Charged particle therapy for cancer: The inheritance of the Cavendish scientists
7
Charged particle therapy for cancer: The inheritance of the Cavendish scientists? Bleddyn Jones a, , Roger G. Dale b , Alejandro Ca ´ rabe-Ferna ´ ndez b a Department of Clinical Oncology, Queen Elizabeth University Hospital, University Hospitals NHS Trust, Birmingham University, Edgbaston, Birmingham B15 2TH, UK b Department of Radiation Physics and Radiobiology, Imperial College Healthcare NHS Trust, Charing Cross Hospital, London W6 8RF, UK abstract The history of developments in atomic physics and its applications follows the decisive input provided by Maxwell and subsequent discoveries by his successors at the Cavendish Laboratory. In medicine the potential applications of particle physics (with the notable exception of the electron) were unfortunately delayed by the disappointing experiences with neutron therapy, which produced long- term scepticism. Neutrons are not appropriate for cancer therapy because not only their physical dose distributions offer no advantages over X-rays, but also their biological dose distributions are worse. The much improved dose distributions achieved with charged particles offer real prospects for better treatment outcomes because of the large reduction in the volume of unnecessarily irradiated tissue in many situations. Charged particle therapy is relatively new and can be applied with increasing confidence due to advances in radiology and computing, but at present there are insufficient numbers of treatment facilities to produce statistically powerful studies to compare treatment outcomes with those of X-rays. Considerable progress has been achieved in Japan and Germany with pilot studies of carbon ions but their efficacy compared with protons needs to be tested: in theory carbon should be better for intrinsically radio-resistant and for the most hypoxic tumours. The optimisation of proton and ion beam therapy in clinical practice remains to be achieved, but there are good scientific reasons why these modalities will be preferred by patients and their physicians in the future. Regrettably, despite hosting many of the momentous discoveries that enabled the development of charged particle therapy, the UK is slow to adopt and implement this very important form of cancer treatment. & 2008 Elsevier Ltd. All rights reserved. 1. Introduction The prodigious physicist James Clerk Maxwell (1831–1879) not only created the mathematical framework that linked electricity and magnetism in the concept of electromagnetic waves that were compatible with the data of Faraday, but was also responsible for advances in colour theory, dimensional analysis and the formation of the National Physical Laboratory in the UK (Mahon, 2004). His last achievement was the establishment of The Cavendish Laboratory in Cambridge. Sadly, he died of abdominal cancer at the age of 48, as had his mother (perhaps indicating deterministic aspects of cancer induction in susceptible individuals due to an inherited tumour suppressor gene). He was succeeded at The Cavendish by another Scottish genius, JJ Thomson, who discovered the electron, followed by Rutherford, who had identified the alpha particle and later coined the term ‘proton’. Chadwick later identified the neutron, a discovery that ultimately allowed the manufacture of the A-bomb (Brown, 1997). The interest in X-ray crystallography initially provided by the Bragg family members— as well as the discovery of the Bragg peak for charged particle dose distribution using radium emissions (Brown and Suit, 2004)—ultimately lead to the identification of the DNA structure by Crick and Watson at The Cavendish and the emergence of the scientific discipline of molecular biology (Wilkins, 2003). This new discipline has used many techniques originally pioneered in physics laboratories to greatly improve our understanding of the deranged chemistry of the cancer cell and provide novel diagnostic and therapeutic methods. 2. Improved technology in physics In X-ray based radiotherapy, the evolutionary sequence towards more powerful X-ray generators followed from conven- tional cathode ray tube designs (from 50–300 kV) through Van der Graff accelerators to cobalt-60 teletherapy using g ray energies that exceeded a megavolt and radio-frequency acceleration in megavoltage linear accelerators. At present, most radiotherapy is given using X-rays in the 6–10MV range. Each development ARTICLE IN PRESS Contents lists available at ScienceDirect journal homepage: www.elsevier.com/locate/apradiso Applied Radiation and Isotopes 0969-8043/$ - see front matter & 2008 Elsevier Ltd. All rights reserved. doi:10.1016/j.apradiso.2008.06.027 Corresponding author. E-mail address: [email protected] (B. Jones). Applied Radiation and Isotopes 67 (2009) 371–377
Transcript of Charged particle therapy for cancer: The inheritance of the Cavendish scientists

ARTICLE IN PRESS
Applied Radiation and Isotopes 67 (2009) 371–377
Contents lists available at ScienceDirect
Applied Radiation and Isotopes
0969-80
doi:10.1
� Corr
E-m
journal homepage: www.elsevier.com/locate/apradiso
Charged particle therapy for cancer: The inheritance of theCavendish scientists?
Bleddyn Jones a,�, Roger G. Dale b, Alejandro Carabe-Fernandez b
a Department of Clinical Oncology, Queen Elizabeth University Hospital, University Hospitals NHS Trust, Birmingham University, Edgbaston, Birmingham B15 2TH, UKb Department of Radiation Physics and Radiobiology, Imperial College Healthcare NHS Trust, Charing Cross Hospital, London W6 8RF, UK
43/$ - see front matter & 2008 Elsevier Ltd. A
016/j.apradiso.2008.06.027
esponding author.
ail address: [email protected] (B. Jones).
a b s t r a c t
The history of developments in atomic physics and its applications follows the decisive input provided
by Maxwell and subsequent discoveries by his successors at the Cavendish Laboratory. In medicine the
potential applications of particle physics (with the notable exception of the electron) were
unfortunately delayed by the disappointing experiences with neutron therapy, which produced long-
term scepticism. Neutrons are not appropriate for cancer therapy because not only their physical dose
distributions offer no advantages over X-rays, but also their biological dose distributions are worse. The
much improved dose distributions achieved with charged particles offer real prospects for better
treatment outcomes because of the large reduction in the volume of unnecessarily irradiated tissue in
many situations. Charged particle therapy is relatively new and can be applied with increasing
confidence due to advances in radiology and computing, but at present there are insufficient numbers of
treatment facilities to produce statistically powerful studies to compare treatment outcomes with those
of X-rays. Considerable progress has been achieved in Japan and Germany with pilot studies of carbon
ions but their efficacy compared with protons needs to be tested: in theory carbon should be better for
intrinsically radio-resistant and for the most hypoxic tumours. The optimisation of proton and ion beam
therapy in clinical practice remains to be achieved, but there are good scientific reasons why these
modalities will be preferred by patients and their physicians in the future. Regrettably, despite hosting
many of the momentous discoveries that enabled the development of charged particle therapy, the UK is
slow to adopt and implement this very important form of cancer treatment.
& 2008 Elsevier Ltd. All rights reserved.
1. Introduction
The prodigious physicist James Clerk Maxwell (1831–1879) notonly created the mathematical framework that linked electricityand magnetism in the concept of electromagnetic waves that werecompatible with the data of Faraday, but was also responsible foradvances in colour theory, dimensional analysis and the formationof the National Physical Laboratory in the UK (Mahon, 2004). Hislast achievement was the establishment of The CavendishLaboratory in Cambridge. Sadly, he died of abdominal cancer atthe age of 48, as had his mother (perhaps indicating deterministicaspects of cancer induction in susceptible individuals due to aninherited tumour suppressor gene). He was succeeded at TheCavendish by another Scottish genius, JJ Thomson, who discoveredthe electron, followed by Rutherford, who had identified the alphaparticle and later coined the term ‘proton’. Chadwick lateridentified the neutron, a discovery that ultimately allowed themanufacture of the A-bomb (Brown, 1997). The interest in X-ray
ll rights reserved.
crystallography initially provided by the Bragg family members—
as well as the discovery of the Bragg peak for charged particledose distribution using radium emissions (Brown and Suit,2004)—ultimately lead to the identification of the DNA structureby Crick and Watson at The Cavendish and the emergence of thescientific discipline of molecular biology (Wilkins, 2003). Thisnew discipline has used many techniques originally pioneered inphysics laboratories to greatly improve our understanding ofthe deranged chemistry of the cancer cell and provide noveldiagnostic and therapeutic methods.
2. Improved technology in physics
In X-ray based radiotherapy, the evolutionary sequencetowards more powerful X-ray generators followed from conven-tional cathode ray tube designs (from 50–300 kV) through Van derGraff accelerators to cobalt-60 teletherapy using g ray energiesthat exceeded a megavolt and radio-frequency acceleration inmegavoltage linear accelerators. At present, most radiotherapy isgiven using X-rays in the 6–10 MV range. Each development

ARTICLE IN PRESS
B. Jones et al. / Applied Radiation and Isotopes 67 (2009) 371–377372
allowed successively improved dose deposition with increasingtissue depth and, at megavoltage energies, the importantachievement of ‘skin sparing’, or reduced superficial tissues doses,as a consequence of the ‘build-up’ of secondary electronequilibrium in the direction of the beam. Improvements inradiotherapy outcomes were noted with each technical advance,although not assessed by randomised clinical trials in mostinstances.
The acceleration of nuclear particles to high energies requiredfor advanced nuclear physics research was achieved with theadvent of cyclotrons and later by synchrotrons. With suchequipment, accelerated protons could be used to bombard aberyllium target, releasing neutrons of sufficient energy to treattumours at modest tissue depths. Much larger cyclotrons werenecessary for proton therapy and there was also a dilemmaregarding whereabouts in the patient to position the Bragg peaksdue to the inadequacies of tumour imaging around 50 years agoand until recent times; the improved tissue definition and 3-Dinformation provided by modern medical imaging has entirelycircumvented this problem.
2.1. Radiobiology suggests new treatment approaches
The neutron aroused interest for clinical use because not onlyrelatively small-sized cyclotrons (using modest proton energies)were required, but also the particles demonstrated interestingbiological properties in terms of their higher cell-killing efficiency.Such a difference can be quantified by the relative biological effect(RBE), which is the ratio of the doses of X-rays and neutronsrequired to produce the same biological effect. Fast neutron RBEvalues of 1.5–5 were found in a variety of biological systemsranging from bacteria and plants to transplanted animal cancers.The immediate inference was that neutrons would be suitable forcancer therapy, yet the first human cancer treatments in the USAwere associated with marked normal tissue toxicity, largelybecause the relevant radiobiology had not been thoroughlyinvestigated.
Further interest arose because of the discovery that radiationswith a high linear energy transfer (LET), such as fast neutrons withincreased ionization events along micrometer distances of theirtracks, are less dependent than X-rays on the presence of oxygento produce cell death. It became clear that many cancerscontained zones of very low oxygen tension, which wereconsidered an important cause of radio-resistance and treatmentfailure. To overcome this problem, high pressure oxygen (HPO)was used in experimental radiotherapy (Gray et al., 1953), but thisproved difficult to administer in the clinic as patients had to beplaced for long durations within HPO tanks and also carriedtechnical disadvantages such as a reduced choice of angular beamarrangements. One attractive alternative to HPO was the usecyclotrons to accelerate protons onto beryllium targets to producefast neutrons of 7–10 MeV (Catterall and Bewley, 1979), but withpoor tissue penetration.
2.2. Differences between X-rays, neutrons and charged particles
Neutrons-like the X-rays used in conventional radiotherapy-pass through the entire thickness of body structures and weredisappointing in clinical applications: this was almost certainlydue to the high RBE delivered to large volumes of tissue. Incontrast, charged particles deposit energy mostly within Braggpeaks, so that accelerated protons and ions can be used toselectively target a deeply situated cancer. Compared with un-charged X-rays (or neutrons), protons deposit between one-half toa tenth of the same radiation energy to the body (Jones, 2006a).
Sharper Bragg peaks and even better dose distributions are foundwith carbon ions and the RBE values in regions exposed to thepeaks are higher than those for protons and are similar to those offast neutrons. This could be an advantage for tumour control but adisadvantage if the peaks were to be misplaced on to excessivevolumes of normal tissues, hence the need for careful positioningof the treatment.
Because of the improved dose distributions, chargedparticle therapy (CPT), from initial experience, allows saferradiotherapy with reduced treatment-related side effects in awide range of tissues; also the option of cancer dose escalation toincrease the cure probability where possible; also there areadvantages in terms of being able to use concurrent or adjuvantcytotoxic chemotherapy regimens more safely since less normalbone marrow is irradiated. In younger patients, there is asubstantial reduction in the risk estimates for radiation-inducedcancer; in older patients there is less risk of causing additionalmorbidities.
2.3. The British and American neutron studies
The UK MRC substantially funded three important projects thatinvestigated neutron therapy. Firstly, at Hammersmith, clinicalstudies, backed by meticulous physics, were conducted withinitial promise (Catterall and Bewley, 1979). But despite the clearevidence obtained there (in a wide variety of animal tissues) thatthe neutron RBE was inversely related to dose per fraction, theclinical dose prescriptions used a fixed RBE, which took noaccount of the increase in RBE in normal tissues that receivedlower doses. Attempts at randomised trials involved controlpatients treated with X-rays or Cobalt beams at other hospitalsusing a wide range of doses. In summary, this experiencegenerated knowledge on how to conduct multi-centre cancertrials with greater rigour (Medical Research Council NeutronTherapy Working Group, 1986). Secondly, at Edinburgh, stricter in-house randomized trials comparing megavoltage X-rays and fastneutrons were carried out, with the advantage that the neutronbeams could be rotated on a gantry. However, the tumour controlrates were disappointing and were accompanied by enhancednormal tissue toxicity, although the dose per treatment used waslower than at Hammersmith (Duncan, 1994). Thirdly, at Clatter-bridge (Liverpool), an extended fast neutron energy (obtainedusing 64-MeV protons) produced depth doses equivalent to5-MeV X-rays in randomized trials, some of which were jointlyundertaken with Seattle (USA) (Errington et al., 1991; Maoret al., 1995) using the Hammersmith fractionation. These trialsshowed that neutrons conferred no clinical advantage. In othercountries, relatively low-energy neutrons had been tried withoutrecourse to formal trials and with little convincing success,although one small trial in Seattle showed that neutron therapyconferred benefit in the control of adenoid-cystic cancers of theparotid gland; but it is possible that a higher dose of X-rays orelectrons in the control arm might have produced the same result(Laramore et al., 1993). Relatively superficial air sinus cancerswere also thought to be better controlled, although there wasalways concern that neutrons were particularly damaging thetissues of the underlying brain, where it had been identified inbrain tumour trials that the RBE was probably around 5 ratherthan 3 (Laramore, 1990).
In retrospect, it is perhaps easy to see what went wrong:
�
More bio-physics studies would have sooner detected thehigher neutron energy released in hydrogen rich tissues suchas white matter in the brain and body fat (which exists invariable amounts around most important organs and is closely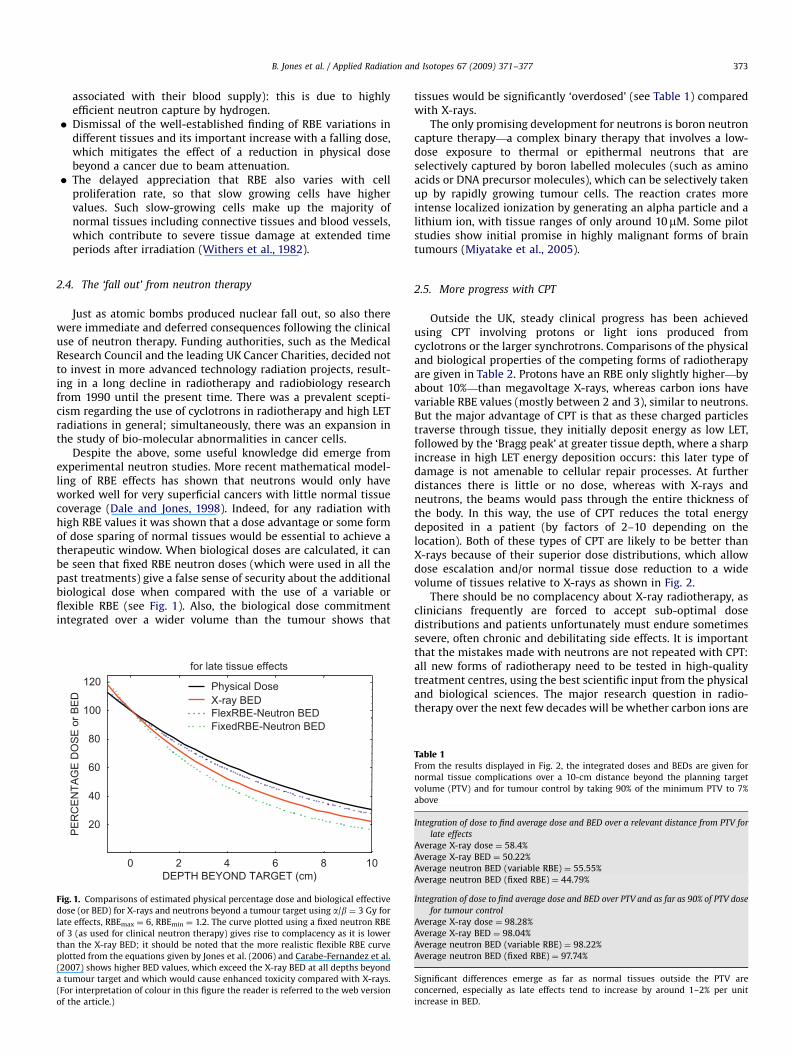
ARTICLE IN PRESS
Figdos
late
of 3
tha
plo
(20
a tu
(Fo
of t
B. Jones et al. / Applied Radiation and Isotopes 67 (2009) 371–377 373
associated with their blood supply): this is due to highlyefficient neutron capture by hydrogen.
� Dismissal of the well-established finding of RBE variations indifferent tissues and its important increase with a falling dose,which mitigates the effect of a reduction in physical dosebeyond a cancer due to beam attenuation.
� The delayed appreciation that RBE also varies with cellproliferation rate, so that slow growing cells have highervalues. Such slow-growing cells make up the majority ofnormal tissues including connective tissues and blood vessels,which contribute to severe tissue damage at extended timeperiods after irradiation (Withers et al., 1982).
2.4. The ‘fall out’ from neutron therapy
Just as atomic bombs produced nuclear fall out, so also therewere immediate and deferred consequences following the clinicaluse of neutron therapy. Funding authorities, such as the MedicalResearch Council and the leading UK Cancer Charities, decided notto invest in more advanced technology radiation projects, result-ing in a long decline in radiotherapy and radiobiology researchfrom 1990 until the present time. There was a prevalent scepti-cism regarding the use of cyclotrons in radiotherapy and high LETradiations in general; simultaneously, there was an expansion inthe study of bio-molecular abnormalities in cancer cells.
Despite the above, some useful knowledge did emerge fromexperimental neutron studies. More recent mathematical model-ling of RBE effects has shown that neutrons would only haveworked well for very superficial cancers with little normal tissuecoverage (Dale and Jones, 1998). Indeed, for any radiation withhigh RBE values it was shown that a dose advantage or some formof dose sparing of normal tissues would be essential to achieve atherapeutic window. When biological doses are calculated, it canbe seen that fixed RBE neutron doses (which were used in all thepast treatments) give a false sense of security about the additionalbiological dose when compared with the use of a variable orflexible RBE (see Fig. 1). Also, the biological dose commitmentintegrated over a wider volume than the tumour shows that
0 2 4 6 8 10
PE
RC
EN
TAG
E D
OS
E o
r BE
D
20
40
60
80
100
120
FixedRBE-Neutron BEDFlexRBE-Neutron BEDX-ray BEDPhysical Dose
DEPTH BEYOND TARGET (cm)
for late tissue effects
. 1. Comparisons of estimated physical percentage dose and biological effective
e (or BED) for X-rays and neutrons beyond a tumour target using a/b ¼ 3 Gy for
effects, RBEmax ¼ 6, RBEmin ¼ 1.2. The curve plotted using a fixed neutron RBE
(as used for clinical neutron therapy) gives rise to complacency as it is lower
n the X-ray BED; it should be noted that the more realistic flexible RBE curve
tted from the equations given by Jones et al. (2006) and Carabe-Fernandez et al.
07) shows higher BED values, which exceed the X-ray BED at all depths beyond
mour target and which would cause enhanced toxicity compared with X-rays.
r interpretation of colour in this figure the reader is referred to the web version
he article.)
tissues would be significantly ‘overdosed’ (see Table 1) comparedwith X-rays.
The only promising development for neutrons is boron neutroncapture therapy—a complex binary therapy that involves a low-dose exposure to thermal or epithermal neutrons that areselectively captured by boron labelled molecules (such as aminoacids or DNA precursor molecules), which can be selectively takenup by rapidly growing tumour cells. The reaction crates moreintense localized ionization by generating an alpha particle and alithium ion, with tissue ranges of only around 10mM. Some pilotstudies show initial promise in highly malignant forms of braintumours (Miyatake et al., 2005).
2.5. More progress with CPT
Outside the UK, steady clinical progress has been achievedusing CPT involving protons or light ions produced fromcyclotrons or the larger synchrotrons. Comparisons of the physicaland biological properties of the competing forms of radiotherapyare given in Table 2. Protons have an RBE only slightly higher—byabout 10%—than megavoltage X-rays, whereas carbon ions havevariable RBE values (mostly between 2 and 3), similar to neutrons.But the major advantage of CPT is that as these charged particlestraverse through tissue, they initially deposit energy as low LET,followed by the ‘Bragg peak’ at greater tissue depth, where a sharpincrease in high LET energy deposition occurs: this later type ofdamage is not amenable to cellular repair processes. At furtherdistances there is little or no dose, whereas with X-rays andneutrons, the beams would pass through the entire thickness ofthe body. In this way, the use of CPT reduces the total energydeposited in a patient (by factors of 2–10 depending on thelocation). Both of these types of CPT are likely to be better thanX-rays because of their superior dose distributions, which allowdose escalation and/or normal tissue dose reduction to a widevolume of tissues relative to X-rays as shown in Fig. 2.
There should be no complacency about X-ray radiotherapy, asclinicians frequently are forced to accept sub-optimal dosedistributions and patients unfortunately must endure sometimessevere, often chronic and debilitating side effects. It is importantthat the mistakes made with neutrons are not repeated with CPT:all new forms of radiotherapy need to be tested in high-qualitytreatment centres, using the best scientific input from the physicaland biological sciences. The major research question in radio-therapy over the next few decades will be whether carbon ions are
Table 1From the results displayed in Fig. 2, the integrated doses and BEDs are given for
normal tissue complications over a 10-cm distance beyond the planning target
volume (PTV) and for tumour control by taking 90% of the minimum PTV to 7%
above
Integration of dose to find average dose and BED over a relevant distance from PTV for
late effects
Average X-ray dose ¼ 58.4%
Average X-ray BED ¼ 50.22%
Average neutron BED (variable RBE) ¼ 55.55%
Average neutron BED (fixed RBE) ¼ 44.79%
Integration of dose to find average dose and BED over PTV and as far as 90% of PTV dose
for tumour control
Average X-ray dose ¼ 98.28%
Average X-ray BED ¼ 98.04%
Average neutron BED (variable RBE) ¼ 98.22%
Average neutron BED (fixed RBE) ¼ 97.74%
Significant differences emerge as far as normal tissues outside the PTV are
concerned, especially as late effects tend to increase by around 1–2% per unit
increase in BED.

ARTICLE IN PRESS
Table 2Comparative aspects of different therapeutic beams in medicine
X-ray Neutron Proton Helium ion Carbon ion
Attenuation with depth Pseudo-exponential Pseudo-exponential Bragg peaka Bragg peakb Bragg peakc
Integral biological dose High Highest Low Lower Lowest
Average RBE 1 3 1.1 1.4 3
Oxygen modification factor 2.5 1.6–1.8 2.4 2.3 1.7
abcRefer to Bragg peak height where c4b4a.
40
80
60 150
50
1500
042
64
84
150150
Fig. 2. Schematic dose distributions for X-rays/neutrons compared with protons
and ions. In each case, the assumed high LET (neutron or ion) radiation dose is
indicated by the bolder typed numbers. The absence of exit dose beyond the black
circular cancer target reduces collateral radiation damage and this will have
several advantages including reduced side effects during and after therapy,
reduced interference with growth and development, better tissue function, a
reduced risk of radiation induced malignancies and more reasonable possibilities
of further treatment if required for other cancers that could arise at later times in
‘low-dose’ or ‘no-dose’ regions. (For interpretation of colour in this figure the
reader is referred to the web version of the article.)
B. Jones et al. / Applied Radiation and Isotopes 67 (2009) 371–377374
superior to protons in specific forms of cancer and how best tointegrate these treatments with the best available molecular-based therapies.
It must be stressed that the dose distribution advantages forCPT discussed above do not equally apply to the newer externalbeam X-ray techniques such as conformal radiotherapy (wherebeams are better shaped) and intensity-modulated radiotherapy,where the beam fluence is considerably modified. IMRT essen-tially leads to a transfer of the same total energy to differentpositions in the body rather than to a wholesale reduction. Forexample, in head and neck cancer, transfer of dose from theparotid gland (to avoid the complication of a dry mouth) to otherareas in the neck such as the carotid arteries, which supply themain source of oxygenated blood to the brain, could result inenhanced risks of stroke. With CPT, such effects are probably moreavoidable since the total energy deposition is smaller.
The UK neutron experience did provide experimental andclinical data, which is now proving useful in the context ofassessing CPT, particularly in the modelling of the radiobiologyassociated with particle therapy: equations have been developedin the UK for the prediction of particle therapy effects in tumoursand normal tissues. It is paradoxical that if an accelerator breaksdown in Japan or Germany, or if a patient defaults from iontherapy for any reason, then British advice on how to correct thedose can be used (Jones and Dale, 2000; Carabe-Fernandez et al.,2007; Jones et al., 2006). Protons and helium ions have a low RBEclose to that of X-rays; the heavier ions such as carbon have RBEvalues close to fast neutrons. There are also opportunities to
explore if ions of intermediate mass between the proton and acarbon ion, such as helium, offer a better solution in specialcircumstances, since the Bragg peak geometry is intermediatebut the RBE increment is relatively small. It is also anticipated thatthe treatment indications will increase with time: this is aconsequence of the fact that only rare forms of cancers wereinitially treated by protons and ions due to restricted access toaccelerators with relatively low particle energies using fixedposition beams; more recently, the increased use of well-designedhospital-based centres with 3601 rotational gantries allowsmuch better opportunities for treating deep seated or awkwardlyplaced cancers.
The treatment of cancer is likely to be very different in adecade or two from now. Improved early cancer diagnosis by non-invasive methods will allow treatment by proton and ion beams ina few (or even single) exposures, with very low collateral radiationdoses to surrounding normal tissues and minimal side effects.Consequently, the need for complex radical surgery, expensiveadjuvant treatments and prolonged palliative care would besharply reduced; also smaller complication probabilities shouldlead to improved quality of life in cured patients.
The UK, for a variety of reasons, presently lags behind othercountries in the procurement of particle therapy facilities, despiteestablishing the first hospital-based proton therapy facility in theworld in 1990 at Clatterbridge. There, the Douglas cyclotron iscapable of treating only as far as the retina of the eye, but has doneso with great success: around 97% local control and a high eye andvisual retention rate (Jones, 2006a). There are already five largefunctioning proton centres in the USA and nearly all the AmericanUniversity Hospitals have advanced business plans or have signedcontracts for such centres, each capable of treating between 400and 3000 patients per year. Japan already has eight workingcentres and Switzerland, France and Germany each have one. Fivemore are being built in Germany (with plans for 20 more), Franceintends to have four centres, Italy three and one each in Austriaand Sweden. The present UK position would be intolerable toMaxwell—a cancer sufferer—and all his scientific followers, whowould have far preferred peaceful applications of their discoveriesin health care rather than in weapons of mass destruction. Thesubsequent careers of Chadwick and other physicists werecertainly coloured by their involvement in the development ofnuclear weapons (Brown, 1997; Frisch, 1979).
2.6. The present UK position
It has taken a long time to persuade the medical establishmentthat the dose distribution advantages of proton therapy may bevery advantageous. The limited published evidence base forimprovements in treatment outcomes exist only for certain rarecancers such as chordomas and sarcomas of the skull base andspine and rare forms of cancer in children.
The recent acknowledgement in the Department of Health’sNational Radiotherapy Advisory Group (NRAG) that at leastone Proton Therapy Centre should be established in England

ARTICLE IN PRESS
Fig. 3. Proton therapy dose distributions for an inoperable meningioma because of
attachment to the cavernous sinus behind the orbit (courtesy of Dr. N.J. Liebsch,
Massachusetts General Hospital). (For interpretation of colour in this figure the
reader is referred to the web version of the article.)
Fig. 4. Proton beam dose plan for a prostate cancer patient with two metal hip
prosthesis achieved at the University Hospital Birmingham using CMS software. A
single anterior field is used here for teaching purposes; further improvements can
be made by the use of a posterior beam or anterior oblique fields. X-ray treatment
dose calculations would be complicated by beam attenuation due to the metal and
by some backscattered radiation, thus leading to unreliable dose distributions
(courtesy of Drs L. Kadiri and S. Green). (For interpretation of colour in this figure
the reader is referred to the web version of the article.)
B. Jones et al. / Applied Radiation and Isotopes 67 (2009) 371–377 375
was a major advance in intent. Although this report probablyunderestimates the eventually anticipated need, it reflects theconcern that the UK has lagged behind other advanced countriesin adopting new technology in medicine and responds to the self-evident threat that many patients may soon prefer to travelabroad for their radiotherapy (Jones, 2006a), which could causepolitical concern if numbers become excessive.
Following public release of the NRAG report (available on theDepartment of Health website), three publications (Lodge et al.,2007; Brada et al., 2007; Olsen et al., 2007) have collated themedical literature and concluded that there is little in the way of aformal medical evidence base for neutron, proton and ion beams,although it is admitted that further research is necessary. Thesepapers represent the conventional wisdom in medicine wherehigh-grade evidence is required for unequivocal proof: the top ofthe scale is represented by large randomised trials, whileanecdotal evidence is at the bottom. Some commentators areprobably not aware of the fact that most proton treatments forskull base tumours have been preceded by many unsuccessfulsurgical attempts or are inoperable; also within the eye, not alltumours are suitable for alternative radioactive plaque therapysince the depth doses achieved from plaques will not coverthe larger tumours and the precise position within the eye(e.g. proximity to optic nerve and macula) can also be acontraindication to plaque therapy. Thus so much patientselection has gone into the proton and plaque studiesthat treatment has been successfully optimised in each case,but the classes of tumour in each are quite different. Anyliterature comparisons are therefore naive attempts to deter-mine a meaningful comparison and must be judged scientifi-cally unsound. Future comparisons between CPT and X-raysmight be more relevant in 5–10 years from now aftersufficient technical development, expansion in the criticalmass of centres that can perform CPT and to allow long-termfollow-up studies of quality of life combined with cure as a singleend point in cancer patients (Jones, 2006b). Most authors havestressed that considerable research is necessary to optimiseparticle therapy in the future (Jones, 2006a; Lodge et al., 2007;Brada et al., 2007; Olsen et al., 2007; Jones, 2006b; Glimeliusand Montelius, 2007; Jones and Burnett, 2005; Taylor, 2006; Joneset al., 2007).
Sufficient clinical research has been performed using fastneutrons and negative conclusions reached (Duncan, 1994);indeed, there is no need to attempt further comparisons. Forprotons, most treatments have involved treatments at physicslaboratories with relatively low energy, horizontal beams, inter-mittent beam availability, compromised fractionation and arestriction to certain rare classes of tumours that were thoughtto be radioresistant and patients who had failed previous surgery(frequently on multiple occasions). The advent of hospital-basedproton services began in the UK in 1990; rotational gantries weredeveloped in Loma Linda University Hospital around 1996followed by Massachussets General around 2000. The experi-mental Tzukuba proton facility in Japan had two gantries in 2001and later developed planning software with dose volumehistograms for proton therapy in Japan. Consequently, it is quiteunscientific to compare the results of the pioneering protontherapies with X-ray data collated in 2006. Strong criticisms of ionbeam therapy are also questionable as there has only been limitedbut meticulously conducted phase I/II studies at Chiba in Japanand a much smaller experience at Darmstadt in Germany. The firstrotational ion beam gantry will only be available in Heidelberg in2008. So, it is quite premature to make detailed comparisons withbest available X-ray treatments.
The conventional approach to medical evidence base isstructured on drug development, which is financially backed by
the drug industry. By using large (often around 3000 patients pertrial) randomised studies that frequently show marginal improve-ments, drug companies can persuade governments to fund theirproducts. A similarly rich industrial base does not exist for particletherapy, so it will be necessary for governments to fund co-operative international trials to provide sufficient data. Thequandary as to whether such trials are necessary and the diffi-culties of randomisation (Glimelius and Montelius, 2007) can beanswered by the fact that the capacity for CPT will be lower thanthe demand for the foreseeable future, so randomisation may bevery appropriate as long as ethical standards are not compromised.
ARTICLE IN PRESS
B. Jones et al. / Applied Radiation and Isotopes 67 (2009) 371–377376
So far it would appear reasonable to expect that the benefits ofcharged particle radiotherapy will be in the following situations:
�
FigHos
use
tion
Figto t
give
Tumours that are well delineated on imaging and that arerelatively radio-resistant, with a low chance of more distantspread.
� Children and younger adult patients: to allow better develop-ment and reduce the risk of radiation induced carcinogenesis.
� To spare CNS tissue/other sensitive organs where cancersare situated in close proximity and are judged inoperable(see Fig. 3).
� To treat cancers in anatomical sites situated close to areas thathave been previously irradiated to high dose (see Fig. 2).
. 5. Single proton beam dose plan for a breast cancer achieved at University
pital Birmingham. It can be seen that opposed tangential breast fields (as are
d conventionally) would cause unnecessary cardiac irradiation. (For interpreta-
of colour in this figure the reader is referred to the web version of the article.)
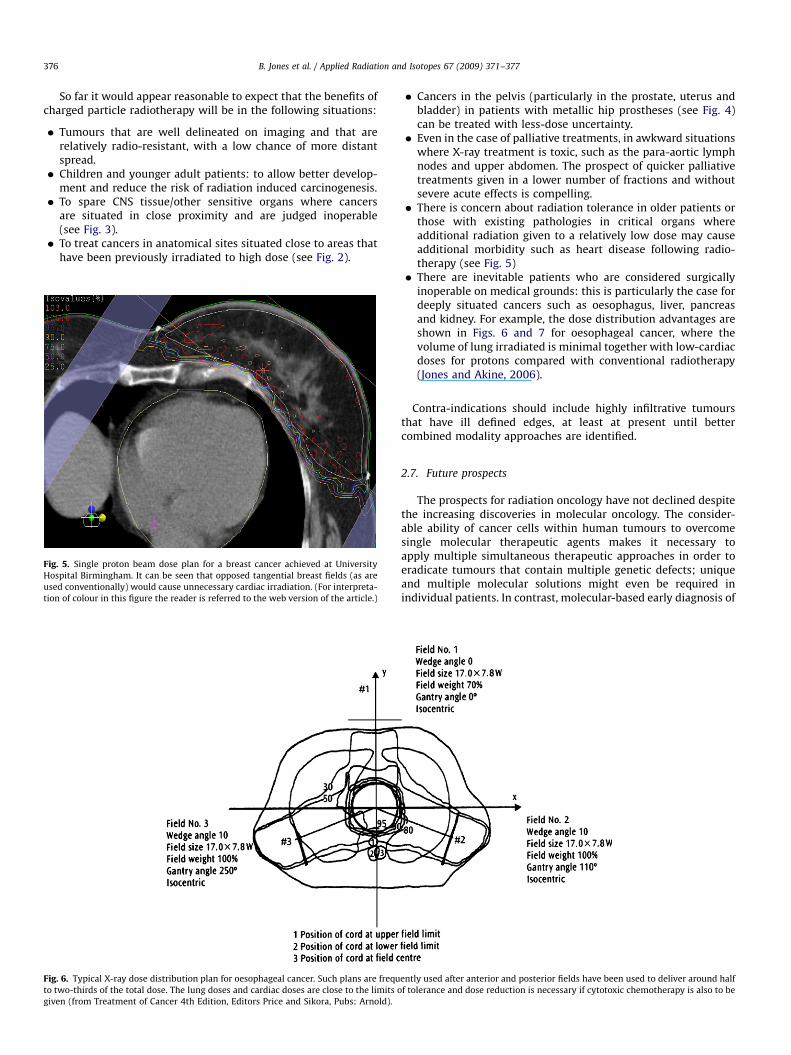
. 6. Typical X-ray dose distribution plan for oesophageal cancer. Such plans are frequ
wo-thirds of the total dose. The lung doses and cardiac doses are close to the limits o
n (from Treatment of Cancer 4th Edition, Editors Price and Sikora, Pubs: Arnold).
�
entl
f to
Cancers in the pelvis (particularly in the prostate, uterus andbladder) in patients with metallic hip prostheses (see Fig. 4)can be treated with less-dose uncertainty.
� Even in the case of palliative treatments, in awkward situationswhere X-ray treatment is toxic, such as the para-aortic lymphnodes and upper abdomen. The prospect of quicker palliativetreatments given in a lower number of fractions and withoutsevere acute effects is compelling.
� There is concern about radiation tolerance in older patients orthose with existing pathologies in critical organs whereadditional radiation given to a relatively low dose may causeadditional morbidity such as heart disease following radio-therapy (see Fig. 5)
� There are inevitable patients who are considered surgicallyinoperable on medical grounds: this is particularly the case fordeeply situated cancers such as oesophagus, liver, pancreasand kidney. For example, the dose distribution advantages areshown in Figs. 6 and 7 for oesophageal cancer, where thevolume of lung irradiated is minimal together with low-cardiacdoses for protons compared with conventional radiotherapy(Jones and Akine, 2006).
Contra-indications should include highly infiltrative tumoursthat have ill defined edges, at least at present until bettercombined modality approaches are identified.
2.7. Future prospects
The prospects for radiation oncology have not declined despitethe increasing discoveries in molecular oncology. The consider-able ability of cancer cells within human tumours to overcomesingle molecular therapeutic agents makes it necessary toapply multiple simultaneous therapeutic approaches in order toeradicate tumours that contain multiple genetic defects; uniqueand multiple molecular solutions might even be required inindividual patients. In contrast, molecular-based early diagnosis of
y used after anterior and posterior fields have been used to deliver around half
lerance and dose reduction is necessary if cytotoxic chemotherapy is also to be

ARTICLE IN PRESS
Fig. 7. Proton dose distributions for a patient with oesophageal cancer: note the
very low cardiac, spinal cord and lung doses. Reproduced by kind permission of
Prof. Y. Akine (Tsukuba University, Japan). (For interpretation of colour in this
figure the reader is referred to the web version of the article.)
B. Jones et al. / Applied Radiation and Isotopes 67 (2009) 371–377 377
cancer—at sufficiently small volumes with low risks of sprea-d—offers a greater potential for application of the safest forms ofablative cancer therapy ranging from surgery to CPT. Even in thecase of larger cancers, the best possible technical advances fromnuclear physics will be required to achieve excellent local cancercontrol, but perhaps then combined with molecular agents toprime the tumour by reversing some of its malignant propertiesand to eradicate low levels of metastatic cancer cells.
Better technology for particle acceleration would improve theapplicability of proton therapy, its space requirements, cost andthe overall patient experience. The recent award of two majorgrants by the Research Councils for novel synchrotrons (BritishAccelerator Science Radiation Oncology Consortium, 2007) andlaser-generated particle beams (Laser Induced Beams of Radiationand their Applications, 2007) provide potential routes for morewidespread expansion in therapeutic centres.
It is certain that the great Cavendish scientists would expect tosee the benefits of their discoveries reflected in better health careand particularly in the treatment of cancer, rather than in atomicweapons. The UK faces a major problem in providing adequatehigh-technology health care, although our world leading physi-cists are eager to help achieve such a mission in cancer therapyusing particle beams. It is ironic, yet perhaps very fitting, thatJapan now leads the world in the applications of nuclear particlesin cancer therapy, with excellent results in both proton and carbonion therapy. The fight against cancer using charged particles is aninternational cause in which many UK scientists and clinicians
wish to participate: but the beneficiaries will be cancer patients,who should be treated by the best dose distributions.
References
Brada, M., Pijls-Johannesma, M., De Ruysscher, D., 2007. Proton therapy in clinicalpractice: current clinical evidence. J. Clin. Oncol. 25, 965–980.
British Accelerator Science Radiation Oncology Consortium, 2007. /www.basroc.org.ukS.
Brown, A.P., 1997. The Neutron and the Bomb: A Biography of James Chadwick.Oxford University Press, Oxford.
Brown, A., Suit, H., 2004. The centenary of the discovery of the Bragg peak.Radiother. Oncol. 73, 265–268.
Carabe-Fernandez, A., Dale, R.G., Jones, B., 2007. The incorporation of the conceptof minimum RBE (RBEmin) into the linear-quadratic model and the potential forimproved radiobiological analysis of high-LET treatments. Int. J. Radiat. Biol.83, 27–39 (Accepted for publication).
Catterall, M., Bewley, D., 1979. Fast Neutrons in the Treatment of Cancer. AcademicPress, London.
Dale, R.G., Jones, B., 1998. The assessment of RBE effects using the concept ofbiologically effective dose. Int. J. Radiat. Oncol. Biol. Phys. 43, 639–645.
Duncan, W., 1994. An evaluation of the results of neutron therapy trials. ActaOncol. 33, 299–306.
Errington, R.D., Ashby, D., Gore, S.M., et al., 1991. High energy neutron treatmentfor pelvic cancers: study stopped because of increased mortality. Br. Med.J. 302, 1045–1051.
Frisch, O.R., 1979. What Little I Remember. Cambridge University Press, Cambridge.Glimelius, B., Montelius, A., 2007. Proton beam therapy—do we need the
randomised trials and can we do them? Radiother. Oncol. 83, 105–109.Gray, L.H., Conger, A.D., Ebert, M., Hornsey, S., Scott, O.C.A., 1953. The concentration
of oxygen dissolved in tissues at the time of irradiation as a factor inradiotherapy. Br. J. Radiol. 26, 638–648.
Jones, B., 2006a. The case for particle therapy. Br. J. Radiol. 79, 24–31.Jones, B., 2006b. Implications of quality adjusted survival for clinical trials in
radiation oncology. Br. J. Radiol. 79, 353–355.Jones, B., Akine, Y., 2006. Letter: dose distribution to the mediastinum and heart.
Br. J. Radiol. 79, 448.Jones, B., Burnett, N.G., 2005. The future for radiotherapy: protons and ions hold
much promise. Br. Med. J. 330, 979–980.Jones, B., Dale, R.G., 2000. Estimation of optimum dose per fraction for high LET
radiations: implications for proton radiotherapy. Int. J. Radiat. Oncol. Biol. Phys.48, 1549–1557.
Jones, B., Crabe-Fernandez, A., Dale, R.G., 2006. Calculation of high-LET radio-therapy dose required for compensation of overall treatment time extensions.Br. J. Radiol. 79, 254–257.
Jones, B., Dale, R.G., Green, S.J., Kirkby, K., Peach, K., 2007. Particle Radiotherapy inthe UK. Editorial, Clinical Oncology. Royal College of Radiologists, UK (acceptedin press).
Laramore, G.E., 1990. Neutron therapy for high grade gliomas: the search for theelusive therapeutic window. Int. J. Radiat. Oncol. Biol. Phys. 19, 493–495.
Laramore, G.E., Krall, J.M., Griffin, T.W., Duncan, W., et al., 1993. Neutron versusphoton irradiation for unresectable salivary gland tumours: final report ofan RTOG-MRC randomized clinical trial. Int. J. Radiat. Oncol. Biol. Phys. 27,235–240.
Laser Induced Beams of Radiation and their Applications, 2007. /www.rcuk.ac.uk/cmsweb/downloads/rcuk/research/basictech/6-2.pdfS.
Lodge, M., et al., 2007. Radiother. Oncol. 83, 110–122.Mahon, B., 2004. The Man Who Changed Everything: The Life of James Clerk
Maxwell. Wiley, New York.Maor, M.H., Errington, R.D., Caplan, R.J., et al., 1995. Fast neutron therapy in
advanced head & neck cancer: a collaborative internal randomised trial.Int. J. Radiat. Oncol. Biol. Phys. 32, 99–604.
Medical Research Council Neutron Therapy Working Group, 1986. Acomparativereview of the hammersmith (1971–75) and Edinburgh (1977–82) neutrontherapy trials of certain cancers of the oral cavity, oropharynx andhypopharynx. Br. J. Radiol. 59, 429–440.
Miyatake, S., Kawabata, S., Kajimoto, Y., Aoki, A., et al., 2005. Modified boronneutron capture therapy for malignant gliomas performed using epithermalneutrons and tow boron compounds with different accumulation mechan-isms: an efficacy study based on findings of neuroimages. J. Neurosurg. 103,1000–1009.
Olsen, D.R., Bruland, O.S., Frykholm, G., Norderhaug, I.N., 2007. Proton therapy—
a systematic review of clinical effectiveness. Radiother. Oncol. 83, 123–132.Taylor, R.E., 2006. Particle matters. Br J. Radiol. 79, 850–851.Wilkins, M., 2003. The Third Man of the Double Helix. Oxford University Press,
Oxford.Withers, H.R., Thames, H.D., Peters, L.J., 1982. Biological basis for high RBE
values for late effects of neutron irradiation. Int. J. Radiat. Oncol. Biol. Phys. 8,2071–2076.