
Chapter 3 - UvA-DARE (Digital Academic Repository)
15
UvA-DARE is a service provided by the library of the University of Amsterdam (https://dare.uva.nl) UvA-DARE (Digital Academic Repository) Imaging of physeal stress in the upper extremity (Ab)normal redefined Kraan, R.B.J. Publication date 2020 Document Version Other version License Other Link to publication Citation for published version (APA): Kraan, R. B. J. (2020). Imaging of physeal stress in the upper extremity: (Ab)normal redefined. General rights It is not permitted to download or to forward/distribute the text or part of it without the consent of the author(s) and/or copyright holder(s), other than for strictly personal, individual use, unless the work is under an open content license (like Creative Commons). Disclaimer/Complaints regulations If you believe that digital publication of certain material infringes any of your rights or (privacy) interests, please let the Library know, stating your reasons. In case of a legitimate complaint, the Library will make the material inaccessible and/or remove it from the website. Please Ask the Library: https://uba.uva.nl/en/contact, or a letter to: Library of the University of Amsterdam, Secretariat, Singel 425, 1012 WP Amsterdam, The Netherlands. You will be contacted as soon as possible. Download date:17 Jul 2022
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Chapter 3 - UvA-DARE (Digital Academic Repository)
UvA-DARE is a service provided by the library of the University of Amsterdam (https://dare.uva.nl)
UvA-DARE (Digital Academic Repository)
Imaging of physeal stress in the upper extremity(Ab)normal redefinedKraan, R.B.J.
Publication date2020Document VersionOther versionLicenseOther
Link to publication
Citation for published version (APA):Kraan, R. B. J. (2020). Imaging of physeal stress in the upper extremity: (Ab)normalredefined.
General rightsIt is not permitted to download or to forward/distribute the text or part of it without the consent of the author(s)and/or copyright holder(s), other than for strictly personal, individual use, unless the work is under an opencontent license (like Creative Commons).
Disclaimer/Complaints regulationsIf you believe that digital publication of certain material infringes any of your rights or (privacy) interests, pleaselet the Library know, stating your reasons. In case of a legitimate complaint, the Library will make the materialinaccessible and/or remove it from the website. Please Ask the Library: https://uba.uva.nl/en/contact, or a letterto: Library of the University of Amsterdam, Secretariat, Singel 425, 1012 WP Amsterdam, The Netherlands. Youwill be contacted as soon as possible.
Download date:17 Jul 2022

3Age related signal intensity changes of the bone
marrow in the healthy adolescent: facilitating interpretation of high resolution 3T MR-images
of the distal forearm
Submitted
Rik B.J. KraanConstantinus F. Buckens
Sjoerd JensLaura S. KoxMario Maas
BNW_Rik_V1.indd 47BNW_Rik_V1.indd 47 23-03-20 11:0823-03-20 11:08
48
Chapter 3
Abstract
PurposeEstablish the presence and characteristics of bone marrow edema-like signal intensity in the distal radius and ulna of healthy adolescents using high resolution 3 Tesla MRI to facilitate interpretation of distal forearm pathology in daily practice.
MethodsHealthy adolescents (aged 12-18 years) underwent 3 Tesla MRI-scans of one wrist. Presence and characteristics of areas with bone marrow edema-like signal intensity in the distal radial and ulnar metaphyses and distal radial epiphysis were assessed by two observers independently using a standardized checklist. Disagreement between observers was settled during a consensus meeting. A hand radiograph was made to evaluate skeletal age.
ResultsTwenty-three children (skeletal age 13.4±1.2 years) were included. Areas of bone marrow edema-like signal intensity of the distal metaphysis were present in the radius in 15 (65%) and in the ulna in 21 participants (91%) and in the distal radial epiphysis in six participants (26%). Signal intensity of all but two areas was graded 1 or 2 out of 5. Participants with bone marrow edema-like signal intensity in the distal radial epiphysis had a lower skeletal age (p<0.05) compared to participants without epiphyseal lesions.
ConclusionBone marrow edema-like signal intensities are prevalent in the distal forearm of healthy children and appear to be age-dependent, presumably the result of physiological (maturation) processes. Simply attributing this high signal intensity to pathology should be prevented. Awareness of the spectrum of normal appearances of the adolescent’s distal forearm on high resolution 3T MRI allows better discrimination between physiologic lesions and true pathology.
BNW_Rik_V1.indd 48BNW_Rik_V1.indd 48 23-03-20 11:0823-03-20 11:08
49
The appearance of the healthy adolescent’s forearm on 3T MRI
Introduction
Magnetic resonance imaging (MRI) is the imaging modality of choice to evaluate the presence of bone marrow pathology including bone marrow edema (BME)-like lesions.1 These lesions appear as ill-defined areas of increased signal intensity on water-sensitive sequences as a result of an increased water content and hypointense signal intensity on T1-weighted images.2 Several pathologic conditions can induce BME-like lesions in the pediatric musculoskeletal system.1 For example, in wrist-loading athletes with stress-related injury periphyseal lesions in the distal radius and ulna are common.3,4 Accurate assessment of the presence and extent of these lesions is important to guide clinical decision making.5,6
However, especially in children focusing solely on the presence of water content is too simple, as maturation-related phenomena can affect the appearance of the bone marrow in the healthy immature skeleton.1,7,8 Therefore, establishing the normal appearance of the bone marrow in the distal forearm and the effect of skeletal age on this appearance is essential to distinguish between physiology and pathology. This is especially relevant in in areas close to unfused physes as early stage physiologic closure can be accompanied by focal periphyseal edema (FOPE).7
BME-like signal intensity in the distal forearm of children has been studied before.9,10 These studies used MRI scanners with a field strength of 1.5T MRI and focused mainly on the presence of BME-like signal intensity.9,10 Our study aims to use the superior image quality of 3T MR images 11,12 to not only evaluate presence, but also extent and signal intensity of the lesions in the epi- and metaphyses of the healthy forearm. These results may facilitate the distinction between maturation dependent and pathology-related increased signal intensity in daily clinical practice.
Methods
Study participants were derived from the Physeal MRI Pilot study; a prospective cohort study in which gymnasts with wrist pain, asymptomatic gymnasts and healthy non-gymnasts were included. To establish the presence of BME-like lesions in healthy skeletally immature distal forearm, participants had to be younger than 18 years old and only non-gymnastic participants were included in the current analysis. The study inclusion ranged from 2015 until 2018 and was approved by the institution’s internal review board.
Healthy participants were included after informed consent was obtained from participants and their parents or guardians. Participants with a history of wrist-fracture or surgery, a fused distal radial physis, growth disturbance or systematic or oncologic disease involving the musculoskeletal system were excluded.
3
BNW_Rik_V1.indd 49BNW_Rik_V1.indd 49 23-03-20 11:0823-03-20 11:08

50
Chapter 3
Patient characteristicsEach participant completed a questionnaire regarding demographic characteristics and the performance and extent of wrist-loading sports activities. Subsequently, a full physical examination of both wrists was performed by a research physician (LSK or RBK), including strength and wrist provocation tests.
ImagingTo determine skeletal age, a digital radiograph of one wrist was obtained. Validated software (BoneXpert, v2.0.1.3; Visiana, Holte, Denmark, www.BoneXpert.com)13 automatically assessed skeletal age of each participant. Subsequently an MRI-scan of the wrist was obtained using an MRI-scanner with a field strength of 3 Tesla (‘Ingenia’, Philips Healthcare, Best, the Netherlands). Participants were placed in feet-first supine position with the wrist placed in a dedicated eight-channel wrist coil next to the body. The scan protocol is depicted in table 1.
Table 1. Overview of the used MRI protocol
Plane Sequence TR (ms) TE (ms) Spatial Resolution (mm)Coronal PD TSE SPAIR 2000 30 0.3*0.3*2.5
PD TSE 2000 20 0.3*0.3*2.5T1 Dixon 639 20
210.32*0.46*2.0
T2 Dixon 2500 7071
0.32*0.43*2.0
3D WATSc 20 5 0.5*0.5*1.5Sagittal PD TSE 2000 20 0.3*0.3*1.5Axial PD TSE 1500 20 0.3*0.3*2.5
T2 TSE SPAIR 2985 60 0.3*0.3*2.5
TR: repetition time; TE: echo time; ms: milliseconds
Image assessmentMR-images of each participant were reviewed by a radiologist specialized in musculoskeletal imaging (CFB, 6 years of experience) and a radiologist-in-training (fifth year) with special interest for musculoskeletal imaging (SJ) using the Amsterdam MRI Assessment of the Physis (AMPHYS) protocol.14 To prevent bias caused by knowing that the participants were healthy non-gymnasts, observers evaluated MRI-scans of all study groups of the Physeal MRI Pilot simultaneously and were blinded for clinical information and study group. Image assessment was done using IMPAX software (AGFA HealthCare N.V., Mortsel, Belgium) on high-resolution monitors.
After the first reading a consensus meeting was held with both readers and a research physician (RBK) to discuss MRI-scans of only the non-gymnasts on which the observers disagreed on the scored items. Observers discussed discrepancies and reached consensus on
BNW_Rik_V1.indd 50BNW_Rik_V1.indd 50 23-03-20 11:0823-03-20 11:08

51
The appearance of the healthy adolescent’s forearm on 3T MRI
all items of the AMPHYS protocol that focused on the appearance of the bone marrow signal intensity. Items included presence of areas with BME-like signal intensity (yes or no) and signal intensity of these areas (scale 1 (minimal increased signal intensity) to 5 (maximum increased signal intensity)) for the distal radial and ulnar metaphyses. For the epiphysis of the distal radius items included presence of areas with BME-like signal intensity (yes or no) and characteristics of these areas including extent (mild, defined as <50% of epiphyseal volume; or severe, defined as >50% of epiphyseal volume), localization (adjacent or not adjacent to the physis), signal intensity (scale 1 to 5) and visibility on the 3D-WATSc sequence (yes or no).
AnalysisPatient characteristics and observations were entered digitally using Castor EDC (Castor Electronic Data Capture, Ciwit BV, Amsterdam, The Netherlands, 2018) and imported for analysis in RStudio (RStudio, Inc., Boston, http://www.rstudio.com/).
Descriptive statistics were used to describe patient demographics, extent of wrist-loading activities, outcomes of physical wrist examinations and observations regarding prevalence and extent of epiphyseal and metaphyseal areas with BME-like signal intensity on MRI. Only observations in which the observers agreed (before or after the consensus meeting) were used. To explore a possible relation between presence BME-like signal intensity and skeletal age, two-sided independent t-tests were used to determine if age differed significantly between participants with and without areas with BME-like signal intensity. P-values below 0.05 were considered statistically significant.
Results
From 2015 to 2018 in total 69 participants were prospectively included of which 23 (12 girls and 11 boys) were healthy non-gymnasts without wrist pain. Participants demonstrated a mean height of 163 (standard deviation (SD) 9) centimeters, a mean weight of 50.9 (SD 11.4) kilograms and a mean calendar- and skeletal age of 13.5 (SD 1.2) years and 13.4 (SD 1.2) years, respectively. Demographic information is depicted in table 2.
Twenty-two of the 23 healthy participants were involved in active sport-participation. Most were involved in sports that did not require wrist-loading (e.g. soccer or korfball). Eight participants reported a primary sport that involved wrist-loading; seven participated in field-hockey and one was a judoka. Two of these eight participated in field-hockey three times per week, the remainder all trained twice per week or less.
3
BNW_Rik_V1.indd 51BNW_Rik_V1.indd 51 23-03-20 11:0823-03-20 11:08

52
Chapter 3
Physical examinationNo abnormalities were observed during inspection of the wrists of included participants. During palpation of the examined (and scanned) wrist, one participant reported pain of the scaphoid bone and one reported pain of the distal radial physis. No pain was reported during active- or passive motion tests, strength tests or provocation tests of the examined wrists.
Table 2. Participant characteristics. Characteristics are illustrated as mean ± standard deviation.
Girls BoysNumber of participants 12 11Height (cm) 164 ± 7 162 ± 12Weight (kg) 52.2 ± 7.6 49.6 ± 14.8BMI (kg/m2) 19.3 ± 2.9 18.8 ± 4.6Calendar age (years) 13.8 ± 1.2 13.3 ± 1.3Skeletal age (years) 13.7 ± 2.0 13.2 ± 1.5Primary sport (n)(including wrist-loading and non-wrist-loading sports)
Field hockey (4)Soccer (2)
Athletics (1)Ice-skating (1)
Judo (1)Karate (1)
Swimming (1)None (1)
Korfball (5)Field hockey (3)
Soccer (2)Rugby (1)
Average sports intensity (hours/week) 3 ± 2 3 ± 1
Metaphyseal BME-like signal intensityIn 15 out of 23 wrists (65%, 8 girls), at least one area with BME-like signal intensity was observed in the distal radial metaphysis. Ten of these 15 areas (67%) had a minimally increased signal intensity (grade 1 out of 5) and in five cases (33%) signal intensity was graded as 2 out of 5. Metaphyseal BME-like signal intensity in the distal ulna was present in 21 out of 23 participants (91%, 10 girls). Signal intensity of these areas was graded as 1 out of 5 in 10 participants, 2 out of 5 in nine participants and 3 out of 5 in two participants. Figure 1 and 2 depict wrists with BME-like signal intensity in the metaphysis of the distal radius and ulna.
Epiphyseal BME-like signal intensityIn six participants (26%, two girls) areas with BME-like signal intensity of the distal radial epiphysis was present. In all six participants the areas occupied less than 50% of the total epiphyseal volume and were thus characterized as mild. In two cases the areas were adjacent to the physis. Signal intensity was mildly increased in all six participants; in three cases signal intensity was scored as 1 (scale 1 to 5) and the remaining cases were scored as signal intensity 2 out of 5. Only one area was observed on the 3D-WATSc sequence. Figure 3 illustrates cases with epiphyseal BME-like signal intensity of the distal radius.
BNW_Rik_V1.indd 52BNW_Rik_V1.indd 52 23-03-20 11:0823-03-20 11:08

53
The appearance of the healthy adolescent’s forearm on 3T MRI
A B
C DFigure 1. A 12.6 years old boy (A & B) and a 13.1 years old boy (C & D) with areas with BME-like signal in-tensity of the metaphysis of the distal radius on coronal PD TSE SPAIR- (A & C) and T2-Dixon (water-only) images (B & D).
A BFigure 2. A 12.4 years old girl with BME-like signal intensity of the metaphysis of the distal ulna on coronal PD TSE SPAIR- (A) and T2-Dixon (water-only) images (B).
3
BNW_Rik_V1.indd 53BNW_Rik_V1.indd 53 23-03-20 11:0823-03-20 11:08
54
Chapter 3
A B
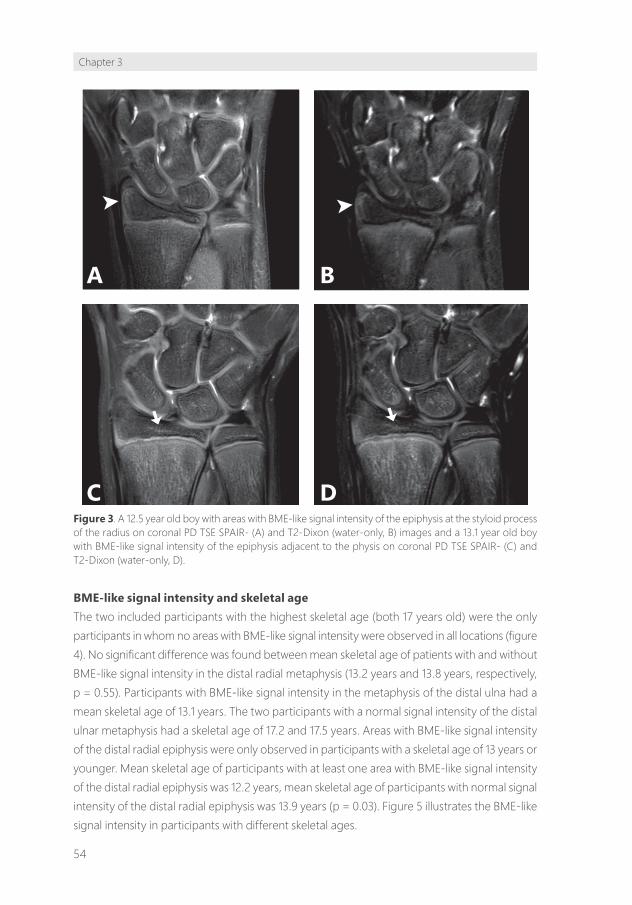
C DFigure 3. A 12.5 year old boy with areas with BME-like signal intensity of the epiphysis at the styloid process of the radius on coronal PD TSE SPAIR- (A) and T2-Dixon (water-only, B) images and a 13.1 year old boy with BME-like signal intensity of the epiphysis adjacent to the physis on coronal PD TSE SPAIR- (C) and T2-Dixon (water-only, D).
BME-like signal intensity and skeletal ageThe two included participants with the highest skeletal age (both 17 years old) were the only participants in whom no areas with BME-like signal intensity were observed in all locations (figure 4). No significant difference was found between mean skeletal age of patients with and without BME-like signal intensity in the distal radial metaphysis (13.2 years and 13.8 years, respectively, p = 0.55). Participants with BME-like signal intensity in the metaphysis of the distal ulna had a mean skeletal age of 13.1 years. The two participants with a normal signal intensity of the distal ulnar metaphysis had a skeletal age of 17.2 and 17.5 years. Areas with BME-like signal intensity of the distal radial epiphysis were only observed in participants with a skeletal age of 13 years or younger. Mean skeletal age of participants with at least one area with BME-like signal intensity of the distal radial epiphysis was 12.2 years, mean skeletal age of participants with normal signal intensity of the distal radial epiphysis was 13.9 years (p = 0.03). Figure 5 illustrates the BME-like signal intensity in participants with different skeletal ages.
BNW_Rik_V1.indd 54BNW_Rik_V1.indd 54 23-03-20 11:0823-03-20 11:08

55
The appearance of the healthy adolescent’s forearm on 3T MRI
12
14
16
Absent PresentPresence of BME-like signal intensity
Skel
etal
age
Radius | EpiphysisA
12
14
16
Absent PresentPresence of BME-like signal intensity
Skel
etal
age
Radius | MetaphysisB
12
14
16
Absent PresentPresence of BME-like signal intensity
Skel
etal
age
Ulna | MetaphysisC
Signal intensity 0 1 2 3
Figure 4. Presence of areas with BME-like signal intensity and signal intensity of the areas in the epiphysis of the distal radius and the metaphyses of the distal radius and ulna compared to skeletal age.
A
DC
B
Figure 5. A 17.5 year old girl without BME-like signal intensity of the distal radius and ulna (A), a 16.2 year old boy with BME-like signal intensity in the metaphysis of the distal radius and ulna (signal intensity (SI) 1 out of 5, B), a 13.8 years old girl with BME-like signal intensity of the metaphysis of the distal radius (SI 1 out of 5) and distal ulna (SI 2 out of 5, C) and a 11.8 year old girl with BME-like signal intensity in the epiphysis (SI 1 out of 5) and metaphysis (SI 2 out of 5) of the distal radius and metaphysis of the distal ulna (SI 3 out of 5).
3
BNW_Rik_V1.indd 55BNW_Rik_V1.indd 55 23-03-20 11:0823-03-20 11:08

56
Chapter 3
Discussion
Results from this study show that areas with BME-like signal intensity observed on high resolution 3T images are prevalent in the distal radius and ulna in healthy adolescents, especially in the metaphysis. All areas had relatively low signal intensity; lesions with severely increased signal intensities were not observed. BME-like signal intensity in the distal radial and ulnar metaphysis were present in all participants with a skeletal age between 12 and 16 years. In the distal radial epiphysis BME-like signal intensity was only observed in children with a skeletal age of 13 years or younger.
Interpretation of findingsNo studies have focused on the appearance of the distal forearm on 3T MR images before. However, several studies have assessed the presence of BME-like signal intensity in the pediatric wrist on 1.5 T MRI-images.9,10,15 Müller et al. evaluated the presence of BME-like signal intensity on 1.5T images in all osseous structures of the wrist, including both the carpal bones and distal radius and ulna, of 84 healthy children (5-15 years old).9 Avenarius et al. evaluated the same cohort again after 4 years.10 Although the overall prevalence of BME-like signal intensity was high in both studies, only two areas with BME-like signal intensity in the distal radius and ulna were reported.9,10
The low prevalence of BME-like signal intensity in the forearm might be attributed to scanning technique as field of view was centered on the carpals, causing the metaphysis to be depicted incompletely. Shabshin et al. evaluated T2-weighted 1.5T images of 31 healthy participants between 7 and 18 years old and reported a prevalence of increased signal intensities of the distal radius and/or ulna of 71%, which is similar to our results. 15 The study also reported a higher prevalence of increased signal intensity among young participants compared to older participants. Although signal intensity of the areas in the distal forearm (mean 2.3 on a scale of 1 to 3) was reported, further characteristics as location (metaphysis or epiphysis) or extent were not described.
Our study has shown these findings to be reproducible in another population, further strengthening the hypothesis that a certain amount of increased signal intensity in the adolescent wrist’s bone marrow is a physiological phenomenon. In addition, the higher resolution of our study’s 3T MR images enabled identification of additional characteristics and establishing the normal appearance of the distal forearm in adolescents in more detail.
MetaphysisSeveral causes may contribute to the observed high prevalence of BME-like signal intensity in the distal radial and ulnar metaphyses. As all participants were healthy and not involved in extensive wrist loading activities, we assume that observed areas of BME-like signal intensity did not result from wrist pathology or traumatic events and are more likely the result of physiologic (maturation related) processes.
BNW_Rik_V1.indd 56BNW_Rik_V1.indd 56 23-03-20 11:0823-03-20 11:08

57
The appearance of the healthy adolescent’s forearm on 3T MRI
During maturation bone marrow converts from hematopoietic active red- to hematopoietic inactive yellow marrow. In long bones the conversion progresses from the diaphysis towards the metaphysis until total conversion is reached at the age of approximately 25 years.8,16 The differences in composition between red (relatively more water) and yellow (relatively more fat) marrow affect signal intensity of the bone marrow on MRI images.8
Despite the fact that bone marrow conversion occurs in a predictable and symmetrical pattern, areas of residual red marrow are frequently observed and can cause local increased signal intensity.1,4,17 In the foot and ankle, presence of these areas of residual red bone marrow were described to be age dependent 17. As the results of our study suggest that BME-like signal intensity is more common in adolescents with a lower skeletal age, it is likely that these lesions are age-dependent in the wrist as well and probably the consequence of residual red marrow.
Furthermore, some participants were in the age range where physeal closure of the distal radius and ulna can take place. During the process of physeal closure focal periphyseal edema (FOPE) can be seen centered at the physis simultaneously in the meta- and epiphysis as a result of decreased flexibility of the bone.7,18 However, this characteristic appearance was not observed in our healthy participants and can therefore not explain the BME-like signal intensity in our participants.
Focal increased signal intensity of the bone marrow can also be the result of reconversion to red bone marrow in circumstances with an increased oxygen demand (e.g. in athletes).1 The participants in our study were healthy and not involved in extensive sports-participation, and therefore it is also unlikely that bone marrow reconversion is an explanation for the reported BME-like signal intensities.
EpiphysisEndochondral ossification of the cartilaginous epiphysis starts centrally with the development of a secondary ossification center and expands more peripherally upon maturation.8 Radiographic ossification of the epiphysis of the distal radius is reached between age 10-13 years in girls and 10-16 years in boys.19 It is known that the epiphyseal ossification process can cause focal areas of high MRI signal intensity on water-sensitive images as a result of reduced bound water molecules in bone marrow. 8,20.
Several areas of increased signal intensity on water-sensitive sequences were reported at the border of the secondary ossification center and cartilaginous epiphysis at the level of the radial styloid process (see figure 1 (A & B)). These lesions all occurred in participants between 11 and 13 years old and can therefore probably be attributed to the physiological ossification processes of the distal radial epiphysis. This also explains the absence of epiphyseal BME-like lesions in older participants.
3
BNW_Rik_V1.indd 57BNW_Rik_V1.indd 57 23-03-20 11:0823-03-20 11:08

58
Chapter 3
Strengths and limitationsThe study’s extensive MRI-protocol obtained at high field strength (3T) and consisting of various sequences ensured optimal evaluation of bone marrow signal intensity and characteristics of areas with BME-like signal intensity and reflects a scanning protocol in daily clinical practice. The performed physical examination and obtained information regarding symptoms decreased the likelihood that observed BME-like signal intensity was caused by pathology. Some of the included participants were involved in wrist-loading activities. Although this might introduce some bias, we assume that in the general population all children load their wrists to some extent, for example during physical education at school. Inclusion of completely unloaded wrists is therefore not feasible, but also undesirable. The fact that the participants in our study reflect the normal pediatric population ensures optimal value of the results for clinical practice. However, extrapolation of the results should be done with caution due to the relatively small sample size. In addition, during the initial evaluation of the MRI-images observers were blinded for study group, however during the consensus meeting only the MRI-images of the non-gymnasts were discussed, possibly introducing some bias.
Clinical implicationsInterpretation of changes in bone marrow signal intensity in the distal radius and ulna remains challenging as BME-like signal intensity is prevalent on MRI-images of the wrist of healthy adolescents. Knowledge of this high prevalence and of the additional characteristics (e.g. signal intensity) may facilitate interpretation of MRI-images in daily practice.
Awareness of physiologic and maturation dependent processes such as bone marrow conversion, FOPE and endochondral ossification that may mimic pathological BME-like signal intensity can prevent clinicians from simply attributing increased water content depicted on MRI to pathology with subsequent unnecessary treatment. This can be particularly relevant in the early diagnosis of physeal stress injury in the wrist, in which the presence of BME can be a sign of injury. Furthermore, as the BME-like lesions appear to be age-dependent, it is important to correlate diagnostic MR-images of the distal radius and ulna with clinical information such as skeletal age to include maturation status in the patient analysis.
As mentioned before, high field strength MRI ensures detailed visibility of the bone marrow and enables evaluation of presence of (subtle) areas of BME-like signal intensity and their characteristics (e.g. extent and signal intensity). In our healthy study population, no areas with severe extent or increase in signal intensity were observed. Further exploration of these characteristics in adolescents with forearm pathology is necessary to determine which characteristics are able to distinguish between physiological and pathological BME like signal intensity.
BNW_Rik_V1.indd 58BNW_Rik_V1.indd 58 23-03-20 11:0823-03-20 11:08

59
The appearance of the healthy adolescent’s forearm on 3T MRI
Conclusion
Areas with bone marrow edema-like signal intensities on MRI are prevalent in the distal radius and ulna of healthy children and appear to be age-dependent, presumably the result of physiological (maturation) processes. Simply attributing this high signal intensity to pathology should be prevented. Awareness of the spectrum of normal appearances of the adolescent’s distal forearm on high resolution 3T MRI allows better discrimination between physiologic lesions and true pathology.
Acknowledgements
The Academic Medical Centre, Amsterdam supported this research by awarding an AMC PhD Scholarship to L.S. Kox. The work was conducted as part of the Sports & Work program of Amsterdam Movement Sciences.
3
BNW_Rik_V1.indd 59BNW_Rik_V1.indd 59 23-03-20 11:0823-03-20 11:08

60
Chapter 3
References
1. Chan BY, Gill KG, Rebsamen SL, Nguyen JC. MR Imaging of Pediatric Bone Marrow. Radiographics. 2016;36(6):1911-1930.
2. Eustace S, Keogh C, Blake M, Ward RJ, Oder PD, Dimasi M. MR imaging of bone oedema: mechanisms and interpretation. Clin Radiol. 2001;56(1):4-12.
3. Bedoya MA, Jaramillo D, Chauvin NA. Overuse injuries in children. Top Magn Reson Imaging. 2015;24(2):67-81.
4. Jaimes C, Chauvin NA, Delgado J, Jaramillo D. MR imaging of normal epiphyseal development and common epiphyseal disorders. Radiographics. 2014;34(2):449-471.
5. Breton S, Jousse-Joulin S, Finel E, et al. Imaging approaches for evaluating peripheral joint abnormalities in juvenile idiopathic arthritis. Semin Arthritis Rheum. 2012;41(5):698-711.
6. Carey J, Spence L, Blickman H, Eustace S. MRI of pediatric growth plate injury: correlation with plain film radiographs and clinical outcome. Skeletal Radiol. 1998;27(5):250-255.
7. Zbojniewicz AM, Laor T. Focal Periphyseal Edema (FOPE) zone on MRI of the adolescent knee: a potentially painful manifestation of physiologic physeal fusion? AJR Am J Roentgenol. 2011;197(4):998-1004.
8. Laor T, Jaramillo D. MR imaging insights into skeletal maturation: what is normal? Radiology. 2009;250(1):28-38.
9. Muller LS, Avenarius D, Damasio B, et al. The paediatric wrist revisited: redefining MR findings in healthy children. Ann Rheum Dis. 2011;70(4):605-610.
10. Avenarius DFM, Ording Muller LS, Rosendahl K. Joint Fluid, Bone Marrow Edemalike Changes, and Ganglion Cysts in the Pediatric Wrist: Features That May Mimic Pathologic Abnormalities-Follow-Up of a Healthy Cohort. AJR Am J Roentgenol. 2017;208(6):1352-1357.
11. Wieners G, Detert J, Streitparth F, et al. High-resolution MRI of the wrist and finger joints in patients with rheumatoid arthritis: comparison of 1.5 Tesla and 3.0 Tesla. Eur Radiol. 2007;17(8):2176-2182.
12. Chhabra A, Soldatos T, Thawait GK, et al. Current perspectives on the advantages of 3-T MR imaging of the wrist. Radiographics. 2012;32(3):879-896.
13. Thodberg HH, Kreiborg S, Juul A, Pedersen KD. The BoneXpert method for automated determination of skeletal maturity. IEEE Trans Med Imaging. 2009;28(1):52-66.
14. Kox LS, Kraan RBJ, van Dijke KF, et al. Systematic assessment of the growth plates of the wrist in young gymnasts: development and validation of the Amsterdam MRI assessment of the Physis (AMPHYS) protocol. BMJ Open Sport Exerc Med. 2018;4(1):e000352.
15. Shabshin N, Schweitzer ME. Age dependent T2 changes of bone marrow in pediatric wrist MRI. Skeletal Radiol. 2009;38(12):1163-1168.
16. Vogler JB, 3rd, Murphy WA. Bone marrow imaging. Radiology. 1988;168(3):679-693.17. Shabshin N, Schweitzer ME, Morrison WB, Carrino JA, Keller MS, Grissom LE. High-signal T2 changes
of the bone marrow of the foot and ankle in children: red marrow or traumatic changes? Pediatr Radiol. 2006;36(7):670-676.
18. Giles E, Nicholson A, Sharkey MS, Carter CW. Focal Periphyseal Edema: Are We Overtreating Physiologic Adolescent Knee Pain? J Am Acad Orthop Surg Glob Res Rev. 2018;2(4):e047.
19. Schmidt S, Baumann U, Schulz R, Reisinger W, Schmeling A. Study of age dependence of epiphyseal ossification of the hand skeleton. Int J Legal Med. 2008;122(1):51-54.
20. Varich LJ, Laor T, Jaramillo D. Normal maturation of the distal femoral epiphyseal cartilage: age-related changes at MR imaging. Radiology. 2000;214(3):705-709.
BNW_Rik_V1.indd 60BNW_Rik_V1.indd 60 23-03-20 11:0823-03-20 11:08




















