Characterization of a Mycobacterium tuberculosis insertion sequence belonging to the IS3 family
12
Characterization of a Mycobacterium tuberculosis Peptide That Is Recognized by Human CD4 and CD8 T Cells in the Context of Multiple HLA Alleles 1 Homayoun Shams, 2 * † Peter Klucar,* Steven E. Weis, § Ajit Lalvani, ¶ Patrick K. Moonan, § Hassan Safi,* † Benjamin Wizel,* † Katie Ewer, ¶ Gerald T. Nepom, David M. Lewinsohn,** Peter Andersen, †† and Peter F. Barnes* †‡ The secreted Mycobacterium tuberculosis 10-kDa culture filtrate protein (CFP)10 is a potent T cell Ag that is recognized by a high percentage of persons infected with M. tuberculosis. We determined the molecular basis for this widespread recognition by identifying and characterizing a 15-mer peptide, CFP10 71– 85 , that elicited IFN- production and CTL activity by both CD4 and CD8 T cells from persons expressing multiple MHC class II and class I molecules, respectively. CFP10 71– 85 contained at least two epitopes, one of 10 aa (peptide T1) and another of 9 aa (peptide T6). T1 was recognized by CD4 cells in the context of DRB1*04, DR5*0101, and DQB1*03, and by CD8 cells of A2 donors. T6 elicited responses by CD4 cells in the context of DRB1*04 and DQB1*03, and by CD8 cells of B35 donors. Deleting a single amino acid from the amino or carboxy terminus of either peptide markedly reduced IFN- production, suggesting that they are minimal epitopes for both CD4 and CD8 cells. As far as we are aware, these are the shortest microbial peptides that have been found to elicit responses by both T cell sub- populations. The capacity of CFP10 71– 85 to stimulate IFN- production and CTL activity by CD4 and CD8 cells from persons expressing a spectrum of MHC molecules suggests that this peptide is an excellent candidate for inclusion in a subunit antitu- berculosis vaccine. The Journal of Immunology, 2004, 173: 1966 –1977. E ight million new cases and 1.8 million deaths annually worldwide are attributed to Mycobacterium tuberculosis, one of the leading causes of death from a single infectious agent (1). The burgeoning epidemic of HIV infection in regions where tuberculosis is common has created a growing population of persons that are highly susceptible to M. tuberculosis. In addition, the continued spread of multidrug-resistant tuberculosis threatens to overwhelm the public health capacity of many jurisdictions (2, 3). These unfavorable factors will cause tuberculosis to remain a major health problem in the coming decades, and increase the ur- gency for development of an effective vaccine. The only available antituberculosis vaccine is bacillus Calmette- Gue ´rin (BCG), 3 a live attenuated Mycobacterium bovis that was created in 1921. Vaccination with M. bovis BCG reduces the se- verity of tuberculosis in children, but does not protect against de- velopment of tuberculosis. Furthermore, vaccination can cause life-threatening disease in immunocompromised patients, such as those with HIV infection (4). T cells play a pivotal role in protection against tuberculosis, and many studies have shown that CD4 T cells are essential for im- munity (5). A growing body of evidence in animals and in humans suggests that CD8 cells also contribute significantly to immune defenses against tuberculosis through lysis of infected cells, pro- duction of IFN-, and direct microbicidal activity (6 –12). There- fore, the most effective vaccine is likely to be one that elicits re- sponses by both CD4 and CD8 T cells (12). Most published evidence indicates that secreted M. tuberculosis Ags stimulate protective immunity (13). Two important secreted proteins are 6-kDa early secretory antigenic target (ESAT-6) and 10-kDa culture filtrate protein (CFP10), which form a tightly bound 1:1 heterodimeric complex (14). The encoding genes are cotranscribed (15) and are part of the RD1 region of the M. tu- berculosis genome, which is deleted from M. bovis BCG. Resto- ration of RD1 enhanced the capacity of BCG vaccination to protect mice against subsequent infection with M. tuberculosis (16). ESAT-6 and CFP10 stimulate T cells to produce IFN- and exhibit CTL activity in animal models and in humans infected with M. tuberculosis, making them excellent candidates for inclusion in an antituberculosis subunit vaccine (17–20). T cells from a high percentage of persons with latent tuberculosis infection recognize ESAT-6 and CFP10 (20, 21), suggesting that they either contain multiple epitopes that are restricted by different MHC molecules, or epitopes that are promiscuously recognized in the context of multiple MHC molecules. Several epitopes for CD4 and CD8 T cells, restricted by different MHC molecules, have been identified *Center for Pulmonary and Infectious Disease Control, and Departments of † Micro- biology, Immunology, and ‡ Medicine, University of Texas Health Center, Tyler, TX 75708; § Department of Internal Medicine, University of North Texas Health Science Center, Fort Worth, TX 76107; ¶ Nuffield Department of Clinical Medicine, Univer- sity of Oxford, John Radcliffe Hospital, Oxford, United Kingdom; Benaroya Re- search Institute, Seattle, WA 98101; **Division of Pulmonary and Critical Care Med- icine, Oregon Health and Science University/Portland Veterans Affairs Medical Center, Portland, OR 97207; and †† Statens Seruminstitut, Copenhagen, Denmark Received for publication December 16, 2003. Accepted for publication May 24, 2004. The costs of publication of this article were defrayed in part by the payment of page charges. This article must therefore be hereby marked advertisement in accordance with 18 U.S.C. Section 1734 solely to indicate this fact. 1 This work was supported by grants from the National Institutes of Health (AI44935), the Cain Foundation for Infectious Disease Research, the Wellcome Trust, and the Center for Pulmonary and Infectious Disease Control. P.F.B. holds the Mar- garet E. Byers Cain Chair for Tuberculosis Research. A.L. is a Wellcome Senior Research Fellow in Clinical Science. 2 Address correspondence and reprint requests Dr. Homayoun Shams, Center for Pul- monary and Infections Disease Control, University of Texas Health Center, 11937 US Highway 271, Tyler, TX 75708. E-mail address: [email protected] 3 Abbreviations used in this paper: BCG, bacillus Calmette-Gue ´rin; BLS, bare lym- phocyte syndrome; CFP, culture filtrate protein; ESAT, early secretory antigenic target. The Journal of Immunology Copyright © 2004 by The American Association of Immunologists, Inc. 0022-1767/04/$02.00
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Characterization of a Mycobacterium tuberculosis insertion sequence belonging to the IS3 family

Characterization of a Mycobacterium tuberculosis Peptide ThatIs Recognized by Human CD4� and CD8� T Cells in theContext of Multiple HLA Alleles 1
Homayoun Shams,2*† Peter Klucar,* Steven E. Weis,§ Ajit Lalvani, ¶ Patrick K. Moonan,§
Hassan Safi,*† Benjamin Wizel,*† Katie Ewer,¶ Gerald T. Nepom,� David M. Lewinsohn,**Peter Andersen,†† and Peter F. Barnes*†‡
The secretedMycobacterium tuberculosis 10-kDa culture filtrate protein (CFP)10 is a potent T cell Ag that is recognized by a highpercentage of persons infected withM. tuberculosis. We determined the molecular basis for this widespread recognition byidentifying and characterizing a 15-mer peptide, CFP1071–85, that elicited IFN-� production and CTL activity by both CD4 � andCD8� T cells from persons expressing multiple MHC class II and class I molecules, respectively. CFP1071–85contained at leasttwo epitopes, one of 10 aa (peptide T1) and another of 9 aa (peptide T6). T1 was recognized by CD4� cells in the context ofDRB1*04, DR5*0101, and DQB1*03, and by CD8� cells of A2� donors. T6 elicited responses by CD4� cells in the context ofDRB1*04 and DQB1*03, and by CD8� cells of B35� donors. Deleting a single amino acid from the amino or carboxy terminusof either peptide markedly reduced IFN-� production, suggesting that they are minimal epitopes for both CD4� and CD8� cells.As far as we are aware, these are the shortest microbial peptides that have been found to elicit responses by both T cell sub-populations. The capacity of CFP1071–85to stimulate IFN-� production and CTL activity by CD4 � and CD8� cells from personsexpressing a spectrum of MHC molecules suggests that this peptide is an excellent candidate for inclusion in a subunit antitu-berculosis vaccine. The Journal of Immunology, 2004, 173: 1966–1977.
Eight million new cases and 1.8 million deaths annuallyworldwide are attributed toMycobacterium tuberculosis,one of the leading causes of death from a single infectious
agent (1). The burgeoning epidemic of HIV infection in regionswhere tuberculosis is common has created a growing population ofpersons that are highly susceptible toM. tuberculosis. In addition,the continued spread of multidrug-resistant tuberculosis threatensto overwhelm the public health capacity of many jurisdictions (2,3). These unfavorable factors will cause tuberculosis to remain amajor health problem in the coming decades, and increase the ur-gency for development of an effective vaccine.
The only available antituberculosis vaccine is bacillus Calmette-Guerin (BCG),3 a live attenuatedMycobacterium bovis that was
created in 1921. Vaccination withM. bovis BCG reduces the se-verity of tuberculosis in children, but does not protect against de-velopment of tuberculosis. Furthermore, vaccination can causelife-threatening disease in immunocompromised patients, such asthose with HIV infection (4).
T cells play a pivotal role in protection against tuberculosis, andmany studies have shown that CD4� T cells are essential for im-munity (5). A growing body of evidence in animals and in humanssuggests that CD8� cells also contribute significantly to immunedefenses against tuberculosis through lysis of infected cells, pro-duction of IFN-�, and direct microbicidal activity (6–12). There-fore, the most effective vaccine is likely to be one that elicits re-sponses by both CD4� and CD8� T cells (12).
Most published evidence indicates that secretedM. tuberculosisAgs stimulate protective immunity (13). Two important secretedproteins are 6-kDa early secretory antigenic target (ESAT-6) and10-kDa culture filtrate protein (CFP10), which form a tightlybound 1:1 heterodimeric complex (14). The encoding genes arecotranscribed (15) and are part of the RD1 region of theM. tu-berculosis genome, which is deleted fromM. bovis BCG. Resto-ration of RD1 enhanced the capacity of BCG vaccination to protectmice against subsequent infection withM. tuberculosis (16).
ESAT-6 and CFP10 stimulate T cells to produce IFN-� andexhibit CTL activity in animal models and in humans infected withM. tuberculosis, making them excellent candidates for inclusion inan antituberculosis subunit vaccine (17–20). T cells from a highpercentage of persons with latent tuberculosis infection recognizeESAT-6 and CFP10 (20, 21), suggesting that they either containmultiple epitopes that are restricted by different MHC molecules,or epitopes that are promiscuously recognized in the context ofmultiple MHC molecules. Several epitopes for CD4� and CD8� Tcells, restricted by different MHC molecules, have been identified
*Center for Pulmonary and Infectious Disease Control, and Departments of†Micro-biology, Immunology, and‡Medicine, University of Texas Health Center, Tyler, TX75708;§Department of Internal Medicine, University of North Texas Health ScienceCenter, Fort Worth, TX 76107;¶Nuffield Department of Clinical Medicine, Univer-sity of Oxford, John Radcliffe Hospital, Oxford, United Kingdom;�Benaroya Re-search Institute, Seattle, WA 98101; **Division of Pulmonary and Critical Care Med-icine, Oregon Health and Science University/Portland Veterans Affairs MedicalCenter, Portland, OR 97207; and††Statens Seruminstitut, Copenhagen, Denmark
Received for publication December 16, 2003. Accepted for publication May 24, 2004.
The costs of publication of this article were defrayed in part by the payment of pagecharges. This article must therefore be hereby markedadvertisement in accordancewith 18 U.S.C. Section 1734 solely to indicate this fact.1 This work was supported by grants from the National Institutes of Health(AI44935), the Cain Foundation for Infectious Disease Research, the Wellcome Trust,and the Center for Pulmonary and Infectious Disease Control. P.F.B. holds the Mar-garet E. Byers Cain Chair for Tuberculosis Research. A.L. is a Wellcome SeniorResearch Fellow in Clinical Science.2 Address correspondence and reprint requests Dr. Homayoun Shams, Center for Pul-monary and Infections Disease Control, University of Texas Health Center, 11937 USHighway 271, Tyler, TX 75708. E-mail address: [email protected] Abbreviations used in this paper: BCG, bacillus Calmette-Gue´rin; BLS, bare lym-phocyte syndrome; CFP, culture filtrate protein; ESAT, early secretory antigenictarget.
The Journal of Immunology
Copyright © 2004 by The American Association of Immunologists, Inc. 0022-1767/04/$02.00

in ESAT-6, providing an explanation for its widespread recogni-tion (18, 22, 23). In contrast, only two CD8 epitopes for CFP10have been identified (24). In this study, we wished to determine themolecular basis for the recognition of CFP10 by most individualswith latent tuberculosis infection. We identified and characterizeda 15-mer peptide of CFP10 that elicited IFN-� production andCTL activity by both CD4� and CD8� T cells from the majorityof persons with latent tuberculosis infection, including those ex-pressing several different MHC class I and class II molecules.
Materials and MethodsStudy subjects
This study was approved by the Institutional Review Boards of the Uni-versity of North Texas Health Science Center (Fort Worth, TX) and theUniversity of Texas Health Center (Tyler, TX). Blood was obtained from10 healthy tuberculin-negative donors without prior contact with tubercu-losis patients, and from 132 donors who were recent contacts of patientswith pulmonary tuberculosis. Seventy-six (58%) donors were Hispanic, 29(22%) were white non-Hispanic, 21 (16%) were African American, and 6(5%) were Asian. All donors had no symptoms of tuberculosis with normalchest radiographs. Donors were classified as having latent tuberculosis in-fection if they had a tuberculin skin test showing at least a 5-mm diameterof induration and their PBMC produced IFN-� in response to CFP10 orESAT-6, based on the ELISPOT assay.
Peptides
We selected 15-mer peptides that overlapped by 10 aa and spanned theCFP10 protein. Truncated peptides were also synthesized, as outlined inthe results. Peptides were synthesized by the Molecular Genetics Instru-mentation Facility at the University of Georgia (Athens, GA) and by In-vitrogen Life Technologies (Carlsbad, CA), using Fmoc chemistry. Peptidepurity was �70%, as assayed by HPLC, and their composition was verifiedby mass spectrometry. Lyophilized peptides were dissolved at 25 mg/ml inDMSO, aliquoted, and stored at 4°C.
Antibodies
We used Abs to framework MHC class I (ATCC clone W6/32; AmericanType Culture Collection (ATCC), Manassas, VA) and MHC class II(ATCC clone 9.3F10; ATCC).
Isolation of PBMC and cell subpopulations
PBMC were obtained by centrifugation over Ficoll-Paque (Pharmacia,Uppsala, Sweden) and cultured in RPMI 1640 (Invitrogen Life Technol-ogies, Gaithersburg, MD), supplemented with 10% heat-inactivated humanAB serum (Atlanta Biologicals, Norcross, GA). In some experiments,
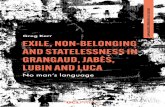
FIGURE 1. Capacity of CFP10 peptides to stimulate IFN-� productionby PBMC from persons with latent tuberculosis infection. PBMC from 49CFP10-responsive persons were cultured overnight on IFN-� ELISPOTplates with 15-mer overlapping peptides spanning the CFP10 protein. Thevalues shown are the percent of CFP10 responders that produced �7IFN-�� cells per 2.5 � 105 cells to each individual peptide. UnstimulatedPBMC showed 0–2 IFN-�� cells per 2.5 � 105 cells.
FIGURE 2. CFP1071–85 and CFP1076–90 stimulate production of IFN-�by PBMC. PBMC from eight CFP10-responsive individuals were stimu-lated with peptides CFP1071–85 and CFP1076–90 for 48 h. PBMC and pos-itively selected CD4� or CD8� cells were then cultured overnight onIFN-� ELISPOT plates. Values shown are the means and SEM of triplicatewells. Unstimulated PBMC showed 0–2 IFN-�� cells per 2.5 � 105 cells.A, B, and C show results for PBMC, CD4� cells, and CD8� cells,respectively.
1967The Journal of Immunology

FIGURE 3. CTL activity of short-term T cell linesstimulated with CFP1071–85 and CFP1076–90. PBMCfrom four donors were stimulated with peptidesCFP1071–85 and CFP1076–90 for 13–14 days. Theseshort-term lines were used as effectors. Positively se-lected CD4� or CD8� cells from these lines were alsoused as effectors. Targets were autologous dendriticcells, either unpulsed or pulsed with relevant pep-tides. A, B, and C show results, using peptide-stimu-lated PBMC, CD4� cells, and CD8� cells as effec-tors, respectively. Values shown are the means andSEM of triplicate wells.
1968 A MYCOBACTERIAL PEPTIDE RECOGNIZED BY CD4� and CD8� T cells

CD4�, CD8�, or CD14� cells were isolated from PBMC by positive se-lection with magnetic beads conjugated to the appropriate Abs (MiltenyiBiotech, Auburn, CA). Positively selected cells were �95% pure, as de-termined by flow cytometry.
Measurement of the frequency of IFN-�-producing cells
To measure the frequency of cells in PBMC that produced IFN-� in re-sponse to mycobacterial Ags or peptides, 2 � 105 cells per well werecultured in RPMI 1640 and 10% heat-inactivated human AB serum, withpurified protein derivative (1 �g/ml; Statens Seruminstitut, Copenhagen,Denmark), CFP10 (10 �g/ml; Lionex, Braunschweig, Germany), ESAT-6(10 �g/ml; Statens Seruminstitut) or CFP peptides (10 �g/ml) for 16–20 hin 96-well plates that were precoated with 15 �g/ml anti-human IFN-�mAb (1-DlK; Mabtech, Nacka, Sweden).
To measure the frequency of IFN-�-producing CD4� or CD8� cells,PBMC were cultured in T-25 flasks at 1.5 � 106 cells/ml, in medium alone,or with peptide (10 �g/ml), or purified protein derivative (1 �g/ml) for48–72 h. Preliminary studies showed that this period of stimulation yieldedthe maximum number of IFN-�� cells. After 48–72 h, cells were washedthree times, and one aliquot was placed on an anti-IFN-�-precoated ELIS-POT plate for 16–20 h. From two other aliquots, CD4� and CD8� cellswere positively selected and placed on an ELISPOT plate for 16–20 h.
ELISPOT plates were washed with PBS plus 0.05% Tween 20, andanti-human IFN-� mAb 7-B6-1 conjugated to alkaline phosphatase(Mabtech) was added as the detection Ab. After 90 min, the plates werewashed and 5-bromo-4-chloro-3-indolyl phosphate/NBT substrate (Moss,Pasadena, MD) was added for 2–5 min or until spots appeared. The spotsin air-dried plates were counted using a stereomicroscope. Responses wereconsidered positive if the Ag-stimulated well contained a mean of at leastfive more spot-forming cells than the mean of the negative control wells,and the Ag-stimulated value was at least twice the mean of the negativecontrol value (20).
In some experiments, freshly isolated CD4� cells (25,000 cells/well) orCD4� clones (100 cells/well) were cultured with transfected bare lympho-cyte syndrome (BLS) cells (25,000 cells/well), expressing a single HLAmolecule (25) as APCs on an ELISPOT plate for 16–20 h. The number ofIFN-�-producing cells was determined, as outlined above.
Expansion of peptide-specific CTLs
PBMC were washed, resuspended in RPMI 1640 containing 10% humanAB serum, 20 mM HEPES, 2 mM L-glutamine, 1 mM sodium pyruvate, 0.1mM nonessential amino acids (all from Invitrogen Life Technologies), 50U penicillin (Sigma-Aldrich, St. Louis, MO), and 10 �g/ml peptide, andseeded in 24-well plates (BD Biosciences, San Jose, CA) at 3 � 106 cells/well. After 3 days, 100 U/ml recombinant human IL-2 (Proleukin; Chiron,Emeryville, CA) was added to each well. After 7 days, 3 � 106 peptide-pulsed irradiated (3300 rad) autologous PBMC and 100 U/ml IL-2 wereadded to each well. Six days later, effector cells were tested for CTL ac-tivity in a 51Cr release assay.
In some cases, positively selected CD4� and CD8� effectors were iso-lated from peptide-expanded short-term lines, using immunomagneticbeads. Purity of these cells was 95–99%, as assessed by flow cytometry.
Generation of peptide-specific T cell clones
Clones were generated by previously described methods (26, 27). Briefly,autologous dendritic cells were generated as described below (preparationof target cells), pulsed with peptide T1, irradiated, and cultured at 104 cellsper well in 96-well round-bottom plates with 300 CD4� T cells in eachwell. Wells that showed visible growth were tested for reactivity with
peptide T1 by ELISPOT. IFN-�� T cell clones were expanded with anti-CD3 mAb (OKT3; Ortho Biotech, Bridgewater, NJ), irradiated allogeneicPBMC, and an EBV-transformed B cell line lymphoblastoid cell lines(LCL).
Assessment of CTL activity
Target cells were autologous dendritic cells, generated by incubating pos-itively selected CD14� macrophages with IL-4 (10 ng/ml; R&D Systems,Minneapolis, MN) and GM-CSF (10 ng/ml; R&D Systems) for 5 day.Dendritic cells were either unstimulated, infected with M. tuberculosisH37Rv for 48 h, or pulsed with a peptide overnight.
Targets were labeled overnight with 100 �Ci of Na251CrO4 (Amersham
Life Science, Arlington Heights, IL) at 37°C. After extensive washing, theywere suspended in complete medium containing 10% FBS, and 104 cells/well were added in triplicate to round-bottom 96-well plates, each wellcontaining 6 � 105 effector cells, an E:T ratio of 60:1. Plates were centri-fuged at 500 � g for 2 min, then incubated for 5 h at 37°C. Supernatantswere collected (Skatron, Sterling, VA), and 51Cr release was expressed asthe mean percent specific lysis, calculated as: 100 � ([experimental re-lease � spontaneous release]/[maximum release � spontaneous release]).Net specific lysis was calculated by subtracting the percent specific lysis ofunpulsed target cells from the percent specific lysis of peptide-pulsed or M.tuberculosis-infected target cells. Maximum and spontaneous release weredetermined in wells containing target cells only, with or without 2% TritonX-100, respectively. Spontaneous release was always �15% of maximumrelease.
MHC typing
DNA was extracted from PBMC, using Wizard Genomic (Promega, Mad-ison, WI). Low resolution HLA typing was performed, using PCR withsequence-specific primers (Combi Tray; GenoVision, West Chester, PA).Briefly, DNA samples (30 ng/�l) were mixed with a master mix containingTaq polymerase (GenoVision), added into the plates containing sequence-specific primers and amplified by PCR. PCR products (10 �l) were elec-trophoresed on a 2% agarose gel containing ethidium bromide. MHC al-leles were identified with the GenoVision version of HELMBERG-SCOREVirtual Sequencing software.
Table I. HLA typing of donors whose T cells recognized CFP1071–85a
Donor CD8�IFN-�� Cells HLA-A HLA-B HLA-C CD4� IFN-�� Cells HLA-DQ HLA-DR
T225 15 � 2 A*01, *24 B*07, *53 Cw*04, *07 78 � 7 B1*05, *06 B1*1001, *15T262 32 � 4 A*24, *31 B*40, *51 Cw*03, *15 85 � 2 B1*03, *04 B1*04, *08T221 314 � 26 A*02, *02 B*39, *40 Cw*03, *07 535 � 58 B1*03, *03 B1*04, *04T193 700 � 52 A*02, *68 B*35, *51 Cw*04, *08 633 � 56 B1*03, *03 B1*04, *04T040 70 � 12 A*26, *68 B*40, *44 Cw*03, *05 223 � 25 B1*03, *03 B1*04, *04T198 223 � 4 A*11, *11 B*15, *3525 Cw*07, *08 39 � 3 B1*03, *03 B1*11, *12T021 15 � 3 A*02, *03 B*40, 58 Cw*03, *06 78 � 2 B1*03, *05 B1*1001, *11
a PBMC were cultured with or without CFP1071–85 for 48 h, and positively selected CD4� and CD8� cells were placed on an ELISPOT plate for 16–20 h to detect IFN-��
cells. The values shown (mean � SEM of triplicate wells) are the number of peptide-stimulated IFN-�� cells per 2.5 � 105 cells. Unstimulated wells contained 0–2 positivecells per 2.5 � 105 cells.
Table II. Truncated peptides derived from CFP1071–85a
CFP1071–85 EISTNIRQAGVQYSRCFP1076–90 IRQAGVQYSRADEEQT1–10 aa IRQAGVQYSRT2–11 aa NIRQAGVQYSRT3–12 aa TNIRQAGVQYSRT4–13 aa STNIRQAGVQYSRT5–14 aa ISTNIRQAGVQYSRT6–9 aa EISTNIRQAT7–9 aa NIRQAGVQYT8–10 aa TNIRQAGVQYT9–10 aa RQAGVQYSRA
a A ladder of 10–14 aa peptides was made from CFP1071–85 (T1-T5). Four otherpeptides (T6-T9) were predicted to bind to 3–8 MHC class I alleles with high affinity,using a scoring system that allocates values to every amino acid in a peptide, basedon the frequency of the respective amino acid in natural ligands, T cell epitopes, orbinding peptides (28).
1969The Journal of Immunology

ResultsTwo CFP10 peptides elicit IFN-� production by T cells frommost persons with latent tuberculosis infection
PBMC from 132 close contacts of patients with pulmonary tuber-culosis were stimulated with the M. tuberculosis-specific proteins,CFP10 and ESAT-6, which have previously been used to identifypersons with latent tuberculosis infection (20, 21, 23). The ELIS-POT assay was used to identify IFN-�-producing cells. Fifty-threesubjects were classified as having latent tuberculosis infection,based on having positive tuberculin skin tests and IFN-�-produc-ing PBMC in response to either ESAT-6 or CFP10. Of these 53, 49responded to CFP10.
To identify the regions of CFP10 that induced IFN-� produc-tion, we tested overlapping 15-aa peptides that spanned CFP10(20). CFP1071–85 and CFP1076–90 were the most potent, and wererecognized by 83 and 91% of responders, respectively (Fig. 1).CFP1071–85 and CFP1076–90 did not elicit IFN-� production byPBMC from 10 tuberculin-negative persons who had no history ofcontact with tuberculosis patients.
CFP1071–85 and CFP1076–90 elicit IFN-� production and CTLactivity by CD4� and CD8� T cells
We stimulated PBMC from eight donors with CFP1071–85 andCFP1076–90. After 48 h, we obtained CD4� and CD8� cells bypositive immunomagnetic selection, and cultured them on ELIS-POT plates overnight. CFP1071–85 induced IFN-� production byPBMC from eight donors (mean 300 � 124 (SE) IFN-�� cells per2.5 � 105 cells; Fig. 2A), by CD4� cells from seven donors (mean205 � 86 IFN-�� cells per 2.5 � 105 cells; Fig. 2B) and by CD8�
cells from eight donors (mean 173 � 85 IFN-�� cells per 2.5 �105 cells; Fig. 2C). CFP1076–90 was recognized by PBMC fromsix donors (mean 320 � 176 IFN-�� cells per 2.5 � 105 cells; Fig.2A), by CD4� cells from seven donors (mean 146 � 64 IFN-��
cells per 2.5 � 105 cells; Fig. 2B), and by CD8� cells from fivedonors (mean 121 � 83 IFN-�� cells per 2.5 � 105 cells; Fig. 2C).
To determine whether CFP1071–85 and CFP1076–90 elicitedCTL activity, PBMC were cultured with either peptide for 7 days,then restimulated for another 6–7 days. This brief period reducedthe likelihood of artifactual induction of peptide-responsive CTL.For four donors, PBMC showed net specific lysis ranging from 6to 45% against peptide-pulsed autologous dendritic cells (Fig. 3A).CD4� T cells isolated from restimulated PBMC showed similarlevels of net specific lysis as PBMC (6–46%; Fig. 3B) and CD8�
T cells showed lower levels of lysis (1–27%; Fig. 3C). Recentstudies show that M. tuberculosis-responsive CD8� T cell clonesare more potent CTL than CD4� T cell clones, using a low E:Tratio and suboptimal peptide concentrations (28). The different re-sults in our experimental system may be due to our use of short-term T cell lines as effectors, a high E:T ratio and high peptideconcentrations. The precursor frequency of CD4� CTL may alsobe higher than that of CD8� CTL in peptide-stimulated PBMC.
CFP1071–85 is recognized by donors expressing different HLAalleles
CFP1071–85 elicited IFN-� production by both CD8� and CD4�
cells from most donors with latent tuberculosis infection, suggest-ing that it is recognized in the context of multiple MHC alleles. Toevaluate these possibilities, we performed MHC typing of sevendonors whose CD4� and CD8� cells produced IFN-� in responseto CFP1071–85 (Table I). No single MHC class I or class II allelewas shared between all donors. However, of these seven individ-uals, six expressed DQB1*03 and four expressed DRB1*04. Thissuggests that CFP1071–85 contains a single epitope that is recog-nized promiscuously in the context of multiple MHC molecules, orthat it contains two or more epitopes, each restricted by differentMHC molecules.
Identification of minimal T cell epitopes within CFP1071–85
To identify the epitopes in CFP1071–85, we first truncated 1–5 aafrom the N terminus (T1-T5, Table II). We also used a motif-basedalgorithm (29) to identify additional sequences in CFP1071–85 thatwere predicted to bind with high affinity (score, �9) to 4–8 MHCclass I alleles (T6-T8, Table II). Finally, we identified a peptidethat was predicted to bind with high affinity to three MHC class Ialleles (T9, Table II).
PBMC from six CFP1071–85-responsive donors were stimulatedwith peptides T1-T9, and the frequency of IFN-�� cells was mea-sured by ELISPOT (Table III). The 9-mer T6 and CFP1071–85
elicited comparable numbers of IFN-�� cells for all donors. The10-mer T1 yielded similar numbers of IFN-�� cells as CFP1071–85
for four donors, and 20–60% fewer IFN-�� cells for two donors.To determine whether peptides T1 and T6 contain minimal
epitopes, we deleted 1–2 amino acids from the N or C terminus ofthese peptides. Removal of a single amino acid from either endof both peptides markedly reduced IFN-� production by PBMC(Table IV).
Table III. Capacity of truncated peptides to stimulate IFN-� production by PBMCa
Donor CFP10 Response T1 (10aa) T2 (11 aa) T3 (12 aa) T4 (13 aa) T5 (14 aa) T6 (9 aa) T7 (9 aa) T8 (10 aa) T9 (10 aa) CFP1071–85 (15 aa)
T221 � 571 671 603 606 590 578 346 384 19 569T225 � 103 190 284 284 240 213 4 6 4 246T262 � 313 325 378 315 381 394 163 228 16 309T267 � 121 119 121 138 146 165 69 82 6 153T283 � 255 266 263 265 305 296 130 171 23 293T294 � 178 141 111 149 179 156 29 62 1 189
T296 � 0 0 0 0 3 0 0 0 0 0T298 � 2 1 0 1 0 2 2 3 1 1T299 � 0 0 0 0 0 1 0 1 0 0T300 � 0 0 0 0 0 0 0 0 0 0T301 � 0 0 0 0 0 0 0 0 0 0T303 � 0 0 0 0 0 0 0 0 0 0T302 � 1 6 1 5 7 0 0 0 1 1T297 � 7 3 6 5 4 6 3 2 2 2
a Freshly isolated PBMC from donors who responded to CFP1071–85 were stimulated overnight on IFN-� ELISPOT plates with peptide (10 �g/ml). For each donor, 2–3experiments were performed. Values shown are the mean number of IFN-�� cells per 2.5 � 105 cells, based on duplicate wells in a representative experiment. Unstimulatedwells contained 0–5 positive cells per 2.5 � 105 cells.
1970 A MYCOBACTERIAL PEPTIDE RECOGNIZED BY CD4� and CD8� T cells

Peptides T1 and T6 are presented by MHC class I and IImolecules
To identify the restriction elements for peptides T1 and T6, wetreated PBMC with anti-MHC class I, anti-MHC class II, or con-trol Ab for 4 h before addition of peptide on the IFN-� ELISPOTplate. Neutralization of MHC class I reduced the mean number ofT1- and T6-responsive IFN-�� cells by 50% (T1, mean 119 � 18vs 51 � 15 cells per 2.5 � 105 cells, p � 0.02; T6, mean 139 �26 vs 65 � 14 cells per 2.5 � 105 cells, p � 0.04; Table V).Anti-MHC class II reduced the number of IFN-�� cells by �90%(T1, mean 119 � 18 vs 9 � 5 cells per 2.5 � 105 cells, p � 0.0001;T6, mean 139 � 26 vs 8 � 2 cells per 2.5 � 105 cells, p � 0.0005;Table V). Isotype control Abs had no effect on the number ofIFN-�� cells (data not shown).
Peptides T1 and T6 elicit IFN-� production and CTL activity byCD4� and CD8� T cells
PBMC from four donors were stimulated with peptides T1 and T6.Forty-eight to 72 h later, positively selected CD4� and CD8� cellswere placed on an IFN-� ELISPOT plate. The frequency of pep-tide-responsive IFN-�� cells was similar in CD4� cells andPBMC (Fig. 4, A and B). The number of IFN-�� CD8� cells waslower than that of CD4� cells, but higher than corresponding val-ues for unstimulated cells in three donors for peptide T1 and fourdonors for peptide T6 (Fig. 4C).
We next evaluated the ability of peptides T1 and T6 to elicitCTL activity. PBMC from five donors were cultured with peptidesT1 and T6 for 7 days and restimulated with peptide for 6–7 moredays. PBMC effectors lysed autologous peptide-pulsed target cells(T1, net specific lysis 8–22%; T6, net specific lysis 6–17%; Fig.4D). Positively selected CD4� T cells showed similar results (T1and T6, net specific lysis 8–39% and 8–20%, respectively; Fig.4E). CD8� T cells also lysed comparable numbers of peptide-pulsed autologous target cells. However, because CD8� cellslysed a high percentage of unpulsed targets, net specific lysis wasrelatively low (T1, 2–14%; T6, 4–10%; Fig. 4F).
Dendritic cells infected with M. tuberculosis express peptides T1and T6
To determine whether peptides T1 and T6 are expressed by APCsduring M. tuberculosis infection in vivo, we cultured PBMC fromthree donors with T1 and T6, and tested their capacity to lyseautologous dendritic cells infected with H37Rv. T1-primed effec-tor PBMC and CD4� cells showed modest lytic activity (net spe-cific lysis 7–13%; Fig. 5, A and C). T6-primed effector PBMC andCD4� cells lysed infected cells from two of three donors (netspecific lysis 0–32%; Fig. 5, B and D). CD8� effector cells pulsedwith T1 or T6 also lysed infected dendritic cells, but nonspecificlysis was higher than for CD4� cells (net specific lysis 2–32%;Fig. 5, E and F).
MHC restriction of T cells that recognize peptides T1 and T6
All nine donors whose T1- or T6-primed CD4� T cells exhibitedCTL activity or produced IFN-� expressed DQB1*03, and sevenof nine also expressed DRB1*04 (Table VI). All five donors whoseT1-primed CD8� T cells showed CTL activity or IFN-� produc-tion were HLA A*02�, whereas all five donors whose T6-primedCD8� T cells showed CTL activity or IFN-� production were HLAB*35�. Three donors whose CD8� T cells responded to T1 and T6expressed both HLA A*02 and B*35 alleles.
To more definitively demonstrate that peptides T1 and T6 arerestricted by DRB1*04 and DQB1*03, we used transfected BLScells expressing a single HLA allele as target cells. Freshly isolatedCD4� T cells were obtained from five persons who responded toCFP10 and were infected with M. tuberculosis, and from threeuninfected persons who did not respond to CFP10. CD4� cellsfrom the CFP10-responsive donors produced IFN-� specifically inresponse to DRB1*0401� or DQB1*0302� targets pulsed withpeptide T1 or T6, but not to unpulsed targets. In contrast, CD4�
cells from CFP10-negative donors did not produce IFN-� in re-sponse to peptide-pulsed targets (Table VII).
The results above suggest that peptides T1 and T6 are recog-nized in the context of more than one MHC class II allele. To
Table IV. Effect of truncation on the capacity of peptides T1 and T6 to elicit IFN-� production by PBMCa
T1(IRQAGVQYSR)
T1–1(RQAGVQYSR)
T1–2(IRQAGVQYS)
T1–3(IRQAGVQY)
T6(EISTNIRQA)
T6–1(ISTNIRQA)
T6–2(EISTNIRQ)
CFP1071–85
(EISTNIRQAGVQYSR)
T225 149 4 3 0 151 0 3 216T262 163 4 18 18 185 0 1 204T267 153 6 18 9 149 4 3 152T283 191 0 63 1 178 1 0 252T294 228 0 60 14 147 1 1 208
a Peptides T1 and T6 were truncated from the amino or carboxy terminus, and the effect of truncation was assessed in the ELISPOT assay. Freshly isolated PBMC fromCFP1071–85-responsive donors were stimulated overnight with 10 �g/ml peptide on IFN-� ELISPOT plates. Values shown are the mean number of IFN-�� cells per 2.5 � 105
cells, based on duplicate wells. Unstimulated PBMC showed 0–4 IFN-�� cells per 2.5 � 105 cells.
Table V. Effect of Abs to MHC class I and MHC class II on peptide-induced IFN-� production by PBMCa
Peptide T1Peptide T1 �Anti-MHC I
Peptide T1 �Anti-MHC II Peptide T6
Peptide T6 �Anti-MHC I
Peptide T6 �Anti-MHC II
T221 100 48 0 139 63 4T225 87 18 4 94 81 5T262 170 108 10 179 94 8T267 123 ND 31 189 ND 18T343 65 35 0 38 15 10T375 168 45 8 195 73 5
a Freshly isolated PBMC from donors responsive to peptides T1 and T6 were incubated with Abs for 4 h, then incubatedovernight with peptide on IFN-� ELISPOT plates. Values shown are the mean number of IFN-�� cells per 2.5 � 105 cells, basedon duplicate wells. Unstimulated PBMC showed 0–4 IFN-�� cells per 2.5 � 105 cells.
1971The Journal of Immunology

confirm these findings at the level of the single cell, we used twoT1-specific CD4� T cell clones as effector cells. BLS cells lackingendogenous MHC class II expression (BLS-1) and six BLS celllines, each expressing a single transfected HLA class II allele,were used as APCs. Significant numbers of IFN-�� cells were
only observed in the presence of peptide, and BLS cells aloneelicited IFN-� production by �10% of the clones (Fig. 6). Thefrequency of IFN-�� cells in both clones was 3- to 6-fold higherwhen BLS cells expressing DRB5*0101 or DRB1*0401 were used,and BLS cells expressing DQB1*0602 yielded a 2-fold higher
FIGURE 4. Peptides T1 and T6 stimulate production of IFN-� and CTL activity. PBMC from four donors were stimulated with peptides T1 and T6 for48 h, and then PBMC (A) and purified CD4� (B) and CD8� T cells (C) were cultured overnight on IFN-� ELISPOT plates. Values shown are the meansand SEM of triplicate wells. Unstimulated cells showed 0–2 cells per 2.5 � 105 PBMC. PBMC from five donors were cultured with peptides T1 or T6for 13–14 days. These short-term lines (D), or positively selected CD4� (E) or CD8� cells (F) from these lines, were used as effectors. Targets wereautologous dendritic cells, either unpulsed or pulsed with relevant peptides. Values shown are the means and SEM of triplicate wells.
1972 A MYCOBACTERIAL PEPTIDE RECOGNIZED BY CD4� and CD8� T cells

response by clone B9. Cells expressing DRB1*0401 induced thestrongest response in both clones.
DiscussionBased on data using purified CD4� and CD8� primary T cells, Tcell lines, and T cell clones, we demonstrated that a 15-mer peptidein the secreted mycobacterial protein CFP10 elicits IFN-� produc-tion and CTL activity by both CD4� and CD8� T cells from a high
proportion of persons with latent tuberculosis infection.CFP1071–85 was recognized by CD4� and CD8� T cells frompersons expressing multiple MHC class II and class I molecules,respectively (Table I), and contains at least two epitopes, one of 10aa (peptide T1) and another of 9 aa (peptide T6). T1 was recog-nized by CD4� cells in the context of at least DRB1*0401,DRB5*0101, and DQB1*0302, and by CD8� cells of A2� donors(Tables VI and VII, and Fig. 6). T6 elicited responses by CD4�
FIGURE 5. CTL activity of effector cells stimulated with peptides T1 and T6 against M. tuberculosis-infected target cells. PBMC from three donors werecultured with peptides T1 (A, C, and E) or T6 (B, D, and F) for 14 days. These short-term lines, and positively selected CD4� or CD8� cells from theselines, were used as effectors. Targets were autologous dendritic cells, either uninfected or infected with H37Rv. Means and SEM of triplicate wells areshown. Effectors used in A and D are peptide-stimulated PBMC, effectors in B and E are CD4� cells, and those in C and F are CD8� cells.
1973The Journal of Immunology

cells in the context of DRB1*0401 and DQB1*0302, and by CD8�
cells of B35� donors (Tables VI and VII). Deleting a single aminoacid from the amino or carboxy terminus of either peptide mark-edly reduced IFN-� production, suggesting that they are minimalepitopes for both CD4� and CD8� cells. As far as we are aware,these are the shortest microbial peptides that are known to stimu-late responses by both T cell subpopulations. The capacity ofCFP1071–85 to stimulate IFN-� production and CTL activity byCD4� and CD8� cells from persons expressing a spectrum ofMHC molecules suggests that this peptide is an excellent candidatefor inclusion in an antituberculosis vaccine.
CD4� and CD8� T cells play complementary roles in protectiveimmunity to many intracellular pathogens, including M. tubercu-losis. CD4� cells are the major source of the macrophage-activat-ing factor IFN-�, whereas CD8� cells predominate in lysing in-fected cells (28). CD4� cells also enhance the CD8� cell responseto Ag through interactions between CD40L on the surface ofCD4� cells and CD40 on APCs and on CD8� cells (30–32), andwe have recently shown that the CD40/CD40L pathway contributes significantly to the human CD8� T cell response to M.tuberculosis (33). To maximize the protective immune response, itis theoretically appealing to vaccinate with peptides that containepitopes for both CD4� and CD8� T cells. Such peptides can bepresented by the same APC to both T cell subpopulations, and theirclose physical proximity may favor CD40/CD40L interactions andcytokine effects that enhance CD8� cell effector function. Admin-istration of a peptide containing a CTL epitope of HIV fused to aTh epitope yielded increased CTL responses (34), and vaccinationwith a 35-mer peptide containing both a CTL and a Th epitope ofhuman papillomavirus completely eradicated papilloma virus-ex-pressing tumors in a murine model (35).
Although epitopes for CD4� cells and those for CD8� cells canbe fused to create chimeric peptides, naturally occurring peptidesrecognized by CD4� and CD8� cells may elicit more effectiveimmunity because they are more likely to undergo appropriate Agprocessing. Fused peptides can also create junctional epitopes thatinhibit the immune response to the desired epitopes (36). Anepitope comprising 15 aa capable of binding to both MHC class Iand class II molecules in a murine model has been identified forHIV (37) and CD8 epitopes within CD4 epitopes are present in
Plasmodium falciparum (38). CD8 epitopes of P. falciparum thatwere nested within CD4 epitopes were more antigenic for humansthan other CD8 epitopes, supporting the enhanced immunogenicityof peptides that stimulate both classes of T cells.
Peptides within the M. tuberculosis proteins Ag 85B, ESAT-6,mce2, and the 16-kDa proteins MPB70 and �-crystallin are rec-ognized by T cells from persons expressing more than one MHCclass II haplotype (39–44). In most of these studies, peptides of16–25 aa were studied, minimal epitopes were not delineated bypeptide truncation, or responses of purified CD4� cells were nottested (39–43). Therefore, these peptides may contain more thanone CD4 epitope, or a CD4 and CD8 epitope, rather than a singlepromiscuous CD4 epitope. Valle and colleagues identified a 12-aapeptide of Ag85 that elicited proliferation by PBMC from 89% ofhealthy tuberculin reactors (44). However, because a proliferativeresponse was defined as only 2-fold that of background levels, andMHC typing of the donors was not performed, it is uncertainwhether this peptide is truly promiscuous. The current study pro-vides the most definitive evidence to date that M. tuberculosispeptides of only 9–10 aa can be recognized by persons expressingmultiple MHC class II alleles. These peptides are shorter than the13–16 aa peptides that have generally been found to bind MHCclass II molecules.
Anti-MHC class I reduced the number of peptide T1- and T6-responsive IFN-�� cells by �50%, whereas anti-MHC class IIalmost completely abrogated the response (Table V). These resultssuggest that MHC class I-restricted CD8� T cells contribute sig-nificantly to IFN-� production induced by M. tuberculosis pep-tides. However, this response depends on the presence of CD4�
cells. These findings extend the results of prior studies indicatingthat the capacity of CD8� T cells to produce IFN-� in response toheat-killed M. tuberculosis requires CD4� cells, probably throughCD40/CD40L interactions (33, 45).
CFP10 is recognized by T cells from the majority of personswith latent tuberculosis infection and by persons with active tu-berculosis, including patients with HIV infection (20, 46, 47). Thecarboxy end of the molecule is highly immunogenic, and peptides71–90 elicit responses by 30–50% of PBMC from CFP10-respon-sive persons in Zambia and India (20, 46). The current resultsconfirm and extend these findings, demonstrating that CFP1071–85
Table VI. HLA typing results and responses of CD4� and CD8� T cells to peptide T1 and peptide T6a
Donor CD4 CTL/IFN-�� DRB1 DQB1 CD8 CTL/IFN-�� HLA-A HLA-B HLA-C
Peptide T1T294 �/ND DRB1□*04, *15 DQB1□*03, *06 �/ND A*24, *3108 B*15, *4406 Cw*01, *05T283 �/ND DRB1□*04, *08 DQB1□*03, *04 �/ND A*24, *68 B*15, *40 Cw*01, *03T295 �/ND DRB1□*04, □*04 DQB1□*03, □*03 �/ND A*01, □*02 B*40, *57 Cw*03, *06T013 �/� DRB1□*04, *08 DQB1□*03, *04 �/� A□*02, *24 B*15, *35 Cw*01, *04T215 �/� DRB1□*04, □*04 DQB1□*03, □*03 �/ND A□*02, *11 B*35, *40 Cw*03, *04T221 �/� DRB1□*04, □*04 DQB1□*03, □*03 �/� A□*02, *02 B*39, *40 Cw*03, *07T193 ND/� DRB1□*04, □*04 DQB1□*03, □*03 ND/� A□*02, *68 B*35, *51 Cw*04, *08T234 ND/� DRB1*03, *13 DQB1*02, □*03 ND/� A*24, *74 B*35, *41 Cw*04, *17T235 �/� DRB1*03, *13 DQB1*02, □*03 �/� A*24, *74 B*35, *41 Cw*04, *17
Peptide T6T294 �/ND DRB1□*04, *15 DQB1□*03, *06 �/ND A*24, *3108 B*15, *4406 Cw*01, *05T283 �/ND DRB1□*04, *08 DQB1□*03, *04 �/ND A*24, *68 B*15, *40 Cw*01, *03T295 �/ND DRB1□*04, □*04 DQB1□*03, □*03 �/ND A*01, *02 B*40, *57 Cw*03, *06T013 �/� DRB1□*04, *08 DQB1□*03, *04 �/� A*02, *24 B*15, □*35 Cw*01, *04T215 �/� DRB1□*04, □*04 DQB1□*03, □*03 �/ND A*02, *11 B□*35, *40 Cw*03, *04T221 �/� DRB1□*04, □*04 DQB1□*03, □*03 �/� A*02, *02 B*39, *40 Cw*03, *07T193 ND/� DRB1□*04, □*04 DQB1□*03, □*03 ND/� A*02, *68 B□*35, *51 Cw*04, *08T234 ND/� DRB1*03, *13 DQB1*02, □*03 ND/� A*24, *74 B□*35, *41 Cw*04, *17T235 �/� DRB1*03, *13 DQB1*02, □*03 �/� A*24, *74 B□*35, *41 Cw*04, *17
a Boxes show HLA class I and class II alleles that appeared to be associated with either CTL activity or IFN-� production by CD8� and CD4� cells, respectively.
1974 A MYCOBACTERIAL PEPTIDE RECOGNIZED BY CD4� and CD8� T cells

contains at least two epitopes for CD4� T cells, and is recognizedin the context of DRB1*0401, DRB5*0101, and DQB1*0302 (Ta-bles VI and VII, and Fig. 6). The responsiveness of CD4� T cellsfrom subject T225 to the CFP10 peptides in the absence ofDRB1*04 or DQB1*03 (Table I) may be due to the expression ofDRB5*0101, which is linked to the DRB1*1501 allele in HLA-DR2� subjects. Peptide T1 contains isoleucine at position 1, ala-nine at position 4, and valine at position 6, conforming to the motifpredicting strong binding to HLAB1*0401, which is the most com-mon subtype of HLAB1*04 in the United States (48). In contrast,peptide T6 shows no features of this motif. Because some donorswhose CD4� T cells produced IFN-� in response to CFP1071–85
expressed other MHC class II alleles (Table I, and data not shown),peptides T1 and T6, or other epitopes on CFP1071–85, are likely tobe presented by additional class II molecules. Our findings areconsistent with previous work demonstrating that certain peptidescan bind to at least seven common DR types, includingDRB1*0401 (49).
Previous work has shown that CFP1085–94 and CFP102–11 areHLA-B14- and HLA-B44-restricted epitopes, respectively, for hu-man CD8� T cell clones (24). We found that CFP1071–85 containsat least two epitopes for CD8� T cells, one recognized by personsexpressing HLA-A*02 and the other by persons expressing HLA-B*35 (Table VI). CD8� T cells from persons expressing otherMHC class I alleles may also recognize these epitopes, as formalrestriction analysis with cells expressing a single allele was notperformed. HLA-A*02 is part of the HLA-A2 supertype, which isexpressed by 39–46% of Caucasians, North American Blacks,Hispanics, and Asians (50). HLA-B*35 is part of the HLA-B7supertype, which is expressed by 43–57% of these ethnic groups.Therefore, CFP1071–85 is likely to be recognized by CD8� T cellsfrom the majority of people in different populations throughout theworld.
The capacity of CFP1071–85 to elicit IFN-� production and CTLactivity by CD4� and CD8� T cells from persons bearing multipleMHC class I and class II alleles makes it an intriguing candidatefor inclusion in an antituberculosis vaccine. DNA vaccines encod-ing short peptides or peptide-based vaccines are attractive becausethey are substantially easier to produce than vaccines based on
whole proteins. In addition, epitopes in proteins that elicit sup-pressive or immunopathogenic responses can be avoided. Peptidessuch as CFP1071–85, perhaps in combination with other immuno-dominant M. tuberculosis peptides, may also be useful to developa diagnostic test for latent tuberculosis infection, based on anELISPOT assay that detects IFN-�-producing cells. However, avaccine that includes CFP1071–85 would limit the clinical utility ofCFP1071–85-based diagnostic tests in the vaccinated population.These potentially contrasting roles will need to be reconciled in thefuture.
FIGURE 6. Peptide T1 is recognized by T cell clones in the context ofdifferent HLA class II alleles. T1-responsive clones B9 and F10 were gen-erated from a donor whose MHC class II alleles were DQB1*03,DQB1*02, DRB1*04, and DRB1*07. Thirty-five percent and 58% of B9and F10 cells produced IFN-� in response to T1-pulsed autologous mac-rophages, respectively. Clones were incubated with BLS cells lacking en-dogenous MHC class II alleles, and with BLS cells expressing single HLAclass II alleles, in the presence or absence of peptide at concentrations of10, 1, and 0.1 �g/ml. Clones without BLS cells were also used as controls.A total of 25,000 BLS cells and 100 clones were placed into each well induplicate, and the number of IFN-�-producing cells was enumerated after16 h. Values shown are the mean of duplicate results obtained with apeptide concentration of 1 �g/ml. A total of 10 �g/ml peptide yieldedessentially identical results. The number of IFN-�� cells was reduced by�90% when the peptide concentration was 0.1 �g/ml.
Table VII. Presentation of peptides T1 and T6 by APC expressing a single HLA allelea
DonorsCFP10
response
Donors HLAType Peptide T1 Peptide T6
DR DQ
DRB1*0401� peptide� CD4
DRB1*0401� CD4
DRB1*0401� peptide
DQB1*0302� peptide �
CD4DQB1*0302
� CD4DQB1*0302� peptide
DRB1*0401� peptide� CD4
DRB1*0401� CD4
DRB1*0401� peptide
DQB1*0302� peptide �
CD4DQB1*0302
� CD4DQB1*0302� peptide
T040 �B1*04 B1*03
80 8 3 45 5 0 113 20 3 110 8 0B1*04 B1*03
T262 �B1*04 B1*03
78 5 3 70 8 0 85 23 3 80 5 0B1*08 B1*04
T283 �B1*04 B1*03
58 18 0 40 0 0 70 13 0 58 8 0B1*08 B1*04
T294 �B1*04 B1*03
68 10 3 65 10 0 120 10 3 55 5 0B1*15 B1*06
T030 �B1*04 B1*03
7 8 0 2 3 0 5 8 0 8 5 0B1*13 B1*06
T062 �B1*01 B1*05
19 14 0 4 7 0 22 16 0 5 5 0B1*13 B1*06
T185 �B1*03 B1*02
3 5 0 2 7 0 4 1 0 5 6 0B1*04 B1*03
T281 �B1*01 B1*05
12 18 0 2 4 0 18 12 0 2 4 0B1*13 B1*05
a BLS cells expressing DRB1*0401 or DQB1*0302 were used as target cells, either unpulsed or pulsed with peptides T1 or T6. Purified CD4� T cells from freshly isolatedPBMC from four donors were added to target cells, and the number of IFN-�� cells was measured by ELISPOT. Values shown are the mean number of IFN-�� cells per 2.5 �105 cells, based on duplicate wells.
1975The Journal of Immunology

AcknowledgmentsWe are grateful to Mabtech and Staffan Paulie for providing us with pre-coated IFN-� ELISPOT plates, and to Ortho Biotech for provision of anti-CD3 mAb. We thank Sharon Kochik for excellent technical assistance inhandling BLS cells and transfectants.
References1. Corbett, E. L., C. J. Watt, N. Walker, D. Maher, B. G. Williams,
M. C. Raviglione, and C. Dye. 2003. The growing burden of tuberculosis: globaltrends and interactions with the HIV epidemic. Arch. Intern. Med. 163:1009.
2. Toungoussova, O. S., P. Sandven, A. O. Mariandyshev, N. I. Nizovtseva,G. Bjune, and D. A. Caugant. 2002. Spread of drug-resistant Mycobacteriumtuberculosis strains of the Beijing genotype in the Archangel oblast, Russia, in1999. J. Clin. Microbiol. 40:1930.
3. Tracevska, T., I. Jansone, V. Baumanis, O. Marga, and T. Lillebaek. 2003. Prev-alence of Beijing genotype in Latvian multidrug-resistant Mycobacterium tuber-culosis isolates. Int. J. Tuberc. Lung Dis. 7:1097.
4. Sterling, T. R., W. T. Brehm, R. D. Moore, and R. E. Chaisson. 1999. Tubercu-losis vaccination versus isoniazid preventive therapy: a decision analysis to de-termine the preferred strategy of tuberculosis prevention in HIV-infected adultsin the developing world. Int. J. Tuberc. Lung Dis. 3:248.
5. Kaufmann, S. H. E. 2001. How can immunology contribute to the control oftuberculosis? Nat. Rev. Immunol. 1:20.
6. Tan, J. S., D. H. Canaday, W. H. Boom, K. N. Balaji, S. K. Schwander, andE. A. Rich. 1997. Human alveolar T lymphocyte responses to Mycobacteriumtuberculosis antigens. J. Immunol. 159:290.
7. Stenger, S., D. A. Hanson, R. Teitelbaum, P. Dewan, K. R. Niazi, C. J. Froelich,T. Ganz, S. Thoma-Uszynski, A. Melian, C. Bogdan, et al. 1998. An antimicro-bial activity of cytolytic T cells mediated by granulysin. Science 282:121.
8. Smith, S. M., R. Brookes, M. R. Klein, A. S. Malin, P. T. Lukey, A. S. King,G. S. Ogg, A. V. S. Hill, and H. M. Dockrell. 2000. Human CD8� CTL specificfor the mycobacterial major secreted antigen 85A. J. Immunol. 165:7088.
9. Geluk, A., K. E. van Meijgaarden, K. L. M. C. Franken, J. W. Drijfhout, S.D’Souza, A. Necker, K. Huygen, and T. H. M. Ottenhoff. 2000. Identification ofmajor epitopes of Mycobacterium tuberculosis AG85B that are recognized byHLA-A*0201-restricted CD8� T cells in HLA-transgenic mice and humans.J. Immunol. 165:6463.
10. Canaday, D. H., R. J. Wilkinson, Q. Li, C. V. Harding, R. F. Silver, andW. H. Boom. 2001. CD4� and CD8� T cells kill intracellular Mycobacteriumtuberculosis by a perforin and Fas/Fas ligand-independent mechanism. J. Immu-nol. 167:2734.
11. Heinzel, A.S., J. E. Grotzke, R. A. Lines, D. A. Lewinsohn, A. L. McNabb,D. N. Streblow, V. M. Braud, H. J. Grieser, J. T. Belisle, and D. M. Lewinsohn.HLA-E-dependent presentation of Mtb-derived antigen to human CD8� T cells.J. Exp. Med. 196:1473.
12. Lazarevic, V., and J. Flynn. 2002. CD8� T cells in tuberculosis. Am. J. Respir.Crit. Care Med. 166:1116.
13. Orme, I. M. 1988. Characteristics and specificity of acquired immunologic mem-ory to Mycobacterium tuberculosis infection. J. Immunol. 140:3589.
14. Renshaw, P. S., P. Panagiotidou, A. Whelan, S. V. Gordon, R. G. Hewinson,R. A. Williamson, and M. D. Carr. 2002. Conclusive evidence that the majorT-cell antigens of the Mycobacterium tuberculosis complex ESAT-6 and CFP-10form a tight, 1:1 complex and characterization of the structural properties ofESAT-6, CFP-10, and the ESAT-6*CFP-10 complex: implications for pathogen-esis and virulence. J. Biol. Chem. 277:21598.
15. Berthet, F. X., P. B. Rasmussen, I. Rosenkrands, P. Andersen, and B. Gicquel.1998. A Mycobacterium tuberculosis operon encoding ESAT-6 and a novel low-molecular-mass culture filtrate protein (CFP-10). Microbiology 144:3195.
16. Pym, A. S., P. Brodin, R. Brosch, M. Huerre, and S. T. Cole. 2002. Loss of RD1contributed to the attenuation of the live tuberculosis vaccines Mycobacteriumbovis BCG and Mycobacterium microti. Mol. Microbiol. 46:709.
17. Arend, S. M., A. Geluk, K. E. van Meijgaarden, J. T. van Dissel, M. Theisen,P. Andersen, and T. H. Ottenhoff. 2000. Antigenic equivalence of human T-cellresponses to Mycobacterium tuberculosis-specific RD1-encoded protein antigensESAT-6 and culture filtrate protein 10 and to mixtures of synthetic peptides.Infect. Immun. 68:3314.
18. Lalvani, A., R. Brookes, R. Wilkinson, A. Malin, A. Pathan, P. Andersen,H. Dockrell, G. Pasvol, and A. Hill. 1998. Human cytolytic and interferon �-se-creting CD8� T lymphocytes specific for Mycobacterium tuberculosis. Proc.Natl. Acad. Sci. USA 95:270.
19. Brandt, L., T. Oettinger, A. Holm, A. B. Andersen, and P. Andersen. 1996. Keyepitopes on the ESAT-6 antigen recognized in mice during the recall of protectiveimmunity to Mycobacterium tuberculosis. J. Immunol. 157:3527.
20. Lalvani, A., P. Nagvenkar, Z. Udwadia, A. A. Pathan, K. A. Wilkinson,J. S. Shastri, K. Ewer, A. V. Hill, A. Mehta, and C. Rodrigues. 2001. Enumer-ation of T cells specific for RD1-encoded antigens suggests a high prevalence oflatent Mycobacterium tuberculosis infection in healthy urban Indians. J. Infect.Dis. 183:469
.
21. Lalvani, A., A. A. Pathan, H. McShane, R. J. Wilkinson, M. Latif, C. P. Conlon,G. Pasvol, and A. V. Hill. 2001. Rapid detection of Mycobacterium tuberculosisinfection by enumeration of antigen-specific T cells. Am. J. Respir. Crit. CareMed. 163:824.
22. Pathan, A. A., K. A. Wilkinson, R. J. Wilkinson, M. Latif, H. McShane,G. Pasvol, A. V. Hill, and A. Lalvani. 2000. High frequencies of circulatingIFN-�-secreting CD8 cytotoxic T cells specific for a novel MHC class I-restrictedMycobacterium tuberculosis epitope in M. tuberculosis-infected subjects withoutdisease. Eur. J. Immunol. 30:2713.
23. Pathan, A. A., K. A. Wilkinson, P. Klenerman, H. McShane, R. N. Davidson,G. Pasvol, A. V. S. Hill, and A. Lalvani. 2001. Direct ex vivo analysis of antigen-specific IFN-�-secreting CD4 T cells in Mycobacterium tuberculosis-infectedindividuals: associations with clinical disease state and effect of treatment. J. Im-munol. 167:5217.
24. Lewinsohn, D. M., L. Zhu, V. J. Madison, D. C. Dillon, S. P. Fling, S. G. Reed,K. H. Grabstein, and M. R. Alderson. 2001. Classically restricted human CD8�
T lymphocytes derived from Mycobacterium tuberculosis-infected cells: defini-tion of antigenic specificity. J. Immunol. 166:439.
25. Kovats, S., G. T. Nepom, M. Coleman, B. Nepom, W. W. Kwok, and J. S. Blum.1995. Deficient antigen-presenting cell function in multiple genetic complemen-tation groups of type II bare lymphocyte syndrome. J. Clin. Invest. 96:217.
26. Lewinsohn, D. M., M. R. Alderson, A. L. Briden, S. R. Riddell, S. G. Reed, andK. H. Grabstein. 1998. Characterization of human CD8� T cells reactive withMycobacterium tuberculosis-infected antigen-presenting cells. J. Exp. Med.187:1633.
27. Lewinsohn, D. M., A. L. Briden, S. G. Reed, K. H. Grabstein, andM. R. Alderson. 2000. Mycobacterium tuberculosis-reactive CD8� T lympho-cytes: the relative contribution of classical versus nonclassical HLA restriction.J. Immunol. 165:925.
28. Lewinsohn, D. A., A. S. Heinzel, J. M. Gardner, L. Zhu, M. R. Alderson, andD. M. Lewinsohn. 2003. Mycobacterium tuberculosis-specific CD8� T cells pref-erentially recognize heavily infected cells. Am. J. Respir. Crit. Care Med.168:1346.
29. Rammensee, H., J. Bachmann, N. P. Emmerich, O. A. Bachor, and S. Stevanovic.1999. SYFPEITHI: database for MHC ligands and peptide motifs. Immunoge-netics 50:213.
30. Bennett, S. R., F. R. Carbone, F. Karamalis, R. A. Flavell, J. F. Miller, andW. R. Heath. 1998. Help for cytotoxic-T-cell responses is mediated by CD40signalling. Nature 393:478.
31. Ridge, J. P., F. DiRosa, and P. Matzinger. 1998. A conditioned dendritic cell canbe a temporal bridge between a CD4� T-helper and a T-killer cell. Nature 393:474.
32. Bourgeois, C., B. Rocha, and C. Tanchot. 2002. A role for CD40 expression onCD8� T cells in the generation of CD8� T cell memory. Science 297:2060.
33. Samten, B., E. K. Thomas, J.-H. Gong, and P. F. Barnes. 2000. Depressed CD40ligand expression contributes to reduced � interferon production in human tu-berculosis. Infect. Immun. 68:3002.
34. Daftarian, P., S. Ali, R. Sharan, S. F. Lacey, C. La Rosa, J. Longmate, C. Buck,R. F. Siliciano, and D. J. Diamond. 2003. Immunization with Th-CTL fusionpeptide and cytosine-phosphate-guanine DNA in transgenic HLA-A2 mice in-duces recognition of HIV-infected T cells and clears vaccinia virus challenge.J. Immunol. 171:4028.
35. Zwaveling, S., S. C. Ferreira Mota, J. Nouta, M. Johnson, G. B. Lipford,R. Offringa, S. H. van der Burg, and C. J. Melief. 2002. Established humanpapillomavirus type 16-expressing tumors are effectively eradicated followingvaccination with long peptides. J. Immunol. 169:350.
36. Wang, Y., J. A. Smith, T. Kamradt, M. L. Gefter, and D. L. Perkins. 1992.Silencing of immunodominant epitopes by contiguous sequences in complex syn-thetic peptides. Cell. Immunol. 143:284.
37. Takahashi, H., R. N. Germain, B. Moss, and J. A. Berzofsky. 1990. An immu-nodominant class I-restricted cytotoxic T lymphocyte determinant of human im-munodeficiency virus type 1 induces CD4 class II-restricted help for itself. J. Exp.Med. 171:571.
38. Wang, R., J. Epstein, F. M. Baraceros, E. J. Gorak, Y. Charoenvit, D. J. Carucci,R. C. Hedstrom, N. Rahardjo, T. Gay, P. Hobart, et al. 2001. Induction of CD4�
T cell-dependent CD8� type 1 responses in humans by a malaria DNA vaccine.Proc. Natl. Acad. Sci. USA 98:10817.
39. Al Attiyah, R., F. A. Shaban, H. G. Wiker, F. Oftung, and A. S. Mustafa. 2003.Synthetic peptides identify promiscuous human Th1 cell epitopes of the secretedmycobacterial antigen MPB70. Infect. Immun. 71:1953.
40. Caccamo, N., A. Barera, C. Di Sano, S. Meraviglia, J. Ivanyi, F. Hudecz,S. Bosze, F. Dieli, and A. Salerno. 2003. Cytokine profile, HLA restriction andTCR sequence analysis of human CD4� T clones specific for an immunodomi-nant epitope of Mycobacterium tuberculosis 16-kDa protein. Clin. Exp. Immunol.133:260.
41. Mustafa, A. S., F. Oftung, H. A. Amoudy, N. M. Madi, A. T. Abal, F. Shaban,K. Rosen, I., and P. Andersen. 2000. Multiple epitopes from the Mycobacteriumtuberculosis ESAT-6 antigen are recognized by antigen-specific human T celllines. Clin. Infect. Dis. 30(Suppl. 3):S201.
1976 A MYCOBACTERIAL PEPTIDE RECOGNIZED BY CD4� and CD8� T cells

42. Mustafa, A. S., F. A. Shaban, R. Al Attiyah, A. T. Abal, A. M. El Shamy,P. Andersen, and F. Oftung. 2003. Human Th1 cell lines recognize the Myco-bacterium tuberculosis ESAT-6 antigen and its peptides in association with fre-quently expressed HLA class II molecules. Scand. J. Immunol. 57:125.
43. Panigada, M., T. Sturniolo, G. Besozzi, M. G. Boccieri, F. Sinigaglia,G. G. Grassi, and F. Grassi. 2002. Identification of a promiscuous T-cell epitopein Mycobacterium tuberculosis Mce proteins. Infect. Immun. 70:79.
44. Valle, M. T., A. M. Megiovanni, A. Merlo, P. G. Li, L. Bottone, G. Angelini,L. Bracci, L. Lozzi, K. Huygen, and F. Manca. 2001. Epitope focus, clonal com-position and Th1 phenotype of the human CD4 response to the secretory myco-bacterial antigen Ag85. Clin. Exp. Immunol. 123:226.
45. Shams, H., B. Wizel, S. E. Weis, B. Samten, and P. F. Barnes. 2001. Contributionof CD8� T cells to � interferon production in human tuberculosis. Infect. Immun.69:3497.
46. Chapman, A. L., M. Munkanta, K. A. Wilkinson, A. A. Pathan, K. Ewer,H. Ayles, W. H. Reece, A. Mwinga, P. Godfrey-Faussett, and A. Lalvani. 2002.
Rapid detection of active and latent tuberculosis infection in HIV-positive indi-viduals by enumeration of Mycobacterium tuberculosis-specific T cells. AIDS16:2285.
47. Skjot, R. L., T. Oettinger, I. Rosenkrands, P. Ravn, I. Brock, S. Jacobsen, andP. Andersen. 2000. Comparative evaluation of low-molecular-mass proteins fromMycobacterium tuberculosis identifies members of the ESAT-6 family as immu-nodominant T-cell antigens. Infect. Immun. 68:214.
48. Livingston, B., C. Crimi, M. Newman, Y. Higashimoto, E. Appella, J. Sidney,and A. Sette. 2002. A rational strategy to design multiepitope immunogens basedon multiple Th lymphocyte epitopes. J. Immunol. 168:5499.
49. Southwood, S., J. Sidney, A. Kondo, M. F. del Guercio, E. Appella, S. Hoffman,R. T. Kubo, R. W. Chesnut, H. M. Grey, and A. Sette. 1998. Several commonHLA-DR types share largely overlapping peptide binding repertoires. J. Immu-nol. 160:3363.
50. Sette, A., and J. Sidney. 1999. Nine major HLA class I supertypes account for thevast preponderance of HLA-A and -B polymorphism. Immunogenetics 50:201.
1977The Journal of Immunology