Changing our lens: seeing the chaos of professional practice as complexity
15
Changing our lens: seeing the chaos of professional practice as complexity MARLENE KRAMER PhD, RN, MSN, FAAN 1 , BARBARA B.BREWER PhD, RN, MALS, MBA 2 , DIANA HALFER MSN, RN, NEA-BC 3 , PAT MAGUIRE RN, MN, NEA-BC 4 , SUMMER BEAUSOLEIL RN, BSN, CCRN 5 , KRISTIN CLAMAN RN 6 , MAURA MACPHEE PhD, RN 7 and JUDY BOYCHUK DUCHSCHER RN, BScN, MN, PhD 8 1 President, Health Science Research Associates, Apache Junction, AZ, 2 Clinical Associate Professor, College of Nursing, University of Arizona, Tucson, AZ, 3 Administrator, Ann & Robert H. Lurie Children’s Hospital of Chicago, Chicago, IL, 4 Senior Kaizen Specialist, MetroWest Medical Center, Framingham, MA, 5 Cath Lab Specialist, Fletcher Allen Health Care, Burlington, VT, 6 Clinical Nurse, Renown Medical Center, Reno, NV USA, 7 Associate Professor, University of British Columbia, Vancouver, British Columbia and 8 Assistant Professor, University of Calgary and Executive Director, Nursing The Future, Calgary, Alberta, Canada Correspondence Marlene Kramer Health Science Research Associates 3285 N. Prospectors Rd. Apache Junction Arizona 85119 USA E-mail: [email protected] KRAMER M., BREWER B.B., HALFER D., MAGUIRE P., BEAUSOLEIL S., CLAMAN K., MACPHEE M. & DUCHSCHER J.B. (2013) Journal of Nursing Management 21, 690–704. Changing our lens: seeing the chaos of professional practice as complexity Aim The purpose of this evidence-based management practice project was to analyse dimensions of the Getting my Work Done issue, the only one of seven issues of highest concern for which 907 nurse interviewees were unable to identify effective strategies, formulate a ‘best management practice’, integrate the practice into clinical settings and evaluate results. Method/process The evidence-based management practice process was used to identify the major impediment to Getting Work Done–assignment to multiple patients with simultaneous complex needs. Best management practice consisted of class presentation of a clinical-management problem scenario to 144 residents in nine Magnet hospitals, a private action commitment, class discussion and terminal action commitments. Results Responses indicated that this ‘best management practice’ was effective in helping newly licensed registered nurses manage and handle multiple patients with simultaneous complex needs. A major avenue of resolution was perception of professional practice responsibilities as a series of complex, interrelated, adaptive systems. Conclusions/implications for nursing management Perception and use of the principles of complexity science assists newly licensed registered nurses in mastering management dilemmas that inhibit professional practice. In many participating hospitals, plans are underway to expand this best practice to include input and perception exchange among experienced nurses, managers and physicians. Keywords: complex adaptive systems, evidence-based management practice, multiple patient/simultaneity complexity, professional practice Accepted for publication: 7 February 2013 Introduction ‘It’s chaotic! I have five patients; often, one or more need care at the same time. How do I decide which patient is more important? What is the ‘right’ thing to do? If it’s life and death, no problem. It’s chaotic then, too, but not because of different patients needing something, rather 690 DOI: 10.1111/jonm.12082 ª 2013 Blackwell Publishing Ltd Journal of Nursing Management, 2013, 21, 690–704
Transcript of Changing our lens: seeing the chaos of professional practice as complexity

Changing our lens: seeing the chaos of professional practiceas complexity
MARLENE KRAMER PhD , RN , M SN , F A AN1, BARBARA B.BREWER PhD , RN , MA L S , M BA
2,DIANA HALFER MSN , RN , N E A - B C
3, PAT MAGUIRE RN , MN , N E A - B C4, SUMMER BEAUSOLEIL RN , B S N ,
C CRN5, KRISTIN CLAMAN RN
6, MAURA MACPHEE P hD , RN7 and JUDY BOYCHUK DUCHSCHER RN ,
B S c N , MN , P h D8
1President, Health Science Research Associates, Apache Junction, AZ, 2Clinical Associate Professor, College ofNursing, University of Arizona, Tucson, AZ, 3Administrator, Ann & Robert H. Lurie Children’s Hospital ofChicago, Chicago, IL, 4Senior Kaizen Specialist, MetroWest Medical Center, Framingham, MA, 5Cath LabSpecialist, Fletcher Allen Health Care, Burlington, VT, 6Clinical Nurse, Renown Medical Center, Reno, NV USA,7Associate Professor, University of British Columbia, Vancouver, British Columbia and 8Assistant Professor,University of Calgary and Executive Director, Nursing The Future, Calgary, Alberta, Canada
Correspondence
Marlene Kramer
Health Science Research
Associates
3285 N. Prospectors Rd.
Apache Junction
Arizona 85119
USA
E-mail: [email protected]
KRAMER M., BREWER B.B., HALFER D., MAGUIRE P., BEAUSOLEIL S., CLAMAN K., MACPHEE M. &
DUCHSCHER J.B. (2013) Journal of Nursing Management 21, 690–704.Changing our lens: seeing the chaos of professional practice as complexity
Aim The purpose of this evidence-based management practice project was to
analyse dimensions of the Getting my Work Done issue, the only one of seven
issues of highest concern for which 907 nurse interviewees were unable toidentify effective strategies, formulate a ‘best management practice’, integrate
the practice into clinical settings and evaluate results.
Method/process The evidence-based management practice process was used toidentify the major impediment to Getting Work Done–assignment to multiple
patients with simultaneous complex needs. Best management practice consisted of
class presentation of a clinical-management problem scenario to 144 residents innine Magnet hospitals, a private action commitment, class discussion and
terminal action commitments.
Results Responses indicated that this ‘best management practice’ was effective inhelping newly licensed registered nurses manage and handle multiple patients with
simultaneous complex needs. A major avenue of resolution was perception of
professional practice responsibilities as a series of complex, interrelated, adaptive systems.Conclusions/implications for nursing management Perception and use of the
principles of complexity science assists newly licensed registered nurses in
mastering management dilemmas that inhibit professional practice. In manyparticipating hospitals, plans are underway to expand this best practice to include
input and perception exchange among experienced nurses, managers and physicians.
Keywords: complex adaptive systems, evidence-based management practice, multiple
patient/simultaneity complexity, professional practice
Accepted for publication: 7 February 2013
Introduction
‘It’s chaotic! I have five patients; often, one or
more need care at the same time. How do I
decide which patient is more important? What is
the ‘right’ thing to do? If it’s life and death, no
problem. It’s chaotic then, too, but not because
of different patients needing something, rather
690DOI: 10.1111/jonm.12082
ª 2013 Blackwell Publishing Ltd
Journal of Nursing Management, 2013, 21, 690–704

the same patient needing multiple things at the
same time. I feel bad, very unprofessional when I
have to consciously decide to withhold needed
care to a patient… Several times, I’ve thought
about leaving nursing… Another cause of the
chaos is constant interruptions by doctors, PT,
lab, other nurses… I’m scared to death I will
harm or kill a patient when I have to make
choices between patients!’.(NLRNs 6–8 months post-hire)*
Newly licensed registered nurses’ (NLRNs) percep-
tions and descriptions of clinical situations as ‘chaotic’
(Cornell et al. 2010) were the major and most frequent
response to adaptation difficulties from 907 nurses
(330 NLRNs, 401 experienced clinical nurses, 138
nurse managers and 38 educators) interviewed in a
qualitative study in 20 US Magnet hospitals (Kramer
et al. 2012a,c). The focus of the previous study was to
ascertain components/strategies of nurse residency pro-
grammes (NRPs) that nurses and managers identify as
effective in helping NLRNs become socialized into the
professional practice role of clinical nurse. This sociali-
zation is accomplished through mastery of seven dilem-
mas repeatedly cited as issues of highest concern for
NLRNs when they leave the dependent, precepted
stage of NRP and enter the independent, clinical prac-
tice role (Kramer 1974, Schmalenberg & Kramer 1979,
Paterson et al. 2001, Krugman et al. 2006, Nursing
Executive Center 2007, Berkow et al. 2009, Pellico
et al. 2009, Kramer et al. 2013a, Kramer et al. 2013b).
Of the seven issues–delegation, clinical autonomy, priori-
tization, registered nurse (RN)–physician collaboration,
restoration of self-confidence through feedback, construc-
tive conflict resolution and Getting Work Done–the last
was identified as the issue of greatest concern and the
only one for which interviewees could not identify effec-
tive NRP strategies/components (Kramer et al. 2012a,c).
This absence of effective strategies is what generated
this evidence-based management practice (EBMP)
project.
Evidence-based practice, a decision-making process
originating with the medical profession to diagnose
and treat illness/injury, has been adopted by nursing
as an approach to practice improvement (Levin 2008).
In contrast to medicine, nursing matured as a profes-
sion within bureaucratic organisations (Kramer &
Schmalenberg 2012,). Although Titler et al.’s (2001)
adaptation of the Iowa model put evidence-based
practice into the context of practice improvement
within an organisation, it did not clearly address inter-
nal data that needs to be gathered or the extent to
which internal data supports and clarifies issues and
their relevance to the organisation. This EBMP study
is descriptive in design. It focuses on the management
component of the clinical nurse role. The EBMP pro-
ject reported here follows Levin’s (2008) adaptation
of the Iowa model: develop answerable questions, col-
lect/analyse best internal (organisational) and external
(literature) data, critically appraise the evidence, and
develop and evaluate effectiveness of implementing a
best management practice.
Purpose and questions
The purpose of this EBMP study was to analyse,
through a critical appraisal of the data, the dimensions
of the Getting Work Done issue. From this, a poten-
tial ‘best management practice’ would be developed,
integrated into practice in nine Magnet Hospitals and
evaluated for effectiveness. The questions to be
answered included: What are the major impediments
to NLRNs getting their work done? What best man-
agement practice will help with this problem?
Four sources of internal data were used to answer
the questions and achieve the objectives of this study.
The first source was digitally recorded responses of
907 nurse interviewees in 20 Magnet hospitals
(Kramer et al. 2012a,c) to the Getting Work Done
issue. These responses have not been reported else-
where as strategies suggested did not meet the criteria
of effectiveness for resolution of the issue. The second
source of internal data was a spontaneously drawn
NLRN sketch (Figure 1) by three of the NLRN inter-
viewees in this same qualitative study, in response to
the question ‘What are similarities and differences in
your nursing practice now (6–8 months post hire)
from when you were with your preceptor?’ After the
site-visits, the NLRN sketch was emailed to the on-
site investigators in the 20 hospitals, requesting them
to present the NLRN sketch to their current group of
NLRNs (n = 348) asking what the sketch said to them
and if there were additions or changes they would like
to make. Ninety-six per cent (n = 334) of the 348
NLRNs confirmed that the sketch accurately depicted
differences in practice ‘between when I was with my
preceptor and now when I am on the staffing roster
and on my own’. The third source of internal data,
collected specifically for this EBMP study, was an
*Unless referenced otherwise, all data in quotes are excerpts from
recorded nurse interviews related to the Getting Work Done issue.
These data have not been published elsewhere. Excerpts related tothe same topic, from multiple interviewees are separated by ellipses
points.
ª 2013 Blackwell Publishing Ltd
Journal of Nursing Management, 2013, 21, 690–704 691
An evidence-based management practice for new graduates

email survey of on-site investigators in the 34 magnet
hospitals participating in the seven-study research
programme (Kramer et al. 2011) requesting informa-
tion regarding the nursing care models and delivery
systems operative in their organisations. The last
source of internal data was 46 personal and email
interviews with Health Science Research Associates
and clinical nurses in the USA and Canada. These in-
terviewees were selected to represent a variety of dif-
ferent clinical units, types of hospitals, and hospital
practice experiences. These nurses provided examples
of NLRN management and clinical dilemmas, as well
as information and insight into the dimensions of the
Getting Work Done issue.
Critical appraisal of data
Dimensions of the issue
Why do NLRNs, 6–9 months post hire, report that
Getting Work Done is the issue of highest concern as
they integrate into the professional practice role of
clinical nurse? Why do more than 5000 front-line
nurse leaders in a NLRN preparation–practice gap
study rank order competencies such as independent
practice, anticipating risks, and keeping track of mul-
tiple responsibilities at the very bottom of 36 needed
NLRN competencies (Berkow et al. 2009)?
Many of the 907 NLRNs and experienced nurse in-
terviewees cited clinical examples, called ‘scenarios’
(Boxes A and B) to illustrate the Getting Work Done
difficulty. These were almost always accompanied by
assessments of how they felt about the decisions they
had made, and doubts as to whether they had made
the ‘right’ or correct decision. These findings, coupled
with the fact that the nurse interviewees in the parent
study (Kramer et al. 2013a) that was carried out in
‘Best of the Best’ Magnet hospitals that had established
NRPs, were unable to identify strategies effective in
addressing the Getting Work Done issue, led to selec-
tion of an EBMP approach for development/testing of
a ‘best practice’.
Components of the professional practice role
According to the literature and the interviewees,
the professional practice role of clinical nurse is responsi-
bility and accountability for providing care and
RN
RN
RN
PT Pt.
Pt.
Pt.
Pt.
Pt.
Preceptor
NLRN
Pa ent FamilyChaplainDie cian
MDPharmacist
Physical TherapistRespiratory Therapist
Social Worker
Pt. Family
NLRN
Pt. Pt.
Pt.Pt.
Pt.
MD
Pa ents’ Families
Transi on Stage(Post-hire to 3 months)
Integra on Stage(4 months to 1 year)
Note: The limited shaded area in theprecepted-NLRN experience means theyhave 'some' responsibility (definitely with the family) for answering ques ons and dealing with other departments etc. butthat the Preceptor "manages" the situa on for virtually all five pa ents--that's why theshaded area is small.
Figure 1: NLRN Sketch of differences between Transition and Integration Stages of Nurse Residency Programs
Figure 1
Differences in Newly Licensed Registered Nurses’ (NLRN) conceptualization of the dominant professional Nurse parctice role during transi-
tion and integration stages of professional socialization.
ª 2013 Blackwell Publishing Ltd
692 Journal of Nursing Management, 2013, 21, 690–704
M. Kramer et al.

managing clinical situations for multiple patients, simul-
taneously (Ebright et al. 2003, Lindberg 2008, Kramer
et al. 2010, 2012a,c). Providing care encompasses all
dimensions of nursing and includes all care interven-
tions–physical, psychological, teaching and technologi-
cal, such as ‘search of a disease or treatment on the
internet for self, patient or physician’. Managing clinical
situations consists of interactions and communications
between/among clinical nurses, patients’ families, physi-
cians, therapists, chaplain, etc. Environmental elements
and interactions–increased technological demands, seem-
ingly unending documentation, multiple health-care pro-
viders, high levels of interdisciplinary coordination and
collaboration and planning for the continuum of care–
are also components of managing clinical situations (Pe-
sut 2008, Kramer et al. 2010).
Simultaneity complexity
This dimension of the professional practice role is
particularly problematic. ‘The difficulty in getting my
work done is because several of my patients need me to
do something at the same time’. Labelled the multiple
patient-simultaneity complexity (MP/SC), MP/SC is
unique to the professional practice role of clinical nurses.
With the possible exception of emergency department
physicians, other health-care professionals provide ser-
vice to clients, sequentially (Kramer et al. 2010).
According to NLRNs, clinical nurses and managerial in-
terviewees, simultaneous means ethical, moral and legal
responsibility, and accountability for assigned patients
‘even when not in the physical presence of the patient’.
This includes on-going caring, concern, proactive moni-
toring of patient status, observation, surveillance, aware-
ness of patient profiles and cognizance of potential
latent failures (Ebright et al. 2003, Lindberg 2008, Kra-
mer et al. 2010, Kramer & Schmalenberg 2012).
Most of the MP/SC scenarios cited by NLRNs and
clinical nurses illustrated difficulties and dilemmas in
the nursing care component of practice (see Box A). In
Box B, a 4-month post-hire NLRN describes a MP/SC
scenario illustrating difficulties involving primarily man-
agement but also care components. This scenario includes
the NLRN’s critique of her clinical reasoning process.
Perceptions of not making the ‘right’ decision, of
not managing MP/SCs correctly are what causes
nurses to judge themselves as ‘poor nurses’ who ‘let
their patients down’. “Fear of not making the ‘right’
decision when faced with competing needs/demands
from several patients is what causes me to not feel
good about myself as a professional nurse”. An expe-
rienced intensive care unit (ICU) nurse, 14 years into
her career, described this memorable experience occur-
ring during her 1st year of practice:
Box A
Joe and Mrs Alstairs multiple patient-simultaneity complexity (MP/SC) scenario
Joe, a 22-year-old hockey player, was one of my five patients. Admitted with a swollen belly, unexplained, recurring fever, weight loss
and itchy skin. A year ago, he was diagnosed with Hodgkin’s disease and had radiation treatment. When I admitted him, he told me, with
a bright, happy smile and tug on the blond curls of his ‘soon-to-be wife’, that he had been ‘cured’. He had been feeling great up to about
a month ago when he was admitted for diagnostic tests. He’d had a slew of them–liver and kidney function, computed tomography (CT)
scans, bone marrow and lymph node biopsies.
Another of my patients was Mrs Alstairs, in her 60s, she has been in and out several times with pancreatic cancer, treated surgically and
with chemo, but still wretched with pain. She was on IV morphine and could barely make it from one administration to the next. When I
did my initial assessment this morning, I sat with her for a while and we talked about distraction methods–a good book on tape to listen
to–that would help her handle the pain a little when it was getting near to her next dose of morphine but not yet time. I read her the sum-
maries of some books and got her recorder and head phones all set up.
The morning had been going fine. At about 10 minutes to 9, as I was on my way to draw up Mrs Alstairs’ IV morphine, which she can
have at 9, Dr Marsh stopped me, says ‘good morning’ and asked if I have Joe today. When I nodded, he said he was on his way in to
see him and asked me to come along. I figured that I had enough time before 9, so I went. After some preliminary ‘how’s the belly today’,
Dr Marstairs said ‘Joe, I have the reports of your tests and it’s not good. Your Hodgkin’s has come back strong; you are already at Stage
IV-b. The outlook is worse when the cancer re-occurs and spreads in less than a year’. As soon as Dr Marsh began his report, I had put
my forearm on Joe’s shoulder and reached for his hand. Joe was absolutely shocked (as was I); his face paled, his eyes got big and
bulgy. Dr Marsh patted him briefly on the arm, said ‘Beth is a good nurse and will take good care of you’. He told Joe to write down ques-
tions that he had and that he’d be back to see him tomorrow and would answer his questions then. And with that, he left! Joe looked at
me with his shocked look, eyes brimming with tears and said: ‘He’s leaving? Please don’t leave me! What did he mean? Am I going to
die? Like now? I’m so young; I have my whole life ahead of me. Marge and I are talking about getting married this summer’.
At the same time that I was trying to listen to and comfort Joe, I was reviewing in my head what I knew about Hodgkin disease (cancer
of the lymph nodes, seen in young adults, prognosis not as bad as it used to be, but very bad if it reoccurs within the 1st year). I also
have to admit that I thought about how I would feel if this were happening to me–I am only 2 years older than he is). Joe was clutching
me like I was a lifeline. I just held on to him and let him cry, and said: ‘Don’t worry, Joe. I’m not leaving you. Go ahead and cry and share
with me whatever you’d like. Let me know if you’d like me to phone Marge or your parents’. In my head, I knew that Mrs Alstairs would
be in severe pain; she needed her IV morphine; it was already past 9.
ª 2013 Blackwell Publishing Ltd
Journal of Nursing Management, 2013, 21, 690–704 693
An evidence-based management practice for new graduates

‘I was working 12-hour nights. Usually in the
ICU, we have two patients. One of my patients
was 28-year old, Carla, with necrotizing pancre-
atitis, who I’d been caring for, for about
two weeks. She was very sick, requiring 1 : 1
care almost the entire time. Multiple vasopres-
sors, continuous renal replacement therapy, an
open fasciotomy in her right arm. After many
family meetings, Carla’s father made the decision
to withdraw care. Her family dynamics were
very difficult and her family was not coming in
to be with her after they withdrew life support.
When I came on at 19:00 hours, Carla had just
been terminally extubated.
My other patient was Miriam, a critically ill
woman who had arrested in the field, and was
continuing to arrest on and off in the unit. Once I
got into her room, I was not really able to leave it
because of constant interventions needed to keep
Box B
Management component multiple patient-simultaneity complexity (MP/SC) scenario
I came on shift and received report from the night nurse for my five patients. One of my patients, Mrs B has chronic obstructive pulmonary dis-
ease (COPD). She’s from _______ and needs home oxygen. She has to be discharged by 11:00 with all necessary supplies (O2 tanks) so
her husband can drive 400 miles, stay overnight and then complete the 800 mile trip the next day. (They only had enough money to stay in a
hotel one night.) An oxygen delivery company had been contacted and oxygen for the trip was due to arrive by 09:00. At 07:30, I called the
oxygen company to confirm the process and the delivery time; everything was set and ready to go. I planned the care of my patients in antici-
pation of Mrs B’s 11:00 discharge by passing medications and charting on her first.
Another of my patients, Mrs S, a diabetic dialysis patient, was to receive dialysis this morning and then be discharged home. When I did my
medication pass and assessments, I noticed that Mrs S’s IV was not flushing well, but I thought it best and to leave it in for now. There was
no point in taking it out and starting a new IV because when she was discharged, she probably wouldn’t need it. I also noticed that she had
not touched her breakfast. I encouraged her to eat, and she said ‘I’m not hungry, I’ll eat later’. I did not give Mrs S her insulin because her fin-
ger-stick blood glucose was not within parameters.
At almost 10:00, Mrs B’s oxygen tanks that had been promised for 09:00 still had not arrived. I called the oxygen company and was told that
they were no longer handling this patient’s case, and that the case had been transferred to a completely different oxygen delivery company.
In my mind, I was frantically thinking, ‘why didn’t you call me and tell me this earlier?!’ Despite my frustration I calmly asked for the contact
information for the ‘new’ oxygen company. But, before calling them, I decided that I needed to inform and reassure Mrs B and her husband
about this new situation. It also occurred to me to ask them how many oxygen tanks they needed and were expecting to receive. They said
they needed five tanks total (for the overnight hotel stay and for the whole trip home). I then called the ‘new’ oxygen company, who said that
they had not received the information about the number of oxygen tanks and why they were to be delivered by 11:00. They said they were set
to deliver only two tanks! I was getting more and more frantic with every phone call and was afraid I might be communicating my anger and
despair to Mr and Mrs B.
At almost 11:00; the dialysis nurse called for Mrs S. I prepared her and transport came to take her to dialysis. I decided that the oxygen tank
situation was getting out of control and that I needed help, so I called the social worker and turned the situation over to her. Finally, at 12:30,
two oxygen tanks were delivered and Mrs B was discharged with a plan that she receives three more at the hotel.
At almost the same time, dialysis called me to say that Mrs S. was hungry and wanted her lunch tray, which was in her room. I informed the
dialysis nurse I did not have time to bring Mrs S’s lunch tray down to the dialysis room because I was in the process of discharging Mrs B, my
COPD patient. I suggested that she call the kitchen and have them bring a lunch tray to dialysis.
Next, I was told to get Mrs B’s former room ready to receive a new patient. The room had been cleaned but there was no bed. I had to search
the whole floor for an empty bed. Meanwhile, I still had to take care of my other three patients, catch up on documentation and grab some
lunch.
About 14:00, as I was trying to get the new patient’s room together, Mrs S, my dialysis patient came back to the floor. At about the same time,
the dialysis nurse called to tells me how much fluid was pulled off and that Mrs S’s vital signs, etc., were stable. I asked if she had eaten her
lunch and the dialysis nurse said that she had obtained the tray from the kitchen but that Mrs S did not touch the food. I went to check on Mrs
S. Her speech was slurred and she showed markedly decreased mentation from my morning assessment. I called the dialysis nurse back to
ask her about the patient’s mentation during dialysis. She said it was normal for patients to be fatigued and somewhat mentally slow post-dial-
ysis. It’s not that I did not believe her, but something (my clinical judgment?) was telling me that this was not normal for Mrs S, particularly as
she had had no breakfast or lunch. I called my charge nurse and we both started assessing Mrs S. About this time, Mrs S became unrespon-
sive; blood glucose level is 61. IV access was compromised from that morning–did I make a mistake in my earlier assessment? Should I have
restarted the IV first thing this morning? A new IV was started and a rapid response was called at 16:15. She was given dextrose 50; by
16:30, she was stable, alert and oriented.
Self-analysis: The most important lessons I learned from the situation with Mr and Mrs B and the oxygen tanks were to make sure you keep
a good line of communication with your patient and keep them informed. I think that my patient and her husband would have been extremely
upset and frustrated if I had not kept them in the loop regarding the changes throughout the morning. If you try to weigh and balance Mrs B’s
situation with the many other possible patients’ needs and situations, it probably doesn’t come out very high on the scale. But it was important
to them. If I could not have gotten this situation straightened out, it would have meant that she would have had to stay another night, and pos-
sibly three more in the hospital (this all happened on a Friday). Neither Medicare nor the hospital would have been happy about that! I alsolearned to use my resources (i.e. social worker). Without using the help of the social worker it may have taken longer to get the patient dis-
charged and on her way home. In hindsight, I should have called the social worker sooner instead of taking my time and attention to contact
the two oxygen companies several times, thus neglecting my other patients.
ª 2013 Blackwell Publishing Ltd
694 Journal of Nursing Management, 2013, 21, 690–704
M. Kramer et al.

her alive. Multiple (5) vasopressors, lots of IV flu-
ids, the need to keep her paralysed in order to
ventilate her. Her ABGs were awful; I had to do a
lot of hand bagging because her O2 saturation
would become very low on the ventilator. I was in
the middle of hand bagging Miriam when the
respiratory therapist came to tell me that Carla
was asystole on the monitor. I had not been in to
see her at all since I had started with Miriam.
There was no one in the room with her when she
died. As her nurse I really should have been there
with her. I felt then, and still feel, very guilty that
I did not know whether she was in pain or not,
and that she died alone. I should have been there
with her, but I had to make a choice. I remember
when I first became a nurse, and a patient would
code and die in the ICU without their family being
around. One of the very experienced night nurses
told me:
“No one ever dies alone here. We’re with them
even if their family can’t be”. That’s always
stuck with me. Carla dying alone and possibly in
pain, still haunts me to this day’.
In addition to negative feelings about self as a nurse,
MP/SCs lead to decreased quality of patient care,
nurse practice satisfaction and increased job turnover.
It is also the number one cause of NLRNs leaving the
profession during their 1st year of clinical practice
(Kramer et al. 2012b).
Nursing care models and care delivery systems
Care models are supposed to answer the question
‘What is nursing?’ Gambino (2008) defines care models
as the philosophy of patient care that guides everyday
practice; he outlines 18 care models operational today.
With outrage in their voices–‘nursing is far more than
that!’–nurse interviewees reported that Webster’s Dic-
tionary (Agnes & Guralnik 2001) defines nursing as the
duties or profession of a nurse/the medical care given
by a nurse.
Lack of agreement on the definition of nursing
affects professional practice in two ways: ‘When we
don’t all define nursing the same there is no frame-
work for decision making to guide/justify nursing care
priorities’. Differences among RN in concepts of ‘what
is nursing’ are reflected in unwillingness to ‘fill in’ or
help one another in MP/SC situations. Clinical nurses
are reluctant to leave their own patients to help a
co-worker when they don’t agree that what the co-
worker intends to do is nursing.
From the perspective of all interview groups, the
dominant care model/definition of nursing is Nightin-
gale’s alterable medium theory: i.e. Nursing is the
planned, scientific alteration in patients’ internal and
external environments enabling the laws of nature to
act, thus facilitating the healing process (Selanders
1998). Not always defined so completely, the essence
of the definition from practicing nurses’ perspectives is
that ‘nursing alters or improves patients’ internal and
external environments so that nature takes its course
and patients get well’:
‘This is what we were taught in undergraduate
and graduate programmes… Florence’s definition
is much more helpful and useful than that defini-
tion about nursing being the diagnosis and treat-
ment of human responses to actual and potential
problems–does that mean if the patient doesn’t
respond negatively to bad news, you can assume
that the news is OK with him?… Some models
like Watson’s, focus mainly on patient’s internal
environment… Primary was supposed to focus on
the continuum of care, but it doesn’t anymore’.
Nightingale was the first to recognize the importance
of relationships and interactions as factors affecting
patient care and health. It is also the model most adapt-
able to the changing world in which we live and is used
by many State Boards of Nursing (Gambino 2008).
Nightingale’s understanding of the relationship between
health and environment not only initiated development
of nursing knowledge through research and theory, it is
also the model used by the Institute of Medicine of the
National Academies (2004) in its definition of clinical
nurses’ professional nursing practice environment
(PNPE). By combining Nightingale’s definition with
Donabedian’s (1988) structure–process–outcome para-
digm, the IOM defines PNPE as an alterable medium in
which structures and processes or practice are altered to
improve quality of patient outcomes.
Nursing care delivery systems answer questions as
to how care is organised and delivered to patients.
Systems often vary by patient unit. Care delivery sys-
tems are necessary to accomplish both the care and
the clinical management components of professional
practice. The care delivery systems most frequently
described were professional teamwork, group practice
or a partnership/buddy system.
There are opposing views as to whether care models
and care delivery systems are the same or different
(Kramer et al. 2012c). Mark (1992) defines them as the
same; Shirey (2008) says they are different. At two
recent Comprehensive Magnet Workshops, the Ameri-
ª 2013 Blackwell Publishing Ltd
Journal of Nursing Management, 2013, 21, 690–704 695
An evidence-based management practice for new graduates

can Nurses Association Credentialing Knowledge Center
(ANCC) offered a programme entitled: What is the
difference between professional practice models and care
delivery systems? (American Nurses Credentialing
Knowledge Center 2012). From the perspective of
NLRNs and experienced nurse interviewees, confusion
and disagreement about care models or care delivery
systems is a problem because each answers a different
question. This is particularly true when the care model
and the delivery system are identified as one and the
same.
The e-mail survey of the on-site investigators in 34
Magnet hospitals (Kramer et al. 2011), including the
20 hospitals in the qualitative interview study and the
nine hospitals participating in this EBMP project indi-
cated that in 18 hospitals, care models and delivery
systems were defined the same: relationship-based
care, family-centred care, patient-centred care or syn-
ergy. In the other 16 hospitals, the dominant care
models were caring, Nightingale and synergy. In these
hospitals, the major delivery systems were modified
primary, modified team, or group practice.
NLRN appraisal of NLRN sketch
The dominant clarifications and additions to the
NLRN sketch suggested by at least half of the 348
NLRNs in 75% of the 20 hospitals is of particular
significance because it suggested a complexity science
approach for resolution of the MP/SC dilemma:
‘Forget the transition drawing on the left: we
grow out of that when we move from our pre-
ceptor. The professional practice role is the one
on the right… You’ve got to show the patients
for all RNs as well as all the people they must
interact with on behalf of their patients… Each
one of these ‘RN–patient assignment circles is an
interconnected whole–what happens in one circle
rebounds or impacts the others… Next, you need
to draw a huge circle around all the RNs and
their group of patients. That’s pictures the unit…A circle around all units would be a picture of the
hospital… Charge nurses and the nurse manager
need to be inside this large circle with lines to all
RNs, to physicians and to other disciplines…’.
Newtonian and complexity sciences
The Newtonian paradigm (Lindberg & Lindberg 2008)
has been the view of the world for more than a century.
Patients are viewed as having broken mechanisms or
parts that can be repaired. Processes are understood
and analysed as linear and predictable. The dawn of
complexity science led to the discovery that the universe
is not stable, closed, predictable or controllable in ways
scientists had thought. New models of thinking assert
interconnection over fragmentation, networks over hier-
archy, influence over control and direction over destina-
tion (Anderson 2003, Baghbanian et al. 2012). The
chief applicability of complexity science to professional
practice is viewing clinical units, agents and hospitals as
complex adaptive systems (CAS) (Institute of Medicine
& Committee on Quality of Healthcare in America
2001, Lindberg 2008, Sturmberg et al. 2012). In CASs,
a system is a structure or object (abstract or concrete)
whose state and variability evolves over time. It is a
group of coordinated elements or agents which, taken
together, constitute a whole. Complex systems are built
up from large numbers of mutually interacting subunits
whose repeated interactions result in rich, collective
behaviour that feeds back into the behaviour of individ-
ual parts. CASs are unstable, non-linear, flexible, con-
tinually evolving and self-organising in response to
feedback. Interactions are focused around the system’s
attractor (for example, shared vision, goals of hospital-
ization), which pull, guide or channel the system. The
stronger the attractor, the more active the system. Dis-
turbances close to the attractor (e.g. loss of a resource,
diagnosis of cancer) create a more active system. When
a system responds adaptively to a disturbance, it allows
for emergence of the best solution for each patient
(Rickles et al. 2007, Lindberg 2008, Sturmberg et al.
2012).
Newtonian and complexity science as reflected in
systems of work organisation
In all industrialized societies, there are basically two
systems for organising work: the part-task model and
the whole-task model. In the first of these models a
worker can be trained, usually in a relatively short
amount of time, to perform a part of the whole task
(for example, making unoccupied patient beds). This
part-task model embraces values of efficiency, speed,
accuracy and safety through repetitive performance of
the same task by the same worker. The degree of
resistance to the task is known and predictable (Cor-
win 1961, Kramer 1974). This system has long been
labelled the bureaucratic system of work largely
because it requires at least one department whose
major goal is to keep the system operating efficiently.
The part-task, bureaucratic system is reductionistic
(i.e. the whole is broken down into discrete, measur-
able parts–departments–and the whole is equal to sum
of parts). It is the system encountered by most NLRNs
in their initial employment in hospitals.
ª 2013 Blackwell Publishing Ltd
696 Journal of Nursing Management, 2013, 21, 690–704
M. Kramer et al.

In academia, NLRNs are taught the whole-task, goal-
oriented, professional model of practice. Practitioners, in
ever-increasing complex, internally controlled disciplines
require extensive, up-to-date knowledge, judgment and
decision-making. They also require a larger, more com-
prehensive context of practice so as to engage in safe,
effective professional practice leading to quality patient
outcomes. The essence of professional practice is moral,
legal, ethical responsibility and accountability for all
aspects of nursing practice (Corwin 1961, Kramer 1974).
The professional system of work organisation is not
synonymous with the complexity science world view par-
adigm, but there are some parallels, specifically emphasis
on ‘whole-task’ work, interconnection over fragmenta-
tion, relationships and interactions over solo perfor-
mance, networks over hierarchy, and influence over
control. Conversely, nursing’s recent emphasis on out-
comes over process is counter to complexity science’s
emphasis on direction over destination. These similarities
and differences illustrate that, in this increasingly complex
world in which we live and practice our profession, we
need to search and reach for the best in both paradigms.
Clinical Examples/Scenarios have long been used by
nurses and researchers to exemplify MP/SCs and other
issues (Kramer 1974, Davis et al. 1975, Kramer &
Schmalenberg 1977 , Schmalenberg & Kramer 1979,).
They are recommended for use in analysis/differentia-
tion of clinical reasoning and critical thinking (Lindberg
& Lindberg 2008, Pesut 2008, University of Newcastle
2009). They also demonstrate differences in practice, in
practice environments and in nurses’ clinical reasoning
and decision-making over time. These are evident when
a 1971 scenario (see below) is compared with a present
day MP/SC scenario (as shown in Box A):
‘It’s 4:30 p.m. You are the only RN on a 20-bed
post cardiac unit. Your nurse aide is on meal
break. While making rounds, you discover a
patient crying because she fears she will have a
repeat post-surgical psychotic break tomorrow
after her surgery. While comforting her, you
hear the dinner cart with its pots of food being
delivered. You know that you need to dish up
food and get trays out to patients, so that they
can eat and cart can be returned for delivery of
food to patients on other floors. What to do?
You need to stay with this patient, but the other
patients need their food… The dominant solu-
tion was to dish up/serve trays as this would
benefit the largest number of patients and dinner
cart is needed on other units’.
(Kramer 1974)
In addition to marked differences in hospital environ-
ments and nurse practice conditions in 1974 and today,
the above scenario also shows the lessening dominance
of Newtonian linear thinking in decision making: care
for 19 patients is more important than care for one
patient and the dinner cart was needed to serve food to
patients on other units. In the above reference, it is also
noted that new graduates indicated that they would get
better performance ratings from the supervisor if they
got the food served and the dinner cart returned.
Development of a potential best managementpractice
Analyses of qualitative interview study data and of the
EBMP project data just presented indicated that about
one-third of the NLRNs, clinical nurses and managers
perceived the complexity of patient RN assignments,
practice settings, patients’ internal and external environ-
ments and interaction among these from a CAS perspec-
tive, although they often did not use those words. The
following interview excerpts contributed to the decision
to utilize MP/SC scenarios and a CAS approach in the
development and testing of a best management practice
for the Getting Work Done issue. The first excerpt from
operating room nurses, illustrates a systems approach to
prioritization:
‘On any given day, a seemingly normal case can
go from routine to chaotic… From the new
grad’s perspective, everything was going fine.
Then the surgeon unexpectedly gets into the liver.
He yells for a ligasure machine. Tech calls for
more suture and lap sponges to mop up the
blood. Anaesthetist calls for more blood and in
the same breath, for a cell saver and heparin… In
a situation like this, new grads panic. Too many
people each wanting something different at the
same time. Truly they don’t know which way to
go first; its sheer chaos for them… Experienced
nurses would have heard blood being sucked into
the suction canister before announcement of the
bleed, and would know that the tech would need
more sponges and that the patient would need
more blood… Most seasoned nurses are giving
supplies to techs before they ask for them. Suc-
tion is high priority and necessary to repair the
vessel or lacerations and to give visualization to
the surgeon so he can see to fix whatever is
wrong… The key to new grads being successful
in situations like this is willingness to use all their
senses, knowledge and connections to learn and
ª 2013 Blackwell Publishing Ltd
Journal of Nursing Management, 2013, 21, 690–704 697
An evidence-based management practice for new graduates

to plan ahead and be able to manage and assess
the situation from a multiple system perspective’.
(Kramer et al. 2012a)
The following description of an effective NRP class
as well as interview data from many nurse managers
illustrates the necessity/value of looking at a clinical
unit as a whole, as a complex system, and helping
NLRNs identify priority systems for the dominant
patient population on the unit:
‘After ABC, for oncology patients–pain control is
top priority… In the ER, after ABC, next priority
is doing what you need to do to get patients home
or transferred out of the ER so there’s room for
other patients. I know that sounds very bureau-
cratic or money hungry, but we are here to provide
a service. You are not doing that if patients are
struggling to breathe or are in severe pain in the
waiting room, while others who have been seen
are lying there waiting to be transferred… I never
thought about it before but, in a way, that’s also
true on rehab. Who’s scheduled first for therapy?
You pass meds, do assessments, and get them
ready so they can make therapy appointments on
time. That’s why those patients are here’.
(Kramer et al. 2012c)
The practice
From all the MP/SC scenarios gathered, the Joe–Mrs
Alstairs dilemma (Box A) was selected for its applicabil-
ity across multiple clinical units. Nine of the 20 qualita-
tive study Magnet hospitals (Kramer et al. 2012a,c)
were selected for representative distribution by geo-
graphic location, type of hospital, and type of residency
program (Kramer et al. 2011). In these hospitals, on-
site investigators worked with nurse educators to
develop/present a NRP class/session for NLRNs about
8 months post-hire. NLRNs were asked to read the
Joe-Mrs. Allstairs (Box 1) scenario and, anonymously,
write down answers to three questions: (1) What would
you do in this situation? (2) How do you think you
would ‘feel about yourself as a nurse’ if you made and
acted on this decision? (3) What, if anything, could you
do to prevent such a situation from happening again?
The reason for this immediate, private commitment
was to stimulate individual, personal clinical reasoning
and decision-making based on data at hand. A private
decision or commitment to an intervention before class
discussion allowed the individual more freedom to
change his/her mind with fewer feelings of embarrass-
ment, defensiveness or inadequacy.
After completing the above, each NLRN placed his/
her anonymous responses into an envelope addressed to
the Health Science Research Associates authors. Educa-
tors then conducted the class discussion focused on the
scenario and the same three questions above. At end of
discussion, the NLRNs were asked to write down what
they thought of this activity–did they enjoy it and what
did they learn? Would they make different decisions
after the class than what they said as the beginning?
Anonymous responses were then placed in the same
envelope for mailing to authors. The only information
provided to educators was that Getting Work Done was
the dilemma or issue of highest concern to NLRNs and
the only one for which 907 nurse interviewees (Kramer
et al. 2012a,c) could not identify effective NRP strate-
gies. The reason for the initial private commitment to a
solution to the MP/SC dilemma, followed by discussion
and then re-evaluation was to ascertain whether the dis-
cussion helped NLRNs consider the possibility of valid
alternative solutions, a better view of themselves as
nurses and the efficacy of viewing the patient care unit as
a series of interrelated, interconnected parts (i.e. CAS).
After the class, educators were asked to complete a
questionnaire citing number of months NLRNs were
post-hire and an estimate of the percentage of NLRNs
who, at the end of the class, favoured the following:
(1) felt that there was one ‘right’ thing to do, (2) felt
bad or unprofessional because of the decision they
had initially made and (3) enjoyed/learned something
from the discussion. Educators were also requested to
provide their assessment of the usefulness of this class
activity in helping NLRN deal with MP/SC dilemmas.
Evaluation of best management practice
Critical appraisal and analysis of internal–particularly
the suggestions for improvement and clarification in
the NLRN sketch–and external data led the investiga-
tors to expect that when presented with a MP/SC sce-
nario, some NLRNs would use systems and
complexity thinking, and lateral rather than vertical
thinking (de Bono 1970) to support their clinical rea-
soning (University of Newcastle 2009, Alfaro-LeFevre
2013), while other would not. Although individual
responses to initial questions might well be along
Newtonian, linear lines (for example, one right answer
that would make NLRNs feel bad if they could not
do their best for both patients), it was expected that
after hearing peer viewpoints, decisions and rationale
for decisions, a larger percentage of NLRNs would
reflect complexity/systems thinking in their post-class
responses and descriptions of what they had learned
ª 2013 Blackwell Publishing Ltd
698 Journal of Nursing Management, 2013, 21, 690–704
M. Kramer et al.

from the class discussion. Analysis of the evidence
indicates that this is what happened.
Ten classes, attended by 144 NLRNs, were held in
nine Magnet hospitals. Class size ranged from four to 45
with 75% of the classes having between 10 and 15
NLRNs. Number of months post-hire ranged from 6 to
12 months with 92% of the NLRNs between 7 and
9 months post-hire. In all but one hospital, the class was
held as a regular part of the integration stage of the NRP.
A total of 27 different solutions/actions were pro-
posed in response to the question: What would you
do in the Joe–Mrs Alstairs (Mrs A) MP/SC? These
were consolidated into five outcomes/goals with a
total of 11 action categories (Table 1). Seventy-five of
the 144 respondents (63%) proposed more than one
goal or solution. In response to the question, ‘How
would you feel about yourself as a nurse if you made
and carried out your decision’, replies from the 144
NLRNs were grouped into five categories from ‘very
positive’ to ‘very negative’ (Table 2). For the third
question, ‘What could you do to prevent such a situa-
tion from occurring again?’, responses were grouped
into four categories with eight actions (Table 3). The
NLRN responses to questions at the end of the class
Table 1
Goals, behavioural descriptions and frequency of selected actions as identified by participants before class discussion intervention
Goal/outcome Description of action/number of citations
A. Both patients receive care needed 1. Stay with Joe; call another RN discretely from within Joe’s room (cell, alert button?) to give
morphine to Mrs A (n = 52)
2. Stay with Joe a short time; explain about give meds to another patient. Give or find other RN to
give morphine to Mrs A. Return to Joe for as long as it takes to provide support he needs (n = 28)
3. Stay with Joe a short time (5 min); acknowledge his shock; ask Joe what support methods he
usually uses. Leave to give morphine to Mrs A, call pastoral care, chaplain, social worker, family
or NP to stay with Joe (n = 13)
4. Notify charge nurse that you will be tied up for some time; have responsibility for Mrs A and your
other patients transferred to other RNs (n = 2)
B. One patient receives care 1. Stay with Joe as long as he needs; write down the questions he has so physician can answer
them (n = 15)
2. Give morphine to Mrs A. Initiate pain consult/PCA pump for Mrs A. (n = 13)
3. Talk to Joe, then tell him you are leaving to get answers to his questions either by getting
physician back into the room or by going on-line and printing out web information for him (n = 6)
C. Both patients receive needed care;
develop ID plan of care
When physician asks you to join him to see Joe, ask physician:
1. Why he wants me? Ask him to wait 5 minutes while you give (or get another RN to give)
morphine to Mrs A; then go with physician to Joe’s room (n = 12)
2. What he is going to do? After he tells you, ask him what his plan of care is? Point out that Joe
will need both psychosocial support and information/answers for his many questions (n = 3)
D. Physician sanction 1. Inform charge nurse/manager about physician’s behaviour/handling of situation. Write physician
up for his behaviour (n = 13)
E. Decrease patient assignment 1. Ask charge nurse to reassign Joe or Mrs A to another nurse (n = 4)
PCA, patient-controlled analgesia; NP, nurse practitioner; RN, registered nurse; ID, interdisciplinary.
Table 2
Categories, descriptions and frequency of ‘how I would feel’ if selected action, as identified by participants before class discussion interven-
tion, is performed
Category Description of feelings/number of citations
A. Very positive* Like a real professional nurse; very good; like I had made the right decision and was able
to help both patients; confident and competent (n = 40)
B. OK, satisfied, comfortable As long as each patient received some of what they needed; satisfied that I had
done the best I could under the circumstances; I had my priorities straight, content
with decision (n = 21)
C. Hopeful that I would learn
‘right’ thing to do, challenged
Have faced these situations many times. I’m embarrassed to ask others what I should
have done first (n = 12)
D. Stressed, anxious, nervous Torn and conflicted between two patient’s needs; unsure of my knowledge and prioritizing,
blindsided by the physician (n = 24)
E. Schizophrenic, guilty, angry, very bad,
sad, heartbroken; blame self for inadequacies
Like a machine, less like a person; no-win situation; disappointed in self and in nursing;
unfeeling; hopeless; both patients clearly in pain; no other choice as I cannot do for both
patients at the same time (n = 47)
*I could really identify with Joe because I am a cancer survivor. Physicians expect nurses to take control of psychosocial support for patients
so this wasn’t as much of a dilemma for me.
ª 2013 Blackwell Publishing Ltd
Journal of Nursing Management, 2013, 21, 690–704 699
An evidence-based management practice for new graduates
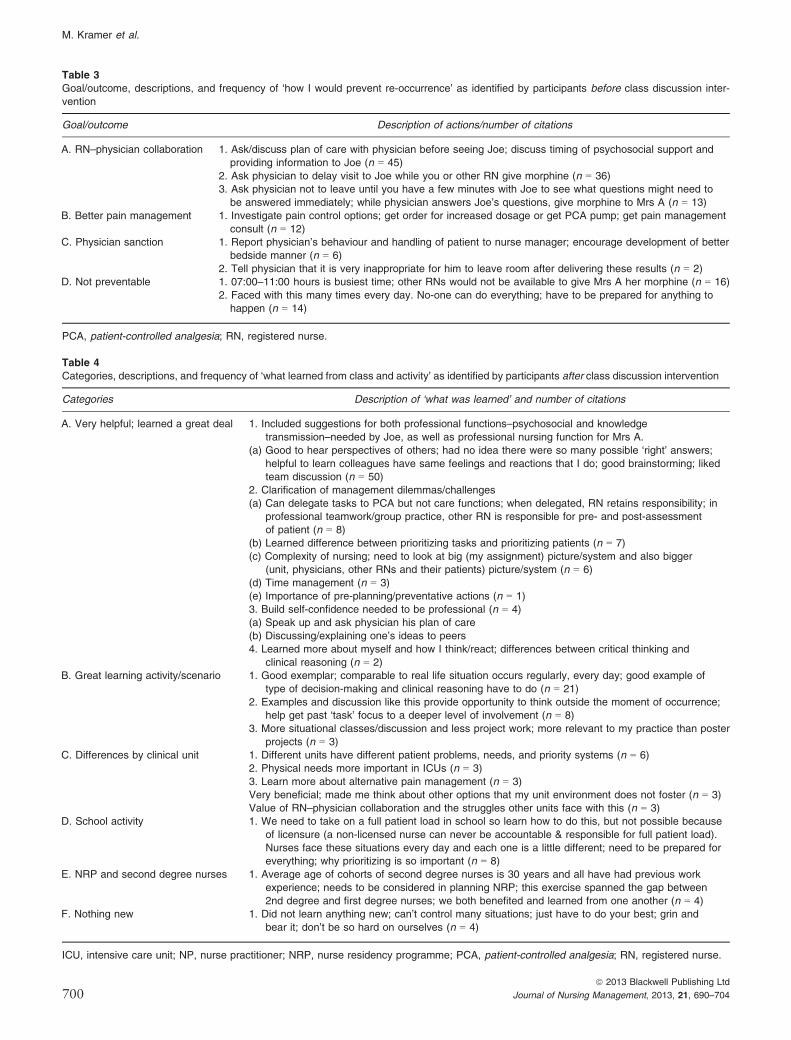
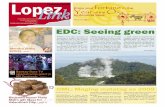
Table 3
Goal/outcome, descriptions, and frequency of ‘how I would prevent re-occurrence’ as identified by participants before class discussion inter-
vention
Goal/outcome Description of actions/number of citations
A. RN–physician collaboration 1. Ask/discuss plan of care with physician before seeing Joe; discuss timing of psychosocial support and
providing information to Joe (n = 45)
2. Ask physician to delay visit to Joe while you or other RN give morphine (n = 36)
3. Ask physician not to leave until you have a few minutes with Joe to see what questions might need to
be answered immediately; while physician answers Joe’s questions, give morphine to Mrs A (n = 13)
B. Better pain management 1. Investigate pain control options; get order for increased dosage or get PCA pump; get pain management
consult (n = 12)
C. Physician sanction 1. Report physician’s behaviour and handling of patient to nurse manager; encourage development of better
bedside manner (n = 6)
2. Tell physician that it is very inappropriate for him to leave room after delivering these results (n = 2)
D. Not preventable 1. 07:00–11:00 hours is busiest time; other RNs would not be available to give Mrs A her morphine (n = 16)
2. Faced with this many times every day. No-one can do everything; have to be prepared for anything to
happen (n = 14)
PCA, patient-controlled analgesia; RN, registered nurse.
Table 4
Categories, descriptions, and frequency of ‘what learned from class and activity’ as identified by participants after class discussion intervention
Categories Description of ‘what was learned’ and number of citations
A. Very helpful; learned a great deal 1. Included suggestions for both professional functions–psychosocial and knowledge
transmission–needed by Joe, as well as professional nursing function for Mrs A.
(a) Good to hear perspectives of others; had no idea there were so many possible ‘right’ answers;
helpful to learn colleagues have same feelings and reactions that I do; good brainstorming; liked
team discussion (n = 50)
2. Clarification of management dilemmas/challenges
(a) Can delegate tasks to PCA but not care functions; when delegated, RN retains responsibility; in
professional teamwork/group practice, other RN is responsible for pre- and post-assessment
of patient (n = 8)
(b) Learned difference between prioritizing tasks and prioritizing patients (n = 7)
(c) Complexity of nursing; need to look at big (my assignment) picture/system and also bigger
(unit, physicians, other RNs and their patients) picture/system (n = 6)
(d) Time management (n = 3)
(e) Importance of pre-planning/preventative actions (n = 1)
3. Build self-confidence needed to be professional (n = 4)
(a) Speak up and ask physician his plan of care
(b) Discussing/explaining one’s ideas to peers
4. Learned more about myself and how I think/react; differences between critical thinking and
clinical reasoning (n = 2)
B. Great learning activity/scenario 1. Good exemplar; comparable to real life situation occurs regularly, every day; good example of
type of decision-making and clinical reasoning have to do (n = 21)
2. Examples and discussion like this provide opportunity to think outside the moment of occurrence;
help get past ‘task’ focus to a deeper level of involvement (n = 8)
3. More situational classes/discussion and less project work; more relevant to my practice than poster
projects (n = 3)
C. Differences by clinical unit 1. Different units have different patient problems, needs, and priority systems (n = 6)
2. Physical needs more important in ICUs (n = 3)
3. Learn more about alternative pain management (n = 3)
Very beneficial; made me think about other options that my unit environment does not foster (n = 3)
Value of RN–physician collaboration and the struggles other units face with this (n = 3)
D. School activity 1. We need to take on a full patient load in school so learn how to do this, but not possible because
of licensure (a non-licensed nurse can never be accountable & responsible for full patient load).
Nurses face these situations every day and each one is a little different; need to be prepared for
everything; why prioritizing is so important (n = 8)
E. NRP and second degree nurses 1. Average age of cohorts of second degree nurses is 30 years and all have had previous work
experience; needs to be considered in planning NRP; this exercise spanned the gap between
2nd degree and first degree nurses; we both benefited and learned from one another (n = 4)
F. Nothing new 1. Did not learn anything new; can’t control many situations; just have to do your best; grin and
bear it; don’t be so hard on ourselves (n = 4)
ICU, intensive care unit; NP, nurse practitioner; NRP, nurse residency programme; PCA, patient-controlled analgesia; RN, registered nurse.
ª 2013 Blackwell Publishing Ltd
700 Journal of Nursing Management, 2013, 21, 690–704
M. Kramer et al.

were grouped into six categories with 15 detailed
actions (Table 4).
Analysis of educators’ post-class questionnaires indi-
cated that educators perceived that a smaller percent-
age of NLRNs felt bad, angry or conflicted about the
decisions they would have made after the class discus-
sion than what NLRNs indicated immediately after
reading the Joe–Mrs Alstairs scenario at the beginning
of the class (22% after compared with 49.3% before
the class discussion). Educators also reported that
after the class, NLRNs demonstrated increased recep-
tivity to the possibility that there was more than one
‘right’ decision depending upon unit, physicians, nurse
colleagues, care delivery system and availability of
other RNs. Educators in all but one hospital indicated
that they would very much like to incorporate this
practice or activity into their NRP.
Summary
There was overwhelming agreement (99%) among
NLRNs and educators that the MP/SC scenario analy-
sis was thought-provoking, beneficial, enlightening and
provoked sharing of many similar MP/SC scenarios.
This best management practice class was less meaning-
ful to NLRNs in specialty (children’s) hospitals, partic-
ularly when the scenario reflected a specialty different
from that of the NLRNs. A class with a mix of
NLRNs from various clinical units in the same hospital
was reported to be exceedingly beneficial for the fol-
lowing reasons. NLRNs learned that: (1) clinical units
defined professional nursing practice in different ways,
(2) priority systems of patient problems and needs var-
ied by units, and (3) support from professional team
members (RNs and physicians) was more the norm on
some units than on others. In two classes, educators
commented that the class discussion stimulated more
participation and contributions from NLRNs who, in
other NRP classes, were usually silent and non-partici-
pative; the reason for this was unknown.
The Joe–Mrs Alstairs scenario was less functional in
hospitals having robust intradisciplinary/interdisciplin-
ary family-centred or relationship-based care delivery
systems. The NLRNs indicated that this was because
these services and systems made the ‘best choice’ obvi-
ous and readily available. Comparison of NLRNs’
comments written immediately after reading the MP/
SC scenario, and educators’ responses to questions on
the post-class questionnaire indicated that two of the
expected outcomes/goals were achieved. At the begin-
ning of the class, almost half of the NLRNs responded
negatively–stressed, angry, conflicted (Categories D &
E in Table 2) – to the question ‘How would you feel
if you had carried out your decision?’ After the class
discussion, in six of the nine hospitals, educators esti-
mated that 100% of the NLRNs in their class would
no longer feel bad because they were unable to meet
the simultaneous needs of both patients.
Complexity systems theory or science was not men-
tioned or suggested to on-site investigators or educators
in any of the project instructions. On-site investigators
did, however, see the NLRN sketch and would know of
the suggestions NLRNs had made for its clarification/
improvement. They were not informed of the suggestions
made by the aggregate 348 NLRNs in the email survey
or that it involved perceiving each RN’s multiple patient
assignment, as well as the unit as a whole, as a complex
system with many interconnected and interrelated agents.
It was anticipated that, with the heavy confirmation from
participants that their MP/SC assignments were perceived
as a whole, as a single complex unit, NLRNs would cite
more than one avenue for resolution of the scenario
dilemma. They would reason that, dependening upon
the severity of the disturbance to the patient’s vortex, and
availability and collaboration with other agents in the
system (other RNs, physicians, management and assistive
personnel), multiple options would need to be consid-
ered. Data indicate that at the end of the class, one-third
of the NLRNs responded that they had learned that there
were multiple, not just one, correct answer to the MP/SC
dilemma. Half of the educators in the 10 classes
estimated the same. In one hospital that had close rela-
tionships with a College of Nursing and many NLRNs
educated by this College, NLRNs were clearly more
familiar with and used complexity concepts, theory and
principles in their clinical reasoning than did NLRNs
from other hospitals.
Conclusions and implications for nursingmanagement
Based on results from this EBMP study, the authors
conclude that this class has considerable potential as a
best management practice for resolving the MP/SC
issue frequently cited as NLRNs’ major problem in
Getting Work Done. Evidence indicates a reduction in
NLRNs’ negative feelings about consequences of their
MP/SC decisions and there was an increase in collabo-
ration with other disciplines after the class discussion.
Twelve years ago, in their analysis of the crisis in
health care quality, the IOM (Institute of Medicine &
Committee on Quality of Healthcare in America, 2001)
recommended viewing health-care organisations as
Complex Adaptive Systems. For those organisations not
ª 2013 Blackwell Publishing Ltd
Journal of Nursing Management, 2013, 21, 690–704 701
An evidence-based management practice for new graduates

already doing so, it is time that systems and complexity
science and its applicability to management of complex
systems be introduced to nurse residents. Porter-O’
Grady et al. (2010) stress that coursework in manage-
ment of complex systems is necessary for clinical nurse
leaders to develop the system thinking, and microsys-
tem-mesosystem level quality improvements that are
necessary to raise the quality of patient outcomes. The
complex systems that clinical nurses must manage also
demand this.
Another suggestion comes directly from NLRNs,
experienced nurses, managers and educators in two of
the hospitals participating in this EBMP project. It
started with several NLRNs verbally relating to their
fellow clinical nurses and managers as much of the
Joe–Mrs Alstairs situation as they could remember and
asking them what decision they would have made:
‘We received the shock of our lives. We thought
we had done such a good job but they brought
up facts and issues we hadn’t even thought of…One RN said: first off, this is probably a medical
diagnostic unit; you knew that Joe had had lots
of tests done. You should have expected that the
physician would be giving Joe the results of those
tests. So, when he asked you to join him, all you
needed to do was raise your eyebrows and he
would have laid out his plan of care. I wouldn’t
be the least bit surprised if it was not a common
practice for this physician to seek out the
patient’s RN when he had bad news to relay…There are two parts to “support” in a situation
like this–psychosocial and relaying specific infor-
mation that the patient asks for. Information
needs to be given in doses the patient can handle.
Most physicians dislike doing the emotional sup-
port bit; many believe that this is the job of the
RN and is an area where nurses excel! What you
need to do is to work out with the physician who
is going to do “what” and “when”. When you
both meet with the patient, you and the physician
discuss the joint plan of care with him. You say
something like: “Look Joe, we know this is a
shock to you. I’m going to stay here with you,
we’ll talk about it, I’ll call anyone you’d like and
then, as you have questions and need more infor-
mation, we’ll write those things down. We’ll
decide if we need to get in touch with Dr __ right
away or if you want to talk with him over the
phone, or if it can wait till he comes in tomor-
row” …You get the idea? Up front and open. All
three of you work out a plan with Joe’.
The final suggestion came from two clinical nurses in
another hospital, both of whom were enrolled in MSN
programs. It’s a take-off from the Nursing Executive
Advisory Center (2011) 15 best practices for enhancing
individual nurse investment in improvement of quality
of patient care. One of the advocated best practices is
‘Inter-assignment Rounding’ (i.e. rounding between
two clinical nurses and the physicians responsible for
the patients assigned to these nurses). Such rounding
provides opportunity for physicians and RNs to coordi-
nate/collaborate on patient plans of care, thereby
improving quality. Clinical nurses also reported that
informal meetings (Kramer et al. 2012a) with physicians
for discussion of clinical scenarios such as the one used
in this EBMP project and development of joint plans of
care ‘are terrific and result in much better patient care.
Acknowledgements
Participation in this evidence-based management
practice project required considerable time, effort and
commitment on the part of the on-site investigators,
clinical educators and residency coordinators in the
nine participating Magnet hospitals where the effective-
ness of this evidence-based best management practice
was evaluated. The authors acknowledge the generous
and enthusiastic participation and wish to thank: Shir-
ley Wiesman, Clinical Nurse Specialist and on-site
investigator, Barb Seliger, Education Specialist, Nurse
Orientation Educator, NICHE Site Coordinator, Aspi-
rus Wausau Hospital, Wausau, WI; Julie Gardner, Resi-
dent & Training Coordinator, Harrison Medical
Center, Bremerton, WA.; Beth A. Smith, Professional
Development Specialist, Nurse Residency Coordinator
and on-site Investigator, Hospital of the University of
Pennsylvania, Philadelphia, PA; Casey O’Brien, Clinical
Education Coordinator, Ann & Robert H. Lurie
Children’s Hospital of Chicago, Chicago, IL; Jane
Jostes-Wanek, Education Nurse Specialist, Donna Po-
duska, ACHE Chief Nurse Executive, Poudre Valley
Hospital, Fort Collins, CO; Roberta Basol, Care Center
Director, Intensive Care/Surgical Care and Clinical
Practice, and on-site Investigator, St Cloud Hospital, St
Cloud, MN; Janet C. Engvall, Graduate Nurse Resi-
dency Coordinator, Center for Professional Practice
Development, The Miriam Hospital, Providence RI; Pat
Horgan, Manager, Clinical Education; Beverly S. Kar-
as-Irwin, Director, Professional Practice and Research,
and on-site investigator, The Valley Hospital, Ridge-
wood NJ; Lauren R. Goodloe, Director of Medical &
Geriatric Nursing, Administrative Director–Nursing
Research and Assistant Dean for Clinical Operations;
ª 2013 Blackwell Publishing Ltd
702 Journal of Nursing Management, 2013, 21, 690–704
M. Kramer et al.

Deborah Fisher, Clinical Director, Pediatric Palliative
Care & Pain Management, Nursing Research Facilita-
tor, Virginia Commonwealth University Medical Cen-
ter, Richmond, VA. We also thank Wendy C. Budin,
Director of Nursing Research and On-site Investigator,
NYU Langone Medical Center, New York City, NY,
for her generous participation in constructing Figure 1
(NLRN sketch) from the e-mail comments and
hand-drawn figures received from NLRNs.
Source of funding
Health Science Research Associates (HSRA) is a volun-
teer, non-profit association of nurse researchers and
mentors who are interested in and conduct research
focused on “Healthy work environments that enable
RNs(and particularly NLRNs) to engage in the profes-
sional practices essential for quality patient outcomes”.
HSRA is unincorporated and ineligible for grants.
Research is supported through honoraria, awards, pre-
sentation and consultation fees.
Ethical approval
The on-site investigators in each of the participating
hospitals obtained Review Board Approval through
their individual organizations.
References
Agnes M. & Guralnik D.B. eds (2001) Webster’s New World
College Dictionary, 4th edn. IDG Books Worldwide, Inc.,
Foster City, CA.
Alfaro-LeFevre R. ed (2013) What is critical thinking, clinical rea-
soning, and clinical judgement? In What is Critical Thinking and
Clinical Reasoning? 5th edn., pp. 1–23. Saunders, St Louis, MO.
American Nurses Credentialing Knowledge Center (2012) Com-
prehensive Magnet Workshops. Available at http://Mwork
[email protected], accessed 26 January 2012.
Anderson R.A. (2003) Nursing homes as complex adaptive
systems. Nursing Research 52 (1), 12–21.
Baghbanian A., Torkfar G. & Baghbanian Y. (2012) Decision-
making in Australia’s health care system and insights from
complex adaptive systems theory. Journal of Health Scope 1
(1), 29–38.
Berkow S., Virkstis K., Stewart J. & Conway L. (2009) Assess-
ing new graduate nurse performance. Nurse Educator 34 (1),
17–22.
de Bono E. (1970) Lateral Thinking: Creativity Step by Step.
Harper & Row, New York.
Cornell P., Herrin-Griffith D., Keim C. et al. (2010) Transform-
ing nursing workflow, part 1: the chaotic nature of nurse
activities. Journal of Nursing Administration 40 (9), 366–373.
Corwin R. (1961) The professional employee: a study of conflict in
nursing roles.American Journal of Sociology 66 (6), 604–615.
Davis M.Z., Kramer M. & Strauss A. (1975) Nurses in Practice:
A Perspective on Work Environments. CV Mosby, St Louis,
MO.
Donabedian A. (1988) The quality of care: how can it be
assessed? Journal of the American Medical Association 260,
1743–1748.
Ebright P.R., Patterson E.S., Chalko B.A. & Render M.L.
(2003) Understanding the complexity of registered nurse work
in acute care settings. Journal of Nursing Administration 33
(12), 630–638.
Gambino M.L. (2008) Complexity and nursing theory: a seismic
shift. In On the Edge: Nursing in the Age of Complexity(C.
Lindberg, S. Nash & C. Lindberg eds), pp. 49–72. Borden-
town, NJ, Plexus Press.
Institute of Medicine and Committee on Quality of Healthcare
in America (2001) Crossing the Quality Chasm: A New
Health Care System for the 21st Century. National Acade-
mies Press, Washington DC.
Institute of Medicine of the National Academies (2004) Keeping
Patients Safe: Transforming the Work Environment of
Nurses. National Academies Press, Washington DC.
Kramer M. (1974) Reality Shock: Why Nurses Leave Nursing.
C.V. Mosby Co., St Louis, MO.
Kramer M. & Schmalenberg C. (1977) Path to Biculturalism:
Conflict Resolution; the Mating of Dreams and Reality.
Contemporary Publishing, Inc., Wakefield, MA.
Kramer M. & Schmalenberg C. (2012) Magnet hospitals: institu-
tions of excellence. kommentar: institutions of excellence. Pflege:
Die Wissenschaftliche Zeitschrift f€ur Pflegeberufe 4, 299–304.
Kramer M., Schmalenberg C. & Maguire P. (2010) Nine struc-
tures and best leadership practices essential for a magnetic
(healthy) work environment. Nursing Administration Quar-
terly 33 (4), 4–17.
Kramer M., Maguire P., Brewer B. & Schmalenberg C. (2011)
Clinical nurses in magnet hospitals confirm productive,
healthy unit work environments. Journal of Nursing Manage-
ment 19, 5–17.
Kramer M., Brewer B. & Maguire P. (2013a) Impact of healthy
unit work environments on new graduate nurses’ environmen-
tal reality shock. Western Journal of Nursing Research 35
(3), 348–383. Available at: http://wjn.sagepub.com/content/
early/recent, accessed 11 March 2011.
Kramer M., Maguire P., Halfer D., Brewer B. & Schmalenberg
C. (2013b) Nurse Residency programs: components and strat-
egies effective in professional socialization of newly licensed
registered nurses. Western Journal of Nursing Research 35
(4), 459–496. Available at: http://wjn.sagebub.com/cgi/
content/abstract/0193945911415555, accessed 4 August 2011.
Kramer M., Maguire P., Halfer D. et al. (2012a) The organiza-
tional transformation power of nurse residency programs.
Presented at the North Star Summit Invitational conference,
June 15, 2011. Nursing Administration Quarterly 36 (2),
155–168.
Kramer M., Halfer D., Maguire P. & Schmalenberg C. (2012b)
Impact of healthy work environments and multistage nurse
residency programs on retention of newly licensed registered
nurses. Journal of Nursing Administration 42 (3), 148–159.
Kramer M., Maguire P., Schmalenberg C. et al. (2012c) Strate-
gies and components of nurse residency programs effective in
new graduate nurses’ integration and management of profes-
sional role responsibilities. Western Journal of Nursing
ª 2013 Blackwell Publishing Ltd
Journal of Nursing Management, 2013, 21, 690–704 703
An evidence-based management practice for new graduates

Research 35 (4), 459–496. Available at: http://wjn.sagebub.
com/cgi/content/abstract/0193945911415555, accessed 4 August
2011.
Krugman M., Bretschneider J., Horn P.B., Krsek C.A., Moutafus
R.A. & Smith M.O. (2006) The national post-baccalaureate
graduate nurse residency program: a model for excellence in
transition to practice. Journal for Nurses in Staff Development
22 (4), 196–205.
Levin R. (2008) Evidence-based practice: if it ain’t broke, don’t
fix it. Research and Theory for Nursing Practice: An Interna-
tional Journal 22 (3), 168–170.
Lindberg C., Nash S. & Lindberg C. (eds) (2008) On the Edge:
Nursing in the Age of Complexity. Plexus Press, Bordentown,
NJ.
Lindberg C. & Lindberg C. (2008) Nurses take note: a primer
on complexity science. In On the Edge: Nursing in the Age of
Complexity(C. Lindberg, S. Nash & C. Lindberg eds),
pp. 23–48. Plexus Press, Bordentown, NJ.
Mark B.A. (1992) Characteristics of nursing practice models.
Journal of Nursing Administration 22 (11), 57–63.
Nursing Executive Advisory Center (2011) Instilling Frontline
Accountability: Best Practices for Enhancing Individual
Investment in Organizational Goals, pp. 61–65. Advisory
Board Company, Washington, DC.
Nursing Executive Center (2007) The Nursing Executive Center
New Graduate Nurse Performance Survey. Advisory Board
Company, Washington, DC.
Paterson B.L., Thorne S.E., Canam C. & Jillings C. (2001)
Meta-Study of Qualitative Health Research: A Practical
Guide to Meta-Analysis and Meta-Synthesis. Sage Publica-
tions, Thousand Oaks, CA.
Pellico L.H., Brewer C.S. & Kovner C.T. (2009) What newly
licensed registered nurses have to say about their first experi-
ences. Nursing Outlook 57 (4), 194–203.
Pesut D.J. (2008) Thoughts on thinking with complexity in
mind. In On the Edge: Nursing in the Age of Complexity
(C. Lindberg, S. Nash & C. Lindberg eds), pp. 211–238.
Plexus Press, Bordentown, NJ.
Porter-O’Grady T., Clark J.S. & Wiggins M.S. (2010) The case
for clinical nurse leaders: guiding nursing practice into the
21st century. Nurse Leader February 8 (1), 37–41.
Rickles D., Hawe P. & Shiell A. (2007) A simple guide to chaos
and complexity. Journal of Epidemiology and Community
Health 61, 933–937.
Schmalenberg C. & Kramer M. (1979) Coping with Reality Shock:
Voices of Experience. Nursing Resources, Wakefield, MA.
Selanders L.C. (1998) The power of environmental adaptation:
Florence Nightingale’s original theory for nursing practice.
Journal of Holistic Nursing 16, 247–263.
Shirey M.R. (2008) Nursing practice models for acute and criti-
cal care: overview of care delivery models. Critical Care
Nursing Clinics of North America 20 (4), 365–373.
Sturmberg J.P., O’Halloran D.M. & Martin C.M. (2012)
Understanding health system reform–a complex adaptive sys-
tems perspective. Journal of Evaluation in Clinical Practice
18, 202–208.
Titler M.G., Kleiber C., Steelman V.J. et al. (2001) The Iowa
model of evidence-based practice to promote quality care. Crit-
ical Care Nursing Clinics of North America 13 (4), 497–509.
University of Newcastle (2009) Clinical Reasoning: Instructor
Resources University of Newcastle. School of Nursing and
Midwifery, Faculty of Health, Newcastle.
ª 2013 Blackwell Publishing Ltd
704 Journal of Nursing Management, 2013, 21, 690–704
M. Kramer et al.