Certified Practice Decision Support Tools (DSTs) - NNPBC
296
1
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of Certified Practice Decision Support Tools (DSTs) - NNPBC

1
2
Certified Practice Decision Support Tools (DSTs)
Registered nurses who are certified by the British Columbia College of Nurses and Midwives (BCCNM) are allowed to perform
certain restricted activities within their autonomous scope of practice. Decision Support Tools (DSTs) set out the activities that are
included in the certified practice guidelines provided by BCCNM. Certified Practice areas include RN First Call, Remote Nursing and
Reproductive Health.
DSTs are regularly reviewed and monitored based on best practices. The information provided is considered current. All certified nurses, RN(C)s, are responsible for following the most current DSTs.
DSTs are not intended to replace the RN(C)'s professional responsibility to exercise independent clinical judgment and use evidence
to support competent, ethical care. The RN(C) must consult with or refer to a physician or nurse practitioner as appropriate, or whenever a course of action deviates from the DST.
TABLE OF CONTENTS
DST Directory .......................................................................................................................................................................... 3
Competencies .......................................................................................................................................................................... 4
RN First Call ............................................................................................................................................................................. 9
Remote Nursing ..................................................................................................................................................................... 87
Contraceptive Management .................................................................................................................................................. 192
Sexually Transmitted Infections ............................................................................................................................................ 212
3
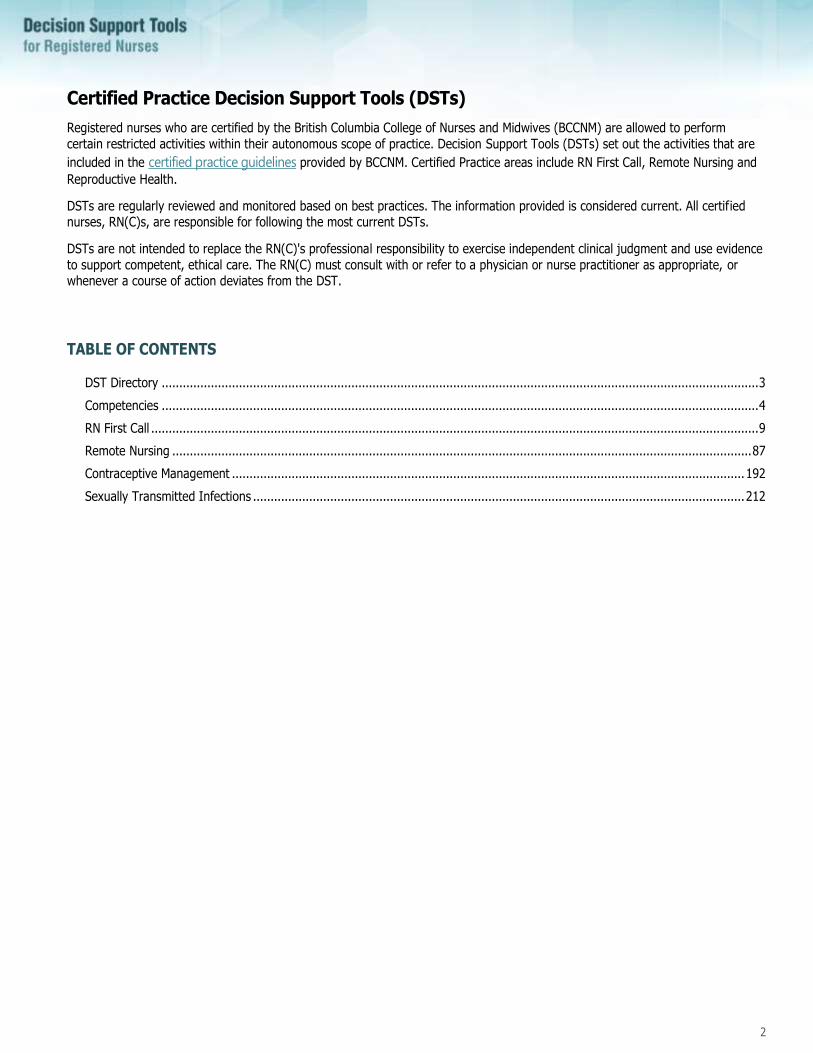
DST Directory
Cross Reference guide to Certification Areas
RN First Call Remote Nursing Contraceptive Management Sexually Transmitted Infections
ID DST name ID DST name ID DST name ID DST name
101 Eye Assessment: Adult 101 Eye Assessment: Adult 900 Contraceptive Management: Assessment
603 Uncomplicated Lower UTI
102 Eye Assessment: Pediatric 102 Eye Assessment: Pediatric 901 Combined Hormonal Contraceptives
1001 STI Assessment
103 Corneal Abrasion Minor: Adult 103 Corneal Abrasion Minor: Adult 902 Progestin-Only Hormonal Contraceptives
1002 Treatment of STI Contacts
104 Corneal Abrasion Minor: Pediatric 104 Corneal Abrasion Minor: Pediatric 1004 Urethritis
105 Conjunctivitis: Adult 105 Conjunctivitis: Adult 1005 Recurrent Urethritis
106 Conjunctivitis: Pediatric 106 Conjunctivitis: Pediatric 1006 Bacterial Vaginosis
201 Ear Nose & Throat Assessment: Adult
201 Ear Nose & Throat Assessment: Adult 1007 Mucopurulent Cervicitis
202 Ear Nose & Throat Assessment: Pediatric
202 Ear Nose & Throat Assessment: Pediatric 1008 Gonorrhea
203 Otitis Media Acute: Adult 203 Otitis Media Acute: Adult 1009 Genital Warts
204 Otitis Media Acute: Pediatric 204 Otitis Media Acute: Pediatric 1010 Chlamydia Trachomatis
206 Pharyngitis: Adult 205 Ceruminosis (Impacted Cerumen: Adult) 1011 Trichomoniasis
207 Pharyngitis: Pediatric 206 Pharyngitis: Adult 1012 Uncomplicated Lower UTI
301 Dental Abscess: Adult 207 Pharyngitis: Pediatric
401 Cardio-Respiratory Assessment: Adult
301 Dental Abscess: Adult
402 Cardio-Respiratory Assessment: Pediatric
401 Cardio-Respiratory Assessment: Adult
501 GI-GU Assessment: Adult 402 Cardio-Respiratory Assessment: Pediatric
601 Lower UTI: Adult 403 Bronchitis Acute: Adult
501 GI-GU Assessment: Adult
502 GI-GU Assessment: Pediatric
601 Lower UTI: Adult
602 Lower UTI: Pediatric
701 Integumentary Assessment: Adult
702 Integumentary Assessment: Pediatric
703 Cellulitis: Adult
704 Cellulitis: Pediatric
705 Impetigo: Adult
706 Impetigo: Pediatric
707 Bites & Scratches: Adult
708 Bites & Scratches: Pediatric
709 Localized Abscess and Furuncle: Adult
801 Use of Nitrous Oxide/Oxygen in Pain Management: Adult

4
Competencies
5
Certified Practice Competencies for RN First Call
Competencies for the BCCNM-certified practice of RN First Call include Section 8 activities for registered nurses. These include diagnosis, care and treatment of adults and/or children with the following diseases and disorders:
• Eye: conjunctivitis, corneal abrasion
• Ear-nose-throat: acute otitis media, pharyngitis, dental abscess (adult only)
• Urinary Tract: lower urinary tract infection (adult females only)
NURSING PRACTICE COMPETENCIES
KNOWLEDGE of: SKILL in: JUDGMENT reasoning in: ATTITUDE by:
• Etiology, pathophysiology, risk factors, predisposing factors, clinical manifestations, communicability, complications, diagnostic findings and management of condition
• Socio-economic determinants of health and risk factors
• Cultural competence and
cultural safety
• Protocols, treatment goals, pharmacological applications and dispensing functions
• Adverse events
• When to consult and/or refer
• Legal framework pertaining to vulnerable populations
• Documentation and reporting requirements
• Engaging with clients using a relational, respectful demeanor
• Recognizing and incorporating cultural wisdom and practices
• Listening to the client and family and gathering a thorough history
• Assessing client’s knowledge
• Performing a relevant physical examination and assessment
• Recognizing circumstances that require immediate consultation or referral
• Collecting specimens, requisitioning tests and interpreting results
• Using clinical reasoning and judgment to make a diagnosis
• Administering/dispensing appropriate medications/treatment
• Engaging in patient and family
education
• Monitoring and follow-up and/or arranging for monitoring and follow-up
• Consulting and/or referring to a physician or NP as appropriate
• Documentation using agency forms
• Assessing the appropriateness of interventions in relation to local cultural beliefs, values and practices
• Taking into account the client’s home environment and context
• Determining client and family capacity to undergo required treatment
• Using clinical reasoning to determine appropriate tests and/or screening
• Requisitioning and/or conducting diagnostic tests, interpreting results and taking appropriate action
• Selecting appropriate treatment regimen
• Recognizing adverse effects of pharmacological or non-pharmacological treatment
• Consulting and referring to appropriate physician, NP or other social and community services
• Using critical thinking for the purpose of delivering care within available resources
• Being self-aware of own beliefs and values
• Being sensitive to the living and working conditions of people living in rural or remote areas
• Working with clients and the community through a lens of cultural safety and cultural competence
• Respecting the lived experience of clients and families
• Promoting capacity building
• Considering the promotion of health and healing as well as the treatment of the current condition
• Taking into account the whole person including their mental, social and psycho-spiritual well-being
• Caring for people on a continuum in community health practice
6
Certified Practice Competencies for Remote Nursing
Competencies for the BCCNM-certified practice of Remote Nursing Practice include Section 8 activities for registered nurses. These include the diagnosis, care and treatment of adults and/or children with the following diseases and disorders:
• Eye: conjunctivitis and corneal abrasion
• Ear-nose-throat: acute otitis media, pharyngitis, ceruminosis (adult only), dental abscess (adult only)
• Genitourinary: urinary tract infection
• Respiratory: acute bronchitis (adult only)
• Skin: abscess and furuncle (adult only), cellulitis, impetigo, bites
• Pain Management: use of a mixture of oxygen and nitrous oxide (adult only).
NURSING PRACTICE COMPETENCIES
KNOWLEDGE of: SKILL in: JUDGMENT reasoning in: ATTITUDE by:
• Etiology, pathophysiology, risk factors, predisposing factors, clinical manifestations, communicability, complications, diagnostic findings and management of
condition
• Socio-economic determinants of health and risk factors
• Cultural competence and cultural safety
• Protocols, treatment goals, pharmacological applications and dispensing functions
• Adverse events
• When to consult and/or refer
• Legal framework pertaining to
vulnerable populations
• Documentation and reporting requirements
• Engaging with clients using a relational, respectful demeanor
• Recognizing and incorporating cultural wisdom and practices
• Listening to the client and family
and gathering a thorough history
• Assessing client’s knowledge
• Performing a relevant physical examination and assessment
• Recognizing circumstances that require immediate consultation or referral
• Collecting specimens, requisitioning tests and interpreting data
• Using clinical reasoning and judgment to make a diagnosis
• Administering/dispensing appropriate medications/treatment
• Engaging in patient and family education
• Monitoring and follow-up and/or arranging for monitoring and follow up
• Consulting and/or referring to a physician or NP as appropriate
• Documenting using agency forms
• Assessing the appropriateness of interventions in relation to local cultural beliefs, values and practices
• Taking into account the client’s home environment and context
• Determining client and family capacity to undergo required treatment
• Using clinical reasoning to determine appropriate tests and/or screening
• Requisitioning and/or conducting diagnostic tests, interpreting results and taking appropriate action
• Selecting appropriate
treatment regimen
• Recognizing adverse effects of pharmacological or non-pharmacological treatment
• Consulting & referring to appropriate physician, NP or other social and community services
• Using critical thinking for the purpose of delivering care within available resources
• Being self-aware of own beliefs and values
• Being sensitive to the living and working conditions of people living in rural and remote areas
• Working with clients and the community through a lens of cultural safety and cultural competence
• Respecting the lived experience of clients and families
• Promoting capacity building
• Considering the promotion of health and healing as well as the treatment of the current
condition
• Taking into account the whole person including their mental, social and psycho-spiritual wellbeing
• Caring for people on a continuum in community health practice

7
Certified Practice Competencies for Reproductive Health: Contraceptive Management
RNs who are BCCNM certified in reproductive health–contraceptive management can autonomously dispense and/or administer combined hormonal contraception and progestin-only hormonal contraception.
NURSING PRACTICE COMPETENCIES
KNOWLEDGE of: SKILL in: JUDGMENT reasoning in: ATTITUDE that:
• Socio-economic determinants of health with a primary focus on accessibility to
services
• gender and sexual diversity
• trauma and violence informed care /practice
• cultural safety including: cultural and spiritual beliefs, generational and community attitudes regarding contraception and pregnancy options
• Contraceptive methods, including effectiveness, pharmacology, indications/contraindications, initial and ongoing management including side
effects.
• Nurse counselling practices as applied to sexuality, reproductive health and pregnancy options
• Available and accessible educational, online resources/services and community services for affected populations and those experiencing barriers to care
• Gathering a thorough history
• Assessing client knowledge
• providing appropriate client centered education, support and resources
• Performing a health assessment
• Confirming pregnancy by urine betaHCG
• Applying nurse counselling practices as applied to sexuality, reproductive health and pregnancy options
• Dispensing and/or administering methods of contraception (prescribing as outlined by BCCNM standards when available)
• Determining the need for specific contraception
• Guiding client through an informed decision making process
• referring clients to appropriate and safe resources/services
• Recognizing the scope and limitations of certified practice
• Consulting and referring to physician/nurse practitioner
• Respects and honours clients’ choices, beliefs,
and values
• Fosters open communication
• Demonstrates self-awareness and self-reflexivity of own beliefs and values, and how this may impact practice
• Reflects creativity and flexibility in supporting client tailored CM care
• Advocates for reducing
stigma and barriers to reproductive health care

8
Certified Practice Competencies for Reproductive Health: Sexually Transmitted Infections
The competencies for Registered Nurse, BCCNM Certified Practice of Reproductive Health - Sexually Transmitted Infections are
documented below. These include Section 8 restricted activities for the diagnosis and treatment of the following diseases and disorders:
1. Chlamydia trachomatis (Reportable)
2. Neisseria gonorrhea (Reportable)
3. Mucopurulent cervicitis
4. Trichomoniasis
5. Bacterial Vaginosis (BV)
6. Urethritis
7. Recurrent Urethritis
8. Lower urinary tract infection
9. Genital Warts
10. Treatment of STI Contacts
NURSING PRACTICE COMPETENCIES
KNOWLEDGE of: SKILL in: JUDGMENT regarding: ATTITUDE that:
• the burden of STIs as it relates to specific populations, syndemics and the determinants of health
• cultural safety
• trauma and violence informed care /practice
• gender and sexual diversity
• etiology, signs & symptoms, testing, complications, diagnostic findings of STIs
• education, counselling, prevention and harm reduction measures
• pharmacology, common side effects, and contraindications related to
medications
• documentation standards, reporting and partner notification requirements
• knowledge of STI epidemiology, local surveillance and affected populations
• Elements that influenceSTI/HIV transmission
• available and accessible
educational and online resources /services and community services for affected populations and those experiencing barriers to accessing care
• assessing the level of plausible risk for acquiring an STI/HIV in relation to the type of exposure
• obtaining a relevant sexual health history
• performing relevant and affirming STI physical assessment, specimen collection and testing
• administering, dispensing and/or recommending STI medication or treatment
• providing appropriate client centred education, support and resources
• facilitating partner notification strategies
• collecting and documenting information for surveillance, reporting, and case management
• determining approach and relevant strategies to assist clients in reducing harm
• testing, treating, and providing follow-up, based on client
assessment, clinical presentation, and laboratory data
• referring clients to appropriate and safe resources/services
• determining appropriate and safe strategies for notifying identified partners
• recognizing the scope and limitations of certified practice
• consulting and referring to physician/nurse practitioner
• respects and honours clients’ choices, beliefs and values
• demonstrates self-awareness and self-reflexivity of own beliefs and values, and how
this may impacts practice
• demonstrates sensitivity regarding impact of STI diagnoses; infectious disease surveillance, reporting, and partner notification
• reflects creativity and flexibility in supporting client tailored STI assessments
• fosters open communication
• advocates for reducing barriers to care
9
Certified Practice Area:
RN First Call
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
RN First Call

10
Certified Practice Area:
RN First Call
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
DST-101 Eye Assessment: Adult
Nurses with Remote Nursing Certified Practice designation (RN(C)s) are able to manage the following eye conditions:
• Conjunctivitis
• Minor corneal abrasion
The following assessment must be completed and documented.
ASSESSMENT
History of Present Illness and Review of System
General
The following characteristics of each symptom should be elicited and explored:
• Onset (sudden or gradual)
• Chronology
• Current situation (improving or deteriorating)
• Location
• Radiation
• Quality
• Timing (frequency, duration)
• Severity
• Precipitating and aggravating factors
• Relieving factors
• Associated symptoms
• Effects on daily activities
• Previous diagnosis of similar episodes
• Previous treatments
• Efficacy of previous treatments
Cardinal Signs and Symptoms
In addition to the general characteristics outlined above, additional characteristics of specific symptoms should be elicited, as follows:
Vision
• Recent changes in vision
• Vision loss including loss of peripheral vision
• Blurring
• Halos around lights
• Floaters
• Flashes of lights
Other Associated Symptoms
• Pain
• Headache
• Sensation of pressure behind eye
• Irritation
DST-101 Eye Assessment: Adult
11
Certified Practice Area:
RN First Call
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
• Foreign-body sensation
• Photophobia
• Diplopia
• Lacrimation
• Itching
• Eye Discharge
• Ear pain
• Nasal discharge
• Sore throat
• Cough
• Nausea or vomiting
• Urethral, vaginal or rectal discharge
• Pain or inflammation of the joints
Medical History (General)
• Medical conditions and surgeries
• Allergies (seasonal as well as medication)
• Medication currently used (prescription, oral contraceptives, over the counter)
• Herbal preparations, vitamins, minerals, supplements and traditional therapies
• Communicable diseases: herpes simplex /zoster
Medical History (Specific to eyes)
• Eye diseases or injuries
• Eye surgery, including corrective
• Use of eyeglasses or contact lenses, corrective or cosmetic
• Change in type of contact lens or solution
• Concurrent infection of the upper respiratory tract
• Other infectious diseases (chicken pox, measles)
• Sexually Transmitted Infections (STIs)
• Immunocompromise
• Exposure to eye irritants (environmental or occupational)
• Current eye medications - homatropine, cylogyl, steroids
• Systemic inflammatory disease (Inflammatory Bowel Disease, Reiter's syndrome, Rheumatoid Arthritis (RA), Lupus)
• Diabetes mellitus
• Hypertension
• Chronic renal disease
• Bleeding disorders
Family History
• Visual disorders (glaucoma, cataract, blindness, etc.)
• Systemic inflammatory disease (i.e., arthritis conditions, lupus)
• Diabetes mellitus
• Others with eye infections
DST-101 Eye Assessment: Adult
12
Certified Practice Area:
RN First Call
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
Personal and Social History (Specific to eyes)
• Occupational and recreational exposure to irritants
• Exposure to ultraviolet radiation from the sun
• Use of protective eyewear for sports and other activities
• Exposure to irritants (chemical, cigarette smoke, wood smoke)
• Housing and sanitation conditions
• Exposure to contagious organisms (e.g. conjunctivitis)
• Sexual activity
PHYSICAL ASSESSMENT OF THE EYE
Vitals
• Temperature
• Pulse
• Respiration
• SpO2
• Blood pressure (BP)
• Pain
General
• Apparent state of health
• Appearance of comfort or distress
• Colour
• Nutritional status
• State of hydration
• Hygiene
• Match between appearance and stated age
Inspection
Test visual acuity, visual field
Inspection
• Bony Orbit: edema, lesions, bruising
• Lids and Lashes: ability to open and close, edema, erythema, crusting, eyelash position, tremors, foreign bodies, lesions.
Evert upper lids as required.
• Lacrimal Apparatus: tearing, size
• Conjunctiva and Sclera: color, pattern of injection, discharge, edema, haemorrhage, pterygium, foreign body
• Cornea: clarity, abrasions or lacerations, arcus senilis (lipid deposition around cornea), foreign body. Fluorescein stain for
corneal integrity.
• Pupil and Iris: color, size, shape, reactivity to light and accommodation
• Lens: transparency, opacities
• Fundi: red reflex, haemorrhage, optic disc, retinal vasculature
• Extraocular muscles: Extra ocular eye movements (EOEM), position and alignment of eyes (i.e., strabismus): use corneal light
reflex test, cover-uncover test
DST-101 Eye Assessment: Adult
13
Certified Practice Area:
RN First Call
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
Palpation
Palpate the bony orbit, forehead, eyebrows, eyelids, lacrimal apparatus and pre-auricular lymph nodes for tenderness, swelling or masses
Do not palpate globe if rupture injury is suspected or if the client has undergone recent eye surgery
Associated Systems
• An ENT examination, including the lymph nodes of the head and neck, should also be performed if there are symptoms of a
systemic condition, such as viral URTI or an STI, (e.g. gonorrhea) is suspected
• Pre-auricular adenopathy might indicate chlamydial, viral or invasive bacterial infection of the eye (e.g., gonorrhea)
Abdomen
Assess liver for tenderness and enlargement if eye symptoms are associated with symptoms of an STI.
Genitourinary System and Rectal Area
Assess for urethral, cervical or vaginal discharge if eye symptoms are associated with symptoms of an STI.
Musculoskeletal System and Extremities
Examine the joints to assess for warmth, redness, pain or swelling.
SYMPTOMS REQUIRING URGENT REFERRAL
The first step is to differentiate major or serious causes of red eye from minor causes.
The following signs and symptoms require urgent referral to a physician or nurse practitioner:
• Unilateral or bilateral eye pain
• Ocular pain
• Ocular injury of any kind
• Severe photophobia of unknown cause
• Persistent blurring of vision
• Recent onset of visual disturbances – light flashes, floaters (recent onset), halos, dimming, visual distortion,
double vision, abnormal colour perception or loss of visual acuity.
• Visual field loss
• Reduced ocular movement
• Exophthalmos (proptosis)
• Ciliary flush
• Scleral icterus
• Hyphema
• Irregular cornea (epithelial defect or opacity, irregular corneal reflection of light)
• Non-reactive pupil
• Treatment failure after 3 days
• Worsening symptoms
• Compromised host (e.g., immuno-suppressed client)
• Signs of preseptal or orbital cellulitis
• Symptoms in conjunction with a communicable disease i.e. chickenpox
• Finger like (dendritic) projections noted on fluorescein stain (herpetic)
DST-101 Eye Assessment: Adult

14
Certified Practice Area:
RN First Call
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
DIAGNOSTIC TESTS
The RN(C) may consider the following diagnostic tests in the examination of the eye to support clinical decision-making:
• Swab drainage for Culture and Sensitivity (C&S) only if there is no resolution of symptoms after an empiric course of
treatment.
ADDITIONAL TESTING
Apply fluorescein stain to test for corneal integrity if there is a possibility that a corneal abrasion has occurred.
DST-101 Eye Assessment: Adult

15
Certified Practice Area:
RN First Call
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
REFERENCES
More recent editions of any of the items in the Reference List may have been published since this DST was published. If you have a newer version, please use it.
American Academy of Ophthalmology. (2014). Policy statement: Guidelines for appropriate referral of persons with possible eye diseases or injury.
American Optometric Association. (2017). Comprehensive eye and vision examination. American Optometric Association.
Ball, J. W., Dains, J. E., Flynn, J. A., Solomon, B. S., & Stewart, R. W. (Eds.). (2015). Seidel’s guide to physical examination (8th ed.). St. Louis, MO: Elsevier.
Boyd, K. (2017). Cataract diagnosis. American Academy of Ophthalmology.
Boyd, K. (2017). Glaucoma. American Academy of Ophthalmology.
Boyd, K. (2016). What you should know about swimming and your eyes. American Academy of Ophthalmology. doi:10.1186/ar96
Canadian Association of Optometrists. (2017). What is a comprehensive eye exam? Canadian Association of Optometrists.
Cleary, G., Nischal, K. K., & Jones, C. a. (2006). Penetrating orbital trauma by stiletto causing complex cranial neuropathies. Emergency medicine journal: EMJ, 23(4), e28.
Dains, J. E., Baumann, L. C., & Scheibel, P. (2012). Advanced health assessment and clinical diagnosis in primary care (4th ed.). St. Louis, MO: Elsevier Mosby.
Estes, M. E. Z. (2014). Health assessment and physical examination (5th ed.). Clifton Park, NY: Cengage Learning.
Eye Physicians & Surgeons of Ontario. (2017). Vision Safety. Canadian Ophthalmological Society.
Jacobs, D. S. (2014). Corneal abrasions and corneal foreign bodies: Clinical manifestations and diagnosis. UpToDate.
Porter, R. S., & Kaplan, J. L. (Eds.). (2011). Approach to the ophthalmologic patient. In The Merck Manual (19th ed.). Whitehouse Station, NJ: Merck Sharpe & Dome Corporation.
Stephen, T. C., Skillen, D. L., Day, R. A., & Bickley L. S. (2010). Canadian Bates’ guide to health assessment for nurses. Philadelphia, PA: Lippincott, Williams & Wilkins.
Waldo, M. H. (Ed.). (2011). Ophthalmic procedures in the office and clinic (3rd ed.). San Francisco, CA: American Society of Ophthalmic Registered Nurses.
Zoric, L. & Stojcic, M. (2013). The influence of ultraviolet radiation on eye. Primary Health Care 3: 133. doi:10.4172/2167-1079.1000133
DST-101 Eye Assessment: Adult
16
Certified Practice Area:
RN First Call
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
DST-102 Eye Assessment: Pediatric
Nurses with Remote Nursing Certified Practice designation (RN(C)s) are able to manage the following eye conditions:
• Conjunctivitis in children 6 months of age and older
• Minor corneal abrasion in children 2 years of age and older
The following assessment must be completed and documented.
ASSESSMENT
History of Present Illness and Review of System
General
The following characteristics of each symptom should be elicited and explored:
• Chronology
• Onset
• Current situation (improving or deteriorating)
• Location
• Radiation
• Quality
• Timing (frequency, duration)
• Severity
• Precipitating and aggravating factors
• Relieving factors
• Associated symptoms
• Effects on daily activities
• Previous diagnosis of similar episodes
• Previous treatments
• Efficacy of previous treatments
Cardinal Signs and Symptoms
In addition to the general characteristics outlined above, additional characteristics of specific symptoms should be elicited as
follows:
Vision
• Recent changes
• Vision loss including loss of peripheral vision
• Blurring
• Halos around lights
• Floaters
Other Associated Symptoms
• Pain
• Sensation of pressure behind the eye
• Irritation
• Foreign-body sensation
• Photophobia
DST-102 Eye Assessment: Pediatric

17
Certified Practice Area:
RN First Call
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
• Diplopia (observed squinting or keeping one eye closed in younger children)
• Lacrimation
• Itching
• Rubbing of eyes
• Eye discharge
• Ear pain
• Nasal discharge
• Sore throat
• Cough
• Nausea or vomiting
• Headache
• Urethral, vaginal or rectal discharge
• Pain or inflammation of the joints
Medical History (General)
• Medical conditions and surgeries
• Allergies (seasonal as well as medication)
• Medication currently used (e.g., prescription, oral contraceptives, over the counter)
• Herbal preparations, vitamins, minerals, supplements and traditional therapies
• Birth and prenatal history if age appropriate
• Communicable diseases: measles, chickenpox (varicella), herpes simplex
• Immunization Status
Medical History (Specific to eyes)
• Eye diseases, defects or injuries
• Eye surgery, including corrective
• Use of eyeglasses or contact lenses, corrective or cosmetic
• Change in type of contact lens or solution
• Concurrent infection of the upper respiratory tract
• Other infectious diseases (chicken pox, measles)
• Sexually Transmitted Infections (STIs)
• Immunocompromise
• Exposure to eye irritants (environmental or occupational)
• Current eye medications - homatropine, cyclogyl, steroids
• Systemic inflammatory disease (Inflammatory Bowel Disease, Reiter's syndrome, Juvenile Rheumatoid Arthritis)
• Diabetes mellitus
• Chronic renal disease
• Bleeding disorders
Family History
• Visual disorders (i.e. glaucoma, blindness, etc.)
• Systemic inflammatory disease (i.e., arthritis conditions, lupus)
• Diabetes mellitus
• Others with eye infections
DST-102 Eye Assessment: Pediatric
18
Certified Practice Area:
RN First Call
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
Personal and Social History (Specific to eyes)
• Concerns reported by parent, caregiver or teacher about child’s vision (i.e. squinting, headaches caused by reading)
• Use of protective eyewear for sports and other activities
• Exposure to irritants (chemicals, cigarette smoke, wood smoke)
• Exposure to ultraviolet radiation from the sun
• Housing and sanitation conditions
• School or day-care exposure to contagious organisms (e.g. conjunctivitis)
• Sexual activity, if applicable
PHYSICAL ASSESSMENT OF THE EYE
Vitals
• Temperature
• Pulse
• Respiration
• SpO2
• Blood pressure (BP)
• Pain
General
• Apparent state of health
• Appearance of comfort or distress
• Colour
• Nutritional status
• State of hydration
• Hygiene
• Match between appearance and stated age
• Character of cry (in infants less than 6 months old)
• Activity level
• Mental status
• Degree of cooperation, consolability
• Emotional reaction to caregiver and examiner
• Difficulty with gait or balance
Inspection
Test visual acuity, visual field
• Visual acuity in children greater than 3 yrs of age
• Using a tumbling E or picture chart for children over 3 yrs of age or who cannot read the alphabet
• Most infants are farsighted, gradually gaining acuity as they develop, attaining approximately 20/50 by one year of age, and
20/20 by 6-8 years of age
• Test visual field in older children if concern about glaucoma
Inspection
• Bony Orbit: edema, lesions, bruising
DST-102 Eye Assessment: Pediatric

19
Certified Practice Area:
RN First Call
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
• Lids and Lashes: ability to open and close, edema, erythema, crusting, eyelash position, tremors, foreign bodies, lesions.
Evert upper lids as required.
• Lacrimal Apparatus: tearing, size
• Conjunctiva and Sclera: color, pattern of injection, discharge, edema, haemorrhage, pterygium, foreign body
• Cornea: clarity, abrasions or lacerations. Corneal cloudiness may be a sign of congenital cataracts, foreign body. Fluorescein
stain to assess for corneal integrity.
• Pupil and Iris: color, size, shape, reactivity to light and accommodation
• Lens: transparency, opacities
• Fundi: red reflex, optic disc, retinal vasculature in older children
• Extraocular muscles: Extra ocular eye movements (EOEM), position and alignment of eyes (i.e., strabismus): use corneal light
reflex test, cover-uncover test
Palpation
Palpate the bony orbit, forehead, eyebrows, eyelids, lacrimal apparatus and pre-auricular lymph nodes for tenderness, swelling or
masses
Do not palpate globe if rupture injury is suspected or if the client has undergone recent eye surgery
Associated Systems
• An ENT examination, including the lymph nodes of the head and neck, should also be performed if there are symptoms of a
systemic condition, such as viral URTI or an STI, (e.g. if gonorrhea is suspected)
• Pre-auricular adenopathy might indicate chlamydial, viral or invasive bacterial infection of the eye (e.g., gonorrhea)
Abdomen
Assess liver for tenderness and enlargement if eye symptoms are associated with symptoms of an STI.
Genitourinary System and Rectal Area
Assess for urethral, cervical or vaginal discharge if eye symptoms are associated with symptoms of an STI.
Musculoskeletal System and Extremities
Examine the joints to assess for warmth, redness, pain or swelling.
DST-102 Eye Assessment: Pediatric
20
Certified Practice Area:
RN First Call
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
SYMPTOMS REQUIRING URGENT REFERRAL
The first step is to differentiate major or serious causes of red eye from minor causes. The following signs and symptoms require urgent referral to a physician or nurse practitioner:
• Unilateral or bilateral eye pain
• Ocular pain
• Ocular injury of any kind
• Severe photophobia of unknown cause
• Persistent blurring of vision
• Recent onset of visual disturbances – light flashes, floaters (recent onset), halos, dimming, visual
distortion, double vision, abnormal colour perception or loss of visual acuity.
• Visual field loss
• Reduced ocular movement
• Exophthalmos (proptosis)
• Ciliary flush
• Scleral icterus
• Hyphema
• Irregular cornea (epithelial defect or opacity, irregular corneal reflection of light)
• Non-reactive pupil
• Treatment failure after 3 days
• Worsening symptoms
• Compromised host (e.g., immuno-suppressed client)
• Signs of preseptal or orbital cellulitis
• Symptoms in conjunction with a communicable disease i.e. chickenpox
• Finger like (dendritic) projections noted on fluorescein stain (herpetic)
DIAGNOSTIC TESTS
The RN(C) may consider the following diagnostic tests in the examination of the eye to support clinical decision-making:
• Swab drainage for Culture and Sensitivity (C&S) only if there is no resolution of symptoms after an empiric course of
treatment.
ADDITIONAL TESTING
• Apply fluorescein stain to test for corneal integrity if there is a possibility that a corneal abrasion has occurred.
DST-102 Eye Assessment: Pediatric
21
Certified Practice Area:
RN First Call
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
REFERENCES
More recent editions of any of the items in the Reference List may have been published since this DST was published. If you have a newer version, please use it.
American Academy of Ophthalmology. (2014). Policy statement: Guidelines for appropriate referral of persons with possible eye diseases or injury.
American Academy of Ophthalmology. (2015). Comprehensive Adult Medical Eye Evaluation.
Ball, J. W., Dains, J. E., Flynn, J. A., Solomon, B. S., & Stewart, R. W. (Eds.). (2015). Seidel’s guide to physical examination (8th ed.). St. Louis, MO: Elsevier.
Eye Physicians & Surgeons of Ontario. (2017). Vision Safety. Canadian Ophthalmological Society.
Dains, J. E., Baumann, L. C., & Scheibel, P. (2012). Advanced health assessment and clinical diagnosis in primary care (4th ed.). St. Louis, MO: Elsevier Mosby.
Estes, M. E. Z. (2014). Health assessment and physical examination (5th ed.). Clifton Park, NY: Cengage Learning.
Gardiner, M. F. (2016). Overview of eye injuries in the emergency department. UptoDate
Jacobs, D. S. (2014). Corneal abrasions and corneal foreign bodies: Clinical manifestations and diagnosis. UptoDate.
Porter, R. S., & Kaplan, J. L. (Eds.). (2011). Approach to the ophthalmologic patient. In The Merck Manual (19th ed.). Whitehouse Station, NJ: Merck Sharpe & Dome Corporation.
Sawyer, S. S. (2012). Pediatric physical examination and health assessment. Sudbury, MA: Jones & Bartlett Learning.
Stephen, T. C., Skillen, D. L., Day, R. A., & Bickley, L. S. (2010). Canadian Bates’ guide to health assessment for nurses. Philadelphia, PA: Lippincott, Williams & Wilkins.
Waldo, M. H. (Ed.). (2011). Ophthalmic procedures in the office and clinic (3rd ed.). San Francisco, CA: American Society of Ophthalmic Registered Nurses.
Zoric, L. & Stojcic, M. (2013). The influence of ultraviolet radiation on eye. Primary Health Care 3: 133.
DST-102 Eye Assessment: Pediatric
22
Certified Practice Area:
RN First Call
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
DST-103 Corneal Abrasion (Minor): Adult
DEFINITION
A minor abrasion is superficial corneal defect due to scraping or rubbing of the corneal epithelium. Corneal abrasions occur in any situation that causes epithelial compromise.
POTENTIAL CAUSES
Usually trauma or foreign body in the eye
• Fingernails
• Animal paws
• Pieces of: paper or cardboard, wood or metal
• Makeup applicators
• Hand tools
• Branches or leaves
• Thermal burns and ultraviolet light burns from: welding, tanning bed use, snow blindness and direct viewing of the sun
TYPICAL FINDINGS OF CORNEAL ABRASION
History
• Trauma
• Sudden unilateral eye pain (sharp or worse with blinking)
• Mild blurred vision (due to tearing) may be present
• Mild photophobia
• Moderate to profuse tearing
• Foreign-body sensation
• Wearing contact lens
Physical Assessment
• Vital signs normal
• Visual acuity may be slightly blurred in affected eye
• Diffuse conjunctival injection1
• Central conjunctival injection or ciliary flush often denotes a more serious problem than slight but diffuse injection
• Pupils round and react briskly to light
• Presence of a foreign body under the upper or lower eyelid must be ruled out. Evert the lids and inspect carefully.
Diagnostic Tests
• Apply fluorescein stain. Corneal cells that are damaged or lost will stain green; cobalt blue light allows easier visualization of
the abrasion.
1 Conjunctival injection refers to redness (bright red or pink) of the conjunctiva fading towards the limbus due to dilatation of the superficial
conjunctival blood vessels occurring in conjunctival inflammations – e.g., conjunctivitis.
DST-103 Corneal Abrasion (Minor): Adult

23
Certified Practice Area:
RN First Call
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
MANAGEMENT AND INTERVENTION
Goals of Treatment
• Preserve vision
• Prevent secondary bacterial infection
• Prevent development of corneal ulceration
• Pain management
Non-pharmacologic Intervention
• Copious irrigation with saline for any foreign body to promote removal
• Do not use contact lens until abrasion healed and antibiotic treatment is finished
• Patching is contra-indicated unless advised by a physician or nurse practitioner
Pharmacologic Interventions
Note: The amount of anesthetic used should be minimal, as these agents have been shown to slow wound healing.
• Instill topical anesthetic eye drop:
o tetracaine 0.5% eye solution (pontocaine) 2 drops stat dose only
Note: The client should not be discharged with topical anesthetics for pain control as they can be toxic to the epithelium and retard healing, increasing the risk of infections and scarring
• Complaints of irritation and foreign-body sensation should resolve in 1 or 2 minutes
• Instill a generous amount of eye lubricant in the lower conjunctival sac
• Analgesics for mild to moderate pain:
o acetaminophen 325mg, 1-2 tabs po q4-6h prn, or
o ibuprofen 200mg, 1-2 tabs po q4-6h prn
Note: Corneal abrasions should never be treated with topical steroids as they slow healing and increase the risk of superinfection.
Note: Tetanus prophylaxis is not recommended unless there is a penetrating injury into the eye, chemical burn, devitalized tissue, or trauma from contaminated material.
Pregnant Women (same dosing as above)
• Eye lubricant and acetaminophen may be used as listed above
• Tetracaine may be used after consulting a physician or nurse practitioner.
• DO NOT USE ibuprofen.
Breastfeeding Women (same dosing as above)
• Eye lubricant and acetaminophen may be used as listed above
• Tetracaine may be used after consulting a physician or nurse practitioner
• Ibuprofen may be used after consulting a physician or nurse practitioner.
POTENTIAL COMPLICATIONS
• Corneal ulceration
• Secondary bacterial infection
• Corneal scarring if abrasion recurs
• Uveitis
• Iritis
DST-103 Corneal Abrasion (Minor): Adult
24
Certified Practice Area:
RN First Call
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
CLIENT EDUCATION /DISCHARGE INFORMATION
• Advise on condition, timeline of treatment and expected course of disease process.
• Advise client that daily follow-up is important to ensure proper healing.
• Counsel client about appropriate use of medications (type, dose, frequency, side effects).
• Counsel client about when they should return back to work.
• Instruct client to return to clinic immediately if pain increases, if vision changes before 24-hour follow-up and if any signs of
infection appear including swelling, discharge, or increased redness.
• Client should return if there are changes such as flashes of light, floaters, a dark veil or vision loss.
• Suggest that client wear protective glasses while working or participating in contact sports, to help prevent similar incidents
in future.
• Do not wear contact lens until healed.
MONITORING AND FOLLOW-UP
• Follow-up at 24 hours to assess healing is imperative.
• If no symptoms or signs, client can be sent home with advice on preventing corneal abrasions.
• If the client is still symptomatic but improving, then the eye should be re-treated as above with lubricant, and re-examined
daily with fluorescein. The uptake of dye should be less than on the previous day. Re-examine daily until the abrasion has
healed completely.
CONSULTATION AND/OR REFERRAL
• Consult a physician or nurse practitioner if
o the abrasion is greater than 4 mm
o the abrasion is located in the center of the cornea
o a penetrating corneal ulcer is found on initial examination,
o pain is severe,
o pupils are not round,
o the abrasion is larger after 24 hours,
o a residual rust ring is evident, or
o there is significant worsening of vision.
• Referral to an optometrist, nurse practitioner or physician is required within 24 hours for large or central defects and in 48-72
hours if there is no response to therapy.
DOCUMENTATION
• According to agency policy
DST-103 Corneal Abrasion (Minor): Adult
25
Certified Practice Area:
RN First Call
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
REFERENCES
More recent editions of any of the items in the Reference List may have been published since this DST was published. If you have a newer version, please use it.
Ahmed, F.,Feldman, H. House, R. MDc, 2015 Corneal Abrasions and Corneal Foreign Bodies. American Academy of Opthalmology. (2012). Corneal Abrasion.
Bashour, M. (2014, March 5). Corneal foreign body. Retrieved from http://emedicine.medscape.com/article/1195581-overview
Canadian Pharmacists Association. (2014). Compendium of Therapeutic Choices (7th ed.). Ottawa, ON: Author
Canadian Pharmacists Association. (2010). E-CPS.
Cash, J. C., & Glass, C. A. (Eds.). (2014). Family practice guidelines (3rd ed.). New York, NY: Springer.
Cronau, H., Kankanala, R. R., & Mauger, T. (2010). Diagnosis and management of red eye in primary care. American Family Physician, 81(2), 137-144.
DynaMed. (2015, December 21). Corneal Abrasion.
Fraenkel A, Lee LR, Lee GA. Managing corneal foreign bodies in office-based general practice ‘ T. 2017;46(3):89-94. Jacobs, D. S. (2015). Corneal abrasions and corneal foreign bodies: Management. UptoDate.
Mitchell L, Grimmer P. Complications & treatment of a red eye. Bpj. 2013;54(54):8-21.
Mukherjee P, Sivakumar A. Tetanus prophylaxis in superficial corneal abrasions. Emerg Med J. 2003;20(1):62-64.
Klostranec, J. M., & Kolin, D. L. (2012). The Toronto notes 2012: Comprehensive medical reference & review for Medical Council of Canada Qualifying Exam Part 1 and the United States Medical Licesnsing Exam Step 2 (28th ed.). Toronto, ON: Toronto Notes for Medical Students.
New Zealand Medicines and Medical Devices Safety Authority. (2008). Minims tetracaine hydrochloride.
Peyman GA, Rahimy MH, Fernandes ML. Effects of morphine on corneal sensitivity and epithelial wound healing: implications for topical ophthalmic analgesia. Br J Ophthalmol. 1994 Feb. 78(2):138-41.
Porter, R. S., & Kaplan, J. L. (2011). Eye Disorders. In The Merck Manual (19th ed). Whitehouse Station, NJ: Merck Sharpe & Dohme Corp.
Verma, A. (2014, February 20). Corneal abrasion.
Wipperman, J. L., & Dorsch, J. N. (2013, January 15). Evaluation and management of corneal abrasions. American Family Physician, 87(2), 114-120.
WHO. Protection Against Exposure to Ultraviolet Radiation | World Health Organization. World Heal Organ. 1994
DST-103 Corneal Abrasion (Minor): Adult
26
Certified Practice Area:
RN First Call
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
DST-104 Corneal Abrasion (Minor): Pediatric
DEFINITION
A superficial corneal defect due to scraping or rubbing of the corneal epithelium.
Corneal abrasions occur in any situation that causes epithelial compromise.
Nurses with Remote Practice Certified Practice designation (RN(C)s) are able to treat children with corneal abrasions who are 2 years of age and older.
POTENTIAL CAUSES
Usually trauma or foreign body in the eye
• Fingernails
• Animal paws
• Pieces of paper, cardboard, metal or wood
• Makeup applicators
• Hand tools
• Branches or leaves
• Thermal burns and ultraviolet light burns from: welding, tanning bed use, snow blindness and direct viewing of the sun
TYPICAL FINDINGS OF CORNEAL ABRASION
History
Trauma
• Sudden unilateral eye pain (sharp or worse with blinking)
• Mild blurred vision (due to tearing) may be present
• Mild photophobia Moderate to profuse tearing
• Foreign-body sensation Contact lens wearing
Physical Assessment
• Vital signs normal
• Weigh for medication calculations
• Visual acuity may be slightly blurred in affected eye
• Diffuse conjunctival injection
• Central conjunctival injection or ciliary flush often denotes a more serious problem than slight but diffuse injection
• Pupils react briskly to light
• Presence of a foreign body under the upper or lower eyelid must be ruled out. Evert the lids and inspect carefully.
• Note: A rust ring: may form around foreign bodies that contain iron, typically those that are metallic.
Diagnostic Tests
• Apply fluorescein stain: corneal cells that are damaged or lost will stain green; cobalt blue light allows easier visualization of
the abrasion
MANAGEMENT AND INTERVENTION
Goals of Treatment
• Preserve vision
DST-104 Corneal Abrasion (Minor): Pediatric
27
Certified Practice Area:
RN First Call
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
• Prevent secondary bacterial infection
• Prevent development of corneal ulceration
• Pain management
Non-pharmacologic Intervention
• Copious irrigation with saline for any foreign body to promote removal
• Do not use contact lens until healed and antibiotic treatment is finished.
• Patching is contraindicated unless advised by a physician or nurse practitioner.
Pharmacologic Interventions
• Weight required for all drug calculations.
• Pediatric doses should not exceed recommended adult doses.
• Instill topical anesthetic eye drop:
• tetracaine 0.5% eye solution (Pontocaine) 2 drops stat dose only
Note: The client should not be discharged with topical anesthetics for pain control as they can be toxic to the epithelium and retard
healing, increasing the risk of infections and scarring.
• Complaints of irritation and foreign-body sensation should resolve in 1 or 2 minutes
• Instill a generous amount of eye lubrication in the lower conjunctival sac.
• Analgesics for mild to moderate pain:
o acetaminophen
o ibuprofen
Note: Corneal abrasions should never be treated with topical steroids as they slow healing and increase the risk of superinfection.
Note: Tetanus prophylaxis is not recommended unless there is a penetrating injury into the eye, chemical burn, devitalized tissue, or trauma from contaminated material.
Pregnant Women (dosing as above)
• Eye lubricant and acetaminophen are safe in pregnancy.
• Tetracaine may be used after consulting a physician or nurse practitioner.
• DO NOT USE ibuprofen.
Breastfeeding Women (same dosing as above)
• Eye lubricant and acetaminophen may be used as listed above
• Tetracaine may be used after consulting a physician or nurse practitioner
• Ibuprofen may be used after consulting a physician or nurse practitioner.
POTENTIAL COMPLICATIONS
• Corneal ulceration
• Secondary bacterial infection
• Corneal scarring if abrasion recurs
• Uveitis
• Iritis
DST-104 Corneal Abrasion (Minor): Pediatric

28
Certified Practice Area:
RN First Call
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
CLIENT/CAREGIVER EDUCATION AND DISCHARGE INFORMATION
• Advise on condition, timeline of treatment and expected course of disease process.
• Advise client that daily follow-up is important to ensure proper healing.
• Counsel client about appropriate use of medications (type, dose, frequency, side effects).
• Counsel client/guardian about when to return to work or school.
• Instruct client to return to clinic immediately if pain increases, if vision decreases before 24-hour follow-up, and if any signs
of infection appear including swelling, discharge, or increased redness. Client should return if there are changes such as
flashes of light, floaters, a dark veil or vision loss.
• Suggest that client wear protective glasses while working or participating in contact sports to help prevent similar incidents in
future.
• If contact lens wearer, do not wear contact lens until healed.
MONITORING AND FOLLOW-UP
• Advise caregiver to follow-up if condition does not improve, deteriorates and for on-going monitoring as necessary. Follow-
up at 24 hours to assess healing is imperative.
• Daily visual acuity test until recovered.
• If no symptoms or signs, client can be sent home with advice on preventing corneal abrasions.
• If client is still symptomatic but improving the eye should be re-treated as above with antibiotic ointment or drops and re-
examined daily with fluorescein. The uptake of dye should be less than on the previous day. Re-examine daily until the
abrasion has healed completely.
CONSULTATION AND/OR REFERRAL
Consult a physician or nurse practitioner if:
• child is under the age of 2 years.
• The abrasion is greater than 4 mm
• The abrasion is located in center of the cornea.
• a penetrating corneal ulcer is found on initial examination,
• pain is severe,
• pupils are not round,
• the abrasion is larger after 24 hours,
• a residual rust ring is evident, or
• there is significant worsening of vision.
• Referral to an optometrist, nurse practitioner or physician is required within 24 hours for large or central defects and in 48-72
hours if there is no response to therapy
DST-104 Corneal Abrasion (Minor): Pediatric

29
Certified Practice Area:
RN First Call
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
REFERENCES
More recent editions of any of the items in the Reference List may have been published since this DST was published. If you have a newer version, please use it.
Ahmed, F.,Feldman, H. House, R. MDc, 2015 Corneal Abrasions and Corneal Foreign Bodies (Safee requested to provide full test article Aug. 3rd) American Academy of Opthalmology. (2012). Corneal Abrasion.
Bashour, M. (2014, March 5). Corneal foreign body.
Canadian Pharmacists Association. (2014). Compendium of Therapeutic Choices (7th ed.). Ottawa, ON: Author
Canadian Pharmacists Association. (2010). E-CPS.
Cash, J. C., & Glass, C. A. (Eds.). (2014). Family practice guidelines (3rd ed.). New York, NY: Springer.
Cronau, H., Kankanala, R. R., & Mauger, T. (2010). Diagnosis and management of red eye in primary care. American Family Physician, 81(2), 137-144.
DynaMed. (2015, December 21). Corneal Abrasion.
Fraenkel A, Lee LR, Lee GA. Managing corneal foreign bodies in office-based general practice ‘ T. 2017;46(3):89-94.
Jacobs, D. S. (2015). Corneal abrasions and corneal foreign bodies: Management. UptoDate. Retrieved from
Klostranec, J. M., & Kolin, D. L. (2012). The Toronto notes 2012: Comprehensive medical reference & review for Medical Council
of Canada Qualifying Exam Part 1 and the United States Medical Licesnsing Exam Step 2 (28th ed.). Toronto, ON: Toronto Notes for Medical Students.
Mitchell L, Grimmer P. Complications & treatment of a red eye. Bpj. 2013;54(54):8-21.
Mukherjee P, Sivakumar A. Tetanus prophylaxis in superficial corneal abrasions. Emerg Med J. 2003;20(1):62-64.
New Zealand Medicines and Medical Devices Safety Authority. (2008). Minims tetracaine hydrochloride.
Peyman GA, Rahimy MH, Fernandes ML. Effects of morphine on corneal sensitivity and epithelial wound healing: implications for topical ophthalmic analgesia. Br J Ophthalmol. 1994 Feb. 78(2):138-41.
Porter, R. S., & Kaplan, J. L. (2011). Eye Disorders. In The Merck Manual (19th ed). Whitehouse Station, NJ: Merck Sharpe & Dohme Corp.
Verma, A. (2014, February 20). Corneal abrasion.
Verma A. (2015, Decemer 15) Corneal abrasion differential diagnoses.
Wipperman, J. L., & Dorsch, J. N. (2013, January 15). Evaluation and management of corneal abrasions. American Family Physician, 87(2), 114-120.
WHO. Protection Against Exposure to Ultraviolet Radiation | World Health Organization. World Heal Organ. 1994.
DST-104 Corneal Abrasion (Minor): Pediatric

30
Certified Practice Area:
RN First Call
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
DST-105 Conjunctivitis: Adult
DEFINITION
Inflammation and erythema of the conjunctiva, caused by hyperemia of tortuous superficial vessels secondary to infection (viral or bacterial) or allergic reaction (histamine).
POTENTIAL CAUSES
• Conjunctivitis is usually viral or bacterial
• The allergic form is more common when accompanied by other allergic symptoms such as rhinitis.
• Wearing contact lenses
• Foreign body, acid or alkali burn to eye
• Other causes include preseptal or orbital cellulitis, corneal injury, uveitis and glaucoma all of which are referred to a physician
or nurse practitioner
Bacterial Pathogens
• Chlamydia
• Haemophilus influenzae (non-typable)
• Neisseria gonorrhoeae
• Pseudomonas Aeruginosa
• Staphylococcus aureus
• Streptococcus pneumoniae
Viral Pathogens (cause up to 80% of all cases of acute conjunctivitis)
• Adenovirus
• Coxsackie virus
• Enterovirus 70
• Herpes simplex virus
Allergic Response
• Seasonal pollens
• Environmental exposure
PREDISPOSING RISK FACTORS
Contact with another person who has conjunctivitis, other atopic (allergic) conditions, and exposure to allergens or exposure to a sexually transmitted infection (STI).
TYPICAL FINDINGS OF CONJUNCTIVITIS
Physical Assessment
Examination should be very brief in the case of a chemical injury to the eye as irrigation of the eye is priority and should begin immediately. A topical anesthetic, e.g. tetracaine, may be used if the examination is uncomfortable for the patient.
• Vital signs and pain assessment
• Visual acuity
• Assess both eyes for symmetry
• Assess eyelids and orbits for crusting, edema, ulceration, nodules, discoloration, inversion of eyelashes, papillary reaction
• Palpate the bony orbit, eyebrows, lacrimal apparatus and pre-auricular lymph nodes for tenderness, swelling or masses
DST-105 Conjunctivitis: Adult

31
Certified Practice Area:
RN First Call
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
• Assess the conjunctiva for erythema, edema, discharge, foreign bodies, phlyctenules (white granules on corneal edge
surrounded by erythema) or other abnormalities
• Note the pattern of injection, such as conjunctival haemorrhage or ciliary flush
• Pupils equal, round, reactive to light and accommodation (PERRLA)
• Examine the anterior segment of the globe with a small penlight
• Assess ocular mobility by checking range of movement
• Use a fluorescein stain to assess for corneal abrasion or ulcers if history or physical findings suggest corneal abrasion.
Corneal cells that are damaged or lost will stain green; cobalt blue light allows easier visualization of the abrasion.
• Perform a general assessment if the client appears systemically ill (i.e., fever) Carefully document all evidence of external
trauma
Bacterial Infection
History
• Eye(s) red, often unilateral initially, may spread to both eyes
• Burning, gritty sensation or foreign body sensation in eyes
• Thick, purulent discharge with crusting
• Complicating bacterial infections, such as otitis media, may be evident
• Recent contact with others with similar symptoms
• Recent sexual activity and possible STI
Common Findings
• Conjunctiva erythematous (unilateral or bilateral)
• Chemosis (swelling of conjunctiva) if severe
• Purulent discharge
• PERRLA
• Visual acuity normal
• Pre-auricular nodes palpable in Neisseria gonorrhea, Chlamydia, and MRSA
Viral Infection
History
• Acute onset of conjunctival injection2 commonly preceded by a viral upper respiratory tract infection
• May begin unilateral, but often bilateral within 24-48 hours.
• No pain, mild to stabbing pain. possibly gritty sensation or mild itching
• Tearing or mucoid discharge
• Systemic symptoms may be present (e.g., sneezing, runny nose, sore throat, preauricular lymphadenopathy)
• Recent contact with others with similar symptoms
Common Findings
• Conjunctiva erythematous (unilateral or bilateral)
• Chemosis and eyelid edema (swelling of conjunctiva due to non-specific irritation) if severe
• Watery or mucoid discharge
DST-105 Conjunctivitis: Adult
32
Certified Practice Area:
RN First Call
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
• PERRLA
• Visual acuity – normal
• Swollen eyelids
• Enlarged, tender preauricular nodes Lasts 1-4 days; infectious for 10-12 days from onset as long as the eyes are red
• Dendritic keratitis on fluorescein staining with herpes simplex virus
Note: clinical factors cannot reliably differentiate viral from bacterial causes
Allergic Response
History
• Seasonal, known, or environmental allergies, allergic rhinitis
• Eczema, asthma, urticaria
• Bilateral watery, red, itchy eyes, without purulent drainage
Common Findings
• Sequential bilateral red eyes,
• Watery discharge and inflammation around the eye and eyelids, which can produce dramatic conjunctival swelling (chemosis)
and lid edema, to the extent that the eye is swollen shut.
• A feeling of grittiness or stabbing pain,
• May have rhinorrhoea or other respiratory symptoms.
• Crusting of the lashes overnight can sometimes be confused for a purulent discharge.
• Enlarged, tender preauricular lymph nodes are often present, and are a useful feature to assist diagnosis.
• PERRLA
• Visual acuity – normal
Diagnostic tests
Specimens should be obtained for culture and smear if inflammation is severe, in chronic or recurrent infections, with atypical conjunctival reactions, and with failure to respond to treatment
MANAGEMENT AND INTERVENTIONS
Note: Review Appendix 1: Algorithm for Diagnosing the Cause of Red Eye
Goals of Treatment
• Relieve symptoms and resolution of infection
• Rule out more serious infections (e.g., uveitis)
• Prevent complications
• Prevent spread of infection to others
Non-pharmacologic Interventions
• Apply warm or cool compresses to eyes, lids and lashes qid for 15 minutes
• Clean eyelids gently of discharge with warm water and a disposable wipe such as cotton swab or tissue
• Avoid rubbing the eye(s)
• Health teaching of good hygiene practices (i.e., frequent hand-washing, use of separate clean face cloth and towels).
Pharmacologic Interventions
Note: Never use steroid or steroid-and-antibiotic combination eye drops, because the infection may progress or a corneal ulcer may rapidly form and cause perforation.
DST-105 Conjunctivitis: Adult
33
Certified Practice Area:
RN First Call
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
Bacterial Infection
• Acute conjunctivitis is frequently self-limiting, and antibiotics are of limited benefit. It may be appropriate to hold antibiotics
for two or three days and start therapy if no improvement or the condition worsens.
• Topical antibiotic eye drop or ointment: bacitracin-polymyxin B ophthalmic solution, 1 drop, every 3 to 4 hours, for 5-7 days,
or
• sulfacetamide 10% ophthalmic solution, 1 to 2 drops, every 2 to 3 hours, for 5-7 days, or
• bacitracin-polymyxin B eye ointment, 1 cm ribbon, QID, for 5-7 days, or
• erythromycin 0.5% eye ointment, 1 cm ribbon, QID, for 5-7 days
• moxifloxacin 0.5% drops, 1 drop TID for 7 days (for treatment of pseudomonas.)
An antibiotic eye ointment may be used at bedtime in addition to the daytime antibiotic eye drops prn:
• erythromycin 0.5% eye ointment for 5-7 nights at bedtime OR
• bacitracin-polymyxin ointment for 5-7 nights at bedtime.
If the infection has been determined to be due to chlamydia or gonorrhea, systemic treatment is required and topical treatment is not necessary. Please refer to the appropriate STI DST.
Viral Infection
• Artificial tears or cool compresses often provide excellent symptomatic relief (antibiotics are not indicated)
o artificial tears, 1 or 2 drops prn
Allergic Response
Artificial tears or cool compresses often provide excellent symptomatic relief (antibiotics are not indicated)
o artificial tears, 1 or 2 drops prn
• Oral antihistamines may be tried if symptoms are severe. Most common side effects are drowsiness, dry mouth, and fatigue.
Use with caution in elderly clients and in clients with known hepatic or renal dysfunction.
o cetirizine 10 mg tab, 1 po daily, or
o loratidine 10 mg tab, 1 po daily, or
o desloratadine 5 mg tab, 1 po daily.
• Topical antihistamine eye drops are recommended if symptoms are not controlled by oral antihistamines or oral
antihistamines cannot be tolerated:
o Cromolyn Na 4% eye drops, 1-2 drops every 4-6 hrs.
Pregnant and Breastfeeding Women (dosing as above)
• Erythromycin eye ointment, polymyxin B gramicidin eye drops, bacitracin-polymyxin eye ointment, artificial tears, cromolyn
Na, cetirizine and loratidine may be used as listed above.
• ONLY USE sulfacetamide if clearly needed.
• DO NOT USE desloratadine
POTENTIAL COMPLICATIONS
• Spread of infection to other eye structures
• Spread of infection to others
DST-105 Conjunctivitis: Adult
34
Certified Practice Area:
RN First Call
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
CLIENT EDUCATION/DISCHARGE INFORMATION
Provide advice regarding:
• the condition, timeline of treatment and expected course of disease process medications (dose, frequency, and instillation)
• avoid using eye cosmetics during acute phase
• contact lenses wearers- discontinue wearing until condition is resolved
• allergic form: recommend that client avoid going outside when pollen count is high. Protective glasses can be worn to
prevent pollen from entering the eyes.
Provide infection control education regarding:
• preventing the spread of infection and hygiene of hands and eyes. Wash hands often.
• preventing contamination of the medication tube or bottle
• not sharing of eye drops or ointments, eye cosmetics, towels or face cloth
• discarding contaminated eye cosmetics which may harbor bacteria and cause recurrent infection.
o For infectious forms, if symptoms or work/school situation requires, recommend school or work restrictions until
improved or there is no further discharge.
o Instruct client/care giver to wash pillowcases, sheets, linens often.in hot water
MONITORING AND FOLLOW-UP
• Clients with moderate or severe symptoms should be seen for follow-up at 24 and 48 hours.
• Follow up appropriately in 2 or 3 days or sooner if symptoms do not improve.
CONSULTATION AND/OR REFERRAL
Consult a physician or nurse practitioner if:
• condition deteriorates, symptoms persist despite treatment, or symptoms recur (see Appendix 1),
• the diagnosis is in doubt and significant ocular infections like uveitis, herpes, and gonorrhea cannot be ruled out,
• there is associated trauma (i.e. blow and/or penetrating eye trauma or serious chemical injury) (high potential for referral),
• visual acuity is decreased or deficit in colour vision,
• moderate or severe pain,
• atypical ocular exam,
• the condition recurs frequently.
DOCUMENTATION
As per agency policy
DST-105 Conjunctivitis: Adult
35
Certified Practice Area:
RN First Call
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
REFERENCES
More recent editions of any of the items in the Reference List may have been published since this DST was published. If you have a newer version, please use it.
Anti-Infective Review Panel. (2013). Anti-infective guidelines for community-acquired infections. Toronto, ON: MUMS Guideline Clearinghouse.
Azari, A. A., & Barney, N. P. (2013). Conjunctivitis: A systematic review of diagnosis and treatment. JAMA: Journal of the American Medical Association, 310(16), 1721-1729.
Blondel-Hill, E., & Fryters, S. (2012). Bugs and drugs: An antimicrobial infectious diseases reference. Edmonton, AB: Alberta Health Services.
Bremond-Gignac, F. Chiambaretta, S. Milazzo. A European Perspective on Topical Ophthalmic Antibiotics: Current and Evolving Options. Ophthalmol Eye Dis. 2011:29.
Canadian Pharmacists Association. (2014). Therapeutic Choices (7th ed.). Ottawa, ON: Author
Canadian Pharmacists Association. (2014). Therapeutic choices for minor ailments. Ottawa, ON: Author.
Cash, J. C., & Glass, C. A. (Eds.). (2014). Family practice guidelines (3rd ed.). New York, NY: Springer.
Chan, P. D., & Johnson, M. T. (2010). Treatment guidelines for medicine and primary care. Blue Jay, CA: Current Clinical Strategies Publishing.
Chen, Y. A., & Tran, C. (Eds.). (2011). The Toronto notes 2011: Comprehensive medical reference and review for the Medical Council of Canada Qualifying Exam Part 1 and the United States Medical Licensing Exam Step 2 (27th ed.). Toronto, ON: Toronto Notes for Medical Students.
Cronau, H., Kankanala, R. R., & Mauger, T. (2010). Diagnosis and management of red eye in primary care. American Family Physician,81(2), 137-144.
DynaMed. (2015, July 31). Allergic conjunctivitis.
DynaMed. (2015, June 9). Infectious conjunctivitis.
Everitt, H. A., & Little, P. S. (2006). A randomized controlled tria of management strategies for acute infective conjunctivitis in general practice. British Medical Journal, 333(321). doi: 10.1136/bmj.38891.551088.7C.
Fraenkel A, Lee LR, Lee GA. Managing corneal foreign bodies in office-based general practice ‘ T. 2017;46(3):89-94.
Friedlaender, M. H. (2011). Ocular allergy. Current Opinion in Allergy and Clinical Immunology, 11(5), 477-482.
Infective conjunctivitis. (2011, September 5). Independent Nurse, 29-30.
Jacobs, D. S. (2015). Conjunctivitis. UptoDate.
Jefferis, J., Perera, R., Everitt, H., van Weert, H., Rietveld, R., Glasziou, P., & Rose, P. (2011). Acute infective conjunctivitis in
primary care: Who needs antibiotics? An individual patient data meta-analysis. British Journal of General Practice, 61(590), e542-e548.
Karpecki, P., Paterno, M., & Comstock, T. (2010). Limitations of current antibiotics for the treatment of bacterial conjunctivitis. Optometry and Vision Science: Official publication of the American Academy of Optometry, 87(11), 908-919.
DST-105 Conjunctivitis: Adult
36
Certified Practice Area:
RN First Call
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
Mitchell L, Grimmer P. Complications & treatment of a red eye. Bpj. 2013;54(54):8-21.
O'Brien, T. P. (2013). Allergic conjunctivitis: An update on diagnosis and management. Current Opinion in Allergy & Clinical Immunology, 13(5), 543-549.
O’Brien TP, Jeng BH, McDonald M, Raizman MB. Acute conjunctivitis: truth and misconceptions. Curr Med Res Opin. 2009;25(8):1953-1961. doi:10.1185/03007990903038269.
Rosario, N., & Bielory, L. (2011). Epidemiology of allergic conjunctivitis. Current Opinion in Allergy & Clinical Immunology, 11(5), 471-476.
Scott, I. MD M. Viral conjunctivitis_ practice essentials, background, etiology medscape April 2017. 2017. http://emedicine.medscape.com/article/1191370-overview.
Sheikh, A., Hurwitz, B., van Schayck, C. P., McLean, S., & Nurmatov, U. (2012). Antibiotics versus placebo for acute bacterial conjunctivitis (review). Cochrane Database of Systematic Reviews, (9).
Shin H, Price K, Albert L, Dodick J, Park L, Dominguez-bello G. Changes in the eye microbiota associated with contact lens wearing. 2016;7(2):1-6. doi:10.1128/mBio.00198-16.
Spering, K. A. (2011). Therapeutic strategies for bacterial conjunctivitis. Clinical Advise Nurse
Practitioners, 14(8), 31-40.
Thanathanee, O., & O'Brien, T. (2011). Conjunctivitis: Systematic approach to diagnosis and therapy. Current Infectious Disease Reports, 13(2), 141-148.Visscher, K. L., Hutnik, C. M. L., & Thomas, M. (2009). Evidence-based treatment of acute infective conjunctivitis: Breaking the cycle of antibiotic prescribing. Canadian Family Physician, 55(11), 1071-1075.
Visscher, K. L., Hutnik, C. M. L., & Thomas, M. (2009). Evidence-based treatment of acute infective conjunctivitis: Breaking the cycle of antibiotic prescribing. Canadian Family Physician, 55(11), 1071-1075.
DST-105 Conjunctivitis: Adult

37
Certified Practice Area:
RN First Call
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
APPENDIX 1: ALGORITHM FOR DIAGNOSING THE CAUSE OF RED EYE
DST-105 Conjunctivitis: Adult

38
Certified Practice Area:
RN First Call
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
DST-106 Conjunctivitis: Pediatric
DEFINITION
Inflammation and erythema of the conjunctiva, caused by hyperemia of tortuous superficial vessels secondary to infection (viral or bacterial) or allergic reaction (histamine).
Nurses with Remote Practice Certified Practice designation (RN(C)s) are able to treat children with conjunctivitis who are 6 months of age and older.
POTENTIAL CAUSES
Conjunctivitis is usually viral or bacterial
The allergic form is more common when accompanied by other allergic symptoms such as rhinitis. Wearing contact lenses
Foreign body, acid or alkali burn to eye
Other causes include preseptal or orbital cellulitis, corneal injury, uveitis and glaucoma all of which are referred to a physician or nurse practitioner
Bacterial Pathogens
• Chlamydia
• Neisseria gonorrhoea
• Haemophilus influenza (non-typable)
• Moraxella Species
• Pseudomonas Aeruginosa1
• Staphylococcus aureus (more common in adults)
• Streptococcus pneumonia
Note: In youth, gonococcal or chlamydial infection should be considered if the history is supportive of this diagnosis and the
adolescent is sexually active.
Viral Pathogens
• Adenovirus (most common virus in children)
• Coxsackie virus
• Enterovirus 70
• Epstein-Barr virus herpes zoster virus (less common)
• Measles and rubella viruses
• Allergic Response Environmental exposure
• Seasonal pollens
PREDISPOSING RISK FACTORS
Contact with another person who has conjunctivitis, other atopic (allergic) conditions and exposure to allergens or exposure to a sexually transmitted infection (STI).
TYPICAL FINDINGS OF CONJUNCTIVITIS
Physical Assessment
Examination should be very brief in the case of a chemical injury to the eye as irrigation of the eye is priority and should begin immediately. A topical anesthetic, e.g. tetracaine, may be used if the examination is uncomfortable for the patient.
Children with mild viral or superficial bacterial conjunctivitis do not usually have significant systemic symptoms. However, assess:
DST-106 Conjunctivitis: Pediatric
39
Certified Practice Area:
RN First Call
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
• Vital signs and pain assessment
• Perform a general assessment if the client appears systemically ill (i.e., fever)
• Weigh (for medication calculations i.e. acetaminophen, ibuprofen)
• Visual acuity if old enough
• Assess both eyes for symmetry
• Assess eyelids and orbits for crusting, edema, ulceration, nodules, discoloration, inversion of eyelashes, papillary reaction
• Palpate the bony orbit, eyebrows, lacrimal apparatus and pre-auricular lymph nodes for tenderness, swelling or masses
• Assess the conjunctiva for erythema, edema, discharge, foreign bodies, phylctenules (white granules on corneal edge
surrounded by erythema) or other abnormalities
• Note the pattern of injection such as conjunctival haemorrhage or ciliary flush
• Pupils equal, round, reactive to light and accommodation (PERRLA)
• Examine the anterior segment of the globe with a small penlight
• Assess ocular mobility by checking range of movement. Use a fluorescein stain to assess for corneal abrasion or ulcers if
history or physical findings suggest corneal abrasion. Corneal cells that are damaged or lost will stain green; cobalt blue light
allows easier visualization of the abrasion.
Carefully document all evidence of external trauma
Bacterial Infection
History
• Eye(s) red, often unilateral initially, may spread to both eyes
• Burning, gritty sensation or foreign body sensation in eyes
• Thick, purulent discharge with crusting in morning
• Complicating bacterial infections, such as otitis media, may be evident
• Recent contact with others with similar symptoms
• Recent sexual activity and possible STI
Common Findings
• Conjunctiva erythematous (unilateral or bilateral)
• Chemosis (swelling of conjunctiva) if severe
• Purulent discharge
• PERRLA
• Visual acuity normal
• Pre-auricular nodes palpable in Neisseria gonorrhea and Chlamydia and MRSA
Viral Infection
History
• Acute onset of conjunctival injection3 commonly preceded by a viral upper respiratory tract infection
• May begin unilateral, but often bilateral within 24-48 hours
• No pain, mild to stabbing pain, possibly gritty sensation or mild itching.
• Tearing or mucoid discharge
• Systemic symptoms may be present (e.g., sneezing, runny nose, sore throat, preauricular lymphadenopathy)
• Recent contact with others with similar symptoms
DST-106 Conjunctivitis: Pediatric
40
Certified Practice Area:
RN First Call
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
Common Findings
• Conjunctiva erythematous (unilateral or bilateral)
• Chemosis (swelling of conjunctiva) if severe
• Watery or mucoid discharge
• PERRLA Visual acuity - normal
• Enlarged, tender preauricular nodes
• Lasts 1-4 days; infectious for up to 2 weeks
• Dendritic keratitis on fluorescein staining with herpes simplex virus
Note: clinical factors cannot reliably differentiate viral from bacterial causes
Allergic Response
History
• Seasonal, known or environmental allergies, allergic rhinitis
• Eczema, asthma, urticaria
• Bilateral watery, red, itchy eyes, without purulent drainage
Common Findings
• Sequential bilateral red eyes
• Watery discharge and inflammation around the eye and eyelids, which can produce dramatic conjunctival swelling (chemosis)
and lid oedema, to the extent that the eye is swollen shut
• A feeling of grittiness or stabbing pain
• May have rhinorrhea or other respiratory symptoms
• Crusting of the lashes overnight can sometimes be confused for a purulent discharge
• Enlarged, tender preauricular lymph nodes are often present, and are a useful feature to assist diagnosis
• PERRLA
• Visual acuity - normal
Diagnostic Tests
• Specimens should be obtained for culture and smear if inflammation is severe, in chronic or recurrent infections, with atypical
conjunctival reactions, and with failure to respond to treatment4
• Swab for gonorrhea or chlamydia
MANAGEMENT AND INTERVENTION
Note: Review Appendix 1: Algorithm for Diagnosing the Cause of Red eye
Goals of Treatment
• Relieve symptoms and resolution of infection
• Rule out more serious infections (e.g., uveitis)
• Prevent complications
• Prevent spread of infection to others
Non-pharmacologic Interventions
• Apply warm or cool compresses to eyes, lids and lashes qid for 15 minutes
• Clean eyelids gently of discharge with warm water and a disposable wipe such as a cotton swab or tissue
• Avoid rubbing the eye(s)
• Public health measures that support good hygiene (i.e., frequent hand-washing, use of separate clean face cloth and towels).
DST-106 Conjunctivitis: Pediatric

41
Certified Practice Area:
RN First Call
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
Pharmacological Interventions
Note:
• Many pediatric drug doses are calculated by weight.
• Topical eye drops and eye ointments may be used as listed below.
• Pediatric doses should not exceed recommended adult doses.
• Never use steroid or steroid-and-antibiotic combination eye drops, because the infection may progress or a corneal ulcer may
rapidly form and cause perforation
Bacterial Infection
Acute conjunctivitis is frequently self-limiting, and antibiotics are of limited benefit. It may be appropriate to hold antibiotics for two
or three days and start therapy if no improvement or the condition worsens.
• Topical antibiotic eye drop or ointment treatment options for children greater than 1 year of age:
o gramicidin- polymyxin B ophthalmic solution, 1 drop, every 3 to 4 hours, for 5-7 days, or
o sulfacetamide 10% ophthalmic solution, 1 to 2 drops, every 2 to 3 hours, for 5-7 days, or
o bacitracin-polymyxin B eye ointment, 1 cm ribbon, QID, for 5-7 days, or
o erythromycin 0.5% eye ointment, 1 cm ribbon, QID, for 5-7 days
o moxifloxacin 0.5% drops, 1 drop TID for 7 days (for treatment of pseudomonas.)
Note: eye ointment may be preferred for younger children and infants.
An antibiotic eye ointment may be used at bedtime in addition to the daytime antibiotic eye drops prn:
• erythromycin 0.5% eye ointment for 5-7 nights at bedtime, or
• bacitracin-polymyxin ointment for 5-7 nights at bedtime.
Viral Infection
• Artificial tears or saline washes often provide excellent symptomatic relief (antibiotics are not indicated)
• artificial tears, 1 or 2 drops prn
Allergic Response
• Artificial tears or saline washes and cool compresses often provide excellent symptomatic relief (antibiotics are not indicated)
• artificial tears, 1 or 2 drops prn
Oral antihistamines may be tried if symptoms are severe. Most common side effects are drowsiness, dry mouth, and fatigue:
• cetirizine (syrup 5 mg/5 mL), Children 2-6 years of age, 5 mL (1 teaspoon) once daily. For twice daily dosing, 2.5 mL (one-
half teaspoon) in the morning and 2.5 mL (one-half teaspoon) of syrup in the evening. Children 6-12 years of age, 10 mL (2 teaspoons) of syrup once daily. For twice daily dosing, 5 mL (one teaspoon) in the morning and 5 mL (one teaspoon) in the evening.
OR
• desloratadine (syrup 0.5 mg/mL), Children 2 Through 5 Years of Age, 2.5 mL (1.25 mg) once a day, regardless of mealtime.
Children 6 Through 11 Years of Age 5 mL (2.5 mg) once a day, regardless of mealtime. 12 years of age or older: 5 mg po
daily
OR
• loratidine: (Oral Solution 1 mg/mL). Children 10 years of age and over (body weight greater than 30 kg): 10 mL (two
teaspoonfuls) once daily. Children 2 through 9 years of age (body weight less than or equal to 30 kg): 5 mL (one
teaspoonful) once daily.
• CLARITIN KIDS should not be administered to children between 2 and 12 years of age for longer than 14 days, unless
recommended by a physician.
o For children 4 years and older, topical antihistamine eye drops are recommended if symptoms are not controlled by oral
antihistamines or oral antihistamines cannot be tolerated:
• cromolyn Na 4% eye drops, 1-2 drops every 4-6 hrs.
DST-106 Conjunctivitis: Pediatric
42
Certified Practice Area:
RN First Call
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
Pregnant and Breastfeeding Youth (dosing as above)
• Erythromycin eye ointment, polymyxin B gramicidin eye drops, bacitracin-polymyxin eye ointment, artificial tears, cromolyn
Na, cetirizine and loratidine may be used as listed above.
• ONLY USE sulfacetamide if clearly needed.
• DO NOT USE desloratadine.
POTENTIAL COMPLICATIONS
• Spread of infection to other eye structures
• Spread of infection to others
CAREGIVER EDUCATION AND DISCHARGE INFORMATION
Provide advice regarding:
• the condition, timeline of treatment and expected course of disease process (dose, frequency, and instillation)
• avoid using eye cosmetics during acute phase
• contact lenses wearers- discontinue wearing until condition is resolved
• allergic form: recommend that child avoid going outside when pollen count is high. Protective glasses can be worn to prevent
pollen from entering the eyes.
Provide infection control education regarding:
• preventing the spread of infection and hygiene of hands and eyes. Wash hands often.
• preventing contamination of the medication tube or bottle
• not sharing of eye drops or ointments, eye cosmetics, towels or face cloth
• discarding contaminated eye cosmetics which may harbor bacteria and cause recurrent infection.
• For infectious forms, recommend school or day care restrictions until improved or there is no further discharge.
INSTRUCT CLIENT/CARE GIVER TO WASH PILLOWCASES, SHEETS, LINENS OFTEN.IN HOT WATER.MONITORING AND FOLLOW-UP
• Clients with moderate or severe symptoms should be seen for follow-up at 24 and 48 hours.
• Follow up appropriately in 2 or 3 days or sooner if symptoms do not improve.
CONSULTATION AND/OR REFERRAL
Consult or referral as indicated under the following circumstances:
• child is less than 6 months of age,
• if condition deteriorates, if symptoms persist despite treatment, or if symptoms recur,
• the diagnosis is in doubt and significant ocular infections like uveitis, herpes and gonorrhea cannot be ruled out,
• there is associated trauma (i.e., blow to eye and or penetrating eye injury (high potential for referral),
• serious chemical eye injury (high potential for referral),
• visual acuity is decreased or deficit in colour vision,
• moderate or severe pain
• atypical ocular exam
• the condition recurs frequently.
DOCUMENTATION
• As per agency policy
DST-106 Conjunctivitis: Pediatric
43
Certified Practice Area:
RN First Call
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
REFERENCES
More recent editions of any of the items in the Reference List may have been published since this DST was published. If you have a newer version, please use it.
Anti-Infective Review Panel. (2012). Anti-infective guidelines for community-acquired infections. Toronto, ON: MUMS Guideline Clearinghouse.
Azari, A. A., & Barney, N. P. (2013). Conjunctivitis: A systematic review of diagnosis and treatment. JAMA: Journal of the American Medical Association, 310(16), 1721-1729.
Blondel-Hill, E., & Fryters, S. (2012). Bugs and drugs: An antimicrobial infectious diseases reference. Edmonton, AB: Alberta Health Services
Canadian Pharmacists Association. (2014). Therapeutic Choices (7th ed.). Ottawa, ON: Author
Canadian Pharmacists Association. (2014). Therapeutic choices for minor ailments. Ottawa, ON: Author.
Cash, J. C., & Glass, C. A. (Eds.). (2014). Family practice guidelines (3rd ed.). New York, NY: Springer.
Council of Canadian Academics. Improving Medicines for Children in Canada. Ottawa: 2014.
Cronau, H., Kankanala, R. R., & Mauger, T. (2010). Diagnosis and management of red eye in primary care. American Family Physician, 81(2), 137-144.
DynaMed. (2015, July 31). Allergic conjunctivitis.
DynaMed. (2015, June 9). Infectious conjunctivitis.
Epling, J. (2010). Bacterial conjunctivitis. American Family Physician, 82(6), 665-666.
Everitt, H.A., Little, P.S., & Smith P.W. (2006). A randomized controlled trial of management strategies for acute infective conjuncitivitis in general practice. British Journal of Medicine, 333(7563): 321.
Esau, R. (Ed.). (2012). British Columbia’s Children’s Hospital pediatric drug dosage guidelines (6th ed.). Vancouver, BC: Children’s & Women’s Health Centre of B.C.
Friedlaender, M. H. (2011). Ocular allergy. Current Opinion in Allergy and Clinical Immunology, 11(5), 477-482.
Gold, R.S. (2011). Treatment of bacterial conjunctivitis in children. Pediatric Annals, 40(2), 95-105.
Golde, K. T., & Gardiner, M. F. (2011). Bacterial conjunctivitis in children: A current review of pathogens and treatment. International Ophthalmology Clinics, 51(4), 85-92.
Infective conjunctivitis. (2011, September 5). Independent Nurse, 29-30.
Jacobs, D. S. (2015). Conjunctivitis. UptoDate.
Jefferis, J., Perera, R., Everitt, H., van Weert, H., Rietveld, R., Glasziou, P., & Rose, P. (2011). Acute infective conjunctivitis in
primary care: Who needs antibiotics? An individual patient data meta-analysis. British Journal of General Practice, 61(590), e542-e548.
Karpecki, P., Paterno, M., & Comstock, T. (2010). Limitations of current antibiotics for the treatment of bacterial conjunctivitis. Optometry and Vision Science: Official publication of the American Academy of Optometry, 87 (11), 908-919.
DST-106 Conjunctivitis: Pediatric
44
Certified Practice Area:
RN First Call
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
Klostranec, J. M., & Kolin, D. L. (2012). The Toronto notes 2012: Comprehensive medical reference and review for the Medical Council of Canada Qualifying Exam Part 1 and the United States Medical Licensing Exam Step 2 (28th ed.). Toronto, ON: Toronto Notes for Medical Students.
La Roche, R., Hamilton J. Vision screening in infants, children and youth. Paediatr Child Heal. 2009;14(4):246-248. Retrieved from. La Rosa, M., Lionetti, E.,
Reibaldi, M., Russo, A., Longo, A., Leonardi, S., & ... Reibaldi, A. (2013, March). Allergic conjunctivitis: A comprehensive review of the literature. Italian Journal of Pediatrics, 39.
Lexicomp Online. Polymxcin, Sulfacetamide etc.. Retrieved from http://online.lexi.com
Mitchell L, Grimmer P. Complications & treatment of a red eye. Bpj. 2013;54(54):8-21.
O'Brien, T. P. (2013). Allergic conjunctivitis: An update on diagnosis and management. Current Opinion in Allergy & Clinical Immunology, 13 (5), 543-549.
O’Brien TP, Jeng BH, McDonald M, Raizman MB. Acute conjunctivitis: truth and misconceptions. Curr Med Res Opin. 2009;25(8):1953-1961.
Pichichero, M. (2011). Bacterial conjunctivitis in children: Antibacterial treatment options in an era of increasing drug resistance. Clinical Pediatrics, 50 (1), 7-13.
Rosario, N., & Bielory, L. (2011). Epidemiology of allergic conjunctivitis. Current Opinion in Allergy & Clinical Immunology, 11(5), 471-476.
Seth, D., & Khan, F. I. (2011). Causes and management of red eye in pediatric ophthalmology. Current Allergy and Asthma Reports, 11(3), 212-219.
Sheikh, A., Hurwitz, B., van Schayck, C. P., McLean, S., & Nurmatov, U. (2012). Antibiotics versus placebo for acute bacterial conjunctivitis (review). Cochrane Database of Systematic Reviews, (9).
Shin H, Price K, Albert L, Dodick J, Park L, Dominguez-bello G. Changes in the eye microbiota associated with contact lens wearing. 2016;7(2):1-6. doi:10.1128/mBio.00198-16.
Spering, K. A. (2011). Therapeutic strategies for bacterial conjunctivitis. Clinical Advisor for Nurse Practitioners, 14(8), 31-40.
Thanathanee, O., & O’Brien T. (2011). Conjunctivitis: Systematic approach to diagnosis and therapy. Current Infectious Disease Reports, 13(2), 141-148.
Visscher, K. L., Hutnik, C. M. L., & Thomas, M. (2009). Evidence-based treatment of acute infective conjunctivitis: Breaking the cycle of antibiotic prescribing. Canadian Family Physician, 55(11), 1071-1075.
DST-106 Conjunctivitis: Pediatric

45
Certified Practice Area:
RN First Call
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
APPENDIX 1: ALGORITHM FOR DIAGNOSING THE CAUSE OF RED EYE
DST-106 Conjunctivitis: Pediatric
46
Certified Practice Area:
RN First Call
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
DST-201 Ear, Nose & Throat Assessment: Adult
Nurses with Remote Nursing Certified Practice designation (RN(C)s) are able to manage the following ear, nose and throat conditions:
• Acute otitis media
• Ceruminosis
• Dental abscess
• Pharyngitis
The following assessment must be completed and documented.
ASSESSMENT
History of Present Illness and Review of System
General
The following characteristics of each symptom should be elicited and explored:
• Onset (sudden or gradual)
• Chronology
• Current situation (improving or deteriorating)
• Location
• Radiation
• Quality
• Timing (frequency, duration)
• Severity
• Precipitating and aggravating factors
• Relieving factors
• Associated symptoms
• Effects on daily activities
• Previous diagnosis of similar episodes
• Previous treatments
• Efficacy of previous treatments
Cardinal Signs and Symptoms
In addition to the general characteristics outlined above, additional characteristics of specific symptoms should be elicited, as follows:
Ears
• Recent changes in hearing
• Compliance with and effectiveness of hearing aid
• Itching
• Earache
• Discharge
• Tinnitus
• Vertigo
• Ear trauma
• Cotton Swab use
DST-201 Ear, Nose & Throat Assessment: Adult
47
Certified Practice Area:
RN First Call
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
Nose and Sinuses
• Rhinorrhea
• Epistaxis
• Obstruction of airflow
• Sinus pain and localized headache
• Itching
• Anosmia
• Nasal trauma
• Sneezing
• Watery eyes
Mouth and Throat
• Hoarseness or recent voice change
• Dental status
• Oral lesions
• Bleeding gums
• Changes of the tongue, e.g. redness, bleeding, lesions
• Sore throat
• Uvula malalignment
• Dysphagia
• White patches on the inner cheeks, tongue, roof of the mouth, and throat
• Redness or soreness
• Cottony feeling in the mouth
• Loss of taste
• Pain while eating or swallowing
• Cracking and redness at the corners of the mouth
Neck
• Pain
• Swelling
• Enlarged lymph glands
• Increasing headache associated with flexing of the neck
Other Associated Symptoms
• Fever
• Malaise
• Nausea or vomiting
Medical History (General)
• Medical conditions and surgeries
• Allergies
• Medication currently used (prescription, oral contraceptives, over the counter)
• Herbal preparations, vitamins, minerals, supplements, and traditional therapies
DST-201 Ear, Nose & Throat Assessment: Adult

48
Certified Practice Area:
RN First Call
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
Medical History (Specific to ENT)
• Frequent ear or throat infections
• Sinusitis
• Trauma to the head or ENT area
• ENT surgery
• Hearing loss or audiometric screening results indicating hearing loss
• Allergies including as seasonal allergies
• Asthma
• Chronic cough
• Meniere’s disease
• ENT cancer
Personal and Social History (Specific to ENT)
• Family and close contacts with similar symptoms
• Smoking including tobacco, cannabis
• Use of chewing tobacco
• Exposure to vapours during “vaping”
• Alcohol use
• Illicit drug use
• Exposure to mould
• Frequent immersion of ears in water (e.g. swimming, bathing)
• Use of foreign object to clean ear
• Use of ear protection
• Crowded living conditions
• Sexual activity
• Personal and dental hygiene habits
• Exposure to cigarette smoke, wood smoke or other respiratory irritants
• Recent air travel or scuba diving
• Occupational exposure to toxins or loud noises
PHYSICAL ASSESSMENT OF THE EARS, NOSE AND THROAT
Vitals
• Temperature
• Pulse
• Respiration
• SpO2
• Blood pressure (BP)
General Appearance
• Apparent state of health
• Appearance of comfort or distress
• Colour
• Nutritional status
DST-201 Ear, Nose & Throat Assessment: Adult
49
Certified Practice Area:
RN First Call
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
• Hydration status
• Hygiene
• Chronological age versus apparent age
• Difficulty with gait or balance
• Piercings and tattoos
Ears
Inspection
• Pinna: look for lesions, abnormal appearance or position. Look at the skin covering the
• mastoid process, behind pinna for redness or swelling, gently pull the pinna forward.
• Canal: discharge, swelling, redness, wax, foreign bodies
• Tympanic membrane: colour, light reflex, landmarks, bulging or retraction, perforation, scarring, air bubbles, fluid level
• Estimate hearing with watch or whisper test
• If whisper test fails, perform Weber and Rinne tests with a 512-hertz tuning fork
Palpation
• Tenderness over tragus or on manipulation of the pinna
• Tenderness on tapping of mastoid process
• Size and tenderness of pre, post auricular and occipital nodes
Nose and Sinuses
Inspection
• External: inflammation, deformity, discharge or bleeding
• Internal: colour of mucosa, edema, deviated or perforated septum, polyps, bleeding
• Observe nasal versus mouth breathing
Palpation
• Sinus and nasal tenderness
Percussion
• Sinus and nasal tenderness
Mouth and Throat
Inspection
• Lips: color, lesions, symmetry
• Oral cavity: breath odour, color, lesions of buccal mucosa
• Teeth and gums: redness, swelling, caries, bleeding
• Tongue: colour, texture, lesions, tenderness of floor of mouth
• Throat and pharynx: colour, exudates, uvula, tonsillar symmetry and enlargement, masses
Neck
Inspection
• Symmetry
• Swelling
• Masses
DST-201 Ear, Nose & Throat Assessment: Adult
50
Certified Practice Area:
RN First Call
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
• Active range of motion
• Thyroid enlargement
Palpation
• Tenderness, enlargement, mobility, contour and consistency of nodes and masses
o Nodes – Pre-and post-auricular, occipital, tonsillar, submandibular, submental, anterior and posterior cervical,
supraclavicular
• Thyroid: size, consistency, contour, position, tenderness
• Parotid: tenderness (diffuse versus discrete), enlargement, mobility, contour and consistency of nodes and masses
Associated Systems for assessment
• A complete assessment should include the respiratory system.
• Face: inspect for asymmetry, skin changes, masses or irregularities
SYMPTOMS REQUIRING URGENT REFERRAL
The first step is to determine if the ENT presentation requires an urgent referral to a physician or nurse practitioner, or can be managed safely by an RN(C).
The following signs and symptoms require referral to a physician or nurse practitioner:
• Positive Brudzinski sign (chin to chest)
• Pain and fever with mastoid tenderness
• Difficulty with secretions, drooling
• Fever of unknown origin
• Treatment failure after 3 days for otitis media, strep throat or peritonsillar abscess
• Displaced uvula
• Uncontrollable epistaxis
• Facial fractures
• Sudden onset of deafness
• Recent ENT surgery
• Hoarseness without fever or illness
• Unexplained vertigo
• Pain out of proportion to clinical findings (consider epiglottitis)
DIAGNOSTIC TESTS
The RN(C) may consider the following diagnostic tests to support clinical decision-making:
• Swab of ear, nose or throat for Culture and Sensitivity (C&S)
DST-201 Ear, Nose & Throat Assessment: Adult
51
Certified Practice Area:
RN First Call
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
REFERENCES
More recent editions of any of the items in the Reference List may have been published since this DST was published. If you have a newer version, please use it.
Ball, J. W., Dains, J. E., Flynn, J. A., Solomon, B. S., & Stewart, R. W. (Eds.). (2015). Seidel’s guide to physical examination (8th ed.). St. Louis, MO: Elsevier.
Carter, S., & Laird, C. (2005). 10 assessment and care of ENT problems. Emergency Medicine Journal, 22, 128-139. doi: 10.1136/emj.2004.021642.
Centers for Disease Control and Prevention. (CDC). (2017). Candida infections of the mouth, throat, and esophagus. CDC.
Dains, J. E., Baumann, L. C., & Scheibel, P. (2012). Advanced health assessment and clinical diagnosis in primary care (4th ed.). St. Louis, MO: Elsevier Mosby.
Estes, M. E. Z. (2014). Health assessment and physical examination (5th ed.). Clifton Park, NY: Cengage Learning.
McCarter, D. F., Courtney, U., & Pollart, S. M. (2007). Cerumen impaction. American Family Physician, 75(10), 1523-1528.
Porter, R. S., & Kaplan, J. L. (2011). Section 5: Ear, nose, throat and dental disorders. In The Merck Manual (19th ed.), (p. 411-534). Whitehouse Station, NJ: Merck Sharp & Dohme Corp.
Stephen, T. C., Skillen, D. L., Day, R. A., & Bickley L. S. (2010). Canadian Bates’ guide to health assessment for nurses. Philadelphia, PA: Lippincott, Williams & Wilkins.
Substance Abuse and Mental Health Services Administration (SAMHSA). 2017. Alcohol,Tobacco, and Other Drugs.
DST-201 Ear, Nose & Throat Assessment: Adult

52
Certified Practice Area:
RN First Call
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
DST-202 Ear, Nose & Throat Assessment: Pediatric
Nurses with Remote Nursing Certified Practice designation (RN(C)s) are able to manage the following ear, nose and throat
conditions:
• acute otitis media in children 6 months of age and older
• pharyngitis in children 1 year of age and older
The following assessment must be completed and documented.
ASSESSMENT
History of Present Illness and Review of System
General
The following characteristics of each symptom should be elicited and explored:
• Onset (sudden or gradual)
• Chronology
• Current situation (improving or deteriorating)
• Location
• Radiation
• Quality
• Timing (frequency, duration)
• Severity
• Precipitating and aggravating factors
• Relieving factors
• Associated symptoms
• Effects on daily activities
• Previous diagnosis of similar episodes
• Previous Trauma
• Previous treatments
• Efficacy of previous treatments
Cardinal Signs and Symptoms
In addition to the general characteristics outlined above, additional characteristics of specific symptoms should be elicited, as
follows:
Ears
• Recent changes in hearing
• Itching
• Earache
• Discharge
• Tinnitus
• Vertigo
• Ear trauma
• Rubbing ears
• Cotton swab use
Nose and Sinuses
• Nasal discharge or postnasal drip
• Epistaxis
DST-202 Ear, Nose & Throat Assessment: Pediatric
53
Certified Practice Area:
RN First Call
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
• Obstruction of airflow
• Sinus pain and localized headache
• Itching
• Anosmia
• Nasal trauma
• Sneezing
• Watery eyes
Mouth and Throat
• Hoarseness or recent voice change
• Dental status
• Oral lesions
• Koplik’s spots (found in oral mucosa)
• Bleeding gums
• Changes of the tongue, e.g. redness, bleeding, lesions
• Sore throat
• Uvula malalignment
• Dysphagia
• White patches on the inner cheeks, tongue, roof of the mouth, and throat
• Redness or soreness
• Cottony feeling in the mouth
• Loss of taste
• Pain while eating or swallowing
• Cracking and redness at the corners of the mouth
Neck
• Pain
• Swelling
• Enlarged lymph glands
• Increasing headache associated with flexing of the neck
Other Associated Symptoms
• Fever
• Malaise
• Nausea and vomiting
Medical History (general)
• Medical conditions and surgeries
• Allergies
• Medication currently used (prescription, oral contraceptives, over the counter)
• Herbal preparations, vitamins, minerals, supplements and traditional therapies
• Birth and prenatal history if age appropriate
• Communicable diseases: measles, chickenpox (varicella), herpes simplex
• Immunization status
Medical History (Specific to ENT)
• Frequent ear or throat infections
• Sinusitis
DST-202 Ear, Nose & Throat Assessment: Pediatric
54
Certified Practice Area:
RN First Call
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
• Trauma to head or ENT area
• ENT surgery
• Hearing loss or audiometric screening results indicating hearing loss
• Allergies including as seasonal allergies
• Asthma
Personal and Social History (Specific to ENT)
• Family and close contacts with similar symptoms
• Smoking including tobacco, cannabis
• Exposure to vapours during “vaping”
• Alcohol use
• Illicit drug use
• Feeding methods (breast or bottle), bottle propping
• Exposure to mould
• Frequent immersion of ears in water (e.g. swimming or bathing)
• Use of foreign object to clean ear
• Insertion of foreign body in ear
• Crowded living conditions
• Sexual activity (if age appropriate)
• Personal and dental hygiene habits
• Exposure to cigarette smoke, wood smoke or other respiratory irritants
• Recent air travel
• Exposure to toxins or loud noises
PHYSICAL ASSESSMENT OF THE EARS, NOSE AND THROAT
Vitals
• Temperature
• Pulse
• Respiration
• SpO2
• Blood pressure (BP)
General
• Apparent state of health
• Appearance of comfort or distress
• Colour
• Nutritional status
• Hydration status
• Hygiene
• Chronological age versus apparent age
• Tripoding
• Character of cry (in infants)
• Activity level
• Mental status
• Degree of cooperation, consolability
DST-202 Ear, Nose & Throat Assessment: Pediatric

55
Certified Practice Area:
RN First Call
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
• Emotional reaction to caregiver and examiner
• Difficulty with gait or balance
• Piercings and tattoos
Safety Tip
For examination, it may be necessary to hold and support a struggling child. For example, lay the child in a supine position and have the parent or caregiver hold the child’s arms extended, in a position close to the sides of the head. This will limit side-to-side movements while you are examining ENT structures. Brace the otoscope, and guard against sudden head movements.
Never restrain a child assuming the tripod position (sitting up and leaning forward) for exam purposes. This may add to their anxiety creating severe respiratory distress.
Ears
Inspection
• External ear: position (in relation to eyes) low-set or small, deformed auricles may indicate associated congenital defects
• Pinna: lesions, abnormal appearance or position, include inspection of tissue behind pinna
• Canal: discharge, swelling, redness, wax, foreign bodies
• Tympanic membrane: colour, light reflex, landmarks, bulging or retraction, perforation, scarring, air bubbles, fluid level.
Check mobility using a pneumatic otoscope
• Estimate hearing by producing a loud noise (i.e., by clapping hands) for an infant or young child (which should elicit a blink
response), or by performing a watch or whisper test for an older child
Clinical tip: For the best view of the eardrum in an infant or a child less than 3 yrs old, pull the outer ear upward, outward and backward
Palpation
• Tenderness over tragus or on manipulation of the pinna
• Tenderness on tapping of mastoid process
• Size and tenderness of pre, post auricular and occipital nodes
Nose and Sinuses
Inspection
• External: inflammation, deformity, discharge, bleeding
• Internal: colour of nasal mucosa, edema, deviated or perforated septum, polyps, bleeding
• Observe nasal versus mouth breathing
Palpation
• Sinus and nasal tenderness (only in older children who can cooperate and provide a response)
Percussion
• Sinus and nasal tenderness (only in older children who can cooperate and provide a response)
Mouth and Throat
Inspection
• Lips: colour, lesions, symmetry, Koplik’s spots
• Oral cavity: breath odour, colour, lesions of buccal mucosa
• Teeth and gums: redness, swelling, caries, bleeding
• Tongue: colour, texture, lesions, symmetry, tenderness of floor of mouth
• Throat and pharynx: colour, exudates, uvula, tonsillar symmetry and enlargement
o A tonsil grade of +2 is normal up to 12 yrs of age
DST-202 Ear, Nose & Throat Assessment: Pediatric
56
Certified Practice Area:
RN First Call
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
Neck and lymph
Inspection
• Symmetry
• Swelling
• Masses
• Active range of motion
• Thyroid enlargement
Palpation
• Tenderness, enlargement, contour, mobility and consistency of nodes and masses
o Nodes – Pre and post auricular, occipital, tonsillar, submandibular, submental, anterior and posterior cervical,
supraclavicular
• Thyroid: size, consistency, contour, position, tenderness
Associate Systems for assessment
• A complete assessment should include the respiratory system
Symptoms requiring urgent referral
The first step is to determine if the ENT presentation requires an urgent referral to a physician or nurse practitioner, or can be managed safely by a nurse with CP designation.
The following signs and symptoms require referral to a physician or nurse practitioner:
• Positive Brudzinski (chin to chest)
• Pain and fever with mastoid tenderness
• Fever of unknown origin
• Treatment failure after 3 days (otitis media, tonsillitis)
• Displaced uvula
• Uncontrollable epistaxis
• Facial fractures
• Sudden onset of deafness
• Recent ear, nose or throat surgery
• Tripoding (sitting up and leaning forward)
• Drooling
• Petechiae
• Pain out of proportion to clinical findings (consider epiglottitis)
DIAGNOSTIC TESTS
The Certified Practice nurse may consider the following diagnostic tests to support clinical decision making:
• Swab of ear, nose or throat for Culture and Sensitivity (C&S)
DST-202 Ear, Nose & Throat Assessment: Pediatric

57
Certified Practice Area:
RN First Call
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
REFERENCES
More recent editions of any of the items in the Reference List may have been published since this DST was published. If you have a newer version, please use it.
Lieberthal, A.S. et al., American Academy of Pediatrics. (2013). Clinical practice guideline: The diagnosis and management of acute otitis media. Pediatrics, 131(3), e964-e999.
Ball, J. W., Dains, J. E., Flynn, J. A., Solomon, B. S., & Stewart, R. W. (Eds.). (2015). Seidel’s guide to physical examination (8th ed.). St. Louis, MO: Elsevier.
Centers for Disease Control and Prevention (CDC). (2017). Candida infections of the mouth, throat, and esophagus. CDC.
Dains, J. E., Baumann, L. C., & Scheibel, P. (2015). Advanced health assessment and clinical diagnosis in primary care (5th ed.). St. Louis, MO: Elsevier Mosby.
Estes, M. E. Z. (2014). Health assessment and physical examination (5th ed.). Clifton Park, NY:Cengage Learning.
Sawyer, S. S. (2014). Pediatric physical examination and health assessment. Sudbury, MA: Jones & Bartlett Learning.
Stephen, T. C., Skillen, D. L., Day, R. A., & Bickley L. S. (2010). Canadian Bates’ guide to health assessment for nurses. Philadelphia, PA: Lippincott, Williams & Wilkins.
Substance Abuse and Mental Health Services Administration (SAMHSA). 2017. Alcohol,Tobacco, and Other Drugs.
DST-202 Ear, Nose & Throat Assessment: Pediatric
58
Certified Practice Area:
RN First Call
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
DST-203 Otitis Media Acute: Adult
DEFINITION
Acute inflammation or infection of the middle ear. It is less common in adults than children.
POTENTIAL CAUSES
• Viral
• Bacterial forms due to Streptococcus pneumoniae, H. influenzae, Moraxella catarrhalis, Group A beta-hemolytic
streptococcus, staphylococcus aureus
• Chlamydia (uncommon)
• Fungal infections such as candida, aspergillis (uncommon)
PREDISPOSING RISK FACTORS
• Eustachian tube dysfunction
• Upper respiratory infection
• Allergies
• Chronic sinusitis
• Cleft palate
• Immunosuppression
• Active or passive smoking
TYPICAL FINDINGS OF OTITIS MEDIA
History
• Otalgia (throbbing)
• Fever
• General malaise
• Sensation of fullness
• Hearing decreased
• Tinnitus or roaring in ear, vertigo
• History of upper respiratory tract symptoms
• Client may feel mildly or moderately ill
Physical Assessment
Refer to end of document, Appendix 1, Guidelines for Pneumatic Otoscopy
• Vital signs. May be febrile.
• Tympanic membrane red, dull, bulging
• Bony landmarks obscured or absent
• Purulent discharge if drum perforated
• Decreased mobility of tympanic membrane (pneumatic otoscope) (appendix 1)
• Bullae seen on tympanic membrane
• Peri-auricular and anterior cervical nodes enlarged and tender
• Wax and other debris should be removed from the ear canal to allow a clear view of the tympanic membrane
DST-203 Otitis Media Acute: Adult
59
Certified Practice Area:
RN First Call
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
Diagnostic Tests
• Swab any drainage for culture and sensitivity
MANAGEMENT AND INTERVENTIONS
Goals of treatment
• Eradicate infection
• Relieve pain
• Prevent complications
Non-Pharmacological Interventions
• None
Pharmacological Interventions
• To relieve pain and fever:
o acetaminophen 325mg, 1-2 tabs po q4-6h prn, or
o ibuprofen 200mg, 1-2 tabs po q4-6h prn
• Oral antibiotic therapy:
o amoxicillin 1 gm, po tid for 5 days, OR
o doxycycline 200 mg PO once, then 100 mg po BID for 5 days
Failure of first line therapy:
• Amoxicillin-clavulanate 875 mg po bid for 10 days
In case of allergies to the above antibiotics, previous antibiotic use within a month, or unavailability of the previously listed antibiotics, consult with or refer to a physician or nurse practitioner.
Pregnant and Breastfeeding Women
• Acetaminophen, amoxicillin, and amoxicillin-clavulanate may be used as listed above.
• DO NOT USE ibuprofen or doxycycline.
POTENTIAL COMPLICATIONS
• Perforated tympanic membrane
• Reduced hearing
• Serous otitis media
• Mastoiditis (rare)
• Chronic otitis media
• Meningitis (rare)
• Epidural (brain) abscess
• Cholesteatoma
CLIENT INFORMATION AND DISCHARGE EDUCATION
• Recommend increased rest if febrile
• Counsel client about appropriate use of medication (dosage compliance and follow up)
• Explain disease course and expected outcome
• Recommend avoidance of flying until symptoms have resolved
• Recommend avoidance of swimming or scuba diving until symptoms have resolved.
• Counsel client to stop smoking
DST-203 Otitis Media Acute: Adult
60
Certified Practice Area:
RN First Call
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
MONITORING AND FOLLOW-UP
• Re-examine patients with persistent pain or fever in 24-48 hours
• Return to clinic in three days if no improvement
• Follow up 10-14 days to look for development of serous otitis
• Assess hearing one to three months after treatment if any symptoms persist
CONSULTATION AND/OR REFERRAL
• No consult or referral needed if uncomplicated and responds to treatment
• If a perforation develops, consult with a physician or nurse practitioner.
DOCUMENTATION
• As per agency policy
DST-203 Otitis Media Acute: Adult
61
Certified Practice Area:
RN First Call
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
REFERENCES
More recent editions of any of the items in the Reference List may have been published since this DST was published. If you have a newer version, please use it.
Alberta Medical Association. (2008). Guideline for the diagnosis and management of acute otitis media. Toward Optimized Practice. Edmonton, AB: TOP Alberta Doctors.
Anti-Infective Review Panel. (2012). Anti-infective guidelines for community-acquired infections. Toronto, ON: MUMS Guideline Clearinghouse.
Blondel-Hill, E., & Fryters, S. (2012). Bugs and drugs: An antimicrobial infectious diseases reference. Edmonton, AB: Alberta Health Services.
Canadian Pharmacists Association. (2014). Therapeutic choices for minor ailments. Ottawa, ON: Author.
Canadian Pharmacists Association. (2014). Therapeutic choices (7th ed.). Ottawa, ON: Author.
Cash, J. C., & Glass, C. A. (Eds.). (2014). Family practice guidelines (3rd ed.). New York, NY: Springer.
Chen, Y. A., & Tran, C. (Eds.). (2011). The Toronto notes 2011: Comprehensive medical reference and review for the Medical Council of Canada Qualifying Exam Part 1 and the United States Medical Licensing Exam Step 2 (27th ed.). Toronto, ON: Toronto Notes for Medical Students.
DynaMed. (2015, August 17). Acute otitis media (AOM).
Limb, C. J., Lustig, L. R., & Klein, J. O. (2014). Acute otitis media in adults (suppurative and serous). UptoDate.
Ramakrishnan, K., Sparks, R. A., & Berryhill, W. E. (2007). Diagnosis and treatment of otitis media. American Family Physician, 76(11), 1650-1658.
APPENDIX 1
Guidelines for Pneumatic Otoscopy
Anyone can learn pneumatic otoscopy, but practice is needed. This method consists of applying air pressure to the tympanic membrane and watching the resultant movement.
• Tools: a battery-operated bright light with a well-charged battery and a hermetically sealed otoscope with pneumatic
attachment
• Client must remain still during the examination (it may be necessary to restrain a child)
• Apply positive pressure (by squeezing a full bulb) and negative pressure (by releasing the bulb), and observe any movement
of the eardrum
• Lack of movement implies the presence of fluid in the middle ear or chronic stiffness of the tympanic membrane
DST-203 Otitis Media Acute: Adult

62
Certified Practice Area:
RN First Call
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
DST-204 Otitis Media Acute: Pediatric
DEFINITION
An acute suppurative infection of the middle ear, often preceded by a viral upper respiratory tract infection (URTI).
Nurses with Remote Practice Certified Practice designation (RN(C)s) are able to treat children with acute otitis media who are 6 months of age and older.
POTENTIAL CAUSES
Viral Organisms
• Respiratory syncytial virus (RSV)
• Picornaviruses (rhinovirus, enterovirus)
• Influenza viruses
• Coronaviruses
• Adenovirus
• Human metapneumovirus.
Common Bacterial Organisms
• Streptococcus pneumoniae
• Moraxella catarrhalis
• Hemophilus influenzae
• Pseudomonas aeruginosa
• Staphylococcus aureus
• Streptococcus pyogenes
Less Common Organisms
• Mycoplasma
• Chlamydia
Other Miscellaneous Causes
• Immunoreactivity
• Allergic rhinitis
PREDISPOSING RISK FACTORS
• Age – most frequent between 3 months to 3 years old (most important risk factor)
• Eustachian tube dysfunction
• Upper respiratory infection
• Allergies
• Cleft palate
• Immunosuppression
• Children exposed to cigarette smoke
• Children with Down syndrome
• Day care environment
• Children of Indigenous origin (eustachian tubes shorter and wider)
• Possibly bottle-fed children, if the child is propped up for feeding or goes to sleep with a bottle of milk at night
DST-204 Otitis Media Acute: Pediatric
63
Certified Practice Area:
RN First Call
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
• Children who use pacifiers when sleeping at night
• Fall and winter months
TYPICAL FINDINGS OF OTITIS MEDIA
History
• Otalgia (pain is absent in 20% of children)
• Fever
• Irritability
• Sensation of fullness
• Hearing decreased
• Tinnitus or roaring in ear
• Vertigo
• History of upper respiratory tract symptoms
• Tugging at ears
• Vomiting or diarrhea may be present
• Restless sleep
• Anorexia
Physical Assessment
• Vital signs. May be febrile.
• Weigh until 12 years of age for medication calculations
• May appear acutely ill
• Tympanic membrane red, dull, bulging
• Bony landmarks obscured or absent
• Purulent discharge if drum perforated
• Decreased mobility of tympanic membrane (pneumatic otoscope) (appendix 1)
• Bullae seen on tympanic membrane
• Peri-auricular and anterior cervical nodes enlarged and tender
• When safe to do so, wax and other debris should be removed from the ear canal to allow a clear view of the tympanic
membrane
• Redness of the tympanic membrane in the absence of other signs may be due to crying, agitation, a common cold,
aggressive examination or manipulation of the external ear canal, or serous otitis media with effusion
Diagnostic Tests
• Swab any drainage for culture and sensitivity
MANAGEMENT AND INTERVENTIONS
Goals of Treatment
• Control pain and fever
• Relieve infection
• Prevent complications
• Avoid unnecessary use of antibiotics
Non-Pharmacologic Interventions
• None
DST-204 Otitis Media Acute: Pediatric
64
Certified Practice Area:
RN First Call
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
Pharmacologic Interventions
Note: All drugs must be calculated by weight. Doses should not exceed recommended adult doses.
To relieve pain and fever: Acetaminophen
PO acetaminophen for pain/fever (calculate 10 – 15 mg/kg/dose; q4-6h)
PR acetaminophen for pain/fever (calculate 10 – 20 mg/kg/dose; q4-6h)
max from all sources: acetaminophen 75 mg/kg in 24 hours or 4,000 mg in 24 hours, whichever is less
To relieve pain and fever: Non Steroidal Anti-Inflammatory Drugs (NSAIDs)
PO ibuprofen for pain/fever [caution-renal]
• Less than 6 months of age: calculate 5 mg/kg/dose; q8h
• Greater than/equal to 6 months to 12 years: calculate 5 – 10 mg/kg/dose; q6-8h; max 400 mg/dose
• Greater than 12 years: 200 – 400 mg/dose; q4-6h; max 400 mg/dose
Max from all sources: ibuprofen 40 mg/kg in 24 hours or 2,400 mg in 24 hours, whichever is less
PO Naproxen BID (calculate 5 – 10 mg/kg/dose; max 500 mg/dose)
Oral Antibiotic Therapy:
In 70% of cases, acute otitis media resolves on its own with supportive care only.
• Do not initially give antibiotics for children 6 months and older:
o If the child is otherwise healthy;
o if the child is easily followed;
o if the symptoms are mild (mild otalgia, untreated fever less than 38.5’ Celsius); and
o if the child is non-toxic.
For these children:
o manage pain aggressively and keep well hydrated; and
o if not improved in 2 days commence antibiotic therapy.
• For children 6 months and older, institute antibiotics without waiting if:
o Severe otalgia and / or irritability lasting longer than 24 hours;
o Fever higher than 38.5’ Celsius;
o Tympanic perforation;
o Bilateral AOM;
o Antibiotic use for AOM in the previous 3 months;
o Presence of co-morbidities such as tonsillitis, which requires treatment; and
o Children who will not be able to be re-examined in 2-3 days,
• Oral antibiotic therapy:
o A 5-day course is appropriate for children greater than 2 years with uncomplicated acute otitis media; for younger
children or children of any age with complications (e.g., perforated eardrum) a 10-day course is appropriate.
amoxicillin (standard dose) 40mg-50mg/kg per day, po divided tid for 5-10 days. Maximum dose 1,500mg/day
OR
amoxicillin-clavulanate (4:1 formulation) 40 mg/kg/day divided TID for 5-10 days. Dosing based on amoxicillin,
max dose 1500 mg/day.
DST-204 Otitis Media Acute: Pediatric
65
Certified Practice Area:
RN First Call
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
o If recurrent infection in less than 3 months or if symptoms fail to respond after 48 hours of treatment with initial
antibiotics then:
amoxicillin (high dose) 80mg/kg/day, po divided tid for 5-10 days. Maximum dose 1,500mg/day
OR
amoxicillin-clavulanate (7:1 formulation) 45 mg/kg/day divided bid for 5-10 days. Maximum amoxicillin dose of
1500 mg/day
• For clients with allergies to the above antibiotics, previous antibiotic use within a month, or unavailability of the previously
listed antibioitics:
azithromycin 10 mg/kg/day once on first day, then 5 mg/kg/day once daily for four days.
Cefuroxime 15mg/kg/dose PO bid. Maximum dose 1,000mg/day
Pregnant
• DO NOT USE ibuprofen
Pregnant and Breastfeeding Women
• Acetaminophen, amoxicillin, amoxicillin-clavulanate and azithromycin may be used as listed above.
POTENTIAL COMPLICATIONS
• Perforated tympanic membrane
• Serous otitis media
• Mastoiditis (rare)
• Meningitis (rare)
• Facial paralysis
CLIENT/CAREGIVER EDUCATION AND DISCHARGE INFORMATION
• Advise on condition, timeline of treatment and expected course of disease process
• Recommend increased rest in the acute febrile phase
• Counsel parents or caregiver about appropriate use of medications (dosage, compliance, follow-up)
• Recommend avoidance of flying until symptoms have resolved
• Avoid feeding in a flat supine position
• Breast feeding recommended
• Avoid tobacco smoke
• Frequent and thorough hand washing
• Update immunizations if necessary
• Antihistamines and decongestants have no proven efficacy in the treatment of acute otitis media and should be avoided.
MONITORING AND FOLLOW-UP
• Advise caregiver of follow up if condition does not improved in 48 hours or sooner if condition deteriorates
• Otherwise, follow up in 14 days:
o If ear is normal, do not give any treatment
o If ear is still dull but asymptomatic (no pain or hearing loss), follow-up again in 6 weeks
o If condition is unresolved, consider treatment with a second-line antibiotic
o Look for development of serous otitis media
• In 70% to 80% of clients, effusion persists after 2 weeks, and 10% still have effusion at 3 months and may exhibit
conductive loss of hearing
DST-204 Otitis Media Acute: Pediatric
66
Certified Practice Area:
RN First Call
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
CONSULTATION AND/OR REFERRAL
• More than 3 infections in 6 months or 4 infections in one year
• Consult with a physician or nurse practitioner if there is no improvement in symptoms or condition worsens within 24-48
hours.
• Hearing should be assessed by audiologist, community health nurse or other appropriate professional 1 month after
treatment is complete if the child has had two or more cases of AOM.
DOCUMENTATION
• As per agency policy
DST-204 Otitis Media Acute: Pediatric
67
Certified Practice Area:
RN First Call
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
REFERENCES
More recent editions of any of the items in the Reference List may have been published since this DST was published. If you have a newer version, please use it.
Acute otitis media: Update on diagnosis and treatment. (2013). Consultant, 53(5), 352-353.
American Academy of Pediatrics. (2013). Clinical practice guideline: The diagnosis and management of acute otitis media. Pediatrics, 131(3), e964-e999.
Anti-Infective Review Panel. (2012). Anti-infective guidelines for community-acquired infections. Toronto, ON: MUMS Guideline Clearinghouse.
Blondel-Hill, E., & Fryters, S. (2012). Bugs and drugs: An antimicrobial infectious diseases reference. Edmonton, AB: Alberta Health Services.
Canadian Pharmacists Association. (2014). Therapeutic choices for minor ailments. Ottawa, ON: Author.
Cash, J. C., & Glass, C. A. (Eds.). (2014). Family practice guidelines (3rd ed.). New York, NY: Springer.
Chen, Y. A., & Tran, C. (Eds.). (2011). The Toronto notes 2011: Comprehensive medical reference and review for the Medical Council of Canada Qualifying Exam Part 1 and the United States Medical Licensing Exam Step 2 (27th ed.). Toronto, ON: Toronto Notes for Medical Students.
DynaMed. (2015, August 17). Acute otitis media (AOM).
Guidelines and Protocols Advisory Committee. (2010). Otitis media: Acute otitis media (AOM) and otitis media with effusion (OME).
Harmes, K. M., Blackwood, R. A., Burrows, H. L., Cooke, J. M., Harrison, R., & Passamani, P. P. (2013). Otitis media: Diagnosis and treatment. American Family Physician, 88(7), 435-440.
Hersh, A. L., Jackson, M., & Hicks, L. A. (2013). Principles of judicious antibiotic prescribing for upper respiratory tract infections in pediatrics. Pediatrics, 132(6), 1146-1154.
Hirst, S., & Neill, S. (2013). Treatment of acute otitis media in childhood. Practice Nursing, 24(8), 407-410.
Jensen, B., & Regier, L. D. (Eds.). (2014). RxFiles: Drug comparison charts (10th ed.). Saskatoon, SK: RxFiles.
Limb, C. J., Lustig, L. R., & Klein, J. O. (2014). Acute otitis media in adults (suppurative and serous). UptoDate.
McWilliams, C. J., & Goldman, R. D. (2011). Update on acute otitis media in children younger than 2 years of age. Canadian Family Physician, 57(11), 1283-1285.
Ramakrishnan, K., Sparks, R. A., & Berryhill, W. E. (2007). Diagnosis and treatment of otitis media. American Family Physician, 76(11), 1650-1658.
Venekamp, R. P., Sanders, S. L., Glasziou, P. P., Del Mar, C. B., Rovers, M. M. (2015). Antibiotics for acute otitis media in children. The Cochrane Database of Systematic Reviews, (6). Doi: 10.1002/14651858.CD000219.pub4.
DST-204 Otitis Media Acute: Pediatric

68
Certified Practice Area:
RN First Call
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
DST-205 Ceruminosis (Impacted Cerumen): Adult
DEFINITION
An accumulation of cerumen causing symptoms, preventing needed assessment of the ear, or both.
SYMPTOMS REQUIRING URGENT REFERRAL OR CONSULTATION
New onset of the following signs and/or symptoms require immediate emergency care and referral to a physician or nurse practitioner
• Ear pain, drainage, and/or bleeding
CARDINAL SIGNS AND/OR SYMPTOMS
• Tinnitus
• Ear fullness
• Hearing loss
• Vertigo
• Cough
• Discharge
• Odour
• Hearing aid feedback or malfunction
• Itching
DIAGNOSTIC TEST
• Greater than 80% obstruction of an ear canal on otoscopy
PHYSICAL ASSESSMENT
• Hardened cerumen in canal
• Red and swollen canal
• Obscured tympanic membrane
• Partial or complete obstruction of ear canal by cerumen
MANAGEMENT
If Tympanic Membrane is Intact
Softening or Emulsifying Cerumen
Soften cerumen with slightly warmed mineral oil or olive oil for several days before attempting irrigation unless there are bothersome symptoms such as pain or vertigo
Administer warm water or saline as ear drops for 10-15 minutes before syringing
Note: triethanolamine polypeptide oleate-condensate (Cerumenex) and carbamide peroxide (Murine) appear no more effective than saline
Irrigation
Inject lukewarm water upwards within ear canal with an ear syringe until cerumen is cleared. After cerumen removal, examine ear for otitis externa or tympanic membrane (TM) perforation
DST-205 Ceruminosis (Impacted Cerumen: Adult)
69
Certified Practice Area:
RN First Call
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
Debridement
Manual debridement should be done by a physician or nurse practitioner
Note 1: Irrigation should not be performed if the TM is known to be perforated, there is a history of ear surgery, the cerumen is not completely occluding the ear canal, if previous irrigations caused pain, or if the client is known to have factors which
increase the risk of complications of irrigation such as anticoagulant therapy, immunocompromised state, diabetes mellitus, prior radiation therapy to the head and neck, ear canal stenosis or exostosis.
Note 2: Clients who are immunocompromised or diabetic have a greater risk for otitis externa following irrigation and should be followed up after the procedure.
POTENTIAL COMPLICATIONS OF IRRIGATION
• Vertigo
• Otitis externa
• TM perforation
• Nystagmus and vertigo
CLIENT INFORMATION AND DISCHARGE EDUCATION
• Explain disease course and expected outcome
• If asymptomatic, cerumen does not need to be removed as it has protective, emollient and bacteriocidal properties
• Suggest not using cotton swabs for ear hygiene (or inserting other objects into the ear)
• Return to clinic if no improvement
• To prevent ceruminosis, suggest client use a bulb syringe with warm water or allow warm water into ears with bathing or
swimming
• 70% isopropyl alcohol or hydrogen peroxide drops reported to reduce cerumen accumulation
MONITORING AND FOLLOW-UP
• Return to clinic in three days if symptoms persist or if immunocompromised (see above)
CONSULTATION AND/OR REFERRAL
• Consult or refer to a physician or nurse practitioner if complicated (TM is not intact), or does not respond to treatment or if
debridement is required
DOCUMENTATION
• As per agency policy
DST-205 Ceruminosis (Impacted Cerumen: Adult)
70
Certified Practice Area:
RN First Call
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
REFERENCES
More recent editions of any of the items in the Reference List may have been published since this DST was published. If you have a newer version, please use it.
Aaron K, Cooper TE, Warner L, Burton MJ. Ear drops for the removal of ear wax. Cochrane ENT Group, ed. Cochrane Database of Systematic Reviews. July 2018. doi:10.1002/14651858.CD012171.pub2
Michaudet C, Malaty J. Cerumen impaction: diagnosis and management. American Family Physician. 2018;98(8):7.
Schwartz SR, Magit AE, Rosenfeld RM, et al. Cerumen impaction: an updated guideline from the AAO-HNSF. Otolaryngol Head Neck Surg. 2017;156(1_suppl):S1-S29. doi:10.1177/0194599816671491
DST-205 Ceruminosis (Impacted Cerumen: Adult)

71
Certified Practice Area:
RN First Call
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
DST-206 Pharyngitis (Sore Throat): Adult
DEFINITION
Inflammation or infection of the mucus membranes of the pharynx. It may also affect the palatine tonsils.
POTENTIAL CAUSES
Infectious
Viruses
• Adenovirus
• Influenza
• Parainfluenza virus
• Epstein-Barr
• Coronavirus
• Rhinovirus
• Enterovirus
• Respiratory synctial virus
• Metapneumovirus
• Herpes simplex virus
Bacterial
• Group A beta-haemolytic strep
• Group C and G streptococci
• Chlamydia pneumoniae
• Diphtheria
• Mycoplasma pneumonia
• Neisseria gonorrhea or chlamydia trachomatis (related to sexual activity)
Fungi
• Candida albicans (immunocompromised)
Non-infectious
• Allergic rhinitis
• Sinusitis with post nasal drip
• Mouth breathing
• Trauma
• GERD (gastroesophageal reflux disease)
PREDISPOSING RISK FACTORS
• Previous episodes of pharyngitis or tonsillitis
• Smoking, exposure to cigarette smoke
• Overcrowding
• Immunocompromised
• Steroids, oral or inhaled
• Diabetes mellitus
• Oral sex
DST-206 Pharyngitis (Sore Throat): Adult
72
Certified Practice Area:
RN First Call
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
TYPICAL FINDINGS OF PHARYNGITIS
Note: Always consider the potential for epiglottitis and airway obstruction when a severely sore throat is out of proportion to the findings of the oropharyngeal exam.
Bacterial
History
• Abrupt onset of sore throat
• Pain with swallowing
• Absence of cough
• Fever or chills
• Malaise
• Headache
• Anorexia
• May have nausea, vomiting and abdominal pain
Physical Assessment
• Fever
• Pulse elevated
• Client appears ill
• Posterior pharynx red and edematous
• Tonsils enlarged, may be asymmetric
• Purulent exudate may be present
• Tonsillar and anterior cervical nodes may be enlarged and tender
• Erythematous “sandpaper” rash of scarlet fever (may be present with streptococcal infection)
• Liver/spleen enlargement +/- tenderness (e.g., mononucleosis)
Viral
History
• Slow progressive onset of sore throat
• Mild malaise
• Cough
• Nasal congestion
Physical Assessment
• Temperature elevated
• Posterior pharynx red and swollen
• Purulent exudate may be present
• Tonsillar and anterior cervical nodes may be enlarged and tender
• Petechiae or purple colour on palate (mononucleosis)
• Vesicles (if herpes)
Non-infectious
• Slow progressive onset of sore throat
• Mild malaise
• Cough
• Persistent, recurrent
DST-206 Pharyngitis (Sore Throat): Adult
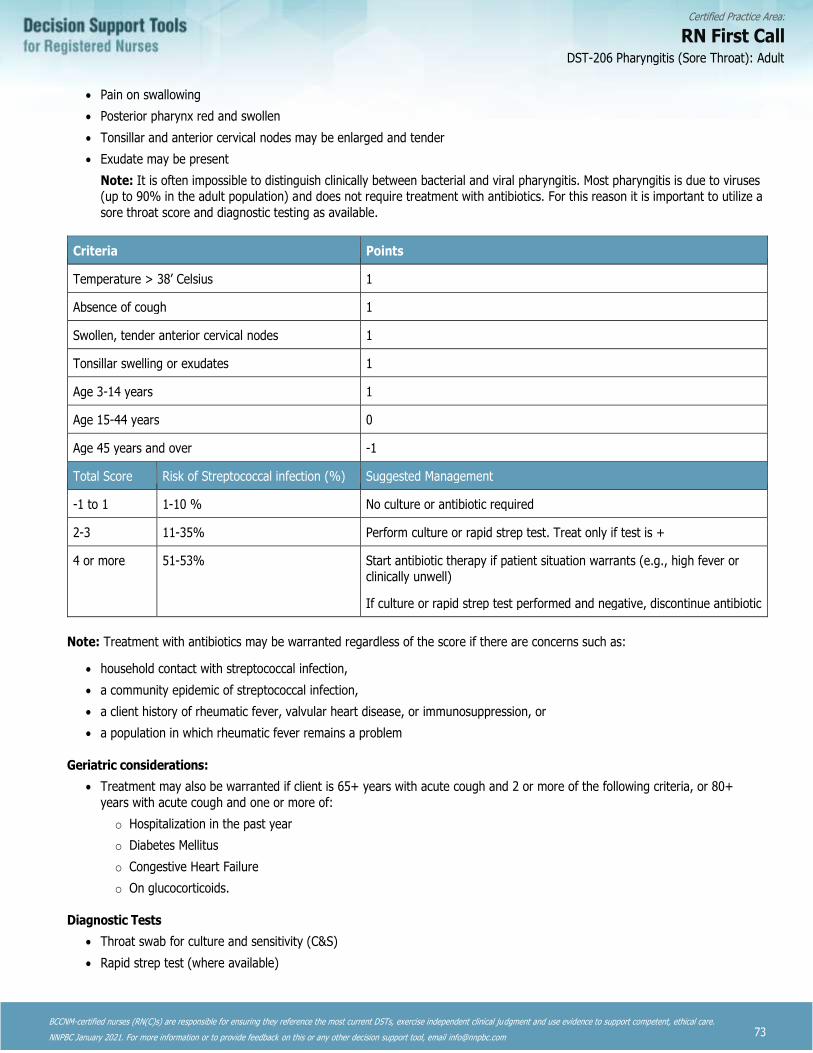
73
Certified Practice Area:
RN First Call
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
• Pain on swallowing
• Posterior pharynx red and swollen
• Tonsillar and anterior cervical nodes may be enlarged and tender
• Exudate may be present
Note: It is often impossible to distinguish clinically between bacterial and viral pharyngitis. Most pharyngitis is due to viruses (up to 90% in the adult population) and does not require treatment with antibiotics. For this reason it is important to utilize a
sore throat score and diagnostic testing as available.
Criteria Points
Temperature > 38’ Celsius 1
Absence of cough 1
Swollen, tender anterior cervical nodes 1
Tonsillar swelling or exudates 1
Age 3-14 years 1
Age 15-44 years 0
Age 45 years and over -1
Total Score Risk of Streptococcal infection (%) Suggested Management
-1 to 1 1-10 % No culture or antibiotic required
2-3 11-35% Perform culture or rapid strep test. Treat only if test is +
4 or more 51-53% Start antibiotic therapy if patient situation warrants (e.g., high fever or clinically unwell)
If culture or rapid strep test performed and negative, discontinue antibiotic
Note: Treatment with antibiotics may be warranted regardless of the score if there are concerns such as:
• household contact with streptococcal infection,
• a community epidemic of streptococcal infection,
• a client history of rheumatic fever, valvular heart disease, or immunosuppression, or
• a population in which rheumatic fever remains a problem
Geriatric considerations:
• Treatment may also be warranted if client is 65+ years with acute cough and 2 or more of the following criteria, or 80+
years with acute cough and one or more of:
o Hospitalization in the past year
o Diabetes Mellitus
o Congestive Heart Failure
o On glucocorticoids.
Diagnostic Tests
• Throat swab for culture and sensitivity (C&S)
• Rapid strep test (where available)
DST-206 Pharyngitis (Sore Throat): Adult

74
Certified Practice Area:
RN First Call
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
MANAGEMENT AND INTERVENTIONS
Goals of Treatment
• Eradicate infection
• Prevent complications
• Prevent spread of group A streptococcus
Non-pharmacologic interventions
• Bed rest during febrile phase
• Adequate oral intake of fluids
• Avoidance of irritants
• Gargling with warm saline (1 tsp. in 1 cup warm water)
Pharmacological Interventions
• Analgesics for mild to moderate pain:
o acetaminophen 325mg, 1-2 tabs po q4-6h prn, or
o ibuprofen 200mg, 1-2 tabs po q4-6h prn
• Treat with oral antibiotics if streptococcal infection is suspected:
o Penicillin VK 600 mg po bid or 300 mg po tid for 10 days
• For clients with penicillin allergy or requiring a suspension (if pen V suspension not available):
o Cephalexin 500 mg po BID for 10 days (DO NOT USE IF CLIENT HAS A SEVERE ANAPHYLACTIC REACTION TO
PENICILLIN)
OR
o Azithromycin 500 mg po daily for 3 days
Pregnant and Breastfeeding Women
• Acetaminophen, penicillin VK, cephalexin and azithromycin may be used as listed above.
• DO NOT use ibuprofen in pregnant patients
If the infection has been determined to be due to chlamydia or gonorrhea, please refer to the appropriate STI DST.
POTENTIAL COMPLICATIONS
• Rheumatic fever (group A strep)
• Acute Glomerulonephritis (group A strep)
• Peritonsillar abscess
• Epiglottitis
• Retropharyngeal abscess
• Otitis media
• Sinusitis
CLIENT EDUCATION AND DISCHARGE INFORMATION
• Gargle frequently with warm salt water (1 tsp. in 1 cup warm water)
• Increase room humidity
• Eat soft bland foods
DST-206 Pharyngitis (Sore Throat): Adult
75
Certified Practice Area:
RN First Call
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
MONITORING AND FOLLOW UP
• Return to clinic if not improved in 24-48 hours
CONSULTATION AND/OR REFERRAL
• A consultation with a physician or nurse practitioner may be necessary if condition is recurrent or persistent or an
undiagnosed underlying pathology is suspected.
• An immunocompromised client, or an unusual presentation of candidiasis, should be referred promptly to a physician or
nurse practitioner.
DOCUMENTATION
• As per agency policy
DST-206 Pharyngitis (Sore Throat): Adult
76
Certified Practice Area:
RN First Call
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
REFERENCES
More recent editions of any of the items in the Reference List may have been published since this DST was published. If you have a newer version, please use it.
Anti-Infective Review Panel. (2012). Anti-infective guidelines for community-acquired infections. Toronto, ON: MUMS Guideline Clearinghouse.
Blondel-Hill, E., & Fryters, S. (2012). Bugs and drugs: An antimicrobial infectious diseases reference. Edmonton, AB: Alberta Health Services.
Cash, J. C., & Glass, C. A. (Eds.). (2014). Family practice guidelines (3rd ed.). New York, NY: Springer.
Canadian Pharmacists Association. (2014). Therapeutic choices (7th ed.). Ottawa, ON: Author.
Canadian Pharmacists Association. (2014). Therapeutic choices for minor ailments. Ottawa, ON: Author.
Carillo-Marquez, M. A. (2015). Bacterial pharyngitis.
Chan, P. D., & Johnson, M. T. (2010). Treatment guidelines for medicine and primary care. Blue Jay, CA: Current Clinical Strategies Publishing.
Chen, A., & Tran, C. (2011). Comprehensive medical reference and review for MCCQE and USMLE II. Toronto notes form medical students. Toronto: Toronto Notes for Medical Students, Inc.
DynaMed. (2016, March 25). Antibiotics for streptococcal pharyngitis.
DynaMed. (2016, March 25). Streptococcal pharyngitis.
DynaMed. (2016, March 25). Pharyngitis.
Gore, J. M. (2013). Acute pharyngitis. JAAPA: Journal of the American Academy of Physician Assistants, 26(2), 57-58.
Jensen, B., & Regier, L. D. (Eds). (2014). RxFiles: Drug comparison charts (10th ed.). Saskatoon, SK: RxFiles
National Institute for Health and Clinical Excellence (NICE). (2008, July). Respiratory tract infections – antibiotic prescribing: Prescribing of antibiotics for self-limiting respiratory tract infections in adults and children in primary care. Manchester, UK: Author.
Shepherd, A. B. (2013). Assessment and management of acute sore throat. Nurse Prescribing, 11(11), 549-553.
Shulman, S.T., Bisno, A.L., Clegg, H.W., Gerber, M.A., Kaplan, E.L., Lee, G.,…Van Beneden, C. (2012). Clinical practice guideline
for the diagnosis and management of group A streptococcal pharyngitis: 2012 update by the Infectious Diseases Society of America. Clinical Infectious Diseases. 55(10), e86-e102.
University of Michigan Health System. (2013, May). Pharyngitis: Guidelines for clinical care: Ambulatory (Rev.). Ann Arbor, MI: Author.
DST-206 Pharyngitis (Sore Throat): Adult
77
Certified Practice Area:
RN First Call
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
DST-207 Pharyngitis (Sore Throat): Pediatric
DEFINITION
A painful condition of the oropharynx associated with infection of the mucus membranes of the pharynx and the palatine tonsils. The peak prevalence is found in children less than 5 years.
Nurses with Remote Practice Certified Practice designation (RN(C)s) are able to treat children with pharyngitis who are 1 year of age and older.
Potential Causes
Infectious
Viruses • Adenovirus
• Parainfluenza virus
• Epstein –Barr
• Coxsackievirus
• Herpes simplex virus
• Enterovirus (more common in children less than 3 years of age)
• Influenza virus
Bacterial • Group A beta-haemolytic strep (GAS) (streptococcus pyogenes)
• Mycoplasma pneumoniae (10% of adolescents)
• Neisseria gonorrhoeae or Chlamydia trachomatis (related to sexual activity)
• Chlamydia pneumoniae
• Diptheriae
Non-infectious
• Allergic rhinitis
• Sinusitis with post nasal drip
• Mouth breathing
• Trauma
• GERD (gastroesophageal reflux disease)
PREDISPOSING RISK FACTORS
• Previous episodes of pharyngitis or tonsillitis
• Smoking, exposure to cigarette smoke
• Overcrowding
• Immunocompromised
• Steroids, oral or inhaled
• Diabetes mellitus
• Oral sex
TYPICAL FINDINGS OF SORE THROAT
See Appendix 1 for pathogens and clinical appearance of tonsils
Note: Always consider the potential for epiglottitis and airway obstruction. If symptoms of airway distress, tripoding, stridor, dysphagia, drooling and anxiety exist, do not exam the child’s mouth or throat, but immediately consult with or refer the client to a physician or nurse practitioner.
DST-207 Pharyngitis (Sore Throat): Pediatric

78
Certified Practice Area:
RN First Call
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
Bacterial
History
• Acute onset
• Very sore throat
• Absence of cough and coryza
• Fever
• Headache
• May have nausea, vomiting, abdominal pain
• General malaise
Physical Assessment
• Significant fever
• Tachycardia
• Weigh until 12 years of age for medication calculations
• Pharyngeal and tonsillar erythema
• Petechiae of soft palate
• Tonsillar exudate (particularly with streptococcal infection, diphtheria or mononucleosis)
• Anterior cervical lymphadenopathy
• Erythematous “sandpaper” rash of scarlet fever (may be present with streptococcal infection)
• Erythematous rash (particularly if child is receiving amoxicillin)
• Lymphadenopathy with splenic enlargement in children with mononucleosis
• Koplik spots
Viral
History
• Acute sore throat combined with symptoms consistent with a viral upper respiratory tract infection (rhinorrhea, cough and
often hoarseness)
Physical Assessment
• Fever (low-grade to significant)
• Tachycardia
• Weigh until 12 years of age for medication calculations
• Pharyngeal and tonsillar erythema and swelling
• Petechiae of soft palate
• Tonsillar exudate similar to that occurring with bacterial infection may be present, particularly in adenovirus
pharyngotonsillitis
• Anterior cervical lymphadenopathy
• Vesicles and ulcers may be present with coxsackievirus infection or herpes
• Hepato- and splenomegaly
Note: It is often impossible to distinguish clinically between bacterial and viral pharyngitis. Most pharyngitis is due to viruses (up to
70% in the pediatric population) and does not require treatment with antibiotics. For this reason, it is important to utilize a sore throat score and diagnostic testing as available.
DST-207 Pharyngitis (Sore Throat): Pediatric

79
Certified Practice Area:
RN First Call
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
Criteria Points
Temperature > 38’ Celsius 1
Absence of cough 1
Swollen, tender anterior cervical nodes 1
Tonsillar swelling or exudates 1
Age 3-14 years 1
Age 15-44 years 0
Total Score Risk of Streptococcal infection (%) Suggested Management
0 to 1 1-10 % No culture or antibiotic required
2-3 11-35% Perform culture or rapid strep test. Treat only if test is +
4 or more 51-53% Start antibiotic therapy if patient situation warrants (e.g., high fever or clinically unwell)
If culture or rapid strep test performed and negative, discontinue antibiotic
Note: Treatment with antibiotics may be warranted regardless of the score if there is a concern such as:
• household contact with streptococcal infection,
• a community epidemic of streptococcal infection,
• a history of rheumatic fever, valvular heart disease, or immunosuppression, or
• a population in which rheumatic fever remains a problem
DIAGNOSTIC TESTS
• Rapid strep test (if available)
• Throat swab for culture and sensitivity
• If the child is greater than 2 years old, culture the throat before treatment or do rapid Strep antigen test (if available); if
negative, do throat culture.
• Monospot if suspect viral
MANAGEMENT AND INTERVENTIONS
Bacterial
Goals of Treatment
• Control pain and fever
• Prevent complications
• Rapid reduction in infectivity
• Prevent spread of Group A Streptococcus
• Decrease antibiotic resistance
Non-Pharmacologic Interventions
• Rest and increase fluid intake
• Avoidance of irritants (smoke)
DST-207 Pharyngitis (Sore Throat): Pediatric
80
Certified Practice Area:
RN First Call
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
• Saline gargles (1tsp of salt in 1 cup of warm water)
• Increase room humidity
Pharmacologic Interventions
Note: All doses must be calculated by weight up until age 12. Pediatric doses should not exceed recommended adult doses.
• To relieve pain:
o acetaminophen 10-15 mg/kg, po q4-6h prn. Maximum dose 75mg/kg/24hr, or a total of 4,000mg/24hr, whichever is
less, or
o ibuprofen 5-10mg/kg, po q6-8h prn. Maximum dose 40mg/kg/24hr
• Pen VK 40mg/kg/day divided bid for 10 days. Amoxicillin is no longer recommended
• In case of unavailability of the previously listed antibiotics, or allergies to the above antibiotics:
o Cephalexin 40 mg/kg/24hr divided bid for 10 days. (DO NOT USE if patient has a severe anaphylactic reaction to
penicillin.)
OR
o Azithromycin 20 mg/kg po daily for 3 days (Maximum dose 500 mg/day)
Pregnant and Breastfeeding Women
• Acetaminophen, penicillin VK, amoxicillin, azithromycin and cephalexin may be used as listed above.
• DO NOT USE ibuprofen in pregnant patients.
• If the infection has been determined to be due to chlamydia or gonorrhea, please refer to the appropriate STI
DST.
Viral
Goals of treatment
• Relieve symptoms
• Supportive care
Non-pharmacological Interventions
• Rest
• Increase oral fluids
• Avoid irritants
• Warm saline gargles qid (1 tsp. of salt in 1 cup of warm water)
Pharmacological Interventions
Note: All doses must be calculated by weight up until age 12. Pediatric doses should not exceed recommended adult doses.
• To relieve pain:
o acetaminophen 10-15 mg/kg, po q4-6h prn. Maximum dose 75mg/kg/24hr or a total of 4,000mg/24hr, whichever is less
OR
o ibuprofen 5-10mg/kg, po q6-8h prn. Maximum dose 40mg/kg/24hr
Pregnant and Breastfeeding Youth
• Acetaminophen may be used in pregnant and breastfeeding youth
• DO NOT use ibuprofen in pregnancy patients.
DST-207 Pharyngitis (Sore Throat): Pediatric
81
Certified Practice Area:
RN First Call
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
POTENTIAL COMPLICATIONS
• Rheumatic fever (group A strep)
• Acute Glomerulonephritis (group A strep)
• Peritonsillar abscess
• Epiglottitis
• Retropharyngeal abscess
• Otitis media
• Sinusitis
• Splenomegaly (Epstein Barr Virus or Infectious Mononucleosis)
• Pneumonia
• Bacterial meningitis
CLIENT/CAREGIVER EDUCATION AND DISCHARGE INFORMATION
• Advise on condition, timeline of treatment and expected course of disease process
• Saline gargles as described above
• Counsel parents/caregiver about appropriate use of medication (dosage, compliance, follow-up)
• If child has any difficulty swallowing, seek help immediately
MONITORING AND FOLLOW-UP
• Return to clinic in 48 hours if awaiting culture results
• Return for care if no improvement in 48 hours
CONSULTATION AND/OR REFERRAL
• Consult a physician or nurse practitioner if child has recurrent bouts of GAS pharyngitis/tonsillitis: greater than 5 episodes in
one year.
DOCUMENTATION
• As per agency policy
DST-207 Pharyngitis (Sore Throat): Pediatric
82
Certified Practice Area:
RN First Call
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
REFERENCES
More recent editions of any of the items in the Reference List may have been published since this DST was published. If you have a newer version, please use it.
Anti-Infective Review Panel. (2012). Anti-infective guidelines for community-acquired infections. Toronto, ON: MUMS Guideline Clearinghouse.
Blondel-Hill, E., & Fryters, S. (2012). Bugs and drugs: An antimicrobial infectious diseases reference. Edmonton, AB: Alberta Health Services.
Campisi, P., & Tewfik, T. L. (2003). Tonsillitis and its complications. Canadian Journal of Diagnosis, 20 (3), 99-105.
Canadian Pharmacists Association. (2014). Therapeutic choices (7th ed.). Ottawa, ON: Author.
Cash, J. C., & Glass, C. A. (Eds.). (2014). Family practice guidelines (3rd ed.). New York, NY: Springer.
Chen, Y. A., & Tran, C. (Eds.). (2011). The Toronto notes 2011: Comprehensive medical reference and review for the Medical Council of Canada Qualifying Exam Part 1 and the United States Medical Licensing Exam Step 2 (27th ed.). Toronto, ON: Toronto Notes for Medical Students.
Chiappini, E., Principi, N., Mansi, N., Serra, A., De Masi, S., Camaioni, A., ... de Martino, M. (2012). Management of acute pharyngitis in children: Summary of the Italian National Institute of Health guidelines. Clinical Therapeutics, 34(6), 1442-1458.
DynaMed. (2016, March 25). Antibiotics for streptococcal pharyngitis.
DynaMed. (2016, March 25). Pharyngitis.
DynaMed. (2016, March 25). Streptococcal pharyngitis.
Esau, R. (Ed.). (2012). British Columbia’s Children’s Hospital pediatric drug dosage guidelines (6th ed.). Vancouver, BC: Children’s & Women’s Health Centre of B.C.
Gore, J. M. (2013). Acute pharyngitis. JAAPA: Journal of the American Academy of Physician Assistants, 26(2), 57-58.
Hersh, A. L., Jackson, M. A., & Hicks, L. A. (2013). Principles of judicious antibiotic prescribing for upper respiratory tract infections in pediatrics. Pediatrics, 132(6), 1146-1154.
Jensen, B., & Regier, L. D. (Eds.). (2014). RxFiles: Drug comparison charts (10th ed.). Saskatoon, SK: RxFiles.
Lexicomp. (2017). Amoxicillin. Lexicomp Online.
Michigan Quality Improvement Consortium. (2013, January). Guideline: Acute pharyngitis in children 2-18 years old (Rev.).
National Institute for Health and Clinical Excellence (NICE). (2008, July). Respiratory tract infections – antibiotic prescribing: Prescribing of antibiotics for self-limiting respiratory tract infections in adults and children in primary care. Manchester, UK: Author.
Nicoteri, J. A. L. (2013). Adolescent pharyngitis: A common complaint with potentially lethal complications. Journal for Nurse Practitioners, 9(5), 295-300.
Shah, U. K. (2015, July 9). Tonsillitis and peritonsillar abscess treatment & management.
Shulman, S.T., Bisno, A.L., Clegg, H.W., Gerber, M.A., Kaplan, E.L., Lee, G.,…Van Beneden, C. (2012). Clinical practice guideline for the diagnosis and management of group A streptococcal pharyngitis: 2012 update by the Infectious Diseases Society of America. Clinical Infectious Diseases. 55(10), e86-e102.
University of Michigan Health System. (2013, May). Pharyngitis: Guidelines for clinical care: Ambulatory (Rev.). Ann Arbor, MI: Author.
DST-207 Pharyngitis (Sore Throat): Pediatric
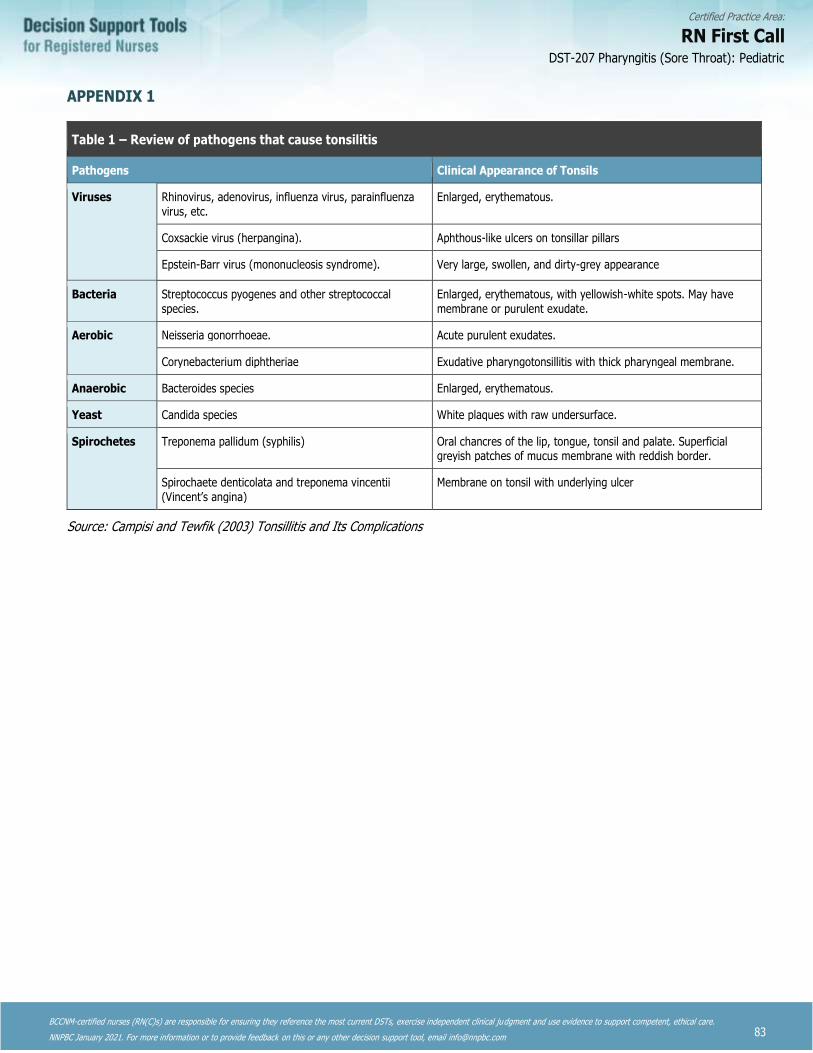
83
Certified Practice Area:
RN First Call
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
APPENDIX 1
Table 1 – Review of pathogens that cause tonsilitis
Pathogens Clinical Appearance of Tonsils
Viruses Rhinovirus, adenovirus, influenza virus, parainfluenza virus, etc.
Enlarged, erythematous.
Coxsackie virus (herpangina). Aphthous-like ulcers on tonsillar pillars
Epstein-Barr virus (mononucleosis syndrome). Very large, swollen, and dirty-grey appearance
Bacteria Streptococcus pyogenes and other streptococcal species.
Enlarged, erythematous, with yellowish-white spots. May have membrane or purulent exudate.
Aerobic Neisseria gonorrhoeae. Acute purulent exudates.
Corynebacterium diphtheriae Exudative pharyngotonsillitis with thick pharyngeal membrane.
Anaerobic Bacteroides species Enlarged, erythematous.
Yeast Candida species White plaques with raw undersurface.
Spirochetes Treponema pallidum (syphilis) Oral chancres of the lip, tongue, tonsil and palate. Superficial greyish patches of mucus membrane with reddish border.
Spirochaete denticolata and treponema vincentii (Vincent’s angina)
Membrane on tonsil with underlying ulcer
Source: Campisi and Tewfik (2003) Tonsillitis and Its Complications
DST-207 Pharyngitis (Sore Throat): Pediatric
84
Certified Practice Area:
RN First Call
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
DST-301 Dental Abscess: Adult
DEFINITION
Infection of the soft tissue surrounding a tooth or gum.
Potential Causes
Progressive dental decay causing pulpitis from gram-positive anaerobes and Bacteroides, Streptococcus viridans
Predisposing Risk Factors
• Dental caries
• Poor dental hygiene
• Dental trauma
Typical Findings of Dental Abscess
History
• Localized, constant, deep, throbbing pain
• Pain worsens with mastication or exposure to extreme temperatures
• Tooth may be mobile
• Gingival or facial swelling and tenderness (or both) may be present
• Fever (rare but possible)
Physical Assessment
• Facial swelling may be present
• Carious tooth
• Tooth tender when tapped
• Gingival edema and erythema
• Tooth may be loose
• Anterior cervical nodes enlarged and tender
• Breath odour
• Fever
Diagnostic Tests
• If uncomplicated, none
MANAGEMENT AND INTERVENTIONS
Goals of Treatment
• Relieve symptoms
• Prevent spread of infection
Non Pharmacologic Interventions
• Warm saline rinses (1 tsp in 1 cup of warm water) qid
• Ice pack wrapped in a towel against the cheek to reduce pain and swelling
DST-301 Dental Abscess: Adult
85
Certified Practice Area:
RN First Call
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
PHARMACOLOGIC INTERVENTIONS
• Analgesics for mild to moderate pain:
o Acetaminophen 325mg, 1-2 tabs po q4-6h prn, or
o Ibuprofen 200mg, 1-2 tabs po q4-6h prn
• Oral antibiotic therapy:
o Penicillin VK 300mg, 1-2 tabs po qid for 7 days
o Amoxicillin 500mg, po bid or tid for 5 days
• For clients with penicillin allergy:
o Clindamycin 150-300 mg, po qid for 7 days
Note: Clindamycin can cause pseudomembranous colitis with diarrhea, severe abdominal cramps and blood or
mucous in the stool. Do not use if there is a history of gastrointestinal disease. Clients must be advised to seek medical attention immediately if they experience persistent diarrhea, stomach pain or cramping, or notice blood or mucous in the stool during and following treatment with clindamycin.
Pregnant and Breastfeeding Women
• Acetaminophen, Penicillin VK and Clindamycin may be used as listed above
• Do not use Ibuprofen
Potential Complications
• Cellulitis
• Recurrent abscess formation
• Systemic infection
• Osteomyelitis
• Sepsis
Client Education and Discharge Information
• Counsel client about appropriate use of medications (dosage and side effects)
• Recommend dietary modifications as indicated – limit consumption of sugary drinks
• Recommend dental hygiene or improvement to dental hygiene
• Make dental appointment
CONSULTATION AND/OR REFERRAL
• Consult a physician or nurse practitioner if a large fluctuant abscess is present
• Refer if client is acutely ill, if the infection has spread to the soft tissues of the neck, or if there is no response in 48-72 hours
• Refer immediately if facial swelling beyond midline or client has intractable pain
• Refer to a dentist for definitive therapy
MONITORING AND FOLLOW-UP
• Follow up in 48-72 hours
DOCUMENTATION
• As per agency policy
DST-301 Dental Abscess: Adult

86
Certified Practice Area:
RN First Call
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
REFERENCES
More recent editions of any of the items in the Reference List may have been published since this DST was published. If you have a newer version, please use it.
Blondel-Hill, E., & Fryters, S. (2012). Bugs and drugs: An antimicrobial infectious diseases reference. Edmonton, AB: Alberta Health Services.
Canadian Dental Association. Antimicrobial treatment options in the management of odontogenic infections.
Cash, J. C., & Glass, C. A. (Eds.). (2014). Family practice guidelines (3rd ed.). New York, NY: Springer.
Chen, A., and Tran, C. (2011). Comprehensive Medical Reference and Review for MCCQE and USMLE II. Toronto Notes for Medical Students. Toronto, On: Toronto Notes for Medical Students, Inc.
Chow, A.W. (2016). Complications, diagnosis, and treatment of odontogenic infections. UpToDate.
Chow, A. W. (2015). Epidemiology, pathogenesis, and clinical manifestations of odontogenic infections. UptoDate [Intranet].
DynaMed. (2015, March 31). Acute apical dental abscess.
Gould, J. M. (2015, April 22). Dental abscess.
Gregoire, C. (2010). How are odontogenic infections best managed? Journal of the Canadian Dental Association.76 (a37).
Peng, L. F. (2015, February 27). Dental infections in emergency medicine.
DST-301 Dental Abscess: Adult

Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
Remote Nursing
Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
DST-401 Cardio-Respiratory Assessment: Adult
This decision support tool is effective as of August 2020. For more information or to provide feedback on this or any other decision support tool, email [email protected]
Nurses with Remote Nursing Certified Practice designation (RN(C)s) are able to manage the following cardio-respiratory condition:
• Acute bronchitis
The following assessment must be completed and documented. Cardiac and respiratory systems can significantly interact, and thus, examination of both systems is presented in this DST.
CARDIO-RESPIRATORY ASSESSMENT
History of Present Illness and Review of Systems
General
The following characteristics of each sign or symptom should be elicited and explored:
• Onset (sudden or gradual)
• Chronology
• Current situation (improving or deteriorating)
• Location
• Radiation
• Quality
• Timing (frequency, duration)
• Severity
• Precipitating and aggravating factors
• Relieving factors
• Associated symptoms
• Current situation (improving or deteriorating)
• Effects on Activities of Daily Living (ADL)
• Previous diagnosis of similar episodes
• Previous treatments and efficacy
Cardinal Signs and Symptoms
In addition to the general characteristics outlined above, additional characteristics of specific symptoms should be elicited, as follows:
Cough
• Quality
• Severity
• Timing
• Duration: If duration greater than 2 weeks screen for tuberculosis (TB)
Sputum
• Colour
• Amount
• Consistency
DST-401 Cardio-Respiratory Assessment: Adult
Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
• Purulence, odour, foul taste
• Time of day when sputum increases
Hemoptysis
• Amount of blood
• Frank blood or frank blood mixed with sputum
• Association with leg pain, chest pain, shortness of breath
Shortness of Breath
• Exercise tolerance (number of stairs client can climb, or distance client can walk)
• Posture – orthopnea or tripoding
• Shortness of breath at rest
• Association with paroxysmal nocturnal dyspnea (PND)
• Associated swelling of ankles or recent weight gain
Cyanosis
• Central vs peripheral
• Frequency and/or triggers of occurrence
• Any recent changes in pattern
• Associated wheeze
Chest Pain
• Associated symptoms such as nausea, sweats, shortness of breath, anxiety, palpitations
• Relation to effort, exercise, meals, bending over
• Explore all aspects of the pain – include location, quality, radiation, severity, timing, and others
Fainting or Syncope
• Weakness, light-headedness, loss of consciousness
• Relation to postural changes, vertigo, or neurological symptoms
Extremities
• Edema:
o site and extent of edema
o relation of edema to activity or time of day
• Intermittent claudication (exercise-induced leg pain)
o distance client can walk before onset of pain related to claudication
o time needed to rest to relieve claudication
o temperature of affected tissue (warm, cool or cold)
• Tingling
• Leg cramps or pain at rest
• Presence of varicose veins
DST-401 Cardio-Respiratory Assessment: Adult
Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
Associated Symptoms
• Fever
• Malaise
• Fatigue
• Night sweats
• Weight loss
• Palpitations
• Nausea and vomiting
• Gastroesophageal reflux
MEDICAL HISTORY
Medical Conditions and Surgeries
• Medical conditions and surgeries
• Allergies (seasonal, environmental, medication)
• Medication currently used:
o Prescription, contraceptive, over-the-counter
o Herbal preparations, vitamins, minerals, supplements and traditional therapies
• Immunizations status (e.g. pneumococcal, annual influenza)
• Medical conditions:
o Frequency of colds and respiratory infections, recent viral illness, joint pain or swelling
o History of rheumatic fever
o Nasal polyps, chronic sinusitis, asthma, bronchitis, pneumonia, chronic obstructive pulmonary disease, TB (disease or exposure), cancer, cystic fibrosis
o Dyslipidemia, hypertension, diabetes mellitus, thyroid disorder, chronic renal disease, systemic lupus erythematosus
o Coronary artery disease, angina, myocardial infarction,
o History of thrombosis, prolonged immobilization
o Cardiac murmurs, valvular heart disease
o Down Syndrome
• Admissions to hospital and/or surgery for respiratory or cardiac illness
• Date and result of last Mantoux test and chest x-ray
• Blood transfusion
Family History
• Others at home with similar symptoms
• Allergies, atopy
• Asthma, lung cancer, TB, cystic fibrosis, bronchitis
• Diabetes mellitus
• Heart disease: hypertension, ischemic coronary artery disease, MI (especially in family members less than 50 years of age), sudden death from cardiac disease, dyslipidemia, hypertrophic cardiomyopathy
DST-401 Cardio-Respiratory Assessment: Adult
Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
Personal and Social History
• Substance use such as smoking tobacco, chewing tobacco, alcohol, cannabis, illicit drugs
• If substance abuse history, note amounts, duration, last used and others
• Exposure to second-hand smoke, wood smoke, pets, mould
• Crowded living conditions
• Poor personal or environmental cleanliness
• High stress levels (personal or occupational)
• Institutional living
• Occupational or environmental exposure to respiratory irritants (miner, firefighter)
• Human immunodeficiency virus (HIV) risks
• Obesity
• Immigration or travel abroad
Physical Assessment
Examination of the ear, nose, and throat should also be carried out because of the interrelatedness between these systems and
structures and the functioning of the lower respiratory tract
Vitals
• Temperature
• Pulse
• Respiration
• SpO2
• Blood pressure
o Orthostatic changes
o Pulsus paradoxus
• Ankle-brachial index (ABI)
• Pain
General
• Apparent state of health
• Appearance of comfort or distress
• Position to aid respiration (e.g. tripod)
• Diaphoresis
• Ability to speak a normal-length sentence without stopping to take a breath
• Colour: skin
• Nutritional status
• Hydration status
• Mental status
• Hygiene
• Match between appearance and stated age
• Acutely or chronically ill
DST-401 Cardio-Respiratory Assessment: Adult
Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
Inspection
• Colour, cyanosis
• Shape of chest
• Symmetry of chest movement
• Rate, rhythm and depth of respiration, respiratory distress
• Intercostal indrawing
• Use of accessory muscles
• Precordium: visible pulsations
• Chest wall scars, bruising, signs of trauma
• Jugular venous pressure
• Colour of conjunctiva
• Extremities
• Hands: edema, cyanosis, clubbing, nicotine stains, cap refill greater than 2 seconds
• Feet and legs:
o Changes in foot colour with changes in leg position (blanching with elevation, rubor of dependency)
o Ulcers, edema (check sacrum if client is bedridden)
o Colour (pigmentation, discolouration)
o Distribution of hair
o Varicose veins
• Skin – rashes, lesions, xanthomas
Palpation
• Tracheal position (midline)
• Chest wall tenderness or crepitus
• Respiratory excursion
• Tactile fremitus
• Spinal abnormality
• Lymph nodes (axillary, supraclavicular, cervical)
• Masses
• Apical beat:
o Point of maximal impulse (PMI) normally located at the fifth intercostal space, mid-clavicular line
o Assess quality and intensity of apical beat
o Apical beat may be laterally displaced, which indicates cardiomegaly
• Identify and assess pulsations and thrills
• Hepatomegaly, right upper quadrant (RUQ) tenderness
• Assess peripheral pulses – radial, brachial, femoral, popliteal, posterior tibial, dorsalis pedis
o Check for synchrony of radial and femoral pulses
• Edema: pitting (grade 1 to 4) and level (how far up the feet and legs the edema extends); sacral edema
DST-401 Cardio-Respiratory Assessment: Adult
Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
Percussion of Lung Fields
• Resonance
o Increased resonance over hyperinflated areas
o Dullness to percussion over areas of consolidation
o Location and excursion of the diaphragm
Auscultation of Lungs
• Listen for sounds of normal air entry before trying to identify abnormal sounds
• Degree of air entry throughout the chest (should be equal)
• Quality of breath sounds (e.g. bronchial, bronchovesicular, vesicular)
• Ratio of inspiration to expiration
• Adventitious sounds:
o Wheezes (rhonchi), crackles (rales), pleural rub, stridor, decreased breath sounds
Auscultation of Heart
• Listen to normal heart sounds before trying to identify murmurs
• Auscultate at aortic, pulmonic, Erb’s point, tricuspid and mitral valve
• Attempt to identify:
o Rate and rhythm
o S1 and S2 sounds and their intensity
o Added heart sounds (S3 and S4), rubs, splitting of S2
o Murmur
• Auscultate carotid arteries, abdominal aorta, renal arteries, iliac arteries, and femoral arteries for bruits
Associated Systems
• A complete respiratory assessment includes the Ear, Nose and Throat (ENT) system
DST-401 Cardio-Respiratory Assessment: Adult
Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
Diagnostic Tests
The RN(C) may consider the following diagnostic tests in the examination of the cardio-respiratory system to support clinical decision making:
• Electrocardiogram (ECG)
• Complete Blood Count (CBC)
• Cardiac troponins
• Sputum for Culture and Sensitivity (C&S)
SYMPTOMS REQUIRING URGENT REFERRAL
The first step is to differentiate acute cardio-respiratory distress and cardio-respiratory conditions that can be managed safely by
RN(C)s.
New onset of the following signs and symptoms require immediate emergency care and referral to a physician or nurse
practitioner:
• Severe dyspnea and inability to lay flat
• Inability to speak or fragmented speech
• Tracheal shift
• Unrelieved chest pain
• Unable to maintain SpO2 92% or greater on room air
• Cyanosis (central or peripheral cyanosis)
• Severe increasing fatigue
• Silent chest or crackles throughout lung fields
• Decreased level of consciousness
• Diminishing respiratory effort
• Nasal flaring or tracheal tug
• Intercostal indrawing
• Recent hospitalization for heart failure (HF)
DST-401 Cardio-Respiratory Assessment: Adult

Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
REFERENCES
More recent editions of any of the items in the Reference List may have been published since this DST was published. If you have a newer version, please use it.
Ashley, Euan A., and Josef Niebauer. Cardiovascular Examination. Cardiology Explained. Remedica, 2004.
Ball, Jane, Joyce E. Dains, John A. Flynn, Barry S. Solomon, and Rosalyn W. Stewart. Seidel’s Guide to Physical Examination: An Interprofessional Approach. Ninth edition. St. Louis, Missouri: Mosby, 2018.
Klostranec, Jesse M., and David L. Kolin, eds. Toronto Notes Medical Reference & Review for MCQE I & USMLE II. 28th ed. Toronto, ON: Toronto Notes for Medical Students, Inc., 2012.
Dains, J. E., Baumann, L. C., & Schiebel, P. (Eds.). (2015). Advanced health assessment and clinical diagnosis in primary care. St. Louis, MO: Elsevier.
Estes, M. E. Z. (2014). Health assessment and physical examination (5th ed.). Clifton Park, NY: Cengage Learning.
Health Canada, First Nations and Inuit Health Branch. (2012). Clinical practice guidelines for nurses in primary care.
Heuer, A. J., & Scanlan, C. L. (2017). Wilkins’ clinical assessment in respiratory care (8th ed.). Maryland Heights, MO: Elsevier Mosby.
Hogan-Quigley, B., Palm, M. L., Bickley, L. S. (2016). Canadian Bates’ guide to health assessment for nurses (2nd ed.). Philadelphia, PA: Lippincott, Williams & Wilkins.
Jarvis, C. (2019). Physical examination and health assessment (3rd Canadian ed.). Toronto, ON: Elsevier Canada.
Provincial Health Services Authority. (2006). Asthma protocol: Health Authority acute asthma management toolkits.
Reese Doyle, Glynda, and Jodie Anita McCutcheon. Section 2.7 Focused Assessments in Chapter 2: Patient Assessment, Version 1.4. In Clinical Procedures for Safer Patient Care- Focused Assessments, 2019.
Shea, Michael J, and Jessica I Gupta. Cardiovascular Examination. In Merck Manual Professional, Version 6. Merck Sharp & Dohme Corp., n.d.
Suneja, M., Szot, J. F., LeBlond R. F., Brown D. D (?). DeGowin’s diagnostic examination (11th ed.). New York, NY: McGraw-Hill Medical.
University of Toronto. Clinical Skills Assessment & Feedback Tool, 2020.
DST-401 Cardio-Respiratory Assessment: Adult
Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
DST-402 Cardio-Respiratory Assessment: Pediatric
Nurses with Remote Certified Practice designation (RN(C)s)4 are able to conduct an assessment,and must consult with and/or refer to a physician or NP as appropriate.
The following assessment must be completed and documented. As a complete respiratory exam includes a cardiovascular exam, these two examinations have been combined.
ASSESSMENT
History of Present Illness and Review of System
General
The following characteristics of each symptom should be elicited and explored:
• Onset – sudden or gradual
• Location – radiation
• Duration – frequency, chronology
• Characteristics – quality, severity
• Associated symptoms
• Aggravating and precipitating factors
• Relieving factors
• Current situation (improving or deteriorating)
• Effects on Activities of Daily Living (ADL)
• Previous diagnosis of similar episodes
• Previous treatments and efficacy
Cardinal Signs and Symptoms
In addition to the general characteristics outlined above, additional characteristics of specific symptoms should be elicited, as
follows:
Cough
• Quality
• Severity
• Timing
• Duration: greater than 2 weeks screen for Tuberculosis (TB)
Sputum
• Colour
• Amount
• Consistency
• Purulence, odour, foul taste
• Time of day worse
4 RN(C) is an authorized title recommended by CRNBC that refers to CRNBC-certified RNs, and is used throughout this Decision
Support Tool (DST).
DST-402 Cardio-Respiratory Assessment: Pediatric
Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
Hemoptysis
• Amount of blood
• Frank blood or mixed with sputum
• Association with leg pain, chest pain, shortness of breath
Shortness of Breath
• Tachypnea, grunting, nasal flaring or retractions
• Shortness of breath at rest
• Posture - orthopnea or tripoding
• Association with paroxysmal nocturnal dyspnea
Cyanosis
• Central vs peripheral
• When does it occur
• Any recent changes in pattern of
• Associated wheeze
Exercise Intolerance
• Infants:
o Eats slowly, tires during feeding
o Cyanosis appears with feeding
o Often described by parents or caregiver as a “good baby”: always quiet, sleeps a lot
• Children:
o Exercise intolerance, inability to keep up with other children same age
Wheeze
• Timing
Chest Pain
• Relation to effort, exercise, meals, bending over
• Explore the pain carefully. Include quality, radiation, severity, timing
Fainting or Syncope
• Weakness, light-headedness, loss of consciousness
• Relation to postural changes, vertigo or neurological symptoms
Other Associated Symptoms
• Fever
• Malaise
• Fatigue
• Anorexia
• Night sweats
• Weight loss
• Palpitations
• Nausea and vomiting
• GI reflux
DST-402 Cardio-Respiratory Assessment: Pediatric
Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
• Runny nose
• Sore throat
• Stridor
Medical History (Specific to Cardio-Respiratory System)
• Allergies, including seasonal and environmental
• Medications currently used (over the counter (OTC), birth control pills (BCP) and prescription including nasal sprays and
inhaled medication (puffers), antihistamines, hormones, steroids, antacids)
• Herbal / traditional preparations
• Growth rate – if failure to thrive, children often exhibit slow weight gain relative to height
• Immunization status including pneumococcal and influenza
• Medical conditions
o Frequency of colds and respiratory infections, recent viral illness, joint pain or swelling
o History of rheumatic fever
o Nasal polyps, chronic sinusitis, asthma (Appendix 1), bronchitis, pneumonia, chronic obstructive pulmonary disease
(COPD), TB (disease or exposure), cancer, cystic fibrosis
o Diabetes mellitus, thyroid disorder, renal disease
o Cardiac murmurs, valvular heart disease
o Down’s syndrome
• Admissions to hospital and/or surgery for respiratory or cardiac illness
• Date and result of last Mantoux test and chest x-ray
• Communicable diseases: measles, chickenpox (varicella), herpes simplex
• Birth and prenatal history if age appropriate
• Exposure to substances while in utero
• Blood transfusion
Family History (Specific to Cardio-Respiratory System)
• Others at home with similar symptoms
• Allergies, atopy
• Asthma (Appendix 1), TB, cystic fibrosis, bronchitis
• Diabetes mellitus
• Sudden Infant Death (SIDS)
• Heart disease
Personal and Social History (Specific to Respiratory System)
• Smoking history (number of packages/day, number of years)
• Exposure to second-hand cigarette smoke, wood smoke, pets, mould
• Crowded living conditions
• Poor personal or environmental cleanliness
• High stress levels
• Institutional living
• Substance use – alcohol, caffeine, street drugs, including injection and inhaled drugs / solvents
• Human immunodeficiency virus (HIV)
• Obesity
• Immigration or travel abroad
DST-402 Cardio-Respiratory Assessment: Pediatric
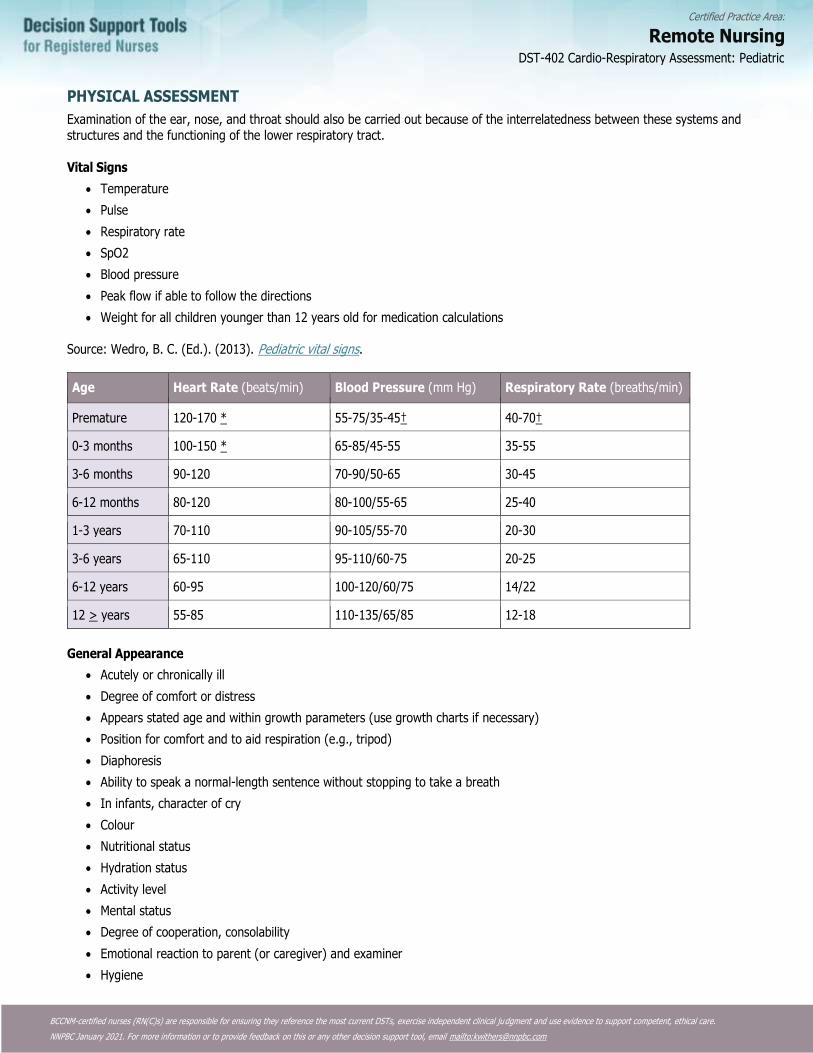
Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
PHYSICAL ASSESSMENT
Examination of the ear, nose, and throat should also be carried out because of the interrelatedness between these systems and structures and the functioning of the lower respiratory tract.
Vital Signs
• Temperature
• Pulse
• Respiratory rate
• SpO2
• Blood pressure
• Peak flow if able to follow the directions
• Weight for all children younger than 12 years old for medication calculations
Source: Wedro, B. C. (Ed.). (2013). Pediatric vital signs.
Age Heart Rate (beats/min) Blood Pressure (mm Hg) Respiratory Rate (breaths/min)
Premature 120-170 * 55-75/35-45† 40-70†
0-3 months 100-150 * 65-85/45-55 35-55
3-6 months 90-120 70-90/50-65 30-45
6-12 months 80-120 80-100/55-65 25-40
1-3 years 70-110 90-105/55-70 20-30
3-6 years 65-110 95-110/60-75 20-25
6-12 years 60-95 100-120/60/75 14/22
12 > years 55-85 110-135/65/85 12-18
General Appearance
• Acutely or chronically ill
• Degree of comfort or distress
• Appears stated age and within growth parameters (use growth charts if necessary)
• Position for comfort and to aid respiration (e.g., tripod)
• Diaphoresis
• Ability to speak a normal-length sentence without stopping to take a breath
• In infants, character of cry
• Colour
• Nutritional status
• Hydration status
• Activity level
• Mental status
• Degree of cooperation, consolability
• Emotional reaction to parent (or caregiver) and examiner
• Hygiene
DST-402 Cardio-Respiratory Assessment: Pediatric
Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
• Bruising, contusions, abrasions (suggestive of trauma)
Inspection
• Anxious appearance or respiratory distress
• Colour, cyanosis
o Acrocyanosis may be normal in infants (< 1month)
• Shape of chest
o An infant’s chest is barrel shaped slowly becoming adult like by 6 yrs
• Symmetry of chest movement
• Rate, rhythm and depth of respiration
• Tripoding, nasal flaring, drooling, grunting
• Intercostal indrawing, tracheal tug
• Accessory muscle use and respiratory distress
• Precordium: visible pulsations may be normal
• Chest wall scars, bruising, signs of trauma
• Tingling
• Leg cramps or pain at rest
• Clubbing of the fingers
• Rashes or eczema
• Audible grunting, wheezing
• Hands - cyanosis, clubbing, nicotine stains, cap refill (<3 seconds)
• Edema
Palpation
• Not as useful in children less than 3 years
• Tracheal position (midline)
• Chest wall tenderness or crepitus
• Respiratory excursion and tactile fremitus in older children
• Spinal abnormality
• Nodes (axillary, supraclavicular, cervical)
• Masses
• Apical beat:
o Point of maximum impulse (PMI) in infants and toddlers at fourth intercostal space and just left of midclavicular line
o PMI in child 7 yrs and older is at fifth intercostals space and just right of midclavicular line
• Identify and assess pulsations and thrills
• Hepatomegaly
• Assess peripheral pulses – radial, brachial, femoral, popliteal, posterior tibial, dorsalis pedis.
o Capillary refill
o Edema – degree of pitting
o Skin temperature, turgor
Percussion
• Useful in children greater than 2 yrs
• Resonance
DST-402 Cardio-Respiratory Assessment: Pediatric
Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
o Increased resonance over hyperinflated areas
o Dullness to percussion over areas of consolidation
Auscultation
• Listen for sounds of normal air entry before trying to identify abnormal sounds
• Degree of air entry throughout the chest (should be equal)
• Quality of breath sounds- vesicular, bronchovesicular and bronchial
o Broncho-vesicular sounds are heard throughout the peripheral lung field up to 5-6 years
• Ratio of inspiration to expiration
• Adventitious Sounds:
o Wheezes (rhonchi), crackles (rales), pleural rub, stridor, decreased breath sounds
• Transmitted upper airway sounds such as nasal congestion are commonly noted in small children
• Listen to normal heart sounds before trying to identify murmurs
• Auscultate at aortic, pulmonic, Erb’s point, tricuspid, and mitral. Attempt to identify:
• Rate and rhythm.
• S1 and S2 sounds and their intensity
• Added heart sounds (S3 and S4), rubs, splitting of S2 and relation to respiration
• Murmurs and if noted, relation to position
• Auscultate carotid arteries, abdominal aorta, renal arteries, iliac arteries, and femoral arteries for bruits
Note: Fifty percent of children develop an innocent murmur at some time in their lives
Associated Systems
• A complete cardio-respiratory assessment includes the ENT system
• Consider GI/GU assessment if appropriate.
Symptoms requiring urgent referral or consultation
Children less than six months require consultation
The first step is to differentiate between acute cardio-respiratory distress and conditions that can be managed safely by RN(C)s.
• The following signs and symptoms require immediate referral to a physician or nurse practitioner:
• Drooling and / or tripoding
• Lethargy and fatigue
• Inability to speak or cry
• SOB and tachypnea greater than 60 breaths/minute
• Diminishing respiratory effort
• Tracheal shift
• Tracheal tugging
• Nasal flaring and head bobbing
• Intercostal indrawing
• Chest pain
• SpO2 less than 92% on room air
DST-402 Cardio-Respiratory Assessment: Pediatric

Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
• Cyanosis (central cyanosis is not detectable until SaO2 is less than 85%)
• Silent chest
• Decreased level of consciousness, blackouts
• Immuno-compromised
• Poor feeding and weight gain in infants and young children
• Extra heart sounds or murmurs
• Apneic or hypoxic spells
• Persistent tachycardia
RN(C)s are able to conduct an assessment. Cardio-respiratory presentations must be assessed and treated in consultation with and/or referral to a physician or nurse practitioner as appropriate.
DST-402 Cardio-Respiratory Assessment: Pediatric
Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
REFERENCES
More recent editions of any of the items in the Reference List may have been published since this DST was published. If you have a newer version, please use it.
Ball, J. W., Dains, J. E., Flynn, J. A., Solomon, B. S., & Stewart, R. W. (Eds.). (2015). Seidel’s guide to physical examination (8th ed.). St. Louis, MO: Elsevier.
Burns, C. E., Dunn, A. M., Brady, M. A., Starr, N. B., & Blosser, C. G. (2009). Pediatric primary care (5th ed.). Philadelphia, PA: Elsevier.
Dains, J. E., Baumann, L. C., & Schiebel, P. (Eds.). (2015). Advanced health assessment and clinical diagnosis in primary care. St. Louis, MO: Elsevier.
Estes, M. E. Z. (2014). Health assessment and physical examination (5th ed.). Clifton Park, NY: Cengage Learning.
Heuer, A. J., & Scanlan, C. L. (2014). Wilkins’ clinical assessment in respiratory care (7th ed.). Maryland Heights, MO: Elsevier Mosby.
Jarvis, C. (2014). Physical examination and health assessment (2nd Canadian ed.). Toronto, ON: Elsevier Canada.
Provincial Health Services Authority. (2009). Asthma protocol: Health Authority acute asthma management toolkits.
Sawyer, S. S. (Ed.). (2014). Pediatric physical examination & health assessment. Mississauga, ON: Jones & Bartlett.
DST-402 Cardio-Respiratory Assessment: Pediatric
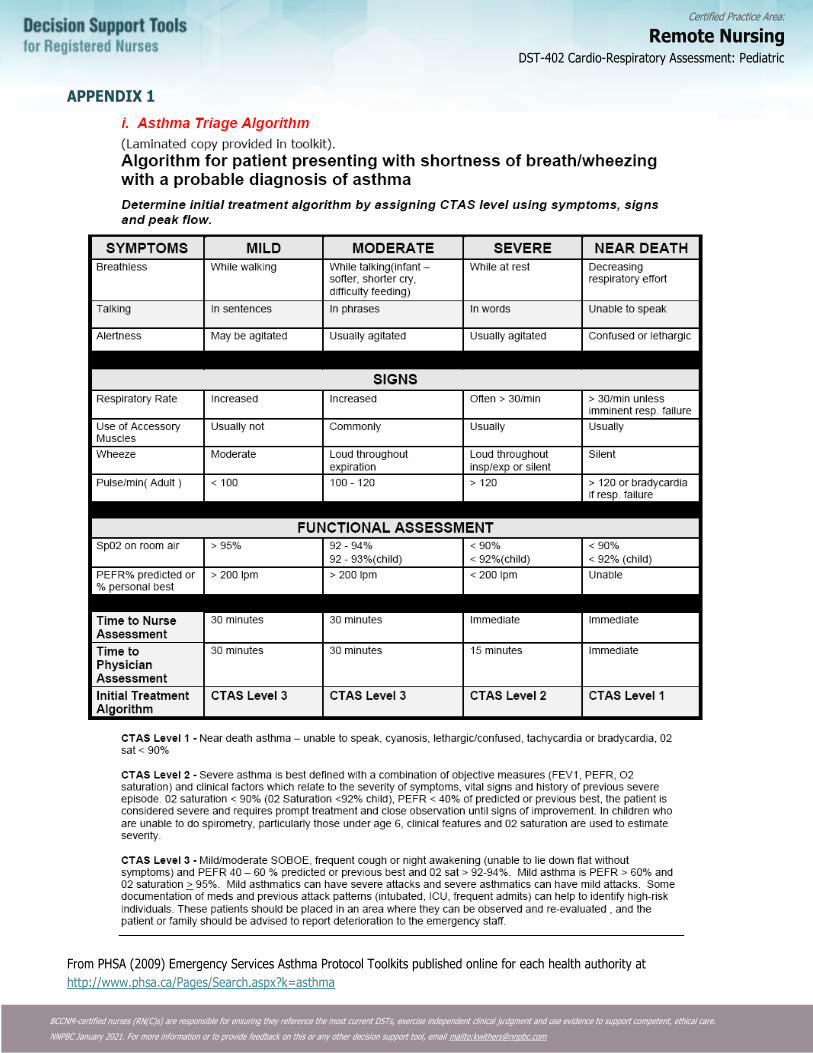
Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
APPENDIX 1
From PHSA (2009) Emergency Services Asthma Protocol Toolkits published online for each health authority at
http://www.phsa.ca/Pages/Search.aspx?k=asthma
DST-402 Cardio-Respiratory Assessment: Pediatric
Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
DST-403 Bronchitis Acute: Adult
DEFINITION
Inflammation of trachea and bronchi (larger airways)
Potential Causes
Viral infection: 90% of cases
• Influenza A or B, adenovirus, rhinovirus, para-influenzae, corona virus, Respiratory Syncytial Virus (RSV), human
metapneumovirus
Bacterial infection: 10% of cases
• Mycoplasma pneumoniae, Chlamydia pneumoniae, Bordetella pertussis possible causes
• Streptococcus pneumoniae and H. Influenziae usually only causative organisms if there is underlying lung disease
Predisposing Risk Factors
• Chronic sinusitis
• Chronic Obstructive Pulmonary Disease (COPD)
• Asthma
• Bronchiectasis
• Immunocompromised (chronic asthma)
• Smoking
• Second hand smoke
• Air pollutants, environmental factors
• Alcoholism
• Gastro Esophageal Reflux Disease (GERD)
• Wood stoves
• Mould
Typical Findings of Acute Bronchitis
Initially the presentation of acute bronchitis is difficult to distinguish from an Upper Respiratory Tract Infection (URTI).
Later the presentation of acute bronchitis and pneumonia are often similar. In general, clients with pneumonia are sicker and usually have more chest abnormalities.
The organisms that cause bronchitis can also cause pneumonia. The difference is in where the infection lies anatomically. Bronchitis involves the larger airways, whereas pneumonia involves the smaller airways and air sacs.
History
• Previous infection of Upper Respiratory Tract (URT)
• General malaise
• Fever
• Cough: initially dry, later productive of white, yellow or green sputum
• Cough for more than 5 days
o Cough often lasts 10-20 days
o 45% still have a cough after two weeks, and 25% still have a cough after 3 weeks
• Muscular aching in the chest wall or discomfort with coughing
• Wheezing may be present
• Dyspnea on exertion may be present
DST-403 Bronchitis Acute: Adult
Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
PHYSICAL ASSESSMENT
• Temperature may be mildly to moderately elevated
• Pulse may be mildly elevated if febrile
• Respirations may be slightly elevated
• Purulent sputum is common in 50% of cases
• Rhinitis may be present
• Expiratory phase may be slightly prolonged
• Wheezes (scattered, low pitched) may be present
• Abnormal vital signs (fever, tachypnea or tachycardia) and signs of consolidation or rales on physical exam suggest the
possibility of pneumonia
Diagnostic tests
• Electrocardiogram (ECG), Culture and Sensitivity (C&S) of sputum
• Consider swab for pertussis, particularly if cough lasts more than 6 days and is accompanied by vomiting
• Consider Tuberculosis (TB) skin test for cough greater than 2 weeks and in high risk or susceptible populations
MANAGEMENT AND INTERVENTIONS
Goals of Treatment
• Relieve symptoms (coughing, fever)
• Prevent pneumonia
Non-pharmacological interventions
• Increased rest (especially if febrile)
• Adequate hydration (8-10 glasses of fluid per day)
• Increased humidity in the environment
• Avoidance of pulmonary irritants (e.g., stop or decrease smoking)
PHARMACOLOGICAL INTERVENTIONS
• To manage fever or pain
o Acetaminophen 325 mg 1-2 tabs po q4-6h prn
OR
o Ibuprofen 200 mg 1-2 tabs po q4-6h prn
• If bronchospasm, dyspnea or wheezing is significant, short-acting ß2-agonist bronchodilators can be used until acute
symptoms resolve
o Salbutamol 100mcg Metered-Dose Inhaler (MDI) 1 or 2 puffs q4h prn via aero chamber-maximum dose of 8 puffs/day
• Avoid antibiotics
In most cases, antibiotics are not recommended for acute bronchitis in an otherwise healthy client, as the cause is usually viral.
• Antibiotics may be considered in those at high risk of serious complications because of pre-existing co-morbidity (heart, lung,
renal, liver, or neuromuscular disease, Congestive Heart Failure, diabetes mellitus, current use of oral glucocorticoids,
immunocompromised)
• In clients with an acute bronchitis overlying chronic bronchitis, antibiotics may be considered for clients who have two or
more of the following symptoms:
o Increased sputum volume
DST-403 Bronchitis Acute: Adult
Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
o Increased sputum purulence
o Increased dyspnea
Choices:
• Amoxicillin 500 mg po tid for 5-7 days
OR
• Doxycycline 200 mg once, then 100 mg po bid for 5-7 days
OR
• Trimethoprim 160 mg / Sulphamethoxazole 800 mg (DS) po bid for 5-7 days
Pregnant or Breastfeeding Women:
• Amoxicillin may be used as listed above.
• DO NOT USE doxycycline and Trimethoprim 160 mg / Sulphamethoxazole 800 mg.
Potential Complications
• Pneumonia
• Post-bronchitis cough
Client Education and Discharge Information
• Recommend hand washing to prevent spread of infection throughout a household
• Inform client that cough may persist for more than 2 weeks
• Inform client that routine antibiotic therapy is not necessary or recommended
Monitoring and Follow-Up
Arrange for follow up in 2-3 days if antibiotics are used and the client’s condition is not resolving.
Consultation and/or Referral
Consult with or refer to physician and/or nurse practitioner if unresponsive to treatment or if pneumonia is suspected.
Documentation
As per agency policy.
DST-403 Bronchitis Acute: Adult

Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
REFERENCES
More recent editions of any of the items in the Reference List may have been published since this DST was published. If you have a newer version, please use it.
Balter, M. S., La Forge, J., Low, D. E., Mandell, L., & Grossman, R. F. (2003). Canadian guidelines for the management of acute exacerbations of chronic bronchitis. Canadian Respiratory Journal, 10 (Suppl B), 3B-32B.
Blondel-Hill, E., & Fryters, S. (2012). Bugs and drugs: An antimicrobial infectious diseases reference. Edmonton, AB: Alberta Health Services.
Blush III, R. R. (2013). Acute bronchitis. Nurse Practitioner, 38(10), 14-20.
Canadian Pharmacists Association. (2014). Therapeutic choices (7th ed.). Ottawa, ON: Author
Carolan, P. L. (2014, March 18). Pediatric bronchitis.
Cash, J. C., & Glass, C. A. (Eds.). (2014). Family practice guidelines (3rd ed.). New York, NY: Springer.
Chen, Y. A., & Tran, C. (Eds.). (2011). The Toronto notes 2011: Comprehensive medical reference and review for the Medical Council of Canada Qualifying Exam Part 1 and the United States Medical Licensing Exam Step 2 (27th ed.). Toronto, ON: Toronto Notes for Medical Students.
DynaMed. (2015, November 20). Acute Bronchitis.
DynaMed. (2015, August 10). Aspiration Pneumonia.
Esherick, J. S., Clark, D. S., & Slater, E. D. (2012). Current practice guidelines in primary care 2012. New York, NY: McGraw-Hill Medical.
Esherick, J. S., Clark, D. S., & Slater, E. D. (Eds.). (2013). Current practice guidelines in primary care. New York, NY: McGraw Hill Medical.
Fayyaz, J. (2015). Bronchitis.
Klostranec, J. M., & Kolin, D. L. (2012). The Toronto notes 2012: Comprehensive medical reference and review for the Medical Council of Canada Qualifying Exam Part 1 and the United States Medical Licensing Exam Step 2 (28th ed.). Toronto, ON: Toronto Notes for Medical Students.
Kuehn, B. M. (2013). Excessive antibiotic prescribing for sore throat and acute bronchitis remains common. JAMA: The Journal of the American Medical Association, 310(20), 2135-2136.
Tackett, K. L., & Atkins, A. (2012). Evidence-based acute bronchitis therapy. Journal of Pharmacy Practice, 25(6), 586-590.
DST-403 Bronchitis Acute: Adult
Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
DST-501 GI-GU Assessment: Adult
GASTROINTESTINAL (GI) - GENITOURINARY (GI) ASSESSMENT
As a complete genitourinary exam includes a gastrointestinal exam, these two examinations have been combined.
Nurses with Remote Nursing Certified Practice designation (RN(C)s) are able to manage the following genitourinary conditions:
• Lower Urinary Tract Infection (UTI)
History of Present Illness and Review of Systems
General Characteristics
The following characteristics of each symptom should be elicited and explored:
• Onset (sudden or gradual)
• Chronology
• Current situation (improving or deteriorating)
• Location
• Radiation
• Quality
• Timing (frequency, duration)
• Severity
• Precipitating and aggravating factors
• Relieving factors
• Associated symptoms
• Effects on daily activities
• Previous diagnosis of similar episodes
• Previous treatments
• Efficacy of previous treatments
Cardinal Signs and Symptoms
In addition to the general characteristics outlined above, additional characteristics of specific symptoms should be elicited, as follows:
Abdominal Pain
• Quality: sharp, burning, cramping
• Quantity: constant, intermittent
• Radiation: localized, generalized
• Timing: related to eating or movement
• Severity
• Consider GU indicators: flank, suprapubic, genital, groin or lower back pain and tenderness
Nausea and Vomiting
• Frequency, amount
• Presence of bile
• Hematemesis (red or coffee ground emesis)
• Force
• Colour
• Relationship to food intake
DST-501 GI-GU Assessment: Adult
Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
Dysphagia
• Solids or liquids
• Site where food gets stuck
• Whether food is regurgitated
Bowel Habits
• Last bowel movement
• Frequency, colour and consistency of stool
• Presence of blood or melena
• Pain before, during or after defecation
• Sense of incomplete emptying after bowel movement
• Use of laxatives: type and frequency
• Tenesmus
• Hemorrhoids
• Belching, bloating and flatulence
• Change in bowel habits
Urinary Symptoms
• Frequency, urgency, quantity
• Dysuria and its timing during voiding (at the beginning or end, throughout)
• Difficulty in starting or stopping urinary stream
• Change in colour and odour of urine
• Hematuria
• Incontinence (including urge and stress)
• Presence of stones or sediment in the urine
• Nocturia (new onset or increase in usual pattern)
• Urinary retention
• For men: post-void dribbling and/or feels bladder is incompletely empty
Jaundice
• Scleral icterus
• Tea-coloured urine
• Clay-coloured bowel movements
• Pruritus (itching)
• History of hepatitis A, hepatitis B or hepatitis C
GU Symptoms – Female
Where appropriate for females to rule-out ectopic pregnancy, Pelvic Inflammatory Disease (PID) or pregnancy as the cause of symptoms:
• Date of last menstrual period (LMP)
• Changes in menstrual period: frequency, amount
• Dyspareunia or post-coital bleeding
• Lesions on external genitalia
• Itching
• Urethral or vaginal discharge
• Sense of pelvic relaxation (pelvic organs feel as though they are falling down or out)
DST-501 GI-GU Assessment: Adult
Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
GU Symptoms – Male
• Testicular pain or swelling
• Discharge from penis, itching
• Lesions on external genitalia
Other Associated Symptoms
• Change in appetite
• Fever
• Malaise
• Headache
• Dehydration
• Recent weight loss or gain that is not deliberate
• Enlarged, painful nodes (axilla, groin)
• Skin: dry, rash, itchy
Medical History Specific to GI - GU Systems
• Allergies (seasonal as well as allergic reactions)
• Past and current use of medications
o Prescription and over-the-counter (OTC) medications
▪ Especially: ASA, antacids, triple therapy for peptic ulcer disease, acetaminophen, antibiotics (particularly clindamycin use within the past 2 months), laxatives, estrogen, progesterone (including birth control),
anticholinergics, antihypertensives, antipsychotics, thiazide diuretics, immunosuppressants, digoxin, codeine
▪ Herbal preparations and traditional therapies
• Immunizations
Diseases – GI
• Hiatus hernia, esophageal cancer
• Documented H. pylori, Gastroesophageal Reflux Disease (GERD) or Peptic Ulcer Disease (PUD)
• Presence of hernia, masses
• Chronic constipation
• Irritable Bowel Syndrome (IBS), Inflammatory Bowel Disease (IBD)
• Diverticulosis
• Liver disease (hepatitis A, hepatitis B, hepatitis C or cirrhosis)
• Gallbladder disease
• Pancreatitis
• Diabetes mellitus
Diseases – GU
• Sexually Transmitted Infections (STI’s), including Human Immunodeficiency Virus (HIV), Human Papilloma Virus (HIV)
• Pelvic Inflammatory Disease (PID)
• Renal disease (pyelonephritis, recurrent cystitis, renal stones)
• Congenital structural abnormalities of GU tract
• Abdominal surgery or exams, including GU such as catheterization, vasectomy, gynaecological procedures
Male
• Hydrocele
• Epididymitis
DST-501 GI-GU Assessment: Adult
Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
• Prostatism
• Varicocele
• Hernia
• Undescended testis
• Spermatocele
• Erectile dysfunction
• Testicular torsion
• Vasectomy
Female
• Menstrual History: menarche, LMP, interval, regularity, duration and amount of flow, premenstrual syndrome (PMS)
symptoms, dysmenorrhea, menopause, postmenopausal bleeding
• Obstetrical History - gravida, term, preterm, abortion, living children (GTPAL), complicated pregnancies and deliveries,
infertility
Other
• Blood transfusion
• Immunocompromised
Family History Specific to GI - GU Systems
• Household contact with hepatitis A or hepatitis B
• Household contact with gastroenteritis, recent GI infections
• Food poisoning
• GERD, PUD
• Gallbladder disease
• Gastric or colon cancer
• Polyps
• Pancreatitis
• Metabolic disease (diabetes mellitus, porphyria)
• Cardiac disease
• Renal disease (renal cancer, polycystic kidneys, renal stones)
• Urinary tract infections
Personal and Social History Specific to the GI - GU Systems
• Substance use (alcohol, smoking tobacco, chewing tobacco, street drugs [including injection drugs] anabolic steroids)
• Dietary recall including foods avoided (and reasons for), fat intake, nitrate intake (smoked foods)
• Obesity, anorexia, bulimia or other eating disorder
• Travel to area(s) where infectious GI conditions are endemic
• Body piercing or tattoos
• Stress at work, home or school
• Quality of drinking water (exposure to pollutants)
• Sanitation problems at home or in the community
• Personal hygiene, toileting habits, use of bubble bath, douches, tight-fitting underwear or other clothing
• Sexual history and practices, including risk behaviours (unprotected oral, anal or vaginal intercourse, multiple partners) and
contraceptives
DST-501 GI-GU Assessment: Adult
Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
• Symptomatic sexual partner
• Sexual or physical assault
• Fear, embarrassment, anxiety
• Missing work, school or social functions because of GU symptoms (incontinence)
Occupational or School Environment
• Healthcare occupation
• Institutional environment
• Environmental exposure
• Chemical exposure
Physical Assessment
Vitals
• Temperature
• Pulse
• Respiration
• SpO2
• Blood pressure
• Pain
General
• Apparent state of health
• Appearance of comfort or distress
• Colour
• Nutritional status
• State of hydration
• Match between appearance and stated age
• Ability to mobilize, gait
Abdominal Inspection
• Abdominal contour, symmetry, scars, dilatation of veins
• Movement of abdominal wall with respiration
• Visible masses, hernias, pulsations, peristalsis
• Guarding and positioning for comfort
Auscultation
• Auscultation should be performed before percussion and palpation so as not to alter bowel sounds
• Presence, character and frequency of bowel sounds
Percussion
• Percuss: resonance, tympany, dull, flat
• Liver: define upper and lower borders, measure span
• Spleen: confirm presence of normal resonance over lowest rib interspace in anterior axillary line
• Bladder: identify distension and fullness
• Costovertebral angle (CVA) percussion for tenderness
DST-501 GI-GU Assessment: Adult
Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
Palpation
• Palpation is performed with the client lying supine, with hands by the sides and relaxed
• The client’s abdomen must be completely exposed
• Examine all four quadrants in succession
• Start with the painless areas, and palpate the painful area last
Light Palpation (perform first)
• Tenderness, muscle guarding, rigidity
• Superficial organs or masses
Deep Palpation
Note: Deep palpation can be conducted by nurses who hold a Remote Nursing Certified Practice designation, demonstrating current certification in this practice.
• Assess for abdominal guarding, tenderness or rigid abdomen
• Feel for organs:
o Liver – assess size, tenderness, smooth or irregular border, firmness or hardness
o Spleen – assess for enlargement, tenderness, consistency
o Kidney – assess for tenderness, enlargement
o Bladder – assess for distension, tenderness
• Masses: location, size, shape, mobility, tenderness, movement with respiration, pulsation, hernias (midline, incisional groin)
• Assess for rebound tenderness (pain that occurs upon suddenly releasing the hand after deep palpation), which indicates
peritoneal irritation
• Assess for referred tenderness (pain that is felt in an area distant to the area being palpated), which can be a clue to the
location of the underlying disease
• Inguinal and femoral lymph nodes: enlargement, tenderness
• Femoral pulses
Abdominal Examination, Peripheral areas
• Spider nevi on face, neck or upper trunk, palmar erythema, Dupuytren’s contracture, clubbing of fingers
GU System – Male
Inspection
• Penis, scrotum and pubic area: inflammation, discharge, lesions, swelling, asymmetrical changes in hair distribution, nits,
warts, position of urethral opening
• Rectum: lesions, discharge, swelling, haemorrhoids
• Inguinal and femoral areas for hernia
Palpation
• Penis: tenderness, induration, nodules, lesions
• Testes and scrotal contents: size, position, atrophy of testes, tenderness, swelling, warmth, masses, hydrocele
• Superficial inguinal ring for hernia
• Cremasteric reflex
GU System – Female
Inspection
• External genitalia: labia majora and labia minora: lesions, ulcerations, masses, induration, and areas of different colour, hair
distribution
• Perineum: lesions, ulcerations, masses, induration, scars
DST-501 GI-GU Assessment: Adult
Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
• Clitoris: size, lesions, ulcerations
• Urethra: discharge, lesions, ulcerations
• Vagina: speculum exam – inflammation, atrophy, discharge, lesions, ulcerations, masses, induration, nodularity, relaxation of
perineum
• Cervix: speculum exam – position, color, shape, size, consistency of discharge, erosions, ulcerations
• Os: multipara or nullipara
Palpation
• Skene’s and Bartholin’s glands: masses, discharge, tenderness
• Cervix: cervical tenderness, bleeding after contact, consistency of cervical tissue
• Uterus: position, size, contour, consistency of uterine tissue, mobility on movement
• Adnexa: ovaries for tenderness, masses, consistency, contour, mobility, pain on movement (Chandelier sign)
Rectal Examination
• For occult blood
• For referred pain
• For masses, haemorrhoids, anal fissures, sphincter tone and others
• Prostate exam in males
Associated Systems
Cardiovascular and Pulmonary Examination
• Cardiovascular and pulmonary exam should also be performed
Eyes, Ears, Nose, Throat
• Assess for pharyngitis and conjunctivitis (chlamydial infection, gonorrhea)
• Lymph nodes (auricular, tonsillar, submandibular, supraclavicular, infraclavicular)
Integumentary
• Assess for skin lesions, rashes, polyarthralgias of disseminated gonorrhea, and hydration status
SYMPTOMS REQUIRING URGENT REFERRAL
The first step is to identify those clients which require urgent referral. The following GI signs and symptoms require immediate referral to a physician or nurse practitioner:
• Severe dehydration (elderly)
• Uncontrolled vomiting
• Recurrent fevers
• Hematemesis
• Frank rectal bleeding or perianal fissures or ulcers
• Melena
• Hematochezia
• Immunocompromised clients (HIV, diabetes, client taking steroids)
• Jaundice
• Ascites
• Distended abdomen
• Rigid painful abdomen (also consider PID, ectopic pregnancy)
• Abdominal bruit or pulsating masses
DST-501 GI-GU Assessment: Adult
Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
Diagnostic Tests
Note: The RN(C) may consider the following diagnostic tests in the examination of the GI - GU systems to support clinical decision-making:
• Stool for occult blood or fecal immunochemical test (FIT), Ova and Parasites (O&P), Culture and Sensitivity (C&S)
• Hemoglobin
• Pregnancy test (urine)
• Pap smear
• Urinalysis – dipstick, R&M, C&S
• C&S – urethral discharge, prostatic secretions, vaginal discharge
• Testing as per the STI Assessment DST
• Random Blood Glucose
• Electrocardiogram (ECG)
DOCUMENTATION
• As per agency policy
• Organomegaly
• Tachycardia and lung crackles
• Localized abdominal pain
• Altered peripheral pulse
• Unequal BP left to right in upper extremities
• Joint edema, erythema, warmth
The following GU signs and symptoms require immediate referral to a physician or nurse practitioner:
• Bleeding from the urethra, male or female
• Urinary retention
• Urethral discharge
• Severe GU pain (consider PID or ectopic pregnancy)
• Scrotal swelling
• Erectile dysfunction (priapism)
• Systemic symptoms (sepsis)
• Incontinence (new onset)
• Recent urologic/renal surgery
• Treatment failure after 3 days
DST-501 GI-GU Assessment: Adult

Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
REFERENCES
More recent editions of any of the items in the Reference List may have been published since this DST was published. If you have a newer version, please use it.
AMN Healthcare Education Services. (2014). Focused gastrointestinal assessment. AMN Healthcare.
Ball, Jane, Joyce E. Dains, John A. Flynn, Barry S. Solomon, and Rosalyn W. Stewart. Seidel’s Guide to Physical Examination: An Interprofessional Approach. Ninth edition. St. Louis, Missouri: Mosby, 2018.
Barad, David H. General Gynecologic Evaluation. In The Merck Manual: Professional Version, 6. Kenilworth, NJ, USA: Merck Sharp & Dohme Corp., 2020.
BC Cancer Agency. (2020). What is the FIT?
Estes, M. E. Z. (2014). Health assessment and physical examination (5th ed.). Clifton Park, NY: Cengage Learning.
Jarvis, C. (2020). Physical examination and health assessment (8th ed.). Toronto, ON: Elsevier Canada.
Moleski, Stephanie M. Evaluation of the Gastrointestinal Patient. In The Merck Manual: Professional Version, 3. Kenilworth, NJ, USA: Merck Sharp & Dohme Corp., 2020.
Reese Doyle, Glynda, and Jodie Anita McCutcheon. Section 2.7 Focused Assessments in Chapter 2: Patient Assessment, Version 1.4. In Clinical Procedures for Safer Patient Care- Focused Assessments, 2019.
Stephen, T. C., Skillen, D. L., Day, R. A., & Bickley L. S. (2010). Canadian Bates’ guide to health assessment for nurses. Philadelphia, PA: Lippincott, Williams & Wilkins.
DST-501 GI-GU Assessment: Adult

Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
DST-502 GI-GU Assessment: Pediatric
Nurses with Remote Nursing Certified Practice designation (RN(C)s)5 are able to manage the following genitourinary condition:
Lower Urinary Tract Infection (UTI) in children 2 years of age and older.
The following assessment must be completed and documented. As a complete genitourinary exam includes a gastrointestinal exam, these two examinations have been combined.
ASSESSMENT
History of Present Illness and Review of Systems
General
The following characteristics of each symptom should be elicited and explored:
• Onset (sudden or gradual)
• Location
• Duration, chronology
• Characteristics/quality of symptom
• Associated symptoms
• Precipitating and aggravating factors
• Relieving factors
• Timing, frequency, and duration
• Current situation (improving or deteriorating)
• Previous diagnosis of similar episodes
• Previous treatments and efficacy
• Effects on daily activities
Cardinal Signs and Symptoms
In addition to the general characteristics outlined above, additional characteristics of specific symptoms should be elicited as follows:
Abdominal Pain (Appendix 1)
• Quality – crampy or constant, sharp or stabbing
• Radiation
• Timing – related to eating
• Severity
• Consider GU location indicators – flank, suprapubic, genital, groin or low back pain and costo-vertebral angle (CVA)
tenderness
Nausea, Vomiting or Regurgitation
• Frequency, amount, timing
• Presence of bile
• Hematemesis
• Force
5 RN(C) is an authorized title recommended by CRNBC that refers to CRNBC-certified RNs, and is used throughout this Decision
Support Tool (DST).
DST-502 GI-GU Assessment: Pediatric
Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
• Color
• Relationship to food intake, i.e., solids or liquids
Dysphagia
• Solids or liquids
• Site where food gets stuck
• Food is regurgitated
Bowel Habits
• Last bowel movement
• Frequency, colour and consistency of stool
• Presence of mucous, blood or melena
• Pain before, during or after defecation
• Sense of incomplete emptying after bowel movement
• Use of laxatives
• Belching, bloating and flatulence
• Change in bowel habits
Urinary Symptoms
• Enuresis (bed wetting)
• New onset incontinence
• Frequency, urgency, quantity
• Dysuria and its timing during voiding (at beginning or end, throughout)
• Change in colour and odour of urine
• Haematuria
• Presence of stones or sediment in the urine
• Toilet training problems
Jaundice
• Scleral icterus
• Tea-coloured urine
• Clay-coloured bowel movements
• Pruritis
• History of hepatitis A, hepatitis B or hepatitis C
GU – Female
• Where appropriate for females to r/o ectopic, pelvic inflammatory disease (PID) or pregnancy as the cause of symptoms:
• Last menstrual period, any change?
• Dyspareunia or post coital bleeding if sexually active
• Lesions, swelling or discoloration of external genitalia
• Urethral or vaginal discharge
• Sense of pelvic relaxation (pelvic organs feel as though they are falling down or out)
GU – Male
• Testicular pain or swelling
DST-502 GI-GU Assessment: Pediatric

Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
• Discharge from penis, itching
• Lesions, swelling or discoloration of external genitalia
Other Associated Symptoms
• Change in appetite
• Fever
• Malaise / activity level
• Headache
• Dehydration
• Usual nutrition and food habits: type of foods eaten, variety of foods in diet, quantity of food eaten, dietary balance, fiber
content of diet
• Food and fluid intake since onset of illness
• Check bottle for content (sour milk)
• Breast feeding mothers (consider diet)
• Unusual weight loss or weight gain
• Skin (e.g., dry, pruritis, rash)
• Unexplained crying, holding of genitals
• Enlarged, painful nodes (axilla, groin)
• Plus the following symptoms associated with nephritic syndrome and glomerulonephritis:
• Swelling of ankles and orbits
• Headaches
• Nosebleeds
• Haematuria
• Decreased urinary output
Medical History Specific to GI / GU Systems
• Allergies (seasonal as well as reactions)
• Medication recently or currently used (prescription, birth control pills (BCP), antibiotics (particularly clindamycin use within
the past 2 months), steroids and over the counter (OTC))
• Herbal preparations
• Immunization status
• Birth and prenatal status if age appropriate (neonate, infant)
• Growth history, obtain measurements if appropriate
• Communicable diseases: measles, chickenpox (varicella), herpes simplex
• Diseases – GI:
o Hiatus hernia
o Documented H. Pylori or gastro esophageal reflux diseases (GERD)
o Presence of hernia or masses
o Irritable bowel syndrome (IBS) / inflammatory bowel disease (IBD)
o Peptic ulcer disease (PUD)
o Diverticulosis
o Liver disease (hepatitis A, hepatitis B, hepatitis C)
o Diabetes mellitus
o Abdominal or GU surgery or procedures
DST-502 GI-GU Assessment: Pediatric
Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
• Diseases – GU:
o Renal disease, cystitis, pyelonephritis, renal stones
o Congenital structural abnormalities in the GU tract
o Human papilloma virus (HPV), sexually transmitted infections (STIs), including human immunodeficiency virus (HIV)
o Male: hydrocele, epididymitis, varicocele, hernia, undescended testis, spermatocele, testicular torsion
o Female: pelvic inflammatory disease (PID)
o Females (if appropriate):
o Menstrual History – menarche, LMP, interval, regularity, duration, amount of flow, premenstrual symptoms (PMS),
dysmenorrhea
o Obstetrical History - gravida, term, para, abortion, live, stillbirth (GTPALS) complicated pregnancies and deliveries
OTHER
• Blood transfusion
• Immunocompromised
Family History Specific to GI / GU Systems
• Household contact with hepatitis A or hepatitis B
• Household contact with gastroenteritis / recent GI infections
• Food poisoning
• GERD, peptic ulcer disease (PUD)
• Gallbladder disease
• Metabolic disease (i.e., diabetes mellitus, porphyria)
• Renal disease (e.g., renal cancer, polycystic kidneys, renal stones)
• Urinary tract infections (UTIs)
Personal and Social History Specific to GI - GU Systems
• Substance use – alcohol, smoking, caffeine, street drugs, including injection drugs, steroids
• Dietary recall including foods avoided (and reasons for), fat intake, nitrate intake (e.g., smoked foods)
• Obesity, anorexia, bulimia, other eating disorders
• Travel to area where infectious GI conditions are endemic
• Body piercing or tattoos
• Stress at home or school, attendance issues
• Exposure to polluted drinking water
• Sanitation problems at home or in the community
• Personal hygiene, toileting habits, use of bubble bath, douches, tight-fitting underwear or other clothing
• If age appropriate, sexual history and practices, including risk behaviours and contraception (unprotected oral, anal or
vaginal intercourse, multiple partners, sexual orientation, symptomatic partner)
• Sexual or physical abuse, inappropriate touch (children must be asked these questions with sensitivity and without the use of
leading questions)
• Fear, embarrassment, anxiety
• Missing work, school or social functions because of GU symptoms (e.g., incontinence)
Occupational or School Environment
• Healthcare occupation
• Institutional environment
DST-502 GI-GU Assessment: Pediatric

Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
• Environmental exposure
• Chemical exposure
PHYSICAL ASSESSMENT
Vital Signs
• Temperature
• Pulse
• Respiratory rate
• SpO2
• Blood pressure (BP)
• Weigh all children under 12 yrs of age for medication calculations
General
• Apparent state of health
• Appearance of comfort or distress
• Color
• Nutritional status
• Hydration
• Match between appearance and stated age
Inspection
• Abdominal size, shape, contour, symmetry, scars, dilatation of veins
• Any distension or asymmetry (in infancy, abdomen is typically protuberant; in early childhood the abdomen is still
protuberant, but flattens when the child is lying down)
• Movement of abdominal wall with respiration
• Visible masses, hernias, pulsations, peristalsis
• Umbilical hernia of up to 2.5 cm may be present up to one year
• Diastasis recti may cause midline bulge (separation of rectus muscles) and usually disappears by early childhood
• Guarding and positioning for comfort (child's behavior can also give very good clues as to the severity of any abdominal pain)
• Ability to mobilize and gait
Auscultation
• Auscultation should be performed BEFORE percussion and palpation so as not to alter bowel sounds
• Note presence, character and frequency of bowel sounds
• Presence of bruits (renal, iliac or abdominal aortic)
Percussion
• General percussion in all four quadrants for normal tympany
• Delineate outline of liver; upper border is in the mid-clavicular line, between the fourth and sixth intercostal spaces; upper
limit of liver span ranges from 8 cm at 5 years of age to 13 cm at puberty
• Determine spleen size
• Costo-vertebral angle (CVA) percussion for tenderness
Palpation
• Ideally, palpation is performed with the child lying supine, with hands by the sides and relaxed
DST-502 GI-GU Assessment: Pediatric
Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
• For some children, having them in their parents lap may be an acceptable alternate
• In reality, it must sometimes be done on the run
• Be sure your hands are warm
• The child's abdomen must be completely exposed
• Examine all four quadrants in succession
• If there is pain, start with the painless areas, and palpate the painful area last
Light Palpation
• Assess tenderness, guarding, superficial masses
• Observe for guarding and abdominal rigidity
• Watch the child's facial expression
Deep Palpation
• Assess for abdominal guarding, tenderness or rigid abdomen
• Feel for organs:
o Liver – assess size, tenderness, smooth or irregular border, firmness or hardness
o Spleen – assess for enlargement, tenderness, consistency
o Kidney – assess for tenderness, enlargement
o Bladder – assess for distension, tenderness
• Masses: location, size, shape, mobility, tenderness, movement with respiration, pulsation, hernias (midline, incisional, groin)
• Assess for rebound tenderness (pain that occurs upon suddenly releasing the hand after deep palpation), which indicates
peritoneal irritation
• Assess for referred tenderness (pain that is felt in an area distant to the area being palpated), which can be a clue to the
location of the underlying disease
• Inguinal lymph nodes: enlargement, tenderness
• Femoral pulses
Genitourinary System – Male
Inspection
• Penis, scrotum and pubic area: inflammation, discharge, lesions, swelling, asymmetry, changes in hair distribution, nits,
warts, position of urethral opening
• Rectum: lesions, discharge, swelling, haemorrhoids
• Inguinal and femoral areas (for hernia)
Palpation
• Penis: tenderness, induration, nodules, lesions, foreskin (retractable by 3 yrs)
• Testes: size, position (undescended), tenderness, masses, swelling, warmth, hydrocele
o Testes are usually descended by one year
• Superficial inguinal ring (for hernia)
• Cremasteric reflex
Genitourinary System – Female
• Child should be in supine frog-leg position for examination
• Spread labia by applying gentle traction toward the examiner and slightly laterally to visualize introitus
DST-502 GI-GU Assessment: Pediatric
Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
Note: Do not perform an internal vaginal examination in a child less than 14 years, prepubescent child or an adolescent
who is not sexually active
Inspection
External genitalia: labia majora and labia minora: lesions, ulcerations, masses, induration, and areas of different color, hair distribution
Perineum: lesions, ulcerations, masses, induration, scars
Clitoris: size, lesions, ulcerations
Urethra: discharge, lesions, ulcerations, irritation
Bleeding (may indicate vaginitis or sexual abuse in a prepubescent girl)
Enlargement of vaginal orifice (may indicate sexual abuse)
If 14 years or older and sexually active, consider a vaginal and internal exam:
o Vagina: speculum exam – inflammation, atrophy, discharge, lesions, ulcerations, excoriation
o Cervix: speculum exam – position, colour, shape, size, consistency discharge, erosions, ulcerations
o Os: multipara or nullipara
Palpation
• Skene’s and Bartholin’s glands: masses, discharge, tenderness
• Cervix: cervical tenderness, bleeding after contact, consistency of cervical tissue
• Uterus: position, size, contour, consistency of uterine tissue, mobility on movement
• Adnexa: ovaries for tenderness, masses, consistency, contour, mobility, pain on movement (Chandelier sign)
Rectal Examination
• Anal patency (check this feature only in newborns)
• Referred pain
• For masses, haemorrhoids, anal fissures, sphincter tone, etc.
• For occult blood
Associated Systems
Cardiovascular and Respiratory Examination
• A cardiovascular and respiratory exam should also be performed
Integumentary
• Assess for skin lesions, rashes, polyarthralgias of systemic gonorrhea and hydration status
Eyes, ears, nose, throat
• Assess for pharyngitis and conjunctivitis (chlamydial infection, gonorrhea)
• Lymph nodes (auricular, tonsillar, submandibular, supraclavicular, infraclavicular)
SYMPTOMS REQUIRING URGENT REFERRAL
The first step is to identify those presentations that require urgent referral
The following GI signs and symptoms require immediate referral to a physician or nurse practitioner:
• Severe dehydration
• Recurrent fever
• Uncontrolled vomiting
DST-502 GI-GU Assessment: Pediatric

Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
• Hematemesis
• Frank rectal bleeding or perianal fissures or ulcers
• Melena
• Hematochezia
• Immunocompromised clients (HIV, diabetes, client taking steroids)
• Jaundice
• Ascites
• Distended abdomen
• Rigid painful abdomen (also consider PID, ectopic pregnancy)
• Abdominal bruit or pulsating masses
• Organomegaly
• Tachycardia and lung crackles along with abdominal pain (may be referred from the lungs in pneumonia)
• Localized abdominal pain
• Altered peripheral pulse
• Unequal BP left to right (difference of approximately 30 mm Hg is indicator of aortic aneurysm)
• Joint edema, erythema, warmth
The following GU signs and symptoms require immediate referral to a physician or nurse practitioner:
• Bleeding from the urethra, male or female
• Urinary retention
• Urethral discharge
• Severe GU pain (consider PID or ectopic pregnancy)
• Scrotal swelling
• Erectile dysfunction (priaprism)
• Systemic symptoms (sepsis)
• Incontinence (new onset)
• Recent urologic/renal surgery
• Treatment failure after 3 days
• Known anatomical abnormality
• All children suspected of sexual assault must be referred to a physician or nurse practitioner
DIAGNOSTIC TESTS
• The certified practice nurse may consider the following diagnostic tests to support decision making:
• Stool for occult blood or fecal immunochemical test (FIT)
• Stool for Ova and Parasites (O&P), Culture and Sensitivity (C&S)
• Hemoglobin
• Pregnancy test (urine)
• Electrocardiogram (ECG)
• Urinalysis – dipstick, R&M, C&S
• C&S – urethral or vaginal discharge
• Random blood glucose
• STI testing as per the STI Assessment DST
• Pap smear
DST-502 GI-GU Assessment: Pediatric
Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
REFERENCES
More recent editions of any of the items in the Reference List may have been published since this DST was published. If you have a newer version, please use it.
AMN Healthcare Education Services. (2014). Focused gastrointestinal assessment. AMN Healthcare.
Ball, J. W., Dains, J. E., Flynn, J. A., Solomon, B. S., & Stewart, R. W. (Eds.). (2015). Seidel’s guide to physical examination (8th ed.). St. Louis, MO: Elsevier.
BC Cancer Agency. (2012). What is the Fecal Immunochemical Test (FIT)?
Chen, Y. A., & Tran, C. (Eds.). (2011). The Toronto notes 2011: Comprehensive medical reference and review for the Medical Council of Canada Qualifying Exam Part 1 and the United States Medical Licensing Exam Step 2 (27th ed.). Toronto, ON: Toronto Notes for Medical Students.
Estes, M. E. Z. (2014). Health assessment and physical examination (5th ed.). Clifton Park, NY: Cengage Learning.
Jarvis, C. (2014). Physical examination and health assessment (2nd Canadian ed.). Toronto, ON: Elsevier Canada.
Porter, R. S., & Kaplan, J. L. (Eds.). (2011). The Merck Manual of Diagnosis and Therapy (19th ed.). Whitehouse Station, NJ: Merck & Co., Inc.
Sawyer, S. S. (2012). Pediatric physical examination and health assessment. Sudbury, MA: Jones & Bartlett Learning.
Stephen, T. C., Skillen, D. L., Day, R. A., & Bickley L. S. (2010). Canadian Bates’ guide to health assessment for nurses. Philadelphia, PA: Lippincott, Williams & Wilkins.
DST-502 GI-GU Assessment: Pediatric
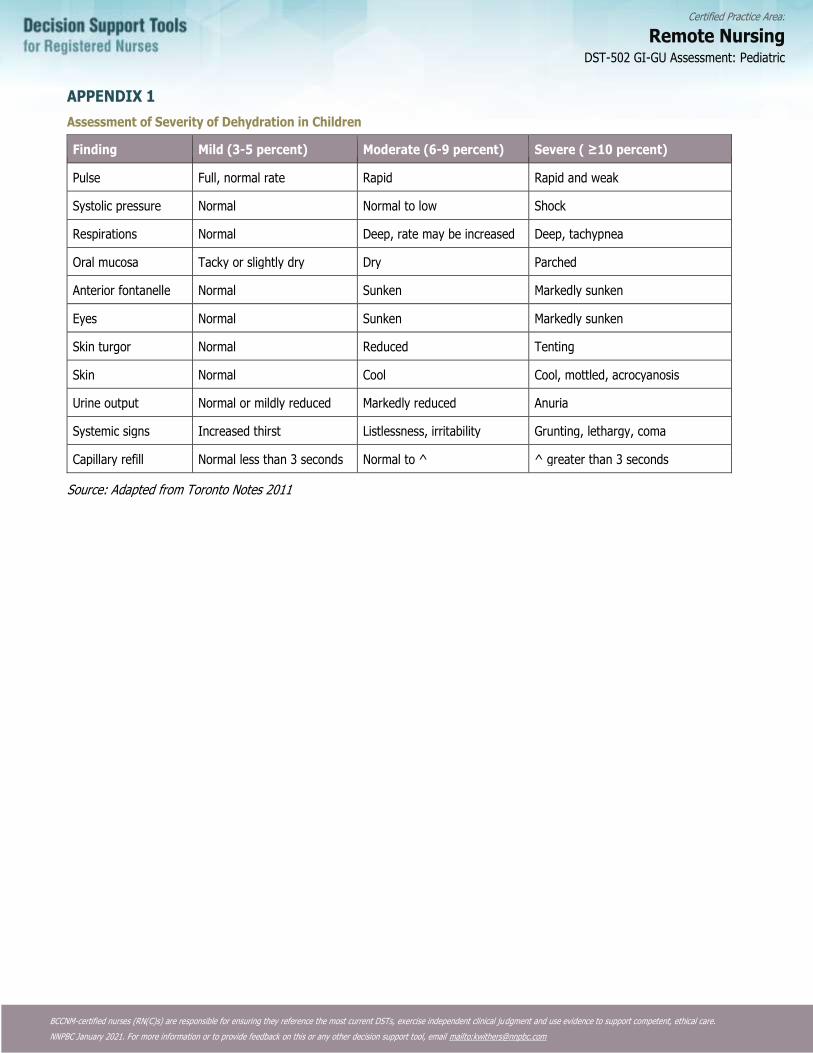
Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
APPENDIX 1
Assessment of Severity of Dehydration in Children
Finding Mild (3-5 percent) Moderate (6-9 percent) Severe ( ≥10 percent)
Pulse Full, normal rate Rapid Rapid and weak
Systolic pressure Normal Normal to low Shock
Respirations Normal Deep, rate may be increased Deep, tachypnea
Oral mucosa Tacky or slightly dry Dry Parched
Anterior fontanelle Normal Sunken Markedly sunken
Eyes Normal Sunken Markedly sunken
Skin turgor Normal Reduced Tenting
Skin Normal Cool Cool, mottled, acrocyanosis
Urine output Normal or mildly reduced Markedly reduced Anuria
Systemic signs Increased thirst Listlessness, irritability Grunting, lethargy, coma
Capillary refill Normal less than 3 seconds Normal to ^ ^ greater than 3 seconds
Source: Adapted from Toronto Notes 2011
DST-502 GI-GU Assessment: Pediatric

Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
DST-601 Lower Urinary Tract Infection (UTI): Adult
DEFINITION
• A lower urinary tract infection (UTI) is a bacterial infection of the bladder, also known as cystitis, caused by bacteria
multiplying in the urine
• Uncomplicated UTIs are acute infections of the bladder in otherwise healthy women
o UTIs are considered complicated in the following circumstances:
▪ All UTIs in men are considered complicated
▪ Anatomic or functional abnormalities of the genitourinary (GU) system, such as obstruction, neurogenic bladder,
stones, prostatic hypertrophy, vesicoureteral reflux
▪ Long term catheterization or recent GU instrumentation
▪ Treatment for a UTI within the previous month
▪ Renal failure, poorly controlled diabetes or patients who are immunocompromised
POTENTIAL CAUSES
• Escherichia coli is the most common organism, found in 80-90% of cases
• Staphylococcus saprophyticus
• Other enterobacteria
PREDISPOSING RISK FACTORS
• Female gender
• Sexual activity
• Previous UTIs
• Pregnancy
• Use of spermicides, diaphragm
• Infrequent voiding
• Dehydration
• Urinary instrumentation (catheterization)
• Renal calculi
• Immunocompromised (human immunodeficiency virus infection)
• Diabetes mellitus
• GU tract anomalies (congenital, urethral stricture, neurogenic bladder, tumour)
• Male specific factors are anal intercourse, intercourse with a female with a UTI, lack of circumcision, and prostatic
hypertrophy.
TYPICAL FINDINGS
• Urinary frequency
• Urinary urgency
• Dysuria
• Mild dehydration
• Afebrile
• Suprapubic discomfort
• Bladder spasm
• Foul smelling urine
• Hematuria
DST-601 Lower Urinary Tract Infection (UTI): Adult
Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
PHYSICAL ASSESSMENT
Vital Signs
• Temperature
• Pulse
• Respiratory rate
• SpO2
• Blood pressure
General Assessment
• Hydration status
• Suprapubic tenderness may be mild to moderate
• If flank pain presents refer or consult with physician or nurse practitioner as suggests ascending infection
• If costovertebral angle (CVA) tenderness presents on percussion refer or consult with physician or nurse practitioner as
suggests ascending infection
Note: In the elderly, symptoms do not always follow the classic triad of urgency, frequency and dysuria. Look for subtle cognitive changes and predisposing factors.
• Sexually Active Female
o If appropriate, perform a pelvic exam and full STI screening if abnormal vaginal discharge or symptoms suggestive of
vaginitis or STI are present
o If appropriate, offer STI screening (see diagnostic tests section below)
• Sexually Active Male
o Assess for urethral symptoms, discharge or genital lesions.
o If present, offer full STI screening (see diagnostic tests section below).
Note: The RN(C) must be certified in STI management in order to carry out activities in the NNPBC STI DSTs. If STI testing is
warranted and the RN(C) is not STI certified, refer to physician or nurse practitioner. If appropriate, offer STI screening (see diagnostic tests section below).
DIAGNOSTIC TESTS
• Urinalysis
• Dipstick test: blood, protein, nitrites, leukocytes
• Consider microscopic urinalysis: white blood cells, red blood cells, bacteria
• Consider labs for renal function: creatinine, BUN, glomerular filtration rate
• Urine culture and sensitivity is generally not required for an uncomplicated UTI
• Collect a urine sample for culture and sensitivity prior to starting antibiotics if:
o This is a complicated UTI
o This is the second presentation of a UTI within a one-year time frame
o Patient presents with treatment failure (persistent UTI symptoms up to 10 days post-treatment)
o Patient presents with fever, chills, rigor, or flank pain (refer or consult physician or nurse practitioner)
o Dipstick urine test is negative, but symptoms are indicative of an UTI
• For complicated UTIs, ensure urine culture and sensitivity is tested 1-2 weeks after antibiotics are completed
• If symptoms or history indicate, offer full STI screening as per the appropriate STI DST, if STI certified
• If full STI screening declined, obtain a urine specimen for CT/GC NAAT
DST-601 Lower Urinary Tract Infection (UTI): Adult
Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
• If STI signs or symptoms are also present ensure follow-up as there may be more than one condition present (e.g. UTI and
STI)
• Consider urine pregnancy test if indicated
Note: If urinary frequency, urgency or dysuria and dipstick is positive for leukocytes and/or nitrites, may treat as lower UTI
MANAGEMENT AND INTERVENTIONS
Goals of Treatment
• Eradicate infection
• Relieve symptoms
• Prevent complications
NON-PHARMACOLOGICAL INTERVENTIONS
• Rest
• Hydrate with 8-10 glasses of fluid per day
PHARMACOLOGIC INTERVENTIONS
Antibiotics: Adult Female, Acute Uncomplicated UTI
Primary Regimen
• Nitrofurantoin 100 mg po four times a day for 5 days OR Macrobid 100 mg po day for 5 days
OR
• Trimethoprim 160 mg/sulfamethoxazole 800 mg, 1 tab PO BID for 3 days
Alternative Regimen
If Allergic or Resistance Risk to Above Medications
• Amoxicillin/clavulanate 875/125 mg, 1 tab PO BID for 5-7 days
If Allergic to Amoxicillin/clavulanate
• Ciprofloxacin 250mg PO BID for 3 days
Antibiotics: Adult Male, UTI (Acute Cystitis)
Note: All UTIs in men are considered complicated.
Primary Regimen
• Trimethoprim 160 mg/sulfamethoxazole 800 mg, 1 tab PO BID for 7 days
OR
• Ciprofloxacin 500 mg PO BID for 7 days
Alternate Regimen
• Amoxicillin/clavulanate 875/125 mg, 1 tab PO BID for 7 days
OR
• Cephalexin 500 mg PO QID for 7 days
DST-601 Lower Urinary Tract Infection (UTI): Adult
Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
Antibiotics: Complicated UTI (e.g. Obstruction, Reflux, Azotemia) or Urinary Catheter-Related Infection
• If low risk of multi-drug resistant infection:
o Ciprofloxacin 500 mg PO BID for 7-14 days
• For high risk of multi-drug resistant infection consult physician or nurse practitioner
Note: Treatment for pyelonephritis is not included in this document as it is an upper UTI.
Note: Ensure sensitivity of organism to the chosen antibiotic once culture and sensitivity result are returned.
If resistant, consult with or refer to a physician or nurse practitioner.
Pregnant and Breastfeeding Person
Pregnant Person
• DO NOT USE: Nitrofurantoin is contraindicated in pregnant patients in third trimester including at term (38 to 42 weeks'
gestation), during labor and delivery, or when the onset of labor is imminent. Alternative antibiotics should be used in
pregnant patients with G-6-PD deficiency
• Use of nitrofurantoin earlier in pregnancy should ONLY be used after consultation with physician or nurse practitioner
• Amoxicillin/clavulanate should ONLY be used during pregnancy after consultation with physician or nurse practitioner
• DO NOT USE trimethoprim/sulfamethoxazole or ciprofloxacin
Breastfeeding Person
• Nitrofurantoin, amoxicillin/clavulanate should only be used during breast feeding after consultation with physician or nurse
practitioner
• DO NOT USE trimethoprim/sulfamethoxazole or ciprofloxacin
POTENTIAL COMPLICATIONS
• Pyelonephritis
• Chronic cystitis
PATIENT EDUCATION AND DISCHARGE INFORMATION
• Advise on condition, treatment and expected course of disease process
• Counsel to return to clinic if fever develops or symptoms do not improve in 48-72 hours
• Counsel on appropriate use of medications (dose, frequency, side effects, need to complete entire course of medications)
• Recommend increasing fluid intake to 8-10 glasses per day
• Counsel on sitting in a warm tub to relieve symptoms of dysuria
• For women, advise regarding wiping front to back after a bowel movement
• Counsel on not using douches
• Counsel on avoidance of bubble baths
• Advise that voiding after intercourse may be beneficial
• Advise as to alternative contraception to avoid spermicide use
• Use appropriate cleaning for sex toys and advise against sharing sex toys
DST-601 Lower Urinary Tract Infection (UTI): Adult
Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
MONITORING AND FOLLOW-UP
• If symptoms do not begin to resolve in 48-72 hours, or if symptoms progress despite treatment, patient should return to the
clinic for reassessment
• Pregnant women who present with symptoms of UTI are recommended to have urine for urinalysis and culture and
sensitivity as indicated
• All pregnant women treated for UTIs are recommended to have a urinalysis and urine for culture and sensitivity 1-2
weeks following treatment and then as indicated
CONSULTATION AND/OR REFERRAL
• Presence of complicating factors suggestive of upper UTI (fever [>38° C] chills, flank pain, CVA tenderness, nausea and
vomiting)
• Women presenting with a second UTI within one month (or a third UTI within two months) or more than three in one year
should be referred to a physician or nurse practitioner
• Women presenting with complicated UTIs require urine for culture and sensitivity and consultation with and/or referral to a
physician or nurse practitioner
• Men who present with an uncertain cause or more than one UTI should be referred to a physician or nurse • practitioner
for further evaluation.
• Men greater than or equal to 50 years of age who present with a true (culture-positive) urinary tract infection for the first
time should be referred to a physician or nurse practitioner for further evaluation.
DOCUMENTATION
• As per agency policy
DST-601 Lower Urinary Tract Infection (UTI): Adult
Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
REFERENCES
More recent editions of any of the items in the Reference List may have been published since this DST was published. If you have a newer version, please use it.
Anti-Infective Review Panel. (2019). Anti-infective guidelines for community-acquired infections. Toronto, ON: MUMS Guideline Clearinghouse.
Antimicrobial Therapy. 50 Stanford Guide. 2020.
Benton, T.J. Urinary tract infections in men. 2018. BMJ. Best Practice.
Blondel-Hill, E., & Fryters, S. (2012). Bugs and drugs: An antimicrobial infectious diseases reference. Edmonton, AB: Alberta Health Services.
Bono, M.J. & Reygaert, W.C. (2020). Urinary Tract Infection. StatPearls Publishing LLC.
British Columbia Centre for Disease Control. (2013). Antimicrobial resistance trend in the province of British Columbia. Vancouver, BC: Author.
Canadian Pharmacists Association. Compendium of Therapeutic Choices. 2019 Edition. Ottawa, ON: Author
Cash, J. C., & Glass, C. A. (Eds.). (2017). Family practice guidelines (4th ed.). New York, NY: Springer.
Dains, J. E., Baumann, L. C., & Schiebel, P. (Eds.). (2019). Advanced health assessment and clinical diagnosis in primary care. St. Louis, MO: Elsevier.
Gupta, K., Hooton, T. M., Naber, K. G., Wullt, B., Colgan, R., Miller, L. G.…Soper D. E. (2011). International clinical practice
guidelines for the treatment of acute uncomplicated cystitis and pyelonephritis in women: A 2010 update by the Infectious
Diseases Society of America and the European Society for Microbiology and Infectious Diseases. Clinical Infectious Diseases, 52(5), e103-e120.
Hooton, T. M. Acute simple cystitis in men. UpToDate, Jul 20, 2020.
Hooton, T. M. & Gupta, K. Acute complicated urinary tract infection (including pyelonephritis) in adults. UpToDate, Aug 21, 2019.
Hooton, T. M. & Gupta, K. Acute simple cystitis in women. UpToDate, Aug 21, 2019.
Lewington, A. Urinary tract infections in women. 2020. BMJ. Best Practice.
Lexicomp. (Lexi-Drugs). Wolters Kluwer Clin Drug Inf Inc. 2020.
Sabih, A. & Leslie, S.W. (2019). Complicated Urinary Tract Infections. StatPearls Publishing LLC.
DST-601 Lower Urinary Tract Infection (UTI): Adult

Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
DST-602 Lower Urinary Tract Infection (UTI): Pediatric
DEFINITION
Bacterial infection of the bladder, also known as cystitis, is caused by bacteria multiplying in the urine.
• UTI is the most common Genito-Urinary (GU) disease in children and the most consistently missed serious bacterial infection
in infants.
• During infancy (less than 1 year of age), UTI’s occur more frequently in boys, but after that time they occur more frequently
in girls.
• In boys, a UTI that occurs after infancy is usually due to a congenital anomaly and requires a referral for investigation.
• Nurses with Remote Practice Certified Practice designation (RN(C)s6) are able to treat children with UTIs who are 2 years of
age and older. Younger children require consultation with or referral to a physician or nurse practitioner.
Potential Causes
• E. coli
• Klebsiella
• Group B Streptococcus
• Proteus
• Staphylococcus epidermis
• Pseudomonas
• H. influenza
• Enterococcus
• Staphylococcus saprophyticus
Predisposing Risk Factors
• Gender – as or more common in boys as neonates
o after neonatal period, incidence higher in females
• Genito-urinary tract anomalies – congenital (vesico-ureteral reflux), urethral stricture, neurogenic bladder, tumour
• Bowel and/or bladder dysfunction, such as infrequent voiding, constipation
• Dehydration
• Previous UTIs
• Sexual activity
• Pregnancy
• Use of spermicides, diaphragm
• Urinary instrumentation (e.g., catheterization)
• Immunocompromise
• Diabetes mellitus
• Male specific factors are insertive anal intercourse, intercourse with a female with a UTI, and lack of circumcision
Typical Findings (Depends on the Age of the Child)
History for Neonates and Infants
• Non-specific, non-urinary symptoms
6 RN(C) is an authorized title recommended by CRNBC that refers to CRNBC-certified RNs, and is used throughout this Decision
Support Tool (DST).
DST-602 Lower Urinary Tract Infection (UTI): Pediatric

Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
• May present with sepsis
• Fever
• Irritability
• Poor feeding
• Vomiting
• Diarrhea or constipation
• Jaundice
• Hypothermia
• Failure to thrive
• Decreased activity, lethargy
History for children less than 3 years old
• Abdominal pain
• Fever
• Vomiting
• Frequency, urgency, dysuria, new onset enuresis
• Strong smelling urine
• Urinary retention
History for children 3 years of age or older
• Frequency
• Dysuria
• Urgency
• Enuresis
• Flank or back pain (upper UTI)
• Vomiting
• Fever
PHYSICAL ASSESSMENT
Vital signs
• Temperature
• Pulse
• Respiration
• SpO2
• Blood pressure (BP)
General
• Hydration status
• Weigh until 12 years of age for medication calculations
• May or may not look ill
• Fever
• Jaundice (neonates)
• Suprapubic tenderness
• Tender abdomen (may need to include reproductive assessment in adolescents)
DST-602 Lower Urinary Tract Infection (UTI): Pediatric
Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
• Costo-Vertebral Angle (CVA) percussion – presence of tenderness suggests ascending infection
• State of circumcision - male
Sexually active Female
If appropriate, perform a pelvic exam if abnormal vaginal discharge or symptoms suggestive of vaginitis or STI are present. If
appropriate, offer STI screening (see below).
Reminder: a referral to a physician or nurse practitioner is required for a pelvic exam for any female who has
not been sexually active or any female less than 14 years of age.
Sexually active Male
Assess for urethral symptoms, discharge or genital lesions. If present, offer full STI screening (see below).
Diagnostic tests
• Urinalysis:
o Dipstick test: blood, protein, nitrites, leukocytes
o Consider microscopic urinalysis: White Blood Cells (WBC), Red Blood Cells (RBC), bacteria
• Urine Culture & Sensitivity (C&S) is generally not required with uncomplicated UTI – consider a urine C&S if:
o This is the second presentation of a UTI within a one-year time-frame
o The client presents with fever, chills, rigor, or flank pain (and refer or consult)
o Dipstick test is negative and symptoms are indicative of a likely UTI
• If symptoms or history indicate, offer full STI screening as per Reproductive Health Certified Practice – Sexually Transmitted
Infections STI Assessment DST. If full STI screening declined, obtain a urine specimen for CT/GC NAAT.
• Consider urine pregnancy test if indicated
Note 1: If dipstick is positive for leukocytes and/or nitrites, may treat as lower UTI
Note 2: If necessary, utilize both the UTI DST and appropriate STI DST as there may be more than one condition
present (e.g. UTI and STI).
Management and Interventions
Goals of treatment
• Relieve symptoms
• Eradicate infection
• Prevent recurrence
• Identify underlying factors
• Prevent complications
Non-pharmacological Interventions
• Rest, if febrile
• Keep hydrated, increase fluids
DST-602 Lower Urinary Tract Infection (UTI): Pediatric

Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
PHARMACOLOGICAL INTERVENTIONS
All drugs must be calculated by weight until age 12 yrs of age. Doses should never exceed adult doses
Antibiotics: Treat only if Routine and Microscopic (R&M) results are positive for nitrites, leukocyte esterase, protein or blood
Children 2 years and older
• Cefixime 8 mg/kg/day PO divided BID for 5-7 days
OR
• if weight appropriate and able to swallow nitrofurantoin tabs, Nitrofurantoin (Macrodantin) 5-7 mg/kg/day PO divided QID for
5 days
Second Line
• Trimethoprim 8 mg/ml - Sulfamethoxazole 40mg/ml. 6-12 mg / kg per day po bid for 3 days. Dosing is based on
Trimethoprim
OR
• Amoxicillin – Clavulanate 40 mg/kg/day po divided tid for 5-7 days.
• Dosing is based on the Amoxicillin component
For Pregnant and Breastfeeding Youth
• Nitrofurantoin (monohydrate/macrocrystal formulation - Macrobid) 100 mg, po bid for 7 days (do not use in third
trimester or labour)
OR
• Nitrofurantoin (macrocrystal formulation - Macrodantin) 50-100 mg, po qid for 7 days
• (do not use in third trimester or labour)
OR
• Cefixime 400 mg PO daily for 7 days.
DO NOT USE Trimethoprim 160 mg / Sulphamethoxazole 800 mg
Consult with a physician or nurse practitioner if client allergic to the above medications.
Potential Complications
• Recurrent UTI
• Sepsis (in neonates and infants)
• Pyelonephritis
• Renal scarring
• Meningitis
Client/Caregiver Education and Discharge Information
• Advise on condition, timeline of treatment and expected course of disease process
• Return to clinic if fever continues or symptoms do not improve in 2 days
• Counsel parent or caregiver about appropriate use of medications (dose, frequency, side effects, need to complete entire
course of medications)
• Increase fluid intake while child is unwell (1.5 times usual intake)
• Sitting in a warm tub may relieve symptoms of dysuria
• For females, advise regarding wiping front to back after a bowel movement
• Do not use douches
DST-602 Lower Urinary Tract Infection (UTI): Pediatric

Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
• Avoid bubble baths
• If sexually active, advise that voiding after intercourse may be beneficial
• Use appropriate cleaning for sex toys and advise against sharing sex toys
Monitoring and Follow-Up
• Follow up in 24-48 hours, make sure that antibiotics are sensitive to organisms
• If symptoms progress despite treatment, client should return to the clinic for reassessment and consultation with a physician
or nurse practitioner
• Arrange follow up for one week after the completion of therapy
• Discuss follow-up urinalysis with physician or nurse practitioner
Consultation and/or Referral
• All infants less than 4 months of age or who look acutely ill must be referred to a physician or nurse practitioner
• Consult a physician or nurse practitioner for treatment failure after 72 hours
• Children presenting with symptoms of pyelonephritis such as high fever, abdomen, flank and CVA tenderness must be
referred to a physician or nurse practitioner
• Following the first UTI, all children should be referred to a physician or nurse practitioner as they may require further
investigation to rule out a congenital anomaly such as vesico-ureteral reflux
DOCUMENTATION
As per agency policy
DST-602 Lower Urinary Tract Infection (UTI): Pediatric

Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
REFERENCES
More recent editions of any of the items in the Reference List may have been published since this DST was published. If you have a
newer version, please use it.
Anti-Infective Review Panel. (2012). Anti-infective guidelines for community-acquired infections. Toronto, ON: MUMS Guideline Clearinghouse.
Blondel-Hill, E., & Fryters, S. (2012). Bugs and drugs: An antimicrobial infectious diseases reference. Edmonton, AB: Alberta Health Services.
Canadian Pharmacists Association. (2014). Therapeutic choices (7th ed.). Ottawa, ON: Author
Cash, J. C., & Glass, C. A. (Eds.). (2014). Family practice guidelines (3rd ed.). New York, NY: Springer.
Chen, Y. A., & Tran, C. (Eds.). (2011). The Toronto notes 2011: Comprehensive medical reference and review for the Medical Council of Canada Qualifying Exam Part 1 and the United States Medical Licensing Exam Step 2 (27th ed.). Toronto, ON: Toronto Notes for Medical Students.
Dains, J. E., Baumann, L. C., & Scheibel, P. (Eds.). (2015). Advanced health assessment and clinical diagnosis in primary care (5th ed.). St. Louis, MO: Elsevier Health Sciences.
DynaMed. (2016, February 1). Urinary tract infection (UTI) in children.
Esau, R. (Ed.). (2012). British Columbia’s Children’s Hospital pediatric drug dosage guidelines (6th ed.). Vancouver, BC: Children’s & Women’s Health Centre of B.C.
Fisher, D. J. (2015, June 18). Pediatric urinary tract infection.
Health Canada, First Nations and Inuit Health Branch. (2012, November). Clinical practice guidelines for nurses in primary care: Pediatric and adolescent care.
White, B. (2011). Diagnosis and treatment of urinary tract infections in children. American Family Physician, 83(4), 409-415.
DST-602 Lower Urinary Tract Infection (UTI): Pediatric

Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
DST-701 Integumentary Assessment: Adult
Nurses with Remote Nursing Certified Practice designation (RN(C)s) are able to manage the following skin conditions:
• Abscess and furuncle
• Cellulitis
• Impetigo
• Bites
ADULT INTEGUMENTARY ASSESSMENT
History of Present Illness and Review of System
General
• The following characteristics of each symptom should be elicited and explored:
o Onset (sudden or gradual)
o Location and spread
o Duration, chronology
o Quality/severity of symptoms
o Associated symptoms
o Precipitating and aggravating factors such as new skin or hair products
o Relieving factors
o Timing and frequency
o Current situation (improving or deteriorating)
o Previous diagnosis of similar episodes
o Previous treatments and efficacy
o Effects on daily activities
Cardinal Signs and Symptoms
• In addition to the general characteristics outlined above, characteristics of specific symptoms should be elicited as follows:
General
o Fever
o Malaise
o Arthralgia
Skin
o Changes in texture or colour
o Unusual dryness or moisture
o Itching, burning, pain or numbness
o Rash
o Bruises, petechiae
o Changes in pigmentation
o Lesions, blisters or crust
o Changes in moles or birthmarks
Hair
o Changes in amount, texture, distribution
Nails
o Changes in texture, structure
DST-701 Integumentary Assessment: Adult DST-701 Integumentary Assessment: Adult
Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
Medical History Specific to Integumentary System
• Allergies (medication, environmental, food)
• Allergic manifestation (photosensitivity, asthma, hay fever, urticaria, Stevens-Johnson Syndrome)
• Medications (over the counter, and prescriptions; tetracycline, steroids, oral contraceptives, antibiotics, anticoagulants,
acetylsalicylic acid)
• Herbal preparations and complimentary therapies
• Immunization status (particularly tetanus and shingles)
• Communicable diseases: measles, chickenpox (varicella), herpes simplex
• Current skin complaint; detailed history
• Diseases:
o Recent or current viral or bacterial illness
o Known methicillin resistant staphylococcus aureus (MRSA) positive
o Immunocompromised
o Seborrheic dermatitis, contact dermatitis, psoriasis, eczema
o Asthma
o Diabetes, rheumatoid arthritis, thyroid disorder, collagen or vascular disorder
o Skin cancer
• Current skin complaint; detailed history
• Sun exposure, tanning beds
• Surgeries or recent Botox, microdermabrasion, chemical peel
• Keloid formation
Family History Specific to Integumentary System
• Allergies (seasonal, food)
• Seborrheic dermatitis
• Psoriasis
• Skin cancer
• Atopic dermatitis
• Autoimmune disorders
Personal and Social History Specific to Integumentary System
• History of sensitive skin
• Obesity
• Hot or humid environment, poor environmental sanitation
• Use of hot tubs, swimming pools
• Tattoos and piercings
• Stress or emotional disturbance (may precipitate flares of chronic skin problem such as psoriasis)
• Exposure to new substances (soaps, foods, plants)
• Recent travel
• Others at home with similar symptoms
• Recent insect bite/sting
• Substance use
Physical Assessment of Integumentary System
Vital Signs
• Temperature
• Pulse
DST-701 Integumentary Assessment: Adult
Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
• Respiration
• SpO2
• Blood Pressure
General Skin Assessment:
• Apparent state of health
• Appearance of comfort or distress
• Colour
• Nutritional status
• State of hydration, older adult at risk
• Hygiene
• Match between appearance and stated age
Inspection and Palpation of Skin
General Skin Examination
• Colour
• Temperature, texture, turgor, tenderness
• Dryness or moisture
• Scaling
• Pigmentation
• Vascularity (erythema, abnormal veins)
• Bruises, petechiae
• Edema
• Induration
• Skin folds
• Hair, nails, mucous membranes
Individual Lesions
• Colour
• Type
• Texture;
• General pattern of distribution
• Shape of single lesions, including the character of lesion edge (whether raised or flat)
• Joint involvement
Note: Examination of patients with darker skin colour requires awareness that pigmentation influences the colour of the lesion and
how certain lesions manifest clinically.
Other Aspects
• Examine lymph nodes
• Examine area distal to enlarged lymph nodes
Major Types and Characteristics of Skin Lesions
• The major types and characteristics of skin lesions are presented in Tables 1 and 2
• Jaundice, spider angioma, palmar erythema or a necklace of telangiectases may indicate liver disease, particularly associated
with alcohol or viral infection
• Petechiae or purpura may suggest a coagulation problem
DST-701 Integumentary Assessment: Adult

Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
Diagnostic Tests
The RN(C) may consider the following diagnostic tests to support clinical decision-making:
• Culture and sensitivity of weeping lesions
• Consider blood glucose and referral/consultation with physician or nurse practitioner if poorly healing wounds
Table 1: Major Types of Skin Lesions
Type of Lesions Feature
Primary Lesion Physical changes caused directly by the disease process
Atrophy (may be secondary) • Skin thin and wrinkled
Macule and patches • Flat, circumscribed, discoloured spot; size and shape variable (mole, port-wine stain),
macules less than 1 cm in diameter, patches greater than 1 cm in diameter
Nodule • Palpable, solid lesion that may or may not be elevated (e.g. keratinous cyst, small lipoma) greater than 1 cm in diameter
Papule • Solid elevated lesion (e.g. wart, syphilitic lesion, pigmented mole) less than/equal to 1 cm in
diameter
Petechiae, ecchymosis and
purpura • Extravasation of blood into skin causing non-blanching red macules and patches
• Petechiae less than 2 mm n diameter, ecchymosis more than 2 mm in diameter
• Purpura are groups of petechiae and/or ecchymosis that may be confluent, macular or raised
Plaque • Well-defined plateau-like elevation compared to its height above the skin (psoriasis)
Pustule • Superficial elevated lesion containing pus (e.g. acne, furuncle, carbuncle)
Telangiectasia • Fine, often irregular red line produced by dilatation of a normally invisible capillary
• Blanches with pressure
Ulcer (may be secondary) • Loss of epidermis and at least part of the dermis
Vesicles and bullae • Circumscribed, elevated lesions less than 5 mm in diameter containing clear fluid
• Larger vesicles are classified as bullae or blisters (e.g. insect bite, sunburn)
Wheal • Transient, irregularly shaped, elevated, indurated, changeable lesion caused by local edema
(e.g. allergic reaction to a drug, a bite, sunlight)
Secondary Lesions • May evolve from primary lesions, or caused by external sources such as trauma, infection, scratching
Crust • Dry exudate
Erosion • Loss of part or all of the epidermis
Excoriation • Superficial linear or hollowed-out crusted area, caused by scratching, or picking
Exudative: Dry (crust or scab) • Dried serum, blood or pus
Exudative: Wet (weeping) • Draining serum, blood or pus
Lichenification • Skin thickened, skin markings accentuated (atopic dermatitis)
Pigmentation changes • Hyperpigmentation (increased skin pigment)
• Hypopigmentation (decreased skin pigment)
• Depigmentation (complete loss of skin pigment)
Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
Scales • Heaping-up of the horny epithelium (e.g. psoriasis, seborrheic dermatitis, fungal infection,
chronic dermatitis)
Scar • Various skin manifestations of healing process (e.g. keloid or acne cicatrisation)
Sources: Suneja, M., Szot, J.F. LeBlond, R.F. & Brown, D. D. (2020).
Wolff, K., Johnson, R., Saavedra, A.P. Roh, E.K. (2017).
Table 2: Major Arrangements of Skin Lesions
Arrangement of Lesions Characteristics of Lesions
Annular Arranged in a circular pattern
Confluent Merge and run together
Discrete Individual, separate and distinct: insect bites
Generalized Scattered over the body: measles
Grouped Clustered: herpes simplex
Linear or serpiginous Forms a line or snakelike shape: poison ivy
Polycyclic Concentric circles resembling a "bull’s-eye": drug reactions, urticaria
Zosteriform Linear arrangement along a nerve root: shingles
Sources: Estes, M. E. Z. (2014).
Suneja, M., Szot, J.F. LeBlond, R.F. & Brown, D. D. (2020).
Signs and Symptoms Requiring Referral or Consultation
• The first step is to differentiate a major skin eruption, infection or event from a minor one that can be managed by nurses
with certified practice designation
• The following require consultation and/or referral to a physician or nurse practitioner:
o Petechiae or widespread purpura
o Unusual bruising
o Palmer erythema
o Spider angioma
o Caput medusae
o Jaundice
o Butterfly rash
o Skin presentation in the presence of systemic disease
o Known or suspected MRSA
o Any cellulitis covering or involving a joint
o Suspicious pigmented lesions
• Urgent referral/consultation: Facial, periorbital and orbital cellulitis are particularly worrisome as they can lead to
meningitis
DOCUMENTATION
• As per agency policy
DST-701 Integumentary Assessment: Adult DST-701 Integumentary Assessment: Adult
Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
REFERENCES
More recent editions of any of the items in the Reference List may have been published since this DST was published. If you have a
newer version, please use it.
Armstrong, C.A. (2019). Approach to the clinical dermatologic diagnosis. UpToDate.
Ball, J. W., Dains, J. E., Flynn, J. A., Solomon, B. S., & Stewart, R. W. (Eds.). (2019). Seidel’s guide to physical examination (9th ed.). St. Louis, MO: Elsevier. ISBN: 9780323481953
British Columbia Centre for Disease Control. (2014). Antimicrobial resistance trends in the Province of British Columbia. Vancouver, BC: Author.
Cash, J. C., & Glass, C. A. (Eds.). (2020). Family practice guidelines (5th ed.). New York, NY: Springer.
Coulson IH, Benton EC, Ogden S. Diagnosis of skin disease. In: Rook's Textbook of Dermatology, Ninth Edition, Griffiths C, Barker J, Bleiker T, et al (Eds), Wiley-Blackwell, Oxford, United Kingdom 2016.
Estes, M. E. Z. (2014). Health assessment and physical examination (5th ed.). Clifton Park, NY: Cengage Learning.
Health Canada, First Nations and Inuit Health Branch. (2012). Clinical practice guidelines for nurses in primary care: pediatric and adolescent care.
Jarvis, C. (2018). Physical examination and health assessment (3rd Canadian ed.). Toronto, ON: Elsevier Canada.
Suneja, M., Szot, J.F. LeBlond, R.F. & Brown, D. D. (2020). DeGowin’s diagnostic examination (11th ed.). New York, NY: McGraw-Hill Medical.
Wolff, K., Johnson, R., Saavedra, A.P. Roh, E.K. (2017). Fitzpatrick's Color Atlas and Synopsis of Clinical Dermatology, (8th Ed.) New York, NY: McGraw-Hill Education.
DST-701 Integumentary Assessment: Adult
Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
DST-702 Integumentary Assessment: Pediatric
Nurses with Remote Practice Certified Practice designation (RN(C)s7) are able to treat children with the following skin conditions:
• Impetigo in children 6 months of age and older
• Cellulitis in children 2 years of age and older
• Bites in children 1 year of age and older
• The following assessment must be completed and documented.
ASSESSMENT
History of Present Illness and Review of Systems
General
The following characteristics of each symptom should be elicited and explored:
• Onset (sudden or gradual)
• Location and spread
• Duration, chronology
• Characteristics /quality/severity of symptoms
• Associated symptoms
• Precipitating and aggravating factors including environmental factors such as skin and hair products
• Relieving factors
• Timing and frequency
• Current situation (improving or deteriorating)
• Previous diagnosis of similar episodes
• Previous treatments and efficacy
• Effects on daily activities
Cardinal Signs and Symptoms
In addition to the general characteristics outlined above, other characteristics of specific symptoms should be elicited, as follows:
General
• Fever
• Malaise
• Arthralgia
Skin
• Changes in texture or colour
• Unusual dryness or moisture
• Itching, burning, pain or numbness
• Rash
• Bruises, petechiae
• Changes in pigmentation
7 RN(C) is an authorized title recommended by BCCNP that refers to BCCNP-certified RNs, and is used throughout this Decision
Support Tool (DST).
DST-702 Integumentary Assessment: Pediatric DST-702 Integumentary Assessment: Pediatric
Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
• Lesions, blisters or crust
• Changes in moles or birthmarks
Hair
• Changes in amount, texture, distribution
Nails
• Changes in texture, structure
Medical History (specific to the Integumentary System)
• Allergies – medication, environmental, food
• Allergic manifestation (e.g., photosensitivity, asthma, hay fever, urticaria, Stevens-Johnson Syndrome)
• Medication (over the counter and prescriptions e.g., tetracycline, sulphonamides, steroids, oral contraceptives, antibiotics,
anticoagulants, acetylsalicylic acid (ASA))
• Herbal preparations and complimentary therapies
• Immunization status (particularly tetanus and shingles)
• Communicable diseases: measles, chickenpox (varicella), herpes simplex
• Current skin complaint; detailed history
• Diseases:
o Recent or current viral or bacterial illness
o Known Methicillin Resistant Staphylococcus Aureus (MRSA) positive
o Immunocompromised
o Seborrheic dermatitis, contact dermatitis, psoriasis, eczema
o Asthma
o Diabetes rheumatoid arthritis, thyroid disorder, collagen or vascular disorder
• Skin cancer, Sun exposure, tanning beds
• Surgeries or recent collagen, Botox, microdermabrasion, chemical peel
• Keloid formation
• Birth and prenatal history, if age appropriate
• Feeding – breast or bottle fed
Family History Specific to Integumentary System
• Allergies (e.g., seasonal, food)
• Seborrheic dermatitis
• Psoriasis
• Skin cancer
• Atopy and asthma
• Autoimmune disorders
Personal and Social History Specific to Integumentary System
• History of sensitive skin
• Obesity
• Hot or humid environment, poor environmental sanitation
• Use of hot tubs, swimming pools
• Tattoos and piercings
• Stress or emotional disturbance (may precipitate flares of chronic skin problem such as psoriasis)
Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
• Self-harm behaviour
• Exposure to new substances (e.g., soaps, foods, pets, plants)
• Recent travel
• Others at home with similar symptoms (e.g., rash)
• Recent insect bite/sting (e.g., bee, tick, mosquito)
PHYSICAL ASSESSMENT OF THE INTEGUMENTARY SYSTEM
Vitals
• Temperature
• Pulse
• Respiration
• SpO2
• Blood pressure (BP)
• Weight for all children under 12 yrs for medication calculations
General
• Apparent state of health
• Appearance of comfort or distress
• Colour
• Nutritional status
• State of hydration
• Hygiene
• Match between appearance and stated age
• Character of cry (in infants less than 6 months old)
• Activity level
• Mental status
• Degree of cooperation, consolability
• Emotional reaction to caregiver and examiner
• Difficulty with gait or balance
Inspection and Palpation of the Skin
• General skin examination
o Colour
o Temperature, texture, turgor, tenderness
o Dryness or moisture
o Scaling
o Pigmentation
o Vascularity, bruises, petechiae
o Edema
o Induration
o Skin folds
o Hair, nails, mucous membranes
• Individual lesions
DST-702 Integumentary Assessment: Pediatric DST-702 Integumentary Assessment: Pediatric
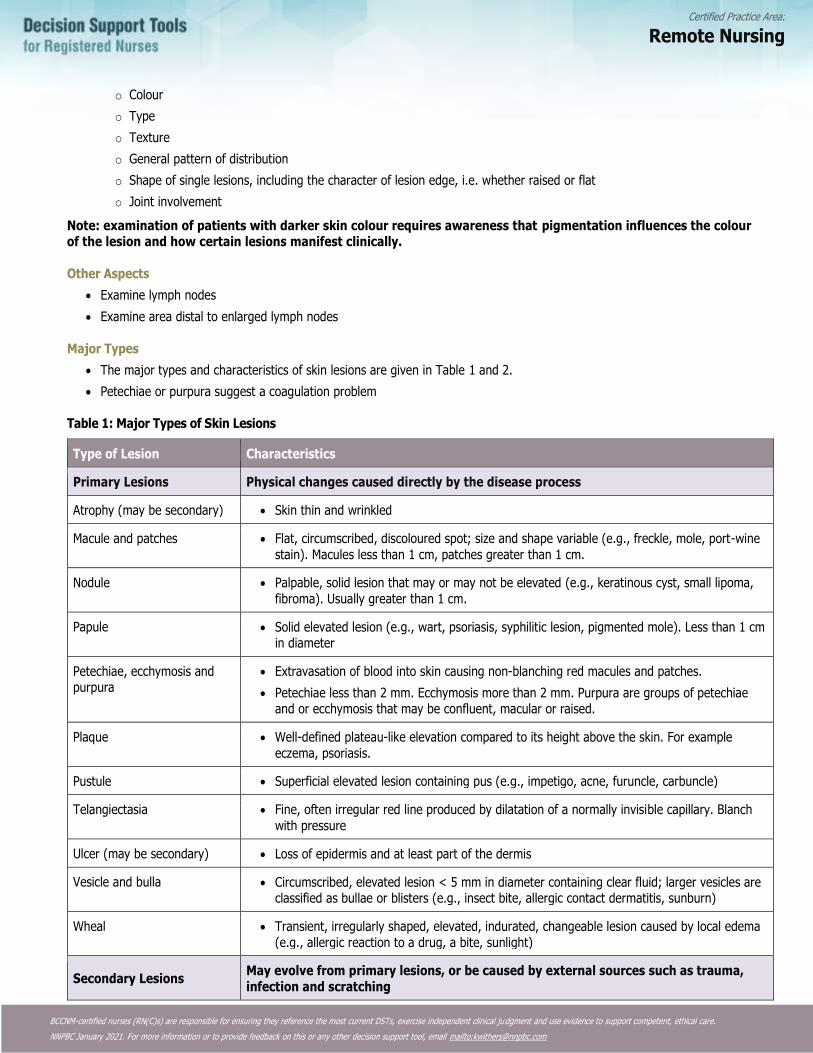
Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
o Colour
o Type
o Texture
o General pattern of distribution
o Shape of single lesions, including the character of lesion edge, i.e. whether raised or flat
o Joint involvement
Note: examination of patients with darker skin colour requires awareness that pigmentation influences the colour of the lesion and how certain lesions manifest clinically.
Other Aspects
• Examine lymph nodes
• Examine area distal to enlarged lymph nodes
Major Types
• The major types and characteristics of skin lesions are given in Table 1 and 2.
• Petechiae or purpura suggest a coagulation problem
Table 1: Major Types of Skin Lesions
Type of Lesion Characteristics
Primary Lesions Physical changes caused directly by the disease process
Atrophy (may be secondary) • Skin thin and wrinkled
Macule and patches • Flat, circumscribed, discoloured spot; size and shape variable (e.g., freckle, mole, port-wine
stain). Macules less than 1 cm, patches greater than 1 cm.
Nodule • Palpable, solid lesion that may or may not be elevated (e.g., keratinous cyst, small lipoma,
fibroma). Usually greater than 1 cm.
Papule • Solid elevated lesion (e.g., wart, psoriasis, syphilitic lesion, pigmented mole). Less than 1 cm in diameter
Petechiae, ecchymosis and purpura
• Extravasation of blood into skin causing non-blanching red macules and patches.
• Petechiae less than 2 mm. Ecchymosis more than 2 mm. Purpura are groups of petechiae and or ecchymosis that may be confluent, macular or raised.
Plaque • Well-defined plateau-like elevation compared to its height above the skin. For example
eczema, psoriasis.
Pustule • Superficial elevated lesion containing pus (e.g., impetigo, acne, furuncle, carbuncle)
Telangiectasia • Fine, often irregular red line produced by dilatation of a normally invisible capillary. Blanch
with pressure
Ulcer (may be secondary) • Loss of epidermis and at least part of the dermis
Vesicle and bulla • Circumscribed, elevated lesion < 5 mm in diameter containing clear fluid; larger vesicles are classified as bullae or blisters (e.g., insect bite, allergic contact dermatitis, sunburn)
Wheal • Transient, irregularly shaped, elevated, indurated, changeable lesion caused by local edema
(e.g., allergic reaction to a drug, a bite, sunlight)
Secondary Lesions May evolve from primary lesions, or be caused by external sources such as trauma,
infection and scratching
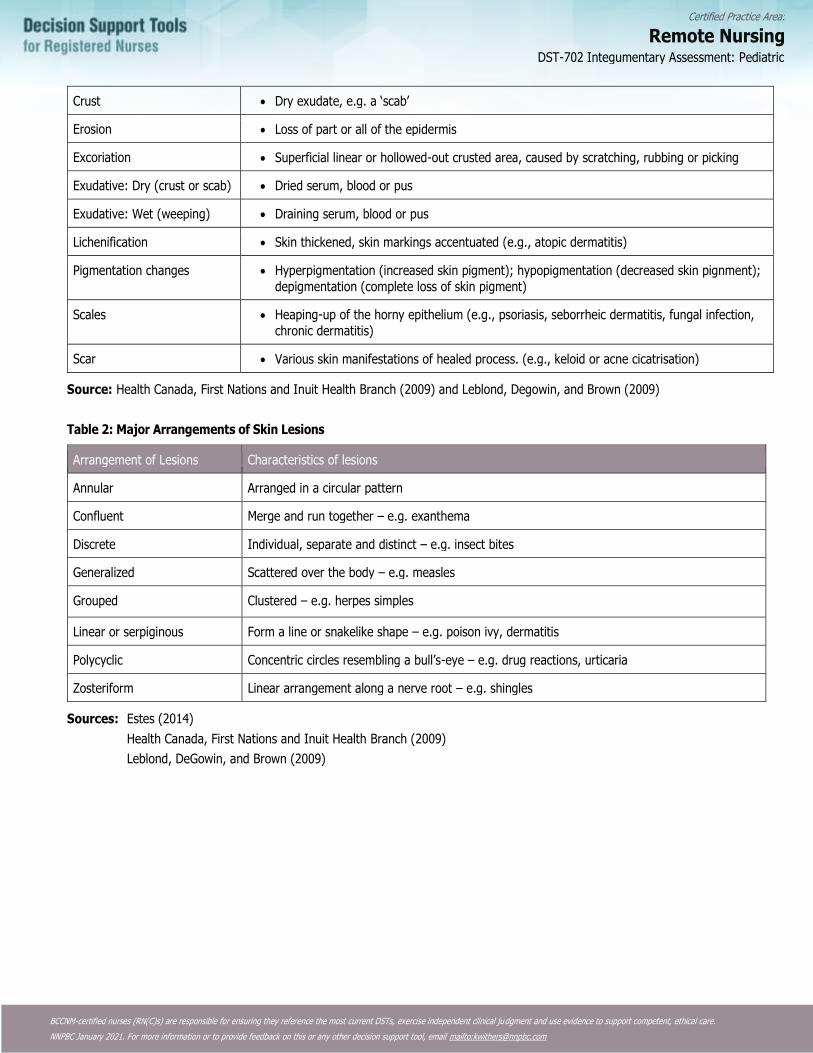
Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
Crust • Dry exudate, e.g. a ‘scab’
Erosion • Loss of part or all of the epidermis
Excoriation • Superficial linear or hollowed-out crusted area, caused by scratching, rubbing or picking
Exudative: Dry (crust or scab) • Dried serum, blood or pus
Exudative: Wet (weeping) • Draining serum, blood or pus
Lichenification • Skin thickened, skin markings accentuated (e.g., atopic dermatitis)
Pigmentation changes • Hyperpigmentation (increased skin pigment); hypopigmentation (decreased skin pignment);
depigmentation (complete loss of skin pigment)
Scales • Heaping-up of the horny epithelium (e.g., psoriasis, seborrheic dermatitis, fungal infection,
chronic dermatitis)
Scar • Various skin manifestations of healed process. (e.g., keloid or acne cicatrisation)
Source: Health Canada, First Nations and Inuit Health Branch (2009) and Leblond, Degowin, and Brown (2009)
Table 2: Major Arrangements of Skin Lesions
Arrangement of Lesions Characteristics of lesions
Annular Arranged in a circular pattern
Confluent Merge and run together – e.g. exanthema
Discrete Individual, separate and distinct – e.g. insect bites
Generalized Scattered over the body – e.g. measles
Grouped Clustered – e.g. herpes simples
Linear or serpiginous Form a line or snakelike shape – e.g. poison ivy, dermatitis
Polycyclic Concentric circles resembling a bull’s-eye – e.g. drug reactions, urticaria
Zosteriform Linear arrangement along a nerve root – e.g. shingles
Sources: Estes (2014)
Health Canada, First Nations and Inuit Health Branch (2009)
Leblond, DeGowin, and Brown (2009)
DST-702 Integumentary Assessment: Pediatric
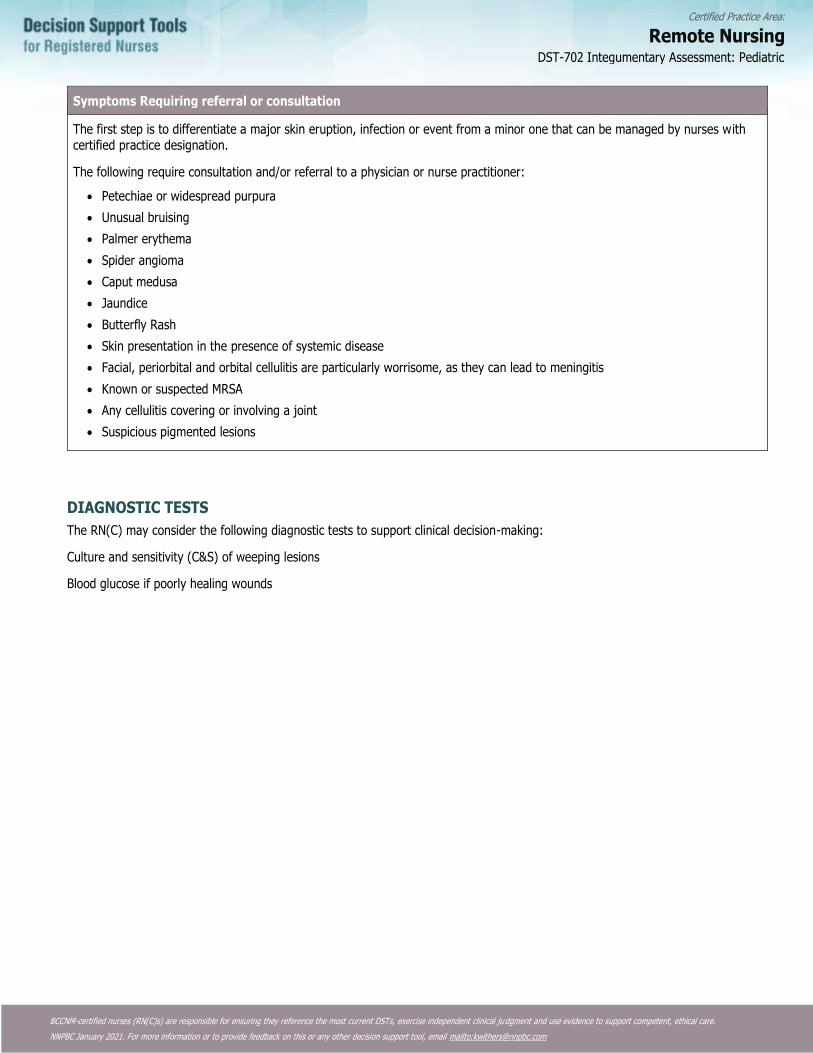
Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
Symptoms Requiring referral or consultation
The first step is to differentiate a major skin eruption, infection or event from a minor one that can be managed by nurses with certified practice designation.
The following require consultation and/or referral to a physician or nurse practitioner:
• Petechiae or widespread purpura
• Unusual bruising
• Palmer erythema
• Spider angioma
• Caput medusa
• Jaundice
• Butterfly Rash
• Skin presentation in the presence of systemic disease
• Facial, periorbital and orbital cellulitis are particularly worrisome, as they can lead to meningitis
• Known or suspected MRSA
• Any cellulitis covering or involving a joint
• Suspicious pigmented lesions
DIAGNOSTIC TESTS
The RN(C) may consider the following diagnostic tests to support clinical decision-making:
Culture and sensitivity (C&S) of weeping lesions
Blood glucose if poorly healing wounds
DST-702 Integumentary Assessment: Pediatric

Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
REFERENCES
More recent editions of any of the items in the Reference List may have been published since this DST was published. If you have a newer version, please use it.
Ball, J. W., Dains, J. E., Flynn, J. A., Solomon, B. S., & Stewart, R. W. (Eds.). (2015). Seidel’s guide to physical examination (8th ed.). St. Louis, MO: Elsevier.
BC Centre for Disease Control. (2014). Guidelines for the management of Community-associated Methicillin-Resistant Staphylococcus aureus (CA-MRSA)-related skin and soft tissue infections in primary care. Vancouver, BC: Author.
Estes, M. E. Z. (2014). Health assessment and physical examination (5th ed.). Clifton Park, NY: Cengage Learning.
Goldstein, B. G., & Goldstein, A. O. (2015). Approach to dermatologic diagnosis. UptoDate.
Health Canada, First Nations and Inuit Health Branch. (2009, July). Clinical practice guidelines for nurses in primary care: Pediatric and adolescent care: Chapter 16: Skin.
Jarvis, C. (2014). Physical examination and health assessment (2nd Canadian ed.). Toronto, ON: Elsevier Canada.
Leblond, R. F., DeGowin, R. L., & Brown, D. D. (2014). DeGowin’s diagnostic examination (10th ed.). New York, NY: McGraw-Hill Medical.
Sawyer, S. S. (2012). Pediatric physical examination and health assessment. Sudbury, MA: Jones & Bartlett Learning.
Stephen, T. C., Skillen, D. L., Day, R. A., & Bickley L. S. (2010). Canadian Bates’ guide to health assessment for nurses. Philadelphia, PA: Lippincott, Williams & Wilkins.
Swetter, S. & Geller, A. C. (2015). Clinical features and diagnosis of cutaneous melanoma.
DST-702 Integumentary Assessment: Pediatric
Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
DST-703 Cellulitis: Adult
DEFINITION
An acute, diffuse, spreading skin infection involving the deeper layers of the skin and subcutaneous tissue.
POTENTIAL CAUSES
• Bacteria: most commonly Staphylococcus species
• In B.C., methicillin resistant staph aureus comprises over 25% of staph aureus infections.
• Local trauma (e.g., lacerations, burns, insect bites, wounds, shaving)
• Skin infections, such as impetigo, scabies, furuncle, tinea pedis
• Underlying skin ulcer
• Fragile skin
• Intravenous drug use
• Immunocompromised host
• Diabetes
• Inflammation (e.g., eczema)
• Edema secondary to venous insufficiency or lymphedema
• Known methicillin resistant staphylococcus aureus (MRSA) positive (family or household member)
Note: If human, cat or dog bite was the original trauma, see Adult Bites DST.
TYPICAL FINDINGS OF CELLULITIS
History
• Presence of predisposing risk factor(s)
• Area increasingly red, warm to touch, painful
• Area around skin lesion also tender but pain localized
• Edema
• Mild systemic symptoms – low-grade fever, chills, malaise and headache may be present
• Known MRSA positive
Physical Assessment
• Local symptoms:
• Erythema and edema of area
• Warm to touch
• Possibly fluctuant (movable and compressible – fluid-
• May resemble peau d’orange
• Advancing edge of lesion diffuse, not sharply demarcated
• Small amount of purulent discharge may be present
• Unilateral
• Systemic indications:
• Increased temperature
• Increased pulse
• Lymphadenopathy of regional lymph nodes and/or lymphangitis
DST-703 Cellulitis: Adult

Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
Diagnostic Tests
• Swab any wound discharge for culture and sensitivity.
• Determine blood glucose level if infection is recurrent or if symptoms are suggestive of diabetes mellitus.
MANAGEMENT AND INTERVENTIONS
Note: Do not underestimate cellulitis. It can spread very quickly and may progress rapidly to necrotizing fasciitis. It should be treated aggressively and monitored on an on-going basis.
Goals of Treatment
• Resolve infection
• Identify formation of abscess
• Check tetanus prophylaxis
Non-pharmacologic Interventions
• Apply warm or cool saline compresses to affected areas qid for 15 minutes for comfort
• Mark border of erythema with pen to monitor spread of inflammation
• Elevate, rest and gently splint the affected limb
Pharmacologic Interventions
Analgesics:
acetaminophen 325 mg 1-2 tabs po q4-6 h prn
OR
ibuprofen 200 mg, 1-2 tabs po q 4-6 h prn
Antibiotics:
Oral antibiotics if MRSA not suspected:
cloxacillin 500 mg po qid for 5-7days,
OR
cephalexin 500 mg po qid for 5-7 days
Clients with penicillin and cephalosporin allergy (e.g. cephalexin):
clindamycin 300 mg PO QID for 5-7 days
Clients with known MRSA:
trimethoprim 160 mg/sulfamethoxazole 800mg (DS) 1 tab po bid for 5-7 days,
OR
doxycycline 100 mg po bid for 5-7 days
Pregnant Women
• Acetaminophen, cloxacillin, cephalexin may be used
• DO NOT USE trimethoprim-sulfamethoxazole or ibuprofen
Breastfeeding Women
• Ibuprofen can be used in breast feeding after consultation with physician or nurse practitioner.
• DO NOT USE trimethoprim/sulfamethoxazole or doxycycline.
DST-703 Cellulitis: Adult

Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
POTENTIAL COMPLICATIONS
• Extension of infection
• Abscess formation
• Sepsis
• Necrotising fasciitis
• Recurrent cellulitis
CLIENT EDUCATION AND DISCHARGE INFORMATION
• Advise on condition, timeline of treatment and expected course of disease process.
• Counsel client about appropriate use of medications (dose, frequency, compliance).
• Encourage proper hygiene of all skin wounds to prevent future infection.
• Stress importance of close follow-up.
• If shaving is the cause, educate the client about shaving with the hair growth.
MONITORING AND FOLLOW-UP
• Follow-up daily until resolving to ensure that infection is controlled.
• Instruct client to return for reassessment immediately if lesion becomes fluctuant, if pain increases or if low grade or high
fever develops.
CONSULTATION AND/OR REFERRAL
• Consult with or refer to a physician or nurse practitioner if:
• New symptoms present or progression of disease is rapid,
• no improvement after 48 hours of antibiotics,
• client is diabetic and /or immunocompromised,
• pain is out of proportion to the clinical findings,
• cellulitis is over or involves a joint, or
• any facial cellulitis.
DOCUMENTATION
As per agency policy
DST-703 Cellulitis: Adult

Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
REFERENCES
More recent editions of any of the items in the Reference List may have been published since this DST was published. If you have a newer version, please use it.
Anti-Infective Review Panel. (2012). Anti-infective guidelines for community-acquired infections. Toronto, ON: MUMS Guideline Clearinghouse.
Blondel-Hill, E., & Fryters, S. (2012). Bugs and drugs: An antimicrobial infectious diseases reference. Edmonton, AB: Alberta Health Services.
Breen, J. O. (2010). Skin and soft tissue infections in immunocompetent patients. American Family Physician, 81(7), 893-899.
British Columbia Centre for Disease Control. (2011). Antimicrobial resistance trends in the Province of British Columbia 2011. Vancouver, BC: Author.
British Columbia Centre for Disease Control. (2014). Guidelines for the management of community-associated methicillin-resistant Staphylococcus aureus (CA-MRSA)-related skin and soft tissue infections in primary care. Vancouver, BC: Author.
Canadian Pharmacists Association. (2017). Therapeutic choices. Ottawa, ON: Author.
DynaMed. (2016). Cellulitis.
DynaMed. (2014, August 12). Treatment of MRSA skin and soft tissue infections.
Herchline, T. E. (2014, August 19). Cellulitis.
Kim, J. & Mukovozov, I. (2017). Toronto notes 2017: Comprehensive medical reference & review for Medical Council of Canada Qualifying Exam Part 1 and the United States Medical Licensing Exam Step 2 th 33rd. Ed.). Toronto, ON: Toronto Notes for Medical Students. Retrieved from https://www.scribd.com/document/351268506/Toronto-Notes-2017-pdf
Liu, C., Bayer, A., Cosgrove, S.E., Daum, R.S., Fridkin, S.K., Gorwitz, R.J.,…Chambers, H.F. (2011). Clinical practice guidel ines by the Infectious Diseases Society of America for the treatment of methicillin-resistant Staphylococcus aureus infections in adults and children. Clinical Infectious Diseases, 52(3), e18-e55.
MacNeal, R. J. (2013). Description of skin lesions. Kenilworth, NJ: Merck & Co.
Napierkowski, D. (2013). Uncovering common bacterial skin infections. Nurse Practitioner, 38(3), 30-37.
Nazarko, L. (2012). An evidence-based approach to diagnosis and management of cellulitis. British Journal of Community Nursing, 17(1), 6-12.
Parnes, B., Fernald, D., Coombs, L., Dealleaume, L., Brandt, E., Webster, B.,…West, D. (2011). Improving the management of skin and soft tissue infections in primary care: A report from State Networks of Colorado Ambulatory Practices and Partners
(SNOCAP-USA) and the Distributed Ambulatory Research in Therapeutics Network (DARTNet). Journal of the American Board of Family Medicine, 24(5), 534-542.
Stevens, D., Bisno, A. L., Chambers, H. F., Dellinger, E. P., Goldstein, E. J. C., Gorbach, S. L.,…Wade, J. C. (2014). Practice guidelines for the diagnosis and management of skin and soft tissue infections: 2014 update by the Infectious Diseases Society of America. Clinical Infectious Diseases, 59(2), e10-e52.
Wolff, K., & Johnson, R. A. (2009). Fitzpatrick’s color atlas and synopsis of clinical dermatology (6th ed.). New York: McGraw-Hill Medical.
DST-703 Cellulitis: Adult
Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
DST-704 Cellulitis: Pediatric
DEFINITION
An acute, diffuse, spreading infection of the skin, involving the deeper layers of the skin and the subcutaneous tissue.
Nurses with Remote Practice Certified Practice designation (RN(C)s8) are able to treat children with non-facial cellulitis who are 2 years of age and older.
POTENTIAL CAUSES
• Bacteria: most commonly Staphylococcus species
• In B.C., methicillin resistant staph aureus comprises over 25% of staph aureus infections.
PREDISPOSING RISK FACTORS
• Local trauma (e.g., lacerations, burns, insect bites, wounds, shaving)
• Skin infections such as impetigo, scabies, furuncle, tinea pedis
• Underlying skin ulcer
• Fragile skin
• Immunocompromised host
• Diabetes
• Inflammation (e.g., eczema)
• Edema secondary to venous insufficiency or lymphedema
• Known methicillin resistant staph aureus (MRSA) positive (family or household member)
Note: If human, cat or dog bite was the original trauma, see Pediatric Bites DST
TYPICAL FINDINGS OF CELLULITIS
History
• Presence of predisposing risk factor
• Area increasingly red, warm to touch, painful
• Area around skin lesion also tender but pain localized
• Edema
• Mild systemic symptoms – low-grade fever, chills, malaise, and headache may be present
• Known MRSA positive
Physical Assessment
• Local symptoms:
o Erythema and edema of area
o Warm to touch
o Possibly fluctuant (movable and compressible – fluid-based)
o May resemble peau d’orange
o Advancing edge of lesion diffuse, not sharply demarcated
8 RN(C) is an authorized title recommended by BCCNP that refers to BCCNP-certified RNs, and is used throughout this Decision
Support Tool (DST).
DST-704 Cellulitis: Pediatric
Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
o Small amount of purulent discharge may be present
o Unilateral
• Systemic indications:
o Increased temperature
o Increased pulse
o Lymphadenopathy of regional lymph nodes and/or lymphangitis
Diagnostic Tests
Swab any wound discharge for culture and sensitivity (C&S)
MANAGEMENT AND INTERVENTIONS
Note: Do not underestimate cellulitis. It can spread very quickly and may progress rapidly to necrotizing fasciitis. It should be treated aggressively and monitored on an on-going basis.
Goals of Treatment for Mild Cellulitis
• Resolve infection
• Identify formation of abscess
• Check tetanus prophylaxis
Non-pharmacologic Interventions
• Apply warm or, if more comfortable, cool saline compresses to affected areas qid for 15 minutes.
• Mark border of erythema with pen to monitor spread of inflammation.
• Elevate, rest and gently splint the affected limb.
PHARMACOLOGIC INTERVENTIONS
Ensure recent weight obtained for medications where dose is dependant on weight
Analgesics
acetaminophen 10-15mg/kg/dose po q4-6 hours prn Do not exceed 75mg/kg in 24 hours, from all acetaminophen sources
OR
ibuprofen 5-10mg/kg/dose po 4-6 hours prn Do not exceed 40mg/kg in 24hr
Antibiotics
Oral antibiotics if MRSA not suspected:
cephalexin 25-50 mg/kg/day po divided qid for 5-7 days
OR
cloxacillin 50 mg/kg per day po divided qid for 5-7 days
Clients with penicillin or cephalosporin allergy (e.g. cephalexin):
clindamycin 25-30 mg/kg/day po divided tid for 5-7 days
Clients with known community acquired MRSA or purulent cellulitis:
trimethoprim-sulfamethoxazole 8-12 mg/kg/day po (dosing is based on trimethoprim component) divided bid for 5-7 days
Pregnant Women (dosing as above)
• Cephalexin, cloxacillin, and acetaminophen may be used as listed above.
• DO NOT USE trimethoprim-sulfamethoxazole or ibuprofen
DST-704 Cellulitis: Pediatric
Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
Breastfeeding Women (dosing as above)
• Ibuprofen can be used in breast feeding after consultation with physician or nurse practitioner.
• DO NOT USE trimethoprim-sulfamethoxazole
POTENTIAL COMPLICATIONS
• Extension of infection
• Abscess formation
• Sepsis
• Necrotising fasciitis
• Recurrent cellulitis
CLIENT/CAREGIVER EDUCATION AND DISCHARGE INFORMATION
• Advise on condition, timeline of treatment and expected course of disease process.
• Counsel client about appropriate use of medications (dose, frequency, compliance).
• Encourage proper hygiene of all skin wounds to prevent future infection.
• Stress importance of close follow-up.
• If shaving is the cause, educate the client about shaving with the hair growth.
MONITORING AND FOLLOW-UP
• Follow-up daily to ensure that infection is controlled.
• Instruct parent or caregiver to return for reassessment immediately if lesion becomes fluctuant, if pain increases, if cellulitis
spreads or if fever develops.
CONSULTATION AND/OR REFERRAL
• Consult with or refer to a physician or nurse practitioner if:
• New systemic symptoms present or progression of disease is rapid,
• no improvement after 48 hours of antibiotics,
• client is diabetic and /or immunocompromised,
• pain is out of proportion to the clinical findings,
• cellulitis is over or involves a joint, or
• any facial cellulitis.
DOCUMENTATION
As per agency policy
DST-704 Cellulitis: Pediatric

Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
REFERENCES
More recent editions of any of the items in the Reference List may have been published since this DST was published. If you have a newer version, please use it.
Anti-Infective Review Panel. (2013). Anti-infective guidelines for community-acquired infections. Toronto, ON: MUMS Guideline Clearinghouse.
Blondel-Hill, E., & Fryters, S. (2012). Bugs and drugs: An antimicrobial infectious diseases reference. Edmonton, AB: Alberta Health Services.
Breen, J. O. (2010). Skin and soft tissue infections in immunocompetent patients. American Family Physician, 81(7), 893-899.
British Columbia Centre for Disease Control. (2014). Antimicrobial resistance trends in the province of British Columbia. Vancouver, BC: Author.
British Columbia Centre for Disease Control. (2014). Guidelines for the management of community-associated methicillin-resistant Staphylococcus aureus (CA-MRSA)-related skin and soft tissue infections in primary care. Vancouver, BC: Author.
British Columbia Centre for Disease Control. (2014). Guidelines for the management of community-associated methicillin-resistant Staphylococcus aureus (CA-MRSA)-related skin and soft tissue infections in primary care. Vancouver, BC: Author.
Canadian Pharmacists Association. (2017). Therapeutic choices. Ottawa, ON: Author.
DynaMed. (2015, July 22). Preseptal cellulitis.
DynaMed. (2015, October 12). Cellulitis.
DynaMed. (2015, September 17). Treatment of MRSA skin and soft tissue infections.
DynaMed. (2015, July 22). Orbital cellulitis.
Esau, R. (Ed.). (2012). British Columbia’s Children’s Hospital pediatric drug dosage guidelines (6th ed.). Vancouver, BC: Children’s & Women’s Health Centre of B.C.
Herchline, T. E. (2017, July 05). Cellulitis.
Kim, J. & Mukovozov, I. 2017). Toronto notes 2017: Comprehensive medical reference & review for Medical Council of Canada Qualifying Exam Part 1 and the United States Medical Licensing Exam Step 2 th 33rd. Ed.). Toronto, ON: Toronto Notes for Medical Students.
Liu, C., Bayer, A., Cosgrove, S.E., Daum, R.S., Fridkin, S.K., Gorwitz, R.J.,…Chambers, H.F. (2011). Clinical practice guidel ines
by the Infectious Diseases Society of America for the treatment of methicillin-resistant Staphylococcus aureus infections in adults and children. Clinical Infectious Diseases, 52(3), e18-e55.
Long, C. B., Madan, R. P., & Herold, B. C. (2010). Diagnosis and management of community-associated MRSA infections in children. Expert Review of Anti-Infective Therapy, 8(2), 183-195.
MacNeal, R. J. (2013). Description of skin lesions. Kenilworth, NJ: Merck & Co.
Methicillin-resistant Staphylococcus aureus in First Nations communities in Canada. (2005). Pediatrics and Child Health, 10(9), 557-559.
DST-704 Cellulitis: Pediatric

Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
Moran, G. J., Krishnadasan, A., Gorwitz, R. J., Fosheim, G. E., McDougal, L. K., Carey, R. B., Talan, D.A. (2006). Methicillin-resistant S. aureus infections among patients in the emergency department. New England Journal of Medicine, 355(7), 666-674.
Napierkowski, D. (2013). Uncovering common bacterial skin infections. Nurse Practitioner, 38(3), 30-37.
NeVille-Swensen, M., & Clayton, M. (2011). Outpatient management of community-associated methicillin- resistant Staphylococcus aureus skin and soft tissue infection. Journal of Pediatric Health Care, 25(5), 308-315.
Rockwell, F., Goh, S. H., Al-Rawahi, G., Hoang, L., Isaac-Renton, J., Gilbert, M.,…Patrick, D. (2005). A report on the emergence of Community-Acquired Methicillin-Resistant Staphylococcus aureus (CA-MRSA) in British Columbia.
Stevens, D., Bisno, A. L., Chambers, H. F., Dellinger, E. P., Goldstein, E. J. C., Gorbach, S. L.,…Wade, J. C. (2014). Practice
guidelines for the diagnosis and management of skin and soft tissue infections: 2014 update by the Infectious Diseases Society of America. Clinical Infectious Diseases, 59(2), e10-e52.
Watkins, J. (2012). Differentiating common bacterial skin infections. British Journal of School Nursing, 7(2), 77-78.
Wolff, K., & Johnson, R. A. (2013). Fitzpatrick’s color atlas and synopsis of clinical dermatology (7thed.). New York: McGraw-Hill Medical.
DST-704 Cellulitis: Pediatric
Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
DST-705 Impetigo: Adult
DEFINITION
A highly contagious, superficial bacterial infection of the skin, it primarily affects children during the summer. Beginning with vesicular lesions, it progresses to honey crusted lesions and is commonly seen on the face, arms, legs and buttocks.
POTENTIAL CAUSES
• S. aureus is the principal pathogen.
• Group A Beta-hemolytic strep presents alone or in conjunction with S. aureus in a minority of cases.
PREDISPOSING RISK FACTORS
• Local skin trauma such as insect bites, wounds
• Skin lesions from other disorders such as eczema, scabies, pediculosis
• Age – more common in pre-school and young children
• Crowded living conditions
• Poor hygiene
• Warm, moist climate
TYPICAL FINDINGS OF IMPETIGO
History
• More common on face, scalp and hands, but may occur anywhere
• Involved area is usually exposed
• Usually occurs during summer
• New lesions usually due to auto-inoculation
• Rash begins as tiny red lesions, which may be itchy
• Lesions rapidly become small vesicles, progressing to pustules, which rupture and drain to form yellow crusts
• Lesions painless
• Fever and systemic symptoms rare – mild fever may be present in more generalized infections
• Known methicillin-resistant staphylococcus aureus (MRSA) positive (client or household member)
Physical Assessment
• Thick, golden yellow, crusted lesion on a red base
• Numerous skin lesions at various stages present (vesicles, pustules, crusts, serous or pustular drainage, ulcers, healing
lesions)
• Bullae may be present, but more common in children
• Lesions and surrounding skin may feel warm to touch
• Regional lymph nodes may be enlarged, tender
Diagnostic Tests
Identification of impetigo may be made upon consideration of clinical features and presentation.
• Culture and Sensitivity of exudate if widespread or treatment failure at 48 hours
• Determine blood glucose level if infection is recurrent or if symptoms suggestive of diabetes mellitus are present
DST-705 Impetigo: Adult
Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
MANAGEMENT AND INTERVENTIONS
Goals of Treatment
• Resolve infection
• Prevent auto-inoculation
• Prevent spread to other household members
Non-pharmacologic Interventions
• Apply warm saline compresses to soften and soak away crusts qid for 15 minutes and prn
Pharmacologic Interventions
• Apply topical antibiotic preparation after each soaking:
o Mupirocin ointment to affected lesions tid for 5 days
• If non-responsive:
o Fusidic acid ointment or cream tid or qid for 7 days
• Topical agents are sufficient when there are only a small number of non-bullous lesions.
• Oral antibiotics may be necessary if there are multiple lesions making topical treatment impractical, the client is febrile and
has systemic symptoms including lymphadenopathy, or if bullous impetigo is present:
Cloxacillin 250-500 mg po qid for 7 days,
OR
Cephalexin 250-500 mg po qid for 7 days
• For clients with allergy to penicillin:
o Erythromycin 250-500 mg/day divided qid po for 7 days
If known MRSA positive or MRSA positive swab result:
Trimethoprim 160 mg /sulfamethoxazole 800mg (DS) 1 tab po bid for 10 days
OR
Doxycycline 100 mg po bid for 5-10 days
Pregnant or Breastfeeding Women (dosing as above)
• Mupirocin, cloxacillin, cephalexin, and erythromycin may be used as listed above.
• Avoid fusidic acid ointment.
• DO NOT USE trimethoprim 160 mg/sulphamethoxazole 800 mg and/or doxycycline.
POTENTIAL COMPLICATIONS
• Localised or widespread cellulitis
• Post-streptococcal glomerulonephritis (uncommon in adults)
• Sepsis
• Acute rheumatic fever
CLIENT EDUCATION AND DISCHARGE INFORMATION
• Counsel client about appropriate use of medications (dose, frequency, compliance).
• Recommend proper hygiene (i.e., daily washing).
• Counsel client about prevention of future episodes.
DST-705 Impetigo: Adult
Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
• Suggest strategies to prevent spread to other household members (e.g., proper hand washing by all household members,
use of separate towels).
• Remain home from work / school for 24 hours after treatment started.
MONITORING AND FOLLOW-UP
• Follow-up in 2-3 days to assess response to treatment.
• Instruct client to return for reassessment if fever develops or infection spreads despite therapy.
CONSULTATION AND/OR REFERRAL
• Consult with a physician or nurse practitioner if no response to treatment.
DOCUMENTATION
As per agency policy
DST-705 Impetigo: Adult

Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
REFERENCES
More recent editions of any of the items in the Reference List may have been published since this DST was published. If you have a newer version, please use it.
Baddour, L. M. (2015). Impetigo. UptoDate.
Blondel-Hill, E., & Fryters, S. (2012). Bugs and drugs: An antimicrobial infectious diseases reference. Edmonton, AB: Alberta Health Services
Breen, J. O. (2010). Skin and soft tissue infections in immunocompetent patients. American Family Physician, 81(7), 893-899.
British Columbia Centre for Disease Control. (2011). Antimicrobial resistance trends in the Province of British Columbia 2011. Vancouver, BC: Author.
British Columbia Centre for Disease Control. (2014). Guidelines for the management of community-associated methicillin-resistant Staphylococcus aureus (CA-MRSA)-related skin and soft tissue infections in primary care. Vancouver, BC: Author.
Canadian Pharmacists Association. (2014). Therapeutic choices (7th ed.). Ottawa, ON: Author.
Canadian Pharmacists Association. (2014). Therapeutic choices for minor ailments. Ottawa, ON: Author.
Cash, J. C., & Glass, C. A. (Eds.). (2014). Family practice guidelines (3rd ed.). New York, NY: Springer.
Klostranec, J. M., & Kolin, D. L. (2012). The Toronto notes 2012: Comprehensive medical reference & review for Medical Council of Canada Qualifying Exam Part 1 and the United States Medical Licensing Exam Step 2 (28th ed.). Toronto, ON: Toronto Notes for Medical Students.
DynaMed. (2015, August 17). Impetigo.
Koning, S., van der Sande, R., Verhagen, A. P., van Suijlekom-Smit, L. W. A., Morris, A. D., Butler, C. C.,…van der Wouden, J. C. (2012). Interventions for impetigo (review). Cochrane Database of Systematic Reviews, (4).
Lawton, S. (2014, March 12-18). Impetigo: Treatment and management. Nursing Times, 110(11), 18-20.
Liu, C., Bayer, A., Cosgrove, S.E., Daum, R.S., Fridkin, S.K., Gorwitz, R.J.,…Chambers, H.F. (2011). Clinical practice guidel ines
by the Infectious Diseases Society of America for the treatment of methicillin-resistant Staphylococcus aureus infections in adults and children. Clinical Infectious Diseases, 52(3), e18-e55.
Napierkowski, D. (2013). Uncovering common bacterial skin infections. Nurse Practitioner, 38(3), 30-37.
Pangilinan, R., Tice, A., & Tillotson, G. (2009). Topical antibiotic treatment for uncomplicated skin and skin structure infections: Review of the literature. Expert Review of Anti-infective Therapy, 7(8), 957-965.
Riain, U. N. (2011). Recommended management of common bacterial skin infections. Prescriber, 22 (15/16), 14-24.
Stevens, D., Bisno, A. L., Chambers, H. F., Dellinger, E. P., Goldstein, E. J. C., Gorbach, S. L.,…Wade, J. C. (2014). Practice guidelines for the diagnosis and management of skin and soft tissue infections: 2014 update by the Infectious Diseases Society of America. Clinical Infectious Diseases, 59(2), e10-e52.
Watkins, J. (2012). Differentiating common bacterial skin infections. British Journal of School Nursing, 7(2), 77-78.
Wolff, K., Johnson, R., & Saavedra, A. (2013). Fitzpatrick’s color atlas and synopsis of clinical dermatology (7th ed.). New York, NY: McGraw-Hill Medical.
DST-705 Impetigo: Adult

Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
DST-706 Impetigo: Pediatric
DEFINITION
A highly contagious, superficial bacterial infection of the skin, it primarily affects children during the summer. Beginning with vesicles, it progresses to honey crusted lesions and is commonly seen on the face, arms, legs and buttocks.
Nurses with Remote Practice Certified Practice designation (RN(C)s9) are able to treat children with impetigo who are 6 months of age and older.
POTENTIAL CAUSES
• S. aureus is the principal pathogen.
• Group A Beta-hemolytic strep presents alone or in conjunction with S aureus in a minority of cases.
PREDISPOSING RISK FACTORS
• Local skin trauma such as insect bites, wounds
• Skin lesions from other disorders such as eczema, scabies, pediculosis
• Age – more common in pre-school and young children (2-5 years)
• Crowded living conditions
• Poor hygiene
• Warm, moist climate
• Children in close contact, e.g. daycare, school
• Known carrier of S. aureus and/or GAS
TYPICAL FINDINGS OF IMPETIGO
History
• More common on face, scalp and hands, but may occur anywhere
• Involved area is usually exposed
• Usually occurs during summer
• New lesions usually due to auto-inoculation
• Rash begins as tiny red lesions, which may be itchy
• Lesions rapidly become small vesicles, progressing to pustules, which rupture and drain to form yellow crusts
• Lesions painless
• Fever and systemic symptoms rare - mild fever may be present in more generalized infections
• Known MRSA positive (client or household member)
Physical Assessment
• Weigh until 12 years of age for medication calculations
• Thick, golden yellow, crusted lesion on a red base
• Numerous skin lesions at various stages present (vesicles, pustules, crusts, serous or pustular drainage, ulcers, healing
lesions)
9 RN(C) is an authorized title recommended by BCCNP that refers to BCCNP-certified RNs, and is used throughout this Decision
Support Tool (DST).
DST-706 Impetigo: Pediatric
Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
• In infants and young children, the bullous form of impetigo may occur. In this case the vesicles continue to enlarge and form
flaccid bullae (blisters) with a clear yellow fluid that slowly darkens. When these rupture they leave a thin brown to golden
yellow coloured crusts.
• Lesions and surrounding skin may feel warm to touch
• Regional lymph nodes may be enlarged and/or tender
Diagnostic Tests
Identification of impetigo may be made upon consideration of clinical features and presentation.
• Culture and Sensitivity of lesion exudate if widespread or not responding to treatment.
• Determine blood glucose level if infection is recurrent or if symptoms suggestive of diabetes mellitus are present.
MANAGEMENT AND INTERVENTIONS
Goals of Treatment
• Resolve infection
• Prevent auto-inoculation
• Prevent spread to other household members
Non-pharmacologic Interventions
• Apply warm saline compresses to soften and soak away crusts qid for 15 minutes and prn
Pharmacologic Interventions
All drugs must be calculated by weight. Do not use more than an adult dose.
Apply topical antibiotic preparation after each soaking:
• mupirocin ointment to affected lesions tid for 7 days
If non-responsive:
• fusidic acid ointment or cream tid or qid for 7 days
Topical agents are sufficient when there are only a small number of non-bullous lesions.
Oral antibiotics may be necessary if there are multiple lesions making topical treatment impractical, the client is febrile and has systemic symptoms including lymphadenopathy, or if bullous impetigo is present:
cephalexin 30-40mg/kg po per day divided qid for 7 days, maximum 2 grams daily
OR
cloxacillin 40-50mg/kg po per day divided qid for 7 days (tastes unpleasant so use cephalexin first)
For clients with allergy to penicillin:
• erythromycin 40mg/kg po per day divided qid for 7 days
• If known MRSA positive or MRSA positive swab:
o Trimethoprim / sulfamethoxazole 8-12 mg / kg per day po bid for 7 days (dosing is based on trimethoprim.)
Pregnant or Breastfeeding Women (dosing as above)
• Mupirocin, cephalexin, cloxacillin and erythromycin may be used.
• Avoid fusidic acid ointment.
• DO NOT USE trimethoprim /sulfamethoxazole.
DST-706 Impetigo: Pediatric
Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
POTENTIAL COMPLICATIONS
• Localised or widespread cellulitis
• Post-streptococcal glomerulonephritis (rare)
• Sepsis
• Acute rheumatic fever
CLIENT/CAREGIVER EDUCATION AND DISCHARGE INFORMATION
• Advise on condition, timeline of treatment and expected course of disease process.
• Counsel parent or caregiver about appropriate use of medications (dose, frequency, compliance).
• Remain home from school/day care for 24 hours after treatment started.
• Recommend proper hygiene (i.e., daily washing).
• Cut fingernails to prevent scratching.
• Counsel client about prevention of future episodes
• Submit strategies to prevent spread to other household members (i.e., proper hand-washing of all household members, use
of separate towels).
MONITORING AND FOLLOW-UP
• Follow-up in 2-3 days to assess response to treatment.
• Instruct client to return for reassessment if fever develops or infection spreads despite therapy.
CONSULTATION AND/OR REFERRAL
• Consult a physician or nurse practitioner if no response to treatment.
DOCUMENTATION
As per agency policy
DST-706 Impetigo: Pediatric

Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
REFERENCES
More recent editions of any of the items in the Reference List may have been published since this DST was published. If you have a newer version, please use it.
Baddour, L. M. (2015). Impetgio. UptoDate.
Blondel-Hill, E., & Fryters, S. (2012). Bugs and drugs: An antimicrobial infectious diseases reference. Edmonton, AB: Alberta Health Services.
Breen, J. O. (2010). Skin and soft tissue infections in immunocompetent patients. American Family Physician, 81(7), 893-899.
British Columbia Centre for Disease Control. (2014). Antimicrobial resistance trends in the province of British Columbia. Vancouver, BC: Author.
British Columbia Centre for Disease Control. (2014). Guidelines for the management of community-associated methicillin-resistant Staphylococcus aureus (CA-MRSA)-related skin and soft tissue infections in primary care. Vancouver, BC: Author.
Canadian Pharmacists Association. (2014). Therapeutic choices (7th ed.). Ottawa, ON: Author.
Cash, J. C., & Glass, C. A. (Eds.). (2014). Family practice guidelines (3rd ed.). New York, NY: Springer.
Klostranec, J. M., & Kolin, D. L. (2012). The Toronto notes 2012: Comprehensive medical reference & review for Medical Council of Canada Qualifying Exam Part 1 and the United States Medical Licensing Exam Step 2 (28th ed.). Toronto, ON: Toronto Notes for Medical Students.
DynaMed. (2015, August 17). Impetigo.
Esau, R. (Ed.). (2012). British Columbia’s Children’s Hospital pediatric drug dosage guidelines (6th ed.). Vancouver, BC: Children’s & Women’s Health Centre of B.C.
Hartman-Adams, H., Banvard, C., & Juckett, G. (2014). Impetigo: Diagnosis and treatment. American Family Physician, 90(4), 229-235.
Koning, S., van der Sande, R., Verhagen, A. P., van Suijlekom-Smit, L. W. A., Morris, A. D., Butler, C. C.,…van der Wouden, J. C. (2012). Interventions for impetigo (review). Cochrane Database of Systematic Reviews, (4).
Lawton, S. (2014, March 12-18). Impetigo: Treatment and management. Nursing Times, 110(11), 18-20.
Liu, C., Bayer, A., Cosgrove, S.E., Daum, R.S., Fridkin, S.K., Gorwitz, R.J.,…Chambers, H.F. (2011). Clinical practice guidel ines by the Infectious Diseases Society of America for the treatment of methicillin-resistant Staphylococcus aureus infections in adults and children. Clinical Infectious Diseases, 52(3), e18-e55.
Long, C. B., Madan, R. P., & Herold, B. C. (2010). Diagnosis and management of community-associated MRSA infections in children. Expert Review of Anti-Infective Therapy, 8(2), 183-195.
Napierkowski, D. (2013). Uncovering common bacterial skin infections. Nurse Practitioner, 38(3), 30-37.
NeVille-Swensen, M., & Clayton, M. (2011). Outpatient management of community-associated methicillin- resistant Staphylococcus aureus skin and soft tissue infection. Journal of Pediatric Health Care, 25(5), 308-315.
Pangilinan, R., Tice, A., & Tillotson, G. (2009). Topical antibiotic treatment for uncomplicated skin and skin structure infections: Review of the literature. Expert Review of Anti-infective Therapy, 7(8), 957-965.
DST-706 Impetigo: Pediatric
Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
Riain, U. N. (2011). Recommended management of common bacterial skin infections. Prescriber, 22 (15/16), 14-24.
Stevens, D., Bisno, A. L., Chambers, H. F., Dellinger, E. P., Goldstein, E. J. C., Gorbach, S. L.,…Wade, J. C. (2014). Practice guidelines for the diagnosis and management of skin and soft tissue infections: 2014 update by the Infectious Diseases Society of America. Clinical Infectious Diseases, 59(2), e10-e52.
Watkins, J. (2012). Differentiating common bacterial skin infections. British Journal of School Nursing, 7(2), 77-78.
Watkins, J. (2013). Bullous and non-bullous impetigo. Practice Nursing, 24(2), 95-96.
DST-706 Impetigo: Pediatric

Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
DST-707 Bites & Scratches: Adult
DEFINITION
An injury or mark caused by an animal or a human being. The primary puncture wounds are caused by teeth that may also tear
tissue and, in some cases, remove tissue in pieces. Wounds frequently become infected.
If a bite has been inflicted on a vulnerable adult consider protection issues and follow local policies for referral of vulnerable adults
considered at risk.
POTENTIAL CAUSES
• Animal bites are common. 60–80% are caused by dogs, and 20–30% by cats; bites by other animals (rabbits, guinea pigs,
hamsters, rats, mice) are much rarer.
• Human bites account for as many as 20% of all bite injuries in some urban areas. Indirect human “bite” wounds caused by a blow from the fist to another person’s teeth have their own specific pattern of injury (known as reverse bite injury, clenched
fist injury, or fight bite).
• The spectrum of injury is broad. Infectious complications are common due to unusual pathogens.
TYPICAL FINDINGS OF A BITE WOUND
History
• Determine cause of injury (human, animal)
• For animal bites: determine if bite was caused by a provoked or unprovoked animal
• Determine vaccination status of the animal (if possible) Refer to BCCDC, Communicable Disease Control, Management of
Specific Diseases, Rabies (May 2017).
• Human bite: assess to determine exposure risk to the bloodborne viruses’ hepatitis B virus (HBV), hepatitis C virus (HCV),
syphilis, and Human Immunodeficiency Virus (HIV). bloodborne viruses’. Refer to BCCDC, Communicable Disease Control,
Blood and Body Fluid Exposure (August 2016).
• Determine time elapsed since injury (after 3 hours, the bacterial count in a wound increase dramatically)
• Determine potential contaminants:
o wound contact with manure, rust, dirt, etc., will increase risk of infection and tetanus
o wounds sustained in barnyards or stables should be considered contaminated (Clostridium tetani is indigenous in
manure)
• Amount of blood lost
• Loss of function in nearby tendons, ligaments, nerves (sensation)
• Immunization status including: tetanus and hepatitis
• Assess if client or household contacts have tested positive for methicillin resistant staphylococcus aureus (MRSA)
PHYSICAL ASSESSMENT
Vital Signs
• Findings may be tachycardia, hypotension if significant blood loss
• General
• Assess wound for:
• Dimensions and depth
• Lacerations versus punctures
• Tissue loss
DST-707 Bites & Scratches: Adult

Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
• Infection (erythema, warmth, tenderness, discharge, local lymphadenopathy)
• Assess integrity of underlying structures (nerves, ligaments, tendons, blood vessels):
o Vascular injury – capillary refill should be checked distally
o Neurologic injury – check distal muscle strength, movement distal to wound and sensation
o Always check sensation before administering anaesthesia
o For hand and finger lacerations check two-point discrimination (Two-point discrimination measures the individual’s
ability to perceive two points of stimuli presented simultaneously. The health care practitioner is interested in the smallest distance between the points that can still be perceived as two points by the individual being tested.), this
should be less than 1 cm at the fingertips
o Tendons – can be evaluated by inspection, but individual muscles and tendons must also be tested for full range of
motion and full strength
o Assess range of motion of all body parts surrounding the wound site
o Bones – check for open fracture or associated fractures, based on mechanism of injury
o Foreign bodies – inspect the area
Diagnostic Tests
• Swab discharge for Culture and Sensitivity (C&S) if infected
• For animal bite injuries follow the British Columbia Centre for Disease Control (BCCDC) Rabies Protocol (see references)
• For human bite injuries follow the British Columbia Centre for Disease Control (BCCDC) Blood and Body Fluid Exposure
Management.
MANAGEMENT AND INTERVENTION
Note: Remove all jewelry from affected area.
• Prophylaxis for tetanus, blood borne pathogens and rabies should be provided when indicated, as per BCCDC. A potential
increased risk of thrombosis (blood clots) has been observed within 24 hours of receipt of immune globulin products, especially when given in large doses (i.e., more than 10 mL). Additional risk factors include: age 45 years and older, history
of thrombosis, or those with risk factors for thrombosis (e.g., obesity, high blood pressure, diabetes, prolonged periods of
immobilization, use of estrogens, a history of heart disease, blood clotting disorders, indwelling central vascular catheters, or
diseases that thicken the blood).4
• As per the BCCDC, The risk of HIV from a human bite is very low and in most circumstances HIV PEP is not required. In
extreme circumstances, if either person is known to be HIV positive and the bite draws blood, causes very deep wounds, or
the viral load is high then post exposure prophylaxis (PEP) could be considered after discussion with a specialist. If HIV PEP is
given, the follow-up blood test should be done. There is no PEP available for HCV.4
Note: People who have experienced the following should not get tetanus immune, those who have:
• had a life - threatening reaction to a previous dose of any immune globulin or any of its components
• a condition called isolated immunoglobulin A deficiency;
• been immunized against measles, mumps, rubella or chickenpox within the past 14 days. 5
Goals of Treatment
• Prevent/control infection
• Preserve function
• Prevent infection from blood borne pathogens, tetanus, or transmission of rabies
• Determine need for tetanus, rabies, and blood borne pathogen diseases prophylaxis
Non-pharmacological Interventions
• Thoroughly cleanse and irrigate with normal saline
DST-707 Bites & Scratches: Adult
Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
• Remove any debris and devitalized tissue
• Consider suture repair of low-risk bite wound lacerations. These are non-infected wounds, have no evidence of damage to
underlying structures and present within 8-12 hours of injury.
Do not suture or close:
• infected wounds
• Deep puncture wounds
• Bite wounds more than 8-12 hours old
• Crush injuries
• Bites in an immunocompromised host
• Cat or human bites
• Bites to the hand or foot
PHARMACOLOGICAL INTERVENTION FOR HUMAN, CAT AND DOG BITES
• Antibiotics are routinely given prophylactically for all human bites if there is moderate to severe tissue damage, deep
puncture wounds or bites to the face, hand, foot or genitals that are more than a simple superficial abrasion.
• Assess for risks of blood borne pathogen transmission and treat appropriately
• Only 3-28% of dog bites become infected and routine prophylaxis is not recommended
• 28-80% of cat bites become infected. Antibiotics are routinely given prophylactically for cat bites as they have a greater
prevalence of anaerobes and infection.
• Prophylaxis is required for elderly unvaccinated or partially vaccinated population
• Prophylaxis:
o Amoxicillin 500 mg/Clavulanate 125mg po tid for 3-5days
OR
o Amoxicillin 875 mg/Clavulanate 125 mg po bid for 3-5 days
• If allergic to penicillin:
o Doxycycline 100 mg po bid for 3-5 days
• Treatment for infected bites or scratches:
o Amoxicillin 500 mg/clavulanate 125mg po tid for 7-14 days
OR
o Amoxicillin 875 mg/clavulanate 125 mg po bid for 7-14 days
o If allergic to penicillin:
▪ Doxycycline 100 mg po bid for 10 days
Pregnant and Breastfeeding Women:
• DO NOT USE doxycycline
• Amoxicillin/clavulanate as outlined above may be used
OR
• Clindamycin 300-450 mg qid for 3-5 days
Potential Complications (All Bites)
• Septic arthritis
• Osteomyelitis
• Abscess formation
DST-707 Bites & Scratches: Adult
Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
• Tendonitis
• Nerve damage
• Compartment syndrome
• Fracture
• Sepsis
• HIV, Syphilis and Hepatitis B and C as a result of exposure to body fluids – human bites only
• Tetanus and or Rabies
CLIENT EDUCATION AND DISCHARGE INFORMATION
• Advise on condition, timeline of treatment and expected course of disease process
• Instruct to keep wound clean and dry
• Keep injured area elevated
• If redness, swelling or pain increases, return to clinic for assessment
• If appropriate, review measures to avoid animal bites
MONITORING AND FOLLOW UP
• Return to clinic in 24 hours for re-assessment
CONSULTATION AND/OR REFERRAL
• Refer all human bite wounds over the knuckle or having the potential to injure underlying structures to a physician or nurse
practitioner
• Refer to a physician or nurse practitioner to consider intravenous (IV) antibiotics if infection has already occurred with a
human bite
• A common location for the human bite is over the knuckles:
o This injury is usually sustained when a closed fist strikes the teeth of an opponent
o There is frequently penetration of the tendon sheath and/or the joint space
o The hand must be examined with the fingers in a flexed position so that the deeper structures are in the identical
position that they were when the injury was sustained
o Only in that position can injury to the underlying structures be visualized through the open skin wound
o Sometimes a foreign body such as a broken tooth is found in the wound
• Refer all facial bites to a physician or nurse practitioner
• Refer any concerns regarding rabies or unprovoked attacks to public health or a local medical health officer
• Encourage client to report a dog attack / bite to RCMP, animal control officer or appropriate official
DOCUMENTATION
As per agency policy. Additional public health reporting may be required in relation to rabies prophylaxis.
DST-707 Bites & Scratches: Adult
Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
REFERENCES
More recent editions of any of the items in the Reference List may have been published since this DST was published. If you have a
newer version, please use it.
Anti-Infective Review Panel. (2012). Anti-infective guidelines for community-acquired infections. Toronto, ON: MUMS Guideline Clearinghouse.
Blondel-Hill, E., & Fryters, S. (2012). Bugs and drugs: An antimicrobial infectious diseases reference. Edmonton, AB: Alberta Health Services.
British Columbia Centre for Disease Control (2015). Blood and body fluid exposure management.
British Columbia Centre for Disease Control. (2014). Guidelines for the management of community-associated methicillin-resistant Staphylococcus aureus (CA-MRSA)-related skin and soft tissue infections in primary care. Vancouver, BC: Author.
British Columbia Centre for Disease Control (2015). Management of specific diseases: Rabies. Vancouver, BC: Author.
British Columbia Centre for Disease Control (2018). Tetanus Immune Globulin (Tig) HyperTET information sheet
Canadian Immunization Guide. (2014). Public Health Agency of Canada
Canadian Pharmacists Association. (2014). Therapeutic choices (7th ed.). Ottawa, ON: Author.
Chrastil, B., Fornage, B. Hymes S. A case of extragenital chancre on a nipple from a human bite during sexual intercourse. Int journal of Dermatology. 2008;1(Cdc):978-980.
Klostranec, J. M., & Kolin, D. L. (2012). The Toronto notes 2012: Comprehensive medical reference & review for Medical Council of Canada Qualifying Exam Part 1 and the United States Medical Licensing Exam Step 2 (28th ed.). Toronto, ON: Toronto Notes for Medical Students.
DynaMed. (2014, April 1). Mammalian bite.
Endom, E. E. (2015). Initial management of animal and human bites. UptoDate.
Kravetz, J. D., & Federman, D. G. (2013). Mammalian bites. In ACP Smart Medicine & AHFS DI Essentials. Retrieved from STAT!Ref database on NurseONE website: [free login for all BC RNs after self-registration on site]
National Guideline Clearinghouse. (2013). Guideline summary: Management of cat and dog bites.
Paschos, N. K., Makris, E. A., Gantsos, A., & Georgoulis, A. D. (2014). Primary closure versus non-closure of dog bite wounds: A randomised controlled trial. Injury, 45(1), 237-240.
Rothe K, Tsokos M, Handrick W. Animal and Human Bite Wounds. Dtsch Arztebl Int. 2015;112(25):433- 443. doi:10.3238/arztebl.2015.0433.
Quinn, J. V., McDermott, D., Rossi, J., Stein, J., & Kramer, N. (2011). Randomized controlled trial of prophylactic antibiotics for dog bites with refined cost models. Western Journal of Emergency Medicine, 11(5), 435-441.
Prevaldi C, Paolillo C, Locatelli C, et al. Management of traumatic wounds in the Emergency Department : position paper from
the Academy of Emergency Medicine and Care (AcEMC) and the World Society of Emergency Surgery (WSES). World J Emerg Surg. 2016;11(1):30. doi:10.1186/s13017-016-0084-3.
Sabhaney, V., & Goldman, R. (2012). Management of dog bites in children. Canadian Family Physician, 58(10), 1094-1096.
DST-707 Bites & Scratches: Adult

Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
Stevens, D., Bisno, A. L., Chambers, H. F., Dellinger, E. P., Goldstein, E. J. C., Gorbach, S. L.,…Wade, J. C. (2014). Practice guidelines for the diagnosis and management of skin and soft tissue infections: 2014 update by the Infectious Diseases Society of America. Clinical Infectious Diseases, 59(2), e10-e52.
Thomas, N., & Brook, I. (2011). Animal bite-associated infections. Expert Review of Anti-Infective Therapy, 9(2), 215-226.
Wolff, K., & Johnson, R. A. (2009). Fitzpatrick’s color atlas and synopsis of clinical dermatology (6th ed.). New York: McGraw-Hill Medical.
DST-707 Bites & Scratches: Adult
Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
DST-708 Bites & Scratches: Pediatric
DEFINITION
An injury or mark caused by an animal or a human being. The primary puncture wounds are caused by teeth that may also tear tissue and, in some cases, remove tissue in pieces. Wounds frequently become infected.
Nurses with Remote Practice Certified Practice designation (RN(C)s10) are able to treat bites in children who are 1 year of age and
older, dependent on the bite severity. If younger than one year or the severity of the bite dictates, the child must be referred to a physician or nurse practitioner.
If a bite has been inflicted on a child, consider child protection issues and follow local policies for referral of children considered at risk.
POTENTIAL CAUSES
• Animal bites are common. 60–80% are caused by dogs, and 20–30% by cats; bites by other animals (rabbits, guinea pigs,
hamsters, rats, mice) are much rarer. The victims tend to be children.
• Human bites account for as many as 20% of all bite injuries in some urban areas. Indirect human “bite” wounds caused by a
blow from the fist to another person’s teeth have their own specific pattern of injury (known as reverse bite injury, clenched
fist injury, or fight bite).
• The spectrum of injury is broad, and infectious complications, generally due to unusual pathogens, are common.
TYPICAL FINDINGS OF A BITE WOUND
History
• Cause of injury (human, animal)
• Animal bite: determine if bite was caused by a provoked or unprovoked animal
• Determine vaccination status of the animal (if possible). Refer to BCCDC, Communicable Disease Control, Management of
Specific Diseases, Rabies (May 2017).
• Human bite: assess to determine exposure risk to the bloodborne viruses’ hepatitis B virus (HBV), hepatitis C virus (HCV), syphilis, and Human Immunodeficiency Virus (HIV). bloodborne viruses’. Refer to BCCDC, Communicable Disease Control,
Blood and Body Fluid Exposure (August 2016).
• Time elapsed since injury (after 3 hours, the bacterial count in a wound increase dramatically)
• Contaminants:
o wound contact with manure, rust, dirt, etc., will increase risk of infection and tetanus wounds sustained in barnyards or
stables should be considered contaminated (Clostridium tetani is indigenous in manure)
• Amount of blood lost
• Loss of function in nearby tendons, ligaments, nerves (sensation)
• Immunization status:
o Tetanus
o Hepatitis
o Known methicillin resistant staphylococcus aureus (MRSA) positive status of client or household contacts
PHYSICAL ASSESSMENT
Pediatric drug doses are calculated by patient weight. Pediatric doses should not exceed recommended adult doses.
10 RN(C) is an authorized title recommended by BCCNP that refers to BCCNP-certified RNs, and is used throughout this Decision
Support Tool (DST).
DST-708 Bites & Scratches: Pediatric

Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
Vital Signs
• Temperature
• Pulse
• Respiration
• SpO2
• Blood pressure (BP)
• Findings may be tachycardia, hypotension if significant blood loss
General
Assess wound for:
• Dimensions and depth
• Lacerations versus punctures
• Tissue loss
• Infection – erythema, warmth, tenderness, discharge, local lymphadenopathy
• Foreign bodies – inspect the area
Assess integrity of underlying structures (nerves, ligaments, tendons, blood vessels):
• Vascular injury – capillary refill should be checked distally
• Neurologic injury – check distal muscle strength, movement distal to wound and sensation
• Always check sensation before administering anaesthesia
• For hand and finger lacerations check two-point discrimination, (Two-point discrimination measures the individual’s ability to perceive two points of stimuli presented simultaneously. The health care practitioner is interested in the smallest distance
between the points that can still be perceived as two points by the individual being tested.), (this should be less than 1 cm at
the fingertips
• Tendons – can be evaluated by inspection, but individual muscles and tendons must also be tested for full range of motion
and full strength
• Assess range of motion of all body parts surrounding the wound site
• Bones – check for open fracture or associated fractures, based on mechanism of injury
Diagnostic Tests
• Swab discharge for Culture and Sensitivity (C&S) if infected
• For animal bite injuries follow the British Columbia Centre for Disease Control (BCCDC) Rabies Protocol (see references)
• For human bite injuries follow the British Columbia Centre for Disease Control (BCCDC) Blood and Body Fluid Exposure
Management.
MANAGEMENT AND INTERVENTION
Note: Remove all jewellery from affected area
• Prophylaxis for tetanus, rabies and blood borne pathogens should be provided when indicated, as per the BCCDC.
• As per the BCCDC, the risk of HIV from a human bite is very low and in most circumstances HIV PEP is not required. In
extreme circumstances, if either person is known to be HIV positive and the bite draws blood, causes very deep wounds, or the viral load is high then post exposure prophylaxis (PEP) could be considered after discussion with a specialist. If HIV PEP is
given, the follow-up blood test should be done. There is no PEP available for HCV.
• Note: People who have experienced the following should not get tetanus immune, those who have:
o had a life-threatening reaction to a previous dose of any immune globulin or any of its components;
o a condition called isolated immunoglobulin A deficiency;
o a history of thrombosis or risk factors for thrombosis; or
o been immunized against measles, mumps, rubella or chickenpox within the past 14 days.
DST-708 Bites & Scratches: Pediatric
Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
Goals of Treatment
• Prevent/control infection
• Preserve function
• Prevent infection from Blood Borne Pathogens, tetanus, or transmission of rabies
Non-pharmacological Interventions
• Thoroughly cleanse and irrigate with normal saline
• Remove any debris and devitalized tissue
• Consider suture repair of low-risk bite wound lacerations. These are non-infected wounds, have no evidence of damage to
underlying structures and present within 8-12 hours of injury.
• Do not suture or close:
o Infected wounds
o Deep puncture wounds
o Bite wounds more than 8-12 hours old
o Crush injuries
o Bites in an immunocompromised host
o Cat or human bites
o Bites to the hand or foot
PHARMACOLOGICAL INTERVENTIONS FOR BITES
Ensure recent weight obtained (for drugs doses dependant on weight)
• Prophylaxis for blood borne pathogens should be provided when indicated. as per BCCDC’s Blood and Body Fluid Exposure
Management. Guideline.
• Antibiotics are routinely given prophylactically for cat bites as they have a greater prevalence of anaerobes and infection
(65% vs. 50%) and P. multocida (75% vs. 50%) than do dog bites.,2 Antibiotics are routinely given prophylactically for all
human bites if there is moderate to severe tissue damage, deep puncture wounds or bites to the face, hand, foot or genitals
that are more than a simple superficial abrasion.
• If infection has already occurred (especially for a bite on the hand) consult with physician or nurse practitioner to consider
intravenous (IV) antibiotics
• Exposure to the face and hands increases the risk of rabies because these body parts are highly innervated, providing greater
and faster opportunity for virus to enter the nervous system.4
Antibiotic prophylaxis is required when:
• The wound has been closed or there is evidence of infection
• It is moderate to severe
• Puncture wounds, particularly if penetrating bone, tendon or joint
• Crush injury / edema
• Preemptive early antimicrobial therapy for 3–5 days is recommended for patients who (a) are immunocompromised; (b) are asplenic; (c) have advanced liver disease; (d) have preexisting or resultant edema of the affected area; (e) have moderate to
severe injuries, especially to the hand or face; or (f ) have injuries that may have penetrated the periosteum or joint capsule.
Note: People who have experienced the following should not get tetanus immune, those who have: had a life-threatening reaction
to a previous dose of any immune globulin or any of its components;
• a condition called isolated immunoglobulin A deficiency;
• a history of thrombosis or risk factors for thrombosis; or
• been immunized against measles, mumps, rubella or chickenpox within the past 14 days.4
DST-708 Bites & Scratches: Pediatric

Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
PHARMACOLOGIC INTERVENTION BITES
Assess for risks of blood borne pathogen and/or rabies transmission and treat appropriately.
Prophylaxis:
• Amoxicillin/clavulanate 40 mg/kg/day po divided tid for 3-5 days (dosing is based on amoxicillin component).
Pregnant and Breastfeeding Youth:
• Amoxicillin/clavulanate may be used as listed above
• DO NOT USE doxycycline
Treatment for infected bites or scratches:
• Amoxicillin/clavulanate 40 mg/kg/day po tid 10 days (dosing is based on amoxicillin component).
Pregnant and Breastfeeding Youth
• Amoxicillin/clavulanate may be used as listed above
• DO NOT USE doxycycline
POTENTIAL COMPLICATIONS (ALL BITES)
• Septic arthritis
• Osteomyelitis
• Abscess formation
• Tendonitis
• Nerve damage
• Compartment syndrome
• Fracture
• Sepsis
• HIV and Hepatitis B and C as a result of exposure to body fluids – (human bites only)
• Tetanus and or Rabies
CLIENT/CAREGIVER EDUCATION AND DISCHARGE INFORMATION
• Advise on condition, timeline of treatment and expected course of disease process
• Instruct to keep wound clean and dry
• Keep injured area elevated
• If redness, swelling or pain increases, return to clinic for assessment
• If appropriate, review measures to prevent animal bites:
MONITORING AND FOLLOW UP
• Return to clinic in 24 hours for re-assessment
CONSULTATION AND/OR REFERRAL
Refer all human bite wounds over the knuckle or having the potential to injure underlying structures to a physician or nurse practitioner
Refer if infection has already occurred with a human bite
A common location for the human bite is over the knuckles
DST-708 Bites & Scratches: Pediatric

Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
• This injury is usually sustained when a closed fist strikes the teeth of an opponent
• There is frequently penetration of the tendon sheath and/or the joint space
• The hand must be examined with the fingers in a flexed position so that the deeper structures are in the identical position
that they were when the injury was sustained
• Only in that position can injury to the underlying structures be visualized through the open skin wound. Sometimes, a foreign
body such as a broken tooth is found in the wound
Refer all facial bites to a physician or nurse practitioner
Refer any concerns regarding rabies or unprovoked attacks to public health or a medical health officer
Encourage client / parent or caregiver to report a dog attack / bite to RCMP, animal control officer or appropriate official
DOCUMENTATION
• As per agency policy
• Additional public health reporting may be required in relation to rabies prophylaxis
DST-708 Bites & Scratches: Pediatric

Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
REFERENCES
More recent editions of any of the items in the Reference List may have been published since this DST was published. If you have a
newer version, please use it.
Anti-Infective Review Panel. (2012). Anti-infective guidelines for community-acquired infections. Toronto, ON: MUMS Guideline Clearinghouse.
Blondel-Hill, E., & Fryters, S. (2012). Bugs and drugs: An antimicrobial infectious diseases reference. Edmonton, AB: Alberta Health Services.
British Columbia Centre for Disease Control. (2015). Communicable Disease Control: Blood and body fluid exposure management. Vancouver, BC: Author.
British Columbia Centre for Disease Control. (2014). Guidelines for the management of community-associated methicillin-resistant Staphylococcus aureus (CA-MRSA)-related skin and soft tissue infections in primary care. Vancouver, BC: Author.
British Columbia Centre for Disease Control. (2015). Management of specific diseases: Rabies. Vancouver, BC: Author.
BC Centre for Disease Control. Communicable Disease Control: Blood and Body Fluid Exposure Management. BC Author.
Canadian Immunization Guide. (2014). Retrieved from Public Health Agency of Canada website.
Canadian Pharmacists Association. (2014). Therapeutic choices (7th ed.). Ottawa, ON: Author
Chrastil, B., Fornage, B. Hymes S. A case of extragenital chancre on a nipple from a human bite during sexual intercourse. Int jJurnal fo Dermatology. 2008;1(Cdc):978-980.Chen, Y. A., & Tran, C. (Eds.). (2011). The Toronto notes 2011: Comprehensive medical reference and review for the Medical Council of Canada Qualifying Exam Part 1 and the United States Medical Licensing Exam Step 2 (27th ed.). Toronto, ON: Toronto Notes for Medical Students.
Davies, H. D. (2000). When your best friend bites: A note on dog and cat bites. Paediatrics and Child Health, 5(7), 381-383.
Endom, E. E. (2015). Initial management of animal and human bites. UptoDate.
Klostranec, J. M., & Kolin, D. L. (Eds). (2012). Toronto Notes 2012: Comprehensive Medical Reference & Review for MCCQE and USMLE II. Toronto, ON: Toronto Notes for Medical Students, Inc.
Kravetz, J. D., & Federman, D. G. (2013). Mammalian bites. In ACP Smart Medicine & AHFS DI Essentials. Retrieved from STAT!Ref database on NurseONE website. [free login for all BC RNs after self-registration on site]
National Guideline Clearinghouse. (2013). Guideline summary: Management of cat and dog bites.
Paschos, N. K., Makris, E. A., Gantsos, A., & Georgoulis, A. D. (2014). Primary closure versus non-closure of dog bite wounds: A randomised controlled trial. Injury, 45(1), 237-240.
Prevaldi C, Paolillo C, Locatelli C, et al. Management of traumatic wounds in the Emergency Department:
position paper from the Academy of Emergency Medicine and Care (AcEMC) and the World
Society of Emergency Surgery (WSES). World J Emerg Surg. 2016;11(1):30. doi:10.1186/s13017-016-0084-3.
Quinn, J. V., McDermott, D., Rossi, J., Stein, J., & Kramer, N. (2011). Randomized controlled trial of prophylactic antibiotics for dog bites with refined cost models. Western Journal of Emergency Medicine, 11(5), 435-441.
DST-708 Bites & Scratches: Pediatric
Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
Rothe K, Tsokos M, Handrick W. Animal and Human Bite Wounds. Dtsch Arztebl Int. 2015;112(25):433- 443. doi:10.3238/arztebl.2015.0433.
Sabhaney, V., & Goldman, R. (2012). Management of dog bites in children. Canadian Family Physician, 58(10), 1094-1096.
Stevens, D., Bisno, A. L., Chambers, H. F., Dellinger, E. P., Goldstein, E. J. C., Gorbach, S. L.,…Wade, J. C. (2014). Practice guidelines for the diagnosis and management of skin and soft tissue infections: 2014 update by the Infectious Diseases Society of America. Clinical Infectious Diseases, 59(2), e10-e52.
Thomas, N., & Brook, I. (2011). Animal bite-associated infections. Expert Review of Anti-Infective Therapy, 9(2), 215-226.
Ward, M. A. (2013). Bite wound infections. Clinical pediatric emergency medicine, 14(2), 88-94.
Wolff, K., & Johnson, R. A. (2013). Fitzpatrick’s color atlas and synopsis of clinical dermatology (7th ed.). New York: McGraw-Hill Medical.
DST-708 Bites & Scratches: Pediatric
Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
DST-709 Localized Abscess and Furuncle: Adult
DEFINITION
• An abscess is a collection of pus in subcutaneous tissues
• A furuncle or boil is an acute, tender perifollicular inflammatory nodule or abscess
• A carbuncle is a deep-seated abscess, formed by a cluster of furuncles, generally larger and deeper
POTENTIAL CAUSES
• Infection with Staphylococcus aureus (25-50% of cases), anaerobes, other microorganisms
• In B.C., Methacillin Resistant Staphylococcus Aureus (MRSA) comprises over 25% of Staphylococcus Aureus infections
PREDISPOSING FACTORS
• Diabetes mellitus
• Immunocompromised or use of systemic steroids
• Previous skin colonisation of client or family with MRSA
• Cellulitis
• Seborrhea
• Trauma such as surgery, cuts, burns, insect or animal bites, slivers, injection drug use, plucking hair
• Excessive friction or perspiration
• Obesity
• Poor hygiene
TYPICAL FINDINGS OF LOCALIZED ABSCESS
History
• Possibly known MRSA positive (client and household members)
• Possible history of injury or trauma
• Local redness, progressing to deep red, swelling, pain, tenderness
• Fever usually absent unless systemic infection
• If opened, purulent, sanguineous material drains
• Folliculitis and carbuncles:
o Usually found on the neck, axilla, breasts, face and buttocks
o Begins as a small nodule, quickly becomes a large pustule 5-30 mm diameter
o May occur singly (folliculitis) or in groups (carbuncles)
o May be recurrent
Physical Assessment
• Localized area of erythema, swelling, warmth and tenderness
• Lesions often indurated and may be fluctuant (may be difficult to palpate if abscess is deep)
• Lesion may spontaneously drain purulent discharge
• Size of abscess often difficult to estimate; abscess usually larger than suspected
• Carbuncle may be present as a red mass with multiple draining sinuses in area of thick, inelastic tissue (i.e., posterior neck,
back, thigh)
• Regional lymph nodes usually not tender or enlarged. If enlarged and tender consider increased risk for systemic infection
• Fever, chills and systemic toxicity are unusual.
DST-709 Localized Abscess and Furuncle: Adult
Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
If client appears toxic, consider the potential for bacteremia and a systemic infection
Diagnostic Tests
• Swab discharge for Culture and Sensitivity (C&S)
• Determine blood glucose level if infection is recurrent or if symptoms suggestive of diabetes mellitus are present
MANAGEMENT AND INTERVENTIONS
For simple, localized abscesses and furuncles that are not ready for lancing, appropriate treatment includes the application of warmth, cleaning and protecting the abscess.
Goals of Treatment
• Resolve infection
• Prevent complications
Non-pharmacologic Interventions
Small, localized abscess / furuncles / carbuncles
• Apply warm saline compresses to area at least qid for 15 minutes (this may lead to resolution or spontaneous drainage if the
lesion or lesions are mild)
• Cover any open areas with a sterile dressing
• Once abscess become fluctuant, if it has not spontaneously begun to drain, lance and continue with heat to facilitate
drainage. Do a C&S of drainage. Rest, elevate and gently splint infected limb
PHARMACOLOGIC INTERVENTIONS
• For pain or fever
o Acetaminophen 325 mg 1-2 tabs po q 4-6 h prn
OR
o Ibuprofen 200 mg, 1-2 tabs po q 4-6 h prn
NOTE: Antibiotics are only recommended if one or more of the following are present;
• The abscess is more than 5 cm,
• There are multiple lesions,
• There is surrounding cellulitis,
• It is located in the central area of the face,
• It is peri-rectal,
• There are systemic signs of infection,
• The client is immunocompromised,
• The client is known to be MRSA positive.
ANTIBIOTICS
First line if MRSA is not suspected:
• Cloxacillin 500 mg po qid for 5-7 days
OR
• Cephalexin 500 mg po qid for 5-7 days
DST-709 Localized Abscess and Furuncle: Adult
Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
If allergic to penicillin and cephalexin, if MRSA positive, or a known MRSA positive diagnosis in the past or in the household
• doxycycline 100 mg po BID for 5-7 days
OR
• trimethoprim 160 mg / sulfamethoxazole 800 mg (DS) 1 tab po bid for 5-7 days
Pregnant or Breastfeeding Women:
Acetaminophen, cloxacillin, and cephalexin may be used as listed above.
DO NOT USE ibuprofen, trimethoprim 160 mg / sulphamethoxazole 800 mg or doxycycline
Potential Complications
• Cellulitis
• Necrotising fasciitis
• Sepsis
• Scarring
• Spread of infection (e.g., lymphangitis, lymphadenitis, endocarditis)
• Recurrence
Client Education/Discharge Information
• Instruct client to keep dressing area clean and dry
• Recommend that client avoid picking or squeezing the lesions
• Return to clinic at any sign of cellulitis or general feeling of illness
• Counsel client about appropriate use of medications (dose, frequency)
• Stress importance of regular skin cleansing to prevent future infection (in clients with recurrent disease, bathe the area bid
with a mild antiseptic soap to help prevent recurrences)
• Do not use public hot tubs or swimming pools
Monitoring and Follow-Up
• Follow up daily until infection begins to resolve
• Instruct client to return immediately for reassessment if lesion becomes fluctuant, if pain increases or if fever develops.
Consultation and/or Referral
Consult with a physician or nurse practitioner promptly for potential intravenous (IV) therapy if:
• Client is febrile or appears acutely ill
• Extensive abscesses, cellulitis, lymphangitis or adenopathy are present
• An abscess is suspected or detected in a critical region (i.e., head or neck, hands, feet, perirectal area, over a joint)
• Immunocompromised client (i.e., diabetic)
• Infection recurs or does not respond to treatment
DOCUMENTATION
As per agency policy
DST-709 Localized Abscess and Furuncle: Adult
Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
REFERENCES
More recent editions of any of the items in the Reference List may have been published since this DST was published. If you have a newer version, please use it.
British Columbia Centre for Disease Control. (2011). Antimicrobial resistance trends in the Province of British Columbia 2011. Vancouver, BC: Author.
British Columbia Centre for Disease Control. (2014). Guidelines for the management of community-associated methicillin-resistant Staphylococcus aureus (CA-MRSA)-related skin and soft tissue infections in primary care. Vancouver, BC: Author.
Blondel-Hill, E., & Fryters, S. (2012). Bugs and drugs: An antimicrobial infectious diseases reference. Edmonton, AB: Alberta Health Services.
Breen, J. O. (2010). Skin and soft tissue infections in immunocompetent patients. American Family Physician, 81(7), 893-899.
Canadian Pharmacists Association. (2011). Therapeutic choices (6th ed.). Ottawa, ON: Author.
Canadian Pharmacists Association. (2014). Therapeutic choices for minor ailments. Ottawa, ON: Author.
Cash, J. C., & Glass, C. A. (Eds.). (2014). Family practice guidelines (3rd ed.). New York, NY: Springer.
DynaMed. (2014, August 12). Skin abscesses, furuncles, and carbuncles.
DynaMed. (2014, August 12). Treatment of MRSA skin and soft tissue infections. Retrieved from http://search.ebscohost.com/login.aspx?direct=true&AuthType=cpid&custid=s5624058&db=dme&AN=900862
Embil, J. M., Oliver, Z. J., Mulvey, M. R., & Trepman, E. (2006). A man with recurrent furunculosis. CMAJ, 175(2), 142-144.
Liu, C., Bayer, A., Cosgrove, S.E., Daum, R.S., Fridkin, S.K., Gorwitz, R.J.,…Chambers, H.F. (2011). Clinical practice guidelines by the Infectious Diseases Society of America for the treatment of methicillin-resistant Staphylococcus aureus infections in adults and children. Clinical Infectious Diseases, 52(3), e18-e55.
NeVille-Swensen, M., & Clayton, M. (2011). Outpatient management of community-associated methicillin- resistant
Staphylococcus aureus skin and soft tissue infection. Journal of Pediatric Health Care, 25(5), 308-315.Singer, A. J., & Talan, D. A. (2014). Management of skin abscesses in the era of methicillin-resistant Staphylococcus aureus. New England Journal of Medicine, 370(11), 1039-1047.
Stevens, D. L., & Eron, L. J. (2013). Cellulitis and soft tissue infections. In ACP Smart Medicine & AHFS DI Essentials. Retrieved from STAT!Ref database on NurseONE website. [free login for all BC RNs after self-registration on site]
Stevens, D. L., Bisno, A. L., Chambers, H. F., Dellinger, E. P., Goldstein, E. J. C., Gorbach, S. L.,…Wade, J. C. (2014). Practice
guidelines for the diagnosis and management of skin and soft tissue infections: 2014 update by the Infectious Diseases Society of America. Clinical Infectious Diseases, 59(2), e10-e52.
Wolff, K., & Johnson, R. A. (2009). Fitzpatrick’s color atlas and synopsis of clinical dermatology (6th ed.). New York: McGraw-Hill Medical.
DST-709 Localized Abscess and Furuncle: Adult
Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
DST-801 Use of Nitrous Oxide/Oxygen in Pain Management: Adult
DEFINITION
A sweet smelling, colourless 50/50 gas mixture of nitrous oxide and oxygen (Canadian product names: Entonox, Alnox Gas, Liqui-
med Analgesic Gas) commonly self-administered by the client through a demand-valve mask and supervised by RN(C)s11. Nitrous
oxide/oxygen supports combustion.
INDICATIONS
Nitrous oxide/oxygen is used in moderate to severe pain management situations when immediate, short-term analgesia and
anxiolysis with minimal sedation is required such as during a difficult dressing change, the application of splints to fracture sites or
during labour.
• The RN(C) may administer nitrous oxide 50% / oxygen 50% to manage pain under the following conditions:
• Stable trauma, such as a minor Motor Vehicle Accident (MVA), fall, recreational injury, or assault
• Burns
• Obstetric clients, particularly labour
• Chest pain
• Abdominal pain
• Painful treatments such as dressing changes or splinting fractures
ACTION
Central nervous system (CNS) depressant action, possibly by partially inhibiting action potentials of the CNS that leads to sedation.
As a mild analgesic, it has an action similar to morphine as it may act on opiate receptors. It does cause some sympathetic
stimulation, which supports blood pressure, systemic resistance and cardiac output. “Spontaneous respirations, airway protective
reflexes, and hemodynamic status are generally preserved at concentrations typically used for sedation and analgesia” (Grant,
2009).
Pharmacokinetics
• Absorption – rapid via the lungs
• Metabolism – body
• Excretion – primarily exhaled. Minimal amount through skin
• Onset – 1-2 minutes. Wears off in 2-8 minutes
Contraindications
• Sensitivity to nitrous oxide
• Any condition or suspected condition involving trapped gas as the nitrous oxide will also diffuse into the airspaces:
o Bowel obstruction
o Air embolism
o Pneumothorax
o Middle ear infection
o Decompression sickness
o Vitreoretinal surgery and intraocular gas bubble
11 RN(C) is an authorized title recommended by CRNBC that refers to CRNBC-certified RNs, and is used throughout this Decision Support Tool
(DST).
DST-801 Use of Nitrous Oxide/Oxygen in Pain Management: Adult

Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
• Head injury with impaired consciousness as nitrous oxide /oxygen will further increase intra cranial pressure (ICP)
• Client inability to comply with instructions
• Suspected inhalation injury with oxygen saturation of less than 100%
• Client has taken nitroglycerin in the last 5 minutes
• Usage in an enclosed treatment area without ventilation
• Use for a continuous period of more than 24 hours
Precautions
Factors that require extra caution in instituting nitrous oxide /oxygen therapy:
• Maxillo-facial injuries which affect ability to hold the mask firmly on the face
• Chronic obstructive pulmonary disease (COPD)
• Distended abdomen
• Shock
• Intoxicated clients
• SCUBA diving within the last 24 hours
Adverse Effects
• CNS – Dizziness, drowsiness, headache, confusion or decreased level of consciousness, or CNS excitation (including seizures),
amnesia, giddiness, tingling
• Gastrointestinal – Nausea and/or vomiting
• Respiratory – Apnea
• Cardiac – Decreased cardiac output and hypotension
• Miscellaneous – Aggravation of middle ear (increased pressure), inhalation by caregiver affects caregiver ability to function;
interference with B12 and folate metabolism
Drug Interactions
• No known significant reactions
Pregnancy Risk Factors
• Considered safe during pregnancy and labor and delivery
Route / Dose
• For mild sedation, anxiolysis and analgesia – nitrous oxide/oxygen for inhalation:
o Self-administered by client using hand-held facemask or mouthpiece. This ensures that if client becomes too drowsy,
they cease to inhale the gas
Availability
Supplied in blue cylinders
Nursing Implications
• Ensure adequate ventilation of the room to avoid bystander effects
• Conduct a history and physical examination to rule out the contraindications for use of nitrous oxide/oxygen. This includes a
cardio-respiratory, gastrointestinal and ear-nose-throat (ENT) exam
• Ensure client is able to follow directions
• Obtain a baseline set of vital signs, including oxygen saturation
• Monitor closely during administration; note patient responsiveness, color, respiratory status
DST-801 Use of Nitrous Oxide/Oxygen in Pain Management: Adult
Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
Client Teaching
• Nitrous oxide/oxygen is self-administered through a demand-valve with face mask or mouthpiece.
• If the pain is spasmodic or episodic, as in labour, encourage the client to stop using the gas during the pain-free periods.
• Review the adverse effects of nitrous oxide /oxygen.
• Do not use while smoking.
Procedure
• Have the client apply the mask or hold mouth piece to own face
• Encourage slow, deep breaths to allow the demand-valve to function
• If the mask falls away as the client becomes sedated, do not replace the mask
• Allow the client to use nitrous oxide/oxygen until the pain is relieved or side-effects appear
• Discontinue if cyanosis develops
Storage
• Tanks should be stored in a horizontal position, preferably above freezing
• Improper storage may lead to separation of N2O2 and O2 (where the N2O2 rises to the top of the cylinder). This includes:
o Tank being stored below -6 C
o Gas is stagnant over a long period of time
o Tank has been stored in a vertical position
• If any of these have occurred, invert the cylinder several times to mix the gases in the cylinder
DOCUMENTATION
As per agency policy
DST-801 Use of Nitrous Oxide/Oxygen in Pain Management: Adult
Certified Practice Area:
Remote Nursing
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email mailto:[email protected]
REFERENCES
More recent editions of any of the items in the Reference List may have been published since this DST was published. If you have a newer version, please use it.
Alai, A. N. (2014, November 10). Nitrous Oxide Administration. Retrieved from http://emedicine.medscape.com/article/1413427-overview
Allman, K. G., & Wilson, I. H. (Eds.). (2011). Oxford handbook of anaesthesia (3rd ed.). Oxford, UK: Oxford University Press.
British Columbia Ambulance Service (2015). Entonox. In BCTG: A mobile reference for the BCAS treatment guidelines.
Canadian Pharmacists Association. (2014). Therapeutic choices (7th ed.). Ottawa, ON: Author.
Ducassé, J. L., Siksik, G., Durand-Béchu, M., Couarraze, S., Vallé, B., Lecoules, N.,...Bounes, V. (2013). Nitrous oxide for early
analgesia in the emergency setting: A randomized, double-blind multicenter prehospital trial. Academic Emergency Medicine, 20(2), 178-184.
DynaMed. (2014, November 18). Comfort measures (pharmacologic) during labor.
Leeman, L., Fontaine, P., King, V., Klein, M. C., & Ratcliffe, S. (2003). The nature and management of labor pain: Part II: Pharmacologic pain relief. American Family Physician, 68(6), 1115-1120.
Lexicomp. (2016). Nitrous oxide: Drug information Lexicomp. UptoDate.
Li, Y. X., Han, W. J., Tang, H. T., Wu, Y. S., Tang, L., Yu, J. Q.,…Zhao, J. J. (2013). Nitrous oxide-oxygen mixture during burn wound dressing: A double-blind randomized controlled study. CNS Neuroscience & Therapeutics, 19(4), 278-279.
Olfert, S.M. (2006). Reproductive outcomes among dental personnel: a review of selected exposures. Journal of the Canadian Dental Association. 72(9), 821-825.
Rooks, J. P. (2011). Safety and risks of nitrous oxide labour analgesia: A review. Journal of Midwifery and Women’s Health, 56(6), 557-565.
Rooks, J. P. (2012). Labor pain management other than neuraxial: What do we know and where do we go next? Birth, 39(4): 318-322.
Rosen, M. A. (2002). Nitrous oxide for relief of labor pain: A systematic review. American Journal of Obstetrics and Gynecology, 186(5 Suppl Nature), S110-S126.
Zier J.L., & Doescher, J.S. (2010). Seizures temporally associated with nitrous oxide administration for pediatric procedural sedation. Journal of Child Neurology. 25(12), 1517-1520.
DST-801 Use of Nitrous Oxide/Oxygen in Pain Management: Adult
192
Certified Practice Area:
Reproductive Health: Contraceptive Management
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
Contraceptive Management

193
Certified Practice Area:
Reproductive Health: Contraceptive Management
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
DST-900 Contraceptive Management: Assessment
A comprehensive contraceptive management assessment is client-centred and includes obtaining informed consent, taking a health
history and completing physical assessment components. When assessing the type of contraception that best meets a client’s needs, the RN(C)12 takes into consideration the individual’s clinical judgment and assessment along with the preferences of the
client. Selection of an appropriate contraceptive method is based on best practice (eg. effectiveness, contraindications, side effects, non-contraceptive benefits), availability, costs, and the desires and prior experience of the client. No single regime is most effective; a variety of regimes can be provided based on client/provider preference.
MANAGEMENT AND INTERVENTIONS
NOTE: For the purpose of this DST, initiation of hormonal contraception is when no hormonal contraception has been used within the last three months or the client is switching from a combined hormonal contraception (CHC) to a progestin only hormonal contraception (POHC) or from a POHC to a CHC.
Intended Client Outcomes
• Client receives safe and effective contraception.
• Unintended pregnancies are prevented through the provision of safe and effective contraception.
• Sexual health education is provided to enhance the client’s capacity to manage their sexual and reproductive health care.
INDICATIONS
RN(C)s practice autonomously to dispense and or administer hormonal contraception for the purpose of contraception when indicated for a client who is seeking a reliable, reversible, coitally-independent method of contraception.
Hormonal contraception is further indicated for a number of menstrual-related problems and the non-contraceptive benefits that they confer. However, clients seeking or using hormonal contraception for purposes other than contraception—see example below—must be referred to a physician or nurse practitioner for a patient specific order or transfer of care.
Other benefits of hormonal contraception include, but are not limited to:
• Decreased acne
• Improvement in some menstrual related conditions such as primary dysmenorrhea, ovarian cysts and premenstrual syndrome
• Decreased risk of ovarian and uterine cancer
• Decreased risk of iron deficiency anemia
• Reduction of ectopic pregnancies
In the absence of contraindications, and with precautions in mind, the choice of contraception is based on client preferences. The RN(C) can assist the client by asking the following sample questions:
• How important is it that you do not get pregnant (efficacy)?
• Which method do you think you would like to use or try?
• How convenient do you want the method to be?
• Do you want to use your contraception daily, weekly, monthly or longer?
• Will you be able to use the method as intended (e.g., take the pills daily, return for regular injection)?
• How important is it to have a discreet method of birth control?
• Are you comfortable touching your own genitals (e.g., ring, female condom)?
• Can you afford the method you wish to use or can you access a program to assist with the cost (pharmacare, extended
health benefits)?
12 Note: RN(C) is an authorized title recommended by BCCNP that refers to BCCNP-certified RNs, and is used throughout this
Decision Support Tool (DST).
DST-900 Contraceptive Management: Assessment
194
Certified Practice Area:
Reproductive Health: Contraceptive Management
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
• Are you or will you be using a birth control method that provides protection against sexually transmitted infections (STIs)?
• How quickly do you want to be able to return to fertility?
Relative and Absolute Contraindications
RN (C)s dispense medications autonomously based on individual client assessment and within the US Medical Eligibility Criteria (US MEC) categories 1 & 2. US MEC categories 3 & 4 require a consult and/or referral.
For complete guidance, see Centers for Disease Control and Prevention. (2016). U.S. medical eligibility criteria for contraceptive use, 2016. Morbidity and Mortality Weekly Report, 65(3), 1-106.
Informed Consent Specific to Contraceptive Management
RNs follow the BCCNP Consent practice standard when assessing informed consent with clients who want to access contraception which included the following:
• Assess the client’s ability to provide consent for hormonal contraception
• Understand the legal requirements for determining if a minor can provide valid consent.
• Know who may give consent if your minor client cannot.
Know your organization's policies about any relevant legislation related to consent. When policies are inadequate or inappropriate, participate in refining and strengthening them.
Health History
Before initiating or continuing a hormonal contraceptive, a thorough medical history is taken or reviewed that includes:
• Potential contraindications - medical conditions, medication use, allergies, smoking, breast/chest feeding
• Assess for strong family history consistent with inherited thrombophilia, such as unprovoked venous thromboembolism (VTE)
in a first or second degree relative under the age of 50.
• Assessment of menstrual patterns that might assist in determining possible benefits of hormonal contraceptive use
• Last menstrual period
• Current or past use of contraception (and any difficulties using the method and or side effects)
• Potential for existing pregnancy and need for pregnancy testing
• Assessment of unexplained vaginal bleeding, including recommendations for additional investigations or referrals
• Assessment of sexual activity (risk factors for STIs and potential need for emergency contraception.
Physical Assessment
The physical assessment includes:
• Initial blood pressure measurement for initiation of all hormonal contraception and at least annually thereafter
• Cervical Cancer Screening, STI Screening, breast/chest exams although important for overall reproductive health, are not
mandatory for provision of hormonal contraception and should not be a requirement to receive contraception.
Diagnostic Testing/Investigations
• No specific diagnostic tests or investigations are required for initiation of hormonal contraception.
• Urine pregnancy testing may be indicated if the client is considered at risk for an existing pregnancy.
PRECAUTIONS AND CONSIDERATIONS
Timing of administration is important for effective contraception.
• Quickstart of a hormonal contraceptive is recommended as it demonstrates improved compliance (especially in youth).
Delaying initiation of hormonal contraception (e.g., Sunday start or start with next menstrual period) could increase the risk
that a client forgets to start, chooses not to start or becomes pregnant while awaiting initiation.
• Inconsistent use of hormonal contraception can result in unintended pregnancy.
DST-900 Contraceptive Management: Assessment

195
Certified Practice Area:
Reproductive Health: Contraceptive Management
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
• Consider use of back-up method(s) and/or emergency contraception (Leonogesterol or Ulipristal acetate) when initiating
hormonal contraception and in situations of missed or late doses. Counsel patient around other options including EC IUD.
• Expense and accessibility can affect a person’s ability to use hormonal contraception effectively.
• Hormonal contraception does not offer protection from STIs
• Youth have been shown to be less tolerant of medication side effects and, therefore, tend to have higher discontinuation rates. As such, proper education and counseling at the time of initiation and follow up of hormonal contraception may help
address youth specific needs. This may include more frequent follow up visits (such as at 3 months).
CLIENT EDUCATION
Use of hormonal contraception is more likely to be successful when client education includes:
• How the method works to prevent pregnancy.
• How to use the method(s) of hormonal contraception.
• Initiation of hormonal contraceptive method and time for onset of contraception (recommend quickstart, first day of next
menstrual period).
• Estimated return to fertility after discontinuing hormonal contraception.
• Storage of hormonal contraceptive products.
• Use of appropriate back-up method(s) and emergency contraception.
• Drug-drug interactions and the need to consult with a health care provider when taking other medications.
• Discussion that hormonal contraception is a medication and should be disclosed to health care providers when asked.
• Hormonal contraceptive methods do not protect against STIs.
• Recognizing and taking appropriate action for:
o transitional and ongoing side effects
o possible serious side effects (e.g., ACHES: abdominal pain, chest pain, headache, eye problems and severe leg pain)
o method failure
o missed or late doses (including vomiting within two hours of ingestion of a contraceptive pill might require repeat
doses)
• Accessing the hormonal contraception (e.g., ability to return to clinic or purchase at pharmacy).
• Planned follow up:
o as per Combined Hormonal Contraceptive (CHC) or Progestin-only Hormonal Contraceptive (POHC) DSTs
o such that the client can contact the clinic/health care provider or return with any questions
o as needed by the client
BREAST/ CHEST FEEDING
Hormonal Contraceptives can be started when the person is medically eligible to use the method and if it is reasonably certain that they are not pregnant, see CHC and POHC DSTs for more information regarding intiation oc contraception during the postpartum period.
Estrogen and progestin are excreted in breastmilk in small quantities, but are unlikely to have an effect on the baby.
DISPENSING AND ADMINISTRATION
The dispensed hormonal contraceptive medication should be labelled with a client-specific label. Labels can be pre-printed, but must be client specific and include the information as outlined in the BCCNP Dispensing Medications Practice Standard.
For specific criteria about the administration of DMPA, please refer to the POHC DST.
DST-900 Contraceptive Management: Assessment

196
Certified Practice Area:
Reproductive Health: Contraceptive Management
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
Expiry dates
• When expiry dates note only the month and year, the date is interpreted as the last day of the noted month.
• The expiry date is the date by which the client should finish the medication in that package.
• When dispensing contraception, the RN(C) must calculate the number of doses required to ensure that the dispensed
method, if used as directed, will be completed prior to the stated expiry date.
DOCUMENTATION
Document on the client’s health record as per agency policy and as per the BCCNP Dispensing Medications Practice Standard.
MONITORING AND FOLLOW UP
• Advise a client to return at any time to discuss side effects or other problems or if they want to change the method being
used. No routine follow-up visit is required.
• To improve continuation rates and enhance a client’s abilities to obtain contraception when needed, health care providers
should prescribe up to a 1- or 2-year supply of COCs at the initial and return visits
IDENTIFYING AND MANAGING SIDE EFFECTS
To manage common side effects, the RN(C) may refer to the following recommended resources:
• SOGC Canadian Contraception Consensus (Part 3 and 4):
Chapter 8 Progestin-Only Contraception
Chapter 9: Combined Hormonal Contraception
• Hatcher, R.A., Trussell, J., Nelson, A.L., Cates, W., Stewart, F., & Kowal, D. (2018). Contraceptive technology (21st Rev.
ED.). New York: Ardent Media Inc.
• Zieman, M., Hatcher, R. A., Allen, A. Z., Lathrop, E. & Haddad, L. (2018). Managing contraception on the go (14th ed). Atlanta, GA: Bridging the Gap Communications.
• RX files https://www.rxfiles.ca/RxFiles/home.aspx (requires subscription))
• Consult with another health care provider for questions [e.g., RN(C), physician, nurse practitioner, pharmacist]
DST-900 Contraceptive Management: Assessment
197
Certified Practice Area:
Reproductive Health: Contraceptive Management
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
REFERENCES
More recent editions of any of the items in the Reference List may have been published since this DST was published. If you have a newer version, please use it.
Centers for Disease Control and Prevention. (2016). U.S. medical eligibility criteria for contraceptive use, 2016. Morbidity and Mortality Weekly Report, 65(3), 1-106.
British Columbia College of Nursing Professionals. (2017). Dispensing Medications: Practice standard for registered nurses and nurse practitioners. Vancouver, BC: Author.
British Columbia College of Nursing Professionals. (2013). Consent: Practice standard for registered nurses and nurse practitioners. Vancouver, BC: Author.
Culwell, K. (2011). WHO Immediate start of hormonal contraceptives for contraception: RHL commentary. Geneva: World Health Organization: WHO Reproductive Health Library.
Dickey, R. P. (2014). Managing contraceptive pill patients (15th ed.). Fort Collins, CO: E. M. I. S. Medical Publishing.
Hatcher, R.A., Nelson, A.L., Trussell, J., Cwiak, C., Cason, P., Policar, M.S., Aiken, A.R.A., Marrazzo, J. & Kowal, D. (2019). Contraceptive technology (21st. ED.). Atlanta: Managing Contraception, LLC.:GA
Infants Act: Chapter 223. (1996). Victoria, BC: Queen’s Printer.
Society of Obstetricians and Gynaecologists of Canada. (2015). SOGC Clinical practice guidelines: Canadian contraception consensus (Part 1 of 4). Retrieved from http://sogc.org/wp-content/uploads/2015/11/gui329Pt1CPG1510E.pdf
Society of Obstetricians and Gynaecologists of Canada. (2013). Position statement: Hormonal Contraceptive and risk of venous thromboembolism (VTE).
World Health Organization. (2016). Selected practice recommendations for contraceptive use, 3rd.edition
Zieman, M., Hatcher, R. A., Allen, A. Z., Lathrop, E. & Haddad, L. (2017-2018). Managing contraception on the go (14th ed). Atlanta, GA: Bridging the Gap Communications
DST-900 Contraceptive Management: Assessment
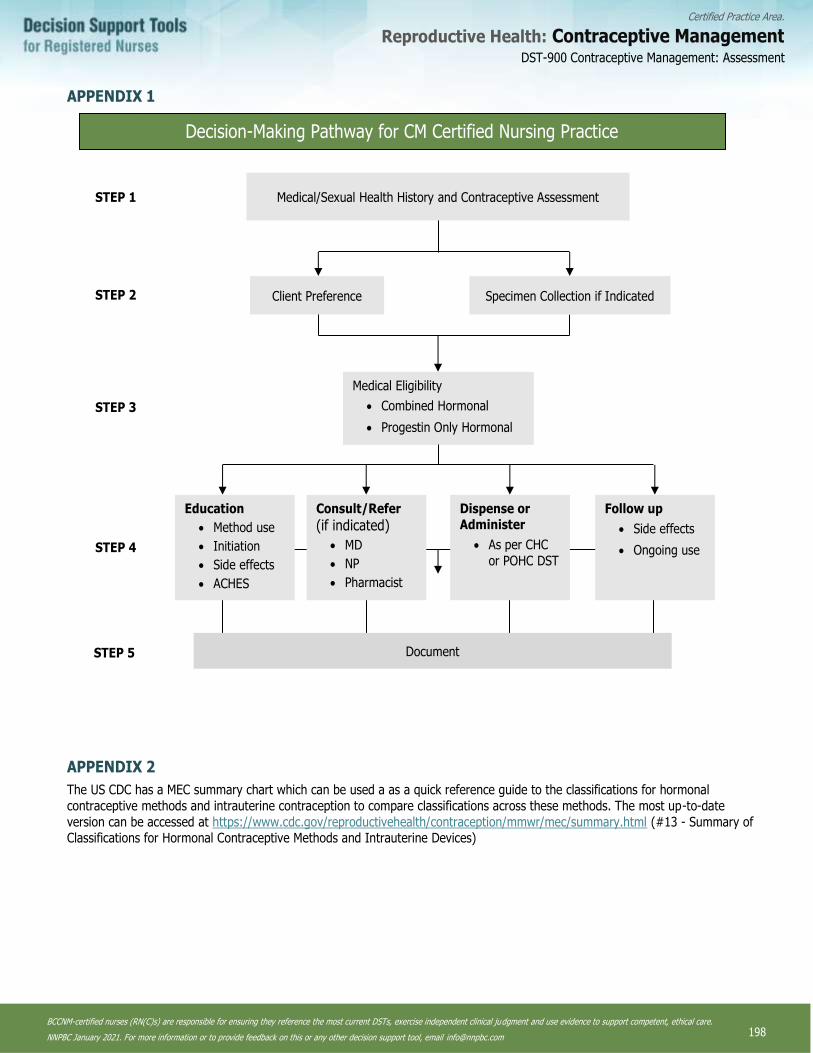
198
Certified Practice Area:
Reproductive Health: Contraceptive Management
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
APPENDIX 1
APPENDIX 2
The US CDC has a MEC summary chart which can be used a as a quick reference guide to the classifications for hormonal
contraceptive methods and intrauterine contraception to compare classifications across these methods. The most up-to-date
version can be accessed at https://www.cdc.gov/reproductivehealth/contraception/mmwr/mec/summary.html (#13 - Summary of Classifications for Hormonal Contraceptive Methods and Intrauterine Devices)
Decision-Making Pathway for CM Certified Nursing Practice
Medical/Sexual Health History and Contraceptive Assessment
Medical Eligibility
• Combined Hormonal
• Progestin Only Hormonal
Client Preference Specimen Collection if Indicated
Education
• Method use
• Initiation
• Side effects
• ACHES
Follow up
• Side effects
• Ongoing use
Dispense or Administer
• As per CHC
or POHC DST
Consult/Refer
(if indicated)
• MD
• NP
• Pharmacist
STEP 1
STEP 3
STEP 2
STEP 4
STEP 5 Document
DST-900 Contraceptive Management: Assessment
199
Certified Practice Area:
Reproductive Health: Contraceptive Management
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
DST-901 Combined Hormonal Contraceptives (CHCs)
This decision support tool (DST) provides clinical guidance for the provision of combined hormonal contraception. It is meant to be used in concert with the Contraceptive Management: Assessment DST.
DEFINITION
Contraception that contains both estrogen and progestin. Three types of combined hormonal contraception are available in Canada: oral contraceptive pills, the transdermal contraceptive patch and the intravaginal contraceptive ring
INDICATIONS
For the purpose of contraceptive management certified practice, CHCs are indicated for any client seeking a reliable, reversible,
coitally-independent method of contraception. RN(C)s independently dispense or administer only CHCs that provide a daily dose of less than 50 mcg of ethinyl estradiol.
RN(C)s only dispense CHCs for the purpose of contraception. Clients seeking or using CHCs for a sole purpose other than contraception must be referred to a physician or nurse practitioner (NP) for a client specific order or transfer of care.
ACTION
The primary method of action of CHCs is through the suppression of gonadotropins induced by the estrogen and progestin effects
on the hypothalamic/pituitary axis, thereby inhibiting ovulation. Progestin supresses luteinizing hormone (LH) secretions, thereby eliminating the LH surge while estrogen supresses follicle stimulating hormone (FSH) secretion, thereby decreasing follicular
maturation. Other mechanisms of action may include the development of endometrial atrophy, making the endometrium unreceptive to implantation and cervical mucus changes that impede sperm transport.
PHARMACOKINETICS
Dose
Combined hormonal contraception contains ethinyl estradiol (EE) and a progestin in various doses and combinations. The amount of EE in CHCsvary. The amount and type of progestin vary and differ in potency and metabolic effect. A low-dose CHC preparation
is preferred to provide effective contraception, acceptable cycle control and the least amount of side effects for that individual. CHCs providing a daily dose of 50 mcg or less of ethinyl estradiol are considered low-dose.
Oral CHC Formulations
Oral CHCs are taken daily, at the same time each day. There are a range of different formulations of oral CHCs available, for example 21-7, 24-4 or extended use packaging.
• Monophasic (each tablet contains a fixed amount of estrogen and progestin)
• Biphasic (each tablet contains a fixed amount of estrogen; the amount of progestin increases in the second half of the cycle)
• Triphasic (the amount of estrogen can be fixed or variable; the amount of progestin increases in three equal phases)
Transdermal CHC Formulations
The transdermal patch is changed once a week for three weeks followed by one week patch-free.
Each transdermal contraceptive patch contains ethinyl estradiol 0.6 mg and norelgestromin 6 mg [releases approximately ethinyl estradiol 35 mcg and norelgestromin 200 mcg per 24 hours]
Intravaginal CHC Formulations
The intravaginal contraceptive ring is worn inside the vagina for three weeks followed by one week ring free.
• Each intravaginal ring delivers ethinyl estradiol 15 mcg/day and etonogestrel 120 mcg/day
DST-901 Combined Hormonal Contraceptives (CHCs)
200
Certified Practice Area:
Reproductive Health: Contraceptive Management
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
Onset
Peak serum concentrations of combined estrogen and progestin vary between products. Contraceptive benefits are realized within seven days of consistent and correct CHC use.
CONSULT OR REFERRAL
RN(C)s are restricted to dispensing or administering CHCs to clients who classify as category 1 or 2 as defined by the U.S. Medical Eligibility Criteria for Contraceptive Use. RN(C)s cannot independently dispense or administer CHCs to women who classify as a category 3 or 4 without an order.
Relative Contraindications
As per U.S. Medical Eligibility Criteria for Contraceptive Use, Category 3
Absolute Contraindications
As per U.S. Medical Eligibility Criteria for Contraceptive Use, Category 4
RN(C)s must refer or consult with a physician or nurse practitioner for the following clients:
• Clients wanting to use CHCs in the presence of relative or absolute contraindications (U.S. Medical Eligibility Criteria for Contraceptive Use, categories 3 and 4).
• Clients whose medical condition has changed so that they might be using combined hormonal contraception in the presence
of relative or absolute contraindications (U.S. Medical Eligibility Criteria for Contraceptive Use, categories 3 and 4).
• Clients with chronic health conditions that increase serum potassium or clients taking medications that increase serum
potassium if considering use of a drosperinone containing CHC.
• Clients who are currently taking CHCs and demonstrate any of the following symptoms: ACHES (abdominal pain, chest pain, headache, eye problems and severe leg pain); unexplained vaginal bleeding; jaundice; syncope; blood pressure >140/>90;
severe migraine headaches (with aura); severe depression; and/or severe allergic skin rash.
• Transvaginal ring users with a history of toxic shock syndrome (TSS). (Rare cases of TSS have been reported by ring users.
Causation has not been determined.)
• Clients reporting headaches that are new and or worsening with the use of hormonal contraception
• Clients taking medications that might be affected by hormonal contraception
Drug Interactions
The following drugs and drug classes are considered MEC category 3 or 4 and could have some effect on CHC absorption. RN(C)s must refer or consult with a physician or nurse practitioner for clients taking any of the following:
• Anticonvulsants: phenytoin, carbamazepine, barbiturates, primidone, topiramate, oxcarbazepine. Lamotrigine alone
(lamotrigine/valproate combo does not interact with hormones).
• Antimicrobials: Rifampicin or Rifabutin therapy
Note: Except for rifampicin, antibiotic use does not affect CHC efficacy.
• Fosamprenavir (antiretroviral).
Drugs that may be affected by CHC use (consult or refer to physician or NP for appropriate management of these clients):
• Clients taking theophylline, tricyclic antidepressants, diazepam or lithium may need dosage adjustments.
• Drospirenone may increase potassium. Clients should be advised to inform their healthcare provider if they have kidney, liver
or adrenal disease because the use of Drospirenone containing CHCs in the presence of these conditions could cause serious heart and health problems. They should also inform their healthcare provider if they are currently on daily, long-term
treatment (NSAIDs, potassium-sparing diuretics, potassium supplementation, ACE inhibitors, angiotensin-II receptor
antagonists, heparin or aldosterone antagonists) for a chronic condition or taking strong CYP3A4 inhibitors.
DST-901 Combined Hormonal Contraceptives (CHCs)
201
Certified Practice Area:
Reproductive Health: Contraceptive Management
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
PREGNANCY AND BREAST/CHEST FEEDING
Pregnancy
There is no known harm to the person, the course of the pregnancy or the fetus if CHCs are inadvertently used during pregnancy.
However, if a CHC is inadvertently initiated with a pregnant client or the client becomes pregnant during CHC use, the CHC should be discontinued immediately.
Postpartum
Initiation of CHC in the post-partum period is dependent on level of risk. A summary is provided but a detailed breakdown can be reviewed in the most upto-date U.S. Selected Practice Recommendations for Contraceptive Use (US SPR).
MEC Category 4
• Less than 21 days post-partum
MEC Category 3
• Breast/chest feeding: 21 to < 30 Days
• Breast/chest feeding: 30–42 days postpartum with other risk factors for VTE (e.g., age ≥35 years, previous VTE, thrombophilia, immobility, transfusion at delivery, peripartum cardiomyopathy, BMI ≥30 kg/m2, postpartum haemorrhage,
postcesarean delivery, preeclampsia, or smoking)
• Non Breast/chest feeding: 21–42 days postpartum with other risk factors for VTE (e.g., age ≥35 years, previous VTE,
thrombophilia, immobility, transfusion at delivery, peripartum cardiomyopathy, BMI ≥30 kg/m2, postpartum hemorrhage,
postcesarean delivery, preeclampsia, or smoking)
Breast/Chest feeding
Conflicting studies suggest theoretical concerns about the effects of CHCs on breastmilk volume. Estrogen and progestin are both excreted in breastmilk in small quantities, but are unlikely to have an effect on the baby.
PRECAUTIONS AND CONSIDERATIONS
In general for all combined Hormonal Contraceptives, the risk of VTE is highest in the first year of CHC use and in first-time users.
The risk of VTE in CHC users remains significantly less than the risk of VTE in pregnancy and the post-partum period. In the
absence of symptoms, routine laboratory screening for thrombophilia or other bleeding disorders is not recommended.13
Precautions and Considerations Specific to the Oral Contraceptive Pill
• Malabsorption related to chronic gastrointestinal inflammation and active diarrhea might cause ineffectiveness of any oral
contraception.
• Repeated vomiting (e.g., bulimia) and/or severe diarrhea can decrease the absorption of the pill and might decrease its
effectiveness. Vomiting within two hours of pill ingestion might require repeated doses.
• The effectiveness of oral CHCs might be slightly decreased among clients who are obese (BMI >30). However, no association has been found between pregnancy risk and body mass index (BMI). It is likely that even a small decrease in effectiveness in
clients who are obese still confers overall effectiveness to be high
Precautions and Considerations Specific to the Transdermal Contraceptive Patch
• The effectiveness of the patch might be slightly decreased among clients weighing greater than 90 kg or who are obese (BMI >30). However, no association has been found between pregnancy risk and body mass index (BMI). It is likely that even a
13 CHCs should not be withheld from women with a family history of venous thromboembolism (VTE) unless they demonstrate symptoms of VTE. Family history of VTE in a first degree relative is a category 2. Some thrombophilia conditions that increase the risk for a deep vein thrombosis (DVP) or pulmonary embolism are heritable. Testing for underlying thrombophilias might be indicated for women with a personal family history of VTE in a first degree relative with a history of spontaneous VTE (i.e., not associated with pregnancy, cancer, airline travel , surgery, obesity, immobilization etc). Screening of asymptomatic women is not recommended.
DST-901 Combined Hormonal Contraceptives (CHCs)

202
Certified Practice Area:
Reproductive Health: Contraceptive Management
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
small decrease in effectiveness in clients who are obese still confers overall effectiveness to be high and therefore should not
be a reason to avoid this method.
• Clients with conditions that affect the skin, such as eczema, psoriasis, cuts, rash or sunburn, should not apply the patch to
these areas.
Precautions and Considerations Specific to the Intravaginal Contraceptive Ring
• Clients who have significant pelvic relaxation, vaginal stenosis or utero-vaginal prolapse and are unable to touch their
genitalia or who have vaginal obstruction are not good candidates for the intravaginal ring.
• Might not be suitable for clients who have conditions that make the vagina more susceptible to irritation or ulceration.
Women who have genital outbreaks of herpes simplex virus are able to use the intravaginal contraceptive ring.
• Should not be used in conjunction with the diaphragm as it could dislodge this barrier.
ADVERSE EFFECTS
Side effects from CHCs are often mild and transient and can respond to a change in formulation. Acknowledgment and management of side effects are crucial to successful continuation of CHCs.
A theoretical understanding of the different side effects implicated by hormones is helpful. The Society of Obstetricians and
Gynecologists of Canada (SOGC) or the US MEC Selected Practice Recommendations for Hormonal Contraceptive Use (2016) have resources for understanding side effects related to contraceptives that can be used as a resource for health care providers.
Common Possible Side Effects
Common side effects of CHCs include, but are not limited to:
• Absence of withdrawal bleed
• Appetite changes (can result in weight gain)
• Breast tenderness
• Breakthrough bleeding/spotting
• Headaches (mild, without aura)
• Nausea
• Mood changes
• Libido changes
• Skin changes
Warning and Precautions
Serious side effects from CHCs are rare. The following symptoms should be investigated immediately, referred to a physician or nurse practitioner and might warrant discontinuation of CHCs:
• ACHES (abdominal pain, chest pain, headache, eye problems and severe leg pain)
• Moderate to Severe Depression
• Jaundice
• Unexplained vaginal bleeding
• Syncope
• Blood pressure >140/>90
• Severe or worsening migraine headaches with or without aura
• Severe allergic reaction
DST-901 Combined Hormonal Contraceptives (CHCs)

203
Certified Practice Area:
Reproductive Health: Contraceptive Management
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
CLIENT EDUCATION SPECIFIC TO CHC USE
Missed or Late CHC Doses
If available, advise the client to follow the product monograph, or advise the client to contact a health care provider or clinic. Some
clinics choose to develop client hand-outs or resources specific to missed or late CHC doses. The Society of Obstetricians and Gynecologists of Canada (SOGC) or the US MEC Selected Practice Recommendations for Hormonal Contraceptive Use (2016) have guidelines for missed hormonal contraceptives that can be used as a resource for health care providers.
Continuous Use, Extended Use and Shortened Hormone Free Intervals
• When determining CHC method of use, the RN(C)s should discuss continuous use, extended use and shortened hormone free
intervals with the client.
• All oral, transdermal and vaginally administered CHCs can be used as continuous, extended use and/or with shortened
hormone free intervals.
• Continuous use, extended use and shortened hormone free intervals increase contraceptive efficacy
• The rate of side effects and adverse events with continuous use regimes is similar to conventional CHC use.
The length of the continuous use or extended use of combined hormonal contraceptive CHC regimens should be administered according to the preference of the client.
Common Side Effects of Continuous and Extended Use
The most common side effect of continuous and extended use of CHCs is irregular bleeding or spotting. This might result in higher
discontinuation rates than 28-day CHC regimes or shortened hormone free interval regimes. Counselling clients on managing these side effects and informing them that the unscheduled bleeding will decrease over time is important.
DISPENSING
For dispensing CHCs, refer to the see Contraceptive Management: Assessment DST
The intravaginal contraceptive ring is a cold chain medication. Once the cold chain has been broken, it is stable at room
temperature for up to four months. The “insert by” expiry date should be indicated on the package as soon as cold-chain storage is broken.
MANAGEMENT AND FOLLOW UP
• After initiation or change of a CHC:
o Advise a client to return at any time to discuss side effects or other problems or if they want to change the method
being used. No routine follow-up visit is required.
• Specific populations that might benefit from more frequent follow-up visits include adolescents, those with certain medical
conditions or characteristics, and those with multiple medical conditions.
• At other routine visits, when seeing combined hormonal contraceptive users RN (C)s should do the following:
o Assess the client’s satisfaction with their contraceptive method and whether they have any concerns about method use.
o Assess any changes in health status, including medications that would change the appropriateness of combined hormonal contraceptives for safe and effective continued use based on U.S. MEC (e.g., category 3 and 4 conditions and
characteristics).
o Assess blood pressure (at least annually).
• Consider assessing weight changes and counselling women who are concerned about weight changes perceived to be
associated with their contraceptive method.
DOCUMENTATION
• Refer to Contraceptive Management: Assessment DST
DST-901 Combined Hormonal Contraceptives (CHCs)
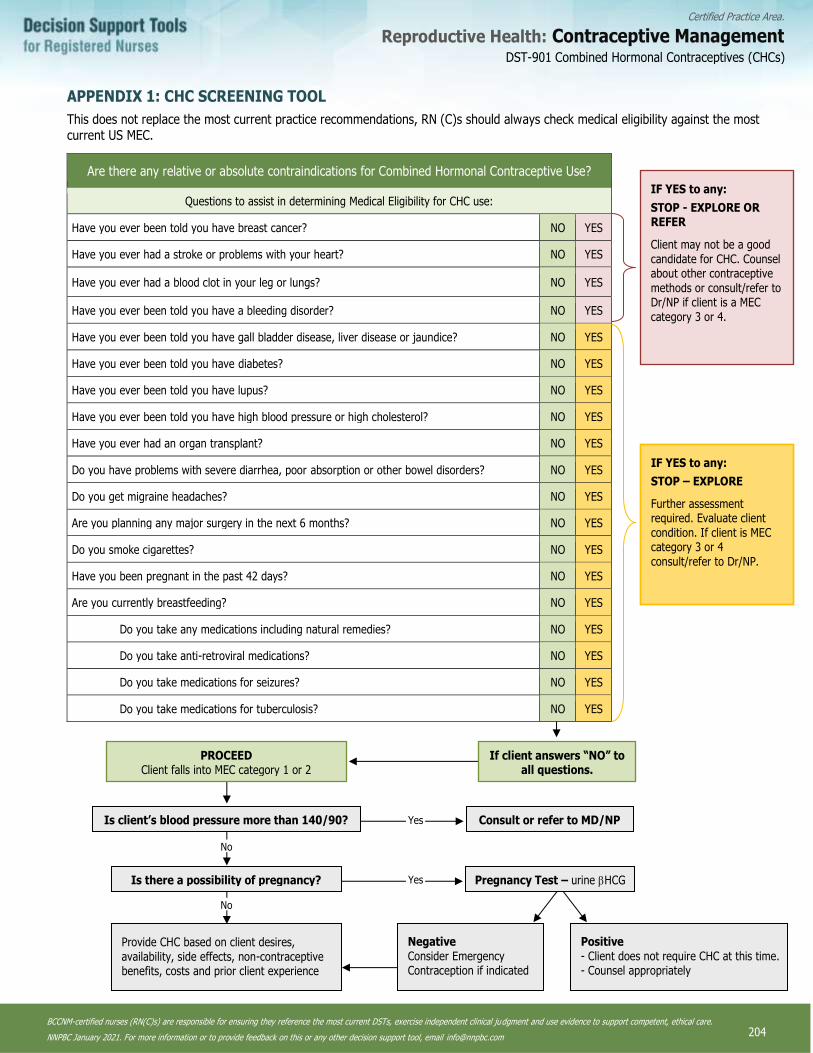
204
Certified Practice Area:
Reproductive Health: Contraceptive Management
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
APPENDIX 1: CHC SCREENING TOOL
This does not replace the most current practice recommendations, RN (C)s should always check medical eligibility against the most current US MEC.
Are there any relative or absolute contraindications for Combined Hormonal Contraceptive Use?
Questions to assist in determining Medical Eligibility for CHC use:
Have you ever been told you have breast cancer? NO YES
Have you ever had a stroke or problems with your heart? NO YES
Have you ever had a blood clot in your leg or lungs? NO YES
Have you ever been told you have a bleeding disorder? NO YES
Have you ever been told you have gall bladder disease, liver disease or jaundice? NO YES
Have you ever been told you have diabetes? NO YES
Have you ever been told you have lupus? NO YES
Have you ever been told you have high blood pressure or high cholesterol? NO YES
Have you ever had an organ transplant? NO YES
Do you have problems with severe diarrhea, poor absorption or other bowel disorders? NO YES
Do you get migraine headaches? NO YES
Are you planning any major surgery in the next 6 months? NO YES
Do you smoke cigarettes? NO YES
Have you been pregnant in the past 42 days? NO YES
Are you currently breastfeeding? NO YES
Do you take any medications including natural remedies? NO YES
Do you take anti-retroviral medications? NO YES
Do you take medications for seizures? NO YES
Do you take medications for tuberculosis? NO YES
IF YES to any:
STOP - EXPLORE OR REFER
Client may not be a good candidate for CHC. Counsel about other contraceptive
methods or consult/refer to Dr/NP if client is a MEC category 3 or 4.
IF YES to any:
STOP – EXPLORE
Further assessment required. Evaluate client condition. If client is MEC category 3 or 4 consult/refer to Dr/NP.
If client answers “NO” to all questions.
PROCEED Client falls into MEC category 1 or 2
Is client’s blood pressure more than 140/90?
Is there a possibility of pregnancy?
No
No
Provide CHC based on client desires, availability, side effects, non-contraceptive benefits, costs and prior client experience
Yes
Yes
Consult or refer to MD/NP
Pregnancy Test – urine HCG
Negative Consider Emergency Contraception if indicated
Positive - Client does not require CHC at this time. - Counsel appropriately
DST-901 Combined Hormonal Contraceptives (CHCs)
205
Certified Practice Area:
Reproductive Health: Contraceptive Management
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
REFERENCES
More recent editions of any of the items in the Reference List may have been published since this DST was published. If you have a newer version, please use it.
Anderson, K.C., Schwartz, M.D. and Lieu, S.O. (2013). Antibiotics and OC effectiveness. Journal of the American Academy of Physician Assistants, 26(1)11.
Blanco-Molina, A. and Montreal, M. (2010). Venous thromboembolism in women taking hormonal contraceptives. Expert Review of Cardiovascular Therapy, 8(2): 211-215.
Centers for Disease Control and Prevention. (2016). U.S. medical eligibility criteria for contraceptive use, 2016. Morbidity and Mortality Weekly Report, 65(3), 1-106.
Centers for Disease Control and Prevention. (2011). Update to CDC’s U.S. medical eligibility criteria for contraceptive Use, 2010: Revised recommendations for the use of contraceptive methods during the postpartum period. Morbidity and Mortality Weekly Report 60(26):878–883.
Dickey, R. P. (2014). Managing contraceptive pill patients (15th ed.). Fort Collins, CO: E. M. I. S. Medical Publishing.
Grossman Barr, N. (2010). Managing Adverse Effects of Hormonal Contraceptives. American Family Physician, 82(12), 1499–1506.
Hatcher, R.A., Nelson, A.L., Trussell, J., Cwiak, C., Cason, P., Policar, M.S., Aiken, A.R.A., Marrazzo, J. & Kowal, D. (2019). Contraceptive technology (21st. ED.). Atlanta: Managing Contraception, LLC.:GA
Martinez, F., Ramirez, I., Perez-Campos, E., Latorre, K. and Lete, I. (2012). Venous and pulmonary thromboembolism and combined hormonal contraceptives. Systematic review and meta-analysis.
Rott, H. (2012). Thrombotic risks of oral contraceptives. Current Opinion in Obstetrics and Gynecology, 24. 235-240
Sridhar, A. & Salcedo, J. (2017). Optimizing maternal and neonatal outcomes with postpartum contraception:impact on breastfeeding and birth spacing. Maternal Health, Neonatology and Perinatology. 3:1 https://doi.org/10.1186/s40748-016-0040-
Society of Obstetricians and Gynaecologists of Canada. (2015). SOGC Clinical practice guidelines: Canadian contraception consensus (Part 1 to 4).
Stewart, M. & Black, K. (2015). Choosing a combined oral contraceptive pill. Aust Prescr 2015:38:6-11.
World Health Organization. (2015). Medical eligibility criteria for contraceptive use, 5th Edition.
Zieman, M., Hatcher, R. A., Allen, A. Z., Lathrop, E. & Haddad, L. (2017-2018). Managing contraception on the go (14th ed). Atlanta, GA: Bridging the Gap Communications
DST-901 Combined Hormonal Contraceptives (CHCs)
206
Certified Practice Area:
Reproductive Health: Contraceptive Management
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
DST-902 Progestin-Only Hormonal Contraceptives
This decision support tool (DST) provides clinical guidance for the provision of progestin-only hormonal contraception. It is meant to be used in concert with the Contraceptive Management: Assessment DST
DEFINITION
Progestin-only hormonal contraception is a hormonal contraceptive method that contains only progestin. Three types of POHCs are
available in Canada: progestin-only oral contraceptive pills, progestin-only injectable (Depo-Medroxyprogesterone Acetate (DMPA) ) and levonorgestrel-releasing intrauterine system. For the purposes of this decision support tool, RN(C)s only autonomously
dispense the first 2 methods and therefore POHCs refer only to the first two progestin-only methods of contraception (oral and injectable).
INDICATIONS
For the purpose of contraceptive management certified practice, POHCs are indicated for any client seeking a reliable, reversible,
coitally-independent method of contraception. POHCs are a reliable and effective contraceptive option for clients unable to use estrogen-containing contraception. POHCs are further indicated for a number of menstrual-related problems and the non-
contraceptive benefits that they might confer. Clients seeking or using POHCs for a sole purpose other than contraception must be referred to a physician or nurse practitioner (NP), for a client specific order or transfer of care.
ACTION
The primary method of action of POHCs is by inhibiting the secretion of pituitary gonadotropins, which then suppresses ovulation.
POHCs also make cervical mucus more viscous, which impedes sperm transport. POHCs also induce endometrial atrophy, making the endometrium unreceptive to implantation.
PHARMACOKINETICS
Oral Dose: POHC oral pills are supplied in packages of 28 tablets, each containing 35mcg of norethindron
Injectable DMPA :DMPA is supplied in vials of 150mg to be injected intramuscularly every 12 – 13 weeks (with a range of 10 to less than 15 weeks being acceptable).
Onset
Contraceptive benefits are realized within seven days of consistent and correct POHC use.
CONSULT OR REFER
RN(C)s14 are restricted to dispensing or administering POHCs to clients who classify as category 1 or 2 as defined by the U.S. Medical Eligibility Criteria for Contraceptive Use. RN(C)s cannot independently dispense or administer POHCs without an order to clients who classify as a category 3 or 4 as defined by the U.S. Medical Eligibility Criteria for Contraceptive Use.
Relative Contraindications
As per U.S. Medical Eligibility Criteria for Contraceptive Use, Category 3
Absolute Contraindications
As per U.S. Medical Eligibility Criteria for Contraceptive Use, Category 4
14 Note: RN(C) is an authorized title recommended by BCCNP that refers to BCCNP-certified RNs, and is used throughout this
Decision Support Tool (DST).
DST-902 Progestin-Only Hormonal Contraceptives

207
Certified Practice Area:
Reproductive Health: Contraceptive Management
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
RN(C)s must refer or consult with a physician or nurse practitioner for the following clients:
Clients wanting to use a POHC in the presence of relative or absolute contraindications (U.S. Medical Eligibility Criteria for Contraceptive Use, categories 3 and 4).
Clients whose medical condition has changed so that they might be using a POHC in the presence of relative or absolute contraindications (U.S. Medical Eligibility Criteria for Contraceptive Use, categories 3 and 4).
Clients who are currently taking POHCs and demonstrate any of the following symptoms: ACHES (abdominal pain, chest pain,
headache, eye problems and severe leg pain); jaundice; syncope; severe depression; unexplained vaginal bleeding; severe or worsening migraine headaches (with or without aura) or severe allergic reaction.
Clients taking medications that might be affected by hormonal contraception
Drug Interactions
The following drugs and drug classes are considered a category 3 or 4 and could have some effect on POHC absorption and
metabolism. Clinicians should always refer to the most current MEC for up to date drug interactions. RN(C)s must refer or consult with a physician or nurse practitioner for clients taking any of the following medications:
Oral
Certain anticonvulsants: phenytoin, carbamazepine, barbiturates, primidone, topiramate, oxcarbazepine
Certain antimicrobial: Rifampicin or Rifabutin therapy (Note: Except for Rifampicin or Rifabutin therapy, antibiotic use does not affect POHC efficacy.)
DMPA
Aminoglutethimide (used to treat Cushing disease) (Not in US MEC but may decrease effectiveness of DMPA)
PREGNANCY AND BREAST/CHEST FEEDING
Pregnancy
There is no known harm to the person, the course of the pregnancy or the fetus if POHCs are inadvertently used during pregnancy. The relation between DMPA use during pregnancy and its effects on the fetus remain unclear. If a POHC is inadvertently initiated with a pregnant client or the client becomes pregnant during POHC use, the POHC should be discontinued immediately.
Postpartum
Initiation of POHCs can occur directly post-partum regardless of breast feeding status.
Breast/Chest feeding
Progestin is excreted in breastmilk in small quantities, but is unlikely to have an effect on the baby. Breastfeeding is not a contraindication for POHC use.
PRECAUTIONS AND CONSIDERATIONS
• Precautions specific to Progestin-Only Oral Contraceptioatients who have undergone malabsortive procedures (such as gastric
bypass or biliopancreaic diversion) are MEC 3
• Malabsorption related to chronic gastrointestinal inflammation and active diarrhea might cause ineffectiveness of any oral
contraception.
• Repeated vomiting (e.g., bulimia) and or severe, persistent diarrhea can decrease the absorption of the pill and might
decrease its effectiveness. Vomiting within two hours of pill ingestion might require repeated doses.
Precautions Specific to DMPA
• DMPA is associated with decreased bone mineral density that is generally temporary and reversible. The advantages of DMPA use generally outweigh theoretical concerns regarding fracture risk. The available evidence does not justify limiting duration
DST-902 Progestin-Only Hormonal Contraceptives
208
Certified Practice Area:
Reproductive Health: Contraceptive Management
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
of DMPA use due to bone density concerns. Use of DMPA in the absence of symptoms or other risk factors (i.e. strong family
history of osteoporosis) is not an indication for bone mineral density testing.
• Clients should be informed about the potential effects of DMPA on bone mineral density and counselled about bone health,
including calcium and vitamin D supplements, smoking cessation, weight-bearing exercise, and decreased alcohol and
caffeine consumption.
• To rule out a rare but possible severe allergic reaction to DMPA, clinicians should recommend that clients wait 15-20 minutes
following injection.
• DMPA might have a slower return to fertility than other hormonal contraceptives. The average return to fertility is 10 months
from the last DMPA injection.
ADVERSE EFFECTS
Side effects from POHCs are often mild and transient and respond to a change in formulation. Acknowledgment and management of side effects are crucial to successful continuation of POHCs.
Common Possible Side Effects
Common side effects of POHCs include, but are not limited to:
• Appetite changes (can result in weight gain)
• Breast tenderness
• Menstrual cyle disturbance: breakthrough bleeding, irregular bleeding, amenorhea
• Headaches (mild, without aura)
• Decreased libido
• Mood changes
• Delayed return to fertility (for DMPA only)
• Weight Gain (for DMPA only)
Warnings and Precautions
Serious complications from POHCs are rare. The following symptoms should be investigated immediately, referred to a physician or nurse practitioner and might warrant discontinuation of POHCs:
• ACHES (abdominal pain, chest pain, headache, eye problems and severe leg pain)
• Moderate to severe depression
• Blood pressure >160/100 (DMPA is MEC category 3 ; POPs RN (c) may dispense but should consider referral for hypertension
assessment).
• Jaundice
• Syncope
• Severe or worsening migraine headaches with or without aura
• Severe allergic reaction
• Unexplained vaginal bleeding
CLIENT EDUCATION SPECIFIC TO POHC USE
• A missed oral POHC pill by more than three hours from the regular time requires use of back up contraception (e.g., condom) for 48 hours. Clients can consider use of emergency contraception if unprotected intercourse occurred within the past 5-7
days.
o If available, advise the client to follow the product monograph, or advise the client to contact a health care provider or clinic. Some clinics choose to develop client hand-outs or resources specific to missed or late POHC doses. The Society
of Obstetricians and Gynecologists of Canada (SOGC) or the US MEC Selected Practice Recommendations for Hormonal
DST-902 Progestin-Only Hormonal Contraceptives
209
Certified Practice Area:
Reproductive Health: Contraceptive Management
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
Contraceptive Use (2016) have guidelines for missed hormonal contraceptives that can be used as a resource for health
care providers.
• Irregular menses is common within the first several months of POHC use. After 6-12 months, amenorrhea is more likely.
• Weight gain is possible with DMPA use and can be used as a teachable moment.
• Clients using DMPA should be counselled regarding calcium intake and or supplementation and encouraged to quit smoking
and perform weight-bearing exercises at least three times a week.
• If it has been 14 weeks or more since the last DMPA injection, a urine pregnancy test should be performed. Use of
emergency contraception can be considered if intercourse has occurred within the last 5-7 days. A back up method (e.g., condoms) should be recommended for the next seven days. Depending on the client’s risk of pregnancy, a repeat urine
pregnancy test may be indicated at two weeks or prior to the next injection.
DISPENSING AND ADMINISTERING
For dispensing POHCs, refer to the Contraceptive Management: Assessment DST
Administering DMPA
Mix the suspension well by shaking the vial before drawing up the medication. Using a 21-23 gauge needle appropriate for muscle
mass, administer 1cc of 150mg/mL DMPA via intramuscular injection into the deltoid or ventrogluteal muscle depending on the client’s preference. The ventrogluteal muscle might be less painful for the client. Do not massage the injection site.
MANAGEMENT AND FOLLOW UP
For the purpose of this DST, initiation of hormonal contraception is when no hormonal contraception has been used within the last three months or the client is switching from a CHC to a POHC or from a POHC to a CHC.
Advise a client to return at any time to discuss side effects or other problems or if she wants to change the method being used. No routine follow-up visit is required.
Specific populations that might benefit from more frequent follow-up visits include adolescents, those with certain medical conditions or characteristics, and those with multiple medical conditions.
At other routine visits, when seeing combined hormonal contraceptive users RN (C)s should do the following:
• Assess the client’s satisfaction with their contraceptive method and whether they have any concerns about method use.
• Assess any changes in health status, including medications, that would change the appropriateness of combined hormonal
contraceptives for safe and effective continued use based on U.S. MEC (e.g., category 3 and 4 conditions )
• Assess blood pressure (at least annually).
• Consider assessing weight changes and counseling women who are concerned about weight changes perceived to be
associated with their contraceptive method
DOCUMENTATION
• Refer to the Contraceptive Management: Assessment DST.
DST-902 Progestin-Only Hormonal Contraceptives
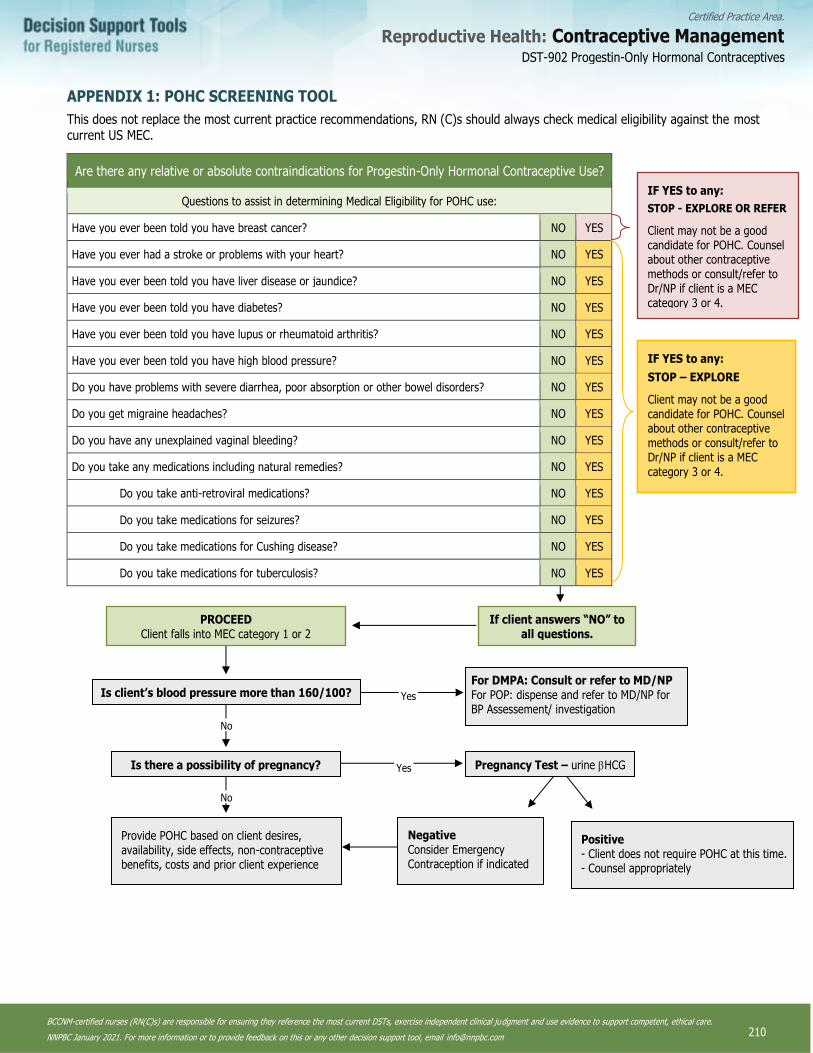
210
Certified Practice Area:
Reproductive Health: Contraceptive Management
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
APPENDIX 1: POHC SCREENING TOOL
This does not replace the most current practice recommendations, RN (C)s should always check medical eligibility against the most current US MEC.
Are there any relative or absolute contraindications for Progestin-Only Hormonal Contraceptive Use?
Questions to assist in determining Medical Eligibility for POHC use:
Have you ever been told you have breast cancer? NO YES
Have you ever had a stroke or problems with your heart? NO YES
Have you ever been told you have liver disease or jaundice? NO YES
Have you ever been told you have diabetes? NO YES
Have you ever been told you have lupus or rheumatoid arthritis? NO YES
Have you ever been told you have high blood pressure? NO YES
Do you have problems with severe diarrhea, poor absorption or other bowel disorders? NO YES
Do you get migraine headaches? NO YES
Do you have any unexplained vaginal bleeding? NO YES
Do you take any medications including natural remedies? NO YES
Do you take anti-retroviral medications? NO YES
Do you take medications for seizures? NO YES
Do you take medications for Cushing disease? NO YES
Do you take medications for tuberculosis? NO YES
If client answers “NO” to all questions.
PROCEED Client falls into MEC category 1 or 2
Is client’s blood pressure more than 160/100?
Is there a possibility of pregnancy?
No
No
Provide POHC based on client desires, availability, side effects, non-contraceptive benefits, costs and prior client experience
Yes
Yes
For DMPA: Consult or refer to MD/NP For POP: dispense and refer to MD/NP for BP Assessement/ investigation
Pregnancy Test – urine HCG
Negative Consider Emergency Contraception if indicated
Positive - Client does not require POHC at this time. - Counsel appropriately
IF YES to any:
STOP - EXPLORE OR REFER
Client may not be a good candidate for POHC. Counsel about other contraceptive methods or consult/refer to Dr/NP if client is a MEC category 3 or 4.
IF YES to any:
STOP – EXPLORE
Client may not be a good candidate for POHC. Counsel about other contraceptive methods or consult/refer to Dr/NP if client is a MEC
category 3 or 4.
DST-902 Progestin-Only Hormonal Contraceptives

211
Certified Practice Area:
Reproductive Health: Contraceptive Management
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
REFERENCES
More recent editions of any of the items in the Reference List may have been published since this DST was published. If you have a newer version, please use it.
Anderson, K.C., Schwartz, M.D. and Lieu, S.O. (2013). Antibiotics and OC effectiveness. Journal of the American Academy of Physician Assistants, 26(1)11.
Centers for Disease Control and Prevention. (2017). Update to CDC’s U.S. Medical Eligibility Criteria for Contraceptive Use, 2016: Revised recommendations for the use of hormonal contraception among women at high risk for HIV infection. Morbidity and Mortality Weekly Report (MMWR), 66(37), 990-994.
Centers for Disease Control and Prevention. (2016). U.S. medical eligibility criteria for contraceptive use, 2016. Morbidity and Mortality Weekly Report, 65(3), 1-106.
Dickey, R. P. (2014). Managing contraceptive pill patients (15th ed.). Fort Collins, CO: E. M. I. S. Medical Publishing.
Freeman, S., & Shulman, L. P. (2010). Considerations for the use of progestin-only contraceptives. Journal of the American Academy of Nurse Practitioners, 22, 81–91.
Grossman Barr, N. (2010). Managing Adverse Effects of Hormonal Contraceptives. American Family Physician, 82(12), 1499–1506.
Hatcher, R.A., Nelson, A.L., Trussell, J., Cwiak, C., Cason, P., Policar, M.S., Aiken, A.R.A., Marrazzo, J. & Kowal, D. (2019). Contraceptive technology (21st. ED.). Atlanta: Managing Contraception, LLC.:GA
Mishra NK, Chowdary KA, Mishra G. Medroxyprogesterone Acetate - A Hormonal Contraceptive. International Journal of Pharmacology and Therapeutics. 2016;6(3):10.
Pfizer Canada. (2011). Depo-Provera Product Monograph. (L3) 26 October 2015.
Society of Obstetricians and Gynaecologists of Canada. (2015). SOGC Clinical practice guidelines: Canadian contraception consensus (Part 1 to 4).
World Health Organization. (2015). Medical eligibility criteria for contraceptive use, 5th Edition
Zieman, M., Hatcher, R. A., Allen, A. Z., Lathrop, E. & Haddad, L. (2017-2018). Managing contraception on the go (14th ed). Atlanta, GA: Bridging the Gap Communications
DST-902 Progestin-Only Hormonal Contraceptives

212
Certified Practice Area:
Reproductive Health: Sexually Transmitted Infections
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
Sexually Transmitted Infections

213
Certified Practice Area:
Reproductive Health: Sexually Transmitted Infections
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
DST-1001 STI Assessment
Within the scope of nursing practice with clients of all genders experiencing or at risk for STI, comprehensive assessment includes:
a sexual health history, a risk assessment, a physical assessment, and screening and/or diagnostic tests. Use of an interpreter is recommended in instances where the clinician does not adequately speak the language of the client.
Guided by three foundational principles, the STI Assessment Decision Support Tool (DST) applies an equity lens to STI assessment.
Through these three principles, the DST takes a new direction towards accommodating and providing more equitable, inclusive and
affirming care for all clients; especially for transgender, gender-diverse and two-spirit peoples. This is of particular importance as inequities are associated with negative stereotypes often leading to higher rates of STIs and non-disclosure of information. As a
consequence, this may hinder relevant testing, diagnosis, treatment, and the provision of targeted client education. The principles below aim to direct clinician-consideration of the diversity in bodies, of the client, their culture, their gender and their context-
specific needs when providing services:
• cultural safety that is trauma- and violence-informed
• knowledge and understanding of the burden of disease as it relates to the social determinants of health (SDOH) and
syndemics
• creative and flexible service provision
The decision to perform a sexual health history may be client-initiated (e.g., client-request, client-reported symptoms or concerns) or clinician-initiated. If a pelvic examination is required as part of the physical assessment, RN(C)s15 must follow PHSA's Pelvic Exam DST (indicated for clients aged 14 years and up). The following criteria apply when providing STI certified practice care:
• consultation and/or referral with a physician or nurse practitioner (NP) is required for:
o all clients 11 years and under
o symptomatic clients aged 12-13 years
o all pregnant clients
o all breast-/chest-feeding clients, depending on required and recommended treatment (see Consultation and/or Referral section of the applicable DST)
Factors Associated with STI Acquisition
Listed below are factors associated with STI acquisition based on syndemic and epidemiological data, and/or social conditions that sustain vulnerability and likelihood of exposure to STI.
• any sexual activity with blood and/or body fluid exchange
• any sexual activity with skin-to-skin contact
• non-use or failure of barriers for oral, genital, and/or anal sex (e.g., condoms, dental dams, etc.)
• sharing sex toys without condoms and/or not cleaning between use
• sexual activity where there is possibility of oral-fecal transmission (e.g., rimming, anal play, etc.)
• previous history of STI
• sexual contact with someone with an STI
• anonymous sexual partner(s) (e.g., internet, bath house, play parties, etc.)
• trade of money, goods, food, and/or shelter for sex
• rough sex causing mucosal tearing
• survivors of sexual assault and sexual abuse
• sexually active youth under 25 years of age
• substance use, such as alcohol or chemicals, in association with having sex
• sharing drug use paraphernalia: pipes, intra-nasal, and injecting equipment
15 Note: RN(C) is an authorized title recommended by BCCNP that refers to BCCNP-certified RNs, and is used throughout this
Decision Support Tool (DST).
DST-1001 STI Assessment DST-1001 STI Assessment
214
Certified Practice Area:
Reproductive Health: Sexually Transmitted Infections
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
Signs and Symptoms Associated with STIs
• often asymptomatic presentation
• abnormal urethral, genital and/or rectal discharge
• pain with intercourse (dyspareunia)
• urinary abnormality – dysuria, frequency, urgency, colour, odour
• ano-genital irritation and inflammation
• ano-genital lesions
• bleeding with intercourse or between menstrual cycles
• fever, lower back pain, deep dyspareunia
Sexual Health History
A sexual health history is the first component of a comprehensive assessment. When conducting a sexual health history, it is necessary to consider the potential for past and present experiences of violence and trauma, both from an interpersonal and a
systemic perspective. Assessments are tailored-based on the information a client discloses (implicit or explicit) about their experiences, exposures, sexual activities, and other risk identifiers.
The sexual health history focuses on information relevant to sexual health, and may include:
• Client concerns
• Demographic information and methods of contacting client
• Assessment of signs and symptoms
• onset
• duration and frequency
• location
• symptom radiation to adjacent areas
• severity
• precipitating and aggravating factors
• relieving factors
• associated symptoms
• effects on daily activities
• previous diagnosis of similar episodes and/or infections (STI, HBV, HCV, HIV)
• previous treatments and outcomes
• Immunization history (e.g., hepatitis A, B and HPV)
• Recent antibiotic use (i.e., date of last dose, reason for use)
• Other medications – prescription and over-the-counter (OTC)
• Allergies (e.g., latex, antibiotics and other medications)
• Sexual contact
• barrier use (e.g., condoms, dental dams, etc.)
• sites of possible exposure
• sexual partners (number, sites of exposure, gender, and most recent sexual contact)
• Previous STI testing and results
• Previous HIV testing and results
• Drug and alcohol use/practices
• Named as an STI contact
• Surgical history (e.g., hysterectomy, vaginoplasty, metoidioplasty, genital cutting, etc.)
DST-1001 STI Assessment

215
Certified Practice Area:
Reproductive Health: Sexually Transmitted Infections
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
• Use of gender-affirming hormones
• Recent (within 28 days) history of sexual assault (refer to PHSA’s Prophylaxis Post Sexual Assault DST)
• Previous and/or current use and/or knowledge of HIV post-exposure prophylaxis (PEP) and/or pre-exposure prophylaxis
(PrEP)
• Reproductive health history
• Pap/cervical screening and results
• date of last menstrual period
• regularity of menses
• pregnancy (risk, intent or current)
• contraception and emergency contraception (including satisfaction with contraception)
• testicular health
Risk Assessment
Building on information collected in the sexual health history, risk assessments provide information regarding the likelihood of exposure to STI. This type of assessment supports clinical judgment regarding:
• screening and diagnostic tests
• sites for specimen collection
• partner notification and referral services
• client education
o Risk assessments draw from essential knowledge regarding modes of STI transmission, and in particular, the
relationships between modes of transmission, sites of exposure (e.g., rectum, oropharynx, genitals), and syndemic evidence for specific populations. While sexual orientation and/or gender may be helpful to clarify sexual behaviours
and sites of exposure, they should not be the primary means by which to inform clinical judgement. In and of
themselves, they are not risk factors for STI acquisition.
In addition to sexual health history, components of the risk assessment include:
• date of last sexual contact (to inform window periods)
• frequency of partners and nature of relationship (e.g., casual, regular, anonymous, etc.)
• gender of contacts (e.g., male, female, transgender, two-spirit, gender-diverse, unsure/questioning, prefer not to answer,
etc.)
• feasibility of contacting sexual partners should they require notification, testing and/or treatment
• how sexual contacts are met (e.g., internet, commercial sex establishments, mobile phone apps, bath houses, etc.)
• sexual and drug use practices of sexual contacts (if known)
• STI and HIV status of sexual contacts (if known)
• possible exposure to blood borne infections (e.g., needle stick) and/or accidental exposures (i.e., exposure to blood during a
fight)
• candidate for and/or client-request for HIV PrEP (see BC CfE’s HIV Pre-exposure Prophylaxis (PrEP) Guidelines)
• candidate for PEP with high risk exposure within past 72 hours (see BC CfE’s HIV Post-exposure Prophylaxis (PEP) Guidelines)
DST-1001 STI Assessment
216
Certified Practice Area:
Reproductive Health: Sexually Transmitted Infections
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
PHYSICAL ASSESSMENT
The physical assessment is a head-to-toe approach in which the clinician uses inspection and palpation to assess potential sites of infection. Physical assessment may include:
• inspection of the mouth and throat (e.g., for lesions, redness, swelling)
• inspection of the trunk, forearms and palms (e.g., for signs of rash, lesions)
• inspection of external genital, pubic, and perianal areas (e.g., for bleeding, discharge, irritation, lesions, rash, etc.)
• palpation of the inguinal nodes (for swelling/tenderness)
Additional Physical Assessments
Penile and Scrotal Anatomy (if applicable)
• inspection of urinary meatus for:
o redness and/or swelling
o discharge (e.g., mucoid, mucopurulent, purulent)
• palpation of testicles for tenderness or abnormal lumps
• if the client is symptomatic or urethral discharge is noted at the meatus, refer to applicable DST and the Screening and Diagnostic Tests section of this DST
Vulvar and Vaginal Anatomy (if applicable)
For internal pelvic exams, please refer to PHSA's Pelvic Exam DST.
• inspect vulva (e.g., redness, swelling, lesions, etc.), introitus, and vagina (e.g., redness, swelling, lesions, hypergranulation)
• assess vaginal discharge for:
o amount, consistency, colour, and odour (e.g., copious, mucoid, purulent, thick, frothy, malodorous, amine odour)
o pH if indicated
• bimanual exam:
o cervical motion tenderness (CMT)
o adnexal tenderness
o fundal tenderness
Screening and Diagnostic Tests
As part of routine screening, all clients should be offered gonorrhea, chlamydia, syphilis and HIV testing. In addition
to this routine screening, further diagnostic testing is completed based on a client’s sexual health history, risk assessment, and presentation of symptoms, such as abnormal genital/urethral symptoms (e.g., discharge, irritation), genital ulcers, lesions, and the sites of the body potentially exposed to infection.
Each method of specimen collection is briefly outlined below. As noted above, tests are indicated based on the sexual health history, risk and physical assessments, client-request, and/or at the discretion of the clinician.
11. Throat swabs
o clinician- or client-collected
12. Urine specimens
o GC/CT and/or trichomonas vaginalis (T. vaginalis or TV) (for further information on testing requirements, refer to
Trichomoniasis DST)
▪ client should not have voided in the previous 1-2 hours
▪ collect approximately 10-20 ml of first-pass urine
▪ used when cervical or vaginal specimens are not desired or appropriate
▪ preferred for clients who have undergone vaginoplasty or hysterectomy
DST-1001 STI Assessment
217
Certified Practice Area:
Reproductive Health: Sexually Transmitted Infections
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
o urine dipstick, urinalysis (micro and/or macroscopic), and/or urine culture & sensitivity (C&S) as indicated by the
Uncomplicated Lower UTI DST
o urine pregnancy test if indicated
13. Urethral specimens
o when visible discharge is present at the meatus, collect discharge (ask client to milk if necessary); insertion of the swab
into the urethra is not required
o collect smear for typical intracellular diplococci (TID) and polymorphonuclear leukoctyes (PMNs) (if immediate
microscopy available) and GC C&S, for symptomatic clients with visible meatal discharge
14. Vaginal specimens
o clinician- or client-collected
o depending on agency lab kits, validation, and facility guidelines, any of the following diagnostic tests may be used for
vaginal specimens:
▪ Nugent score/gram stain for bacterial vaginosis (BV)
▪ vaginal smear for BV and yeast
▪ gram stain or culture for yeast and/or T. vaginalis
▪ T. vaginalis NAAT
▪ T. vaginalis antigen detection (if available)
▪ T. vaginalis C&S (if applicable)
▪ wet-mount of T. vaginalis; wet-mount and/or clue cells, BV, and/or yeast if immediate microscopy available
▪ GC/CT NAAT
▪ vaginal pH
▪ vaginal KOH whiff test (if available – see Safe Use of 10% Potassium Hydroxide in STI Screening located in the
BCCDC Communicable Disease (CD) Manual Chapter 5: Sexually Transmitted Infections)
o vaginal specimens are indicated with any of the following:
▪ abnormal odour
▪ abnormal vaginal discharge
▪ vaginal irritation and/or inflammation
▪ symptoms of pelvic inflammatory disease (PID)
▪ clients determined to be at potential higher risk (based on risk assessment)
15. Cervical Specimens
o may be indicated in the following:
▪ Pap/cervical screening test
▪ symptoms (e.g., lesion)
▪ GC C&S
▪ pelvic or internal exam
16. Rectal Swabs
o clinician- or client-collected
DST-1001 STI Assessment

218
Certified Practice Area:
Reproductive Health: Sexually Transmitted Infections
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
Certified Practice Testing Options for Site-based STI Screening1
All clients testing for STIs should be offered tests for the following:
• gonorrhea
• chlamydia
• syphilis
• HIV
Site Asymptomatic Symptomatic Notes
Throat GC/CT NAAT (when indicated; see notes)
GC C&S Collect C&S first, then NAAT for contacts to GC (asymptomatic and symptomatic clients).
GC/CT NAAT Indicated for clients who have given oral sex on a penis.
Penile urethra
(with or without
phalloplasty or metoidioplasty
with urethral lengthening)
GC/CT NAAT urine GC C&S Collect visible discharge from the meatus (ask client to milk if necessary); insertion of the swab into the urethra is not required.
Smear (of meatal discharge) for TID and PMN Recommended but may not be offered in all clinical settings (only where immediate microscopy is available).
GC/CT NAAT urine
1 Unless otherwise indicated, all tests are listed in the order they should be collected
DST-1001 STI Assessment
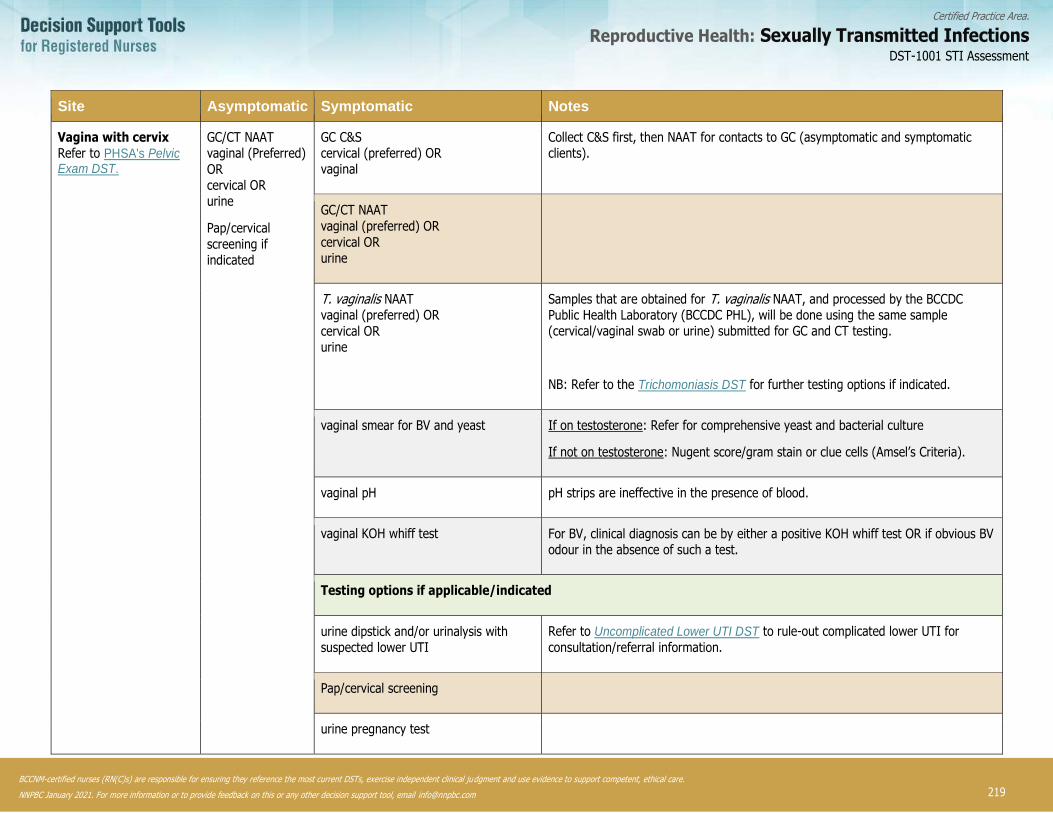
219
Certified Practice Area:
Reproductive Health: Sexually Transmitted Infections
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
Site Asymptomatic Symptomatic Notes
Vagina with cervix Refer to PHSA's Pelvic Exam DST.
GC/CT NAAT vaginal (Preferred)
OR cervical OR urine
Pap/cervical
screening if indicated
GC C&S cervical (preferred) OR vaginal
Collect C&S first, then NAAT for contacts to GC (asymptomatic and symptomatic clients).
GC/CT NAAT
vaginal (preferred) OR
cervical OR urine
T. vaginalis NAAT vaginal (preferred) OR
cervical OR urine
Samples that are obtained for T. vaginalis NAAT, and processed by the BCCDC Public Health Laboratory (BCCDC PHL), will be done using the same sample (cervical/vaginal swab or urine) submitted for GC and CT testing.
NB: Refer to the Trichomoniasis DST for further testing options if indicated.
vaginal smear for BV and yeast If on testosterone: Refer for comprehensive yeast and bacterial culture
If not on testosterone: Nugent score/gram stain or clue cells (Amsel’s Criteria).
vaginal pH pH strips are ineffective in the presence of blood.
vaginal KOH whiff test For BV, clinical diagnosis can be by either a positive KOH whiff test OR if obvious BV odour in the absence of such a test.
Testing options if applicable/indicated
urine dipstick and/or urinalysis with suspected lower UTI
Refer to Uncomplicated Lower UTI DST to rule-out complicated lower UTI for
consultation/referral information.
Pap/cervical screening
urine pregnancy test
DST-1001 STI Assessment
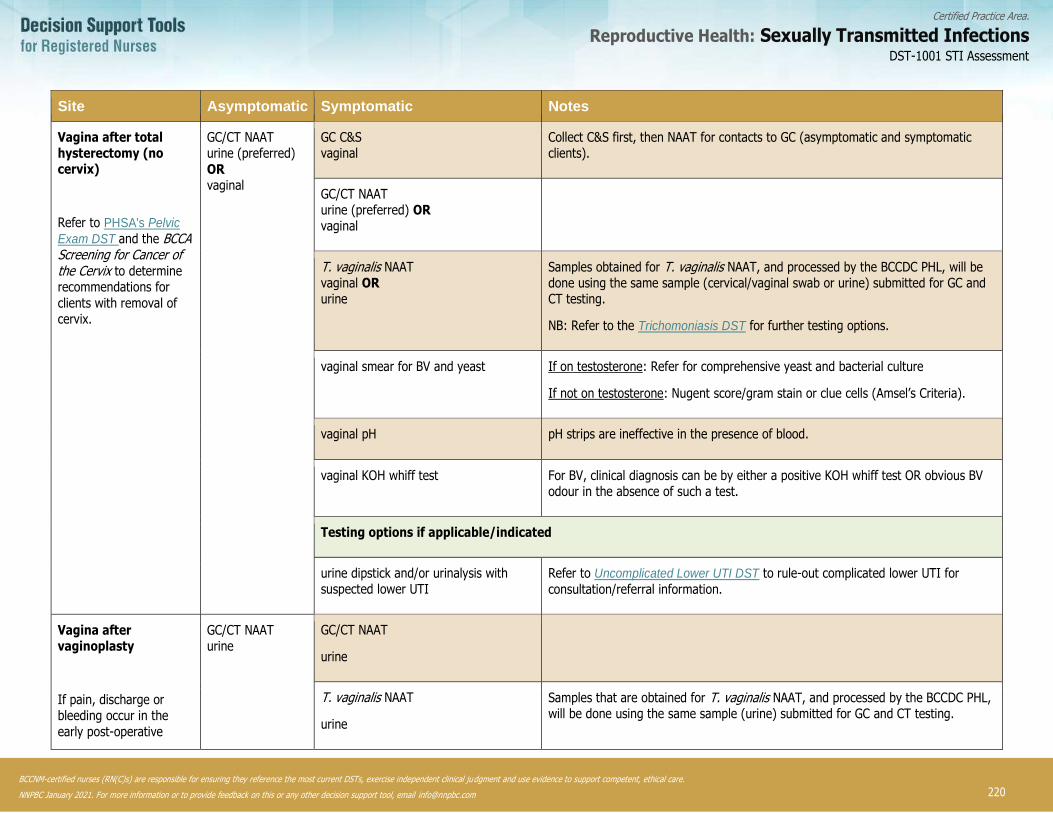
220
Certified Practice Area:
Reproductive Health: Sexually Transmitted Infections
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
Site Asymptomatic Symptomatic Notes
Vagina after total hysterectomy (no cervix)
Refer to PHSA's Pelvic
Exam DST and the BCCA Screening for Cancer of the Cervix to determine recommendations for
clients with removal of cervix.
GC/CT NAAT urine (preferred)
OR vaginal
GC C&S vaginal
Collect C&S first, then NAAT for contacts to GC (asymptomatic and symptomatic clients).
GC/CT NAAT urine (preferred) OR vaginal
T. vaginalis NAAT vaginal OR urine
Samples obtained for T. vaginalis NAAT, and processed by the BCCDC PHL, will be done using the same sample (cervical/vaginal swab or urine) submitted for GC and CT testing.
NB: Refer to the Trichomoniasis DST for further testing options.
vaginal smear for BV and yeast If on testosterone: Refer for comprehensive yeast and bacterial culture
If not on testosterone: Nugent score/gram stain or clue cells (Amsel’s Criteria).
vaginal pH pH strips are ineffective in the presence of blood.
vaginal KOH whiff test For BV, clinical diagnosis can be by either a positive KOH whiff test OR obvious BV odour in the absence of such a test.
Testing options if applicable/indicated
urine dipstick and/or urinalysis with suspected lower UTI
Refer to Uncomplicated Lower UTI DST to rule-out complicated lower UTI for
consultation/referral information.
Vagina after vaginoplasty
If pain, discharge or bleeding occur in the
early post-operative
GC/CT NAAT urine
GC/CT NAAT
urine
T. vaginalis NAAT
urine
Samples that are obtained for T. vaginalis NAAT, and processed by the BCCDC PHL, will be done using the same sample (urine) submitted for GC and CT testing.
DST-1001 STI Assessment
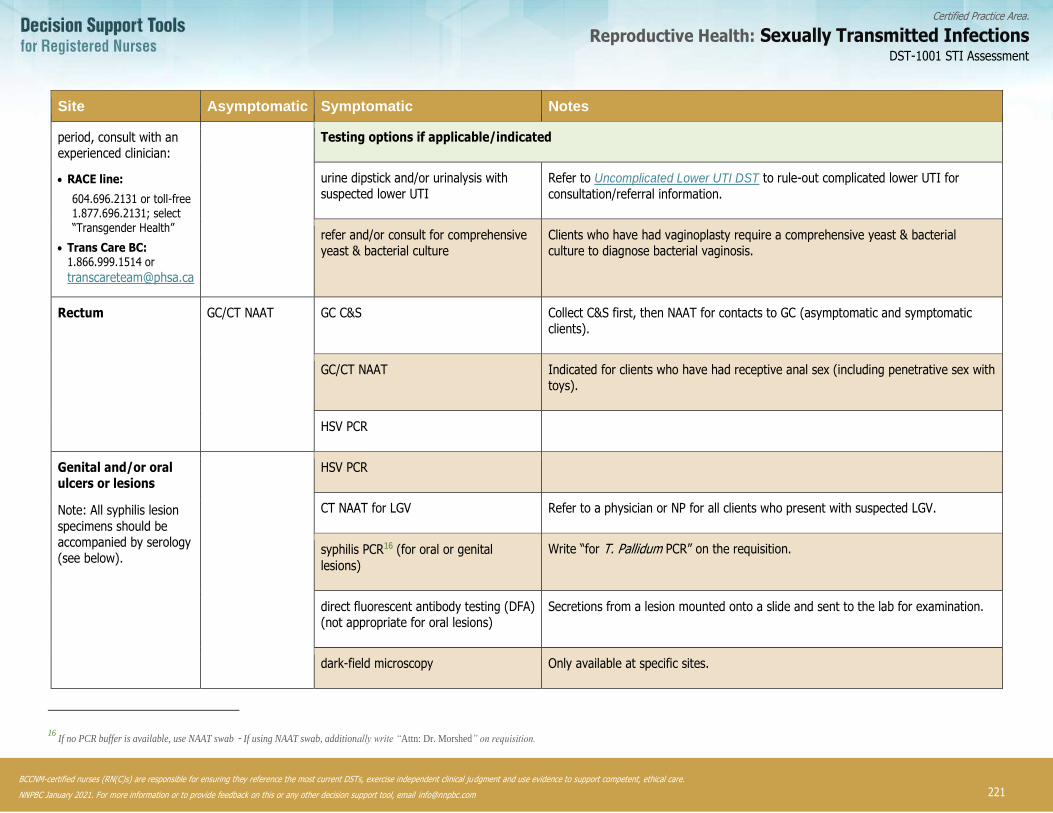
221
Certified Practice Area:
Reproductive Health: Sexually Transmitted Infections
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
Site Asymptomatic Symptomatic Notes
period, consult with an experienced clinician:
• RACE line:
604.696.2131 or toll-free 1.877.696.2131; select “Transgender Health”
• Trans Care BC: 1.866.999.1514 or
Testing options if applicable/indicated
urine dipstick and/or urinalysis with suspected lower UTI
Refer to Uncomplicated Lower UTI DST to rule-out complicated lower UTI for
consultation/referral information.
refer and/or consult for comprehensive yeast & bacterial culture
Clients who have had vaginoplasty require a comprehensive yeast & bacterial culture to diagnose bacterial vaginosis.
Rectum GC/CT NAAT GC C&S Collect C&S first, then NAAT for contacts to GC (asymptomatic and symptomatic clients).
GC/CT NAAT Indicated for clients who have had receptive anal sex (including penetrative sex with toys).
HSV PCR
Genital and/or oral ulcers or lesions
Note: All syphilis lesion
specimens should be accompanied by serology (see below).
HSV PCR
CT NAAT for LGV Refer to a physician or NP for all clients who present with suspected LGV.
syphilis PCR16 (for oral or genital
lesions)
Write “for T. Pallidum PCR” on the requisition.
direct fluorescent antibody testing (DFA) (not appropriate for oral lesions)
Secretions from a lesion mounted onto a slide and sent to the lab for examination.
dark-field microscopy Only available at specific sites.
16
If no PCR buffer is available, use NAAT swab - If using NAAT swab, additionally write “Attn: Dr. Morshed” on requisition.
DST-1001 STI Assessment
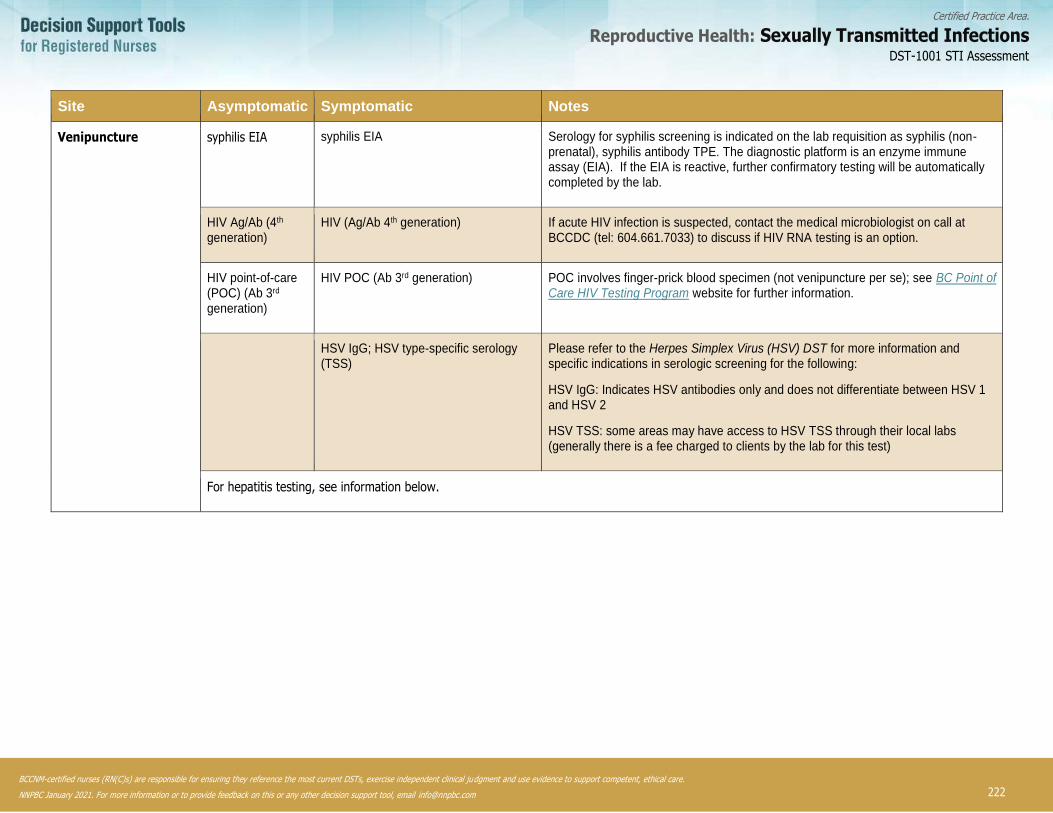
222
Certified Practice Area:
Reproductive Health: Sexually Transmitted Infections
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
Site Asymptomatic Symptomatic Notes
Venipuncture syphilis EIA
syphilis EIA Serology for syphilis screening is indicated on the lab requisition as syphilis (non-prenatal), syphilis antibody TPE. The diagnostic platform is an enzyme immune assay (EIA). If the EIA is reactive, further confirmatory testing will be automatically completed by the lab.
HIV Ag/Ab (4th generation)
HIV (Ag/Ab 4th generation) If acute HIV infection is suspected, contact the medical microbiologist on call at BCCDC (tel: 604.661.7033) to discuss if HIV RNA testing is an option.
HIV point-of-care (POC) (Ab 3rd generation)
HIV POC (Ab 3rd generation) POC involves finger-prick blood specimen (not venipuncture per se); see BC Point of Care HIV Testing Program website for further information.
HSV IgG; HSV type-specific serology (TSS)
Please refer to the Herpes Simplex Virus (HSV) DST for more information and specific indications in serologic screening for the following:
HSV IgG: Indicates HSV antibodies only and does not differentiate between HSV 1 and HSV 2
HSV TSS: some areas may have access to HSV TSS through their local labs (generally there is a fee charged to clients by the lab for this test)
For hepatitis testing, see information below.
DST-1001 STI Assessment

223
Certified Practice Area:
Reproductive Health: Sexually Transmitted Infections
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
Hepatitis A, B, C Serology
The decision to test for acute or chronic infection or immunity should take into consideration past or current risk factors, risk for future exposure, and/or prior testing and vaccination history.
• Hepatitis A Virus (HAV)
HAV infection is primarily transmitted by the fecal-oral route. The most common transmission pathway is through the
consumption of food or water contaminated with infected feces. Transmission can also occur through close physical contact
resulting in the oral ingestion of contaminated feces (e.g., rimming).
HAV serologic testing is only recommended in the following scenarios where there has been no prior hepatitis A vaccine
series:
o Presenting with signs and symptoms suggestive of acute hepatitis
o Chronic hepatitis B or hepatitis C infection
o Chronic liver disease (e.g., cirrhosis)
o Individuals with haemophilia A or B receiving plasma-derived replacement clotting factors and testing negative for anti-
HAV IgG
Include the following serologic tests:
o Signs and symptoms: anti-HAV Total and anti-HAV IgM
o Screening: anti-HAV Total
For further information, see BCCDC CDC Manual: Chapter 1 - Hepatitis A and BCCDC CDC Manual: Chapter 2 - Immunization.
• Hepatitis B Virus (HBV)
HBV is a blood-borne virus that is highly transmissible via perinatal, percutaneous or sexual exposure to a HBV infected
person’s blood and/or body fluids. HBV infection is most commonly acquired through sexual contact, injection drug use, and
perinatal exposure from mother-to-infant.
Indications for HBV serologic testing in the absence of a prior full hepatitis B vaccine series includes:
o HIV or HCV infection
o individuals who engage in illicit drug use
o sexual partner or household contact of someone with acute or chronic HBV infection
o recent sexual assault (refer to PHSA’s Prophylaxis Post Sexual Assault DST)
o unprotected sex and/or multiple sex partners
Include the following serologic tests:
o HBsAg
o Anti-HBs
o Anti-HBc Total
For further information or HBV screening, risk factors and/or laboratory and testing information, refer to the BCCDC CDC Manual: Chapter 1 - Hepatitis B and BCCDC CDC Manual: Chapter 2 - Immunization.
• Hepatitis C Virus (HCV)
HCV is a blood-borne virus that is highly transmissible via percutaneous exposures to infectious blood. Permucosal
transmission may occur if blood is present but is not as efficient.
Indications for testing in a sexual health/harm reduction context may include:
o sharing of injection and/or non-injection drug equipment (e.g., crack pipes, cocaine straws)
DST-1001 STI Assessment

224
Certified Practice Area:
Reproductive Health: Sexually Transmitted Infections
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
o diagnosis of HBV (chronic or acute), HIV, or STIs where sores and lesions are present such as Lymphogranuloma venereum (LGV) and syphilis
o repeated condomless sexual contact with person(s) where there is a possibility of blood exchange (e.g., rough sex
causing mucosal tearing)
o tattooing, body piercing, and/or acupuncture in unregulated premises where unsterile equipment and/or improper
technique is used
o recent sexual assault (refer to PHSA’s Prophylaxis Post Sexual Assault DST)
For individuals with ongoing hepatitis C related risk factors, annual screening is recommended.
Include the following serologic tests:
o Anti-HCV
o HCV RNA – only if previous anti-HCV positive
For further information on HCV, screening, risk factors pand/or laboratory and testing information, refer to the BCCDC CDCManual: Chapter 1 - Hepatitis C
DST-1001 STI Assessment

225
Certified Practice Area:
Reproductive Health: Sexually Transmitted Infections
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
REFERENCES
More recent editions of any of the items in the reference list may have been published since this DST was published. If you have a newer version, please use it.
Bachmann, L.H., Johnson, R. E., Chen, H., Markowitz, L., Papp, J. R., Palella, J., Hook, E. W. (2010). Nucleic acid amplification tests for diagnosis of Neissieria gonorrhoeae and Chlamydia trachomatis rectal infections. Journal of Clinical Microbiology. 48(5):1827.
Bauer, G. R., Hammond, R., Travers, R., Kaay, M., Hohenadel, K. M., & Boyce, M. (2009). “I don’t think this is theoretical; this is
our lives”: How erasure impacts health care for transgender people. Journal of the Association of Nurses in AIDS Care, 20(5), pp.348-361.
Bauman, D. (2012). Diagnostic methods in pediatric and adolescent gynecology. Endocrine Development, 22, p. 2240-2255. doi: 10.1159/000326633.
Bell, C., Hough, E., Smith, A., Greene, L. (2007). Targeted screening for Trichomonas vaginalis in women, a pH-based approach. International Journal of STD & AIDS. (18) pp.402-403.
British Columbia Centre for Disease Control (BCCDC). (2014). British Columbia treatment guidelines. Sexually transmitted infections in adolescent and adults. STI/HIV Prevention and Control Division, B.C. Centre for Disease Control.
BCCDC. (2018). Management of specific infections. Hepatitis A. Communicable Disease Control Manual. Not yet released.
BCCDC. (2017). Management of specific infections. Hepatitis B. Communicable Disease Control Manual.
BCCDC. (2016). Management of specific infections. Hepatitis C. Communicable Disease Control Manual.
British Columbia Centre for Excellence in HIV/AIDS (BC-CfE). (2017a). HIV post-exposure prophylaxis (PEP) Guidelines.
BC-CfE. (2017b). Guidance for the use of pre-exposure prophylaxis (PrEP) for the prevention of HIV acquisition in British Columbia.
British Columbia Public Health Microbiology & Reference Laboratory (BPHMRL). (2014). Automated Syphilis Screening Implementation.
British Columbia College of Nursing Professionals (BCCNP). (2014). Competencies for CRNBC Certified Practice: Reproductive Health – Sexually Transmitted Infections.
BCCNP. (2018). Scope of Practice Standards for Registered Nurses.
Brook, G. et al. (2013). 2013 UK national guideline for consultations requiring sexual history taking. International Journal of STD & AIDS, 0(0), p. 1-14.
Cheikhelard. A., Chaktoura, Z., Thibaud, E. (2012). Gynecologic clinical examination of the child and adolescent. Endocrine Development, 221-10.
Grennan, T. (2017). Update on syphilis testing via polymerase chain reaction (PCR). Email distribution of practitioner alert, BC Centre for Disease Control.
Hathorn, E., Ng, Andrea., Page, M., Hodson, J., Gaydos, C., Ross, J.D. (2015). A service evaluation of the Gen-Probe Aptima
nuclei acid amplification test for Trichomonas vaginalis: should it change whom we screen for infection? Sexually Transmitted Infections 91(2); pp.81-86.
DST-1001 STI Assessment
226
Certified Practice Area:
Reproductive Health: Sexually Transmitted Infections
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
Helms, D. J., Mosure, D. J., Metcalf, C. A., Douglas, J. M., Malotte, C. K., Paul, S. M., Peterman, T. A. (2007). Risk factors for prevalent and incident Trichomonas vaginalis among women attending three sexually transmitted disease clinics. Sexually Transmitted Diseases. (35) 5 pp.484-488.
Jain, A. & Bradbeer, C. (2007). Recurrent bacterial vaginosis of neovagina after gender reassignment surgery. International Journal of STD & AIDS, 18, pp.140-141.
Lindroth, M. (2016). ‘Competent persons who can treat you with competence, as simples as that’ – An interview study with transgender people on their experiences of meeting health care professionals. Journal of Clinical Nursing, 25, pp.3511-3521.
Petricevic, L., Kaufmann, U., Domig,K., Kraler, M., Marschalek, J., Kneifel W. & Kiss, H. (2014). Molecular detection of lactobacillus species in the neovagina of male-to-female transsexual women. Scientific reports, 4(3746), pp.1-4.
Provincial Health Services Authority’s Trans Care BC. (2017). Caring for trans and gender diverse clients in BC: A primary care toolkit.
Public Health Agency of Canada (PHAC). 2016 updates summary in: Canadian guidelines on sexually transmitted infections.
PHAC. (2016). Canadian guidelines on sexually transmitted infections (Revised December, 2016).
PHAC. (2014). Canadian guidelines on sexually transmitted infections (Revised October, 2014). Section 6 - Specific Populations.
Rich, A., et al. (2017). Sexual HIV risk among gay, bisexual and queer transgender men: Findings from interviews in Vancouver, Canada. Culture, Health and Sexuality, 19(11), pp.1197-1209.
Schacter, J., Moncada, J., Liska, S., Shayevich, C., Klausner, J. D. (2008). Nucleic acid amplification tests in the diagnosis of
chlamydial and gonococcal infections of the oropharynx and rectum in men who have sex with men. Sexually Transmitted Diseases, 35(7), pp.637-642.
Schacter, J., McCormack, W.W., Chernesky, M.A., Martin, D. H., Van Der Pol, B., Rice, P., Chow, J.M. (2003). Vaginal Swabs are
appropriate specimens for diagnosis of genital tract infection with Chlamydia trachomatis. Journal of Clinical Microbiology, 41(8), pp.3784-3789.
Sherrard, J., Ison, C., Moody, J., Wainwright, E., Wilson, J., Sullivan, A. (2014). United Kingdom national guideline on the management of Trichomonas vaginalis. International Journal of STI & AIDS, 25(8), pp.541-549.
Shafer, M., Moncada, J., Boyer, C. B., Betsinger, K., Flinn, S. D., Schachter, J., (2003). Comparing first-void urine specimens, self-collected vaginal swabs, and endocervical specimens to detect Chlamydia trachomatis and Neisseria gonorrheoeae by a nucleic acid amplification test. Journal of Clinical Microbiology, 41 (9). pp.4395-4399.
Singer, M. & Clair, S. (2003). Syndemics and public health: reconceptualizing disease in bio-social context. Medical Anthropology Quarterly, 17(4), pp.423-441.
Stewart, C.M., Shoeman, S.A., Booth, A.R., Smith, S. D., Wilcox M. H., Wilson, J. D. (2012). Assessment of self-taken swabs versus clinician taken swab cultures for diagnosing gonorrheoea in women: single centre, diagnostic accuracy study. BMJ 2012; 34; e8107.
University of California San Francisco (UCSF) (2016). Center of Excellence for Transgender Health, Guidelines for the primary and gender-affirming care of transgender and gender non-binary people.
van Liere G., Hoebe C., Wolffs P., & Dukers-Muijrers, N. (2014). High co-occurrence of anorectal chlamydia with urogenital
chlamydia in women visiting an STI clinic revealed by routine universal testing in an observational study: A recommendation towards a better anorectal chlamydia control in women. BMC Infectious Diseases, 14(274), pp.1-7.
DST-1001 STI Assessment

227
Certified Practice Area:
Reproductive Health: Sexually Transmitted Infections
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
Verteramo, R., Calzolari, E., Degener, A. M., Masciangelo, R., Patella, A. (2008). Trichomonas vaginalis infection: Risk indicators among women attending for routine gynecologic examination. Japan Society of Obstetrics and Gynecology. (34) 2, pp.233-237.
Weyers, S, Verstraelen, H., Gerris, J., Monstrey, S., Lopes Santiago, G.S., Saerens, B., Verhelst, R. (2009). Microflora of the penile skin-lined neovagina of transsexual women. BMC Microbiology, 9(102), pp.1-10.
World Professional Association for Transgender Health. (2011). Standards of care for the health of transsexual, transgender, and gender-nonconforming people, Version 7.
DST-1001 STI Assessment
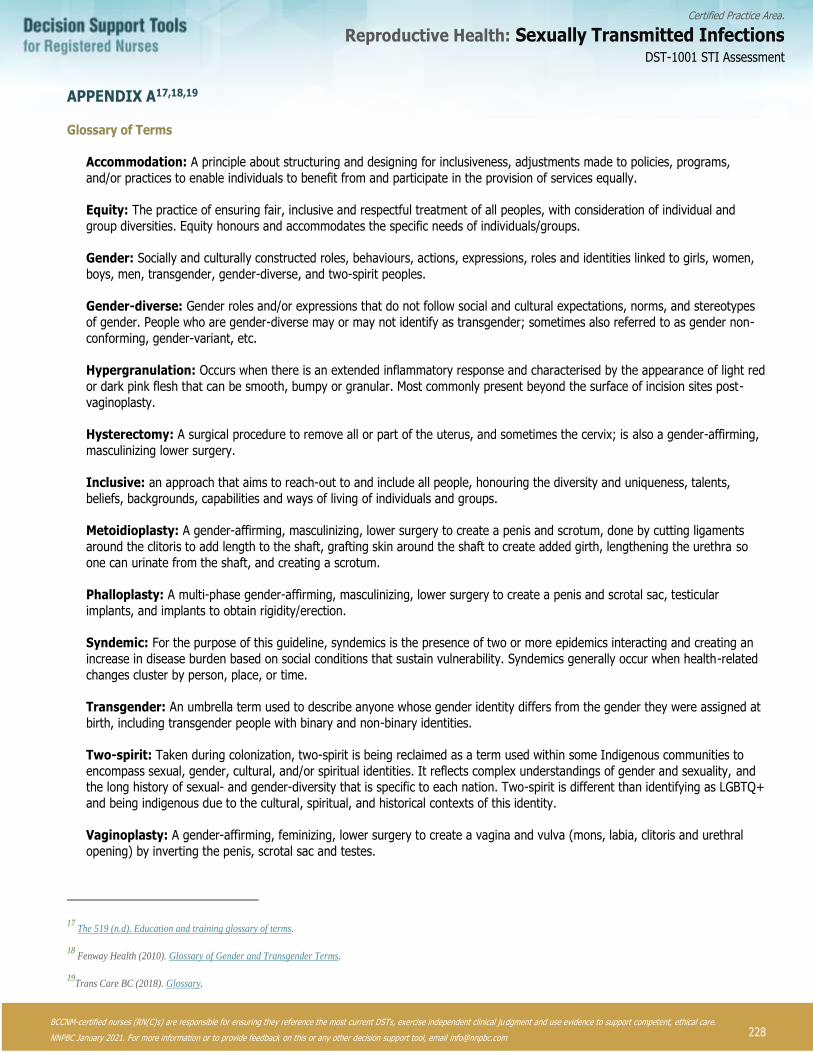
228
Certified Practice Area:
Reproductive Health: Sexually Transmitted Infections
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
APPENDIX A17,18,19
Glossary of Terms
Accommodation: A principle about structuring and designing for inclusiveness, adjustments made to policies, programs,
and/or practices to enable individuals to benefit from and participate in the provision of services equally.
Equity: The practice of ensuring fair, inclusive and respectful treatment of all peoples, with consideration of individual and
group diversities. Equity honours and accommodates the specific needs of individuals/groups.
Gender: Socially and culturally constructed roles, behaviours, actions, expressions, roles and identities linked to girls, women,
boys, men, transgender, gender-diverse, and two-spirit peoples.
Gender-diverse: Gender roles and/or expressions that do not follow social and cultural expectations, norms, and stereotypes
of gender. People who are gender-diverse may or may not identify as transgender; sometimes also referred to as gender non-
conforming, gender-variant, etc.
Hypergranulation: Occurs when there is an extended inflammatory response and characterised by the appearance of light red
or dark pink flesh that can be smooth, bumpy or granular. Most commonly present beyond the surface of incision sites post-
vaginoplasty.
Hysterectomy: A surgical procedure to remove all or part of the uterus, and sometimes the cervix; is also a gender-affirming,
masculinizing lower surgery.
Inclusive: an approach that aims to reach-out to and include all people, honouring the diversity and uniqueness, talents,
beliefs, backgrounds, capabilities and ways of living of individuals and groups.
Metoidioplasty: A gender-affirming, masculinizing, lower surgery to create a penis and scrotum, done by cutting ligaments
around the clitoris to add length to the shaft, grafting skin around the shaft to create added girth, lengthening the urethra so
one can urinate from the shaft, and creating a scrotum.
Phalloplasty: A multi-phase gender-affirming, masculinizing, lower surgery to create a penis and scrotal sac, testicular
implants, and implants to obtain rigidity/erection.
Syndemic: For the purpose of this guideline, syndemics is the presence of two or more epidemics interacting and creating an
increase in disease burden based on social conditions that sustain vulnerability. Syndemics generally occur when health-related
changes cluster by person, place, or time.
Transgender: An umbrella term used to describe anyone whose gender identity differs from the gender they were assigned at
birth, including transgender people with binary and non-binary identities.
Two-spirit: Taken during colonization, two-spirit is being reclaimed as a term used within some Indigenous communities to
encompass sexual, gender, cultural, and/or spiritual identities. It reflects complex understandings of gender and sexuality, and the long history of sexual- and gender-diversity that is specific to each nation. Two-spirit is different than identifying as LGBTQ+
and being indigenous due to the cultural, spiritual, and historical contexts of this identity.
Vaginoplasty: A gender-affirming, feminizing, lower surgery to create a vagina and vulva (mons, labia, clitoris and urethral
opening) by inverting the penis, scrotal sac and testes.
17
The 519 (n.d). Education and training glossary of terms.
18 Fenway Health (2010). Glossary of Gender and Transgender Terms.
19Trans Care BC (2018). Glossary.
DST-1001 STI Assessment

229
Certified Practice Area:
Reproductive Health: Sexually Transmitted Infections
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
DST-1002 Treatment of STI Contacts
This decision support tool (DST) provides RN(C)s20 with clinical guidance for treatment of clients who are contacts to an STI and
require treatment with schedule 1 medications. STIs described in both the certified practice and non-certified practice DSTs are included in this DST.
Refer to the corresponding infection-specific certified and/or non-certified practice STI DST to ensure the client has received the
recommended sexual health history/risk assessments, education and, if appropriate, screening. For symptomatic clients who are
contacts to an STI, refer to the appropriate STI DST to determine if consultation with or referral to a physician or nurse practitioner (NP) is required based on DST recommendations, assessment and diagnostic findings.
Consultation with or referral to a physician or NP is required for all pregnant clients and may be required for breast-/chest-feeding clients depending upon the recommended treatment. Refer to the specific STI DST for further information.
BCCNP STI DSTs are not indicated for clients who are less than 12 years old and RN(C)s must follow the PHSA Pelvic Exam DST (indicated for clients aged 14 years and up) when providing STI care (see the STI Assessment DST for further screening and
treatment recommendations). Clients 12-13 years of age who are symptomatic require consultation with or referral to a physician or NP.
DEFINITION
The process of offering testing and treatment to the sexual contacts of a person diagnosed with an STI or STI syndrome.
POTENTIAL CAUSES
Bacterial:
• Neisseria gonorrhoeae (GC)
• Chlamydia trachomatis (CT)
• Bacterial Vaginosis (BV)
• Treponema pallidum (syphilis)
Protozoan:
• Trichomonas vaginalis (TV)
Syndromes:
• urethritis
• mucopurulent cervicitis (MPC)
• pelvic inflammatory disease (PID)
• epididymitis
• proctitis
PREDISPOSING RISK FACTORS
• sexual contact with someone with an STI
• vaginal, anal or oral sexual contact
20 Note: RN(C) is an authorized title recommended by BCCNP that refers to BCCNP-certified RNs, and is used throughout this
Decision Support Tool (DST).
DST-1002 Treatment of STI Contacts
230
Certified Practice Area:
Reproductive Health: Sexually Transmitted Infections
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
STI CONTACT ASSESSMENT
Offer full comprehensive STI assessment and screening. If declined, provide treatment appropriate to the type of contact and/or symptoms. See the STI Assessment DST for further information.
Sexual Health History
• complete a sexual health history and risk assessment – typical findings include:
o sexual contact with at least one partner
o identified as a sexual contact to someone with confirmed positive laboratory test for STI
o identified as a sexual contact to STI syndrome (e.g., urethritis NYD)
Physical Assessment
• offer focused physical assessment
• if symptoms present, refer to the corresponding STI DST, and consult with or refer to physician or NP as needed
SCREENING DIAGNOSTIC TESTS
• provide screening and diagnostic testing for STI contact based on the type of exposure and presenting symptoms
MANAGEMENT AND INTERVENTIONS
Goals of Treatment
• treat potential infection
• prevent potential complications due to untreated or undiagnosed infection
• prevent the spread of infection
DST-1002 Treatment of STI Contacts

231
Certified Practice Area:
Reproductive Health: Sexually Transmitted Infections DST-1002 Treatment of STI Contacts
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
TREATMENT OF CHOICE FOR STI CONTACTS
The treatment required for an STI contact may differ from treatment provided for the index case. When recommended treatment for the contact is the same as the index, refer to the specific STI DST for information regarding treatment options including pharmaceutical and therapeutic suitability.
STI or Syndrome Contact Management and Trace Back Period Treatment of Contact Notes
Bacterial Vaginosis (BV)
• offer assessment to all applicable contacts
• treatment of male contacts is not indicated and
does not prevent recurrence
See Bacterial Vaginosis DST.
1. There may be an increased incidence of concordant BV infection in
sexual partnering and/or sexual behaviours where BV could flourish.
2. Where relevant, sexual partners of people diagnosed with BV may benefit from assessment and testing for BV. If clinical assessment
and/or lab testing results are positive for BV, then treat as per the
BV DST.
3. Refer to the BV DST for client education, screening
recommendations, alternate treatments and further medication
information.
Chlamydia (CT) 60 days
• test and treat all contacts in the last 60 days
• if there are no sexual contacts in the last 60 days,
then recommend testing and treatment for the last sexual contact
See Chlamydia DST.
1. Advise to abstain from sexual activity during the 7-day course of
treatment or for 7 days post-single-dose therapy.
2. Refer to the CT DST for client education, screening recommendations, alternate treatments and further medication
information.
Lympho-granuloma venereum (LGV)
60 days
• test and treat all contacts in the last 60 days
• if there are no sexual contacts in the last 60 days,
then recommend testing and treatment for the
last sexual contact
First Choice:
doxycycline 100 mg PO BID for 21 days
Alternate Choice:
Consult with or refer to physician or NP.
1. Empiric LGV treatment is recommended for all partners of confirmed
or probable cases. Completion of treatment is recommended
regardless of results.
2. Contacts should abstain from sexual activity for 7 days after initiation
of treatment.
3. Testing of all exposed sites (e.g., throat, suspicious lesions, urine, vagina, cervix, rectum) is recommended. Indicate “contact to LGV”
on requisition.
4. Consult with or refer to physician or NP if client is symptomatic, and
all confirmed cases.
5. For confirmed LGV cases, please contact the Provincial STI Clinic’s
syphilis/LGV nursing desk (604.707.5607) for further management.
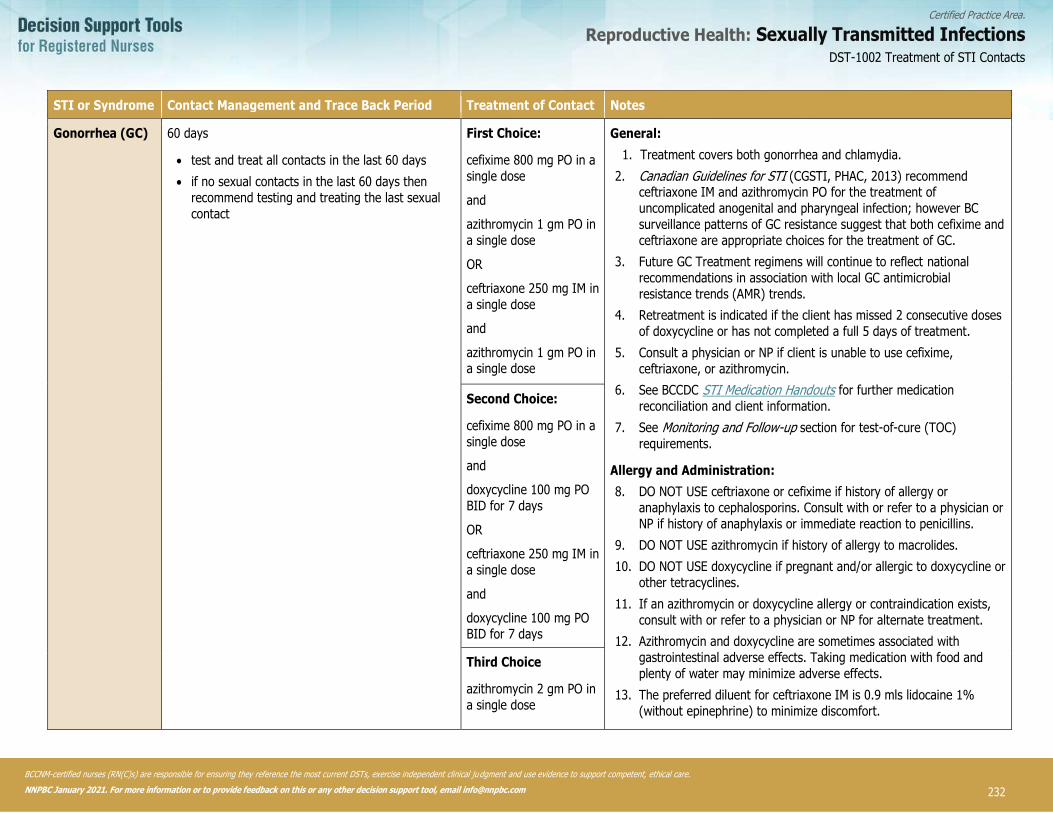
232
Certified Practice Area:
Reproductive Health: Sexually Transmitted Infections DST-1002 Treatment of STI Contacts
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
STI or Syndrome Contact Management and Trace Back Period Treatment of Contact Notes
Gonorrhea (GC) 60 days
• test and treat all contacts in the last 60 days
• if no sexual contacts in the last 60 days then
recommend testing and treating the last sexual
contact
First Choice:
cefixime 800 mg PO in a
single dose
and
azithromycin 1 gm PO in
a single dose
OR
ceftriaxone 250 mg IM in
a single dose
and
azithromycin 1 gm PO in a single dose
General:
1. Treatment covers both gonorrhea and chlamydia.
2. Canadian Guidelines for STI (CGSTI, PHAC, 2013) recommend ceftriaxone IM and azithromycin PO for the treatment of
uncomplicated anogenital and pharyngeal infection; however BC
surveillance patterns of GC resistance suggest that both cefixime and
ceftriaxone are appropriate choices for the treatment of GC.
3. Future GC Treatment regimens will continue to reflect national
recommendations in association with local GC antimicrobial
resistance trends (AMR) trends.
4. Retreatment is indicated if the client has missed 2 consecutive doses
of doxycycline or has not completed a full 5 days of treatment.
5. Consult a physician or NP if client is unable to use cefixime,
ceftriaxone, or azithromycin.
6. See BCCDC STI Medication Handouts for further medication
reconciliation and client information.
7. See Monitoring and Follow-up section for test-of-cure (TOC)
requirements.
Allergy and Administration:
8. DO NOT USE ceftriaxone or cefixime if history of allergy or
anaphylaxis to cephalosporins. Consult with or refer to a physician or
NP if history of anaphylaxis or immediate reaction to penicillins.
9. DO NOT USE azithromycin if history of allergy to macrolides.
10. DO NOT USE doxycycline if pregnant and/or allergic to doxycycline or
other tetracyclines.
11. If an azithromycin or doxycycline allergy or contraindication exists,
consult with or refer to a physician or NP for alternate treatment.
12. Azithromycin and doxycycline are sometimes associated with
gastrointestinal adverse effects. Taking medication with food and
plenty of water may minimize adverse effects.
13. The preferred diluent for ceftriaxone IM is 0.9 mls lidocaine 1%
(without epinephrine) to minimize discomfort.
Second Choice:
cefixime 800 mg PO in a
single dose
and
doxycycline 100 mg PO
BID for 7 days
OR
ceftriaxone 250 mg IM in
a single dose
and
doxycycline 100 mg PO BID for 7 days
Third Choice
azithromycin 2 gm PO in
a single dose
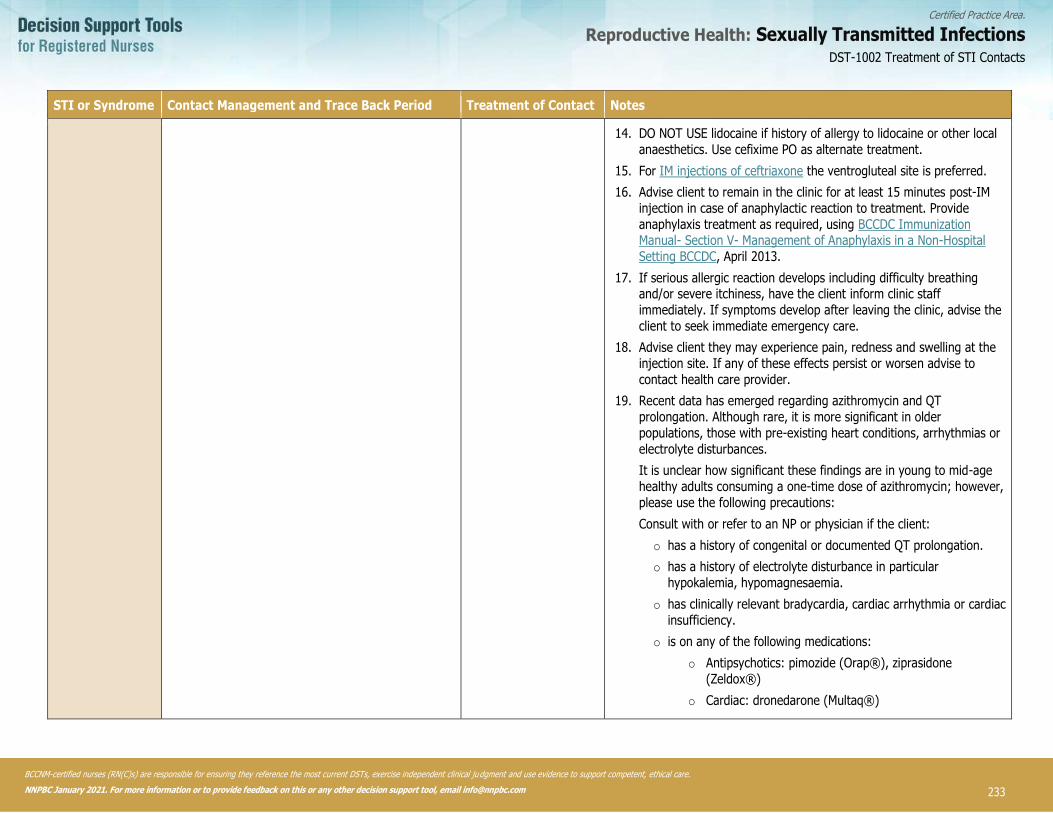
233
Certified Practice Area:
Reproductive Health: Sexually Transmitted Infections DST-1002 Treatment of STI Contacts
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
STI or Syndrome Contact Management and Trace Back Period Treatment of Contact Notes
14. DO NOT USE lidocaine if history of allergy to lidocaine or other local
anaesthetics. Use cefixime PO as alternate treatment.
15. For IM injections of ceftriaxone the ventrogluteal site is preferred.
16. Advise client to remain in the clinic for at least 15 minutes post-IM
injection in case of anaphylactic reaction to treatment. Provide
anaphylaxis treatment as required, using BCCDC Immunization Manual- Section V- Management of Anaphylaxis in a Non-Hospital
Setting BCCDC, April 2013.
17. If serious allergic reaction develops including difficulty breathing and/or severe itchiness, have the client inform clinic staff
immediately. If symptoms develop after leaving the clinic, advise the
client to seek immediate emergency care.
18. Advise client they may experience pain, redness and swelling at the
injection site. If any of these effects persist or worsen advise to
contact health care provider.
19. Recent data has emerged regarding azithromycin and QT
prolongation. Although rare, it is more significant in older
populations, those with pre-existing heart conditions, arrhythmias or
electrolyte disturbances.
It is unclear how significant these findings are in young to mid-age
healthy adults consuming a one-time dose of azithromycin; however,
please use the following precautions:
Consult with or refer to an NP or physician if the client:
o has a history of congenital or documented QT prolongation.
o has a history of electrolyte disturbance in particular
hypokalemia, hypomagnesaemia.
o has clinically relevant bradycardia, cardiac arrhythmia or cardiac
insufficiency.
o is on any of the following medications:
o Antipsychotics: pimozide (Orap®), ziprasidone
(Zeldox®)
o Cardiac: dronedarone (Multaq®)
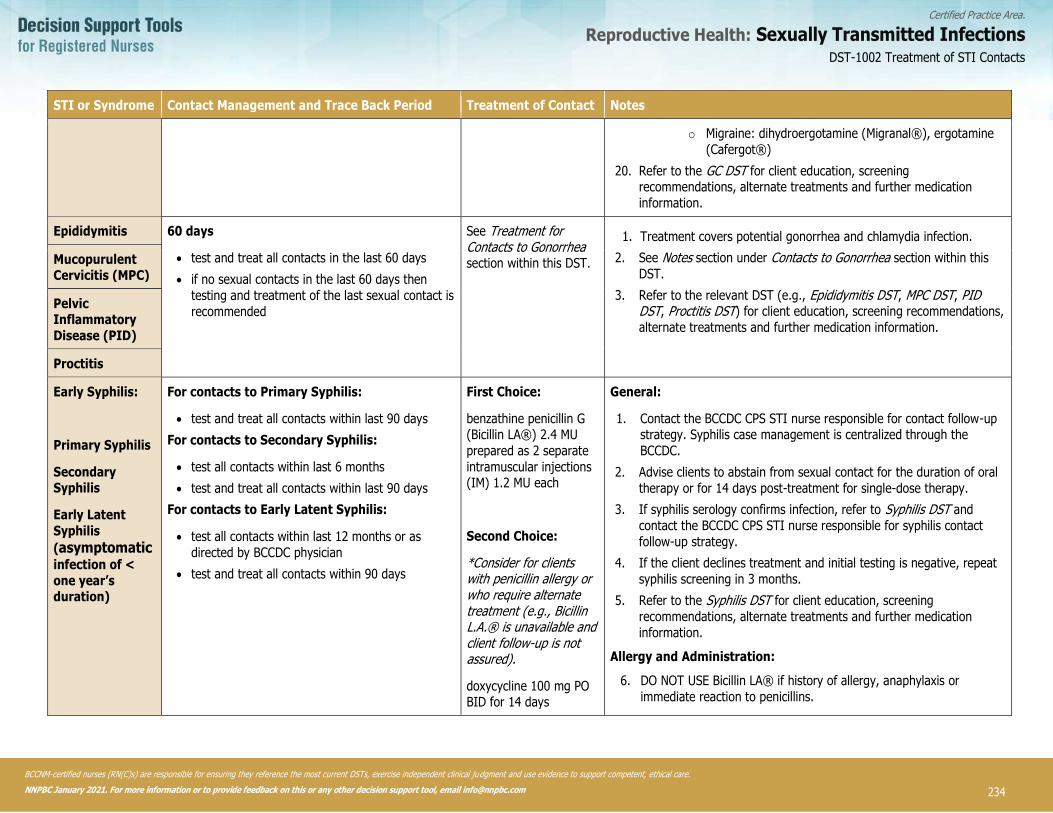
234
Certified Practice Area:
Reproductive Health: Sexually Transmitted Infections DST-1002 Treatment of STI Contacts
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
STI or Syndrome Contact Management and Trace Back Period Treatment of Contact Notes
o Migraine: dihydroergotamine (Migranal®), ergotamine
(Cafergot®)
20. Refer to the GC DST for client education, screening recommendations, alternate treatments and further medication
information.
Epididymitis 60 days
• test and treat all contacts in the last 60 days
• if no sexual contacts in the last 60 days then
testing and treatment of the last sexual contact is
recommended
See Treatment for Contacts to Gonorrhea section within this DST.
1. Treatment covers potential gonorrhea and chlamydia infection.
2. See Notes section under Contacts to Gonorrhea section within this
DST.
3. Refer to the relevant DST (e.g., Epididymitis DST, MPC DST, PID DST, Proctitis DST) for client education, screening recommendations,
alternate treatments and further medication information.
Mucopurulent Cervicitis (MPC)
Pelvic Inflammatory
Disease (PID)
Proctitis
Early Syphilis:
Primary Syphilis
Secondary Syphilis
Early Latent
Syphilis
(asymptomatic
infection of <
one year’s duration)
For contacts to Primary Syphilis:
• test and treat all contacts within last 90 days
For contacts to Secondary Syphilis:
• test all contacts within last 6 months
• test and treat all contacts within last 90 days
For contacts to Early Latent Syphilis:
• test all contacts within last 12 months or as
directed by BCCDC physician
• test and treat all contacts within 90 days
First Choice:
benzathine penicillin G (Bicillin LA®) 2.4 MU
prepared as 2 separate
intramuscular injections (IM) 1.2 MU each
Second Choice:
*Consider for clients with penicillin allergy or who require alternate treatment (e.g., Bicillin L.A.® is unavailable and client follow-up is not assured).
doxycycline 100 mg PO BID for 14 days
General:
1. Contact the BCCDC CPS STI nurse responsible for contact follow-up strategy. Syphilis case management is centralized through the
BCCDC.
2. Advise clients to abstain from sexual contact for the duration of oral
therapy or for 14 days post-treatment for single-dose therapy.
3. If syphilis serology confirms infection, refer to Syphilis DST and
contact the BCCDC CPS STI nurse responsible for syphilis contact
follow-up strategy.
4. If the client declines treatment and initial testing is negative, repeat
syphilis screening in 3 months.
5. Refer to the Syphilis DST for client education, screening
recommendations, alternate treatments and further medication
information.
Allergy and Administration:
6. DO NOT USE Bicillin LA® if history of allergy, anaphylaxis or
immediate reaction to penicillins.

235
Certified Practice Area:
Reproductive Health: Sexually Transmitted Infections DST-1002 Treatment of STI Contacts
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
STI or Syndrome Contact Management and Trace Back Period Treatment of Contact Notes
Late Latent Syphilis
(asymptomatic infection > one year’s duration)
Test (do not treat) contacts to latent syphilis:
all long term sexual contacts; and
children whose mother has a late latent syphilis diagnosis
Treat only if serology is reactive.
7. Administer Bicillin LA® into the ventral (preferred) or dorsal gluteal
sites on the same visit, at 2 separate sites. (See here)
8. Provide client education about the potential for a Jarisch-Herxheimer reaction which may occur soon after treatment and is expected to
resolve within 24 hours. This is not a sign of a drug allergy.
9. If syphilis serology is confirms infection, refer to Syphilis DST and
contact the BCCDC CPS STI nurse responsible for syphilis contact follow-up strategy. Syphilis case management is centralized in BC
through the BCCDC.
10. Refer to the Syphilis DST for client education, screening recommendations, alternate treatments and further medication
information.
Trichomoniasis 60 days
• treat all contacts in the last 60 days
• testing is also offered to certain contacts within
the past 60 days as per Trichomoniasis DST
• if no sexual contacts in the last 60 days then
recommend treatment of the last sexual contact
See Trichomoniasis DST. 1. Advise to abstain from sexual contact until completion of multi-dose
treatment or for 7 days after single-dose therapy.
2. Refer to the Trichomoniasis DST for client education, screening
recommendations, alternate treatments and further medication
information.
Urethritis –
presumptive Gonorrhea
60 days
• test and treat all contacts case in the last 60 days
• if no sexual contacts, then testing and treatment
of the last sexual contact is recommended
See Treatment for Contacts to Gonorrhea section within this DST.
1. Treatment covers potential gonorrhea and chlamydia infection.
2. See Notes section under Contacts to Gonorrhea section within this
DST.
3. Refer to the GC DST for client education, screening recommendations, alternate treatments and further medication
information.
Non-gonococcal Urethritis (NGU)
60 days
• test and treat all contacts in the last 60 days
• if no sexual contacts then testing and treatment
of the last sexual contact is recommended
See Treatment for Contacts to Chlamydia section within this DST.
1. Treatment covers potential chlamydia infection.
2. See Notes section under Contacts to Chlamydia section within this
DST.
3. Refer to the CT DST for client education, screening recommendations, alternate treatments and further medication
information.
236
Certified Practice Area:
Reproductive Health: Sexually Transmitted Infections
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
CLIENT EDUCATION
Counsel client regarding:
• returning for follow-up assessment if symptoms occur.
• the appropriate use of medications (dosage, side effects, and need for re-treatment if dosage not completed, or symptoms
do not resolve).
• avoiding sexual contact until treatment is completed as indicated in the treatment table.
• harm reduction (condom use significantly reduces the risk of transmission).
• cleaning sex toys between use and using condoms if sharing sex toys
• the benefits of routine STI screening.
• the potential complications of untreated STI.
• co-infection risk for HIV when another STI is present.
• the asymptomatic nature of STI.
DOCUMENTATION
• as per agency policy
DST-1002 Treatment of STI Contacts
237
Certified Practice Area:
Reproductive Health: Sexually Transmitted Infections
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
REFERENCES
More recent editions of any of the items in the reference list may have been published since this DST was published. If you have a newer version, please use it.
Australasian Sexual Health Alliance (ASHA). (n.d.). Australian STI management guidelines for use in primary care.
British Association for Sexual Health and HIV (BASHH). (n.d.). BASHH guidelines.
Barbee, L.A., Kerani, R.P., Dombrowski, J.C., Soge, O. & Golden, M.R. (2013). A retrospective comparative study of 2-drug oral
and intramuscular cephalosporin treatment regimens for pharyngeal gonorrhea. Clinical Infectious Diseases, 56(11), pp.1539-1545.
British Columbia Centre for Disease Control (BCCDC). (2014). British Columbia treatment guidelines: Sexually transmitted infections in adolescent and adults. STI/HIV Prevention and Control Division, BCCDC.
BCCDC Public Health Laboratory (BCCDC PHL). (2016). Laboratory trends. Vancouver, BC.
Briggs, G.G., Freeman, R.K. & Yaffe, S.J. (2001). Drugs in pregnancy and lactation: A reference guide to fetal and neonatal risk. 6th ed. Philadelphia: Lippincott Williams & Wilkins.
Centers for Disease Control and Prevention (CDC). (2015). 2015 Sexually transmitted diseases treatment guidelines.
Forcey, D.S., Vodstrcil, L.A., Hocking, J.S., Fairley, M.L., McNair, R.P. & Bradshaw, C.S. (2015). Factors associated with bacterial vaginosis among women who have sex with women: A systematic review. PLoS One 10(12): e0141905-e0141905.
Holmes, K., Sparling, P., Stamm, W., Piot, P., Wasserheit, J., Corey, L., Cohen, M. & Watts, H. (2008). Sexually transmitted disease (4th ed). Toronto, ON: McGraw Hill Medical.
Hottes, T.S., Lester, R.T., Hoang, L., McKay, R., Gilbert, M., Patrick, D.M., Wong, T., Martin, R. & Ogilvie, G. (2013). Cephalosporin and azithromycin susceptibility in Neissieria gonorrheoeae isolates by site of infection, British Columbia, 2006 to 2011. Sexually Transmitted Diseases, 40(1), pp.46-51.
Public Health Agency of Canada (PHAC). (2012). Canadian guidelines on sexually transmitted infections.
PHAC. (2017). 2016 Updates summary. In: Canadian guidelines on sexually transmitted infections.
PHAC. (2017). Supplementary statement for the management of Lymphogranuloma venereum (LGV) cases and contacts. In: Canadian guidelines on sexually transmitted infections.
Society of Obstetricians and Gynecologists. (SOGC). (2008). Screening and management of bacterial vaginosis in pregnancy. JOGC, 211, pp.702-708.
DST-1002 Treatment of STI Contacts
238
Certified Practice Area:
Reproductive Health: Sexually Transmitted Infections
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
DST-1004 Urethritis
DEFINITION
Term Definition
Urethritis Inflammation of the urethra caused by any etiology that manifests as
urethral discharge, dysuria, urethral itching or meatal erythema.
Presumptive gonococcal urethritis (e.g. Neisseria
gonorrhoeae)
Urethritis with microscopy confirmed typical intracellular diploccoci (TID).
Non-gonococcal urethritis (NGU) Urethritis with increased polymorphonuclear leukocytes (PMNs) and the
absence of a positive laboratory test for Neisseria gonorrhea or TID.
Urethritis not yet diagnosed (NYD) Urethritis without immediate microscopy diagnosis.
Recurrent urethritis* Persistence of urethral symptoms when the onset of treatment was at least
two weeks prior, treatment was taken as directed, and there has been no
re-exposure or new exposure (e.g., new or untreated partner).
*For clients with recurrent urethritis refer to the Recurrent Urethritis Decision Support Tool DST.
POTENTIAL CAUSES
Bacterial:
• Neisseria gonorrhoeae (GC)
• Chlamydia trachomatis (CT)
• Mycoplasma genitalium
• Ureaplasma urealyticum
Viral:
• adenovirus
• herpes simplex virus (HSV)
Protozoan:
• Trichomonas vaginalis (TV)
Non-STI:
• secondary to catheterization or other instrumentation or trauma of the urethra
• in association with other factors that contribute to urinary tract infection (e.g., prostate or cystitis unrelated to STI)
• underlying anatomical issue (e.g., urethral stricture, fistulae, post-operative complications)
PREDISPOSING RISK FACTORS
• sexual contact where there is transmission through the exchange of body fluids
DST-1004 Urethritis
239
Certified Practice Area:
Reproductive Health: Sexually Transmitted Infections
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
TYPICAL FINDINGS
Sexual Health History
• sexual contact with at least one partner
• may report sexual contact with a partner infected with HSV
• sexual contact with someone with confirmed positive laboratory test for STI
Physical Assessment
• urethral discharge
• painful urination (dysuria)
• urethral itch, irritation or awareness
• meatal erythema
DIAGNOSTIC TESTS
Full STI screening is recommended. See the STI Assessment DST.
• Urethral swab. For symptomatic clients. Collect the following specimens from visible discharge at the urethral opening,
insertion into the urethra is not required:
o smear for TID and PMNs (collect only if immediate microscopy is available) and
o GC culture and sensitivity (C&S)
• Urine specimen. For all clients. Collect urine for GC/CT NAAT. Ideally the client should not have voided in the previous 1-
2 hours, collect the first voided 10-20 ml. Note the following:
o if urethral swabs are indicated, the urine specimen is collected after the urethral swab
o may be collected as the only diagnostic test in agencies or circumstances where:
▪ GC C&S is unavailable
▪ the client declines urethral swab
DST-1004 Urethritis

240
Certified Practice Area:
Reproductive Health: Sexually Transmitted Infections
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
MANAGEMENT AND INTERVENTIONS
Goals of Treatment
• treat infection
• prevent complications
• prevent spread of infection
• alleviate symptoms
TREATMENT OF CHOICE
Treatment is warranted in the following cases:
• presumptive gonorrhea– diagnosis is based on microscopy results
• non-gonococcal urethritis (NGU) – diagnosis is based on microscopy results
• urethritis not yet diagnosed (NYD) – when microscopy results are not immediately available
• sexual contacts of clients diagnosed with urethritis (see Treatment of STI Contacts DST)
DST-1004 Urethritis

241
Certified Practice Area:
Reproductive Health: Sexually Transmitted Infections
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
CLINICAL EVALUATION/CLINICAL JUDGMENT
Urethral Symptoms
Urethritis Algorithm
Meatal dischargeNo meatal discharge
Immediate microscopy
results
No immediate microscopy
results
1) Swab meatal discharge for:• Smear for TID/PMNs• GC C&S
2) Urine for GC/CT NAAT
1) Swab meatal discharge for GC C&S
2) Urine for GC/CT NAAT
Urine for GC/CT NAAT
Diagnosis: Urethritis NYD
Treat for gonorrhea and chlamydia
Smear:• ≥ 5 PMNs• TID positive
Smear:• ≥ 5 PMNs• TID negative
Smear:• ≤ 5 PMNs• TID negative
Diagnosis: Presumptive gonorrhea
Treat for gonorrhea and chlamydia
Diagnosis: Non-gonococcal urethritis (NGU)
Treat for chlamydia
Await diagnostic results
OR
If client is unable to return for results or is experiencing significant symptoms, refer to or consult with physician/NP
NOTE:
If symptoms persist after completion of treatment – see Recurrent Urethritis DST
DST-1004 Urethritis
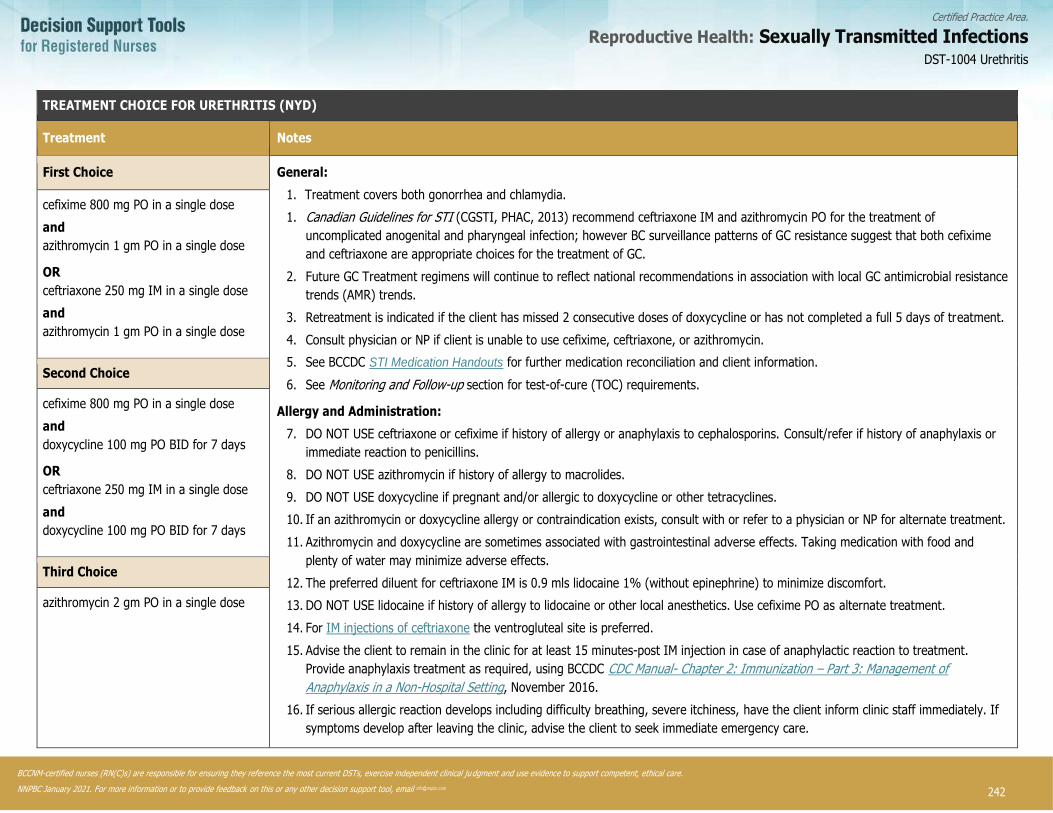
242
Certified Practice Area:
Reproductive Health: Sexually Transmitted Infections DST-1004 Urethritis
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
1. NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
TREATMENT CHOICE FOR URETHRITIS (NYD)
Treatment Notes
First Choice General:
1. Treatment covers both gonorrhea and chlamydia.
1. Canadian Guidelines for STI (CGSTI, PHAC, 2013) recommend ceftriaxone IM and azithromycin PO for the treatment of
uncomplicated anogenital and pharyngeal infection; however BC surveillance patterns of GC resistance suggest that both cefixime
and ceftriaxone are appropriate choices for the treatment of GC.
2. Future GC Treatment regimens will continue to reflect national recommendations in association with local GC antimicrobial resistance
trends (AMR) trends.
3. Retreatment is indicated if the client has missed 2 consecutive doses of doxycycline or has not completed a full 5 days of treatment.
4. Consult physician or NP if client is unable to use cefixime, ceftriaxone, or azithromycin.
5. See BCCDC STI Medication Handouts for further medication reconciliation and client information.
6. See Monitoring and Follow-up section for test-of-cure (TOC) requirements.
Allergy and Administration:
7. DO NOT USE ceftriaxone or cefixime if history of allergy or anaphylaxis to cephalosporins. Consult/refer if history of anaphylaxis or
immediate reaction to penicillins.
8. DO NOT USE azithromycin if history of allergy to macrolides.
9. DO NOT USE doxycycline if pregnant and/or allergic to doxycycline or other tetracyclines.
10. If an azithromycin or doxycycline allergy or contraindication exists, consult with or refer to a physician or NP for alternate treatment.
11. Azithromycin and doxycycline are sometimes associated with gastrointestinal adverse effects. Taking medication with food and
plenty of water may minimize adverse effects.
12. The preferred diluent for ceftriaxone IM is 0.9 mls lidocaine 1% (without epinephrine) to minimize discomfort.
13. DO NOT USE lidocaine if history of allergy to lidocaine or other local anesthetics. Use cefixime PO as alternate treatment.
14. For IM injections of ceftriaxone the ventrogluteal site is preferred.
15. Advise the client to remain in the clinic for at least 15 minutes-post IM injection in case of anaphylactic reaction to treatment.
Provide anaphylaxis treatment as required, using BCCDC CDC Manual- Chapter 2: Immunization – Part 3: Management of
Anaphylaxis in a Non-Hospital Setting, November 2016.
16. If serious allergic reaction develops including difficulty breathing, severe itchiness, have the client inform clinic staff immediately. If
symptoms develop after leaving the clinic, advise the client to seek immediate emergency care.
cefixime 800 mg PO in a single dose
and
azithromycin 1 gm PO in a single dose
OR
ceftriaxone 250 mg IM in a single dose
and
azithromycin 1 gm PO in a single dose
Second Choice
cefixime 800 mg PO in a single dose
and
doxycycline 100 mg PO BID for 7 days
OR
ceftriaxone 250 mg IM in a single dose
and
doxycycline 100 mg PO BID for 7 days
Third Choice
azithromycin 2 gm PO in a single dose

243
Certified Practice Area:
Reproductive Health: Sexually Transmitted Infections DST-1004 Urethritis
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
1. NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
TREATMENT CHOICE FOR URETHRITIS (NYD)
17. Advise client they may experience pain, redness and swelling at the injection site. If any of these effects persist or worsen, advise to
contact health care provider.
18. Recent data has emerged regarding azithromycin and QT prolongation. Although rare, it is more significant in older populations,
those with pre-existing heart conditions, arrhythmias or electrolyte disturbances.
19. It is unclear how significant these findings are in young to mid-age healthy adults consuming a one-time dose of azithromycin;
however, please use the following precautions:
Consult with or refer to an NP or physician if the client:
• has a history of congenital or documented QT prolongation.
• has a history of electrolyte disturbance in particular hypokalemia, hypomagnesaemia.
• has clinically relevant bradycardia, cardiac arrhythmia or cardiac insufficiency.
• is on any of the following medications:
o Antipsychotics: pimozide (Orap®), ziprasidone (Zeldox®)
o Cardiac: dronedarone (Multaq®)
o Migraine: dihydroergotamine (Migranal®), ergotamine (Cafergot®)
TREATMENT CHOICE FOR URETHRITIS – Non-gonococcal (NGU)
Diagnosis - Type Treatment Notes
Non-gonococcal urethritis (NGU) – when immediate
microscopy is available and results include:
• urethral swab for smear is negative for TID
• urethral swab for smear ≥ 5 PMNs
First Choice See Notes section on previous two pages.
doxycycline 100 mg PO BID for 7 days
OR
azithromycin 1 gm PO in a single dose

244
Certified Practice Area:
Reproductive Health: Sexually Transmitted Infections
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
PARTNER COUNSELLING AND REFERRAL
Counsel clients to notify people who may have been exposed through sexual contact within the previous 60 days that they require testing and treatment to cover chlamydia and gonorrhea. If no sexual contact in the past 60 days then the client may notify their last sexual contact regarding testing and treatment (see Treatment of STI Contacts DST).
MONITORING AND FOLLOW-UP
• Follow-up is based on test results or recurrence of symptoms. If test results positive for STI, refer to appropriate STI DST for
monitoring and follow-up.
POTENTIAL COMPLICATIONS
• persistent or recurrent urethritis (see Recurrent Urethritis DST)
• epididymitis
• sexually-acquired reactive arthritis
• stricture (rare)
• prostatitis (rare)
CLIENT EDUCATION
Counsel client regarding:
• abstaining from sexual activity during the 7-day course of treatment or for 7 days post single-dose therapy for clients and
their contacts.
• informing last sexual contact AND any sexual contacts within the last 60 days that they require testing and treatment.
• methods of partner notification
• the appropriate use of medications (dosage, side effects, and need for re-treatment if dosage not completed, or symptoms
do not resolve).
• harm reduction (e.g., condom use significantly reduces the risk of transmission).
• the benefits of routine STI screening.
• the potential complications from untreated urethritis.
• co-infection risk for HIV when another STI is present.
• the asymptomatic nature of STI.
• the importance of revisiting the clinic if symptoms persist or recur 14 days or more after treatment has been initiated.
• repeat testing is not necessary unless symptoms do not resolve 14 days or more after antibiotic treatment has been initiated.
• urethritis can be transmitted through oral, vaginal and anal sexual contact. Organisms responsible for the infection may
reside in the throat, vagina or rectum of sexual partners, and may not be detectable with testing.
CONSULTATION AND/OR REFERRAL
Consult or refer to physician or NP, if the client is experiencing complications associated with urethritis (e.g., epididymitis – see BCCDC’s non-certified practice Epididymitis DST).
DOCUMENTATION
• urethritis is not reportable
• as per agency policy
DST-1004 Urethritis

245
Certified Practice Area:
Reproductive Health: Sexually Transmitted Infections
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
REFERENCES
More recent editions of any of the items in the reference list may have been published since this DST was published. If you have a newer version, please use it.
Australasian Sexual Health Alliance (ASHA). (2016). Urethritis – male. In Australian STI Management Guidelines for use in Primary Care.
Barbee, L.A., Kerani, R.P., Dombrowski, J.C., Soge, O. & Golden, M.R. (2013). A retrospective comparative study of 2-drug oral and intramuscular cephalosporin treatment regimens for pharyngeal gonorrhea. Clinical Infectious Diseases, 56(11), pp.1539-1545.
British Columbia Centre for Disease Control (BCCDC). (2014). British Columbia treatment guidelines: Sexually transmitted infections in adolescent and adults. STI/HIV Prevention and Control Division, BCCDC.
BCCDC. (2013). BCCDC’s videos on injection landmarking and technique. BCCDC.
BCCDC Public Health Laboratory (BCCDC PHL). (2016). PHSA Laboratories Guide to Programs and Services. Vancouver, BC.
Centers for Disease Control and Prevention (CDC). (2015). Urethritis. 2015 Sexually Transmitted Diseases Treatment Guidelines. Atlanta, GA.
Holmes, K., Sparling, P., Stamm, W., Piot, P., Wasserheit, J., Corey, L., Cohen, M. & Watts, H. (2008). Sexually transmitted disease (4th ed). Toronto, ON: McGraw Hill Medical.
Horner, P.J., Blee, K., O'Mahony, C., Muir, P., Evans, C. & Radcliffe, K. (2015). UK national guideline on the management of non-gonococcal urethritis. Int J STD AIDS, pp.1-12.
Hottes, T.S., Lester, R.T., Hoang, L., McKay, R., Gilbert, M., Patrick, D.M., Wong, T., Martin, R. & Ogilvie, G. (2013).
Cephalosporin and azithromycin susceptibility in Neissieria gonorrheoeae isolates by site of infection, British Columbia, 2006 to 2011. Sexually Transmitted Diseases, 40(1), pp.46-51.
Lunny, C., Taylor, D., Hoang, L., Wong, T., Gilbert, M., Lester, R. & Greub, G. (2014). Self-collected versus clinician-collected sampling for chlamydia and gonorrhoea screening: A systemic review and meta-analysis. PLoS ONE, 10(7), pp.1-23.
Manhart, L.E., Gillespie, C.W., Lowens, M.S., Khosropour, C.M., Colombrara, D.V., Golden, M.R., Hakhu, N.R., Thomas, K.K.
Hughes, J.P., Jensen, N.L. & Totten, P.A. (2013). Standard treatment regimens for nongonoccoccal urethritis have similar but declining cure rates: A randomized controlled trial. Clinical Infectious Diseases, 56(7), pp.934-942.
Papp, J. et al. (2014). Recommendations for the laboratory-based detection of Chlamydia trachomatis and Neisseria gonorrhoeae. Morbidity and Mortality Weekly Report, 63(1).
Pattman, R., Snow, M., Handy, P., Sankar, K.N. & Elawad, B. (2005). Oxford Handbook of Genitourinary Medicine, HIV, and AIDS, 1st Edition, Copyright (c) 2005 Oxford University Press.
Public Health Agency of Canada (PHAC). (2013). Urethritis. In: Canadian guidelines on sexually transmitted infections.
PHAC. (2014). Supplementary statement for recommendations related to the diagnosis, management, and follow-up of urethritis. In: Canadian guidelines on sexually transmitted infections.
PHAC. (2017). 2016 Updates Summary. In: Canadian guidelines on sexually transmitted infections.
University of California San Francisco (UCSF) & Center of Excellence for Transgender Health. (2016). Guidelines for the primary and gender-affirming care of transgender and gender non-binary people.
DST-1004 Urethritis
246
Certified Practice Area:
Reproductive Health: Sexually Transmitted Infections
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
DST-1005 Recurrent Urethritis
DEFINITION
Persistence of urethral symptoms when the onset of treatment for urethritis was at least two weeks prior, treatment was taken as
directed, there has been no re-exposure or new exposure to infection through sexual contact (e.g., new sexual contact or untreated
contact), and test results for chlamydia and gonorrhea were negative. Urethritis refers to inflammation of the urethra that is caused by any etiology that manifests as urethral discharge, dysuria, urethral itching or meatal erythema.
For those clients who present with urethral symptoms, but do not fit the definition for recurrent urethritis use the Urethritis Decision Support Tool (DST).
POTENTIAL CAUSES
Bacterial:
• Neisseria gonorrhoea (GC)
• Chlamydia trachomatis (CT)
• Mycoplasma genitalium
• Ureaplasma urealyticum
Viral:
• adenovirus
• herpes simplex virus (HSV)
Protozoan:
• Trichomonas vaginalis (TV)
Non-STI:
• secondary to catheterization or other instrumentation, or trauma of the urethra
• in association with other factors that contribute to urinary tract infection (e.g., prostate or cystitis unrelated to STI)
• underlying anatomical issue (e.g., urethral stricture, fistulae, post-operative complications)
PREDISPOSING RISK FACTORS
• sexual contact with a new partner
• sexual contact with an untreated partner
• interventions or manipulations that may cause urethral irritation such as, catheterization or inserting foreign objects into the
urethra
• incomplete or inappropriate treatment for previous urethritis diagnosis
• organisms resistant to previous antibiotic treatment choice
TYPICAL FINDINGS
Sexual Health History
• recent history of treatment for urethritis
• persistent urethral symptoms
o dysuria, urethral discharge, urethral itching/irritation, or meatal erythema and
▪ all medication has been taken as directed
▪ onset of treatment was ≥ 2 weeks prior
▪ no re-exposure to untreated sexual contact
DST-1005 Recurrent Urethritis
247
Certified Practice Area:
Reproductive Health: Sexually Transmitted Infections
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
▪ no exposure to new sexual contact
▪ test results were negative for gonorrhea and chlamydia
Note: If above criteria are not met, then refer to Urethritis DST.
Physical Assessment
• urethral discharge
• urethral itch, irritation or awareness
• painful urination (dysuria)
• meatal erythema
DIAGNOSTIC TESTS
• repeat urethral swab, if discharge is present for:
o smear for typical intracellular diplococci (TID) and polymorphonuclear leukocytes (PMNs) (if available) and
o GC culture & sensitivity (C&S)
Note: Collect the discharge from the meatal opening without inserting the swab directly into the urethra.
AND
• urine specimen for GC/CT NAAT (ideally the client should not have voided in the previous 1-2 hours; collect first 10-20 ml)
Interpreting Microscopy Results
See Recurrent Urethritis Algorithm (page 4).
DST-1005 Recurrent Urethritis

248
Certified Practice Area:
Reproductive Health: Sexually Transmitted Infections
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
CLINICAL EVALUATION/CLINICAL JUDGMENT
Persistent urethral symptoms AND
• All medication has been taken as directed• Onset of treatment was ≥ 2 weeks prior• No re-exposure to an untreated partner• No exposure to new partner(s)• Test results were negative for gonorrhea and chlamydia
If above criteria are not met – then refer to Urethritis DST
Tests positive
Recurrent Urethritis Algorithm
Meatal dischargeNo meatal discharge
Immediate microscopy
results
No immediate microscopy
resultsUrine for GC/CT NAAT
1) Swab meatal discharge for:• Smear for TID/PMNs• GC C&S
2) Urine for GC/CT NAAT
1) Swab meatal discharge for GC C&S
2) Urine for GC/CT NAAT
Smear:• ≥ 5 PMNs• TID positive
Smear:• ≥ 5 PMNs• TID negative
Smear:• ≤ 5 PMNs• TID negative
Diagnosis: Presumptive gonorrhea
Treat for gonorrhea and chlamydia
Diagnosis: Recurrent urethritis
Treat as per DST
Consult with or refer to physician or NP
Client follow-up not assured
Client follow-up assured
Treat as per DSTWait for
diagnostic results
Symptoms resolve
Symptoms persist
Tests negative
Consult and/or refer to
physician or NP
Treat according to results
Consult and/or refer to
physician or NP
DST-1005 Recurrent Urethritis
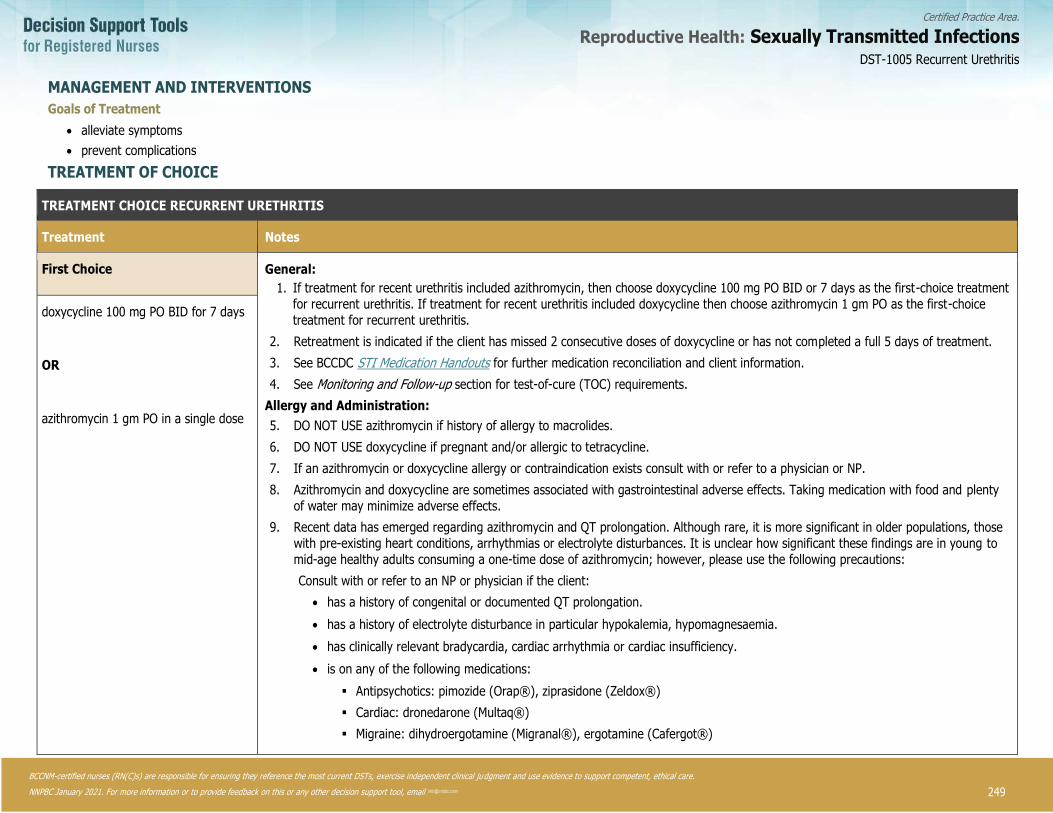
249
Certified Practice Area:
Reproductive Health: Sexually Transmitted Infections DST-1005 Recurrent Urethritis
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
2. NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
MANAGEMENT AND INTERVENTIONS
Goals of Treatment
• alleviate symptoms
• prevent complications
TREATMENT OF CHOICE
TREATMENT CHOICE RECURRENT URETHRITIS
Treatment Notes
First Choice General:
1. If treatment for recent urethritis included azithromycin, then choose doxycycline 100 mg PO BID or 7 days as the first-choice treatment
for recurrent urethritis. If treatment for recent urethritis included doxycycline then choose azithromycin 1 gm PO as the first-choice
treatment for recurrent urethritis.
2. Retreatment is indicated if the client has missed 2 consecutive doses of doxycycline or has not completed a full 5 days of treatment.
3. See BCCDC STI Medication Handouts for further medication reconciliation and client information.
4. See Monitoring and Follow-up section for test-of-cure (TOC) requirements.
Allergy and Administration:
5. DO NOT USE azithromycin if history of allergy to macrolides.
6. DO NOT USE doxycycline if pregnant and/or allergic to tetracycline.
7. If an azithromycin or doxycycline allergy or contraindication exists consult with or refer to a physician or NP.
8. Azithromycin and doxycycline are sometimes associated with gastrointestinal adverse effects. Taking medication with food and plenty
of water may minimize adverse effects.
9. Recent data has emerged regarding azithromycin and QT prolongation. Although rare, it is more significant in older populations, those
with pre-existing heart conditions, arrhythmias or electrolyte disturbances. It is unclear how significant these findings are in young to
mid-age healthy adults consuming a one-time dose of azithromycin; however, please use the following precautions:
Consult with or refer to an NP or physician if the client:
• has a history of congenital or documented QT prolongation.
• has a history of electrolyte disturbance in particular hypokalemia, hypomagnesaemia.
• has clinically relevant bradycardia, cardiac arrhythmia or cardiac insufficiency.
• is on any of the following medications:
▪ Antipsychotics: pimozide (Orap®), ziprasidone (Zeldox®)
▪ Cardiac: dronedarone (Multaq®)
▪ Migraine: dihydroergotamine (Migranal®), ergotamine (Cafergot®)
doxycycline 100 mg PO BID for 7 days
OR
azithromycin 1 gm PO in a single dose

250
Certified Practice Area:
Reproductive Health: Sexually Transmitted Infections
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
PARTNER COUNSELLING AND REFERRAL
Sexual contacts of clients who have recurrent urethritis do not require notification or treatment.
MONITORING AND FOLLOW-UP
Consult with or refer to a physician or NP if tests are negative and symptoms persist.
POTENTIAL COMPLICATIONS
• epididymitis
• sexually-acquired reactive arthritis
• stricture (rare)
• prostatitis (rare)
CLIENT EDUCATION
Counsel client regarding:
• the appropriate use of medications (dosage, side effects, and need for re-treatment if dosage not completed, or symptoms
do not resolve).
• harm reduction (condom use significantly reduces the risk of transmission).
• the importance of revisiting clinic if symptoms persist after treatment has been completed for one week.
• sexual contacts of clients with recurrent urethritis do not require treatment.
CONSULTATION AND/OR REFERRAL
Consult with or refer to a physician or NP in the following situations:
• if symptoms persist or recur after completed therapy for recurrent urethritis, and all tests results are negative.
• for allergies or contraindications related to the treatment outlined in this DST.
DOCUMENTATION
• recurrent urethritis is not reportable
• as per agency policy
DST-1005 Recurrent Urethritis

251
Certified Practice Area:
Reproductive Health: Sexually Transmitted Infections
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
REFERENCES
More recent editions of any of the items in the reference list may have been published since this DST was published. If you have a newer version, please use it.
British Columbia Centre for Disease Control (BCCDC). (2014). British Columbia treatment guidelines: Sexually transmitted infections in adolescent and adults.
Bradshaw, C.S., Chen, M.Y., et al. (2008). Persistence of Mycoplasma genitalium following azithromycin therapy. PLoS One, 3(11), p.e3618.
Holmes, K., Sparling, P., Stamm, W., Piot, P., Wasserheit, J., Corey, L., Cohen, M. & Watts, H. (2008). Sexually transmitted disease (4th ed). Toronto, ON: McGraw Hill Medical.
Pattman, R., Snow, M., Handy, P., Sankar, K.N. & Elawad, B. (2005). Oxford Handbook of Genitourinary Medicine, HIV, and AIDS, 1st Edition, Copyright (c) 2005 Oxford University Press.
Public Health Agency of Canada. (PHAC). (2010). Section 4 – Management and treatment of specific syndromes: Urethritis. In: Canadian guidelines on sexually transmitted infections.
PHAC. (2017). 2016 Updates Summary. In: Canadian guidelines on sexually transmitted infections.
University of Washington. (2013). The Practitioner’s handbook for the management of sexually transmitted diseases.
DST-1005 Recurrent Urethritis
252
Certified Practice Area:
Reproductive Health: Sexually Transmitted Infections
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
DST-1006 Bacterial Vaginosis
Note: For clients who are on gender-affirming testosterone therapy or who have had gender-affirming vaginoplasty, who have
signs/symptoms of BV, consult with and/or refer to a nurse practitioner (NP) or physician as clients may require additional tests and
alternate treatment. See Trans Care BC’s Gender-affirming Care for Trans, Two-Spirit and Gender Diverse Patients in BC: A Primary Care Toolkit.
DEFINITION
A common imbalance of the vaginal flora caused by an overgrowth of vaginal bacteria (especially anaerobic, gram negative bacilli) with a possible a depletion of lactobacilli.
POTENTIAL CAUSES
Bacterial:
• Gardnerella vaginalis
• Prevotella species
• Mobiluncus species
• Ureaplasma urealyticum
• Mycoplasma hominis
PREDISPOSING RISK FACTORS
• sexual contact with at least one partner
• new/multiple sexual partners
• other STI (e.g., herpes simplex virus type 2 (HSV-2), chlamydia, gonorrhea)
• intrauterine device (IUD)
• cigarette smoking
• douching
TYPICAL FINDINGS
Sexual Health History
• often asymptomatic (>50%)
• change in normal patterns of discharge
• odour (fishy)
• irritation
• recurrent BV is common. Individuals should be re-evaluated to reconfirm diagnosis and for consult/referral if indicated.
Physical Assessment
Cardinal Signs
• Client-reported changes in vaginal discharge which may include:
o moderate to profuse amount
o homogenous (i.e., not clumpy)
o greyish or white colour
o thin
o fishy odour
o amine (fishy) odour before or after a positive KOH whiff test
o pH greater than (>) 4.5
DST-1006 Bacterial Vaginosis

253
Certified Practice Area:
Reproductive Health: Sexually Transmitted Infections
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
DIAGNOSTIC TESTS
Full STI screening is recommended. See the STI Assessment DST.
If signs or symptoms of BV are present, the following methods are available for BV diagnosis:
• Nugent scoring: from gram stain lab results
• Amsel’s criteria: clinical diagnosis including microscopy
• Modified Amsel’s Criteria: clinical diagnosis when microscopy not available
The following specimens are collected from the vaginal wall through clinician- or client-collected blind swab or during a speculum exam:
• swab for microscopy: smear on slide for gram stain and/or clue cells
• swab for pH
• swab for KOH whiff test
Notes:
1. Prepare glass slide for microscopy prior to using for pH or whiff test.
2. pH strips are ineffective in the presence of blood.
3. The KOH whiff test involves adding 10% KOH solution (not exceeding 0.5 ml) to collected vaginal secretions and briefly
sniffing (1-2 seconds) the vapour to assess for an amine odour. Detection of an amine odour constitutes a positive whiff
test. For more information on KOH whiff testing see: Safe Use of 10% Potassium Hydroxide in STI Screening located in the
BCCDC Communicable Disease (CD) Manual Chapter 5: Sexually Transmitted Infections.
CLINICAL EVALUATION/CLINICAL JUDGMENT
Nugent Score/Gram Stain
Determined by lab testing of vaginal smear with three possible scoring outcomes and interpretations (see Bacterial Vaginosis Nugent Scoring (Gram Stain) algorithm):
• negative (0-3)
• intermediate (4-6)
• positive (7-10)
Amsel’s Criteria
Clinical criteria requiring 3 of the following symptoms or signs for BV diagnosis:
• pH greater than (>) 4.5
• presence of moderate-profuse grey-white discharge – may be thin and homogenous (non-clumping)
• positive KOH whiff test OR obvious BV odour (in the absence of KOH whiff test)
• lab slide of smear result is positive for clue cells**
**Can be used if immediate microscopic evaluation is available.
Modified Amsel’s Criteria
This method is useful for clinical management of BV when microscopic evaluation for clue cells is not immediately available, and the client reports abnormal changes in vaginal discharge plus at least 2 of the following are present:
• pH greater than (>) 4.5
• presence of homogenous, moderate-profuse grey-white discharge
• positive KOH whiff test OR obvious BV odour in the absence of the KOH whiff test
DST-1006 Bacterial Vaginosis
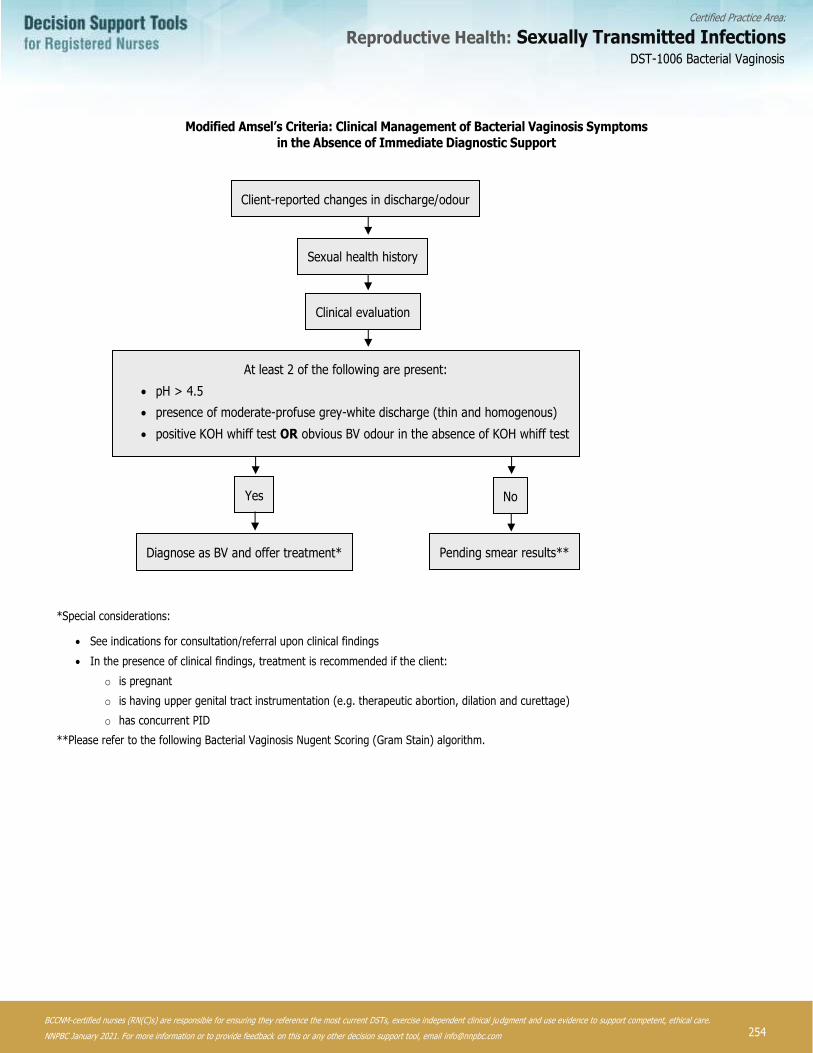
254
Certified Practice Area:
Reproductive Health: Sexually Transmitted Infections
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
Modified Amsel’s Criteria: Clinical Management of Bacterial Vaginosis Symptoms
in the Absence of Immediate Diagnostic Support
Yes
Sexual health history
Client-reported changes in discharge/odour
Clinical evaluation
At least 2 of the following are present:
• pH > 4.5
• presence of moderate-profuse grey-white discharge (thin and homogenous)
• positive KOH whiff test OR obvious BV odour in the absence of KOH whiff test
No
Pending smear results** Diagnose as BV and offer treatment*
*Special considerations:
• See indications for consultation/referral upon clinical findings
• In the presence of clinical findings, treatment is recommended if the client:
o is pregnant
o is having upper genital tract instrumentation (e.g. therapeutic abortion, dilation and curettage)
o has concurrent PID
**Please refer to the following Bacterial Vaginosis Nugent Scoring (Gram Stain) algorithm.
DST-1006 Bacterial Vaginosis

255
Certified Practice Area:
Reproductive Health: Sexually Transmitted Infections
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
Bacterial Vaginosis Nugent Scoring (Gram Stain)
No
Interpretation: intermediate
(Nugent score: 4 – 6)
Do the following apply?
• pregnancy*
upper genital tract gynecological procedure
(e.g., therapeutic abortions, dilation and curettage)
• concurrent PID
Yes
Treatment recommended to prevent PID and pregnancy*
complications
Assess risk, offer treatment
& explain transient nature of BV
Interpretation: negative
(Nugent score: 0 – 3)
Interpretation: positive
(Nugent score: 7 – 10)
Do not offer treatment
No Yes
Offer treatment
*Consult with or refer to a physician or NP.
Smear results
Current or persistent symptoms
DST-1006 Bacterial Vaginosis
256
Certified Practice Area:
Reproductive Health: Sexually Transmitted Infections
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
MANAGEMENT AND INTERVENTIONS
Goals of Treatment
• treat infection
• prevent complications
• alleviate symptoms
TREATMENT OF CHOICE
Treatment Notes
First Choice General:
1. Though demonstrated to have a lower efficacy in treating BV
(primarily due to recurrence), metronidazole 2 gm PO as a single dose
may be given in instances where completion of treatment is a concern.
2. Intravaginal metronidazole gel and clindamycin cream/ovules/oral
formulations are not included in the BCCDC Provincial STI Drug Program. RN(C)s may need to consult with a physician or NP to obtain
a prescription for the client.
3. Clindamycin cream may weaken latex condoms and diaphragms for up
to 5 days after use.
4. The efficacy of probiotic (lactobacillus or lactic acid formulations),
antiseptics, or boric acid preparations as treatments for BV has, to
date, not been conclusively demonstrated despite promising results. Until there is more published data, it is premature to make a
judgement as to their recommended use.
Allergy and Administration:
5. Alcohol must be avoided 12 hours pre-treatment, during treatment and
24-48 hours post-treatment with metronidazole.
6. Metronidazole 500 mg PO BID for 7 days is acceptable and safe to
administer in breast-/chest-feeding clients. Consult/refer for other first
choice or alternate treatment recommendations in pregnant clients.
metronidazole 500 mg PO BID for 7 days
OR
metronidazole gel 0.75%, one applicator (5 g) once a day intravaginally for 5 days
OR
clindamycin cream 2%, one applicator (5 g) intravaginally once a day for 7 days
Alternate Treatment
metronidazole 2 gm PO in a single dose
OR
clindamycin 300 mg PO BID for 7 days
OR
clindamycin ovules 100 mg intravaginally once at bedtime for 3 days
PREGNANT OR BREAST-/CHEST-FEEDING CLIENTS
For clients who are pregnant consult with or refer to physician or NP. For clients who are breast-/chest-feeding, metronidazole 500 mg PO BID for 7 days is acceptable and safe to administer.
PARTNER COUNSELLING AND REFERRAL
Where relevant (clients with vaginas, clients with vaginoplasty), sexual partners of people diagnosed with BV benefit from assessment and testing for BV. If clinical assessment and/or lab testing results are positive for BV, treat as per BV DST.
MONITORING AND FOLLOW-UP
If symptoms resolve, follow-up is not required. If symptoms persist following initial treatment, ensure treatment compliance and re-evaluate to re-confirm diagnosis.
DST-1006 Bacterial Vaginosis

257
Certified Practice Area:
Reproductive Health: Sexually Transmitted Infections
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
POTENTIAL COMPLICATIONS
• presence of BV during an invasive procedure (e.g., dilation and curettage), has been associated with post-procedure pelvic
inflammatory disease (PID)
• BV may be associated with premature rupture of membranes in clients with a history of previous complicated pregnancy
CLIENT EDUCATION
Counsel client regarding:
• the appropriate use of medications (dosage, side effects, and need for re-treatment if dosage not completed, or symptoms
do not resolve).
• special precautions for taking metronidazole: avoid alcohol 12 hours prior to starting treatment, during the course of
treatment and for 24-48 hours after treatment completion.
• refraining from sexual activity or use condoms consistently during treatment.
• vaginal flora and pH balance. Advise that certain practices such as intra-vaginal cleansing (douching) can alter vaginal flora
and pH balance.
• promising results in the investigation of available probiotic (lactobacillus or lactic acid formulations), antiseptics, and boric
acid preparations for use in the treatment of BV; however, their exact efficacy as treatments for BV is unknown.
• IUD use being associated with BV.
• cleaning sex toys between use and using condoms if sharing sex toys
• the presence of BV can increase the likelihood of HIV transmission.
• the presence of BV can increase the likelihood of STI acquisition (e.g., HIV, GC, CT, HSV).
• if symptoms do not resolve with treatment, they will require referral to a physician or NP.
• BV may occur without having had sexual contact.
CONSULTATION AND/OR REFERRAL
Consult with or refer to a physician or NP in the following situations:
• whenever first choice and alternate treatment is contraindicated
• if the client is unable to abstain from alcohol during treatment period
• when prescription for treatment is required
• if the client is pregnant
• recurrent BV (RBV); RBV is defined as persistent symptoms after treatment of:
o 2 or more episodes of BV within a 4-week time frame
o 4 or more episodes of BV within a 1-year period
• for breast-/chest-feeding clients where metronidazole first choice treatment is not being used
DOCUMENTATION
• BV is not reportable
• as per agency policy
DST-1006 Bacterial Vaginosis

258
Certified Practice Area:
Reproductive Health: Sexually Transmitted Infections
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
REFERENCES
More recent editions of any of the items in the reference list may have been published since this DST was published. If you have a newer version, please use it.
Australasian Sexual Health Alliance (ASHA). (2016). Australian STI management guidelines for use in primary care: Bacterial vaginosis.
Bradshaw, C.S. & Brotman, R.M. (2015). Making inroads into improving treatment of bacterial vaginosis: Striving for long-term cure. BMC Infectious Diseases.15; p.292.
British Association for Sexual Health and HIV (BASHH). (2012). UK national guideline for the management of bacterial vaginosis.
Centers for Disease Control and Prevention (CDC). (2015). Sexually transmitted diseases treatment guidelines: Diseases characterized by vaginal discharge – bacterial vaginosis. MMWR Recommendations and Reports. 64:3; pp.104-110.
Forcey, D.S., Vodstrcil, L.A., Hocking, J.S., Fairley, C.K., Law, M., McNair, R.P. & Bradshaw, C.S. (2015). Factors associated with bacterial vaginosis among women who have sex with women: A systematic review. PLOS ONE | DOI:10.1371/journal.pone.0141905.
Heczk, P.B., Tomusiak, A., Adamski, P., Jakimiuk, A.J., Stefański, G., Mikołajczyk-Cichońska, A., Suda-Szczurek, M. & Strus, M.
(2015). Supplementation of standard antibiotic therapy with oral probiotics for bacterial vaginosis and aerobic vaginitis: A randomised, double-blind, placebo controlled trial. BMC Women's Health. 15:115.
Machado, D., Castro, J. & Palmei, A. (2016). Bacterial vaginosis biofilms: Challenges to current therapies and emerging solutions. Frontiers in Microbiology. 6:1528.
Madden, T., Grentzer, J.M., Secura, G.M., Allsworth, J.E., & Peipert, J.F. (2012). Risk of bacterial vaginosis in users of the intrauterine device: A longitudinal study. Sexually Transmitted Diseases. 39(3); pp.217-222.
Mullins, M.Z. & Trouton, K.M. (2015). BASIC study: is intravaginal boric acid non-inferior to metronidazole in symptomatic
bacterial vaginosis? Study protocol for a randomized controlled trial. Mullins and Trouton Trials (2015). 16:315 DOI 10.1186/s13063-015-0852-5.
Nyirjesy, P. (2014). Management of persistent vaginitis. Obstetrics and Gynecology. 124:6
Provincial Health Services Authority (PHSA) & Trans Care BC. (2017). Caring for trans and gender diverse clients in BC: A primary care toolkit.
Public Health Agency of Canada (PHAC). (2010). Vaginal discharge (bacterial vaginosis, vulvovaginal candidiasis, trichomoniasis). In: Canadian guidelines on sexually transmitted infections.
PHAC. (2014). Supplementary statement for recommendations related to the diagnosis, management, and follow-up of vaginal discharge. In: Canadian guidelines on sexually transmitted infections.
Reichman O, Akins R & Sobel J (2009). Boric acid addition to suppressive antimicrobial therapy for recurrent bacterial vaginosis. Sexually Transmitted Diseases. 36:11.
Sobel, R. & Sobel, J.D. (2015). Metronidazole for the treatment of vaginal infections. Expert Opinion on Pharmacotherapy. 16:7; pp.1109-1115.
Society of Obstetricians & Gynecologist of Canada (SOGC). (2014). Best practices to minimize risk of infection with intrauterine device insertion. J Obstet Gynaecol Can 2014; 36 (3); pp.266–274.
DST-1006 Bacterial Vaginosis
259
Certified Practice Area:
Reproductive Health: Sexually Transmitted Infections
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
van Schalkwyk, J. & Yudin, M.H. (2015). Vulvovaginitis: screening for and management of trichomoniasis, vulvovaginal candidiasis, and bacterial vaginosis. Journal of Obstetrics and Gynaecology of Canada. 37(3); pp.266–274.
Weyers, S., Verstaelen, H., Gerris, J., Monstrey, S., dos Santos Lopes Santiago, G., Sarens, B., De Backer, E., Gerrt, C.,
Vaneechoutte, M., Verhelst, R. (2009). Microflora of the penile skin-lined neovagina of transsexual women. BMC Microbiolody. 9:102. doi: 10.1 186/1471-2180-9-102.
DST-1006 Bacterial Vaginosis
260
Certified Practice Area:
Reproductive Health: Sexually Transmitted Infections
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
DST-1007 Mucopurulent Cervicitis (MPC)
DEFINITION
Inflammation of the cervix with mucopurulent or purulent discharge from the cervical os.
POTENTIAL CAUSES
Bacterial:
• Chlamydia trachomatis (CT)
• Neisserria gonorrhoeae (GC)
Viral:
• herpes simplex virus (HSV)
Protozoan:
• Trichomonas vaginalis (TV)
Non-STI:
• chemical irritants
• vaginal douching
• persistent disruption of vaginal flora
PREDISPOSING RISK FACTORS
• sexual contact where there is transmission through the exchange of body fluids
• sexual contact with at least one partner
• sexual contact with someone with confirmed positive laboratory test for STI
• incomplete STI medication treatment
• previous STI
TYPICAL FINDINGS
Sexual Health History
• may be asymptomatic
• sexual contact with at least one partner
• increased abnormal vaginal discharge
• dyspareunia
• bleeding after sex or between menstrual cycles
• external or internal genital lesions may be present with HSV infection
• sexual contact with someone with confirmed positive laboratory test for STI
Physical Assessment
Cardinal Signs
• mucopurulent discharge from the cervical os (thick yellow or green pus) and /or friability of the cervix (sustained bleeding
after swabbing gently)
DST-1007 Mucopurulent Cervicitis (MPC)
261
Certified Practice Area:
Reproductive Health: Sexually Transmitted Infections
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
The following may also be present:
• abnormal change in vaginal discharge
• cervical erythema/edema
Other Signs
• cervicitis associated with HSV infection:
o cervical lesions usually present
o may have external genital lesions with swollen inguinal nodes
Notes:
4. Clients may experience mild to moderate bleeding during cervical screening with spatula, cytobrush and/or endocervical nucleic acid amplification testing (NAAT) for gonorrhea (GC) and chlamydia (CT). This is common and does not necessarily
indicate mucopurulent cervicitis (MPC). Friability, which includes frank and sustained bleeding post-cervical screening, is a
potential sign of MPC.
5. Clients who present with symptoms of MPC should also be assessed for signs of pelvic inflammatory disease (PID) through bimanual exam for tenderness. If PID is present, consult with or refer to a physician or nurse practitioner (NP) for further
assessment.
6. A bimanual exam may be too uncomfortable for clients with cervical lesions due to HSV infection; they should be referred
to a physician or NP for further assessment and treatment.
DIAGNOSTIC TESTS
Full STI screening is recommended, including:
• vaginal swabs for:
o yeast
o bacterial vaginosis
o GC/CT/trichomonas NAAT
AND
• cervical swabs for:
o GC culture and sensitivity (C&S)
o GC/CT NAAT – if vaginal specimen not collected
o HSV polymerase chain reaction (PCR), if lesions are present on the cervix
CLINICAL EVALUATION/CLINICAL JUDGMENT
• treat all clients with MPC, as indicated by mucopurulent discharge visible from the cervical os, even when no laboratory
results are available
• treat all persons identified as a sexual contact
• if PID or HSV is clinically suspected; see PID DST or HSV DST
MANAGEMENT AND INTERVENTIONS
Goals of Treatment
• treat infection
• prevent complications
• prevent the spread of infection
DST-1007 Mucopurulent Cervicitis (MPC)
262
Certified Practice Area:
Reproductive Health: Sexually Transmitted Infections
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
TREATMENT OF CHOICE
Treatment Notes
First Choice General:
1. Treatment covers both gonorrhea and chlamydia.
2. Future GC Treatment regimens will continue to reflect national recommendations in
association with local GC antimicrobial resistance trends (AMR) trends.
3. Retreatment is indicated if the client has missed 2 consecutive doses of doxycycline
or has not completed a full 5 days of treatment.
4. Consult physician or NP if client is unable to use cefixime, ceftriaxone, or
azithromycin.
5. See BCCDC STI Medication Handouts for further medication reconciliation and client
information.
6. See Monitoring and Follow-up section for test-of-cure (TOC) requirements.
Allergy and Administration:
7. DO NOT USE ceftriaxone or cefixime if history of allergy or anaphylaxis to
cephalosporins. Consult with or refer to a physician or NP if history of anaphylaxis or
immediate reaction to penicillins.
8. DO NOT USE azithromycin if history of allergy to macrolides.
9. DO NOT USE doxycycline if pregnant and/or allergic to doxycycline or other
tetracyclines.
10. If an azithromycin or doxycycline allergy or contraindication exists, consult with or
refer to a physician or NP for alternate treatment.
11. Azithromycin and doxycycline are sometimes associated with gastrointestinal
adverse effects. Taking medication with food and plenty of water may minimize
adverse effects.
12. The preferred diluent for ceftriaxone IM is 0.9 mls lidocaine 1% (without
epinephrine) to minimize discomfort.
13. DO NOT USE lidocaine if history of allergy to lidocaine or other local anesthetics.
Use cefixime PO as alternate treatment.
14. For IM injections of ceftriaxone the ventrogluteal site is preferred.
15. Advise the client to remain in the clinic for at least 15 minutes-post IM injection in
case of anaphylactic reaction to treatment. Provide anaphylaxis treatment as
required, using BCCDC CDC Manual- Chapter 2: Immunization – Part 3:
Management of Anaphylaxis in a Non-Hospital Setting, November 2016.
16. If serious allergic reaction develops including difficulty breathing, severe itchiness,
have the client inform clinic staff immediately. If symptoms develop after leaving
the clinic, advise the client to seek immediate emergency care.
17. Advise client they may experience pain redness and swelling at the injection site. If
any of these effects persist or worsen advise to contact health care provider.
cefixime 800 mg PO in a single dose
and
azithromycin 1 gm PO in a single dose
OR
ceftriaxone 250 mg IM in a single dose
and
azithromycin 1 gm PO in a single dose
Second Choice
cefixime 800 mg PO in a single dose
and
doxycycline 100 mg PO BID for 7 days
OR
ceftriaxone 250 mg IM in a single dose
and
doxycycline 100 mg PO BID for 7 days
Third Choice
azithromycin 2 gm PO in a single dose
DST-1007 Mucopurulent Cervicitis (MPC)
263
Certified Practice Area:
Reproductive Health: Sexually Transmitted Infections
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
Treatment Notes
18. Recent data has emerged regarding azithromycin and QT prolongation. Although
rare, it is more significant in older populations, those with pre-existing heart
conditions, arrhythmias or electrolyte disturbances.
It is unclear how significant these findings are in young to mid-age healthy adults
consuming a one-time dose of azithromycin; however, please use the following
precautions:
Consult with or refer to an NP or physician if the client:
o has a history of congenital or documented QT prolongation.
o has a history of electrolyte disturbance in particular hypokalemia,
hypomagnesaemia.
o has clinically relevant bradycardia, cardiac arrhythmia or cardiac insufficiency.
o is on any of the following medications:
a) Antipsychotics: pimozide (Orap®), ziprasidone (Zeldox®)
b) Cardiac: dronedarone (Multaq®)
c) Migraine: dihydroergotamine (Migranal®), ergotamine (Cafergot®)
PREGNANT OR BREAST-/CHEST-FEEDING CLIENTS
For all pregnant or breast-/chest-feeding clients, consult with or refer to a physician or NP.
PARTNER COUNSELLING AND REFERRAL
Counsel clients to notify people who may have been exposed through sexual contact within the previous 60 days that they require
testing and treatment to cover chlamydia and gonorrhea. If no sexual contact in the past 60 days then the client may notify their last sexual contact regarding testing and treatment (see Treatment of STI Contacts DST).
MONITORING AND FOLLOW-UP
Follow-up is based on test results or recurrence of symptoms. If test results positive for STI, refer to appropriate STI DST for monitoring and follow-up.
POTENTIAL COMPLICATIONS
• pelvic inflammatory disease (PID)
• infertility
• ectopic pregnancy
• chronic pelvic pain
• sexually-acquired reactive arthritis
• disseminated gonococcal infection (DGI)
CLIENT EDUCATION
Counsel client regarding:
• abstaining from sexual activity during the 7-day course of treatment or for 7 days post-single-dose therapy for clients and
their contacts.
• informing last sexual contact AND any sexual contacts within the last 60 days that they require testing and treatment.
DST-1007 Mucopurulent Cervicitis (MPC)

264
Certified Practice Area:
Reproductive Health: Sexually Transmitted Infections
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
• the appropriate use of medications (dosage, side effects, and need for re-treatment if dosage not completed, or symptoms
do not resolve).
• harm reduction (condom use significantly reduces the risk of transmission).
• cleaning sex toys between use and using condoms if sharing sex toys
• the benefits of routine STI screening.
• the potential complications of untreated cervicitis.
• co-infection risk for HIV when another STI is present.
• the asymptomatic nature of STI.
• the importance of revisiting a health care provider if symptoms persist.
CONSULTATION AND/OR REFERRAL
Consult with or refer to a physician or NP in the following situations; when:
• assessment indicates PID
• HSV infection is suspected
• syphilis infection is suspected
• client is pregnant and/or breast-/chest-feeding
• recurrent MPC is suspected
• symptoms persist following MPC treatment completion
DOCUMENTATION
• MPC is not reportable
• as per agency policy
DST-1007 Mucopurulent Cervicitis (MPC)
265
Certified Practice Area:
Reproductive Health: Sexually Transmitted Infections
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
REFERENCES
More recent editions of any of the items in the reference list may have been published since this DST was published. If you have a newer version, please use it.
Atashili, J., Poole, C., Ndumbe, P.M., Adimora, A.A. & Smith, J.S. (2008). Bacterial vaginosis and HIV acquisition: A mete-analysis of published studies. AIDS, 22(12), pp.1493-1501.
Australasian Sexual Heatlh Alliance (ASHA). (2016). Cervicitis. In: Australian STI Management Guidelines for Use in Primary Care [Internet].
British Columbia Centre for Disease Control (BCCDC). (2014). British Columbia treatment guidelines. Sexually transmitted infections in adolescent and adults. Clinical Prevention Services, BCCDC.
BCCDC. (2009). Communicable Disease Manual: Chapter 2: Immunization Program. Vancouver: BCCDC.
BCCDC. (2013). Vaccine administration. BCCDC.
BCCDC Public Health Laboratory (BCCDC PHL). (2016). Laboratory trends. Vancouver, BC.
Centre of Excellence for Transgender Health (CoE). (2016). Guidelines for the primary and gender-affirming care of transgender and gender nonbinary people.
Centers for Disease Control (CDC). (2015). Diseases characterized by urethritis and cervicitis. In: 2015 Sexually Transmitted Diseases Treatment Guidelines [Internet]. Atlanta, GA.
Holmes, K., Sparling, P., Stamm, W., Piot, P., Wasserheit, J., Corey, L., Cohen, M., & Watts, H. (2008). Sexually transmitted diseases (4th ed). Toronto, ON: McGraw Hill Medical.
Marrazzo, J.M., & Martin, D.H. (2007). Management of women with cervicitis. Clinical Infectious Diseases, 44, pp.S102-S110.
Marrazzo, J., Wiesenfeld, H., Murray, P., Busse, B., Meyn, L., Krohn, M. & Hillier, S. (2006). Risk factors for cervicitis among women with bacterial vaginosis. The Journal of Infectious Diseases, 193(5), pp.617-624.
Marrazzo, J. (2005). Mucopurulent cervicitis: no longer ignored, but still misunderstood. Infectious Disease Clinics of North America, 19(2), p.333.
Pattman, R., Snow, M., Handy, P., Sankar, K.N. & Elawad, B. (2005). Oxford Handbook of Genitourinary Medicine, HIV, and AIDS, 1st Edition, Copyright (c) 2005 Oxford University Press.
Public Health Agency of Canada (PHAC). (2014). Supplementary statement for the recommendations related to the diagnosis, management, and follow-up of vaginal discharge. In: Canadian Guidelines on Sexually Transmitted Infections [Internet].
PHAC. (2017). 2016 Updates Summary. In: Canadian guidelines on sexually transmitted infections.
Taylor, S., Lensing, S., Schwebke, J., Lillis, R., Mena, L., Nelson, A. & Lee, J. (2013). Prevalence and treatment outcome of cervicitis of unknown etiology. Sexually Transmitted Diseases, 40(5), pp.379-385.
DST-1007 Mucopurulent Cervicitis (MPC)
266
Certified Practice Area:
Reproductive Health: Sexually Transmitted Infections
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
DST-1008 Gonorrhea (Reportable)
DEFINITION
Bacterial infection caused by the transmission of Neisseria gonorrhoeae (N. gonorrhoeae or GC) during sexual contact in which body fluids are exchanged.
CAUSE
Bacterial: Neisseria gonorrhoeae
PREDISPOSING RISK FACTORS
• sexual contact where there is transmission through the exchange of body fluids
TYPICAL FINDINGS
Sexual Health History
• sexual contact with at least one partner
• may be asymptomatic
• sexual contact with someone with confirmed positive laboratory test for STI
• short incubation period (e.g., urethritis and discharge may develop within one week of sexual contact)
Physical Assessment
GC infection can be asymptomatic in all sites; however, urethral GC infections are often symptomatic, while pharyngeal, vaginal and rectal infections are often asymptomatic.
• inflammation of the tissues around the eye including: acute redness, purulent discharge and crusting (symptoms of
conjunctivitis); can be caused from gonococcal infection in the eye; consult with or refer to physician or nurse practitioner
(NP) for symptoms of conjunctivitis
• sore throat (throat infection is most often asymptomatic)
• urethral symptoms such as, discharge (usually purulent, may be copious), itch or awareness
• painful (dysuria) or difficult urination
• testicular pain and/or swelling (symptoms of epididymitis)
• abnormal change in vaginal discharge
• abnormal vaginal bleeding:
o vagina with or without cervix: after intercourse or between menstrual period
o vagina after vaginoplasty: abnormal vaginal bleeding is not always STI-related as longer post-operative symptoms of
bleeding could be indicative of hypergranulation; refer to the STI Assessment DST for more information, and especially
for clients experiencing pain, discharge, or bleeding in the first 3 to 4 month post-operative period
• lower abdominal pain (symptom of pelvic inflammatory disease)
• dyspareunia
• inflammation of the rectum, rectal pain and anal discharge (symptoms of proctitis)
DIAGNOSTIC TESTS
Full STI screening is recommended. See the STI Assessment DST.
GC C&S is indicated for all clients who are symptomatic and/or are a contact to gonorrhea.
• Throat:
o for clients who are symptomatic and/or are a contact to GC, collect:
DST-1008 Gonorrhea (Reportable)
267
Certified Practice Area:
Reproductive Health: Sexually Transmitted Infections
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
▪ GC culture & sensitivity (C&S) swab
▪ GC NAAT swab
o for asymptomatic clients who require screening only, collect:
▪ GC NAAT swab, if indicated in sexual health history
• Penile urethra (with or without phalloplasty or metoidioplasty with urethral lengthening):
o for clients who are symptomatic with urethral discharge and/or are a contact to GC, collect specimen from visible
discharge at the meatus - insertion into the urethra is not required:
▪ GC C&S swab
▪ smear for typical intracellular diploccoci (TID) and polymorphonuclear leukocytes (PMNs) (collect only if immediate
microscopy is available)
▪ GC NAAT urine. Ideally the client should not have voided in the previous 1-2 hours; collect first void 10-20 ml
• Vagina:
o With cervix:
▪ asymptomatic – GC NAAT vaginal (preferred) or cervical swab
▪ symptomatic or contact to GC – a full pelvic examination is recommended to collect GC C&S cervical (preferred) or
vaginal swab (when unable to perform pelvic exam) and GC NAAT vaginal (preferred) or cervical swab
o After total hysterectomy (no cervix):
▪ asymptomatic – GC NAAT urine (preferred) or vaginal swab
▪ symptomatic or contact to GC – GC C&S vaginal swab and GC NAAT urine specimen (preferred) or vaginal swab
o After vaginoplasty: GC NAAT urine. Ideally the client should not have voided in the previous 1-2 hours; collect first
void 10-20 ml
▪ asymptomatic/symptomatic-GC NAAT urine
• Rectum:
o for clients who are symptomatic and/or are a contact to GC, collect:
▪ GC C&S swab
▪ GC NAAT swab
o for asymptomatic clients who require screening only, collect:
▪ GC NAAT swab, if indicated in sexual health history
Notes:
7. If urethral swabs are indicated (e.g., for symptomatic clients), the urine specimen is collected after the urethral swab.
8. GC NAAT urine specimens may be collected as the only diagnostic test in agencies or circumstances where:
o GC C&S is unavailable, and the client is symptomatic
o client is asymptomatic
o if client declines recommended testing of cervical or vaginal sites
9. In general, self-collected vaginal swabs are indicated when a full or partial pelvic examination is not required or appropriate. Clinician-collected vaginal swabs are generally done when a partial or full pelvic examination is required or
requested by the client.
10. Recent data show that NAAT vaginal swabs for C. trachomatis and N. gonorrhoeae identify as many or more infections over
cervical, urethral, or urine specimens.
DST-1008 Gonorrhea (Reportable)

268
Certified Practice Area:
Reproductive Health: Sexually Transmitted Infections
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
• NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
CLINICAL EVALUATION/CLINICAL JUDGMENT
Treat all clients with confirmed gonorrhea by positive laboratory result.
If providing treatment for a client with confirmed positive cervical, vaginal or urine laboratory test for Neisseria gonorrhoeae; assess for signs of pelvic inflammatory disease (PID) through symptoms inquiry and/or physical assessment (bimanual exam), if indicated.
Treat all persons identified as a sexual contact within the past 60 days to a confirmed gonorrhea or case. If there are no sexual contacts in the previous 60 days, then follow-up should occur for the last sexual contact.
MANAGEMENT AND INTERVENTIONS
Goals of Treatment
• treat infection
• prevent complications
• prevent the spread of infection
DST-1008 Gonorrhea (Reportable)

269
Certified Practice Area:
Reproductive Health: Sexually Transmitted Infections DST-1008 Gonorrhea (Reportable)
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
a) NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
TREATMENT OF CHOICE
Treatment Notes
First Choice General:
1. Treatment covers both gonorrhea and chlamydia.
2. Canadian Guidelines for STI (CGSTI, PHAC, 2013) recommend ceftriaxone IM and azithromycin PO for the treatment of
uncomplicated anogenital and pharyngeal infection; however, BC surveillance patterns of GC resistance suggest that both
cefixime and ceftriaxone are appropriate choices for the treatment of GC.
3. Future GC Treatment regimens will continue to reflect national recommendations in association with local GC antimicrobial
resistance trends (AMR) trends.
4. Retreatment is indicated if the client has missed 2 consecutive doses of doxycycline or has not completed a full 5 days of
treatment.
5. Consult a physician or NP if client is unable to use cefixime, ceftriaxone, or azithromycin.
6. See BCCDC STI Medication Handouts for further medication reconciliation and client information.
7. See Monitoring and Follow-up section for test-of-cure (TOC) requirements.
Allergy and Administration:
8. DO NOT USE ceftriaxone or cefixime if history of allergy or anaphylaxis to cephalosporins. Consult with or refer to a physician or
NP if history of anaphylaxis or immediate reaction to penicillins.
9. DO NOT USE azithromycin if history of allergy to macrolides.
10. DO NOT USE doxycycline if pregnant and/or allergic to doxycycline or other tetracyclines.
11. If an azithromycin or doxycycline allergy or contraindication exists, consult with or refer to a physician or NP for alternate
treatment.
12. Azithromycin and doxycycline are sometimes associated with gastrointestinal adverse effects. Taking medication with food and
plenty of water may minimize adverse effects.
13. The preferred diluent for ceftriaxone IM is 0.9 mls lidocaine 1%
14. DO NOT USE lidocaine if history of allergy to lidocaine or other local anesthetics. Use cefixime PO as alternate treatment.
cefixime 800 mg PO in a single dose
and
azithromycin 1 gm PO in a single dose
OR
ceftriaxone 250 mg IM in a single dose
and
azithromycin 1 gm PO in a single dose
Second Choice
cefixime 800 mg PO in a single dose
and
doxycycline 100 mg PO BID for 7 days
OR
ceftriaxone 250 mg IM in a single dose
and
doxycycline 100 mg PO BID for 7 days
Third Choice
azithromycin 2 gm PO in a single dose

270
Certified Practice Area:
Reproductive Health: Sexually Transmitted Infections DST-1008 Gonorrhea (Reportable)
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
a) NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
Treatment Notes
15. For IM injections of ceftriaxone the ventrogluteal site is preferred.
16. Advise the client to remain in the clinic for at least 15 minutes-post IM injection in case of anaphylactic reaction to treatment.
Provide anaphylaxis treatment as required, using BCCDC CDC Manual- Chapter 2: Immunization – Part 3: Management of
Anaphylaxis in a Non-Hospital Setting, November 2016.
17. If serious allergic reaction develops including difficulty breathing and/or severe itchiness, have the client inform clinic staff
immediately. If symptoms develop after leaving the clinic, advise the client to seek immediate emergency care.
18. Advise client they may experience pain redness and swelling at the injection site. If any of these effects persist or worsen advise
to contact health care provider.
19. Recent data has emerged regarding azithromycin and QT prolongation. Although rare, it is more significant in older populations,
those with pre-existing heart conditions, arrhythmias or electrolyte disturbances.
It is unclear how significant these findings are in young to mid-age healthy adults consuming a one-time dose of
azithromycin; however, please use the following precautions:
Consult with or refer to an NP or physician if the client:
o has a history of congenital or documented QT prolongation.
o has a history of electrolyte disturbance in particular hypokalemia, hypomagnesaemia.
o has clinically relevant bradycardia, cardiac arrhythmia or cardiac insufficiency.
o is on any of the following medications:
▪ Antipsychotics: pimozide (Orap®), ziprasidone (Zeldox®)
▪ Cardiac: dronedarone (Multaq®)
▪ Migraine: dihydroergotamine (Migranal®), ergotamine (Cafergot®)
271
Certified Practice Area:
Reproductive Health: Sexually Transmitted Infections
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
PREGNANT OR BREAST-/CHEST-FEEDING CLIENTS
For all pregnant or breast-/chest-feeding clients, consult with or refer to a physician or NP. Test-of-cure (TOC) is recommended for pregnant and/or breast-/chest-feeding clients and should be performed at 3-4 weeks after completion of treatment.
PARTNER COUNSELLING AND REFERRAL
People who have confirmed laboratory tests positive for Neisseria gonorrhoeae are offered partner counselling and referral to identify all the people who may have been exposed through sexual contact in the previous 60 days. If no sexual partner in the previous 60 days then follow up should occur for the last sexual contact (see Treatment of STI Contacts DST).
MONITORING AND FOLLOW-UP
Repeat testing at 6 months is recommended due to potential high risk of re-infection.
Perform TOC in the following situations:
• if symptoms persist
• for all pregnant and/or breast-/chest-feeding clients
• for all pharyngeal infections
• if treatment was other than the recommended first choice
• for clients who received antibiotics linked to a case who had treatment failure or demonstrated resistance to the same
antibiotic
TOC using GC culture (C&S) should be performed a minimum 3-7 days post-treatment completion. TOC using GC NAAT (if culture is not available), should be performed 3-4 weeks post-treatment completion.
POTENTIAL COMPLICATIONS
• epididymitis
• infertility
• sexually-acquired reactive arthritis
• disseminated gonococcal infection (DGI)
• pelvic inflammatory disease (PID)
• ectopic pregnancy
• chronic pelvic pain
CLIENT EDUCATION
Counsel client regarding:
• abstaining from sexual activity during the 7-day course of treatment or for 7 days post-single-dose therapy for clients and
their contacts.
• informing last sexual contact AND any sexual contacts within the last 60 days that they require testing and treatment.
• methods of partner notification.
• the appropriate use of medications (dosage, side effects, and need for re-treatment if dosage not completed, or symptoms
do not resolve).
• harm reduction (condom use significantly reduces the risk of transmission).
• cleaning sex toys between use and using condoms if sharing sex toys
• the benefits of routine STI screening.
• the potential complications from untreated gonorrhea.
• co-infection risk for HIV when another STI is present.
DST-1008 Gonorrhea (Reportable)
272
Certified Practice Area:
Reproductive Health: Sexually Transmitted Infections
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
• the asymptomatic nature of STI.
• repeating STI screening which includes testing for Neisseria gonorrhoeae in 6 months’ time as re-infection rate is high.
• the importance of revisiting a health care provider if symptoms persist.
CONSULTATION AND/OR REFERRAL
Consult with or refer to a physician or NP for all clients who are pregnant or breast-/chest-feeding. Consult with or refer to physician or NP for allergy/contraindications to treatment outlined in this DST.
DOCUMENTATION
• Neisseria gonorrhoeae is reportable
• complete H208 form as per reporting procedures
• as per agency policy
DST-1008 Gonorrhea (Reportable)
273
Certified Practice Area:
Reproductive Health: Sexually Transmitted Infections
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
REFERENCES
More recent editions of any of the items in the reference list may have been published since this DST was published. If you have a newer version, please use it.
Barbee, L.A., Kerani, R.P., Dombrowski, J.C., Soge, O.O. & Golden, M.R. (2013). A retrospective comparative study of 2-drug oral and intramuscular cephalosporin treatment regimens for pharyngeal gonorrhea. Clinical Infectious Diseases, 56(11), pp.1539 1545.
British Columbia Centre for Disease Control (BCCDC). (2014). British Columbia treatment guidelines: Sexually transmitted infections in adolescent and adults. STI/HIV Prevention and Control Division, BCCDC.
BCCDC. (2009). BCCDC Communicable disease manual Chapter 2: Immunization program. Vancouver: BCCDC.
BCCDC. (2013). BCCDC’s videos on injection landmarking and technique.
BCCDC Public Health Laboratory (BCCDC PHL). (2016). Laboratory trends. Vancouver, BC.
Centers for Disease Control and Prevention (CDC). (2015). Sexually transmitted diseases treatment guidelines. Atlanta, GA.
Hottes, T.S., Lester, R.T., Hoang, L., McKay, R., Gilbert, M., Patrick, D.M., Wong, T. Martin, R. & Ogilvie, G. (2013).
Cephalosporin and azithromycin susceptibility in Neissieria gonorrheoeae isolates by site of infection, British Columbia, 2006 to 2011. Sexually Transmitted Diseases, 40(1), pp.46-51.
Lunny, C., Taylor, D., Hoang, L., Wong, T., Gilbert, M., Lester, R. & Greub, G. (2014). Self-collected versus clinician-collected sampling for chlamydia and gonorrhoea screening: A systemic review and meta-analysis. PLoS ONE, 10(7), pp.1-23.
Papp, J. et al. (2014). Recommendations for the laboratory-based detection of Chlamydia trachomatis and Neisseria gonorrhoeae. Morbidity and Mortality Weekly Report, 63(1).
Pattman, R., Snow, M., Handy, P., Sankar, K.N. & Elawad, B. (2005). Oxford Handbook of Genitourinary Medicine, HIV, and AIDS, 1st Edition, Copyright (c) 2005 Oxford University Press.
Public Health Agency of Canada (PHAC). (2013). Gonococcal infections. In: Canadian guidelines on sexually transmitted infections.
PHAC. (2017). 2016 Updates Summary. In: Canadian guidelines on sexually transmitted infections.
PHAC. (2017). Treatment of N. gonorrhoeae in response to the discontinuation of spectinomycin: Alternative treatment guidance statement. In: Canadian guidelines on sexually transmitted infections.
Shafer, M., Moncada, J., Boyer, C.B., Betsinger, K., Flinn, S.D. & Schachter, J. (2003). Comparing first-void urine specimens,
self-collected vaginal swabs, and endocervical specimens to detect Chlamydia trachomatis and Neisseria gonorrheoeae by a nucleic acid amplification test. Journal of Clinical Microbiology, 41(9), pp 4395-4399.
Schacter, J., Moncada, J., Liska, S., Shayevich, C. & Klausner, J.D. (2008). Nucleic acid amplification tests in the diagnosis of
chlamydial and gonococcal infections of the oropharynx and rectum in men who have sex with men. Sexually Transmitted Diseases, 35(7), pp.637-642.
Stewart, C.M., Shoeman, S.A., Booth, A.R., Smith, S.D., Wilcox, M.H. & Wilson, J.D. (2012). Assessment of self-taken swabs versus clinician taken swab cultures for diagnosing gonorrhoea in women: single centre, diagnostic accuracy study. BMJ, 34, e8107.
DST-1008 Gonorrhea (Reportable)
274
Certified Practice Area:
Reproductive Health: Sexually Transmitted Infections
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
DST-1009 Genital Warts
DEFINITION
Genitals warts refer to skin or mucosal infection caused by the genotypes of human papillomavirus (HPV). HPV is readily transmissible and one of the most common STIs worldwide. The estimated lifetime likelihood of HPV infection is upwards of 75%.
There are over 40 types of HPV known to reside in the anogenital tract, oral cavity and oropharynx. Persistent infection with one or
more of the high-risk HPV types (e.g., HPV-16, -18) may lead to precancerous or cancerous lesions of the cervix, vulva, vagina, penis, anus, oral cavity, oropharynx and larynx. Infection with low risk HPV types (e.g., HPV-6, -11) is associated with low or no
cancer risk, rather can lead to anogenital warts or other benign lesions (e.g., low-grade squamous intraepithelial lesion [LSIL] of the cervix or anal canal).
CAUSE
Viral: human papillomavirus (HPV)
PREDISPOSING RISK FACTORS
• sexual contact where there is transmission through skin-to-skin with an individual who has HPV infection
• immunosuppression (e.g., HIV infection, organ transplant and immunosuppressive drug therapy)
TYPICAL FINDINGS
Sexual Health History
• change in the affected area from “normal” to a wart-like or bumpy appearance
• sexual contact with at least one partner
• may report either current or past partner as having HPV infection presently or in the past, though often there is no
reported/known history
• may describe bumps that are painless
• may report itching/irritation to affected area (particularly when perianal warts are present)
Physical Assessment
• usually painless
• may cause bleeding and pruritus (perianal)
• may appear on the genitals and perineum in clusters or as single bumps as:
o flat
o cauliflower-like
o flesh-coloured
o darker in colour than surrounding skin
Note: Most anogenital HPV infections are asymptomatic and/or subclinical.
DIAGNOSTIC TESTS
Full STI screening is recommended upon initial assessment for genital warts to rule-out other STI presentations such as syphilis (e.g., condylomata lata looks very similar to genital warts).
• diagnosis is confirmed through clinical findings from visual inspection
• routine diagnostic testing for genital HPV is not currently available
• routine Pap testing as per British Columbia Cancer Agency’s Screening for Cancer of the Cervix guidelines
o the presence of genital warts is not an indication for a change in routine Pap screening recommendations
DST-1009 Genital Warts
275
Certified Practice Area:
Reproductive Health: Sexually Transmitted Infections
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
CLINICAL EVALUATION/CLINICAL JUDGMENT
• when clinical findings of HPV are evident, review all treatment options with client
• treatment of internal warts (e.g., intravaginal, cervical, and rectal) requires referral to a physician or NP
MANAGEMENT AND INTERVENTIONS
Goals of Treatment
• mainly aesthetic, to remove visible warts
• reduce the spread of infection
TREATMENT OF CHOICE
Review anogenital wart treatment options with the client, including benefits and risks of each. The treatment of anogenital warts
are carried out by RN(C)s according to the BCCNP Standard for Acting Within Autonomous Practice. For use of alternate cryotherapeutic agents, follow agency-specific guidelines and policies.
The treatment options are:
• defer treatment and monitor – many genital warts will resolve spontaneously
• client-applied: These options can be expensive. Consultation and/or referral to a physician or NP is required to obtain a
prescription for:
o imiquimod 5% or 3.75% cream
o podofilox 0.5% solution
o sinecatechins 10% ointment
• provider-applied:
o First Choice: Cryotherapy with liquid nitrogen (preferred) or alternate cryotherapy regimens approved for the
treatment of genital warts (e.g., dimethyl ether propane (Histofreezer®, see package insert for treatment details)
o Alternate Treatment:
o podophyllin 10% tincture or 25% resin
o trichloracetic acid (TCA)
First Choice: Cryotherapy with liquid nitrogen
Note: Over-the-counter (OTC) cryotherapeutic remedies for wart treatment are not recommended for the treatment of genital warts. Clinical diagnosis is required prior to treatment recommendation.
Method of Use
11. Apply using spray canister. Adjust lighting and use magnification as needed.
12. Stretch the area to be sprayed. Hold the spray nozzle approximately 1 cm away from the skin. Distance may vary slightly
dependent on amount of freezing required.
13. Spray intermittently to create and maintain a whitish frozen area involving the wart, with a halo of 1-2 mm around the
wart. Freezing should be maintained for 5-10 seconds post-application.
14. Allow for the skin to thaw. This occurs when the frozen whitish area returns to normal colour (may be slightly reddened).
15. Repeat steps 2 to 4 for 2-3 treatment cycles total for each wart.
16. Treatment is repeated every 7 to 14 days for 6 to 8 treatment visits. Ensure previously treated areas are completely healed
prior to subsequent treatment.
17. If warts have not resolved by the 8th treatment session, consult/refer with a physician or NP to determine next steps.
Alternate Treatments
• Podophyllin 10% or 25%
DST-1009 Genital Warts
276
Certified Practice Area:
Reproductive Health: Sexually Transmitted Infections
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
For use only in the absence of other treatment options given concerns about local and systemic safety, and low efficacy.
DO NOT USE podophyllin:
o in pregnancy
o for the treatment of any internal warts – cervical, meatal, vaginal, or anal. Podophyllin may be used around, but not in
the meatus, around the introitus, but not in the vagina or on the cervix, and around, but not in the anus
o on open sores or excoriated skin
o on clients who have diabetes
Method of Use
1. Measure out 0.5 ml podophyllin using syringe/needle.
2. Dab podophyllin on warts with cotton swab – limit the area of application to < 5cm². The dose per visit is should not
exceed 1.0 mL.
3. Allow the area to fully dry prior to the client dressing after treatment.
4. Remind the client to wash off the first application (first-time treatment) in 1 hour; and if there is no adverse reaction then
wash off subsequent applications in 4-6 hours.
5. Podophyllin application may be repeated at seven-day (weekly) intervals for up to 6 treatment sessions.
6. If warts have not resolved after 6 treatment sessions, consult/refer with a physician or NP to determine next steps.
Notes:
1. Side effects of treatment may include mild to moderate local skin reactions which may include discomfort, tenderness, stinging or pain at the site. Blistering, erythema and itching may also occur. Reactions are managed by decreasing the
intensity of future treatments.
2. If there is no improvement in the warts after 3 provider-applied treatment sessions, consider adding additional treatment
options (e.g., cryotherapy first, then apply podophyllin).
Trichloracetic acid (TCA)
DO NOT USE TCA:
o for the treatment of any internal warts – cervical, meatal, vaginal, or anal
o on open sores or excoriated skin
Method of Use
1. Measure out small amount using syringe/needle.
2. Apply petroleum jelly or 2% xylocaine ointment to the surrounding area to protect healthy skin.
3. Use a cotton swab to dab the acid preparation on. Apply sparingly.
4. Allow area to dry until a “white frosting” appearance is noted. Do not need to wash off.
5. Can be used weekly for up to 6-8 weeks.
Notes:
1. TCA is a highly caustic solution that can cause blistering and ulcerations if used in excess. The viscosity is lower than water
and can spread very quickly.
2. If painful, soap or sodium bicarbonate can be used to neutralize the area. Powder the area with talc or sodium bicarbonate
or apply soap to any un-reacted acid.
DST-1009 Genital Warts

277
Certified Practice Area:
Reproductive Health: Sexually Transmitted Infections
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
PREGNANT OR BREAST/CHEST-FEEDING CLIENTS
For all pregnant or breast-/chest-feeding clients consult with or refer to a physician or NP. Podophyllin is contraindicated in pregnancy.
PARTNER COUNSELLING AND REFERRAL
Counsel clients to recommend their sexual partners have an examination for genital warts.
MONITORING AND FOLLOW-UP
Refer to specific treatment section in this DST for monitoring and follow-up recommendations.
POTENTIAL COMPLICATIONS
• pre-cancerous or cancerous lesions from co-infection with specific HPV subtypes
• overgrowth of external warts in immunocompromised individuals
• perinatal transmission (rare)
• recurrent episodes of growth after treatment
CLIENT EDUCATION
Counsel client regarding:
• genital warts are common and the likelihood of genital infection with HPV, over the lifespan, is upwards of 75%.
• routine Pap testing is recommended, and clinical findings of genital warts is not an indication for a change in the frequency of
Pap testing.
• eligibility for a HPV vaccine which can protect against some strains of HPV.
• external visible warts are generally not associated with cancers of the cervix, anus, or genitals, as they are considered low-
risk and are usually benign.
• warts often resolve on their own within 18-24 months even without treatment.
• that while most genital HPV infections resolve, whether or not HPV infection itself completely clears after visible warts have
resolved, is unknown. Diagnostic testing to determine clearance is neither recommended nor routinely available.
• treatment is mainly aesthetic to remove visible warts; a small risk of recurrence remains.
• genital warts are sexually transmitted through skin–to-skin contact (condoms are helpful in reducing transmission when they
cover the area of skin that is affected by HPV).
• HPV is transmissible – though likely to a lesser degree – even when visible warts are not present on the skin.
• Re-infection with the same strain is possible.
• if they are HIV positive, to follow-up with their HIV health care provider for potential further follow-up and/or screening (e.g.,
anal Paps).
• that it is possible and very common to have more than one strain of HPV.
• the fact that most people are asymptomatic and that partners who are both infected with HPV can have different clinical
manifestations (e.g., one person may be asymptomatic while the other may experience visible affects such as warts).
• the side effects of treatment may include: mild to moderate local skin reactions which may include discomfort, tenderness,
stinging or pain at the site. Blistering, erythema, itching and changes to skin pigmentation may also occur. Reactions are
managed by decreasing the intensity of future treatments.
• avoiding irritants to the area, including shaving, which can promote the warts spreading.
DST-1009 Genital Warts
278
Certified Practice Area:
Reproductive Health: Sexually Transmitted Infections
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
CONSULTATION AND/OR REFERRAL
Consult with or refer to a physician or NP in the following situations; clients who:
• have reached maximum treatment duration, administered as recommended without resolution of symptoms.
• are pregnant and/or breast-/chest-feeding.
• have warts that are atypical in appearance, are larger than 1-2 cm or have suspicious pigmentation.
• have internal genital warts (anal, vaginal, or urethral).
• have an unusual, unexpected or severe reaction to genital wart treatment.
• are unable to tolerate cryotherapy or other provider-applied treatment and require a prescription for client-applied treatment.
• have diabetes and opting for or require topical podophyllin treatment.
DOCUMENTATION
• HPV is not reportable
• as per agency policy
DST-1009 Genital Warts
279
Certified Practice Area:
Reproductive Health: Sexually Transmitted Infections
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
REFERENCES
More recent editions of any of the items in the reference list may have been published since this DST was published. If you have a newer version, please use it.
Baumann, L.S. (2016). Update on green tea. Dermatology News, 47, p.26.
British Association for Sexual Health and HIV (BASHH). (2015). UK National guidelines on the management of anogenital warts. pp.1-24.
British Columbia College of Nursing Professionals (BCCNP). (2018). Scope of Practice for Registered Nurses: Standards, Limits and Conditions.
Brunk, D. (2016). Expert shares treatment tips for molluscum contagiosum and warts. Pediatric News, 50, p.S12+.
Centers for Disease Control and Prevention (CDC). (2013). Human papillomavirus (HPV) and oropharyngeal cancer.
CDC. (2015). Anogenital warts. In 2015 Sexually Transmitted Diseases Treatment Guidelines.
CDC. (2015). HPV-associated cancers and precancers. In 2015 Sexually Transmitted Diseases Treatment Guidelines.
CDC. (2015). Human papillomavirus (HPV) infection. In 2015 Sexually Transmitted Diseases Treatment Guidelines.
Cervical Cancer Screening Program & BC Cancer Agency. (2017). Screening for cancer of the cervix: An office manual for health care providers.
Denny, L. (2016). Epidemiology and burden of disease associated with HPV infection. Current Obstetrics and Gynecology Reports, 5(3), pp.189-195. doi: 10.1007/s13669-016-0174-y.
Gravitt, P.E. (2011). The known unknowns of HPV natural history. Journal of Clinical Investigation, 121(12), pp.4593-4599. doi: 10.1172/JCI57149.
Hutter, J. & Decker, C. (2016). Human papillomavirus infection. Disease-a-Month, 62, pp.294-300. doi: 10.1016/j.disamonth.2016.03.014.
Park, I., Introcaso, C. & Dunne, E. (2015). Human papillomavirus and genital warts: a review of the evidence for the 2015
Centers for Disease Control and Prevention sexually transmitted diseases treatment guidelines. Clinical Infectious Diseases, 61(suppl 8), pp.S849-S855. doi: 10.1093/cid/civ813.
Passmore, J. & Williamson, A. (2016). Host immune responses associated with clearance or persistence of human papillomavirus infections. Current Obstetrics and Gynecology Reports, 5(3), pp.177-188. doi: 10.1007/s13669-016-0163-1.
Petrosky, E., Bocchini Jr., J.A., Hariri, S., Chesson, H., Curtis, C.R., Saraiya, M. & Markowitz, L.E. (2015). Use of 9-valent human papillomavirus (HPV) vaccine: Updated HPV: vaccination recommendations of the advisory committee on immunization practices. Morbidity and Mortality Weekly Report, 64(11), p.300.
Public Health Agency of Canada (PHAC). (2014). Human papillomavirus (HPV) infections. In: Canadian Guidelines on Sexually Transmitted Infections. Ottawa, ON.
Seyferth, E., Bratic, J. & Bocchini Jr., J. (2016). Human papillomavirus epidemiology and vaccine recommendations: selected review of the recent literature. Current Opinion in Pediatrics, 28(3), pp.400-406. doi: 10.1097/MOP.0000000000000354.
Stanley, M. (2016). Preventing cervical cancer and genital warts - How much protection is enough for HPV vaccines? Journal of Infection, 72, pp.S23-S28. doi: 10.1016/j.jinf.2016.04.018.
DST-1009 Genital Warts
280
Certified Practice Area:
Reproductive Health: Sexually Transmitted Infections
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
Taylor, S., Bunge, E., Bakker, M. & Castellsague, X. (2016). The incidence, clearance and persistence of non-cervical human papillomavirus infections: a systematic review of the literature. BMC Infectious Diseases, 16(293), pp.1-21. doi: 10.1153/s12879-016-1633-9.
Yang, L., Zhu, D., Dang, Y. & Zhao, X. (2016). Treatment of condyloma acuminata in pregnant women with cryotherapy
combined with proanthocyanidins: outcome and safety. Experimental and Therapeutic Medicine, 11, pp.2391-2394. doi: 10.3892/etm.2016.3207.
Yanofsky, V., Patel, R. & Goldenberg, G. (2012). Genital warts: A comprehensive review. Journal of Clinical and Aesthetic Dermatology, 5(6), pp.25-36.
Yong, M., Parkinson, K., Goenka, N. & O'Mahony, C. (2010). Diabetes and genital warts: an unhappy coalition. International Journal of STD & AIDS, 21(7), pp.457-459.
DST-1009 Genital Warts
281
Certified Practice Area:
Reproductive Health: Sexually Transmitted Infections
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
DST-1010 Chlamydia Trachomatis (Reportable)
DEFINITION
Bacterial infection caused by the transmission of Chlamydia trachomatis (C. trachomatis or CT) during sexual contact in which body fluids are exchanged.
Note: Lymphogranuloma venereum (LGV) is a bacterial infection also caused by C. trachomatis serovars L1, L2 or L3. LGV serovars of C. trachomatis typically causes more severe and/or complicated infection and are tropic to the lymph tissue. STI RN(C) must refer to a physician or nurse practitioner (NP) for all clients who present with suspected LGV. For management of contacts to LGV, see the Treatment of STI Contacts DST.
CAUSE
Bacterial: Chlamydia trachomatis
PREDISPOSING RISK FACTORS
• sexual contact where there is transmission through the exchange of body fluids
TYPICAL FINDINGS
Sexual Health History
• sexual contact with at least one partner
• often asymptomatic
• sexual contact with someone with confirmed positive laboratory test for STI
Physical Assessment
• often asymptomatic
• inflammation of the tissues around the eye including: acute redness, purulent discharge and crusting (symptoms of
conjunctivitis); can be caused from chlamydial infection in the eye; consult with or refer to physician or nurse practitioner
(NP) for symptoms of conjunctivitis
• sore throat (throat infection is most often asymptomatic)
• urethral symptoms such as, discharge, itch or awareness
• painful (dysuria) or difficult urination
• testicular pain and/or swelling (symptoms of epididymitis)
• abnormal change in vaginal discharge
• abnormal vaginal bleeding:
o vagina with or without cervix: after intercourse or between menstrual period
o vagina after vaginoplasty: abnormal vaginal bleeding is not always STI-related as longer post-operative symptoms of
bleeding could be indicative of hypergranulation; refer to the STI Assessment DST for more information, and especially
for clients experiencing pain, discharge, or bleeding in the first 3 to 4 month post-operative period
• lower abdominal pain (symptom of pelvic inflammatory disease)
• dyspareunia
• inflammation of the rectum, rectal pain and anal discharge (symptoms of proctitis)
DIAGNOSTIC TESTS
Full STI screening is recommended. See the STI Assessment DST.
• Throat: CT NAAT swab, if indicated in sexual health history
DST-1010 Chlamydia Trachomatis (Reportable)

282
Certified Practice Area:
Reproductive Health: Sexually Transmitted Infections
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
• Penile urethra (with or without phalloplasty or metoidioplasty with urethral lengthening): CT NAAT urine. Ideally
the client should not have voided in the previous 1-2 hours; collect first void 10-20 ml
• Vagina:
o With cervix: Vaginal CT NAAT swab. Vaginal specimens may be clinician- or self-collected by swabbing the posterior
fornix of the vaginal wall
▪ If vaginal swab is declined, urine CT NAAT can be collected
▪ Cervical CT NAAT swab can also be collected but is not the preferred mode of collection
o After total hysterectomy (no cervix): CT NAAT urine (preferred) or vaginal CT NAAT swab
o After vaginoplasty: CT NAAT urine. Ideally the client should not have voided in the previous 1-2 hours; collect first
void 10-20 ml
• Rectum: CT NAAT swab, if indicated in sexual health history
Notes:
3. In general, self-collected vaginal swabs are indicated when a full or partial pelvic examination is not required or
appropriate. Clinician-collected vaginal swabs are generally done when a partial or full pelvic examination is required or
requested by the client.
4. Recent data show that vaginal swabs for C. trachomatis and N. gonorrhoeae NAATs identify as many or more infections
over cervical, urethral swabs or urine specimens.
CLINICAL EVALUATION/CLINICAL JUDGMENT
Treat all clients with confirmed chlamydia by positive laboratory result.
When providing treatment for a client with confirmed positive cervical, vaginal or urine laboratory test for Chlamydia trachomatis; assess for signs of pelvic inflammatory disease (PID) through symptoms inquiry and/or physical assessment (bimanual exam), if indicated.
Treat all persons identified as a sexual contact within the past 60 days to a confirmed chlamydia or case. If there are no sexual contacts in the previous 60 days then follow-up should occur for the last sexual contact.
MANAGEMENT AND INTERVENTIONS
Goals of Treatment
• treat infection
• prevent complications
• prevent the spread of infection
DST-1010 Chlamydia Trachomatis (Reportable)

283
Certified Practice Area:
Reproductive Health: Sexually Transmitted Infections
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
a. NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
TREATMENT OF CHOICE
Treatment Notes
First Choice General:
1. Treatment covers general CT infection but does not cover LGV. Referral to a physician or NP is required for LGV diagnosis and treatment.
2. Retreatment is indicated if the client has missed 2 consecutive doses of doxycycline or has not completed a full 5 days of treatment.
3. See BCCDC STI Medication Handouts for further medication reconciliation and client information.
4. See Monitoring and Follow-up section for test-of-cure (TOC) requirements.
Allergy and Administration:
5. DO NOT USE azithromycin if history of allergy to macrolides.
6. DO NOT USE doxycycline if pregnant and/or allergic to doxycycline or other tetracyclines.
7. If an azithromycin or doxycycline allergy or contraindication exists, consult with or refer to a physician or NP for alternate treatment.
8. Azithromycin and doxycycline are sometimes associated with gastrointestinal adverse effects. Taking medication with food and plenty of
water may minimize adverse effects.
9. Recent data has emerged regarding azithromycin and QT prolongation. Although rare, it is more significant in older populations, those with
pre-existing heart conditions, arrhythmias or electrolyte disturbances.
It is unclear how significant these findings are in young to mid-age healthy adults consuming a one-time dose of azithromycin; however,
please use the following precautions:
Consult with or refer to an NP or physician if the client:
o has a history of congenital or documented QT prolongation.
o has a history of electrolyte disturbance in particular hypokalemia, hypomagnesaemia.
o has clinically relevant bradycardia, cardiac arrhythmia or cardiac insufficiency.
o is on any of the following medications:
▪ Antipsychotics: pimozide (Orap®), ziprasidone (Zeldox®)
▪ Cardiac: dronedarone (Multaq®)
▪ Migraine: dihydroergotamine (Migranal®), ergotamine (Cafergot®)
doxycycline 100 mg PO BID
for 7 days
OR
azithromycin 1 gm PO in a
single dose
DST-1010 Chlamydia Trachomatis (Reportable)
284
Certified Practice Area:
Reproductive Health: Sexually Transmitted Infections
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
3. NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
PREGNANT OR BREAST-/CHEST-FEEDING CLIENTS
For all pregnant or breast-/chest-feeding clients, consult with or refer to a physician or NP. Test-of-cure (TOC) is recommended for pregnant and/or breast-/chest-feeding clients and should be performed at 3-4 weeks after completion of treatment.
PARTNER COUNSELLING AND REFERRAL
People who have confirmed laboratory tests positive for Chlamydia trachomatis require partner counselling to identify people who may have been exposed through sexual contact in the previous 60 days. If no sexual partner in the previous 60 days then follow-up should occur for the last sexual contact (see Treatment of STI Contacts DST).
MONITORING AND FOLLOW-UP
Repeat testing at 6 months due to potential high risk of re-infection.
TOC is only recommended 3-4 weeks post-treatment completion for pregnant and/or breast-/chest-feeding clients or if symptoms persist following treatment.
POTENTIAL COMPLICATIONS
• epididymitis
• sexually-acquired reactive arthritis
• pelvic inflammatory disease (PID)
• infertility
• ectopic pregnancy
• chronic pelvic pain
CLIENT EDUCATION
Counsel client regarding:
• abstaining from sexual activity during the 7-day course of treatment or for 7 days post-single-dose therapy for clients and
their contacts.
• informing last sexual contact AND any sexual contacts within the last 60 days that they require testing and treatment.
• methods of partner notification.
• the appropriate use of medications (dosage, side effects, and need for re-treatment if dosage not completed, or symptoms
do not resolve).
• harm reduction (condom use significantly reduces the risk of transmission).
• cleaning sex toys between use and using condoms if sharing sex toys
• the benefits of routine STI screening.
• the potential complications of untreated chlamydia.
• co-infection risk for HIV when another STI is present.
• the asymptomatic nature of STI.
• repeating STI screening, which includes testing for Chlamydia trachomatis, in 6 months’ time as re-infection rate is high.
• the importance of revisiting a health care provider if symptoms persist.
CONSULTATION AND/OR REFERRAL
Consult with or refer to a physician or NP for all clients who are pregnant or breast-/chest- feeding. Consult with or refer to physician or NP for symptoms of conjunctivitis. Consult with or refer to physician or NP for allergy/contraindications to treatment outlined in this DST.
DST-1010 Chlamydia Trachomatis (Reportable)

285
Certified Practice Area:
Reproductive Health: Sexually Transmitted Infections
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
3. NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
DOCUMENTATION
• Chlamydia trachomatis is reportable
• complete H208 form as per reporting procedures
• as per agency policy
DST-1010 Chlamydia Trachomatis (Reportable)

286
Certified Practice Area:
Reproductive Health: Sexually Transmitted Infections
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
3. NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
REFERENCES
More recent editions of any of the items in the reference list may have been published since this DST was published. If you have a newer version, please use it.
Australasian Sexual Heatlh Alliance (ASHA). Chlamydia. 2016. In: Australian STI Management Guidelines [Internet].
Bachmann, L.H., Johnson, R. E., Chen, H., Markowitz, L., Papp, J. R., Palella, J., & Hook, E. W. (2010). Nucleic acid
amplification tests for diagnosis of Neissieria gonorrhoeae and Chlamydia trachomatis rectal infections. Journal of Clinical Microbiology, 48(5), p.1827.
British Association for Sexual Health and HIV (BASHH). Chlamydia. 2015. In: BASHH Guidelines [Internet].
British Columbia Centre for Disease Control (BCCDC). (2014). British Columbia treatment guidelines: Sexually transmitted infections in adolescent and adults. STI/HIV Prevention and Control Division, BCCDC.
BCCDC. (2015). Lymphogranuloma venereum in BC: An update on a re-emerging STI.
Centers for Disease Control (CDC). (2015). Chlamydia infections. In: 2015 Sexually Transmitted Diseases Treatment Guidelines [Internet]. Atlanta, GA; [55-9].
Public Health Agency of Canada (PHAC). (2013). Chlamydial infections. In: Canadian Guidelines on Sexually Transmitted Infections.
PHAC. 2017. 2016 Updates Summary. In: Canadian guidelines on sexually transmitted infections.
PHAC. 2016. Laboratory Diagnosis of Sexually Transmitted Infections – Revised December 2016. In Canadian guidelines on sexually transmitted infections.
Schacter, J., Moncada, J., Liska, S., Shayevich, C. & Klausner, J.D. (2008). Nucleic acid amplification tests in the diagnosis of chlamydial and gonococcal infections of the oropharynx and rectum in men who have sex with men. Sexually Transmitted Diseases, 35(7), pp.637-642.
Schater, J., McCormack, W.W., Chernesky, M.A., et al. (2003). Vaginal Swabs are appropriate specimens for diagnosis of genital tract infection with Chlamydia trachomatis. Clin Microbiol, 41, pp.3784-3789.
Shafer, M., Moncada, J., Boyer, C.B., Betsinger, K., Flinn, S.D. & Schachter, J. (2003). Comparing first-void urine specimens, self-collected vaginal swabs, and endocervical specimens to detect Chlamydia trachomatis and Neisseria gonorrheoeae by a nucleic acid amplification test. Journal of Clinical Microbiology, 41(9), pp.4395-4399.
Stewart, C.M., Shoeman, S.A., Booth, A.R., Smith, S.D., Wilcox M.H., & Wilson, J.D. (2012). Assessment of self-taken swabs
versus clinician taken swab cultures for diagnosing gonorrhoea in women: single centre, diagnostic accuracy study. BMJ, 34, p.e8107.
van Liere, G.A.F.S., Hoebe, C.J.P.A., Wolffs, P.F.G., Dukers-Muijrers, N.H.T.M. (2014). High co-occurrence of anorectal chlamydia with urogenital chlamydia in women visiting an STI clinic revealed by routine universal testing in an observational study: A recommendation towards a better anorectal chlamydia control in women. BMC infectious diseases. 2014;14(1):274.
DST-1010 Chlamydia Trachomatis (Reportable)
287
Certified Practice Area:
Reproductive Health: Sexually Transmitted Infections
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
3. NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
DST-1011 Trichomoniasis
DEFINITION
Infection caused by the transmission of Trichomonas vaginalis (T. vaginalis or TV) during sexual contact in which body fluids are exchanged.
CAUSE
Protozoan: Trichomonas vaginalis
PREDISPOSING RISK FACTORS
• sexual contact where there is transmission through the exchange of body fluids
TYPICAL FINDINGS
Sexual Health History
• sexual contact with at least one partner
• sexual contact with someone with confirmed positive laboratory test for STI
Physical Assessment
• generally asymptomatic
• vaginal and/or urethral irritation
• abnormal change in vaginal discharge (frothy, whitish yellow in colour)
• painful (dysuria) or difficult urination
• vulvar erythema
• cervical erythema (“strawberry cervix”)
• pH greater than (>) 4.5 (not applicable after vaginoplasty)
DIAGNOSTIC TESTS
Full STI screening is recommended. See the STI Assessment DST.
Diagnostic testing is not available for men unless specifically called into the BCCDC Public Health Laboratory (BCCDC PHL) by an
ordering physician or nurse practitioner (NP). For transgender clients, some laboratories in British Columbia will accept specimens if
“transgender client” is indicated on the requisition. There are currently no provincial recommendations for routine trichomoniasis screening in BC. Screening should be offered to all clients with vaginal symptoms and considered in high prevalence populations.
Diagnostic tests used for trichomoniasis will depend on the lab testing platform and/or workplace guidelines and may include the following:
• trichomoniasis NAAT vaginal swab
• trichomoniasis NAAT urine
• trichomoniasis C&S vaginal swab
• trichomoniasis antigen vaginal swab
• wet-mount microscopy
CLINICAL EVALUATION/CLINICAL JUDGMENT
Treat all clients with confirmed trichomoniasis by positive laboratory result. May treat based on microscopy results if trichomoniasis is identified on wet-mount.
DST-1011 Trichomoniasis
288
Certified Practice Area:
Reproductive Health: Sexually Transmitted Infections
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
3. NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
MANAGEMENT AND INTERVENTIONS
Goals of Treatment
• treat infection
• prevent complications
• prevent the spread of infection
TREATMENT OF CHOICE
Treatment Notes
First Choice General:
1. Clients treated with metronidazole 500 mg PO BID for 7 days for
presumptive bacterial vaginosis (BV) clinical management at the time of
assessment and testing; do not require further treatment with
metronidazole if the diagnostic test results are positive for trichomoniasis.
Allergy and Administration:
2. Alcohol must be avoided 12 hours pre-treatment, during treatment and 24-
48 hours post-treatment with metronidazole.
3. Metronidazole 500 mg PO BID for 7 days is acceptable and safe to
administer in breast-/chest-feeding clients. Consult/refer for other first
choice or alternate treatment recommendations in pregnant clients.
metronidazole 2 gm PO in a single dose
Alternate Treatment
metronidazole 500 mg PO BID for 7 days
PREGNANT OR BREAST-/CHEST-FEEDING CLIENTS
For clients who are pregnant, consult with or refer to physician or NP. For clients who are breast-/chest-feeding, metronidazole 500 mg PO BID for 7 days is acceptable and safe to administer.
PARTNER COUNSELLING AND REFERRAL
People who have confirmed laboratory test for trichomoniasis should notify all the people who may have been exposed through
sexual contact in the previous 60 days. If no sexual contact in the previous 60 days then the client should notify their last sexual contact (see Treatment of STI Contacts DST).
MONITORING AND FOLLOW-UP
Clients who continue to experience symptoms, and have not been re-exposed to an untreated partner after completing treatment, should be referred to a physician or NP.
POTENTIAL COMPLICATIONS
• infertility or lower sperm count in men
• premature rupture membranes in pregnant clients
DST-1011 Trichomoniasis
289
Certified Practice Area:
Reproductive Health: Sexually Transmitted Infections
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
3. NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
CLIENT EDUCATION
Counsel client regarding:
• abstaining from sexual activity during the 7-day course of treatment or for 7 days post-single-dose therapy for clients and their contacts.
• all sexual partners within the last 60 days require treatment; testing and treatment is indicated for contacts with vaginas; if no sexual partners within the past 60 days, the last sexual partner requires follow-up for treatment and testing if appropriate.
• the appropriate use of medications (dosage, side effects, and need for re-treatment if dosage not completed, or symptoms do not resolve).
• special precautions for taking metronidazole: avoid alcohol 12 hours prior to starting treatment, during the course of treatment and for 24-48 hours after treatment completion.
• harm reduction (condom use significantly reduces the risk of transmission).
• cleaning sex toys between use and using condoms if sharing sex toys
• the benefits of routine STI screening.
• the potential complications of untreated trichomoniasis.
• co-infection risk for HIV when another STI is present.
• the asymptomatic nature of STI.
CONSULTATION AND/OR REFERRAL
Consult with or refer to a physician or NP in the following situations; clients who:
• are pregnant
• are allergic to metronidazole
• have persistent symptoms after receiving treatment with no re-exposure to untreated partner(s)
• is unable to abstain from alcohol during recommended treatment period
DOCUMENTATION
• trichomoniasis is not reportable
• as per agency policy
DST-1011 Trichomoniasis

290
Certified Practice Area:
Reproductive Health: Sexually Transmitted Infections
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
3. NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
REFERENCES
More recent editions of any of the items in the reference list may have been published since this DST was published. If you have a newer version, please use it.
Bell, C., Hough, E., Smith, A. & Greene, L. (2007). Targeted screening for Trichomonas vaginalis in women, a pH-based approach. International Journal of STD & Aids, (18), pp.402-403.
British Association for Sexual Health and HIV (BASHH). (2014). United Kingdom national guideline on the management of Trichomonas vaginalis. BASHH Guidelines.
British Columbia Centre for Disease Control (BCCDC). (2011). Safe Use of 10% Potassium Hydroxide in STI Screening. In: BCCDC Communicable Disease Manual: Chapter 5.
BCCDC. (2014). British Columbia treatment guidelines: Sexually transmitted infections in adolescent and adults.
Centers for Disease Control and Prevention (CDC). (2015). Trichomoniasis - diseases characterized by vaginal discharge. In: 2015 Sexually Transmitted Diseases Treatment Guidelines.
Coleman, J.S., Gaydos, C.A. & Witter, F. (2013). Trichomonas vaginalis: Vaginitis in obstetrics and genecology practice: New concepts and controversies. Obstet Gynecol Surv, 68(1), pp.43-50.
Hegazy, M.M., El-Tantawy, N.L., Soliman M.M., El-Sadeek, E.S. & El-Nagar, H.S. (2012). Performance of rapid
immunochromatographic assay in the diagnosis of Trichomonas vaginalis. Diagnostic Microbiology Infectious Disease, 74(1), pp.49-53.
Helms, D. J., Mosure, D. J., Metcalf, C. A., Douglas, J. M., Malotte, C. K., Paul, S. M. & Peterman, T.A. (2007). Risk factors for prevalent and incident Trichomonas vaginalis among women attending three sexually transmitted disease clinics. Sexually Transmitted Diseases, 5(35), pp.484-488.
Holmes, K., Sparling, P., Stamm, W., Piot, P., Wasserheit, J., Corey, L., Cohen, M. & Watts, H. (2008). Sexually transmitted diseases (4th ed). Toronto: McGraw Hill Medical.
Huppert, J.S., Joel, E., Mortensen, J.L., Reed, J.K., Kimberly, D., William, R., Miller, C. & Hobbs, M. (2007). Rapid antigen
testing compares favourably with transcription-mediated amplification assay for the detection of Trichomonas vaginalis in young women. Clinical Infectious Diseases, (45), pp.194-198.
Klebanoff, M.A., Carey, J.C., Hauth, J.C., et al. (2001). Failure of metronidazole to prevent preterm delivery among pregnant women with asymptomatic Trichomonas vaginalis infection. N Engl J Med, 345, pp.487–493.
Public Health Agency of Canada (PHAC). (2010). Section 4 - Management and treatment of specific syndromes. Vaginal
discharge (bacterial vaginosis, vulvovaginal candidiasis, trichomoniasis). In: Canadian Guidelines on Sexually Transmitted Infections.
PHAC. (2014). Supplementary statement for recommendations related to the diagnosis, management, and follow-up of vaginal discharge: March 2014. In: Canadian Guidelines on Sexually Transmitted Infections.
Weyers, S, Verstraelen, H., Gerris, J., Monstrey, S., Lopes Santiago, G.S., Saerens, B., Verhelst, R. (2009). Microflora of the penile skin-lined neovagina of transsexual women. BMC Microbiology, 9(102), p. 1-10.
Verteramo, R., Calzolari, E., Degener, A.M., Masciangelo, R. & Patella, A. (2008). Trichomonas vaginalis infections: risk
indicators among women attending for routine gynaecologic examination. Japan Society of Obstetrics and Gynecology, 2(34), pp.233-237.
DST-1011 Trichomoniasis
291
Certified Practice Area:
Reproductive Health: Sexually Transmitted Infections
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
3. NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
DST-1012 Uncomplicated Lower UTI
DEFINITION
Bacterial infection of the bladder, also known as cystitis, is caused by bacteria multiplying in urine. A lower urinary tract infection (UTI) occurs in the urethra and the bladder and is a common infection is young sexually active people.
Uncomplicated lower UTI is an acute infection of the bladder in an otherwise healthy person. RN(C)s21 are limited to the treatment of uncomplicated lower UTI in sexually active people with vaginas.
See Consultation and/or Referral section for specific information regarding consultation with and referral to a physician or nurse practitioner (NP).
POTENTIAL CAUSES
Bacterial:
• Escherichia coli (E. coli)
• Enterococcus Faecalis
• Staphylococcus saprophyticus
• Staphylocossus aureus
• other enterobacteriaceae (e.g., Proteus mirabilis, Klebsiella pneumoniae)
PREDISPOSING RISK FACTORS
• anatomical (e.g., shorter urethra)
• foreign body (e.g., catheterization)
• previous UTI
• sexual activity, especially recent new sexual partner
• genito-urinary tract anomalies – congenital, urethral stricture, neurogenic bladder, tumor
• diaphragm or spermicide use
• urinary instrumentation (e.g., catheterization) – refer to physician or NP
• diabetes mellitus
• renal or urethral calculi
• immunocompromised (e.g., HIV infection)
• pregnancy
• trauma
• strictures
21 Note: RN(C) is an authorized title recommended by BCCNP that refers to BCCNP-certified RNs, and is used throughout this
Decision Support Tool (DST).
DST-1012 Uncomplicated Lower UTI

292
Certified Practice Area:
Reproductive Health: Sexually Transmitted Infections
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
3. NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
TYPICAL FINDINGS
Sexual Health History
• urinary frequency or urgency
• vaginal irritation
• dysuria
• suprapubic pain or discomfort
• hematuria
• mild dehydration
Physical Assessment
• suprapubic tenderness – may be mild to moderate
• flank pain – if present consult or refer – suggests upper UTI
• fever, rigor, chills – if present consult or refer – suggests upper UTI
• hydration status
DIAGNOSTIC TESTS
• urinalysis:
o dipstick test for:
▪ nitrites, leukocytes (most predictive of lower UTI)
▪ blood, protein
o consider microscopic urinalysis: WBC, RBC, bacteria
Note: While positive dipstick test for nitrites and leukocytes are the most predictive of lower UTI; positive findings for blood and
protein, in the absence of positive results for nitrites and leukocytes, may also indicate lower UTI. Consult with a physician or NP for
clients with symptoms of lower UTI with negative results for nitrites and leukocytes.
• urine culture & sensitivity (C&S) is generally not a required test when managing uncomplicated lower UTI – consider a urine
C&S if:
o this is the second presentation of a UTI within a one-year time-frame
o evidence of an upper UTI; i.e., the client presents with fever, chills, rigor, or flank pain (refer or consult)
o dipstick test is negative and symptoms are indicative of a likely UTI
• offer full STI screening
• consider pregnancy test if indicated
CLINICAL EVALUATION/CLINICAL JUDGMENT
May treat as lower urinary tract infection if:
• frequency, urgency or dysuria are present
AND
• urine dipstick test is positive for leukocytes and/or nitrites
DST-1012 Uncomplicated Lower UTI
293
Certified Practice Area:
Reproductive Health: Sexually Transmitted Infections
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
3. NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
MANAGEMENT AND INTERVENTIONS
Goals of Treatment
• alleviate symptoms
• prevent complications and ascending infection
• treat infection
TREATMENT OF CHOICE
Treatment Notes
First Choice General:
1. Nitrofurantoin demonstrates less resistance to E. coli and E. Faecalis than
trimethoprim/sulphamethoxazole, and is recommended as first choice for treatment of Lower UTI.
2. See BCCDC STI Medication Handouts for further medication reconciliation
and client information. Allergy and Administration:
3. DO NOT USE nitrofurantoin if there is a history of renal impairment or
allergy to nitrofurantoin or dantrolene.
4. DO NOT USE trimethoprim or sulphamethoxazole if there is a history of allergy to sulpha drugs.
5. Consult physician or NP if the client is unable to use first or second choice
treatment recommendations.
6. If serious allergic reaction develops including difficulty breathing and/or severe itchiness, have the client inform clinic staff immediately. If
symptoms develop after leaving the clinic, advise the client to seek
immediate emergency care.
nitrofurantoin 100 mg PO BID for 5 days
Second Choice
trimethoprim 160 mg/sulphamethoxazole 800 mg tab PO BID for 3 days
PREGNANT OR BREAST-/CHEST-FEEDING CLIENTS
Refer all pregnant or breast-/chest-feeding clients to a physician or NP for treatment.
PARTNER COUNSELLING AND REFERRAL
Partner follow-up is not required.
MONITORING AND FOLLOW-UP
If symptoms do not begin to resolve in 48-72 hours or if symptoms persist despite treatment, the client should return to be re-
assessed by a physician or NP.
POTENTIAL COMPLICATIONS
• ascending infection - pyelonephritis
• chronic UTI
• interstitial cystitis
DST-1012 Uncomplicated Lower UTI
294
Certified Practice Area:
Reproductive Health: Sexually Transmitted Infections
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
3. NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
CLIENT EDUCATION
Counsel client regarding:
• the appropriate use of medications (dosage, side effects, and need for re-treatment if dosage not completed, or symptoms
do not resolve).
• returning to the clinic if fever develops or symptoms do not improve in 48-72 hours.
• the potential causes of lower UTI; having a new sexual partner and/or recent intercourse, and the use of spermicides.
• behavioral measures that may help to reduce uropathogens or irritants from entering the urethra including:
o routine cleaning with warm water
o using mild and non-irritant bath products, especially for bubble baths
o voiding before and after intercourse
o condom use during intercourse
o changing barrier methods (e.g., gloves, condoms, dental dams) or cleaning hands/toys/genitals between anal and
vaginal play
o cleaning sex toys between use and using condoms if sharing sex toys
o maintaining fluid intake at 8-10 glasses per day
o avoiding douching and commercial ‘vaginal cleaning products’
o wiping from front-to-back after voiding
CONSULTATION AND/OR REFERRAL
Consult with or refer to a physician or NP in the following situations:
• who are pregnant or breast-/chest-feeding
• under the age of 14 years
• for clients with symptoms of lower UTI with negative results for nitrites and leukocytes
• who have symptoms suggestive of an upper urinary tract infection, including some or all of the following:
o flank pain, severe back or abdominal pain
o chills, fever >38ºC, rigor
o nausea or vomiting
• with recurrent lower UTI; the second episode of lower UTI within one month or more than 3 episodes in one year
• recent urinary tract instrumentation or the presence of indwelling catheter, stents or nephrostomy tubes
• with a history of urologic or renal anomaly, impairment, surgery, transplant, or kidney stones
• with chronic health concerns – uncontrolled diabetes, neurogenic bladder, renal disease, long-term catheterization, spinal
cord injury, immunocompromised
• who have had symptoms of lower UTI for 7 days or longer
• with hospital-acquired infection
DOCUMENTATION
• uncomplicated lower UTI is not reportable
• as per agency policy
DST-1012 Uncomplicated Lower UTI
295
Certified Practice Area:
Reproductive Health: Sexually Transmitted Infections
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
3. NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
REFERENCES
More recent editions of any of the items in the reference list may have been published since this DST was published. If you have a newer version, please use it.
British Columbia Centre for Disease Control (BCCDC). (2015). Antimicrobial Resistance Trends in the Province of British Columbia 2014.
British Columbia College of Nursing Professionals (BCCNP). (2016). Adult (female) Lower Urinary Tract Infection (UTI). In: Certified Practice Remote Nursing Decision Support Tool.
British Columbia Medical Association & BC Ministry of Health Services. (2009). Macroscopic and microscopic urinalysis and the investigation of UTI. In: BC Guidelines. BC Ministry of Health Guidelines and Protocols Advisory Committee.
Blondel-Hill, E., & Fryters, S. (2006). Bugs & Drugs. Capital Health.
Car, J. (2006). Urinary tract infections in women: diagnosis and management in primary care. BMJ, 332, pp.94-97.
Christiaens, T., De Meyere, M., Verschraegan, G. Peersman, W., Heytens, S., & De Maeseneer, J. (2002). Randomized controlled trial of nitrofurantoin versus placebo in the treatment of uncomplicated urinary tract infection in women. British Journal of General Practice, pp.729-734.
Colman, R., & Somgyi, R. (2008). Toronto Notes 2008. Comprehensive medical reference and review for MCCQE and USMLE II. Toronto Notes for Medical Students: Toronto, ON.
Dorland, W.A. (1994). Cystitis. In: Dorland’s Illustrated Medical Dictionary (28th ed). W.B. Saunders Company.
Fihn, S. (2003). Acute uncomplicated urinary tract infection in women. The New England Journal of Medicine, 349, pp.259-26.
Grude, N., Tveten, Y., Jenkins, A., & Kristiansen, B. (2005). Uncomplicated urinary tract infections: Bacterial findings and efficacy of empirical antibacterial treatment. Scandinavian Journal of Primary Health Care, (23), pp.115-119.
Gupta, K., & Trautner, B. W. (2013). Diagnosis and management of recurrent urinary tract infections in non-pregnant women. BMJ, 346(7910), pp.30-33.
Gupta, K., Hooton, T., Naber, K., Wullt, B., Colgan, R., Miller, L., Moran, G., Nicolle, L., Schaeffer, A., & Soper, D. (2011).
International clinical practice guidelines for the treatment of acute uncomplicated cystitis and pyelonephritis in women: A 2010 update by the Infectious Diseases Society of America and the European Society for Microbiology and Infectious Diseases.
Hanno, P. M., Erickson, D., Moldwin, R., Faraday, M. M., & American Urological Association. (2015). Diagnosis and treatment of interstitial Cystitis/Bladder pain syndrome: AUA guideline amendment. Journal of Urology, the, 193(5), 1545-1553
Heng, M., & Greenwald, J. (2007). The Toronto note 2007 clinical management handbook. Toronto, Canada; Toronto Notes for Medical Students, Inc.
Hoebeke, P., Selvaggi, G., Ceulemans, P., De Cuypere, G., T’Sjoen, G., Weyers, S., & Monstrey, S. (2005). Impact of sex reassignment surgery on lower urinary tract function. European Urology, 47(3), p. 398-402.
Hooton, T., & Stamm, W. (2009). Acute cystitis in women.
Hooton, T. M., & Gupta, K. (2013). Recurrent urinary tract infection in women. In: D.S. Basow (Ed.). UpToDate.
Jackson, M. (2007). Evidence-based practice for evaluation and management of female urinary tract infection. Urologic Nursing, 27(2), pp.133-136.
DST-1012 Uncomplicated Lower UTI

296
Certified Practice Area:
Reproductive Health: Sexually Transmitted Infections
BCCNM-certified nurses (RN(C)s) are responsible for ensuring they reference the most current DSTs, exercise independent clinical judgment and use evidence to support competent, ethical care.
3. NNPBC January 2021. For more information or to provide feedback on this or any other decision support tool, email [email protected]
Jensen, B., & Regier, L. (2008). The Rx Files. Drug Comparison Charts. 7th Edition. Rx Files.
Katchman, M., Christiaens, T., Baerheim, A., & Leibovici, L. (2009). Duration of antibacterial treatment for uncomplicated urinary tract infection in women (Review). The Cochrane Library (3). The Cochrane Collaboration. John Wiley & Sons Ltd.
Mehnert-Kay, S. (2005). Diagnosis and management of uncomplicated urinary tract infections. American Family Physician,72(3), pp.451-456.
Nicolle, L., Anderson, P., Conly, J., Mainprize, T., Meuser, J., Nickel, J., Senikas, V., & Zhanel, G. (2006). Uncomplicated urinary tract infection in women. Canadian Family Physician, (52), pp.612-618.
Nosseir, S. B., Lind, L. R., & Winkler, H. A. (2012). Recurrent uncomplicated urinary uract infections in women: A review. Journal of Women's Health, (15409996), 21(3), pp.347-354.
Petricevic, L., Kaufmann, U., Domig,K., Kraler, M., Marschalek, J., Kneifel W. & Kiss, H. (2014). Molecular detection of lactobacillus species in the neovagina of male-to-female transsexual women. Scientific reports, 4(3746), pp.1-4.
Provincial Health Services Authority’s Trans Care BC. (2017). Caring for trans and gender diverse clients in BC: A primary care toolkit.
Tanagho, E. A., McAninch, J. W. (1995). Smith’s general urology. 14th Edition. Appleton & Lange. Norwalk, CT.
University of California San Francisco (UCSF) & Center of Excellence for Transgender Health. (2016). Guidelines for the primary and gender-affirming care of transgender and gender non-binary people.
Weyers, S, Verstraelen, H., Gerris, J., Monstrey, S., Lopes Santiago, G.S., Saerens, B., & Verhelst, R. (2009). Microflora of the penile skin-lined neovagina of transsexual women. BMC Microbiology, 9(102), pp. 1-10.
DST-1012 Uncomplicated Lower UTI