Changing systems by changing individuals: the incubation approach to systems change
15
ORIGINAL PAPER Changing systems by changing individuals: the incubation approach to systems change Susan L. Staggs Marlita L. White Paul A. Schewe Erica B. Davis Ebony M. Dill Published online: 5 April 2007 Ó Springer Science+Business Media, LLC 2007 Abstract This article describes and evaluates the imple- mentation of an innovative approach to systems change, the incubation approach, which was developed on a systems change project designed to increase the capacity of multi- ple systems (e.g., law enforcement, child protection, domestic violence, mental health, early education) to re- spond to children’s exposure to violence. The incubation approach encourages change agents to collaborate with project staff to gently nurture, or ‘‘incubate,’’ feasible and warranted change in target systems. Project staff gain concrete commitment from motivated and accessible change agents and collaborate with those agents to imple- ment change actions. This approach works well with committed, executive-level change agents in target sys- tems, with stable systems that have low turnover and well- integrated subsystems, and when seed funds are provided to key organizations. Keywords Children’s exposure to violence Á Systems change Á Intervention theory Á Intervention method Á Non-profit organizations The incubation approach: changing systems by changing individuals Child exposure to violence is the result of a child expe- riencing violence, whether through their direct experience in the cases of child abuse and neglect, or as a bystander or witness. This violence may include intimate partner violence, family or community violence, sexual assault, or child abuse/neglect. This is an astonishing amount of violence, given that each year, 10–20% of the children in the United States are exposed to intimate partner violence alone (Carlson, 2000). Although the impact of children’s exposure to violence (CEV) varies as a function of indi- vidual, familial, and environmental factors, its effects can include severe and long-term neurological, developmen- tal, academic, social, and psychological difficulties (Ehrensaft et al., 2003; Fantuzzo & Mohr, 1999; Margolin & Gordis, 2000; Osofsky, 1995; Whitfield, Anda, Dube, & Felitti, 2003). Yet despite the serious impact of CEV, services for the ‘‘forgotten victims’’ who are ‘‘caught in the crossfire’’ of violent events are virtually non-existent (Ceballo, Ramirez, Maltese, & Bautista, 2006; Johnson, 1998, p. 271; Rivett & Shaun, 2006). Clinical practice has historically focused on treating victims of violence; unless child witnesses have diagnosable (i.e., reimbursable) psychological problems, services for these children are largely unavailable (Graham-Bermann & Hughes, 2003; Groves, 1997; Lynch, 2003). Thus, although exposure to violence has been documented as a major public health problem, many exposed children do not have access to needed services, which may serve to perpetuate the in- tergenerational transmission of violence by leaving a population of children with psychological and relational vulnerabilities unidentified and untreated (Rivett & Shaun, 2006). S. L. Staggs (&) Á P. A. Schewe Department of Psychology (MC 285), University of Illinois at Chicago, 1007 W. Harrison St., Chicago, IL, USA60607 e-mail: [email protected] M. L. White Á E. B. Davis Á E. M. Dill Office of Violence Prevention, Chicago Department of Public Health, 333 South State Street, Suite 320, Chicago, IL 60604, USA 123 Am J Community Psychol (2007) 39:365–379 DOI 10.1007/s10464-007-9103-6
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Changing systems by changing individuals: the incubation approach to systems change

ORIGINAL PAPER
Changing systems by changing individuals: the incubationapproach to systems change
Susan L. Staggs Æ Marlita L. White Æ Paul A. Schewe ÆErica B. Davis Æ Ebony M. Dill
Published online: 5 April 2007
� Springer Science+Business Media, LLC 2007
Abstract This article describes and evaluates the imple-
mentation of an innovative approach to systems change, the
incubation approach, which was developed on a systems
change project designed to increase the capacity of multi-
ple systems (e.g., law enforcement, child protection,
domestic violence, mental health, early education) to re-
spond to children’s exposure to violence. The incubation
approach encourages change agents to collaborate with
project staff to gently nurture, or ‘‘incubate,’’ feasible and
warranted change in target systems. Project staff gain
concrete commitment from motivated and accessible
change agents and collaborate with those agents to imple-
ment change actions. This approach works well with
committed, executive-level change agents in target sys-
tems, with stable systems that have low turnover and well-
integrated subsystems, and when seed funds are provided
to key organizations.
Keywords Children’s exposure to violence �Systems change � Intervention theory � Intervention method �Non-profit organizations
The incubation approach: changing systems by
changing individuals
Child exposure to violence is the result of a child expe-
riencing violence, whether through their direct experience
in the cases of child abuse and neglect, or as a bystander
or witness. This violence may include intimate partner
violence, family or community violence, sexual assault, or
child abuse/neglect. This is an astonishing amount of
violence, given that each year, 10–20% of the children in
the United States are exposed to intimate partner violence
alone (Carlson, 2000). Although the impact of children’s
exposure to violence (CEV) varies as a function of indi-
vidual, familial, and environmental factors, its effects can
include severe and long-term neurological, developmen-
tal, academic, social, and psychological difficulties
(Ehrensaft et al., 2003; Fantuzzo & Mohr, 1999; Margolin
& Gordis, 2000; Osofsky, 1995; Whitfield, Anda, Dube,
& Felitti, 2003). Yet despite the serious impact of CEV,
services for the ‘‘forgotten victims’’ who are ‘‘caught in
the crossfire’’ of violent events are virtually non-existent
(Ceballo, Ramirez, Maltese, & Bautista, 2006; Johnson,
1998, p. 271; Rivett & Shaun, 2006). Clinical practice has
historically focused on treating victims of violence; unless
child witnesses have diagnosable (i.e., reimbursable)
psychological problems, services for these children are
largely unavailable (Graham-Bermann & Hughes, 2003;
Groves, 1997; Lynch, 2003). Thus, although exposure to
violence has been documented as a major public health
problem, many exposed children do not have access to
needed services, which may serve to perpetuate the in-
tergenerational transmission of violence by leaving a
population of children with psychological and relational
vulnerabilities unidentified and untreated (Rivett & Shaun,
2006).
S. L. Staggs (&) � P. A. Schewe
Department of Psychology (MC 285), University of Illinois at
Chicago, 1007 W. Harrison St., Chicago, IL, USA60607
e-mail: [email protected]
M. L. White � E. B. Davis � E. M. Dill
Office of Violence Prevention, Chicago Department of Public
Health, 333 South State Street, Suite 320, Chicago, IL 60604,
USA
123
Am J Community Psychol (2007) 39:365–379
DOI 10.1007/s10464-007-9103-6

Here we provide an overview of the problem of CEV,
describe the implementation of an innovative approach to
systems change designed to enhance capacity to respond to
the problem of exposure to violence in systems that touch
the lives of children and/or their caregivers, such as law
enforcement and court services, child welfare services,
domestic violence service providers, family and mental
health support service providers, and early education sys-
tems. We describe the theoretical and methodological basis
of the approach and evaluate its effectiveness.
The problem of children’s exposure to violence
CEV involves children who directly observe, hear, or learn
about the abuse of another person (child, relative, care-
giver, or individual) as well as those children who directly
experience abuse and neglect in the community or in the
home. The effects of exposure to violence on young chil-
dren can negatively impact individuals across the lifespan.
Childhood impacts include a higher risk of neurological
dysfunction, cognitive and behavioral problems, and post-
traumatic stress disorder, while adult impacts include in-
creased risk of future abuse perpetration or victimization
(Edelson, 1999; Mabanglo, 2002; Whitfield et al., 2003).
A 20-year prospective study found that exposure to
violence as a child was the strongest predictor of domestic
violence victimization as an adult and a strong predictor of
perpetration as an adult, and a recent review of 21 studies
found that exposed children were at increased risk of
developing violence-condoning attitudes, internalizing
problems such as depression and anxiety, and externalizing
problems such as aggressiveness and antisocial behavior
(Ehrensaft et al., 2003; Edelson, 1999). Very young chil-
dren (ages 0–6) may be especially traumatized as result of
their exposure to violence. Even before they have the
ability to verbalize, infants and young children are found to
be sensitive and responsive to the fears and emotions of
their caregivers and may suffer anxiety, increased aggres-
siveness, and developmental delays (Shonokoff & Phillips,
2000); Zeaneah, 1993). Yet research also documents a
severe lack of services available for such children and
their families, especially for infants and toddlers (Graham-
Bermann & Hughes, 2003; Groves, 1997; Lynch, 2003;
Osofsky, 2003).
Most service providers are not aware of the impact of
exposure to violence or how to identify children who have
been exposed, and few are currently equipped to intervene
with children exposed. Further compromising effective
response efforts are limited specialized intervention and
treatment resources addressing CEV, and a limited public
policy focus on the issue (Benjamin, 1998). A complicating
factor is that the most important resource protecting
children from the negative effects of exposure to violence
may be a strong relationship with a competent, caring,
positive adult, most often a parent. Yet when parents are
themselves witnesses to or victims of violence, they may
have difficulty fulfilling their caregiver roles and lack ac-
cess to appropriate services (Osofsky, 2003).
The impact of exposure to violence on children and the
current dearth of available system resources for addressing
this problem indicate the urgent need to build capacity to
address exposure within and across a vast, diverse array of
existing systems that touch the lives of these children and
their caregivers. However, introducing additional programs
into over-worked, resource-poor government and nonprofit
systems, many entrenched in highly bureaucratic and
deeply ingrained ways of working that often center on
service delivery to niche populations, is a daunting task
indeed. This article details one such initiative and presents
an evaluation of methodological and theoretical compo-
nents of an innovative method of systems change, the
incubation approach.
Method
Intervention description
In recognition of the need to increase systemic respon-
siveness to CEV, the National Institutes of Justice’s
Department of Juvenile Justice created the Safe Start Ini-
tiative and requested proposals for demonstration project
grants in 2000. These grants provided about five years of
funding for eleven grantees to address problems faced by
young children exposed to violence within homes, schools
and communities. A large midwestern city’s Department of
Public Health received funding as one of the eleven sites
and aimed to reduce the impact of exposure to violence on
children ages zero to six in two low-income, high-crime,
predominantly African American communities. The
department applied for the grant based on its access to a
large infrastructure capable of housing a multi-system
collaborative, its history of and commitment to health
advocacy, and its existing relationships with key target
systems.
A system is defined for the purposes of this project as a
group of organizations with similar missions that are for-
mally or informally attached to each other. For systems
change to occur, at least one of seven incubation actions
must be implemented and likely to impact multiple orga-
nizations within the system. For example, providing CEV
training to one domestic violence service organization
would not qualify as domestic violence system change
because it would not impact multiple organizations in the
domestic violence system. But CEV training in the city’s
366 Am J Community Psychol (2007) 39:365–379
123

police department would count as systems change in the
first responder system, because the police department
comprises several organizations (i.e., divisions) throughout
the city. The project’s system change goal was to incubate
‘‘CEV responsiveness’’ in existing systems by implanting
in those systems the notion that CEV responsiveness can
and should be part of the target system’s mission. That
notion would then be grown, nurtured, and protected until
it reached maturity and was translated into concrete and
lasting systems change. The project collaborates with
change agents in target systems to embed feasible, war-
ranted CEV incubation into those systems in a relational,
non-coercive fashion.
Internal project structure
The project was housed in the city’s Department of Public
Health. Project staffing at its largest consisted of 3 full-time
positions (Project Director, Education Coordinator, and
Implementation Coordinator) and 3 part-time consulting
positions (Evaluation, Implementation/Systems and Tech-
nology/Information). Implementation activities were coor-
dinated through an Implementation Advisory Board (IAB),
a large collaborative composed of representatives from, on
average, 24 child and family serving systems. There were
about 200 people on the official IAB roll, although about
30 people comprised the core group of stakeholders. Par-
ticipation of the other official members waxed and waned
over the years depending on their connection to the issue,
access to funding, and ability to balance many competing
priorities. These partners were recruited based on their
understanding of cross-system issues and their ability to
facilitate change processes within their own systems. The
project capitalized on existing relationships with system
representatives and existing commitments to violence
prevention, children’s mental health, and related concerns
to recruit people onto the IAB. The IAB has met on a
quarterly basis since its inception and organized eight
workteams, each with a specific charge. Each team met
monthly or bi-monthly, and meetings were facilitated and
documented by the project staff. The Direct Service
Implementation Team defined the components of the
family support services and mental health services to be
provided. The First Responder/Incident-Based Implemen-
tation Team developed procedures and protocols for first
responders to identify and refer children for treatment. The
Training Collaborative developed curricula and collabo-
rated with potential institutional partners to carry out re-
search, training, and capacity building activities for service
providers and first responders. The Evaluation and Data
Collection Implementation Team provided consultation
and support to the local evaluation team, ensuring that
appropriate outcomes were evaluated. The Court Action
Implementation Team advocated for program and policy
development across various court offices and initiatives.
Protection of human participants on the project was en-
sured by review and approval of all project protocol by the
Department of Public Health’s Institutional Review Board
as well as review boards for participating service providers,
which included board members from the target communi-
ties as well as research and treatment professionals.
Systems change theory
The project’s approach to systems change was to work with
influential and motivated individuals in target systems to
create within those individuals a personal commitment to
becoming ‘‘personal incubators’’ for change in their sys-
tems. These individuals worked with project staff to
spearhead a drive within and, when appropriate, across
their systems to incubate CEV responsiveness into target
systems. At first, such changes could be small, but would
snowball to become progressively larger and more im-
pactful as more and more individuals in the target systems
were engaged in CEV-related actions.
Dunphy’s (1996) five components of a comprehensive
systems change theory provide theoretical insight into
this approach. Dunphy states that although organizational
change theory is at a nascent developmental state where
many theoretical orientations and diverse approaches are
advocated by leading change theorists, five components
appear essential to any comprehensive theory of systems
change: (1) a metaphor for the nature of the change and
organization, (2) an analytical framework for under-
standing change, (3) a model of the ideal organization,
(4) an intervention theory, and (5) a definition of the role
of change agents. The incubation approach possesses
each of these components; the nature of each is described
below.
The use of metaphor to communicate with and engage
system representatives in change efforts is a necessary and,
if compelling, powerful way to change individual minds
about the need for change in a static system. Metaphors
work by connecting the change effort to existing schema in
the minds of those involved, which helps them to easily
grasp the essential purpose of the change. For example, if
the objective of a change effort is to ‘‘fix’’ a ‘‘broken’’
organization, change agents could be thought of as
‘‘maintenance workers’’ and the system could be thought
of as a ‘‘repair shop’’ (Akin & Palmer, 2000; Armenakis &
Bedeian, 1992; Armenakis, Fredenberger, Giles, & Cher-
ones, 1996; Dunphy, 1996; Marshak, 1993, p. 49). The
metaphor for change on the project was, clearly, the idea of
change agents and systems as incubators for change, a
‘‘build and grow’’ metaphor consistent with the develop-
mental nature of the approach (Marshak, 1993, p. 49).
Am J Community Psychol (2007) 39:365–379 367
123

The framework for understanding the change process
must describe the structures, relationships, and processes
critical to the change process (Dunphy, 1996). The key
structure in this change process was the IAB and its
workteams, but relationships were critical and the key
leverage points for change. Existing relationships, both
personal and professional, were seen as instrumental in
recruiting individuals from target systems to serve on the
IAB, and in motivating individuals to take personal and
professional risks in what was anticipated to be a lengthy,
protracted struggle to change their systems. Three pro-
cesses were seen as critical to the intervention, two of
which were interpersonal, reflecting the importance of
relationships to the change effort. Interpersonal relation-
ship processes between IAB members and decisionmakers
in target systems were important in securing ongoing par-
ticipation in the change effort. The outcome of negotiation
processes between change agents and decisionmakers in
their systems was hypothesized to be a major factor in
determining the ultimate success of the intervention in
particular systems. Lastly, we hoped that mutually sup-
portive interpersonal processes among fellow change
agents would foster cross-system collaboration and keep
commitment levels high.
An ideal model suggests the direction of change and
how the success of the change effort should be evaluated
(Dunphy, 1996). The Incubation approach’s ideal model of
an effectively functioning system is reflected in the seven
incubation actions. An effectively functioning incubation
system has implemented one or more incubation actions, as
evaluated by transmission to the project of relevant data
such as the number and characteristics of children identi-
fied as exposed to violence, the number of referrals to CEV
service providers, and the outcomes of CEV screenings.
Directionality is specified through the stipulation that an
incubation action must build system capacity for address-
ing CEV – systems must commit to go beyond what they
already do. For example, domestic violence service agen-
cies providing play therapy to children residing in shelters
would have to increase their capacity to address CEV be-
yond the provision of therapy by instituting a CEV
screening protocol for children or implementing some
other incubation action.
Intervention theorists have outlined two basic ap-
proaches to systems change into which most existing the-
ories of change can fit: evolutionary, or continuous,
approaches and revolutionary, or episodic, approaches.
Revolutionary, episodic approaches seek to radically
change the status quo by creating a temporary but signifi-
cant upheaval, whereas evolutionary, continuous ap-
proaches seek to implement slow, continuous, non-
disruptive change processes (Corrigan & Boyle, 2003;
Weick & Quinn, 1999).
The incubation approach is an evolutionary, continuous
approach to change rather than a revolutionary, episodic
approach. The project’s reliance upon a large multi-system
collaborative for guidance reflects its embrace of the evo-
lutionary approach, a ‘‘slow process that requires consen-
sus among all levels of stakeholders.’’ Contrasted with the
chaotic, abrupt, seemingly irrational revolutionary ap-
proach to change, the evolutionary approach is develop-
mental in nature, logical and rational, requiring a change in
content rather than context (Corrigan & Boyle, 2003, p.
381; Weick & Quinn, 1999). This fits with the incubation
metaphor of slow, nurtured growth of CEV responsiveness
and its desire to embed CEV responsiveness within the
existing protocols of target systems.
Also at work in understanding the change process are
the concepts of relational systems change (Markoff, Fin-
kelstein, Kammerer, Kreiner, & Prost, 2005) and the
learning lens perspective (Rajagopalan & Spreitzer,
1997). Relational systems change uses relationships (ra-
ther than, say, executive directives) as the primary change
vehicle, which the project has done by working through a
large collaborative and concentrating on developing last-
ing relationships with system representatives. The col-
laborative nature of the incubation approach relationally
bonds system representatives to the project in a shared
ideological commitment to help vulnerable children. It is
a friendly, cooperative approach rather than adversarial,
confrontational approach. The project also uses a rela-
tional approach by capitalizing on the relationships its
more powerful collaborative members have with influen-
tial people outside the immediate project network to
incubate change. The ‘‘learning lens’’ theory also illu-
minates the incubation approach’s understanding of the
change process. In contrast to a rational lens perspective
on change as a ‘‘sequential, planned search for optimal
solutions to well-defined problems based on previously
defined firm objectives,’’ the learning lens perspective
sees change as an incremental series of small steps
undertaken from within a dynamic, ever-changing system
environment (Rajagopalan & Spreitzer, 1997, p. 50). The
steps of the incubation approach reflect its incremental
nature. Target systems are encouraged to choose from a
diverse menu of possible change actions requiring more
or less of a firm commitment on the part of the target
system. Something as simple as a one-time commitment
to train system representatives on CEV qualifies as a
change action under the incubation approach, but the
approach also encompasses more pervasive goals for
change such as instituting a referral protocol for children
exposed to violence throughout the service network of the
public health system. But even the most substantive
change actions in the incubation approach usually occur
in a staged, incremental manner.
368 Am J Community Psychol (2007) 39:365–379
123

Definition of change agent role
The definition of the change agent in the incubation ap-
proach depends on the personal commitment of individual
representatives from target systems to creating change in
their systems. Sometimes, the IAB workteams or the pro-
ject staff functioned as change agents in systems where no
representative from the target system could be engaged.
But the preferred role of change agents was as ‘‘tempered
radicals,’’ or ‘‘individuals who identify with and are
committed to their organizations, and are also committed to
a cause, community, or ideology that is fundamentally
different from, and possibly at odds with, the dominant
culture of their organization (Meyerson & Scully, 1995, p.
586).’’ This was thought to be the case with many potential
change agents. While target systems were generally seen as
sympathetic to the notion that addressing CEV was
important, CSS was concerned that system representatives
might not view becoming a CEV incubator as a high pri-
ority. As result, we anticipated a need to steward the pro-
cess with the agency representative if needed. Additionally,
the IAB was very conscious of documenting and adver-
tising the gains of any system as a way of encouraging
similar efforts across the board.
Incubation procedure
The incubation procedure is a multi-level procedure;
individuals, organizations within target systems, and entire
systems may become incubators. Individuals become
incubators by making a written, personal commitment,
usually at the end of a training session, to complete the
steps on a personal action plan for CEV advocacy. Orga-
nizations become incubators when they either implement
one of seven incubation actions and/or sign a memorandum
of understanding to become an incubator. Systems-level
incubation is defined as two or more organizations within a
target system working together to create change across
organizations, as evidenced by documentation of the cross-
organizational working arrangement.
Incubation is defined as a supported effort to integrate
heightened awareness of and responsiveness to young
children’s (0–6 years) exposure to violence into standard
and ongoing practices of individuals, target systems, and
organizations within those systems. The project began
using the incubation approach in 2002 and continues to
refine it in current systems change work. Individuals,
organizations, or whole systems can become incubators for
change by entering into a thoughtful, collaborative process
wherein the project staff partner with at least one system
representative for the express purpose of developing and
implementing a plan to integrate heightened awareness
of and responsiveness to young children’s (0–6 years)
exposure to violence. The incubation approach emerged
organically as the most appropriate method for systems
change because it is relational and non-threatening, has
been embraced by key system representatives, and is
equally suitable for use both with bureaucratic govern-
mental systems that have entrenched ways of working as
well as with smaller and more agile systems.
While the incubation process varies depending on the
unique needs of each target system, it generally includes
five commitment steps and seven incubation actions. The
five commitment steps are: (1) identify target system (2)
engage change agents in preliminary planning process (3)
gain formal commitment to the change process from the
target system (4) collaborate with systems representatives
to develop and implement an action plan and (5) Develop
monitoring and evaluation processes for each selected ac-
tion. The seven incubation actions are: (1) Assess current
(baseline) policy and/or practice (2) identify policies that
might be enhanced or changed (3) Host CEV training or
train-the-trainer sessions (4) enhance capacity to identify
exposed or at-risk children (5) enhance capacity to refer
exposed or at-risk children for CEV services (6) enhance
capacity to screen exposed or at-risk children and (7) en-
hance capacity to treat children exposed to violence or their
caregivers.
Commitment steps
In the first step, the project collaborative identified seven-
teen target systems based upon the system’s connection to
the issue, to the client population (age or type of need), or
to communities that are impacted by the issue. Interested
persons may also emerge to facilitate the linkage between
the project’s efforts and systems not previously identified.
Systems were targeted for change and categorized based on
their potential to identify, refer, screen, or treat CEV, to
implement policy, or to provide funding. State government
agencies, county and city government agencies, and
grantmaking foundations were targeted as systems that
could implement policy or provide funding. Systems with
the potential to identify, refer, screen, or treat CEV were
subdivided into non-mutually exclusive categories based
on their capacity to provide initial identification/referral/
screening, initial treatment, or ongoing treatment. Systems
with the potential to identify/refer/screen were subdivided
into incident-based, symptoms-based, or both, depending
on their point of contact with children and/or their care-
givers. Incident-based systems included first responders
(e.g., law enforcement, fire/emergency management ser-
vices, hospital emergency rooms). Symptom-based systems
included non-emergency mental and physical health care
organizations, community and faith-based organizations,
child care providers and organizations, and early childhood
Am J Community Psychol (2007) 39:365–379 369
123

education providers (e.g., Head Start). Systems with the
potential to handle incident- and symptoms-based identi-
fication included child welfare, the court system, hospital
emergency rooms, and domestic violence service provid-
ers. Systems with the potential to provide initial treatment
such as crisis intervention included child welfare, domestic
violence service providers, substance abuse treatment
providers, and child care/early education providers. Sys-
tems with the potential to provide ongoing treatment in-
cluded family support service providers and mental health
service providers.
Engagement and preliminary planning activities domi-
nate the second step. The project director stated that the
project pitched the incubation metaphor to system repre-
sentatives by communicating with them that, ‘‘Our systems
are all connected in some way with children, and every
individual in these systems can help make life better for
children. There is a way for you to personally maximize the
chances that one child, child X, will have a better life, and
that is by helping us create a CEV incubator in your sys-
tem.’’ To engage change agents and promote planning, we
used a series of group activities to allow partners to suggest
actions that they could take. A matrix was distributed that
had each IAB member’s name as a row and each commit-
ment step and incubation action as a column. IAB members
were asked to list what they thought they could do (rea-
sonably and within a three-month time frame) as individuals
or as change agents to further their organization’s com-
mitment to CEV or implementation of incubation actions.
Some IAB members, for example, indicated that they could
review their organization’s intake procedures to identify
places where CEV screening might be feasible, or schedule
train-the-trainer sessions on CEV for educators in their
organizations. Following this exercise, the team developed
a chart of commitments and continued to distribute this list
and update it as partners met their commitments throughout
the program year. Where possible, project staff also worked
with change agents to conduct feasibility studies, identify
points of entry (CEV inclusion) in standard practice, clarify
the decision-making hierarchy, devise an initial approach to
gain institutional support, and suggest an incubation time-
line and action items.
The third step formalizes the process and cements the
system’s commitment to become a CEV incubator.
Working with and through the system representative, pro-
ject staff gain formal commitment to the change process
from the target organization or system, usually in the form
of a Memorandum of Understanding that clarifies a time-
line for a launch date and initial change activities, clarifies
accountability expectations (who does what when), stipu-
lates funding to be provided, if any, and identifies public
awareness and education activities that should be con-
ducted to support the launch. We sought commitment at the
executive level, but became more flexible in cases where it
was clear that incubation could occur at lower levels.
Step Four finds the incubation team developing a plan
for implementing change. The plan itself is not a prescribed
template. Here we were looking for the partners to simply
commit to a process and an outcome. Usually, incubator
actions began to be implemented in this step.
As the last commitment step in the incubation approach,
the project works with all incubation sites to monitor and
evaluate the effectiveness of the incubation change effort.
Again, efforts are made to integrate evaluation into the
organizations’ standard operating procedures, and time,
money, and other resource commitments are taken into
consideration when developing a monitoring and evalua-
tion plan for each participating organization.
Incubation actions
Incubation actions can occur at any commitment step, but
usually occur during Steps 4 and 5. There are seven incu-
bation actions, the first two of which are needs assess-
ments: (1) Conduct a pre-incubation assessment to
document current (baseline) policy and/or practice (2)
Review and identify policies that may be enhanced or
changed to better support CEV responsiveness (3) Offer
staff training on CEV (4) Enhance the identification of
exposed or at-risk children (5) Enhance the screening of
exposed or at-risk children (6) Enhance the referral of
exposed or at-risk children, and (7) Enhance the services
delivered to exposed and at-risk children.
Incubation actions 1 and 2
Systems that are unsure of the best way for their systems to
become incubators may elect to work with the project staff
to conduct strategic planning activities, such as a pre-
incubation assessment to document current (baseline) pol-
icy and/or practice, culminating in a written assessment
and recommendations document that can be used for future
decisionmaking. Systems may also choose to conduct a
policy review to identify policies that may be enhanced or
changed to better support CEV responsiveness. Such a
review considers the political environment of the system
and attempts to ascertain where additional advocacy and
external support for the change effort may be required.
Incubation action 3
One of the most basic incubation actions a system can take
is to train their personnel on CEV. System representatives
may receive training in CEV and may also choose to par-
ticipate in the project’s Train-the-Trainer program by
attending a three-to-six hour orientation program to learn
370 Am J Community Psychol (2007) 39:365–379
123

how to train others on CEV responsiveness. Training can be
a one-time event, but the preferred solution is for CEV
training to be incorporated into an organization’s annual
professional development curriculum. Another less-inten-
sive incubation action is for a system to promote CEV
awareness and integrate into their existing internal and
external communications and social marketing materials
messages on CEV. Actions include displaying CEV specific
posters and brochure in close to consumers and other staff.
Incubations actions 4–7
The last four incubation actions are more involved and
constitute a more comprehensive commitment to integrat-
ing CEV responsiveness into policies, procedures, and
practices. Systems can become incubators by enhancing
their ability to (4) identify (5) refer (6) screen and/or (7)
serve children exposed to violence. Prior to 2006, the only
actions that were explicitly funded by the project were
actions 4–7. In some instances, program partners provided
the necessary funding to produce materials and/or deliver
the CEV training. Nevertheless, from the program’s per-
spective, only three service providers in the target com-
munities were funded to identify, refer, screen, and treat
children exposed to violence and their caregivers. These
service providers collected intake information and con-
ducted post-treatment assessments. Apart from these three
funded providers, the project usually attempted to enhance
systemic responsiveness in the least invasive way possible
– the way that requires the least amount of change, dis-
ruption, or funds expenditures from the target system. For
example, the project considered how both internal and
external referrals are currently made in target systems and
worked with change agents to identify the least disruptive
way to integrate identification and referral for CEV into
domestic violence and family support service organiza-
tions. For current child service providers, system change
efforts might focus on the service content, such as building
knowledge of CEV and trauma-sensitive care into existing
clinical protocols and enhancing eligibility for treatment to
include children exposed to violence.
Measures and data analysis
Qualitative interviewing, participant observation, focus
groups, document content analyses, and collection of
quantitative process data were used to evaluate the effec-
tiveness of the incubation approach. Qualitative data were
analyzed using Glaser’s (1992) grounded theory approach,
while quantitative process data (e.g., number of organiza-
tions trained, number of children referred) were summed
across years, organizations, or systems to determine sys-
tem- or project-level outcomes. We evaluated the success
of each commitment step through a series of unstructured
qualitative interviews and focus groups with project staff
and IAB members, who responded to questions about les-
sons learned and facilitators and barriers at each step.
Responses to these questions were compiled and organized
by theme. Only events mentioned by a majority of
respondents and affirmed in focus groups with core project
staff were included as commitment step successes, chal-
lenges, facilitators, or barriers.
To evaluate the success of incubation actions, we used a
mixed-methods approach that included conducting quali-
tative interviews and exercises with project staff and IAB
members, reviewing relevant documents, and collecting
quantitative process data. For example, to get an under-
standing of our progress toward meeting each systems
change goal, project staff collaboratively rated progress on
each goal’s activities using a five-point rating scale, where 1
was ‘‘no progress,’’ 2 was ‘‘a little progress,’’ 3 was ‘‘some
progress,’’ 4 was ‘‘a lot of progress’’ and 5 was ‘‘activity
completed’’. We then averaged the activity ratings by goal
to determine progress on each goal. The results of this
exercise were summarized in a progress report and used to
inform a focus group in which project staff discussed suc-
cesses, challenges, facilitators and barriers for each action.
We measured the success of the first two incubation
actions by reviewing project progress documents devel-
oped by project staff that detailed their efforts, successes,
and challenges in implementing these actions in target
systems. For action 3, we collected quantitative process
and outcome data on training effectiveness, including the
number of people trained and participant increases in CEV
knowledge and skills. For actions 4–7, we collected
quantitative process data from the three contracted service
providers and from other organizations that had committed
to identify and refer children for treatment to the funded
service providers. The funded service providers transmitted
information on the number of referrals received and the
source of each referral to project evaluators each month. At
termination of treatment, service providers completed end-
of-treatment forms detailing the number of caregivers and
children that had received services, the types of services
they had received, and the number of sessions each par-
ticipant attended. From this data we determined the total
numbers of, for example, needs assessments completed,
training sessions conducted, and number of children and
adults referred, screened, and provided with services.
Results and discussion
Table 1 describes outcomes for each commitment step –
the types and number of systems changed, examples of
successes and challenges, and facilitators and barriers. As
Am J Community Psychol (2007) 39:365–379 371
123

Table 1 Commitment outcomes
Commitment
step
Type of system (# of
organizations) changed
Successes Challenges Facilitators and barriers
Identify target
systems
n/a Categorizing systems as
incident-based, symptoms-
based, or both was helpful
in identifying systems and
the organizations within
them. This categorization
scheme also served as a
template from which to
recruit IAB members.
There were so many systems
that touched either children
exposed to violence or their
caregivers that managing
the scope of the
intervention was difficult.
Some systems had
hundreds of organizations
within them, but had to be
targeted because of their
relevance, such as domestic
violence service providers.
The scope of the intervention
was larger than its
capacity, so there were
problems in the beginning
because too many
organizations (over 300 at
one point) were targeted
for intervention. As the
project progressed, the
number of systems targeted
remained the same, but the
number of organizations
within each system that
were targeted for
intervention was decreased
to make the project more
manageable and more in
line with existing capacity.
Engage change
agents in
preliminary
planning
process
Courts (1), domestic violence
(2), early education (2),
family support (2), first
responders (1), funding (3),
government (2), higher
education (1), mental and
physical health (1),
violence prevention (2)
The city’s police department
had an accessible and
invested representative;
through her the project
gained the support and
endorsement of decision-
makers that led to a change
in police protocol for
responding to incidents of
domestic and community
violence.
We attempted to do the same
with the city’s Fire Dept.
The change agent was fully
on board, but we did not
get a wholehearted
endorsement from the
executive office to move
forward. Consequently, we
had to reconsider our
planned timeline for
incubating within this
organization.
Change agents who held
executive-level positions in
target system organizations
were most able to commit
to systems-level
engagement. Other
individual change agents,
while not at the executive
level, often had high
personal commitments to
the project, but were not
always able to secure
organizational commitment
to becoming a CEV
incubator. In some cases,
other members of the
collaborative were able to
encourage CEV
commitments across
systems.
Gain formal
commitment
to the change
process from
the target
system
Clinical practice (2), courts
(1), domestic violence (1),
early education (1), family
support (1), first responders
(1), funding (2), violence
prevention (1)
About half of our IAB
voluntarily and quickly
signed the formal
memorandum of
understanding and
institutionally endorsed
IAB participation and plans
to move the CEV work
forward.
Some of the partners were
unable to get executive
approval of the proposed
actions from their
executive officers, and we
had to settle for conducting
basic training at the
organization, whereas we
would have preferred a
more far reaching
commitment.
Again, we were most likely to
secure organizational
commitment from change
agents with
decisionmaking authority
in their organizations. We
discovered that we needed
to be more flexible in
requiring executive
authorization in cases
where certain actions could
be institutionalized at
lower levels. Monetary
support may have helped
secure institutional-level
commitment by offsetting
the use of limited
resources.
372 Am J Community Psychol (2007) 39:365–379
123

can be seen, having a change agent at the executive level in
an organization within a target system was key in obtaining
commitment at the organizational level. Barriers to com-
mitment included commitment at the change agent level
that did not translate into commitment at the organization
level, capacity constraints within organizations, and the
lack of funding available for needs assessment tasks, and
engagement disruptions due to sweeping organizational
change. Data collection capacity in five systems, including
the city’s police department, the domestic violence hotline,
and the three contracted service providers, was enhanced to
allow collection of previously uncaptured data on the
prevalence of CEV and the characteristics of violent
events, victims and perpetrators.
Table 1 continued
Commitment
step
Type of system (# of
organizations) changed
Successes Challenges Facilitators and barriers
Collaborate with
systems
representatives
to develop and
implement an
action plan
clinical practice (2),
community and faith-based
(1), domestic violence (1),
family support services (1),
first responder (1), funding
(2), violence prevention (1)
We have made it this far with
only a few of the partners
as our second stage was to
gather commitments at the
IAB level. One notable
success is that an ex-
offender reentry service
program has identified two
staff persons to join with
project staff in designing
and conducting incubation
actions 1 and 2.
An early education service
organization offered the
project multiple years of
funding to deliver CEV
training, but organizational
restructuring and staff
changes has interrupted
consistent contact with
organization
representatives. Their
commitment to the issue is
high, however.
The implementation plan
itself does not need to hold
to a prescribed template,
which promotes flexibility.
Nevertheless, this stage can
seem overwhelming, as
change agents are faced
with conducting
comprehensive, unfunded,
and time-consuming
analyses. Thus, we lowered
our expectations at this
step and are now simply
looking for target systems
to commit to a change-
oriented process with a
traceable outcome.
Facilitators include
executive-level
involvement and/or
consent in the process;
barriers include lack of
system capacity,
consistency, or interest.
Develop a
monitoring
and feedback
plan
Domestic violence (1), first
responder (1), family
support services (2),
clinical practice (2)
The police department
changed their policies and
procedures in the target
communities. The police
documented the number of
identifications and referrals
they made and forwarded
this information to project
evaluators on a quarterly
basis along with descriptive
data on victim and offender
age, gender and
relationship, and number
and ages of children
present on each call.
An early education
organization underwent
train-the-trainer sessions,
but we were not able to
establish a reliable protocol
to receive training counts
on a regular basis. For
different reasons, we faced
a similar barrier getting
some of the 1st responder
partners to document
counts for the training they
delivered.
While some of the system
partners received funding
to ensure that they had the
capacity to support the data
exchange functions, others
donated staff time. In the
latter case, CEV actions
may have to yield to allow
the organization to address
its other fiduciary
responsibilities.. In cases
where we had knowledge
that the organizations were
implementing incubation
actions, we did not insist
on monitoring and
feedback commitments.
Another potential barrier is
the absence of evaluation
and technical consultants.
The program will lack the
statistical and interpretive
expertise necessary to
appropriately process and
disseminate the data we
collect.
Am J Community Psychol (2007) 39:365–379 373
123
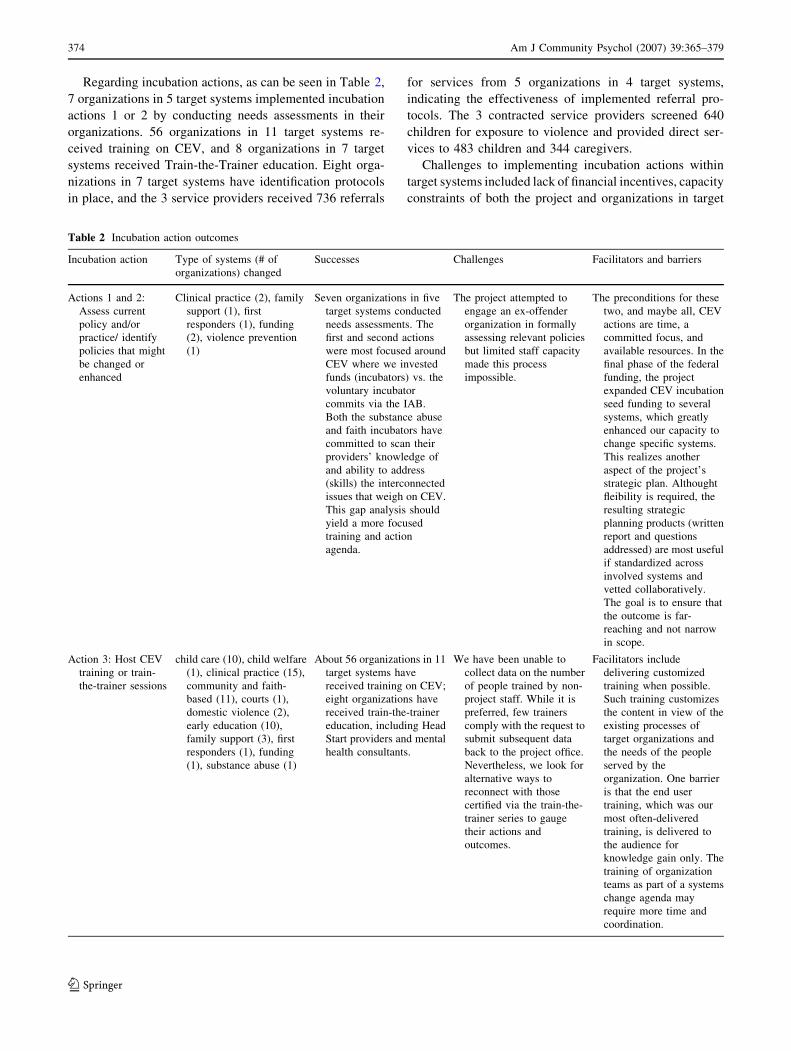
Regarding incubation actions, as can be seen in Table 2,
7 organizations in 5 target systems implemented incubation
actions 1 or 2 by conducting needs assessments in their
organizations. 56 organizations in 11 target systems re-
ceived training on CEV, and 8 organizations in 7 target
systems received Train-the-Trainer education. Eight orga-
nizations in 7 target systems have identification protocols
in place, and the 3 service providers received 736 referrals
for services from 5 organizations in 4 target systems,
indicating the effectiveness of implemented referral pro-
tocols. The 3 contracted service providers screened 640
children for exposure to violence and provided direct ser-
vices to 483 children and 344 caregivers.
Challenges to implementing incubation actions within
target systems included lack of financial incentives, capacity
constraints of both the project and organizations in target
Table 2 Incubation action outcomes
Incubation action Type of systems (# of
organizations) changed
Successes Challenges Facilitators and barriers
Actions 1 and 2:
Assess current
policy and/or
practice/ identify
policies that might
be changed or
enhanced
Clinical practice (2), family
support (1), first
responders (1), funding
(2), violence prevention
(1)
Seven organizations in five
target systems conducted
needs assessments. The
first and second actions
were most focused around
CEV where we invested
funds (incubators) vs. the
voluntary incubator
commits via the IAB.
Both the substance abuse
and faith incubators have
committed to scan their
providers’ knowledge of
and ability to address
(skills) the interconnected
issues that weigh on CEV.
This gap analysis should
yield a more focused
training and action
agenda.
The project attempted to
engage an ex-offender
organization in formally
assessing relevant policies
but limited staff capacity
made this process
impossible.
The preconditions for these
two, and maybe all, CEV
actions are time, a
committed focus, and
available resources. In the
final phase of the federal
funding, the project
expanded CEV incubation
seed funding to several
systems, which greatly
enhanced our capacity to
change specific systems.
This realizes another
aspect of the project’s
strategic plan. Althought
fleibility is required, the
resulting strategic
planning products (written
report and questions
addressed) are most useful
if standardized across
involved systems and
vetted collaboratively.
The goal is to ensure that
the outcome is far-
reaching and not narrow
in scope.
Action 3: Host CEV
training or train-
the-trainer sessions
child care (10), child welfare
(1), clinical practice (15),
community and faith-
based (11), courts (1),
domestic violence (2),
early education (10),
family support (3), first
responders (1), funding
(1), substance abuse (1)
About 56 organizations in 11
target systems have
received training on CEV;
eight organizations have
received train-the-trainer
education, including Head
Start providers and mental
health consultants.
We have been unable to
collect data on the number
of people trained by non-
project staff. While it is
preferred, few trainers
comply with the request to
submit subsequent data
back to the project office.
Nevertheless, we look for
alternative ways to
reconnect with those
certified via the train-the-
trainer series to gauge
their actions and
outcomes.
Facilitators include
delivering customized
training when possible.
Such training customizes
the content in view of the
existing processes of
target organizations and
the needs of the people
served by the
organization. One barrier
is that the end user
training, which was our
most often-delivered
training, is delivered to
the audience for
knowledge gain only. The
training of organization
teams as part of a systems
change agenda may
require more time and
coordination.
374 Am J Community Psychol (2007) 39:365–379
123
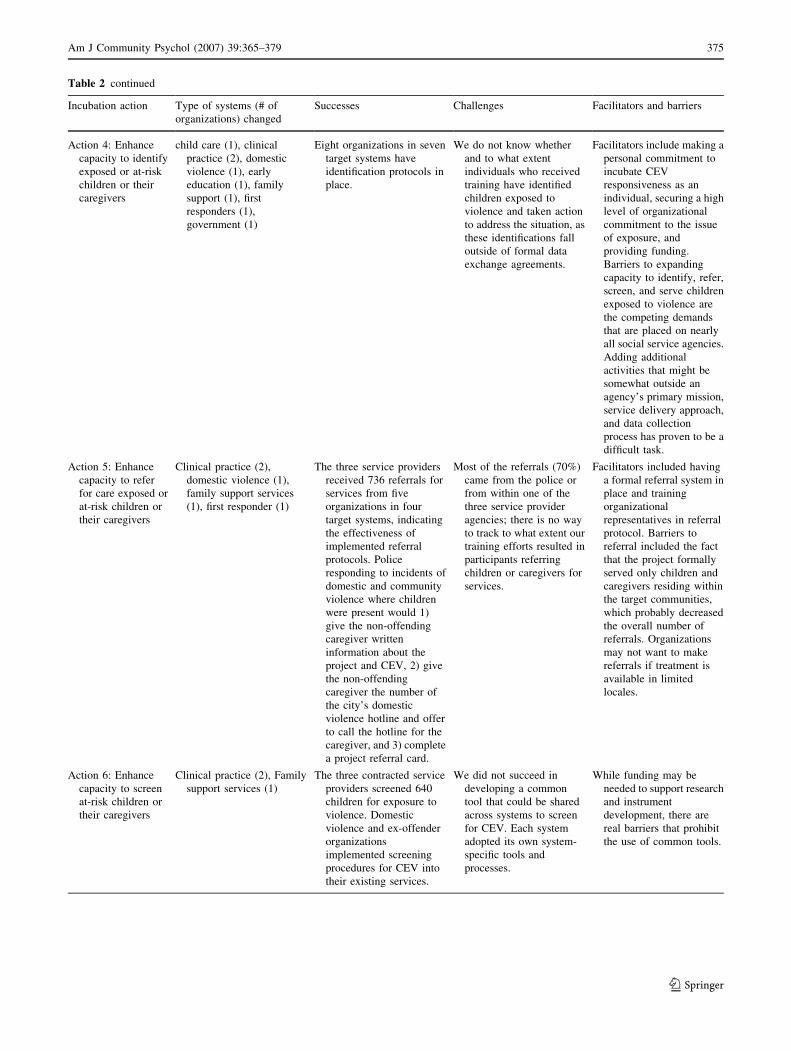
Table 2 continued
Incubation action Type of systems (# of
organizations) changed
Successes Challenges Facilitators and barriers
Action 4: Enhance
capacity to identify
exposed or at-risk
children or their
caregivers
child care (1), clinical
practice (2), domestic
violence (1), early
education (1), family
support (1), first
responders (1),
government (1)
Eight organizations in seven
target systems have
identification protocols in
place.
We do not know whether
and to what extent
individuals who received
training have identified
children exposed to
violence and taken action
to address the situation, as
these identifications fall
outside of formal data
exchange agreements.
Facilitators include making a
personal commitment to
incubate CEV
responsiveness as an
individual, securing a high
level of organizational
commitment to the issue
of exposure, and
providing funding.
Barriers to expanding
capacity to identify, refer,
screen, and serve children
exposed to violence are
the competing demands
that are placed on nearly
all social service agencies.
Adding additional
activities that might be
somewhat outside an
agency’s primary mission,
service delivery approach,
and data collection
process has proven to be a
difficult task.
Action 5: Enhance
capacity to refer
for care exposed or
at-risk children or
their caregivers
Clinical practice (2),
domestic violence (1),
family support services
(1), first responder (1)
The three service providers
received 736 referrals for
services from five
organizations in four
target systems, indicating
the effectiveness of
implemented referral
protocols. Police
responding to incidents of
domestic and community
violence where children
were present would 1)
give the non-offending
caregiver written
information about the
project and CEV, 2) give
the non-offending
caregiver the number of
the city’s domestic
violence hotline and offer
to call the hotline for the
caregiver, and 3) complete
a project referral card.
Most of the referrals (70%)
came from the police or
from within one of the
three service provider
agencies; there is no way
to track to what extent our
training efforts resulted in
participants referring
children or caregivers for
services.
Facilitators included having
a formal referral system in
place and training
organizational
representatives in referral
protocol. Barriers to
referral included the fact
that the project formally
served only children and
caregivers residing within
the target communities,
which probably decreased
the overall number of
referrals. Organizations
may not want to make
referrals if treatment is
available in limited
locales.
Action 6: Enhance
capacity to screen
at-risk children or
their caregivers
Clinical practice (2), Family
support services (1)
The three contracted service
providers screened 640
children for exposure to
violence. Domestic
violence and ex-offender
organizations
implemented screening
procedures for CEV into
their existing services.
We did not succeed in
developing a common
tool that could be shared
across systems to screen
for CEV. Each system
adopted its own system-
specific tools and
processes.
While funding may be
needed to support research
and instrument
development, there are
real barriers that prohibit
the use of common tools.
Am J Community Psychol (2007) 39:365–379 375
123

systems, and lack of data collection protocol for capturing
identifications and referrals from outside key organizations.
Theoretical implications
We evaluated the effectiveness of the project’s five theo-
retical components (Dunphy, 1996) through participant
observation and qualitative interviews with project staff
and IAB members. The incubation metaphor was effective
in that it increased the chances that individuals would make
personal commitments to become incubators themselves.
The incubation metaphor appealed to the nurturing, caring
personalities of people who work in public and social
service systems and care about the mental and physical
health of fragile children. The use of the incubation met-
aphor helped individuals mentally connect the change ef-
fort to something good and positive – an incubator where
vulnerable children could be helped by nurturing system
representatives. The incubation metaphor, which carries
with it the promise of technical support, may have also
helped ease fears about implementing change in the minds
of skeptical or ambivalent change agents.
The change process on this project was understood to
occur primarily through personal and professional rela-
tionships, and data from qualitative interviews with project
staff suggest that relationships were a key factor in getting
the IAB and workteams up and running and securing per-
sonal commitments to the project and to CEV advocacy in
general. The relational approach worked well for recruit-
ment and creating change in individuals, but not as well for
gaining commitment or implementing incubator actions in
target systems unless the change agent was an executive in
his or her organization. Although the project, at times
through staff and others via collaborative members, was
able to gain an audience with the state governor and county
court judges by capitalizing on the existing relational net-
works of IAB members, the project’s inability to intervene
in negotiation processes between motivated change agents
and decisionmakers in their organizations in some places
may have hampered our efforts to convert individual
change into organizational change. The incubation process
often stalled when change agents attempted to create
change in their organizations absent financial or other re-
source commitments from the project. For example, as a
federal initiative, project staff cannot actively lobby elected
officials. Additionally, all lobbying efforts are coordinated
across the host department, which means the project can
not independently approach decision makers. The legisla-
tive agenda for the department is developed and promoted
through a central government affairs office and then
through the city Mayor’s office. Lastly, some incubator
commitments were unable to be sustained because of a lack
of resources to continue even effective efforts.
There is disagreement on the effectiveness of the IAB
and workteam structure. First, the IAB remained the hub to
which all workteams reported. Various workteams experi-
enced some tension when its decisions were not fully
supported by the IAB. Nevertheless, most of the imple-
mentation teams satisfied their charge to develop and
implement aspects of the project that included issues of
information dissemination and review of project materials
such as training curricula and evaluation protocol. A cri-
tique of the IAB could be that the absence of an articulated
decisionmaking process made moving beyond areas of
Table 2 continued
Incubation action Type of systems (# of
organizations) changed
Successes Challenges Facilitators and barriers
Action 7: Enhance
capacity to provide
services to exposed
or at-risk children
or their caregivers
Clinical practice (2), Family
support services (1)
The three contracted social
service agencies have
provided direct services to
483 children and 344
caregivers.
The challenge here is
convincing non-delegate
organizations to offer
additional services
without a guarantee that
those services are
reimbursable.
Facilitators include
providing monetary
support, training,
measurement protocol,
and ongoing evaluation
and technical
consultation. Absent
monetary support,
organizations are unable
to support the provision of
non-reimbursable
services. To fit into
existing service systems,
children must either be
diagnosed with a
psychological disorder
before treatment will
reimbursable or attached
to early education issues.
376 Am J Community Psychol (2007) 39:365–379
123

disagreement difficult. Further, the administrative tasks of
preparing for, facilitating, and documenting IAB and
workteam meetings became one of the main tasks of the
project. But the project did not always realize a return on
its considerable investment of resources into managing
these meetings, when the outcomes of the meeting did not
in general move the project forward in its systems change
goals.
This large, collaborative structure helped establish and
maintain relationships and commitment to the project, but
the collaborative decisionmaking expected within such a
structure bogged the project down; the key decisionmaker
on the project was not one individual but a group of indi-
viduals from different target systems who participated on
the project for very different reasons. Consensus was not
often forthcoming, which sent project staff ‘‘back to the
drawing board’’ on multiple occasions in an attempt to
develop solutions that would satisfy all project members.
As a result, it was not uncommon for some decisions such
as which evaluation instrument to use or how to format a
training evaluation form to stretch out over multiple
months. Another drawback of this approach was that while
in theory the project was a collaborative one, when divisive
issues such as how to sustain the project beyond its initial
funding period arose, decisionmaking was hampered by the
absence of a formal voting process.
Our model of an ideal organization as an organization
implementing one or more incubation actions resulted in a
somewhat skewed view of change, because the majority of
incubation actions took place through training on CEV at
organizations within target systems. As noted, the purpose
of the basic training was to increase knowledge of CEV
and ability to take action to help children exposed to vio-
lence, which are individual rather than organizational
change outcomes. Thus although training was one of the
most successful aspects of the project, it did not necessarily
foster change at the organization and system level, al-
though it did result in a number of individuals becoming
personal incubators. On the other hand, the delivery of
CEV training was viewed as a fundamental starting point to
allow individuals - within organizations - to gain a better
understanding of CEV, which would inform decisions
about organizational behavior.
The intervention theory used on the project of slow,
evolutionary, non-coercive change was embraced by
change agents who often represented systems in which the
wheels of change turned slowly indeed. An evolutionary
theory of change may be the most appropriate theory to
adapt when attempting to change existing systems that are
entrenched in bureaucracy and slow decisionmaking pro-
cesses. The downside to this, however, as evidenced by the
many small changes but few large changes made by the
project, is that the inroads made using this approach may
be too small to make a difference at a systems level, or that
change efforts may lose momentum over the long term.
The goal is to leverage smaller improvements into greater
commitments, which are supported by the collaborative
base.
The role of the change agent as ‘‘tempered radical’’
worked best when the change agent was an executive in a
target system, but also when the change agent had suffi-
cient access to executives with the power and authority to
drive through potentially controversial changes. For
example, a citywide service program to help ex-offenders
reintegrate into society has incorporated CEV training,
screening, and referral into their client assessment and
service planning protocol even though addressing CEV was
not initially seen as one of the primary goals of the system.
Through the efforts of one motivated mid-management
change agent, the system embraced CEV responsiveness as
a vital aspect of its mission.
Facilitators and barriers to the incubation approach
As shown in Tables 1 and 2, several key facilitators and
barriers to using the incubation approach to systems change
emerged. Perhaps the most important facilitator was pro-
viding seed funds to organizations within target systems to
support the implementation of incubation actions. The fact
that CEV is emerging as a new issue means that existing
systems have to be retrofit to accommodate CEV actions.
This requires a substantial commitment of staff time, which
is often scarce. Few of the partner organizations had re-
sources to dedicate to the project, so all donations of time
(and there were many) and funds meant that something else
went undone. Other facilitators included recruiting pow-
erful, executive-level system representatives for leadership
positions in the project collaborative and challenging
individuals to engage in CEV activism. Barriers included
high staff turnover at target systems, systems in chaos, and
systems with autonomously operating subsystems.
The incubation approach appears best-suited to use with
stable systems that have low turnover and well integrated
subsystems. In some cases, project staff spent a great deal
of time and effort working with individual system repre-
sentatives only to have those representatives leave the
target systems without fully orienting their replacements on
the project. The incubation approach’s focus on working
through individual system representatives is vulnerable to
staff turnover and reassignment.
Another identified vulnerability of the approach was that
it did not seem to work well in systems with unintegrated
subsystems. Systems in which subsystems operated as
autonomous units and did not interact with other subsys-
tems was a barrier to incubation in the overall system,
because incubation seeds planted in one subsystem tended
Am J Community Psychol (2007) 39:365–379 377
123

to remain in that subsystem and did not necessarily per-
meate throughout the organization due to the lack of in-
frastructural integration among subsystems. The sub-
systems were approached as separate entities requiring the
requisite level of attention as though they were in fact
independent organizations. Lastly, systems undergoing
reorganizations or executive reshufflings are not suited to
the incubation approach, because their lack of stability
precludes gaining an incubation foothold.
Conclusion
The Incubator Approach’s results thus far show that it may
be a viable approach to embedding change in existing
systems by capitalizing on interpersonal relationships and
leveraging individual change to change systems, although
clearly the approach does have shortcomings, chief among
these being its ability to catalyze individual change into
systems change in the short term. However, the approach is
consistent with community psychology values of collabo-
ration and promotion of wellness, and is thus recommended
as a potentially attractive approach for use by community
psychologists working for change in existing human ser-
vice systems. Evaluation results suggest that capitalizing
on the power of metaphor, creating small pockets of
change in target systems, and maximizing the use of
executive-level ‘‘tempered radicals’’ as change agents
while minimizing the politicization and slow work pro-
cesses that often occur in collaboratives can make for a
successful strategy for creating change in existing
bureaucratic human service systems.
Acknowledgements This project was supported by Grant #
2000JWVXK004 awarded by the Office of Juvenile Justice and
Delinquency Prevention, Office of Justice Programs, US Department
of Justice. Points of view or opinions in this document are those of the
authors and do not necessarily represent the official position or pol-
icies of the US Department of Justice.
References
Akin, G., & Palmer, I. (2000). Putting metaphors to work for change
in organizations. Organizational Dynamics, 28(3), 67–79
Armenakis, A. A., & Bedeian, A. G. (1992). The role of metaphors in
organizational change: Change agent and change target perspec-
tives. Group & Organization Management, 17, 242–248
Armenakis, A., Fredenberger, W., Giles, W., & Cherones, L. (1996).
Symbolism use by business turnaround change agents. Interna-tional Journal of Organizational Analysis, 4, 123–134
Benjamin, M. P. (1998). The psychological impact of violence on
children and families: Assessment and service system strategies.
In M. Hernandez & M. R. Isaacs (Eds.), Promoting culturalcompetence in children’s mental health services. Systems of carefor children’s mental health (pp. 169–183). Baltimore, MD: Paul
H. Brookes Publishing Co.
Carlson, B. E. (2000). Children exposed to intimate partner violence:
Research findings and implications for intervention. Trauma,Violence, and Abuse, 1, 321–342
Ceballo, R., Ramirez, C., Maltese, K. L., & Bautista, E. M. (2006). A
bilingual ‘‘neighborhood club’’: Intervening with children
exposed to community violence. American Journal of Commu-nity Psychology, 37, 167–174
Corrigan, P. W. & Boyle, M. G. (2003). What works for mental health
system change: Evolution or revolution? Administration &Policy in Mental Health, 30, 379–395
Dunphy, D. (1996). Organizational change in corporate settings.
Human Relations, 49(5), 541–552
Edelson, J. L. (1999). Children’s witnessing of adult domestic
violence. Journal of Interpersonal Violence, 14, 839–870
Ehrensaft, M. K., Cohen, P., Brown, J. Smailes, E., Chen, H., &
Johnson, J. G. (2003). Intergenerational transmission of partner
violence: A 20-year prospective study. Journal of Consulting &Clinical Psychology, 71, 741–753
Fantuzzo, J. W., & Mohr, W. K. (1999). Prevalence and effects of
child exposure to domestic violence. Future of Children 9, 21–
32
Glaser, B. (1992). Basics of Grounded Theory Analysis. Mill Valley,
CA: Sociology Press
Graham-Bermann, S. A., & Hughes, H. M. (2003). Intervention for
children exposed to interparental violence (IPV): Assessment of
needs and research priorities. Clinical Child & Family Psychol-ogy Review, 6, 189–204
Groves, B. M. (1997). Growing up in a violent world: The impact of
family and community violence on young children and their
families. Topics in Early Childhood Special Education, 17, 74–
102
Johnson, L. D. (1998). Caught in the crossfire: Examining legislative
and judicial response to the forgotten victims of domestic
violence. Law & Psychology Review, 22, 271–286
Lynch, M. (2003). Consequences of children’s exposure to commu-
nity violence. Clinical Child & Family Psychology Review, 6,
265–274
Mabanglo, M. A. G. (2002). Trauma and the effects of violence
exposure and abuse on children: A review of the literature. SmithStudies in Social Work, 72, 231–251
Margolin, G., & Gordis, E. B. (2000). The effects of family and
community violence on children. Annual Review of Psychology,
51, 445–479
Markoff, L. S., Finkelstein, N., Kammerer, N., Kreiner, P., & Prost,
C. A. (2005). Relational systems change: Implementing a model
of change in integrating services for women with substance
abuse and mental health disorders and histories of trauma.
Journal of Behavioral Health Services & Research, 32(2), 227–
240
Marshak, R. J. (1993). Managing the metaphors of change. Organi-zational Dynamics, 22(1), 44–56
Meyerson, D. E., & Scully, M. A. (1995). Tempered radicalism and
the politics of ambivalence and change. Organization Science,6(5), 585–600 Sep-Oct
Osofsky, J. D. (2003). Prevalence of children’s exposure to domestic
violence and child maltreatment: Implications for prevention and
intervention. Clinical Child & Family Psychology Review,6,161–170
Osofsky, J. D. (1995). The effects of exposure to violence on young
children. American Psychologist, 50, 782–788
Rajagopalan, N., & Spreitzer, G. M. (1997). Toward a theory of
strategic change: A multi-lens perspective and integrative
framework. Academy of Management Review, 22(1), 48–79
Rivett, M., & Shaun, K. (2006). From awareness to practice:
Children, domestic violence, and child welfare. Child AbuseReview, 15, 224–242
378 Am J Community Psychol (2007) 39:365–379
123

Shonokoff, J. P., & Phillips, D. A. (Eds.) (2000). From neurons toneighborhoods: The science of early childhood development.Washington, DC: National Academies Press.
Weick, K. E., & Quinn, R. E. (1999). Organizational change
and development. Annual Review of Psychology, 50, 361–
386
Whitfield, C. L., Anda, R. F., Dube, S. R., & Felitti, V. J. (2003).
Violent childhood experiences and the risk of intimate partner
violence in adults: Assessment in a large health maintenance
organization. Journal of Interpersonal Violence, 18, 166–185
Zeanah, C. H. (1993). Handbook of infant mental health. New York:
Guilford Press
Am J Community Psychol (2007) 39:365–379 379
123