Carpentier-Edwards Standard Porcine Bioprosthesis: Primary Tissue Failure (Structural Valve...
8
Carpentier-Edwards Standard Porcine Bioprosthesis: Primary Tissue Failure (Structural Valve Deterioration) by Age Groups W. R. E. Jamieson, M.D., L. J. Rosado, M.D., A. I. Munro, M.D., A. N. Gerein, M.D., L. H. Burr, M.D., R. T. Miyagishima, M.D., M. T. Janusz, M.D., and G. F. 0. Tyers, M.D. ABSTRACT Primary tissue failure (structural valve dete- rioration) has been documented as the most prominent complication of porcine bioprostheses. The influence of age on primary tissue failure has received limited consid- eration. From 1975 to 1986, 1,301 Carpentier-Edwards standard porcine bioprostheses were implanted in 1,183 patients in 1,201 operations. Of the total number of prostheses, 97.7% were implanted prior to 1983. The mean follow-up was 5.6 years and was 97.5% complete. Primary tissue failure was identified in 96 patients (98 operations) at reoperation (95) or autopsy (3). One hundred four (104) prostheses were involved. Thirty-one failed after aortic valve replacement (AVR), 49 after mitral valve replacement (MVR), and 24 after multiple-valve replacement (18 pa- tients). There were 47 male and 49 female patients. The mean age at implantation was 47 years (range, 8 to 72 years). The mean implantation time was 74.0 months. The freedom from primary tissue failure at 10 years is 77.0 f 2.9% overall; for AVR, 83.1 f 3.7%; for MVR, 72.1 f 4.9%; and for multiple-valve replacement, 65.5 f 7.8%. The freedom from deterioration for patients less than 20 years of age is significantly less than that for other age groups. The freedom from deterioration increased by decades; the greatest freedom was noted in patients 70 to 80 years old and 80 years old or older. The freedom from deterioration at 10 years for patients less than 30 years of age is 26.8 f 17.2%; 30 to 59 years, 77.4 f 3.0%; and 60 years and older, 83.1 f 4.2%. The aortic valve prosthesis performed superiorly in the younger and older age groups while in the intermediate group there was no difference in the performance of aortic and mitral valve prostheses. Primary tissue failure (structural valve deterioration) has been the most prominent valve-related complication of biological prostheses [ 1-22]. Structural valve deteriora- From Vancouver General Hospital and St. Paul's Hospital, The Univer- sity of British Columbia, Vancouver, BC, Canada. Presented at the Twenty-third Annual Meeting of The Society of Tho- racic Surgeons, Toronto, Ont, Canada, Sept 21-23, 1987. Address reprint request to Dr. Jamieson, Division of Cardiovascular and Thoracic Surgery, Department of Surgery, The University of British Col- umbia, 910 W 10th Ave, Vancouver, BC, Canada V5Z 4E3. tion has influenced long-term durability. Data concern- ing primary tissue failure by age groups will facilitate clinical decisions. There is substantial documentation of an increased incidence of primary tissue failure in chil- dren and adolescents [I, 3, 8, 9, 12, 17, 19, 201. At the University of British Columbia-affilia ted teaching hospi- tals, bioprostheses have been the prostheses of choice in approximately 93% of patients undergoing valve re- placement over the past 12 years. This analysis is limited to the influence of age in structural deterioration of Car- pentier-Edwards standard porcine bioprostheses im- planted at Vancouver General Hospital and St. Paul's Hospital since 1975. Material and Methods From 1975 to 1986, 1,301 Carpentier-Edwards standard porcine bioprostheses were implanted in 1,183 patients in 1,201 operations. Of the total number of biopros- theses, 97.7% were implanted prior to 1983. There were 572 aortic valve replacements (AVR), 509 mitral valve replacements (MVR), 111 multiple-valve replacements, 8 tricuspid valve replacements, and 1 pulmonary valve re- placement (Table 1). Structural valve deterioration, by definition, incorpo- rates primary tissue failure. Structural valve deteriora- tion is generally defined as any abnormality in a prosthe- sis that causes stenosis or regurgitation and is found at autopsy or reoperation, including leaflet disruption, calcification, or strut malfunction. Dysfunction due to prosthetic valve endocarditis or periprosthetic leak is not considered structural valve deterioration according to the defined criteria. Follow-up of the total patient population was 97.5% complete; 30 patients were lost to follow-up. The evalua- tion was conducted by direct communication with the patient and communication with attending physicians, family physicians, and specialists. The closing period was the 6 months from November, 1986, to April, 1987. Values are expressed as the mean * the standard er- ror of the mean unless otherwise noted. Freedom from structural valve deterioration is expressed by actuarial methods. The linearized occurrence rates are expressed as percent per patient-year. The hazard rates are ex- pressed as linearized rates for each individual postop- erative year. The evaluation of the significance of the freedom curves was determined by the Lee-Desu test. Two-tailed p values of less than 0.05 were considered significant. 155 Ann Thorac Surg 46:155-162, Aug 1988. Copyright 0 1988 by The Society of Thoracic Surgeons
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Carpentier-Edwards Standard Porcine Bioprosthesis: Primary Tissue Failure (Structural Valve...

Carpentier-Edwards Standard Porcine Bioprosthesis: Primary Tissue Failure (Structural Valve Deterioration) by Age Groups W. R. E. Jamieson, M.D., L. J. Rosado, M.D., A. I. Munro, M.D., A. N. Gerein, M.D., L. H. Burr, M.D., R. T. Miyagishima, M.D., M. T. Janusz, M.D., and G. F. 0. Tyers, M.D.
ABSTRACT Primary tissue failure (structural valve dete- rioration) has been documented as the most prominent complication of porcine bioprostheses. The influence of age on primary tissue failure has received limited consid- eration. From 1975 to 1986, 1,301 Carpentier-Edwards standard porcine bioprostheses were implanted in 1,183 patients in 1,201 operations. Of the total number of prostheses, 97.7% were implanted prior to 1983. The mean follow-up was 5.6 years and was 97.5% complete. Primary tissue failure was identified in 96 patients (98 operations) at reoperation (95) or autopsy (3). One hundred four (104) prostheses were involved. Thirty-one failed after aortic valve replacement (AVR), 49 after mitral valve replacement (MVR), and 24 after multiple-valve replacement (18 pa- tients). There were 47 male and 49 female patients. The mean age at implantation was 47 years (range, 8 to 72 years). The mean implantation time was 74.0 months. The freedom from primary tissue failure at 10 years is 77.0 f 2.9% overall; for AVR, 83.1 f 3.7%; for MVR, 72.1 f 4.9%; and for multiple-valve replacement, 65.5 f 7.8%. The freedom from deterioration for patients less than 20 years of age is significantly less than that for other age groups. The freedom from deterioration increased by decades; the greatest freedom was noted in patients 70 to 80 years old and 80 years old or older. The freedom from deterioration at 10 years for patients less than 30 years of age is 26.8 f 17.2%; 30 to 59 years, 77.4 f 3.0%; and 60 years and older, 83.1 f 4.2%. The aortic valve prosthesis performed superiorly in the younger and older age groups while in the intermediate group there was no difference in the performance of aortic and mitral valve prostheses.
Primary tissue failure (structural valve deterioration) has been the most prominent valve-related complication of biological prostheses [ 1-22]. Structural valve deteriora-
From Vancouver General Hospital and St. Paul's Hospital, The Univer- sity of British Columbia, Vancouver, BC, Canada.
Presented at the Twenty-third Annual Meeting of The Society of Tho- racic Surgeons, Toronto, Ont, Canada, Sept 21-23, 1987.
Address reprint request to Dr. Jamieson, Division of Cardiovascular and Thoracic Surgery, Department of Surgery, The University of British Col- umbia, 910 W 10th Ave, Vancouver, BC, Canada V5Z 4E3.
tion has influenced long-term durability. Data concern- ing primary tissue failure by age groups will facilitate clinical decisions. There is substantial documentation of an increased incidence of primary tissue failure in chil- dren and adolescents [I, 3, 8, 9, 12, 17, 19, 201. At the University of British Columbia-affilia ted teaching hospi- tals, bioprostheses have been the prostheses of choice in approximately 93% of patients undergoing valve re- placement over the past 12 years. This analysis is limited to the influence of age in structural deterioration of Car- pentier-Edwards standard porcine bioprostheses im- planted at Vancouver General Hospital and St. Paul's Hospital since 1975.
Material and Methods From 1975 to 1986, 1,301 Carpentier-Edwards standard porcine bioprostheses were implanted in 1,183 patients in 1,201 operations. Of the total number of biopros- theses, 97.7% were implanted prior to 1983. There were 572 aortic valve replacements (AVR), 509 mitral valve replacements (MVR), 111 multiple-valve replacements, 8 tricuspid valve replacements, and 1 pulmonary valve re- placement (Table 1).
Structural valve deterioration, by definition, incorpo- rates primary tissue failure. Structural valve deteriora- tion is generally defined as any abnormality in a prosthe- sis that causes stenosis or regurgitation and is found at autopsy or reoperation, including leaflet disruption, calcification, or strut malfunction. Dysfunction due to prosthetic valve endocarditis or periprosthetic leak is not considered structural valve deterioration according to the defined criteria.
Follow-up of the total patient population was 97.5% complete; 30 patients were lost to follow-up. The evalua- tion was conducted by direct communication with the patient and communication with attending physicians, family physicians, and specialists. The closing period was the 6 months from November, 1986, to April, 1987.
Values are expressed as the mean * the standard er- ror of the mean unless otherwise noted. Freedom from structural valve deterioration is expressed by actuarial methods. The linearized occurrence rates are expressed as percent per patient-year. The hazard rates are ex- pressed as linearized rates for each individual postop- erative year. The evaluation of the significance of the freedom curves was determined by the Lee-Desu test. Two-tailed p values of less than 0.05 were considered significant.
155 Ann Thorac Surg 46:155-162, Aug 1988. Copyright 0 1988 by The Society of Thoracic Surgeons
156 The Annals of Thoracic Surgery Vol 46 No 2 August 1988
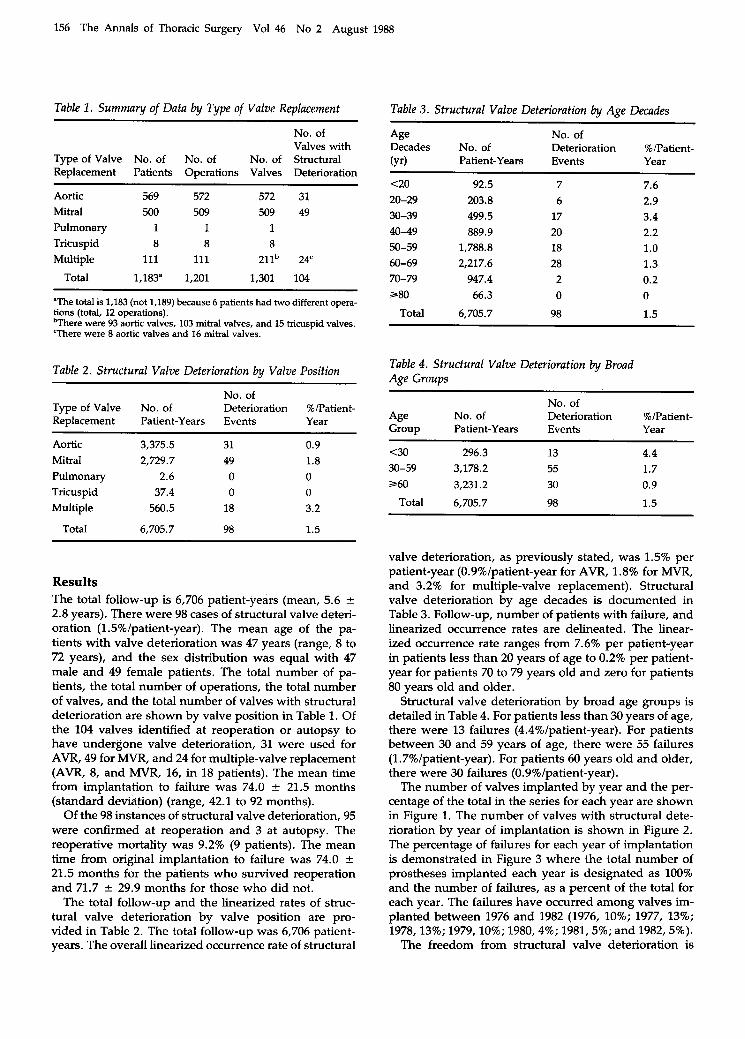
Table 1. Summary of Data by Type of Valve Replacement
No. of Valves with
Type of Valve No. of No. of No. of Structural Replacement Patients Operations Valves Deterioration
~
Aortic 569 572 572 31 Mitral 500 509 509 49 Pulmonary 1 1 1 Tricuspid 8 8 8 Multiple 111 111 211b 24'
Total 1,183" 1,201 1,301 104
"The total is 1,183 (not 1,189) because 6 patients had two different opera- tions (total, 12 operations). bThere were 93 aortic valves, 103 mitral valves, and 15 tricuspid valves. 'There were 8 aortic valves and 16 mitral valves.
Table 2. Structural Valve Deterioration by Valve Position
No. of Type of Valve No. of Deterioration %/Patient- Replacement Patient-Years Events Year
Aortic 3,375.5 31 0.9 Mitral 2,729.7 49 1.8 Pulmonary 2.6 0 0 Tricuspid 37.4 0 0 Multiple 560.5 18 3.2
Total 6,705.7 98 1.5
Table 3. Structural Valve Deterioration by Age Decades
Age No. of Decades No. of Deterioration %/Patient- (Yr) Patient-Years Events Year
<20 92.5 7 7.6 20-29 203.8 6 2.9 30-39 499.5 17 3.4 40-49 889.9 20 2.2 50-59 1,788.8 18 1.0 60-69 2,217.6 28 1.3 70-79 947.4 2 0.2 280 66.3 0 0
Total 6,705.7 98 1.5
Table 4. Structural Valve Deterioration by Broad Age Groups
No. of Age No. of Deterioration %/Patient- Group Patient-Years Events Year
<30 296.3 13 4.4 30-59 3,178.2 55 1.7 260 3,231.2 30 0.9
Total 6,705.7 98 1.5
Results The total follow-up is 6,706 patient-years (mean, 5.6 * 2.8 years). There were 98 cases of structural valve deteri- oration (1.5%/patient-year). The mean age of the pa- tients with valve deterioration was 47 years (range, 8 to 72 years), and the sex distribution was equal with 47 male and 49 female patients. The total number of pa- tients, the total number of operations, the total number of valves, and the total number of valves with structural deterioration are shown by valve position in Table 1. Of the 104 valves identified at reoperation or autopsy to have undergone valve deterioration, 31 were used for AVR, 49 for MVR, and 24 for multiple-valve replacement (AVR, 8, and MVR, 16, in 18 patients). The mean time from implantation to faildre was 74.0 f 21.5 months (standard deviation) (range, 42.1 to 92 months).
Of the 98 instances of structural valve deterioration, 95 were confirmed at reoperation and 3 at autopsy. The reoperative mortality was 9.2% (9 patients). The mean time from original implantation to failure was 74.0 f 21.5 months for the patients who survived reoperation and 71.7 f 29.9 months for those who did not.
The total follow-up and the linearized rates of struc- tural valve deterioration by valve position are pro- vided in Table 2. The total follow-up was 6,706 patient- years. The overall linearized occurrence rate of structural
valve deterioration, as previously stated, was 1.5% per patient-year (0.9%/patient-year for AVR, 1.8% for MVR, and 3.2% for multiple-valve replacement). Structural valve deterioration by age decades is documented in Table 3. Follow-up, number of patients with failure, and linearized occurrence rates are delineated. The linear- ized occurrence rate ranges from 7.6% per patient-year in patients less than 20 years of age to 0.2% per patient- year for patients 70 to 79 years old and zero for patients 80 years old and older.
Structural valve deterioration by broad age groups is detailed in Table 4. For patients less than 30 years of age, there were 13 failures (4.4%/patient-year). For patients between 30 and 59 years of age, there were 55 failures (1.7%/patient-year). For patients 60 years old and older, there were 30 failures (0.9%/patient-year).
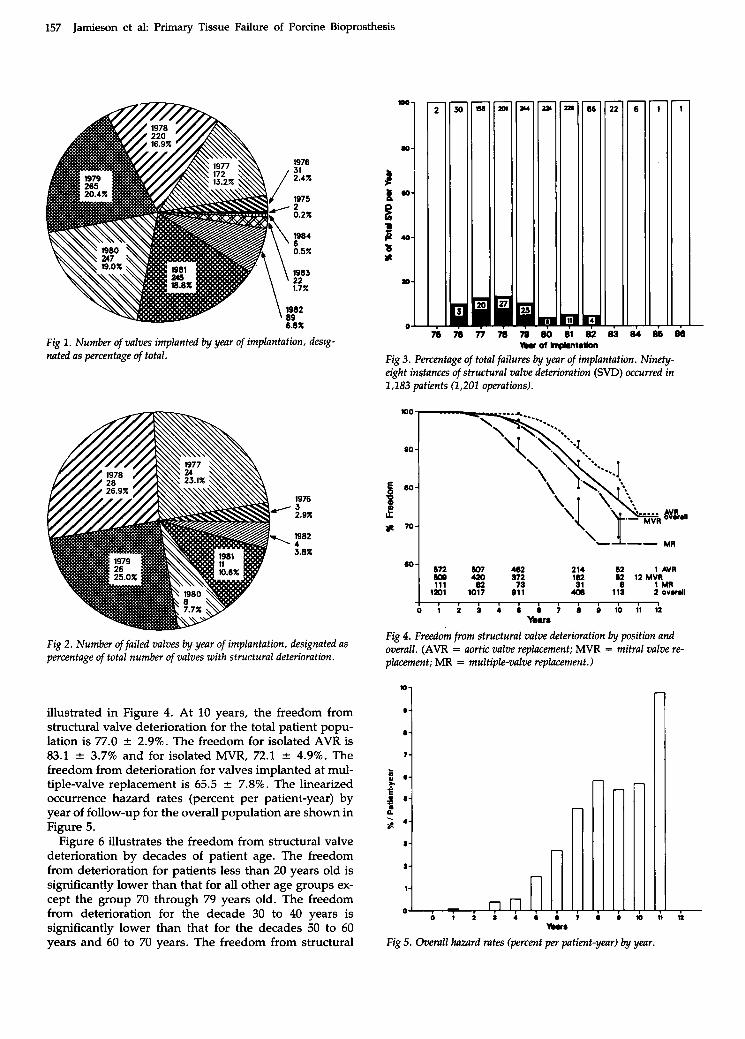
The number of valves implanted by year and the per- centage of the total in the series for each year are shown in Figure 1. The number of valves with structural dete- rioration by year of implantation is shown in Figure 2. The percentage of failures for each year of implantation is demonstrated in Figure 3 where the total number of prostheses implanted each year is designated as 100% and the number of failures, as a percent of the total for each year. The failures have occurred among valves im- planted between 1976 and 1982 (1976, 10%; 1977, 13%; 1978,13%; 1979,10%; 1980,4%; 1981,5%; and 1982,5%).
The freedom from structural valve deterioration is
157 Jamieson et al: Primary Tissue Failure of Porcine Bioprosthesis
lo-
@ -
a-
7-
Fig 1. Number of valves implanted by year of implantation, desig- nated as percentage of total.
2 3 0 -1 a t
1 40-
B a- 1 X
zo-
o- . . m m
W r n Y
T j m m muofmp*nt.tkn
Fig 3. Percentage of total failures by yenr of implantation. Ninety- eight instances of structural valve deterioration (SVD) occurred in 1,183 patients (1,201 operations).
1976 3 2.9%
1982 4 3.8%
672 607 482 214 62 1 AVR
111 (I? 73 la2 31 8 1 MR 6W 420 372 "1 imi 1017 011
62 12 MVR
44) 113 2 overall
Fig 2 . Number of failed valves by year of implantation, designated as percentage of total number of valves with structural deterioration.
illustrated in Figure 4. At 10 years, the freedom from structural valve deterioration for the total patient popu- lation is 77.0 f 2.9%. The freedom for isolated AVR is 83.1 f 3.7% and for isolated MVR, 72.1 * 4.9%. The freedom from deterioration for valves implanted at mul- tiple-valve replacement is 65.5 f 7.8%. The linearized occurrence hazard rates (percent per patient-year) by year of follow-up for the overall population are shown in Figure 5.
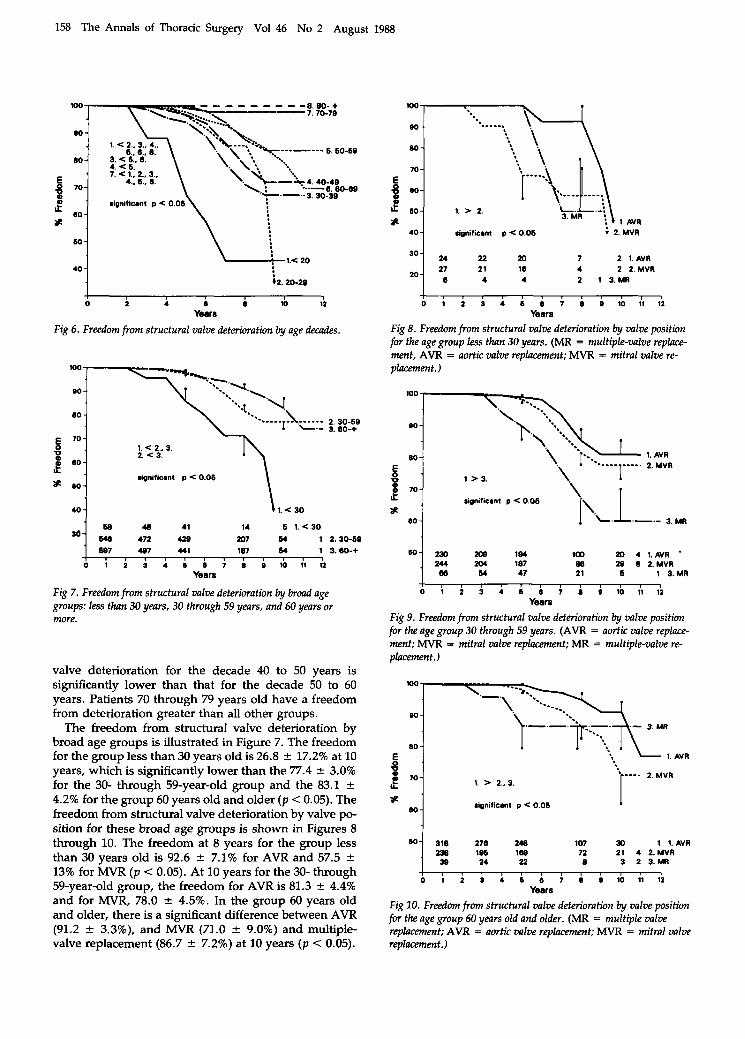
Figure 6 illustrates the freedom from structural valve deterioration by decades of patient age. The freedom from deterioration for patients less than 20 years old is significantly lower than that for all other age groups ex- cept the group 70 through 79 years old. The freedom from deterioration for the decade 30 to 40 years is significantly lower than that for the decades 50 to 60 years and 60 to 70 years. The freedom from structural
I I
0 1 2 9 4 6 ~ 7 8 0 1 0 1 1 1 2 Yeam
Fig 4. Freedom from structural valve deterioration by position and overall. (AVR = aortic valve replacement; MVR = mitral valve re- placement; M R = multiple-valve replacement.)
M u 8
Fig 5. Overall hazard rates (percent per patient-year) by year.
r U
158 The Annals of Thoracic Surgery Vol 46 No 2 August 1988
60-
.
- & 4 . 4 0 - 4 0
1-39
318 278 248 107 30 1 1. AVR ao l a6 iw 72 21 4 2.MVR 39 24 21 8 3 2 3.MR
80 - * W -
4 0 - v2.20-29
0 i i 9 8 m ri Years
Fig 6. Freedom from structural valve deterioration by age decades.
48 41 14 6 1.<30 m7 64 1 2.30-60 187 64 1 3.80-+
0 1 2 3 4 6 8 7 8 0 10 11 12 Years
Fig 7. Freedom from structural valve deterioration by broad age groups: less than 30 years, 30 through 59 years, and 60 years or more.
valve deterioration for the decade 40 to 50 years is significantly lower than that for the decade 50 to 60 years. Patients 70 through 79 years old have a freedom from deterioration greater than all other groups.
The freedom from structural valve deterioration by broad age groups is illustrated in Figure 7. The freedom for the group less than 30 years old is 26.8 f 17.2% at 10 years, which is significantly lower than the 77.4 2 3.0% for the 30- through 59-year-old group and the 83.1 f 4.2% for the group 60 years old and older (p < 0.05). The freedom from structural valve deterioration by valve po- sition for these broad age groups is shown in Figures 8 through 10. The freedom at 8 years for the group less than 30 years old is 92.6 ? 7.1% for AVR and 57.5 f 13% for MVR (p < 0.05). At 10 years for the 30- through 59-year-old group, the freedom for AVR is 81.3 2 4.4% and for MVR, 78.0 ? 4.5%. In the group 60 years old and older, there is a significant difference between AVR (91.2 * 3.3%), and MVR (71.0 f 9.0%) and multiple- valve replacement (86.7 ? 7.2%) at 10 years (p < 0.05).
100
eo - 80 - 70 - 1 80-
3 60- 1. > 2. * 1 AVR 4 0 significant p < 0.06 ; 2.MVR
m 7 2 1.AVR 4 2 2.MVR
4 4 2 1 3.MR 20
- l , r , 1 1 , 1 1 1 1 1
0 1 2 3 4 6 8 7 8 0 10 11 12 Years
Fig 8. Freedom from structural valve deterioration by valve position for the age group less than 30 years. ( M R = multiple-valve replace- ment, AVR = aortic valve replacement; MVR = mitral valve re- placement.)
90 -
80 -
$ 70- LL Significant p < 0.06 *
1. 2
AVR . MVR
80 1 L.L.-.-
m 4 ~ A V R * W
28 8 2.MVR 1 3.MR
0 1 2 3 4 6 0 7 0 0 10 11 12 Year8
Fig 9. Freedom from structural valve deterioration by valve position for the age group 30 through 59 years. (AVR = aortic valve replace- ment; MVR = mitral valve replacement; M R = multiple-valve re- placement.)
100 \
iignificant p < 0.06 I
159 Jamieson et al: Primary Tissue Failure of Porcine Bioprosthesis
m-
D-
o-
7-
m-
8 -
D-
7 -
i 0 -
t
c e c 6- -
n lu o m I U
Mu.
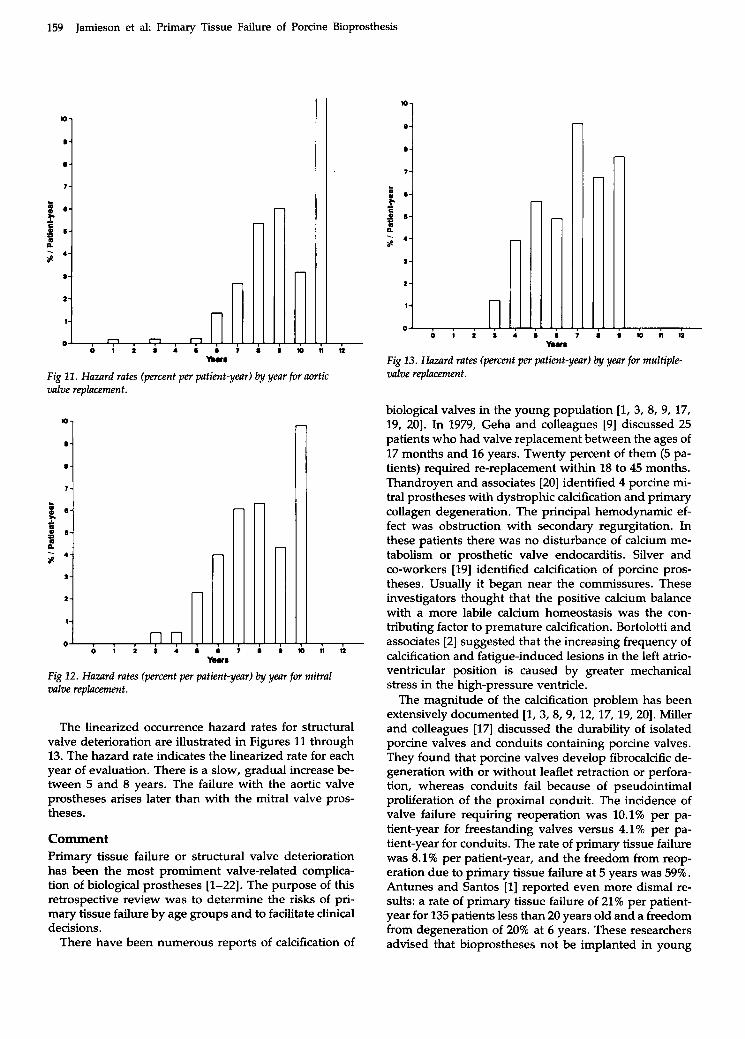
Fig 1 1 . Hazard rates (percent per patient-year) by year for aortic valve replacement.
1 r i
y.ur
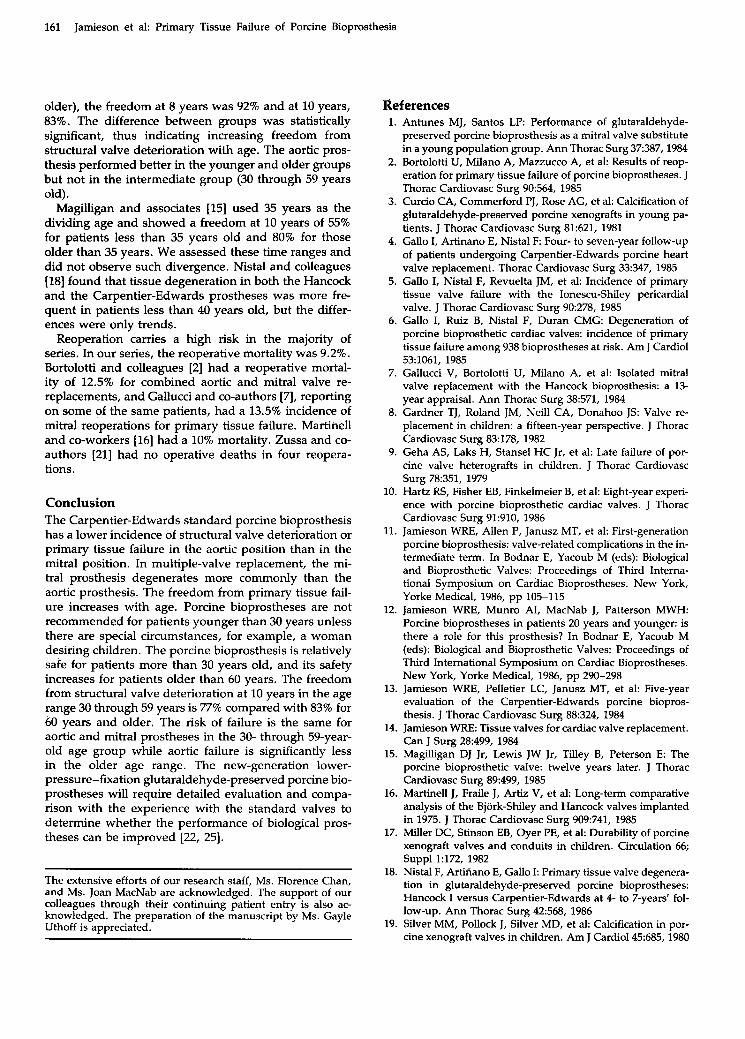
Fig 12. Hazard rates (percent per patient-year) by year for mitral valve replacement.
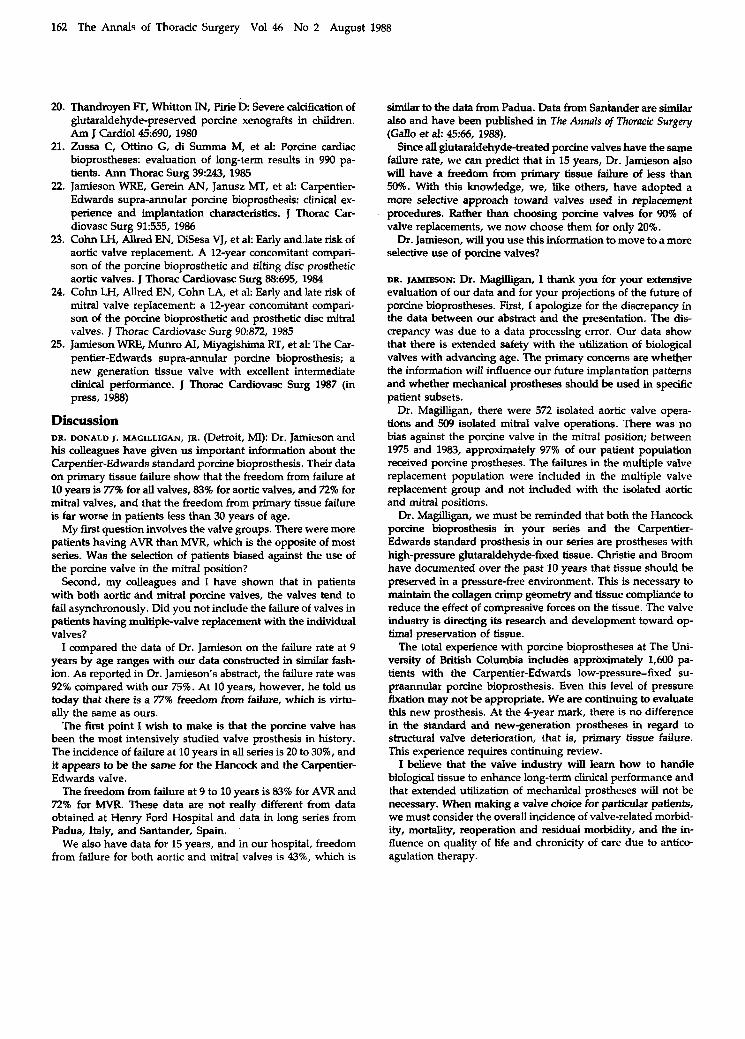
The linearized occurrence hazard rates for structural valve deterioration are illustrated in Figures 11 through 13. The hazard rate indicates the linearized rate for each year of evaluation. There is a slow, gradual increase be- tween 5 and 8 years. The failure with the aortic valve prostheses arises later than with the mitral valve pros- theses.
Comment Primary tissue failure or structural valve deterioration has been the most promiment valve-related complica- tion of biological prostheses [l-221. The purpose of this retrospective review was to determine the risks of pri- mary tissue failure by age groups and to facilitate clinical decisions.
There have been numerous reports of calcification of
m
.i
1 ‘ # I to n ti
Fig 13. Hazard rates (percent per patient-year) by year for multiple- valve replacement.
biological valves in the young population [I, 3, 8, 9, 17, 19, 201. In 1979, Geha and colleagues [9] discussed 25 patients who had valve replacement between the ages of 17 months and 16 years. Twenty percent of them (5 pa- tients) required re-replacement within 18 to 45 months. Thandroyen and associates [20] identified 4 porcine mi- tral prostheses with dystrophic calcification and primary collagen degeneration. The principal hemodynamic ef- fect was obstruction with secondary regurgitation. In these patients there was no disturbance of calcium me- tabolism or prosthetic valve endocarditis. Silver and co-workers [ 191 identified calcification of porcine pros- theses. Usually it began near the commissures. These investigators thought that the positive calcium balance with a more labile calcium homeostasis was the con- tributing factor to premature calcification. Bortolotti and associates [2] suggested that the increasing frequency of calcification and fatigue-induced lesions in the left atrio- ventricular position is caused by greater mechanical stress in the high-pressure ventricle.
The magnitude of the calcification problem has been extensively documented [l, 3, 8, 9, 12, 17, 19, 201. Miller and colleagues [17] discussed the durability of isolated porcine valves and conduits containing porcine valves. They found that porcine valves develop fibrocalcific de- generation with or without leaflet retraction or perfora- tion, whereas conduits fail because of pseudointimal proliferation of the proximal conduit. The incidence of valve failure requiring reoperation was 10.1% per pa- tient-year for freestanding valves versus 4.1% per pa- tient-year for conduits. The rate of primary tissue failure was 8.1% per patient-year, and the freedom from reop- eration due to primary tissue failure at 5 years was 59%. Antunes and Santos [l] reported even more dismal re- sults: a rate of primary tissue failure of 21% per patient- year for 135 patients less than 20 years old and a freedom from degeneration of 20% at 6 years. These researchers advised that bioprostheses not be implanted in young

160 The Annals of Thoracic Surgery Vol 46 No 2 August 1988
patients or in patients with a life expectancy exceeding 10 years. This opinion has been shared by many clinical investigators [3, 8, 201.
Our experience with this age group, though limited, is similar. The incidence of structural valve deterioration was 7.6% per patient-year among patients less than 20 years old (no patient was less than 8 years old), the highest in the series. The freedom at 6 years was 57% and at 8 years, 43%. This rate is significantly lower than for all other age groups by decade. However, we believe the use of bioprostheses in adolescent women is war- ranted, as it avoids the difficulties of anticoagulation during pregnancy [ 121.
For the age groups older than children and adoles- cents, there has been limited documentation of the risk of structural valve deterioration by age [15]. In 1985, Magilligan and colleagues [15] reported that among 951 patients who had valve implantation since 1971, valves in patients 35 years of age and younger had a signifi- cantly greater rate of degeneration. The prosthesis in that series was the original Hancock valve.
Primary tissue failure is also the major concern with bioprosthetic valves in the adult population, but the con- tinuing influence of age has received limited review [15]. It is believed that patients younger than 50 to 60 years have an increased incidence of primary tissue degenera- tion. This degeneration takes the form of tears and per- forations with or without calcification. Calcification can be the only source of degeneration, but this is less fre- quent.
The long-term experience with the standard high- pressure-fixed glutaraldehyde-preserved porcine bio- prostheses has been reviewed continually. The majority of the reports involve the Hancock prosthesis, which was introduced in 1971. The Carpentier-Edwards valve was not introduced until 1975, and documented experi- ence is shorter. In a 12-year experience with the Hancock valve, Magilligan and co-workers [15] reported 71% free- dom from primary tissue failure at 10 and 12 years for the aortic prosthesis and 71% at 10 years and 67% at 12 years for the mitral prosthesis.
Gallucci and colleagues [2, 71 have one of the longest documented experiences with the Hancock valve. In 1984, they [7] presented the results of MVR performed between 1970 and 1981 in 476 patients. Actuarial free- dom from primary tissue failure was 58% at 13 years. In 1985, they [2] reported that the freedom from primary tissue failure at 12 years was 61% for AVR and 69% for MVR with the standard high-pressure-fixed glutaralde- hyde-preserved prosthesis. The modes of failure were stenosis due to calcification and cusp stiffening, and in- competence due to commissural detachment at the site of calcium infiltration. Cohn and colleagues [23, 241 re- ported a 20% incidence of primary tissue failure at 10 years.
In our experience, the overall freedom from primary tissue failure with the Carpentier-Edwards porcine bio- prosthesis was 77% at 10 years; it was 83% for AVR and 72% for MVR (see Fig 4). To our knowledge, the superior
performance of the porcine prosthesis in the aortic posi- tion has not been previously documented. The flexible Elgiloy wireform support structure might contribute to this improved performance by reducing the stress on the leaflets. The results with the mitral prosthesis were simi- lar to those in the Hancock experience.
The documentation for pericardial prostheses is lim- ited. Gallo and colleagues [5] showed a 79% freedom from tissue degeneration at 7 years with the Ionescu- Shiley pericardial prosthesis.
The “explantation interval” has been used as an index of durability in some series. The overall linearized occur- rence rates between series are influenced by several fac- tors. Because primary tissue failure does not remain constant throughout the total observation period, com- parisons of this variable of performance are less mean- ingful. Gallucci and associates [7l documented an inci- dence of 1.7% per patient-year for patients having MVR, a mean age of 53 years, a mean follow-up of 5.2 years, and a mean explantation time of 8 years. In a later report by the same group [2], the overall incidence of primary tissue failure was 2.0% per patient-year (2.3% for AVR and 1.8% for MVR) for patients with a mean age of 37 years, a mean follow-up of 5.6 years, and a mean time to explantation of 7.7 years.
The experience with structural valve deterioratiop in our series is 1.5% per patient-year overall (0.9% in the aortic position and 1.8% in the mitral position); the mean follow-up was 5.6 years, the mean age was 47 years, and the mean time to explantation was 6 years. Martinell and colleagues [16] had a higher incidence with the Hancock prostheses (2.9% per patient-year overall, and 2% for AVR, 3% for MVR, and 4.6% for multiple-valve replace- ment), but the mean age was lower at 39 years. On the other hand, Zussa and co-workers [21] had an overall incidence of 0.2% per patient-year at a mean follow-up of 21 months with various porcine prostheses. Nistal and co-authors [18] reported an incidence of primary tissue valve failure of 0.49% per patient-year for the Hancock prosthesis and 0.97% per patient-year for the Carpentier-Edwards prosthesis in patients with a mean age of 49 and 50 years, a mean follow-up of 59 and 56 months, and a mean time to failure of 58 and 49 months, respectively. The Ionescu-Shiley pericardial valve had an incidence of primary tissue failure of 2.1% per patient-year; the mean age at implantation was 36 years, and the explantation interval was 54 months [5].
Age has been extensively considered in our review of the Carpentier-Edwards standard porcine prosthesis. The linearized rate of occurrence of structural valve de- terioration for patients less than 30 years old was 4.4% per patient-year, 1.7% per patient-year for patients 30 through 59 years old, and 0.9% per patient-year for pa- tients 60 years old and older (see Table 4). The overall incidence was 1.5% per patient-year. The freedom in the younger age range was 72% at 8 years (see Fig 7). In the 30- through 59-year-old group, the freedom from pri- mary tissue failure was 82% at 8 years and 77% at 10 years, while in the elderly group (60 years old and
161 Jamieson et al: Primary Tissue Failure of Porcine Bioprosthesis
older), the freedom at 8 years was 92% and at 10 years, 83%. The difference between groups was statistically significant, thus indicating increasing freedom from structural valve deterioration with age. The aortic pros- thesis performed better in the younger and older groups but not in the intermediate group (30 through 59 years old).
Magrlligan and associates [15] used 35 years as the dividing age and showed a freedom at 10 years of 55% for patients less than 35 years old and 80% for those older than 35 years. We assessed these time ranges and did not observe such divergence. Nistal and colleagues [18] found that tissue degeneration in both the Hancock and the Carpentier-Edwards prostheses was more fre- quent in patients less than 40 years old, but the differ- ences were only trends.
Reoperation carries a high risk in the majority of series. In our series, the reoperative mortality was 9.2%. Bortolotti and colleagues [2] had a reoperative mortal- ity of 12.5% for combined aortic and mitral valve re- replacements, and Gallucci and co-authors [7], reporting on some of the same patients, had a 13.5% incidence of mitral reoperations for primary tissue failure. Martinell and co-workers [16] had a 10% mortality. Zussa and co- authors (211 had no operative deaths in four reopera- tions.
Conclusion The Carpentier-Edwards standard porcine bioprosthesis has a lower incidence of structural valve deterioration or primary tissue failure in the aortic position than in the mitral position. In multiple-valve replacement, the mi- tral prosthesis degenerates more commonly than the aortic prosthesis. The freedom from primary tissue fail- ure increases with age. Porcine bioprostheses are not recommended for patients younger than 30 years unless there are special circumstances, for example, a woman desiring children. The porcine bioprosthesis is relatively safe for patients more than 30 years old, and its safety increases for patients older than 60 years. The freedom from structural valve deterioration at 10 years in the age range 30 through 59 years is 77% compared with 83% for 60 years and older. The risk of failure is the same for aortic and mitral prostheses in the 30- through 59-year- old age group while aortic failure is significantly less in the older age range. The new-generation lower- pressure-fixation glutaraldehyde-preserved porcine bio- prostheses will require detailed evaluation and compa- rison with the experience with the standard valves to determine whether the performance of biological pros- theses can be improved [22, 251.
The extensive efforts of our research staff, Ms. Florence Chan, and Ms. Joan MacNab are acknowledged. The support of our colleagues through their continuing patient entry is also ac- knowledged. The preparation of the manuscript by Ms. Gayle Uthoff is appreciated.
References 1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
Antunes MJ, Santos LP: Performance of glutaraldehyde- preserved porcine bioprosthesis as a mitral valve substitute in a young population group. Ann Thorac Surg 37387,1984 Bortolotti U, Milano A, Mazzucco A, et al: Results of reop- eration for primary tissue failure of porcine bioprostheses. J Thorac Cardiovasc Surg 90:564, 1985 Curcio CA, Commerford PJ, Rose AG, et al: Calcification of glutaraldehyde-preserved porcine xenografts in young pa- tients. J Thorac Cardiovasc Surg 81:621, 1981 Gallo I, Artinano E, Nistal F: Four- to seven-year follow-up of patients undergoing Carpentier-Edwards porcine heart valve replacement. Thorac Cardiovasc Surg 33:347, 1985 Gallo I, Nistal F, Revuelta JM, et al: Incidence of primary tissue valve failure with the Ionescu-Shiley pericardial valve. J Thorac Cardiovasc Surg 90:278, 1985 Gallo I, Ruiz B, Nistal F, Duran CMG: Degeneration of porcine bioprosthetic cardiac valves: incidence of primary tissue failure among 938 bioprostheses at risk. Am J Cardiol 53:1061, 1985 Gallucci V, Bortolotti U, Milano A, et al: Isolated mitral valve replacement with the Hancock bioprosthesis: a 13- year appraisal. Ann Thorac Surg 38:571, 1984 Gardner TJ, Roland JM, Neil1 CA, Donahoo JS: Valve re- placement in children: a fifteen-year perspective. J Thorac Cardiovasc Surg 83:178, 1982 Geha AS, Laks H, Stansel HC Jr, et al: Late failure of por- cine valve heterografts in children. J Thorac Cardiovasc Surg 78:351, 1979 Hartz RS, Fisher EB, Finkelmeier B, et al: Eight-year experi- ence with porcine bioprosthetic cardiac valves. J Thorac Cardiovasc Surg 91:910, 1986 Jamieson WRE, Allen P, Janusz MT, et al: First-generation porcine bioprosthesis: valve-related complications in the in- termediate term. In Bodnar E, Yacoub M (eds): Biological and Bioprosthetic Valves: Proceedings of Third Interna- tional Symposium on Cardiac Bioprostheses. New York, Yorke Medical, 1986, pp 105-115 Jamieson WRE, Munro AI, MacNab J, Patterson MWH: Porcine bioprostheses in patients 20 years and younger: is there a role for this prosthesis? In Bodnar E, Yacoub M (eds): Biological and Bioprosthetic Valves: Proceedings of Thud International Symposium on Cardiac Bioprostheses. New York, Yorke Medical, 1986, pp 290-298 Jamieson WRE, Pelletier LC, Janusz MT, et al: Five-year evaluation of the Carpentier-Edwards porcine biopros- thesis. J Thorac Cardiovasc Surg 88:324, 1984 Jamieson WRE: Tissue valves for cardiac valve replacement. Can J Surg 28499, 1984 Magdligan DJ Jr, Lewis JW Jr, Tilley B, Peterson E: The porcine bioprosthetic valve: twelve years later. J Thorac Cardiovasc Surg 89499, 1985 Martinell J, Fraile J, Artiz V, et al: Long-term comparative analysis of the Bjork-Shiley and Hancock valves implanted in 1975. J Thorac Cardiovasc Surg 909:741, 1985 Miller DC, Stinson EB, Oyer PE, et a1 Durability of porcine xenograft valves and conduits in children. Circulation 66; Suppl 1:172, 1982 Nistal F, Artiiiano E, Gallo I: Primary tissue valve degenera- tion in glutaraldehyde-preserved porcine bioprostheses: Hancock I versus Carpentier-Edwards at 4- to 7-years’ fol- low-up. Ann Thorac Surg 42:568, 1986 Silver MM, Pollock J, Silver MD, et al: Calcification in por- cine xenograft valves in children. Am J Cardiol45:685, 1980
162 The Annals of Thoracic Surgery Vol 46 No 2 August 1988
20. Thandroyen IT, Whitton IN, pirie D. Severe calcification of glutaraldehyde-preserved porcine xenografts in children. Am J Cardiol45:690, 1980
21. Zussa C, Ottino G, di Summa M, et ak Porcine cardiac bioprostheses: evaluation of long-term results in 990 pa- tients. Ann Thorac Surg 39243, 1985
22. Jamieson WRE, Gerein AN, Janusz MT, et a1 Carpentier- Edwards supra-annular porcine bioprosthesis: clinical ex- perience and implantation characteristics. J Thorac Car- diovasc Surg 91:555, 1986
2% Cohn LH, Allred EN, DiSesa VJ, et al: Early and late risk of aortic valve replacement. A 12-year concomitant compari- son of the porcine bioprosthetic and tilting disc prosthetic aortic valves. J Thorac Cardiovasc Surg 88:695, 1984
24. Cohn LH, Allred EN, Cohn LA, et al: Early and late risk of mitral valve replacement: a 12-year concomitant compari- son of the porcine bioprosthetic and prosthetic disc mitral valves. J Thorac Cardiovasc Surg 902372, 1985
25. Jamieson WRE, Mum0 AI, Miyagishima RT, et al: The Car- pentier-Edwards supra-annular porcine bioprosthesis; a new generation tissue valve with excellent intermediate clinical performance. J Thorac Cardiovasc Surg 1987 (in press, 1988)
Discussion DR. DONALD J. MAGILLIGAN, JR. (Detroit, MI): Dr. Jamieson and his colleagues have given us important information about the Carpentier-Edwards standard porane bioprosthesis. Their data on primary tissue failure show that the freedom from failure at 10 years is 77% for all valves, 83% for aortic valves, and 72% for mitral valves, and that the freedom from primary tissue failure is far worse in patients less than 30 years of age.
My first question involves the valve groups. There were more patients having AVR than MVR, which is the opposite of most series. Was the selection of patients biased against the use of the porcine valve in the mitral position?
Second, my colleagues and I have shown that in patients With both aortic and mitral porcine valves, the valves tend to fail asynchronously. Did you not include the failure of valves in patients having multiple-valve replacement with the individual valves?
I compared the data of Dr. Jamieson on the failure rate at 9 years by age ranges with our data constructed in similar fash- ion. As reported in Dr. Jamieson’s abstract, the failure rate was 924 compared with our 75%. At 10 years, however, he told us today that there is a 77% freedom from failure, which is virtu- ally the same as ours.
The first point I wish to make is that the porcine valve has been the most intensively studied valve prosthesis in history. The incidence of failure at 10 years in all series is 20 to 30%, and it appears to be the same for the Hancock and the Carpentier- Edwards valve.
The freedom from failure at 9 to 10 years is 83% for AVR and 72% for MVR. These data are not really different from data obtained at Henry Ford Hospital and data in long series from Padua, Italy, and Mtander, Spain.
We also have data for 15 years, and in our hospital, freedom from failure for both aortic and mitral valves is 43%, which is
similar to the data from Padua. Data from Santander are similar also and have been published in The Annals of Thoracic Surgery (Gallo et al: 4556, 1988).
Since all glutaraldehyde-treated porcine valves have the same failure rate, we can predict that in 15 years, Dr. Jamieson also will have a freedom from primary tissue failure of less than 50%. With this knowledge, we, like others, have adopted a more selective approach toward valves used in replacement procedures. Rather than choosing porcine valves for 90% of valve replacements, we now choose them for only 20%.
Dr. Jamieson, will you use this infonnation to move to a more selective use of porcine valves?
DR. IAMIBSON: Dr. MagiEgan, I thank you for your extensive evaluation of our data and for your projections of the future of porcine bioprostheses. First, I apologize for the discrepancy in the data between our abstract and the presentation. The dis- crepancy was due to a data processing error. Our data show that there is extended safety with the utilization of biological valves with advancing age. The primary concerns are whether the information will influence our future implantation patterns and whether mechanical prostheses should be used in specific patient subsets.
Dr. Magilligan, there were 572 isolated aortic valve opera- tions and 509 isolated mitral valve operations. There was no bias against the porcine valve in the mitral position; between 1975 and 1983, approximately 97% of our patient population received porcine prostheses. The failures in the multiple valve replacement population were included in the multiple valve replacement group and not included with the isolated aortic and mitral positions.
Dr. Magilligan, we must be reminded that both the Hancock porcine bioprosthesis in your series and the Carpentier- Edwards standard prosthesis in our series are prostheses with high-pressure glutaraldehyde-fixed tissue. Christie and Broom have documented over the past 10 years that tissue should be preserved in a pressure-free environment. This is necessary to maintain the collagen crimp geometry and tissue compliance to reduce the effect of compressive forces on the tissue. The valve industry is directing its research and development toward op- timal preservation of tissue.
The total experience with porcine bioprostheses at The Uni- versity of British Columbia includes approximately 1,600 pa- tients with the Carpentier-Edwards low-pressure-Fled su- praannular porcine bioprosthesis. Even this level of pressure fixation may not be appropriate. We are continuing to evaluate this new prosthesis. At the 4-year mark, there is no difference in the standard and new-generation prostheses in regard to structural valve deterioration, that is, primary tissue failure. This experience requires continuing review.
I believe that the valve industry will learn how to handle biological tissue to enhance long-term clinical performance and that extended utilization of mechanical prostheses will not be necessary. When making a valve choice for particular patients, we must consider the overall incidence of valve-related morbid- ity, mortaiity, reoperation and residual morbidity, and the in- fluence on quality of life and chronicity of care due to antico- agulation therapy