
Characteristics of hospitalised patients with 2009 H1N1 influenza in Chile
8
UNCORRECTED PROOF Respiratory Medicine (]]]]) ], ]]]–]]] Characteristics of hospitalised patients with COPD in the Nordic countries Christer Janson a, , Thorarinn Gislason b , Charlotte Suppli Ulrik c , Markku M. Nieminen d , Runa Hallin a , Eva Lindberg a , Gunnar Gudmundsson b , Tiina Aine d , Per Bakke e a Department of Medical Sciences: Respiratory Medicine and Allergology, Uppsala University, Akademiska Sjukhuset, Uppsala SE 751 85 , Sweden b Department of Respiratory Medicine and Allergology, Landspitali-University Hospital, Reykjavik, Iceland c Department of Respiratory Diseases, Hvidovre Hospital, University of Copenhagen, Copenhagen, Denmark d Department of Respiratory Medicine, Tampere University Hospital, Tampere, Finland e Haukeland University Hospital, Bergen, Norway KEYWORDS ’; ’; ’ Summary The objective of the present study was to examine differences in the characteristics and management of hospitalised patients with chronic obstructive pulmonary disease (COPD) and to determine factors related to the duration of the hospital stay in the Nordic countries. The study comprised 416 patients from five University Hospitals (Bergen, Reykjavik, Uppsala, Tampere and Copenhagen). The patients were interviewed and spirometry was performed. Psychological status was assessed with the Hospital Anxiety and Depression questionnaire and quality of life with the St. Georges’ Hospital Respiratory Questionnaire. The mean age was 69 years, 51% were women. The majority of the patients (76%) had severe COPD (GOLD stage III and IV) and 24% were on long-term oxygen therapy. Forty five % of the patients had cardio-vascular disease and 11% diabetes. In Bergen, Uppsala and Tampere over half of the patients had anxiety and depression but the prevalence of psychiatric co-morbidity was lower in Reykjavik and Copenhagen. The median length of the hospitalisation was 7–8 days in four of the five centres but two times higher in Reykjavik. The independent predictors for a longer hospitalisation was living alone (+3 days), being on long-term oxygen (+8 days) and having diabetes (+5 days). In conclusion, this study revealed substantial differences in the characteristics and management of hospitalised COPD patients between departments of respiratory 1 3 5 7 9 11 13 15 17 19 21 23 25 27 29 31 33 35 37 39 41 43 45 47 49 51 53 55 ARTICLE IN PRESS 3B2v8:06a=w ðDec 5 2003Þ:51c XML:ver:5:0:1 YRMED : 2335 Prod:Type:FTP pp:18ðcol:fig::NILÞ ED:PabitraBorah PAGN:anu 0954-6111/$ - see front matter & 2006 Published by Elsevier Ltd. doi:10.1016/j.rmed.2006.03.022 Corresponding author. Tel.: +46186114115, fax: +46186110228. E-mail address: [email protected] (C. Janson).
Transcript of Characteristics of hospitalised patients with 2009 H1N1 influenza in Chile

1
3
5
7
9
11
13
15
17
19
21
23
25
27
29
31
33
35
37
39
41
43
45
47
49
51
53
55
ARTICLE IN PRESS
3B2v8:0XML:ve
Respiratory Medicine (]]]]) ], ]]]–]]]
U
6a=w ðDec 5 20r:5:0:1
0954-6111/$ - sdoi:10.1016/j.r
�CorrespondiE-mail addr
Characteristics of hospitalised patients with COPDin the Nordic countries
Christer Jansona,�, Thorarinn Gislasonb, Charlotte Suppli Ulrikc, MarkkuM. Nieminend, Runa Hallina, Eva Lindberga, Gunnar Gudmundssonb,Tiina Ained, Per Bakkee
ROOFaDepartment of Medical Sciences: Respiratory Medicine and Allergology, Uppsala University, AkademiskaSjukhuset, Uppsala SE 751 85 , SwedenbDepartment of Respiratory Medicine and Allergology, Landspitali-University Hospital, Reykjavik, IcelandcDepartment of Respiratory Diseases, Hvidovre Hospital, University of Copenhagen, Copenhagen, DenmarkdDepartment of Respiratory Medicine, Tampere University Hospital, Tampere, FinlandeHaukeland University Hospital, Bergen, Norway
KEYWORDS’;’;’
NCO
03Þ:51c YRMED
ee front matter & 2006med.2006.03.022
ng author. Tel.: +46 186ess: christer.janson@me
RRECTED PSummary The objective of the present study was to examine differences in thecharacteristics and management of hospitalised patients with chronic obstructivepulmonary disease (COPD) and to determine factors related to the duration of thehospital stay in the Nordic countries.
The study comprised 416 patients from five University Hospitals (Bergen,Reykjavik, Uppsala, Tampere and Copenhagen). The patients were interviewedand spirometry was performed. Psychological status was assessed with the HospitalAnxiety and Depression questionnaire and quality of life with the St. Georges’Hospital Respiratory Questionnaire.
The mean age was 69 years, 51% were women. The majority of the patients (76%)had severe COPD (GOLD stage III and IV) and 24% were on long-term oxygen therapy.Forty five % of the patients had cardio-vascular disease and 11% diabetes. In Bergen,Uppsala and Tampere over half of the patients had anxiety and depression but theprevalence of psychiatric co-morbidity was lower in Reykjavik and Copenhagen. Themedian length of the hospitalisation was 7–8 days in four of the five centres but twotimes higher in Reykjavik. The independent predictors for a longer hospitalisationwas living alone (+3 days), being on long-term oxygen (+8 days) and having diabetes(+5 days).
In conclusion, this study revealed substantial differences in the characteristicsand management of hospitalised COPD patients between departments of respiratory
: 2335 Prod:Type:FTPpp:1�8ðcol:fig::NILÞ
ED:PabitraBorahPAGN:anu
Published by Elsevier Ltd.
114115, fax: +46 186110228.dsci.uu.se (C. Janson).

1
3
5
7
9
11
13
15
17
19
21
23
25
27
29
31
33
35
37
39
41
43
45
47
49
51
53
55
57
59
61
ARTICLE IN PRESS
C. Janson et al.2
disease in five Nordic university hospitals. Living alone, concurrent diseases likediabetes and long-term oxygen therapy are predictors of more prolongedhospitalisation periods.& 2006 Published by Elsevier Ltd.
E
63
65
67
69
71
73
75
77
79
81
83
85
87
89
91
93
95
97
99
101
103
105
107
109
111
UNCORRECT
Introduction
Acute exacerbations of chronic obstructive pul-monary disease (COPD) is becoming one of the mostcommon causes for hospitalisations in the Nordiccountries.1 As an effect the cost for the manage-ment of COPD is increasing and the total cost forCOPD in Sweden 1999 was estimated to 982 millionEuro.2 Exacerbations account for 35–45% of thetotal per capita health-care costs for COPD and thecost for an COPD exacerbations that requires a visitto an emergency care unit or a night in hospital wasin 1999 estimated to be on average 2400 Euro perpatient in Sweden.3
During the last decades international guidelineson the management of COPD have been developed4
and these guidelines have been implemented in allthe Nordic countries. Despite the socio-economicsimilarities and the common guide lines data fromofficial statistics have shown considerable differ-ences in hospitalisation rates for COPD and asthmabetween the Nordic countries with a variation from533 discharged patients per 100,000 inhabitants inDenmark to 147/100,000 inhabitants in Finland.5
This may to some extent be explained by differ-ences in the prevalence of smoking and COPD in theNordic countries,5–8 but may also reflect nationaldifferences in the management of COPD.
In a retrospective study covering 500 patientswith obstructive lung disease from five universityteaching hospitals in the Nordic countries we foundthat there were large differences in the diagnosticprocedures and the length of hospitalisationsbetween the hospitals.9 The retrospective studyalso underlined that there is a high readmissionrate in hospitalised patients with obstructive lungdisease with 50% of the patients having beenreadmitted within 12 months after being dischargefrom hospital.6 In year 2000–2002, a prospectiveNordic multicenter study was performed.10 The aimof this investigation was to study the managementand prognosis in hospitalised patients with COPD inthe Nordic countries.
The aim of this investigation was to compare thecharacteristics and management of hospitalisedCOPD patients from one departments of respiratorymedicine in each of the five Nordic countries. A
YRMED
secondary aim was to analyse risk factors ofprolonged hospitalisations.
D PROOF
Method
The study aimed to include 100 patients each fromfive University Hospitals (Bergen, Reykjavik, Up-psala, Tampere and Copenhagen) in the Nordiccountries (Fig. 1). The departments included were:The Department of Respiratory Medicine andAllergology, Akademiska sjukhuset, Uppsala, Swe-den; The Department of Thoracic Medicine, Hauke-land University Hospital, Bergen, Norway; TheDepartment of Respiratory Medicine, TampereUniversity Hospital,Tampere, Finland; The Depart-ment of Respiratory Medicine, Vifilstadir UniversityHospital, Gardabaer, Iceland and The Departmentof Respiratory Medicine, Hvidovre Hospital, Copen-hagen Denmark.
Consecutive patients from each of the partici-pating hospitals were included provided that theyhad been admitted with acute exacerbations ofobstructive lung disease (asthma, chronic bronchi-tis, chronic obstructive bronchitis or emphysema)during the year 2000–2001. As the majority of thepatients had COPD all patients with asthma(n ¼ 66) were excluded and reported are only datafrom the 416 patients that fulfilled the criteria forCOPD according to the Global Initiative for ChronicObstructive Pulmonary Disease stage 1 or higher.4
The following data were collected at dischargefrom the respective pulmonary departments:
1.
Questionnaire that included information on thefollowing: age, gender, length of hospital stay,smoking history, education, and family situation(living at home, assisted at home, nursing home,with spouse, alone or with others).2.
Spirometry, body weight and height. Predictedvalues for forced expiratory volume in 1 s (FEV1)and forced vital capacity (FVC) were calculatedbased on the European Coal and Steel Unionreference values.113.
Health Related Quality of Life was assessed usingthe disease-specific St. George’s RespiratoryQuestionnaire (SGRQ). It has three components:symptoms, activity and impact, in addition to: 2335

ROOF
1
3
5
7
9
11
13
15
17
19
21
23
25
27
29
31
33
35
37
39
41
43
45
47
49
51
53
55
57
59
61
63
65
67
69
71
73
75
77
79
81
83
85
ARTICLE IN PRESS
Copenhagen
Uppsala
BergenTampere
Reykjavik
Figure 1 Location of the study centres.
Characteristics of hospitalised patients with COPD in the Nordic countries 3
total score.12 Higher scores indicate worsehealth status.
4.
8789
91
93
CTAnxiety and depression were evaluated with theHospital Anxiety and Depression Scale (HADS).13
It is composed of two parts, one with 7 questionsthat are related to anxiety and another with 7questions that are related to depression. A scoreof 8 or greater on either part was used as thecut-off point for diagnosing anxiety and depres-sion, respectively.
5.
9597
99
101
103
NCORREFrom the patient records information wascollected on treatment at discharge, includinglong-term oxygen therapy and medications.Assessment of co-morbidity was based on thediagnosis used by the treating physician. Dia-betes mellitus was considered to be present ifthe patient was using medications for diabetes.Hypertension, ischaemic heart disease or atrialfibrillation were considered to be present whendiagnosed by the attending physician and thepatient was using appropriate medications. U 105107
109
111
Statistics
Statistical analyses were performed using StatView5.0 (SAS Institute Inc, Cary, NC, USA). Chi-squaredtest and one-way analysis of variation were used
YRMED
ED Pwhen analysing differences between the hospitals.Multiple linear regression was used to analysedeterminants for the length of hospitalisation. Inthis analysis the duration of hospitalisation was logtransformed. A P-valueo0.05 was considered sta-tistically significant.
Results
The analysis included 205 men and 211 women,mean (7SD) age 69710 years. The characteristicsof the 416 patients in the different hospitals aredisplayed in Table 1. Many of the patients wereliving alone (52.1%) and cardio-vascular co-morbid-ity (45.0%) and diabetes (10.6%) was common.Significant differences in the characteristics of thepatients between the hospitals were found for allvariables except age, lung function and theprevalence of diabetes (Table 1).
A large majority of the patients (76.0%) hadsevere COPD (GOLD stage III and IV) with nosignificant difference between the centres (Fig.2). In Bergen, Uppsala and Tampere over half of thepatients had anxiety and depression but theprevalence of psychiatric co-morbidity was lowerin Reykjavik and Copenhagen (Fig. 3). Many of thepatients had low health-related quality of life, but
: 2335

RECTED PROOF
1
3
5
7
9
11
13
15
17
19
21
23
25
27
29
31
33
35
37
39
41
43
45
47
49
51
53
55
57
59
61
63
65
67
69
71
73
75
77
79
81
83
85
87
89
91
93
95
97
99
101
103
105
107
109
111
ARTICLE IN PRESS
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%I II III IV P=0.29
Bergen Uppsala Reykjavik Tampere Copenhagen
Figure 2 Severity classification according to the GOLD criteria in hospitalised COPD patients.
Table 1 Characteristics of the patients (mean+SD or %).
Bergen(n ¼ 100)
Uppsala(n ¼ 87)
Reykjavik(n ¼ 81)
Tampere(n ¼ 60)
Copenhagen(n ¼ 88)
P-value
Age 70711 69711 6979 67711 70710 0.22Women 46 60 54 32 57 0.007Smokers 27 33 13 27 28 0.04Pack years 25717 35725 44723 34726 40721 o0.0001Living alone 39 53 59 40 68 0.0003FEV1 (% of predicted) 40717 36718 43721 39718 35717 0.07Cardio-vasculardisease
40 67 42 50 28 o0.0001
Diabetes 15 9 16 5 6 0.06
C. Janson et al.4
UNCORpatients in Uppsala and Reykjavik had higherquality of life than patients from the three otherhospitals (Fig. 4).
A majority of the patients were on maintenancetreatment with inhaled corticosteroids but therewhere considerable difference in the use of otherpharmacological agents (Table 2). Patients inReykjavik were using ipratropium and nebulisedtreatment considerably less often than patientsfrom the other hospitals. The number of patients onlong-term oxygen was 98 (23.6%).
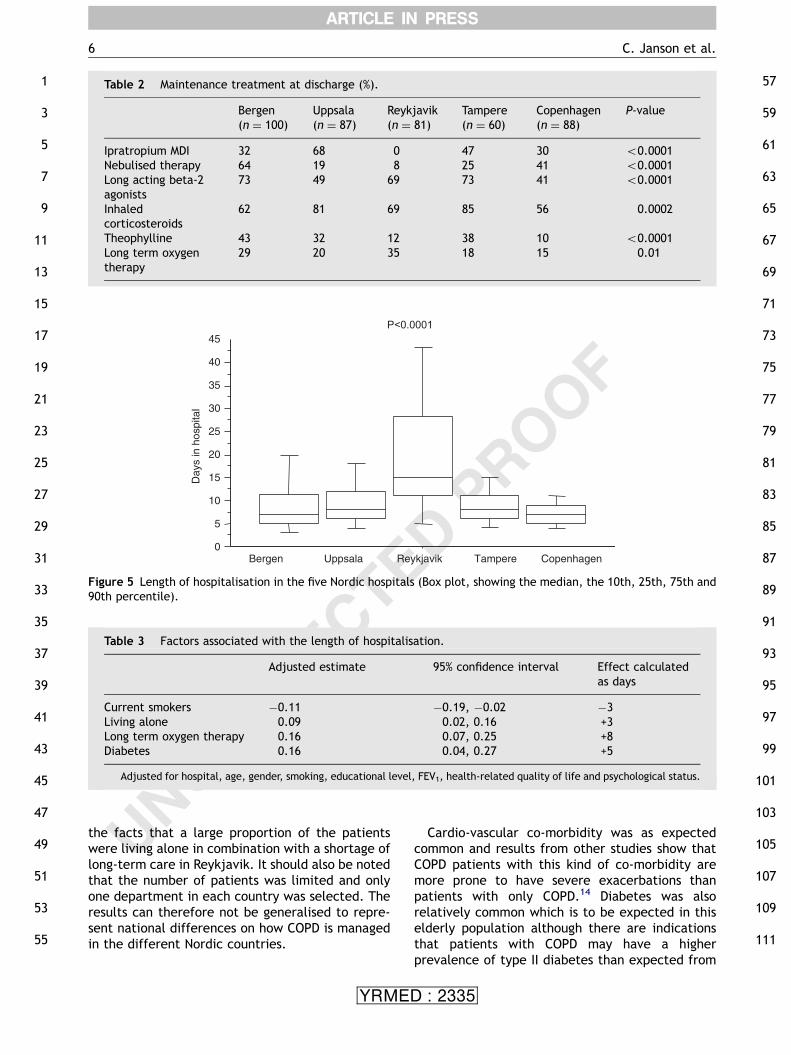
The median length of the hospitalisation was 7–8days in four of the five centres. The only exceptionwas Reykjavik were the median length of hospita-lisation was two times higher than in the other
YRMED
hospitals (Fig. 5). The independent predictors for alonger hospitalisation was living alone, being onlong-term oxygen and having diabetes, whilepatients that were current smokers had a signifi-cantly shorter length of hospitalisation (Table 3).
Discussion
The main result of this investigation is that therewere quite large differences in the characteristicsand treatment of COPD patients between these fiveNordic university hospitals. There was a widevariation in the length of hospital stay. Patients
: 2335

UNCORRECTED PROOF
1
3
5
7
9
11
13
15
17
19
21
23
25
27
29
31
33
35
37
39
41
43
45
47
49
51
53
55
57
59
61
63
65
67
69
71
73
75
77
79
81
83
85
87
89
91
93
95
97
99
101
103
105
107
109
111
ARTICLE IN PRESS
0%
20%
40%
60%
80%
100%
Bergen Uppsala Reykjavik Tampere Copenhagen
P<0.0001
None Anxiety Depression Both
Figure 3 Anxiety and depression in patients hospitalised because of COPD.
20
30
40
50
60
70
80
90
Tota
l score
Bergen
P<0.0001
Uppsala Reykjavik Tampere Copenhagen
Figure 4 Health-related quality of life measured as total score using the St. George Respiratory Questionnaire (Boxplot, showing the median, the 10th, 25th, 75th and 90th percentile).
Characteristics of hospitalised patients with COPD in the Nordic countries 5
who are old, have concurrent diseases like diabetesand patients on long-term oxygen therapy hadprolonged hospitalisation periods.
Like in our previous retrospective study9 thelength of hospital stay was longest in Reykjavik.
YRMED
This is also in accordance with official statisticswere the mean hospital stay for patients withobstructive lung diseases in year 2002 was 8 days inIceland compared to 5–6 days in the other Nordiccountries.5 The difference might have to do with
: 2335
CORRECTED PROOF
1
3
5
7
9
11
13
15
17
19
21
23
25
27
29
31
33
35
37
39
41
43
45
47
49
51
53
55
57
59
61
63
65
67
69
71
73
75
77
79
81
83
85
87
89
91
93
95
97
99
101
103
105
107
109
111
ARTICLE IN PRESS
Table 2 Maintenance treatment at discharge (%).
Bergen(n ¼ 100)
Uppsala(n ¼ 87)
Reykjavik(n ¼ 81)
Tampere(n ¼ 60)
Copenhagen(n ¼ 88)
P-value
Ipratropium MDI 32 68 0 47 30 o0.0001Nebulised therapy 64 19 8 25 41 o0.0001Long acting beta-2agonists
73 49 69 73 41 o0.0001
Inhaledcorticosteroids
62 81 69 85 56 0.0002
Theophylline 43 32 12 38 10 o0.0001Long term oxygentherapy
29 20 35 18 15 0.01
0
5
10
15
20
25
30
35
40
45
Bergen Reykjavik
Day
s in
hos
pita
l
P<0.0001
Uppsala Tampere Copenhagen
Figure 5 Length of hospitalisation in the five Nordic hospitals (Box plot, showing the median, the 10th, 25th, 75th and90th percentile).
Table 3 Factors associated with the length of hospitalisation.
Adjusted estimate� 95% confidence interval Effect calculatedas days
Current smokers �0.11 �0.19, �0.02 �3Living alone 0.09 0.02, 0.16 +3Long term oxygen therapy 0.16 0.07, 0.25 +8Diabetes 0.16 0.04, 0.27 +5
�Adjusted for hospital, age, gender, smoking, educational level, FEV1, health-related quality of life and psychological status.
C. Janson et al.6
UNthe facts that a large proportion of the patientswere living alone in combination with a shortage oflong-term care in Reykjavik. It should also be notedthat the number of patients was limited and onlyone department in each country was selected. Theresults can therefore not be generalised to repre-sent national differences on how COPD is managedin the different Nordic countries.
YRMED
Cardio-vascular co-morbidity was as expectedcommon and results from other studies show thatCOPD patients with this kind of co-morbidity aremore prone to have severe exacerbations thanpatients with only COPD.14 Diabetes was alsorelatively common which is to be expected in thiselderly population although there are indicationsthat patients with COPD may have a higherprevalence of type II diabetes than expected from
: 2335

1
3
5
7
9
11
13
15
17
19
21
23
25
27
29
31
33
35
37
39
41
43
45
47
49
51
53
55
57
59
61
63
65
67
69
71
73
75
77
79
81
83
85
87
89
91
93
95
97
99
101
103
105
ARTICLE IN PRESS
Characteristics of hospitalised patients with COPD in the Nordic countries 7
UNCORRECT
age alone.15 In our study patients with diabetes hadlonger hospitalisation periods probably due to theproblems with maintaining a glucose balance duringsystemic corticosteroid treatment.
In three of the centre over half of the patientshad probable anxiety and depression which is muchhigher than found in a study of a Swedish generalpopulation.16 The high prevalence of psychiatricco-morbidity may be important as anxiety anddepression has been found to be associated to anincreased risk of readmissions in emergency-trea-ted patients with asthma and COPD.17
While it was expected that patients living aloneand patients on long-term oxygen therapy wouldhave increased hospital stays the finding of sig-nificantly shorter hospitalisations in COPD patientsthat still are smokers is surprising. One possibleexplanation could be that smoking is prohibited inmost hospitals in the Nordic countries and patientsthat are addicted may therefore be more moti-vated to leave the hospitals earlier. Neverthelessefforts to motivate hospitalised smoking COPDpatients to quite smoking should be encouragedas the risk of new hospital admissions was reducedby about 40% in COPD patients that managed toquite smoking in a Danish study.18
The data on maintenance treatment showed bothdifferences and similarity between the hospitals.Like in our previous study very few of the Icelandicpatients were using ipratropium, while the use ofinhaled corticosteroids and long acting beta2-agonist was relatively widespread in all thehospitals. The majority of the patients had severeCOPD and the use of inhaled corticosteroids istherefore in accordance with the guidelines,4 asthis treatment has been showed to reduce the riskof rehospitalisations although the effect is not verylarge.19
In conclusion there was a wide variation in thecharacteristics, treatment and length of hospitalstay between the hospitals. Patients that livealone, have concurrent diseases like diabetes andpatients on long-term oxygen therapy often havemore prolonged hospitalisation periods. The pa-tients have now been followed for 12 months andanalyses of this data will give an assessment of thedifferent risk factors for readmission of COPD in theNordic countries. This information may also giveindications on how to lower the health economicburden of COPD in Northern Europe.
107
109
111
Uncited reference[20]
YRMED
Acknowledgements
The authors wish to thank all the participants in thestudy, and also Boehringer Ingelheim Denmark,Norway, Sweden and Finland, as well as the SwedishHeart and Lung association for financial support.
ED PROOF
References
1. The National Board of Health and Welfare, Stockholm,Sweden. Halso- och sjukvardsstatistisk arsbok, 2002. http://www.sos.se) (upp datera).
2. Jansson S-A, Andersson F, Borg S, Ericsson Å, Jonsson E,Lundback B. Costs of COPD in Sweden according to diseaseseverity. Chest 2002;122:1994–2002.
3. Anderson F, Borg S, Jansson SA, Jonsson AC, Ericsson A, PrutzC, et al. The costs of exacerbations in chronic obstructivepulmonary disease. Resp Med 2002;96:700–8.
4. Global Initiative For Chronic Obstructive Lung Disease.Global strategy for the diagnosis, management, and pre-vention of chronic obstructive pulmonary disease (Updated2003). www.goldcopd.com.
5. Nordic Medico-Statistical Committee. Health statistics in theNordic countries, 2002, www.nom-nos.dk.
6. Frosig A, Johnsen CR, Vestergaard Pedersen B, Taudorf E.Effects of low-level airpolution on asthma and chronicbronchitis in Nordic cities. Research Report, The NordicCouncil of Ministers, 1993.
7. Siafakas NM, Vermeire P, Pride NB, Paoletti P, Gibson J, et al.Optimal management of chronic obstructive pulmonarydisease (COPD). Eur Respir J 1995;8:1398–423.
8. De Marco R, Accordini S, Cerveri I, Corsico A, Sunyer J,Neukirch F, et al. An international survey of chronicobstructive pulmonary disease in young adults according toGOLD stages. Thorax 2004;59:120–5.
9. Janson C, Bakke P, Haahtela T, Gislason T, Suppli Ulrik C,Nettelbladt M, et al. Obstructive lung disease in patientswithin the hospital in the Nordic countries. Eur Respir Rev2000;10:428–31.
10. Suppli Ulrik C. Genindlæggelse af patienter med obstruktivlungesygdom i de nordiske lande. Lungeforum 200; 36–37.
11. European Community for Coal and Steel. Standardisation oflung function tests. Clin Respir Phys 1983;19(Suppl. 5):22–7.
12. Jones PW, Quirk FH, Baveystock CM, Littlejohns P. A self-complete measure of health status for chronic airflowlimitation. The St. George’s Respiratory Questionnaire. AmRev Respir Dis 1992;145:1321–7.
13. Zigmond AS, Snaith RP. The hospital anxiety and depressionscale. Acta Psyciatr Scand 1983;67:361–70.
14. Pistelli R, Lange P, Miller DL. Determinants of prognosis ofCOPD in the elderly: mucus hypersecretion, infections,cardiovascular comorbidity. Eur Respir J 2001;21(Suppl40):10s–4s.
15. Rana JS, Mittleman MA, Sheikh J, Hu FB, Manson JE, ColditzGA, et al. Chronic obstructive pulmonary disease, asthma,and risk of type 2 diabetes in women. Diabetes Care2004;27:2478–84.
16. Lisspers J, Nygren A, Soderman E. Hospital anxiety anddepression scale (HAD): some psychometric data for aSwedish sample. Acta Psychiatr Scand 1997;96:281–6.
17. Dahlen I, Janson C. Anxiety and depression are related tothe outcome of emergency treatment in patients
: 2335

1
3
5
7
9
11
13
15
ARTICLE IN PRESS
C. Janson et al.8
with obstructive pulmonary disease. Chest 2002;122:1633–7.
18. Godtfredsen NS, Vestbo J, Osler M, Prescott E. Risk ofhospital admission for COPD following smoking cessation andreduction: a Danish population study. Thorax2002;57:967–72.
19. Alsaeedi A, Sin DD, McAlister FA. The effects of inhaledcorticosteroids in chronic obstructive pulmonary disease: a
UNCORRECTE
YRMED
systematic review of randomized placebo-controlled trials.Am J Med 2002;113:59.
20. Brusasco V, Hodder R, Miravitlles M, Korducki L, Towse L,Kesten S. Health outcomes following treatment for sixmonths with once daily tiotropium compared with twicedaily salmeterol in patients with COPD. Thorax2003;58:399–404.
D PROOF
: 2335




















