
Childhood Behavior Precursors of Schizotypal Personality ...
11
Childhood Behavior Precursors of Schizotypal Personality Disorder by Su'chin Serene Olin, Adrian Raine, Tyrone D. Cannon, Josef Pamas, Fini Schulsinger, and Sarnoff A. Mednick Abstract No study has yet reported specifically on the early behavior of individuals later diagnosed with schizo- typal personality disorder (SPD). This study examines prospectively collected teacher reports on school behavior as a means of assessing childhood precursors of SPD. Thirty-six DSM-IU-R diagnosed schizotypal subjects were compared with four other groups: 31 schizophrenia patients, 37 diagnosed as nonpsychotic mentally ill, 68 who were not mentally ill but had mothers with schizophrenia, and 60 who were not mentally ill and had normal parents. These individuals were compared on a teachers' school report question- naire obtained when the subjects averaged 15.1 years old. Those who later developed SPD were found to be more passive and unengaged and more hypersensitive to criticisms compared with the nonschizophrenia groups. Similar results were found when males and females were examined separately, except that males who developed SPD were found to be less disruptive and hyperexcitable compared with males with schizo- phrenia; females with SPD did not differ from females with schizophrenia. A receiver operating characteristic analysis found these factors to predict 73.5 percent of future SPDs; the ability of these factors to predict future SPDs is comparable for males and females. These findings suggest that preschizotypal traits may be identified in late childhood or adolescence. Schizophrenia Bulletin, 23(l):93-103, 1997. Bleuler (1911/1950) recognized a mild form of schizo- phrenia in the relatives of his schizophrenia patients. Early studies (e.g., Kety et al. 1968, 1978) using Danish samples confirmed Bleuler's observations in the biologi- cal relatives of adoptees with schizophrenia. Such individ- uals were described as having borderline or latent schizo- phrenia. The concept of borderline or latent schizophrenia was operationalized later by Spitzer et al. (1979) and termed schizotypal personality disorder (SPD) in DSM-1II (American Psychiatric Association 1980). The association between SPD and schizophrenia has been demonstrated. Several studies have found SPD and schizotypal traits to be more prevalent in the families of schizophrenia sub- jects (e.g., Baron et al. 1983; Squires-Wheeler et al. 1992; Kendler et al. 1993, 1994; Parnas et al. 1993). Recent analyses of the Danish samples also reported SPD to be elevated in the biological families of adoptees with schiz- ophrenia (Kety 1988; Kendler et al. 1994). The consistent association of SPD and schizophrenia in family and adop- tion studies implicates both a familial and a genetic rela- tionship between SPD and schizophrenia. Although some researchers consider schizophrenia to be the primary disorder and SPD to be the secondary form, an alternative perspective (e.g., Mednick et al. 1987) views SPD as the basic disorder. According to the latter perspective, which posits a diathesis-stress model, schizophrenia and SPD are "schizotypes" that share the same genetic liability (the diathesis) for schizophrenia. Interactions with the environment determine which of these schizotypes later decompensate to schizophrenia. Schizotypes who experience greater environmental stres- sors (e.g., perinatal complications, family instability) are more likely to develop overt schizophrenia symptoms (Mednick et al. 1987). Based on this perspective, SPD is considered a life-long disorder, suggesting that behavioral precursors of SPD could be identified. Many studies have investigated premorbid behavioral indicators of schizo- phrenia and schizophrenia-spectrum disorders, including some well-known, high-risk, longitudinal projects such as the Rochester Longitudinal Study (Sameroff et al. 1987), Emory University Project (Goodman 1987), Israeli Reprint requesls should be sent to Dr. S.S. Olin. Social Science Research Institute, Allan Hancock Foundation. Rm. B67. University of Southern California. Los Angeles, CA "00X9-0375. 93 Downloaded from https://academic.oup.com/schizophreniabulletin/article/23/1/93/1880751 by guest on 25 January 2022
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Childhood Behavior Precursors of Schizotypal Personality ...

Childhood Behavior Precursors of SchizotypalPersonality Disorder
by Su'chin Serene Olin, Adrian Raine, Tyrone D. Cannon, Josef Pamas,Fini Schulsinger, and Sarnoff A. Mednick
Abstract
No study has yet reported specifically on the earlybehavior of individuals later diagnosed with schizo-typal personality disorder (SPD). This study examinesprospectively collected teacher reports on schoolbehavior as a means of assessing childhood precursorsof SPD. Thirty-six DSM-IU-R diagnosed schizotypalsubjects were compared with four other groups: 31schizophrenia patients, 37 diagnosed as nonpsychoticmentally ill, 68 who were not mentally ill but hadmothers with schizophrenia, and 60 who were notmentally ill and had normal parents. These individualswere compared on a teachers' school report question-naire obtained when the subjects averaged 15.1 yearsold. Those who later developed SPD were found to bemore passive and unengaged and more hypersensitiveto criticisms compared with the nonschizophreniagroups. Similar results were found when males andfemales were examined separately, except that maleswho developed SPD were found to be less disruptiveand hyperexcitable compared with males with schizo-phrenia; females with SPD did not differ from femaleswith schizophrenia. A receiver operating characteristicanalysis found these factors to predict 73.5 percent offuture SPDs; the ability of these factors to predictfuture SPDs is comparable for males and females.These findings suggest that preschizotypal traits maybe identified in late childhood or adolescence.
Schizophrenia Bulletin, 23(l):93-103, 1997.
Bleuler (1911/1950) recognized a mild form of schizo-phrenia in the relatives of his schizophrenia patients.Early studies (e.g., Kety et al. 1968, 1978) using Danishsamples confirmed Bleuler's observations in the biologi-cal relatives of adoptees with schizophrenia. Such individ-uals were described as having borderline or latent schizo-phrenia. The concept of borderline or latent schizophrenia
was operationalized later by Spitzer et al. (1979) andtermed schizotypal personality disorder (SPD) in DSM-1II(American Psychiatric Association 1980). The associationbetween SPD and schizophrenia has been demonstrated.Several studies have found SPD and schizotypal traits tobe more prevalent in the families of schizophrenia sub-jects (e.g., Baron et al. 1983; Squires-Wheeler et al. 1992;Kendler et al. 1993, 1994; Parnas et al. 1993). Recentanalyses of the Danish samples also reported SPD to beelevated in the biological families of adoptees with schiz-ophrenia (Kety 1988; Kendler et al. 1994). The consistentassociation of SPD and schizophrenia in family and adop-tion studies implicates both a familial and a genetic rela-tionship between SPD and schizophrenia.
Although some researchers consider schizophrenia tobe the primary disorder and SPD to be the secondaryform, an alternative perspective (e.g., Mednick et al.1987) views SPD as the basic disorder. According to thelatter perspective, which posits a diathesis-stress model,schizophrenia and SPD are "schizotypes" that share thesame genetic liability (the diathesis) for schizophrenia.Interactions with the environment determine which ofthese schizotypes later decompensate to schizophrenia.Schizotypes who experience greater environmental stres-sors (e.g., perinatal complications, family instability) aremore likely to develop overt schizophrenia symptoms(Mednick et al. 1987). Based on this perspective, SPD isconsidered a life-long disorder, suggesting that behavioralprecursors of SPD could be identified. Many studies haveinvestigated premorbid behavioral indicators of schizo-phrenia and schizophrenia-spectrum disorders, includingsome well-known, high-risk, longitudinal projects such asthe Rochester Longitudinal Study (Sameroff et al. 1987),Emory University Project (Goodman 1987), Israeli
Reprint requesls should be sent to Dr. S.S. Olin. Social ScienceResearch Institute, Allan Hancock Foundation. Rm. B67. University ofSouthern California. Los Angeles, CA "00X9-0375.
93
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/23/1/93/1880751 by guest on 25 January 2022

Schizophrenia Bulletin, Vol. 23, No. 1, 1997 S.S. Ol incta l .
Kibbutz-City Study (Marcus et al. 1987), Stony BrookHigh-Risk Project (Weintraub 1987), New York High-Risk Project (Erlenmeyer-Kimling and Cornblatt 1987),Finnish Adoptive Family Study (Tienari et al. 1987),Copenhagen High-Risk Project (Mednick et al. 1987), andUniversity of California, Los Angeles High-Risk Project(Goldstein 1987). Followback studies also have been con-ducted to identify behaviors that may predict later schizo-phrenia. Such followup and followback studies foundpreschizophrenia subjects to be emotionally labile, ner-vous, and withdrawn (Watt 1972, 1978; Watt andLubensky 1976; John et al. 1982; Weintraub 1987; Hanset al. 1992). Additionally, disruptive classroom behaviorappeared to be associated with later schizophrenia, partic-ularly in males (Watt 1972, 1978; Watt and Lubensky1976; John et al. 1982; Watt et al. 1982; Janes et al. 1983;Kohlberg et al. 1984; Schwartzman et al. 1985; Olin et al.1995). In contrast, fewer studies have focused on precur-sors of SPD, and no longitudinal study has yet looked sys-tematically at the childhood behaviors of diagnosedschizotypals.
In contrast to the childhood schizophrenia behaviorof both externalizing (i.e., undercontrolled, aggressive)and internalizing (i.e., overcontrolled, anxious, inhibited)behaviors, adult symptoms of SPD include more internal-izing behaviors (Achenbach and Edelbrock 1978). Forexample, schizotypal traits include social anxiety and noclose friends, which may have analogs with internalizingchildhood behavior. Patterns such as passivity and with-drawal may be characteristic of preschizotypals. If SPDtruly is a life-long personality disorder, then analogs toadult SPD symptoms should be found in adolescence. Infact, one study assessing schizotypal traits in nondiag-nosed offspring of psychiatric parents found stability ofschizotypal features across time, supporting the idea thatadult-diagnosed schizotypal individuals may have earlyindicators of their potential for SPD in adulthood(Squires-Wheeler et al. 1992). If behaviors differentiatingpreschizotypals from other children and adolescents canbe identified, they can be used to target such individualsfor early intervention. Furthermore, behaviors distinguish-ing SPD and schizophrenia may elucidate current theorieson the relationship between schizophrenia and SPD.
The present study set out to test these hypotheses in alongitudinal format using teacher reports of school behav-ior in the Copenhagen high-risk sample of offspring ofmothers with schizophrenia. Teacher reports of schoolbehavior of 36 children and adolescents who laterreceived a lifetime DSM-III-R (American PsychiatricAssociation 1987) diagnosis of SPD were compared withschool reports of individuals later diagnosed as havingschizophrenia, being nonpsychotic but mentally ill, or
normal. Based on a knowledge of preschizophreniabehavior and the similarities between SPD and schizo-phrenia features, some tentative hypotheses were made.
1. Internalizing behaviors:a. SPD versus nonschizophrenia outcomes:
Preschizotypals are expected to be more withdrawn andpassive than children with nonpsychotic psychiatric andnormal outcomes. Relative to these children, preschizo-typals also are expected to be more socially anxious.
b. SPD versus schizophrenia: No hypothesis wasformed on this relationship because preschizotypal indi-viduals are expected to be similar to those with preschizo-phrenia with regard to internalizing behaviors.2. Externalizing behaviors:
a. SPD versus nonschizophrenia outcomes: Nohypothesis was made on this relationship becausepreschizotypals are not expected to be different from chil-dren with nonschizophrenia outcomes with regard toexternalizing behaviors.
b. SPD versus schizophrenia: Preschizotypals arehypothesized to exhibit less externalizing behavior prob-lems, compared with preschizophrenia subjects.
Because males and females have been found toexhibit different precursor behaviors in schizophrenia(Watt 1972, 1978; Watt and Lubensky 1976; Schwartzmanet al. 1985; Asarnow et al. 1991; Olin et al. 1995), thequestion of sex differences in preschizotypal behaviorsalso was examined in this study.
Methods
Subjects. The sample comprises 162 high-risk subjectsand 60 low-risk subjects from the Danish high-risk studyof 311 individuals followed since 1962. The originalDanish high-risk prospective study included 207 high-risksubjects who had a mother with severe schizophrenia.They were matched to 104 low-risk subjects on variablesthat included age, sex, father's occupation, rural-urbanresidence, and institutional upbringing versus family life(Mednick and Schulsinger 1968). At the time of the 1962study, the subjects were between the ages of 9 and 20,with a mean age of 15.1 years. None of the subjectsincluded in the project had a psychiatric diagnosis in1962. Two major diagnostic followup studies have beenconducted since 1962. The first diagnostic followup wasin 1972 when subjects averaged 25 years old. The secondfollowup took place when these subjects averaged 39 to42 years old and were largely past the risk period fordeveloping schizophrenia. The lifetime diagnoses used inthe present study are based on DSM-lll-R.
Only four SPDs in the low-risk group had complete
94
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/23/1/93/1880751 by guest on 25 January 2022

Childhood Behavior Precursors of Schizotypal Disorder Schizophrenia Bulletin, Vol. 23, No. 1, 1997
school reports. Consequently, these subjects were notincluded in the analyses.
DSM-IH-R Diagnoses. Between 1972 and 1974, thefirst major diagnostic followup was conducted by HanneSchulsinger (1976) and consisted of the Present StateExamination (PSE), PSE Etiology Scale, PSE syndromechecklist (Wing et al. 1974), Current and PastPsychopathology Scales (Endicott and Spitzer 1972), andother items assessing schizophrenia characteristics. Inaddition, hospital records were screened and relevant hos-pital charts were reviewed and scored for symptoms.Schulsinger completed a summary of the interview andhospital records, including social, occupational, and otherpsychiatric information. This information recently wasconverted to DSM-III-R diagnoses through carefulreview of the interview summaries.
Between 1986 and 1989, Bjorn Jacobsen conductedthe second diagnostic followup. The subjects were evalu-ated using three structured psychiatric interviews: theSchedule for Affective Disorders and Schizophrenia—Lifetime Version (Spitzer and Endicott 1978), the PSE, andthe Personality Disorders Examination (Loranger et al.1985). Again, the hospital records of all subjects werescreened for relevant information. Jacobsen completed asummary on each subject, including social, occupational,and psychiatric information. Based on this assessment, eachsubject was assigned diagnoses using DSM-III-R criteria.
Blind, independent reviews of the interview sum-maries from each assessment were conducted. This reviewindicated a high degree of diagnostic reliability (mean Kcoefficient = 0.965) (Parnas et al. 1993). More recently,the interview summaries of the SPD subjects werereviewed. All SPD subjects in the high-risk group evi-denced at least five of the nine features of SPD describedin DSM-IV (American Psychiatric Association 1994).
Subjects were assigned a primary lifetime diagnosisrepresenting the most severe Axis I or II diagnosis ateither assessment. The diagnostic outcomes of all the sub-jects in the Copenhagen high-risk sample have been dis-cussed in a separate article (Parnas et al. 1993). For thepresent study, the high-risk group included 36 schizotypalsubjects; SPD was considered primary to all disordersexcept schizophrenia. The SPD group was compared withthree groups of children from the high-risk group: (1)31children who later developed schizophrenia; (2) 37 non-psychotics including individuals diagnosed with nonpsy-chotic depression, substance abuse, and other Axis I andII disorders; and (3) 68 not mentally ill (NMI) individuals.They were also compared with 60 NMI individuals fromthe low-risk sample. Ten of the high-risk subjects did notreceive complete school reports (2 SPD, 1 schizophrenia,5 nonpsychotic, 2 NMI). Several psychotic disorders in
the high-risk group were not included in these analysesbecause they occurred at low rates (1 delusional disorder,1 schizophreniform disorder, 7 atypical psychosis, 6organic brain syndrome, 5 paranoid personality disorder);15 high-risk subjects were excluded because of missingdiagnoses.
School Report. In 1962, subjects were assessed exten-sively on several measures, including a teacher report ofschool behavior. Subjects were asked for their permissionto send the questionnaire to the teachers. All subjects gavetheir oral agreement to the full day of assessment andteacher ratings. Teachers who knew the students bestcompleted a school report questionnaire. School reportsfor older subjects were done retrospectively. For everysubject, the teacher who completed the questionnaire hadknown the subject for at least 3 years. The school reportwas not completed for 12 (10 high-risk, 2 low-risk) sub-jects. The rest received complete or nearly completeschool reports. Missing items on the questionnaire werenonsystematically distributed across all items.
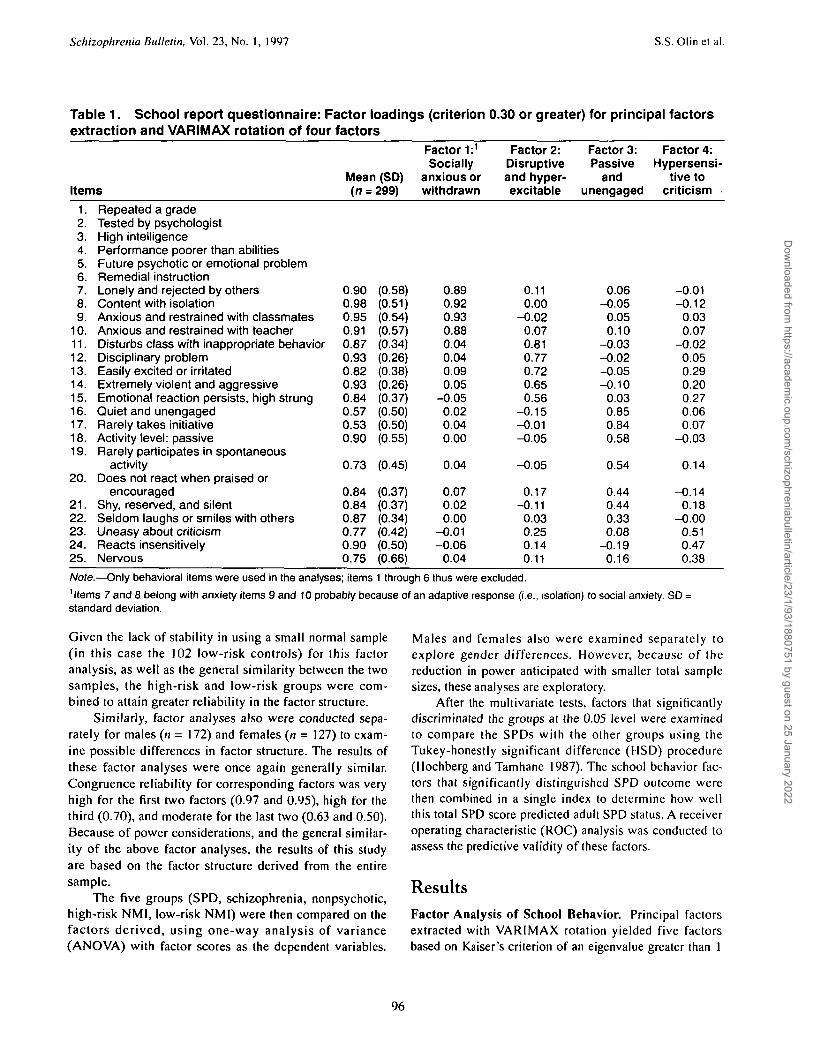
Table 1 presents the school report questionnaire. Onlybehavioral items were included in the analyses; thus,items 1 through 6 were excluded. These items requiredteachers to make a true-false response about the subject'sclassroom behavior. For all items, teachers were allowed a"don't-know" response.
Analyses. An exploratory factor analysis was the methodof choice for the following reasons: (1) The literaturerelated to precursors of SPD is sparse. This article isintended to explore and identify possible precursors ofadult SPD. Given that little is known about early SPDbehaviors, exploratory factor analysis is appropriate(Bollen 1989). (2) The school report questionnaire had notbeen factor analyzed before, and consequently, anexploratory factor analysis is useful in suggesting under-lying patterns in the teacher school report questionnaire(Bollen 1989). Principal axis factoring with VARIMAXrotation was employed using Statistical Package for theSocial Sciences (SPSS-X; Norusis 1988). Factor scoreswere summed using the regression method (Norusis1988). All individuals (n = 299) of the Copenhagen High-Risk Study with school data were used. Missing data for aspecific item (ranging from 5.1% to 10.6%) were replacedwith the group mean to maximize sample size.
Of concern was the question of the probable bias inusing an ascertained sample in factor analysis. Factoranalyses were conducted separately using the high-riskgroup (n = 197) and the low-risk group (n - 102).Congruence reliability (Harman 1976) for correspondingfactors was very high for the first three factors (0.93, 0.88,and 0.80) and moderate for the last two (0.56 and 0.42).
95
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/23/1/93/1880751 by guest on 25 January 2022
Schizophrenia Bulletin, Vol. 23, No. 1, 1997 S.S. Olin et al.
Table 1. School report questionnaire: Factor loadings (criterion 0.30 or greater) for principal factorsextraction and VARIMAX rotation of four factors
Items
1.2.3.4.5.6.7.8.9.
10.11.12.13.14.15.16.17.18.19.
20.
21.22.23.24.25.
Repeated a gradeTested by psychologistHigh intelligencePerformance poorer than abilitiesFuture psychotic or emotional problemRemedial instructionLonely and rejected by othersContent with isolationAnxious and restrained with classmatesAnxious and restrained with teacherDisturbs class with inappropriate behaviorDisciplinary problemEasily excited or irritatedExtremely violent and aggressiveEmotional reaction persists, high strungQuiet and unengagedRarely takes initiativeActivity level: passiveRarely participates in spontaneous
activityDoes not react when praised or
encouragedShy, reserved, and silentSeldom laughs or smiles with othersUneasy about criticismReacts insensitivelyNervous
Mean (SD)(n = 299)
0.90 (0.58)0.98 (0.51)0.95 (0.54)0.91 (0.57)0.87 (0.34)0.93 (0.26)0.82 (0.38)0.93 (0.26)0.84 (0.37)0.57 (0.50)0.53 (0.50)0.90 (0.55)
0.73 (0.45)
0.84 (0.37)0.84 (0.37)0.87 (0.34)0.77 (0.42)0.90 (0.50)0.75 (0.66)
Factor 1:1
Sociallyanxious orwithdrawn
0.890.920.930.880.040.040.090.05
-0.050.020.040.00
0.04
0.070.020.00
-0.01-0.06
0.04
Factor 2:Disruptiveand hyper-excitable
0.110.00
-0.020.070.810.770.720.650.56
-0.15-0.01-0.05
-0.05
0.17-0.11
0.030.250.140.11
Factor 3:Passive
andunengaged
0.06-0.05
0.050.10
-0.03-0.02-0.05-0.10
0.030.850.840.58
0.54
0.440.440.330.08
-0.190.16
Factor 4:Hypersensi-
tive tocriticism
-0.01-0.12
0.030.07
-0.020.050.290.200.270.060.07
-0.03
0.14
-0.140.18
-0.000.510.470.38
Note.—Only behavioral items were used in the analyses; items 1 through 6 thus were excluded.1ltems 7 and 8 belong with anxiety items 9 and 10 probably because of an adaptive response (i.e., isolation) to social anxiety. SD =standard deviation.
Given the lack of stability in using a small normal sample(in this case the 102 low-risk controls) for this factoranalysis, as well as the general similarity between the twosamples, the high-risk and low-risk groups were com-bined to attain greater reliability in the factor structure.
Similarly, factor analyses also were conducted sepa-rately for males (n = 172) and females (n = 127) to exam-ine possible differences in factor structure. The results ofthese factor analyses were once again generally similar.Congruence reliability for corresponding factors was veryhigh for the first two factors (0.97 and 0.95), high for thethird (0.70), and moderate for the last two (0.63 and 0.50).Because of power considerations, and the general similar-ity of the above factor analyses, the results of this studyare based on the factor structure derived from the entiresample.
The five groups (SPD, schizophrenia, nonpsychotic,high-risk NMI, low-risk NMI) were then compared on thefactors derived, using one-way analysis of variance(ANOVA) with factor scores as the dependent variables.
Males and females also were examined separately toexplore gender differences. However, because of thereduction in power anticipated with smaller total samplesizes, these analyses are exploratory.
After the multivariate tests, factors that significantlydiscriminated the groups at the 0.05 level were examinedto compare the SPDs with the other groups using theTukey-honestly significant difference (HSD) procedure(Hochberg and Tamhane 1987). The school behavior fac-tors that significantly distinguished SPD outcome werethen combined in a single index to determine how wellthis total SPD score predicted adult SPD status. A receiveroperating characteristic (ROC) analysis was conducted toassess the predictive validity of these factors.
ResultsFactor Analysis of School Behavior. Principal factorsextracted with VARIMAX rotation yielded five factorsbased on Kaiser's criterion of an eigenvalue greater than 1
96
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/23/1/93/1880751 by guest on 25 January 2022

Childhood Behavior Precursors of Schizotypal Disorder Schizophrenia Bulletin, Vol. 23, No. 1, 1997
(Kaiser 1958). The criterion for significant loadings was setat 0.30 or greater; these factor loadings are shown in table1. Factor 1 accounted for 19.8 percent of the variance: thisfactor included items 7 through 10 and was labeled"socially anxious or withdrawn." Factor 2 accounted for anadditional 18.6 percent of the variance: this factor includeditems 11 through 15 and was labeled "disruptive and hyper-excitable." Factor 3 accounted for 16 percent of the vari-ance: this factor, consisting of items 16 through 22, waslabeled "passive and unengaged." Factor 4 accounted for anadditional 6.8 percent of the variance: this factor, consist-ing of items 23 through 25, was labeled "hypersensitive tocriticism." The fifth factor consisted of items 19 and 22 andwas dropped from further analyses for four reasons: (1)Factor 5 meets only the minimal criterion of an eigenvaluegreater than 1 (eigenvalue = 1.011) and only accounts foran additional 5.3 percent of the variance. (2) Only twoitems loaded on this factor. (3) Both items were alreadyaccounted for in factor 3. (4) Removing the fifth factorresulted in simple structure as outlined by Thurstone(1947). Thus, further analyses were based on a four-factorsolution. The regression method was used to create factorscores for all four factors.
The five diagnostic groups were compared on thefour factors. The means and standard deviations of thefour factor scores are shown in table 2. The five groupswere significantly different from one another on three fac-tors (factors 2, 3, and 4).
1. Testing of Hypotheses—Internalizing Behaviors:a. SPD versus other nonschizophrenia outcomes: The
one-way ANOVA indicated that factor 3 (passive andunengaged) significantly differentiated among the fivegroups (F - 3.67; df = 4,216; p - 0.007). Pairwise com-parisons using the Tukey HSD procedure supported thehypothesis that preschizotypals would be more passiveand unengaged than other children. Specifically, pre-schizotypals were significantly more passive and unen-gaged compared with the low-risk NMIs (p < 0.05). Noneof the other pairwise comparisons was significant. Thehypothesis that preschizotypals would exhibit greatersocial anxiety (factor 1) was not supported.
b. SPD versus schizophrenia: Preschizotypals werenot significantly different from preschizophrenia subjectson factor 1 (socially anxious or withdrawn) or factor 3(passive and unengaged).
Table 2. Means (standard deviations) of factor scores on the four factors derived from the schoolreport questionnaire
Groups (n)
Factor 1:Socially
anxious orwithdrawn
Factor 2:Disruptive
andhyperexcitable
Factor 3:Passive
andunengaged
Factor 4:Hypersensitive
tocriticism
Males and females combinedSPD (34)SZ (30)NPD (32)HR-NMI (66)LR-NMI (60)
MalesSPD (24)SZ(18)NPD (18)HR-NMI (30)LR-NMI (34)
FemalesSPD (10)SZ(12)NPD (14)HR-NMI (36)LR-NMI (26)
0.09 (0.40)0.16 (0.44)
-0.002 (0.31)0.11 (0.40)0.01 (0.35)
0.040.180.070.120.03
0.210.13
-0.090.11
-0.02
(0.24)(0.46)(0.39)(0.34)(0.38)
(0.64)(0.43)(0.02)(0.45)(0.31)
-O.020.630.20
-0.12-0.22
0.051.00.59
-0.03-0.11
-0.190.07
-0.32-0.21-0.35
(0.65)1
(1.4)2
(1.2)(0.76)1
(0.64)1
(0.71 )1
(1.5)2
(1.5)(0.82)1
(0.74)1
(0.48)(1.0)(0.39)(0.70)(0.44)
0.290.20
-0.290.14
-0.24
0.250.16
-0.34-O.08-0.28
0.390.26
-0.220.33
-0.18
(0.93)2
(1.0)(0.79)(0.92)(0.81)1
(0.90)(1.0)(0.78)(0.93)(0.84)
(1.0)(1.0)(0.84)(0.88)(0.78)
0.460.050.10
-0.09-0.09
0.40-0.07
0.18-0.18-0.09
0.620.230.00
-0.01-0.08
(1.1)2
(0.88)
(0.62)
(0.53)1
(0.58)1
(1.1)2
(0.81)
(0.67)
(0.49)1
(0.63)
(1.0)2
(0.98)(0.57)(0.57)(0.51)1
Note.—SPD = schizotypal personality disorder; SZ = schizophrenia; NPD = nonpsychotic disorder; HR-NMI = high-risk not mentally ill;LR-NMI = low-risk not mentally ill.1This group is significantly different from the group having the most deviant score for that factor,^ h i s group had the most deviant score for that factor.
97
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/23/1/93/1880751 by guest on 25 January 2022

Schizophrenia Bulletin, Vol. 23, No. 1, 1997 S.S. Olinetal.
2. Testing of Hypotheses—Externalizing Behaviors:a. SPD versus other nonschizophrenia outcomes:
Factor 2 (disruptive and hyperexcitable) distinguished thefive groups (F = 5.26; df = 4,216; p - 0.0005). Pairwisecomparison using Tukey's procedure indicated, however,that the preschizotypals were not different from the non-preschizophrenia groups on this factor.
b. SPD versus schizophrenia: Pairwise comparisonindicated that preschizotypals were significantly (p <0.05) less disruptive and hyperexcitable (factor 2) than thepreschizophrenia subjects. In fact, the preschizophreniasubjects were the most disruptive group (Olin et al. 1995).They were significantly more disruptive and hyper-excitable than the preschizotypals and the high-risk NMIand low-risk NMI groups (p < 0.05).
Exploratory Hypotheses. No hypothesis was made forfactor 4 (hypersensitive to criticism). This factor, however,distinguished the five groups (F - 4.11; df - 4,216; p =0.003). Preschizotypals were more hypersensitive to criti-cism than other children (table 2). Specifically, Tukey'sprocedure showed that preschizotypals were significantlymore hypersensitive to criticism compared with high-riskand low-risk children with NMI (p < 0.05). The other pair-wise comparisons were not significantly different.
Analyses by Sex. These analyses were replicated formales and females separately to explore gender differ-ences. In general, except for changes in p values resultingfrom the reduced power associated with smaller samplesizes, the results for males and females were similar tothose of the combined sample. Preschizotypal males andfemales were found to be more passive and unengagedand more hypersensitive to criticism. The results of theanalyses for males and females are shown in table 2.
Factor 1 (socially anxious or withdrawn). This fac-tor did not distinguish the males or the females.
Factor 2 (disruptive and hyperexcitable).Preschizotypal males were less disruptive and hyperex-citable than the preschizophrenia males (F - 4.80; df- 4;p = 0.001). In fact, the preschizophrenia males also werefound to be more disruptive and hyperexcitable than thehigh-risk NMI and low-risk NMI males. Preschizotypalfemales were not significantly different from their femalepreschizophrenia peers on this factor. Compared withtheir male nonschizophrenia peers, preschizotypal malesdid not differ on this factor; similarly, preschizotypalfemales did not differ from their female nonschizophreniapeers on this factor.
Factor 3 (passive and unengaged). The differencebetween preschizotypal males and the low-risk NMImales approached significance (F - 1.98; df - 4; p =
0.10). Similarly, the difference between the preschizotypalfemales and the low-risk NMI females also approachedsignificance (F = 2.11; df= 4; p = 0.09). The lack of sig-nificant findings when the sexes were separated is proba-bly caused by the decreased power associated withsmaller sample sizes. As can been seen in table 2, themean factor 3 scores for the SPDs and the low-risk NMIsare comparable when the groups are combined or sepa-rated by sex.
Factor 4 (hypersensitive to criticism). Preschizo-typal males were found to have significantly higher scoresthan high-risk NMI males (F = 2.54; df = 4; p = 0.04),whereas preschizotypal females were found to have sig-nificantly higher scores than the low-risk NMI females(F = 2.53; <//= 4;/> = 0.046).
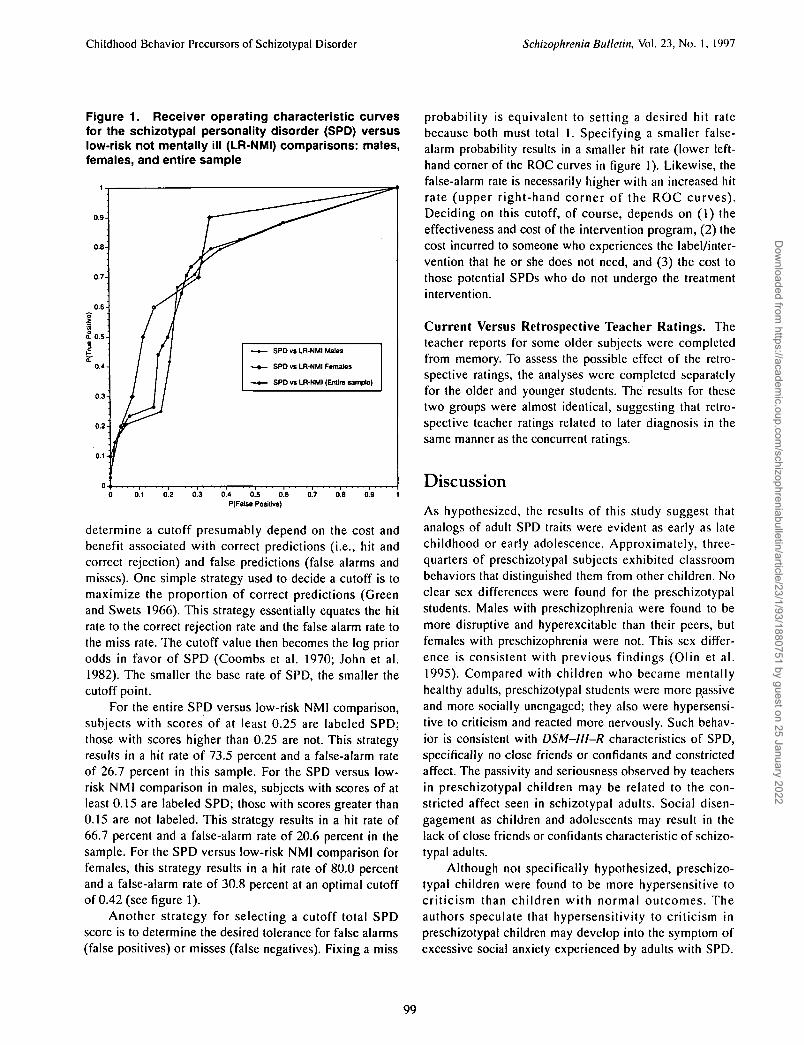
Assessing the Predictive Value of the SPD Factors: AnROC Analysis. To assess the predictive value of the SPDfactors, an index was developed by summing the signifi-cant differentiating factor scores derived from the entiresample to obtain a total SPD score for each subject (inthis case, factors 3 and 4; factor 2 was not included in thisindex because it distinguished only the male SPD fromthe male schizophrenia subjects). An ROC analysis(Swets and Pickett 1982; Hsiao et al. 1989; Mossman andSomoza 1989) was used to evaluate the efficacy of thetotal SPD score for differentiating preschizotypals fromnormals. In the absence of a general population sample,the low-risk normal control (i.e., NMI) group is used toexamine the positive and negative predictive power of thistotal SPD score. Figure 1 shows rates for true-positive andfalse-positive reports corresponding to various cutoffs inthe total SPD score for the entire sample. The points formales and females are also plotted separately—includingendpoints (0,0) and (1,1)—and are connected to producetwo ROC curves (Egan 1975; Swets and Pickett 1982),one for each sex. The ROC curve shows the tradeoffbetween the probability of true-positive and false-positivereports as the decision criterion changes. A conservativecriterion would result in low true- and false-positive rates,represented by a point near the lower left-hand corner offigure 1. In contrast, a lenient criterion would result inhigh true- and false-positive rates, represented by a pointnear the upper right-hand corner of the graph. The true-positive rate corresponds to the sensitivity of the totalSPD score, whereas the false-positive rate corresponds to1 minus the specificity of the total SPD score. As seen infigure 1, the ROC for both males and females is compara-ble to that of the entire sample.
In essence, the ROC curve represents all possible dis-crimination rules that can be obtained by selecting differ-ent total SPD score cutoffs. Decision rules developed to
98
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/23/1/93/1880751 by guest on 25 January 2022
Childhood Behavior Precursors of Schizotypal Disorder Schizophrenia Bulletin, Vol. 23, No. 1, 1997
Figure 1. Receiver operating characteristic curvesfor the schizotypal personality disorder (SPD) versuslow-risk not mentally ill (LR-NMI) comparisons: males,females, and entire sample
0.8-
SPD vs LR-NMI Males
SPO vs LR-NMI Females
SPD vs LR-NMI (Entire sample)
0.3 0.4 0.5 0.6
P(False Positive)0.7 o.e
determine a cutoff presumably depend on the cost andbenefit associated with correct predictions (i.e., hit andcorrect rejection) and false predictions (false alarms andmisses). One simple strategy used to decide a cutoff is tomaximize the proportion of correct predictions (Greenand Swets 1966). This strategy essentially equates the hitrate to the correct rejection rate and the false alarm rate tothe miss rate. The cutoff value then becomes the log priorodds in favor of SPD (Coombs et al. 1970; John et al.1982). The smaller the base rate of SPD, the smaller thecutoff point.
For the entire SPD versus low-risk NMI comparison,subjects with scores of at least 0.25 are labeled SPD;those with scores higher than 0.25 are not. This strategyresults in a hit rate of 73.5 percent and a false-alarm rateof 26.7 percent in this sample. For the SPD versus low-risk NMI comparison in males, subjects with scores of atleast 0.15 are labeled SPD; those with scores greater than0.15 are not labeled. This strategy results in a hit rate of66.7 percent and a false-alarm rate of 20.6 percent in thesample. For the SPD versus low-risk NMI comparison forfemales, this strategy results in a hit rate of 80.0 percentand a false-alarm rate of 30.8 percent at an optimal cutoffof 0.42 (see figure 1).
Another strategy for selecting a cutoff total SPDscore is to determine the desired tolerance for false alarms(false positives) or misses (false negatives). Fixing a miss
probability is equivalent to setting a desired hit ratebecause both must total 1. Specifying a smaller false-alarm probability results in a smaller hit rate (lower left-hand corner of the ROC curves in figure 1). Likewise, thefalse-alarm rate is necessarily higher with an increased hitrate (upper right-hand corner of the ROC curves).Deciding on this cutoff, of course, depends on (1) theeffectiveness and cost of the intervention program, (2) thecost incurred to someone who experiences the label/inter-vention that he or she does not need, and (3) the cost tothose potential SPDs who do not undergo the treatmentintervention.
Current Versus Retrospective Teacher Ratings. Theteacher reports for some older subjects were completedfrom memory. To assess the possible effect of the retro-spective ratings, the analyses were completed separatelyfor the older and younger students. The results for thesetwo groups were almost identical, suggesting that retro-spective teacher ratings related to later diagnosis in thesame manner as the concurrent ratings.
Discussion
As hypothesized, the results of this study suggest thatanalogs of adult SPD traits were evident as early as latechildhood or early adolescence. Approximately, three-quarters of preschizotypal subjects exhibited classroombehaviors that distinguished them from other children. Noclear sex differences were found for the preschizotypalstudents. Males with preschizophrenia were found to bemore disruptive and hyperexcitable than their peers, butfemales with preschizophrenia were not. This sex differ-ence is consistent with previous findings (Olin et al.1995). Compared with children who became mentallyhealthy adults, preschizotypal students were more passiveand more socially unengaged; they also were hypersensi-tive to criticism and reacted more nervously. Such behav-ior is consistent with DSM-lll-R characteristics of SPD,specifically no close friends or confidants and constrictedaffect. The passivity and seriousness observed by teachersin preschizotypal children may be related to the con-stricted affect seen in schizotypal adults. Social disen-gagement as children and adolescents may result in thelack of close friends or confidants characteristic of schizo-typal adults.
Although not specifically hypothesized, preschizo-typal children were found to be more hypersensitive tocriticism than children with normal outcomes. Theauthors speculate that hypersensitivity to criticism inpreschizotypal children may develop into the symptom ofexcessive social anxiety experienced by adults with SPD.
99
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/23/1/93/1880751 by guest on 25 January 2022

Schizophrenia Bulletin, Vol. 23, No. 1, 1997 S.S. Olinetal.
In DSM-IV, the SPD feature of excessive social anxiety isassociated with paranoid ideation, which may beexpressed as hypersensitivity in childhood or adolescence.
In this context, it is interesting that preschizotypalchildren were not found to be more socially anxious (fac-tor 1) compared with the other groups. The adult schizo-typal trait of social anxiety may develop later, as a conse-quence of passivity and hypersensitivity. The inability ofthese children to initiate and participate in activities, com-pounded by their sensitivity to criticism and anxiety inother classroom situations, may result in a lack of social-izing opportunities. This lack of socialization in childhoodmay later lead to social anxiety as adults and explain thelack of close friends and confidants characteristic ofschizotypal adults. Alternatively, social anxiety mayunderlie many disorders and may not be specific to SPD.
The ROC analysis showed that the total SPD scorehad some predictive efficacy. When a total SPD score waschosen to maximize the proportion of SPD predictions,approximately three-quarters of future SPDs were tar-geted. Some nonschizotypals were falsely classified usingthese total SPD scores in childhood, however, which indi-cates that some behaviors identified by the school reportmay not be specific to schizotypy.
Of particular interest in this study were behaviors thatdistinguished preschizophrenia sufferers and preschizotyp-als, and these may elucidate differences in the etiologies ofthe two disorders. In this study, children with preschizo-phrenia were found to be more hyperexcitable and disrup-tive than those who were preschizotypal. This etiologicaldifference may be explained by Meehl's diathesis-stressmodel of schizophrenia. According to Meehl (1962, 1989,1990), schizotypals and persons with schizophrenia are"schizotypes" who share a common genetic diathesis.Schizophrenia is postulated to develop as a result of theinteractions of these schizotypes with the environment. Inparticular, schizotypes who suffer stressful experiencesmay develop overt schizophrenia, whereas those who donot suffer stressful experiences develop SPD. The childrenwith preschizophrenia in the sample studied experienceddelivery complications and poor rearing environments,such as family instability, early institutionalization, andparental separations (Mednick et al. 1987; more recentunpublished analyses of schizophrenia replicate earlierfindings). Such early stressful experiences also have beenassociated with later antisocial behavior (Raine 1993).Consequently, the poor impulse control and disruptivebehaviors exhibited by children with preschizophreniamay be related to their more stressful environments.
Of note is the somewhat higher rate of SPD in thestudy sample than that reported in other studies. In thecurrent study, 17.4 percent of the children of parents with
schizophrenia developed SPD. In the Roscommon FamilyStudy, Kendler et al. (1993) reported a lifetime prevalenceof 13.9 percent SPD in parents of children with schizo-phrenia. Among the first-degree relatives, the parent-childconcordance rate was twice that of sibling-siblingconcordance. In the provincial and national samples of theDanish Adoption Study of Schizophrenia (Kendler et al.1993), SPD was reported in 10.7 percent of first-degreerelatives of those with schizophrenia. Concordance ratesfor parent-child versus sibling-sibling concordance werenot distinguished. The concordance between schizophre-nia and SPD in the Copenhagen High-Risk Study is some-what higher than that in other studies. Several differencesbetween the current sample and other studies may explainthis difference in prevalence rates. First, the sample ischaracterized by offspring of mothers with severe schizo-phrenia. Only mothers who qualified as having severe ortypical schizophrenia in Europe and the United Stateswere selected. In 1962, these mothers had been hospital-ized for at least 5 years or had three separate hospitaliza-tions of at least 3 month's duration with no sign ofimprovement at discharge (Mednick and Schulsinger1968). Second, the concordance rate of SPD is based onparent-child concordance rather than sibling-sibling con-cordance. The latter concordance rates have been shownto be lower (Kendler et al. 1993). Third, there is a signifi-cant amount of assortive mating in the sample (Parnas1985). The high-risk subjects were more likely than thelow-risk (control) subjects to have a father with a schizo-phrenia-spectrum diagnosis. This factor increases geneticliability and the chance of developing schizophrenia-spec-trum disorders. Fourth, most of the subjects in this studyhad significant contact with their mothers with schizo-phrenia, unlike the adoptees in the Danish adoption study.Many of the children in the current study were reared inpublic institutions when the mother broke down. Thestress and instability in the environments of the offspringof parents with schizophrenia might account for thegreater prevalence of both schizophrenia and SPD in thesample, compared with adoption studies.
Advantages and Limitations. This study is potentiallyimportant for several reasons. First, this study is the first,to our knowledge, to examine behavior precursors of SPDbased on a sizable number of DSM-III-R diagnosedSPDs. Second, teacher ratings were made prospectively,before any of the subjects received a psychiatric diagno-sis. Although teachers might have been aware of parentalillnesses—an awareness that could potentially lead toincreased SPD scores in the high-risk group, the studyresults indicate that the SPD group scored at a higherlevel than even the high-risk NMI group. These findings
100
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/23/1/93/1880751 by guest on 25 January 2022

Childhood Behavior Precursors of Schizotypal Disorder Schizophrenia Bulletin, Vol. 23, No. 1, 1997
suggest that teacher ratings were fairly accurate, despitepossible biases. Third, the student characteristics wererated more than 30 years before the diagnosis, indicating acontinuity in the disorder.
There are some inherent limitations, however. First,the findings were constrained by items in the school reportquestionnaire. Because the questionnaire did not collectinformation relating to the more positive traits of SPD (e.g.,odd beliefs or magical thinking, odd behavior, odd speech,unusual perceptual experiences, and paranoia), this studycould not determine if precursors of these traits aredetectable before overt onset of the disorder. The predictivepower of the school report ratings may be limited if suchtraits have detectable early precursors. This limitationpoints to the need for further research that investigates early(preschool) analogs of the positive traits of SPD in futurelongitudinal research. The development of a childhoodmeasure tapping positive schizotypal traits would be essen-tial. Second, some nonschizotypal children had total SPDscores that would classify them as potential SPDs. Thislack of specificity indicates the need to delineate further theearly behaviors that may be more specific to preschizotypy,such as the more positive traits of SPD. Third, the SPDsample in this study is a high-risk group, a factor that maylimit the ability to generalize from the findings. Fourth, theuse of an ascertained sample in the factor analysis may biasthe total SPD score distribution. Future studies ideallyshould use an unselected general population. Finally, thelack of theoretical background in this area necessitated amore exploratory approach. The findings reported in thisstudy thus should be considered preliminary and call forreplication, preferably in a general population.
Conclusions
Precursors of schizotypy that are analogs of some of theadult symptomatology are identifiable in late childhood orearly adolescence. This finding could have potentiallyimportant implications: (1) Diagnostically, the existence ofchildhood precursors of SPD suggests that such precursorsmight be considered in future DSM criteria for SPD. (2)Childhood analogs of adult schizotypal symptoms indicatethat SPD does not develop suddenly in adulthood butrather has its roots in late childhood, or even earlier. Theearly signs of SPD suggest that genetic and/or environ-mental factors existing before school age play an impor-tant role in the development of this life-long disorder.
References
Achenbach, T.M., and Edelbrock, C. The classification of
child psychopathology: A review and analysis of empiri-cal efforts. Psychological Bulletin, 85:1275-1301,1978.
American Psychiatric Association. DSM-W: Diagnosticand Statistical Manual of Mental Disorders. 3rd ed.Washington, DC: The Association, 1980.
American Psychiatric Association. DSM-Hl-R: Diag-nostic and Statistical Manual of Mental Disorders. 3rded., revised. Washington, DC: The Association, 1987.
American Psychiatric Association. DSM-IV: Diagnosticand Statistical Manual of Mental Disorders. 4th ed.Washington, DC: The Association, 1994.
Asarnow, J.R.; Asarnow, R.F.; Hornstein, N.; and Russell,A. Childhood onset schizophrenia: Developmental per-spectives on schizophrenic disorders. In: Walker, E.F., ed.Schizophrenia: A Life Course Developmental Perspective.San Diego, CA: Academic Press, 1991. pp. 95-122.
Baron, M.; Gruen, R.; Asnis, L.; and Kane, J.M. Familialrelatedness of schizophrenic and schizotypal states.American Journal of Psychiatry, 140:1437-1442, 1983.
Bleuler, E. Dementia Praexox or the Group of Schizo-phrenias. (1911) Translated by J. Zinkin. New York, NY:International Universities Press, 1950.
Bollen, K.A. Structural Equation Modeling With LatentVariables. New York, NY: John Wiley & Sons, 1989.
Coombs, C.H.; Dawes, R.M.; and Tversky, A. Mathe-matical Psychology: An Elementary Introduction. Engle-wood Cliffs, NJ: Prentice-Hall, 1970.
Egan, J.P. Signal Detection Theory and ROC Analysis.New York, NY: Academic Press, 1975.
Endicott, J., and Spitzer, R. Current and past psycho-pathology scales (CAPPS). Archives of GeneralPsychiatry, 27:678-687, 1972.
Erlenmeyer-Kimling, L, and Cornblatt, B. The New YorkHigh-Risk Project: A followup report. SchizophreniaBulletin, 13(3):451^62,1987.
Goldstein, M.J. The UCLA High-Risk Project. Schizo-phrenia Bulletin, 13(3):505-514, 1987.
Goodman, S.H. Emory University Project on children ofdisturbed parents. Schizophrenia Bulletin, 13(3):411-423,1987.
Green, D.M., and Swets, J.A. Signal detection theory andpsychophysics. Huntington, NY: Drieger, 1966.
Hans, S.L.; Marcus, J.; Henson, L; Auerbach, J.G.; andMirsky, A.F. Interpersonal behavior of children at risk forschizophrenia. Psychiatry, 55:314-335, 1992.
Harman, H.H. Modern Factor Analysis. 3rd ed. Chicago,IL: University of Chicago Press, 1976.
Hochberg Y., and Tamhane, A.C. Multiple Comparison
101
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/23/1/93/1880751 by guest on 25 January 2022

Schizophrenia Bulletin, Vol. 23, No. 1, 1997 S.S. Ol inc ta l .
Procedures. New York, NY: John Wiley & Sons, 1987.
Hsiao, J.K.; Bartko, J.J.; and Potter, W.Z. Diagnosingdiagnoses. Archives of General Psychiatry, 44:664—668,1989.
Janes, C.L.; Weeks, D.G.; and Worland, J. School behav-ior in adolescent children of parents with mental disorder.Journal of Nervous and Mental Disease, 171:234-240,1983.
John, R.J.; Mednick, S.A.; and Schulsinger, F. Teacherreports as a predictor of schizophrenia and borderlineschizophrenia: A Bayesian decision analysis. Journal ofAbnormal Psychology, 91:399—413, 1982.
Kaiser, H.F. The varimax criterion for analytic rotation infactor analysis. Psychometrika, 23:187-200, 1958.
Kendler, K.S.; Gruenberg, A.M.; and Kinney, D.K.Independent diagnoses of adoptees and relatives asdefined by DSM-UI in the provincial and national sam-ples of the Danish Adoption Study of Schizophrenia.Archives of General Psychiatry, 51:456-468, 1994.
Kendler, K.S.; McGuire, M.; Gruenberg, A.M.; O'Hare,A.; Spellman, M.; and Walsh, D. The Roscommon FamilyStudy: III. Schizophrenia-related personality disorders inrelatives. Archives of General Psychiatry, 50:781-788,1993.
Kety, S.S. Schizophrenic illness in the families of schizo-phrenic adoptees: Findings from the Danish national sam-ple. Schizophrenia Bulletin, 14(2):217-222, 1988.
Kety, S.S.; Rosenthal, D.; Wender, P.H.; and Schulsinger,F. The types and prevalence of mental illness in the bio-logical and adoptive families of adopted schizophrenics.Journal of Psychiatric Research, 6:345-362, 1968.
Kety, S.S.; Rosenthal, D.; Wender, P.H.; Schulsinger, F;and Jacobsen, B. The biologic and adoptive families ofindividuals who became schizophrenic: Prevalence ofmental illness and other characteristics. In: Wynne, L.C.;Cromwell, R.L.; and Matthysse, S., eds. The Nature ofSchizophrenia. New York, NY: John Wiley & Sons, 1978.pp. 25-37.
Kohlberg, L.; Ricks, D.; and Snarey, J. Childhood devel-opment as a predictor of adaptation in adulthood. GeneticPsychology Monographs, 110:91-172, 1984.
Loranger , A.W.; Sussman , V.L.; Oldman, J .M.; andRussakoff, L.M. Personality Disorder Examination: AStructured Interview for Making Diagnosis of DSM-Ilf-RPersonality Disorders. White Plains, NY: Cornell MedicalCollege, 1985.
Marcus, J.; Hans, S.L.; Nagler, S.; Auerbach, J.G.;Mirsky, A.F.; and Aubrey, A. Review of the NIMH IsraeliKibbutz-City Study and the Jerusalem Infant
Development Study. Schizophrenia Bulletin, 13(3):425-438, 1987.
Mednick, S.A.; Parnas, J.; and Schulsinger, F. TheCopenhagen High-Risk Project, 1962-1986. Schizo-phrenia Bulletin, 13(3):485^t95, 1987.
Mednick, S.A., and Schulsinger, F. Some premorbid char-acteristics related to breakdown in children with schizo-phrenic mothers. Journal of Psychiatric Research,6:267-291, 1968.
Meehl, P.E. Schizotaxia, schizotypy, schizophrenia.American Psychologist, 17:827-838, 1962.
Meehl, P.E. Schizotaxia revisited. Archives of GeneralPsychiatry, 46:935-944, 1989.
Meehl, P.E. Toward an integrated theory of schizotaxia,schizotypy, and schizophrenia. Journal of PersonalityDisorders, 4:1-99, 1990.
Mossman, D., and Somoza, E. Maximizing diagnosticinformation from the dexamethasone suppression test.Archives of General Psychiatry, 46:653-660, 1989.
Norusis, M.J. SPSS-X Advanced Statistics Guide. 2nd ed.Chicago, IL: SPSS Inc., 1988.
Olin, S.S.; John, R.J.; and Mednick, S.A. Assessing thepredictive value of teacher reports in a high risk samplefor schizophrenia: An ROC analysis. SchizophreniaResearch, 16:53-66, 1995.
Parnas, J. Mates of schizophrenic mothers: A study ofassortive mating from the American-Danish High RiskProject. British Journal of Psychiatry, 146:490-497,1985.
Parnas, J.; Cannon, T.D.; Jacobsen, B.; Schulsinger, H.;Schulsinger, F; and Mednick, S.A. Lifetime DSM-III-Rdiagnostic outcomes in offspring of schizophrenic moth-ers: Results from the Copenhagen High-Risk Study.Archives of General Psychiatry, 50:707-714, 1993.
Raine, A. The Psychopathology of Crime: Criminal Be-havior as a Clinical Disorder. San Diego, CA: AcademicPress, 1993.
Sameroff, A.; Seifer, R.; Zax, M.; and Barocas, R. Earlyindicators of developmental risk: Rochester LongitudinalStudy. Schizophrenia Bulletin, 13(3):383-394, 1987.
Schulsinger, H. A ten-year follow-up of children of schiz-ophrenic mothers: Clinical assessment. Ada PsychiatricaScandinavica, 53:371-386, 1976.
Schwartzman, A.E.; Ledingham, J.E.; and Serbin, L.A.Identification of children at risk for adult schizophrenia: Alongitudinal study. International Review of AppliedPsychology, 34:363-380, 1985.
Spitzer, R.L., and Endicott, J. Schedule for Affective
102
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/23/1/93/1880751 by guest on 25 January 2022

Childhood Behavior Precursors of Schizotypal Disorder Schizophrenia Bulletin, Vol. 23, No. 1, 1997
Disorders and Schizophrenia—Lifetime Version. NewYork, NY: New York Psychiatric Institute, 1978.
Spitzer, R.L.; Endicott, J.; and Gibson, M. Crossing theborder into borderline personality and borderline schizo-phrenia: The development of criteria. Archives of GeneralPsychiatry, 36:17-24, 1979.
Squires-Wheeler, E.; Skodol, A.E.; and Erlenmeyer-Kimling, L. The assessment of schizotypal features overtwo points in time. Schizophrenia Research, 6:75-85,1992.
Swets, J.A., and Pickett, R.M. Evaluation of diagnosticsystems: Methods from signal detection theory. NewYork, NY: Academic Press, 1982.
Thurstone, L.L. Multiple Factor Analysis. Chicago, IL:University of Chicago Press, 1947.
Tienari, P.; Sorri, A.; Lahti, I.; Naarala, M.; Wahlberg,K.E.; Moring, J.; Pohjola, J.; and Wynne, L.C. Geneticand psychosocial factors in schizophrenia: The FinnishAdoptive Family Study. Schizophrenia Bulletin,13(3):477-484, 1987.
Watt, N.F. Longitudinal changes in the social behavior ofchildren hospitalized for schizophrenia as adults. Journalof Nervous and Mental Disease, 155:42—54, 1972.
Watt, N.F. Patterns of childhood social development inadult schizophrenics. Archives of General Psychiatry,35:160-165,1978.
Watt, N.F.; Grubb, T.W.; and Erlenmeyer-Kimling, L.Social, emotional, and intellectual behavior at schoolamong children at high risk for schizophrenia. Journal ofConsulting and Clinical Psychology, 50:171-181, 1982.
Watt, N.F., and Lubensky, A.W. Childhood roots of schiz-ophrenia. Journal of Consulting and Clinical Psychology,44:363-375, 1976.
Weintraub, S. Risk factors in schizophrenia: The StonyBrook High-Risk Project. Schizophrenia Bulletin,13(4):439^t50, 1987.
Wing, J.K.; Cooper, J.E.; and Sartorious, N. TheMeasurement and Classification of Psychiatric Symptoms.London, England: Cambridge University Press, 1974.
Acknowledgment
This research was supported by grants MH-46014 andMH-00619 to Dr. Sarnoff A. Mednick from the NationalInstitute of Mental Health.
The Authors
Su-chin Serene Olin, M.A., is Senior Research Assistant,Department of Psychology and the Social ScienceResearch Institute, University of Southern California, LosAngeles, CA; Adrian Raine, D.Phil., is Professor,Departments of Psychology and Psychiatry and the SocialScience Research Institute, University of SouthernCalifornia, Los Angeles, CA; Tyrone D. Cannon, M.D., isAssistant Professor, Departments of Psychology andPsychiatry, University of Pennsylvania, Philadelphia, PA;Josef Parnas, M.D., is Associate Director, Department ofPsychiatry, Hvidovre University, and Associate Professor,Department of Psychiatry, University of Copenhagen,Denmark; Fini Schulsinger, M.D., is Professor,Department of Psychiatry, University of Copenhagen,Denmark; Sarnoff A. Mednick, Ph.D., is Professor,Department of Psychology and the Social ScienceResearch Institute, University of Southern California, andis on the Board of Directors at the Institute for PreventiveMedicine, Copenhagen Health Services, Denmark.
103
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/23/1/93/1880751 by guest on 25 January 2022




















