing health facilities and to build the capacity of a trained team of evaluators to assess risk. These efforts will build on ex-periences from similar initiatives in South America and the Caribbean. The ultimate goal is to obtain a commit-ment at the political level to establishing a safe hospitals program to follow through and to raise public awareness of the need to protect health infrastructure in the most vulnerable communities in Central America.
Tools and Training Protecting hospitals and health facilities from the
impact of disasters is too big a job for the health sector alone. It requires the commitment and active support of a variety of sectors, agencies and individuals. It requires the development of targeted training initiatives in a vari-ety of technical areas that many health professionals still consider new. It seeks to gain the buy-in from non-health professionals as well. They are critical to the outcome of this objective by expanding the pool of the Region’s hu-man resources in disaster risk reduction through coordi-nation and networking.
Tools that Contribute to the Safe Hospitals Initiative
The key for supporting this strategy is the Hospital Safety Index. This simple, low cost tool helps countries to carry the carrying out of a preliminary analysis of the safety level of their hospitals in disaster situations and set priorities for action. In 2008, a group of experts from
countries throughout the Region who had field tested the Checklist in more than 200 hospitals, revisited the methodology, technical aspects and results of the appli-cation of the hospital safety index tools. After a some-times-difficult debate centered around new knowledge, country-specific standards, and evidence-based informa-tion, the group made many substantial changes to the Checklist, under PAHO’s leadership, and it was formally published in 2008. It will continue to be modified over time to meet needs as they arise.
The Hospital Safety Index is made up of three com-ponents:
• Evaluation forms: the first of which includes general information on the health facility; the second is the Safe Hospitals Checklist which is used by a trained team of evaluators to assess the safety level of 145 aspects or fac-tors in the health facility, categorized under four components: location with regard to hazards in the hospital of a structural, non-structural, func-tional or organizational nature.
• TheGuide for Evaluators, the prin-cipal training tool, was developed to guide and standardize assessment cri-teria for health facilities, both in an individual context as well as in rela-tion to the health services network. The Guide explains the methodology and the conceptual basis of the Hos-pital Safety Index, gives guidance for the make up of the multi-disciplinary team and the assessment work to be carried out. It also describes and ex-plains the questions included in the Checklist to fa-cilitate the work of the team.
• Safety Index Calculator. The levels of safety assigned to each item on the Checklist are recorded in an excel spreadsheet which uses formulas to calculate automatically the numeric value for each one of the 145 components under assessment, placing them within one of three safety categories: high, medium or low.
Determining a hospital’s safety index is a new way of managing risk. The Index can be applied at regular inter-vals, making it possible to continuously monitor safety and measure progress achieved. In that way, safety is not

16
A n n u a l R e p o r t 2 0 0 8
a state of ‘yes-or-no’ or ‘all-or-nothing,” but rather a con-dition that can be improved gradually. All these materials are available online and in print format. The Hospital Safety Index has been distributed as a package to PAHO member countries and to other WHO regions, where PAHO has provided experts from member countries to conduct training sessions.
Successful application of the Hospital Safety Index requires setting up and training assessment teams in all countries, and PAHO/WHO has already carried out and/or scheduled regional and national courses. To sup-port these courses, training materials were created. These include a series of multimedia presentations that review the concept of a ‘safe hospital’ (identification and loca-tion of hazards, as well as the structural, non-structural and functional factors) and the essential aspects for plan-ning hospital assessments, and explain how to apply the safe hospitals Checklist and calculate the Hospital Safety Index. The materials include special practical recom-mendations for instructors, with a view toward creating a sustainable body of trainers in-country and thus reduce dependency on PAHO.
Once these courses are concluded, participants should be able to carry out assessment of health facilities and discuss the findings with health authorities in order to set disaster mitigation or preparedness priorities to improve hospital safety. The Hospital Safety Index does not re-place costly and detailed vulnerability studies. However, because it is relatively inexpensive and easier to apply, it is an important first tool for national authorities to use to set priorities for investment in hospital safety.
Building disaster-resilient hospitals and health facili-ties in hurricane-prone areas requires a sound knowledge of wind hazards. Yet the Caribbean was still using wind hazard maps that were almost 40 years old, which led to uninformed and sometimes counterproductive decisions on appropriate wind speeds for selected projects and in some Caribbean countries. Regional building standards for wind resistance were laid out in the 1985 Caribbean Uniform Building Code (CUBiC). Because a great deal of reliable data had become available since the maps were last produced and thanks to advances in science and technology related to the long-term forecasting of hur-ricane activity in the North Atlantic (including the Ca-ribbean), new state-of-the-art wind hazard maps for Ca-ribbean islands and nearby coastal areas of Central and South America were developed in 2008 by a researcher, under an arrangement with PAHO/WHO, using data from the U.S. National Hurricane Center and with in-put from stakeholders such as engineers, architects and meteorological officials. (More in Annex 7).
The wind hazards maps alone provide just the back-ground information required to build infrastructure to resist the impact of natural hazards. In order to facilitate the work of engineers and project managers who design and construct critical infrastructure such as hospitals, a “Caribbean Application” document was developed to allow use of the American Society of Civil Engineers (ASCE) codes, which some Caribbean countries such as the Bahamas and the Dominican Republic have ad-opted. However, because the ASCE code (ASCE -7) was written for the U.S., which has a mixture of hurricane-prone regions and non-hurricane regions, the Caribbean application document eliminates all references to non-hurricane regions.) More than 45 engineers and archi-tects from the English-speaking Caribbean have been trained to use the wind hazard maps.
Now it is possible to take a virtual tour of a ‘safe’ hospital, thanks to a new multimedia tool that has been used to create a vir-tual learning environment. For several years PAHO has opted to use new technologies to produce educational materials and techni-cal information resources, mak-ing them easier to use and more versatile. The new DVD pro-gram on the virtual safe hospital is divided into modules that can be used independently or together to provide an overview. The technical guide or the structure of the content has been arranged in large part on the concepts and issues in the Hospital Safety Index, given that ex-perts have agreed that these are the key determinants of the safety of a hospital or health facility. However, the tool is flexible—it can support training courses for evaluators, but is can also be used by anyone who wants to know more about safe hospitals. Users can navigate through the virtual hospital can always adapt their jour-ney, choosing the preferred route and repeating or skip-ping the subjects. A complete journey can take almost three hours, but the viewing of the general introductory video will take only 15 minutes and facilitates a quick understanding of all the components. See Annex 8 for the contents of this new CD, which made its debut on World Health Day 2009.
Training for application of the Hospital Safety Index
In the Caribbean, 58 professionals from 15 countries were trained in two courses in 2008 to apply the Safe Hospitals Checklist, assign a score, use the score to calcu-late the index, and write a summary report on the assess-

17
ment. Of those trained, 18 have already participated in the actual evaluation of hospitals in the Region. A third course is planned for 2009 in order to establish a cadre of safe hospital evaluators in the English-speaking Carib-bean. Participants in the courses included civil engineers, architects, biomedical technicians, and disaster manage-ment specialists.
Paraguay developed a national team of safe hospitals evaluators after participating in a regional evaluators’ course. The Minister of Health demonstrated commit-ment to a ‘safe hospitals’ program by hosting a confer-ence for directors of the nation’s general hospitals, at which the health experts who had participated in the regional Evaluators training had a national audience at which to speak about the issues. This sparked so much interest that Paraguay committed to joining efforts with PAHO/WHO to create a national Safe Hospitals Evalu-ation Team who, by the end of 2008, had visited four hospitals near the capital, Asunción, to begin the process of evaluating and making safety recommendations to all general hospitals in Paraguay by the end of 2009.
Other Training for Safe Health Services
As a result of limited human, material and financial resources in the Caribbean, communities rely heavily on preparedness efforts to ensure health services can con-tinue functioning after a disaster. However, in spite of individual achievements, actions have been insufficient and unsustainable over time. Consultations with na-tional authorities and assessments of the hospitals’ emer-gency response capacity have highlighted weaknesses in emergency preparedness in these institutions. There is an underlying need to implement detailed programs to im-prove, update and test emergency plans in the main and community health facilities in the Caribbean.
To address this need, a course on hospital emergency planning was implemented in early 2008 and hospital personnel from eight countries participated. In addition
to enhancing their technical competence, participants were also able to review and make improvements to their own national preparedness plans during the course and in follow-up country visits. Grenada, Anguilla and Dominica, three of the countries that participated in the course, were subsequently supported in drills to test and further update plans.
Partnerships, Networks and Coordination
The Disaster Mitigation Advisory Group (DiMAG) is a key partner in the development of strategies to safe-guard health services in the Americas from the impact of disasters. This multidisciplinary network of Latin Ameri-can and Caribbean experts is available to provide inde-pendent advice to PAHO/WHO and its Member States on a variety of issues related to disaster mitigation and risk reduction in the health sector. It was the DiMAG that originally developed the idea of the Hospital Safety Index, which is gaining acceptance as a global tool for assessing the likelihood that a hospital can remain func-tioning in disaster situations.
Currently, more than 20 persons are part of the DiMAG. In 2008, they provided technical support to a variety of new initiatives, including the application of the Hospital Safety Index in Latin America and the Ca-ribbean and in WHO’s Eastern Mediterranean Region, and the development and testing of a package of training materials for Safe Hospitals Evaluators.
Another important contribution of DiMAG mem-bers in 2008 was support provided at the request of China’s National Commission of the Council of State, following the May earthquake, which destroyed 50% of the health facilities in the Province of Sichuan. The capacity of health personnel was also affected. At least 4,000 health professionals were victims themselves—either killed or injured. The World Health Organization
C h a p t e r 2 - P r o t e c t i n g H e a l t h S e r v i c e s f r o m t h e I m p a c t o f D i s a s t e r s
After taking part in a regional training course in early 2008 for evaluators of safe hospitals, Trinidad pre-
pared a two-phase plan to assessing the safety of selected health facilities. Phase one included develop-
ing the policy approach, evaluators, conducting assessments and determining priorities for intervention,
while phase two included implementing the recommendations from phase one. A primary outcome of the plan
was the creation of Regional Health Authority assessment teams to assess hospitals in their respective regions.
By mid-2008, authorities had conducted training in four of the five health regions, established evaluation
teams and assessed seven hospitals and health facilities. These hospitals and health facilities are slated for a sec-
ond round of more in-depth assessments to gauge progress.
Trinidad Developed Teams of Safe Hospital Evaluators for Regional Health Authorities

A n n u a l R e p o r t 2 0 0 8
18
organized an interdisciplinary mission which included the participation of experts from the DiMAG and PAHO, together with the World Bank, to recommendations regarding public health, health services, infrastructure and reform of the health system.
PAHO/WHO sponsors annual meetings of the DiMAG to discuss scientific and technical advances and to make recommendations on issues
for future. At its latest annual meeting in December 2008, the DiMAG made a number of recommendations that will be followed up in the coming year and beyond. Below are some of the issues debated at the two-day meeting, held in Panama on December 11-12, 2008.
• Inconsistencies exist among regional seismichazardmaps, thereby limiting their effective use. Consensus should be sought for Caribbean Basin seismic hazard maps. DiMAG recognizes the work currently being undertaken by the Caribbean Development Bank and looks forward to new Caribbean seismic hazard maps for design purposes.
• Astrategyshouldbedevelopedtosustaincurrentef-forts to apply the Hospital Safety Index, including training the evaluators who use the Safe Hospitals Checklist to assess health facilities. The Checklist will be revised for use in smaller health facilities by review-ing the weighted formulas in the Safety Index Calcu-lator. DiMAG will also promote the creation and use of learning tools and methodologies.
• DiMAGproposesthatfuturesafehospitalsmeasurestake into account the risks associated with climate change (e.g. flooding, stronger hurricanes and storm surge) and increase awareness regarding these haz-ards.
• Informationwillbecollectedandpublishedtodem-onstrate the need for strong motion sensors in hos-pitals and health care facilities located in highly vul-nerable areas. A fire safety guide for hospitals will be developed and published and will include procedures for evacuation exercises, as part of the hospital pre-paredness program.
• Astep-by-step,non-technicalguidewillbedevelopedfor the political level and decision makers to promote integration and use of existing tools in the design and construction of hospitals and health facilities.
PAHO and DiMAG will encourage and lend support to the June 2009 IStructE—Caribbean Division Con-ference on Safe Hospitals.
Advocacy for Safer Health Services
The International Strategy for Disaster Reduction (UNISDR) organizes and leads biennial World Disas-ter Reduction Campaigns. At the beginning of 2008, launched a global two-year campaign whose theme is Hospitals Safe from Disasters—Reduce Risk, Protect Health Facilities, Save Lives. PAHO and WHO are the ISDR’s key technical partners in this campaign, which will continue until the end of 2009.
The Campaign aims to raise awareness of the need to: protect the lives of patients and health workers through structural strengthening of medical facilities, to insure buildings and health services, and to train workers to prepare plans that will maintain the functionality of their health systems before, during, and after disasters. PAHO participated enthusiastically in this campaign during 2008 because it raised the profile of this issue which PAHO has worked on with countries for more than a decade. With the growing support of other UN agencies and the World Bank, the key financing partner of the campaign, PAHO was able to step up efforts to protect health facilities and ensure that they continue to function during and after a disaster. Governments regionwide were encouraged to develop strategic action plans to ensure that hospitals and health facilities are safe from disasters, and to make risk reduction an integral part of health policies.
The global launch of the Campaign took place in January 2008 in Switzerland, but in the Americas it was marked with a variety of activities, including formal ceremonies and training opportunities. For example, to mark the beginning of the campaign in Quito, Ecuador, the Minister of Health introduced the country’s national Policy on Safe Hospitals. In Central America, the Cam-paign was launched in Panama in March and in El Salva-dor at the regional meeting of the Coordination Center for Disaster Prevention in Central America (CEPRE-DENAC). Similar activities took place throughout the Region.
It is important to promote these objectives at political summits and technical meetings; to document and share good practices on how to make hospitals safer; and to include essential health services such as primary care cen-ters, blood banks, laboratories, and emergency services in

19
the campaign. It is also necessary to involve professionals from different disciplines (engineers, architects, mainte-nance workers) in risk identification and reduction, and to identify those health services where strategic action plans can be implemented, involving governments, the health sector, and other actors.
Several years ago, PAHO had created a specialized website to serve as a collective repository of regional in-formation on the topic of safe hospitals. However, with the advent of the World Disaster Reduction Campaign, PAHO converted it into an interagency (PAHO, WHO and ISDR) information and resource hub on ‘Hospitals Safe from Disasters,’ the theme of the current World Di-saster Reduction Campaign. The new website— www.safehospitals.info—contains details on the launch of the campaign, distribution of promotional materials, the hospital safety index, PAHO/WHO publications related to the subject of safe hospitals, news items, and a photo gallery. In addition to contributing the name (URL), PAHO completed all the programming and
trained WHO and ISDR staff to use this new content management system.
C h a p t e r 2 - P r o t e c t i n g H e a l t h S e r v i c e s f r o m t h e I m p a c t o f D i s a s t e r s
20
A n n u a l R e p o r t 2 0 0 8
21
Supporting Countries to Respond to Disaster Events in the Health Sector
Chapter 3
Overview
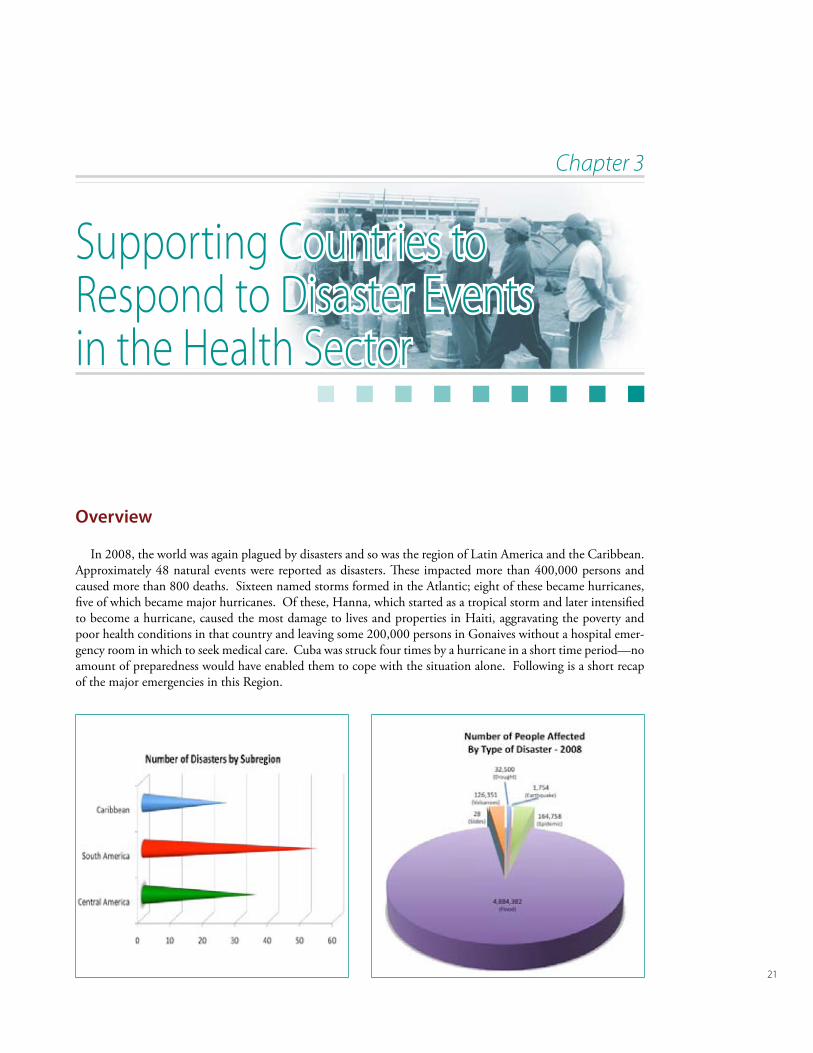
In 2008, the world was again plagued by disasters and so was the region of Latin America and the Caribbean. Approximately 48 natural events were reported as disasters. These impacted more than 400,000 persons and caused more than 800 deaths. Sixteen named storms formed in the Atlantic; eight of these became hurricanes, five of which became major hurricanes. Of these, Hanna, which started as a tropical storm and later intensified to become a hurricane, caused the most damage to lives and properties in Haiti, aggravating the poverty and poor health conditions in that country and leaving some 200,000 persons in Gonaives without a hospital emer-gency room in which to seek medical care. Cuba was struck four times by a hurricane in a short time period—no amount of preparedness would have enabled them to cope with the situation alone. Following is a short recap of the major emergencies in this Region.
22
A n n u a l R e p o r t 2 0 0 8
January
February
March/April
May / June
July/August
September/October
November/December
January
February
March/April
May / June
July/August
September/October
November/December
January
February
March/April
May / June
July/August
September/October
November/December
In 2008, the Tungurahua and Galeras volcanoes erupted. Ecuador’s Tungurahua volcano generally follows a ten-year cycle of eruption, where periods of intense activity are followed by periods of relative calm. In this latest eruption, nearly 1,000 people from high-risk locations were evacuated. PAHO/WHO helped national authorities to activate a health situation room for con-stant monitoring and surveillance and to ensure that the local Emergency Op-erations Committees were on permanent alert.
In Colombia, the eruption of the Galeras volcano also triggered a height-ened alert in hospitals and health facilities, forcing the evacuation of 150 people from Genio and Mapachico near the city of Pasto. PAHO/WHO took part in local Emergency Committee meetings and worked closely with the INGEOMINAS, Colombia’s na-tional institute of geology and mining, to monitor this and possible future eruptions.
Highlights: Natural Hazards
Bolivia declared a state of emergency following widespread flooding in the departments of Santa Cruz, Cochabamba, Beni and La Paz that affected some 55,000 families. In the city of Trinidad alone, 97,500 people were evacuated
due to rains and the elevated risk of water-borne diseases. PAHO/WHO deployed disaster and mental health specialists, helped to provide safe drinking water, and installed the LSS/SUMA system to manage humanitar-ian aid. PAHO/WHO also supported the Ministry of Health and Emergen-cy Operations Centers to coordinate relief operations.
Since early March and extending into early April, heavy rainfall and flooding affected near-ly 1.8 million people in the coastal provinces of Ecuador. This emergency prompted national authorities to relocate some 14,000 people into 331 shelters. Although six of the 43 hospitals in the affected area were impacted, only one had to be evacuated temporarily. PAHO/WHO held a surveillance and diagnostic workshop with local epidemiologists and laboratory tech-nicians to increase national capacity. An action plan was also prepared for safe water, situation rooms and risk communications. LSS/SUMA was installed to help manage humanitarian aid, including the arrival of 48,000 impregnated mosquito nets, 18 fumigation machines and water containers and treatment supplies, which were delivered to temporary shelters.
23
January
February
March/April
May / June
July/August
September/October
November/December
January
February
March/April
May / June
July/August
September/October
November/December
Hurricane season normally be-gins each year in early June and lasts through November. However, in 2008 the pattern changed with the early arrival of Tropical Storms Alma and Arthur in May, which caused heavy rainfall in most of Central America. In the low-lying and coastal areas of Belize, 10 inches of rain in 36 hours affected more than 10,000 people. Inaccessible roads hampered the delivery of essential food supplies and medical care. PAHO/WHO provided technical and logisti-
cal support to the MOH to conduct damage and needs assessment in water and sani-tation and environmental health and to purchase water purification tablets. Equip-ment and supplies were also acquired to support vector control activities to prevent possible outbreaks.
In Guatemala, three days of intense rain in late July caused severe flood-ing and landslides in the municipality of La Union in the province of Zacapa. Access to this area was only possible by air and difficult alternate roads, mak-ing relief operations much more complicated. In response to the emergency, PAHO/WHO mobilized an assessment team to evaluate damage and health risks and several field specialists supported relief operations together with the Ministry of Health and other national entities.
Tropical Storm Gustav moved across Jamaica in the last days of August with heavy rainfall and strong winds. Extensive flooding caused most of the damage, which resulted in loss of prop-erty, crops and livelihood in 160 communities. Several communities in St Thomas, Portland, St Andrew and St Catherine were cut off due to
landslides and health teams had to be flown into these areas to conduct medical and health assessments and provide care. Responding to a request from the Ministry of Health, PAHO/WHO deployed a water and sanitation advisor and an LSS/SUMA team to provide much needed support in damage assessments and needs analysis for health facilities and environmental health. Technical support was also provided in the Ministry’s national Emergency Opera-tions Center in general coordination, epidemiological surveillance and environmental health.
C h a p t e r 3 - S u p p o r t i n g C o u n t r i e s t o R e s p o n d t o D i s a s t e r E v e n t s i n t h e H e a l t h S e c t o r
24
A n n u a l R e p o r t 2 0 0 8
Hurricane Ike passed over the Turks and Caicos Islands as a Category 4 hur-ricane, less than one week after Tropical Storm Hanna affected the islands in early September. In Grand Turk, an estimated 95% of houses had roof damage. The hos-pital in Grand Turk suffered damage in all areas, and 75% of the hospital was severely damaged. Authorities found it challenging to maintain the appropriate level of staff-ing, as the hospital staff themselves were victims of the storm. PAHO/WHO deployed an expert in water and sanitation following TS Hanna, who was later joined by a disaster specialist to provide sup-
port to the Hurricane Ike response. PAHO/WHO also mobilized health staff from other countries in the region to complement those in the Turks and Caicos.
Halfway through the 2008 hurricane sea-son, several Caribbean countries had already fallen victim to the destructive hurricanes Gustav, Hanna and Ike.
In Haiti, the situation became complex. In 2008, four hurri-canes and tropical storms struck the island (Gustav and Hanna within a two-week period). The city of Gonaives was completely flooded, affecting nearly 800,000 people, prompting the relocation of 80,000 to temporary shelters. The local health system was unable to function and services had to be delivered by mobile clinics. (See next section on complex disasters in Haiti for additional informa-tion.)
In the final stretch of hurricane season, persistent rains from tropical depressions resulted in widespread flooding and landslides. In Honduras, more than 300,000 people were affected and nearly 100,000 had no access to safe drinking water. PAHO/WHO pro-cured emergency and medical supplies and provided technical assistance in water and sanitation, disaster management and coordination of humanitarian aid, through the LSS/SUMA systems. In Belize, communi-ties were still flooded up to a month after the rains had passed. National authorities identified access to clean water as a major problem and asked PAHO/WHO to deploy an expert in water and sanitation to support the MOH in its response activities. PAHO also helped Belize reduce the risk of water-borne diseases by pro-viding essential supplies to disinfect drinking water reservoirs and household water storage containers and to train water authorities in quality monitoring.
January
February
March/April
May / June
July/August
September/October
November/December
25
January
February
March/April
May / June
July/August
September/October
November/December
Hurricane season officially ends each year at the end of November, and it is rare to see major hurricanes so late in the season. Hurricane Paloma was one of them. A powerful Category 4 storm with winds reaching 225 km/h (140mph), Paloma struck the Cay-man Islands and later lashed Cuba. Approximately 1.2 million people in Cuba (almost 11% of the population) were evacuated in anticipation of the hurricane. Another 220,000 were relo-cated to 1,448 shelters, while the rest were housed in the homes of relatives and friends. Three family doctor clin-ics and a pharmacy in the area were af-fected as well. Safe drinking water was a concern.
At the same time, parts of the Caribbean were also still experiencing wide-spread flooding as a result of heavy rainfall. Guyana’s capital, Georgetown, is
vulnerable to floods because of its low lying topogra-phy. In early December, 20,000 families were affected as communities along the east banks of the Demerara River and parts of Georgetown were flooded. Sanita-tion became a major issue, as latrines and septic tanks were all inundated. The Ministry of Health with the assistance of PAHO/WHO and the Caribbean Disas-ter Emergency Response Agency (CDERA) deployed field specialists to assess the situation and facilitate the response operations.
C h a p t e r 3 - S u p p o r t i n g C o u n t r i e s t o R e s p o n d t o D i s a s t e r E v e n t s i n t h e H e a l t h S e c t o r

26
A n n u a l R e p o r t 2 0 0 8
Complex Emergencies
Haiti
For many years, PAHO/WHO has worked with Haiti’s Ministry of Health to strengthen its disaster manamement capacity and improve health sector co-ordination, following the cluster approach. The cre-ation of decentralized emergency operations centers (EOCs) in the southern peninsula departments of Sud, Sud-Est, and Grand Anse was a major success for early warning and to reduce the impact of disasters on the already vulnerable population. Following this example, the Haitian Civil Protection (DPC) began to establish EOCs in departments previously without such Centers (Nord, Nord-Ouest and Artibonite). PAHO coordinated closely with the Civil Defense to ensure these new EOCs would be organized and set up in a similar manner. Training activities continued throughout 2008.
Hurricanes Fay, Gustav, Hanna and Ike – within a time span of just three weeks in August-September 2008 – once again demonstrated the incomparable ad-vantage of having trained and experienced health pro-fessionals in the country at the moment of a disaster. The Emergency Operations Centers were immediately activated and PAHO staff based in these departments coordinated the health response at departmental level,
providing information to the health cluster coordinator in the capital, Port-au-Prince. In addition to functioning as health information centers for each department, these EOCs also functioned as de facto multi-sectoral coordi-nation points. The health cluster coordinator analyzed and disseminated the infor-mation, first daily and later
three times per week, to health partners at the health cluster coordinators meeting and through a listserv es-tablished for health cluster partners. The health cluster met at PAHO/WHO’s office in Port-au-Prince, with more than 20 agencies providing information. This allowed the Ministry of Health and PAHO/WHO to have a better picture of what was really going on in the country. After the first month, the Ministry of Health hosted the Cluster meetings.
During the acute emergency phase, PAHO/WHO placed a disaster expert in Gonaives, who organized health cluster meetings and coordinated health re-
sponse with the principal health partner in Gonaives, Medecins sans Frontiere-Belgium. Work-ing with the Ministry of Health and the U.S. Centers for Disease Prevention and Control, surveil-lance forms were developed and distributed with a 24-hour phone number provided for outbreak early warning. PAHO/WHO and the Ministry of Health managed the investigations when neces-sary. Basic drugs were provided to a number of hospitals and a team was mobilized to clean the prison, where 240 inmates lived in shocking health conditions. Advice on the management of dead bodies was provide by a forensic expert who visited cemeteries and the private mortu-aries in Gonaives (107 bodies where already buried in rudimentary graves, only 20cm deep). The same expert visited Cabaret’s private mortuaries where he assisted with the management of cadavers.
Fuel shortages hampered the ability of the main hospitals in Cape Haitian (Justinien) and Fort Liberte to function; PAHO purchased 4,000 gallons of diesel through its office in the Dominican Republic. This fuel was sufficient to keep the two hospitals function-ing for thirty days. Fuel was also provided to MSF field hospital in Gonaives and some health clinics that were still functioning.
The process of creating Emergency Operations Centers demonstrated how difficult it is to keep phys-ical and human resources in Haiti, especially in the field (outside Port-au-Prince). The EOCs are difficult to staff and the risk of equipment disappearing is high. The EOC in Les Cayes was looted just before the first hurricane, and identifying qualified human resources for the EOCs became a bigger challenge following the disasters, as NGOs and other agencies competed for staff, leaving the Ministry of Health with no techni-cal staff.
Recognizing the difficulty of sustaining disaster preparedness and risk reduction activities and recog-nizing that our long-term objective is to have a fully functioning disaster management program in the Ministry of Health, PAHO/WHO will focus the next phase of its work in Haiti on disaster response and institutional readiness, which yield more immediate results and have direct live-saving results. PAHO/WHO will also promote the establishment of a health coordination response mechanism, under the chair-

27
manship of the Ministry of Health. This group would serve as the health cluster in case of a UN response and as the health preparedness group in non-crisis situations.
Colombia
PAHO continues to work with national and local health authorities to improve the health of internal-ly displaced populations (IDP) in Colombia and in neighboring countries. In 2008, activities were man-aged through five field offices in the departments of Norte de Santander, Choco, Valle del Cauca, Huila and Nariño. These five field offices cover a total of eight departments and foster collaboration with local authorities, international agencies, and NGOs.
From 2005 to 2008, a total of 1,115,408 persons were registered as IDP. During 2008, a total of around 359,000 persons were registered nationwide as IDP. Existing official registers show that in more than a decade, in Colombia, 2,760,808 people have been displaced, which is more than 6% of the country’s population.
During the past year, PAHO/WHO continued to hold regular Health Round Table meetings. A strat-egy developed at the beginning of the project, these “mesas” allow all health partners and stakeholders to discuss current issues related to displaced populations and exchange concerns and ideas. Once topics are dis-cussed, participants create a plan of action and assign responsibilities in order to ensure efficient response in any emergency that may affect IDP or refugees as well as a mechanism for follow up and evaluation.
In addition to regular activities, some of the spe-cific achievements in 2008 include:
• IncollaborationwiththeDepartmentofHealthofChocó, PAHO/WHO published the first epidemio-logical bulletin for Chocó including essential health
indicators and information captured by SIGA (the system for the management of health information). This bulletin is fundamental for decision-making and planning as well as for evaluating risks and the health status of populations in different municipalities. Chocó has the highest rate of poverty and some of the worst indicators for health in the country. This publica-tion not only includes vital health, demographic and poverty statistics, but also, demonstrates the affect of the armed conflict as Chapter 4 is devoted to populations in a state of displacement. The docu-ment is 142 pages, including many tables, and can be used as point of reference for the development of many activities and to monitor changes in the area. This effort serves as a baseline for future work and a cornerstone in order to construct the improvement in the health of the Chocó.
• PAHO/WHOcontinuestodisseminateandapplythe Access Route to Healthcare, a tool created at the beginning of the pro-gram to help IDPs under-stand how and where they can access health care. This tool is adapted according to the population (indigenous, afro-Colombian) and the lo-cation or department. In or-der to enhance sustainability and collaboration with local communities, a strategy is now being applied to create local community oversight groups called ‘comités de veeduría comunitario.’ Local leaders receive train-ing on the Access Route and volunteer to represent their community at meetings and trainings within municipalities and departments. The involvement of local leaders empowers communities by provid-ing them a voice and allowing them to be involved in processes that affect displaced populations direct-ly. Through this strategy, IDP can interact directly at meetings or trainings with health providers and other authorities or organizations to communicate and express concerns regarding their rights.
• RapidResponseTeams:ThecreationoftheEmer-gency and Immediate Response (ERI) teams rep-resents a significant advancement in strengthening local capacity for the evaluation of and timely re-
C h a p t e r 3 - S u p p o r t i n g C o u n t r i e s t o R e s p o n d t o D i s a s t e r E v e n t s i n t h e H e a l t h S e c t o r
28
A n n u a l R e p o r t 2 0 0 8
sponse to emergency and displacement situations. ERI’s are multidisciplinary teams composed of a doctor, nurse, water and sanitation expert, psy-chologist and others. At its onset, this initiative in-tended to support responses for only specific cases, however, progress has advanced and it has been pos-sible establish these teams more formally.
The National Immediate Response Team was cre-ated in order to respond to the needs for institutional strengthening in the event of complex emergencies resulting from mass displacements or during other emergencies. The National ERI provides technical support to local levels when needed as well as promotes standardized protocols and procedures. It ensures that various institutions communicate and respond ef-fectively to the different phases of the emergencies. Given the constant increase of mass displacements in the different areas of the country, PAHO/WHO pro-motes the initiative to have ERIs on a regional level. To date, 6 Immediate Response Teams have been cre-ated at the regional level. Immediate response teams are now being formed at the municipal level as well.
• Commission on Water, Sanitation and Hygiene(CASH): During the last year, PAHO/WHO, in collaboration with the Government of Colombia, International Organizations, universities, the pri-vate sector and other UN Agencies, has promoted the creation of Technical Working Groups. One working group that was created was the Commis-sion on Water, Sanitation and Hygiene. CASH’s purpose is to contribute to the strengthening of risk management in water, basic sanitation and hy-giene, favoring inter-institutional work directed at the most vulnerable communities and/ or in acute crisis situations. PAHO/WHO provided material on water and sanitation in emergency situations to CASH. This working group is essential given that a study of gaps (2006-2007) in healthcare for dis-placed populations showed that water quality is one of the areas with major needs.
Epidemics
Yellow Fever Outbreak in Paraguay
Epidemics as well as natural disas-ters require a coordinated response. An outbreak of yellow fever in Para-guay required an important mobili-zation of national and international resources. By the end of March 2008,
26 cases were con-firmed; of these, eight people died and seven were hos-pitalized. PAHO/WHO organized the procurement of almost 3.5 mil-lion doses of yel-low fever vaccine from neighbor-ing countries and from WHO’s global stock of yel-low fever vaccine and by mid-March 2008, more than 1.5 million people in at-risk areas, in-cluding along the border with Brazil, Bolivia and Argen-tina, had been vac-cinated, which in some departments, reached a 95% coverage rate. Vec-tor control activi-ties were coordi-nated to fumigate infected areas and destroy breeding grounds. The plan was successful in reducing larva in-festation to refer-ence levels for con-trolling the spread of the disease.
Health situation rooms are set up to collect and update information on emergency situations, there-by enabling authorities to make decisions based on the most reliable data. PAHO/WHO provided sup-port to national authorities in Paraguay to produce a variety of information products, including situation
reports and epidemiological bulletins. A committee was ap-pointed to follow up confirmed cases of yellow fever. PAHO/WHO also organized a number of workshops to update medi-cal staff on the timely diagnosis and treatment of patients in-
Y ellow fever is caused by infection with yellow fever virus, which is transmitted
by the bite of infected mos-quitoes. Jungle yellow fever is mainly a disease of monkeys. It is spread from infected mosqui-toes to monkeys in the tropical rain forest. People get jungle yellow fever when they are bitten by mosquitoes that have been infected after feeding on infected monkeys. Jungle yellow fever is rare and occurs mainly in persons who live or work in tropical rain forests.
Urban yellow fever is a disease of humans. It is spread by mosquitoes that have been infected by other people. Aedes aegypti is the type of mosquito that usually carries yellow fever from human to human. These mosquitoes have adapted to living among humans in cities, towns, and villages. Their larvae grow in discarded tires, flower pots, oil drums, and water stor-age containers close to human dwellings. Urban yellow fever is the cause of most yellow fever outbreaks and epidemics.
Source: U.S. Centers for Disease
Prevention and Control
What is Yellow Fever?
29
fected with yellow fever. The confirmation of cases of yellow fever requires a laboratory diagnosis, and laboratories—a critical part of the health services network—were over-extended. PAHO/WHO do-nated reagents and equipment which helped to re-duce the time needed to obtain the test results.
Concurrently, treatment protocols were published and disseminated through a variety of means to reach the largest number possible of health workers. Community participation was critical to controlling the disease: eliminating breeding grounds, spraying in and around their homes; a willingness to be vac-cinated and learning to recognize the symptoms of the disease and to seek help quickly. PAHO/WHO worked with regional health specialists in risk com-munications to develop a communications plan to achieve the desired impact.
The Regional Health Emergency Response Team
Members of the Regional Health Emergency Re-sponse Team were deployed to most disasters in the re-gion, albeit sometimes in limited numbers, depending on the magnitude of the situation. Epidemics as well as natural disaster required active support from the team and PAHO/WHO.
Despite the fact that sometimes countries are able to manage disaster situations on their own, international pressure and visi-bility given to the situation in the media can result in deployment of international staff to support the various coordination mecha-nisms in place at national level. For ex-ample, the Emergency Response Team was deployed twice to Bolivia, despite the fact that during the April 2009 flood, regional authorities in Beni knew very well how to deal with the situation. However, the influx of external actors made coordination much more difficult. On the other hand, deploy-ment of the Emergency Response Team to Haiti was essential, not only for coordina-tion issues but also to implement activities related to the health sector
In 2008, training was conducted to in-corporate epidemiologists into the Health Emergency Response Team. The team con-sists of medical epidemiologists, clinicians and disaster specialists that would respond
to any health emergency in the Americas, includ-ing suspected human cases of avian influenza or pandemic influenza. Participants were drawn from Ministries of Health and PAHO offices from South and Central Amer-ica and the Caribbean. The establishment of such a regional team is one of the activities in support of the International Health Reg-ulations (2005) which came into effect in 2007. These regulations are a body of laws designed to help the world remain alert and ready to respond to the challenge of epidemics and pandemics brought about by emerging and reemerging infectious diseases and by the increasing movement of persons and goods in an era of globaliza-tion. Compliance with these modern regulations will ensure that the world is not taken by surprise when out-breaks occur and that disruption to travel, commerce, and business activities are minimized.
Other response team training included the incorpora-tion of a group of persons trained in risk communica-tions (see box) and health logistics—a specialty that is still not fully recognized by the Organization. For Haiti, WHO/HAC provided the support of an extra logistics specialist.
M ore than two decades ago, PAHO/WHO member states asked the Organization to create a Regional Emergency Response Team composed of experts with varied backgrounds in public health and disasters. Although health communicators had
accompanied the Response Team on an ad hoc basis, PAHO/WHO recognized the need to formally incorporate communications and media experts to act as a bridge between technical and public information in emergency situations and to clearly demonstrate the health impact of disasters.
In 2008, experts in the field of communications and information management (includ-
ing journalists) came together to review and approve procedures, methodologies, tools
and strategies for communications and information management in emergencies.
The 25 participants took part in an earthquake simulation exercise designed to bring to
light the political and technical challenges that unfold in the aftermath of many large-scale
emergencies, many of which can be resolved with well-developed communications and
information management strategies. They also reviewed and made recommendations to
improve guidelines on communications and information management in emergency situ-
ations. Once all recommendations are consolidated, these guidelines will be published and
incorporated into the PAHO/WHO Emergency Response Team Manual.
Communications Expert Incorporated into Response Team
C h a p t e r 3 - S u p p o r t i n g C o u n t r i e s t o R e s p o n d t o D i s a s t e r E v e n t s i n t h e H e a l t h S e c t o r

30
A n n u a l R e p o r t 2 0 0 8
Support for managing humanitarian assistance and lo-gistics will continue as an important subset of the Health Emergency Response Team. Team members were de-ployed to most disasters in the Region which involved the mobilization of humanitarian aid. Although LSS/SUMA (the Logistics Support System) is well-known in the Americas, more and more requests are received from other regions, such as WHO’s Eastern Mediterra-nean Regional Office for courses or deployment of the SUMA experts to Tunisia or in support of the conflict in Gaza. Most requests originate in the countries or from WHO offices and until now, despite verbal support from OCHA, no training or post-disaster action was requested by OCHA or another UN agency. However, on a posi-tive note, NGOs such as World Vision and the White Helmets use LSS/SUMA in their response operations.
WHO held its fifth Public Health Pre-Deployment (PHPD) Course in Canada, organized together with PAHO/WHO and sponsored by the government of Canada. The course helps to prepare public health and other professionals, who are already experts in their specific fields or experienced in emergency settings, to work effectively and safely in emergency and crisis situ-ations. In this particular course, emphasis was given to crises situations that could affect countries in Latin America and the Caribbean, and placed in the context of how emergency response mechanisms at various lev-els complement to address priority public health needs of affected populations. Over 25 participants attended the course, including 12 persons from the region of the Americas. The course was extremely well received and some of the participants will be included into the PAHO regional response team. Two persons from South Amer-ica also attended the WHO Health Cluster coordination course organized by WHO in Tunisia. They will serve as important reference facilitators when a similar course is organized in the Americas in Spanish.
PAHO/WHO Headquarters Emergency Operations Center
The Headquarters’ Emergency Operations Center provides the physical environment for staff from several technical departments in PAHO/WHO to work togeth-er to provide the Organization and Member States with accurate and timely information on public health events. In disaster/crisis situations, the EOC leads the Organiza-tion’s operational emergency response and can operate 24 hours a day/7days a week. It is monitored remotely in normal times.
The EOC has various functions as part of its ongoing activities, including monitoring, alert, and risk assess-
ment. In the event of an emergency, it will oversee the organization’s disaster response, response management and coordination and logistics in support of deployment of technical teams, equipment and supplies to the field. Underpinning this work, the EOC has other functions of readiness and training, liaison, reporting and informa-tion dissemination and knowledge management.
Although mentioned elsewhere in this report, sev-eral emergencies in 2008 highlighted the importance of the PAHO/WHO’s EOC in support of disaster response ef-forts. As the Gov-ernment of Paraguay faced the outbreak of yellow fever in the ur-ban area, the ensuing high demand for vac-cines, immunization services, investigation and treatment of cas-es, and environmen-tal sanitation coordi-nation required that all the resources of PAHO be called into play, from a direct ap-peal for vaccines from neighboring countries and the world stock-pile in France, to the deployment of highly specialized technical experts to the field and the establishment of a national emer-gency team to assist the government in crisis management and logistics. The EOC deployed a crisis management team to the country and provided daily reports on the progress of the event in headquarters.
In August, the EOC participated in a multi-agency simulation exercise, CONVEX-3, which was organized by the International Atomic Energy Agency (IAEA). Under the technical leadership of the PAHO/WHO focal point for Radio-nuclear Medicine, the EOC was activated and provided technical support to the exercise with the preparation of situation reports and briefings. During the exercise, the focal point for the International Health Regulations (IHR) was based at the EOC to in-tegrate information received from that system with other communications.
31
During the five-week period that the Caribbean was hit by four hurricanes which caused severe damage to several countries, Haiti was the hardest hit with over 600 deaths and the flooding of the city of Gonaives and destruction of one its hospitals. Cuba sustained massive damage to agricultural lands, buildings and infrastruc-ture; however, the government evacuated more than 2 million people with little loss of life. The Dominican Republic also sustained agricultural damage and some infrastructure loss. The only hospital in Grand Turk Is-
land, in the Turks and Caicos Islands, was significantly damaged and the island sustained flooding. During this period, the Emergency Operation Center received and collated information on the various storms and damages and provided constant information on the various coun-try situations and the response of the organization. It or-ganized briefings of the Disaster Task Force and hosted a special ambassadors briefing for the OAS and other agencies that support humanitarian relief.
C h a p t e r 3 - S u p p o r t i n g C o u n t r i e s t o R e s p o n d t o D i s a s t e r E v e n t s i n t h e H e a l t h S e c t o r
32
A n n u a l R e p o r t 2 0 0 8
33
Forging Stronger Partnerships at National, Regional and Global Level
Chapter 4
PAHO’s Strategic Direction for Disaster Preparedness and Risk Reduction
For many decades, PAHO was one of the few international health sector actors working in emer-gencies and disasters in the Americas. However, this situation has changed dramatically in recent years, requiring greater outreach work with international development partners and humanitarian agencies, ranging from regional disaster management bodies, to donors and UN agencies, while being mindful of our underlying mandate to support the national capacity of the health sector in Member States.
In 2008, PAHO initiated a new five-year plan-ning cycle for disasters and emergencies. One of the first tasks was to clearly communicate our goals and strategy to our partners. In response to the evolving regional scenario and drawing on lessons gleaned from past experiences, the new five-year Strategic Plan addressed two broad aspects of disaster manage-ment. The first related to disaster risk reduction,2 the development side of our technical cooperation, which involve both day-to-day and long-term activities. The
second is related to humanitarian response aspects of technical cooperation that requires lean, fast, and flexible mechanisms for short-term but effective inter-ventions. The Strategic Plan defines PAHO’s overall corporate strategy for enabling the health sector to reduce risk, prepare for and respond to disasters and emergencies, while at the same time creating a body of knowledge and lines of action that also benefits the health sector beyond this Region.
The preparation of the 2008-2012 ‘Strategic Plan for a Secure and Di-saster-resilient Health Sector’ coin-cided with PAHO’s organization-wide Strategic Plan 2008-2012 (approved by Member States in October 2007), which reflects an even greater level of commitment to disaster risk re-duction. The fact that this topic has become a collective responsibility of many technical divisions and country office programs was due, in part, to the establishment of a high-level stra-tegic objective by the World Health Organization.3
2 For PAHO, “disaster risk reduction” refers to actions aimed at reducing the hazard, the vulnerability or both. It encompasses prevention and mitigation. ‘Disaster management’ covers the full range of interventions: prevention, preparedness, mitigation, response, recovery and reconstruction. Although this is not the ISDR definition, PAHO uses disaster risk reduction in this sense due to the characteristics of its clients.
3 Strategic Objective 5 (SO5): ‘To reduce the health consequences of emergencies, disasters, crises and conflicts and minimize their social and economic im-pact’; Strategic Plan of the Pan American Health Organization 2008-2012. October 2007

34
A n n u a l R e p o r t 2 0 0 8
In April, 2008, PAHO convened a meeting of high-level experts (including Canada and the U.S.) to look at changes in the humanitarian environment in Latin America and the Caribbean and discuss their implica-tions on regional institutions. A number of impor-tant recommendations stemmed from this meeting on issues ranging from changes in funding patterns to humanitarian response vs. recovery to the UN hu-manitarian reform and the Cluster mechanism. The background document prepared to guide this meeting and the excellent recommendations put forth by the high-level group of experts is attached in Annex 9.
Ultimately, this expert body endorsed PAHO’S new ‘Strategic Plan for a Secure and Disaster-resilient Health Sector,’ which will govern the Organization’s wide ranging involvement in disaster preparedness, risk reduction and response. See Annex 10.
Partnerships in Training
Training for Public Health Deployment in Disasters and Emergencies
Although most countries have national, inter-country and regional response mechanisms, often international assistance is still required. In emergen-cies and disasters, the humanitarian community needs an adequate pool of qualified and experienced health professionals, armed with public health knowledge and skills and trained to support countries.
To meet this need, WHO offers annual (and sometimes biannual) Public Health Pre-Deployment
(PHPD) courses. The purpose of the course is to prepare professionals with knowledge and experience in a variety of public health and related fields to work effectively in the design, imple-mentation, management and/or coor-dination of emergency response and early recovery. The Canadian Interna-tional Development Agency support-ed the 2008 course, which was held in Ontario, Canada. It was delivered by a
pool of experienced humanitarian and health experts, drawn from member states, the UN system, academic and technical institutions and NGOs and PAHO pro-vided a number of instructors as well as participants from the Americas (see agenda in Annex 11). PAHO was also responsible for the organization of the course, which provided an important complement to the UN Disaster Assessment and Coordination (UNDAC)
training conducted by OCHA for humanitarian gen-eralists, and to the Health Cluster Field Coordinator training (see below).
The intensive two-week residential course helped participants (half of whom were from this Region) to understand the health sector’s core functions in emer-gencies, and the principles and approaches needed to assist national/local authorities to address health priorities through a coordinated and all-inclusive sec-toral/cluster approach.
Deployment of Experts from LAC to other Regions
A World Health Organization/World Bank team was deployed to Sichuan Province, China after the May 2008 earthquake. The multisectoral team, which was led by a for-mer PAHO/WHO disas-ter specialist and included a member of DiMAG, pre-pared a report setting forth a number of recommendations for the public health system, health services and infrastructure. The recommendations called for public health programs serving populations in the earthquake-affected areas to be fully financed with public funds, and to take into account the chang-ing population profile, including the major diseases and disabilities. It was also recommended that stake-holders involved in the health system reconstruction have access to data in order to improve coordinated care, monitoring and evaluation. Preparedness plans developed for the health sector (and beyond) must have an all-hazards approach and be tested through drills and exercises. Individual and community-based mental health services must be provided to the affect-ed population and earthquake responders.
Early retrofitting or reconstruction of primary health facilities (i.e. village health stations/clinics, township health centers) should be given top priority, and the reconstruction strategy should keep in mind the needs at the county and provincial levels. For ex-ample, some facilities and laboratories could be closed or merged to reduce unnecessary competition and re-dundant spending, and to focus on service provision. Robust needs assessments of healthcare, damages to health facility infrastructure and functions, and the

35
C h a p t e r 4 - F o r g i n g S t r o n g e r P a r t n e r s h i p s a t N a t i o n a l , R e g i o n a l a n d G l o b a l L e v e l
health workforce should be carried out in a timely fashion to inform planning. Strategies should provide a bridge between the emergency phase and the recon-struction phase and should also address the environ-mental impact of clinical waste in the transitional pe-riod and during the planning of new facilities.
Several key recommendations fell closely in line with policies suggested by PAHO for many years un-der its ‘Safe Hospitals’ initiative (which most of the member states are carrying forth). For example, it is important that existing and planned health facilities recognize the special requirements hospitals have (in-cluding essential infrastructure such as water supply, communications, electricity and transport) and em-brace the PAHO/WHO ‘Safe Hospitals Initiative’, which requires hospitals (especially secondary and tertiary facilities) to remain functional after earth-quakes. The creation of a technical working group to advise the construction or relocation of future health infrastructure is recommended as well as employing independent reviewers (review consultants) for the design of all healthcare facilities (modeled on the DiMAG—see Chapter 2). For existing health facili-ties in Sichuan and the rest of China, it is important to carry out vulnerability assessments, and consider using the PAHO/WHO Hospital Safety Index (see Chapter 2).
Collaboration among national, regional and international actors
PAHO’s ongoing work with governments in the Region places the Organization in a unique position to take advantage of opportunities and initiatives at the global and regional level and to support the main-streaming of health issues into broader overall disaster management structures. The following initiatives il-lustrate this.
U.N. Humanitarian Reform and the Cluster initiative
The UN Cluster approach is implemented to co-ordinate all actors working in a certain field such as health, following a large-scale disaster. The issue of the Cluster mechanism and its importance to coun-tries in Latin America and the Caribbean has gener-ated significant discussion. Countries in this Region and PAHO have noted that it is important to avoid a negative impact on national institutions in situations where the humanitarian reform is implemented with-out consultation or adjustments in the most advanced
of developing countries. In addition, under the hu-manitarian reform, the lead responsibility for health is disaggregated into four distinct Clusters. In LAC, there are definite advantages as well as precedents for consolidating the number of the health-related Clus-ters, according to the structure and role of the Minis-try of Health.
Clusters are headed by the UN agencies, who are members of the U.N. Inter-Agency Standing Com-mittee and at the end of 2008, two PAHO staff at-tended the training for future leaders of the health cluster should it be activated in this Region. This was an important opportunity, as it has provided the ini-tial entry point to gain a clearer understanding of the implication of the mechanism and to share with other experts the content and methodology. This also pro-vided a clearer understanding of the U.N. humanitar-ian reform and WHO’s expected role as lead cluster agency. See summary of duties and qualifications for health Cluster leads in Annex 12.
International Day for Disaster Reduction
Each year, the world marks the International Day for Di-saster Reduction on the sec-ond Wednesday in October. Because the theme of the cur-rent World Disaster Reduction Campaign is “Hospitals Safe from Disasters”, global celebra-tions of this day focused on protecting critical infrastruc-ture such as health facilities. The PAHO/WHO disaster of-fice in Panama partnered with the UN International Strategy (whose regional office for the Americas shares office facilities with PAHO/WHO in Pana-ma) launched a photography contest and engaged in outreach activities with regional hospitals and health facilities.
PAHO collaborated closely with the UNISDR to mark the global celebration of the International Day for Disaster Reduction at the UN Headquarters in New York, where the occasion was marked with a high level panel discussion (including the participation of the Governor of the British Virgin Islands who spear-headed the country’s preparation of a national disaster plan) for UN Ambassadors and the launch of a global web site (see following section.) Coincidentally, the

36
A n n u a l R e p o r t 2 0 0 8
International Day fell on the third anniversary of the massive 2005 South Asian earthquake that devastated an entire region of Pakistan.
Technical information and resources“How to make Donations” Initiative
The issue of good donations is of concern to many agencies and countries. A scenario in which large quantities of humanitarian relief arrives in a disaster-affected country, only to create a second disaster, is
common. In addition to technical and logistical problems, the situa-tion is further complicated by dona-tions that are inappropriate or arrive too late to meet the real needs of the disaster victims. This is recurrent and widespread in emergencies and therefore requires an interagency, multidisciplinary and participatory approach. To help solve this problem, PAHO led an interagency group4 to develop a campaign on Good Prac-tices in International Donations: public awareness and advocacy for the media and donor community.
The pilot initiative focused on four countries in the region which recently experienced emergency situations or significant disasters: Guatemala, the Do-minican Republic, Peru and Ecuador and produced information designed to influence three target groups: (1) national and international media, (2) embassies in donor countries and international organizations and (3) authorities in countries receiving aid, primarily ministries of foreign affairs, civil defense, ministries of health and others. The purpose is not to establish regulations or international standards, but rather to promote and disseminate practical guidelines to up-date or improve existing national guidelines and stan-dards in this field.
By the end of 2008, the information produced was all available on a Spanish-language web site called SaberDonar (Know How to Donate -- www.Saber-Donar.info), including a brief guide that summarizes general principles of donations in different sectors; a public information kit on how to both provide and receive more effective donations; and posters. Com-munication among partners and target groups took
place electronically, via the Internet, e-mail and on the web, using social networking tools.
Given that it is not the exclusive problem of one agency, country or disaster, and that it is a recur-rent common problem in many emergencies, this work took on an inter-agency, multi-disciplinary and participatory approach. Under the coordination of PAHO/WHO, an inter-agency group was estab-lished which applied the same approach, time-frame and main objectives of the campaign and was made up of the following agencies: OCHO, INTERMON/OXFAM, the International Federation of Red Cross and Red Crescent Societies (both the regional office and the Disaster Response Unit for the Americas), the World Food Programme (WFP) and the Regional Di-saster Information Center (CRID), with the financial support of the Spanish Agency for International De-velopment Cooperation (AECID).
The following products were produced:
• Ashortpublicationentitled“HowtomakeDona-tions: practical recommendations for Humanitar-ian Donations” received technical input from all agencies. Printing and distribution of the guide was also collective work: PAHO printed 1,000 copies, but OXFAM and the WFP have each printed an-other thousand copies with their agencies’ funds. The guide has been translated into English and publication in English will be funded by the In-ternational Federation of Red Cross and Red Cres-cent Societies.
• Postersandshortradiospotsinwhichclear,practi-cal messages are summarized about good practices for humanitarian donations (these can be seen via the Radio Network on the web at http://www.ra-dioteca.net/verserie.php?id=5209. A short video on the same issue is on the website at http://www.saberdonar.info/materiales.php.
• Thewebpagewww.Saberdonar.info was launched to promote the information produced and allow users to download all materials produced for the campaign, as well as offer links to other information sources and resources (in English and Span-ish) about donations
4 The members of the interagency group are of PAHO/WHO, INTERMON/OXFAM, PADRU/IFRC, OCHA, UNICEF, WFP, the CRID, The Communi-cation Initiative and the Alas Foundation, with the support of the Spanish International Cooperation Agency.

37
C h a p t e r 4 - F o r g i n g S t r o n g e r P a r t n e r s h i p s a t N a t i o n a l , R e g i o n a l a n d G l o b a l L e v e l
and humanitarian assistance which make up a practical information kit on the subject.
The issue of humanitarian donations was also the focus of work in the Andean Region. The An-dean Disaster Prevention and Response Committee (CAPRADE), which is part of the Andean Commu-nity, worked with PAHO and the International Fed-eration of Red Cross and Red Crescent Societies to publish guidelines on the topic. The Andean Region has a sustained and successful track record working on these issues. Several years ago, the Andean Region Council of Ministers of Foreign Affairs approved an Andean Strategy of Disaster Prevention and Re-sponse. One of the five strategic lines was promot-ing mutual assistance in disaster situations – a policy which PAHO has supported for years for the health sector and which now has become mainstreamed into the policy of multisector agencies.
Global Website Highlights Regional Achievements
As mentioned in Chapter 2, “Hospitals Safe from Disaster” website was re-launched in 2008 (http://safehospitals.info/) to coincide with the Interna-tional Day for Disaster Reduction. The website was transformed into a truly global website on the issue in terms of outlook and content, becoming a global vehicle for change and information on making health facilities safe from disasters. A key strategy of the new site is to aggregate, link up, and promote the work and online resources of a variety of partners in one convenient location, including each of the six WHO Regional Offices as well as the ISDR and its regional focal points. Regions now have access to the site and autonomy to upload material of their choice in the languages they prefer it to appear. (By the time of the relaunch, selected key site content, including naviga-tion buttons, were available in English, French and Spanish). The aim is for some material to be available online in each of the six official UN languages. At the conclusion of the two-year World Disaster Reduction Campaign (December 2009), PAHO will continue to manage and run the site.
Mainstreaming disaster preparedness and risk reduction across institutional partners
The goal of disaster risk reduction is to ‘disaster-proof ’ the development process. To reach this goal,
the health sector itself must take disaster risk into ac-count in all aspects of its planning, design, investment and operational activities. It is equally as important that international and regional partners recognize the importance of and take steps to reduce disaster risk in the health sector through their own development and humanitarian activities.
Following are some examples of mainstreaming disaster preparedness, risk reduction and response across the work of PAHO’s other technical divisions and with national and international partners:
• CEPREDENAC,theCenterforDisasterPreven-tion in Central America is an inter-governmental body and part of the Central American Integration System (SICA). CEPREDENAC developed proce-dures to improve the coordination of humanitarian aid in disaster situations among member countries and is promoting the use of the PAHO-led Logis-tics Support System (LSS/SUMA) as the standard for management of international assistance.
• IntheCaribbean,thehealthdisastercoordinatorsfrom the Ministries of Health initiated contribu-tions to the development of a comprehensive di-saster management strategy at country level. This stragegy is being spearheaded by the Caribbean Di-saster Response Agency (CDERA), CARICOM’s specialized disaster management agency.
• RESSCAD is themeeting of healthministers inCentral America and the Dominican Republic. RESCAAD is responsible for the Health Agenda for Central America and the Dominican Republic 2009-2018, which is a collective roadmap to im-proving regional health conditions. The Agenda lays out 10 strategic objectives for political action, around which plans are drawn up and resources assigned (both regional and international). One of the 10 strategic objectives is to reduce vulnerability to natural and manmade disasters and the effects of climate change. (See Annex 13).
• In emergency situations, theboundaries betweenthematic responsibilities are often blurred. On the positive side, this contributes to mainstream-ing of many aspects of disaster management and contributes to coordination. At international lev-el, although PAHO/WHO is the Cluster lead for health issues, UNICEF is responsible for water and sanitation. Despite this division of labor between organizations, the two clusters must and do work closely in emergency management and response.

38
A n n u a l R e p o r t 2 0 0 8
• ThesameistruewithinPAHO/WHO.TheAreaon Sustainable Development and Environment (SDE) is traditionally responsible for water and sanitation. However, some experts from this tech-nical area serve as PAHO/WHO disaster focal points throughout the Americas, contributing to improving national capacity in emergency plan-ning and preparedness and to guaranteeing access to safe drinking water and sanitation for millions of people. In 2008, these two technical areas de-veloped a joint plan of action and held two work-shops to provide the technical content needed for SDE staff to serve as national emergency focal points and to contribute to regional disaster pre-paredness and response efforts, particularly in the context of the UN Humanitarian Reform. Strate-gies were also developed to increase the participa-tion and input of PAHO’s SDE experts when the WASH Cluster is activated in Latin America and the Caribbean and to increase their involvement in all aspects of risk management.
• ImprovingthecapacityofPAHO/WHOcountryoffices to contribute to the management of health aspects of disasters was an important focus in 2008 in Central America. The PAHO/WHO Offices in Honduras and Costa Rica held training workshops that included a simulation exercise, using a flood
scenario that required the activation of PAHO plans and procedures to assist the ministries of health. Thanks to the exercise, the offices real-ized they needed to update their emergency plans. The exercises also pointed out the need for PAHO to review many of its formal standard operating procedures—a lengthy process that was initiated in 2008. Later in 2008, widespread flooding hit Costa Rica and Honduras and country offices suc-cessfully implemented their revised country plans, which proved to have improved most processes at national level for the mobilization and/or purchase of resources and goods to support the affected countries.
The success drawn from old and new partnerships as well as the collaborative activities implemented throughout 2008 demonstrate that working with ac-tors at the local, national and international level is essential when preparing countries for disasters and responding to emergencies. Whether it’s improving donations or enhancing the capacity of countries and the international community to respond, PAHO/WHO will continue to strengthen current relation-ships and foster new partnerships in order to reduce the risk in the health sector to emergencies and disasters.
39
Annex 1 ................Report of the meeting of Caribbean health disaster coordinators
Annex 2 ................Health Sector Disaster Management Self-Assessment Tool
Annex 3 ................PAHO/WHO White Paper on climate change, prepared for the 48th Directing Council of the Pan American Health Organization, October 2008
Annex 4 ................Workshop on the elderly in disaster situations
Annex 5 ..................Resolution CSP 27.R14, Pan American Sanitary Conference, October 2007
Annex 6 ..................Safe Hospitals Checklist
Annex 7 ..................New wind hazard maps developed for Caribbean islands and nearby coastal areas of Central and South America
Annex 8 ..................Contents of the DVD-based Virtual Tour of a Safe Hospital
Annex 9 ..................Consultation on Global Humanitarian Trends and their Implications on Institutions in Latin America and the Caribbean
Annex 10 ...............PAHO Strategic Plan 2008-2012 for a Secure and Disaster-Resilient Health Sector
Annex 11 ...............Public Health Pre-deployment Course
Annex 12 ...............Duties and qualifications of humanitarian health Cluster leads
Annexes

40
41
ACINDESCANDHICAPRADECARECCARICOMCDCCDERACDMCEPREDENACCERFCETESBCIDACREDCRIDDFIDDiMAGEARECATECHOEDANEOCFLACSOIACNDRIDBIDP
Argentinian Association for Health Research and DevelopmentCentral American Network for Disaster Health InformationAndean Committee for Disaster Prevention and AssistanceCaribbean Epidemiology CenterCaribbean Community SecretariatU.S. Centers for Disease Control and PreventionCaribbean Disaster Emergency Response AgencyCaribbean Disasters Management FrameworkCoordination Center for Natural Disaster Prevention in Central AmericaCentral Emergency Response FundEnvironmental Health Technology Company (São Paulo, Brazil)Canadian International Development AgencyCenter for Research on the Epidemiology of DisastersRegional Disaster Information CenterUK Department for International DevelopmentDisaster Mitigation Advisory GroupEpidemic Alert ResponseEmergency Care and TreatmentEuropean Commission’s Humanitarian Aid Office Emergency Damage and Needs AssesstentEmergency Operations CenterLatin American Social Sciences FacultyInter-American Committe for Natural Disaster ReductionInter-American Development BankInternally Displaced Population
Acronyms
42
A n n u a l R e p o r t 2 0 0 8
IFRCIHRINDECIISDRLEADERSLSSMCMMERCOSURMoHMOUNGOOASOCHAOPDEMOFDAPADFPAHOPHCPEDPHEICPREDECANPWRREDLAC
REMSAARTASELASESPASSINAPREDSUMAUNUNDACUNDPUNHRDWFPWHO
International Federation of Red Cross and Red Crescent SocietiesInternational Health RegulationsPeruvian Civil Defense InstituteInternational Strategy for Disaster ReductionInternational Course for Managers on Health, Disasters and DevelopmentLogistics Support SystemMass Casualty ManagementSouthern Common MarketMinistry of HealthMemorandum of UnderstandingNon-governmental OrganizationOrganization of American StatesUN Office for the Coordination of Humanitarian AffairsOffice of Disaster Preparedness and Emergency Management (Jamaica)Office of U.S. Foreign Disaster AssistancePan American Development FoundationPan American Health OrganizationPrimary Health CareArea on Emergency Preparedness and Disaster ReliefPublic Health Emergencies of International ConcernDisaster Prevention in the Andean CommunityPAHO/WHO RepresentativeRisk, Emergency, and Disasters Task Force of the Regional Inter-Agency Standing Committee for Latin America and the CaribbeanMeeting of the Andean Region Ministers of HealthRegional Trade AgreementLatin American Economic System Public Health and Social Services Secretariat (Dominican Republic)National System for Disaster Prevention, Mitigation and Response (Nicaragua)Supply Management SystemUnited NationsUnited Nations Disaster Assessment and Coordination TeamUnited Nations Development ProgramUnited Nations Humanitarian Response Depot (under the WFP)World Food ProgramWorld Heatlh Organization
ANNEX 1
13th Health Disaster Coordinators Meeting
SUMMARY REPORT
Kapok Hotel, Trinidad1 – 3 July 2008
Summary Report of the 13th Health Disaster Coordinators Meeting
Page 2 of 25
1.0 Executive SummaryDuring the first three days of July 2008, PAHO/WHO met with health disaster coordinators from Caribbean Ministries of Health in Trinidad. The thirty nine participants includingrepresentatives from 22 countries examined a number of issues crucial to the region. Theseincluded the Impact of Climate Change in Caribbean Countries, Disease Surveillance in Disasters, Regional Coordination Mechanisms for Health and Pandemic Influenza. The recently launched Wind Hazard Maps for Caribbean Islands and nearby coastal areas of Central and South America was also featured as was the Safe Hospital Initiative in the Caribbean.
The countries agreed to the following common work plan to be implemented over the next year, with technical support from PAHO/WHO. It was also agreed that country representatives and PAHO/WHO will report on the progress made in implementing activities, during the 2009 HDC meeting.
National Level Sub-regional Level (PAHO)Preparedness - review and update national health
sector disaster plans- conduct at least one simulation exercise (drill or desktop)- identify two issues that need improvement (plan/simulation)
- develop an outline for the inclusion of elderly in the health disaster plan- advance the development of the health sector disaster preparedness self assessment tool
Mitigation - apply the safe hospital checklist in at least one hospital- implement safety improvement measures in those hospitals that applied the checklist
- conduct at least three trainings on the use of wind hazard maps- conduct training on the application of the safety index
Response - form a outbreak containment team- strengthen the regional emergency response team by identifying two persons as potential members (expertise: epidemiology, water and sanitation, communication, logistics, health services)-
- develop protocols for containment of epidemiological outbreaks- train new members of the regionalemergency response team
Partnerships - establish links and formalize agreements and partnerships for disaster risk reduction- contribute to the development of comprehensive disaster management at country level-
- mobilize resources to support country level disaster risk reduction initiatives
A training schedule for MCM/ICS, ECAT and LSS courses was also developed based on requestsfrom the countries. PAHO/WHO agreed to support these activities by providing instructors and course material.
PAHO/WHO has brought the coordinators together in these meetings annually since 1995. Theyprovide a forum for consultation and priorities setting on health disaster management in the region.
Summary Report of the 13th Health Disaster Coordinators Meeting
Page 3 of 25
2.0 Meeting ObjectivesThe 13th meeting of health disaster coordinators (HDC) for the Caribbean Sub Region was convened with the objective of reviewing developments and performances in the last year, and identifying main areas of cooperation in health disaster risk reduction in the Caribbean for 2008-2009.The specific objectives were to:
1. Provide participants with information and tools for strategic
management, advocacy and leadership in health disaster risk reduction
2. Share relevant risk, hazard and emergency-related experiences, promote
networking, and introduce robust coordination mechanisms at the sectoral,
national, regional and international levels
3. Introduce participants to the concepts, mechanisms and issues involved in risk
identification, management and reduction at the sectoral and national levels.
The meeting was successful in achievement of its overall objective. In fact, the countries and PAHO/WHO agreed to a minimum set of activities to be implemented at the national and sub-regional levels over the next year, in the areas of preparedness, mitigation, response andpartnerships. The specific objectives were also achieved to varying degrees. Objective #1 could have had greater achievement via the provision of more tools for advocacy and leadership, and objective #3, with more discussions on the issues involved in risk management.
3.0 Meeting Organization and ParticipantsAs indicated on the agenda (annex 1), the meeting utilized a mixture of approaches towards achievement of its objectives, that of technical presentations, sharing of country case studies, group work/plenary and a desktop simulation exercise. This structure was adapted in keeping with recommendations from HDC meeting 2007.
With multidisciplinary and multinational representation, the meeting was successful in its reach. Twenty two countries were represented and there were 39 participants who included healthdisaster coordinators, PAHO/WHO disaster focal points and resource persons (annex 2). The need for easily accessible training, to prepare and orient HDCs for their job functions was highlighted, in that, at least twenty percent of HDCs were new in their post and did not have prior training or experience in disaster management.
PAHO/WHO TRT provided excellent support and collaboration before and during the meeting. The Ministry of Health TRT were also extremely gracious co-hosts and their commitment to the meeting and disaster management in general, was evident through amongst other ways, theattendance of officials from the highest level (Minister of Health, Permanent Secretary and Chief Medical Officer) at the Opening Ceremony of the meeting and again at the Reception (above mentioned plus the Parliamentary Secretary) which they hosted for the participants.
Summary Report of the 13th Health Disaster Coordinators Meeting
Page 4 of 25
4.0 Summary of Group Work /Plenary Sessions
One group work and two plenary sessions were conducted during the meeting as follows:
4.1 Group Work: Health Sector Disaster Preparedness Assessment
ObjectiveThe objective of this session was to develop an outline (questions/indicators and format) for the health sector disaster preparedness self assessment tool
OrganizationParticipants were divided into four groups in keeping with the four areas of the health disaster management framework, which was proposed in the earlier presentation on health sector disaster programme development and management. These areas were preparedness, mitigation, response, and partnerships. Groups were asked to develop the outline for their area of focus.Before the breakout groups, participants were provided with information on the guidelines for thedevelopment of a self assessment tool for the Caribbean (see Presentation CD orhttp://www.disaster-info.net/carib/hdc2008.htm). This was intended to set the tone for the group work.
OutputThe groups proposed formats and a number of questions for inclusion in the assessment tool. Thegroup transcripts with these are presented in Annex 3. The following were also recommended for finalizing the assessment tool:
- Revision of the disaster section of the Essential Public Health Functions- Revision of similar instruments- In the first instance, convening a two days consultation or stakeholders’ meeting to
consider relevant issues such as standards and/or benchmarks, scope and objectives for the tool.
4.2 Group Work: Comprehensive Disaster Management (CDM) and the Health Sector Committee
ObjectiveThe objective of this session was to obtain input from participants on the composition and operation of a Health Disaster Risk Reduction Committee for the Caribbean.
OrganizationThe session was conducted as a plenary. It followed the presentation by the CDERA presenter,which provided an overview of the Comprehensive Disaster Management Strategy andProgramming Framework. The CDERA presenter spoke about CDM and the health sector in the Caribbean – the related outcomes and the governance process for implementation. As part of the governance structure, leads were identified for health and other sectors. These sector leads will be supported by a Sector Sub-committee to facilitate wider inclusion of relevant stakeholders in the CDM planning and implementation process at the sectoral level.During the plenary session, participants were informed that CDERA had invited PAHO/WHOto lead the mainstreaming of CDM in the health sector. The recommended members of the healthsub-committee were CEHI, CAREC, CFNI, CHRC and St. Kitts and Nevis, the lead country for health in CARICOM.

Summary Report of the 13th Health Disaster Coordinators Meeting
Page 5 of 25
Participants were also advised that PAHO/WHO will be spearheading a five year CIDA fundedhealth disaster risk reduction (DRR) project in the Caribbean, which requires a similarcoordinating committee as the CDM Health Sub-Committee.PAHO/WHO’s proposed strategy to address both of these needs (and more) is to establish one umbrella coordinating committee for health disaster risk reduction in the Caribbean. Thiscommittee will include representatives from the English, Dutch and French islands and willjustifiably have strong country level representation, since activities are primarily implemented at that level.
OutputThe following suggestions emanated from the plenary session:
Suggestions
� Cluster countries based on similarities, select one representative from each cluster for the committee, and rotate leadership among clusters. Cluster formation criteria should be disaster-oriented. Proposed criteria included:
o Geographical locationo Population sizeo Types of hazards present/affecting the countryo Spatial extent of countryo Political relatedness (among countries)
� Change fifty percent of persons on the committee every two years. This will be achieved via a change in clusters representative. Countries within the clusters will select therepresentative to sit on the committee
� Use the annual HDC meeting as the forum where the committee is re-constituted and the leadership rotated
� Define clearly the scope, roles and purpose of the committee� Revise the TOR proposed by CDERA for the CDM health sector sub-committee, to
determine aspects that can be adopted and adapted� Develop reporting mechanisms� Develop monitoring and evaluation systems for the committee and implementation of
health DRR activities in the region
Clusters Resulting from Plenary DiscussionsOECSCountries
UKOverseasTerritories
French and DutchDepts.
Land based Countries
OtherEnglishSpeaking
RegionalHealthInstitutions
InternationalInstitution
St. Lucia BVI Aruba Belize JamaicaSt. Vincent &GrenadinesSt Kitts &Nevis
TCI Curacao Guyana Trinidad & Tobago
Antigua CI GuadeloupeDominica Bermuda MartiniqueGrenada MonsterratBarbados Anguilla
Suriname Bahamas
CEHI PAHO -PED
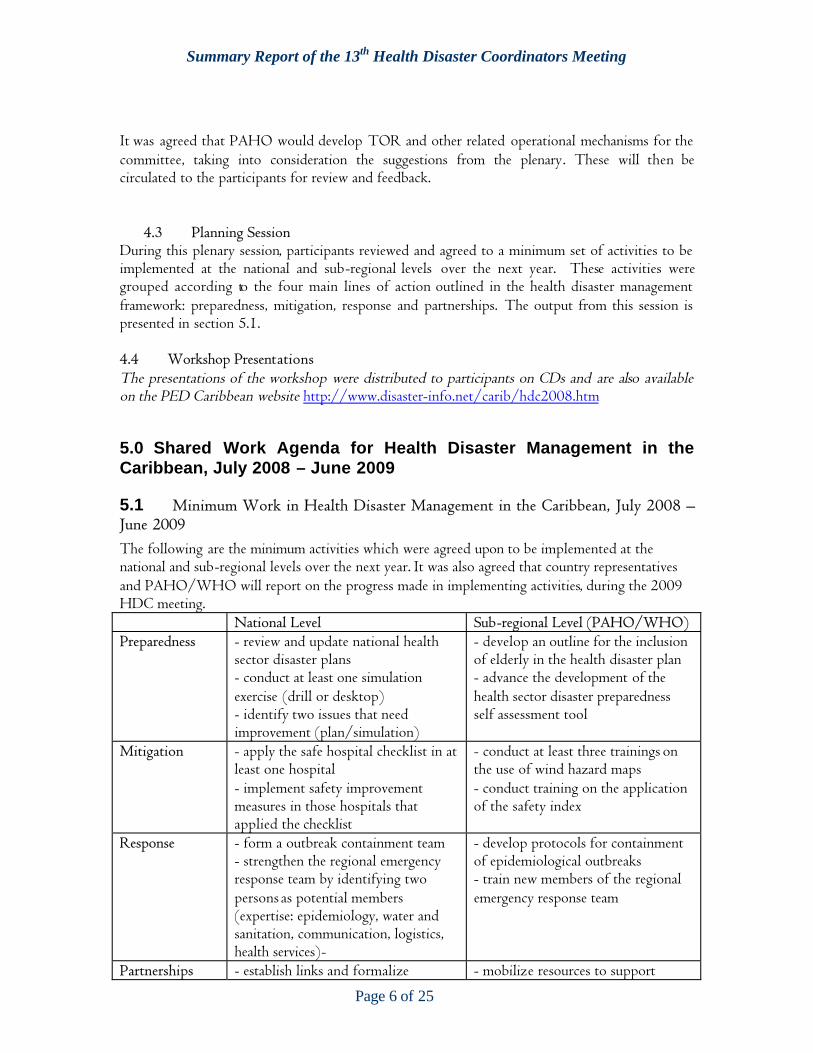
Summary Report of the 13th Health Disaster Coordinators Meeting
Page 6 of 25
It was agreed that PAHO would develop TOR and other related operational mechanisms for the committee, taking into consideration the suggestions from the plenary. These will then becirculated to the participants for review and feedback.
4.3 Planning SessionDuring this plenary session, participants reviewed and agreed to a minimum set of activities to be implemented at the national and sub-regional levels over the next year. These activities weregrouped according to the four main lines of action outlined in the health disaster management framework: preparedness, mitigation, response and partnerships. The output from this session is presented in section 5.1.
4.4 Workshop PresentationsThe presentations of the workshop were distributed to participants on CDs and are also available on the PED Caribbean website http://www.disaster-info.net/carib/hdc2008.htm
5.0 Shared Work Agenda for Health Disaster Management in theCaribbean, July 2008 – June 2009
5.1 Minimum Work in Health Disaster Management in the Caribbean, July 2008 –June 2009The following are the minimum activities which were agreed upon to be implemented at the national and sub-regional levels over the next year. It was also agreed that country representatives and PAHO/WHO will report on the progress made in implementing activities, during the 2009 HDC meeting.
National Level Sub-regional Level (PAHO/WHO)Preparedness - review and update national health
sector disaster plans- conduct at least one simulation exercise (drill or desktop)- identify two issues that need improvement (plan/simulation)
- develop an outline for the inclusion of elderly in the health disaster plan- advance the development of the health sector disaster preparedness self assessment tool
Mitigation - apply the safe hospital checklist in at least one hospital- implement safety improvement measures in those hospitals that applied the checklist
- conduct at least three trainings on the use of wind hazard maps- conduct training on the application of the safety index
Response - form a outbreak containment team- strengthen the regional emergency response team by identifying two persons as potential members (expertise: epidemiology, water and sanitation, communication, logistics, health services)-
- develop protocols for containment of epidemiological outbreaks- train new members of the regionalemergency response team
Partnerships - establish links and formalize - mobilize resources to support
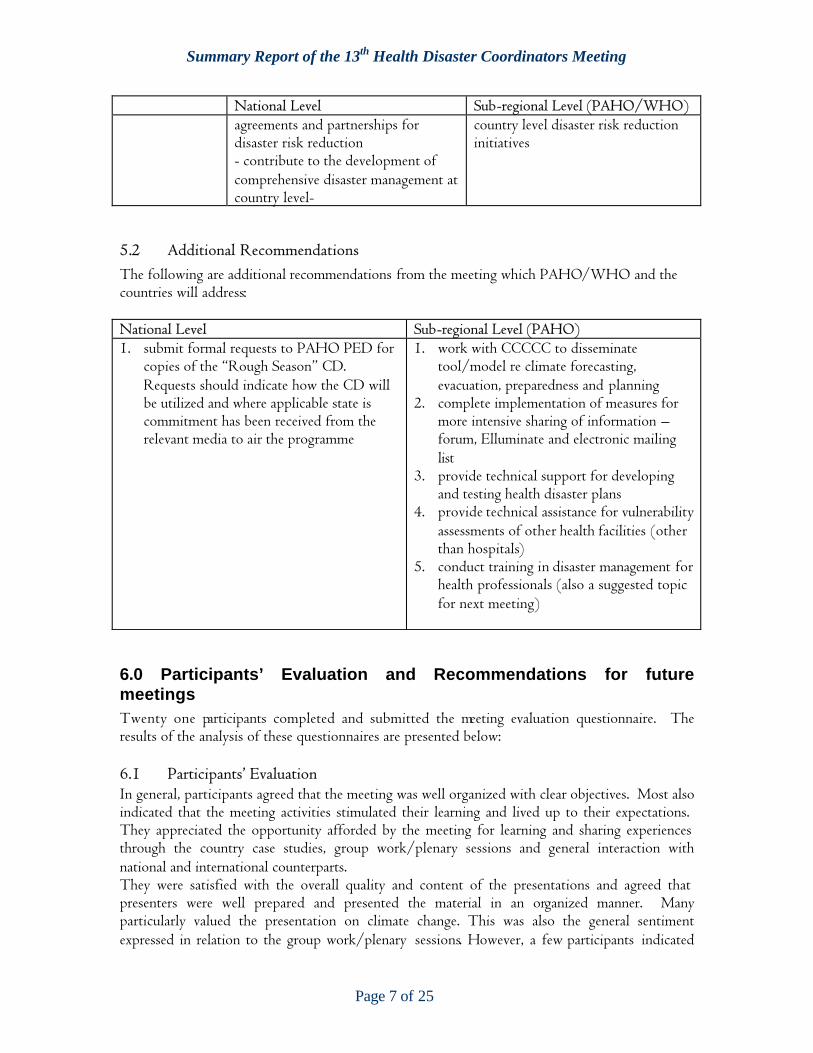
Summary Report of the 13th Health Disaster Coordinators Meeting
Page 7 of 25
National Level Sub-regional Level (PAHO/WHO)agreements and partnerships for disaster risk reduction- contribute to the development of comprehensive disaster management at country level-
country level disaster risk reduction initiatives
5.2 Additional RecommendationsThe following are additional recommendations from the meeting which PAHO/WHO and the countries will address:
National Level Sub-regional Level (PAHO)1. submit formal requests to PAHO PED for
copies of the “Rough Season” CD.Requests should indicate how the CD will be utilized and where applicable state is commitment has been received from the relevant media to air the programme
1. work with CCCCC to disseminate tool/model re climate forecasting, evacuation, preparedness and planning
2. complete implementation of measures for more intensive sharing of information –forum, Elluminate and electronic mailing list
3. provide technical support for developing and testing health disaster plans
4. provide technical assistance for vulnerabilityassessments of other health facilities (otherthan hospitals)
5. conduct training in disaster management for health professionals (also a suggested topic for next meeting)
6.0 Participants’ Evaluation and Recommendations for futuremeetingsTwenty one participants completed and submitted the meeting evaluation questionnaire. Theresults of the analysis of these questionnaires are presented below:
6.1 Participants’ EvaluationIn general, participants agreed that the meeting was well organized with clear objectives. Most also indicated that the meeting activities stimulated their learning and lived up to their expectations.They appreciated the opportunity afforded by the meeting for learning and sharing experiences through the country case studies, group work/plenary sessions and general interaction withnational and international counterparts.They were satisfied with the overall quality and content of the presentations and agreed that presenters were well prepared and presented the material in an organized manner. Manyparticularly valued the presentation on climate change. This was also the general sentimentexpressed in relation to the group work/plenary sessions. However, a few participants indicated
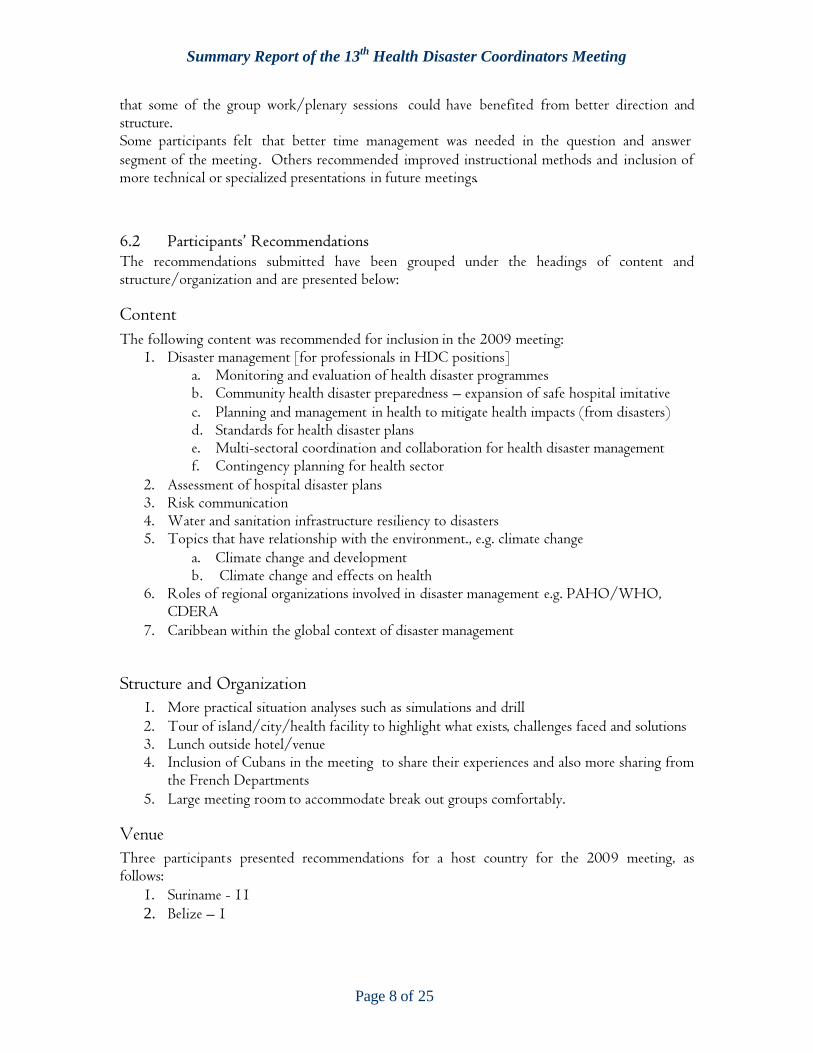
Summary Report of the 13th Health Disaster Coordinators Meeting
Page 8 of 25
that some of the group work/plenary sessions could have benefited from better direction andstructure.Some participants felt that better time management was needed in the question and answer segment of the meeting. Others recommended improved instructional methods and inclusion of more technical or specialized presentations in future meetings.
6.2 Participants’ RecommendationsThe recommendations submitted have been grouped under the headings of content andstructure/organization and are presented below:
ContentThe following content was recommended for inclusion in the 2009 meeting:
1. Disaster management [for professionals in HDC positions] a. Monitoring and evaluation of health disaster programmesb. Community health disaster preparedness – expansion of safe hospital imitativec. Planning and management in health to mitigate health impacts (from disasters)d. Standards for health disaster planse. Multi-sectoral coordination and collaboration for health disaster managementf. Contingency planning for health sector
2. Assessment of hospital disaster plans3. Risk communication4. Water and sanitation infrastructure resiliency to disasters5. Topics that have relationship with the environment., e.g. climate change
a. Climate change and developmentb. Climate change and effects on health
6. Roles of regional organizations involved in disaster management e.g. PAHO/WHO,CDERA
7. Caribbean within the global context of disaster management
Structure and Organization1. More practical situation analyses such as simulations and drill2. Tour of island/city/health facility to highlight what exists, challenges faced and solutions 3. Lunch outside hotel/venue4. Inclusion of Cubans in the meeting to share their experiences and also more sharing from
the French Departments5. Large meeting room to accommodate break out groups comfortably.
VenueThree participants presented recommendations for a host country for the 2009 meeting, asfollows:
1. Suriname - 112. Belize – 1
Sum
mar
y Re
port
of th
e 13
th H
ealth
Dis
aste
r Coo
rdin
ator
s Mee
ting
Page
9 of
25Th
e P
an A
mer
ican
Hea
lth
Org
aniz
atio
n
in c
olla
bor
atio
n w
ith
The
Min
istr
y of
Hea
lth
Trin
idad
& T
obag
o
pres
ents
th
e
13th
Hea
lth
Dis
aste
r C
oord
inat
ors
Mee
tin
g
OP
ENIN
G C
EREM
ON
Y
Kap
ok H
otel
, Tri
nid
ad
1st
Jul
y, 2
008
Min
istry
of H
ealth
Gov
ernm
ent o
f the
Rep
ublic
of T
rinid
ad a
nd T
obag
o
Sum
mar
y Re
port
of th
e 13
th H
ealth
Dis
aste
r Coo
rdin
ator
s Mee
ting
Page
10 o
f 25
Obj
ectiv
esPr
ogra
m
The
over
all
obje
ctiv
e of
the
mee
ting
is t
o re
view
dev
elop
men
ts a
nd
perf
orm
ance
in th
e la
st y
ear
and
iden
tify
mai
n ar
eas
of c
oope
ratio
n in
heal
th d
isas
ter r
isk
redu
ctio
n in
the
Car
ibbe
an fo
r 200
8 –
2009
.
The
spec
ific
obje
ctiv
es a
re to
:
1.Pr
ovid
e pa
rtic
ipan
ts w
ith i
nfor
mat
ion
and
tool
s fo
r st
rate
gic
man
agem
ent,
advo
cacy
an
d le
ader
ship
in
he
alth
di
sast
er
risk
redu
ctio
n
2.Sh
are
rele
vant
ri
sk,
haza
rd
and
emer
genc
y-re
late
d
expe
rien
ces,
pr
omot
e ne
twor
king
, an
d in
trod
uce
robu
st
coor
dina
tion
mec
hani
sms
at t
he s
ecto
ral,
natio
nal,
regi
onal
and
inte
rnat
iona
l lev
els
3.In
trod
uce
part
icip
ants
to th
e co
ncep
ts, m
echa
nism
s an
d is
sues
invo
lved
in
risk
ide
ntifi
catio
n, m
anag
emen
t an
d re
duct
ion
at
the
sect
oral
an
d na
tiona
l le
vels
8:30
amR
egis
trat
ion
9:00
amO
peni
ngC
erem
ony
Mrs
. Mon
ica
Zacc
arel
li D
avol
i,D
isas
ter R
educ
tion
Adv
isor
PA
HO
Bar
bado
s
Wel
com
e an
d O
peni
ngR
emar
ks
Dr.
Car
ol B
oyd-
Scob
ie,
PAH
O/W
HO
Rep
rese
ntat
ive,
Tri
nida
d an
d To
bago
Key
note
Add
ress
Hon
. Mr.
Jerr
y N
arac
e,M
inis
ter o
f Hea
lth,
Tr
inid
ad a
nd T
obag
o
10:0
0 am
Clo
sing
Dr A
vril
Siun
g-C
hang
Envi
ronm
enta
l Hea
lth
Adv
isor
PA
HO
Tri
nida
d
Sum
mar
y Re
port
of th
e 13
th H
ealth
Dis
aste
r Coo
rdin
ator
s Mee
ting
Page
11 o
f 25
Obj
ectiv
esTh
e ov
eral
l obj
ectiv
e of
the
mee
ting
is to
revi
ew d
evel
opm
ents
and
perf
orm
ance
in
the
last
yea
r an
d id
entif
y m
ain
area
s of
coop
erat
ion
in h
ealth
dis
aste
r ri
sk r
educ
tion
in th
e C
arib
bean
for 2
008
– 20
09.
The
spec
ific
obje
ctiv
es a
re to
:
1.Pr
ovid
e pa
rtic
ipan
ts w
ith i
nfor
mat
ion
and
tool
s fo
r
stra
tegi
c m
anag
emen
t,ad
voca
cy
and
lead
ersh
ip
in
heal
th d
isas
ter r
isk
redu
ctio
n
2.Sh
are
rele
vant
ri
sk,
haza
rd
and
emer
genc
y-re
late
d
expe
rien
ces,
prom
ote
netw
orki
ng,
and
intr
oduc
e
robu
st
coor
dina
tion
mec
hani
sms
at
the
sect
oral
,
natio
nal,
regi
onal
and
inte
rnat
iona
l lev
els
3.In
trod
uce
part
icip
ants
to
the
conc
epts
, m
echa
nism
s
and
issu
es in
volv
ed in
ris
k id
entif
icat
ion,
man
agem
ent
and
redu
ctio
n at
the
sect
oral
and
nat
iona
l lev
els.
THE
PA
N A
MER
ICA
N H
EA
LTH
OR
GA
NIZ
ATI
ON
In c
olla
bora
tion
wit
h
The
Min
istr
y of
Hea
lth
Trin
idad
& T
obag
o
Pre
sent
s th
e
13th
Hea
lth
Dis
aste
r C
oord
inat
oM
eeti
ng
AG
END
A
Kap
ok H
otel
, Tri
nid
ad1
– 3
Ju
ly 2
008
Sum
mar
y Re
port
of th
e 13
th H
ealth
Dis
aste
r Coo
rdin
ator
s Mee
ting
Page
12 o
f 25
DA
Y01
10:0
0W
orks
hop
Intr
oduc
tion
?In
trod
uctio
n of
Par
ticip
ants
?Re
view
of M
eetin
g O
bjec
tives
?Rev
iew
of W
orks
hop
Agen
da
Ms.
Nic
ole
Wyn
ter,
PED
, PAH
O
10:3
0~
BR
EAK
~
11:0
0Fe
edba
ck o
n A
ctiv
itie
s fr
om H
DC
200
7?
Rep
ort
on la
st y
ear’s
act
iviti
es?
Regi
onal
/inte
rnat
iona
l per
spec
tives
and
up
date
s
Mrs
. Mon
ica
Zac
care
lli D
avol
i, PE
D, P
AHO
Mod
erat
or:
Mrs
. Nic
ole
Slac
k Li
burd
11:3
0Im
pac
t of
Clim
ate
Ch
ang
e in
C
arib
bean
Cou
ntr
ies
Dr.
Ulri
c Tr
otz,
Carib
bean
Com
mun
ity C
limat
e Ch
ange
Cen
ter
12:3
0~
LUN
CH
~
Mod
erat
or:
Dr.
Earl
Bes
t1:
30H
ealt
h Se
ctor
Dis
aste
r P
rogr
amm
e D
evel
opm
ent
and
Man
agem
ent
?Ke
y de
finiti
ons
and
conc
epts
?St
ruct
urin
g H
ealth
Dis
aste
rM
anag
emen
t Pr
ogra
mm
es?
Coun
try
case
stu
dy (
Hai
ti)
Dr.
Dan
a Va
n Al
phen
, PED
, PAH
O
Dr.
Phi
lippe
Des
man
gles
3:30
Gro
up
Wor
kH
ealth
sec
tor
disa
ster
pre
pare
dnes
sas
sess
men
tM
rs. J
oyce
Tho
mas
, PED
, PAH
O
4:30
Wra
p u
p an
d A
djou
rnm
ent
��
�D
AY
02
Mod
erat
or:
Dr.
Bal
kara
n S
hiv
nau
th8:
30Sa
fe H
ospi
tal I
nit
iati
ve in
th
e C
arib
bean
: R
egio
nal
an
d N
atio
nal
P
ersp
ecti
ves
?D
IPEC
HO
Pro
ject
?Co
untr
y ca
se s
tudi
es (
Trin
idad
, D
omin
ica,
St. Vi
ncen
t an
d th
e G
rena
dine
s)
?W
ind
Haz
ard
map
s
Mrs
. Joy
ce T
hom
asM
s. J
oann
e Pe
rsau
d,M
s. S
andr
a Ch
arte
r-Ro
lle &
Dr.
Sim
one
Keiz
er-B
each
e
Dr.
Dan
a Va
n Al
phen
10:3
0~
BR
EAK
~
11:0
0M
oder
ator
:D
r. E
lizab
eth
Ferd
inan
dD
isea
se S
urv
eilla
nce
in D
isas
ters
�Te
chni
cal P
rese
ntat
ion
�Co
untr
y ca
se s
tudy
(Ja
mai
ca)
Dr.
Eld
onna
Boi
sson
, CAR
EC
Dr.
Mar
ion
Bullo
ck-D
ucas
se,
Min
istr
y of
Hea
lth, J
amai
ca12
:00
Mec
hani
sms
for
mor
e in
tens
ive
shar
ing
of in
form
atio
n o
n h
ealt
h d
isas
ter
redu
ctio
n
Ms.
Nic
ole
Wyn
ter
/D
r. A
vril
Siun
g-Ch
ang,
PAH
O T
RT12
:30
~LU
NC
H ~
1:30
Mod
erat
or:
Mr.
And
rew
Ske
rrit
Reg
iona
l Coo
rdin
atio
n M
echa
nism
s fo
r H
ealt
h�
Com
preh
ensi
veD
isas
ter
Man
agem
ent
�Co
untr
y ca
se s
tudi
es (
BVI
and
Trin
idad
)
�G
rou
p W
ork:
CDM
and
the
H
ealth
Se
ctor
CD
M h
ealth
sect
or c
omm
ittee
Mrs
. And
ria G
rosv
enor
, CD
ERA
Mrs
. Daw
n Le
onar
d &
M
s. J
oann
e Pe
rsau
dM
s. M
onic
a Za
ccar
elli
Dav
oli
4:30
Wra
p u
p an
d A
djou
rnm
ent
��
�D
AY
03
8:30
Mod
erat
or:
Dr.
Wim
Bak
ker
Pan
dem
ic I
nfl
uen
za�
Upd
ates
, Upc
omin
g ac
tiviti
es a
nd r
epor
t of
last
yea
r’s s
imul
atio
ns�
Coun
try
case
stud
ies
(St. L
ucia
, Guy
ana
and
Gua
delo
upe)
Dr.
Rob
ert
Lee,
PED
, PAH
O
Mr.
Aug
ustin
e Co
mpt
on,
Dr.
Asho
k So
okde
o,D
r. M
arie
-Fra
nce
Pet
chy
10:0
0~
BR
EAK
~
10:3
0Ea
rth
quak
e Si
mu
lati
on E
xerc
ise
Dr.
Rob
ert
Lee
12:3
0~
LUN
CH
~
1:30
Pla
nnin
g Se
ssio
nRe
visi
on o
f co
oper
atio
n pr
iorit
ies
in h
ealth
di
sast
er r
isk
redu
ctio
n in
the
Car
ibbe
anM
rs. M
onic
a Za
ccar
elli-
Dav
oli
3:00
Wor
ksho
p Ev
alua
tion
Ms.
Nic
ole
Wyn
ter
3:15
Con
clu
sion
of
wor
ksh
op
Summary Report of the 13th Health Disaster Coordinators Meeting
Page 13 of 25
ANNEX 2LIST OF PARTICIPANTS
13TH HEALTH DISASTER COORDINATOR’S MEETINGKAPOK HOTEL TRINIDAD
1ST – 3RD JULY 2008.
COUNTRY NAMEANGUILLA Mr. Lynrod Brooks
Health PlannerMinistry of HealthP.O. Box 60The ValleyAnguilla AI 2690Tel: 1-264-497-3042 / 3940 ( W) 1-264-235-8583 ( H ) 1-264-497-5695 (Fax)Email : [email protected]
ANTIGUA Mr. Gary ThomasHospital AdministratorHolberton HospitalQueen Elizabeth HighwaySt. John’s Antigua W.I.Tel: 1-268-462-0251 /2 ( W) 1-268-464-9505 (Cell) 1-268-462-4067 (Fax & Direct)Email: [email protected]
BAHAMAS Mr. Moses DeveauxHospital Administrator/ Disaster CoordinatorMinistry of HealthP.O. Box 3729Nassau NP BahamasTel: 1- 242-502-4730 ( W)
1-242-325-7947 (Private) 1-242-364-6134 (H)Email: [email protected]
BARBADOS Dr. Elizabeth FerdinandHealth Disaster CoordinatorMinistry of HealthJemmotts LaneBridgetown, BarbadosTel: 1-246-427-8326 (W) 1-246-436-2497 (H)Email: [email protected]
BELIZE Mr. John BoddenSenior Public Health Inspector
Summary Report of the 13th Health Disaster Coordinators Meeting
Page 14 of 25
Ministry of HealthEast Block BuildingIndependence Plaza, Belmopan,Cayo Dist, Belize, CA.Tel: 011-5018222325 Ext. 81386(W) 011-501-222-4196 (H) 011-501-822-2942 (Fax)Email: [email protected]
BERMUDA Mr. David KendellChief Environmental Health Officer,Gov’t of BermudaP.O. Box Hm 1195Hamilton, Bermuda HMEXTel: 441-3369385 (W) 441-7374577 (H) 441-2321941 (Fax)Email: [email protected]
BRITISH VIRGIN ISLANDS
Mrs. Dawn LeonardHealth Disaster CoordinatorMinistry of Health and Social Development (BVI)RG Hodge BuildingRoad Town ,TortolaBritish Virgin Islands VG1110Tel: 284-494-3701 Ext.2168 (W)284-540-0451 & 284-495-4987 (H)284-494-5287 (F) 284-540-0451(C)Email: [email protected]
CAYMAN ISLANDS Ms. Michelle ReidHealth & Safety Officer / Disaster CoordinatorHealth Services Authority1 Hospital Road, P.O. Box 915Georgetown Grand CaymanCayman Islands.Tel: 345-244-2582 (W) 345-949-9549 (H) 345- 949- 2998 (Fax)Email: [email protected]
CURACAO Dr. Earl BestMedical DirectorDirectorate Health,P.O. Box 3447 Curacao,Netherlands AntillesTel: 5999-7368496 (W) 5999-7366749 (H) 5999-7363845 (Fax) 5999-5600745 ( Cell)Email: [email protected]
Summary Report of the 13th Health Disaster Coordinators Meeting
Page 15 of 25
DOMINICA Mrs. Sandra Charter – RolleCoordinator /NHC Ministry of HealthGov’t Headquarters, RoseauDominica.Tel: 767-266-3522 (W) 767-449-2464 (H)Email: [email protected]
GRENADA Mr. Osbert CharlesHealth Disaster CoordinatorMinistry of HealthBotanical GardensTanteen, St. Georges,Grenada.Tel: 1-473-440-2485 (W) 440-3485 (W) 1-473-438-5433 (H)
1-473-406-7738 (Cell) 1-473-405-3212 (Cell)Email: [email protected]
GUADELOUPE Dr. Marie – France PetchyEmergency MDCHU Pointe-a-Pitre / AbymesService des urgencesBP 465, Route de Chauvel97159 Ponte-a-Pitre CedexGuadeloupe (FWI)Tel: 590-590-891-120 (W) 590-590-982-965 (H) 590-690-716-890 (Cell) 590-590-891-108 (Fax)Email: [email protected]
GUYANA Dr. Ashok SookdeoDirector Environmental Health Unit,Ministry of Health ,Upper Brickdam,Georgetown GuyanaTel: 592-621-3778 (W) 592-233-5857 (H)Email : [email protected]
HAITI Dr. Philippe DesmanglesFocal Point Disaster / EmergencieServicesMSPP / VPE (Haiti)Palais des Ministeres HaitiPort-Au-Prince.Tel: 509- 3454-7817 (W) 509-3737-7955 (W)
Summary Report of the 13th Health Disaster Coordinators Meeting
Page 16 of 25
Email: [email protected] Mr. Trevor Howe
Health Disaster CoordinatorMinistry of HealthP.O. Box 24 Brades,Monsterrat.Tel: 664-491-6057 (W) 664-491-5219 (H)Email: [email protected]
NEVIS Ms. Nicole Slack – LiburdHealth PlannerMinistry of Health / HDCMain Street, ChrlestownNevis.Tel: 869-469-5521 Ext. 2192 (W) 869-469-9093 (H) 869-469-5629 (Fax)Email: [email protected]
[email protected]. KITTS Mr. Andrew Skerritt
HDC / Health PlannerMinistry of HealthP.O. Box 186,Bladen’s Commercial Development ,Basseterre,St. KittsTel: 869-467-1171 (W) 869-662-3087 (H)Email: [email protected]
ST. LUCIA Mr. Augustin ComptomProjects OfficerMinistry of Health2nd Floor Stanislaus James Bldg,Waterfront CastriesSt. LuciaTel: 1-758-468-5300 (W) 1-758-721-5199 (H)Email: [email protected]
ST. VINCENT Dr. Simone Keizer- BeacheHealth Disaster CoordinatorMinistry of Health St. Vincentc/o Milton Cato Memorial HospitalKingstown, St. VincentTel: 784-456-1185 (W) 784-457-9700 (H) 784-457-1014 (Fax)Email: [email protected]
SURINAME Dr. Willem Jan Bakker
Summary Report of the 13th Health Disaster Coordinators Meeting
Page 17 of 25
Medical Epidemiologist /PhysicianMinistry of Health, Bureau of PublicHealth,Rode Kruislaan no.22Paramaribo, SurinameTel: 597-499-596 (W)
597-432-510 (H)Email: [email protected]
TURKS AND CAICOS ISLANDS
Dr. Daren N. HallGeneral Physician / HDC DesignateMedical Department TCI Gov’tMnistry of HealthMyrtle Rigby Health ComplexLeeward HighwayProvidenciales, Turks & Caicos Islands.Tel: 649-941-3991 (W) 649-231-7723 (H) 649-941-8480 (Fax)Email: [email protected]
TRINIDAD AND TOBAGO
Dr. Balkaran ShivnauthMedical Officer, Mgr Emergency Services and Disaster Preparedness Coordination,Ministry of HealthFrench VillageEric Williams Medical ComplexMount HopeTel: 1-868-645-9175/ 6844 (W) 1-868-657-6665 (H) 1-868-647-9175 (Fax)Email: [email protected][email protected]
TRINIDAD ANDTOBAGO
Ms. Joanne PersadResearch OfficerEmergency Services and Disaster Preparedness Coordinating Unit,French Village, Eric Wiliams Medical Complex, Mount Hope.Tel: 1-868-645-6844 (W) 1-868-643-3668 (H) and Fax. 1-868-645-9175 (Fax)Email: [email protected]
TRINIDAD AND TOBAGO
Mr. Phillip PedroSafety OfficerMinistry of HealthDisaster Command CentreFrench Village,Eric Williams Medical Sciences Complex, Mount Hope.Tel: 1-868-645-9175 (W)Email: [email protected]
Summary Report of the 13th Health Disaster Coordinators Meeting
Page 18 of 25
PRESENTERS AND PAHO STAFF
BARBADOS Ms. Joyce ThomasProject Manager,PAHODayrells Rd. & Navy Gardens,Christ Church,BarbadosTel: 246-264-3860Fax:246-436-6447Email: [email protected]
BARBADOS Mrs. Andria GrosvenorTechnical Manager, Preparedness & Country SupportCDERABLDG #1 Manor Lodge Complex,Lodgehill , St. MichaelBarbados.Tel: 246-425-0386 (W) 246-428-0489 (H)Email: [email protected]
BARBADOS Mrs. Monica ZaccarelliSub-regional Advisor, Disaster Risk ReductionPAHODayrells Rd. & Navy Gardens,Christ Church,BarbadosTel: 246-264-3860Fax:246-436-6447Email: [email protected]
BARBADOS Ms. Nicole WynterDisaster Preparedness & Response OfficerPAHODayrells Rd. & Navy Gardens,Christ Church,BarbadosTel: 246-264-3860Fax:246-436-6447Email: [email protected]
BELIZE Dr. Ulric TrotzScience AdvisorCaribbean Community Climate Change Center,2nd Floor, Lawrence Nicholas Building,P.O. Box 563, Bliss ParadeBelmopan, Belize.Tel: 501-822-1094 / 1004 (W) 501-822-1340 (H)

Summary Report of the 13th Health Disaster Coordinators Meeting
Page 19 of 25
501-822-1365 (Fax)Email: [email protected]
BELIZE Mr. Jose PerezEnvironmental Health AdvisorPAHO / WHO168 Newtown Barracks,Belize City, BelizeTel: 501-224-4885 (W) 501-607-9662 (H)Email: [email protected]
HAITI Dr. Oliver KleitzProgram On Emergency Preparedness and Disaster ReliefPAHO WHO295 Avenue John BrownPort-Au-Prince, HaitiTel: 509-3699-9245 (Cell)Email: [email protected]
JAMAICA Dr. Silva HomeroEnvironmental Health AdvisorPAHO Jamaica2-4-King Street , 7th FloorKingston.Tel: 876-967-4626(W) 876-544-8598 (H) 876- 967-8598 (Fax)Email: [email protected]
PANAMA Dr. Dana Van AlphenRegional AdvisorPAHO / WHOCasa 142, Ave ArodemenaCiudad del SabeClayton Panama CityPanama.Tel: 507-317-0669 (W)
507-6677-6401 (H)Email: [email protected]
ST. LUCIA Adriannus VlugmanEnvironmental Health AdvisorPAHO /WHO c/o CE40 Box 1111Castries, St. LuciaTel: 758-489-8007 (W)Email: [email protected]
SURINAME Mr. Guno van der JagtAdminstrative OfficerPAHO , Burenstr 33Paramaribo , Suriname.
Summary Report of the 13th Health Disaster Coordinators Meeting
Page 20 of 25
Tel: 597-471-676 Ext. 233 (W) 597-853-8485 (H) 597-471-568 (Fax)Email: [email protected]
TRINIDAD AND TOBAGO
Dr. Avril Siung – ChangEnvironmental Health AdvisorPAHO49 Jeringham Avenue,Port –of-SpainTel: 1-868-624-7524 (W) 1-868-663-5800 (H) 1-868-624-5643 (Fax)Email: [email protected]
TRINIDAD AND TOBAGO
Dr. Eldonna BoissonEpidemiologistCaribbean Epidemiology CentreCAREC / PAHO / WHO16 – 18 Jamaica Boulevard,Federation Park,Port – of – SpainTel: 1-868-622-4261 Ext. 344 (W) 1-868-622-1008 (Fax)Email: [email protected]
UNITED STATES OF AMERICA
Dr. Robert LeeEOC Manager HQPAHOWashington, DCTel: 202-974-3704 (W)Email: [email protected]
TRINIDAD AND TOBAGO
Mrs. Carol – Ann Saunders- CarringtonAdministrative AssistantPAHOTel: 1-868-777-8992 (Cell)Email: [email protected]
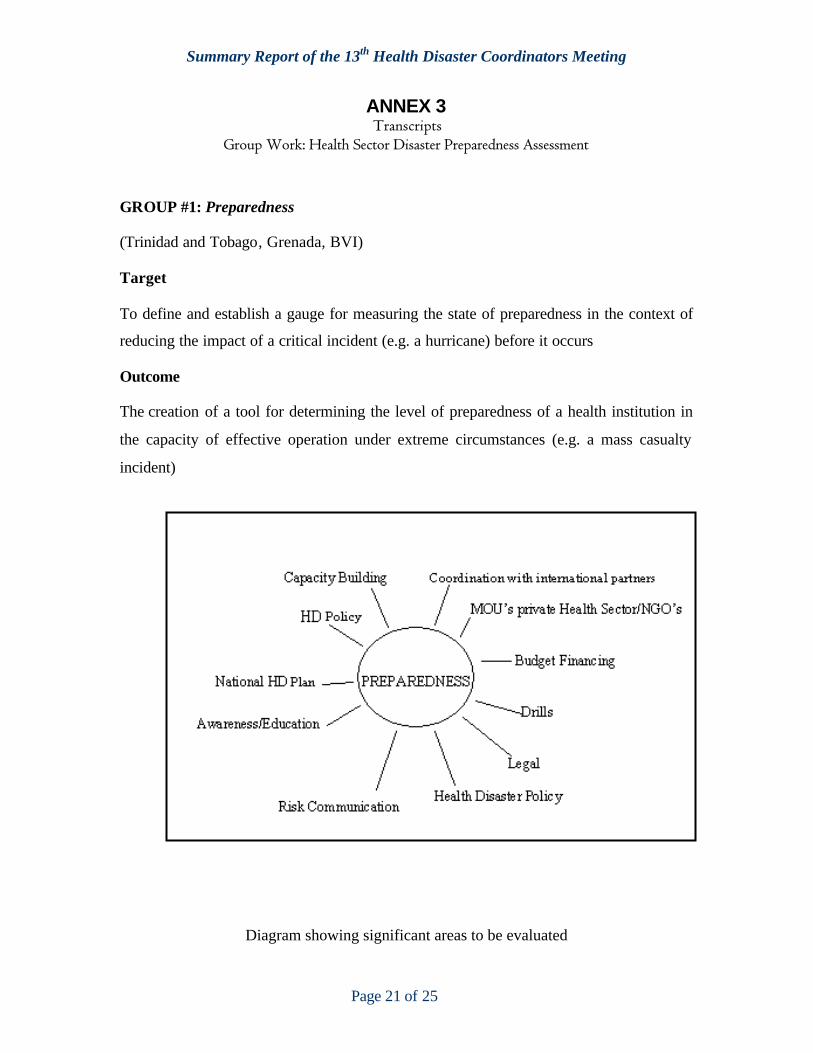
Summary Report of the 13th Health Disaster Coordinators Meeting
Page 21 of 25
ANNEX 3Transcripts
Group Work: Health Sector Disaster Preparedness Assessment
GROUP #1: Preparedness
(Trinidad and Tobago, Grenada, BVI)
Target
To define and establish a gauge for measuring the state of preparedness in the context of
reducing the impact of a critical incident (e.g. a hurricane) before it occurs
Outcome
The creation of a tool for determining the level of preparedness of a health institution in
the capacity of effective operation under extreme circumstances (e.g. a mass casualty
incident)
Diagram showing significant areas to be evaluated
Summary Report of the 13th Health Disaster Coordinators Meeting
Page 22 of 25
Strategy
Each area must be examined for completeness
Boxes along side each question will indicate…
Y = yes I = incomplete N = no
A value will be given to each box (e.g. Y =2 I = 1 N = 0 )
At the end of the exercise a grade (e.g. A, B or C) will be ascribed for attaining certain
numbers –TO BE DETERMINED.
1) HD POLICY
� Has HD policy been established and accepted? Y ? ?I ? ?N?
� Drafted? Y ? ?I ? ?N?
2) HD PLAN
� Responsible person? Y ? ?I ? ? N?
� Resources available? Y ? ?I ? ?N?
� Material? Y ? ?I ? ?N?
� Financial? Y ? ?I ? ?N?
� Human? Y ? ?I ? ?N?
� Stakeholders identified? Y ? ?I ? ?N?
� Roles and responsibilities clearly defined? Y ? ?I ? ?N?
� Vulnerabilities determined and risks analyzed? Y ? ?I ? ?N?
� Coordination mechanism in place? Y ? ?I ? ?N?
Group Members
Dr. Balkaran Shivnauth – Trinidad and Tobago
Mr. Phillip Pedro – Trinidad and Tobago.
Osbert A. Charles – Grenada
Dawn Leonard – BVI
Ton Vlugman – PAHO
Summary Report of the 13th Health Disaster Coordinators Meeting
Page 23 of 25
GROUP #2: Mitigation
(Barbados, Cayman Islands, Nevis, Montserrat, Curacao, Trinidad)
Definition
Set of actions aimed at reducing damage resulting from interaction between hazard and vulnerability
Headings for Self Assessment Tool 1. Structural e.g. walls, roof, building material and foundation
2. Non structural e.g. utilities, plumbing, equipment, electrical3. Functional, fire escapes, supplies and staff and planning
4. Environmental e.g. location, geologic conditions, soil accessibility5. Health education and awareness 6. Ambulances and vehicles-maintenance programme
(Unsure if some of these fall under mitigation or under preparedness but they must be considered.)
IndicatorsStructural:-a) mechanisms established to ensure building code standards are applied to all new health facilitiesb) All major repair projects include disaster mitigation measures that comply withbuilding codesc) One health facility to be selected for retro fitting per year “process for retro fitting followed”, i.e. assessment, design of corrective measures, and implementation.”
Non structural: a) 100% of health facilities should have sufficient utilities e.g. water, electricity for at least 3 daysb) 100% of health facilities should have sufficient supplies, i.e. food, drugs, medical supplies for 7 days
Functional – a) At least one simulation exercise conducted annually for all healthfacilitiesb) Annual review of health institutional disaster plans conducted and updated asnecessary
Summary Report of the 13th Health Disaster Coordinators Meeting
Page 24 of 25
Environmental: a) There are hazard maps for all health facilitiesHealth education and awareness: - short term a) 100% of health care staff made aware of health mitigation strategies in first yearMedium term a) 20-30% of public trained in health disaster preparedness in 2 years
Long term a) 60-70% of public trained with in 5 years
Ambulance and vehicles:-a) provisions in place for adequate parking/garaging and protection for 100% of the vehicular fleet.
The group briefly reviewed the standards used for assessment for hospitals and felt that many of the questions could be applied to all the health facilities in regard to mitigation. However these would have to be ranked and weighted accordingly. Time did not permit this.
Summary Report of the 13th Health Disaster Coordinators Meeting
Page 25 of 25
GROUP #4: Partnerships
(Belize, St. Kitts, Dominica, TCI, St. Vincent and the Grenadines)
Questions- Is there a structure responsible for communication to all stakeholders and the
general Public in the national health committee? (Communication Officer/ Sub-committee)
- Is there a listing of key persons and organization responsible for disasterpreparedness? (Contact/mailing list). Key sectors include private sector,government departments, UN Agencies
o Security, food production, utilities and public works, health sector, media- Is there a structure for mobilization and management of financial /Technical
resources?
- Health (Private/ Government/Volunteer)o Does each have an Institution Disaster Plan?
o Is it incorporated into the national plano Does the Institution have a MOU with the MOH?o Does each institution have a Disaster Management Committee?
o Does each institution participate in multi-sectoral drills?
ANNEX 2
GUIDELINES FOR DEVEOPMENT OF SELF
ASSESSMENT TOOL FOR THE HEALTH SECTOR
Presenter – Joyce Thomas
BACKGROUND
• Work on the development of a self assessment tool started with a survey in 2006
• Twelve of the twenty-three countries responded
• The responses were opened ended and were difficult to compare
Background con’t
• The development of the self assessment tool was included as an activity under the “Safe Hospital Project”
• USAID completed and tested a B-Tool with the OECS Member countries
• The persons involved in the preparation and testing of the tool was consulted to learn from their experience
The USAID B-TOOLIt is an objective instrument which can be used by
countries to:• a) assess their vulnerability to natural and man
made hazards, • b) evaluate the adequacy of existing institutions
and policies to address the current disaster situation facing the country, and
• c) guide the prioritization of resources to address critical needs at the developmental level.
B-Tool con’t
• The BTool covers the six areas of disaster management as identified in the Inter-American Development Bank Action Plan. These are; Risk Identification, Risk Mitigation, Risk Transfer, Disaster Preparedness, Emergency Response and Rehabilitation and Reconstruction
B-Tool con’t• It can be used to prioritize national and regional
programs of activities.• It can be used as an incentive at the political
level to stimulate action due to the comparative nature of its scores against another country.
• It provides information, in a consistent manner, on the state of readiness of each country. This information can be used by regional and international funding agencies to define or redefine programmes of assistance to the region.
Process of development • The tool was developed in six stages. These
are: • Selection of a comprehensive disaster
management framework• Identification of disaster risk management tools
and resources• Design of assessment questions• Stakeholder review and modification of the tool• Pilot testing and modification of the tool• Adaptation of the tool by local and regional
stakeholders
Selection of a comprehensive disaster management framework
PAHO has signed on to Comprehensive Disaster Management
All CDERA member states have either developed a comprehensive disaster management framework or is in the process of developing one
Identification of disaster risk management tools and resources
• The next stage in the design process was the selection of tools and resources required to effectively and efficiently manage the components of the framework.
The following are some tools and resources that were selected for review:
• Policies and plans• Integration of plans and activities• Involvement of the private sector• Involvement of the regional & international agencies• Legislation/Regulations• Financial resources /Human resources • Interagency-Coordination
Design of assessment questions
The formulation of a series of management questions that aim to explore the adequacy and content of current disaster risk management tools and resources of the country in each of the six disaster management phases and the design of a scoring system.
The Questions
The questions were phrased to highlight best practices recommendations in disaster risk management activities. It contains a list of easily understood questions that were chosen through extensive review of risk management literature and broad-based consultation.

ANNEX 3
PAN AMERICAN HEALTH ORGANIZATION WORLD HEALTH ORGANIZATION
48th DIRECTING COUNCIL 60th SESSION OF THE REGIONAL COMMITTEE
Washington, D.C., USA, 29 September-3 October 2008
Provisional Agenda Item 4.12 CD48/16 (Eng.) 22 August 2008 ORIGINAL: ENGLISH
ROUNDTABLE ON CLIMATE CHANGE AND ITS IMPACT ON PUBLIC HEALTH: A REGIONAL PERSPECTIVE
Background 1. In recent years, PAHO’s Directing Council has maintained a trend of including a roundtable as an agenda item related to that year’s World Health Day (WHD) theme. WHD is celebrated annually on April 7, which marks the founding of the World Health Organization (WHO) and serves as an opportunity to draw worldwide attention to a subject of major importance to global health. “Protecting Health from Climate Change” was selected as the 2008 WHD theme and PAHO has convened a roundtable on the topic to be held during the 48th Directing Council in September 2008. 2. The United Nations Framework Convention on Climate Change (UNFCCC) defines climate change as “change of climate which is attributed directly or indirectly to human activity that alters the composition of the global atmosphere and which is in addition to natural climate variability observed over comparable time periods.”1 The United Nations (UN) and the Intergovernmental Panel on Climate Change (IPCC) have devoted considerable time to analyzing the issue of climate change. Summary of the Theme 3. The adverse health impacts of climate change can be both direct and indirect. Direct impacts result from climatic extremes such as thermal stress and weather disasters. Indirect impacts result from climatic influences on vector-borne disease transmission, water- and food-borne disease transmission, and food and water security. Indirect impacts also include the consequences of social and economic dislocation, including population displacement.
1 Article 1, paragraph 2 of the Convention, UN, 1992.

CD48/16 (Eng.) Page 2 4. In the Region of the Americas, major areas of concern relate to increases in extreme weather events, subsequent changes in food supply and nutritional security, as well as changes in water supply, in the range and distribution of vector-borne diseases, and in rising sea levels. The impacts of climate change on cities will become increasingly important and in some countries will be made worse as a result of rapid and poorly planned urbanization. 5. Current population vulnerability influences the capacity to respond to the impact of climate change. Effective adaptation strategies should identify population groups that are unable to cope with the effects of climate variability and extremes. At risk populations live in areas prone to floods, droughts, and heat waves. The most vulnerable groups include children under five, pregnant and lactating women, older adults, marginalized, rural, urban, indigenous populations, and displaced populations. Vulnerability can further be exacerbated by other stress factors such as poverty, food insecurity, conflict, and disease. 6. The two ways in which societies can actively respond to climate change are through mitigation and adaptation. Mitigation aims to reduce, delay or avoid impact through interventions that reduce the sources of greenhouse gases or those that enhance gas-absorbing "sinks." In the sphere of public health, this involves primary prevention aimed at preventing the onset of injury or illness. Adaptation is defined as an adjustment in the natural or human system in response to changes produced by climatic stimuli. Mitigation and adaptation must be addressed by civil society, industry, government and other sectors, while taking into consideration the cultural diversity of the Region and the need to increase the awareness of many of our citizens. PAHO/WHO Collaborative Efforts 7. PAHO and WHO are closely collaborating on the topic of climate change in the Americas and worldwide, in an effort to increase awareness of its health consequences, assess country-specific risks, strengthen health systems to ensure adequate protection from climate-related risks, and enhance the inclusion of a public health perspective on climate change decision-making in other sectors. The Organization is in the process of developing a plan of action based on the regional country profiles reviewed during a Regional Workshop on Climate Change and its Effects on Health in the Americas, held in Brazil from 9 to 11 April 2008. 8. PAHO has prepared a White Paper on Climate Change and Public Health to be analyzed during the Roundtable (Annex A).
CD48/16 (Eng.) Page 3
Proposed Structure for the Roundtable Participants In addition to delegates from the Member States attending the 48th Directing Council, there will be participation of representatives of academia, UN agencies and civil society organizations. Format Introduction - in plenary (25 minutes)
The theme will be introduced, with a keynote address
Discussion Groups (1 hr 45 minutes)
Participants will choose between three discussion groups, each of which will be provided with the same guidelines on climate change and its impacts on public health.
Interpretation will be provided in English, French, Portuguese and Spanish for groups 1 and 2, and in English and Spanish for group 3. Each group will include a chair, a motivational speaker and a rapporteur. Sign up sheets for each group will be available at the registration desk as of the first day of the Council.
The rapporteurs of each discussion group will synthesize the discussions and conclusions of their group and produce a combined report.
Presentation of Report-in plenary on the following day (30 minutes)
The combined report prepared by the rapporteurs will be presented to the Council. It is hoped that this report will guide the future work of the countries and strengthen PAHO’s White Paper on Climate Change and Human Health.
Annexes

CD48/16 (Eng.) - 1 - Annex A
White Paper
Protecting Health from the Effects of Climate Change in the Region of the Americas: Moving from Evidence to Action
1. The objective of this White Paper is to present the evidence that climate change is a phenomenon that is increasingly affecting human health. It also aims to describe a set of actions that are needed in order to protect people from current and expected climate related health impacts. 2. Climate change is not new to the health sector. The first scientific report on climate change and health was released by World Health Organization in 1990. In 1995, PAHO presented the issue at the National Academy of Sciences during a conference on climate change and human health. Since then, PAHO has worked to increase awareness, information and initiate risk assessments in the Member States. Nowadays, these actions must be scaled up. Climate change is a more serious threat than anticipated in the early 90s, affecting mostly vulnerable populations with the worst health conditions, and those threatened by multiple environmental risk factors. The impact of climate change on health could seriously challenge the public health advances made, and thus calls for heightened awareness and preparation to face emerging threats. This fact is reflected in the agreements made during the 61st World Health Assembly in its Resolution WHA61.19 (2008). There is scientific evidence of climate change 3. There is scientific evidence showing that the world’s climate is changing and there is consensus on this within the scientific community. This change is due, in great part, to diverse human activities related to the burning of fossil fuels. In 2007, the Intergovernmental Panel on Climate Change (IPCC) concluded that the warming of the climate—which includes an increase in climatic variability—is unequivocal based on observed increases in global average air and ocean temperatures, the widespread melting of snow and ice, and rising global average sea level. 4. The ambient temperatures of the globe increased 0.74°C over the period 1906-2005. The rate of warming averaged over the past 50 years (0.13°C + 0.03°C per decade) is nearly twice that of the last 100 years. Evidence from around the world demonstrates that rising temperatures are changing and disrupting the balance of natural systems that supply the basic needs of life.

CD48/16 (Eng.) Annex A - 2 - There is evidence of health risks from climate change 5. During the 61st World Health Assembly in 2008, Member States expressed concern over the impact of rising temperatures being observed in some aspects of health. Observed changes in the precipitation and rainfall patterns are affecting the geographic range and incidence of many climate-sensitive health determinants and the consequences resulting from these factors. The health effects associated with climatic conditions can be divided into three broad categories: effects that are directly related to weather or climate; effects that result from environmental changes that occur in response to climate change; and effects resulting from consequences of climate-induced economic dislocation, environmental decline, and conflict. Changes in the frequency and intensity of thermal extremes and other extreme weather events (i.e., floods and droughts) directly influence population health. In addition, indirect impact due to changes in the intensity and variety of infectious diseases and food- and water-borne diseases have been noted. Increases in the prevalence of respiratory diseases are associated with air pollutants and aero-allergens. Saline intrusion from rising sea levels and retreating glaciers can greatly affect local water supplies. Other impacts include the health consequences of social and economic dislocation and of population displacement. 6. Globally, people at greatest risk include the very young, the elderly, the infirm, migrant populations, indigenous populations, poor communities, and poor women in particular. Low-income countries and areas where under-nutrition is widespread, education is poor and infrastructure is weak, will have the most difficulty in adapting to climate change and the related health consequences. Vulnerability is also determined by geography, and is higher in areas with a high endemicity of climate-sensitive diseases, water scarcity, low food production and isolated populations. Moreover, populations considered to be at greatest risk are those living in small-island developing states, mountainous regions, water-stressed areas, mega cities and coastal areas in developing countries, as well as the poor in urban and rural areas and those lacking access to health services. The evidence highlights the need of effective responses 7. Climate change affects some of the most important risk factors for health, such as the availability of fresh water and food. It also affects several climate-sensitive diseases, including those with the highest global disease burden—malnutrition, diarrhea and malaria, amongst others—which in turn mostly affect children.
CD48/16 (Eng.) - 3 - Annex A
8. Some climate change is inevitable. This means that it will be necessary to make changes in the health sector to adapt to such changes, and for health systems to be prepared to protect peoples’ health from increased climate-associated risks. In particular, it will be necessary to strengthen core public health interventions, paying greater attention to environmental and socioeconomic determinants of health. Effective responses in the health sector represent opportunities to protect public health, interacting in synergy with initiatives such as “Healthy Places” and “Faces, Voices and Places.” In addition, responses need to consider the numerous experiences acquired during decades by the health sector in the management of environmental risks and emergencies, such as those resulting from hurricanes and El Nino preparedness. 9. Considering the high rate of urbanization, the Region of the Americas should focus on urban health determinants, including the provision of water. However, rural areas, where some of the most vulnerable populations live cannot be overlooked. Furthermore, due to the many island states in the Region, concern over rising sea levels and the availability of potable water in small islands needs to be addressed, as do health actions related to preparedness and response to emergencies in countries that are experiencing extreme climate-related phenomena. The availability of food and crop yields may suffer in some countries, impacting nutrition and bringing about the displacement of populations. Climate sensitive vector-borne diseases, such as dengue, yellow fever and malaria, require particular attention. These are just some of the health concerns which a comprehensive plan of action should address. The health sector needs coordinated action 10. Following consultation with Member States, PAHO is proposing a Regional Plan of Action to Protect Health from the Effects of Climate Change in the Region of the Americas. The Plan could serve as a model for the development of national plans of action in the countries, adapted to local needs. Elements that should be addressed in a plan of this nature are detailed below. Goals, strategic objectives and actions 11. A Regional Plan of Action on climate change should ensure that concerns about public health security be placed at the center of the response to climate change. It should support the development and implementation of adaptation strategies at local, national, and regional levels to minimize the health impacts of climate change, and encourage the adoption of energy measures to mitigate climate change and avoid further and potentially disastrous impacts on health. A plan would need to be regularly evaluated in order to remain effective with regards to this emerging phenomenon.

CD48/16 (Eng.) Annex A - 4 - 12. The goals of the proposed plan would seek to empower, equip and strengthen the capacity of health systems locally and nationally to protect human health from risks related to climate change. 13. The strategic objectives to be achieved would include: Evidence: Promote and support the generation of knowledge on health risks associated with climate change and on the response of the public health sector to this phenomenon. Sensitization: Create awareness of the effects of climate change on health among both the general public and in different sectors including health sector personnel, by promoting communication and dissemination of information in a multidisciplinary approach. Resources: Promote the strengthening and development of human resources, financial resources, institutional development, and policy development. Adaptation: Strengthen and develop the capacity of health systems to design, implement, monitor, and evaluate adaptation measures with the aim of improving response capacity to prepare for and effectively respond to the risks of climate change. Partnerships: Promote, articulate and establish cross-disciplinary, interagency and intersectoral partnerships to ensure that health protection and promotion is central to climate change policies. 14. The following actions are needed to facilitate the achievement of these objectives, most of which need to be carried out with the participation of other sectors. Evidence: Promote and support the generation of knowledge on health risks associated with climate change and on the response of the public health sector to this phenomenon. • Observatory of climate and health: Support the establishment of observatories on
climate change and human health where no surveillance system exists, and strengthen existing systems, specifically integrating reliable information systems.
(a) Develop, adapt or adopt vulnerability indicators, establish the degree of
vulnerability and monitor advances and progress in adaptation measures, as well as the efficacy and efficiency of the interventions.
(b) Harmonize health indicators within the United Nations system, in
CD48/16 (Eng.) - 5 - Annex A
particular the achievement of the targets of the United Nations Framework Convention on Climate Change (UNFCCC).
(c) Develop a uniform methodology or tools to evaluate vulnerability that
provides information on the necessary actions for adaptation, to include the use of climatologist-prepared scenarios.
(d) Develop research based on epidemiological and statistical methods to
analyze and interpret multisectoral data and the impacts of climate change.
(e) Carry out quantitative and qualitative evaluations of the effects of climate change on health.
(f) Establish networks of experts and institutions to share information on
climate change and health that contributes to the regional integration of adaptation activities.
(g) Disseminate the information that is generated through communication
networks, such as web pages and the virtual library.
(h) Systematize local experiences salvaging health promotion initiatives, with community participation.
• Surveillance systems: Create and strengthen health and health determinant
surveillance systems, with an emphasis on environmental health and climate sensitive diseases.
• Research promotion: Support research to gather evidence on the impacts of
climate change on health.
(a) Promote applied research to evaluate the impact of climate change on the health of vulnerable populations, including children, the elderly, people with preexisting illnesses and poor people, in particular among women.
(b) Promote studies on the calculation of the cost of actions and of lack of
action, in order to guarantee an appropriate and transparent use of resources invested in protecting public health from climate change.
CD48/16 (Eng.) Annex A - 6 -
(c) Promote the use of evaluation, integrated health and environment action methods (such as GEO-Health, the ecosystem approach, and panoramic epidemiology, among others) to develop comprehensive actions to minimize the negative effects of climate change on human health and wellbeing.
(d) Promote the evaluation of greenhouse gas mitigation strategies proposed
in other sectors such as energy, transport and urban design, to minimize the negative effects of climate change on human health and wellbeing.
• Generation of information: Promote technical cooperation and provide national
and regional support to evaluate the health consequences of climate change:
(a) Support the academic sector and promote research to determine to what extent the weather and the climate affect geographic reach, and the incidence of climate sensitive diseases, taking into account multi-causality, confounding factors and effect modifiers.
(b) Prepare guidelines on how to evaluate vulnerability and adaptation at
local, national and regional scales. These evaluations would need to provide a better understanding of current and future health risks due to climate change and uncertainties related to these risks, as well as point to interventions that can increase the population’s resilience in the face of climate change.
(c) Determine what approach and tools should be used to quantify climate
change-attributable burden of disease; determine particularly vulnerable populations and regions; assess existing health systems capacity to cope with the projected effects on health, and prioritize additional interventions needed to increase the adaptation capacity to climate change.
(d) Systematize adaptation experiences among indigenous, rural and
traditional communities to generate mechanisms that adequately address different cultures.
(e) Evaluate achievements, failures, areas of opportunity and lessons learned,
in climate change-related areas, such as emergency response and health services, and improve regional, national and local capacity to evaluate actions.
CD48/16 (Eng.) - 7 - Annex A
• Exchange of Information: Promote and facilitate the exchange of knowledge between sectors, and support collaborative efforts to strengthen action capacity:
(a) Promote the creation of regional networks to disseminate health risks
caused by climate change and responses on the part of the health sector, as well as of other disciplines in light of these changes.
(b) Strengthen situation rooms and emergency operations centers.
(c) Establish or strengthen subregional databases on climate change and
health.
• Sensitization: Create awareness of the effects of climate change on health among
both the general public and in different sectors including health sector personnel, by promoting communication and dissemination of information in a multidisciplinary approach.
(a) Increase awareness: Sensitize decision-makers to the projected negative
outcomes for human health as the result of climate change and the need to reduce risks associated with climate change in the field of public health, and promote the health system response in the face of this phenomenon.
(b) Promote strategies: Promote education, information and risk
communication strategies related to climate change and human health within health personnel and the general population.
(c) Develop guides: Develop education, training and information guides for
the incorporation of climate change adaptation mechanisms to protect human health.
• Resources: Promote the strengthening and development of human resources,
financial resources, institutional development, and policy development.
(a) Strengthen the national regulatory framework to include climate change in health sector policies in a cross-cutting manner.
(b) Strengthen human resources: Strengthen and continue the work of
WHO/PAHO in supporting countries in environmental health training and, specifically, in climate change and health.
(c) Identify funds at the national and regional level for all the activities
identified in this plan.
CD48/16 (Eng.) Annex A - 8 -
i. Identify international funds for research on the effects of climate change on human health.
ii. Procure financing of health adaptation using resources of regional
funds and other regional financing mechanisms.
iii. Systematize successful experiences for the financing of health adaptation measures for climate change, using resources generated from mitigation as a base.
iv. Include climate change and health in PAHO workplans.
v. Facilitate greater financing from donor organizations to execute
programs and activities that address health risks of climate change. For example, national or regional proposals could be developed, financed by the Adaptation Fund from the Global Environment Facility.
• Adaptation: Strengthen and develop the capacity of health systems to design,
implement, monitor, and evaluate adaptation measures with the aim of improving response capacity to prepare for and effectively respond to the risks of climate change
(a) Adaptation evaluations: Provide technical cooperation and national and
regional support to design and to execute national plans of action in order to address the health risks of climate change, to manage such risks in an effective way and to provide them with follow up, such as quantifying the costs and benefits of the interventions.
(b) Adaptation priorities: Implement and evaluate adaptation measures in
critical health matters. Implement adaptation measures based on vulnerability assessments already made or being undertaken.
(c) Work with other sectors: Evaluation of the health implications of actions
of other sectors.
i. Provide technical cooperation and modify the necessary instruments—like cost benefit analyses and evaluations of the health effects—to evaluate, at the national and regional level, health implications of policies adopted in sectors such as agriculture, energy, transportation, water and sanitation, education, finance and the environment.
CD48/16 (Eng.) - 9 - Annex A
ii. Incorporate climate change in risk management plans, in preparedness, and in response to emergency and disaster situations.
(d) Emergency response related to climate change: Work at different levels of
government to improve regional, national and local capacity to support health systems, and respond to public health and emergency problems that result from climate change.
i. Improve regional, national and local capacity to respond to public
health needs in emergencies caused by increased frequency and intensity of disasters related to modifications in hydro-meteorological patterns, and to wide-reaching epidemics.
ii. Strengthen health systems response to the damage caused by extreme
climatic events, and survey consequences, including effects on mental health, infectious disease outbreaks and other adverse impact on health.
• Partnerships: Promote, articulate and establish cross-disciplinary, inter-agency
and intersectoral partnerships to ensure that health protection and promotion is central to climate change policies.
(a) Mitigation policies in the health sector: Facilitate the preparation and
dissemination of technical guidelines on best ways to reduce greenhouse gas emissions in the health sector.
(b) Strengthening the health sector: Promote the formation of information
centers within Ministries of Health and other health institutions, to identify, evaluate, reduce and eliminate health risks, as well for sharing information with centers in other counties:
i. Promote the establishment of focal points within ministries of health to
focus on issues of climate change and health, considering existing the institutional base in each country.
ii. Strengthen health systems by means of the Essential Public Health
Functions, specifically health promotion and primary health care, with the aim of being able to act on the effects of climate change on health.
iii. Strengthen health programs related to risk, emergency and disaster
management.
iv. Include the health sector in National Climate Change Commissions.

CD48/16 (Eng.) Annex A - 10 -
(c) Network of experts: Promote the formation of multidisciplinary expert groups and networks that will contribute to the strengthening of the health sector in the implementation of actions due to climate change.
(d) Intersectoral work: Promote and strengthen the exchange of information
between sectors, minimizing the costly duplication of initiatives. Partner with civil society and the private sector, among others.
(e) Evaluate the benefits of measures applied in other sectors: Prepare and
provide technical cooperation for the calculating costs and benefits to health of mitigation strategies proposed in other sectors.
(f) Interinstitutional action: Provide technical cooperation to countries to
ensure their active participation in processes related to climate change within the UNFCCC
(g) Cooperation between countries: Promote technical cooperation projects
between countries to study and mitigate the effects of climate change in border and among vulnerable populations.
(h) Subregional cooperation: Promote the theme within the subregional
integration mechanisms (MERCOSUR, Andean Nations Community—CAN, the Central American integration system—SICA, and the Caribbean Community—CARICOM).
(i) Regional forum: Promote the creation of a regional forum on climate
change and health with intersectoral participation.
(j) Collaborating centers: Identify and establish WHO/PAHO Collaborating Centers in the Region in the area of climate change and health, to support national and regional capacity development.
PAN AMERICAN HEALTH ORGANIZATION Pan American Sanitary Bureau, Regional Office of the
WORLD HEALTH ORGANIZATION
CD48/16 (Eng.) Annex B
ANALYTICAL FORM TO LINK AGENDA ITEM WITH ORGANIZATIONAL AREAS
1. Agenda Item: 4.12
2. Agenda Title: Roundtable on Climate Change and Its Impact on Public Health: A Regional Perspective
3. Responsible Unit: Risk Assessment ad Global Environmental Change Team Sustainable Development and Environmental Health Area (SDE) 4. Preparing Officers: Luiz A. Galvão and Samuel Henao 5. List of collaborating centers and national institutions linked to this Agenda item:
Centers for Disease Control and Prevention (CDC), United States Institut national de santé publique du Québec (INSPQ-CHUQ-DSP), Canada Oswaldo Cruz Foundation (FIOCRUZ), Brazil) University of Wisconsin, Human Ecology/Atmospheric and Oceanic Sciences, United States University of Harvard/Department of Environmental Health, United States
6. Link between Agenda item and Health Agenda of the Americas: Item (b) Tackling Health Determinants - Paragraph 40 The determinants of health should be tackled in order to effectively protect poor, marginalized, and vulnerable populations. This refers to determinants that are related to (a) social exclusion, (b) exposure to risks, (c) unplanned urbanization, and (d) the effects of climate change. This approach requires revision of legislative frameworks, which currently provide adverse incentives for the improvement of health determinants. Notes and References - Paragraph 32 The variables included in this grouping are the following: (a) social exclusion: income, gender, education, ethnic origin, and disability; (b) exposure to risks: poor living and working conditions, unhealthy lifestyles, lack of information, difficulty in accessing food and water, soil, water and air pollution, and contaminated food; (c) unplanned urbanization exacerbates the inadequate water services, sanitation, and housing; and (d) among the consequences of climate change are floods, droughts, and vector-borne diseases, which affect poor population with higher intensity. 7. Link between Agenda item and Strategic Plan 2008-2012: SO 8: To promote a healthier environment, intensify primary prevention and influence public policies in all sectors so as to address the root causes of environmental threats to health.
RER 8.2: Member States supported through technical cooperation for the implementation of primary prevention interventions that reduce environmental health risks; enhance safety; and promote public health, including in specific settings and among vulnerable population groups (e.g. children, older adults).
IND 8.2.5: Number of countries following WHO’s guidance to prevent and mitigate emerging occupational and environmental health risks, promote equity in those areas of health and protect
- 2 -
vulnerable populations. RER 8.3: Member States supported through technical cooperation to strengthen occupational and environmental health policy-making, planning of preventive interventions, service delivery and surveillance.
IND 8.3.1: Number of countries receiving technical and logistical support for developing and implementing policies for strengthening the delivery of occupational and environmental health services and surveillance.
RER 8.4: Guidance, tools, and initiatives created to support the health sector to influence policies in priority sectors (e.g. energy, transport, agriculture), assess health impacts, determine costs and benefits of policy alternatives in those sectors, and harness non-health sector investments to improve health.
IND 8.4.4: Number of regional or national events conducted with PASB’s technical cooperation with the aim of building capacity and strengthening institutions in health and other sectors for improving policies relating to occupational and environmental health in at least 3 sectors.
SO 5: To reduce the health consequences of emergencies, disasters, crises and conflicts, and minimize their social and economic impact.
RER 5.5: Member States supported through technical cooperation to strengthen national preparedness and establish alert and response mechanisms for food safety and environmental health emergencies.
IND 5.5.2: Number of countries with national plans for preparedness, and alert and response activities with respect to chemical, radiological and environmental health emergencies.
8. Best practices in this area and examples from other countries within AMRO: 1. Country Profiles on Climate Change and Health of the Americas – 2008 2. Workshop on Climate Change and Health – Brazil, April 2008 3. Regional Communication Initiative on Climate Change and Health – April-November 2008 9. Financial implications of Agenda item: PAHO should allocate enough funds to support the Regional Plan of Action on Climate Change and Health, particularly to the SDE Area/Vector Control and Disaster Emergency when it is developed. Funds needed approximately US$ 300,000 (consultants and activities) to be mobilized through WHO and direct PAHO efforts.
- - -
PAN AMERICAN HEALTH ORGANIZATION WORLD HEALTH ORGANIZATION
48th DIRECTING COUNCIL 60th SESSION OF THE REGIONAL COMMITTEE
Washington, D.C., USA, 29 September-3 October 2008
Provisional Agenda Item 4.12 CD48/16, Add. II (Eng.) 30 September 2008 ORIGINAL: ENGLISH
ROUNDTABLE ON CLIMATE CHANGE AND ITS IMPACT ON PUBLIC HEALTH: A REGIONAL PERSPECTIVE
FINAL REPORT
Climate Change and Health 1. For several years, PAHO’s Directing Council has included a roundtable as an agenda item related to a given year’s World Health Day (WHD) theme. WHD is celebrated annually on April 7, which marks the founding of the World Health Organization (WHO) and serves as an opportunity to draw worldwide attention to a subject of major importance to global health. “Protecting Health from Climate Change” was selected as the 2008 WHD theme and a roundtable on the topic was held during the 48th Directing Council in September 2008. 2. The United Nations Framework Convention on Climate Change (UNFCCC) defines climate change as “change of climate which is attributed directly or indirectly to human activity that alters the composition of the global atmosphere and which is in addition to natural climate variability observed over comparable time periods.”1 The United Nations (UN) and the Intergovernmental Panel on Climate Change (IPCC) have devoted considerable time to analyzing the issue of climate change and have concluded that the effects of rising temperature on some aspects of human health are already being observed; that the net global effect of projected climate change on human health is expected to be negative, especially in developing countries, small island developing States, and vulnerable local communities which have the least capacity to prepare for and adapt to such change, and that exposure to projected climate change could affect the health status of millions of people, through increases in malnutrition, death, disease, and injury due to extreme weather events, in the burden of diarrheal disease, in the frequency
1 Article 1, paragraph 2 of the Convention, UN, 1992.
CD48/16, Add. II (Eng.) Page 2 of cardio-respiratory diseases, and through changes in the distribution of some infectious disease vectors. 3. In the Region of the Americas, major areas of concern relate to an increase in extreme weather events, subsequent changes in food supply and nutritional security, as well as changes in water supply, in the range and distribution of vector-borne diseases, and in rising sea levels. The impacts of climate change on cities will become increasingly important, and in some countries will be made worse as a result of rapid and poorly planned urbanization. 4. In light of the strong, global scientific consensus that warming of the climate system is unequivocal and is affecting human health, the World Health Assembly in 2008 adopted a resolution (WHA61.19) requesting, inter alia, the Director General " to consult Member States on the preparation of a workplan for scaling up WHO’s technical support to Member States for assessing and addressing the implications of climate change for health and health systems, including practical tools and methodologies and mechanisms for facilitating exchange of information and best practice and coordination between Member States, and to present a draft workplan to the Executive Board at its 124th session.” 5. The Pan American Health Organization is in the process of developing a plan of action, which is based on a Regional Workshop on Climate Change and its Effects on Health in the Americas, held in Brazil from 9 to 11 April 2008, a series of country consultations, and regional country profiles prepared during March 2008. The objective of the White Paper on Climate Change and Public Health is to present the evidence that climate change is a phenomenon that is increasingly affecting human health and to describe a set of actions that are needed in order to protect people from current and expected climate related health impacts. 6. The goals of the proposed plan would seek to empower, equip, and strengthen the capacity of health systems locally and nationally to protect human health from risks related to climate change, ensuring that concerns about public health security are placed at the center of the response to climate change. It should support the development and implementation of adaptation strategies at local, national, and regional levels to minimize the health impacts of climate change, and encourage the adoption of energy measures to mitigate climate change and avoid further and potentially disastrous impacts on health. 7. The strategic objectives to be achieved can be summarized as Evidence, Sensitization, Resources, Adaptation, and Partnerships. There are numerous actions needed to facilitate the achievement of these objectives, most of which need to be carried out with the participation of other sectors.
CD48/16, Add. II (Eng.) Page 3
8. PAHO and WHO are closely collaborating on the topic of climate change in the Americas and worldwide, in an effort to increase awareness of its health consequences, assess country-specific risks, strengthen health systems to ensure adequate protection from climate-related risks, and enhance the inclusion of a public health perspective on climate change decision-making in other sectors. 9. The most relevant themes analyzed during the three discussion groups of the roundtable are presented in the following points: (a) Most of the countries of the Region participated in group discussions. There was
consensus among these countries that climate change is already causing health impacts. This makes the proposed Regional Plan of Action relevant and timely for the Member States.
(b) Moral and ethical questions were raised related to the causes of climate change,
where the largest effects are being seen, and compensation for the impacts. Issues of environmental justice and human rights mean that mitigation and adaptation actions need to be undertaken.
(c) The development and economic models followed by some of the countries of the
Region are unsustainable. Lack of planning, deforestation, waste management (including the lack of recycling), and infrastructure development all have impacts on the environment, agriculture, tourism, and health.
(d) Current production and consumption patterns, and the reliance on fossil fuels,
impact the environment and exacerbate climate change. These are the central causes of the problem. However, because climate change is a long-term phenomena, countries need to take actions to minimize the problem and allocate necessary resources. The proposed Plan of Action addresses these concerns.
(e) The proposal of a Regional Observatory on climate change and health was
supported. Further research, including vulnerability assessments, should be conducted where this information currently does not exist. It was emphasized that this observatory should include not only health information but also data from other related sectors in order to make comprehensive assessments and promote preventive action.
(f) Education and information programs, targeted to different groups, should focus on
raising public awareness and the actions which individuals should take to minimize their impacts on the environment and on how they can protect themselves from climate change.
CD48/16, Add. II (Eng.) Page 4 (g) Green ecological strategies need to be implemented at every level. (h) PAHO needs to work with countries in the identification and mobilization of
resources for action on climate change and health. The creation of a regional fund was suggested.
(i) The proposed Regional Plan of Action is very comprehensive in its lists of
actions, and these need to be translated into national plans of actions focused on individual country priorities and local needs using the national profiles on climate change and health. The proposal to establish focal points on climate change within the ministry of health was supported. The tools mentioned in the proposed Plan of Action are still under development.
(j) Alignment and integrated cooperation within the national ministries and also
within the areas and programs of PAHO is needed for a comprehensive response to the proposed Plan of Action.
(k) It is suggested that indicators be developed for evaluating the achievement of the
goal of the proposed Plan of Action. (l) Partnerships need to be expanded and supplemented to share the existing
expertise and experiences of countries. Skills that are currently lacking can also be developed through such partnerships.
(m) Current population movements spread diseases into areas now susceptible to their
transmission. Large-scale population movements can also be a result of climate change.
(n) Although National Plans of Actions need to be developed, there are aspects of the
proposed Regional Plan of Action that can be put into implementation immediately.
- - -
ANNEX 4
Pan American Health Organization in collaboration with the
Department of Disaster Management, British Virgin Islands
WORKSHOP REPORT
Maria’s by the Sea Hotel and Restaurant Road town, Tortola, British Virgin Islands
July 14 – 15, 2008
Report on the Elderly in Disasters Workshop
Page 2
TABLE OF CONTENTS
1.0 INTRODUCTION................................................................................... 3 2.0 OPENING CEREMONY........................................................................... 4 3.0 OBJECTIVES AND ORGANISATION OF THE SEMINAR ............................. 4 4.0 REPORT OF SESSIONS ......................................................................... 5
Report on the Elderly in Disasters Workshop
Page 3
Elderly in Disasters WORKSHOP REPORT
Maria’s by the Sea Hotel and Restaurant Road town, Tortola, British Virgin Islands
July 14 – 15, 2008
1.0 INTRODUCTION Disasters affect every part of society, from young to old, able bodied to disabled. However the burden from a disaster is not shared equally throughout society. Disasters are known to have a disproportionately high impact on the elderly. This is due to a variety of factors including increased vulnerability from physical factors such as chronic disease and disability as well as multiple social factors. Globally, the proportion of older people is growing faster than any other age group. In 2000, one in ten or about 600 million people were 60 years or older. By 2050 this figure is expected to reach around 1.9 billion people. In the Caribbean, the UN estimates that the over 60 population will increase from 11.1% (4,500,000) in 2005 to 24.6% (12,400,000) in 2050. In recognition of these issues, the Emergency Preparedness and Disaster Relief Area of the Pan American Health Organization in collaboration with the British Virgin Islands Department of Disaster Management hosted a workshop on the Elderly in Disasters at Maria’s by the Sea Hotel, British Virgin Islands from July 14 – 15, 2008. A copy of the Workshop Agenda is attached as Annex I. The workshop brought policy makers from disaster management and social development together with nursing home managers and international and local NGO’s such as HelpAge International and VOICE. CDERA and CARICOM were also in attendance. Participants at this workshop reviewed the challenges involved in providing care for the elderly before, during and after a disaster and identified potential strategies which can help to address these challenges. A copy of the list of participants is attached at Annex II.
Report on the Elderly in Disasters Workshop
Page 4
2.0 OPENING CEREMONY
The Workshop’s Opening Ceremony was held at 0900 hrs on July 14, 2008 and was chaired by Evan Inniss from PAHO, Barbados. Territorial-at-Large Representative, The Honourable Irene Penn-O’Neal delivered remarks on behalf of the Deputy Premier and Minister for Health and Social Development, Honourable Dancia Penn, QC, OBE, who was currently away from BVI on official business. The opening of the workshop also included remarks from Monica Zaccarelli Davoli, Deputy Director of the BVI Department of Disaster Management (DDM), Mr. Zebelon McLean, Coordinator of the CDERA, Mr. Jeremy Collymore and the Director of BVI DDM Sharleen DaBreo. Copies of The Honourable Penn-O’Neal and Jeremy Collymore’s remarks are attached.
Approximately 35 persons attended the opening ceremony including BVI’s newly appointed acting Permanent Secretary in the Ministry of Health and Social Development, Ms. Petrona Smith also attended the opening of the workshop.
3.0 OBJECTIVES AND ORGANISATION OF THE SEMINAR
3.1 Workshop Objectives
The Workshop sought to: 1. Review the impact of disasters on the elderly 2. Increase awareness of their specific vulnerabilities and needs. 3. Identify challenges in caring for the elderly before, during and after a
disaster. 4. Make recommendations to guide the development of tools and materials
to address the specific needs of the elderly. 5. Identify training needs to ensure proper management of the elderly
before, during and after a disaster 3.2 Organization of the Workshop
The Workshop was organized into plenary sessions and working group sessions. Plenary 1, Impact of disasters on the elderly, set the stage for the discussions by presenting the epidemiology of disasters, indicating the vulnerability of the population and highlighted the specific needs of the elderly. Presentations were made on the following: I. Elderly in Disasters II. Challenges in providing humanitarian aid to the elderly III. Care of elderly in disasters in the Caribbean Plenary 2, Responding to the needs of the Elderly, focussed on sharing the experience and challenges faced in caring and planning for the elderly before, during and after a disaster.
Report on the Elderly in Disasters Workshop
Page 5
Presentations included:
I. Hurricane Katrina in USA: Experiences of the management of the Elderly
II. Hurricane Ivan in Grenada: Case Study on the needs and challenges of dealing with the Elderly
III. Results of the BVI Elderly and Disabled Emergency Preparedness & Response Assessment
IV. Trinidad’s National Policy on Ageing Working Groups identified challenges faced in and proposed strategies for caring for the elderly before, during and after disasters.
A copy of the Workshop Agenda is attached.
4.0 REPORT OF SESSIONS
4.1 Plenary 1 - Impact of disasters on the elderly
1. Impact of Disasters on the Elderly Dr Dana van Alphen, Pan American Health Organization
Dr van Alphen in her presentation highlighted the importance of considering the particular needs of the elderly in disasters. It was noted that PAHO, in its role in supporting countries to ensure systems are better prepared to cope with disasters, is working to identify the scope of the issue and suitable actions for the future. The presentation outlined the impact disasters had on the elderly namely • Heat wave in France - 70% of deaths were in over 70’s age group • Hurricane Katrina in the USA - 74% of the dead were over the age of
60, and nearly half were over 75. The results of a telephone survey conducted by PAHO Barbados of nursing homes in Barbados, Trinidad and Tobago, BVI and Jamaica were shared and the following issues were noted. I. Between 1.2 and 3.24% of the elderly population in the Caribbean
countries sampled lived in homes.
II. Approximately 2/3 of residents in homes are women.
III. The majority of residents are disabled or require help mobilizing
IV. The governance arrangements for homes varied in each Caribbean country
V. There is little available information on disaster response plans in homes or their capacity to cope with a disaster.
Report on the Elderly in Disasters Workshop
Page 6
2. Challenges in providing humanitarian aid to the elderly in
disasters Mary Lee Ellis, International Federation of Red Cross and Red Crescent Societies
In highlighting some challenges in providing humanitarian aid to the elderly in disasters, the IFRC Capacity Building Officer suggested that some these challenges were exacerbated by misconceptions that the elderly will be cared for by family and other agencies and discrimination caused by the prejudices held by individuals, communities, government and aid organizations. There was general agreement from the Workshop participants that challenges in caring for the elderly during a disaster included: • Lack of mobility • Chronic Poor Health • Nutritional Needs • Isolation
Good practices to address some of these challenges included:
• Training health and response staff to the particular needs of the elderly during a disaster
• Including simple mobility aids in relief packages for those are less mobile
• Establishing food kitchens for the elderly with specific supplementary food in sizes that can be easily carried
The Vulnerability and Capacity Assessment (VCA) as a tool to help communities address the root causes of vulnerability was discussed and its potential usefulness acknowledged by the workshop participants.
3. Care of the Elderly in Disasters in the Caribbean Jeff James, HelpAge International
In this presentation, Mr James highlighted that although the elderly were a resilient and valuable community resource, emergency interventions failed to notice or acknowledge their contribution. The results of the 2005 Caribbean Regional Development Centre Needs Assessments carried out by HelpAge in communities in St Vincent and the Grenadines, St Lucia and Grenada were noted.
Report on the Elderly in Disasters Workshop
Page 7
These assessments highlighted the following as reasons that make the elderly more vulnerable to disasters: • They lived in highly vulnerable areas • Their low literacy levels prevented them from fully benefiting from
printed disaster preparedness materials • Absence of communications tools which would allow them to be
alerted to imminent disasters
4. Plenary 1 discussion
The discussion following presentations in Plenary 1 raised the following:
• Strategies that were used or could be used in responding to the needs of the elderly after a disaster impact.
• The vulnerability of nursing and elderly homes etc that cater for the elderly as it relates to the location and structure of homes for the elderly.
• The need to mainstream disaster management into all sectors
• The importance of working at community level e.g. linking parishes together.
• The need to highlight the impact of disasters on elderly men as they often do not have social support structures.
4.2 Plenary 2 - Impact of disasters on the elderly
Plenary 2 focused on sharing the experience and challenges faced in caring and planning for the elderly before, during and after a disaster. The first two presentations were case studies illustrating the impact of two different hurricanes on the elderly. 1. Hurricane Katrina in USA: Experiences of the Management Of
The Elderly - Sam Vigersky
This presentation highlighted lessons learnt in dealing with the elderly in the aftermath of Hurricane Katrina in the USA and how new technology could be used in the future. Key observations made after visiting shelters in the affected area were: • The elderly were disproportionately affected • Community support for the elderly was disaggregated • The elderly were least likely to ask for help • Issues with intimidation, isolation and transportation • The lack of a policy to accommodate the elderly or disabled at the
service centre
Report on the Elderly in Disasters Workshop
Page 8
Mr Vigersky proposed the use of Wiki technology as a tool that could help to address some of these challenges as it would allow the exchange of information over the internet.
2. Hurricane Ivan in Grenada: Case Study on the Needs and Challenges of dealing with the Elderly
Winnifred Gilbert, Richmond Hill Home This presentation was a very powerful and personal account of Matron
Gilbert’s experience on how the Richmond Hill Home dealt with Hurricane Ivan’s impact. The presenter gave a very graphic account of challenges and issues faced during and in the aftermath of the hurricane’s impact which included:
• Lack of preparedness of the staff to deal with a hurricane even
though there were adequate warnings • Absence of a Disaster Plan that could be followed especially after the
impact • The vulnerability of the building and the lack of provisions to handle
such emergencies
The workshop noted that the lessons learnt from the Hurricane Ivan experience has been reviewed and are being used to initiate activities aimed at improving the level of preparedness at the Richmond Hill Home in Grenada including the retrofitting of the building and its roof.
3. Results of the BVI Elderly and Disabled Emergency Preparedness
& Response Assessment Kimberlee Mobley, BVI Department of Disaster Management (DDM) BVI DDM conducted a survey of BVI’s Disabled and Elderly Homes and in presenting the results of the Survey, the consultant highlighted the following: • Majority of residents have limited/no mobility and/or disabilities that
require assistance continually. • The facilities are older structures with a number of noted safety
concerns and operational deficiencies. • Two (2) of the facilities were leased by the government and need
modifications for safety and welfare issues • Few of the facilities had Disaster Plans The main recommendations coming out of this Assessment related to the training for persons who work in the facilities, scheduling of emergency drills and the development of Disaster Plans for all the facilities. The workshop participants also noted that the BVI DDM has already started to implement some of the recommendations through the
Report on the Elderly in Disasters Workshop
Page 9
development of a Disaster Plan Template which would be used to guide all the facilities in BVI to develop a Disaster Plan. A copy of the template was shared with the workshop participants.
4. Trinidad’s Draft National Policy on Ageing Gaynelle Abraham-Brathwaite, Ministry of Social Development,
The Workshop noted that Trinidad and Tobago had developed a National Policy on Ageing using a multi-disciplinary committee with representation from the public and private sectors, non-governmental organizations and the input from public consultations. The policy was passed in Cabinet in September 2006. The overall goal of the policy is to promote the well being of older persons in a sustainable manner and provide older persons with the opportunity to be integrated into the mainstream of society. The policy has the following 12 priority areas: 1. Social Security 2. Income security and Employment 3. Participation, involvement and social inclusion 4. Dignity and respect for older persons 5. Healthcare and standards for care facilities 6. Housing 7. Education and training 8. Recreation 9. Legislation 10. Transportation 11. Disaster Preparedness 12. Research
In presenting this policy, Ms Abraham-Brathwaite highlighted some of the institutional and administrative arrangements that need to be put in place to effectively implement the policy. These included • The need for utilizing a community-based multi-sectoral approach • Utilization of existing institutions and the importance of networking • The need for the government, the private sector and civil sector to
work together
Copies of the policy were provided to workshop participants. 5. Plenary 2 - Discussion
Discussion following Plenary 2 focused on the mitigative and preventative measures that should have been employed in Grenada to help the

Report on the Elderly in Disasters Workshop
Page 10
Richmond Hill Home mitigate and respond the adverse effects of Hurricane Ivan. The need for national disaster offices and elderly homes to work together was strongly highlighted and was seen as a critical step in bring the issue of elderly in disasters to the forefront. The workshop noted that a Disaster Plan had been developed for the Adina Donovan Home in the British Virgin Islands and that work was ongoing for all the homes in BVI to have such a plan. Much discussion ensued on the National Policy on Ageing for Trinidad and Tobago as the workshop participants viewed it as a model that could be considered by other Caribbean states. Whilst acknowledging the appropriateness of the 12 priority areas, participants highlighted the potential interconnectivity of some of the priority areas and urged Trinidad and Tobago to ensure that disaster preparedness is not seen as a stand-alone area but that activities be undertaken to mainstream disaster preparedness throughout the various priority areas.
4.3 Results of Working Group Activity 1. Identification of Needs and Challenges
The working groups on day 1 allowed further exploration of the needs and identified challenges in caring for the elderly before, during and after a disaster. The groups concurred with the needs the elderly as highlighted by the various presentations and proposed that the following challenges needed to be addressed if countries were to adequately care for the elderly during a disaster. • Absence of baseline data on the elderly population • Lack of groups advocating the rights of the elderly • Absence of established mandates and legislation ensuring the
provision of care to older persons • Recognition by policy makers that although older people are
vulnerable they have special skills and can be a valuable resource. • Lack of proper coordination and communication to ensure that the
needs of the elderly are adequately addressed before, during and after a disaster
• Limited financial and human resources • Recognition of the nutritional needs of the elderly and including this
consideration in the relief supplies that are provided • Erosion of social responsibility which leads to inadequate community
response mechanisms • Political inference in the distribution of humanitarian aid
Report on the Elderly in Disasters Workshop
Page 11
2. Identification of strategies to address the challenges in caring for the elderly
The working groups on day 2 made recommendations and agreed to undertake specific activities that would address the specific needs of the elderly highlighted in the presentations and the Working Group activity on Day 1. 2.1 Agreements were made to undertake the following activities by
December 2008
I. Barbados Elderly Care Association to work with at least 2 Nursing Homes in Barbados to develop Disaster Plans
II. Richmond Hill Home will work with NaDMA and other disaster management officials in Grenada to draft a Disaster Plan for the Nursing Home
III. National Disaster Coordinators from the British Virgin Islands and Jamaica to seek to table the issue of elderly in disasters at the next Annual Meeting of National Disaster Coordinators of the Caribbean Disaster Emergency Management Agency
IV. BVI Department of Disaster Management to finalize the National Disaster Plans for all the Elderly/Disabled/Children Homes in BVI and have a table top exercise to test some of the plans
V. Pan American Health Organization – PED to revise Caribbean DANA instruments to ensure that the issues related to the elderly are part of the DANA assessment tool.
VI. VOICE, Belize will bring the issues raised at the workshop to private elderly homes in Belize
2.2 The specific recommendations are detailed below
2.2.1 Civil Society/Community/Non-governmental
Agency Level
Short to medium term mechanisms
1. Be the champion to ensure that persons who have to work with the elderly during a disaster are appropriately trained
2. Ensure that disaster preparedness activities and literature cater for the literacy levels of the elderly
Report on the Elderly in Disasters Workshop
Page 12
by recognizing their unique vulnerabilities and contributions
Long term mechanisms
1. Develop advocacy programmes aimed at increasing awareness of policy makers and the donor community
2. Work with the relevant authorities to ensure that official baseline data on the elderly exist prior to an emergency.
3. Strength community networks for the elderly and develop tools to improve disaster management and building capacity at the community level
4. Collaborate with communities to develop strategies to strengthen community support to older people and reduce their levels of risk during disasters
2.2 National Disaster Organizations
Short to medium term mechanisms
1. Work with Nursing and Elderly Homes to develop National Disaster Plans and have these plan appropriately exercised
2. Train disaster relief staff to recognize older people’s needs and rights.
Long term mechanisms
3. Review National Relief, Search and Rescue, Evacuation and Shelter policies and plans to ensure that the needs of the elderly are included particularly as it relates to the particular risk factors and issues affecting the nutritional status of the elderly
4. Include the elderly in emergency needs assessments, targeting, planning, implementation, monitoring and evaluation.
2.3 Pan American Health Organization
Short to medium term mechanisms
1. Facilitate a working group comprising PAHO, CDERA, IFRC, HelpAge and other stakeholders to champion the issue of elderly in disaster and follow-up on the workshop recommendations.
Report on the Elderly in Disasters Workshop
Page 13
2. Revise the Emergency Response Team guidelines to ensure that the issues related to the care for the elderly are appropriately addressed.
3. Work with the Ministries of Health/Health Disaster Coordinators to develop an outline for the inclusion of elderly needs in national Health Disaster Plans.
Long term mechanisms
4. Work with the Ministries of Health and other partners to develop health and nutritional standards/guidelines for elderly in emergencies particularly in emergency shelters.
5. Develop programmes to raise awareness among agencies and organizations concerning physical and health issues specific to older people and of ways to adapt basic need support to their requirements
6. Facilitate the development of training for health staff to ensure knowledge of geriatric nutritional, health and medical care needs.
Caribbean Community
7. Include the issues of elderly in disasters on the agenda of Council for Human and Social Development (COHSOD)
5.0 CONCLUDING COMMENT
Key short term plans were the development of plans for nursing homes and assessment of homes using the template developed by BVI. The need for good quality baseline assessments and vulnerability assessments before a disaster was outlined as well as needs assessments focusing on the elderly in the aftermath of a disaster. The provision of training in managing the elderly and suitable storage of supplies for the elderly in shelters was mentioned as a priority as well as the use of community leadership and capacity building.
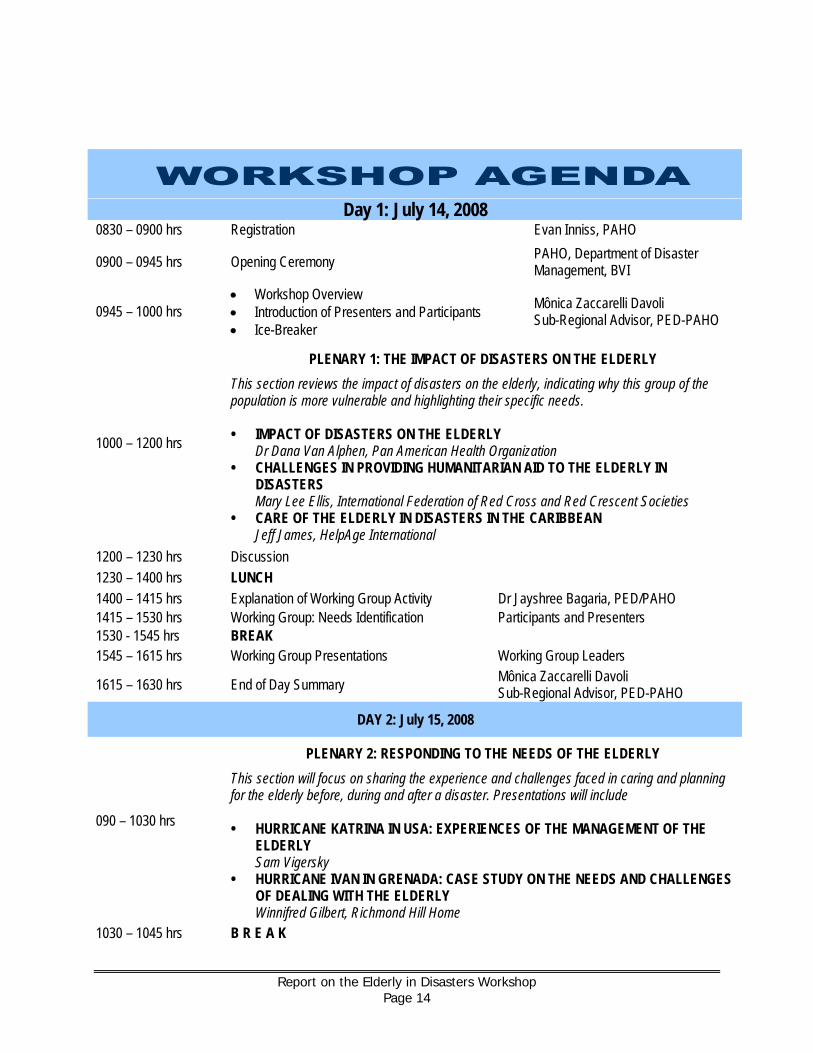
Report on the Elderly in Disasters Workshop
Page 14
Day 1: July 14, 2008 0830 – 0900 hrs Registration Evan Inniss, PAHO
0900 – 0945 hrs Opening Ceremony PAHO, Department of Disaster Management, BVI
0945 – 1000 hrs • Workshop Overview • Introduction of Presenters and Participants • Ice-Breaker
Mônica Zaccarelli Davoli Sub-Regional Advisor, PED-PAHO
1000 – 1200 hrs
PLENARY 1: THE IMPACT OF DISASTERS ON THE ELDERLY This section reviews the impact of disasters on the elderly, indicating why this group of the population is more vulnerable and highlighting their specific needs. • IMPACT OF DISASTERS ON THE ELDERLY Dr Dana Van Alphen, Pan American Health Organization • CHALLENGES IN PROVIDING HUMANITARIAN AID TO THE ELDERLY IN
DISASTERS Mary Lee Ellis, International Federation of Red Cross and Red Crescent Societies • CARE OF THE ELDERLY IN DISASTERS IN THE CARIBBEAN Jeff James, HelpAge International
1200 – 1230 hrs Discussion 1230 – 1400 hrs LUNCH 1400 – 1415 hrs Explanation of Working Group Activity Dr Jayshree Bagaria, PED/PAHO 1415 – 1530 hrs Working Group: Needs Identification Participants and Presenters 1530 - 1545 hrs BREAK 1545 – 1615 hrs Working Group Presentations Working Group Leaders
1615 – 1630 hrs End of Day Summary Mônica Zaccarelli Davoli Sub-Regional Advisor, PED-PAHO
DAY 2: July 15, 2008
090 – 1030 hrs
PLENARY 2: RESPONDING TO THE NEEDS OF THE ELDERLY This section will focus on sharing the experience and challenges faced in caring and planning for the elderly before, during and after a disaster. Presentations will include • HURRICANE KATRINA IN USA: EXPERIENCES OF THE MANAGEMENT OF THE
ELDERLY Sam Vigersky • HURRICANE IVAN IN GRENADA: CASE STUDY ON THE NEEDS AND CHALLENGES
OF DEALING WITH THE ELDERLY Winnifred Gilbert, Richmond Hill Home
1030 – 1045 hrs B R E A K
Report on the Elderly in Disasters Workshop
Page 15
1045 – 1200 hrs
PLENARY 2: RESPONDING TO THE NEEDS OF THE ELDERLY • RESULTS OF THE BVI ELDERLY AND DISABLED EMERGENCY PREPAREDNESS &
RESPONSE ASSESSMENT Kimberlee Mobley, Department of Disaster Management, British Virgin Islands
13. TRINIDAD’S DRAFT NATIONAL POLICY ON AGEING Gaynelle Abraham-Brathwaite, Ministry of Social Development, Trinidad and Tobago
1200 – 1230 hrs Discussion
1230 – 1330 hrs L U N C H
1330 – 1530 hrs Working Groups Discussions: Development of Recommendations and Strategies Participants and Presenters
1530 – 1545 hrs B R E A K
1545 – 1615 hrs Working Group Presentations Working Group Leaders
1615 – 1645 hrs Workshop Wrap Up and Closing Mônica Zaccarelli Davoli Sub-Regional Advisor, PAHO
Report on the Elderly in Disasters Workshop
Page 16
ELDERLY IN DISASTERS WORKSHOP - LIST OF PARTICIPANTS NAME JOB TITLE AGENCY ADDRESS TEL NO FAX NO EMAIL
Monica Zaccarelli Davoli
Disaster Preparedness Advisor
Pan American Health Organization
No. 8 Upton St Michael Barbados
246 436 6448 246 436 6447 [email protected]
Kimberlee Mobley (Presenter) Consultant BVI Department of
Disaster Management P.O.Box 712 St. John USVI 00831
352 346 4501 284 544 3639 [email protected]
Dana van Alphen (Presenter) Regional Advisor PAHO/WHO
c/o OPS/OMS Panama City Panama
507 66776401 507 317 0669 [email protected]
Zebalon McLean Deputy Director Department of Disaster Management
3 Wailing Road, McNamara Tortola, BVI VG 1110
284 468 4200 284 494 2024 [email protected]
Rev Clement E Francis
Coordinator for the Elderly
Ministry of Social Development
Botanical Gardens, Tanteen, St. George’s, Grenada
473 435 7680 473 440 6037 473 405 1162
473 444 1234
[email protected] [email protected]
Jennifer L Dunn Coordinator VOICE/National Council on Aging
20 Narguster Street, Belmopan, Belize 501 822-2421
Lindy Jeffery Executive Director
National Council on Ageing/ Ministry of Human Development and Social Transformation
#35 Mussel Creek Street P.O.Box 372 Belmopan Belize
501 822 1546 501 822 3978 [email protected]
Report on the Elderly in Disasters Workshop
Page 17
NAME JOB TITLE AGENCY ADDRESS TEL NO FAX NO EMAIL
Sam Vigersky (Presenter)
Emergency Management Specialist
University of Michigan – Office of Emergency Management
407-5 Nob Hill CT Ann Arbor, MI 48103 917 400 3310 [email protected]
Beverly Hall-Taylor Executive Director National Council for Senior Citizens Ministry of Labour and Social Security
11 West Kings House Road Kingston 10 Jamaica
876 926 2374-5 876 906 9277-8 876 926 2374 [email protected]
Anya Thomas Senior Project Officer, Sustainable Development
CARICOM Secretariat P.O.Box 10827 Turkeyen Greater Georgetown, Guyana
592 222 0001-75 Ext 2625
292 222 0155 [email protected]
Ronald Jackson Director General Office of Disaster Preparedness & Emergency Management
12 Camp Road Kingston 4 Jamaica
876 928 5111 876 360 7322 876 928 5503 [email protected]
Juleth Donovan Assistant Manager Adina Donovan Home for the Elderly
Main Street Road Town Tortola, BVI, VG 1110
284 494 4690
Patricia Marylee Ellis (Presenter)
Capacity Building Manager
International Federation of Red Cross and Red Crescent Societies
Picton Street Port of Spain Trinidad & Tobago
868 628 2439 868 628 7289 868 708 2957
868 628 9715 [email protected]
Winnifred Gilbert (Presenter) Registered Nurse Richmond Hill Home
Mardigras St. Paul’s Grenada
876 435 1090 876 440 2869 876 416 6949
Maureen Ward President Barbados Elderly Care Association Friendly Hall, St. Lucy 246 439 8198 246 439 8198 [email protected]
Brenda Hall Matron Cave’s Nursing Home Brydens Avenue Brittons Hill St. Michael
246 426-4382 246 427-1303 246 230-4714
246 429-8055
Report on the Elderly in Disasters Workshop
Page 18
NAME JOB TITLE AGENCY ADDRESS TEL NO FAX NO EMAIL
Dawn Leonard Health Disaster Coordinator
Ministry of Health and Social Development
R. G Hodge Building Road Town Tortola British Virgin Islands
284 494 3701 Ext 2168 [email protected]
Jeremy Collymore Coordinator Caribbean Disaster Emergency Response Agency
Building #1 Manor Lodge Lodge Hill, St Michael Barbados
246 425 0386 246 425 8854 [email protected]
Jeff James (Presenter)
Regional Representative HelpAge International 11 ½ Swallowfield Road
Kingston 5, Jamaica 876 906 3658 876 333 0147 876 906 4678 [email protected]
Gaynelle Abraham-Brathwaite (Presenter)
Project/Programme Officer
Division of Ageing Ministry of Social Development
78 Independence Square Port of Spain Trinidad and Tobago
868 623 7242 868 800 6742
Marcia Sinclair-Alexander
Director of Emergency Services
International Federation of Red Cross and Red Crescent Societies
Central Village, St. Catherine, Jamaica 876 984 7860-2 876 984 8272 malexander@jamaicaredcro
ss.org
Dr Jayshree Bagaria Short term Consultant Pan American Health
Organization Dayrells Road, Christ Church, Barbados 246 436 6448 246 436 6447 [email protected]
Evan Inniss Administrative Assistant
Pan American Health Organization
Dayrells Road, Christ Church, Barbados 246 436 6448 246 436 6447 [email protected]
ANNEX 5
PAN AMERICAN HEALTH ORGANIZATION WORLD HEALTH ORGANIZATION
27th PAN AMERICAN SANITARY CONFERENCE 59th SESSION OF THE REGIONAL COMMITTEE
Washington, D.C., USA, 1-5 October 2007
CSP27.R14 (Eng.) ORIGINAL: ENGLISH 5 October 2007
RESOLUTION
CSP27.R14
SAFE HOSPITALS: A REGIONAL INITIATIVE ON DISASTER-RESILIENT HEALTH FACILITIES
THE 27th PAN AMERICAN SANITARY CONFERENCE, Having considered the report of the Director on Safe Hospitals: A Regional Initiative on Disaster-resilient Health Facilities (Document CSP27/12) and aware of the benefit of joining forces to reduce health disaster risk; Considering that the 45th Directing Council of the Pan American Health Organization (2004) approved Resolution CD45.R8 urging Member States to adopt “Hospitals Safe from Disasters” as a national risk reduction policy and that 168 countries adopted the same goal at the World Conference on Disaster Reduction as one of the priority actions to be implemented by 2015; Aware that, according to data provided by PAHO/WHO Member States, 67% of their health facilities are located in disaster risk areas and that in the last decade nearly 24 million people in the Americas lost health care for months, and sometimes years, due to damage to health facilities directly related to disasters; Taking into account that functional collapse is the main cause of hospitals being out of service after a disaster and that access to health services is a critical need in saving lives, especially during emergencies, and is a main responsibility of the health sector and also one of the Essential Public Health Functions;
CSP27.R14 (Eng.) Page 2 Considering that the UN International Strategy for Disaster Reduction (ISDR) decided to organize, for 2008-2009, the global safe hospitals campaign as an example of a complex entity that requires the collaboration of all sectors, including financial institutions, in order to make hospitals resilient to disasters, and that the World Health Organization is the technical entity responsible for the campaign; and
In order to significantly contribute to reducing disaster risk in the Region and taking into account that the safe hospital campaign will make a major contribution to comprehensive hospital safety, including patient safety and health of workers,
RESOLVES: 1. To urge the Member States to: (a) Ensure that a specific entity in each ministry of health has the responsibility to
develop a disaster risk reduction program; (b) Actively support the 2008-2009 ISDR safe hospitals campaign through: • Establishment of partnerships with stakeholders within and beyond the health
sector, such as national disaster management organizations, planning, national and international financial institutions, universities, scientific and research centers, local authorities, communities, and other key contributors;
• Sharing and implementing best practices in order to achieve practical and
significant progress on the safe hospitals initiative at the country level; • Encouraging assessment of the existing health facilities and the potential
vulnerabilities to disasters, in order to develop long-term plans to eliminate such vulnerabilities;
• Ensuring that all new hospitals are built with a level of protection that better
guarantees that they will remain functional in disaster situations, and implementing appropriate mitigation measures to reinforce existing health facilities;
(c) Develop national policies on safe hospitals, adopt appropriate national and
international norms and standards, and monitor the safety of the health facility network;

CSP27.R14 (Eng.) Page 3
(d) To promote the inclusion of risk reduction as part of the accreditation process for health facilities.
2. To request the Director to: (a) Develop new tools to assess the likelihood that health facilities remain functional
during and after a disaster and assist Member States in their implementation; (b) Support countries in documenting and sharing best practices as well as achieving
progress on the safe hospital initiative; (c) Promote and strengthen coordination and cooperation with regional and
subregional agencies related to the issue of disasters.
(Eighth plenary meeting, 4 October 2007)
ANNEX 6
11
Elements relating to the geographic location ................................................................................... 13
Elements related to the structural safety of the facility .................................................................. 16
Elements related to non-structural safety ........................................................................................... 18
Functional capacity of the hospital ....................................................................................................... 26
Form 2
Safe Hospitals Checklist
Notice:
This form should be distributed to all members of the evaluating team. If necessary, you may photocopy this form or print additional copies from the CD-ROM included in the folder.
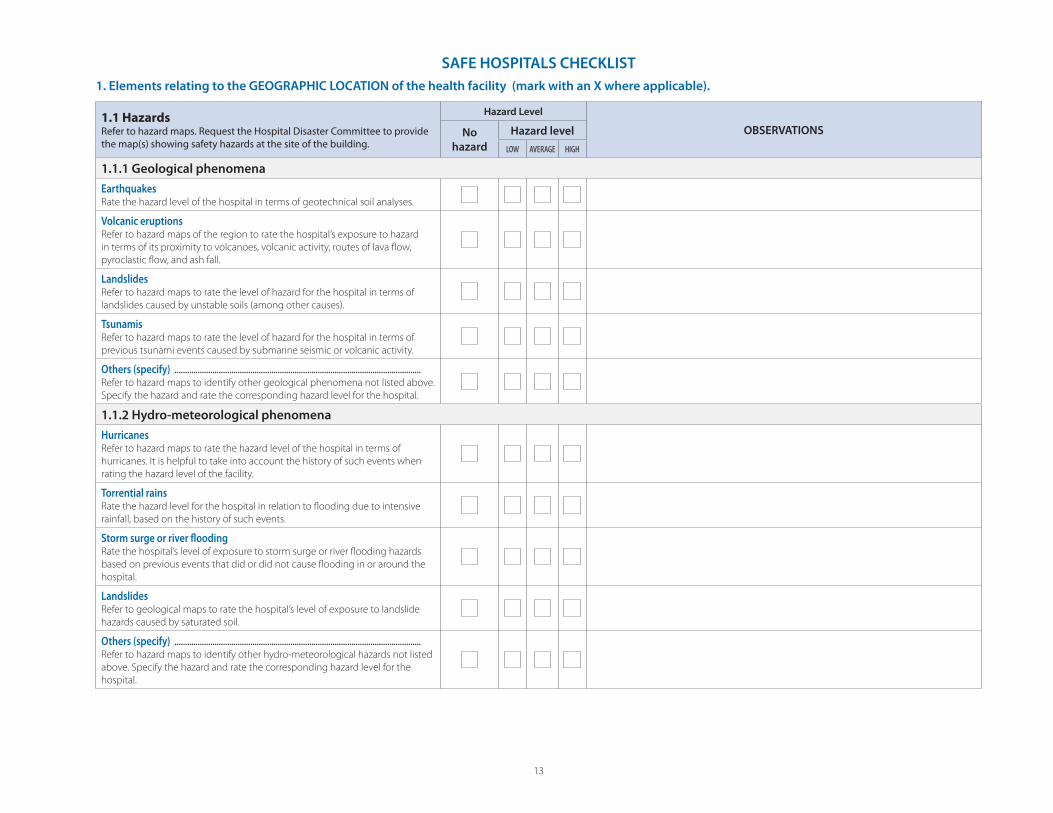
13
1. Elements relating to the GEOGRAPHIC LOCATION of the health facility (mark with an X where applicable).
1.1 Hazards Refer to hazard maps. Request the Hospital Disaster Committee to provide the map(s) showing safety hazards at the site of the building.
Hazard Level
OBSERVATIONSNo
hazard
Hazard level
LOW AVERAGE HIGH
1.1.1 Geological phenomena
EarthquakesRate the hazard level of the hospital in terms of geotechnical soil analyses.
Volcanic eruptionsRefer to hazard maps of the region to rate the hospital’s exposure to hazard
in terms of its proximity to volcanoes, volcanic activity, routes of lava fl ow,
pyroclastic fl ow, and ash fall.
LandslidesRefer to hazard maps to rate the level of hazard for the hospital in terms of
landslides caused by unstable soils (among other causes).
TsunamisRefer to hazard maps to rate the level of hazard for the hospital in terms of
previous tsunami events caused by submarine seismic or volcanic activity.
Others (specify) .....................................................................................................................Refer to hazard maps to identify other geological phenomena not listed above.
Specify the hazard and rate the corresponding hazard level for the hospital.
1.1.2 Hydro-meteorological phenomena
HurricanesRefer to hazard maps to rate the hazard level of the hospital in terms of
hurricanes. It is helpful to take into account the history of such events when
rating the hazard level of the facility.
Torrential rainsRate the hazard level for the hospital in relation to fl ooding due to intensive
rainfall, based on the history of such events.
Storm surge or river fl oodingRate the hospital’s level of exposure to storm surge or river fl ooding hazards
based on previous events that did or did not cause fl ooding in or around the
hospital.
LandslidesRefer to geological maps to rate the hospital’s level of exposure to landslide
hazards caused by saturated soil.
Others (specify) .....................................................................................................................Refer to hazard maps to identify other hydro-meteorological hazards not listed
above. Specify the hazard and rate the corresponding hazard level for the
hospital.
SAFE HOSPITALS CHECKLIST
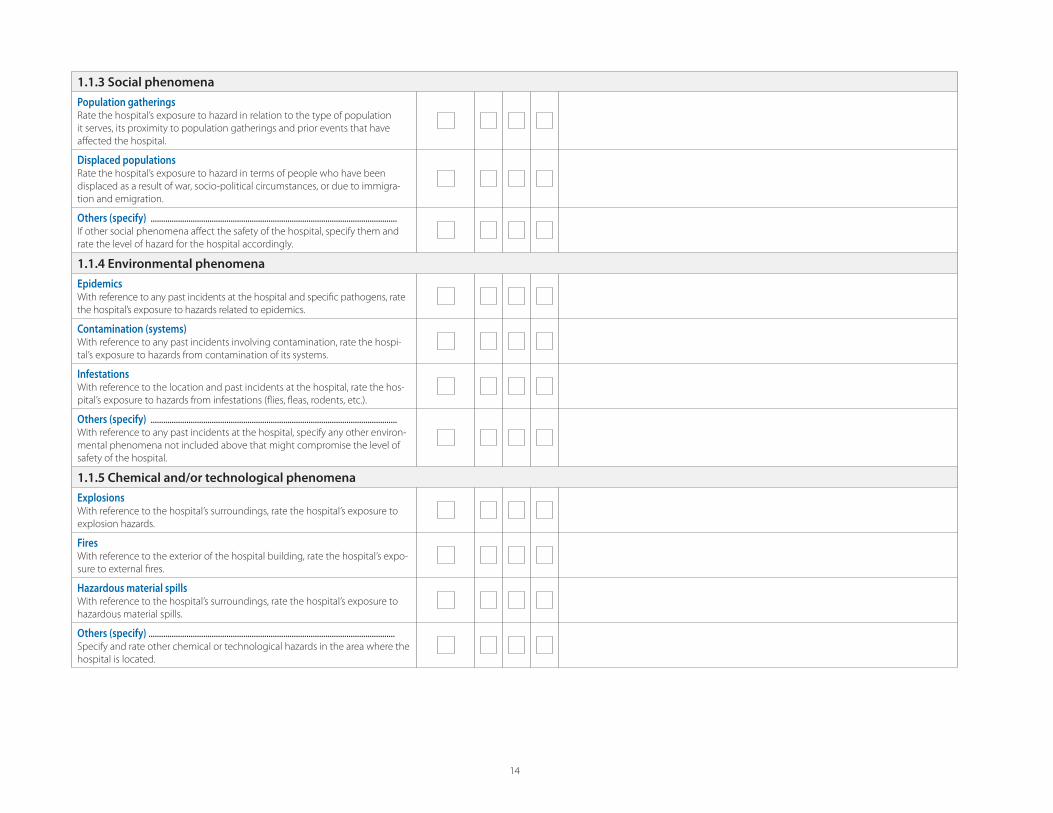
14
1.1.3 Social phenomena
Population gatheringsRate the hospital’s exposure to hazard in relation to the type of population
it serves, its proximity to population gatherings and prior events that have
aff ected the hospital.
Displaced populationsRate the hospital’s exposure to hazard in terms of people who have been
displaced as a result of war, socio-political circumstances, or due to immigra-
tion and emigration.
Others (specify) .....................................................................................................................If other social phenomena aff ect the safety of the hospital, specify them and
rate the level of hazard for the hospital accordingly.
1.1.4 Environmental phenomena
EpidemicsWith reference to any past incidents at the hospital and specifi c pathogens, rate
the hospital’s exposure to hazards related to epidemics.
Contamination (systems)With reference to any past incidents involving contamination, rate the hospi-
tal’s exposure to hazards from contamination of its systems.
Infestations With reference to the location and past incidents at the hospital, rate the hos-
pital’s exposure to hazards from infestations (fl ies, fl eas, rodents, etc.).
Others (specify) .....................................................................................................................With reference to any past incidents at the hospital, specify any other environ-
mental phenomena not included above that might compromise the level of
safety of the hospital.
1.1.5 Chemical and/or technological phenomena
Explosions With reference to the hospital’s surroundings, rate the hospital’s exposure to
explosion hazards.
Fires With reference to the exterior of the hospital building, rate the hospital’s expo-
sure to external fi res.
Hazardous material spills With reference to the hospital’s surroundings, rate the hospital’s exposure to
hazardous material spills.
Others (specify) .....................................................................................................................Specify and rate other chemical or technological hazards in the area where the
hospital is located.
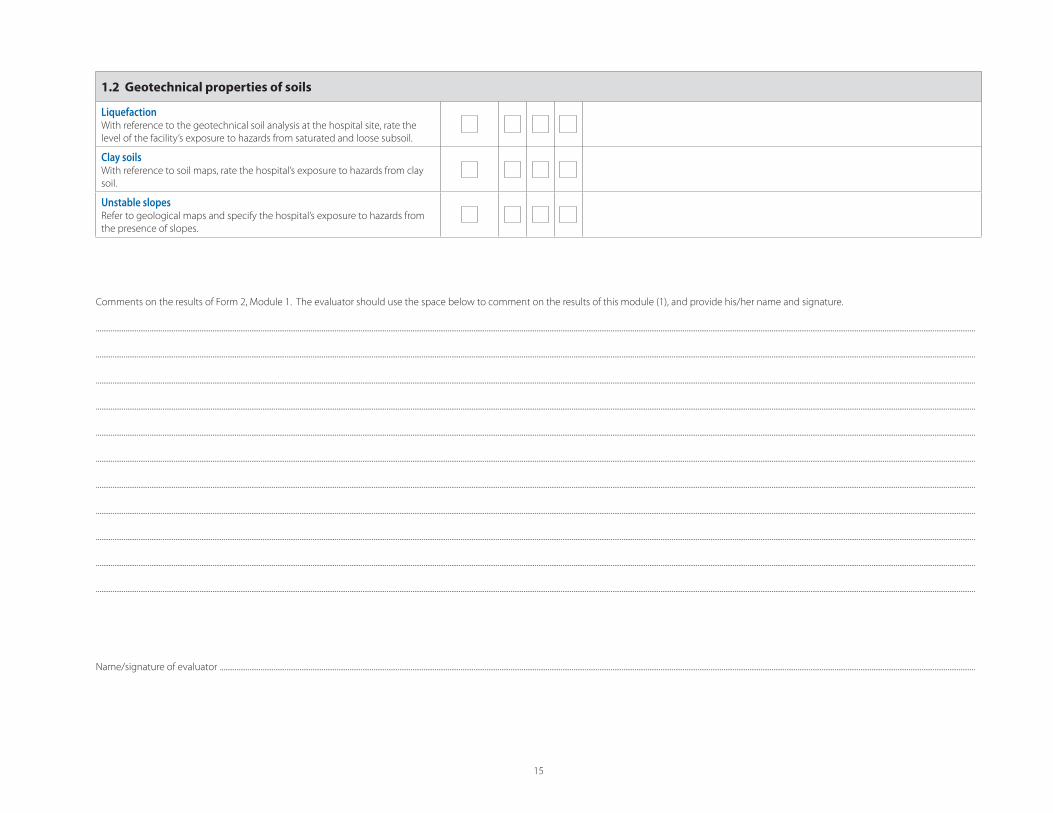
15
1.2 Geotechnical properties of soils
LiquefactionWith reference to the geotechnical soil analysis at the hospital site, rate the
level of the facility’s exposure to hazards from saturated and loose subsoil.
Clay soilsWith reference to soil maps, rate the hospital’s exposure to hazards from clay
soil.
Unstable slopes Refer to geological maps and specify the hospital’s exposure to hazards from
the presence of slopes.
Comments on the results of Form 2, Module 1. The evaluator should use the space below to comment on the results of this module (1), and provide his/her name and signature.
...........................................................................................................................................................................................................................................................................................................................................................................................................................................................................................
...........................................................................................................................................................................................................................................................................................................................................................................................................................................................................................
...........................................................................................................................................................................................................................................................................................................................................................................................................................................................................................
...........................................................................................................................................................................................................................................................................................................................................................................................................................................................................................
...........................................................................................................................................................................................................................................................................................................................................................................................................................................................................................
...........................................................................................................................................................................................................................................................................................................................................................................................................................................................................................
...........................................................................................................................................................................................................................................................................................................................................................................................................................................................................................
...........................................................................................................................................................................................................................................................................................................................................................................................................................................................................................
...........................................................................................................................................................................................................................................................................................................................................................................................................................................................................................
...........................................................................................................................................................................................................................................................................................................................................................................................................................................................................................
...........................................................................................................................................................................................................................................................................................................................................................................................................................................................................................
Name/signature of evaluator ........................................................................................................................................................................................................................................................................................................................................................................................................................
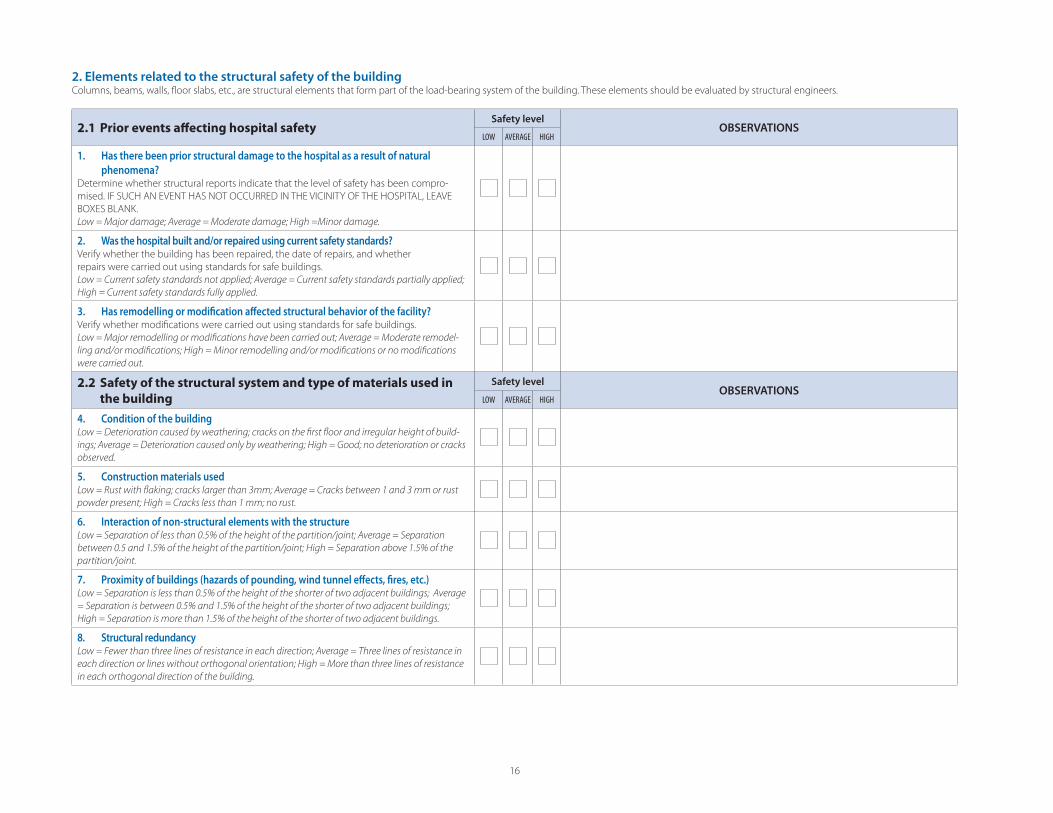
16
2. Elements related to the structural safety of the buildingColumns, beams, walls, fl oor slabs, etc., are structural elements that form part of the load-bearing system of the building. These elements should be evaluated by structural engineers.
2.1 Prior events aff ecting hospital safety Safety level
OBSERVATIONSLOW AVERAGE HIGH
1. Has there been prior structural damage to the hospital as a result of natural
phenomena?Determine whether structural reports indicate that the level of safety has been compro-
mised. IF SUCH AN EVENT HAS NOT OCCURRED IN THE VICINITY OF THE HOSPITAL, LEAVE
BOXES BLANK.
Low = Major damage; Average = Moderate damage; High =Minor damage.
2. Was the hospital built and/or repaired using current safety standards?Verify whether the building has been repaired, the date of repairs, and whether
repairs were carried out using standards for safe buildings.
Low = Current safety standards not applied; Average = Current safety standards partially applied;
High = Current safety standards fully applied.
3. Has remodelling or modifi cation aff ected structural behavior of the facility?Verify whether modifi cations were carried out using standards for safe buildings.
Low = Major remodelling or modifi cations have been carried out; Average = Moderate remodel-
ling and/or modifi cations; High = Minor remodelling and/or modifi cations or no modifi cations
were carried out.
2.2 Safety of the structural system and type of materials used in
the building
Safety levelOBSERVATIONS
LOW AVERAGE HIGH
4. Condition of the buildingLow = Deterioration caused by weathering; cracks on the fi rst fl oor and irregular height of build-
ings; Average = Deterioration caused only by weathering; High = Good; no deterioration or cracks
observed.
5. Construction materials usedLow = Rust with fl aking; cracks larger than 3mm; Average = Cracks between 1 and 3 mm or rust
powder present; High = Cracks less than 1 mm; no rust.
6. Interaction of non-structural elements with the structureLow = Separation of less than 0.5% of the height of the partition/joint; Average = Separation
between 0.5 and 1.5% of the height of the partition/joint; High = Separation above 1.5% of the
partition/joint.
7. Proximity of buildings (hazards of pounding, wind tunnel eff ects, fi res, etc.)Low = Separation is less than 0.5% of the height of the shorter of two adjacent buildings; Average
= Separation is between 0.5% and 1.5% of the height of the shorter of two adjacent buildings;
High = Separation is more than 1.5% of the height of the shorter of two adjacent buildings.
8. Structural redundancy Low = Fewer than three lines of resistance in each direction; Average = Three lines of resistance in
each direction or lines without orthogonal orientation; High = More than three lines of resistance
in each orthogonal direction of the building.
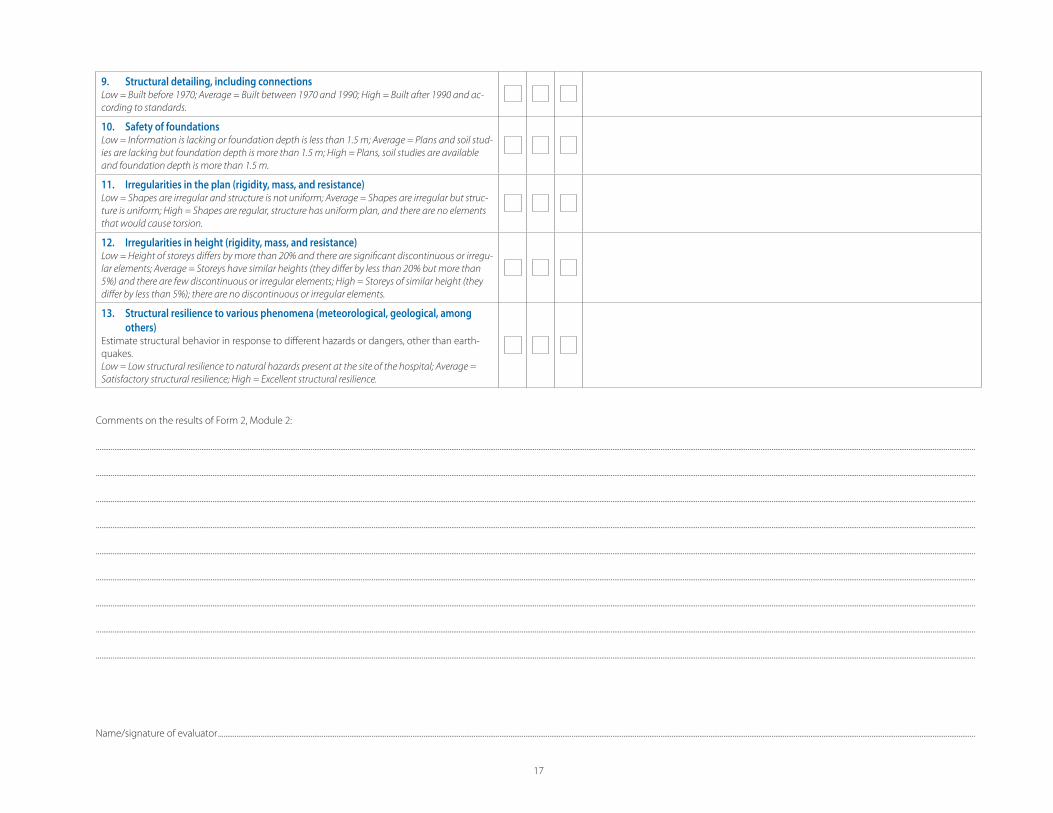
17
9. Structural detailing, including connectionsLow = Built before 1970; Average = Built between 1970 and 1990; High = Built after 1990 and ac-
cording to standards.
10. Safety of foundationsLow = Information is lacking or foundation depth is less than 1.5 m; Average = Plans and soil stud-
ies are lacking but foundation depth is more than 1.5 m; High = Plans, soil studies are available
and foundation depth is more than 1.5 m.
11. Irregularities in the plan (rigidity, mass, and resistance)Low = Shapes are irregular and structure is not uniform; Average = Shapes are irregular but struc-
ture is uniform; High = Shapes are regular, structure has uniform plan, and there are no elements
that would cause torsion.
12. Irregularities in height (rigidity, mass, and resistance)Low = Height of storeys diff ers by more than 20% and there are signifi cant discontinuous or irregu-
lar elements; Average = Storeys have similar heights (they diff er by less than 20% but more than
5%) and there are few discontinuous or irregular elements; High = Storeys of similar height (they
diff er by less than 5%); there are no discontinuous or irregular elements.
13. Structural resilience to various phenomena (meteorological, geological, among
others)Estimate structural behavior in response to diff erent hazards or dangers, other than earth-
quakes.
Low = Low structural resilience to natural hazards present at the site of the hospital; Average =
Satisfactory structural resilience; High = Excellent structural resilience.
Comments on the results of Form 2, Module 2:
...........................................................................................................................................................................................................................................................................................................................................................................................................................................................................................
...........................................................................................................................................................................................................................................................................................................................................................................................................................................................................................
...........................................................................................................................................................................................................................................................................................................................................................................................................................................................................................
...........................................................................................................................................................................................................................................................................................................................................................................................................................................................................................
...........................................................................................................................................................................................................................................................................................................................................................................................................................................................................................
...........................................................................................................................................................................................................................................................................................................................................................................................................................................................................................
...........................................................................................................................................................................................................................................................................................................................................................................................................................................................................................
...........................................................................................................................................................................................................................................................................................................................................................................................................................................................................................
...........................................................................................................................................................................................................................................................................................................................................................................................................................................................................................
Name/signature of evaluator .........................................................................................................................................................................................................................................................................................................................................................................................................................
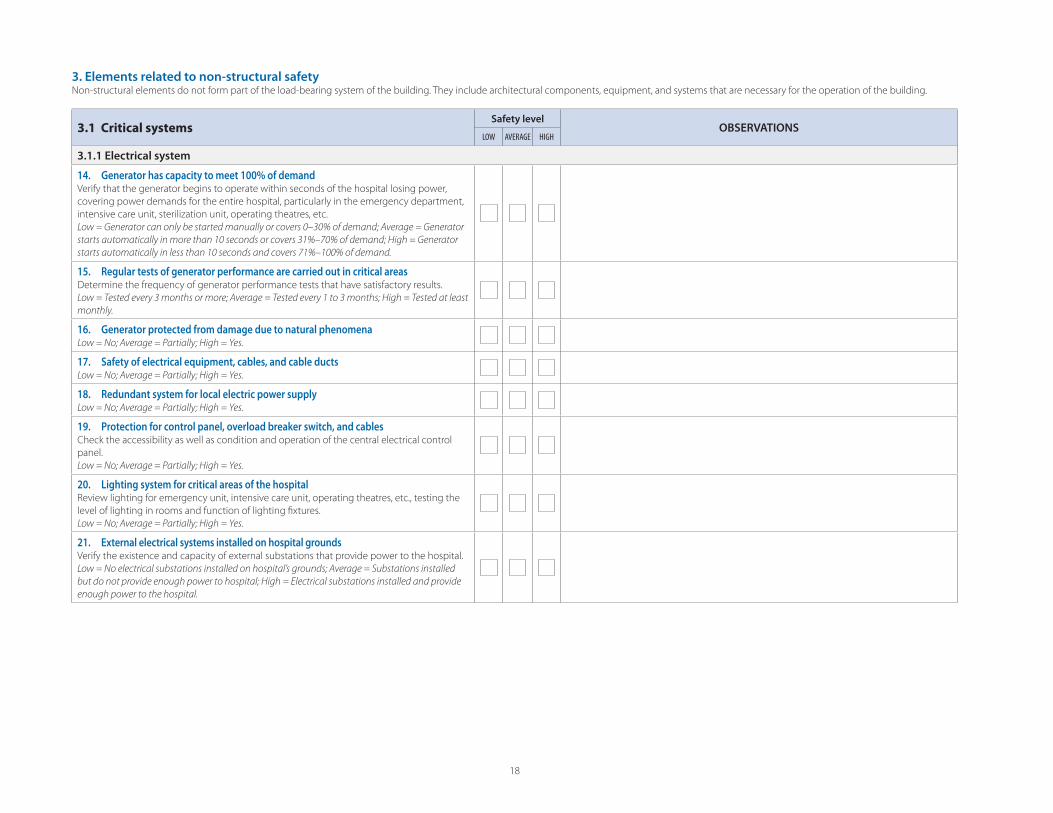
18
3. Elements related to non-structural safetyNon-structural elements do not form part of the load-bearing system of the building. They include architectural components, equipment, and systems that are necessary for the operation of the building.
3.1 Critical systemsSafety level
OBSERVATIONSLOW AVERAGE HIGH
3.1.1 Electrical system
14. Generator has capacity to meet 100% of demandVerify that the generator begins to operate within seconds of the hospital losing power,
covering power demands for the entire hospital, particularly in the emergency department,
intensive care unit, sterilization unit, operating theatres, etc.
Low = Generator can only be started manually or covers 0–30% of demand; Average = Generator
starts automatically in more than 10 seconds or covers 31%–70% of demand; High = Generator
starts automatically in less than 10 seconds and covers 71%–100% of demand.
15. Regular tests of generator performance are carried out in critical areas Determine the frequency of generator performance tests that have satisfactory results.
Low = Tested every 3 months or more; Average = Tested every 1 to 3 months; High = Tested at least
monthly.
16. Generator protected from damage due to natural phenomena Low = No; Average = Partially; High = Yes.
17. Safety of electrical equipment, cables, and cable ductsLow = No; Average = Partially; High = Yes.
18. Redundant system for local electric power supplyLow = No; Average = Partially; High = Yes.
19. Protection for control panel, overload breaker switch, and cablesCheck the accessibility as well as condition and operation of the central electrical control
panel.
Low = No; Average = Partially; High = Yes.
20. Lighting system for critical areas of the hospitalReview lighting for emergency unit, intensive care unit, operating theatres, etc., testing the
level of lighting in rooms and function of lighting fi xtures.
Low = No; Average = Partially; High = Yes.
21. External electrical systems installed on hospital groundsVerify the existence and capacity of external substations that provide power to the hospital.
Low = No electrical substations installed on hospital’s grounds; Average = Substations installed
but do not provide enough power to hospital; High = Electrical substations installed and provide
enough power to the hospital.
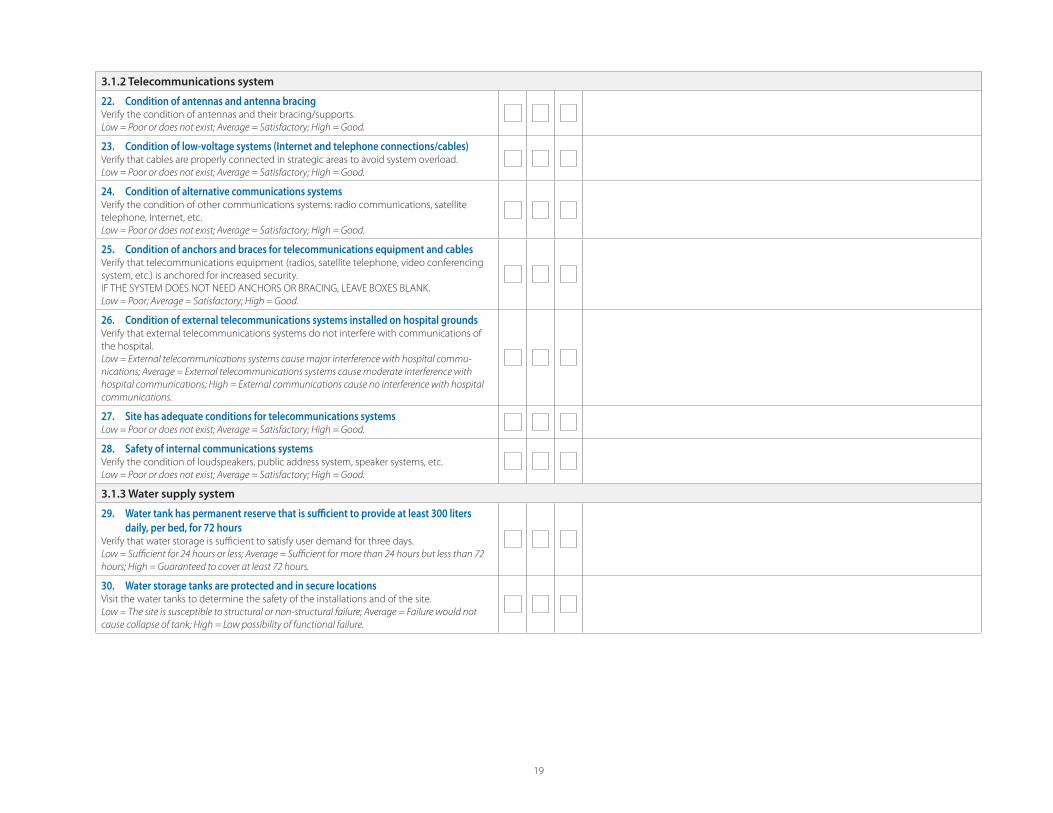
19
3.1.2 Telecommunications system
22. Condition of antennas and antenna bracing Verify the condition of antennas and their bracing/supports.
Low = Poor or does not exist; Average = Satisfactory; High = Good.
23. Condition of low-voltage systems (Internet and telephone connections/cables)Verify that cables are properly connected in strategic areas to avoid system overload.
Low = Poor or does not exist; Average = Satisfactory; High = Good.
24. Condition of alternative communications systemsVerify the condition of other communications systems: radio communications, satellite
telephone, Internet, etc.
Low = Poor or does not exist; Average = Satisfactory; High = Good.
25. Condition of anchors and braces for telecommunications equipment and cables Verify that telecommunications equipment (radios, satellite telephone, video conferencing
system, etc.) is anchored for increased security.
IF THE SYSTEM DOES NOT NEED ANCHORS OR BRACING, LEAVE BOXES BLANK.
Low = Poor; Average = Satisfactory; High = Good.
26. Condition of external telecommunications systems installed on hospital groundsVerify that external telecommunications systems do not interfere with communications of
the hospital.
Low = External telecommunications systems cause major interference with hospital commu-
nications; Average = External telecommunications systems cause moderate interference with
hospital communications; High = External communications cause no interference with hospital
communications.
27. Site has adequate conditions for telecommunications systemsLow = Poor or does not exist; Average = Satisfactory; High = Good.
28. Safety of internal communications systemsVerify the condition of loudspeakers, public address system, speaker systems, etc.
Low = Poor or does not exist; Average = Satisfactory; High = Good.
3.1.3 Water supply system
29. Water tank has permanent reserve that is suffi cient to provide at least 300 liters
daily, per bed, for 72 hoursVerify that water storage is suffi cient to satisfy user demand for three days.
Low = Suffi cient for 24 hours or less; Average = Suffi cient for more than 24 hours but less than 72
hours; High = Guaranteed to cover at least 72 hours.
30. Water storage tanks are protected and in secure locationsVisit the water tanks to determine the safety of the installations and of the site.
Low = The site is susceptible to structural or non-structural failure; Average = Failure would not
cause collapse of tank; High = Low possibility of functional failure.
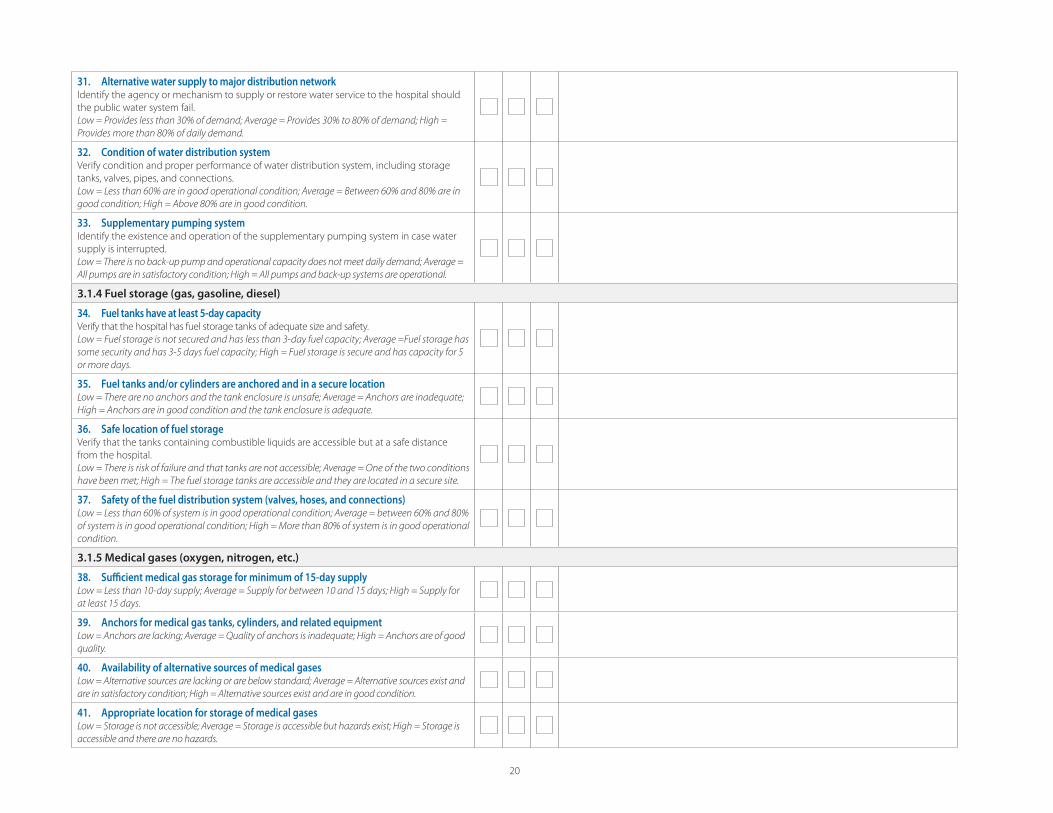
20
31. Alternative water supply to major distribution networkIdentify the agency or mechanism to supply or restore water service to the hospital should
the public water system fail.
Low = Provides less than 30% of demand; Average = Provides 30% to 80% of demand; High =
Provides more than 80% of daily demand.
32. Condition of water distribution systemVerify condition and proper performance of water distribution system, including storage
tanks, valves, pipes, and connections.
Low = Less than 60% are in good operational condition; Average = Between 60% and 80% are in
good condition; High = Above 80% are in good condition.
33. Supplementary pumping systemIdentify the existence and operation of the supplementary pumping system in case water
supply is interrupted.
Low = There is no back-up pump and operational capacity does not meet daily demand; Average =
All pumps are in satisfactory condition; High = All pumps and back-up systems are operational.
3.1.4 Fuel storage (gas, gasoline, diesel)
34. Fuel tanks have at least 5-day capacityVerify that the hospital has fuel storage tanks of adequate size and safety.
Low = Fuel storage is not secured and has less than 3-day fuel capacity; Average =Fuel storage has
some security and has 3-5 days fuel capacity; High = Fuel storage is secure and has capacity for 5
or more days.
35. Fuel tanks and/or cylinders are anchored and in a secure locationLow = There are no anchors and the tank enclosure is unsafe; Average = Anchors are inadequate;
High = Anchors are in good condition and the tank enclosure is adequate.
36. Safe location of fuel storageVerify that the tanks containing combustible liquids are accessible but at a safe distance
from the hospital.
Low = There is risk of failure and that tanks are not accessible; Average = One of the two conditions
have been met; High = The fuel storage tanks are accessible and they are located in a secure site.
37. Safety of the fuel distribution system (valves, hoses, and connections)Low = Less than 60% of system is in good operational condition; Average = between 60% and 80%
of system is in good operational condition; High = More than 80% of system is in good operational
condition.
3.1.5 Medical gases (oxygen, nitrogen, etc.)
38. Suffi cient medical gas storage for minimum of 15-day supply Low = Less than 10-day supply; Average = Supply for between 10 and 15 days; High = Supply for
at least 15 days.
39. Anchors for medical gas tanks, cylinders, and related equipment Low = Anchors are lacking; Average = Quality of anchors is inadequate; High = Anchors are of good
quality.
40. Availability of alternative sources of medical gasesLow = Alternative sources are lacking or are below standard; Average = Alternative sources exist and
are in satisfactory condition; High = Alternative sources exist and are in good condition.
41. Appropriate location for storage of medical gasesLow = Storage is not accessible; Average = Storage is accessible but hazards exist; High = Storage is
accessible and there are no hazards.
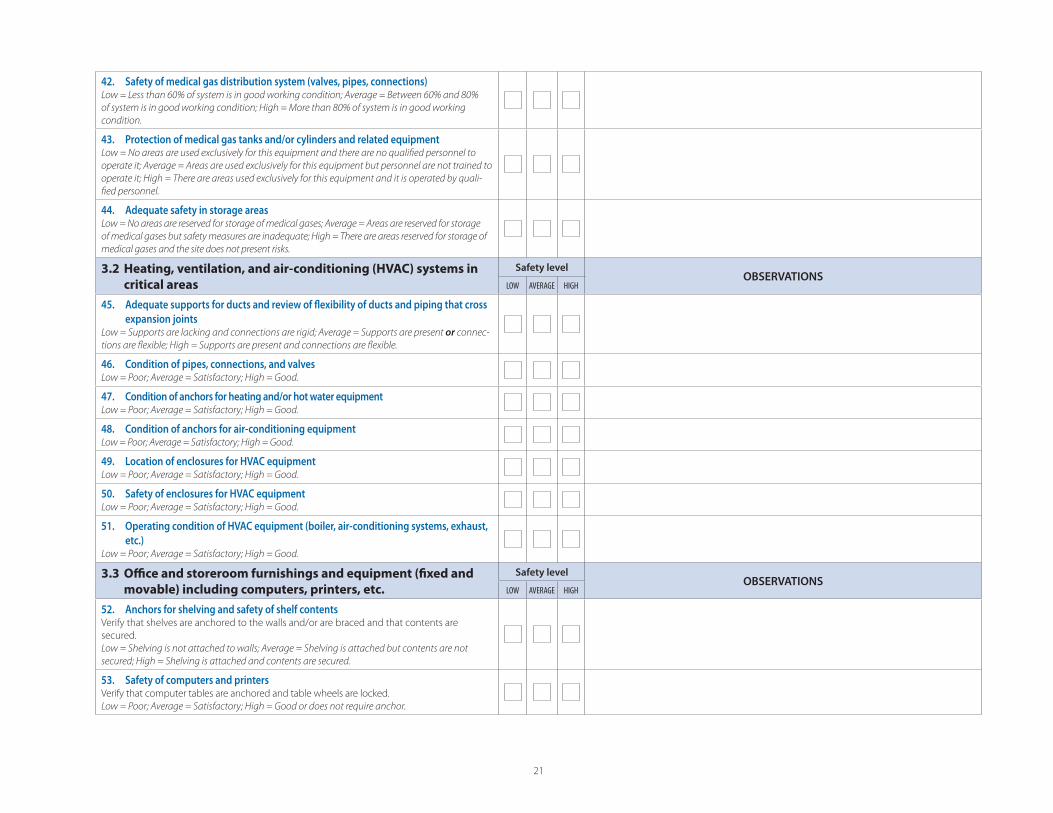
21
42. Safety of medical gas distribution system (valves, pipes, connections)Low = Less than 60% of system is in good working condition; Average = Between 60% and 80%
of system is in good working condition; High = More than 80% of system is in good working
condition.
43. Protection of medical gas tanks and/or cylinders and related equipmentLow = No areas are used exclusively for this equipment and there are no qualifi ed personnel to
operate it; Average = Areas are used exclusively for this equipment but personnel are not trained to
operate it; High = There are areas used exclusively for this equipment and it is operated by quali-
fi ed personnel.
44. Adequate safety in storage areas Low = No areas are reserved for storage of medical gases; Average = Areas are reserved for storage
of medical gases but safety measures are inadequate; High = There are areas reserved for storage of
medical gases and the site does not present risks.
3.2 Heating, ventilation, and air-conditioning (HVAC) systems in
critical areas
Safety levelOBSERVATIONS
LOW AVERAGE HIGH
45. Adequate supports for ducts and review of fl exibility of ducts and piping that cross
expansion joints Low = Supports are lacking and connections are rigid; Average = Supports are present or connec-
tions are fl exible; High = Supports are present and connections are fl exible.
46. Condition of pipes, connections, and valves Low = Poor; Average = Satisfactory; High = Good.
47. Condition of anchors for heating and/or hot water equipment Low = Poor; Average = Satisfactory; High = Good.
48. Condition of anchors for air-conditioning equipment Low = Poor; Average = Satisfactory; High = Good.
49. Location of enclosures for HVAC equipmentLow = Poor; Average = Satisfactory; High = Good.
50. Safety of enclosures for HVAC equipmentLow = Poor; Average = Satisfactory; High = Good.
51. Operating condition of HVAC equipment (boiler, air-conditioning systems, exhaust,
etc.) Low = Poor; Average = Satisfactory; High = Good.
3.3 Offi ce and storeroom furnishings and equipment (fi xed and
movable) including computers, printers, etc.
Safety levelOBSERVATIONS
LOW AVERAGE HIGH
52. Anchors for shelving and safety of shelf contentsVerify that shelves are anchored to the walls and/or are braced and that contents are
secured.
Low = Shelving is not attached to walls; Average = Shelving is attached but contents are not
secured; High = Shelving is attached and contents are secured.
53. Safety of computers and printersVerify that computer tables are anchored and table wheels are locked.
Low = Poor; Average = Satisfactory; High = Good or does not require anchor.
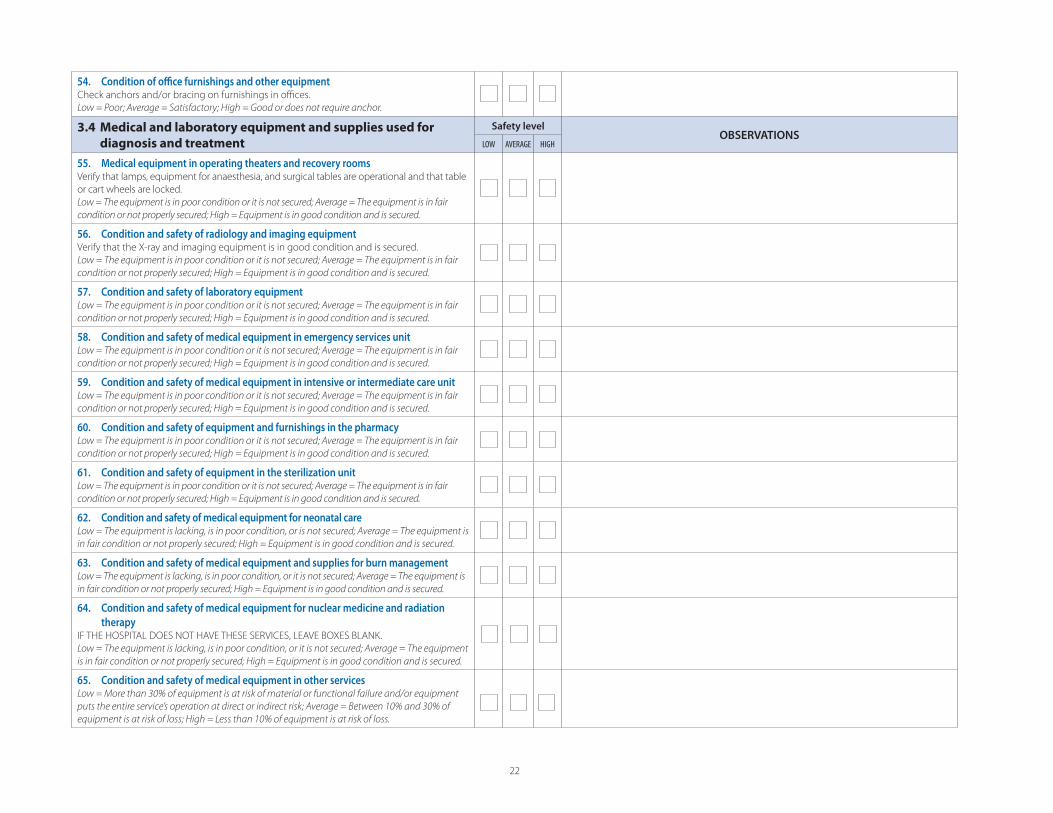
22
54. Condition of offi ce furnishings and other equipmentCheck anchors and/or bracing on furnishings in offi ces.
Low = Poor; Average = Satisfactory; High = Good or does not require anchor.
3.4 Medical and laboratory equipment and supplies used for
diagnosis and treatment
Safety levelOBSERVATIONS
LOW AVERAGE HIGH
55. Medical equipment in operating theaters and recovery roomsVerify that lamps, equipment for anaesthesia, and surgical tables are operational and that table
or cart wheels are locked.
Low = The equipment is in poor condition or it is not secured; Average = The equipment is in fair
condition or not properly secured; High = Equipment is in good condition and is secured.
56. Condition and safety of radiology and imaging equipmentVerify that the X-ray and imaging equipment is in good condition and is secured.
Low = The equipment is in poor condition or it is not secured; Average = The equipment is in fair
condition or not properly secured; High = Equipment is in good condition and is secured.
57. Condition and safety of laboratory equipmentLow = The equipment is in poor condition or it is not secured; Average = The equipment is in fair
condition or not properly secured; High = Equipment is in good condition and is secured.
58. Condition and safety of medical equipment in emergency services unitLow = The equipment is in poor condition or it is not secured; Average = The equipment is in fair
condition or not properly secured; High = Equipment is in good condition and is secured.
59. Condition and safety of medical equipment in intensive or intermediate care unitLow = The equipment is in poor condition or it is not secured; Average = The equipment is in fair
condition or not properly secured; High = Equipment is in good condition and is secured.
60. Condition and safety of equipment and furnishings in the pharmacy Low = The equipment is in poor condition or it is not secured; Average = The equipment is in fair
condition or not properly secured; High = Equipment is in good condition and is secured.
61. Condition and safety of equipment in the sterilization unitLow = The equipment is in poor condition or it is not secured; Average = The equipment is in fair
condition or not properly secured; High = Equipment is in good condition and is secured.
62. Condition and safety of medical equipment for neonatal careLow = The equipment is lacking, is in poor condition, or is not secured; Average = The equipment is
in fair condition or not properly secured; High = Equipment is in good condition and is secured.
63. Condition and safety of medical equipment and supplies for burn managementLow = The equipment is lacking, is in poor condition, or it is not secured; Average = The equipment is
in fair condition or not properly secured; High = Equipment is in good condition and is secured.
64. Condition and safety of medical equipment for nuclear medicine and radiation
therapy IF THE HOSPITAL DOES NOT HAVE THESE SERVICES, LEAVE BOXES BLANK.
Low = The equipment is lacking, is in poor condition, or it is not secured; Average = The equipment
is in fair condition or not properly secured; High = Equipment is in good condition and is secured.
65. Condition and safety of medical equipment in other servicesLow = More than 30% of equipment is at risk of material or functional failure and/or equipment
puts the entire service’s operation at direct or indirect risk; Average = Between 10% and 30% of
equipment is at risk of loss; High = Less than 10% of equipment is at risk of loss.
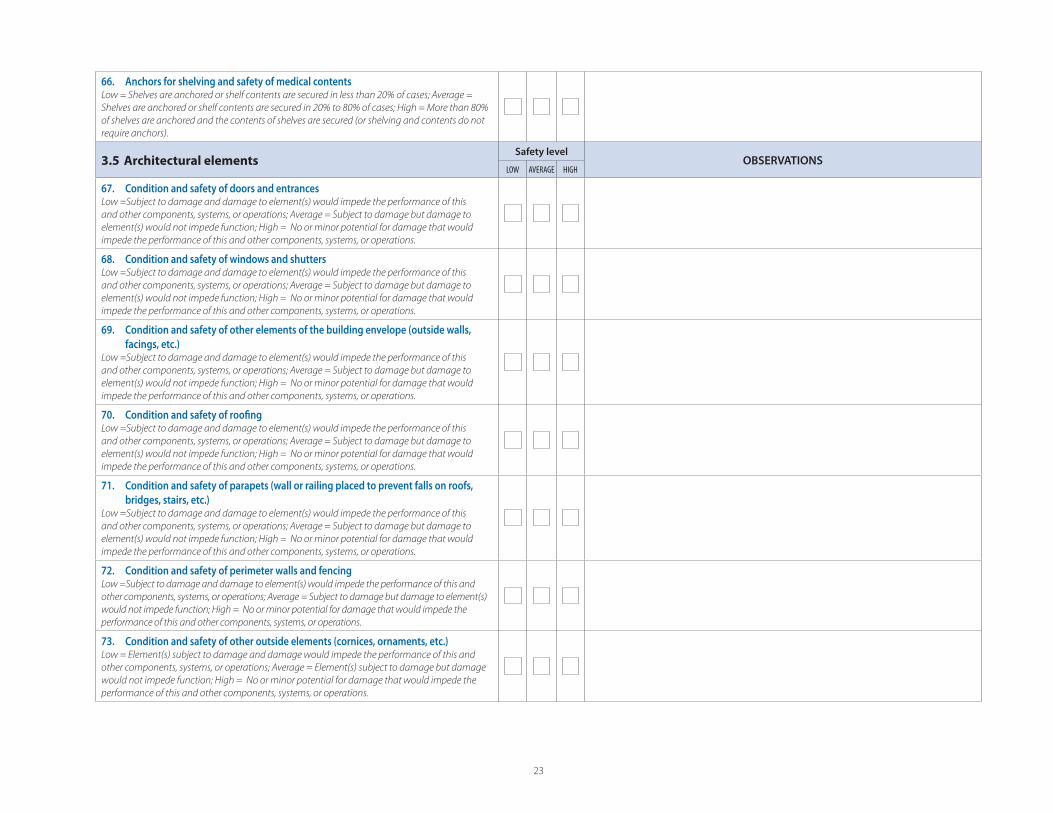
23
66. Anchors for shelving and safety of medical contentsLow = Shelves are anchored or shelf contents are secured in less than 20% of cases; Average =
Shelves are anchored or shelf contents are secured in 20% to 80% of cases; High = More than 80%
of shelves are anchored and the contents of shelves are secured (or shelving and contents do not
require anchors).
3.5 Architectural elementsSafety level
OBSERVATIONSLOW AVERAGE HIGH
67. Condition and safety of doors and entrancesLow =Subject to damage and damage to element(s) would impede the performance of this
and other components, systems, or operations; Average = Subject to damage but damage to
element(s) would not impede function; High = No or minor potential for damage that would
impede the performance of this and other components, systems, or operations.
68. Condition and safety of windows and shuttersLow =Subject to damage and damage to element(s) would impede the performance of this
and other components, systems, or operations; Average = Subject to damage but damage to
element(s) would not impede function; High = No or minor potential for damage that would
impede the performance of this and other components, systems, or operations.
69. Condition and safety of other elements of the building envelope (outside walls,
facings, etc.)Low =Subject to damage and damage to element(s) would impede the performance of this
and other components, systems, or operations; Average = Subject to damage but damage to
element(s) would not impede function; High = No or minor potential for damage that would
impede the performance of this and other components, systems, or operations.
70. Condition and safety of roofi ngLow =Subject to damage and damage to element(s) would impede the performance of this
and other components, systems, or operations; Average = Subject to damage but damage to
element(s) would not impede function; High = No or minor potential for damage that would
impede the performance of this and other components, systems, or operations.
71. Condition and safety of parapets (wall or railing placed to prevent falls on roofs,
bridges, stairs, etc.)Low =Subject to damage and damage to element(s) would impede the performance of this
and other components, systems, or operations; Average = Subject to damage but damage to
element(s) would not impede function; High = No or minor potential for damage that would
impede the performance of this and other components, systems, or operations.
72. Condition and safety of perimeter walls and fencingLow =Subject to damage and damage to element(s) would impede the performance of this and
other components, systems, or operations; Average = Subject to damage but damage to element(s)
would not impede function; High = No or minor potential for damage that would impede the
performance of this and other components, systems, or operations.
73. Condition and safety of other outside elements (cornices, ornaments, etc.)Low = Element(s) subject to damage and damage would impede the performance of this and
other components, systems, or operations; Average = Element(s) subject to damage but damage
would not impede function; High = No or minor potential for damage that would impede the
performance of this and other components, systems, or operations.
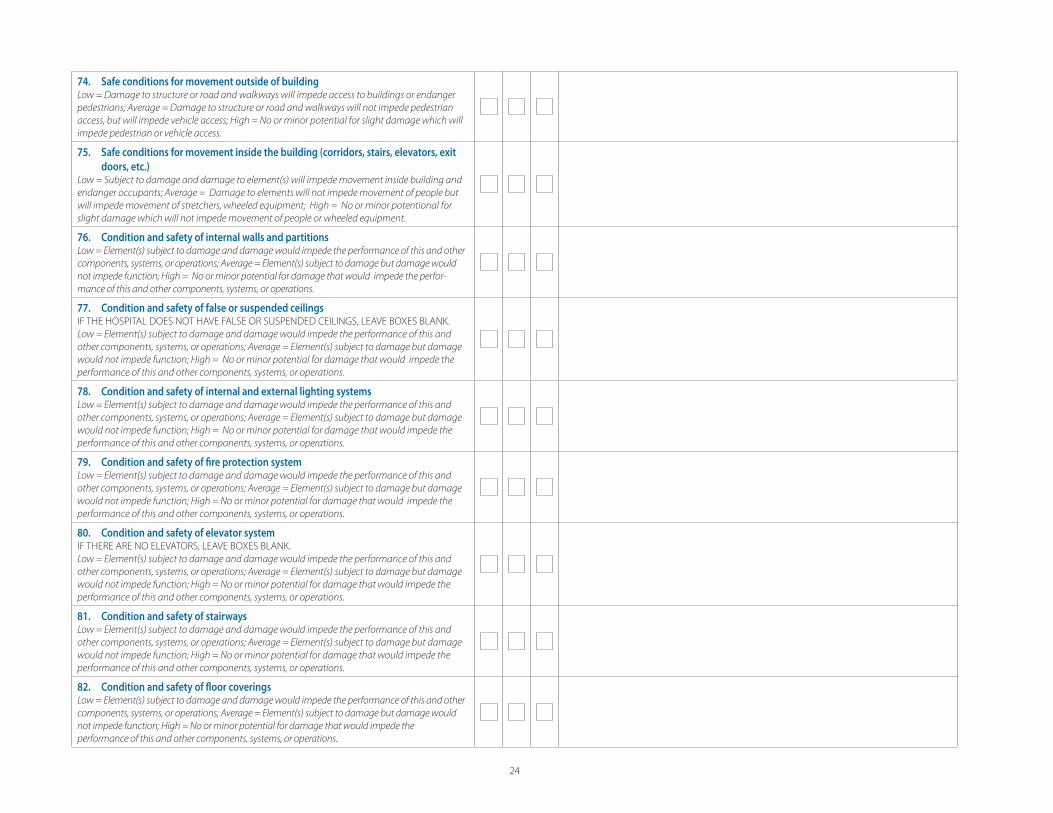
24
74. Safe conditions for movement outside of buildingLow = Damage to structure or road and walkways will impede access to buildings or endanger
pedestrians; Average = Damage to structure or road and walkways will not impede pedestrian
access, but will impede vehicle access; High = No or minor potential for slight damage which will
impede pedestrian or vehicle access.
75. Safe conditions for movement inside the building (corridors, stairs, elevators, exit
doors, etc.)Low = Subject to damage and damage to element(s) will impede movement inside building and
endanger occupants; Average = Damage to elements will not impede movement of people but
will impede movement of stretchers, wheeled equipment; High = No or minor potentional for
slight damage which will not impede movement of people or wheeled equipment.
76. Condition and safety of internal walls and partitionsLow = Element(s) subject to damage and damage would impede the performance of this and other
components, systems, or operations; Average = Element(s) subject to damage but damage would
not impede function; High = No or minor potential for damage that would impede the perfor-
mance of this and other components, systems, or operations.
77. Condition and safety of false or suspended ceilingsIF THE HOSPITAL DOES NOT HAVE FALSE OR SUSPENDED CEILINGS, LEAVE BOXES BLANK.
Low = Element(s) subject to damage and damage would impede the performance of this and
other components, systems, or operations; Average = Element(s) subject to damage but damage
would not impede function; High = No or minor potential for damage that would impede the
performance of this and other components, systems, or operations.
78. Condition and safety of internal and external lighting systemsLow = Element(s) subject to damage and damage would impede the performance of this and
other components, systems, or operations; Average = Element(s) subject to damage but damage
would not impede function; High = No or minor potential for damage that would impede the
performance of this and other components, systems, or operations.
79. Condition and safety of fi re protection systemLow = Element(s) subject to damage and damage would impede the performance of this and
other components, systems, or operations; Average = Element(s) subject to damage but damage
would not impede function; High = No or minor potential for damage that would impede the
performance of this and other components, systems, or operations.
80. Condition and safety of elevator systemIF THERE ARE NO ELEVATORS, LEAVE BOXES BLANK.
Low = Element(s) subject to damage and damage would impede the performance of this and
other components, systems, or operations; Average = Element(s) subject to damage but damage
would not impede function; High = No or minor potential for damage that would impede the
performance of this and other components, systems, or operations.
81. Condition and safety of stairwaysLow = Element(s) subject to damage and damage would impede the performance of this and
other components, systems, or operations; Average = Element(s) subject to damage but damage
would not impede function; High = No or minor potential for damage that would impede the
performance of this and other components, systems, or operations.
82. Condition and safety of fl oor coveringsLow = Element(s) subject to damage and damage would impede the performance of this and other
components, systems, or operations; Average = Element(s) subject to damage but damage would
not impede function; High = No or minor potential for damage that would impede the
performance of this and other components, systems, or operations.

25
83. Hospital access routesLow = Element(s) subject to damage and damage would impede the performance of this and
other components, systems, or operations; Average = Element(s) subject to damage but damage
would not impede function; High = No or minor potential for damage that would impede the
performance of this and other components, systems, or operations.
84. Other architectural elements, including emergency signsLow = Element(s) subject to damage and damage would impede the performance of this and
other components, systems, or operations; Average = Element(s) subject to damage but damage
would not impede function; High = No or minor potential for damage that would impede the
performance of this and other components, systems, or operations.
Comments on the results of Form 2, Module 3:
...........................................................................................................................................................................................................................................................................................................................................................................................................................................................................................
...........................................................................................................................................................................................................................................................................................................................................................................................................................................................................................
...........................................................................................................................................................................................................................................................................................................................................................................................................................................................................................
...........................................................................................................................................................................................................................................................................................................................................................................................................................................................................................
...........................................................................................................................................................................................................................................................................................................................................................................................................................................................................................
...........................................................................................................................................................................................................................................................................................................................................................................................................................................................................................
...........................................................................................................................................................................................................................................................................................................................................................................................................................................................................................
...........................................................................................................................................................................................................................................................................................................................................................................................................................................................................................
...........................................................................................................................................................................................................................................................................................................................................................................................................................................................................................
...........................................................................................................................................................................................................................................................................................................................................................................................................................................................................................
...........................................................................................................................................................................................................................................................................................................................................................................................................................................................................................
Name/signature of evaluator ........................................................................................................................................................................................................................................................................................................................................................................................................................
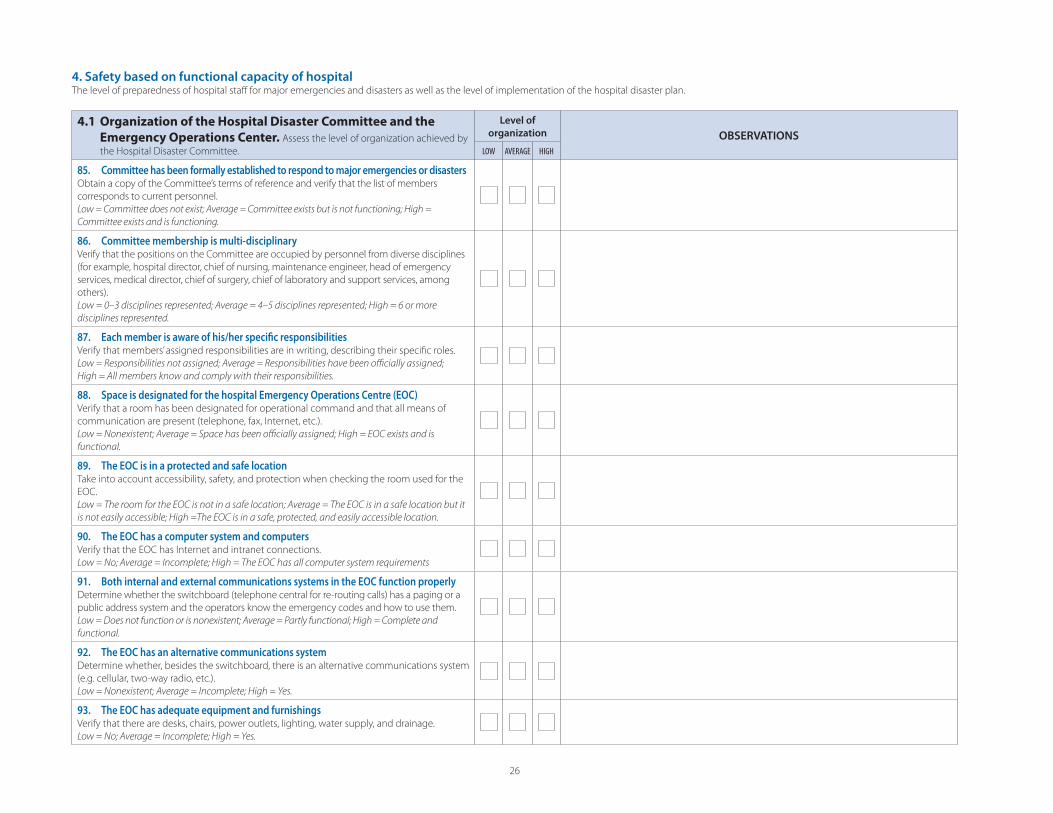
26
4.1 Organization of the Hospital Disaster Committee and the
Emergency Operations Center. Assess the level of organization achieved by
the Hospital Disaster Committee.
Level of
organization OBSERVATIONS
LOW AVERAGE HIGH
85. Committee has been formally established to respond to major emergencies or disasters Obtain a copy of the Committee’s terms of reference and verify that the list of members
corresponds to current personnel.
Low = Committee does not exist; Average = Committee exists but is not functioning; High =
Committee exists and is functioning.
86. Committee membership is multi-disciplinaryVerify that the positions on the Committee are occupied by personnel from diverse disciplines
(for example, hospital director, chief of nursing, maintenance engineer, head of emergency
services, medical director, chief of surgery, chief of laboratory and support services, among
others).
Low = 0–3 disciplines represented; Average = 4–5 disciplines represented; High = 6 or more
disciplines represented.
87. Each member is aware of his/her specifi c responsibilitiesVerify that members’ assigned responsibilities are in writing, describing their specifi c roles.
Low = Responsibilities not assigned; Average = Responsibilities have been offi cially assigned;
High = All members know and comply with their responsibilities.
88. Space is designated for the hospital Emergency Operations Centre (EOC)Verify that a room has been designated for operational command and that all means of
communication are present (telephone, fax, Internet, etc.).
Low = Nonexistent; Average = Space has been offi cially assigned; High = EOC exists and is
functional.
89. The EOC is in a protected and safe locationTake into account accessibility, safety, and protection when checking the room used for the
EOC.
Low = The room for the EOC is not in a safe location; Average = The EOC is in a safe location but it
is not easily accessible; High =The EOC is in a safe, protected, and easily accessible location.
90. The EOC has a computer system and computers Verify that the EOC has Internet and intranet connections.
Low = No; Average = Incomplete; High = The EOC has all computer system requirements
91. Both internal and external communications systems in the EOC function properlyDetermine whether the switchboard (telephone central for re-routing calls) has a paging or a
public address system and the operators know the emergency codes and how to use them.
Low = Does not function or is nonexistent; Average = Partly functional; High = Complete and
functional.
92. The EOC has an alternative communications system Determine whether, besides the switchboard, there is an alternative communications system
(e.g. cellular, two-way radio, etc.).
Low = Nonexistent; Average = Incomplete; High = Yes.
93. The EOC has adequate equipment and furnishings Verify that there are desks, chairs, power outlets, lighting, water supply, and drainage.
Low = No; Average = Incomplete; High = Yes.
4. Safety based on functional capacity of hospitalThe level of preparedness of hospital staff for major emergencies and disasters as well as the level of implementation of the hospital disaster plan.
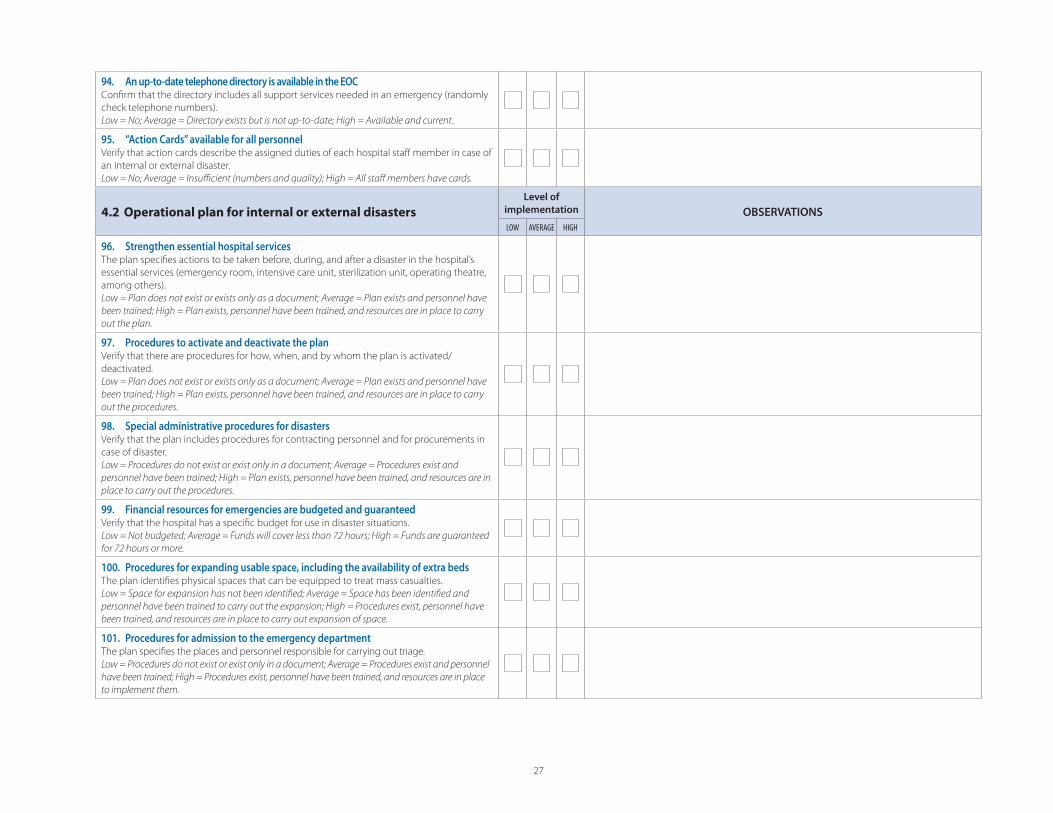
27
94. An up-to-date telephone directory is available in the EOCConfi rm that the directory includes all support services needed in an emergency (randomly
check telephone numbers).
Low = No; Average = Directory exists but is not up-to-date; High = Available and current.
95. “Action Cards” available for all personnelVerify that action cards describe the assigned duties of each hospital staff member in case of
an internal or external disaster.
Low = No; Average = Insuffi cient (numbers and quality); High = All staff members have cards.
4.2 Operational plan for internal or external disasters
Level of
implementation OBSERVATIONS
LOW AVERAGE HIGH
96. Strengthen essential hospital servicesThe plan specifi es actions to be taken before, during, and after a disaster in the hospital’s
essential services (emergency room, intensive care unit, sterilization unit, operating theatre,
among others).
Low = Plan does not exist or exists only as a document; Average = Plan exists and personnel have
been trained; High = Plan exists, personnel have been trained, and resources are in place to carry
out the plan.
97. Procedures to activate and deactivate the planVerify that there are procedures for how, when, and by whom the plan is activated/
deactivated.
Low = Plan does not exist or exists only as a document; Average = Plan exists and personnel have
been trained; High = Plan exists, personnel have been trained, and resources are in place to carry
out the procedures.
98. Special administrative procedures for disastersVerify that the plan includes procedures for contracting personnel and for procurements in
case of disaster.
Low = Procedures do not exist or exist only in a document; Average = Procedures exist and
personnel have been trained; High = Plan exists, personnel have been trained, and resources are in
place to carry out the procedures.
99. Financial resources for emergencies are budgeted and guaranteedVerify that the hospital has a specifi c budget for use in disaster situations.
Low = Not budgeted; Average = Funds will cover less than 72 hours; High = Funds are guaranteed
for 72 hours or more.
100. Procedures for expanding usable space, including the availability of extra beds The plan identifi es physical spaces that can be equipped to treat mass casualties.
Low = Space for expansion has not been identifi ed; Average = Space has been identifi ed and
personnel have been trained to carry out the expansion; High = Procedures exist, personnel have
been trained, and resources are in place to carry out expansion of space.
101. Procedures for admission to the emergency departmentThe plan specifi es the places and personnel responsible for carrying out triage.
Low = Procedures do not exist or exist only in a document; Average = Procedures exist and personnel
have been trained; High = Procedures exist, personnel have been trained, and resources are in place
to implement them.
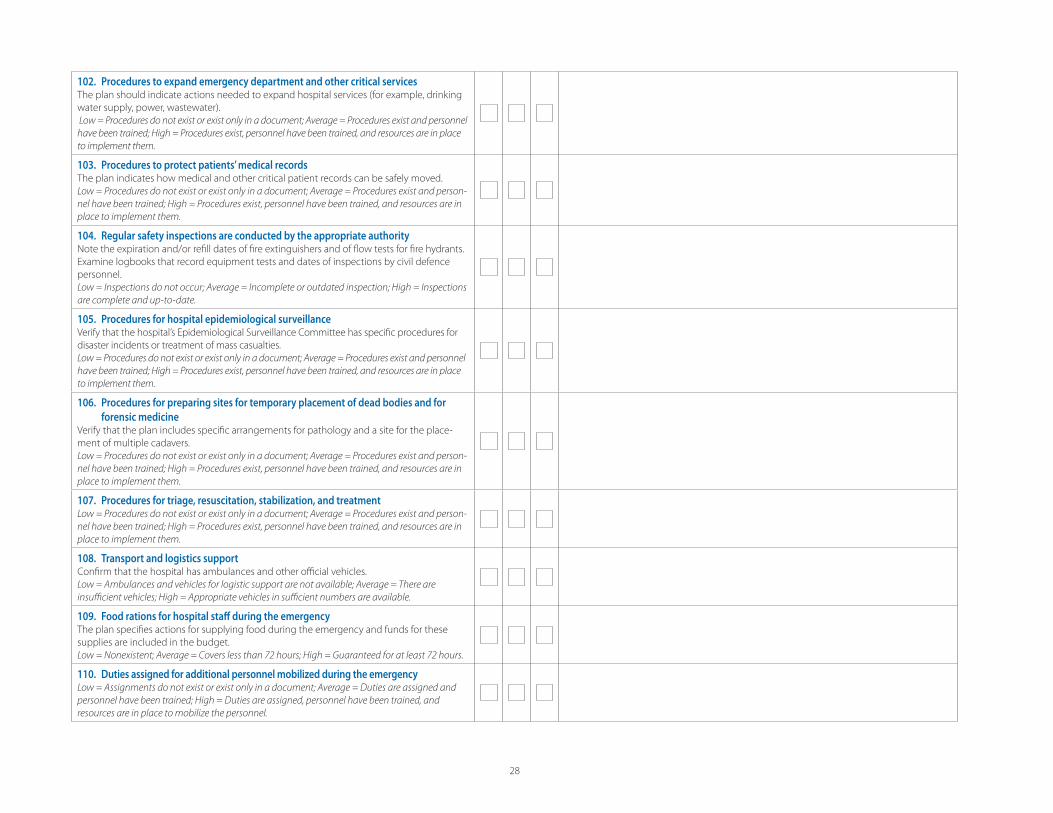
28
102. Procedures to expand emergency department and other critical services The plan should indicate actions needed to expand hospital services (for example, drinking
water supply, power, wastewater).
Low = Procedures do not exist or exist only in a document; Average = Procedures exist and personnel
have been trained; High = Procedures exist, personnel have been trained, and resources are in place
to implement them.
103. Procedures to protect patients’ medical recordsThe plan indicates how medical and other critical patient records can be safely moved.
Low = Procedures do not exist or exist only in a document; Average = Procedures exist and person-
nel have been trained; High = Procedures exist, personnel have been trained, and resources are in
place to implement them.
104. Regular safety inspections are conducted by the appropriate authorityNote the expiration and/or refi ll dates of fi re extinguishers and of fl ow tests for fi re hydrants.
Examine logbooks that record equipment tests and dates of inspections by civil defence
personnel.
Low = Inspections do not occur; Average = Incomplete or outdated inspection; High = Inspections
are complete and up-to-date.
105. Procedures for hospital epidemiological surveillanceVerify that the hospital’s Epidemiological Surveillance Committee has specifi c procedures for
disaster incidents or treatment of mass casualties.
Low = Procedures do not exist or exist only in a document; Average = Procedures exist and personnel
have been trained; High = Procedures exist, personnel have been trained, and resources are in place
to implement them.
106. Procedures for preparing sites for temporary placement of dead bodies and for
forensic medicineVerify that the plan includes specifi c arrangements for pathology and a site for the place-
ment of multiple cadavers.
Low = Procedures do not exist or exist only in a document; Average = Procedures exist and person-
nel have been trained; High = Procedures exist, personnel have been trained, and resources are in
place to implement them.
107. Procedures for triage, resuscitation, stabilization, and treatment Low = Procedures do not exist or exist only in a document; Average = Procedures exist and person-
nel have been trained; High = Procedures exist, personnel have been trained, and resources are in
place to implement them.
108. Transport and logistics supportConfi rm that the hospital has ambulances and other offi cial vehicles.
Low = Ambulances and vehicles for logistic support are not available; Average = There are
insuffi cient vehicles; High = Appropriate vehicles in suffi cient numbers are available.
109. Food rations for hospital staff during the emergency The plan specifi es actions for supplying food during the emergency and funds for these
supplies are included in the budget.
Low = Nonexistent; Average = Covers less than 72 hours; High = Guaranteed for at least 72 hours.
110. Duties assigned for additional personnel mobilized during the emergencyLow = Assignments do not exist or exist only in a document; Average = Duties are assigned and
personnel have been trained; High = Duties are assigned, personnel have been trained, and
resources are in place to mobilize the personnel.
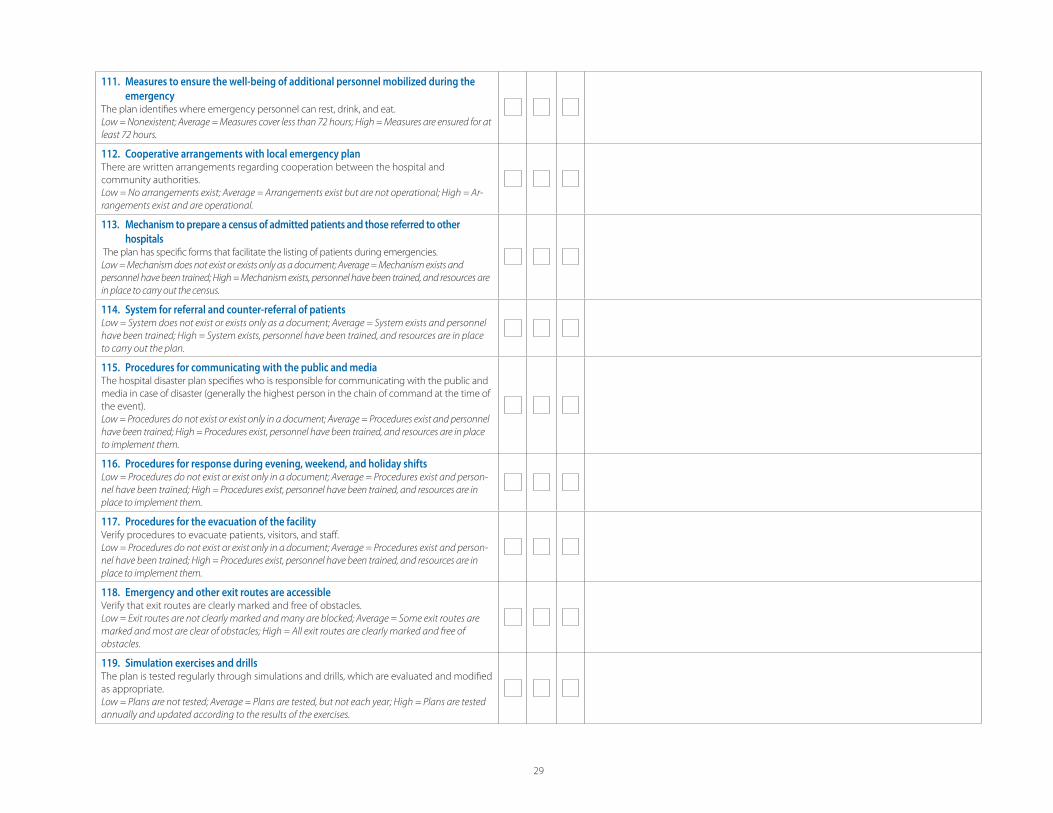
29
111. Measures to ensure the well-being of additional personnel mobilized during the
emergencyThe plan identifi es where emergency personnel can rest, drink, and eat.
Low = Nonexistent; Average = Measures cover less than 72 hours; High = Measures are ensured for at
least 72 hours.
112. Cooperative arrangements with local emergency planThere are written arrangements regarding cooperation between the hospital and
community authorities.
Low = No arrangements exist; Average = Arrangements exist but are not operational; High = Ar-
rangements exist and are operational.
113. Mechanism to prepare a census of admitted patients and those referred to other
hospitals The plan has specifi c forms that facilitate the listing of patients during emergencies.
Low = Mechanism does not exist or exists only as a document; Average = Mechanism exists and
personnel have been trained; High = Mechanism exists, personnel have been trained, and resources are
in place to carry out the census.
114. System for referral and counter-referral of patientsLow = System does not exist or exists only as a document; Average = System exists and personnel
have been trained; High = System exists, personnel have been trained, and resources are in place
to carry out the plan.
115. Procedures for communicating with the public and mediaThe hospital disaster plan specifi es who is responsible for communicating with the public and
media in case of disaster (generally the highest person in the chain of command at the time of
the event).
Low = Procedures do not exist or exist only in a document; Average = Procedures exist and personnel
have been trained; High = Procedures exist, personnel have been trained, and resources are in place
to implement them.
116. Procedures for response during evening, weekend, and holiday shifts Low = Procedures do not exist or exist only in a document; Average = Procedures exist and person-
nel have been trained; High = Procedures exist, personnel have been trained, and resources are in
place to implement them.
117. Procedures for the evacuation of the facility Verify procedures to evacuate patients, visitors, and staff .
Low = Procedures do not exist or exist only in a document; Average = Procedures exist and person-
nel have been trained; High = Procedures exist, personnel have been trained, and resources are in
place to implement them.
118. Emergency and other exit routes are accessibleVerify that exit routes are clearly marked and free of obstacles.
Low = Exit routes are not clearly marked and many are blocked; Average = Some exit routes are
marked and most are clear of obstacles; High = All exit routes are clearly marked and free of
obstacles.
119. Simulation exercises and drills The plan is tested regularly through simulations and drills, which are evaluated and modifi ed
as appropriate.
Low = Plans are not tested; Average = Plans are tested, but not each year; High = Plans are tested
annually and updated according to the results of the exercises.
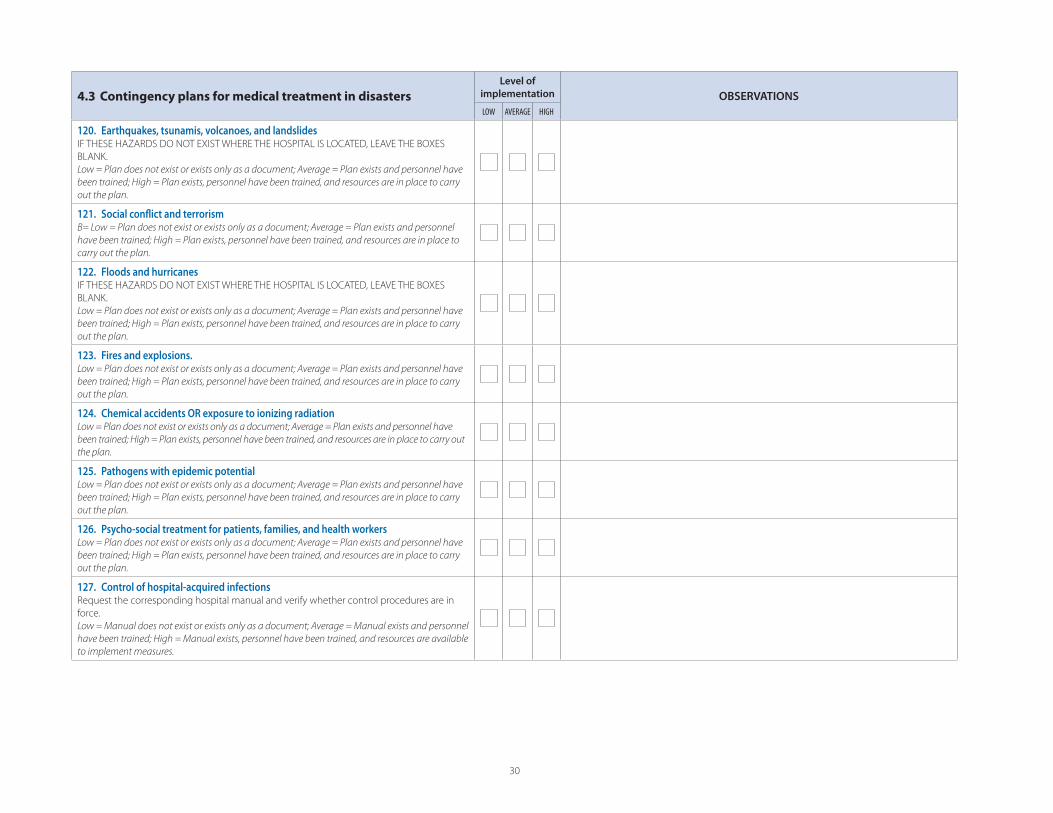
30
4.3 Contingency plans for medical treatment in disasters
Level of
implementation OBSERVATIONS
LOW AVERAGE HIGH
120. Earthquakes, tsunamis, volcanoes, and landslidesIF THESE HAZARDS DO NOT EXIST WHERE THE HOSPITAL IS LOCATED, LEAVE THE BOXES
BLANK.
Low = Plan does not exist or exists only as a document; Average = Plan exists and personnel have
been trained; High = Plan exists, personnel have been trained, and resources are in place to carry
out the plan.
121. Social confl ict and terrorismB= Low = Plan does not exist or exists only as a document; Average = Plan exists and personnel
have been trained; High = Plan exists, personnel have been trained, and resources are in place to
carry out the plan.
122. Floods and hurricanesIF THESE HAZARDS DO NOT EXIST WHERE THE HOSPITAL IS LOCATED, LEAVE THE BOXES
BLANK.
Low = Plan does not exist or exists only as a document; Average = Plan exists and personnel have
been trained; High = Plan exists, personnel have been trained, and resources are in place to carry
out the plan.
123. Fires and explosions.Low = Plan does not exist or exists only as a document; Average = Plan exists and personnel have
been trained; High = Plan exists, personnel have been trained, and resources are in place to carry
out the plan.
124. Chemical accidents OR exposure to ionizing radiationLow = Plan does not exist or exists only as a document; Average = Plan exists and personnel have
been trained; High = Plan exists, personnel have been trained, and resources are in place to carry out
the plan.
125. Pathogens with epidemic potentialLow = Plan does not exist or exists only as a document; Average = Plan exists and personnel have
been trained; High = Plan exists, personnel have been trained, and resources are in place to carry
out the plan.
126. Psycho-social treatment for patients, families, and health workersLow = Plan does not exist or exists only as a document; Average = Plan exists and personnel have
been trained; High = Plan exists, personnel have been trained, and resources are in place to carry
out the plan.
127. Control of hospital-acquired infectionsRequest the corresponding hospital manual and verify whether control procedures are in
force.
Low = Manual does not exist or exists only as a document; Average = Manual exists and personnel
have been trained; High = Manual exists, personnel have been trained, and resources are available
to implement measures.
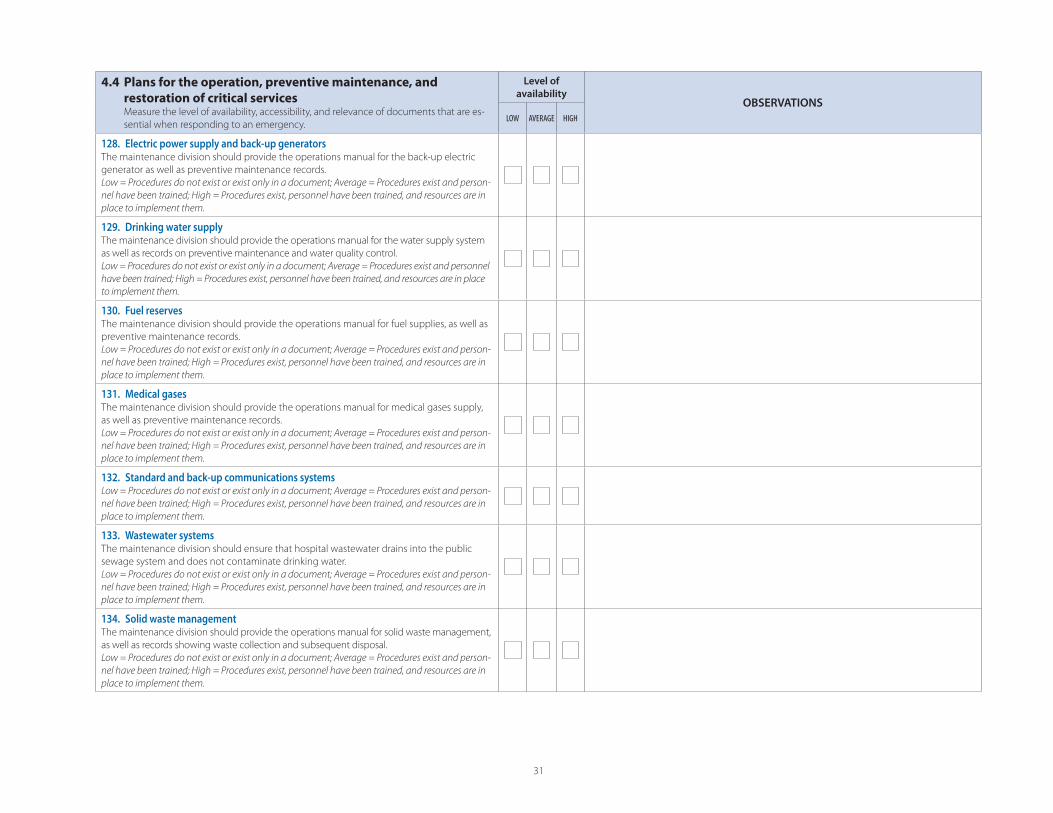
31
4.4 Plans for the operation, preventive maintenance, and
restoration of critical services Measure the level of availability, accessibility, and relevance of documents that are es-
sential when responding to an emergency.
Level of
availabilityOBSERVATIONS
LOW AVERAGE HIGH
128. Electric power supply and back-up generatorsThe maintenance division should provide the operations manual for the back-up electric
generator as well as preventive maintenance records.
Low = Procedures do not exist or exist only in a document; Average = Procedures exist and person-
nel have been trained; High = Procedures exist, personnel have been trained, and resources are in
place to implement them.
129. Drinking water supplyThe maintenance division should provide the operations manual for the water supply system
as well as records on preventive maintenance and water quality control.
Low = Procedures do not exist or exist only in a document; Average = Procedures exist and personnel
have been trained; High = Procedures exist, personnel have been trained, and resources are in place
to implement them.
130. Fuel reservesThe maintenance division should provide the operations manual for fuel supplies, as well as
preventive maintenance records.
Low = Procedures do not exist or exist only in a document; Average = Procedures exist and person-
nel have been trained; High = Procedures exist, personnel have been trained, and resources are in
place to implement them.
131. Medical gases The maintenance division should provide the operations manual for medical gases supply,
as well as preventive maintenance records.
Low = Procedures do not exist or exist only in a document; Average = Procedures exist and person-
nel have been trained; High = Procedures exist, personnel have been trained, and resources are in
place to implement them.
132. Standard and back-up communications systemsLow = Procedures do not exist or exist only in a document; Average = Procedures exist and person-
nel have been trained; High = Procedures exist, personnel have been trained, and resources are in
place to implement them.
133. Wastewater systemsThe maintenance division should ensure that hospital wastewater drains into the public
sewage system and does not contaminate drinking water.
Low = Procedures do not exist or exist only in a document; Average = Procedures exist and person-
nel have been trained; High = Procedures exist, personnel have been trained, and resources are in
place to implement them.
134. Solid waste managementThe maintenance division should provide the operations manual for solid waste management,
as well as records showing waste collection and subsequent disposal.
Low = Procedures do not exist or exist only in a document; Average = Procedures exist and person-
nel have been trained; High = Procedures exist, personnel have been trained, and resources are in
place to implement them.
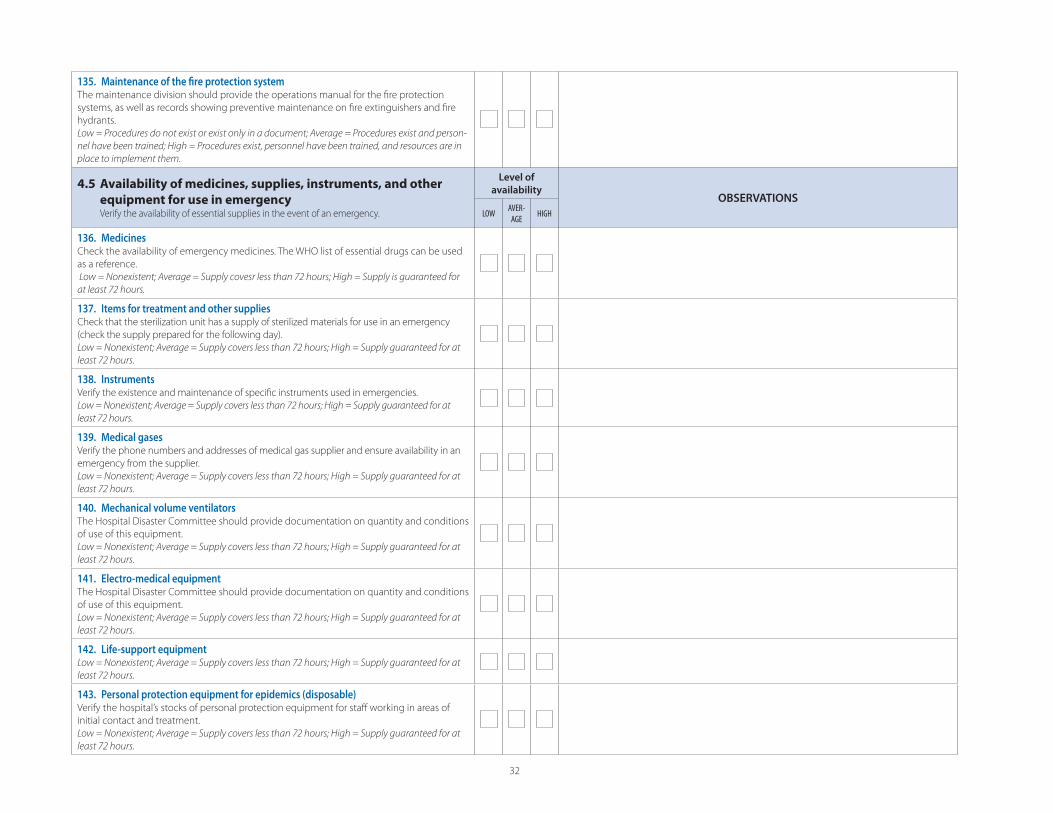
32
135. Maintenance of the fi re protection systemThe maintenance division should provide the operations manual for the fi re protection
systems, as well as records showing preventive maintenance on fi re extinguishers and fi re
hydrants.
Low = Procedures do not exist or exist only in a document; Average = Procedures exist and person-
nel have been trained; High = Procedures exist, personnel have been trained, and resources are in
place to implement them.
4.5 Availability of medicines, supplies, instruments, and other
equipment for use in emergency Verify the availability of essential supplies in the event of an emergency.
Level of
availabilityOBSERVATIONS
LOWAVER-AGE
HIGH
136. MedicinesCheck the availability of emergency medicines. The WHO list of essential drugs can be used
as a reference.
Low = Nonexistent; Average = Supply covesr less than 72 hours; High = Supply is guaranteed for
at least 72 hours.
137. Items for treatment and other suppliesCheck that the sterilization unit has a supply of sterilized materials for use in an emergency
(check the supply prepared for the following day).
Low = Nonexistent; Average = Supply covers less than 72 hours; High = Supply guaranteed for at
least 72 hours.
138. InstrumentsVerify the existence and maintenance of specifi c instruments used in emergencies.
Low = Nonexistent; Average = Supply covers less than 72 hours; High = Supply guaranteed for at
least 72 hours.
139. Medical gasesVerify the phone numbers and addresses of medical gas supplier and ensure availability in an
emergency from the supplier.
Low = Nonexistent; Average = Supply covers less than 72 hours; High = Supply guaranteed for at
least 72 hours.
140. Mechanical volume ventilatorsThe Hospital Disaster Committee should provide documentation on quantity and conditions
of use of this equipment.
Low = Nonexistent; Average = Supply covers less than 72 hours; High = Supply guaranteed for at
least 72 hours.
141. Electro-medical equipmentThe Hospital Disaster Committee should provide documentation on quantity and conditions
of use of this equipment.
Low = Nonexistent; Average = Supply covers less than 72 hours; High = Supply guaranteed for at
least 72 hours.
142. Life-support equipment Low = Nonexistent; Average = Supply covers less than 72 hours; High = Supply guaranteed for at
least 72 hours.
143. Personal protection equipment for epidemics (disposable)Verify the hospital’s stocks of personal protection equipment for staff working in areas of
initial contact and treatment.
Low = Nonexistent; Average = Supply covers less than 72 hours; High = Supply guaranteed for at
least 72 hours.

33
144. Crash cart for cardiopulmonary arrestThe Hospital Disaster Committee should provide documentation on quantity, conditions of
use, and locations of crash carts for treatment of cardiopulmonary arrest.
Low = Nonexistent; Average = Supply covers less than 72 hours; High = Supply guaranteed for at
least 72 hours.
145. Triage tags and other supplies for managing mass casualtiesThe emergency department distributes and uses triage tags in case of mass casualties.
Evaluate the supply in terms of the maximum capacity of the hospital.
Low = Nonexistent; Average = Supply covers less than 72 hours; High = Supply guaranteed for at
least 72 hours.
Comments on the results of Form 2, Module 4:
...........................................................................................................................................................................................................................................................................................................................................................................................................................................................................................
...........................................................................................................................................................................................................................................................................................................................................................................................................................................................................................
...........................................................................................................................................................................................................................................................................................................................................................................................................................................................................................
...........................................................................................................................................................................................................................................................................................................................................................................................................................................................................................
...........................................................................................................................................................................................................................................................................................................................................................................................................................................................................................
...........................................................................................................................................................................................................................................................................................................................................................................................................................................................................................
...........................................................................................................................................................................................................................................................................................................................................................................................................................................................................................
...........................................................................................................................................................................................................................................................................................................................................................................................................................................................................................
...........................................................................................................................................................................................................................................................................................................................................................................................................................................................................................
...........................................................................................................................................................................................................................................................................................................................................................................................................................................................................................
Name/signature of evaluator ........................................................................................................................................................................................................................................................................................................................................................................................................................
ANNEX 7
Development of Design Wind Speed Maps for the Caribbean for Application with the Wind Load
Provisions of ASCE 7
Area on Emergency Preparedness and Disaster Relief Coordination 525 23rd Street, N.W.
Washington, DC 20037-2875

This study was prepared by:
P. J. Vickery and D. Wadhera
Applied Research Associates, Inc. 8540 Colonnade Centre Drive, Suite 307
Raleigh NC 27615 ARA Report 18108-1
Under a special grant from the Office of Foreign Disaster Assistance of the United States Agency for International Development (OFDA/USAID).
The study has been made possible through the financial support of the Division of Humanitarian Assistance, Peace and Security of the Canadian International Development Agency (HAPS/CIDA) and the Office of Foreign Disaster Assistance of the United States
Agency for International Development (OFDA/USAID).
Development of Design Wind Speed Maps for the Caribbean for Application with the Wind Load Provisions of ASCE 7
1
1. INTRODUCTION
The objective of this study is to develop estimates of wind speeds as a function of
return period for locations in the Caribbean Basin that can be used in conjunction with the design wind provisions used in the US wind loading standards that reference ASCE 7-98 and later. Maps of hurricane induced wind speeds are developed using a peer reviewed hurricane simulation model as described in Vickery et al. (2000a, 2000b, 2006, 2008a, 2008b), and Vickery and Wadhera (2008). The hurricane simulation model used here is an updated version of that described in Vickery et al. (2000a, 2000b) which was used to produce the design wind speeds used in ASCE 7-98 through to the ASCE 7-05, the current version.
Section 2 of the report describes the simulation methodology and model
validation results, and section 3 presents the wind speed results and provides some guidance as to how these wind speeds should be used in conjunction with the requirements of the ASCE 7. A summary is presented in section 4.

Development of Design Wind Speed Maps for the Caribbean for Application with the Wind Load Provisions of ASCE 7
2
2. METHODOLOGY The hurricane simulation approach used to define the hurricane hazard in the Caribbean consists of two major components. The first component comprises a hurricane track model that reproduces the frequency and geometric characteristics of hurricane tracks as well as the variation of hurricane size and intensity as they move along the tracks. The second portion of the model is the hurricane wind field model, where given key hurricane parameters at any point in time from the track model, the wind field model provides estimates of the wind speed and wind direction at an arbitrary position. The meteorological inputs to the wind field model include the central pressure difference, Δp, translation speed, c, radius to maximum winds (RMW) and the Holland B parameter. (For computing Δp, the far field pressure is taken as 1013 mbar, and thus Δp is defined as 1013 minus the central pressure, pc.) The geometric inputs include storm position, heading and the location of the site where wind speeds are required. The following sections describe the verification of the track model for the Caribbean and a summary of the wind field model is also presented. 2.1 Track and Intensity Modelling
The hurricane track and intensity simulation methodology used to define the hurricane hazard in the Caribbean follows that described in Vickery et al. (2000, 2008), but the coefficients used in the statistical models have been calibrated to model the variation in storm characteristics throughout the Caribbean basin.
Track and Relative Intensity Modelling The over water hurricane track
simulation is performed in two steps. In the first step, the hurricane position at any point in time is modelled using the approach given in Vickery et al. (2000a). In the second step, the relative intensity, I, of the hurricane is modelled using a modified version of the approach given in Vickery et al. (2000a) as described in Vickery et al. (2008a) The relative intensity is then used to compute the central pressure, as described in Vickery et al (2000a). Then, using this central pressure, the RMW and B are computed as described in Vickery and Wadhera (2008) and Vickery et al (2008a). A simple one dimensional ocean mixing model, described in Emanuel et al. (2006), is used to simulate the effect of ocean feedback on the relative intensity calculations. The ocean mixing model returns an estimate of a mixed layer depth which is used to compute the reduction in sea surface temperature caused by the passage of a hurricane. This reduced sea surface temperature is used to convert historical pressures to relative intensity values. The historical relative intensity values are then used to develop regional statistical models of the form of Equation 2-1, where the relative intensity at any time is modelled as a function of relative intensity at last three steps and the scaled vertical wind shear, Vs, (DeMaria and Kaplan, 1999).
ε++++= −−+ siiii VcIcIcIcI 4231211 )ln()ln()ln()ln( (2-1)
where c1, c2, etc. are constants that vary with region in the Atlantic Basin, and ε is
a random error term. If a storm crosses land, the central pressure is computed using a

Development of Design Wind Speed Maps for the Caribbean for Application with the Wind Load Provisions of ASCE 7
3
filling model, where the central pressure t hours after landfall is dependent on the storm pressure at the time of landfall and the number of hours that the storm has been over land. Storm Filling Unlike hurricanes making landfall along the US mainland coastline, in the case of the Caribbean there is insufficient historical data available to develop island specific hurricane weakening (or filling) models for hurricanes passing over islands in the Caribbean. The limited data available to develop a statically based hurricane filling model is primarily a result of the 6 hour temporal resolution associated with HURDAT data, coupled with the fact that there is no additional information on landfall and exit pressures for those storms that do cross islands. In the storm intensity model described herein, we found that the filling model described in Vickery (2005) originally developed for use with hurricanes making landfall along the New England coast results in a variation in storm intensity statistics across islands that best matched the historical data. The use of the New England coast filling model provided the best model-data comparisons of storm central pressure statistics, with the other models described in Vickery (2005) yielding overestimates of storm intensity (as defined by central pressure) for regions on the lee sides of larger landmasses (Hispaniola, Cuba, Yucatan Peninsula). This overestimate of intensity indicates that storms crossing these land masses fill more rapidly than is predicted using any of the other (Gulf of Mexico, Florida Peninsula or Atlantic Coast) filling models given in Vickery (2005). 2.1.1 Model Validation
In the model validation/calibration process we compared the statistics of storm heading, translation speed, c, distance of closest approach, central pressure and annual occurrence rates for modelled and historical storms passing within 250 km of a grid-point. The distance of closest approach, dmin, is defined as positive if a storm passes to the left of a site (centre of the circle) and negative if the storm passes to the right. Storm heading, θ, is measured clockwise from true north, such that a heading of 0 degrees represents a storm heading due north, 90 degrees represents a storm heading due east and -90 degrees represents a storm moving towards the west. The annual storm occurrence rate, λ, is defined as the total number of storms that enter the circle during the period of record divided by the record length. All storms in the HURDAT data base are used in the development of the model, not just those that reach hurricane intensity. The parameters c, dmin, and θ are all computed at the point of closest approach to the centre of the circle. The central pressure values used in the validation procedure are the minimum values measured or modelled at any time while the storm is in the circle. For this study, we perform the comparisons using overlapping 250 km radius circles centred on a 2 degree grid spanning from 10o N to 26o N, and 59o W to 91o W. Figure 2-1 shows the location of the 140 grid points and the extent of the 250 km radius circles used in the validation/calibration process.
The HURDAT data set used in the model validation includes all tropical cyclones encompassing the period 1900 through 2007. However, central pressure data is only available for about 40% of the data points in the Caribbean. As noted in Georgiou et al. (1983), Georgiou (1985), and Vickery et al. (1995), we assume that the missing central
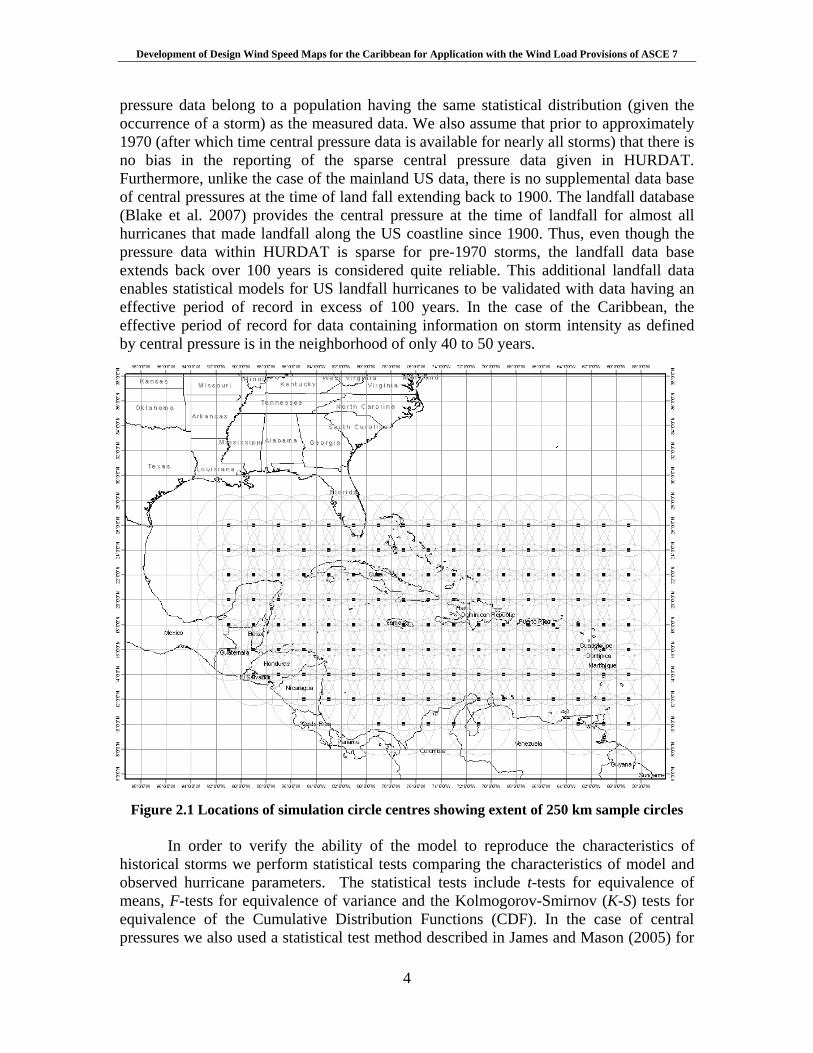
Development of Design Wind Speed Maps for the Caribbean for Application with the Wind Load Provisions of ASCE 7
4
pressure data belong to a population having the same statistical distribution (given the occurrence of a storm) as the measured data. We also assume that prior to approximately 1970 (after which time central pressure data is available for nearly all storms) that there is no bias in the reporting of the sparse central pressure data given in HURDAT. Furthermore, unlike the case of the mainland US data, there is no supplemental data base of central pressures at the time of land fall extending back to 1900. The landfall database (Blake et al. 2007) provides the central pressure at the time of landfall for almost all hurricanes that made landfall along the US coastline since 1900. Thus, even though the pressure data within HURDAT is sparse for pre-1970 storms, the landfall data base extends back over 100 years is considered quite reliable. This additional landfall data enables statistical models for US landfall hurricanes to be validated with data having an effective period of record in excess of 100 years. In the case of the Caribbean, the effective period of record for data containing information on storm intensity as defined by central pressure is in the neighborhood of only 40 to 50 years.
Figure 2.1 Locations of simulation circle centres showing extent of 250 km sample circles
In order to verify the ability of the model to reproduce the characteristics of
historical storms we perform statistical tests comparing the characteristics of model and observed hurricane parameters. The statistical tests include t-tests for equivalence of means, F-tests for equivalence of variance and the Kolmogorov-Smirnov (K-S) tests for equivalence of the Cumulative Distribution Functions (CDF). In the case of central pressures we also used a statistical test method described in James and Mason (2005) for
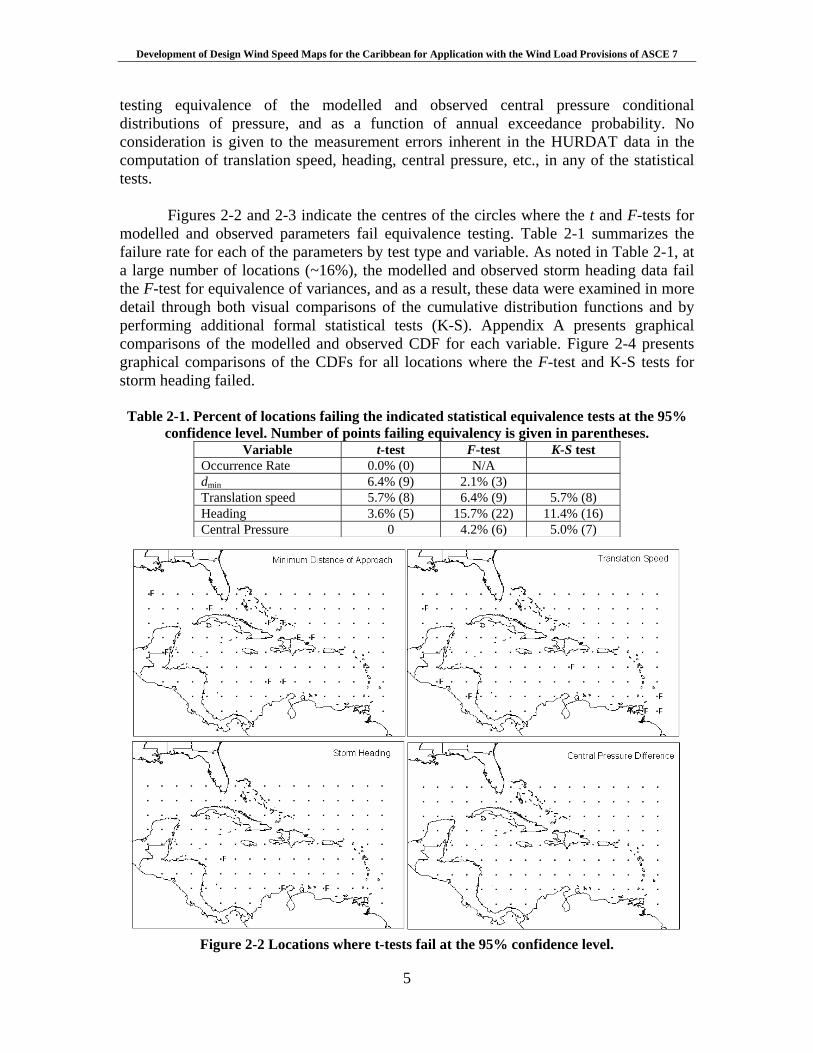
Development of Design Wind Speed Maps for the Caribbean for Application with the Wind Load Provisions of ASCE 7
5
testing equivalence of the modelled and observed central pressure conditional distributions of pressure, and as a function of annual exceedance probability. No consideration is given to the measurement errors inherent in the HURDAT data in the computation of translation speed, heading, central pressure, etc., in any of the statistical tests.
Figures 2-2 and 2-3 indicate the centres of the circles where the t and F-tests for modelled and observed parameters fail equivalence testing. Table 2-1 summarizes the failure rate for each of the parameters by test type and variable. As noted in Table 2-1, at a large number of locations (~16%), the modelled and observed storm heading data fail the F-test for equivalence of variances, and as a result, these data were examined in more detail through both visual comparisons of the cumulative distribution functions and by performing additional formal statistical tests (K-S). Appendix A presents graphical comparisons of the modelled and observed CDF for each variable. Figure 2-4 presents graphical comparisons of the CDFs for all locations where the F-test and K-S tests for storm heading failed.
Table 2-1. Percent of locations failing the indicated statistical equivalence tests at the 95% confidence level. Number of points failing equivalency is given in parentheses.
Variable t-test F-test K-S test Occurrence Rate 0.0% (0) N/A dmin 6.4% (9) 2.1% (3) Translation speed 5.7% (8) 6.4% (9) 5.7% (8) Heading 3.6% (5) 15.7% (22) 11.4% (16) Central Pressure 0 4.2% (6) 5.0% (7)
Figure 2-2 Locations where t-tests fail at the 95% confidence level.
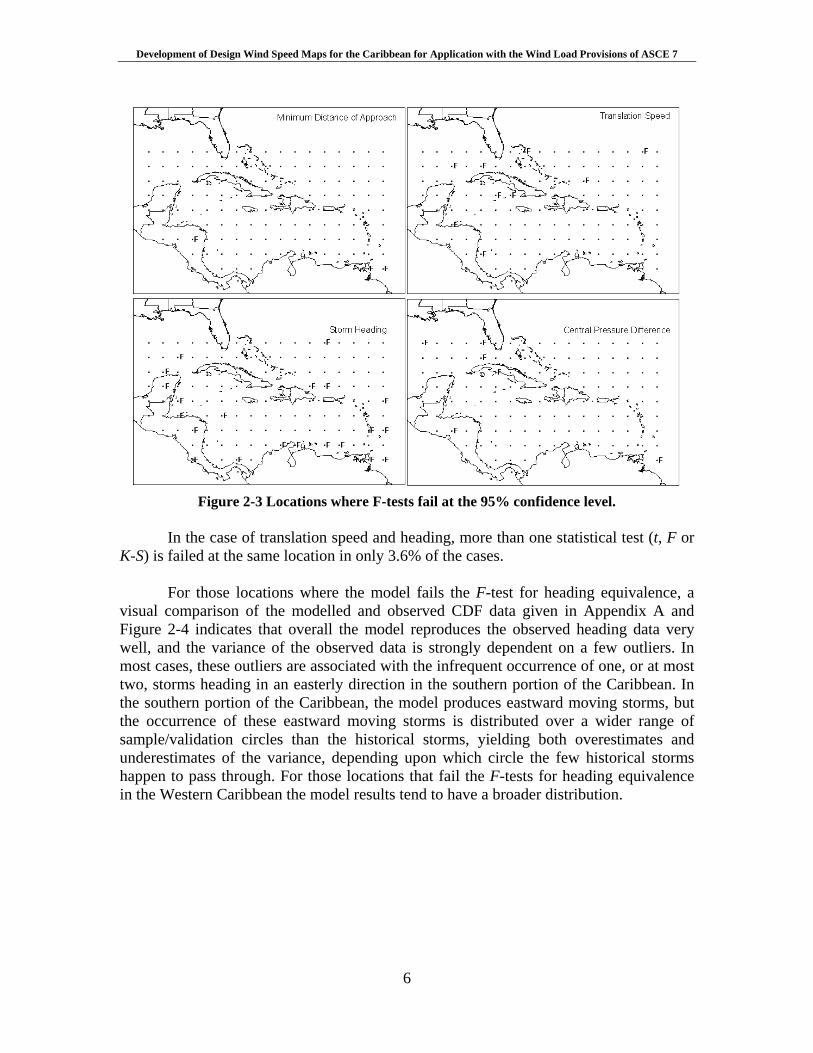
Development of Design Wind Speed Maps for the Caribbean for Application with the Wind Load Provisions of ASCE 7
6
Figure 2-3 Locations where F-tests fail at the 95% confidence level.
In the case of translation speed and heading, more than one statistical test (t, F or
K-S) is failed at the same location in only 3.6% of the cases. For those locations where the model fails the F-test for heading equivalence, a
visual comparison of the modelled and observed CDF data given in Appendix A and Figure 2-4 indicates that overall the model reproduces the observed heading data very well, and the variance of the observed data is strongly dependent on a few outliers. In most cases, these outliers are associated with the infrequent occurrence of one, or at most two, storms heading in an easterly direction in the southern portion of the Caribbean. In the southern portion of the Caribbean, the model produces eastward moving storms, but the occurrence of these eastward moving storms is distributed over a wider range of sample/validation circles than the historical storms, yielding both overestimates and underestimates of the variance, depending upon which circle the few historical storms happen to pass through. For those locations that fail the F-tests for heading equivalence in the Western Caribbean the model results tend to have a broader distribution.
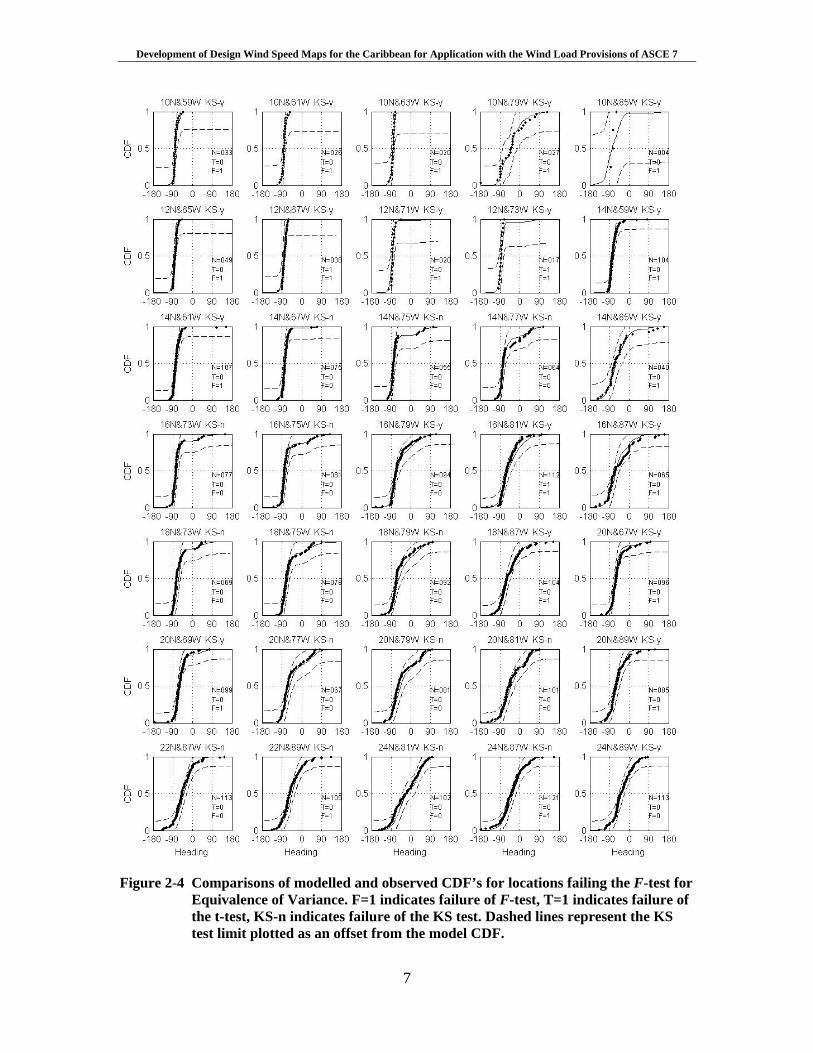
Development of Design Wind Speed Maps for the Caribbean for Application with the Wind Load Provisions of ASCE 7
7
Figure 2-4 Comparisons of modelled and observed CDF’s for locations failing the F-test for
Equivalence of Variance. F=1 indicates failure of F-test, T=1 indicates failure of the t-test, KS-n indicates failure of the KS test. Dashed lines represent the KS test limit plotted as an offset from the model CDF.

Development of Design Wind Speed Maps for the Caribbean for Application with the Wind Load Provisions of ASCE 7
8
Figure 2-5 presents a comparison of modelled and observed central pressures plotted versus return period for 35 locations in the Caribbean. The 35 locations follow along the Lesser and Greater Antilles, the Bahamas, Aruba, and coastal Central America, and thus encompass most of the populated region of the Caribbean. The observed central pressures plotted vs. return period were computed assuming the Np pressure data points obtained from a total of N tropical cyclones that pass through the circle are representative of the full population of N storms. With this assumption, the CDF for the conditional distribution for storm central pressure is computed, where each pressure has a probability of 1/(Np+1). The return period associated with a given central pressure is obtained from
)](exp[1/1 cc PpPRP <−−= λ (2-2) where )( cc PpP < is the probability that the central pressure pc is less than Pc given the occurrence of any one storm, and λ is the annual occurrence rate defined as N/NY where NY is the number of years in the historical record, taken here as 108 years (1900 through 2007). The model estimates of central pressure versus return period are computed using Equation 2-2, where λ is simply the number of storms that enter the circle during the 100,000 simulated years divided by 100,000 and the probability distribution for central pressure is obtained by rank ordering the simulated central pressures.
In addition to the mean model estimates of pressure vs. return period, each of the plots given in Figure 2-5 also presents the 2.5th and 97.5th percentile (95% confidence range) values of central pressures derived by sampling Np different values of central pressure from the simulated storm set and computing the CDF and then the pressure RP curve using the model value of λ. This process was repeated 1000 times, yielding 1,000 different RP curves based on sampling Np pressures randomly from the simulated storm set. The 1,000 different RP curves are then used to define the 95% confidence range for the mean pressure RP curves. Testing for equivalence of empirical distributions using this re-sampling approach is presented in James and Mason (2005), who indicate that for sample sizes of the order of 20, the method is as powerful as either the Cramer-von Mises or Anderson-Darling tests for equivalence. Of the 35 pc-RP curves given in Figure 2-5, two cases fail the empirical distribution equivalence testing method, as indicated by the notation JM=n at the top of the plot. Failure is defined as one or more observed values falling outside the bounds of the 2.5th and 97.5th percentile curves. In our testing, we only include tropical cyclones with central pressures less than 990 mbar. The equivalence testing of the pc-RP curves yields a comparison that includes the combined effects of the modelling of both the central pressures and the frequency of occurrence of the storms.
Figure 2-6 presents a qualitative comparison of the modelled and observed
extreme central pressures in the Caribbean. The observed values are presented as contours of the minimum observed central pressure anywhere within 250 km of the indicated point. The modelled values represent the minimum pressures anywhere within 250 km of the indicated point, likely to be exceeded, on average, once every 50 years
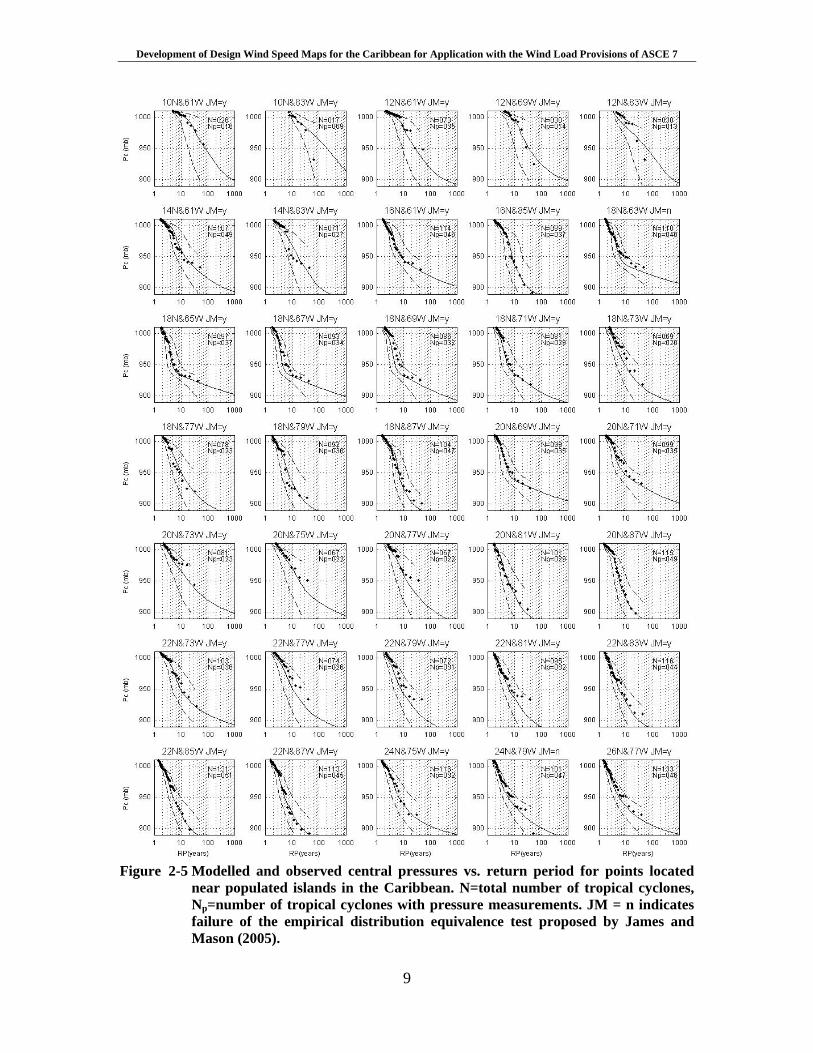
Development of Design Wind Speed Maps for the Caribbean for Application with the Wind Load Provisions of ASCE 7
9
Figure 2-5 Modelled and observed central pressures vs. return period for points located
near populated islands in the Caribbean. N=total number of tropical cyclones, Np=number of tropical cyclones with pressure measurements. JM = n indicates failure of the empirical distribution equivalence test proposed by James and Mason (2005).
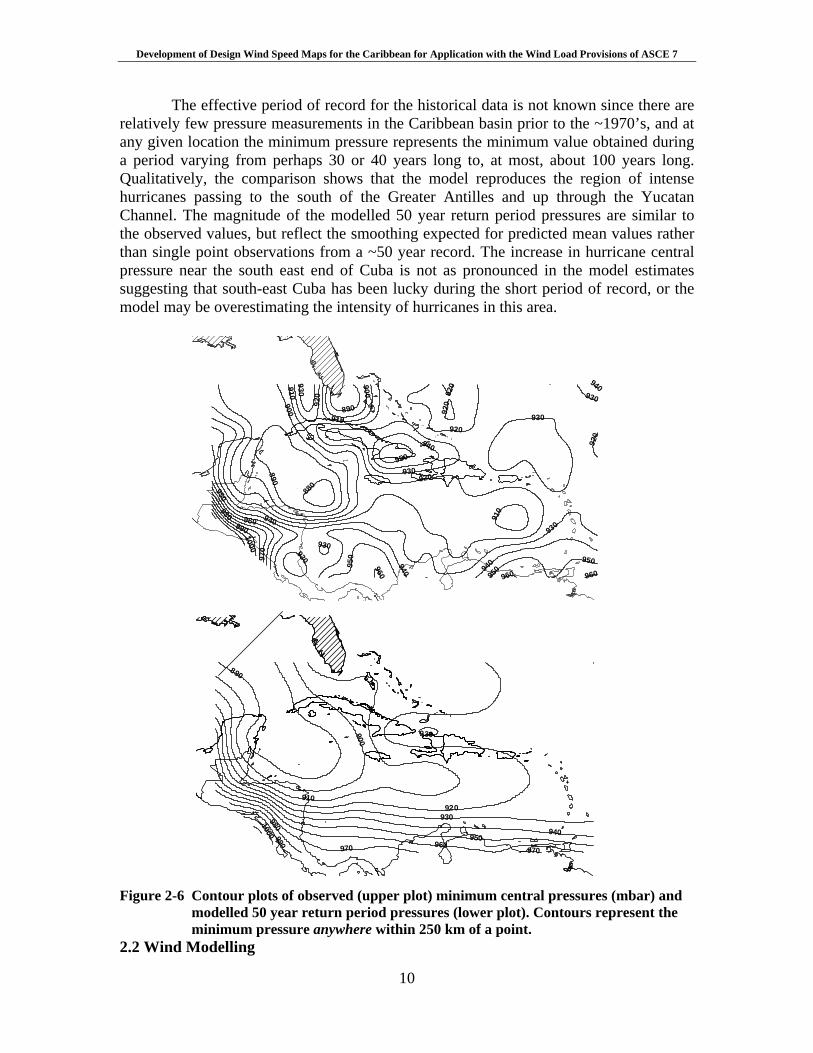
Development of Design Wind Speed Maps for the Caribbean for Application with the Wind Load Provisions of ASCE 7
10
The effective period of record for the historical data is not known since there are relatively few pressure measurements in the Caribbean basin prior to the ~1970’s, and at any given location the minimum pressure represents the minimum value obtained during a period varying from perhaps 30 or 40 years long to, at most, about 100 years long. Qualitatively, the comparison shows that the model reproduces the region of intense hurricanes passing to the south of the Greater Antilles and up through the Yucatan Channel. The magnitude of the modelled 50 year return period pressures are similar to the observed values, but reflect the smoothing expected for predicted mean values rather than single point observations from a ~50 year record. The increase in hurricane central pressure near the south east end of Cuba is not as pronounced in the model estimates suggesting that south-east Cuba has been lucky during the short period of record, or the model may be overestimating the intensity of hurricanes in this area.
930
920
940900
910
950
890
960
970
980
9901000
880
960
890
920
960
920
950
930
920
940
930
930
930
940
930
940900
910
950
920
910
920
940
950
930
950
960
940
930
950960
920
970
910
900
890
980990
1000
930
970
Figure 2-6 Contour plots of observed (upper plot) minimum central pressures (mbar) and
modelled 50 year return period pressures (lower plot). Contours represent the minimum pressure anywhere within 250 km of a point.
2.2 Wind Modelling
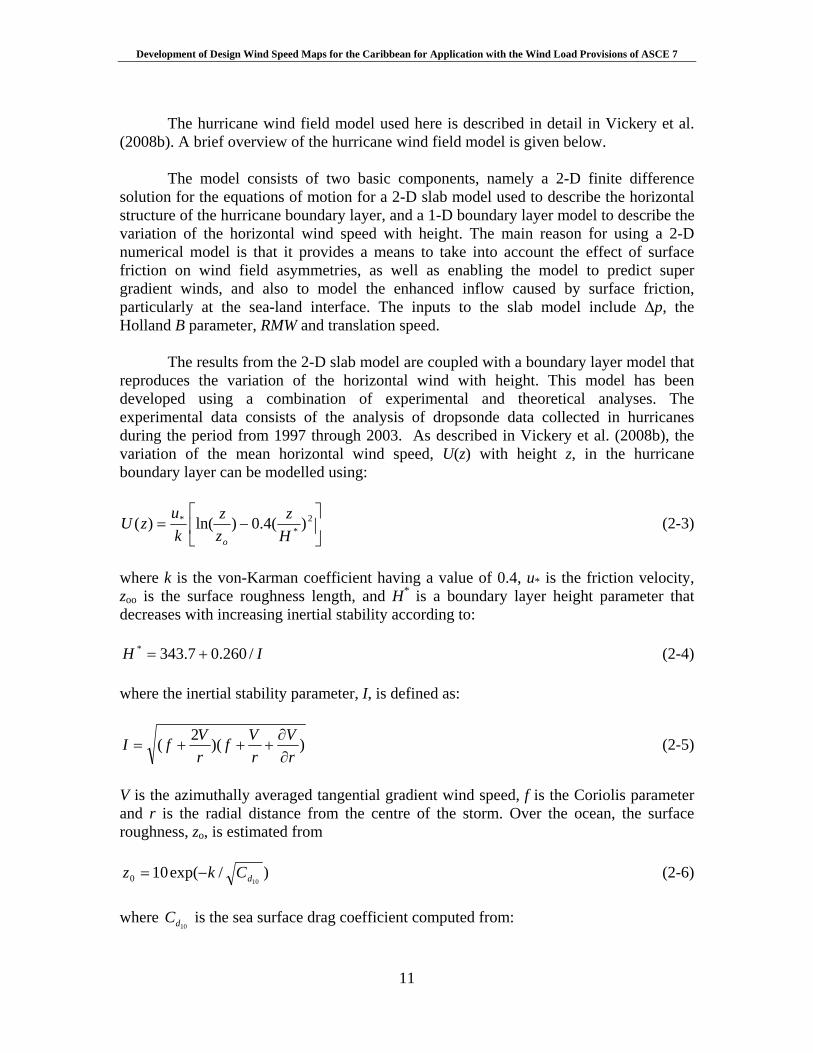
Development of Design Wind Speed Maps for the Caribbean for Application with the Wind Load Provisions of ASCE 7
11
The hurricane wind field model used here is described in detail in Vickery et al.
(2008b). A brief overview of the hurricane wind field model is given below. The model consists of two basic components, namely a 2-D finite difference
solution for the equations of motion for a 2-D slab model used to describe the horizontal structure of the hurricane boundary layer, and a 1-D boundary layer model to describe the variation of the horizontal wind speed with height. The main reason for using a 2-D numerical model is that it provides a means to take into account the effect of surface friction on wind field asymmetries, as well as enabling the model to predict super gradient winds, and also to model the enhanced inflow caused by surface friction, particularly at the sea-land interface. The inputs to the slab model include Δp, the Holland B parameter, RMW and translation speed.
The results from the 2-D slab model are coupled with a boundary layer model that
reproduces the variation of the horizontal wind with height. This model has been developed using a combination of experimental and theoretical analyses. The experimental data consists of the analysis of dropsonde data collected in hurricanes during the period from 1997 through 2003. As described in Vickery et al. (2008b), the variation of the mean horizontal wind speed, U(z) with height z, in the hurricane boundary layer can be modelled using:
⎥⎦
⎤⎢⎣
⎡−= 2
** )(4.0)ln()(
Hz
zz
ku
zUo
(2-3)
where k is the von-Karman coefficient having a value of 0.4, u* is the friction velocity, zoo is the surface roughness length, and H* is a boundary layer height parameter that decreases with increasing inertial stability according to:
IH /260.07.343* += (2-4) where the inertial stability parameter, I, is defined as:
))(2(rV
rVf
rVfI
∂∂
+++= (2-5)
V is the azimuthally averaged tangential gradient wind speed, f is the Coriolis parameter and r is the radial distance from the centre of the storm. Over the ocean, the surface roughness, zo, is estimated from
)/exp(10100 dCkz −= (2-6)
where
10dC is the sea surface drag coefficient computed from:
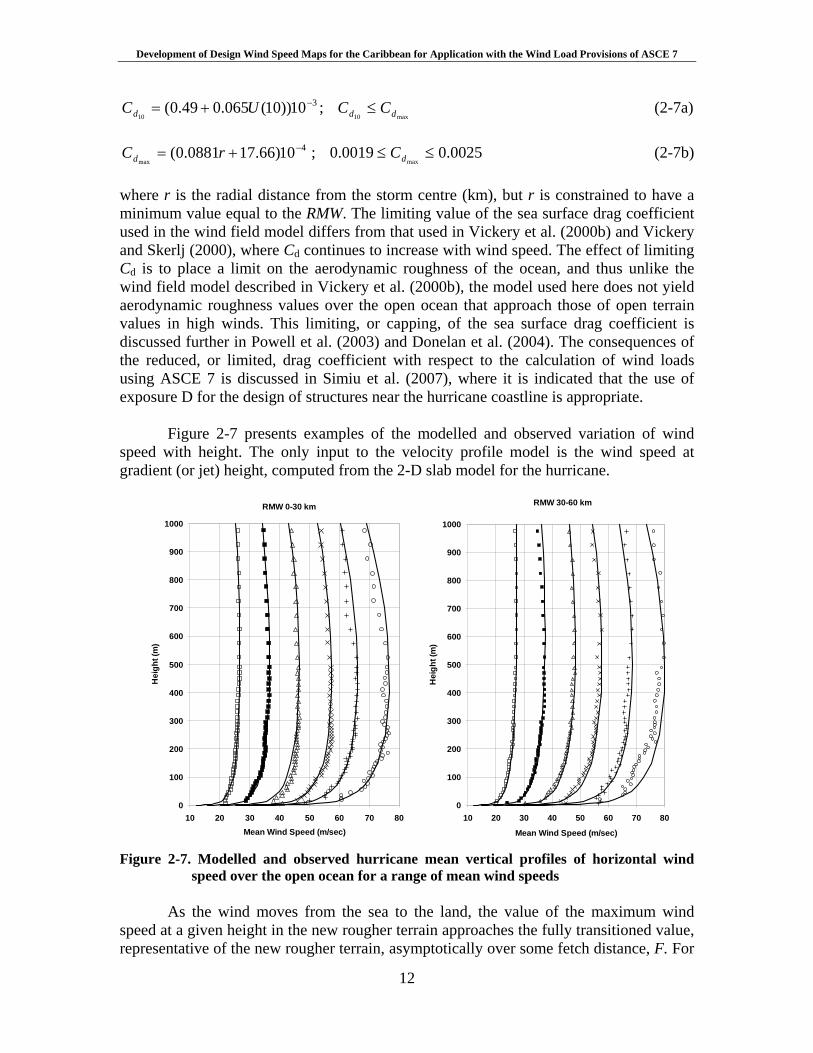
Development of Design Wind Speed Maps for the Caribbean for Application with the Wind Load Provisions of ASCE 7
12
310))10(065.049.0(10
−+= UCd ; max10 dd CC ≤ (2-7a)
410)66.170881.0(
max
−+= rCd ; 0025.00019.0max
≤≤ dC (2-7b) where r is the radial distance from the storm centre (km), but r is constrained to have a minimum value equal to the RMW. The limiting value of the sea surface drag coefficient used in the wind field model differs from that used in Vickery et al. (2000b) and Vickery and Skerlj (2000), where Cd continues to increase with wind speed. The effect of limiting Cd is to place a limit on the aerodynamic roughness of the ocean, and thus unlike the wind field model described in Vickery et al. (2000b), the model used here does not yield aerodynamic roughness values over the open ocean that approach those of open terrain values in high winds. This limiting, or capping, of the sea surface drag coefficient is discussed further in Powell et al. (2003) and Donelan et al. (2004). The consequences of the reduced, or limited, drag coefficient with respect to the calculation of wind loads using ASCE 7 is discussed in Simiu et al. (2007), where it is indicated that the use of exposure D for the design of structures near the hurricane coastline is appropriate.
Figure 2-7 presents examples of the modelled and observed variation of wind
speed with height. The only input to the velocity profile model is the wind speed at gradient (or jet) height, computed from the 2-D slab model for the hurricane.
RMW 30-60 km
0
100
200
300
400
500
600
700
800
900
1000
10 20 30 40 50 60 70 80
Mean Wind Speed (m/sec)
Hei
ght (
m)
RMW 0-30 km
0
100
200
300
400
500
600
700
800
900
1000
10 20 30 40 50 60 70 80Mean Wind Speed (m/sec)
Hei
ght (
m)
Figure 2-7. Modelled and observed hurricane mean vertical profiles of horizontal wind
speed over the open ocean for a range of mean wind speeds As the wind moves from the sea to the land, the value of the maximum wind
speed at a given height in the new rougher terrain approaches the fully transitioned value, representative of the new rougher terrain, asymptotically over some fetch distance, F. For
Development of Design Wind Speed Maps for the Caribbean for Application with the Wind Load Provisions of ASCE 7
13
modelling the transition from sea to land, the ESDU (1982) boundary layer transition model is used, but the limiting fetch distance of about 100 km used in ESDU (1982) is reduced to 20 km. This smaller fetch distance is consistent with the lower boundary layer heights associated with tropical cyclones (~600 m) compared to the larger values (~3000 m) used in ESDU for winds not produced by tropical cyclones. Figure 2-8 presents a plot showing the percentage the wind speed has transitioned (reduced) from the overwater values to the overland values as a function of distance from the coast. Note that at a distance of about 1 km from the coast, the peak gust wind speed has transitioned to about 70% of the fully reduced value. In a typical strong hurricane, the surface roughness, zo will be about 0.003m, and the open terrain value is 0.03m. From ESDU (1982) the full transitioned values of the peak 3 second gust and hourly mean wind speeds are about 89% and 83% of the marine winds, respectively.
Hourly Average
0%
20%
40%
60%
80%
100%
1 10 100 1000 10000 100000Fetch (m)
Deg
ree
Tran
sitio
ned Modified ESDU
ESDU
3 Second Gust
0%
20%
40%
60%
80%
100%
1 10 100 1000 10000 100000Fetch (m)
Deg
ree
Tran
sitio
ned Modified ESDU
ESDU
Figure 2-8. ESDU and modified ESDU wind speed transition functions at 10 m elevation.
Figure 2-9 presents a summary comparison of the maximum peak gust wind speeds computed using the wind field model described in Vickery et al. (2008b) to observations for both marine and land based anemometers. There are a total of 245 comparisons summarized in the data presented in Figure 2-9 (165 land based measurements and 80 marine based measurements). The agreement between the model and observed wind speeds is good, however there are relatively few measured gust wind speeds greater than 100 mph. The largest observed gust wind speed is only 128 mph. The differences between the modelled and observed wind speeds is caused by a combination of the inability of the wind field model to be adequately described by single values of B and RMW, errors in the modelled boundary layer, errors in height, terrain and averaging time adjustments applied to measured wind speeds (if required) as well as storm track position errors and errors in the estimated values of Δp, RMW and B. Estimates of the wind field model error obtained from the information given in Figure 2-9 are used in the estimates of wind speed as a function of return period as described in Section 3.
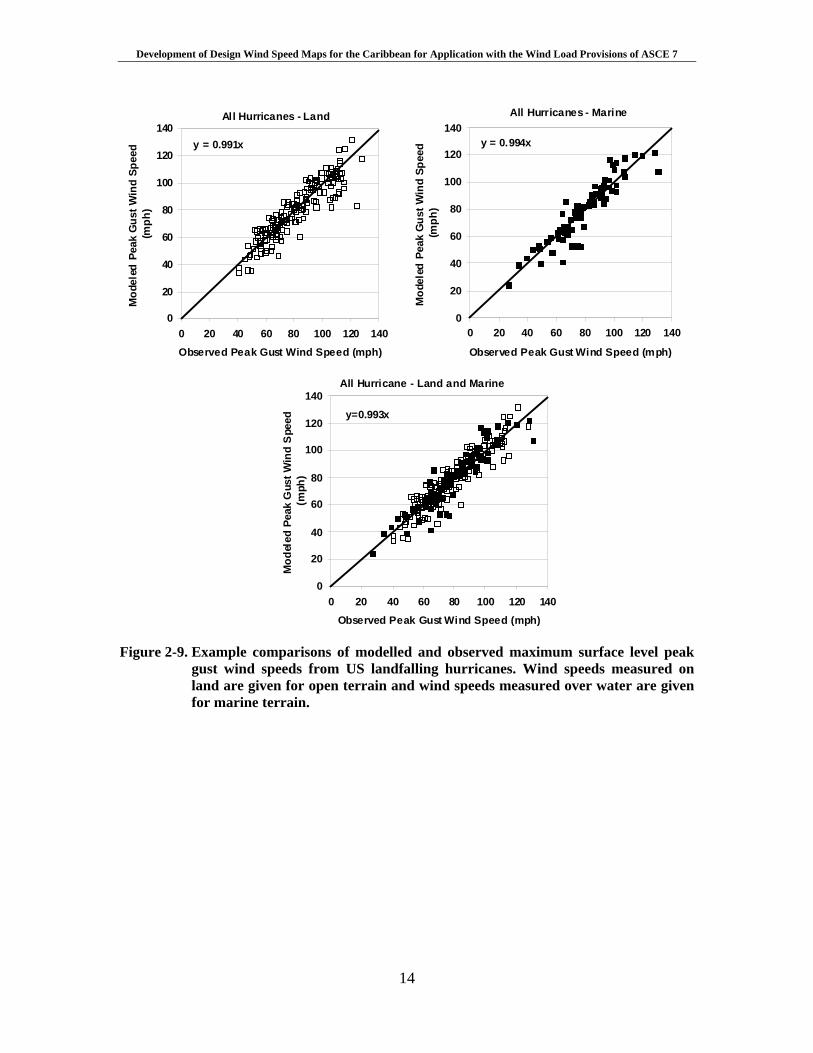
Development of Design Wind Speed Maps for the Caribbean for Application with the Wind Load Provisions of ASCE 7
14
All Hurricanes - Marine
y = 0.994x
0
20
40
60
80
100
120
140
0 20 40 60 80 100 120 140
Observed Peak Gust Wind Speed (mph)
Mod
eled
Pea
k G
ust W
ind
Spee
d (m
ph)
All Hurricanes - Land
y = 0.991x
0
20
40
60
80
100
120
140
0 20 40 60 80 100 120 140Observed Peak Gust Wind Speed (mph)
Mod
eled
Pea
k G
ust W
ind
Spee
d (m
ph)
All Hurricane - Land and Marine
y=0.993x
0
20
40
60
80
100
120
140
0 20 40 60 80 100 120 140Observed Peak Gust Wind Speed (mph)
Mod
eled
Pea
k G
ust W
ind
Spe
ed
(mph
)
Figure 2-9. Example comparisons of modelled and observed maximum surface level peak
gust wind speeds from US landfalling hurricanes. Wind speeds measured on land are given for open terrain and wind speeds measured over water are given for marine terrain.

Development of Design Wind Speed Maps for the Caribbean for Application with the Wind Load Provisions of ASCE 7
15
3. DESIGN WIND SPEEDS The hurricane simulation model described in section 2 was used to develop estimates of peak gust wind speeds as a function of return period in the Caribbean. All speeds are produced as values associated with a 3 second gust wind speed at a height of 10 m in flat open terrain. The wind speeds can be used in conjunction with the methods outlined in Chapters 2 and 6 of ASCE editions 7-98 and later for the purposes of estimating design wind pressures. As will be discussed in more detail below, the basic wind speed to be used in the design of Category II structures is the 700-year wind speed divided by 6.1 . For Category III and IV structures, the wind speed to be used is the 1,700-year wind speed divided by 6.1 . The use of 1,700-year wind speed divided by
6.1 replaces the need to use the 700 year values with an importance factor of 1.15 as given in ASCE 7-98 and later. For buildings located near the coast, the wind speeds presented herein should be used with the procedures given in ASCE 7 including the use of Exposure D. The use of exposure D is required because of the limit in the sea surface drag coefficient. The following sections discuss the development of the wind speed maps and the use of the resulting wind speeds in conjunction with the wind load provisions as given in ASCE 7-98 and later. 3.1 Design Wind Speed Maps
Predictions of wind speed as a function of return period at any point in the Caribbean are obtained using the hurricane simulation model described in Section 2 using a 100,000 year simulation of hurricanes. Upon completion of the 100,000-year simulation, the wind speed data are rank ordered and then used to define the wind speed probability distribution, P(v>V), conditional on a storm having passed within 250 km of the site and producing a peak gust wind speed of at least 20 mph. The wind speed associated with a given exceedance probability is obtained by interpolating from the rank ordered wind speed data. The probability that the tropical cyclone wind speed (independent of direction) is exceeded during time period t is,
∑∞
=
<−=>0
)()|(1)(x
tt xpxVvPVvP (3-1)
where )|( xVvP < is the probability that the velocity v is less than V given that x storms occur, and pt(x) is the probability of x storms occurring during time period t. From Equation 3-1, with pt(x) defined as having a Poisson distribution and defining t as one year, the annual probability of exceeding a given wind speed is,
)](exp[1)( VvPVvPa >−−=> λ (3-2)
where λ (annual occurrence rate) represents the average annual number of storms approaching within 250 km of the site and producing a minimum 20 mph peak gust wind speed, and )( VvP > is the probability that the velocity v is greater than V given the occurrence of any one storm.
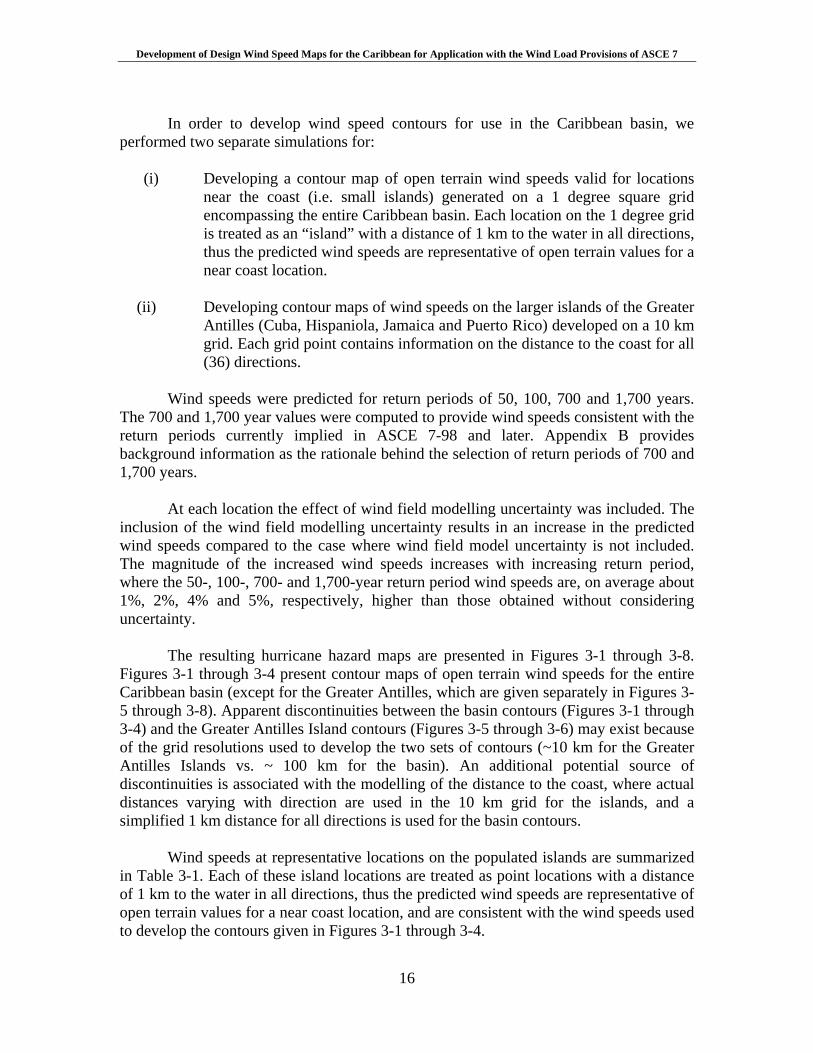
Development of Design Wind Speed Maps for the Caribbean for Application with the Wind Load Provisions of ASCE 7
16
In order to develop wind speed contours for use in the Caribbean basin, we
performed two separate simulations for:
(i) Developing a contour map of open terrain wind speeds valid for locations near the coast (i.e. small islands) generated on a 1 degree square grid encompassing the entire Caribbean basin. Each location on the 1 degree grid is treated as an “island” with a distance of 1 km to the water in all directions, thus the predicted wind speeds are representative of open terrain values for a near coast location.
(ii) Developing contour maps of wind speeds on the larger islands of the Greater
Antilles (Cuba, Hispaniola, Jamaica and Puerto Rico) developed on a 10 km grid. Each grid point contains information on the distance to the coast for all (36) directions.
Wind speeds were predicted for return periods of 50, 100, 700 and 1,700 years.
The 700 and 1,700 year values were computed to provide wind speeds consistent with the return periods currently implied in ASCE 7-98 and later. Appendix B provides background information as the rationale behind the selection of return periods of 700 and 1,700 years.
At each location the effect of wind field modelling uncertainty was included. The
inclusion of the wind field modelling uncertainty results in an increase in the predicted wind speeds compared to the case where wind field model uncertainty is not included. The magnitude of the increased wind speeds increases with increasing return period, where the 50-, 100-, 700- and 1,700-year return period wind speeds are, on average about 1%, 2%, 4% and 5%, respectively, higher than those obtained without considering uncertainty.
The resulting hurricane hazard maps are presented in Figures 3-1 through 3-8.
Figures 3-1 through 3-4 present contour maps of open terrain wind speeds for the entire Caribbean basin (except for the Greater Antilles, which are given separately in Figures 3-5 through 3-8). Apparent discontinuities between the basin contours (Figures 3-1 through 3-4) and the Greater Antilles Island contours (Figures 3-5 through 3-6) may exist because of the grid resolutions used to develop the two sets of contours (~10 km for the Greater Antilles Islands vs. ~ 100 km for the basin). An additional potential source of discontinuities is associated with the modelling of the distance to the coast, where actual distances varying with direction are used in the 10 km grid for the islands, and a simplified 1 km distance for all directions is used for the basin contours.
Wind speeds at representative locations on the populated islands are summarized
in Table 3-1. Each of these island locations are treated as point locations with a distance of 1 km to the water in all directions, thus the predicted wind speeds are representative of open terrain values for a near coast location, and are consistent with the wind speeds used to develop the contours given in Figures 3-1 through 3-4.
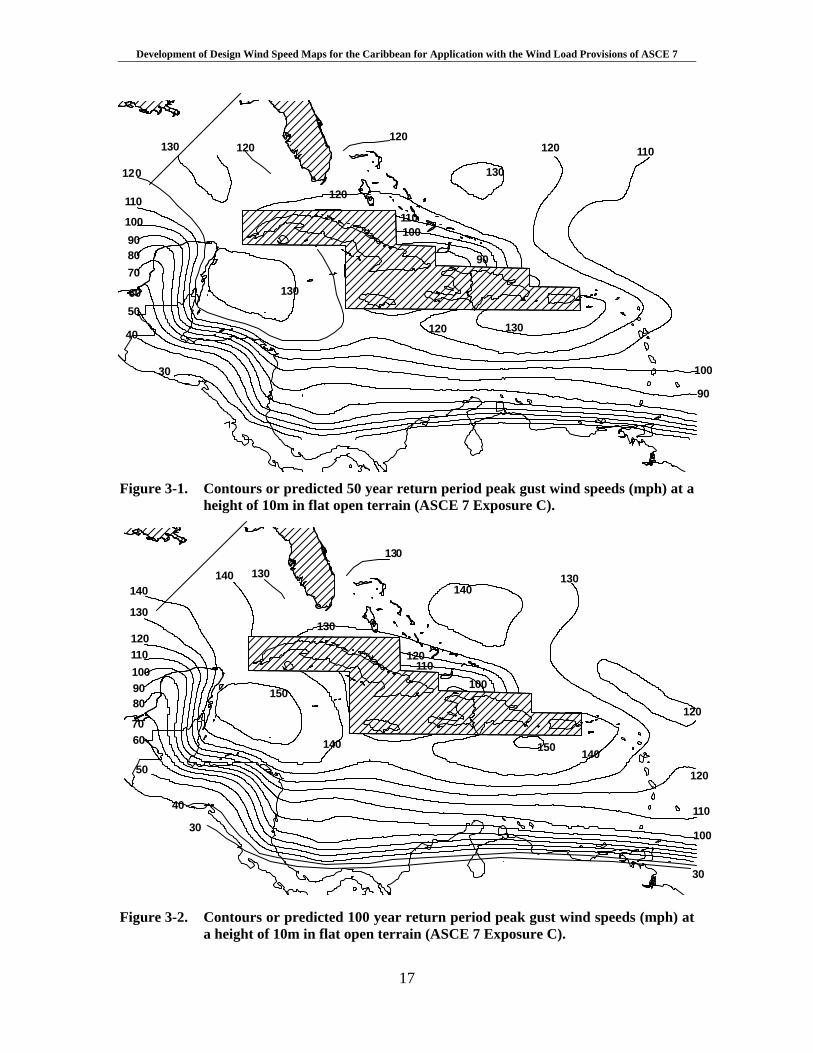
Development of Design Wind Speed Maps for the Caribbean for Application with the Wind Load Provisions of ASCE 7
17
130
120
110
100908070
6050
40
30
130
120120
130
120 110
120 130
100
90
120
110100
90
Figure 3-1. Contours or predicted 50 year return period peak gust wind speeds (mph) at a
height of 10m in flat open terrain (ASCE 7 Exposure C).
140
130
1201101009080
7060
50
40
30
140
140
150
130
130
140130
120
110
100
30
130
120110
100
150 140
120
Figure 3-2. Contours or predicted 100 year return period peak gust wind speeds (mph) at
a height of 10m in flat open terrain (ASCE 7 Exposure C).
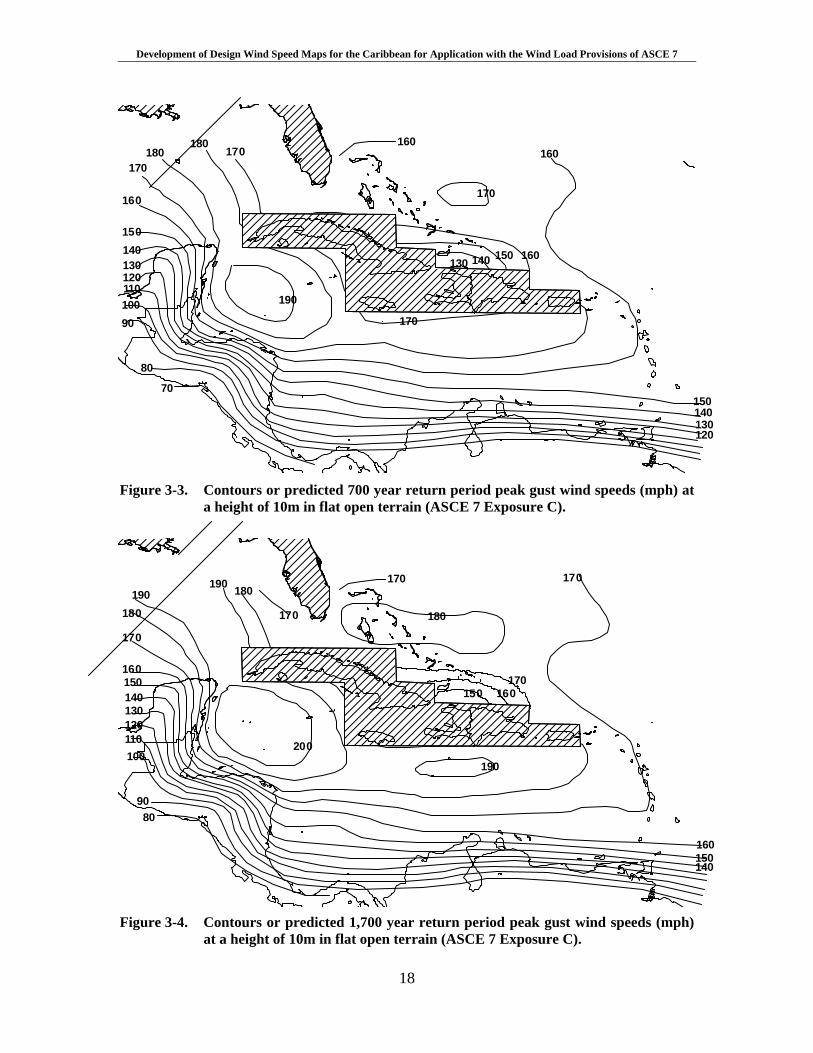
Development of Design Wind Speed Maps for the Caribbean for Application with the Wind Load Provisions of ASCE 7
18
180180
170170
15014013012011010090
80
70
160
190
160
170
160
150140130120
170
160150140130
Figure 3-3. Contours or predicted 700 year return period peak gust wind speeds (mph) at
a height of 10m in flat open terrain (ASCE 7 Exposure C).
190180
170
160150140130120110100
9080
190 180
170
170
180
200
190
160150140
170
170160150
Figure 3-4. Contours or predicted 1,700 year return period peak gust wind speeds (mph)
at a height of 10m in flat open terrain (ASCE 7 Exposure C).
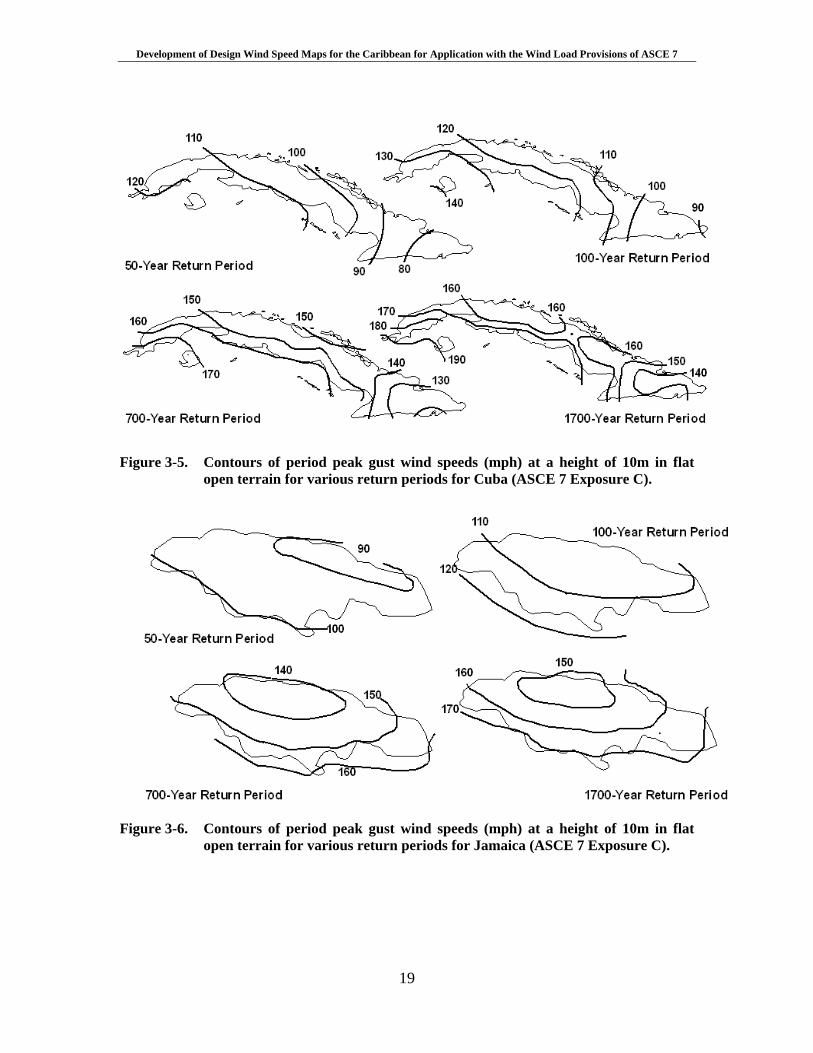
Development of Design Wind Speed Maps for the Caribbean for Application with the Wind Load Provisions of ASCE 7
19
Figure 3-5. Contours of period peak gust wind speeds (mph) at a height of 10m in flat
open terrain for various return periods for Cuba (ASCE 7 Exposure C).
Figure 3-6. Contours of period peak gust wind speeds (mph) at a height of 10m in flat
open terrain for various return periods for Jamaica (ASCE 7 Exposure C).

Development of Design Wind Speed Maps for the Caribbean for Application with the Wind Load Provisions of ASCE 7
20
Figure 3-7. Contours of period peak gust wind speeds (mph) at a height of 10m in flat
open terrain for various return periods for Puerto Rico (ASCE 7 Exposure C).
Figure 3-8. Contours of period peak gust wind speeds (mph) at a height of 10m in flat
open terrain for various return periods for the island of Hispaniola(ASCE 7 Exposure C).
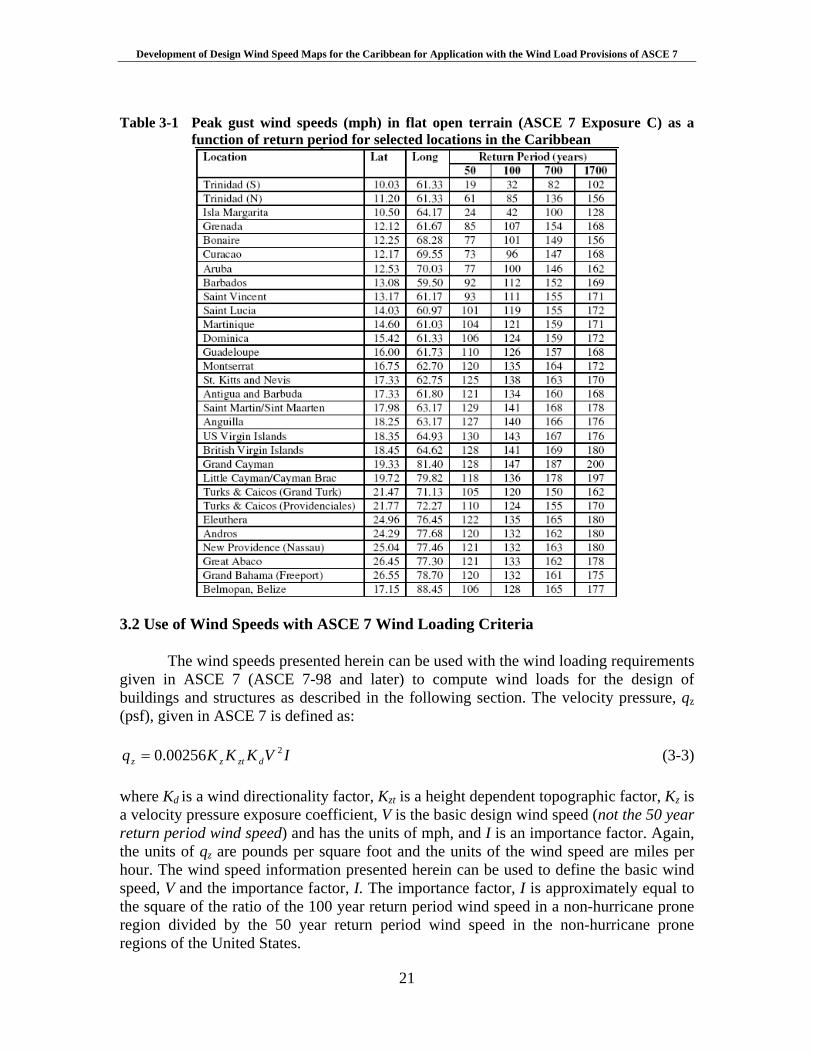
Development of Design Wind Speed Maps for the Caribbean for Application with the Wind Load Provisions of ASCE 7
21
Table 3-1 Peak gust wind speeds (mph) in flat open terrain (ASCE 7 Exposure C) as a
function of return period for selected locations in the Caribbean
3.2 Use of Wind Speeds with ASCE 7 Wind Loading Criteria The wind speeds presented herein can be used with the wind loading requirements given in ASCE 7 (ASCE 7-98 and later) to compute wind loads for the design of buildings and structures as described in the following section. The velocity pressure, qz (psf), given in ASCE 7 is defined as:
IVKKKq dztzz200256.0= (3-3)
where Kd is a wind directionality factor, Kzt is a height dependent topographic factor, Kz is a velocity pressure exposure coefficient, V is the basic design wind speed (not the 50 year return period wind speed) and has the units of mph, and I is an importance factor. Again, the units of qz are pounds per square foot and the units of the wind speed are miles per hour. The wind speed information presented herein can be used to define the basic wind speed, V and the importance factor, I. The importance factor, I is approximately equal to the square of the ratio of the 100 year return period wind speed in a non-hurricane prone region divided by the 50 year return period wind speed in the non-hurricane prone regions of the United States.

Development of Design Wind Speed Maps for the Caribbean for Application with the Wind Load Provisions of ASCE 7
22
As discussed in the commentaries of ASCE 7-98, ASCE 7-02 and ASCE 7-05, and Appendix B of this report, the basic wind speed used in ASCE 7 is the 500-year return period wind speed divided by 5.1 . In the non-hurricane prone region of the US, the resulting basic wind speed is a 50-year return period value. In the hurricane prone regions of the continental United States the return period associated with the basic wind speed varies with location, but is typically in the range of 70 to 100 years.
Here, the basic wind speed is the 700-year return period wind speed divided
by 6.1 , which yields a design wind speed that is consistent with the intent of the developers of the ASCE 7 wind speed map. Thus the wind speed to be used in Equation 3-3 and subsequently the wind load calculations given in ASCE 7 is
6.1/700VV =
Appendix B provides information as to the reason for using a 700-year return
period wind speed divided by 6.1 , as compared to the 500 year return period wind speed divided by 5.1 as presented in ASCE 7-98 through ASCE 7-05. Appendix B also provides the rationale for replacing the IV 2 term (where I =1.15) in Equation 3-3 with
21700 )6.1/(V for the design of Category III and IV structures.
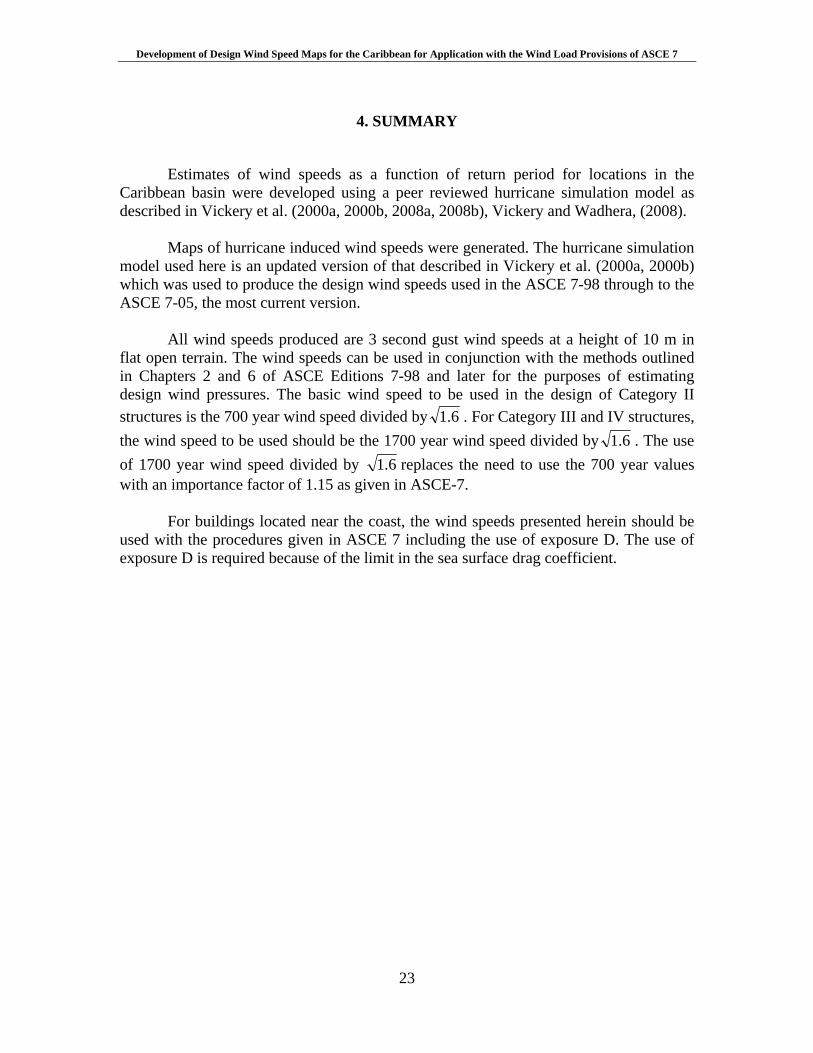
Development of Design Wind Speed Maps for the Caribbean for Application with the Wind Load Provisions of ASCE 7
23
4. SUMMARY
Estimates of wind speeds as a function of return period for locations in the
Caribbean basin were developed using a peer reviewed hurricane simulation model as described in Vickery et al. (2000a, 2000b, 2008a, 2008b), Vickery and Wadhera, (2008).
Maps of hurricane induced wind speeds were generated. The hurricane simulation
model used here is an updated version of that described in Vickery et al. (2000a, 2000b) which was used to produce the design wind speeds used in the ASCE 7-98 through to the ASCE 7-05, the most current version.
All wind speeds produced are 3 second gust wind speeds at a height of 10 m in
flat open terrain. The wind speeds can be used in conjunction with the methods outlined in Chapters 2 and 6 of ASCE Editions 7-98 and later for the purposes of estimating design wind pressures. The basic wind speed to be used in the design of Category II structures is the 700 year wind speed divided by 6.1 . For Category III and IV structures, the wind speed to be used should be the 1700 year wind speed divided by 6.1 . The use of 1700 year wind speed divided by 6.1 replaces the need to use the 700 year values with an importance factor of 1.15 as given in ASCE-7.
For buildings located near the coast, the wind speeds presented herein should be
used with the procedures given in ASCE 7 including the use of exposure D. The use of exposure D is required because of the limit in the sea surface drag coefficient.
Development of Design Wind Speed Maps for the Caribbean for Application with the Wind Load Provisions of ASCE 7
24
5. REFERENCES
Donelan, M.A., B.K. Haus, N. Reul, W.J. Plant, M. Stiassnie, H.C. Graber, O.B. Brown, and E.S. Saltzman, (2004). “On the limiting aerodynamic roughness in the ocean in very strong winds” Geophys. Res. Lett., 31, L18306
Emanuel, K.A, S. Ravela, E. Vivant and C. Risi, (2006), “A statistical–deterministic approach to hurricane risk assessment”, Bull. Amer. Meteor. Soc., 19, 299-314.
ESDU, (1982), “Strong Winds in the Atmospheric Boundary Layer, Part 1: Mean Hourly Wind Speed”, Engineering Sciences Data Unit Item No. 82026, London, England, 1982.
Georgiou, P.N., (1985), “Design Windspeeds in Tropical Cyclone-Prone Regions”, Ph.D. Thesis, Faculty of Engineering Science, University of Western Ontario, London, Ontario, Canada, 1985.
Georgiou, P.N., A.G. Davenport and B.J. Vickery, (1983) “Design wind speeds in regions dominated by tropical cyclones”, 6th International Conference on Wind Engineering, Gold Coast, Australia, 21-25 March and Auckland, New Zealand, 6-7 April.
Holland, G.J., (1980), “An analytic model of the wind and pressure profiles in hurricanes, Mon. Wea. Rev., 108 (1980) 1212-1218.
James, M. K. and L.B. Mason, (2005), “Synthetic tropical cyclone database”, J. Wtrwy, Port, Coast and Oc. Engrg., 131, 181-192
Jarvinen, B.R., C.J. Neumann, and M.A.S. Davis, (1984), “A Tropical Cyclone Data Tape for the North Atlantic Basin 1886-1983: Contents, Limitations and Uses”, NOAA Technical Memorandum NWS NHC 22, U.S. Department of Commerce, March, 1984. DeMaria, M., and J. Kaplan (1999), “An updated Statistical Hurricane Intensity Prediction Scheme (SHIPS) for the Atlantic and Eastern North Pacific Basins”, Weather and Forecasting, 14, 326–337. Powell, M.D., P.J. Vickery, and T.A. Reinhold, (2003), “Reduced drag coefficient for high wind speeds in tropical cyclones”, Nature, 422, 279-283. Simiu, E., P. J. Vickery, and A Kareem, (2007), “Relations between Saffir-Simpson hurricane scale wind speeds and peak 3-s gust speeds over open terrain”, J. Struct. Eng, 133, 1043-1045 Vickery, P.J. and D. Wadhera, (2008), “Statistical Models of Holland Pressure Profile Parameter and Radius to Maximum Winds of Hurricanes from Flight Level Pressure and H*Wind Data”, submitted to J. Appl. Meteor.
Development of Design Wind Speed Maps for the Caribbean for Application with the Wind Load Provisions of ASCE 7
25
Vickery, P.J.; D. Wadhera, L.A. Twisdale Jr., and F.M. Lavelle, (2008a), “United States hurricane wind speed risk and uncertainty”, submitted to J. Struct. Eng.. Vickery, P.J., D. Wadhera, M.D. Powell and Y. Chen, (2008b) “A Hurricane Boundary Layer and Wind Field Model for Use in Engineering Applications”, accepted for publication in J. Appl. Meteor. Vickery, P.J., J. X. Lin, P. F. Skerlj, and L. A. Twisdale Jr., (2006), “The HAZUS-MH hurricane model methodology part I: Hurricane hazard, terrain and wind load modelling”, Nat. Hazards Rev., 7, 82-93 Vickery, P.J., (2005), “Simple empirical models for estimating the increase in the central pressure of tropical cyclones after landfall along the coastline of the United States”, J. Appl. Meteor., 44, 1807-1826. Vickery, P.J., P.F. Skerlj and L.A. Twisdale Jr., (2000a) “Simulation of hurricane risk in the U.S. using an empirical track model,” J. Struct. Eng., 126, 1222-1237 Vickery, P.J., P.F. Skerlj, A.C. Steckley and L.A. Twisdale Jr., (2000b) Hurricane wind field model for use in hurricane simulations, J. Struct. Eng., 126. 1203-1221 Vickery, P.J. and P.F. Skerlj, (2000), “Elimination of exposure D along hurricane coastline in ASCE 7”, J. Struct. Eng.. 126, 545-549 Vickery, P.J., and L.A. Twisdale, (1995), “Prediction of hurricane wind speeds in the U.S.,” J. Struct. Eng., 121, 1691-1699

Development of Design Wind Speed Maps for the Caribbean for Application with the Wind Load Provisions of ASCE 7
A-1
Appendix A
Comparisons of modelled and observed cumulative frequency distributions of central pressure, heading, and translational speed
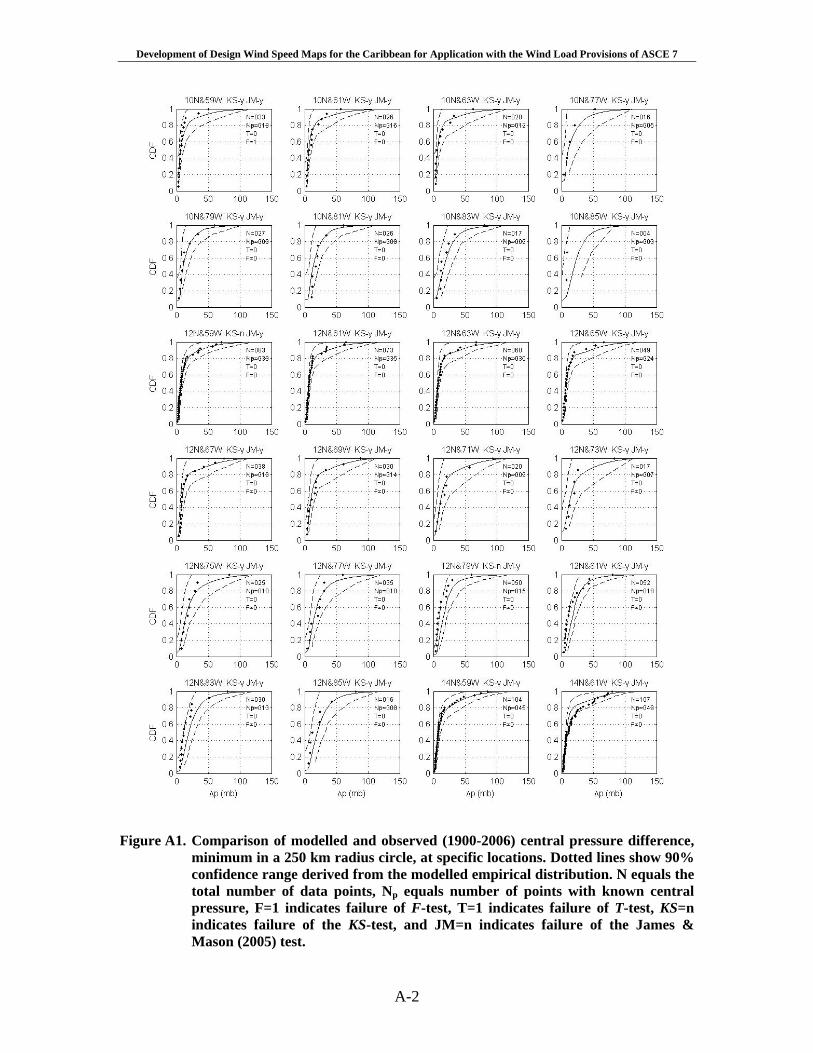
Development of Design Wind Speed Maps for the Caribbean for Application with the Wind Load Provisions of ASCE 7
A-2
Figure A1. Comparison of modelled and observed (1900-2006) central pressure difference,
minimum in a 250 km radius circle, at specific locations. Dotted lines show 90% confidence range derived from the modelled empirical distribution. N equals the total number of data points, Np equals number of points with known central pressure, F=1 indicates failure of F-test, T=1 indicates failure of T-test, KS=n indicates failure of the KS-test, and JM=n indicates failure of the James & Mason (2005) test.
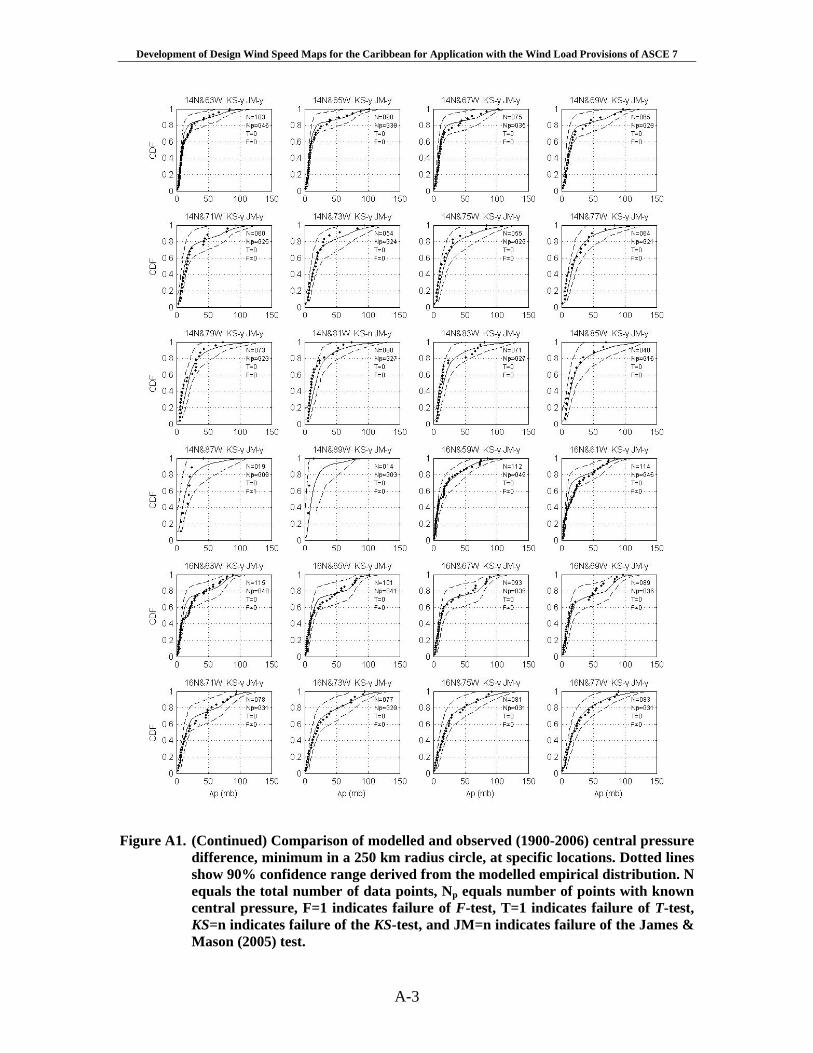
Development of Design Wind Speed Maps for the Caribbean for Application with the Wind Load Provisions of ASCE 7
A-3
Figure A1. (Continued) Comparison of modelled and observed (1900-2006) central pressure
difference, minimum in a 250 km radius circle, at specific locations. Dotted lines show 90% confidence range derived from the modelled empirical distribution. N equals the total number of data points, Np equals number of points with known central pressure, F=1 indicates failure of F-test, T=1 indicates failure of T-test, KS=n indicates failure of the KS-test, and JM=n indicates failure of the James & Mason (2005) test.
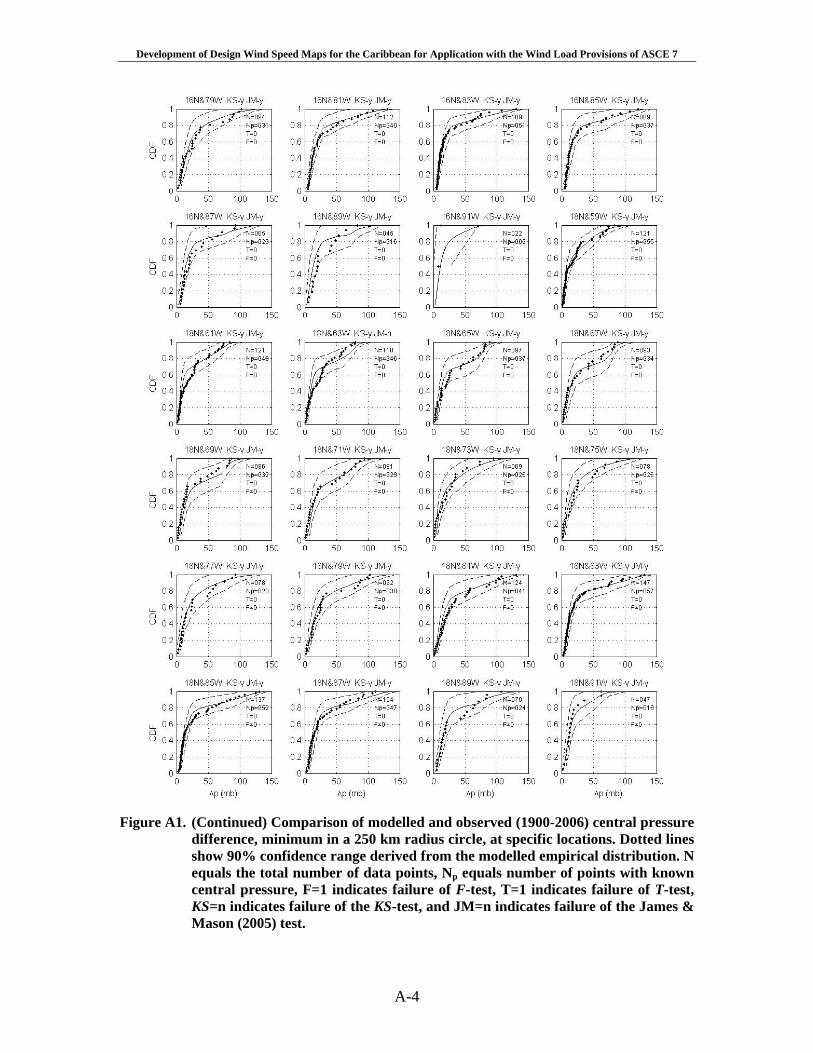
Development of Design Wind Speed Maps for the Caribbean for Application with the Wind Load Provisions of ASCE 7
A-4
Figure A1. (Continued) Comparison of modelled and observed (1900-2006) central pressure
difference, minimum in a 250 km radius circle, at specific locations. Dotted lines show 90% confidence range derived from the modelled empirical distribution. N equals the total number of data points, Np equals number of points with known central pressure, F=1 indicates failure of F-test, T=1 indicates failure of T-test, KS=n indicates failure of the KS-test, and JM=n indicates failure of the James & Mason (2005) test.
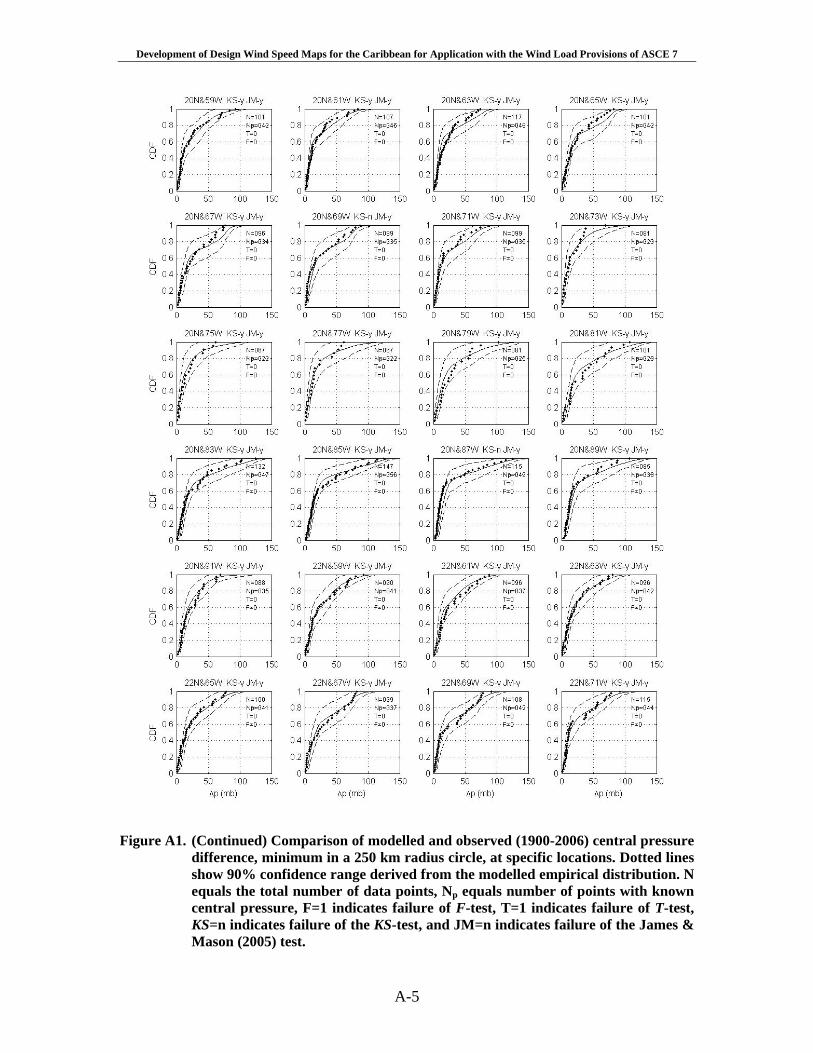
Development of Design Wind Speed Maps for the Caribbean for Application with the Wind Load Provisions of ASCE 7
A-5
Figure A1. (Continued) Comparison of modelled and observed (1900-2006) central pressure
difference, minimum in a 250 km radius circle, at specific locations. Dotted lines show 90% confidence range derived from the modelled empirical distribution. N equals the total number of data points, Np equals number of points with known central pressure, F=1 indicates failure of F-test, T=1 indicates failure of T-test, KS=n indicates failure of the KS-test, and JM=n indicates failure of the James & Mason (2005) test.
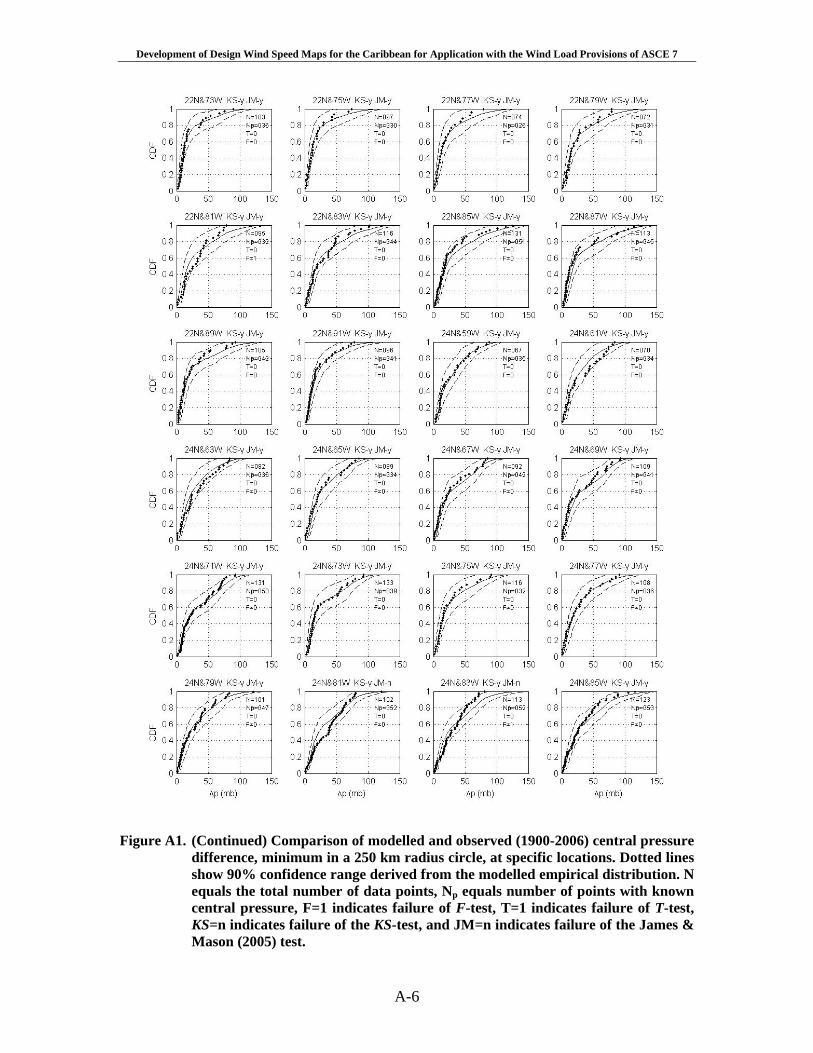
Development of Design Wind Speed Maps for the Caribbean for Application with the Wind Load Provisions of ASCE 7
A-6
Figure A1. (Continued) Comparison of modelled and observed (1900-2006) central pressure
difference, minimum in a 250 km radius circle, at specific locations. Dotted lines show 90% confidence range derived from the modelled empirical distribution. N equals the total number of data points, Np equals number of points with known central pressure, F=1 indicates failure of F-test, T=1 indicates failure of T-test, KS=n indicates failure of the KS-test, and JM=n indicates failure of the James & Mason (2005) test.
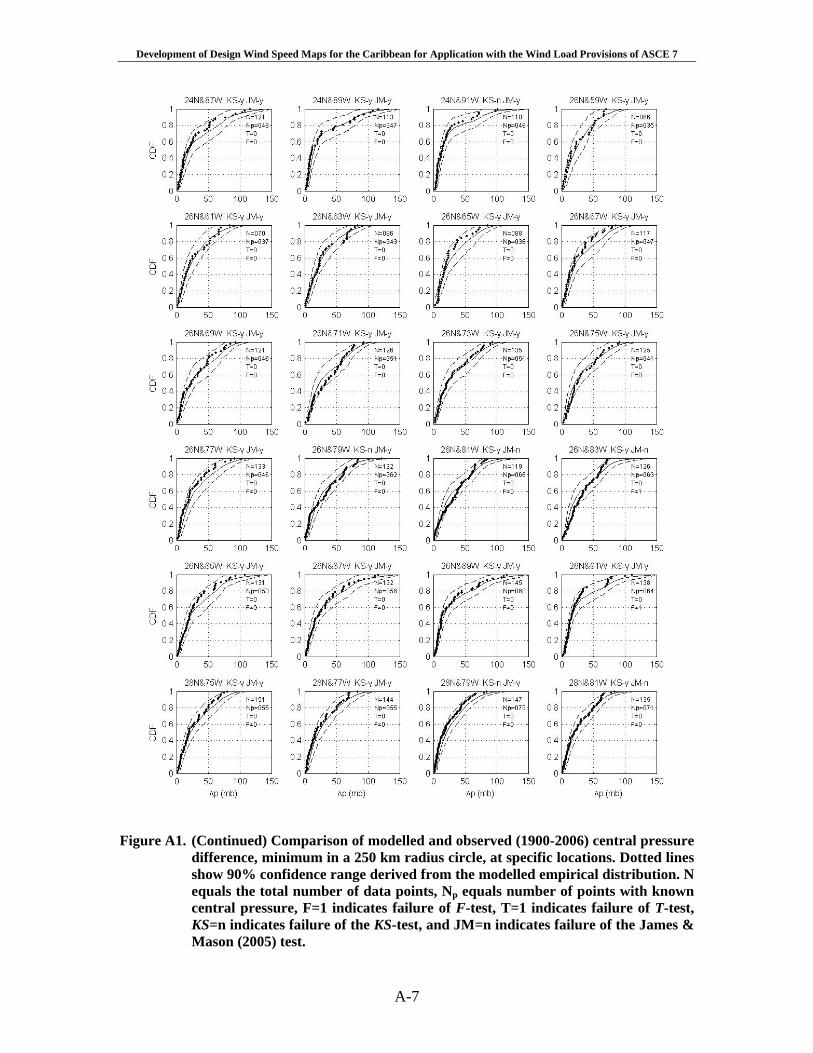
Development of Design Wind Speed Maps for the Caribbean for Application with the Wind Load Provisions of ASCE 7
A-7
Figure A1. (Continued) Comparison of modelled and observed (1900-2006) central pressure
difference, minimum in a 250 km radius circle, at specific locations. Dotted lines show 90% confidence range derived from the modelled empirical distribution. N equals the total number of data points, Np equals number of points with known central pressure, F=1 indicates failure of F-test, T=1 indicates failure of T-test, KS=n indicates failure of the KS-test, and JM=n indicates failure of the James & Mason (2005) test.
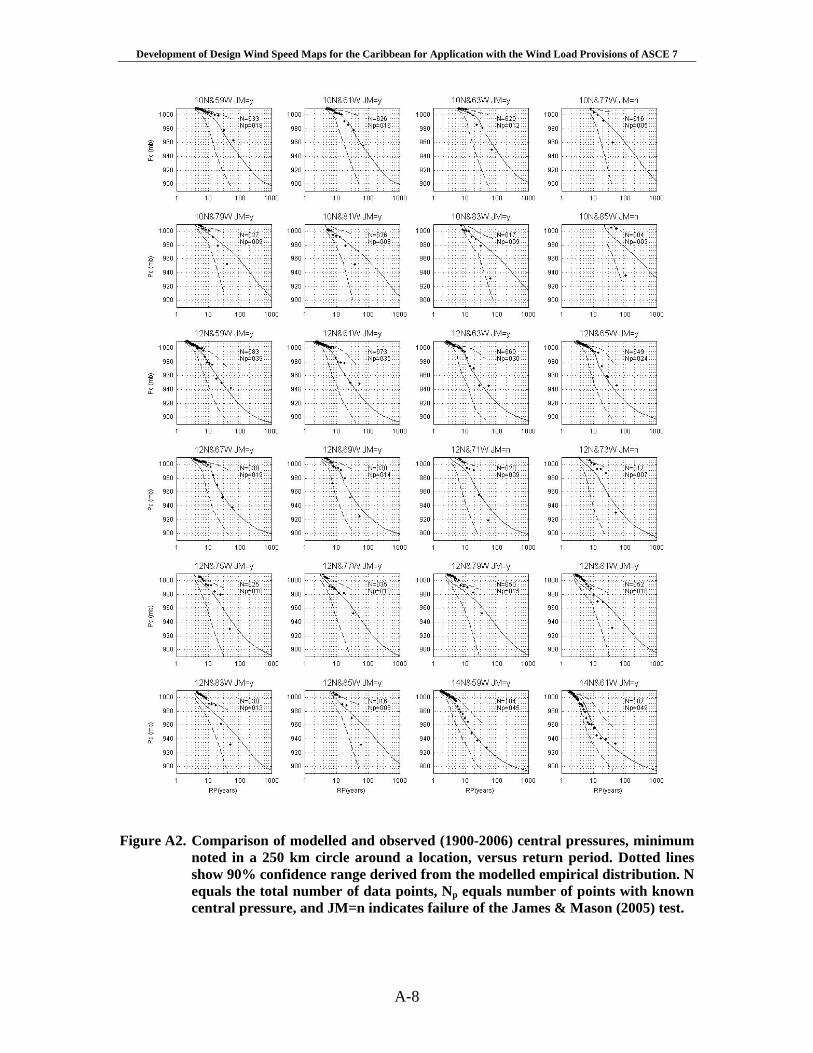
Development of Design Wind Speed Maps for the Caribbean for Application with the Wind Load Provisions of ASCE 7
A-8
Figure A2. Comparison of modelled and observed (1900-2006) central pressures, minimum
noted in a 250 km circle around a location, versus return period. Dotted lines show 90% confidence range derived from the modelled empirical distribution. N equals the total number of data points, Np equals number of points with known central pressure, and JM=n indicates failure of the James & Mason (2005) test.
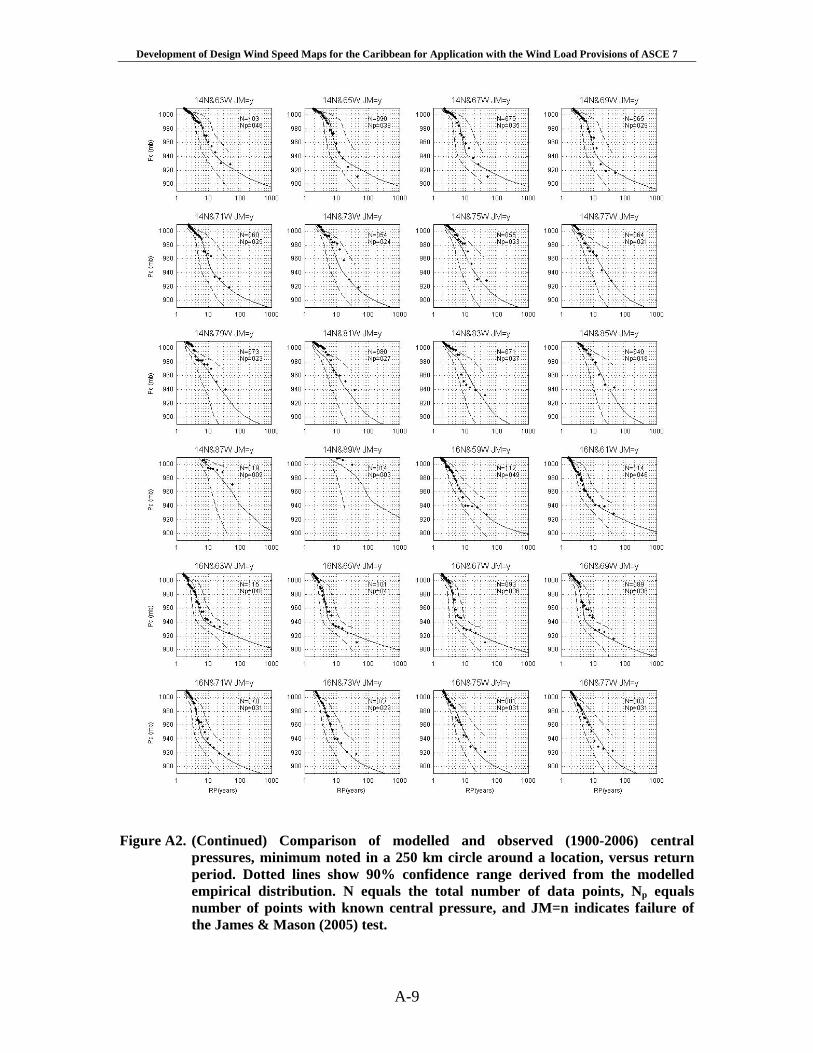
Development of Design Wind Speed Maps for the Caribbean for Application with the Wind Load Provisions of ASCE 7
A-9
Figure A2. (Continued) Comparison of modelled and observed (1900-2006) central
pressures, minimum noted in a 250 km circle around a location, versus return period. Dotted lines show 90% confidence range derived from the modelled empirical distribution. N equals the total number of data points, Np equals number of points with known central pressure, and JM=n indicates failure of the James & Mason (2005) test.
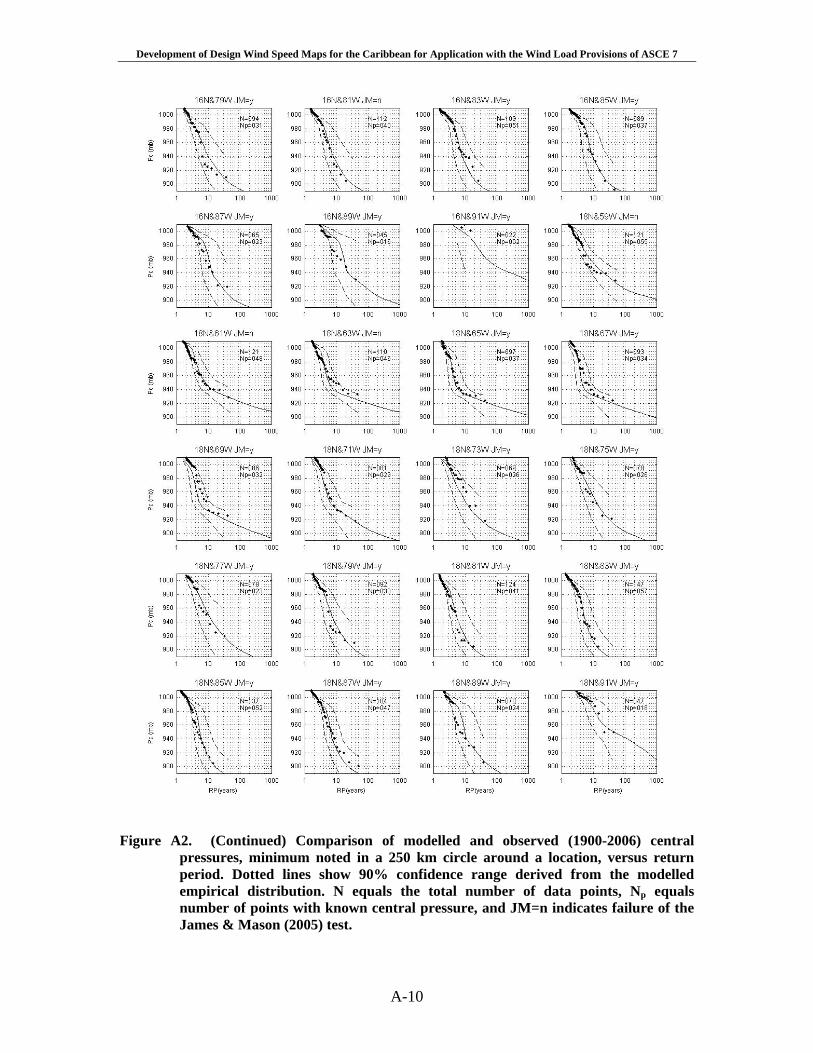
Development of Design Wind Speed Maps for the Caribbean for Application with the Wind Load Provisions of ASCE 7
A-10
Figure A2. (Continued) Comparison of modelled and observed (1900-2006) central
pressures, minimum noted in a 250 km circle around a location, versus return period. Dotted lines show 90% confidence range derived from the modelled empirical distribution. N equals the total number of data points, Np equals number of points with known central pressure, and JM=n indicates failure of the James & Mason (2005) test.
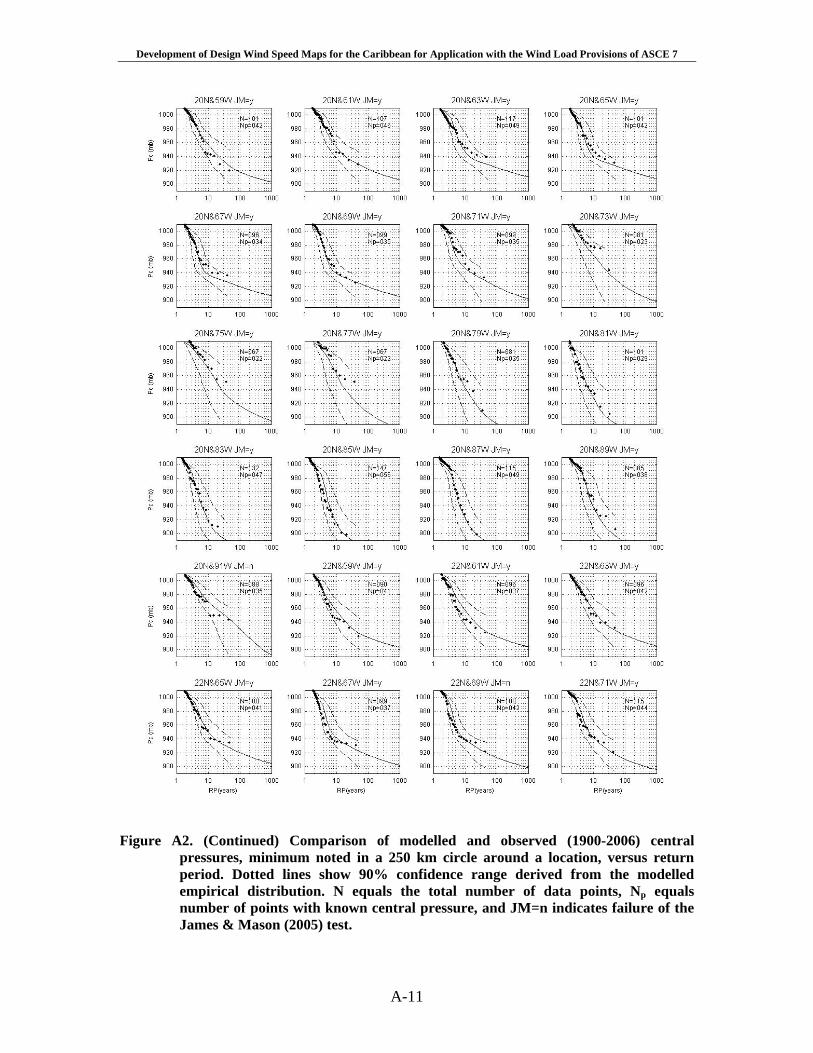
Development of Design Wind Speed Maps for the Caribbean for Application with the Wind Load Provisions of ASCE 7
A-11
Figure A2. (Continued) Comparison of modelled and observed (1900-2006) central
pressures, minimum noted in a 250 km circle around a location, versus return period. Dotted lines show 90% confidence range derived from the modelled empirical distribution. N equals the total number of data points, Np equals number of points with known central pressure, and JM=n indicates failure of the James & Mason (2005) test.
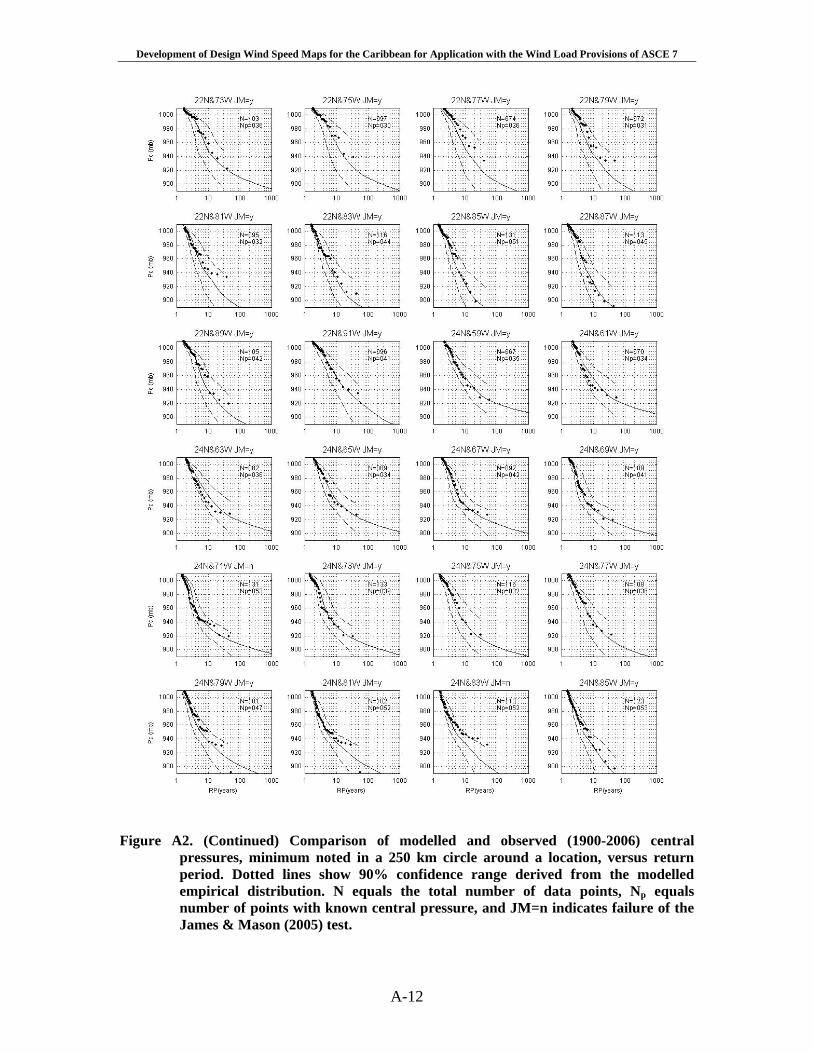
Development of Design Wind Speed Maps for the Caribbean for Application with the Wind Load Provisions of ASCE 7
A-12
Figure A2. (Continued) Comparison of modelled and observed (1900-2006) central
pressures, minimum noted in a 250 km circle around a location, versus return period. Dotted lines show 90% confidence range derived from the modelled empirical distribution. N equals the total number of data points, Np equals number of points with known central pressure, and JM=n indicates failure of the James & Mason (2005) test.
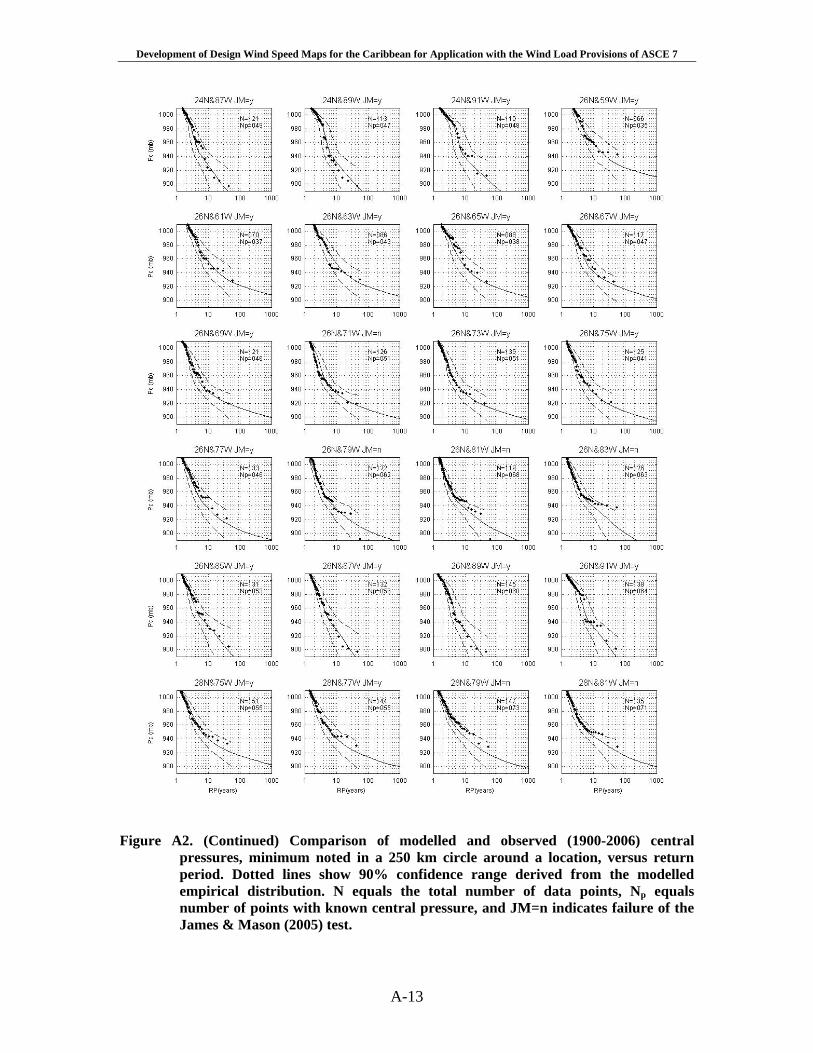
Development of Design Wind Speed Maps for the Caribbean for Application with the Wind Load Provisions of ASCE 7
A-13
Figure A2. (Continued) Comparison of modelled and observed (1900-2006) central
pressures, minimum noted in a 250 km circle around a location, versus return period. Dotted lines show 90% confidence range derived from the modelled empirical distribution. N equals the total number of data points, Np equals number of points with known central pressure, and JM=n indicates failure of the James & Mason (2005) test.
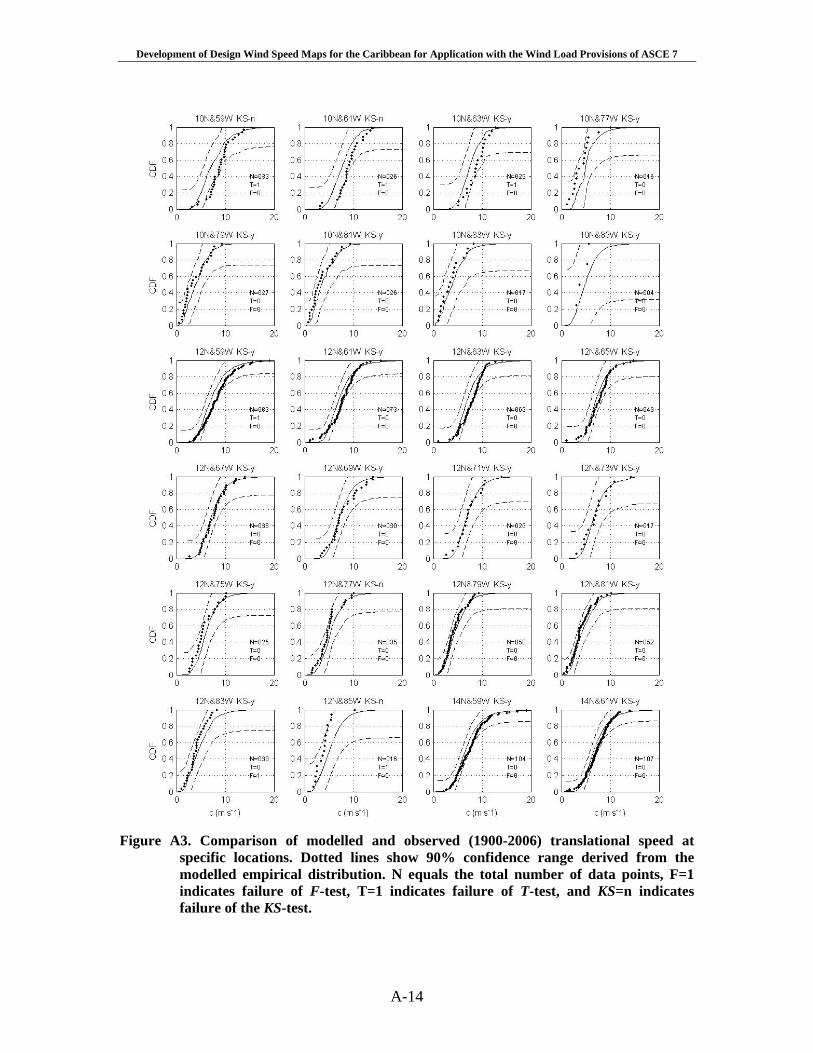
Development of Design Wind Speed Maps for the Caribbean for Application with the Wind Load Provisions of ASCE 7
A-14
Figure A3. Comparison of modelled and observed (1900-2006) translational speed at
specific locations. Dotted lines show 90% confidence range derived from the modelled empirical distribution. N equals the total number of data points, F=1 indicates failure of F-test, T=1 indicates failure of T-test, and KS=n indicates failure of the KS-test.
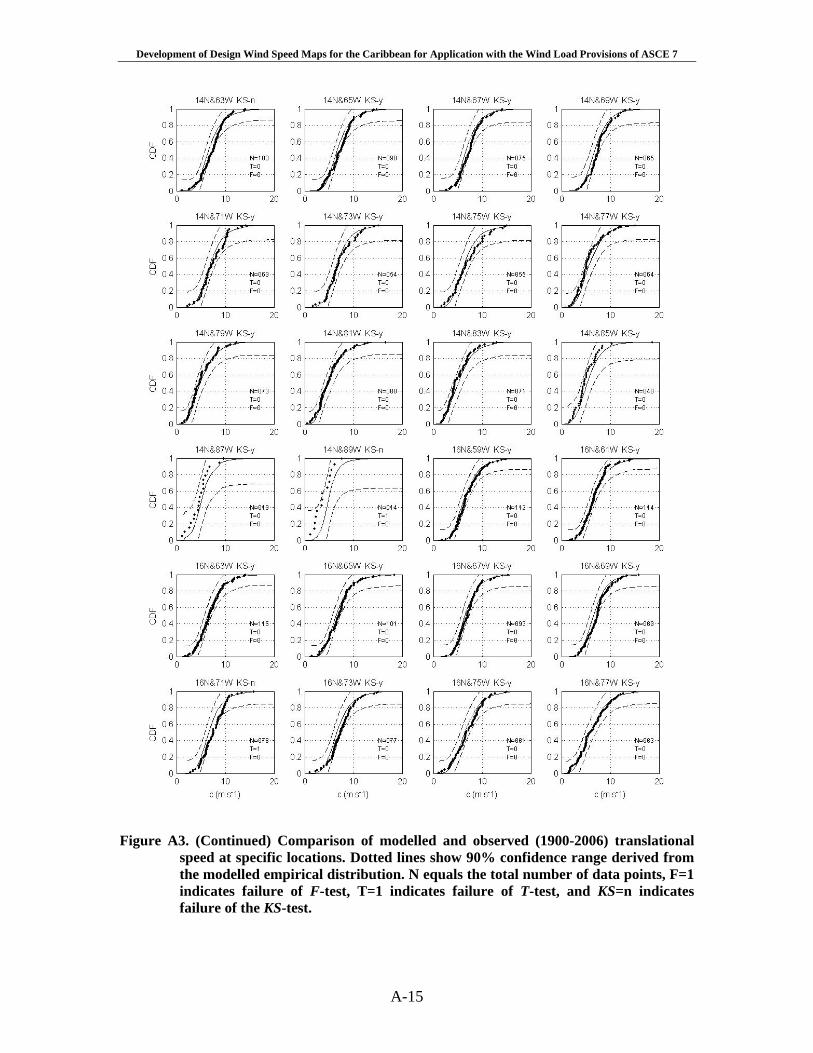
Development of Design Wind Speed Maps for the Caribbean for Application with the Wind Load Provisions of ASCE 7
A-15
Figure A3. (Continued) Comparison of modelled and observed (1900-2006) translational
speed at specific locations. Dotted lines show 90% confidence range derived from the modelled empirical distribution. N equals the total number of data points, F=1 indicates failure of F-test, T=1 indicates failure of T-test, and KS=n indicates failure of the KS-test.
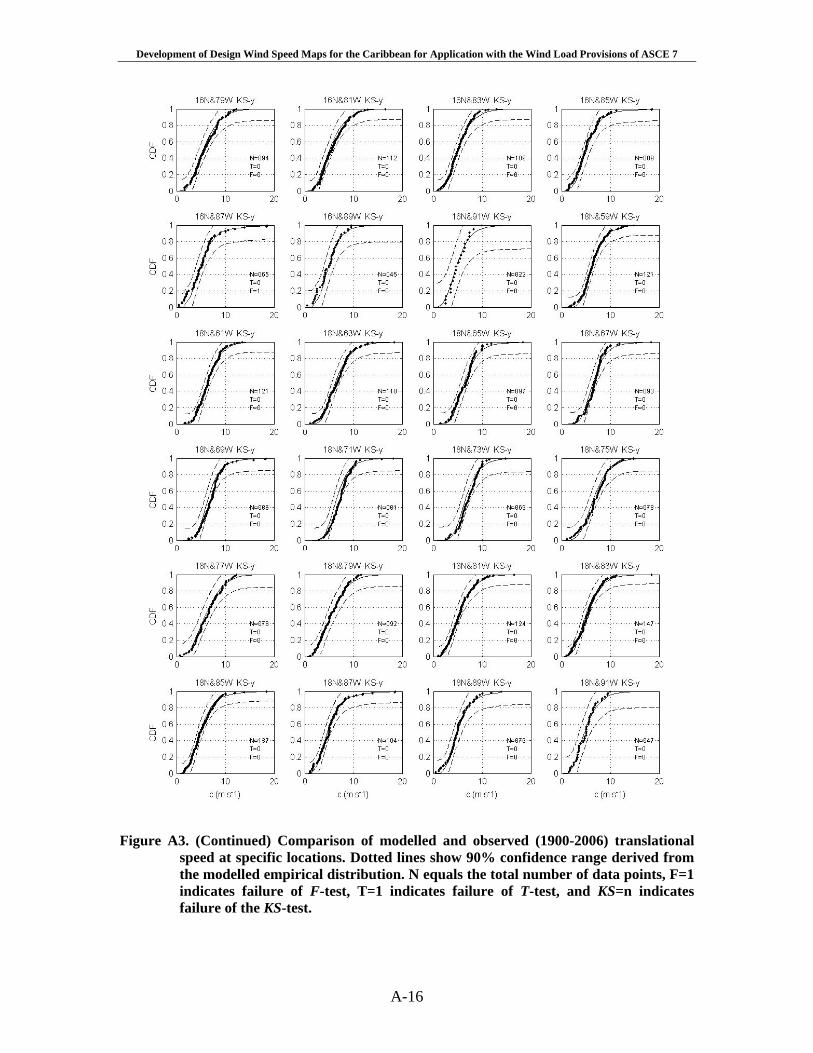
Development of Design Wind Speed Maps for the Caribbean for Application with the Wind Load Provisions of ASCE 7
A-16
Figure A3. (Continued) Comparison of modelled and observed (1900-2006) translational
speed at specific locations. Dotted lines show 90% confidence range derived from the modelled empirical distribution. N equals the total number of data points, F=1 indicates failure of F-test, T=1 indicates failure of T-test, and KS=n indicates failure of the KS-test.
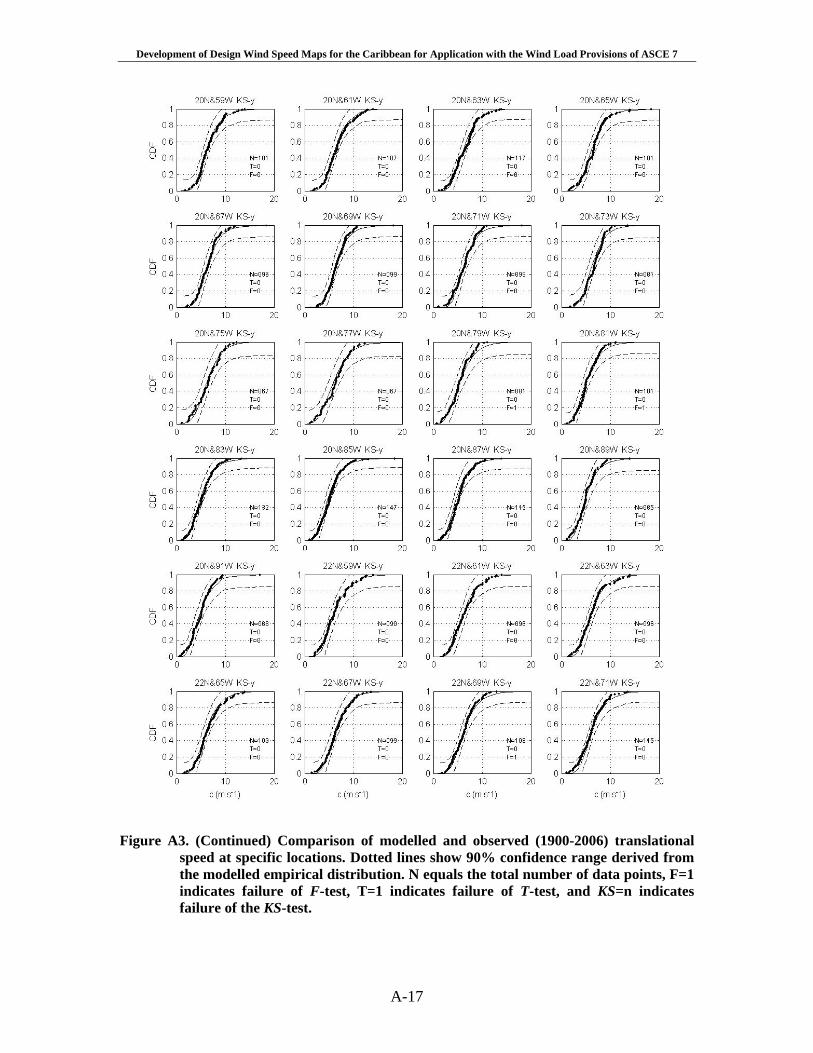
Development of Design Wind Speed Maps for the Caribbean for Application with the Wind Load Provisions of ASCE 7
A-17
Figure A3. (Continued) Comparison of modelled and observed (1900-2006) translational
speed at specific locations. Dotted lines show 90% confidence range derived from the modelled empirical distribution. N equals the total number of data points, F=1 indicates failure of F-test, T=1 indicates failure of T-test, and KS=n indicates failure of the KS-test.
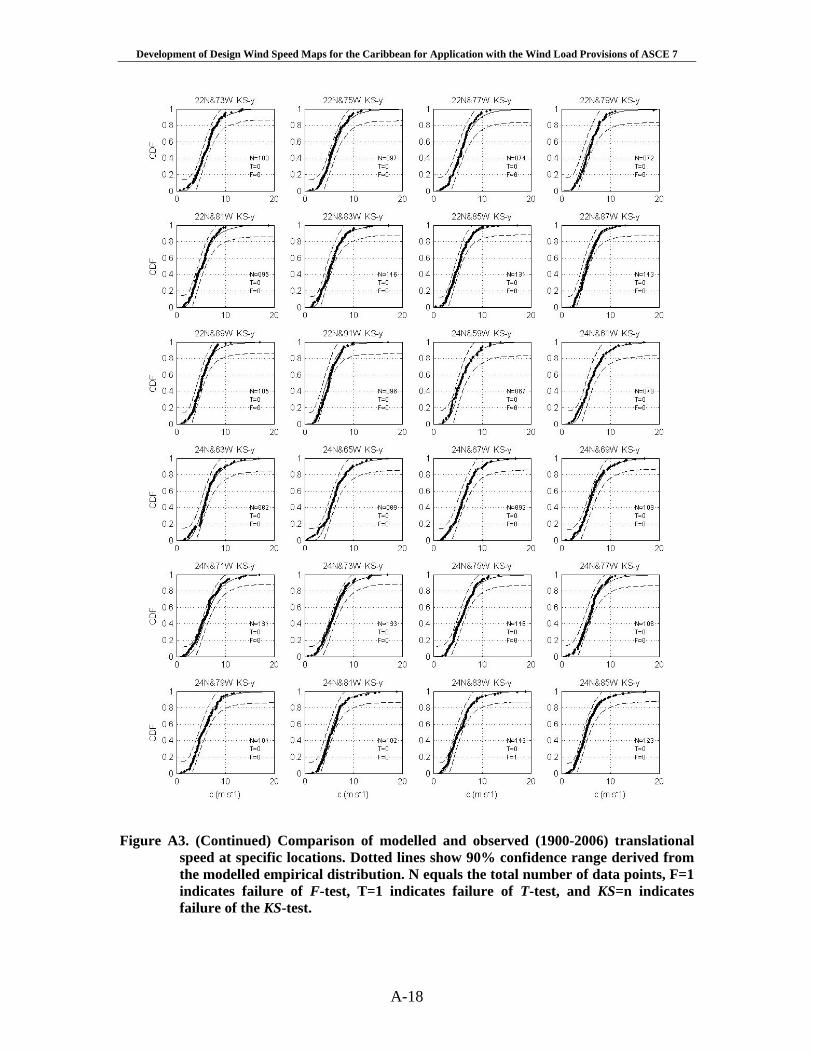
Development of Design Wind Speed Maps for the Caribbean for Application with the Wind Load Provisions of ASCE 7
A-18
Figure A3. (Continued) Comparison of modelled and observed (1900-2006) translational
speed at specific locations. Dotted lines show 90% confidence range derived from the modelled empirical distribution. N equals the total number of data points, F=1 indicates failure of F-test, T=1 indicates failure of T-test, and KS=n indicates failure of the KS-test.
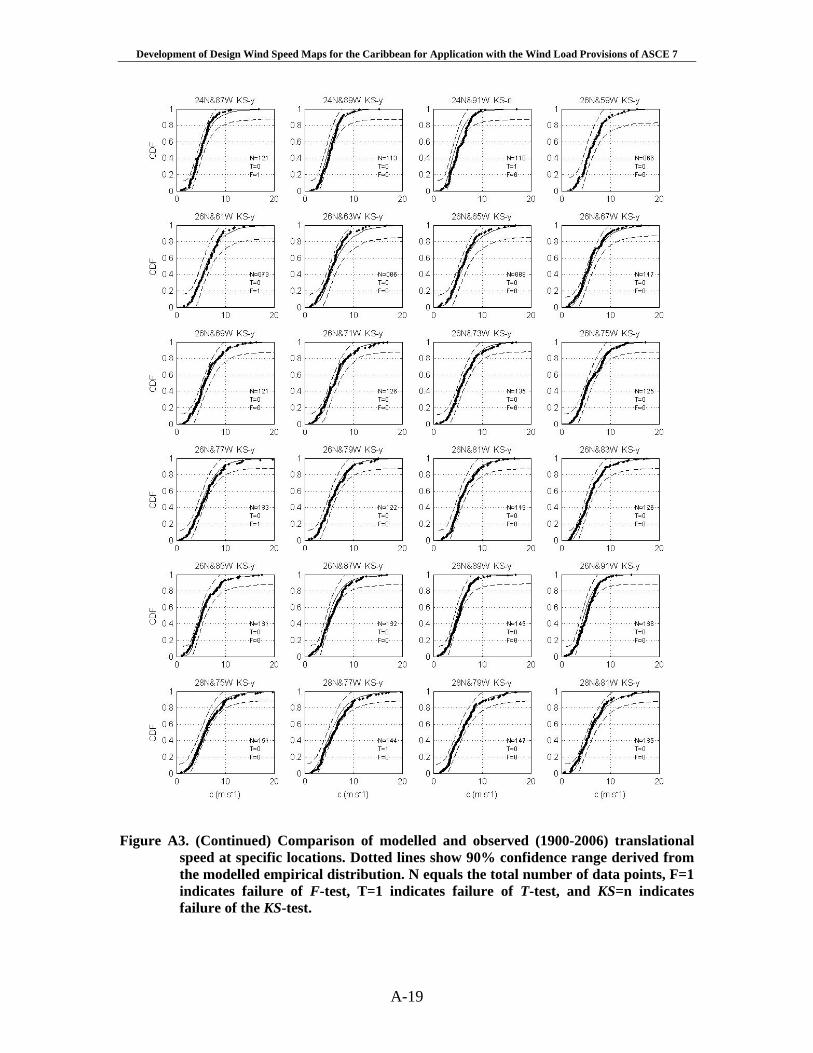
Development of Design Wind Speed Maps for the Caribbean for Application with the Wind Load Provisions of ASCE 7
A-19
Figure A3. (Continued) Comparison of modelled and observed (1900-2006) translational
speed at specific locations. Dotted lines show 90% confidence range derived from the modelled empirical distribution. N equals the total number of data points, F=1 indicates failure of F-test, T=1 indicates failure of T-test, and KS=n indicates failure of the KS-test.
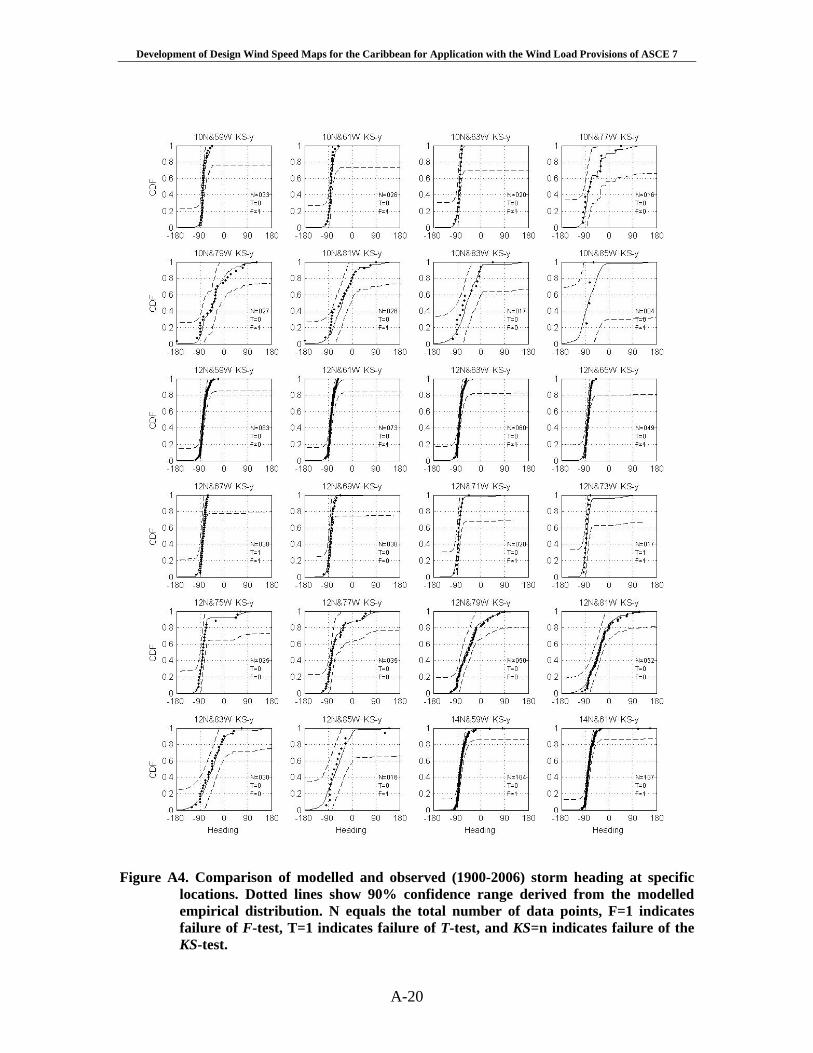
Development of Design Wind Speed Maps for the Caribbean for Application with the Wind Load Provisions of ASCE 7
A-20
Figure A4. Comparison of modelled and observed (1900-2006) storm heading at specific
locations. Dotted lines show 90% confidence range derived from the modelled empirical distribution. N equals the total number of data points, F=1 indicates failure of F-test, T=1 indicates failure of T-test, and KS=n indicates failure of the KS-test.
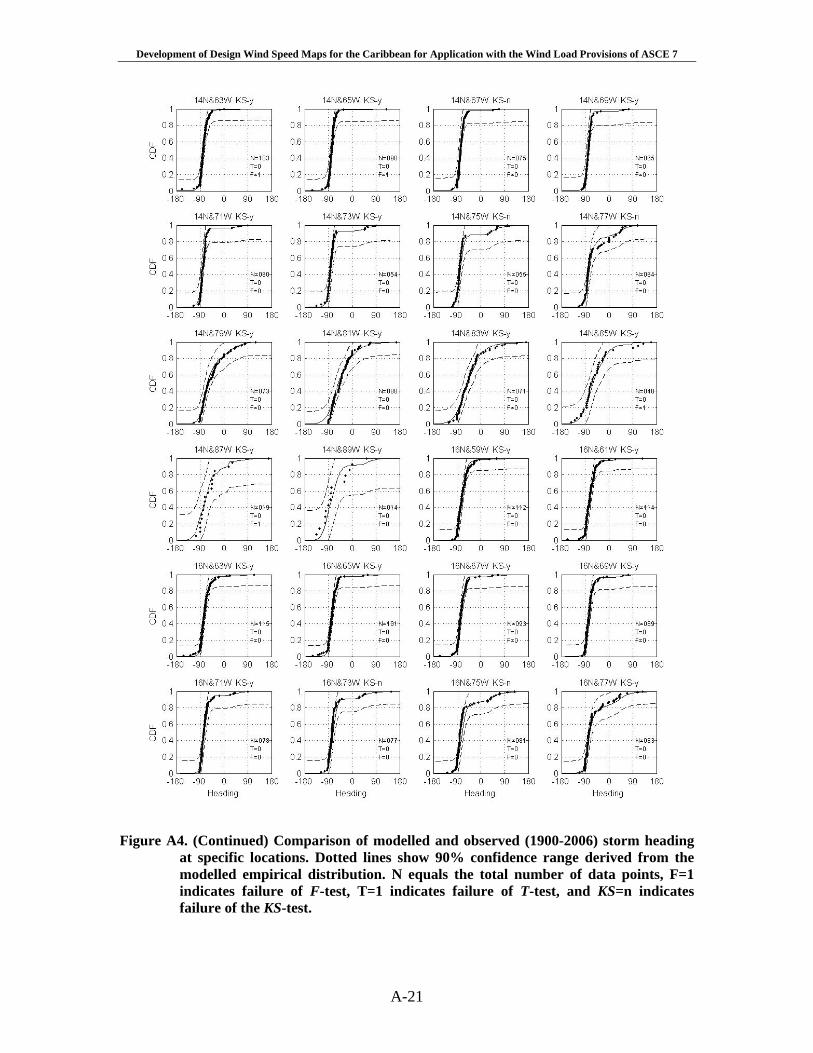
Development of Design Wind Speed Maps for the Caribbean for Application with the Wind Load Provisions of ASCE 7
A-21
Figure A4. (Continued) Comparison of modelled and observed (1900-2006) storm heading
at specific locations. Dotted lines show 90% confidence range derived from the modelled empirical distribution. N equals the total number of data points, F=1 indicates failure of F-test, T=1 indicates failure of T-test, and KS=n indicates failure of the KS-test.
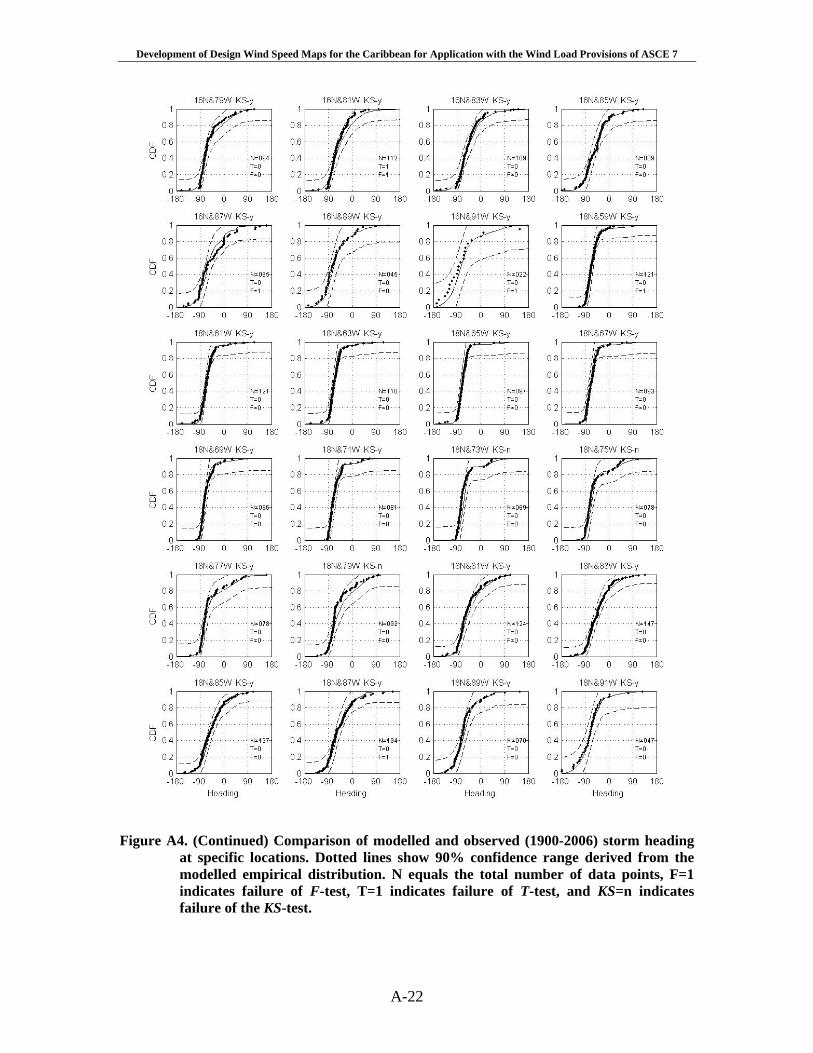
Development of Design Wind Speed Maps for the Caribbean for Application with the Wind Load Provisions of ASCE 7
A-22
Figure A4. (Continued) Comparison of modelled and observed (1900-2006) storm heading at specific locations. Dotted lines show 90% confidence range derived from the modelled empirical distribution. N equals the total number of data points, F=1 indicates failure of F-test, T=1 indicates failure of T-test, and KS=n indicates failure of the KS-test.
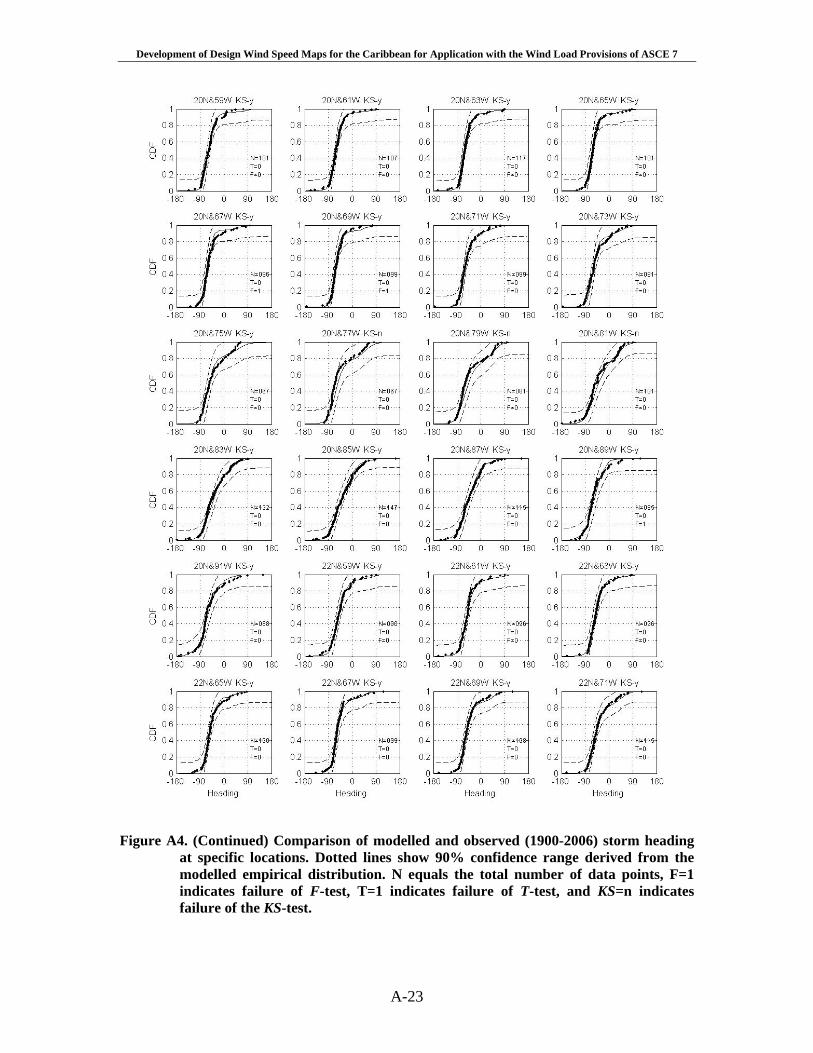
Development of Design Wind Speed Maps for the Caribbean for Application with the Wind Load Provisions of ASCE 7
A-23
Figure A4. (Continued) Comparison of modelled and observed (1900-2006) storm heading at specific locations. Dotted lines show 90% confidence range derived from the modelled empirical distribution. N equals the total number of data points, F=1 indicates failure of F-test, T=1 indicates failure of T-test, and KS=n indicates failure of the KS-test.
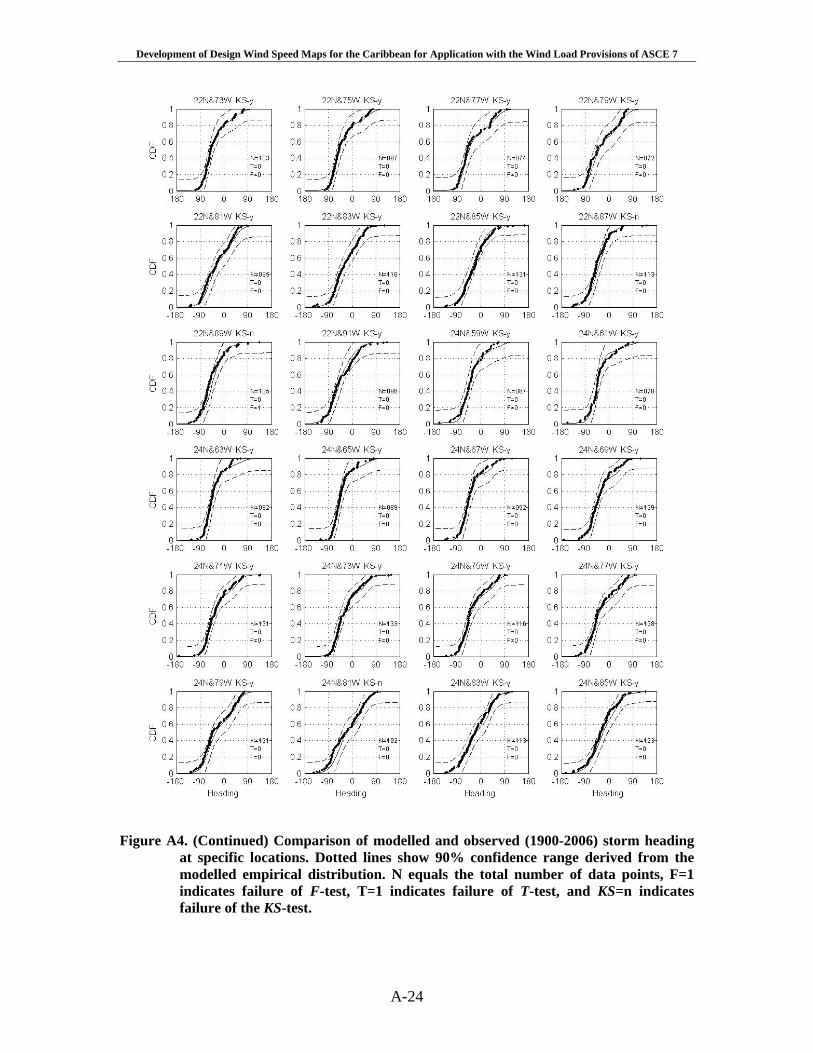
Development of Design Wind Speed Maps for the Caribbean for Application with the Wind Load Provisions of ASCE 7
A-24
Figure A4. (Continued) Comparison of modelled and observed (1900-2006) storm heading
at specific locations. Dotted lines show 90% confidence range derived from the modelled empirical distribution. N equals the total number of data points, F=1 indicates failure of F-test, T=1 indicates failure of T-test, and KS=n indicates failure of the KS-test.
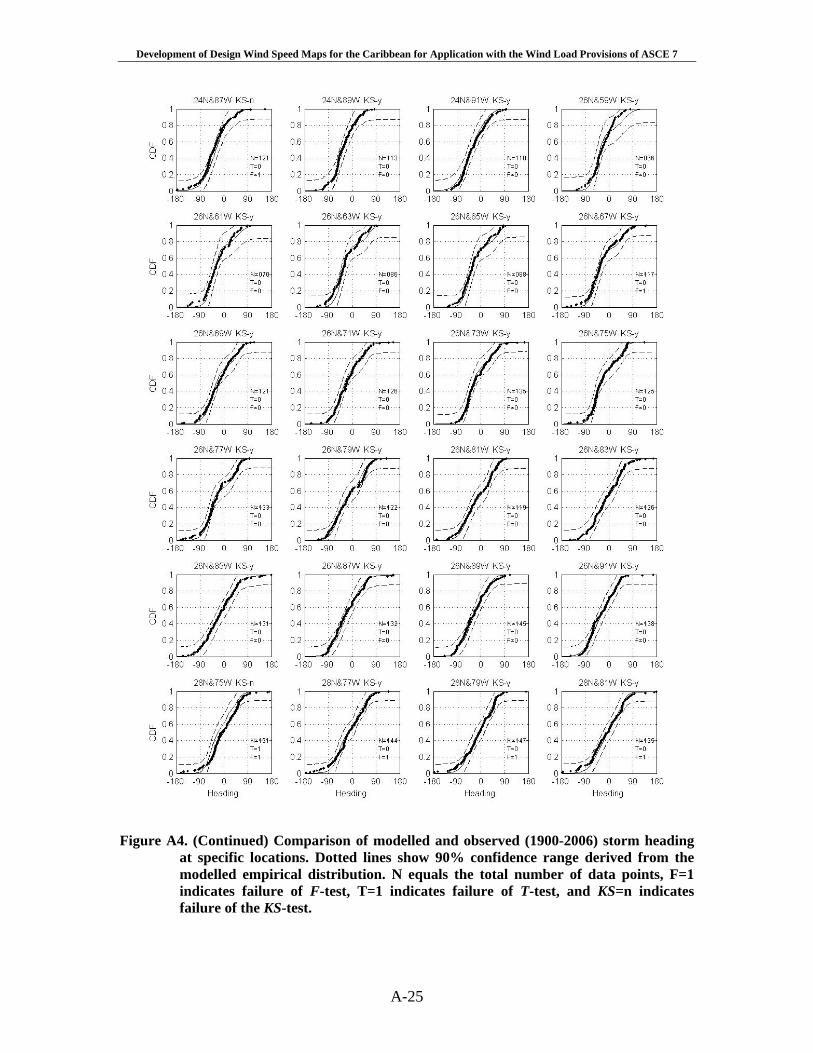
Development of Design Wind Speed Maps for the Caribbean for Application with the Wind Load Provisions of ASCE 7
A-25
Figure A4. (Continued) Comparison of modelled and observed (1900-2006) storm heading
at specific locations. Dotted lines show 90% confidence range derived from the modelled empirical distribution. N equals the total number of data points, F=1 indicates failure of F-test, T=1 indicates failure of T-test, and KS=n indicates failure of the KS-test.
Development of Design Wind Speed Maps for the Caribbean for Application with the Wind Load Provisions of ASCE 7
B-1
Appendix B
Definition of Basic Wind Speeds Used in ASCE 7
The purpose of this appendix is to review the process used by ASCE 7 Wind Load Task Committee (WLTC) in the development of the wind speed map given in ASCE 7-98 and beyond that presents a design wind speed map that is defined by wind speed contours that represents the 500 year return period wind speed divided by the square root of the load factor (i.e. 5.1 ). The goal of the WLTC was to develop a wind speed map that yielded approximately risk consistent designs (for wind resistance) in hurricane and non-hurricane prone regions of the United States. To reach this objective the WLTC developed an approach that, while approximate, resulted in a design wind speed map that incorporated a hurricane importance factor into the specification of the design wind speeds. The approach essentially involved equating the return period associated with exceeding the ultimate wind load in both the non-hurricane and hurricane prone regions of the United States. The methodology allowed for the implied hurricane importance factor to vary with location rather than using a single value as had been used in prior editions of the standard. The approach taken by the WLTC is extended here for the case where the wind load factor is equal to 1.6 rather than 1.5, and is further extended to determine the effective return period associated with the ultimate design of Category III and IV structures (as defined in ASCE 7).
Prior to the introduction of ASCE 7-95, the design wind load equations in ASCE
7 included a multiplicative term in the form of a hurricane importance factor. This hurricane importance factor was introduced to take into account the fact that the tails of the wind speed exceedance probability distributions for hurricane winds are longer than those associated with non-hurricane winds. The hurricane importance factor varied from about 1.05 at the coast and decayed linearly to 1.0 at a distance of 100 miles inland. The hurricane importance factor in ASCE 7 and it predecessor (ANSI A58.1) was applied to the 50-year return period wind speed given in the standard, not the resulting velocity pressure. Thus, using the ASCE and ANSI provisions, buildings and structures located near the coast were designed using a wind speed that had a longer return period than those located 100 miles or more inland.
In the development of the wind speed map given in ASCE 7-95, the hurricane importance factor was incorporated directly into the wind speed map (i.e. wind speeds along the hurricane prone at the coast were increased by 5% and wind speeds 100 miles inland were left unchanged, and those in between were adjusted through linear interpolation of the hurricane importance factor).
In the development of the design wind speed map used in ASCE 7-98 the WLTC
re-visited the hurricane importance factor that had been in use in the US standards since 1982. The primary reasons for re-visiting the hurricane factor was the recognition that the importance factor likely varied with location along the coast and using a constant value of 1.05 was not appropriate.

Development of Design Wind Speed Maps for the Caribbean for Application with the Wind Load Provisions of ASCE 7
B-2
The approach taken to develop a varying importance factor began with the premise that the nominal wind load computed using the methods given in ASCE 7, when multiplied by the wind load factor, was representative of an “ultimate” load. Furthermore, it was assumed that the variability of the wind speed dominates the calculation of the wind load factor. The ultimate wind load, W, is given as
LFHF WVICW 2)(= B-1
where CF is a building/component specific coefficient that includes the effects building height, building geometry, terrain, gust factors, etc., as computed using the procedures outlined in ASCE 7, V is the design wind speed, WLF is the wind load factor, and IH is the hurricane importance factor.
In order to estimate the value of the hurricane importance factor, IH, the
committee required that the annual probability of exceeding the ultimate wind load in the hurricane and non-hurricane regions of the US should be the same. Note that requiring the annual probability of exceeding the ultimate load in the two areas (hurricane vs. non-hurricane) to be the same does not mean that the annual probabilities of failure are the same. Recalling that the nominal design wind speed in the non-hurricane regions of the United States is associated with a return period of 50 years, the WLTC sought to determine the return period associated with the wind speed producing the “ultimate” load in a representative non-hurricane prone region. As defined in ASCE 7-98, over most of the non-hurricane prone coastline of the United States, the wind speed for any return period can be computed from:
)]12ln(1.036.0[50 TVVT += B-2
where T is the return period in years and, VT is the T year return period wind speed. In the non-hurricane prone regions of the United States, the ultimate wind load occurs when:
LFFTFT WVCVCW 250
2 == B-3 thus
LFT WTVV =+= )]12ln(1.036.0[50 B-4 and from B-4, the return period T associated with the ultimate wind speed in the non-hurricane prone portion of the United States is:
)10exp(00228.0 LFWT = B-5
Using the wind load factor of 1.6 as is currently specified in ASCE 7-05, from (B-5) we get T = 709 years.
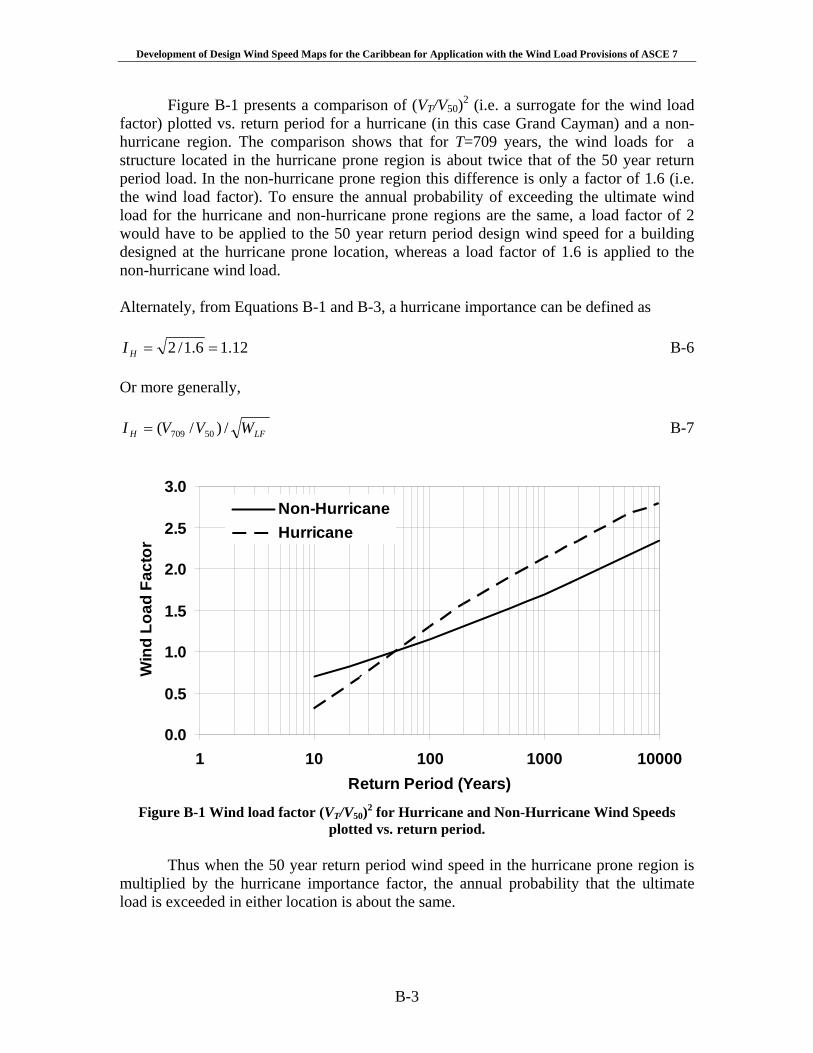
Development of Design Wind Speed Maps for the Caribbean for Application with the Wind Load Provisions of ASCE 7
B-3
Figure B-1 presents a comparison of (VT/V50)2 (i.e. a surrogate for the wind load factor) plotted vs. return period for a hurricane (in this case Grand Cayman) and a non-hurricane region. The comparison shows that for T=709 years, the wind loads for a structure located in the hurricane prone region is about twice that of the 50 year return period load. In the non-hurricane prone region this difference is only a factor of 1.6 (i.e. the wind load factor). To ensure the annual probability of exceeding the ultimate wind load for the hurricane and non-hurricane prone regions are the same, a load factor of 2 would have to be applied to the 50 year return period design wind speed for a building designed at the hurricane prone location, whereas a load factor of 1.6 is applied to the non-hurricane wind load. Alternately, from Equations B-1 and B-3, a hurricane importance can be defined as
12.16.1/2 ==HI B-6 Or more generally,
LFH WVVI /)/( 50709= B-7
0.0
0.5
1.0
1.5
2.0
2.5
3.0
1 10 100 1000 10000Return Period (Years)
Win
d Lo
ad F
acto
r
Non-HurricaneHurricane
Figure B-1 Wind load factor (VT/V50)2 for Hurricane and Non-Hurricane Wind Speeds
plotted vs. return period. Thus when the 50 year return period wind speed in the hurricane prone region is
multiplied by the hurricane importance factor, the annual probability that the ultimate load is exceeded in either location is about the same.
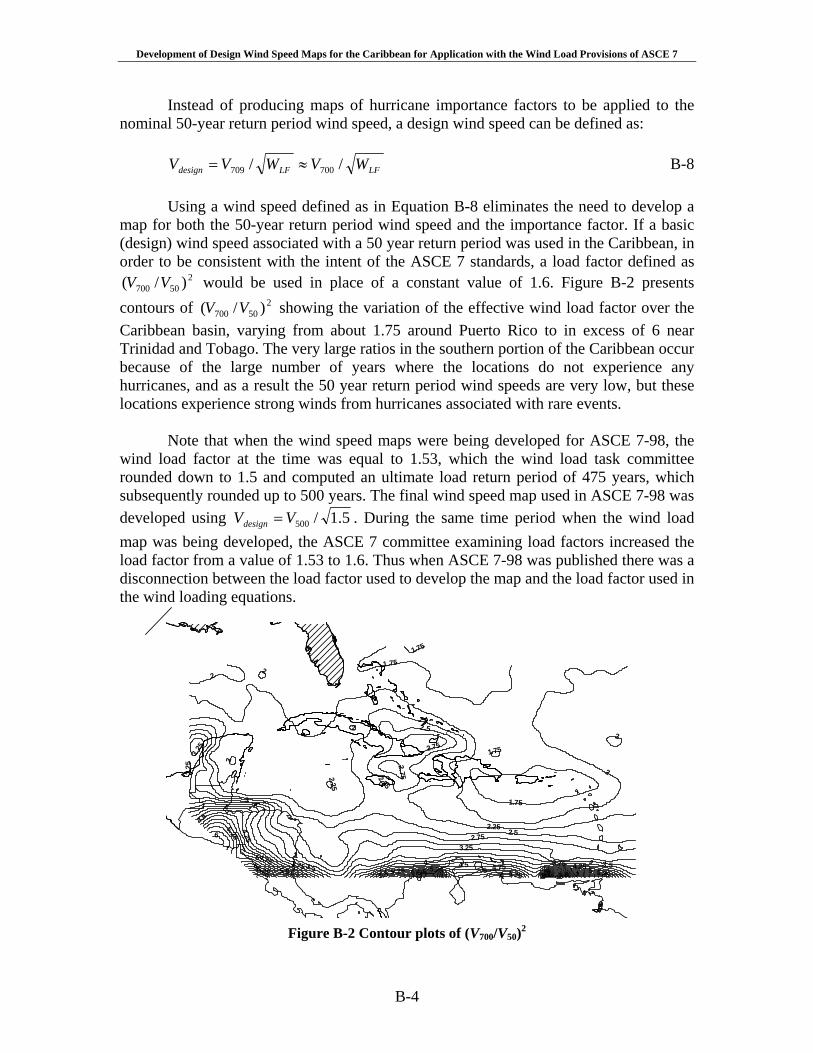
Development of Design Wind Speed Maps for the Caribbean for Application with the Wind Load Provisions of ASCE 7
B-4
Instead of producing maps of hurricane importance factors to be applied to the nominal 50-year return period wind speed, a design wind speed can be defined as:
LFLFdesign WVWVV // 700709 ≈= B-8
Using a wind speed defined as in Equation B-8 eliminates the need to develop a
map for both the 50-year return period wind speed and the importance factor. If a basic (design) wind speed associated with a 50 year return period was used in the Caribbean, in order to be consistent with the intent of the ASCE 7 standards, a load factor defined as
250700 )/( VV would be used in place of a constant value of 1.6. Figure B-2 presents
contours of 250700 )/( VV showing the variation of the effective wind load factor over the
Caribbean basin, varying from about 1.75 around Puerto Rico to in excess of 6 near Trinidad and Tobago. The very large ratios in the southern portion of the Caribbean occur because of the large number of years where the locations do not experience any hurricanes, and as a result the 50 year return period wind speeds are very low, but these locations experience strong winds from hurricanes associated with rare events.
Note that when the wind speed maps were being developed for ASCE 7-98, the wind load factor at the time was equal to 1.53, which the wind load task committee rounded down to 1.5 and computed an ultimate load return period of 475 years, which subsequently rounded up to 500 years. The final wind speed map used in ASCE 7-98 was developed using 5.1/500VVdesign = . During the same time period when the wind load map was being developed, the ASCE 7 committee examining load factors increased the load factor from a value of 1.53 to 1.6. Thus when ASCE 7-98 was published there was a disconnection between the load factor used to develop the map and the load factor used in the wind loading equations.
3
2
4
2.5
5
2.752.25
3.25
3.54.5 3.75 4.256
4.755.25
1.75
75.5 85.75
6.56.25 9
2
4
2
5.75
3.75
3.25 2.75
5.25
2
66.5
2.25
2
4.75
6
1.75
1.75
5.5
2.752.25
53.5
4.25
6
2
5
3.25
5.25
4.5
1.75
2.5
Figure B-2 Contour plots of (V700/V50)2

Development of Design Wind Speed Maps for the Caribbean for Application with the Wind Load Provisions of ASCE 7
B-5
As indicated above, when the correct load factor of 1.6 is used, a design wind speed defined as 6.1/700VVdesign = is appropriate. This design wind speed is equivalent to designing a structure using the 700 year return period wind speed and a load factor of unity.
The importance factor used in ASCE 7 for the computation of wind loads for the
design of category III and IV structures is defined so that the nominal 50-year return period non-hurricane wind speed is increased to be representative of a 100-year return period value. This importance factor is not the hurricane importance factor, IH, but rather a factor used to increase the wind loads based on an occupancy classification. The importance factor is applied to the design of all category III and IV buildings whether or not they are located in a hurricane prone region. Following the approach used above to estimate the resulting ultimate load return period associated with the 100 year design wind speed in the non-hurricane prone regions we find that:
])/(10exp[00228.0 50100 LFWVVT = B-9
where for 50100 /VV computed from B-4 and WLF = 1.6, we find that T=1,697 years. In the
development of Equation B-9, the term LFWVV )/( 50100 replaces the LFW used in Equation B-5, effectively resulting in a higher load factor for category III and IV structures equal to 2
50100 )/( VVWLF . Thus for Category III and IV structures, a design wind
speed of 6.1/1700V is appropriate. In the versions of ASCE 7 since 1993 (i.e., ASCE 7-95 and beyond), the
importance factor has been applied to the velocity pressure, not, the wind velocity as was the case in prior editions. The design pressure in ASCE 7-95 and later is
IVKKKq dztzz200256.0= B-10
where the importance factor I is equal to 1.15 for category III and IV structures. For consistency in the hurricane prone regions, the importance factor should be defined as:
27001700 )/( VVI = B-11
Figure B-3 presents contour plots of 2
7001700 )/( VVI = where a large gradient of I from north to south is evident, but over most of the region, I, is consistent with the 1.15 value given in ASCE 7. In the case of the Category II buildings where a 700 year return period wind speed represents an ultimate design wind speed for these Category II buildings, we find that for Category III and IV buildings a 1,700 year return period wind speed is representative of the ultimate wind load. Both approaches inherently include the variation in the hurricane importance factor in hurricane prone regions, but are tied back to a wind load factor equal to 1.6 as applied to the non-hurricane prone region of the United States.
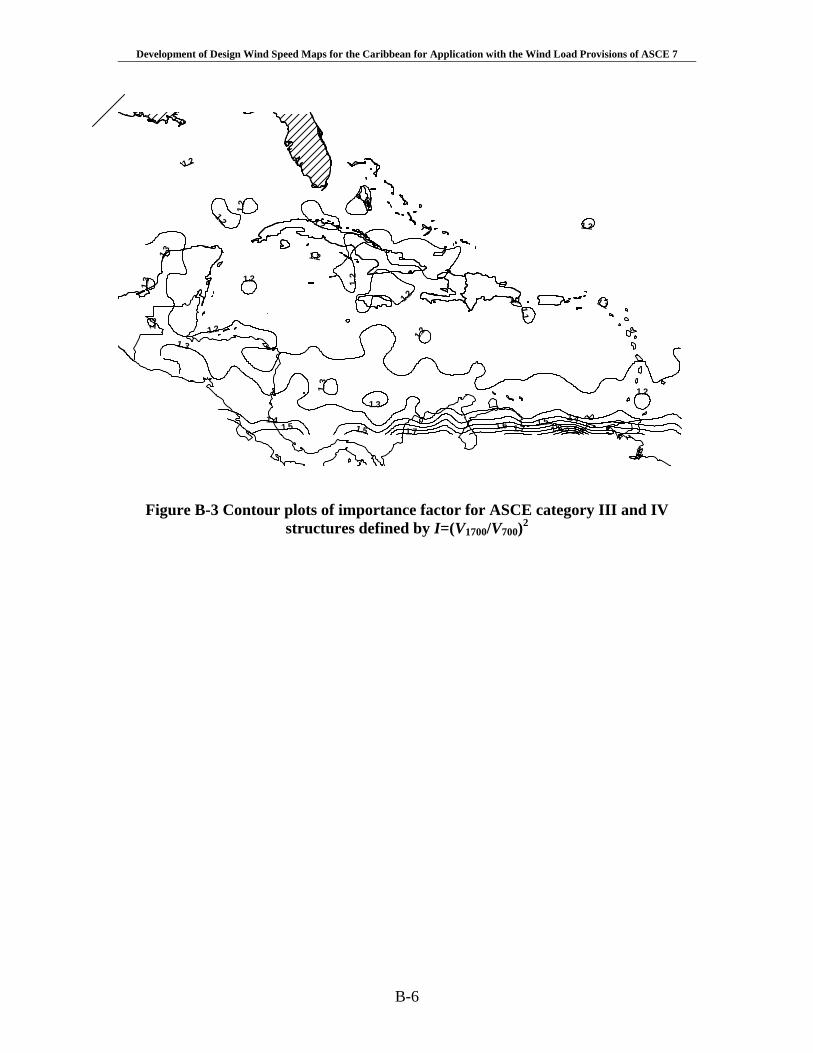
Development of Design Wind Speed Maps for the Caribbean for Application with the Wind Load Provisions of ASCE 7
B-6
1.21.3
1.41.51.6 1.7 1.8 2 1.9
1.11.11.2
1.2
1.2
1.2
1.2
1.5
1.1
1.2
1.3
1.3 1.2
1.2
1.3
1.7
1.2
1.2
1.3
1.2
1.31.4
1.2
1.5
Figure B-3 Contour plots of importance factor for ASCE category III and IV structures defined by I=(V1700/V700)2
ANNEX 8
Preparación para el viaje
Virtual Journey through a Safe HospitalMultimedia Training Program on Hospitals Safe from Disasters
© Pan American Health Organization, 2009
USER’S GUIDE
2
© Pan American Health Organization, 2009
Virtual Journey through a Safe Hospital is a multimedia training tool produced by the Area on Emergency Preparedness and Disaster Relief of the Pan American Health Orga-nization, Regional Office of the World Health Organization (PAHO/WHO). This production is part of a DIPECHO project on Safe Hospitals in disasters, financed by the European Commission’s Humanitarian Aid Office (ECHO).
The opinions expressed and recommendations made in this publication do not necessa-rily reflect the current policies and opinions of the Pan American Health Organization or its Member States.
The Pan American Health Organization will give favorable consideration to requests for authorization to reproduce or translate all or part of this material. Requests for informa-tion should be directed to the Area on Emergency Preparedness and Disaster Relief, Pan American Health Organization, 525 23rd Street, Washington, D.C. 20037, U.S.A.; Fax (202) 775 4578; e-mail: [email protected].
Production of this program has been made possible with the financial support of the Eu-ropean Commission’s Humanitarian Aid Office (ECHO), the Division of Humanitarian As-sistance, Peace and Security of the Canadian International Development Agency (CIDA), and the Office for Foreign Disaster Assistance of the U.S. Agency for International Deve-lopment (OFDA/AID). The Regional Office for the Americas of the United Nations Interna-tional Strategy for Disaster Reduction (UNISDR) supported the duplication of this DVD as part of its inter-agency initiative for the 2008–2009 World Disaster Reduction Campaign, “Hospitals Safe from Disasters.”
3
Introduction
The multimedia training program, Virtual Journey through a Safe Hospital, introduces the technical elements involved in keeping hospitals (or any health facility) safe when fa-ced with natural disasters or disasters caused by human activity.
With the innovative and interactive use of video, animation, images, sound, text, graphic presentations, and technical content, this program will help you to understand all aspects of Hospital Safety.
The Virtual Journey through a Safe Hospital is divided into modules that can be used in-dividually to gain in-depth understanding of specific topics. Viewing the general introduc-tion will take only 15 minutes and provides a quick understanding of all the components of a Safe Hospital. Viewing all of the modules can take up to three hours and will provide a full representation of the subject.

4
Contents
While navigating with Virtual Journey through a Safe Hospital, you will learn what makes a hospital safe in disaster situations, the components that can make a hospital vulnerable, and elements that can make it safe when exposed to hazards. Each of the following modules emphasizes different aspects of Hospital Safety:
• Preparationforthejourney• WhatisaSafeHospital?• Locationandmainhazards• Let’sstudythestructuralcomponents• Let’sanalyzethenon-structuralcomponents• Let’sanalyzethefunctionalcomponents• TheHospitalSafetyIndex• TheHospitalDisasterPlanning
Inaddition,intheLibrarysectionyoucanbrowsethrough(anddownload)technicaldocuments, supporting material, videos, and photographs that PAHO/WHO has pro-duced about Safe Hospitals.
If you have any problems, remember that you can consult the Help Section in the general navigation bar (horizontal menu), where you will find answers to frequently asked questions about using this tool and about Safe Hospitals.

5
Preparation for the journey
This is a short, animated presentation that will help you to use effectively this multimedia trainingtool.ItexplainshowtousethemenustoaccesstheContentsSection,theLibrarySection (that includes photographs, videos, technical guidelines, training material, promo-tional material, and the Safe Hospital Index), the Help Section and the Frequently Asked Questions Section, with answers about how to use this tool as well as answers about Safe Hospitals. It also explains how to use the interactive graphics, animations, and virtual visits that you will find in several sections.
The general navigation bar (horizontal menu) takes you to the Main
Menu,theLibrary,Contents, and the
Help sections.
The Main Menu (vertical menu) shows the general contents.
You can access any specific issue by
clicking on it.
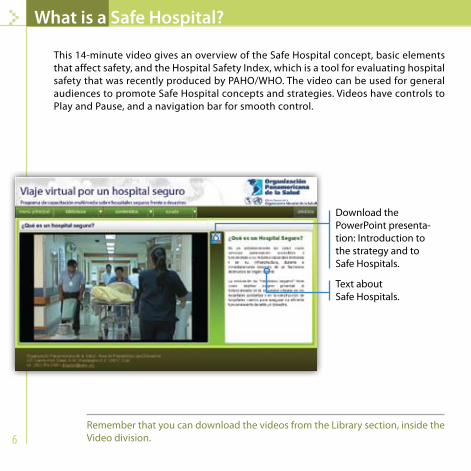
6
What is a Safe Hospital?
This 14-minute video gives an overview of the Safe Hospital concept, basic elements that affect safety, and the Hospital Safety Index, which is a tool for evaluating hospital safety that was recently produced by PAHO/WHO. The video can be used for general audiences to promote Safe Hospital concepts and strategies. Videos have controls to Play and Pause, and a navigation bar for smooth control.
Download the PowerPoint presenta-tion: Introduction to the strategy and to Safe Hospitals.
Text about Safe Hospitals.
RememberthatyoucandownloadthevideosfromtheLibrarysection,insidetheVideo division.

7
Location and main hazards
In this section, animations depict the main natural hazards or those caused by human activity that can have an impact on health facilities. At the end of the presentation, you will be able to identify and evaluate external risk factors and the most common types of damage caused by hazards in health care centers.
In this section: animations show
different phenomena that can affect
a hospital.
Download the PowerPoint presen-tation: Identify and
evaluate main hazards.
Virtual tour. During the introduc-tory video, move the
mouse over the screen and click on the red flags to access more
information about hazards that can affect
a hospital.
Text about the location of hospitals and main hazards that can have an impact on health facilities.
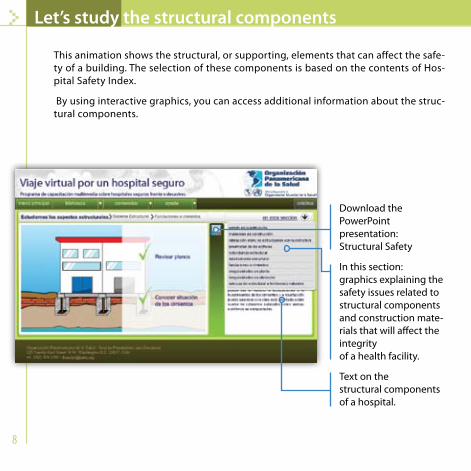
8
Let’s study the structural components
This animation shows the structural, or supporting, elements that can affect the safe-ty of a building. The selection of these components is based on the contents of Hos-pital Safety Index.
By using interactive graphics, you can access additional information about the struc-tural components.
Download the PowerPoint presentation: Structural Safety
In this section: graphics explaining the safety issues related to structural components and construction mate-rials that will affect the integrity of a health facility.
Text on the structural components of a hospital.
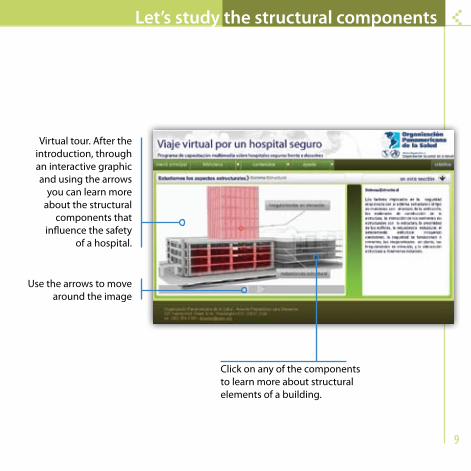
9
Let’s study the structural components
Virtual tour. After the introduction, through an interactive graphic and using the arrows
you can learn more about the structural
components that influence the safety
of a hospital.
Use the arrows to move around the image
Click on any of the components to learn more about structural elements of a building.
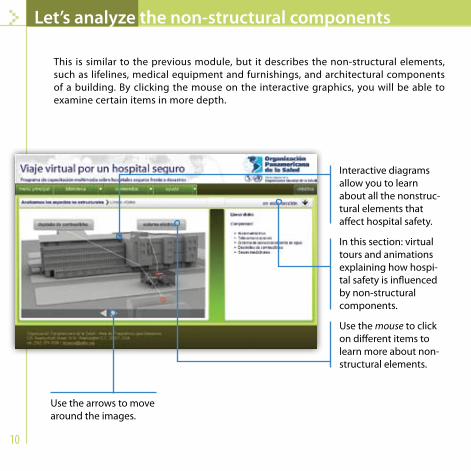
10
Let’s analyze the non-structural components
This is similar to the previous module, but it describes the non-structural elements, such as lifelines, medical equipment and furnishings, and architectural components of a building. By clicking the mouse on the interactive graphics, you will be able to examine certain items in more depth.
Interactive diagrams allow you to learn about all the nonstruc-tural elements that affect hospital safety.
In this section: virtual tours and animations explaining how hospi-tal safety is influenced by non-structural components.
Use the mouse to click on different items to learn more about non-structural elements.
Use the arrows to move around the images.

11
Let’s analyze the non-structural components
Download the PowerPoint presenta-tion on non-structural
components.
A virtual 360° tour. You can click on the green thumb-tacks
to learn about special safety measures to
protect non-structural components in a building.
Text describing nonstructural elements that must be evaluated to ensure the safety of hospitals.
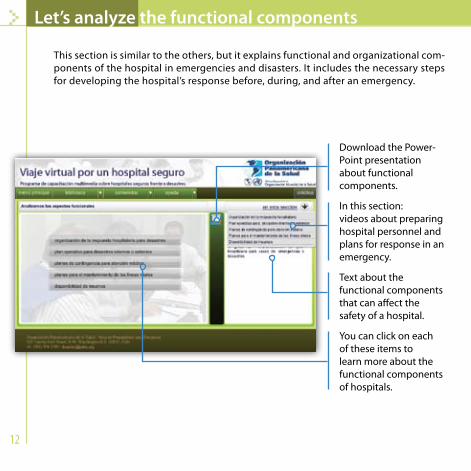
12
Let’s analyze the functional components
This section is similar to the others, but it explains functional and organizational com-ponents of the hospital in emergencies and disasters. It includes the necessary steps for developing the hospital’s response before, during, and after an emergency.
Download the Power-Point presentation about functional components.
In this section: videos about preparing hospital personnel and plans for response in an emergency.
Text about the functional components that can affect the safety of a hospital.
You can click on each of these items to learn more about the functional components of hospitals.
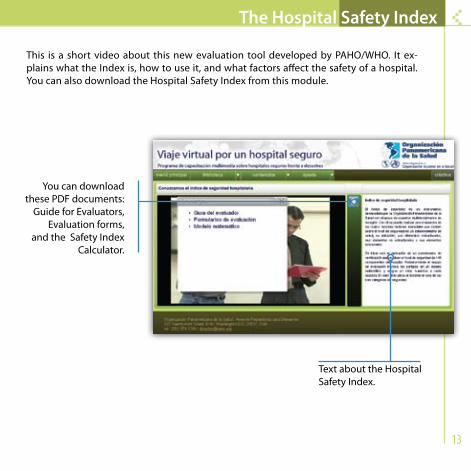
13
The Hospital Safety Index
This is a short video about this new evaluation tool developed by PAHO/WHO. It ex-plains what the Index is, how to use it, and what factors affect the safety of a hospital. You can also download the Hospital Safety Index from this module.
You can download these PDF documents:
Guide for Evaluators, Evaluation forms,
and the Safety Index Calculator.
Text about the Hospital Safety Index.
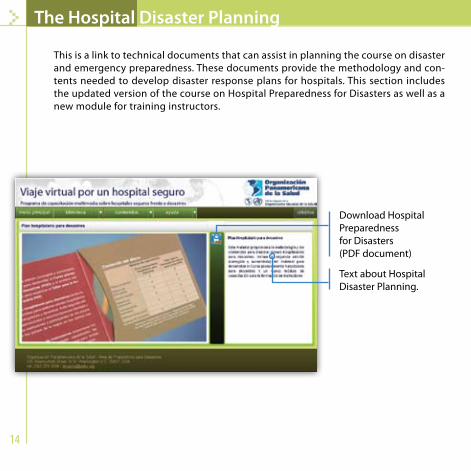
14
The Hospital Disaster Planning
This is a link to technical documents that can assist in planning the course on disaster and emergency preparedness. These documents provide the methodology and con-tents needed to develop disaster response plans for hospitals. This section includes the updated version of the course on Hospital Preparedness for Disasters as well as a new module for training instructors.
Download Hospital Preparedness for Disasters (PDF document)
Text about Hospital Disaster Planning.
15
Library
The Virtual Journey through a Safe Hospital includes a Virtual Library section. You can view and download the most important materials that PAHO/WHO has produced about this issue. These include publications, promotional and training material, technical guidelines, videos, graphics, and photographs that will assist in your study and analysis of Safe Hospi-tals in emergency situations.
© Pan American Health Organization, 2009
More information is also available on the PAHO/WHO website: www.paho.org/disasters
and the website of the Regional Disaster Documentation Center: www.crid.or.cr (visit the Safe Hospitals section).
Virtual Journey through a Safe Hospital Multimedia Training Program on Hospitals Safe from Disasters.
Made possible with the financial support of:
Pan American Health Organization Area on Emergency Preparedness and Disaster Relief
y Socorro en Casos de Desastres 525 Twenty-third Street, N.W.
Washington, D.C. 20037
ANNEX 9
Executive Report of the
Consultation on Global
Humanitarian Trends
and their Implications on
Institutions in the Americas
Airlie Center, Warrenton, VA 3-4 April 2008
The topic of disaster management has grown steadily and gained an increasingly important place on the health agenda of countries in Latin America and the Caribbean. However, the increasing number of actors, the improved capacity at local and regional level and globalization is quickly changing how we deal with risk reduction and disaster management. To address these realities, the Pan American Health Organization, regional office for the Americas of the World Health Organization, organized a high-level consultation on global humanitarian trends and their implications on institutions in the Americas. Over a two-day period, from 3-4 April 2008, experts discussed some of the broad issues that are driving these changes at global level and their implications at country level. This Consultation came at a particularly critical time, providing rich input into the Pan American Health Organization’s next strategic plan (2008-2012) for a secure and disaster resilient health sector in the Americas. This following document includes an Executive Report of the deliberations of this meeting, a list of participants and the revised position paper on global humanitarian trends and their implications for on institutions in the Americas.
Additional copies on the web at www.paho.org/disasters
Executive Report of the Consultation on Global Humanitarian Trends
and their Potential Implications on Countries in the Americas
Airlie Center, Warrenton, VA 3-4 April 2008
The objectives of the meeting were to:
Review and validate the potential implications of global humanitarian changes for national health or disaster institutions in Latin America and the Caribbean (LAC).
Suggest possible courses of action for the Pan American Health Organization (PAHO/WHO) and other interested partners to maximize the positive impact of the global changes on the disaster management capacity of the LAC.
High level participants (listed in Annex 1) from a broad range of agencies reviewed the discussion paper (Annex 2) prepared by a group of disaster management experts and provided recommendations to PAHO/WHO on these and other issues. They shared their experience on a personal basis. The opinions expressed did not necessarily reflect those of their organizations.
1. Relevance of the discussion paper on Global Humanitarian Trends and their
Implications on Institutions in the Americas
There was consensus that the diagnosis made regarding changes in the humanitarian field and their potential implications on national institutions in LAC was relevant and appropriate. In the introduction, experts suggested stressing the importance of emerging threats such as the Pandemic Influenza and climatic changes. Although addressing the challenges resulting from these changes will require additional commitment from the health sector in LAC countries, the current commitment to risk reduction and preparedness alone is still seen as insufficient. It was perceived that the discussion paper presented a somewhat negative perception of the impact of humanitarian changes on national institutions. This should be balanced with the potential gains for beneficiaries (i.e. the victims) that result from more efficient fund raising and response.
Pan American Health Organization Executive Report of the
Consultation on Global Humanitarian Trends and their Potential Implications on Countries in the Americas
3
These points have been addressed in the revised discussion paper, which is attached to this report or available on request from [email protected].
2. Changes in funding patterns
a. Conclusions The lack of access by governments of disaster-affected countries and/or attempts to influence how aid is used are valid issues that should be addressed internationally. The root of the problem lies in the varying levels of performance of Ministries of Health when it comes to managing and accounting for external relief funds. Bilateral donors in the Region have shown openness and flexibility in channeling funding directly to national institutions that are clearly competent and transparent. The case of the Ministry of Health in Ecuador is an example of one success story. The participants recognized the risk of marginalizing national authorities, given the current procedures for allocating CERF and other pooled funding. The evaluation of the CERF that is currently ongoing should take into consideration this point. Ministries of Health also lack knowledge and understanding of existing funding mechanisms for humanitarian response. The Inter-American Development Bank, for instance, has significant funding for risk assessment for climate change, yet the health sector in LAC countries has not availed itself of this funding source. An imbalance exists between funding that is available for disaster response and what is available for preparedness and risk reduction (DRR). Participants discussed at length the matter of assigning a percentage of humanitarian funding for DRR. Participants felt the allocation of relief funds for preparedness, or at least the flexibility to do so, should be encouraged, but stopped short of recommending a pre-determined percentage. It is more important to include DRR as an item in all national development budgets and projects rather than only in post-disaster external relief assistance. Finally, it was noted that some UN agencies have a flexible pass-through mechanism to transfer funds rapidly for a nominal fee to other partners: NGOs or national institutions. WHO does not have such a procedural mechanism.
b. Recommendations
The debate on funding patterns and their implications, which took place at this meeting in April 2008, should be repeated at subregional levels in Latin

Pan American Health Organization Executive Report of the
Consultation on Global Humanitarian Trends and their Potential Implications on Countries in the Americas
4
America and the Caribbean and involve subregional organizations, the health sector, the Ministries of Foreign Affairs and other actors. Development funds allocated by international financial institutions (IFIs) should be more fungible, that is, reprogrammable to areas at greatest risk or in need. LAC countries should improve perceptions regarding their ability to manage funds by utilizing, as appropriate, the OECD Principles of Corporate Governance. PAHO/WHO should help to improve the capacity of the Ministries of Health to manage and report on humanitarian response projects. PAHO/PED should inform and train national counterparts on the existing funding mechanisms (CERF and others) and priorities. PAHO/WHO should develop a flexible pass-through administrative mechanism for rapidly channeling external funds to MoH and possibly NGOs. Participants should brief the OCHA-commissioned team that is currently evaluating the CERF.
3. Humanitarian response vs. recovery/reconstruction
a. Conclusions
The phases of the disaster cycle form part of a continuum. Following the impact, recovery and reconstruction must begin immediately. Increasingly, the World Bank and the Inter-American Development Bank are ready to begin the recovery process immediately following the disaster impact – concurrently with emergency response. Response actors and coordinators must take this factor into account. Humanitarian and development actors differ on who is best equipped to lead the recovery process. The experts at this meeting see recovery as primarily a development activity rather than a humanitarian activity. However, in practice, this process is initially driven by the availability of humanitarian (response) funding and managed by humanitarian responders, who may not necessarily have the skills and development experience needed. The health sector is one of the weak links in recovery/ reconstruction. The lack of recovery plans and shortcomings in terms of the participation of the Ministries of Health in the reconstruction process were noted. Early recovery is the time to (re)introduce disaster risk reduction in the planning process.
Pan American Health Organization Executive Report of the
Consultation on Global Humanitarian Trends and their Potential Implications on Countries in the Americas
5
b. Recommendations
Humanitarian actors should consider the developmental nature of recovery activities and take advice from agencies that specialize in recovery and reconstruction. IFIs should make risk management an early component of any recovery process. LAC countries, in particular the Ministries of Health, should discuss recovery plans prior to disasters.
4. The Humanitarian Reform and the Cluster initiative
a. Conclusions
The participants recognized the need to improve coordination of humanitarian response and the importance of the Humanitarian Reform for the beneficiaries, especially in complex disaster situations. They noted that some disaster-affected governments and experts have expressed reservations regarding a potentially negative impact on national institutions in situations where the humanitarian reform is implemented without consultation or adjustments in the most advanced of developing countries . The Cluster mechanism is not meant to replace governments, especially in the case of sudden-onset natural disasters in advanced countries. In the health field, donor representatives recalled the comprehensive nature of PAHO’s health coordination in past disasters, in line with WHO’s holistic definition of health as a state of physical, social and mental wellbeing. They also noted that, under the humanitarian reform, the lead responsibility for health is disaggregated into four distinct Clusters. In LAC, there are definite advantages as well as precedents for consolidating the number of the health-related Clusters according to the structure and role of the Ministry of Health. As recognized by the Eastern Caribbean Donor Group, “if the national system is working, we should support it.” Finally, participants determined that the increasing use of English as the working humanitarian language in recent disasters further hampers the active involvement of local authorities from non-English speaking countries.

Pan American Health Organization Executive Report of the
Consultation on Global Humanitarian Trends and their Potential Implications on Countries in the Americas
6
b. Recommendations The UN should adapt its Cluster structure to the organization of the affected country, not the reverse. In LAC, a sectoral/cluster approach, consolidating all health activities into one mechanism, with the Ministry of Health as lead agency, may be more appropriate in most cases. PAHO/WHO, in line with its mandate and past experience, should continue to provide technical guidance and coordination on all matters related to health. LAC countries should request the humanitarian community and OCHA to adopt Spanish as the only working language for Cluster and coordination meetings in Latin America (or Spanish-speaking Caribbean countries such as the Dominican Republic and Cuba), to facilitate leadership and participation from the national institutions.
5. A comprehensive risk reduction approach
a. Conclusions
The International Strategy for Disaster Reduction (ISDR) has developed inter-agency groups and a joint program of work, with a system to track investments in disaster risk reduction. However, in most cases, the health sector is not one of the most active members of ISDR National Platforms. The Hyogo Framework of Action (HFA) is an important entry point for the LAC countries. However, LAC may not have insufficient information on the HFA and this might be the cause of a perceived lack of commitment. Most Ministries of Health in LAC are weak when it comes to advocacy and outreach. Most often, they do not have a budget line for risk reduction. Their focus remains on response / preparedness and communicable diseases.
b. Recommendation
PAHO/WHO and the Ministries of Health should take advantage of the ISDR regional meeting of National Platforms in February 2009 to stimulate health sector awareness and commitment to HFA goals.
Pan American Health Organization Executive Report of the
Consultation on Global Humanitarian Trends and their Potential Implications on Countries in the Americas
7
6. Awareness and capacity building
a. Conclusions National authorities in LAC are not sufficiently aware of the potential benefits as well as the unintended consequences of the global humanitarian changes, including the Humanitarian Reform, International Health Regulations 2005, the CERF and other mechanisms. If the population of LAC and its institutions are to benefit from these changes, decision makers in health, foreign affairs and other sectors must become more familiar with the issues. All participating agencies should make it a priority to keep them well informed. Sustainable improvements in disaster risk reduction (from prevention to response and recovery) are contingent upon strong and committed institutions. Marginalizing (and thereby weakening) national institutions is counter-productive in the long run. Along the same lines, simply demonstrating commitment on the part of LAC countries is insufficient, given the magnitude of the problem.
b. Recommendations PAHO should place the highest priority on building awareness and capacity in the Ministries of Health and Foreign Affairs to understand international mechanisms and the potential benefit of their proactive use, as well as the cost of not asserting national leadership in this field. These sessions should be multisectorial and carried out with the collaboration of relevant partners. A sustained effort to educate countries could include:
i. A mapping of all instruments available to assist governments, not only in response but also in disaster risk reduction
ii. A comprehensive training package on these tools
iii. Case studies / success stories (possibly Ecuador)
iv. A situation analysis for briefing Ministers of Health at the PAHO/WHO Directing Council Meting (September 2008).
PAHO should target decision makers throughout the Region and in PAHO/WHO to seek additional commitment to DRR and engagement in the reform process. PAHO should raise selected issues from the discussion paper at the next meeting of UN Regional Directors.
Pan American Health Organization Executive Report of the
Consultation on Global Humanitarian Trends and their Potential Implications on Countries in the Americas
8
7. Emerging threats: Climate change and pandemic influenza
a. Conclusions Neither the discussion paper nor the PED Strategic Plan sufficiently addresses the issue of new threats, in particular climate change. Climactic changes are likely to impact public health and manifest themselves through an escalating number of events over time, including more severe hydrometeorological disasters, food scarcity and increased transmission of communicable diseases. Some events will have severe consequences that will activate PED’s disaster management mandate and intersectoral coordination mechanisms. There is a lack of health studies and impact assessments in LAC. IFI funding is available but not used by countries. When it comes to pandemic influenza, a functional distribution of tasks exists within PAHO/WHO. However, this is not yet the case for climate change. b. Recommendations PAHO/PED and the ministries health should develop partnerships with agencies that conduct impact assessments related to climate change. Ministries of health must build stronger linkages with national climate change commissions. PAHO/WHO should clarify its internal distribution of roles and responsibilities using disaster scenarios resulting from climate change.
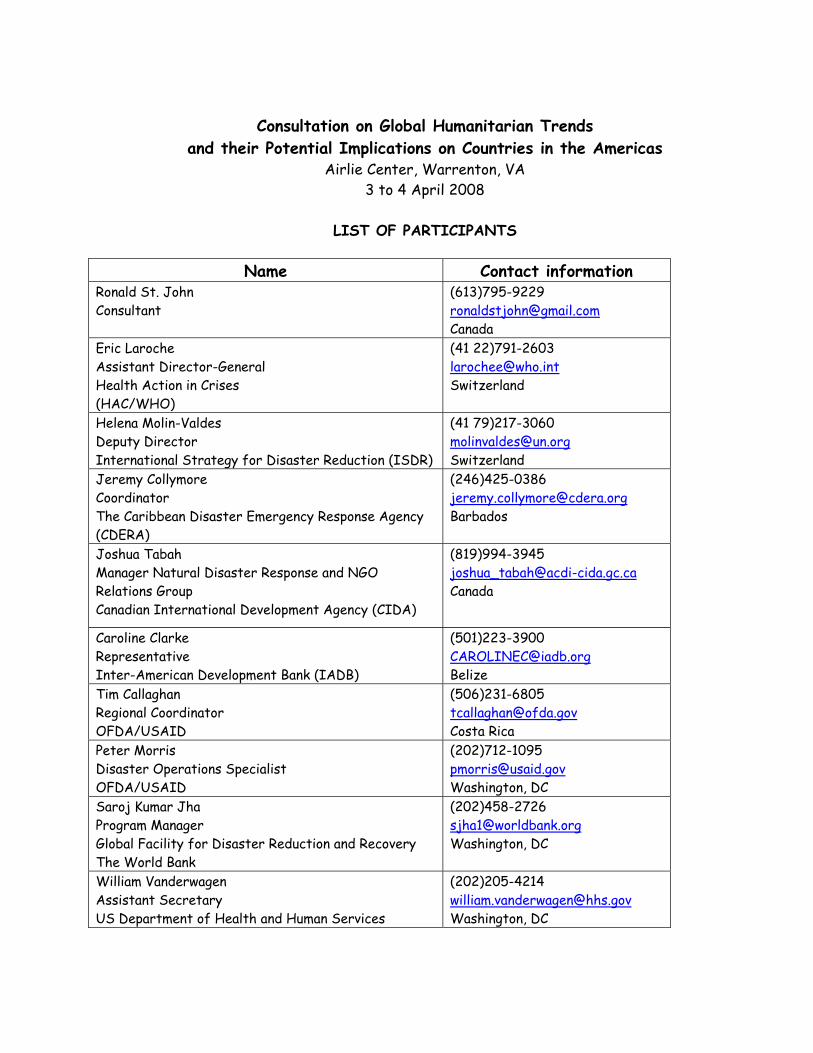
Consultation on Global Humanitarian Trends
and their Potential Implications on Countries in the Americas Airlie Center, Warrenton, VA
3 to 4 April 2008
LIST OF PARTICIPANTS
Name Contact information Ronald St. John Consultant
(613)795-9229 [email protected] Canada
Eric Laroche Assistant Director-General Health Action in Crises (HAC/WHO)
(41 22)791-2603 [email protected] Switzerland
Helena Molin-Valdes Deputy Director International Strategy for Disaster Reduction (ISDR)
(41 79)217-3060 [email protected] Switzerland
Jeremy Collymore Coordinator The Caribbean Disaster Emergency Response Agency (CDERA)
(246)425-0386 [email protected] Barbados
Joshua Tabah Manager Natural Disaster Response and NGO Relations Group Canadian International Development Agency (CIDA)
(819)994-3945 [email protected] Canada
Caroline Clarke Representative Inter-American Development Bank (IADB)
(501)223-3900 [email protected] Belize
Tim Callaghan Regional Coordinator OFDA/USAID
(506)231-6805 [email protected] Costa Rica
Peter Morris Disaster Operations Specialist OFDA/USAID
(202)712-1095 [email protected] Washington, DC
Saroj Kumar Jha Program Manager Global Facility for Disaster Reduction and Recovery The World Bank
(202)458-2726 [email protected] Washington, DC
William Vanderwagen Assistant Secretary US Department of Health and Human Services
(202)205-4214 [email protected] Washington, DC
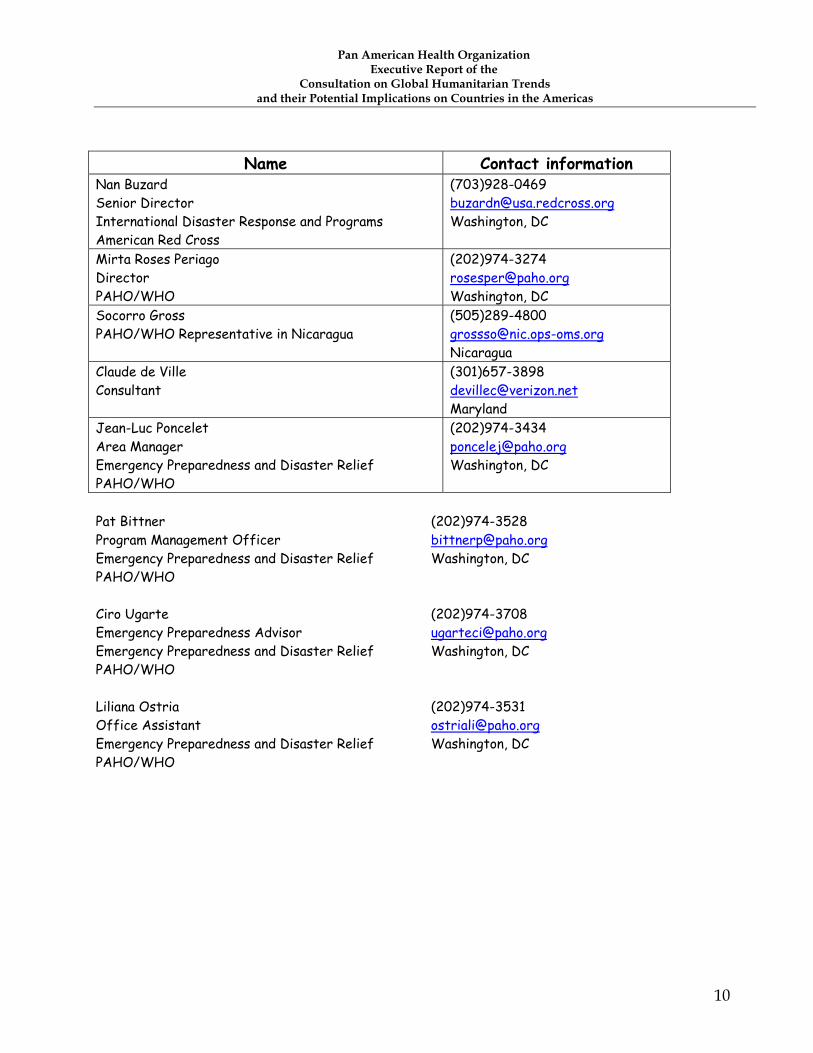
Pan American Health Organization Executive Report of the
Consultation on Global Humanitarian Trends and their Potential Implications on Countries in the Americas
10
Name Contact information Nan Buzard Senior Director International Disaster Response and Programs American Red Cross
(703)928-0469 [email protected] Washington, DC
Mirta Roses Periago Director PAHO/WHO
(202)974-3274 [email protected] Washington, DC
Socorro Gross PAHO/WHO Representative in Nicaragua
(505)289-4800 [email protected] Nicaragua
Claude de Ville Consultant
(301)657-3898 [email protected] Maryland
Jean-Luc Poncelet Area Manager Emergency Preparedness and Disaster Relief PAHO/WHO
(202)974-3434 [email protected] Washington, DC
Pat Bittner (202)974-3528 Program Management Officer [email protected] Emergency Preparedness and Disaster Relief Washington, DC PAHO/WHO Ciro Ugarte (202)974-3708 Emergency Preparedness Advisor [email protected] Emergency Preparedness and Disaster Relief Washington, DC PAHO/WHO Liliana Ostria (202)974-3531 Office Assistant [email protected] Emergency Preparedness and Disaster Relief Washington, DC PAHO/WHO
Discussion Paper on
Global Humanitarian Trends
and their Implications on Institutions
in the Americas
Meeting of Experts convened by PAHO/WHO
Airlie Center, Warrenton, VA 3-4 April 2008
Introduction The countries of Latin America and the Caribbean (LAC) have long been leaders in the field of disaster preparedness and response (disaster management). In the 1980s and 1990s, unparalleled progress was made in convincing governments and agencies to take seriously the risks posed by natural disasters and to plan ahead to reduce risk and prepare to respond to the health consequences. Many countries established full-time disaster management offices and the ministries of health appointed National Health Disaster Coordinators. The collapse of Hospital Juarez in the 1985 Mexico earthquake triggered a progressive shift from preparedness and response toward a more comprehensive risk reduction approach in the health sector, which ultimately led to the adoption of “Hospitals Safe from Disasters” as the theme the ISDR-WHO World Disaster Reduction Campaign for 2008-2009. Today, the situation is distinct:
New threats, such as terrorism, SARS, pandemic influenza and climate change are becoming more prominent;
The pace of change within the global humanitarian community has accelerated. These changes, which are partly the result of explosive growth in this sector, can also be potentially beneficial at country level. The focus of this paper is on the potential impact of these humanitarian trends and reforms—both positive and negative—on the capacity of national institutions and in particular, ministries of health;
Institutions in LAC may not be fully aware of these global changes and consequently are slow to adjust and take maximum benefit of all they have to offer for disaster-affected populations.
Humanitarian changes at global level include:
Increased awareness of disaster risk reduction, thanks in part to the adoption of the Hyogo Framework of Action;
Changes in humanitarian funding patterns;
The involvement of new actors;
The adoption of minimum standards for humanitarian assistance;
Overlapping between relief, recovery and reconstruction;
Redefining disasters and emergencies: shifting priorities;
The changing role of financial institutions;
The revised International Health Regulations;
The United Nations Humanitarian Reform. It is questionable whether countries in this Region are sufficiently aware of and ready to adapt to these changes. Justifiably proud of their early pioneering efforts, the countries of LAC and their inter-country or regional disaster institutions tend to remain in isolation, fostered by a common language and culture.
Pan American Health Organization Global Humanitarian Trends and their Implications
on Institutions in the Americas
2
Humanitarian changes at global level of potential importance for LAC and its inter-country institutions
Increased awareness of disaster risk reduction: the Hyogo Framework of Action (2005-2015) The United Nations deemed the decade of the 1990s as the International Decade for Natural Disaster Reduction. As a result, political and public awareness of the socioeconomic cost of disasters rose dramatically. It culminated with the Hyogo Framework for Action (HFA), adopted at the World Conference on Disaster Reduction (January 2005). The catastrophic impact of the tsunami in December 2004, just a few weeks before this global conference, focused world attention on prevention and preparedness. The HFA’s emphasis on sustainable development, mainstreaming of risk reduction and above all, on national responsibilities are very positive:
“each State has the primary responsibility for its own sustainable development and for taking effective measures to reduce disaster risk, including for the protection of people on its territory, infrastructure and other national assets from the impact of disasters. At the same time, in the context of increasing global interdependence, concerted international cooperation and an enabling international environment are required…”1
Changes in humanitarian funding patterns
The amount of funding Global funding for risk reduction has undoubtedly increased as a result of the adoption of the HFA, but to a far lesser degree than funding for immediate response. In the aftermath of the tsunami, US$14 billion were pledged and, for the most part, delivered. Almost 40% came from private contributions to NGOs and the Red Cross system, as compared to an average of 15% in most disasters. The customary coordination mechanisms and national authorities in affected countries had minimal influence on how this funding was used. The Tsunami Evaluation Coalition (TEC) conducted a study on the funding of the response to the tsunami in late 2004 and early 2005. Without taking into consideration funds received for disaster prevention, mitigation or risk reduction, the TEC study found that the overly generous funding had a perverse effect on the humanitarian community:
1 Hyogo Framework for Action, paragraph 13. Online at www.unisdr.org/eng/hra/hfa.htm.
Pan American Health Organization Global Humanitarian Trends and their Implications
on Institutions in the Americas
3
The evaluators concluded that “Much of the implementation response was driven by the availability of funds, or by contextual opportunism, rather than by needs.”
Of greater relevance to LAC is the potential for a negative impact on local institutions.2 In another TEC study, a different group of evaluators noted that: “By ignoring local capacity, the role of external aid is made to seem all the more important. The more external aid there is, the more that local capacity is undermined.”3
Although the tsunami in South Asia may be an extreme example, the response to the Pakistan earthquake followed a similar pattern of very generous short-term donations in the immediate aftermath, reflecting a definite trend in international response, especially in high-profile media events.
Funding mechanisms
Mechanisms for funding humanitarian response have also evolved. With the establishment of the Central Emergency Response Fund in March 2006,4 UN organizations, and through them international NGOs and the IFRC, now have access to large amounts of funding for life-saving activities or chronically underfunded response operations. International NGOs have suggested that they also should have direct access to CERF funding, and one suggested that 50% of CERF allocations should go to NGOs5. Government and health authorities have no direct access to CERF, and there is no requirement that country authorities are consulted in the definition or implementation of CERF-funded projects. The ministry of health is not formally a part of the process to formulate priorities or review health proposals, despite the fact that the UN General Assembly Resolution (A/RES/60/124) approving the CERF reaffirmed the guiding principles of Resolution 46/182 of 19 December 1991.6 Since its launch, the CERF has committed US$ 619.1 million to humanitarian projects in 60 countries affected by natural disasters and armed conflicts. Bilateral humanitarian funding also tends to concentrate on a few global agencies, either through direct support to those international partners or through pooled funding under
2 In most disasters, including in Latin America (Costa Rica, El Salvador, Peru) and the Caribbean the health personnel are also heavily affected by the impact. 3 TEC Impact of the tsunami response on local and national capacities, p. 11. 4 A/RES/60/124 5 OXFAM Briefing Paper 100. The UN Central Emergency Response Fund One Year On. 6 Guiding principle 4: “Each State has the responsibility first and foremost to take care of the victims of natural disasters and other emergencies occurring on its territory. Hence, the affected State has the primary role in the initiation, organization, coordination, and implementation of humanitarian assistance within its territory.” A/RES/46/182
Pan American Health Organization Global Humanitarian Trends and their Implications
on Institutions in the Americas
4
UN management. Based on recent PAHO/WHO experience, bilateral funding through regional/subregional partners appears to have decreased.
Ineligibility of MoH for humanitarian funds Funding partners and the public prefer to direct their increasing contributions toward NGOs, Red Cross and UN agencies for the immediate response. Government institutions, even those with good track records when it comes to transparency and disaster management, are not eligible to manage relief funds and deliver services. Donors do not sufficiently differentiate between countries with an emerging economy and considerable human resources for rapid response to a natural disaster and the so-called ‘failed states,’ where authorities lack transparency and good governance and may be part of the problem in a conflict. However, active participation on the part of the Ministries of Health may provide the necessary legitimacy; strengthening national capacity should be a key strategy of the global response system.
The involvement of new actors With the availability of generous funding in search of a project or an implementing partner, the number of humanitarian agencies and actors is increasing dramatically. As the IFRC correctly stated, humanitarian response is now the “largest unregulated industry”.7 The involvement of many new actors can be, in itself, a positive development that reflects mainstreaming of the topic. However, it poses a difficult challenge to coordinating health authorities (and international organizations) in terms of differentiating among NGOs with skills and expertise from the growing number of amateur-like, unprofessional groups. The NGO community is not the only “new actor” that brings potentially valuable assets and contributions to the table. The private sector, in particular the pharmaceutical or food industry, now provides direct “technical assistance” and support, occasionally under the banner of the UN. However, there is little, if any, interaction with national authorities, including the Ministries of Health. A lack of coordination with and guidance from the Ministry of Health only contributes to a further blurring of the lines between non-profit and for-profit undertakings in the aftermath of disasters. On the one hand, the pharmaceutical or information industries have much to contribute in terms of knowledge, skills and material donations. On the other hand, there is always a question of conflict of interest when commercial proprietary products (software, drugs or vaccines) are promoted and introduced by “humanitarian actors” with little oversight from the Ministries of Health and UN technical agencies. Foreign militaries in LAC have always been a major actor in international response. Now the trend is gaining strength globally, at times making this institution the dominant player, 7 World Disaster Report, International Federation of Red Cross and Red Crescent Societies, 2004

Pan American Health Organization Global Humanitarian Trends and their Implications
on Institutions in the Americas
5
at the expense of traditional mechanisms and the health sector’s coordination role (Ministry of Health). Government-sponsored Civil Brigades may offer very effective and appropriate assistance (medical or other), provided they respond to actual needs and adjust to the socio-political context of the affected country. In the UN system, specialized inter-agency mechanisms or services have been established or strengthened: from the well established UNDAC,8 to the Humanitarian Information Center (HIC) and the UN Joint Logistic Center (UNJLC), which are lesser well known in LAC. These mechanisms, when mobilized, assume de facto, the leadership in their respective areas. This situation was observed in Indonesia, Sri Lanka and Pakistan, as well as in the recent floods in Bolivia.9 Although local authorities are often unprepared to claim their coordinating role, substituting them with relatively well- equipped and focused mechanisms, which have been endorsed by the donor community, may turn out to be counterproductive.
The adoption of minimum standards for humanitarian assistance Humanitarian assistance must follow some principles and apply some kind of measurable standards for accountability and quality control. For this purpose, the SPHERE Project was launched in 1997 by a group of humanitarian NGOs and the Red Cross and Red Crescent movement. The principle and widely-used SPHERE product is a handbook detailing Minimum Standards in Disaster Response (health, water, shelter, etc) that people affected by disasters have a right to expect from humanitarian assistance. 10 Although the formulation of universal standards is an achievement, these “minimum” standards are unrealistically high. For instance, 15 liters of quality drinking water/person/day in many poor rural areas may be far above what was available prior the disaster or could be sustained. In the medical care field, staffing guidelines are also rarely attained under non-emergency circumstances in developing countries.11 The result is the temporary and costly
8 The participation of experts from the Americas in the UNDAC mechanism is a model for other regions. 9 In January 2006, the Bolivian highlands experienced intense, prolonged rainfall. Thousands of families were affected. Although a general lack of leadership was observed among national institutions responsible for emergency management, the situation was aggravated when the UN established an external structure, headed by the UNDP. This group, known as UNETE (United Nations Emergency Team), was designed to convene and coordinate UN agencies that have a country presence. The fact that UNETE assumed a role well beyond coordination resulted in the “drawing back” of national institutions. This situation at the national level was repeated at the department level, where the OSSOC displaced the emergency operations committee in the Department of Santa Cruz. 10 http://www.sphereproject.org/content/view/27/84/lang,English/ 11 For instance:
a. At community level: one community health worker per 500-1,000 population; one skilled/traditional birth attendant per 2,000 population; one supervisor per 10 home visitors... b. Peripheral health facility (for approximately 10,000 population): total of two-five staff; minimum of one qualified health worker, based on one clinician per 50 consultations per day; non-qualified staff for administering oral rehydration therapy (ORT), dressings, etc. and for registration, administration, etc.
Pan American Health Organization Global Humanitarian Trends and their Implications
on Institutions in the Americas
6
delivery of an unsustainable level of services to selected groups,12 creating new inequities and a conflict with the more realistic objectives of the long-term recovery programs. The challenge is to adjust the response to a disaster to the local context. Consistency and sustainability should prevail.
Overlapping between relief, recovery and reconstruction Ten years ago, the response to an earthquake triggered immediate life-saving efforts that would taper off after four to five weeks, leaving behind those agencies or NGOs with a development approach to handle recovery. Reconstruction funds would not materialize for several years, leaving the delayed health needs poorly met due to the lack of specific funding for transition from relief to reconstruction (recovery). The traditional phases of the disaster cycle (prevention, preparedness, response and recovery) were always represented as a continuum. Today however, the post-impact phases overlap more than ever and compete for resources, whether financial or human. Today, the economic valuation conducted by financial institutions of the damage caused by a disaster is being made just days after the impact, rather than weeks or months later,13 and consequently, the timeline for receiving pledges for reconstruction has also shortened significantly. At the same time, the generous (and in cases, excessive) funding for humanitarian immediate response in well-publicized disasters encourages first responders to expand the definition of ‘emergency relief activities’ to match the duration of available humanitarian funding. Relief teams may remain active for years. Governments’ efforts to declare an emergency over and initiate the recovery process may be defeated by humanitarian actors.14 In most cases, the availability of unused relief funds plays a major role in overextending the relief phase. Mandates are also stretched, resulting in IFRC and WHO leading a process of monitoring “recovery” indicators,15 which traditional lead agencies for reconstruction (the financial institutions) consider as duplicative of their effort. In addition multiple parallel efforts by
12 In this instance, the selected group may be the displaced population rather than the host community, for example. 13 Conducting early surveys of economic damage (as opposed to emergency needs) presents an additional challenge for the ministry of health, which, during the first few weeks, is deeply involved in the response and has scarce resources to spare for an economic assessment. 14 In Aceh province, Indonesia, WHO extended its emergency response long after the government had shifted to developmental mode (recovery and reconstruction). In Pakistan, official plans for the return of displaced populations to their place of origin at the end of the winter met withresistance, not from the affected population but from international actors who insisted that displaced families be given the choice of whether or not to continue in camps, with full services including education. Indeed, agencies had extended the doctrine of “voluntary repatriation” beyond conflicts to natural disasters. 15 Tsunami Recovery Impact Assessment & Monitoring System (TRIAMS) http://www.humanitarianinfo.org/sumatra/reliefrecovery/livelihood/docs/doc/inforesources/ConceptPaperonTRIAMSImpactMonitoringSystem.pdf
Pan American Health Organization Global Humanitarian Trends and their Implications
on Institutions in the Americas
7
humanitarian agencies, reconstruction institutions and government to redevelop the health system lead to duplication and inconsistencies.
Redefining disasters and emergencies: shifting priorities The prevention and management of the effects of climate change, terrorism and other security issues cannot be ignored, and indeed, are medium to long-term priority issues that deserve more action. LAC countries are, however, more vulnerable to natural disasters and technological accidents. However, since September 11, 2001, too much focus has shifted from common technological or natural disasters to terrorism. There is little rationale to abandon a multi-hazard, multi-phase approach to disaster mitigation, preparedness and response at regional and country level. Global political concerns and the availability of earmarked funds should influence, but not dictate, country action.
The changing role of financial institutions The interest and role of regional and global banks (Inter-American Development Bank and the World Bank) have evolved over the last several years. The World Bank (WB):16
A new policy aims to facilitate the WB’s support to “social aspects of recovery within the relief-to-recovery continuum.”…“In today’s emergencies, the Bank is being asked to step in earlier and under a wider variety o f situations, often as part o f integrated international support for a country’s emergency recovery plan. This means that the Bank’s first response-the needs assessments and technical assistance-is often carried out while relief activities are under way”17
The Global Facility for Disaster Reduction and Recovery (GFDRR), established in June 2006, is already a major player in the disaster management field through its support of UNISDR. Australia, Canada, Denmark, European Union, Italy, Japan, Spain, Sweden, Switzerland, UK and World Bank are contributing to the GFDRR. In brief, the WB is asserting its role (and leadership) in the early recovery, an area where the humanitarian community was rapidly expanding, often without the necessary development expertise.
16 An “Evaluation of the World Bank Assistance for Natural Disasters” by the Independent Evaluation Group (IEG) of the WB, 2006, led to the document entitled Toward a New Framework for Rapid Bank Response to Crises and Emergencies (R2007-00 10), made public in April 2007. Online at www.worldbank.org (search using the title for a link to the PDF document.) 17 (R2007-00 10) Changing Role of the World Bank, p.3.
Pan American Health Organization Global Humanitarian Trends and their Implications
on Institutions in the Americas
8
The Inter-American Development Bank (IDB)
The IDB approved its Disaster Risk Management Policy in 2007.18 The purpose of this policy is to improve the Bank's ability to assist the borrowing member countries in the attainment of their development goals in sustainable economic growth, poverty reduction and promotion of social equity, by supporting their efforts to proactively manage disaster risk.19 The new policy has two interrelated objectives:
i) “To strengthen the Bank’s effectiveness in supporting its borrowers to systematically manage risks related to natural hazards by identifying these risks, reducing vulnerability and by preventing and mitigating related disasters before they occur; and
ii) “To facilitate rapid and appropriate assistance by the Bank to its borrowing member countries in response to disasters in an effort to efficiently revitalize their development efforts and avoid rebuilding vulnerability”20
The policy adopted by the IDB’s Immediate Response Facility, which links eligibility for emergency funding to a country’s commitment to preparedness, is a positive step.
The revised International Health Regulations (IHR 2005) The IHR, which were initially adopted in 1969, were revised in 2005 to include any “illness or medical condition, irrespective of origin or source, that presents or could present significant harm to humans,” including therefore issues resulting from the natural, accidental or deliberate release of chemical or radionuclear material. The management of technological disasters is potentially becoming an international concern.21 In 2007, WHO dedicated World Health Day to “Health Security” and upgraded its department of communicable diseases at headquarters to cover emergencies caused by chemicals and other environmental hazards as well as climate change. How IHR 2005 and the redistribution of roles within WHO will reflect on the Ministries of Health in the Region remains unclear.
18 Disaster Risk Management Policy, 28 February 2007. Online at http://www.iadb.org/sds/doc/ENV-DRMPolicy.pdf 19 Quoted from http://www.iadb.org/sds/ENV/site_2970_e.htm 20 IDB Disaster Risk Management Policy p.3 21In English: http://www.who.int/csr/ihr/IHRWHA58_3-en.pdf or in Spanish: www.who.int/csr/ihr/WHA58_3-sp.pdf
Pan American Health Organization Global Humanitarian Trends and their Implications
on Institutions in the Americas
9
The Humanitarian Reform Few practitioners doubt that the international humanitarian system was in need of serious reform. The lack of clear mandates “has repeatedly led to ad hoc, unpredictable humanitarian responses, with inevitable capacity and response gaps in some areas.” “Humanitarian reform seeks to improve the effectiveness of humanitarian response by ensuring greater predictability, accountability and partnership.” In September 2005 the UN Inter-Agency Standing Committee (IASC) agreed to designate global “cluster leads” – specifically for humanitarian emergencies – in nine sectors or areas of activity. “The approach is designed around the concept of partnerships between UN agencies, the International Red Cross and Red Crescent Movement, international organisations and NGOs.22 Partners work together towards agreed common humanitarian objectives both at the global level (preparedness, standards, tools, stockpiles and capacity-building) and at the field level (assessment, planning, delivery and monitoring).” 23 One concern for LAC is the fact that the voting membership in the IASC, the governing mechanism for the humanitarian reform, is limited to UN agencies, with other key humanitarian actors (ICRC, NGOs etc.) serving as non-voting members. Donor governments have been instrumental in this reform. What has been missing in the design and implementation of the proposed partnership is a voice from the affected countries, which are responsible for directing humanitarian assistance to their population. Due to a lack of awareness, the humanitarian reform process is perceived as a mechanism of the United Nations System and not of national and regional actors. Leadership for issues in the health sector is also distributed among several Clusters: nutrition, water and sanitation, mental health (as a topic under the Protection Cluster) and finally ‘health’ per se. The former two are led by UNICEF and the latter by WHO. It is a major and regrettable departure from the holistic definition of health as it appears in the WHO constitution and a step backward from coordination practices in LAC. Fortunately, an increasing number of States with an emerging economy and working institutions are reclaiming their responsibility and demanding adjustments to a mechanism that is designed primarily for response in failed or ineffective states.24
22 It is noteworthy that local governments are not mentioned as part of the partnerships. 23 Inter Agency Standing Committee (IASC). Guidance note on using the cluster approach to strengthen humanitarian response 24 November 2006 24 For example, in recent disasters, Mexico, Nicaragua and Peru chose not to accept the activation of the Cluster mechanism.

Pan American Health Organization Global Humanitarian Trends and their Implications
on Institutions in the Americas
10
Implications at country and sub-regional levels
At country level Changes in the humanitarian system are not merely operational, but strategic and political as well. They redefine whose disaster it is and establish rules of accountability. These changes may affect all countries of the Americas. Although most of the changes are intended to benefit the affected population, the implications for countries in LAC may be profound in the case of large scale disasters. The disadvantages may partly offset the expected benefits.
The Ministries of Health will find it difficult to influence how the large amount of available funding is allocated.
Few Ministries of Health are familiar with the mandates, roles, strengths and weaknesses of an increasing number of actors (civil or military, private or public).
The Cluster approach, if not guided by the health authorities, may result in a transfer of leadership from the national level to a donor-driven international system, further marginalizing health coordinators in Latin America and the Caribbean.
In the absence of national humanitarian assistance standards adapted to the level of development and preexisting services in the affected country, unrealistically high “minimum standards” are applied for the duration that humanitarian funds are available.
A post-disaster assessment of impact (economic valuation), using the ECLAC methodology, is taking place much earlier, while the health sector is still fully absorbed in the immediate medical and public health response. The earlier the economic valuation takes place, the greater the shortage of qualified health assessors.
International humanitarian relief agencies are undertaking the reconstruction of health facilities, housing and income-generating activities independently from national development and reconstruction calendars and priorities. The skills and approaches required for emergency relief and response are not necessarily appropriate for development-like recovery.25
International emphasis on immediate (external) response is overshadowing the need for increased efforts in risk reduction and national preparedness. Funds for preparedness and risk reduction are not a standard feature of humanitarian relief grants.
• Ultimately, national institutions may lose credibility and the respect of the population.
25 Conversely, development entities are not necessary competent to lead relief and rehabilitations initiatives.
Pan American Health Organization Global Humanitarian Trends and their Implications
on Institutions in the Americas
11
At subregional level The LAC region has long-standing subregional organizations: CEPREDENAC, created in 1987,26 CDERA, created in 1991,27 and CAPRADE, created in 2002.28 All three are implementing inter-country risk reduction and preparedness initiatives. Because the mandate, resources and ownership of each organization is not the same, their role in emergency response differs greatly. In preparedness and risk reduction, each agency has developed its own approach and political balance when it comes to securing support from donors and civilian or military actors. Most agencies, including the three subregional agencies, have adopted an opportunistic pragmatism in order to grow and provide services. There is little precedent in other regions to assess the impact of global changes on sub-regional entities. At the time of major disaster, one can anticipate that:
Sub-regional organizations are likely to be dramatically understaffed and under-resourced as compared to a fully mobilized global coordination capacity.
The quality of prior relationships with main actors (donors, UN agencies, NGOs and the military) will determine to what extent the subregional entity will be able to advocate for a meaningful participation of the government in the actual management of international assistance (Cluster leadership, assessment of needs, coordination and timing/planning of recovery).
A dependency on external funding (in particular bilateral or military sources) may limit the sub regional agencies’ ability to take a firm stand before the international community and donors and call for an effective leadership role for the Disaster Management and Civil Protection agencies and the Ministries of Health firmly over external interventions.
Conclusions The international community’s renewed assertiveness in humanitarian response aims to improve a rapid and unimpeded access to external relief assistance by the affected population. It is essentially directed toward the beneficiaries, to whom many humanitarian stakeholders express direct accountability. Indeed, few, if any countries have the capacity to provide large-scale immediate assistance to a population stricken by a major disaster. The approach, however, is justified often by the lack of sustained investment on the part of the countries in their own preparedness and response capacity. The inability of national
26 Centro de Coordinación para la Prevención de los Desastres Naturales en América Central 27 The Caribbean Disaster Emergency Response Agency 28 Andean Committee for Disaster Prevention and Assistance

Pan American Health Organization Global Humanitarian Trends and their Implications
on Institutions in the Americas
12
institutions to effectively manage external resources and be accountable for their response to immediate needs of the affected population is widely perceived and sometimes well-documented. However, sidetracking national institutions once past the extremely short lifesaving relief in order to mitigate shortcomings is a short-term approach that will not increase capacity in the next disaster, nor will it stimulate countries in LAC to assume responsibilities and international commitments and make a political and financial investment in disaster risk reduction. It is only through the strengthening of national and regional capacity that the potential for humanitarian reform and the changes taking place globally will be fully applied to benefit affected groups in the Americas. Leadership for response and for recovery is different. For the latter, a long-term development perspective is required. The health sector is seen as lagging behind in recovery/reconstruction. In brief, national institutions in LAC and other regions have the resources, knowledge and skills to carry out successful programs. They should be persuaded and strengthened to act rather than be substituted by international actors.
ANNEX 10
FOREWORD “If you do something for me and you do it without me, then you do it against me.” This quote from Jawaharlal Nehru aptly describes the philosophy behind this strategic plan developed by the Area on Emergency Preparedness and Disaster Relief of the Pan American Health Organization, regional office for the Americas of the World Health Organization. The aim of the Area on Emergency Preparedness and Disaster Relief is to make an increasing difference in helping countries in the Americas and other Regions to reduce the health sector’s risk to all types of disasters, with the ultimate goal of reducing morbidity and mortality following such emergency events, while at the same time improving the health of the population of the Americas. It has been more than 30 years since PAHO/WHO’s Member Countries requested the Organization to help strengthen their national response capacity through the efficient use of existing resources. We look back at 1976 as a pivotal year, when the Directing Council made the decision to include the topic of disaster response in the health sector agenda. Over the years, this initiative has expanded to include preparedness, mitigation and other risk reduction activities. Today, it is common to see disaster preparedness, mitigation, response and risk reduction reflected in PAHO/WHO policy documents and decisions. The Health Agenda for the Americas clearly points to natural and manmade disasters as factors that limit the achievement of health sector goals and the PAHO/WHO strategic plan for 2008-12 reflects an even greater level of commitment on the part of the Organization to disaster risk reduction. The recent decision of the WHO General Assembly to consider disaster preparedness as one of the Organization’s 16 Strategic Objectives and the subsequent decision to elevate Health Action in Crises to the Organization’s highest administrative level—a Cluster—only confirms the visionary approach taken by the countries of the Americas more than three decades ago. This area of work is also critical to the advancement of the health agenda in the Americas and the achievement of the Millennium Development Goals. There is no doubt that any major event that impacts a country in this Region has the potential to significantly constrain the entire Organization’s goals and objectives. Disaster risk reduction is not the concern of any one single entity within PAHO but rather it is now a corporate priority. Within the context of this Region, the following strategic plan for a secure and disaster-resilient health sector in the Americas establishes a clear vision and delineates our priorities of reducing disaster risk and mitigating the impact of disasters on the population’s health and well-being, a collective responsibility and commitment of the Pan American Health Organization. Mirta Roses Periago Director, Pan American Health Organization
Jean Luc Poncelet Area Manager, Emergency Preparedness and Disaster Relief

A secure and disaster-resilient health sector in the Americas Strategic Plan 2008 – 2012 of the Pan American Health Organization
ii
Table of Contents
1. Background 1
2. Strategy 3
2.1 Vision 3
2.2 Our strategic objectives 3
2.3 How will we work? 5
2.4 Who will our partners be? 6
2.5 Where will we work? 8
2.6 Who are our intended beneficiaries? 8
3. Situation and Vulnerability Analysis 9
3.1 The Latin American and Caribbean context 9
3.2 Changing profile of hazards and risk 12
3.3 Climate change 13
3.4 International humanitarian reform 13
3.5 Changing profile of member states 13
4. PED Program Strategic Lines of Action 14
4.1 Improving disaster preparedness capacity in the health sector 14
4.2 Protecting health services from the risk of disasters 15
4.3 Supporting countries to respond to disaster events in the health sector 17
4.4 Forging stronger partnerships with national, regional and global partners 18
4.5 Mainstreaming DRR across all our institutional partners 19
5. Structure and Program Management 20
5.1 PAHO corporate commitment to DRR 20
5.2 PED Program staffing and structure 21
5.3 Partnerships for health preparedness 22

A secure and disaster-resilient health sector in the Americas Strategic Plan 2008 – 2012 of the Pan American Health Organization
iii
6. Monitoring and Evaluation 23
6.1 Internal PAHO monitoring and reporting 23
6.2 PED Program monitoring 23
6.3 External evaluations 24
7. Assumptions and risks 25
Annex 1: PAHO/PED Organizational chart 27
Annex 2: List of acronyms 27
1. Background
In 1976, the Member States requested the Pan American Health Organization, regional office for the Americas of the World Health Organization (PAHO/WHO), to establish a Program on Emergency Preparedness and Disaster Relief (PED) to help strengthen the countries’ response capacity to natural disasters through the efficient use of existing resources. Over the last three decades, the scope of this initiative has expanded to include risk reduction and to improve the resilience of the health sector to disasters.
PAHO/WHO recognizes that disaster prevention, risk reduction, preparedness and
recovery form parts of a continuum of activities and that most often these phases overlap. In fact, the only moment that is clearly defined in time is the moment in which a disaster occurs, shifting the continuum from preparedness into response (and subsequently recovery) mode.
Within this framework, and in the current planning cycle, the range of technical
cooperation activities has expanded to encompass an ‘all- hazards’ approach. Examples include the methanol intoxication in Nicaragua (2006), the multisectoral crises due to hemorrhagic dengue and yellow fever in Paraguay (2006/2008), the population displacement in Colombia (ongoing), the incidents of civil strife in Bolivia (2007) and the demands to prepare for phases 5 and 6 of pandemic influenza. The health issues stemming from these emergencies are now becoming an important part of national public agendas as a priority of many governments.
This trend will continue, perhaps at a faster pace, as the public’s expectations of the
state’s ability to respond and even prevent all type of disasters increases. This reality, coupled with expectations on the part of the international community that countries will have institutions capable of handling all aspects of disaster management, even in mega-events on the scale of the Asian tsunami, requires the Organization to re-position itself. New challenges such as climate change are emerging, which will require us to re-assess the risks to public health and levels of vulnerability of populations in the Region over the next five years and beyond.
The countries of Latin America and the Caribbean have made considerable progress
in reducing the health impact of major emergencies and disasters. Many ministries of health have a stable disaster preparedness and response unit or office with responsibility for covering all types of disasters (multi-hazard), and in most countries, they can count on strong political support. They have a permanent structure as well as a minimal full-time professional staff and a defined (although insufficient) budget. In the hierarchy of the

A secure and disaster-resilient health sector in the Americas Strategic Plan 2008 – 2012 of the Pan American Health Organization
2
ministry, they have access to the highest level of decision making and clearly reach out to other sectors.1
Although national level disaster preparedness is relatively well-advanced in the
Americas, historically our work has tended to progress in isolation from initiatives in other regions of the world. The last five years has shown us that more and more institutional players are becoming active in the health preparedness and risk reduction field and that we can no longer be an ‘island’, separated from the broader international health community. During the next strategic period, the Organization must take into account this new situation and look more systematically at initiatives taking place in other parts of the world. We will also continue to focus on new and innovative areas to which this Region and the Organization can contribute, as part of global efforts to improve risk reduction in the health sector.
In response to the evolving regional scenario and drawing on lessons gleaned from past experiences, this Strategic Plan addresses two broad aspects of institutional disaster management. The first relates to aspects of disaster risk reduction,2 the developmental aspects of our technical cooperation, which involve both day-to-day and long-term activities. The second is related to the humanitarian response side of technical cooperation, which requires lean, fast, and flexible mechanisms for short-term but highly effective measures. We recognize that the Organization must engage in both modes of operation to fulfill its mandate.
This 2008-2012 Strategic Plan for the Area on Emergency Preparedness and Disaster
Relief coincides and is in line with PAHO/WHO’s organization-wide Strategic Plan 2008-2012 (approved by Member States in October 2007). The PAHO/WHO strategic plan reflects an even greater level of commitment to disaster risk reduction. This enhanced corporate involvement has been due, in part, to WHO’s establishment of a high-level strategic objective. 3 This commitment must now become a collective responsibility of many technical divisions and country office programs. We must also focus on this Region’s unique challenges and opportunities. These enable us to move beyond a common set of objectives and to continue building country capacities in accordance with the commitments and requests of the member states in benefit of the most vulnerable populations.
The objective of this document is to define PAHO/WHO’s corporate strategy for
delivering effective technical cooperation to enable the health sector in the countries of Latin America and the Caribbean to reduce risk, prepare for and respond to disasters and emergencies, while at the same time creating a body of knowledge and lines of action that benefit the health sector beyond the Americas.
1 Progress Report on National and Regional Health Disaster Preparedness and Response presented to the Pan American Health Organization, 47th Directing Council., September 2006. 2 For PAHO, “disaster risk reduction” refers to actions aimed at reducing the hazard, the vulnerability or both. It encompasses prevention and mitigation. ‘Disaster management’ covers the full range of interventions: prevention, preparedness, mitigation, response, recovery and reconstruction. Although this is not the ISDR definition, PAHO uses disaster risk reduction in this sense due to the characteristics of its clients. 3 Strategic Objective 5 (SO5): ‘To reduce the health consequences of emergencies, disasters, crises and conflicts and minimize their social and economic impact’; Strategic Plan 2008-2012, October 2007.
A secure and disaster-resilient health sector in the Americas Strategic Plan 2008 – 2012 of the Pan American Health Organization
3
2. Strategy 2.1 Vision
Natural and other man-made events will always occur and we will never be able to prevent them from happening completely. But there is much that can be done to reduce the risk and to better prepare for disaster events to limit the impact on the population’s health, especially the poorest and most vulnerable. It is also our duty to our member states to be as well prepared as possible to respond to any event, be it a localized emergency or a multi-country ‘mega-disaster’. Our long-term vision for Latin America and the Caribbean is therefore of a future when there is adequate, nationally-led and sustained capacity to reduce disaster risk in the health sector, both to prevent damage to infrastructure and service delivery and to provide a timely and effective response to disasters. To achieve this vision, PED will maintain its cooperation in the traditional areas of disaster preparedness, mitigation and response, which form the core pillars of our programming. We will continue to approach everything we do with the constant and underlying aim of supporting our member states and their health sectors. However, developments in the international humanitarian framework and the regional context of operations as well as evolving risks outlined above require new initiatives and ways of working to meet the challenges of this coming five year plan.
2.2 Our strategic objectives
a. Improving disaster preparedness capacity in the health sector We will strive to support our national partners in developing a well-prepared health sector disaster program with leadership, credibility and coordinating authority within the national context, which encourages the engagement and participation of a wide variety of partners, such as NGOs and the private sector. To achieve this, we will contribute to building national preparedness through a range of interventions and approaches including: advocacy and technical support for updating and improving sector policy and legislation; continuous training of new partner organization staff as well as personnel of Ministries of Health; the provision of scientific information to inform preparedness; support for improved plans and procedures; and the provision of targeted financial and human resources to improve preparedness and the facilitation of partnerships. b. Protecting health services from the risk of disasters We will work toward improving the safety of health services. These measures will focus on ensuring the functional continuity of health service delivery during and following a specific event; it also will seek to better protect health personnel, equipment, infrastructure and non-structural assets from the impact of disasters. It is essential that health services, buildings and physical facilities are better protected from locally relevant hazards. We include here the full range of health services, from
A secure and disaster-resilient health sector in the Americas Strategic Plan 2008 – 2012 of the Pan American Health Organization
4
large complex hospitals in urban centers to small, single-room health posts serving dispersed rural communities. Our focus is always on the continuity of service, including in instances of outbreaks of disease or epidemics, rather than solely on infrastructure. We will provide expert technical support and develop new tools for assessing risk and to better train the health workforce. We will also work with our major development partners in the Region to encourage greater investment in mitigation. We will actively lobby at global level for the promotion of the World Disaster Reduction Campaign “Hospitals Safe from Disasters.” c. Supporting countries to respond to disaster events in the health sector Our mission is to strengthen national capacity to respond to all types of emergencies and disasters that have public health consequences—whether natural, manmade (including acts of terrorism and/or conflict) or technological in nature. PAHO is a development agency, not a humanitarian agency that distributes supplies. However, in emergency situations we must be ready to respond quickly and comprehensively and be able to operate using procedures similar to humanitarian agencies. We will continue to support our member states by ensuring their effectiveness and readiness as first line responders to any emergency situation. We will also seek to improve our own readiness to respond by investing in systems and capacities to take direct action in situations where national capacity is overwhelmed. We will ensure that PAHO/WHO is capable to lead the health cluster for the Western Hemisphere when called upon. d. Forging stronger relationships with our national, regional and global partners Over the last decade, humanitarian response to disasters has become a growth industry, with many new actors entering the field or old ones renewing and strengthening their involvement. The time when PAHO was the only international health actor in the Region in the aftermath of disasters is past. Member countries now have a greater number of partners in the health sector, and international organizations are developing new approaches and initiatives all the time. We must develop and deepen our partnerships, both within the Region and globally, to learn more effectively and contribute to the Region’s own valuable experiences and lessons. Today more than ever, PAHO must clearly demonstrate its value added and must reach out to be part of the global network of multisectoral actors in disaster risk management. We will achieve this by increasing our collaboration with partners within and outside the health sector, and by establishing new communication mechanisms and networks with governments, donors, civil society groups and other UN Agencies. We will move away from direct delivery of services and towards a more brokering or facilitating role in support of our member states. e. Mainstreaming health disaster risk reduction across all our institutional
partners There is now a growing recognition that disaster risk reduction is a development concern, and should not be seen only in the context of a humanitarian response to an

A secure and disaster-resilient health sector in the Americas Strategic Plan 2008 – 2012 of the Pan American Health Organization
5
emergency. To have truly sustained impact at scale, we must advocate for the integration of elements of risk reduction that address health concerns across the day-to-day activities of both our own organization and those of our partners. We will approach the objective of mainstreaming by improving our internal and external communication strategies and by promoting common language and clear concepts about disaster risk reduction as primarily a development concern. We will strive to elevate the disaster risk reduction agenda to the highest levels of the Public Health Forum by developing technical and operational capacities across PAHO/WHO in support of countries in crises. We will use our technical expertise and leverage to influence the thinking of our major partners, both Ministries of Health and others at national and regional levels, to better address risk reduction and to ensure that risk reduction principles and activities form part of and support other health initiatives such as primary health care, patient safety, workers’ health and other efforts that contribute to the Millennium Development Goals.4 f. Changing attitudes and behaviors surrounding emergencies and disasters Misperceptions and inaccurate information abound with regard to the public health impact and management of emergency and disaster situations and have been major factors leading to inefficient and ineffective post-disaster actions that have diverted time as well as human and financial resources away from areas for which they were most needed. In the past, PAHO/WHO has worked to educate health decision makers and the public about what is and what is not appropriate international health relief assistance, what is involved in the management of dead bodies, or how disasters can affect communicable disease patterns. We will continue to work with organizations and agencies as well as the media to replace common disaster myths with authoritative health information. By helping to change how people react to and behave in disasters and by improving the public’s overall understanding of the health impact of these events, we hope to contribute to building disaster-resilient communities.
2.3 How will we work?
Each member country has different needs and varying capacities and levels of resources available to its respective health sector. As a consequence, we recognize that there is no one blueprint way of working that can be applied to all country contexts. We also must work with our regional and international partners, which will require yet other ways of working. In order to meet these demands and to achieve our strategic objectives, we will select from a range of functional approaches, which can be grouped into the following categories:
a. technical support: much of our core business is aimed at training and capacity building of national level partners, with a focus on government Ministries of Health. We will continue to support our public sector partners, but increasingly reach out
4 Indeed, it would be difficult if not impossible for any major health initiative to reach its goal if dramatically affected by a disaster.
A secure and disaster-resilient health sector in the Americas Strategic Plan 2008 – 2012 of the Pan American Health Organization
6
through programs of technical support and advisory services to new partners, including civil society networks and the private sector; b. advocacy: we are mindful that we cannot achieve our objectives on our own, especially when these rely on changing underlying policy, legislation and investment decision-making processes. Therefore, we will proactively lobby key development partners such as the International Financing Institutions and Ministries of Planning and Finance, and others to promote disaster management at all levels;
c. information and knowledge management: based on many years of experience, we know that information is a powerful, relatively inexpensive and indispensable tool for decision making by all actors. We will continue to conduct, learn from and share the results of post-disaster lessons learned exercises and produce authoritative information on health issues, both in developmental and emergency situations. We will continue to set regional standards through guidelines and publications and to develop new and innovative mechanisms for dissemination, making appropriate use of evolving technologies;
d. facilitation and coordination: we recognize the increasing importance of partnerships in the health sector and the need for strong coordination, particularly in the fast-moving humanitarian response context. We will use our extensive networks and access to key decision-making fora in the Region to contribute to coordination efforts. Our leading role in the U.N. health Cluster will be instrumental in this effort;
e. direct action: in situations where there is the need for direct intervention (situations that exceed the local capacity to respond), the PED program will continue to be involved in providing services on the ground, both through our regular staff based in headquarters and sub-regional offices as well as through our specialist response teams. Although we may intervene directly in such cases, we will always work in support of our member states and relevant health authorities. Our focus will be on the crisis management aspects of all hazards, while the Organization’s other subject matter experts will aid with the technical aspects.
2.4 Who will our partners be?
PAHO has a core mandate to support and provide services to member states in the health sector. As such the PED program has historically focused on key government partners, most notably the ministries of health in the Region. This will continue to be the case, but in addition we will seek to expand partnerships and collaboration over the coming five years to include a broader range of actors in the health sector as well as those outside the sector, who nonetheless are critical for achieving our strategic objectives. Health sector partners
PAHO country offices: through our network of disaster focal points, but also
working across all relevant technical departments, such as communicable diseases, health services, mental health and environmental health;

A secure and disaster-resilient health sector in the Americas Strategic Plan 2008 – 2012 of the Pan American Health Organization
7
Ministries of Health: supporting the Disaster Management Programs or Units within ministries, but also providing training and technical support to other departments dealing with preparedness and rapid response at both central and decentralized levels, including the national focal points for International Health Regulations (IHR) and other subject matter experts;
NGOs and civil society networks: we will make increasing efforts to engage with and provide support to civil society organizations that are active in the health sector, both at national and regional levels;
Other health providers sharing common strategic objectives: social security, security forces and private providers operate in all countries, either formally or informally; in a number of countries they are legislated to provide services. We must work harder to reach them and advocate for them to make greater efforts to address disaster risk as in many countries they are the most important health care providers;
International organizations: we will continue to collaborate with agencies that are important players in the health sector, such as the International Federation of the Red Cross and Red Crescent Societies, UNICEF, and others.
Other partners
Ministries of finance and planning: we will continue to engage key ministries
as part of our efforts to integrate risk management into the everyday business of government, especially to improve investment in mitigation measures;
Police, civil defense and military forces: we recognize the critical role that these forces play, particularly in rapid response, and will continue to provide training and technical support;
Media and journalist networks: the way in which disaster events are portrayed to the public is increasingly important and the media has a key role in presenting a balanced view of the importance of risk reduction. We will make new efforts to engage with the media and provide technical information and orientation;
Universities and other research centers: we already collaborate with a range of academic institutions, particularly in the area of information management; these efforts will continue with an increasing shift in the development and dissemination of technical information from regional to country level. We will seek out new partners, such as meteorological offices, to be better informed about the likely impact of climate change;
International financial institutions: we will build on our existing relationships with the main IFIs, including the World Bank and the Regional Development Banks and look to establish more structured and systematic relationships to improve our advocacy work. Our close working relations with ISDR will facilitate this process;
National and regional disaster management coordination bodies: PAHO was instrumental in the creation of CDERA, CEPREDENAC and CAPRADE and we will continue to play a prominent role in these important sub-regional disaster reduction mechanisms. We will continue in our privileged role as coordinator of the disaster preparedness and response working group of the Organization of American States;
International humanitarian agencies: we are part of a broader network of humanitarian agencies and will continue to work with UN agencies, international
A secure and disaster-resilient health sector in the Americas Strategic Plan 2008 – 2012 of the Pan American Health Organization
8
NGOs and the Red Cross National Societies and the IFRC, both during emergency response and on a regular basis. When called upon, we will act as the health sector Cluster lead within the framework of the IASC coordination system.
2.5 Where will we work?
PAHO is responsible for providing services in support of the health sector to all member countries in the Region. As such, the PED program will continue to work in all sub-regions. However, we recognize that individual countries have differing capacities and needs and that they may require different types of technical support for a number of reasons, including underlying health indicators, development of the health sector and level of vulnerability to hazards. There may also be priorities based on underlying structural or political problems. Specific populations may also be at higher risk, for example, indigenous groups that make up significant minorities in certain countries. Therefore, we will continue to provide a base level of support and engagement in all member countries, including maintaining a response capacity in all parts of the Region. We will focus additional attention and resources on a number of priority countries identified on the basis of their high exposure to hazards, high vulnerability to disasters, high levels of poverty and lower levels of preparedness. These are countries that the Organization has also identified as priority countries based on current health indicators: Bolivia, Guyana, Haiti, Honduras and Nicaragua. PAHO will also work closely with countries that have been particularly successful in disaster management in the health sector, in order to enhance their capacity to share experiences and experts before, during and after disasters.
2.6 Who are our intended beneficiaries?
The disaster management programs of national health authorities (ministries of health) and other health sector institutions will continue to be our main target in the coming strategic plan period. We will target our assistance both at central or national level and at sub-national levels where appropriate. The extent to which we target our assistance to sub-national entities will be determined on a case-by-case basis, depending on capacity and progress toward decentralization in each country. Given the connections between health and social and economic factors such as income, education, housing, labor, and social status, we will place emphasis on the most vulnerable populations in both urban and rural areas. Special consideration will be given to the identification of and support to socially excluded groups, such as marginalized indigenous populations, displaced people and low income families, among others, in areas that are more likely to be affected by disasters. We will identify these vulnerable and marginalized groups in consultation with central government authorities, ministries of health and other partners who may represent the special interests of these populations, such as NGOs and civil society organizations, stressing the importance of respect for intercultural beliefs and the
A secure and disaster-resilient health sector in the Americas Strategic Plan 2008 – 2012 of the Pan American Health Organization
9
incorporation of human rights-based perspectives into all activities and program implementation Given that disasters impact women and men differently, special attention will be given to gender issues during the implementation of this strategic plan. Gender equality mandates have emanated from global and inter-American conferences, where governments committed to promoting gender equality in the formulation of all public policies and programs. Responding to the these mandates and in line with this long standing commitment, PAHO’s Directing Council adopted a Gender Equality Policy in September 2005 that applies to all facets of its work. The policy calls for including gender-sensitive focus and analysis in all aspects of technical cooperation, development of national policy frameworks and management of human resources. PED will develop a stronger commitment to collect and analyze humanitarian data disaggregated by age and gender. This will be achieved through development of forms that include this variable and including this requirement in all training of disaster experts on needs assessments (Regional Health Disaster Response Team, national counterparts, etc.). We will also promote gender in health issues with our partners and in the development of our technical information.
3. Situation and Vulnerability Analysis 3.1 The Latin America and Caribbean context
Latin America and Caribbean countries are extremely vulnerable to a wide variety of natural hazards Each year, an average of 130 natural disasters of varying degrees of magnitude occurs in the Region. In the period 2001-2005, the impact of these destructive phenomena left a death toll of some 20,000, and 28 million victims.5 Although it is becoming increasingly more difficult to pinpoint with precision how exposed the population is to these threats, it is widely estimated that 73% of the population and 67% of health clinics and hospitals in 19 countries6 in the Region are located in high risk areas.7 Natural and man-made disasters also have a devastating impact on countries’ economies. In 2005 alone, hurricanes were responsible for more than US$ 205 billion in losses, with 7 million people affected in the Region of the Americas8. Damage to the small countries and economies of Central America and the Caribbean was estimated at more than US$ 2.22 billion, revealing their vulnerability and the need for
5 Health in the Americas 2007, Regional Volume. Coping with Disasters. Pan American Health Organization. 6 The countries included are: Anguilla, Argentina, the Bahamas, Belize, Chile, Colombia, Costa Rica, the Dominican Republic, Ecuador, El Salvador, French Guiana, Guadeloupe, Guatemala, Guyana, Haiti, Honduras, Martinique, Nicaragua, and the Turks and Caicos Islands. 7 Source: Survey on the Health Sector State of Preparedness and Mitigation to Disasters, prepared by the Area on Emergency Preparedness and Disaster Relief – March to July 2006. 8 Preliminary Overview of the Economies of Latin America and the Caribbean. Economic Commission for Latin America and the Caribbean (ECLAC): Santiago de Chile, 2005.

A secure and disaster-resilient health sector in the Americas Strategic Plan 2008 – 2012 of the Pan American Health Organization
10
prevention and mitigation plans and measures. In Grenada alone, economic losses from Hurricane Ivan (2004) represented 253% of the country’s GDP.9
The vulnerability of urban populations is growing fast and rural people remain at risk
Disparate socio-economic development drives people to migrate from rural to urban areas or to emigrate in search of jobs and a better life. Overall, the urban population in Latin America and the Caribbean grew from 65 to 78% between 1980 and 2005; the rate of growth was less in Central America and the Spanish-speaking Caribbean and Haiti. The uncontrolled growth of urban areas in the Region is a matter of urgent concern. In most cases, urbanization is not accompanied by a well designed development plan and in some cases with a complete lack thereof. In the 1950s, only two cities had more than 10 million people. Today, more than 20 cities meet this criterion and most are in poor countries. As urbanization continues, much of it poorly planned, the vulnerability of urban populations is of increasing concern. Higher population density and more complex physical infrastructure have the potential for a greater disaster impact, while at the same time, urban populations often have a poor understanding of their vulnerability. Rural areas also suffer from ongoing problems of poverty, limited resources, and a lack of access to health services and environmental degradation. Latin America and the Caribbean is often considered as a middle-income region, but much of its population still lives in extreme poverty After years of stagnation, economic growth in Latin America and the Caribbean has resumed. Notwithstanding, there is an enormous gap in income distribution in the Region (measured by the Gini coefficient) 10 and this gap has not closed to any degree between 1990 (Gini of 0.383) and 2002 (Gini of 0.403). These inequalities result in poverty and their intensity is exacerbated in vulnerable segments of the population such as households headed by women, certain ethnic groups, rural populations or migrant communities. An estimated 41% of the population in Latin America and the Caribbean is poor and 17% is indigent.11 Economic disparity has caused pockets of extreme poverty that, in certain circumstances, may breed violence in the aftermath of natural disasters (looting, theft, domestic violence, etc.). Despite past progress, the Region suffers from a lack of trained human resources
Despite all the effort put into disaster management training over the past years in the health sector, there continues to be a lack of human resources. Where staff has been trained, it is often difficult to track individuals due to high levels of turnover in the civil service, particularly following political change in governments. Wholesale turnover following elections and other management changes can be a very significant constraint to building sustained human resource capacity within ministries. Hence, new health personnel and other key actors need to be continuously trained to ensure they are in place and available when needed for the development of activities involving mitigation, preparedness and response.
9 Economic Damages: Share of GDP, by Natural Disaster and Country (2005), International Strategy for Disaster Reduction. www.unisdr.org/disaster-statistics/top50.htm. 10 The Gini coefficient measures the inequality of income distribution or inequality of wealth distribution. 11 Data from the Strategic Plan of the Pan American Health Organization 2008-2012.

A secure and disaster-resilient health sector in the Americas Strategic Plan 2008 – 2012 of the Pan American Health Organization
11
In some Caribbean countries with small populations and limited government capacity, it is common for one person to have to perform a range of different duties with multiple responsibilities. In such cases, where there is insufficient staffing and budget, it is unreasonable to expect the designation of a full-time disaster manager in the health services.
Vulnerability to disasters constrains development efforts and reinforces poverty Vulnerability to disasters is a significant constraining factor to the achievement of the Millennium Development Goals (MDG) in the Region. Exposure to disasters increases the vulnerability of the poor, deepening their poverty and preventing them from taking advantage of economic opportunities, thereby reinforcing their poverty in a downward spiral. As well as impacting individuals and households through the destruction or loss of assets, disasters can have a devastating impact on macro-economic performance and can set back development gains by decades. For example, the devastation caused by Hurricane Mitch in Central America in 1998 resulted in US$ 58 million of damage in Honduras alone; this equated to the loss or disruption of access to drinking water for 75% of the population, or approximately 4.5 million people.12 But even developed countries are not immune. Hurricane Katrina was the most destructive natural disaster in U.S. history. The overall destruction wrought by Hurricane Katrina, which was both a large and powerful hurricane as well as a catastrophic flood, vastly exceeded that of any other previous US major disaster. Estimates vary but, considering property damage alone, Hurricane Katrina is America’s most costly disaster—natural or man-made—with a price tag that approached the $100 billion mark.13 PAHO’s disaster risk management activities are designed to contribute to human well-being, minimizing the negative effect of disasters and maintaining achievements in public health by responding to the health needs of vulnerable populations affected by such events.
Conflict and insecurity are a significant issue in some parts of the region Social and economic inequalities and poverty are known factors that contribute to internal conflicts and civil strife and have a direct impact on the health of the population. Despite the relatively stable situation of the Region, a number of internal conflicts that caused significant internal population displacement have created new challenges for the health sector. These events may increase over the next five years.
As well as the conventional notion of insecurity and the threat of violent conflict, we are seeing a new development in terms of the collective fear of pandemic outbreaks of communicable diseases, which are now perceived as ‘national emergencies’ and as significant threats to security in a broader sense.
12 Global Water Supply and Sanitation Assessment 2000 Report; WHO 13 “The Federal Response to Hurricane Katrina: Lessons Learned.” Online at www.whitehouse.gov/reports/katrina-lessons-learned.pdf

A secure and disaster-resilient health sector in the Americas Strategic Plan 2008 – 2012 of the Pan American Health Organization
12
There is an increasingly crowded field of actors working in health emergencies in the Region
In past decades, PAHO was one of the very few, if only truly international organization working in health emergencies and humanitarian response. This situation has changed dramatically, with Hurricane Mitch perhaps marking the threshold into a new era, characterized by a proliferation of actors in disaster preparedness and response. These include an expanded UN system, international NGOs, the Red Cross and Red Crescent movement and increasingly active bilateral donors. The effective coordination of so many agencies is becoming a major challenge, especially at the interface between the international community and national government authorities; competition for funding is progressively increasing. We must adapt to this changing operational environment and provide effective leadership and coordination in our core technical discipline.
3.2 Changing profile of hazards and risk
Although natural hazards remain the most common threat to countries in the Region, we will face new and more challenging hazards emerging in the coming years. In the last few years, for the first time governments declared national emergencies for previously unrecognized reasons such as the ethanol intoxication in Nicaragua, ethylene glycol in Panama, SARS in Canada or dengue in Paraguay. These emergency situations had the potential to overwhelm national health services and presented challenges in areas such as clinical management, information and communications. The emerging threat of pandemic influenza in 1997 and later in 2003 revealed that epidemics do not constitute a sufficiently important part of national disaster plans. Despite recent planning, the health sector is still inadequately prepared to face this type of threat. Another very significant change is the public’s perception of these situations. Diseases such as dengue, which were until recently considered only as a medical issue, are increasingly viewed through the same lens as bioterrorism or pandemic flu: they cause fear and are increasingly seen as a threat to security, the economy, tourism or other non-health areas. Therefore, perhaps the strongest contribution a disaster management expert can make is to assist society, during phase 5 and 6 of a potential pandemic, to use all available resources to reduce, to the extent possible, the impact on health. This coincides with our definition of coordination.
Exposure to toxic chemicals is a serious public health problem in the Region. The volume and variety of these substances has increased, and WHO estimates that per capita exposure to some, such as pesticides, is two times higher than the global average. Although improving, the reporting of morbidity and mortality from acute and chronic poisoning does not reflect the magnitude of the problem.
Technological hazards pose significant potential risks for countries that have reached a certain level of industrial development. Little has been done in terms of regulation and prevention, and the health sector is poorly prepared to face a large-scale chemical, radiological or other technological disaster. This risk will most probably increase in tandem with economic development and the globalization of trade.
A secure and disaster-resilient health sector in the Americas Strategic Plan 2008 – 2012 of the Pan American Health Organization
13
3.3 Climate change
Climate change has implications for disaster risk management, as it impacts the exposure to hydro-meteorological hazards such as storms, floods and drought and also modulates underlying risk factors, which influence the vulnerability to environmental hazards and therefore the probability of disaster occurring.14 The effects of climate change—direct or indirect—also have an impact on disease vector distribution and subsequent changes in the distribution of infectious diseases. Planning for improved disaster risk reduction must recognize that climate change alters the magnitude and frequency of extreme events and that we can no longer rely solely on historical patterns of hazard and risk profiles. Response mechanisms and economic planning for disasters therefore must take these new variables into account.
Disaster response planning must engage in a much more proactive way with the meteorological sector to factor in local and global environmental issues that change risk patterns and increase vulnerability. In Guyana, for instance, the government has begun discussing the relocation of the capital further inland to cope with anticipated rising sea levels due to global warming. The capital, Georgetown, is below sea level and regularly floods after heavy rains or storms.
3.4 International humanitarian reform
The UN Inter-Agency Standing Committee (IASC) is the primary mechanism for inter-agency coordination of humanitarian assistance. The IASC, composed of UN and other humanitarian agencies, has changed the way in which humanitarian assistance is coordinated and delivered. Assistance is now organized around nine clusters, each of which is responsible for all activities related to its topic, regardless of whether the government, an NGO or a UN agency is implementing them.
PAHO/WHO is the recognized leader for the health Cluster in the Americas. Within PAHO, the PED program is the liaison office for OCHA and all other humanitarian actors and remains the focal point for the humanitarian reform initiatives.
The responsibilities of the health Cluster leader in cases involving a large international response are complex and far-reaching and require certain skills that not all PAHO staff have. In these situations, the Director will assign a senior disaster specialist whose functions will be to exclusively ensure independent coordination. While giving a key role to government/local authorities, PAHO will focus specifically on the Cluster responsibility in health coordination, but will ensure that the Organization’s public health subject matter experts actively collaborate in other Clusters, such as nutrition and water and sanitation, without which health interventions would fail or be seriously compromised.
3.5 Changing profile of member states
Several countries such as Argentina, Brazil, Chile, Cuba, Mexico and Venezuela, are increasingly developing their external cooperation strategies, offering human and
14 Sperling F., Szekely F. Disaster Risk Management in a Changing Climate, May 2005.
A secure and disaster-resilient health sector in the Americas Strategic Plan 2008 – 2012 of the Pan American Health Organization
14
other resources during emergencies. These countries are essentially becoming new contributors in the Region and are taking on some aspects of more traditional donors. However, this is an evolving process and these countries are still in the early stages of learning how to function as a provider of assistance; it is likely to be some time in the future (five years or more), before these countries move to direct large-scale funding possibilities.
PAHO has many years of experience in interacting with international donors and as the interface between international assistance and national government recipients; we will therefore support the process of the changing role of these emerging regional donor countries through engagement with both national health authorities and Ministries of Foreign Affairs.
4. PED Program Strategic Lines of Action
4.1 Improving disaster preparedness capacity in the health sector
‘A health sector disaster program with the leadership, credibility and coordinating authority within the national context, which also integrates the participation of a wide range of partners, including NGOs and private sector operators.’ Although emergency preparedness is an important pillar of PAHO’s technical cooperation and a prerequisite for effective emergency response, the issue continues to be ‘politely’ overlooked by the international community and on national political agendas. PAHO is in a unique position to continue to promote the need for a strong national disaster program in Ministries of Health, including staff and a funded work plan that serves as the nation’s centerpiece for all health issues related to disasters. In order to protect what has already been achieved and to maintain a strong institutional “disaster” memory (which can be easily lost due to high staff turnover), the strengthening of the health disaster programs will remain our strategic priority. We will accomplish this by continuously lobbying to maintain these offices, provide adequate budget and staff, allow access to the Ministry’s highest decision making level and providing access to the most up-to-date training opportunities and information.
Over the next five years we also will reach out beyond our core constituency of the Ministries of Health and make a concerted effort to engage with and support other health players, such as NGOs and private sector operators. We will make technical information and some training available to them and provide coordination and facilitation services to improve communication and learning both across these groups and with government health authorities. We will adopt the following lines of action:
Strengthen health disaster programs in Ministries of Health: increase the focus
on multi-hazards and previously un-addressed risks such as chemical accidents and pandemic influenza; develop scientific linkages to better understand the potential impacts of climate change on both disaster risk and health; promote the
A secure and disaster-resilient health sector in the Americas Strategic Plan 2008 – 2012 of the Pan American Health Organization
15
adoption of benchmarks to demonstrate institutional commitment to DRR; assist member countries to better monitor and evaluate progress; support drills and simulations and improve response to mass casualty events;
Improve partnerships for disaster preparedness: enhance the Ministries of Health leadership roles at national level by improving coordination within the health sector and with other sectors (i.e., reviewing and testing plans); contribute to improving international humanitarian assistance focusing on health;
Support continued training efforts: develop the management and technical skills of health professionals by ensuring access to specialized training; develop a web based tool, freely accessible and containing an inventory of available training opportunities in health disaster management; incident management systems, etc.;
Provide authoritative technical information and publications: develop new and innovative methodological designs and guidelines; prepare and disseminate training tools and information products that are specifically adapted to country/target audience needs; improve access to sources of technical information through both conventional and digital means.
4.2 Protecting health services from the risk of disasters
‘Better protected health services – including staff, management systems, equipment, assets and physical infrastructure - that are safe and remain functional during and after a disaster event’ The devastating effects of natural hazards are not due exclusively to nature. They are also due to failures in the development process, resulting from the lack of consideration of the impact of existing natural hazards. In other words, a disaster could potentially be avoided if all necessary measures were taken to ensure that whatever is planned, designed, built or maintained is done in such a way so as to ensure that it can continue to function following high-intensity events.
Evidence has shown that the cost of building a new disaster-safe hospital or health facility is negligible when measures are included in early design considerations. For the vast majority of new health facilities, incorporating comprehensive disaster protection from earthquake and weather events into designs from the beginning will only add up to 4% to the cost.15 Public health professionals have the scientific and institutional responsibility to ensure that all health development projects are “hazard-proof.” Although the health sector has successfully instilled the concept that “prevention is better than cure,” much remains to be done to ensure that this applies to disaster risk reduction.
The concept of reducing vulnerability is appealing, but to achieve this requires that all levels of the Organization look at new ways of delivering technical cooperation that are safe from disasters. Because the scope of this task is vast and the resources
15 Protecting New Health Facilities from Disasters: Guidelines for the Promotion of Disaster Mitigation, Washington D.C., PAHO/WHO 2003.
A secure and disaster-resilient health sector in the Americas Strategic Plan 2008 – 2012 of the Pan American Health Organization
16
of the Organization and the member countries are limited, it is recommended that PAHO concentrate its efforts on the initiative “Hospitals Safe from Disasters”; the target identified by its 2004 Directing Council and endorsed by 168 countries at the 2005 World Conference on Disaster Reduction (Kobe, Hyogo, Japan, 2005). The hospitals safe from disasters initiative focuses on a specific, easy to identify target that is simple to measure, visible and multisectoral in nature. To transform the theoretical concept of health sector risk reduction into practice, health disaster coordinators, ministers of health and other health professionals have agreed to concentrate on making all new hospitals and other health care systems disaster-resilient, as an indicator of progress in risk reduction.
WHO and International Strategy for Disaster Reduction, with the support of the World Bank and technical assistance from PAHO, have jointly launched a two-year (2008-2009) World Disaster Reduction Campaign whose theme is “Hospitals Safe from Disasters.” We will have a full-time staff member working on this initiative and will continue collaborating with the ISDR in this endeavor. To achieve this goal we will adopt the following actions:
provide technical support to member countries: to identify and develop
Hospitals Safe from Disasters as a national policy; technical cooperation for the development of a national disaster mitigation program; develop and promote new tools (such as the hospital safety index, an inventory of safe hospitals, and multimedia training tools) that help countries to identify risk; assist countries to adapt and apply national benchmarks for risk reduction in the health sector in order to measure, monitor, and report on progress toward reaching the goals of the Hyogo Framework for Action;
support the development of human resources and networks: expand the Region’s human resources base for disaster risk reduction; strengthen and render operational a regional network of technical experts in disaster mitigation, the DiMAG – Disaster Mitigation Advisory Group - and other new networks for chemical and radio-nuclear emergencies, making their services available to any region of the world; support and develop training initiatives in disaster mitigation, such as a course that leads to certification in disaster mitigation;
facilitate partnerships and coordinate: strengthening partnerships with scientific and technical institutions and professional associations to facilitate access to the latest scientific knowledge by health professionals; spearhead a regional initiative to make hospitals safe from disasters; establish an inter-regional mechanism (at global level) for mutual exchange of successful experiences in disaster risk reduction in the health sector;
advocate for safer health services: promote integration of health disaster mitigation measures into the regular procedures of financial institutions, mainly in investment loans and grants (World Bank, Inter-American Development Bank, Economic Commission for Latin America and the Caribbean, Caribbean Development Bank, Andean Finance Corporation, etc.); lobby for recognition of the issue of disaster risk reduction in the health sector; actively promote activities within the scope of the World Disaster Reduction Campaign “Hospitals Safe from Disasters” at country level.

A secure and disaster-resilient health sector in the Americas Strategic Plan 2008 – 2012 of the Pan American Health Organization
17
4.3 Supporting countries to respond to disaster events in the health sector
‘A health sector disaster program with the capacity to respond quickly and effectively to events, with the guarantee of timely and appropriate regional support in cases when national capacity is overwhelmed ’
PAHO’s primary mandate in disaster situations focuses on national and international coordination, the quick and independent assessment of health needs and the immediate provision of specialized public health advice. In certain cases, the Organization implements public health projects that no other agency or institution is in a position to do, providing support to other areas in PAHO/WHO whose subject matter experts are better positioned to take the lead. The Organization will also forge alliances with and provide support to various national partners. PAHO/WHO as Cluster lead for the health sector in the Western Hemisphere will ensure that a coordinated response is provided and that the Ministries of Health retain a leading role. PAHO/WHO will coordinate with other UN agencies and it will support countries to make use of the Central Emergency Response Fund (CERF) when necessary.
We will focus on strengthening the Emergency Operations Center (EOC) that has been established at PAHO Headquarters, whose main responsibility is to channel emergency information. The EOC captures and analyzes information and provides it to the Executive Management. It also serves as a physical space to promote communication among all parties active in the response and to facilitate rapid decision making. The speed with which information is received is critical to the task of an EOC. In the event of a major disaster, PAHO will make full use of support available from WHO Geneva, but will give priority to a response team consisting of nationals from the Region.
During the next five years we will promote the Logistics Support System (LSS) for adoption by other humanitarian organizations such as OCHA, with the expectation that other agencies will take the lead in the implementation of LSS in post-disaster situations. The future of LSS will have to be decided at the end of the next five-year period.
For the most part, countries are now self-sufficient in responding to small disasters. Future efforts will focus on dealing with medium-size emergencies, with support from neighboring countries, recognizing that outside support is, and always will be, needed if a major disaster strikes. Sometimes international assistance overshadows national authorities, even when they are able to manage the response. We will always strive to assist and to strengthen our member states’ response capacity. PAHO will assist member states to ensure quick recovery of the population following major disasters. We will work with the World Bank to mainstream preparedness and mitigation measures into health sector reconstruction activities. We will adopt the following lines of action:
facilitation and coordination for improved response capacity: support Member
Countries in mobilizing human and financial resources to address the health impact of disasters; assist countries to coordinate the health response through the establishment of mechanisms such as Emergency Operations Centers; coordinate

A secure and disaster-resilient health sector in the Americas Strategic Plan 2008 – 2012 of the Pan American Health Organization
18
with communicable disease experts in the implementation of the IHR; facilitate decision making at national and international level by providing timely and accurate information on the health impact and priorities; activate and lead the health Cluster as part of the international response when the Cluster approach is implemented by the UN; contribute to WHO global efforts in disaster response by promoting the exchange of experts between the Pan American Health Response Team and other regions; ensure that the health sector impact is reflected in post-disaster socioeconomic assessments conducted by ECLAC and other institutions;
training and building of national capacity to respond: practical and updated tools, guidelines, and technical advice for an authoritative diagnosis of the health situation in the aftermath of disasters; promote the systematic documentation and analysis of the health impact of disasters, including lessons learned exercises;
direct intervention to support a national response: mobilize logistical teams for management of humanitarian supplies and health equipment and a pool of experts in health logistics as part of the Pan American Regional Health Emergency Response Team; promote transparency and efficient management of humanitarian assistance LSS/SUMA and its use by other agencies and countries; deploy the Pan American Health Emergency Response Team in case of disasters and increase the participation of national experts through agreements (MOU) with specialized agencies or institutions; support the organization and set up national response teams; identify members for specialized subsets of the Regional Health Emergency Response Team (mental health, epidemiology, etc); coordinate and execute emergency and recovery projects following the immediate response, by developing a team of qualified project managers.
4.4 Forging stronger partnerships with our national, regional and global partners
‘A well-informed and coordinated network of health sector and other partners at national and international level that share a common vision of nationally-led and sustained capacity to reduce disaster risk.’
For many decades, PAHO has worked in the Americas as one of the few international health sector actors. This situation has changed dramatically in recent years and we now must do more to reach out and work with our international development partners and humanitarian agencies. We will be more proactive in our collaboration with external partners – ranging from regional disaster management bodies, to donors and UN agencies – but we will always be mindful of our underlying mandate, which is to support the national capacity of our Member State health sectors. There must be better and more open communication among all actors to ensure that we do not duplicate efforts, leave gaps in our assistance, or place inappropriate demands on our national partners, who already function with limited resources. One of the first tasks for us will be to clearly communicate our goals and this strategy to our partners. We will rely on existing coordination and collaboration mechanisms, such as the REDLAC (Risk, emergencies and disasters in the LAC region), which comprises key humanitarian players such as OCHA, UNICEF, ISDR, IFRC and international NGOs. We will also work in support of the ISDR work plan. To improve our relationships with partners we will adopt the following lines of action:
A secure and disaster-resilient health sector in the Americas Strategic Plan 2008 – 2012 of the Pan American Health Organization
19
support and facilitate coordination networks: investigate the development of a
thematic platform with partners on health and disasters; actively participate in national, sub-regional and regional fora in the health and disaster management sectors; provide targeted financial support to enable facilitation and coordination efforts;
act as a broker between our national partners and international actors: PAHO will act as broker between other actors and the government; support the mainstreaming of health issues into broader disaster management structures; develop joint plans and incorporate health entities (i.e. health disaster coordinators in the Americas) into the strategic plans of regional and sub-regional disaster institutions (such as CEPREDENAC, CAPRADE and CDERA); incorporate disaster issues into sub-regional health bodies (such as REMSAA, RESSCAP, and CCH); research, develop and negotiate formal agreements with other institutions (universities, NGOs, etc.);
provide technical information and resources: continue to support the Regional Disaster Information Center (CRID) that was developed with the support of PAHO, ISDR, MSF, the IFRC and the Government of Costa Rica; provide new technical information and funding of short-term technical staffing requirements or training in support of networks in the Region.
4.5 Mainstreaming disaster risk reduction across all our institutional partners
‘A national health sector that takes disaster risk into account in all aspects of their planning, design, investment and operational activities, supported by international partners that also recognize the importance of reducing disaster risk in the health sector through developmental and humanitarian assistance. ’
Hazards such as drought, hurricanes and earthquakes occur naturally and may or may not result in a disaster. The potential for a natural hazard to cause a disaster is a function of the magnitude of the event itself, the vulnerability of a population and its coping capacity. Disaster risk reduction is fundamentally about tackling the underlying elements of risk from natural and technological hazards. Its aim is to reduce the vulnerability of individuals, communities and societies, and to build their resilience or capacity to prepare for and withstand the impacts of disasters. Disaster risk reduction seeks to integrate disaster preparedness and hazard mitigation measures into longer-term development. The goal of disaster risk reduction is to ‘disaster-proof’ development processes.
We understand disaster preparedness, risk reduction and response as crosscutting issues that require proper marketing and mainstreaming if they are to be incorporated into all levels and activities. Mainstreaming requires changing how people react to and behave in disasters and improving the public’s overall understanding of the health impact of these events in order build disaster-resilient communities. Mainstreaming also requires repackaging how disasters are conceptualized and presented in order to ensure a comprehensive policy and practical action plans. External communication includes working together with donors and other actors to present common messages to our national health sector partners and to the public.
A secure and disaster-resilient health sector in the Americas Strategic Plan 2008 – 2012 of the Pan American Health Organization
20
We will address the mainstreaming of risk reduction within the health sector both internally by promoting integration across the work of PAHO’s other technical divisions and with our national and international partners. We will work in the following lines of action:
provide technical support to better address risk reduction: develop technical and
operational capacities across PAHO/WHO in support of countries in crisis, particularly for conducting health assessments, mobilizing resources, coordinating health action, providing guidance and monitoring the performance of humanitarian action in relation to the health and nutrition of affected populations;
make available technical information regarding risk reduction: provide targeted information products to different partners to inform decisions regarding development of policy and operational guidelines to better address risk reduction (health disaster management policies, investment and lending criteria, risk assessment criteria);
training and orientation of key decision-makers: continue and expand the PAHO Corporate Capacity Building initiative; orientation of key IFIs and donor staff active in the health sector in the Region regarding preparedness and disaster management priorities.
5. Structure and Program Management
5.1 PAHO corporate commitment to disaster risk reduction
PAHO was the first WHO Region to formally establish a Disaster Preparedness Unit; (Resolution CD24.R10 following the earthquake in Guatemala in 1976). From that time on, the Organization’s commitment to disaster risk management has increased and expanded through a network of sub-regional offices, Country Office Focal Points and disaster focal points in every PAHO area, unit and center.
The strategic plan of the Pan American Health Organization for 2002-2007 named disaster preparedness, mitigation and response as one of its eight priority areas. The Organization’s Strategic Plan for the period 2008 -2012 includes Strategic Objective 5 (SO5): “to reduce the health consequences of emergencies, disasters, crisis and conflicts, and minimize their social and economic impact.”
The high priority PAHO/WHO places on disaster risk management within the Organization is not only reflected by the weight given to disaster activities within the strategic plans, but also by the different resolutions adopted by member states in support of such activities. These include: ‘Disaster-Resilient Health Facilities’ (2007), ‘Disaster Preparedness and Response’ (2004), and a wide variety of Directives issued on the subject. In addition, PAHO helped countries to prepare the Health Agenda for the Americas 2008–2017, launched in Panama in June 2007 by all ministries of health of the Americas. The Health Agenda recognizes disasters as a limiting factor in achieving health sector goals as well as an impediment to the normal functioning

A secure and disaster-resilient health sector in the Americas Strategic Plan 2008 – 2012 of the Pan American Health Organization
21
of health services. The Pan American Health Organization’s 47th Directing Council endorsed this Health Agenda.
Corporate Capacity Building initiative
Whether in normal times or emergency situations, the decision-making process no longer adheres to a strict hierarchy. The process relies on an increasingly complex and fluid network. In emergencies, all PAHO/WHO staff may, at some point, be linked to critical decisions that impact public health, and this requires everyone to have a common understanding of the Organization’s key risk management priorities. In the best interest of both disaster victims and PAHO’s national and regional agenda, it also requires consultation, sharing of information, commitment among all hierarchical levels of the Organization and a consideration of differing perspectives and points of view. Risk reduction is a cross-cutting area of technical cooperation, similar to others in PAHO/WHO. Each technical area within the Organization has its specific responsibilities. PED’s role is to provide technical guidance with and for countries and to PAHO’s other technical divisions and units. PAHO initiated a corporate capacity building initiative in 2007 to harness the Organization’s wide ranging public health expertise and to mainstream disaster management across the Organization. More than 90 high level staff received training on risk management, emergency preparedness and increased their knowledge of the UN Humanitarian Reform. Although administrative procedures regarding disasters are in place, it is still necessary to clarify or define roles and responsibilities of the PAHO/WHO Representatives (PWR) and senior and executive management in the disaster response phase, particularly in relation to the new Cluster approach. We must also further examine particular issues to ensure a more harmonized approach and to maintain our comparative advantage, fill gaps and address hurdles for internal collaboration. Based on positive experiences to date, we will continue with the corporate capacity building initiative in the next strategic planning period as an integral part of our in-house mainstreaming efforts and to communicate the importance of disaster risk management across the Organization.
5.2 PED Program staffing and structure
In order to implement this strategic plan and to contribute to PAHO’s internal mandate, we will work to ensure that each PWR and Area of Work has at least one expected result that contributes to making the health sector safer from disasters. The PED program will continue working from its Regional Office in Washington and its three sub-regional offices (South America – Quito, Ecuador; Central America – Panama City, Panama and Caribbean – Barbados); we will maintain our two special initiatives: the Internally Displaced Persons project in Colombia and the Emergency Preparedness project in Haiti. A functional organizational chart is included as Annex 1.
A secure and disaster-resilient health sector in the Americas Strategic Plan 2008 – 2012 of the Pan American Health Organization
22
The magnitude and the number of disaster management issues facing the countries are increasing constantly. This has resulted in more projects, more short-term, earmarked funding, and more partners and activities, all of which must be handled with the existing PED staff and structure. In order to face these growing responsibilities, PED has reorganized responsibilities in line with the new PAHO strategic planning and organization. We will:
create three Project Coordinators, responsible for identifying expected results,
indicators and milestones for each project, for monitoring progress of plans and outputs and for supporting advisors;
assign new responsibilities and reporting lines for all Sub-regional Advisors who will report to the three Project Coordinators, liaise with PAHO country offices and manage the sub-regional office staff;
have a regional Information and Publications Advisor responsible for the overall strategic direction of all technical information, publications, multimedia, and communications;
assign direct responsibility to the PED Area Manager for oversight of the Sub-regional Advisors and the Project Coordinators.
To better respond to disasters, PAHO created a Disaster Task Force in HQ and a Regional Health Emergency Response Team that reports to the Director. The team leader of Regional Response Team is the counterpart of similar positions in other international organizations or clusters. The command and control mode of operation is different from the business-as-usual approach of the Organization and requires flexibility, good will and seniority on the part of the response team leader, the PWR and the Administration. The change of mode is especially important, as disasters are highly emotional and politically-charged situations. In a matter of days or even minutes, key priorities must be determined. When necessary, the PAHO/WHO country office will ensure that arrangements are made to establish new sub-offices in an affected area for the duration of the emergency. The size of the sub-office will vary accordingly to the event, but a field response coordinator requires logistic and administrative support as well as technical experts to carry out response activities. In addition to our own direct staff and the Disaster Focal Points within PAHO country offices, the success of the PED Program depends heavily on the Health Disaster Coordinators within national Ministries of Health. We will continue to support these key staff and to provide them with the highest level of technical training and access to the information and tools that they need to build sustained capacity in their ministries.
5.3 Partnerships for health preparedness
The Area on Emergency Preparedness and Disaster Relief will continue to promote liaison and dialogue with donors and agencies that support health emergency preparedness in Latin America and the Caribbean. PAHO will continue to host periodic meetings, extending invitations to agencies that express interest in making a
A secure and disaster-resilient health sector in the Americas Strategic Plan 2008 – 2012 of the Pan American Health Organization
23
commitment to health preparedness or mitigation in the Region. Both internal (e.g. core corporate capacity building process, etc.) and external consultation mechanisms (e.g. sub-regional plans, country cooperation strategy processes, etc.) will also continue to take place. The direction of PED's future actions will be guided by its relationship with the cooperation activities of other agencies and the expectation of a broader network of experts. PED will expand its alliances with a growing number of important regional actors in health (both in quality and quantity). In the next strategic planning period, we will create a broader consultation mechanism to serve as a Technical Advisory Group, to advise or comment on general trends and the direction that technical cooperation should follow. In addition, we will work to influence other health and disaster reduction entities to work toward common regional objectives and benchmarks for assessing progress.
6. Monitoring and Evaluation We recognize that monitoring and evaluation of progress and impact in this technical area form a critical part of our work and we will seek to improve these functions. To achieve this we will seek to approach monitoring through two separate mechanisms or streams. 6.1 Internal PAHO monitoring and reporting
We will monitor progress through our internal reporting systems, which are part of the regular corporate program management procedures, based on the Bi-annual Work Plans, or BWPs. Staff will monitor and collect data and information regarding progress against planned activities in the work plans and assess progress on the basis of indicators and milestones set out in the BWPs. This information will be utilized by the Organization to inform the Region-wide Expected Results, as established in the new WHO Strategic Objective 5.
6.2 PED Program monitoring
In addition to internal monitoring, we will use a more in-depth set of monitoring instruments that is specific to the PED Program itself and which seek to assess the impact of our work. Through this monitoring process, we will seek to address much more qualitative aspects of the program that can help us better understand the true impact of our work. More importantly, we must try to understand the quality of these plans and what impact they have had on improving the continuity of health service delivery during a disaster event.
A secure and disaster-resilient health sector in the Americas Strategic Plan 2008 – 2012 of the Pan American Health Organization
24
We took a big step forward in this direction in 2006 when a region-wide survey was carried out by PAHO on the status of health preparedness in the Americas.16 Although there were limitations to the survey, we consider that the resulting report represents the first attempt toward an objective description of the realty across the Region, focusing on more qualitative aspects of the state of heath service delivery and disaster management. This first survey was a major breakthrough in terms of achieving consensus among countries of the need to measure the overall level of disaster preparedness and risk reduction. The baseline data from this survey was used to develop this current strategic plan and in the future we will look to improve the methodology itself and to transform this as the reference tool for regional planning and benchmarking. Ideally, the health data will be used to improve the planning and knowledge of all regional partners.
In addition to the survey, this current Strategic Plan 2008-2012 contains expected
results with measurable indicators (i.e. SMART–specific, measurable, achievable, realistic and time bound). This will be PED’s main planning instrument and activities will be undertaken as described in this document. A Logical Framework will outline expected results and indicators for the main program components. Each year, PED will prepare a comprehensive annual report that will measure the level of progress toward the achievement of the expected results based on the selected indicators.
We will continue to submit disaster-specific reports as requested and additional informal information throughout the course of the implementation period. We will also report to the Governing Bodies through PAHO’s monitoring system. The experience gained during implementation of this Plan may require adjustments to the expected results. External changes in the environment may also require changes in the expected results or activities.
6.3 External evaluations
Building on the monitoring activities outlined above, we will continue to encourage the use of external evaluations. We value the independence and objective rigor that these evaluations have provided in the past. For example, this Strategic Plan has been revised taking into consideration the recommendations from the last Evaluation carried out in 2007 and financed by DFID/CHASE. We would welcome an external evaluation before the end of the implementation of this 2008-2012 Strategic Plan. As the 2007 evaluation was comprehensive, we propose that shorter evaluations be undertaken at some point mid-way through the planning period to allow for an assessment and adjustment of the plan, based on changes to the operating environment and developments in the health sector and in disaster management in the Region.
16 Survey on the Health Sector State of Preparedness and Mitigation to Disasters, prepared by the Area on Emergency Preparedness and Disaster Relief – March to July 2006 (http://www.paho.org/english/dd/ped/CD47-34-e%5B1%5D.pdf).
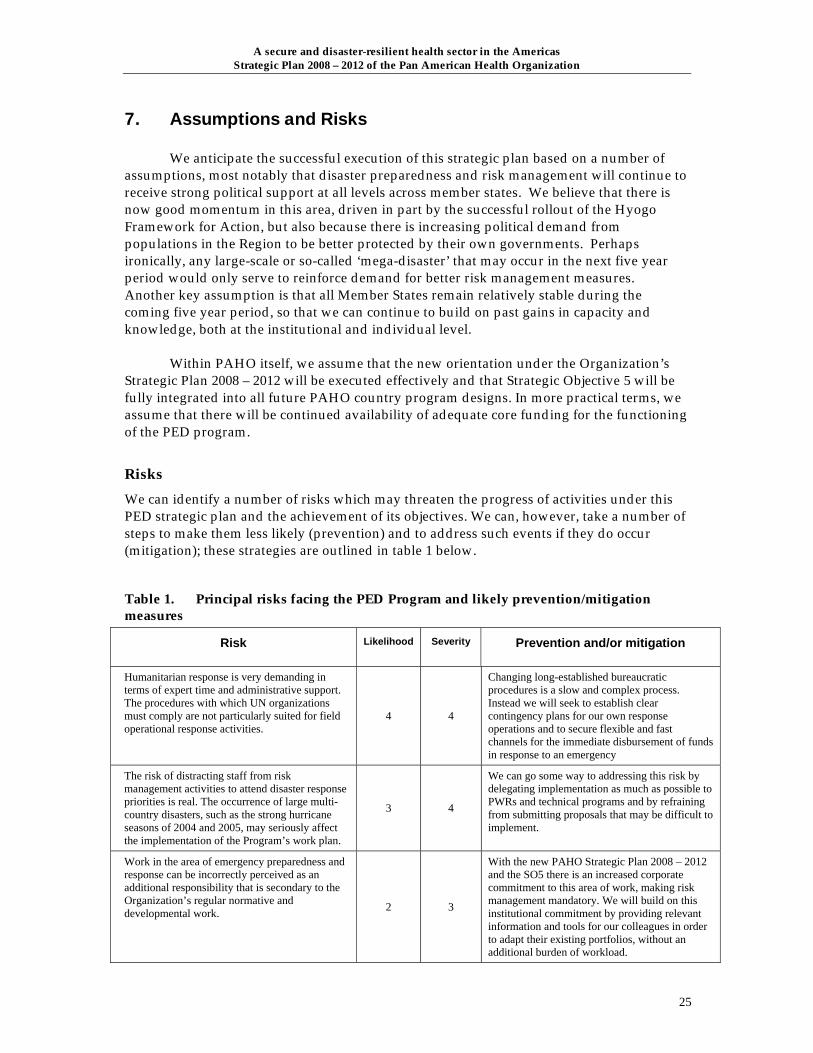
A secure and disaster-resilient health sector in the Americas Strategic Plan 2008 – 2012 of the Pan American Health Organization
25
7. Assumptions and Risks We anticipate the successful execution of this strategic plan based on a number of assumptions, most notably that disaster preparedness and risk management will continue to receive strong political support at all levels across member states. We believe that there is now good momentum in this area, driven in part by the successful rollout of the Hyogo Framework for Action, but also because there is increasing political demand from populations in the Region to be better protected by their own governments. Perhaps ironically, any large-scale or so-called ‘mega-disaster’ that may occur in the next five year period would only serve to reinforce demand for better risk management measures. Another key assumption is that all Member States remain relatively stable during the coming five year period, so that we can continue to build on past gains in capacity and knowledge, both at the institutional and individual level. Within PAHO itself, we assume that the new orientation under the Organization’s Strategic Plan 2008 – 2012 will be executed effectively and that Strategic Objective 5 will be fully integrated into all future PAHO country program designs. In more practical terms, we assume that there will be continued availability of adequate core funding for the functioning of the PED program.
Risks We can identify a number of risks which may threaten the progress of activities under this PED strategic plan and the achievement of its objectives. We can, however, take a number of steps to make them less likely (prevention) and to address such events if they do occur (mitigation); these strategies are outlined in table 1 below.
Table 1. Principal risks facing the PED Program and likely prevention/mitigation measures
Risk Likelihood
Severity Prevention and/or mitigation
Humanitarian response is very demanding in terms of expert time and administrative support. The procedures with which UN organizations must comply are not particularly suited for field operational response activities.
4 4
Changing long-established bureaucratic procedures is a slow and complex process. Instead we will seek to establish clear contingency plans for our own response operations and to secure flexible and fast channels for the immediate disbursement of funds in response to an emergency
The risk of distracting staff from risk management activities to attend disaster response priorities is real. The occurrence of large multi-country disasters, such as the strong hurricane seasons of 2004 and 2005, may seriously affect the implementation of the Program’s work plan.
3 4
We can go some way to addressing this risk by delegating implementation as much as possible to PWRs and technical programs and by refraining from submitting proposals that may be difficult to implement.
Work in the area of emergency preparedness and response can be incorrectly perceived as an additional responsibility that is secondary to the Organization’s regular normative and developmental work. 2 3
With the new PAHO Strategic Plan 2008 – 2012 and the SO5 there is an increased corporate commitment to this area of work, making risk management mandatory. We will build on this institutional commitment by providing relevant information and tools for our colleagues in order to adapt their existing portfolios, without an additional burden of workload.
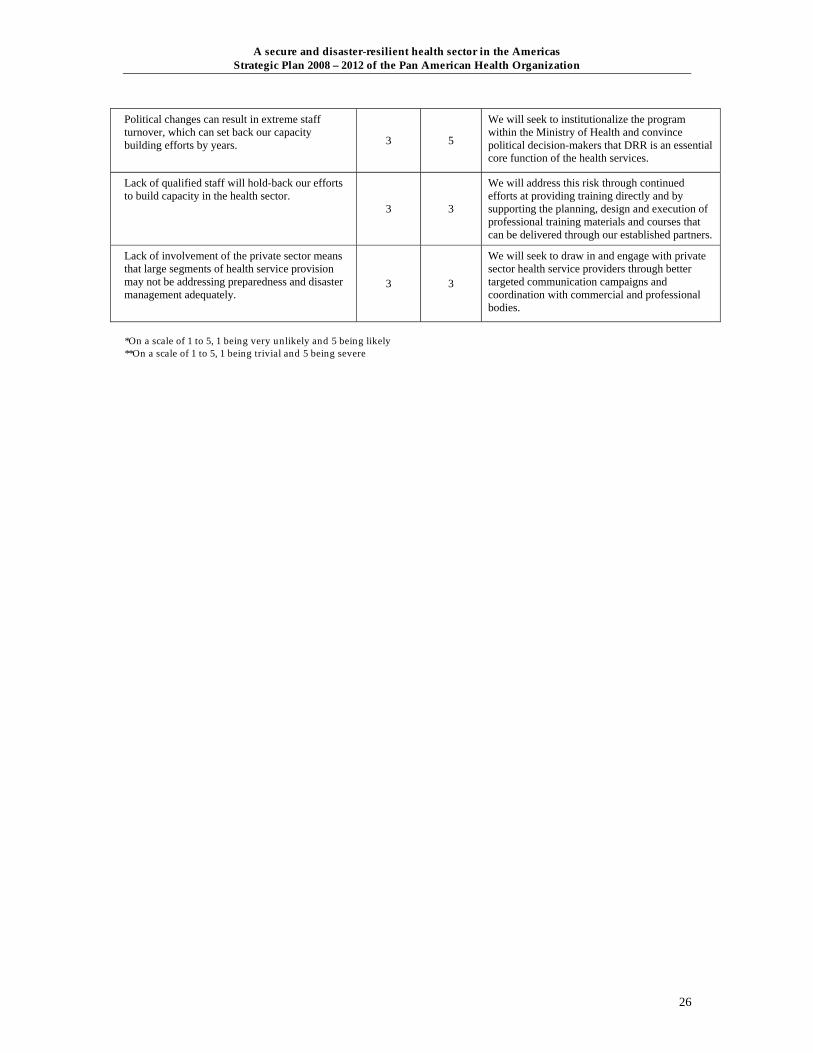
A secure and disaster-resilient health sector in the Americas Strategic Plan 2008 – 2012 of the Pan American Health Organization
26
Political changes can result in extreme staff turnover, which can set back our capacity building efforts by years.
3 5
We will seek to institutionalize the program within the Ministry of Health and convince political decision-makers that DRR is an essential core function of the health services.
Lack of qualified staff will hold-back our efforts to build capacity in the health sector. 3 3
We will address this risk through continued efforts at providing training directly and by supporting the planning, design and execution of professional training materials and courses that can be delivered through our established partners.
Lack of involvement of the private sector means that large segments of health service provision may not be addressing preparedness and disaster management adequately.
3 3
We will seek to draw in and engage with private sector health service providers through better targeted communication campaigns and coordination with commercial and professional bodies.
*On a scale of 1 to 5, 1 being very unlikely and 5 being likely **On a scale of 1 to 5, 1 being trivial and 5 being severe

A secure and disaster-resilient health sector in the Americas Strategic Plan 2008 – 2012 of the Pan American Health Organization
27
Annex 1: PAHO/PED Organizational Chart
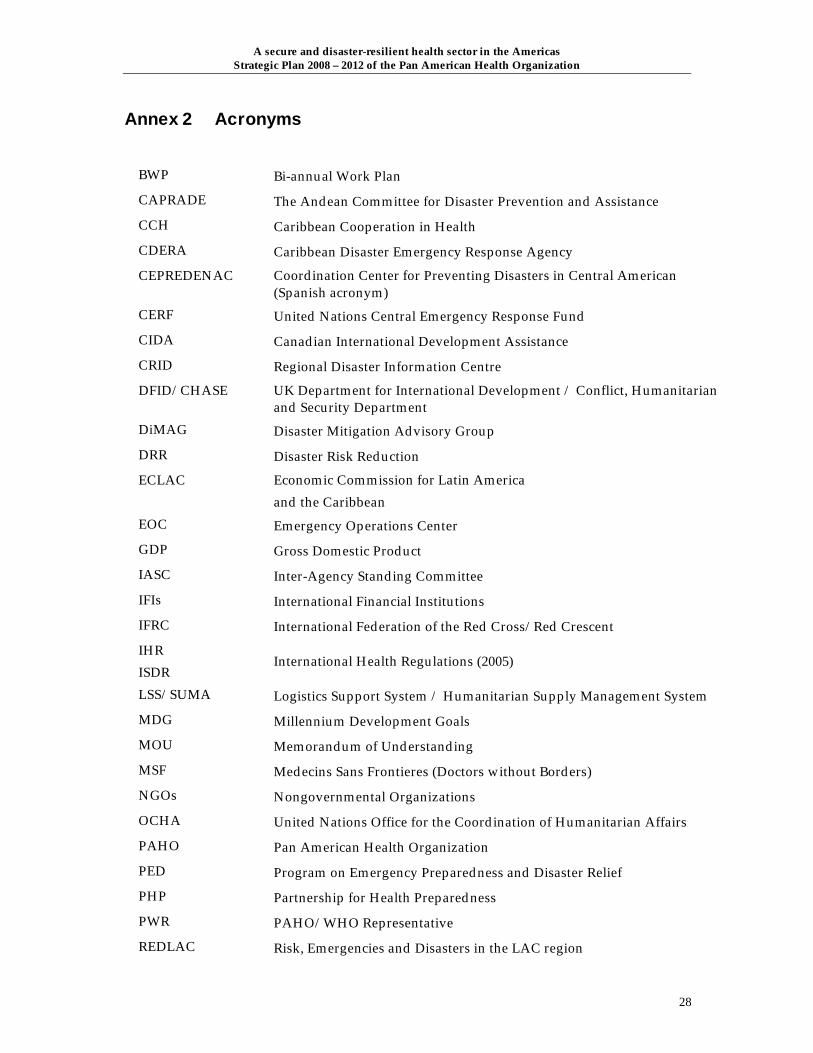
A secure and disaster-resilient health sector in the Americas Strategic Plan 2008 – 2012 of the Pan American Health Organization
28
Annex 2 Acronyms
BWP Bi-annual Work Plan
CAPRADE The Andean Committee for Disaster Prevention and Assistance
CCH Caribbean Cooperation in Health
CDERA Caribbean Disaster Emergency Response Agency
CEPREDENAC Coordination Center for Preventing Disasters in Central American (Spanish acronym)
CERF United Nations Central Emergency Response Fund
CIDA Canadian International Development Assistance
CRID Regional Disaster Information Centre
DFID/CHASE UK Department for International Development / Conflict, Humanitarian and Security Department
DiMAG Disaster Mitigation Advisory Group
DRR Disaster Risk Reduction
ECLAC Economic Commission for Latin America and the Caribbean
EOC Emergency Operations Center
GDP Gross Domestic Product
IASC Inter-Agency Standing Committee
IFIs International Financial Institutions
IFRC International Federation of the Red Cross/Red Crescent
IHR ISDR
International Health Regulations (2005)
LSS/SUMA Logistics Support System / Humanitarian Supply Management System
MDG Millennium Development Goals
MOU Memorandum of Understanding
MSF Medecins Sans Frontieres (Doctors without Borders)
NGOs Nongovernmental Organizations
OCHA United Nations Office for the Coordination of Humanitarian Affairs
PAHO Pan American Health Organization
PED Program on Emergency Preparedness and Disaster Relief
PHP Partnership for Health Preparedness
PWR PAHO/WHO Representative
REDLAC Risk, Emergencies and Disasters in the LAC region

A secure and disaster-resilient health sector in the Americas Strategic Plan 2008 – 2012 of the Pan American Health Organization
29
REMSAA Meeting of the Ministers of Health in the Andean Region , (Spanish acronym)
RESSCAP Meeting of the Health Sectors in Central America and Panama (Acronym in Spanish)
SARS Severe Acute Respiratory Syndrome
SMART Expected Results: Specific, Measurable, Achievable, Realistic and Time bound
UNICEF United Nations Children’s Fund
USAID/OFDA U.S. Agency for International Development / Office of U.S. Foreign Disaster Assistance
WHO World Health Organization

ANNEX 11

Public Health Pre-Deployment Course
16 - 29 November 2008 I Ontario, Canada
Course agenda Page 1 of 4
PHPD Course agenda
Week 1 - Module 1: Health in the broader humanitarian context; and Module 2: Public health issues in emergencies TIME/DAY SUN I 16 NOV MON I 17 NOV TUES I 18 NOV WED I 19 NOV THUR I 20 NOV FRI I 21 NOV SAT I 22 NOV
Module 1: Health in the broader humanitarian context
Module 2: Public health issues in emergencies
8:30-8:45 Module 1 overview Recap/Admin Admin Recap/Admin Recap/Admin Recap/Admin
9.00-10:30 M1.S1 International humanitarian system Dr. Jean-Luc Poncelet (PAHO)
M1.S3 In-country health partnerships in emergencies Mr. Ciro Ugarte (PAHO)
Module 2 Overview M2.S1 Introduction to public health in disasters: Communicable Diseases Dr. Francesco Checchi (WHO)
M2.S3 Health Services in Natural Disasters and Complex Emergencies Dr. Altaf Musani (EMRO)
M2.S5 Chronic diseases in emergencies Dr. Gilbert Burnham & Dr. Joy Cook (HOPKINS)
M2.S7 Reproductive Health during crisis Dr. Zaitoon Qazi (WHO) and Dr. Lisa Thomas (WHO)
10:30-11:00
Break Break Break Break Break Break
11:00-12:30
Arrival Hotel check-in
M1.S1 International humanitarian system Dr. Altaf Musani (EMRO)
M1.S3 WHO in country and field reality Dr. Altaf Musani (EMRO)
M2.S1 Introduction to public health in disasters: (cont from above) Dr. Francesco Checchi (WHO)
M2.S3 Public health management of acute-onset natural disasters (simulation) Dr. Gilbert Burnham & Dr. Joy Cook (HOPKINS)
M2.S5 ICE STORM CANADA Mr. Frank Welsh (PHAC)
M2.S7 Reproductive health during crises cont Dr. Zaitoon Qazi (WHO) and Dr. Lisa Thomas (WHO)
12:30-13:30
Lunch
Lunch
Lunch
Lunch
Lunch
Lunch
Lunch

Public Health Pre-Deployment Course
16 - 29 November 2008 I Ontario, Canada
Course agenda Page 2 of 4
13:30-15:00
M1.S2 Humanitarian Reforms Mr Douglas Reimer (OCHA Panama)
M1.S3 Financing Reporting Exercise, Write a CERF Mr. Jukka Sailas (WHO Geneva) & Mr Nicolas Lagomarsino (PAHO)
M2.S2 Contexts and impacts of acute-onset natural disasters [1] Water & Sanitation Ms. Ana Treasure ((PAHO/HON)
M2.S4 SIMULATION cont Dr. Gilbert Burnham & Dr. Joy Cook (HOPKINS)
M2.S6 Nutrition and emergencies Dr. Hélène Delisle (TRANSNUT)
M2.S8 First aid course Canadian Red Cross
15:00-15:30
M0.S1 Welcome, Introductions
Break Break Break Break Break Break
M2.S8 First aid course Canadian Red Cross
15:30-17:00
M0.S2 Introduction to the course Expectations check
M1.S2 HUMANITARIAN GUIDING PRINCIPLES Ms Isabelle Doust (Canadian Red Cross)
M1.S3 EXERCISE ON HOW TO WRITE A CERF Mr Nicolas Lagomarsino (PAHO)
M2.S2 Infection diseases in emergency setting Dr. Francesco Checchi (WHO)
M2.S4 Simulation cont Dr. Gilbert Burnham & Dr. Joy Cook (HOPKINS)
M2.S6 Writing a sitrep Exercise Dr. Dana Van Alphen (PAHO) & Dr. Rudi Coninx (WHO)
17:00-17:30
Review of the day Review of the module
Review of the day Review of the day Technical Issues Raised by Participants & Facilitators Rudi, Dana, Francesco
19:00 Welcome reception
Optional evening session Student presentations
Optional evening session Student presentations
Optional evening session Sexual and Gender Based Violence
Optional evening session Family Planning
Optional evening session HIV and Sexually Transmitted Infections

Public Health Pre-Deployment Course
16 - 29 November 2008 I Ontario, Canada
Course agenda Page 3 of 4
Week 2 - Module 3: Operational and personal effectiveness [OPE]; and Field simulation exercise [SIMEX]
TIME/DAY SUN I 23 NOV
MON I 24 NOV TUES I 25 NOV WED I 26 NOV THUR I 27 NOV FRI I 28 NOV SAT I 29 NOV
Module 3: Operational and personal effectiveness Field simulation exercise [SIMEX]
8:30-8:45 Module 3 overview Recap/Admin Recap/Admin Admin M3.S1a Intro to UN security: phases, role of WHO security
8:45-10:30
M3.S1b Weapons and effects of explosions
M3.S3 Personal safety Travel safety in the field
M3.S9 Risk communication ROBERTA WALKER
MC.S1 Course evaluation and individual feedback (at CRC)
10:30-11:00 Break Break Break Break
11:00-12:30 M3.S1c UN security plan (inc office security plan)
M3.S4 Health and hygiene in the field JO MORRIS
M3.S10 Mission readiness, and stress management Shappell-fgi (Danielle Martin)
MC.S2 cont
12:30-13:30 Lunch Lunch
Field exercise
Closing/Lunch
13:30-15:00 M3.S2 Standard operating procedures in emergencies [1] NICOLAS LAGOMARSINO
M3.S5 Map reading and GPS
15:00-15:30
Course Off Day
Break Break
M3. ME Round robin/ multiple exercises: 1. Radio exercise 2. Vehicle search 3. Sketch mapping 4. Survival in the field/personal kits 5. ITT exercise
Brief operations team Security briefing Depart for 'Zambre' Field exercise
Hot Debrief LUNCH
Departures
Public Health Pre-Deployment Course
16 - 29 November 2008 I Ontario, Canada
Course agenda Page 4 of 4
15:30-17:00 M3.S6 Media management ROBERTA WALKER
17:00-17:30
M3.S2 Standard operating procedures in emergencies [2]
6. SatComms exercise 7. HMS exercise
Video Debrief (At CRC)
19:00
M3.S7 PPE M3.S8 ITT - Satcomms, networking, radios
Deployment preparation exercise
Field exercise [overnight in exercise site]
ANNEX 12
DRAFT for FIELD CONSULTATION
[Health Cluster Guide – draft, 30 June 2008] 1
Health Cluster Guide
A practical guide for Health Cluster Coordinators and participants
Note for users and reviewers of this draft
This draft is intended for field consultation, to capture field experience and ensure that the final product will meet field needs. It is planned to issue a provisional version in Nov. 2008. A final version will be produced late-2009 after one year of use of the provisional version and extensive consultation with health cluster participants in the field and partners at global level.
Users and reviewers are requested to provide specific suggestions for improving the accuracy and usefulness of the draft by:
• indicating what you think needs to be modified, added or deleted;
• providing “Lessons & practical hints from field experience” to be included in the various sections;
• providing examples (mini-case studies) that can be included in specific sections to illustrate key points: positive and negative examples – examples of successes and problems.
The present draft is edited in A4 format but it is envisaged that the document will finally be printed in a smaller format, e.g. A5 or similar. Selecting “2 pages per sheet” when printing will give you a rough idea of what the final product might look like if produced in A5 format.
IASC Global Health Cluster
Draft 30 June 2008

DRAFT for FIELD CONSULTATION
[Health Cluster Guide – draft, 30 June 2008] 2
Contents
About this Guide.......................................................................................................................................4
Acronyms and abbreviations...................................................................................................................5
1 Role and functioning of a health cluster............................................................................................6 1.1 The cluster approach at country level ...................................................................................................... 10 1.2 What is expected of the cluster lead, coordinator and participants......................................................... 12 1.3 Relationship with the government/MoH and other clusters ..................................................................... 15 1.4 Cluster activities during different phases of health response.................................................................. 16
2 What’s needed for an effective health cluster .................................................................................19 2.1 The challenge for the cluster coordinator ................................................................................................ 21 2.2 Organizing cluster meetings..................................................................................................................... 24 2.3 Cooperating with other clusters and coordinating entities....................................................................... 26
3 Health information in Crisis ..............................................................................................................27 3.1 Crisis and Health Information Management ............................................................................................ 29 3.2 Key Health Information Needs in Crisis and associated tools................................................................. 33 3.3 The need for initial / rapid assessment and monitoring tools .................................................................. 38 3.4 From an initial to a comprehensive and from an assessment based to a monitoring based approach . 40 3.5 IRA Initial Rapid Assessment................................................................................................................... 44 3.6 HeRAMS Health Resources Availability Mapping System ...................................................................... 45 3.7 Crisis and Routine Health Information and Surveillance Systems - to be updated…………....…………50
4 Strategy development and planning ...............................................................................................49 4.1 Defining overall objectives and strategies; preparing a health sector action plan ................................. 52 4.2 Preparing a health cluster/sector response plan ..................................................................................... 56 4.3 Preparing the health components of a CHAP.......................................................................................... 59 4.4 Taking account of cross-cutting concerns .............................................................................................. 62 4.5 Developing contingency plans ................................................................................................................ 63
5 Mobilizing and managing resources ................................................................................................64 5.1 Preparing health inputs to flash appeals ................................................................................................. 65 5.2 Preparing and reviewing a consolidated appeal ...................................................................................... 66 5.3 Proposing CERF applications for the health sector................................................................................. 68 5.4 Working with donors; accessing funds from other sources ..................................................................... 69 5.5 Provision of last resort.............................................................................................................................. 71
6 Monitoring health action plan implementation; evaluating & learning lessons............................72 6.1 Monitoring implementation of the health cluster/sector response plan .................................................. 74 6.2 Monitoring the performance of health services ....................................................................................... 75 6.3 Evaluating health sector response; organizing a lesson-learned exercise ............................................ 77
7 Managing and disseminating information .......................................................................................79 7.1 Managing information .............................................................................................................................. 80 7.2 Disseminating information – managing external communications .......................................................... 82
8 Standards and protocols...................................................................................................................83 8.1 Promoting – and building consensus on – evidence-based best practices ........................................... 85 8.2 Promoting adherence to agreed standards and protocols ..................................................................... 88
9 Promoting recovery...........................................................................................................................89 9.1 Protecting and reinforcing local capacities from the outset ..................................................................... 90
DRAFT for FIELD CONSULTATION
[Health Cluster Guide – draft, 30 June 2008] 3
9.2 Supporting health system recovery.......................................................................................................... 91
Annexes
A1: Generic terms of reference for a sector/cluster lead at country level............................................93
A2: Terms of reference for a health cluster coordinator......................................................................95
B: Role and activities of the Global Health Cluster ...........................................................................97
C: Mapping the availability of health services ...................................................................................98
D: Levels of care and sub-sectors for initial analysis and planning .................................................102
E: Health actor mapping: Who-What-Where-When ........................................................................103
F: Types and phases of assessment in a humanitarian crisis.........................................................105
G: General principles for all data collection activities – assessments, surveys and surveillance.....107
H: Drawing up an assessment plan, schedule and budget .............................................................110
I: Indicators for surveillance ..........................................................................................................115
J: Collecting and interpreting mortality and morbidity data.............................................................117
K: Stakeholder analysis..................................................................................................................118
L: Needs Analysis Framework (NAF) .............................................................................................119
M: Priority cross-cutting concerns ...................................................................................................120
N: Analysing response options; examples of negative effects ........................................................123
O: Common problems and challenges in health system recovery...................................................125
(to be created…) Important technical reference and guidance materials
Useful websites
… ?
Glossary of key terms (and concepts).....................................................................................................128

DRAFT for FIELD CONSULTATION
[Health Cluster Guide – draft, 30 June 2008] 4
About this Guide
Its purpose (and target audience)
This Guide suggests how the Health Cluster lead agency, coordinator and participants can work together during a humanitarian crisis to achieve the aims of reducing avoidable mortality, morbidity and disability, and restoring the delivery of and access to preventive and curative health care as quickly as possible.
It highlights key principles of humanitarian health action in each phase of the response and how coordination and joint efforts among health sector actors �– partners – can increase the effectiveness and efficiency of health interventions. It draws on IASC and other documents but also includes lessons from field experience.
Although addressed to “Health Cluster Coordinators” and “Health Cluster Participants”, the guidance is equally valid for coordinators and members of health sector coordination groups that seek to achieve effective coordinated health action in countries where the cluster approach has not been adopted. It should also be useful in cases where, at county level, it has been decided to combine health with nutrition in a single cluster or sector group.
Its structure
Chapter 1 explains the role of a health cluster at national and, where needed, sub-national levels, and suggests what needs to be done to establish and sustain an effective cluster. It also outlines the principal actions that need to be taken during different phases of response.
Chapters 2 to 9 focus on specific functions and issues that a health cluster/sector is expected to fulfil and address. Each chapter highlights the key principles, summarizes what needs to be done and considered, lists the tools and guidelines that are available, indicates the challenges likely to be faced, and provides practical hints and references for further guidance. The tools and guidelines referred to include, but are not limited to, those developed by the Global Health Cluster.1
The annexes and additional documents on the accompanying CD-ROM provide essential complementary information.
Different bullets indicate different types of information or guidance:
= principles; what needs to be kept in mind
= action points; what needs to be done
= what to avoid
= reference documents; where to look for further guidance
• = components of the issue being discussed
1 The “common gaps” boxes at the start of several of the chapters are reproduced from Gap guidance materials: assisting the health sector coordination mechanism to identify and fill gaps in the humanitarian response, GHC, version 1.0 for field testing, October 2007. They present common gaps found in ten country case studies covering field operations during the period 2004 to 2007.
DRAFT for FIELD CONSULTATION
[Health Cluster Guide – draft, 30 June 2008] 5
Acronyms and abbreviations CAP consolidated appeal process (sometimes also [mis]used for consolidated appeal)
CERF Central Emergency Response Fund
CHAP common humanitarian action plan (component of a consolidated appeal document)
EmOC emergency obstetric care
GHC Global Health Cluster
HC Humanitarian Coordinator
HCC Health Cluster Coordinator
IASC Inter-Agency Standing Committee2
MISP minimum initial service package (for reproductive health)
MoH Ministry of Health
MYR mid-year review (of a consolidated appeal)
NAF needs analysis framework (for preparing a CHAP)
OCHA UN Office for the Coordination of Humanitarian Affairs
TOR terms of reference
WHO World Health Organization
3W Who-What-Where (analysis of the activities of humanitarian partners)
4W Who-What-Where-When
2 The IASC includes: OCHA, UNICEF, UNHCR, WFP, UNDP, UNFPA, FAO and WHO. Standing invitees are ICRC, IFRC, IOM, ICVA (International Council of Voluntary Agencies), Inter-Action, SCHR (Steering Committee for Humanitarian Response), RSGIDP (the Representative of the Secretary-General on Internally Displaced Persons), UNHCHR and the World Bank.
DRAFT for FIELD CONSULTATION
[Health Cluster Guide – draft, 30 June 2008] 6
1 Role and functioning of a health cluster
Key points: The cluster should enable participating organizations to work together, harmonize efforts and use
available resources efficiently within the framework of agreed objectives, priorities and strategies.
The cluster lead agency is responsible to the Humanitarian Coordinator for ensuring the satisfactory functioning of the cluster.
The health cluster coordinator facilitates and leads the work of the cluster, and ensures coordination with other clusters in relation to activities relevant to public health as well as the cross-cutting issues.
Participating organizations are expected to be proactive partners in assessing needs, developing strategies and plans for the overall health sector response, implementing agreed priority activities, and adhering to agreed standards to the maximum extent possible.
The cluster itself serves as a mechanism for coordinated assessments, joint analyses, the development of agreed overall priorities, objectives, strategies and a health sector (strategic) action plan, and the monitoring and evaluation of the implementation and impact of that plan …?
N.B. The cluster approach (and humanitarian reform more generally) is a relatively new and still evolving concept and, as of early 2008, the associated guidance is not yet fully developed – there remain some grey areas.
Decisions on the clusters required at country level are made on a case-by-case basis by the Humanitarian Coordinator in close consultation with the IASC agencies present and following consultations with national authorities. They are approved by the UN Emergency Relief Coordinator in consultation with the IASC principals. Cluster leads are designated taking account of the capacities of the different agencies in country to fulfil the required functions (including that of provider of last resort). They may, or may not, coincide with cluster leadership at the global level.
The country-level cluster lead agency assigns a health cluster coordinator and is responsible to provide the administrative and other support services required for the coordinator and the cluster to function effectively. In general, the HCC should be a full-time position without any responsibility for the lead agency’s own programmes or activities.
The relationships among the cluster lead agency representative, the HCC, the cluster and the HC is shown in Figures 1a and 1b. The relationship between the country-level cluster and sub-national level “zonal” clusters is shown in Figure 1c.3
Question to reviewers: Which of these diagrams is the most useful, 1a or 1b…?
3 N.B. These diagrams are drafts that are presently being discussed with OCHA…
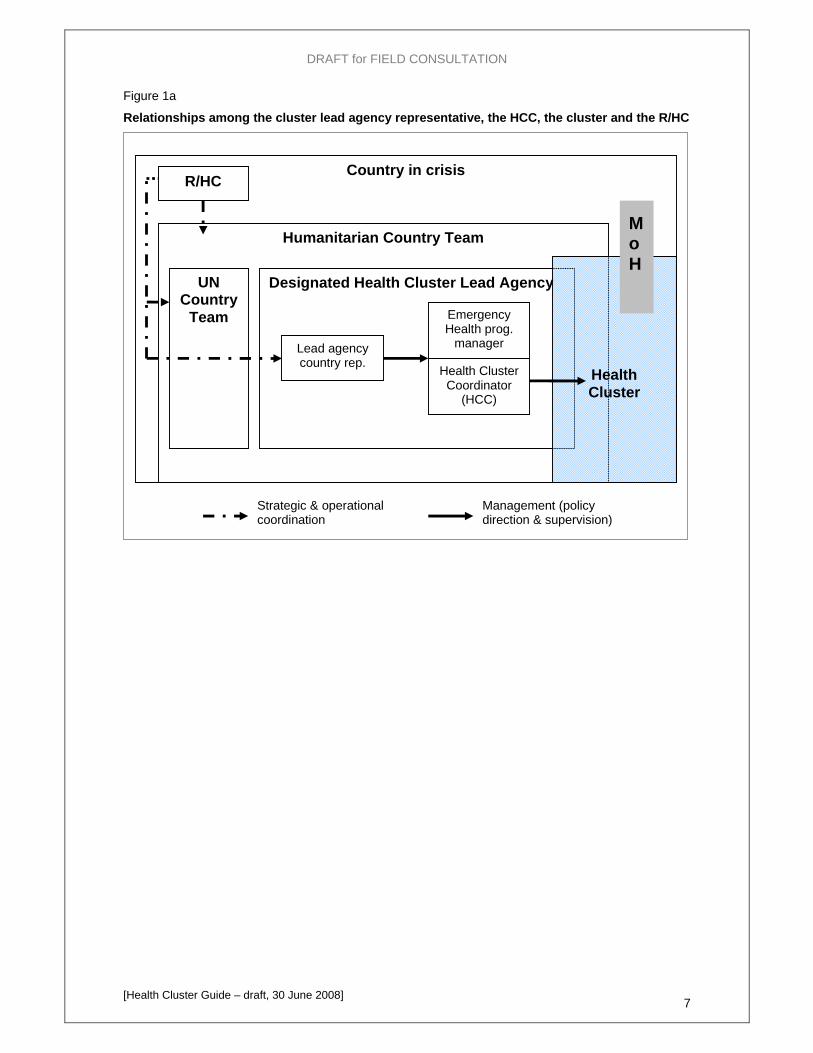
DRAFT for FIELD CONSULTATION
[Health Cluster Guide – draft, 30 June 2008] 7
Figure 1a
Relationships among the cluster lead agency representative, the HCC, the cluster and the R/HC
Humanitarian Country Team
UN Country
Team
Country in crisis
Designated Health Cluster Lead Agency
Health Cluster
R/HC
Lead agency country rep.
Emergency Health prog.
manager
Health Cluster Coordinator
(HCC)
MoH
Strategic & operational coordination
Management (policy direction & supervision)
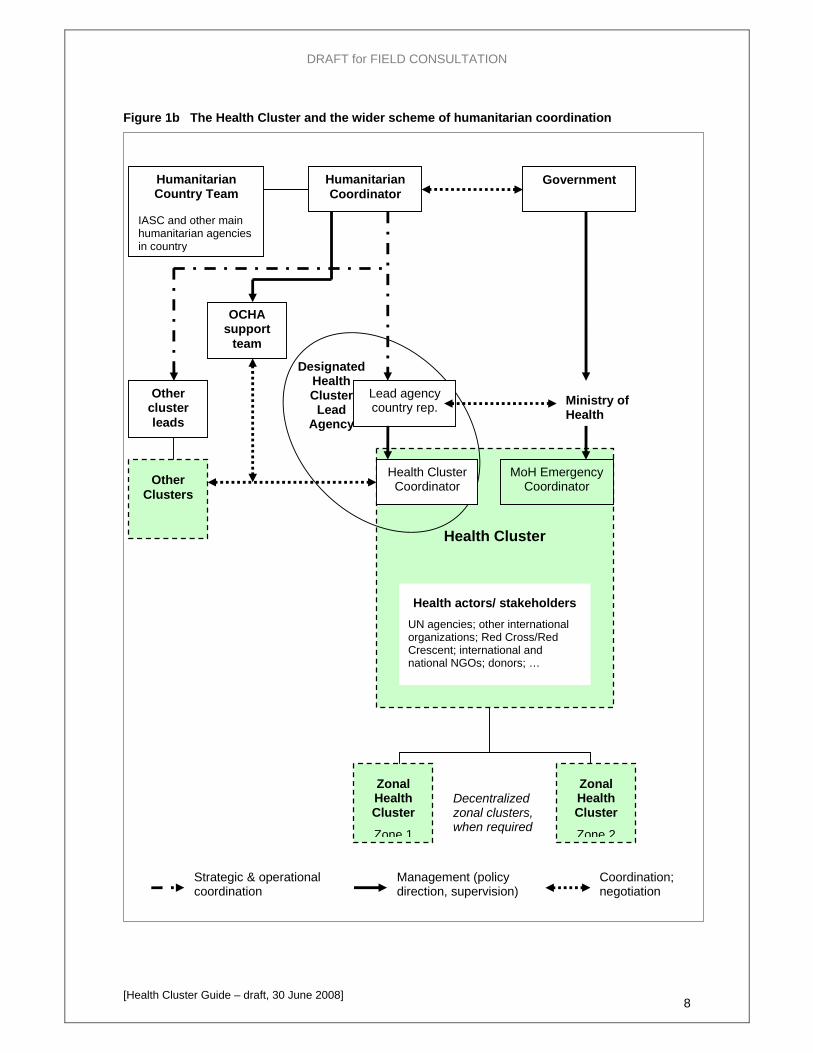
DRAFT for FIELD CONSULTATION
[Health Cluster Guide – draft, 30 June 2008] 8
Figure 1b The Health Cluster and the wider scheme of humanitarian coordination
Health Cluster
Designated Health Cluster
Lead Agency
Health Cluster Coordinator
Lead agency country rep. Ministry of
Health
Health actors/ stakeholders UN agencies; other international organizations; Red Cross/Red Crescent; international and national NGOs; donors; …
Humanitarian Coordinator
Government
Other cluster leads
Coordination; negotiation
Management (policy direction, supervision)
Humanitarian Country Team
IASC and other main humanitarian agencies in country
MoH Emergency Coordinator
Strategic & operational coordination
Zonal Health Cluster
Zone 1
Zonal Health Cluster
Zone 2
Decentralized zonal clusters, when required
Other Clusters
OCHA support
team
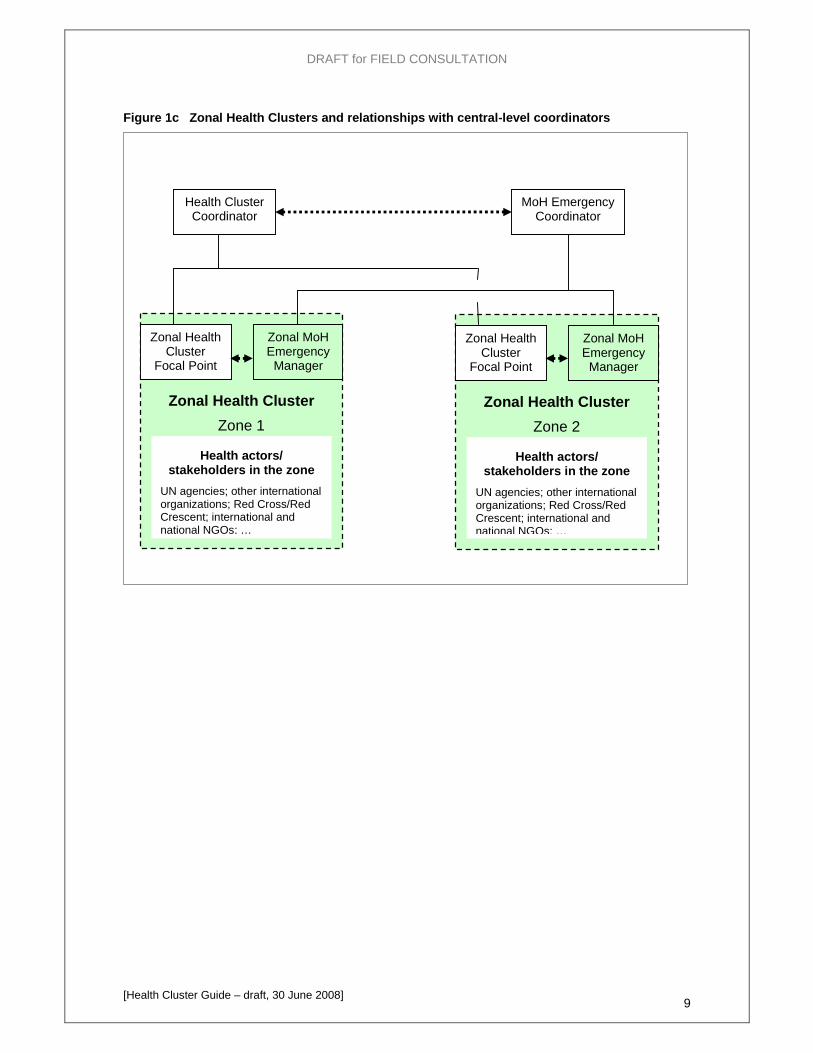
DRAFT for FIELD CONSULTATION
[Health Cluster Guide – draft, 30 June 2008] 9
Figure 1c Zonal Health Clusters and relationships with central-level coordinators
Zonal Health Cluster Zone 2
Zonal Health Cluster Zone 1
Zonal Health Cluster
Focal Point
Health actors/ stakeholders in the zone
UN agencies; other international organizations; Red Cross/Red Crescent; international and national NGOs; …
Zonal MoH Emergency Manager
Health Cluster Coordinator
MoH Emergency Coordinator
Zonal Health Cluster
Focal Point
Health actors/ stakeholders in the zone
UN agencies; other international organizations; Red Cross/Red Crescent; international and national NGOs; …
Zonal MoH Emergency
Manager
DRAFT for FIELD CONSULTATION
[Health Cluster Guide – draft, 30 June 2008] 10
1.1 The “Cluster approach”
What is the cluster approach
At country level, the cluster approach establishes a clear system of leadership and accountability within each sector of international humanitarian response activity under the overall leadership of the humanitarian coordinator, and provides a framework for effective partnerships among humanitarian actors in each sector and good cooperation among international organizations, national authorities, NGOs and other stakeholders.
It strengthens, rather than replaces, existing coordination mechanisms.
Why was it introduced
An independent review commissioned by the UN Emergency Relief Coordinator in 2005 found significant gaps in humanitarian response. The Cluster Approach was adopted by the IASC the same year to: • improve the efficiency and effectiveness of humanitarian response to crises; • increase predictability and accountability in all the main sectors of international
humanitarian response; and • ensure that gaps in response do not go unaddressed.
When should it be used
It should be used in any sudden major new emergency requiring a multi-sectoral response with the participation of a wide range of international humanitarian actors. It should be introduced progressively in all countries where a Humanitarian Coordinator has been appointed (by adapting current working methods to conform to cluster approach guidance). 4 It should be used for (inter-agency) contingency planning for major new emergencies.
How is it different from a traditional “sector” approach
In most major humanitarian operations, sectoral groups have existed for many sectors but “coordination” has often been limited to information exchange and few sectors had clearly a designated lead agency accountable for the sector response. The cluster approach: (i) provides for a clear system of leadership and accountability for all the key sectors or areas of humanitarian activity, under the overall leadership of the Humanitarian Coordinator; and (ii) envisages a commitment from all participating organizations to harmonize efforts and work in partnership for the benefit of the affected population(s).
The aim of all health action during a humanitarian crisis/emergency is to reduce avoidable mortality, morbidity and disability, and restore the delivery of and equitable access to preventive and curative
health care as quickly as possible.
The country-level health cluster should enable participating organizations to work together to harmonize efforts and use available resources efficiently within the framework of agreed objectives, priorities and strategies to achieve the above aim through joint/coordinated action.
Any health sector coordination group implementing the “cluster approach” should serve as a mechanism for:
• collaboration among participating organizations in assessments and analysis, and in assuring an effective, integrated health information system;
• agreement on evidence-based priorities, objectives and strategies for response, and common standards and protocols, and the adoption of these by all partners as a basis for their own activities;
• coordinated action by all partners to implement agreed strategies, make effective use of available resources, identify and fill gaps in services, promote sustainable recovery, and address urgent health problems as and when they arise; and
4 As of April 2008, the cluster approach has been adopted in 13 countries with protracted/chronic emergencies (Liberia, Somalia, Uganda, Columbia, DRC, Ethiopia, Chad, CAR, Guinea, Tajikistan, Zimbabwe, Kenya), and in 8 major acute emergencies since then, starting with the Pakistan earthquake of October 2005.
DRAFT for FIELD CONSULTATION
[Health Cluster Guide – draft, 30 June 2008] 11
• collaboration among all partners in sector-level monitoring, evaluation, learning lessons, capacity building and preparedness.
The key document on the cluster approach, developed after extensive consultation among agencies at the international level and endorsed by the IASC principals is:
IASC - Guidance Note on using the Cluster Approach to Strengthen Humanitarian Response, 24 Nov. 2006
The generic terms of reference for sector/cluster leads at the country level, annex I to the above guidance note, are reproduced in Annex A1.
For additional, complementary information, see:
IASC - Operational Guidance on designating Sector/Cluster Leads in Major New Emergencies, 2007
IASC - Operational Guidance on designating Sector/Cluster Leads in Ongoing Emergencies, 2007 IASC Working Group 5-7 November 2007, Rome Statement on Cluster Roll-Out IASC - Strengthening NGOs Participation in the IASC, A Discussion Paper, 24 April 2006 IASC - Principles of Partnership, A Statement of Commitment, 28 March 2007 IASC – Operational Guidance on responsibilities of cluster/sector Leads and OCHA in Information
Management, IASC Task Force on Cluster Approach, Oct. 2007
For information about the role and activities of the Global Health Cluster (GHC), see Annex B.
The cluster approach is one of the three pillars of Humanitarian Reform the other two being the strengthening of the Humanitarian Coordinator (HC) system and strengthening of humanitarian financing (through improved appeals and the Central Emergency Response Fund, CERF). OCHA has established a Humanitarian Reform Support Unit (HRSU) based in Geneva, to support HCs and IASC partners in implementing the reform and to monitor the progress. OCHA is also working to improve its support to HCs.
For information about Humanitarian Reform, see: http://www.humanitarianreform.org/

DRAFT for FIELD CONSULTATION
[Health Cluster Guide – draft, 30 June 2008] 12
1.2 Roles of the cluster lead, coordinator and participants
Role of the country-level Cluster Lead Agency
The cluster lead has to ensure the establishment and proper functioning of the Cluster. This includes appointing a country-level cluster coordinator, designating cluster focal points at sub-national level, when needed, and assuring information management and other support services necessary for the satisfactory functioning of the cluster.
Specifically, the sector/cluster lead at the country level is accountable to the Humanitarian Coordinator for facilitating a process at the sectoral level aimed at ensuring the following:
Inclusion of key humanitarian partners Establishment and maintenance of appropriate humanitarian coordination mechanisms Coordination with national/local authorities, State institutions, local civil society and other relevant
actors Participatory and community-based approaches Attention to priority cross-cutting issues Needs assessment and analysis Emergency preparedness Planning and strategy development Application of standards Monitoring and reporting Advocacy and resource mobilization Training and capacity building Provision of assistance or services as a last resort (see section 5.5)
For more detail, see: IASC - Guidance Note on using the Cluster Approach to Strengthen Humanitarian Response, 24 Nov. 2006, Annex I, Generic terms of reference for sector/cluster leads at the country level.
What is expected of the Health Cluster Coordinator
The generic TOR for a Health Cluster Coordinator (HCC) are reproduced in Annex A. They mirror the TOR of the Sector/Cluster leads referred to above, covering the tasks that the cluster as a whole is expected to accomplish. In a nutshell, the coordinator is expected to:
Enable cluster participants to be more effective by working together, in coalition, than they could individually, and to maximize the benefit for the target population of the Cluster participants’ individual inputs and efforts.
Provide leadership to and work on behalf of the Cluster as a whole, facilitating all Cluster activities and maintaining a strategic vision.
Ensure that needs – and risks, capacities and opportunities – are assessed and understood as best possible at all stages of the humanitarian response, and that information is shared.
Generate the widest possible consensus on priorities and an overall strategic/action plan for humanitarian (and early recovery) action that addresses the priority needs and risks in the sector, incorporates appropriate strategies, and promote appropriate standards.
Work with Cluster members collectively and individually to identify gaps in response and try to ensure that available resources are directed to addressing priority problems and that assistance and services are provided equitably and impartially to different areas population groups on the basis of need.
Ensure coordination with other clusters in all activities relevant to public health.
The role is to “facilitate” and “lead” (not to “direct”).
DRAFT for FIELD CONSULTATION
[Health Cluster Guide – draft, 30 June 2008] 13
What is expected of Cluster Participants
Cluster participants are expected to be proactive partners in assessing needs, developing strategies and plans for the sector, and implementing agreed priority activities. This implies:
shared responsibility for assessing needs, establishing overall priorities, developing strategies and a common overall plan for action by cluster participants, and for accomplishing agreed objectives to the maximum extent possible within the limits of available resources; and
individual agency responsibilities for implementing activities for which they commit themselves, and for adhering to agreed standards and protocols as much as possible.
Coordination – coordinated action – cannot be achieved by a “coordinator”, only by all participants working together as a team – see the Principles of Partnership box below.
Role of sub-national-level clusters and focal points
… to be developed …
Principles of Partnership
Equality Equality requires mutual respect between members of the partnership irrespective of size and power. The participants must respect each other's mandates, obligations and independence and recognize each other's constraints and commitments. Mutual respect must not preclude organizations from engaging in constructive dissent.
Transparency Transparency is achieved through dialogue (on equal footing), with an emphasis on early consultations and early sharing of information. Communications and transparency, including financial transparency, increase the level of trust among organizations.
Result-oriented approach Effective humanitarian action must be reality-based and action-oriented. This requires result-oriented coordination based on effective capabilities and concrete operational capacities.
Responsibility Humanitarian organizations have an ethical obligation to each other to accomplish their tasks responsibly, with integrity and in a relevant and appropriate way. They must make sure they commit to activities only when they have the means, competencies, skills, and capacity to deliver on their commitments. Decisive and robust prevention of abuses committed by humanitarians must also be a constant effort.
Complementarity The diversity of the humanitarian community is an asset if we build on our comparative advantages and complement each other’s contributions. Local capacity is one of the main assets to enhance and on which to build. Whenever possible, humanitarian organizations should strive to make it an integral part in emergency response. Language and cultural barriers must be overcome.
[A Statement of Commitment, Global Humanitarian Platform, July 2007, http://www.icva.ch/ghp.html]
Accountability of country-level cluster leads and participants
“While sector/cluster lead agencies at the country level cannot be held accountable for the performance of all humanitarian partners operational in that sector, they are accountable to the Humanitarian Coordinator for ensuring, to the extent possible, the establishment of adequate coordination mechanisms for the sector or area of activity concerned, adequate preparedness, as well as adequate strategic planning for an effective operational response…
“While the cluster approach encourages strong partnerships and joint planning amongst humanitarian
DRAFT for FIELD CONSULTATION
[Health Cluster Guide – draft, 30 June 2008] 14
actors, it is up to individual agencies to determine levels of participation in the work of the different sectoral groups. The cluster approach itself does not require that humanitarian actors be held accountable to sector leads. Likewise, it does not demand accountability of non-UN actors to UN agencies. Individual humanitarian organizations can only be held accountable to sector leads in cases where they have made specific commitments to this effect.”
[IASC - Guidance Note on using the Cluster Approach to Strengthen Humanitarian Response, 24 Nov. 2006]
DRAFT for FIELD CONSULTATION
[Health Cluster Guide – draft, 30 June 2008] 15
1.3 Relationships with the government/MoH and other clusters
Relationships with national and local health authorities
“Each State has the responsibility first and foremost to take care of the victims of natural disasters and other emergencies occurring on its territory. Hence, the affected State has the primary role in the initiation, organization, coordination, and implementation of humanitarian assistance within its territory.” [UN General Assembly Resolution 46/182]
“… States have primary responsibility for meeting the assistance and protection needs of people affected by natural disasters and other emergencies (including conflict-related ones) occurring on their territories: International actors should therefore be reliable and predictable partner for governments and other relevant local and national actors and should support national efforts to meet the humanitarian needs of affected populations and to complement national efforts including in cases where national authorities are unable or unwilling to lead the response. “Local government structures and existing capacities should be taken into account when rolling out of the cluster and determining response structures at the country level should remain flexible.” [IASC Working Group, Rome 5-7 November 2008]
The health cluster lead serves as a bridge between the MoH/national health authorities and international and NGO humanitarian health actors.
A key responsibility of the health cluster lead at the country level is to ensure that (international) humanitarian actors build on local capacities and that they develop and maintain appropriate links with relevant government and local authorities (notably the MoH) and local civil society organizations active in health-related activities. The nature of these links will depend on the situation in each country and on the willingness and capacity of each of these organisations to lead or participate in humanitarian activities:
• Where the MoH is in a strong position to lead the overall humanitarian health response, the cluster should organize the international humanitarian response in support of the host Government’s efforts. This would typically be the case following a natural disaster.
• In other cases, particularly in a situation of ongoing conflict, the willingness or capacity of the Government or State institutions – including the MoH – to lead or contribute to humanitarian activities may be compromised, and this will clearly influence the nature of the relationships which it establishes with international humanitarian actors. [IASC - Guidance Note on using the Cluster Approach to Strengthen Humanitarian Response, 24 Nov. 2006]
Practical arrangements may vary accordingly. It has often been found appropriate for an MoH representative and the cluster lead to co-chair meetings at both national and sub-national levels.
Relationships with other clusters/sector groups
At the global level, several key aspects and determinants of public health are covered by the Nutrition, Shelter, and WASH (water, sanitation and hygiene) clusters. When there are similar arrangements at country level, close coordination among the health cluster and the other clusters concerned is essential.
Meetings of all cluster leads and cluster coordinators facilitate such coordination but direct coordination with the other clusters is also essential, see section 2.3.

DRAFT for FIELD CONSULTATION
[Health Cluster Guide – draft, 30 June 2008] 16
1.4 Cluster activities during different phases of health response
Figure 2 below summarizes the programme planning and management process that Cluster participants need to keep in mind and that the coordinator must facilitate. Note that:
• Overall situation analysis, the development of agreed objectives, priorities, strategies and a strategic framework/action plan for health sector action, monitoring the implementation of the agreed health interventions, and evaluating health sector performance is the responsibility of the Cluster as a whole and the coordinator in particular.
• Detailed planning, implementation, monitoring and evaluation of individual projects are the responsibility of the individual organization concerned. However, where the “cluster approach” is fully adopted and organizations work in partnership, the cluster coordinator and cluster participants may organize joint/independent monitoring and evaluation of individual projects, including real-time evaluations, under the leadership of the HCC.
• The process of assessment, situation analysis, planning and monitoring is iterative with refinements and adjustments being made as more, up-dated information becomes available.
Joint training can contribute to the effectiveness of collective action and the establishment and maintenance of broadly similar standards across projects managed by different organizations in different areas.
Figure 3 lists the main actions to be taken during four distinct phases of response. The time frame and the focus of response for each phase depend on the nature of the disaster/crisis. For some emergencies, there may be an early warning phase in advance of the onset of the crisis. Note that:
• The “first steps” need to be completed more quickly in case of a sudden-onset disaster than a slow-onset crisis, but the activities are similar.
• In some cases, particularly in case of a complex (conflict) emergency, the situation may evolve differently in different parts of the country; the acute phase last longer in some areas than others.
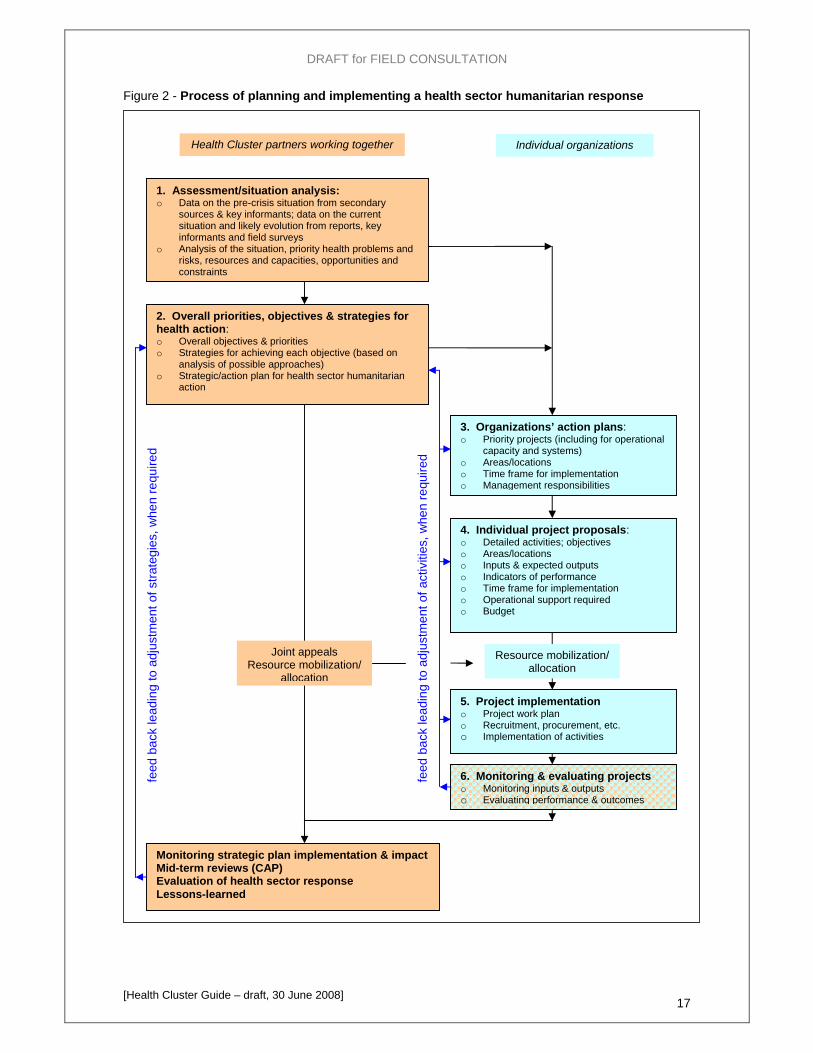
DRAFT for FIELD CONSULTATION
[Health Cluster Guide – draft, 30 June 2008] 17
Figure 2 - Process of planning and implementing a health sector humanitarian response
feed
bac
k le
adin
g to
adj
ustm
ent o
f act
iviti
es, w
hen
requ
ired
feed
bac
k le
adin
g to
adj
ustm
ent o
f stra
tegi
es, w
hen
requ
ired
1. Assessment/situation analysis: o Data on the pre-crisis situation from secondary
sources & key informants; data on the current situation and likely evolution from reports, key informants and field surveys
o Analysis of the situation, priority health problems and risks, resources and capacities, opportunities and constraints
2. Overall priorities, objectives & strategies for health action: o Overall objectives & priorities o Strategies for achieving each objective (based on
analysis of possible approaches) o Strategic/action plan for health sector humanitarian
action
3. Organizations’ action plans: o Priority projects (including for operational
capacity and systems) o Areas/locations o Time frame for implementation o Management responsibilities
Individual organizations
4. Individual project proposals: o Detailed activities; objectives o Areas/locations o Inputs & expected outputs o Indicators of performance o Time frame for implementation o Operational support required o Budget
5. Project implementation o Project work plan o Recruitment, procurement, etc. o Implementation of activities
Resource mobilization/ allocation
Monitoring strategic plan implementation & impact Mid-term reviews (CAP) Evaluation of health sector response Lessons-learned
Joint appeals Resource mobilization/
allocation
6. Monitoring & evaluating projects o Monitoring inputs & outputs o Evaluating performance & outcomes
Health Cluster partners working together
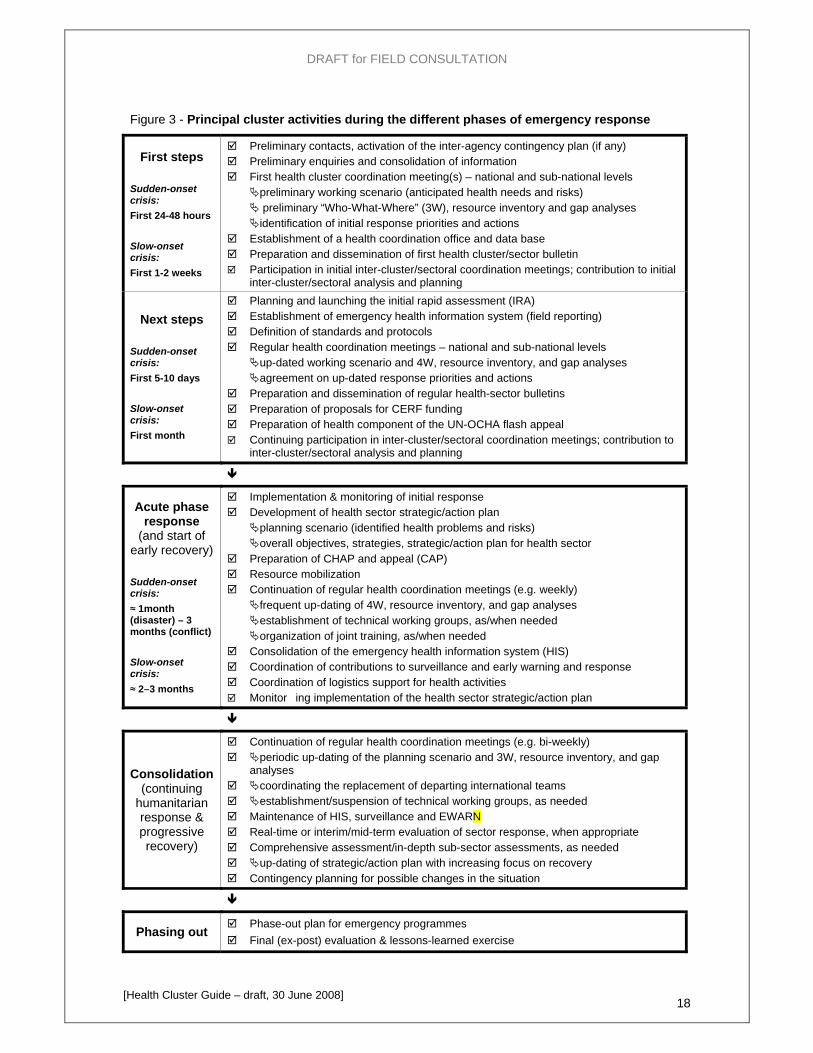
DRAFT for FIELD CONSULTATION
[Health Cluster Guide – draft, 30 June 2008] 18
Figure 3 - Principal cluster activities during the different phases of emergency response
First steps Sudden-onset crisis: First 24-48 hours Slow-onset crisis: First 1-2 weeks
Preliminary contacts, activation of the inter-agency contingency plan (if any) Preliminary enquiries and consolidation of information First health cluster coordination meeting(s) – national and sub-national levels
preliminary working scenario (anticipated health needs and risks) preliminary “Who-What-Where” (3W), resource inventory and gap analyses identification of initial response priorities and actions
Establishment of a health coordination office and data base Preparation and dissemination of first health cluster/sector bulletin Participation in initial inter-cluster/sectoral coordination meetings; contribution to initial
inter-cluster/sectoral analysis and planning
Next steps Sudden-onset crisis: First 5-10 days Slow-onset crisis: First month
Planning and launching the initial rapid assessment (IRA) Establishment of emergency health information system (field reporting) Definition of standards and protocols Regular health coordination meetings – national and sub-national levels
up-dated working scenario and 4W, resource inventory, and gap analyses agreement on up-dated response priorities and actions
Preparation and dissemination of regular health-sector bulletins Preparation of proposals for CERF funding Preparation of health component of the UN-OCHA flash appeal Continuing participation in inter-cluster/sectoral coordination meetings; contribution to
inter-cluster/sectoral analysis and planning
Acute phase response
(and start of early recovery) Sudden-onset crisis: ≈ 1month (disaster) – 3 months (conflict) Slow-onset crisis: ≈ 2–3 months
Implementation & monitoring of initial response Development of health sector strategic/action plan
planning scenario (identified health problems and risks) overall objectives, strategies, strategic/action plan for health sector
Preparation of CHAP and appeal (CAP) Resource mobilization Continuation of regular health coordination meetings (e.g. weekly)
frequent up-dating of 4W, resource inventory, and gap analyses establishment of technical working groups, as/when needed organization of joint training, as/when needed
Consolidation of the emergency health information system (HIS) Coordination of contributions to surveillance and early warning and response Coordination of logistics support for health activities Monitor�ing implementation of the health sector strategic/action plan
Consolidation (continuing
humanitarian response & progressive recovery)
Continuation of regular health coordination meetings (e.g. bi-weekly) periodic up-dating of the planning scenario and 3W, resource inventory, and gap
analyses coordinating the replacement of departing international teams establishment/suspension of technical working groups, as needed Maintenance of HIS, surveillance and EWARN Real-time or interim/mid-term evaluation of sector response, when appropriate Comprehensive assessment/in-depth sub-sector assessments, as needed up-dating of strategic/action plan with increasing focus on recovery Contingency planning for possible changes in the situation
Phasing out Phase-out plan for emergency programmes Final (ex-post) evaluation & lessons-learned exercise
DRAFT for FIELD CONSULTATION
[Health Cluster Guide – draft, 30 June 2008] 19
2 What’s needed for an effective health cluster
Key points: The aim of the health cluster is to achieve the best possible coverage of health interventions focusing on the priority health needs of the population(s) affected by the crisis. “Coordination” can contribute to this but is only one (albeit crucial) aspect of the work of a health cluster; it is not an end in itself.
Coordinated action can be achieved in different ways depending on the situation and existing capacities but the following are essential in all cases:
joint assessment, analysis, planning and monitoring that generates agreement on priorities, objectives and strategies and results in the preparation and regular up-dating of an agreed strategic/action plan for health sector action and agreed priorities for the resource allocations (applications to CERF, use of pooled funds, etc.);
regular exchanges of information, shared/common basic data, and regular meetings that are well planned and managed.
The health cluster lead must ensure:
Appropriate facilities for cluster coordinator and support staff. Appropriate support services and budget for cluster activities. Specific project proposal for donor funding, if needed.
The HCC must be a facilitator and, at the same time, provide leadership and ensure:
Broad participation – all health actors including new arrivals. Appropriate involvement of MoH.
Regular, well-prepared meetings that are well-managed and focus on problem solving and joint planning (not just information sharing). Prompt issuing of summary minutes.
Up-to-date contact lists available to everyone.
Who-What-Where-When (4W) data collected early and kept up-to-date. The provider of last resort function activated when needed.
Technical assistance.
Health information system (linked to and complementing any OCHA-managed humanitarian information centre, HIC).
Arrangements for dialogue and coordination with other public-health-related clusters (especially nutrition and WASH).
Regular, direct communications with cluster participants individually, the representative of the health cluster lead, and the MoH.
DRAFT for FIELD CONSULTATION
[Health Cluster Guide – draft, 30 June 2008] 20
Common “gaps” in relation to health sector coordination findings from 10 country case studies (2004-07)
Examples Proposed remedies
Ineffective health sector coordination mechanism, failing to include affected community, national and local governments, donor governments, multilateral agencies, national and international NGOs, academic institutions, military and the media, as well as the private sector and organised religion.
Poor coordination of plans and communication of activities between the capital and the field coordination mechanism.
Multiple coordination mechanisms operating simultaneously. Meetings time-consuming, resulting in information sharing rather than action planning.
Unclear distinction between health leadership roles of different UN agencies.
Inadequate inter-sectoral coordination.
Deploy authoritative lead with group facilitation skills to act as dedicated coordinator with no additional implementation responsibilities early in an acute crisis.
Nominate field level coordinator(s) as well as central coordinator as indicated by the situation. Consider putting in place a decentralised Cluster approach with a Cluster lead agency in the field, conducting field–level sector-wide planning which is then forwarded to central level for review and support.
Orient meetings towards common actions; disseminate standards, guidelines and country planning documents (e.g. on CD) to partners.
Establish interagency Letters of Understanding covering field operations to clarify agreed roles and responsibilities where confusion exists.
Conduct regular inter-sectoral coordination meetings, ensuring attendance by sectoral representatives with decision making capacity.
DRAFT for FIELD CONSULTATION
[Health Cluster Guide – draft, 30 June 2008] 21
2.1 The challenge for the cluster coordinator
Some basic principles
Build on what exists: use and build on existing coordination mechanisms, to the extent possible.
Address the key health priorities of the affected populations, starting with what is most feasible and expand incrementally to address other concerns as soon as possible: start with modest objectives, demonstrate value added and build trust, hence get buy-in, then broaden the scope (see the box below).
Make sure all participants have something to gain: for a cluster/sector coordination group to be successful, it must offer tangible benefits to participants such as access to more/better information or expertise, opportunities for common strategizing and planning, facilitated access to the affected areas, access to resources (transport, funds, etc.) from a common pool or through the identification of opportunities for sharing.
Acknowledge constraints: constraints to coordinated action include different mandates and agendas, competition among agencies for donor resources, and competing demands on the time of participating individuals. (More barriers to coordination are highlighted in the box below.)
Learn from the past: find out how health sector coordination processes operated in previous emergencies in the country, what worked well and what didn’t, and why.
What to do
Be inclusive: the coordinator and already-participating organizations should be proactive in identifying other health actors (current or potential) and encouraging them to join/attend meetings.
Build relationships – “network”: achieving coordination is primarily an issue of behaviour and inter-personal skills (even though demonstrated technical competence can help); the coordinator must build personal relationships with all health actors and facilitate direct contacts and relationships among them.
Conduct a quick stakeholder analysis to identify the interests that will facilitate and those that will hinder the establishment and effective functioning of the health cluster. Hence identify ways to build on the positive factors and gradually reduce the negative ones.
Use existing mechanisms for the preparation of an OCHA flash appeal, a CHAP and CAP, and other inter-agency planning processes, as opportunities to build this culture of collaboration, participation and partnership.
Involve participants in formulating the agendas for meetings and identifying areas requiring specific work, and ensure that all partners participate in and contribute to the definition of priorities (and consequent decisions on the allocation of resources).
Ensure that local knowledge and know-how are harnessed, and ensure translation at meetings.
Ensure that the meetings focus on problem solving, prioritization and planning, and do not simply become a forum for information sharing. Keep meetings as short as possible and adjust their frequency to the needs of phase of operation.
Arrange for a few designated individuals to work on specific problematic issues and bring a recommendation back to the next cluster meeting, when necessary, but avoid a proliferation of meetings. Ask for email feed back on drafts and limit discussion in cluster meetings to the key issues only.
Make sure that information about meetings, decisions and current health issues are readily available to all actors.
Respect the mandates and characteristic orientations of different organizations and recognize the diversity of perspectives, approaches and methodologies that may exist. Seek to build consensus on needs, risks, objectives, and how available resources can best be applied.
Recognize the different levels of expertise and resources available to different partners and ensure that all are able to contribute to and benefit from cluster.

DRAFT for FIELD CONSULTATION
[Health Cluster Guide – draft, 30 June 2008] 22
Adopt a problem-solving and solution-oriented mindset; seek input and encourage dialogue.
Understand participants’ expectations and constraints; ensure that expectations are realistic and seek ways to help them overcome constraints.
Ensure transparency in all Cluster activities and the use of resources.
Seek feedback from cluster members on the effectiveness of the Cluster and how it could be enhanced.
A progressive approach to effective “coordination”
Coordination is teamwork: make each partner feel part of it. Without being too strict on the sequence, you can adopt a progressive approach.
1. As a start, have the partners sharing information
• on their mandates, objectives, roles and responsibilities • on their resources and capabilities • on the type and quantity of assistance that they can provide • on their areas of operations • on the priorities that they want to address • on their projects • on their sources of data • on their perception of the general context.
2. As next step, have the partners working together
• at assessing needs • at setting the standards of assistance • at mobilising external resources • at ensuring access to the beneficiaries • at building local and national capacities • at training their own staff.
3. In a more advanced phase, you will find that the team can share plans and resources:
• through joint contingency planning ('..what if ?') • through joint strategic planning • through joint operational planning • by implementing joint operations • by sharing their experts • by sharing security systems • by sharing logistics (communication and transport)
Some common barriers to coordination Tips to overcome them
The perception that coordination will limit autonomy and that the freedom to make decisions and run programs as desired will be circumscribed.
Informing the cluster stakeholders on coordination mechanism and issues. Have frank and open discussions on the goals expected to be reached through the coordination efforts
Too many decision-makers and/or too many organizations involved in the coordination mechanism will complicate the process and make any consensus and/or agreement, difficult to achieve.
Identify the key actors who should be part of the coordination and decide whom to invite according to the aim of the meeting
Diversification and specification of each implementing agency, resulting in different expectations or beliefs about what is important for the beneficiaries and/or stakeholders
Promote an understanding of the mandates of the collaborating organizations

DRAFT for FIELD CONSULTATION
[Health Cluster Guide – draft, 30 June 2008] 23
Lack of resources (both human and financial) allocated to coordination might be seen as a low priority given limited time
Make sure that adequate budgets in the Flash Appeal and UNCAP are allocated for the management and coordination of the cluster team
Limited “field-based” decision-making authority such that no decisions can be made without HQ approval thus resulting in delays or having an agreement overturned.
Establish a decentralized coordination mechanism, represented at country and field level Establish deadlines for HQ decisions and that action will take place regardless of the outcome after the deadline
Staff turnover where new staff lacks a commitment to coordination or are unaware of coordination agreements
Delegate part of your work and hand over functions to others, preferably to senior national staff in order to assure and guarantee the continuation and memory of the activities implemented
Unilateral actions that ignore established coordination mechanisms of the coordination body whether by donors or member organizations.
Clarify coordination parameters and activities with partner organizations and call for a meeting to find solution how to overcome such unilateral actions in future. Get support from some donors or partner organization on that. That such actions can divert effective coordination by establishing norms of coordination
Ineffectual or inappropriate coordination leadership, for example, when the coordination body exercises autocratic leadership and imposes decisions on others without a transparent process of involvement.
Evaluate periodically how the coordination process is going and how it might be improved (involve different stakeholders in this process) Involve partners in the coordination process
A coordination process that is not working well, has unclear objectives, and is seen to waste time without obvious benefits to those participating in it.
Provide useful information and services Provide concrete actionable deliverables
DRAFT for FIELD CONSULTATION
[Health Cluster Guide – draft, 30 June 2008] 24
2.2 Organizing cluster meetings
Organizing a first meeting
If there is an existing, effective cluster/sector coordination group, it should be easy to organize a first meeting quickly after the onset of a crisis. If there is an existing inter-agency contingency plan, the meeting should be able to get down to business and take decisions rapidly.
If there is no existing coordination group, the designated lead agency for health should contact the MoH and the other main health actors to arrange a first meeting with as many participants as possible.
In all cases:
Include all relevant governmental and other national entities.
Get the MoH to chair or co-chair the meeting, if possible.
Ensure that the health cluster lead agency emergency programme manager attends.
Prepare a realistic agenda – see the example in the box below; focus on key issues identified and agreed in advance with the MoH.
Prepare as handouts the information, including maps, available from preliminary enquiries.
Prepare formats and/or flip charts to record the information you want to get from others during or after the meeting. This includes, in particular, information on who is doing what, where (see section 2.4)
Ensure that the chair (or co-chairs) keep discussions focused and enforce time-keeping.
Ensure the rapid preparation and distribution of a concise record of key items of information shared in the meeting, decisions reached, and follow up actions required with responsibilities.
The first meeting must be convened by the lead agency within the first 24-48 hours for a sudden-onset crisis (the first 2-3 days for a slow-onset crisis) even if the individual designated as coordinator has not yet arrived. An agenda is suggested in the box below.
It may be useful to present the generic health cluster coordinator TOR (Annex A) and ask for quick comments as to whether and how they might need to be amended to suit the context of the country and the current emergency.
Possible agenda for a first Health Cluster meeting
1. Welcome, introductions (if needed); explanation of the purpose of the cluster; agreement on the agenda
2. Short briefing by MoH and the HCC (or the Cluster Lead representative if the HCC is not yet in place) on what is known about the situation, health needs, and actions already taken or planned
3. Sharing information: what each participating organization knows, is doing, plans to do (when and where), and the problems and constraints faced
4. Information gaps: identification of any major gaps in information concerning specific areas and/or health aspects; discussion and agreement on how critical information gaps will be filled (who will do what when)
5. Service gaps: identification of major, life-threatening health risks and gaps in measures and services to address those risks; discussion and agreement on how those gaps will be filled (who will do what when)
6. Assessment: arrangements for a (collaborative) initial rapid assessment
7. Information clearing house: agreement for an emergency health information focal point to receive and collate information from all participants
8. Bulletin: arrangements for the production and dissemination of an emergency health bulletin
9. Next meeting: date, place, time, agenda items and anything participants are requested to prepare

DRAFT for FIELD CONSULTATION
[Health Cluster Guide – draft, 30 June 2008] 25
Organizing follow-up/ongoing meetings
Agenda items for a subsequent meeting may be based on that proposed for a first meeting – focusing on up-dates – and include establishing agreement on case definitions, treatment protocols, standard drug and equipment lists, and reporting systems.
All meetings should be announced/re-confirmed – and the agenda issued – several days ahead of time.
DRAFT for FIELD CONSULTATION
[Health Cluster Guide – draft, 30 June 2008] 26
2.3 Cooperating with other clusters and coordinating entities
Working with other clusters
Invite other clusters/sector groups to assign representatives to attend health Cluster meetings.
Assign representatives of the health Cluster to attend the other Cluster meetings and report back to the HCC and the next health Cluster meeting.
Organize joint activities such as a tri-cluster (health, nutrition & WASH) Initial Rapid Assessment (IRA), see section 3.4.
Identify as early as possible the cross-cutting issues that have particular significance for the health sector and use the inter-cluster coordination meetings and mechanisms to plan joint (or complementary) activities to address them appropriately.
Establish joint plans with relevant other clusters (notably WASH and nutrition) for addressing issues relating to specific priority public health problems of common concern (such as preparing for or responding to a cholera outbreak) and HIV/AIDS (a cross-cutting concern).
Working with other coordinating entities
Work closely with any UNDAC or OCHA team present.
Provide the RC/HC and OCHA with information on the health situation. Get from OCHA (and the humanitarian information centre, HIC, when established) information compiled on other sectors, especially shelter, nutrition and WASH.

DRAFT for FIELD CONSULTATION
[Health Cluster Guide – draft, 30 June 2008] 27
3 Health Information in Crisis
3.1 Crisis & Health Information Management
Crisis result in a disruption of Health Systems, inducing a disruption of existing Routine Health Information and Surveillance Systems. The particularities of a crisis moreover generate specific needs in terms of Health Information usually not accounted for in National HIS or Routine Surveillance Systems.
Crisis therefore call for the adoption and deployment of specific Assessment & Monitoring tools that will ensure health information needs are met throughout the crisis while simultaneously preparing the ground for the rehabilitation and, whenever needed, upgrade of Routine Health Information and Surveillance Systems.
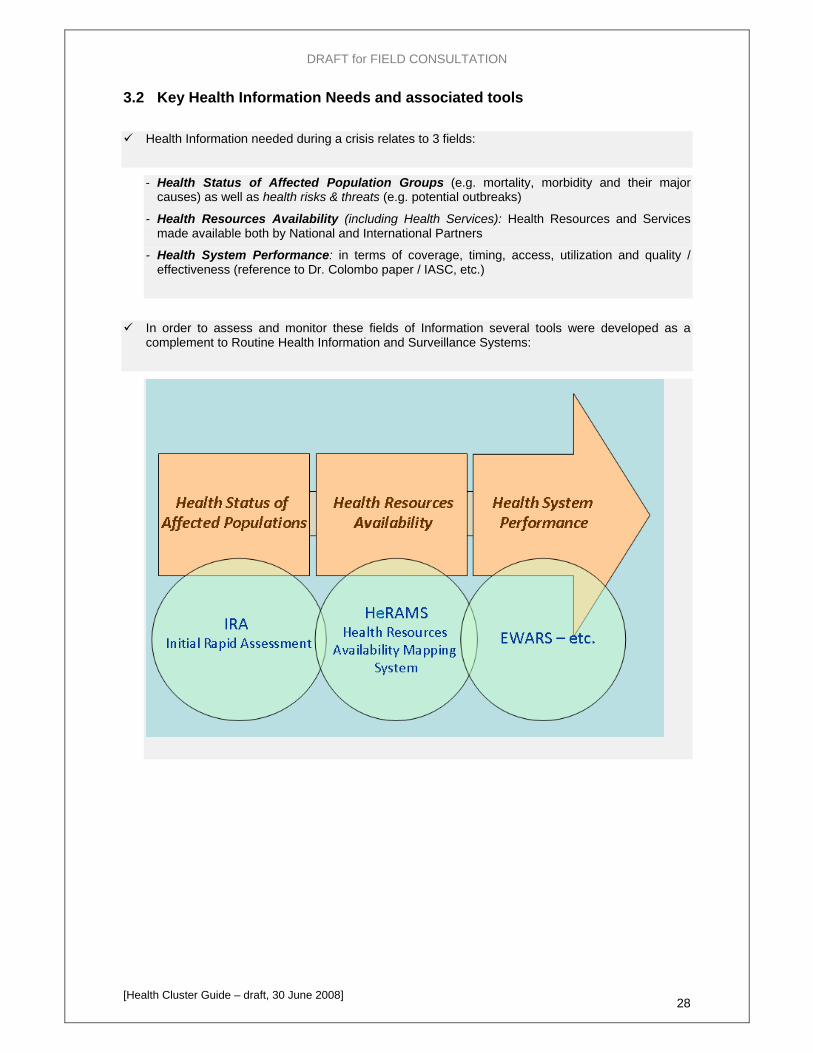
DRAFT for FIELD CONSULTATION
[Health Cluster Guide – draft, 30 June 2008] 28
3.2 Key Health Information Needs and associated tools
Health Information needed during a crisis relates to 3 fields:
- Health Status of Affected Population Groups (e.g. mortality, morbidity and their major causes) as well as health risks & threats (e.g. potential outbreaks)
- Health Resources Availability (including Health Services): Health Resources and Services made available both by National and International Partners
- Health System Performance: in terms of coverage, timing, access, utilization and quality / effectiveness (reference to Dr. Colombo paper / IASC, etc.)
In order to assess and monitor these fields of Information several tools were developed as a complement to Routine Health Information and Surveillance Systems:
DRAFT for FIELD CONSULTATION
[Health Cluster Guide – draft, 30 June 2008] 29
3.3 The need for initial / rapid Assessment and Monitoring tools Both IRA and HeRAMS were originally developed with the ambition of meeting decision makers' information needs comprehensively. The onset of a crisis however seldom allows for such assessments mainly because of:
limited access to affected areas
limited availability of adequate resources (qualified data collectors, data analysts, etc.)
limited time for decision making and action
Such limitations strengthened the need for the development of so-called "Initial" or "Rapid" versions of existing tools. These should tackle issues specific to the onset of crisis by allowing :
- situation assessment and monitoring at larger scales
- fast and eased implementation
- low resource requirements
3.4 From an initial to a comprehensive and from an assessment based to a monitoring based approach
Assessments provide information on the situation at a particular point in time. Repeating
Assessments over time allows to measure change in time, an essential dimension for decision makers.
Similarly as the situation evolves and moves into a transition phase, more and more
information becomes necessary for fine tuning humanitarian interventions.
Evolving from Initial to more Comprehensive and from Assessment based to Monitoring based Approaches should therefore constitute a priority objective in Information Management in Crisis.
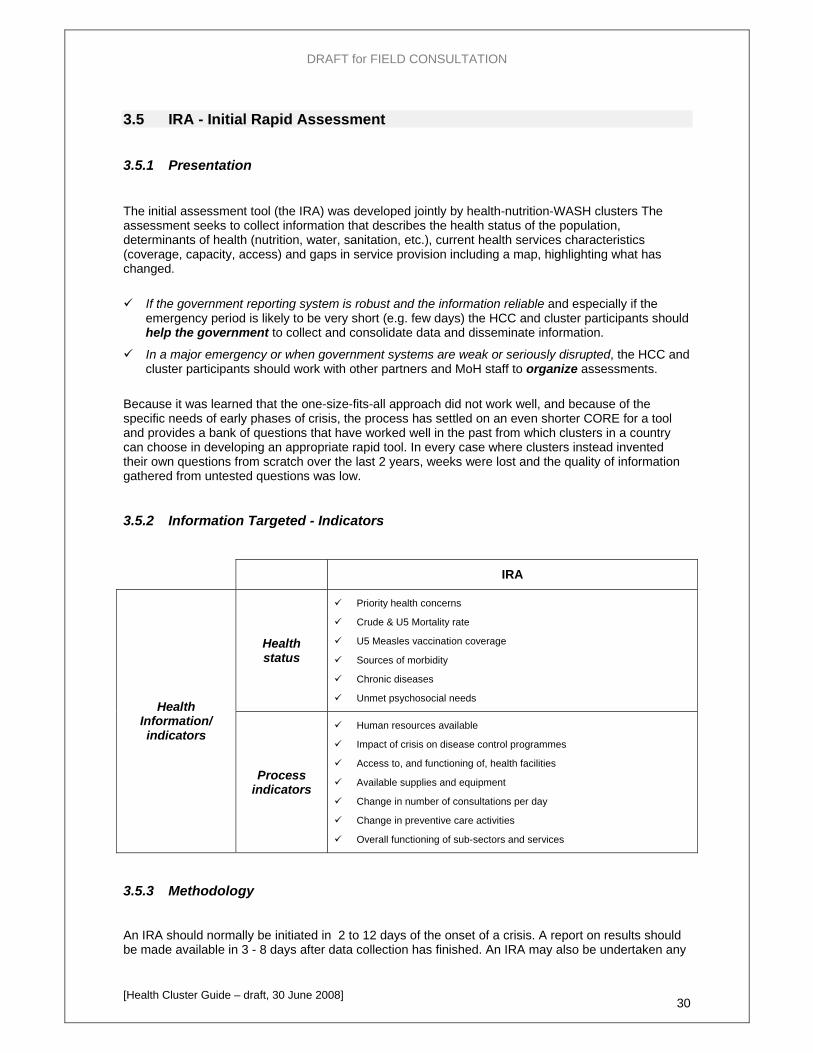
DRAFT for FIELD CONSULTATION
[Health Cluster Guide – draft, 30 June 2008] 30
3.5 IRA - Initial Rapid Assessment
3.5.1 Presentation The initial assessment tool (the IRA) was developed jointly by health-nutrition-WASH clusters The assessment seeks to collect information that describes the health status of the population, determinants of health (nutrition, water, sanitation, etc.), current health services characteristics (coverage, capacity, access) and gaps in service provision including a map, highlighting what has changed.
If the government reporting system is robust and the information reliable and especially if the emergency period is likely to be very short (e.g. few days) the HCC and cluster participants should help the government to collect and consolidate data and disseminate information.
In a major emergency or when government systems are weak or seriously disrupted, the HCC and cluster participants should work with other partners and MoH staff to organize assessments.
Because it was learned that the one-size-fits-all approach did not work well, and because of the specific needs of early phases of crisis, the process has settled on an even shorter CORE for a tool and provides a bank of questions that have worked well in the past from which clusters in a country can choose in developing an appropriate rapid tool. In every case where clusters instead invented their own questions from scratch over the last 2 years, weeks were lost and the quality of information gathered from untested questions was low.
3.5.2 Information Targeted - Indicators
IRA
Health status
Priority health concerns
Crude & U5 Mortality rate
U5 Measles vaccination coverage
Sources of morbidity
Chronic diseases
Unmet psychosocial needs Health
Information/ indicators
Process indicators
Human resources available
Impact of crisis on disease control programmes
Access to, and functioning of, health facilities
Available supplies and equipment
Change in number of consultations per day
Change in preventive care activities
Overall functioning of sub-sectors and services
3.5.3 Methodology
An IRA should normally be initiated in 2 to 12 days of the onset of a crisis. A report on results should be made available in 3 - 8 days after data collection has finished. An IRA may also be undertaken any

DRAFT for FIELD CONSULTATION
[Health Cluster Guide – draft, 30 June 2008] 31
time when a previously inaccessible area can be reached or, when reassessment is indicated following a significant change in the overall humanitarian context.
The key elements of planning, undertaking and reporting on an assessment are indicated in Figure 8. There are three main stages – planning, field work, and analysis and reporting. The success of an assessment and the value of the report are heavily dependent on the quality of the planning – steps 1 to 10 – done before the field visits. In most cases, steps 3 to 10 will be undertaken more-or-less concurrently.
Figure 8
Principal steps in organizing & undertaking a rapid assessment
(1) Initial decision Agreement among health-related agencies and the MoH that an assessment is needed.
(2) Planning the assessment
1-2 days
Half-day planning meeting and follow-up work by individuals and sub-groups to: 1. compile available data and agree a working scenario; 2. agree the objectives, scope of work and timeframe (dates) for the assessment, and its
relationship to other assessment activities; 3. agree information requirements, data collection and criteria for deciding where to go
(site selection procedures) and whom to talk with; 4. design/customize interview guides, questionnaires, and analysis sheets; translate the
questionnaires into local language(s) if necessary; 5. identify personnel (and interpreters, if required) for fieldwork; 6. prepare maps, supplies, equipment (including tents, food, if necessary) and
background information kits for field teams; 7. assemble and train fieldwork teams; 8. arrange transport (including fuel), security and communications for teams; 9. inform key persons (MoH and others) in areas to be visited; and 10. plan (arrange for) the processing and analysis of data during and after the fieldwork.
(3) Field work
5-6 days
Visits by teams to purposively-selected areas/sites to: • interview and collect data from officials and other key informants in administrative
centres and health facilities; and • interview community groups and households.
(4) Analysis and
reporting 3-4 days
Processing and analysis of data (primary and secondary) Identification of priority problems, needs and risks Analysis of possible strategies and development of recommendations Preparing the report ; Disseminating the report
DRAFT for FIELD CONSULTATION
[Health Cluster Guide – draft, 30 June 2008] 32
HCC and Health Cluster action:
Where there is an inter-agency contingency plan, activate it and organize a joint, multi-sector assessment with partners as foreseen.
Whenever it’s possible to organize a “joint” assessment in the first few days:
Liaise with the Nutrition and WASH clusters and invite as many as possible of the main health actors, together with key actors from the other sectors, to a planning meeting to be held on day 1:
o Agree the purpose/objectives hence the time frame for the assessment.
o Define responsibilities and timeframes for all preparatory actions (see Figure 7).
o Adapt the IRA format to the local context, if necessary.5
Rapidly review health-related secondary data available at national level (unless this has already been done as a part of contingency planning) – see ISA guidance note 2.3 especially table 2.
Then, jointly with the other clusters:
Assemble field assessment teams – see ISA guidance note 2.4. Ensure that teams are balanced in terms of expertise and gender, and between national and international personnel; prioritize general public health experience – see box below.
Select the areas to be visited. Use stratified sampling to select not only areas that are believed to be particularly badly affected but also ones covering a range of different conditions and population groups that may be differently affected and face different health problems and risks.6
Define the criteria and procedures to be applied by assessment teams in selecting individual sites to be visited within the selected areas.
Specify the (few, key) items of data on other sectors that health members of assessment teams should collect in the absence of team members for the other sectors, and vice-versa.
Provide guidance notes (including case definitions) and organize rapid training – and security briefing, where needed – for all field assessment teams.
Provide field teams with a maximum of available secondary data on the areas they will visit before they start field visits, so that interviews and primary data collection can be appropriately focused.
Plan logistics carefully and ensure that all teams have necessary permits (where needed), transport (including fuel, etc.), communications (radios and/or access to telephones), GPS (and are trained in its use), and access to accommodation (camping equipment, if necessary), water and food.
Make arrangements to receive and rapidly collate and analyse incoming reports from assessment teams, health facilities, relief teams and other sources. (These arrangements must be made in advance, as part of the planning for the assessment. Too often, analysis of data from “rapid” assessments has taken several weeks!)
Prepare a realistic budget for the whole assessment process – including field travel and the analysis of the data – and secure funds.
5 Adaptation may be necessary if significant urban populations are involved or a variety of population groups (e.g. refugees, IDPs and residents), or to take account of locally-endemic diseases [IRA form section 6.2] and the structure of local health services [section 7.5]). Modifications should focus on clarification, removing items that are clearly inappropriate or highly-sensitive, or adding content. The core structure of the form should be preserved. 6 Where time and consideration permit, plan to visits areas and sites in different livelihood or agro-ecological zones, both urban and rural areas, and both resident and non-resident populations (the latter may include third-country nationals, refugees or internally displaced persons). Additional criteria for stratifying and selecting sites may include socio-economic status and characteristics, sites with more/less access to services, sites with higher/lower levels of poverty, sites with higher/lower prevalence of chronic malnutrition, and minority as well as majority population groups. [Adapted from IRA guidance note 2.5]

DRAFT for FIELD CONSULTATION
[Health Cluster Guide – draft, 30 June 2008] 33
The above should be possible in case of a slow-onset crisis or when an inter-agency contingency plan had already been prepared and arrangements for assessment agreed in advance.
If such joint planning is not feasible in the first few days:
Call a quick meeting…try to agree on a standard, common core for a data collection formats and a standard approach to data collection…try to ensure reasonable coverage of all main areas…and then compile data from different organizations’ assessments and facilitate a joint analysis exercise.
Assessment team composition
Multi-disciplinary teams with a maximum of experienced public health generalists are needed. Balanced team composition is crucial, especially with regard to:
• Knowledge and expertise: primarily public health generalists but specialists may be included where specific aspects are clearly important during the initial period, e.g. mass casualty management (but be careful to ensure that the assessment is not unduly biased towards the concerns of individual specialists)
• Organisational representation: representatives from the government/MoH, UN and other international organisations, the Red Cross and Red Crescent Movement and NGOs should be included)
• Gender for both team members and interpreters, where needed • National and international experts: the former are familiar with the context, but may bring preconceptions; the
latter lack familiarity, but can provide a useful unbiased perspective and experience from elsewhere [Adapted from IRA guidelines, draft, Global Health Cluster, 2007]
Additional guidance
Intersectoral Rapid Assessment tool (form and guidelines), Global Health-Nutrition-WASH Clusters, 2008
Annex F, Types and phases of assessment in a humanitarian crisis Annex G, Guiding principles for all data collection activities – assessments, surveys & surveillance Annex H - Drawing up an assessment plan, schedule and budget, from Emergency Food Security
Assessment Handbook, first edition, WFP 2005 IASC Gender handbook in humanitarian action, IASC Geneva, 2006
http://www.humanitarianinfo.org/iasc/content/documents/subsidi/tf_gender/IASC%2520Gender%2520Handbook%2520%2528Feb%25202007%2529.pdf
UNHCR Tool for participatory assessment in operations, UNHCR Geneva, 2006 http://www.unhcr.org/publ/PUBL/450e963f2.html
IASC - Need Analysis Framework, April 2007 (www.ochaonline.un.org/OchaLinkClick.aspx?link=ocha&docid=1039803)
Darcy & Hofmann, According to need? Needs assessment and decision-making in the humanitarian sector , HPG Report # 15, Sept 2003 (www.odi.org.uk/HPG/papers/hpgreport15.pdf)
DRAFT for FIELD CONSULTATION
[Health Cluster Guide – draft, 30 June 2008] 34
3.6 HeRAMS - Health Resources Availability Mapping System
3.6.1 Presentation
HeRAMS is a package of tools developed in the frame of the GHC with the aim of supporting the collection, collation, analysis and management of information related to Health Resources (and Services) Availability throughout a Crisis.
HeRAMS more precisely stands for :
• Health Resources Availability in terms of:
Health Infrastructures
Health Personnel
Health Services
• Mapping in terms of:
Assessment
Monitoring
Georeferencing
• System in terms of:
Analytical Framework
Technical Support Tools
HeRAMS Package is composed of:
- An Analytical Framework
- A User's / Developers Guidelines
- Automated Data Collection Forms
- A Central DB System for Data Management and Analysis
It is a Monitoring tool that may however, depending on needs, be used as a one-time assessment tool. A initial / rapid version (i-HeRAMS) is also under development to cover specific needs and answer specific challenges posed during the onset phase of crisis.
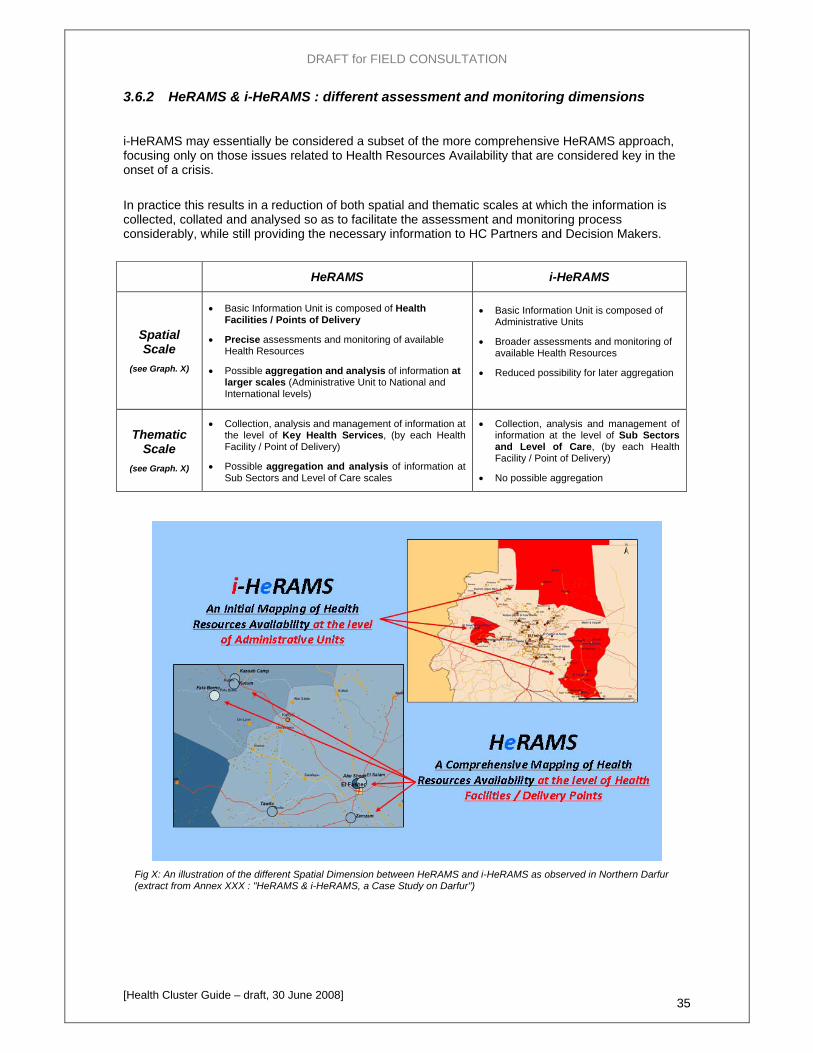
DRAFT for FIELD CONSULTATION
[Health Cluster Guide – draft, 30 June 2008] 35
3.6.2 HeRAMS & i-HeRAMS : different assessment and monitoring dimensions
i-HeRAMS may essentially be considered a subset of the more comprehensive HeRAMS approach, focusing only on those issues related to Health Resources Availability that are considered key in the onset of a crisis.
In practice this results in a reduction of both spatial and thematic scales at which the information is collected, collated and analysed so as to facilitate the assessment and monitoring process considerably, while still providing the necessary information to HC Partners and Decision Makers.
HeRAMS i-HeRAMS
Spatial Scale
(see Graph. X)
• Basic Information Unit is composed of Health Facilities / Points of Delivery
• Precise assessments and monitoring of available Health Resources
• Possible aggregation and analysis of information at larger scales (Administrative Unit to National and International levels)
• Basic Information Unit is composed of Administrative Units
• Broader assessments and monitoring of available Health Resources
• Reduced possibility for later aggregation
Thematic Scale
(see Graph. X)
• Collection, analysis and management of information at the level of Key Health Services, (by each Health Facility / Point of Delivery)
• Possible aggregation and analysis of information at Sub Sectors and Level of Care scales
• Collection, analysis and management of information at the level of Sub Sectors and Level of Care, (by each Health Facility / Point of Delivery)
• No possible aggregation
Fig X: An illustration of the different Spatial Dimension between HeRAMS and i-HeRAMS as observed in Northern Darfur (extract from Annex XXX : "HeRAMS & i-HeRAMS, a Case Study on Darfur")
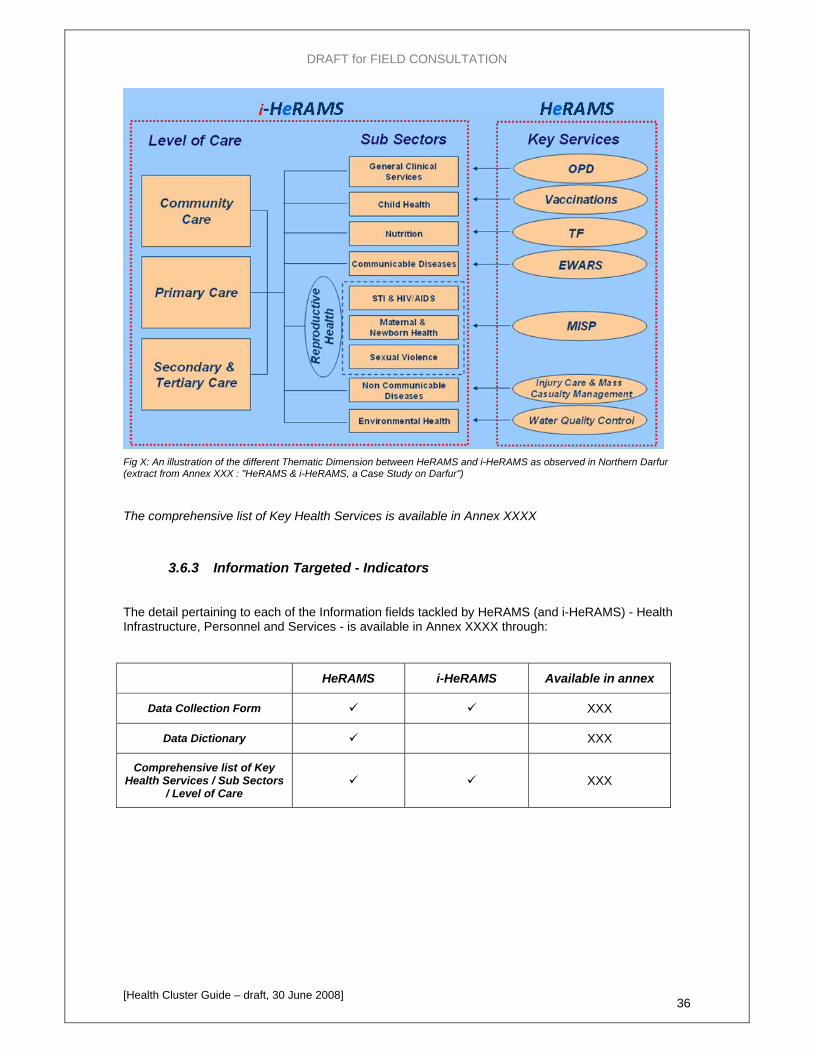
DRAFT for FIELD CONSULTATION
[Health Cluster Guide – draft, 30 June 2008] 36
Fig X: An illustration of the different Thematic Dimension between HeRAMS and i-HeRAMS as observed in Northern Darfur (extract from Annex XXX : "HeRAMS & i-HeRAMS, a Case Study on Darfur")
The comprehensive list of Key Health Services is available in Annex XXXX
3.6.3 Information Targeted - Indicators
The detail pertaining to each of the Information fields tackled by HeRAMS (and i-HeRAMS) - Health Infrastructure, Personnel and Services - is available in Annex XXXX through:
HeRAMS i-HeRAMS Available in annex
Data Collection Form XXX
Data Dictionary XXX
Comprehensive list of Key Health Services / Sub Sectors
/ Level of Care XXX
DRAFT for FIELD CONSULTATION
[Health Cluster Guide – draft, 30 June 2008] 37
3.6.4 Methodology
The Concept of Point of Delivery
Points of Delivery were defined as both geographical and thematic entities (settlements, IDP Camps, etc.) against which health facilities are mapped.
Introducing the concept of Point of Delivery into HeRAMS brought major benefits in the way data was gathered and increased substantially it's potential for analysis.
Points of Delivery are first of all a highly time and resource efficient way of ascertaining the geographical location of health facilities. Equally importantly, they allow for doing so in inaccessible areas.
In addition this allows bridges to be built much more efficiently between HeRAMS and other existing Information Systems developed and maintained by other clusters, thus efficiently preparing the ground for cross cluster data dissemination, collation and analysis.
A practical advantage of this built-in inter-operability is the possibility of relating HF to Point of Delivery's population in qualitative and quantitative.
Data Collection
HeRAMS was developed so as to allow data collection at a centralized level.
Data should be collected through structured surveys between an Information Management Focal Point, and partners' focal points. Such interviews may be added to the agenda of already existing inter cluster meetings and should take no longer than 20-30mn on average.
Appointing this task to Primary Health Officers generates noticeable benefits, but also implies training is provided up front by Information Management Specialists.
Specific Data Collection Forms were designed under Excel, with many features being developed so as to answer two main objectives:
ease the data collection process as much as possible.
ensure data quality and consistency from the first step of information generation.
Centralizing Managing and Analysis Data: HeRAMS Central DB System (CDBS)
The Data Collection Forms developed also include features allowing a direct import of the information gathered in the field through function embedded in the CDBS, thus allowing for a transfer of information from Excel Data Collection Forms to the central Access based System, while always ensuring quality and consistency are preserved.
The CDBS primarily allows for the storage and management of the information gathered to establish the baseline of Health Resources Availability during the first HeRAMS assessment. It however also includes the necessary features to store and maintain the results of subsequent assessments and therefore track the evolution of HeRAMS indicators over time.
Most importantly, a large section was devoted to standardized Canned Reports allowing non specialist users to automatically generate information based on HeRAMS Indicators.
This section currently allows for the generation of Reports based on the following four thematic fields:
DRAFT for FIELD CONSULTATION
[Health Cluster Guide – draft, 30 June 2008] 38
- Health Facilities Characteristics
- Health Personnel
- Health Services
- Health Partner's Mapping
These reports can moreover be generated at all temporal and spatial scales available, allowing for trend analysis as well as spatial analysis such as the comparison of indicator values across districts, sub districts or states and help both:
- Identify priority areas for interventions
- Evaluate the impact of health interventions in time
It should finally be noted that the possibility of accessing raw data is still made available for more advanced users wishing to carry out in-depths analysis.
The CDBS used in Darfur and containing the baseline information for North and South Darfur was added as an attached file for testing.
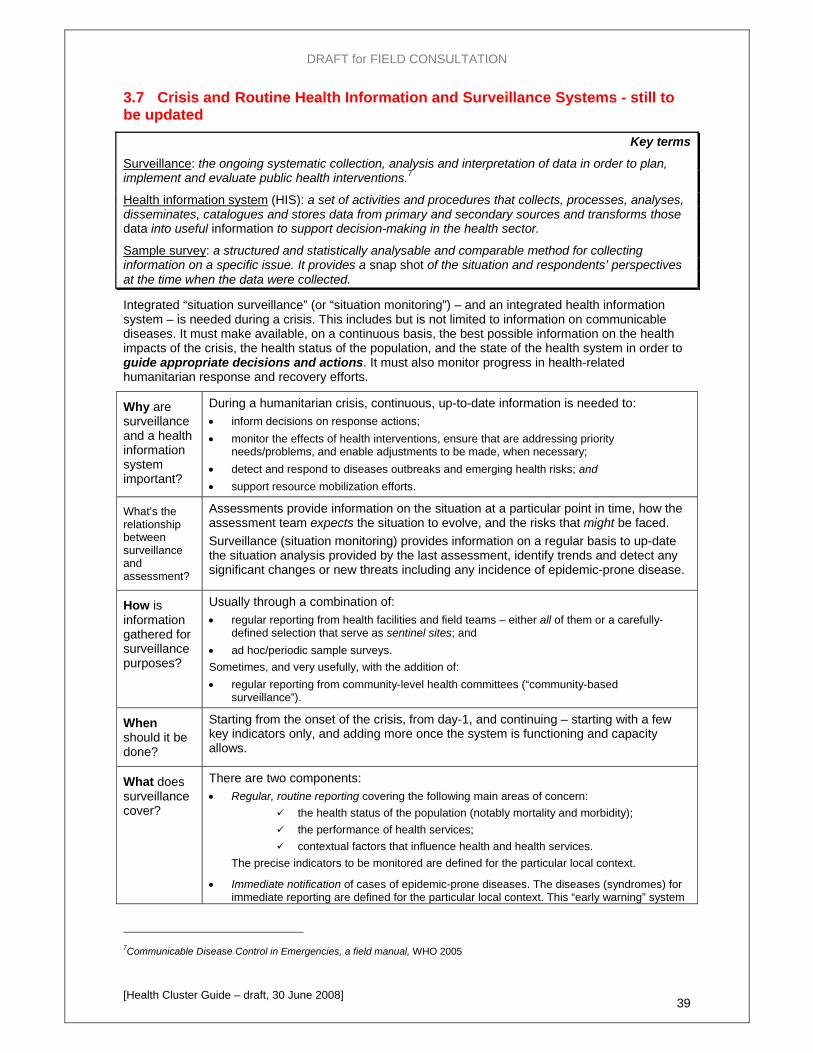
DRAFT for FIELD CONSULTATION
[Health Cluster Guide – draft, 30 June 2008] 39
3.7 Crisis and Routine Health Information and Surveillance Systems - still to be updated
Key terms
Surveillance: the ongoing systematic collection, analysis and interpretation of data in order to plan, implement and evaluate public health interventions.7
Health information system (HIS): a set of activities and procedures that collects, processes, analyses, disseminates, catalogues and stores data from primary and secondary sources and transforms those data into useful information to support decision-making in the health sector.
Sample survey: a structured and statistically analysable and comparable method for collecting information on a specific issue. It provides a snap shot of the situation and respondents’ perspectives at the time when the data were collected.
Integrated “situation surveillance” (or “situation monitoring”) – and an integrated health information system – is needed during a crisis. This includes but is not limited to information on communicable diseases. It must make available, on a continuous basis, the best possible information on the health impacts of the crisis, the health status of the population, and the state of the health system in order to guide appropriate decisions and actions. It must also monitor progress in health-related humanitarian response and recovery efforts.
Why are surveillance and a health information system important?
During a humanitarian crisis, continuous, up-to-date information is needed to: • inform decisions on response actions; • monitor the effects of health interventions, ensure that are addressing priority
needs/problems, and enable adjustments to be made, when necessary; • detect and respond to diseases outbreaks and emerging health risks; and • support resource mobilization efforts.
What’s the relationship between surveillance and assessment?
Assessments provide information on the situation at a particular point in time, how the assessment team expects the situation to evolve, and the risks that might be faced. Surveillance (situation monitoring) provides information on a regular basis to up-date the situation analysis provided by the last assessment, identify trends and detect any significant changes or new threats including any incidence of epidemic-prone disease.
How is information gathered for surveillance purposes?
Usually through a combination of: • regular reporting from health facilities and field teams – either all of them or a carefully-
defined selection that serve as sentinel sites; and • ad hoc/periodic sample surveys. Sometimes, and very usefully, with the addition of: • regular reporting from community-level health committees (“community-based
surveillance”).
When should it be done?
Starting from the onset of the crisis, from day-1, and continuing – starting with a few key indicators only, and adding more once the system is functioning and capacity allows.
What does surveillance cover?
There are two components: • Regular, routine reporting covering the following main areas of concern:
the health status of the population (notably mortality and morbidity); the performance of health services; contextual factors that influence health and health services.
The precise indicators to be monitored are defined for the particular local context.
• Immediate notification of cases of epidemic-prone diseases. The diseases (syndromes) for immediate reporting are defined for the particular local context. This “early warning” system
7Communicable Disease Control in Emergencies, a field manual, WHO 2005
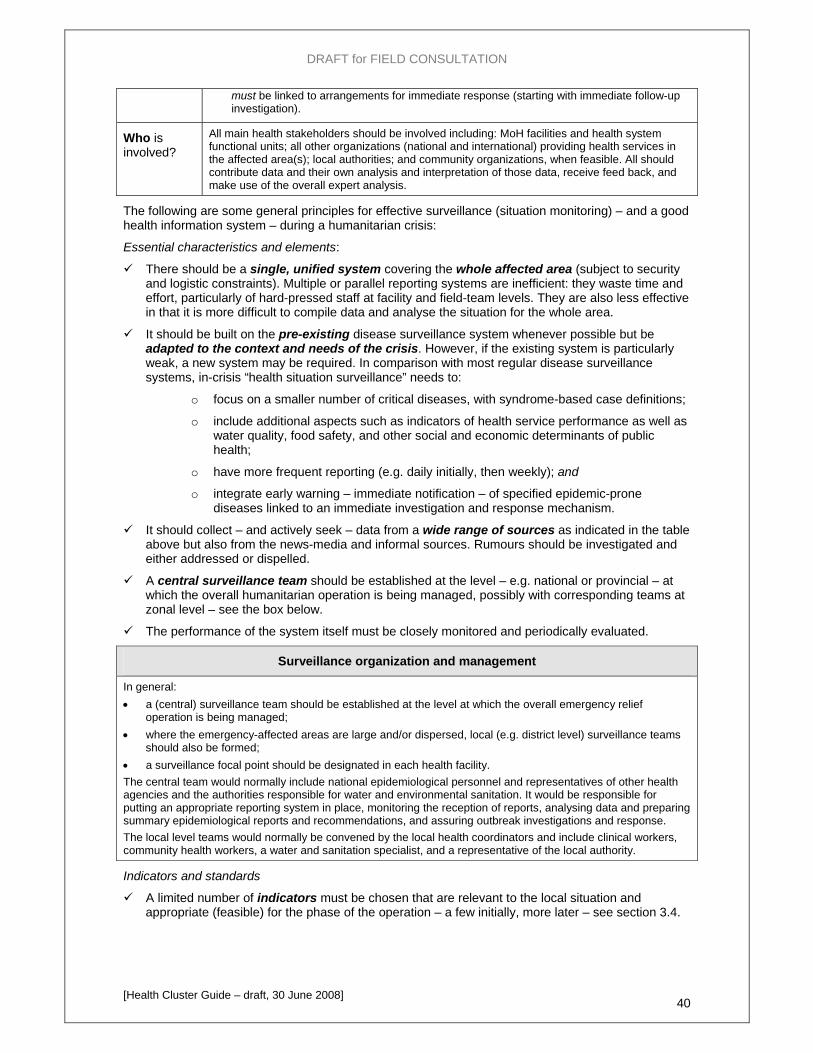
DRAFT for FIELD CONSULTATION
[Health Cluster Guide – draft, 30 June 2008] 40
must be linked to arrangements for immediate response (starting with immediate follow-up investigation).
Who is involved?
All main health stakeholders should be involved including: MoH facilities and health system functional units; all other organizations (national and international) providing health services in the affected area(s); local authorities; and community organizations, when feasible. All should contribute data and their own analysis and interpretation of those data, receive feed back, and make use of the overall expert analysis.
The following are some general principles for effective surveillance (situation monitoring) – and a good health information system – during a humanitarian crisis:
Essential characteristics and elements:
There should be a single, unified system covering the whole affected area (subject to security and logistic constraints). Multiple or parallel reporting systems are inefficient: they waste time and effort, particularly of hard-pressed staff at facility and field-team levels. They are also less effective in that it is more difficult to compile data and analyse the situation for the whole area.
It should be built on the pre-existing disease surveillance system whenever possible but be adapted to the context and needs of the crisis. However, if the existing system is particularly weak, a new system may be required. In comparison with most regular disease surveillance systems, in-crisis “health situation surveillance” needs to:
o focus on a smaller number of critical diseases, with syndrome-based case definitions;
o include additional aspects such as indicators of health service performance as well as water quality, food safety, and other social and economic determinants of public health;
o have more frequent reporting (e.g. daily initially, then weekly); and
o integrate early warning – immediate notification – of specified epidemic-prone diseases linked to an immediate investigation and response mechanism.
It should collect – and actively seek – data from a wide range of sources as indicated in the table above but also from the news-media and informal sources. Rumours should be investigated and either addressed or dispelled.
A central surveillance team should be established at the level – e.g. national or provincial – at which the overall humanitarian operation is being managed, possibly with corresponding teams at zonal level – see the box below.
The performance of the system itself must be closely monitored and periodically evaluated.
Surveillance organization and management
In general: • a (central) surveillance team should be established at the level at which the overall emergency relief
operation is being managed; • where the emergency-affected areas are large and/or dispersed, local (e.g. district level) surveillance teams
should also be formed; • a surveillance focal point should be designated in each health facility. The central team would normally include national epidemiological personnel and representatives of other health agencies and the authorities responsible for water and environmental sanitation. It would be responsible for putting an appropriate reporting system in place, monitoring the reception of reports, analysing data and preparing summary epidemiological reports and recommendations, and assuring outbreak investigations and response. The local level teams would normally be convened by the local health coordinators and include clinical workers, community health workers, a water and sanitation specialist, and a representative of the local authority.
Indicators and standards
A limited number of indicators must be chosen that are relevant to the local situation and appropriate (feasible) for the phase of the operation – a few initially, more later – see section 3.4.

DRAFT for FIELD CONSULTATION
[Health Cluster Guide – draft, 30 June 2008] 41
Standards should be defined establishing the minimum acceptable level of achievement for each indicator in order to provide a basis for interpreting and the findings and explaining their relevance to decision-makers. See section 8.1.
Tools, guidelines, training and support
Appropriate reporting formats, guidelines and training must be provided for all health facilities, field teams and others who are expected to report.
Reporting formats must be simple, designed to facilitate completion and subsequent data extraction, with precise language and appropriate translation.
Training and guidelines should clearly explain the purpose and importance of the reports, describe the format (and any other tools) in detail, and provide practical instructions to promote consistently good reporting – and preliminary analysis and interpretation of the data – by all facilities and teams. They should cover, amongst other things:
o What are the tools used for data collection? o Who is responsible for collecting the data? o What data should be collected and how? o How and when should the data be reported? o How should the data be interpreted and used?
Members of the central (and any decentralized) surveillance team should visit health facilities and teams whenever possible to provide encouragement, explanations and advice, to resolve problems, and identify ways in which the system might be improved.
Transmission, processing and analysis of data
Prompt, regular reporting from health facilities and field teams is essential. Reliable means – and budgets – must be assured for communicating data. (Means might include the use of mobile phones, radios [where permitted by the relevant authorities], and/or hard copies carried by bus or transport companies/drivers.)
Capacity must be available with the central surveillance team to receive and rapidly screen (“clean”) the data received, compile and analyse them with a focus on identifying trends and changes, and divergences from the established standards.
Analysis should focus on aggregate figures initially, and be refined to disaggregate by age and sex as and when feasible.
Data analysis should start at field level. Zonal health cluster focal points supported by epidemiologists or other experienced data analysts, when available, should assure quick, local analysis in collaboration with district/provincial health authorities and other stakeholders. This should identify priorities for immediate action and provide the central surveillance/HIS team with local interpretation together with the raw data.
Regular feedback must be provided by the central surveillance team to all data providers.
The findings must be published promptly, and delivered regularly to decision-makers in all the main stakeholder entities – MoH, the national relief coordination body, international agencies, the main national NGOs, donors, news-media, etc. (Reports may be distributed in conjunction with the regular health bulletin, see section 7.2.)
HCC and Health Cluster action:
Work with the MoH to ensure that an appropriate health information system and arrangements for surveillance of the health situation are in place; establish suitable arrangements, if necessary. This includes:
o a central HIS/surveillance team with dedicated (full-time) staff, an appropriate ; workspace, dedicated computers, telephones and other equipment (e.g. radios), as needed; and
o where appropriate, zonal level HIS/surveillance teams.
In all cases, ensure that adequate resources are dedicated to HIS and surveillance.
DRAFT for FIELD CONSULTATION
[Health Cluster Guide – draft, 30 June 2008] 42
Establish clear procedures – or ensure that clear procedures exist – for the rapid clearance of surveillance/HIS reports, and that they are understood by all concerned. (Bureaucratic delays in producing and issuing information can greatly reduce the validity and usefulness of the information.)
Ensure appropriate links with the data bases of the OCHA-managed humanitarian information centre (HIC), where there is one.
Monitor the performance of the HIS.
Ensure that information is handled and used responsibly, see box below.
Handling and using data and information responsibly
Verify and record the sources and probable reliability of all data and information received. Cross-check – “triangulate” – data from different sources, whenever possible. Consider possible margins of error in data and the implications for decisions. Specify the sources – and the limitations – of any data issued or disseminated. When quoting data or reporting information, always provide analysis of its significance. Respect the confidentiality of medical records: ensure that any copies of documents that contain patients’
names are stored securely and not copied, distributed or left lying around. In any situation of conflict or repression, respect the confidentiality of informants who do not wish their
identities to be revealed.
Lessons & practical hints from field experience
In Uganda, the health cluster uses Village Health Teams (VHTs) to conduct Community-based Disease Surveillance (CBDS) to monitor disease trends at community level …add few details from recent report from HC in Uganda … Such an innovative approach might be replicated in other settings once the situation has stabilized.
.…
Additional guidance
UNHCR – Health Information System (HIS) Project, 2008. www.unhcr.org/his Guidelines for prioritization of disease surveillance, WHO-CDS, 2007 Communicable Disease Control in emergencies, WHO 2005, chapter 3 Natural Disasters – protecting the public’s health, PAHO 2000, chapter 7 Epidemiological surveillance after natural disaster, PAHO 1982 WHO recommended surveillance standards, WHO, 1999
…
3.2 TOOLS COMPLEMENTARITY (To be developed and included before tools presentation)
DRAFT for FIELD CONSULTATION
[Health Cluster Guide – draft, 30 June 2008] 43
Response Planning
Key points: Planning includes deciding on priorities, objectives and strategies. Clarity and agreement on
objectives, strategies and an overall health cluster/sector response plan are essential for coherent, coordinated humanitarian health action. All main health actors should be engaged in defining these elements and they must be understood by all stakeholders. They must be agreed with the national and local health authorities, whenever possible.
There must be clear, demonstrated links among the situation analysis, priority problems, objectives and chosen strategies. All must be reviewed and up-dated together as and when needed:
o Initial objectives, strategies and plans should all be reviewed and adjusted in the subsequent days as the situation evolves or additional information becomes available.
o A detailed health cluster/sector response plan should be drawn up as soon as the initial rapid assessment has been completed.
o That plan should be reviewed regularly and up-dated as needed as the situation evolves and the focus shifts from the humanitarian goal (reducing excess mortality and morbidity) to that of recovery (rebuilding essential health services) and following any significant change in the situation. 8
Alternative options for addressing the priority problems must be examined and the reasons for the choice of particular strategies explained/recorded.
Efforts must be made to use and strengthen existing structures and (re-)build local capacities, whenever possible. Recovery should be promoted from the earliest possible moment (see 9.1). Potential negative effective must be considered, and minimized.
Objectives, strategies and response plans for humanitarian health response should be agreed with national and local health authorities, whenever possible.
The cluster/sector health response plan should be phased to ensure effective coverage of minimum initial services before providing broader essential services. It should address all aspects: human resources, facilities, equipment and supplies.
Cross-cutting concerns such as gender, HIV/AIDS, the environment and protection must be integrated into the cluster/sector planning process.
Contingency plans should be drawn up to deal with foreseeable threats to health or health services.
The HCC should guide partners in their choice of areas to work and activities to prioritize (as well as standards and protocols to use – see 8.1).
Common “gaps” in relation to response planning findings from 10 country case studies (2004-07)
Examples Proposed remedies
8 Planning including the choice of strategies is a dynamic process. Von Molkte the Elder, a Field Marshal in the Prussian army in the mid-19th century and one of the greatest strategists, warned against the risk of too detailed, rigid strategies and plans saying: "No battle plan survives contact with the enemy".
DRAFT for FIELD CONSULTATION
[Health Cluster Guide – draft, 30 June 2008] 44
No implementation plan relevant to the phase of the response (particularly structural rehabilitation) addressing the whole affected area. Implementation driven by agency capacities and mandates, availability of funds, and ‘contextual opportunism’, rather than needs (eg support to hospital capacity and tertiary care over primary care).
Conduct a joint evidence-based prioritization exercise, identifying major causes of morbidity and mortality, prioritizing preventive and curative health services to these causes.
Agree on a minimum package of health services (including reproductive health) to be delivered by each level of health facility, appropriate to the phase of the emergency.
Develop a common action plan together with NGOs, affected community, and MOH, focused on health priorities, within the principles of primary health care, and, particularly in the early recovery phase, finding the balance between urgent service delivery needs and longer term system building.
The following questions are examples of broad issues that need to be examined when setting priorities and deciding on strategies:
What are the principal causes of avoidable mortality and morbidity at present?
What are the principal health risks in the coming months?
Which of these problems affect the greatest number of people?
Which are the key health sector problems that need to be addressed?
Which of the issues above represent the absolute priorities? List the 5 top, justify why and set realistic objectives for the next 6, 12 and 36 months
What options are available to address these problems, what resources would be required, and what impact could be expected?
What is the existing and future capacity to effectively address the priority issues?
Focus on dealing with the immediate, most pressing public health hazards and risks first, as well as the most critical health systems issues, but put them in a longer-term perspective. Start with broad questions – like those above –and then progressively go into greater detail. Map out the issues and possible response options before taking decisions and embarking on planning,
The process of response planning – defining objectives, selecting strategies and preparing a health cluster/sector response plan – based on the situation analysis is shown schematically in Figure 8 (next page). The context analysis, including issues of capacities, resources and constraints, is critical to the definition of objectives (which must be realistic), the analysis of response options and selection of strategies (which must be both appropriate and feasible), and the preparation of the health cluster/sector response plan (which must also be realistic).
The planning process described in this chapter and outlined in Figure 8 corresponds to step 2 in the overall process of planning and implementing an emergency programme outlined in Figure 2, in section 1.4. That ideal process of agreeing a cluster/sector response plan (step 2) and individual organizations then producing their own action plans in the context of that cluster/sector plan (step 3) should be feasible from the outset in two situations: (i) in case of a slow-onset crisis; (jj) when an inter-agency contingency plan exists and includes an outline sector response plan.
In other cases, steps 2 and 3 will be undertaken in parallel during the initial stages:
• the HCC will have to work to bring together as many as possible of the main health actors to share information and progressively develop a shared analysis of the situation and needs, and agreement on overall goals, response strategies and, eventually, an overall health cluster/sector response plan; while, at the same time,
• individual organizations (cluster participants) draw up their own initial action plans taking account of what is known about the response plans of other actors and remain flexible to adjust their plans, if/when needed, to better address the priority needs identified within the overall cluster/sector plan and minimize duplication with the activities of other health actors.

DRAFT for FIELD CONSULTATION
[Health Cluster Guide – draft, 30 June 2008] 45
Figure 8
Analysis of health problems & risks
Prioritized list of health problems & risks
Definition of objectives (realistic; focused on priority problems, and maximizing health benefits
Analysis of response options (advantages/disadvantages)
Analysis of context capacities, resources, constraints
Health cluster/sector response plan
Selection of response strategies
(appropriate & feasible)
From analysis to a health cluster/sector response plan
DRAFT for FIELD CONSULTATION
[Health Cluster Guide – draft, 30 June 2008] 46
4.1 Defining objectives and selecting strategies Key terms
An objective is the desired state that it is intended to achieve – the desired outcome. Objectives are defined at different levels: overall objectives (or “goals”) of the emergency programme, and specific objectives (or “purposes”) of individual projects that contribute to achieving the higher goals.
Strategies are the methods used to achieve specific objectives. Where alternative approaches are possible, a choice has to be made among the different options.
Defining objectives
All objectives should be defined in relation to the priority health problems and risks identified in the situation analysis and within the overall framework of reducing excess mortality, morbidity and disability and restoring the delivery of, and equitable access to, preventive and curative health care as quickly as possible. They should focus on addressing:
• the main causes of death and illness in the local context; and
• the major constraints to delivery of and access to health care services.
Specific objectives may include improving information and reinforcing systems as well as achieving direct health outcomes. While many will concern aspects that are the responsibility of the MoH (and the Health Cluster/sector coordination group), some may relate to aspects that are the responsibility of other ministries (and other cluster/sector coordination groups).
Objectives must be “SMART” – Specific, Measurable, Accurate, Realistic and Time-bound (e.g. “the risk of diarrhoea reduced by 50% in the target population in 6 months”). They must:
• address coherently the priority problems and risks identified in assessments;
• be tailored for specific phases of the response;
• take account of the context, the capacities and resources available, any protection and human rights issues, the impact of HIV/AIDS, security conditions, any limitations on access, and any other constraints on people and the delivery of services; and
• differentiate among men and women, girls and boys, when appropriate.
They may also need to take account of expectations that must be met – the policies and values of the various stakeholders that will affect the evolution of the overall situation and the implementation of health-related activities.
Objectives may need to be reviewed and refined if there are significant changes in the situation or the resources available (including the number, interests and competencies of the health actors present), or when new information becomes available from assessment or monitoring activities.
Initially the focus will be on ensuring that life-threatening humanitarian needs are met, while always looking for opportunities to promote recovery and rebuild systems. As soon as life-threatening needs are met, the focus should shift progressively towards re-building national systems and capacities while ensuring that any remaining humanitarian needs are met.
Selecting response strategies
Selecting strategies is deciding how to address the priority problems and risks in order to achieve the objectives. For example, to limit the risk of a measles outbreak, one option would be a mass immunisation campaign against the disease. But, if you deem that the current coverage is good enough, it may be better to strengthen the routine immunisation systems while focusing effort and resources on other health priorities.
Strategies should be chosen on the basis of the situation analysis and an explicit, recorded analysis of the advantages and disadvantages of the available response options – the possible alternative ways of addressing specific problems and accomplishing particular objectives. Response strategies must be:
DRAFT for FIELD CONSULTATION
[Health Cluster Guide – draft, 30 June 2008] 47
appropriate – address the priority problems and risks effectively, coherently and efficiently in a manner suited to the local context; and
feasible – able to be implemented in the local context and with the resources expected to be available.
Annex N includes examples of some typical problems and the kinds of alternative strategies that could be possible and amongst which choices must be made. The box below suggests some important considerations involved in determining appropriateness and feasibility.
What is appropriate? What is feasible?
To be appropriate, response strategies must:
effectively address the identified priority problems within the intended time period; build on existing and potential capacities; be adapted to the context (including the geographical extent, causes of the crisis, the pre-crisis
situation, whether people are displaced, current trends and processes towards recovery, etc.); take account of:
o national health policy and international standards, and the characteristics and status of the health system;
o the interests and expectations of health-sector stakeholders; o any protection and human rights issues – not increase risks for the population but, if
possible, contribute to reducing them; and o any potential unintended, negative effects that particular strategies might have (see
Annex N). be “gender-aware” – take account of the different situation and needs of men and women, girls
and boys, where appropriate – and culturally sensitive; seek to protect and expedite the recovery and rebuilding of national systems and capacities as
much as possible, especially once life-threatening needs have been met; make services accessible equitably to all population groups including marginalized and
disadvantaged groups (disabled people, minorities, etc.); and be as cost-effective as possible (because resources are almost always a constraint).
To the extent possible, they should also, from the outset:
build on existing systems and optimize the use of existing resources; promote community participation and community-based planning; enhance the capacities and reduce the vulnerabilities of people and health services; complement – be in synergy with – other activities in the health or related sectors; and avoid creating, or reinforcing, dependency.
To be feasible, they must be:
technically feasible, and the expertise required be available; politically and culturally acceptable; and able to be implemented in the prevailing security conditions and in spite of other operational
constraints.
Careful analysis is necessary to identify the most appropriate strategies, ones that will achieve the defined objectives while minimizing any potential negative effects. Note that short-term actions taken to address an immediate systemic problem in service delivery may have significant distorting effects on the entire health system in the longer term – see the examples in Annex N.
However, the preliminary analysis to establish initial objectives and define initial responses can – and should – be very rapid, when undertaken by experienced individuals because:
• some of the main problems and risks that arise in particular types of situation are well-known;
DRAFT for FIELD CONSULTATION
[Health Cluster Guide – draft, 30 June 2008] 48
• the range of response options is often limited and, for certain risks in specific contexts, experience has shown that a particular response is almost always needed.
For example, in crowded conditions there is often a high risk of measles, “minimizing the risk of a measles outbreak” will almost always be a priority objective, and mass measles vaccination will be an appropriate response in most crowded environments, especially when routine systems have been disrupted. In such cases, the preliminary assessment should automatically – and rapidly – check whether there is indeed such a risk and, if so, establish this as a priority to be addressed, specify a corresponding objective, and indicate the strategy.
Never-the-less, most response decisions need careful consideration and it will be important to ensure that assessment teams and decision-makers avoid jumping to conclusions without a necessary minimum of evidence that a particular intervention is a priority, appropriate and feasible.
Identifying and choosing among alternative response options requires an analysis of the context as well as relevant health sector information. It also requires abilities to compare the current situation with other, similar contexts, to learn from the past, and to engage with a broad range of stakeholders possibly including new players (military, non-state actors, etc). It involves value judgements requires diplomacy and political wisdom to ensure that the perspectives of all main stakeholders are recognized in the process of analysis and taken into account in the final response plan.
Draw on experience in previous crises in the same area or among similar populations in neighbouring countries. If actions are proposed on the basis of experiences further afield, ensure a thorough analysis of the differences as well as the similarities between the two contexts. What worked (or failed) in one context will not necessarily work (or fail) in another!
The reasons for the adoption of a particular approach, or set of strategies, should be explained clearly and concisely in the health cluster/sector response plan.
The context of a crisis is often fluid; strategies should be kept under review and changed if they prove ineffective in achieving the established objectives. If necessary, the objectives themselves may need to be re-defined, possibly reducing their ambition and scope.
“Strategy” and “strategies”
The term “strategy” used in different ways by different institutions and individuals:
(i) It is sometimes used to refer to the overall approach to be used to accomplish overall goals, such as “minimising avoidable mortality and morbidity”. In this usage, a “strategy” is developed to accomplish the goals taking account of contextual factors, and strategy development includes deciding on the main areas of intervention, corresponding objectives, and the broad approaches to be used to accomplish them.
(ii) It is sometimes used to refer to the particular (micro-level) approaches to be used to accomplish specific objectives, such as “minimising the risk of a measles epidemic” or “assuring the adequate availability of drugs”. In this usage, objectives are developed in relation to the priority problems and risks, and “strategies” are selected to accomplish each objective based on an analysis of the options available and taking account of the contextual factors and cross-cutting concerns.
Be careful to avoid the unnecessary misunderstandings that can occur when people use and interpret the term “strategy” differently!
In the present draft, the term is used as in ii above.
HCC and Health Cluster action:
During the first few days
Where an inter-agency/health-sector contingency plan exists for the type of crisis concerned, review the objectives and strategies envisaged in that plan and adjust them to the current initial working scenario.
Where no relevant contingency plan exists, develop initial objectives and strategies from scratch based on the initial working scenario.
DRAFT for FIELD CONSULTATION
[Health Cluster Guide – draft, 30 June 2008] 49
Ensure that the initial objectives defined for the first few weeks of response are realistic and focus on life-threatening humanitarian needs while capitalizing on any opportunities that may exist to initiate recovery straight away.
Once the initial assessment has been completed
Elaborate objectives for the coming 6 to 12 months on the basis of the initial rapid assessment and as new information becomes available. Include both continuing humanitarian response and a progressively increasing focus on recovery.
Review objectives and strategies at regular intervals in the context of periodic progress reviews. Check whether they are still appropriate and realistic. Revise/refine them if and when necessary in agreement with all concerned stakeholders.
A matrix such as the one below may be helpful to map out the main issues/problems and response options.
Problem/ risk/ issue
Key situation analysis points
Specific objectives
Response options
Advantages (arguments for)
Disadvantages (arguments
against)
Relevant experience from similar
contexts
Lessons & practical hints from field experience
.…
Additional guidance
IASC - Need Analysis Framework, Strengthening the analysis and presentation of Humanitarian Needs in the CAP, CAP Sub-working group, April 2007 (www.ochaonline.un.org/OchaLinkClick.aspx?link=ocha&docid=1039803)
Global Health Cluster Recovery Strategy Guidance, expected late 2008 WHO - Analysing Disrupted Health Systems Manual UN - Transitional Strategy Guidance Note IASC - Implementing Early Recovery Guidelines, expected late 2008 UN - Integrated Mission Planning Process Guidelines UNDP - Post-Disaster Recovery Guidelines An Operational Note on Transitional Results Matrix …?
DRAFT for FIELD CONSULTATION
[Health Cluster Guide – draft, 30 June 2008] 50
4.2 Preparing a health cluster/sector response plan The health sector/cluster response plan is the principal tool for ensuring that the actions of all health actors are coordinated and, in particular, that the actions of external health actors are well coordinated with, and appropriately support, those of the national and local health authorities and other local actors.
The initial response plan following the preliminary assessment is the basis for the flash appeal (see section 5.1). The more refined plan based on the more thorough initial assessment is the core of the health component of the common humanitarian action plan (CHAP) and, thus, of the consolidated appeal (see section 5.2).
In a crisis, planning tends to become fragmented and short-term, with different entities developing projects in isolation. The development of an overall health response plan based on agreed objectives and strategies can help reduce the fragmentation.
An overall plan provides a framework for health response throughout the affected area(s), including the allocation of resources among areas. Within that framework, specific, local plans should be prepared for each distinct area.
Planning is an iterative process, not a one-off exercise. Plans should be prepared for specific time periods and be up-dated whenever needed:
• Focus on ensuring the delivery of essential services initially; plan to broaden the scope only when essential services have been assured. It is easier to scale up the provision of health care than scale it down.
• When resources are insufficient to meet all needs – as is almost always the case – concentrate effort and resources where they can make difference. Diluting scarce resources across the board can be ineffective.
• Produce an initial response plan rapidly and improve it and make it more specific as more solid information becomes available, consensus with stakeholders is reached and resources materialize. Don’t waste time preparing very-detailed, comprehensive plans that can quickly become irrelevant.
Two key elements should guide the development of plans: priority needs and capacity (existing and projected financial resources and implementation capacity). A plan that does not address priority needs or does not take account of resource/capacity constraints, is a useless document!
The response plan is based on the objectives and strategies defined as described in section 4.1 and should focus on:
• addressing priority health problems needs and filling critical gaps in specific services and the health system as a whole; and
• achieving the maximum health benefit for the maximum number of people in disaster/crisis-affected districts and populations.
The plan must include an explanation of the objectives and why particular response strategies have been chosen. The rationale must be concise but provide the reason – the justification – for the proposed actions. This will be very brief for the initial response plan, more detailed for subsequent plans. It should:
• provide a concise analysis of the situation including the prioritized list of the main problems and their underlying causes;
• present the objectives for each main area of intervention (e.g. prevention and control of communicable diseases, injury rehabilitation, surveillance, drug supplies management) and the strategies proposed to achieve the objectives, showing how the objectives and strategies derive from the assessment findings and situation analysis; and
• highlight the operational constraints and inter-sectoral cross-cutting concerns that have been identified as being particularly important for health in the current situation and explain how they have been taken into account, and show how general emergency programming principles have been applied.
DRAFT for FIELD CONSULTATION
[Health Cluster Guide – draft, 30 June 2008] 51
N.B. This is not a restatement of the needs assessment! It takes the situation analysis as a basis and develops the rationale for the precise response plan.
The plan should include, as annexes, contingency plans to deal with new crises that could arise in the course of the planned humanitarian operation (see section 4.5).9
Phased plans and incremental approaches
In some situations it may be possible to define – and agree – from the outset a phased plan to address a particular problem. For example: “In a particular recovery context, there is a serious imbalance in the workforce, with a large shortfall of midwives, mainly in rural areas. A substantial investment is required to accelerate the training of new staff in this category. In the meantime, a package of incentives is envisaged for midwives willing to move to underserved areas for the next 3 years, when new midwives will have been trained. A comprehensive human resource development plan for the next 10 years will be launched with technical assistance provided by donor X.”
In many cases, especially where there are conflicting perspectives and pressures, it is necessary to adopt an incremental approach and proceed gradually towards the set goals, taking into account the resistance and opportunities that emerge during the process. This involves getting consensus on intermediate objectives, achieving them, and then moving to a higher objective as soon as the context is conducive. Good monitoring, and perhaps a real-time evaluation, is essential to track the intermediate outcomes and facilitate agreement on the next, follow-on phase.
HCC and Health Cluster action:
Preparing an initial response plan during the first few days
Prepare a very concise statement of the overall goals of the cluster/sector response, the priority problems to be addressed during the initial plan period (perhaps 1 month?), the specific objectives for that period, the principal strategies to be applied, who will do what where, and the principal gaps (uncovered priority needs/activities).
Focus on filling gaps in critical life-sustaining services in areas where large numbers of people are known, or believed, to be seriously affected, and filling gaps in information that is critical for determining needs and planning an appropriate response.
Try to make sure each organization taking responsibility for a particular area or activity has, or will have, the capacity and systems to support the anticipated field activities.
Planning once the initial assessment has been completed
Prepare a concise but more comprehensive response plan for the next 3/6/12 months.
Include projects/activities to consolidate or enhance, where needed, the capacity assure and manage health information and facilitate coordination while working to progressively reduce dependence on external assistance, as and when possible.
Build on any opportunities for recovery and building the capacities of people, health facilities and the health system in general.
Prepare contingency plans for events (contingencies) that could impact on the health of the population and/or the ongoing humanitarian assistance operations of health-sector actors during the coming months. See section 4.5.
Lessons & practical hints from field experience
.…
9 The contingency plans referred to here are “in-crisis” contingency plans, prepared to deal with events (“contingencies”) that could further complicate the current situation.
DRAFT for FIELD CONSULTATION
[Health Cluster Guide – draft, 30 June 2008] 52
Additional guidance
Annex C, Mapping the availability of health services provides a list that may also help in putting together overall objectives and a health sector response/action plan.
…
DRAFT for FIELD CONSULTATION
[Health Cluster Guide – draft, 30 June 2008] 53
4.3 Preparing the health component of a CHAP The CHAP is an overall strategic plan for humanitarian response covering all relevant sectors. It constitutes the core of a consolidated appeal (see section 5.3) but can also serve as a reference for organisations that decide not to participate in such an appeal. A CHAP includes the following elements:
• an analysis of the context and humanitarian consequences (humanitarian needs and risks taking account of the capacities and vulnerabilities of different affected population groups);
• scenarios – best, worst, and most likely scenarios;
• strategic priorities including clear statements of longer-term objectives and goals; and
• prioritised response plans for each sector (of which health is one).
The CHAP is developed by the IASC/Humanitarian Country Team under the leadership of the Humanitarian Coordinator. Non-IASC members, such as national NGOs, can be included, and other key stakeholders in humanitarian action, in particular the host government and donors, should be consulted.
There are two principal aspects: contributing to overall, inter-sectoral elements (which is primarily the responsibility of the health cluster lead), and drawing up a health response plan (which should be a “cluster” effort, led by the HCC)
HCC and Health Cluster action:
Contributing to overall, inter-sectoral elements
The cluster lead agency will contribute to the development of: (i) the section on the overall context and humanitarian consequences; (ii) strategic priorities for the humanitarian operation as a whole, and (iii) general criteria for selecting and prioritizing projects.
In doing so, the cluster lead should consult with cluster participants as needed and ensure that:
all current and potential health consequences are adequately taken into account;
inter-relationships among public-health-related needs and risks are clearly recognized; and
the situation and vulnerabilities of all distinct population sub-groups are taken into account.
Drawing up a health response plan
The cluster should agree a 2-page response plan for the health sector (including psycho-social needs). The summary from a health sector NAF report may be used – see Annex M – or information from an alternative, evidence-based, inter-agency needs and response analysis.
Projects to support critical health system elements (and health coordination) should be included, when needed, as well as projects for the delivery of supplies and services.
Selecting and prioritizing projects (for inclusion in the CHAP)10
Arrange a special meeting to select and prioritize projects for inclusion in the CHAP and consolidated appeal. If the cluster is large, it may be useful to form a technical working group for this purpose including representatives each main group of stakeholders, e.g. government, large INGOs, large NNGOs, small INGOs, small NNGOs, other national institutions, donors. Elect a chair and co-chair at least one of which from an NGO or the Red Cross/Crescent.
Review the criteria established by the IASC/Humanitarian Country Team for the selection and prioritization of projects in general and agree on the specific criteria to be used for health projects.
Ask organizations participating in the cluster/sector group to prepare 1-page project sheets following the CAP technical guidelines and submit them to the chair and co-chair. Emphasize that the projects should address agreed priority needs and support the implementation of the agreed health sector strategy.
10 Edited from Guidance for CAP Project Selection and Prioritization, IASC June 2004
DRAFT for FIELD CONSULTATION
[Health Cluster Guide – draft, 30 June 2008] 54
Review the proposals – discussion facilitated by the designated chair and co-chair. Send back to the originating organizations any proposals that do not meet the agreed criteria.
Submit the selected proposals to the Humanitarian Coordinator/OCHA. The chair and co-chair should then participate in a peer (inter-cluster) review to ensure overall consistency in the proposals for different sectors.
The HC makes the final decision and is accountable to the Emergency Relief Coordinator for ensuring that projects included in the appeal are in line with the agreed overall humanitarian needs and strategic priorities.
Note that any support needed to assure the effective functioning of the health cluster, and the ability of the cluster lead agency and coordinator to fulfil their responsibilities, must be included in the package. Budget lines may be needed for, e.g. information management, communications and evaluations.
What should be included in a health response plan for a CAP/CHAP
A CHAP – section 3 of a CAP – should normally include:
the priority health needs and risks; a corresponding health response plan with no more then five objectives for the health sector
and no more then five key health indicators for measuring progress towards objectives; a list of the organisations that will contribute to this health response plan, and a outline or
chart showing the complementarity between proposed activities; a brief explanation of how the cluster/sector group will monitor implementation and the
achievement of objectives; the implications if the health response plan is not implemented.
The strategy must be evidence-based and clearly linked to one or more of the agreed overall strategic humanitarian priorities, and include the main organizations working in the health sector.
Individual projects must be reviewed and agreed upon by the health cluster/sector group and support the defined health response strategy (see below).
[Adapted from Technical Guidelines for Consolidated Appeals, IASC 2006]
Sample criteria for project selection/prioritisation
Health response strategy: the project helps to achieve the agreed health objectives, addressing agreed priority needs.
Organisational capacity: the appealing organisation has the technical expertise in country, capacity, and mandate to implement the project, or can mobilize this operational capacity as required.
Population: the project targets – will benefit – one or more of the priority, vulnerable population groups identified by the IASC country team.
Geographic area: the project will be implemented in a region that is considered to be a priority.
Timing: the project can make a measurable impact in the time-frame of the appeal (usually one year).
Other context-specific criteria: e.g. projects that include a focus on HIV/AIDS, help to build local capacity, and/or promote gender equality.
[Adapted from Guidance on CAP Project Selection and Prioritisation, IASC June 2004]
Lessons & practical hints from field experience
.…

DRAFT for FIELD CONSULTATION
[Health Cluster Guide – draft, 30 June 2008] 55
Additional guidance
www.humanitarianinfo.org/iasc/content/subsidi/swg_cap/cap.asp
For an example (Liberia 2007), see: http://ochaonline.un.org/cap2005/webpage.asp?Page=1546
DRAFT for FIELD CONSULTATION
[Health Cluster Guide – draft, 30 June 2008] 56
4.4 Taking account of cross-cutting concerns
All activities must be planned taking account of human rights, gender and environmental concerns and risks and constraints related to HIV/AIDS.
Checklist for cross-cutting concerns 11
Human rights and protection:
Do proposed strategies and implementation modalities assure equality of access to assistance and services for ALL population groups and adequate protection for beneficiaries and humanitarian/health workers?
Might they reinforce existing patterns of discrimination or increase risks?
Could activities or implementation modalities be modified to better assure respect for human rights and protection, especially for groups determined to be at particular risk (e.g. women, people with HIV/AIDS, adolescent boys)?
Gender:
Do proposed strategies and implementation modalities promote gender equality?
Might they increase existing inequalities?
Could activities or implementation modalities be modified to better promote gender equality?
HIV/AIDS:
Do proposed strategies take account of the prevalence of HIV/AIDS and minimize the risks of transmission in a culturally appropriate manner?
Could activities or implementation modalities be modified to better provide for people suffering from HIV/AIDS and reduce risks of transmission?
Are standard precautions being effectively implemented in all areas (the first priority before considering any other measures)?
Are arrangements in place to assure continuing treatment for patients already on ART?
Environment:
Do proposed strategies and implementation modalities assure protection of the environment and natural resource base?
Might they create additional unnecessary waste?
Could activities or implementation modalities be modified to better protect the environment?
Annex E summarizes the main issues in relation to these concerns.
For further guidance, see:
Proposal Checklist on Health and Human Rights for Humanitarian Action, draft
IASC Guidelines for Gender-based Violence Interventions in Humanitarian Settings: Focusing on Prevention and Response to Sexual Violence in Emergencies
IASC Guidelines for HIV/AIDS interventions in emergency settings
11 The following checklist is based on key questions in the CHAP guidelines + add-ons for HIV/AIDS
DRAFT for FIELD CONSULTATION
[Health Cluster Guide – draft, 30 June 2008] 57
4.5 Developing contingency plans
Events that could further impact on the health of the population or on the ongoing humanitarian assistance operations during the coming months must be anticipated. Contingency plans must be prepared to respond to possible new health threats and to ensure, as much as possible, the continuity of services and humanitarian assistance to the target populations. They should be included as annexes to the health cluster/sector response plan.
Events (contingencies) that might need to be anticipated include, for example:
• secondary disasters: recurrence of the primary hazard or secondary phenomena such as epidemics of communicable diseases or a forthcoming cyclone season;
• deterioration of the security situation, notably the possibility that renewed conflict could affect certain health facilities or disrupt supply corridors;
• breakdown of in-country supply chains due to overburdened provincial services;
• rumours and misinformation impairing relief activities.
HCC and Health Cluster action:
Identify and prioritize possible contingencies that, during the coming months, could impact on:
o the health of the population; or
o the ongoing humanitarian assistance operations in the health sector actors.
Decide within the cluster, in coordination with the MoH and other main health actors, how such events will be managed – the health needs responded to and operational support and services maintained if/when such events occur.
Specify what additional resources – human, material, financial – would be needed.
Lessons & practical hints from field experience
.…
Additional guidance
Inter-agency Contingency Planning guidelines, IASC Working Group, 2008
Case example
Contingency planning for a possible cholera outbreak during floods in Uganda
…to be completed by IMC…
DRAFT for FIELD CONSULTATION
[Health Cluster Guide – draft, 30 June 2008] 58
5 Mobilizing and managing resources
Key points: Advocate for health sector priorities and needs among partners and donors. Keep all those
concerned informed on health issues using opportunities like IASC and donor meetings to highlight the health situation and ask for support.
Facilitate the process of preparing and providing health inputs into flash appeals and consolidated appeals.
When indicators show that the health situation is deteriorating and there is a need for emergency intervention, the HCC, in agreement with health cluster participants, should approach the humanitarian coordinator to request activation of the CERF rapid response window. The HCC should also consolidate health cluster inputs for applications to the CERF under-funded emergencies window.
Since NGOs are not eligible to access CERF funds directly, the country-level health cluster lead is responsible for ensuring that CERF funds allocated to NGO projects are passed through to the NGOs concerned.
Common “gaps” in relation to resources findings from 10 country case studies (2004-07)
Examples Proposed remedies
Inadequate resources to implement essential actions to minimize avoidable mortality and morbidity. In the acute phase, compounded by inflexibility of emergency funding, and lack of transparency in disbursement to NGOs. Resource gaps often reported when moving from emergency to early recovery phase.
Advocate with donors and national governments for greater, more transparent resource allocation. Improve the evidence-base for advocacy such as through joint assessment or evaluation, and disseminate results. Encourage popular media coverage, including by high profile personalities as ‘roving ambassadors’.
Avoid the introduction of user fees, which in most settings will not liberate adequate funds to improve quality and coverage and will disproportionately affect the poor.
… examples of CERF applications, flash appeals and CAP project sheets may be included on the CD-ROM…
DRAFT for FIELD CONSULTATION
[Health Cluster Guide – draft, 30 June 2008] 59
5.1 Preparing health inputs to a “flash” appeal
The flash appeal is a tool for structuring a coordinated humanitarian response for the first three to six months of an emergency. It contains an analysis of the context and of humanitarian needs (citing whatever specific needs assessments are available), response plans (at the general strategic level as well as sectoral plans including specific proposed projects), and statements on roles and responsibilities. It contains early estimates and best guesses, focusing on urgent life-saving needs plus whatever early recovery projects can be assessed and implemented within the first few months.
The Humanitarian Coordinator triggers a flash appeal in consultation with all stakeholders and defines the time frame for preparation. Normally, the draft should be completed in country within five days of the onset of an emergency (and issued by OCHA-Geneva no more than 48 hours later).
Usually, there is a scheduled revision about a month later to incorporate fuller information and more recovery projects (especially connecting to government plans as they crystallize). The flash appeal may be developed into a consolidated appeal if an inter-agency response is needed beyond six months.
The Health Cluster/sector Lead is responsible for preparing and submitting to the HC a response plan for the health sector.
HCC and Health Cluster action:
The cluster/sector lead should:
Bring together all organisations working significantly in the health sector and facilitate of process to:
o analyse available assessment information and agree a general, initial response strategy;
o vet projects proposed by individual organizations; and
o build consensus on project inclusion, ensuring that all those listed in the appeal are relevant, high-priority, coordinated and feasible.
Write up the plan in the required appeal document format.
Normally, the health sector draft should be submitted to the HC within 72 hours of the decision to launch a flash appeal; the actual deadline will be specified by the HC in each case.
The Flash Appeal may include projects from UN agencies, international organizations, and NGOs. It may include project partnerships with the Red Cross or Red Crescent National Society of the country of operation. Government ministries cannot appeal for funds directly in a flash appeal, but can be partners in UN or NGO projects. Government officials as well as local donor representatives may be consulted.
Lessons & practical hints from field experience
.…
Additional guidance
IASC - Flash Appeal Guidance English version (ochaonline.un.org/cap2005/GetBin.asp?DocID=1397 -) French Version (ochaonline.un.org/cap2005/GetBin.asp?DocID=1954 -) Cheat Sheet …

DRAFT for FIELD CONSULTATION
[Health Cluster Guide – draft, 30 June 2008] 60
5.2 Preparing, monitoring and reviewing a consolidated appeal
The consolidated appeal is a tool – a document – used to plan, coordinate, fund, implement and monitor humanitarian activities in response to a major or complex emergency or natural disaster.
A consolidated appeal is usually developed through a month of consultations among agencies in the field, led by the HC, in which assessment information is analysed and priorities and strategies are agreed upon. The process of developing a consolidated appeal helps to ensure a thoughtful and thorough approach to humanitarian action.
A consolidated appeal is prepared following agreement by the Emergency Relief Coordinator (ERC) and IASC, in consultation with the Humanitarian Coordinator and the IASC Country Team may that an emergency is either complex or major and necessitates consolidated approach to resource mobilization. It is prepared according to the Technical Guidelines for Consolidated Appeals.
Preparing a consolidated appeal
Prepare the health section of a Common Humanitarian Action Plan (CHAP) as described in section 4.3.
Organizations participating in a Consolidated Appeal should one-page Project Sheets according to CAP Technical Guidelines and submit them to the Chair and Co-Chair of the Health Cluster Planning meeting/group. The projects should address agreed priority needs and support the implementation of specific sector objectives.
Reference Bibliography:
IASC - UN CAP Appeal Guidance - English version - http://ochaonline.un.org/FundingFinance/ConsolidatedAppealsProcess/tabid/1106/Default.aspx. French version - http://ochaonline.un.org/cap2005/DocView.asp?DocID=1396
IASC WG - Guidance for CAP Project Selection and Prioritization, June 2004
Tracking contributions against an appeal
The Financial Tracking Service is a global, on-line, real-time database of humanitarian funding needs and contributions. It serves to improve resource allocation decisions and advocacy, by clearly indicating to what extent populations in crisis receive humanitarian aid, and in what proportion to needs. The FTS offers a series of analytical tables that show humanitarian aid flows to specific crises, and also allows users to produce custom tables on demand.
Reference Bibliography:
UN - UN Agency Field Office and the Financial Tracking Service (FTS) http://ocha.unog.ch/fts/exception-docs/AboutFTS/guidesheets/FTS_&_UN_agency_Field_Office_guide.pdf
Conducting a mid-year review (MYR)
The Mid-Year Review (MYR) aims to:
• Measure progress made in achieving the goals and objectives of the Common Humanitarian Action Plan (CHAP) and report findings to stakeholders;
• Determine whether or not the agreed strategy is having the desired impact, and if necessary change the strategy to adapt to new conditions;
• Update the portfolio of projects;
• Reprioritize humanitarian response activities and projects;
• Analyse funding; and
DRAFT for FIELD CONSULTATION
[Health Cluster Guide – draft, 30 June 2008] 61
• Advocate for donor support.
One of the main tasks of the health cluster lead, and HCC, is to highlight the needs and priorities of the health sector.
The cluster, including include all of the organizations engaged in humanitarian health action (i.e. NGOs, the Red Cross and Red Crescent Movement, UN agencies, donors, and host authorities) must:
review all proposed projects in the CAP and validate that each is relevant, feasible, not redundant, and economically budgeted; all proposed projects that do not meet these requirements should be deleted;
highlight any important new information or strategy; and
prioritize remaining unfunded or under-funded projects using at least a two-tier system (top and medium priority).
The cluster/sector lead has a pivotal role: their responsibility is to review their health sector response plan and reconfirm that all health project proposals counted in the CAP are still relevant (if not, the proposing organisation should either delete or revise them), and that all suitable proposals are counted (especially NGO proposals). Projects already funded but not yet counted in the CAP should be counted in it as part of the MYR (as long as they are consistent with the CHAP), in order to accurately measure funding according to need.
Individual agencies should give their headquarters an early look at their new or revised projects during the MYR process, to minimise misunderstandings and last-minute changes.
Ideally, joint planning and the coordinated implementation of agreed activities would be followed by joint reporting back to donors – the preparation of a joint narrative report to be submitted to all donors together with the separate financial reports of each organization to each donor. The health cluster lead and HCC should propose this to cluster participants and donors and, where agreed, take the lead in preparing an overall narrative report based on the strategy and expected results presented in the flash or consolidated appeal.
Lessons & practical hints from field experience
.…
Additional guidance
OCHA – Humanitarian Appeal – Guidelines for Mid-Year Review 2008 - http://ochaonline.un.org/humanitarianappeal/webpage.asp?MenuID=9198&Page=1481
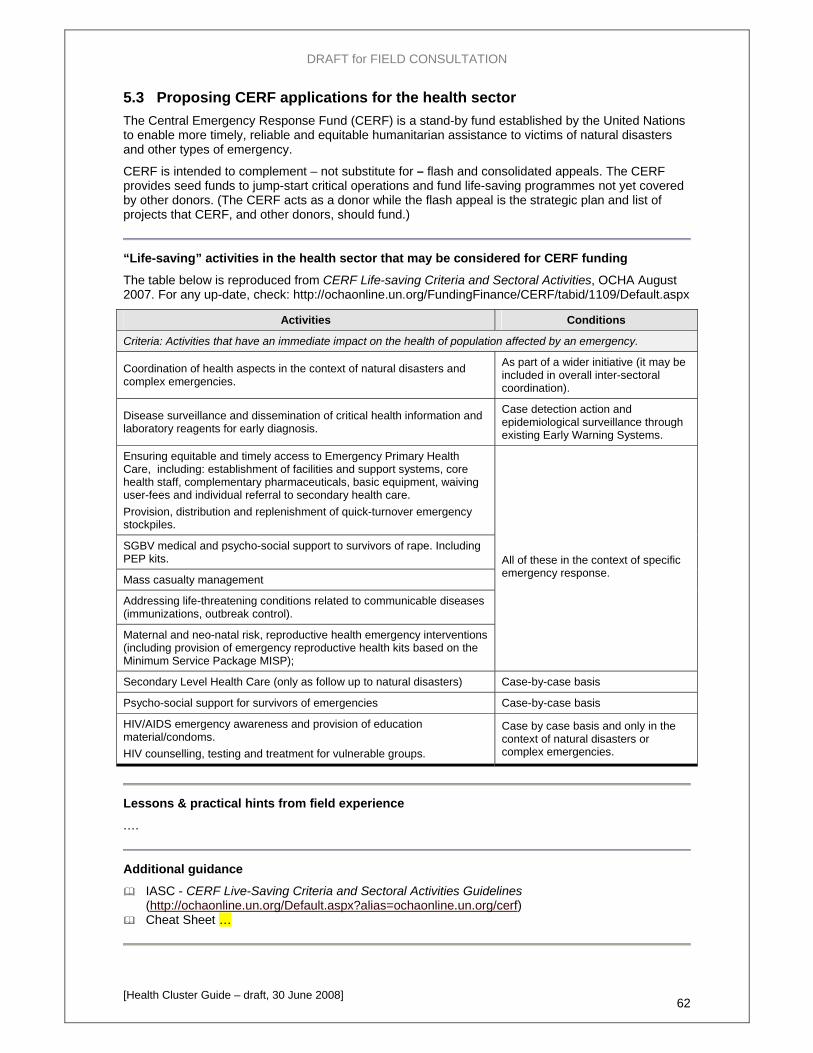
DRAFT for FIELD CONSULTATION
[Health Cluster Guide – draft, 30 June 2008] 62
5.3 Proposing CERF applications for the health sector The Central Emergency Response Fund (CERF) is a stand-by fund established by the United Nations to enable more timely, reliable and equitable humanitarian assistance to victims of natural disasters and other types of emergency.
CERF is intended to complement – not substitute for – flash and consolidated appeals. The CERF provides seed funds to jump-start critical operations and fund life-saving programmes not yet covered by other donors. (The CERF acts as a donor while the flash appeal is the strategic plan and list of projects that CERF, and other donors, should fund.)
“Life-saving” activities in the health sector that may be considered for CERF funding
The table below is reproduced from CERF Life-saving Criteria and Sectoral Activities, OCHA August 2007. For any up-date, check: http://ochaonline.un.org/FundingFinance/CERF/tabid/1109/Default.aspx
Activities Conditions
Criteria: Activities that have an immediate impact on the health of population affected by an emergency.
Coordination of health aspects in the context of natural disasters and complex emergencies.
As part of a wider initiative (it may be included in overall inter-sectoral coordination).
Disease surveillance and dissemination of critical health information and laboratory reagents for early diagnosis.
Case detection action and epidemiological surveillance through existing Early Warning Systems.
Ensuring equitable and timely access to Emergency Primary Health Care, including: establishment of facilities and support systems, core health staff, complementary pharmaceuticals, basic equipment, waiving user-fees and individual referral to secondary health care. Provision, distribution and replenishment of quick-turnover emergency stockpiles.
SGBV medical and psycho-social support to survivors of rape. Including PEP kits.
Mass casualty management
Addressing life-threatening conditions related to communicable diseases (immunizations, outbreak control).
Maternal and neo-natal risk, reproductive health emergency interventions (including provision of emergency reproductive health kits based on the Minimum Service Package MISP);
All of these in the context of specific emergency response.
Secondary Level Health Care (only as follow up to natural disasters) Case-by-case basis
Psycho-social support for survivors of emergencies Case-by-case basis
HIV/AIDS emergency awareness and provision of education material/condoms. HIV counselling, testing and treatment for vulnerable groups.
Case by case basis and only in the context of natural disasters or complex emergencies.
Lessons & practical hints from field experience
.…
Additional guidance
IASC - CERF Live-Saving Criteria and Sectoral Activities Guidelines (http://ochaonline.un.org/Default.aspx?alias=ochaonline.un.org/cerf)
Cheat Sheet …
DRAFT for FIELD CONSULTATION
[Health Cluster Guide – draft, 30 June 2008] 63
5.4 Working with donors; accessing funds from other sources
Working with donors
The Cluster Lead and HCC, on behalf of the cluster and health sector as a whole, should:
Take initiative to contact local donor representatives, any foundations and potential private-sector donors represented in the country to explain health sector priorities and resource needs. Keep them informed on a regular basis.
Encourage potential donors to participate in cluster coordination meetings and briefings.
Invite donors to join assessment missions and project site visits. Support joint donor fact-finding missions.
Prepare concise, “donor-friendly” briefing materials and presentations, including graphics. Prepare and provide detailed technical material and presentations only when requested by a particular donor.
Establish system to record contacts with donors (proposals given, indications of interest received).
Accessing funds from other (non-traditional) sources
In certain circumstances, funds for humanitarian and/or early recovery activities may be sought from:
• Common Humanitarian Funds (established for specific countries)
• Multiple Donors Trust Fund
• Community Peace and Stability Fund
or, for recovery activities, through the mechanism of the UN Development Assistance Framework (UNDAF).
Funds may also be sought from foundations and the private sector…
Sharing resources
When “pooled” resources are available for health action:
agree within the cluster – in a cluster meeting – on criteria for the selection of project activities in priority areas and the allocation of resources to individual agencies;
invite agencies to submit proposals (e.g. using the CERF application format) in accordance with the agreed criteria;
form a project appraisal group including representatives from each main group of stakeholders (e.g. government, large INGOs, large NNGOs, small INGOs, small NNGOs, other national institutions and donors) to review proposals and select projects to be funded.12
Ensure that the procedures for transferring funds (e.g. from CERF) to the concerned implementing organizations are clear and understood by all concerned.13
Lessons & practical hints from field experience
.…
12 The same appraisal group may also screen and select proposals for inclusion in a Flash Appeal or a CAP, and applications for CERF funds. 13 For example, when WHO is cluster lead, CERF funds will be transferred initially to WHO-HAC in Geneva and from there to the international headquarters of the organizations concerned after signature of a corresponding agreement. (This normally enables the organization concerned to begin operations more quickly than if funds were transferred directly to an account in the country of operations.)

DRAFT for FIELD CONSULTATION
[Health Cluster Guide – draft, 30 June 2008] 64
Additional guidance
Center in International Cooperation New York University, in collaboration with The Humanitarian Policy Group, Overseas Development Institute - Common Funds for Humanitarian Action in Sudan and the Democratic Republic of Congo: Monitoring and Evaluation Study, Draft 1, November 2006
UNDP - Memorandum of Understanding regarding Operational Aspects of the Peacebuilding Funds
UNDP - Multi-donors Trust Fund (MDTF) Development Initiatives, Review of Trust Fund Mechanisms fro Transition Financing, Phase 2
Report, 28 April 2006

DRAFT for FIELD CONSULTATION
[Health Cluster Guide – draft, 30 June 2008] 65
5.5 Provision of Last Resort Where necessary, and depending on access, security and availability of funding, the cluster lead, as provider of last resort, must be ready to ensure the provision of services required to fill critical gaps identified by the cluster. This includes gaps in relation to early recovery needs within the sector.
Where critical gaps persist in spite of concerted efforts to address them, the cluster lead is responsible for working with the national authorities, the Humanitarian Coordinator and donors to advocate for appropriate action to be taken by the relevant parties and to mobilize the necessary resources for an adequate and appropriate response. [IASC Operational Guidance on the Concept of “Provider of Last Resort”, Draft May 2008]
The “Provision of Last Resort” should be activated when:
1. the Health Cluster agrees that there is an important life-threatening gap in the Health sector response, and
2. one or more of the agreed benchmarks for the health sector response as a whole is not being met, and
3. evidence suggests that a significant proportion of the target population is at risk of avoidable death if the gap is not filled urgently.
The Health Cluster Lead must therefore at all times:
be sufficiently aware of its own capacities and limitations;
be ready to take credible stop-gap measures;
be prompt in identifying alternatives; and
be ready to delegate responsibilities to fill the ultimate mission-critical gap without feeling for this challenged in its leadership role…?
Serving as provider of last resort is to be satisfied, and to have all partners satisfied, that all possible efforts have been undertaken to fill agreed priority gaps calling on additional local and international partners and advocating for additional donor commitment.

DRAFT for FIELD CONSULTATION
[Health Cluster Guide – draft, 30 June 2008] 66
6 Monitoring health action plan implementation; evaluating & learning lessons
Key points: The principal focus is on monitoring the implementation of the overall health cluster/sector
response plan and evaluating the performance of the overall health sector response.
When the cluster approach is fully implemented and participating health actors work together in partnership, the cluster may – and is encouraged to – organize joint monitoring and evaluation of individual projects.
A multi-partner working group should provide input and achieve consensus on indicators, target selection and other aspects of M&E design and implementation right at the beginning of the emergency. M&E should be included in the health response plan.
Participatory monitoring and evaluation (PM&E) is a useful approach to a wide range of stakeholders in the process. The more participatory M&E activities the more likely they will represent the real situation and opinions of the health sector stakeholders (including community organizations/local people),.
M&E should be as simple as possible. (Most programmes collect far more data than they use.)
Monitoring should be initiated from the early stages of response. It can be refined and extended later; the start must not be delayed while waiting for a sophisticated monitoring system to be developed.
A real-time evaluation (RTE) can be very useful in the early stages of response and the health cluster should be ready to organize one or, better, to participate in an inter-sectoral RTE.
M&E are management tools used to:
• assess programme implementation (efficiency) • assess programme effectiveness (value and impact) • track changes in population needs and ensure the effective allocation of scare resources • ensure accountability to key stakeholders (donors, implementers, managers, service users) • extract lessons from a given programme or project and inform decisions about future programme
development
The success of health interventions often depends on these "direction setting" activities.
Take care to ensure that “effectiveness” and “efficiency” are properly distinguished, and are assessed separately:
• Effectiveness is a measure of the extent to which an intervention’s intended outcomes (its specific objectives) have been achieved.
• Efficiency is a measure of the relationship between outputs (the products produced or services provided by an intervention) and inputs (the resources it uses).
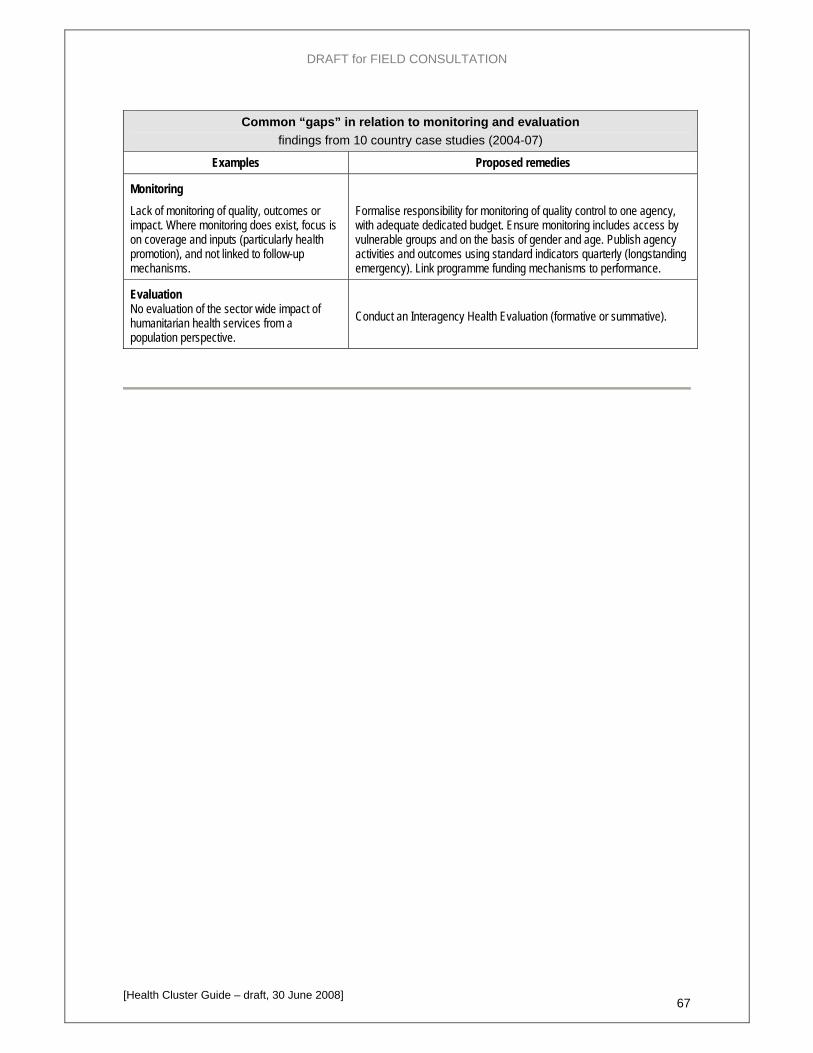
DRAFT for FIELD CONSULTATION
[Health Cluster Guide – draft, 30 June 2008] 67
Common “gaps” in relation to monitoring and evaluation findings from 10 country case studies (2004-07)
Examples Proposed remedies
Monitoring Lack of monitoring of quality, outcomes or impact. Where monitoring does exist, focus is on coverage and inputs (particularly health promotion), and not linked to follow-up mechanisms.
Formalise responsibility for monitoring of quality control to one agency, with adequate dedicated budget. Ensure monitoring includes access by vulnerable groups and on the basis of gender and age. Publish agency activities and outcomes using standard indicators quarterly (longstanding emergency). Link programme funding mechanisms to performance.
Evaluation No evaluation of the sector wide impact of humanitarian health services from a population perspective.
Conduct an Interagency Health Evaluation (formative or summative).
DRAFT for FIELD CONSULTATION
[Health Cluster Guide – draft, 30 June 2008] 68
6.1 Monitoring implementation of health cluster response Project/programme monitoring is an integral part of day-to-day management. It provides information by which management can identify and solve implementation problems, and assess progress in implementing the planned activities.
The HCC and health cluster are concerned with monitoring the implementation of the health cluster plan or the cluster participants’ collective contribution to the overall health sector response plan.
Arrangements are needed for standard implementation reporting by all cluster participants – by all health actors, if possible – and for receiving, collating and analysing the reports. This should be done in collaboration with the MoH (or other relevant national authorities); there should not be separate, parallel reporting to the cluster and the MoH!
Period joint reviews are essential. All concerned health actors should be involved and examine not only the progress of specific kinds of activity but also whether the cluster is meeting its objectives in terms of partnerships, standards, and gap filling. Reviews should examine data from both programme monitoring and situation surveillance (see section 3.4).
The mid-year reviews (MYR) of the consolidated appeal are important exercises but intermediate reviews every 2 or 3 months may also be useful in some cases.
Some questions to be addressed during monitoring and reviews14
Which activities are underway and what progress has been made?
At what rate are resources being used and how does usage compare with progress in implementation (outputs)? How do costs incurred compare with the budget? [efficiency]
Are the desired results being achieved (e.g. quarterly update)? [effectiveness]
To what extent are these results furthering the purposes of the health response plan (e.g. half-yearly analysis)?
What changes have occurred in the overall contest? Do the original assumptions hold true?
HCC and Health Cluster action:
Up-date status of activities – and the who-what-where actor map – at every coordination meeting by getting participants to enter new information into formats provided (not lengthy statements in plenary!)
Organize MYRs on the required schedule, and intermediate reviews if agreed by cluster participants to be useful.
…
Include reporting by partners …
Lessons & practical hints from field experience
.…
Additional guidance
IASC - Guidelines CAP Mid-Year Review
The Sphere Project. Humanitarian Charter and Principles of Humanitarian Response, revised edition 2004. Geneva, 2004 http://www.sphereproject.org/index.htm
14 Manual Project Cycle Management, June 2005, European Commission, ECHO
DRAFT for FIELD CONSULTATION
[Health Cluster Guide – draft, 30 June 2008] 69
6.2 Monitoring the performance of health services Monitoring of performance of health services is central to assessing the effectiveness of the health response plan or individual service-delivery projects at any point in time. It can be used to report on performance trends over time. In many cases the health service quality was already weak due repeated disasters and inadequate periods for ’recovery’ and the capacity of national HIS to support monitoring may also be limited. Support to assure an adequate HIS will be an important component of the health cluster/sector response plan in many cases and one organization (the cluster lead or another cluster participant) take responsibility of leading the provision of international assistance in this area.
The performance of health services in crisis is measured by coverage, timeliness, access, utilization and quality/effectiveness. Coverage provides the percentage of affected population reached by humanitarian aid, There should be universal coverage for the most essential services. Timeliness is a major benchmark of effectiveness, particularly in sudden-onset natural disasters.
Some possible indicators of performance are shown in Annex C. Coverage is one important measure, see the box below. Performance can also be measured against the Sphere standards.
N.B. Ongoing performance measurement (i.e. monitoring) does not address the issues of how or why an outcome was (or was not) realised. This is determine though the evaluation.
Estimating coverage [Synthesized from Tracking health performance and humanitarian outcomes, background conference paper,
A. Griekspoor, A Loretti & S Colombo, WHO 2005]
Coverage, for epidemiological purposes, is “a measure of the extent to which the services rendered cover the potential need for these services in a community. It is expressed as a % in which the numerator is the number of services rendered and the denominator is the number of instances in which the service should have been rendered”15.
Coverage estimates are usually calculated as a percentage:
Population coverage (%) = No. of people with access to service × 100 Total population concerned (N)
In a humanitarian crisis, coverage can be calculated in relation to the total affected population, the total affected population that can be reached, or, for an intervention is targeted, the total targeted population. These different coverage rates may be expressed as:
• potential humanitarian coverage, where N = Total affected population. • operational humanitarian coverage, where N = Total affected population that can be reached • targeted population coverage, where N = Total target population
Changes in coverage can be used to monitor how well a programme is performing in reaching its target population. For purposes of evaluation, a change in coverage is a simple measure of the difference between coverage levels at different time points:
% Change in coverage = Coverage at Time2 – Coverage at Time1 × 100 Coverage at Time1
For the comparison between estimates to be valid, coverage levels must be estimated using the same (standardized) methodology at each time point.
15 Last JM: A Dictionary of Epidemiology, Oxford University Press, 2001

DRAFT for FIELD CONSULTATION
[Health Cluster Guide – draft, 30 June 2008] 70
Sphere standards for health services
All people have access to health services that are prioritized to address the main causes of excess mortality and morbidity (example of indicator: all members of the community, including vulnerable groups, have access to priority health interventions)
Health services are designed to support existing health systems structures and providers (example: local health facilities are supported and strengthened by responding agencies)
People have access to health services that are coordinated across agencies and sectors to achieve maximum impact (ex: specific responsibility of each agency clarified)
Health services are based on relevant primary health care principles (ex: a standardized referral system is established by the lead health authority and utilised by health agencies) suitable transportation is organised for patients to reach the referral facility.
People have access to clinical services that are standardized and follow accepted protocols and guidelines (adequate staffing 50 patients/day)
The design and development of health services are guided by the on-going coordinated collection, analysis and utilization of relevant public health data (ex health facilities and agencies submit data on a regular basis)
HCC and Health Cluster action:
Work with the MoH and other important health actors, as appropriate, to:
Identify a minimum set of performance indicators relevant to the country situation, including gender-sensitive indicators, through a consultative process (M&E group, workshop, etc).
Ensure the inclusion of these indicators in the general HIS reporting system.
Organize sample surveys, where/when needed.
….
Lessons & practical hints from field experience
.…
…include an example of a set of indicators used in a particular emergency…?
Additional guidance
Sphere Handbook Tracking health performance and humanitarian outcomes, background conference paper, A.
Griekspoor, A Loretti & S Colombo, WHO 2005 …
DRAFT for FIELD CONSULTATION
[Health Cluster Guide – draft, 30 June 2008] 71
6.3 Evaluating health sector response; organizing a lesson-learned exercise
Evaluation is an assessment, as systematic and objective as possible, of an ongoing or completed project, programme or policy, its design, implementation and results.
A widely-accepted OECD definition established 5 basic evaluation criteria: the relevance and fulfilment of objectives, efficiency, effectiveness, impact, and sustainability. ALNAP has suggested 3 more for the evaluation of humanitarian actions: connectedness, coherence and coverage.
An evaluation should provide information that is credible and useful, enabling the incorporation of lessons learned into the decision-making process of both recipients and donors. An evaluation can be done during implementation (“mid-term”), at its end (“final evaluation”) or afterwards (“ex post evaluation”), either to help steer the project or to draw lessons for future projects and programming.16
Evaluating humanitarian assistance programmes is not an easy task. While qualitative methods are more likely to capture the intricate nature of disaster responses, those evaluating such programmes should be prepared to use different methods and compare and weigh the results to arrive at valid conclusions (Sphere).
Joint evaluations or lessons-learning exercises should be organized – usually separately – at appropriate moments. They must be organized at a time when it is feasible to generate information that is accurate, reliable and useful.
They may be organized at national level or within particular operational zones. They must identify critical health and operational issues and fine-tune the strategies to address them. Areas of weakness must be identified so that steps can be taken to rectify them. The findings should lead to policy, operational and technical recommendations.
A real-time evaluation may be appropriate during the early stages of a major humanitarian operation. The purpose will be to help ensure the best possible outcomes for the affected population by identifying – and suggestions solutions to – any problems in the coordination, planning and management of the response, and ensuring accountability.
For any major crisis, a final lessons-learning exercise should be undertaken not later than one month after the end of humanitarian operations. It should cover both programme and operational aspects. This should be included in the work plan and budget of the Cluster/sector coordination group.
The purpose of each evaluation or lessons exercise must be clearly defined, the terms of reference (TOR) drawn up with care – see box below – and an adequate budget established.
A key success factor in sector programme evaluation is the involvement of all sector partners, including the MoH, in the planning of the evaluation to ensure their ownership of the results. All the main health actors should be involved in planning the exercise and agree the TOR. (A sector programme evaluation is more complex than a single-intervention evaluation!)
An evaluation manager must be designated for each evaluation or lessons exercise. S/he must be able to devote sufficient time to managing the process. Evaluation teams should include a mix of relevant skills and experience, and be gender-balanced.
Reports, findings and recommendations must be promptly disseminated to all concerned and brought to the attention of the managers who need to know and take action.
Drawing up terms of reference for an evaluation or lessons exercise
Whatever the purpose and approach, well-thought-out TOR are important. They should be directly relevant to the decisions to be taken by intended users. The time and effort invested in preparing good TOR have big payoffs in terms of resulting quality, relevance and usefulness.
The TOR should spell out the objectives (purposes) of the exercise, the methodology to be used, the steps to
16 Manual Project Cycle Management, June 2005, European Commission, ECHO
DRAFT for FIELD CONSULTATION
[Health Cluster Guide – draft, 30 June 2008] 72
be gone through, and the roles and responsibilities of all concerned parties.
Limit questions to the most important issues and ones that can realistically be answered in the prevailing circumstances; prioritize them.
• Do not overload the TOR! Overloading is a frequent problem when many people add their own questions, especially in joint agency evaluations. The need to focus requires a prioritisation of the diverse needs of the various possible users or stakeholders.
• Be cautious about combining lesson-learning and accountability purposes in a single evaluation – the issues and the intended users are different and it may result in ambiguity in emphasis and approach.
TOR are as important for internal teams as they are for external teams, although external teams may require more detail on background context and on intended audiences and uses. TOR may need to be translated for in-country use. For a sector-wide evaluation, the TOR must be agreed among all stakeholders. The methodologies and tools to be used may need to be adapted/developed and piloted during an initial design phase.
Role of an evaluation manager
The evaluation manager is part of the evaluation team, albeit with a special role and perspective. S/he must, amongst other things:
Ensure financial and logistical preparation: careful budgeting and thorough logistics preparations are essential – don’t under-estimate the cost, time and resources required, especially the field work component of an evaluation
Devote adequate time to the process, be systematic (in planning and supervising), sensitive (to the needs of the team and others involved), and solutions-oriented (anticipate and respond promptly to the problems that will inevitably arise)
Ensure that sufficient time is given to\building the appropriate level of interaction and ongoing reporting back between the evaluation team, the evaluation manager, operational personnel and other stakeholders
Ensure follow-up – that the report/findings and recommendations are promptly disseminated to all concerned and brought to the attention of the managers who need to know and take action.
HCC and Health Cluster action:
Work with the MoH and other important health actors, as appropriate, to:
Identify the appropriate timing for a joint evaluation or lessons-learning exercise, and get support for the proposal from the main stakeholders.
Organize a consultative process to: (i) identify both the issues (the broad areas that need to be explored) and the specific questions that need to be answered; and (ii) agree on TOR and a plan.
Ensure the designation of an evaluation manager and support him/her as needed.
Lessons & practical hints from field experience
.…
Additional guidance
ALNAP 2006 - Evaluating humanitarian action using the OEDC-DAC criteria, T Beck: see http://www.alnap.org/publications/eha_dac/index.htm
IASC - Proposal of a Pilot Initiative to test Inter-Agency Real-Time Evaluation Interagency Health and Nutrition Evaluations in Humanitarian Crises (IHE) Initiative. Guidelines for
Implementing Interagency Health and Nutrition Evaluations in Humanitarian Crises (forthcoming) Report of the real-time evaluation of response to the Nargis cyclone disaster in Myanmar,
expected late 2008
DRAFT for FIELD CONSULTATION
[Health Cluster Guide – draft, 30 June 2008] 73
7 Managing and disseminating information
Key points: Disaggregated data on the situation and health response activities (disaggregated by area,
population group, age and sex, as much as possible) must be collected, collated, analysed, stored in a readily-retrievable manner, and made available to all stakeholders.
Agreement is needed on the information that is required from cluster participants and other health actors, in what form and how often it should be presented.
A central registry of organizations involved in health activities must be kept up to date, including information on operations and capacities.
Information on the health situation, health-related activities and outstanding (unmet) needs should be issued regularly to all stakeholders (including donors) and the news-media.
…
Common “gaps” in relation to health service delivery standards findings from 10 country case studies (2004-07)
Examples Proposed remedies
Lack of data for monitoring and planning including malnutrition, mortality, and morbidity.
Health Information System inappropriate to the phase of the response. For example, continued use of sentinel site surveillance rather than population based data in the early recovery phase.
Establish a common health information system coordinated by one agency aiming for timely complete reporting from all facilities. Put in place effective mortality data collection system (such as community-based mortality data collection using community health workers). Conduct mortality survey where indicated.
Implement population-based Health Information System in early recovery (as appropriate).
DRAFT for FIELD CONSULTATION
[Health Cluster Guide – draft, 30 June 2008] 74
7.1 Managing information
“Information management” is the process of receiving and storing data in a way in which they can be quickly retrieved whenever needed, and systematically compiling and analysing data to generate information for early warning, programme planning, management and evaluation, and advocacy purposes.
Good information and good information management are essential for coordination and the key to successful emergency response. They are also necessary to support requests for resources. A good information management system is needed from day-1.
A full-time information manager is needed in many cases, and space to manage the receipt and organization of information, to display it in an accessible manner, and to manage dissemination.
Information should be collected from the health surveillance system but also from agencies' reports and the news media. Non-confirmed rumours should not be discounted: they should be checked out and addressed or dispelled.
The health information system must be linked with the humanitarian information centre (HIC), where there is one, especially for access to information on the potential causes of health problems, e.g. shortage of water, pollution of sources, lack of sanitation, etc. as well as basic demographic data, etc.
Documents containing background information should be assembled including reports of previous emergency operations, epidemiological studies, country briefs, etc.
HCC and Health Cluster action:
….
Lessons & practical hints from field experience
.…
Additional guidance
…
Operational Principles for Humanitarian Information Management and Exchange
Accessibility. Humanitarian information and data should be made accessible to all humanitarian actors by applying easy-to-use formats and by translating information into common or local languages when necessary. Information and data for humanitarian purposes should be made widely available through a variety of online and offline distribution channels, including the media.
Inclusiveness. Information management and exchange should be based on a system of collaboration, partnership and sharing with a high degree of participation and ownership by multiple stakeholders, especially representatives of the affected population.
Inter-operability. All sharable data and information should be made available in formats that can be easily retrieved, shared and used by humanitarian organizations.
Accountability. Users must be able to evaluate the reliability and credibility of data and information by knowing its source. Information providers should be responsible to their partners and stakeholders for the content they publish and disseminate.
Verifiability. Information should be accurate, consistent and based on sound methodologies, validated by external sources and analysed within the proper contextual framework.
Relevance. Information should be practical, flexible, responsive, and driven by operational and decision-making needs throughout all phases of a crisis.
Objectivity. Information managers should consult a variety of sources when collecting and analysing information so as to provide varied and balanced perspectives for addressing problems and recommending solutions.
Humanity. Information should never be used to distort, to mislead or cause harm to affected or at-risk populations
DRAFT for FIELD CONSULTATION
[Health Cluster Guide – draft, 30 June 2008] 75
and should respect the dignity of victims.
Timeliness. Humanitarian information must be kept current and should be collected, analysed and disseminated efficiently.
Sustainability. Humanitarian information and data should be preserved, catalogued and archived so that it can be retrieved for future use, such as for preparedness, analysis, lessons learned and evaluation.
[Source: …]

DRAFT for FIELD CONSULTATION
[Health Cluster Guide – draft, 30 June 2008] 76
7.2 Disseminating information – managing external communications
Information on the health situation, health-related activities and outstanding (unmet) needs should be issued regularly.
HCC and Health Cluster action:
Arrange for the regular production of a Health Bulletin (presenting health data and trends) and newsletter (providing technical and general information on health, cross-cutting issues) with procedures and deadlines for the submission of information and articles, and the rapid clearance of drafts by a small, cluster-appointed editorial board. (Don’t under-estimate the time required for the compilation and preparation of material.)
Disseminate the bulletin widely – to MoH facilities at all levels, all other relevant government entities, UN agencies, NGOs, donors, news-media, etc.
Establish and regularly up-date a “health” website, or provide inputs to be integrated in another, inter-sectoral news and reporting forum. Where there is a humanitarian information centre (HIC), for example, health sector issues may be integrated in the HIC website.
Establish and cultivate contacts with local and international journalists/news-media representatives.
Prepare press releases and organize press briefings whenever there is important information to publicize.
Organize question-and-answer briefings and field visits for national and international journalists.
Establish a photo-library and systematically collect and catalogue photos of the health situation and significant events.
…
Lessons & practical hints from field experience
In Uganda, the health cluster issues a quaterly Newsletter and Bulletin. In addition, monthly cluster reports, and daily or weekly situation reports are disseminated. Distribution channels include: mailing list, cluster website, and a Google share group.
.…
Additional guidance
…
…template for a health bulletin to be inserted as an annex …

DRAFT for FIELD CONSULTATION
[Health Cluster Guide – draft, 30 June 2008] 77
8 Standards and protocols
Key points: Aim for high coverage with quality
Build consensus on the application of best practices
Monitor the application/implementation of evidence-based interventions
Promote an enabling environment for implementation/adoption of evidence-based practices
Common “gaps” in relation to health service delivery standards findings from 10 country case studies (2004-07)
Examples Proposed remedies
Malnutrition Global acute malnutrition among children 6-59 months of age often excessive, even in longstanding emergencies and early recovery situations.
Health care for the malnourished not always in line with international standards, particularly routine malaria treatment in therapeutic feeding centres. For example, deaths due to malaria were very high in one therapeutic feeding centre. Promotion of breast feeding inadequate.
Create linkages between the health sector and the nutrition coordination mechanism. Ensure adequate data for decision making on prevalence of malnutrition.
Disseminate operational guidance to partners, together with nutrition partners, with focus on community based care (including community based therapeutic care and promotion of breast feeding).
Water-borne diseases Lack of prevention, hygiene promotion, and standardized clinical management of diarrhea, with linkages to the WASH activities. Inadequate access to adequate quantities of safe water in many settings.
Create linkages between the health sector and the Water, Sanitation and Hygiene (WASH) coordination mechanism to ensure access to water meets minimum international standards, and to develop and disseminate standards and operational guidance on hygiene promotion and the management of diarrhea.
Measles Measles vaccination coverage not in line with international standards, particularly in non-camp situations.
Organize well monitored mass measles vaccination together with agencies and national authorities where indicated. Reinforce routine vaccination programme as indicated by phase of response.
Outbreaks Lack of standard reporting and case definition, no real time analysis and slow feedback. Delayed laboratory confirmation of outbreak. Slow response times (greater than 48 hours).
Appoint one agency to coordinate disease surveillance, outbreak detection and response. Plan for outbreak response, including identification of laboratories (local, national, international) for confirmation. Prompt establishment of Early Warning Alert and Response System. Establish contingency supply stock for emergency response.

DRAFT for FIELD CONSULTATION
[Health Cluster Guide – draft, 30 June 2008] 78
Malaria Lack of standardized prevention and treatment of malaria, appropriate to the epidemiological setting and phase of response, and for special groups such as severely malnourished.
Develop and disseminate standards and operational guidelines, advocate for evidence-based treatment guidelines, and plan for additional support to drug and materials supply as necessary.
Reproductive health (incl. obstetrics) High maternal mortality, with limited access to emergency obstetric care and comprehensive reproductive health care.
Disseminate phase-specific minimum package of care among partners (including distribution of clean delivery kits to pregnant women in acute emergencies and promoting deliveries in a health facility with a trained practitioner in more stable settings).
Appoint a dedicated reproductive health coordinator or coordinating agency.
Gender-based violence (GBV) Absent comprehensive effective inter-sectoral prevention and response to GBV.
Ensure that the health sector participates in an inter-sectoral strategy for preventing and responding to GBV.
Develop and disseminate standard operating procedures for GBV including standardized reporting, referral and clinical management, coordinated by dedicated reproductive health coordinator.
HIV/AIDS & sexually-transmitted infections Services for HIV/AIDS prevention and care neglected, inadequate, or not integrated into health service delivery. Lack of age- and gender- appropriate prevention and treatment of STIs and HIV/AIDS, coordinated with other sectors.
Waste disposal not always safe.
Blood transfusion not always safe.
Initiate a community based minimum service package for STI and HIV prevention, sensitive to gender and age.
Provide adequate supplies for prevention, diagnosis and treatment, including antiretroviral drugs where rolled out.
Develop and disseminate standards and operational guidelines for implementation and monitoring of safe waste disposal and blood transfusion.
Mental health & psycho-social support Stage-specific planning for mental health and psycho-social support disorganized or absent, particularly for the management of alcohol dependence. Lack of community based approach to mental health.
Define a ‘global framework’ for mental health early in the emergency response. In the emergency phase, actions should be mainly psychosocial, with community health workers delivering social support and psychological first aid.
Disposal of dead bodies (forensics)
Socially and culturally inappropriate burial of corpses, mass graves.
Disseminate standards and operational guidelines.
Advocate with national authorities for culturally appropriate burial as indicated.
DRAFT for FIELD CONSULTATION
[Health Cluster Guide – draft, 30 June 2008] 79
8.1 Promoting – and building consensus on – evidence-based best practices Quality is essential if emergency health response is to decrease mortality and morbidity. For example, if a measles vaccination campaign doesn’t achieve 95% coverage it would have failed to prevent the risk of a measles outbreak. The HCC has the duty to promote and facilitate the implementation of quality health care responses in all the priority sub-sectors identified for health cluster action.
• Where national treatment policies and guidelines are different from recommended ‘global’ best practices, it is suggested that the HCC take the opportunity to promote best practices and the enhancement of the relevant national policies and guidelines.
• Where guidelines and protocols exist but are not widely implemented, or practised, at community and facility levels, it is recommended that most of the HCC’s effort be directed to facilitating and monitoring the implementation of the activities at facility and community levels.
Sub-sector Good practices & recommended reference materials
There is at a minimum 1 basic health unit per 10,000 people There is a basic emergency obstetric care (EmOC), with 6 signal functions, at health centre level,
with 1 health centre per 30,000 people 1 comprehensive EmOC and 4 basic EmOC for 500,000 people is the recommended standard
but, in a conflict setting, services should be available as near to the population as possible as referral might be impossible
Mid-level medical practitioner’s (nurse, midwife, health officer) role in the provision of curative health services enhanced
Role of CHW in provision of curative care for childhood illness e.g. community-case management of pneumonia in remote locations, a potential strategy to reach remote scattered communities and inaccessible displacement camps
Risk assessment for disease outbreaks
Gen
eral
Hea
lth S
ervi
ces
Sphere minimum standards, available at: www.sphereproject.org Reproductive Health in refugee situations: an inter-agency field manual www.iawg.net/resources/field_manual.html
Refugee Health; an approach to emergency situations www.refbooks.msf.org/msf_docs\ Children with pneumonia have access to adequate treatment within 24-48 hours of symptoms Zinc supplementation for treatment of childhood diarrhoea Vitamin A supplementation for all children under the age of 5yrs ORS – available at home level, for the treatment of dehydration Malaria treatment – recommended Artemsinin-based combination therapy (ACT), with RDT or
microscopic diagnosis
Chi
ld H
ealth
Child health in complex emergencies www.books.nap.edu/catalog.php Malaria control in complex emergencies : an interagency field handbook http://www.who.int/malaria/docs/ce_interagencyfhbook.pdf Clinical guidelines: diagnosis and treatment manual (MSF) www.refbooks.msf.org/msf_docs/en/Clinical_Guide/CG_en.pdf
Management of cases with severe acute malnutrition at health center level If acute malnutrition level is above national standard or >10 GAM, & >1 SAM – coordinate with
nutrition cluster for possible initiation of community case management of acute malnutrition (CMAM)
Nut
ritio
n Management of severe malnutrition: a manual for physicians and senior health workers: www.who.int/nutrition/publications/malnutrition Community-based Therapeutic Care: a field manual www.fantaproject.org/downloads/pdfs/CTC_Manual_v1_Oct06.pdf
Early Warning and Response (EWR) system established, including data collection from service providers, data analysis, and dissemination
Outbreak response initiated within 24-48 hours of case reporting Case Fatality Rate during cholera and measles outbreaks <1% Measles vaccination campaign conducted with the objective to achieve >95% coverage among
children 6-59months
Com
mun
icab
le
Dis
ease
s
Management of A Measles Epidemic, MSF
DRAFT for FIELD CONSULTATION
[Health Cluster Guide – draft, 30 June 2008] 80
Management of epidemic meningococcal meningitis www.refbooks.msf.org/msf_docs/en/Meningitis/Mening_en.pdf Communicable diseases control in emergencies: field manual http://whqlibdoc.who.int/publications/2005/9241546166_eng.pdf Cholera guidelines, WHO www.who.int/foodsafety/publications/foodborne_disease/cholera/en/
Standard precautions at facility level Continuity of ARTs for those who are on treatment (restocking) Safe blood transfusion Condoms available and accessible to the community Syndromic case management of STIs Rapid test for syphilis as part of focused ANC Initiate PMTCT in contexts where HIV/AIDS is the main cause of death (e.g. sub-Saharan Africa)
STIs
& H
IV/A
IDS
Sexually transmitted & other reproductive tract infections http://www.who.int/reproductive-health/publications/rtis_gep/index.htm Practical guidelines for infection control in health care facilities: www.who.int/water_sanitation_health/emergencies/infcontrol/en/
Provision of clean delivery kits to pregnant women with counselling on how to use the kit and birth preparedness plan
Immediate postnatal (maternal & newborn) care within 24-48 hours after delivery by medical personnel (or trained community health workers)
Provision of basic EmOC signal functions at health centre level Availability of a referral facility for comprehensive EmOC Availability of referral mechanism Neonatal resuscitation, materials available at all health service delivery points and staff trained on
essential newborn care including neonatal resuscitation Aim to increase proportion of deliveries at facility level
Mat
erna
l & N
ewbo
rn H
ealth
MSF Obstetrics in remote settings: a guide for non-specialized health care www.refbooks.msf.org/msf_docs/en/Obstetrics/Obstetrics_en.pdf Integrated Management of Pregnancy, childbirth, and newborn care: www.who.int/reproductive-health/publications/pcpnc/pcpnc.pdf Minimum Initial Service Package for Reproductive Health in Crisis Situations: www.rhrc.org/MISP/english/
Medical staff have the skills to medically manage cases of sexual violence PEP for HIV/AIDS, STI treatment, Hepatitis B vaccine, EC – available at basic health unit level
with minimum stock-out Provision of, or programme link with, psychosocial support
Sexu
al V
iole
nce
Clinical management of rape survivors www.who.int/reproductive-health/publications/clinical_mngt_rapesurvivors.pdf IASC Gender-based-violence www.humanitarianinfo.org/iasc/content/subsidi/tf_gender/gbv.asp
Rescue and evacuation, first aid, and surgical care needs are immediately available following natural disasters like earthquakes
Re-stocking of supplies for chronic diseases in circumstances where the burden of chronic diseases is high
Non
-co
mm
unic
abl
e di
seas
es
Safe sharp & medical waste disposal system in place in all facilities Health facility staff trained on standard precautions
Envi
ron
men
tal
HCC action:
Ensure that national guidelines are known by all main stakeholders.
Where the national guidelines are not in line with the latest global evidence or recommended practices, facilitate dialogue among stakeholders to ensure that the latest evidence is applied.
Promote the application (implementation) of the latest guidelines.
DRAFT for FIELD CONSULTATION
[Health Cluster Guide – draft, 30 June 2008] 81
Ensure an enabling environment for the implementation of the best clinical and public health practices.
Facilitate consensus building on standards and protocols.
Facilitate and promote adherence to best practices and standard of care.
Where there is disagreement on standard of care, facilitate dialogue with the aim of ensuring that the local communities get the ‘best’ care.
Expected result: Emergency-affected communities have access to quality health services (high coverage with quality) – with success shown in reduced levels of mortality and morbidity.
Lessons & practical hints from field experience
.…
Additional guidance
See references in the table above.
DRAFT for FIELD CONSULTATION
[Health Cluster Guide – draft, 30 June 2008] 82
8.2 Promoting adherence to agreed standards and protocols
HCC and Health Cluster action:
Create forums for sharing programme learning among stakeholders.
Create the opportunity to share collated, analyzed data from health facilities in the coverage area for joint analysis and development of public health action.
Engage stakeholders in identification of model practices for cross-learning.
The Cluster lead/HCC may also:
Monitor the indicators of health status and public health service provision and, when necessary, draw attention to national standards and international best practice and suggest what could be done to improve standards.
Make sure that international NGOs and all other cluster participants are aware of national health policies and priorities, and international protocols and best practice, and their relevance in the prevailing situation. Encourage them to respect those policies and protocols and to preserve and strengthen local capacity with a view to developing services (including health information/warning systems and health facilities) that are sustainable in the long term.
Discourage any organization from actions not consistent with the established standards.
Arrange for the preparation and dissemination of technical guidelines and organize training for cluster participants, if needed.
Encourage all health actors to look for and exploit all opportunities to protect and (re-)build national health systems and capacities.
Emphasize the importance of maintaining and, where possible, strengthening the MoH and sub-national level health structures, and not denuding these structures.
Arrange briefings for new organizations arriving in the country to work in the health sector; when required, help the MoH to arrange such briefings. This may include:
o the country’s epidemiological profile, national health policies and programmes, and pre-emergency health service coverage;
o national and international expertise available (e.g. for tropical diseases specific to the country which may be beyond the capacities of some foreign NGOs);
o the structure of the MoH and the list of health focal points on other organizations;
o details of arrangements for emergency health coordination.
The cluster lead/HCC may also provide foreign relief teams that are new to the country with advice on measures to protect their own health and try to ensure that they have arrangements for emergency medical evacuations.
Lessons & practical hints from field experience
.…
Additional guidance
…
DRAFT for FIELD CONSULTATION
[Health Cluster Guide – draft, 30 June 2008] 83
9 Promoting recovery
Key points - to be revised/up-dated Strengthen the capacity of national stakeholders including government, civil society and local
organizations and institutions in health service delivery, emergency preparedness, risk reduction, response and recovery.
Ensure that, from the outset, the humanitarian response protects and, wherever possible, contributes to strengthening and rebuilding local health systems and capacities.
Make sure that national health personnel are involved in all activities, including participating in assessments, analyses, decision-making, project design, implementation and monitoring of interventions, preparing joint reports and co-chairing meetings, as a conscious effort of on-the job training.
Support the role of the Line Ministry to manage the sector.
…
<Common “gaps” in relation to health service delivery standards findings from 10 country case studies (2004-07)
Examples Proposed remedies
Failure to link with existing capacities, including district and national authorities, local non-government and private sector. For example, a tented clinic was set up within walking distance of unsupported local health centre.
Failure to involve communities in assessment, planning, monitoring and evaluation of interventions. For example, in one emergency, international responders failed to recognize that most of the life-saving activity was conducted by local communities prior to the arrival of international support. In another emergency, beneficiary ‘participation’ was limited to paying for labour.
Develop local partnerships from the outset. Integrate humanitarian facilities with nearby local facilities. Invite a Ministry of Health representative as co-chair of the health cluster / health sector coordination mechanism. In early recovery, conduct district health management training.
Strengthen linkages between community, community health workers, and health facilities. Take a human rights based approach to programming.
DRAFT for FIELD CONSULTATION
[Health Cluster Guide – draft, 30 June 2008] 84
9.1 Protecting and reinforcing local capacities from the outset
The strengthening/re-building of local health systems and capacity can be initiated from day-1 by designing and implementing all emergency health programmes and activities in ways that contribute to that objective. The recovery phase after a disaster provides a window of opportunity for building preparedness systems and capacity and instituting vulnerability reduction measures. These opportunities must be seized.
HCC and Health Cluster action:
Work together and with the MoH, as appropriate, to ensure that all emergency health programmes and activities are designed and implemented in ways that contribute to re-building local capacities. Tray, in particular, to ensure that:
• existing facilities and systems are used, reactivated and repaired, whenever possible – and that new, parallel systems are avoided, unless absolutely necessary;
• existing in-country competencies are identified and used as much as possible;
• local personnel are involved in all assessment, planning and response activities;
• (re)training needs are identified and appropriate, task-oriented training provided as early as possible.
Try to get agreement among all the main health actors on:
• the importance of maintaining and, where possible, strengthening the MoH and sub-national level health structures; and
• how to avoid denuding these structures. (Possibilities might include paying incentives to MoH staff to stay at their posts. Use imagination to find ways, together with partners.)
Identify existing in-country competencies and try to make sure that they are used to good effect.
Discourage all health actors from creating new parallel systems, unless absolutely necessary.
Facilitate international/ national partnerships with and among NGOs to help build local capacity.
Promote the Principles of Partnership reproduced in section 1.2.
When the emergency is over and external health actors are leaving, handover of health services to the government should be carefully planned – sequenced progressively, step-by-step over a defined period of time.
Lessons & practical hints from field experience
.…
Additional guidance
…
For detailed guidance in relation to re-building national capacity and systems possible, see Analysing Disrupted Health Systems, WHO 2008, and the Health Cluster Guide, draft 2008.

DRAFT for FIELD CONSULTATION
[Health Cluster Guide – draft, 30 June 2008] 85
9.2 Supporting health system recovery – to be edited
After a prolonged crisis, or, towards the end of one, recovery is the complex and long process during which internal and external partners need to work together to rebuild the State capacity to deliver health and other essential services such as security and other social services while also re-establishing economic activities.
The recovery phase is crucial. This is when solid foundations for reconstruction should be laid. It is a period fraught by many problems and endowed with many opportunities. Planning recovery and reconstruction should start early.
Formulating sound policies, adequate strategies and flexible plans, are essential steps to provide a framework for action in a highly fragmented environment.
Guiding Principles
The following are a few guiding principles:
Pay careful attention to the local context and be aware of international experiences. Blanket generalizations must be avoided.
Take a systemic approach to the health sector, trying to anticipate the effect of individual interventions on the whole health system (this should be done at national level but, also, at a sub-national level – a region or district). The health system is part of the wider national system: think and work in collaboration with other sectors: water, education, roads, etc.
Do no harm: some interventions have the potential of introducing distortions that will be difficult to correct. For instance, a salary policy unconcerned with the local economic situation or a lavish investment in infrastructure with no thought of future recurring costs.
Take care of the process as much as of the result: policies, strategies and plans should not be elaborated in isolation but be the result of intensive, extended and iterative discussions with all the concerned partners. In many situations, there are non-state actors whose involvement, although politically delicate, is essential and whose exclusion is a recipe for failure.
Be aware of the political implications: a post-conflict period is, often, in a fragile equilibrium. Ethnic, religious, social and territorial sensibilities must be known and understood.
Act in the short term but think in the long term: urgent actions are needed and important. At the same time, immediate post-conflict interventions may have long term impacts. Reconstructing a State, not only its infrastructure, is a decades-long process.
Communicate widely, clearly, frequently and regularly.
Opportunities for Change
Often, the recovery period offers important opportunities. The enthusiasm for reconstruction may be high, the generosity of donors considerable, the resistance to change reduced.
If the health system before the crisis contained (as it is often the case) distortions and inequities, the recovery phase may offer the possibility of laying the ground for improvements.
Given the scarcity of information, the basis for sound policy decisions must be:
• Knowledge of the health system as it was before the crisis • Knowledge of health systems of similar countries • Knowledge of the international public health debate and its most updated and evidence based
conclusions • Identifying the decisions that can be taken immediately and those that can be postponed • Identifying the studies needed to provide the most urgent, relevant and precise information to
formulate more refined strategies and plans.
DRAFT for FIELD CONSULTATION
[Health Cluster Guide – draft, 30 June 2008] 86
At the early stage, plans should not be too detailed (they would become rapidly outdated) and should allow a high degree of flexibility, for continuous fine-tuning as more, and more precise, information becomes available.
When planning the reconstruction of a health system, the following aspects must be considered at the same time:
• the health network, in relation to population distribution and settlements • the human resources needed to manage it • the management systems to make it work • the financial resources needed and likely to become available
Main steps in planning and implementing support to recovery
In the majority of cases, the recovery of a disrupted health system requires:
1. Putting together a sound information base (accuracy more important than precision)
2. Formulating policies and strategies (negotiation and sharing as important as final product)
3. Planning the restoration of service delivery, including expansion to underserved areas (difficult balance between politics, equity and efficiency)
4. Introducing new service delivery models (important to mix lessons from elsewhere and understanding of local context)
5. Training new cadres and retraining (or retrenching) old ones (long term planning for pre-service training is essential)
6. Introducing strong management systems (an all too often neglected cornerstone of recovery)
7. Ensuring equity, effectiveness and efficiency (compromises are inevitable)
HCC and Health Cluster action:
….
Lessons & practical hints from field experience
.…
Additional guidance
WHO, Pavignani & Colombo, Analysing Disrupted Health Sectors, a Modular Manual, expected 2008
WHO, J.-J. Guilbert, Educational Handbook for Health Personnel, WHO Offset Publication No 35, Revised and Updated 1998
Establishing Human Resource Systems for Health during Post-conflict Reconstruction, Management Sciences For Health (MSH), occasional paper No. 3 (2006) http://www.msh.org/resources/publications/pdf/HRH_Postconflict.pdf
DRAFT for FIELD CONSULTATION
[Health Cluster Guide – draft, 30 June 2008] 87
Annex A 1 Generic Terms of Reference for Sector/Cluster Leads at the Country Level [Reproduced from: IASC Guidance Note on Using the Cluster Approach to Strengthen Humanitarian Response, Nov. 2006, Annex 1. The full guidance note is on the CD-ROM.]
Sector/cluster leads at the country level are accountable to the Humanitarian Coordinator for facilitating a process at the sectoral level aimed at ensuring the following:
Inclusion of key humanitarian partners
• Ensure inclusion of key humanitarian partners for the sector, respecting their respective mandates and programme priorities
Establishment and maintenance of appropriate humanitarian coordination mechanisms
• Ensure appropriate coordination with all humanitarian partners (including national and international NGOs, the International Red Cross/Red Crescent Movement, IOM and other international organizations), through establishment/maintenance of appropriate sectoral coordination mechanisms, including working groups at the national and, if necessary, local level;
• Secure commitments from humanitarian partners in responding to needs and filling gaps, ensuring an appropriate distribution of responsibilities within the sectoral group, with clearly defined focal points for specific issues where necessary;
• Ensure the complementarity of different humanitarian actors’ actions;
• Promote emergency response actions while at the same time considering the need for early recovery planning as well as prevention and risk reduction concerns;
• Ensure effective links with other sectoral groups;
• Ensure that sectoral coordination mechanisms are adapted over time to reflect the capacities of local actors and the engagement of development partners;
• Represent the interests of the sectoral group in discussions with the Humanitarian Coordinator and other stakeholders on prioritization, resource mobilization and advocacy;
Coordination with national/local authorities, State institutions, local civil society and other relevant actors
• Ensure that humanitarian responses build on local capacities;
• Ensure appropriate links with national and local authorities, State institutions, local civil society and other relevant actors (e.g. peacekeeping forces) and ensure appropriate coordination and information exchange with them.
Participatory and community-based approaches
• Ensure utilization of participatory and community based approaches in sectoral needs assessment, analysis, planning, monitoring and response.
Attention to priority cross-cutting issues
• Ensure integration of agreed priority cross-cutting issues in sectoral needs assessment, analysis, planning, monitoring and response (e.g. age, diversity, environment, gender, HIV/AIDS and human rights); contribute to the development of appropriate strategies to address these issues; ensure gender-sensitive programming and promote gender equality; ensure that the needs, contributions and capacities of women and girls as well as men and boys are addressed;
Needs assessment and analysis
• Ensure effective and coherent sectoral needs assessment and analysis, involving all relevant partners
Emergency preparedness
• Ensure adequate contingency planning and preparedness for new emergencies;
DRAFT for FIELD CONSULTATION
[Health Cluster Guide – draft, 30 June 2008] 88
Planning and strategy development
Ensure predictable action within the sectoral group for the following:
• Identification of gaps;
• Developing/updating agreed response strategies and action plans for the sector and ensuring that these are adequately reflected in overall country strategies, such as the Common Humanitarian Action Plan (CHAP);
• Drawing lessons learned from past activities and revising strategies accordingly;
• Developing an exit, or transition, strategy for the sectoral group.
Application of standards
• Ensure that sectoral group participants are aware of relevant policy guidelines, technical standards and relevant commitments that the Government has undertaken under international human rights law;
• Ensure that responses are in line with existing policy guidance, technical standards, and relevant Government human rights legal obligations.
Monitoring and reporting
• Ensure adequate monitoring mechanisms are in place to review impact of the sectoral working group and progress against implementation plans;
• Ensure adequate reporting and effective information sharing (with OCHA support), with due regard for age and sex disaggregation.
Advocacy and resource mobilization
• Identify core advocacy concerns, including resource requirements, and contribute key messages to broader advocacy initiatives of the HC and other actors;
• Advocate for donors to fund humanitarian actors to carry out priority activities in the sector concerned, while at the same time encouraging sectoral group participants to mobilize resources for their activities through their usual channels.
Training and capacity building
• Promote/support training of staff and capacity building of humanitarian partners;
• Support efforts to strengthen the capacity of the national authorities and civil society.
Provision of assistance or services as a last resort
• As agreed by the IASC Principals, sector leads are responsible for acting as the provider of last resort (subject to access, security and availability of funding) to meet agreed priority needs and will be supported by the HC and the ERC in their resource mobilization efforts in this regard. (This concept is to be applied in an appropriate and realistic manner for cross-cutting issues such as protection, early recovery and camp coordination.)
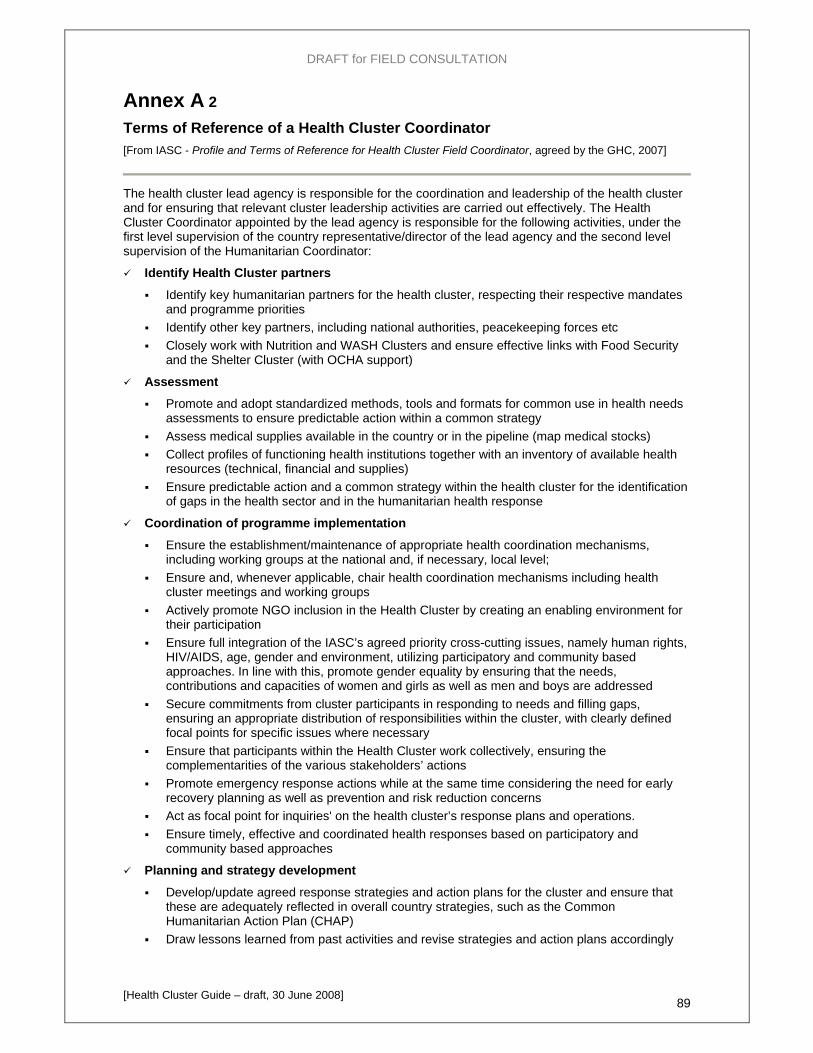
DRAFT for FIELD CONSULTATION
[Health Cluster Guide – draft, 30 June 2008] 89
Annex A 2 Terms of Reference of a Health Cluster Coordinator [From IASC - Profile and Terms of Reference for Health Cluster Field Coordinator, agreed by the GHC, 2007]
The health cluster lead agency is responsible for the coordination and leadership of the health cluster and for ensuring that relevant cluster leadership activities are carried out effectively. The Health Cluster Coordinator appointed by the lead agency is responsible for the following activities, under the first level supervision of the country representative/director of the lead agency and the second level supervision of the Humanitarian Coordinator:
Identify Health Cluster partners
Identify key humanitarian partners for the health cluster, respecting their respective mandates and programme priorities
Identify other key partners, including national authorities, peacekeeping forces etc Closely work with Nutrition and WASH Clusters and ensure effective links with Food Security
and the Shelter Cluster (with OCHA support)
Assessment
Promote and adopt standardized methods, tools and formats for common use in health needs assessments to ensure predictable action within a common strategy
Assess medical supplies available in the country or in the pipeline (map medical stocks) Collect profiles of functioning health institutions together with an inventory of available health
resources (technical, financial and supplies) Ensure predictable action and a common strategy within the health cluster for the identification
of gaps in the health sector and in the humanitarian health response
Coordination of programme implementation
Ensure the establishment/maintenance of appropriate health coordination mechanisms, including working groups at the national and, if necessary, local level;
Ensure and, whenever applicable, chair health coordination mechanisms including health cluster meetings and working groups
Actively promote NGO inclusion in the Health Cluster by creating an enabling environment for their participation
Ensure full integration of the IASC’s agreed priority cross-cutting issues, namely human rights, HIV/AIDS, age, gender and environment, utilizing participatory and community based approaches. In line with this, promote gender equality by ensuring that the needs, contributions and capacities of women and girls as well as men and boys are addressed
Secure commitments from cluster participants in responding to needs and filling gaps, ensuring an appropriate distribution of responsibilities within the cluster, with clearly defined focal points for specific issues where necessary
Ensure that participants within the Health Cluster work collectively, ensuring the complementarities of the various stakeholders’ actions
Promote emergency response actions while at the same time considering the need for early recovery planning as well as prevention and risk reduction concerns
Act as focal point for inquiries' on the health cluster’s response plans and operations. Ensure timely, effective and coordinated health responses based on participatory and
community based approaches
Planning and strategy development
Develop/update agreed response strategies and action plans for the cluster and ensure that these are adequately reflected in overall country strategies, such as the Common Humanitarian Action Plan (CHAP)
Draw lessons learned from past activities and revise strategies and action plans accordingly
DRAFT for FIELD CONSULTATION
[Health Cluster Guide – draft, 30 June 2008] 90
Initiate, as soon as appropriate, preparatory work and a strategy for the recovery phase and the handover to national and local health authorities
Application of standards
Ensure that health cluster participants are aware of relevant policy guidelines, technical standards and relevant commitments that the Government has undertaken under international human rights law
Ensure that health responses are in line with existing (IASC) policy guidance, technical standards, and relevant Government human rights legal obligations
Monitoring and Evaluation
Ensure common monitoring mechanisms are in place to review impact of the cluster and progress against implementation plans
Promote and adopt standardized methods, tools and formats for common use in monitoring health trends, activities and outcomes to support strategic decision-making
Establish participatory mechanisms for monitoring of health programmes and outcomes Promote the adoption of a health performance and humanitarian outcomes tracking service
using agreed benchmarks, indicators, and data (disaggregated by age and sex) so as to provide a systematic accountable arrangement to assess the timeliness, coverage, and appropriateness of humanitarian health action, as well as the impact of health and wider humanitarian assistance, in relation to the targeted populations
Promote a common and joint system of reviews and evaluations conducted with due transparency , accountability and objectivity
Information management and reporting
Develop common health information management strategy and tools including the regular production of a Health Cluster Bulletin
Ensure adequate reporting and effective information sharing (with OCHA support), to effectively communicate cluster activities, progress, reports, data and other relevant information to partners and stakeholders
Promote common software for health data collection and analysis such as, but not limited to, Epi-info, Health Mapper, LSS, etc.
Advocacy and resource mobilization
Represent the interests of the health cluster in discussions with the Humanitarian Coordinator on prioritization, resource mobilization and advocacy
Identify common strategies for communicating with public, media, and policy makers, including for the marketing and advocacy of appeals to donors
Identify core advocacy concerns, including resource requirements, and contribute key messages to broader advocacy initiatives of the Humanitarian Coordinator and other actors
Advocate for donors to fund health cluster participants to carry out priority activities while at the same time encouraging cluster participants to mobilize resources for their activities through their usual channels
Establish channels and mechanisms for resources mobilized at cluster level to facilitate transfer of funds for projects implementation if donors prefer to fund the cluster lead
Training and capacity building of national authorities and civil society
Promote and support training of humanitarian personnel and capacity building of humanitarian partners
Support efforts to strengthen the capacity of the national authorities and civil society Develop and implement a common strategy within the health cluster for capacity building and
training
Acting as provider of last resort
Demonstrate that all possible efforts and initiatives have been undertaken to fill gaps and agreed priority needs, call on additional local and international partners, and advocate for additional donor commitment.
DRAFT for FIELD CONSULTATION
[Health Cluster Guide – draft, 30 June 2008] 91
Annex B Role and activities of the Global Health Cluster The mission of the Global Health Cluster (GHC), led by WHO, is to provide the strategic, technical and normative support to the Health Clusters at country level in order to achieve a predictable health sector leadership during the response to and recovery from acute as well chronic crisis, in order to:
• prevent and reduce crisis related excess morbidity and mortality; • ensure evidence-based actions, • gap filling and sound coordination; • enhance accountability, predictability and effectiveness of humanitarian health actions.
The GHC has taken a number of initiatives aimed at contributing to more coordinated and effective health responses. These include amongst other things:
• gap guidance materials including an analysis of health sector gaps in ten recent crises (Oct. 2007);
and, ongoing in 2008:
• joint Initial Rapid Assessment (IRA) tool for health, nutrition, water and sanitation together with the Nutrition Cluster and the Water, Sanitation and Hygiene (WASH) Cluster;
• health partners' mapping, including assessment and monitoring of health services availability;
• guidance on health sector recovery following acute or protracted crisis situations; and
• the preparation of this Guide.
Reference bibliography: for more details, see (on the CD-ROM):
IASC - Guidance Note on using the Cluster Approach to Strengthen Humanitarian Response, 2006
IASC - Strengthening NGOs Participation in the IASC, A Discussion Paper, 24 April 2006 IASC - Principles of Partnership, A Statement of Commitment, 28 March 2007 IASC - Operational Guidance on designating Sector/Cluster Leads in Major New Emergencies,
2007 IASC - Operational Guidance on designating Sector/Cluster Leads in Ongoing Emergencies, 2007 IASC - Working Group 5-7 November 2007, Rome Statement on Cluster Roll-Out
and: http://www.humanitarianreform.org/

DRAFT for FIELD CONSULTATION
[Health Cluster Guide – draft, 30 June 2008] 92
Annex C Mapping the availability of health services This annex presents: (i) a list of the basic data that should be collected on individual health facilities, whenever possible, and the format of a corresponding Excel spreadsheet for storing the data; and (ii) standard components of health service sectors and sub-sectors.
Ci) Basic data on health facilities Partner Name State the name of the Partner interviewed
Facility identification
Health Facility Name State the name of the HF
State State where the HF is located
Locality Locality where the HF is located
Administrative Unit Administrative Unit where the HF is located
Latitude Latitude of the HF in DECIMAL DEGREES – with min. 5 decimals - ( xx,xxxxx)
Fixe
d da
ta
Longitude Longitude of the HF in DECIMAL DEGREES – with min. 5 decimals - ( xx,xxxxx)
Point of delivery characteristics
Delivery Point Type
IDPC (HF located in IDP Camp and serving exclusively IDPs) – S (HF located in Settlement and serving exclusively Residents – IDPC/S (HF located in IDP Camp but also serving Residents) – S/IDPC (HF located in Settlement but also serving IDPs)
Delivery Point Name Name of the IDP camp/settlement that is delivering the service
Health Facility Type RH (Rural Hospital) – PHCC (Primary Health Care Center) – PHCU (Primary Health Care Unit) – Mob_clinic (Mobile Clinic)
Health Facility Status F (functioning), NF (Non functioning), UR (Under Rehabilitation), P (Planned)
Building Specify the status of the building if it is Permanent (P) or Temporary (T)
Ownership State the entity (ies) owning of the facility
Management State the entity (ies) in charge of running the facility
Support State the entity (ies), if any, supporting the operations of the facility
EWARS Reporting Site Y/N - Is the facility reporting regularly as part of the Early Warning System?
Inpatient Capacity Number of beds in the HF
Facility-based personnel
Medical Officers Number of Medical Officers in the HF
Medical Assistant Number of Medical Assistants in the HF
Nurse Number of Nurses in the HF
Primary Health Officer Number of Primary Health Officers in the HF
Midwife Number of Midwives in the HF
Vaccinator Number of Vaccinators in the HF
Laboratory Personnel Number of Laboratory personnel; i.e., Lab Assistant or Lab Technician
Village Volunteer Number of village volunteers (with no salary)
Community –based personnel
Community Health Workers Number of Community Health Workers (with salary)
Dat
a to
be
up-d
ated
regu
larly
Traditional Birth Attendant
Number of Traditional Birth Attendant, or other Reproductive Health Practitioners with LOW training and no/low salary

DRAFT for FIELD CONSULTATION
[Health Cluster Guide – draft, 30 June 2008] 93
Village Trained Midwife Number of Village Trained Midwife, or other Reproductive Health Practitioners with GOOD training and salary
New Delivery Point State name of Point of Delivery if it is not available in the list

DRAFT for FIELD CONSULTATION
[Health Cluster Guide – draft, 30 June 2008] 94
Cii) Health service sectors, sub-sectors and components The following table presents standard components of health service sectors and sub-sectors that should be assured, to the maximum extent possible, for a crisis-affected population. It may be used during assessment and situation monitoring to check the availability of health services by level of care and by point of delivery. The categories may be used in 4W (Who-What-Where-When) recording and analysis.
Level of Care
Areas of Service / sub-sectors Health Services (in bold the RH MISP Services) Yes/
No A11 Deaths & births A1 Collection of
Vital Statistics A12 Others: eg.: population movements;registry of pregnant women and new-born A21 IMCI community component: IEC of child care taker+active case findings A22 Home based treatment of: fever/malaria, ARI/pneumonia, dehydration due to acute diarrhooea A2 Child Health
A23 Community mobilization for and support to mass vaccination campaigns and/or mass drug administration/treatments
A31 Screening of acute malnutrition (MUAC) A32 Follow up of children enrolled in supplementary/therapeutic feeding (trace defaulters) A3 Nutrition
A33 Community Therapeutic Care of Severe Acute Malnutrition A41 Vector control (IEC+impregnated bed nets+in/out door insecticide spraying) A42 Community mobilization for and support to mass vaccinations and/or drug administration/treatments A4 Communicable
Diseases A43 IEC on TB self referral A51 Community leaders advocacy on STI/ HIV A52 IEC on prevention of STI/HIV infections and behavioural change communication A5 STI &
HIV/AIDS A53 ensure access to free condoms
A6 Maternal & newborn health A61 Clean home delivery, including distribution of Clean Delivery (CD) kit to visible pregnant women,
IEC & behaviour change communication, knoledge of danger signs & where/when to go for help
A7 Non-
Communic. Diseases
A71 Psyco-social support for: mental health disorders, terminal patients including AIDS patients, rape survivors, orphan & unaccompanied children, unaccompanied elders
A
Com
mun
ity C
are
A8 Environmental Health A81 IEC on hygiene promotion & on water and sanitation, community mobilization for clean up
campaigns and/or other sanitation activities B11 Outpatient Services B12 Basic Laboratory B13 Short hospitalization capacity (5-10 beds)
B1 General Clinical
Services
B14 Referral capacity 3 Transportation, 2 means of communication 4 referral proceedure B21 EPI : Routine Immunization against all national target diseases & adequate cold chain in place B2 Child Health B22 Under 5 Clinic conducted by IMCI trained health staff B31 Management of Moderate Acute Malnutrition B3 Nutrition B32 Management of Severe Acute Malnutrition B41 Sentinel site of Early Warning System of epidemic prone diseases, outbreak response B42 Diagnosis & treatment of Malaria B43 Diagnosis & treatment of TB
B4 Communicable Diseases
B44 Other local relevant communicable diseases (eg: sleeping sickness) B51 Syndromic Management of Sexual Transmitted Infections B52 Standard Precautions B53 Availability of free condoms B54 Prophylaxis & Treatment of Opportunistic Infections B55 VCT B56 PMTCT
B5 STI &
HIV/AIDS
B57 ART B61 Family Planning
B62 Antenatal Care, 1) assess pregnant, pregnancy stools, birth & emergency plan2) respond to observed signs3)family planning 4) Advise/counsel on nutrition & self care
B63 Post Care 1) Postpartum examination of of mother (up to 6 weeks) 2)respond to observed signs 3) Family planning
B
Prim
ary
Car
e
SEXU
AL
REP
RO
DU
CTI
VE H
EALT
H
B6 Maternal & Newborn Health
B64 Clean & Safe Normal Delivery
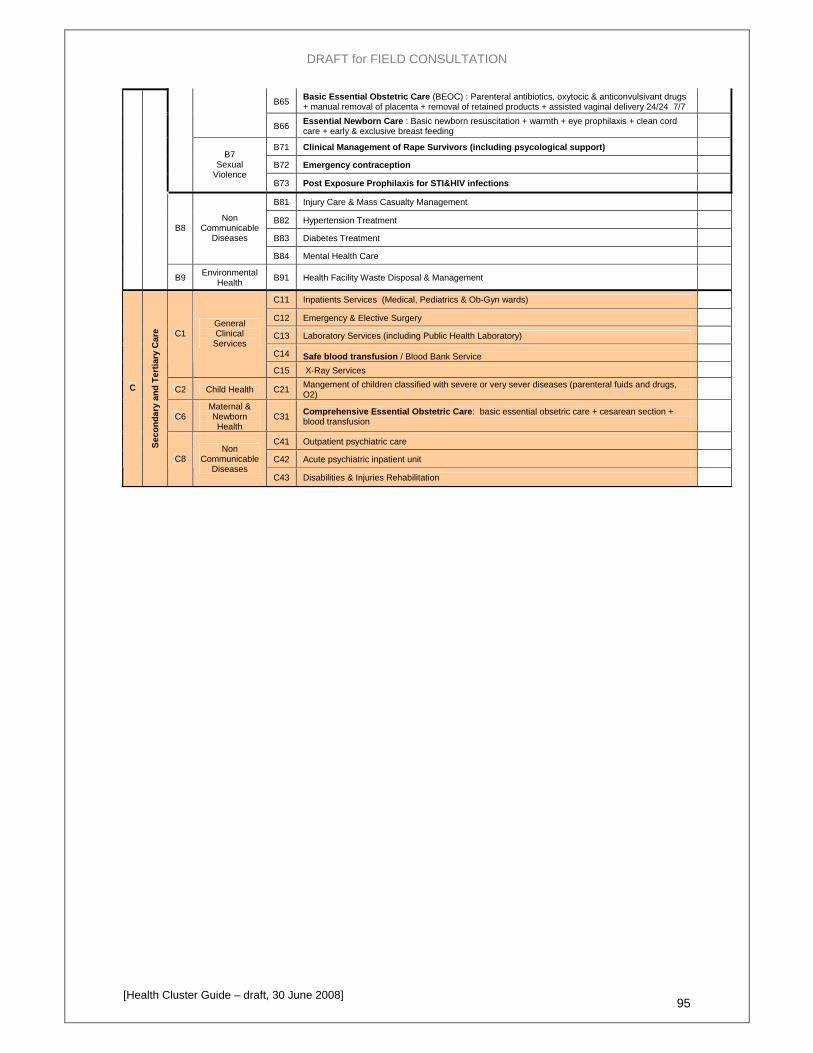
DRAFT for FIELD CONSULTATION
[Health Cluster Guide – draft, 30 June 2008] 95
B65 Basic Essential Obstetric Care (BEOC) : Parenteral antibiotics, oxytocic & anticonvulsivant drugs + manual removal of placenta + removal of retained products + assisted vaginal delivery 24/24 7/7
B66 Essential Newborn Care : Basic newborn resuscitation + warmth + eye prophilaxis + clean cord care + early & exclusive breast feeding
B71 Clinical Management of Rape Survivors (including psycological support) B72 Emergency contraception
B7 Sexual
Violence B73 Post Exposure Prophilaxis for STI&HIV infections B81 Injury Care & Mass Casualty Management B82 Hypertension Treatment B83 Diabetes Treatment
B8 Non
Communicable Diseases
B84 Mental Health Care
B9 Environmental Health B91 Health Facility Waste Disposal & Management
C11 Inpatients Services (Medical, Pediatrics & Ob-Gyn wards) C12 Emergency & Elective Surgery C13 Laboratory Services (including Public Health Laboratory) C14 Safe blood transfusion / Blood Bank Service
C1 General Clinical
Services
C15 X-Ray Services
C2 Child Health C21 Mangement of children classified with severe or very sever diseases (parenteral fuids and drugs, O2)
C6 Maternal & Newborn Health
C31 Comprehensive Essential Obstetric Care: basic essential obsetric care + cesarean section + blood transfusion
C41 Outpatient psychiatric care C42 Acute psychiatric inpatient unit
C
Seco
ndar
y an
d Te
rtia
ry C
are
C8 Non
Communicable Diseases
C43 Disabilities & Injuries Rehabilitation

DRAFT for FIELD CONSULTATION
[Health Cluster Guide – draft, 30 June 2008] 96
Annex D Levels of care and sub-sectors for initial analysis and planning The schema below presents the main health sub-sectors as agreed within the Global Health Cluster and identifies the key services that must be assured (in place) from the onset of any crisis. A list of key services must be established taking account of the context.
Level of Care Sub Sectors Initial Services
Levels of Care & Sub-sectors for Initial Analysis and Planning including Health Partners' Mapping
OPD
Vaccinations CommunityCare
Primary Care
Secondary & Tertiary Care
General Clinical Services
Child Health
Nutrition
Communicable Diseases
STI & HIV/AIDS
Maternal & Newborn Health
Sexual Violence
Non Communicable Diseases
Environmental Health
Rep
rodu
ctiv
e
Hea
lth
TF
EWARN
MISP
Injury Care & Mass Casualty Management
Water Quality
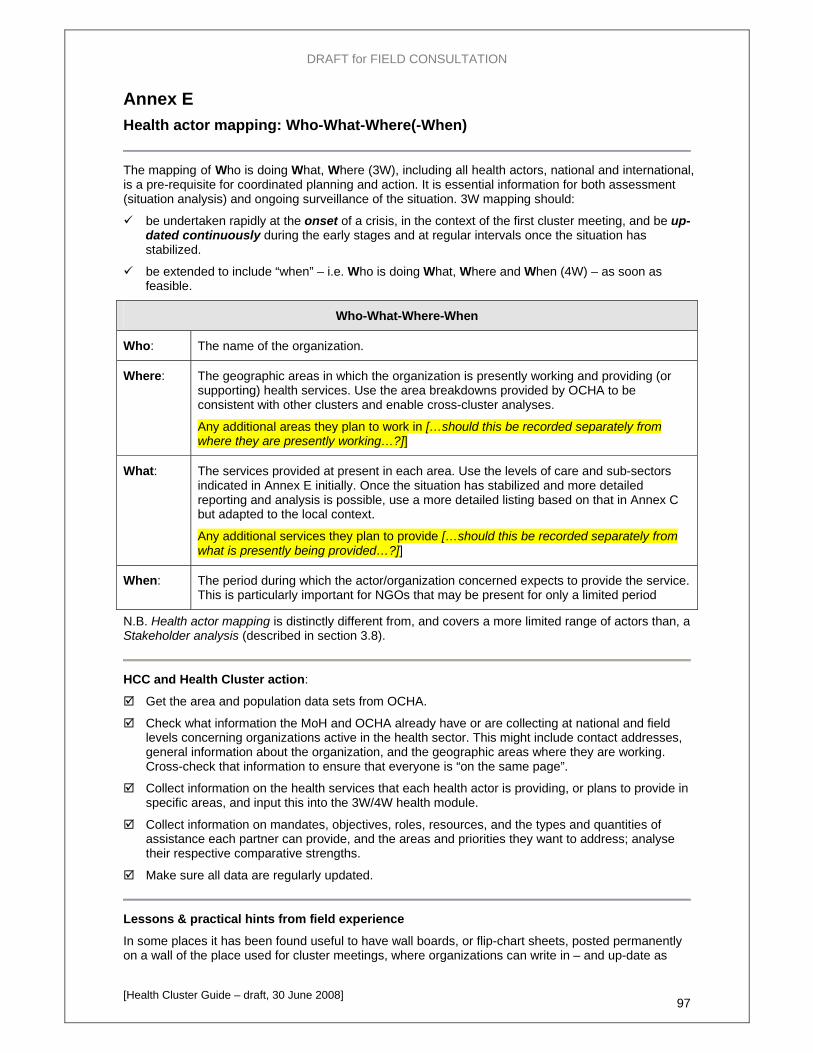
DRAFT for FIELD CONSULTATION
[Health Cluster Guide – draft, 30 June 2008] 97
Annex E Health actor mapping: Who-What-Where(-When)
The mapping of Who is doing What, Where (3W), including all health actors, national and international, is a pre-requisite for coordinated planning and action. It is essential information for both assessment (situation analysis) and ongoing surveillance of the situation. 3W mapping should:
be undertaken rapidly at the onset of a crisis, in the context of the first cluster meeting, and be up-dated continuously during the early stages and at regular intervals once the situation has stabilized.
be extended to include “when” – i.e. Who is doing What, Where and When (4W) – as soon as feasible.
Who-What-Where-When
Who: The name of the organization.
Where: The geographic areas in which the organization is presently working and providing (or supporting) health services. Use the area breakdowns provided by OCHA to be consistent with other clusters and enable cross-cluster analyses.
Any additional areas they plan to work in […should this be recorded separately from where they are presently working…?]]
What: The services provided at present in each area. Use the levels of care and sub-sectors indicated in Annex E initially. Once the situation has stabilized and more detailed reporting and analysis is possible, use a more detailed listing based on that in Annex C but adapted to the local context.
Any additional services they plan to provide […should this be recorded separately from what is presently being provided…?]]
When: The period during which the actor/organization concerned expects to provide the service. This is particularly important for NGOs that may be present for only a limited period
N.B. Health actor mapping is distinctly different from, and covers a more limited range of actors than, a Stakeholder analysis (described in section 3.8).
HCC and Health Cluster action:
Get the area and population data sets from OCHA.
Check what information the MoH and OCHA already have or are collecting at national and field levels concerning organizations active in the health sector. This might include contact addresses, general information about the organization, and the geographic areas where they are working. Cross-check that information to ensure that everyone is “on the same page”.
Collect information on the health services that each health actor is providing, or plans to provide in specific areas, and input this into the 3W/4W health module.
Collect information on mandates, objectives, roles, resources, and the types and quantities of assistance each partner can provide, and the areas and priorities they want to address; analyse their respective comparative strengths.
Make sure all data are regularly updated.
Lessons & practical hints from field experience
In some places it has been found useful to have wall boards, or flip-chart sheets, posted permanently on a wall of the place used for cluster meetings, where organizations can write in – and up-date as
DRAFT for FIELD CONSULTATION
[Health Cluster Guide – draft, 30 June 2008] 98
and when necessary – their own data as well as see what others have entered. The information is transcribed into the Health Cluster 3W/4W module and printouts distributed periodically by the HCC.
…
Additional guidance
…
DRAFT for FIELD CONSULTATION
[Health Cluster Guide – draft, 30 June 2008] 99
Annex F Types and phases of assessment in a humanitarian crisis
The table below (adapted from Emergency Food Security Assessment Handbook, first edition, WFP 2005) summarizes the typical main data collection and analysis processes involved in responding to the health aspects of a humanitarian crisis/emergency.
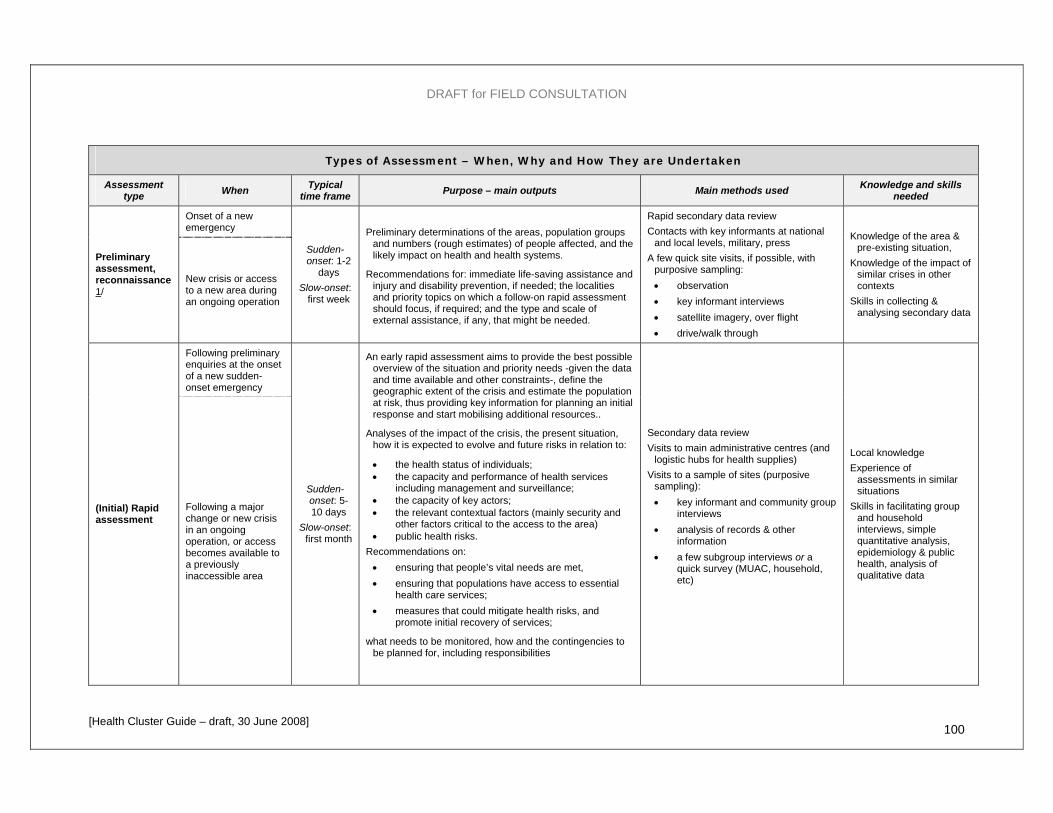
DRAFT for FIELD CONSULTATION
[Health Cluster Guide – draft, 30 June 2008] 100
Types of Assessment – When, Why and How They are Undertaken
Assessment type When Typical
time frame Purpose – main outputs Main methods used Knowledge and skills needed
Onset of a new emergency
Preliminary assessment, reconnaissance 1/
New crisis or access to a new area during an ongoing operation
Sudden-onset: 1-2
days Slow-onset:
first week
Preliminary determinations of the areas, population groups and numbers (rough estimates) of people affected, and the likely impact on health and health systems.
Recommendations for: immediate life-saving assistance and injury and disability prevention, if needed; the localities and priority topics on which a follow-on rapid assessment should focus, if required; and the type and scale of external assistance, if any, that might be needed.
Rapid secondary data review Contacts with key informants at national
and local levels, military, press A few quick site visits, if possible, with
purposive sampling: • observation • key informant interviews • satellite imagery, over flight • drive/walk through
Knowledge of the area & pre-existing situation,
Knowledge of the impact of similar crises in other contexts
Skills in collecting & analysing secondary data
Following preliminary enquiries at the onset of a new sudden-onset emergency
(Initial) Rapid assessment
Following a major change or new crisis in an ongoing operation, or access becomes available to a previously inaccessible area
Sudden-onset: 5-10 days
Slow-onset: first month
An early rapid assessment aims to provide the best possible overview of the situation and priority needs -given the data and time available and other constraints-, define the geographic extent of the crisis and estimate the population at risk, thus providing key information for planning an initial response and start mobilising additional resources..
Analyses of the impact of the crisis, the present situation, how it is expected to evolve and future risks in relation to:
• the health status of individuals; • the capacity and performance of health services
including management and surveillance; • the capacity of key actors; • the relevant contextual factors (mainly security and
other factors critical to the access to the area) • public health risks.
Recommendations on: • ensuring that people’s vital needs are met, • ensuring that populations have access to essential
health care services; • measures that could mitigate health risks, and
promote initial recovery of services;
what needs to be monitored, how and the contingencies to be planned for, including responsibilities
Secondary data review Visits to main administrative centres (and
logistic hubs for health supplies) Visits to a sample of sites (purposive
sampling): • key informant and community group
interviews • analysis of records & other
information • a few subgroup interviews or a
quick survey (MUAC, household, etc)
Local knowledge Experience of
assessments in similar situations
Skills in facilitating group and household interviews, simple quantitative analysis, epidemiology & public health, analysis of qualitative data
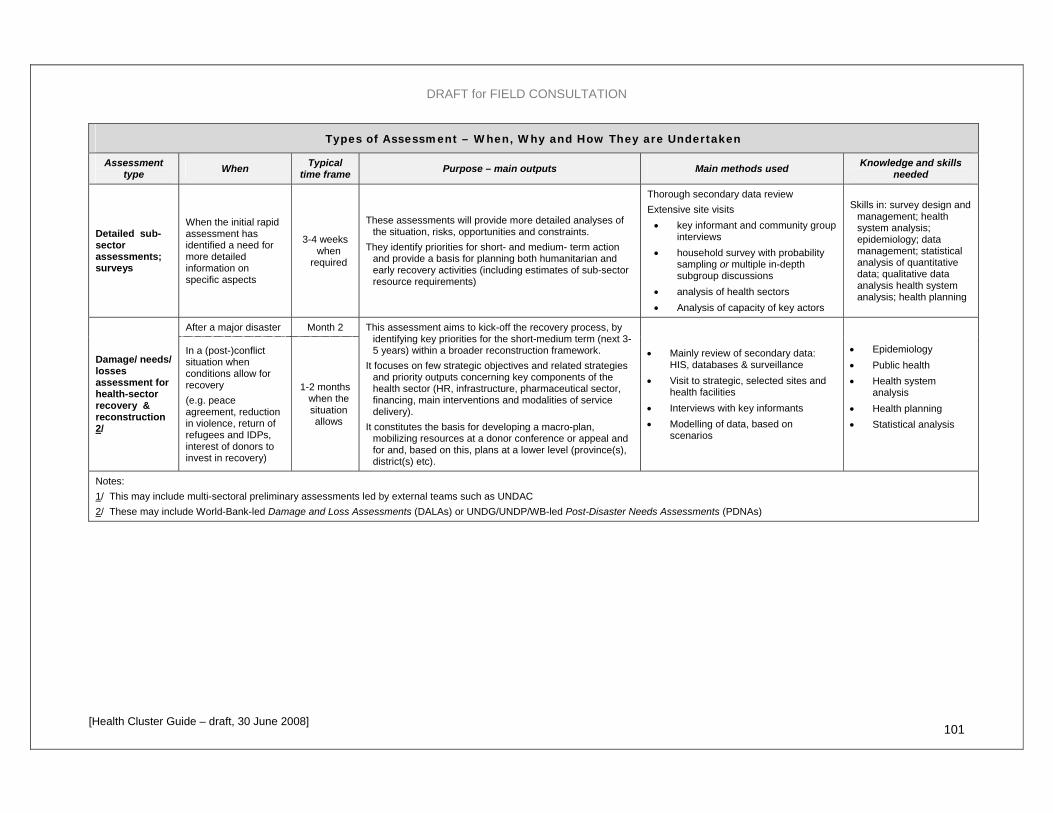
DRAFT for FIELD CONSULTATION
[Health Cluster Guide – draft, 30 June 2008] 101
Types of Assessment – When, Why and How They are Undertaken
Assessment type When Typical
time frame Purpose – main outputs Main methods used Knowledge and skills needed
Detailed sub-sector assessments; surveys
When the initial rapid assessment has identified a need for more detailed information on specific aspects
3-4 weeks when
required
These assessments will provide more detailed analyses of the situation, risks, opportunities and constraints.
They identify priorities for short- and medium- term action and provide a basis for planning both humanitarian and early recovery activities (including estimates of sub-sector resource requirements)
Thorough secondary data review Extensive site visits • key informant and community group
interviews • household survey with probability
sampling or multiple in-depth subgroup discussions
• analysis of health sectors • Analysis of capacity of key actors
Skills in: survey design and management; health system analysis; epidemiology; data management; statistical analysis of quantitative data; qualitative data analysis health system analysis; health planning
After a major disaster Month 2
Damage/ needs/ losses assessment for health-sector recovery & reconstruction 2/
In a (post-)conflict situation when conditions allow for recovery (e.g. peace agreement, reduction in violence, return of refugees and IDPs, interest of donors to invest in recovery)
1-2 months when the situation allows
This assessment aims to kick-off the recovery process, by identifying key priorities for the short-medium term (next 3-5 years) within a broader reconstruction framework.
It focuses on few strategic objectives and related strategies and priority outputs concerning key components of the health sector (HR, infrastructure, pharmaceutical sector, financing, main interventions and modalities of service delivery).
It constitutes the basis for developing a macro-plan, mobilizing resources at a donor conference or appeal and for and, based on this, plans at a lower level (province(s), district(s) etc).
• Mainly review of secondary data: HIS, databases & surveillance
• Visit to strategic, selected sites and health facilities
• Interviews with key informants • Modelling of data, based on
scenarios
• Epidemiology • Public health • Health system
analysis • Health planning • Statistical analysis
Notes: 1/ This may include multi-sectoral preliminary assessments led by external teams such as UNDAC 2/ These may include World-Bank-led Damage and Loss Assessments (DALAs) or UNDG/UNDP/WB-led Post-Disaster Needs Assessments (PDNAs)
DRAFT for FIELD CONSULTATION
[Health Cluster Guide: working draft] 102
Annex G General principles for all data collection activities – assessments, surveys and surveillance The following reminders focus on initial rapid assessments but many are equally relevant for follow-on detailed sub-sector assessments and surveys.
Good planning and preparation prior to field visits are essential for all assessments – see the
principal steps outlined in the schema below. Responsibilities and timeframes for all preparatory actions must be defined and fulfilled in advance.
Broad participation including as many current health actors as can be quickly brought together:
o a joint assessment, when possible (when contingency plans and arrangements for assessments are already in place at the moment of crisis onset);
o otherwise, maximum feasible coordination among individual agencies’ assessment efforts in different areas, sharing of data, and joint analysis
Focus on identifying and prioritizing health problems (including gaps/losses in staff, facilities, supplies and service coverage as well as health risks), their causes and likely evolution – not just describing the situation and “needs”.
o For resident populations: focus in particular on what has changed and on current and foreseeable health risks. Get pre-crisis data on epidemiology and the health system and health seeking behaviours from existing secondary sources.
o For displaced populations: examine the current health situation and current and foreseeable risks.
Keep clearly in mind the purpose – to inform early decisions – and the trade-offs that therefore have to be made between timeliness (speed), accuracy and comprehensiveness. But make a conscious effort to get an overall picture (not just snap-shots of the worst localities) through careful sampling of sites for field visits and triangulation of data from a variety of sources.
Maximum use should be made of available secondary data – see box below. Primary data collection should focus on determining what has changed, filling gaps in information, and identifying feasible options for response.
Standard data collection formats and methods should be used by all field teams. For rapid assessments, they may be based on the multi-sectoral Interagency Rapid Assessment tool and guidelines or local equivalents that adequately cover all essential elements and are familiar to in-country partners.
Assessment teams should be balanced in terms of gender, professional backgrounds and skills with a maximum of experienced public health "all-rounders". (Specialists almost inevitably focus their attention and recommendations on aspects relevant to their specialization and are not always able to take a broad overview and prioritize among the range of needs.)
Prompt reporting and dissemination of assessment findings are essential to ensure that responses are timely and appropriate, recognizing that the situation can change rapidly. Reports should meet the minimum standards outlined in the box below. They should be finalized and circulated to all stakeholders – government departments, donors, UN and NGO partners – within a few days of completion of the field visits.
To the extent possible, the whole process should be managed in a way that contributes to enhancing national and local capacities for future assessments.
Note that the IRA format may be used not only for an initial rapid assessment in the first few days following a sudden-onset crisis but also for recording of basic data by non-specialist personnel at any time…
DRAFT for FIELD CONSULTATION
[Health Cluster Guide: working draft] 103
Using both secondary and primary data
Much secondary data on the pre-crisis situation and the effects of the crisis will often be available at national level and this will provide the basis for finalizing the data collection instrument (the IRA format or other) to be used by the field assessment teams and selecting the areas/localities to be visited.
Additional, more recent and/or more detailed secondary data should be collected in the affected area by the assessment teams before starting site visits and primary data collection in order to:
• fill gaps in information on pre-crisis conditions; and
• finalize the choice of sites to be visited.
The collection of primary data (both qualitative and quantitative) at community level is required to:
• validate or up-date information provided by the available secondary data;
• provide an understanding of impacts of the crisis and the current situation at community level, the underlying causes, and the influence of contextual factors; and
• enable the affected populations to participate in identifying priorities for response.
Secondary and primary data together provide the basis for developing a situation analysis and identifying the priority problems and areas for humanitarian (and early recovery) response.
SPHERE standards for (initial) assessments
“Assessments provide an understanding of the disaster situation and a clear analysis of threats to life, dignity, health and livelihoods to determine, in consultation with the relevant authorities, whether an external response is required and, if so, the nature of the response.” Key indicators include:
• Information is gathered using standardised procedures and made available to allow for transparent decision-making.
• Through consultation, the assessment takes into account the response of the local and national authorities and other actors and agencies.
• Local capacities and strategies to cope with the disaster, both those of the affected population and the surrounding population, are identified.
• The assessment takes into account the responsibility of relevant authorities to protect and assist the population on the territory over which they have control, and takes into account national law, standards and guidelines applicable where the affected population is found, as they conform with international law.
• The assessment includes an analysis of the operating environment, including factors affecting the personal safety and security of the affected population and of humanitarian staff.
• Estimates of population numbers are cross-checked and validated with as many sources as possible, and the basis of the estimate made known.
• Assessment findings are made available to other sectors, national and local authorities and representatives of the affected population. Recommendations are made on the need for external assistance, and on appropriate response that should be linked with exit or transition strategies.
[SPHERE handbook, 2004, common standard 2]
DRAFT for FIELD CONSULTATION
[Health Cluster Guide: working draft] 104
Annex H Drawing up an assessment plan, schedule and budget [section 10.1 from Emergency Food Security Assessment Handbook, first edition, WFP 2005]
Required output: A written plan that specifies: (i) what will be done to prepare for and undertake data collection in the field and to complete the assessment process; (ii) how, when and by whom it will be done, and (iii) the resources required and from where they will be obtained.
Why? To ensure that all necessary preparatory steps are taken in time and that the field surveys, proceed as smoothly as possible and the assessment produces the required outputs on time.
When? Planning should start as soon as the objectives of the assessment have been defined. The schedule prepared at this stage will have to be reviewed, and may need to be revised, once the data collection and sampling methods are defined in activity 6 (see figure 10d).
By whom?
A designated working group of individuals from […the lead/responsible agency…] and partners collaborating in the assessment.
How? Based on the refined ‘working’ scenario, the agreed objectives and timeframe for the assessment, and the decisions on methods and sampling procedures, particularly the number of sites to be visited, draw up: • a schedule in the form of a bar chart showing when the various steps will be
undertaken, and when they must be completed; • an action plan specifying, briefly (probably in the form of a matrix), what is to be
done for each step, the human and material resources required, and who is responsible for completing the action within the specified time frame; and
• a preliminary budget.
Drawing up a schedule The assessment plan must clearly specify how the remaining activities of the process will be completed and assign responsibilities for everything that needs to be done. The plan must be written down and available to all concerned. Figure 10b provides an example of a possible schedule for planning and implementing a rapid assessment in the 3-week period. For completeness, it includes the previous activities 1 to 4. In case of a crisis in a confined geographic area, the whole process may be compressed into a single week. In a major crisis covering a large area, it may be stretched over six weeks. In practice, it may be found that the assessment cannot be completed as proposed, within the specified timeframe, with the human and material resources available. If so, the problem must be discussed with all collaborating parties and more resources must be mobilized or a decision be made to either extend the timeframe or cut back on some aspects, with a clear understanding of the possible consequences in terms of the quality and reliability of the data and the conclusions that will be able to be drawn. The schedule will need to be updated accordingly. In fact, the schedule should be considered as a working document that is refined on an ongoing basis especially during the first few days of planning. However, once methods have been decided, every effort should be made to adhere to the schedule agreed at that point.
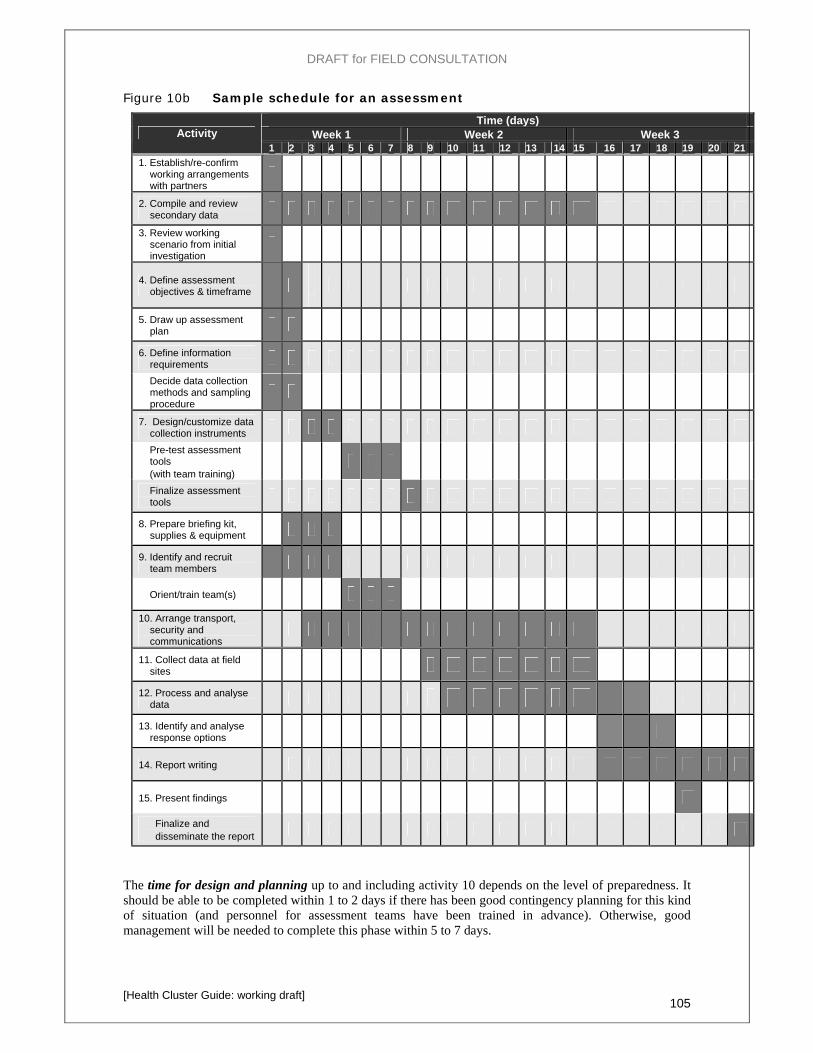
DRAFT for FIELD CONSULTATION
[Health Cluster Guide: working draft] 105
Figure 10b Sample schedule for an assessment Time (days)
Week 1 Week 2 Week 3 Activity 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21
1. Establish/re-confirm working arrangements with partners
2. Compile and review secondary data
3. Review working scenario from initial investigation
4. Define assessment objectives & timeframe
5. Draw up assessment plan
6. Define information requirements
Decide data collection methods and sampling procedure
7. Design/customize data collection instruments
Pre-test assessment tools
(with team training)
Finalize assessment tools
8. Prepare briefing kit, supplies & equipment
9. Identify and recruit team members
Orient/train team(s) 10. Arrange transport,
security and communications
11. Collect data at field sites
12. Process and analyse data
13. Identify and analyse response options
14. Report writing
15. Present findings
Finalize and disseminate the report
The time for design and planning up to and including activity 10 depends on the level of preparedness. It should be able to be completed within 1 to 2 days if there has been good contingency planning for this kind of situation (and personnel for assessment teams have been trained in advance). Otherwise, good management will be needed to complete this phase within 5 to 7 days.
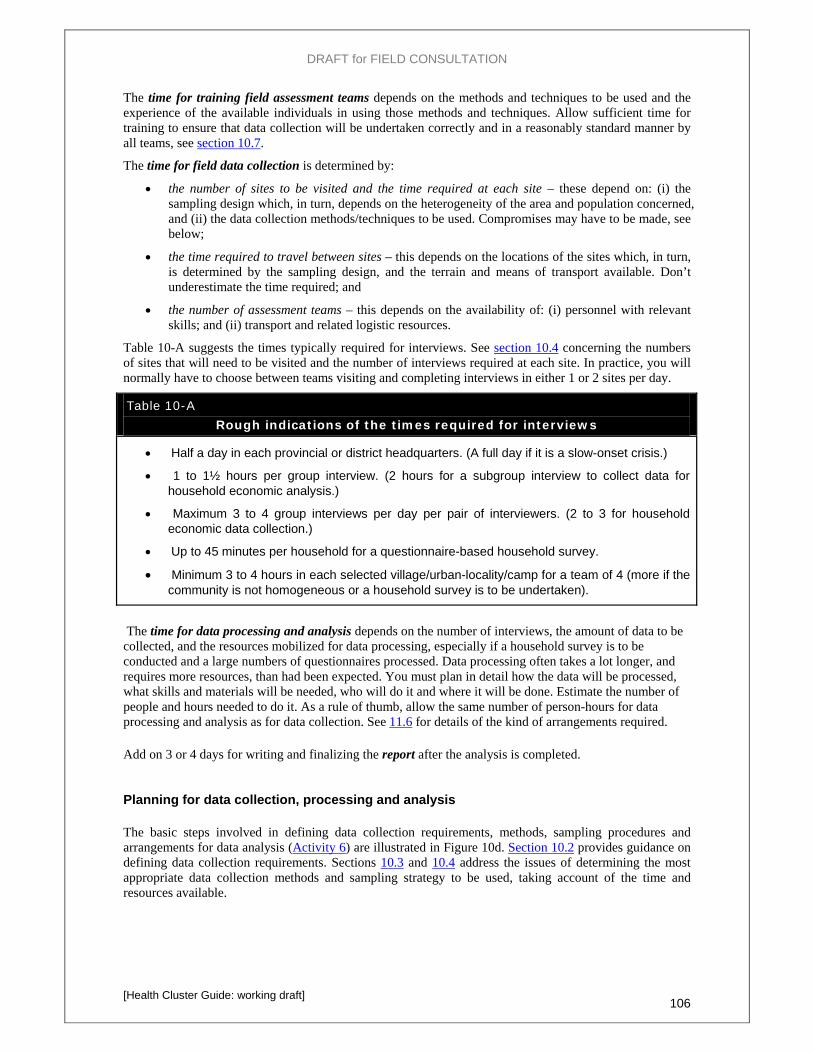
DRAFT for FIELD CONSULTATION
[Health Cluster Guide: working draft] 106
The time for training field assessment teams depends on the methods and techniques to be used and the experience of the available individuals in using those methods and techniques. Allow sufficient time for training to ensure that data collection will be undertaken correctly and in a reasonably standard manner by all teams, see section 10.7. The time for field data collection is determined by:
• the number of sites to be visited and the time required at each site – these depend on: (i) the sampling design which, in turn, depends on the heterogeneity of the area and population concerned, and (ii) the data collection methods/techniques to be used. Compromises may have to be made, see below;
• the time required to travel between sites – this depends on the locations of the sites which, in turn, is determined by the sampling design, and the terrain and means of transport available. Don’t underestimate the time required; and
• the number of assessment teams – this depends on the availability of: (i) personnel with relevant skills; and (ii) transport and related logistic resources.
Table 10-A suggests the times typically required for interviews. See section 10.4 concerning the numbers of sites that will need to be visited and the number of interviews required at each site. In practice, you will normally have to choose between teams visiting and completing interviews in either 1 or 2 sites per day.
Table 10-A Rough indications of the times required for interviews
• Half a day in each provincial or district headquarters. (A full day if it is a slow-onset crisis.) • 1 to 1½ hours per group interview. (2 hours for a subgroup interview to collect data for
household economic analysis.) • Maximum 3 to 4 group interviews per day per pair of interviewers. (2 to 3 for household
economic data collection.) • Up to 45 minutes per household for a questionnaire-based household survey. • Minimum 3 to 4 hours in each selected village/urban-locality/camp for a team of 4 (more if the
community is not homogeneous or a household survey is to be undertaken).
The time for data processing and analysis depends on the number of interviews, the amount of data to be collected, and the resources mobilized for data processing, especially if a household survey is to be conducted and a large numbers of questionnaires processed. Data processing often takes a lot longer, and requires more resources, than had been expected. You must plan in detail how the data will be processed, what skills and materials will be needed, who will do it and where it will be done. Estimate the number of people and hours needed to do it. As a rule of thumb, allow the same number of person-hours for data processing and analysis as for data collection. See 11.6 for details of the kind of arrangements required.
Add on 3 or 4 days for writing and finalizing the report after the analysis is completed. Planning for data collection, processing and analysis
The basic steps involved in defining data collection requirements, methods, sampling procedures and arrangements for data analysis (Activity 6) are illustrated in Figure 10d. Section 10.2 provides guidance on defining data collection requirements. Sections 10.3 and 10.4 address the issues of determining the most appropriate data collection methods and sampling strategy to be used, taking account of the time and resources available.
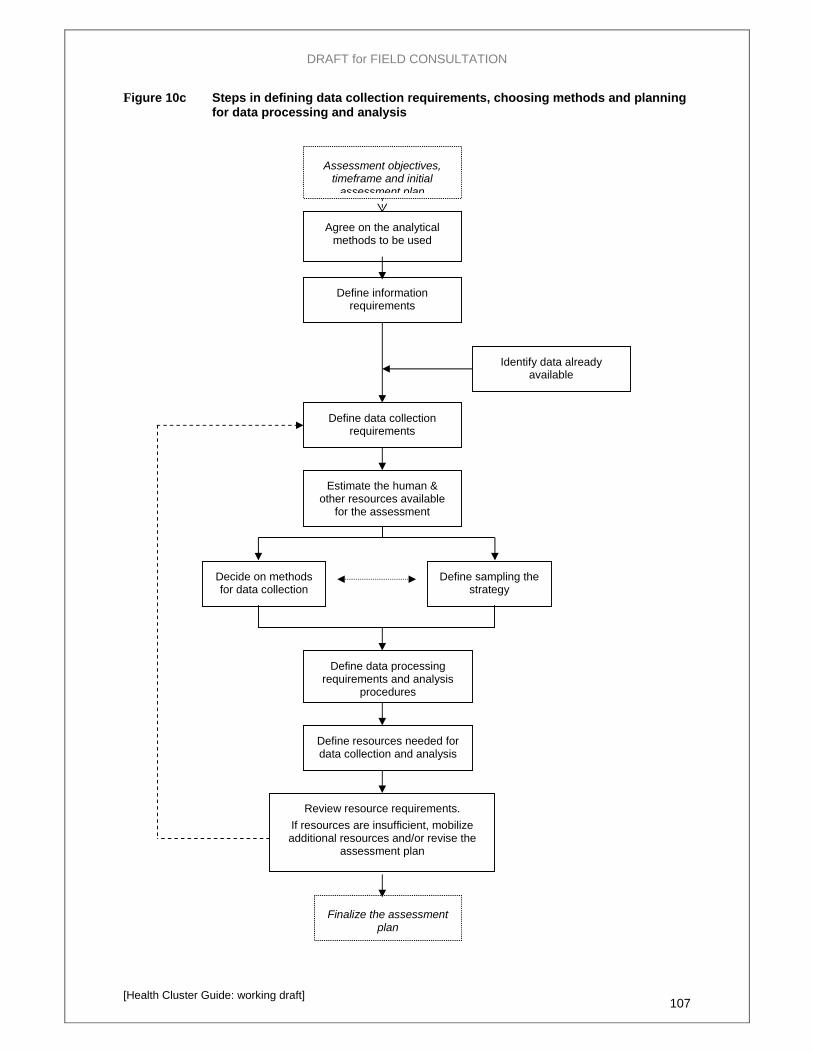
DRAFT for FIELD CONSULTATION
[Health Cluster Guide: working draft] 107
Figure 10c Steps in defining data collection requirements, choosing methods and planning for data processing and analysis
Agree on the analytical methods to be used
Define information requirements
Define sampling the strategy
Decide on methods for data collection
Define resources needed for data collection and analysis
Review resource requirements. If resources are insufficient, mobilize additional resources and/or revise the
assessment plan
Estimate the human & other resources available
for the assessment
Assessment objectives, timeframe and initial
assessment plan
Finalize the assessment plan
Define data collection requirements
Identify data already available
Define data processing requirements and analysis
procedures
DRAFT for FIELD CONSULTATION
[Health Cluster Guide: working draft] 108
Once you have defined the methods to be used, you must specify the procedures to be used for processing and analysing the data collected by field assessment teams and the resources and time that will be needed:
• Section 11.6 provides guidance on the processing of data (both quantitative and qualitative data). For data collected using rapid appraisal techniques you must develop – specify – the initial summary matrices that each team is required to produce. For household survey data, planning will focus on where and by whom the completed questionnaires will be processed, and how they will be submitted by each field team.
• Chapter 12 provides general guidance on analysis while chapters 4 to 7 provide guidance in relation to each theme. At the planning stage, you should draw up an analysis plan. For the analysis of data collected using rapid appraisal techniques, you should specify: (i) the basic analyses (cross-tabulations) to be made at the first stage of the analysis on a team-by-team basis; (ii) whether you will be able to arrange for an independent analyst to work with each field assessment team without unduly delaying the analysis process; and (iii) how and by whom the final overall analysis will be undertaken. For the analysis of household survey data you must also envisage the initial cross-tabulations to be made and specify who will undertake the detailed analysis and interpretation of the data and then combine the household survey data with that from community group and key informant interviews.
The value of an independent eye in analysing rapid appraisal data An analyst who did not participate in the data collection brings a fresh mind and an unbiased perspective to the analysis of the recorded data. This can help to identify relationships suggested by the data and issues that may benefit from discussion within the team, while avoiding bias arising from team members’ impressions for which evidence may be limited. The team and the analyst can then discuss and agree on findings – the story that the data tell.
Preparing a budget for the assessment Ensure that you have a realistic budget before the field work begins. A rapid assessment may cost anything up to US$ 30,000 depending on the geographic extent and topography of the area and the variety of livelihood zones and socio-economic groups affected. As a starting point, consider the following line items:
• per diem/DSA costs for government and other participants (if unable to be borne by their own organization);
• transport costs (fares, rental and/or fuel and maintenance costs for vehicles, boats, helicopters, aircraft, as required, DSA for drivers);
• security costs (in case it is necessary to hire guards or escorts); • training costs (rental of premises/accommodation; transport; materials; honoraria for trainers; DSA
for trainees, etc); • telecommunications expenses (telephone bills, including sat-phones if needed; acquisition of
radios, etc.) • incidental costs for teams while in the field; • equipment including camping gear, if necessary (purchase or rental if borrowing is not possible);
and • photocopying costs for briefing kits, data collection instruments, the final report, etc.
Encourage all participating agencies to participate in covering the costs, at least by paying the costs (including per diems) of their own staff.
DRAFT for FIELD CONSULTATION
[Health Cluster Guide: working draft] 109
Annex I Indicators for surveillance and performance monitoring
This annex provides:
(i) the generic performance indicators suggested by WHO; and
(ii) an example – indicators used in Sudan in 2008.
Indicators must be selected relevant to the situation in each case.
Generic (performance) indicators suggested by WHO, 2005 [from Tracking the performance of essential health and nutrition services in humanitarian response, background paper for a WHO workshop: “Tracking Health Performance and Humanitarian Outcomes”, Geneva, Dec. 2005]
Availability of and access to primary and secondary health services: • availability of primary and secondary health facilities in relation to population • utilisation rate of outpatients services
Measles vaccination: • coverage of measles vaccination (as a priority prevention program, and as one of the proxies
for the performance of the health system) Selective feeding programmes:
• coverage of nutrition rehabilitation centres and one indicator on their performance like aggregated recovery rate or case fatality ratios,
Provision of emergency obstetric care: • coverage of emergency obstetric care (as performance by itself to explain Maternal mortality
rate, and as proxy for access to secondary care) Health surveillance:
• coverage/catchment area, regularity of data flow • morbidity pattern (and surveillance of epidemic prone diseases) • some performance indicators with regards to outbreaks: coverage of the outbreak
detection/surveillance system, and quality of response through timeliness, Attack Rate and Case Fatality Rate.
The choice of the critical services – and thus of the related indicators for performance that need to be tracked – will need appropriate discussion in the different contexts. General issues that deserve to be addressed are related to coverage, access, utilisation, thresholds and timeliness.
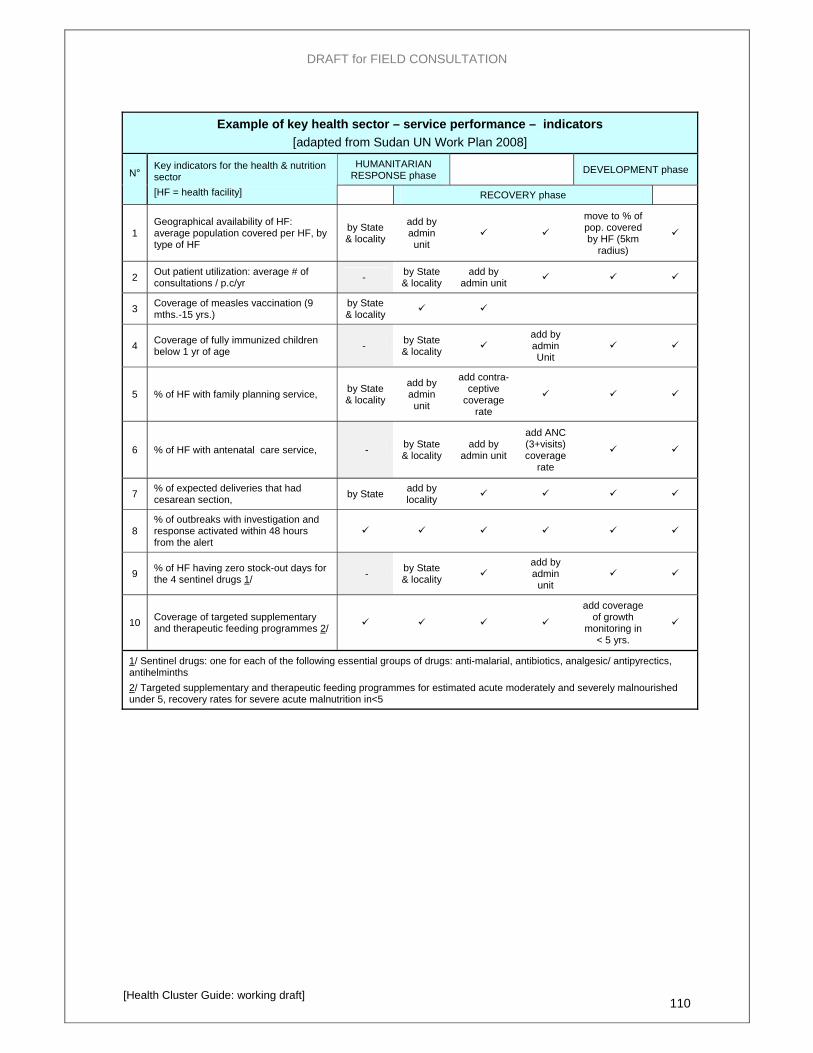
DRAFT for FIELD CONSULTATION
[Health Cluster Guide: working draft] 110
Example of key health sector – service performance – indicators [adapted from Sudan UN Work Plan 2008]
HUMANITARIAN RESPONSE phase DEVELOPMENT phase N°
Key indicators for the health & nutrition sector [HF = health facility] RECOVERY phase
1 Geographical availability of HF: average population covered per HF, by type of HF
by State & locality
add by admin unit
move to % of pop. covered by HF (5km
radius)
2 Out patient utilization: average # of consultations / p.c/yr - by State
& locality add by
admin unit
3 Coverage of measles vaccination (9 mths.-15 yrs.)
by State & locality
4 Coverage of fully immunized children below 1 yr of age - by State
& locality add by admin Unit
5 % of HF with family planning service, by State & locality
add by admin unit
add contra-ceptive
coverage rate
6 % of HF with antenatal care service, - by State & locality
add by admin unit
add ANC (3+visits) coverage
rate
7 % of expected deliveries that had cesarean section, by State add by
locality
8 % of outbreaks with investigation and response activated within 48 hours from the alert
9 % of HF having zero stock-out days for the 4 sentinel drugs 1/ - by State
& locality add by admin
unit
10 Coverage of targeted supplementary and therapeutic feeding programmes 2/
add coverage of growth
monitoring in < 5 yrs.
1/ Sentinel drugs: one for each of the following essential groups of drugs: anti-malarial, antibiotics, analgesic/ antipyrectics, antihelminths 2/ Targeted supplementary and therapeutic feeding programmes for estimated acute moderately and severely malnourished under 5, recovery rates for severe acute malnutrition in<5
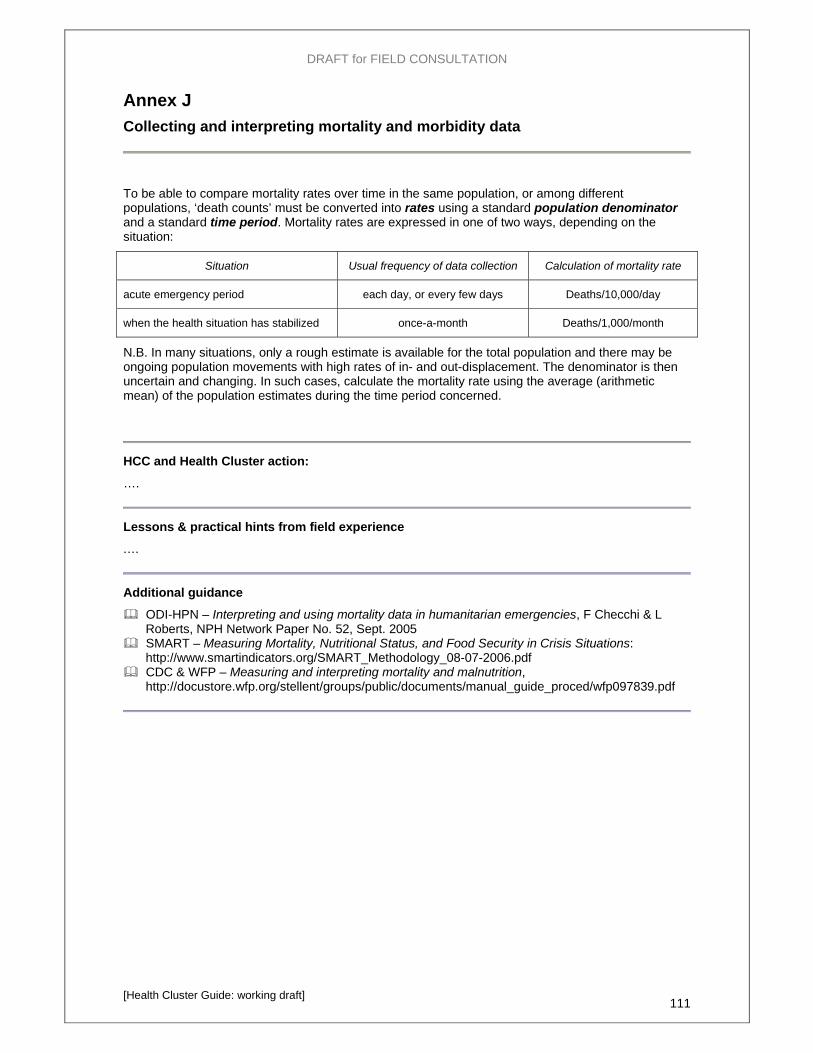
DRAFT for FIELD CONSULTATION
[Health Cluster Guide: working draft] 111
Annex J Collecting and interpreting mortality and morbidity data
To be able to compare mortality rates over time in the same population, or among different populations, ‘death counts’ must be converted into rates using a standard population denominator and a standard time period. Mortality rates are expressed in one of two ways, depending on the situation:
Situation Usual frequency of data collection Calculation of mortality rate
acute emergency period each day, or every few days Deaths/10,000/day
when the health situation has stabilized once-a-month Deaths/1,000/month
N.B. In many situations, only a rough estimate is available for the total population and there may be ongoing population movements with high rates of in- and out-displacement. The denominator is then uncertain and changing. In such cases, calculate the mortality rate using the average (arithmetic mean) of the population estimates during the time period concerned.
HCC and Health Cluster action:
….
Lessons & practical hints from field experience
.…
Additional guidance
ODI-HPN – Interpreting and using mortality data in humanitarian emergencies, F Checchi & L Roberts, NPH Network Paper No. 52, Sept. 2005
SMART – Measuring Mortality, Nutritional Status, and Food Security in Crisis Situations: http://www.smartindicators.org/SMART_Methodology_08-07-2006.pdf
CDC & WFP – Measuring and interpreting mortality and malnutrition, http://docustore.wfp.org/stellent/groups/public/documents/manual_guide_proced/wfp097839.pdf
DRAFT for FIELD CONSULTATION
[Health Cluster Guide: working draft] 112
Annex K Stakeholder analysis 17
A stakeholder analysis should be undertaken at the onset of a crisis, in the context of the first cluster/sector coordination group meeting but should then be up-dated continuously during the early stages and at regular intervals once the situation has stabilized.
“Stakeholders” include all agencies, organizations, groups or individuals who have a direct or indirect interest in a health, health services and the activities of the health cluster, and whose attitudes and actions could have an influence on health and the outcomes of humanitarian health activities.
A stakeholder analysis can help the health cluster stakeholders identify:
• The interests of all stakeholders that may affect or be affected by health response actions;
• Potential conflicts or risks that could limit the feasibility of particular response strategies (and any possible strategies for overcoming such factors).
• Opportunities and relationships that can be built on during implementation of the response;
• Groups that should be encouraged to participate in different stages of the process;
• Appropriate strategies and approaches for stakeholder engagement; and
• Ways to reduce negative impacts on vulnerable and disadvantaged population.
The full participation of stakeholders in both project design and implementation of is a key to – but not a guarantee of – success. Stakeholder participation:
• Gives stakeholders some say over how their interventions may affect the response;
• Is essential for sustainability;
• Generates a sense of ownership if initiated early in the process;
• Provides opportunities for learning for the stakeholders themselves; and
• Builds capacity and enhances responsibility.
N.B. Stakeholder analysis is distinctly different from, and covers a larger range of interested parties than, a Who-What-Where-When analysis of health service providers (described in section 2.4).
Reference Bibliography: For further guidance, see:
Ruairi Brugha and Zsuzsa Varvasovszky, Stakeholder analysis: a review, Health Policy and Planning; 15(3): 239-246, Oxford University Press 2000
Kammi Schmeer, Stakeholder Analysis Guidelines, Policy Toolkit for Strengthening Health Sector Reform, section 2, Latin America and Caribbean Regional Health Sector Reform Initiative, www.lachsr.org/documents/policytoolkitforstrengtheninghealthsectorreformpartii-EN.pdf
Resources for Implementing the WWF Standards, Cross-Cutting Tool, Stakeholder Analysis, October 2005 http://assets.panda.org/downloads/1_1_stakeholder_analysis_11_01_05.pdf
World Bank - Social Analysis, Stakeholder Analysis and Stakeholder Analysis pagebrief (www1.worldbank.org/publicsector/politicaleconomy/November3Seminar/Stakehlder%20Readings/WB%20Stakeholders%20Analysis%201-page%20brief.pdf)
DFID, 1995. Guidance Note on how to do Stakeholder Analysis of Aid Projects and Programmes, London
DFID, 1993. Note on Enhancing Stakeholder Participation in Aid Activities, London, DFID
17 Adapted from WWF, Cross-Cutting Tool, Stakeholder Analysis, October 2005,

DRAFT for FIELD CONSULTATION
[Health Cluster Guide: working draft] 113
Annex L Needs Analysis Framework (NAF)
The “NAF” is proposed, by OCHA, as a multi-sectoral tool for use by country teams. It includes a section on health which probably needs to be improved.
Needs Analysis Framework (NAF)18
What is the Needs Analysis Framework?
The Needs Analysis Framework is a tool to help Humanitarian Coordinators and IASC country teams to organise and present existing information on humanitarian needs in a coherent and consistent manner. It helps to strengthen the joint analysis of needs within and among sectors. Combining evidence and judgment, it helps country teams reach a common understanding of humanitarian needs, set priorities, and ensure that nothing important is overlooked. (N.B. the NAF does call for any additional assessments and does not propose/impose any particular methodologies for data collection and analysis.)
When should a health cluster use (prepare) a NAF, and why
The health cluster – coordinator and participants – should use the relevant sections of the NAF to analyse the health situation and needs when so requested by the HC or the IASC country team, e.g. as the first step towards preparing a Consolidated Humanitarian Action Plan (CHAP).19 It may also be used at any time when the cluster decides to up-date its own analysis of the situation and identify gaps in information and/or service coverage. The process also provides evidence for advocacy and resource mobilization for public health action, and contributes to assuring accountability to stakeholders.
How to use the NAF Adapt the framework to the context by removing headings that are not relevant and adding others that are.
Use it as a blueprint to consolidate and analyse existing information – baseline and assessment data from all sources – and to identify any gaps in information and understanding that need to be filled by further enquiries/data collection.
Assess and record judgements on the reliability of the various items of information. Use the framework to identify problems and interdependencies among problems and
underlying causal factors. Ensure that the final document is analytical, not merely descriptive!
All cluster partners are expected to contribute assessment and other relevant information. The HCC and the cluster lead agency with selected individuals from the MoH and a few other agencies should undertake the compilation and initial drafting. The cluster as a whole should review and approve the final document.
18 Adapted from Needs Analysis Framework, IASC CAP sub-working group, April 2007 19 The overall, multi-sectoral NAF report should be no more than 25 pages with a 2-page summary that will be incorporated in the CHAP.
DRAFT for FIELD CONSULTATION
[Health Cluster Guide: working draft] 114
Annex M Priority Cross-cutting Issues
Human Rights20 The International Covenant on Economic Social and Cultural Rights recognizes the right of everyone to the enjoyment of the highest attainable standard of physical and mental health. (ICESCR- Art. 12). Hence, States are obliged to ensure the use of the maximum of its available resources for this purpose, even in the face of humanitarian crisis.
The right to health (short expression for "the right to enjoyment of the highest attainable standard of health") is an inclusive right extending to timely and appropriate health care and to the underlying determinants of health, such as access to safe and potable water and adequate sanitation, an adequate supply of safe food, nutrition and housing, healthy occupational and environmental conditions, and access to health-related education and information, including on sexual and reproductive health. A further important aspect is the participation of the population in all health-related decision making at the community, national and international levels.
The right to health contains the following interrelated and essential elements:
Availability
Accessibility (non-discrimination, physical -, economic -, and information accessibility)
Acceptability
Quality
The human rights principles are:
• Equality and non-discrimination: Different groups are often affected in different ways, particularly women, children, minorities, persons living with HIV/AIDS, the urban or rural poor, an others who face different forms of discrimination and exclusion. In many cases entire communities are displaced, livelihoods are destroyed, many are forced to escape violence or death, and local communities in the receiving end also struggle in the face of new constraints to access to health goods, services and facilities.
• Legal Protection and Accountability: From a human rights perspective, prevention of violations of human rights is essential. States and Humanitarian Actors must receive support to understand their obligations and incorporate them in all phases of their programming in order to guarantee standards are kept to the best of their capacities. Security of individuals and groups ought to be guaranteed with specific policies, authorities and mechanisms at the earliest possible. State actors, whether decision makers or those in charge of the delivery of health goods, services and facilities, and other actors on site must be accountable for such violations.
• Participation: For human rights based approach in health, the process (how things are done and decided) is as relevant as the final outcome (individuals in a healthier physical and mental state). Participation is more than general consultation to a few members of the displaced community. It is rather the incorporation throughout the programming process of diverse groups and perspectives in relation to health priorities, risks, potential partnerships, including in the decision making process. In other words, it is about finding ways and mechanisms to allow for bottom-up proposals to be taken into account.
• Information and Training: Access to periodic information is crucial in the managing of a crisis. Additionally, the right to information implies the provision to the general public with information which is accurate and easy to understand. Such information must be presented in different formats to allow children, persons with disabilities, diverse language groups, as well as the illiterate poor access to health and life saving information, to understand health-risks, prevention mechanisms, and finally to know about the existence and use of complaint and redress mechanisms.
20 Introductory Note, Draft Proposal Checklist on Health and Human Rights for Humanitarian Action
DRAFT for FIELD CONSULTATION
[Health Cluster Guide: working draft] 115
Gender21 The term Gender refers to the social differences between females and males that are learned, and though deeply rooted in every culture, are changeable and have wide variations both within and between cultures. Gender determines the roles, power, and access to resources for females and males in any culture. In emergencies, women and men, boys and girls are affected differently. Available data suggest that there is a pattern of gender differentiation at all stages of the emergency process.
Due to gender norms and their interaction with biological factors, women and children-especially girls- may face increased risk for adverse effects and violence. They may be unable to access assistance safely and/or to make their needs known. Additionally, women are often insufficiently inclided in community consultation and decision-making processes resulting in the needs of women not being met. Understanding gender differences, inequalities, and capacities and responding to them, improves the effectiveness of our humanitarian actions. The overall goal of mainstreaming gender is to achieve gender equality.
Protecting human rights and promoting gender equality must be seen as central to the humanitarian community’s responsibility to protect and provide assistance to those affected by emergencies. Two main strategies are needed to reach the goal of gender equality, namely gender mainstreaming and targeted actions in response to a gender analysis, as well as a number of programmes which together make up a gender equality programme.
HIV/AIDS22 During a crisis, the effects of poverty, powerlessness and social instability are intensified, increasing people’s vulnerability to HIV/AIDS. As the emergency and the epidemic simultaneously progress, fragmentation of families and communities occurs, threatening stable relationships.
The social norms regulating behavior are often weakened. In such circumstances, women and children are at increased risk of violence, and can be forced into having sex to gain access to basic needs such as food, water or even security. Displacement may bring populations, each with different HIV/AIDS prevalence levels, into contact. This is especially true in the case of populations migrating to urban areas to escape conflict or disaster in the rural areas. As a consequence, the health infrastructure may be greatly stressed; inadequate supplies may hamper HIV/AIDS prevention efforts.
During the acute phase of an emergency, this absence or inadequacy of services facilitates HIV/AIDS transmission through lack of universal precautions and unavailability of condoms. In war situations, there is evidence of increased risk of transmission of HIV/AIDS through transfusion of contaminated blood. The presence of military forces, peacekeepers, or other armed groups is another factor contributing to increased transmission of HIV/AIDS. These groups need to be integrated in all HIV prevention activities.
From the information available to date, the thinking on HIV transmission in emergency settings is that:
• The risk of HIV transmission appears to be low in places with low HIV prevalence rates at the beginning of an emergency, and where populations remain isolated. This appears to remain true even when there are high levels of risk behaviours such as rape.
• War can accelerate the transmission of HIV in places where rape and sexual exploitation are superimposed on high levels of HIV before the beginning of an emergency. Causality, however, is difficult to determine, as it is almost impossible to know if survivors of rape became infected because of the rape, or were already infected.
• In areas affected by natural disaster, the impact of HIV depends on existing HIV prevalence rates and the capacity of the government, international agencies, donors and civil society to respond.
21 IASC Guidelines for Gender-based Violence Interventions in Humanitarian Settings: Focusing on Prevention and Response to Sexual Violence in Emergencies 22 IASC Guidelines for HIV/AIDS interventions in emergency settings

DRAFT for FIELD CONSULTATION
[Health Cluster Guide: working draft] 116
6.2.4 Environment23 Why do you need to be concerned about the environment in emergencies?
When a disaster strikes or a conflict unfolds, humanitarian actors have to move quickly to save lives, meet basic needs and protect survivors. In the rush to provide a rapid humanitarian response, addressing the environmental threats caused by the emergency may seem to be secondary. They are not. Conflicts and Disasters, as well as relief and recovery operations, impact the environment in ways that threaten human life, health, livelihoods and security. Failure to address these risks can undermine the relief process through additional loss of life, displacement, aid dependency and increased vulnerability.
There is a strong link between the environment and disasters. Environmental pre-conditions often contribute to disasters. Disasters can result in negative environmental impacts. Emergency response can have positive or negative environmental impact. The cost of ignoring these links include: 1. secondary environmental threats with real or potential negative impacts on human life, health, welfare, livelihoods, environment, 2. short-term responses that do not deal with longer-term environmental effects, 3. emergency solutions that unnecessarily add garbage and waste materials to the environment, 4. loss of important ecological resources.
What are potential environmental impacts in an emergency?
As natural resources play a key role in meeting relief needs, six humanitarian response clusters can be directly affected by environmental impacts: health; water, sanitation and hygiene; shelter; camp management and coordination; logistics and early recovery. As these risks can undermine the effective delivery of humanitarian assistance and compound the crisis, they should be assessed and identified as early as possible. Activities supported or put in place by these clusters can also create unintended environmental impacts. These impacts can further compound or exacerbate the emergency situation or undermine long term recovery.
23 Cross-cutting Issues, Key things to Know, Humanitarian Reform
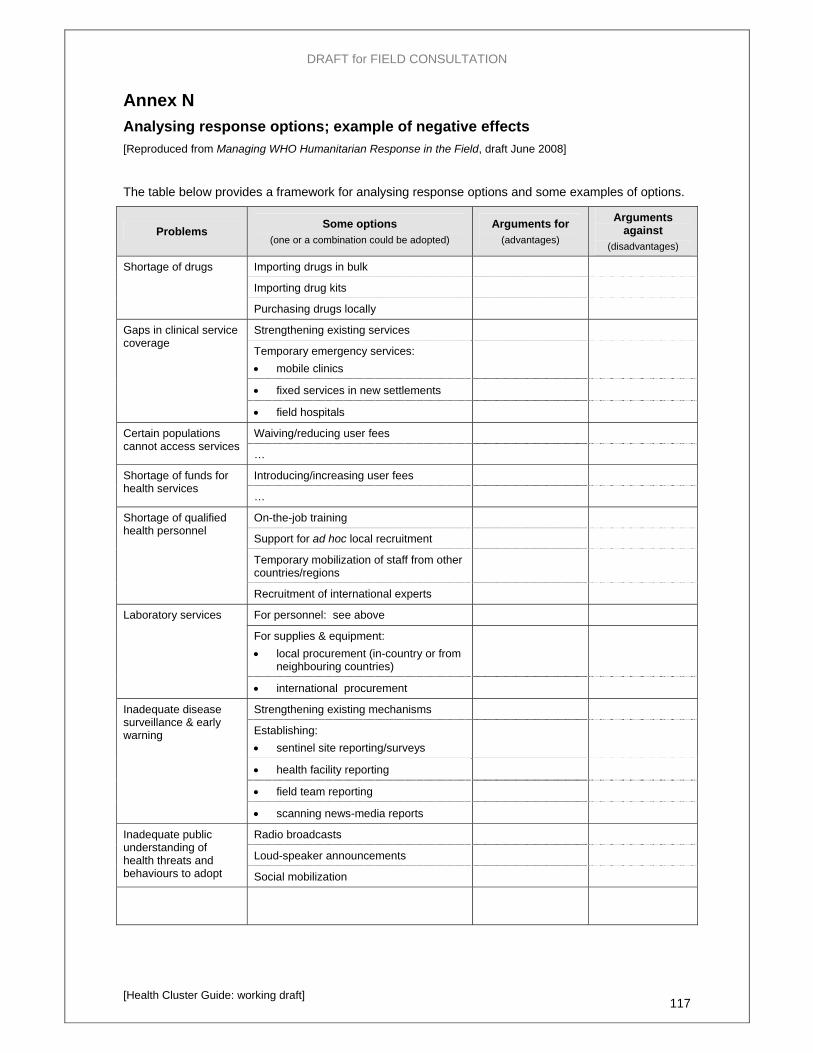
DRAFT for FIELD CONSULTATION
[Health Cluster Guide: working draft] 117
Annex N Analysing response options; example of negative effects [Reproduced from Managing WHO Humanitarian Response in the Field, draft June 2008]
The table below provides a framework for analysing response options and some examples of options.
Problems Some options (one or a combination could be adopted)
Arguments for (advantages)
Arguments against
(disadvantages)
Importing drugs in bulk
Importing drug kits
Shortage of drugs
Purchasing drugs locally
Strengthening existing services
Temporary emergency services: • mobile clinics
• fixed services in new settlements
Gaps in clinical service coverage
• field hospitals
Waiving/reducing user fees Certain populations cannot access services
…
Introducing/increasing user fees Shortage of funds for health services
…
On-the-job training
Support for ad hoc local recruitment
Temporary mobilization of staff from other countries/regions
Shortage of qualified health personnel
Recruitment of international experts
For personnel: see above
For supplies & equipment: • local procurement (in-country or from
neighbouring countries)
Laboratory services
• international procurement
Strengthening existing mechanisms
Establishing: • sentinel site reporting/surveys
• health facility reporting
• field team reporting
Inadequate disease surveillance & early warning
• scanning news-media reports
Radio broadcasts
Loud-speaker announcements
Inadequate public understanding of health threats and behaviours to adopt Social mobilization
DRAFT for FIELD CONSULTATION
[Health Cluster Guide: working draft] 118
Examples of alternative strategies and unintended negative consequences
Alternative strategies
In a refugee camp, a specific objective may be to reduce the risk of an outbreak of severe diarrhoea. Possible strategies that might be considered include: public education for improved hygiene; improved water supplies; improved sanitation facilities; mass vaccination. In this case, the first three strategies would probably be adopted simultaneously but not the last one (as mass cholera vaccination is not recommended by WHO).
Following a disaster, the assessment reveals that there will be a shortage of drugs. Possible strategies include: importing drug kits; importing drugs in bulk, purchasing drugs locally. The arguments for and against each of these options must be carefully examined before deciding on the strategy to adopt. (Note that even establishing the fact that there is, or will be, a real shortage of drugs can be problematic, but importing drugs because it "seems" there could be a shortage can be very damaging – see below).
Unintended negative consequences
Provision of drugs: Large volumes of donated/imported drugs can have unintended negative consequences. Following the tsunami December 2005, large quantities were imported into Aceh, Indonesia and given out free by relief agencies. The local market for pharmaceuticals was totally disrupted forcing local private pharmacies to close and move to other provinces. The result was that:
o people with chronic diseases could no longer buy their insulin, blood pressure medicine, etc. (items that were not considered “emergency” drugs so not provided by the relief agencies); and
o the overall recovery of the health sector was compromised because, as relief NGOs closed their operations and left, local people had nowhere to buy medicines anymore.
Waiving user fees: User-fees can be a major financial obstacle to access to health care, especially during a crisis. However, in many countries, the managers of government health facilities in many countries depend on user fees (and selling drugs) to supplement their meagre budgets for staff costs and salaries. In Aceh, once the Government waived user fees and NGOs gave out free drugs, there was a big migration of government health staff out of the province. This created a long-term problem of manpower shortage that still persisted several years later.
DRAFT for FIELD CONSULTATION
[Health Cluster Guide: working draft] 119
Annex O Common problems and challenges in health system recovery
The box below summarizes the most common problems in post-conflict situations and some broad policy suggestions. The paragraphs that follow discuss in slightly more detail a few of the major problems mentioned.
Common systemic flaws and possible policy responses in the recovery phase [Adapted from: Analysing Disrupted Health Sectors, a Modular Manual, Pavignani & Colombo, WHO expected 2008]
Common flaws and distortions Possible policy answer
Workforce oversized in relation to Health Network and under-skilled
Freeze recruitment of unskilled and low-skilled staff Expand training of high skilled cadres Retrain / Upgrade existing staff Introduce incentives to facilitate layoffs
Rigid civil service regulations resulting in an inefficient and unresponsive workforce
Introduce fixed-term, performance-related contracts Devolve hiring and firing to local health authorities
Deregulated privatisation of service provision
Contract out service delivery to NGOs, charities, etc. Contract out regulatory functions
Hospital-biased system Close down some redundant and derelict hospitals Alternatively: downsize and downgrade them while rehabilitating them Build new lower level health units in underserved areas (and new first referral hospitals where they are lacking)
Fragmented and expensive pharmaceutical sector
Establish a centralized purchasing system of generic drugs through international competitive bidding Promote the essential drugs concept Introduce standardized treatment protocols
Large portions of the population without access to basic health services
Invest in underserved areas Design and introduce realistic service delivery packages Introduce incentives to encourage staff redeployment to hard-to-reach-hard-to-stay areas Remove or reduce formal and informal user charges
Insufficient financing (absolute or against stated goals)
Propose less ambitious goals Advocate for additional internal and external funding
Ineffective management systems Encourage training and emergence of professional managers Introduce regular and transparent external audits
A plethora of actors
Often, the abundance of "actors" in the recovery phase is a more of a problem than a blessing.
In the absence of a strong Government, UN Agencies, International and National NGOs, religious organizations, all act in an uncoordinated manner, through fragmented interventions and with different agendas. All this inevitably creates a chaotic situation, full of inefficiencies, inconsistencies, duplications and waste.
In Kosovo, in 1999, more than 400 foreign NGOs flocked "to help". Many of them offered what they had, not what was needed. Most of them where, conceptually and technically, equipped for interventions in much poorer countries. Their approach was inadequate and, often, resented by the local population.
Beating a bit of common sense (usually not common at all) in this plethora of actors, often with their own open or hidden agendas, is a task as daunting as it is necessary.
DRAFT for FIELD CONSULTATION
[Health Cluster Guide: working draft] 120
An elusive solution: Coordination
Coordination during this phase is as important as it is elusive. According to the World Bank, many recovery processes were hampered by " … a lack of an overarching nationally-driven plan to which all donors agree, resulting in fragmentation, gaps or duplication in aid-financed programs."24
The unpalatable truth is that everybody wants to coordinate but nobody wants to be coordinated.
The presence of a "Lead Actor", leading with a clear and shared vision, inspiring and overseeing joint assessments, helping to draft policies, strategies and broad plans, would be instrumental. The National Government should do this. If it is still too fragile, a major donor or, better still, a respected International Organization could/should play this role. To ensure meaningful levels of real coordination, and not a mere and futile exchange of irrelevant details on fragmented activities, whoever is in charge must be trusted and respected for technical competence, political clout, and track history of success.
Such essential and instrumental "Leading Role" cannot be "taken" by any Agency. It can only be "granted" by the other actors. Given the abundance of rivalries, disagreements, sometimes open mistrust between various "actors", this isn't an easy thing to happen. And it cannot happen by decree. It can only happen on the basis of a solid, proven and recognized background of field successes. The "Leading Agency" must enjoy universal respect (from Government, NGOs, Donors) and, continuously, show that it deserves it.
Not sufficient but necessary: Policies, Strategies and Plans
Early formulation of sound policies, strategies and plans, is necessary to provide direction and a common framework for action.
There are obstacles. After long crises, often, governments lack the capacity of formulating sound policies and strategies. The information basis is fragile and grossly incomplete. The political clout of the Ministry of Health is, usually, insignificant. This could make more difficult to consider potentially controversial choices: introducing or not introducing user fees; going for decentralization or waiting to strengthen the central government first, expanding the health network or consolidating the existing (often dysfunctional) one.
Fragmented and dispersed knowledge
In an environment where everything is fragmented, from actors to interventions, from policies to strategies, knowledge is no exception.
What is known, what has been understood, what has been gained through the analysis of previous experiences, is often stored in the mind of individuals or in their drawers and shelves. Little is done to share this wealth. Territorial and cultural fragmentation, language barriers, and political implications, make things worse. This leads many newcomers to think that they have to start from scratch, that nothing has been done and nothing is actually known. This is an obvious and harmful mistake.
The structure and the nature of the Aid Architecture
The imposition of corporate policies and strategies by powerful organizations is commonplace. Preconceived ideas, experiences successful elsewhere but inappropriate to the local context, are presented, often imposed, as if they were purely technical and free of political considerations. Short term programming, rapid turnover of staff and short assignments of many consultants, compound the situation.
Often overlooked: Finances and human resources
At the beginning of the recovery process it is of paramount importance to make as much as possible accurate estimates of the costs of the recovery process and of the resources likely to be available for it, from donors as well as from domestic sources of revenues.
Elaborating strategies and formulating plans without linking them to the resources realistically going to be available, is a futile exercise. It is also a deceptive one. "Be obsessed with resources" is a commandment never to be neglected.
24 World Bank and United Nations Development Programme, An operational Note on Transitional Results matrices: Using results Based Frameworks in Fragile States, New York, 2005

DRAFT for FIELD CONSULTATION
[Health Cluster Guide: working draft] 121
Human resources are another essential aspect to be kept in mind when planning.
Today's plans for human resources development are likely to yield results in about ten years time.
Neglecting a sound reflection on and analysis of these essential aspects may lead to an unduly expansion of the health network (without the human resources to manage it adequately) or to a flurry of inadequate ad hoc training activities.
Even more often overlooked: Management Systems
During the recovery phase, when urgent and important activities are carried out and policies, strategies and plans are formulated, management systems are often neglected.
Yet, they are an essential part of the engine that will keep the system going.
Planning for sound management systems (Health Management Information System, Drugs and Supplies procurement and Distribution Systems, Human Resource Management Systems, Supervision and Support System, Quality Assurance System, etc.) is an essential step to ensure medium and long term success of short term decisions and actions.
An unavoidable necessity: Not linear but broadly logical approach
In an ideal world, the first logical step would be to gather accurate (and precise) information for the sound formulation of policies, strategies and plans. In reality, it is rarely possible to proceed in this way.
More often, several steps will have to be taken at the same time. Policies and strategies must be formulated on fragile and incomplete information basis, and plans will have to be broad, keeping a high degree of flexibility.
Information gathering will continue, through surveys, ad hoc studies and the slow initiation of a routine Health Management Information System. This must be elaborated and thought of at the early stages of Recovery.
A few important and urgent actions can be taken on the basis of imprecise but accurate information, sufficient to make sure that the right direction has been taken. For instance, the rehabilitation of important secondary level hospitals in populated areas is an undisputed priority.
Starting important operations early will boost the morale of health workers and the public as well. And will contribute to give legitimacy to the (new) government.
DRAFT for FIELD CONSULTATION
[Health Cluster Guide: working draft] 122
Glossary of key terms (and concepts) …these generic terms are to be agreed with other clusters, if possible…
Assessment a structured process of collecting and analyzing data to measure the impact of the crisis, and provide an understanding of the situation and any related threats, in order to determine whether a response is required and, if so, the nature of that response. An assessment is a time-bound exercise that produces a report and recommendations to inform decision-making at a particular point in time.
Cluster Cluster approach
A group of organizations and other stakeholders working together address needs in a particular sector (such as health). The cluster approach is a way of organizing coordination and cooperation among humanitarian actors to facilitate joint strategic planning. At country level, it: (i) establishes a clear system of leadership and accountability for international response in each sector, under the overall leadership of the humanitarian coordinator; and (ii) provides a framework for effective partnerships among international and national humanitarian actors in each sector. The aim is to ensure that international responses are appropriately aligned with national structures and to facilitate strong linkages among international organizations, national authorities, national civil society and other stakeholders.
Coordination A process (set of activities) that brings different elements into a harmonious or efficient relationship. [from Oxford English Dictionary]
In the context of humanitarian response, the aim is to have all participating organizations working together in partnership to harmonize efforts and use available resources efficiently within the framework of agreed objectives, priorities and strategies, for the benefit of the affected population(s). …The proactive process by which allocation of material, human, financial, and technical resources is made more efficient and effective…? [Shelter cluster tool kit]
Effectiveness a measure of the extent to which an intervention’s intended outcomes (its specific objectives) have been achieved.
Efficiency a measure of the relationship between outputs (the products produced or services provided by an intervention) and inputs (the resources it uses).
Evaluation A systematic and impartial examination (of humanitarian action) intended to draw lessons to improve policy and practice and enhance accountability. [ALNAP]
Evaluation answers the questions: Have we achieved what we set out to achieve? If not, why not, and what might we need to change? [Tear Fund]
Impact The effect on the affected population (e.g. reduction in measles incidence) [Guidelines for CAP Mid-year Review]
Output The actions completed to date by a project (e.g. 10,000 children vaccinated) [Guidelines for CAP Mid-year Review]
Monitoring The process/act of observing and checking over a period of time; maintaining regular surveillance over something. [from Oxford English Dictionary] In the context of humanitarian operations, two forms of monitoring are distinguished: (i) Monitoring (surveillance) of the situation – regularly gathering and analysing data on health conditions, risks, access to services, etc. to detect and measure changes. (ii) Monitoring the implementation and programmes and projects – regularly gathering and analysing data on project inputs and outputs to answer the questions: Have we done the things we said we were going to do? If not, why not, and what needs to change? [Tear Fund]

DRAFT for FIELD CONSULTATION
[Health Cluster Guide: working draft] 123
Partners Partnership
Individuals and organizations that collaborate to achieve mutually agreed upon objectives. The concept of “partnership” connotes shared goals, common responsibility for outcomes, distinct accountabilities and reciprocal obligations. Partners may include governments, civil society, non-governmental organizations, universities, professional and business associations, multi-lateral organizations, private companies, etc. [WFP Programme Guidance Manual]
Sector A distinct part of an economy, society or sphere of activity. [Oxford English Dictionary] In the context of humanitarian response, key sectors include: agriculture; food; health; nutrition; protection; shelter; water, etc. See also “cluster”.
Stakeholder Stakeholder analysis
An agency, organization, group or individual who has direct or indirect interest in a particular activity, or its evaluation.
Stakeholder analysis is an analysis of the interests and relative influence of the various stakeholders involved.
Strategy Strategic plan
The approach that will be used to achieve one or more defined objectives – how the objective(s) will be achieved. A strategic plan is a concise document that outlines the actions to be taken to achieve the defined objective, or set of objectives, specifying time frames and responsibilities for implementation. [WHO, Managing WHO Humanitarian Response in the Field, draft Jan 08]
Surveillance The systematic collection, analysis and interpretation of data in order to plan, implement and evaluate public health interventions. [WHO]
Pan American Health OrganizationRegional O ff ice of the
World Health OrganizationArea on Emergency Preparedness and Disaster Relief525 23rd Street, N.W.Washington, D.C. 20037, USAwww.paho.org/[email protected]
2008ANNUAL REPORT








